







Bahasa
Halaman
Hukum

A STUDY ON
VATHA PITHAM
Dissertation Submitted To
THE TAMIL NADU DR.M.G.R Medical University
Chennai – 32
F or the Partial fu lfillm ent in A w arding the D egree of
DOCTOR OF MEDICINE (SIDDHA)
(Branch – I Pothu Maruthuvam)
Department of Pothu Maruthuvam
Government Siddha Medical College
Palayamkottai – 627 002
APRIL – 2012
CONTENTS
Page No
ACKNOWLEDGEMENT
I. INTRODUCTION 1
II. AIM AND OBJECTIVES 5
III. ABSTRACT 7
IV. REVIEW OF LITERATURE
a. SIDDHA ASPECTS 8
b. MODERN ASPECTS 55
V. MATERIALS AND METHODS 81
VI. RESULTS AND OBSERVATION 85
VII. DISCUSSION 103
VIII. SUMMARY 112
IX. CONCLUSION 115
X. ANNEXURES
� PREPARATION AND PROPERTIES OF
THE TRIAL MEDICINE 117
� BIO-CHEMICAL ANALYSIS 124
� PHARMACOLOGICAL ANALYSIS 127
� TOXICOLOGICAL STUDY 129
� CASE SHEET PROFORMA 133
XI. BIBLIOGRAPHY 148
Acknowledgement
ACKNOWLEDGEMENT
First, I thank Almighty for his showered blessings which is the
ultimate source of my success.
I express my gratitude to our Siddhars for all their manifold mercies.
I would like to offer my reverence to My Beloved Parents who are
an epitome of Love, Sacrifice, Encouragement and inspiration.
I wish to express gratitude and acknowledgement to the
Vice-Chancellor, The TamilNadu Dr.M.G.R. Medical University, Chennai,
The Special Commissioner, Director of Indian Medicine and Homeopathy,
Chennai and Joint Director of Indian Medicine and Homeopathy, Chennai.
I also wish to convey my deep gratitude to
Prof. Dr.N.Chandramohan Doss M.D.(s)., Principal, Government Siddha
Medical College, Palayamkottai for patronizing the work by providing all
the necessary facilities.
I also wish to convey my deep gratitude to
Prof. Dr. S.Soundarrajan M.D.(s)., Vice Principal, Government Siddha
Medical College, Palayamkottai for patronizing the work by providing all
the necessary facilities.
I express my deep sense of gratitude to Dr.S.Mohan, M.D.(s)., Head
of the Department, P.G. Pothu Maruthuvam, Government Siddha Medical
College, Palayamkottai for his valuable guidance and suggestion in caring
out the dissertation.
I express my deep sense of gratitude to Dr. R.Thangamoney,
M.D.(S), former HOD Department of PG Pothu Maruthuvam, Government
Siddha Medical College, Palayamkottai, for him guidance and suggestions
in the selection of topic.
I am extremely grateful to Assistant Lecturer
Dr. S. Justus Antony M.D.(s)., Department of P.G Pothu Maruthuvam,
Government Siddha Medical college, Palayamkottai for their kind and
affectionate encouragement to my work.
I am extremely grateful to Assistant Lecturer
Dr. G.Subash Chandran M.D.(s)., Department of P.G Pothu Maruthuvam,
Government Siddha Medical college, Palayamkottai for their kind and
affectionate encouragement to my work throughout the study period.
I am extremely grateful to Reader Dr.A.Manoharan M.D.(s).,
Department of P.G Pothu Maruthuvam, Government Siddha Medical
college, Palayamkottai for his valuable guidance to my work.
It is my responsibility to express my thanks to Dr.V.Sree Loganathan
B.I.M., RMO, GSMC, Palayamkottai for offering his suggestion and advices
whenever needed.
I extend my deep sense of gratitude to Dr.S.Nazer, M.D General
Medicine Former Professor, Department of Modern Medicine for their
valuable suggestion in this study.
I express my deep sense of gratitude to
Prof. Dr.V. Thiru Neelakandan M.B.B.S., M.D, HOD, Modern Medicine,
Government Siddha Medical College, Palayamkottai for his Valuable
guidance in modern aspects.
I thank Dr. S. Bageerathy for the help rendered in analysing urine
and blood for my patients in Laboratory during the study.
I thank to staff nurses, pharmacist and attenders for their help in
varius stage of my study.
I express my heartfelt thanks to Mr. R.Parthasarathy, former in the
salem districy for the collection of herbal drug for my dissertation work.
I take this opportunity to express my deep sense of gratitude to
Mr. M. Kalaivanan M.Sc., M.Phil., Lecturer and other staffs of Modern
Pharmacology Department, Government Siddha Medical College,
Palayamkottai for their help during the entire course of my work.
I would like thanks to Mrs. T. Poongodi, M.L.I.S., M.Phil., for
permitting me to utilize the college library for my dissertation work.
I would like thanks to Mr.Chelladurai, M.Sc., Botany, for their
identification of herbal drung for my dissertation work.
I also thanks to Mrs. N. Nagaprema M.Sc. M.Phil., Lecturer Head
of the Department and all the staffs of Department of Bio-Chemistry, for
their help in Biochemical Analysis for this work.
I wish to thank Mrs. M.Alagammal M.Sc., Head of the Department
and Mrs.S.Sudha M.Sc., Ph.D., Lecturer., Department of herbal botany and
pharmacognosy Government Siddha Medical College for her kind help in
botanical aspect of my study.
I would like to convey my thanks to Shakthi Diagnostics,
Vannarpet, Tirunelveli , for their Co-operation to diagnostic the disease.
Finally I convey my thanks to Mr. M.Maharaja, Maharaja DTP Services, Palayamkottai for his expertise typing and printing work.
Introduction
INTRODUCTION
“ngv!Lkz!wPk<okz<zil<!Nkq!
hgue<!Lkx<Ox!dzG/”!
! ! ! ! ! ! ! .!kqVg<Gxt<!himz<.2!
! ‘Man is the most wonderful creature of ‘Nature’. When discussing the
issue of health, it is common for people in all cultures to talk just about their
body, its ailments and the medicines they right to treat these ailments.
However health is not merely a matter of the state of the body, since it is
obvious we are much more than just this material forms.
A system of health that only takes into account the structure and the
functioning of the physical body can not effectively address human health in
its totality. “Siddha” is not just a medical approach to health, rather it is a
complete philosophy of life. It gives equal importance to the parts of life,
which are more subjective and intangible as well as those, which are
objective and material, those aspects we can observe with out physical
senses. In fact, it is a view of life which understands that the non-material
components of our life, our consciousness, mind, thoughts and emotions
animate and direct our more physical parts.
The term “Siddhar” has been derived from the word “Siddhi” which
literally means accomplished, achieved or perfected success and so it referes
to one who had attained his end in spiritual goal. They were mystics, yogis,
poets, devotees and medical men of various combinations.
In “Siddha” system of medicine we can save our body from diseases
and attain our soul to the “Nature”. The Siddha system of medicine is the
ancient system of medicine, which has been presented by the ‘siddhars’. The
unique nature of this system is its continuous service to humanity in
computing diseases and in maintaining the physical, mental and moral
health, while many of these contemporaries had completed their forces long
ago. The Siddha system of medicine is purely scientific and the peculiar
complex system of science and philosophy. It provides rational methods for
the treatment of many diseases, which are considered to be obstinate and
incurable in other system of medicine.
The “Siddha” focuses on maintaining a balanced integrated
relationship among them. In balance, whether physical, mental or emotional
arises when there is a disconnection between the subjective and objective
areas of life.
More over they labored much in the field of alchemy and medicines
and also attained success in Yoga and Philosophy. They were of extra sense
perception and highly spiritual, having complete control over all the
elements. They had full awareness of the nature and activities of all objects
on the planets of all times past, present and future.
They were said to be mostly “Tamilians” who were familiar with the
wonderful properties of rare drugs peculiar to south India in their both
physiological & psychological aspects. They choose not only to keep their
bodies and souls together but also prolong their lives to a considerable
extent. Their motive life was the service of god through humanity.
“Nature cures everything”
– Hippocrates
Hipprocates, famous Greek Physician and Philosopher (460-367 B.C)
is considered to be the “Father of Medicine”. Even earlier than Hipprocates,
Vedas and Puranas of ancient India especially in Tamilnadu, a system of
Medicine called “Siddha” system was evolved. The basic principle of
Siddha medicine states that the entire body, both physical and mental, is
made up of “96 Thathuvas” and “Tri-Dhosas”. The three aspects are Vatha,
Pitha, Kabha. Tri-Dhosa or mukkutrangal forms the basic of the human body
and character. The Tri-Dhosas are maintained in the body in a particular
ratio (ie) vatha-1 unit, pitha-1/2 unit and kabha-1/4 unit. Imbalance or any
derangements in Tri-Dhosas cause diseases.
From the verse’s “Theraiyar Maruthuva Bharatam”
! “uiklib<h<!hjmk<Kh<!hqk<k!ue<eqbib<g<!gik<Ks<!Osm<h!
! ! sQklib<k<!Kjmk<K…//”!
! It is clearly understood that Vatha is constructive in nature, Pitha is
protective in nature and Kabha is destructive in nature.In general all systems
of medicine, the combination of various herbs and minerals are used in
judicious proportion activate Vatha, Pitha, Kabha doshas (defects) and bring
about the needed balance of these three to the human body.
For instance the combination of herbs or roots is done in such a
fashion that one herb adverse action will be neutralized by the other herb.
“Siddhars” who had experienced with very many herbs and found-out
the efficacy of each and every herb in the human system.
The cure from intake of herbal medicines is astonishing; So it has
attracted the attention of people world over.
Luckily the Siddhars were all Tamil Saints and so Tamilnadu has the
previlage of possessing the knowledge of Siddha system. The Siddhars have
thoroughly studied the human Psychology and the mind set is important for
cure.
The mind, soul and the body have to have the absolute coordination
for keeping the health, intact.
Faith in the medicine is necessary before taking them. Mental health
is necessary for Physical well being. That is why the popular Tamil Saint.
Agathiyar Says….
“ lelK!osl<jlbieiz<!lf<kqvR<!oshqg<g!Ou{<mi!
! ! lelK!osl<jlbieiz<!uiBju!dbi<k<k!Ou{<mi!
! ! lelK!osl<jlbieiz<!uisqjb!fqXk<k!Ou{<mi!
! ! lelK!osl<jlbieiz<!lf<kqvR<!osl<jlbiOl”
Manmurikiyam states that
“hqk<kf<!kiOe!GVkqbqx<!Oxie<Xl<”!
1. Vatha pitham is similarly compare in modern science as systemic
Hypertension.
2. Systemic Hypertension are produced several risk facters. It affects all
the organs.
3. The normal level of Systolic Blood Pressure is 120-140/mmHg and
diastolic Blood Pressure is 80-90mmHg.
4. Any alternation of systolic and diastolic pressure may leads to
systemic hypertension.
This dissetation work has selected “Vatha Pitham” under the Pitha
diseases by “Yugi Vaidhya Chinthamani - 800” and a clinical entity
comparable to “Hypertension” in modern medicine. The incidence of this
disease as mentioned above is increasing, so I have tried to formulate a
treatment methodology to treat this disease.
The choice of drugs for clinical study was
1.IRUVELI KIYALAM – Internally,
Ref: Agathiar Vaithiya Pooranam - 205
The drug was prepared personally by me and tried in 20 selected cases
of vatha pitham in IP and OP. The clinical study was undertaken in the post
graduate department of Pothu Maruthuvam at Government Siddha Medical
College, Palayamkottai. Those cases were treated with trial drug.
Aims and Objectives
AIM AND OBJECTIVES
Vatha Pitham (Hypertension) - “The silent killer of the society is
probably most important public health problem. Because according to
current report, about 15% of the population can be regarded as hypertensive
and 7% of death occur due to this. So as a preliminary effect, Vatha Pitham
(Hypertension) was selected for the dissertation. IRUVELI KIYALAM
was selected for evaluating its clinical efficacy in patients with Essential
Hypertension.
Vatha Pitham (Hypertension) is a staggering public health problem for
three reasons.
1. It is very common.
2. Its effects are sometimes devastating (Myocardial infarction,
stroke).
3. It remains asymptomatic until late in its clinical course.
Hypertension is an important cause of death. There deaths are due to
cerebral haemorrhage or dissecting aneurysm or heart failure. They are
important because, they are almost entirely prevented by treatment. But the
great majority of deaths due to Hypertension are caused by coronary artery
Heart disease (CAHD).
If the hypertension patients remain untreated, it affects all the organs
in the body. To bring a light and hope in the lives of the hypertensive
individuals with the siddha medicines. Vatha Pitham (Hypertension) was
selected for the dissertation work as a maiden attempt.
The ultimate aim of the present study on Vatha Pitham is:
� To make a clinical study on the course of the disease under careful
examination on the Aetiology, Pathogenesis, Treatment and
Prognosis by making use of Siddha concept.
� To explore the unique diagnostic methods mentioned by Siddhars.
� To have an idea of the incidence of the Vatha Pitham with regards
to Age, Sex, Socio-economic status, Family history and Personal
history.
� To know how the disease Vatha Pitham alters the normal
conditions under the topic Mukkutram, Poripulangal, Udalkattugal,
Envagai thervugal, Naadi, Neerkuri, Neikuri.
� To know the extend of correlation of Aetiology, Signs, Symptoms
and Complications of Vatha Pitham in Siddha aspect with
Hypertension in modern aspect.
� To have a clinical trial on Vatha Pitham patients with Iruveli
Kiyalam in the post-graduate studies and Research Centre,
Govt.Siddha Medical College Hospital, Palayamkottai, under the
guidance of the staff of the post-graduate department of Pothu
Maruthuvam.
� To use modern parameters to confirm the diagnosis, progress of the
disease.
� To evaluate and to produce pharmacological and biochemical
analysis reports of the test drugs.
� To estimate the toxic effects of the drugs.
Abstract
ABSTRACT
Since the commonest disease in the society, number of sufferers
increasing day by day, I have chosen the disease “Vatha Pitham” for my
dissertation work.
20 patients of either sex were selected as In patients and 20 patients of
either sex as Out patient were selected and administered with the trial
medicine .
IRUVELI KIYALAM- 90ml internally twice a day during the whole
study period.
The trial medicine was subjected to Biochemical, pharmacological and
toxicological analyis
At the end of the trial study, the majority of the cases show good
results.
Siddha Aspect

REVIEW OF SIDDHA LITERATURE
Definition of Pitha
Pitha is one of three major Uyir thathukkal namely Vatha, Pitha and
Kabha Otherwise called as MUKKUTRAM.
“fqzl<!fQi<kQutq!uqSl<Ohijmf<Kl<!
gzf<klbg<!gLzgl<!Nkzqe<”!!
- Sadhaga naadi
According to this lines, the world is made up of five elements known
as “PANCHA BOOTHA”.
These are
1. Prithivi - Earth
2. Appu - Water
3. Theyu - Fire
4. Vayu - Air
5. Aahayam - Space
In these, pitha consists the element Thee (Fire).
The relation between Uyir thathukkal and Pancha bootha is as follows,
Uyir thathuikkal Pancha bootha
Vatha Vayu (Air)
Aahayam (space)
Pitha Theyu (Fire)
Kabha Appu (Water)
Prithivi (Earth)
Thus Vayu and Aahayam combine to become vatha uyir thathu, which
controls all aspects of movements. The words dry, light, cold, quick, rough
minute and mobile describe the characteristics for Vatha Uyir thathu.
Theyu alone becomes pitha Uyir thathu, which controls all the body’s
conversion processes, produce heat and energy producing capacities. The
words hot, pungent, aggressive, liquid, mobile and acid describe the
characteristics, of Pitha Uyir thathu.
Appu supported by Prithivi becomes Kabha Uyir thathu and controls
liquifaction, lubrication and cohesion. It is also responsible for giving
solidity and structure to the body. Kabha Uyir thathu primarily reflects the
qualities of the water but also some traits of the earth element, consequently
kabha is heavy, slow, cold, steady, solid and oily.
Formation of Muthoda
“NglK!fic!fvl<H!obPhk<kQvibqvl<!
-Vh<hi!fic!WPh!OkiOvi!
bqvlie!Okgk<kqz<!gzh<Oh!fic!
Wg<gs<!slk<!okipqz<!Dg<g!sguiB!
kg<g!fic!we<Ox!siM” !
- Yugi Vaidhya Chinthamani - 800
“-Vh<hie!fic!WPhOkiCvi!
bqvlie!Okgk<kqz<!Wzh<!ohVfic!
yg<gkslk<!okipqjz!Dg<g!ks!uiBg<gt<!
kg<ghc!we<Ox!siVl<” !
!
“siVf<ks!fic!ke<eqz<!&zl<!&e<X!
OhVlqml<!hqr<gjzBl<!hqe<eZme<!.!liXl<!
djvg<guqvx<!gix<oxim<Mek<KOl!fisq!!
ujvs<!SpqObi!jlbk<kqz<!uf<K!gjz!&e<xqz<!uiBuil!
hieEme<!
kf<k!hqvi{e<!slieEg<GR<!sf<klxg<!!
%m<MxU!Ovgqk<kz<!dXl<!uikl<!hqk<kl<!
fim<Mr<!ghOlbil<!fiM” !
- Kannusamiyam
According to this verse, the human body is composed of 72,000 naadi
narambugal.
Among this 72,000 naadies, ten are prominent naadies (Dasa naadies).
Of these ten naadies 3 are known as moolathara naadies.
These are
� Edagalai.
� Pingalai.
� Suzhumunai.
Ten Vayus present in the body are
1. Piranan.
2. Abhaanan.
3. Udhanan.
4. Viyanan.
5. Samanan.
6. Nagan.
7. Koorman.
8. Kirugaran.
9. Devathathan.
10. Thananjeyan.
Among these Abhaanan conjugates with edagalai to form ‘Vatha’.
Piranan conjugates with pingalai to form ‘Pitha’.
Samanan conjugates with suzhumunai to form ‘Kabha’.
These three humours vatha, pitha and kabha are more or less
correlated with excrete, gastric juice, and saliva respectively.
They circulate in the body system in different proportions and help in
the digestion of food and other general physiological functions of the body.
Each of them has different functions.
The right proportion of each in proper combination are responsible for
maintaining the good health.
When some of the environmental factors like diet, weather etc.,
disturb pitha, it looses its control, which may be diminished or exaggerated.
So the other two Uyir thathus are also disturbed which are in peculiar
equilibrium state. Finally this may leads to pitha diseases.
Natural Characteristics of Pitha
Locations
Generally pitha lives in
1. Piranan.
2. Pingalai.
3. Head.
4. Heart.
5. Blood.
6. Stomach.
7. Urinary bladder.
8. Sweat.
9. Eye.
10. Skin.
11. Umblicus.
12. Saliva.
1. According to Thiru Moolar,
! “hqiqf<kqMl<!hqk<kl<!OhviR<szk<kqeqz<”!
! It means, ‘pitha’ lives in urine.
2. According to Yugi muni,
“Ohiole<x!hqk<kk<Kg<!gqVh<hqmOl!Ogtib<!
! ! Ohvie!g{<mk<kqe<!gQpkiGl<”!
! ! It means, place of the ‘pitha’ in body is below the neck.
NATURAL PROPERTIES
Pitha in its natural habit may cause
1. Digestion.
2. Hunger or hungry (poly phagia).
3. Taste.
4. Thirst.
5. Vision.
6. Light.
7. Concentration.
8. Knowledge.
9. Softness.
10. Warm.
11. Hardness.
12. Heat production in the body.
13. Bluish colour formation.
14. Production of heat during digestion.
15. Memory power.
QUALITIES OF PITHA
Own Qualities – 6
1. Akkini - Hot
2. Kaaram - Pungent
3. Kurooram - agressive
4. Salaroopam - Liquid
5. Oodumthanmai - Mobile
6. Pulippu - Acid
Opposite qualities – 6
1. Kulirchi - Cold
2. Getti - Solid
3. Santham - Mild or harmless
4. Kasappu - Bitter
5. Inippu - Sweet
6. Nilaitthiruthal - Immobile
Hyper Pitha - Signs
1. Yellowish discolouration of eye, skin urine and motion.
2. Poly phagia and poly dypsia.
3. Burning sensation all over the body.
4. Sweating.
5. Giddiness.
6. Haemorrhage.
7. Angry.
8. Immovable.
9. Emaciation.
10. All taste to be like sour or bitter.
Hypo Pitha - Signs
1. Cold.
2. Decrease in colour.
3. Disturbance in natural growth of Iyam.
4. Less heat.
Pitha Thegi - Natural Characterestics
Physical characters
� The person has high thee thoda.
� The muscle content can be less beyond the bones and joints.
� Body may appear always with heat, sweating and with unpleasent
smell.
� Wrinkled skin.
� Colour of the skin can be yellowish red with shining.
� Face, palm and sole are reddish yellow in colour.
� Thin eyelids.
� Reddish discoluration of eyes due to heat, anger and hungry.
� Black moles with pimples.
� More heat in the body.
� Yellow or red colour of the body.
� Reddishness in upper and Lower limbs.
� Lesser hair in body.
� Giddiness.
Behavioural characters :
� Willing to take sweet, astringent, bitter and cold foods.
� Lesser intake of food.
� Intolerence to appetite, thirst, heat, angry and fear.
� Willing to be garlanded.
� Low sukkilam.
� Low kaamam.
� Reduced lust.
� Hatefullness, respect, courage, clear knowledge, talkative, good
habits, discipline and love with others.
� In dream, there will be sun, wind, light of fire, lightening and
kongu tree with flowers, caeasapenia tree (Sarakkondrai)
Murukkan tree are found.
� Happier and has good education.
� Age will be 65 years and has 3/4 vitality.
� Higher appetite.
� Willing to eat more.
Pitha thega kuri
“nxquie!hqk<kk<kiozMk<k!Okgl<!
! bxolzqU!fqxl<!out<jt!biqjuObiM!
hqiqbik!SgzQjzbx<h!U{<c!
! ohVl<Htqh<!H{U!ogit<tz<!ohiqObii<!kl<jl!
Gxqbik!uisivl<!h{<{z<!Hk<kq!
! Gpl<hqh<!hqe<!Okxz<!gjzg<!Rie!Ohikl<!
ofxqbigg<!gx<xxqU!osiz<zz<!uQvl<!
! !! fqjzh<H!lkqbqz<!glkq!bxuliOl”!
!! ! ! ! ! ! .!Noi Naadal noi mudhal naadal
According to this verse, the natural characteristics of pitha thegi are
� Emaciation.
� White coloured skin.
� Low intake of food.
� Willing to take sour taste foods.
� Confused minds.
� Interest in Arts.
� Respect to elders.
� Intelligency.
� Courage.
� Excessive lust.
Place and function of pitha
“kieie!hqk<kl<!hqr<gjzjbh<!hx<xqs<!
! ! sib<uie!hqvi{!uiBU!ke<jes<!osi<f<K!!
! Deie!fQi<h<jhbqz<!n[gq!!&zk<!
! ! Kkqk<okPf<k!ug<gqeqjb!dxU!osb<K!
! liOeOgtqVkbk<kqzqVh<H!ligq!
! ! lbzigq!fqjeuigq!lbg<gligq!
! gieie!sqvf<keqOz!-vg<gligqg<!
! ! ogi{<M!fqe<x!hqk<kfqjz!%xqOeiOl”!
- Noinaadal Noi Mudhal Naadal
According to this verse, pitha is associated with piranan and pingalai,
goes to urinary bladder and mix with seevakkini to lives in heart and head
SYMPTOMS DUE TO EXCESS IN PITHA
“dXkqBt<t!hqk<klK!Okie<xqz<!ouh<H!
! d]<{uiBuk<kq!Svlkq!sivir<gt<!!
lxkqBme<!gqXgqXh<H!hbqk<kqb!Ovigl<!
! uti<!Osijg!bpoziqU!gif<kz<!jgh<H!
-Vkbk<kqz<!gzg<glK!lxh<H!kigl<!
! wPr<geU!OlbjeU!lbg<g!&i<s<js!
sqxqK!ohVl<hiM!vk<kl<!hqvOlgr<gt<!
! Osi<f<K!lqG!hq{q!hzUR<!sqxg<Gf<!kiOe”!
.!Sadhaga Naadi
According to this verse, , the symptoms due to excess in pitha are
� Excess heat.
� Fever.
� Dysentry.
� Loss of memory.
� Giddiness.
� Mental disorders.
� Dropsy, burning.
� Palpitation, thirst, dreams.
� Loss of consciousness.
� Menorrhogia.
� Gonorrhoea.
“hqk<kOl!oseqk<kix<!S,M!
ohzk<Km!Zzvs<!osb<Bl<!
hqk<kOl!lqGf<kizQjt!
bqVlZl<!ohzk<K!fqx<Gl<!
hqk<kOl!lqGf<k!kieiz<!ohzr<!Gjxf<Kl<!hPk<Kl<!
hqk<kOl!kqvm<cF~zqx<!
Ohsqeii<!ohiqObii<!kiOl”
.!GunaVaagada Naadi
!
“hqk<kOl!gkqk<k!OhiK!ohVf<kqMl<!uikL{<mil<!
hqk<kOl!gkqk<k!OhiK!ohVf<kqMl<!ubqx<xqz<!uiB!
hqk<kOl!gkqk<k!OhiK!hqkx<xqMl<!hqk<Ok!OgT!
hqk<kOl!gkqk<k!OhiK!hqxf<kqMl<!hq{qbOegl</” !
.!GunaVaagada Naadi
According to this verse the excess in pitha may cause symptoms as follows
� Increase in heat leads to dryness of body.
� Cough and expectoration.
� Loss of strength.
� Increase in Vatha.
� Excess gas in abdomen.
� Unwanted talkativeness.
� A state of delirium.
“ hGk<kqcx<!hqk<kl<!hzhz!sqf<jkbil<!
uVk<kqMl<!uif<kqBl<!uib<!fQi<lqg!U,Xl<!
lGk<kqM!Oleqbqz<!lim<c!wiqh<OhXl<!
lqGf<k!ue<eqg<G!lqg!uqmr<jgg<GOl” !
. kqV&zi<!
According to this verse the symptoms due to excess in pitha are
� Many thinkings.
� Vomiting.
� Excess secretion of saliva.
� Burning sensation in body.
� Bitter taste in tongue.
“%xqmOu!uqk<klK!lQxqx<xieiz<!
! ogiMr<gik<k!Zm!zpx<sq!fMg<g!L{<mil<!
lQxqmOu!Ovisqbf<kie<!fiuxm<sq!
! Olzie!OgihlK<!uqg<gz<!&i<s<js!
K~xqmOu!!gqX!gqXh<H!gikjmh<H!
! okif<klir<!gsh<HmOe!l{<jmg<!Gk<K!
NOl!kie<!bk<kq!Svl<!hi{<M!Osijg!
! Nmie!uqmis<!SvLl<!hqvOlgf<kie<!
OhiOlkie<!gilijz!hqk<k!oum<jm!
! ohiz<zik!hi{<MmOe!squf<k!fQvil<!
OkgOl!kie<!squh<hiB!lR<stiBR<!!
! sqX!sqXk<KbqV{<M!uVr<Gpq!uqPf<K!
fiOl!kie<!osie<OeiOl!hqk<kg<!%X!!
fuqe<!xqm<hii<!uisLeq!fuqe<!xqm<miOv”!
- Agathiyar
In these verse, Agathiyar says the symptoms of excess pitha are the
follows:
� Heat.
� Allergy.
� Shivering.
� Dryness of tongue.
� Angry.
� Hiccough.
� Loss of consciousness.
� Giddiness.
� Hearing loss.
� Bitter taste in tongue, headache.
� Fever, continuous fever.
� Oedema, anaemia.
� Jaundice.
� Leucorrhoea.
� Red coloured urine.
� Red or yellow coloured skin.
� Emaciation.
“hqk<k!Ovigq!ohVLmz<!S,miGl<!
!fqk<kli!Lgl<!Ofi<!uqpq!fiU!hz<!
!Lk<k!fQV!Lbi<k<k!sqh<hiGl<!
!Sk<k!lR<stib<k<!Okie<xqmg<!g{<cOm”!
- Kali Virutham
According to this verse the excess in pitha leads to following symptoms
1. Excessive body heat.
2. Red and yellowish discolouration of face, eyes, teeth, tongue and urine.
“Wzuib<!Gpzib<!hqk<kR<!osb<G{l<!uqtl<hg<!Ogtib<!
!Ogiz!Ouz<!uqpq!squf<K!Gtqi<f<kqciqVg<G!lz<ziz<!
!sQzOu!fQi<!gMk<K!ofif<K!SXg<oges<sq!uf<K!uQPl<!
!RizOl!gqXgqoxe<X!fiUzi<f<kqVg<Gr<!giO{”!
.!Raththina churukka naadi
According to this verse, the excess in pitha cause the following symptoms
� Reddish discolouration and feverishness.
� Burning micturition with pain and pricking.
� Giddiness.
� Dryness of tongue.
“hqk<kk<kqz<!hqk<kligqz<!hqkx<xqMr<!gqXgqXg<Gl<!
!sk<kqBlkqg!liGR<!siQvk<kqjth<!H{<mig<Gl<!
!nk<kqbiBzVOleq!bigLl<!OuxkiGl<!
!ux<xqObouTk<Kg<!gibl<!oux{<M!hqe<!uQg<gL{<mil<”!!
- Agathiyar Naadi
According to this verse, the excess in pitha may cause the symptoms
� Unwanted talking.
� Giddiness.
� Vomiting.
� Breathlessness.
� Dryness of body.
� Paleness and oedema of body can occur. !
“kioee<x!hqk<k!lQxz<!smolz<zir<!gif<kz<!gi[l<!
!Doee<x!uif<kq!uib<!fQ'xqOb!YPGR<!siuie<!
!uioee<x!lm<cz<!ouGl{<jmbqz<!Gk<K{<miGl<!
!Okoee<x!uqg<gz<!&i<s<js!osuqbjmh<H{<mil<!hiOv” !!!
- Kavviyaththin Naadi
According to this verse, the excess in pitha may cause the symptoms such as,
� Burning sensation all over the body.
� Vomiting.
� Excess secretion of Saliva.
� Pricking pain in head.
� Hiccough.
� Unconsciousness.
� Loss of hearing.
� Death.
Relation with taste
Taste, in common is divided into 6 types, called as Aru Suvai (6 taste)
Those are
1. Inippu - Sweet
2. Pulippu - Sour
3. Uppu - Salt
4. Kaippu - Bitter
5. Kaarppu - Pungent
6. Thuvarppu - Astringent
All 6 tastes are formed by the combination of two boothams from
pancha bootham, these are
Inippu = Prithivi + Appu
Pulippu = Prithivi + Theyu
Uppu = Appu + Theyu
Kaippu = Vayu + Aahaayam
Kaarpu = Vayu + Theyu
Thuvarppu = Prithivi + Vayu
Like that in Mukkutra, Except Azhal, the other two kutra (Vali, Iyam)
has the combination of two boothams. Azhal is formed by one bootha that is
Vali = Vayu + Aahaayam
Azhal = Thee or Theyu
Iyam = Appu + Prithivi
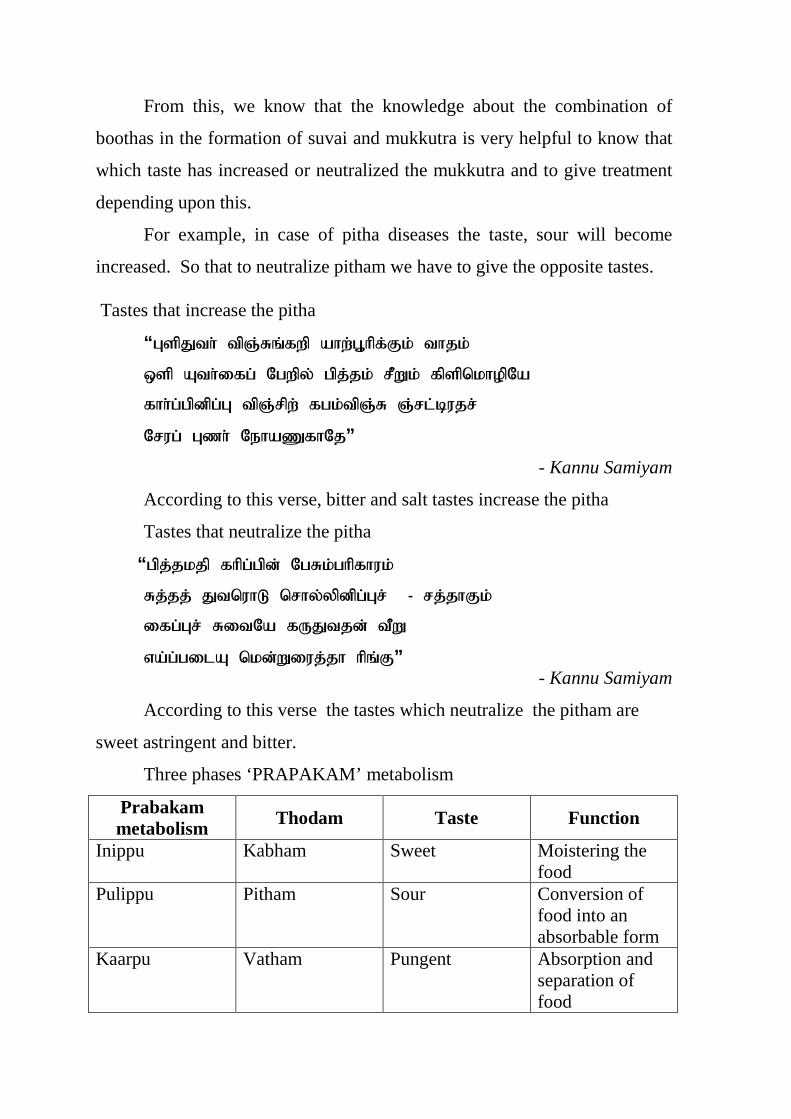
From this, we know that the knowledge about the combination of
boothas in the formation of suvai and mukkutra is very helpful to know that
which taste has increased or neutralized the mukkutra and to give treatment
depending upon this.
For example, in case of pitha diseases the taste, sour will become
increased. So that to neutralize pitham we have to give the opposite tastes.
Tastes that increase the pitha
!! “ HtqKui<!uqR<Sr<gxq!bix<H,iqg<Gl<!uikl<!
!! ytq!Bui<jgh<!Ohxqz<!hqk<kl<!sQXl<!gqtqolipqOb!
!! gii<h<hqeqh<H!uqR<sqx<!ghl<uqR<S!R<sm<cvks<!
!! Osvh<!H{i<!Ofib[giOk”!
- Kannu Samiyam
According to this verse, bitter and salt tastes increase the pitha
Tastes that neutralize the pitha
“hqk<klkq!giqh<hqe<!OhSl<hiqgivl<!
Sk<kk<!KuoviM!osiz<zqeqh<Hs<!!.!sk<kiGl<! !
jgh<Hs<!SjuOb!gVKuke<!uQX!
wb<h<hjmB!ole<Xjvk<ki!iqr<G” !- Kannu Samiyam
According to this verse the tastes which neutralize the pitham are
sweet astringent and bitter.
Three phases ‘PRAPAKAM’ metabolism
Prabakam metabolism Thodam Taste Function
Inippu Kabham Sweet Moistering the food
Pulippu Pitham Sour Conversion of food into an absorbable form
Kaarpu Vatham Pungent Absorption and separation of food

