Medicinal Chemistry of Antifungal drugs
34
Medicinal Chemistry of Antifungal drugs By: Dr. Rasha Saad Department of Pharmaceutical Chemistry at MSU
Transcript of Medicinal Chemistry of Antifungal drugs

Medicinal Chemistry of Antifungal drugs
By:
Dr. Rasha Saad
Department of Pharmaceutical Chemistry at MSU

Types of fungal infections
1. Superficial : Affect skin – mucous membrane.
• Tinea versicolor, Dermatophytes : Fungi that affect keratin layer of skin, hair, nail.e.g.tinea pedis ,ring worm infection
• Candidiasis : Yeast-like, oral thrush, vulvo-vaginitis , nail infections.
Affect internal organs as : lung ,heart , brain leading to pneumonia , endocarditis , meningitis.
2. Deep infections
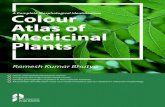
• Fungal infections classification:
– Superficial infections: Ringworm (tinea) → skin and mucous membrane. Incidence rate is high.
– Systemic infections: Candida albicans →
opportunist infections. Fatality rate is high.
Superficial infections
Systemic infections

• Antifungal agents classification:
– Antibiotics: ---Amphotericin B;
– Azole: ----------Ketoconazole;
– Allylamine: ---Terbinafine;
– Pyrimidine: ---Flucytosine. Superficial infections
Systemic infections

The discovery that some infectious diseases could be attributed to fungi actually preceded the pioneering work of Pasteur and Koch in the early of nineteens with pathogenic bacteria by several years. Gruby isolated the fungus responsible for favus on potato slices, rubbed it on the head of a child, and produced the disease. Hence, he fulfilled Koch’s postulates 40 years before they were formulated. In spite of its earlier beginnings, medical mycology was quickly overshadowed by bacteriology, and it has only recently begun to receive