
Medicinal Chemistry - CCS University
150
Medicinal Chemistry Dr Moira Bode and Dr Amanda Rousseau Dr Moira Bode and Dr Amanda Rousseau C403 and C503 An introduction to drug design and development, and understanding how drugs work
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Medicinal Chemistry - CCS University
Medicinal Chemistry
Dr Moira Bode and Dr Amanda RousseauDr Moira Bode and Dr Amanda Rousseau
C403 and C503
An introduction to drug design and development, and
understanding how drugs work

• 14 Lectures
− Introduction
− Antiviral agents
− Antibacterial agents
− Cancer and chemotherapy
− Malaria
• Useful textbook: “An Introduction to Medicinal Chemistry”
Graham L Patrick
Course Overview
Graham L Patrick
• Afternoon “labs”: 20 Sep: Excursion to CPT
26/27 Sep: Student presentations on CPT visit
• Course assessment: Assignment (30% of class record)
Presentation (20% of class record)
Class Test (50% of class record)
Exam

• “Medicinal Chemistry is the science that deals with the discovery and design of
new therapeutic chemicals and their development into useful medicines.”
- RB Silverman in “The Organic Chemistry of Drug Design and Drug Action”
What is Medicinal Chemistry?
• Medicinal Chemistry broadly involves:
- Isolation of compounds from Nature, or synthesis of new molecules
- Investigation of the relationship between structure and biological activity
- Elucidation of interactions with biological receptors
- Determination of pharmacokinetic and pharmacodynamic properties

What are Drugs?
• Drugs are compounds that
• All drugs show
• The safety of a drug is indicated by • The safety of a drug is indicated by
• Drugs should have more
Where do drugs act?
• Drugs act on
• The majority of drug targets are
Generally, the drug interacts with the target by:• Generally, the drug interacts with the target by:
• The study of how drugs interact with their target is known as

Chinese
• Health Science Anthology 13th century BC
Where did it all start?
Egyptian
• Ebers Papyrus, 16th century BC, describes ~ 900 prescriptions
• Health Science Anthology 13th century BC
• Pen Ts’ao, a book of herbs, 4th century BC
− Dichroa febrifuga prescribed for fevers
− Ma Huang (Ephedra sinica) used
as heart stimulant, treatment of asthma

How were “medicines” developed?
Originally, all therapeutic agents were
R = R’= H; Morphine
R = Me, R’ = H; Codeine
R = R’ = Ac; Heroin
• Opium
− Use in China recorded over 2000 years ago
− Contains about 25 alkaloids
− 10% is morphine

• Digitalis from foxglove
− Discovered by William Withering in 1775
− Active component is digoxin (1930)
− Sold as Lanoxin by GSK for treatment of congestive heart failure
and atrial arrhythmias
Chemical and Engineering News, 2005, 83, 3
• Aspirin• Aspirin
− 400BC: Hippocrates prescribes bark and leaves of
willow tree to relieve pain and fever
− 1763: Rev. Edmund Stone recorded use of willow bark
− Early 1800’s: salicin was isolated in pure form by various chemists
− 1860: Salicylic acid first synthesised by Kolbe
− 1898 : Acetyl salicylate, “aspirin” was released on market by Bayer
thanks to work by Felix Hoffman
G Westmann, Scientific American, January 1991, 58

How does Aspirin work?
• Mechanism of action only elucidated in 1970’s by
• Prostaglandins are local hormones formed by
• Prostaglandins have
• Vane established that Aspirin blocks

How does Aspirin work?
PG synthases
Lipoxygenase
Leukotrienes
Thromboxane synthase
Platelets
Arachidonic acid
Prostacyclin
Prostacyclin synthase
PGI2 PGE2
ProstaglandinsThromboxane
Platelets
Endothelial cells
How were “medicines” developed?
• Originally, all therapeutic agents were natural extracts - containing mixtures of
compounds
• Opium from poppy
• Digitalis from foxglove
• Extract from crushed bark of willow tree

How were “medicines” developed?
• 1891, two malaria patients cured with
− First time that a was used in humans
• 1910, Salvarsan (compound 606) was introduced as a remedy for syphilis
• Paul Ehrlich is known as the founder of chemotherapy, as he recognised that
molecules acted by binding to receptors in the body,
SHE Kaufmann, Nature Reviews, Drug Discovery, 2008, 7, 373
Chemical and Engineering News, 2005, 83, 3

• Largely, therapeutic agents divided into two classes:
Major Class:
Minor Class:
- Vaccines
- Proteins
- Antibodies
Therapeutic agents - where are we today?
• Natural products still the most important source of drugs:
S/NM S* S*/NM
N
ND
S
S/NM S* S*/NM N ND S
Sources of small molecule drugs, 1981-2006
DJ Newman, Journal of Medicinal
Chemistry, 2008, 51, 2589
Drug Discovery How are new drugs discovered?
• “In general, drugs are not discovered. What is more likely discovered is a lead
compound” RB Silverman
• What is a lead?
- The lead is a
- Ideally, a lead should display some
- Must allow for
Drug Discovery
• Salicylic acid – early example of a “lead” molecule
O OH
OH
• The lead compound is modified to

• Two approaches:
- Identification of a small molecule that displays biological
activity
- Knowledge of a potential biological target that could be
How is a lead discovered?
- Knowledge of a potential biological target that could be
exploited to cure a disease
• Both approaches require , and that
their activity be evaluated in a
• Screening of natural products
• Medical folklore
• Screening synthetic compound libraries
• Utilising structures of existing drugs (me-too and SOSA)
• Starting from the natural ligand
• Combinatorial synthesis
How is a lead discovered?
• Combinatorial synthesis
• Computer-aided design
• Computer-aided screening of virtual libraries
• Serendipity and the prepared mind

• A means of determining if a compound has the desired activity in a biological
system, relative to a control compound
- Activity is the
What are Bioassays?
- Potency is the
• The primary screen is usually an

• In general, a “hit” compound is identified from the primary screen. The hit:
• Hit to lead process may involve
• Data from the primary screen is often expressed as IC50
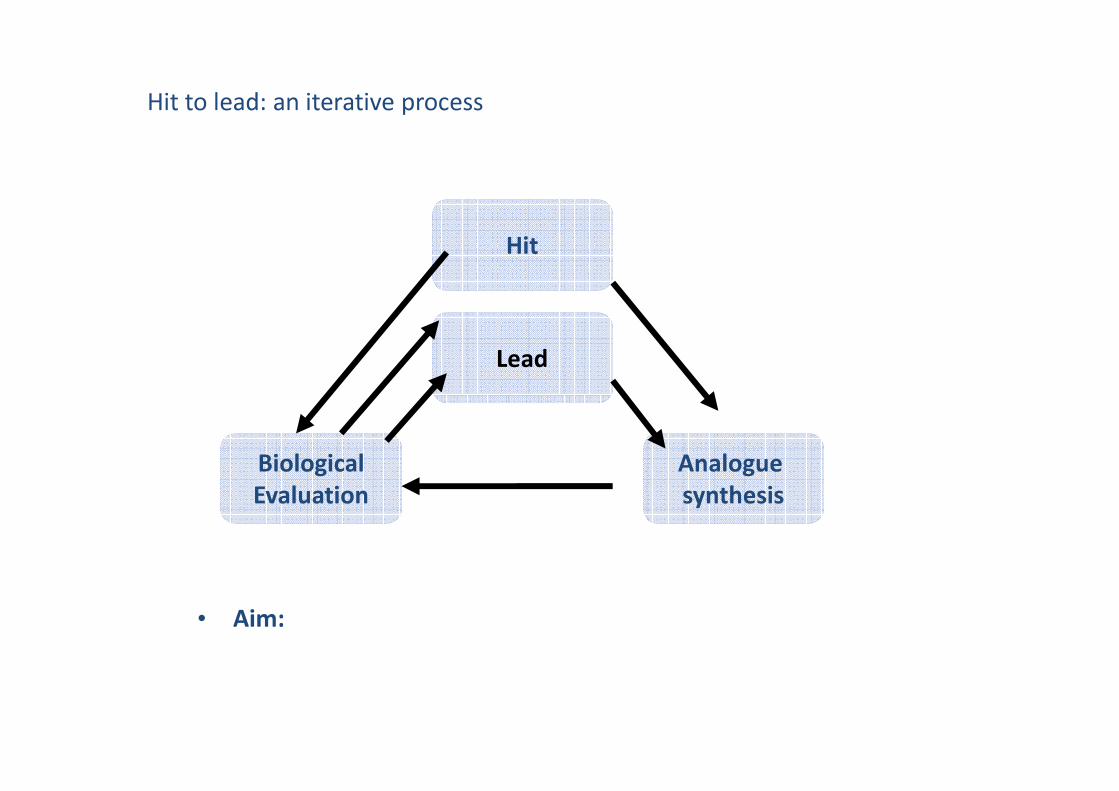
Hit to lead: an iterative process
Hit
Lead
• Aim:
Analogue
synthesis
Biological
Evaluation
• Favourable properties for a “drug-like” compound depend on
• For orally active compounds, these properties are summarised by Lipinski’s
Drug-likeness?
• Poor absorption and permeation are likely when
CA Lipinski, Drug Discovery Today, 2004, 1, 337;
CA Lipinski et al., Advanced Drug Delivery Reviews, 1997, 23, 3

• Passing the RO5 is no guarantee that a compound is drug-like
• Exceptions: antibiotics, antifungals, vitamins, cardiac glycosides
Drug-likeness?
• The RO5 says nothing about specific structural features found in drugs or non-
drugs eg:

• Summarised as ADME
Pharmacokinetics
What the body does to the drug

• The passage of a drug from
Absorption
• Influenced by mode of drug administration
• The extent to which a drug is absorbed is often referred to as
• pH of digestive tract NB factor influencing absorption of drugs:
− pH of stomach varies between
− pH of duodenum varies between
− pH of intestine stabilises at
• Properties of the drug important for absorption:
Absorption
•• Orally taken drugs must cross
• Most orally active drugs pass through
• Thus, drugs are required to cross
• Balance of
• Orally active drugs usually obey
• Polar drugs can be
Absorption
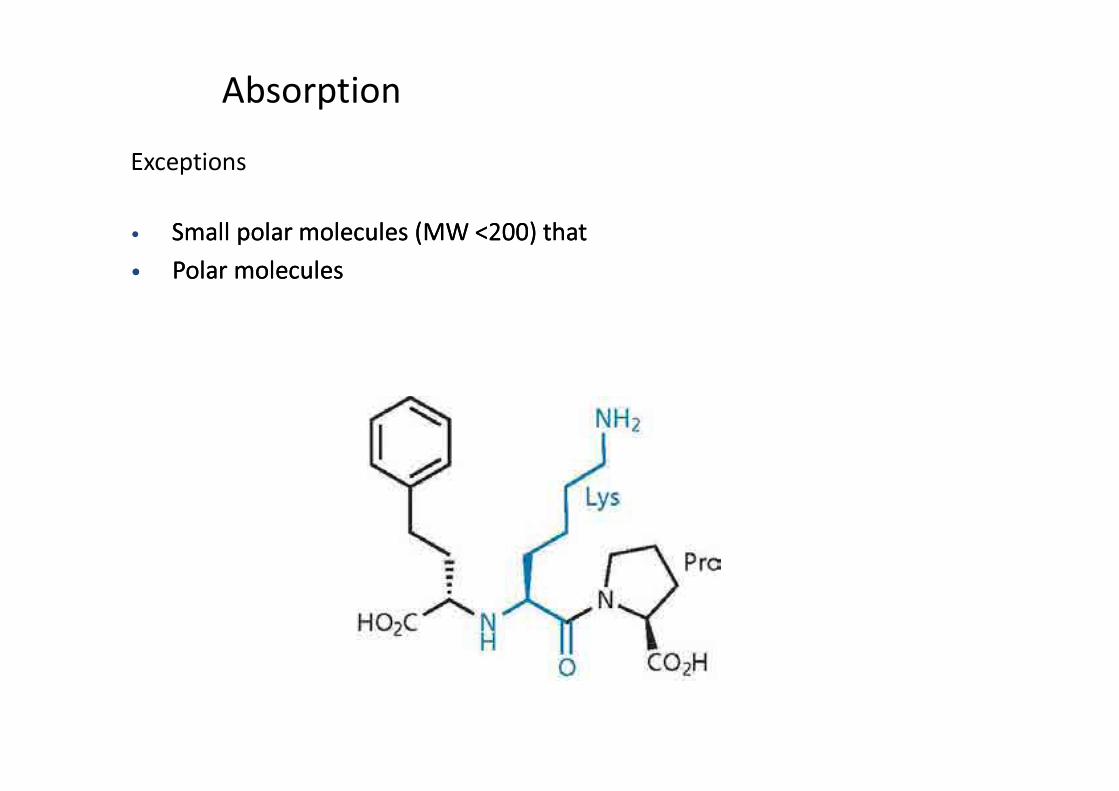
Exceptions
• Small polar molecules (MW <200) Small polar molecules (MW <200) thatthat
•• Polar Polar moleculesmolecules
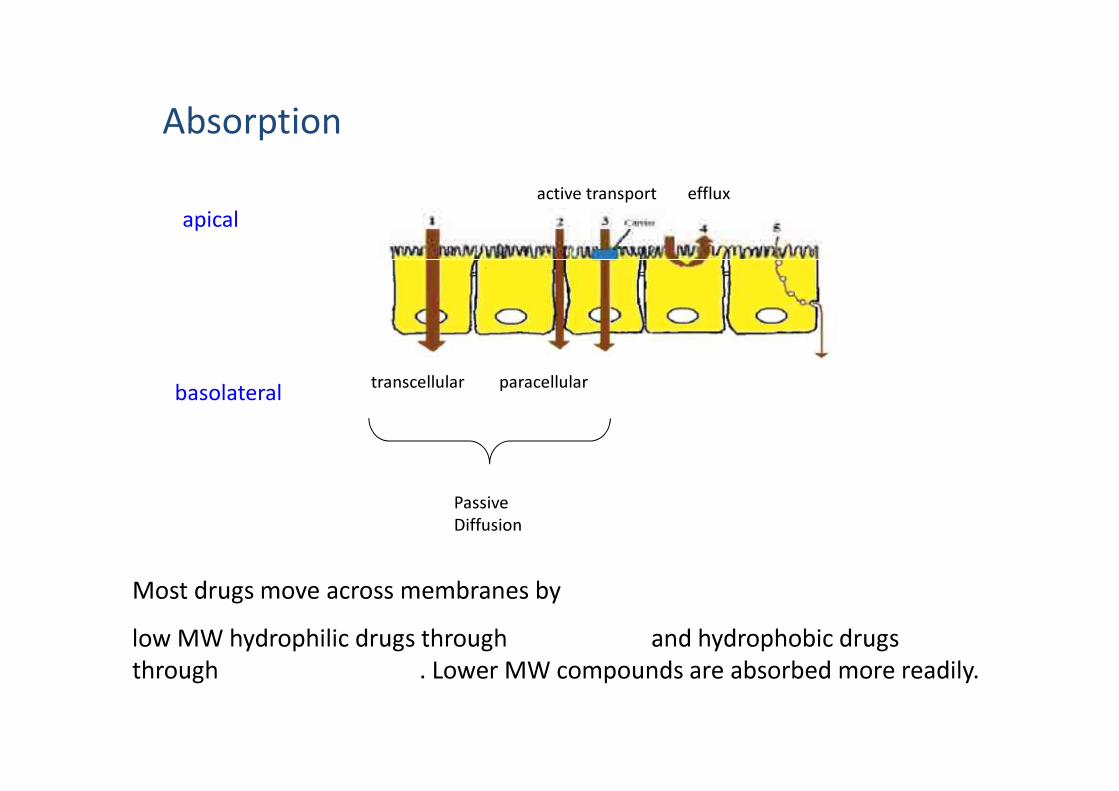
What influences permeability?
apical
basolateraltranscellular paracellular
effluxactive transport
Absorption
basolateral
Passive
Diffusion
Most drugs move across membranes by
low MW hydrophilic drugs through and hydrophobic drugs
through . Lower MW compounds are absorbed more readily.
• After absorption, drugs are distributed from
• Influenced by:
Distribution
• For lipid-soluble drugs, tissue membranes present , rapid equilibration • For lipid-soluble drugs, tissue membranes present , rapid equilibration
between plasma and tissues occurs
− However,
• Properties of the drug important for good distribution:
• The chemical alteration of a drug by a biological system with the principle
purpose of eliminating it from the system
- Phase I:
- Phase II:
Metabolism
• Mostly occurs in• Mostly occurs in
• Extent of metabolism largely determined by
- Oral: absorption from intestine into hepatic portal vein, taken
to liver, undergoes
• In general, lipophilic drugs are more prone to metabolism
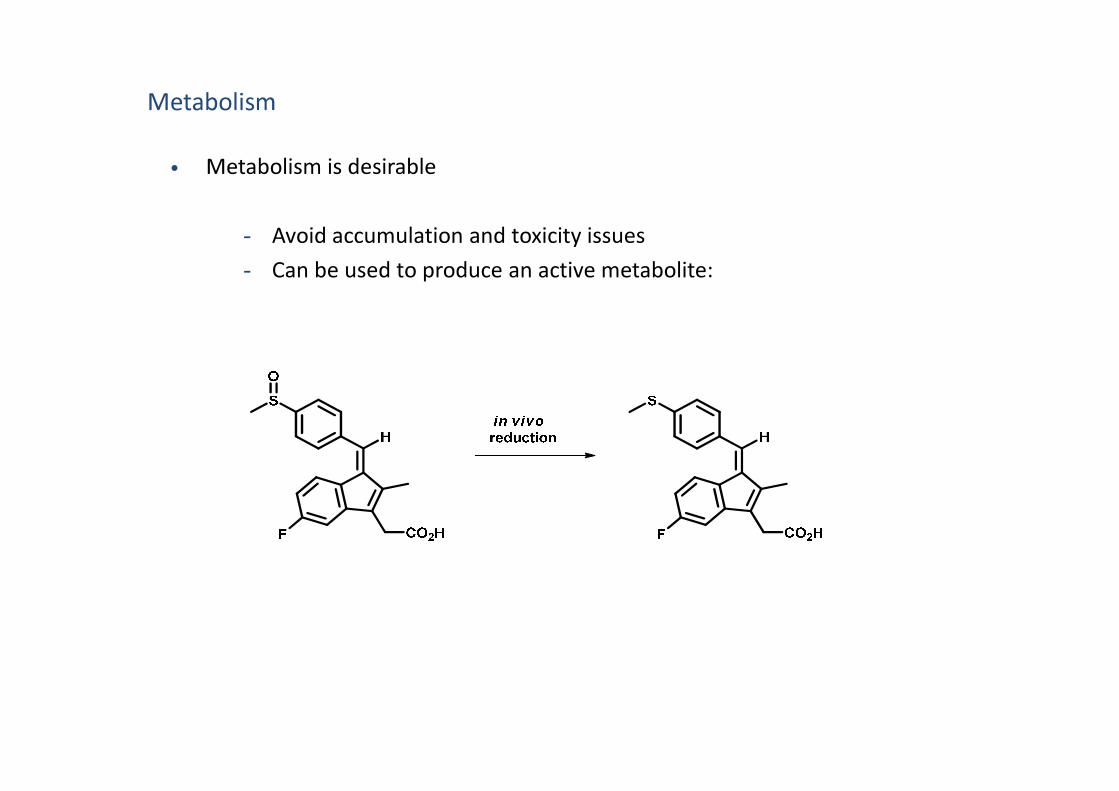
• Metabolism is desirable
- Avoid accumulation and toxicity issues
- Can be used to produce an active metabolite:
Metabolism
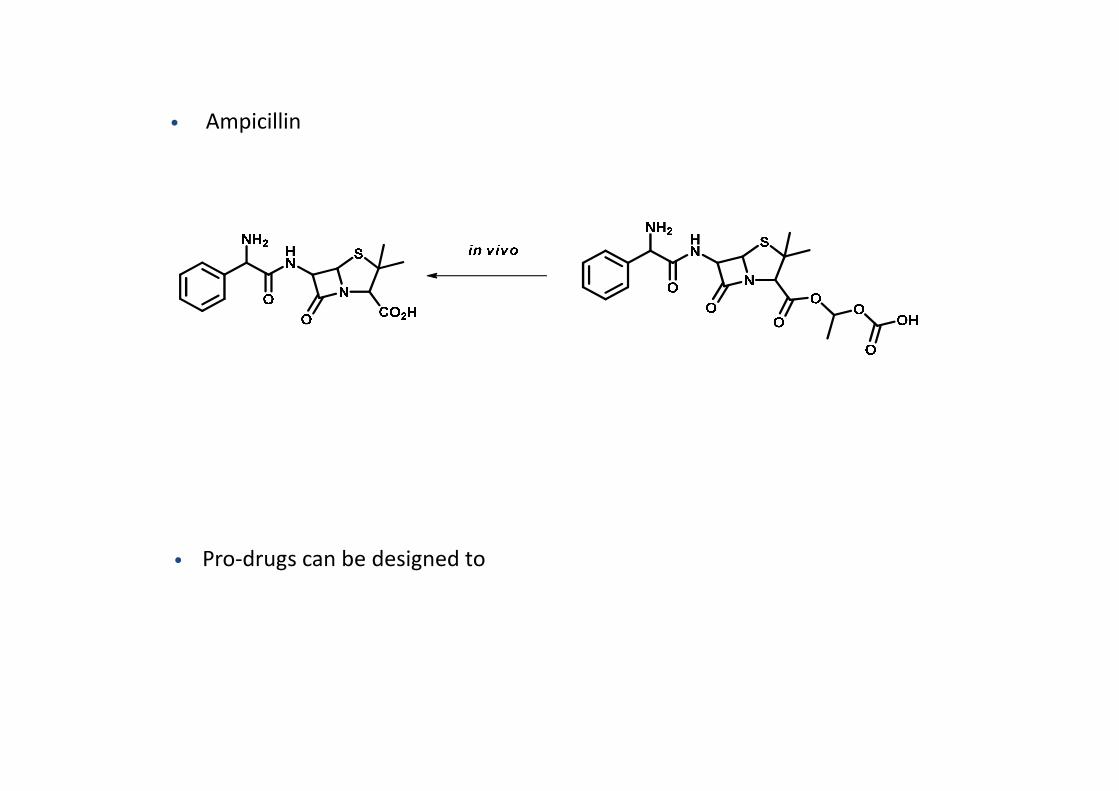
• Ampicillin
• Pro-drugs can be designed to