ALTERATIONS OF PITHA
The three humours are affected either themselves or with udal
thaathukkal, pathologically.
The types of alteration of pitha
Thannilai Valarchi
Definition : A Kutram which is provoked in its own location is called
Thannilai valarchi
Limitation : Hatefullness of the things which are causing Thannilai
valarchi and likeness of the things which are getting
opposite properties are the limitations of Thannilai valarchi.
Period : Pitha gets thannilai valarchi during Kaar Kaalam -
Aavani and purattasi.
II. Vetrunilai Valarchi
Definition : A kurtram which is provoked to other locations is called
Vetrunilai valarchi.
Limitation : Signs and Symptoms of the affected kutram and the
pathological conditions of the udal thaathukkal give the
details of the limitations.
Period : Pitham gets Vetrunilai valarchi during koothir kaalam
Iyppasi and Kaarthigai.
III. Thannilai Adiadhal
Definition : A provoked kutram, which is neutralized in its own
location is called Thannilai Adaidhal.
Period : The provoked pitha neutralizes during Mun Pani Kaalam
Margazhi and Thai.
Types of pitham
The siddha classical texts divide pitham into five subsidiary forms that
differ from other by their localization in the body (Anatomical and by their
particular functions (Physiological).
They are
� Anal pitham.
� Eranjaga Pitham.
� Saadhaga Pitham.
� Aalosga Pitham.
� Prasaga Pitham.
Anal pitham
� It gives appetite and helps in digestion.
� It has the character of thee or fire.
� It lies between abdomen and scrotum. Pitham dries the liquid form
things and digests the food we take.
Eranjaga Pitham:
� Which colours the blood.
� It increases the quality of blood.
� It lives in intestine and gives red colour to the essence which seperate
from the food we take.
Saadhaga Pitham:
� It controls the whole body.
� It has the ccomplishing property.
� It lies in heart and accomplish the work, via knowledge, mind and
desire.
Aalosaga Pitham:
� It brightens the eyes.
� It shows the things to eyes.
� It lies in eyes and shows the shape of all things.
Prasaga Pitham:
� It gives complexion to the skin.
� It lies in skin and brightens the skin.
Classificatin of Pitha diseases
According to Yugi Vaidhya Chinthamani- 800 Pitha diseases are
classified into 42 types . According to this classification, the symptoms of
VATHA PITHAM gives us a picture more or less similar to Hypertension.
Classification
“fim<cOee<!hqk<kk<kqe<!ohbjvk<kiEl<!
! ! fix<hk<kqv{<mie!G{iG{r<gt<!
! Nm<cOeeiUV!hqk<kf<ke<OeiM!
! ! Nlzhqk<k!lkOeiMe<lik!hqk<kf<!!
! kim<cOee<!klf<k!hqk<kl<!uik!hqkkf<!
! ! keqk<Okii<!he<eqhqk<kR<!sqOzm<l!hqk<kf<!
! K~m<cOee<!SOvi{qk!hqk<kf<!uqgiv!hqk<kf<!
! ! Kcbie!uqv{!hqk<kf<!okijgjbg<!OgOt”!
!!!!“okijgbie!Uvk<khqk<k!lqvk<k!hqk<kR<!
! ! Spqgish<!hqk<koliP!Suish<!hqkkl<!
! ujgbie!sqOzm<l!hqk<kr<!gVl<hqk<kf<kie<!
! ! ligvh<hie<!hqk<kk<Okim!sQv{!hqk<kl<!
! njgbie!uVsqhqk<k!oliqhqk<kf<kie<!
! ! npz<uqk<kf<!Kch<hqk<kl<!uq]h<hqk<kf<kie<!
! Ljgbie!nkqsivh<!hqk<kf<kiEl<!
! ! &zh<hqk<k!Lkqi<uqk<k!LjxjlbiOl!
! Ljxjlbir<!g{<m!hqk<kOliM!hqk<kl<!
! ! &Mhqk<k!fMg<Gh<!hqk<kr<!ghizhqk<kl<!
! kqxjlbiR<!si<k<kq!hqk<kf<kigh<!hqk<kf<!
! ! kVg<gie!uqg<gz<!hqk<kl<!!]bhqk<kf<kie<!
! kqxjlbif<!kqlqi<hqk<kl<!uzqhqk<kOliM!
! ! sQkhqk<kr<!gqVlqhqk<kl!sik<b!hqk<kl<!
! lxjlbil<!lii<g<g!hqk<klVk<kQM!hqk<kl<!
! ! ujgbK!fix<hk<kqv{<M!lgqp<f<K!hiOv/” !
- Yugi Vaidhya Chinthamani- 800
According to this verse, pitha diseases are classified into 42 types
� Aavuru pitham
� Amalaga pitham
� Unmadha pitham
� Thamandha pitham
� Vatha pitham
� Vanni pitham
� Silathma pitham
� Suronitha pitham
� Vigara pitham
� Virana pitham
� Uraththa pitham
� Raththa pitham
� Kaasa pitham
� Swasa pitham
� Semipitham
� Karum pitham
� Karappan pitham
� Aseerana pitham
� Aroosi pitham
� Eri pitham
� Azhal pitham
� Thudi pitham
� Athisaara pitham
� Moola pitham
� Vida pitham
� Muthir pitham
� Kanda pitham
� Oodu pitham
� Moodu pitham
� Naaduku pitham
� Kabaala pitham
� Sarthi pitham
� Thaga pitham
� Vikkal pitham
� Shaya pitham (Kaya pitham)
� Thimir pitham
� Vali pitham
� Seetha pitham
� Kirumi pihtam
� Asathiya pitham
� Markkap pitham
� Marumdeedu pitham
According to Pararasa Sekaram
The pitha diseases are classified into 40 types in Pararasekaram
“ux<xqMr<!gis!hqk<k!Olikqb!uikhqk<kl<!
osix<xqMl<!uxm<sq!hqk<kf<!KbVX!Spx<X!hqk<kl<!
osx<xqMR<!sk<kq!hqk<kR<!Osx<he!hqk<kf<!Okgl<!
ux<xqM!Lzi<k<K!hqk<kl<!uslxh<!hqkx<Xl<!hqk<kl<!
hqk<kli!obMg<Gl<!hqk<kl<!Okqk<K!fMg<Gl<!hqk<kl<!
sk<kli!lUe!hqk<kr<!KbVx!OuiMl<!hqk<kl<!
sk<klii<!gcb!hqk<kR<!six<xqb!uiBh<!hqk<kl<!
sqk<kli!Bxr<Gl<!hqk<kl<!osl<hqk<kR<!sQk!hqk<kl<!
sQklib<!lbg<Gl<!hqk<kR<!osh<hqb!uOgiv!hqk<kl<!
Ohkli!bzm<Ml<!hqk<kl<!ohVk<K!uiB,Xl<!hqk<kl<!
Wkli!ObXl<!hqk<k!bqzr<Gf<!kvk<kqx<!hqk<kl<!
ghizlii<!H,khqk<kl<!hVl<hqk<k!LOvig!hqkkl<!
nhiblii<!vkqg!hqk<k!lMl<hqk<k!lOvisq!hqk<kl<!
Ghiblii<!oghik!hqk<kr<!%XLm<!h{Olii<!hqk<kl<!
yVkeq!uqmik!hqk<k!OlikqMl<!uqsiqe<!hqk<kl<!
kVl!uqgib!hqk<kR<!sii<sbqk<kq!bk<kqe<!hqk<kl<!
DVlqG!lf<khqk<k!Olikqe!lqeqOl!zqh<hiz<!
uVlkqe<!G{LR<!osb<b!uGk<kqM!lVf<KR<!osiz<uil<”!
!! ! ! ! .!Pararasasekaram
� According to the Therayar, the pitha diseases are classfied into 21
types in Therayar Vaagadam
� According to Dhanvandhiri, in the book Dhanvandhiri Vaidhyam
pitha diseases are classified into 40 types including vatha pitham.
VATHA PITHAM
Definition
It is one of the 42 Pitha diseases as mentioned in Yugi Vaidhya
Chinthamani - 800. The disease is caused by pitham having symptoms like
Giddiness, Fatigue, Headache, Blurring of vision.
uikhqk<kl<!
! kiqh<hie!g{<kjeOb!lqg!ljxg<Gf<!
! ! kiqbik!lqguqjvs<sz<!Hjgs<s!Z{<mi!
! lqiqh<hie!g{<lqe<!lqeqbib<!Spe<X!
! ! lqg<gfQI!kKl<hqOb!gzr<gq!fqx<Gl<!
! uiqh<hie!lqe<Eml<H!uqbi<ju!hiG!
! ! lbg<golim!kqbg<glib<!uif<kq!biGu<!
! Gxqh<hie!ogil<OhPl<!ne<el<!Ou{<mir<!
! ! %xqOeil<!uikhqk<k!ogit<jg!kiOe!
- b,gq!juk<kqb!sqf<kil{q!
g{<Hjgs<sz<?! wiqs<sjzB{<mig<gqg<! g{<j{! ljxg<Gl<!
g{<lqe<lqeqh<! H,s<sqjbh<! Ohiz! Spzs<! osb<K! g{<{QI! ucBl<?!
g{<gzr<Gl<?! dml<hqz<! uqbi<ju?! lbg<gl<?! kbg<gl<?! uif<kq?! d{U!
Ou{<mijl!wEl<!GxqG{r<jgtg<!gim<Ml</!
!
� Excessive sweating.
� Giddiness.
� Fatigue.
� Vomitting.
� Loss of appetite.
� Blurring of vision.
According to Thanvanthiri Vaidhyam – I higl<?!!
Symptoms of Vatha pitham are !
!! “osizx<giq!kieOleq!Svr<Gtqi<!KbvL{<mil<!
!! ! uqbg<giq!kie!ue<el<!ouXk<kqMl<!nVsqB{<mil<!
!! szqk<Km!zbi<f<K!ofif<K!kti<s<sqbib<!!dkvf<!ke<je!
!! ! uzqk<kpe<!oxiqk<Kg<!gif<kq!uikk<kqx<!hqk<kliOl!”
(himz<!w{<!;!29!*!!
)hg<g!w{<!;!78*!
!! dmzqz<! Gtqi<Svl<! Oukje! -jugT{<miGl</! ! Ngikvk<jkk<!
kt<Tl</! nVsq! Wx<hMl</! dmz<! uim<ml<! njmBl<?! ! ubqx<xqz<! uzq?!
wiqs<sz<!LkziejugTl<!d{<miGl</!-ju!uikhqk<kg<!GxqgtiGl</! !
� Fever.
� Loss of appetite.
� Tiredness.
� Abdominal pain.
According to Pararasasekaram, Vathapitham is mentioned as
“ohiVlqMl<!siQvLx<Xl<!OhikofR<!sqck<Kk<!okib<uib<!
!! -VlqM!LgLl<!uQr<G!Olklib<g<!gMg<GOleq!
lVuqMl<!hsqBlqe<xq!lzg<gqM!fMg<g!L{<mil<”!
!! ohVgqM!uik!hqk<kR<!osb<G{l<!OhSr<giOz!
)hvvisOsgvl<!hg<g!w{<!;!8*!
� Body pain.
� Cough.
� Swelling of face.
� Loss of appetite.
AETIOLOGY
According to Yugi Vaidhya Chinthamani - 800
lgqp<f<KOl!hqk<kf<kie<!uVGl<!uiX!
! lsOkui<!kjlh<h{qb!lim<mi!kii<g<Gl<!
lgqpf<KOl!GVucjb!u{r<gi!kig<Gl<!
! likiuqe<!lelgqpi!lii<g<gk<!kii<g<Gl<!
lgqp<f<KOl!kf<jkjb!uR<sqk<k!Ohi<g<Gl<!
!! lkizbr<gt<!!okiPkqmi!lii<g<gk<!kii<g<Gl<!
lgqp<f<K!squ!kqvuqbk<jk!bhgiqk<!Okii<g<Gl<!
! lihi!kgi<g<G!uf<K!lVUl<!hiOv!
!
lVUOl!Htqh<H!djvh<!Hzh<H!lqR<sz<!
!! lekqOz!Kg<gr<gtjmk!ziZ!
ofVUOl!ofVh<H!oub<bqz<!Ogihf<!ke<eqz<!
!! fqk<kqjv!kieqz<zieiz<!uqVk<kq!Vg<gqz<!
nVUOl!ng<gqeqbqx<!ohisqg<g!uqm<hiz<!
! nkqglib<h<!oh{<Ohig!lEhuqk<k!
fVUOl!ficg<Gl<!OlOz!fqe<X!
! ficOb!g{<mlm<mibq!Vg<Gl<!hiOv!
.!B,gq!Leq!
From this verse, the Aetiological factors which cause pitha diseases
including vatha pitham are
� Persons do not pay respect to good,
� Persons who do not give due respect to guru,
� Persons who do not make their mother happy,
� Persons who cheated their father,
� Persons who do not go to temple,
� Persons who steal “Siva diraviyam”
� High in take of sour and salt foods,

� Having feelings in mind,
� Walking in sunlight and heat,
� Loss of sleep,
� Excessive indulgence in sex.
According to Pararasasekaram,!
hqk<kOki]lkqgiqk<kx<G!WK!
!
“oub<bqzq!emg<jg!biZl<!oul<hsq!lqGk<k!ziZl<!
Kb<bOkiz<!vZofb<!bie<hiz<!Kb<k<kjz!uqMk<k!ziZl<!
jfbOu!uVr<Ogi!hk<jk!f{<j{bix<!gsh<jh!fiTl<!
jgBx!d{<{!ziZr<!gkqk<kqMl<!hqk<k!Oki]l<”!
!
“hqk<kk<jk!uqjtg<G!ole<X!Ohsqb!U{ju!fiTl<!
olk<kOu!bVf<k!ziZ!lqGf<kqMl<!Kbvk<!!kiZl<!
fqk<kqjv!bqzijl!biZ!fqjeUg{<!lqGk<k!ziZl<!
lx<Xt!OuK!uiZl<!ui<k<kqg<Gl<!hqk<k!Oki]l<”!
.!hvvisOsgvl<!
!
This verse, says the aetiological factors that, lead to pitha diseases.
These are
� Walking in sunlight.
� Excessive appetite.
� Avoiding in take of milk and ghee.
� Increasing anger.
� Excessive intake of sour foods.
� High intake of food which increase pitham.
� Increased sorrow.
� Loss of sleep.
� Vedhu- Excessive use of steam bath.
According to Danvandhiri vaidhiyam,
“ngiz!fqk<kqjvbqeiZl<!nkqsr<g!Oligk<kiZg<!
! kgik!oul<!hsqbqeiZf<!kVuqm!Olx<jgbiZl<!
! hgikue<!gqOzsk<kiZl<!hbqk<kqb!hkii<k<kk<kiZl<!
! sqgv!kir<!gz<jgbiZf<k!Osi<f<kqMl<!hqk<kf<kiOe”!!
“-Vlz!lmg<!jgbiZl<!oliVlz!lqjpg<jgbiZl<!
uVl<!oubqz<!ohVg<jgbiZ!leLX!Ogihk<kiZR<!
SvlK!kiqg<jgbiZR<!SMhq{!fix<xk<kiZf<!
kqvuqbr<!ogMjgbiZf<!Osi<f<kqMl<!hqk<kk<!kiOe” !! ! ! ! ! ! ! ! ! !
This verse, says
� Irregular sleeping habit.
� Increased appetite.
� Lust on women.
� Excessive in take of foods that increase Pitham.
� Improper disposal of waste by the body.
� By the ill effects of sun’s rays.
� Angry.
� Fever.
� Smell of the decaying dead body.
� Spoil of Diraviyam. !
“ fqk<kqjv!kuqi<kziZl<!ofMOfvl<!fqx<jgbiZl<!
!Gk<kqv!uqkk<kqeiZr<!ogil<heii<!lVf<kQm<miZl<!
!Sk<kqbqz<!ziOk!ogi{<m!nUuqk!Okiuqk<kiZl<!
!hqk<kOl!hqvOgihqk<Kh<!ohVf<Kbi<!osb<Br<giO{”!!
! ! ! ! ! .!Dhanvandhiri vaidhyamm
According to this verse, the aetiological factors which cause pitha
diseases ae sleeplessness standing, for a long time in a place, and consuming
drugs which contain unpurified raw drugs.
PATHOLOGY (Mukkutra Verupaadugal)
“dx<xOkii<!dmzqe<!%X!
! dXh<Hme<!uqvuq!fqe<X!
! Lx<Xl<l!Ofib<gt<!wz<zil<!
! LgzkqeqOz!Okie<Xl<!OhiK!!
! hx<XOl!uikhqk<kl<!
!! sqOzx<hef<kef<ke<eqz<!ye<jxh<!
! hx<xqOb!Okie<X!ole<X”!
! !! ! ! ! .Agathiyar Gurunaadi
In Siddha sysem of medicine, disease have been classified in the basis
of mukkutram. Vatha pitham Noi is one of the pitha dominent disease. In
this disease the azhal kutram is elevatd from its normal plane. The elevation
of pitha from its normal unit and therby increase the heat of the body, Then
the normal function of Dhasavayu have been affected. Due to increased
azhal and the elevated function of vayu the disease arise. Though the prime
causative factor is azhal kutram, the other two humour vatha and kaba are
also affected simultaneiously. Because of that only the disease is classfied on
the basis of 3 dhosas.
The three thosa theory has a strong hold on the study of Guna.
1. Sattuva
It is the illuminating pure and good quality.
2. Rajo
It is the quality of mobility of activity. It makes a person active and
energetic tense and willful.
3. Thamo
It is the dark and restraining quality.
Of these three gunas the Rajo Guna is of pitha type. A man in whom
Rajo Guna predominates has inner thrist and affectionate.
As he is passionate and covetous, he hurts others. He is unsteady,
fickle, easily distracted as well as ambition and acuisitive, He shrinks from
unpleasant things and clings to plasant ones. His speech is sour and his
stomach greedy. These are the normal qualities are Roja Guna individuals.
All the human beings are affected by these Guna factor. Unless the bad
qualities of Gunas are controlled disease like Vatha Pitham Noi will occur
due to humoral changes in the body as a stress factor.
Naadi Pathology:
!!!!“ohiVtie!uikk<kqz<!hqk<kR<!Osi<f<K!
! ! ohiVf<K!G{r<gtiL]<{uiB!sk<kq!
! osiqbijl!Htqk<Okh<hl<!ohiVlz<!fQiqx<!
! ! squh<H!lzl<hqck<kZVf<!kiK!fm<ml<!
! gVuie!OkglkqZjts<sz<!Osil<hz<!
! ! jg!giz<!kxqh<H!fig<gsg<G!le<el<!
! hiquie!U,{<!Gjxkz<!Vsq!Ogmikz<!
! ! hz!OfiBl<!uVk<kq!jug<Gl<!hir<GkiOe”!
! ! ! ! ! ! .!skgfic/!
!!!!“dXkqBt<t!hqk<klK!Okie<xqz<!ouh<H!
! ! d]<{uiBux<xq!Svlkq!sivr<gt<!
! lxkqBme<!gqXgqXh<H!hbqk<kqb!Ovigl<!
! ! uti<!OsijgbpoziqU!gif<kz<!jgh<H!
! -Vkbk<kqz<!gzg<glK!lxh<H!kigl<!
! ! wPr<gtU!Olb!jeU!lbg<g!&Is<js!
! sqxqK!ohVl<hiM!vk<kl<!hqvOlgr<gt<!
! ! Osi<f<K!lqG!hq{q!hzUR<!sqxg<Gf<kiOe”!
! ! ! ! ! ! .!skgfic!
! !
!!!!“hqk<kk<kqz<!hqk<kligqz<!hqkx<xqMr<!gqXgqXg<Gl<!
! sk<kqBlkqgliGR<!siQvk<kqjeh<!H{<miGl<!
nk<kqbiBzVOleq!bigLl<!OuxkiGl</!
ux<xqOb!ouTk<Kg<!gibl<!ux{<M!hqe<!uQg<gL{<mil<”!
! ! ! ! .!ngk<kqbi<!fic
In Vatham, Pranan, Abanan, Viyanan, Uthanan, Samanan, Nagan,
Kirukaran and Devathathan are affected.
Altered Pranan causes dyspnoea.
Altered Abanan causes oliguria, constipation.
Altered Viyanan causes malaise, neuralgic pain, fatigue.
Altered Uthanan causes nausea, vomitting.
Altered Samanan causes loss of appetite, taste disturbances.
Altered Koorman causes altererd sensorium, horipliatation,
blurring of vision.
Altered Kirukaran causes cough, sneezing.
Altered Devathathan causes malaise, fatigue, sleeplessness, anxiety.
In Pitham
Altered Analam causes loss of appetite.
Altered Ranjagam causes pallor of nailbed, conjuctiva and
reduced Hb.
Altered Sathagam causes mental confusion, difficulty in
concentration.
Altered Alosagam causes difficulty in differentiating colour,
blurring of vision.
Altered prasagam causes pallor of skin.
In Kabam
Altered Avalambagam causes derangement of other kabas
Altered Kiletham causes loss of appetite
Altered Santhigam causes joint pain
Complication of Vatha Pitham
According to “Agasthiyar Gunavagadam”
“ Ogtmi!-Vkbk<kqz<!Kch<!H{<miGl<!
! ! ogcbie!&s<SLm<mz<!Okie<X!lh<hi!
! fQtmi!Ouglib<!fmg<g!ouim<mi!
! ! fqslie!-mKhg<g!-vk<ki!sbk<kqz<!
! uitmi!OukjeBl<!d{i<s<sq!Ge<xq!
! ! utlie!sqvsqeqz<kie<!uzqBl<!gim<Ml<!
! Oktmi!ncg<gckie<!lbg<gl<!d{<mil<!
! ! oktquie!-Vkbk<kqz<!giK!juk<Kg<!OgOt/!
! giKjuk<Kg<!Ogm<mig<giz<!-Vk!bk<kqe<!
! ! gelie!sk<kr<gt<!Ogm<c!miK!
! fqkqbib<g<!jgjbjuk<Kh<!hiIk<ki!bieiz<!
! ! fqs<sblib<!-Vkbk<kqe<!Kch<H!nh<Ohi!
! Oukjebib<h<!hzlig!ncg<Gl<!hiV!
! ! ouGK~vl<!hvuqbK!uqjvuib<h<!OhiGl<!
! Osikqk<k!sqgqs<jsjbfie<!osiz<Oue<!hiV!
! ! Sglig<g!ujgbxqbs<!osiz<Oue<!hiOv”!
! ! ! ! ! ! ! .!Agathiyar Gunavagadam!!
� Palpitation.
� Breathlessness.
� Difficulty in walking.
� Pain in the left sided chest.
� Head ache.
� Fainting
� Muffled heart-sounds on auscultation.
� Heaving apical impulse on palpation.
!
According to Pararasa Sekaram,! !
hqk<klkqgiqk<kziz<!hqxg<Gl<!OuX!Ofib<gt<!
!! “hqk<kOl!bkqg!iqk<kix<!ohVk<kqMr<!gsLr<!gisl<!
!! !! olk<kOu!uQg<gf<!Okie<X!lqGk<kqM!Lzi<f<K!S,jz!
!! yk<kOki!fqvk<k!Ge<l!Olicb!Gmz<ui!kr<gt<!
!!!!!!! wb<k<kqM!osr<g{<!liiq!bqe<eL!lOeg!Ofib<gt</”
� Pulmonary disease.
� Oedema.
� Peripheral neuritis.
� Persistent gastric ulcer.
DIFFERENTIAL DIAGNOSIS:
sQkhqk<kl<!
! ue<jlbi!Bml<ohr<Gl<!ucBf<!k{<{QI!
! ! lbg<gli!!Bmz<gek<Kh<!hivliGl<!
! H{<jlbib<h<!hqmiqkeq?!zqsqU{<!hiGl<!
! ! ohiVlqOb!ubqXh<!hqsf<kieiGl<!
! kq{<jlbi!Bmz<gek<Ks<!osig<G!OhiziR<!
! ! sQxqOb!lqg!uqVlqs<!sqf<jk!OgmiR<!
! os{<jlbib<!uib<fQIkie<!dh<H!jxg<Gf<!
! ! sqXfQVR<!sqgh<hiGf<!sQkhqk<kl<!
! ! ! ! ! ! ! )B,gq!sqf<kil{q*!
! dmzqz<!uqbi<juk<!k{<{QI!lqGkqbigg<!ogim<Ml<!lbg<gl<?!dmz<!
gek<kz<?! hTuibqVk<kz<?! Hxr<gPk<kqz<! -sqU?! ubqX! ohiVlq!Dkz<?!
hzlq<e<jl?! -Vlz<?! ofR<S! H{<{ikz<! Lkzqb! GxqG{r<gjt!
gim<MuOkiM?! uib<fQI! dh<Hgiqk<kz<?! sqXfQI! squf<K! -pqkzigqb!
GxqG{r<gjtBl<!d{<mig<Gl</!
According to Yugi Vaidhya Chinthamani - 800 the clinical features
of seetha pitham are
� Excess sweating.
� Giddiness
� Pain in the neck.
� Abdominal distention.
� Tiredness.
� Cough.
� Redness of urine.
Eventhough, the symptoms of seetha pitham are related to vatha
pitham. Cough, redness of urine, pain in the neck are not present in vatha
pitham.
According to Theraiyar Vagadam, Thalaichuzhal Pitham belongs
to Pitha disease.
kjzs<$pz<!hqk<kl<;!
“npz<!hqk<k!Lml<!ohz<zi!lezib<!uQSl<!nkqglkib<!kigL!!!
lqgU{<miGl<!
!!Spz<!hqk<kl<!fmg<jgbqOz!gqX!gqXoue<X!!
!!Sx<xquqPg<!gim<Mole!lVuXg<Gl<”!
. Okjvbi<!uigml</!himz<!w{<!37:/!)h/w{<;87*!
The above symptoms are after the complications of diabetes mellitus
i.e. diabetic neuropathy.
According to Yugi muni, Uraktha pitham belongs to pitha diseases,
“&Ig<glir<!OgihlK!lqgU{<!miG!
! ! Ljebig!ucgcg<Gs<!s{<jm!ogit<Tl<!
! NIg<glibg<!%uqOb!uqjvs<s!ziG!
! ! likie!hikitl<!Ohkq!biGl<!
! fiIg<glib<!fe<jlKe<jl!Okie<xi!lx<xie<!
! ! fzg<glig!g{<squg<Gf<!K~g<g!lqz<jz! !
! DIg<gli!Bmp<K~!zqg<G!Lh<H!
! ! Lvk<khqk<k!uikk<kq!Z{<jl!kiOe”!
! ! ! ! ! ! ! .!B,gq!juk<kqb!sqf<kil{q!

� Frequent angerness.
� Aggressive behaviour.
� Speaking in high-pitched voice.
� Frequent diarrhoea.
� Inability to differentiate good- things
� Redness of the eyes.
� Insomnia.
� Obesity.
The same features are mentioned under Uraktha pitham in
Sarabendra Vaidhya Muraigal also which more or less correlate with
hypertension.
“kjzuzq!Spx<sq!uqpqgt<!lbr<gz<!
! utqLkz<!&e<Xl<!lQxq!fqx<xz<!
! fvl<Hgt<!okxqk<kz<!lbg<gf<!Okie<xz<!
! dml<hqjtk<!kqMkz<!dvepqf<!kqMkz<!
! GjzOfi!BXkz<!GVkq!osxqkz<!
! gVg<gt<!hqxU!olzqf<K!kti<kz<!
! GVkq!ogikqh<hqe<!lVuqM!ole<h”!
Frequent diarrhoea, Insomnia, Obesity are not present in vatha pitham.
Piniyari muraimai (Diagnosis)
Diagnosis is the very important thing for a physician by which he
deals the disease by finding its cause and is helpful to undertake a correct
line of treatemnt and also prognosis. The diagnosis is based on
� Poriyalarithal (Inspection).
� Pulanalarithal (Palpation).
� Vinathal (Interrogation) and
� Envagai thervugal.
1. Poriyal arithal
Porigal are the five organs of perception. They are nose, tongue, eyes,
skin and ears.
Poriyalarithal is examining the pori of the patient by pori of the
physician.
2. Pulanal arithal
Pulangal are the five object of senses namely smell, taste, sight,
sensation and sound.
3. Vinathal (Interrogation):
By vinathal, the physician knows about the patient’s name, age,
occupation, native place (thinai), family history, socio economic status,
dietary habits, complaints, history of past illness, relevant history of
treatment and habits etc.,
Envagai thervugal:
It is the basis diagnostic principle and the unique speciality of the
siddha system of medicine. The following verse’s reveals this as follows
“fich<hiqsl<!fi!fqxl<!olipq!uqpq!
!lzl<!&k<kqvlqju!lVk<KuviBkl<” ! ! .!Okjvbi<!
Envagai thervugal are
� Naadi (pulse).
� Sparisam (palpation).
� Naa (tongue).
� Niram (colour of the skin).
� Mozhi (speech).
� Vizhi (eyes).
� Malam (motion).
� Moothiram (urine).
Envagai thervugal gives a definite idea to diagnose Vatha pitham. This
is explained as follows.
1.Naadi
In the Noi Nadal Noi Mudhal Nadal text it is defined as follows,
dmzqz<!dbqi<!kiqk<kqVh<hkx<Gg<!giv{lie!sQu!sg<kq!wKOui!
! nKOu!kiK!nz<zK!fic!weh<hMl<!
Genesis of Naadi:
The three thathukkal are formed by the combination of three naadies
with three vayus.
Idakalai + Abanan = Vatham
Pinkalai + Piranan = Pitham
Suzhumunai + Samanan = Kabham
These can be felt one inch above the wrist on the radial side by means
of palpation with the tips of index, middle and ring finger corresponding to
vatham, pitham and kabham respectively
!!!!“giqLgecjb!uip<k<kqg<!jgkeqz<fic!hii<g<gqz<!
! ohVuqvzr<Gzkk<qz<!hqck<kc!fMOu!okim<miz<!
! yV!uqvOzicz<!uikLbi<!fMuqvzqx<!hqk<kl<!!
! kqVuqvz<!&e<xqOzicz<!Osk<Kl!fickiOe”!
!! ! ! ! ! ! ! .! juk<kqbsivsr<gqvgl<!
According to Thirumoolar’s Naadi Nool
“kiKLjxOgt<!keqk<!kGkqs<!sf<OkiM!
! YKXgilqb!Lf<kq!ofMlii<H!
! giK!OfM&g<Gg<!g{<ml<!gvl<HVul<!
! OhiKXLs<sqHgp<!hk<Kl<!hii<k<kqOm”!
� Inner aspect of the ankle joint.
� Genital organs.
� Abdomen.
� Thorax.

� Ear.
� Nose.
� Neck.
� Hands.
� Eye-brows.
� Vertex are the sites for pulse reading.
Among them, the pulses read from hands are considered to be the best
for diagnosing diseases.
2. Sparisam (palpation) :
By sparisam, the temperature of skin (heat or cold), smoothness, sweat,
dryness, hard patches, swelling, abnormal growth, tenderness, ulcers,
enlargements, nourishment can be noted.
3.Naa (Tongue) :
In the examination of tongue, it's colour, coating, dryness, deviation and
movement, variations in taste and the conditions of teeth and gums can be
noted.
4. Niram (colour) :
By examining the niram, the type of udal (body) whether vatham (black),
pitham (red or yellow) and kabam (white) or mixed, cyanosis and pallor of
the body can be noted.
5. Mozhi (speech or voice) :
In the examination of mozhi, high or low pitched voice, slurring and
incoherant speech, nasal or crying, hoarseness of voice can be noted .
6. Vizhi (Eye) :
In the examination of vizhi, the change in the colour of the eye such as
redness, yellowishness, pallor etc may be noted. With these dryness,
lacrimation, sharpness of vision, response of the pupil, falling of hair in eye-
lashes, inflammations and ulcerations may also be noted.
7. Malam (stools) :
In the examination of malam, it's nature (whether it is solid, semisolid
or liquid), its colour, it's quantity (increased or decreased) can be noted.
Other examinations like diarrhoea, presence of blood, mucus, undigested
matter in the stools and odour should be studied .
8. Moothiram (urine) :-
In the examination of urine, the colour, odour, quantity of urine, the
presence of froath, deposits, blood, pus, small stones, abnormal constituents
such as sugar, proteins etc and the frequency of urination can be noted.
Neerkuri and Neikuri are the two methods used to diagnose the
disease. They are discussed below.
Neerkuri :
According to this verse, the general features of urine, i.e niram, edai,
manam, nurai and enjal are analysed.
� Niram indicates the colour of the urine voided.
� Edai indicates the specific gravity of the urine voided
� Manam indicates the smell of the urine voided.
� Nurai indicates the frothy nature of the urine voided.
� Enjal indicates the quantity (increased or decreased) of the urine
voided.
Neikuri :
For this examination, urine is collected in the early morning in a pure
glass vessel. The patient should be prepared specially for this before a day in
a manner of not taking excessive diet in irregular timing etc.
A drop of gingelly oil is dropped on a wide vessel containing the
urine to be tested and placed in the sunlight in a calm place. The
derangement of the three thathuvas and the disease can be diagnosed by
the behaviour of gingelly oil on the surface of the urine.
Seven Udal kattugal:
1. Saram :
This is the product which assimilate in the digestive process- It
strengthens the body and mind.
2. Senneer :
The rasam after absorption is converted into senneer. It is responsible
for knowledge, strength, boldness and healthy complexion.
3. Oon :
It gives a structure to the body and is responsible for the movement of
the body.
4. Kozhuppu :
When the organs of the body do their works this. Thathu helps for
lubrication and facilitates their functions.
5. Enbu :
It gives shape to the body and is responsible for protection of vital
organs.
6. Moolai :
It is present in the core of the bone which strengthens and maintains
the normal condition of the bones.
7. Sukkilam/Suronitham:
It is responsible for reproduction.
When the seven udal thathukkal increases or decreases from the
normal level, the normal functioning of the body is affected.
Thingal or nilam
Thinai or Nilam is classified into five types
They are
� Kurinji - Mountain and its surroundings
� Mullai - Forest and its surroundings
� Marutham - Field and its surroundings
� Neithal - Sea and its surroundings
� Paalai - Desert and its surroundings
1. Kurinji
“GxqR<sq!uV!fqzk<kqx<!ogix<xL{<c!vk<kl<!
dxqr<sq!uV!SvL!L{<mil<!.!!nxqRjvg<!!
jgbOl!kr<Gk!vk<kijl!uz<jz!Br<gkqg<Gl<!
JbOl!kr<G!lxq”!
- Pathartha guna chinthamani
According to this verse, in Kurinji, kabha diseases, fever which cause
anaemia tumour in stomach (Aamai katti) are common.
2. Mullai
!!!!“Lz<jz!fqzk<kjlb!Lf<fqjv!OluqElu<!
ouz<jz!fqjzk<k!hqk<k!olb<Kxr<gi{<!.!nz<zoueqe<!
uikolipq!bikkE{<!le<E!lju!upqOfib<h<!!
Ohkolipq!bikjxbh<!hqe<H”!
- Pathartha guna chinthamani
According to this verse, in Mullai, pitha diseases, liver diseases and
vatha diseases commonly occur.
3. Marutham
“lVkfqz!fe<eQi<!utolie<jxg<!ogi{<Om!
! ohiV!kfqz!likqbOfib<!Ohig<Gr<!!.!gVkfqzk<!
! kixqmkR<!S,p!uVf<Kuove<!xix<!hq{qobz<!
! WxqvkR<!S,p<uqg<G!lqz<”!!
- Pathartha guna chinthamani
According to this verse, in Marutham, Vatha, Pitham and Kabha
diseases all get cured. It is the best place to live.
4. Neithal
“ofb<keqz!OlZui<h<jh!fQr<gi!KxqElK!!
! oub<keqz!Olkr<G!uQmiGl<!.!ofib<kQe<!
! lVr<G!mjz!Lg<gig<gq!uz<ZXh<jh!uQg<Gr<!
! gV!r<Gmjzg<!gQpqxg<Gr<!gi{<”!!
According to this verse, in Neithal, pitha vayu, filariasis and Hernia
occur commonly.
5. Paalai
“ hijz!fqzl<Ohix<!hmjvh<!hqxh<hqg<g!
! Oljzfqz!lQbiK!uqiqk<kx<G!.!!Oujzfqz!
! Lh<hq{qg<G!lqz<zil<!LjxOb!bux<xzil<!
wh<hq{qg<G!!lqz<zi!lg<oke<”!!
According to this verse, in paalai, vatham, pithtam and kabham get
deranged and lead to various diseases.
GxqR<sq!fqzOl!uiklir<!gi[l<!hijz!hqk<kliR<!
! osxqf<k!lVkR<!sqOzk<llir<!sqOzk<luik!Lz<jzbkil<!
! fqjxf<k!ofb<kz<!uikhqk<kl<!fqzr<gtkje!lbg<gi!
! Zjxf<k!uqbikq!gzf<kqVg<G!Lhiblxqf<K!osb<uQOv!
- Padhinen Siddhar naadi saasthiram
According to this verse, the diseases that develop in each land in as
follows
Kuringi - Vatha diseases
Mullai - Kabha vatha diseases
Marutham - Kabha diseases
Neithal - Vatha pitha disease
Palali - Pitha diseases
Paruva Kaalangal
A year is classified into six seasons eachy consitutes two months ,
they are
Season Months Kaarkaalam Aavani and Purattasi
Koodhir kaalam Iyppasi and Kaarththigai Munpani Kaalam Maargazhi and thai Pin pani kaalam Maasi and panguni Elavenir Kaalam Chiththirai and Vaigaasi
Muthu venir kaalam Aani and Aadi
Udal Vanmai
It means the strength and vitality of the body and is classified into
three types
1. Iyrarkai vanmai
It is formed naturally from mukkunam. These are sathuva, rajotha and
thamo gunaas.
2. Kaala vanmai
It is due to year (Age) and the paruva kalangal.
3. Seyarkai vanmai
It secure the body which is formed through the mukkunam by proper
day to day diet according to that ‘gunam’ and by drug intake without
disturbing the vitality of the body.
Prognosis:
If the patient had good B.P control, then the prognosis will be a good
one. But if the level of blood pressure is fluctuated it will end in lots of
complication.
Line of treatment:
In siddha system, the treatment is based on the deranged three doshas.
“uqOvsek<kiz<!uikf<kiPl<!
! ! ulek<kiz<!hqk<kl<!kiPl<!
! ! fsqb!nR<sek<kiz<!ghl<!kiPl<” /!
! Pitha disease can be brought down by “vamanam” with the emetic
drugs. This emetic drugs are given according to the disease and patient’s
tolerance to drug.
The line of treatment of Vatha Pitham noi is as follows:
1. Internal medicines - To bring down the vitiated Pitham
2. Diet - To maintain Tridoshas.
3. Yoga therapy - To maintain Dhasavayukal and to improve
mental and body health
4. Prevention methods - To relieve anxiety and stress.
Administration of internal medicines to normalize pitham:
For the treatment of Vatha Pitham noi, several remedies are suggested
in ancient siddha literatures. Among these remedies,
Iruveli Kiyalam – 90ml B.D was given before meals.
2. DIET:
Siddhars advice the diet regimen for pitha patients and they are
explained below:
Diet to be added:
� -VLjx!uck<k!OsiX!)Double boiled rice).
� gR<sq)Rice water).
� nk<kqh<hqR<S)Ficus glomavata)
� nujvh<hqR<S)Dolichos lab-lab)
� l{k<kg<gitq!gQjv!)Solanum rubrum)
� ohie<eir<gi{q!)Alternanthera sessilis)
� sqXgQjv!(Amaranthus gangeticus)
� hsjzg<gQjv!)Portulaca quadrifolia)
� Htqbijv!)Oxalis korniculatus).
� Sg<gie<gQjv!(Rumex vesicarius).

Diet restriction :
Siddhars advice to avoid sour, salty and pungent food for Vatha
Pitham noi. Nowadays all the patient were advised to take low sodium diet
(less than 5mg per day) and to take low fatty diet (especially oils containing
mono-unsaturated fatty acids (MUFA).
Yoga therapy:
Yogasanam is one of the part of Astanga Yogam. It controls mind and
body by various mechanisms. So it has been applied to control various
stress-related diseases nowadays as an adjuvant therapy.
Mechanism:
Every asanas require the spine to be kept erect and to keep riched
blood supply to the pelvic region. This stimulates kundalini, which controls
the mind and body.
In modern study, it seems to stimulation of psycho-neuro hormonal
axis which controls the sympathetic overactivity. This in turn eliminates free
radicals, catecholamines and secrets endorphins and encephalins which is a
natural steroidal hormone which helps to maintain the body and mind active
and releive the stress.
Asanas beneficial in hypertension:
� Padmasanam
� Pranayamam
� Vajrasanam
� Savasanam.
Relaxation Therapy:
It is particularly useful for anxiety disorders, psychosomatic disorders
(e.g hypertension) and in other conditions where anxiety is associated (e.g.
smoking, sexual disturbances, sleeplessness). It is usually done in a calm
room with a relaxed mind in the lying down posture with palms facing
upwards for about 15 to 20 minutes twice daily. The underlying principle is
the counterproductive nature of relaxation towards anxiety. So the cycle
(anxiety leading to muscle tension which in turn aggravates anxiety) is
broken by this approach.
In schulz method, relaxation is done through concentration on certain
thoughts by autogenous training. In the commonly used Jacobson’s method,
the client is taught to relax one group of muscles at a particular time (by
alternate contraction and relaxation) which progresses slowly from head to
foot until the whole body is relaxed.
The person also knows the adverse, effect of muscle contraction. For
example, the relaxation of head muscles will often correct tension headache.
So it is a simple and highly useful technique.
Transcendental Meditation:
It is an unusual state of consciousness taking qualities of both sleep
and wakefulness with a profound state of rest. It decreases the oxygen
consumption, heart rate, respiratory rate and sympathetic overactivity. So it
reduces tension and anxiety. It improves interpersonal relationships and
concentration power.
There are number of meditative processes like attending to a mental
repetation of a sound or mantra etc.
In our programme, the patient was asked to repeat a word (as he likes)
silently for about 20 minutes twice daily in a relaxed, calm, comfortable
position with eyes closed, It removes the inner conflicts, anxiety and mental
stress very effectively. So a sense of well-being and mental relaxation with
good sleep was observed in patients who do this mediation regularly.
Prevention:
� Relieving the tension or the stress and stain of life by reducing
unnecessary burden and responsibilities.
� Transforming the attitudes and belief systems so as to reduce
anxiety and excitement.
� Good sleep.
� Low sodium chloride intake (less than 5gm per day).
� Totally avoiding intake of tabacco.
� Stopping alcohol consumption or reducing it considerable.
� Overcoming obesity.
� Avoiding constipation.
� Light regular exercise (avoid undue physical strain and exertion).
� Practice of relaxation and positive thinking.
Modern Aspect

