







Bahasa
Halaman
Hukum

Magnetic Resonance Im
Estimation of the content of fat and parenchyma in breast tissue
using MRI T1 histograms and phantomsB
Raymond C. Bostona, Mitchell D. Schnallb, Sarah A. Englanderb,
J. Richard Landisc, Peter J. Moatea,TaSchool of Veterinary Medicine, New Bolton Center, University of Pennsylvania, Kenneth Square, PA 19348, USA
bSchool of Radiology, New Bolton Center, University of Pennsylvania, Kenneth Square, PA 19348, USAcSchool of Epidemiology, New Bolton Center, University of Pennsylvania, Kenneth Square, PA 19348, USA
Received 21 September 2004; accepted 3 February 2005
Abstract
Mammographic breast density has been correlated with breast cancer risk. Estimation of the volumetric composition of breast tissue using
three-dimensional MRI has been proposed, but accuracy depends upon the estimation methods employed. The use of segmentation based on
T1 relaxation rates allows quantitative estimates of fat and parenchyma volume, but is limited by partial volume effects. An investigation
employing phantom breast tissue composed of various combinations of chicken breast (to represent parenchyma) and cooking fats was
carried out to elucidate the factors that influence MRI T1 histograms. Using the phantoms, T1 histograms and their known fat and
parenchyma composition, a logistic distribution function was derived to describe the apportioning of the T1 histogram to fat and parenchyma.
This function and T1 histograms were then used to predict the fat and parenchyma content of breasts from 14 women. Using this method, the
composition of the breast tissue in the study population was as follows: fat 69.9F22.9% and parenchyma 30.1F22.9%.
D 2005 Elsevier Inc. All rights reserved.
Keywords: MRI; Breast tissue; Fat; Parenchyma; Estimation
1. Introduction
A mammographically dense breast refers to a breast
which appears to more intensely attenuate the X-ray beam
and is regarded as depicting mostly parenchyma, while a
breast which is not dense appears radiolucent and is
regarded as being composed of mostly fatty tissue [1]. In
1976, Wolfe [2] found a relationship between mammo-
graphic breast density and breast cancer risk. Since then,
there have been a substantial number of reports that have
shown that the odds ratio for developing breast cancer for
the most dense compared with the least dense breast tissue
categories ranges from 1.8 to 6.0, with most studies
yielding an odds ratio of 4.0 or greater [3]. Despite the
undoubted importance of breast density in the etiology and
the detection of breast cancer, it has been described as
0730-725X/$ – see front matter D 2005 Elsevier Inc. All rights reserved.
doi:10.1016/j.mri.2005.02.006
B This work was supported by grants from the NIH (CA82707-01,
CA090699-0182) and by a grant from the Susan G. Komen Breast Cancer
Foundation (IMG 2000-224).
T Corresponding author. Tel.:+1 6109256146; fax: +1 6109258123.
E-mail address: [email protected] (P.J. Moate).
bperhaps the most undervalued and underutilized risk
factor in studies investigating the causes of breast cancerQ[4]. Technical reasons are probably partly responsible for
the limited utilization of breast density in cancer research.
Mammographic density is commonly estimated by
delineating the radiographically dense areas on the mam-
mogram from the entire breast area, and the percentage
breast density is calculated as the area of high radiographic
density divided by the total breast area [5,6]. Although
digital segmentation with either interactive [7] or automated
[8] thresholding has been employed to differentiate between
fat and parenchyma, the entire notion of a threshold means
that the differentiation is somewhat subjective. Another
limitation of the current mammography methodology is that
pixels are identified as either fat or parenchyma, and no
account is taken of the actual depth of the pixel being imaged.
Variation in the thickness of breasts during compression,
variations in positioning of the breast, nonlinear character-
istics of film and film digitizers, and variations in X-ray flux
have also been suggested as factors that could influence the
apparent density of a mammogram [9]. Given these
aging 23 (2005) 591–599

R.C. Boston et al. / Magnetic Resonance Imaging 23 (2005) 591–599592
confounding factors, it is not surprising that recent research
has demonstrated the high degree of inaccuracy of mam-
mography for estimating the fat and parenchyma content of
breasts [10]. Despite these problems, there is now evidence
that there is large variation in the parenchyma/fat tissue in
women [11] and that this ratio declines with age [1,12] and
can be expected to decline as the compressed thickness of the
breast increases [13]. Breast composition also undergoes
cyclic changes during the menstrual cycle [14] and may be
influenced by diet (intakes of polyunsaturated fat, vitamins C,
E and B12, and by intake of alcohol) [15] and by hormone
replacement therapy [16].
Despite the importance of breast composition to the
etiology and diagnosis of breast cancer, there have been only
a few studies that have made direct chemical measurements
of parenchyma and fat in breast tissue, and these involved
only a small number of fresh mastectomy specimens [17,18].