• NB to avoid
• Primary route of excretion:
• Liver –
• Lungs –
Excretion
• Lungs –
• Skin –
• Breastmilk and saliva

ADME summary
Systemic Circulation
GI tract Tissues IV
Serum
ORAL IM or SC
Drug Systemic Circulation
KidneysGI tractLiver
proteinsDrug
Hepatic portal vein
Bile
duct
faeces urine
Drug + metabolites

• Arises due to:
• Therapeutic index is a measure of the safety of a drug
LD50
ED50
Toxicity
ED50
• Toxicity levels tolerated vary for different diseases

• Ideal: Complete selectivity: target receptor/enzyme etc is absent in humans,
doesn’t interfere with any other pathways
• Selective toxicity: drug is toxic to pathogen but tolerated by host
Drug selectivity
• More than one pathway in host to compensate for interference in particular
biosynthetic route
• Usually easier when targeting an invading organism (eg bacteria) rather than
viruses, cancer, autoimmune etc

• Thalidomide
- 1950’s Marketed as
- Gained popularity as an effective drug for morning sickness
• Major medical disaster:
• Link with thalidomide only made in 1961
• Drug is a mixture of
Toxic metabolites/stereochemistry
O
O
N
NH
O
O
• Drug is a mixture of
• Only one enantiomer causes teratogenic effects
• Optimise target interactions
• Optimise access to the target
Lead Modification
• Reduce toxicity

• Doesn’t exist!
• Ideally should have a combination of the following properties:
Summary: The perfect drug?
• Responsible for major epidemics throughout history:
• Smallpox
− Weakened Roman Empire AD 165- 180 and AD 251-266
− Decimated indigenous tribes in North and South America
during European colonisation
Viruses
during European colonisation
• Influenza
− “Spanish flu” killed > 20 million people 1918-1919
• Concerns that terrorists will use viruses as weapons:

• Viruses are
What are viruses?
• Protein package (capsid) containing nuclear material
and enzymes essential for replication
• Nuclear material codes for
• They take over a host cell to
Taken from “An Introduction to Medicinal Chemistry”, GL Patrick
• Through the air
- influenza, chicken pox, measles, mumps, viral pneumonia, rubella,
smallpox
• Food- or water-borne
- Viral gastroenteritis, Poliomyelitus, hepatitis A, E
How are viruses transmitted?
- Viral gastroenteritis, Poliomyelitus, hepatitis A, E
• Through insects, eg ticks, mosquitoes
- Yellow fever, Colorado tick fever
• Through physical contact
- AIDS, cold sores, common cold, rabies

Life cycle of viruses
Host cell
Taken from “An Introduction to Medicinal Chemistry”, GL Patrick
Vaccination
• Preferred method of protection against viral infections
• 1st done in 1700’s by Edward Jenner (smallpox)
• Introduce foreign material bearing
but lacking
How do we target viral infections? Prevention
but lacking
• Body’s immune system recognises the molecular fingerprint of the
virus
BUT: Difficult for viruses that mutate readily
Ineffective as treatment, only for
Ineffective in

Antiviral drugs
How do we target viral infections? Treatment
• Viruses are effectively hidden in the host cell from
• Host machinery is used to carry out • Host machinery is used to carry out
• Most research into antiviral drugs began as a result of
• Generally, target proteins

Antiviral drugs
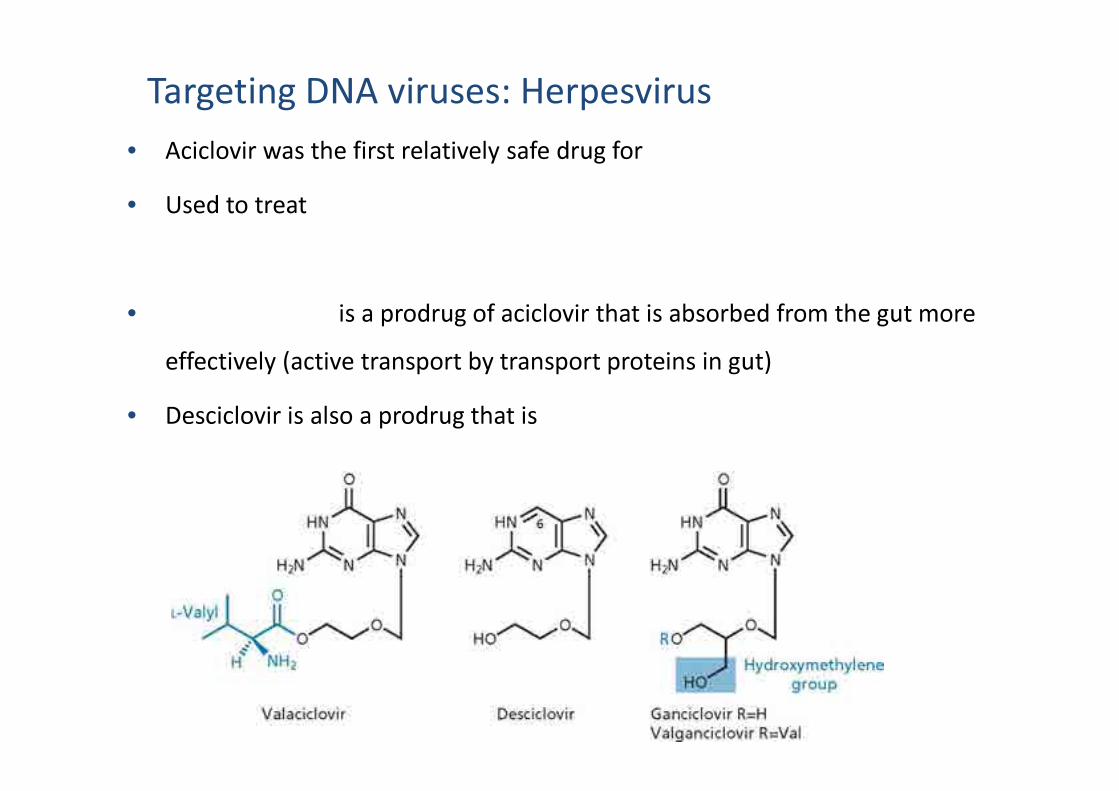
Targeting DNA viruses: Herpesvirus
• The most successful viral target to date:
• Aciclovir was discovered by compound screening,
• It is
Targeting DNA viruses: Herpesvirus
• Aciclovir was the first relatively safe drug for
• Used to treat
• is a prodrug of aciclovir that is absorbed from the gut more
effectively (active transport by transport proteins in gut)
• Desciclovir is also a prodrug that is
HIV
• Retrovirus:
• No vaccine available
• Antiviral drugs target NB viral proteins:• Antiviral drugs target NB viral proteins:
• Reverse transcriptase: converts ss RNA to ds DNA (both an RNA- and
DNA- dependent DNA polymerase)
• Protease: converts viral protein prepared in host cell into functional viral
proteins (maturation)
• Integrase: integrates viral DNA into host’s DNA (provirus)
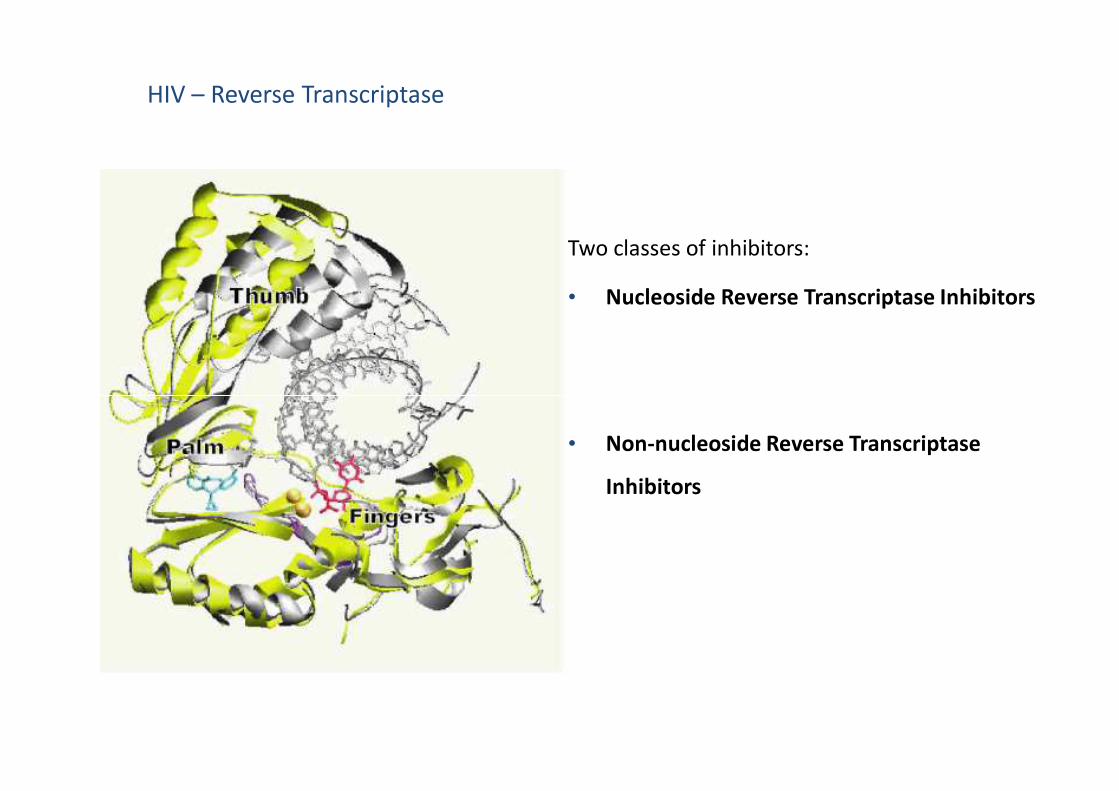
HIV – Reverse Transcriptase
Two classes of inhibitors:
• Nucleoside Reverse Transcriptase Inhibitors
• Non-nucleoside Reverse Transcriptase
Inhibitors
Nucleoside Reverse Transcriptase Inhibitors (NRTI’s)
• Mimic natural substrate
• Bind at enzyme
• Terminate
• All inhibitors are phosphorylated
• All lack
• Tenofovir has a stable

HIV – Reverse Transcriptase
Nucleoside Reverse Transcriptase Inhibitors (NRTIs)
N
NN
N
NH2
O
OH
O
Primer strand
OO
PO
OOP
O
O
OP
O
O
ONH
O
ON
Tem
plate
strand
O
OH
N
NN
N
NH2
O
O
O
Primer strand
P OO
O
O
OH
NH
O
ON
Tem
plate
strand

HIV – Reverse Transcriptase
• Nucleoside Reverse Transcriptase Inhibitors (NRTIs)
N
NH
O
OO
HO N
NH
O
OO
HO N
NHF
O
O
S
OHO
N3
S S
AZT (Zidovudine) 3TC (Lamivudine) FTC (Emtricitabine)
Tenofovir

