







Bahasa
Halaman
Hukum

Role of medicinal plants in healthcare in Africa and related
issues: special emphasis to Ethiopia as an example.
M.I.Zuberi Ph.D (U.K), Professor of Environmental Science,
Ambo University, Ethiopia [[email protected]]
Introduction
In all the developing countries, especially in the Continent of
Africa (Fig 1), the majority of the common people continue to
rely heavily on the use of medicinal plants as their primary
source of healthcare. About 70-80% of Africa’s population rely
on traditional medicine, for example, in Tanzania an estimated
30 000 - 40 000 traditional practitioners provide health service
in comparison with 600 modern medical doctors (Hedberg et al.,
1982; 1983); also in Malawi, there were an estimated 17 000
traditional practitioners and only 35 medical doctors (Anon.,
1987). The International Development Research Centre (IDRC) gave
one estimate which puts the number of Africans who routinely use
the traditional medicinal services for primary health care as
high as 85% in Sub-Saharan Africa.
The fact is use of medicinal plants was as old as human society,
in the written record, the study of herbs dates back over 5,000
years to the Sumerians, who created clay tablets with lists of
hundreds of medicinal plants. In 1500 B.C., the Ancient
Egyptians wrote the Ebers Papyrus, which contains information on
over 850 plant medicines. In India, Ayurveda medicine has used
many plants possibly as early as 1900 BC as the earliest
Sanskrit writings such as the Rig Veda, and Atharva Veda are some
of the earliest available documents detailing the medical
knowledge that formed the basis of theAyurveda system later
described by ancient Indian herbalists such
as Charaka and Sushruta during the 1st millennium BC. The
Sushruta Samhita attributed to Sushruta in the 6th century BC
describes 700 medicinal plants. Also noted that the
first Chinese pharmacopoeia, the Shennong Ben Cao Jing lists 365
medicinal plants and their uses, while the succeeding generations
augmented on the Shennong Bencao Jing, as in the Yaoxing Lun (Treatise on
the Nature of Medicinal Herbs), a 7th-century Tang Dynasty treatise on
herbal medicine (eg Daly et al , 2000).
However, following the course of economic development, there has
been a shift from using traditional medicines to consulting
modern medical doctors, but with a very slow socio-economic and
cultural change taking place in Africa, this shift is mostly
confined to the urban areas. The vast rural populations, being
poor and having little access to modern medical system, still
rely on the medicinal plants used in the traditional system of
healthcare (Bannerman, 1983) . Even recent reports suggest
that 60%-80% of the people in Africa rely on traditional
remedies to treat themselves for various diseases (van Wyk,
2008), also a large percentage of the people in Africa use
traditional remedies to treat their animals for various diseases.
The African continent have a long history of use of plants
for curing diseases and ailments, and in some African
countries up to 90% of the population rely on medicinal plants as
a source of drugs (Hostettmann et al 2000). Traditional medicines
in Africa are generally not adequately researched, and are weakly
regulated (WHA 1988 ). There is a lack of detailed
documentation of the traditional knowledge associated with the
use of medicinal plants, which is generally transferred orally
(WHO,2000). Also, there may be serious adverse effects
resulting from misidentification or misuse of healing plants.
Now, all developing countries have begun to realize that the high
costs of modern health care systems and the technologies that are
required will be difficult to obtain for the majority of the
people, thus supporting Africa's dependence to traditional
medical system a positive aspect (WHO, 2001). Due to this,
interest has recently been expressed in integrating traditional
African medicine into the continent's national health care
systems (Farnsworth et al, 1985). For these reasons, there is a
need to document the plant resources, conserve and develop
traditional medical system incorporating it into the national
healthcare systems of all African countries through training and
evaluation of effective remedies and by documenting the knowledge
of plants utilized, giving recognition and proper emphasis on
their contribution to the primary healthcare (Akerele, 1987;
Anyinam, 1987; Good, 1987).
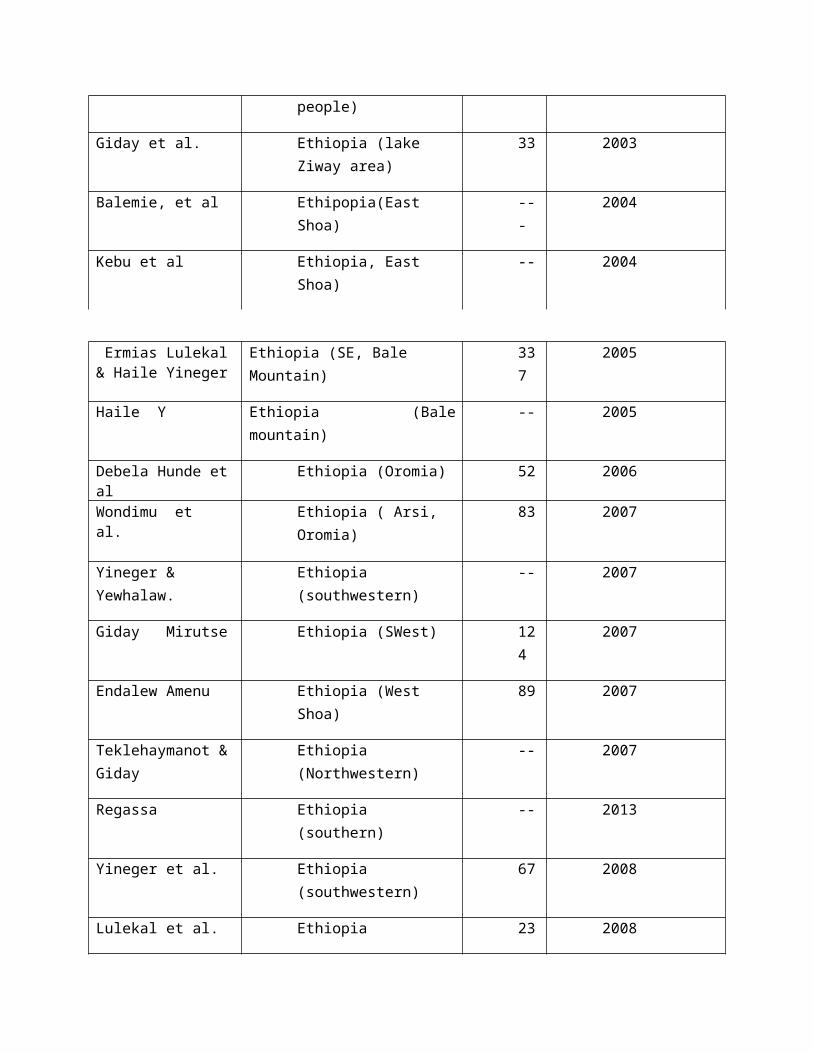
