WORLD HEALTH ASSEMBLY
222
OFFICIAL RECORDS OF THE WORLD HEALTH ORGANIZATION No. 127 SIXTEENTH WORLD HEALTH ASSEMBLY GENEVA, 7 - 23 MAY 1963 PART I RESOLUTIONS AND DECISIONS ANNEXES WORLD HEALTH ORGANIZATION GENEVA September 1963
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of WORLD HEALTH ASSEMBLY

OFFICIAL RECORDSOF THE
WORLD HEALTH ORGANIZATION
No. 127
SIXTEENTH
WORLD HEALTH ASSEMBLYGENEVA, 7 - 23 MAY 1963
PART I
RESOLUTIONS AND DECISIONS
ANNEXES
WORLD HEALTH ORGANIZATION
GENEVA
September 1963
The following abbreviations are used in the Official Records of the World Health Organization:
ACABQ
ACC
BTAO
CCTA
CIOMS
ECA
ECAFE
ECE
ECLA
FAO
IAEA
ICAO
ILO
IMCO
ITU
MESA
OIHP
OPEX
PAHO
PA SB
SMF
TAB
TAC
UNESCO
UNICEF
UNRWA
Advisory Committee on Administrative and Budgetary Questions
Administrative Committee on Co- ordination
Bureau of Technical Assistance Operations
Commission for Technical Co- operation in Africa
Council for International Organizations of Medical Sciences
Economic
Economic
Economic
Economic
Food and
Commission for Africa
Commission for Asia and the Far East
Commission for Europe
Commission for Latin America
Agriculture Organization
- International Atomic Energy Agency
- International Civil Aviation Organization
- International Labour Organisation (Office)
- Inter -Governmental Maritime Consultative Organization
- International Telecommunication Union
- Malaria Eradication Special Account
- Office International d'Hygiène Publique
- Programme (of the United Nations) for the provision of operational, executive andadministrative personnel
- Pan American Health Organization
- Pan American Sanitary Bureau
- Special Malaria Fund of PAHO
- Technical Assistance Board
- Technical Assistance Committee
- United Nations Educational, Scientific and Cultural Organization
- United Nations Children's Fund
- United Nations Relief and Works Agency for Palestine Refugees in the Near East
UNSCEAR - United Nations Scientific Committee on the Effects of Atomic Radiation
WFUNA - World Federation of United Nations Associations
WMO - World Meteorological Organization
The designations employed and the presentation of the material in this volume do not imply the expressionof any opinion on the part of the Director -General concerning the legal status of any country or territoryor of its authorities, or concerning the delimitation of its frontiers.
PRINTED IN SWITZERLAND

The Sixteenth World Health Assembly, held at the Palais des Nations, Geneva, from
7 to 23 May 1963, was convened in accordance with resolution WHA15.28 of the Fifteenth
World Health Assembly and resolution EB30.R9 of the Executive Board (thirtieth session).
The proceedings of the Sixteenth World Health Assembly are being published in two
parts. The resolutions, with annexes, are contained in this volume. The records ofplenary
and committee meetings will be printed, along with the list ofparticipants, agenda and other
material, in Official Records No. 128.
56502

In this volume the resolutions are reproduced in the numerical order in which they were adopted. However,in order to facilitate the use of the volume in conjunction with the Handbook of Resolutions and Decisions,they have been grouped by title in the table of contents under the subject -headings of the Handbook. Therehas also been added, beneath each resolution, a reference to the section of the Handbook containing previousresolutions on the same subject. The sixth edition of the Handbook -which is indexed both by subjectand by resolution symbol- contains most of the resolutions adopted up to and including the FourteenthWorld Health Assembly and the twenty- eighth session of the Executive Board.
The following reference list of sessions of the Health Assembly and Executive Board shows the resolutionsymbol applicable to each session and the Official Records volume in which the resolutions were originallypublished.
First World Health AssemblyExecutive Board, First SessionExecutive Board, Second SessionExecutive Board, Third Session
Held
24 June - 24 July 194816 -28 July 194825 October - 11 November 194821 February - 9 March 1949
Resolutionsymbol
OfficialRecords No.
13
14
14
17
Second World Health Assembly 13 June - 2 July 1949 WHA2.- 21
Executive Board, Fourth Session 8 -19 July 1949 22Executive Board, Fifth Session 16 January - 2 February 1950 25
Third World Health Assembly 8 -27 May 1950 WHA3.- 28
Executive Board, Sixth Session 1 -9 June 1950 EB6.R- 29
Executive Board, Seventh Session 22 January - 5 February 1951 EB7.R- 32
Fourth World Health Assembly 7 -25 May 1951 WHA4.- 35
Executive Board, Eighth Session 1 -8 June 1951 EB8.R- 36
Executive Board, Ninth Session 21 January - 4 February 1952 EB9.R- 40Fifth World Health Assembly 5 -22 May 1952 WHA5.- 42
Executive Board, Tenth Session 29 May - 3 June 1952 EB10.R- 43Executive Board, Eleventh Session 12 January - 4 February 1953 EB11.R- 46
Sixth World Health Assembly 5 -22 May 1953 WHA6.- 48Executive Board, Twelfth Session 28 -30 May 1953 EB12.R- 49Executive Board, Thirteenth Session 12 January - 2 February 1954 EB13.R- 52
Seventh World Health Assembly 4 -21 May 1954 WHA7.- 55
Executive Board, Fourteenth Session 27 -28 May 1954 EB14.R- 57
Executive Board, Fifteenth Session 18 January - 4 February 1955 EB15.R- 60
Eighth World Health Assembly 10 -27 May 1955 WHA8.- 63
Executive Board, Sixteenth Session 30 May 1.955 EB16.R- 65
Executive Board, Seventeenth Session 17 January - 2 February 1956 EB17.R- 68
Ninth World Health Assembly 8 -25 May 1956 WHA9.- 71
Executive Board, Eighteenth Session 28 -30 May 1956 EB18.R- 73
Executive Board, Nineteenth Session 15 -30 January 1957 EB19.R- 76Tenth World Health Assembly 7 -24 May 1957 WHA10.- 79
Executive Board, Twentieth Session 27 -28 May 1957 EB20.R- 80
Executive Board, Twenty -first Session 14 -28 January 1958 EB21.R- 83
Eleventh World Health Assembly 28 May - 13 June 1958 WHA11.- 87
Executive Board, Twenty- second Session 16 -17 June 1958 EB22.R- 88
Executive Board, Twenty -third Session 20 January - 3 February 1959 EB23.R- 91
Twelfth World Health Assembly 12 -29 May 1959 WHAl2.- 95Executive Board, Twenty- fourth Session 1 -2 June 1959 EB24.R- 96Executive Board, Twenty -fifth Session 19 January - 1 February 1960 EB25.R- 99
Thirteenth World Health Assembly 3 -20 May 1960 WHA13.- 102
Executive Board, Twenty -sixth Session 25 October - 4 November 1960 EB26.R- 106
Executive Board, Twenty- seventh Session 30 January - 2 February 1961 EB27.R- 108
Fourteenth World Health Assembly 7 -24 February 1961 WHA14.- 110
Executive Board, Twenty- eighth Session 29 May - 1 June 1961 EB28.R- 112
Executive Board, Twenty -ninth Session 15 -26 January 1962 EB29.R- 115
Fifteenth World Health Assembly 8 -25 May 1962 WHA15.- 118
Executive Board, Thirtieth Session 29 -30 May 1962 EB30.R- 120
Executive Board, Thirty -first Session 15 -28 January 1963 EB31.R- 124Sixteenth World Health Assembly 7 -23 May 1963 WHA16.- 127
Executive Board, Thirty- second Session 27 -28 May 1963 EB32.R- 129
- IV.. s"+i
l.+i / sfka! _
Index to resolutions: page 211
CONTENTS
RESOLUTIONS AND DECISIONSPage
Resolutions on Programme
WHA16.31 Continued Assistance to Newly Independent States 15
BIOLOGY AND PHARMACOLOGY
WHA16.36 Clinical and Pharmacological Evaluation of Drugs 18
WHA16.38 Clinical and Pharmacological Evaluation of Drugs : Standards of Drugs 19
MALARIA
Malaria EradicationWHA16.23 Report on the Development of the Malaria Eradication Programme 10
COMMUNICABLE DISEASES
Virus and Rickettsial Diseases
WHA16.37 Smallpox Eradication Programme 19
International QuarantineWHA16.34 Additional Regulations of 23 May 1963 amending the International Sanitary Regula-
tions, in particular with respect to Notifications 16
WHA16.35 Committee on international Quarantine : Eleventh Report 18
HEALTH PROTECTION AND PROMOTION
Mental HealthWHA16.25 Television Influence on Youth 1 l
Nutrition
WHA16.42 Joint FAO /WHO Programme on Food Standards (Codex Alimentarius) 21
REPORTS AND EVALUATION
Annual Report of the Director - General
WHA16.12 Annual Report of the Director- General fór 1962 6
Resolutions on Programme and Budget
CONSIDERATION AND APPROVAL OF PROGRAMME AND BUDGET ESTIMATES
WHA16.6 Supplementary Budget Estimates for 1963 2
WHA16.8 Addition to Schedule A to the Appropriation Resolutions for the Financial Years1962 and 1963 3
-V -
Page
WHA16.13 Effective Working Budget and Budget Level for 1964 6
WHA16.28 Appropriation Resolution for the Financial Year 1964 12
Resolutions concerning the World Health Assembly and Executive Board
WORLD HEALTH ASSEMBLY
Time and PlaceWHA16.16
EXECUTIVE BOARD
Selection of the Country in which the Seventeenth World Health Assembly will be held 7
Membership of the Board
WHA16.11 Election of Members entitled to designate a Person to serve on the Executive Board 5
Minutes, Resolutions and ReportsWHA16.44 Reports of the Executive Board on its Thirtieth and Thirty -first Sessions 22
Resolutions on Regional Matters
INDIVIDUAL REGIONS
Africa
WHA16.9WHA16.43
Accommodation for the Regional Office for Africa 3
Meetings of the Regional Committee for Africa 21
Resolutions on Constitutional and Legal Matters
MEMBERSHIP
Decisions Concerning Individual States and Territories
WHA16.3WHA16.4
Admission of New Associate Members : Mauritius 1
Admission of New Associate Members : Kenya 1
Resolutions on Financial and Administrative Matters
FINANCIAL MATTERS
Assessments and
WHA16.10WHA16.7WHA16.20
Financing of the
WHA16.17
WHA16.18
Contributions
Scale of Assessment for 1964Assessments of New Members for 1962 and 1963Status of Collection of Annual Contributions and of Advances to the Working Capital
Fund
4
3
8
Malaria Eradication Programme - Malaria Eradication Special AccountMalaria Eradication Special Account 7
Malaria Eradication Postage Stamps 7
Voluntary Fund for Health Promotion
WHA16.26
WHA16.27
Voluntary Fund for Health Promotion : Medical Research 11
Voluntary Fund for Health Promotion : Community Water Supply 12
- VI -
Page
Accounts and External AuditWHA16.14 Appointment of the External Auditor 6
WHA16.5 Financial Report on the Accounts of WHO for the Year 1962 and Report of theExternal Auditor 2
STAFF MATTERS
Staff Regulations and RulesWHA16.15 Amendments to the Staff Rules 6
Pension FundWHA16.19 Annual Report of the United Nations Joint Staff Pension Board for 1961 8
WHA16.21 Appointment of Representatives to the WHO Staff Pension Committee 9
Director - General
WHA16.1 Appointment of the Director -General 1
WHA16.2 Contract of the Director -General 1
WHO HEADQUARTERS
Construction of Separate WHO BuildingWHA16.22 Headquarters Accommodation : Progress Report 9
ORGANIZATIONAL STUDIES
WHA16.29 Organizational Study on Measures for providing Effective Assistance in MedicalEducation and Training to meet Priority Needs of the Newly Independentand Emerging Countries 14
WHA16.30 Organizational Study on Methods of Planning and Execution of Projects 15
Resolutions on Co- ordination and External Relations
UNITED NATIONS AND ITS AGENCIES
GeneralWHA16.32 Decisions of the United Nations, Specialized Agencies and IAEA affecting WHO's
Activities : Administrative, Budgetary and Financial Matters; Inter -organizationMachinery for Matters of Pay and Allowances 15
WHA16.33 Decisions of the United Nations, Specialized Agencies and IAEA affecting WHO'sActivities : Conference Arrangements 16
WHA16.39 Decisions of the United Nations, Specialized Agencies and IAEA affecting WHO'sActivities : Programme Matters 20
Social and Economic Matters
WHA16.40 United Nations Development Decade 20
Health of Children - Co- operation with UNICEFWHA16.24 Developments in Activities assisted jointly with UNICEF 11
Co- operation with the United Nations on Other Subjects
WHA16.41 Extension of the Agreement with UNRWA 20
- VII -

Page
Procedural Decisions
(i) Composition of the Committee on Credentials 23
(ii) Composition of the Committee on Nominations 23
(iii) Verification of Credentials 23
(iv) Election of Officers of the Sixteenth World Health Assembly 24
(v) Election of Officers of the Main Committees 24
(vi) Establishment of the General Committee 24
(vii) Adoption of the Agenda 24
ANNEXES
1. International Quarantine :I. Eleventh Report of the Committee on International Quarantine 27
2. Discussion by the Executive Board on the Eleventh Report of the Committee on Inter-national Quarantine 60
2. Financial Report on the Accounts of WHO for 1962 and Report of the External Auditor : Reportof the Ad Hoc Committee of the Executive Board 63
3. Supplementary Budget Estimates for 1963 :1. Report of the Ad Hoc Committee of the Executive Board 65
2. Report by the Director -General 66
4. Accommodation for the Regional Office for Africa :
1. Report of the Ad Hoc Committee of the Executive Board 71
2. Report by the Director- General 72
5. Malaria Eradication Special Account 74
6. Malaria Eradication Postage Stamps 79
7. Headquarters Accommodation :1. Report of the Ad Hoc Committee of the Executive Board 87
2. Progress Report by the Director -General 89
8. Development of the Malaria Eradication Programme in 1962 92
9. Review and Approval of the Programme and Budget Estimates for 1964 :
1. Report of the Ad Hoc Committee of the Executive Board 157
2. Report by the Director -General 158
10. Summary of Budget Estimates for the Financial Year 1 January - 31 December 1964 161
11. Decisions of the United Nations, Specialized Agencies and the International Atomic Energy Agencyaffecting WHO's Activities (Administrative, Budgetary and Financial Matters) 165
12. Clinical and Pharmacological Evaluation of Drugs 166
13. United Nations Development Decade 168
14. Meetings of the Regional Committee for Africa 180
15. Organizational Study on Measures for Providing Effective Assistance in Medical Education andTraining to meet Priority Needs of the Newly Independent and Emerging Countries 182
16. Smallpox Eradication Programme 195
Index to Resolutions and Decisions 211
- viii -

RESOLUTIONS AND DECISIONS
WHA16.1 Appointment of the Director -General
The Sixteenth World Health Assembly,
On the nomination of the Executive Board,
REAPPOINTS Dr M. G. Candau as Director -General of the World Health Organization.
Handb. Res., 6th ed., 7.3.10.2 Fourth plenary meeting, 8 May 1963
WHA16.2 Contract of the Director -General
The Sixteenth World Health Assembly,
1. Pursuant to Article 31 of the Constitution and Rule 106 of the Rules of Procedure of the World HealthAssembly,
APPROVES the contract establishing the terms and conditions of appointment, salary and other emolumentsfor the post of Director -General; 1 and
II. Pursuant to Rule 110 of the Rules of Procedure of the World Health Assembly,AUTHORIZES the President of the Sixteenth World Health Assembly to sign this contract in the name
of the Organization.
Handb. Res., 6th ed., 7.3.10.2 Fourth plenary meeting, 8 May 1963
WHA16.3 Admission of New Associate Members : Mauritius
The Sixteenth World Health Assembly
ADMITS Mauritius as an Associate Member of the World Health Organization, subject to notice beinggiven of acceptance of associate membership on behalf of Mauritius in accordance with Rules 115 and 116of the Rules of Procedure of the World Health Assembly.
Handb. Res., 6th ed., 6.2.1.2 Sixth plenary meeting, 9 May 1963
WHA16.4 Admission of New Associate Members : Kenya
The Sixteenth World Health Assembly
ADMITS Kenya as an Associate Member of the World Health Organization, subject to notice beinggiven of acceptance of associate membership on behalf of Kenya in accordance with Rules 115 and 116of the Rules of Procedure of the World Health Assembly.
Handb. Res., 6th ed., 6.2.1.2 Sixth plenary meeting, 9 May 1963
1 Of. Rec. WO Hlth Org. 124, Annex 16, Appendix.
- 1 -
SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
WHA16.5 Financial Report on the Accounts of WHO for the Year 1962 and Report of the External Auditor
The Sixteenth World Health Assembly,
Having examined the Financial Report of the Director -General for the period 1 January to 31 December1962 and the Report of the External Auditor for the same financial period, as contained in Official RecordsNo. 126; and
Having considered the report of the Ad Hoc Committee of the Executive Board on its examination ofthese reports,'
ACCEPTS the Director -General's Financial Report and the Report of the External Auditor for the financialyear 1962.
Handb. Res., 6th ed., 7.1.11.3
WHA16.6 Supplementary Budget Estimates for 1963
Seventh plenary meeting, 14 May 1963 (Committeeon Administration, Finance and Legal Matters, firstreport)
The Sixteenth World Health Assembly,
Having considered the proposals of the Director -General and the recommendations of the ExecutiveBoard concerning supplementary budget estimates for 1963, 21. APPROVES the supplementary estimates for 1963;2. DECIDES to amend the Appropriation Resolution for 1963 (resolution WHA15.42) by increasing theamounts voted under paragraph I as follows :
Appropriation Purpose of Appropriation AmountSection US $
PART II : OPERATING PROGRAMME
4. Programme Activities 95 2505. Regional Offices 23 7007. Other Statutory Staff Costs 142 180
Total - Part II 261 130
PART III: ADMINISTRATIVE SERVICES
8. Administrative Services 27 3509. Other Statutory Staff Costs 36 620
Total - Part III 63 970
PART IV : OTHER PURPOSES
10. Headquarters Building Fund 113 000
Total - Part IV 113 000
TOTAL - PARTS II, III AND 1V 438 100
' See Annex 2.2 See Annex 3.

RESOLUTIONS AND DECISIONS 3
3. DECIDES further to amend paragraph III of resolution WHA15.42 by increasing the amounts undersub -paragraphs (i) and (iii) as follows :
(i) the amount of $ 35 990 available by reimbursement from the Special Account of the ExpandedProgramme of Technical Assistance
(iii) the amount of $ 402 110 representing miscellaneous income available for the purpose
$ 438 100
H ando. Res., 6th ed., 2.1 Seventh plenary meeting, 14 May 1963 (Committeeon Administration, Finance and Legal Matters, firstreport)
WHA16.7 Assessments of New Members for 1962 and 1963
The Sixteenth World Health Assembly,
Noting that several States became Members of the Organization during 1962 and 1963 by depositingwith the Secretary -General of the United Nations a formal instrument of acceptance of the WHO Consti-tution,
DECIDES that these Members shall be assessed as follows :
Member State 1962Per cent.
1963Per cent.
Algeria 0.04 0.04Burundi 0.04 0.04Rwanda 0.04 0.04Trinidad and Tobago 0.04Uganda 0.04Jamaica 0.04
Handb. Res., 6th ed., 7.1.2.2 Seventh plenary meeting, 14 May 1963 (Committeeon Administration, Finance and Legal Matters, firstreport)
WHA16.8 Addition to Schedule A to the Appropriation Resolutions for the Financial Years 1962 and 1963
The Sixteenth World Health Assembly
DECIDES that, since Algeria, Burundi, Rwanda, Trinidad and Tobago, Uganda, Jamaica, Kenya, andMauritius are carrying out malaria programmes, they are eligible for credits in 1962 and /or 1963 in thesame way as those Members listed in Schedule A attached to the Appropriation Resolutions for the financialyears 1962 and /or 1963.1
Handb. Res., 6th ed., 2.1; 2.1.15 Seventh plenary meeting, 14 May 1963 (Committeeon Administration, Finance and Legal Matters, firstreport)
WHA16.9 Accommodation for the Regional Office for Africa
The Sixteenth World Health Assembly,
Having considered the report of the Director -General on accommodation for the Regional Office forAfrica and the report of the Executive Board thereon; 2
1 Resolutions WHA14.43 and WHA15.42.2 See Annex 4.
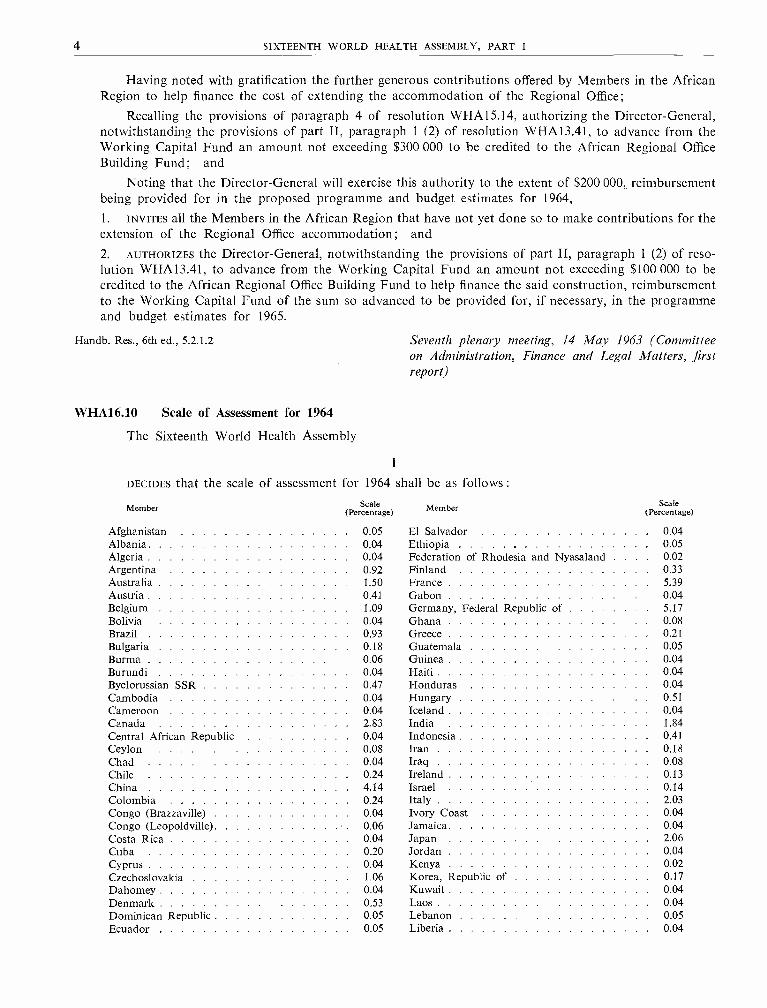
4 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Having noted with gratification the further generous contributions offered by Members in the AfricanRegion to help finance the cost of extending the accommodation of the Regional Office;
Recalling the provisions of paragraph 4 of resolution WHA15.14, authorizing the Director -General,notwithstanding the provisions of part II, paragraph 1 (2) of resolution WHA13.41, to advance from theWorking Capital Fund an amount not exceeding $300 000 to be credited to the African Regional OfficeBuilding Fund; and
Noting that the Director -General will exercise this authority to the extent of $200 000, reimbursementbeing provided for in the proposed programme and budget estimates for 1964,1. INVITES all the Members in the African Region that have not yet done so to make contributions for theextension of the Regional Office accommodation; and
2. AUTHORIZES the Director -General, notwithstanding the provisions of part II, paragraph 1 (2) of reso-lution WHA13.41, to advance from the Working Capital Fund an amount not exceeding $100 000 to becredited to the African Regional Office Building Fund to help finance the said construction, reimbursementto the Working Capital Fund of the sum so advanced to be provided for, if necessary, in the programmeand budget estimates for 1965.
Handb. Res., óth ed., 5.2.1.2
WHA16.10 Scale of Assessment for 1964
The Sixteenth World Health Assembly
Seventh plenary meeting, 14 May 1963 (Committeeon Administration, Finance and Legal Matters, firstreport)
I
DECIDES that the scale of assessment for 1964 shall be as follows :
Member (Percentage) Member (Perscentage)
Afghanistan 0 05 El Salvador 0 04Albania 0 04 Ethiopia 0 05Algeria 0 04 Federation of Rhodesia and Nyasaland . . 0.02Argentina 0 92 Finland 0 33Australia 1 50 France 5 39Austria 0 41 Gabon 0 04Belgium 1 09 Germany, Federal Republic of 5 17Bolivia 0 04 Ghana 0 08Brazil 0 93 Greece 0 21Bulgaria 0 18 Guatemala 0 05Burma 0 06 Guinea 0 04Burundi 0 04 Haiti 0 04Byelorussian SSR 0 47 Honduras 0 04Cambodia 0 04 Hungary 0 51Cameroon 0 04 Iceland 0 04Canada 2 83 India 1 84Central African Republic 0 04 Indonesia 0 41Ceylon 0 08 Iran 0 18Chad 0 04 Iraq 0 08Chile 0 24 Ireland 0 13China 4 14 Israel 0 14Colombia 0 24 Italy 2 03Congo (Brazzaville) 0 04 Ivory Coast 0 04Congo (Leopoldville) 0 06 Jamaica 0 04Costa Rica 0 04 Japan 2 06Cuba 0 20 Jordan 0 04Cyprus 0 04 Kenya 0 02Czechoslovakia 1 06 Korea, Republic of 017Dahomey 0 04 Kuwait 0 04Denmark 0 53 Laos 0 04Dominican Republic 0 05 Lebanon 0 05Ecuador 0 05 Liberia 0 04
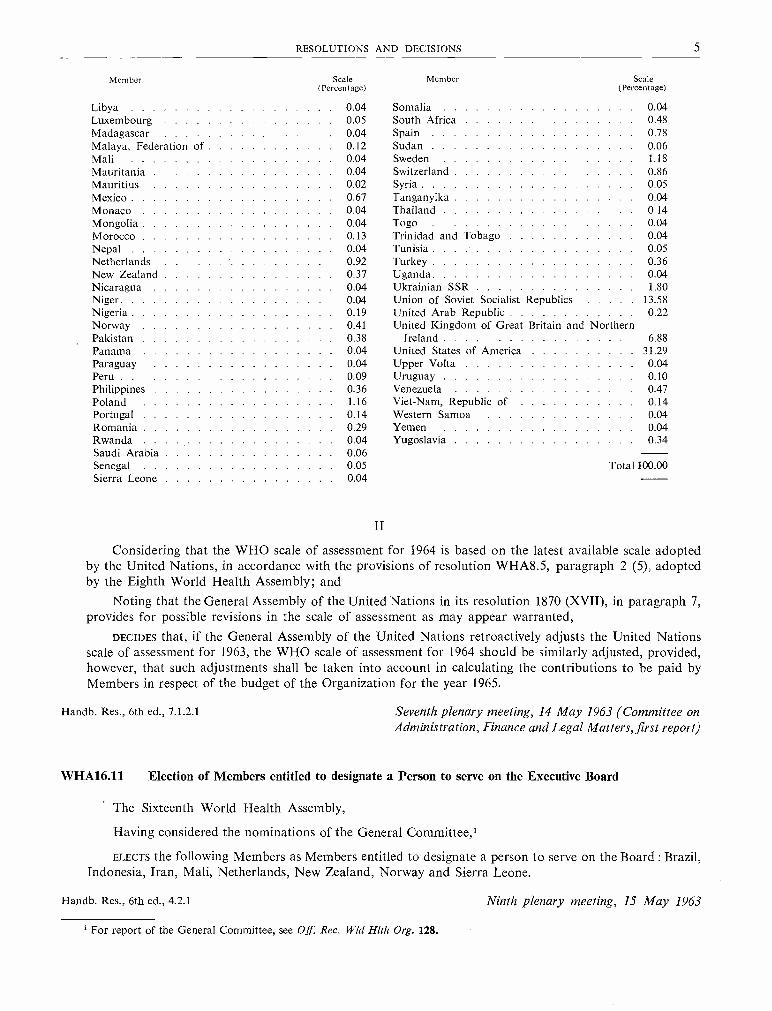
RESOLUTIONS AND DECISIONS 5
Member - Scale(Percentage)
Member Scale(Percentage)
Libya 0 04 Somalia 0 04
Luxembourg 0 05 South Africa 0 48
Madagascar 0 04 Spain 0 78Malaya, Federation of 0 12 Sudan 0 06Mali 0 04 Sweden 1 18Mauritania 0 04 Switzerland 0 86Mauritius 0 02 Syria 0 05Mexico 0 67 Tanganyika 0 04Monaco 0 04 Thailand 0 14
Mongolia 0 04 Togo 0 04
Morocco 0 13 Trinidad and Tobago 0 04
Nepal 004 Tunisia 0 05Netherlands 0 92 Turkey 0 36New Zealand 0 37 Uganda 0 04Nicaragua 0 04 Ukrainian SSR 1 80Niger 0 04 Union of Soviet Socialist Republics 13 58Nigeria 0 19 United Arab Republic 0 22Norway 0 41 United Kingdom of Great Britain and NorthernPakistan 0 38 Ireland 6 88Panama 0 04 United States of America 31 29Paraguay 0 04 Upper Volta 004Peru 0 09 Uruguay 0 10Philippines 0 36 Venezuela 0 47Poland 1 16 Viet -Nam, Republic of 014Portugal 0 14 Western Samoa 0 04
Romania 0 29 Yemen 0 04
Rwanda 0 04 Yugoslavia 0 34Saudi Arabia 0 06
100.00Senegal 0 05 TotalSierra Leone 0 04
II
Considering that the WHO scale of assessment for 1964 is based on the latest available scale adoptedby the United Nations, in accordance with the provisions of resolution WHA8.5, paragraph 2 (5), adoptedby the Eighth World Health Assembly; and
Noting that the General Assembly of the United Nations in its resolution 1870 (XVII), in paragraph 7,provides for possible revisions in the scale of assessment as may appear warranted,
DECIDES that, if the General Assembly of the United Nations retroactively adjusts the United Nationsscale of assessment for 1963, the WHO scale of assessment for 1964 should be similarly adjusted, provided,however, that such adjustments shall be taken into account in calculating the contributions to be paid byMembers in respect of the budget of the Organization for the year 1965.
Handb. Res., 6th ed., 7.1.2.1 Seventh plenary meeting, 14 May 1963 (Committee onAdministration, Finance and Legal Matters, first report)
WHA16.11 Election of Members entitled to designate a Person to serve on the Executive Board
The Sixteenth World Health Assembly,
Having considered the nominations of the General Committee,1
ELECTS the following Members as Members entitled to designate a person to serve on the Board : Brazil,Indonesia, Iran, Mali, Netherlands, New Zealand, Norway and Sierra Leone.
Handb. Res., 6th ed., 4.2.1 Ninth plenary meeting, 15 May 1963
1 For report of the General Committee, see Off. Rec. Wld Hith Org. 128.
6 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
WHA16.12 Annual Report of the Director -General for 1962
The Sixteenth World Health Assembly,
Having reviewed the Report of the Director -General on the work of WHO during 1962,'
1. NOTES with satisfaction the manner in which the programme was planned and carried out in 1962, inaccordance with the established policies of the Organization; and
2. COMMENDS the Director -General for the work accomplished.
Handb. Res., 6th ed., 1.14.1 Tenth plenary meeting, 16 May 1963
WHA16.13 Effective Working Budget and Budget Level for 1964
The Sixteenth World Health Assembly
DECIDES that :
(1) the effective working budget for 1964 shall be US $34 065 100;(2) the budget level for 1964 shall be established in an amount equal to the effective working budgetas provided in paragraph (1) above, plus the assessments represented by the Undistributed Reserve; and
(3) the budget for 1964 shall be financed by assessments on Members after deducting(i) the amount of US $756 990 available by reimbursement from the Special Account of theExpanded Programme of Technical Assistance; and(ii) the amount of US $849 100 available as casual income for 1964.
Handb. Res., 6th ed., 2.1 Tenth plenary meeting, 16 May 1963 (Committee onProgramme and Budget, first report)
WHA16.14 Appointment of the External Auditor
The Sixteenth World Health Assembly
RESOLVES that Mr Uno Brunskog be appointed external auditor of the accounts of the World HealthOrganization for the three financial years 1964 to 1966 inclusive, to make his audits in accordance with theprinciples incorporated in Article XII of the Financial Regulations, with the provision that, should thenecessity arise, he may designate a representative to act in his absence.
Handb. Res., 6th ed., 7.1.11.1
WHA16.15 Amendments to the Staff Rules
Eleventh plenary meeting, 18 May 1963 (Committee onAdministration, Finance and Legal Matters, secondreport)
The Sixteenth World Health Assembly
NOTES the amendments to the Staff Rules made by the Director -General and confirmed by the ExecutiveBoard.2
Handb. Res., 6th ed., 7.3.1.2 Eleventh plenary meeting, 18 May 1963 (Committee onAdministration, Finance and Legal Matters, secondreport)
1 Off. Rec. Wld Hlth Org. 123.2 Of Rec. Wld Hlth Org. 124, resolution EB31.R37 and Annex 6.
RESOLUTIONS AND DECISIONS 7
WHA16.16 Selection of the Country in which the Seventeenth World Health Assembly will be held
The Sixteenth World Health Assembly,
Considering the provision of Article 14 of the Constitution with regard to the selection of the countryor region in which the next Health Assembly will be held,
DECIDES that the Seventeenth World Health Assembly shall be held in Switzerland.
Handb. Res., 6th ed., 4.1.1.2
WHA16.17 Malaria Eradication Special Account
Eleventh plenary meeting, 18 May 1963 (Committee onAdministration, Finance and Legal Matters, secondreport)
The Sixteenth World Health Assembly,
Having considered the report of the Director - General on the Malaria Eradication Special Account;Having noted that the financing of the " regular " malaria eradication programme for the year 1963
is assured and that, according to resolution WHA14.15, the full cost of the " regular " malaria eradicationprogramme for the year 1964 is included in the proposed regular budget estimates;
Realizing, however, that funds are available only for financing a portion of the " accelerated " malariaeradication programme planned for 1963 and 1964;
Noting further that the " accelerated " programme will be financed through funds set aside by theDirector -General not only for the current year's obligations but also for continuing commitments in theensuing year either up to the full completion of any individual activity approved for implementation withina period of two years, or to such appropriate phase of the activity as would be decided in each instancedepending upon its nature,
1. REQUESTS the Director - General to transmit this resolution together with the report of the Director -General to all Members of the Organization, calling particular attention to the Assembly's expression ofappreciation to the donors to the Malaria Eradication Special Account; and2. REITERATES its appeal to Members in a position to do so, and especially to economically more developedMembers, to make voluntary contributions to the Malaria Eradication Special Account in order to enablethe Organization to carry out planned " accelerated " operations.
Handb. Res., 6th ed., 7.1.8
WHA16.18 Malaria Eradication Postage Stamps
Eleventh plenary meeting, 18 May 1963 (Committee onAdministration, Finance and Legal Matters, secondreport)
The Sixteenth World Health Assembly,
Having considered the Director -General's report on the malaria eradication postage stamp campaign," The World United against Malaria "; 2 and
Taking into account the final list of participants, with the dates of issue of their stamps and relatedphilatelic material, under the World Health Organization's malaria eradication postage stamp plan, as shownin Appendix 2 of the report,
1. NOTES with satisfaction the results obtained through this philatelic campaign in publicizing the worldmalaria eradication programme and in raising funds for the Malaria Eradication Special Account;
1 See Annex 5.2 See Annex 6.

8 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
2. THANKS the governments that have participated in the project;
3. EXPRESSES its appreciation to those governments that have offered donations either in stamps and otherphilatelic material or in cash;
41 NOTES that the sale of stamps and related philatelic material will close during the year 1963 and that anyunsold philatelic material will be duly destroyed by the Organization in the manner described in the reportof the Director -General; and
5. REQUESTS the Director -General to submit a final financial report on this project to a subsequent sessionof the Executive Board or the World Health Assembly.
Handb. Res., 6th ed., 7.1.8 Eleventh plenary meeting, 18 May 1963 (Committee onAdministration, Finance and Legal Matters, secondreport)
WHA16.19 Annual Report of the United Nations Joint Staff Pension Board for 1961
The Sixteenth World Health Assembly
NOTES the status of the operation of the Joint Staff Pension Fund as indicated by the annual report forthe year 1961 and as reported by the Director -General.
Handb. Res., 6th ed., 7.3.7.2 Eleventh plenary meeting, 18 May 1963 (Committee onAdministration, Finance and Legal Matters, secondreport)
WHA16.20 Status of Collection of Annual Contributions and of Advances to the Working Capital Fund
The Sixteenth World Health Assembly,
1
Having considered the report of the Director -General on the status of collection of contributions and ofadvances to the Working Capital Fund as at 30 April 1963;
Noting with satisfaction that a large number of Members have paid their annual contributions andadvances to the Working Capital Fund,
1. CALLS THE ATTENTION of Members to the importance of paying their contributions as early as possiblein the Organization's financial year;
2. REQUESTS Members which have not done so to provide in their national budgets for regular payment tothe World Health Organization of their annual contributions; and
3. URGES those Members concerned to make special efforts to liquidate their arrears in the shortest possibletime;
II
Considering that the continued non -payment of arrears could make it necessary to abandon or curtailapproved programmes of the Organization;
Noting further with regret that the arrears of Bolivia, Guatemala, Haiti, Panama and Uruguay make itnecessary for the Assembly to consider, in accordance with Article 7 of the Constitution and the provisionsof paragraph 2 of resolution W HA8.13, whether or not their right to vote should be suspended at the SixteenthWorld Health Assembly,
1. DECIDES not to suspend the voting rights of the delegations concerned at the Sixteenth World HealthAssembly;

RESOLUTIONS AND DECISIONS 9
2. REQUESTS the Executive Board, at its sessions when the agenda of the World Health Assembly is prepared,to make specific recommendations, with the reasons therefor, to the Health Assembly with regard to anyMembers in arrears in the payment of contributions to the Organization to an extent which would invokethe provisions of Article 7 of the Constitution;
3. INVITES Members that are in arrears to an extent which would invoke the provisions of Article 7 of theConstitution to submit to the Executive Board a statement of their intentions as to payment of their arrears, sothat the Health Assembly, when it considers the matter in accordance with the provisions of reso-lution WHA8.13, will be able to make its decision on the basis of the statements of such Members and therecommendations of the Executive Board;
4. REQUESTS the Director - General to study with the Member States concerned the difficulties of thesecountries and to report to the appropriate sessions of the Executive Board and the World Health Assembly;
5. REQUESTS further the Director -General to communicate this resolution to the Members which may beconcerned.
Handb. Res., 6th ed., 7.1.2.4; 7.1.3.3 Eleventh plenary meeting, 18 May 1963 (Committee onAdministration, Finance and Legal Matters, thirdreport) .
WHA16.21 Appointment of Representatives to the WHO Staff Pension Committee
The Sixteenth World Health Assembly
RESOLVES that the member of the Executive Board designated by the Government of Mali be appointedas member of the WHO Staff Pension Committee, and that the member of the Board designated by theGovernment of New Zealand be appointed as alternate member, the appointments being for a period of threeyears.
Handb. Res., 6th ed., 7.3.7.3 Eleventh plenary meeting, 18 May 1963 (Committee onAdministration, Finance and Legal Matters, third.report)
WHA16.22 Headquarters Accommodation : Progress Report
The Sixteenth World Health Assembly,
Noting the reports and recommendations of the Executive Board,' its Standing Committee on Head-quarters Accommodation,' and its Ad Hoc Committee,' as well as the report of the Director -General onheadquarters accommodation;'
Noting the substantial increase in construction costs since the Thirteenth World Health Assemblyauthorized the construction of a headquarters building;
Recognizing the importance of adhering to good quality standards of construction in the interest of staffefficiency and of long -term economy in maintenance;
Taking into account that making a reasonable provision for underground parking at this stage in theconstruction programme will result in an economy for the Organization over a period of years; and
Considering therefore that it is necessary to re- establish such provision as was included in the originalarrangement for the building,
1. EXPRESSES its appreciation to the Executive Board, and to its Standing Committee on HeadquartersAccommodation, for the continuing surveillance of this undertaking;
' Of Rec. Wld Hlth Org. 124, resolutions EB31.R22 and EB31.R25 and Annex 15.' Of Rec. Wld Hith Org. 124, Annex 15, part 1.3 See Annex 7.

10 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
2. ACKNOWLEDGES with appreciation the action of those Member governments which have contributedto the building project and invites other Member governments to do likewise;
3. DECIDES to revise operative paragraph 1 of resolution WHA13.46 by authorizing the construction of thebuilding at a cost not exceeding Sw. fr. 60 000 000;
4. DECIDES furthermore that, subject to the total authorization of funds for the building project, provisionfor underground parking for about 300 vehicles should be made;
5. REAFFIRMS its expressions of appreciation to the Government of the Swiss Confederation and of theRepublic and Canton of Geneva for the generous assistance already provided toward the realization of theheadquarters building;
6. EXPRESSES its hope that the host government will find it possible to provide on an interest -free basis theremaining credits required; and
7. REQUESTS the Executive Board and the Director - General to report further to the Seventeenth WorldHealth Assembly, including a report on the definitive arrangements for the financing of the additional costs.
Handb. Res., 6th ed., 7.4.2.1 Eleventh plenary meeting, 18 May 1963 (Committee onAdministration, Finance and Legal Matters, thirdreport)
WHA16.23 Report on the Development of the Malaria Eradication Programme
The Sixteenth World Health Assembly,
Having considered the report of the Director -General on the development of the malaria eradicationprogramme; 1
Noting that the objectives of the co- ordinated plan for continental Europe had been successfully fulfilledin that all the remaining malarious areas had reached the consolidation phase by the end of 1962;
Noting the outstanding progress towards eradication during the past year, in which areas inhabited bymillions of people passed from the attack to the consolidation phase, mainly in South -East Asia and in theAmericas; and
Recognizing that administrative and technical problems such as inadequate health services, particularepidemiological patterns, insecticide resistance or changes in the behaviour of the vectors, as well as parasiteresistance to drugs, may delay the effective development of malaria eradication in certain areas,
1. INVITES governments to undertake preliminary operations or to pursue with vigour the eradication pro-grammes to their planned conclusion and to collaborate with neighbouring countries on a regional basis topermit progress to be made on a broad geographical area and for mutual protection against reintroduction of thedisease;
2. RECOMMENDS, in countries without the administrative and public health facilities for full implementationof malaria eradication programmes, the parallel development in a flexible way of a minimum public healthservice on the basis of total coverage, to support effectively such programmes especially during the consolida-tion and maintenance phases;
3. REQUESTS the Director - General to provide appropriate assistance for the study and solution of thetechnical difficulties found in problem areas and to pursue research into the development of methods toovercome the technical difficulties encountered in malaria eradication;
4. REQUESTS the Director -General to study the present position in regard to the implementation of themalaria eradication programme, its achievements, shortcomings and prospects, including the provision ofadequate staff and finances for the global eradication programme, and to submit a report on the matter tothe World Health Assembly as early as possible; and
1 See Annex 8.
RESOLUTIONS AND DECISIONS 11
5. REQUESTS the Director -General to report further progress in the malaria eradication programme to theSeventeenth World Health Assembly.
Handb. Res., 6th ed., 1.4.2 Eleventh plenary meeting, 18 May 1963 (Committee onProgramme and Budget, second report)
WHA16.24 Developments in Activities assisted jointly with UNICEF
The Sixteenth World Health Assembly,
Having considered the report of the Director - General on developments in activities assisted jointlywith UNICEF,
1. NOTES the report of the Director -General;
2. ENDORSES the views expressed by the Executive Board at its thirty -first session,' with particular emphasison UNICEF's continued support of programmes for the establishment of basic health services, educationand training, and for mass control and eradication campaigns against communicable diseases, and theimportance of assistance to malaria eradication activities, particularly in Africa;
3. EXPRESSES its satisfaction with the continuing close and efficient co- operation between the two organi-zations in jointly- assisted programmes; and
4. REQUESTS the Director -General to transmit to UNICEF the concern of WHO in that any reduction inmaterial assistance to joint UNICEF /WHO activities would adversely affect the health and welfare of children.
Handb. Res., 6th ed., 8.1.4.1 Eleventh plenary meeting, 18 May 1963 (Committee onProgramme and Budget, second report)
WHA16.25 Television Influence on Youth
The Sixteenth World Health Assembly,
Aware of the great influence of television programmes and of the risk that those based on violence andcrime may adversely affect mental health, particularly of the younger viewers;
Taking into account the need to obtain a scientific assessment of the effects of such programmes; andMindful of the different measures taken by governments to secure the avoidance of harmful influences,
1. STRESSES the educational value of television, with special regard to programmes in the field of healtheducation and medical training; and
2. RECOMMENDS that national health authorities encourage the study of television influence on mental health,particularly of children and young adults.
Handb. Res., 6th ed., 1.7.2 Twelfth plenary meeting, 22 May 1963 (Committee onProgramme and Budget, third report)
WHA16.26 Voluntary Fund for Health Promotion : Medical Research
The Sixteenth World Health Assembly,
Considering that the programme planned under the Special Account for Medical Research as set forthin Official Records No. 121, Annex 4, is satisfactory;
1 Resolution EB31.R32.
12 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Noting that this programme is complementary to the research programme included in the regular budgetof the Organization; and
Emphasizing the world -wide importance of medical research,
1. EXPRESSES the hope that more countries will make voluntary contributions to the Special Account;
2. REQUESTS the Director - General to implement the medical research programme, within the broad conceptof the third general programme of work for a specific period, to the extent that funds become availablethrough voluntary contributions to the Special Account; and
3. INVITES the Director - General to take such further action as would most effectively contribute to thedevelopment of the medical research programme.
Handb. Res., 6th ed., 7.1.9; 1.11 Twelfth plenary meeting, 22 May 1963 (Committee onProgramme and Budget, third report)
WHA16.27 Voluntary Fund for Health Promotion : Community Water Supply
The Sixteenth World Health Assembly,
Considering that the programme planned under the Special Account for Community Water Supplyas set forth in Official Records No. 121, Annex 4, is satisfactory; and
Believing that this programme is of considerable importance in stimulating and assisting countries todevelop plans for community water supply systems,
1. EXPRESSES the hope that more countries will make voluntary contributions to the Special Account;
2. REQUESTS the Director- General to implement the planned programme, within the broad concept of thethird general programme of work for a specific period, to the extent that funds become available throughvoluntary contributions to the Special Account; and
3. INVITES the Director- General to take such further action as would most effectively contribute to thedevelopment of the community water supply programme.
Handb. Res., 6th ed., 7.1.9; 1.8 Twelfth plenary meeting, 22 May 1963 (Committee onProgramme and Budget, third report)
WHA16.28 Appropriation Resolution for the Financial Year 1964 1
I.
The Sixteenth World Health Assembly
RESOLVES to appropriate for the financial year 1964 an amount of US $36 288 230 as follows :
Appropriation Purpose of Appropriation AmountSection US $
PART I : ORGANIZATIONAL MEETINGS
1. World Health Assembly 317 2102. Executive Board and its Committees 189 0903. Regional Committees 100 530
Total - Part I 606 830
1 See Annex 9. For analysis of these appropriations under chapters, see Annex 10.

