MKDU - Ilmu Sosial dan Perilaku dalam Kesehatan Masyarakat...
63
MKDU - Ilmu Sosial dan Perilaku dalam Kesehatan Masyarakat (ISP) Kuliah Pendahuluan Pendekatan Ilmu Sosial dan Perilaku dalam Kesehatan Masyarakat 2017 Disampaikan oleh: Yayi Suryo Prabandari PROGRAM STUDI S2 ILMU KESEHATAN MASYARAKAT FAKULTAS KEDOKTERAN UNIVERSITAS GADJAH MADA
Transcript of MKDU - Ilmu Sosial dan Perilaku dalam Kesehatan Masyarakat...

MKDU - Ilmu Sosial danPerilaku dalam
Kesehatan Masyarakat(ISP)
Kuliah Pendahuluan Pendekatan Ilmu Sosial danPerilaku dalam Kesehatan Masyarakat 2017
Disampaikan oleh:Yayi Suryo Prabandari
PROGRAM STUDI S2 ILMU KESEHATAN MASYARAKAT FAKULTAS KEDOKTERAN
UNIVERSITAS GADJAH MADA

Tujuan Umum mata kuliah
• Formulate socio-anthro-psychological theories and approach in understanding health social problem comprissing how to function, conflict and interaction, promotion, prevention and curative delivery in health services, management and policy decision making process.
• Evaluate the social, behavioral and cultural aspects related to community health status and the role of health workforce function in controlling community health
Tujuan Umum mata kuliah
• Analyze the reasons and causes of people in accepting or refusing healthy behavior in perspective and context of individual, family, social structure and culture.
• Debate global and international health issues related to social determinant of health
Tujuan khusus
• Explain rationale to learn about social behavioral approach in public health, trans-disciplinary perspective and the complexity of social behavioral science
• Debate main behavioral theories to learn about healthy and unhealthy behavior (Group assignment and discussion)
• Appraise the main principle of anthropological approach to understand health
• Debate main anthropological principles to sharp human approach in public health (Group assignment and discussion)
Tujuan khusus
• Review sociological theories and perspective in understanding health
• Debate main sociological theories in public health (Group assignment and discussion)
• Analyze social determinant of health, equity and public health program
• Review new paradigm health promotion and the application of social behavioral theories for promoting health
Tujuan khusus• Appraise behavior change theories and its
application of selected theories on tobacco control
• Analyze dimension of social culture on health and illness including gender perspective
• Debate the health seeking behavior of the community in relation to health and illness (Group assignment and discussion)
• Appraise the shift of health organization, services, and health workforces, in relation to social change
Tujuan khusus• Debate the shift of health organization and services –
observation from the field (group assignment and discussion)
• Appraise society action and the application of ecological theory in particular public health issues: a case ofcommunity empowerment and local policy application for tackling NCD
• Appraise social anthropological perspective related to public health in particular issues – International and Global Health – case of communicable disease AIDS and TB (including stigma)
• Appraise social behavior approach related to public health in particular issues-occupational and environment health

LATAR BELAKANG PERLUNYA KOMPETENSI SOSIAL PERILAKU:
SOCIAL DETERMINANTS OF HEALTH

SDG – Sustainable Development Goals

Kondisi dasar Kesehatan (WHO)
Pendidikan
PenghasilanPerumahan
Kedamaian
keadilansosial dankesetaraan
Sumber yang berkelanjutan
Ekosistemyg stabil
10

Penentu Sosial Kesehatan
Penghasilan
Status sosialPendidikan
STATUS
SEHAT
WHO Commission on Social Determinants of Health (2008)
• The determinants of health include the social, physical and economic environments, as well as individual characteristics and behaviors.
• The context of people’s lives determines their health, not less than their genetic inheritance and their personal choices and way of life thus, health is inappropriate
KEY DEFINITIONS
• Social determinants of health These refer to the social, economic, and political situations that affect the health of individuals, communities, and populations.
• Inequity in health and health care
• Inequity in health is a normative concept and refers to those inequalities that are judged to be unjust or unfair because they result from socially derived processes.
• Equity in health care requires active engagement in planning, implementation, and regulation of health systems to make unbiased and accountable arrangements that address the needs of all members of society.
*

WHO’s Commission on Social Determinants of Health (2008) established the following overarching recommendations:
improve the conditions of daily life - the circumstances in which people are born, grow, live work and age
tackle the inequitable distribution of power, money and resources - the structural drivers of those conditions of daily life – globally, nationally and locally;
measure the problem, evaluate action, expand the knowledge base, develop a workforce , that is trained in the social determinants of health, and raise public awareness about the social determinants of health.

WHO’s Commission on Social Determinants of Health (2008) established the following overarching recommendations:
• to tackle the health inequities within and across countries
through political commitment on the main principles of 'closing the gap in a generation’ as a national concern,
as is appropriate, and to coordinate and manage intersectoral action for health in order to mainstream health equity in all policies, where appropriate, by using health and health equity impact assessment tools;
• to develop and implement goals and strategies to improve public
health with a focus on health inequities;

What is socioeconomic of illness?
• Social determinant of health
• Economic and macro situation in a country
Socioeconomic
• Communicable disease
• Non communicable disease
Illness• Burden of illness to
the sites (district/city, province, nation)
• Social impact of illness to the family
Socioeconomic

