







Bahasa
Halaman
Hukum

High-Dose Probiotics for the Treatmentof Active PouchitisPaolo Gionchetti, M.D.,1 Fernando Rizzello, M.D.,1 Claudia Morselli, M.D.,1
Gilberto Poggioli, M.D.,2 Rosi Tambasco, M.D.,1 Carlo Calabrese, M.D.,1
Patrizia Brigidi, M.D.,3 Beatrice Vitali, M.D.,3 Giulia Straforini, M.D.,1
Massimo Campieri, M.D.1
1 Department of Internal Medicine and Gastroenterology, University of Bologna, Bologna, Italy2 Department of Clinical Surgery, University of Bologna, Bologna, Italy3 Department of Pharmaceutical Sciences, University of Bologna, Bologna, Italy
PURPOSE: Pouchitis is the major long-term complicationafter ileal-pouch anal anastomosis for ulcerative colitis.Broad-spectrum antibiotics are the mainstay of treatment inthis condition. Recently, we have shown the efficacy of ahighly concentrated probiotic preparation (VSL#3, 900billions/sachet lyophilized viable bacteria) in preventingrelapses of chronic pouchitis and in preventing pouchitisonset. This study was designed to evaluate the efficacy ofhigh-dose VSL#3 in the treatment of mildly active pouchitis.METHODS: Twenty-three consecutive patients with mildpouchitis, defined as a score of between 7 and 12 in thePouchitis Disease Activity Index, which includes clinical,endoscopic, and histological criteria, were treated withVSL#3, 2 sachets b.i.d. (3600 billion bacteria/day) forfour weeks. Symptomatic, endoscopic, and histologicevaluations were undertaken before and after treatmentaccording to Pouchitis Disease Activity Index. Remissionwas defined as a combination of a Pouchitis DiseaseActivity Index clinical score of e2, endoscopic score ofe1, and total Pouchitis Disease Activity Index score of e4.Patients in remission after treatment were treated withVSL#3, 1 sachet b.i.d. (1800 billion bacteria), as mainte-nance treatment for six months. The quality of life wasassessed with the Inflammatory Bowel Disease Question-naire. RESULTS: Sixteen of 23 patients (69 percent) were inremission after treatment. The median total PouchitisDisease Activity Index scores before and after therapywere 10 (range, 9–12) and 4 (range, 2–11), respectively
(P<0.01). The median Inflammatory Bowel Disease Ques-tionnaire score also significantly improved from 110(range, 90–140) to 200 (range, 95–220; P<0.001). All 16patients who went into remission maintained remissionduring maintenance treatment. Only one patient experi-enced a transient bloating at the beginning of treatment.CONCLUSIONS: High doses of the probiotic VSL#3 areeffective in the treatment of mild pouchitis. Furthercontrolled studies are warranted. [Key words: Ulcerativecolitis; Pouchitis; Probiotics]
T otal proctocolectomy with ileal pouch-anal
anastomosis (IPAA) has emerged during the
past 15 years as the surgical procedure of choice for
the management of ulcerative colitis (UC). Pouchitis,
a nonspecific idiopathic inflammation of the ileal
reservoir, has become the most frequent long-term
complication after pouch surgery for UC.1 The
reported incidence of pouchitis is variable, largely
because of differences in the type and duration of
follow-up and, particularly, because myriad diagnostic
criteria have been used to define this syndrome.2–7
Most patients who develop acute pouchitis do so
within the first year, but some may suffer their first
attack some years after surgery.4
The etiology is still unknown, but both a history of
UC and increased bacterial concentrations are the
main factors.1,8 The importance of bacteria is further
emphasized by the evident efficacy of antibiotics.9–11
This syndrome is clinically characterized by vari-
able symptoms, including increased stool frequency
and fluidity, rectal bleeding, abdominal cramping,
Correspondence to: Paolo Gionchetti, M.D., Department ofInternal Medicine and Gastroenterology, Policlinico S. Orsola, ViaMassarenti 9, Bologna 40138, Italy, e-mail: [email protected].
Dr. Pardi does consulting and research for Salix.
Dis Colon Rectum 2007; 50: 2075–2084DOI: 10.1007/s10350-007-9068-4* The American Society of Colon and Rectal SurgeonsPublished online: 13 October 2007
2075

urgency and tenesmus, incontinence, fever, and
extraintestinal manifestations.8 A clinical diagnosis
should be confirmed by endoscopy and histology.
The endoscopic features of pouchitis include muco-
sal erythema, edema, friability, petechiae, granulari-
ty, loss of vascular pattern, erosions, and superficial
ulceration. Histologic examination shows an acute
inflammatory infiltrate with crypt abscesses and
ulceration in addition to chronic inflammation,
including villous atrophy, and crypt hyperplasia,
which is almost universal and probably represents
an adaptive response of the pouch mucosa to fecal
stasis.12 The absence of clear and universally accept-
ed criteria for the diagnosis, classification, and
definition of activity has created variability in the
reported incidence of pouchitis and in the assess-
ment of therapy. To overcome this problem, Sand-
born and colleagues developed the Pouchitis Disease
Activity Index (PDAI).13 This 18-point index is based
on clinical symptoms and endoscopic appearance, as
well as acute histologic findings, and represents an
objective and reproducible scoring system for
pouchitis. Active pouchitis is defined as a score Q7,
and remission is defined as a score <7.
Probiotics are defined as living microorganisms,
which on ingestion in adequate amounts, exert
health effects beyond inherent basic nutrition.14
Bacteria associated with probiotic activity are most
commonly lactobacilli, bifidobacteria, and strepto-
cocci, but other nonpathogenic bacteria, such as
some strains of Escherichia coli, and nonbacterial
organisms, such as the yeast Saccharomyces boular-
dii, have been used. The rationale for using pro-
biotics in inflammatory bowel disease is based on
convincing evidence implicating intestinal bacteria in
the pathogenesis of the disease.15,16
Good results have been obtained with probiotic
therapy in experimental colitis. Administration of
Lactobacillus reuteri reduced inflammation signifi-
cantly in acetic acid- and methotrexate induced-
colitis in rats.17,18 More recently, Lactobacillus sp.
was shown to prevent the development of sponta-
neous colitis in interleukin (IL)-10–deficient mice 19;
continuous feeding with Lactobacillus plantarum
could attenuate an established colitis in the same
knockout model.20 In IL-10–deficient mice, Lactoba-
cillus salivarius subsp. salivarius reduced the rate
of inflammation progression through dysplasia and
colonic cancer.21 Bifidobacterium infantis and
Lactobacillus salivarius attenuated inflammation,
reducing the production of Th1-type cytokines in
the IL-10 knockout model.22 Probiotics were shown
to be effective in maintenance therapy of UC.23–25
We have used a probiotic preparation (VSL#3)
with a high bacterial concentration and a cocktail
of eight different bacterial species. It has been
shown to be effective in maintenance therapy of
chronic pouchitis,26,27 in prevention of the onset of
pouchitis,28 in maintenance therapy of UC,29 and in
treatment of active mild-to-moderate UC.30 This
study was designed to evaluate the efficacy of
VSL#3 in the treatment of mildly active pouchitis.
