0319 aog journal - Dental Link
32
Towards Perfect Practice THE SUMMER 2001 JOURNAL Volume 16 Issue 1 AOG AOG CHARITY BALL 17th November 2001 At The Radisson Portman IS AMALGAM ‘SAFE’ AS A RESTORATIVE MATERIAL? - PATHWAYS TO PROFESSIONAL POWER - A MILLENNIUM OF ENDODONTICS: A HISTORICAL PERSPECTIVE PART 1 - CLINICAL GOVERNANCE - TAX ADVANTAGED INVESTMENTS FOR ACCELERATED GROWTH
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of 0319 aog journal - Dental Link
To w a r d s P e r f e c t P r a c t i c e
T H E
SUMMER 2001
JOURNALVolume 16 Issue 1
AOG
AOG CHARITY BALL17th November 2001 At The Radisson PortmanIS AMALGAM ‘SAFE’ AS A RESTORATIVE MATERIAL? - PATHWAYS TOPROFESSIONAL POWER - A MILLENNIUM OF ENDODONTICS:A HISTORICAL PERSPECTIVE PART 1 - CLINICAL GOVERNANCE -TAX ADVANTAGED INVESTMENTS FOR ACCELERATED GROWTH

“MCINTYRE, DOESN’T SOUND AVERY ASIAN NAME”With the abovecomment one of mycolleagues aptlydescribed the lack ofunderstanding aboutthe role andmembership of theAnglo AsianO d o n t o l o g i c a lGroup - the Anglosdon’t have to beAsian. As the President and the firstCaucasian to be elected to that honour I woulddearly love to see the AOG broadening itsmembership to encompass all of those likeminded people within the wider dentalcommunity. Yes, of course the focus of theAOG is on the ethnic minority communities athome and less wealthy members of the dentalprofession overseas, they are the groups forwhom so much needs to be done and who areso often overlooked. I believe that the AOG isunique among dental societies in puttingcharity and assistance to the less fortunate atthe head of its agenda - we have no specific orlimited clinical interest groups, no politicalagenda and no wish to advance our personalinterests. We simply aim to illustrate thecaring and compassionate side of dentistry thatrarely if ever gets noticed. You only have tolook at the £5,000 raised for Charity at themagnificent ball held at the Café Royal lastyear, or the recent Charity Ball and auction toraise money for the Gujarat EarthquakeAppeal to see the visible proof of that.
As members of course we know about all ofthis, so who better to spread the word aboutthe benefits of membership than those of uswho enjoy it now? It is an obvious fact, but ifwe all recruit just one new member the AOGwill double in size and our potential influencewill grow with it.
I am very fortunate to have taken over fromsuch a hard working man as Jatin, he handedover a society in good heart with soundfinancial status and a dynamic and enthusiasticcommittee who are always coming up withideas to improve the benefits available tomembers. I look forward to serving you thisyear as your President and enjoying yoursupport at our many functions.
Air Vice-Marshal Ian McIntyre
THE JOURNAL OF THE ANGLO-ASIAN ODONTOLOGICAL GROUP (AOG)PresidentIan McIntyre
President ElectAbhay Soneji
Secretary GeneralRishi Mehrotra
Minutes SecretaryPinkoo Bose
TreasurerMahesh Patel
Membership SecretaryNishan Dixit
Seminar SecretaryKishore Soneji
Social SecretaryPomi Datta
Sponsorship SecretaryDipak Joshi
EditorSubir Banerji
Awards SecretariesAshok SongraUlpi Darbar
Golfing SecretaryBhupi Bhogal
Committee MembersDinesh JaniParvin AmijiRuss Ladwa
Co-opted Committee MembersRaj MajithiaSudhir RadiaSuresh Sharma
Journal SponsorThe Dental Directory
Welcome to anotherissue of the AOGjournal. It has been avery active year forthe committee andmembers of oursociety. This year
saw another very successful collaboration withBSGDS at the conference in South Africa.Pictures are included to remind the ones whowere there and evoke regret for the ones whoweren’t. This year also saw our President, Ian
McIntyre, receive The Probe’s LifetimeAchievement Award. With his characteristicmodesty, Ian was quick to mention the manyothers who were worthy of distinction.
On January 26th however, there was agruesome reminder of the destructive forces ofthe elements. Nature shook Gujarat till 30,000lay dead and wastelands blossomed wherepeople’s dreams once stood. Much hashappened and the state machinery is often inthe way. Rehabilitation is yet to touch tens ofthousand of people.
In April over 5,000 marched from Bhachau tothe collector’s office in Bhuj — a distance ofsome 67 km in scorching heat to protest aboutthe delays in receiving aid. Pictures of asmiling eight year old boy being fitted with anartificial leg, and a family making it’s waythrough the rubble every Sunday stoppingmomentarily to pay respects in Anjar streetwhere 250 school children perished, reflectsthe strength of the human spirit. “We go tovisit them just to remind ourselves that we arethe fortunate ones who are left here to be goodhuman beings and keep alive the Kutchi spirit”says 11 year old Parth Bhinde.
So it is good that help both corporate andindividual is coming through. Manjul andRashmi have to be congratulated on organisingan event which has raised about £50,000 forthe relief fund and pledges still keep coming inwith the total increasing. No doubt therebuilding process will take a few years. Theearthquake of 1995 in Kobe, Japan whichkilled over 5,000 took 5 years forrehabilitation, so help is still required.
In this latest issue I have endeavoured to puttogether some articles which I hope will be ofinterest. The first part of a three part article bySanjeev Bhanderi ‘A Millennium ofEndodontics’ is a very interesting featurewhich will give a complete overview ofendodontics. Contributions of both clinical andfinancial interest are also featured and as ever,my warm thanks goes out to all thecontributors. Please send in your commentswhich are always an enormous source of helpand encouragement.
Wishing you all the very best for the summer.Subir Banerji.Editor.E-mail: [email protected]
From The Editor

South AfricaThe happy Couple
Steve Perry’s &
Rash Patels
Products
The Dean and the Green
The President and Wife
Sheila Farell, Manny Vasant & Edger Gordon

The question of mercury toxicity is frequentlyraised, not least by the media and inevitably afew days later by our patients who have readthe articles. The specific fears that such articlesraise are often simplistic and unequivocal.Links with Multiple Sclerosis (MS), severesoft tissue reactions and amalgam corrosionwhen placed in contact with other metallicrestorations, even fine gold.....
Perhaps the layperson should, quite sensibly,be cautious – in light of such information – intheir approach to amalgam, but how shouldwe, as professionals, respond when they cometo seek our advice?
A review of some relevant literature is detailedbelow and may help in our advice to those whoseek it.
It is certain that mercury is toxic. The role thatthe mercury component of dental amalgamplays in the total mercury insult to those whocome into contact with it, and the ill effectsattributable to this material, has been underdebate for years. In order to determine thesignificance of mercury from its use in clinicaldentistry, the following need to be considered.
1. THRESHOLD LEVELSRELATING TO MERCURYEXPOSURE:
Two levels are used in assigning industrial andother thresholds for mercury (Hg)concentration in the air and these relate tolevels at which ill effects appear or fail toappear (1). They are:1. Lowest observed adverse effect level(LOAEL); and2. No observed adverse effect level (NOAEL).Hg threshold levels have been drawn up on thebasis of toxicity studies carried out onindustrial workers exposed to Hg vapour.Threshold levels suggested for the generalpublic are based on these, having includedgenerous allowances for safety and for the factthat industrial workers are subjected tocontinuous exposure (a 40hr working week).
The WHO has recommended a health-basedoccupational exposure limit for air of 25microgram/cubic m. Gerstner & Huff-’77 (11)suggested a NOAEL threshold for air exposureof 1 microgram/ cubic m. for children,
restorations. It has been shown that gutbacteria can form and degrade methyl mercury.b). The corrosion process results in Hgreaching the surface of the restoration where aconcentration gradient exists. The Hg is thenreleased in the vapour form; the Hg may alsodissolve into saliva and be swallowed.Toothbrushing and chewing will accelerate therate of release. Berglund estimated from his daily dose equation the mean amount swallowed at approximately 10microgram/day. This Hg is oxidised to the lesstoxic mercuric ion form and 5-10% is absorbed(2). Hence, less than 1 microgram/day will beabsorbed through this route.
iii). Pulp and the peridontium:a).Studies have shown that Hg may reach thepulp through dentinal tubules in the absence ofa lining.b). Particles may be implanted unintentionallyduring retrograde obturation of a root-canal, orinadvertent placement into a socket.
Studies of such inclusions by electronmicroscopy and energy dispersive x-raymicroanalysis show that these particlesundergo progressive degradation to theirconstituent elements, which, when dispersed,eventually accumulate in the kidneys, or areexcreted through faeces. However, thequantities of Hg passing through this route isconsidered negligible in terms of totalexposure. Sandborg-Englund(13) concluded in1996 (in a study of renal function before andafter amalgam fillings were removed in 10volunteers) that there was no signs of renaltoxicity from dental amalgam sources.
In assessing the role of dental amalgam in theoverall toxic effects of Hg, one needs toconsider the other sources of Hg challenge tothe body. These include seafood andenvironmental pollution, e.g. the burning offossil fuels. One Swedish study showed thatthe consumption of 1 saltwater seafood mealper week raised blood Hg levels from 2.3-5.1ng/l; whilst another study comparing averageHg levels in patients with amalgam fillings(0.7 ng/l) to those without (0.3 ng/l) shows thatdental amalgam made a difference of only 0.4ng/l (9) (two German studies actually found nodifference in the Hg levels of blood and urinesamples when comparing subjects withamalgam fillings to controls without). It could
Is amalgam‘safe’asa restorative material? A review of some relevant literature on the subject of mercury toxicity
pregnant women and the infirm. It wasconsidered that below this level, Hg vapour inambient air posed no health hazards. Assigninga ventilation rate of 22 cubic m. /day, a lowestthreshold of 1 microgram/cubic m. of Hgproduces a safety threshold of 20microgram/day through the lungs (assuming100% absorption). This figure may bemultiplied by a factor of 10 to estimate thedaily absorption through the GI tract due topoorer absorption by this route and a furthertwo-fold for the lower toxicity of mercuriccompounds (1). This gives a safe threshold of400 microgram/day for GI absorption.Hg exposure, from a dental source, may beviewed against these thresholds to assess therisks.
2. QUANTIFYING THEMERCURY CHALLENGE TO APATIENT OR DENTAL WORKER:
The routes of absorption of Hg from a dentalsource into the body include:i). Lungs:This is in the form of Hg vapour. Potentialsources include:a). Use of Hg in the dental surgery at any stagebefore the amalgam has set, e.g. duringtrituration of amalgam in the amalgamator;exposure of Hg (due to its volatile nature);spillages.b). Vapour release from amalgam restorationsas a result of corrosion. This is much reducedby the use of high- Copper alloys which arefree of the Gamma II phase.c). During the insertion and removal ofamalgam restorations, e.g. duringcondensation or cutting of amalgam with airturbines.One study using vapour detectors over a 24hr.period reported only 1.7 microgram/dayinhaled(9). Three other studies showed Hgvapour exposure, for patients with 8-10amalgam restorations, of between 1.1-4.4microgram/day(9). It may be seen that theselevels, taken on their own, are well below thethresholds considered safe for Hg absorbedthrough respiration.
ii). GI tract:This may be in the form of amalgam particlesor in ionic form:a). Particles of amalgam may be swallowedduring treatment, or through the fracture of
AOG
5

AOG
be argued, therefore, that dietary sources canhave a 7 times higher effect on blood Hg levelsthan amalgam restorations.Jones (3) wrote in1999:i). The average daily intake of methylated Hg(mainly in the form of seafood) needed to be inthe region of 300 micrograms to causediscernible effects in even the most sensitiveindividual.ii). Due to the low amount of Hg released fromamalgam, he estimated that a patient wouldhave to have 490 amalgam surfaces for thelevels of Hg vapour and mercuric ions to reachmaximum safety levels.iii). The dietary form of Hg (methylated Hg) ismore toxic and its uptake some 6-7 timeshigher when compared to Hg from amalgamsources.Eley (1) also wrote that:i). Estimates of average daily intake of Hgfrom sources such as water, food, air and fossilfuels range up to 20 microgram/day; most of itin the more toxic methylated form. Thiscompares to estimates of 1 microgram/daythrough the lungs and 1 microgram/daythrough the GI tract attributable to amalgam.
When assessing the risks to the general public,it should be noted that dental workers have amuch higher exposure to Hg vapour (Wirz etal. (5) found that although the blood and urinesamples in dental workers were twice that ofcontrol groups- with and without amalgamrestorations-there was no evidence of any Hgtoxicity in any of the groups).Osborne in ‘92 (4) concluded that there was noavailable evidence to show that dental workerswere adversely affected by Hg use.Another study in 1993 involving Japaneseschool children showed that the presence ofamalgam fillings made a difference of only1.5% to a mean urine level of 2 ng/l.It may be concluded that:i). The absorption of Hg from a dental sourceis very small in relation to levels that wouldcause ill effect or threshold levels set to protectthe public.ii). Hg release from amalgam is smallcompared to exposure from other sources.
3. TOXICITY OF MERCURY INRELATION TO AMALGAMRESTORATIONS:
It is possible to show the derivation ofelemental Hg and inorganic Hg salts fromamalgam; the link between dental amalgamand organic Hg compounds, however, is very
tenuous. The main source of such compounds(in the form, primarily, of methylated Hg)come from the diet.
Exposure to inorganic Hg can lead toMercurialism with CNS symptoms andreproductive disorders. Organic Hgcompounds, e.g. alkyl Hg compounds, cancross the blood-brain barrier and accumulate inhigh concentrations in the brain. They cancause toxic neurocephalopathy. Eley & Cox(6) wrote that, to date, there is no evidence ofmethyl Hg from dental sources detected in theoral cavity.
Many of the symptoms stated in the reportslinking amalgam with Hg toxicity do not fitwith any one pattern of Hg poisoning. Somerelate to inorganic, others to organic Hg, whilstanother group of symptoms are notcharacteristic of either form (7).
The main body of evidence implicating dentalHg has come from anecdotal reporting ofsymptom resolution after the removal ofamalgam restorations. In such cases, it has notbeen possible to show a causal relationshipbetween amalgam and the symptoms. Stenman& Grans (8) concluded from a study of 348patients (some of whom were self-selectedbecause of their fear of amalgam Hg toxicity)that many of those whose reported symptomsresolved post-removal of amalgam hadsymptoms that were primarily ‘mental’!
4. MERCURYHYPERSENSITIVITY:
It is associated with a Coombs type IVhypersensitivity in < 1% of the treatedpopulation. Symptoms involve hyperemia,edema and vesicle formation. Evaluation by adermatologist should precede assumption ofallergy. A skin patch-test is available but deemedunreliable and Mackert-’85 (14) stronglyadvised against its use as a definitive test.
5. AMALGAM’S IMPLICATIONIN MULTIPLE SCLEROSIS (MS):
There has been many attempts to link thepresence of dental amalgam to MS. But sinceMS is characterised by spontaneous bouts ofremission, the anecdotal reports of symptomresolution on amalgam removal cannot betaken to show a causal relationship betweenthe two events.
Clausen-’93 (15) found no significantdifferences in the post-mortem brain total Hglevels in studies of patients who had sufferedMS and those who had not. The lipid-solubleHg was in fact significantly lower in MSsufferers, therefore, it could be seen that MS isnot connected with increased Hg levels in thebrain.
6. ENVIRONMENTALCONSIDERATIONS:
In September 1992 the Swedish NationalBoard of Health & Welfare issued a report thatproposed a plan for the discontinuation of theuse of Hg in dentistry. This was based entirelyon environmental concerns, as opposed to anyproven health risks in its clinical dentalapplication. The Swedish government hadalready planned for the cessation of Hg use inindustry. This was a culmination of researchinto the paper processing industry’s pollutionin the ‘50s and ‘60s.