Fakta
* Beberapa slide diambil dari presentasi Promkes DinkesPropinsi Yogyakarta

Laporan WHO 2011
Perbandingan Penyebab kematian 2000-2011
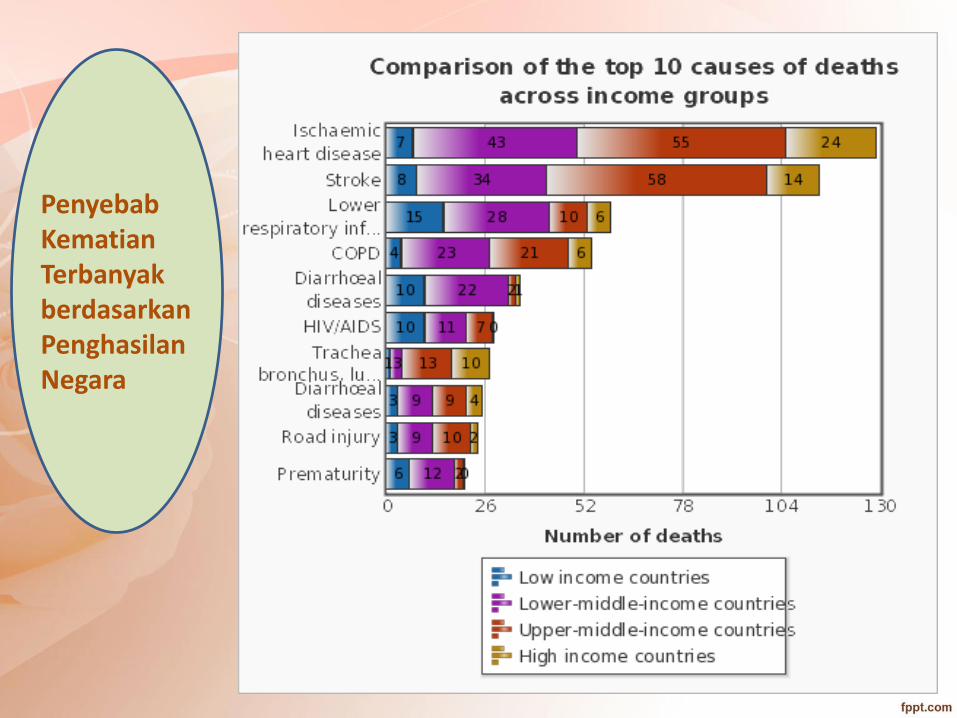
PenyebabKematianTerbanyakberdasarkanPenghasilanNegara
Impact of Non-Communicable Diseases on Productivity
• Countries throughout the world are expected to lose significant amounts of national income as a result of chronic disease’s negative impact on labor supplies and a reduction in GDP.
• Labor supplies are reduced as a result of premature death or illness causing inability to work.
• In 2005, heart disease, stroke and diabetes caused an estimated loss in national income of 18 billion international dollars in China, 9 billion in India and 3 billion in Brazil These losses accrue over time because more people die each year so estimates for 2015 are three to six times that of 2005 for the same countries.
Costs of Absenteeism and Presenteeism
• Absenteeism is defined as absence from work due to illness while presenteeism is defined as productivity lost from ill employees coming to work and performing below the normal standard.
• In 2006, the United Kingdom had a working population of 37.7 million individuals. There were 175 million days lost in 2006 to absence from illness.
This amounts to 4.64 days lost due to illness per person. In the UK, the estimated cost – both direct and indirect – of absences due to illness was 20.2 billion pounds in 2006.
• It is widely accepted that presenteeism has a larger effect than absenteeism, causing some to state that presenteeism is “1.8 times as important as absenteeism.” The science of understanding
metrics and costs of presenteeism are still being developed, however controlling presenteeism and absenteeism is an area that will save employers money and also will contribute to the national economy
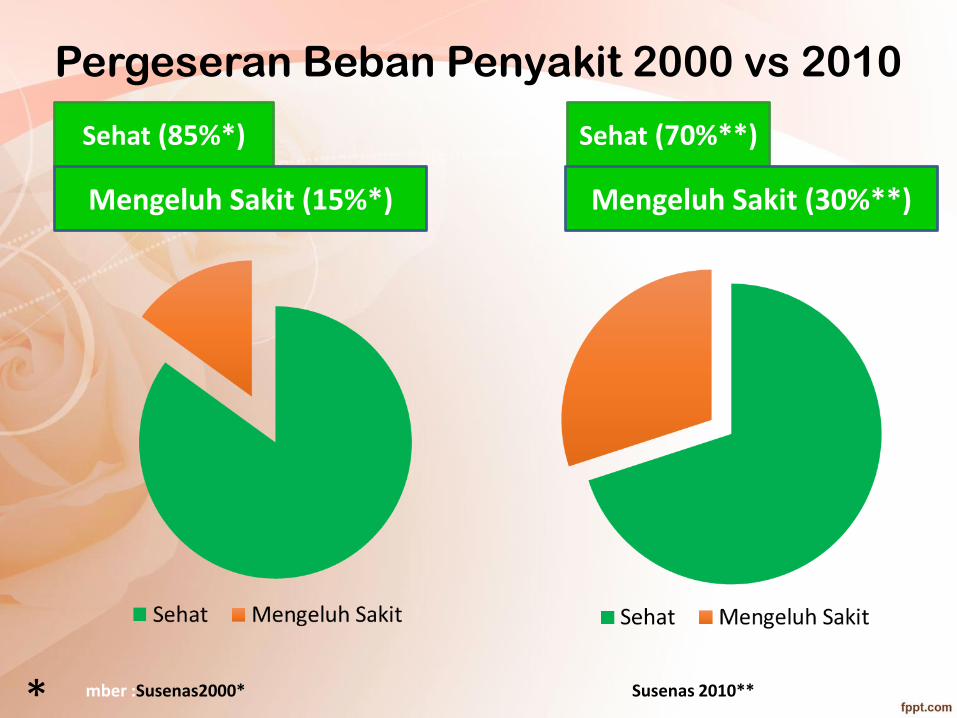
Sehat (85%*) Sehat (70%**)
Pergeseran Beban Penyakit 2000 vs 2010
Mengeluh Sakit (30%**)Mengeluh Sakit (15%*)
mber :Susenas2000* Susenas 2010***
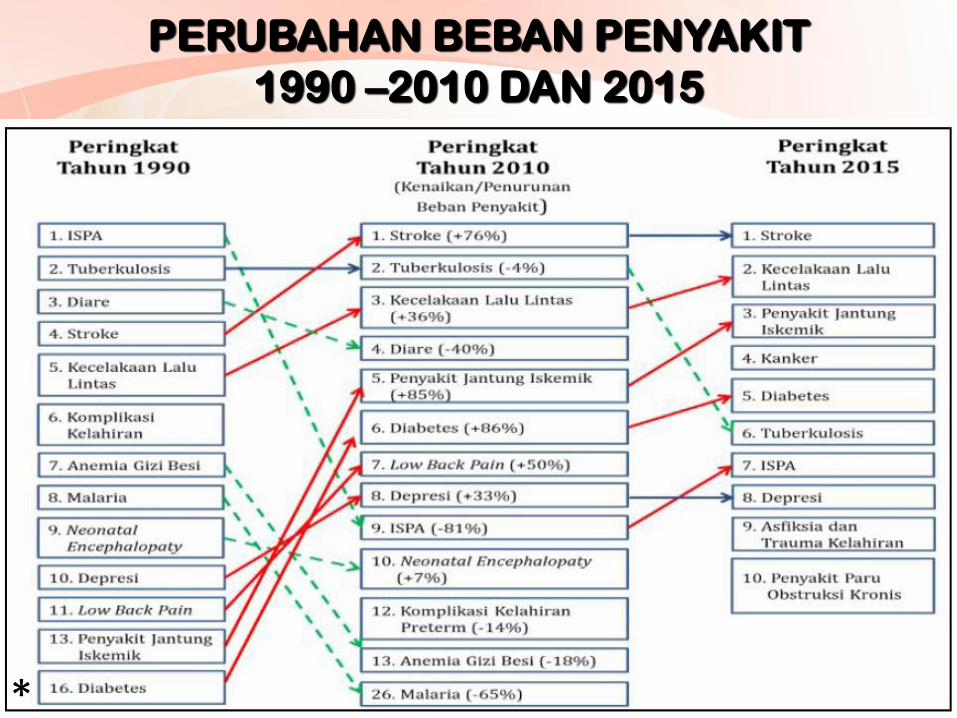
PERUBAHAN BEBAN PENYAKIT
1990 –2010 DAN 2015
*