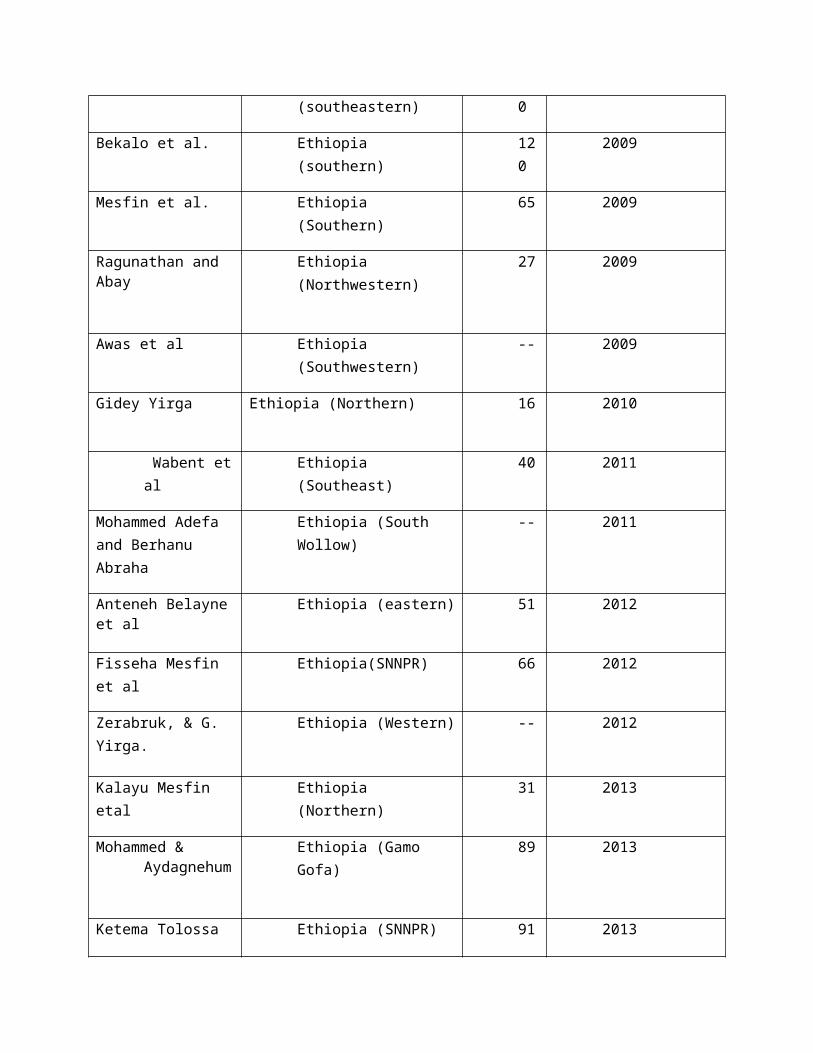
Only until recently, ethnobotanical studies are being carried
out throughout Africa confirming that native plants are the main
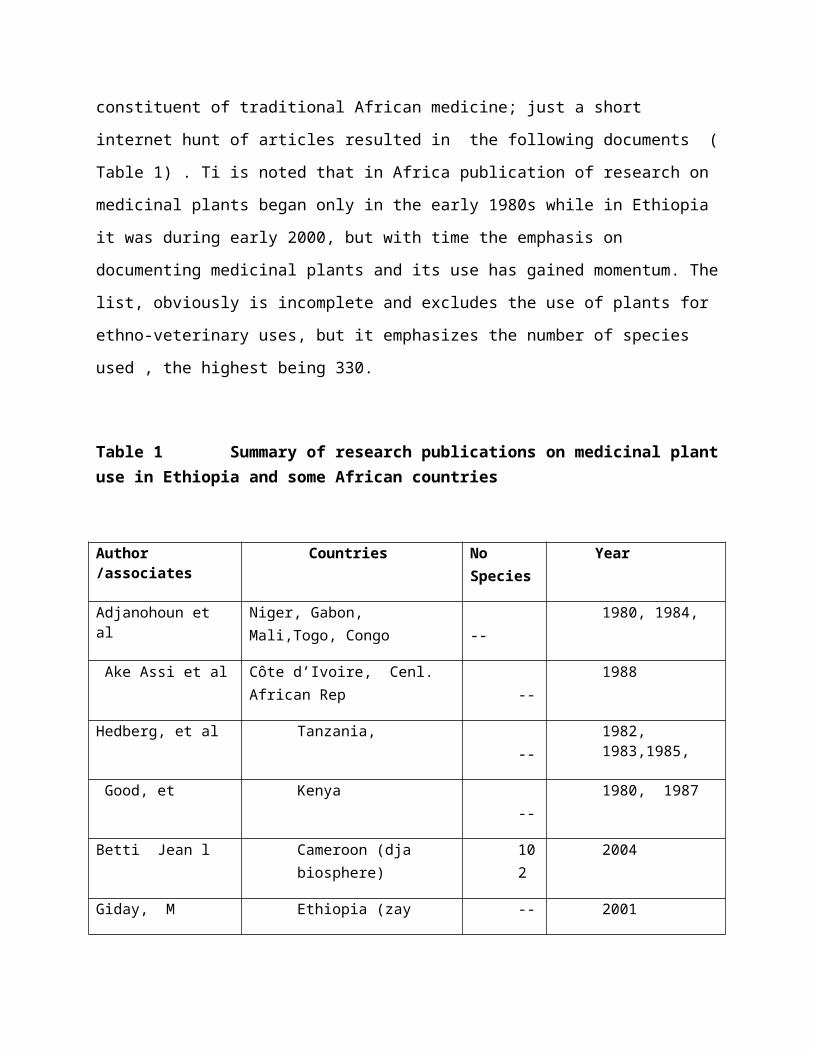
constituent of traditional African medicine; just a short
internet hunt of articles resulted in the following documents (
Table 1) . Ti is noted that in Africa publication of research on
medicinal plants began only in the early 1980s while in Ethiopia
it was during early 2000, but with time the emphasis on
documenting medicinal plants and its use has gained momentum. The
list, obviously is incomplete and excludes the use of plants for
ethno-veterinary uses, but it emphasizes the number of species
used , the highest being 330.
Table 1 Summary of research publications on medicinal plantuse in Ethiopia and some African countries
Author /associates
Countries No Species
Year
Adjanohoun et al
Niger, Gabon, Mali,Togo, Congo
--
1980, 1984,
Ake Assi et al Côte d’Ivoire, Cenl. African Rep
--
1988
Hedberg, et al Tanzania, --
1982,1983,1985,
Good, et Kenya --
1980, 1987
Betti Jean l Cameroon (dja biosphere)
102
2004
Giday, M Ethiopia (zay -- 2001
people)
Giday et al. Ethiopia (lake Ziway area)
33 2003
Balemie, et al Ethipopia(East Shoa)
---
2004
Kebu et al Ethiopia, East Shoa)
-- 2004
Ermias Lulekal& Haile Yineger
Ethiopia (SE, Bale Mountain)
337
2005
Haile Y Ethiopia (Balemountain)
-- 2005
Debela Hunde etal
Ethiopia (Oromia) 52 2006
Wondimu et al.
Ethiopia ( Arsi, Oromia)
83 2007
Yineger & Yewhalaw.
Ethiopia (southwestern)
-- 2007
Giday Mirutse Ethiopia (SWest) 124
2007
Endalew Amenu Ethiopia (West Shoa)
89 2007
Teklehaymanot &Giday
Ethiopia (Northwestern)
-- 2007
Regassa Ethiopia (southern)
-- 2013
Yineger et al. Ethiopia (southwestern)
67 2008
Lulekal et al. Ethiopia 23 2008
(southeastern) 0
Bekalo et al. Ethiopia (southern)
120
2009
Mesfin et al. Ethiopia (Southern)
65 2009
Ragunathan and Abay
Ethiopia (Northwestern)
27 2009
Awas et al Ethiopia (Southwestern)
-- 2009
Gidey Yirga Ethiopia (Northern) 16 2010
Wabent etal
Ethiopia (Southeast)
40 2011
Mohammed Adefa and Berhanu Abraha
Ethiopia (South Wollow)
-- 2011
Anteneh Belayneet al
Ethiopia (eastern) 51 2012
Fisseha Mesfin et al
Ethiopia(SNNPR) 66 2012
Zerabruk, & G. Yirga.
Ethiopia (Western) -- 2012
Kalayu Mesfin etal
Ethiopia (Northern)
31 2013
Mohammed &Aydagnehum
Ethiopia (Gamo Gofa)
89 2013
Ketema Tolossa Ethiopia (SNNPR) 91 2013

et al
Zewdu Birhanu Ethiopia(Northwestern)
41 2013
Fisseha Mesfinet al
Ethiopia (SNNPR) 56 2014
Balcha Abera Ethiopia (Southwest)
49 2014
Mesfin, Fissehaet al
Ethiopia (Amaro) 56 2014
Now, with 70-80% of Africa’s population relying on traditional
medicines, the importance of the role of medicinal plants in the
healthcare system being enormous, also Africa is endowed with
many plants that can be used for medicinal purposes in the future
. In fact, out of the approximated 6400 plant species in tropical
Africa, more than 4000 are used as medicinal plants (WHO, 2007).
As most of the modern drugs have been developed from knowledge
and materials from medicinal plants use, serious attention has
now been given on this sector, as is evidenced by the
recommendation of the World Health Organization in 1970
(Wondergem et al., 1989) . As a result, proven traditional
remedies are being incorporated within national drug policies,
some moves towards a greater professionalism within African
medicine are being initiated (Last and Chavunduka, 1986). Little
attention however, has so far been paid to the socio-economic and
conservation aspects of medicinal plant resources, probably due
to lack of resources and the relatively scattered nature and
small volumes involved, also the specialist nature of the
informal trade is there. Although the high rate of population
growth, wide degradation of forests and rapid urbanization have
generated a heavy pressure on the plant-based raw materials with
wide and intensive collection and marketing with the trade
networks expanding from rural to urban to international levels.
This shift from the collection of raw plant materials from the
traditional experts to commercial exploiters with purely
commercial and short term interest has resulted in a disregard
for traditional conservation practice and a breakdown of taboos
and customs in the matter. This, in addition to a very rapid and
substantial decline in the area of natural vegetation and
forest , the natural home for medicinal plants, has exacerbated
the crisis.