Non-Nucleoside Reverse Transcriptase Inhibitors (NNRTIs)
• No
• Many structural classes,
• Bind at
• There is no cavity in the
• Prone to develop
HN
N
N NH
CN
CN
O
N
N NH
CNCN
NH2
Br
etravirine rilpivirine
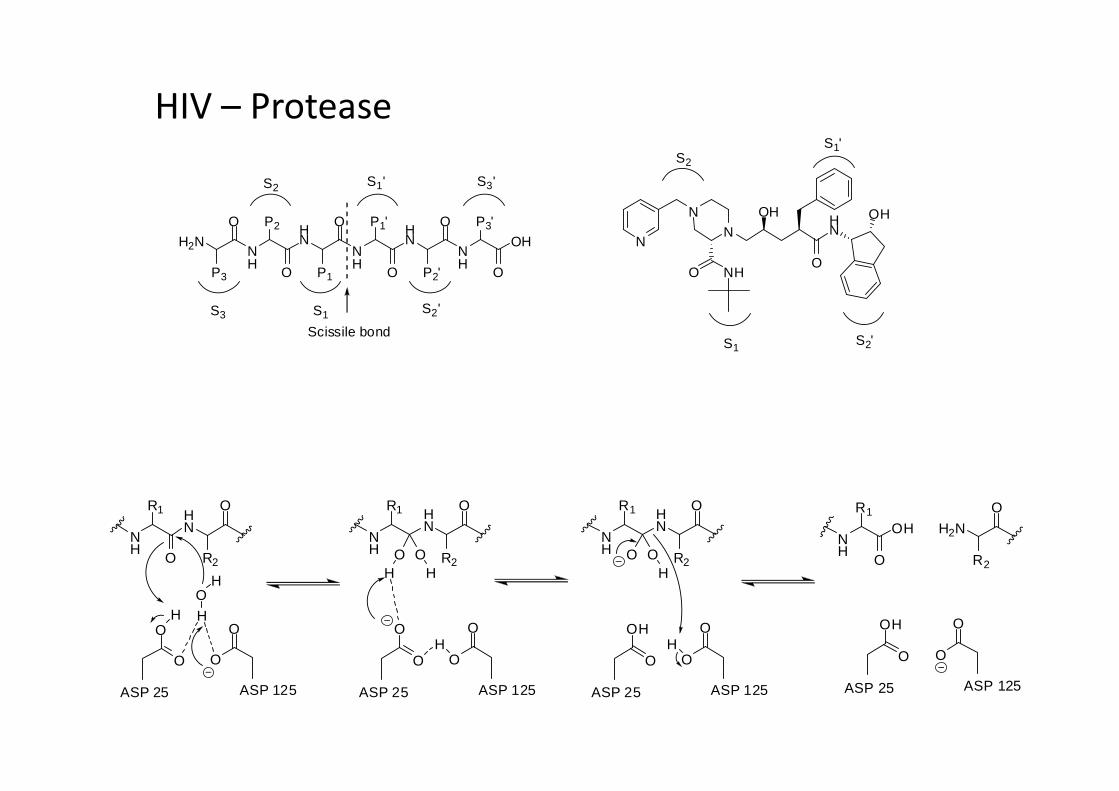
HIV – Protease
• Inhibitors mimic
• Contain a non-scissile
• Do not obey RO5!
• Highly metabolised, use
Protease - Peptidomimetic inhibitors
N
N
N
NHO
HN
OH
O
OH
H2NNH
HN
NH
HN
NH
OH
P3
O P2
O P1
O P1'
O P2'
O P3'
O
Scissile bond
S1
S2
S3
S1'
S2'
S3'
S1
S2
S2'
S1'
HIV – Protease
NH
HN
O
R2O
R1
O
O
HO
O
H
OH
ASP 25 ASP 125
NH
HN
O
R2
R1
O
O
O
O
ASP 25 ASP 125
O OHH
H
NH
HN
O
R2
R1
OH
O
O
O
ASP 25 ASP 125
O OH
H
O
R2
OH
O
O
O
ASP 25 ASP 125
H2NNH
OH
R1
O
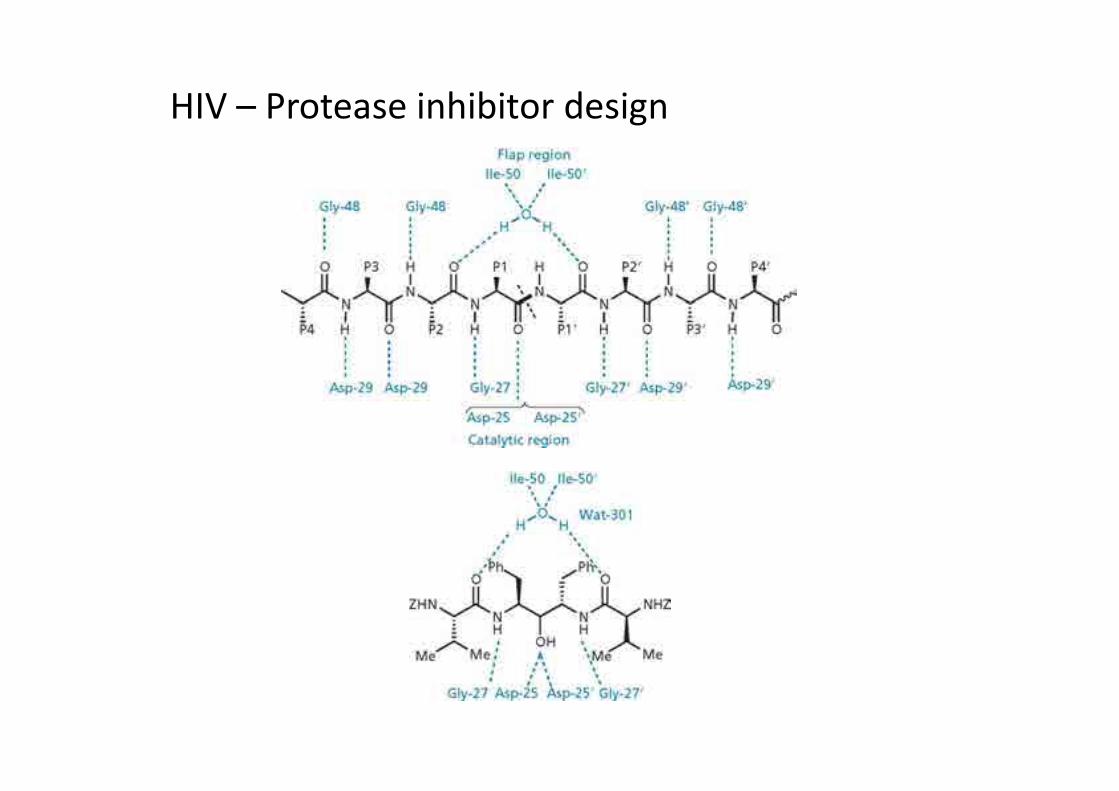
ProteaseHIV – Protease inhibitor design

CH3
CH3
OHN
NH
N
O
OH O
NH
O
N
N
N
NHO
HN
OH
O
Lopinavir Indinavir
OH
N
S N NH
HN
CH3
O
O
NH
O
OH
O
S
N
Ritonavir

HIV – Integrase
• Integrates
• Only one FDA approved drug
• Relatively new area of research
O O
OH
NN
O
HN
N
NHN
F
OO
O-K+
raltegravir
OF
Cl
OH
O
elvitegravir
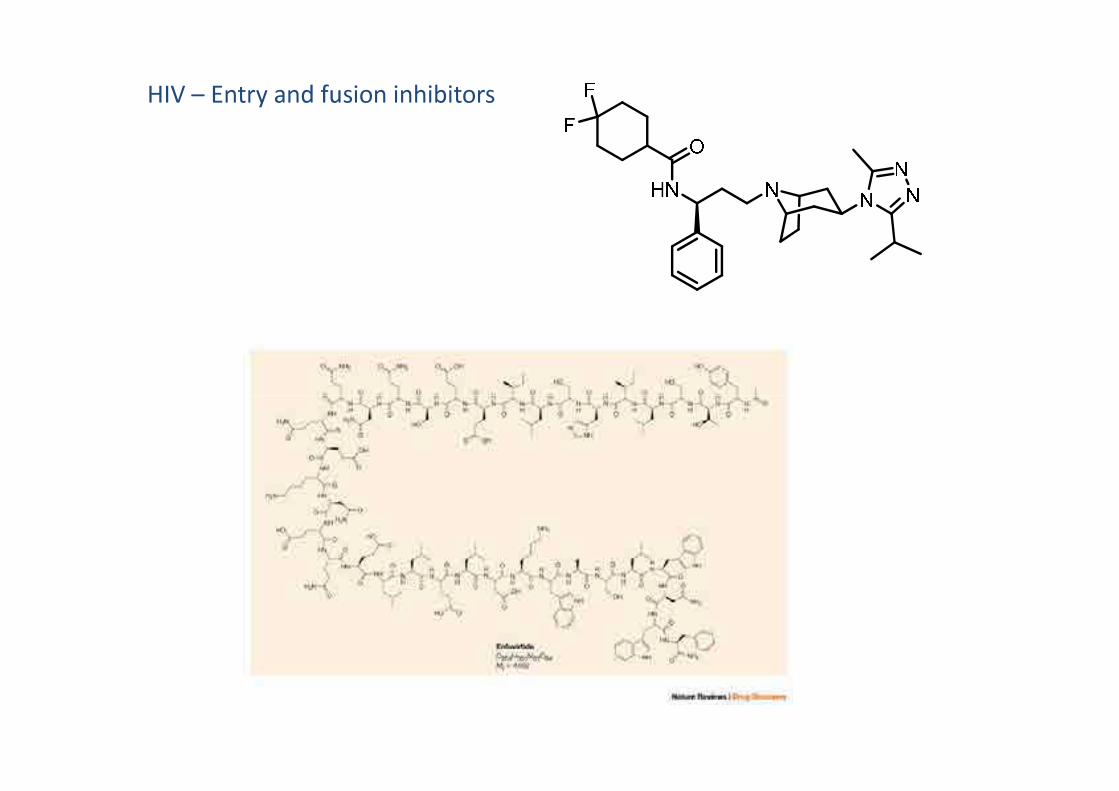
HIV – Entry and fusion inhibitors

HIV: New targets/ approaches: New targets/
approaches• Bevirimat –
• Bryostatin –
OHO
O
O
H
H H
H
H
H
OH
O
Bevirimat
• Microbicides –

Targeting RNA viruses: Influenza A
• Airborne, respiratory disease
• Caused by an
• Nucleocapsid contains
• Membrane envelope surrounding nucleocapsid contains
• NA is an enzyme that

Influenza A- Vaccines?
• Antigenic variation: the virus changes the amino acids in HA and NA
• RNA polymerase is error prone
• Sub-types of influenza are defined based on the antigenic variants of HA and
NA
• Vaccines are based on recent (most virulent) antigenic variants

H1N1 pandemic
• Often called “swine flu”
• Caused about 17 000 deaths between June 2009 and January 2010
• Confirmed cases in 214 countries around the world • Confirmed cases in 214 countries around the world
• First pandemic (worldwide epidemic) since 1968 Hong Kong flu
• Can cause pulmonary embolism- leading cause of death
• Systemic inflammatory response syndrome causes pulmonary oedema
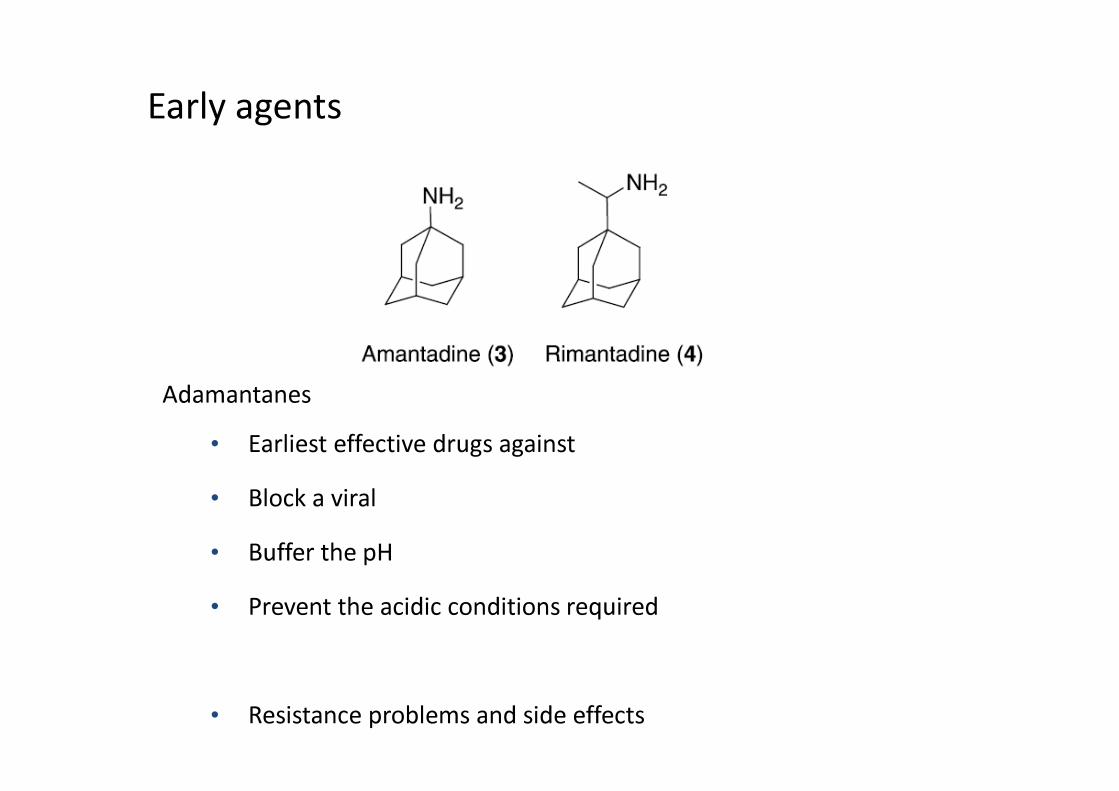
Early agents
AdamantanesAdamantanes
• Earliest effective drugs against
• Block a viral
• Buffer the pH
• Prevent the acidic conditions required
• Resistance problems and side effects

Neuraminidase (NA) inhibitors
• NA crucial to
• Although shape of protein changes,
• NA inhibitors mimic natural substrate:

Neuraminidase (NA) inhibitors
• NB regions for binding:

Neuraminidase (NA) inhibitors
• NB regions for binding:
Sialic acid

Neuraminidase (NA) inhibitors
R = H,
R = Et,)
Sialic acid
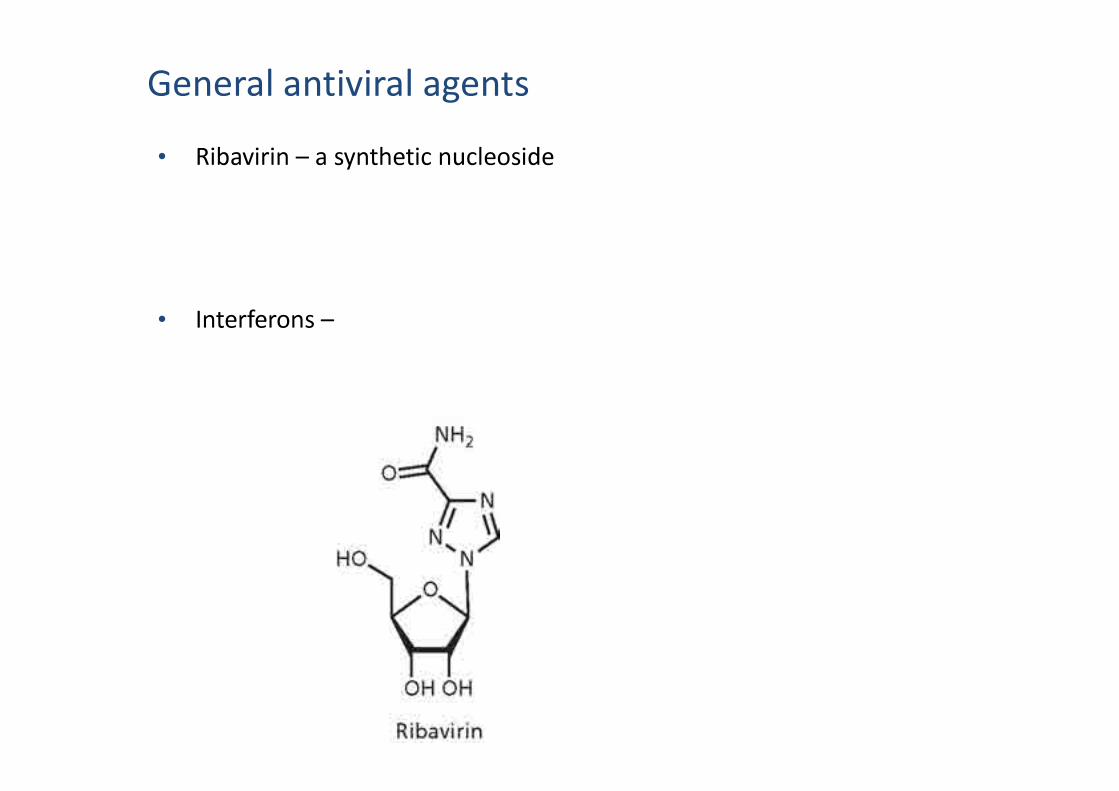
General antiviral agents
• Ribavirin – a synthetic nucleoside
• Interferons –

• Bacteria are first identified in 1670’s
(Leeuwenhoek)
Antibacterials: history
• The link between bacteria and disease was only made in the mid 1800’s
(Pasteur)
• “Germ theory” of disease advocated by Lister
• 1930’s: prontosil and sulfa drugs- first drugs effective against systemic bacterial
infections
• “Magic bullet” theory (Ehrlich)- use of salvarsan (1910) for treatment of syphilis:
birth of chemotherapy