PENYEBAB KEMATIAN UTAMA UNTUK SEMUA UMUR DI INDONESIA
24
Penyebab kematian utama di Indonesia 2015 SRS adalahStroke, Kardiovaskulair, DM Komplikasi (6,7), TB,
Sumber: Litbangkes*
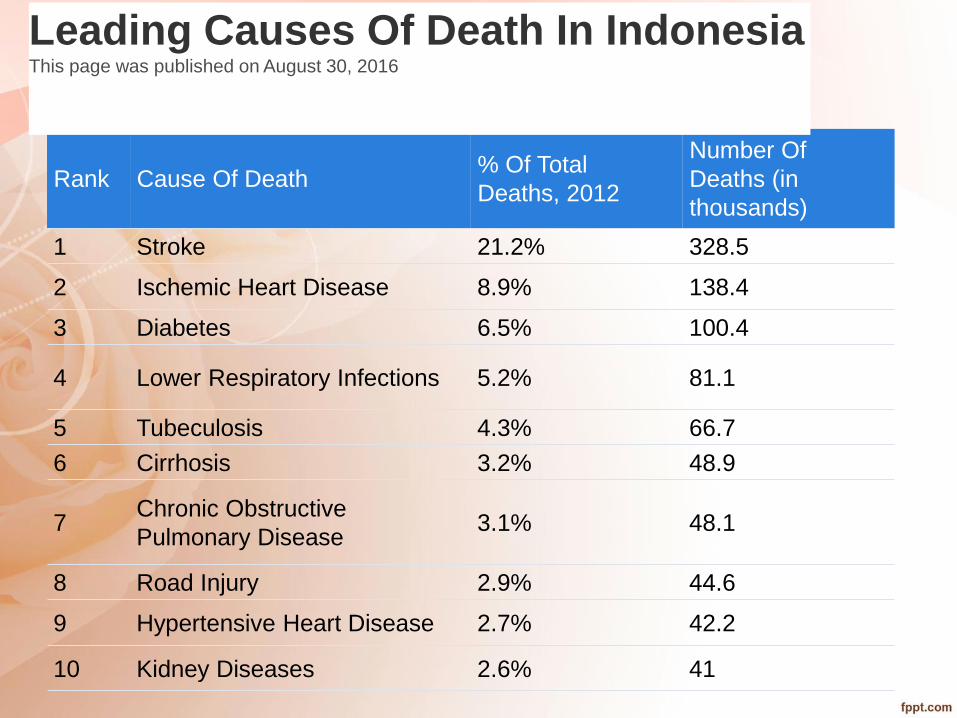
Rank Cause Of Death% Of Total
Deaths, 2012
Number Of
Deaths (in
thousands)
1 Stroke 21.2% 328.5
2 Ischemic Heart Disease 8.9% 138.4
3 Diabetes 6.5% 100.4
4 Lower Respiratory Infections 5.2% 81.1
5 Tubeculosis 4.3% 66.7
6 Cirrhosis 3.2% 48.9
7Chronic Obstructive
Pulmonary Disease3.1% 48.1
8 Road Injury 2.9% 44.6
9 Hypertensive Heart Disease 2.7% 42.2
10 Kidney Diseases 2.6% 41
Leading Causes Of Death In IndonesiaThis page was published on August 30, 2016