An alternative modality for estimating the fat and
parenchyma content of tissues in animals and humans
involves MRI [19-21]. Moreover, a significant correlation
has already been shown between X-ray mammography
percent density and two MRI parameters: mean T2 relaxation
time and relative water content [22]. A number of different
methods have been used to estimate fat and parenchyma
content of tissues from MRI data. Kover et al. [19], when
estimating the fat content of live chickens, used a mouse to
manually draw around areas of adipose tissue and thus
f
f
A
C
f
D
0
1000
2000
3000
4000
5000
0 500 1000 1500 2000
Time (ms)
f
0
10000
20000
30000
40000
50000
0 500 1000 1500 2000
Time (ms)
f
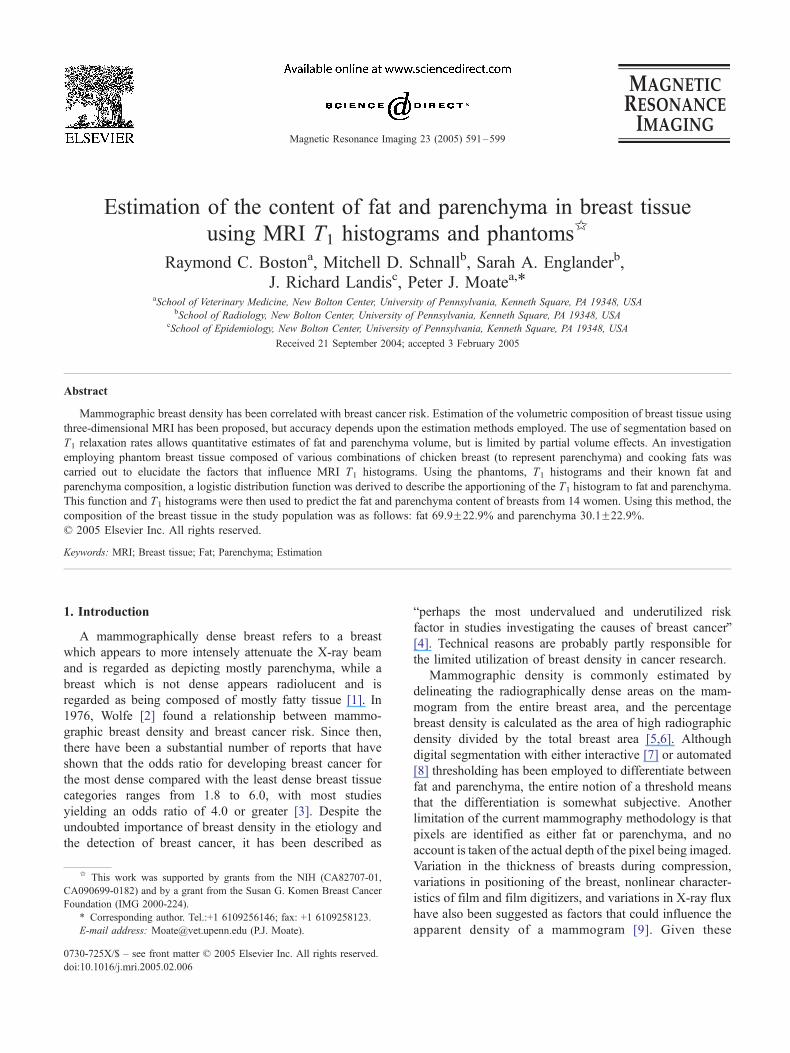
Fig. 1. T1 histograms of individual breasts from four subjects (A, B, C and
segment theMR image into fat and parenchyma. Baulain [20]
used both gray value distribution (histogram) of the pixels
and also cluster analysis methods to estimate body compo-
sition of live pigs and sheep. In human breast tissue, fat is
often diffusely dispersed throughout parenchymal tissue, and
it may not necessarily be practical or possible to manually
outline in a MR image distinct regions of adipose tissue.
Therefore, a variety of methods have been used to segment
MR images and to classify the tissue in the different segments
[23]. There are two distinct approaches that rely on unique
NMR properties of fat relative to the fibroglandular tissues:
chemical shift and T1. Although chemical shift techniques
may be more specific in identifying fat, T1-based techniques
are easier to implement over a wide variety of scanner
platforms and field strengths. This is a technique currently
being employed in a study at the University of Pennsylvania.
T1-based techniques take advantage of the fact that
inversion recovery images with different T1 times, or T1
weighted images with different TR values, will have a gray
scale such that the signal in each voxel is related to the T1
relaxation time of the voxel (or cube of tissue) that the pixel
depicts. A T1 image or map can be calculated from a series
of images produced using an inversion recovery pulse
sequence. The gray scale of a specific pixel is related to the
T1 relaxation time of the voxel (or cube of tissue) which that
pixel depicts. T1 histograms depict the number of voxels
that have specific T1 relaxation times. Fig. 1A–D depicts a
0 500 1000 1500 2000
Time (ms)
f
0
2000
4000
6000
8000
10000
0 500 1000 1500 2000
Time (ms)
0
300
600
900
1200
1500
f
B
D). f is the frequency or number of pixels that have a value of T1.
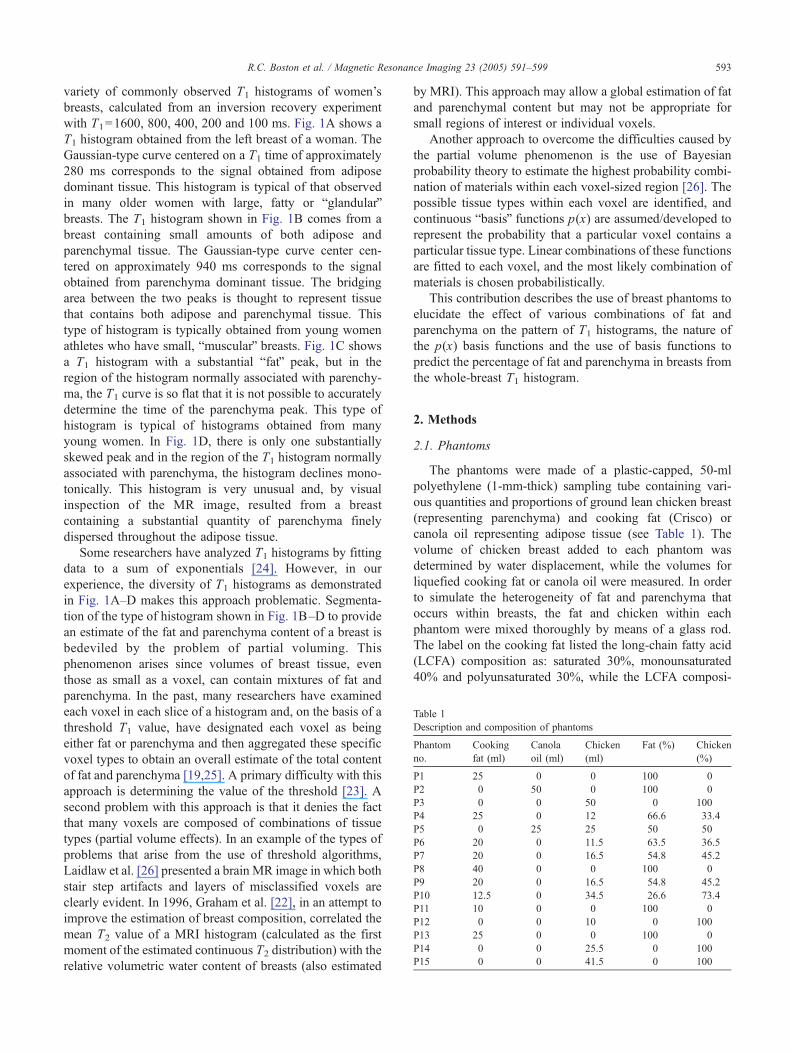
able 1
escription and composition of phantoms
hantom
o.
