kuliah farSP(1)kbk

of 59
-
Upload
yuhumaqyu6841 -
Category
Documents
-
view
220 -
download
0
Transcript of kuliah farSP(1)kbk
-
7/28/2019 kuliah farSP(1)kbk
1/59
Pharmacokinetics
Nur Permatasari
-
7/28/2019 kuliah farSP(1)kbk
2/59
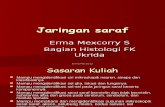
Site of Action
Dosage EffectsPlasmaConcen.
Pharmacokinetics Pharmacodynamics
PHARMACOKINETICS PHARMACODYNAMICS
The drug acts on the body,the body work on the drug
-
7/28/2019 kuliah farSP(1)kbk
3/59
-
7/28/2019 kuliah farSP(1)kbk
4/59
-
7/28/2019 kuliah farSP(1)kbk
5/59
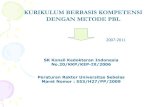
Bound Free Free Bound
Therapeutics site of actionRECEPTORS
TISSUE
RESERVOIRS
SYSTEMICCIRCULATION
Free Drug
Bound Drug
ABSORPTION/LIBERATION
EXCRETION
BIOTRANSFORMATION
Unwanted ofsite of actionFREE BOUND
METABOLITE
-
7/28/2019 kuliah farSP(1)kbk
6/59
In order to reach their site of action, drugshave to pass through several membranes transmembrane transport AND
the plasma membrane represents thecommon barrier to drug distribution.
-
7/28/2019 kuliah farSP(1)kbk
7/59
Structure of the plasma membrane
The plasma membrane consists of a bilayer and membrane proteins
embedded in the bilayer
-
7/28/2019 kuliah farSP(1)kbk
8/59
Mechanisms of transmembran transport
Passive diffusion: passage of drugs through thelipid surface (major mechanism of drugabsorption) directly proportional to the magnitude of the concentration gradient across the membrane
Lipid-soluble drugsSmall water-soluble drugsNoncharged form of weak electrolytes
Drug absorption is depend on physicochemical properties of drug
-
7/28/2019 kuliah farSP(1)kbk
9/59
The rate of absorption is related to
the oil:water partition coefficient
The greater the partition coefficient, thehigher the lipid-solubility of the drug, andthe greater its diffusion across membranesor the faster its absorption
-
7/28/2019 kuliah farSP(1)kbk
10/59
Water-soluble drugs
Cell membranes are relatively permeable towater either by diffusion or by flow
resulting from hydrostatic or osmoticdifferences across the membrane, butbulk-flow transport is limited when themolecular mass of the solute exceeds 100to 200 daltons
-
7/28/2019 kuliah farSP(1)kbk
11/59
Weak electrolytes and membrane permeability
Most drugs are small (MW < 1000) weak electrolytes (acids/bases). In solution
exist in a non-ionized and an ionizedforms of drugs .
The fraction of drug that is non-ionized
depends on its chemical nature, its
pKa, and the local biophase pH...
-
7/28/2019 kuliah farSP(1)kbk
12/59
-
7/28/2019 kuliah farSP(1)kbk
13/59
% Ionized vs. pH
For HA acids:% ionization = 100/(1 + 10 (pKa pH))
For BH + acids:% ionization = 100/(1 + 10 (pH
pKa))
Example: Percentage ionized pseudoephedrine HCl(pKa 9.9) in the small intestine at pH 8.0?
-
7/28/2019 kuliah farSP(1)kbk
14/59
-
7/28/2019 kuliah farSP(1)kbk
15/59
Filtration: bulk flow of water-soluble drugsthrough pores (glomerular, capillary)
Facilitated diffusion: carrier-mediated,ATP not required (e.g., glucose)
Active transport: carrier-mediated, ATPrequired (e.g., Na +, K+, Ca++)
Endocytosis and exocytosis: (e.g., for verylarge compounds)
Other transmembrane transport
-
7/28/2019 kuliah farSP(1)kbk
16/59
-
7/28/2019 kuliah farSP(1)kbk
17/59
Per oral is a major route of drugadministration .. Why ??
Relatively Fast Painless (usually)
Easy Safe No need for equipment or help Most drugs can be given orally
But. Some physiologic factors determinedthe drug absorption
-
7/28/2019 kuliah farSP(1)kbk
18/59
ORAL INGESTION , governed by:
surface area for absorption, blood flow,physical state of drug, concentration.
occurs via passive process.
In theory: weak acids optimally absorbed in
stomach, weak bases in intestine.
In reality: the overall rate of absorption ofdrugs is always greater in the intestine(surface area, organ function).