MODERN ASPECTS
BLOOD PRESSURE
Anatomy of Hypertension:
The effects of hypertension are widespread no organ in the body is
spared.
In the heart, there is gradual concentric hypertrophy of the left
ventricle.
Degenerative lesions develop in both the heart and arteries and lead to
the lethal consequences, of hypertension. The coronary arteries develop
atheromatous lesions which aggregate the development of Ischaemic heart
disease or even frank myocardial Infarction.
Hypertension is an important risk factor for the development of
aneurysm of aorta especially dissecting aneurysm of aorta
Arterioles called as the resistant vessels of the bdoy. So deposition of
a hyaline material, thickness of the vessel wall, medial and intimal
hypertrophy, reduplication of elastical lamina and intimal proliferation.
Hypertension is implicated in the aneurysmal dilatation of small
arteries in the brain (CHARCOT BOUCHARD ANEURYSM) which
precipitate haemorrhagic stroke)
History of Blood pressure:
The first determination of arterial Blood Pressure was done in 1733 by
Rev Stephen Hales by inserting brass cannula into the central end of the
femoral artery of a horse.
Definition:
Blood pressure means the lateral force exerted by the blood column
against any unit area of the vessel wall which is expressed in mm of Hg.
It is expressed as systolic and diastolic pressure.Palpatory method of BP
recording is always precede the auscultatory method.
Systolic blood pressure:
It is defined as the maximal pressure exerted during systole. The
normal range is 89 – 100 mm Hg.
Significance:
It reflects the distensibility characteristic of the arterial system as it
receives blood from the left ventricle. It can be altered by the stress and
strain of day-to-day life.
Diastolic blood pressure:
It is defined as the minimum pressure exerted during diastole. The
normal range is 70 – 89 mm Hg.
Blood Pressure must be recorded in lying, sitting and standing
positions especially when postural hypotension is suspected. When there is
fall in systolic pressure of > 20mm Hg after standing for 3 minutes from
lying posture the patient is said to have postural hypotension.
Significance :
It represents the state of the peripheral vessels and determines the
filling of the coronary vessels.
Pulse pressure :
It is defined as the difference between systolic and diastolic pressure.
Normal range = 30 – 60mmHg
Significance :
It is caused by the ejection of blood into the aorta during systole.
A rise in systolic or fall in diastolic will increase the pulse pressure.
Mean arterial pressure :
It is the product of cardiac output and total peripheral resistance.
MAP = Diastolic blood pressure + 1/3 of pulse pressure
Normal -100mm Hg.
Significance :
It determines the tissue perfusion pressure.
To confirm the presence of hypertension, multi Blood Pressure
recordings should be taken with a mercurial mmetre on several occasions.
Home monitoring, ambulatory monitoring are preferable.
Classification of Hypertension
(The seventh report of the joint national committee on preventic detection,
evaluation and treatment of high blood pressure)
Category Systolic pressure Diastolic pressure
Normal <120 mmHg <80 mmHg
Pre – hypertension 120 – 139 mmHg 80 – 89 mmHg
Hypertension
a) Stage 1 140 – 159 mmHg 90 – 99 mmHg
b) Stage 2 > 160 mmHg > 100 mmHg
Definition and classification of blood pressure levels (WHO)
Category Systolic pressure Diastolic pressure
Optimal <120 mmHg <80 mmHg
Normal <130 mmHg < 85 mmHg
High Normal 130 – 139 mmHg 85 – 89 mmHg
ANOTHER CLASSIFICATION
Category Systolic pressure Diastolic pressure
Grade / Stage I / Mild 140 – 159 mmHg 90 – 99 mmHg
Grade / Stage II / Moderate
160 – 179 mmHg 100 – 109 mmHg
Grade / Stage III / Severe
≥ 180 mmHg ≥ 110 mmHg
When the diastolic pressure is below 90 mm Hg, a
� Systolic pressure below 140 mm Hg indicates normal blood
pressure
� between 140-149 mm Hg indicates borderline isolated systolic
hypertension
� 140 mm Hg or higher indicates isolated systolic hypertension.
When there is an elevation of systolic pressure > 30 mm Hg and a
diastolic pressure of > 20 mmHg from the basal original level, it indicates
presence of hypertension.
Factors maintaining arterial blood pressure:
� Cardiac output.
� Peripheral resistance.
� Elasticity of arterial walls.
� Blood volume.
� Capacity of vascular bed.
CARDIAC CYCLE
Among these, cardiac output and peripheral resistance are considered
to be more important . So blood pressure is the product of cardiac output
and peripheral resistance.
B.P = CO * PR
Cardiac output :
It depends upon venous return, blood volume, heart rate and force of
heart beat. If cardiac output increases it rises, Blood Pressure and if it
decreases, it reduces Blood Pressure.
As per Frank sterlings law, force of contraction of heart is directly
proportional to initial length of muscle fibres.
Peripheral resistance :
The peripheral resistance depends on viscosity of blood, size of the
lumen of the blood vessel and viscosity of blood flow.
If the peripheral resistance is increased due to high viscosity and
reduced blood vessel size, the blood pressure rises.
Venous return:
If venous return is more, increased in ventricular filling and cardiac
output, results in increased Blood Pressure.
Elasticity of the arterial walls :
The elastic recoil is responsible for the maintenance of peripheral
resistance. It is mainly concerned with the origin and maintenance of
diastolic pressure.
Blood volume :
Increase in blood volume increases both systolic and diastolic
pressures. It maintains Blood Pressure through venous return and cardiac
output.
Capacity of the vascular Bed :
When the arterioles and capillaries dilate, it increases the capacity of
vascular bed and it decreases B.P and vice-versa.
Regulation of B.P :
The regulation of blood pressure is necessary for the proper blood
supply to various organs according to the needs.
The regulation of B.P is controlled by four important mechanisms.
They are
1. Nervous mechanism.
2. Renal mechanism.
3. Endocrine mechanism.
4. Capillary fluid shift mechanism.
Nervous mechanism :
It rapidly re adjust the B.P in a few seconds. These are useful during
exercise, emotional states and change in posture. The desired effects are
due to
� Pressoreceptor sino aortic mechanism.
� Increased sympathetic activity and
� Central nervous system ischaemic response.
a. Sino aortic mechanism :
This mechanism works through the baroreceptor or pressoreceptor
mechanism. These receptors are spray-type nerve endings that lie in the
walls of the large arteries especially in the walls of the internal carotid artery,
carotid sinus and the wall of the aortic arch.
If these receptors stretches due to rise in pressure, it transmits signals
into the central nervous system, and “feedback” signals are then sent back
through the autonomic nervous system to reduce blood pressure normally.
Baroreceptors are not stimulated by pressures between
0 and 60mmHg. But above 60mm Hg they respond progressively more
rapidly and reach a maximum at about 180 mm Hg.
In Chronic hypertension, the baroreceptor reflex mechanism is ‘reset’
to maintain the high rather than a normal blood pressure.
b. Increased sympathetic activity :
This mechanism mainly works through adrenergic receptors namely α
and β receptors. These are present in post ganglionic sympathetic nerve
endings.
A receptors are further classified into α1 and α2. α1 receptors
present in the vascular smooth muscle leads to constriction. α2 receptors are
present in the human leucocytes and platelets and it helps to release renin
from the kidney.
Receptors are further classified into β1 and β2. β1 receptors present
in the heart, increases the force and rate of contraction. β2 receptor present
in the bronchus leads to relaxation of bronchus.
c. Ischaemic response of the C.N.S :
Ischaemic leads to sensitisation of vasomotor centre. When B.P falls
very low below 90mm, the Vaso Motor Centre produces vasocontriction of
vessels throughout the body. Thereby the B.P will be raised.
2. Renal Mechanism :
Kidneys regulate blood pressure various mechanisms. The important are
� Extracellular Fluid Volume theory.
� Salt retention theory.
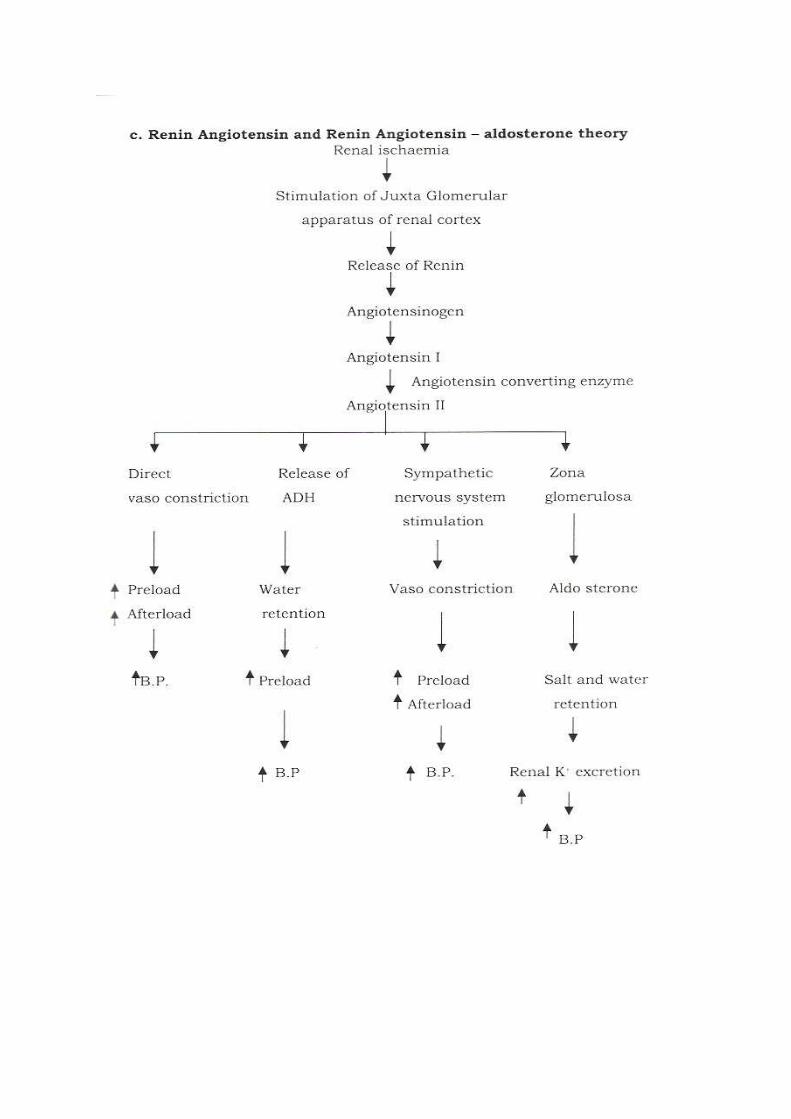
� Renin Angiotensin theory and Renin Angiotensin-aldosterone theory.
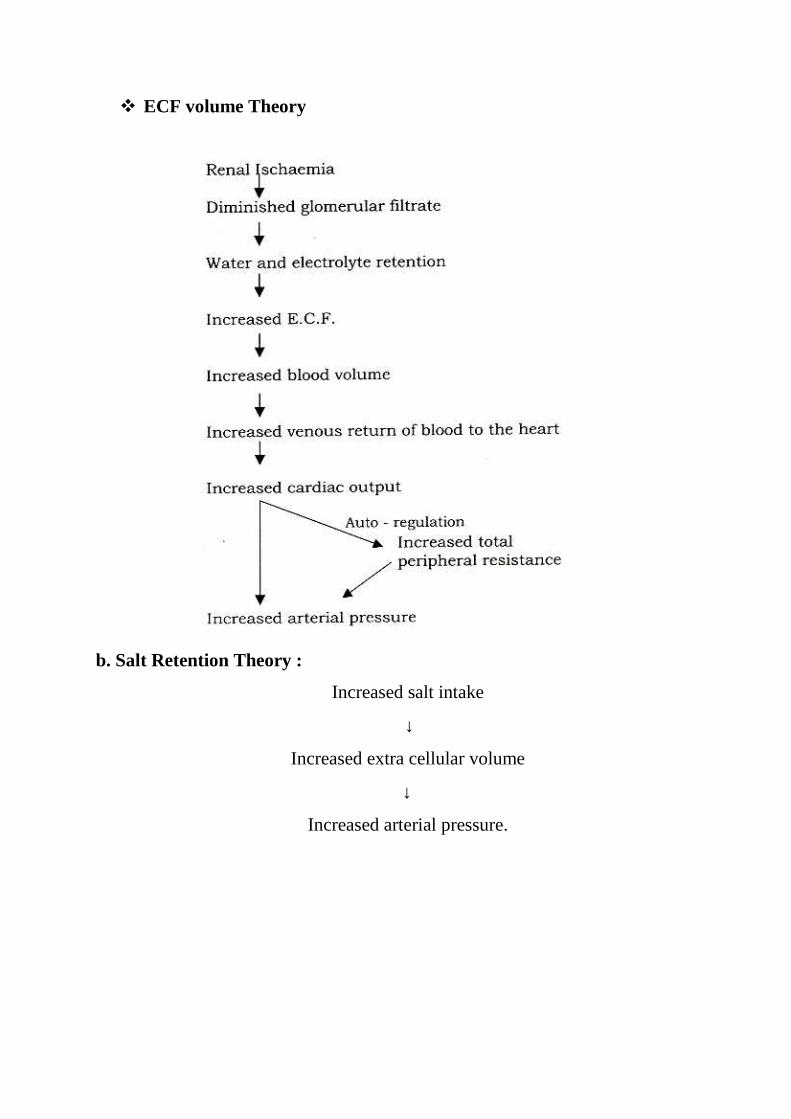
� ECF volume Theory
b. Salt Retention Theory :
Increased salt intake
↓
Increased extra cellular volume
↓
Increased arterial pressure.
The hormones concerned in the regulation of B.P are
� Catecholamines, adrenaline and nor-adrenaline.
� Aldosterone
� Vasopressin
a. Catecholamines, adrenaline and nor-adrenaline :
These are excessively secreted during stress and strain which in turn
leads to stimulation of adrenergic receptors. It leads to increased Blood
Pressure.
b. Aldosterone :
It regulates the sodium content of ECF and ECF volume which in turn
influence Blood Pressure.
c. Vasopressin :
It promotes the retention of water.
4. The capillary fluid shift mechanism :
If the capillary hydrostatic pressure is increased, Blood Pressure is
rised and vice versa.
MEASUREMENT OF BLOOD PRESSURE :
Shortly after Riva-Rocci had invented the sphymomanometer, the
Russian surgeon Korotkoff suggested that by placing a stethoscope over the
brachial artery at the antecubital fossa distal to the Riva-Rocci cuff, sounds
could be heard. The origin of these sounds is still not clear. Vibratory and
flow phenomenon are probably responsible.
The phases are
Phase I :
The first appearance of faint clear tapping sounds (Thuds) which
gradually increase in intensity represents the systolic Blood Pressure.
Phase II :
The softening of the sounds, which may become swishing or blowing.
Phase III :
The return of sharper softer sounds, which become crisper, but never
fully regain the intensity of phase I sounds.
Neither phase II or phase III have any known clinical significance.
Phase IV :
Distinct abrubt muffling of sounds which become soft and blowing.
The fourth phase is 7 – 10mm Hg above the true diastolic pressure.
Phase V :
The point at which all sounds disappear completely.
Phase I is taken as systolic pressure and phase V as diastolic pressure.
For an adult, the standard cuff width is 12 cm.
Korotkoff Sounds
Korotkoff sounds should be examined preferably with bell of the
stethoscope. There are five phases of korotkoff sounds, i.e. the sounds
produced by the flow of blood as the constricting Blood Pressure cuff is
gradually released.
Diastolic pressure closely corresponds to phase V. However, in aortic
regurgitation, the disappearance point is extremely low, sometimes 0 mm Hg
and so phase IV is taken as diastolic Blood Pressure in adults as well as
children.
When Korotkoff sounds are not heard while recording Blood Pressure,
ask the patient to raise the cuffed upper limb and ask him to open and close
the fist of that hand repeatedly and then record the Blood Pressure.
The length of the bladder is approximately twice that of the width. The
average length of the rubber bag is 25 cm.
The air bag within the cuff should extend for at least 2/3rd of the arm
length and circumference.
The midportion of the rubber bag within the cuff should lie over the
brachial artery.
After inflation, the cuff should be deflated at a rate of 2-3 mm Hg per
second.
Auscultatory Gap
Occasionally, after the initial appearance of the Korotkoff sounds,
indicating the systolic pressure, the sounds disappear for sometime, to re-
appear again and finally disappear at the diastolic pressure.
This phenomenon of a silent gap is found in certain patients with
hypertension. It overestimates the diastolic pressure and underestimates the
systolic pressure thereby necessitating the palpatory method of Blood
Pressure recording to always precede the auscultatory method.
Auscultatory gap occurs when there is venous distension or reduced
velocity of arterial flow in the arm.
Various Cuff Sizes for Blood Pressure Measurement
Age in Years Width of the bladder of the cuff < 1 yr 2.5cm
1 – 5 yrs 5cm 6 -10 years 10cm
Normal adult 12.5cm Obese adult 14cm
Thigh 20 – 25 cm
Apparatus :
1. Mercury Sphygmomanometer:
Here the pressure changes are reflected by a rise of mercury. It is an
accurate method of taking Blood pressure. However, the instrument is bulky
and heavy.
2. Aneroid meter :
Here the pressure changes are reflected by a change in the needle
which is connected to the spring. Though the instrument is small and non-
bulky, it has to be frequency reset to ensure accuracy.
3. Electronic Blood Pressure meter :
Here the pressure changes are measured electronically. They are not
very accurate.
Technique :
1. Clothing should be removed from the arm. If it cannot be removed, it
is better to leave it as it is, rather than fold the clothing into tight
constricting bands.
2. The cuff should be encircled around the arm. If the bladder does not
encircle the arm completely, the centre of the bladder should be over
the brachial artery. The rubber tubes from the bladder are usually
placed inferiorly at the site of the brachial artery, but it would be better
to place it superiorly or posteriorly so that the antecubital fossa is
easily for auscultation.
3. The bell gives better sound reproduction but a diaphragm is easier to
secure with the finger of one’s hand and covers a large area.
4. To measure Blood Pressure in the legs a thigh cuff containing large
bladder (18*24 cms) for adults should be wrapped around the thigh of
the prone patient and the korotkoff sounds auscultated in the popliteal
fossa in the usual way. Blood Pressure in the legs is equal to that in
the arms provided the bladder is adequate in size.
5. For children, pediatric size cuff should be used.
Precautions :
1. Explain the procedure to the patient to allay anxiety.
2. Avoid exertion, meals or smoking for 30 minutes before Blood
Pressure is measured. The patient must be allowed to rest for 5
minutes before Blood Pressure is measured. He should not have
consumed coffee, tea for the preceding one hour or smoked for the
preceding 15 minutes. He should no bladder distension.
3. The room should be warm and quiet.
4. High Blood Pressure may be erroneously recorded in an obese person
because the inflatable rubber bladder may be too short for the obese
arm (recommended dimensions are 12 * 35 cms). When the bladder
does not completely encircle the arm the centre of the bladder must be
placed directly over the brachial artery.
5. The arm must be supported to the heart level. In the supine position
the arm is usually at the heart level. In sitting and standing positions
the arm must be horizontal with fourth intercostal space at the heart
level. Some antihypertensive agents cause postural hypotension and
when this is expected, Blood Pressure must be measured in both lying
and standing positions.
6. It is desirable to record the Blood Pressure in both the arms as the
differences in systolic pressure exceeding 10 mm Hg between the two
arms when measured simultaneously or in rapid sequence suggest
obstructive lesions of aorta, innominate or subclavian arteries.
7. In vertebrobasilar insufficiency, a difference in pressure between the
arms may signify that a subclavian steal is responsible for
cerebrovascular symptoms.
8. Normally systolic pressure in the legs is up to 20 mm Hg higher than
in the arms, but diastolic Blood Pressure is the same.When systolic
pressure in the popliteal artery exceeds that in brachial artery by > 20
mm Hg (Hill's sign), AR is usually present.
9. Measuring lower limb Blood Pressure is useful in detecting
coarctation of aorta or obstructive disease of the aorta or its immediate
branches..
10. The Blood Pressure may be higher in right arm by 2-10 mm Hg. Most
pressures in practice are measured on the right arm. However if the
Blood Pressure is higher by 10 mm Hg in one arm further
measurements should be made in that arm.
11. The cuff should be snugly fitted to the arm. A cuff which is too tight
may give a false lower blood pressure and a loose cuff may give a
false higher Blood Pressure.
12. Repeated inflation of the cuff may cause venous congestion of the
limb and elevate both systolic and diastolic Blood Pressure. To avoid
this the cuff should be inflated as rapidly as possible and deflated
completely between successive readings. At least 15 seconds should
be allowed between successive measurements.
Postural or Orthostatic Hypotension
Blood Pressure must be recorded in lying, sitting and standing
positions especially when postural hypotension is suspected.
When there is a fall in systolic pressure of > 20 mm Hg after standing
for 3 minutes, from the lying posture, the patient is said to have postural
hypotension
Causes
� Hypovolaemia (blood or fluid loss).
� Autonomic neuropathy (diabetes mellitus, old age).
� Drugs (ganglion blocking agents, centrally acting anti-hypertensives).
� Myocardial pump failure.
� Secondary hypertension (pheochromocytoma).
In atrial fibrillation, an average of three Blood Pressure recordings in
the same limb must be taken.
HYPERTENSION
An elevated arterial pressure is probably the most important public
health problem in developed countries, being common, asymptomatic,
readily detectable, usually easily treatable and often leading to lethal
complications if left untreated.
Definition :
Since there is no dividing line between normal and high blood
pressure, arbitrary levels have been established to define those who have an
increased risk of developing a morbid cardio-vascular event and / or will
clearly benefit from medical therapy. This definition should consider not
only the level of diastolic pressure but also systolic pressure, age, sex and
race.
Hypertension is thus not a disease or abnormality but if it
progresses it leads to end organ damages.
Incidence:
It is present in 10-15% of the individuals in the Indian population.
The prevalence of individuals prone to have hypertension are more in Asian
migrants especially Indians due to the presence of increased Lipo-protein (a)
in their blood.
Aetiology :
The causes of elevated arterial pressure is unknown in most cases.
The prevalence of various forms of secondary hypertension depends on the
nature of the population studied and how extensive the evaluation is. There
are no available data to define the frequency of secondary hypertension in
the general population.
Classification :
Arterial hypertension may be classified into
1. Primary or idiopathic or essential hypertension.
2. Secondary hypertension.
Essential hypertension :
Patients with arterial hypertension and with no definable cause are
said to have primary or essential or idiopathic hypertension. Moreover
individuals who may have generalised or functional abnormalities causing
the hypertension are defined as having essential hypertension.
Factors influencing the development of essential hypertension :
1. Genetic and Familial.
2. Socio – economic
3. Dietary factors :
• Obesity.
• High salt intake.
• High alcohol, caffeine.
4. Hormonal factors.
• High renin.
• Reduced nitric oxide etc.
5. Neurotransmitters
• Acetyl choline.
• Nor-adrenaline.
• Substance-p.
• Serotonin.
• Dopamine etc.

Factors modifying the course of essential hypertension :
• Age.
• Race.
• Sex.
• Smoking.
• Excessive salt intake.
• Serum Cholesterol.
• Glucose intolerance.
• Weight.
• Renin activity.
Aetiology :
Common causes of hypertension
� Essential or primary hypertension 94%
� Secondary hypertesion 6%
1. Renal 4%
2. Endocrine 1%
3. Misselaneous 1%
About 95% of the causes have no specific underlying causes. In most of
the cases, the causes are multifactorial.
Pathogenesis :
It is not clearly understood. However it is known that the underlying
defect is an increasing peripheral vascular resistance. This is due to an
increase in sympathetic nervous activity or a fundamental defect in the
vascular smooth muscle.

PATHOPHYSIOLOGY OF HYPERTENSION
Pathophysiology:
In larger arteries (> 1mm diameter) the internal elastic lamina is
thickened, smooth muscle hypertrophied, fibrous tissue deposited. So the
vessels dilate and become tortuous and their walls become less compliant.
Atheroma is perpetuated.
In smaller arteries (< 1 mm diameter) hyaline arterio-sclerosis occurs
in the wall, the lumen narrows and aneurysms may develop. These structural
changes lead to an increase in peripheral vascular resistances, a further rise
in blood pressure and acceleration of atheroma within the vessel walls.
Classification :
Essential hypertension may be classified into
I Clinically :
• Isolated systolic hypertension.
• Accelerated hypertension.
• Benign hypertension.
• Malignant hypertension.
• Hyper tensive urgency
• Hypertensive emergency
• White coat hypertesnion
• Pseudohypertension
• Transistent hypertension
• Episodic or Paroxysmal hypertension.
• Labile Hypertension
• Paradoxical Hypertension
1. Isolated Systolic Hypertension
This is said to be present when systolic blood pressure is > 140 mm
Hg and diastolic blood pressure is < 90 mr Hg. It is commonly seen in old
age (above 65 years).
2. Accelerated Hypertension
A Significant recent increase in blood pressure over previous
hypertensive levels, associated with evidence vascular damage on
fundoscopic examination, but without papilloedema.
3.Benign Hypertension
Hypertension remains fairly stable over many years. It is compatible
with long life.
4. Malignant Hypertension
A triad of blood pressure of > 200/140 mm Hg, grade retinopathy
(papilloedema) and renal dysfunction.
5. Hypertensive Urgency
This is a situation in which the Blood Pressure is markedly elevated,
but without any evidence of end organ damage. In this condition, the control
of the elevated Blood Pressure can be done gradually.
6. Hypertensive Emergency
This is a situation in which the Blood Pressure is markedly elevated,
but with evidence of some end organ damage. In this condition, the control
of the elevated Blood Pressure has to be done immediately in order to
prevent further end organ damage.
7. White Coat Hypertension
A transient increase in blood pressure in normal individuals, when
Blood Pressure is recorded in a physician's consulting room, or in a hospital.

8. Pseudohypertension
A false increase in blood pressure recording due to stiff and
noncompliant vessels (Osier's sign), occurring in old age. In these
individuals, actual intra-arterial Blood Pressure is lower than the Blood
Pressure measured by a sphygmomanometer.
9. Transient Hypertension
This may be seen in
• Acute cerebrovascular accidents
• Acute myocardial infarction
• Acute glomerulonephritis
• Pregnancy
• Acute intermittent porphyria.
It is systemic hypertension seen for a transient phase of the time when
the patient is under stress or when he is having a disorder with a transient
hypertensive phase, may occur in the above-mentioned conditions.
10. Episodic or Paroxysmal Hypertension
This seen in pheochromocytoma. However, a patient with
pheochromocytoma may be normotensive, hypotensive or hypertensive.
11. Labile Hypertension
Patients, who sometimes, but not always have arterial pressure within
the hypertensive range, are classified as having labile hypertension.
12. Paradoxical Hypertension
In this form of hypertension, patients paradoxically show an increase
in Blood Pressure, even when on antihypertensive drugs.
Examples
1. Patients with DM and HTN, on β blockers, on developing hypoglycaemia
show a paradoxical rise over previously well-controlled Blood Pressure.
This is because the excess adrenaline released secondary to hypo-
glycaemia, acts unopposed on the α1 receptors and thereby raises the
Blood Pressure.
2. With high doses of clonidine, the peripheral α 1 receptors are stimulated,
apart from its central action, thereby raising the Blood Pressure.
3. ln patients with bilateral renal artery stenosis,administration of ACE
inhibitors, results in a para doxical rise in Blood Pressure.
4. Administration of β blockers in patients with pheochromocytoma leads to
uninhibited α receptor stimulation by epinephrine leading to paradoxical
rise in Blood Pressure
II According to the severity :
• Mild hypertension.
• Moderate hypertension.
• Severe hypertension.
In adults, a diastolic pressure below 85mmHg is considered to be
normal;
• between 85 to 89 mm Hg is high normal,
• 90-104mmHg mild hypertensive;
• 105 to 114mmHg; moderate hypertensive
• 115mmHg or greater to severe hypertensive.
When the diastolic pressure is below 90mmHg,
• a systolic pressure below 140mmHg indicates normal blood pressure,
• between 140 to 159mmHg is border-line isolated systolic
hypertension;
• 160mmHg or higher is isolated systolic hypertension.
Clinical features :
Symptoms :
Most of the patients are asymptomatic
• Occipital headache usually in the early morning.
• Easy fatigability.
• Giddiness.
• Lack of concentration.
• Loss of memory.
• Insomnia.
• Palpitation.
• Breathlessness.
• Flashes of light before the eyes.
• Epistaxis.
Signs :
Most of the patients have no abnormal physical signs apart from the
hypertension.
• Apical heave (left ventricular hypertrophy).
• Accentuation of aortic component of second heart sound
(loud or ringing A2).
• Fourth heart sound (S4).
• Pulse-high bounding pulse.
Complications :
Central nervous system complications :
• Transient ischaemic attacks.
• Cerebro-vascular accidents due to cerebral thrombosis or
haemorrihage.
• Sub-arachnoid haemorrhage.
• Hypertensive encephalopathy.
It is characterized by very high Blood Pressure, neuralgic
manifestations including transient disturbances in speech and vision,
paraesthesiae, fits, disorientation, loss of consciousness and papilloedema.
The neuralgic deficits are easily reversible with control of blood pressure.
Cardio-vascular complications :
• Coronary artery disease (Angina, myocardial infarction).
• Left ventricular failure.
• Aortic aneurysm.
• Aortic dissection.
Renal complications :
• Proteinuria.
• Progressive renal failure.
Maligant hypertension :
Sometimes hypertensive renal damage results in an increased release
of renin which in turn accelerates hypertension. There is worsening of renal
failure and very severe hypertension.
Opthalmic complications :
• Hypertensive retinopathy.
• It is charaterized by thickening of the walls of the retinal arterioles and
it can cause visual field defects and blindness.
• Granding of hypertensive retinopathy according to KEITH-
WAGENER-BARKER classification
Stage I : Arteriolar narrowing and vessel irregularity.
Stage II : AV nipping.
Stage III : Flame shaped haemorrhages, hard exudates, cotton wool spots.
Stage IV : Papilloedema.
Prognosis :
Factors indicating an adverse, prognosis in hypertension :
• Black race.
• Youth.
• Male.
• Persistent diastolic pressure > 115 mmHg.
• Smoking.
• Diabetes mellitus.
• Obesity.
• Evidence of end organ damage.
A. Cardiac :
• Cardiac enlargement.
• ECG changes of ischaemic or left ventricular strain.
• Myocardial infarction.
• Congestive heart failure.
B. Eyes :
• Retinal exudates and hemorrhages.
• Papilloedema.
C. Renal :
Impaired renal function.
D. Nervous system :
Cerebrovascular accident.
HYPERTENSIVE CRISIS
Hypertensive emergency :
It is an acute clinical condition and it should be controlled within
minutes. If not, it leads to end organ damage.
Causes :
• Abrupt drug withdrawal.
• Renal problems (eg.Acute Glomerula Nephritis).
• Catecholamine excess (pheochromocytoma).
• Drugs (steroids, sympathomimetics).
• Events involving CNS (eg. Cerebro Vascular Accident).
• After coronary bye-pass surgery.
Hypertensive urgency :
This is also an acute clinical condition and the B.P should be
controlled within hours. There is no end organ damage.
Causes :
• Accelerated / malignant hypertension.
• Brain infarct.
• Surgical (post operative, renal transplant, severe body burns).
• Sudden withdrawal of treatment.
• Eclampsia.
Hypertensive States
These are situations in which there is a marked increase in both
systolic and diastolic Blood Pressure, occurring in normal individuals, as
during sexual intercourse or on diving into cold water.
Measurement of Blood Pressure may be useful in detecting
• Pulsus paradoxus
• Pulsus alternans.
Pulsus Paradoxus
Inflate the Blood Pressure cuff to suprasystolic level and deflate
slowly at a rate of 2 mm Hg per heart beat. The peak systolic pressure during
expiration is noted. The cuff is then deflated even more slowly, and the
pressure is again noted when Korotkoff sound becomes audible throughout
the respiratory cycle. Normally the difference between the two pressures
should not exceed 10 mm Hg during quiet respiration. If it is more than 10
mm Hg, pulsus paradoxus is said to be present."
Pulsus Alternans
Inflate the Blood Pressure cuff to suprasystolic level and deflate
slowly. Pulsus alternans is present if there is an alterlation in the intensity of
Korotkoff sound.
Investigations :
Since essential hypertension has no obvious cause, the causes for
secondary hypertension must be ruled out.
Basic investigations :
• Urine analysis for blood, protein and glucose.
• Blood urea and creatinine (to assess renal fuction).
• Serum electrolytes (for hypokalaemia and alkalosis in
hyperaldosteronism).
• Fasting and post-prandial blood glucose (for hyperglycaemia).
• Serum cholesterol and tri-glycerides (to rule out atherosclerosis).
• Serum calcium and uric acid.
• Electrocardiogram and ECHO to rule out cardiac pathology.
• Chest – radiograph (for cardiac size, failure and aortic dilatation).
Secondary studies :
• Plasma catecholamine levels and 24 hours urinary Vanillylmandalic
acid.
o Pheochromocytoma.
• Plasma cortisol levels, 24 hours urinary cortisol and dexamethasone
suppression test
o Cushing’s syndrome.
• Intra-venous urogram, renal angiogram, ultrasonagraphy
o Renal artery stenosis, polycystic renal disease.
• Hypokalaemia, high aldosterone levels, low plasma renin
o Primary aldosteronism.
• Growth Harmone levels and x-ray of the skull
o Acromegaly.
• T3, T4, TSH levels
o Primary hypothyroidism.
• Chest radiography for rib notching and catheterization
o Coarctation of aorta.

Materials and Methods
MATERIALS AND METHODS
The disease vatha pitham noi has been described in Yugi Vaidhya
Chinthamani - 800. Approach towards the patient were made according to
the signs and symptoms mentioned in the verse Vathapitham as well as the
Blood Pressure levels.
Selection of the patients:
20 patients were admitted in the inpatient ward
20 patients were treated in outpatient ward.
• Both sexes were selected.
• Patients with the age group between 35 – 75 were selected.
• Patients mostly with mild to moderate hypertension were selected.
Patients with secondary hypertension ( Renal, hormonal, pregnancy
and drug induced) were excluded.
• Only essential hypertension patients were selected for the study.
For this purpose, a case sheet was prepared based on both siddha and
modern aspects and was maintained separately for all the patients.
Iruveli kiyalam is the drug selected for the research work. The
medicine was prepared by the author in the post-graduate Gunapadam
practical hall with the knowledge and guidelines of staff of the post-graduate
department. The preparation of these drugs are mentioned below.
PREPARATION OF DRUG
-VOuzq!gqbipl<!
!
wz<zif<!kie<!OhigouiV!gqbipR<osiz<Ou!
! eqVOuzq!lKvLmeqR<sq!&e<XR<!
osiz<zilz<!ujgg<Gg<!gix<!hzlib<k<K~g<gqs<!!
! Sglig!uqVfipq!fQiqzqm<M!
ouz<zOu!kQobiqk<K!obm<Omie<xig<gq!
! uQxigh<!hk<Kfim<!ogit<uibieiz<!
uz<zokiV!uikhqk<kR<!Osijg!hi{<M!
! uir<gquqMl<!nOvisqgLl<!uivioke<Oe!"!
!! ! ! ! ! ! .!ngk<kqbi<!juk<kqb!H,v{l<!316!
Ingredients
• Roots of Iruveli (Coleus Forskholii)
• Adhimadhuram (Glycyrhyza Glabra)
• Ingi (Zingiber Officinale)
All the above drugs are taken in equal parts
Preparation:
The drugs Adhimadhuram and Ingi were bought from the pharmacy
raw drug store Government Siddha Medical College and Hospital they are
cleaned and dried under shade. The roots of Iruveli are purchased from the
field. The raw drugs are authenticated by medical botanist of Govt. Siddha
Medical College Palayamkottai.
200gm of each items are ground into small pieces. Mixed well. 5gms
of mixture was taken in 720 ml of water. It is boiled in a reduced flame to
the final volume of 1/8th measure i.e 90ml and filtered.
Dosage :
90ml twice a day
Indications:
Vatha pitham (Hypertension), Sobai, Pandu
Life Span:
3 hours
Reference:
Agathiyar Vaithya Pooranam - 205 (Pg. No. 154)
Administration of drug:
The trial drug, Iruveli Kiyalam 90ml was given twice daily before
meals for minimum 40 days.
Patients were advised to consume restricted diet including minimum
salt and fat intake.
Evaluation of the drugs:
The herbal drugs selected for dissertation work were subjected to
pharmacological, Bio-chemical and Toxicological analysis. These analysis
were made in the Pharmacology department and Bio-Chemistry department,
Govt. Siddha medical college, Palayamkottai.
Parameters of Assessment:
During the trial studies, the parameters adopted for the assessment of
the role of Iruveli Kiyalam in the management of vatha pitham are described
below.
1. Subjective improvement:
Here the patient’s sense of well being was noted.
2. Patterns of changes in systolic and diastolic B.P:
The B.P of all the patients were recorded twice daily regularly.
Clinical improvement:
Here reduction of patient’s symptoms like sleep pattern, emotional
disturbances, giddiness, headache, fatigue has been noted.
Investigations :
The signs and symptoms of vatha pitham almost correlates with
hypertension in modern medicine. Siddha parameters like Envagaithervugal,
Poriyalarithal, Pulanalarithal, 7 Udal thathukkal and Vinathal were applied.
Investigations meant for hypertension in modern medicine were sought for
Vatha pitham also.
Lab investigations:
Lab investigations were done in the Government Siddha Medical
College and Hospital which include routine blood investigations like T.C,
D.C, ESR, HB, Blood Sugar, Blood Urea, Uric acid and Serum Cholesterol.
Other investigations include X- ray - Chest P.A view.
Diagnosis:
Siddha methods of diagnosis were employed based on the Tridhosa
theory, Envagai thervugal and Seven udal kattugal.
Modern method of diagnosis were employed on the basis of daily
recordings of Blood Pressure by sphygmomanometer, blood, urine and
radiological investigations.
Results and Observation

RESULTS AND OBSERVATIONS
Results were observed with respect to the following criteria
1. Sex Distribution
2. Age Distribution
3. Thegi
4. Kaalam Distribution
5. Religion Distribution
6. Thinai Distribution
7. Paruva Kaalam Distribution
8. Sirupoludhu Distribution
9. Occupation Distribution
10. Socio-economic status
11. Risk factors
12. Clinical features
13. Duration of Illness
14. Other System involvement
15. Family history
16. Diet factor
17. Habitual History
18. Gnanendhiriyam (Imporigal)
19. Kanmendhiriyam
20. Kosam
21. Mukkutram a)Vadham b)Pitham c) Kabam
22. Ezhu Udal Kattugal
23. Envagai Thervugal
24. Neerkuri
25. Neikuri
26. Clinical Assessment
27. Effect on Blood Pressure
28. Laboratory Analysis and ECG
29. Echo Report
30. Gradation of Results
For this study 20 In-patients and 20 Out-patients were selected.
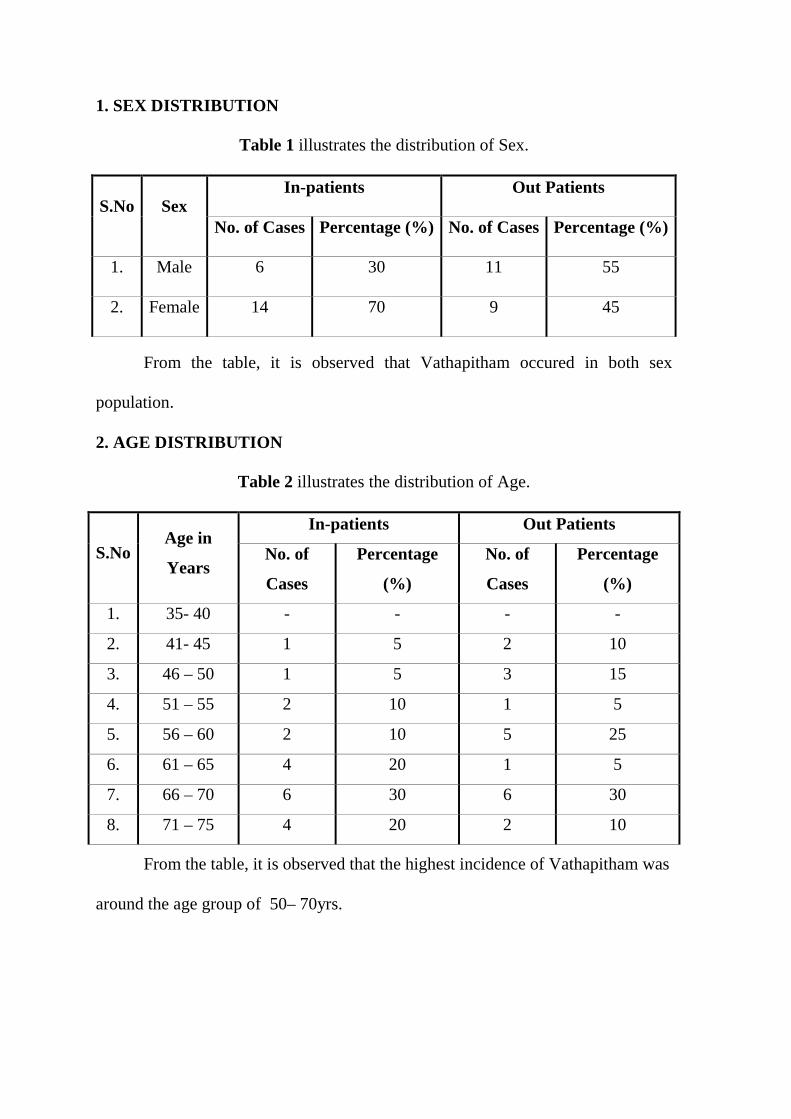
1. SEX DISTRIBUTION
Table 1 illustrates the distribution of Sex.
In-patients Out Patients S.No Sex
No. of Cases Percentage (%) No. of Cases Percentage (%)
1. Male 6 30 11 55
2. Female 14 70 9 45
From the table, it is observed that Vathapitham occured in both sex
population.
2. AGE DISTRIBUTION
Table 2 illustrates the distribution of Age.
In-patients Out Patients
S.No Age in
Years No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. 35- 40 - - - -
2. 41- 45 1 5 2 10
3. 46 – 50 1 5 3 15
4. 51 – 55 2 10 1 5
5. 56 – 60 2 10 5 25
6. 61 – 65 4 20 1 5
7. 66 – 70 6 30 6 30
8. 71 – 75 4 20 2 10
From the table, it is observed that the highest incidence of Vathapitham was
around the age group of 50– 70yrs.

