Dr Vivi_farmakotx Obat Git 2,2013
52
Farmakoterapi Farmakoterapi OBAT-OBAT YANG BEKERJA PADA SISTEM PENCERNAAN 2 OBAT-OBAT YANG BEKERJA PADA SISTEM PENCERNAAN 2 Fathiyah Safithri
-
Upload
erinageraldi -
Category
Documents
-
view
220 -
download
6
description
farmakologi
Transcript of Dr Vivi_farmakotx Obat Git 2,2013
-
FarmakoterapiFarmakoterapiFarmakoterapiFarmakoterapi
OBAT-OBAT YANG BEKERJAPADA
SISTEM PENCERNAAN 2OBAT-OBAT YANG BEKERJA
PADASISTEM PENCERNAAN 2
OBAT-OBAT YANG BEKERJAPADA
SISTEM PENCERNAAN 2OBAT-OBAT YANG BEKERJA
PADASISTEM PENCERNAAN 2
Fathiyah Safithri
-
PROKINETIK AGENT
-
Indikasi
memotilitas gastermengosongkanlambung lbh cepatTx Gatroparesis
me tonus spinkter bawah esofagusspinkter bisa menutup sempurna TxGERD
memotilitas gastermengosongkanlambung lbh cepatTx Gatroparesis
me tonus spinkter bawah esofagusspinkter bisa menutup sempurna TxGERD
-
DRUGS PROMOTE GI MOTILITY
Stimulate R/Muscarinic- choline esters cholinomimetics (betanechol)
Prokinetic agents selective motility stimulants
(metoclopramide, cisapride, erythromycin)
Stimulate R/Muscarinic- choline esters cholinomimetics (betanechol)
Prokinetic agents selective motility stimulants
(metoclopramide, cisapride, erythromycin)
-
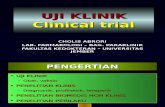
Conceptual model of prokinetic agentsDopaminergicneuron
(-)
(+)(-) D2
2 3
3
serotoninserotonin Ach
5HT45 HT3
1(+)
Effectororgan GI
-
Mech. Of action General pharm. class Example of drug Usedmedications
Aktivasi R/ Musc. Cholinergic agents Betanecholneostigmin
Costipationpseudoobstruction
Classification of prokinetic agents
Inhibisi R/D2 Antagonis R/Dopamin MetoclopramideDomperidone
GERD
Aktivasi R/5HT4Inhibisi R/5HT3
Agonis R/SerotoninAntagonis R/ Serotn
CisaprideMetoclopramide
Gastroparesis
Aktivasi R/Motilin Motilin like agents Erytromycin Gastroparesis
-
OBAT ANTI MUNTAH
-
Differential diagnosis of nausea and vomiting
-
10, Issue 12, December 2009, Anaesthesia &Intensive Care Medicine Volume Pages 597601
-
Paediatrics and Child HealthVolume 20, Issue 3, March 2010,Pages 129134
-
Anaesthesia & Intensive Care MedicineVolume 13, Issue 12, December 2012, Pages 613616
-
Anaesthesia & Intensive Care MedicineVolume 7, Issue 12, December 2006, Pages 453455
-
Chemotherapeutic drugs can trigger emesis by twoways: Direct activation of the medullarychemoreceptor trigger zone. 5-HT3(serotonin3), D2 (dopamine) and NK-1 receptorsplay a critical role as neurotransmitters.
Cell damage of the GI tract. This causesserotonin release from the enterochromaffincells, this molecule activates 5-HT3 receptors onvagal and splanchnic afferent fibers that sendimpulses to the medulla, activating the CTZ whichstimulates the vomiting center.
Chemotherapeutic drugs can trigger emesis by twoways: Direct activation of the medullarychemoreceptor trigger zone. 5-HT3(serotonin3), D2 (dopamine) and NK-1 receptorsplay a critical role as neurotransmitters.
Cell damage of the GI tract. This causesserotonin release from the enterochromaffincells, this molecule activates 5-HT3 receptors onvagal and splanchnic afferent fibers that sendimpulses to the medulla, activating the CTZ whichstimulates the vomiting center.