RESOLUTIONS AND DECISIONS 13
Appropriation Purpose of AppropriationSection
PART II : OPERATING PROGRAMME
AmountUS $
4. Programme Activities 16 439 8195. Regional Offices 2 663 7066. Expert Committees 226 6007. Other Statutory Staff Costs 5 521 280
Total - Part II 24 851 405
PART III : ADMINISTRATIVE SERVICES
8. Administrative Services 1 925 1829. Other Statutory Staff Costs 618 683
Total - Part III 2 543 865
PART IV: OTHER PURPOSES
10. Headquarters Building Fund 500 00011. Transfer to the Malaria Eradication Special Account 5 363 00012. Reimbursement of the Working Capital Fund 200 000
Total - Part IV 6 063 000
SUB -TOTAL - PARTS I, II, III AND IV 34 065 100
PART V : RESERVE
13. Undistributed Reserve 2 223 130
Total - Part V 2 223 130
TOTAL - ALL PARTS 36 288 230
II. Amounts not exceeding the appropriations voted under paragraph I shall be available for the paymentof obligations incurred during the period 1 January to 31 December 1964 in accordance with the provisionsof the Financial Regulations.
Notwithstanding the provisions of this paragraph, the Director -General shall limit the obligations to beincurred during the financial year 1964 to the effective working budget established by the World HealthAssembly, i.e. Parts I, II, III and IV.
III. The appropriations voted under paragraph I shall be financed by contributions from Members afterdeduction of :
(i) the amount of $ 756 990
(ii) the amount of $ 98 860(iii) the amount of $ 454 733(iv) the amount of $ 295 507
Total $1 606 090
available by reimbursement from the Special Account of theExpanded Programme of Technical Assistancerepresenting assessments on new Members from previous yearsrepresenting miscellaneous income available for the purposeavailable by transfer from the cash portion of the Assembly SuspenseAccount
thus resulting in assessments against Members of $34 682 140.

14 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
IV. The Director -General is authorized to transfer an amount not exceeding US $190 060 from the cashbalance available in the Malaria Eradication Special Account to cover the credits towards the payment ofcontributions of Members in accordance with Schedule A attached.
SCHEDULE ATO THE APPROPRIATION RESOLUTION FOR THE FINANCIAL YEAR 1964
Members eligible for credits of 25 per cent.' towards the payment of their contributions in respect of that portion of their assess-ments corresponding to the total amount voted for Appropriation Section 11 under Part IV (Other Purposes) of paragraph I of theAppropriation Resolution :
Afghanistan Ecuador Laos RwandaAlbania El Salvador Lebanon Saudi ArabiaAlgeria Ethiopia Liberia Senegal
* Argentina Federation of Rhodesia and Libya Sierra LeoneBolivia Nyasaland Madagascar Somalia
* Brazil Gabon Malaya, Federation of South AfricaBulgaria Ghana Mali * SpainBurma Greece Mauritania SudanBurundi Guatemala Mauritius SyriaCambodia Guinea * Mexico TanganyikaCameroon Haiti Morocco ThailandCentral African Republic Honduras Nepal TogoCeylon * India Nicaragua Trinidad and TobagoChad Indonesia Niger Tunisia
* China Iran Nigeria TurkeyColombia Iraq Pakistan UgandaCongo (Brazzaville) Israel Panama United Arab RepublicCongo (Leopoldville) Ivory Coast Paraguay Upper VoltaCosta Rica Jamaica Peru VenezuelaCuba Jordan Philippines Viet -Nam, Republic ofDahomey Kenya Portugal YemenDominican Republic Korea, Republic of Romania Yugoslavia
Handb. Res., 6th ed., 2.1 Twelfth plenary meeting, 22 May 1963 (Committee onProgramme and Budget, third report)
WHA16.29 Organizational Study on Measures for providing Effective Assistance in Medical Education andTraining to meet Priority Needs of the Newly Independent and Emerging Countries
The Sixteenth World Health Assembly,
Having considered the report of the Executive Board on its organizational study on " Measures forproviding effective assistance in medical education and training to meet priority needs of the newly independentand emerging countries ",2 prepared at the request of the Fifteenth World Health Assembly,3
1. THANKS the Board for the study made; and
2. REQUESTS the Director- General to develop the education and training programme further, taking intoaccount the contents of the report and the comments of the Committee on Programme and Budget of theSixteenth World Health Assembly.
Handb. Res., 6th ed., 7.5 Twelfth plenary meeting, 22 May 1963 (Committee onProgramme and Budget, fourth report)
* Eligible under resolution WHA15.35.' In accordance with resolution WHA14.15.2 See Annex 15.3 Resolution WHA15.59.
RESOLUTIONS AND DECISIONS 15
WHA16.30 Organizational Study on Methods of Planning and Execution of Projects
The Sixteenth World Health Assembly
NOTES the report on the progress of the organizational study on the methods of planning and executionof projects.
Handb. Res., 6th ed., 7.5 Twelfth plenary meeting, 22 May 1963 (Committee onProgramme and Budget, fourth report)
WHA16.31 Continued Assistance to Newly Independent States
The Sixteenth World Health Assembly,
Having studied the report of the Director -General on continued assistance to newly independent States ;
Noting resolution EB31.R39 adopted by the Executive Board at its thirty -first session;
Recognizing the urgent need to accelerate the assistance to newly independent and emerging Statesin accordance with the programme laid down by the Fifteenth World Health Assembly in resolu-tion WHA15.22; and
Realizing that the implementation of such an accelerated programme requires larger resources than arecurrently available to the Organization,
1. NOTES the report of the Director -General;
2. ENDORSES the actions taken by the Director- General to implement an accelerated programme for assistingnewly independent and emerging States; and
3. INVITES Members that are in a position to do so to make voluntary contributions to the Special Accountfor Accelerated Assistance to Newly Independent and Emerging States, as established by the Fifteenth WorldHealth Assembly in its resolution WHA15.22.
Handb. Res., 6th ed., 1.1.4; 7.1.9 Twelfth plenary meeting, 22 May 1963 (Committee onProgramme and Budget, fourth report)
WHA16.32 Decisions of the United Nations, Specialized Agencies and IAEA affecting WHO's Activities :Administrative, Budgetary and Financial Matters; Inter -organization Machinery for Matters ofPay and Allowances
The Sixteenth World Health Assembly,
Having considered the report of the Director -General 1 on decisions of the United Nations, specializedagencies and the International Atomic Energy Agency affecting WHO's activities;
Having taken into account the views expressed in resolution EB31.R43 adopted by the Executive Boardat its thirty -first session,
1. NOTES with satisfaction that progress continues to be made in the co- ordination of administrative,budgetary and financial matters;
2. EXPRESSES its satisfaction that the Administrative Committee on Co- ordination has agreed that, subjectto the views of the Board itself, the International Civil Service Advisory Board might serve as an independentbody to make recommendations to the appropriate authorities on problems arising in the administrationof the common system of salaries and allowances;
1 See Annex 11.

16 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
3. CONSIDERS that, if new terms of reference and authorities extending the competence of the InternationalCivil Service Advisory Board are approved by all concerned, this will become one of the most importantactions thus far taken to improve co- ordination on administrative matters; and
4. REQUESTS the Director -General, in the further consideration of this matter in the Administrative Com-mittee on Co- ordination, to take into account the views expressed in the discussion in the World HealthAssembly.
Handb. Res., 6th ed., 8.1.1.5; 7.3.4 Twelfth plenary meeting, 22 May 1963 (Committee onAdministration, Finance and Legal Matters, fourthreport)
WHA16.33 Decisions of the United Nations, Specialized Agencies and IAEA affecting WHO's Activities :Conference Arrangements
The Sixteenth World Health Assembly,
Having considered the report of the Director -General ' on decisions of the United Nations, specializedagencies and the International Atomic Energy Agency affecting WHO's activities;
Noting that the Administrative Committee on Co- ordination has established arrangements to facilitatethe exchange of information regarding the scheduling of conferences by the various organizations;
Considering that such inter -secretariat co- ordination, while useful, can only be effective if those concernedtake full account of established recurring requirements for scheduled conferences;
Considering further that disruption of established conference schedules results in unnecessary expenseto governments;
Recalling that the World Health Assembly has always met in the Palais des Nations in the month of Maywhen it has been convened in Geneva,
1. EMPHASIZES the necessity for facilitating annual assemblies of organizations such as the World HealthOrganization at the normal time in order to avoid disruption of the established cycle of operations of theOrganization ;
2. EXPRESSES the hope that there will be continuing and improved co- ordination and co- operation in thescheduling of meetings among the agencies concerned;
3. REQUESTS the Director -General to transmit this resolution to the Secretary -General of the United Nationswith the request that he transmit it to the Economic and Social Council; and
4. EXPRESSES the hope that the Economic and Social Council will, in the exercise of its responsibility underArticle 63, paragraph 2, of the Charter of the United Nations, take into account the requirements of thespecialized agencies when it considers conference schedules.
Handb. Res., 6th ed., 8.1.1.5 Twelfth plenary meeting, 22 May 1963 (Committee onAdministration, Finance and Legal Matters, fourthreport)
WHA16.34 Additional Regulations of 23 May 1963 amending the International Sanitary Regulations, in particularwith respect to Notifications
The Sixteenth World Health Assembly,
Considering the need for the amendment of certain of the provisions of the International SanitaryRegulations, as adopted by the Fourth World Health Assembly on 25 May 1951, in particular with respect tonotifications;
Having regard to Articles 2 (k), 21 (a) and 22 of the Constitution of the World Health Organization,ADOPTS, this 23rd day of May 1963, the following Additional Regulations :
' See Annex 11.

RESOLUTIONS AND DEOISIONS ".. : . 17
ARTICLE IIn Articles 1, 3, 36 and 97 of the International Sanitary Regulations, there shall be made the following
amendments :
Article 1Imported case: Delete this definition and replace by :
" ` imported case ' means an infected person arriving on an international voyage : ".Infected local area. Delete paragraph (a) and replace by :
" (a) a local area where there is a case of plague, cholera, yellow fever, or smallpox that is neither animported case nor a transferred case; or ".
Transferred case. Add the following definition :" ' transferred case' means an infected person whose infection originated in another local area underthe jurisdiction of the same health administration; ".
Article 3Insert as paragraph 2:
" 2. In addition each health administration shall notify the Organization by telegram within twenty-four hours of its being informed
(a) that one or more cases of a quarantinable disease have been imported or transferred into anon- infected local area -the notification to include information on the origin of infection;(b) that a ship or aircraft has arrived with one or more cases of a quarantinable disease on board-the notification to include the name of the ship or the flight number of the aircraft, its previousand subsequent ports -of -call, and whether the ship or aircraft has been dealt with."
Re- number paragraph 2 as paragraph 3.Article 36Insert as paragraph 3:
" 3. Where a health administration has special problems constituting a grave danger to public health aperson on an international voyage may, on arrival, be required to give a destination address in writing."
Article 97In paragraph 1, after the words Appendix 6 ", insert the words :
" except when a health administration does not require it ".
ARTICLE HThe period provided in execution of Article 22 of the Constitution of the Organization for rejection or
reservation shall be three months from the date of the notification by the Director - General of the adoptionof these Additional Regulations by the World Health Assembly.
ARTICLE HIThese Additional Regulations shall come into force on the first day of October 1963.
ARTICLE IVThe following final provisions of the International Sanitary Regulations shall apply to these Additional
Regulations : paragraph 3 of Article 106, paragraphs 1 and 2 and the first sentence of paragraph 5 of 107,108 and paragraph 2 of 109, substituting the date mentioned in Article III of these Additional Regulationsfor that mentioned therein, 110 to 113 inclusive.
IN FAITH WHEREOF we have set our hands at Geneva this 23rd day of May 1963.M. A. MAJEKODUNMI
President of the Sixteenth World Health Assembly
M. G. CANDAUDirector- General of the World Health Organization
Handb. Res., 6th ed., 1.5.7.5 Thirteenth plenary meeting, 23 May 1963 (Committeeon Programme and Budget, fifth report)
18 SIXTEENTH WORLD HEALTH ASSEMBLY, PART 1
WHA16.35 Committee on International Quarantine : Eleventh Report
The Sixteenth World Health Assembly,
Having considered the eleventh report of the Committee on International Quarantine,'
1. THANKS the members of the Committee for their work; and
2. ADOPTS the eleventh report of the Committee on International Quarantine.
Handb. Res., 6th ed., 1.5.7.6 Thirteenth plenary meeting, 23 May 1963 (Committeeon Programme and Budget, fifth report)
WHA16.36 Clinical and Pharmacological Evaluation of Drugs
The Sixteenth World Health Assembly,
Having noted the resolution of the Executive Board on the clinical and pharmacological evaluationof drugs; 2
Having examined the report by the Director -General on the clinical and pharmacological evaluation ofdrugs; 3
Considering that international co- operation is essential for the achievement of the best possible protectionagainst hazards for man arising out of the use of drugs;
Agreeing to the definition of a " drug " as any substance, or mixture of substances, destined for use inthe diagnosis, treatment, mitigation or prevention of disease in man, as set out in the report of the StudyGroup on the Use of Specifications for Pharmaceutical Preparations;
Realizing the technical and administrative difficulties of securing regular exchange of information onall drugs,
1. REAFFIRMS the need for early action in regard to rapid dissemination of information on adverse drugreactions;
2. REQUESTS Member States
(a) to communicate immediately to WHO(i) any decision to prohibit or limit the availability of a drug already in use,(ii) any decision to refuse the approval of a new drug,(iii) any approval for general use of a new drug when accompanied by restrictive provisions,
if these decisions are taken as a result of serious adverse reactions; and(b) to include in this communication as far as possible the reasons for the action taken and the non-proprietary and other names, and the chemical formula or the definition;
3. (a) RECOGNIZES the importance of accurate appraisal, at the national level, of the toxic effects of drugs;and
(b) INVITES Member States to arrange for a systematic collection of information on serious adversedrug reactions observed during the development of a drug and, in particular, after its release for generaluse
4. REQUESTS the Director -General
(a) to transmit immediately to Member States the information received under paragraph 2;
1 See Annex 1.2 Resolution EB31.R6.3 See Annex 12.4 Wld Huth Org. techa. Rep. Ser. 1957, 138, 14.
RESOLUTIONS AND DECISIONS 19
(b) to study the value and feasibility, including the administrative and financial implications, of WHOcollecting from and disseminating to Member States
(i) the non -proprietary and other names, chemical formulae and definitions of new drugs releasedor approved,(ii) the information contained in 3 (b) above;
(c) to continue the study of the possibility of formulating, and of seeking international acceptance of,basic principles and requirements applicable to the toxicological, pharmacological and clinical evaluationof drugs; and(d) to pursue action in the matter and report to the Executive Board and to the Seventeenth WorldHealth Assembly.
Handb. Res., 6th ed., 1.3 Thirteenth plenary meeting, 23 May 1963 (Committeeon Programme and Budget, fifth report)
WHA16.37 Smallpox Eradication Programme
The Sixteenth World Health Assembly,
Having considered the report of the Director -General on the progress so far achieved in the world -wideprogramme of smallpox eradication, 1
1. NOTES
(i) that smallpox continues to be a serious health problem in the endemic areas, and exposes the restof the world to risk, of infection;(ii) that the implementation of many national eradication programmes is making slow progress owingto inadequacy of national resources, particularly in transport, equipment, and the potent and stablevaccine so necessary for tropical and sub -tropical areas;
2. INVITES Member States to make voluntary contributions in cash or in kind to enable the Organizationto provide assistance to requesting countries to meet their deficiencies of transport, equipment and vaccine;
3. RECOMMENDS to those countries where the disease is still present
(i) that they intensify their control programmes aiming at eradication and take the necessary stepsto ensure the provision of a potent and stable vaccine;(ii) that neighbouring countries, and particularly contiguous ones, co- ordinate their smallpox controlactivities and /or eradication campaigns in order to diminish the risk of spread of the disease between theirrespective territories during their programmes; and
4. REQUESTS the Director -General to submit a further report on the progress of the smallpox eradicationprogramme to the Seventeenth World Health Assembly.
Handb. Res., 6th ed., 1.5.4 Thirteenth plenary meeting, 23 May 1963 (Committeeon Programme and Budget, sixth report)
WHA16.38 Clinical and Pharmacological Evaluation of Drugs : Standards of Drugs
The Sixteenth World Health Assembly,
Recognizing the urgent need of securing a high standard of drugs for human use in all countries,
1 See Annex 16.
20 SIXTEENTH WORLD HEALT,H ASSEMBLY, PART I
I. REQUESTS the Executive Board to examine ways and means of ensuring that drugs exported from aproducing country comply with the drug control requirements which apply in that country for domestic use;and
2. REQUESTS the Executive Board to report thereon to the Seventeenth World Health Assembly.
Handb. Res., 6th ed., 1.3 Thirteenth plenary meeting, 23 May 1963 (Committeeon Programme and Budget, sixth report)
WHA16.39 Decisions of the United Nations, Specialized Agencies and IAEA affecting WHO's Activities :Programme Matters
The Sixteenth World Health Assembly,
Having considered the report of the Director -General on the decisions of the United Nations, specializedagencies and the International Atomic Energy Agency affecting WHO's activities on programme matters,
NOTES the report.
Handb. Res., 6th ed., 8.1.1.6 Thirteenth plenary meeting, 23 May 1963 (Committeeon Programme and Budget, sixth report)
WHA16.40 United Nations Development Decade
The Sixteenth World Health Assembly,
Having studied the report of the Director -General i on the United Nations Development Decade;
Reaffirming the decisions on the Development Decade set forth in resolution WHA15.57 of the FifteenthWorld Health Assembly; and
Mindful of the aims of the United Nations Development Decade and the contribution which the WorldHealth Organization can make to their achievement, particularly through assistance to governments, ontheir request, in national health planning and the education and training of professional and auxiliary healthstaff,
I. NOTES the report of the Director -General;
2. EMPHASIZES the importance of investment in health as a vital component of economic and social develop-ment; and
3. STRESSES the need for expanding WHO activities in keeping with the health objectives of the UnitedNations Development Decade, both through the Organization's regular programme and the use of otheravailable resources.
Handb. Res., 6th ed., 8.1.2 Thirteenth plenary meeting, 23 May 1963 (Committeeon Programme and Budget, sixth report)
WHA16.41 Extension of the Agreement with UNRWA
The Sixteenth World Health Assembly,
Considering that, on 29 September 1950, an agreement was concluded between the Director -Generalof the World Health Organization and the Director of the United Nations Relief and Works Agency forPalestine Refugees in the Near East (UNRWA) on the basis of principles established by the Third WorldHealth Assembly;
1 See Annex 13.

RESOLUTIONS AND DECISIONS 21
Considering that the Thirteenth World Health Assembly, in resolution WHA13.62, extended the dura-tion of this agreement until 30 June 1963;
Considering that, subsequently, the General Assembly of the United Nations, at its seventeenth session,extended the mandate of UNRWA until 30 June 1965; 1 and
Considering that the World Health Organization should continue the technical direction of the healthprogramme administered by UNRWA,
AUTHORIZES the Director -General to extend the duration of the agreement with UNRWA until 30 June1965.
Handb. Res., 6th ed., 8.1.5.1 Thirteenth plenary meeting, 23 May 1963 (Committeeon Programme and Budget, sixth report)
WHA16.42 Joint FAO /WHO Programme on Food Standards (Codex Alimentarius)
The Sixteenth World Health Assembly
1. APPROVES the establishment of a joint FAO /WHO programme on food standards whose principal organwill be the Codex Alimentarius Commission;
2. ADOPTS the statutes of the Codex Alimentarius Commission; 2
3. AGREES to the calling of the first session of the Codex Alimentarius Commission in June 1963;
4. EXPRESSES the hope that the Codex Alimentarius Commission will give priority to the health aspects ofits work and will further preparatory work on a regional basis wherever this appears desirable in order toachieve the fundamental aims laid down for the Commission;
5. REQUESTS the Director- General to ensure the fullest participation of WHO in the joint food standardsprogramme; and
6. FURTHER REQUESTS the Director -General to report to the thirty -third session of the Executive Board onthe progress made by the Codex Alimentarius Commission, and on the outcome of the review of the methodof financing the work of the Commission to be made by the FAO Conference in November 1963.
Handb. Res., '6th ed., 1.7.3; 8.1.6.2 Thirteenth plenary meeting, 23 May 1963 (Committeeon Programme and Budget, sixth report)
WHA16.43 Meetings of the Regional Committee for Africa
The Sixteenth World Health Assembly,
Having considered the report of the Director -Generals on meetings of the Regional Committee forAfrica and the request of the Regional Committee for Africa to the World Health Assembly;
Noting that the Government of the Republic of South Africa, in spite of a number of resolutions adoptedover several years, and in particular resolution 1761 (XVII) of 6 November 1962, by the General Assemblyof the United Nations on the policies of apartheid of the Government of the Republic of South Africa,has not complied with those resolutions;
Taking into account the humanitarian principles and the objective enunciated in the Constitution ofthe World Health Organization and especially with reference to the control of communicable diseases, whichdo not recognize national boundaries;
Taking into account, in addition, that the resolution of the Regional Committee for Africa calls atten-tion to the necessity of safeguarding the health rights of all African populations concerned;
1 General Assembly resolution 1856 (XVII).2 See Off. Rec. Wld Hlth Org. 124, 74.3 See Annex 14.
22 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Considering that the conditions imposed upon the non -white populations of South Africa seriouslyprejudice their physical, mental and social health, and are contrary to the principles of the Organization;
Considering the necessity to avoid any action that may hamper the proper functioning of the RegionalOrganization for Africa; and
Noting that the Director of the African Regional Office, after consultation with the Director -General,has notified the Member States in the Region that the thirteenth session of the Regional Committee forAfrica will be held in September- October 1963 at the African Regional Office because of the circumstanceswhich have not made it possible to convene it at the place previously selected by the Regional Committeeat its eleventh session,
1. APPROVES the actions taken by the Regional Director and by the Director -General to ensure the func-tioning of the African Regional Organization and the fulfilment of the constitutional functions of the AfricanRegional Committee for the protection of the health rights of all populations of the Region;
2. CALLS ATTENTION to General Assembly resolution 1761 (XVII) of 6 November 1962, and invites theGovernment of the Republic of South Africa to renounce the policy of apartheid in the interests of thephysical, mental and social well -being of the population;
3. UNDERTAKES, within the provisions of the Constitution of the World Health Organization, to supportall measures that may be taken to contribute towards the solution of the problem of apartheid;
4. INVITES the Government of the Republic of South Africa to take appropriate measures so that all thepopulations of South Africa shall benefit by the public health services of that country;
5. EXPRESSES the hope that Members of the Region will do whatever is possible to further the effectivefunctioning of the African Regional Organization, promote the humanitarian goals of the World HealthOrganization, and protect the health rights of the South African population;
6. REQUESTS the Director -General to transmit this resolution to the Secretary -General of the UnitedNations with the request that it will be made available to the Special Committee appointed under the termsof General Assembly resolution 1761 (XVII) of 6 November 1962;
7. REQUESTS further that the Director -General report to each session of the World Health Assembly onthis matter until such time as it is resolved to the satisfaction of the Regional Committee for Africa and theWorld Health Assembly.
Handb. Res., 6th ed., 5.2.1.4 Thirteenth plenary meeting, 23 May 1963 (Committeeon Administration, Finance and Legal Matters, fifthreport)
WHA16.44 Reports of the Executive Board on its Thirtieth and Thirty -first Sessions
The Sixteenth World Health Assembly
1 NOTES the reports of the Executive Board on its thirtieth' and thirty -first sessions; 2 and
2. COMMENDS the Board on the work it has performed.
Handb. Res., 6th ed., 4.2.5.2 Thirteenth plenary meeting, 23 May 1963
1 Off Rec. Wld Hlth Org. 120.2 Off Rec. Wld Hlth Org. 124; 125.
RESOLUTIONS AND DECISIONS 23
PROCEDURAL DECISIONS
(i) Composition of the Committee on Credentials
The Sixteenth World Health Assembly appointed a Committee on Credentials consisting of delegatesof the following twelve Members : Australia, Bulgaria, Canada, Cyprus, Federation of Malaya, Ghana,Madagascar, Nepal, Peru, Spain, Sweden, Syria.
First plenary meeting, 7 May 1963
(ii) Composition of the Committee on Nominations
The Sixteenth World Health Assembly appointed a Committee on Nominations consisting of delegatesof the following twenty -four Members : Argentina, Cambodia, Congo (Leopoldville), France, Gabon, India,Iran, Israel, Jamaica, Lebanon, Mexico, Morocco, Netherlands, New Zealand, Nigeria, Norway, Romania,Thailand, Tunisia, Union of Soviet Socialist Republics, United Arab Republic, United Kingdom of GreatBritain and Northern Ireland, United States of America, Venezuela.
First plenary meeting, 7 May 1963
(iii) Verification of Credentials
The Sixteenth World Health Assembly recognized the validity of the credentials of the followingdelegations :
Members
Afghanistan, Albania, Algeria, Argentina, Australia, Austria, Belgium, Bolivia, Brazil, Bulgaria, Burma,Burundi, Cambodia, Cameroon, Canada, Central African Republic, Ceylon, Chad, Chile, China, Colombia,Congo (Brazzaville), Congo (Leopoldville), Cuba, Cyprus, Czechoslovakia, Dahomey, Denmark, Ecuador,Ethiopia, Federal Republic of Germany, Federation of Malaya, Finland, France, Gabon, Ghana, Greece,Guatemala, Guinea, Hungary, Iceland, India, Indonesia, Iran, Iraq, Ireland, Israel, Italy, Ivory Coast,Jamaica, Japan, Jordan, Kuwait,' Laos, Lebanon, Liberia, Libya, Luxembourg, Madagascar, Mali, Mauri-tania, Mexico, Monaco, Mongolia, Morocco, Nepal, Netherlands, New Zealand, Nicaragua, Niger, Nigeria,Norway, Pakistan, Panama, Paraguay, Peru, Philippines, Poland, Portugal, Republic of Korea, Republicof Viet -Nam, Romania, Rwanda,' Saudi Arabia, Senegal, Sierra Leone, Somalia, South Africa, Spain,Sudan, Sweden, Switzerland, Syria, Tanganyika,' Thailand, Togo,' Trinidad and Tobago, Tunisia, Turkey,Uganda, Union of Soviet Socialist Republics, United Arab Republic, United Kingdom of Great Britainand Northern Ireland, United States of America, Upper Volta, Venezuela, Western Samoa, Yemen,Yugoslavia.
Associate Members
Kenya, Mauritius.First, third, seventh and thirteenth plenary meetings,7, 8, 14 and 23 May 1963
' Credentials provisionally accepted.
24 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
(iv) Election of Officers of the Sixteenth World Health Assembly
The Sixteenth World Health Assembly, after considering the recommendation of the Committee onNominations, elected the following officers :
President: Dr M. A. Majekodunmi (Nigeria);Vice- Presidents: Professor R. Gerie (Yugoslavia), Dr Sushila Nayar (India), Mr Abdul Rahman bin Haji
Talib (Federation of Malaya).
(v) Election of Officers of the Main Committees
(vi)
Second plenary meeting,. 7 May 1963
The Sixteenth World Health Assembly, after considering the recommendations of the Committee onNominations, elected the following officers of the main committees :COMMITTEE ON PROGRAMME AND BUDGET : Chairman, Dr V. V. Olguín (Argentina);
COMMITTEE ON ADMINISTRATION, FINANCE AND LEGAL MATTERS : Chairman, Mr I. T. Kittani (Iraq).
Second plenary meeting, 7 May 1963
The main committees subsequently elected the following officers :
COMMITTEE ON PROGRAMME AND BUDGET : Vice- Chairman, Dr S. P. Tchoungui (Cameroon); Rapporteur,Dr M. Sentici (Morocco);
COMMITTEE ON ADMINISTRATION, FINANCE AND LEGAL MATTERS : Vice- Chairman, Dr J. Vysohlíd (Czecho-slovakia); Rapporteur, Dr A. L. Bravo (Chile).
Establishment of the General Committee
The Sixteenth World Health Assembly, after considering the recommendations of the Committee onNominations, elected the delegates of the following fourteen countries as members of the GeneralCommittee : Cambodia, Canada, Congo (Leopoldville), Dahomey, France, Indonesia, Iran, Israel,Mexico, Sweden, Tanganyika, Union of Soviet Socialist Republics, United Kingdom of Great Britain andNorthern Ireland, United States of America.
Second plenary meeting, 7 May 1963
(vii) Adoption of the Agenda
The Sixteenth World Health Assembly adopted the provisional agenda prepared by the Executive Boardat its thirty -first session.'
Third plenary meeting, 8 May 1963
' Two items (3.13, Housing of staff of the Regional Office for Africa, and 3.15, Working Capital Fund) were deleted because theywere no longer necessary.

ANNEXES

Annex 1
INTERNATIONAL QUARANTINE
[A16 /P &B /2 -8 March 1963]
In accordance with resolution EB31.R2, the Director -General has the honour tosubmit to the Sixteenth World Health Assembly the eleventh report of the Committeeon International Quarantine, together with the minutes of the discussion which took placeduring the thirty -first session of the Executive Board.
1. ELEVENTH REPORT OF THE COMMITTEE ON INTERNATIONAL QUARANTINE
Composition of the Committee
IntroductionGeneral Aspects
The International Sanitary Regulatiors
[WHO /IQ /134 - 19 Oct. 1962CONTENTS
Page Page
27 Part VI. Sanitary Documents 53
28 Part VII. Sanitary Charges 5429 Part VIII. Various Provisions 5430
Part I. Definitions 30Appendices 55
Part II. Notifications and Epidemiological Informa-tion 32
Part III. Sanitary Organization 35 Appendix I Cases of Quarantinable Disease (Smallpox)imported by International Traffic
Part IV. Sanitary Measures and Procedure 36
Part V. Special Provisions relating to each of the 1. Cases imported by Ship 57
Quarantinable Diseases 37 2. Cases imported by Aircraft 58
Plague 37
Cholera 37Yellow Fever 43 Appendix 2 - Divergent Opinion on the Question ofSmallpox 45 Amendment to the International Certificate of Vaccina-Typhus 53 tion or Revaccination against Smallpox 58
Composition of the Committee
The Committee on International Quarantine heldits eleventh meeting in the Palais des Nations, Geneva,from 15 to 19 October 1962.
Members
Dr O. B. Alakija,2 Acting Chief Medical Adviser tothe Federal Government, Federal Ministry ofHealth, Lagos, Nigeria
Dr A. Allard, Director of Medical Services, SabenaAirlines, Brussels, Belgium
1 See resolutions WHA16.34 and WHA16.35.2 Unable to attend. Health Service, Rio de Janeiro, Brazil
Dr J. C. Azurin, Director, Bureau of Quarantine,Department of Health, Manila, Philippines
Dr M. H. El Bitash, Under - Secretary of State, Ministryof Public Health, Cairo, United Arab Republic
Dr W. A. Karunaratne,2 Director of Health Services,Colombo, Ceylon
Dr L. H. Murray, Principal Medical Officer, Ministryof Health, London, United Kingdom of GreatBritain and Northern Ireland
Dr H. M. Penido, Superintendent, Special Public
- 27 -

28 SIXTEENTH WORLD HEALTH ASSEMBLY, PART 1
Dr G. M. Redshaw, Assistant Director -General ofHealth, Commonwealth Department of Health,Canberra, Australia
Dr J. G. Telfer, Medical Director, Division of ForeignQuarantine, United States Public Health Service,Department of Health, Education and Welfare,Washington, D.C., United States of America
Representative of the International Civil AviationOrganization
Mr H. A. Seidelmann, Technical Officer, Facilitationand Joint Financing Branch
Representative of the International Air TransportAssociation
Mr R. W. Bonhoff
Secretariat
Dr R. I. Hood, Chief Medical Officer, InternationalQuarantine, Division of Communicable Diseases(Secretary)
The Committee met on the morning of 15 October1962. Dr P. M. Kaul, Assistant Director -General,opened the meeting on behalf of the Director -General,and welcomed the members and representatives ofICAO and IATA. He recalled that at the WorldHealth Assembly in May 1962 some concern hadbeen expressed by delegates about the importation ofeight smallpox cases into Europe in the precedingmonths. During the discussion on this matter somequestions had been raised about the status of smallpoximmunity after revaccination and about the need forrevising the present procedures. He further recalledthat, in 1951, in resolution WHA4.80, the WorldHealth Assembly had expressed the opinion that " theInternational Sanitary Regulations ... represent onlypart of the action required to remove the international
threat of quarantinable diseases ". That resolutionalso stated that it was believed that " health administra-tions by improving sanitary conditions and expandingtheir health and medical services . .. are therebysecuring their own protection against the entry andestablishment of quarantinable diseases ", and that" the freest possible movement of internationaltraffic is highly desirable in the interests of worldeconomic and social, including health, progress ",and recommended to all governments that " they .. .raise the level of protection, by vaccination ...against ... smallpox ". He informed the Committeethat, as the Organization continued to assist countriesin smallpox eradication programmes, more was beinglearned about vaccines, procedures and reactionsto vaccination. The Organization was also supportingcertain research studies relating to smallpox and hadalready proposed further studies. Those includedresearch on the comparative value of different animalsfor the production of smallpox vaccine, on theprotective and therapeutic value of antivacciniagamma -globulin of human and animal origin, on thecorrelation between vaccination reactions and anti-body levels at the time of vaccination, and on otherepidemiological and immunological problems con-nected with smallpox. In his programme for 1964,the Director -General had proposed an expert com-mittee on smallpox.
Dr H. M. Penido was unanimously elected Chairmanand Dr M. H. El Bitash Vice -Chairman. The Chair-man was requested to act as Rapporteur.
The draft agenda was approved.The Committee considered the annual report by
the Director -General on the functioning of the Inter-national Sanitary Regulations during the period from1 July 1961 to 30 June 1962. This report is reproducedbelow, the various sections being followed, whereappropriate, by the comments and recommendationsof the Committee (in italics).
INTRODUCTION
1. This report on the functioning of the InternationalSanitary Regulations and their effects on internationaltraffic is prepared in accordance with the provisionsof Article 13, paragraph 2, of the Regulations. Itcovers the period from 1 July 1961 to 30 June 1962.
2. Previous reports cover the period beginningwith the time of entry- into -force of the Regulations(1 October 1952).
' Off. Rec. Wld Hith Org. 56, 3; 64, 1; 72, 3; 79, 493; 87, 397;95,471;102,35;110,31;118,35.
3. This report follows the same general lines as itpredecessors and considers the application of theRegulations from three aspects : as seen by the Organi-zation in its administrative role of applying theRegulations; as reported by Member States inaccordance with Article 62 of the Constitution ofthe Organization and Article 13, paragraph 1, of theRegulations; and as reported by other organizationsdirectly concerned with the application of the Regula-tions. For ease of reference the three aspects areconsolidated and presented in the numerical order ofthe articles of the Regulations.

ANNEX 1 29
4. By reason either of their importance or of theprocedure leading to their study, other questionshave necessitated the preparation of special documents,independently of this report. They are neverthelessbriefly mentioned in it.5. The ninth report of the Committee on Inter-national Quarantine was adopted by the FifteenthWorld Health Assembly on 23 May 1962 (resolutionWHA15.37). On the same day the Fifteenth Health
Assembly also adopted, in resolution WHA15.38,the tenth report of the Committee on InternationalQuarantine -on its special meeting held on 3 May1962.2 These reports and the proceedings of theAssembly relating to international quarantine matterswere published in Official Records Nos 118 and 119respectively. An offprint of the ninth and tenth reportsof the Committee on International Quarantine is
available.
GENERAL ASPECTS
Position of States and Territories under the Inter-national Sanitary Regulations
6. Information showing the position of States andterritories under the Regulations as of 1 January 1962was included in the Weekly Epidemiological Record,1962, No. 7. Since that date one more State hasbecome a party to the Regulations -the MongolianPeople's Republic, on 18 July 1962; the informationwas published in Weekly Epidemiological RecordNo. 29 of 20 July 1962.
Countries not bound by the Regulations 1
7. Australia, Burma, Chile and Singapore, althoughnot parties to the Regulations, apply their provisionsin nearly all respects.
Administration of the Regulations
8. In its previous report the Committee noted thedecision of the Director- General that headquartersshould assume sole responsibility for the administra-tion of the Regulations as from 1 January 1962.During a six months' transition period beginning on1 July 1961, the WHO quarantine offices in Alexandria,Singapore and Washington continued to carry outsome of the functions previously delegated to them.Largely owing to their extensive efforts, the change-over at the end of 1961 operated smoothly. TheSingapore Weekly Epidemiological Report, whichbegan publication on 1 March 1925, ceased to bepublished with the issue dated 28 December 1961.The Weekly Epidemiological Bulletin of the RegionalOffice for the Eastern Mediterranean ended publicationon 29 December 1961. The Weekly EpidemiologicalReport of the Pan American Sanitary Bureau /WHORegional Office for the Americas continued publica-tion, but ceased in 1962 to be a mechanism fordissemination of information under the Regulations.
For the most part States have become accustomedto direct communication with headquarters on allmatters concerning the Regulations.
' See also sections 29, 69 and 106.
The Singapore Naval Radio Station and otherstations in Asia began in the first week of January1962 to retransmit the text of the daily epidemio-logical radiotelegraphic bulletin issued from Genevaand covering the whole world. The Abu -Zabal(Cairo) Station retransmitted the Geneva bulletinfor the first six months of 1962 and then ceased todo so; during this period it was determined that theStates that received the retransmission from Abu -Zabal (Cairo) could easily and effectively receive thedirect transmission from Geneva -Prangins.
Periodicity of Meetings of the Committee on Inter-national Quarantine
9. The Fifteenth World Health Assembly (in reso-lution WHA15.36) authorized the Director -General(a) to postpone as from 1963, at his discretion, theannual meeting of the Committee to the followingyear, provided that the Committee is convened atleast every other year; and (b) to convene a meetingof the Committee at other times when he considers itnecessary. The Assembly further requested theDirector -General to submit for review to the Com-mittee, in 1966, the question of periodicity of itsmeetings and to present the report and recommend-ations of the Committee to the Twentieth WorldHealth Assembly.
International Protection against Malaria
10. At its ninth session the Committee on Inter-national Quarantine recommended a meeting ofmalaria and international quarantine experts to reviewthe situation as regards international protectionagainst malaria.' The Expert Committee on Malariain its ninth report made a similar recommendation.'
An Expert Committee on Malaria is scheduled for1963 to consider international protection against
2 See section 18.3 Off. Rec. Wld Hlth Org. 118, 37, section 11.
Wld Hlth Org. techn. Rep. Ser., 1962, 243, 24, 40,
30 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
malaria, and to recommend procedures for establishingeffective protective measures.
The attention of the Committee is invited especiallyto sections 4.2 and 9.5 (Prevention of re- introductionof infection) of the ninth report of the Expert Com-mittee on Malaria.'
The Committee notes the ninth report of the ExpertCommittee on Malaria.
Aircraft Disinsection
11. At its ninth session the Committee recommended,inter alia, further trials on aircraft disinsection at the" blocks away " period in tropical areas where con-ditions of high humidity or - extreme dryness arepresent.2 Results of such trials are reported in aseparate document.
The Committee noted the extract from a documententitled °i Studies on Aircraft Disinsection at ` blocksaway ' in Tropical Areas " and especially that dis-insection of aircraft carried out at the " blocks away "period was biologically effective in the tropics. TheCommittee reaffirms the opinion given in its eighthreport that the operation referred to as " blocks away "disinsection is regarded as a " technically acceptablealternative method for disinsection of the passengercabin with aerosols ",3 and recommends that healthauthorities, together with operators of internationalflights, examine the possibilities for the early applicationof this procedure for aircraft disinsection.
The Committee recommends that single -use type ofaerosol dispensers should be used for disinsection of thepassenger cabin of aircraft, and that this type of dispensershould be made widely available.
The Committee notes that the procedures andformulations at present recommended are those con-
Article 1
tamed in the seventh and eleventh reports of the ExpertCommittee on Insecticides. The Committee drawsespecial attention to the recommendations concerning" blocks away " disinsection contained in the eleventhreport of the Expert Committee.'
The Committee understands that in aviation termi-nology the words " in flight " mentioned in Article 73,paragraph 2, include the time an aircraft begins movingon the ground before its actual take -off, and con-sequently disinsection carried out at the " blocks away "period can be considered as disinsection in flight.
The Committee was informed that the Director -General is prepared to furnish technical assistance toStates, on request, with any aircraft disinsectionproblems.
Mosquito Vectors of Disease
12. At its ninth session the Committee requested theDirector -General to inform it at its next session aboutaction on circular letter No. 14 of 5 May 1961.6 Thenumber of replies by States has in the interim beenmore satisfactory.
Information on the Aedes aegypti situation atinternational airports will be published in the WeeklyEpidemiological Record at an early date. Informationon other mosquito vectors of disease, particularlyanophelines, will follow.
International Protection against Trachoma
13. The attention of the Committee is invited tosection 10 of the third report of the Expert Committeeon Trachoma, dealing with prophylaxis of trachomain international traffic.'
The Committee notes the third report of the ExpertCommittee on Trachoma, and particularly section 10.
THE INTERNATIONAL SANITARY REGULATIONS
PART I. DEFINITIONS
14. Imported Case and Transferred Case. In previousreports the Committee has stated that the terms of thedefinition of an " imported case " are intended toapply only to a case introduced into a territory fromoutside that territory.¢ The word " territory " hasoccasionally been misunderstood. In practice the
1 Wld Hlth Org. techn. Rep. Ser., 1962, 243, 23, 40.
2 Off Rec. Wld Hlth Org. 118, 38, section 14.
3 Off Rec. Wld Hlth Org. 110, 33, section 8.
4 Off Rec. Wld Hlth Org. 64, 32; 110, 34.
words " imported case " have been interpreted toinclude an infected person (see definition) in theincubation period. Thus an " imported case " hasmeant an infected person who has arrived on aninternational voyage, i.e., an infected person comingfrom another territory under the jurisdiction of anothernational health administration.
' Wld Hlth Org. techn. Rep. Ser., 1961, 206, 8 (reproduced inAnnex VII of the second annotated edition, 1961, of the Inter-national Sanitary Regulations, p. 106, paras 1-4).
6 Off Rec. Wld Hlth Org. 118, 38, section 17.' Wld Hlth Org. techn. Rep. Ser., 1962, 234, 38.