Medicinal plants use in Ethiopia
A country with a wide range of climatic and ecological
conditions supporting an enormous diversity of fauna and flora,
(Pankhurst, 2001), Ethiopia, possesses a wide range of
potentially useful medicinal plants (Fig 2). Ethiopia is
believed to be home for about 6500 species of higher plants,
with approximately 12% of these endemic (UNEP 1995).
Traditional medicinal practices are common in Ethiopia,
about 80% of the population in the country use plant based
traditional medicine for primary health care (Dawit , 2001).
It has been estimated that 95% of traditional medical
preparations in Ethiopia are of plant origin (Dawit, 1986), there
is a rich reservoir of local indigenous knowledge on medicinal
plant use. Medicinal plants used by the Ethiopian were estimated
to be over 700 species, but later were revised to about 1000
(Edwards, 2001), more than 300 of which are frequently
mentioned in many sources ( Edwards, 2001; Giday et al, 2010 and
in table 1).
The knowledge on medicinal plants is largely oral, however,
Ethiopia’s ancient church practices have documented some of the
knowledge as inscribed in Parchments which partly characterize
the traditional medical system usually described as medico
religious written in Geez manuscripts of the 15th century
(Gelahun Abate, 1989; Dawit Abebe and Ahadu Ayehu, 1993). Many
cultural groups in the country have their own written or oral
traditions that could be associated with individual clans or
groups as partly stated by Amare Getahun (1976) and Abbink
(1995). The greater concentration of medicinal plants are found
in the south and south western Ethiopian parts of the country
following the concentration of biological and cultural diversity
(Edwards, 2001; Belayneh et al.2012 ). For a very long time, 80%
of the human population and 90% of livestock in Ethiopia rely
on traditional medicine, as most plants species have shown
very effective medicinal value for some ailments of human beings
and domestic animals (Abebe 2001). Formal recognition to
traditional medicine in Ethiopia was given in 1942 where the
legality of the practice is acknowledged as long as it does not
have negative impact on health, this was reaffirmed in the 1943
and 1948 in Medical Registration Proclamations. The Ethiopian
Penal Code (512/1957) and the Civil Code (8/1967) provide
guidelines for the practice of traditional medicine, there was no
stipulation of any requirement for registration. Although
registration and licensing was introduced in 1950 (Ministry of
Health, 1984), yet this is not in practice.
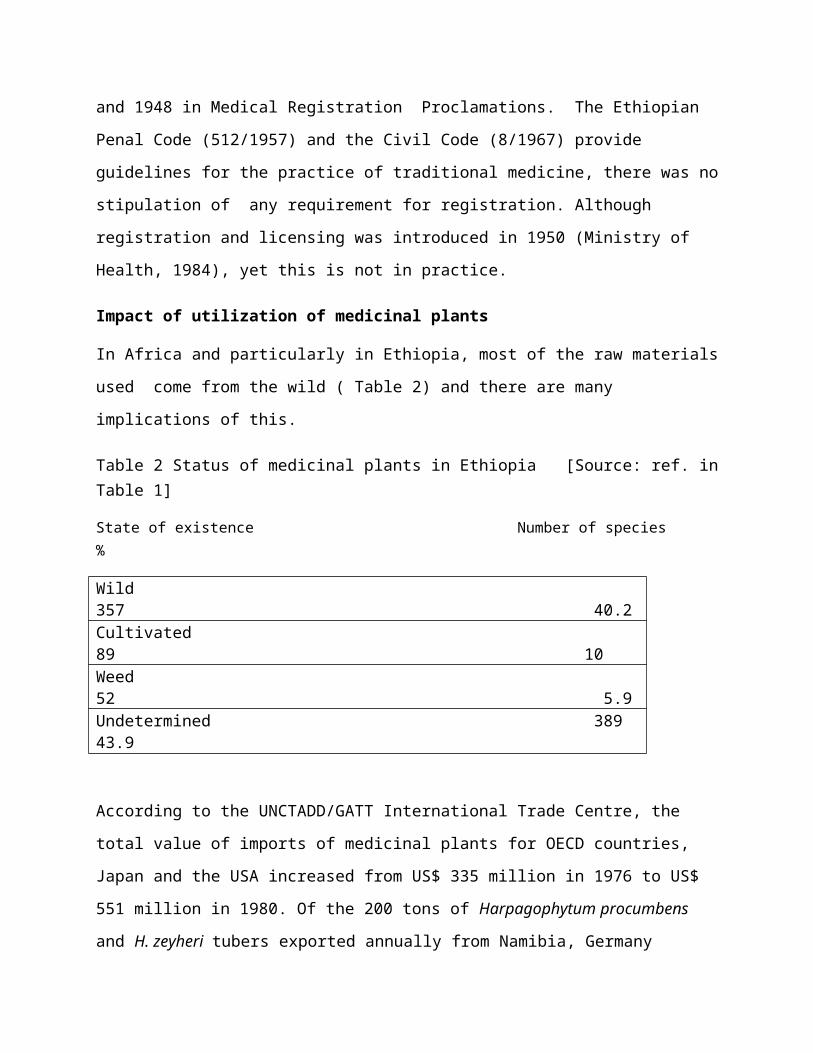
Impact of utilization of medicinal plants
In Africa and particularly in Ethiopia, most of the raw materials
used come from the wild ( Table 2) and there are many
implications of this.
Table 2 Status of medicinal plants in Ethiopia [Source: ref. inTable 1]
State of existence Number of species %
Wild 357 40.2Cultivated 89 10 Weed 52 5.9Undetermined 389 43.9
According to the UNCTADD/GATT International Trade Centre, the
total value of imports of medicinal plants for OECD countries,
Japan and the USA increased from US$ 335 million in 1976 to US$
551 million in 1980. Of the 200 tons of Harpagophytum procumbens
and H. zeyheri tubers exported annually from Namibia, Germany
imported 80.4%, with the remaining sold to France, Italy, USA,
Belgium and to South Africa (Nott, 1986). There are numerous
examples, eg. Maytenus buchananii, around 27.2 tons of plant
material were collected by the American National Cancer Institute
(NCI) from a conservation area in the Shimba Hills of Kenya for
screening purposes as a potential treatment for pancreatic
cancer, but when additional material was required four years
after the first harvesting in 1972, regeneration was so poor that
collectors struggled to obtain the additional material needed.
Others like 75-80 t of Griffonia simplicifolia seed exported each year
to Germany from Ghana (Abbiw, 1990) or the medicinal plant
material exported from Cameroon to France (Voacanga africana seed
(575 tons); Prunus Africana bark (220tons), Pausinystalia johimbe
bark (15 t) (United Republic of Cameroon, 1989) all testify how
the raw materials are harvested from nature. Also alarming that
no useful survey or research are known on the social or
environmental consequences of this harvesting, especially when
the harvesting process remains very destructive like cutting or
uprooting the plants for collecting fruits/seeds or bulbs (Rifai
and Kartawinata, 1991) as the trading agent or pharmaceutical
company are willing to pay a high price for a very large
amounts. There also are numerous records how many species of
medicinal plants became endangered or even extinct because for
uncontrolled harvest of important parts like root, fruits, seeds
or bark . As listed in Table 3, high proportions of the parts
used have been roots, whole plants, fruits, bark stem and seeds ,
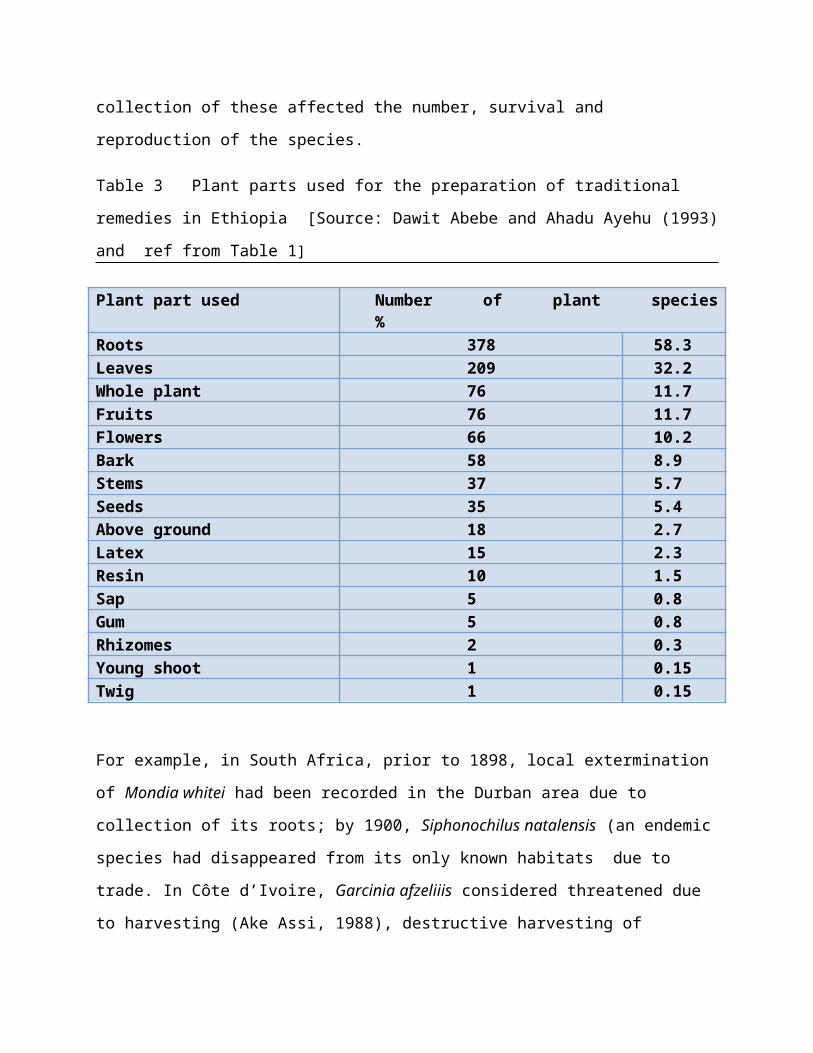
collection of these affected the number, survival and
reproduction of the species.