-
General classification of antiemetic agentsAntiemetic class Examples Type vomiting
most effective5 HT3-antagonist Ondansetron Cytotoxic drugCentrally acting dopamineantagonist
Metoclopramide(5HT3)Promethazine(antimusc&antihist)
Cytotoxic drugMetoclopramide(5HT3)Promethazine(antimusc&antihist)
H1- antagonist Cyclizine Vestibular(motionsickness)
Muscarinic antagonist Scopolamine Motion sickness
Neurokinin rec Investigational Cytotoxic drug
Cannabinoid rec antag Drobabinol Cytotoxic drug
-
AntiemetikAntiemetikAntiemetikAntiemetik
Serotonin (5HT) Antagonists Dopamine (DA) Antagonists Anticholinergics (muscarinic blockers) Cannabinoids
Serotonin (5HT) Antagonists Dopamine (DA) Antagonists Anticholinergics (muscarinic blockers) Cannabinoids
Serotonin (5HT) Antagonists Dopamine (DA) Antagonists Anticholinergics (muscarinic blockers) Cannabinoids
Serotonin (5HT) Antagonists Dopamine (DA) Antagonists Anticholinergics (muscarinic blockers) Cannabinoids
-
Dopamine AntagonistsDopamine AntagonistsDopamine AntagonistsDopamine Antagonists
Phenothiazines prochloraperazine (Compazine) promethazine (Phenergan)
Butyrophenones haloperidol (Haldol) droperidol (Inapsine)
metoclopramide (Reglan)
Phenothiazines prochloraperazine (Compazine) promethazine (Phenergan)
Butyrophenones haloperidol (Haldol) droperidol (Inapsine)
metoclopramide (Reglan)
Phenothiazines prochloraperazine (Compazine) promethazine (Phenergan)
Butyrophenones haloperidol (Haldol) droperidol (Inapsine)
metoclopramide (Reglan)
Phenothiazines prochloraperazine (Compazine) promethazine (Phenergan)
Butyrophenones haloperidol (Haldol) droperidol (Inapsine)
metoclopramide (Reglan)
-
Serotonin AntagonistsSerotonin AntagonistsSerotonin AntagonistsSerotonin Antagonists
Indikasi : mengatasi ES penggunaan kemoterapiyg menginduksi muntah
Ondansetron (Zofran) Tidak mempengaruhi R/ dopamine tdk ada
efek ekstrapiramidal Granisetron (Kytril)
Indikasi : mengatasi ES penggunaan kemoterapiyg menginduksi muntah
Ondansetron (Zofran) Tidak mempengaruhi R/ dopamine tdk ada
efek ekstrapiramidal Granisetron (Kytril)
Indikasi : mengatasi ES penggunaan kemoterapiyg menginduksi muntah
Ondansetron (Zofran) Tidak mempengaruhi R/ dopamine tdk ada
efek ekstrapiramidal Granisetron (Kytril)
Indikasi : mengatasi ES penggunaan kemoterapiyg menginduksi muntah
Ondansetron (Zofran) Tidak mempengaruhi R/ dopamine tdk ada
efek ekstrapiramidal Granisetron (Kytril)
-
ANTIEMETIC AGENT
-
ANTIEMETIC AGENT
-
Farmakoterapi Obatsistem hepato-bilier
-
LIVERAliran Darah Hepar:a. vena portal (80%) nutrients & xenobiotics dari GIT
b. arteri hepatic (20%) oxygen, metabolite & circulating xenobiotics
potensial mengalami kerusakanakibat intoksikasi
Aliran Darah Hepar:a. vena portal (80%) nutrients & xenobiotics dari GIT
b. arteri hepatic (20%) oxygen, metabolite & circulating xenobiotics
potensial mengalami kerusakanakibat intoksikasi
-
LIVERPhysiological role* Nutrients metabolism
carbohydrates, lipids and proteins
* Synthesis and secretes bilewater, ions, lipids (bile salts), and bile pigments(bilirubin).