PATIENTS AND METHODS
The study was performed in accordance with the
Declaration of Helsinki and was approved by the
ethical committee of our hospital; written, informed
consent was obtained from the patients. Patients
were included if they had current active mild
pouchitis, defined as a score between 7 and 12,
using the 18-point PDAI.13 All patients had J-shaped
constructed pouches; three-stage IPAA was per-
formed in 18 patients and two-stage IPAA in 5
patients.
Patients were excluded from entry if they 1) had
chronic pouchitis; 2) had received any treatment for
pouchitis, including antibiotics, steroids or immuno-
suppressants, within two weeks before participation;
3) had taken nonsteroidal anti-inflammatory drugs;
4) had previously taken VSL#3; 5) had a history of
epilepsy or convulsions; 6) had perianal disease
(including abscess, fissure, stricture, or anal sphincter
weakness); 7) had severe cardiovascular, respiratory,
hepatic (including primary sclerosing cholangitis) or
renal conditions; or 8) were pregnant or breast feeding.
Concurrent use of antidiarrheals, probiotics, or
narcotic drugs also excluded them from the study.
Study Medication
VSL#3 (VSL#3 Pharmaceuticals, Inc, Ft. Lauderdale,
FL) consisted of packets containing 900 billion viable
lyophilized bacteria of 4 strains of Lactobacillus (L. casei,
L. plantarum, L. acidophilus, and L. delbrueckii subsp.
bulgaricus), 3 strains of Bifidobacterium (B. longum,
L. breve, and B. infantis), and 1 strain of Streptococcus
salivarius subsp. thermophilus, designated as S. ther-
mophilus throughout this article.
Patients received VSL#3 2 packets b.i.d. for four
weeks. Patients who obtained remission were treated
with VSL#3 one sachet b.i.d. (1800 billion bacteria
2076 GIONCHETTI ET AL Dis Colon Rectum, December 2007

per day) for six months as maintenance treatment.
The medications were dispensed by the investigator
at the initial visit; compliance was assessed by
counting returned bags and questioning the patients.
Evaluation and Scheduling
Demographics and pouchitis risk factors (recent
tobacco cessation, sclerosing cholangitis, extraintesti-
nal manifestation, pancolitis) were assessed at baseline.
Symptom assessment (stool frequency, rectal bleeding,
fecal urgency, abdominal cramps, fever) and endo-
scopic examination of the ileal pouch and the ileum for
several centimeters proximal to the pouch, with
mucosal biopsies and histologic assessment of biopsy
specimens were performed at baseline and after four
weeks and six months according to the PDAI.
Mild pouchitis was defined as a total PDAI score of
Q7 and e12. Remission was defined as a clinical score
of e2 (total possible range, 0–6), endoscopic PDAI
score of e1 (total possible range, 0–6), and total PDAI
of e4.
Patients were assessed according to whether they
had achieved remission. Health-related quality of life
was assessed at baseline and after four weeks, by
using the Inflammatory Bowel Disease Questionnaire
(IBDQ),31 which considers bowel, systemic, and
emotional symptoms as well as social function. The
IBDQ ranges from 32 (worst quality of life) to 224
(best quality of life).
Safety Assessment
All unfavorable, unexpected symptoms were
recorded in the diary kept by patients during the
study. Laboratory studies, including a complete
blood count and blood chemistry measurements,
were performed at baseline and at the end of
treatment.
Microbiologic Determinations
Fecal sample collection. Fecal samples of patients
were examined before starting treatment (T0) and
after one month of treatment (T1). The specimens
were collected with sterile plastic containers,
immediately stored at j20-C, and analyzed within
ten days for evaluating their bacterial microflora
composition.
Isolation and enumeration of fecal bacterial
groups. Anaerobic culture techniques, isolation
procedures, and identification methods were
performed following the Wadsworth Anaerobic
Bacteriology Manual 5th edition.32 One gram of each
fecal sample was homogenized in 99 ml of prereduced
half-strength Wilkins Chalgreen Anaerobic Broth
(Oxoid, Basingstoke, UK) and serially diluted in an
anaerobic cabinet (Anaerobic System, Mod. 2028,
Forma Scientific Co, Marietta, OH). The dilutions
were spread onto plates containing the following
agar media: LAMVAB33 for Lactobacillus; RB34 for
Bifidobacterium; Schaedler anaerobe (Oxoid,
Basingstoke, UK) plus defibrinated horse blood
(50 g/l), menadione (5 mg/l), vancomycin (28 mg/l),
and kanamycin (100 mg/l) for Bacteroides; and Oxoid
Perfringens Agar (Oxoid, Basingstoke, UK) for
Clostridium perfringens. Plates were anaerobically
incubated in triplicate at 37-C for 24 to 48 hours. The
same dilutions were removed from the anaerobic
glove box and used to inoculate the following media:
Azide Maltose (Biolife, Milan, Italy) for enterococci;
MacConkey (Merck, Darmstadt, Germany) for
coliforms; and ST agar,35 slightly modified by adding
bromocresole purple (30 mg/l), bromocresole green
(100 mg/l), and nalidixic acid (30 mg/l) for S.
thermophilus. Plates were aerobically incubated in
triplicate at 37-C for 24 to 36 hours. The lower limit
of detection was 1,000 microorganisms/g feces, and
bacterial concentrations were expressed as colony-
forming units (CFU) per gram of dry feces. Represen-
tative colonies of each selective medium were
identified to genus level by standard bacteriological
procedures, such as Gram_s stain reaction, colonial and
cellular morphology, and biochemical reactions.