Table 3 Plant parts used for the preparation of traditional
remedies in Ethiopia [Source: Dawit Abebe and Ahadu Ayehu (1993)
and ref from Table 1]
Plant part used Number of plant species%
Roots 378 58.3 Leaves 209 32.2 Whole plant 76 11.7 Fruits 76 11.7 Flowers 66 10.2 Bark 58 8.9 Stems 37 5.7 Seeds 35 5.4 Above ground 18 2.7 Latex 15 2.3 Resin 10 1.5 Sap 5 0.8 Gum 5 0.8 Rhizomes 2 0.3 Young shoot 1 0.15 Twig 1 0.15
For example, in South Africa, prior to 1898, local extermination
of Mondia whitei had been recorded in the Durban area due to
collection of its roots; by 1900, Siphonochilus natalensis (an endemic
species had disappeared from its only known habitats due to
trade. In Côte d’Ivoire, Garcinia afzeliiis considered threatened due
to harvesting (Ake Assi, 1988), destructive harvesting of
Griffonia simplicifolia, Voacanga thuoarsii and Voacanga Africana fruits for
the international pharmaceutical market is also of high concern;
in Nigeria, despite traditional restrictions the Okoubaka
aubrevillei trees (a very rare species in West Africa) were being
harvested . There appears to be nothing published on the
current status of many of these species. Some other examples are
Prunus Africana , Pausinystalia johimbe bark harvesting in Cameroon and
Madagascar, fruit harvesting of Griffonia simplicifolia, Voacanga thuoarsii
and Voacanga africana for the international pharmaceutical market.
Taverniera abyssinica whose slender roots are marketed is a
popular traditional medicine but the species is labeled as
critically endangered in the Red List of Endemic Trees and Shrubs
of Ethiopia (Vivero et al., 2003).
There are many reasons for the lack of management of these
resources, one major issue is the low prices paid for the raw
materials do not cover the costs of replacement or resource
management , and there is no such attempts in field. Instead,
the major traders/ importers especially from the developed
countries continue to demand high volumes of plant material
contributing to the decline of medicinal plant species in Africa.
Fortunately, in most of the African countries having high rural
population and low urbanization, collection of raw materials
for ordinary species is often on the small scale, still keeping
some wild populations going. But where a species is popular and
the demand is high but supplies are low and specially if the
species is already rare due to habitat destruction and
agricultural expansion, the damage to the population will be very
rapid and high, needing quick attention. Also important is the
part used, the common sale and use of medicinal plant leaves as a
source of medicine in many countries (like Côte d’Ivoire) leaves
less pressure on the plants; which differs markedly from the
high frequency of roots, bark or bulbs, fruits and seeds at
markets (Table 3). Throughout Lesotho, Malawi, Mozambique,
Swaziland, Zambia, Zimbabwe, and particularly South Africa,
herbal material that is dried (roots or bark), or has a long
shelf-life (bulbs ,seeds and fruits) dominates herbal medicine
markets.
Although there is very limited information on the population
biology of medicinal plants, it is possible to classify target
plant species according to demand, plant life-form, part used,
distribution and abundance (Cunningham, 1990). From a
conservation viewpoint, African medicinal plants can be divided
into two categories that are of concern:
(1) Species with slow growth/reproduction with a limited
distribution but high in demand for commercial gathering
where demand exceeds supply ( eg. Warburgia salutaris in east
and Southern Africa and Siphonochilus aethiopicus in Swaziland
and South Africa.
(2) Popular species which are not endangered because they
have a wide distribution, but where habitat change and
intense commercial harvesting (eg. Trichilia emetica and Albizia
adianthifolia in southern Africa ).
Research, documentation and dissemination
As emphasized above, tropical and subtropical Africa contains
more than 40,000 species of plant with a potential for
development and out of which only 5000 species are used
medicinally and , in spite of this huge potential and
diversity, the African continent has only contributed 83 of
the 1100 blockbuster drugs globally (Rukangira, 2004). A few
plant species that provide medicinal herbs have been
scientifically evaluated for their possible medical
applications. Some plants used in traditional medicines, such
as taenicides, are widely known to be toxic. For example,
blindness and changes in central nervous system function have
repeatedly been found in people who took over dosage of
Hagenia abyssinica (Rokos, 1969). Many cases
of Podophyllum poisoning have been reported from Hong Kong
following the inadvertent use of the roots because of
similarity in the morphology of roots. Also cases of
cardiotoxicity resulting from the ingestion of Aconitum species
used in complementary medicine for acute infections and panic
attacks have been reported also from Hong Kong (WHO, 2004).
There are increasing number of reports of patients
experiencing negative health consequences caused by the use of
herbal medicines. Among many, one of the major cause of
diverse effects is directly linked to the poor quality of
herbal medicines, including raw medicinal plant materials, and
to the wrong identification of plant species. Cultivating,
collecting and classifying plants correctly are therefore of
the utmost importance for the quality and safety of products.
Not only patient safety issues, there is a huge risk that a
growing herbal market and its great commercial benefit might
pose a threat to biodiversity through over-harvesting of the
raw materials for herbal medicines and other natural health
care products. If not controlled, these practices may lead to
the extinction of endangered species and the destruction of
natural habitats and resources. The WHO guidelines on good
agricultural and collection practices (GACP) for medicinal
plants are an important initial step to ensure good quality,
safe herbal medicines and ecologically sound cultivation
practices for future generations (WHO,2004). In an easy-to-
understand style they cover the spectrum of cultivation and
collection activities, including site selection, climate and
soil considerations and identification of seeds and plants.
Guidance is also given on the main post-harvest operations and
includes legal components such as national and regional laws
on quality standards, patent status and benefits sharing.
The safety and efficacy data are available for even fewer herbs,
their extracts and active ingredients and the preparation
containing them. Also in most African countries, the herbal
medicines market is poorly regulated and herbal products are
often neither registered nor controlled. So, the assurance of
safety, quality and efficacy of medicinal plants and plant
products has now become the key issue among the users in urban
areas and in other developed/ developing countries. For
ensuring the efficacy of traditional medicine, both the general
consumer and health care professionals need reliable, up to date
and authoritative information on the safety and efficacy of the
medicinal plant products.
Research and documentation are important for allowing reliable
information exchange between the sources and users of the
medicinal plants. Without well documented reliable information
on the safety, efficacy and phytochemical characteristics of
different constituent/products, it is difficult for users and
buyers to assess the utility or value of the raw materials and
extracts of African origin. Consequently, the level of use and
world trade in Indian and Chinese medicinal plants and extracts
are far more extensive than those of the African Region.
Although, in recent years there has been an upsurge in research
and development in African universities and research centres on
ethnobotany and medicinal products ( eg Table 1), only a few
plant products have been commercialized and still much of the
basic scientific information is not available (Newmann,2005;
AAMPS, 2010).

Also, much of valuable information on reproductive system,
seed/seedling survival and population dynamics are not available
for decision making in management, so is on the quantities of
traditional medicines being harvested or sold, whether for the
local use, trade or for export and the extraction of active
ingredients. For example, in South Africa, harvesting from wild
populations of certain species is on a scale that cause concern
amongst conservation organizations and rural herbalists, and a
listing of priority species is available (Cunningham, 2001).
