








Bahasa
Halaman
Hukum


The Neonatal Airway
and Neonatal Intubation

Goals of Presentation
Recognize differences between neonatal
and adult airway
Review neonatal intubation technique and
equipment
Review common mistakes and
complications of intubation
Examine syndromes commonly associated
with difficult neonatal airways

Why do we care?
Prompt intubation of a distressed neonate
can be life-saving
Increasingly premature population
Residents are getting less training at this
RRC limitation of intensive care training
(1994)
Revision of NRP protocols (2000)

Why do we care? Database of all neonatal intubations at UCSD
from 1992-2002 9190 attempts recorded
What did they find? Successful intubation on each attempt
• PGY1 33%, PGY2 40%, PGY3 40%
Total intubations attempted during residency • 1994 – 38(+/- 19), 2002 – 12(+/- 6)
Total intubations successful during residency • 1994 – 24(+/- 14), 2002 – 4(+/-2)
Conclusion “Pediatric trainees are currently provided inadequate
experience to allow development of proficiency at neonatal intubation.”
NN Finer, et al. Neonatal Intubation: Success of Pediatric Trainees. J Peds 2005;146:638-41.
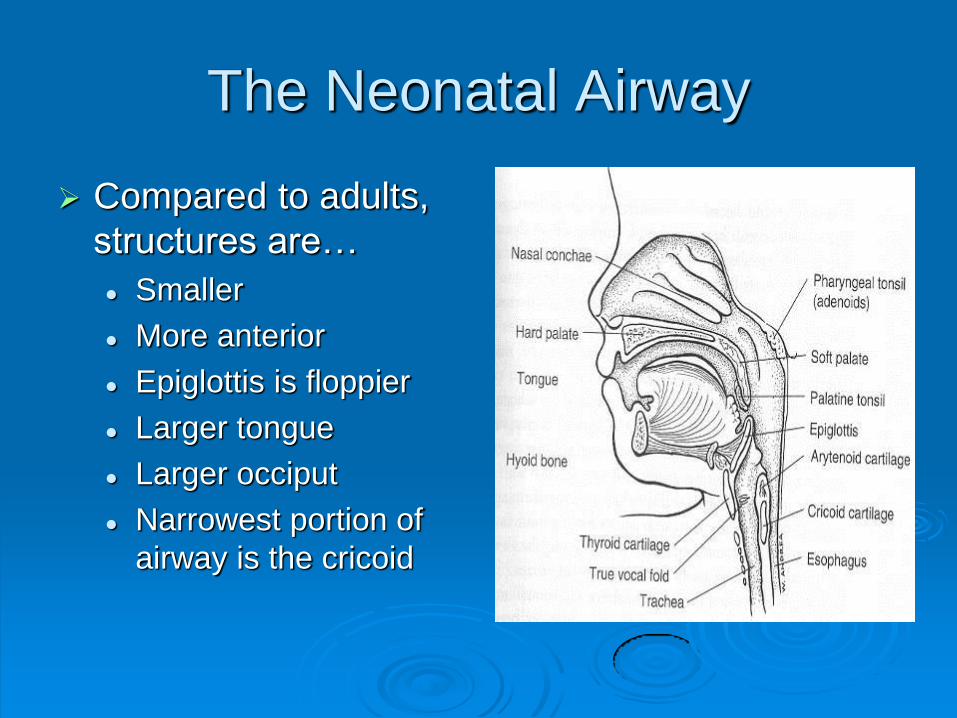
The Neonatal Airway
Compared to adults,
structures are…
Smaller
More anterior
Epiglottis is floppier
Larger tongue
Larger occiput
Narrowest portion of
airway is the cricoid

Airway Anatomy
Embryology
Larynx from 4th and 5th
arches
Primitive larynx altered
by hypobranchial
eminence, epiglottis,
arytenoids
Laryngeal lumen
obliterated and
recanalized

Indications for Intubation
In delivery room
Cardiorespiratory instability
Meconium during birth, with a depressed
infant
Prematurity requiring need for surfactant
therapy
Congenital malformations

Indications for Intubation
In NICU
Unable to protect airway
Hypercarbic respiratory failure
Hypoxic respiratory failure
Therapeutic indication

What do you need?
Monitors - Cardiac and pulse oximetry
Suction - Yankauer or catheter
Machine - Laryngoscope, ventilator or
bag/mask
Airway - Endotracheal tube
Intravenous - Peripheral or central line
Drugs --
Sedation/analgesia/paralysis/atropine