However, their Medical Research Councilconcluded that Hg pollution from dentistrycould be successfully controlled by the use ofamalgam separators, many of which haveefficiencies in excess of 99%. At present,discarded household batteries account for themajority of Hg in municipal waste. A 1992U.S. Environmental Protection Agency report(12) stated that batteries accounted for 86% ofdiscarded Hg, whilst dental amalgamaccounted for 0.56%.
7.COST IMPLICATIONS OF THEUSE OF AMALGAM AND ITSALTERNATIVES:
These include:i). Additional dentists would need to be trainedto provide the same level of dental care, due tothe operator intensive nature of thealternatives.ii). The long term costs of amalgamalternatives will rise with time due to the lowerlife expectancies of some alternatives e.g.composites.iii). More frequent replacement of restorationswill result in tooth substance loss; thedownward restorative spiral will incur a costthat is harder to quantify.iv). Theoretical calculations of the long termcosts of a 2 or 3 surface gold/ compositerestoration is about 4 times that of amalgam; 5times more for small gold restorations.v). As the alternatives improve, these costs willfall.vi). The continued use of amalgam, itself,incurs costs in the:a). handling of the separated amalgam,b). raising of the specifications of the dentalequipment, e.g. capsule amalgam and modernamalgamators; and in the surgery set-up costse.g. clean air systems.
Is amalgam ‘safe’as arestorative material?Continued from previous page
6

AOG
8. NATIONAL GOVERNMENTPOSITIONS ON MERCURY INDENTISTRY:
1). In 1993, a two year U.S. Public HealthService review involving a wide range ofmedical experts concluded that there was nopersuasive evidence to compel a change toamalgam alternatives.Their conclusions were based on thefollowing findings (in brief):i). The amount of elemental Hg released fromamalgam was minute.ii). Existence of specific adverse responses tothese minute amounts had not been demonstrated.iii). Even if adverse responses existed, theywere so subtle as to be undetectable andtherefore no harm could be shown.iv). True hypersensitivity was very rare. Only50 or so reported cases since the early 1900s.v). There is no persuasive evidence that showsa causal relationship between amalgam andmany of the symptoms attributed to Hgtoxicity from a dental source.vi). The benefits of amalgam include:a). Cost effectiveness compared to existingalternatives.b). Absence of an alternative of comparableproperties that may be used as a viablesubstitute in all situations.
2). The German authorities haverecommended:The use of amalgam should be avoided ifpossible in:i). Children under 6 years old; who theyconsidered to have a higher sensitivity to Hg. However the WHO clearly stated thatthere is no evidence to show age-related sensitivity in humans.ii). Patients with renal complaints.iii). Pregnant women. However, a study byEricson & Kallen (4) in ‘89 did not find any significant differences between dentalworkers and control groups for spontaneous abortions, low birth weight oftheir babies, congenital abnormalities or infant survival. Studies with conflictingconclusions do exists on this issue.
3). The Canadian government have set a limit95% below the level that may cause ill-effectsand have lowered the recommendedmaximum daily exposure to Hg for women ofchild bearing age and children under 10 years.This has not been based on any scientificevidence but confirms a tendency forgovernment health authorities to ‘err’ on theside of caution.Schuurs- ‘99 (10) concluded that the negativeeffects on reproduction due to Hg exposure inthe dental office are unproven. Unless verypoor Hg hygiene measures were employed,the Hg concentration in the air will not exceedthe female’s time-weighted long-termThreshold Limit Value.
Therefore, in view of the lower amounts of Hgthat will emanate from amalgam restorations,the public should be at an even lower risk fromHg of a dental source compared to dentalworkers.
9. MERCURY HYGIENE IN THE DENTAL SURGERYENVIRONMENT:
i). Hand condensation of amalgam will reducemean air levels to 15-320 microgram/cubic m. compared to levels of 770 microgram/cubicm. with mechanical condensation.ii). ‘Wet’ cutting of amalgam in one studyreduced:a). mean Hg vapour levels to 15microgram/cubic m. (compared to 50-190microgram/cubic m. without water cooling).b). mean particulate matter to 30-60microgram/cubic m (compared to 270-520microgram/cubic m. without water cooling.iii). Use of rubber-dam will reduce:a). the GI tract exposure through swallowing,b). moisture contamination of the unsetamalgam leading to lower corrosion – asignificant source of Hg release and loweredrestoration life-expectancy.iv). Correct handling and hygiene measures:a). Avoid skin contact. The routine use ofprocedure gloves now eliminate almost alloperator skin contact.b). Use of protective clothing/ footwear willreduce exposure (e.g. absorption throughnailbed of toes).c). Correct storage of unused amalgam under asolution of Potassium Permanganate pending proper disposal.d). Use of capsule amalgam and moderntriturators.e). Use of high Copper alloys to eliminate theGamma II phase.f). Instigation of prompt recovery proceduresin the event of Hg spillage.g). Hard surgery flooring with rounded lineangles at the walls and cabinetry to prevent accumulation of undetected spillages.h). Uni-directional air-flow systems thatreplaces the surgery air constantly to reduce the air concentration of Hg vapour.i). Refraining from the dry-polishing ofamalgam.
It may be concluded that provided the handlingand use of amalgam is carried out with care,there is no convincing evidence that, from aHg toxicity or environmental viewpoint, towarrant the cessation of its use.
N. Poon
References(1). Eley B.M.The future of dental amalgam: A review of theliterature.Br. Dent. J. 1997; 182: 373-381.
(2). Mackert J.R. Jr.Factors affecting estimations of dental amalgammercury exposure from measurements of mercuryvapour levels in intra-oral and expired air.J Dent Res. 1987; 66: 1775-1780.
(3). Jones D.W.Exposure or absorption and the crucial question oflimits for mercury.Journal l’Association Dentaire Canadienne.65(1):42-6, 1999 Jan.
(4). Jones D.W.The enigma of amalgam in dentistry.Br Dent J 1994; 177:159-170.
(5). Wirz J., Ivanovic D., Schmidli F.Mercury loading from amalgam fillings.Schweizer Montasschrift fur Zahnmedizin.100(11): 1292-8, 1990.
(6). Eley B.M., Cox S.W.Mercury from dental amalgam fillings in patients.Br Dent J 1987; 163: 221-226.
(7). Eley B.M., Cox S.W.Mercury poisoning from dental amalgam- anevaluation of the evidence.J Dent 1998; 16: 90-95.
(8). Stenman S., Grans L.Symptoms and differential diagnosis of patientsfearing mercury toxicity from amalgam fillings.Scandinavian Journal of Work, Environment &Health. 23 Suppl 3: 59-63, 1997.
(9). Anusavice K.Phillip’s Science of Dental Materials.10th edition, 1996; WB Saunders, Philadelphia.
(10). Schuurs A.H.Reproductive toxicity of occupational mercury. Areview of the literature.Journal of Dentistry. 27(4): 249-56, 1999 May.
(11). Gerstner H., Huff.Clinical toxicology of mercury.J. Toxicol Environ Health. 1997;2:491-526.
(12). E.P.A.Characterisation of products containing mercury inmunicipal solid waste in the U.S.EPA report. Mar.1992.
(13). Sandborg-Englund G., Nygren A.,Ekstrand., Elinder c.No evidence of renal toxicity from amalgamfillings.Am J Physiol 1996;271:R941-945.
(14). Mackert J.Hypersensitivity to mercury from dentalamalgams.J. Am. Acad. Dermatol. 1985;12:877-880.
(15). Clausen J.Mercury and multiple sclerosis.Acta Neurologica Scand. 1993;87(6):461-464.
7

AOG
8
Presented at a joint AOG/BSGDS meeting at The Wilderness Hotel, Western Cape, S.A.April 2001 by Edgar Gordon
Governance of the professions is one of thehottest media topics around at themoment. All regulatory bodies are
reviewing their arrangements either by choice orthrough government intervention with regulationof the General Medical Council taking the highestpriority. Reform of the GMC is at the very heartof modernising the NHS. It is only natural thatthe public debate is very focused on doctorsbecause of Bristol, the Ledward case and ofcourse Dr. Shipman. The inflammatory languageused by Alan Milburn of the Alder Hey organscandal adds gist to the mill and because of thehistorical relationship between our profession andmedicine, dentistry is inevitably the seconddomino. What happens at the General MedicalCouncil today will inevitably happen to theGeneral Dental Council tomorrow.
The title of my presentation is privatepatients’ complaints. Technically – I should referto them as non-NHS complaints. The reason isthat the NHS general practice, the communityand the hospital service all have a well tried andtested system that was updated as recently as1995. I am also excluding capitation plans,insurance and dental corporate bodies. All three,for purely marketing reasons, have reasonablyeffective complaint mechanisms in place.
Dental private patient complaints occupy aunique place in the UK health care system. Thisis because there is virtually no private medicalpractice in family doctoring. Today, one in fourGDPs treat 70% or more of their patientsprivately and there still is no formal mechanismfor these patients to complain in the absence oflegally defined personal injury or professionalmisconduct. Granted the General Dental Councilhas recently become more pro-active in theirapproach to complaints. A recent high profilesuspension of a private practitioner caused anunprecedented furore in the dental press. It is amatter of debate on whether the GDC acted asthey did to forestall a greater degree ofgovernmental surveillance.
Why do patients complain?It is often said by organisations acting for patientsthat when things go wrong, patients are notprimarily interested in money. What they want isto be told the truth, an apology where appropriateand changes in practice to prevent other peoplefrom suffering. This view is almost wholly basedon dealing with complaints in the NHS hospitaltrust sector and very little in primary care. It doesnot apply in dentistry and certainly is it atcomplete variance with the experiences of thedental defence organisations. Item of service feeshas always been central to the culture of dentistry.Moreover, in the private sector, manyinterventions are elective, there are alternativesand many are lifestyle procedures with eithermarginal or no effect on health gain. Otherfactors contribute to the rising tide of dentalcomplaints. A patient is more likely to complainif they have expectations, have absorbed
the culture of a consumer society and are better educated.
It is also much easier to complain aboutdental than medical care. Dentistry is far moremeasurable both quantitatively and qualitatively.Most interventions are essentially invasive,irreversible and visible. They are elective and notlife threatening. It follows that consumers havechoices and enhanced levels of consent arerequired. Since dental care is provided in cottageindustry conditions it is easier to focus on a singleidentifiable person who is both the clinician andthe owner of the business. This contrasts with thedifficulty of dealing with a large diverseorganisation like a hospital where care is given bya multi-disciplinary hierachial managed staff.
The majority of dental private patientcomplaints are specific. They ask that followingunsatisfactory treatment some sort of offer orarrangement be made to carry out remedial workat no further charge. Irrespective of whethercomplainants go back to the same practitionerthey may seek common law damages. This is thefinancial compensation for their perceived harmtogether with the costs of repairing any damage.Inter-personal wrong doing is the tort known asclinical negligence. For this to succeed it mustpass all three criteria of the Bolam test – a duty ofcare, a breach of that duty and damage arisingfrom that breach. Private practice also generatessome – but not many – breach of contract claimssuch as a poorly fitting denture or a crown ofincorrect colour.
Another common objective is the desire tofind an explanation of why the dental treatmentwent wrong. Where there has been an adverseresult, dentists are often suspected of being lessthan completely open and honest with theirexplanations. Some consumers will try and use acomplaints system as a discovery procedure.Another reason often given is to preventunsatisfactory outcomes happening to otherpatients. This is a laudable attitude by a cynicwould find it hard to believe that a patient whohad crowns fall out after only six months is moreconcerned about other people’s crowns than theirown. Lastly complaints can be prompted by thethreat of debt collection. A fee may remainunpaid but the dentist is unaware that theconsumer is dissatisfied. When later faced withthe threat of civil proceedings to recover the debt,they may respond by counter-claiming for breachof contract as well as alleged negligence.
Irrespective of whether the complaintconcerns a clinical or contractual matter the firstpiece of advice to any complainant that any otherresponsible practitioner or other authority wouldgive, statutory or voluntary, would be to go backand voice their concerns with the practitionerconcerned…and quickly. It has long beenrecognised that a dentist’s manner and attitude tothe patient at the time of complaint can have a far-reaching effect on how vigorously the complaintis pursued. Dentists know themselves thatsympathetic handling of an aggrieved patient,together with helpful explanations of whathappened, can go a long way to defusing thesituation. The dentist must be given theopportunity of putting things right. This issupported by the GDC whose guidance to
dentists is that if a patient has cause to complainabout the service provided every effort should bemade to resolve the matter at practice level. ForNHS treatment it is part of a dentist’s term ofservice to record complaints in writing,acknowledge them either orally or in writingwithin three days and in ten days forward theirdefinitive comments.
Trying to discover whether dental treatmentwas private or NHS has always been difficult.The term ‘independent dentistry’ has not helped.Patients are still confused and there is still littledocumentary evidence such as a treatment plan,estimate or receipt. This has long been aconsumerist problem and led to the governmentintroducing the FP17DC in 1990.
There is evidence that many practitioners donot follow the FP17DC procedure. Moreover,Health Authority complaint managers give theform of low priority. Not a single dentaldisciplinary hearing has ever been heardregarding a practitioner’s failure give thismandatory information. It becomes part of adisciplinary hearing only as a adjunct to othermore serious matters.
There are further difficulties. Althoughprivate contract dentistry is presently growingexponentially the actual number of purely privatepractices is still only 800 amongst approximately20,000 generalists. This relatively small grouphave no administrative links with any HealthAuthority. The majority of practitioners refer totheir practices not as private practices but asindependent practices where both NHS andprivate contract services are provided. Thepictures become more confusing because NHSregistered patients may elect to have part of acourse of treatment carried out privately.
Understanding the nature of the contract isabsolutely vital for a patient who wants tocomplain. This is because a NHS registeredpatient, even though part of the treatment wascarried out privately, can still avail themselves ofthe NHS complaints machinery. This allowsthem to present their complaint to a layIndependent Review Panel whose HealthAuthority may, in certain circumstances refer tothe matter for a disciplinary hearing. However –and here we come to the crunch – this second tierNHS disciplinary hearing has nothing to do withcompensation. Technically, the patient is not thecomplainant – it is the Health Authority. Thepatient is just a witness. At a hearing they will beasked to leave the room after giving evidence.All they will get is their bus fare. In very rarecircumstances a patient may get a refund of theirstatutory co-payment and told to find anotherNHS dentist to carry out the remedial work. Theycertainly will not be told the result of the hearing.The Health Authority is only concerned with thedentist’s terms of service. Should the dentistappeal against an adverse finding the patient maybe asked to go over their complaint for a secondtime without even been told why. It is no smallwonder that many complainants have given up bythen.
Not only does the NHS complaints take agreat deal of time but if, before the IndependentReview Panel considers the complaint, the patientchanges their mind and decides to proceed to
Dental Private Patient Complaints

AOG
9
litigation, the NHS complaints machinery isimmediately aborted.
From this you might have gathered that thereis not much percentage for the patient to gothrough the NHS complaints machinery if theyare looking for some financial redress. It may justbe an outlet for letting off steam which can betherapeutic in itself. There is also the possibility– for the really sophisticated and knowledgeable– that the NHS procedure might provide a usefullitmus test as to the strength of a negligenceaction before a complainant spends their ownmoney.
Then where does a wholly privatepatient go to make a complaintagainst a practitioner?An obvious port of call is the General DentalCouncil whose primary duty is to protect thepublic and to discipline dentists who fall seriouslyshort of the standards expected of them. But likethe NHS complaints machinery the one thing thata complainant will not get from a GDCinvestigation is compensation. However, unlikethe NHS system they will get a report of theoutcome and the sanctions – if any – against thedentist. This, of course, can form the basis of asubsequent claim in the civil courts. It is alsopossible to make a complaint to the GDCconcurrently with civil litigation. It has also beenknown for complainants to reverse the procedureand make a complaint after an out of courtsettlement has been made denying liability.