Studies and research information which identify threatened
medicinal plants should
be circulated through the International Board for Plant Genetic
Resources (IBPGR) to regional gene banks and IUCN, also
information should be disseminated to rural communities on
appropriate conservation / cultivation methods for medicinal
plants which are in local demand. Very little goes unnoticed in
communally owned areas so that if problems arise regarding the
depletion of valued local resources, the traditional medicinal
groups / associations or community leaders are likely to be
effective for immediate action. Information relating to adverse
toxic properties in medicinal plants should also be circulated
particularly to practitioners/traders and in Primary healthcare
training (Akerele, 1987; Anyinam, 1987; Good, 1987).
Market related research and information sharing should also be
emphasized, a rapid development of alternative supply sources
through buffer stock/cultivation in large quantities and at a
low price to compete with prices obtained by gatherers of wild
stocks can reduce the pressure on wild resource base. This will
satisfy market demands, result in more secure jobs and provide
fewer incentives to gather from the wild. If this does not occur,
key species will disappear from the wild, thereby undermining the
local medicinal resource base. Also important are in information
on plant biology and reproduction, as many of the vulnerable
category of species, by their very nature, may not be grown
profitably due to their slow growth rates or especial habitat
requirements, especially as the land which is most likely to be
available for medicinal plant cultivation is likely to be less
productive.
Information and codes on effectiveness, precision and standards
are important too. In Ethiopia, Amare Getahun (1976), Sofowora
(1982), and Dawit Abebe (1986) discussed the lack of
precision and standardization as one drawback for the
recognition of the traditional health care system. One of
the constraints which are hindering proper development and use
of medicinal plants is the lack of suitable technical
specifications and quality control standards for African
medicinal plants and extracts. This makes it extremely difficult
for users and buyers whether local or overseas to compare batches
of products from different places or years. Lack of trading
standards also implies that Good Agricultural and Collecting
Practices (WHO, 2003) and Good Manufacturing Practices (WHO,
2007) are not adhered to. This is in marked contrast with
countries such as China and India where traditional formulations
have not only been recorded but are evaluated both at the local
and national level and used in their health centres.
Problems with medicinal plant use: Management for safe &
sustainable use
With the progress in modern science, concerns on the safety
and quality of raw plant materials and finished products from
medicinal plants became a major issue (WHO, 2001, 2007). The
quality of plant products not only depend on genetic or on
environment of the plant, but also on collection methods,
cultivation, harvest, post-harvest processing, transport and
storage practices. There remains a high probability of
contamination by microbial or chemical agents during any of
the production stages resulting in deterioration in safety and
quality. Most of the medicinal plants being collected from the
wild may be contaminated by other species or plant parts
through misidentification, accidental contamination or
intentional adulteration, all of which may have unsafe
consequences.
Also important are the interaction between medicinal plant use
and modern medicines among the urban and immigrant
populations. The Ethiopian immigrant population is more
diffuse in the USA and other developed countries and often

without access to traditional medicinal practitioners, often
use herbal remedies (Hodes, 1997). In many cases Ethiopian
patients in urban and foreign areas use traditional remedies
in combination with prescribed modern medications for related
or unrelated health conditions without informing their
physician (Fullas,2001). Ethiopian patients who use
traditional medicine and do not inform their health care
providers may do this for several reasons including cultural
differences ( Jackson,2008) . Many herbal substances that are
used in Ethiopian traditional medicine are also used as
ingredients and spices in Ethiopian food (Fullas, 2003; Zuberi
et al , 2014). Consumption of these herbs and spices as part
of a normal diet is not likely to cause adverse herb-drug
interactions as consumed in relatively small quantities but
when utilized for medicinal purposes there may be an
increased likelihood of adverse interactions with modern
medicines (Jackson, 2008).
Therefore, the management of traditional medicinal plant
resources is probably the most complex African resource
management issue facing conservation agencies, healthcare
professionals and resource users. As pressure is increasing on
diminishing medicinal plant supplies, constructive resource
management and conservation actions must be identified, based
upon a clear understanding of the surrounding medicinal plant
use. Among others, three central issues to be considered: (1)
What are the causes behind the depletion of wild populations of
medicinal plant species in Africa? (2) Which species are of
particular concern and should be given priority for positive
action? (3) What can be done to ensure the effective conservation
of all medicinal plant species? As medicinal plant resource
management problems exist not in these areas alone but also in
the processing, standardization, quality control, marketing and
consumption not only the rural areas but in densely populated and
rapidly urbanizing regions, efficient management and control
reaching a balance between human needs and medicinal plant
resources is most urgent.
Giving emphasis to the plant resources, identification of habitat
with a high density of endemic families, genera and species with
medicinal properties; management effort around core conservation
areas through interaction with resource users and provision of
alternatives to wild populations of threatened species are
important. For those which are nearly extinct or seriously
endangered, seed and gene banks should be maintained as
precaution and backup against extinction. It is important for the
gene bank to collect information on uses and efficacy of
medicinal plants than collect material for ex-situ conservation.
Where the local habitats of these medicinal plants are
threatened there is the need to be established in field gene
banks until technology is available for reestablishing the
indigenous habitat. But ultimate goal of the conservation process
is certainly to preserve the natural habitats of vulnerable
medicinal plant species and to achieve sustainable exploitation

in less vulnerable areas. So, permanent forest areas/ large plots
should be set up in selected sites to monitor the status of the
endangered species like Warburgia salutaris, Garcinia afzeliiand Okoubaka
aubrevillei in Africa. Also, collections for seed and gene banks
should be undertaken according to the principles of conservation
biology and population genetics, the sample size , population
size and distribution, genetic diversity and reproductive biology
should be kept in mind for future stability, medicinal property
and evolutionary changes. Also attention be given in order to
select for commercially beneficial properties such as growth
rate, adaptation to different habitats and highest levels of
active ingredients for pharmaceutical use. Moreover,
establishment of ex-situ populations of threatened and endangered
species in more than one locations, botanical gardens under the
existing framework of the IUCN Botanical Gardens Programme should
be considered. The
potential for the clonal production of medicinal plants with
desired qualities or known toxicities. Are good options. The
conservation of medicinal plants is by necessity a long term
project requiring the development of traditional medicinal
practitioner groups/associations, trained technical staff
supported by organizations/universities and a general public that
is aware of
the issues at stake. Improvement in national education standards
especially in the fields of natural resource management is a key
factor in the conservation issue which will come about only as a
result of economic development in the African nations.
The need in Africa for institution building, organizing the
stakeholder groups and better staffing and funding of traditional
medical institutions, herbaria, research and evaluation centers,
chemical analytical facilities, drug testing are well known
(Hedberg et al, 1982;1983). Along with medicinal plant
conservation, there should be expansion of cultivation of
medicinal plants especially those with high demand, the rural
communities, commercial growers, government decision-makers,
pharmaceutical companies should come forward.
Traditional medicinal practitioners in most cases are working in
isolation and neglect, though are very aware of the conservation
status and needs of the local medicinal plants can do very
little. It is true, they can be influential in changing local
opinion so as to limit over-exploitation and in conservation only
if they are organized and supported. It is recommended that
support is given to the formation of rural traditional medical
practitioners’ associations which might be easily possible
through local health services providing system of the country
with the support of the national governments and WHO.
Realizing the needs of institutions, as early as in 1979, the
Office for the Coordination of Traditional Medicine was
established in Ethiopia which arranged meetings, workshops and
conducted chemical assays and biomedical studies of some herbal
medicines and a total of 6,000 traditional practitioners were
registered and a monograph describing 260 medicinal plants was
prepared (Ministry of Health, 1984, GoE, 1993; Beshaw, 1991).
There were targets of the drug policy include conducting
coordinated research on traditional medicines and for development
into pharmaceutical drugs, general strategies for strengthening
the health sector through research and development, creating
favorable conditions for the development of safe and effective
drugs and involving private providers ( Ministry of Health,
1993; GoE, 1993). Laws and regulations on traditional medicine
were issued , the national drug program was formulated through
Drug Administration and Control Authority (DACA) but little
progress could be obtained till 2006 (Kebede Deribe Kassaye et
al, 2006).
Cultivation of medicinal plants: an alternative
As the demand on medicinal plants multiply with expansion of the
pharmaceutical industries, cultivation as an alternative to
overexploitation of scarce traditional medicinal plants was
suggested over 50 years ago in South Africa for scarce and
effective species such as Alepidea amatymbica and Warburgia salutaris.
But even just few years ago, no large scale cultivation had
taken place. There are two main reasons for this, and both apply
elsewhere in Africa:
(1) lack of institutional support for production and
dissemination of key species for cultivation;
(2) the low prices paid for traditional medicinal plants by
herbal medicine traders and urban herbalists.