* Synthesis protein enzymesalbumin, cytochrome P450s, transaminase
Physiological role* Nutrients metabolism
carbohydrates, lipids and proteins
* Synthesis and secretes bilewater, ions, lipids (bile salts), and bile pigments(bilirubin).
* Synthesis protein enzymesalbumin, cytochrome P450s, transaminase
-
LIVERLIVER Nutrient metabolism :a. Carbohydrate metabolism
synthesis glycogen from glucose and reverse
b. Lipid metabolismtriglyceride, FFA, HDL, LDL, VLDL
c. Protein metabolismenzymes, albumin, amino acid
Nutrient metabolism :a. Carbohydrate metabolism
synthesis glycogen from glucose and reverse
b. Lipid metabolismtriglyceride, FFA, HDL, LDL, VLDL
c. Protein metabolismenzymes, albumin, amino acid
-
LIVERxenobiotic metabolism :a. enhance excretionby change any substance become polar,hydrophilic.
b. inactivate detoxicationit is often (but not always) achieved,sometime activation.
xenobiotic metabolism :a. enhance excretionby change any substance become polar,hydrophilic.
b. inactivate detoxicationit is often (but not always) achieved,sometime activation.
-
Parasetamol
NABQI conjugation(N-aetylbenzoquinoneimine) (sulphate or glucuronate)
conjugation
(sulphate or glucuronate)
renal excretion renal excretion
7 10% 90 93%
glutathione
oxidation
Parasetamol
NABQI conjugation(N-aetylbenzoquinoneimine) (sulphate or glucuronate)
conjugation
(sulphate or glucuronate)
renal excretion renal excretion
NABQI : hepatotoxic
-
Liver Diseases - Disorders1. Acute hepatitis (acute viral hepatitis, alcoholic
hepatitis)2. Chronic hepatitis (chronic persistent hepatitis,
chronic active hepatitis autoimmune type)3. Liver cirrhosis (compensated and non-compensated cirrhosis, liver cirrhosisencephalopathy, cirrhosis edema and ascites,bleeding from esophageal varices, and cirrhosisrenal failure)
1. Acute hepatitis (acute viral hepatitis, alcoholichepatitis)
2. Chronic hepatitis (chronic persistent hepatitis,chronic active hepatitis autoimmune type)
3. Liver cirrhosis (compensated and non-compensated cirrhosis, liver cirrhosisencephalopathy, cirrhosis edema and ascites,bleeding from esophageal varices, and cirrhosisrenal failure)
-
Liver Diseases - Disorders
4. Special liver cirrhosis(hemochromatosis, Wilson disease,primary biliary cirrhosis)
5. Gallstones
4. Special liver cirrhosis(hemochromatosis, Wilson disease,primary biliary cirrhosis)
5. Gallstones
-
Drugs in Hepatitis1. Acute hepatitis Symptomatic teraphy cholestyramine, reduce pruritus but may cause
hepatotoxicity use this drug as it really needed corticosteroids no benefit active immunization hepatitis-B vaccine passive immunization immune serum globulin
(HBIG) effective? side effects?2. Chronic hepatitis corticosteroids or other immunosuppressant avoid
1. Acute hepatitis Symptomatic teraphy cholestyramine, reduce pruritus but may cause
hepatotoxicity use this drug as it really needed corticosteroids no benefit active immunization hepatitis-B vaccine passive immunization immune serum globulin
(HBIG) effective? side effects?2. Chronic hepatitis corticosteroids or other immunosuppressant avoid
-
Cholestyramine Acid bile chelator Bind to acid bile in the intestine lumen block acid bile reabsorption
serum bilirubin pruritus Unpleasant taste May causes diarrhea and abdominal
discomfort If pruritus is not controlled by
cholestyramine antihistamine isrecommended
Acid bile chelator Bind to acid bile in the intestine lumen block acid bile reabsorption
serum bilirubin pruritus Unpleasant taste May causes diarrhea and abdominal