The second option is a solicitor, preferablyone who specialises in personal injury andclinical negligence. Here, as already stated, anallegation of negligence can only succeed if it canbe demonstrated that a dentist has failed in theirduty of care and that as a result of this failure theyhave suffered damage. This is known ascausation and it is sometimes very difficult toestablish. Going to a solicitor and litigation, orthe threat of litigation, is the only way to receivecompensation not only for any harm done butalso to fund remedial treatment that will put theclaimant in as near a position as possible asexisted before the damage. Settlements alsoinclude any future dental treatment that might berequired as a result of the negligence.
Exactly two years ago – in April 1999 – wehad radical changes in the Civil Procedure Rulesas a result of the Lord Wolff’s ‘Access to Justice’report. Today the litigation process is highlystreamlined and claims for less than £15K areincluded in what is known as a fast trackprocedure. This is a timetable that is controlledby the Court and not by solicitors. It iscomparatively rare that a dental claim does notfall into the fast track category.
Successful litigation depends almost entirelyon a dental expert’s report whose duty is to theCourt and not to the claimant or instructingsolicitor and who may be a single joint expert.The report will be wholly based on what thedental records show and the claimant’s statement.The conclusion will be based on whether aresponsible body of other general dentalpractitioners, not hospital consultants orConsultants in Dental Public Health, but otherHigh Street dentists, would have adopted thesame procedures under similar circumstances.Just because dental treatment fails it does notfollow that it was done negligently. Anecdotal
evidence from dental experts is that over 70% ofall alleged claims are completely without anymerit. A further number of marginal claims areabandoned after a conference with Counsel.Causation is the usual sticking point. A dentistmight have failed in their duty of care but thetooth or teeth were at risk in any event due tosome other variable. Currently 99% of claimsthat can be supported are settled without anadmission of liability although there is oftenskirmishing between solicitors to arrive at thelevel of damages.
Until a year ago Legal Aid Board claimantswere in a strong financial position as they hadlittle to lose. Now conditional fee arrangementspermits solicitors to enter into a contract with theclaimant which provides for fees to be paid onlyif a case succeeds. In addition there is apercentage uplift if they win. If successful, theclaimants costs, the uplift and a premium forinsurance can all be recovered. An unsuccessfulclaimant will only lose their premium and thesolicitor will remain unpaid. From these reforms,fast track and conditional fee arrangements, thetwo big barriers to litigation, time and costs, havepartly been removed.
A very quick word about AlternativeDispute Resolution know as ADR. This includesarbitration which is legally binding and almost asexpensive as going to Court, mediation which isless expensive but not binding and conciliationwhich requires a certain minimum fund ofgoodwill which is normally lacking in clinicaldisputes. For this reason ADR is little used inhealth complaints. It is seen in commercialdisputes such as construction and shipping as isconciliation in family matters. It is also useful ininter-professional disputes which is outsidetoday’s remit.
So what are we left with? We are left withthe private patient who has a complaint –legitimate or otherwise – but one that falls shortof legally defined negligence. It can beunnecessary pain, poor out-of-hours emergencyservices, being kept waiting, locums, poor recordkeeping, lost x-rays and reports, staff that areeither incompetent or rude – or both – it can beabout anything – the colour of the wallpaper or theabsence of girlie magazines in the waiting room.Remember – the definition of a complaint is ‘anexpression of dissatisfaction requiring a response’.
Why does it require a response? Surely if thepatient/client/consumer is dissatisfied they willgo elsewhere. Water finds its own level. Thereason that all private patient complaints requirea response is because we need to reassure thepublic that we are a caring profession. The covertreason is simply to preserve our self-regulationalbeit a heavily reformed one.
The view of the British Dental Association isthat there should be one unified mechanism todeal with all dental complaints that fall short ofnegligence and that the current NHS procedureshould be extended. To quote a BDAspokesperson ‘We want one front door’. The ideais to treat private patient complaints as a fact-finding exercise totally divorced from anyclinical assessments. It would give a patient theopportunity to be taken seriously and for theirgrievance to be acknowledged and respected.This would satisfy many complainants. Theenquiry would satisfy any ‘day in court’ attitude.It would be entirely non-judgemental with noneed of professional assessors. However, the
BDA want the GDC to deal with complaints onan agency basis. I would suggest a publiclyfunded independent review type mechanism.
My reason is that notwithstandingconstitutional changes in the GDC and theuncertain composition of the Fitness to PracticeCommittee (or whatever elected or appointedbody replaces it) the Council should not beallowed to be put in the position of sleuth, judgeand jury. The dangers of serendipity in aninvestigation is too great. With the best will in theworld I cannot envisage Chinese walls working inWimpole Street. Even if it was possible dentistswould have no confidence in such a system. Thisleaves the GDC with only one concern – that ofprocess rather than praxis – to be concerned withthe methodology and procedure rather than theoutcome. To this end paragraph 3.13 of‘Maintaining Standards’ should be expanded toinclude that copies of an acknowledgement of acomplaint followed by a definitive response beforwarded to the Council. This to be carried outwithin a set time frame and failure to do so wouldlead to a charge of serious professionalmisconduct. Should the mandatory reply fail tosatisfy the complainant then a type of localindependent panel could be asked to investigateand that these panels be financed from publicexpenditure.
I feel that these simple proposals will go along way. Complainants will have theopportunity of making sense of their complaintwith the knowledge that the process has beenmonitored. I think it can be predicted withreasonable accuracy who will be draftingpractitioner’s responses. It is obvious that thedental defence organisations would be majorstakeholders in this type of operation. I say thisnot because of the competition between them –which is largely illusory – but their obsessionwith control.
My conclusions are:• The present crisis in professional self-regulation has little to do with private generaldental practice.
• Nevertheless the absence of a dental privatepatients complaints procedure is still damagingpublic confidence in the dental profession.
• Complaint mechanisms for NHS dentaltreatment, managed capitation, insurance anddental corporate bodies exists.
• That the General Dental Council shouldexpand paragraph 3.13 ‘Maintaining Standards’with respect to responding to private patientcomplaints and support complainants withinformation.
• That the General Dental Council audit theprocess of private patient complaints.
• An acceptance that the civil procedure rulesnow in place make alleged clinical negligencematters less expensive than hitherto, thatconditional fee arrangements have made accessto justice easier and an acknowledgement thatthis is the only way successful claimants canreceive damages.
• For the private patient complaint that fallsshort of clinical negligence local independentreview type panels should be convened financedby public expenditure.
ConclusionNow, the BDA has stronger leadership thanever. This is reflected in the 3 top officialsJohn Renshaw, John Craig and Ian Wylie,respectively the Chairman, the Vice Chairmanand Chief Executive. I do not believe that thisterrific trio would present ‘glass ceilings’ foraspirants from the opposite sex or ethnicbackgrounds. From my perspective I have nohesitation in stating how supportive they havebeen to me.
So, if you have a talent to contribute to aprogressive BDA, which then benefits us all, Ibelieve that these men in particular willsupport you in your endeavours. Clearly weneed to make the top more representative ofthe profession but that can only happen if morepeople are encouraged to enter.
So what is my personal view. When I firstcame on board I was surprised to learn that thiswas never run as the £5 million operation, it is.
The internal view was it didn’t need to havea business like efficiency, because that
conflicted with being a membershiporganisation and perhaps that led to
the huge operating losses. Thefirst year of having the BDA
board of directors neatlycoincides with
makinga small profit!Hopefully next yearwill show that this will be the trend to be proudof. As you know you need profit to create newservices/products, otherwise the subs have torise and we wouldn’t want that, would we!
In conclusion, there is a real conflict betweenbeing a truly democratic organisation andhaving a business like efficiency. But I reallybelieve that this is the best it’s been and nowthere is general acknowledgement that changeis necessary to evolve. However, if you couldhelp move it one stage further and join in the revolution, then that would be great.Become a voting member and join us as a branch rep on the Rep Body. I’ll happilytry to guide you. If you want to ask me something specific then please contact me on email [email protected] tel. no. 0777 6138616.
I hope this helps you to understand more aboutthe BDA and help you feel comfortableinputting into its work, of looking after thedentists’ interests. If you don’t go for that,then tell me how to make it better and then letssee what happens.
AOG
10
BackgroundMany of us are too busy to have devoted timeto understanding how the BDA hierarchyworks. Generally, there is very little need toacquire this knowledge. But we live in timeswhere coping with change in our profession isa routine matter, rather than an exceptionalglitch. In an acknowledgement of this and tospeed up the decision making process, theBDA has just finished its own modernisationprocess. Below there is a summary of how theBDA works.
StructureThere is the new BDA board of Directors, whoall began their jobs in the year 2000. Theyhave the responsibility to set the strategy andto react to any big issues. There is also adetermination to effect some leadership inlooking after the needs of the dentists.
Now with a bunch of well motivated but onlypart time dentists, progress has to be slower aswe try to become business like. To fullyappreciate this, reflect on how you cope withnew implementing initiatives like clinicalgovernance, within your practice. I guaranteeyou’ll empathise as you try and change theculture of your practice!
Like any democratic organisation most areelected into position and in this case the powerbase is the Representative Body. Surprisingly,getting to be on the Rep Body is not difficult atall, as some of the positions are simplyunopposed. That cannot be good fordemocracy and has to reflect on a lack ofknowledge or just pure apathy. The role onlyrequires you to attend a minimum of 2meetings a year in London and feeding back tothe colleagues you’ll represent.
So the Rep Body will elect from within itselfand add to the other Board of Directors, whoare the Chairs of GDS, Private Communityand Hospital committees.
Rep BodyThis has approximately 80 dentists andgenerally meets twice a year to debate andcomment on the Executive Boards work and
recommendations. This work in usually doneon a Saturday so you don’t need to take a dayoff work, but it doesn’t help the weekendstretch further either!
These RB members choose most of the Boardand should hold them accountable for theirperformance. The ultimate accountability iseffected on election day! They also contribute
to the working groups that sort outissues like Education and
Standards, or Ethics and puta Rep or two onto the
main BDACommittees.
Executive BoardA lot of the ‘behindthe scenes’ discussionabout the BDA’s work isoverseen here, to ensure thatwe are meeting the needs ofmembers, i.e. surveys, producingadvice guidelines, development ofthe website etc. Over the last 3 yearsthe BDA’s made substantial losses andso the finances now play a bigger role tominimise this from becoming a regularforfeit. The last financial year saw a profit forthe first time in years.
Other routine work includes finalisingresponses to other agencies such as theDepartment of Health, GDC, The Faculty etc.This can revolve around issues on how todevelop General Professional Training, anational Private Practice ComplaintsProcedure, and stopping other Governmentdepartments from inadvertently becominginvolved in Dentistry. For example, we havenearly had private dentistry getting lumpedinto a new quango. This agency wouldregulate the provision of this private healthcare service and charge us hundreds ofpounds more for that interference, sorry I domean pleasure. This type of activity doesn’t generate any media activity so it would naturally escape ones notice.
Other work includes creating new benefits formembers and although the highly successfulinsurance service is established, newerservices that offer the convenience of a travel agency or lower costs of utilities, i.e. gas, electricity and phones are now offered. 2001 should witness the launch of a practice valuation scheme and a capitation scheme with all the insurance and direct debiting facility, for members to ‘badge’ as an in-house service to offer their patients.
Amarjit Gillgives an insightinto the BDA.
Pathways to Professional Power!
CHARITY BALLThe Charity ball has already raised half the target
through your generous donations. The cheques are
still coming in. Should you still wish to help the
victims, it is still not too late! Every penny counts!
DONATIONS:The Gift Aid Declaration overleaf will enhance the valueof your contribution. Special forms are available forcompanies and partnerships.
I enclose a cheque for £1,000
Please send me a DD form to be able to pay 10 instalments @ £100 per month
I have enclosed a donation to the value of £
Cheques made payable to: Sewa International (India Quake Appeal)
Name:
Address:
Phone: Fax:
e-mail:
For further information or to send donations:
Dr Manny Vasant1210 London Road, London SW16 4DNTel: 020 8764 1424. Fax: 020 8679 3126
or
Dr Rashmi Patel156a Haverstock Hill, London NW3 2ATTel: 020 7722 4405. Fax: 020 7483 3603
Gujarat (India) has been devastated by a powerful
earthquake this January. For those of us remote
from the tragedy, it is difficult to appreciate the
scale of the damage, suffering and pain.
For those who survived, slowly, very slowly, it
dawns upon them that they have their life – a life
that has changed forever. Some will never see their
parents, nor, any relatives again – ever again!
For some parents, the last they heard of their
children was a near but not so near scream when
they could not reach them. This scar will last
their lifetime.
This is yesterday’s news, tomorrow’s news, it is
news for a very long time until people find their
feet on the ground.
We are the fortunate ones whocan help, so please be generous.
INDIA QUAKE APPEALAnglo-Asian Odontological Group (AOG) and
SEWA INTERNATIONAL (Registered Charity No 267309 www.sewainernational.com)
Appeal to the dental trade and profession at large
Charity Ball andFund Raising Event (target £100,000)
AOGAnglo-Asian Odontological Group
✁
AOG
12
SEWA International (Registered Charity No. 267309)46/48 Loughborough Road, Leicester LE4 5LD. Tel: 0116 266 5665
I would like all gifts to Sewa International, paid on or after the date ofthis declaration to be Gift Aid Donations.
I pay tax at: Basic Rate
Higher Rate (please tick as appropriate)
Signed Date:
PLEASE NOTE: You should have paid an amount of UK Income Tax or Capital Gains Tax equal tothe tax deducted from your donations for your gifts to be eligible for Gift Aid.
The sum of £
For: India Quake Appeal Project
Name
Address
Postcode
Please complete and post to:
Anglo-Asian Odontological Group (India Quake Appeal)at:
Dr Manny Vasant1210 London Road, London SW16 4DNTel: 020 8764 1424. Fax: 020 8679 3126
or
Dr Rashmi Patel156a Haverstock Hill, London NW3 2ATTel: 020 7722 4405. Fax: 020 7483 3603Gif
t Aid
Dec
lara
tion
✁


By Parimal Chaudhuri
My experience indealing with dentalpractitioners confirmwhen it comes to investing the
uppermost in their mind is tax saving andgrowth. One of the purposes of personalfinancial planning is to create wealth, preserveit, enjoy it in need, and then to transfer thesurplus to your succeeding generationpreferably without or minimal tax paid to theExchequer. This article will concern in briefhow to create wealth in a tax efficient manner.
Individual Savings Account ( ISA ). This is the first port of call. This is a tax freewrapper to encourage investors to save fortheir future financial well being or retirement.There are different variants of ISAs availabledepending on ones financial circumstances ;the one suitable for high net worthprofessionals is known as ‘Maxi ISA’. One caninvest up to maximum of £7,000 per tax yearin a maxi ISA. The investment is free of bothincome and capital gains tax. Unlike pension,a tax credit of 10% only will be recoverable in
respect of UKdividends until April2004. The approvedproviders of ISAs arei n s u r a n c ecompanies, banks,building societies
and unit trusts managers / companies. Thereare wide varieties of funds available to chosefrom for investment. You will have to be verycareful in choosing the funds, market sectorand the provider in terms of (financialstrength), past performance, and your owninvestment risk profile. It is advisable youconsult a good Independent Financial Adviserto guide you through the maze of ISAs.
Personal or / Stakeholder Pensions.One of the primary incentives to invest inprivate pensions is its generous tax breaks. On6 April 2001, Government introduced newrules giving tax breaks on pensioncontributions to individuals without taxableearnings. This the government expects willrevolutionise the savings market forretirement. Almost anyone can now contribute £2808, andthe government will top it up to £3600, peryear to a Stakeholder Pension regardless of ageor earnings. This makes it possible for the firsttime to contribute to a pension for the yearswhen you have no income (during a careerbreak), and also on behalf of non – earningspouse or children.