Risk factors of NCD in Indonesia

FACTORSINTERNATIONAL
Development
Globalization
of
markets
School
Food &
Activity
WORK/SCHOOL/
HOME
Infections
Labor
Worksite
Food &
Activity
Leisure
Activity/
Facilities
Agriculture/
Gardens/
Local markets
COMMUNITY
LOCALITY
Health
Care
System
Public
Safety
Public
Transport
Manufactured/
Imported
Food
Sanitation
NATIONAL/REGIONAL
Food &
Nutrition
Urbanization
Education
HealthO
SITY
PREVALEN
E
INDIVIDUAL
Energy
Expenditure
Modified from Ritenbaugh C, Kumanyika S, Morabia A, Jeffery R, Antipathies V. IOTF website 1999: http://www.iotf.org
POPULATION
%
OBESE
OR
UNDER
WT
Social security
Media
Transport
Family &
Home
National
perspective
Media &
Culture
Food
intake :
Nutrient
density
Media
programs
& advertising
Societal policies and processes influencing the
population prevalence
of obesity

PROPORSI PENDUDUK DENGANFAKTOR RISIKO PTM DI INDONESIA
FAKTOR RISIKO PTM 2007(%)
2013(%)
1 Merokok (usia ≥ 15 th) 34,7 36,3
2Aktifitas fisik kurang
(usia ≥ 10 th)48,2 26,1
3Kurang konsumsi sayur &
buah (usia ≥ 10 th)93,6 93,5
4Konsumsi minuman
beralkohol4,6 n.a
5Konsumsi minuman beralkohol
berbahaya0,3 n.a
6Obesitas sentral
(usia ≥ 18 th)18,8 26,6
7Obesitas (usia >15 th,
IMT >25)19,1 15,4
Sumber: Riskesdas 2007; Riskesdas 2013
Mengubah perilakumerupakantantangan utamadalam pencegahandan pengendalianPTM
*

Determinan
penyebab remaja
menjadi perokok*
*Prabandari, YS, 2012

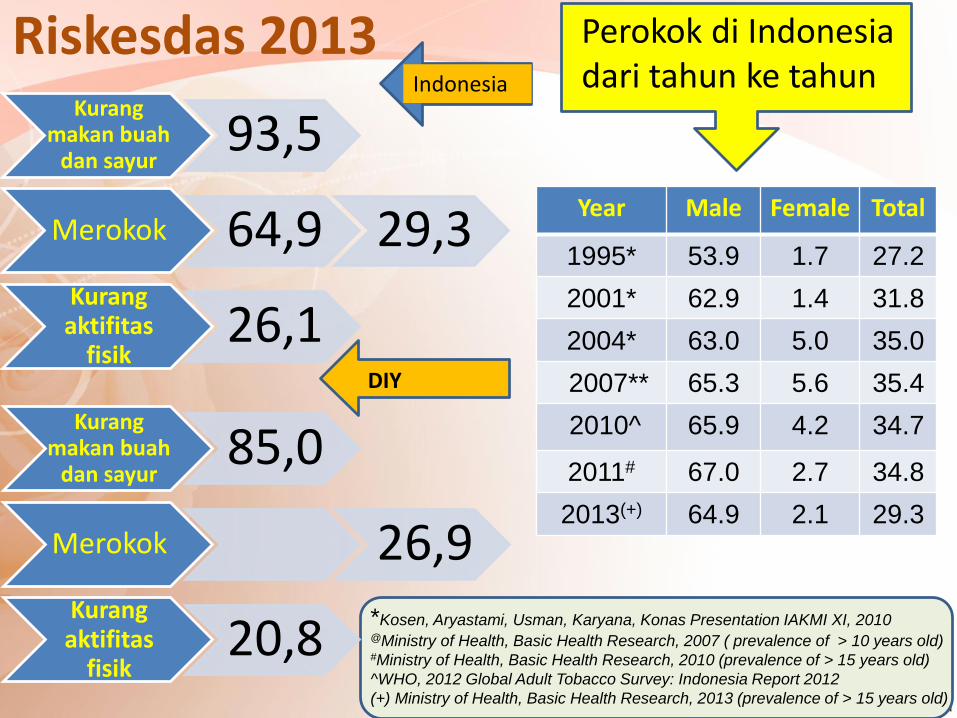
Riskesdas 2013Kurang
makan buahdan sayur
93,5
Merokok 64,9 29,3Kurangaktifitas
fisik26,1
Kurangmakan buah
dan sayur85,0
Merokok 26,9Kurangaktifitas
fisik20,8
Indonesia
DIY
Perokok di Indonesia dari tahun ke tahun
*Kosen, Aryastami, Usman, Karyana, Konas Presentation IAKMI XI, 2010 @Ministry of Health, Basic Health Research, 2007 ( prevalence of > 10 years old)#Ministry of Health, Basic Health Research, 2010 (prevalence of > 15 years old)
^WHO, 2012 Global Adult Tobacco Survey: Indonesia Report 2012
(+) Ministry of Health, Basic Health Research, 2013 (prevalence of > 15 years old)
Year Male Female Total
1995* 53.9 1.7 27.2
2001* 62.9 1.4 31.8
2004* 63.0 5.0 35.0
2007** 65.3 5.6 35.4
2010^ 65.9 4.2 34.7
2011# 67.0 2.7 34.8
2013(+) 64.9 2.1 29.3
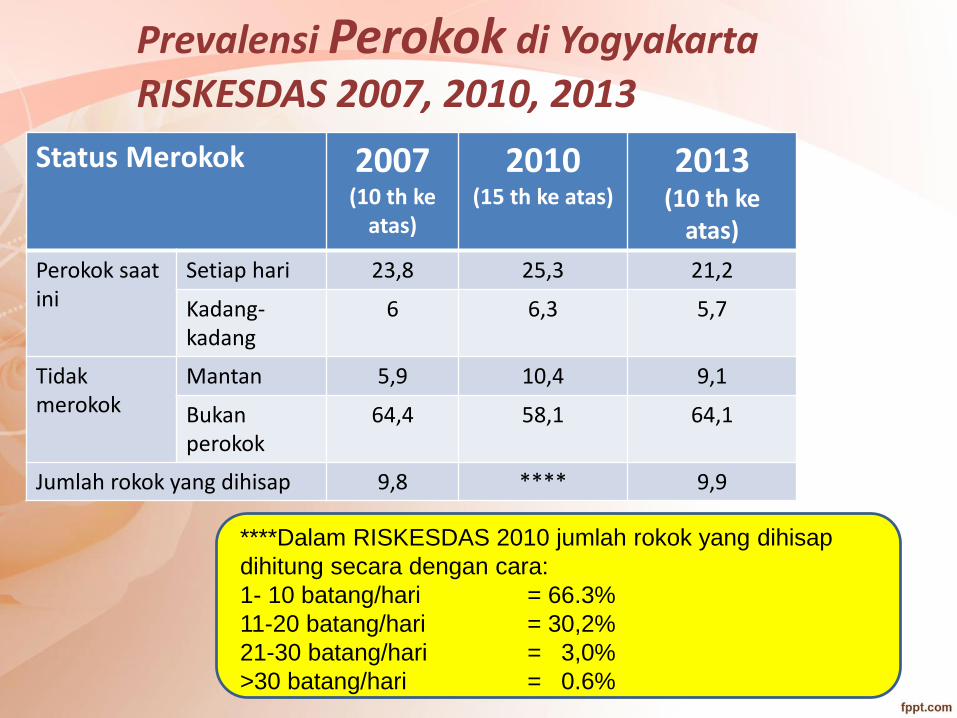
Prevalensi Perokok di Yogyakarta
RISKESDAS 2007, 2010, 2013
Status Merokok 2007(10 th ke
atas)
2010(15 th ke atas)
2013(10 th ke
atas)
Perokok saatini
Setiap hari 23,8 25,3 21,2
Kadang-kadang
6 6,3 5,7
Tidakmerokok
Mantan 5,9 10,4 9,1
Bukanperokok
64,4 58,1 64,1
Jumlah rokok yang dihisap 9,8 **** 9,9
****Dalam RISKESDAS 2010 jumlah rokok yang dihisap
dihitung secara dengan cara:
1- 10 batang/hari = 66.3%
11-20 batang/hari = 30,2%
21-30 batang/hari = 3,0%
>30 batang/hari = 0.6%