the serious attention that it deserves. This is perhaps attributable to the relatively benign nature of the common mycoses, the rarity of the most serious ones, and the need for a morphological basis for differential identification of these structurally complex forms.
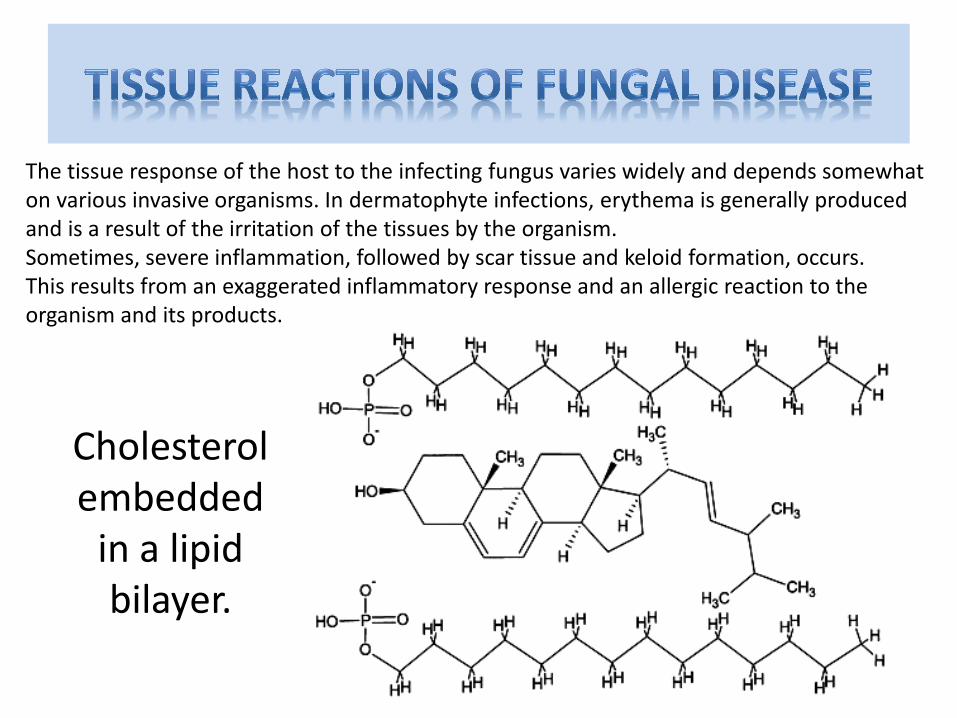
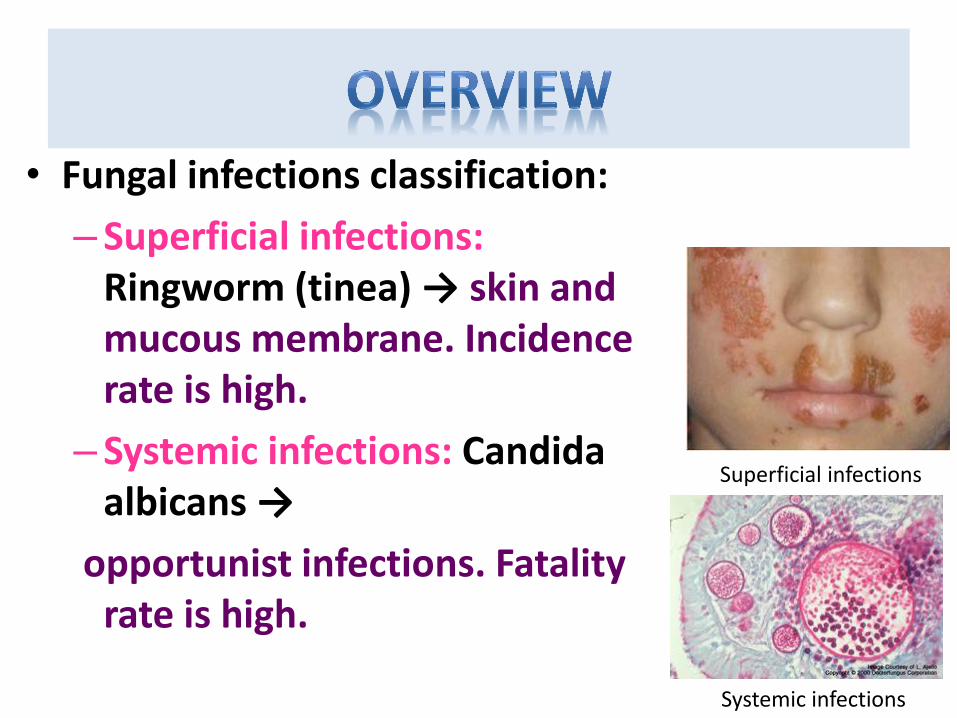
The tissue response of the host to the infecting fungus varies widely and depends somewhat on various invasive organisms. In dermatophyte infections, erythema is generally produced and is a result of the irritation of the tissues by the organism. Sometimes, severe inflammation, followed by scar tissue and keloid formation, occurs. This results from an exaggerated inflammatory response and an allergic reaction to the organism and its products.
Cholesterol embedded
in a lipid bilayer.

Squalen
Squalen epoksidase
O
Squalen epoksid-syklase
HO
Lanosterol
Lanosterol14a-demetylase
Antimycotic azoles
HO
Ergosterol
HO
H
H
HO
Kolesterol
H
H
H
Antimycotic allylic amines
Component of
fungus cell walls

With organisms that invade living tissue, such as those responsible for subcutaneous and systemic disease, there is generally a uniform acute pyogenic reaction that gives way to various chronic disease outcomes. Grnuloma with caseation and fibrocaseous pulmonary granuloma are potential outcomes of infection with Histoplasma capsulatum, and thrombotic arteritis, a thrombosis characterized by a purulent coagulative necrosis and invasion of blood vessels, may be caused during aspergillosis and mucormycosis. The large numbers of fungal species of many morphotypes, their disease etiology, and the diversity of outcomes make medical mycology a complex field.
Ergosterol embedded in a lipid bilayer.