The only groups who are excluded from takingadvantage of the new £3,600 “pensionallowance” for themselves are: those aged over
75; and those earning more than £30,000 ayear and contributing to an employer – runpension scheme.
At the same time a new government -approved personal pension known as“Stakeholder Pension” was launched.Stakeholder labelled pension must be flexibleand portable. Annual management charge mustnot exceed 1%, allow stop and startcontribution as you please, and switching offunds between managers must be free ofcharge.
Whether you choose a stakeholder – labelledscheme or non – stakeholder pension is up toyou. The stakeholder variety may becompetitive and flexible; some non –stakeholder schemes may offer additionalfeatures such as wider range of investmentfunds to choose from.
All personal pensions, stakeholder orotherwise, benefit from tax relief at the basicrate the moment the contributions are made.So a contribution of £2,808 will be “grossedup” by the government to the £3,600 limit.Higher rate tax relief can also be claimedthrough the tax return if the person in whosename the scheme is taken out (not the personsupplying the funds) is a higher rate tax payer.This will cut the net cost of a £3,600contribution to just £2,160. The fund will growfree from income and capital gains tax just likeany other Inland Revenue approved pensionfund. At the time of vesting, 25% of the fundvalue can be taken as tax free cash; the balancemust be used to buy an annuity to provideincome for life.
The downside of the pension is that thebeneficiary can not get their hands on theassets until they retire or aged 50 at the earliestas the law stands.
National Savings National Savings have a wide range of
Gro
wth
.A
ccel
erat
ed
Tax-
Adv
anta
ged
Inve
stm
ents
for
14
AOG
It is interesting how the face of dentistry inthis country has changed in the last fifteenyears. The aesthetic demands and the need
to feel and look good has done a service to theprofession. One of the biggest impacts inmodern dentistry has to be the need to restorewith fixed prosthesis on Dental Implants. Thisarea has been researched far beyond any othersubject in dentistry as you are fully aware andthis is the area where my passion lies. Havingseen the benefits over the twelve years in myown practice, I decided to move to a dedicatedImplant Centre.
Dental Implantology brings a mixed bag ofgoodies, as with any highly complex work thefees are always deemed to be attractive and itbrings in the profession to want to provide thisin general practice. This is not bad as itincreases the consumption and delivery, andhopefully decrease the cost of implantology inthe long run at the consumer level. There is avery steep learning curve and things cansometimes go wrong, this causes distress to noend and with intricate and expensive work theconsumer led society will always look atpunitive damages.
There are always cases which can be treatedwith Dental Implants in general practicewithout much difficulty. In an ideal situationthere is sufficient bone height and widthwithout any soft tissue deficiency and wellaway from any vital structures the finaloutcome can remain unobtrusive. These cases,even though rare, are a great practice builderand help the patient in a variety of situations,from a missing single tooth, free-end saddlesor an overdenture.
There will always be cases which are farbeyond the comfort zones of the generalpractitioner. This requires either an outsidehelp to treat the cases or further, detaileddiagnostic tools in the shape of tomographs.
Until now the majority of the Dentistsproviding Dental Implants or carrying out anyform of hard tissue reconstruction has beenrelying on CT scans. The logistics, time, costand the amount of radiation has always made ita tool occasionally used. One has to weigh the
radiation against the benefit and this makes thetool available but seldom used. The othersimilar tools are the Scanora and the transverseslices on certain OPG machines which takeless time and the radiation dose is low, but they suffer from unproportional distortion and ‘noise’.
About a year ago I came across a scannerwhich is dedicated to the dentomaxillofacialarea. The equipment is a Digital VolumeTomogram employing cone beam technologysimilar to an OPG machine. This thereforereduces the exposure and minimises the scantime. Compared to a normal CT scanner whichtakes 15 to 20 minutes, this machine willgather the data in 70 seconds. This alsoreduces the patient exposure to 5-10 timeslower than the CT scanner. What a benefit!
Once the data is gathered, the information canbe processed to get OPGs, axials, transaxialsand 3D images. With these advantages there isno reason not to carry out the scan so that thetreatment can be planned well. This works atreat for the Centre.
We at the Centre now provide a service notonly for the scans but help with treatmentplanning or interpretation of the data.
The other added benefits of the scan is toassess periodontal prognosis by looking at the3Ds of the bone, endodontics with thetransaxial cut at 0.5 mm intervals, orthodonticassessment of buried teeth and TMJ 3Ds.
Kish Soneji BSc (Hons) MSc BDS LDS RCS61 Harley StreetLondon
DigitalVolume Tomography
By Kish Soneji
investment vehicles suitable for every age and tax status. They are also one of the safest formsof investment as they are provided by, andunderwritten by the government.
The products which will be of interest tohigher rate tax payers are National SavingCertificates. These certificates provide tax freeincome. Two types of certificates are available;index linked and fixed.
The maximum investment allowed in eachtype is £10,000 per person for a term of 5years. No interest is payable if cancelled in
the first year. There is no limit to thereinvestment of matured certificates. After 5years you will get back your capital plus theaccumulated interest.
The certificates in issue at the moment are 19th
Index – Linked and 57th Fixed Rate carryinginterest rate of 1.65% plus retail price index (RPI ) and 3.55% compoundrespectively over 5 years.
You can buy the certificates through your localPost Office and there are no charges. National Savings do not pay any commissionto the advisers.
Venture Capital Trusts ( VCTs ) This falls into a very high risk category ofinvestment. While it offers substantial taxbreaks and potentially high returns on your investment it carries risk so much so thatyou may end up loosing your capital if the market goes against you. You should seek expert advice before entering into thisarea of investment.
A VCT is a quoted company which invests atleast 70% in qualifying unquoted companieswhich may include AIM (alternativeinvestment market) listed ones. Generous taxbreaks are designed to attract capital topromote innovative new entrepreneurs tolaunch themselves into the business.
An investment in VCT shares will entitle oneaged 18 or over to an income tax refund upto20% of the amount subscribed. The maximuminvestment is £100,000 in any one tax year.Your investment will be committed for 5 yearsto take the full benefit of the tax advantage.
The rules governing VCTs are complex andwith limited space available in this article Iwill not be able to go into further details.
The tax efficient investments discussed aboveare by no means exhaustive but the productssuitable for high net worth investors I hope toaddress in my future articles.
Parimal Chaudhuri is an Independent FinancialConsultant and a freelance writer. Tel /Fax: 020 8906 3454 ; Mobile : 07956 589416.
15
AOG
AOG
16
By 8p.m. The Café Royal one of London’smost prestigious venues was buzzing as theguests arrived to a champagne reception andfor those who preferred fizz of a differentvariety Cobra beer flowed nicely.
The President Jatin Desai accompanied by hiswife Gopa greeted the guests and were soonjoined by a very contingent accompanying thePresident Elect Air Vice-Marshal IanMcIntyre. The uniforms of the airforce andthe armed forces were not only colourful butalso most impressive.
The guests for the evening included one of ourown Raj Rayan who attended in his capacityas the Dean of the Faculty of the GeneralDental Practitioners of the Royal College ofSurgeons of England along with his mostcharming wife Ahila. The Chief Guest wasnone other than the Surgeon GeneralLieutenant Robert Menzies accompanied byhis wife Joan.
The food provided by Madhus brilliant ofSouthall was as usual brilliant! In fact it didsurpass previous efforts as there was anexcellent selection for vegetarians, the qualitywines which again were supplied by ourfriends at The Dental Directory wereoutstanding, the excellent desserts roundedoff a splendid feast.
The Surgeon General Robert Menzies wasvery kind in his address and complimentedthe AOG and its role within the DentalProfession and also for its unique capacity forcharity and support for noteworthy causes allover the world. He recommended the ArmedForces as a career route for Dentistsparticularly for those of the ethnic minorities.
AOG CHARITY BALL 2000
The President thanked his committee fortheir tireless enthusiasm and efforts to takethe AOG from strength to strength.
Then an imputual charity auction was held,where Mike Volk of The Dental Directoryraised a further £6,000 on the night for yourcommittee to pledge to one of the manycharities the AOG supports.
After the formalities, the band took over,the band took over and almost all were onthe floor dancing, cavorting and enjoyingthemselves to the early hours.
Truly a night to remember.
ON THE 18TH NOVEMBER 2000, THE AOG GLITTERATI, THEIRFRIENDS AND COLLEAGUES, THE GREAT AND GOOD OF THEDENTAL PROFESSION DESCENDED ON THE WEST END OFLONDON FOR A NIGHT TO REMEMBER.
Presidents Address
Café Royal, London
Ex President Mayur Bhatt, Mrs Bhattand Dr Jatin Desai
Jatin Desai, Air Vice-Marshal Ian McIntyre, Abhay Soneji–President Elect and Kish Soneji.
Jyoti Soneji presents flowers to Gopa Desai
Mike Volk
Center – Dr Saif Najefi, Ex president.President Jatin Desai and Gopa Desaileading the dance.
AOG President Dr Jatin Desai, Robert Menzies Surgeon Generaland Air Vice-Marshal Ian McIntyre president elect.
Contingent from Armed Forces
Flowers for Pammi Dutta presented by Dr Rashmi Patel– Ex president
The top table of the President
Lieutenant GeneralRobert Menzies Surgeon General on Behalf of the guests
AOGAOG
18
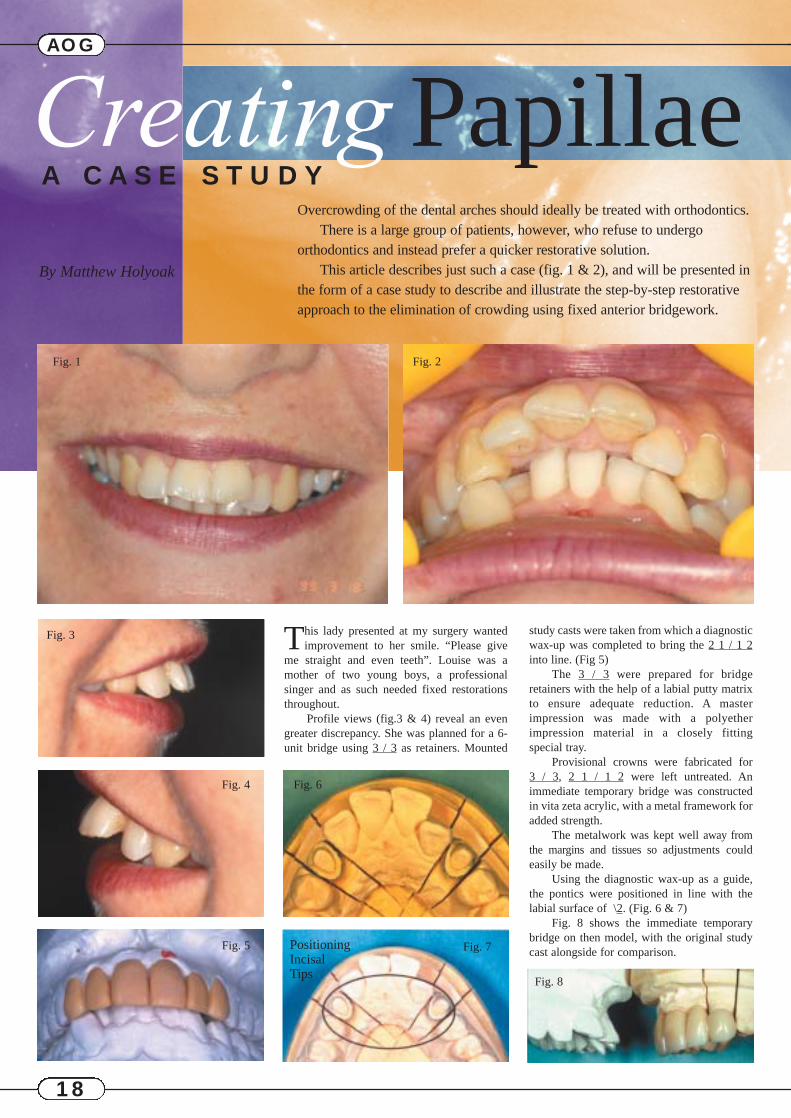
study casts were taken from which a diagnosticwax-up was completed to bring the 2 1 / 1 2into line. (Fig 5)
The 3 / 3 were prepared for bridgeretainers with the help of a labial putty matrixto ensure adequate reduction. A masterimpression was made with a polyetherimpression material in a closely fitting special tray.
Provisional crowns were fabricated for 3 / 3, 2 1 / 1 2 were left untreated. Animmediate temporary bridge was constructedin vita zeta acrylic, with a metal framework foradded strength.
The metalwork was kept well away fromthe margins and tissues so adjustments couldeasily be made.
Using the diagnostic wax-up as a guide,the pontics were positioned in line with thelabial surface of \2. (Fig. 6 & 7)
Fig. 8 shows the immediate temporarybridge on then model, with the original studycast alongside for comparison.
Creating PapillaeA C A S E S T U D Y
Overcrowding of the dental arches should ideally be treated with orthodontics.There is a large group of patients, however, who refuse to undergo
orthodontics and instead prefer a quicker restorative solution.This article describes just such a case (fig. 1 & 2), and will be presented in
the form of a case study to describe and illustrate the step-by-step restorativeapproach to the elimination of crowding using fixed anterior bridgework.
By Matthew Holyoak
Fig. 1 Fig. 2
Fig. 3
Fig. 4
Fig. 5
Fig. 6
Fig. 7PositioningIncisal Tips
This lady presented at my surgery wantedimprovement to her smile. “Please give
me straight and even teeth”. Louise was amother of two young boys, a professionalsinger and as such needed fixed restorationsthroughout.
Profile views (fig.3 & 4) reveal an evengreater discrepancy. She was planned for a 6-unit bridge using 3 / 3 as retainers. Mounted
Fig. 8
AOG
19
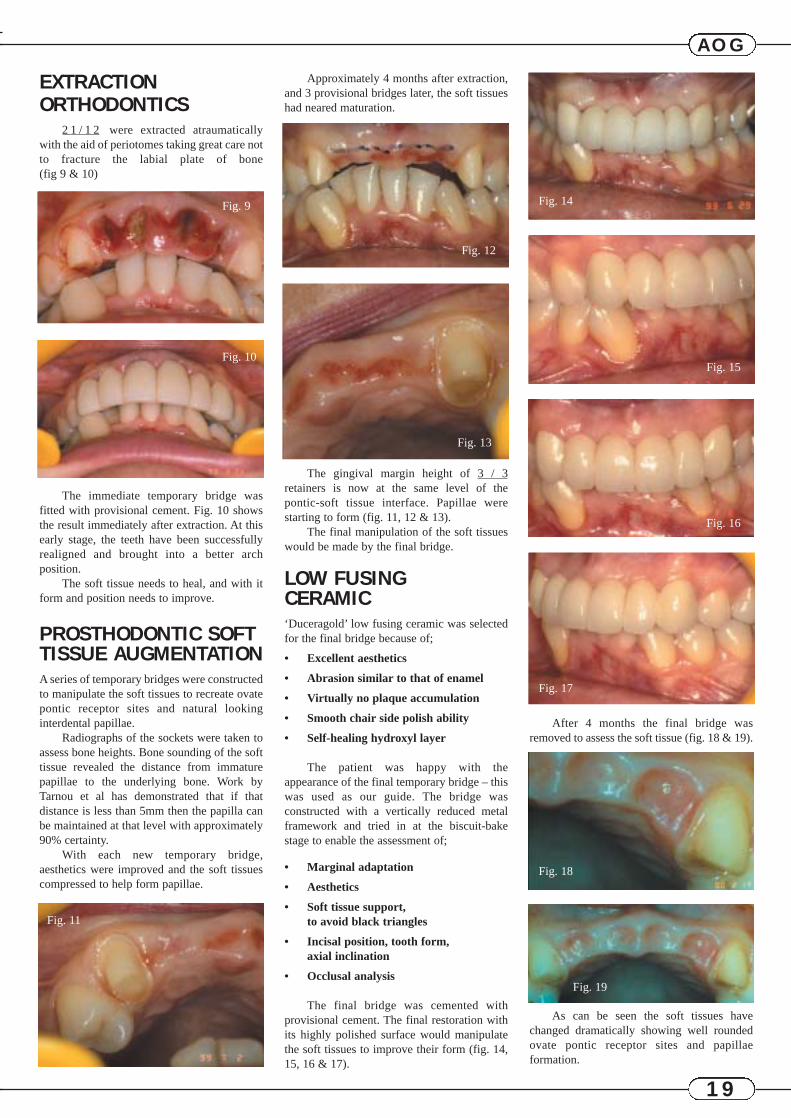
EXTRACTIONORTHODONTICS
2 1 / 1 2 were extracted atraumaticallywith the aid of periotomes taking great care notto fracture the labial plate of bone (fig 9 & 10)
The immediate temporary bridge wasfitted with provisional cement. Fig. 10 showsthe result immediately after extraction. At thisearly stage, the teeth have been successfullyrealigned and brought into a better archposition.