ANNEX 1 31
The Committee recommends that, in Article 1, thedefinition of " imported case " should be amended toread:
" imported case " means an infected person arrivingon an international voyage.The Committee further recommends that Article 1
be amended by adding the following definition:" transferred case " means an infected person whoseinfection originated in another local area under thejurisdiction of the same health administration.
15. Infected Local Area. According to paragraph (a)of the definition, a plague, cholera, yellow -fever orsmallpox infected local area is a local area in whichthere is a non -imported case. The Committee, in itsthird report,' has given its opinion that when a case ishospitalized in an area other than the actual infectedlocal area the local area of hospitalization does notbecome an infected local area solely because of thehospitalized case. It is to be noted, however, thatsuch hospitalized cases are usually non -imported.They are sometimes referred to as transferred cases,in that they have been first notified from the localarea actually infected. In practice the Director -General has interpreted the above opinion to coverthe following circumstances : a person infected inone local area A of a State and moving to anotherlocal area B within the same State before being notifiedas a case is, of course, a non -imported case. However,it has been considered that local area E, which waspreviously free from infection, is not an infected localarea solely on the basis of such a case having beenintroduced into it. In most instances local area B hasbeen a hundred or more kilometres from the infectedlocal area A.
The Committee recommends that, in Article 1, thedefinition of " infected local area" be amended byadding, in paragraph (a), the words " or non-trans-ferred" after the word " non-imported".
16. Infected Local Area - Size. In its fourthreport 2 the Committee stated that one of the basicprinciples of the International Sanitary Regulationsis the acceptance by all States of local areas designatedby any national health administration. When severallocal areas are adjacent to one another in heavilypopulated sections of a country and it is known thatthere is considerable daily movement of populationwithin these sections, some States believe that it isunrealistic to consider as infected only one such localarea. These States have been apt to consider asinfected the entire heavily populated section in theother State, although only one local area within such
' Off Rec. Wld Hlth Org. 72, 38, section 27.2 Off. Rec. Wld Huth Org. 79, 497, section 22.
a section had been declared infected, or is infected bydefinition. This question rarely arises in respect ofinternational travellers who have complied with theprovisions of Article 34.
The Committee recommends to health administrationsthat, in heavily populated sections of a State, thedesignation of local areas should take into considerationthe extent of movement of population within severaladjacent administrative districts.
17. Infected Local Area - Cholera: Hong Kong.The Government sends the following comments :
" The size of an area to be declared a cholera' infected local area ' has an important bearing onthe epidemiology. Where more than one prefectureor county of a country is declared infected, restrictionsshould apply to the whole country ideally or to atleast a distinct geographical area, for example, anisland or other geographical unit which can beregarded as such. The declaration of infected localareas on a district basis, where borders are contiguousand where there is free movement of people to andfro, pays no heed to the epidemiology of cholera."
18. Quarantinable Diseases - Cholera. On 23 May1962,3 the Fifteenth World Health Assembly adoptedthe tenth report of the Committee on InternationalQuarantine, which met in Geneva on 3 May 1962 toconsider the question of El Tor infection and itsrelationship to the International Sanitary Regulations.Extracts from the Committee's report are givenbelow :
The Committee recalls that in 1957, at the time of its fifthsession and for some decades before that time, all reported casesof the disease due to El Tor vibrios had been limited to theCelebes. It was on this basis that the Committee was of theopinion that this disease should not be included in the termcholera, a quarantinable disease under the International SanitaryRegulations.4 The Eleventh World Health Assembly endorsedthis opinion.5
The Committee studied the detailed reports of the severaloutbreaks of El Tor infection (in Indonesia, in Sarawak (July1961), in Macao (August 1961), in Hong Kong (August 1961),in the Philippines (September 1961) and in North Borneo(January 1962)) and considered the views of the experts on theseoutbreaks, including the conclusions and recommendations ofthe Scientific Group on Cholera Research 8 and the findings ofthe meeting in Manila 7 . . .
The Committee, noting that the Scientific Group on CholeraResearch "having given very careful consideration to all theavailable evidence about the epidemiology and clinical features
3 Resolution WHA15.38.4 Off. Rec. Wld Hlth Org. 87, 400, section 17.
Resolution WHA11.44.6 Scientific Group on Cholera Research, Geneva, 2 -6 April
1962.
Meeting for the Exchange of Information on Cholera El Tor,Manila, 16 -19 April 1962.

32 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
of El Tor infection, recommends that this disease be regardedas essentially identical with classical cholera and . . . dealtwith as such ", is of the opinion that, in the light of the bestinformation and knowledge available, cholera El Tor does notdiffer from classical cholera in its epidemiological, clinical andpathological aspects and in measures of treatment. The Com-mittee endorses the recommendation of the Scientific Groupon Cholera Research that: " In regard to the use of prophy-lactic vaccines . . . classical cholera vaccines be used untilsuch time as evidence is produced from experimental or fieldvaccine studies of the absence of cross -protection betweenclassical cholera and El Tor vaccines ".
The Committee is therefore now of the opinion that cholera,under the definition of quarantinable diseases inArticle 1 of the Regulations, should include cholera due to theEl Tor vibrio, and recommends that its opinion given at its fifthsession and endorsed by the Eleventh World Health Assemblyshould be amended accordingly.
The Committee recognizes that there are several gaps infundamental knowledge, both in relation to El Tor and classicalcholera, and that the World Health Organization is engaged in
studies of cholera and cholera El Tor, including standards forand efficacy of the vaccine, which will, it is hoped, supply thenecessary information to enable the Committee to keep underreview its opinion stated above).
Beginning with the issue dated 25 May 1962,notifications of cholera El Tor have been includedin the Weekly Epidemiological Record. In the currentnotifications section of the Record a suitable footnotehas been added to indicate that the disease was choleraEl Tor. In the infected area list of the Record no suchdifferentiation has been made.
The Committee noted the method of disseminationof information on cholera El Tor made in the WeeklyEpidemiological Record. The Committee was informedthat in the daily epidemiological radiotelegraphicbulletin no differentiation is made between cholera andcholera El Tor. The Committee is in agreement withthe practices described above for the dissemination ofinformation -on cholera El Tor.
PART II. NOTIFICATIONS AND EPIDEMIOLOGICAL INFORMATION
19. No notifications required by the Regulations(Articles 3 to 6 and Article 9) have been received from :
the Democratic People's Republic of Korea (since1956);
the Democratic Republic of Viet -Nam (since 1955);
China (mainland) (since March 1951);Yemen (since March 1958) (an annual report on the
working of the Regulations for the year underreview has been received from Yemen).
20. For many decades it has been routine practice,especially in Asia, to notify cases of quarantinablediseases disembarked from ships. Telegraphicinformation includes date and port of arrival, name ofship, previous ports of call, name of disease, numberof cases among crew or passengers, the fact that allnecessary measures have been taken to deal with theship, and subsequent ports of call, with expected datesof arrival. Table 9 of the WHO CODEPID wasconstructed to facilitate such telegraphic notifications.Subsequent airmail notifications confirm the tele-graphic notification and include details on the shipitself, previous ports of call, with dates, subsequentports of call, with dates, sanitary measures taken andparticulars on each case, including probable sourceof infection and vaccination certificate. In recent yearssimilar notifications have been made for infectedaircraft. These notifications have facilitated inter-national traffic; the Organization knows of noinstance where carriers or persons at subsequentports of call have been subjected to unnecessarysanitary measures. These notifications have assistedother health administrations to carry out permitted
surveillance operations of persons, especially whenthe disease is smallpox.
The notifications described above are not providedfor in the International Sanitary Regulations. TheCommittee will wish to consider whether such notifica-tions and subsequent dissemination of information bythe Organization should be an obligation under theRegulations.
Information is given in separate documents onimported cases and related matters . and on cases ofquarantinable diseases imported by ship and aircraft.See also the recommendation of the Comm ittee undersection 21.
Article 3
21. In its ninth report the Committee urged allhealth administrations to notify the Organizationby telegram within twenty -four hours when one ormore cases of a quarantinable disease have beenimported into a non -infected local area.2 In thediscussion on this report at the Fifteenth WorldHealth Assembly it was requested that the Committeeconsider making such notifications an obligation underthe Regulations.3 Both in the Committee and at theHealth Assembly it was clearly stated and definitelyagreed that such notifications of themselves wouldnot mean that the non -infected local area therebybecame an infected local area.
. Off: Rec. Wld Hlth Org. 118, 61-62.2 Off: Rec. Wld Hlth Org. 118, 39, section 19.3 Off. Rec. Wld Hlth Org. 119, 196.

ANNEX 1 33
The Committee recommends that Article 3 should beamended by adding the following paragraph after thefirst paragraph:
2. In addition each health administration shall notifythe Organization by telegram within twenty-four hoursof its being informed
(a) that one or more cases of a quarantinabledisease have been imported or transferred into anon- infected local area -the notification shallinclude information on the origin of infection;
(b) that a ship or aircraft has arrived with one ormore cases of a quarantinable disease on board-the notification shall include the name of the shipor the flight number of the aircraft, its previous andsubsequent ports of call, and whether the ship oraircraft has been dealt with.
The present paragraph 2 of Article 3 should be re-numbered paragraph 3.
Article 6
22. In previous reports the Committee has statedthat the time- limits in Article 6, paragraph 2 (a),equal to twice the incubation period of the disease,are minimum limits, and health administrations mayextend them before declaring an infected local area intheir territory free from infection and continue for alonger period their measures of prophylaxis to preventthe recurrence of the disease or its spread to otherareas.'
It is recalled that the health administration of Indiahas for some years extended these minimum limitsto three times the incubation period in respect ofcholerà. Because notifications are normally submittedon a weekly basis, three times the incubation period offive days (fifteen days) in practice usually meansthree weeks. The health administrations of thePhilippines, Hong Kong and China (Taiwan) haveinformed the Organization that they will also useat least this extended period before declaring acholera- infected local area free from infection.
The Committee notes the policy of India, Hong Kong,China (Taiwan) and the Philippines, and commendsthis practice to other health administrations.
23. The provisions of Article 6 permit a healthadministration to notify a local area as free of infectionwhen, inter alia, " twice the incubation period of thedisease... has elapsed since the last case identifiedhas died, recovered or been isolated ".
1 Off. Rec. Wld Hlth Org. 72, 38, section 23; 79, 499, section28; 110, 36, section 17.
In the past year a case of smallpox developed in anurse who had already been isolated in hospital withclose contacts of an imported case. Isolation beganon the 1st of the month, she fell ill on the 12th anddied on the 20th. Since she had been isolated on the1st, the health administration, with the concurrenceof the Director -General, notified the area as freefrom infection on the 30th of the month. Threedays later a nurse in a ward adjoining but separatedfrom the isolation ward fell ill, developed smallpoxand died. The second nurse had been vaccinated onthe 1st of the previous month and had had a papularreaction (read as successful).
The Committee will wish to consider the policydescribed above in relation to the provisions ofArticle 6.
The Committee is of the opinion that the periodstipulated in Article 6 should begin when the last caseis identified as a case, irrespective of the time that thisperson may have been isolated.
Article 8
24. Ethiopia. The Government reports as follows :" As personnel available in embassies, legations or
consulates usually are not able to understand quaran-tine questions and interpret the International SanitaryRegulations, it is recommended that VaccinationCertificate Requirements for International Travel beput at the disposal of all airline services and alldiplomatic missions, and that it be stressed that onlythe quarantine services in the countries where thediplomatic missions or airlines are located have theauthority to interpret the International SanitaryRegulations. Any case of dispute should be referredto these quarantine services and not settled bydiplomatic missions or the employees of airlines."
The Committee urges health administrations toarrange that diplomatic missions of their governmentsare kept up to date on national requirements forvaccination certificates for international travel.
Article 9
25. The provisions of Article 9 require a weeklytelegraphic report of the number of cases of thequarantinable diseases and deaths therefrom in townsand cities adjacent to a port or airport. In the absenceof such cases airmail reports are required for certainspecified periods. It is the opinion of the Director -General that these provisions apply also to anyimported cases and cases transferred into such towns
34 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
or cities, e.g., for hospitalization, from another localarea within the same territory.
The Committee is in agreement with this opinion.
Article 11
26. From 1 January 1962 the obligations of theOrganization under Article 11 for dissemination ofall epidemiological and other information which ithas received under Articles 3 to 9 inclusive have beenthe responsibility of headquarters. These obligations,as well as those to disseminate other information onthe Regulations, have been carried out by head-quarters by means of the Weekly EpidemiologicalRecord, the daily epidemiological radiotelegraphicbulletins, telegrams, telephone calls, and airmailmemoranda giving advance information which willsubsequently appear in the Record. For reasons ofeconomy and accuracy, telegrams are usually sent inCODEPID (WHO Epidemiological Cable Code andits 1961 revised Geographical Index).
The Geneva -Prangins transmission of the dailyepidemiological radiotelegraphic bulletin (a textcovering the whole world) is retransmitted free ofcharge by fourteen stations in Asia. One -third ofthese retransmissions are made more than once a week.
See section 8 for the situation from 1 July 1961 to31 December 1961.
27. The Weekly Epidemiological Record, in the section" Epidemiological Notes ", published a summary,including maps, of the reported occurrence of cholera,'plague,2 smallpox,' and yellow fever 4 during 1961.
Information on imported cases and outbreaks ofquarantinable diseases in the following countrieswas also published in this section :
Cholera: in Burma, Hong Kong, Macao andSarawak;
Cholera El Tor: in Indonesia, North Borneo and thePhilippines;
Plague: in United States of America, and Venezuela;
Smallpox: in Basutoland, Belgium, Central AfricanRepublic, Congo (Brazzaville), Congo (Leopold-ville), Federal Republic of Germany, Muscat andOman, Poland, Trucial Oman, Union of SovietSocialist Republics, and United Kingdom of GreatBritain and Northern Ireland.A summary of the smallpox situation in Europe
was followed by the recommendations of the Com-
' Wkly epidem. Rec., 1962, 21, 254.2 Wkly epidem. Rec., 1962, 29, 355.3 Wkly epidem. Rec., 1962, 25, 306.
4 Wkly epidem. Rec., 1962, 27, 333.
5 Wkly epidem. Rec., 1962, 3, 37.
mittee on International Quarantine at its seventhsession 6 on the need for the use of potent vaccines,correct vaccination procedures, and the importancefor medical and other personnel who come in contactwith travellers to maintain a high level of immunityby repeated vaccination.
The section " Epidemiological Notes " continuedto present summaries of reports on influenza outbreaks.
28. Separate publications were :(í) the revised Geographical Index of CODEPID,which came into force on 1 October 1961;
(ii) Yellow -Fever Vaccinating Centres for Inter-national Travel: situation as on 28 July 1961;(iii) Vaccination Certificate Requirements for Inter-national Travel: situation as on 20 December 1961;
(iv) Ports designated in Application of the Inter-national Sanitary Regulations: situation as on 6 April1962.
Amendments to publications (ii), (iii) and (iv)appeared as usual in the Weekly EpidemiologicalRecord. In addition, seven lists of amendments toVaccination Certificate Requirements for InternationalTravel were issued for those addressees (mainly travelagencies) which do not receive the Weekly Epidemio-logical Record.
Article 13
29. In accordance with Article 13, paragraph 1, ofthe Regulations and Article 62 of the Constitution, thefollowing 123 States and territories have submittedinformation concerning the occurrence of cases ofquarantinable diseases due to or carried by inter-national traffic, and /or on the functioning of theRegulations and difficulties encountered in theirapplication :Afghanistan Central African RepublicAlbania CeylonAngola ChadAustralia ChileAustria ChinaBarbados ColombiaBasutoland Comoro ArchipelagoBechuanaland Congo (Brazzaville)Belgium Congo (Leopoldville)Bermuda Cook IslandsBritish Guiana CubaBritish Solomon Islands Pro- Cyprus
tectorate CzechoslovakiaBritish Virgin Islands DahomeyBurma DenmarkBurundi DominicaCambodia EcuadorCanada El SalvadorCape Verde Islands Ethiopia
6 Of Rec. Wld Huth Org. 102, 47, section 59.

ANNEX 1 35
Falkland IslandsFederal Republic of GermanyFederation of Rhodesia and
NyasalandFijiFinlandFrance (including French
Guiana, Guadeloupe, Mar-tinique and Réunion)
French PolynesiaFrench SomalilandGabonGambiaGhanaGibraltarGilbert and Ellice IslandsGuatemalaHondurasHong KongHungaryIndiaIndonesiaIraqIcelandIsraelJamaicaJapanJordanKenyaKuwaitLaosLebanon
LibyaMacaoMaliMauritaniaMauritiusMexicoMongoliaMontserratMoroccoMozambiqueNepalNetherlands, Kingdom of the
(including Netherlands, Su-rinam, Netherlands Antilles,as well as Netherlands NewGuinea)
New CaledoniaNew HebridesNew ZealandNigerNigeriaNorth BorneoNorwayParaguayPhilippinesPolandPortuguese GuineaPortuguese TimorPuerto RicoRepublic of KoreaRomaniaSao Tomé and Principe
SarawakSeychellesSierra LeoneSouth AfricaSpainSt HelenaSt Kitts -Nevis -AnguillaSt LuciaSt Pierre and MiquelonSt VincentSudanSwazilandSwedenSwitzerlandTanganyikaThailand
TogoTongaTrinidad and TobagoTurkeyUgandaUnion of Soviet Socialist
RepublicsUnited Kingdom of Great
Britain and NorthernIreland
United States of AmericaVenezuelaWestern SamoaYemenYugoslaviaZanzibar
The Committee notes with concern that the numberof States submitting annual reports in accordance withArticle 13 of the Regulations and Article 62 of theConstitution of the Organization has decreased for theyear under review, and requests the Director - General tocontinue his efforts to obtain annual reports on thefunctioning of the Regulations from all States andterritories.
30. Details of cases of quarantinable diseases due toor carried by international traffic are given in Part V,in Appendix 1, and also in a separate document.
PART III. SANITARY ORGANIZATION
31. Yemen. The Government states that, with thehelp of the Organization, quarantine services inYemen have recently been well organized and areworking satisfactorily.
Article 14
32. Information on the provision of pure drinking -water at international ports and airports has beenreceived from thirty -eight countries in reply to circularletter No. 17 of 18 May 1961. The informationreceived from countries will be published in the WeeklyEpidemiological Record. Four countries have reportedthat water supplies in all their ports and airports aresatisfactory. Fifteen countries have indicated thatall the ports and airports listed by them have satis-factory water supplies. For the remaining countries,some of their ports and airports are satisfactory,but others fail to meet international standards in onerespect or another, and in some cases the data availableare insufficient.
Article 19
33. The International Air Transport Association(TATA) informed the Organization that its recent
Annual General Meeting approved the recommend-ation of its Medical Committee that WHO be askedto carry out a world -wide survey of internationalairports to ensure implementation of recommendationscontained in the WHO Guide to Hygiene and Sanitationin Aviation.'
The Committee requests the Director -General to referthis question to appropriate bodies of the Organization.
The Committee notes that the Director -General hasalready invited the attention of health administrationsto the recommendations of the Expert Committee onHygiene and Sanitation in Aviation and is prepared toassist States on request.
The Committee urges health administrations to makea review of the airports designated as sanitary airportsin order to determine whether they meet the presentconditions of traffic.
Article 21
34. Health administrations of 104 States and terri-tories have notified the Organization that 649 ports
' World Health Organization (1960) Guide to hygiene andsanitation in aviation, Geneva.

36 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
have been approved under Article 17 for the issue ofDeratting Certificates and /or Deratting ExemptionCertificates; of those, 145 have been approved forthe issue of Deratting Exemption Certificates only.'
35. Notifications of 222 sanitary airports have beenreceived from ninety -nine health administrations.
Article 27
Airports with direct transit areas number twenty -eightin twenty -one States and territories.'
Article 22
36. Ghana. The Government states that the situationin ports and airports of entry has remained as reportedpreviously.¢
PART IV. SANITARY MEASURES AND PROCEDURE
37. Canada. The Government reports as follows :" As reported in previous years 2 surveillance as
provided in Article 27 of the International SanitaryRegulations is impossible to enforce in Canada.Over one -fifth of persons placed under surveillancefail to report, give fictitious addresses, or cannot betraced at the destination they have reported."
Article 30
38. Spain. The Government reports as follows(translation from the Spanish) :
" It is pointed out in connexion with the disquietingsituation created in Western Europe by the appearanceof smallpox foci (which started at the end of December1961, following the importation of cases of the diseasein the incubation period, and persisted over the firstsix months of 1962), that the fact that no casesappeared outside the countries affected may beconsidered as proof of the efficacy of the frontierquarantine services. The same may be said of theWHO quarantine service, thanks to which we receivedtimely information concerning the international healthsituation and data concerning the evolution of the fociin question.
" In short, it may be said that the abnormal situationreferred to provided satisfactory proof of the efficacyof the present protective measures against quaran-tinable diseases in general and smallpox in particular.This result is all the more worthy of mention becausethe quarantinable disease concerned is perhaps themost dangerous on account of its epidemiologicalcharacteristics and prolonged period of incubation,and also because of the intensity of air traffic.
" In this connexion it is true that the present practiceof demanding a smallpox vaccination certificate frompassengers arriving by air upsets the smooth flow ofsuch traffic. On the other hand, in the case of airtraffic, it is usually difficult to tell, in the countries of
1 World Health Organization (1962) Ports designated inapplication of the International Sanitary Regulations, Geneva -as brought up to date on 31 August 1962.
2 Off Rec. Wld Huth Org. 118, 45, section 55.
arrival, whether or not passengers have come from agiven infected local area -knowledge which couldbe provided accurately and easily by the healthauthorities of the country of origin.
" In view of the foregoing, it is suggested that,without prejudice to the present provisions of theRegulations, the health authorities of countries inwhich smallpox infected local areas exist should berequired to take the responsibility of preventing thedeparture of any person who has not been vaccinated(and who therefore does not possess a valid vaccinationcertificate) or who is suspected of having had contactwith the infection during the fourteen days precedinghis intended departure by air."
The Committee emphasizes that under the provisionsof Article 30 the health authority for a local area whichis an infected local area has the obligation to take allpracticable measures to prevent the departure of anyinfected person or suspect. At its eighth session theCommittee stated that in areas where smallpox ispresent, " health administrations may, in partialfulfilment of these obligations, require a smallpoxvaccination certificate of departing travellers ".5
The Committee further recalls that persons undersurveillance may move to another territory, but inthat instance the provisions of Article 27, paragraph 2apply.
Article 34
39. See section 62.
Article 35
40. Seychelles. The Government reports that,during the epidemic of smallpox in Karachi, grantingof pratique by radio to ships was temporarilysuspended.
Article 36; Article 4841. See sections 96 and 93 respectively.
' World Health Organization (1960) Airports designated inapplication of the International Sanitary Regulations, Geneva -as brought up to date on 31 August 1962.
4 Off. Rec. Wld Filth Org. 118, 43, section 46.5 Of . Rec. Wld Hlth Org. 110, 47, section 68.
ANNEX 1 37
PART V. SPECIAL PROVISIONS RELATING TO EACH OF THE QUARANTINABLE DISEASES
42. Information, including maps, on plague, cholera,yellow fever and smallpox notified for the calendaryear 1961, is given in a separate document, consistingof extracts from the Weekly Epidemiological Record.'
Plague
Article 52
43. A health administration has stated that difficultiesarise when certain other countries insist that whenderatting is done the fumigation agents must be hydro-cyanic acid or sulfur dioxide.
The Director -General has replied quoting the opiniongiven by the Committee at its third session that" Deratting Certificates should be held to be validirrespective of the agent used, provided it is ofrecognized effectiveness and inspection of the shipafter deratting shows it to be free from rats ".2
The Committee reaffirms its opinion given at itsthird session and quoted above.
44. United States of America. The Governmentreports as follows :
" Evidence of appreciable numbers of rats wasfound on only a small percentage of ships enteringUnited States ports. This was attributed to improvedsanitation, more extensive use of rat -proof construc-tion, wider practice of rat trapping carried on con-tinuously at sea and in port, and rodent control inport areas.
" The over -all sanitation improvement programmehas resulted in considerable improvements on manyvessels. Four foreign flag vessels received certificatesof sanitary vessel operation this past year. It is anti-cipated that this number will more than double in thenext year."
Cholera
45. In a communication to the Organization a healthadministration has raised the following questions,which are submitted to the Committee for con-sideration.
The wide spread of cases of cholera El Tor in anumber of countries of Asia in 1961 is arousinganxiety as to the possibility of their further spread ifprophylactic quarantine measures are not introducedagainst them.
It is considered desirable to supplement the systemof prophylactic measures against cholera laid down
1 Wkly epidem. Rec., 1962, 21, 254; 25, 306; 27, 333; 29, 355.2 Of Rec. Wld Hlth Org. 72, 37, section 13.
in the Regulations by an item calling for isolation, formedical observation, of persons who have been indirect contact with a cholera patient during an inter-national journey, regardless of whether on not theypossess valid vaccination certificates.
This suggestion is based on the fact that vaccinationagainst cholera provides immunity for a very shortperiod (six months) and it is impossible to be certainthat a person who has been in close contact with apatient will escape infection, particularly in the laterpart of the " guaranteed " vaccination period. In anycase, it should be possible to authorize the healthauthorities to settle this question in accordancewith the epidemiological circumstances.
46. Sanitary measures in respect of cholera taken byone State against arriving international travellersexceeded those permitted by the Regulations. Thisaction occurred after cases of cholera El Tor werenotified in China (Taiwan) in July 1962 and in HongKong in August 1962. Crew and passengers on healthyships coming from these two areas were submittedto stool examination or rectal swabbing and whenone or more carriers were found all travellers wereplaced in isolation until three consecutive negative
the ship, which hadbeen in quarantine during this period, was then givenfree pratique. An aircraft having stopped in Taipeiwas subsequently quarantined for nearly twenty -fourhours, together with its crew and passengers, althoughall except a few were in possession of valid internationalcertificates of vaccination against cholera. Two ofthose without vaccination certificates, who had somediarrhoea, had embarked at Taipei, but were shownby examination after arrival not to have cholera.47. Canada. The Government reports as follows :
" Due to the prevalence of cholera in certaincountries, it was necessary during the early monthsof 1962 to regard El Tor cholera as true cholera.Persons entering Canada from areas infected withEl Tor cholera were held subject to the same require-ments as persons from areas infected with cholera.Canada's deviation from the International SanitaryRegulations in regard to El Tor cholera was, ofcourse, corrected by the action subsequently taken bythe Organization to interpret the Regulations withrespect to El Tor cholera." $
48. Hong Kong. The Government reports as follows :" During the period 1 July 1961 to 30 June 1962,
Hong Kong in common with certain other countriesin the region was infected with cholera El Tor. An
3 Resolution WHA15.38.

38 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
account of the outbreak in Hong Kong has beenpublished as a White Paper and copies of this WhitePaper have already been forwarded to the Director -General of WHO...
" From the experience gained of the epidemiologyof cholera during the outbreak in Hong Kong, it issuggested that Articles 60 to 69 ... of the InternationalSanitary Regulations should be reviewed. Despite theconsiderable powers conveyed by these articles, it hasnot proved possible to prevent the entry of Vibriocholerae infections into countries in the region despiterigid application of the quarantine measures allowedby the Regulations.
" The role of the contact -carrier in the disseminationof cholera is not fully understood, but there is evidenceto support the view that the contact -carrier withoutclinical symptoms of the disease may be the agentof dissemination from country to country, particularlythose contact -carriers moving by sea in small vesselsover short distances which do not normally go throughquarantine inspections.
" It is evident that the powers at present given underthe Regulations are not wide enough to prevent thedissemination of cholera for the following reasons : 1
In the past, passengers travelling by air were notnormally of the socio- economic group likely to beinfected. This no longer applies and increasing useis being made of air transport, particularly charterflights, to move groups of people in the lowerincome groups. Accordingly, the risk of introducingthe infection through contact -carriers withoutsymptoms is a very real one.
Before action can be taken under the existingRegulations, a ship or aircraft can only be suspectedif a case of cholera has occurred on board duringthe voyage. With the speed of modern travel this isnot realistic and passengers embarking on a ship oraircraft calling at a port in an infected country arenot subject to any quarantine restrictions if that portoccurs in, but has been excluded from, an infectedlocal area. Where a port or airport is surroundedby or is adjacent to an infected local area, that portshould be regarded as infected and only transitpassengers who have been accommodated in adirect transit area should be excluded from restric-tions. The tendency not to declare ports and airportsas infected areas other than for use as transit areasgives a very wide loophole in the powers of protec-tion by receiving countries. Both ports and airportsare usually surrounded by infected local areas;as a result the tendency is for passengers embarkingat these ports to claim they are not subject to
1 See further reasons given by the Government of Hong Kongunder sections 17, 55, 59 and 61.
quarantine restrictions on account of cholera, eventhough they may have come from an infected areato the airport.
The place of oral antibiotics in the treatment ofthe contact -carrier state requires intensive investiga-tion with a view to determining whether or nottheir use could replace surveillance or isolation ofsuspected or proved contact- carriers."
49. Japan. The Government reports as follows :" 1. At the time of the epidemic of cholera due toEl Tor vibrio in Indonesia, Sarawak, North Borneo,Hong Kong and the Philippines toward the end of1961, we came to the conclusion that cholera due toEl Tor vibrio is a communicable disease whichmerited the same treatment as the cholera under theInternational Sanitary Regulations and such aconclusion was based on actual observation by ourscholars and various information accumulated. Itwas under such a conviction that the Japanese membersof the WHO Expert Advisory Panel, as well as theMinistry of Health and Welfare, proposed therevision of the Regulations in this respect. We werecertainly glad about the action of the Fifteenth WorldHealth Assembly adopting the tenth report of the Com-mittee on International Quarantine thus including thecholera due to El Tor vibrio under the Regulations.
paved way for us rely on the epidemio-logical information from the WHO headquarters andto be prepared not only in our quarantine policy butalso in the prevention of the spread of this disease ifand when it entered this country. These preparationsconsisted of inoculating approximately 600 000 personsof priority groups, such as seamen, port workers, etc.in about forty ports which were likely to be called atby ships from the Philippines, etc.
" 2. We were thus prepared when, on 21 July 1962,we obtained information on the outbreak of cholerain Taiwan, generally speaking at a distance from ourcountry of two or three days' voyage by ship. We thencarefully watched arrivals from Taiwan. A Japanesecargo ship, MIKAGE -MARU, arrived at Kanmon Porton 31 July, after calling at the port of Kaohsiung,Taiwan, from 19 to 27 July. At the time of routinequarantine inspection it was learned that there wasat least one crew member who had diarrhoea whilethe ship was calling at Kaohsiung Port. Therefore,as a precaution, with the consent of the captain, thestools of the entire crew were examined. However,since the entire crew had been inoculated againstcholera, and also since Kaohsiung Port was not notifiedby WHO as a cholera infected local area, the ship wasgiven a provisional pratique under Article 18 of theJapanese Quarantine Law, and the entire crew wasplaced under surveillance. On 1 August, in the

ANNEX 1 39
evening, three patients and fourteen carriers weredetected out of thirty -eight crew members. Measureswere taken to invalidate the provisional pratique, theentire crew were isolated, and the ship was disinfected.Disinfection as well as stool examination was extendedto cover 2400 contacts and some 100 houses whichwere visited by the crew. In order to deal with possiblecontamination of the sea water, fishing as well asswimming was forbidden over a certain expanse of thesea and beaches. Drastic measures were taken toforestall a secondary infection, and as a result thedisease did not extend beyond these imported cases.However, it must be noted that on the second stoolexamination five additional carriers were detected fromamong the crew who had been negative at the time ofthe first stool examination, and placed under sur-veillance.
" 3. From the experience stated above, and alsofrom the consideration that the invasion of Taiwanby cholera must be a sizeable one, we reached theconclusion that the mere presentation of a validcertificate of inoculation did not safeguard thiscountry and that in order to prevent the invasion ofcholera into this country we would have to adopt aformula of ascertaining the presence or absence ofcarriers. Accordingly, we started on 2 Augustrequiring stool examination and closure of lavatory(toilet cans to be used instead), as well as prohibitingdischarge of waste matter and waste water, withrespect to ships arriving from Taiwan.
" 4. In connexion with the stool examination, in nocase has rectal swabbing been ordered, locally orfrom the Ministry, in compliance with the provisionof the International Sanitary Regulations. However,it has been undertaken on some occasions in which acrew member or a passenger has voluntarily requestedsuch a recourse.
" 5. On 10 August, the Chinese cargo ship Ru-YUNGarrived at Kobe Port. This ship had left KaohsiungPort on 7 August and Keelung Port on 8 August.While the result of the first stool examination wasnegative, one carrier was detected by the secondexamination. A Japanese cargo ship, HIRASHIMA-MARU, arrived at Kanmon Port on 21 August afterleaving Kaohsiung Port on 15 August. Four carrierswere detected at the time of the first stool examinationand one additional carrier was detected at the timeof the second examination. Both ships were imme-diately quarantined and disinfected and crews wereisolated or placed under surveillance. These andrelated disease prevention measures enabled us tostop the invasion. It is worthy of attention that thelatter case demonstrates that carriers were detected
on the sixth day after sailing from the locally infectedarea.
" 6. Information was obtained from WHO head-quarters that on 23 August a case of cholera occurredin Hong Kong. We then required one stool exami-nation with respect to ships arriving from Hong Kong.Thus we detected two carriers on board the UnitedStates cargo ship HONG KONG BEAR which arrivedat Hakata Port on 27 August, sailing from HongKong on 24 August, arriving at Naha Port in Okinawaon 26 August, and leaving the same on 27 August.Isolation of the two carriers and other necessarymeasures were taken.
" 7. On 28 August, we obtained information froma reliable source in Okinawa that one case of choleraoccurred, although United States authority maintainedthis was merely a carrier, and together with the con-sideration of the case of HONG KONG BEAR, weadopted a policy of dealing with Okinawa in thesame way as we did with Hong Kong from 1 Sep-tember. Three carriers were detected on board theJapanese cargo ship FUYO-MARU and one carrieron another Japanese cargo ship SHOZUI-MARU,both arriving at Tsukumi Port on 1 September. Thecrew was isolated at the Hikoshima detention quartersof the Moji Quarantine Station. The measures againstarrivals from Okinawa were lifted and replaced by thenormal procedure starting on 11 September, afterbeing satisfied that there was no case following thefirst one, and such a fact was ascertained by amission who went there to study the situation.
" 8. On 29 August, the Japanese cargo ship KYOTO -
MARU arrived at Tokyo Port leaving Cagayan deOro, a Philippines port in a locally infected area, on23 August. There was a crew member who haddiarrhoea when the ship arrived, and stool examinationwas conducted. The first examination revealed threecarriers and the second examination three additionalcarriers outside the one who had diarrhoea. This isnoteworthy as a case of detection of carriers after sixdays beyond the incubation period of five days.
" 9. In order to observe the actual situation inTaiwan and co- ordinate our measures with the effortsin Taiwan, and also in response to the invitationextended through the diplomatic channel, we dis-patched four persons representing the cholera scholars'group and two administrators from the Ministry ofHealth and Welfare to Taiwan on 28 August. Throughthis visit we ascertained that the cholera epidemic hadby then been controlled to the extent that the locallyinfected areas had been narrowed down to the fiveprovinces in the south, namely Yunlin, Chiayi,Tainan, Kaohsiung, and Pingtung, and the two cities
40 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
of Tainan and Kaohsiung. Therefore, the quarantinemeasures were brought back to normal routine withrespect to ships leaving Keelung, Taipei and otheruninfected areas in Taiwan on and after 14 September,and arriving at our shores.
" On 19 September Taiwan was declared free fromcholera infection, the information about whichreached us on 20 September. In compliance with theRegulations, we withdrew the special measuresagainst arrivals from Taiwan departing from Taiwanon and after 20 September.
" 10. With respect to ships arriving from HongKong also, on the basis of information as of 9 Sep-tember that only four cases and four carriers ofcholera existed, without showing a sign of furtherspread, and in consideration of the fact that preventiveinoculation of the inhabitants has covered a greaterportion of the population, normal routine measuresare applied to ships sailing from Hong Kongon and after 15 September, so long as they meetcertain conditions, such as the presence of a ship'sdoctor on board, good health management on board,etc.
" In summary, the initial experience with MIKAGE-MARU was that of discovering at the time of theroutine quarantine procedure no suspected case amongthe entire crew who had had preventive inoculation.However, when the stool examination was conductedwith the consent of the captain, three patients andfourteen carriers were detected. As stated in para-graph 2 above, the crew had been permitted to goashore, and a very drastic measure had to be takenaffecting many citizens. This gave rise to a greatshock and anxiety to the Japanese people in general,and to criticism that the quarantine measure was notsufficient.
" In connexion with this experience, we came to theconclusion that under the prevailing condition ofenvironmental sanitation and of food habits in thiscountry, the adherence to the International SanitaryRegulations, in particular the provisions of Article 69,paragraph 2, would not safeguard this country againstthe invasion and spread of cholera. Therefore, wewere forced to take recourse to administering theleast necessary measures of stool examination. Theresults have been, as stated in paragraphs 5 through8 above, the discovery of eighteen carriers withrespect to six ships following the discovery withMIKAGE -MARU. It is our belief that by such detectionwe were barely able to forestall the invasion of thiscountry by cholera.
" The measures taken have been temporary andemergency measures under very pressing circumstances.For the reasons stated above, we would wish that the
Regulations be reviewed with a view to amending thequarantine formula to deal more adequately withpreventing the spread of cholera by internationaltraffic.
" Now, here are the facts about aircraft. Theparticular aircraft, TG 600, Thai Airways, undet jointoperation with SAS, arrived from Taipei on 20 Augustwith eleven crew members and fifty -eight passengers :one from Bangkok, eleven from Hong Kong andtwenty -three from Taipei. Two of the passengers fromTaipei had diarrhoea at the time of arrival and volun-tarily underwent stool examination from fear that theymight have contracted cholera. There were sevenother passengers from Taipei and six from HongKong, who did not possess valid vaccination certificates.We judged them to be possible suspects, and they alsounderwent stool examination. We did not order theaircraft to be detained. However, we accepted theoffer to let passengers stay overnight on the plane,until the results of the examination were known."50. Japan. The following further communicationhas been received from the Government :
" PROPOSAL FOR THE AMENDMENTOF THE INTERNATIONAL SANITARY REGULATIONS
WITH RESPECT TO QUARANTINE PROCEDURE AGAINST CHOLERA
" In facing the outbreak of epidemic of choleradue to El Tor vibrio in Indonesia and the WesternPacific Region since last year, the health administrationin Japan has actively exerted itself, in compliancewith the provisions of the International SanitaryRegulations, in an effort to prevent the spread of thisdisease through international voyage. On the basisof our experience of the incidence of the Japanesecargo ship MIKAGE -MARU on 31 July, and the sub-sequent quarantine policy adopted, about whichexplanation has been separately presented, it is herebyrequested that the International Sanitary Regulationsbe partially amended with respect to the followingpoints and thereby improve the existing quarantineformat.
" I. ' Infected local area'" The definition of the ` infected local area ' provided
for in Article 1 of the International Sanitary Regula-tions is liable to variable interpretation from countryto country, specifically there may be wider andnarrower delineation of the area in the absence ofuniformity of its application. Some country maydelimit its boundary to an extremely small area, andthere have been instances that such delimitation wasnot conducive to the prevention of the spread of thedisease. It is proposed that the definition of the` local area ' be amended to include the port or theairport as a matter of course and that it would be
ANNEX 1 41
defined as an area of province, prefecture, city,town, etc., which may include the neighbouring areaswhich are judged to be liable directly or indirectlyto affect the ship or the aircraft present in the port orthe airport.
" The reasons:" The information on the outbreak of cholera in
Yunlin, Chiayi and Tainan in Taiwan reached ourhealth administration through radio from Genevaon 20 July. A cable was also received from the WorldHealth Organization on 23 July : the same information,with additional information that the seaports andthe airport were not infected. In the meantime, theJapanese ship MIKAGE -MARU, which left KaohsiungPort on 27 July, arrived at Kanmon Port on 31 July,and, out of its thirty -eight crew, three patients andnineteen carriers were detected. From the Organi-zation, however, we received information on 9 and11 August that Kaohsiung City had been designatedas infected on 28 July. In the same information, theport of Kaohsiung was still excluded from the infectedlocal area, and it was by the Organization's informationdated 17 August that the port of Kaohsiung had beendesignated as locally infected.
" Again in the meantime, one carrier was detectedon board the Chinese ship Ru -YuNG which had leftKaohsiung Port on 7 August, Keelung Port on8 August and arrived at Kobe Port on 10 August.
" The above instances form the basis of our requestfor' the amendment of the provisions with respect tothe definition of the ` infected local areas '.
" II. On the measures with respect to carriers" Under the current International Sanitary Regula-
tions, the quarantine measures are provided foragainst the dangers of cases of cholera, as in Article 63wherein it is implied that on arrival of an infectedship or aircraft any person in possession of a validcertificate of vaccination will have to be permittedto go ashore or leave the aircraft, although undersurvei11ar e, or, as in Article 69, under which onlya person who has symptoms indicative of choleramay be subjected to stool examination. The Regula-tions lack any provision for measures to preventthe spread of cholera through carriers. With the beliefthat there is a great danger of spread of cholerathrough carriers, we would request the amendment ofthe Regulations to provide for the following :
(1) to treat the carrier, once detected, similarlyas the case -for instance, the carrier, once detected,should be reported as such together with the case,if any, and treated similarly as the case as far asquarantine measures are concerned ;(2) to enable isolation of any person arriving onboard an infected ship or aircraft even if one
possesses a valid vaccination certificate because itis possible that he may be a carrier;
(3) to enlarge the scope of requirement for sub-mission to stool examination to include any personarriving from an infected local area within a certainperiod of time.
" In the instance of the Japanese ship MIKAGE -MARUabout which reference has been made above, Kaoh-siung Port had not been declared an infected localarea, and the entire crew had been vaccinated againstcholera, and further there was no suspicion as to theirhealth at the time of arrival. However, on learningthat at least one member of the crew had diarrhoeawhen the ship was calling at Kaohsiung Port, theentire crew was subjected to stool examination withthe consent of the captain. The provisional pratiquehad been given to the ship which docked and the crewwas permitted to go ashore. The result of examinationrevealed the presence of vibrio in twenty -two out ofthirty -eight crew (in fact, three patients and nineteencarriers). Fortunately, secondary cases have beenforestalled through rigorous preventive measures.
" If these patients and carriers had not been detectedand were permitted to move about freely a disastroussituation might have been brought about affectingour citizens. Through the policy adopted on therequirement of stool examination vibrios have beendetected in a total of forty persons (namely threepatients and thirty -seven carriers) out of seven shipsconcerned. It is our belief that such an experiencereveals the importance of quarantine policy in whichthe stool examination plays the major role and alsothe necessity for applying quarantine measures topersons who possess valid vaccination certificates.
" It has been pointed out and emphasized at thetime of the conference for the exchange of informationon paracholera due to El Tor vibrio, held in Manilain April this year, that the presence of many carriersplayed an important role in the spread of infectionin the epidemic of El Tor cholera in the WesternPacific Region. It is our submission that the samemeasures should be applied to carriers as with thepatients.
" For your information, Annex I 1 gives the listof cholera infected ships and the way in which thepatients and carriers have been detected.
" III. On the period of time during which stoolexamination may be required the present InternationalSanitary Regulations delimit the requirement forstool examination to a person arriving from an infectedlocal area within the incubation period of cholera.However, on a number of occasions it has been found
1 Not reproduced in this volume.
42 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
that the presence of vibrio may be detected beyondthe limit of five days. It is therefore submitted that theRegulations be amended to enable requirement for stoolexamination up to fifteen days after departure from aninfected local area for the following reasons.
" The reasons:" As quoted from many reports in the WHO
Monograph `Cholera" by Pollitzer, over 90 per cent.of instances of vibrio discharge terminate within tendays. Also, as shown in Annexes II 2 and I11,2 thefirst dealing with the survey on the period of vibriodischarge among the patients and carriers found inTaiwan in 1962, and the second dealing with thenumber of days since the departure from infectedlocal areas and the date on which carriers weredetected, the period in which stool examination maybe required in the quarantine measures againstcholera should be extended to fifteen days maximumsince the date of departure from an infected localarea, on the basis of the incubation period of fivedays plus ten days in which vibrio discharges maycontinue."
51. North Borneo. The Government reports asfollows :
" ... there can be no doubt that infection by choleraEl. Tor was introduced to North Borneo by inter-national traffic -not on large vessels, but on smallkumpits travelling between the Sulu Province(Philippines) and North Borneo. Difficulties havebeen experienced in applying Article 62, since kumpitsdo not land only at recognized ports, but also atsmall places along the coast. Furthermore thejourney is so short that even if persons did not sufferfrom cholera El Tor during the voyage, they could beincubating it. Article 62 also does not meet the dangerof healthy carriers. Therefore the North BorneoQuarantine Rules (under the Quarantine Ordinance)were enforced which gave powers to quarantine theseboats and their passengers in the quarantine anchor-ages for the duration of the incubation period, eventhough no case had occurred on them before arrival ..In addition mass vaccination with anticholera vaccinewas given to large sections of the local population,notably in coastal areas exposed to risk. The Philip-pine Republic was declared a locally infected areawith cholera El Tor and inoculation regulationsenforced for travellers (vide Gazette NotificationNo. 57 of 20 January 1962).
"It was only recently that cholera El Tor was declaredto be the same as cholera under the InternationalSanitary Regulations. Before then this country's
1 Pollitzer, R. (1959) Cholera, Geneva (World Health Organ-ization: Monograph Series No. 43).
2 Not reproduced in this volume.
only recourse was to invoke powers under its Quaran-tine Ordinance. Cholera El Tor was declared to bea dangerous infectious disease under that Ordinanceand the quarantine measures described ... abovewere enforced whenever possible.
" Between 17 January and 31 May, there were 46definite cases of cholera El Tor in North Borneo, sixof them were fatal. In addition, some 100 deathsoccurred at remote coastal and island places duringthe first half of the year, which, from inquiries anddescriptions, were very likely caused by cholera El Torvibrio. The peak of North Borneo's epidemic occurredduring the period 1 March to 10 March and the areamost severely affected was the Semporna districtwhich reported more than half of the confirmed cases,and about half of the deaths probably due to thedisease. All other cases occurred in coastal areas inthe north and east of the territory, with the exceptionof one small focus along the Sugut river, some 25 milesupstream."
52. Philippines. The Government reports as follows :" Cases of cholera El. Tor first appeared in Manila
on 22 September 1961, and from this focus the diseasespread to areas in island groups comprising Luzon,Visayas and Mindanao. Up to the week ending30 June 1962, a total of 16 616 cases and 2223 deathshave been reported from 45 of the 56 provinces and33 of the 39 cities of the archipelago. The El Torvibrio has been identified in about 50 per cent. of thecases in Manila and suburbs, and in 20 per cent. ofall cases.
" It is possible that this disease has been introducedinto the country from any of the neighbouring El Torinfected areas ... From the time cholera El Tor hasbeen considered a quarantinable disease (23 May 1962),Article 30 of the Regulations has been complied with."
53. Sarawak. The Government reports that duringan outbreak of cholera El Tor, which started on12 July, the following cases were recorded :
First Division . .
Second Division . .
Third Division . .
Fourth Division . .
Fifth Division . . .
226 cases, with 45 deaths33 cases, with 15 deaths41 cases, with 10 deaths1 case, with 0 death0 case
Total 301 cases, with 70 deaths
The last case was reported on 5 October 1961 andthe country was declared free from the disease on19 October. No cases have been notified since thatdate.
54. United States of America. The Governmentreports as follows :
" The inclusion of El Tor type of cholera in thedefinition of quarantinable diseases in the Inter-

ANNEX 1 43
national Sanitary Regulations resolved the questionof Member countries exceeding the Regulations inrespect to the application of certain quarantinemeasures to persons arriving from areas in whichthis disease became epidemic during the past year.The World Health Organization is to be con-gratulated for its diplomatic handling of this problemand for facilitating its resolution."
Article 60
55. Hong Kong. The Government submits the follow-ing comments :
" In view of the knowledge of the duration of thecontact -carrier state, for quarantine purposes con-sideration might be given to a review of the durationof the incubation period."
Article 61
56. Philippines. The Government reports that,contrary to Article 61, paragraph 2, two injectionsof cholera vaccine within one week's interval wererequired by the health authorities of certain countries.
Article 63
57. Philippines. The Government reports that shipsof Philippine registry were regarded by the healthauthorities of certain countries as cholera- infectedships; the water on board was removed (without priorlaboratory examination) and replaced by fresh waterbefore the ships were given free pratique.
Article 68
58. Under the conditions specified in Article 68 ahealth authority may, inter alia, prohibit the importof fruit which is to be consumed uncooked. Duringthe cholera El Tor outbreaks in Asia some healthadministrations, in exercise of their rights underArticle 68, have prohibited the import of bananas andmangoes. These and other similar fruit, althougheaten uncooked, have a thick skin or rind which is noteaten and which is normally intact when the fruit isexported. There would appear to be little if any dangerof the spread of cholera by international traffic in thistype of fruit. However, no controlled studies areknown which would give an authoritative answer tothis hypothesis.
59. Hong Kong. The Government sends the follow-ing comments :
" Article 68 has been widely and variously inter-preted by the countries concerned during the yearunder review, and sanitary measures have been appliedwithout relation to the present state of knowledge ofthe epidemiology of cholera and of the vehicles likely
to carry infection. Signatory countries should beurged to respect the spirit and intention of Article 68."
60. Philippines. The Government states that onecountry banned the importation of all foodstuffs fromthe Philippines.
Article 69
61. Hong Kong. The Government comments asfollows :
" Article 69 should be revised to give powers torequire a non -vaccinated individual without symptomsindicative of cholera to submit to stool examinationif coming from an infected local area and disembarkingin a non- infected country, provided that the disembar-kation takes place within the incubation period."
Sections 45 -61. The Committee notes that severalStates have proposed, have taken, or are taking measuresin excess of the Regulations and invites the attentionof health administrations to the provisions of Article 23of the Regulations.
The Committee understands the difficult situationcreated in the area where cholera outbreaks are nowoccurring, but is not prepared at present to recommendany amendment to the Regulations.
The Committee recognizes that while the gaps infundamental knowledge continue to exist, difficultieswill in large part remain. The Committee considers,however, that many of the practical difficulties for healthadministrations would be eased to a great extent if, inaddition to fulfilment of obligations under Article 8,full and frequent consultations and exchange of informa-tion, particularly on preventive measures, were to takeplace between the health administrations concerned.Notification of measures should be made as far inadvance of their application as possible.
The Committee notes, as mentioned in its ninth report,that the Organization is engaged in research on cholera.The Committee stresses again the need for research toclose the gaps in fundamental knowledge and requeststhe Director- General to pursue such research vigorouslyand energetically.
Yellow Fever
62. (a) In adopting the ninth report of the Com-mittee on International Quarantine the World HealthAssembly excepted section 74 of that report andrequested the Director -General to refer this sectionto the Committee for reconsideration.' It reads :
Many travellers coming directly from Réunion by air areobliged by the Egyptian sanitary authorities at Cairo airport toproduce a yellow -fever vaccination certificate or are put in qua-
Resolution WHAI 5.37.