PCR detec t ion of S . thermophi lus and
Bifidobacterium. Amplification reactions were
carried out in a Biometra Thermal Cycler II
(Biometra, Gottingen, Germany). Dynazyme II
(Celbio, Milan, Italy) was used as a thermostable
polymerase as suggested by the supplier. The total
volume of each reaction mixture was 25 ml, and cells
from plate colonies were used directly as template,
wi thout i so la t ion of chromosomal DNA.
Amplification of S. thermophilus was obtained using
the species-specific primer set ThI/ThII, based on
the 16S–23S rDNA internal transcribed region.36 The
expected size of the PCR product was 250 bp. The
reaction mixture consisted of 200 mM each dNTP, 1
mM of ThI and ThII primer, and 1 U of Dynazyme II.
The amplification profile was at 95-C for 1 minute,
55-C for 30 seconds, and 72-C for 1 minute. This was
repeated for 40 cycles. The program also included
preincubation at 95-C for 5 minutes before the first
Vol. 50, No. 12 PROBIOTICS IN ACTIVE POUCHITIS 2077

cycle and a final incubation at 72-C for 5 minutes.
Bifidobacteria were amplified by using the 16S rDNA
genus-specific primer set Bif164/Bif662,37 obtaining
an amplicon of 523 bp. The VSL#3 strains B. infantis
and B. breve were detected specifically by the strain-
specific primer sets InfY-BV.L/R and BreY-BV.R/L
16S–23S rDNA,38 designed on the 16S–23S rDNA
sequences. The PCR product sizes were 330 and 340 bp
for B. infantis and B. breve strains, respectively. The
following experimental conditions were used: PCR
reaction mixture was composed of 200 mM each
dNTP, 0.5 mM of each primer, and 1 unit of
Dynazyme II. The thermocycle program consisted of
the following time and temperature profile: 1) 95-C for
5 minutes; 2) 40 cycles of 1 minute at 95-C, 30 seconds
at a specific annealing temperature, and 1 minute at
72-C; and 3) 5 minutes at 72-C. The annealing
temperature was 55-C for the primer sets Bif164/
Bif662 and InfY-BV.L/R and 64-C for the primer set
BreY-BV.R/L.
Enumeration of S. thermophilus and VSL#3 strains
B. infantis and B. breve was performed by direct
amplification of 30 to 50 colonies randomly selected
from the highest dilutions of ST modified and RB
agar plates. Aliquots (5–10 ml) of the amplified
products were subjected to gel electrophoresis in
2 percent agarose gels and were visualized by
ethidium bromide staining.
Statistical Analysis
Statistical analysis was performed with Prism Version
2.0 (GraphPad Inc., San Diego, CA). For descriptive
data, the median and range were calculated. The
Wilcoxon_s signed-rank test (paired, two-tailed) was
used to compare pretreatment and posttreatment
bowel frequency, PDAI scores, and IBDQ scores.
The primary measure of efficacy was the compar-
ison between the pretreatment and posttreatment
PDAI scores, with remission defined as a combination
of a clinical score of e2, endoscopic PDAI score of e1,
and total PDAI of e4. Comparison of fecal concentra-
tion of bacteria before treatment and after one month
was performed by using the Student_s t test.
RESULTS
Patient Characteristics
Twenty-three patients with mildly active pouchitis
participated in this trial. Characteristics of the patients are
shown in Table 1. Six patients had experienced their
first episode of pouchitis, whereas 17 had relapsing
pouchitis. No patients withdrew from the trial.
Clinical Results
Sixteen (69 percent) of 23 treated patients went
into remission, whereas 7 were unchanged. Four of
16 patients who went into remission had experienced
their first episode of pouchitis and 12 had relapsing
pouchitis. The median bowel frequency significantly
decreased from 10 (range, 8–15) to 6 (range, 3–12)
after probiotic treatment (P<0.001), as did the median
total PDAI score from 10 (range, 9–12) to 4 (range,
2–11; P<0.001); this significant decrease was the
result of a significant reduction in clinical, endoscop-
ic, and histologic scores of PDAI (Table 2). Figure 1
shows the changes in total PDAI scores in all patients.
All 16 patients who went into remission were still in
remission at the end of six months_ maintenance
therapy, with median bowel frequency of 4 (range,
2–8) and median PDAI scores of 3 (range, 2–4). The
median IBDQ score, at the end of the study, was
Table 1.Demographic and Clinical Characteristics
of Patients (N=23)
Male/Female ratio 13/10
Mean age (yr) 31.8Smoking habits
Smokers 5Ex-smokers 3Nonsmokers 15
Extension of colitisExtensive 20Distal 3
Extraintestinal manifestations 4Time since ileal-pouch anal
anastomosis (mo)43.5T26.3
Onset of pouchitis after surgery (mo) 21.3T13.5
Data are numbers or means T standard deviations.