Cooking
fat (ml)
Canola
oil (ml)
Chicken
(ml)
Fat (%) Chicken
(%)
1 25 0 0 100 0
2 0 50 0 100 0
3 0 0 50 0 100
4 25 0 12 66.6 33.4
5 0 25 25 50 50
6 20 0 11.5 63.5 36.5
7 20 0 16.5 54.8 45.2
8 40 0 0 100 0
9 20 0 16.5 54.8 45.2
10 12.5 0 34.5 26.6 73.4
11 10 0 0 100 0
12 0 0 10 0 100
13 25 0 0 100 0
14 0 0 25.5 0 100
15 0 0 41.5 0 100
R.C. Boston et al. / Magnetic Resonance Imaging 23 (2005) 591–599 593
variety of commonly observed T1 histograms of women’s
breasts, calculated from an inversion recovery experiment
with T1=1600, 800, 400, 200 and 100 ms. Fig. 1A shows a
T1 histogram obtained from the left breast of a woman. The
Gaussian-type curve centered on a T1 time of approximately
280 ms corresponds to the signal obtained from adipose
dominant tissue. This histogram is typical of that observed
in many older women with large, fatty or bglandularQbreasts. The T1 histogram shown in Fig. 1B comes from a
breast containing small amounts of both adipose and
parenchymal tissue. The Gaussian-type curve center cen-
tered on approximately 940 ms corresponds to the signal
obtained from parenchyma dominant tissue. The bridging
area between the two peaks is thought to represent tissue
that contains both adipose and parenchymal tissue. This
type of histogram is typically obtained from young women
athletes who have small, bmuscularQ breasts. Fig. 1C shows
a T1 histogram with a substantial bfatQ peak, but in the
region of the histogram normally associated with parenchy-
ma, the T1 curve is so flat that it is not possible to accurately
determine the time of the parenchyma peak. This type of
histogram is typical of histograms obtained from many
young women. In Fig. 1D, there is only one substantially
skewed peak and in the region of the T1 histogram normally
associated with parenchyma, the histogram declines mono-
tonically. This histogram is very unusual and, by visual
inspection of the MR image, resulted from a breast
containing a substantial quantity of parenchyma finely
dispersed throughout the adipose tissue.
Some researchers have analyzed T1 histograms by fitting
data to a sum of exponentials [24]. However, in our
experience, the diversity of T1 histograms as demonstrated
in Fig. 1A–D makes this approach problematic. Segmenta-
tion of the type of histogram shown in Fig. 1B–D to provide
an estimate of the fat and parenchyma content of a breast is
bedeviled by the problem of partial voluming. This
phenomenon arises since volumes of breast tissue, even
those as small as a voxel, can contain mixtures of fat and
parenchyma. In the past, many researchers have examined
each voxel in each slice of a histogram and, on the basis of a
threshold T1 value, have designated each voxel as being
either fat or parenchyma and then aggregated these specific
voxel types to obtain an overall estimate of the total content
of fat and parenchyma [19,25]. A primary difficulty with this
approach is determining the value of the threshold [23]. A
second problem with this approach is that it denies the fact
that many voxels are composed of combinations of tissue
types (partial volume effects). In an example of the types of
problems that arise from the use of threshold algorithms,
Laidlaw et al. [26] presented a brain MR image in which both
stair step artifacts and layers of misclassified voxels are
clearly evident. In 1996, Graham et al. [22], in an attempt to
improve the estimation of breast composition, correlated the
mean T2 value of a MRI histogram (calculated as the first
moment of the estimated continuous T2 distribution) with the
relative volumetric water content of breasts (also estimated
by MRI). This approach may allow a global estimation of fat
and parenchymal content but may not be appropriate for
small regions of interest or individual voxels.
Another approach to overcome the difficulties caused by
the partial volume phenomenon is the use of Bayesian
probability theory to estimate the highest probability combi-
nation of materials within each voxel-sized region [26]. The
possible tissue types within each voxel are identified, and
continuous bbasisQ functions p(x) are assumed/developed to
represent the probability that a particular voxel contains a
particular tissue type. Linear combinations of these functions
are fitted to each voxel, and the most likely combination of
materials is chosen probabilistically.
This contribution describes the use of breast phantoms to
elucidate the effect of various combinations of fat and
parenchyma on the pattern of T1 histograms, the nature of
the p(x) basis functions and the use of basis functions to
predict the percentage of fat and parenchyma in breasts from
the whole-breast T1 histogram.