44 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
rantine when they are in transit at Cairo or their aircraft touchesthere. However, according to the requirements in regard tovaccination certificates notified to the Organization by the UnitedArab Republic, the Department of Réunion is not considered asan endemic or infected area. Thus, passengers coming directlyfrom Réunion who have merely been in transit through NairobiAirport (Kenya) under the conditions laid down in Articles 34and 75 of the Regulations should not be required to produce acertificate.
The Committee notes that the Department of Réunion is not ayellow fever infected area, that the airport local area of Nairobi(Embakasi) has been removed from the endemic zone under theprovisions of Article 70, paragraph 2, unamended, and that thisairport is provided with a direct transit area.
Consequently the Committee is of the opinion that the measurestaken at Cairo are in excess of the provisions of the Regulations.'
(b) The yellow -fever vaccination requirements ofthe United Arab Republic, as published by the Organi-zation in 1962, read as follows :
Air passengers in transit coming from an endemiczone or infected area, and not holding a certificate,shall be detained in the precincts of the airport untilthey resume their journey. The following countriesand territories are regarded as endemic zones orinfected areas : Africa : ... Kenya .. .
(c) The following information has been providedby the United Arab Republic : 2
The United Arab Republic " did not in factdemand vaccination certificates in the circumstancesdescribed in the complaint, but it had to ensure thatpassengers had not left the transit area in Nairobi.All that was required was a certificate to that effectfrom the health authorities of the airport. A ` directtransit area' was defined in Article 1 of the Interna-tional Sanitary Regulations as ' a special areaestablished in connexion with an airport, approvedby the health authority concerned and under itsdirect supervision, for accommodating direct transittraffic and, in particular, for accommodating, insegregation, passengers and crews breaking their airvoyage without leaving the airport ' ".The Committee recalls that, under the Regulations,
airport direct transit areas are for the purpose offacilitating international traffic. The Committee is ofthe opinion that, especially where areas outside a directtransit area or outside an airport may present a dangerof transmission of a quarantinable disease, the airporthealth authority has the obligation to ensure that transitpassengers do not leave the designated direct transitarea. When the airport is not yet provided with a directtransit area, the same obligation applies as regards thesegregation and transfer of persons referred to underArticle 34 (b).
1 Off. Rec. Wld Hlth Org. 118, 48, section 74.2 Statement made by the delegate of the United Arab Republic
at the Fifteenth World Health Assembly (Off. Rec. Wld HlthOrg. 119, 195).
The Committee recalls its opinion given at its firstsession that the procedure for establishing that directtransit of passengers at airports in yellow fever infectedlocal areas fulfils the required conditions should consistof direct contact between the governments concerned.If agreement cannot be reached the Organization may,on request, make any appropriate investigation, but theOrganization does not thereby assume responsibility forthe fulfilment of the conditions required.3
63. India. The Government reports as follows... since monkeys can act as reservoir of yellow-
fever infection and play an important part in interna-tional spread of yellow -fever infection, it is suggestedthat suitable provisions may be made in case oftransport of monkeys from one country to another.The International Sanitary Regulations already containprovisions relating to vectors of quarantinable diseasesand as such there cannot be any objection to theinclusion of such provisions of quarantine measuresagainst monkeys."
The Committee takes note of the communication fromthe Government of India on the question of monkeyscarried in international traffic and reaffirms its opiniongiven in its ninth report that this problem could best besolved by agreements between the States concerned,outside the provisions of the Regulations.'
Article 70
64. Notifications of areas considered as receptive orno longer receptive under Article 70 were publishedin the Weekly Epidemiological Record. An up -to -datelist of yellow -fever receptive areas appeared in WeeklyEpidemiological Record, 1962, No. 8, and in Vaccina-tion Certificate Requirements for International Travel,1962.
Article 70 (unamended)
65. Information, including maps, on the delineationof the yellow -fever endemic zones in Africa and inAmerica was published in Vaccination CertificateRequirements for International Travel, 1962. Quarterlyreports received on the Aedes aegypti index in localitiesexcluded from these endemic zones were also publishedin the Weekly Epidemiological Record.
66. Ethiopia. The Government reports that theEthiopian Quarantine Services are often blamed formeasures imposed on their services by the countrieswhich consider Ethiopia as a yellow -fever endemiczone. Passengers from North America and Europecannot understand why they have not been requested
3 Off Rec. Wld Huth Org. 56, 58, section 66.4 Off Rec. Wld Hlth Org. 118, 54, section 117.

ANNEX 1 45
to be vaccinated before leaving their countries forEthiopia while they are required to produce a certificatewhen leaving Ethiopia for some countries.
The Committee recommends that health administra-tions should advise travellers that the requirements ofcountries are related not only to the health conditionsprevailing in the country of departure but also toconditions in countries in which the traveller disembarksor transits during his journey except in so far as hefollows the provisions of Article 34.
Article 73
67. Philippines. The Government again reportsthat insects, including mosquitos, are found in aircraftarriving at Manila Airport. This may be due to thefact that disinsection is not carried out or that thetechniques used are inadequate.
The Committee invites attention to its commentsunder section 11 and is of the opinion that the " blocksaway " procedure for aircraft disinsection may helpto solve the problem raised.
Article 74
68. Seychelles. The Government reports as follows :" It has been deemed advisable to amend the
vaccination certificate requirements in respect ofyellow fever because of delays in obtaining informationconcerning infected local areas.2 The recognizedconcession for children under one year of age, however,has been introduced in respect of yellow -fever andcholera inoculations."
Article 75
69. Burma. The Organization was informed by theGovernment on 19 September 1962 that the arrange-ments concluded between Burma and India andbetween Burma and Pakistan were terminated on1 September 1962.
Smallpox
70. Basutoland. The Government reports that, bythe end of July 1962, the epidemic of smallpox 3 whichstarted in 1961 appeared to have been controlled.
71. Belgium. The Government reports that one caseof smallpox was imported from the Congo (Leopold-ville),' but thanks to the energetic isolation and pro-
1 For previous report, see Off. Rec. Wld Hlth Org. 118, 49,section 81.
2 The Government of Seychelles decided to require a yellow -fever vaccination certificate from arrivals from the endemiczones; previously the requirement applied to arrivals frominfected local areas. The Organization is in communicationwith the health administration concerned.
3 Off. Rec. Wld Hlth Org. 118, 50, section 90.' See Appendix 1.
phylactic measures adopted no secondary case wasreported. Details concerning this imported case aregiven below :
On 12 October 1961, a child aged seventeen monthsand his mother arrived at Brussels Airport fromLeopoldville, via Rome. The child had been vaccinatedsix months and again eight days before arrival. On14 October he was hospitalized; the diagnosis ofsmallpox was established on 16 October, and he diedon 18 October. Before her departure from the Congo,the mother was working in a hospital at Bakwanga,where smallpox patients were treated.
In connexion With smallpox outbreaks in Europe,the Government reports as follows (translation fromthe French):
" During the period in question special quarantinemeasures -in particular the requirement of a validsmallpox vaccination certificate -were applied inregard to persons coming from Düsseldorf, Simmerath-Montjoie, Aix -la- Chapelle (Federal Republic of Ger-many); Bradford, Tipton, Hornchurch, Ilkley, Wool-wich, Llantrisant, Rhondda, Pennybont (UnitedKingdom of Great Britain and Northern Ireland) andNowy Port -Gdansk (Poland) when there were casesof smallpox in these areas.
" While these smallpox foci were present in neigh-bouring countries, we met with some difficulties inapplying the International Sanitary Regulations andasked the opinion of the Organization on certainpoints, in particular on the :
(1) interpretation of Article 6, 2 (a) of the Regula-tions, relating to the date when an infected localarea may again be considered as being free frominfection (letters of 19 February and 14 March1962);
(2) interpretation of the definition of ' infectedlocal area' (letter of 12 April 1962) ; 6
(3) interpretation of the terms primary vaccina-tion and revaccination (letters of 2 May and 31 July1962).
" Furthermore, experience of smallpox epidemicson our land frontiers has shown that there should bespecial provisions for frontier areas where the popula-tion of the two countries is mixed, particularly, measuresto ensure the rapid and direct notification through thelocal health authorities in the border areas of any caseof quarantinable disease, with indications of theorigin and evolution of the case, and of the measurestaken."
72. Ceylon. The Government reports that it was notpossible to trace the source of infection of the three
See section 23.6 See section 16.

46 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
outbreaks which occurred during the period underreview. A total of sixty -six cases, with twelve deaths,was reported.
73. Dahomey. The Government states that eighty -four cases of smallpox, with fourteen deaths, occurredin the country during the period under review; nocases, however, were reported by the health authoritiesof the airport and the port of entry.
74. Denmark. The Government reports as follows :" ... only in one instance we had reason to believethat a case of smallpox, originating in Nigeria, wascarried to our country. However, the ... clinicalpicture was most doubtful and no secondary caseshave occurred. We would not consider it to havebeen a case of modified smallpox."
75. Federal Republic of Germany. The Governmentreports as follows :
" . there occurred one outbreak of smallpox eachin Düsseldorf (Regierungsbezirk Düsseldorf) and inLammersdorf /Simmerath (Regierungsbezirk Aachen),both situated in the Land of Northrhine -Westphalia.'The smallpox outbreak in Düsseldorf was initiatedby a German engineer, returning on 2 December 1961from Liberia. The outbreak in the Regierungsbezirk ofAachen occurred in the rural district of Monschauand was caused by a German mechanic, who returnedon 23 December 1961 from India. In Dusseldorf therewere five cases, two of which ended fatally, whereasin the rural district of Monschau and in the townborough of Aachen thirty -three cases were noted, oneof which ended fatally.
" Both outbreaks had their source in travellersreturning from tropical areas where smallpox isendemo- epidemic. At the time of their arrival in theFederal Republic both travellers did not show anysymptoms of the disease. Both were in possession ofvalid international vaccination certificates. Thus, theimportation of smallpox could not be prevented byapplying the measures provided for in the Interna-tional Sanitary Regulations.
" However, in both cases the spread of the diseasecould be checked efficiently. That an outbreak ofsmallpox occurred among the patients in the Sim-merath hospital, where the first case within theMonschau area was isolated and treated, must beattributed to the fact that, up to now, too little atten-tion has been devoted to the spread of smallpoxthrough the air. In the Simmerath hospital it hasbeen observed that the smallpox virus, which wascontinually spread by a highly infectious child sufferingfrom pharyngitis variola and from a barking cough,
' See Appendix 1.
infected persons who had approached the child nomore than at a distance of about twenty metres.
" The measures for combating the disease followednormal routine regarding isolation and protectivevaccination. The persons who had been in contactwith smallpox cases were placed under a more or lesssevere isolation according to the intensity of theirprevious contact. Thus, the endeavours to check thespreading of the disease from its focus to the popula-tion in general were successful. Immediately followingthe confirmation of smallpox by laboratory tests,large -scale vaccination campaigns were started. InDüsseldorf about 150 000 people and in the districtof Monschau and in Aachen about 208 000 peoplewere vaccinated against smallpox.
" The evaluation of the measures taken by othercountries following the smallpox outbreaks in theFederal Republic has shown that some countries donot adhere to the measures admissible pursuant tothe International Sanitary Regulations, but exceedby far the limits set by these instructions. Thus,travellers by air or rail were more or less forced tosubmit to protective vaccinations, requirements wereplaced upon international vaccination certificateswhich find no support in the International SanitaryRegulations, health certificates for goods were requiredand the whole territory of the Federal Republic wasconsidered as a ' local infected area '. These incidentsmay be attributed partly to inadequate co- operationbetween the officials of the frontier control and ofthe health authorities .. .
" In addition hereto, the two smallpox outbreakshave given rise to a number of fundamental problems.These concern the accommodation of persons sufferingfrom smallpox and of suspect cases and their personaland material care as well as the prevention of casesand their spread by international traffic.
" The accommodation of smallpox cases and ofsuspect persons in the ward for infectious diseaseswithin a general hospital, where the ward is notlocated in a special isolation house or, still worse, inisolated rooms of a ward for internal diseases, mustbe considered as fully inadequate. In future, smallpoxcases will have to be kept in special isolation hospitals.For their care and treatment medical and nursingpersonnel must be available who dispose of a satisfac-tory protection by vaccination, i.e., these personsmust be revaccinated at regular intervals. Theirsuitability for working in quarantine wards will alsodepend upon the degree of their reaction to vaccina-tion. Considering the training of doctors and auxiliarymedical personnel, the treatment of smallpox willbe paid more attention to and the diagnostic methodswill be improved.
ANNEX 1 47
" In addition, the question has been raised whethersmallpox might be spread by mail traffic and whichmeasures against this hazard might be taken. Whetherand in how far the measures admissible in accordancewith Article 48 of the International Sanitary Regula-tions should be considered as satisfactory is still thesubject of thorough tests ..
" Apart from these two outbreaks of smallpox, nofurther cases of quarantinable diseases occurred in theFederal Republic of Germany during the period underreview."
76. Federation of Rhodesia and Nyasaland. TheGovernment reports that smallpox infection wasintroduced into Luapula Province from the adjacentarea of the Congo (Leopoldville). It is not certain,however, that cases carried across a river frontiercan be considered as being due to international traffic.
77. Ghana. The Government reports the followingimported cases :
(1) Nigerian, aged 16 years. He arrived in Ghanaon 8 December 1961, from Northern Nigeria, by land,through Togo; developed smallpox on 16 Decemberand was isolated on 19 December.(2) Ghanaian, aged 32 years; resident in Bouake,Ivory Coast. He became sick with high fever andwas brought back home; a rash appeared en route toGhana. He was isolated on 21 January 1962 and diedon 23 January.(3) Ghanaian girl, aged 9 years; resident in Palime,Togo. She arrived home at Avloto on 25 February1962; developed smallpox on 27 February and wasisolated on 5 March.(4) Togolese, aged 46 years; resident in Ghana. Hetravelled to Togo on 26 January 1962 and returnedon 30 January; developed smallpox on 10 Februaryand was isolated, on 19 February.(5) Togolese woman aged 24 years. She travelledfrom Togo to Ghana while already suffering fromthe disease; detected during traffic checking at AkrosoFerry and isolated on the same day (22 March).
(6) Togolese woman, aged 39 years. She arrivedfrom Palime, Togo, on or about 22 April and developedsmallpox a few days after arrival. The patient wasfound concealed in a house on 12 May and wasisolated on the same day.
All cases except the second recovered.
78. Kenya. The Government reports that the shipLOCH ALVIE coming from Karachi arrived at Mombasaon 17 December 1961 with a case of smallpox onboard.
1 See Appendix 1.
79. Libya. The Government reports that fullattention was given to the development of the smallpoxoutbreaks in the Federal Republic of Germany andin the United Kingdom of Great Britain and NorthernIreland, and that Libya depended a great deal on thenotifications and information received from theOrganization.
80. Mauritania. The Government reports that nocases of quarantinable diseases due to internationaltraffic were recorded, and adds the following com-ments (translation from the French):
" It should however be noted that there is a move-ment of persons between Mauritania and Senegal andbetween Mauritania and Mali which cannot becontrolled : periodic migration of shepherds in searchof water and pasturage; crossing of rivers by personsworking on one side and living on the other. Thesepopulation movements were certainly the cause ofa number of cases of smallpox which appeared inJune 1962, but their nature and the extent of thefrontiers make control impossible."
81. Poland. The Government reports that between21 March and 9 June 1962 there was an outbreak ofsmallpox due to international traffic at Gdarísk..No deaths were reported.2
82. Togo. The Government states that 465 cases ofsmallpox, with eighteen deaths, were observed inTogo during the period under review, and adds thefollowing comments (translation from the French) :
" Some cases of smallpox are imported owing to thenumerous exchanges between Ghana and Dahomeyacross the Togo frontiers -where control is impossible.
" The best way of ensuring mass vaccination is bythe well -tried method of using mobile teams. At thepresent time, vaccinations are performed at fixedunits in the principal hospital centres. When anepidemic occurs, a team goes out and puts a cordonround the markets and vaccinates the greater partof the population."
83. Trucial Oman. In a report dated 19 February1962, on the smallpox outbreak in Dubai, the Govern-ment stated that, through the foresight of the SeniorMedical Officer, all schoolchildren of Dubai hadbeen vaccinated as soon as the news reachedTrucial Oman that smallpox in Pakistan was causingconcern. Therefore, by the time the first case in Dubaiwas reported on 20 January, a large proportion of themost vulnerable section of the population had beengiven protection. With one or two exceptions, all casesin Dubai were among pilgrims on their way to SaudiArabia.
2 See section 92 and Appendix 1.

48 SIXTEENTH WORLD HEALTH ASSEMBLY, . PART I
84. Union of Soviet Socialist Republics. The Govern-ment states that, in February 1962, a suspected caseof smallpox was found in the Kizyl Atreks rayon of theTurkmenian S SR. The diagnosis of smallpox wasnot confirmed, but all necessary measures had beentaken.
85. United Kingdom of Great Britain and NorthernIreland. The Government reports as follows :
" The fact that some twenty out of sixty -four personswho were seen by smallpox consultants during 1961had recently arrived from abroad indicates that therisk of importations of smallpox is continually present.
On 28 December 1961, the first of what was to bea series of five separate importations of smallpox 1came to light.
" _Airport Health Control. The airport health controlaspects which are of interest were as follows :
" Under the system of health control at LondonAirport normally in operation during the year allpersons arriving on an aircraft by direct flight from asmallpox endemic or epidemic area (this includesIndia, Pakistan, as well as countries in South -EastAsia, Central and South America and parts of Africa)were given a yellow warning card. While a certificateof vaccination against smallpox was not formallyrequired from people arriving in this country fromsmallpox infected areas, all were asked if they had aninternational certificate of vaccination againstsmallpox. If the scrutiny of the certificate was satis-factory, no further action was taken. If the certificatedid not satisfy scrutiny or the passenger did not holdone, the name and destination address of the travellerwas taken and filed at the airport in case it was needed,should an importation later be traced to that aircraft.
" This practice originated in 1952 when the Inter-national Sanitary Regulations came into force.These Regulations did away with the personaldeclaration of origin and health which was a form onwhich arriving travellers were requested to state theirdestination addresses. The Regulations did not permithealth authorities to obtain a written statement fromarriving travellers.
" Also in force was an arrangement concluded bythe Western European Union whose health functionshave now been taken over by the Council of Europe(Partial Agreement). Under this arrangement, aircraftflying solely within the territory of the States partyto this agreement, i.e., the United Kingdom, Ireland,France, Belgium, Netherlands, Luxembourg, FederalRepublic of Germany and Italy, were free from healthcontrol. It was known by the parties to the agreementthat on such aircraft there would be persons frominfected areas who had changed planes in transit or
1 See Appendix 1.
had a short stop -over within Western Europe andtravelled further on an aircraft free from healthcontról. This category had been accepted as a risk.
" Smallpox had been present in Karachi during1961. In mid- December a significant increase in thenumber of cases occurred. Five Pakistani immigrantsamong the many who entered this country throughLondon Airport between 16 December 1961 and12 January 1962 developed smallpox after arrival.Two of them died. All five had valid internationalcertificates of recent revaccination. Three arrived bydirect flight, two by indirect flights which were notsubject to formal health control on arrival here.
" More stringent controls were, as an emergencymeasure, progressively put into effect as evidence cameto hand that revaccinations taking place in Karachiwere not taking effect in an appreciable number ofpersons. When the third importation had beenidentified special arrangements were made on15 January 1962 to regard as ' suspects ' travellers whohad been in Karachi within fourteen days prior toarrival. The measures taken included clinical examin-ation of vaccination sites and, where necessary, offeringvaccination and subsequent isolation for fourteen daysor until the vaccination had taken. Destinationaddresses of disembarking passengers were taken andthey were put under formal surveillance. The Depart-ment advised that these precautions should be takenat all ports and airports throughout the country atthis time. Checks made during February and Marchshowed that some 67 per cent. of arrivals fromPakistan came on direct flights. The remainder(33 per cent.) came by ' indirect flight '- havingchanged their aircraft at one of nine different airports,four of them being within the ` excepted area '.
" From 15 January until 9 March while thesestringent measures were in force, ninety -six suspectsout of the 4138 arrivals from Karachi were isolatedeither in Denton Hospital or the Eastern Hospital.Thirty -seven of these suspects showed evidence, by asuccessful revaccination at the airport or at thehospital, that they were susceptible to vaccinia andpresumably also to smallpox on arrival. (This numberrepresents less than one per cent. of the arrivals fromKarachi during the time the measures were in force.)
" During the period when arrivals from Karachiwere being placed under formal surveillance oppor-tunity was taken to check its effectiveness. In severalcities and towns in the Midlands the percentage ofimmigrants from Karachi who were later traced to thedestination addresses which they gave on arrival laybetween 85 per cent. and 100 per cent. The impressionwas gained that the higher rates reflected the timeand effort which local authorities spent on followingrecently arrived immigrants through several changes

ANNEX 1 49
of address. A comparable figure of 33 per cent. fromone London borough was the result of immigrants notknowing their destination address and giving theaddress of an embassy or an hotel to which they didnot go. These results must be looked at against thefact that many of the immigrants were illiterate, wereunable to speak English and had arrived without anyfirm knowledge of their subsequent movements.
" Cases of Smallpox in England and Wales. In order,briefly, to complete the description of the importationsthe details of the imported cases and the outbreaksthey caused are given below :
" A. Imported Cases. Arranged in the order inwhich they were recognized to be suffering fromsmallpox these fivé imported cases are shown inTable I by dates of arrival, onset of illness and removalfrom the community.
TABLE I
Im-ports-tionNo.
District
Date of
arrivalat
Londononset ofillness
removal fromcommunity
1 St Pancras 25.12.61 25.12.61 28.12.61Metrop. Borough (died 6.1.62)
2 West Bromwich 19.12.61 21.12.61 28.12.61County Borough
3 Bradford 16.12.61 29.12.61 30.12.61County Borough (died unre-
cognized)
4 Birmingham 4.1.62 8.1.62 15.1.62County Borough
5 Cardiff 12.1.62 13.1.62 16.1.62County Borough
" Importation No. 3 first came to light with therecognition of secondary cases on 11 January 1962.
"B. Indigenous Cases. From 11 January 1962indigenous cases began to be recognized. The totalwas sixty -two cases of whom twenty -five died. Thesefigures include two persons who died of illnessesdiagnosed retrospectively as smallpox without labora-tory confirmation and one person confirmed as a caseof smallpox who died of another cause.
" The relationship of the indigenous to the importedcases was as follows :
" Importation No. 1. No secondary case occurredamong persons known to have been in contact. Twoapparently sporadic cases in the Greater Londonarea were taken ill during January. Both were knownto have been working not far from Long Reach
Smallpox Hospital at a relevant time. The mode oftransmission was not determined.
" Importation No. 2. One secondary case only, amedical officer of health who had examined theimported case.
" Importation No. 3. This patient sickened withsmallpox in Bradford Children's Hospital, where shewas under treatment for another condition. She diedwithin twenty -four hours of onset, and, during life,infected seven other children in the same ward of thehospital, a visitor and one of the hospital cooks.A pathologist who performed the post -mortemexamination also acquired the infection and sub-sequently died. The total number of cases in the firstgeneration was ten, of whom five died.
" One of the children developed smallpox aftertransfer to a long -stay hospital, where the infectionwas transmitted to one other child. The visitor toBradford Children's Hospital was admitted, beforethe diagnosis was established, to St Luke's GeneralHospital where he infected two other patients. Thetotal number of cases in the second generation wasthree, of whom one died, though this death was notassigned to smallpox.
" Importation No. 4. No secondary case developed.
" Importation No. 5. This patient, who was taken illin Cardiff on 13 January 1962, was admitted on16 January to a smallpox hospital situated in theRhondda Valley. No secondary case occurred amongpersons known to have been in contact.
" On 25 February it became evident that cases ofsmallpox were occurring in the Rhondda district. Inretrospect the first case of the outbreak was recognizedto be a young married woman whose home was at adistance of about half a mile from the smallpoxhospital. This woman died on 9 February, the dayafter she had been delivered of a still -born child.Smallpox was not suspected as the cause of death.Subsequent events showed that this woman infectedfour persons with whom she had been in contactduring life. A gynaecologist who attended the post-mortem examination also acquired the infection andsubsequently died.
" During the period 9 February to 15 March thetotal number of cases in the Rhondda and neigh-bouring district of Llantrisant was twenty -five, out ofwhom six died. These figures include the womanwho died on 9 February. The cases fell into severalgroups of close contacts, but the links between someof the groups were tenuous and the possibility of amissed case or cases was considered. Vaccination wasoffered on a very wide scale throughout the affectedarea.

50 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
" After it was hoped that the outbreak had ended,a further incident came to light during the first weekin April when a number of patients who were occupy-ing a ward in a mental hospital, near Bridgend, werefound to be suffering from smallpox. This outbreak,which has been confined to the one ward of thehospital, was also related to a death recognized as dueto smallpox only in retrospect. An elderly womanwho had been in the ward for more than a year diedon 25 March after a short febrile illness. During theperiod 25 March to 15 April a total of twenty -onecases occurred, all confirmed by laboratory investiga-tion, of whom thirteen died. These figures includethe woman who died on 25 March. The hospital waseffectively closed to outside contact from 7 Apriland the whole hospital remained in quarantine until30 April. The method by which the infection wasintroduced into the ward remains unknown.
" The total number of cases in the two outbreaksin South Wales was forty -six, of whom nineteen died.
" The importations and indigenous cases areanalysed in Table II.
TABLE 11
Importation England Wales
No. Cases Deaths Second-ary cases Deaths Second-
ary cases Deaths
1 I 1 2 - - -2 1 - 1 - - -3 1 1 13 6* - -4 1 - - - - -5 1 - - - 46 19
Including one death from other causes.
England and Wales were declared free from small-pox on 20 May 1962.
" Vaccination. While mass vaccination was notadvocated for the population generally as a controlmeasure, the demand for vaccination increased duringthe outbreaks. No accurate figures are available of thenumber of vaccinations carried out but some indicationis given from the fact that over seven million dosesof vaccine lymph were distributed.
" As regards complications of vaccination pro-visional information was received of :
3 cases of vaccinia gangrenosa with nil deaths;39 cases of eczema vaccinatum with 10 deaths;40 cases of post -vaccinal encephalomyelitis with
4 deaths;91 cases of generalized vaccinia with 3 deaths.
In addition, in five other deaths the death certifi-cate mentioned vaccination.
CONCLUSION
1. The risk of importations of smallpox willcontinue so long as smallpox remains endemic inseveral countries of the world. The risk appears tohave increased in recent years consistent with changesin the nature, volume and speed of internationalair traffic. It seems necessary, therefore, to concentrateon eradication of endemic foci by mass vaccinationcampaigns using a potent vaccine and a method whichgives immunity against smallpox.
" 2. The International Certificate of Vaccinationagainst Smallpox is the evidence an internationaltraveller carries that he has an immunity againstsmallpox. It may be false evidence because revaccina-tion performed was not successful and hence gave noimmunity or because the certificate issued was bogusand fraudulent or because the patient was alreadyincubating smallpox.
" The fraudulent certificate when it occurs is amatter for national action, but it is felt that the WorldHeálth Organization can make the certificate ofvaccination against smallpox better evidence of success-ful revaccination by requiring it to show the result ofrevaccination. Indeed it is a matter for considerationwhether the certificate of revaccination should not onlyrecord the result and a second insertion if no resultof the first is seen, but require also that the firstinsertion be made at least fourteen days before thecertificate of revaccination becomes valid.
" It is fully realized that this return to a form andmodel on the lines of the certificate issued under the1944 Conventions would impose delays and diffi-culties on international travel, but these could in somemeasure be reduced if the requirements of a validcertificate could be demanded under the InternationalSanitary Regulations only from arrivals from aninfected area and not, as at present, quite illogically,from arrivals from anywhere in the world."
86. United States of America. The Governmentreports that State and local health officers co- operatedin smallpox vaccination programmes at ports of entryfor persons in the port area and adjacent communitywho would have contact at some time with interna-tional traffic because of the nature of their employment.
87. Zanzibar. The Government reports as follows :" On 7 July 1961, S.S. AMRA arrived from Bombay
via Mombasa, after having landed a suspected caseof smallpox at Mombasa... The fifty -two passengersdisembarking at Zanzibar were placed under sur-veillance for fourteen days." 1
1 The diagnosis of this suspected case was not confirmed.

ANNEX 1 51
Article 83
88. St Kitts -Nevis -Anguilla. The Government reportsas follows :
" The outbreak of smallpox in the United Kingdomearlier this year necessitated quarantine measures tobe instituted on all ships arriving in the territory inso far as disembarking passengers were concerned."
89. France. The Government reports as follows(translation from the French) :
" The appearance in Great Britain and the FederalRepublic of Germany of several smallpox foci ledthe French administration to apply the provisions ofArticle 83, paragraph 2, to travellers coming frominfected local areas ...
" The application of these provisions in the cir-cumstances mentioned above gave rise to certaindifficulties.
" Pursuant to these provisions, an internationalcertificate of vaccination against smallpox wasrequired on arrival in France of all travellers comingfrom an infected local area either directly or withinfourteen days of being in such an area. However,since the countries involved were neighbouring oneswith which there is a great deal of traffic and the localareas were, for the most part, small, with no ports orairports, control operations on arrival proved difficult.In order to make sure that all travellers arriving inFrance from an infected local area or within fourteendays of being in such an area do in fact possess aninternational certificate of vaccination against small-pox, it is necessary to question a very large numberof travellers."
90. United States of America. The Governmentreports that sixty -five persons were detained longenough for a differential diagnosis for smallpox orcholera, or for development of satisfactory evidenceof vaccination or immunity among persons arrivingfrom infected local areas. All but three arrived by air.In contrast to the sixty -five, only eleven persons weredetained the previous year.
Sections 70 -90. The Committee continues to viewas a major threat to world health the reintroduction ofsmallpox from the several foci of this disease about theworld into territories where it is no longer present.Aware of the Organization's objective that smallpox beeradicated from all territories and of the problems whichwill delay attainment of this objective for at leastseveral years, the Committee fully realizes its greatresponsibility for making appropriate recommendationsto the Assembly with the aim of providing the varioushealth administrations with International SanitaryRegulations which will allow effective prevention of thepassage of smallpox in international traffic. The Corn-
mittee has reviewed present knowledge of the disease,the status of susceptibility among various populations,and the methods for the prevention of spread includingthe methods and practicabilities of immunization pro-cedures. The Committee has reached a conclusion thata good degree of protection against the importation ofsmallpox into a territory is available to the healthadministration of the territory within the terms of theexisting International Sanitary Regulations. TheCommittee is ever anxious for improvements in thisprotection. It recognizes that absolute protection is notattainable within present limits of knowledge withoutmarked interference with international traffic.
The Committee invites the attention of healthadministrations to their obligations under the provisionsof Article 30 to take all practicable measures to preventthe departure of any infected person or suspect. TheCommittee urges such health administrations, in partial
fulfilment of these obligations, to require a valid inter-national certificate of vaccination or revaccinationagainst smallpox of departing travellers.
The Committee recalls that international vaccinationcertificates are issued under the authority of a govern-ment and consequently governments have the responsi-bility to ensure that potent vaccines and proper pro-cedures are used, so that smallpox vaccination willresult in an adequate immunity to smallpox.
The Committee was informed that some States issueto travellers arriving from a smallpox infected area awarning card stating that if they fall ill they should seekmedical advice and present the warning card. TheCommittee believes this could be a useful procedure.
The Committee again stresses the need for medicaland other personnel who come in contact with travellersto maintain a high level of immunity against smallpoxby repeated vaccination.'
The Committee is extremely concerned with therecord of importation of smallpox in internationaltraffic and the secondary spread which has occurredsince its last meeting. The Committee recalls thatadditional sanitary measures may be applied to thespecial groups listed in Artcile 103 of the Regulationsand notes that several of the imported cases were ofthese categories.
One member of the Committee, as a direct result ofrecent importations into Western Europe, has proposeda recommendation for a series of changes in the Inter-national Sanitary Regulations, intended to lessen therisk of such importations. The Committee has con-sidered this proposal at length and in detail. TheCommittee believes that greater knowledge of smallpoxand vaccination is necessary to permit a practicableand effective solution. Accordingly, the Director-
1 Off. Rec. Wld Hlth Org. 102, 47, section 59.
52 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
General is requested to refer this problem to appropriateexperts and provide the Committee with recommenda-tions at an early date. It has concluded that the specificterms of the proposal might interfere with world trafficwithout any proportionate degree of enhancement ofprotection, and without, in fact, providing for completeprotection against all importations of the sort recentlyexperienced.
The member referred to above is of the opinion thatthis procedure does not offer early hope of additionalsafeguards to those countries at risk, and accordinglyhas recorded his divergent opinion in Appendix 2.'
The Committee invites the attention of healthadministrations to the recommended requirements forsmallpox vaccine 2 drawn up by a WHO study groupand again stresses the advantages of dried smallpoxvaccine.3
The Committee was informed that the Organization isprepared to arrange for the potency testing of smallpoxvaccine, on request of the country producing it.
91. India. In connexion with the outbreak of small-pox on board the INDIAN RESOLVE,4 the Governmentgives the following information
" ... twenty-five cases were confirmed as smallpoxby laboratory examination; eight cases were diagnosedclinically 5 and thirty -seven were classified as suspects.The first case which broke out on 5 March 1962 wasdiagnosed as chickenpox by the port health officersat Aden, Suez and Kiel. Before leaving Calcutta on19 February, most of the persons on board wererevaccinated by the company's medical officer withfresh vaccine obtained the same day from the VaccineInstitute of Calcutta Corporation. Those who werenot vaccinated before they left Calcutta were inpossession of valid certificates. Since it is the practicein India to enforce vaccination of all crew membersonce in three years, these vaccinations were not thefirst of their kind but were probably the second, thirdor fourth vaccinations in their lives. The occurrence ofso many cases of smallpox among the crew membersrevaccinated on different days with the differentbatches of fresh potent vaccine, unanimous diagnosisof chickenpox made by three port health officers andtotal absence of any secondary case among the non -immune population coming in contact with the ship atthe previous ports give rise to certain doubts aboutthe correctness of the clinical and laboratory diagnosisarrived at ....
' See p. 58.2 Wld Hlth Org. techn. Rep. Ser., 1959, 180.3 For previous comment of the Committee on this subject, see
Off. Rec. Wld Hlth Org. 102, 47, section 59.' See section 92 and Appendix 1.5 Four of them were later confirmed.
" 1 n view of such contradictory evidence and also fromthe point of view of judicious application of quarantinemeasures, it is considered most desirable that facilitiesshould be provided to get the diagnosis confirmed ata WHO approved referral laboratory and a numberof such laboratories distributed all over the worldmay be approved by WHO. Specimens could be sentby the port health authorities either on behalf of theshipping companies who may so request, or on theirown behalf in case facilities are not locally available.Reports from the referral laboratories may similarlybe. sent direct to the port health authority concerned.Shipping companies will perhaps have no objectionto meeting the expenditure involved in regard to casesreferred from their ships. It is highly probable thatfavourable findings of an internationally reputedlaboratory will at least have the effect of mitigatingthe rigid quarantine measures which some countriesare only too apt to apply, if not of completely elimin-ating them."
See comments of the Committee under section 92.
92. Poland. The following communication has beenreceived from the Government (translation from theFrench):
" With reference to your letter of 13 September1962 concerning smallpox cases among members ofthe crew of the ship INDIAN RESOLVE,6 I can give youthe following information :
(1) the smallpox cases notified to the World HealthOrganization were confirmed both clinically and inthe laboratory (isolation of the virus);(2) the diagnosis of varicella in the case of thefirst patient on the boat, made by the port medicalofficers at Aden, Suez and Kiel, was not confirmedby the laboratory' examination;(3) cases of smallpox among persons recentlyvaccinated against the disease, or revaccinatedseveral times, are possible, since vaccination doesnot exclude the possibility of smallpox of a clinicallymild or abortive nature, a fact we have confirmedhere among the staff of the quarantine service whohave been revaccinated several times ;
(4) we fully agree that there is a need to create adiagnosis reference centre approved by WHO, whichcould collaborate with the laboratory centres in thedifferent countries and place standardized strains,sera and antigens for diagnostic purposes at theirdisposal."
The Committee was informed that the Organizationhas assisted countries to set up diagnostic laboratories,has conducted one course in the laboratory diagnosis
6 See sections 81 and 91.