Table 2.Median Total PDAI Score and Each Component
PDAI Score Variation
PDAI score Baseline Four Weeks Six Months
Total 10 (9–12) 4 (2–11). 3 (2–4).Clinical 3 (2–4) 1 (0–4)* 0 (0–2)*Endoscopic 4 (2–5) 1 (1–4)* 1 (0–1)*Histologic 3 (2–4) 1 (1–3)* 1 (0–2)*
PDAI = Pouchitis Disease Activity Index.Results are medians with ranges in parentheses.*P<0.002; .P<0.001 vs. baseline.Data at six months refer only to the 16 patients
who went into remission after four weeks
2078 GIONCHETTI ET AL Dis Colon Rectum, December 2007
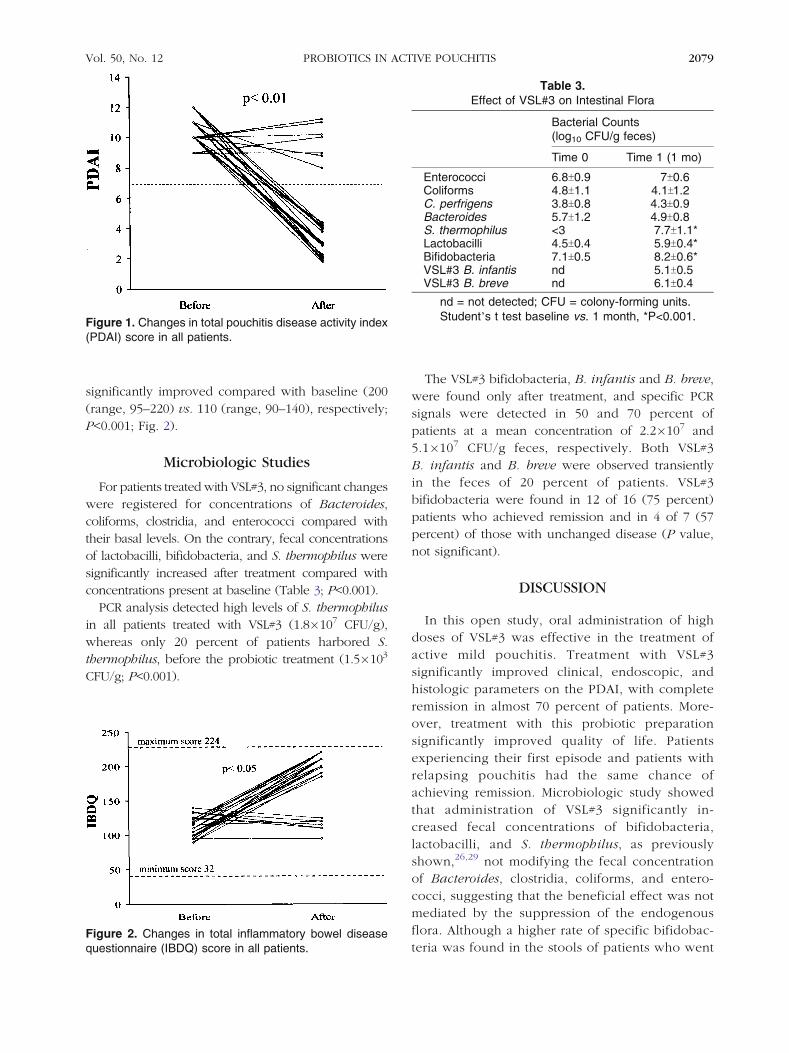
significantly improved compared with baseline (200
(range, 95–220) vs. 110 (range, 90–140), respectively;
P<0.001; Fig. 2).
Microbiologic Studies
For patients treated with VSL#3, no significant changes
were registered for concentrations of Bacteroides,
coliforms, clostridia, and enterococci compared with
their basal levels. On the contrary, fecal concentrations
of lactobacilli, bifidobacteria, and S. thermophilus were
significantly increased after treatment compared with
concentrations present at baseline (Table 3; P<0.001).
PCR analysis detected high levels of S. thermophilus
in all patients treated with VSL#3 (1.8�107 CFU/g),
whereas only 20 percent of patients harbored S.
thermophilus, before the probiotic treatment (1.5�103
CFU/g; P<0.001).
The VSL#3 bifidobacteria, B. infantis and B. breve,
were found only after treatment, and specific PCR
signals were detected in 50 and 70 percent of
patients at a mean concentration of 2.2�107 and
5.1�107 CFU/g feces, respectively. Both VSL#3
B. infantis and B. breve were observed transiently
in the feces of 20 percent of patients. VSL#3
bifidobacteria were found in 12 of 16 (75 percent)
patients who achieved remission and in 4 of 7 (57
percent) of those with unchanged disease (P value,
not significant).
DISCUSSION
In this open study, oral administration of high
doses of VSL#3 was effective in the treatment of
active mild pouchitis. Treatment with VSL#3
significantly improved clinical, endoscopic, and
histologic parameters on the PDAI, with complete
remission in almost 70 percent of patients. More-
over, treatment with this probiotic preparation
significantly improved quality of life. Patients
experiencing their first episode and patients with
relapsing pouchitis had the same chance of
achieving remission. Microbiologic study showed
that administration of VSL#3 significantly in-
creased fecal concentrations of bifidobacteria,
lactobacilli, and S. thermophilus, as previously
shown,26,29 not modifying the fecal concentration
of Bacteroides, clostridia, coliforms, and entero-
cocci, suggesting that the beneficial effect was not
mediated by the suppression of the endogenous
flora. Although a higher rate of specific bifidobac-
teria was found in the stools of patients who went
Figure 1. Changes in total pouchitis disease activity index(PDAI) score in all patients.
Figure 2. Changes in total inflammatory bowel diseasequestionnaire (IBDQ) score in all patients.
Table 3.Effect of VSL#3 on Intestinal Flora
Bacterial Counts(log10 CFU/g feces)
Time 0 Time 1 (1 mo)
Enterococci 6.8T0.9 7T0.6Coliforms 4.8T1.1 4.1T1.2C. perfrigens 3.8T0.8 4.3T0.9Bacteroides 5.7T1.2 4.9T0.8S. thermophilus <3 7.7T1.1*Lactobacilli 4.5T0.4 5.9T0.4*Bifidobacteria 7.1T0.5 8.2T0.6*VSL#3 B. infantis nd 5.1T0.5VSL#3 B. breve nd 6.1T0.4
nd = not detected; CFU = colony-forming units.Student_s t test baseline vs. 1 month, *P<0.001.
Vol. 50, No. 12 PROBIOTICS IN ACTIVE POUCHITIS 2079

into remission, compared with patients who did
not respond to probiotic treatment, the difference
was not statistically significant, because of the
small sample size.