2. Methods
2.1. Phantoms
The phantoms were made of a plastic-capped, 50-ml
polyethylene (1-mm-thick) sampling tube containing vari-
ous quantities and proportions of ground lean chicken breast
(representing parenchyma) and cooking fat (Crisco) or
canola oil representing adipose tissue (see Table 1). The
volume of chicken breast added to each phantom was
determined by water displacement, while the volumes for
liquefied cooking fat or canola oil were measured. In order
to simulate the heterogeneity of fat and parenchyma that
occurs within breasts, the fat and chicken within each
phantom were mixed thoroughly by means of a glass rod.
The label on the cooking fat listed the long-chain fatty acid
(LCFA) composition as: saturated 30%, monounsaturated
40% and polyunsaturated 30%, while the LCFA composi-
T
D
P
n
P
P
P
P
P
P
P
P
P
P
P
P
P
P
P

R.C. Boston et al. / Magnetic Resonance Imaging 23 (2005) 591–599594
tion of the canola oil was as follows: saturated 7.8%,
monounsaturated 55.3% and polyunsaturated 32.4%. The
USDA National Nutrient Database (http://www.nal.usda.
gov/fnic/cgi-bin/nut_search.pl) lists lean chicken breast
without skin as containing 1.24% fat and the LCFA
composition (as % of total LCFA) as: saturated 36.3%,
monounsaturated 33.0% and polyunsaturated 30.7%.
2.2. Human subjects
Magnetic resonance imaging was performed on both left
and right breasts of 14 Caucasian women patients as part of
standard procedures for the investigation of possible breast
cancer. The meanFstandard deviation and range for their
ages (years) were 48.1F8.6 and 38–70, and for body-
weights (kg) were 65.9F15.6 and 46.4–104.1. Approval
from our institutional review board was obtained prior to
the start of this study.
2.3. Instrumentation and imaging protocol
MR imaging was performed on a 1.5-T Signa scanner
(General Electric Medical Systems, Milwaukee, WI). After
informed consent, patients were placed in the scanner in the
prone position. Total imaging time for both breasts was
approximately 20 min. Briefly, the MRI protocol employed
was as follows: the field of view (FOV) was generally
180 to 240 mm, and sagittal slice thickness ranged from 2.2
to 3.5 mm depending on the size of particular breasts. The
number of data points (D), i.e., pixels per FOV on the
computer screen used in this investigation, was 250. With
FOV=180 mm, S=2.2 mm and D=250, a voxel will have
the following dimensions: height=180/250=0.72 mm,
width=0.72 mm, thickness=2.2 mm.
Three-dimensional bilateral slab interleaved spoiled
gradient echo inversion recovery sequence was used to
acquire data (TR/TE 17.6/1.4 ms, flip angle=558, F64 kHz
sampling bandwidth, 64 slices). Five data sets were obtained
using a nonselective inversion pulse at 1600, 800, 400,
200 and 100 ms prior to the start of the imaging sequence.
The total acquisition time for the data acquired for each
patient exam was 20 min; however, more recent implemen-
tation of SENSE encoding has reduced this to 10 min. These
inversion recovery data were used to calculate T1 maps of
each slice [27]. The protocol for imaging the phantoms was
similar to that used for the patients except that the phantoms
were imaged at room temperature (258C), sagittal slice
thickness was 3.5 mm (to reproduce the worst case scenario
in terms of partial volume effects), and 14 slices/phantom
were made.
2.4. Analysis of MR imaging data
Images were masked by hand to remove the chest wall.
Breast tissue was identified visually by qualified person-
nel. Breast tissue could clearly be distinguished from the
chest wall and the axilla. We used a graphical user
interface (GUI)-based program — written in-house.
Functionality of this GUI-based program included adding
or removing area, dilating or eroding, and selecting a
cutoff threshold. T1 maps were constructed by fitting the
data acquired using five inversion times with a function
derived from the solution of the Bloch equations for the
MR pulse sequence. Histograms of the masked images
were produced. Calculations were performed on the T1
histogram data using a Microsoft Excel spreadsheet.
STATA software was used to estimate spline functions
and their derivatives, and to perform regressions and
statistical analyses [28]. In the studies described here, the
mean T1 value (T̂1) of each histogram was calculated from
the first moment of the T1 distribution:
T̂T 1 ¼
Pi¼1
i¼n
fi 4 T1i
n 4 f̂f ið1Þ
where fi is the frequency or signal count that has a value
of T1i, f̂ i is the average count or frequency for the
histogram, i is the bin number centered on time T1i, n is
the number of bins used for the histogram and, in all the
histograms in this investigation, n was set at 200 and the
bin width was 10 ms.
Using the phantom T1 histograms, a linear regression
equation was determined as a calibration equation to relate
parenchyma percentage in the phantoms to T̂1 (Eq. (2)):
P% ¼ � 33:1F7:3þ 0:153F0:0127 4 T̂T 1;
R2 ¼ 0:91 ð2Þ
Although Eq. (2) has a high R2 value, from a practical
point of view, the fact that the T̂1 values for pure fat and
pure chicken breast (parenchyma) may not closely match
the times of the corresponding peaks in T1 histograms of
breast tissue in vivo makes the use of this specific equation
for predicting breast composition somewhat problematic.
However, since in phantoms there is a high degree of
concordance with respect to T̂1 and the peak times of both
pure fat (P1, ms) and pure parenchyma (P2, ms) (this
finding presented in the Results section), it is likely that this
concordance would also occur in breast tissue in vivo. We
therefore surmised that the parenchyma % (P%) of a breast
could be approximately estimated from the total T1
histogram by:
P% ¼ � P1 4 100
P2� P1
� �þ 100
P2� P1
� �4 T̂T 1 ð3Þ
where in this case, P1 refers to the population mean time of
the fat peak (P1, ms) and P2 refers to the population mean
time of the parenchyma peak (P2, ms) of breast tissue.