The soft tissue needs to heal, and with itform and position needs to improve.
PROSTHODONTIC SOFTTISSUE AUGMENTATIONA series of temporary bridges were constructedto manipulate the soft tissues to recreate ovatepontic receptor sites and natural lookinginterdental papillae.
Radiographs of the sockets were taken toassess bone heights. Bone sounding of the softtissue revealed the distance from immaturepapillae to the underlying bone. Work byTarnou et al has demonstrated that if thatdistance is less than 5mm then the papilla canbe maintained at that level with approximately90% certainty.
With each new temporary bridge,aesthetics were improved and the soft tissuescompressed to help form papillae.
Approximately 4 months after extraction,and 3 provisional bridges later, the soft tissueshad neared maturation.
The gingival margin height of 3 / 3retainers is now at the same level of the pontic-soft tissue interface. Papillae werestarting to form (fig. 11, 12 & 13).
The final manipulation of the soft tissueswould be made by the final bridge.
LOW FUSING CERAMIC‘Duceragold’ low fusing ceramic was selectedfor the final bridge because of;
• Excellent aesthetics
• Abrasion similar to that of enamel
• Virtually no plaque accumulation
• Smooth chair side polish ability
• Self-healing hydroxyl layer
The patient was happy with theappearance of the final temporary bridge – thiswas used as our guide. The bridge wasconstructed with a vertically reduced metalframework and tried in at the biscuit-bakestage to enable the assessment of;
• Marginal adaptation
• Aesthetics
• Soft tissue support, to avoid black triangles
• Incisal position, tooth form, axial inclination
• Occlusal analysis
The final bridge was cemented withprovisional cement. The final restoration withits highly polished surface would manipulatethe soft tissues to improve their form (fig. 14,15, 16 & 17).
After 4 months the final bridge wasremoved to assess the soft tissue (fig. 18 & 19).
As can be seen the soft tissues havechanged dramatically showing well roundedovate pontic receptor sites and papillaeformation.
Fig. 9
Fig. 12
Fig. 13
Fig. 14
Fig. 15
Fig. 16
Fig. 17
Fig. 18
Fig. 19
Fig. 10
Fig. 11
AOG
20
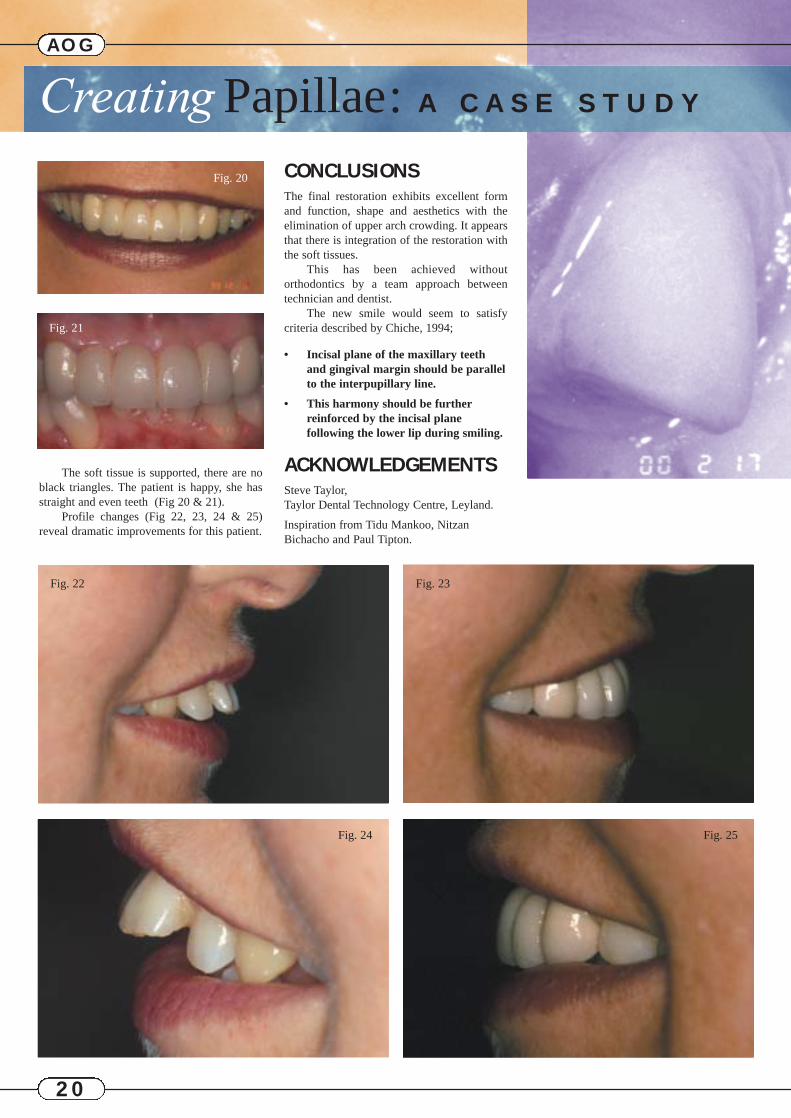
The soft tissue is supported, there are noblack triangles. The patient is happy, she hasstraight and even teeth (Fig 20 & 21).
Profile changes (Fig 22, 23, 24 & 25)reveal dramatic improvements for this patient.
CONCLUSIONSThe final restoration exhibits excellent formand function, shape and aesthetics with theelimination of upper arch crowding. It appearsthat there is integration of the restoration withthe soft tissues.
This has been achieved withoutorthodontics by a team approach betweentechnician and dentist.
The new smile would seem to satisfycriteria described by Chiche, 1994;
• Incisal plane of the maxillary teeth and gingival margin should be parallel to the interpupillary line.
• This harmony should be furtherreinforced by the incisal plane following the lower lip during smiling.
ACKNOWLEDGEMENTSSteve Taylor, Taylor Dental Technology Centre, Leyland.
Inspiration from Tidu Mankoo, NitzanBichacho and Paul Tipton.
AOG
Fig. 21
Fig. 22 Fig. 23
Fig. 24 Fig. 25
Fig. 20
Creating Papillae: A C A S E S T U D Y
AOG
21
During 1998 one of the guest speakers at MillHill Rotary Club gave a talk on “VoluntaryServices Being Offered by the RotariansOverseas”. In response to that talk, RotarianHardev Singh Coonar offered his services as avolunteer and explored the possibilities ofsetting up a Pain Relief Clinic in North India.
In August 1998, during his summer vacation,he explored the possibilities of establishing aPain Relief Clinic at a rural location withineasy reach from Chandigarh, which is thecapital of Punjab, India. Baba Ajit Singh ofHansali very kindly agreed to finance theproject. Rotary Club of Mill Hill UK andRotary Club Sirhind, Punjab, sponsored theproject. Rotarian Hardev Singh Coonar spentthe last week of January and four weeks ofFebruary 1999 in setting up this which is nowfully functional. The first patient was seen onMonday 8th February 1999 and at the end oftwo weeks, official inauguration took place onSunday 21st February 1999. The clinic wasinaugurated by Baba Ajit Singh and thisfunction was attended by several members ofthe Rotary Club, Sirhind, Mr Bhatnagar,Secretary of Health, Government of Punjab,Dr S S Sidhu, Director, Sri Guru Ram DassDental Institute Amritsar, and a large numberof local dignitaries.
LocationDera Baba Ajit Singh is 23 miles fromChandigarh and surrounded by very fertileagricultural land. Chandigarh isapproximately 150 miles from New Delhi.The best way to travel from Delhi toChandigarh is by train, and the journey iscovered in three hours. Dera Baba Ajit Singhcan also be approached by road travelling onthe National Highway from Delhi to Amritsar.Approximately 120 miles from Delhi, anapproach road from a small town calledSadhoogarh leads to Dera Baba Ajit Singhwhich is approximately three miles from themain road.
AccommodationThe Pain Relief Clinic is situated in anindependent block and the surgery occupies alarge room. There is ample waiting space for
the patients. There is living accommodation inthe vicinity, which can be used by visitingdoctors, and has the usual modern facilities.The clinic itself is equipped with a dental unitand has its own autoclave for sterilisation.
StaffAt present there is one Dental Surgeon whoworks six days a week from 10.00 a.m. to 2.30p.m. She is paid a nominal salary by themanagement of Dera Baba Ajit Singh. TheDental Surgeon is assisted by an operatingroom assistant, who is under training.
ObjectivesThe clinic is designed to provide diagnosis ofthe conditions in the mouth, pain relief frominflammatory and non inflammatoryconditions of the mouth. Routine dentalextractions are carried out under localanaesthetic to relieve pain. For a limitednumber of patients, oral prophylaxis is carriedout and oral hygiene instructions are given.This service is provided free of charge butpatients can make donations according to theirwishes into the cash box, which is only openedby the management.
ManagementThe Pain Relief Clinic at Hansali is under thecontrol of the management of Dera Baba AjitSingh. The management is advised by Dr P SCoonar who is the medical adviser and by DrH S Coonar, and Dr S S Sidhu as dentaladvisers. The financial matters are dealt withby Baba Ajit Singh himself or by MrGursharan Singh, Financial Controller.
The RotaryClub’sContributionThe Rotary Club of Sirhind hasagreed to provide local hospitalityto visiting dental surgeons and hasalso provided the usual publicityincluding the preparation of thesign boards.
PAIN RELIEF CLINIC AT DERA BABA AJIT SINGH HANSALI
HimachalPradesh
Haryana
Rajasthan
Pakistan Punjab
Chandigarh
N
The Rotary Club of Mill Hill has pledged toprovide services of Rotarian Hardev SinghCoonar and has contributed to the cost ofstationery and a certain amount of medicines.
Future PlansThe Rotary and other volunteer DentalSurgeons from overseas will be encouraged tovisit and work at the Pain Relief Centre byprior arrangements. Efforts have been made tofind one Senior Dental Surgeon to visit theclinic once a week in order to provideconsultant support to the dental surgeon. Thisperson would have to be paid a salary andfunds may also be needed for providing airconditioning during the summer and heatingduring the winter months. Although theprimary role of the clinic is to provide aservice to the poor people in the area, there isa considerable potential in impartingknowledge to local dental surgeons by visitingdoctors and dental surgeons. There is scope indeveloping the Pain Relief Clinic to cope withpain in other parts of the body providedvolunteers are available who specialise indisciplines other than dental surgery.
Clinics in other parts of rural India, Sri Lanka,Pakistan and Bangladesh are also set to start.Accommodation and food will be provided forvolunteers. For more details contact
Hardev Singh CoonarRoyal Free HospitalPond StreetLondonNW3 2QG
Tel 020 7794 0500Fax 020 7830 2754
Quite often the reasons for the bank’sapproach to your practice’s financialneeds is not one of purposely adopting a
negative approach but stems from a lack ofknowledge of how your profession operates,compounded by an inability to communicatewith it’s customers. The results are an idealenvironment to foster misgivings andmisunderstandings.
Getting a good service from you bank ismuch easier if you know your bank managerand he knows about you and understands yourbusiness. It’s obvious, but it is all aboutcommunicating effectively.
A bank takes time to understand theirparticular needs and that evaluates yourpotential, as well as your current performance,will undoubtedly nurture a relationship based onmutual, co-operation and information sharing.
But what sort of things do we look for?Why do we ask for certain information andwhat relevance does it have? Here are a few tipsto help you develop a good workingrelationship with your bank manager.
Meetings with your bank manager occur ina variety of circumstances but they all have asimilar format and requirements. In all of thesemeetings, whether for a practice purchase orbecause you have decided to review your bankingarrangements, certain information will berequested, details of which will be covered later.
ARE YOU IN BUSINESS ORJUST PRACTISING?
It is generally true that bankers know aboutbanking and dentists know about teeth. It’sobvious (that word again) but it is still the singlebiggest cause of problems. There can and willbe no mutual comprehension unless both sidesmake a particular effort. Looking at it from theBanker’s perspective, we are interestedprimarily in the practice as a business. If youunderstand that before making an approach tothe bank you’ll be more successful. Most ofwhat follows merely serves to reinforce thispoint and suggests how to put the lesson intopractice.
IS YOUR’S A SYMPATHETICBANKER?
For a bank manager to understand the practiceas a business, he or she (we’ll assume it is a man
from now on) needs to understand what makesa dental practice tick. So does your bankmanager know what capitation fees are? Whatan intra oral camera is? And does a hygienistmake you money?
If the answer is no, make sure he does assoon as you can. Invite him to the practice andinvest some time in explaining the way thebusiness works. This is an investment and not awaste of time and effort, it really does help. Ifyou can do this at a time when you don’t needan immediate cash injection it would bepreferable as bank managers are as cynical asthe next man. Even if the next man has just wonthe cynic’s Oscar.
An hour or two with no pressure on eitherside will help considerably when you do needsome assistance. Just be careful that your bankdoes not see this as an opportunity to elicit amanagement charge from you, checkbeforehand.
PREPARATIONBecause the banker is looking at your practiceas a business, you have to come across as abusinessman. And that means preparation andpresentation.
Firstly, think about what the banker wantsto know. Then contact him or his assistant wellbefore the meeting to check. Find out exactlyhow he needs the information presented as thiswill aid his assessment of your requirements. Itis on the quality of this information, yourattitude, and responses to questions in themeeting that the manager will base his decisionon. He may also have to justify it to seniormanagers.
Make sure you spend time compiling theinformation, allocate yourself more time thanyou think it will take. This can often be a timeto consider your practice management. Ifgetting the information ready for the meeting isa trial, perhaps you do not have the rightmanagement information? Before you meet thebanker, perhaps you should meet youraccountant?
PRESENTATIONA set of figures that have been written illegiblywill not have the same immediate impact as aproperly typed set. It’s not right but it’s humannature.
And try going to the meeting with yourown agenda ready. Get on the front foot bystating what you want from the meeting andthen using your agenda suggest the way thatyou would like to structure the meeting. Suggesthow much time you would like to spend on eachsubject and overall. Check to make sure thatyour suggestions are well met. Then do try tostick to your timetable.
It will help the meeting progress smoothlybut it also lets the banker know that you knowabout making time effective. A prerequisite of asuccessful practice. After all bankers haveplenty of ineffective meetings.
It may be useful to ‘rehearse’your proposalwith a colleague to detect and eliminate any‘gaps’ or discrepancies which you can then fill.