ANNEX 53
of smallpox, is prepared to furnish consultants for thispurpose and, for difficult cases, is prepared to arrangefor the examination of laboratory specimens at therequest of the countries concerned. The Organizationis also considering the designation of a WHO referencelaboratory for the study and characterization of poxviruses.
93. International Transport of MailInformation on this subject was presented to the
Committee in a separate document.
Article 97
The Committee is not aware of any evidence of trans-mission of smallpox by mail since the Regulationsentered into force, and consequently, at present, doesnot recommend any change in the provisions of Article 48,but requests the Director - General to study this questionand report to a subsequent meeting of the Committee.
Typhus
94. Republic of Korea. The Government states thatduring the period under review fifty -two cases oftyphus (with one death) occurred in the territory.
PART VI. SANITARY DOCUMENTS
95. (a) The provisions of paragraph 1 of Article 97appear to make it mandatory for the pilot, or hisauthorized agent, to complete and deliver the healthpart of the Aircraft General Declaration; this to bedone whether or not there is anything of epidemio-logical significance to report and independently ofwhether the health authority wishes to receive thisdocument.
(b) One arrangement among States under Article 104,in establishing an " excepted area " for sanitarymeasures under the Regulations, has eliminated theobligation to submit the health part of the. AircraftGeneral Declaration under conditions laid down in thearrangement.' It is assumed that this action has beentaken in view of the general policy stated in Article 23that " the sanitary measures permitted by theRegulations are the maximum measures applicableto international traffic ", and the basic purpose of theagreement - to facilitate international traffic and thesimplification of sanitary measures.
(e) Except for abnormal circumstances, it is con-sidered that for many parts of the world the routinesubmission of the health part of the Aircraft GeneralDeclaration may be an unnecessary formality.
(d) The Committee's opinion is desired on whetherthe provisions of Article 97 require the routinesubmission of this document or whether healthadministrations can in normal circumstances foregothis requirement. It would be understood that, ifthis document is no longer required routinely, itwould still remain the duty of the pilot to arrange for
' These conditions provide as follows : "An aircraft whichbegins its flight at any place within the ' excepted area ' anddoes not call during its voyage at any place outside that area,is not subjected to health control on its arrivals at any otherplace within the ' excepted area '." The arrangement containsa temporary suspension clause for abnormal circumstances.
its submission when there are any persons on boardknown to be suffering from illness other than air-sickness or the effects of accidents, when cases ofillness have been disembarked during the flight, orwhen there is any condition on board which may leadto the spread of disease.
The Committee recommends that Article 97 shouldbe amended in paragraph 1 by adding, after the words" Appendix 6 ", the words " except when a healthadministration does not require it ".
Article 100
96. United Kingdom. The Government reports asfollows :
" The World Health Organization should ... giveconsideration to the difficulties imposed on healthadministrations in tracing arrivals from infected areaswithout documentary evidence of their intendeddestination. The volume and nature of internationaltraffic now warrants a re- examination of the decisiontaken by the World Health Assembly in 1952 whensuch documentary evidence was made illegal under theInternational Sanitary Regulations. A destinationaddress is important. To obtain it from the passengerfrom an infected area on a form completed during thevoyage or flight would save time and obviate the delaysand inefficiency which will continue if the limitationsimposed by the International Sanitary Regulations aremaintained."
Information on proposed sanitary documents isgiven in a separate document; see also section 89.
The Committee discussed the question of permittinghealth administrations to require in writing fromarriving travellers details of their travel before arrivaland a destination address.
The Committee concluded that health administrations,other than those of States whose reservations have
54 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
already been accepted, should not be permitted to requirein writing from travellers on an international voyage, onarrival, details of their travel during the days beforetheir arrival and, consequently, no amendment to theRegulations is proposed.
The Committee then considered the desirability of
granting power to a health authority to require adestination address in writing from arriving travellers.The Committee notes that Article 103 does allow sucha requirement to be enforced for special groups. TheCommittee appreciates the desire of some healthadministrations to have destination addresses fromarriving travellers but realizes that to permit it as a
Article 101
general requirement would impose delays on inter-national traffic. The Committee recommends that, wherea health administration has special problems, arrivingpassengers may be required to give a destinationaddress in writing.
The Committee therefore recommends the additionof a third paragraph to Article 36 as follows:
3. Where a health administration has specialproblems constituting a grave danger to publichealth a person on an international voyage may,on arrival, be required to give a destination addressin writing.
PART VII. SANITARY CHARGES
97. The provisions of Article 101, paragraph 3,require States to notify the Organization immediatelyof tariffs for sanitary charges and of any amendmentsthereto. States are also required to publish the tariffat least ten days in advance of any levy thereunder.
Although not required by the Regulations todisseminate such information, the Organization hasdone so. A review of the small amount of informationreceived and disseminated by the Organization in thepast year and of older information shows clearlythat much of the information is undoubtedly out ofdate. Shipping companies and airlines which require
Article 104
this information presumably . obtain it from thepublished tariffs of States.
The Organization has used the information receivedto answer inquiries of other health administrations and,as necessary, to invite attention to excessive tariffs.
The Organization plans now to cease routinedissemination of information received on tariffs ofsanitary charges.
The Committee notes the action proposed.
98. Netherlands. The Government reports thatcharges are still levied which do not conform withArticle 101.2
PART VIII. VARIOUS PROVISIONS
99. (a) An arrangement for the direct and rapidexchange of epidemiological information was con-cluded between the Governments of Ceylon andIndia; 1 it came into force on 1 January 1962.
(b) On 2 February 1962, recommendations for theunification of the sanitary rules applicable to theDanube River traffic were adopted in Budapest bythe Danube River Commission. These recom-mendations had been drawn up with the assistance ofthe Organization. By 18 September 1962 two of thecountries concerned (Czechoslovakia and the USSR)had notified their adoption of these recommendations.
(c) The arrangement of 15 June 1956, formerlyunder the aegis of the Western European Union, has
been transferred to the aegis of the Council of Europe.Countries parties to this arrangement are : Belgium,the. Federal Republic of Germany, France, Greece(as from 1 February 1962), Ireland, Italy, Luxembourg,the Netherlands and the United Kingdom (includingthe Channel Islands and the Isle of Man).
(d) At a meeting called in Manila in April 1962, bythe Regional Director for the Western Pacific, forexchange of information on cholera El Tor it wasagreed that bilateral or multilateral arrangementsunder Article 104 would undoubtedly facilitateapplication of the Regulations in Asia in respect ofcholera El Tor. As requested, the Organizationsuggested to States concerned a number of items forconsideration.
2 The Organization took up the matters mentioned in the1 See Wkly epidem. Rec., 1962, 8, 102. report of the Netherlands directly with the countries concerned.

ANNEX 1 55
APPENDICES
Appendix 2
100. Philippines. The Government reports that insome countries travellers were required to possesscertificates of vaccination showing that seven insteadof six days had elapsed after the first injection of thevaccine.'
Appendices 2, 3 and 4
101. Philippines. The Government reports again thatarrivals are not always in possession of the requiredvaccination certificates. In some cases, the certificatesare not issued on the international form,2 or they aresigned by registered nurses and do not carry theapproved stamp.
102. Union of Soviet Socialist Republics. TheGovernment states that a considerable number oftravellers do not carry the required vaccinationcertificates.
103. Ethiopia. The Government reports that theEthiopian Airlines have included in their OperationsManual information obtained from the diplomaticmissions in Addis Ababa for visa and vaccinationrequirements. As travellers cannot obtain their visasif they do not comply with the other requirements ofthe diplomatic services, the airlines have to follow" diplomatic information " on quarantine rather thanthe International Sanitary Regulations and theVaccination Certificate Requirements for InternationalTravel.
As an example, information given by one embassyin Addis Ababa for travel to a nearby country wasdirectly contrary to the stated requirement of thathealth administration. It took the Ministry of Healthabout six months to get the situation corrected.'
Appendix 3
104. Ethiopia. The Government reports that arelatively high percentage of yellow -fever vaccinationcertificates issued in those parts of the world whereyellow fever does not exist and cannot develop arenot fully completed and therefore not valid.
1 When the Committee met, this excessive measure had beenwithdrawn.
2 See previous recommendation of the Committee; secondannotated edition, 1961, of the International Sanitary Regula-tions, pp. 42 -43, footnotes (4), (9) and (10).
3 The difficulty described above is not restricted to Ethiopia.The WHO Secretariat in Geneva is often questioned aboutinformation given by a consulate, since this information isdifferent from that notified to the Organization by the healthadministration concerned. See also section 24.
105. Uganda. The Government reports as follows :" Difficulties were again experienced due to the
Government of India's insistence on children underthe age of one year being inoculated against yellowfever.
" This problem has been overcome by requiringshipping companies to refuse passages on ships boundfor India to anyone not in possession of a valid inter-national certificate."
The Committee notes that the Government of Ugandaitself requires a yellow fever vaccination certificate fordeparting travellers proceeding to India. The Committeenotes that since the legal relationships between Ugandaand India are governed by the reservations made byIndia to the Additional Regulations of 1955, the Govern-ment of Uganda has an obligation under Article 72to require " any person leaving an infected local area onan international voyage and proceeding to a yellow feverreceptive area " to possess a certificate of vaccinationagainst yellow fever.
The Committee reaffirms the opinion given in itseighth report that it is the responsibility of each healthadministration to inform prospective travellers, travelagencies, shipping firms and airlines of its own require-ments.'
Appendix 4
106. Australia. The Government reports as followsas regards age for smallpox vaccinations :
" It is again stressed 6 that the World HealthOrganization should issue an authoritative statementon requirements so that a lead can be given to allauthorities concerned with international travel becausethe present variations create confusion and embarrass-ment for international travellers."
The Committee was informed of research in progresswhich, it is hoped, will reduce or eliminate the reportedincidence of complications.
d Off. Rec. Wld Huth Org. 110, 50, section 85.e The question of possible amendment to the form of the
certificate has been raised by several health administrations.The previous report of Australia on this subject read as
follows : " It would appear that countries in Southern Europemaintain the attitude that vaccination against smallpox is notdesirable under the age of twelve months and that recentlycountries in Central Europe have adopted the attitude of pre-venting vaccination after the age of three years. For inter-national travellers these variations create great confusion andembarrassment, and it is essential that the World Health Organ-ization publish in the immediate future an authoritative state-ment on requirements so that a lead can be given to all authoritiesconcerned with international travel." (Of. Rec. Wld Hlth Org.118, 55, section 118).
56 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
107. Ireland. The Government reports that duringthe outbreak of smallpox in Europe some problemshave arisen in regard to the dependability of somevaccination and revaccination certificates.
108. Seychelles. The Government reports that, duringthe epidemic of smallpox in Karachi, all arrivingpassengers from Pakistan were required to showevidence of a recent successful vaccination againstsmallpox rather than to possess a vaccination certifi-cate. This was deemed necessary in view of the factthat the travellers who introduced the disease intothe United Kingdom possessed valid smallpoxvaccination certificates. Disembarking travellerswho could not show evidence of a successful vaccin-ation were revaccinated before landing and kept undersurveillance. Transit passengers -whether or not inpossession of certificates -were not allowed todisembark. These emergency regulations were inforce for approximately two months.
109. United States of America. The Governmentreports as follows :
" A uniform ' approved stamp ' was adopted foruse by state and local health departments on inter-national certificates of vaccination against smallpoxand cholera. It is anticipated that such stamps willbe in effect at the end of this year in all states andpossessions of the United States, the Trust Territoryand the Commonwealth of Puerto Rico. Other' approved stamps ' of the United States include thestamp of the Department of Defense, the stampassigned to official yellow -fever vaccination centres,the seal of the Public Health Service, and the special` S -C ' stamp approved by the Public Health Service."
Appendix 6
110. United States of America. The Governmentreports as follows :
" There were a number of cases of failure to reportillness on aircraft, in the health part of the AircraftGeneral Declaration, Appendix 6 of the InternationalSanitary Regulations. An outstanding example wasfailure to report ten cases of chickenpox in infantKorean orphans who were accompanied by a physicianand four nurses. One case developed during flight.There was also failure to report measles and anindividual with prostration accompanied by diarrhoeaand dehydration. These specific problems werebrought to the attention of the airlines involved.There have been instances also where crew membershave refused to sign the declaration.
" To help provide that significant illness on anaircraft will be brought promptly to the attention ofthe port health authority, the following amendmentto the health part of the Aircraft General Declaration,Appendix 6, page 60, International Sanitary Regula-tions, 1961, is recommended :
" 1. Delete first paragraph and insert -Persons on board with known or suspected illness
other than airsickness or the effects of accidents, aswell as those cases of illness disembarked duringthe flight (include persons with any possible signof illness, for example, chills, fever, rash, collapse). .
" 2. Insert ` by the country of entry ' after ` Signa-ture, if required,'."The Committee was informed that some airlines
provide instructions to their aircrews on significantsigns of illness to be reported and recommends that allairlines pursue the same policy.
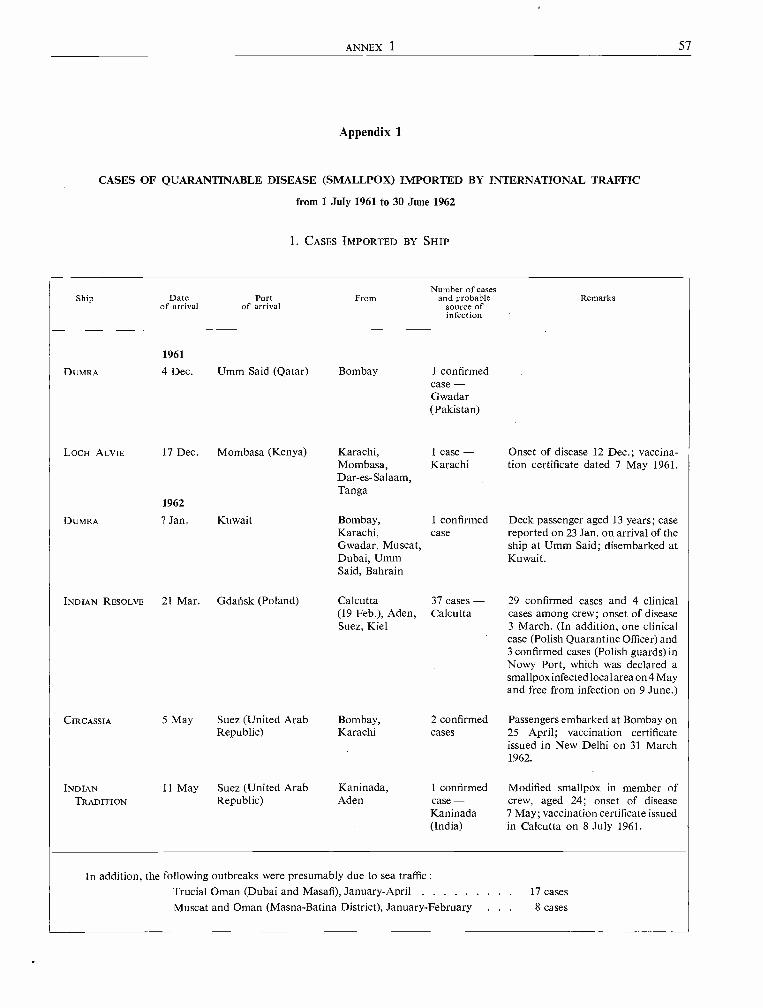
ANNEX 1 57
Appendix 1
CASES OF QUARANTINABLE DISEASE (SMALLPDX) IMPORTED BY INTERNATIONAL TRAFFIC
from 1 July 1961 to 30 June 1962
1. CASES IMPORTED BY SHIP
Ship Date Portof arrival of arrival
DUMRA
FromNumber of cases
and probablesource ofinfection
Remarks
1961
4 Dec. Umm Said (Qatar) Bombay 1 confirmedcase -Gwadar(Pakistan)
LOCH ALVIE 17 Dec. Mombasa (Kenya) Karachi, 1 case - Onset of disease 12 Dec.; vaccina -Mombasa, Karachi tion certificate dated 7 May 1961.Dar -es- Salaam,Tanga
DUMRA
1962
? Jan. Kuwait Bombay, 1 confirmed Deck passenger aged 13 years; caseKarachi, case reported on 23 Jan. on arrival of theGwadar, Muscat, ship at Umm Said; disembarked atDubai, Umm Kuwait.Said, Bahrain
INDIAN RESOLVE 21 Mar. Gdalísk (Poland) Calcutta 37 cases - 29 confirmed cases and 4 clinical(19 Feb.), Aden, Calcutta cases among crew; onset of diseaseSuez, Kiel 3 March. (In addition, one clinical
case (Polish Quarantine Officer) and3 confirmed cases (Polish guards) inNowy Port, which was declared asmallpox infected localarea on 4 Mayand free from infection on 9 June.)
CIRCASSIA 5 May Suez (United Arab Bombay, 2 confirmed Passengers embarked at Bombay onRepublic) Karachi cases 25 April; vaccination certificate
issued in New Delhi on 31 March1962.
INDIAN 11 May Suez (United Arab Kaninada, 1 confirmed Modified smallpox in member ofTRADITION Republic) Aden case - crew, aged 24; onset of disease
Kaninada 7 May; vaccination certificate issued(India) in Calcutta on 8 July 1961.
In addition, the following outbreaks were presumably due to sea traffic :Trucial Oman (Dubai and Masafi), January -April 17 cases
Muscat and Oman (Masna -Batina District), January- February 8 cases
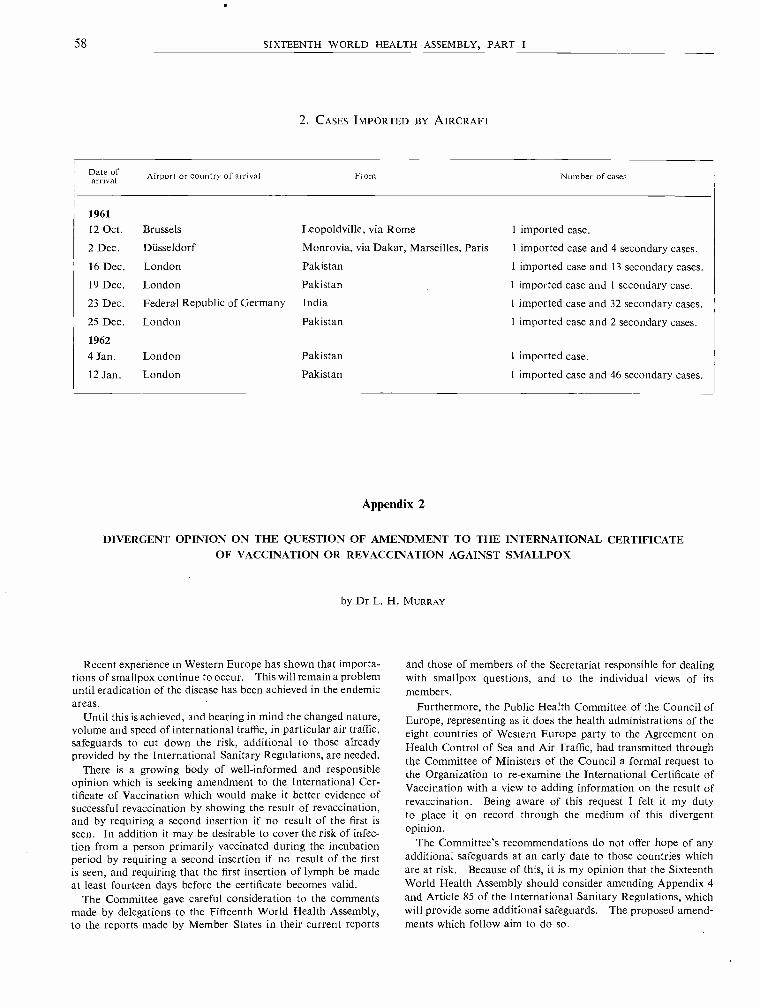
58 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
2. CASES IMPORTED BY AIRCRAFT
Date ofarrival Airport or country of arrival From Number of cases
1961
12 Oct. Brussels Leopoldville, via Rome 1 imported case.
2 Dec. Düsseldorf Monrovia, via Dakar, Marseilles, Paris 1 imported case and 4 secondary cases.
16 Dec. London Pakistan 1 imported case and 13 secondary cases.
19 Dec. London Pakistan 1 imported case and 1 secondary case.
23 Dec. Federal Republic of Germany India I imported case and 32 secondary cases.
25 Dec. London Pakistan 1 imported case and 2 secondary cases.
1962
4 Jan. London Pakistan 1 imported case.
12 Jan. London Pakistan 1 imported case and 46 secondary cases.
Appendix 2
DIVERGENT OPINION ON THE QUESTION OF AMENDMENT TO THE INTERNATIONAL CERTIFICATEOF VACCINATION OR REVACCINATION AGAINST SMALLPDX
by Dr L. H. MURRAY
Recent experience in Western Europe has shown that importa-tions of smallpox continue to occur. This will remain a problemuntil eradication of the disease has been achieved in the endemicareas.
Until this is achieved, and bearing in mind the changed nature,volume and speed of international traffic, in particular air traffic,safeguards to cut down the risk, additional to those alreadyprovided by the International Sanitary Regulations, are needed.
There is a growing body of well- informed and responsibleopinion which is seeking amendment to the International Cer-tificate of Vaccination which would make it better evidence ofsuccessful revaccination by showing the result of revaccination,and by requiring a second insertion if no result of the first isseen. In addition it may be desirable to cover the risk of infec-tion from a person primarily vaccinated during the incubationperiod by requiring a second insertion if no result of the firstis seen, and requiring that the first insertion of lymph be madeat least fourteen days before the certificate becomes valid.
The Committee gave careful consideration to the commentsmade by delegations to the Fifteenth World Health Assembly,to the reports made by Member States in their current reports
and those of members of the Secretariat responsible for dealingwith smallpox questions, and to the individual views of itsmembers.
Furthermore, the Public Health Committee of the Council ofEurope, representing as it does the health administrations of theeight countries of Western Europe party to the Agreement onHealth Control of Sea and Air Traffic, had transmitted throughthe Committee of Ministers of the Council a formal request tothe Organization to re- examine the International Certificate ofVaccination with a view to adding information on the result ofrevaccination. Being aware of this request I felt it my dutyto place it on record through the medium of this divergentopinion.
The Committee's recommendations do not offer hope of anyadditional safeguards at an early date to those countries whichare at risk. Because of this, it is my opinion that the SixteenthWorld Health Assembly should consider amending Appendix 4and Article 85 of the International Sanitary Regulations, whichwill provide some additional safeguards. The proposed amend-ments which follow aim to do so.
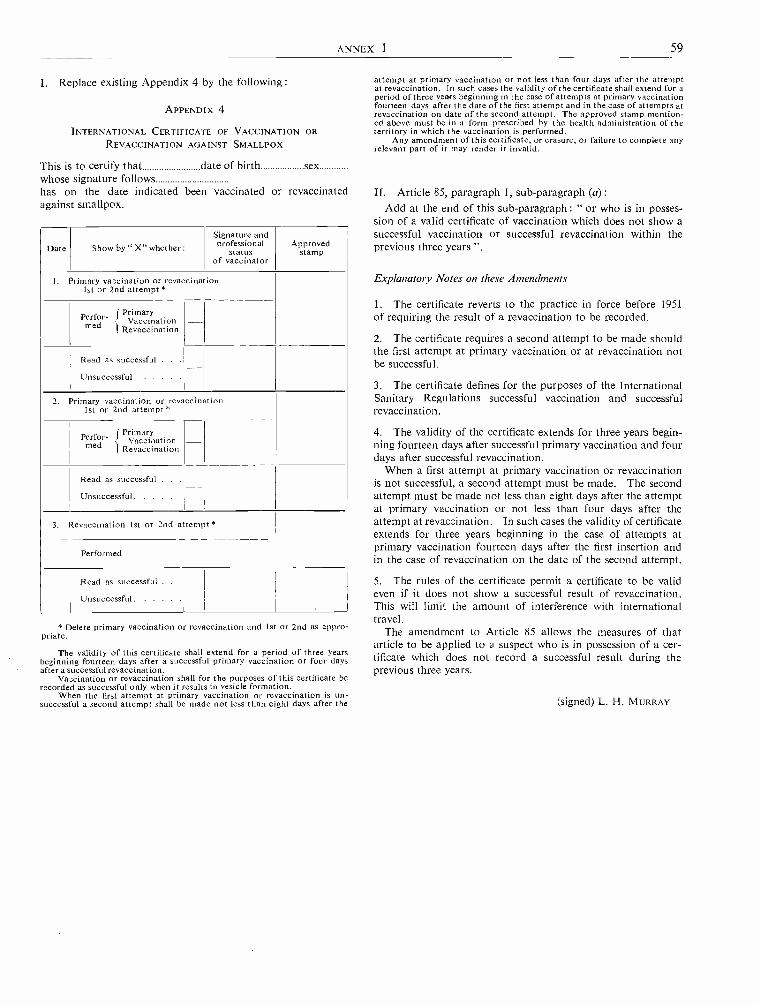
ANNEX 1 59
I. Replace existing Appendix 4 by the following:
APPENDIX 4
INTERNATIONAL CERTIFICATE OF VACCINATION ORREVACCINATION AGAINST SMALLPDX
This is to certify that date of birth sexwhose signature followshas on the date indicated been vaccinated or revaccinatedagainst smallpox.
Date Show by " X" whether :Signature andprofessional
statusof vaccinator
Approvedstamp
1. Primary vaccination or revaccination1st or 2nd attempt
Perfor- f Primarymed Vaccination
t Revaccination
Read as successful . .
Unsuccessful
2. Primary vaccination or revaccination1st or 2nd attempt *
Perfor- f Primarymed Vaccarination
i Revaccination
Read as successful .
Unsuccessful
3. Revaccination 1st or 2nd attempt
Performed
Read as successful . .
Unsuccessful.
* Delete primary vaccination or revaccination and 1st or 2nd as appro-priate.
The validity of this certificate shall extend for a period of three yearsbeginning fourteen days after a successful primary vaccination or four daysafter a successful revaccination.
Vaccination or revaccination shall for the purposes of this certificate berecorded as successful only when it results in vesicle formation.
When the first attempt at primary vaccination or revaccination is un-successful a second attempt shall be made not less than eight days after the
attempt at primary vaccination or not less than four days after the attemptat revaccination. In such cases the validity of the certificate shall extend for aperiod of three years beginning in the case of attempts at primary vaccinationfourteen days after the date of the first attempt and in the case of attempts atrevaccination on date of the second attempt. The approved stamp mention-ed above must be in a form prescribed by the health administration of theterritory in which the vaccination is performed.
Any amendment of this certificate, or erasure, or failure to complete anyrelevant part of it may render it invalid.
II. Article 85, paragraph 1, sub -paragraph (a):Add at the end of this sub -paragraph : " or who is in posses-
sion of a valid certificate of vaccination which does not show asuccessful vaccination or successful revaccination within theprevious three years ".
Explanatory Notes on these Amendments
1. The certificate reverts to the practice in force before 1951of requiring the result of a revaccination to be recorded.
2. The certificate requires a second attempt to be made shouldthe first attempt at primary vaccination or at revaccination notbe successful.
3. The certificate defines for the purposes of the InternationalSanitary Regulations successful vaccination and successfulrevaccination.
4. The validity of the certificate extends for three years begin-ning fourteen days after successful primary vaccination and fourdays after successful revaccination.
When a first attempt at primary vaccination or revaccinationis not successful, a second attempt must be made. The secondattempt must be made not less than eight days after the attemptat primary vaccination or not less than four days after theattempt at revaccination. In such cases the validity of certificateextends for three years beginning in the case of attempts atprimary vaccination fourteen days after the first insertion andin the case of revaccination on the date of the second attempt.
5. The rules of the certificate permit a certificate to be valideven if it does not show a successful result of revaccination.This will Iimit the amount of interference with internationaltravel.
The amendment to Article 85 allows the measures of thatarticle to be applied to a suspect who is in possession of a cer-tificate which does not record a successful result during theprevious three years.
(signed) L. H. MURRAY
60 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
2. DISCUSSION BY THE EXECUTIVE BOARD ON THE ELEVENTH REPORTOF THE COMMITTEE ON INTERNATIONAL QUARANTINE
(Extracts from the Minutes of the First Meeting of the Thirty-first Session, 15 January 1963)
[From EB31 /Min /1 Rev. 1 - 11 March 1963]
5. Eleventh Report of the Committee on InternationalQuarantine
Agenda, 2.3
Dr KAUL, Assistant Director -General, introducingdocument EB31/26, which submitted the eleventhreport of the Committee on International Quarantine(WHO/IQ/134),1 said that the Committee had con-sidered the annual report of the Director -General,prepared in accordance with the provisions ofArticle 13 of the International Sanitary Regulations,on the functioning of the Regulations and their effecton international traffic, and its recommendations onthe annual report were contained in the document.In considering the administration of the InternationalSanitary Regulations, the Committee had reviewedthe adequacy of certain definitions used for the purposeof the International Sanitary Regulations. In sec-tions 14 and 15, the Committee recommended to theAssembly certain amendments whose purpose was toachieve clarification and epidemiological realismregarding quarantinable diseases and to establishformally the practice in use in the administration ofthe Regulations. The definitions involved concernedimported cases, and a new phrase -" transferredcase " -was introduced and defined.
The Committee proposed to the Assembly (section21) that Article 3 be amended by adding a new para-graph whose purpose was to provide more currentinformation on the movement of the quarantinablediseases.
Information was given in sections 45 -61 concerningcholera El Tor. The Committee had discussed thepresent situation in great detail but, because of thegaps in fundamental knowledge about the spread ofthat disease, it had felt that it had not yet reached thetime to recommend any amendments to the Regula-tions. The Committee was fully informed of theOrganization's programme of research in the fieldof cholera.
In sections 70 -90, a very full record could be found ofthe development of cases of smallpox imported intoEurope during 1962. The Committee had discussedthat situation in considerable detail, and had alsoreviewed the International Sanitary Regulations in
1 See part 1 of this annex.
relation to the importation of such infection, and itsconclusions were recorded in the paragraphs followingthose sections. The Committee had not been con-vinced that any amendments to the Regulations inrespect of smallpox should be made at that time, andit had noted especially that the Director- General hadproposed an expert committee on smallpox in hisprogramme for 1964. That expert committee mightprovide the opportunity for experts to review thedevelopment in scientific knowledge with regard tosmallpox. The Board would also note that, as men-tioned on page 52 of the report, one member of theCommittee on International Quarantine had recordedhis divergent opinion (Appendix 2 to the report) onthe decision of the Committee not to make any amend-ments at that stage.
The Committee had discussed (section 96) whetherany additional sanitary documents in respect ofarriving international travellers were justified, andhad concluded that the health administrations shouldnot be permitted generally to require any additionaldetails in writing. It did, however, recommend to theWorld Health Assembly the amendment of Article 36by the addition of a third paragraph permitting healthadministrations with special problems constituting agrave danger to public health to require a destinationaddress in writing of arriving international travellers.
The report of the Committee on InternationalQuarantine was usually discussed and noted by theExecutive Board and transmitted to the HealthAssembly for its consideration.
Sir George GODBER, referring to Appendix 2 to thereport of the Committee on International Quarantine,expressed regret that the Committee had not found itpossible to make any recommendations to ensuregreater reliability of the international certificate ofvaccination, which was described (on page 50) as" the evidence an international traveller carries thathe has an immunity against smallpox ". For instance,six separate importations of smallpox had beenintroduced into the United Kingdom during 1962, inevery case of which the patients had carried a validinternational certificate of revaccination. The certificateof revaccination as it stood was therefore certainlynot reliable evidence. The primary concern was not,
ANNEX 1 61
of course, with producing certificates, but with gettingpeople effectively vaccinated. From the point ofview of countries to which many people might travelfrom areas where infection occurred, the absence ofreliable evidence was a much more serious difficultynow than it had been ten years ago. Large numbersmight arrive by air within the incubation period, ashad happened in the United Kingdom during theearlier part of 1962, and in spite of the efforts made inthe countries of origin to secure that travellers werevaccinated it was quite inevitable that some of themshould be unsuccessful. At a later stage, when effortshad been intensified, 98 per cent. of the travellershad been effectively vaccinated or revaccinated, andof the remaining 2 per cent., half were susceptible tovaccination and the remaining half resistant. Hecould only express regret that the Committee had notgiven more weight to that point. It might be that thesuggestion embodied in the minority report ofDr Murray (which appeared in Appendix 2 to thereport of the Committee on International Quarantine)to try and secure a reliable certificate would imposedelays that would be very difficult for travellers to sus-tain, but he considered it at least desirable to try to makethe certificate more reliable evidence than at present.
Mr SAITO, alternate to Dr Omura, said thatDr Omura had asked him to emphasize the importancehe attached to the work of the Committee on Inter-national Quarantine and to express appreciation of thework of the Secretariat. He hoped that the Committeeand the Secretariat would continue with that mostimportant aspect of the Organization's work byutilizing all the available knowledge and experienceof countries.
Professor ZDANOV expressed regret that the construct-ive proposals contained in Appendix 2 to the reportfor the amendment of Appendix 4 to the Regulationshad not been reflected in the Committee's own pro-posals. They were of value since they would remindphysicians and authorities concerned with quarantinethat it was not sufficient to make vaccines but thattheir efficacy must also be ensured. He asked that theCommittee on International Quarantine be notifiedof the Board's discussions, since he was concernedthat smallpox was so widespread throughout theworld, possibly because vaccination was not properlycarried out.
He would repeat his recommendation made at theFifteenth World Health Assembly that smallpoxshould receive more publicity. There were manypossibilities of influencing the quality of vaccinationand of quarantine measures and thus of contributingto the reduction of smallpox, and the more that waspublished on the subject the more public opinion
would be brought to bear in countries where theproblem received insufficient attention.
He suggested that maps giving data on the distribu-tion of smallpox might be regularly published by theOrganization as a further means of maintainingawareness of the problem.
Dr WATT said that the report emphasized a pointdiscussed by the Fifteenth World Health Assembly -the importance of the Committee's meeting regularly,so that it could consider the effects of changes in theworld travel situation. The key issue in the wholeproblem was the effectiveness of the vaccinator and ofthe vaccine used. The certificate would not change theminds and attitudes of those who did not treatvaccination with the importance it deserved. Therewere two effective lines of approach to the problem.The first was to ensure effective vaccines and properproduction and storage facilities, etc., and the secondwas to make it fully clear to those using the vaccinethat there must be effective use of the material. Toenlarge the certificate would merely penalize theconscientious and do nothing to change the omissionsof those who were not so meticulous and careful.The issue of the certificate itself could easily divertattention from the important point to be kept in mind,and he would strongly urge that in considering theproblem the Committee should concern itself withthe basic issue rather than with the certificates.
Professor AUJALEU said he fully shared Sir GeorgeGodber's regret that the modifications in the vaccina-tion certificate proposed by Dr Murray had notbeen accepted by the Committee. The vaccine wasimportant but -and here he was sorry that he couldnot agree with Dr Watt -the certificate was also ofgreat importance.
The CHAIRMAN drew attention to the fact that thesupplementary agenda contained an item on smallpoxeradication, under which the subject could be dealtwith more fully. The report under consideration hadbeen prepared, in fact, for submission to the HealthAssembly and remarks made by Board members on itwere transmitted to the Health Assembly to be takeninto account. In bringing those facts to the Board'sattention, he was not trying to restrict the presentdiscussion.
Professor ZDANOV said that, following the Chair-man's explanation, he would reserve his furthercomments until discussion of the item on smallpoxeradication.
Dr VANNUGLI, although recognizing that smallpoxcontrol was not effected simply by the issue of vaccina-tion certificates, nevertheless shared the opinion that
62 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
there would be great advantage in thoroughly studyingthe possibility of improving their content. He saw nomajor difficulty in adding a note stating the result ofvaccination, which would be of particular advantageto countries like his own where the disease had longsince disappeared.
Dr KAUL, Assistant Director- General, answeringpoints raised in the discussion, said that the problem ofsmallpox had been a major subject for discussion bythe Committee on International Quarantine at itseleventh session. It had devoted a considerable partof its time to that problem and had thus given dueweight to its importance.
Secondly, in the course of discussing protection ofpopulations from the risk of imported smallpoxinfection, attention had been given to certain scientificdata that were pertinent, in addition to the vaccinationcertificate. Such questions as the exact constitutionof a successful vaccination, primary or secondary;period before immunity was established after primaryvaccination and revaccination, and duration of suchimmunity; and avoidance of interference withinternational traffic through use of the vaccinationcertificate until there was adequate scientific justifica-tion therefor, had been thoroughly reviewed. TheCommittee had felt that it had had no new knowledgebefore it on those questions, and that was one of thereasons that had led the Director -General to proposethe convening of an expert committee on problems ofsmallpox in 1964 -the earliest date he could suggestfor such a meeting. The experts who would review thesituation then would be able to make recommendationson those scientific matters and in the meantime theOrganization might perhaps take action to stimulateinquiry into them.
The Committee on International Quarantine hadin addition to considering the suggestions put forwardfor improving the vaccination certificate reviewed therelevant International Sanitary Regulations to seeto what extent immediate action could be taken witha view to strengthening them. Its conclusions andrecommendations, as set out in the paragraphsfollowing sections 70 - 90 of the report, had beenreached only after that review, and they showed thatthe Committee had been deeply concerned with theproblem and would take it up again at a future sessionwhen further information might be expected to beavailable.
Professor AUJALEU said he was well aware that, asDr Kaul had said, all the scientific problems connectedwith the outward appearance of immunity throughsmallpox vaccination had not as yet been resolved.
On the other hand, it should not be assumed thatnational officials responsible for verifying vaccinationcertificates and interviewing travellers were completelydevoid of knowledge. The request put forward to theCommittee by Dr Murray had been that the vac-cination certificate should show what happened aftervaccination so that national officials might draw theirown conclusions. To diverge for a moment, he wouldagain point out that there was no difference between aso- called " immune " reaction and complete absenceof vaccination; therein lay the trouble and the reasonfor the view that the vaccination certificate should,without any reference whatsoever to scientific data,show exactly what happened after vaccination.
Professor GAY PRIETO remarked that a very highpercentage of negative results was obtained in revac-cination and there was good reason to believe thatroutine methods of revaccination by scarification wereresponsible for that result. The percentage of positiveresults was infinitely higher where revaccination wasdone by intradermal injection. The general objectionput forward to adoption of that procedure was simplythat scarification was a much easier process. It wouldbe worth while for the Organization to organizestudies to determine the percentage of positive resultsobtained by each method; he was sure their resultswould be highly significant.
Dr SERPA- FLÓREZ said that the speed of present -day travel, especially by air, added daily to theimportance of the Organization's world campaign forthe eradication of smallpox. But the problem couldnot be separated into two component parts, relatingrespectively to the countries where the disease wasendemic and those that had succeeded after tremendousefforts in stamping it out. Accordingly, it wouldbe worth while for the Board to request those countriesthat had had no case of smallpox over many years toensure that every effort was made to maintain a highimmunity level in their populations.
Dr FARAH, Rapporteur, read out the following draftresolution for the Board's consideration :
The Executive Board1. NOTES the eleventh report of the Committeeon International Quarantine;2. THANKS the members of the Committee fortheir work; and3. TRANSMITS the report, together with the minutesof the discussion which took place at the ExecutiveBoard, to the Sixteenth World Health Assembly forits consideration.Decision: The draft resolution was adopted (reso-lution EB31.R2).