• Current antibiotics
Why do we need new antibacterial agents?
• Bacterial infections still a major cause of death worldwide, but particularly in
• DRUG
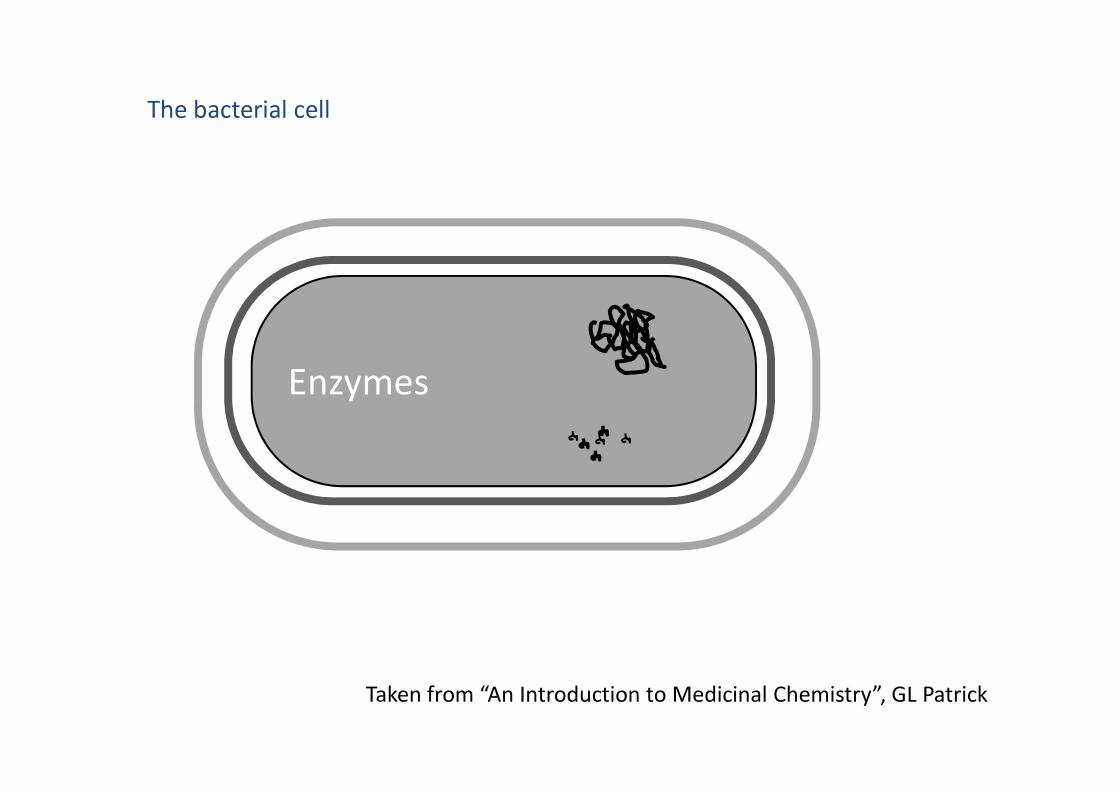
The bacterial cell
Enzymes
Taken from “An Introduction to Medicinal Chemistry”, GL Patrick
Enzymes
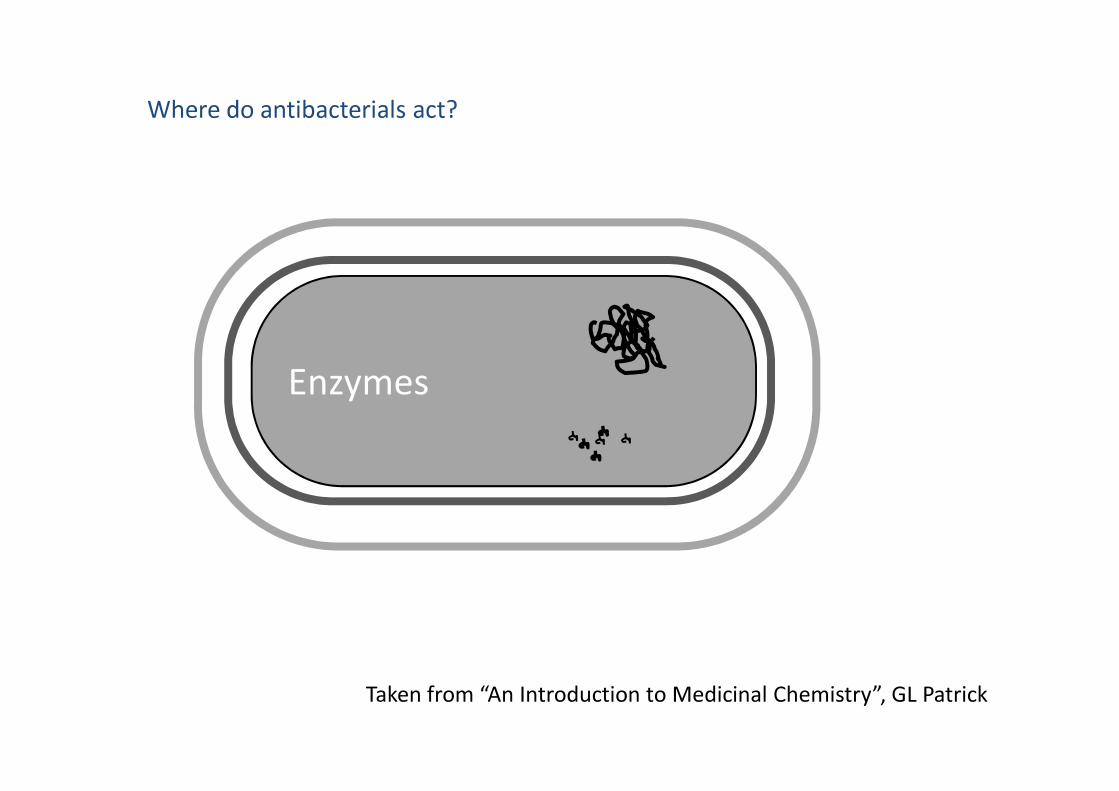
Where do antibacterials act?
Enzymes
Taken from “An Introduction to Medicinal Chemistry”, GL Patrick
Enzymes

Inhibitors of cell metabolism (antimetabolites) - Sulfonamides
• 1935, prontosil effective against bacteria
• First synthetic antibacterial agent
• Led to the development of numerous analogues
• But: Ineffective against
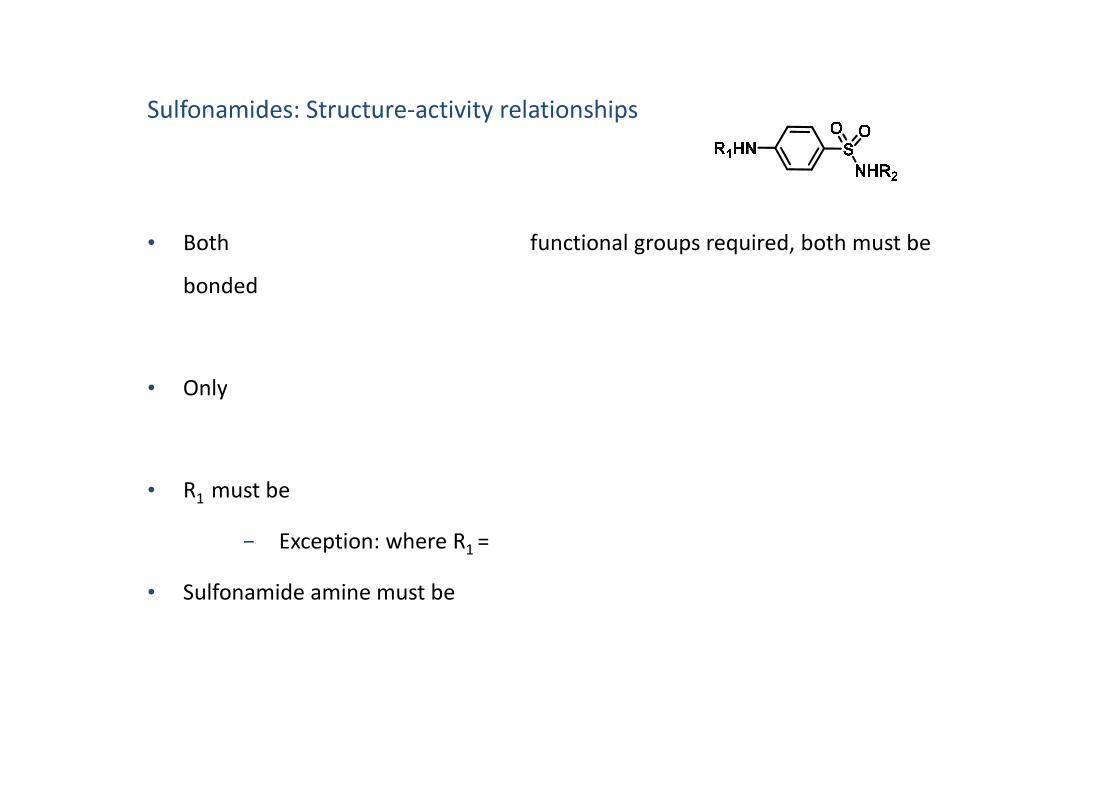
Sulfonamides: Structure-activity relationships
• Both functional groups required, both must be
bonded
• Only• Only
• R1
must be
− Exception: where R1
=
• Sulfonamide amine must be

Sulfonamides: Structure-activity relationships
• Varying R2
affects
1) Affects the extent of binding to
2) Affects
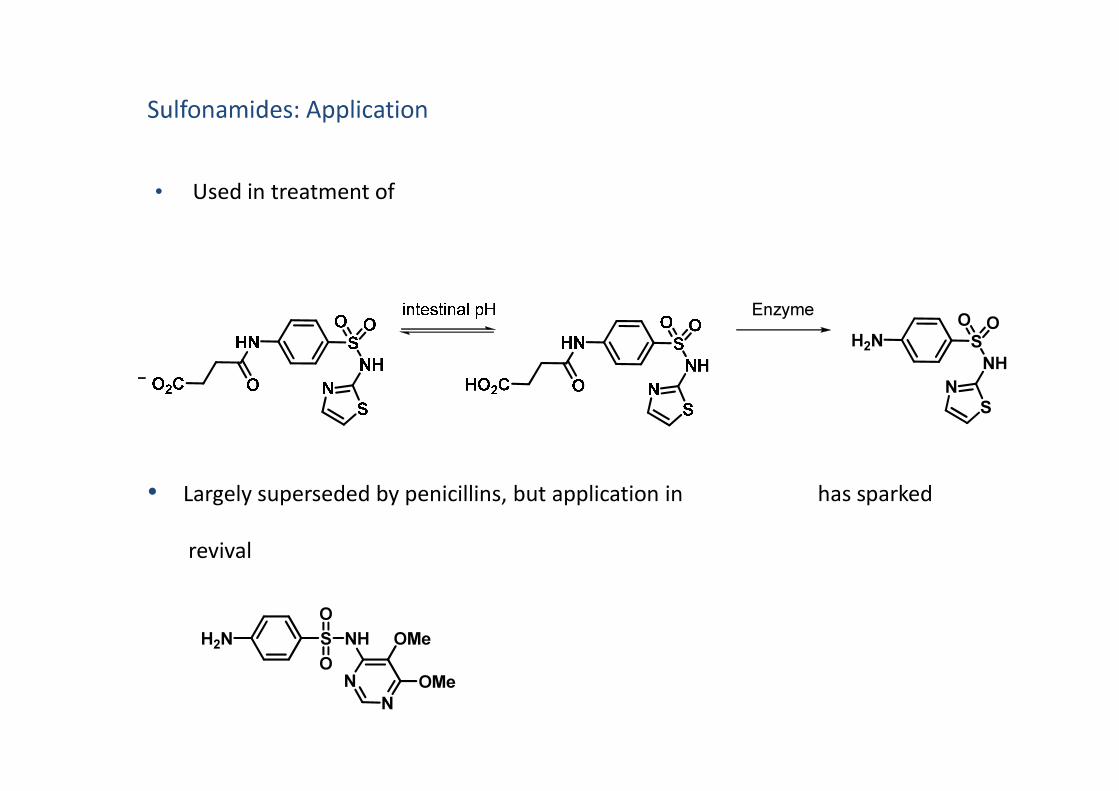
• Used in treatment of
Sulfonamides: Application
H2N SO
NH
O
N
Enzyme
• Largely superseded by penicillins, but application in has sparked
revival
S
H2N S
O
NH
O
N
N OMe
OMe

Sulfonamides: Mechanism of Action
• Act as of dihydropteroate synthase
• Block pathway responsible for
• THF essential for• THF essential for
• They are (inhibit cell growth and reproduction) not
• Rely on to kill remaining bacterial cells

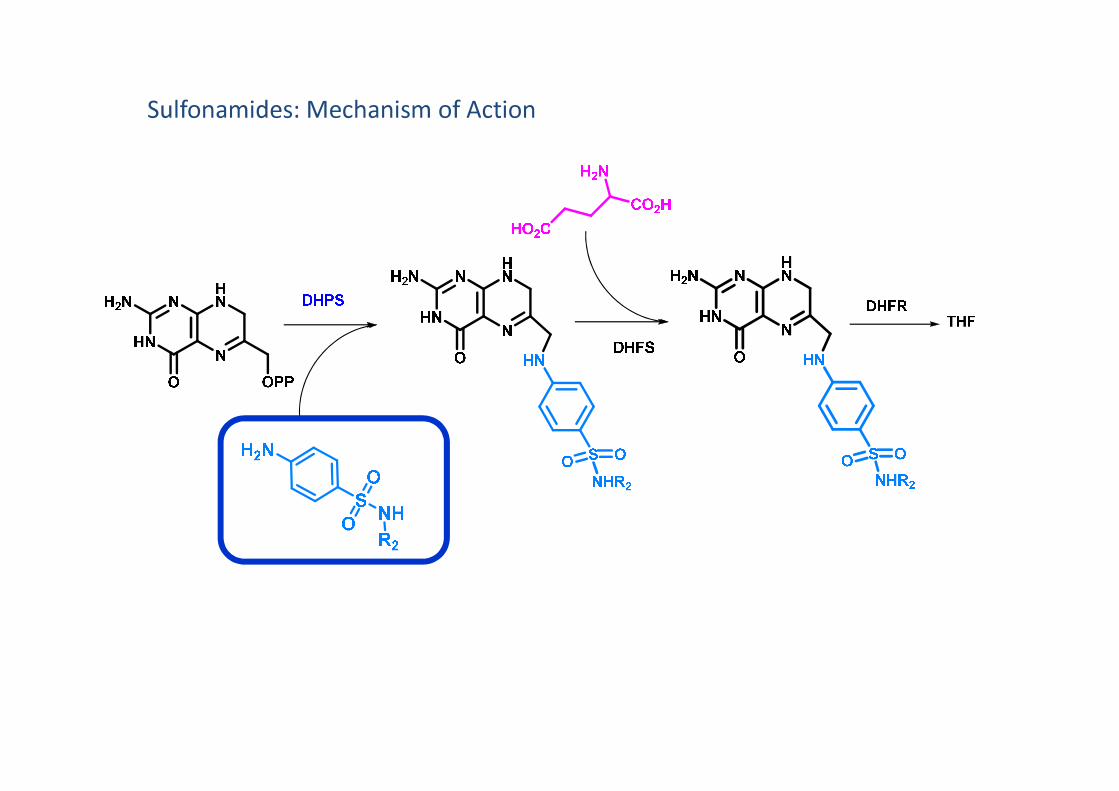
Sulfonamides: Mechanism of Action

Penicillins: history
• 1877 Moulds produce substances that kill bacteria (Pasteur)
• 1941 first clinical trials
• 1928 Fleming discovers antibacterial properties of penicillin
• 1938 Florey and Chain isolate penicillin by freeze-drying and chromatography
• 1941 first clinical trials
• 1945 Structure determined by X-ray crystallography (Hodgkins)
• 1957 First total synthesis (Sheehan)
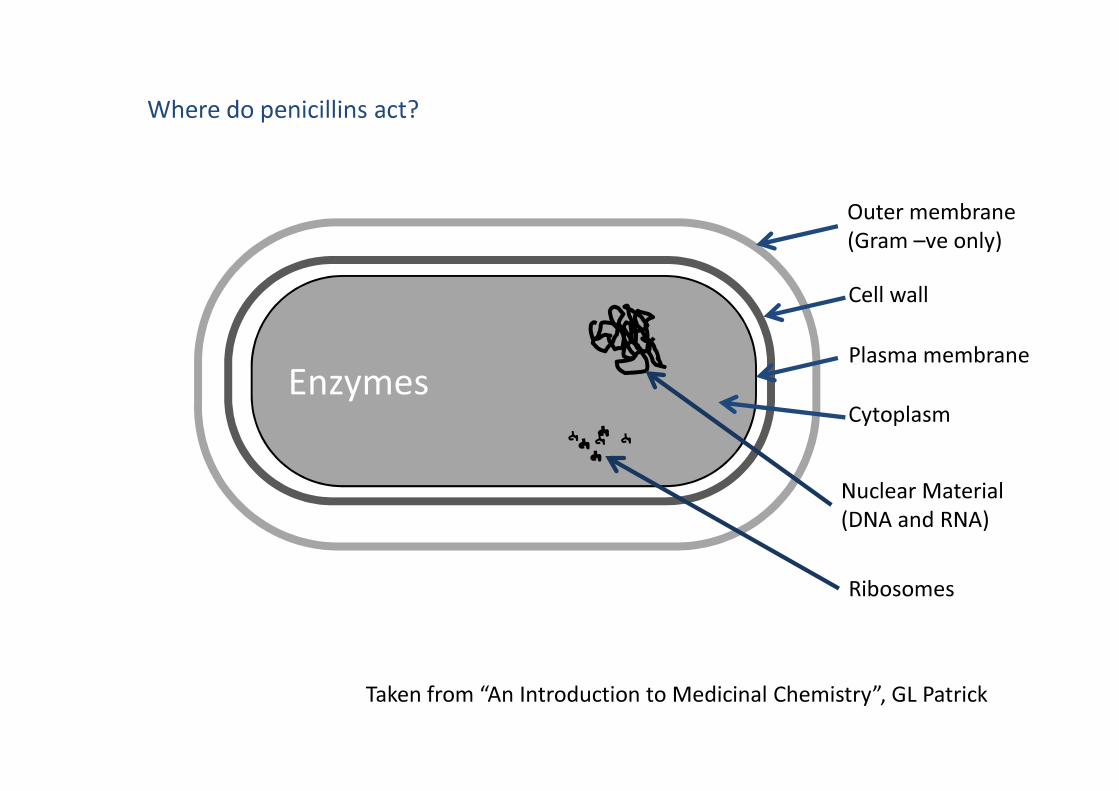
Where do penicillins act?
Enzymes
Cell wall
Outer membrane
(Gram –ve only)
Plasma membrane
Taken from “An Introduction to Medicinal Chemistry”, GL Patrick
Enzymes
Nuclear Material
(DNA and RNA)
Cytoplasm
Ribosomes