DON’T HIDE IT, DON’TAVOID IT… DEAL WITH THE
DOWNSIDEAt any meeting with the bank, whether it is thefirst or one of many, do not forget yourrelationship with each other is built on thefoundation of mutual trust and respect. Raise anynegatives before he does, explain, rationalise andthen if possible dismiss them, this shows thatyou have considered all the angles.
For instance your 12 months cashflow doesnot include rent because you have a rent freeperiod. You know this but it could be consideredas an omission especially if you have notmentioned it. Bank manager’s training is one ofcritical assessment to safeguard yours and othercustomer’s money and their experienceoccasionally leads them to make negativeassumptions being unaware of all of the facts.
A good example of this is when asked tofinance a surgery purchase it was apparent fromthe information provided that their were goodpractice profits, low borrowings but no
Getting the most outof your Bank
How often do you hear comments like “my bank manager just doesn’tunderstand my personal or practice financial needs” and “I can’tunderstand why the bank won’t help me”.
There are no doubts that these views are commonly held,especially as they are heard frequently from potential new customersaround the country and to a certain extent they are justified. However there are always two sides to any story.
£££££
22
AOG

accumulation of assets. This was queried andwe were categorically informed that nothinghad been omitted. The assumption was that theprofits had been spent wantonly and we allknow how hard it is to ‘cut back’ expenditure,no matter how easy it looks on paper. The resultwas a declined loan. As you would expect thisdecision was not received enthusiastically andwhen the reasoning was explained, a set ofbuilding society pass books showing the‘missing’ profits was provided. An approvedloan proposal followed.
THE BACKGROUND....WHAT’S WANTED & WHY?
(The questions that should be asked by aknowledgeable banker)
Dental Qualifications and HistoryA detailed dental CV to show your experience.Like you the banker is unsure of the futurechanges to dentistry in the UK, specifically thefunding of the NHS. By keeping up to date withdental technology we take some comfort in yourcontinued earning ability.
Personal Financial Position Detailed personal and practice asset and liabilitysummary, these are required to assess youroverall financial position as this materiallyaffects your needs and requirements from yourpractice. Consideration should have be given toyour drawings policy, if you have one, as this iskey to the amount of spare capacity you have tomeet any funding request. In certain cases apersonal income and expenditure is useful toconfirm the minimum level of drawings thatyou need. Confirmation of your tax positionwill also be required.
Practice DetailsNumber of ‘chairs’, active patient list, the ‘split’between NHS and private, level of capitationfees, number of exempt cases, staff numbers,premises terms, i.e. rental and review period.Comments on any future capital expenditureand how you intend or currently market yourpractice are required. Knowledge of thecompetition e.g. their policy to NHS patientsand the demographics of your area, is it suitablefor private dentistry are also useful.
Track Record Evidenced via your accounts, your personalfinancial position, DPB schedules, bankstatements. It is unlikely that you will beprovided with bank statements on a practicebeing purchased, but you can always ask. Theothers are prerequisites as they are the bank’sonly way of financially assessing the deal andlevel of risk. The perceived risk is the key factorin deciding the interest rate to be levied.
Financial Requirements Your current and future requirements whetheroverdraft, loan or leasing and how the costs willimpact on the practice. A cashflow forecast isuseful in that it provides an insight into theoperation of the practice and it also shows thatyou have carefully considered your needs. A
note of caution, if you put an item in thecashflow make sure you know why it is there.There is nothing worse then reviewing acashflow, prepared by the accountant, withwhich the dentist is unfamiliar and is unable tocomment on it’s contents. What does thisconvey to the banker? Once prepared use itregularly to gauge your success and accuracy asit is a valuable management tool. Whenpurchasing a practice where there are to bechanges in the number of associates a projectedprofit and loss and cashflow is a great benefit.
Practice ManagementDo you know what your practice profit is on amonthly basis, if not you should do. Show andexplain your management information.
Your CommitmentWe lend you other people’s money and we willlook to reduce their risk. This will be by aninput from you as a cash contribution orsecurity, which one is immaterial but in mostcases necessary and expected.
The knowledgeable bank’s approach to arequest for funding can be surmised:-
Who is this person? A detailed dental C.V.clearly showing your experience. Asset andliability statement, do not be vague or blasé andprovide evidence.
How much does he/she want? Costing ofproposal to include accounts, cashflow and so on.
What for? Explain the rationale for the request.
How is it to be repaid? Know your ownpersonal and practice financial position. If youcannot explain your practice profitability whatdoes this convey to your manager.
Can they afford the repayments? Projectionsand reference to existing accountinginformation.
What are the risks? Consider the possibledownsides then resolve them.
What is the bank’s ‘fall back’ position?Quality and income generating ability of dentistand security.
If you follow these guidelines things will beachieved quicker and an understanding willdevelop between the bank and yourself.
To continue what you have achievedalready started, talk to the bank manager duringthe year. Update him with any changes, positiveas well as the negative ones. If you foresee aproblem contact the bank, this shows anappreciation and knowledge of your practice. Italso allows more time for the bank’s input. Asan accountancy colleague once said, if you havea problem and ask a bank manager for animmediate answer it is usually no.
It is in everybody’s interest for you tosucceed and the bank should be considered as afinancial partner not the inconvenient, uncaringbanker.
A good, caring bank will recommend anannual review irrespective whether you borrowfunds. This enables all aspects of your practice
and the bank’s services to be discussed ‘face toface’ to reinforce the mutual respect that shouldbe developing. Be mindful that there could be acost for this, depending on who are yourbankers. To keep it simple:-
Be honest
Keep in contact
Avoid surprises
THE CHOICE IS YOURSYou can present your case effectively andinvolve your bank in your practice but whichbank to choose?
It is not as straight forward as it seems asall banks offer varying levels of service,different products and contrary to popular beliefnot all banks are the same.
Choose your banker with care. Try testinghim against the following criteria:
Knowledge of dentistryIs there a specialised unit? If so does it providenationwide coverage? What you do not want isone bank with one policy interpreted differentlyby individual managers around the country.
Does the bank manager visit you?This is a cost in addition to any bank fees as youare unable to earn during the time at his office,include travelling time.
Practice bank accountCan it fulfil the standard requirements of apractice, e.g. standing orders, cheque books andso on.
Credit interestDoes the current account earn Credit interest, isit tiered and can it be individually tailored toyour practice as we do. Our practice accountcan combine the current and deposit accounts inone account at a preferential interest rate. Thissaves time, effort and maximises income.
Practice FundingDo they provide practice finance at competitiverates, is any price differential possible betweensecured and unsecured lending? What value dothey assign the security? We recognise the valueof your income stream and this effects our viewof security.
Is there a policy of continued customercontact?Annual review at a minimum.
Charges Not all banks are the same, consider them allbefore committing yourself. Remember the bestway of ensuring you enjoy painless banking isby talking to the bank and using us and ourcontacts. We may not be able to help but wenormally know someone who can.
Jay PatelProfessions Unit Bank of Ireland36 Queen Street, London EC4R 1HJTel: 020 7634 5064
23
AOG
MannyVasant
Man is stronger than thestrongest beast, not physically,but in inner wisdom. Failures and disappointmentsin life are just common andsometimes may be evenrewards in disguise by theway of future successes.Don’t let this littledisappointment involving adelay of six months, in yourgoal, rob you of your “peaceof mind”– so vital for yourmany battles in future.
Excerpt from a letter written by Manny’sfather to his brother Kishor during a temporarydisappointment during his medical course.
These words are a constant source of strengthand solace to Manny at all times. As hesuccessfully made it to the Gillmans Point, theofficial certification point at the top of MountKilimanjaro, these words were still echoingthrough his mind as they always do. Hebelieves that a man’s job is to do one’s best -the result, to a certain extent, is irrelevant andcertainly out of one’s control.
Despite a busy schedule Manny found time tomeet with us. Over dinner we chatted freelyand he was very generous about sharing hismany stories, both good and bad! Hisexperiences through life, it seemed, have actedto catalyse his strength to achieve the successhe now has and rightfully deserves.
Manjul believes that the Asian OdontologicalGroup (AOG), as it was called then, wasofficially launched in 1982 at a socialgathering at the YMCA Croydon whichManny had organised for Asian dentists. Some70 or so dentists attended this function. Asocial event at Guy’s Hospital paved the wayfor regular events in the AOG’s calendar. Soon
after this event, Raj Rayan launched anewsletter which really became the voice ofthe AOG. It was Manny, who wrote a letter inthis newsletter and suggested that the name bechanged to Anglo-Asian Odontological Group.Even in the early days he had the vision thatthis group would one day be prominent in thenational scene, indeed with potential forinternational recognition.
Born and brought up in Tanzania, Mannyobtained a place to read dentistry in Bombay atone of the oldest dental schools in the country-The Nair Hospital Dental College, a colonialBritish institution. At the University, bycoincidence, he met his old high school class-mate from home, Meena who was to laterbecome his wife. On qualification in 1972, dueto the political climate in East Africa, Mannywas forced to come to England and re-qualifyto be able to register in the UK. This, he did ina record time of four months. The difficultiesof overseas graduates wanting to register topractice in this country was experienced firsthand. Many of his contemporaries could nottake the stress. Many sought other jobs such asbus conductors or clerks for survival. Somequalified up to 20 years later – others were notso lucky. One or two even lost their bottlecompletely. The stress and the frustration wastoo much. For a man of high principles, it wasonly natural that he take up their cause.
On qualification, he got married in Croydon,Surrey and set up a home there. This was tobecome a meeting, eating and teaching placefor those who followed him. To this day,Manny continues to run courses for them-albeit, these have now progressed to better andbigger venues. Manny quietly, but persistently,continued his crusade for a level playing field.This could not have gone unnoticed. TheInternational Qualifying Examinationlaunched in year 2001, by the General DentalCouncil is a welcome change.
Manny was president of the AOG in 1994 andamongst others, along with Raj Rayan andRuby Austin, a founder member of the CentralLondon MGDS Study Group. He has remaineda strong advocate of postgraduate educationwith a career pathway for general practitionersfirmly in mind. Running two busy practiceshimself, how he finds the time to fulfil his
many commitments of being a vocationaltrainer, VT advisor, lecturer, examiner forvarious examinations — the list is endless andis highly commendable. Since 1997 Mannyhas been appointed to become a RegionalAdvisor (University of London SW ThamesVT Scheme). Fighting against all oppositionfor his principles and beliefs seems to be thedriving force behind this dynamic man.
A committed family man, his daughter is anoptometrist and his son is now following inhis footsteps, at GKT Medical and DentalSchool, London. Manny has been andcontinues to be, a mentor to manypractitioners, guiding them through theFaculty examinations. He also lends thebenefit of his considerable experience to helpcolleagues write articles, organise lectures orset up practices. He remains grateful to hisfirst principal Dr Harris Yee-chong ofMitcham Surrey for offering him anopportunity of a job after (unsuccessfully)having knocked on several doors.Subsequently, his second principal, Dr LalitBandlish London, encouraged him to carry onwith his passion of taking post-graduateeducation and allowed him to make hisfrequent journeys to the USA.
Successful in the American BoardExaminations and having obtained a licenceto practice in the state of New York, early inhis career, he has friends on either side of theAtlantic. When asked for advice fromprofessional colleagues, one can always saythat “I don’t know the answer to that but Iknow a man who does” and then refer them toManny who is willing to help. Whether he ison a squash court, golf course, at surgery orlecture podium, the essential ingredient is thathe “enjoys” what he does, this seems to be thecommon denominator for his success. Heremains highly respected in the professionaland academic circles.
Sharing time with him at a restaurant acrossthe road from his practice was a highlypleasurable and informative experience.Achieving what he has so far one wouldexpect that he has deserved to take thingseasy. Hearing what he has planned for thefuture however, it seems that he is not one torest on his laurels.
Subir Banerji & Russ Ladwa share anevening with Manny (Manjul) Vasant
A N E V E N I N G W I T H
24
BENEFITS TO ALL AOGMEMBERS WHEN USINGTHE DENTAL DIRECTORY
Every AOG member can benefit from the following discounts:
10% DISCOUNT off branded products shown in The Dental Directory Master Catalogue*
11.5% DISCOUNT on all orders sent via The Desktop Directory computer ordering system onbranded products
12.5% DISCOUNT off our house preferredUnoDent, Perfection Plus and Degussa Dental products
14% DISCOUNT on all orders sent via The Desktop Directory on house preferred products.*Excludes the PriceWatch Mini Catalogues.
The above AOG discounts coupled with our low published prices
represent substantial savings for every AOG member when you
buy your dental materials, sundries and consumables from
The Dental Directory.
The Dental Directory also offers AOG members a unique Product
Audit service. This should save your practice 5-7% on your
annual materials spend, even before your AOG discount is added.
The Dental Directory has had the privilege of being the Preferred
Dental Dealer to the AOG since 1994. In that time, we have
donated 1% of each members monthly spend to the AOG
Committee to help further the Groups aims, objectives and
ambitions.
If you would like a copy of our latest catalogue, or would like to
find out more about how a Product Audit can save your practice
up to 7% off your annual materials spend, simply call us FREE on
0800 585 586.
DELIVERING THE FUTUREOFDENTISTRY
On the 29th of June 2001 at The Institute ofPhysics in London prominent clinicians andacademics from both sides of the Atlantic werebrought together for a stimulating meeting. RajRayan, Dean of the Faculty, set the tone.“Where is the scientific evidence?” he asked.As clinicians we carry out forms of treatmenteveryday on our patients which would notstand up to scientific scrutiny. Using exampleshe challenged the basis of the rationales usedfor dental treatment. Where do we stand as aprofession? As scientists? Technicians? Or artists? The bottom line — “Do the patientno harm!!”
Senator Rawson from Las Vegas put forwardthe scientific basis of bite marks as used inforensic pathology. The bite marks left at thescene of a crime are so unique that it isregarded as strong evidence to prove theinnocence or guilt of an individual. His flightat least was not delayed unlike the otherAmerican delegates led by Dr Arun Nayyar.
Larry Holt stressed the financial virtues of feeper item based dental treatment against theInsurance based system of payments in theUSA. Clinical freedom and a set up to providehigh quality dental treatment at a pace whichbest suited the clinician were described as thedesirable advantages. The comparison of theNHS system to the insurance system becameinevitable and was discussed at length withcontributions from the delegates chaired byRash Patel.
Under the guidance of Dr Arun Nayyar, DrRandy Muecke and Dr Leever presented anoverview of a technique to predictably andrepeatedly mount the maxillary andmandibular casts of a patient usingcephalometric radiographs. The technique, forwhich the patent is pending, appears toincrease the accuracy and reproducibility ofadvanced restorative work.
With the knowledge that the revenue for dental
treatment in this country of 2.5 billion is thesame as that spent by this population onChicken Tikka Masala, the meeting drew to aclose.
At the Pierre Fauchard Academy (PFA)Dinner, which followed later that evening,several new fellows were inducted. Amongstthem were Amolok Singh, Raj Majithia, JatinDesai, Paul Howard and Tony Kilcoyne.Organised in 1936 the PFA is an InternationalHonour Dental Organisation and one of itsprimary objectives was the extension ofcontrol by the dental profession over its ownliterature. This control has remained animportant function of the Academy. It is arecognition for ethical dentists who have madecontributions to the art and science of dentistryor to society. Membership to this Academy isby invitation and no doubt the newly inductedfellows felt privileged to be a part of such anorganisation.
DENTAL CONTROVERSIES ACROSS THE PONDTHE INTELLECTUALA JOINT MEETING BY THE PIERRE FAUCHARD ACADEMYAND THE FACULTY OF GENERAL DENTAL PRACTITIONERS (UK) THE ROYAL COLLEGE OF SURGEONS OF ENGLAND. DEBATE.
25

AOG
26
NEWNEWSRAJ RAYAN & AMALOK SINGH.Re-elected in to he GDC.
AOG PRESIDENT.AOG president Ian McIntyre receives Probe lifetime achievement award.