-
7/28/2019 kuliah farSP(1)kbk
19/59
Unique characteristics of the oral route
Influences of gastric emptying (acceleratesgastric emptying increase the rate ofabsorption)
Small intestine usually most important becauseof large surface area (folds of Kerckring, villi,microvilli)
The motility of the small intestineDrug inactivation important for oral routestomach (acid), small intestine (ester/other enzyme), distal small intestine/colon (gut bact)
-
7/28/2019 kuliah farSP(1)kbk
20/59
Ingestion of a solid dosage form with aglass of cold water, fasting, lying on theright side, hyperthyroidism accelerategastric emptying
Ingestion with a fatty meal, acidic drink, orwith another drug with anticholinergicproperties, lying on the left side,hypothyroidism, sympathetic output (as instress) retard gastric emptying.
-
7/28/2019 kuliah farSP(1)kbk
21/59
First-Pass Metabolism
Extent of metabolism occurring beforedrug enters systemic circulationMain site: Liver
Decrease in drug efficacy (orally) can beovercome by using a greater doseExample: Propranolol (5 mg vs. 100 mg)
Extensive metabolism may render oral
admin. impossibleExample: Lidocaine
-
7/28/2019 kuliah farSP(1)kbk
22/59
The fraction of drug eliminated fromportal blood during absorption hepaticextraction ratio (ER H)
ERH = ClH/ Q H
Bioavaibilty (F) F = 1- ERH
-
7/28/2019 kuliah farSP(1)kbk
23/59
Absorption describes the rate and extentat which a drug leaves its site ofadministration.
Bioavailability (F) is the extent to which adrug reaches its site of action, or to abiological fluid (such as plasma) from whichthe drug has access to its site of action.
Drug Absorption & Route of
administration
-
7/28/2019 kuliah farSP(1)kbk
24/59
AUCinjected I.v.
AUCoral
time
p l a s m a c o n c e n
t r a
t i o n o
f d r u g
Bioavailability = AUC oral
AUC injected i.v.X 100
AUC = area under the curve
-
7/28/2019 kuliah farSP(1)kbk
25/59
Important Properties Affecting
Drug AbsorptionChemical properties
acid or base
degree of ionization polaritymolecular weightlipid solubility or...
partition coefficient
Physiologic variablesgastric motility
pH at the absorption sitearea of absorbing surface
blood flow pre absorptive hydrolysisingestion w/wo food
-
7/28/2019 kuliah farSP(1)kbk
26/59
Advantage Relatively Fast Painless (usually) Easy Safe No need for equipment
or help Most drugs can begiven orally
E.g., medications in pill form, barbiturates, LSD,caffeine, alcohol
Disadvantage Not very fast Some drugs dont
withstand stomach/GIconditions (insulin,cocaine)
Drug absorption morevariable May cause GI distress Not suitable for
uncooperative, vomiting,unconscious
FIRST PASS through liver
-
7/28/2019 kuliah farSP(1)kbk
27/59
INJECTION
subcutaneous, intramuscular absorbed bydiffusion and affected by blood flow
intravenous, intraarterial injection avoidsabsorption
Other Injection types Intraperitoneal = (I.P.) into stomach cavity (between
organs). Faster than P.O.
Intrathecal = into subdural spaces of the spinal cord; bypasses blood- brain barrier but invasive
Intracerebroventricular = into the ventricles (wherecerebrospinal fluid is produced) in the brain;bypasses blood- brain barrier but extremelyinvasive Intracerebral = into the brain itself
-
7/28/2019 kuliah farSP(1)kbk
28/59
Injection, in general
Advantage Fast Bypasses first pass Bypasses digestion More accurate dose Can be done by
person with training
Disadvantage Painful Too fast to respond if
bad reaction or overdose Potential for infection Unless planning IV, must
be careful to avoid veins No recall of drug
-
7/28/2019 kuliah farSP(1)kbk
29/59
-
7/28/2019 kuliah farSP(1)kbk
30/59
MUCOUS MEMBRANEsublingual, buccal, nasal, vaginal or rectalmucosa: passive diffusion
Advantage Quick absorption Easy and discreet Little chance of
infection or tissueharm (except with
vasoconstrictors)
Disadvantage Can taste bad or
irritate membranes Not all drugs absorbed readily
Ease and speed exacerbate abuseliabledrugs potential for abuse
-
7/28/2019 kuliah farSP(1)kbk
31/59
SKINTransdermal
Advantage Easy Not painful
Slow, sustainedrelease Bypasses GI tract
& first pass Only have to change
every few days /weeks
Disadvantage Can fall off Potential toxicity to
children and pets Very few drugsabsorbed sufficiently,low permeability ofskin
Local irritation possible Toxicity if additional
drug consumed
-
7/28/2019 kuliah farSP(1)kbk
32/59
DistributionOnly that fraction of drug which is non-protein-bound can bind to cellular receptors and pass across tissuemembranes, thus being distributed to other body
tissues, metabolized, and excreted.