3. DISTRIBUTION OF THEGI
Table 3 illustrates the distribution of Thegi.
In-patients Out Patients
S.No Thegi No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Vatha Thegi 2 10 4 20
2. Pitha Thegi 14 70 14 70
3. Kabha Thegi 4 20 2 10
From the table, it is observed that the highest incidence of vatha pitham was
pitha thegi.
4. KAALAM DISTRIBUTION
Table 3 illustrates the distribution of Kaalam
In-patients Out Patients
S.No Kaalam No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Vadha Kaalam
1 – 33 years - - - -
2. Pitha Kaalam
34 – 66 years 10 50 17 85
3. Kaba Kaalam
67 – 100 years 10 50 3 15
The table showed that, the highest incidence of Vathapitham in Pitha
Kaalam.
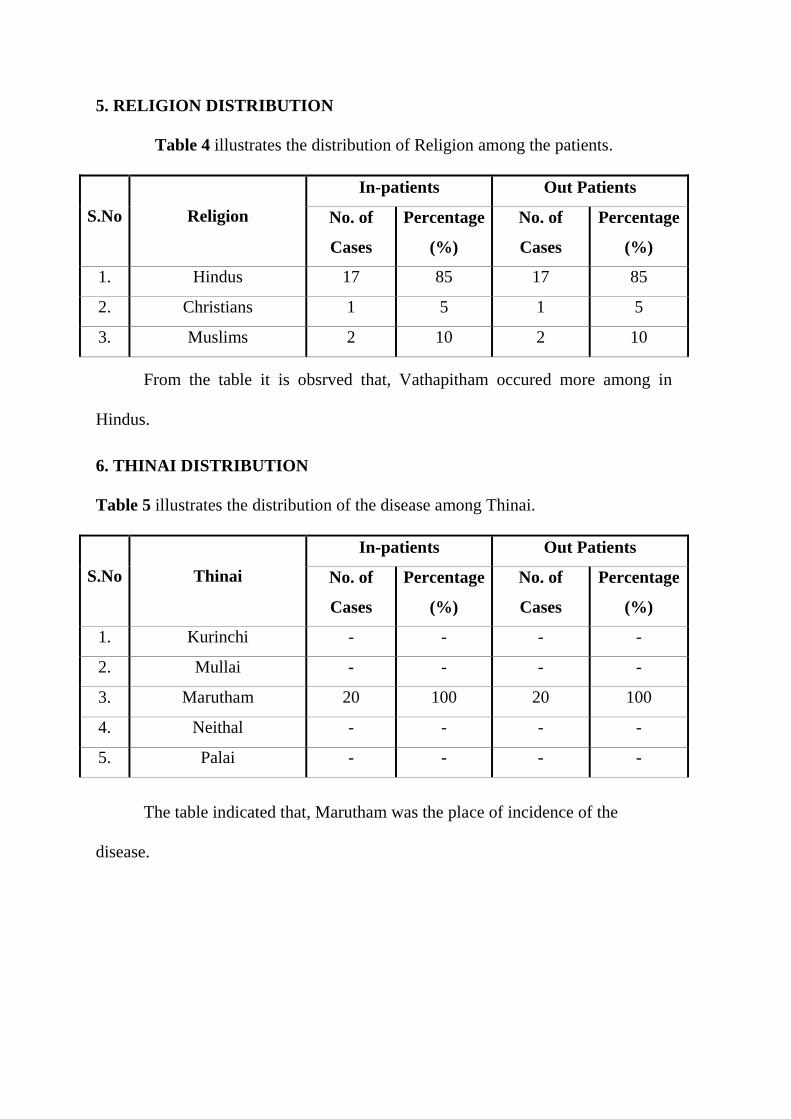
5. RELIGION DISTRIBUTION
Table 4 illustrates the distribution of Religion among the patients.
In-patients Out Patients
S.No Religion No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Hindus 17 85 17 85
2. Christians 1 5 1 5
3. Muslims 2 10 2 10
From the table it is obsrved that, Vathapitham occured more among in
Hindus.
6. THINAI DISTRIBUTION
Table 5 illustrates the distribution of the disease among Thinai.
In-patients Out Patients
S.No Thinai No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Kurinchi - - - -
2. Mullai - - - -
3. Marutham 20 100 20 100
4. Neithal - - - -
5. Palai - - - -
The table indicated that, Marutham was the place of incidence of the
disease.
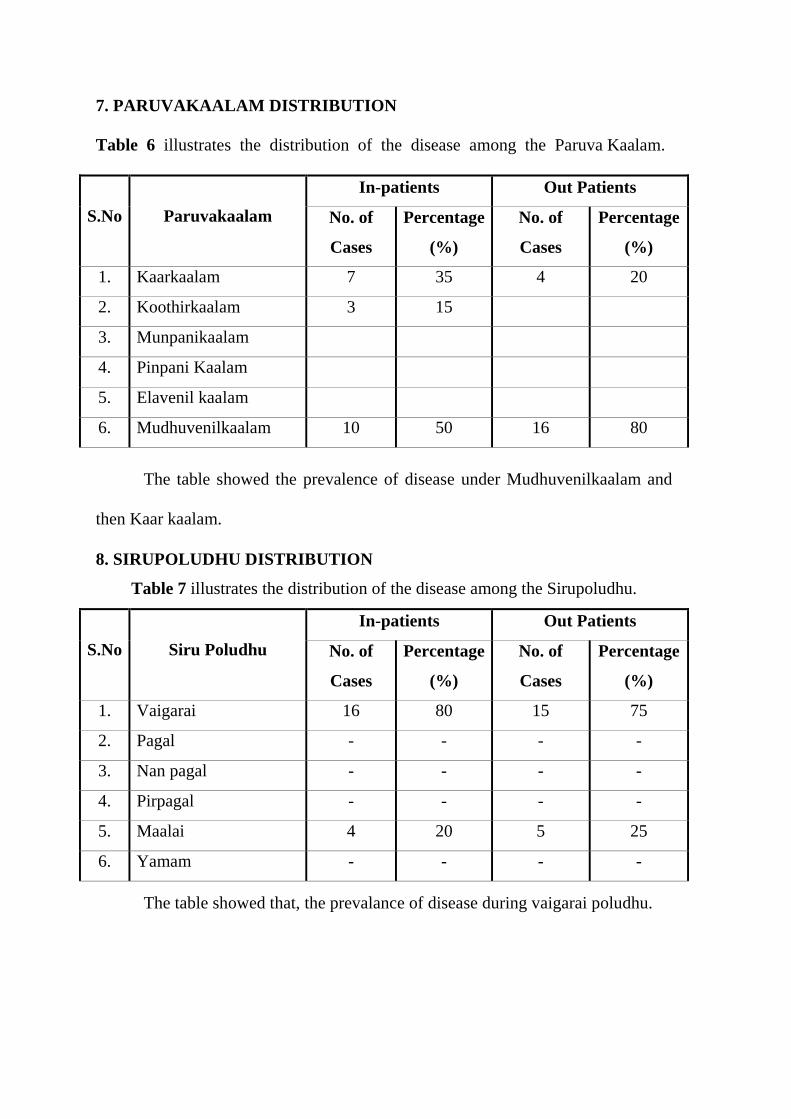
7. PARUVAKAALAM DISTRIBUTION
Table 6 illustrates the distribution of the disease among the Paruva Kaalam.
In-patients Out Patients
S.No Paruvakaalam No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Kaarkaalam 7 35 4 20
2. Koothirkaalam 3 15
3. Munpanikaalam
4. Pinpani Kaalam
5. Elavenil kaalam
6. Mudhuvenilkaalam 10 50 16 80
The table showed the prevalence of disease under Mudhuvenilkaalam and
then Kaar kaalam.
8. SIRUPOLUDHU DISTRIBUTION
Table 7 illustrates the distribution of the disease among the Sirupoludhu.
In-patients Out Patients
S.No Siru Poludhu No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Vaigarai 16 80 15 75
2. Pagal - - - -
3. Nan pagal - - - -
4. Pirpagal - - - -
5. Maalai 4 20 5 25
6. Yamam - - - -
The table showed that, the prevalance of disease during vaigarai poludhu.
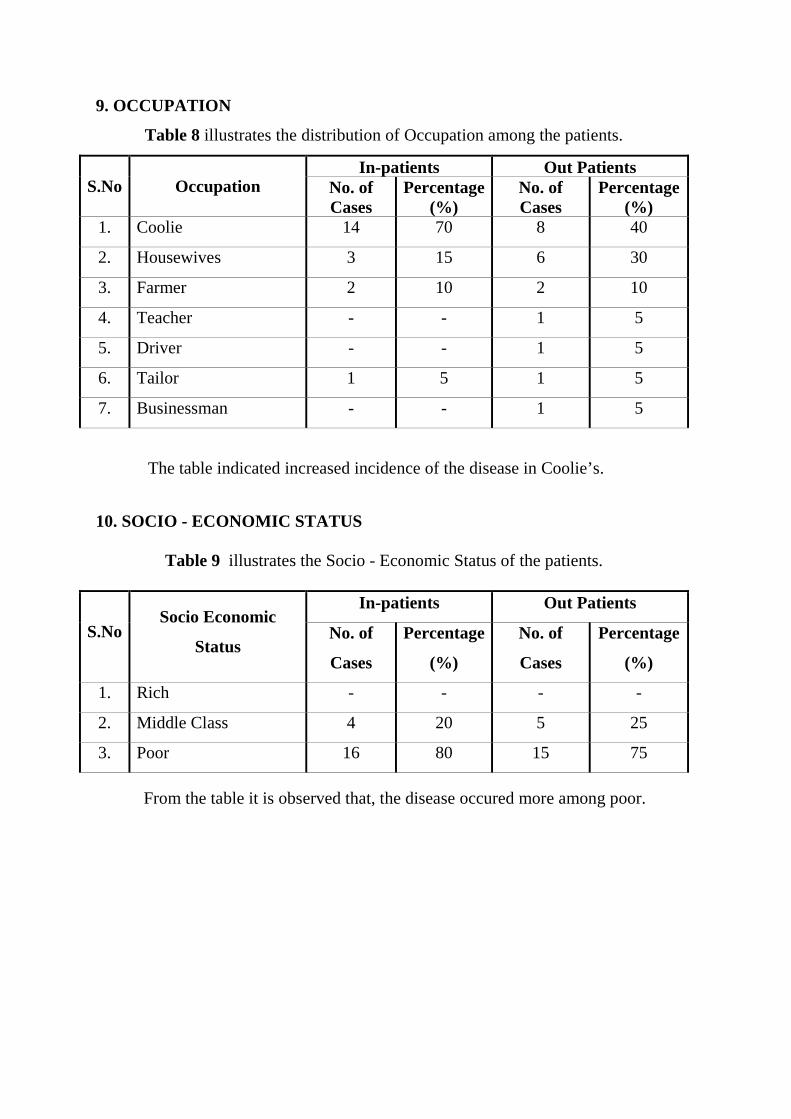
9. OCCUPATION
Table 8 illustrates the distribution of Occupation among the patients.
In-patients Out Patients S.No Occupation No. of
Cases Percentage
(%) No. of Cases
Percentage (%)
1. Coolie 14 70 8 40
2. Housewives 3 15 6 30
3. Farmer 2 10 2 10
4. Teacher - - 1 5
5. Driver - - 1 5
6. Tailor 1 5 1 5
7. Businessman - - 1 5
The table indicated increased incidence of the disease in Coolie’s.
10. SOCIO - ECONOMIC STATUS
Table 9 illustrates the Socio - Economic Status of the patients.
In-patients Out Patients
S.No Socio Economic
Status No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Rich - - - -
2. Middle Class 4 20 5 25
3. Poor 16 80 15 75
From the table it is observed that, the disease occured more among poor.
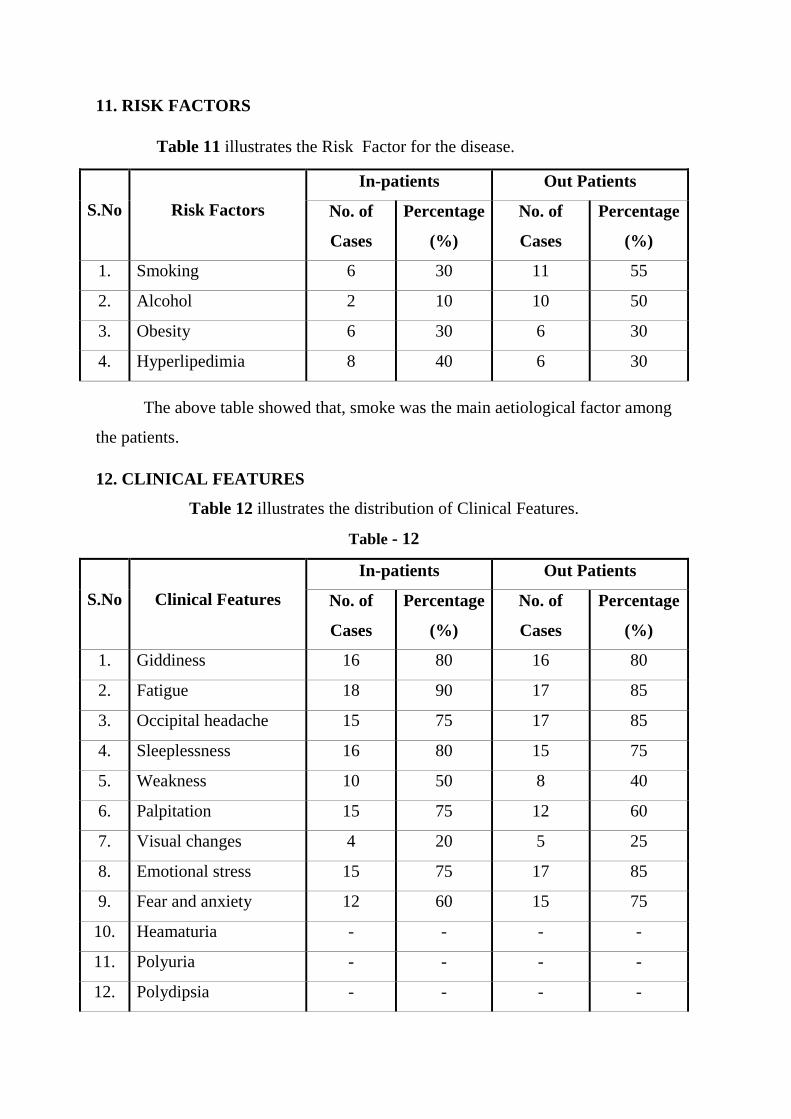
11. RISK FACTORS
Table 11 illustrates the Risk Factor for the disease.
In-patients Out Patients
S.No Risk Factors No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Smoking 6 30 11 55
2. Alcohol 2 10 10 50
3. Obesity 6 30 6 30
4. Hyperlipedimia 8 40 6 30
The above table showed that, smoke was the main aetiological factor among
the patients.
12. CLINICAL FEATURES
Table 12 illustrates the distribution of Clinical Features.
Table - 12
In-patients Out Patients
S.No Clinical Features No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Giddiness 16 80 16 80
2. Fatigue 18 90 17 85
3. Occipital headache 15 75 17 85
4. Sleeplessness 16 80 15 75
5. Weakness 10 50 8 40
6. Palpitation 15 75 12 60
7. Visual changes 4 20 5 25
8. Emotional stress 15 75 17 85
9. Fear and anxiety 12 60 15 75
10. Heamaturia - - - -
11. Polyuria - - - -
12. Polydipsia - - - -
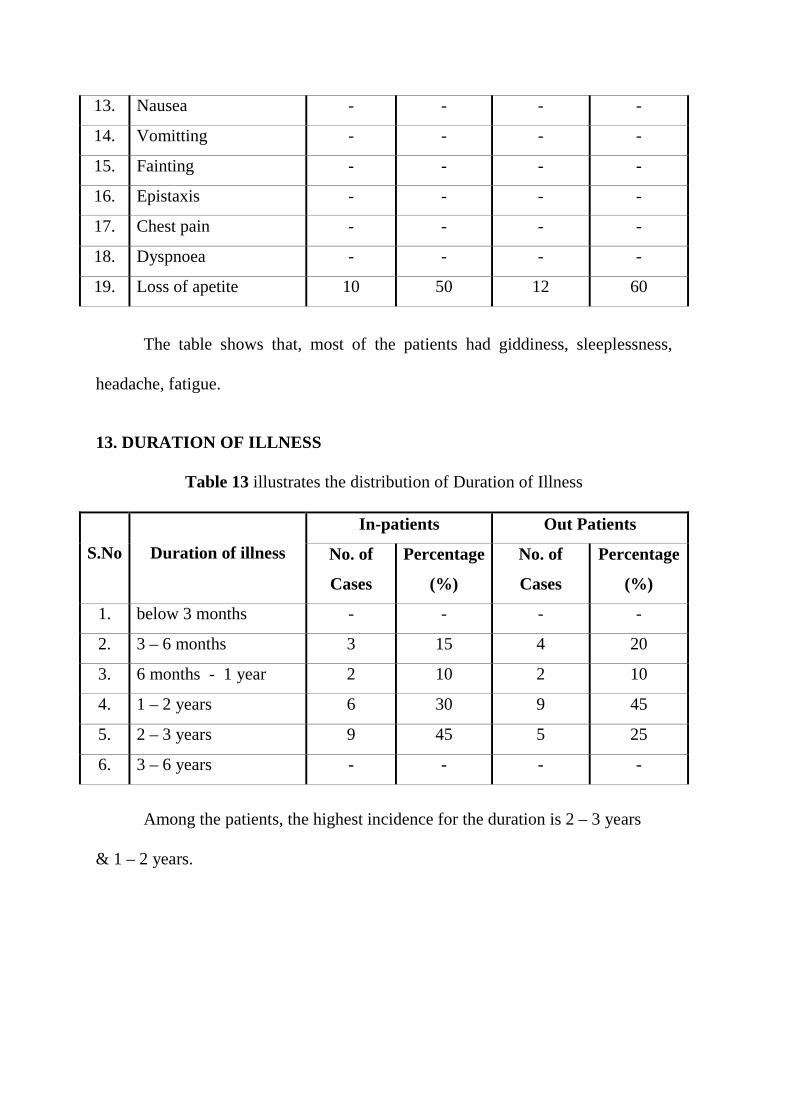
13. Nausea - - - -
14. Vomitting - - - -
15. Fainting - - - -
16. Epistaxis - - - -
17. Chest pain - - - -
18. Dyspnoea - - - -
19. Loss of apetite 10 50 12 60
The table shows that, most of the patients had giddiness, sleeplessness,
headache, fatigue.
13. DURATION OF ILLNESS
Table 13 illustrates the distribution of Duration of Illness
In-patients Out Patients
S.No Duration of illness No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. below 3 months - - - -
2. 3 – 6 months 3 15 4 20
3. 6 months - 1 year 2 10 2 10
4. 1 – 2 years 6 30 9 45
5. 2 – 3 years 9 45 5 25
6. 3 – 6 years - - - -
Among the patients, the highest incidence for the duration is 2 – 3 years
& 1 – 2 years.
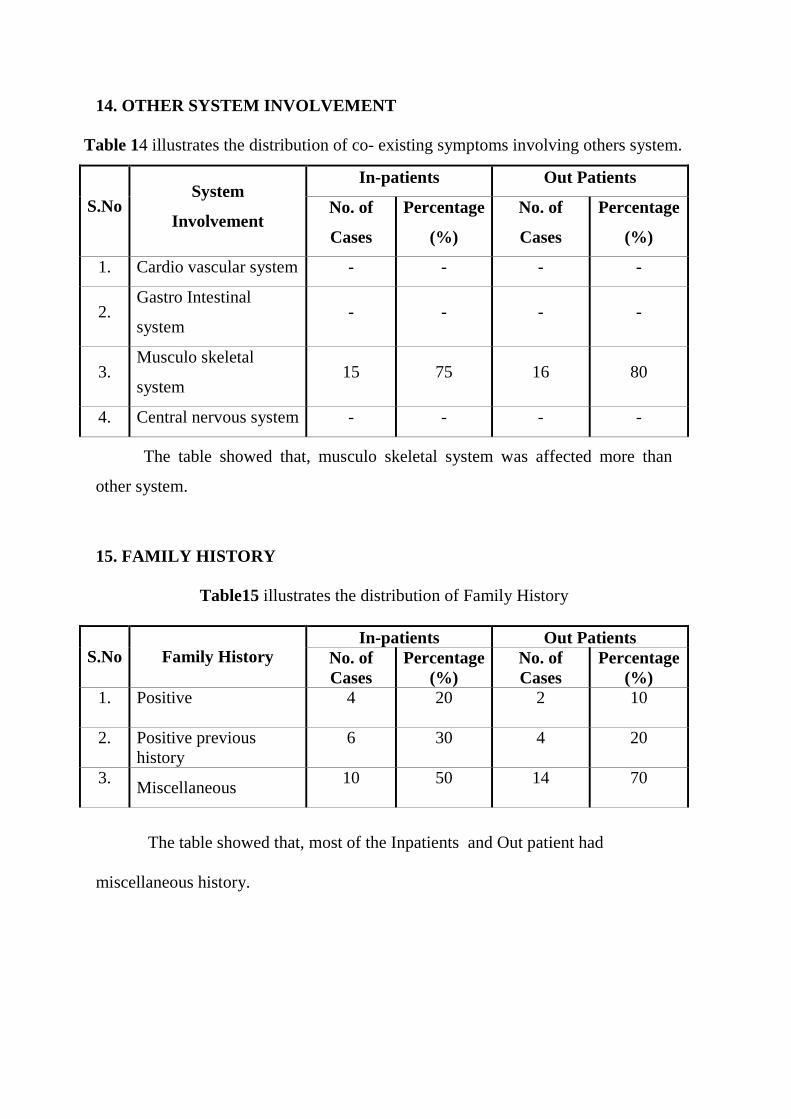
14. OTHER SYSTEM INVOLVEMENT
Table 14 illustrates the distribution of co- existing symptoms involving others system.
In-patients Out Patients
S.No System
Involvement No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Cardio vascular system - - - -
2. Gastro Intestinal
system - - - -
3. Musculo skeletal
system 15 75 16 80
4. Central nervous system - - - -
The table showed that, musculo skeletal system was affected more than
other system.
15. FAMILY HISTORY
Table15 illustrates the distribution of Family History
In-patients Out Patients S.No Family History No. of
Cases Percentage
(%) No. of Cases
Percentage (%)
1. Positive 4 20 2 10
2. Positive previous history
6 30 4 20
3. Miscellaneous
10 50 14 70
The table showed that, most of the Inpatients and Out patient had
miscellaneous history.
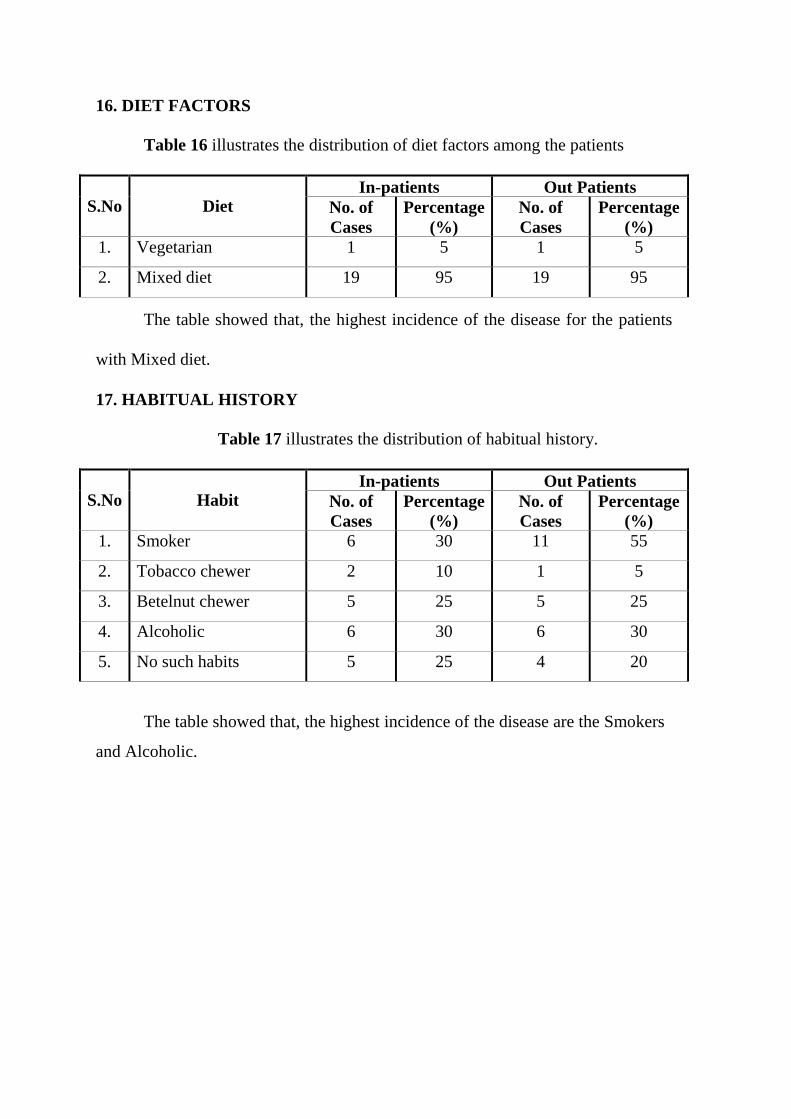
16. DIET FACTORS
Table 16 illustrates the distribution of diet factors among the patients
In-patients Out Patients S.No Diet No. of
Cases Percentage
(%) No. of Cases
Percentage (%)
1. Vegetarian 1 5 1 5
2. Mixed diet 19 95 19 95
The table showed that, the highest incidence of the disease for the patients
with Mixed diet.
17. HABITUAL HISTORY
Table 17 illustrates the distribution of habitual history.
In-patients Out Patients S.No Habit No. of
Cases Percentage
(%) No. of Cases
Percentage (%)
1. Smoker 6 30 11 55
2. Tobacco chewer 2 10 1 5
3. Betelnut chewer 5 25 5 25
4. Alcoholic 6 30 6 30
5. No such habits 5 25 4 20
The table showed that, the highest incidence of the disease are the Smokers
and Alcoholic.
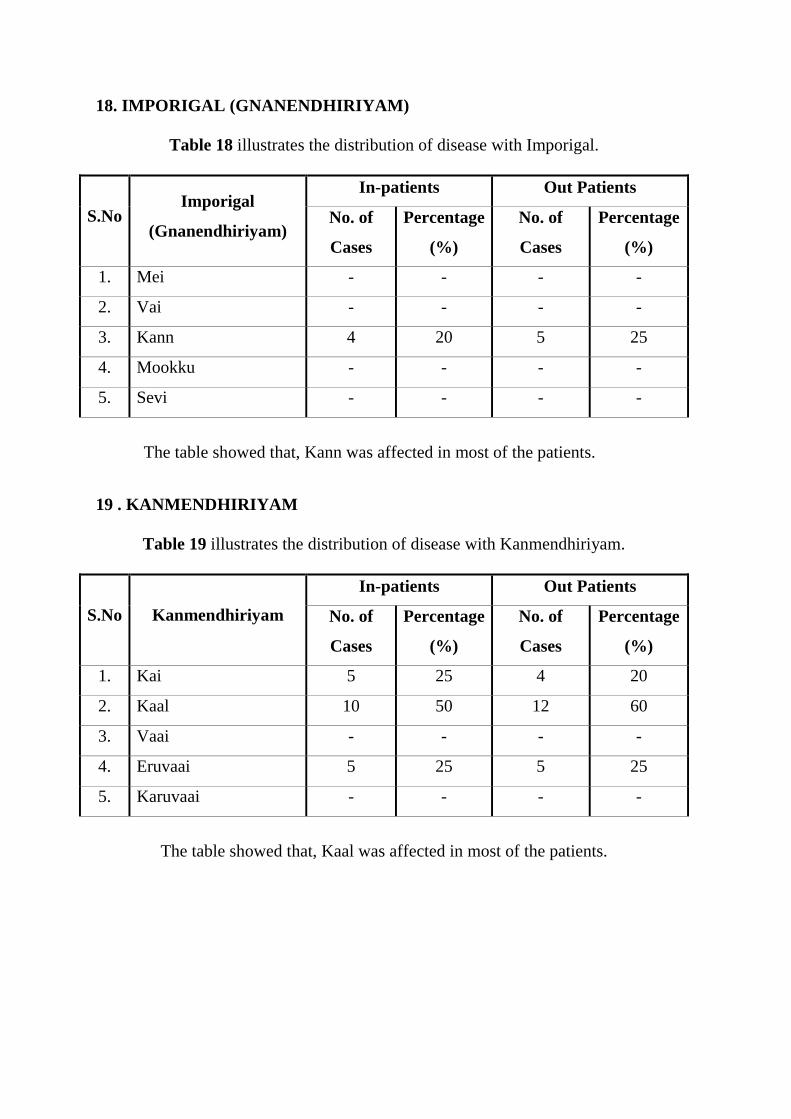
18. IMPORIGAL (GNANENDHIRIYAM)
Table 18 illustrates the distribution of disease with Imporigal.
In-patients Out Patients
S.No Imporigal
(Gnanendhiriyam) No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Mei - - - -
2. Vai - - - -
3. Kann 4 20 5 25
4. Mookku - - - -
5. Sevi - - - -
The table showed that, Kann was affected in most of the patients.
19 . KANMENDHIRIYAM
Table 19 illustrates the distribution of disease with Kanmendhiriyam.
In-patients Out Patients
S.No Kanmendhiriyam No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Kai 5 25 4 20
2. Kaal 10 50 12 60
3. Vaai - - - -
4. Eruvaai 5 25 5 25
5. Karuvaai - - - -
The table showed that, Kaal was affected in most of the patients.
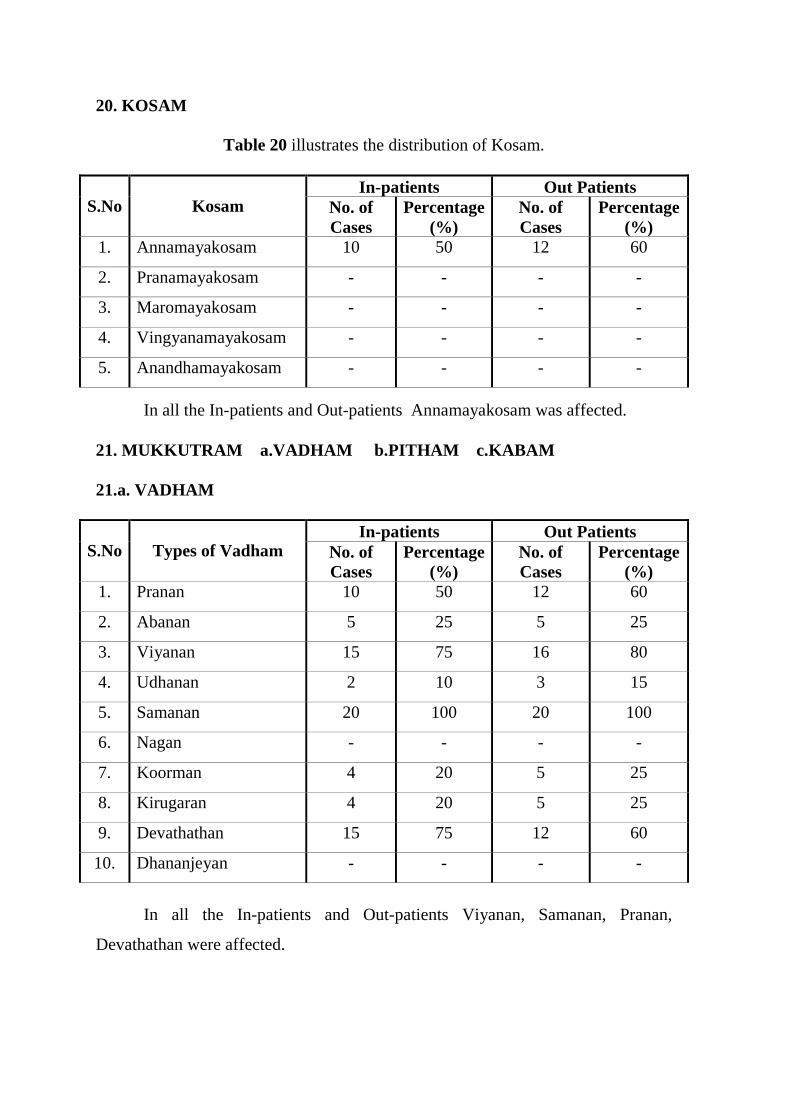
20. KOSAM
Table 20 illustrates the distribution of Kosam.
In-patients Out Patients S.No Kosam No. of
Cases Percentage
(%) No. of Cases
Percentage (%)
1. Annamayakosam 10 50 12 60
2. Pranamayakosam - - - -
3. Maromayakosam - - - -
4. Vingyanamayakosam - - - -
5. Anandhamayakosam - - - -
In all the In-patients and Out-patients Annamayakosam was affected.
21. MUKKUTRAM a.VADHAM b.PITHAM c.KABAM
21.a. VADHAM
In-patients Out Patients S.No Types of Vadham No. of
Cases Percentage
(%) No. of Cases
Percentage (%)
1. Pranan 10 50 12 60
2. Abanan 5 25 5 25
3. Viyanan 15 75 16 80
4. Udhanan 2 10 3 15
5. Samanan 20 100 20 100
6. Nagan - - - -
7. Koorman 4 20 5 25
8. Kirugaran 4 20 5 25
9. Devathathan 15 75 12 60
10. Dhananjeyan - - - -
In all the In-patients and Out-patients Viyanan, Samanan, Pranan,
Devathathan were affected.
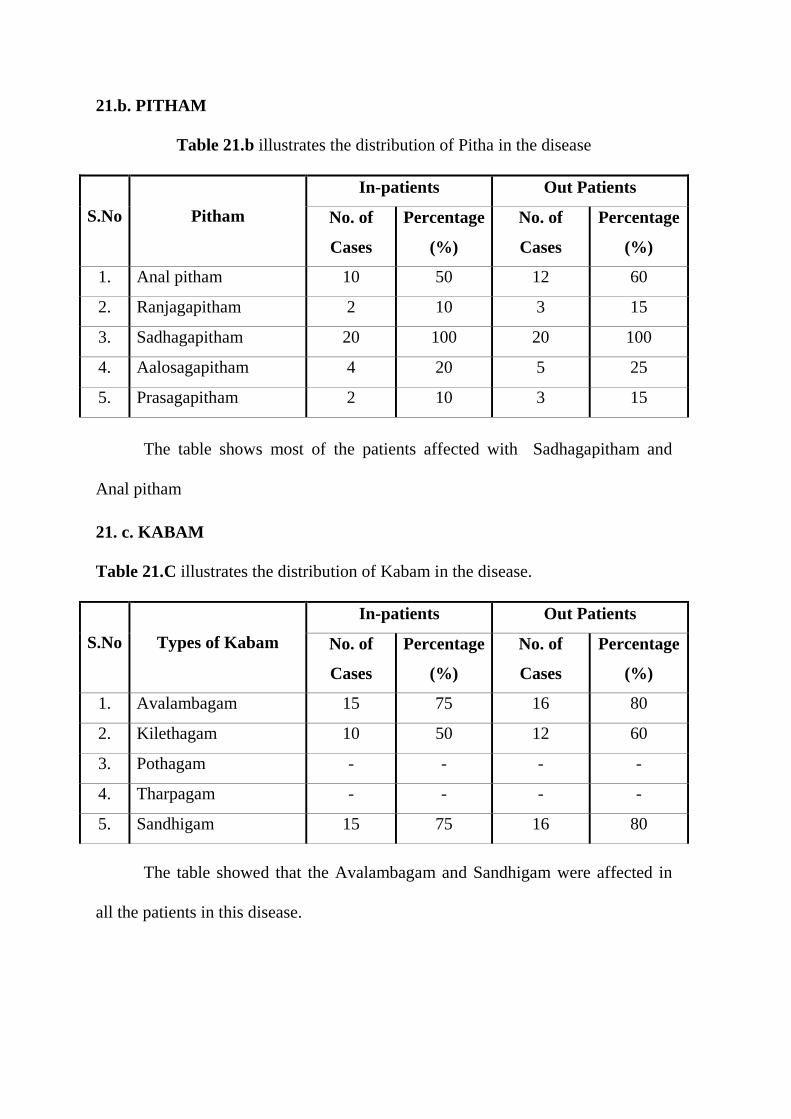
21.b. PITHAM
Table 21.b illustrates the distribution of Pitha in the disease
In-patients Out Patients
S.No Pitham No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Anal pitham 10 50 12 60
2. Ranjagapitham 2 10 3 15
3. Sadhagapitham 20 100 20 100
4. Aalosagapitham 4 20 5 25
5. Prasagapitham 2 10 3 15
The table shows most of the patients affected with Sadhagapitham and
Anal pitham
21. c. KABAM
Table 21.C illustrates the distribution of Kabam in the disease.
In-patients Out Patients
S.No Types of Kabam No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Avalambagam 15 75 16 80
2. Kilethagam 10 50 12 60
3. Pothagam - - - -
4. Tharpagam - - - -
5. Sandhigam 15 75 16 80
The table showed that the Avalambagam and Sandhigam were affected in
all the patients in this disease.
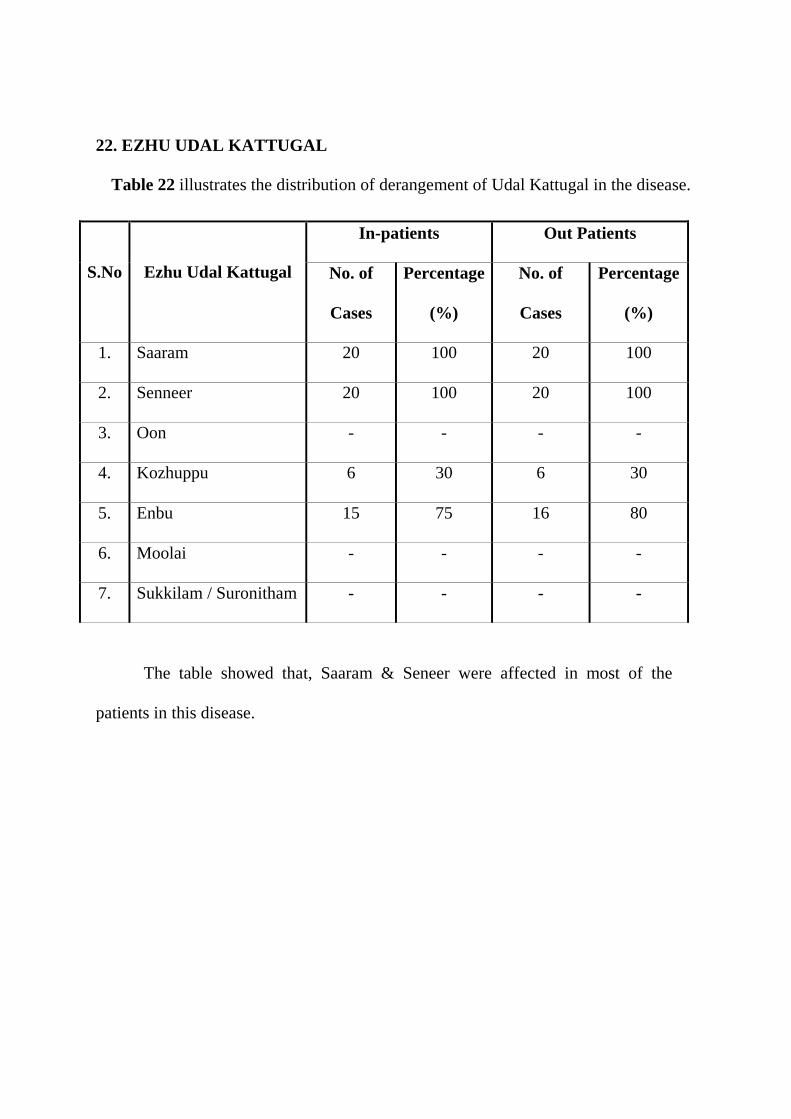
22. EZHU UDAL KATTUGAL
Table 22 illustrates the distribution of derangement of Udal Kattugal in the disease.
In-patients Out Patients
S.No Ezhu Udal Kattugal No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Saaram 20 100 20 100
2. Senneer 20 100 20 100
3. Oon - - - -
4. Kozhuppu 6 30 6 30
5. Enbu 15 75 16 80
6. Moolai - - - -
7. Sukkilam / Suronitham - - - -
The table showed that, Saaram & Seneer were affected in most of the
patients in this disease.
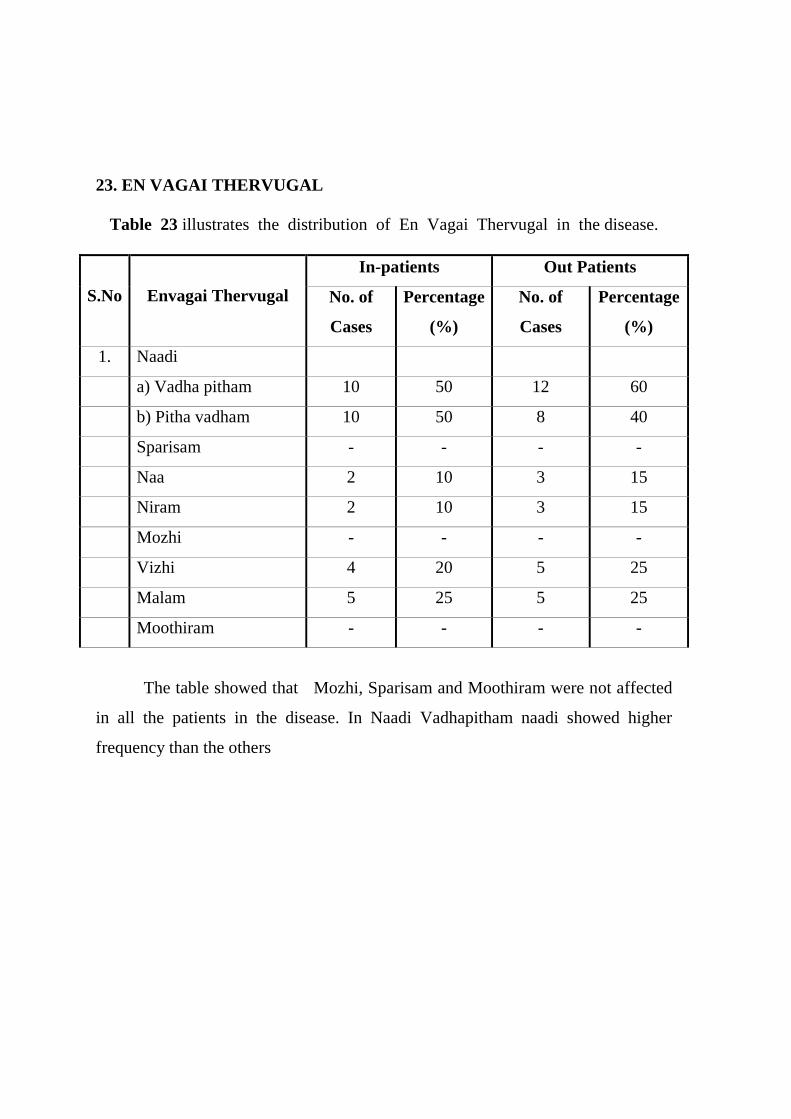
23. EN VAGAI THERVUGAL
Table 23 illustrates the distribution of En Vagai Thervugal in the disease.
In-patients Out Patients
S.No Envagai Thervugal No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Naadi
a) Vadha pitham 10 50 12 60
b) Pitha vadham 10 50 8 40
Sparisam - - - -
Naa 2 10 3 15
Niram 2 10 3 15
Mozhi - - - -
Vizhi 4 20 5 25
Malam 5 25 5 25
Moothiram - - - -
The table showed that Mozhi, Sparisam and Moothiram were not affected
in all the patients in the disease. In Naadi Vadhapitham naadi showed higher
frequency than the others
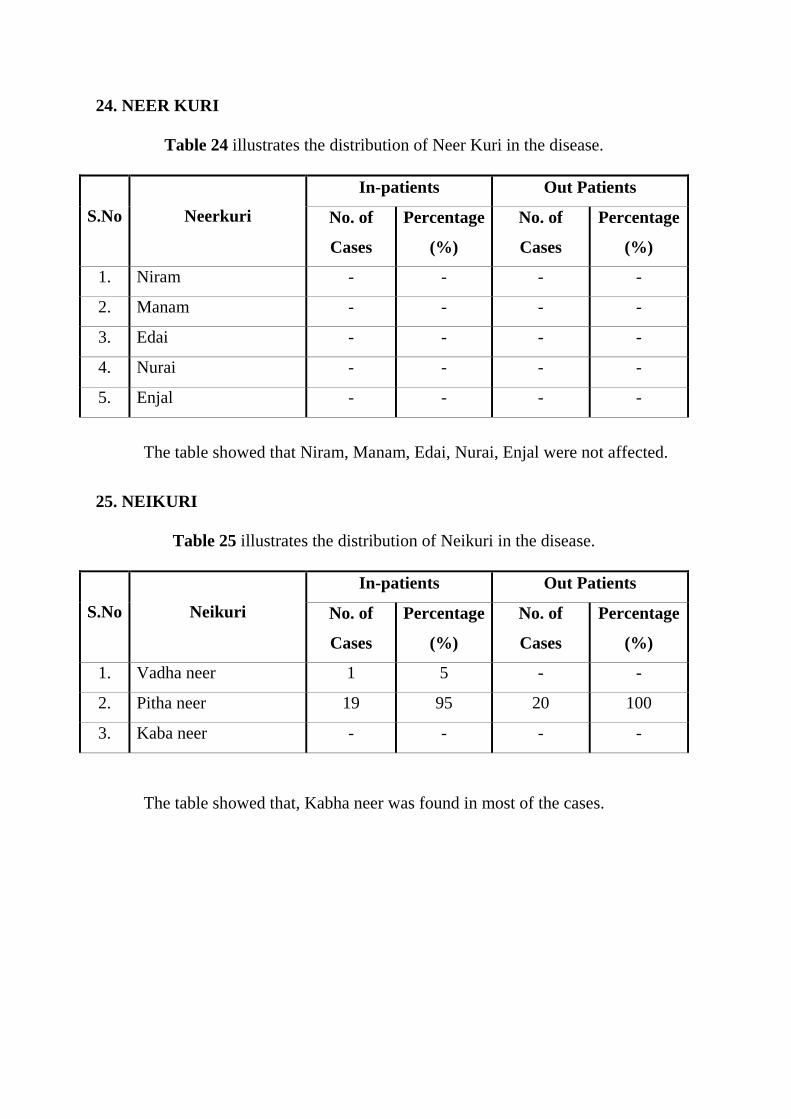
24. NEER KURI
Table 24 illustrates the distribution of Neer Kuri in the disease.
In-patients Out Patients
S.No Neerkuri No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Niram - - - -
2. Manam - - - -
3. Edai - - - -
4. Nurai - - - -
5. Enjal - - - -
The table showed that Niram, Manam, Edai, Nurai, Enjal were not affected.
25. NEIKURI
Table 25 illustrates the distribution of Neikuri in the disease.
In-patients Out Patients
S.No Neikuri No. of
Cases
Percentage
(%)
No. of
Cases
Percentage
(%)
1. Vadha neer 1 5 - -
2. Pitha neer 19 95 20 100
3. Kaba neer - - - -
The table showed that, Kabha neer was found in most of the cases.
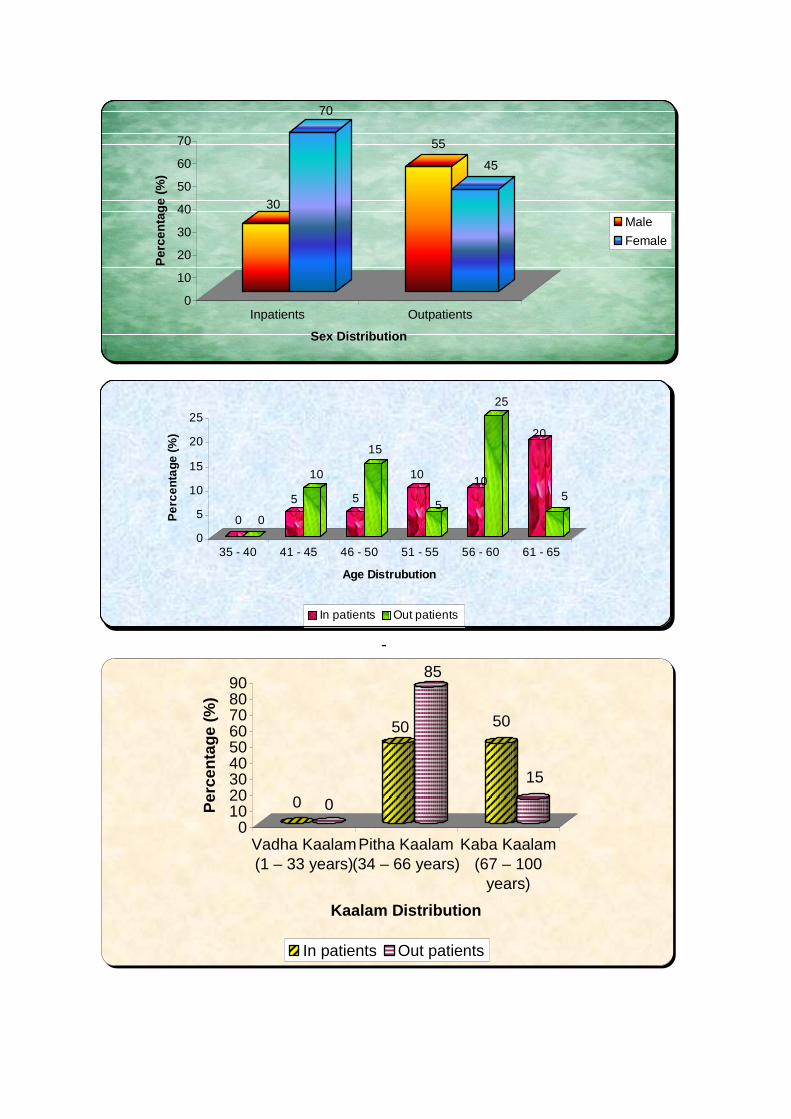
30
70
55
45
0
10
20
30
40
50
60
70
Per
cent
age
(%)
Inpatients Outpatients
Sex Distribution
Male
Female
-
0 0
50
85
50
15
0102030405060708090
Per
cent
age
(%)
Vadha Kaalam(1 – 33 years)
Pitha Kaalam(34 – 66 years)
Kaba Kaalam(67 – 100
years)
Kaalam Distribution
In patients Out patients
0 0
5
10
5
15
10
5
10
25
20
5
0
5
10
15
20
25
Per
cent
age
(%)
35 - 40 41 - 45 46 - 50 51 - 55 56 - 60 61 - 65
Age Distrubution
In patients Out patients
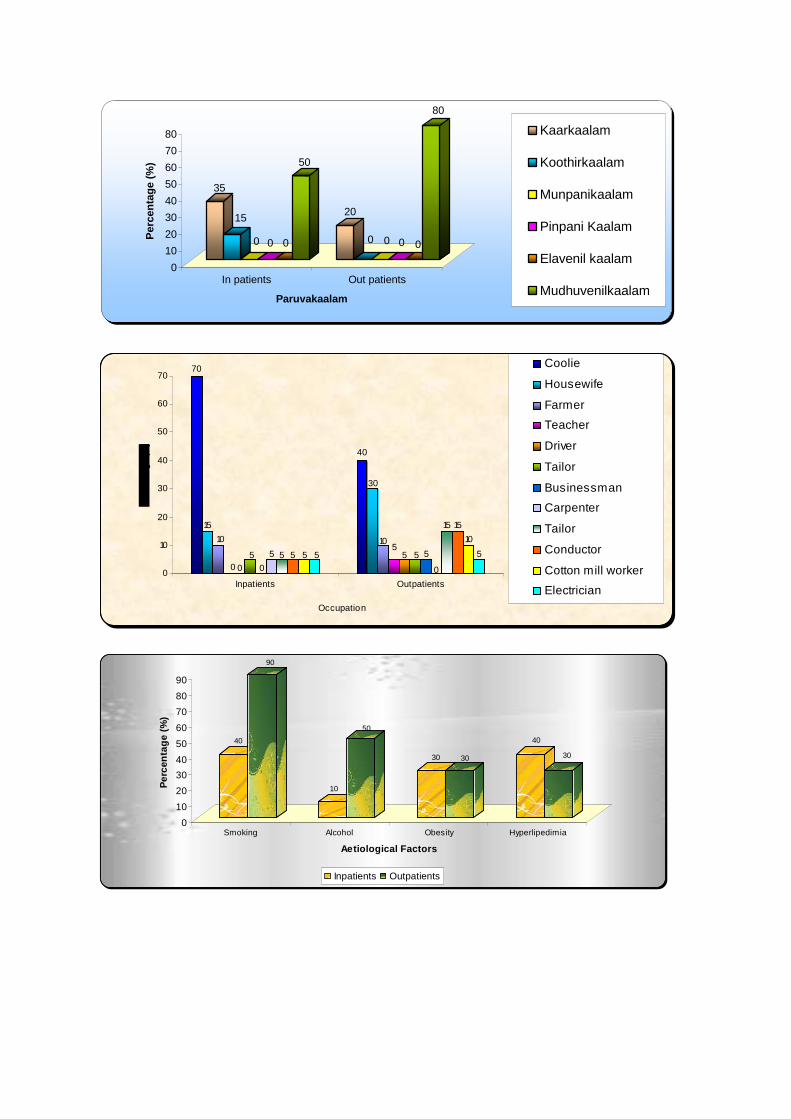
35
15
0 0 0
50
20
0 0 0 0
80
0
10
20
30
40
50
60
70
80P
erce
ntag
e (%
)
In patients Out patients
Paruvakaalam
Kaarkaalam
Koothirkaalam
Munpanikaalam
Pinpani Kaalam
Elavenil kaalam
Mudhuvenilkaalam
70
15
10
0 05
0
5 5 5 5 5
40
30
105
5 5 5
0
15 15
10
5
0
10
20
30
40
50
60
70
Inpatients Outpatients
Occupation
Coolie
Housewife
Farmer
Teacher
Driver
Tailor
Businessman
Carpenter
Tailor
Conductor
Cotton mill worker
Electrician
40
90
10
50
30 30
40
30
0
10
20
30
40
50
60
70
80
90
Per
cent
age
(%)
Smoking Alcohol Obesity Hyperlipedimia
Aetiological Factors
Inpatients Outpatients
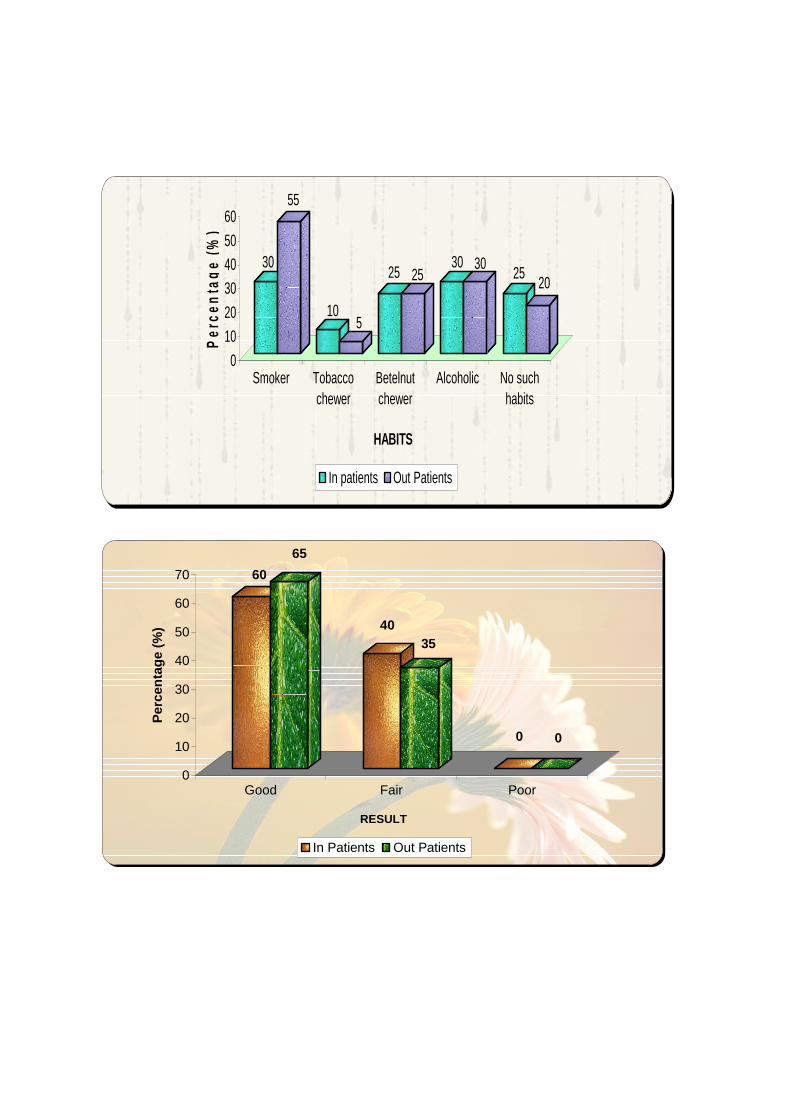
30
55
105
25 2530 30
2520
0
10
20
30
4050
60P
erce
ntag
e (%
)
Smoker Tobaccochewer
Betelnutchewer
Alcoholic No suchhabits
HABITS
In patients Out Patients
60
65
4035
0 0
0
10
20
30
40
50
60
70
Per
cent
age
(%)
Good Fair Poor
RESULT
In Patients Out Patients
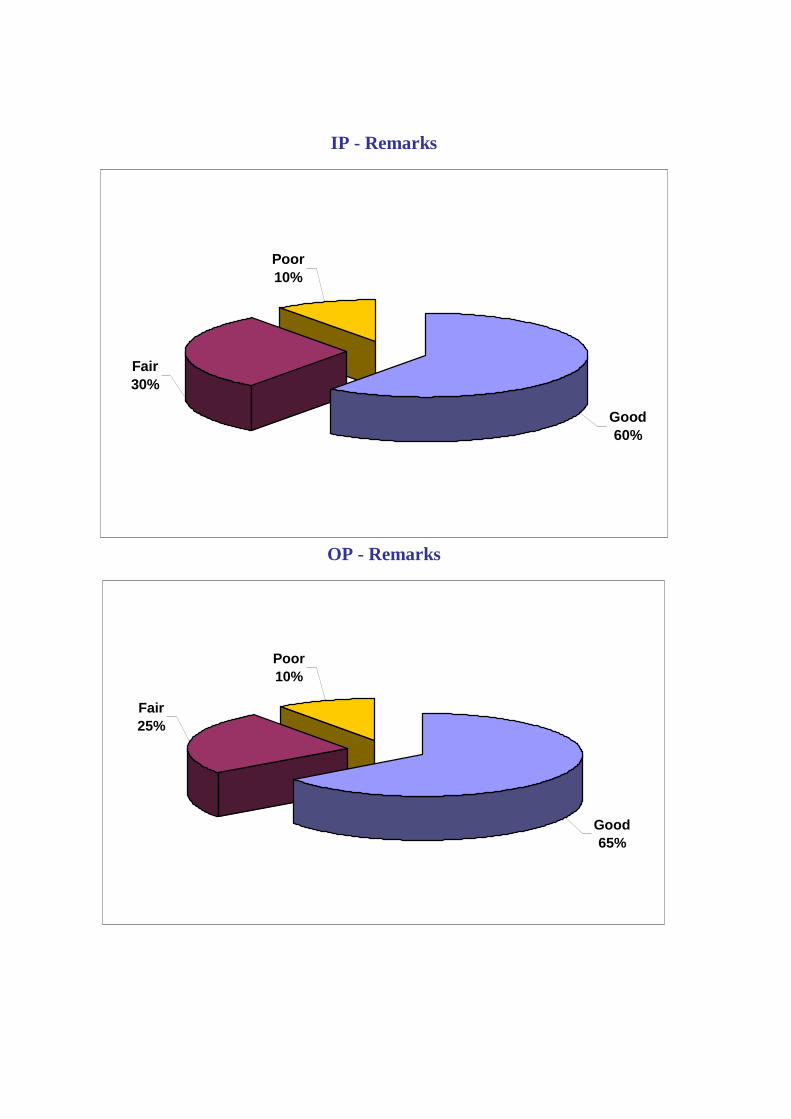
IP - Remarks
Good60%
Poor10%
Fair30%
OP - Remarks
Good65%
Poor10%
Fair25%
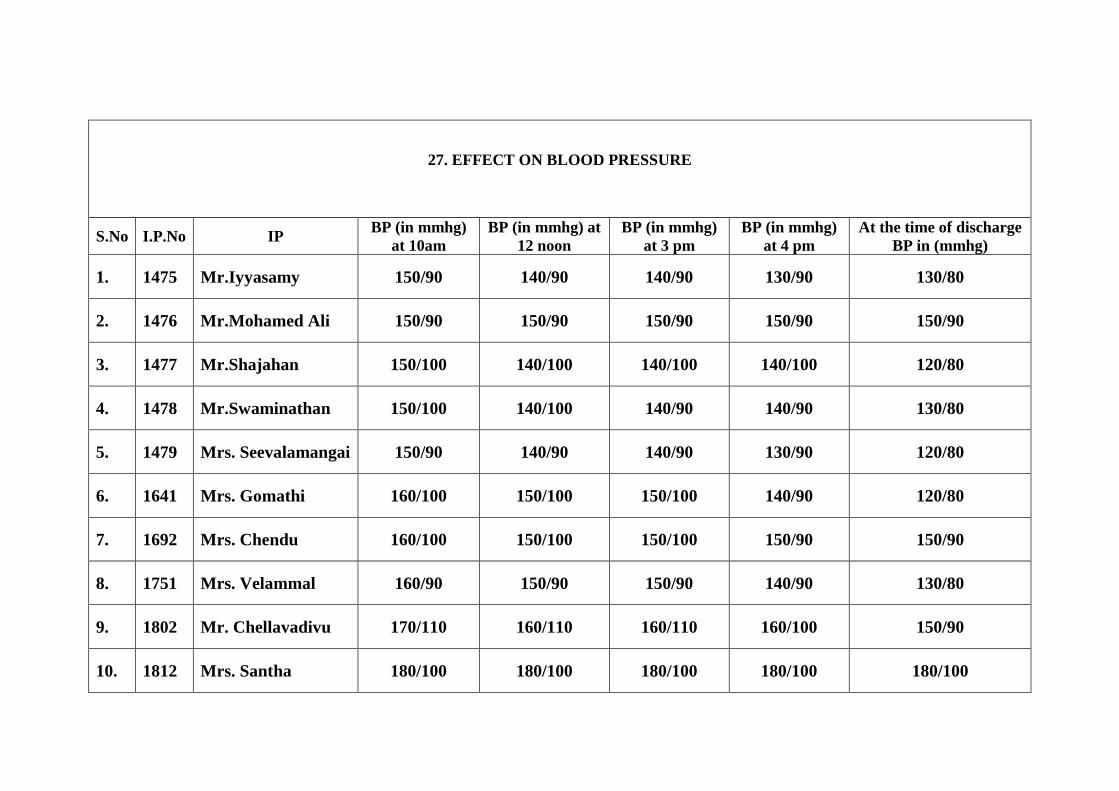
27. EFFECT ON BLOOD PRESSURE
S.No I.P.No IP BP (in mmhg) at 10am
BP (in mmhg) at 12 noon
BP (in mmhg) at 3 pm
BP (in mmhg) at 4 pm
At the time of discharge BP in (mmhg)
1. 1475 Mr.Iyyasamy 150/90 140/90 140/90 130/90 130/80
2. 1476 Mr.Mohamed Ali 150/90 150/90 150/90 150/90 150/90
3. 1477 Mr.Shajahan 150/100 140/100 140/100 140/100 120/80
4. 1478 Mr.Swaminathan 150/100 140/100 140/90 140/90 130/80
5. 1479 Mrs. Seevalamangai 150/90 140/90 140/90 130/90 120/80
6. 1641 Mrs. Gomathi 160/100 150/100 150/100 140/90 120/80
7. 1692 Mrs. Chendu 160/100 150/100 150/100 150/90 150/90
8. 1751 Mrs. Velammal 160/90 150/90 150/90 140/90 130/80
9. 1802 Mr. Chellavadivu 170/110 160/110 160/110 160/100 150/90
10. 1812 Mrs. Santha 180/100 180/100 180/100 180/100 180/100
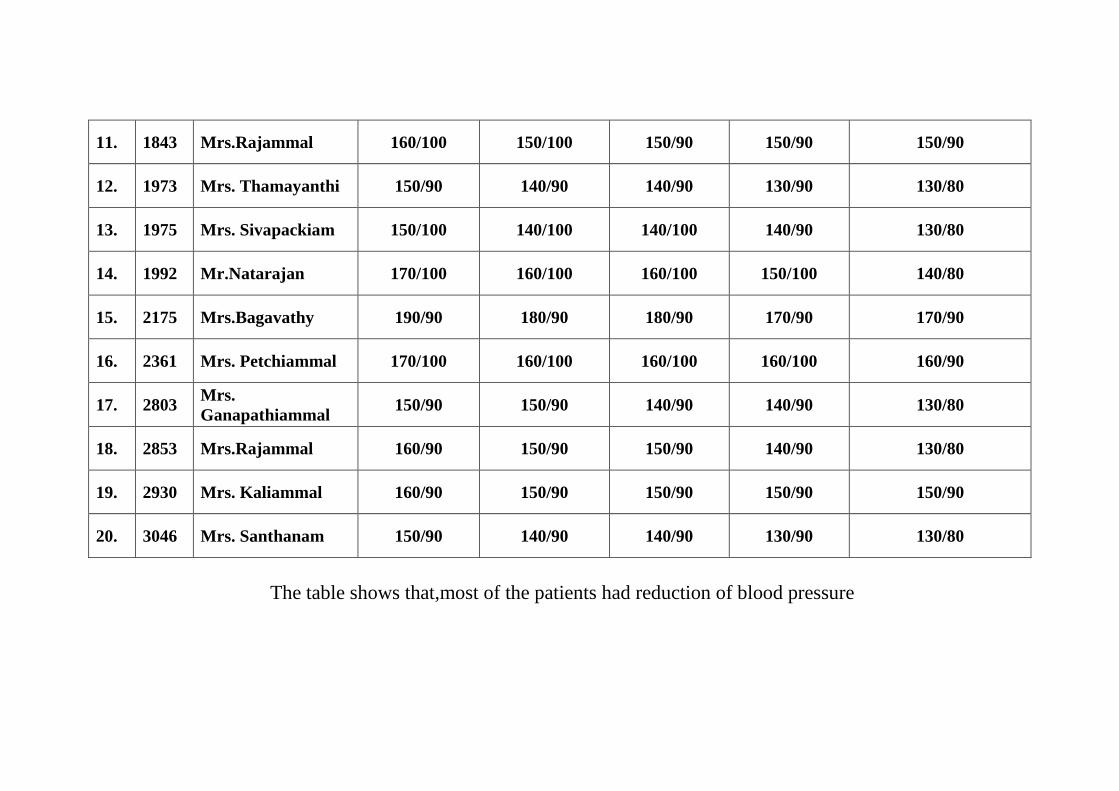
11. 1843 Mrs.Rajammal 160/100 150/100 150/90 150/90 150/90
12. 1973 Mrs. Thamayanthi 150/90 140/90 140/90 130/90 130/80
13. 1975 Mrs. Sivapackiam 150/100 140/100 140/100 140/90 130/80
14. 1992 Mr.Natarajan 170/100 160/100 160/100 150/100 140/80
15. 2175 Mrs.Bagavathy 190/90 180/90 180/90 170/90 170/90
16. 2361 Mrs. Petchiammal 170/100 160/100 160/100 160/100 160/90
17. 2803 Mrs. Ganapathiammal
150/90 150/90 140/90 140/90 130/80
18. 2853 Mrs.Rajammal 160/90 150/90 150/90 140/90 130/80
19. 2930 Mrs. Kaliammal 160/90 150/90 150/90 150/90 150/90
20. 3046 Mrs. Santhanam 150/90 140/90 140/90 130/90 130/80
The table shows that,most of the patients had reduction of blood pressure
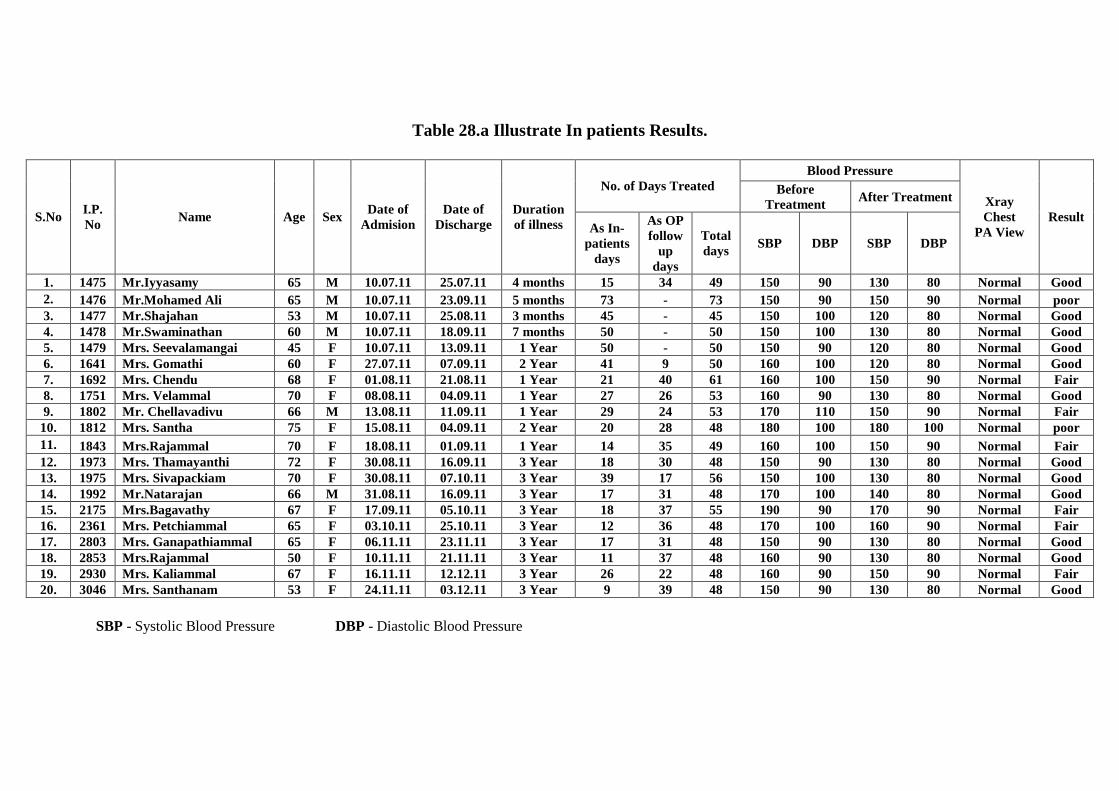
Table 28.a Illustrate In patients Results.
Blood Pressure No. of Days Treated Before
Treatment After Treatment
S.No I.P. No
Name Age Sex Date of
Admision Date of
Discharge Duration of illness As In-
patients days
As OP follow
up days
Total days
SBP DBP SBP DBP
Xray Chest
PA View Result
1. 1475 Mr.Iyyasamy 65 M 10.07.11 25.07.11 4 months 15 34 49 150 90 130 80 Normal Good 2. 1476 Mr.Mohamed Ali 65 M 10.07.11 23.09.11 5 months 73 - 73 150 90 150 90 Normal poor 3. 1477 Mr.Shajahan 53 M 10.07.11 25.08.11 3 months 45 - 45 150 100 120 80 Normal Good 4. 1478 Mr.Swaminathan 60 M 10.07.11 18.09.11 7 months 50 - 50 150 100 130 80 Normal Good 5. 1479 Mrs. Seevalamangai 45 F 10.07.11 13.09.11 1 Year 50 - 50 150 90 120 80 Normal Good 6. 1641 Mrs. Gomathi 60 F 27.07.11 07.09.11 2 Year 41 9 50 160 100 120 80 Normal Good 7. 1692 Mrs. Chendu 68 F 01.08.11 21.08.11 1 Year 21 40 61 160 100 150 90 Normal Fair 8. 1751 Mrs. Velammal 70 F 08.08.11 04.09.11 1 Year 27 26 53 160 90 130 80 Normal Good 9. 1802 Mr. Chellavadivu 66 M 13.08.11 11.09.11 1 Year 29 24 53 170 110 150 90 Normal Fair 10. 1812 Mrs. Santha 75 F 15.08.11 04.09.11 2 Year 20 28 48 180 100 180 100 Normal poor 11. 1843 Mrs.Rajammal 70 F 18.08.11 01.09.11 1 Year 14 35 49 160 100 150 90 Normal Fair 12. 1973 Mrs. Thamayanthi 72 F 30.08.11 16.09.11 3 Year 18 30 48 150 90 130 80 Normal Good 13. 1975 Mrs. Sivapackiam 70 F 30.08.11 07.10.11 3 Year 39 17 56 150 100 130 80 Normal Good 14. 1992 Mr.Natarajan 66 M 31.08.11 16.09.11 3 Year 17 31 48 170 100 140 80 Normal Good 15. 2175 Mrs.Bagavathy 67 F 17.09.11 05.10.11 3 Year 18 37 55 190 90 170 90 Normal Fair 16. 2361 Mrs. Petchiammal 65 F 03.10.11 25.10.11 3 Year 12 36 48 170 100 160 90 Normal Fair 17. 2803 Mrs. Ganapathiammal 65 F 06.11.11 23.11.11 3 Year 17 31 48 150 90 130 80 Normal Good 18. 2853 Mrs.Rajammal 50 F 10.11.11 21.11.11 3 Year 11 37 48 160 90 130 80 Normal Good 19. 2930 Mrs. Kaliammal 67 F 16.11.11 12.12.11 3 Year 26 22 48 160 90 150 90 Normal Fair 20. 3046 Mrs. Santhanam 53 F 24.11.11 03.12.11 3 Year 9 39 48 150 90 130 80 Normal Good
SBP - Systolic Blood Pressure DBP - Diastolic Blood Pressure
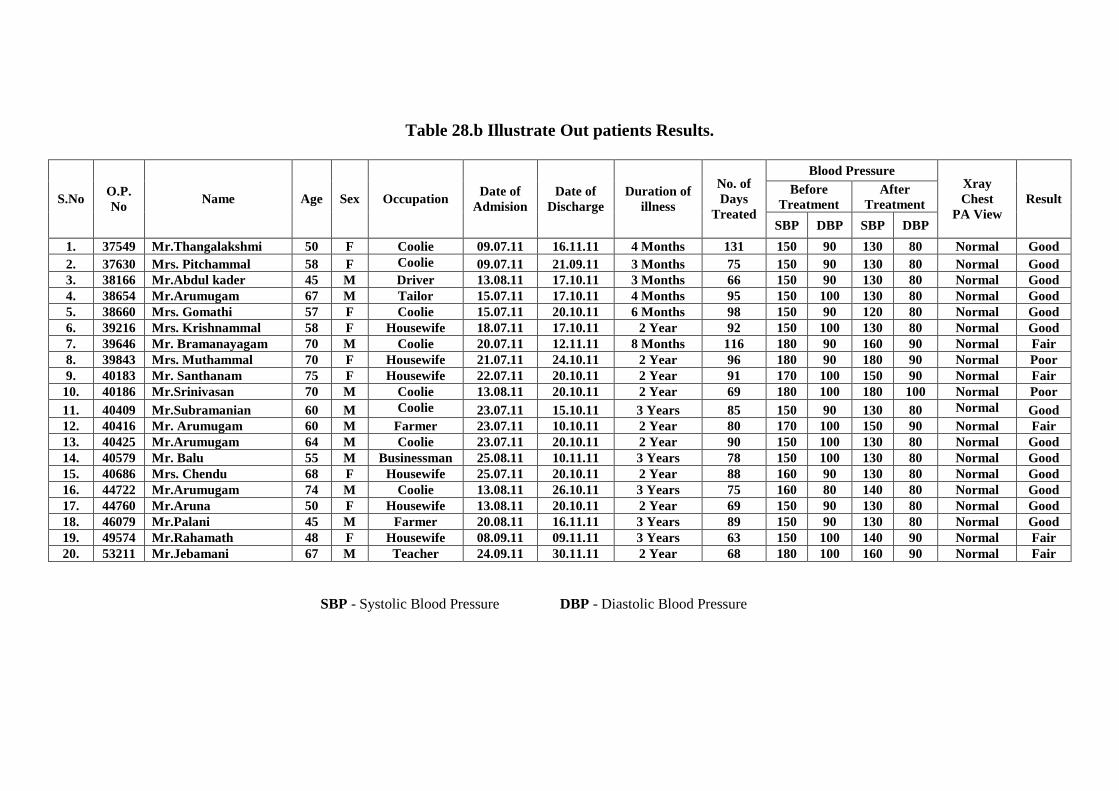
Table 28.b Illustrate Out patients Results.
Blood Pressure Before
Treatment After
Treatment S.No O.P. No
Name Age Sex Occupation Date of
Admision Date of
Discharge Duration of
illness
No. of Days
Treated SBP DBP SBP DBP
Xray Chest
PA View Result
1. 37549 Mr.Thangalakshmi 50 F Coolie 09.07.11 16.11.11 4 Months 131 150 90 130 80 Normal Good 2. 37630 Mrs. Pitchammal 58 F Coolie 09.07.11 21.09.11 3 Months 75 150 90 130 80 Normal Good 3. 38166 Mr.Abdul kader 45 M Driver 13.08.11 17.10.11 3 Months 66 150 90 130 80 Normal Good 4. 38654 Mr.Arumugam 67 M Tailor 15.07.11 17.10.11 4 Months 95 150 100 130 80 Normal Good 5. 38660 Mrs. Gomathi 57 F Coolie 15.07.11 20.10.11 6 Months 98 150 90 120 80 Normal Good 6. 39216 Mrs. Krishnammal 58 F Housewife 18.07.11 17.10.11 2 Year 92 150 100 130 80 Normal Good 7. 39646 Mr. Bramanayagam 70 M Coolie 20.07.11 12.11.11 8 Months 116 180 90 160 90 Normal Fair 8. 39843 Mrs. Muthammal 70 F Housewife 21.07.11 24.10.11 2 Year 96 180 90 180 90 Normal Poor 9. 40183 Mr. Santhanam 75 F Housewife 22.07.11 20.10.11 2 Year 91 170 100 150 90 Normal Fair 10. 40186 Mr.Srinivasan 70 M Coolie 13.08.11 20.10.11 2 Year 69 180 100 180 100 Normal Poor 11. 40409 Mr.Subramanian 60 M Coolie 23.07.11 15.10.11 3 Years 85 150 90 130 80 Normal Good 12. 40416 Mr. Arumugam 60 M Farmer 23.07.11 10.10.11 2 Year 80 170 100 150 90 Normal Fair 13. 40425 Mr.Arumugam 64 M Coolie 23.07.11 20.10.11 2 Year 90 150 100 130 80 Normal Good 14. 40579 Mr. Balu 55 M Businessman 25.08.11 10.11.11 3 Years 78 150 100 130 80 Normal Good 15. 40686 Mrs. Chendu 68 F Housewife 25.07.11 20.10.11 2 Year 88 160 90 130 80 Normal Good 16. 44722 Mr.Arumugam 74 M Coolie 13.08.11 26.10.11 3 Years 75 160 80 140 80 Normal Good 17. 44760 Mr.Aruna 50 F Housewife 13.08.11 20.10.11 2 Year 69 150 90 130 80 Normal Good 18. 46079 Mr.Palani 45 M Farmer 20.08.11 16.11.11 3 Years 89 150 90 130 80 Normal Good 19. 49574 Mr.Rahamath 48 F Housewife 08.09.11 09.11.11 3 Years 63 150 100 140 90 Normal Fair 20. 53211 Mr.Jebamani 67 M Teacher 24.09.11 30.11.11 2 Year 68 180 100 160 90 Normal Fair
SBP - Systolic Blood Pressure DBP - Diastolic Blood Pressure
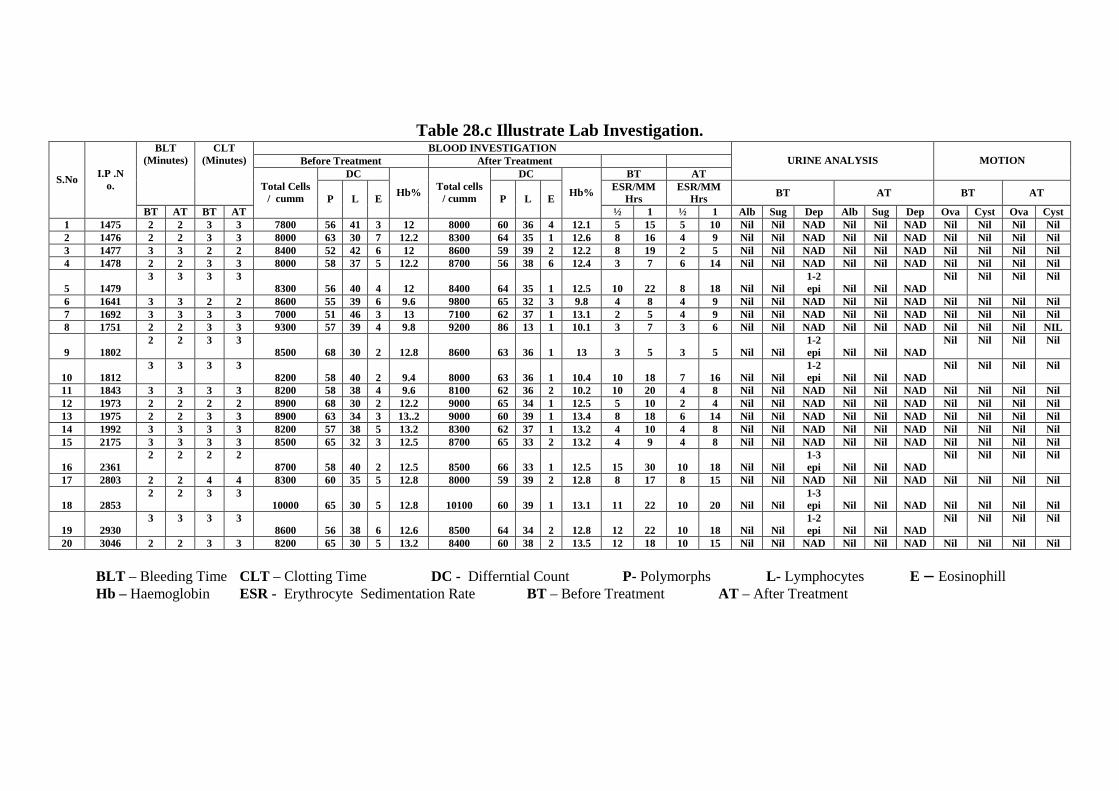
Table 28.c Illustrate Lab Investigation.
BLOOD INVESTIGATION Before Treatment After Treatment
DC DC BT AT URINE ANALYSIS MOTION
BLT (Minutes)
CLT (Minutes)
ESR/MM Hrs
ESR/MM Hrs BT AT BT AT
S.No I.P .N o.
BT AT BT AT
Total Cells / cumm P L E
Hb% Total cells / cumm P L E
Hb%
½ 1 ½ 1 Alb Sug Dep Alb Sug Dep Ova Cyst Ova Cyst 1 1475 2 2 3 3 7800 56 41 3 12 8000 60 36 4 12.1 5 15 5 10 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 2 1476 2 2 3 3 8000 63 30 7 12.2 8300 64 35 1 12.6 8 16 4 9 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 3 1477 3 3 2 2 8400 52 42 6 12 8600 59 39 2 12.2 8 19 2 5 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 4 1478 2 2 3 3 8000 58 37 5 12.2 8700 56 38 6 12.4 3 7 6 14 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil
5 1479 3 3 3 3
8300 56 40 4 12 8400 64 35 1 12.5 10 22 8 18 Nil Nil 1-2 epi Nil Nil NAD
Nil Nil Nil Nil
6 1641 3 3 2 2 8600 55 39 6 9.6 9800 65 32 3 9.8 4 8 4 9 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 7 1692 3 3 3 3 7000 51 46 3 13 7100 62 37 1 13.1 2 5 4 9 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 8 1751 2 2 3 3 9300 57 39 4 9.8 9200 86 13 1 10.1 3 7 3 6 Nil Nil NAD Nil Nil NAD Nil Nil Nil NIL
9 1802 2 2 3 3
8500 68 30 2 12.8 8600 63 36 1 13 3 5 3 5 Nil Nil 1-2 epi Nil Nil NAD
Nil Nil Nil Nil
10 1812 3 3 3 3
8200 58 40 2 9.4 8000 63 36 1 10.4 10 18 7 16 Nil Nil 1-2 epi Nil Nil NAD
Nil Nil Nil Nil
11 1843 3 3 3 3 8200 58 38 4 9.6 8100 62 36 2 10.2 10 20 4 8 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 12 1973 2 2 2 2 8900 68 30 2 12.2 9000 65 34 1 12.5 5 10 2 4 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 13 1975 2 2 3 3 8900 63 34 3 13..2 9000 60 39 1 13.4 8 18 6 14 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 14 1992 3 3 3 3 8200 57 38 5 13.2 8300 62 37 1 13.2 4 10 4 8 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 15 2175 3 3 3 3 8500 65 32 3 12.5 8700 65 33 2 13.2 4 9 4 8 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil
16 2361 2 2 2 2
8700 58 40 2 12.5 8500 66 33 1 12.5 15 30 10 18 Nil Nil 1-3 epi Nil Nil NAD
Nil Nil Nil Nil
17 2803 2 2 4 4 8300 60 35 5 12.8 8000 59 39 2 12.8 8 17 8 15 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil
18 2853 2 2 3 3
10000 65 30 5 12.8 10100 60 39 1 13.1 11 22 10 20 Nil Nil 1-3 epi Nil Nil NAD Nil Nil Nil Nil
19 2930 3 3 3 3
8600 56 38 6 12.6 8500 64 34 2 12.8 12 22 10 18 Nil Nil 1-2 epi Nil Nil NAD
Nil Nil Nil Nil
20 3046 2 2 3 3 8200 65 30 5 13.2 8400 60 38 2 13.5 12 18 10 15 Nil Nil NAD Nil Nil NAD Nil Nil Nil Ni l
BLT – Bleeding Time CLT – Clotting Time DC - Differntial Count P- Polymorphs L- Lymphocytes E – Eosinophill Hb – Haemoglobin ESR - Erythrocyte Sedimentation Rate BT – Before Treatment AT – After Treatment
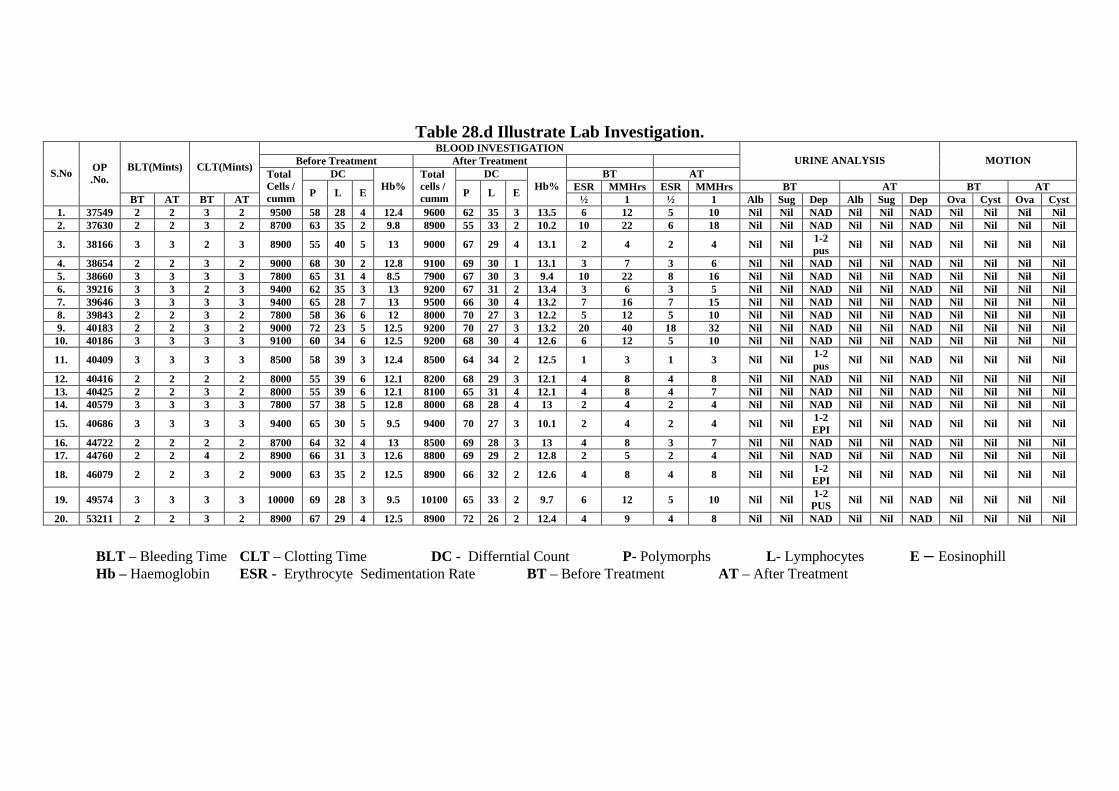
Table 28.d Illustrate Lab Investigation. BLOOD INVESTIGATION
Before Treatment After Treatment DC DC BT AT
URINE ANALYSIS MOTION BLT(Mints) CLT(Mints)
ESR MMHrs ESR MMHrs BT AT BT AT S.No OP
.No.
BT AT BT AT
Total Cells / cumm P L E
Hb% Total cells / cumm P L E
Hb% ½ 1 ½ 1 Alb Sug Dep Alb Sug Dep Ova Cyst Ova Cyst
1. 37549 2 2 3 2 9500 58 28 4 12.4 9600 62 35 3 13.5 6 12 5 10 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 2. 37630 2 2 3 2 8700 63 35 2 9.8 8900 55 33 2 10.2 10 22 6 18 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil
3. 38166 3 3 2 3 8900 55 40 5 13 9000 67 29 4 13.1 2 4 2 4 Nil Nil 1-2 pus
Nil Nil NAD Nil Nil Nil Nil
4. 38654 2 2 3 2 9000 68 30 2 12.8 9100 69 30 1 13.1 3 7 3 6 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 5. 38660 3 3 3 3 7800 65 31 4 8.5 7900 67 30 3 9.4 10 22 8 16 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 6. 39216 3 3 2 3 9400 62 35 3 13 9200 67 31 2 13.4 3 6 3 5 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 7. 39646 3 3 3 3 9400 65 28 7 13 9500 66 30 4 13.2 7 16 7 15 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 8. 39843 2 2 3 2 7800 58 36 6 12 8000 70 27 3 12.2 5 12 5 10 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 9. 40183 2 2 3 2 9000 72 23 5 12.5 9200 70 27 3 13.2 20 40 18 32 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 10. 40186 3 3 3 3 9100 60 34 6 12.5 9200 68 30 4 12.6 6 12 5 10 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil
11. 40409 3 3 3 3 8500 58 39 3 12.4 8500 64 34 2 12.5 1 3 1 3 Nil Nil 1-2 pus
Nil Nil NAD Nil Nil Nil Nil
12. 40416 2 2 2 2 8000 55 39 6 12.1 8200 68 29 3 12.1 4 8 4 8 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 13. 40425 2 2 3 2 8000 55 39 6 12.1 8100 65 31 4 12.1 4 8 4 7 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 14. 40579 3 3 3 3 7800 57 38 5 12.8 8000 68 28 4 13 2 4 2 4 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil
15. 40686 3 3 3 3 9400 65 30 5 9.5 9400 70 27 3 10.1 2 4 2 4 Nil Nil 1-2 EPI
Nil Nil NAD Nil Nil Nil Nil
16. 44722 2 2 2 2 8700 64 32 4 13 8500 69 28 3 13 4 8 3 7 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil 17. 44760 2 2 4 2 8900 66 31 3 12.6 8800 69 29 2 12.8 2 5 2 4 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil
18. 46079 2 2 3 2 9000 63 35 2 12.5 8900 66 32 2 12.6 4 8 4 8 Nil Nil 1-2 EPI
Nil Nil NAD Nil Nil Nil Nil
19. 49574 3 3 3 3 10000 69 28 3 9.5 10100 65 33 2 9.7 6 12 5 10 Nil Nil 1-2 PUS Nil Nil NAD Nil Nil Nil Nil
20. 53211 2 2 3 2 8900 67 29 4 12.5 8900 72 26 2 12.4 4 9 4 8 Nil Nil NAD Nil Nil NAD Nil Nil Nil Nil
BLT – Bleeding Time CLT – Clotting Time DC - Differntial Count P- Polymorphs L- Lymphocytes E – Eosinophill Hb – Haemoglobin ESR - Erythrocyte Sedimentation Rate BT – Before Treatment AT – After Treatment
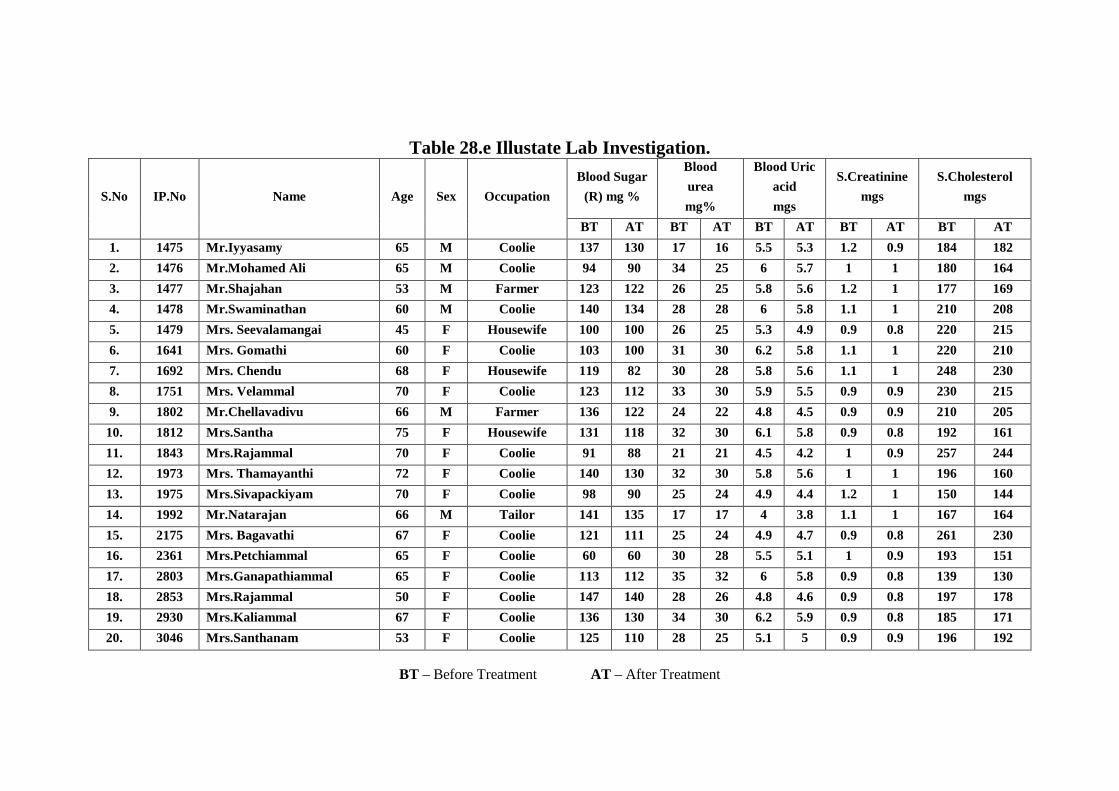
Table 28.e Illustate Lab Investigation.
Blood Sugar
(R) mg %
Blood
urea
mg%
Blood Uric
acid
mgs
S.Creatinine
mgs
S.Cholesterol
mgs S.No IP.No Name Age Sex Occupation
BT AT BT AT BT AT BT AT BT AT
1. 1475 Mr.Iyyasamy 65 M Coolie 137 130 17 16 5.5 5.3 1.2 0.9 184 182
2. 1476 Mr.Mohamed Ali 65 M Coolie 94 90 34 25 6 5.7 1 1 180 164
3. 1477 Mr.Shajahan 53 M Farmer 123 122 26 25 5.8 5.6 1.2 1 177 169
4. 1478 Mr.Swaminathan 60 M Coolie 140 134 28 28 6 5.8 1.1 1 210 208
5. 1479 Mrs. Seevalamangai 45 F Housewife 100 100 26 25 5.3 4.9 0.9 0.8 220 215
6. 1641 Mrs. Gomathi 60 F Coolie 103 100 31 30 6.2 5.8 1.1 1 220 210
7. 1692 Mrs. Chendu 68 F Housewife 119 82 30 28 5.8 5.6 1.1 1 248 230
8. 1751 Mrs. Velammal 70 F Coolie 123 112 33 30 5.9 5.5 0.9 0.9 230 215
9. 1802 Mr.Chellavadivu 66 M Farmer 136 122 24 22 4.8 4.5 0.9 0.9 210 205
10. 1812 Mrs.Santha 75 F Housewife 131 118 32 30 6.1 5.8 0.9 0.8 192 161
11. 1843 Mrs.Rajammal 70 F Coolie 91 88 21 21 4.5 4.2 1 0.9 257 244
12. 1973 Mrs. Thamayanthi 72 F Coolie 140 130 32 30 5.8 5.6 1 1 196 160
13. 1975 Mrs.Sivapackiyam 70 F Coolie 98 90 25 24 4.9 4.4 1.2 1 150 144
14. 1992 Mr.Natarajan 66 M Tailor 141 135 17 17 4 3.8 1.1 1 167 164
15. 2175 Mrs. Bagavathi 67 F Coolie 121 111 25 24 4.9 4.7 0.9 0.8 261 230
16. 2361 Mrs.Petchiammal 65 F Coolie 60 60 30 28 5.5 5.1 1 0.9 193 151
17. 2803 Mrs.Ganapathiammal 65 F Coolie 113 112 35 32 6 5.8 0.9 0.8 139 130
18. 2853 Mrs.Rajammal 50 F Coolie 147 140 28 26 4.8 4.6 0.9 0.8 197 178
19. 2930 Mrs.Kaliammal 67 F Coolie 136 130 34 30 6.2 5.9 0.9 0.8 185 171
20. 3046 Mrs.Santhanam 53 F Coolie 125 110 28 25 5.1 5 0.9 0.9 196 192
BT – Before Treatment AT – After Treatment
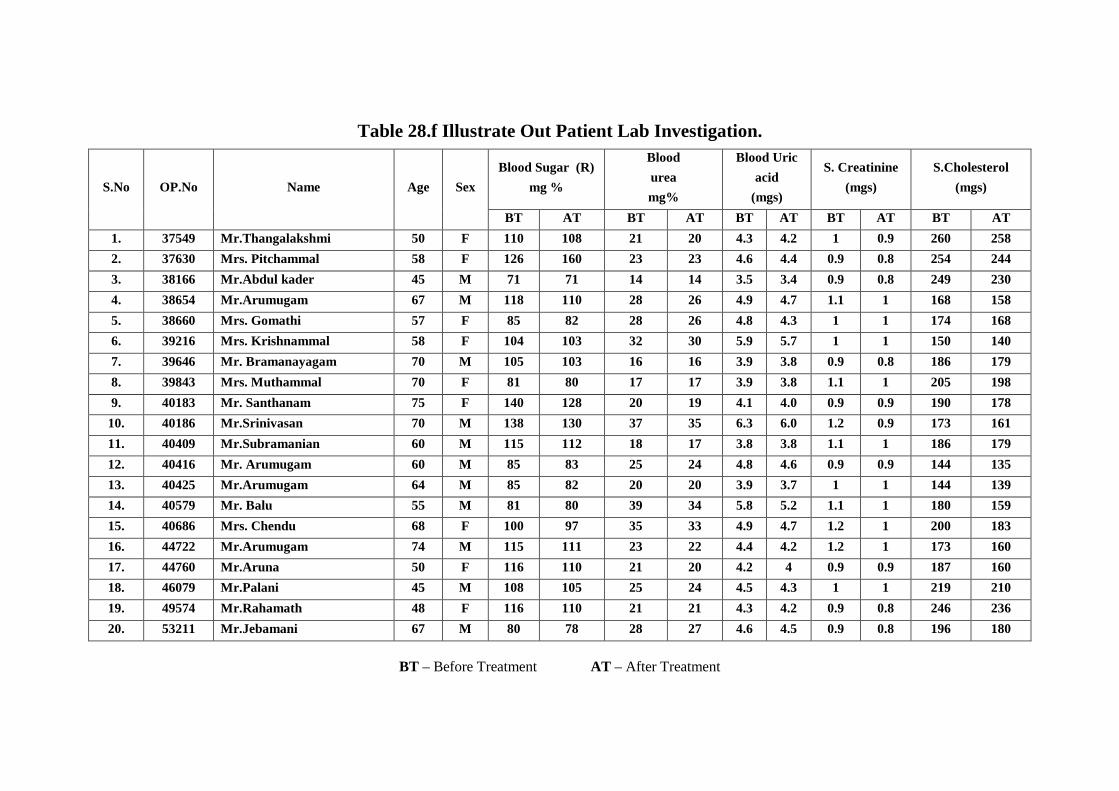
Table 28.f Illustrate Out Patient Lab Investigation.
Blood Sugar (R)
mg %
Blood
urea
mg%
Blood Uric
acid
(mgs)
S. Creatinine
(mgs)
S.Cholesterol
(mgs) S.No OP.No Name Age Sex
BT AT BT AT BT AT BT AT BT AT
1. 37549 Mr.Thangalakshmi 50 F 110 108 21 20 4.3 4.2 1 0.9 260 258
2. 37630 Mrs. Pitchammal 58 F 126 160 23 23 4.6 4.4 0.9 0.8 254 244
3. 38166 Mr.Abdul kader 45 M 71 71 14 14 3.5 3.4 0.9 0.8 249 230
4. 38654 Mr.Arumugam 67 M 118 110 28 26 4.9 4.7 1.1 1 168 158
5. 38660 Mrs. Gomathi 57 F 85 82 28 26 4.8 4.3 1 1 174 168
6. 39216 Mrs. Krishnammal 58 F 104 103 32 30 5.9 5.7 1 1 150 140
7. 39646 Mr. Bramanayagam 70 M 105 103 16 16 3.9 3.8 0.9 0.8 186 179
8. 39843 Mrs. Muthammal 70 F 81 80 17 17 3.9 3.8 1.1 1 205 198
9. 40183 Mr. Santhanam 75 F 140 128 20 19 4.1 4.0 0.9 0.9 190 178
10. 40186 Mr.Srinivasan 70 M 138 130 37 35 6.3 6.0 1.2 0.9 173 161
11. 40409 Mr.Subramanian 60 M 115 112 18 17 3.8 3.8 1.1 1 186 179
12. 40416 Mr. Arumugam 60 M 85 83 25 24 4.8 4.6 0.9 0.9 144 135
13. 40425 Mr.Arumugam 64 M 85 82 20 20 3.9 3.7 1 1 144 139
14. 40579 Mr. Balu 55 M 81 80 39 34 5.8 5.2 1.1 1 180 159
15. 40686 Mrs. Chendu 68 F 100 97 35 33 4.9 4.7 1.2 1 200 183
16. 44722 Mr.Arumugam 74 M 115 111 23 22 4.4 4.2 1.2 1 173 160
17. 44760 Mr.Aruna 50 F 116 110 21 20 4.2 4 0.9 0.9 187 160
18. 46079 Mr.Palani 45 M 108 105 25 24 4.5 4.3 1 1 219 210
19. 49574 Mr.Rahamath 48 F 116 110 21 21 4.3 4.2 0.9 0.8 246 236
20. 53211 Mr.Jebamani 67 M 80 78 28 27 4.6 4.5 0.9 0.8 196 180
BT – Before Treatment AT – After Treatment
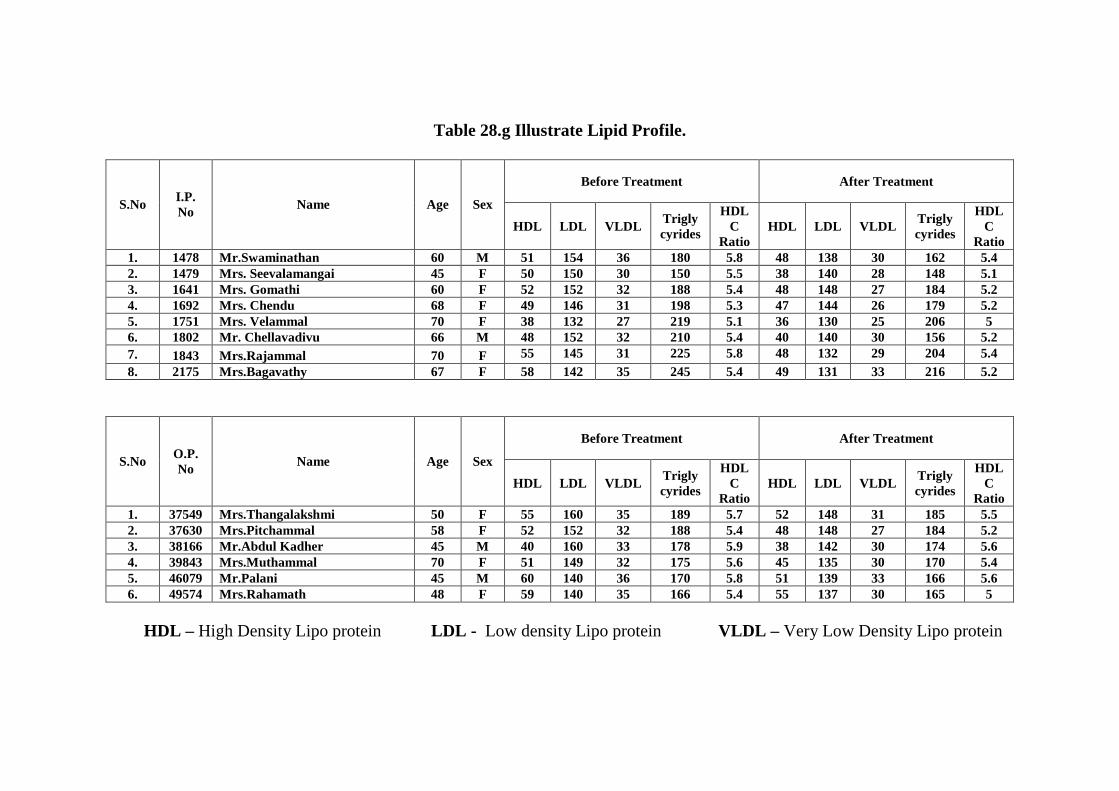
Table 28.g Illustrate Lipid Profile.
Before Treatment After Treatment
S.No I.P. No
Name Age Sex
HDL LDL VLDL Trigly cyrides
HDL C
Ratio HDL LDL VLDL
Trigly cyrides
HDL C
Ratio 1. 1478 Mr.Swaminathan 60 M 51 154 36 180 5.8 48 138 30 162 5.4 2. 1479 Mrs. Seevalamangai 45 F 50 150 30 150 5.5 38 140 28 148 5.1 3. 1641 Mrs. Gomathi 60 F 52 152 32 188 5.4 48 148 27 184 5.2 4. 1692 Mrs. Chendu 68 F 49 146 31 198 5.3 47 144 26 179 5.2 5. 1751 Mrs. Velammal 70 F 38 132 27 219 5.1 36 130 25 206 5 6. 1802 Mr. Chellavadivu 66 M 48 152 32 210 5.4 40 140 30 156 5.2 7. 1843 Mrs.Rajammal 70 F 55 145 31 225 5.8 48 132 29 204 5.4 8. 2175 Mrs.Bagavathy 67 F 58 142 35 245 5.4 49 131 33 216 5.2
Before Treatment After Treatment
S.No O.P. No
Name Age Sex
HDL LDL VLDL Trigly cyrides
HDL C
Ratio HDL LDL VLDL
Trigly cyrides
HDL C
Ratio 1. 37549 Mrs.Thangalakshmi 50 F 55 160 35 189 5.7 52 148 31 185 5.5 2. 37630 Mrs.Pitchammal 58 F 52 152 32 188 5.4 48 148 27 184 5.2 3. 38166 Mr.Abdul Kadher 45 M 40 160 33 178 5.9 38 142 30 174 5.6 4. 39843 Mrs.Muthammal 70 F 51 149 32 175 5.6 45 135 30 170 5.4 5. 46079 Mr.Palani 45 M 60 140 36 170 5.8 51 139 33 166 5.6 6. 49574 Mrs.Rahamath 48 F 59 140 35 166 5.4 55 137 30 165 5
HDL – High Density Lipo protein LDL - Low density Lipo protein VLDL – Very Low Density Lipo protein
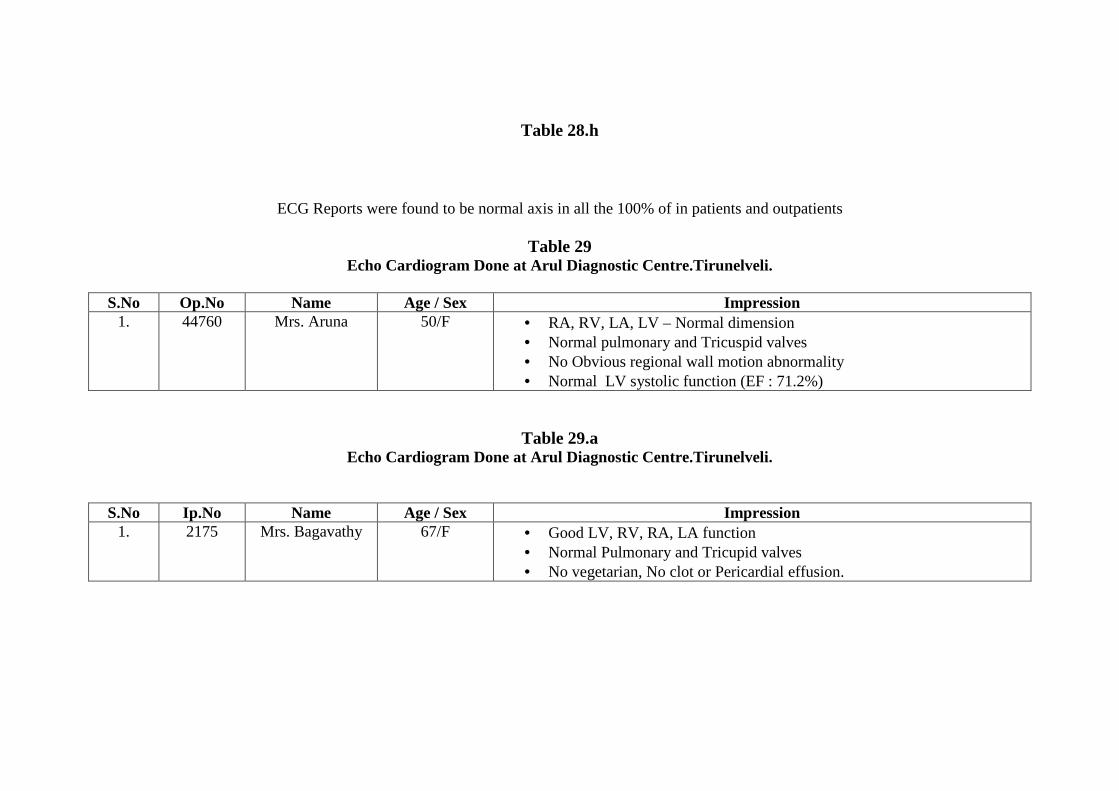
Table 28.h
ECG Reports were found to be normal axis in all the 100% of in patients and outpatients
Table 29 Echo Cardiogram Done at Arul Diagnostic Centre.Tirunelveli.
S.No Op.No Name Age / Sex Impression
1. 44760 Mrs. Aruna 50/F • RA, RV, LA, LV – Normal dimension • Normal pulmonary and Tricuspid valves • No Obvious regional wall motion abnormality • Normal LV systolic function (EF : 71.2%)
Table 29.a Echo Cardiogram Done at Arul Diagnostic Centre.Tirunelveli.
S.No Ip.No Name Age / Sex Impression 1. 2175 Mrs. Bagavathy 67/F • Good LV, RV, RA, LA function
• Normal Pulmonary and Tricupid valves • No vegetarian, No clot or Pericardial effusion.

