Inggris Bu Ana
4
A. Determining staffing mix The same data used to determine FTSs are used to identify staffing mix. For example, for patient care needs involving general hygiene care, feeding, transferring, or turning patients, unlicensed assitive personnel (UAPs) can be used. For patient care needs involving frequent assessments, patient education, or discharge planning, RNs will be needed because of the skilla required. A high RN-skill mix allows for greater staffing flexibility. Again , information on typical or usual patientneeds is obtained by using trends from the patient classification system. For many patient care units, the distribution of staff varies from shift to shift and by days of the week. Patient census on a surgical unit will probably fluctuate throughout the week, with a higher census Monday through Thursday and a lower census over the weekend. In addition, some surgical units may have more complex cases earlier in the week and short-stay surgical casses later in the week. Surgical patients may have a shorter length of stay (LOS) than many medical patients. The patient census on a medical unit rarely fluctuates Monday through Friday , but may be less on weekends, when diagnostic tests are not done. The workload on many units also varies within the 24-hour period. The care demands on a surgical unit will be heavicst early in the morning hours prior to the start of the surgical schedule; midmorning , when the unit receives patients from cretical care unit(s); late in the
-
Upload
bambangsujana -
Category
Documents
-
view
212 -
download
0
description
td
Transcript of Inggris Bu Ana

A. Determining staffing mix
The same data used to determine FTSs are used to identify staffing mix. For example,
for patient care needs involving general hygiene care, feeding, transferring, or turning
patients, unlicensed assitive personnel (UAPs) can be used. For patient care needs
involving frequent assessments, patient education, or discharge planning, RNs will be
needed because of the skilla required. A high RN-skill mix allows for greater staffing
flexibility. Again , information on typical or usual patientneeds is obtained by using
trends from the patient classification system. For many patient care units, the
distribution of staff varies from shift to shift and by days of the week. Patient census
on a surgical unit will probably fluctuate throughout the week, with a higher census
Monday through Thursday and a lower census over the weekend. In addition, some
surgical units may have more complex cases earlier in the week and short-stay
surgical casses later in the week. Surgical patients may have a shorter length of stay
(LOS) than many medical patients. The patient census on a medical unit rarely
fluctuates Monday through Friday , but may be less on weekends, when diagnostic
tests are not done.
The workload on many units also varies within the 24-hour period. The care demands
on a surgical unit will be heavicst early in the morning hours prior to the start of the
surgical schedule; midmorning , when the unit receives patients from cretical care
unit(s); late in the afternoon, when patients return from the postanes-thesia recovery
unit; and in the evening hours, when same-day surgical patients are discharged.
Critical care units may have greater care needs in the mornings when transferring
patients to medical or surgical units and in the early afternoon hours when admitting
new surgical cases. Medical units usually have the heaviest care needs in the morning
hours, when patients’ daily care needs are being met and physicians are making
rounds. On skilled nursing and immediately after mealtimes and in the evening hours;
during other times of the day, patients are often away from the unit and involved in
various therapeutic activities. In contrast with the medical, surgical, critical care, and
rehabilitation units that have definite patterns of patient care needs, labor-and-delivery
and emergency department areas cannot predict when patient care needs will be most
intense. Thus, labor-and-delivery and emergency department areas must rely on block
staffing to ensure that adequate nursing staff are available at all times.
Block staffing involves scheduling a set staff mix for every shift. However, there may
be trends in peak workload hours in emergency departments, when additional staff
(RN, UAP, or secretary ) beyound the block staff are necessary. Examples of peak
workload hours within the emergency department may be from 6:00 p.m.TO 10.00
p.m to accommodate patient needs after physicians affices close or from 12:00 A.M.
to 3:00 A>M> to accommodate alcohol-related injuries. Ali these patienst of care
needs must be known when staffing, requirements and work scheduies are
established. Data reflecting peak workload times must be continously monitored to
maintain the appropriate levels and mix of staff.