The actual pattern of drug distribution reflects variousphysiological factors (blood perfusing organ, capillary
permeability ) and physicochemical properties (proteinplasma binding, lipid solubility) of the drug.
-
7/28/2019 kuliah farSP(1)kbk
33/59
Phases of Distribution
first phasereflects cardiac output and regionalblood flow. Thus, heart, liver,kidney & brain receive most of thedrug during the first few minutesafter absorption.
next phase
delivery to muscle, most viscera,skin and adipose is slower, andinvolves a far larger fraction of thebody mass.
-
7/28/2019 kuliah farSP(1)kbk
34/59
Central nervous system: permeable to lipid-solubledrugs only; limited permeability to water-solubledrugs when inflamed, that are highly bound toplasma proteins , that are weak acids (are highlyionized at the pH of blood, 7.4)
The view that the placenta is an absolute barrier todrugs is, however, completely inaccurate (in partbecause a number of influx transporters are alsopresent.The fetus is to some extent exposed to alldrugs taken by the mother.
-
7/28/2019 kuliah farSP(1)kbk
35/59
Plasma proteinalbumin- binds many acidic drugs
a1-acid glycoprotein for basic drugs
The fraction of total drug in plasma that isbound is determined by :
* its concentration,* its binding affinity,
* and the number of binding sites
Binding of drugs to plasma proteins such asalbumin is nonselective
-
7/28/2019 kuliah farSP(1)kbk
36/59
Drug Reservoirs
Body compartments where a drug canaccumulate are reservoirs. They havedynamic effects on drug availability.
GIT plasma proteins as reservoirs (binddrug)cellular reservoirs
Adipose (lipophilic drugs)Bone (crystal lattice)Transcellular (ion trapping)
-
7/28/2019 kuliah farSP(1)kbk
37/59
-
7/28/2019 kuliah farSP(1)kbk
38/59
Bone Reservoir
Tetracycline antibiotics (and otherdivalent metal ion-chelating agents) andheavy metals may accumulate in bone.They are adsorbed onto the bone-crystalsurface and eventually becomeincorporated into the crystal lattice.
Bone then can become a reservoir forslow release of toxic agents (e.g., lead,radium) into the blood.
-
7/28/2019 kuliah farSP(1)kbk
39/59
Adipose Reservoir
Many lipid-soluble drugs are stored infat. In obesity, fat content may be as
high as 50%, and in starvation it maystill be only as low as 10% of bodyweight.
70% of a thiopental dose may befound in fat 3 hr after administration.
-
7/28/2019 kuliah farSP(1)kbk
40/59
GI Tract as Reservoir
Weak bases are passively concentrated inthe stomach from the blood because ofthe large pH differential.Some drugs are excreted in the bile inactive form or as a conjugate that can behydrolyzed in the intestine and
reabsorbed.In these cases, and when orallyadministered drugs are slowly absorbed,the GI tract serves as a reservoir.
-
7/28/2019 kuliah farSP(1)kbk
41/59
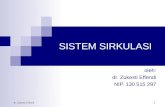
Redistribution
Termination of drug action is normallyby biotransformation/excretion, butmay also occur as a result ofredistribution between variouscompartments.
Particularly true for lipid-solubledrugs that affect brain and heart.
-
7/28/2019 kuliah farSP(1)kbk
42/59
Redistribution of thiopental after intravenous injection
T h i o p e n
t a l c o n c e n
t r a
t i o n
( a s p e
r c e n
t o
f i n i t i a l d o s e
)
100
50
0
minutes
1 10 100 1000
blood
brainmuscle adipose
-
7/28/2019 kuliah farSP(1)kbk
43/59
Drug Biotransformation
Usually inactivates the drug.Can generate active metaboliteCan generate toxic metabolite (isoniazid).Often generates polar, highly ionizedmetabolites.Conversion rate influences pharmacologicalactivity.Some drugs are eliminated unchanged (digoxin).