140
GRADATION OF RESULTS Table 30
In-patients Out Patients S.No Result
No. of Cases Percentage (%) No. of Cases Percentage (%) 1. Good 12 60 13 65 2. Fair 6 30 5 25 3. Poor 2 10 2 10
This table showed that In Ip 60% of the patient had Good result,30% had Fair result,10% had Poor result.In Op,65% of the patient had
Good result,25% had Fair result and 10%had Poor result.
Assessment of result
GOOD : Complete dissaperance of giddiness, restoration of normal Blood Pressure. FAIR : Moderate disapperance of giddness, moderate control of
Blood Pressure.
POOR : Uncontrlled Blood Pressure.
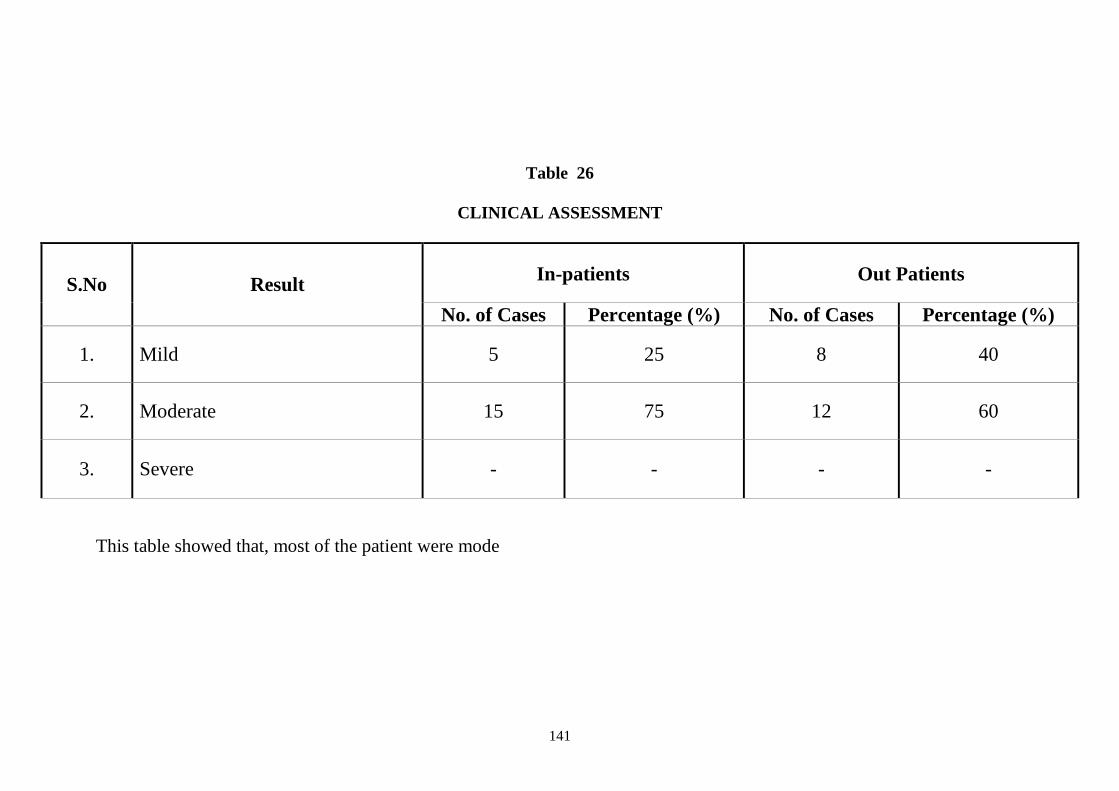
141
Table 26
CLINICAL ASSESSMENT
In-patients Out Patients S.No Result
No. of Cases Percentage (%) No. of Cases Percentage (%)
1. Mild 5 25 8 40
2. Moderate 15 75 12 60
3. Severe - - - -
This table showed that, most of the patient were mode
142
117
118