The use of a molecular method to distinguish
between endogenous and exogenous ingested bifi-
dobacteria confirmed that the bifidobacteria strains
administered with VSL#3 survived the gastric acid
and bile and influenced the gut flora composition.Furthermore, the specific detection of VSL#3
strains B. infantis and B. breve confirmed that the
increase of the total fecal bifidobacteria population
after probiotic consumption was caused by the
presence of VSL#3 bifidobacteria strains. The dif-
ferent colonization behavior in terms of size and
frequency of detection of the exogenous bifidobac-
terial strains in the patients treated with VSL#3
emphasizes the complexity of the relationships
between exogenous bacteria and the human host
and supports the importance of a mixture of pro-
biotic strains.The etiology of pouchitis is still unknown and is
likely to be multifactorial; however, the immediate
response to antibiotic treatment suggests a patho-
genic role of microflora, and recently pouchitis has
been associated with a decreased ratio of anaerobic
to aerobic bacteria, reduced fecal concentrations of
lactobacilli and bifidobacteria, and increased luminal
pH.39 Treatment of pouchitis is largely empiric and
only a few small placebo-controlled trials have been
conducted. Antibiotics are the mainstay of treatment,
and metronidazole and ciprofloxacin are most com-
monly used initially, with a rapid and dramatic
response. Small randomized trials have suggested
that antibiotic therapy with metronidazole and cipro-
floxacin may be effective in treating active pouchi-
tis.9–11 Both drugs significantly lowered PDAI scores,
but patients treated with ciprofloxacin experienced
significantly greater reductions in the PDAI scores
and fewer adverse effects than those treated with
metronidazole.11
Recent studies have supported the potential thera-
peutic role of probiotics in IBD. Encouraging results
have been obtained with probiotic therapy in experi-
mental colitis.17–22 In three controlled studies, capsules
containing a nonpathogenic strain of Escherichia coli,
the Nissle 1917, were shown to be as effective as
mesalamine in maintenance treatment of UC.23–25
In open studies, VSL#3 was shown to be effective
in preventing relapses in patients with UC, who were
intolerant or allergic to sulphasalazine or 5-amino-
salicylic acid.29 VSL#3 induced remission in 53
percent of patients with active mild-to-moderate
UC, with a further 24 percent improvement in a six-
week trial.30
In three double-blind studies, VSL#3 was shown to
be significantly superior to placebo in maintaining
remission in patients with chronic pouchitis and
preventing the onset of pouchitis.26–28
Regarding the mechanism of action, recent studies
have shown that treatment with VSL#3 significantly
increases tissue levels of the anti-inflammatory cyto-
kine IL-10, with a significant decrease of tissue levels
of proinflammatory cytokines IL-1, TNF-a, and IFN-g;
a reduction of matrix metalloproteinase activity; and
a modulation of dendritic cell function.40,41
CONCLUSIONS
The study results indicate that the use of a highly
concentrated mixture of probiotic bacterial strains is
effective in the treatment of active mild pouchitis, is
well tolerated, and improves significantly the quality
of life of patients with pouchitis. This treatment may
represent a possible alternative to antibiotics for
patients with mild pouchitis. Currently, the only
limiting factor for the expanded use of VSL#3 in
patients with pouchitis is the relatively high cost,
which is not covered by health insurance or govern-
ment agencies. The efficacy of this new probiotic
preparation may be related to the increase of
concentrations of protective bacteria, as demonstrat-
ed by the microbiologic data, and further support the
potential role for probiotics in IBD therapy.
REFERENCES
1. Sandborn WJ. Pouchitis following ileal pouch-anal
anastomosis: definition, pathogenesis, and treatment.
Gastroenterology 1994;107:1856–60.
2. Svaninger G, Nordgren S, Oresland T, Hulten L.
Incidence and characteristics of pouchitis in the Koch
continent ileostomy and the pelvic pouch. Scand J
Gastroenterol 1993;28:695–700.
3. Penna C, Dozois R, Tremaine W, et al. Pouchitis after
ileal pouch-anal anastomosis for ulcerative colitis occurs
with increased frequency in patients with associated
primary sclerosing cholangitis. Gut 1996;38:234–9.
4. Stahlberg D, Gullberg K, Liljeqvist L, Hellers G, Lofberg R.
Pouchitis following pelvic pouch operation for ulcerative
colitis. Incidence, cumulative risk, and risk factors. Dis
Colon Rectum 1996;39:1012–8.
2080 GIONCHETTI ET AL Dis Colon Rectum, December 2007
5. Meagher AP, Farouk R, Dozois R, Kelly KA, Pemberton
JH. J-ileal pouch-anal anastomosis for CUC: complica-
tions and long-term outcome in 1310 patients. Br J Surg
1998;85:800–3.
6. Fazio VW, O’Riordain MG, Lavery IC, et al. Long-term
functional outcome and quality of life after stapled
restorative proctocolectomy. Ann Surg 1999;230:575–84.
7. Simchuk EJ, Thirlby RC. Risk factors and true incidence
of pouchitis in patients after ileal pouch-anal anasto-
moses. World J Surg 2000;24:851–6.
8. Sandborn WJ. Pouchitis: definition, risk factors,
frequency, natural history, classification, and public
perspectives. In: McLeod RS, Martin F, Sutherland LR,
Wallace JL, Williams CN, eds. Trends in inflammatory
bowel disease 1996. Lancaster, England: Kluwer
Academic Publishers, 1997:51–63.
9. Madden M, McIntyre A, Nicholls RJ. Double-blind cross-
over trial of metronidazole versus placebo in chronic
unremitting pouchitis. Dig Dis Sci 1994;39:1193–6.
10. Gionchetti P, Rizzello F, Venturi A, et al. Antibiotic
combination therapy in patients with chronic, treat-
ment-resistant pouchitis. Aliment Pharmacol Ther
1999;13:713–8.
11. Shen B, Achkar JP, Lashner BA, et al. A randomized
clinical trial of ciprofloxacin and metronidazole to treat
acute pouchitis. Inflamm Bowel Dis 2001;7:301–5.
12. Sheperd NA, Jass JR, Duval I, Moskowitz RL, Nicholls
RJ, Morson BC. Restorative proctocolectomy with ileal
reservoir: pathological and histochemical study of
mucosal biopsy. J Clin Pathol 1987;40:601–7.
13. Sandborn WJ, Tremaine WJ, Batts KP, Pemberton JH,
Phillips SF. Pouchitis after ileal pouch-anal anastomo-
sis: a pouchitis disease activity index. Mayo Clin Proc
1994;69:409–15.
14. Schaafsma G. State of the art concerning probiotic
strains in milk products. IDF Nutr Newsl 1996;5:234.
15. Campieri M, Gionchetti P. Probiotics in inflammatory
bowel disease: new insight to pathogenesis or a
possible therapeutic alternative? Gastroenterology
1999;116:1246–9.
16. Shanahan F. Probiotics in inflammatory bowel diseases.
Gut 2001;48:609.
17. Fabia R, Ar_Rajab A, Johansson M-L, et al. The effect of
exogenous administration of Lactobacillus reuteri R2LC
and oat fiber on acetic acid-induced colitis in the rat.
Scand J Gastroenterol 1993;28:155–62.
18. Mao Y, Nobaek S, Kasravi B, et al. The effects of
Lactobacillus strains and oat fibre on methotrexate-
induced enterocolitis in rats. Gastroenterology
1996;111:334–44.
19. Madsen KL, Doyle JS, Jewell LD, Tavernini MM,
Fedorak RN. Lactobacillus species prevents colitis in
interleukin-10 gene-deficent mice. Gastroenterology
1999;116:1107–14.