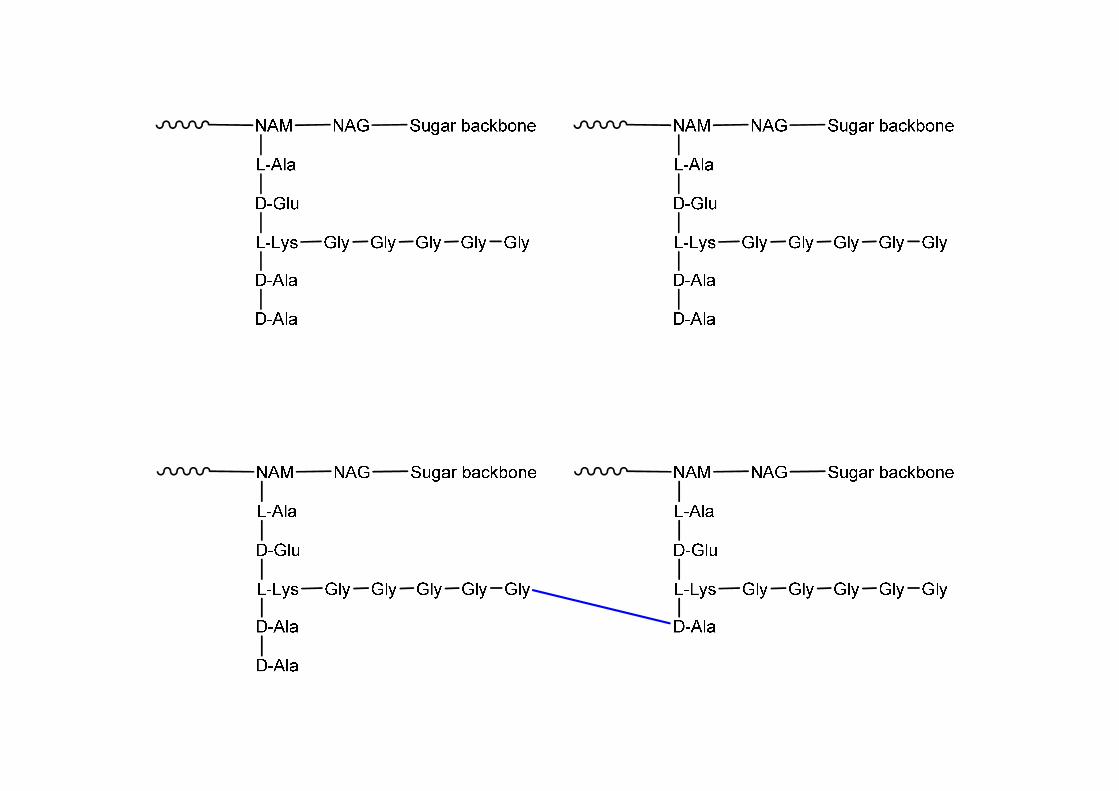
How do penicillins inhibit cell wall synthesis?
• Cell wall is a peptidoglycan structure:
• Parallel series of sugar backbones consisting of two types of sugars:
•
• and• and
• Peptide chains are bound to the
• Final stage of cell wall synthesis: D-alanine of one chain displaced by glycine of
another chain
• Penicillin blocks this final

How do penicillins inhibit cell wall synthesis?
-proposed mechanism of action
OH NH3
Ser Lys
ONH
OHNPeptide
chain
PeptideChain
PeptideChain
O
NH2
Gly
D-Ala-D-Ala

Bacterial resistance to penicillins
Bacterial strains vary in their susceptibility to penicillins:
• Physical barriers:
• β-lactamases
OH
Ser
• High levels of transpeptidase enzyme, binding affinity to transpeptidase, efflux
pumps, mutations
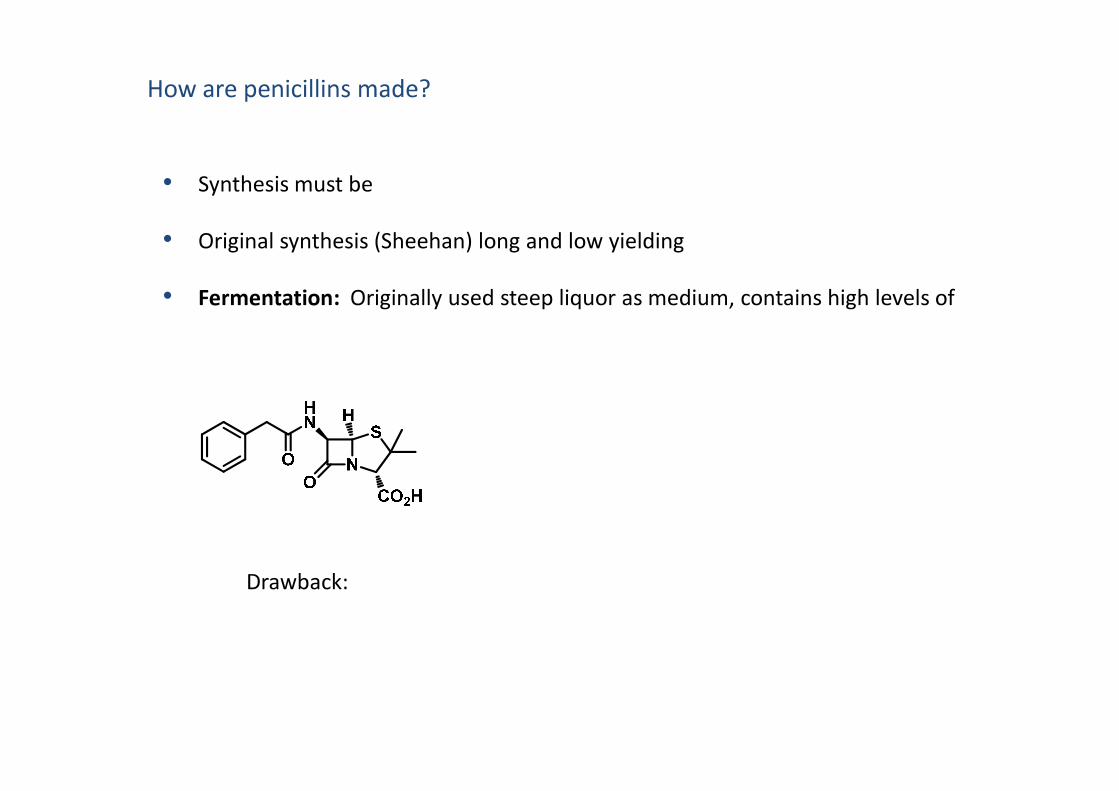
How are penicillins made?
• Synthesis must be
• Original synthesis (Sheehan) long and low yielding
• Fermentation: Originally used steep liquor as medium, contains high levels of
Drawback:

• Semi-synthesis: 1959 Biosynthetic intermediate is isolated from fermentation
Intermediate treated with
• Alternatively, isolate penicillin G and
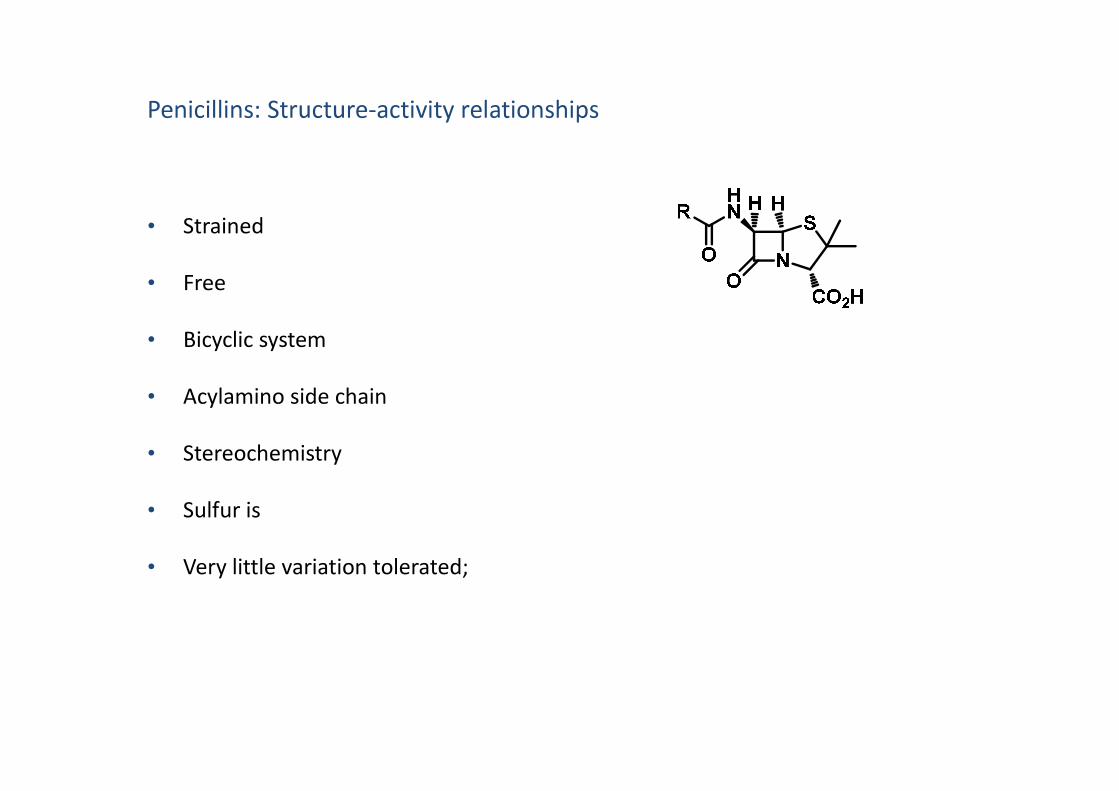
Penicillins: Structure-activity relationships
• Strained
• Free
• Bicyclic system
• Acylamino side chain• Acylamino side chain
• Stereochemistry
• Sulfur is
• Very little variation tolerated;

Penicillin analogues
Why do we need analogues of penicillin G?
1) Reduce
•
•
•

Penicillin analogues
How do we design analogues of penicillin G to be acid stable?
•• Varying
N
S
O
HN H
CO2H
O
X

Why do we need analogues of penicillin G?
2) Reduce
• 1960’s 80% of all Staphylococcus aureus infections were
How do we design analogues of penicillin G to
•
N
S
O
HN H
CO2H
O
OEt
R1
= R2
= H; Oxacillin
R1
= Cl, R2
= H; Cloxacillin
R1
= Cl, R2
= F; Flucloxacillin
R1
= Cl, R2
= Cl; Dicloxacillin
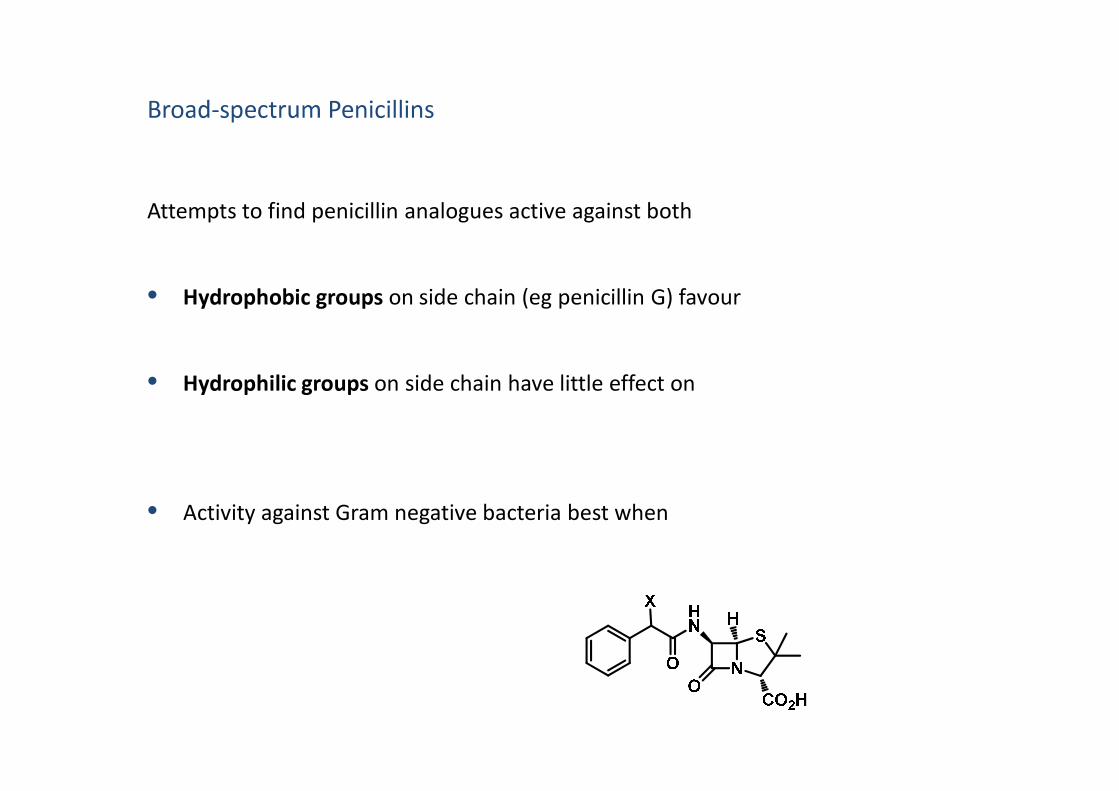
Broad-spectrum Penicillins
Attempts to find penicillin analogues active against both
• Hydrophobic groups on side chain (eg penicillin G) favour
• Hydrophilic groups on side chain have little effect on• Hydrophilic groups on side chain have little effect on
• Activity against Gram negative bacteria best when

Aminopenicillins
• Ampicillin and amoxicillin
N
S
O
HN H
CO2H
O
H2N H
HO
• Orally active, used as
•
But:
• Sensitive to
•

Broad-spectrum Penicillins
Pro-drugs of Aminopenicillins R =
R =
R =
O
O
• Esters mask the carboxylic acid functional group:

• Metabolism in vivo

Broad-spectrum Penicillins
Carboxypenicillins
• Carbenicillin • Pro-drugs of Carbenicillin
• Broad spectrum activity
But:
•••
•
R = Ph;
R = ;
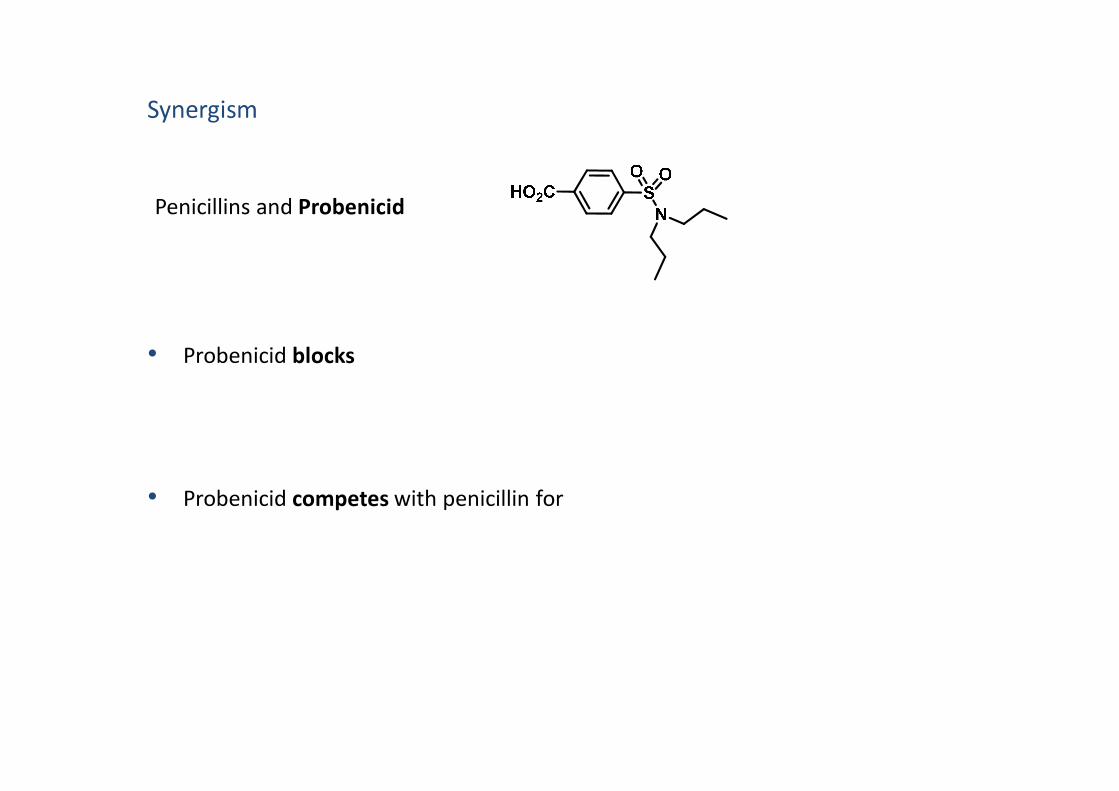
• Probenicid blocks
Penicillins and Probenicid
Synergism
• Probenicid competes with penicillin for

• 1976 Clavulanic acid isolated from Streptomyces clavuligerus,
•
Penicillins and Clavulanic acid
Synergism
• Shown to have weak antibiotic activity, but:
• Used in combination with
•
•