APPEAL TO THE TRADE AND PROFESSION FROM -MANJUL .Donation and materials to a Hospital inMwanza, Tanzania.
Access to dental services even in Mwanza,the second largest town in Tanzania, arevery limited. For the disadvantaged, elderlyand poor the suffering and pain can beterrible. YOUR help would alleviate muchpain and suffering.
We are helping to set up a dental clinicwithin a hospital to serve the localcommunity in this town. The services willbe available to all at very subsidised costsand will be run by a local charity. A localdentist to run the clinic has been identified.I have personally visited the hospital andwould endorse the project. There will be anopportunity for any volunteers (own travelexpenses but free accommodation possible)to go and help once the clinic is running.
Simple serviceable dental equipment (in working condition) and materials are required.
PLEASE HELP! Please send details of any availableequipment to:
Dr Manny VasantAppeal co-ordinator1210 London RoadLondon SW16 4DNFax: 020 8679 3126Phone: 020 8764 1424 (please fax or e mail)e mail: [email protected]
At the end of a long day while negotiating adifficult root canal, I thought that the phonecall from “Nicola of ITN” was somebodytrying to sell me something so I asked thereceptionist to take a message. When, out ofcuriosity, I returned the telephone call thenext day, it was indeed somebody from the news channel wanting me for aninterview but by that time they had foundsomebody else. My teenage daughters weremost upset that I had missed out on anopportunity to be on TV.
Personally I was relieved because I wouldn’thave been prepared. For any mediaencounter one has to be prepared and go withconfidence. As a BDA media spokesperson(and hoping to speak for the FGDP too!) Ihad a fascinating training day with someother aspirants recently at Wimpole Street,conducted by the thoroughly professionalmedia consultant, Kim McLoughlin (whoamong other things was involved withproducing the Kilroy programme).
You must check your facts beforehand(NEVER LIE). For a telephone interview,stall for time to prepare, rather than gostraight into it. Have three short, simplepositive “messages” you want to get acrossplanned and get them in in the first fewminutes because “waffle” and timeconstraints will edit out quite a lot.
Be warned that there is no “off the record”remark with a journalist. If you do not wantsomething recorded just do not say it. I haveknown colleagues get into trouble for tryingto be honest and fair. That’s another thing, asa professional person you may feel you haveto give a balanced argument - DON’T. Yougive your/the professions side. The journalistwill do the opposition.
An interview in the practice can bedisruptive. Two minutes of airtime couldtake hours to record! But do not be temptedto be filmed on the golf course or by an
expensive sports car. Television is apowerful medium. Remember the greatestimpact is not made by what you say, butyour body language first, then your voiceand the actual words the least. So smile,look positive and sympathetic; wear sensiblecomfortable clothes (no garish colours orchecks) without bits of paper to distract. Donot make casual remarks even if theinterview has formally ended.
In any interview the journalist has anagenda, so learn to deflect some questionsso that you can get your message in. Avoidacronyms and jargon. Rule of thumb is thatwhat you say should be in words that onaverage a 15-year-old can understand. Wepractitioners tend to speak too much of thetechnical language which may impress ourcolleagues, but not the lay audience.
As an interviewee you have some rights.You are allowed to ask what the format/typeof programme is, the audience, the otherparticipants, recorded/live etc. Interestinglyyou can also guess what the first questionwill be, but not a detailed list of all thequestions. You also have the right to go backand correct something, even if theprogramme has been recorded. Never beafraid to correct a mistaken statement thatthe interviewer is making but be sure of yourfacts.
Avoid any negative aspects or unfavourablewords to creep into the interview. Always be confident, upbeat and well prepared. In this age of spin doctors, advertising andaccountability the media can be a powerfultool for you and your profession if used wisely. Any media encounter shouldtherefore be welcomed as a goldenopportunity to promote your profession andpractice. So go and fly the flag positivelywith pride, power and professionalism.
Russ Ladwa.
So you want to be a
TV StarAsks Russ Ladwa.

Clinical Governance is the subject of moreconfusion and suspicion than it merits; justbecause it is a Government initiative does notautomatically make it a bad thing for the GDSpractitioner. Recent articles in the dental presshas even suggested that it is going to becomesome malign influence by those dry fingereddentists seeking to control the real workers.Perhaps as one newly arrived in the dryfingered brigade and working in HealthAuthority, I can put some of theseapprehensions at rest.
Essentially CG is a means for a clinician tomonitor the effectiveness of their ownprofessional practices, both medical anddental, their conduct and performance. Themain aim is to standardise the perceived widedifferences in the quality of clinical carethroughout the country and to build uponaccepted common best practice. While HealthAuthorities may be able to help with theprocess, for it to be successful it must be“owned” and run by the participatingclinicians themselves.
In my opinion, there are 5 main buildingblocks to CG:1) Clinical Audit2) Clinical Effectiveness - Evidence Based
Dentistry 3) Risk Management4) Quality Assurance5) Practice organisation
and staff development.
Quality assurance, improvement andmanagement can be addressed by:
• Greater use of research in clinical practice •
Measuring performance against acknowledged and agreed standards
• Providing career development for the whole dental team
• Learning from complaints• Strategic Priority Areas
Clinical Excellence - Evidence Based Decision Making. Three critical areas:• The dentist’s expertise, skill and judgement• The needs and preferences of patients• Acting on the best available evidence
Clinical Excellence - Clinical EffectivenessClinical effectiveness is an umbrella term foractivities ensuring that the best care is given.It involves finding the evidence, acting upon it,monitoring and evaluating the results.Because so little scientific evidence exists tosupport most dental procedures this is an areawhere standards could and should be set bypractitioners themselves through audit ledclinical guidelines and evidence basedpractice. Clearly from the outset audit projectsmust have strict criteria and standard settingmust be based on current best evidence
Clinical Excellence - Clinical AuditCA is the systematic critical analysis of thequality of dental care, including the proceduresused for diagnosis and treatment, the use ofresources and the outcome from the patient’spoint of view.
Clinical Excellence - Research and DevelopmentNever an easy area for busy dentists requiringtime energy and resources. Encouragementwill be necessary at a national level before thiscan become a reality outside universities.
Clinical Excellence - Patient ExperiencesClinical Governance requires a change ofattitude from the “participant-Recipient” styleof practice to one where there is a genuinepartnership with the patient. It is morerelevant in medicine perhaps, but an importantfactor in Government thinking nevertheless.
Clinical Excellence - Quality AssuranceQuality assurance is based on setting andmeeting standards; setting the standards is thehard part. Quality assurance and clinicalgovernance are linked through the riskmanagement process.
Standards Of Care
Standards of Care - Quality Improvement Quality improvement links quality assuranceand audit so that having met the standard inquality assurance and measured the outcome
by audit you then aim for an improvement - theaudit cycle. Quality improvement is supportedby:• Leadership by the team leader, usually but
not exclusively the dentist• Continuing professional development -
meeting the GDC guidelines• Sharing of information
Standards of Care - Continuing Professional DevelopmentCPD is about developing yourself and yourstaff in a process of “lifelong learning”. It supports CG by:• Ensuring skills are up to date and effective• Ensuring that skills are appropriate to the
services being offered.
For staff CPD should include a training anddevelopment plan based on needs rather thaninterests, appraisal, encouragement fromsenior staff and time. The resourceimplications of CPD require decisions at anational level.
Reducing Risk
Risk management should include:• Reporting incidents• Risk assessment and prevention strategies• Handling complaints• Clinical supervision• Dealing with poor performance• CPD
The booklets produced by the ProtectionSocieties to assist in the development of a RiskManagement regime are excellent and shouldbe used as guidance for individualpractitioners.
There are packages available from the BDAand others to assist practitioners in preparingfor Clinical Governance, but I personallyfavour a more local approach where eachpractice thinks about it for itself. Using acookbook approach from a third party mightget a tick in the CG box but is less likely togenerate the change in practicing behaviourthat should produce lasting benefits for boththe patient and the practice.
And what about the threat that “Big Brother” issomehow going to use CG to impose theGovernments standards and interfere with yourclinical freedom. I believe that nothing couldbe further from the truth. Used properly CGcould be about setting new and higherstandards for general dental practice. If theevidence were there we dry fingered operatorswould be hard pushed to argue against it, thetrick will be to use CG to generate theevidence that the Department of Health can notignore. The reins are now firmly in thepractitioners hands if they have the courage totake control.
CLINICALGOVERNANCE
Air Vice-Marshal Ian McIntyre
AOG
27

A Millennium of Endodontics:A Historical Perspective-Part 1
Endodontics had its humble beginningsin the bizarre ideas and treatments thatwere provided in ignorance of the
pathological processes involved. Much painwas endured by the patient at the experimentalhands of our predecessors in history as theyderived the theories we can now take forgranted as the principles of modernEndodontic therapy.
The signs and symptoms of infection of dentalorigin were documented as early as 3700 BCby the Egyptian civilizations. Around the eraof the ancient Chinese Dynasties aphenomenon was described, that could belikened to an alveolar abscess, resulting frominfection by a mystical “white worm with ablack spot on its head” (probably describingthe appearance of non-vital fibrous pulptissue). This “worm” theory remainedestablished for thousands of years, through theages of the great Greek and Roman scholarsand physicians, beyond the Middle Ages, untilquite early on in the 19th century. Otherattempts were made in order to identify thecauses of toothache with diagnoses often beingquite outrageous as: ‘Fungus’ of a nerve (aclinical description probably that of a pulp‘polyp’); and, ‘vicarious menstruation’ from atooth in a case of a young women!1
Work by Sixteenth century anatomists beganto challenge the ‘worm-theory’ of dental pain.In 1746, the maverick ideas of a certain PierreFauchard may have started the birth ofoperative endodontics in a form familiar to ustoday, based on accurate descriptions of pulpcavity and root canals of different teeth. It wasslowly becoming appreciated that it was dentaldecay that caused much of pulp-disease and soeventually displaced the ‘worm-theory’ onceand for all. Then, towards the end of the 19thcentury, Roentgen was to discover X-rays (in1895). The implementation of this latterdiscovery in clinical dentistry was rapidly seento give endodontic therapy a more scientificfoundation together with irrefutable diagnosticevidence of bony disease that could now bedirectly associated with periapical (andperiodontal) pathology. Also around this time,the introduction of topical cocaine analgesiafueled a surge in popularity for root canaltreatment of the day and became moreaccepted by patients.
The treatments evolved still without any sounddiagnoses and so remained only palliative.Arabian physicians would brutally sever thenerve of the offending tooth by subluxating it,which apparently would resolve the persistentpain!2. Techniques for ‘capping’ exposednerves in order to treat them superficially butalso attempting to maintain its healthbecame the vogue. In the 17th and 18thcenturies, each dental ‘physician’ had hisown favourite exotic concoction for thepulp-capping technique: oil of cloves,arsenic, opium, nitric acid, creosote, andeven red-hot instruments for cautery. Fromthis, materials that could provide amechanical barrier within the treated rootwere used (approaching today’s concept of‘obturation’): gold foil, lead plates, asbestos,and Hill’s stopping (gutta percha).
Within our lifetimes (and still today!), ‘pulpcapping’ still remains present albeit with lesstoxic agents (e.g. steroid-antibiotic andcalcium hydroxide cements). However,unfortunately such treatment is ofteninappropriately given in an attempt to ‘avoid’conventional endodontic intervention andshould be regarded as pulp “crapping” ratherthen capping! Also, other biologically‘offensive’ materials based on phenolic andparaformaldehyde compounds have, only untilrecently, been popular as root fillers or sealersuntil their toxic effects were discovered.Today, the philosophy of root canal ‘fillings’has changed towards providing purely apassive mechanical barrier, initially, with theimplementation of silver cones, stainless steelpoints, and acrylic cones. Currently, GuttaPercha has proved to be the material of choice.
ROOT CANAL PREPARATIONConcepts fundamentally changed in 1955,when Ingle3 showed that endodontic failureswere consistently resulting from poorly filledcanals and this was somehow closely related totheir initial instrumentation. He developed theStandardised Technique that aimed to create anideal conical preparation by the grindingaction of reamers into the root canal.Although groundbreaking at the time, certainshortcomings were encountered concerningthe reaming technique. Difficulties were seenin treating curved canals, with ledging-formation and perforation of canal walls near
the apex. As a solution, smaller more flexiblefiles were then advocated, but this would thenpotentially underprepare the canal walls andleave infected and necrotic material beyondthe curvature or where anatomic aberrationsremain inaccessible (Fig. 1).
This led in 1958 to a establishment of astandard which eventually was taken up by theFederation de Dentale Internationale (FDI) andthen by the International StandardsOrganisation, encompassing size, shape andnomenclature of a wide range of endodonticinstruments (ISO Standard No. 3630)4, to giveus the familiar 2% tapered instrument.Improvements in handpiece-technology in thelate 1960’s also saw the emergence of power-driven intracanal preparation claiming tofacilitate the procedure (e.g. the Giromaticreciprocating handpiece5). Such methods,however, had serious dangers concerning theloss of tactile-feedback, extrusion of debristhrough the canal apex and aggressive cuttingaction especially around curvatures. Recentimprovements in instrument and electric-motor design have paved the way for a newerinterest and hope in their re-emerged use(discussed in the next article).
EMERGING CONCEPTS“We do not believe that all teeth can be saved,nor do we believe that all pulpless teethshould be extracted ....” (Moffit 1922)14
THE ROLE OF MICROBIOLOGICALINFECTIONIn 1894, Miller6 published his findings on therole of bacteria in dental disease. He was oneof the first to suggest that elimination ofdamaging bacteria by removal of the pulp tothe apex was the most satisfactory treatmentfor affected teeth. From this, much researchwas done particularly in the mid- to late 20thcentury on establishing the vital of role of
Fig 1.
Instrument
InaccessibleDebris
ORIGINALCANAL WALLS
PREPAREDCANAL SPACE
AOG
28
By Sanjeev L. Bhanderi BDS Lon. MSc
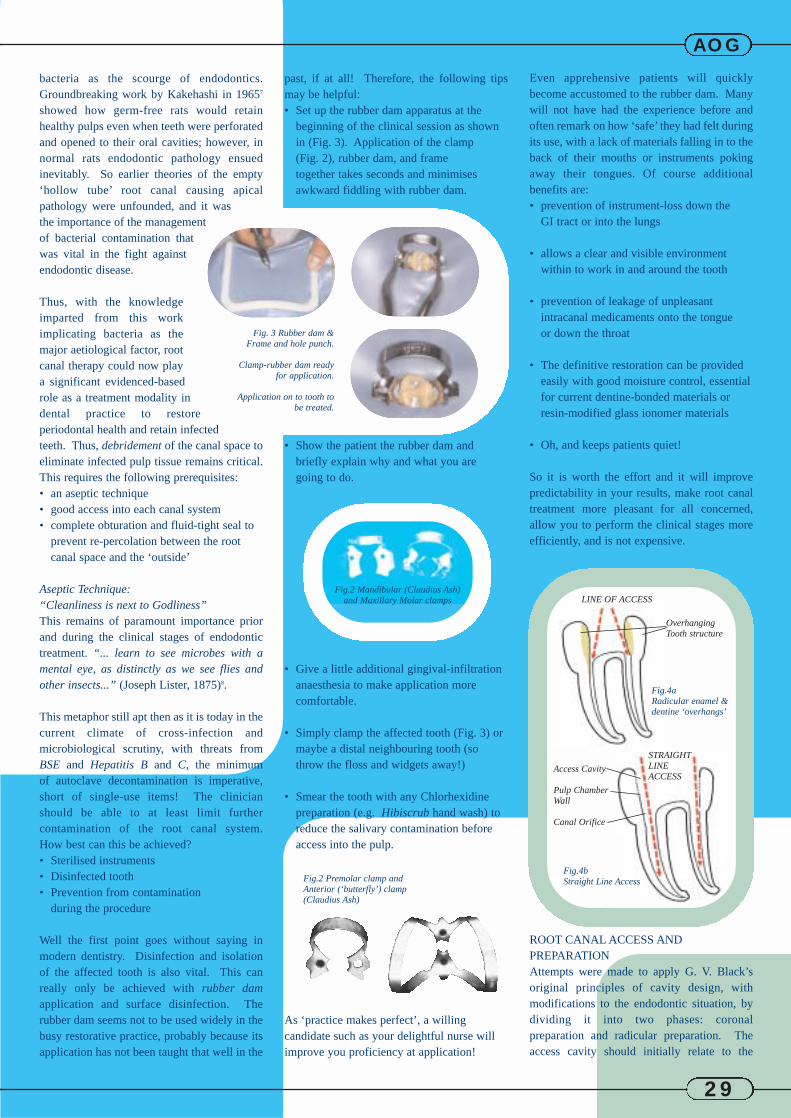
bacteria as the scourge of endodontics.Groundbreaking work by Kakehashi in 19657
showed how germ-free rats would retainhealthy pulps even when teeth were perforatedand opened to their oral cavities; however, innormal rats endodontic pathology ensuedinevitably. So earlier theories of the empty‘hollow tube’ root canal causing apicalpathology were unfounded, and it wasthe importance of the managementof bacterial contamination thatwas vital in the fight againstendodontic disease.