Unfortunately, when using this equation to predict breast
composition, if a particular breast were to have a T̂1 less
than the mean P1 value or greater than the mean P2 value,
then infeasible predictions of P% (i.e., P%b0 or P%N100)

0
10
20
30
40
50
60
0 10 20 30 40 50 60
Measured tissue volume (ml)
Pre
dic
ted
tis
sue
volu
me
(ml)
Fig. 2. The standard curve derived from phantoms used to predict the
volumes (ml) of fat (empty squares) and parenchyma (solid triangles) in
breast histograms. The solid line is the line of identity.
Time (ms)
1.
Fat
or
par
ench
yma
pro
po
rtio
n i
n T
1 si
gn
al
1
0
0.2
0.4
0.6
0.8
2
0 500 1000 1500 2000
Fig. 3. The logistic functions (thick line for parenchyma, thin line for fat)
used to segment breast T1 histograms. The vertical dotted lines (at T1
times 457.85, 565.43, 654.57 and 762.36 ms) segment the histogram
into quintiles.
R.C. Boston et al. / Magnetic Resonance Imaging 23 (2005) 591–599 595
could occur. This problem was circumvented by introducing
the modifications shown in Eq. (4):
P% ¼ 0 if T̂T 1VP1
P% ¼ � P1 4 100
P2� P1
� �þ 100
P2� P1
� �4 T̂T 1 for P1V T̂T1VP2
P% ¼ 100 if T̂T 1zP2 ð4Þ
In order to utilize Eq. (4) to predict the parenchyma
content of breasts, the population mean estimates of P1 and
P2 were estimated from our sample of subjects. First, ten-
knot quadratic spline functions were used to obtain smooth,
continuous-distribution functions to describe the T1 histo-
grams of each breast. The first derivative of the spline
functions was used to identify the times of the fat and
parenchyma peaks.
2.5. Prediction of breast composition using a logistic
equation
A logistic function [29] was used to describe the
proportion (Pxp(i)) of the T1 signal that originates from
voxels composed of parenchyma. Alternatively, Pxp(i)) can
be thought of as a function that approximates the probability
that a particular voxel will contain parenchyma.
Pxp ið Þ ¼ 1
1þ exp � P3 4 T1 �P1þ P2
2
� �� �� �� � ð5Þ
where T1 is the relaxation time of a specific voxel, P1 is the
mean T1 time of the fat peak, P2 is the mean T1 time of the
parenchyma peak and P3 is the maximum slope of the
logistic curve. We chose a logistic function as this type of
curve has the desired shape attributes and good parameter
estimability due to their intrinsic dimensionality and domain
of influence [30]. Since we assume that breast tissue
contains only fat and parenchyma, the function used to
describe the proportion of fat in a specific voxel (Pxf) is
described by Eq. (6):
Pxf ið Þ ¼ 1� Pxp ið Þ ð6Þ
It follows that the total amount of parenchyma (TP, ml)
that caused the T1 histogram can be described by:
TP ¼Xnl
FOV 4 FOV 4 S 4 fi 4 Pxp ðiÞD 4D 4 1000
ð7Þ
where FOV is the field of view in millimeters, S is
the slice thickness in millimeters and D represents the
number of pixels per FOV. Similarly, the total amount
of fat (ml) responsible for the T1 histogram can be
described by:
TF ¼Xnl
FOV 4 FOV 4 S 4 fi 4 Pxf ðiÞD * D * 1000
ð8Þ
In the case of phantoms, P1 and P2 were taken to be
the mean peak times of the phantoms composed of pure
fat and pure chicken breast, respectively.
In order to estimate parameter P3 in Eq. (5), Eqs. (7)
and (8) were coded into an Excel spreadsheet so as to
predict the amount of fat and parenchyma in each phantom.
By utilizing the bsolverQ optimizer available in Excel to
minimize the sum of squares of the differences between
the predicted quantities of fat and parenchyma with the
measured quantities of fat and parenchyma in each
phantom, P3 was estimated to be 0.009102 ms�1. The
calibration line resulting from this optimization procedure
and which relates the known and predicted volumes of fat
and parenchyma is shown in Fig. 2. Eqs. (7) and (8) were
also used to estimate the volumes of fat and parenchyma
present in breasts. The value of parameter P3 determined
using phantoms was assumed to apply to breasts, but the
mean P1 and P2 values of breasts per se were employed.
The logistic equations used to estimate the proportions of
parenchyma and fat in breasts are shown in Fig. 3.

R.C. Boston et al. / Magnetic Resonance Imaging 23 (2005) 591–599596
3. Results and discussion
3.1. Phantom histograms
T1 histograms of cooking fat, canola oil, chicken breast
and mixtures of chicken breast and fat are shown in
Fig. 4A–D. The histogram of cooking fat was Gaussian in
form and closely resembled the fat peak that occurs in
typical breast T1 histograms (compare with Fig. 1A). The
histogram from the canola oil had a much smaller peak and
was more platykurtotic than the histogram obtained from the
cooking fat. The histograms produced from phantoms
containing mixtures of fat and chicken had reduced peak
heights for both fat and chicken relative to histogram peak
heights obtained from phantoms containing either pure fat
or chicken (compare Fig. 4A with B and C). Phantoms that
contained mixtures of fat and chicken had T1 histograms
with substantial bbridgingQ between the fat and parenchyma
peak (Fig. 4B and C). We interpret this observation as
evidence of the bpartial volumeQ phenomenon.
3.2. Comparison of phantom T1 histograms with breast T1
histograms
The five phantoms that were 100% fat had (meanFS.D.)
T̂1 of 228F12.4 ms and their peak times (P1) occurred at
208F25.7 ms. In contrast to fat or adipose tissue, the four
phantoms that were composed of 100% chicken had T̂1 of
818F102.9ms and peak times (P2) occurred at 810F95.0ms.