• Second largest cause of death in developed world
Cancer
• Cancer cells form when normal cells lose
• Eventually, cancer cells lose characteristics of the
• If the cancer has spread and formed tumours elsewhere in the body
• If the cancerous cells are localised (in one place) the tumour is
• Up to 30% of cancers may be caused
What causes cancer?
• Further 30% of cancers may be
Lifestyle
• have been implicated in about 15% of cancers
•
•
Genetic faults
• Proto-oncogenes
What causes cancer?
Cellular level
This results in:
abnormal growth due to defective signalling pathways, insensitivity to growth-
inhibitory signals, abnormal cell cycle regulation, immortality and the ability to
avoid programmed cell death (apoptosis), ability to develop blood vessels
(angiogenesis)
• Inactivation of

• Surgery
• Radiation therapy
• Chemotherapy
What are the treatments for cancer?
− Drugs acting on
− Drugs acting on − Drugs acting on
− Drugs acting on
Intrinsic resistance
•
Drug Resistance
Acquired resistance
•

Causes of resistance:
− Slow growth rate
− Poor uptake
− Overproduction
− Mutations
− Alternative
− Mixture of
− Efflux

Cancer chemotherapy: Drugs acting on nucleic acids
Intercalating agents
• Contain
• They slip in between the layers of
• This distorts the structure of
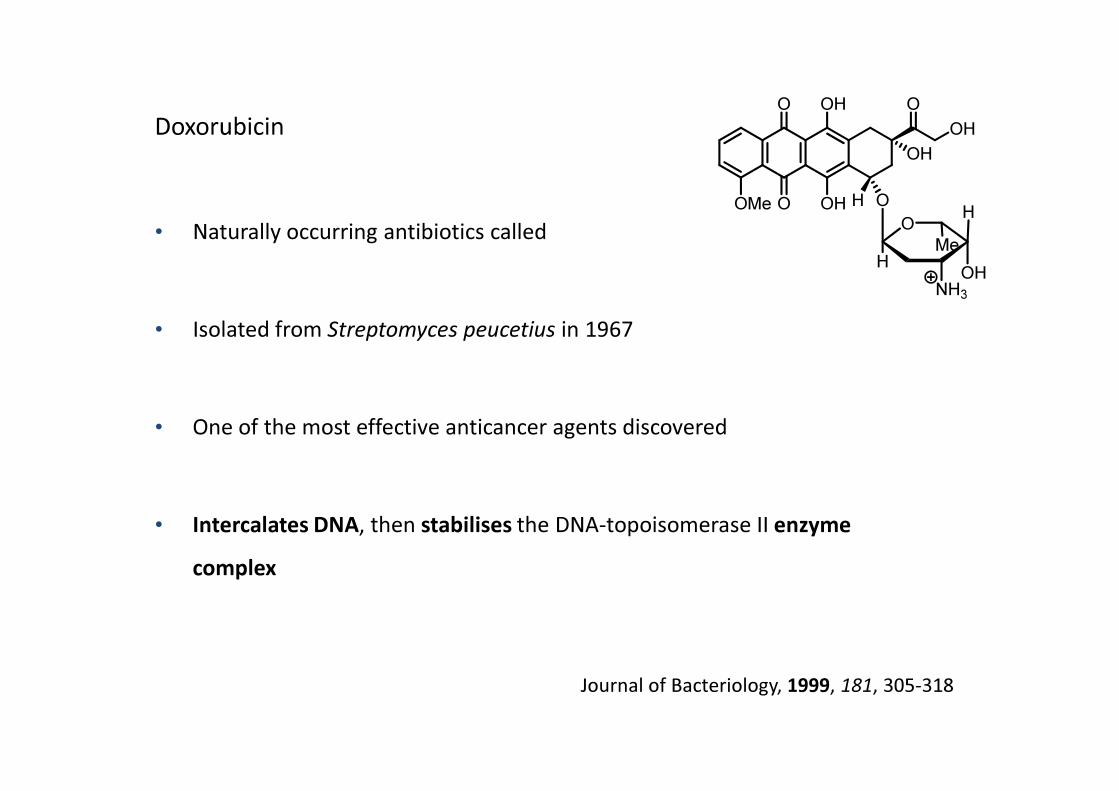
Doxorubicin
• Naturally occurring antibiotics called
• Isolated from Streptomyces peucetius in 1967
OMe
O
O
OH
OH H
OH
O
OH
O
O
H
H
OH
Me
NH3
• One of the most effective anticancer agents discovered
• Intercalates DNA, then stabilises the DNA-topoisomerase II enzyme
complex
Journal of Bacteriology, 1999, 181, 305-318

Cancer chemotherapy: Drugs acting on nucleic acids
Intercalating agents
Doxorubicin
OMe
O
O
OH
OH H
OH
O
OH
O
O
H
H
OH
Me
NH3
• Once bound, stabilises complex formed between Topoisomerase II and the DNA
strand
• Topoisomerase II responsible for
• This may trigger
• Administered
•
• Susceptible to resistance by

Cancer chemotherapy: Drugs acting on nucleic acids
Alkylating and metallating agents
• Highly
• They react with to form strong• They react with to form strong
(in partcular N-7 of guanine)
• Disrupts
• BUT: can alkylate

Cisplatin
• Most frequently used anticancer drug
• Discovered accidentally during research into the effects of electric current on
bacterial growth (1960’s)
• Structure activated in cells to produce reactive positively charged species which
act as
• Bind at regions of DNA containing adjacent
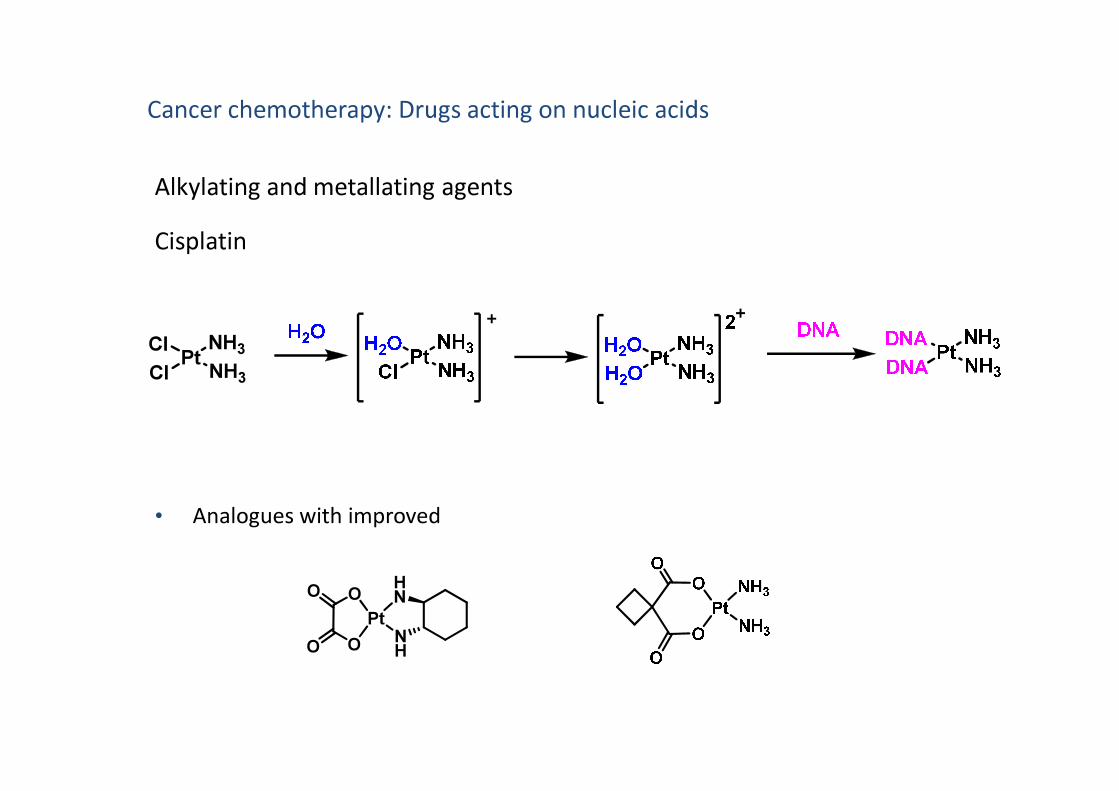
Cancer chemotherapy: Drugs acting on nucleic acids
Alkylating and metallating agents
Cisplatin
PtCl NH3
NH3Cl
• Analogues with improved
PtNH
HNO
OO
O

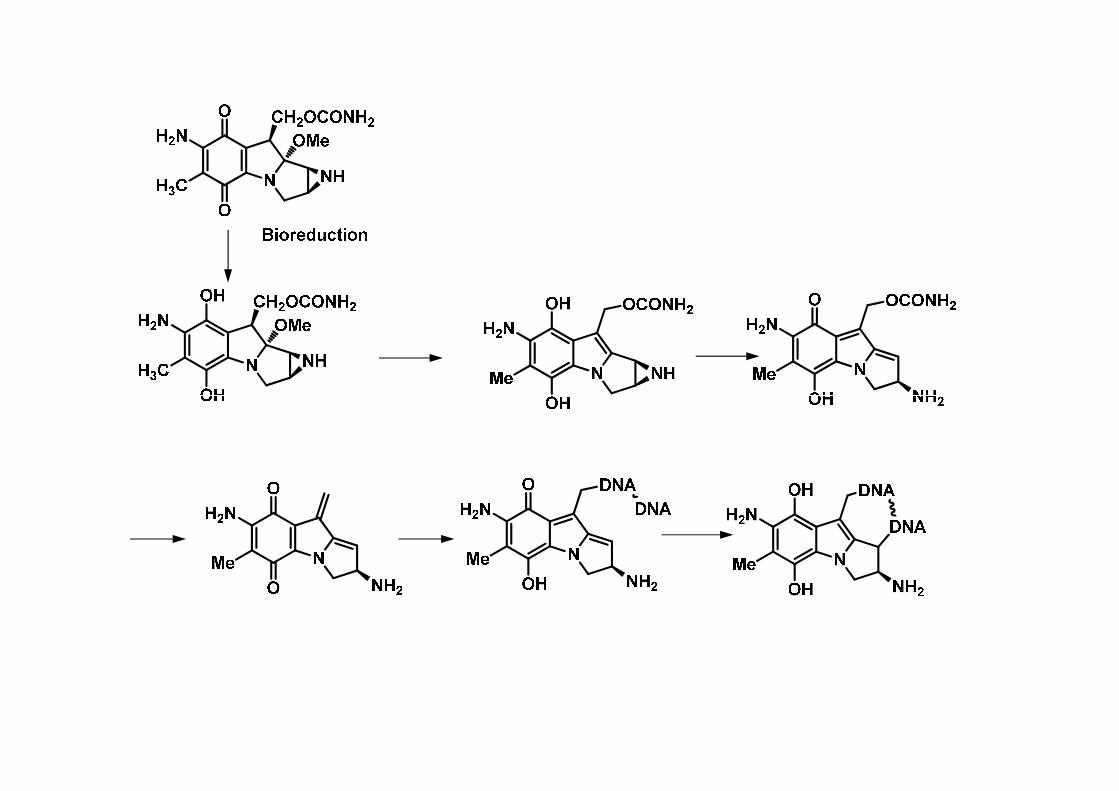
Cancer chemotherapy: Drugs acting on nucleic acids
Alkylating and metallating agents
Mitomycin C
• Discovered in 1950’s
• Isolated from Streptomyces caespitosus
• Toxic
• Pro-drug, undergoes
• Cross links DNA
• As reduction step is required, thought to be active in
Antimetabolites
• Inhibit enzymes involved in the
Cancer chemotherapy: Drugs acting on enzymes
• May result in the formation of

DHF = Dihydrofolate
DHFR = Dihydrofolate reductase
THF = Tetrahydrofolate
SHMT = Serine hydroxymethyl
transferase
TS = Thymidylate synthase

Cancer chemotherapy: Drugs acting on enzymes
Antimetabolites - inhibitors of DHFR
• Dihydrofolate reductase maintains
• THF essential co-factor for many cellular processes, including
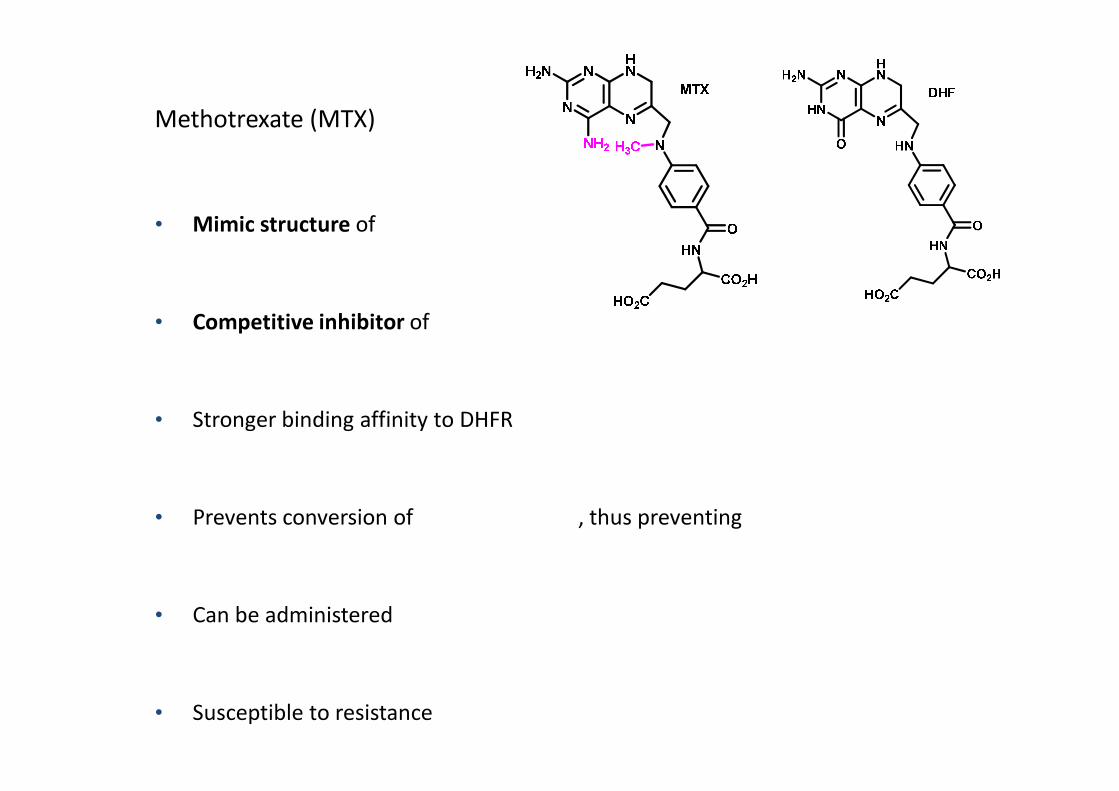
Methotrexate (MTX)
• Mimic structure of
• Competitive inhibitor of
• Stronger binding affinity to DHFR
• Prevents conversion of , thus preventing
• Can be administered
• Susceptible to resistance

Cancer chemotherapy: Drugs acting on enzymesDHF = Dihydrofolate
DHFR = Dihydrofolate reductase
THF = Tetrahydrofolate
SHMT = Serine hydroxymethyl
transferase
TS = Thymidylate synthase
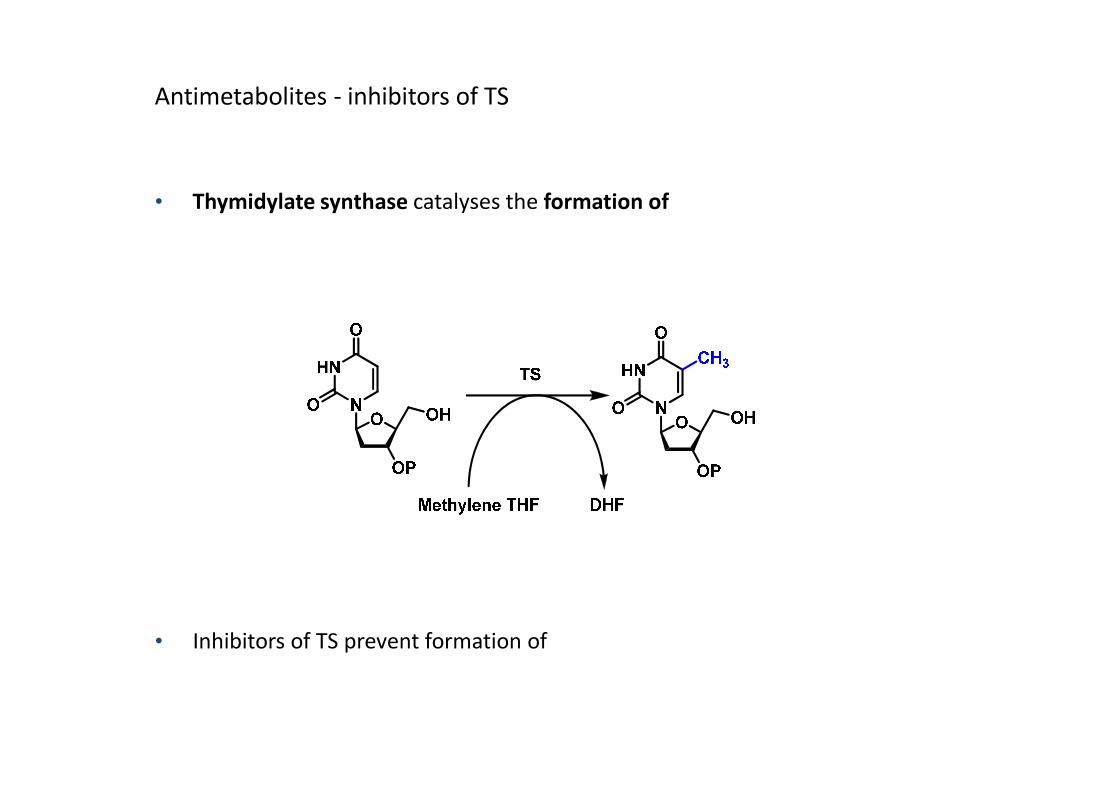
Antimetabolites - inhibitors of TS
• Thymidylate synthase catalyses the formation of
• Inhibitors of TS prevent formation of