20. Schultz M, Veltkamp C, Dieleman LA, et al. Lactobacil-
lus plantarum 299Vs in the treatment and prevention
of spontaneous colitis in interleukin-10-deficient mice.
Inflamm Bowel Dis 2002;8:71–80.
21. O’Mahony L, Feeney M, O’Halloran S, et al. Probiotic
impact on microbial flora, inflammation and tumour
development in IL-10 knockout mice. Aliment Pharma-
col Ther 2001;15:1219–25.
22. McCarthy J, O’Mahony L, O’Callaghan L, et al. Double-
blind, placebo-controlled trial of two probiotic strains
in interleukin 10 knockout mice and mechanistic link
with cytokine balance. Gut 2003;52:975–80.
23. Kruis W, Schuts E, Fric P, Fixa B, Judmaier G, Stolte M.
Double-blind comparison of an oral Escherichia coli
preparation and Mesalazina in maintaining remission of
ulcerative colitis. Aliment Pharmacol Ther 1997;11:853–8.
24. Rembacken BJ, Snelling AM, Hawkey PM, Axon AT.
Non-pathogenic Escherichia coli versus mesalazine for
the treatment of ulcerative colitis: a randomized trial.
Lancet 1999;354:635–9.
25. Kruis W, Fric P, Pokrotnieks J, et al. Maintaining
remission of ulcerative colitis with Escherichia Coli
Nissle 1917 is as effective as with standard mesalazine.
Gut 2004;53:1617–23.
26. Gionchetti P, Rizzello F, Venturi A, et al. Oral
bacteriotherapy as maintenance treatment in patients
with chronic pouchitis: a double-blind, placebo-
controlled trial. Gastroenterology 2000;119:305–9.
27. Mimura T, Rizzello F, Helwig U, et al. Once daily high
dose probiotic therapy for maintaining remission in
recurrent or refractory pouchitis. Gut 2004;53:108–14.
28. Gionchetti P, Rizzello F, Helvig U, et al. Prophylaxis of
pouchitis onset with probiotic therapy: a double-blind
placebo controlled trial. Gastroenterology 2003;
124:1202–9.
29. Venturi A, Gionchetti P, Rizzello F, et al. Impact on the
faecal flora composition of a new probiotic prepara-
tion. Preliminary data on maintenance treatment of
patients with ulcerative colitis (UC) intolerant or
allergic to 5-aminosalicylic acid (5-ASA). Aliment
Pharmacol Ther 1999;13:1103–8.
30. Bibiloni R, Fedorak RN, Tannock GW, et al. VSL#3
probiotic mixture induces remission in patients with
active ulcerative colitis. Am J Gastroenterol 2005;100:
1539–46.
31. Guyatt G, Mitchell A, Irvine EJ, et al. A new measure of
health status for clinical trials in inflammatory bowel
disease. Gastroenterology 1989;96:804–10.
32. Summanen P, Baron EJ, eds. Wadswort anaerobic
bacteriology manual. 5th ed. Singapore: STAR Publishers
Co., 1993.
33. Hartemink R, Domenech VR, Rombouts FM. LAMVAB-
A new selective medium for the isolation of lactobacilli
from feces. J Microb Meth 1997;29:77–84.
Vol. 50, No. 12 PROBIOTICS IN ACTIVE POUCHITIS 2081
34. Hartemink R, Kok BJ, Weenk GH, Rombouts FM.
Raffinose-Bifidobacterium (RB) agar, a new selective
medium for bifidobacteria. J Microb Meth 1996;27:33–43.
35. Dave RI, Shah NP. Evaluation of media for selective
enumeration of Streptococcus thermophilus, Lactobacil-
lus delbrueckii subsp. bulgaricus, Lactobacillus acid-
ophilus, and bifidobacteria. J Dairy Sci 1996;76:1529–36.
36. Timisjarvi AT, Alatossava T. Development of oligonu-
cleotide primers from the 16S23S rRNA intergenic
sequences for identifying different dairy and probiotic
lactic acid bacteria by PCR. Int J Food Microbiol
1997;35:49–56.
37. Kok RG, De Wall A, Schut F, Welling GW, Weenk G,
Hellingwerf KJ. Specific detection and analysis of a
probiotic Bifidobacterium strain in infant faeces. Appl
Environ Microbiol 1996;62:3668–72.
38. Brigidi P, Vitali B, Swennen E, Altomare L, Rossi M,
Matteuzzi D. Specific detection of Bifidobacterium
strains in a new probiotic preparation and in human
feces by polymerase chain reaction. Syst Appl Micro-
biol 2000;23:391–9.
39. Ruseler-van-Embden JG, Schouten WR, van Lieshout
LM. Pouchitis: result of microbial imbalance? Gut
114;35:658–64.
40. Ulisse S, Gionchetti P, D’Alo S, et al. Expression of
cytokines, inducible nitric oxide synthetase and matrix
metalloproteinases in pouchitis: effects of probiotic
treatment. Am J Gastroenterol 2001;96:2691–9.
41. Hart AL, Lammers K, Brigidi P, et al. Modulation of
human dendritic cell phenotype and function by pro-
biotic bacteria. Gut 2004;53:1602–9.
INVITED COMMENTARY
To the Editor—Total proctocolectomy with restorative
ileal pouch-anal anastomosis (IPAA) is the surgery of
choice for patients with medically refractory ulcerative
colitis or a complication, such as dysplasia.1 Approximately
30 percent of patients with ulcerative colitis eventually
require colectomy, and the majority will have an IPAA.