At present, cultivation of medicinal plants is chiefly
restricted to temperate areas and with the exception of India
and Nepal, few tropical countries have investigated the potential
of cultivating medicinal plants on a commercial scale. As
commercial cultivation depends on many aspects especially the
price of the raw materials, cost of cultivation, market stability
and the price for favoured species , all determining whether
cultivation is a viable option, under uncontrolled market when
the supply exceeds demand, then price falls.
In spite of the above constraints, cultivation has replaced
wild collection for the supply of some essential drugs used in
modern medicine, eg. the Madagascar rosy periwinkle,
Catharanthus roseus, which is widely cultivated in Spain and the
United States for its properties in treating childhood
leukaemia and Hodgkin’s disease. Another traditional medicine
for which demand is greater than the potential for supply is
the African tree Pygeum (Prunus africana), bark being very
popular as natural remedy for prostate disorders in some
European countries. As it is harvested from wild trees growing
in the mountain forests of Africa and in Madagascar which is
unsustainable under current practices, so the International
Centre for Research in Agroforestry (ICRAF) and others are
working to establish sustainable sources of Prunus
africana through conservation of wild tree populations and
assistance to smallholders to grow the tree also helping
increasing farmers’ incomes. Another example, is Devil’s
Claw, Harpagophytum procumbens, a popular medicinal plant used
as a tonic, a treatment for arthritis and rheumatism, to
reduce fever, ease sore muscles, reduce cholesterol, and
externally the ointment is used to treat sores, boils, and
ulcers has been unsustainably harvested and may become extinct
in the wild under current practices. Now Devil’s Claw is
produced in southern Africa and Namibia providing local
people with a sustainable product at a guaranteed and fair
price.
Though ethnobotanical studies conducted in Ethiopia (Table 1)
indicated that most medicinal plant species used to treat human
ailment were wild, implies that the majority of plants of
medical importance were not yet identified and describe,
to be under cultivation will require important information about
their biology, reproduction and management. Although some of
these species are threatened in the wild (e.g. Garcinia afzelii and
Warburgia salutaris), low prices provided by the traders/exporters
fails to ensure that they can be profitably cultivated without
well coordinated, well supported and organized program.
An interesting model is provided in Thailand where a project for
cultivation of medicinal plant of known efficacy has been
initiated in about 1000 villages and traditional household
remedies, with improved formulae, are produced as compressed
tablets packed in foil and distributed to “drug co-operatives”
set up through a Drug and Medical Project Fund in more than 45
000 villages as well as in community hospitals ( Wondergem et al.
1989; WHO, 1977) have already drawn on the Thailand experience in
making recommendations regarding primary healthcare in Ghana.
WHO’s efforts toward sustainable medicinal plant use
The importance of medicinal plants in the health care systems in
many developing countries including those of Africa has been
underscored by various resolutions of the World Health Assembly
and WHO Regional Committees. The Resolution WHA41.19 of 1988 on
Traditional medicine and medicinal plants (WHA, 1988) urged
Member States to examine the situation with regard to their
indigenous medicinal plants and to take effective measures to
ensure their conservation and encourage their sustainable
utilization. That resolution requested WHO to promote inter-
country meetings for the dissemination of knowledge and the
exchange of experience on the subject; and to collaborate with
Member States in the design and implementation of programs for
the conservation and sustainable utilization of medicinal plants.
The resolution AFR/RC 50/ R5 of 1999 on Essential drugs in the
WHO African Region situation and trends analysis (WHO, 2000)
requested WHO to support the African member states to carrying
out research on medicinal plants and promoting their use in
health care systems; while resolution AFR/RC 5//R3 of 2000 was on
promoting the traditional medicine in health systems. A Strategy
for the African Region (WHO,2001) urged Member States to actively
promote, in collaboration with all other partners, the
conservation of medicinal plants and requested WHO to strengthen
WHO Collaborating Centres and other research institutions to
carry out research and develop monographs of medicinal plants and
disseminate results on safety and efficacy of traditional
medicines. Following these efforts, many countries including
Benin, Burkina Faso, Cameroon, Cote d’Ivoire, Ghana, Guinea,
Madagascar, Mali, Mauritius, Nigeria, Senegal, Seychelles and
South Africa have developed monographs of medicinal plants,
while Benin, Cameroon, Chad, Cote d’Ivoire have developed
inventories of medicinal plants and documented traditional
medical drugs. WHO also helped in developing monographs on some
commonly used medicinal plants (WHO, 1999-2000). Also some
countries like Ghana and Nigeria have published national herbal
pharmacopoeias, other countries have been conducting research on
traditional medicines used for the treatment of priority
diseases. The WHO has released guidelines for good agricultural
and collection practices for medicinal plants - an industry
estimated worth more than US$ 60 billion (WHO,2004). The
guidelines are intended for national governments to ensure
production of herbal medicines is of good quality, safe,
sustainable and poses no threat to either people or the
environment.
Following WHO’s initiatives (WHO,2005), the Ethiopian authorities
also undertook attempts to regularize this sector. Laws and
regulations on traditional medicine under the Drug Administration
and Control Proclamation No. 176/99 was introduced, national
drug program was adopted, one of the responsibilities of the Drug
Administration and Control Authority (DACA) which was to prepare
standards of safety, efficacy and quality of traditional
medicine, and evaluate laboratory and clinical studies and
giving license for the use of traditional medicine in the
official health services. But even in 2006, there was no
registered traditional practitioner and way of registration in
the Federal Ministry of Health but numerous herbal medicines
being sold on the streets with medical claims (Kebede Deribe
Kassayeet al, 2006). Also, no regulatory requirements exist for
the manufacturing or safety assessment of traditional medicines
and herbal medicines are not included in the essential medicines
list, there being neither a post market surveillance system, a
restriction on the sale of herbal medicines nor a guideline for
clinical trials using traditional medicines. By early 2006 DACA
had not yet carried out any activity on traditional medicines and
no traditional drug was registered and licensed although
guidelines are being prepared (Kebede Deribe Kassayeet al, 2006).
Conclusion
It is indicated from the above discussion that to sustain the
use of medicinal plants in Ethiopia but also in all other
developing countries like India, China and South Africa, it is
important to create a long term relationship and collaboration
among all the stakeholders of the traditional medicine system
and with the modern medicine system including the pharmaceutical
industry, aiming at the wellbeing of the common people. To do
this, it is required that the national governments and the
international organizations like the WHO should take very
concrete steps keeping all the actors of the traditional medicine
in the fore.
Fig 1. AFRICA POLITICAL MAP [http://www.worldatlas.com/]
Fig 2 Ethiopia showing natural areas [https://www.google.com.et/]
ReferencesAAMPS (Association of African Medicinal Plants Standards) available at: http://www.aamps.orgAbebe, D. 2001. The role of medicinal plants in healthcare coverage ofEthiopia, the possible benefits of integration. Pp. 6–21 in Conservation and Sustainable Use of Medicinal Plants in Ethiopia, Proceedings of the National Workshop, 28 April–01 May 1998. Edited by M. Zewdu. Demissie A. Institute of Biodiversity Conservation and Research, Addis Ababa, Ethiopia.
Abebe D and Ayehu A 1993. Medicinal plants and enigmatic health practices of Northern Ethiopia. Addis Ababa, Ethiopia: B S P E; 1993.
Abbink J. 1995. Medicinal and ritual plants of Ethiopia southwest: An account of recent research. Indigenous Knowledge and Development Monitor. 1995; 3(2): 6-8
Adjanohoun, E.J. ; Ahyi, A. M. R.; Ake Assi,L.; Dan Dickto, L.; Daounda, H.; Delams,M.; de Sousa, L.; Garba, M.; Guinko, S.;Kayonga, A.; N’Golo, D.; Raynal, J.L.;Saadou, M. 1980. Médecine traditionnelle et pharmacopée: contribution aux etudes ethnobotaniques et
floristiques au Niger.Paris, Agence de Cooperation Culturelleet Technique.
Adjanohoun, E.J.; Ake Assi, L.; Chibon, P.; deVecchy, H.; Duboze, E.; Eyme, J.; Gassita,J.-N.; Goudote, E.; Guinko, S.; Keita, A.;Koudogbo, B.; le Bras, M.; Mourambou,I.; Mve-Mengome, E.; Nguema, M-G.;Ollome, A.N.; Posso, P.; Sita, P. 1984.Contribution aux études ethnobotaniqueset floristiques au Gabon. Paris, Agence deCoopération Culturelle et Technique.