RISKESDAS 2010
ASI eksklusif 15,3 – 39,8
Akses terhadap air minum yang baik 67,5
Kepemilikan fasilitas BAB pribadi 69,7
Buang sampah sembarangan 9,0;
dibuang di laut/sungai/parit 10,2
Gizi buruk 4,9; Gizi kurang 13,0; Gizi lebih 5,8

RISKESDAS 2013
ASI eksklusif 38,0%, Inisiasi menyusui dini 34,5%
Akses terhadap air minum yang improved 66,8%
BAB dengan benar 82,6%
Buang sampah sembarangan 9,0;
dibuang di laut/sungai/parit 10,2
Kurus 8,7%; Gizi lebih 13,5%; Obes 15,4%

35
Gaya Hidup dan Kesehatan
• Evolusi Budaya: perubahan adaptif budayauntuk menghadapi tekanan lingkungan
• Gaya Hidup: perilaku seseorang, carahidup seseorang
Adanya evolusi budaya menyebabkanperubahan gaya hidup

36
Global trends• Demografi dan tekanan sosial• Kondisi ekologi• Pertumbuhan dan perkembangan ekonomi• Kesenjangan kemiskinan• Social fabric• Perkembangan teknologi• Perkembangan, konflik dan perdamaian• Beban ganda penyakit• Pekerjaan• Kecenderungan sistem kesehatan yg spesifik

37
Siapakah yang “menderita”akibatperubahan sosial?
• Pendidikan rendah
• Sosial ekonomi rendah
Miskin
Banyak penyakit
THE HEALTH HIRARCHY
HIRARKI
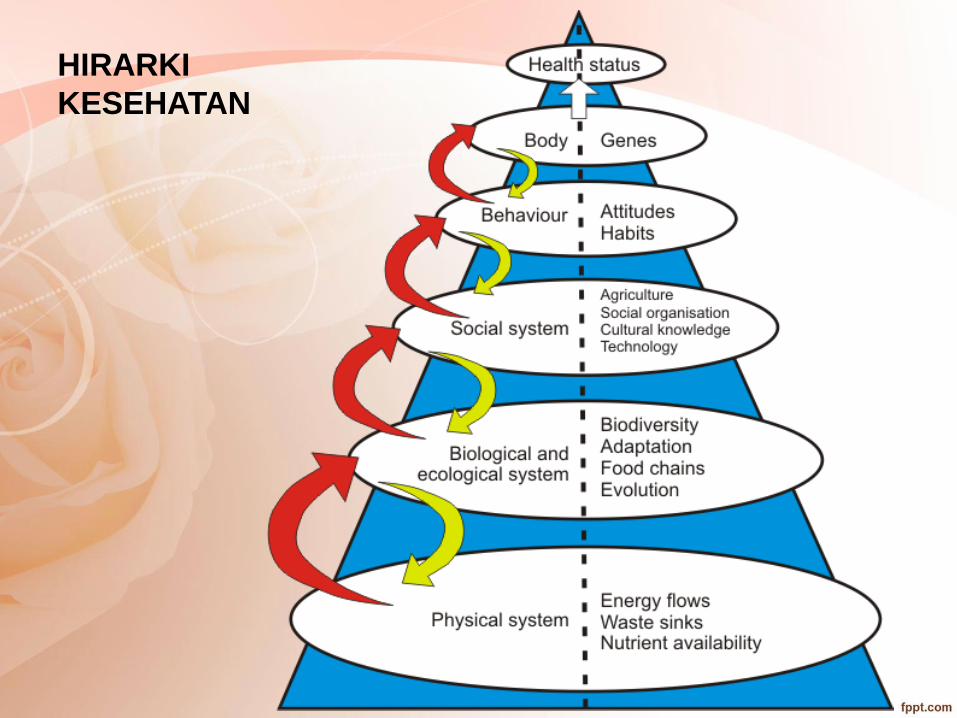
KESEHATAN