Pouchitis is an idiopathic inflammatory condition that
occurs in the ileal pouch in up to 60 percent of these
patients.2 In some reports, most pouchitis occurs within a
few years of the IPAA,3 whereas in others, the risk
continues to increase with longer follow-up.4 The
majority of patients have acute pouchitis that responds to
antibiotics, but approximately 60 percent have at least one
recurrence, 5 to 10 percent develop chronic pouchitis that
requires chronic medications, and a small subset has
refractory pouchitis that may require pouch excision or
exclusion.2
The pathophysiology of pouchitis is not known. The fact
that pouchitis occurs almost exclusively in patients who
had IPAA for ulcerative colitis and not for familial
adenomatous polyposis (FAP) suggests an underlying
immune dysregulation. Furthermore, the fact that
pouchitis typically does not occur until the diverting
ileostomy is closed, and that pouchitis typically responds
to antibiotic therapy, suggest that bacteria drive the
inflammatory process. However, it is not clear whether
pouchitis occurs because of overgrowth of normal bacteria
or the presence of abnormal bacteria (dysbiosis).5
Regarding the bacteriology of pouch effluent, levels of
various bacteria from pouches in ulcerative colitis patients
were similar to that in FAP in one study,6 and may
resemble normal colonic flora, 7 whereas other studies
have shown that the flora in pouch effluent has more
anaerobes,8 or an increase in strict anaerobes compared
with facultative anaerobes,9 or more bacteroides and
bifidobacteria, than from subjects with an end
ileostomy.3,10 Despite these findings, one study showed
that the increase in anaerobes did not correlate with
subsequent pouch mucosal inflammation.9 Finally, sulfate-
reducing bacteria, which produce the mucosal toxin
hydrogen sulfide, have been seen exclusively in pouches
of ulcerative colitis patients.6,9
In pouchitis, total aerobes and some pathogenic
bacteria, such as clostridia and sulfate-reducing bacteria,
may be increased, while total anaerobes and specific
bacteria, such as bacteroides, bifidobacteria, and
lactobacilli, may be decreased.7,11–15 Yet another study
showed that patients developing pouchitis had low
bacterial and high fungal diversity.16 However, the
differences in anaerobic bacteria were less pronounced in
one study that assessed mucosa-associated flora,17 and
three other studies have shown no significant changes in
effluent bacteriology in patients with pouchitis,3,18,19
although these studies have been criticized for
methodologic flaws.5
Antibiotic therapy decreases total bacterial counts and
may eradicate certain pathogens,7,19,20 although the effect
of ciprofloxacin may be different than metronidazole.7
Other investigators have shown no difference in the
bacterial milieu in those with or without pouchitis and
little change in the microflora after antibiotics.3,19 Given
this disparate data, the role of specific bacteria, or ratios of
different types of bacteria, in the pathogenesis of pouchitis
is not clear.
Open-label studies or case series suggest that most
patients with pouchitis respond promptly to antibiotic
therapy.2,3,21 Patients who fail to respond to a single
antibiotic may respond to combination antibiotics,20,22
and patients with relapsing or chronic pouchitis may
need continuous maintenance antibiotics. However, few
randomized, controlled, antibiotic trials have been
performed.23–25 Although clinical experience confirms that
antibiotics are effective in most patients with pouchitis,
adverse effects with even short-term use of metronidazole
occur in 33 to 57 percent of patients, including nausea,
vomiting, dysgeusia, abdominal discomfort, headache, and
2082 GIONCHETTI ET AL Dis Colon Rectum, December 2007

skin rash.23–27 The incidence of these side effects and
others, such as peripheral neuropathy, increases with
chronic use. Thus, patients who require chronic antibiotic
therapy often are treated with ciprofloxacin. However,
even with this relatively safe and well-tolerated drug, there
is concern that chronic use of a single antibiotic may select
for resistant organisms and thus lead to more difficult to
treat pouchitis or other infections.
Recent reports have suggested that altering the pouch
flora with probiotic bacteria may be an alternative to
repeated or chronic antibiotic use. Several studies have
shown that a mixed-flora oral probiotic preparation (VSL
#3) can maintain remission in chronic pouchitis 26,27 or
prevent the development of pouchitis in the first place.28
This probiotic, which contains four strains of lactobacilli,
three strains of bifidobacteria, and a streptococcus, also has
shown promise in treatment and maintenance of remission
in ulcerative colitis.29 In the antibiotic withdrawal studies in
chronic pouchitis, remission was maintained in 85 percent
of patients treated with VSL #3 compared with 0 to 6
percent in those receiving placebo.26,27 In another
controlled trial, VSL #3 or placebo were given
prophylactically after IPAA.28 After one year of follow-up,
the incidence of pouchitis was 10 percent in the VSL #3
group and 40 percent in the placebo group. In this study,
VSL #3 also reduced the stool frequency of patients without
pouchitis. However, an open-label study of VSL #3 in
patients with antibiotic-dependent chronic pouchitis
treated at a referral center was less encouraging.30 In this
uncontrolled study, which did not assess for compliance
with probiotic treatment, <20 percent of patients were able
to maintain remission on VSL #3 during eight months of
follow-up.
The probiotic Lactobacillus rhamnosus GG also seems
to decrease the risk of developing pouchitis after IPAA
when given prophylactically,31 but was no better than
placebo for treatment of mild active pouchitis.32
In the current issue of Diseases of the Colon & Rectum,
the report by Gionchetti and colleagues extends the use of
VSL #3 from these prior studies of primary and secondary
prophylaxis to treatment. In this open-label study in 23
patients with mild pouchitis, four weeks of treatment with
high-dose VSL #3 was well tolerated and resulted in
remission in 69 percent, accompanied by significant
improvement in endoscopy, histology, and quality of life
scores. Response was seen in patients with their first
episode of pouchitis and in those with recurrent disease.
All patients who went into remission maintained remission
during six months of follow-up on a lower-dose VSL #3.
Given the results of this study, and the previous studies
using VSL #3, is it time to stop prescribing antibiotics for
patients with acute pouchitis? No. Although these results
are encouraging, the study was small and uncontrolled,
and the patients had mild pouchitis, which may be more
likely to experience random variation in symptom intensity
and a placebo response. This regimen or other probiotics
should be tested in well-designed, properly powered,
randomized, blinded, controlled trials. If the exciting
results reported in the Gionchetti article can be
confirmed, we may witness the end of the antibiotic era
for treatment of pouchitis, or at least a significant reduction
in the need for antibiotic therapy in this patient group in
lieu of probiotics. Furthermore, if the prophylactic efficacy
of VSL #3 or Lactobacillus GG are confirmed, we may
routinely place all of our colitis patients on probiotics after
IPAA, resulting in a significant reduction in the incidence of
pouchitis, and therefore the need for active treatment.
REFERENCES
1. Fazio VW, Ziv Y, Church JM, et al. Ileal pouch-anal
anastomosis: complications and function in 1005
patients. Ann Surg 1995;222:120–7.
2. Pardi DS, Sandborn WJ. Management of pouchitis.
Aliment Pharmacol Ther 2006;23:1087–96.
3. Shepherd NA, Hulten L, Tytgat GN, et al. Workshop:
Pouchitis. Int J Colorectal Dis 1989;4:205–29.