discomfort If pruritus is not controlled by
cholestyramine antihistamine isrecommended
-
Corticosteroids May have a benefit in cholestasis secondary to hepatitis-A viral infection(not for other type of viral hepatitis)
May suppress RES decrease self protection towardinfection
May have a benefit in cholestasis secondary to hepatitis-A viral infection(not for other type of viral hepatitis)
May suppress RES decrease self protection towardinfection
-
Chronic active hepatitis Autoimmune hepatitischaracterized by histopathologicalfeature : chronic hepatitis, presence ofautoantibody
Interferon-a inhibit viral replication (+ 40% ofchronic hepatitis-B) may cause influenza like symptom,bone marrow suppression, depression,irritable
Autoimmune hepatitischaracterized by histopathologicalfeature : chronic hepatitis, presence ofautoantibody
Interferon-a inhibit viral replication (+ 40% ofchronic hepatitis-B) may cause influenza like symptom,bone marrow suppression, depression,irritable
-
LIVER CIRRHOSIS
-
Liver cirrhosis A pathological features caused by irreversible chronic injury of the hepaticparenchyma
Extensive fibrosisin association with regenerative nodules
As a final common pathwayof many types of chronic liver injury,
Clinical featuresreflect the severity of hepatic damage rather than theetiology of underlying liver diseases
A pathological features caused by irreversible chronic injury of the hepaticparenchyma
Extensive fibrosisin association with regenerative nodules
As a final common pathwayof many types of chronic liver injury,
Clinical featuresreflect the severity of hepatic damage rather than theetiology of underlying liver diseases
-
Clinical features ofClinical features of
Liver cirrhosis Loss of functioning hepatocellular mass jaundice, edema, coagulopathy, metabolicabnormalities,
Fibrosis and distorted vasculature portal hypertension and its sequelae(gastroesophagel varices and splenomegaly)
Ascites and hepatic encephalopathy resulted from both hepatocellularinsufficiency and portal hypertension
Loss of functioning hepatocellular mass jaundice, edema, coagulopathy, metabolicabnormalities,
Fibrosis and distorted vasculature portal hypertension and its sequelae(gastroesophagel varices and splenomegaly)
Ascites and hepatic encephalopathy resulted from both hepatocellularinsufficiency and portal hypertension
-
Alcohol induced hepatic lesion1. Alcoholic fatty liver
accumulation of fat in the liver result from an impairment of fatty acid oxidation,
increase uptake and esterification to formtriglyceride and diminished lipoprotein biosynthesis
2. Alcoholic hepatitishepatocyte degeneration and necrosis balloonedcells, infiltrate alcoholic hyaline
3. Alcoholic cirrhosisdestruction of hepatocytes and fibroblastcollagenization
1. Alcoholic fatty liveraccumulation of fat in the liver result from an impairment of fatty acid oxidation,
increase uptake and esterification to formtriglyceride and diminished lipoprotein biosynthesis
2. Alcoholic hepatitishepatocyte degeneration and necrosis balloonedcells, infiltrate alcoholic hyaline
3. Alcoholic cirrhosisdestruction of hepatocytes and fibroblastcollagenization
-
Liver cirrhosis compensated cirrhosis
- regularly reviewed for sign of hepatocellularfailure serum analysis for LFT
- long term care includes control of ascites- avoid drugs that induce coma do not give unnecessarily drugs
compensated cirrhosis- regularly reviewed for sign of hepatocellularfailure serum analysis for LFT