A
0
500
1000
1500
2000
2500
0 200 400 600 800 1000
f
B
f
C
0
100
200
300
400
500
0 200 400 600 800 1000
f
DTime (ms)
Time (ms)
f
Fig. 4. T1 histograms of phantoms: (A) fats: solid dots represent cooking fat (25
chicken breast (25 ml). (C) Solid dots represent a mixture of cooking fat (25 ml) a
and chicken (25 ml). Note that in each case the frequency axis has been rescaled
The slight discrepancies between the T̂1 values and the time
of the corresponding peak result from the fact that the
histograms of these bpureQ phantoms cannot be described by
pure Gaussian-type equations and reflect the fact that the
histograms are slightly skewed. The P1 values for fat in
phantoms are less than the P1 values (280F14 ms) that we
have observed in T1 histograms of in vivo breasts (Table 2)
and slightly less than the 230F10 ms mean value for ex vivo
breasts reported by Graham et al. [31]. In addition, the peak
time for parenchyma in phantoms (810F95.0 ms) is smaller
than the peak times we have observed for parenchymal
breast tissue in vivo 945F108 (ms) (see Table 2) and
substantially smaller than the value of 1330F240 ms
reported for parenchymal breast tissue ex vivo [31].
There are a number of factors that could account for these
apparent discrepancies between the observed times of fat
and parenchyma peak heights for phantoms and the
observed times of peak heights for corresponding peaks in
breast tissue. Firstly, the phantoms were at room tempera-
ture when the MRI was conducted, and this would have
caused a substantial shortening of the T1 relaxation times,
especially that of parenchyma [32]. Secondly, in vivo, both
adipose and parenchymal breast tissue are highly vascular-
ized and contain approximately 5–8% blood by weight.
Thus, it can be expected that in the phantoms, the absence of
the water (in blood) would tend to slightly decrease the T1
relaxation times of both the adipose and the parenchymal
0
200
400
600
800
1000
0 200 400 600 800 1000
Time (ms)
0
200
400
600
800
1000
0 200 400 600 800 1000
Time (ms)
ml); hollow circles represent canola oil (50 ml). (B) Solid dots represent
nd chicken (12 ml). (D) Solid dots represent a mixture of canola oil (25 ml)
for display purposes.

Table 2
Characteristics of T1 histograms of breasts and estimated fat and
parenchyma content of breasts of 14 Caucasian women
Parameter Left breast Right breast Breasts
Number 14 14 28
Total area under the
curve*106 (counts ms)
1.76F0.96 1.70F0.85 1.73F0.90
Time of fat peak (P1) (ms) 276F12 282F15 279F14
Time of parenchyma peak
(P2) (ms)
910F114 972F114 941F110
T̂1 (ms) 443F155 480F198 461F176
Fat (%) by T̂1 69.5F29.4 64.8F32.7 67.1F30.6
Parenchyma (%) by T̂1 30.5F29.4 35.2F32.7 32.9F30.6
Fat (%) by logistic equation 71.3F22.4 68.6F24.1 69.9F22.9
Parenchyma (%) by
logistic equation
28.7F22.4 31.4F24.1 30.1F22.9
Breast volume (ml) by
logistic equation
472F381 449F352 460F360
Fat volume (ml) by
logistic equation
394F378 369F358 381F362
Parenchyma volume (ml) by
logistic equation
78F50 80F49 79F49
R.C. Boston et al. / Magnetic Resonance Imaging 23 (2005) 591–599 597
peaks in our phantoms. Thirdly, as shown in Fig. 4A, the
degree of saturation of fat can influence the time of the fat
peak. In breast cancer patients, the breast LCFA composi-
tion has been reported to be as follows: saturated 33.3F3.9,
monounsaturated 48.0F2.2 and polyunsaturated 16.6F3.7
A B
C D
0
1000
2000
3000
4000
0 500 1000 1500 2000
Time (ms)
ff
0
10000
20000
30000
40000
50000
0 500 1000 1500 2000
f
Time (ms)
f
2
4
6
8
f
Fig. 5. Segmentation of four breast T1 histograms using the logistic function. The g
the parenchyma signal. (A) 93.3% fat; (B) 22.8% fat; (C) 60.9% fat; (D) 67.6%
[33]. In comparison, the LCFA composition of canola oil
was as follows: saturated 7.8%, monounsaturated 55.3%
and polyunsaturated 32.4%, while for the LCFA composi-
tion of the cooking fat was saturated 30%, monounsaturated
40% and polyunsaturated 30%. Clearly, these differences in
LCFA composition could contribute towards the discrepan-
cy between phantoms and breasts in the mean times for the
fat peak.
3.3. Prediction of breast composition based on the T1
histogram
The mean fat and P% of breasts as predicted by Eq. (4)
are shown in Table 2. It should be noted that for some
individual breasts, the use of Eq. (4) resulted in a prediction
of 0% parenchyma. Since breasts are likely to contain at
least some parenchyma, this extreme type of prediction is
likely to have some error and this type of prediction could
lead to discontinuities and step artifacts in imaging.
As can be seen in Fig. 5, the use of Eqs. (7) and (8) to
predict parenchyma and fat in breast tissue resulted in
distribution curves without discontinuities. Indeed, all fat
and parenchyma distribution curves calculated using this
function appeared plausible in that they generally showed
strong symmetry typical of the Gaussian-type curves ob-
tained from phantoms of bpureQ fat and bpureQ parenchyma.
1500
Time (ms)
0
300
600
900
1200
0 500 1000 1500 2000
0
000
000
000
000
0 500 1000 1500 2000
Time (ms)
ray line depicts the histogram, the long dash the fat signal and the short dash
fat.