Ake Assi, L. 1988. Espèces rares et en voied’extinction de la flore dela Côted’Ivoire. Monogr. Syst. Bot. Missouri Bot.Gard., 25, 461 - 463.
Akerele, O. 1987. The best of both worlds:bringing traditional medicine up to date. Soc. Sci. Med., 24, 177 - 181.
Amare G (1976). Some Common Medicinal and Poisonous Plants Used in Ethiopia Folk Medicine. Addis Ababa University pp. 3-63.
Anyinam, C. 1987. Availability, accessibility, acceptability and adaptability: four attributes of African ethnomedicine. Soc.Sci. Med.,25, 803 - 811.Anonymous. 1987. Statement of Development Policies 1987 - 1996. Republic of Malawi.Zomba, Government Printer.Anteneh Belayneh, Zemede Asfaw, Sebsebe Demissew, and Negussie Bussa (2012) Medicinal plants potential and use by pastoral and agro-pastoral communities in Erer Valley of Babile Wereda, Eastern Ethiopia. Journal of Ethnobiology and Ethnomedicine,8:42
Awas Tesfaye, Sebsebe Demissew (2009). Ethnobotanical study of medicinal plants in Kafficho people, south-western Ethiopia. J. In: Proceedings of the 16th International Conference of Ethiopian Studies, ed. by SveinEge, Harald Aspen, BirhanuTeferra and ShiferawBekele, Trondheim Trondheim, NorwayBalcha Abera. 2014.Medicinal plants used in traditional medicine by Oromo people, Ghimbi District, Southwest Ethiopia. Journal of Ethnobiology and Ethnomedicine 2014, 10:40
Balemie, K., E. Kelbessa & Z. Asfaw. 2004. Indigenous medicinal plantutilization, management and threats in Fentalle area, Eastern Shewa, Ethiopia. Ethiopian Journal of Biological Sciences3:37–58Bannerman RH (1983). The Role of Traditional Medicine in Primary Health Care, Traditional Medicine and Health Care Coverage." World Health Organization, Geneva pp. 318-327.
Bekele, E. 2007. Study on Actual Situation of Medicinal Plants in Ethiopia. Prepared for Japan Association for International Collaboration of Agriculture and Forestry, Addis Ababa, Ethiopia.
Belayneh, A., Z. Asfaw, S. Demissew, & N. Bussa. 2012. Medicinal plants potential and use by pastoral and agropastoral communities inErer Valley of Babile Wereda, Eastern Ethiopia. Journal of Ethnobiology and Ethnomedicine8:42
Bekalo, T.H., S.D. Woodmatas & Z.A. Woldemariam. 2009. An ethnobotanical study of medicinal plants used by local people in the lowlands of Konta Special Woreda, southern nations, nationalities and peoples regional state, Ethiopia. Journal of Ethnobiology and Ethnomedicine5:26Beshaw M.1991. Promoting traditional medicine in Ethiopia: A brief historical overview of government Policy. Soc. Sci and Med, 33:193-200.
Cragg G, Newmann DJ (2005). Biodiversity: A continuing source of noveldrug leads. Pure and Appl. Chem., 77, 7-24.
Daly, Walter J.; Brater, D. Craig (2000). "Medieval contributions to the search for truth in clinical medicine". Perspectives in Biology and Medicine 43 (4): 530–540
Dawit A (1986). Traditional medicine in Ethiopia. The attempt being made to promote it for effective and better utilization.SINET: Ethiop.J. Sci. 9: 61-69.Dawit A. (2001). Plants as primary source of drugs in the traditional health care practices of Ethiopia. Plant genetic resourceof Ethiopia, 6,101 - 113.
Dawit Abebe and Ahadu Ayehu 1993. Medicinal plants and enigmatic health practices of northern Ethiopia, BSPE, Addis Ababa.
Edwards, S. 2001. The ecology and conservation status of medicinal plants on Ethiopia. What do we know? pp. 46-55, In: medhin Zewdu and Abebe Demissie (eds.) Conservation and Sustainable use of medicinal plants in Ethiopia,
Proceedings of National Workshop on Biodiversity Conservation and Sustainable use of medicinal plants in Ethiopia, Instsitute of Biodiversity Conservation and Research, Addis Ababa.Fisseha Mesfin, Talemos Seta, and Abreham Assefa. 2014. An Ethnobotanical Study of Medicinal Plants in Amaro Woreda, Ethiopia. Ethnobotany Research &Applications 12:341-354.
Fullas, F. (2003). Spice plants in Ethiopia: their culinary and medicinal applications. Iowa, USA: Library Congress Cataloging.
Gelahun Abate (1989).Etse Debdabe (Ethiopian Traditional Medicine ).Sebsebe Demissew (ed.),Research and Publications Office, Addis AbabaUniversity.(In amharic)
Giday, M. 2001. An Ethnobotanical Study on Medicinal Plants used by the Zay People in Ethiopia. M.S. Thesis, Centrum för Biologisk Mångfald, Uppsala, Sweden
Giday M, Asfaw Z, Elmqvist T, Woldu Z (2003). An ethnobotanical study of medicinal plants used by the Zay people in Ethiopia. J. Ethnopharmacol., 85(1): p 43-52.
Gidey, Y. (2010). Assessment of indigenous knowledge of medicinal plants in Central zone ofTigray, Northern Ethiopia. African Journal of Plant scinces. 4, 006-011.
Giday M, Asfaw, Z.Woldu Z (2009). Medicinal Plants of the Meinit Ethnic Group of Ethiopia: An Ethnobotanical Study. J. Ethnophamacol., 124(3): 513-521
GoE . 1993. The Transitional Government of Ethiopia Office of the Council of Ministers. Report of the National Health Policy Task Force,Social and Administration Affairs. Addis Ababa, Ethiopia. February 1993.
Good, C. M. 1987. Ethnomedical systems in Africa: patterns of traditional medicine in rural and urban Kenya. Kenya. The Guildford Press.
Haile Y (2005). A study of the Ethno botany of medicinal plants and floristic composition of the dry Afromontane Forest at
Bale Mountains National Park. MSc Thesis. Department of Biology,Addis Ababa University.
Hedberg, I.; Hedberg, O.; Madati, P.J.;Mshigeni, K.E.; Mshiu, E.N.; Samuelson,G. 1982. Inventory of plants used in traditional medicine inTanzania. 1. Plants of the families Acanthaceae -Cucurbitaceae. J. Ethnopharmacology, 6,29 - 60.
Hedberg, I., Hedberg, O.; Madati, P.J.;Mshigeni, K.E.; Mshiu, E.N.; Samuelson,G.. 1983a. Inventory of plants used in traditional medicine in Tanzania. 2. Plants of the families Dilleniaceae - Opiliaceae.J. Ethnopharmacology, 9, 105 - 128.
Haile Yineger and Delenasaw Yewhalaw (2007). Traditional medicinal plant knowledge and use by local healers in Sekoru District, Jimma Zone, southwest. Ethiop. J.Ethnobiol. and Ethnomed. 3 (24)
Hostettmann K, Marston A, Ndjoko K, Wolfender J-L. The Potential of African Medicinal Plants as a Source of Drugs. Current Organic Chemistry. 2000; 4:973–1010.
Hunde, D., Z. Asfaw & E. Kelbessa. 2006. Use of traditional medicinal plants by people of ‘Boosat’ sub district, Central Eastern Ethiopia. Ethiopian Journal of Health Sciences16(2):141–155Hodes, R. (1997). Cross-cultural medicine and diverse health beliefs Ethiopians abroad. Western Journal of Medicine, 166, 29-36.
Jackson, J.C. (2008) Personal interview with Medical Director of International Medicine Clinic (HMC) on topic of Ethiopian traditional medicine use in immigrant patients (Haborview Medical Center, Seattle,WA).
Kalayu Mesfin,Gebru Tekle, Teklemichael Tesfay. 2013. Ethnobotanical Study of Traditional Medicinal Plants Used by Indigenous People of Gemad District, Northern Ethiopia. Journal of Medicinal Plants Studies.1( 4), 32-37.
Kebu,B., K.Ensermu and A. Zemede, 2004.Indigenous medicinal utilization , management and threats in Fen tale area, Eastern Shewa, Ethiopia. Ethi. J. Biol.Sci.,3: 1-7.
Mesfin, Fisseha; Seta, Talemos; Assefa, Abreham 2014. An Ethnobotanical Study of Medicinal Plants in Amaro Woreda, Ethiopia. Ethnobotany Research & Applications 12: 341-354.
Mohammed Adefa and Berhanu Abraha 2011. Ethnobotanical Survey of Traditional Medicinal
Plants in Tehuledere District, South Wollo, Ethiopia Journal of Medicinal Plants Research. 5(26),6233-6242.