119
Discussion
120
DISCUSSION
Vatha Pitham as said in Yugi Vaidhya Chinthamani – 800 more or
less clinically correlate with Hypertension.
Hypertension is evolving high mortality especially as cardio-vascular
and cerebro-vascular diseases. Nowadays most of this problems are due to
increased stress and strain, lack of exercise, irregular dietary habits,
sedantary life etc.
As per recent studies, both systolic and diastolic pressures are equally
important and treated carefully.
The present study is a preliminary study. 20 patients of both sex were
admitted in the In-patient and 20 patients of both sex were treated in Out
patient in Post Graduate department of Govt. Siddha Medical college,
Palayamkottai and they were given the trial drug.
1.Sex distribution :
In IP, Out of 20 cases, 30% belong to Male and 70% belong to female.
In OP, Out of 20 cases, 55% belongs to male and 45% belongs to
female. It indicates that Vatha Pitham was common in both sex.
2.Age distribution :
In IP out of 20 cases, 5% cases were in the age between 41-45yrs,
5% between 46-50yrs, 10% between 51-55yrs and 10% between 56-60yrs,
and 20% between 61-65yrs, 30% between 66-70yrs and 20% between 71 –
75 years.
In OP out of 20 cases, 10% cases were in the age between 41-45yrs,
15% between 46-50yrs, 5% between 51-55yrs and 25% between 56-60yrs,
and 5% between 61-65yrs,30% between 66-70yrs and 10% between
71 – 75 years.
So the incidence of this disease was common in the elderly people age
group 50 – 70 years.
121
3. Constitution of body :
In IP out of 20 cases 10% of the patients were Vadha theki,
70% Pitha theki and 20% Kaba theki.
In OP out of 20 cases 20% of the patients were Vadha theki,
70% Pitha theki and 10% Kaba theki.So most of the patients wee pitha thegi.
4.Mukutra Kaalagal :
In IP Among 20 cases, 50% were found in the Pitha Kaalam and 50% in
the Kaba Kaalam.
In OP Among 20 cases, 85% were found in the Pitha Kaalam and 15% in
the Kaba Kaalam
So the disease was predominantly found in Pitha Kaalam.
5. Religious distribution :
In OP and IP 85% were Hindus, 10% Muslims and 5% were
Christians.
So Vatha pitham was commonly affected in Hindus.
6.Thinai :
In OP and IP 100% cases belonged to Marutham. So most of the cases
were found Marutham.
7.Paruva Kaalam :
In IP out of 20 cases, 35% were admitted in the Kaar Kaalam and
15% in the Koothir Kaalam, 50% were admitted in Muduvenil Kaalam
In OP out of 20 cases, 20% were admitted in the Kaar Kaalam,
80% were admitted in Muduvenil Kaalam
So most of the cases were admitted in the Mudhuvenil Kaalam.
8. Sirupozhuthu:
In IP out of 20 cases, 80% of the patients showed the prevalence of
disease during vaigarai pozhuthu, 20% of the patients shouwed the
prevalence of disease during malai pozhuthu.
In OP out of 20 cases, 75% of the patients showed the prevalence of
disease during vaigarai pozhuthu, 25% of the patients shouwed the
prevalence of disease during malai pozhuthu.
122
So the prevalence of disease during vaigarai poluthu.
9.Occupational Status:
In IP Out of 20 cases, 70% belonged to coolies, 15% house-wives,
10% farmer and 5% tailor.
In OP Out of 20 cases, 40% belonged to coolies, 30% house-wives,
5% driver, 10% farmer, 5% tailor, 5% teacher and 5% businessman.
So Vatha pitham was found increased incidence in coolies
10.Socio-economic status :
In IP 20% belonged to middle class and 80% belonged to poor class.
In OP 25% belonged to middle class and 75% belonged to poor class.
So this disease can occur in poor class of the society.
11. Risk factors:
In IP 40% of the cases were smokers, 10% Alcoholic, 30% Obese,
40% hyper lipedimic.
In OP 90% of the cases were smokers, 50% Alcoholic, 35% Obese,
30% hyper lipedimic.
So Smoking was the main risk factor among the patients.
12. Clinical features:
In IP 80% had giddiness, 90% had fatigue, 75% had Occipital
headache, 80% had sleeplessness, 50% had weakness, 75% had palpitation,
20% had visual defects, 75% had emotional stress, 60% had fear& anxiety
and 50% had loss of appetite.
In OP 80% had giddiness, 85% had fatigue, 85% had Occipital
headache, 75% had sleeplessness, 40% had weakness, 60% had palpitation,
25% had visual defects, 85% had emotional stress, 75% had fear& anxiety
and 60% had loss of appetite.
So Vatha Pitham can be presented as a spectrum of symptoms but
commonly giddiness, fatigue and sleeplessness.
123
13. Duration of illness
In IP Out of 20 cases, 15% of patients have the incidence for the
duration of 3- 6 months, 10% of the patient have the incidence for the
duration of 6 months to 1 year, 30% of the patients have the incidence for
the duration of 1-2 years, 45% of the patients have the incidence for the
duration of 2 – 3 years.
In OP Out of 20 case, 20% of patients have the incidence for the
duration of 3- 6 months, 10% of the patient have the incidence for the
duration of 6 months to 1 year, 45% of the patients have the incidence for
the duration of 1-2 years, 25% of the patients have the incidence for the
duration of 2 – 3 years.
So among the patients, the highest incidence of the disease is from 1-
2yrs & 2-3yrs.
14. Other systems involved :
In IP out of 20 cases 75% of cases co-existed with musculo skeletal
system involvement.
In OP out of 20 cases 80% of cases co-existed with musculo skeletal
system involvement.
15. Family History:
In IP out of 20 cases, 20% of the cases had positive family history,
30% of cases had positive previous history, 50% of the cases had
miscellaneous history
In OP 10% of the patients had positive family history, 20% of patients
had positive previous history, 70% of the patients had miscellaneious
history.So most of the patient had miscellaneous history.
16. Diet factors:
In OP and IP 95% were mixed diet. and 5% vegetarian. So most of
the cases were mixed diet.
124
17.Habitual history:
In IP out of 20 cases, 30% were smoker, 10% were tobaco chewer,
25% were betel nut chewer, 30% were alchoholic, 25% were no such a
habit.
In OP out of 20 cases, 55% were smoker, 5% were tobaco chewer,
25% were betel nut chewer, 30% were alchoholic, 20% were no such a
habit.So the highest incidence is smoker and alcoholic.
18. Imporigal (Gnanenthirium)
In IP out of 20 cases, 20% of the patient affected with Kann.
In OP out of 20 cases, 25% of the patient affected with Kann.
So Kann was affected in most of the patients.
19.Kanmenthriam:
In IP out of 20 cases, 25% patients were affected with kai, 50% of the
patients were affected with kaal, 25% of the patients were affected with
eruvai.
In OP out of 20 cases, 20% patients were affected with kai, 60% of
the patients were affected with kaal, 20% of the patients were affected with
eruvai.
So Kaal was affected in most of the patients.
20. Kosam:
In IP out of 20 cases, 50% of patients were affected with
annamayakosam, In OP 60% of cases were affected with annamayakosam.
So annamayakosam was affected in most of the patients.
21. Tridhosa theory:
a. Disturbances in vatham :
In IP 50% cases had derangement in Pranan, 25% Abanan, 75% Viyanan
100% Samanan, 10% Udanan, 20% Koorman, 20% Kirukaran and 75%
Devathathan.
125
In OP 60% cases had derangement in Pranan, 25% Abanan, 80%
Viyanan, 15% Udanan, 100% Samanan, 25% Koorman, 25% Kirukaran and
60% Devathathan.
• Affected Pranan can produced loss of appetite.
• Affected Abanan can produced constipation.
• Affected Viyanan can produced malaise, fatigue, neuralgic pain etc.
• Affected Uthanan can produced nausea and vomiting.
• Affected Samanan can produced loss of appetite and taste
disturbances.
• Affected Koorman can produced altered sensorium, horipliation and
blurring of vision.
• Affected Kirukaran produced body pain and tiredness.
• Affected Devathathan can produced malaise, fatigue, sleeplessness
and anxiety.
B. Disturbances in pitham :
In IP 50% had derangement in Anal pitham, 10% Ranjagam, 100%
Sathagam, 20% Alosagam and 10% Prasagam.
In OP 60% had derangement in Anal pitham, 15% Ranjagam, 100%
Sathagam, 25% Alosagam and 15% Prasagam.
• Affected Anal pitham can producesdloss of appetite.
• Affected Ranjaga pitham can produced pallor of nailbed, skin and
conjunctiva, reduced haemoglobin.
• Affected Sathaga pitham can produced mental confusion and difficulty
in concentration.
• Affected Alosaga pitham can produced blurring of vision.
• Affected Prasaga pitham can produced pallor of skin.
126
c. Disturbances in Kabam :
In IP 75% had derangement in Avalambagam, 50% Kilethagam, 75%
Santhigam
In OP 80% had derangement in Avalambagam, 60% Kilethagam, 80%
Santhigam
• Affected Avalambagam can produced derangement of other kabhas
• Affected Santhigam can produced difficulty in joint movements.
• Affected Kilethagam can produced loss of apetite.
22. Seven udal kattugal :
In IP Out of 20 cases, 100% had disturbances in saaram and senneer,
30% kozhuppu, 75% enbu.
In OP Out of 20 cases, 100% had disturbances in saaram and senneer,
30% kozhuppu, 80% enbu.
• Affected saaram can produced weakness of the body and mind, fear
and anxiety.
• Affected senneer can produced derangements in pitham.
• Affected kozhuppu can produced obesity, hypercholesteraemia.
• Affected Enbu can produced difficulty in range of movements, joint
pain.
23. Envagai thervugal :
In IP 50% of the cases had pitha vatha nadi, 50% had vatha pitha
nadi, 10% naa and niram, 20% vizhi and 25% malam were affected.
In OP 40% of the cases had pitha vatha nadi, 60% had vatha pitha
nadi, 15% naa and niram, 25% vizhi and 25% malam were affected.
• Affected naa and niram can produced paleness.
• Affected vizhi can produced blurring of vision, redness of eyes.
• Affected malam can produced constipation.
127
24. Neerkuri
In neerkuri, miram, manam, edai, nurai and enjal were not affected in
all the patients.
25. Neikuri
In IP neikuri, 95% had pitha neer and 5% had vatha neer.
In OP 100% had pitha neer.
26. Clinical Assessment
In IP out of 20 cases 25% mild blood pressure, 75% Moderate blood
pressure
In OP out of 20 cases 40% mild and 60% Moderate blood pressure.
27. Effect of blood pressure:
From the table 27,In Ip and Op, it is observed that,all the patients had
marked reduction of blood pressure at the time of discharge
28. Lab investigation and ECG report:
From the table 28a to 28h illustrate lab investigation.
29. ECHO:
From the table 29,it is observed that normal impression in the Echo-
cardiogram
30. Gradation of results:
In IP 60% of the patients had good results, 30% of the patients had fair
and 10% of the patients had poor results.
In OP 65% of the patients had good results, 25% of the patients had
fair and 10% of the patients had poor results.
Investigations :
Routine investigation of blood and urine were done during the time
of admission and discharge for all cases.
128
Urine examination in Ip & Op showed,Nil aibumin. 30% of patients
had deposits in before treatment. After treatment there was NAD(Nothing
Abnormal Deposits).
Blood investigation showed that, 30% raised Blood Urea and Serum
cholesterol before treatment.
After treatment, blood investigation showed that, moderate reduction
in Blood urea and mild reduction in Serum cholesterol .
Radiological investigation :
X-ray chest P.A. view was done for 80% of patients. For remaining
20% of the patients, X-ray was not taken due to inevitable conditions.No
abnormal findings can find out in all Chest X-Rays.
Modern Medicine comparision :
The signs and symptoms of Vatha Pitham as said in Yugi vaidhya
chindhamani-800 are closely matched with hypertension.
According to modern medicine literature survey, the causes of primary
hypertension may be smoking, alcohol, high fatty diet, altered life-style,
increased stress and strain both physically and mentally, Type-A personality
etc.
In siddha literature survey also the above causes are mentioned in the
Vatha pitham.
Management :
All the selected patients were administered to take the trial medicine
Iruveli Kiyalam 90 ml was given internally twice a day before food daily, till
discharge.
Clinically,My drug has proven, no side effects and no adverse effects
were observed.
129
Summary