R.C. Boston et al. / Magnetic Resonance Imaging 23 (2005) 591–599598
Furthermore, in contrast to the moments approach, when
using the logistic approach (Eqs. (7) and (8)), we did not
obtain any implausible predictions of the composition of
individual breasts (i.e., none with zero parenchyma). More
importantly, the strong concordance of the known and
predicted volumes of fat and parenchyma in the phantoms
(Fig. 4) gives us reason to have confidence in the same
logistic equation approach for predicting the composition of
breasts. The mean percentages of fat and parenchyma in
breasts as estimated by the logistic equation are similar to
the corresponding values as estimated by the moments
approach. Both methods may be useful for predicting the fat
and P% of breasts, but the logistic approach more readily
lends itself to imaging since the logistic curve enables the
imager to identify a number of ranges, e.g., quintiles (see
Fig. 3), which could allow an MR image to be segmented
into a limited number of gray scales representing defined
composition ranges of fat and parenchyma.
In this investigation, a number of experimental issues
could have introduced some error into this empirical
calibration approach. Firstly, the phantoms were of much
smaller volume than breasts. Since we employed phantoms
that ranged in volume from only 10.0 to 50 ml, this
necessarily introduced some errors. The determination of fat
and chicken volume by displacement probably involved an
error of up to 10% for the determination of individual
phantom volumes. Furthermore, in small phantoms, the ratio
of edge effects to binternalQ voxels is greater than in larger-
size breasts, and it is problematic to consider that bedgeQvoxels that contain some fat, chicken and air may or may
not be detected by MRI. The relatively large slice thickness
(3.5 mm), which was chosen to match the slice thickness
employed for the majority of breast MRI, probably resulted
in inappropriate resolution for the small volumes of the
phantoms. For these reasons, we concur with Clarke et al.
[23] who have said bFor a true indication of the maximum
accuracy of the segmentation methods, the phantom
volumes should be comparable to the anatomical or
pathologic structures of interest.QWe surmise that spatial scale of the phantom mixture
may greatly impact on the type of histogram obtained. We
speculate that for a phantom composed of both fat and
chicken, if the lumps of chicken breast were very much
larger than the voxel size, bimodal histograms would likely
result. However, even when the lumps of chicken breast are
larger than the voxel size, due to edge effects (chicken
abutting fat), there would still be voxels that contain both fat
and chicken, and bridge effects (like those seen in Fig. 4C
and D) would result. Experimental difficulties also impinge
on the type of histograms we obtain. We have found that
even when chicken is chopped and ground to a fine
consistency, it will naturally tend to clump, especially when
mixed with oil. These difficulties acknowledged, with
phantoms composed of fat and ground chicken breast, we
were nevertheless able to obtain a diverse range of histo-
grams that mimicked the types of histograms obtained from
breasts in vivo. This suggests that we had indeed replicated
the spatial scale of the fat/parenchyma distribution that
occurs in vivo.
As mentioned earlier, the phantoms were imaged at room
temperature instead of body temperature. As also discussed
earlier, cooking fat, and especially canola oil, may not
necessarily be the best simulacra to human body fat. Indeed
it could be expected that pork fat would more closely
chemically resemble human fat, and there is experimental
precedent for using pork fat as phantoms in MRI inves-
tigations [34]. Furthermore, the fat and oil used in these
phantoms may have contained some moisture, and the
chicken breast almost certainly contained some fat. For
these reasons, the work presented here must be regarded as
preliminary in nature. Nevertheless, although the estimated
volumes of fat and parenchyma in breasts in this investi-
gation may not be absolutely correct, their relative ranking
would still be useful for quantifying the effects of
experimental drugs or investigating the time course changes
in breast composition. Graham et al. [22], working with a
population of asymptomatic patients, have shown associa-
tions between relative water content of breasts (as measured
by MRI) and socio-demographic and anthropometric risk
factors for breast cancer. The possibility that the empirical
approach to the estimation of parenchyma and fat content of
breasts as described here could provide a more direct and
perhaps enhanced measure of risk could have important
implications for epidemiological studies of breast cancer
and for models that predict risk of breast cancer [35].
4. Conclusion
The empirical logistic model presented here has the
flexibility to accurately and plausibly segment all of the
MRI T1 histograms that we have encountered.
References
[1] Stomper P, D’Souza D, DiNitto P, Arredondo M. Analysis of
parenchymal density on mammograms in 1353 women 25–79 years
old. AJR Am J Roentgenol 1996;167(5):1261–5.
[2] Wolfe JN. Breast patterns as an index of risk for developing breast
cancer. AJR Am J Roentgenol 1976;126:1130–9.
[3] Harvey JA, Bovbjerg VE. Quantitative assessment of mammographic
breast density: relationship with breast cancer risk. Radiology
2004;230(1):29–41.
[4] Byrne C. Studying mammographic density: implications for under-
standing breast cancer. J Natl Cancer Inst 1997;89(8):531–3.
[5] Shepherd JA, Kerlikowske KM, Smith-Bindman R, Genant HK,
Cummings SR. Measurement of breast density with dual X-ray
absorptiometry: feasibility. Radiology 2002;223(2):554–7.
[6] Ursin G, Parisky YR, Pike MC, Spicer DV. Mammographic density
changes during the menstrual cycle. Cancer Epidemiol Biomark Prev
2001;10(2):141–2.
[7] Byng JW, Yaffe MJ, Jong RA, Shumak RS, Lockwood GA, Tritchler
DL, et al. Analysis of mammographic density and breast cancer risk
from digitized mammograms. Radiographics 1998;18(6):1587–98.
[8] Sivaramakrishna R, Obuchowski NA, Chilcote WA, Powell KA.
Automatic segmentation of mammographic density. Acad Radiol
2001;8(3):250–6.

R.C. Boston et al. / Magnetic Resonance Imaging 23 (2005) 591–599 599
[9] Wang XH, Good WF, Chapman BE, Chang YH, Poller WR, Chang
TS, et al. Automated assessment of the composition of breast tissue
revealed on tissue-thickness-corrected mammography. AJR Am J
Roentgenol 2003;180(1):257–62.