Antimetabolites - inhibitors of TS
5-Fluorouracil
Pro-drug for a
Cancer chemotherapy: Drugs acting on enzymes
• Activated in the body to form
• Binds
• Prevents any further
• Administered

HN
N
O
O
HO
OP
O
X
HN
N
N
HN
NO
H2N
Ar
MethyleneTHF
X=H, dUMP
X = F, 5-Fluorouracil
HN
N
O
O
HO
OP
O
HSEnzyme
HN
N
N
HN
HNO
H2N
Ar
H
X=H, dUMP
X = F, 5-Fluorouracil
Tubulin
• Tubulin is a
• Building block for microtubules which are
Cancer chemotherapy: Drugs acting on structural proteins
• Drugs can bind to
• Majority of drugs targeting tubulin polymerisation/depolymerisation are
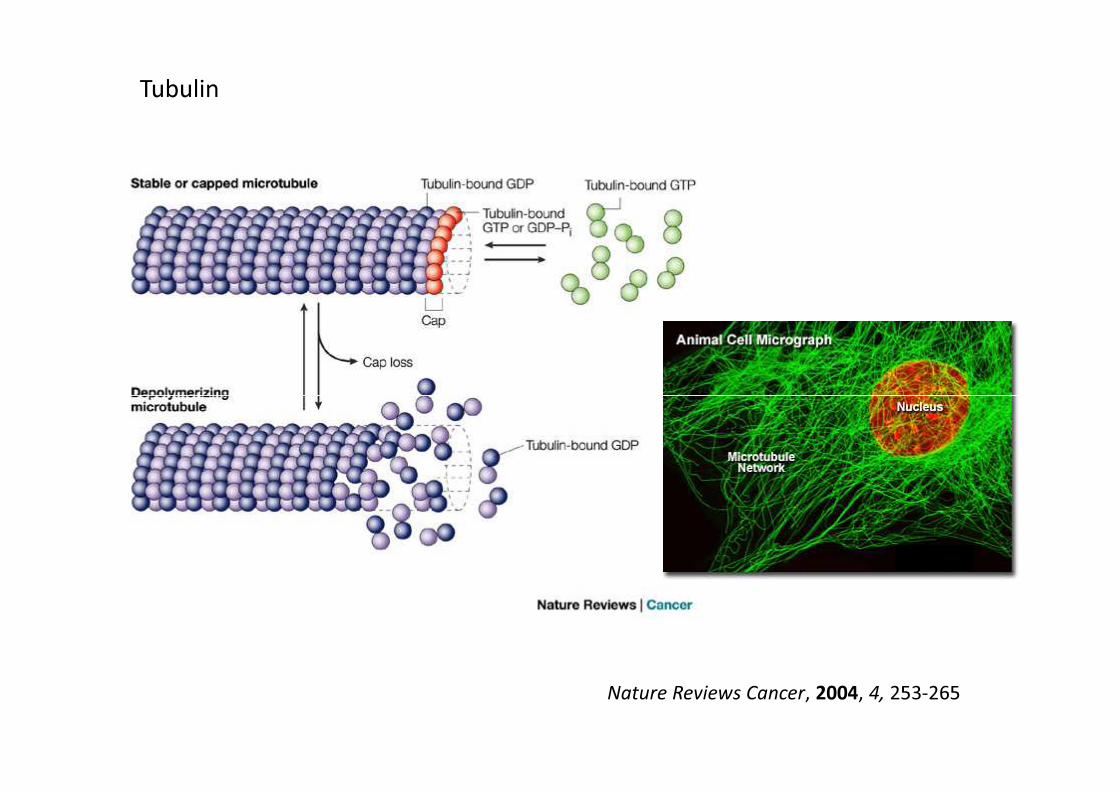
Tubulin
Nature Reviews Cancer, 2004, 4, 253-265
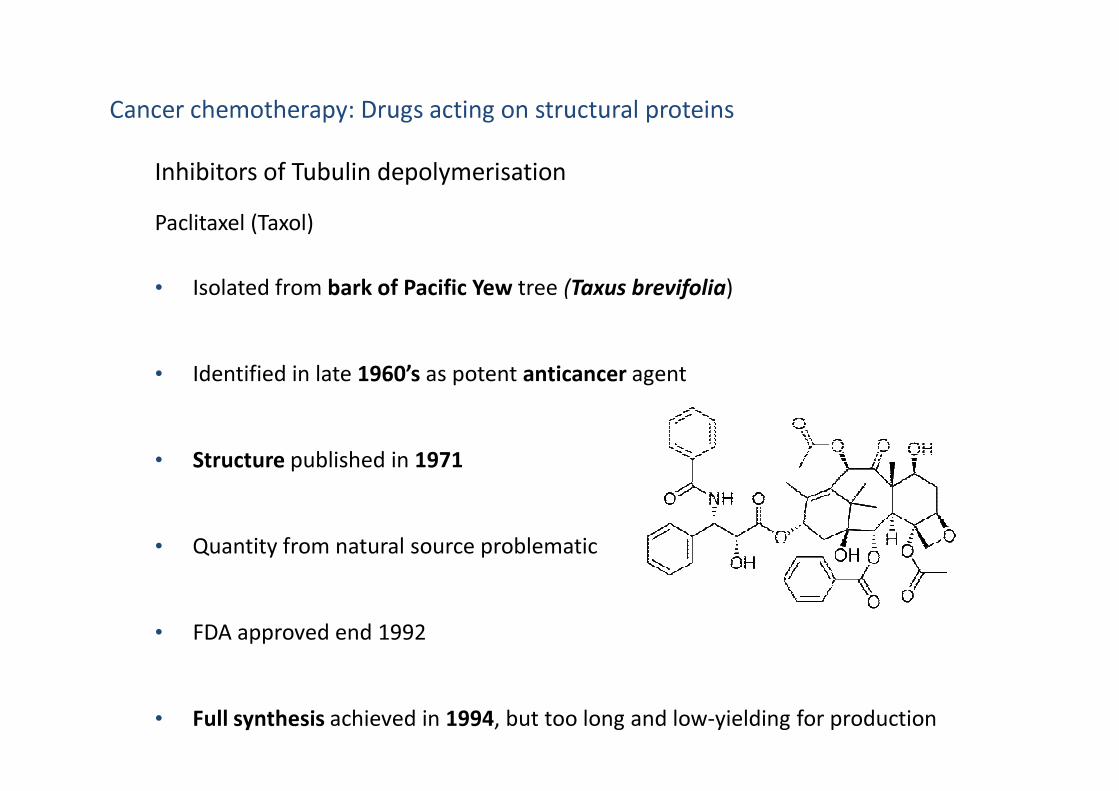
Inhibitors of Tubulin depolymerisation
Paclitaxel (Taxol)
• Isolated from bark of Pacific Yew tree (Taxus brevifolia)
• Identified in late 1960’s as potent anticancer agent
Cancer chemotherapy: Drugs acting on structural proteins
• Structure published in 1971
• Quantity from natural source problematic
• FDA approved end 1992
• Full synthesis achieved in 1994, but too long and low-yielding for production

• 10-deacetylbaccatin isolated from• 10-deacetylbaccatin isolated from
• Semi-synthetic route from 10-deacetylbaccatin developed, used in production
• Advanced precursor isolated from
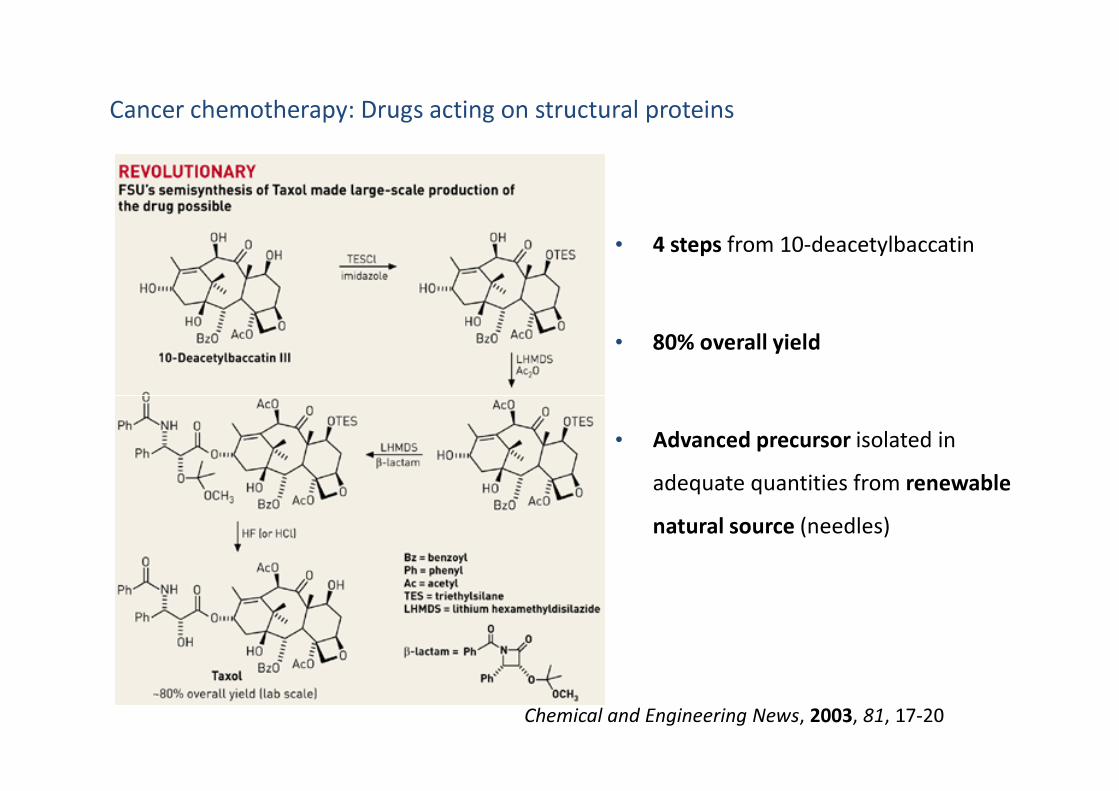
Cancer chemotherapy: Drugs acting on structural proteins
• 4 steps from 10-deacetylbaccatin
• 80% overall yield
Chemical and Engineering News, 2003, 81, 17-20
• Advanced precursor isolated in
adequate quantities from renewable
natural source (needles)

Inhibitors of Tubulin depolymerisation
Paclitaxel (Taxol)
• Mechanism of action determined early 1990’s
• Taxol binds to
• Stabilises microtubule,
• Halts
Annals of Oncology, 1994, 5 Suppl 6, S3-6; SB Horwitz

Inhibitors of Tubulin depolymerisation
Paclitaxel (Taxol)
• Areas NB for binding to tubulin:
Cancer chemotherapy: Drugs acting on structural proteins
• Introduce variations to improve pharmacokinetics on other side of molecule:
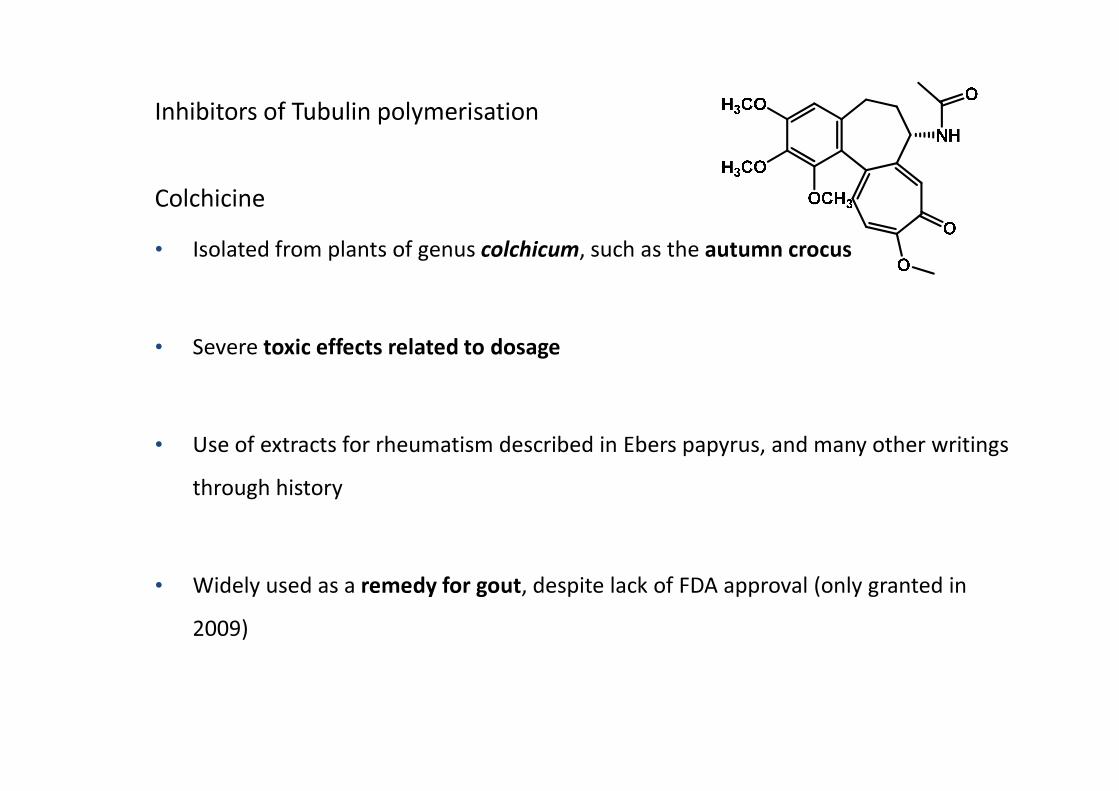
Inhibitors of Tubulin polymerisation
Colchicine
• Isolated from plants of genus colchicum, such as the autumn crocus
• Severe toxic effects related to dosage
• Use of extracts for rheumatism described in Ebers papyrus, and many other writings
through history
• Widely used as a remedy for gout, despite lack of FDA approval (only granted in
2009)
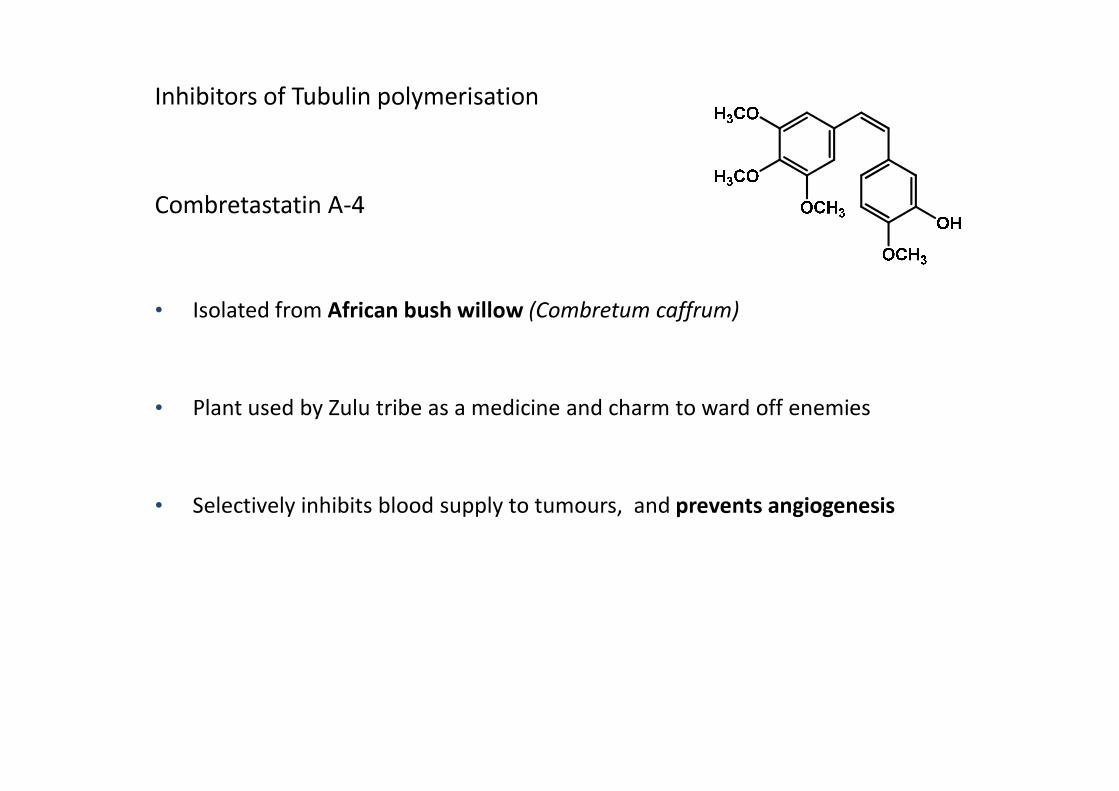
Inhibitors of Tubulin polymerisation
Combretastatin A-4
• Isolated from African bush willow (Combretum caffrum)
• Plant used by Zulu tribe as a medicine and charm to ward off enemies• Plant used by Zulu tribe as a medicine and charm to ward off enemies
• Selectively inhibits blood supply to tumours, and prevents angiogenesis

• Similar structure:
• Two
• cis geometry of alkene in Combretastatin A-4 NB for
•
• Both drugs bind to tubulin, prevent formation of