Classification of Antifungal Drugs
• 1- Antifungal Antibiotics :
• Griseofulvin
• Polyene macrolide : Amphotericin- B & Nystatin
• 2- Synthetic :
• Azoles :
– A) Imidazoles : Ketoconazole , Miconazole
– B) Triazoles : Fluconazole , Itraconazole
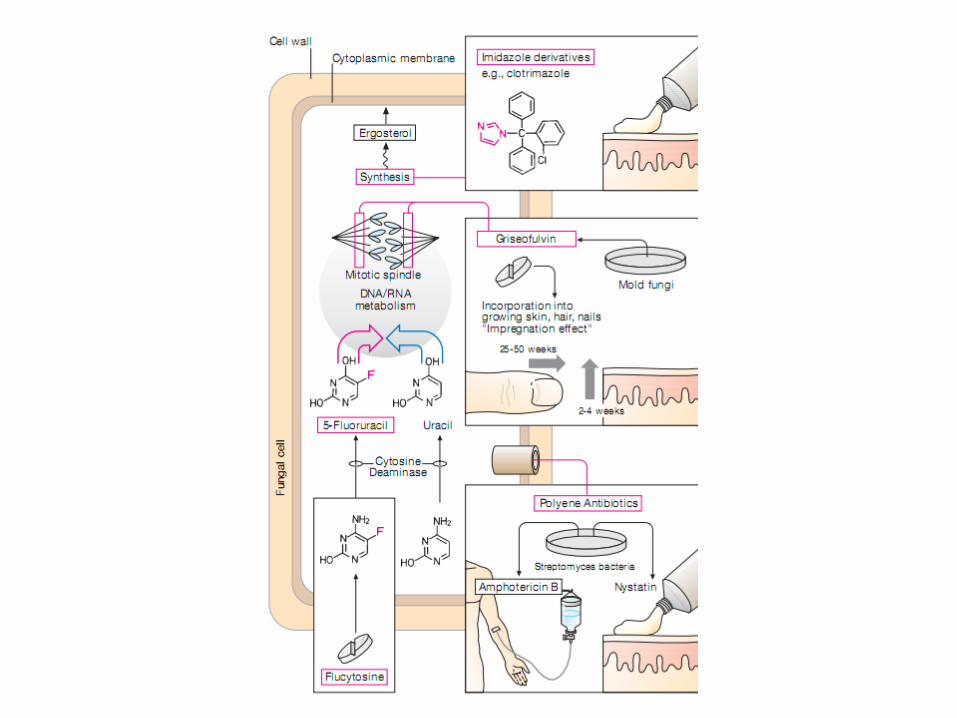
• Polyene antibiotic • The polyene antibiotics bind with sterols in the fungal cell membrane,
principally ergosterol. This causes the cell's contents to leak out and the cell dies. Animal cells contain cholesterol instead of ergosterol and so they are much less susceptible.
– Nystatin
– Amphotericin B (may be administered liposomally) – Natamycin
– Rimocidin
– Filipin
– Pimaricin
– The antifungal agents that are used are listed in this particular slide. Amphotericin B and Liposomal Amphotericin B will be discussed as well as the azoles that are listed on this slide. Nystatin is also used primarily as a topical agent for different uses. Finally Flucytosine is used adjunctively in addition to some other agents for systemic fungal infection.
I. Antifungals damaging permeability
of the cell membrane
•Imidazoles: Bifonazole, Clotrimazole, Econazole,
Ketoconazole, Miconazole
•Triazoles: Fluconazole, Itraconazole, Voriconazole
•Allylamines: Terbinafine, Naftifine
•Morpholines: Amorolfine
•Thiocarbamates: Tolciclate, Tolnaftate
•Substituted pyridones: Ciclopirox
•Polyene antibiotics: Amphotericin B, Nystatin
II. Antifungals inhibiting chitin synthesis in the cell wall
•Caspofungin, Griseofulvin
III. Antifungals inhibiting synthesis of nucleic acids
•Flucytosine
1. Polyene antibiotics
Amphotericin B and Nystatin bind to the fungal
cell membrane component ergosterol, leading to
increased fungal cell membrane permeability and
the loss of intracellular constituents. Amphotericin has
a lesser affinity for the mammalian cell membrane
component cholesterol, but this interaction does
account for most adverse toxic effects.
Amphotericin B has activity against Candida spp.,
Cryptococcus neoformans, Blastomyces dermatitidis,
Histoplasma capsulatum, Sporothrix schenckii,
Coccidioides immitis, Paracoccidioides braziliensis,
Aspergillus spp., Penicillium marneffei, etc.