Annex 2
FINANCIAL REPORT ON THE ACCOUNTS OF WHO FOR 1962AND REPORT OF THE EXTERNAL AUDITOR 1
[A16 /AFL /15 - 8 May 1963]
REPORT OF THE AD Hoc COMMITTEE OF THE EXECUTIVE BOARD
1. At its thirty -first session, the Executive Board (inresolution EB31.R52) established an Ad Hoc Com-mittee, consisting of Dr M. K. Afridi, ProfessorE. Auialeu and Dr A. Nabulsi, to meet on 6 May1963 to consider the report of the External Auditoron the accounts of the Organization for the year 1962,and to submit to the Sixteenth World Health As-sembly, on behalf of the Board, such comments as itdeemed necessary.
2. The Committee met on 6 May 1963 in the Palaisdes Nations and Dr Afridi was elected Chairman.3. Mr Uno Brunskog, the External Auditor, in-troduced his report and commented on the moreimportant matters raised therein and in the FinancialReport of the Director- General.2
4. The Committee then reviewed the report of theExternal Auditor in detail and received, either fromthe External Auditor or from representatives of theDirector -General, explanations on various pointsraised by the members of the Committee.
5. On the basis of its review, the Committee desiresto bring the following items to the attention of theAssembly :
5.1 In paragraph 1.1 of his report, the ExternalAuditor comments on the scope and character of hisaudit and states : " The scope and character of theaudit in 1962 has been essentially the same as in earlieryears. Transactions, accounts and inventories wereexamined to the extent necessary to satisfy myself asto their correctness. The financial statements submittedto me for audit have been certified accordingly. I havealso examined the reports of the internal auditors andreviewed their work, which has given me completesatisfaction. In connexion with the 1962 audit, I wishto state specifically that to my knowledge there havebeen no cases of fraud or presumptive fraud."5.2 In paragraphs 1.2 and 1.3 of his report, theExternal Auditor states : " During 1962 I visited two
1 See resolution WHA16.5.2 Off. Rec. Wld Huth Org. 126.
regional offices and formed the opinion that the finan-cial and administrative aspects of the work in theseoffices were being performed satisfactorily. As aresult of my audit of the accounts of the Organizationas a whole, I can state that they are well kept andcomply with established policies, rules and regulationsof the Organization and the Health Assembly. Inkeeping with past practice I have during 1962 drawnattention to minor errors, discovered during thecourse of the audit, which have immediately beenadjusted and therefore call for no further auditobservation. Such minor errors, involving for instancesmall calculating mistakes, are unavoidable in anyinternational organization with fairly large operations.It is the frequency of errors that would be of signifi-cance, but I am pleased to report that in the WorldHealth Organization the number of such errors hasbeen negligible. In fact, it has given me great satis-faction to see that one of the regional offices, withsudden considerable expansion of activities in 1962,while not fully staffed was nevertheless able withsubstantial overtime to carry out its financial andadministrative work very efficiently indeed."
5.3 The Committee desires to bring to the attentionof the Assembly the following comment by the ExternalAuditor in paragraph 1.4 of his report : " Again thisyear the result of my audit leads me to confirm thatthe different funds of the Organization have been wellmanaged."
5.4 In paragraph 2.2 of his report, the ExternalAuditor noted that the total obligations incurred in1962 amounted to $24 164 650, representing 97.19 percent. of the effective working budget for that year.The comparable figure for 1961 was 97.07 per cent.
5.5 In paragraph 2.3 of his report, the ExternalAuditor remarks on the cost of the administrativeservices of the Organization as follows : "From the abovetable it will be seen that, while the percentage of theobligations for the operating programme increasedby 2.4 per cent., that relating to administrativeservices decreased by 1 per cent. in 1962. Taking into
- 63 -
64 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
account the total obligations incurred by the Organi-zation in 1962 from all its resources, amounting tosome $35.7 million (as shown in Appendix 1 to theFinancial Report), obligations for administrativeservices represented 6.02 per cent. only. This doesnot include the activities carried out by the Organi-zation in the Congo (Leopoldville) against reimburse-ment by the United Nations. Disbursements totalled$2.58 million in 1962. If these disbursements areadded to the above total obligations, the percentagefor administrative services would be 5.6."
5.6 In section 5 of his report, the External Auditorcomments on the position of the Working CapitalFund. He advised the Committee that he intended tomake a further study of the position of this Fundduring 1963. The Committee also noted that, inresolution WHA13.41, the Assembly had requestedthe Executive Board to review the situation of theWorking Capital Fund at its first session in 1965.
5.7 In paragraph 6.3 of his report, the ExternalAuditor noted that there were proceeds of $181 303from the postage stamp project of WHO's malariaeradication programme and stated : " I have reviewedthe Agreement between WHO and the Inter- Govern-mental Philatelic Corporation, the guarantee from thebank in New York acting as custodian of the stamps,and related material, and also the quarterly accountscovering payments and inventory of stamps etc. Ihave found all these arrangements satisfactory insafeguarding the interests of the Organization andhave no observation to make on the accounts."5.8 In summing up his report on the regular fundsof the Organization, the External Auditor drew specialattention to paragraph 9 of his report, which states :
" In my audit report concerning the accounts for1957, I stated inter alla : ` ... the control exercisedover all transactions has attained such a standard thatI feel obliged to felicitate the World Health Organi-zation on the occasion of its Tenth Anniversary onits very good and sound financial administration '.Now, fifteen years after the inception of WHO, duringwhich time the activities of the Organization haveincreased by about nine times, I am pleased to statethat what I said in 1958 is still valid. Good adminis-tration in an organization of WHO's structure isparticularly important to enable the technical activ-ities to be carried out efficiently."
6. The Committee wishes to commend the ExternalAuditor on his report and to express its appreciationof the explanations given by him and by the represen-tatives of the Director -General during the review ofthe report.
7. The Committee recommends to the SixteenthWorld Health Assembly the adoption of the followingresolution :
The Sixteenth World Health Assembly,Having examined the Financial Report of the
Director -General for the period 1 January to31 December 1962 and the Report of the ExternalAuditor for the same financial period, as containedin Official Records No. 126; and
Having considered the report of the Ad HocCommittee of the Executive Board on its examin-ation of these reports,
ACCEPTS the Director -General's Financial Reportand the Report of the External Auditor for thefinancial year 1962.
Annex 3
SUPPLEMENTARY BUDGET ESTIMATES FOR 1963
1. REPORT OF THE AD Hoc COMMITTEE OF THE EXECUTIVE BOARD
[A16 /AFL /8 Add. 1 Rev. 1 -9 May 1963
1. At its thirty -first session the Executive Board, inresolution EB31.R52, established " an Ad HocCommittee of the Executive Board consisting of :Dr M. K. Afridi, Professor E. Aujaleu, andDr A. Nabulsi, to meet on Monday, 6 May 1963,to ... report to the Sixteenth World Health Assemblyon the minor adjustments reported by the Director -General in the cost estimates for the supplementarybudget for 1963 ".2. The Committee met on 6 May 1963 in the Palaisdes Nations, Geneva, and Dr Afridi was electedChairman.
3. In considering the adjustments reported by theDirector -General, the Committee noted that theywere of two kinds -first, those which are mandatoryunder the Staff Regulations and Staff Rules of theOrganization (set forth in paragraphs 2, 3 and 4 ofthe Director -General's report) (part 2 of this annex)and, secondly, those of a discretionary nature (setforth in paragraphs 5 and 6 of that report).
4. With regard to the former, the Ad Hoc Committee,following its review of these items, considered theestimates to be satisfactory and recommends theirapproval by the Sixteenth World Health Assembly.5. In the course of its review of the provisions of adiscretionary nature proposed, the Committee wasinformed that the provision of $40 000 for services tonew Members and Associate Members and to Mem-bers resuming active participation was intended tomeet such minimum requests for services as may beforthcoming from such Members. In this connexionthe Committee recalled that since the Fifteenth WorldHealth Assembly the following new Members (someof which were previously Associate Members) hadjoined the Organization : Algeria, Burundi, Jamaica,Rwanda, Trinidad and Tobago, and Uganda. TheCommittee was also informed that applications forAssociate Membership were before the SixteenthWorld Health Assembly for Kenya and Mauritius
I See resolution WHA16.6.
and that one Member had resumed active participationin the work of the Organization.6. As a result of its study of the proposals made bythe Director -General for provision to assist in meetingsome of the additional costs of the headquartersbuilding, the Committee concluded that the stepsproposed by the Director- General were prudent anddesirable. In reply to a question as to why, at thetime of the preparation of the proposed programmeand budget estimates for 1963, it had not been foreseenthat a deferment might be possible with regard to therepayment of loans for the headquarters building,it was explained that the loan agreement with the SwissConfederation stipulates that the first instalment ofrepayment of the loans should take place on 31 Decem-ber 1963. At that time also it could not be foreseenthat delay in the construction work to the extentwhich has now taken place would necessarily occur.For these reasons the Director - General was boundto include provision in the proposed programme andbudget estimates for 1963 for repayment of the loansfrom the Swiss Confederation and the Republic andCanton of Geneva. As explained in his report, noportion of the loans has yet been used and thereforeno difficulties should be experienced in arranging adeferment of the repayment.
7. The Committee decided to recommend to theSixteenth World Health Assembly that it also approvethe inclusion in the supplementary estimates for 1963of the provisions proposed by the Director -Generalfor the purposes referred to in paragraphs 5 and 6above.
8. The Committee noted that sufficient income wasavailable to meet the financing of the total supple-mentary estimates of $438 100 for 1963 by using(a) $35 990 representing an increase in the amountof the lump -sum allocation to WHO from the SpecialAccount of the Expanded Programme of TechnicalAssistance towards the administrative and operationalservices costs of that programme, and (b) $402 110available from casual income over and above the
- 65 -
66 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
amount recommended by the Director -General tobe used to help finance the proposed programme andbudget estimates for 1964.9. Should the Sixteenth World Health Assemblyaccept the above recommendations of the Ad HocCommittee on behalf of the Board, it may wish toadopt the following resolution in place of that setforth in paragraph 2 of resolution EB31.R13:
The Sixteenth World Health Assembly,Having considered the proposals of the Director -General and
the recommendations of the Executive Board concerning sup-plementary budget estimates for 1963,
1. APPROVES the supplementary estimates for 1963;
2. DECIDES to amend the Appropriation Resolution for 1963(resolution WHA15.42) by increasing the amounts voted underparagraph I as follows :
Appropriation Purpose ofSection Appropriation
PART II : OPERATING PROGRAMME
4. Programme Activities5. Regional Offices7. Other Statutory Staff Costs
1. Introduction
AmountUS$
95 25023 700
142 180
Total - Part II 261 130
Appropriation Purpose ofSection Appropriation
AmountUS $
PART III : ADMINISTRATIVE SERVICES
8. Administrative Services 27 3509. Other Statutory Staff Costs 36 620
Total - Part III 63 970
PART IV : OTHER PURPOSES
10. Headquarters Building Fund 113 000
Total - Part IV 113 000
TOTAL - Parts II, III and IV 438 100
3. DECIDES further to amend paragraph III of resolutionWHA15.42 by increasing the amounts under sub -paragraphs (i)and (iii) as follows :
(i) the amount of $35 990 available by reimbursement fromthe Special Account of theExpanded Programme of Tech-nical Assistance
(ii) the amount of $402 110 representing miscellaneous in-come available for the purpose
Total $438 100
2. REPORT BY THE DIRECTOR - GENERAL
1.1 In accordance with the provisions of FinancialRegulation 3.10, the Director -General submitted tothe Executive Board at its thirty -first session sup-plementary estimates for 1963 1 in the amount of$162 000 including :
(a) $120 000 required to meet the costs of a changein the post- adjustment classification for Genevafrom class 1 to class 2; and
(b) $42 000 to meet additional costs anticipatedbecause of changes in post- adjustment classificationsfor some of the regional offices, where cost -of- livingsurveys are in progress or about to be undertaken.
1.2 Having considered these supplementary estimatesand the recommendation of the Director -Generalconcerning their financing, the Executive Board, inresolution EB31.R13, recommended to the SixteenthWorld Health Assembly that it approve the supple-mentary estimates for 1963 and their financing asproposed by the Director -General, subject to minoradjustments in cost estimates, to be reported by theDirector -General to the Sixteenth World Health
I Off Rec. Wld Hlth Org. 124, Annex 11.
[A16 /AFL /8 - 3 May 1963]
Assembly through the Ad Hoc Committee of theExecutive Board, meeting on 6 May 1963.
1.3 The adjustments to the estimates which theDirector -General finds it necessary to report resultfrom :
(a) increases in post- adjustment classificationswhich have become effective in 1963;
(b) increases in the salary scales for general servicestaff in certain locations;
(c) increased payment to pensioners of the OfficeInternational d'Hygiène Publique;
(d) provision for services to new Members andMembers resuming active participation; and
(e) provision toward increased costs of the head-quarters building.
Details of these adjustments are set forth below.
2. Increases in Post -adjustment Classifications
As reported to the Executive Board 1 $120 000 isrequired in consequence of the change from class 1
to class 2 in the post- adjustment classification forGeneva, which became effective as from 1 November
ANNEX 3 67
1962. The Director - General now reports that afurther amount of $41 200 is required to meet theadditional expenditure resulting from increases inthe post- adjustment classifications for New Delhiand Copenhagen, as follows :
New Delhi (Regional Office for South -East Asia)
Estimatedadditional
CostsUS $
Changed from class 2 to class 3 as from 1 April 1963 10 100
Copenhagen (Regional Office for Europe)Changed from class 0 to class 1 as from 1 January
and from class 1 to class 2 as from 1 March 1963 31 100
41 200
3. Increases in the Salary Scales for General ServiceStaff in Certain Locations
Increases in the salary scales for general servicestaff in the employ of international organizationsin certain centres will result in increased costs to WHOunder the regular budget in 1963, as follows :
Geneva (headquarters)
US$
From 1 March 1963 and from 1 September 1963 85 400
Copenhagen (Regional Office for Europe)From 1 January 1963 25 400
New Delhi (Regional Office for South -East Asia)From 1 January 1963 10 700
121 500
4. Increased Payments to Pensioners of the OfficeInternational d'Hygiène Publique (OIHP)
In resolution EB27.R24 the Executive Board at itstwenty- seventh session, believing that the WorldHealth Organization " as the successor organizationto the OIHP, has a moral responsibility to amelioratethe situation of the OIHP pensioners in a mannerconsistent with that approved by the General Assem-bly of the United Nations for pensioners of the UnitedNations Joint Staff Pension Fund ", authorized" the Director - General to make future adjustmentsin the payments to those pensioners should furtheradjustments be made in the Joint Staff PensionFund by the General Assembly of the United Nations ".In exercise of this authority, the Director -General,in consideration of increases in the payments topensioners of the United Nations Joint Staff PensionFund approved by the General Assembly of the UnitedNations with effect from 1 January 1963, has accordedsimilar increased payments to OIHP pensioners atan estimated total cost in 1963 of $2400.
5. Provision for Services to New Members and toMembers resuming Active Participation
The Director- General proposes that an amountof $40 000 be included in the supplementary estimatesfor 1963 for the purpose of meeting requests from newMembers and Associate Members, as well as fromMembers resuming active participation in the workof the Organization.
6. Provision towards Increased Costs of the Head-quarters Building
The Director -General is submitting a progressreport on headquarters accommodation under pro-visional agenda item 3.11 to the Sixteenth WorldHealth Assembly,' which refers inter alia to theincreased costs. The Executive Board at its thirty -first session adopted resolution EB31.R25, paragraph 5of which requested " the Director - General to examinewith the authorities of the Swiss Confederation anincrease in the amount of the interest -free loan offeredto the Organization, with a view to the financing ofthe additional cost foreseen ", and paragraph 6 ofwhich requested the Director -General to report onthis matter " through the Ad Hoc Committee of theExecutive Board ". At the time of the preparation ofthis report information was not available to enablethe Director -General fully to report on this matter.However, it is clear that the increase in cost of theheadquarters building will require a number of stepsto be taken. There are two steps which the Director -General believes can be taken now. First, in view ofthe fact that no portion of the loan has yet been usedbecause of delay in the construction work, the Director-General has reason to believe that arrangements canbe made with the Swiss Confederation to defer until1965 or 1966 the first instalment on the repayment ofthe loan. The terms of the loan agreement with theRepublic and Canton of Geneva are such that in thelight of construction progress it is not now anticipatedthat repayment will have to be started until 1965 atthe earliest. The Director -General, therefore, proposesthat the amount of $387 000 appropriated by theFifteenth World Health Assembly under Appropria-tion Section 10, " Headquarters Building : Repaymentof Loans ", of the Appropriation Resolution for theFinancial Year 1963 (WHA15.42) be used for a creditto the Headquarters Building Fund, the title ofAppropriation Section 10 being changed to read" Headquarters Building Fund ". Secondly, theDirector -General proposes that the amount of$387 000 be increased to $500 000 by including anadditional amount of $113 000 in the supplementary
' See Annex 7, part 2.
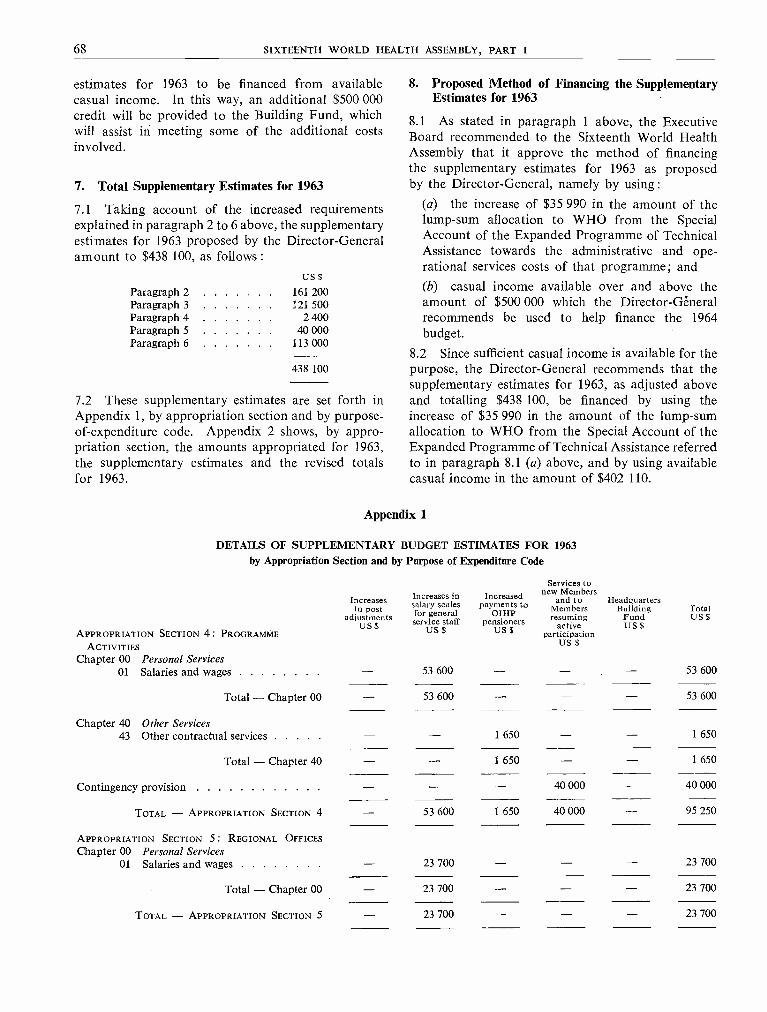
68 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
estimates for 1963 to be financed from availablecasual income. In this way, an additional $500 000credit will be provided to the Building Fund, whichwill assist in meeting some of the additional costsinvolved.
7. Total Supplementary Estimates for 1963
7.1 Taking account of the increased requirementsexplained in paragraph 2 to 6 above, the supplementaryestimates for 1963 proposed by the Director - Generalamount to $438 100, as follows :
uS $
Paragraph 2 161 200Paragraph 3 121 500Paragraph 4 2 400Paragraph 5 40 000Paragraph 6 113 000
438 100
7.2 These supplementary estimates are set forth inAppendix 1, by appropriation section and by purpose -of- expenditure code. Appendix 2 shows, by appro-priation section, the amounts appropriated for 1963,the supplementary estimates and the revised totalsfor 1963.
8. Proposed Method of Financing the SupplementaryEstimates for 1963
8.1 As stated in paragraph 1 above, the ExecutiveBoard recommended to the Sixteenth World HealthAssembly that it approve the method of financingthe supplementary estimates for 1963 as proposedby the Director -General, namely by using :
(a) the increase of $35 990 in the amount of thelump -sum allocation to WHO from the SpecialAccount of the Expanded Programme of TechnicalAssistance towards the administrative and ope-rational services costs of that programme; and(b) casual income available over and above theamount of $500 000 which the Director- Gëneralrecommends be used to help finance the 1964budget.
8.2 Since sufficient casual income is available for thepurpose, the Director -General recommends that thesupplementary estimates for 1963, as adjusted aboveand totalling $438 100, be financed by using theincrease of $35 990 in the amount of the lump -sumallocation to WHO from the Special Account of theExpanded Programme of Technical Assistance referredto in paragraph 8.1 (a) above, and by using availablecasual income in the amount of $402 110.
Appendix 1
DETAILS OF SUPPLEMENTARY BUDGET ESTIMATES FOR 1963by Appropriation Section and by Purpose of Expenditure Code
APPROPRIATION SECTION 4: PROGRAMMEACTIVITIES
Increasesin post
adjustmentsUS $
Increases insalary scalesfor general
service staffUS $
Increasedpayments to
OIHPpensioners
US $
Services tonew Members
and toMembersresuming
activeparticipation
US $
HeadquartersBuilding
FundUS $
TotalUS $
Chapter 00 Personal Services01 Salaries and wages 53 600 53 600
Total - Chapter 00 53 600 53 600
Chapter 40 Other Services43 Other contractual services 1 650 1 650
Total - Chapter 40 1 650 1 650
Contingency provision 40 000 40 000
TOTAL - APPROPRIATION SECTION 4 53 600 1 650 40 000 95 250
APPROPRIATION SECTION 5: REGIONAL OFFICESChapter 00 Personal Services
01 Salaries and wages 23 700 23 700
Total - Chapter 00 23 700 23 700
TOTAL - APPROPRIATION SECTION 5 23 700 23 700

ANNEX 3 69
APPROPRIATION SECTION 7: OTHER STATUTORYSTAFF COSTS
Increasesin post
adjustmentsUS $
Increases insalary scalesfor generalservice staff
US $
Increasedpayments to
OIHPpensioners
US $
Services tonew Members
and toMembersresuming
activeparticipation
US $
HeadquartersBuilding
FundUS $
TotalUS $
Chapter 10 Personal Allowances12 Pension fund 7 560 7 56013 Insurance 1 590 1 59015 Other allowances 129 200 3 830 133 030
Total - Chapter 10 129 200 12 980 142 180
TOTAL - APPROPRIATION SECTION 7 129 200 12 980 142 180
APPROPRIATION SECTION 8: ADMINISTRATIVESERVICES
Chapter 00 Personal Services01 Salaries and wages 26 600 26 600
Total - Chapter 00 26 600 26 600
Chapter 40 Other Services43 Other contractual services 750 750
Total - Chapter 40 750 750
TOTAL - APPROPRIATION SECTION 8 26 600 750 27 350
APPROPRIATION SECTION 9: OTHER STATUTORYSTAFF COSTS
Chapter 10 Personal Allowances12 Pension fund 3 080 3 08013 Insurance - 560 56015 Other allowances 32 000 980 32 980
Total - Chapter 10 32 000 4 620 36 620
TOTAL - APPROPRIATION SECTION 9 32 000 4 620 36 620
APPROPRIATION SECTION 10: HEADQUARTERS
BUILDING FUNDChapter 80 Acquisition of Capital Assets
83 Land and buildings 113 000 113 000
Total - Chapter 80 - 113 000 113 000
TOTAL - APPROPRIATION SECTION 10 113 000 113 000
GRAND TOTAL 161 200 121 500 2 400 40 000 113 000 438 100

70 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Appendix 2
AMOUNTS APPROPRIATED FOR 1963, SUPPLEMENTARY ESTIMATES, AND REVISED TOTALS FOR 1963UNDER THE REGULAR BUDGET
AppropriationSection Purpose of appropriation
PART I : ORGANIZATIONAL MEETINGS
Amountsappropriated
for 19631US$
Supplementaryestimates for
1963US$
Revisedtotals
for 1963US$
1. World Health Assembly 326 110 326 1102. Executive Board and its Committees 189 090 189 0903. Regional Committees 84 420 84 420
Total - Part I 599 620 599 620
PART II : OPERATING PROGRAMME
4. Programme Activities 14 823 216 95 250 14 918 4665. Regional Offices 2 517 489 23 700 2 541 1896. Expert Committees 220 400 - 220 4007. Other Statutory Staff Costs 4 573 268 142 180 4 715 448
Total - Part II 22 134 373 261 130 22 395 503
PART III: ADMINISTRATIVE SERVICES
8. Administrative Services 1 716 432 27 350 1 743 7829. Other Statutory Staff Costs 536 575 36 620 573 195
Total - Part III 2 253 007 63 970 2 316 977
PART IV : OTHER PURPOSES
10. Headquarters Building Fund 387 000 113 000 500 00011. Contribution to the Malaria Eradication Special Account 4 000 000 - 4 000 00012. African Regional Office : Building Fund 100 000 100 00013. African Regional Office : Staff Housing 482 000 482 000
Total - Part IV 4 969 000 113 000 5 082 000
Sub -total - Parts I, II, III and IV 29 956 000 438 100 30 394 100
PART V : RESERVE
14. Undistributed Reserve 2 149 570 2 149 570
Total - Part V 2 149 570 2 149 570
TOTAL - Au. PARTS 32 105 570 438 100 32 543 670
1 Appropriation Resolution WHA15.42, taking into account transfers between sections concurred in by the Executive Boardin resolution EB31.R10.

ANNEX 4 71
Annex 4
ACCOMMODATION FOR THE REGIONAL OFFICE FOR AFRICA 1
1. REPORT OF THE AD Hoc COMMITTEE OF THE EXECUTIVE BOARD
[A16 /AFL /7 Add. 1 - 8 May 1963]
1. At its thirty -first session the Executive Board (inresolution EB31.R52) established " an Ad HocCommittee of the Executive Board, consisting of :Dr M. K. Afridi, Professor E. Aujaleu, andDr A. Nabulsi, to meet on Monday, 6 May 1963, to .. .(c) report to the Sixteenth World Health Assemblysuch further information as is submitted by theDirector -General on accommodation for the RegionalOffice for Africa ... including the budgetary andfinancial aspects ".
2. The Committee met on 6 May 1963 in the Palaisdes Nations, Geneva, and Dr Afridi was electedChairman.
3. The Committee had before it a report of theDirector -General on the accommodation for theRegional Office for Africa (as contained in part 2of this annex). From this report the Committee notedthat the Director -General had included an amountof $200 000 in the proposed programme and budgetestimates for 1964 for reimbursement of the WorkingCapital Fund, in pursuance of the authority vestedin him by the Fifteenth World Health Assembly inresolution WHA15.14, " to advance from the WorkingCapital Fund an amount not exceeding $300 000 tobe credited to the African Regional Office BuildingFund, to help finance the said construction, reimburse-ment to the Working Capital Fund of the sum soadvanced to be provided for, if necessary, in theprogramme and budget estimates for 1964 ". At thetime those estimates were prepared, taking into accountthe $100 000 appropriated by the Fifteenth WorldHealth Assembly for 1963, the amount of contribu-tions and pledges from Members and the estimatedcost of the construction of the extension, the Director -General had anticipated that $200 000 only would berequired.
4. The revised preliminary estimates in the light ofcurrent construction costs in Brazzaville indicate thatthe total estimated cost will be approximately$700 000. Contributions and pledges from Membergovernments as at 25 April 1963 amounted to
1 See resolution WHAI6.9.
$301 846, as reflected in the appendix to the Director -General's report (part 2 of this annex).
5. The Committee noted that, subject to additionalcontributions becoming available from Members,the Director -General would have to have recourseto the full authorization of advancing $300 000 fromthe Working Capital Fund. However, since cons-truction work can hardly begin before early 1964, theCommittee agrees with the proposal of the Director -General that the Sixteenth World Health Assemblyauthorize him to withdraw $100 000 from theWorking Capital Fund, such advance to be reimbursedto the Working Capital Fund by provision in theproposed programme and budget estimates for 1965.The Committee therefore recognized that no actionwas necessary with regard to the provision in theproposed programme and budget estimates for 1964.
6. The Committee was informed that, with regardto paragraph 4 of resolution EB31.R20, the Director -General had communicated with the Government ofthe Republic of South Africa and that he would reportany further developments to the Sixteenth WorldHealth Assembly (see part 3 of this annex).
7. Should the Sixteenth World Health Assemblyaccept the proposal of the Director -General, theAd Hoc Committee, on behalf of the ExecutiveBoard, recommends for the approval of the HealthAssembly the following draft resolution :
The Sixteenth World Health Assembly,Having considered the report of the Director -
General on accommodation for the Regional Officefor Africa and the report of the Executive Boardthereon;
Having noted with gratification the furthergenerous contributions offered by Members in theAfrican Region to help finance the cost of extendingthe accommodation of the Regional Office;
Recalling the provisions of paragraph 4 ofresolution WHA15.14, authorizing the Director -General, notwithstanding the provisions of Part II,paragraph 1 (2) of resolution WHA13.41, toadvance from the Working Capital Fund an

72 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
amount not exceeding $300 000 to be credited tothe African Regional Office Building Fund;
Noting that the Director -General will exercisethis authority to the extent of $200 000, reimburse-ment being provided for in the proposed programmeand budget estimates for 1964,1. INVITES all the Members in the African Regionthat have not yet done so to make contributionsfor the extension of the Regional Office accom-modation ;
2. AUTHORIZES the Director -General, notwith-standing the provisions of Part II, paragraph 1 (2)of resolution WHA13.41, to advance from theWorking Capital Fund an amount not exceeding$100 000 to be credited to the African RegionalOffice Building Fund to help finance the said cons-truction, reimbursement to the Working Capital Fundof the sum so advanced to be provided for, ifnecessary, in the programme and budget estimatesfor 1965.
2. REPORT BY THE DIRECTOR- GENERAL
1. In his report on this subject to the FifteenthWorld Health Assembly 1 the Director -General statedthat the transfer of property rights in the Djoué Estatefrom the French Government to the World HealthOrganization had taken place. He drew attention tothe need for an extension of the regional office building,indicating that such extension was tentatively estimatedto cost about $600 000. Toward the cost of thisextension certain governments of Africa had at thatdate pledged slightly more than $182 000 and provisionin the amount of $100 000 had been included in theproposed programme and budget estimates for 1963.2. The Health Assembly, in resolution WHA15.14,authorized the Director -General " to proceed withthe construction of an extension to the existingbuilding for the Regional Office for Africa " and " toadvance from the Working Capital Fund an amountnot exceeding $300 000 to be credited to the AfricanRegional Office Building Fund, to help finance thesaid construction, reimbursement to the WorkingCapital Fund of the sum so advanced to be providedfor, if necessary, in the programme and budgetestimates for 1964 ".3. In the Appropriation Resolution for the financialyear 1963 (WHA15.42) the Fifteenth World HealthAssembly included the sum of $100 000 requestedby the Director -General toward the constructioncost.4. Since the Fifteenth World Health Assembly thearchitect has been developing detailed plans for theextension of the building in consultation both withregional office officials and those at headquartersconcerned with the planning of office space. Thearchitect has also prepared revised preliminaryestimates of the cost of the work in the light of currentconstruction costs in Brazzaville. Because of risingcosts for such work in Africa, as elsewhere, and becauseof certain modifications in the original plans in the
3 Off. Rec. Wld Hllh Org. 118, Annex 10.
[AI 6/AFL/7 - 29 April 1963]
interest of the most effective utilization of the addi-tional space, the total estimated cost of the work isnow approximately $700 000.5. The revised preliminary plans are virtually com-pleted and it is anticipated that detailed drawings willbe finished during 1963; on the basis of these it willbe possible to obtain bids. At that time the finalcost can be more accurately determined.
6. As of 25 April contributions from Member govern-ments had been received or pledged in a total amountof $301 846, as set forth in the appendix to this report.These contributions, together with the $100 000provided for in the 1963 budget, represent total creditsof $401 846 towards the presently anticipated cost of$700 000. The balance required remains within thesum of $300 000 which the Assembly authorized theDirector -General to advance as necessary from theWorking Capital Fund.7. It appears clear now that recourse to this autho-rization will have to be had, and the Director -Generalhas made provision in the 1964 budget to reimburse theWorking Capital Fund in that year in the amount of$200 000, which was the amount estimated to berequired when the proposed programme and budgetestimates were prepared. Since construction workcan hardly begin before early 1964, it is assumedthat the balance of the authorization, i.e., $100 000,which it might be necessary to advance from the Work-ing Capital Fund could be reimbursed in 1965. Sinceit appears that a new authorization should be providedfor this purpose, the Director -General would suggestthat the Health Assembly consider a resolution alongthe lines of resolution WHA15.14 with the amountof $100 000 being substituted for the figure of $300 000and the year 1965 replacing 1964. Obviously, to theextent that additional contributions become available,and depending upon the ultimate cost of the work,these advances from the Working Capital Fund andconsequent reimbursements would be reduced.
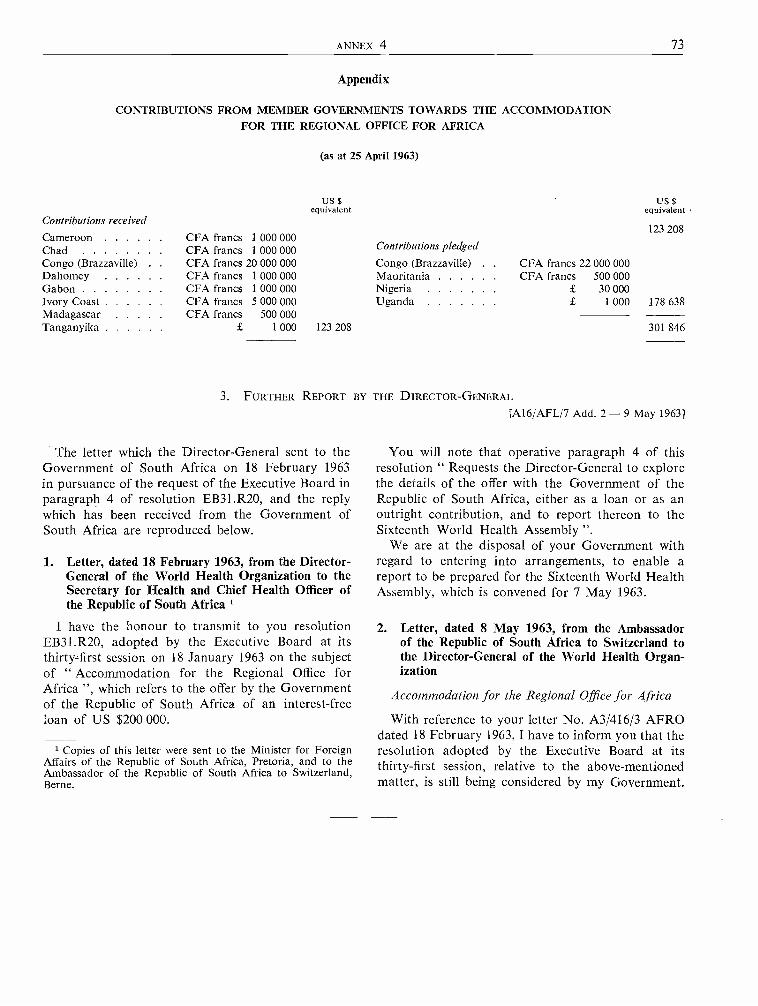
ANNEX 4 73
Appendix
CONTRIBUTIONS FROM MEMBER GOVERNMENTS TOWARDS THE ACCOMMODATIONFOR THE REGIONAL OFFICE FOR AFRICA
(as at 25 April 1963)
Contributions received
US $equivalent
Us$equivalent
123 208Cameroon CFA francs 1 000 000Chad CFA francs 1 000 000 Contributions pledged
Congo (Brazzaville) CFA francs 20 000 000 Congo (Brazzaville) . . CFA francs 22 000 000Dahomey CFA francs 1 000 000 Mauritania CFA francs 500 000Gabon CFA francs 1 000 000 Nigeria £ 30 000Ivory Coast CFA francs 5 000 000 Uganda £ 1 000 178 638Madagascar CFA francs 500 000
301 846Tanganyika £ 1 000 123 208
3. FURTHER REPORT BY THE DIRECTOR - GENERAL
[A16 /AFL /7 Add. 2 -9 May 1963]
The letter which the Director -General sent to theGovernment of South Africa on 18 February 1963in pursuance of the request of the Executive Board inparagraph 4 of resolution EB31.R20, and the replywhich has been received from the Government ofSouth Africa are reproduced below.
1. Letter, dated 18 February 1963, from the Director -General of the World Health Organization to theSecretary for Health and Chief Health Officer ofthe Republic of South Africa 1
I have the honour to transmit to you resolutionEB31.R20, adopted by the Executive Board at itsthirty -first session on 18 January 1963 on the subjectof " Accommodation for the Regional Office forAfrica ", which refers to the offer by the Governmentof the Republic of South Africa of an interest -freeloan of US $200 000.
1 Copies of this letter were sent to the Minister for ForeignAffairs of the Republic of South Africa, Pretoria, and to theAmbassador of the Republic of South Africa to Switzerland,Berne.
You will note that operative paragraph 4 of thisresolution " Requests the Director -General to explorethe details of the offer with the Government of theRepublic of South Africa, either as a loan or as anoutright contribution, and to report thereon to theSixteenth World Health Assembly ".
We are at the disposal of your Government withregard to entering into arrangements, to enable areport to be prepared for the Sixteenth World HealthAssembly, which is convened for 7 May 1963.
2. Letter, dated 8 May 1963, from the Ambassadorof the Republic of South Africa to Switzerland tothe Director -General of the World Health Organ-ization
Accommodation for the Regional Office for Africa
With reference to your letter No. A3/416/3 AFROdated 18 February 1963, I have to inform you that theresolution adopted by the Executive Board at itsthirty -first session, relative to the above -mentionedmatter, is still being considered by my Government.
74 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Annex 5
MALARIA ERADICATION SPECIAL ACCOUNT 1
REPORT BY THE DIRECTOR - GENERAL
1. Introduction
The Fifteenth World Health Assembly, in para-graph 3 of resolution WHA15.34, reiterated " itsconviction that continued voluntary contributionsin cash and in kind are essential for accelerating themalaria eradication programme " and in paragraph 5requested " the Director - General to continue hisefforts as in the past for increasing voluntary contri-butions to the Malaria Eradication Special Accountand to report on this matter regularly to the HealthAssembly ".
2. Status of the Malaria Eradication Special Account
2.1 Contributions received or pledged from theinception of the Special Account up to 30 April 1963are shown in Appendix 1 to this report.2.2 To complete the information on the voluntarycontributions made to finance the world malariaeradication programme, the contributions receivedby and /or pledged to the Pan American Health Organi-zation's Special Malaria Fund up to 30 April 1963are shown in Appendix 2.2.3 As at 30 April 1963 the status of the MalariaEradication Special Account was as follows :
Balance carried forward on 1 January
Us$ Uss
1963 1 241 874Contributions received from 1 January to
30 April 1963 1 565 441Contributions from the regular budget for
1963 4 000 000Income from the Malaria Eradication
Postage Stamp Plan from 1 January to30 April 1963 2 10520 6 817 835
Less:
Estimated obligations for " regular "malaria eradication field operationsin 1963 5 518 000
Estimated balance available 1 299 835
1 See resolution WHA16.17.2 Derived from promised donations in cash; excludes proceeds
from the sale of stamps through the Organization in 1963 forwhich the return has not yet been received.
[A16 /AFL /11 -3 May 1963]
2.4 In addition, as shown in Appendix 1, there arepledges amounting to $1 169 698 ($1 035 700 in cashand $133 998 in kind); the cash portion includes$1 000 000 pledged by the United States of America.2.5 The financing of the " regular " malaria eradi-cation operations for the year 1963 is thus assured.As for the year 1964, the full cost of the " regular "eradication operations is included in the proposedregular budget estimates in accordance with resolutionWHA14.15.
2.6 The estimated balance of $1 299 835 shown inparagraph 2.3 is available for implementing a portionof the " accelerated " programme, estimated at$2 115 000 in 1963 3 and at $4 360 000 in 1964.3 Theimplementation of projects of the programme desig-nated as " accelerated " will depend upon theamounts available from voluntary contributions. TheDirector -General will set aside funds not only for thecurrent year's obligations, but also for continuingcommitments for the ensuing year. Consequently fundsin hand will be used to meet obligations either up to thecompletion of any individual activity approved forimplementation within a period of two years, or upto such appropriate phase of the activity as is decidedin each instance, depending upon its nature. Byfinancing " accelerated " activities in this manner, theOrganization will avoid a situation whereby anyfuture costs of such activities started would ipsofacto have to be financed by recourse to the regularbudget.
3. Importance of Continued Voluntary Contributions
3.1 The funds for financing the " regular " malariaeradication field operations for the year 1963 beingassured, and assuming that the Sixteenth WorldHealth Assembly will implement the recommendationscontained in resolution WHA14.15 concerning theincorporation in the regular budget of the full costof the " regular " malaria eradication field programmefor the year 1964, voluntary contributions will continueto be necessary for financing the " accelerated "portion of the programme3.2 The advantages of a more rapid and broader im-
3 Off: Rec. Wld Hlth Org. 121, 402.

ANNEX 5 75
plementation of the eradication campaign have been re-cognized by the Fourteenth and Fifteenth World HealthAssemblies (resolutions WHA14.27, WHA15.20 andWHA15.34). The Executive Board at its thirty -firstsession, recalling the relevant provisions of resolutionsWHA15.20 and WHA15.34 on the acceleration ofthe malaria eradication programme from continuedvoluntary contributions, appealed " to Members whoare in a position to do so to make voluntary contri-butions to the Malaria Eradication Special Accountin order to make it possible to implement the pro-gramme operations planned to be financed fromthat account " (resolution EB31.R26).
3.3 Mention was made in paragraph 2.6 above ofthe expenditure planned for the " accelerated "operations in 1963 and in 1964, which total $6 475 000.These funds, if obtained, would contribute primarilyto the promotion of pre- eradication projects inAfrica; they would also be used for the undertakingof new malaria eradication projects and the speeding -up of some projects already under way.
3.4 It will be recognized that any increased assistancewhich the Organization is in a position to offer to themalarious countries encourages them to make addi-tional efforts in the health field. There is no need toemphasize the importance of this as the health needsand the requirements for health investments in thedeveloping countries are well known.
4. Fund- raising
4.1 As requested by the Executive Board in reso-lutions EB29.R27 and EB31.R26, and by the WorldHealth Assembly in resolution WHA15.34, theDirector -General has pursued his efforts to obtainvoluntary contributions from governments, voluntaryhealth organizations, foundations, industries, labourorganizations, institutions and individuals, along thelines described in his earlier reports on the SpecialAccount.
4.2 A limited number of countries have respondedto WHO's reiterated appeals for voluntary funds.It is thanks to their generosity that the carrying -outof the malaria eradication programme was madepossible during the period when the programme waswholly financed from voluntary contributions; theircontributions have also assisted in the transfer of theprogramme to the regular budget by stages. It ishoped now that all Members of the Organization,and particularly the economically more advancedcountries, realizing the advantages of a more rapidimplementation of the global eradication programmein terms of its final outcome and of eventual savingsin the total cost of eradication, will make an effort toprovide the Malaria Eradication Special Accountwith the necessary means for financing the " accele-rated " operations as planned.
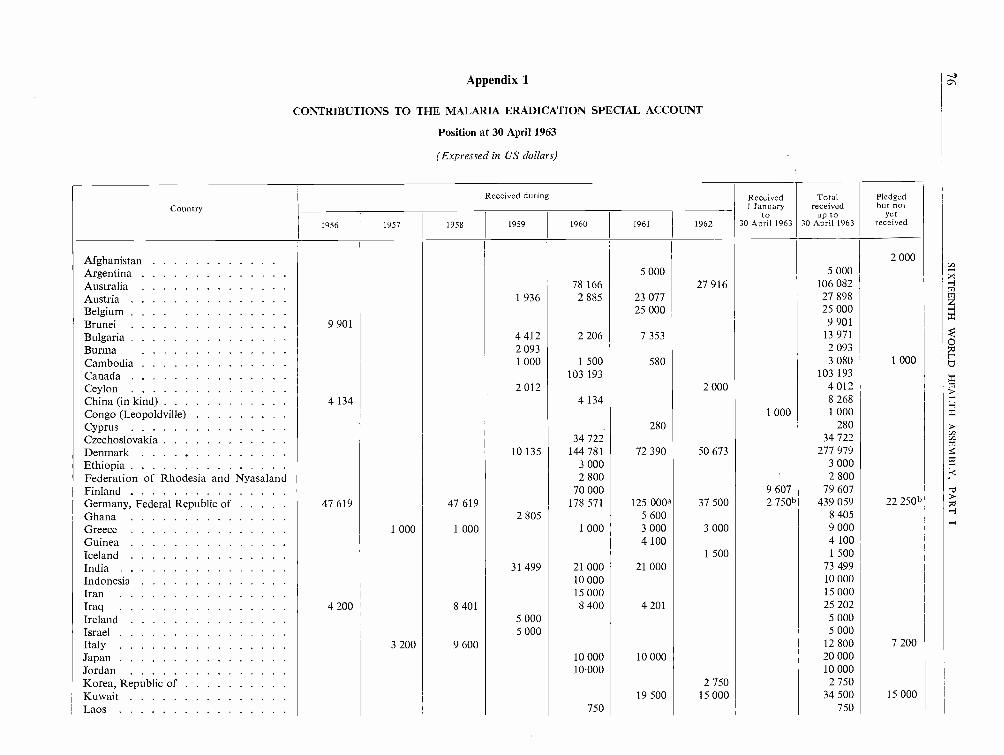
Appendix 1
CONTRIBUTIONS TO THE MALARIA ERADICATION SPECIAL ACCOUNT
Position at 30 April 1963
(Expressed in US dollars)
Country
Received during Received1 January
to30 April 1963
Totalreceived
up to30 April 1963
Pledgedbut not
yet
received1956 1957 1958 1959 1960 1961 1962
Afghanistan 2 000
Argentina 5 000 5 000
Australia 78 166 27 916 106 082
Austria 1 936 2.885 23 077 27 898
Belgium 25 000 25 000
Brunei 9 901 9 901
Bulgaria 4 412 2 206 7 353 13 971
Burma 2 093 2 093
Cambodia 1 000 1 500 580 3 080 1 000
Canada 103 193 193
Ceylon 2 012 2 000 4 012
China (in kind) 4 134 4 134 8 268
Congo (Leopoldville) 1 000 1 000
Cyprus 280 280
Czechoslovakia 34 722 34 722
Denmark 10 135 144 781 72 390 50 673 277 979
Ethiopia 3 000 3 000
Federation of Rhodesia and Nyasaland 2 800 2 800
Finland 70 000 9 607 79 607
Germany, Federal Republic of 47 619 47 619 178 571 125 000a 37 500 2 750b 439 059 22 250b
Ghana 2 805 5 600 8 405
Greece 1 000 1 000 1 000 3 000 3 000 9 000
Guinea 4 100 4 100
Iceland 1 500 1 500
India 31 499 21 000 21 000 73 499
Indonesia 10 000 10 000
Iran 15 000 15 000
Iraq 4 200 8 401 8 400 4 201 25 202
Ireland 5 000 5 000
Israel 5 000 5 000
Italy 3 200 9 600 12 800 7 200
Japan 10 000 10 000 20 000
Jordan 10"000 10 000
Korea, Republic of 2 750 2 750
Kuwait 19 500 15 000 34 500 15 000
Laos 750 750

LebanonLibyaLuxemburgMalaya, Federation ofMoroccoNepal
2 242 1
1
577500
1
2
581
000
2
4
262
257
1
4
1
598
217
000
4
2
3
524
000
000
13 7841 5002 0008 4745 0001 000
Netherlands 27 624 27 624
New Zealand 28 000 28 000 2 800 58 800
Nigeria 280 8 512 17 020 25 812
Norway 100 140 100 140
Pakistan 10 000 20 000 30 000
Philippines 5 000 5 000
Poland (in kind) 83 333 83 333
Portugal 10 000 10 000
Romania 20 000 20 000
Saudi Arabia 4 500 5 000 5 000 14 500
Sierra Leone 280 280
Sudan 3 012 2 869 5 000 10 881
Sweden 19 331 135 318 154 649
Switzerland 23 256 46 296 46 296 115 848
Thailand 1 507 2 007 3 514
Tunisia 2 000 2 000 2 000 2 000 2 017 10 017
Turkey 35 714 7 111 42 825
Union of Soviet Socialist Republics (in kind) 82 500 250 000 164 474 496 974 57 748
United Arab Republic 22 523 22 523
United States of America 5 000 000 6 000 000 4 000 000 1 500 000 16 500 000 1 000 000Upper Volta 4 069 4 069
Viet -Nam, Republic of 2 000 1 000 3 000
Yugoslavia 3 000 25 000 2 000 30 000
Holy See 1 000 1 000 2 000 4 000
Totals - Countries 68 096 5 046 003 167 620 6 260 880 1 157 570 4 356 495 571 664 1 561 670 19 189 998 1 105 198
Miscellaneous gifts :MISEREOR (German Bishops' cam-
paign) 100 000 100 000
German Red Cross in the GermanDemocratic Republic (in kind) . . . 1 400 1 400 54 000
Sundry 906 1 886 23 886 44 747 7 599 10 473 3 771 93 268 10 500
United Kingdom Committee for WHO 6 900 6 900
Totals - Voluntary Contributions 68 096 5 046 909 169 506 6 284 766 1 202 317 4 464 094 590 437 1 565 441 19 391 566 1 169 698
Transfer from the regular budget . . . . 2 000 000 ° 4 000 000d 6 000 000
GRAND TOTALS 68 096 5 046 909 169 506 6 284 766 1 202 317 4 464 094 2 590 437 5 565 441 25 391 566 1 169 698
a Of which $37 500 in kind.b In kind.C In accordance with resolution WHA14.43.d In accordance with resolution WHA15.42.

Appendix 2
CONTRIBUTIONS TO THE SPECIAL MALARIA FUND OF THE PAN AMERICAN HEALTH ORGANIZATION
Position at 30 April 1963
(Expressed in US dollars)
Country
1956
Colombia aDominican RepublicHaitiUnited States of AmericaVenezuela
Totals (cash)
GRAND TOTAL (cash and pledged)
Received during Totalreceived
up to30 April 19631957 1958 1959 1960 1961 1962 1963
5 000 5 000100 000 100 000 200 000
5 000 5 000
3 500 000 5 000 000 1 500 000 1 000 000 1 000 000 12 000 000
299 400 299 400
3 899 400 105 000 5 000 000 1 505 000 1 000 000 1 000 000 12 509 400
Pledgedbut not
yetreceived
300 000
300 000
12 809 400
a This contribution was reported to the Fourteenth World Health Assembly as a pledge to the Malaria Eradication Special Account of the World Health Organization,but it was subsequently ascertained that the contribution was intended for the Special Malaria Fund of the Pan American Health Organization.