130
SUMMARY
Vatha Pitham (Hypertension) is very common and its prevalence is
very much increased now. Most of the cases are not yet diagnosed. Most of
the cases present their symptoms in the later stage only. Vatha Pitham as
compared with Hypertension in Modern, should be properly screened,
diagnosed and treated as early as possible. If neglected, it produces
urgencies and emergencies.
So the author had worked on this subject very thoroughly and more
enthuciastically to help the suffering society.
Iruveli Kiyalam was taken as a trial drug for this clinical study.
The Aetiology, pathology, patho-physiology, classification, clinical
features, complication, prognosis, diagnosis, treatment and prevention of the
disease were collected from various literatures from Siddha system and
Modern system of Medicine.
In this study, 20 patients of both sex of varying age groups were
selected as In-patients and 20 patients as Out-patients.
From the observations and results, we were clear that, the disease was
common in the following aspects.
Age incidence was commonly found in 50-70yrs and it occurs in all
classes of people and mostly in mixed diet.
Hindus were affected more than the other religions. All the cases were
belong to marutha nilam. The patients suffered from giddiness, head ache,
fatiguability and sleeplessness.
In Uyir thathukal,
• Vatham had deranged. Vyanan was affected in all the patients.
• Pitham had deranged especially Analam, Ranjagam, Sathagam and
Alosagam.
131
• Kabam had deranged especially Avalambagam, Kiletham and
Santhigam.
In Seven udal kattugal, most of the cases had disturbances in saaram,
senneer and kozhuppu.
Signs and symptoms as mentioned in the case sheets was dealt in the
discussion.
Siddha diagnosis were made with the help of Envagai thervugal,
Neerkuri and Neikuri had showed derangement in Tri-dhosas. Naadi had
showed pitha vatham and vatha pitham.
The efficacy of the test drug, iruveli kiyalam was observed during the
period of study.
Iruveli kiyalam – 90ml twice daily before meals.
� Majority of the cases had shown marked reduction of blood pressure
and symptoms.
� The results of this clinical trial were found to be very encouraging in
almost every cases and there was marked improvement.
� All the In patients were instructed to follow up the treatment in the
Out patient.
� No recurrence occur during the treatment schedule.
� No side effects and adverse effects were noted during this period of
study.
� The trial drugs were found to play the major role to correct the
deranged three humours therby correcting Pranan, Abanan, Udhanan,
Vyanan, Samanan, Koorman, Kirugaran and Devathathan vayus and
Pitham such as Analam, Ranjagam, Sathagam, Aalosagam and
kabham such as Avalambagam, Kiletham and Santhigam is restored to
the normal.
� All the patient were advised to follows strict diet restrictions and
adviced to practice yoga and meditation therapy
132
� No cases had evidence of secondary hypertension clinically.
In modern views, routine B.P readings were taken regularly to assess
the improvement. Moreover routine blood, urine investigations were done.
Serum cholesterol, Blood urea, Blood sugar, Serum creatinine were also
done. ECG was taken in some patients. In radiological investigations, x-ray
chest P-A view.
Pharmacological evalution showed that the drug has got significant
diuretic action and there is no toxic effect in acute toxicity study.
Biochemical analysis showed the presence of starch, iron in ferrous
form, unsaturated compounds, reducing sugar amino-acids, calcium,
sulphate and chloride.
133
Conclusion
134
CONCLUSION
60% of In patient showed good results in this trial, 30% showed fair
results and the remaining 10% showed poor results. Among the out patients,
which are under this trail 65% of the subjects showed good results 25%
showed fair results and the remaining 10% showed poor results. The trial
drugs,
1. Iruveli Kiyalam has got the taste of Inippu and Kaarpu suvaigal.
2. Iruveli Kiyalam has got Thanmai - Thatpam
3. Iruveli Kiyalam has got Inippu pirivu.
The identification of suvai, thanmai and pirivu are on the basis of
individual ingredients of these preparations.
According to the basic principles of Siddha medicines as described by
the ancient sage Siddhars.
The taste, vital humours, the universal Pancha Boothas are closely
ralated to each other.
In this trial, the drug has got Inippu and Kaarpu suvaigal.
The Inippu suvai which decrease the excess of vatham & pitham.
‘gizpz<!fs<Sr<!!gckgx<Xl<”!
- sqk<k!lVk<Kuir<g!SVg<gl</!
The kaarpu suvai has got the principle to dilate the blood vessels and
prevent the obstruction in the blood vessel and to regulates the blood
circulation.
“ogiPh<jhBl<!yPg<gQcz<!upuPk<kqms<!osb<!
!ofb<h<jhBl<!ypqk<kqMl<!Jb!uqgivl<!
!npqk<kqMl<!fic!fit!njmh<hqjeg<!
!gpx<xqOb!kml<ohx!uqbx<Xr<!giIhiR<!
!Sjukjeg<!g{g<Ogi!M{<{qz<!
!fjubqjz!fzlil<!fzqbqjz!flg<Og”!
- sqk<k!lVk<Kuir<g!SVg<gl</!
135
Iruveli Kiyalam has got Thanmai Thatpam. The Thatpam has got the
action to decrease the excessive pitham those who are suffering from vitiated
pitham.
After the ingestion, these trial drug enter into gartric juice, it will
change into the vibagam. This in turn to change the taste into inippu and
kaarpu.
Inippu suvai which neutralize excessive vatha pitham.
Also Inipu suvai which neutralize excessive pitham.
‘gizpz<!fs<Sr<!gckgx<Xl<”!!
- sqk<k!lVk<Kuir<g!SVg<gl<!
!
The role of Thanmai veeriyam has got the action of antipitha effect.
In this trial the drugs present in Iruveli kiyalam has got significent
efficiency to treat vathapitham on the basis of their anti pitha prinicple.
I observed in many patients that, the blood pressure remained normal
even after 10 days of cessation of treatment. It shows the high bio-
availability of the kiyalam. So it can be used as one of the effective durgs to
treat high blood pressure in the siddha hospitals.
!
136
Annexure
Preparation and Properties
of The Trial Medicine
137
ANNEXURES - I
-VOuzq!gqbipl<!
! “wz<zif<!kie<!OhigouiV!gqbipR<osiz<Ou!
! ! eqVOuzq!lKvLmeqR<sq!!&e<Xf<!
! osiz<zilz<!ujgg<Gg<gix<!hzlib<k<K~g<gqs<!
! ! Sglig!uqVfipq!fQiqzqm<M!
! ouz<zOu!kQobiqk<K!obm<omie<xig<gq!
! ! uQxigh<!hk<Kfim<!ogit<uibieiz<!
! uz<zokiV!uikhqk<kR<!Osijghi{<M!
! ! uir<gquqMl<!nOvisqgLl<!uiviokie<Oe!”
- ngk<kqbi<!juk<kqb!H,v{l<!316!
Preparation of the trial drug:-
Ingredients:
Roots of Iruveli (Coleus Forskholii)
Adhimadhuram (Glycyrhiza Glabra)
Ingi (Zingiber officinale)
All the above drugs taken equal parts
Preparation:
The drugs Adhimadhuram and ingi were bought from the pharmacy
raw drug store GSMCH. They are cleaned and dried under shade. The roots
of Iruveli are purchased from the field. Raw drugs are authenticated by
medicinal botanist of Government Siddha Medical College, Palayamkottai.
200gm of each items are ground into small pieces. Mixed well. 5gms
of mixture was taken in 720ml of water. It is boiled in a reduced flame to
the final volume of 1/8th measure that is 90ml and filtered.
Dosage : 90ml – twice a day
Indications : Giddiness, Vatha pitham, obesity, anemia and arosigam.
Life span : 3 hours
Reference : Agathiayar Vaithia Poornam 205 (P.No:154).
138
Properties of the trial drug: -VOuzq!
! “-VOuzq!OhiqEm!bqbg<gr<!OgT!
! ! bqxqOhil!bxq!Ogsv///////!kqs<sqbliGl<!
! uVOuzq!uiegR<!szLliGl<!
! ! lgk<kie<!Ogsvl<!Heig!uqbiGl<!
! kqVOuzq!sQktf<!kQI<k<k!hqk<kR<!
! ! sqOv]<mi!Osx<hisg<!gvLliGl<!
! SVOuzq!Sv!gisei!seqBliGl<!
! ! Sbl<hie!bqVOuzqs<!$]liGl</”
-Bogar Nigandu!
Botanical Name : Coleus forskholii
Tamil Name : Iruveli
Family : Lamiaceae
Useful part : Roots
Suvai : Inippu
Thanmai : Seetham
Pirivu : Inippu.
Habitat : A perennial herb, branched, aromatic
Chemical constituents:
Major : Forskohlin – 10 to 18%
Diterpenoids like forskolin, coleonols, coleons, barbatusin,
cyclobutatusin, coleosol, coleol, coleonone, deoxycoleonol,
7-deacetylforskolin and 6-acety-7-deacetylforskolin.
Properties and activity:
Coleus has basic cardiovascular action and lower blood pressure due
to forskohlin’s cyclic AMP elevating ability, which results in relaxation of
arteries and increaed force of contraction of the heart muscle. If may be
beneficial in cerebro vascular insufficiency and in enhancing post storke
139
recovery, Platelet aggregation inhibitory effect also used in cardiovascular
disorders.
Forskohlin the alkaloid used extract from tuburous root of Coleus
Forskohlin are being as a drug for Hyper Tension, glaucoma, asthma,
hypothyroidism, weight loss, immune enhancement, congestive heart failure
an certain types of cancer.
It is spasmolytic, CNS active, hypothermic, diuretic and vasodilator
Pharmacology:
Forskohlin was found to be a direct cerbral vasodilator. It lowers
intraoccular pressure in rabbit and in normal volunteers free from eye
disease.
Uses:
Coleus has been used as a medical herb to treat heart and lung
diseases, intestinal spasms, insomnia and convulsions. It also lowers blood
pressure, antipasmodic, dilates the blood vessels. Uterine cramps as well as
painful urination. It accelerates the breakdown of existing fat stores.
-Quality standard of Indian Medicinal Plant Vol.4 P-107
-eqh<hqe<!G{l<;!
� dmx<gm<MgTg<G! ue<jlBl<?! dmZg<G! Dm<mk<jkBl<!
ytqjbBl<?!-f<kqiqb!hzk<jkBl<!kVl</!
� uikl<?!uikhqk<k!Okimr<gt<!ke<eqjz!uti<s<sqbjmbqe<!nux<jx!
ke<eqjzh<hMk<kUl<?! hqk<kl<?! uiB?! uq]l<! Ngqbux<jx! fQg<gUl<!
-kje!dhObigqg<gzil</!
ke<jl!uQiqb!okipqz<;!
! leg<gtqh<H?!NBt<!uqVk<kq!kl<hel<!Ngqbux<jx!osb<Bl<!vk<kl<?!
hqk<kl<!Ohig<Gl</!
hqiqU;!
!! -eqh<H.uikhqk<kk<jk!slh<hMk<Kl</!

140
nkqlKvl<!
!
Botanical Name : Glycyrrhiza glabra
Tamil Name : Adhimadhuram
Trade Name : Liquorice
Habitat : Perrenial herb
Family : Fabaceae
Usefullpart : Root
Suvai : Inippu
Thanmai : Seetham
Pirivu : Inippu
ohiKG{l<;!
!!!!“gk<kqbiq!Lh<hq{qbiz<!uVH{<!kigr<!
! g{<O{ib<de<!likl<uqg<gz<!uzqou{<!Gm<ml<!
! hqk<kolZl<!HVg<gq!gqiqs<svl<!Nui<k<k!
! hqk<klk!&Is<js!uqmhigl<!ouh<hf<!
! kk<kquV!uikOsi!{qkr<gi!lijz!
! sVuuqmr<!gilqbOfib<!kiK!fm<mr<!
! Gk<kqVlz<!Nsqbr<gl<!-kp<Ofib<!-f<K!
! Gbh<H{<[l<!Ohil<!lK~goleg<!%Xr<!giOz”!
! ! ! ! ! ! .!Okjvbi<!G{uigml<!h{<H;!2/ -K! Lh<hq{qbiz<! uVl<! H{<?! fQI! Oum<jg?! g{<Ofib<gt<?!
ouxqOfib<?!ouh<HOfib<gt<!Ohig<Gl</!
3/ kQg<Gx<xk<kqe<!ue<jljb!kips<!osb<Bl</!
Chemical constituents:
The dried roots and underground stems of this plant constitute the
drug. Liquorice roots consists of triterpenids and flavonoid, starch, glucose,
sucrose, asparagine, fat, resins, mannitol and bitter principles.
Chemistry-contain glycoside Glycerrhizin.
141
Properties and Action:
The liquorice roots are useful in medicine as well as flavour. It is
known as demulcent, expectorant, laxative and sweetener.
Various preparation of liquorice are administered in Gastric &
Duodenal ulcers, Cardiac asthma, Hypertension, Rheumatoid arthritis &
Dermititis.
. Hand book of medicinal plants (P.No: 171)
Prof. S.K.Bhattacharjee
Properties & Uses:
Refrigerent, Demulcent, Expectorant, Mild laxative, Tonic, Diuretic
-Drient longman
-Indian Medicinal plants-3 P.84
!
-eqh<hqe<!G{l<;!
! dmx<gm<MgTg<G! ue<jlBl<?! dmZg<G! Dm<mk<jkBl<!
ytqjbBl<?!-f<kqiqb!hzk<jkBl<!kVl</!
! uikl<?!uikhqk<k!Okimr<gt<!ke<eqjz!uti<s<sqbjmbqe<!nux<jx!
ke<eqjzh<hMk<kUl<?!hqk<kl<?!uiB?!uq]l<!Ngqbux<jx!fQg<gUl<!-kje!
dhObigqg<gzil</!
!
ke<jl!uQiqb!okipqz<;!
! leg<gtqh<H?!NBt<!uqVk<kq!kl<hel<!Ngqbux<jx!osb<Bl<!vk<kl<?!
hqk<kl<!Ohig<Gl</!!
hqiqU;!
!! -eqh<H!.!uikhqk<kk<jk!slh<hMk<Kl</!
!
142
-R<sq!
!
Botanical Name : Zingiber officinale
Family : Gingiberaceae.
Useful part : Rhizome
Suvai : Karppu
Thanmai : Veppam
Pirivu : Karppu.
ohiKG{l<;!
! -R<sqbqe<!G{Ol!oke<xqbz<!HmEjvg<gg<!OgtQI!
! nR<sqMl<!se<eqobz<zi!lge<xqMl<!hqk<kOkiml<!
! ofR<sqeq!zqVlx<!Ogijp!ofgqp<f<kqMl<!ghr<gt<!ke<jl!
! lqR<sqeq!uVoli!oue<X!uqtl<hqMl<!Oku!F~Oz/!
! ! ! ! ! ! .!WM/!&zqjg!uGh<H.!G{himl</!
h{<H;!
!! se<eq?!hqk<k!Okiml<!fQr<Gl</!
! -Vlz<!Ogijp?!ghg<gm<M!kQVl</!
! hqk<k!lbg<gk<kqx<G!-kje!keqbigUl<!upr<gzil</!
ZINGIBER
Constituents:
Indian ginger contains an aromatic acid, volatile oil, camphene,
phallendrene, zingiberine, cineol and borneol.
An oleo recin: Gingerin, active principle. Others resins and starch.
- Indian Materia Medica. (P.No:1310)
Action:
The raw zinger is acrid, thermogenic, appetiser, laxative, stomachic
and carminative.
143
Uses :
It is useful in anorexia, diarrhoea, vomitting, dyspepsia.
It removes obstruction in the vessels.
gii<h<hqe<!G{l<!;!
!
“ ////////////////////////!hVleil<!
ogiPh<jhBl<!yPg<gQcz<!uPuPk<kqms<!osb<!
ofb<h<jhBl<!ypqk<kqMl<!Jb!uqgivl<!
npqk<kqMl<!fic!fit!njmh<hqjeg<!
gpx<xqOb!kml<ohx!uqbx<Xr<!giIh<hiR<!
Sjukjeg<!g{g<Ogi!M{<{qz<!
fjubqjz!fzlil<!fzqbqjz!flg<Og”!
! ! ! ! ! ! .!lVk<Ku!keqh<himz<!
! !
!! dmZg<Gh<! hVljek<! kVl<! ogiPh<hqe<! osxqjuBl<?!
upuph<Ht<t! ofb<h<jhBl<! ypqk<KuqMl</! ! dmzqZt<t! ficgtqZl<!
GVkqfitl<! Lkzie! fitr<gtqZl<! lzqer<gt<! kr<gq! njugtqz<!
YmOu{<cb! fQIh<! ohiVm<gjt! Ymouim<milz<! njmk<Kg<!
ogi{<Mt<tjugjtBl<! njvk<K! nu<uqmlqVf<K! nh<hix<! osz<z!
-bx<xqBl<!fic!fvl<Hgtqz<!sk<Kgjt!uqsizqg<gUl<!osb<Bl</! !
!
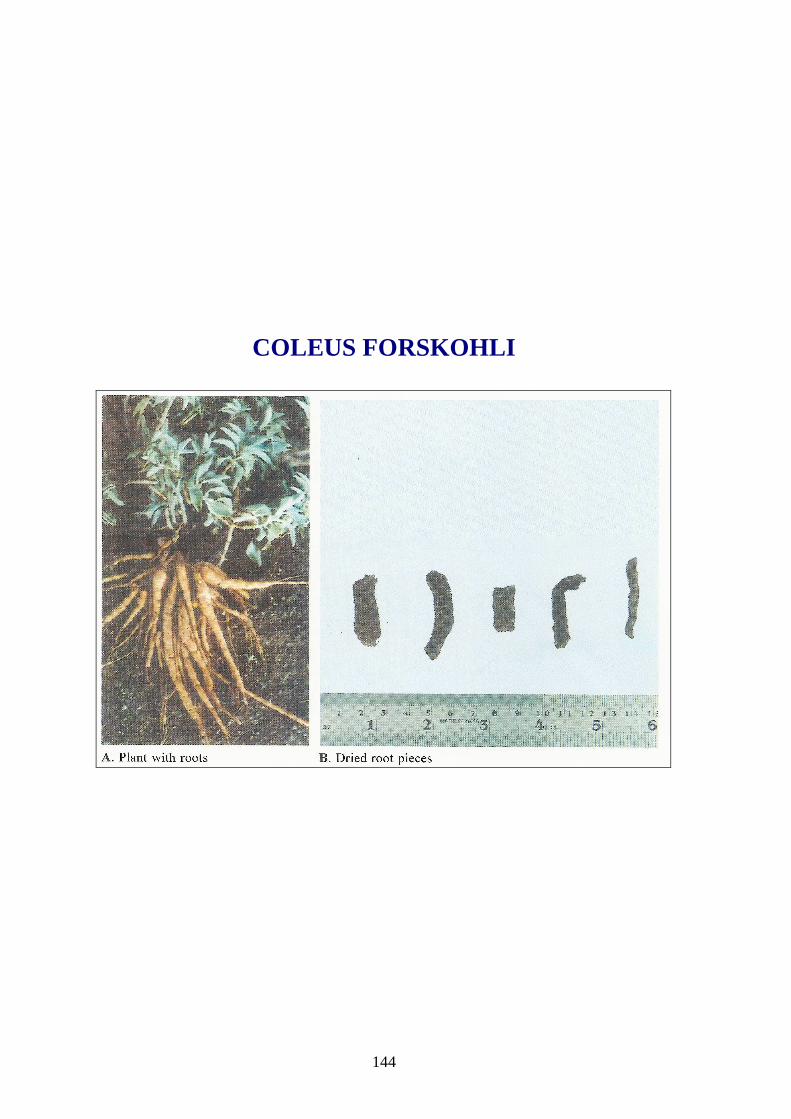
144
COLEUS FORSKOHLI

145
INJI – Zingiber officinale
ATHIMATHURAM – Glycyrrhiza glabra
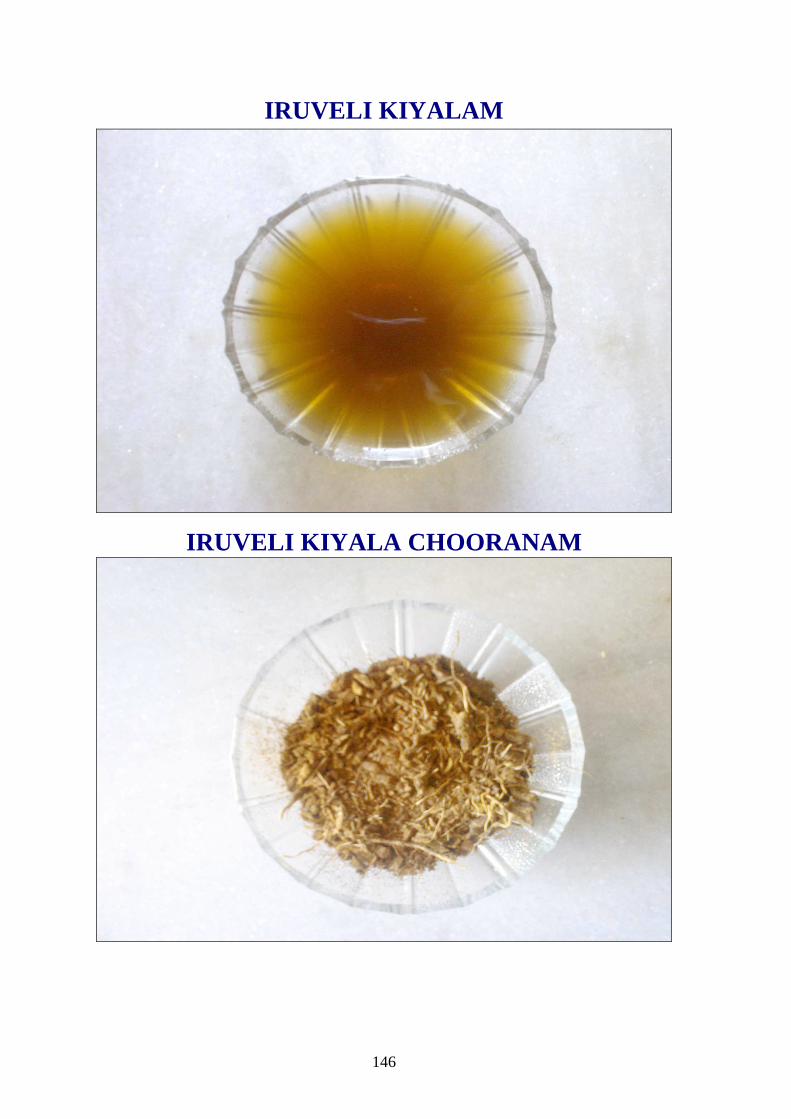
146
IRUVELI KIYALAM
IRUVELI KIYALA CHOORANAM
147
Bio-Chemical Analysis

148
ANNEXURE – II
A. BIO-CHEMICAL ANALYSIS OF IRUVELI KIYALAM
PREPARATION OF THE EXTRACT
5gms of the drug was weighed accurately and placed in a 250ml clean
beaker. The 50ml of distilled water is added and dissolved well. Then it is
boiled well for about 10 minutes. It is cooled and filtered in a 100ml
volumetric flask and then it is make up to 100ml with distilled water. This
fluid is taken for analysis.
QUALITATIVE ANALYSIS
S.NO. EXPERIMENT OBSERVATION INFERENC
E
1. TEST FOR CALCIUM
2ml of the above prepared extract is
taken in a clean test tube. To this add
2ml of 4% Ammonium oxalate solution
A white precipitate
is formed
Indicates the
presence of
calcium
2. TEST FOR SULPHATE:
2ml of the extract is added to 5%
barium chloride solution.
A white precipitate
is formed
Indicates the
presence of
sulphate
3. TEST FOR CHLORIDE
The extract is treated with silver nitrate
solution
A white precipitate
is formed
Indicates the
presence of
chloride
4. TEST FOR CARBONATE
The substance is treated with
concentrated Hcl.
No brisk
effervessence is
formed
Absence of
Carbonate
5. TEST FOR STARCH
The extract is added with weak iodine
solution.
Blue colour is
formed
Indicates the
presence of
Starch
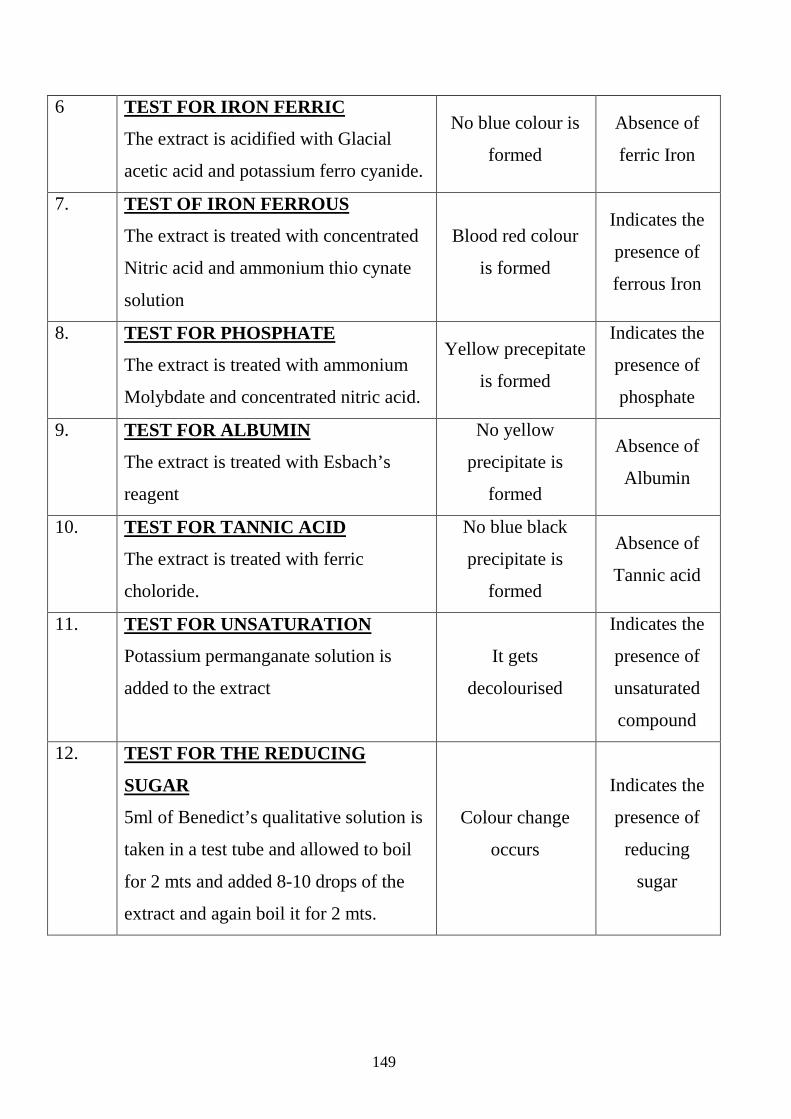
149
6 TEST FOR IRON FERRIC
The extract is acidified with Glacial
acetic acid and potassium ferro cyanide.
No blue colour is
formed
Absence of
ferric Iron
7. TEST OF IRON FERROUS
The extract is treated with concentrated
Nitric acid and ammonium thio cynate
solution
Blood red colour
is formed
Indicates the
presence of
ferrous Iron
8. TEST FOR PHOSPHATE
The extract is treated with ammonium
Molybdate and concentrated nitric acid.
Yellow precepitate
is formed
Indicates the
presence of
phosphate
9. TEST FOR ALBUMIN
The extract is treated with Esbach’s
reagent
No yellow
precipitate is
formed
Absence of
Albumin
10. TEST FOR TANNIC ACID
The extract is treated with ferric
choloride.
No blue black
precipitate is
formed
Absence of
Tannic acid
11. TEST FOR UNSATURATION
Potassium permanganate solution is
added to the extract
It gets
decolourised
Indicates the
presence of
unsaturated
compound
12. TEST FOR THE REDUCING
SUGAR
5ml of Benedict’s qualitative solution is
taken in a test tube and allowed to boil
for 2 mts and added 8-10 drops of the
extract and again boil it for 2 mts.
Colour change
occurs
Indicates the
presence of
reducing
sugar
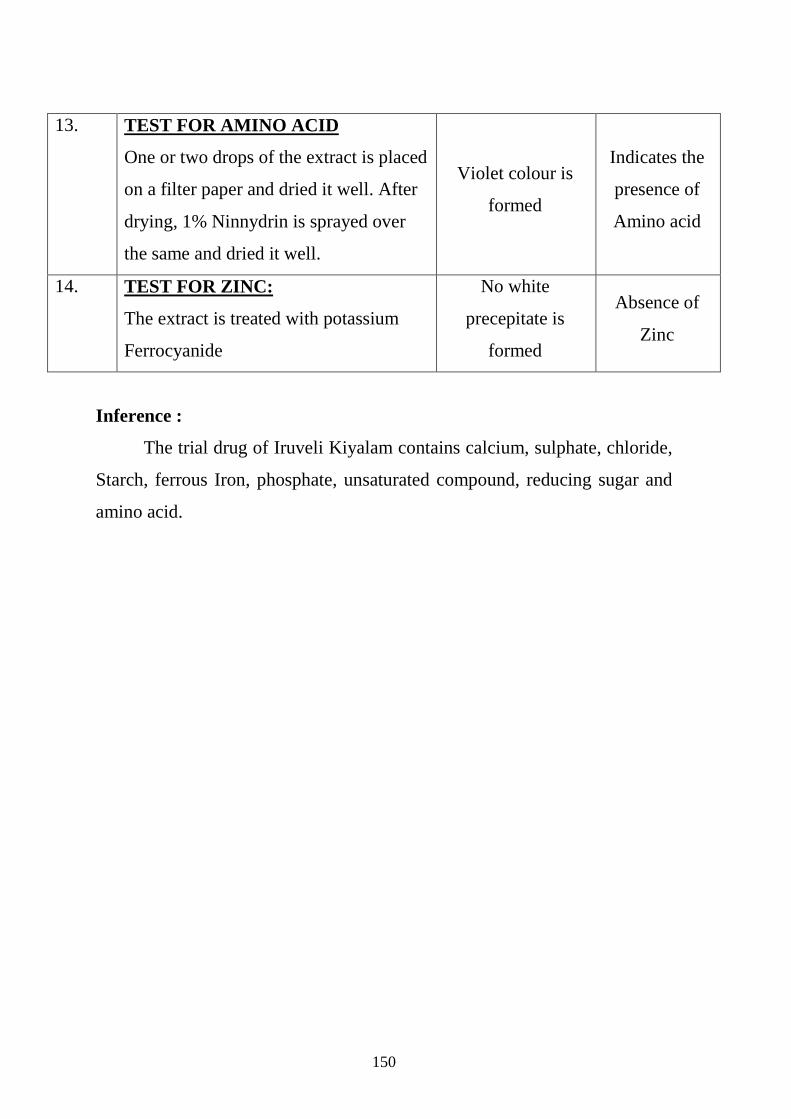
150
13. TEST FOR AMINO ACID
One or two drops of the extract is placed
on a filter paper and dried it well. After
drying, 1% Ninnydrin is sprayed over
the same and dried it well.
Violet colour is
formed
Indicates the
presence of
Amino acid
14. TEST FOR ZINC:
The extract is treated with potassium
Ferrocyanide
No white
precepitate is
formed
Absence of
Zinc
Inference :
The trial drug of Iruveli Kiyalam contains calcium, sulphate, chloride,
Starch, ferrous Iron, phosphate, unsaturated compound, reducing sugar and
amino acid.
151
Pharmacological Analysis

152
B. PHARMACOLOGICAL ANALAYSIS
EVALUATION OF DIURETIC EFFECT OF IRUVELI KIYALAM
Aim:
To study the diuretic effect of Iruveli Kiyalam in albino rats.
Preparation of the test drug:
Iruveli Kiyalam:
5 gms of Iruveli Kiyala Chooranam was boiled in a reduced flame in
100ml of water and reduced to 50ml.
Procedure :
Two groups of rats each weighing 100-150 gms were taken. Each
group contain 3 rats. They were kept deprived of food and water for an
overnight period.
In the first group, each animal received 5ml of distilled water orally.
They were kept in a metabolic cage and taken as control group.
In the second group, each animal received 5ml of the test drug orally.
They were kept in another metabolic cage.
For both the groups, urine was collected in a pure glass vessel
separately and the quantity was measured after 1 ½hrs , 3 hrs and 4 ½ hrs
The readings were Sl.No. Time in hours Control group in ml Test drug group
in ml 1. 1 ½ 7 8 2. 3 11 15 3. 4 ½ 15 27
Then the urine electrolytes were measured. The measurement was done
Krishna Computerised Clinical Laboratory, Palayamkottai.
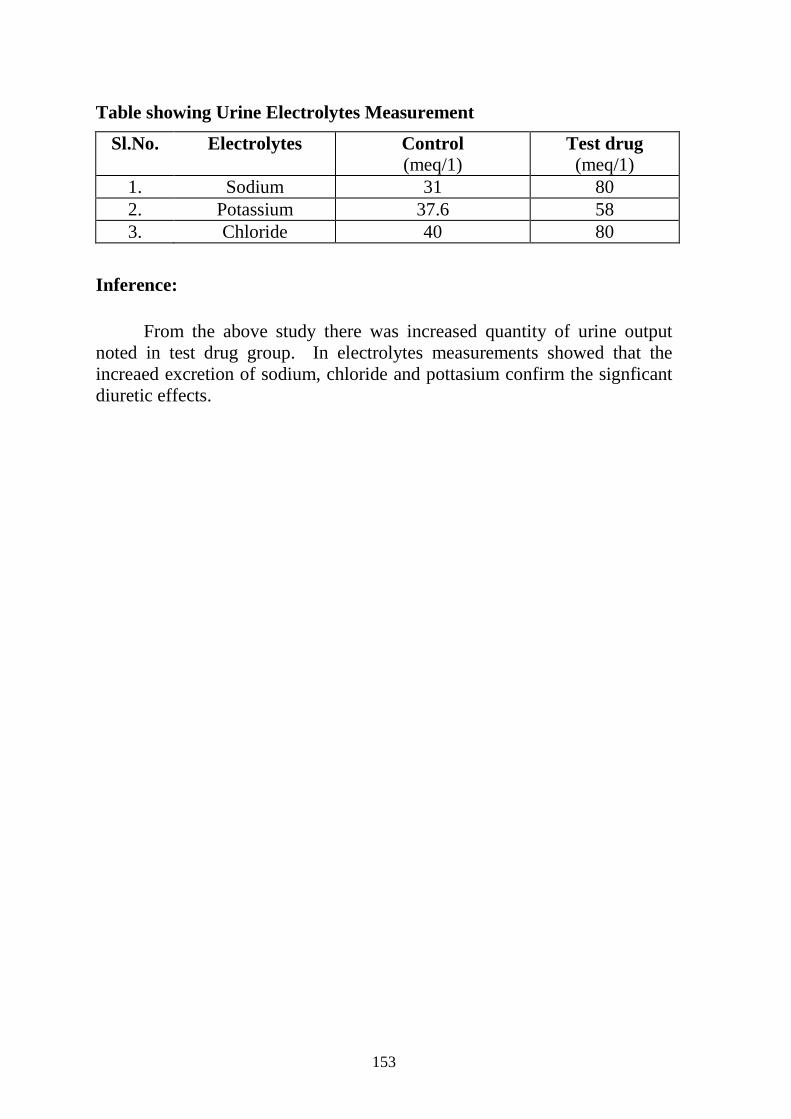
153
Table showing Urine Electrolytes Measurement
Sl.No. Electrolytes Control (meq/1)
Test drug (meq/1)
1. Sodium 31 80 2. Potassium 37.6 58 3. Chloride 40 80
Inference:
From the above study there was increased quantity of urine output noted in test drug group. In electrolytes measurements showed that the increaed excretion of sodium, chloride and pottasium confirm the signficant diuretic effects.
154
Toxicological Study
155
ACUTE TOXICITY STUDIES
Toxicity study:
The toxicity evaluation of IRUVELI KIYALA CHOORANAM is
carried out in phase.
Phase I - Acute toxicity study
Animal:
Wistar albino rat bred in the animal house attached to the
Post Graduate, Pharmacology Department, Government Siddha Medical
College, palayamkottai were used.
Sex:
Animals of both sexes were used.
Weight:
Animals weighing between 80-120 gms were selected.
Feeding of the animals:
The animals were randomly selected and kept in their cages.
Conventional laboratory diet was used with unlimited supply of drinking
water.
Separation of animals into groups:
30 rats were divided into 6 groups, each group consists of 5 rats. One
group is kept as control, by giving water alone.
156
Dose levels of the drug:
Since it is difficult to proceed the toxicity study with Iruveli Kiyalam
basis, it is better to study with Iruveli Kiyala Chooranam basis. The Iruveli
Kiyala chooranam contained in the Iruveli Kiyalam having the following
ascending dose levels were fixed by presuming a range of atleast toxic to
high toxic doses.
I Group - Control
II Group - 200mg / 100gm body weight of animal
III Group - 400mg / 100gm body weight of animal
IV Group - 800mg / 100gm body weight of animal
V Group - 1600mg / 100gm body weight of animal
VI Group - 3200mg / body weight of animal
Route of administration:
Oral administration.
Drug preparation:
The drug was weighted and taken and suspended in water, which is
heated and melted, as a suspending agent. The mixture was ground well
before the administration. The preparation owas done in such a way that 1ml
of suspension contains dose ranging from 200mg to 3200mg of IRUVELI
KIYALA CHOORANAM which is given to the respective groups, as
classified above in the dose level. The drug was administered in morning and
observed.
Observation:
The following details are recorded.
I. Stimulation:
• Hyperactivity
• Pyloerection
157
• Twitching
• Rigidity
• Irritability
• Jumping
• Clonic convulsion
• Tonic convulsion
II. Depression:
Ptosis
Sedation
Sleep
Loss of Pinna reflex
Ataxia
Loss of muscle tone
Analgesia.
III. Autonomic effect :
Straub tail
Laboured Respiration
Cyanosis
Blanching
Reddening
158
IV. Number of animals dead:
At the end of 24 hours, the number of animals live or dead in each
group was noted and approximate ED50 is tried to determine. The tabular
column was made and the results was analysed.
Result:
The said parameters in acute toxicity study were observed on various
6 groups (Group I, II, III, IV, V and VI) Group I – is the control and Group
II-VI were treated with the drug such as 200mg, 400mg, 800mg, 1600mg
and 3200mg / 100gm body weight of the animal respectively. The results
were tabulated in Table I to VI.
From the table I-VI it is being found that the drug IRUVELI
KIYALA CHOORANAM did not produce any mortality even upto the
dose level of 3200mg/ 100gm body weight of the animal. The same
procedure in acute toxicity study was done for 7 days and after the study
period it is found that the drung did not reduce any mortality. and
abnormalities in behavioural pattern Since it is practically difficult to give morethan 3200mg/ 100gmbody
weight of the animal in this small species (wistar albino rats) it is unable to
calculate the lethal dose in this preliminary acute toxicity study. So it is
inferred that the drug is safe upto 3200 mg/ 100gm body weight of the
animal.