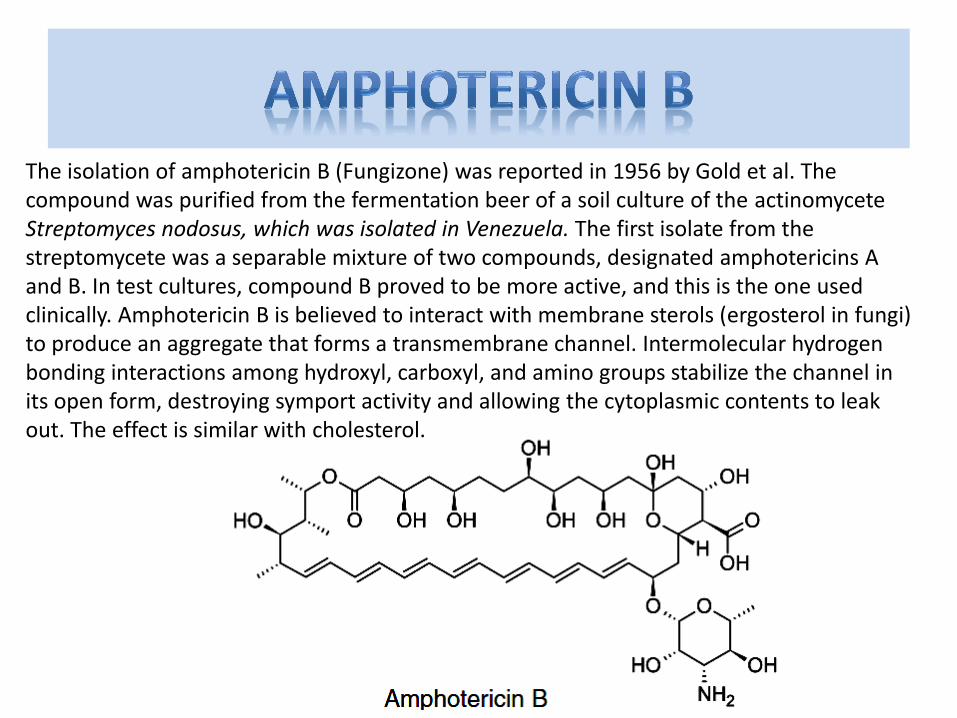
The isolation of amphotericin B (Fungizone) was reported in 1956 by Gold et al. The compound was purified from the fermentation beer of a soil culture of the actinomycete Streptomyces nodosus, which was isolated in Venezuela. The first isolate from the streptomycete was a separable mixture of two compounds, designated amphotericins A and B. In test cultures, compound B proved to be more active, and this is the one used clinically. Amphotericin B is believed to interact with membrane sterols (ergosterol in fungi) to produce an aggregate that forms a transmembrane channel. Intermolecular hydrogen bonding interactions among hydroxyl, carboxyl, and amino groups stabilize the channel in its open form, destroying symport activity and allowing the cytoplasmic contents to leak out. The effect is similar with cholesterol.

Amphotericin B
• Amphotericin A & B are antifungal antibiotics.
• Amphotericin A is not used clinically.
• It is a natural polyene macrolide
• (polyene = many double bonds )
• (macrolide = containing a large lactone ring )

Resistance to amphotericin B
• Resistance occurred when ergosterol binding is impaired either by :
– Decreasing the membrane concentration of ergosterol.
– Or by modyfing the sterol target molecule.