ANNEX 6 79
Annex 6
MALARIA ERADICATION POSTAGE STAMPS[A16 /AFL /13 Rev. 1 - 11 May 1963]
REPORT BY THE DIRECTOR -GENERAL
1. Background and Purpose
1.1 The plan for the issue of malaria eradicationpostage stamps was conceived as a part of the con-tinuing efforts to disseminate information on andstimulate interest in the campaign against malaria.2In addition to this main objective, the plan wasdeveloped with a secondary objective, i.e., as apotential source of income for the world malariaeradication programme. The date of issue recom-mended was 7 April 1962, but any other date before31 December 1962 was considered satisfactory. Inaccordance with the decisions of the Executive Board 3and the Fifteenth World Health Assembly 4 the issuesmade after 31 December 1962 are not consideredas part of the Organization's malaria eradicationpostage stamp plan.
2. Participation
2.1 The total number of participants was 114. Outof these, ninety -eight postal administrations issuedone or more postage stamps commemorating themalaria eradication programme; some of them alsoissued related philatelic material, e.g., souvenirsheets, first -day covers, etc.; sixteen postal administra-tions participated by providing special cancellations.Eighty -three countries and territories made or promiseddonations either in stamps, philatelic material, and /orin cash.
2.2 The number of Members of the Organizationthat participated is shown by regions, in Appendix 1,part 1.
2.3 The list of the participants, with the dates ofissue of their stamps and related philatelic materialunder the World Health Organization's malariaeradication postage stamp plan, is given in Appendix 1,part 2.
1 See resolution WHA16.18.2 Resolutions EB26.R10, WHA14.27 and EB28.R27.3 Resolutions EB29.R28 and EB31.R41.4 Resolution WHA15.47.
3. Publicity for the Malaria Eradication Programme
3.1 Thanks to the large participation in this philatelicproject, millions of stamps and special cancellationshave been transmitting to all parts of the world anappeal for united efforts against the world's mostwidespread and costliest disease, as nearly all of themcarry the slogan " The World United AgainstMalaria ". The special cancellation slogan in theUnited Kingdom of Great Britain and NorthernIreland only, according to the official estimates, wasapplied on about 200 million items of mail; over100 000 items of mail were daily imprinted with theantimalaria slogan in Geneva during the week7 -14 April 1962; the United States of America issued100 million antimalaria stamps, the Republic ofViet -Nam 7 million, Nigeria 4.8 million, Czecho-slovakia 4.45 million, Poland 3.75 million, India3.5 million -to give but a few illustrations. Whiledrawing the attention of the populations of the moreprivileged nations to the problem of malaria, thesenumerous philatelic items, at the same time, have beentelling the peoples of the malarious countries that therest of the world does not forget their struggle forbetter health.
3.2 The issue of antimalaria postage stamps receivedconsiderable coverage in the press. Items in the pressranged from articles and features to official statementson and announcements of individual issues. Medicalpublications also carried articles in connexion withantimalaria stamps. A review of the clippings receivedin headquarters gives an indication of the publicityobtained in the press. In 1958, the year of the extensionof malaria eradication operations on a world -widescale, the clippings received in headquarters fromthirty -three countries contained 371 articles aboutmalaria. In 1962, the Division of Public Informationhas recorded, in the press of thirty countries fromwhich the Division receives clippings, 1529 articleson the malaria eradication stamp campaign and theeradication programme or the problem of malariain general.
3.3 Many postal administrations, in advertising theirmalaria eradication commemorative issues, includedinformation and data about malaria and the eradica-tion programme in their respective bulletins and

80 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
pamphlets. The narratives on malaria were usuallyprepared with the assistance of WHO staff. Thousandsof such bulletins and pamphlets were distributedthroughout the world.
3.4 The International Boy Scout Movement, Canada,and the Hobbies Committee in the United Statesof America endeavoured, through their own meansand channels, to publicize the malaria eradicationstamp plan as an illustration of the world solidarityin combating malaria.
3.5 Several chemical and pharmaceutical companiescontributed to the efforts to spread information aboutmalaria by printing and distributing brochures orillustrated features relating to the issue of malariaeradication stamps, coloured stamp illustrated folders,articles with coloured stamp reproductions, advertise-ments with the design of the model stamp, etc.
3.6 Twelve press releases on the malaria eradicationstamp plan, prepared by headquarters, were distributedin 42 000 copies. Regional offices and the LiaisonOffice with the United Nations also issued a numberof press releases. The extra issue of the magazineWorld Health, devoted to malaria, which was printedin November 1961 in 97 000 copies, was exhaustedby early 1962. A new special issue was printed inJune 1962 to meet the increased demand for documen-tation on malaria. As at 31 December 1962, 103 000copies of the latter had been distributed.
3.7 Other mass information media also gave a greatdeal of attention to malaria eradication stamps.Radio and television stations all over the world carriedthe message " The World United Against Malaria "and arranged for special programmes, the centraltheme of which was the battle against malaria. Forthis purpose, headquarters sent printed and visualmaterial and included items concerning malaria inWHO feature programmes. The Philatelic Agencyfor Malaria Eradication Postage Stamps, the Organi-zation's sales agent, at its own expense, produced720 short television films and 3810 phonographrecords. The Agency distributed, mostly to radio andtelevision stations for the " Stamp Out Malaria "programme, thousands of kits containing copies ofthese films, records, slides, information material, etc.
3.8 The Advertising Council in the United States ofAmerica (a non -profit, public service organization)authorized and recommended the malaria eradicationstamp programme to be broadcast by radio andtelevision stations throughout the country. As aresult, during 1962 radio and television stations in theUnited States, including the major national networks,daily publicized the malaria eradication programmeand appealed to the public to support antimalaria
work. A thirty- minute programme produced by theSwiss Broadcasting Corporation (Société romandede Radio -diffusion, Studio de Lausanne), withrecorded material collected on the spot in Africa,was broadcast by thirty -two national networks totallingforty -five transmitters of the Communauté des pro-grammes de langue française (including France,Belgium, Switzerland, Luxembourg, Monaco, Canada,countries and territories in Africa, Asia, Oceania,Latin America and the Caribbean area). Althoughno appeal for funds was made, a sum of Sw. Fr. 6132.20was donated by listeners and placed to the credit ofthe Malaria Eradication Special Account. A similartelevision programme of the same duration, entitledLes Esclaves de la Fièvre (The Slaves of Fever) wasdistributed by Eurovision to be shown in the UnitedKingdom (BBC), Sweden, Denmark, the Netherlandsand Switzerland. The opening of the " MALAREX" ex-hibition in the Palais des Nations was covered by theSwiss and French television, the latter having sent a teamfrom Paris to prepare a special programme on the sub-ject. A radio feature on the malaria eradication opera-tions in North Borneo, with an on- the -spot report, wasaccepted by nineteen radio stations in different partsof the world. The estimated advertising value of thesebroadcasts, if paid for at the current commercialrates, would amount to several hundred thousanddollars.
3.9 Exhibitions of the malaria eradication postagestamps and related philatelic material commemoratingthe world malaria eradication programme includedthose organized in Belgium (Brussels and Charleroi);the Federal Republic of Germany (Essen, Hamburg,Munich); France (Evian); the Republic of Korea(Seoul); India (Madras); Iran (Teheran); Philippines(Manila); Switzerland (Geneva); United States ofAmerica (Baltimore, Chicago, Los Angeles, Minnea-polis, New York, Philadelphia, Washington). Otherstamps and philatelic material displayed on theoccasion of some of those exhibitions illustrated thehistory of WHO and its daily, often little known, work.
3.10 Arrangements were made for the exhibition ofantimalaria stamps at the Century -21- Exhibition inSeattle, the Do- It- Yourself Exhibition in Londonand the Great Toronto Stamp and Coin Show inToronto. Antimalaria stamps were also exhibited attraditional philatelic exhibitions, such as ASDAStamp Show in New York, Europa 62 in Naples,Italy, INTERPEX in New York, NASPEX in LongIsland, PRAGA 62 World Exhibition of PostageStamps in Prague, SOJEX 1962 in Atlantic City,STAMPEX in London. Some of those world- famousphilatelic events were held in 1962 under the sloganof the antimalaria campaign. A number of other
ANNEX 6 81
philatelic exhibitions displayed antimalaria stamps,such as : EXPHISALM -62 in Vielsalm, Belgium;BEPEX in Bergen County, United States of America;the exhibition of the Philatelic Club in Ypres, Belgium;the First Philatelic Exhibition in Bangalore, India;the Dundee and District Philatelic Society in Dundee,United Kingdom, etc. Malaria eradication stampswere also displayed in various Brazilian towns,Multan Cantonment in Pakistan, in Manatee CountyStamp Club and Eureka Stamp Society in Bradenton,United States of America, in Venezuela, etc. All thesedisplays, attended by hundreds of thousands of visitors,highlighted the problem of malaria and the effortsmade to free the world from this disease.
3.11 Ceremonies took place in some capital citieson the day of issue, and at the United Nations head-quarters in New York on the occasion of the issueof the United Nations antimalaria stamps on 30 March1962. A special message from the President of theUnited States of America was read at the ceremonyheld in Washington. In Teheran a donation ceremonywas organized at which the stamps were handed to theWHO representative. The Government of the Republicof Viet -Nam indicated its interest in setting up apermanent exhibition of malaria eradication stampsin its malaria headquarters.
3.12 The foregoing account of the publicity activitiesand events resulting from the malaria eradicationstamp plan is far from being exhaustive, but it issufficient evidence that this plan has made anappreciable contribution to the spreading of informa-tion on malaria and the stimulation of public interestin the battle against malaria. The intensified world-wide publicity about the problem of malaria coincideswith the Organization's efforts to obtain continuingvoluntary support for the acceleration of the eradica-tion programme, as approved by the Fourteenth andFifteenth World Health Assemblies.
4. Donations
4.1 Of the eighty -three countries and territorieswhich made or promised donations in connexionwith the issue of antimalaria stamps, sixty -one donatedquantities of stamps and some quantities of relatedphilatelic material; one country, which did notissue antimalaria stamps, donated envelopes with aspecial cancellation; twenty -one promised the proceedsfrom the surcharge or a percentage of the proceedsfrom the sale of stamps. The list showing the donorcountries and territories, the denominations andnumber of series received as well as donations incash promised and /or received is given in Appendix 2.
4.2 The value of the postage stamps and relatedphilatelic items sold as at 31 March 1963 amounted toUS $203 271, from which there is to be deducted thesales agent's commission of $30 491. Thus, US$172 780was transferred to the Malaria Eradication SpecialAccount, together with US $22 094 representing thecash donations received, making a total of US$194 874.
4.3 There still remain quantities of unsold stampsand related philatelic items. This in part is due to thefact that in many instances the donated stampsreached the Organization's consignee in New Yorklong after the date of issue, when the demand on thephilatelic market was already met to a large extent.The sale of this material continues, but the saleprospects do not seem particularly promising. Theclosing date for sale will be fixed some time in 1963and will be announced at least one month in advance.
5. Planning and Execution of the Malaria EradicationStamp Plan
5.1 Some information on the organizational andadministrative aspects of this undertaking and thework involved is given in Appendix 3.
6. Termination of the Project
6.1 In a report to the thirty -first session of theExecutive Board the Director -General outlined theaction to be followed for the termination of theOrganization's malaria eradication postage stampplan. Subsequently that report was transmittedto all Members. The final list of participants, with thedates of issue of their stamps and related philatelicmaterial making part of this stamp plan, and the listof donations (Appendices 1 and 2) have beenestablished according to the envisaged procedure.As mentioned in paragraph 4.3 above, the closure ofthe sale will take place during 1963.
6.2 The countries which withdraw their antimalariastamps before the closing date of the sale are expectedto inform the Organization, which will then alsowithdraw the stamps concerned from its own sale.
6.3 All stamps and related philatelic items remainingunsold on the closing date of the WHO sale will bedestroyed in accordance with Article V(a) of theAgreement between WHO and the Inter -GovernmentalPhilatelic Corporation in the presence of a witnessappointed by WHO. A copy of the relevant certificatewill be transmitted to the governments concerned.
6.4 The final financial account of income and expend-iture is expected to be submitted to the thirty -thirdsession of the Executive Board and to the SeventeenthWorld Health Assembly.
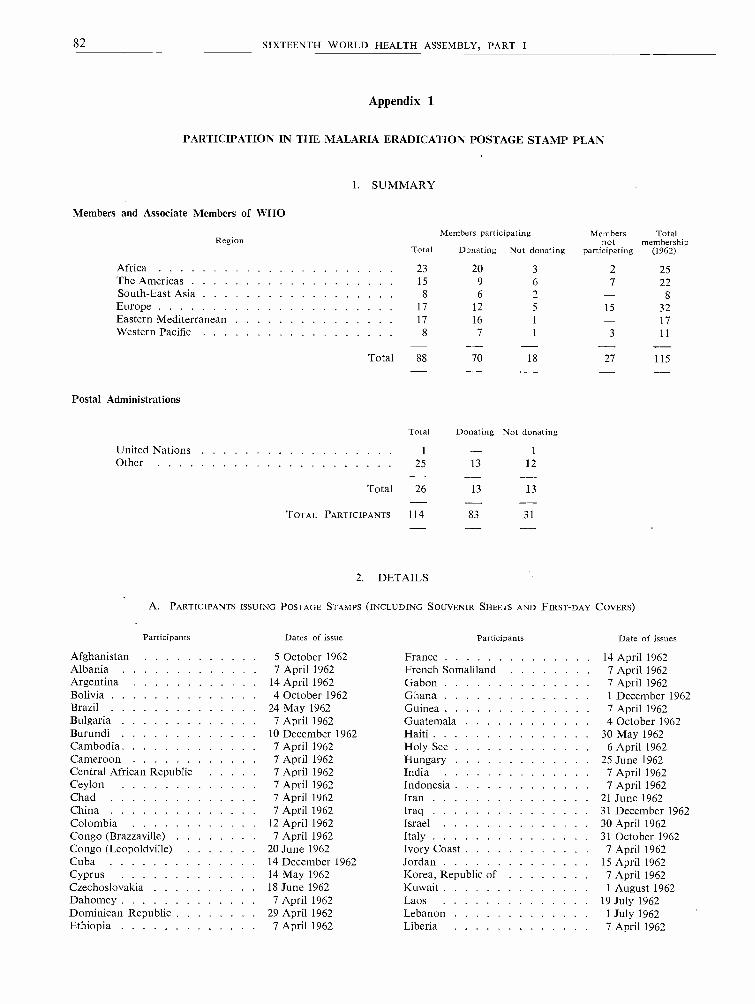
82 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Appendix 1
PARTICIPATION IN THE MALARIA ERADICATION POSTAGE STAMP PLAN
I. SUMMARY
Members and Associate Members of WHO
RegionTotal
Members participating
Donating Not donating
Membersnot
participating
Totalmembership
(1962)
Africa 23 20 3 2 25The Americas 15 9 6 7 22South -East Asia 8 6 2 - 8Europe 17 12 5 15 32Eastern Mediterranean 17 16 1 - 17Western Pacific 8 7 1 3 11
Total 88 70 18 27 115
Postal Administrations
United Nations
Total
1
Donating
-Not donating
1
Other 25 13 12
Total 26 13 13
TOTAL PARTICIPANTS 114 83 31
2. DETAILS
A. PARTICIPANTS ISSUING POSTAGE STAMPS (INCLUDING SOUVENIR SHEETS AND FIRST -DAY COVERS)
Participants Dates of issue Participants Date of issues
Afghanistan 5 October 1962 France 14 April 1962Albania 7 April 1962 French Somaliland 7 April 1962Argentina 14 April 1962 Gabon 7 April 1962Bolivia 4 October 1962 Ghana 1 December 1962Brazil 24 May 1962 Guinea 7 April 1962Bulgaria 7 April 1962 Guatemala 4 October 1962Burundi 10 December 1962 Haiti 30 May 1962Cambodia 7 April 1962 Holy See 6 April 1962Cameroon 7 April 1962 Hungary 25 June 1962Central African Republic 7 April 1962 India 7 April 1962Ceylon 7 April 1962 Indonesia 7 April 1962Chad 7 April 1962 Iran 21 June 1962China 7 April 1962 Iraq 31 December 1962Colombia 12 April 1962 Israel 30 April 1962Congo (Brazzaville) 7 April 1962 Italy 31 October 1962Congo (Leopoldville) 20 June 1962 Ivory Coast 7 April 1962Cuba 14 December 1962 Jordan 15 April 1962Cyprus 14 May 1962 Korea, Republic of 7 April 1962Czechoslovakia 18 June 1962 Kuwait 1 August 1962Dahomey 7 April 1962 Laos 19 July 1962Dominican Republic 29 April 1962 Lebanon 1 July 1962Ethiopia 7 April 1962 Liberia 7 April 1962

ANNEX 6 83
Participants
LibyaLiechtensteinMadagascarMalaya, Federation ofMaldive IslandsMaliMauritaniaMexicoMonacoMongoliaMoroccoNepalNicaraguaNigerNigeriaPakistanPanamaPanama Canal ZonePapua and New GuineaParaguayPhilippinesPolandPortugal 1Ryukyu Islands
Dates of issue
7 April 19622 August 19627 April 19627 April 19627 April 19627 April 19627 April 1962
30 May 19626 June 19628 July or August 19623 September 19627 April 1962
27 July 19627 April 19627 April 19627 April 19623 May 1962
24 September 19627 April 1962
23 May 196224 October 1962
1 October 196212 March 19627 April 1962
Participants Dates of issue
Saudi Arabia 7 May 1962Senegal 7 April 1962Sierra Leone 7 April 1962Somalia 25 October 1962Spain 21 December 1962Sudan 7 April 1962Surinam 2 May 1962Swaziland 2 24 April 1962Switzerland 19 March 1962Syria 7 April 1962Thailand 7 April 1962Togo 2 June 1962Tunisia 7 April 1962Turkey 7 April 1962Union of Soviet Socialist Republics 6 May 1962United Arab Republic 20 June 1962United Nations Postal
Administration 30 March 1962United States of America 30 March 1962Upper Volta 7 April 1962Venezuela 20 December 1962Viet -Nam, Republic of 7 April 1962Yemen 20 June 1962Yugoslavia 7 April 1962
B. PARTICIPANTS ISSUING SPECIAL CANCELLATIONS ONLY
Austria (Bregenz Post Office) . . .
British GuianaBritish Solomon Islands ProtectorateBurmaCanada
Denmark
East African Postal Administration -Kenya, Tanganyika and Uganda .
Country
Afghanistan
3 September 19627 April 19628 May 19627 April 19621 April 1962
17 April 196216 August 1962
AlbaniaBoliviaBrazilBulgariaBurundi
CambodiaCeylonChinaColombia
2 April 1962
Federation of Rhodesia and NyasalandFrench PolynesiaMaltaNew ZealandSingaporeUnited Kingdom of Great Britain and
Northern IrelandZanzibar
Appendix 2
DONATIONS TO WHO UNDER THE PLAN
A. STAMPS AND RELATED PHILATELIC MATERIAL
Denominations of stamps
2, 2, 5, 10 and 15 puts25, 50, 75, 100 150 and 175 puts0.10, 0.11, 1.50 and 2.50 leks600 and 2 000 bolivianos21 cruzeiros5 and 20 stotinki8 and 50 francs58 francs (first -day covers)2, 4 and 6 riels0.25 Ceylonese rupee0.80 and 3.60 new Taiwan dollars0.20, 0.40, 0.50, 1 and 1.45 pesos(first -day covers) without stamps
1 Eight overseas provinces each issued one postage stamp.2 Malaria control.
7 April 19622 April 19627 April 19626 April 19627 April 1962
1 August 1962April 1962
Number ofseries donated
1 040800
1 0002 000
100 00010 0003 000
4906 000
100 000100 000
10 0001 000

84 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Country Denominations of stampsNumber of
series donated
Cuba 1, 2 and 3 centavos 100 000Cyprus 10 and 30 mils 25 000Czechoslovakia 0.60 and 3 korunas 5 000
0.60 and 3 korunas (souvenir sheets) 4 9980.60 and 3 korunas (first -day covers) 10 000
Denmark 12 ore envelopes 4 967Ethiopia 0.15, 0.30 and 0.60 Ethiopian dollars 30 000Guinea 25, 50 and 100 Guinea francs 15 000
100 Guinea francs (souvenir sheets) 2 000Haiti 50 centimes 99 960
50 centimes (airmail) 100 0645 centimes 96 00010 centimes 99 96420 centimes 99 8561 gourde 100 0042 gourdes (souvenir sheets) 25 000
Holy See 15, 40, 70 and 300 lire 100 00015, 40, 70 and 300 lire (first -day covers) 35 000
Hungary 2.5 forints 2 0004 stamps at 2.5 forints (souvenir sheets) 1 000
Indonesia 0.40, 1.50, 3 and 6 Indonesian rupiahs 100 000Iran 2, 6 and 10 rials 16 650
18 rials (first -day covers) 11 627envelopes with cancelled 18 rials stamps 16 435
Israel " 0.25 Israeli pound 20 0000.25 Israeli pound (first -day covers) 5 000
Jordan 0.015 and 0.035 Jordanian dinar 165 0000.050 Jordanian dinar (first -day covers) 34 837
Korea, Republic of 40 hwan 100 00040 hwan (souvenir sheets) 100 000
Kuwait 4 and 25 fils 40 000Laos 4, 9 and 10 kips 20 000Lebanon 30 and 70 piastres 24 999Liberia 25 cents and 25 cents airmail 20 000Libya 15 and 50 milliemes 60 000
15 and 50 milliemes (imperforated stamps) 4 00015 and 50 milliemes (souvenir sheets) 3 000
Liechtenstein 0.50 Swiss franc 100 0000.50 Swiss franc (first -day covers) 10 000
Malaya, Federation of 0.25, 0.30 and 0.50 Malayan dollar 50 000Maldive Islands 2, 3, 5, 10, 15, 25, 50 larees and 1 rupee 5 000Mexico 0.40 peso 40 000
0.20 peso (mental health stamps) 20 000Mongolia 1, 5, 10, 15, 20, 30, 40, 50 mongo 1 000 *Morocco 0.20 and 0.50 dirham 100 000Nepal 12 paisas 50 000
1 Nepalese rupee 1 680Pakistan 10 and 13 paisas 93 478
10 and 13 paisas (first -day covers) 49 995Poland 0.60, 1.50 and 2.50 zlotys 100 000
4.60 zlotys (first -day covers) 34 8003 zlotys (souvenir sheets) 50 0003 zlotys (first -day covers, souvenir sheets) 35 200
Portuguese Overseas Provinces:Angola 2.50 escudos 25 000Cape Verde Islands 2.50 escudos 25 000Portuguese Guinea 2.50 escudos 25 000Portuguese India 2.50 escudos 25 000Mozambique 2.50 escudos 25 000São Tomé and Principe 2.50 escudos 25 000Timor 2.50 escudos 25 000Macao 0.40 ayo 25 000
* Not yet received.
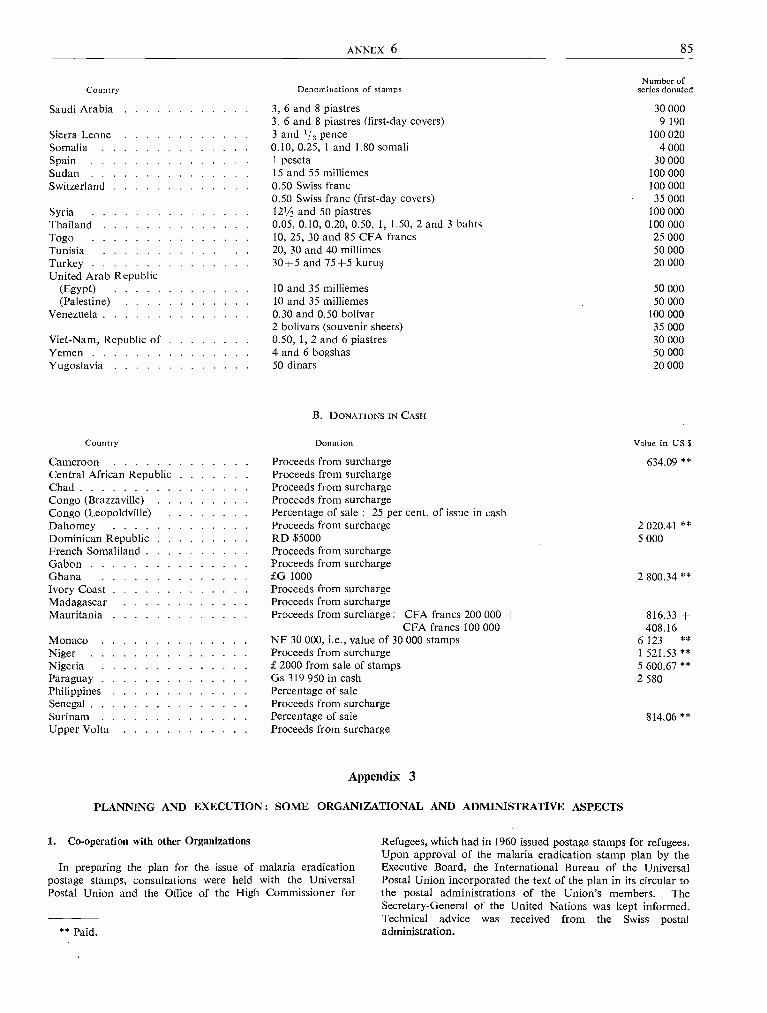
ANNEX 6 85
Country Denominations of stamps
Saudi Arabia 3, 6 and 8 piastres3, 6 and 8 piastres (first -day covers)
Sierra Leone 3 and 1/, penceSomalia 0.10, 0.25, 1 and 1.80 somaliSpain 1 pesetaSudan 15 and 55 milliemesSwitzerland 0.50 Swiss franc
0.50 Swiss franc (first -day covers)Syria 121/2 and 50 piastresThailand 0.05, 0.10, 0.20, 0.50, 1, 1.50, 2 and 3 bahtsTogo 10, 25, 30 and 85 CFA francsTunisia 20, 30 and 40 millimesTurkey 30 +5 and 75+5 kurusUnited Arab Republic
(Egypt) 10 and 35 milliemes(Palestine) 10 and 35 milliemes
Venezuela 0.30 and 0.50 bolívar2 bolivars (souvenir sheets)
Viet -Nam, Republic of 0.50, 1, 2 and 6 piastresYemen 4 and 6 bogshasYugoslavia 50 dinars
Country
B. DONATIONS IN CASH
Donation
Number ofseries donated
30 0009 190
100 0204 000
30 000100 000100 00035 000
100 000100 00025 00050 00020 000
50 00050 000
100 00035 00030 00050 00020 000
Value in US $
Cameroon Proceeds from surcharge 634.09 **Central African Republic Proceeds from surchargeChad Proceeds from surchargeCongo (Brazzaville) Proceeds from surchargeCongo (Leopoldville) Percentage of sale : 25 per cent. of issue in cashDahomey Proceeds from surcharge 2 020.41 **Dominican Republic RD $5000 5 000French Somaliland Proceeds from surchargeGabon Proceeds from surchargeGhana £G 1000 2 800.34 **Ivory Coast Proceeds from surchargeMadagascar Proceeds from surchargeMauritania Proceeds from surcharge : CFA francs 200 000 + 816.33 +
CFA francs 100 000 408.16Monaco NF 30 000, i.e., value of 30 000 stamps 6 123 **Niger Proceeds from surcharge 1 521.53 **Nigeria £ 2000 from sale of stamps 5 600.67 **Paraguay Gs 319 950 in cash 2 580Philippines Percentage of saleSenegal Proceeds from surchargeSurinam Percentage of sale 814.06 **Upper Volta Proceeds from surcharge
Appendix 3
PLANNING AND EXECUTION : SOME ORGANIZATIONAL AND ADMINISTRATIVE ASPECTS
1. Co- operation with other Organizations
In preparing the plan for the issue of malaria eradicationpostage stamps, consultations were held with the UniversalPostal Union and the Office of the High Commissioner for
** Paid.
Refugees, which had in 1960 issued postage stamps for refugees.Upon approval of the malaria eradication stamp plan by theExecutive Board, the International Bureau of the UniversalPostal Union incorporated the text of the plan in its circular tothe postal administrations of the Union's members. TheSecretary- General of the United Nations was kept informed.Technical advice was received from the Swiss postaladministration.
86 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
2. Preparation of the Emblem and the Model Stamps
Four artists were invited to submit drawings for both theemblem and the model stamps under conditions speciallyestablished for that purpose. An advisory committee wasconvened to recommend the selection of the emblem and designsof model stamps prepared by the artists. The committee wascomposed of experts in the matter coming from three MemberStates of the Organization (other than those from which theartists had been selected) and two members from the Secretariat.
3. Arrangements for the Sale of Donated Stamps
For the sale of the stamps and other related philatelic materialwhich would be donated to the Organization, an agreement wasconcluded with the Inter -Governmental Philatelic Corporation.Under this agreement the Corporation was appointed to act asthe exclusive agent of the Organization and to sell the stampscontributed to WHO at their face value, through its speciallyestablished subsidiary - the Philatelic Agency for MalariaEradication Postage Stamps. The stamps and other contribu-ted material were to be consigned to the J. Henry SchroderBanking Corporation, New York, which acted as custodian ofsuch donations on behalf of the Organization. These arrange-ments relieved the Organization of complex operations ofreceiving, handling, distributing, advertising, accounting fordonations, etc. The agreement was transmitted to all Members(by circular letter C.L.32. 1961, of 4 October 1961), and sub-sequently to other participants, and noted by the ExecutiveBoard in resolution EB29.R28.
4. Communications with Participants
The carrying -out of the plan required voluminous communica-tions with Members and other participants. Communicationsranged from general information about the plan to individualletters dealing with various administrative, financial and technicaldetails. Regional offices also followed up the development ofthe plan and assisted in solving many problems. The same istrue for the field staff in a number of the participating countriesand territories. The delays in the dispatch of donated stampsand related material caused a considerable amount of additionalcorrespondence. In a number of cases the donations were
delivered to the field staff or sent to the respective regionaloffice or headquarters, and they in turn had to arrange for for-warding them to New York.
Whenever it was noted that stamps and /or, more specifically,some denominations, souvenir sheets or first -day covers wereissued in limited quantities, the Director -General drew theattention of the countries concerned to the desirability that theyissue adequate quantities to ensure wide and easy distribution.
5. Philatelic Organizations, Stamp Trade and Collectors
Various philatelic organizations, including the InternationalPhilatelic Federation, showed varying degrees of interest in theplan and communicated with the Organization. Some stamptrade circles, presumably dissatisfied with the efforts which theOrganization was making in order to implement this project inconformity with its objectives and its humanitarian character,engaged in active propaganda against it, and it was necessaryfor the Organization to take measures to counteract suchpropaganda.
Numerous private letters were received requesting informationin respect of the stamps; they were referred for action to thePhilatelic Agency for Malaria Eradication Postage Stamps orits sub -agents. The letters requesting information on themalaria programme itself were answered by WHO staff.
6. Preparation of Exhibition
The exhibition of malaria eradication postage stamps inGeneva was organized by WHO staff in co- operation with thePhilatelic Agency for Malaria Eradication Postage Stamps,which bore most of the expenditure involved. This exhibitionalso included other stamps and philatelic material illustratingthe history of the Organization and its daily work. TheOrganization contributed to other exhibitions by sending stampsprepared for display according to the established technicalrequirements and by providing visual material and informationmaterial about WHO and malaria. In most cases informationwas also sent to radio, press and television in the cities wheresuch exhibitions were held. The Philatelic Agency for MalariaEradication Postage Stamps participated in the preparation andarrangements of almost all the exhibitions held outside Geneva.

ANNEX 7 87
Annex 7
HEADQUARTERS ACCOMMODATION 1
1. REPORT OF THE AD Hoc COMMITTEE OF THE EXECUTIVE BOARD
1. At its thirty -first session the Executive Board, inresolution EB31.R52, established " an Ad Hoc Com-mittee of the Executive Board consisting of : Dr M. K.Afridi, Professor E. Aujaleu, and Dr A. Nabulsi ".By resolution EB31.R25 the Board delegated to thiscommittee responsibility for examining on behalf ofthe Board the Director- General's report to theAssembly on headquarters accommodation, specificallywith reference to the anticipated increased cost of thebuilding project and its financing.
2. The Committee met on 8 May 1963 in the Palaisdes Nations, Geneva, to deal with this subject.3. The Committee had before it a progress report bythe Director -General (see part 2 of this annex) anda working paper containing the Director -General'slatest calculation of the anticipated cost of theconstruction project. The Committee decided to dealwith the subject in three parts : (1) the problem ofparking, (2) the anticipated increased cost of thebuilding project, and (3) the financing of the additionalcost.
Parking
4. The Committee reviewed the history of provisionsregarding parking since the inception of the proposalto construct the headquarters building, referring forthis purpose to the report which the Director -Generalhad made to the Standing Committee on HeadquartersAccommodation in November 1962,2 to the con-sideration given to the subject by the Standing Com-mittee at that time as reflected in its report 3 to theExecutive Board at its thirty -first session, and to thereport made by the Director -General to the samesession of the Executive Board.4 The Committeenoted that the original project for the building hadincluded provision for underground parking for aportion of the total anticipated number of vehicles,since this was considered essential to preserve thedignity of the building. For a staff of approximately
1 See resolution WHAI 6.22.2 Off: Rec. Wld Hlth Org. 124, Annex 15, part 1, Appendix.3 Off Rec. Wld Hlth Org. 124, Annex 15, part 1.4 Off Rec. Wld Hlth Org. 124, Annex 15, part 2.
[A16 /AFL /12 Add.1 - 9 May 1963]
one thousand it was assumed that provision wouldneed to be made for about six hundred vehicles intotal, and of these some four hundred were to beparked underground.5. Among the various measures adopted to bringthe original building project within the limits of theAssembly authorization of Sw. fr. 40 000 000 was theelimination of the provision for underground parking.At that time it was hoped that sufficient land areawould be available to permit surface parking entirely,without too serious prejudice to the appearance of thebuilding. The actual land area made available, however,had been less than originally hoped and this had ledthe Director -General to the conclusion, which hereported to the Standing Committee on HeadquartersAccommodation, that reintroduction into the pro-gramme of work of the provision for an undergroundgarage for about four hundred vehicles was essential.
6. The Standing Committee on Headquarters Accom-modation, after reviewing the situation in detail,concluded that " while it was already clear that acertain number of underground garages would benecessary, the area to be provided underground couldbe reduced if additional land could be made avail-able ".5 The Standing Committee had therefore askedthe Director -General to investigate the possibilities ofobtaining extra land from the authorities of theCanton of Geneva.
7. These several considerations had led the ExecutiveBoard in January 1963, in adopting resolutionEB31.R25, to record the conclusion.
3. CONCURS in the view of the Director -Generalthat reasonable provision for underground parkingshould be explored with reference to the construc-tion programme.
While the Ad Hoc Committee considered that underthe terms of resolution EB31.R25 it need not formulateany further conclusions about the parking, it didbelieve that it would be useful to draw the attention ofthe Assembly to the contents of paragraph 4.5 of theDirector -General's progress report, in which he reportsthe results of his explorations with the authorities of
Off. Rec. Wld Hlth Org. 124, Annex 15, part 1, para. 7.3.

88 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
the Canton of Geneva with regard to the availability ofadditional land areas which might be made availablefor parking. The Committee noted that only one sucharea, which could provide for about one hundredvehicles, was to be put at the disposal of the Organi-zation. The Committee also noted from explanationsgiven by the representatives of the Director -Generalthat there are no present indications of an intention toconvey this land to the Organization permanently.Rather it is the Director -General's understanding thatthe use of it would be granted to the Organizationunder an arrangement whereby, should future develop-ments so warrant, the authorization to use this landcould be withdrawn.
Costs
8. The Committee transmits, as an appendix to thisreport, for the information of the Assembly the latestcost estimates of the building project prepared by theDirector -General. These estimates have been preparedin the same form as those presented by the Directo r-General to the Standing Committee on HeadquartersAccommodation in November 1962,1 thus enabling adirect comparison to be made between the twoestimates at two different points in time.9. The Committee noted that the current estimates,which of the furtheras well as the amounts of the contracts for the secondsection of the work, fully confirm the earlier predictionsof a total cost of approximately Sw. fr. 60 000 000. Infact, the figure is slightly more than Sw. fr. 60 000 000if the underground garage to be constructed is forapproximately four hundred vehicles. It is slightlyless than Sw. fr. 60 000 000 if the underground garagecapacity is reduced to approximately three hundredplaces.
10. The Committee noted the fact that price increasesduring the past twelve months on the contracts for thefirst section of work had in fact amounted to approxi-mately 7 per cent., whereas the rate of increase foreseenin the estimates last autumn was 5 per cent. per annum.The Committee noted that the Director -Generalwas still maintaining in his new estimates an assump-tion of an overall average price increase of 5 per cent.
1 Off. Rec. Wld Hlth Org. 124, Annex 15, part 1, Appendix.
per annum throughout the entire construction period.It noted explanations given by the representative of theDirector - General that the allowance of an averageincrease of 5 per cent. per annum over the total periodis intended to cover somewhat higher rates that mayprevail during a portion only of the total constructionperiod.
11. It is the opinion of the Ad Hoc Committee thatthe situation as at 30 April 1963 has not altered thebasis of the recommendation of the Executive Board,in paragraph 4 of resolution EB31.R25, which readsas follows :
4. RECOMMENDS to the Sixteenth World HealthAssembly, in consequence, that the financialauthorization for the accomplishment of the newheadquarters building project be increased to aboutsixty million Swiss francs, the revised amount to bedetermined by the Health Assembly in the light of thesituation at the time of that Assembly.
Financing
12. The Ad Hoc Committee noted the explorationswhich the Director - General had undertaken with theauthorities of the Swiss Confederation with regard toan increase in the amount of the interest -free loantoward the cost of the building project the letterwhich had been received from the Head of the SwissFederal Political Department (see part 2 of thisannex).
13. The Ad Hoc Committee would draw the attentionof the Assembly to the recommendations which theCommittee is making in its reports on the supplemen-tary budget estimates for 1963 2 and on the review andapproval of the programme and budget estimates for1964.2 For the reasons indicated in these reports, theCommittee is proposing that the Assembly adoptbudgetary adjustments for both years 1963 and 1964which, if approved by the Health Assembly, wouldassist in the financing of the additional constructioncost, with the result that the remaining needs to befinanced would be approximately Sw. fr. 15 680 000(US $3 629 630), i.e., Sw. fr. 20 000 000 less Sw.fr. 4 320 000 (US $1 000 000).
2 See Annex 3.3 See Annex 9.

ANNEX 7 89
Appendix
COST ESTIMATES FOR HEADQUARTERS BUILDING
as at 30 April 1963
Contracts already awarded (honoraria included), value at 30 April 1963 :Sw.fr. Sw.fr.
Section I (including adjustments) 23 353 056
Section II (contracts awarded up to 30 April 1963) 4 623 264
Total of awarded contracts, value at 30 April 1963 27 976 320
Contracts remaining to be let (honoraria included) :Section II 8 415 576
Section III, value at 17 July 1961 9 119 390
Increase, Section III, up to 30 April 1963 based on 5 per cent. per annum 767 854
Total of contracts to be let at 30 April 1963 18 302 820
TOTAL VALUE OF CONTRACTS AT 30 APRIL 1963 46 279 140
Garages (approximately 400 places), value in April 1962 4 000 000
Increase, garages, at 30 April 1963 based on 5 per cent. per annum 200 000
Total, garages, at 30 April 1963 4 200 000
Total, all constructions, at 30 April 1963 50 479 140
Contingencies :5 per cent. of Sw.fr. 50 479 140 2 523 957
Increase to be foreseen in the construction cost (5 per cent. per annum) :between 30 April 1963 and 31 December 1963 1 765 000
between 1 January 1964 and 31 December 1964 2 738 405
between 1 January 1965 and 30 November 1965 2 635 714
7 139 119
Other costs 400 000
GRAND TOTAL 60 542 216
Approximate savings if the capacity of the garages were reduced to about 300 places: Sw.fr. 1 000 768
2. PROGRESS REPORT BY THE DIRECTOR -GENERAL
1. Building Progress
1.1 On 24 May 1962, Dr S. V. Kurasov, President ofthe Fifteenth World Health Assembly, laid the founda-tion stone of the future headquarters building.Immediately afterwards earth -moving operations andthe main building work began. However, unfortuna-tely, from the very beginning, the contractor re-sponsible for the main building work fell behind histime -table.
1.2 Despite the undeniable efforts made by thecontractor to speed up progress, the work was already
[A16 /AFL /12 - 6 May 1963]
about three months behind schedule when, in Januaryand February 1963, the exceptional severity of thewinter completely or partly prevented work on thesite for a few weeks. Since the resumption of activitieson 18 February the main building work has progressedat a satisfactory rate. Since March the firm has beenworking in two shifts from 4 a.m. until 9.30 p.m.As a result of these special efforts the building isbeginning to rise above ground, the larger part of thebasements now having been finished.1.3 During all this period the films to which contractshave been awarded for heating and air -conditioning,

90 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
plumbing, electricity and lifts have been producingthe equipment, which they will begin to install as soonas the main building work is sufficiently advanced.
2. Tenders and the Award of Contracts for theSecond Section of the Work
2.1 For the purpose of letting the contracts, the varioustypes of work involved in the building of the new head-quarters were divided into several sections, of whichthe first is now under way; the second section consistsof the following:
proofing and metal fittings;metal façades;light metal door- and window -frames;glass;movable partitions;metal ceilings and light fittings ;doors and door -frames,
In accordance with the " Procedure for the Invitingof Tenders and the Award of Contracts ",1 drawn upby the Standing Committee on Headquarters Accom-modation, the tender documents for this work weresent out on 15 December 1962 to ninety -one firmsfrom ten countries, two of them outside Europe.2.2 The public opening of the tenders received tookplace as planned on 1 March 1963 in the presence ofrepresentatives of the architect, the consultant electricalengineer and the tendering firms. The tenders openedcame from firms in six countries. Four tenders werereceived for proofing and metal fittings, eleven formetal façades, six for the external light metal door- andwindow- frames, two for glass, twelve for movablepartitions, twelve for metal ceilings and light fittings,and seven for doors and door -frames.2.3 After these tenders had been examined andreports from the architect and the consultant electricalengineer had been studied, the Director -General, inaccordance with paragraph 11 of the " Procedure "mentioned in paragraph 2.1, awarded the contractsfor proofing and metal fittings, light metal door-frames and window- frames, glass, metal ceilings,light fittings and doors and door -frames to the firmswhich had submitted the lowest acceptable tenders.
At the date of this report no decision had yet beenmade regarding the award of contracts for metalfaçades and movable partitions.
3. Gifts from Governments
3.1 The December 1962 report submitted to theExecutive Board by the Standing Committee on Head-quarters Accommodation 2 lists the gifts from govern-
1 Off Rec. Wld Hlth Org. 106, 47.2 Off. Rec. Wld Hith Org. 124, Annex 15, part 1.
ments in cash or in kind received, offered or con-templated as of 7 November 1962. Some governmentshave since offered gifts in kind or stated that they arethinking of doing so in the near future. Discussionsare in progress with these governments with a view toobtaining details of their proposed contributions tothe headquarters building. The Standing Committee,within whose competence falls the acceptance of giftsin kind, will be informed of all these cases at its nextmeeting.3.2 Apart from certain offers of marble, tropicaltimber and decorative panels and sculptures, the giftsare concerned with the furnishing of the offices for theDirector -General, the Deputy Director- General andthe Assistant Directors -General, and of the stafflounge. There are still, however, offices, halls andmeeting rooms whose furnishing and decoration couldusefully be the subject of government donations. Inparticular, there are the Executive Board Room, thefour committee rooms, the entrance hall, etc. Stillother possibilities were mentioned in the list attachedto a letter sent by the Director -General on 31 October1962 to the governments that had not already at thatdate indicated their intention to contribute.
4. Cost of the Building
4.1 As on HeadquartersAccommodation and the Director- General pointedout in their reports to the Executive Board at its thirty -first session,3 building costs in Geneva increased byabout 25 per cent. between 1959 and 1962. Thereis reason to believe that building costs will continueto increase by at least 5 per cent. per annum, whichwould involve a further increase of about 15 per cent.before completion of the work, which is expected atthe end of 1965.4.2 This constantin crease in building costs hashad important repercussions on the cost of the head-quarters building. All earlier forecasts of the costhave been upset. The original project, which formedthe basis for the authorization to build given in 1960by the Thirteenth World Health Assembly (resolutionWHA13.46) has had to be revised several times tokeep the cost within the limits fixed by that Assembly.The report of the Standing Committee 4 referred toabove summarizes the various reductions made inthe original project.4.3 With the report of the Director -General on thefinancial situation as of 2 November 1962 s beforeit, the Standing Committee " discussed whether it
3 Of Rec. Wld Hlth Org. 124, Annex 15, parts 1 and 2.4 Of Rec. Wld Hlth Org. 124, Annex 15.3 Of Rec. Wld Hith Org. 124, Annex 15, part 1, Appendix.