- long term care includes control of ascites- avoid drugs that induce coma do not give unnecessarily drugs
-
Liver cirrhosis decompensated cirrhosis- diet should be as nutritious as possible. high protein diet
(provided that there is no evidence of precoma orcoma)
- oral vitamin K if there is high prothrombin time avoid unnecessarily drugs
decompensated cirrhosis- diet should be as nutritious as possible. high protein diet
(provided that there is no evidence of precoma orcoma)
- oral vitamin K if there is high prothrombin time avoid unnecessarily drugs
-
Liver cirrhosis Edema and ascites- mobilise intraperitoneal fluid decrease Na+ dietary intake
(1 1,5 g/day : 40 60 mmol/day)- diuretics (furosemide, or spironolacton if needed) avoid dehydration if diuretic isused
Edema and ascites- mobilise intraperitoneal fluid decrease Na+ dietary intake
(1 1,5 g/day : 40 60 mmol/day)- diuretics (furosemide, or spironolacton if needed) avoid dehydration if diuretic isused
-
Hepatic encephalopathy- oral lactulose acidifying the colonic contents
(reducing absorption of ammonia and possibletoxins)the dose is increased until desired effect isobtained
- neomycin (reduce urease producing intestinalbacteria) avoid unnecessarily drugs
Liver cirrhosis Hepatic encephalopathy
- oral lactulose acidifying the colonic contents
(reducing absorption of ammonia and possibletoxins)the dose is increased until desired effect isobtained
- neomycin (reduce urease producing intestinalbacteria) avoid unnecessarily drugs
-
HEPATOTOXICITY
-
Manifestation ofHEPATOTOXICITY
1. Fatty liver2. Hepatitic reactions3. Obstructive jaundice cholestatic jaundice
4. Liver necrosis5. Liver cirrhosis6. Liver cancer
1. Fatty liver2. Hepatitic reactions3. Obstructive jaundice cholestatic jaundice
4. Liver necrosis5. Liver cirrhosis6. Liver cancer
-
Drug induced Fatty LiverDrug induced Fatty Liver
1. Carbontetrachloride (CCl4)2. Tetracycline3. Ethionine4. Ethanol chronic5. Phalotidine alkaloids
1. Carbontetrachloride (CCl4)2. Tetracycline3. Ethionine4. Ethanol chronic5. Phalotidine alkaloids
-
Intrahepatic cholestasis1. Carbimazole, methylthiouracil (antithyroiddrugs)
2. Benzodiazepines (anxiolytics, anticonvulsant)3. Clavulanic acid (b-lactamase inhibitor)4. Imidazole (i.e. ketokonazole antimycotics)5. Sulphonylurea (oarl antidiabetics tolbutamide,
glibenclamide, chlopropamide)6. Tricyclic antidepressants (imipramine,
amitryptiline, desipramine, iprindole)7. Phenothiazines (i.e. chlorpromazineantipsychotics)
1. Carbimazole, methylthiouracil (antithyroiddrugs)
2. Benzodiazepines (anxiolytics, anticonvulsant)3. Clavulanic acid (b-lactamase inhibitor)4. Imidazole (i.e. ketokonazole antimycotics)5. Sulphonylurea (oarl antidiabetics tolbutamide,
glibenclamide, chlopropamide)6. Tricyclic antidepressants (imipramine,
amitryptiline, desipramine, iprindole)7. Phenothiazines (i.e. chlorpromazineantipsychotics)
-
Intrahepatic cholestasis
1. Anabolic steroids (methyltestosterone,norethindrolone)
2. Azatrioprine (antiviral)3. Mercaptopurine (antimetabolite for acute leukemia)
4. Oestrogen (contraceptive agents)
1. Anabolic steroids (methyltestosterone,norethindrolone)
2. Azatrioprine (antiviral)3. Mercaptopurine (antimetabolite for acute leukemia)
4. Oestrogen (contraceptive agents)
-
DrugDrug // toxin inducedtoxin inducedLIVER NECROSIS
1. Aflatoxin2. INH3. Carbontetrachloride4. Paracetamol5. Chloroform6. Tetracycline7. Dinitrophenol8. Ethionine9. Halothane10. Ibuprofen11. Indomethacin12. Amanita phaloides