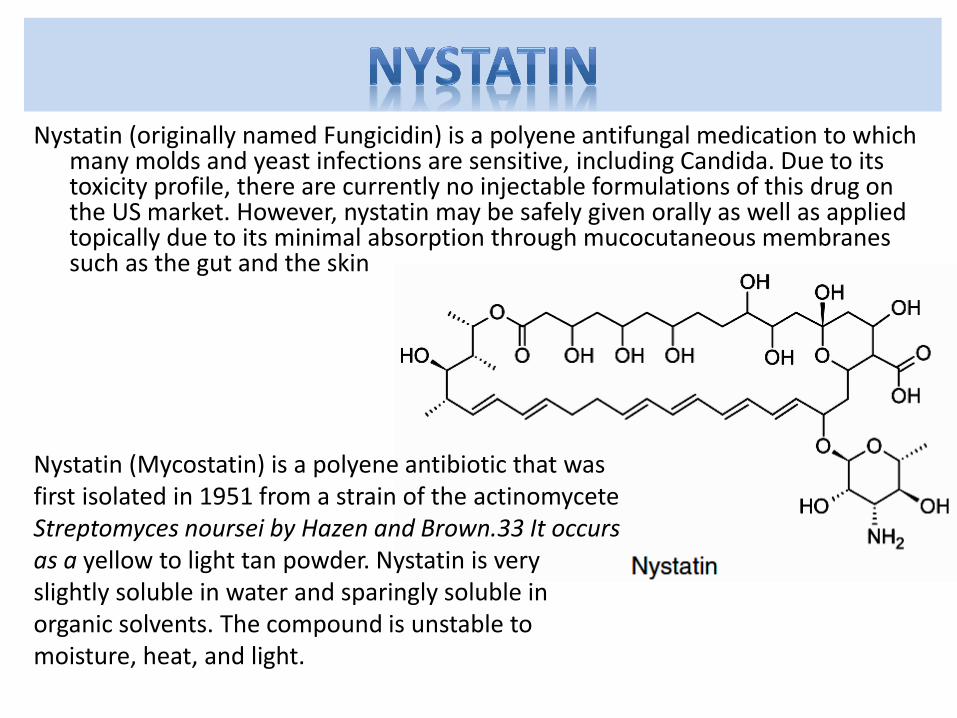
Nystatin (originally named Fungicidin) is a polyene antifungal medication to which many molds and yeast infections are sensitive, including Candida. Due to its toxicity profile, there are currently no injectable formulations of this drug on the US market. However, nystatin may be safely given orally as well as applied topically due to its minimal absorption through mucocutaneous membranes such as the gut and the skin
Nystatin (Mycostatin) is a polyene antibiotic that was first isolated in 1951 from a strain of the actinomycete Streptomyces noursei by Hazen and Brown.33 It occurs as a yellow to light tan powder. Nystatin is very slightly soluble in water and sparingly soluble in organic solvents. The compound is unstable to moisture, heat, and light.
Nystatin
• It is a polyene macrolide ,similar in structure &
mechanism to amphotericin B.
• Too toxic for systemic use.
• Used only topically.
• It is available as creams, ointment , suppositories & other preparations.
• Not significantly absorbed from skin, mucous membrane, GIT .
Clinical uses
• Prevent or treat superficial candidiasis of mouth, esophagus, intestinal tract.
• Vaginal candidiasis
• Can be used in combination with antibacterial agents & corticosteroids.
• Allylamines
• Allylamines inhibit the enzyme squalene epoxidase, another enzyme required for ergosterol synthesis:
• Terbinafine - marketed as Lamisil
• Amorolfine
• Naftifine
• Butenafine
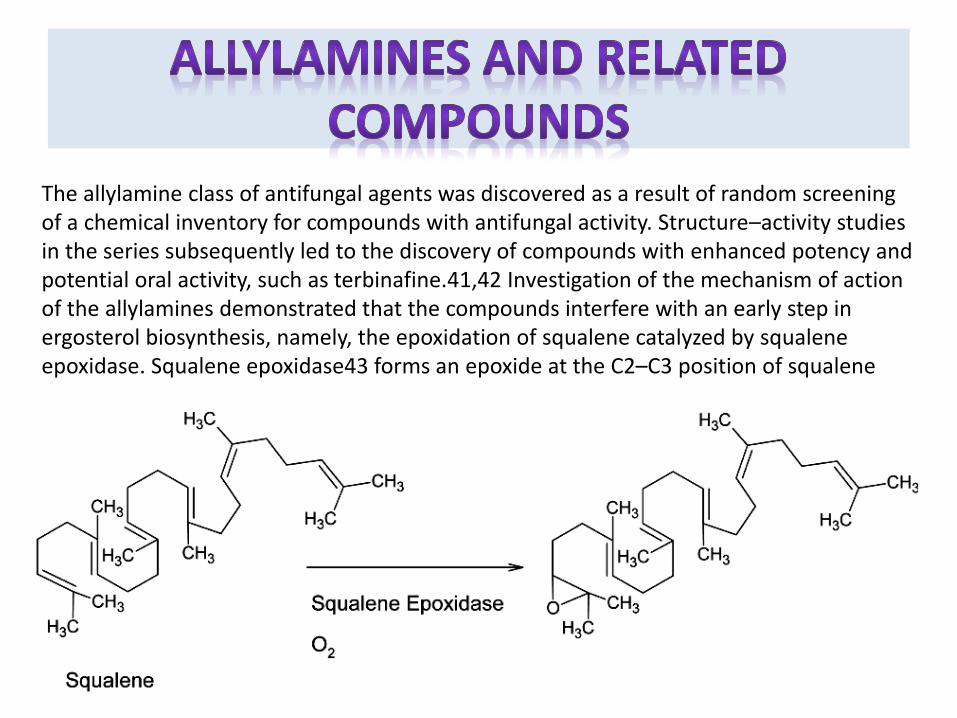