Thus, with the knowledgeimparted from this workimplicating bacteria as themajor aetiological factor, rootcanal therapy could now playa significant evidenced-basedrole as a treatment modality indental practice to restoreperiodontal health and retain infectedteeth. Thus, debridement of the canal space toeliminate infected pulp tissue remains critical.This requires the following prerequisites: • an aseptic technique • good access into each canal system • complete obturation and fluid-tight seal to
prevent re-percolation between the root canal space and the ‘outside’
Aseptic Technique: “Cleanliness is next to Godliness” This remains of paramount importance priorand during the clinical stages of endodontictreatment. “... learn to see microbes with amental eye, as distinctly as we see flies andother insects...” (Joseph Lister, 1875)8.
This metaphor still apt then as it is today in thecurrent climate of cross-infection andmicrobiological scrutiny, with threats fromBSE and Hepatitis B and C, the minimum of autoclave decontamination is imperative,short of single-use items! The clinician should be able to at least limit furthercontamination of the root canal system. How best can this be achieved?• Sterilised instruments• Disinfected tooth• Prevention from contamination
during the procedure
Well the first point goes without saying inmodern dentistry. Disinfection and isolationof the affected tooth is also vital. This canreally only be achieved with rubber damapplication and surface disinfection. Therubber dam seems not to be used widely in thebusy restorative practice, probably because itsapplication has not been taught that well in the
past, if at all! Therefore, the following tipsmay be helpful:• Set up the rubber dam apparatus at the
beginning of the clinical session as shown in (Fig. 3). Application of the clamp (Fig. 2), rubber dam, and frame together takes seconds and minimises awkward fiddling with rubber dam.
• Show the patient the rubber dam and briefly explain why and what you are going to do.
• Give a little additional gingival-infiltration anaesthesia to make application more comfortable.
• Simply clamp the affected tooth (Fig. 3) or maybe a distal neighbouring tooth (so throw the floss and widgets away!)
• Smear the tooth with any Chlorhexidine preparation (e.g. Hibiscrub hand wash) to reduce the salivary contamination before access into the pulp.
As ‘practice makes perfect’, a willing candidate such as your delightful nurse will improve you proficiency at application!
Even apprehensive patients will quicklybecome accustomed to the rubber dam. Manywill not have had the experience before andoften remark on how ‘safe’ they had felt duringits use, with a lack of materials falling in to theback of their mouths or instruments pokingaway their tongues. Of course additionalbenefits are:• prevention of instrument-loss down the
GI tract or into the lungs
• allows a clear and visible environment within to work in and around the tooth
• prevention of leakage of unpleasant intracanal medicaments onto the tongue or down the throat
• The definitive restoration can be provided easily with good moisture control, essentialfor current dentine-bonded materials or resin-modified glass ionomer materials
• Oh, and keeps patients quiet!
So it is worth the effort and it will improvepredictability in your results, make root canaltreatment more pleasant for all concerned,allow you to perform the clinical stages moreefficiently, and is not expensive.
ROOT CANAL ACCESS ANDPREPARATIONAttempts were made to apply G. V. Black’soriginal principles of cavity design, withmodifications to the endodontic situation, bydividing it into two phases: coronalpreparation and radicular preparation. Theaccess cavity should initially relate to the
Fig. 3 Rubber dam &Frame and hole punch.
Clamp-rubber dam readyfor application.
Application on to tooth tobe treated.
Fig.2 Premolar clamp and Anterior (‘butterfly’) clamp (Claudius Ash)
AOG
29
Fig.2 Mandibular (Claudius Ash)and Maxillary Molar clamps
Fig.4a Radicular enamel &dentine ‘overhangs’
LINE OF ACCESS
OverhangingTooth structure
Access Cavity
Pulp ChamberWall
Canal Orifice
Fig.4b Straight Line Access
STRAIGHTLINE ACCESS

canal. Thus, the digital action is: 1 a passive restricted clockwise angle that is
sufficient only to engage the blades into thedentine wall;
2 then, a counterclockwise rotation with apical pressure that is sufficient to cut and load the cleaved dentine-chips into the flutes-spaces;
3 finally, this is followed by a slight clockwise turn to release the file and allow removal of the debris from the canal.
This allows the reaction forces against the dentine-cutting blades to resolve or“balance” towards the centre of the instrumentshaft. Thus, the instrument is notpreferentially deflected towards any particularwall and so the central axis of the canal ismaintained (Fig 7).
This is a technique that can only really beappreciated if demonstrated and practiced andmost endodontic hands-on courses provide anopportunity for this. But when mastered it isfar more predictable and efficient than the‘round-the-clock’ filing technique that has been traditionally taught. It can beimplemented right away in practice, asconventional K-type hand files are all that arerequired.
THE ROOT CANAL FILLINGThe root canal is being prepared for obturationby virtue of the fact that it has been sufficientlydisinfected, opened-up, and is of a satisfactoryshape which it can be filled in threedimensions. Why fill once the bacteria havebeen removed? Root canals must be filled inthree-dimensions in order to secure a fluid-tight seal from the apical tissues and lateralaccessory canals, which will allow re-growthof retained intra-canal flora. But, moreimportantly is the fact that the coronal aspect iswhere the seal is paramount as this is the mostlikely source of potential contamination15,16.The ‘obturation’ should be consideredcomplete only when the definitive restoration
internal pulp chamber walls and then ‘project’the root canal orifices coronally. This may beinfluenced by site, shape, curvature, anddirection of the root canals taking due accountof deposition of secondary/reparative dentine.Thus, from a mechanical viewpoint, thisconcept of coronal flaring allows initial rootcanal preparation to be performed
• It will straighten the path of access into curved or calcified canals (Fig. 4)
• Removal of the majority of endodontic infection from the contaminated coronal zone of the canal15
• Apical instrumentation is thus made more predictable and effective in finely curved canals, reducing the risk of gouging (or ‘zipping’) the wall of the outer curvature
• Deeper delivery of irrigants and debridement
• Improved resistance-form for the final Gutta Percha obturation and penetration of condensation implements towards the working length.
The overall aim is to achieve straight-line access (Fig. 4a & 4b) Irrigation plays is an equally significant role incanal cleaning. They achieve more than simplywashing out debris:
• chemical dissolution of tissue remnants• antimicrobial effect• lubrication of the canal walls to facilitate
instrumentation.
Sodium hypochlorite (0.25-5.25 per cent) isthe solution of choice and easily available as a
standard 4% solution (Fig 5). In addition, upto 17% ethyl-diamine-tetraacetic acid (EDTA,Fig. 6) is suggested as a chelating agent, whichremoves calcium ions from dentine and thesmear layer thereby softening their organic-inorganic complex rendering their removaleasier. Other agents such as 0.02%chlorhexidine gluconate (mouth wash) maybehelpful during emergency root canal cleansingwhen rubber dam is not used, prior to arranging the definitive endodonticappointment.
CONTEMPORARY PREPARATIONTECHNIQUESOver the latter part of the century, varioustechniques had been developed for thepreparation and shaping of the curved canal toachieve an acceptable tapered form.
• Serial Step-back (1969)9 - which aims to achieve a smooth taper from apex to orifice.
• Crown-down Approach (1984)10- as its name suggested, is broadly considered as step-back ‘in- reverse’.
• Modified Double-flared Technique (1983)11- is a combination of both step-back and crown-down. It therefore has with the benefits of pre-coronal flaring
• Graduating/Greater Taper (1996)12 - will be discussed in the next article
All these techniques (except the latter)advocate that instruments should be used in‘scraping’ or filing action. This can pushdebris apically and cause shaping errorsparticularly in curved canals. As a possiblesolution, James Roane in 198512 developed theBalanced Force technique and suggested thatthe file may maintain the central axis of acurved canal if a rotational force was appliedto it, so eliminating canal transportation. Thisworks best with a file of a triangular cross-section such as a K-type file. Such balance offorces is generated by rotating the file with allits cutting blades in contact with the dentine, asoccurs in the narrow apical region of a root
AOG
30
Fig. 5 4% Sodium Hypochlorite preparations (available from your local Supermarket)
Fig. 6 EDTApreparations: gels (Optident& Dentsply-Maillefer) &Liquid(Pulpdent)
R
R
R - inward forces reacting
against the cutting of the
file-blades into dentine
canal wall, all equally
resolving into the centre
of the file
(A filing ‘scraping’ action would not be balanced
and canal wall is cut unevenly and ledging or
transportation may result.)
Fig. 7 The balanced force Technique
R
has been secured at the crown of the tooth,otherwise this remains ‘the weakest link’(!).
Gutta Percha remains the material of choicewithin the root canal as it possesses the mostdesirable properties and is relatively versatilein application. Traditionally, cold lateralcondensation has been the technique of choicebut with the realisation that gutta percha can bemade to flow when heated, a plethora of newthermoplastic techniques have been developedand will be discussed in a later article.
So, throughout history ‘root-treatment’ hasdeveloped from a mere crude palliativeprocedure into a more biologically baseddiscipline. Contemporary endodontics is nowviewed to aim for the restoration of a healthyperiodontal ligament, free of infection andinflammation and so keeping a tooth infunction. Resolution of endodontic pathologyinvolves chemo-mechanical debridement in anaseptic environment with judicious use of filesthat ‘surgically’ remove pathologicallyaffected pulp tissue. It is impossible tocompletely sterilise the endodontium of a toothso the aim is to decrease the microbial count toan insignificant (non-pathological) level andthen incarcerate the residual flora, removetheir nutrient supply, and prevent re-growth ofthe flora.
So what’s in store for the new millennium?Now that we are equipped with the knowledgeof the principles of Endodontics, the nextarticle will enlighten on how technology hasflooded the discipline with a plethora of newand exciting methods and materials that can beused to attain the highest predictability inclinical results with efficiency.
REFERENCES:1 Hullihen SP. “Odontalgia. Observations on toothache”1839. Amer. J. Dent. Sci. 1:105-111
2 Curson I. “History and Endodontics” 1965. The Dental Pract. & Dent Record.15(12):435-9
3 Ingle JL. “The Need for Endodontic InstrumentStandardisation” 1955. OS.OM.OP. 8:1211-1213
4 Ingle JL. “A Standardised endodontic techniqueutilising newly designed instruments andfiling materials” 1961. OS.OM.OP. 14(1): 83-91
5 Frank AL. “An evaluation of the Giromatic endodontichandpiece” 1967. OS.OM.OP. 24:419-421
6 Miller WD. “An introduction in the study of thebacteriopathology of the dental pulp” 1894. Dent. Cos. 36:505
7 Kakehashi S. et al “The effect of surgical exposures of dentalpulps in germ-free and conventionallaboratory rats” OS. OM. OP. 20:340-349
8 Lister J. “Demonstration of antiseptic surgery beforemembers of the British Medical Association” 1875. Edin. Med. J. 21:193-205
9 Clem WH. “Endodontics in the adolescent patient”1969. Dent. Clin. N. Amer. 13:483-7
10 Morgan LF. & Montgomery S. “An evaluation of the crown-downpressureless technique” 1984. J. Endo. 10(10):491-8
11 Fava LRG. “The double-flared technique: an alternativefor biomechanical preparation” 1983. J. Endo. 9:76-80
12 Roane JB., et al. “The balanced force concept forinstrumentation of curved canals” 1985. J. Endo. 11:203-11
13 Buchanan LS., “The Art of Endodontics: Files of GreaterTaper” Feb. 1996. Dentistry Today
14 Moffit JJ. “Procedure in root canals” Dec 1922. Dent. Cos. 11:1133-1148
15 Shovelton DS. “The presence and distribution of micro-organisms within non-vital teeth” 1964. Brit. Dent. J. 117:101-107
16 Saunders WP. & Saunders EM. “Coronal leakage as a cause of failure in root canal therapy: a review” 1994. Endo. & Dent. Traumat. 10(3):105-8
DATES FORTHE DIARY
AOG
31
Do not forget -
The AOG Charity Ball17th November 2001
at the magnificent
Radisson Portman 22
Portman Square
London W1.
Again we advise you
to book early to avoid
disappointment as this
event is always a huge
success.
So reserve this date in
your diary now for a
guaranteed enjoyable
evening.

Working as One to Benefit Our Patients
Management ServicesHelp LinePractice BenchmarkingDiscountsRepresentationTrainingInternet Services
For an information pack Call Tanya now on01409 254 354www.codeUK.com
As Dentists our primary motivation is always for the care our patients and how to offer them the most suitable and up-to-date treatments.However we are working in an increasinglycommercial and competitive environment. Now more than ever modern business techniquesmust be combined with the caring provision of dentistry.
CODE was established in 1978 to offer dentalpractice owners management support andservices. We have hundreds of members acrossthe United Kingdom, our members range fromowners of large groups of multiples to singlehanded practitioners.
Dental practice owners are under increasingpressure from the expansion of corporatedentistry, the difficulties of working within the NHSand the expansion of legislation from Europe.
CODE Management Services are designed toenhance the business of running a dentalpractice, offering independent dentists thebenefits and economies of scale previouslyavailable only to the larger groups. It has alwaysbeen CODE's view that a well-run business willresult in better service to our patients.
CODE Business Partners offer discounted orunique services to members ranging fromaccountancy, surveying, and law to new practicedesign and build. Business Partners also offermembers free initial advice on relevant topics. All of CODE's professionals are chosen through our years of experience of dental practice management.
CODE discounts not only more than cover thecost of membership, but can really improve theprofitability of your practice.
Benchmarking is a way to measure the results ofyour practice against similar ones around the country. Using this information you can target the areas in your business that are 'under performing' and make improvementswhere they are really necessary.
Help-Line operators are there every working dayto assist you with the day-to-day problemsencountered running your business. Commonissues include: Employment problems, disputesbetween colleagues or principals and staff,contract issues and health and safety concerns.The CODE team will answer your questions orpoint you in the right direction for you to find thesolution. Our Network Professionals will often beable to answer simple questions without chargingyou a fee. However if you have a serious problem,you may need to instruct a professional to act onyour behalf.
We represent over 1000 dentists working inindependent practices. CODE is keen to improvethe relationship between practice owners and thedental establishment. Our close links with theBDA, GDC, DPB and other bodies are key toensuring that practice owners' interests are putforward at every available forum.
CODE on the Road training is a Nationwideprogramme of business seminars. Topics rangefrom Practice Management, Computer andInternet Usage to Benchmarking and Marketing.
CODESupporting Dental Practice Owners
For membership enquiries or for further information please contact the CODE office.