HIRARKI KESEHATAN DAN SAKIT PADA MANUSIA

HIRARKI KESEHATAN SERTA DISIPLIN DAN TEORI DALAM KESEHATAN
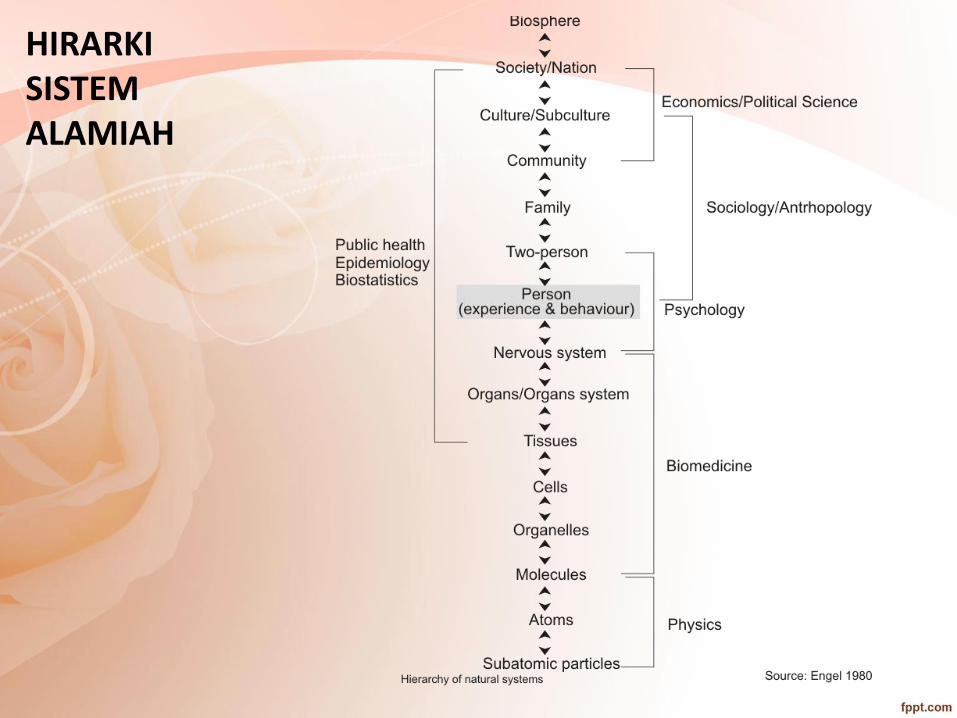
HIRARKI SISTEM ALAMIAH
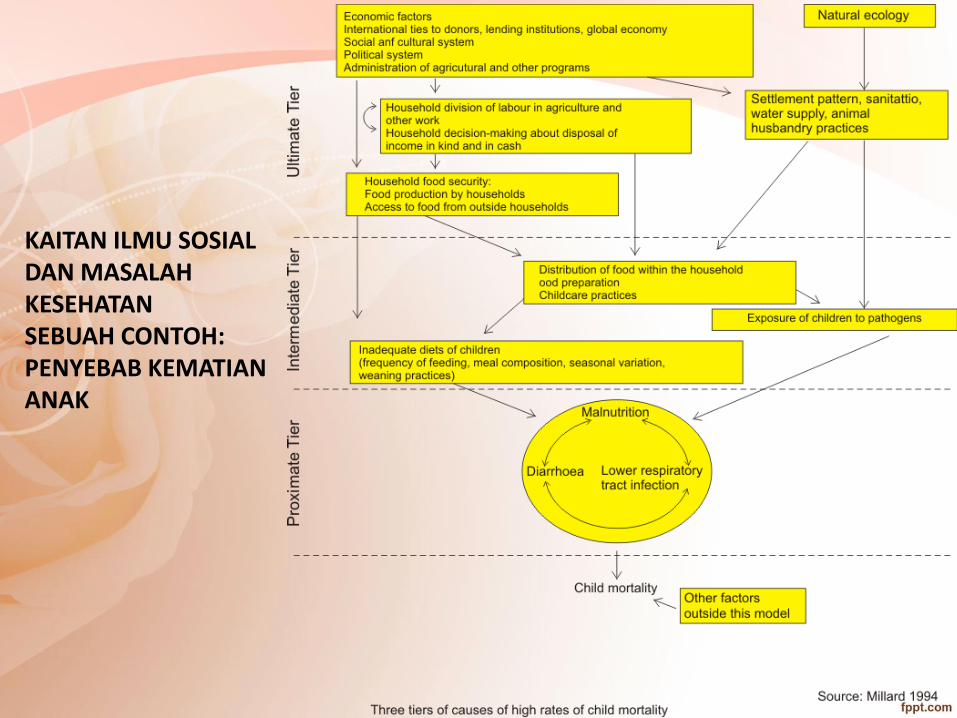
KAITAN ILMU SOSIAL DAN MASALAH KESEHATAN SEBUAH CONTOH:PENYEBAB KEMATIAN ANAK


45
Maternal death determinant:Indonesian case
Education Economy Gender Social Culture
P
r
e
g
n
a
n
t
w
o
m
e
n
Nutrition
Infectious
disease
4 T’s
Behavior
C
o
m
p
l
i
c
a
t
i
o
n
Late to identify of
red flag and make
decision
Late in reach health
facilities
Late in get
services in health
facilities
Human resources Facilities Medication
Death
Demand side
Supply side

BEHAVIORAL AND SOCIAL SCIENCES : DEFINITIONS, DOMAINS, CONTRIBUTION AND INTERVENTION

Social Sciences• Anthropology (and archaeology)
• Demography
• Economics
• Geography
• History
• Law
• Education
• Linguistics
• Political science
• Psychology
• Sociology

The social and behavioral sciences provide tools for:
• Analyzing health and illness
• Developing greater competencies (especially cultural competence)
• Developing a more critical and discerning science.