The allylamine class of antifungal agents was discovered as a result of random screening of a chemical inventory for compounds with antifungal activity. Structure–activity studies in the series subsequently led to the discovery of compounds with enhanced potency and potential oral activity, such as terbinafine.41,42 Investigation of the mechanism of action of the allylamines demonstrated that the compounds interfere with an early step in ergosterol biosynthesis, namely, the epoxidation of squalene catalyzed by squalene epoxidase. Squalene epoxidase43 forms an epoxide at the C2–C3 position of squalene
2. Allylamines – reversible noncompetitive
inhibitors of the fungal enzyme squalene
monooxygenase, which converts squalene to lanosterol.
With a decrease in lanosterol production, ergosterol
production is also diminished, affecting fungal cell
membrane synthesis and function. These agents
exhibit fungicidal activity against dermatophytes
and fungistatic activity against yeasts.
Naftifine is available for topical use only in the treat-
ment of cutaneous dermatophyte and Candida infections.
Terbinafine (Lamisil®) is available for
topical and systemic use (oral tablet) in
the treatment of dermatophyte skin and
nail infections.
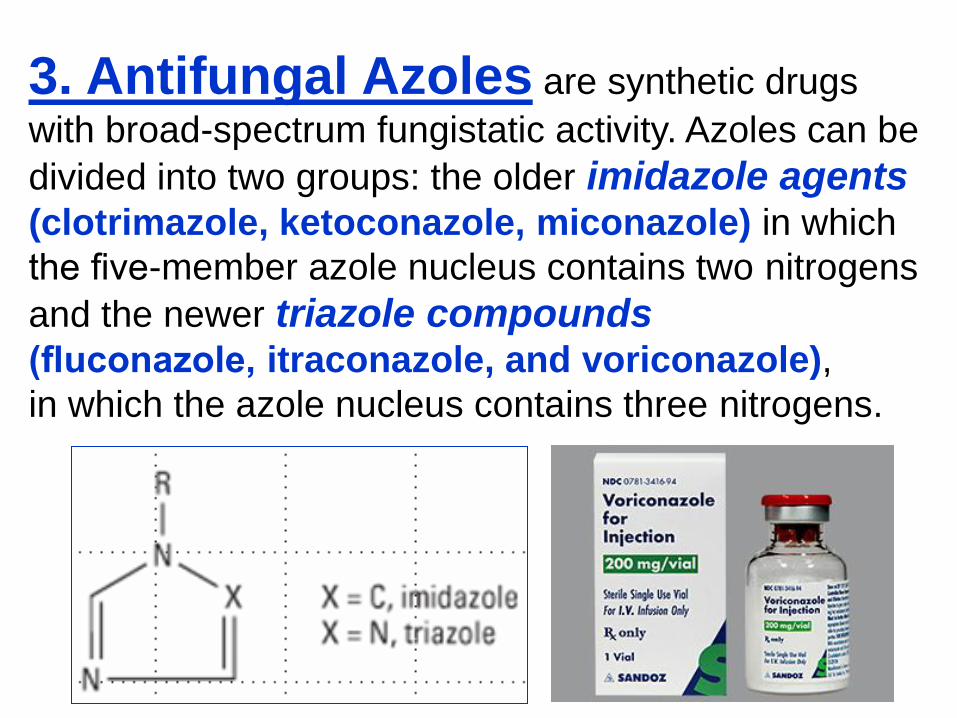
3. Antifungal Azoles are synthetic drugs
with broad-spectrum fungistatic activity. Azoles can be
divided into two groups: the older imidazole agents
(clotrimazole, ketoconazole, miconazole) in which
the five-member azole nucleus contains two nitrogens
and the newer triazole compounds
(fluconazole, itraconazole, and voriconazole),
in which the azole nucleus contains three nitrogens.