[10] Lee NA, Rusinek H, Weinreb J, Chandra R, Toth H, Singer C, et al.
Fatty and fibroglandular tissue volumes in the breasts of women
20–83 years old: comparison of X-ray mammography and computer-
assisted MR imaging. AJR Am J Roentgenol 1997;168(2):501–6.
[11] Costanza ME. Breast cancer screening in older women. Cancer Suppl
1992;69(7):1925–31.
[12] Byrne C, Schairer C, Wolfe J, Parekh N, Salane M, Brinton L, et al.
Mammographic features and breast cancer risk: effects with time, age,
and menopause status. J Natl Cancer Inst 1995;87(21):1622–9.
[13] Gentry JR, DeWerd LA. The measurement of in vivo mammographic
exposures and the calculated mean glandular dose across the United
States. Med Phys 1996;23(6):899–903.
[14] Soderqvist G, Isaksson E, von Schoultz B, Carlstrom K, Tani E, Skoog
L. Proliferation of breast epithelial cells in healthy women during the
menstrual cycle. Am J Obstet Gynecol 1997;176(1 Pt 1):123–8.
[15] Vachon CM, Kushi LH, Cerhan JR, Kuni CC, Sellers TA. Association
of diet andmammographic breast density in theMinnesota breast cancer
family cohort. Cancer Epidemiol Biomark Prev 2000;9(2):151–60.
[16] Rutter CM, Mandelson MT, Laya MB, Seger DJ, Taplin S. Changes in
breast density associated with initiation, discontinuation, and con-
tinuing use of hormone replacement therapy [see comment]. JAMA
2001;285(2):171–6.
[17] Hammerstein G, Miller D, White D, Masterson M, Woodard H,
Laughlin J. Absorbed radiation dose in mammography. Radiology
1979;130(2):485–91.
[18] Woodard H, White D. The composition of body tissues. Br J Radiol
1986;59(708):1209–18.
[19] Kover G, Romvari R, Horn P, Berenyi E, Jensen JF, Sorensen P. In
vivo assessment of breast muscle, abdominal fat and total fat volume
in meat-type chickens by magnetic resonance imaging. Acta Vet Hung
1998;46(2):135–44.
[20] Baulain U. Magnetic resonance imaging for the in vivo determination
of body composition in animal science. Comput Electron Agric
1997;17(2):189–203.
[21] Poon CS, Bronskill MJ, Henkelman RM, Boyd NF. Quantitative
magnetic resonance imaging parameters and their relationship to
mammographic pattern. J Natl Cancer Inst 1992;84(10):777–81.
[22] Graham SJ, Bronskill MJ, Byng JW, Yaffe MJ, Boyd NF. Quantitative
correlation of breast tissue parameters using magnetic resonance and
X-ray mammography. Br J Cancer 1996;73(2):162–8.
[23] Clarke LP, Velthuizen RP, Camacho MA, Heine JJ, Vaidyanathan M,
Hall LO, et al. MRI segmentation: methods and applications. Magn
Reson Imaging 1995;13(3):343–68.
[24] Kroeker RM, Stewart CA, Bronskill MJ, Henkelman RM. Continuous
distributions of NMR relaxation times applied to tumors before and
after therapy with X-rays and cyclophosphamide. Magn Reson Med
1988;6(1):24–36.
[25] Graham SJ, Stanchev PL, Lloyd-Smith JO, Bronskill MJ, Plewes DB.
Changes in fibroglandular volume and water content of breast tissue
during the menstrual cycle observed by MR imaging at 1.5 T. J Magn
Reson Imaging 1995;5(6):695–701.
[26] Laidlaw DH, Fleischer KW, Barr AH. Partial-volume Bayesian
classification of material mixtures in MR volume data using voxel
histograms. IEEE Trans Med Imaging 1998;17(1):74–86.
[27] Englander SA, Quing Yuan Schnall M. A 3D technique to determine
global contrast pharmacokinetics and parenchyma volume in breasts
[Abstract]. Glasgow (Scotland)7 International Society of Magnetic
Resonance in Medicine; 2001 [April 23–27].
[28] Stata. Stata statistical software. Release 7.0 ed. College Station (Tex)7
Stata Corporation; 2001.
[29] Hill AV, Lupton H. Muscular exercise, lactic acid, and the supply and
utilization of oxygen. Q J Med 1923;16:135–71.
[30] Moate PJ, Dougherty L, Schnall MD, Landis RJ, Boston RC. A
modified logistic model to describe gadolinium kinetics in breast
tumors. Magn Reson Imaging 2004;22(4):467–73.
[31] Graham SJ, Ness S, Hamilton BS, Bronskill MJ. Magnetic resonance
properties of ex vivo breast tissue at 1.5 T. Magn Reson Med
1997;38(4):669–77.
[32] Bohris C, Schreiber WG, Jenne J, Simiantonakis I, Rastert R,
Zabel HJ, et al. Quantitative MR temperature monitoring of high-
intensity focused ultrasound therapy. Magn Reson Imaging 1999;
17(4):603–10.
[33] Chajes V, Niyongabo T, Lanson M, Fignon A, Couet C, Bougnoux P.
Fatty-acid composition of breast and iliac adipose tissue in breast-
cancer patients. Int J Cancer 1992;50(3):405–8.
[34] Poon CS, Szumowski J, Plewes DB, Ashby P, Henkelman RM. Fat/
water quantitation and differential relaxation time measurement using
chemical shift imaging technique. Magn Reson Imaging 1989;7(4):
369–82.
[35] Gail MH, Costantino JP. Validating and improving models for
projecting the absolute risk of breast cancer. J Nat Cancer Inst
2001;93(5):334–5.
Top Related
Copyright © 2022 FDOKUMEN