WORKING DEFINITION OF THE BEHAVIORAL AND SOCIAL SCIENCES (ADAPTED FROM THE OFFICE OF BEHAVIORAL AND SOCIAL SCIENCE RESEARCH OF THE NIH)
• The Behavioral and Social Sciences are defined as the sciences of behavior, including individual psychological processes and behavioral interactions, and the sciences of social interaction, including familial, cultural, economic, and demographic.
• The core areas focus on the understanding of behavioral or social processes and on the uses of these processes to predict or influence health outcomes or risk factors
#

HEALTH CARE CHALLENGES AMENABLE TO BEHAVIORAL AND SOCIAL SCIENCE INQUIRY
• Behavioral & Social Determinants of Morbidity and Mortality
• Health and Health Care Disparities
• Medical Error Reduction
• Patient Safety
• Primary Care Shortage
• Physician Discontent and Burn-out
• Unequal Access to Care
#

Behavioral and Social Science Domains related to Health and Health Care
• Patient Behavior
• Mind-Body Interaction
• Physician Role & Behavior
• Physician-Patient Interaction
• Health Policy, Economics, and Systems (including Population Health)
• Social and Cultural Context
#
• Dra. Yayi Suryo Prabandari, M.Si., Ph.D (Koordinator) – psikolog (klinis & kesehatan), promotor kesehatan
• Dr. Fatwa Sari Tetra Dewi, MPH., Ph.D – dokter, epidemiolog dan promotor kesehatan
• Dr. Ratna Siwi Padmawati, MA – antropolog, antropologkesehatan dan kebijakan
• Dr. Mubasyisyir Hasan Basri, MA (dokter, kesehatan masyarakat, sosiologi
• Supriyati, S.Sos., M.Kes., Ph.D (can) – sosiolog, promotor kesehatan
Pengajar
PENUGASAN INDIVIDU DAN KELOMPOK

Penugasan Individu
Penu-
gasan
1
Buatlah diagram penentu sosial sebuah penyakit yang dilaporkan tinggi
prevalensi atau insidensinya di daerah asal karyasiswa
Gunakan minimal 3 artikel jurnal terbitan 5 tahun terakhir sebagai dasar
pembahasan selain laporan kasus dari daerahnya. Jurnal minimal terdiri 1
artikel jurnal internasional reputasi (ambil data base yang dilanggan UGM)
dan 2 artikel jurnal nasional terakreditasi.
Jawaban diketik dalam kertas A4 maksimal 3 halaman termasuk judul dan
daftar pustaka, gunakan font times roman, dikumpulkan pada sekretaris
masing-masing minat paling lambat 1 minggu setelah kuliah sesi 5.
Penugasan IndividuPenu-
gasan
2
Pilih salah satu kasus berikut:
- Mengapa orang yang berpendidikan cenderung mengonsumsi
pil/obat tinggi serat daripada makan buah dan sayur segar?
- Mengapa kawasan tanpa rokok tidak efektif di Indonesia?
- Mengapa terdapat 70% penduduk Indonesia yang mengonsumsi mie
instant setiap hari meskipun hal tersebut tidak sehat?
- Mengapa mahasiswa senang makanan ”sampah” (junk food)
Jawaban maksimal 2000 kata dan didasarkan minimal 5 artikel jurnal terbitan
5 tahun terakhir (3 artikel jurnal nasional terakreditasi Ristekdikti atau
Litbangkes dan 2 artikel jurnal internasional bereputasi – gunakan data base
yang dilanggan UGM).
Jawaban diketik dalam kertas A4, gunakan font times
roman/arial/Calibri/cambria, dikumpulkan pada sekretaris masing-masing
minat paling lambat 1 minggu setelah kuliah sesi 6.
Penugasan IndividuPenu-
gasan
3
Pilihlah salah satu pesan kesehatan yang ada di media cetak
atau web/virtual atau media berbasis teknologi lainnya dan
reviulah pesan kesehatan tersebut berdasar teori komunikasi,
perilaku, sosial atau antropologi, serta efektivitas media.
Jawaban maksimal 2000 kata dan didasarkan minimal 5 artikel
jurnal terbitan 5 tahun terakhir (3 artikel jurnal nasional
terakreditasi Ristekdikti atau Litbangkes dan 2 artikel jurnal
internasional bereputasi – gunakan data base yang dilanggan
UGM).
Jawaban diketik dalam kertas A4, gunakan font times
roman/arial/Calibri/cambria, dikumpulkan pada sekretaris
masing-masing minat paling lambat 1 minggu setelah kuliah
sesi 6.
PENUGASAN KELOMPOK 1Tugas:
Penugasan dan diskusi kelompok (Kelas dibagi beberapa kelompok, satu kelompok terdiri
dari 4 atau 5 mahasiswa)
Dalam penugasan kelompok, karyasiswa diharuskan:
1. Melakukan wawancara semi struktur pada temannya di luar Prodi S2 IKM, masing-
masing mahasiswa mewawancara 2 orang tentang perilaku sehat dan tidak sehat
2. Setelah wawancara, hasil dianalisis untuk memahami terbentuknya perilaku berdasar
teori perilaku
3. Melakukan reviu langkah pertama dan kedua dengan referensi yang diwajib dan
anjurkan di kuliah sesi 2
4. Hasil wawancara individu dan analisis digabung dalam satu kelompok, dikomparasi
dan disimpulkan
5. Setiap kelompok presentasi dalam diskusi kelompok yang dipandu fasilitator.
Presentasi disajikan dalam PPT atau lainnya (video pendek dsb). Setiap kelompok wajib
presentasi selama 10 menit dan dilanjutkan 10 menit diskusi.
6. Hasil presentasi kelompok dikumpulkan pada fasilitator masing-masing paling lambat 1
minggu setelah presentasi. Laporan penugasan kelompok diketik pada kertas A4, huruf
arial/times roman/Calibri/Garamond, minimal font 11, spasi 1.5 and maksimum 7
halaman, termasuk cover dan daftar pustaka. Gunakan pustaka artikel jurnal 5 tahun
terakhir, minimal 3 artikel jurnal nasional terakreditasi Ristekdikti atau Litbangkes dan 2
jurnal internasional bereputasi (gunakan data dasar EBSCO, PubMed, Cochrane,
Scopus, dan yang dilanggan oleh UGM
Penugasan Kelompok ke 2
Penugasan:
Kelas dibagi kelompok dan lanjutkan dengan kelompok yang sama pada penugasan
sebelumnya (penugasan 1).
Dalam penugasan kelompok, karyasiswa diharuskan:
Melakukan evaluasi prinsip antropologi yang berkaitan dengan sehat dan sakit
Melakukan debat prinsip antropologi yang berkaitan dengan kesehatan masyarakat
Reviu langkah 1 dan 2 dengan referensi yang wajib dan dianjurkan dalam kuliah sesi 3
Setiap kelompok presentasi dalam diskusi kelompok yang dipandu fasilitator. Presentasi
disajikan dalam PPT atau lainnya (video pendek dsb). Setiap kelompok wajib presentasi
selama 10 menit dan dilanjutkan 10 menit diskusi.
Hasil presentasi kelompok dikumpulkan pada fasilitator masing-masing paling lambat 1
minggu setelah presentasi. Laporan penugasan kelompok diketik pada kertas A4, huruf
arial/times roman/Calibri/Garamond, minimal font 11, spasi 1.5 and maksimum 7 halaman,
termasuk cover dan daftar pustaka. Gunakan pustaka artikel jurnal 5 tahun terakhir, minimal
3 artikel jurnal nasional terakreditasi Ristekdikti atau Litbangkes dan 2 jurnal internasional
bereputasi (gunakan data dasar EBSCO, PubMed, Cochrane, Scopus, dan yang dilanggan
oleh UGM)