1. Aflatoxin2. INH3. Carbontetrachloride4. Paracetamol5. Chloroform6. Tetracycline7. Dinitrophenol8. Ethionine9. Halothane10. Ibuprofen11. Indomethacin12. Amanita phaloides
-
Liver NecrosisLiver NecrosisParasetamol
NABQI conjugation(N-cetylbenzoquinoneimine) (sulphate or glucuronate)
conjugation(sulphate or glucuronate)
renal excretion renal excretion
7 10% 90 93%
Parasetamol
NABQI conjugation(N-cetylbenzoquinoneimine) (sulphate or glucuronate)
conjugation(sulphate or glucuronate)
renal excretion renal excretion
-
NABQI (n(n--acetylbenzoquinoneimineacetylbenzoquinoneimine))NABQI
binding (covalent) to celluler hepatic proteins
damage endoplasmic reticulumswelling mitochondriadestruction of nucleus
mesruption of plasma membrane
cell necrosis
NABQI
binding (covalent) to celluler hepatic proteins
damage endoplasmic reticulumswelling mitochondriadestruction of nucleus
mesruption of plasma membrane
cell necrosis
-
Acutehepatocellular damage(non dose dependent)(non dose dependent)
1. INH, pyrazinamide, rifampicin(antituberculosis)
2. Carbamazepine (muscle realxant,anticonvulsant)
3. Halothane (inhalant general anesthetics)4. Imidazole (i.e. ketokonazole antimycotics)5. Ibuprofen, indomethacin (NSAIDs)6. Methyldopa (antihypertensive)7. MAO inhibitor (i.e. desipramineantidepresant)
8. Barbiturate (hypnotics, anticonvulsant)7. Sulfonamide (sulfamethoxazolchemotherapeutics)
1. INH, pyrazinamide, rifampicin(antituberculosis)
2. Carbamazepine (muscle realxant,anticonvulsant)
3. Halothane (inhalant general anesthetics)4. Imidazole (i.e. ketokonazole antimycotics)5. Ibuprofen, indomethacin (NSAIDs)6. Methyldopa (antihypertensive)7. MAO inhibitor (i.e. desipramineantidepresant)
8. Barbiturate (hypnotics, anticonvulsant)7. Sulfonamide (sulfamethoxazolchemotherapeutics)
-
1. Alcohol (beverage)2. Amiodarone (cardiac stimulant)3. Azatrioprine (antiviral)4. Chlorambucil (alkylating agent for CLL)5. Hydrocarbons (glue glue sniffing)6. Overdose iron salt (antianemics)a7. Methotrexate (antimetabolite, antifolic acid for cancer)8. Acetaminophen (analgesics antipyretics)7. Tetracycline (intravenous large dose)
Acutehepatocellular damage( dose dependent)( dose dependent)
1. Alcohol (beverage)2. Amiodarone (cardiac stimulant)3. Azatrioprine (antiviral)4. Chlorambucil (alkylating agent for CLL)5. Hydrocarbons (glue glue sniffing)6. Overdose iron salt (antianemics)a7. Methotrexate (antimetabolite, antifolic acid for cancer)8. Acetaminophen (analgesics antipyretics)7. Tetracycline (intravenous large dose)
-
Previous cholecystitis Rapid weight loss during treatment of overweight, morbid-obesity cholesterol is the main substance forms the stone
Ursodiol decrease cholesterol secretion into the bile decrease intestine cholesterol absorption increase bile flow cholesterol stone disolve
Opioid analgesics analgesia, increase duct smooth muscle tonemasking effect stone captures duct rupture spasmolytics (hyoscin, papaverin)
Antibiotics, antiinflammatory drugs
CHOLELITHIASIS Previous cholecystitis Rapid weight loss during treatment of overweight, morbid-obesity cholesterol is the main substance forms the stone
Ursodiol decrease cholesterol secretion into the bile decrease intestine cholesterol absorption increase bile flow cholesterol stone disolve
Opioid analgesics analgesia, increase duct smooth muscle tonemasking effect stone captures duct rupture spasmolytics (hyoscin, papaverin)
Antibiotics, antiinflammatory drugs
-
Drug Induced Liver Injury andIts Patterns
Navarro, V. J. et al. N Engl J Med 2006;354:731-739