Ketema Tolossa, Etana Debela, Spiridoula Athanasiadou, Adugna Tolera,Gebeyehu Ganga, and Jos GM Houdijk, 2013. Ethno-Medicinal Study OfPlants Used For Treatment Of Human And Livestock Ailments ByTraditional Healers In South Omo, Southern Ethiopia. Journal ofEthnobiology and Ethnomedicine ; DOI: 10.1186/1746-4269-9-32
Kebede Deribe Kassaye, Alemayehu Amberbir, Binyam Getachew, Yunis Mussema.2006. Historical overview of traditional medicine practices and policy in Ethiopia Ethiop.J.Health Dev. 20(2). 127-134.
Last, M.and Chavunduka, G.L. 1986. The Professionalization of AfricanMedicine. Manchester, Manchester University Press.
Lulekal, E., E. Kelbessa, T. Bekele & H. Yineger. 2008. An ethnobotanical study of medicinal plants in Mana Angetu District, southeastern Ethiopia. Journal of Ethnobiology and Ethnomedicine4:10.
Mesfin, F., S. Demissew & T. Teklehaymanot. 2009. An ethnobotanical study of medicinal plants in Wonago Woreda, SNNPR, Ethiopia. Journal of Ethnobiology and Ethnomedicine5:28 1–18
Ministry of Health. 1984. History of Ethiopian Health Service. Addis Ababa, Ethiopia. January 1984
Mohammed Adefa Seid and Seyoum Getaneh Aydagnehum. 2013. Medicinal Plants Biodiversity and Local Healthcare Management System in Chencha District; Gamo Gofa, Ethiopia. Journal of Pharmacognosy and Phytochemistry. 2( 1 ).284-293.
Nasir Tajure Wabe, Mohammed Adem Mohammed and Nandikola Jaya Raju. 2011. Ethnobotanical survey of medicinal plants in the Southeast Ethiopia used in traditional medicine. Spatula DD.1(3): 153-158.
Pankhurst, R. (2001). The status and availability of oral and written knowledge on traditional healthcare. In: Conservation and Sustainable
Use of Medicinal Plants in Ethiopia Proceeding of The National Workshop on Biodiversity Conservation and Sustainable Use of MedicinalPlants in Ethiopia, 28 April-01 May 1998, pp.92-106 (Medhin Zewdu and Abebe Demissie eds.). IBCR, AA.
Regassa, R. 2013. Assessment of indigenous knowledge of medicinal plant practice and mode of service delivery in Hawassa city, southern Ethiopia. Journal of Medicinal Plants Research7(9):517–535.
Rokos L. 1969. Eye complications in poisoning caused by "Kosso" (Hagenia abyssinica). Ethiop Med J.7:11.
Rukangira (2004) Overview on Medicinal Plants and Traditional Medicinein Africa.
Sebsebe, D., Ermias. D. (2001). Basic and Applied Research in Medicinal Plants. In: Conservation and Sustainable Use of Medicinal Plants in Ethiopia Proceeding of The National Workshop on BiodiversityConservation and Sustainable Use of Medicinal Plants in Ethiopia, 28 April-01 May 1998, pp.29-33. (Medhin Zewdu and Abebe Demissie eds.). IBCR, AA.
Sofowora A (1982). Medicinal plants and traditional medicine in Africa. John Wiley, Chichester pp. 179.
Teklehaymanot, T. & M. Giday. 2007. Ethnobotanical study of medicinal plants used by people in Zegie Peninsula, Northwestern Ethiopia. Journal of Ethnobiology and Ethnomedicine 3:12
UNEP (United Nations Environment Program). 1995. Global Biodiversity Assessment. United Nations Environment Program, Nairobi, Kenya.van Wyk, B-E (2008). A broad review of commercially important southernAfrican medicinal plants. J. Ethnopharmacol., 119, 342-355.
Vivero, J.L. Ensermu Kelbessa and Sebsebe Demessew 2003. The red list of endemic trees and shrubs of Ethiopia and Eritrea. IUCN.Wabe NT, Mohammed MA, Raju NJ. An ethnobotanical survey of medicinal plants in the Southeast Ethiopia used in traditional medicine. SpatulaDD. 2011; 1(3): 153-158.
WHA (World Health assembly) 1988. Resolution WHA41.19 on Traditional medicine and medicinal plants. The Forty-First World Health Assembly, Geneva, 2-13 May 1988.
WHO (World Health Organization) (2000) Essential Drugs in the WHO African Region: Situation and Trend Analysis. Final Report of the WHO Regional Committee for Africa, Windhoek, Namibia, 1999. (Document reference, AFR/RC49/R5).WHO(World Health Organization). 2001 Resolution Promoting the Role of Traditional Medicine in Health Systems: A Strategy for African Countries. World Health Organization. Regional Office for Africa, (Document reference AFR/RC50/R3).World Health Organization (WHO) (2001). Legal Status of Traditional Medicine and Complementary/ Alternative Medicine: A Worldwide Review. WHO, Geneva.WHO (World Health Organization).1999/2002. WHO Monographs on selected medicinal plants. Volume 1&2. World Health Organization, Geneva.WHO Traditional Medicine Strategy". WHO. 2002. p. 1WHO (World Health Organization) 2003. Guidelines on good agricultural and collection practices (GACP) for Medicinal Plants. WHO, Geneva (Document reference, WHO/EDM/ TRM/2003).WHO,2004. The WHO guidelines on good agricultural and collection practices (GACP) for medicinal plants Medicinal plants – guidelines to promote patient safety and plant conservation for a US$ 60 billion industry. [http://www.who.int/mediacentre/news/notes/2004/np3/en/]
World Health Organization (2003). Guidelines on good agricultural and collection practices (GACP) for Medicinal Plants. WHO, Geneva (Document reference, WHO/EDM/ TRM/2003).World Health Organization (2007). WHO Guidelines on Good ManufacturingPractices (GMP) for herbal medicines http:// apps.who.int/medicinedocs/documents/s14215e/s14215e.pdf (accessed 30/8/10) ISBN 9789241547161.WHO(World Health Organization. 2007. WHO Guidelines on Good Manufacturing Practices (GMP) for herbal medicines http:// apps.who.int/medicinedocs/documents/s14215e/s14215e.pdf (accessed 30/8/10) ISBN 9789241547161.WHO.2005. National Policy on Traditional Medicine and regulation of Herbal medicines, Report of a WHO Global Survey, Geneva, Switzerland May 2005WHO.2001. Legal Status of Traditional Medicine and Complementary/Alternative Medicine: A World Wide Review. Geneva 2001. WHO.2003 Fact Sheet, Traditional Medicine, Geneva, May 2003.
Wondimu,T., Asfaw, Z. and Kelbessa, E. 2007. Ethnobotanical study of medicinal plants around Dheeraa town, Arsi Zone, Ethiopia. Journal of Ethno-Pharmacology. 112: 152-161
Wondergem, P.; Senah, K.A.; Glover, E.K.1989. Herbal Drugs in Primary Healthcare. Ghana: An Assessment of the Relevance of Herbal Drugs in PHC and Some Suggestions for Strengthening PHC.Amsterdam, Royal Tropical Institute.
Wondimu T, Asfaw Z, Kelbessa E (2007). Ethnobotanical study of medicinal plants around 'Dheeraa' town, Arsi zone, Eth. J. Ethnopharmacol., 112(1): 152-161
Yineger, H. & D. Yewhalaw. 2007. Traditional medicinal plant knowledge and use by local healers in Sekoru District, Jimma Zone, Southwestern Ethiopia. Journal of Ethnobiology and Ethnomedicine 3:24
Yineger, H., D. Yewhalaw & D. Teketay. 2008. Ethnomedicinal plant knowledge and practice of the Oromo ethnic group in southwestern Ethiopia. Journal of Ethnobiology and Ethnomedicine 4:11
Yirga Gidey (2010). Ethnobotanical Study of Medicinal Plants inand Around Alamata, Southern Tigray, Northern Ethiopia. Current Res. J. Biol. Sci., 2(5): 338-344
Zerabruk, S. & G. Yirga. 2012. Traditional knowledge of medicinal plants in Gindeberet district, Western Ethiopia. South African Journalof Botany78:165–169.
M.I. Zuberi, Birhanu Kebede, Teklu Gosaye & Olika Belachew. 2014. Species of herbal spices grown in the poor farmers’ home gardens of West Shoa, Highlands of Ethiopia: an Ethnobotanical account. Journal of Biodiversity and Environmental Sciences (JBES). 4(4), 164-185
Top Related
Copyright © 2022 FDOKUMEN