Penugasan Kelompok ke 3Tugas:
Penugasan dan diskusi kelompok (Kelas dibagi beberapa kelompok, satu kelompok
terdiri dari 4 atau 5 mahasiswa)
Dalam penugasan kelompok, karyasiswa diharuskan:
Melakukan reviu teori utama sosiologi yang berkaitan dengan kesehatan secara umum
dan kesehatan masyarakat
Melakukan depat perbandingan teori-teori sosiologi
Melakukan reviu langkah pertama dan kedua dengan referensi yang diwajib dan anjurkan
di kuliah sesi 4
Setiap kelompok presentasi dalam diskusi kelompok yang dipandu fasilitator. Presentasi
disajikan dalam PPT atau lainnya (video pendek dsb). Setiap kelompok wajib presentasi
selama 10 menit dan dilanjutkan 10 menit diskusi.
Hasil presentasi kelompok dikumpulkan pada fasilitator masing-masing paling lambat 1
minggu setelah presentasi. Laporan penugasan kelompok diketik pada kertas A4, huruf
arial/times roman/Calibri/Garamond, minimal font 11, spasi 1.5 and maksimum 7
halaman, termasuk cover dan daftar pustaka. Gunakan pustaka artikel jurnal 5 tahun
terakhir, minimal 3 artikel jurnal nasional terakreditasi Ristekdikti atau Litbangkes dan 2
jurnal internasional bereputasi (gunakan data dasar EBSCO, PubMed, Cochrane,
Scopus, dan yang dilanggan oleh UGM)

Reminding
GROUP WORK AND
SMALL DISCUSSION
(3 ASSIGNMENT)
INDIVIDUAL
ASSIGNMENT (3)
Session 2Session 3Session 4
Session 5Session 6Session 7
Mini Quiz diadakan 5 menitsebelum kuliah dimulai –berdasar Main Reference

Penilaian• MINI QUIZ …………………………………………………… 15%
• Group assignment ………………………………………….. 25%
• Individual assignment ……………….……………… 25%
• Final exam ………………………………………………….. 35%

NO TOPIK BAHASAN PENGAJAR1 Session 1 – Social behavioral approach in public health, trans-disciplinary
perspective and the complexity of social behavioral science YSP
2 Session 2 – Behavioral theories underlying healthy and unhealthy behavior YSP
3 Diskusi kelompok 1 Fasilitator4 Session 3 – The main principle of anthropological approach to understand health RSP
5 Diskusi kelompok 2 Fasilitator6 Session 4 – Sociological theories and perspective in understanding health SP
7 Diskusi kelompok 3 Fasilitator8 Session 5 – Social determinant of health, equity and public health program MBS
9 Session 6 – Communication & Behavior change theories and its application of selected theories on tobacco control
YSP
10 Session 7 – New paradigm on Health Promotion and the use of Technology for promoting health
FST
11 Session 8 – Dimension of social culture on health, illness and gender perspective RSP
12 Session 9 – Social change and the shift of health organization, services and workforces
MBS
13 Session 10 – Society action and the application of ecological theory in particular public health issues: a case of Community empowerment and local policy application for tackling NCD
FST
14 Session 11 – Social behavior related to public health in particular issues –International and Global Health – case of communicable disease AIDS and TB, including stigma
RSP
15 Session 12 – Social behavior related to public health in particular issues (delivered on each department)
departemen terkait
FINAL EXAMINATION (TAKE HOME)
Satuan Acara Pengajaran ISP 2017

Terima kasih