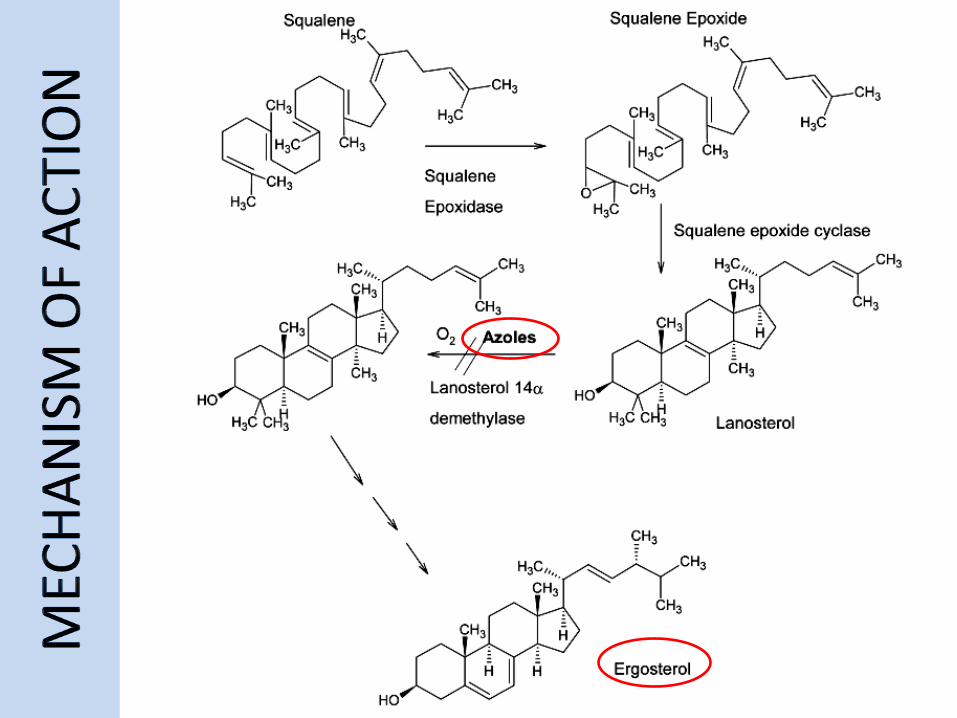
All azoles exert antifungal activity by inhibiting
cytochrome P450 enzymes responsible for the
demethylation of lanosterol to ergosterol.
Reduced fungal membrane ergosterol concen-
trations result in damaged, leaky cell membranes.
The toxicity of these drugs depends on
their relative affinities for mammalian and fungal
cytochrome P450 enzymes.
The triazoles tend to have fewer side effects,
better absorption, better drug distribution in
body tissues, and fewer drug interactions.

Fluconazole does not require an acidic
environment, as does ketoconazole, for GI absorption.
About 80 to 90% of an orally administered
dose is absorbed, yielding high serum drug levels. The
t1/2 of the drug is 27 to 37 h, permitting once-daily
dosing in patients with normal renal function. Only 11%
of the circulating drug is bound to plasma proteins.
The drug penetrates widely into most body tissues.
Cerebrospinal fluid levels are 60 to 80% of serum levels,
permitting effective treatment for fungal meningitis.
About 80% of the drug is excreted unchanged in the
urine. Dosage reductions are required in the presence
of renal insufficiency.