159
Case sheet Proforma
160
GOVERNMENT SIDDHA MEDICAL COLLEGE AND HOSPITAL
PALAYAMKOTTAI
POST- GRADUATE DEPARTMENT OF POTHU MARUTHUVAM
AN OPEN CLINICAL TRIAL FOR THE DISEASE VATHA PITHAM USING THE SIDHA DRUG “IRUVELI KIYALAM” INTERNAL
FORM I –SCREENING FORM
1. OP/ IP No: 2. BED No: 3. Sl. No:
4. NAME: 5. AGE: 6. GENDER:
7. OCCUPATION: 8. SOCIO ECONOMIC STATUS
9. DATE OF ADMISSION: 10. DATE OF DISCHARGE:
11. POSTAL ADDRESS:
------------------------------------------------------------------------------------------------------------
II. EXCLUSION CRITERIA:
� Renal hypertension
� Hormonal hypertension
� Pregnancy induced
hypertension
� Drug induced hypertension.
� Left ventricular failure.
� Cerebro vascular accident.
� Pulmonary Hypertension
� Sanni naadi nilai.
� Kaba vatha dhontham
� Asathiya neikuri.
� Patients with infective
diseases.
I. INCLUSION CRITERIA:
� Age : 35 – 75 Yrs
� Sex : Both Male and Female
� Patients having symptoms of
giddiness, headache, palpitation
sleeplessness, fatiguability
� Mild Moderate and Accelerated
hypertensive patients
134
nvsqei<!sqk<k!lVk<Kug<!gz<Z~iq!lx<Xl<!lVk<Kulje?!
hijtbr<Ogim<jm?!!!
hm<mOlx<hch<H!ohiK!lVk<Kuk<Kjx/!
uik!hqk<kl<!Ofib<g<G!lVf<kig!-VOuzq!gqbipl<!
hiqgiqh<Hk<kqxjeg<!g{<mxqBl<!lVk<Ku!Nb<U/!
!
!xg;Gjy; gbtk;
Ma;thsuhy; rhd;wspf;fg;gl;lJ
ehd; ,e;j Ma;T Fwpj;j midj;J tpguq;fisAk; Nehahspf;F GhpAk;
tifapy; vLj;Jiuj;Njd; vd cWjpaspf;fpNwd;.
Njjp : ifnahg;gk; :
,lk; : ngah; :
Nehahspapd; xg;Gjy;
vd;dplk; ,e;j kUj;Jt Ma;tpd; fhuzj;ijAk; kUe;jpd; jd;ik kw;Wk;
kUj;Jt topKiwiag; gw;wpAk; njhlh;e;J vdJ cly; ,af;fj;ij
fz;fhzpf;fTk;> mjidg; ghJfhf;fTk; gad;gLk; kUj;Jt Ma;Tf;$l
ghpNrhjidfs; gw;wp jPUg;jp mspf;Fk; tifapy; Ma;T kUj;Jtuhy; tpsf;fpf;
$wg;gl;lJ.
ehd; ,e;j kUj;Jt Ma;tpd; NghJ fhuzk; vJTk; $whky; vg;nghOJ
Ntz;LkhdhYk; ,e;j ma;tpypUe;J vd;id tpLtpj;Jf; nfhs;Sk; chpikia
njhpe;jpUf;fpNwd;.
ehd; vd;Dila Rje;jpukhf Njh;T nra;Ak; chpikiaf; nfhz;L ‘thj
gpj;j Neha;f;fhd ,UNtyp fpahok;” ghpfhpg;Gj;jpwidf; fz;lwpAk; kUj;Jt
Ma;tpw;F vd;id cl;gLj;j xg;Gjy; mspf;fpNwd;.
Njjp : ifnahg;gk;: ,lk; : ngah; : Njjp: rhl;rpf;fhuh; ifnahg;gk; : ,lk;: ngah;: cwTKiw :
135
GOVERNMENT SIDDHA MEDICAL COLLEGE AND HOSPITAL
PALAYAMKOTTAI
POST- GRADUATE DEPARTMENT OF POTHU MARUTHUVAM
AN OPEN CLINICAL TRIAL FOR THE DISEASE VATHA PITHAM USING THE SIDHA DRUG “IRUVELI KIYALAM” INTERNAL
Form: II CONSENT FORM
CERTIFICATE BY INVESTIGATOR
I certify that I have disclosed all the details about the study in the terms readily understood by
the patient.
Signature…………………. Date……… Name…………………… CONSENT BY PATIENT
I have been informed to my satisfaction, by the attending physician, the purpose of
the clinical trial, and the nature of drug treatment and follow-up including the laboratory
investigations to be performed to monitor and safeguard my body functions.
I am aware of my right to opt out of the trial at any time during the course of the trial
without having to give the reasons for doing so.
I, exercising my free power of choice, hereby give my consent to be included as a
subject in the clinical trial of ‘Iruveli Kiyalam’ (Internal drug) for the treatment of ‘Vatha
Pitham’
Signature………………… Name……………………..
Date…………………..
136
GOVERNMENT SIDDHA MEDICAL COLLEGE AND HOSPITAL
PALAYAMKOTTAI
POST- GRADUATE DEPARTMENT OF POTHU MARUTHUVAM
AN OPEN CLINICAL TRIAL FOR THE DISEASE VATHA PITHAM USING THE SIDHA DRUG “IRUVELI KIYALAM” INTERNAL
FORM III – CASE PROFORMA (IP/OP)
1. OP/ IP No: 2. BED No: 3. Sl. No:
4. NAME: 5. AGE: 6. GENDER:
7. OCCUPATION: 8. SOCIO ECONOMIC STATUS
9. DATE OF ADMISSION: 10. DATE OF DISCHARGE:
11. POSTAL ADDRESS: Prognosis : Good / Fair / Poor
------------------------------------------------------------------------------------------------------------
12. COMPLAINTS & DURATION:
13. HISTORY OF PRESENT ILLNESS:
14. PAST HISTORY:
15. FAMILY HISTORY:
16. MENSTRUAL HISTORY (If applicable):
Lecturer HOD
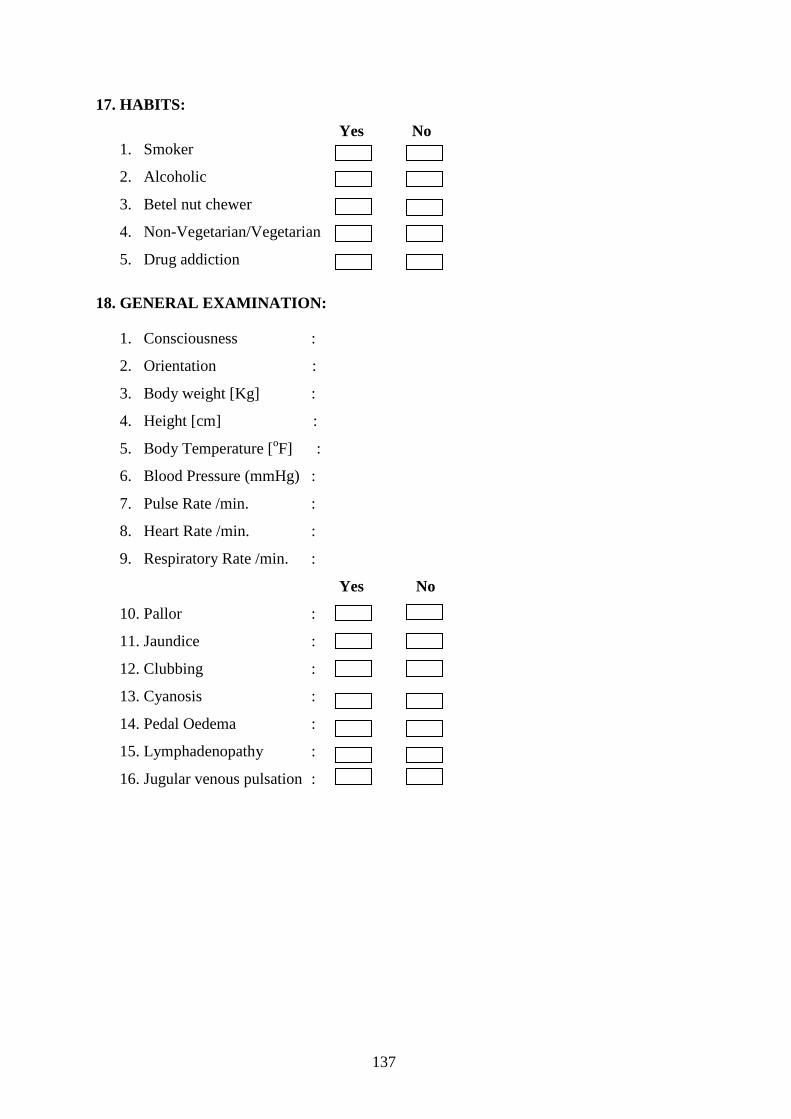
137
17. HABITS:
Yes No 1. Smoker
2. Alcoholic
3. Betel nut chewer
4. Non-Vegetarian/Vegetarian
5. Drug addiction
18. GENERAL EXAMINATION:
1. Consciousness :
2. Orientation :
3. Body weight [Kg] :
4. Height [cm] :
5. Body Temperature [oF] :
6. Blood Pressure (mmHg) :
7. Pulse Rate /min. :
8. Heart Rate /min. :
9. Respiratory Rate /min. :
Yes No
10. Pallor :
11. Jaundice :
12. Clubbing :
13. Cyanosis :
14. Pedal Oedema :
15. Lymphadenopathy :
16. Jugular venous pulsation :
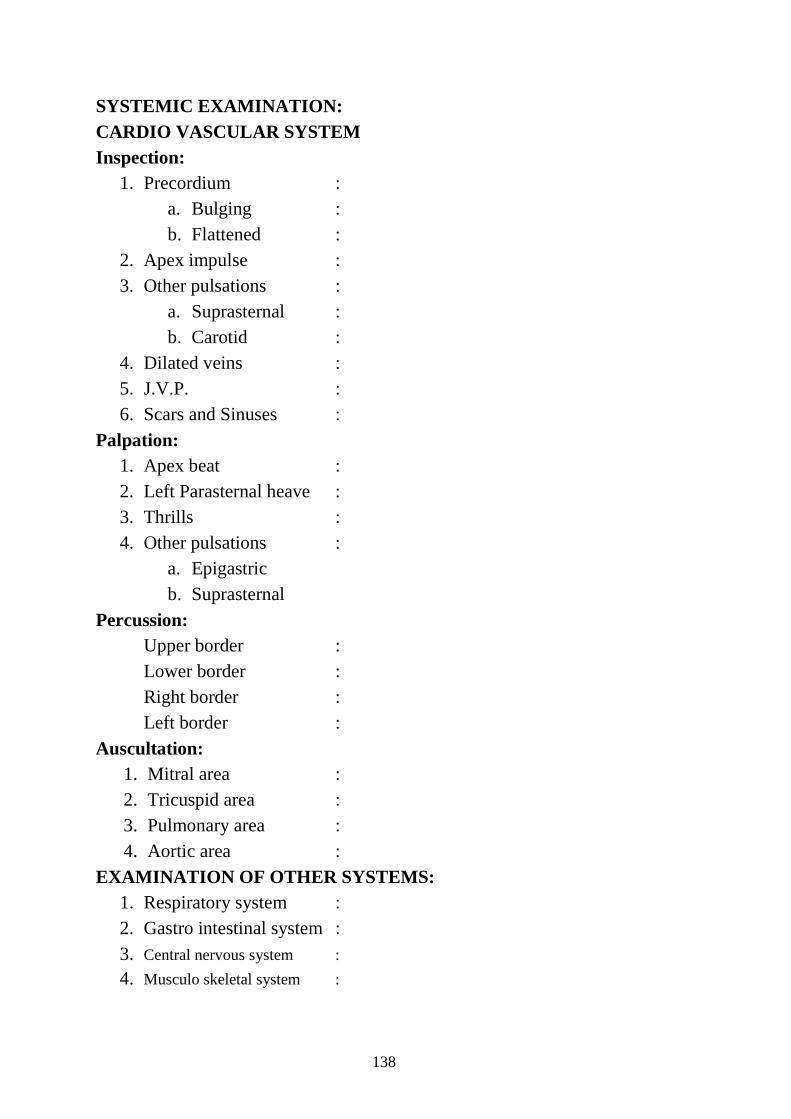
138
SYSTEMIC EXAMINATION: CARDIO VASCULAR SYSTEM Inspection:
1. Precordium : a. Bulging : b. Flattened :
2. Apex impulse : 3. Other pulsations :
a. Suprasternal : b. Carotid :
4. Dilated veins : 5. J.V.P. : 6. Scars and Sinuses :
Palpation: 1. Apex beat : 2. Left Parasternal heave : 3. Thrills : 4. Other pulsations :
a. Epigastric b. Suprasternal
Percussion: Upper border : Lower border : Right border : Left border : Auscultation:
1. Mitral area : 2. Tricuspid area : 3. Pulmonary area : 4. Aortic area :
EXAMINATION OF OTHER SYSTEMS: 1. Respiratory system : 2. Gastro intestinal system : 3. Central nervous system : 4. Musculo skeletal system :
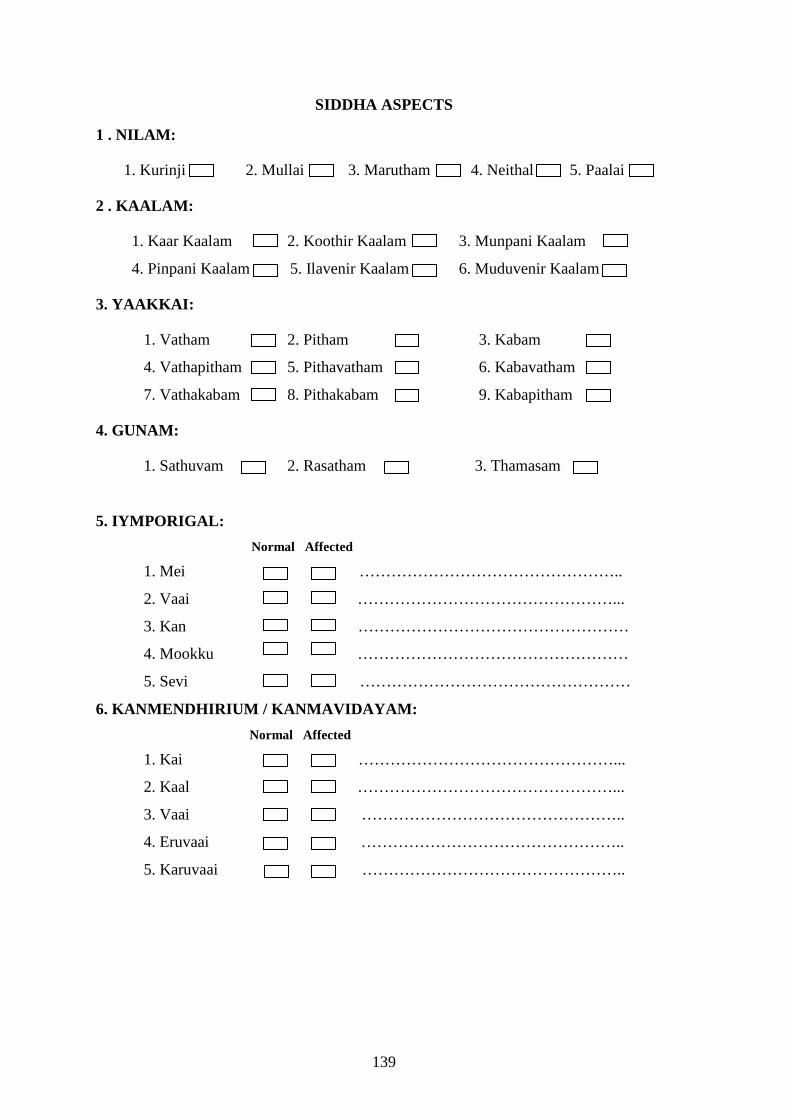
139
SIDDHA ASPECTS
1 . NILAM:
1. Kurinji 2. Mullai 3. Marutham 4. Neithal 5. Paalai
2 . KAALAM:
1. Kaar Kaalam 2. Koothir Kaalam 3. Munpani Kaalam
4. Pinpani Kaalam 5. Ilavenir Kaalam 6. Muduvenir Kaalam
3. YAAKKAI:
1. Vatham 2. Pitham 3. Kabam
4. Vathapitham 5. Pithavatham 6. Kabavatham
7. Vathakabam 8. Pithakabam 9. Kabapitham
4. GUNAM:
1. Sathuvam 2. Rasatham 3. Thamasam
5. IYMPORIGAL:
Normal Affected
1. Mei …………………………………………..
2. Vaai …………………………………………...
3. Kan ……………………………………………
4. Mookku ……………………………………………
5. Sevi ……………………………………………
6. KANMENDHIRIUM / KANMAVIDAYAM:
Normal Affected
1. Kai …………………………………………...
2. Kaal …………………………………………...
3. Vaai …………………………………………..
4. Eruvaai …………………………………………..
5. Karuvaai …………………………………………..

140
7. UYIR THATHUKKAL:
I. VATHAM: Normal Affected
1. Piraanan …………………………………………
2. Abaanan …………………………………………
3. Viyaanan …………………………………………
4. Uthaanan …………………………………………
5. Samaanan ………………………………………….
6. Naagan ………………………………………….
7. Koorman ………………………………………….
8. Kirukaran …………………………………………
9. Devathathan …………………………………………
10. Dhananjeyan …………………………………………
II. PITHAM : Normal Affected
1. Analam ………………………………………….
2. Ranjagam ………………………………………….
3. Saathagam …………………………………………..
4. Aalosagam ………………………………………….
5. Prasagam ………………………………………….
III. KABAM: Normal Affected
1. Avalambagam ……………………………………………
2. Kilethagam ……………………………………………
3. Pothagam ……………………………………………
4. Tharpagam ……………………………….…………...
5. Santhigam ……………………………………………
8. UDAL THAATHUKKAL: Normal Affected
1. Saaram …………………………………..
2. Senneer …………………………………..
3. Oon …………………………………..
4. Kozhuppu …………………………………..
5. Enbu …………………………………...
6. Moolai .…………………………………..
7. Sukkilam/Suronitham …………………………………...
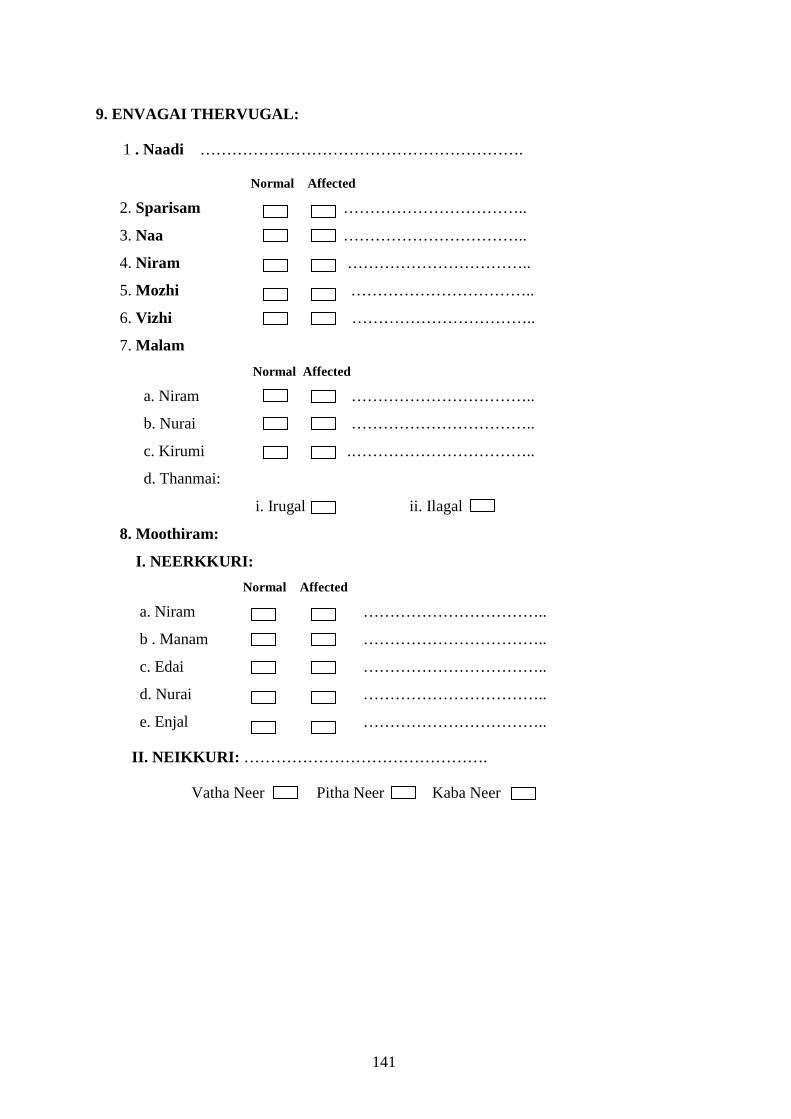
141
9. ENVAGAI THERVUGAL:
1 . Naadi …………………………………………………….
Normal Affected
2. Sparisam ……………………………..
3. Naa ……………………………..
4. Niram ……………………………..
5. Mozhi ……………………………..
6. Vizhi ……………………………..
7. Malam
Normal Affected
a. Niram ……………………………..
b. Nurai ……………………………..
c. Kirumi .……………………………..
d. Thanmai:
i. Irugal ii. Ilagal
8. Moothiram:
I. NEERKKURI:
Normal Affected
a. Niram ……………………………..
b . Manam … ……………………………..
c. Edai ……………………………..
d. Nurai ……………………………..
e. Enjal ……………………………..
II. NEIKKURI: ……………………………………….
Vatha Neer Pitha Neer Kaba Neer
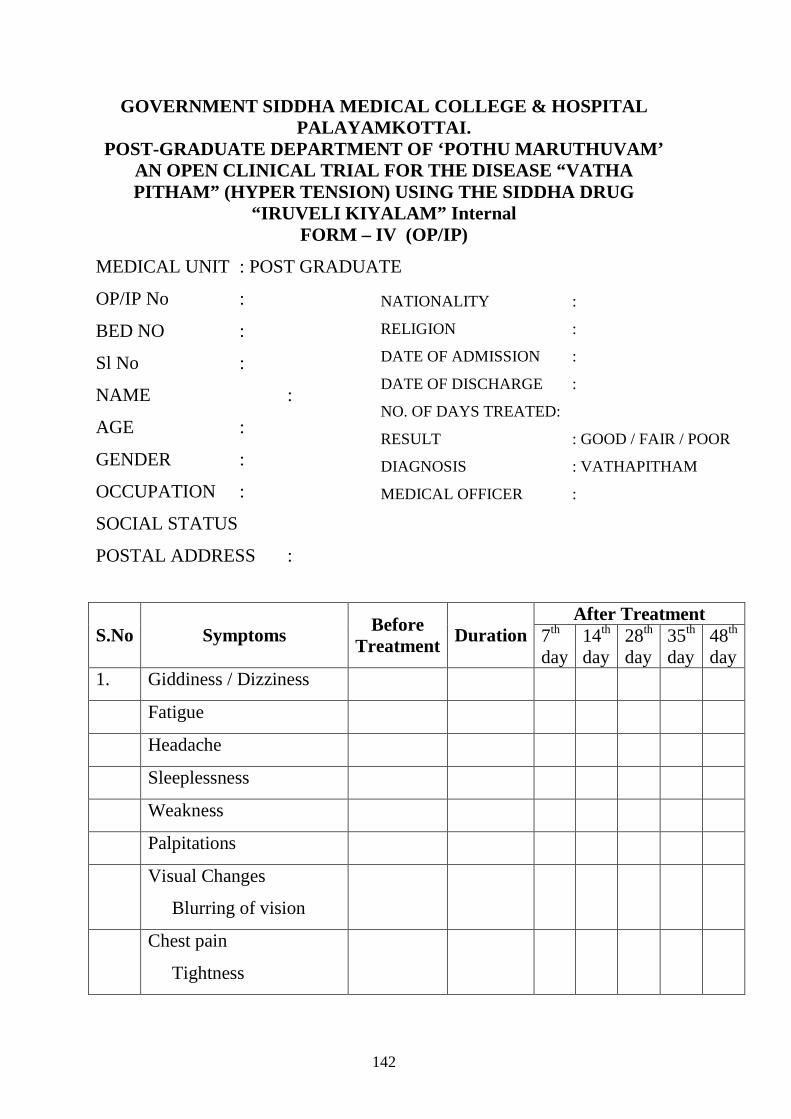
142
GOVERNMENT SIDDHA MEDICAL COLLEGE & HOSPITAL PALAYAMKOTTAI.
POST-GRADUATE DEPARTMENT OF ‘POTHU MARUTHUVAM’ AN OPEN CLINICAL TRIAL FOR THE DISEASE “VATHA PITHAM” (HYPER TENSION) USING THE SIDDHA DRUG
“IRUVELI KIYALAM” Internal FORM – IV (OP/IP)
MEDICAL UNIT : POST GRADUATE
OP/IP No :
BED NO :
Sl No :
NAME :
AGE :
GENDER :
OCCUPATION :
SOCIAL STATUS
POSTAL ADDRESS :
After Treatment S.No Symptoms Before
Treatment Duration 7th day
14th day
28th day
35th day
48th day
1. Giddiness / Dizziness
Fatigue
Headache
Sleeplessness
Weakness
Palpitations
Visual Changes
Blurring of vision
Chest pain
Tightness
NATIONALITY :
RELIGION :
DATE OF ADMISSION :
DATE OF DISCHARGE :
NO. OF DAYS TREATED:
RESULT : GOOD / FAIR / POOR
DIAGNOSIS : VATHAPITHAM
MEDICAL OFFICER :

143
Heaviness or chest
Oedema
Peripheral
Lumbosacral
Generalised
Pitting / Non
Pitting
Nausea
Frequent
Occasional
Associated with
vomiting
Vomitting
Frequent
Occasional
Stained with blood
Haematuria
Polyuria
Polydipsia
Fainting
Epistaxis
Dyspnoea
On Exertion
Rest
Loss of apetite
Emotional stress
Fear / Anxiety
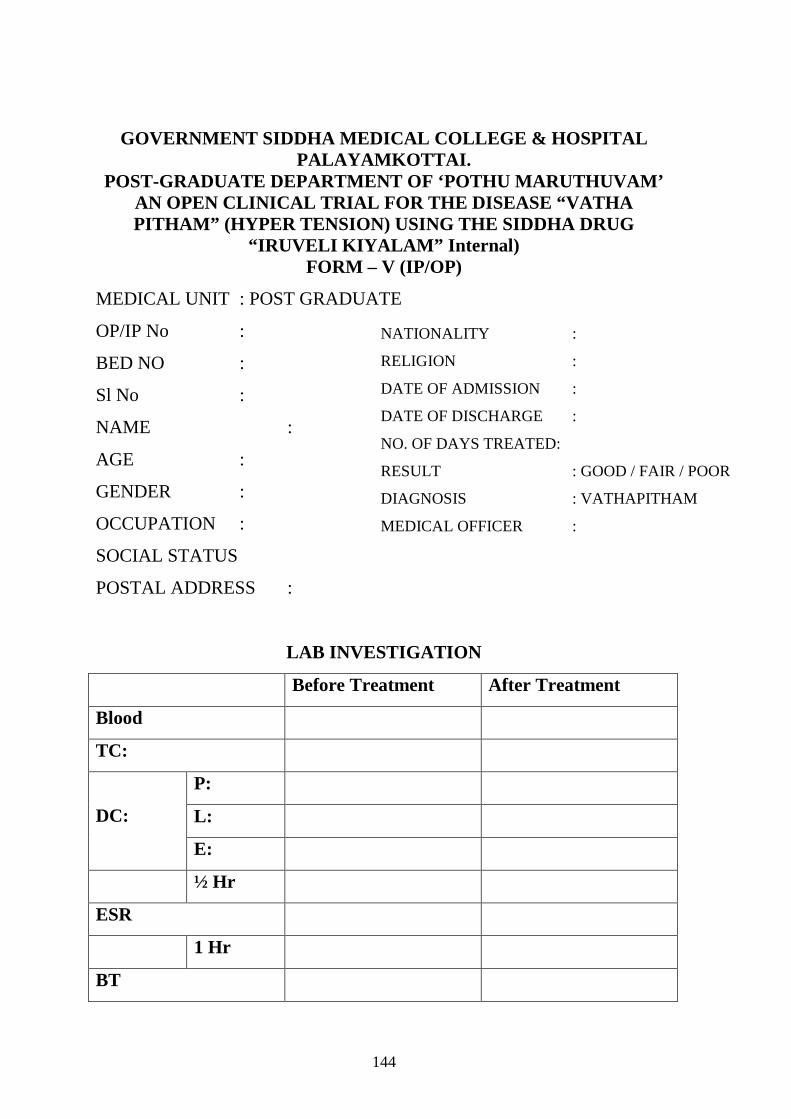
144
GOVERNMENT SIDDHA MEDICAL COLLEGE & HOSPITAL PALAYAMKOTTAI.
POST-GRADUATE DEPARTMENT OF ‘POTHU MARUTHUVAM’ AN OPEN CLINICAL TRIAL FOR THE DISEASE “VATHA PITHAM” (HYPER TENSION) USING THE SIDDHA DRUG
“IRUVELI KIYALAM” Internal) FORM – V (IP/OP)
MEDICAL UNIT : POST GRADUATE
OP/IP No :
BED NO :
Sl No :
NAME :
AGE :
GENDER :
OCCUPATION :
SOCIAL STATUS
POSTAL ADDRESS :
LAB INVESTIGATION
Before Treatment After Treatment
Blood
TC:
P:
L: DC:
E:
½ Hr
ESR
1 Hr
BT
NATIONALITY :
RELIGION :
DATE OF ADMISSION :
DATE OF DISCHARGE :
NO. OF DAYS TREATED:
RESULT : GOOD / FAIR / POOR
DIAGNOSIS : VATHAPITHAM
MEDICAL OFFICER :
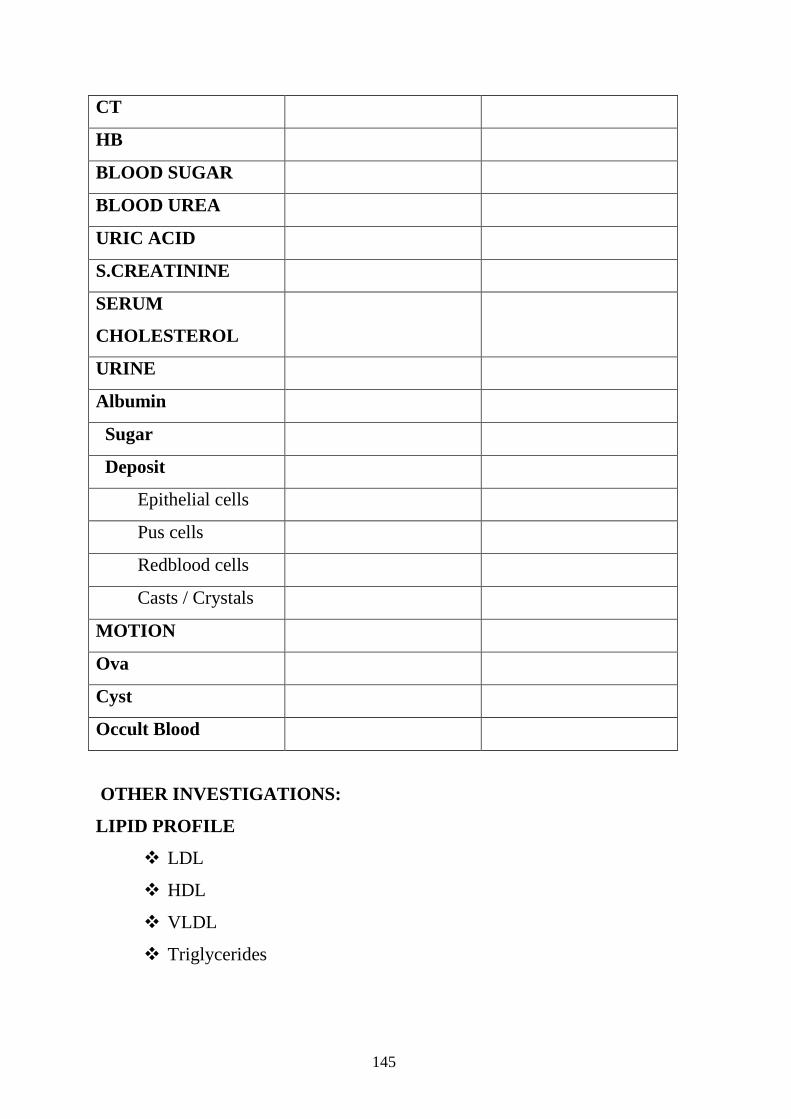
145
CT
HB
BLOOD SUGAR
BLOOD UREA
URIC ACID
S.CREATININE
SERUM
CHOLESTEROL
URINE
Albumin
Sugar
Deposit
Epithelial cells
Pus cells
Redblood cells
Casts / Crystals
MOTION
Ova
Cyst
Occult Blood
OTHER INVESTIGATIONS:
LIPID PROFILE
� LDL
� HDL
� VLDL
� Triglycerides
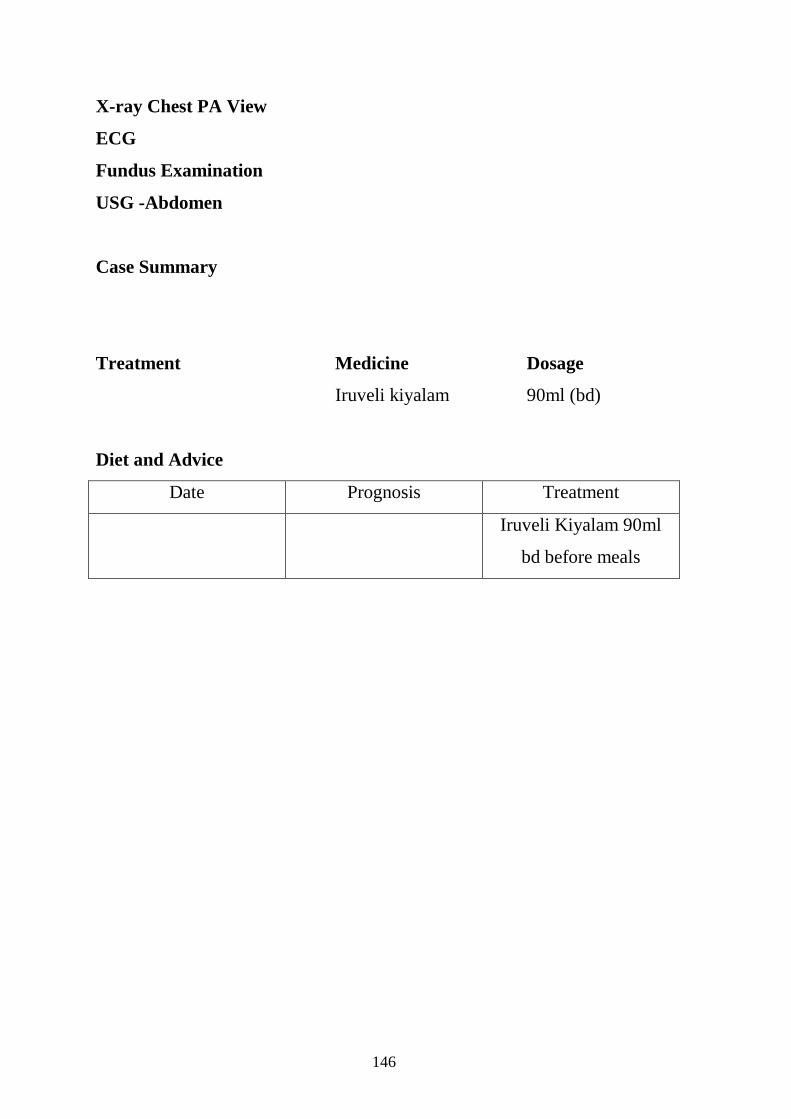
146
X-ray Chest PA View
ECG
Fundus Examination
USG -Abdomen
Case Summary
Treatment Medicine Dosage
Iruveli kiyalam 90ml (bd)
Diet and Advice
Date Prognosis Treatment
Iruveli Kiyalam 90ml
bd before meals
147
GOVERNMENT SIDDHA MEDICAL COLLEGE AND
HOSPITAL PALAYAMKOTTAI
POST- GRADUATE DEPARTMENT OF POTHU MARUTHUVAM AN OPEN CLINICAL TRIAL OF IRUVELI KIYALAM FOR VATHA PITHAM
FORM - VI PATIENT WITHDRAWAL FORM (OP/IP) 1. OP / IP No …………… 2. S.No. …………… 3. Date: ……………
4. Name …………… 5. Age …………… 6. Gender …………
7. Postal address:
------------------------------------------------------------------------------------------------------------
Complaints and Duration:
Irregular treatment:
Other causes:
148
Bibliography
149
BIBLIOGRAPHY
1. Yugi vaidhya chinthamani. - R.Thiyagarajan. 2. Siddha Maruthuvam.
- K.M. Kuppuswamy Mudhaliar. HPIM. 3. Agathiyar Vaithiya Rathina Churukkam
- K.B.Thiyagarajan 4. Agathiyar Vaithiya Kaviyam - 1500
- S.P.Ramachandran 5. Agathiyar Naadi Sasthiram
- S.P. Ramachandran 6. Theraiyar Vaithyam - 1000 1st part
- S.P.Ramachandran 7. Theraiyar Vagadam
- S.P.Ramachandran 8. Theraiyar Neerkuri and Neikuri Nool
- S.P.Ramachandran 9. Thanvandhiri Vaidhayam
- S.P.Ramachandran 10. Agathiyar Gunavagadam
11. Pararasasekaram - Ponnaiyapillai
12. Pathinen Siddhar Naadi Sasthiram
13. Thirukkural - Thiruvalluvar
14. Agathiyar paripooranam - 1200 - S.P.Ramachandran
15. Noi Naadal Noi mudhal Naadal Thirattu. - I & II volume. - Dr. M. Shanmugavelu. HPIM. 16. Uyir Kakkum siddha maruthuvam @ Athma Ratchamirtham.
- S.P.Ramachandran.
17. T.V.Sambasivampillai Tamil & English Dictionary
18. Siddha maruthuvanga churukkam. - Dr.C.S.Uthamarayan. 19. Thotrakirama Araichium Siddha Maruthuva varalarum. - Dr.C.S.Uthamarayan. 20. Gunapadam - mooligai vaguppu.
- Dr.S.Murugesa mudhaliyar.

150
21. Siddha Maruthuvam sirappu. - Dr.R.Thiyagarajan C.I.M.
22. Maruthuva Thavara Iyal. - Dr.Somasundaram .
23. Sikicha Rathna Dheepam @ vaidhya chinthamani – I & II volume.
- C.Kannusamy pillai.
24. Thanvandhiri Vaidhyam- I volume.- Dr.S.Venkatarajan.
25. Angiosperms Vagaipadu. - Dr.S.Soma sundaram
26. Padhartha Guna Vilakkam. - C. Kannusamy Pillai.
Modern Books:
27. Indian Materia Medica-Vol I & II - Dr.K.M. Natkarni.
28. Quality standard Indian Medicinal Plants ICMR 2003
29. Materia Medica of India and their therapeutics.
30. Ross and Wilson’s Anatomy and Physiology.
31. Essential of Medical Physiology.
- Dr.K.Sembulingam and Prema Sembulingam. Ph.D.,
32. Robbinson’s Pathologic Basis of Disease.
33. Medicinal plants in India - T. Pullaiah
34. Indian Medicinal Plants Vol. I & II - Orient Longmann.no
35. Davidson’s Principle and Practice of Medicine.
36. Manual of Practical Medicine.
- Dr. R. Alagappan
37. Hutchison’s Clinical Methods.
38. Pharmacology and Pharmacotherapeutics
- K.D.Tripathi
39. www. icmr.nic.in
40. www.openmed.nic.in
41. www.wikipedia.org
Top Related
Copyright © 2022 FDOKUMEN