Laryngoscope Blades
Straight blades are
placed under the
epiglottis and used to
lift anteriorly to
expose the cords.
Curved blades are
placed in the valecula
and lifted anteriorly to
expose the cords.
Macintosh
Miller
Wisconsin

Endotracheal Tubes
Endotracheal tubes are divided by the size
of their internal diameter
For neonates endotracheal tube size
roughly corresponds to 1/10th of
gestational age rounded down to the
nearest size.
For example
• A 36 week premie would get a 3.5 ETT
• A 28 week premie would get a 2.5 ETT
Intubation Procedure
Proper positioning
Equipment • Bed and patient at comfortable height
• Suction and meconium aspirator readily available
• Endotracheal tubes not under warmer
• All equipment tested and working just prior to use
Patient • Shoulder roll
• Head in sniffing position Too much hyperextension can make visualization difficult

Intubation Procedure
Pre-oxygenate with 100% bag valve mask ventilation
Contraindicated in known congenital diaphragmatic hernia
Apply monitors
Give drugs
Remember minimum atropine dose
Ensure ability to bag/mask ventilate before paralysis

Intubation Procedure
Inserting the
laryngoscope blade
Hold laryngoscope in
left hand
While standing above
the patient, insert the
blade in the right side
of the mouth
WITHOUT trying to
visualize the cords.

Intubation Procedure
Take a step back
Lower your head to
the level of the label
Slowly advance
laryngoscope until
you visualize the
epiglottis
Use straight or curved
blade appropriately

Intubation Procedure
Visualize the vocal
cords
Meconium below
cords?
Both moving if not
paralyzed?
Structurally normal?
Pick up endotracheal
tube and pass
between vocal cords

Assessing Endotracheal Tube
Placement
Direct visualization
End tidal CO2 monitoring
Chest rise
Auscultation
ETT vapor
Less reliable
Chest X-ray

Intubation Procedure
Secure endotracheal tube to lip with tape
Do not let go of tube until secure
Reassess that endotracheal tube is still in place.
Assess the neonate –
Improving? More pink? Heart rate increasing?
Continue resuscitation – proceed to B and C….

Common Problems
Esophageal Intubation
Blade placed too deep, cords not visualized
Tongue obscures visualization
Sweep tongue to one side with blade
More anterior lift
Tape on blade
Cannot see cords
Head is hyper-extended - reposition

Common Problems
Cannot intubate
Most neonates can be bag valve mask
ventilated easily
Call early for anesthesiology assistance
• “Bag ventilating with oxygen can prolong life for a
long time, repeatedly attempting and failing
intubation will not.”
Surgical airway

Difficult Neonatal Airways
Must always be prepared for something
abnormal
Increasing awareness of problems
beforehand because of neonatal
ultrasound
“Things you can see” versus “Things you
may find”

Difficult Neonatal Airways
Congenital malformations
“Things you can see”
Predictable from looking at the patient
• Cleft lip and palate
• Pierre Robin syndrome
• Treacher Collins syndrome
• Goldenhar syndrome
• Apert and Crouzon Syndrome

Congenital Malformations
Cleft Lip and Palate
Most common
congenital face
malformation
Pierre Robin
Sequence
Obstruction is usually
at the nasopharyngeal
level

Congenital Malformations
Apert and Crouzon
Maxillary hypoplasia
Nasopharyngeal
airway compromise
Goldenhar syndrome
Unilateral anomalies
Higher incidence of
airway anomalies

Congenital Malformations
Treacher Collins
Choanal
atresia/stenosis more
common
Down’s Syndrome
Subglottic stenosis
more common
Remember
atlantoaxial instability

Difficult Neonatal Airways
Congenital Malformations
“Things you may find”
• Laryngomalacia
• Hemangioma or
Lymphangioma
• Tracheal web
• Laryngeal atresia
• Subglotic stenosis

Congenital Malformations
Laryngomalacia
A sequence between
fully formed to atresia

Congenital Malformations
Laryngeal Web
Tracheal Atresia
Survive only if
tracheoesophageal
fistula or emergent
trach

Congenital Malformations
Hemangioma or
Lymphangioma
Only about 30%
present at birth

Congenital Malformations
Subglottic Stenosis

In Review
Proper positioning is critical for successful
neonatal intubation
Call for help early if unable to intubate or for any
congenital anomalies
Continue to provide oxygen with bag valve mask
ventilation
Practice makes perfect
It is estimated that you need to perform at least 90
intubations to be able to intubate successfully on the
first or second attempt at least 80% of the time
Top Related
Copyright © 2022 FDOKUMEN