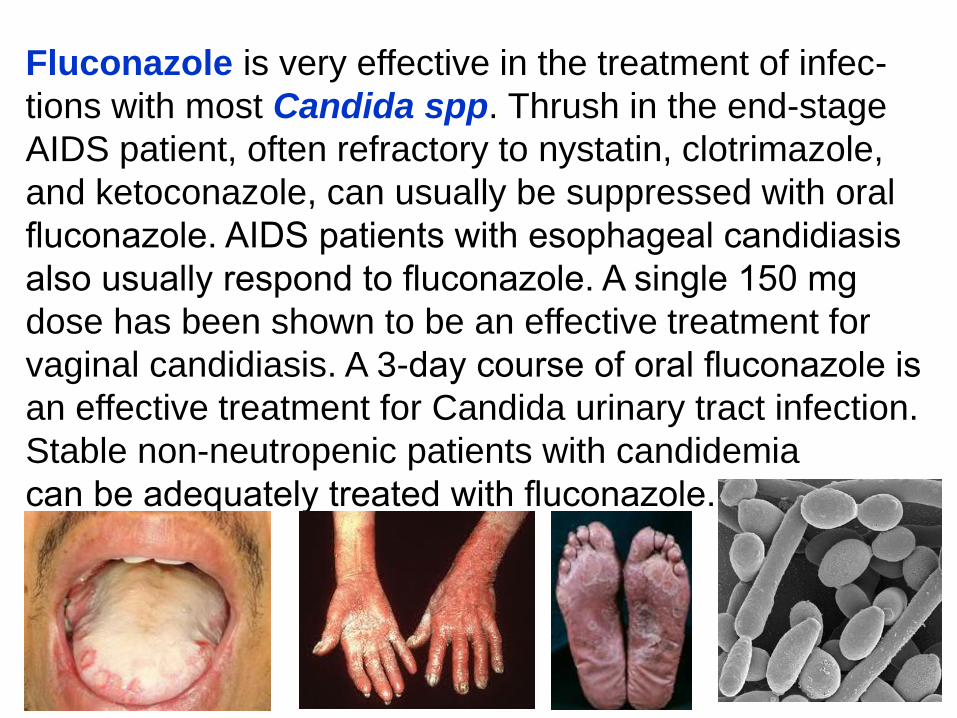
Fluconazole is very effective in the treatment of infec-
tions with most Candida spp. Thrush in the end-stage
AIDS patient, often refractory to nystatin, clotrimazole,
and ketoconazole, can usually be suppressed with oral
fluconazole. AIDS patients with esophageal candidiasis
also usually respond to fluconazole. A single 150 mg
dose has been shown to be an effective treatment for
vaginal candidiasis. A 3-day course of oral fluconazole is
an effective treatment for Candida urinary tract infection.
Stable non-neutropenic patients with candidemia
can be adequately treated with fluconazole.

4. Fluorinated pyrimidines Flucytosine (5-flucytosine, 5-FC)
is an analogue of cytosine that was originally
synthesized for possible use as an antineoplastic
agent. 5-FC is converted to 5-fluorouracil inside the cell
by the fungal enzyme cytosine deaminase. The active
metabolite 5-fluorouracil interferes with fungal DNA
synthesis by inhibiting thymidylate synthetase.
Incorporation of these metabolites into fungal RNA
inhibits protein synthesis.
Flucytosine has a significant antifungal activity against
Candida spp. and the fungal organisms responsible
for chromomycosis.

5. Echinocandins
Caspofungin is a semisynthetic lipopeptide. It
inhibits the synthesis of beta-D-glucan, a cell wall
component of filamentous fungi. Caspofungin is
approved for the treatment of invasive aspergillosis
in patients not responding to
amphotericin B, and itraconazole.
Adverse effects are mediated through histamine
release: facial flushing, rash, fever, and pruritus.
Dose reductions are required in the presence of
moderate hepatic insufficiency.

6. Pyridones Ciclopirox olamine is a pyridone derivative
for the treatment of cutaneous dermatophyte
infections, cutaneous C. albicans infections,
and tinea versicolor caused by Malassezia furfur.
It interferes with fungal growth by inhibiting
macromolecule synthesis.
7. Thiocarbamates Tolnaftate is an antifungal agent effective
in the topical treatment of dermatophyte
infections and tinea.
8. Nonpolyene antibiotics Griseofulvin is an oral fungistatic agent used
in the long-term treatment of dermatophyte infections
caused by Epidermophyton, Microsporum, and
Trichophyton spp. Produced by Penicillium
griseofulvin, it inhibits fungal growth by binding to the
microtubules responsible for mitotic spindle formation.
The drug binds to keratin precursor cells
and newly synthesized keratin in the stratum corneum
of the skin, hair, and nails, stopping the progression of
dermatophyte infection. In the treatment of ringworm
of the beard, scalp, and other skin surfaces, 4 to 6
weeks of therapy is often required.