• Fifth leading cause of death worldwide
• Widespread infectious disease: half the world population
• 800 000 people die annually,
Malaria
• Historically, more soldiers died of malaria than in battle action
• Most research into development of antimalarials conducted by military institutions
(eg Walter Reed Army Institute of Research)
• Direct link to poverty: US$ 12 billion lost every year in GDP
• Malaria is caused by
• Malaria is contracted when a person is
• Five species of Plasmodium capable of transmitting malaria in humans:
How is malaria contracted?
P. falciparum -
P. vivax -
-
P. ovale
P. malariae
P. knowlesi -
-

Malaria: Lifecycle of the parasite

Vector Control:
• Indoor Residual Spraying (IRS) of insecticides
• Long-Lasting Insecticide Treated Nets (LLITN)
Malaria: Treatment and control
Prophylaxis and Drug Therapy:
• Chloroquine and other quinolines
• Antifolates
• Atovaquone
• Artemisinin derivatives
• Antibiotics
Antimalarials - Inhibitors of Folate metabolism
• Plasmodium species rely heavily on
• These are obtained two ways:
••
•
• Antifolates target enzymes of
• Target

DHF = Dihydrofolate
DHFR = Dihydrofolate reductase
THF = Tetrahydrofolate
SHMT = Serine hydroxymethyl
transferase
TS = Thymidylate synthase
Antimalarials - Folate salvage pathway
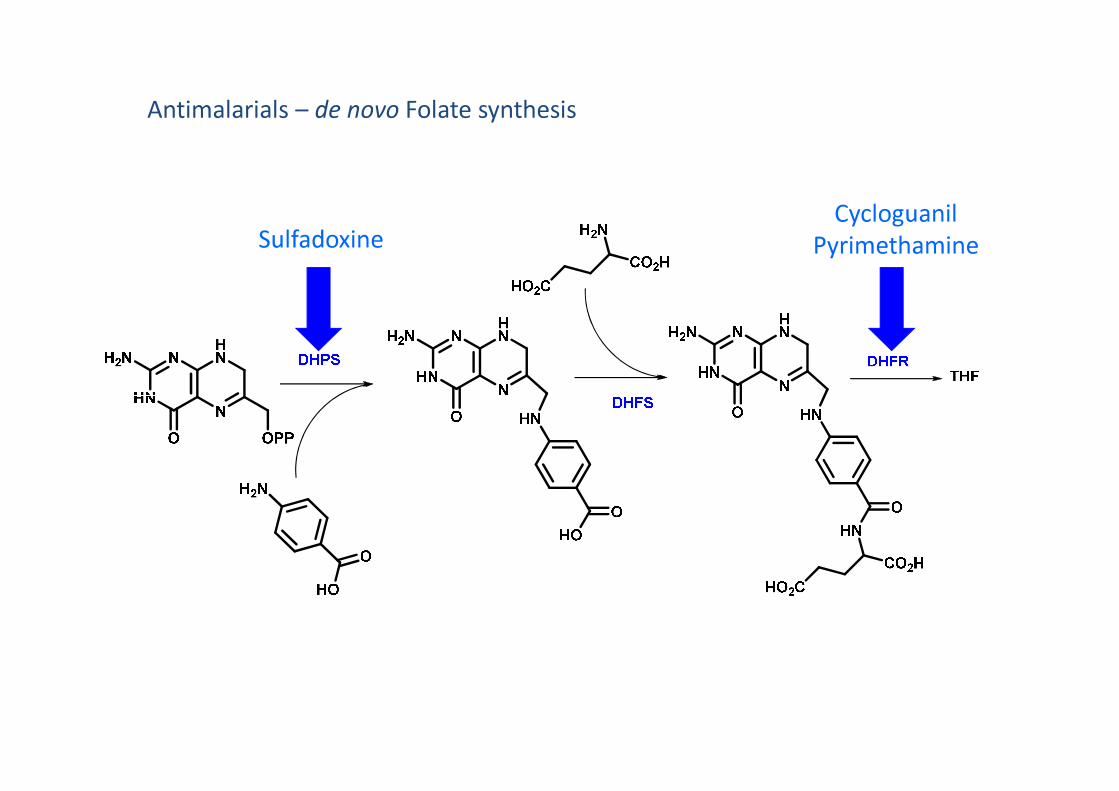
SulfadoxineCycloguanil
Pyrimethamine
Folate metabolism- de novo synthesisAntimalarials – de novo Folate synthesis
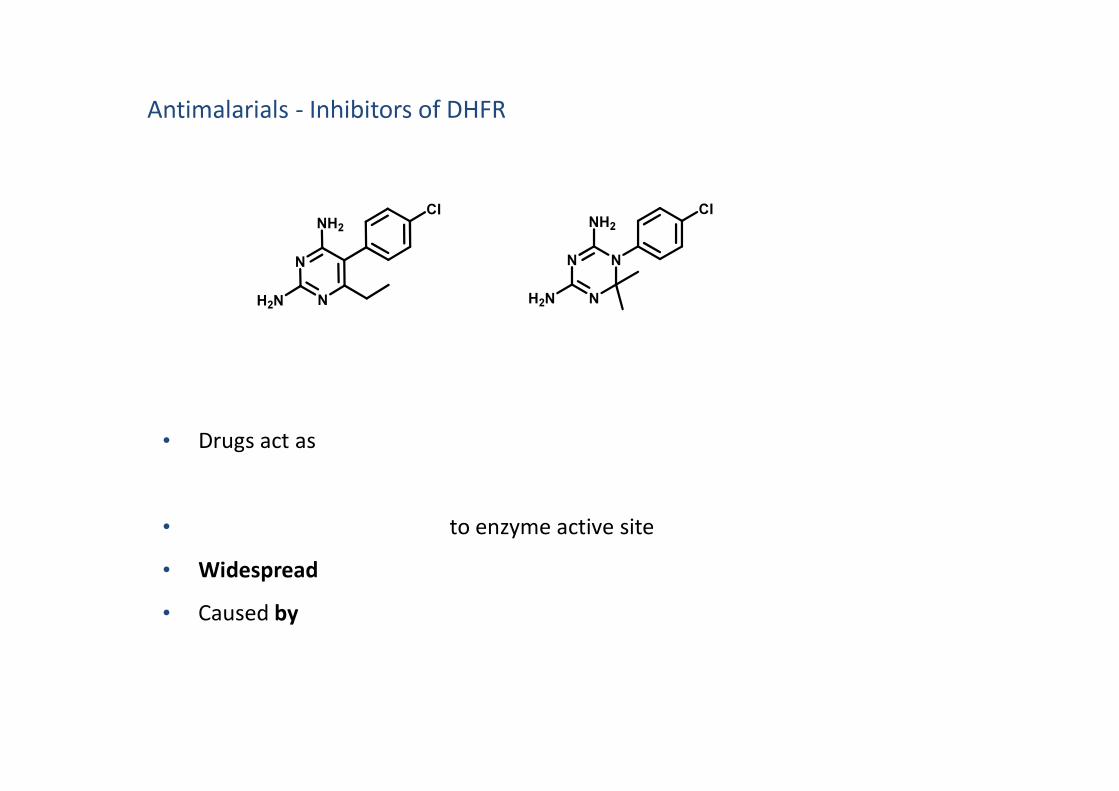
Antimalarials - Inhibitors of DHFR
N
N
NH2
H2N
Cl
NN
NH2
Cl
NH2N
• Drugs act as
• to enzyme active site
• Widespread
• Caused by

DHF = Dihydrofolate
DHFR = Dihydrofolate reductase
THF = Tetrahydrofolate
SHMT = Serine hydroxymethyl
transferase
TS = Thymidylate synthase
Antimalarials - Inhibitors of DHFR
OR
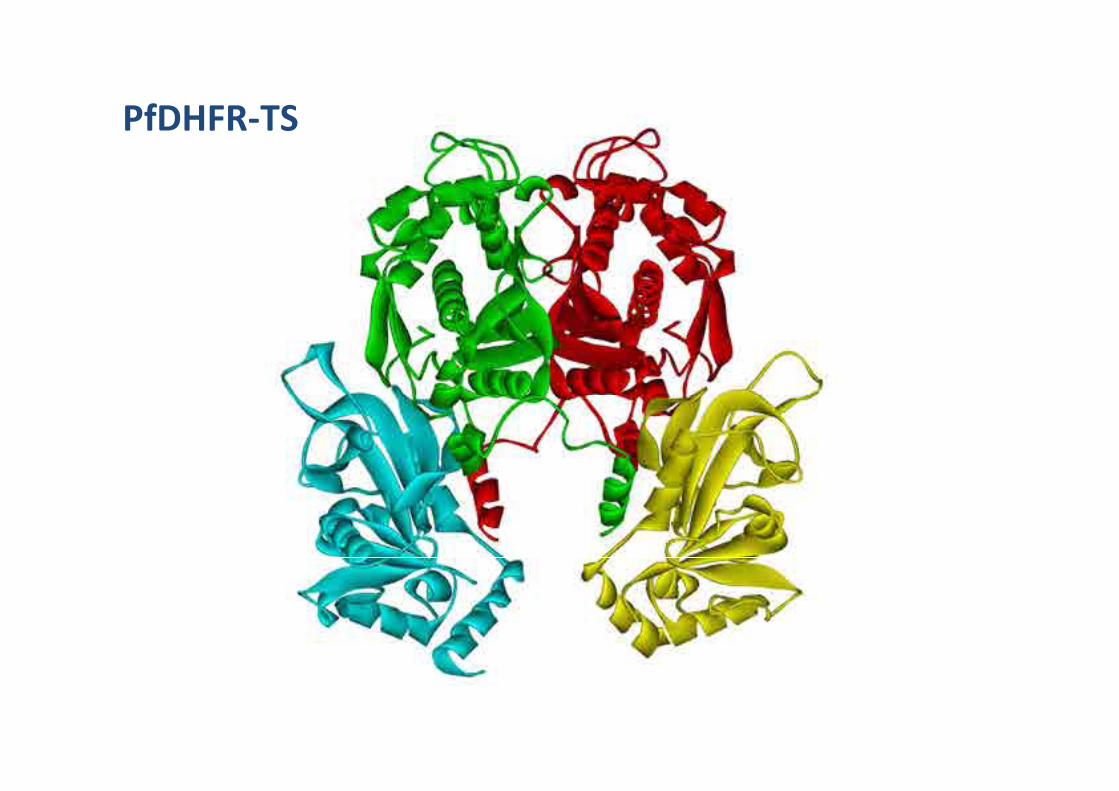
PfDHFR-TS
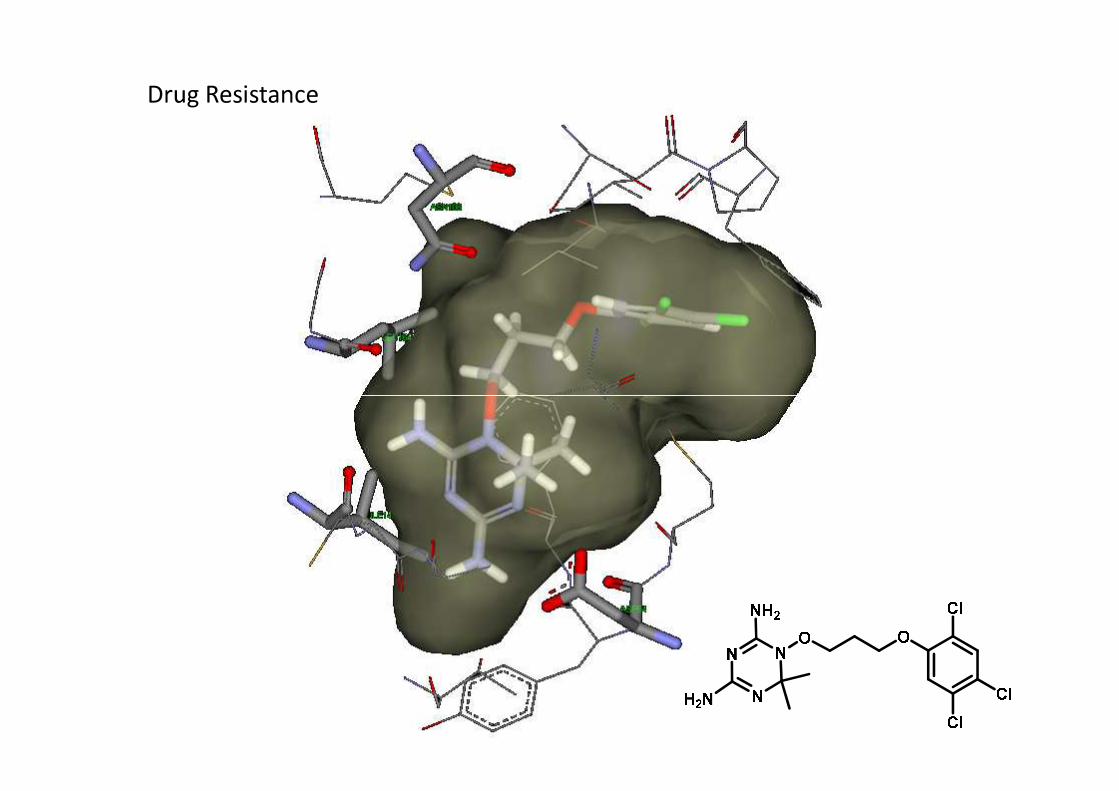
Drug Resistance

Antimalarials - Inhibitors of DHFR
N
N
NH2
H2N
Cl
NN
NH2
Cl
NH2N
• Design new drugs with
N
N
N O
H
NH2
H2N
HCl
X
“Triazine Derivates for Use in the Treatment of Malaria”, 2010, WO2011018742 (A1)
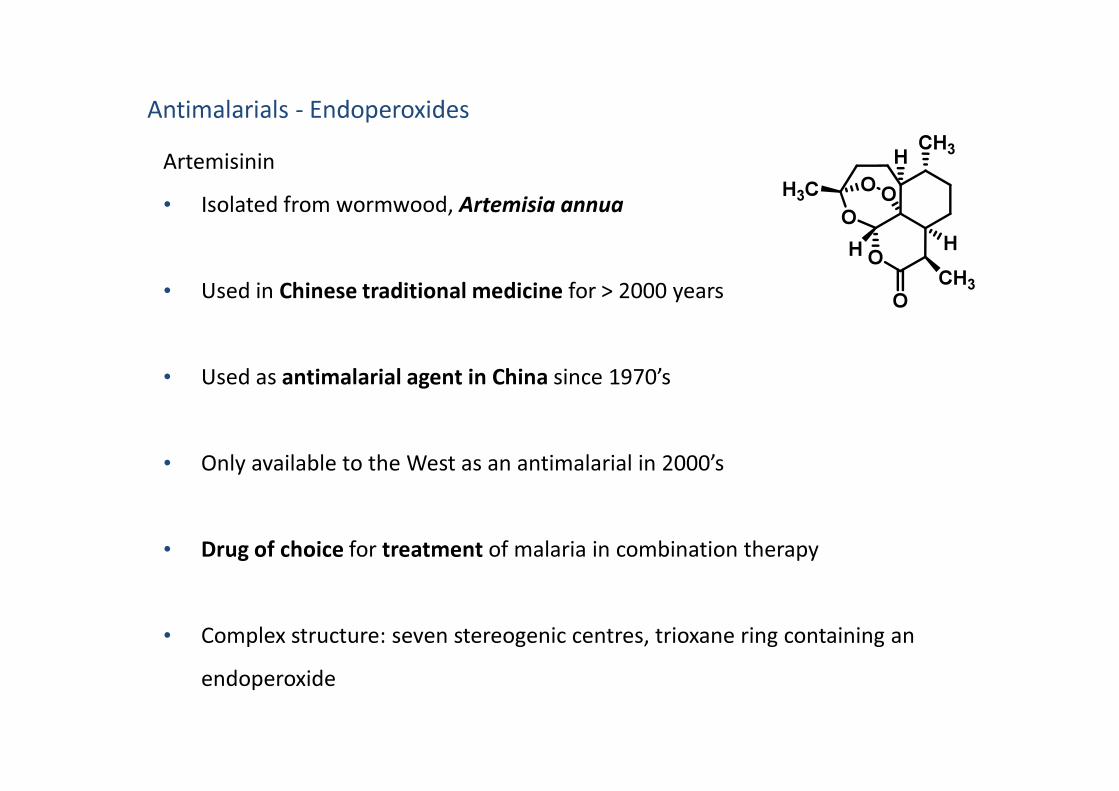
Antimalarials - Endoperoxides
Artemisinin
• Isolated from wormwood, Artemisia annua
• Used in Chinese traditional medicine for > 2000 years
• Used as antimalarial agent in China since 1970’s
O
O
CH3H
H
CH3
O
H
OOH3C
• Only available to the West as an antimalarial in 2000’s
• Drug of choice for treatment of malaria in combination therapy
• Complex structure: seven stereogenic centres, trioxane ring containing an
endoperoxide

Drawbacks:
• Artemisinin poorly soluble in water and oil,
• Short plasma half life in body
• Ideally, need better PK properties

Artemisinin
• Reduction to give
• DHA and derivatives of DHA also
O
O
CH3H
H
CH3
O
H
OOH3C
Antimalarials - Endoperoxides
O
O
CH3H
H
CH3
OH
H
OOH3C
O
O
CH3H
H
CH3
OR
H
OOH3C
• DHA and derivatives of DHA also
• NB feature for activity:

• Mechanism not fully understood
• Thought to involve radical mechanism, after activation by Fe(II)
O
CH3H
OOH3C
Antimalarial Endoperoxides: mechanism of action
O
O
H
CH3
O
H
O
O
CH3H
H
CH3
O
H
O
H3C 1) H
2) - FeIIIOH




