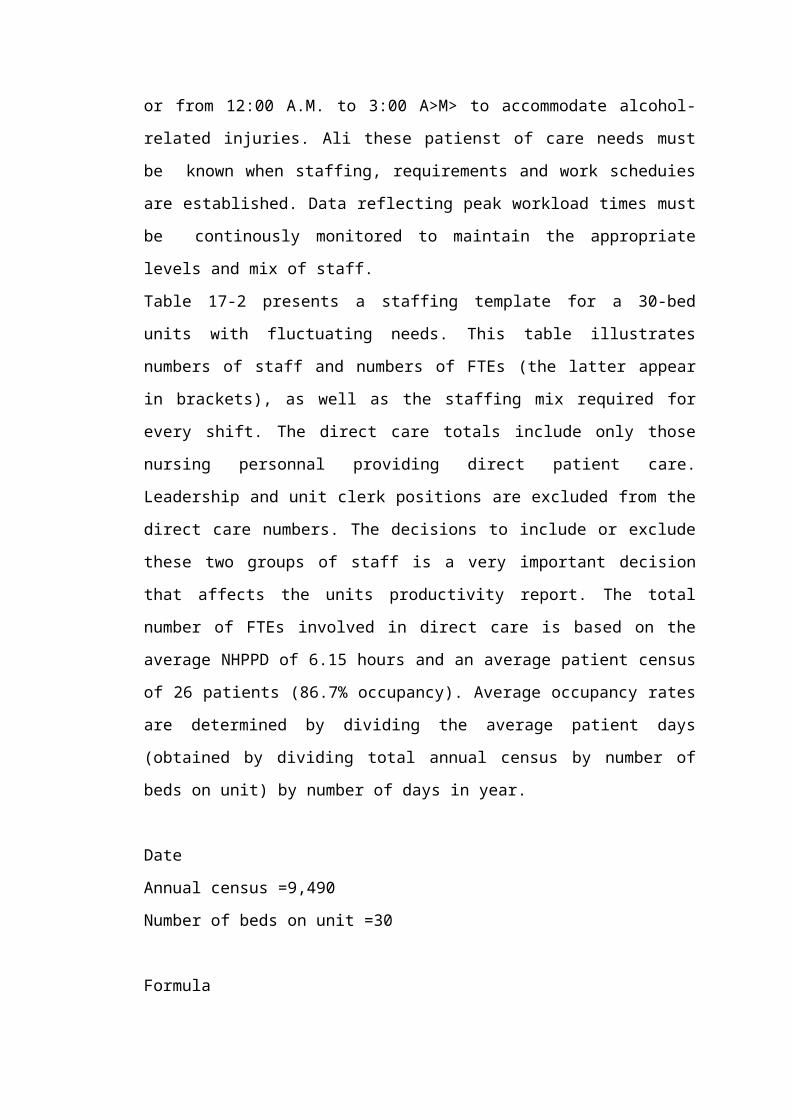
Table 17-2 presents a staffing template for a 30-bed units with fluctuating needs. This
table illustrates numbers of staff and numbers of FTEs (the latter appear in brackets),
as well as the staffing mix required for every shift. The direct care totals include only
those nursing personnal providing direct patient care. Leadership and unit clerk
positions are excluded from the direct care numbers. The decisions to include or
exclude these two groups of staff is a very important decision that affects the units
productivity report. The total number of FTEs involved in direct care is based on the
average NHPPD of 6.15 hours and an average patient census of 26 patients (86.7%
occupancy). Average occupancy rates are determined by dividing the average patient
days (obtained by dividing total annual census by number of beds on unit) by number
of days in year.
Date
Annual census =9,490
Number of beds on unit =30
Formula
Average patient days ¿annual censusnumber of beds
Occupancy rate¿Average patient days
Days∈ year
Average patient days =9490
30 =316.33
Occupancy rate =316365
=86.7 %