-
7/28/2019 kuliah farSP(1)kbk
44/59
-
7/28/2019 kuliah farSP(1)kbk
45/59
Phase I functionalization reactions(oxidation, reduction, hydrolysis) introduce orexpose a functional group on the parentcompound result in loss of pharmacologicalactivity
Phase II conjugation reactions lead tocovalent linkage of a functional group on theparent drug or phase I metabolite withendogenously derived glucuronic acid, sulfate,methyl, glutathione, amino acids, acetate,acetylate etc result in highly polarconjugates
-
7/28/2019 kuliah farSP(1)kbk
46/59
Biotransformation of Major Functional
Groups
(-OH) oxidation, methylation, glucuronideconjugation, sulfate conjugation.
(-COOH) oxidation, glucuronideconjugation, glycine conjugation.
(-NH 2) deamination (and aldehydeformation), glucuronide conjugation,methylation.
-
7/28/2019 kuliah farSP(1)kbk
47/59
Phase I and Phase II Metabolic
Reactions
Drug
Phase I Absorption
Metabolite withmodified activity
Inactive metabolite
Metabolism
Lipophilic Hydrophilic
Phase II
Conjugate
Conjugate
Excretion
-
7/28/2019 kuliah farSP(1)kbk
48/59
Some Drugs Stimulate and SomeInhibit the drug metabolizing enzymes
Stimulation is via induction, which means anincrease in enzyme synthesis (oxidation,reduction, glucoronide formation).Phenobarbital and polycyslic aromatichydrocarbon (cigarette smoke) inducersInhibition is via competition, prodruginhibition or a decrease in the activity ofexisting enzyme.Cimetidine inhibitor
-
7/28/2019 kuliah farSP(1)kbk
49/59
Enzyme Induction
No induction
Phenobarbitalinduction
Benzopyreneinduction
Time (hrs)1
10
100
P l a s m a
L e v e
l
Z o x a z o
l a m
i n e
(m g
/ m l )
(Classic barbiturateeffect)
(Generated fromgrilling meat)
-
7/28/2019 kuliah farSP(1)kbk
50/59
ACETAMINOPHENMETABOLISM
1. Oxidation
2. Reactive Intermediate3. Glutathione Conjugation
4. Hepatic Cell Death
-
7/28/2019 kuliah farSP(1)kbk
51/59
Acetominophen Metabolism
Ac-glucuronide Ac Ac-sulfate
Cytochrome P-450
Reactive electrophiliccompound (Ac*)
Ac*-protein
Hepat ic c el l death
GSH
GS-Ac*
Ac-mercapturate
Good Bad
-
7/28/2019 kuliah farSP(1)kbk
52/59
Elimination Of Drugs
Metabolism: Liver
Excretion: KidneyLiver (bile)Lungs
Others : Feces, Saliva, Sweat, Milk
-
7/28/2019 kuliah farSP(1)kbk
53/59
Renal Excretion of Drugs
Filtration (Glomerulus)Secretion - Active Transport (Tubule)
Transporter for Organic AcidsTransporter for Organic Bases
Reabsorption - Passive Transport (Tubule)
-
7/28/2019 kuliah farSP(1)kbk
54/59
-
7/28/2019 kuliah farSP(1)kbk
55/59
Glomerular Filtration
Only unbound drug is filtered.
Plasma Protein Binding of drug preventsfiltration: Thyroxine is 99% bound.Molecular Size:
Albumin (70,000) is not filtered.Inulin (5,500) is freely filtered; can beused to estimate GFR.
-
7/28/2019 kuliah farSP(1)kbk
56/59
Tubular Secretion
Active TransportOrganic Acids (inhibited by probenecid)
Organic BasesNo effect of protein binding on this processThe clearance of drug eliminated by tubularsecretion is a function of renal blood flow
-
7/28/2019 kuliah farSP(1)kbk
57/59
Tubular Reabsorption
Passive Transport:pH, concentration, size, lipid solubility,
ionization.acid urine favors reabsorption of weakacid, basic urine favors reabsorption ofweak base.pH urine is affected by diet,drugs, diurnal,condition of patients (respiratory andmetabolic acidosis)
-
7/28/2019 kuliah farSP(1)kbk
58/59
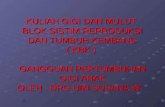
Enterohepatic Cycle
Liver
Common bile duct
Small intestine
Portal vein
3
4 1
2
-
7/28/2019 kuliah farSP(1)kbk
59/59
Factors affecting drug metabolism
reversible binding to plasma proteinslocalization of drugs (e.g., fat)hepatic blood flowAgegenetics-related deficiency or alteration in drugmetabolizing enzyme (e.g., acetylator,pseudocholinesterase deficiency and succinylcholine)pathologyinhibition / inductionof drug metabolizing enzyme (e.g.,by erythromycin, phenobarbital)Diet (carb-protein, vegetables, charcoal-broiled beef)Enviromental chemicals (alcohol, cigarette smoking,other chemicals)