4. Simchuk EJ, Thirlby RC. Risk factors and true incidence
of pouchitis in patients after ileal pouch-anal anasto-
moses. World J Surg 2000;24:851–6.
5. Lim M, Sagar P, Finan P, et al. Dybiosis and pouchitis.
Br J Surg 2006;93:1325–34.
6. Duffy M, O’Mahony L, Coffey JC, et al. Sulfate-reducing
bacteria colonize pouches formed for ulcerative colitis
but not for familial adenomatous polyposis. Dis Colon
Rectum 2002;45:384–8.
7. Gosselink MP, Schouten WR, van Lieshout LM, et al.
Eradication of pathogenic bacteria and restoration of
normal pouch flora: comparison of metronidazole and
ciprofloxacin in the treatment of pouchitis. Dis Colon
Rectum 2004;47:1519–25.
8. Santavirta J, Mattila J, Kokki M, Matikainen M. Mucosal
morphology and fecal bacteriology after ileoanal
anastomosis. Int J Colorect Dis 1991;6:38–41.
9. Smith FM, Coffey JC, Kell MR, et al. A characterization
of anaerobic colonization and associated mucosal
adaptations in the undiseased ileal pouch. Colorectal
Dis 2005;7:563–70.
10. Nasmyth DG, Godwin PG, Dixon MF, et al. Ileal
ecology after pouch-anal anastomosis or ileostomy. A
study of mucosal morphology, fecal bacteriology, fecal
volatile fatty acids, and their interrelationship. Gastro-
enterology 1989;96:817–24.
11. Nicholls RJ, Belliveau P, Neill M, et al. Restorative
proctocolectomy with ileal reservoir: a pathopysiolog-
ical assessment. Gut 1981;22:462–8.
12. Ruseler-van Embden JG, Schouten WR, van Leieshout
LM. Pouchitis: result of microbial imbalance? Gut
1994;35:658–64.
Vol. 50, No. 12 PROBIOTICS IN ACTIVE POUCHITIS 2083
13. Brandi G. Chaussade S, Ladire M, et al. Analysis of ileal
bacterial flora in patients with ileal-anal anastomosis
with and without pouchitis. Gut 1992;33(Suppl 2):S41.
14. Ohge H, Furne JK, Springfield J, et al. Association
between fecal hydrogen sulfide production and pou-
chitis. Dis Colon Rectum 2005;48:469–75.
15. Iwaya A, Iiai T, Okamoto H, et al. Change in the
bacterial flora of pouchitis. Hepatogastroenterology
2006;53:55–9.
16. Kuhbacher T, Ott SJ, Helwig U, et al. Bacterial and
fungal microbiota in relation to probiotic therapy
(VSL#3) in pouchitis. Gut 2006;55:833–41.
17. Onderdonk AB, Dvorak AM, Cisneros RL, et al.
Microbial assessment of tissue biopsy samples from
ileal pouch patients. J Clin Microbiol 1992;30:312–7.
18. O’Connell PR, Rankin DR, Weiland LH, Kelly KA.
Enteric bacteriology, absorption, morphology and
emptying after ileal pouch-anal anastomosis. Br J Surg
1986;73:909–14.
19. Kmiot WA, Youngs D, Tudor R, et al. Mucosal
morphology, cell proliferation and faecal bacteriology
in acute pouchitis. Br J Surg 1993;80:1445–9.
20. Gionchetti P, Rizzello F, Venturi A, et al. Antibiotic
combination therapy in patients with chronic, treat-
ment-resistant pouchitis. Aliment Pharmacol Ther
1999;13:713–8.
21. Hurst RD, Molinari M, Chung TP, et al. Prospective
study of the incidence, timing and treatment of
pouchitis in 104 consecutive patients after restorative
proctocolectomy. Arch Surg 1996;131:497–500.
22. Mimura T, Rizzello F, Helwig U, et al. Four-week open-
label trial of metronidazole and ciprofloxacin for the
treatment of recurrent or refractory pouchitis. Aliment
Pharmacol Ther 2002;16909–17.
23. Madden MV, McIntyre AS, Nicholls RJ. Double-blind
crossover trial of metronidazole versus placebo in chronic
unremitting pouchitis. Dig Dis Sci 1994;39:1193–6.
24. Shen B, Achkar JP, Lashner BA, et al. A randomized
clinical trial of ciprofloxacin and metronidazole to treat
acute pouchitis. Inflamm Bowel Dis 2001;7:301–5.
25. Sambuelli A, Boerr L, Negreira S, et al. Budesonide
enema in pouchitis—a double-blind, double-dummy,
controlled trial. Aliment Pharmacol Ther 2002;16:27–34.
26. Gionchetti P, Rizzello F, Venturi A, et al. Oral
bacteriotherapy as maintenance treatment in patients
with chronic pouchitis: a double-blind, placebo-con-
trolled trial. Gastroenterology 2000;119:305–9.
27. Mimura T, Rizzello F, Helwig U, et al. Once daily
high dose probiotic therapy (VSL#3) for maintaining
remission in recurrent or refractory pouchitis. Gut
2004;53:108–14.
28. Gionchetti P, Rizzello F, Helwig U, et al. Prophylaxis
of pouchitis onset with probiotic therapy: a double-
blind, placebo-controlled trial. Gastroenterology
2003;124:1202–9.
29. Chapman TM, Plosker GL, Figgitt DP. VSL#3 probiotic
mixture: a review of its use in chronic inflammatory
bowel disease. Drugs 2006;66:1371–87.
30. Shen B, Brzezinski A, Fazio VW, et al. Maintenance
therapy with a probiotic in antibiotic-dependent pou-
chitis: experience in clinical practice. Aliment Pharma-
col Ther 2005;22:721–8.
31. Gosselink M, Schouten WR, van Lieshout LM, et al.
Delay of first onset of pouchitis by oral intake of the
probiotic strain Lactobacillus rhamnosus GG. Dis Colon
Rectum 2004;47:876–84.
32. Kuisma J, Mentula S, Jarvinen H, et al. Effect of
Lactobacillus rhamnosus GG on ileal pouch inflamma-
tion and microbial flora. Aliment Pharmacol Ther
2003;17:509–15.
Darrell S. Pardi, M.D.Rochester, Minnesota
2084 GIONCHETTI ET AL Dis Colon Rectum, December 2007
Top Related
Copyright © 2022 FDOKUMEN