ANNEX 7 91
would be possible to recommend to the Board sub-stantial amendments to the building programme "but concluded " that any further large -scale changein the programme might seriously affect the utilityof the building ".1
4.4 At the same time the Committee, at the suggestionof the Director -General, reconsidered the questionof the underground garages, which had been eliminatedfor reasons of economy even before the originalproject had been submitted to the Thirteenth WorldHealth Assembly. Since the land area made availableto the Organization by the Canton of Geneva hasproved too small to provide for the estimated sixhundred vehicles to be parked without detracting toomuch from its appearance, an underground garage forabout four hundred vehicles was included in theestimate of the building costs in paragraph 5 of theDirector -General's above -mentioned report on thefinancial situation.2
4.5 The Standing Committee concurred in theDirector- General's view that an underground garagefor a certain number of vehicles would be necessaryin addition to the surface parking. In pursuance of thesuggestion made by the Standing Committee whenit considered this question, the Director -Generalapproached the authorities of the Canton of Geneva inorder to explore every possibility that might arise ofusing additional land to increase the available outsideparking areas. The only immediate result of thediscussions was that authorization was received fromthe Department of Public Works to use an area ofadjacent land which would provide parking forabout a hundred vehicles.
4.6 The Executive Board, after considering at itsthirty -first session the report of the Standing Com-mittee on Headquarters Accommodation,3 and thereport by the Director- General on the progress ofwork,4 adopted the resolution EB31.R25.
4.7 Since January 1963 new indications have con-firmed the tendency for building costs to rise. Thusthe various firms awarded contracts in 1962 havenotified new price changes which increase by 4.78per cent. the total amount of their contracts for theperiod between 1 January and 30 April 1963 alone,and bring up to 7.06 per cent. the increase in theamount of those contracts resulting from contrac-
tually valid price increases since the contracts weresigned in 1962.
4.8 The same tendency was also noted when thetenders for the second section of the work wereopened. Although in all these cases the lowestacceptable tender was approved, the total of thecontracts already awarded for this section of the workby 30 April 1963 was 9.15 per cent. higher than theestimates made by the architect in 1961. As to thetwo large contracts for the metal façades and movablepartitions, which have not yet been awarded, theoffers received forecast an even more importantincrease.
4.9 This latest information can leave no doubt thatthe recommendation made by the Executive Boardto the World Health Assembly that the sum envisagedfor completing the building should " be increased toabout sixty million Swiss francs " was well founded.
5. Finance
5.1 In accordance with the Executive Board'srequest (in resolution EB31.R25), the Director -General initiated discussions with the authorities of theSwiss Confederation with a view to examining thepossibilities of increasing the amount of the interest -free loan offered to the Organization, in order tocover these additional costs.5.2 A letter, dated 4 May, from the Head of theSwiss Federal Political Department to the Director -General is reproduced below (translation from theFrench):
With reference to our correspondence and variousinterviews concerning the additional financialmeans requested from Switzerland for the construc-tion of the headquarters building of the WorldHealth Organization in Geneva, we have the honourto inform you that this question is now being studiedby the competent federal and cantonal authorities.We can assure you that it will be given sympatheticconsideration; nevertheless, since no decision inregard to the extent and conditions of our possibleparticipation has so far been reached, we are un-fortunately not yet in a position to give youfuller information. However, we hope to be able todo so in the near future.
1 Off. Rec. Wld Hlth Org. 124, Annex 15, part 1, para. 7.2.2 Off. Rec. Wld Hlth Org. 124, Annex 15, part 1, Appendix.3 Off Rec. WId Hlth Org. 124, Annex 15, part 1.4 Off. Rec. Wld Hlth Org. 124, Annex 15, part 2.
92 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Annex 8
DEVELOPMENT OF MALARIA ERADICATION PROGRAMME IN 1962
[A16 /P &B /3 - 12 March 1963]
REPORT BY THE DIRECTOR - GENERAL
CONTENTS
Page Page
Introduction 92 7. Problems facing Malaria Eradication 109
1. General Progress and Prospects 93 7.1 Problem Areas 1097.2 Resistance of Malaria Parasites to Drugs . 110
1.1 The Over -all Picture 93 7.3 Vector Reactions to Insecticides 1101.2 Global Epidemiological Assessment 94
8. Research 1172. Training of National Malaria Eradication Staff . 97
8.1 Parasitology of Malaria 1183. WHO Technical Services in the Field of Malaria 8.2 Chemotherapy 118
Eradication 99 8.3 Immunology 1198.4 Epidemiology 119
4. General Health Services and Malaria Eradication 8.5 Entomology 120Programmes 100 8.6 Developments in Insecticides 120
5. Operational Aspects 101 9. Co- ordination 1215.1 Eradication Programmes 101
5.1.1 Planning, Organization and Management 101 10. Status of Malaria Eradication, by Regions . 122
5.1.2 Spraying Operations 101 10.1 African Region 1225.1.3 Drug Administration 102 10.2 Region of the Americas 1245.1.4 Epidemiological Evaluation and Surveil- 10.3 South -East Asia Region 128
lance Operations 103 10.4 European Region 1315.2 Pre- eradication Programmes 104 10.5 Eastern Mediterranean Region 134
5.2.1 Planning 105 10.6 Western Pacific Region 1395.2.2 Health Infrastructure 1065.2.3 National Malaria Service and Antimalaria Appendix 1. Detailed Status of Malaria Eradication as
Activities 106 at 31 December 1962 1445.2.4 Progress in Pre -eradication Programmes . 107
Appendix 2. Professional Staff employed in National6. Registration of Areas where Malaria has been Eradi- Malaria Eradication Services as at 31
cated, and Maintenance of Achieved Eradication . 108 December 1962 154
INTRODUCTION
A giant stride in 1962 has been the transfer to theconsolidation phase of the 168 million people livingin areas where transmission of malaria has ceasedfor a sufficient time to allow the reservoir of infectionin the population to reach such a low level thatspraying operations could safely be stopped andreplaced by surveillance. Most of these 168 million
1 See resolution WHA16.23.
people are covered by the Indian programme, but13 million are in the Americas and 2 million inthe Eastern Mediterranean Region. Another stimu-lating event has been the addition of 13 millionpeople to the total of those living in areas from whichmalaria is considered to have been eradicated.
After the attainment of the consolidation phaseprogress is sometimes handicapped by a slackeningof interest and by a premature reduction of financial

ANNEX 8 93
support to the campaign, just when the mopping upof the last hidden cases and foci demands the greatestscreening effort and deployment of talent and ima-gination.
Considerable preparatory progress is also beingmade in areas not yet ready for malaria eradicationprogrammes. The formulation of the policy of pre -eradication programmes has found enthusiastic accep-tance in the less developed countries. Such pro-grammes are now being developed in twenty -threecountries of Africa and Asia. A marked impetushas been given to the development of these program-mes by the Organization's readiness to accelerate theglobal malaria eradication programme. Unfortunately,the progress of such momentum is dependent on thecontinuation of voluntary contributions.
1.1 The Over -all Picture
The Expert Committee on Malaria, which includedexperts on public health administration, met inApril 1962 and, after considering a report by aconsultant, made important recommendations 1 on theparallel development of an adequate health infra-structure as being essential for the achievement ofmalaria eradication. It laid special stress on thenecessity for the closer relationship between thegeneral health services and the malaria eradicationservices at all stages of the malaria eradication pro-grammes. WHO is putting great emphasis on theimplementation of these recommendations, whichwill stimulate and speed up the organization of thepublic health services of the developing countries toa level at which they will be able to assist in thedevelopment of the malaria eradication programme.
1. GENERAL PROGRESS AND PROSPECTS
Achievements in 1962 have been apparent in everyaspect of the global malaria eradication programme.The greatest advance has been in the population inareas under consolidation, which has increased to243 million in 1962, as compared with 75 million in1961. Table A gives a summary of the status of malariaeradication by regions as at 31 December 1962.Early in 1963, the whole of continental Europereached the consolidation phase of the programme,thus achieving the aims of the Co- ordinated Planestablishing Priority for the Eradication of Malariain Continental Europe, which was formulated at theFirst European Conference on Malaria Eradication,held at Palermo in 1960.
As the all -out attack phase advances, problemsemerge here and there. Besides the administrativedifficulties, due to either organizational deficienciesor financial shortcomings, the technical difficulties ininterrupting transmission, sometimes leading to thedevelopment of so- called " problem areas " (seesection 7.1, page 109), require special local study andsupplementary attack measures. In one country atleast (El Salvador), malaria transmission in certainareas has defied all residual insecticides. A combina-tion of physiological resistance and behaviouristicchanges has made the vector refractory to the ima-gocidal attack, and while a more appropriate, alter-native remedy is being looked for, the malaria incidenceis returning to the original pre -DDT levels. In oneway this failure is a serious and regrettable setback;it is also a far -reaching event which amply confirmsthe foresight of the Eighth World Health Assemblyin urging the eradication of malaria on a global
basis, and which gives strong justification for thepursuit of the programme with unrelenting vigourand determination until the final goal is reached.
Following resolution WHA15.20 of the FifteenthWorld Health Assembly, calling for acceleration ofthe development of basic public health and organiz-ational facilities to shorten the time needed fortotal malaria eradication, particular emphasis hasbeen placed on pre- eradication programmes in 1962.By the end of the year there were twenty -threecountries with this type of programme, either startedor at the advanced planning stage.
The demand for adequately trained national andinternational staff of every speciality, particularly forthe African and Western Pacific Regions, continuedand increased in 1962. The established malaria erad-ication training centres at Belgrade (Yugoslavia),Sao Paulo (Brazil), Kingston (Jamaica) and inVenezuela were supplemented by two courses inMoscow, one in English and one in French. The newmalaria eradication training centre at Lagos, Nigeria,held its first course in October 1962. Training shouldbegin in Lomé (Togo) during the second half of1963 and should recommence in Manila (Philippines)about the same date. In 1962, national training centresin Ethiopia, India, Indonesia, Pakistan and Sudancontinued their activities.
The scheme for exchange of scientific workersagain proved extremely valuable in 1962 in enablingsenior officials concerned in national malaria eradi-cation activities to visit other programmes and relatedscientific centres and thus gain additional experienceand solve problems.
1 See ninth report of the Expert Committee on Malaria(Wld Hlth Org. techn. Rep. Ser., 1962, 243).

94 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
TABLE A. SUMMARY OF STATUS OF MALARIA ERADICATION, BY REGION, AT 31 DECEMBER 1962
Region
Population, in thousands,
Total
of areas wheremalaria neverindigenous ordisappeared
without specificantimalariameasures
oforiginal
malariousareas
of areaswheremalaria
eradicationclaimed
(mainten-ance phase)
of areas where eradication programmes in progressof areas
whereeradication
programmesnot yetstarted
in theconsolida-
tionphase
in theattackphase
in thepreparatory
phaseTotal
AfricaThe Americas . .
South -East Asia .
EuropeEastern
Mediterranean . .
Western Pacific(excluding China(mainland), NorthKorea and NorthViet -Nam) . . .
Total
172 434429 726634 678698 861
212 546
215 573
14 815275 835
35 238391 937
36 419
137120
157 619153 891599 440306 924
176 127
78 453
3 27859 3261467
245 744
1 884
17 367
143530 436
162 02830 026
14 486
4 766
1 15549 386
381 06012 987
12 705
3 809
-13 7539 191-
10 077
280
2 59093 575
552 27943 013
37 268
8 855
151 751990
45 69418 167
136 975
52 231
2 363 818(3 058 930)*
891 364 1 472 454 329 066 243 177 461 102 33 301 737 580 405 808
* The figure in brackets includes the estimated population (of 695 112 thousand) of China (mainland), North Korea and North Viet -Nam fromwhich no other information is available.
1.2 Global Epidemiological Assessment
The global epidemiological assessment is basedmainly on information received through the WHO -promoted quarterly reports on surveillance operations.The general adoption of this system would providethe basis for an effective and comprehensive assess-ment. By the end of 1962, the number of countriessubmitting quarterly reports on surveillance opera-tions had reached thirty -eight (including four coun-tries in the attack phase only). This is fourteen morethan in 1961, most of them in the Region of theAmericas. The situation at the end of 1962 withregard to countries wholly or partly in the consoli-dation phase can be seen by regions in Table B.
TABLE B. REPORTING OF SURVEILLANCEOPERATIONS IN 1962
RegionCountries with
programmes in theconsolidation phase
Countries submittingquarterly reportson surveillance
Africa 4 2The Americas . . . . 22 13
South -East Asia . . 5 3
Europe 9 7
Eastern Mediterranean 7 6Western Pacific . . . 5 3
By the end of 1962 the population of originallymalarious areas that had reached the consolidation
TABLE C. POPULATION OF ORIGINALLY MALARIOUSAREAS IN THE MAINTENANCE AND CONSOLIDATION
PHASES IN 1961 AND 1962
Region Year
Populationof originallymalariousareas (in
thousands)
Populationin areas
under con-solidation
andmaintenance
(inthousands)
Percentageof
populationof originally
malariousareas underconsolida-tion and
maintenance.
Africa 1961 152 557 4 581 3.01962 157 619 4 713 3.0
The Americas . . 1961 146 592 74 158 50.61962 153 891 89 762 58.4
South -East Asia . 1961 570 759 8 073 1.51962 599 440 163 495 27.2
Europe 1961 302 420 270 363 89.41962 306 924 275 770 89.8
EasternMediterranean . 1961 172 284 14 421 8.4
1962 176 127 16 370 9.3
Western Pacific . . 1961 75 311 25 495* 33.91962 78 453 22 133 28.2
Total 1961 1 419 923 397 091 27.71962 1 472 454 572 243 38.8
* Corrected figure.
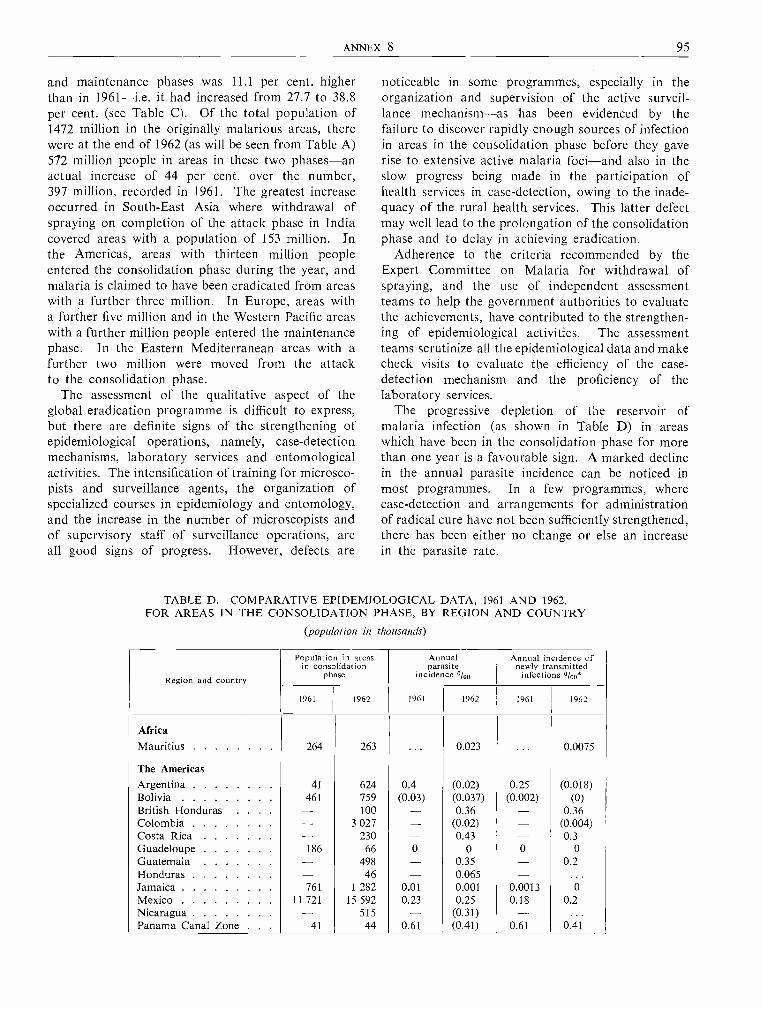
ANNEX 8 95
and maintenance phases was 11.1 per cent. higherthan in 1961 -i.e. it had increased from 27.7 to 38.8per cent. (see Table C). Of the total population of1472 million in the originally malarious areas, therewere at the end of 1962 (as will be seen from Table A)572 million people in areas in these two phases -anactual increase of 44 per cent. over the number,397 million, recorded in 1961. The greatest increaseoccurred in South -East Asia where withdrawal ofspraying on completion of the attack phase in Indiacovered areas with a population of 153 million. Inthe Americas, areas with thirteen million peopleentered the consolidation phase during the year, andmalaria is claimed to have been eradicated from areaswith a further three million. In Europe, areas witha further five million and in the Western Pacific areaswith a further million people entered the maintenancephase. In the Eastern Mediterranean areas with afurther two million were moved from the attackto the consolidation phase.
The assessment of the qualitative aspect of theglobal eradication programme is difficult to express,but there are definite signs of the strengthening ofepidemiological operations, namely, case -detectionmechanisms, laboratory services and entomologicalactivities. The intensification of training for microsco-pists and surveillance agents, the organization ofspecialized courses in epidemiology and entomology,and the increase in the number of microscopists andof supervisory staff of surveillance operations, areall good signs of progress. However, defects are
noticeable in some programmes, especially in theorganization and supervision of the active surveil-lance mechanism -as has been evidenced by thefailure to discover rapidly enough sources of infectionin areas in the consolidation phase before they gaverise to extensive active malaria foci -and also in theslow progress being made in the participation ofhealth services in case -detection, owing to the inade-quacy of the rural health services. This latter defectmay well lead to the prolongation of the consolidationphase and to delay in achieving eradication.
Adherence to the criteria recommended by theExpert Committee on Malaria for withdrawal ofspraying, and the use of independent assessmentteams to help the government authorities to evaluatethe achievements, have contributed to the strengthen-ing of epidemiological activities. The assessmentteams scrutinize all the epidemiological data and makecheck visits to evaluate the efficiency of the case -detection mechanism and the proficiency of thelaboratory services.
The progressive depletion of the reservoir ofmalaria infection (as shown in Table D) in areaswhich have been in the consolidation phase for morethan one year is a favourable sign. A marked declinein the annual parasite incidence can be noticed inmost programmes. In a few programmes, wherecase -detection and arrangements for administrationof radical cure have not been sufficiently strengthened,there has been either no change or else an increasein the parasite rate.
TABLE D. COMPARATIVE EPIDEMIOLOGICAL DATA, 1961 AND 1962,FOR AREAS IN THE CONSOLIDATION PHASE, BY REGION AND COUNTRY
(population in thousands)
Region and country
Population in areasin consolidation
phase
Annualparasite
incidence o /oo
Annual incidence ofnewly transmitted
infections o /oo*
1961 1962 1961 1962 1961 1962
AfricaMauritius 264 263 ... 0.023 ... 0.0075
The AmericasArgentina 41 624 0.4 (0.02) 0.25 (0.018)Bolivia 461 759 (0.03) (0.037) (0.002) (0)British Honduras . . . . - 100 - 0.36 - 0.36Colombia - 3 027 - (0.02) - (0.004)Costa Rica - 230 - 0.43 - 0.3Guadeloupe 186 66 0 0 0 0Guatemala - 498 - 0.35 - 0.2Honduras - 46 - 0.065 - ...Jamaica 761 1 282 0.01 0.001 0.0013 0Mexico 11 721 15 592 0.23 0.25 0.18 0.2Nicaragua - 515 - (0.31) - ...Panama Canal Zone . . . 41 44 0.61 (0.41) 0.61 0.41

96 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Region and country
Population in areasin consolidation
phase
Annualparasite
incidence loo
Annual incidence ofnewly transmitted
infections o /oo*
1961 1962 1961 1962 1961 1962
Peru 47 864 0.021 0.02 ... 0.002Surinam 115 125 0 0.008 0 0Trinidad and Tobago. . . 197 877 0.005 0.001 0 0Venezuela 173 150 0.63 0.35 0.17 0.09
South -East Asia
Afghanistan 86 87 0.035 (0.08) 0 0Burma 3 500 4 100 (0.035) 0.19 (0.004) .. .
Ceylon 1 260 1 294 (0.011) 0.003 (0.001) 0India 1 800 154 887 0.01 0.017 0.007 ...Thailand - 1 660 - 0.95 ** - 0.9
Europe
Albania 786 1 053 0.052 0.018 0.032 0Bulgaria 55 48 0 0 0 0Greece 2 437 2 167 0.05 0.046 0.024 0.027Portugal 631 678 (0.027) (0.02) (0.008) (0.004)Romania 5 747 6 326 0.002 0.002 0 0Spain 294 298 0.06 0.003 0.017 0Turkey 17 959 18 268 0.05 0.055 0.04 0.038Union of Soviet Socialist
Republics 2 000 890 0.033 0.15 0.025 0.1Yugoslavia 258 298 0.05 0.003 0 0
Eastern Mediterranean
Iran 5 500 6 000 0.13 0.42 0.09 0.3Iraq 3 300 4 163 0.002 0.097 0 0.086Israel 1 499 1499 (0.029) (0.024) (0.003) (0.003)Jordan 480 851 0.067 0.28 0 0.22Lebanon 683 683 0.009 0.28 0 0.14Libya 14 25 ... 0.72 ** ... 0.68
Syria 1123 1 265 0.021 0.027 0.0035 0.006
Western Pacific
China (Taiwan) 800 945 0.14 0.021 0.087 0.001North Borneo 13 13 0.3 0.23 0 0Philippines 3 261 3 261 0.69 0.82 ** 0.35 ...Sarawak 571 505 0.32 0.42 0.1 0.29
0 Negative result.- Not applicable.
... No information received.* Incidence of cases grouped under indigenous, introduced and unclassified.
** The annual parasite incidence exceeds the maximum permissible level of 0.5 per thousand population for aconsolidation phase area.
() Figures in brackets refer to areas where case -detection was inadequate; thus the annual parasite incidenceis of limited value.
The progress in continental Europe and the qualityof the epidemiological work performed there has beenimpressive. In the whole of Europe, 4518 cases ofmalaria were reported during 1962, of which 3594were in Turkey. No indigenous malaria case wasreported in Spain in 1962, and none in Bulgariain 1961 and 1962.
In Venezuela, eradication was certified in 1961 ashaving been achieved in an area with a populationof 4 325 000, and the excellent results obtained in
most of the countries of Zone I of the Region of theAmericas, namely Venezuela and seven Caribbeanisland administrations (Dominica, Grenada, Guade-loupe, Jamaica, Martinique, St Lucia and Trinidadand Tobago), promise imminent achievement oferadication in the whole Zone. In the seven islandadministrations, no indigenous malaria case due toPlasmodium falciparum or P. vivax was reportedduring 1962.
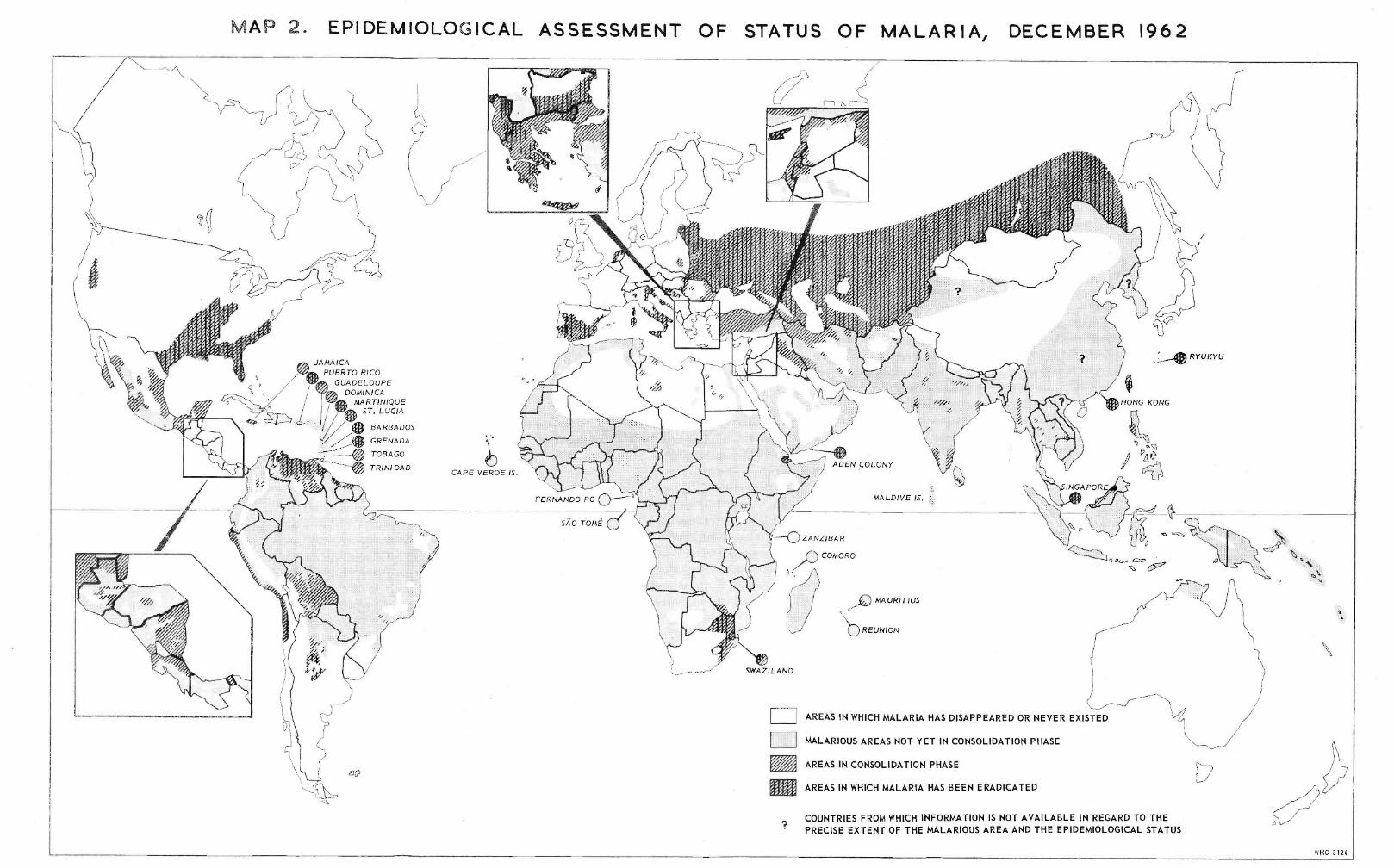
MAP 2. EPIDEMIOLOGICAL ASSESSMENT OF STATUS OF MALARIA, DECEMBER 1962
:1/6,6/611>11/11/11,/i,/1//1/
1/ ,/1 ,1 /1 ¡/1111/1'/11111/11%::ii%;:%;:%s%%::%%/1,11,/1,/1i111/11:///
/11:111111//1/1111'/1/1//1 i/1i111111/11ii1/1:i1/////i, 0/.0,:;:01/ / I // /,1 ! //// ,//////¡,// /,////
/11/11//11/11 /11//11/11 r11 "/,,////1///,r 4:1/1//li/% 4/111/1,/1,///1/1: 11//1111,// 111'/1/1111111//1//111/') ///,/,,11 //,/,,,,,, /, /, ,,l,/,,/' /'/,//¡/,,/ /,/sl//////11i11i/1//111/ .;ll/11111i/ ,
A';! 1/11111//1;1/111>1,J///¡11/1111//11//l'//l'/1i/1/11111/:' 11/11/11111//11/111/11;!.1 111////1//1/!11l11/>1,/1/1111/11° '/! / / // // // // /> / // // /1'/11'//11/1/1/11//1/1/ i1'/i1//1//1/////111//'//'/1/1////111i1///¡i/¡i/1¡11¡/`iï//¡/¡!1¡!1¡/1¡/1'çi/1/11/11''ifj11%1/11111j1111111111111111111'11l11/11/
%iii1/'y ¡¡1¡¡1'¡' /;%1%,' :,;11111/111111111>
'"'s'1 '0%!,:'
000/0/0/1!1/;$/1¡11 /',11111/1i'/!% / '// i11'il'/ 1111 ii/f'//Ikt/% i1/1:Îi/11fd/ .
alqi /,
,.
,tJAMAICAPUERTO RICO
GUADELOUPEDOMINICA
MARTINIQUEST. LUCIA
BARBADOS
GRENADA
TOBAGO
TRINI DAD
SÁO TOMÉ - ZANZIBAR
COMORO 4:21:10643e. CL'zV
MAURITIUS
REUNION
OSWAZILAND
op /.f1 ¡ ¡1
AREAS IN WHICH MALARIA HAS DISAPPEARED OR NEVER EXISTED
MALARIOUS AREAS NOT YET IN CONSOLIDATION PHASE
AREAS IN CONSOLIDATION PHASE
AREAS IN WHICH MALARIA HAS BEEN ERADICATED
COUNTRIES FROM WHICH INFORMATION IS NOT AVAILABLE IN REGARD TO THEPRECISE EXTENT OF THE MALARIOUS AREA AND THE EPIDEMIOLOGICAL STATUS
WHO 3126
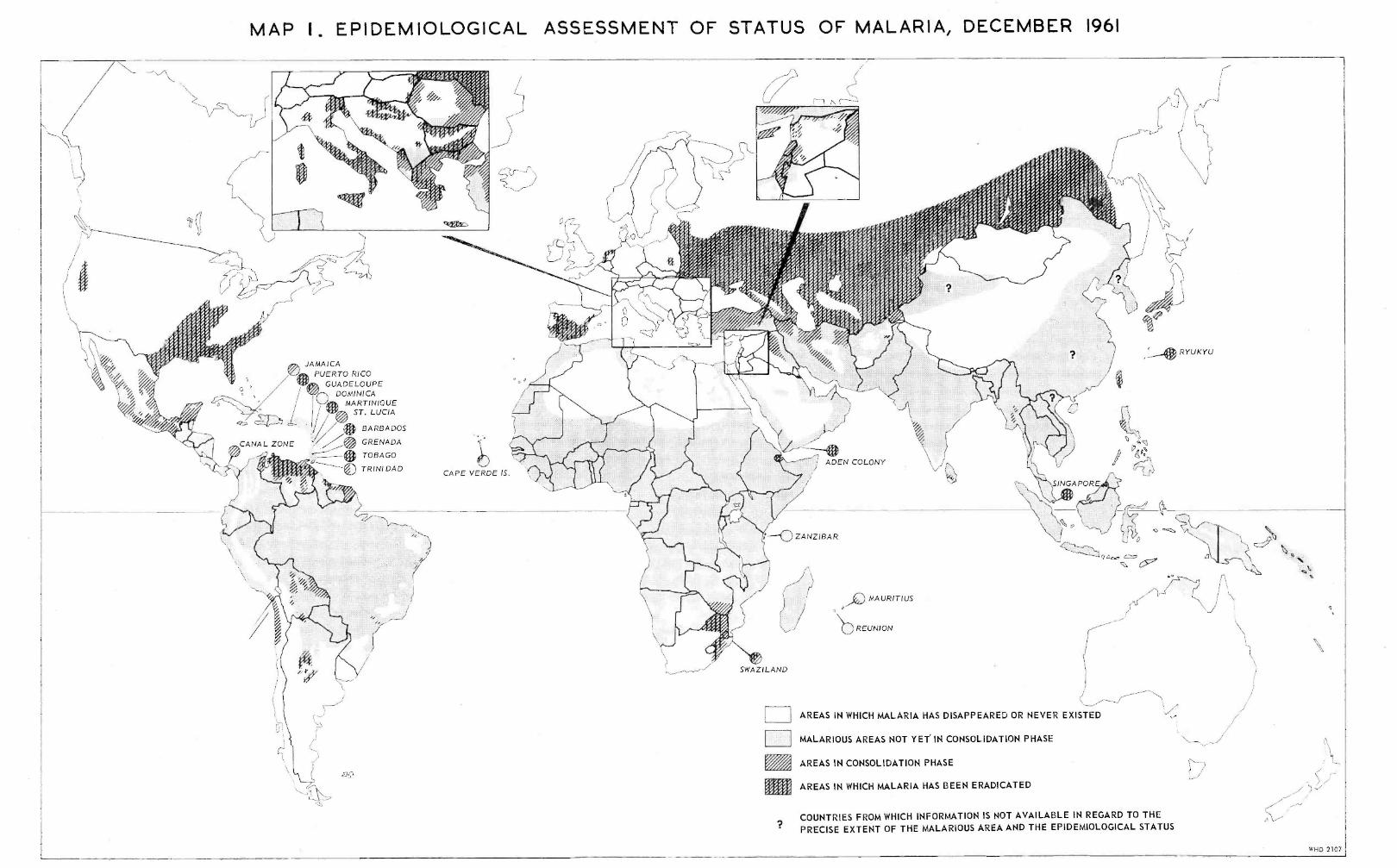
/'MAP I. EPIDEMIOLOGICAL ASSESSMENT OF STATUS OF MALARIA, DECEMBER 1961
r-1 r\-
/4
!! !
1i1IfJ//%!/1/f/¡//'
/
!!r
f / 1
i/// iJ1¡I#i/
'¡11/s///
¡//
1, 1%1///
/l1j1¡//%1///i
1/111111i///¡
//
/// /r ! f7
%
111/J / i/ 1///i¡
j 1
/1/ 1 1i/'1/1;;11e1/
1
;1i11111/11°1
111111111¡:iy;11111 1111;
11,/ 1/ /./j j%/4'11iú01 /
GUADELOUPEDOMINICA
MARTINIQUEST. LUCIA G
RYUKYU
SINGAPORE
l-o ZANZIBAR
cup
J
SWAZILAND
MAURITIUS
REUNION
AREAS IN WHICH MALARIA HAS DISAPPEARED OR NEVER EXISTED
MALARIOUS AREAS NOT YET IN CONSOLIDATION PHASE
AREAS IN CONSOLIDATION PHASE
AREAS IN WHICH MALARIA HAS BEEN ERADICATED
COUNTRIES FROM WHICH INFORMATION IS NOT AVAILABLE IN REGARD TO THEPRECISE EXTENT OF THE MALARIOUS AREA AND THE EPIDEMIOLOGICAL STATUS
?
O
WHO 2107

ANNEX 8 97
In Ceylon and India the surveillance activities inareas in the consolidation phase are satisfactory. InIndia, of the 140 units that entered the consolidationphase in 1962, only two reverted to the attack phase,and seventy -eight more units have already beenscheduled for withdrawal of spraying in 1963 and itis expected that the total population under the conso-lidation phase in India in 1963 will be about 250million.
Some active malaria foci occurred during 1962 inareas in the consolidation phase in neighbouringcountries of the Eastern Mediterranean Region (Iraq,Israel, Jordan, Lebanon, Syria) and, although thesereflected some weakness in the case -detection me-chanism, yet the quality of the epidemiological workcarried out to delimit and eliminate the foci wassatisfactory.
In the Western Pacific Region, the eradication pro-gramme in China (Taiwan) suffered a temporarysetback, owing to the appearance of active foci ofmalaria following the importation of malaria infec-tions from abroad. The visit of the WHO team forcertifying the achievement of eradication, scheduledfor 1963, has had to be deferred until there is animprovement in the case -detection mechanism, espe-cially by medical institutions, and by better controland follow -up of arrivals from overseas.
Under the assessment of the global malaria eradi-cation programme it is appropriate to refer to thestrategy adopted in the planning and implementationof this programme. The conviction of public healthleaders of the soundness of the eradication policyand their determination to achieve this goal are very
favourable signs. The strengthening of WHO technicalservices in the epidemiological field by the establish-ment of regional posts for epidemiologists during1962, the organization of a refresher course on ad-vanced epidemiological methodology in 1963, and theissue by WHO, in December 1962, of a Manual onEpidemiological Evaluation and Surveillance in MalariaEradication, will certainly contribute to raising thestandard of all epidemiological activities. Govern-ments requesting WHO teams to certify and registerthat eradication has been achieved are stimulated tostrengthen their rural health services, since adequatecoverage by these services and their proficiency indetecting and eliminating malaria infections are amongthe main criteria to be fulfilled. Other favourablesigns are the promotion of the development of anetwork of rural health services synchronized with thedevelopment of the malaria service, as conceived inthe planning and execution of pre- eradication pro-grammes in developing countries, and the efforts toaccelerate these programmes in Africa in order toshorten the time needed for total malaria eradication.
In the global malaria eradication programme, oncethe spectacular victories associated with the attackphase are over, progress will appear slower and beless obvious. The management of the later partsof the consolidation phase and dealing with so -calledproblem areas will certainly be a challenge to malario-logists and public health workers, but through deeperknowledge of the epidemiology of malaria, throughintensified research and studies to perfect epidemio-logical operations and, above all, through man's willand determination to achieve the goal, the finalbattle against this scourge will be won.
2. TRAINING OF NATIONAL MALARIA ERADICATION STAFF
Throughout the year the Organization has continuedto assist in a vitally important aspect of all malariaeradication programmes -the training of staff. Thisassistance has been given in a variety of forms, andis aimed at providing enough adequately trained peopleat every level.
Every effort is made to arrange wherever possiblefor the various categories of personnel -particularlynon -professional staff -to be trained in their owncountries. Not only is this more economical thantraining elsewhere, especially if large numbers areinvolved, but also training adapted to the environmentin which the personnel are employed is of far greatervalue.
For limited numbers of staff at the professionallevel and for personnel holding the more responsiblepositions in large programmes, training abroad maybe necessary and desirable : it gives staff with direc-
tional responsibility the opportunity of comparingoperating programmes under different epidemiological,physical and administrative conditions. Thus, inaddition to acquiring a knowledge of basic malariaeradication techniques, these future executives gainexperience of operational and administrative proce-dures which they can later adapt for use in their owncountry programmes.
During the year the Organization has helped toprovide these opportunities in a variety of ways.Existing international centres have been maintainedand new ones have been established, or plans for theirestablishment have been well advanced. Assistancewith training within Member countries has includedadvisory staff to help with teaching and managementof national training centres and supplies and equip-ment. In addition to the award of fellowships toenable staff of national malaria services to attend
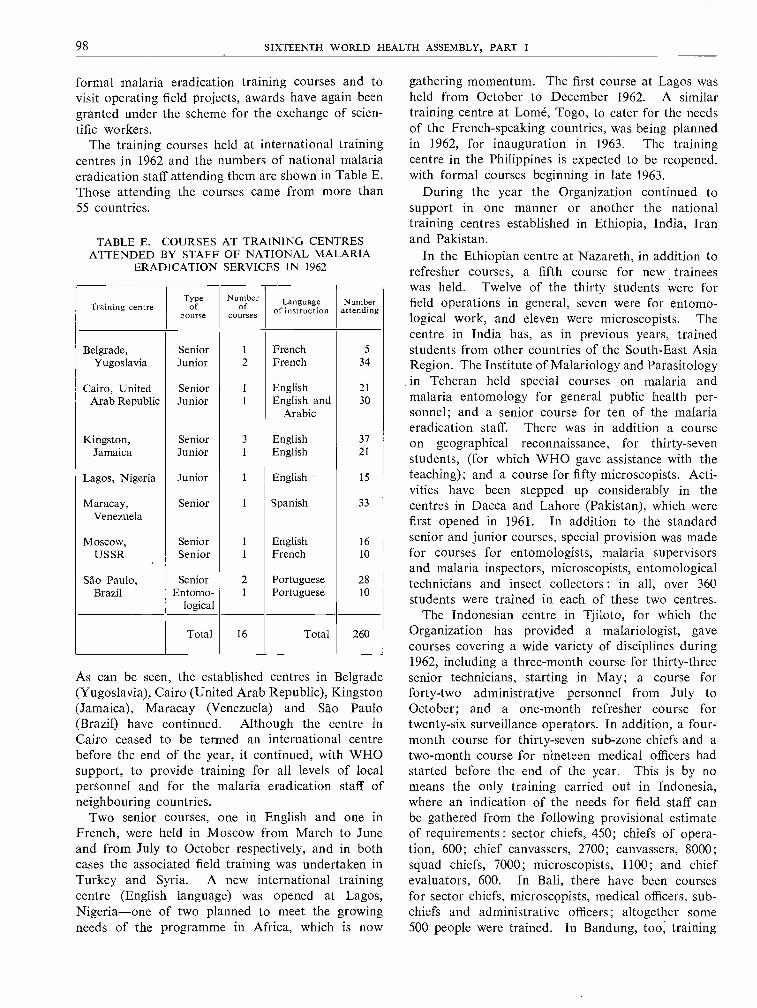
98 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
formal malaria eradication training courses and tovisit operating field projects, awards have again beengranted under the scheme for the exchange of scien-tific workers.
The training courses held at international trainingcentres in 1962 and the numbers of national malariaeradication staff attending them are shown in Table E.Those attending the courses came from more than55 countries.
TABLE E. COURSES AT TRAINING CENTRESATTENDED BY STAFF OF NATIONAL MALARIA
ERADICATION SERVICES IN 1962
Training centreType
ofcourse
Numberof
coursesLanguage
of instructionNumber
attending
Belgrade,Yugoslavia
SeniorJunior
1
2FrenchFrench
5
34
Cairo, United Senior 1 English 21
Arab Republic Junior 1 English and 30Arabic
Kingston,Jamaica
SeniorJunior
3
1
EnglishEnglish
3721
Lagos, Nigeria Junior 1 English 15
Maracay, Senior 1 Spanish 33
Venezuela
Moscow,USSR
SeniorSenior
1
1
EnglishFrench
1610
São Paulo,Brazil
SeniorEntorno-
logical
21
PortuguesePortuguese
2810
Total 16 Total 260
As can be seen, the established centres in Belgrade(Yugoslavia), Cairo (United Arab Republic), Kingston(Jamaica), Maracay (Venezuela) and Sdo Paulo(Brazil) have continued. Although the centre inCairo ceased to be termed an international centrebefore the end of the year, it continued, with WHOsupport, to provide training for all levels of localpersonnel and for the malaria eradication staff ofneighbouring countries.
Two senior courses, one in English and one inFrench, were held in Moscow from March to Juneand from July to October respectively, and in bothcases the associated field training was undertaken inTurkey and Syria. A new international trainingcentre (English language) was opened at Lagos,Nigeria -one of two planned to meet the growingneeds of the programme in Africa, which is now
gathering momentum. The first course at Lagos washeld from October to December 1962. A similartraining centre at Lomé, Togo, to cater for the needsof the French -speaking countries, was being plannedin 1962, for inauguration in 1963. The trainingcentre in the Philippines is expected to be reopened,with formal courses beginning in late 1963.
During the year the Organization continued tosupport in one manner or another the nationaltraining centres established in Ethiopia, India, Iranand Pakistan.
In the Ethiopian centre at Nazareth, in addition torefresher courses, a fifth course for new traineeswas held. Twelve of the thirty students were forfield operations in general, seven were for entomo-logical work, and eleven were microscopists. Thecentre in India has, as in previous years, trainedstudents from other countries of the South -East AsiaRegion. The Institute of Malariology and Parasitologyin Teheran held special courses on malaria andmalaria entomology for general public health per-sonnel; and a senior course for ten of the malariaeradication staff. There was in addition a courseon geographical reconnaissance, for thirty -sevenstudents, (for which WHO gave assistance with theteaching); and a course for fifty microscopists. Acti-vities have been stepped up considerably in thecentres in Dacca and Lahore (Pakistan), which werefirst opened in 1961. In addition to the standardsenior and junior courses, special provision was madefor courses for entomologists, malaria supervisorsand malaria inspectors, microscopists, entomologicaltechnicians and insect collectors : in all, over 360students were trained in each of these two centres.
The Indonesian centre in Tjiloto, for which theOrganization has provided a malariologist, gavecourses covering a wide variety of disciplines during1962, including a three -month course for thirty -threesenior technicians, starting in May; a course forforty -two administrative personnel from July toOctober; and a one -month refresher course fortwenty -six surveillance operators. In addition, a four -month course for thirty -seven sub -zone chiefs and atwo -month course for nineteen medical officers hadstarted before the end of the year. This is by nomeans the only training carried out in Indonesia,where an indication of the needs for field staff canbe gathered from the following provisional estimateof requirements : sector chiefs, 450; chiefs of opera-tion, 600; chief canvassers, 2700; canvassers, 8000;squad chiefs, 7000; microscopists, 1100; and chiefevaluators, 600. In Bali, there have been coursesfor sector chiefs, microscopists, medical officers, sub -chiefs and administrative officers; altogether some500 people were trained. In Bandung, too, training
ANNEX 8 99
has been given special emphasis and 609 of the staffwere trained, including chiefs of sectors and theirdeputies, microscopists and other field operationalstaff. Two new training centres are planned forSumatra.
In Sudan the WHO- assisted centre was completedtowards the end of the year and courses are expectedto begin in 1963.
Apart from the specifically designated malariaeradication training centres referred to above, theOrganization has assisted, wherever possible, with thetraining aspects of individual country programmes,large and small. In some instances the assistance hasbeen the actual organization of a specific course ofstudy, such as that held for senior technicians inChina (Taiwan) for the benefit of the countries inthe Western Pacific Region. A similar type of coursewas held in the Philippines for field operationalstaff at the senior squad or sector chief level. Earlyin 1963 a special course for entomologists took placeat Kuala Lumpur for personnel in the WesternPacific Region. In other cases, WHO assistance hasbeen given through the advisory service staff attachedto specific projects, or regional or headquarters staff
have been made available to give specific teachingassistance. In Afghanistan, for example, courseswere held throughout the year for junior and seniormalaria inspectors, and some 150 were trained.In Nepal, too, several training courses, lasting fromone week to three months, have given training to anadditional 190 personnel.
Brief reference has been made above to the teachingof malaria to public health personnel not directlyassociated with the malaria programme. It is presumedthat such people will indirectly support the programmeby their association, for example, with the develop-ment of a country's health infrastructure. Allied tothese are the voluntary collaborators whose servicesare utilized extensively in many countries in surveil-lance activities and for whose training no little efforthas been made. Indication of this effort can begauged from the fact that in Haiti alone 500 ofthese people received training in one month.
The WHO advisory staff, in addition to givingdirect aid in the preparation and presentation ofspecific courses, have helped national staff to prepareteaching media. The use of such manuals and teachingaids is strongly advocated by the Organization.
3. WHO TECHNICAL SERVICES IN THE FIELD OF MALARIA ERADICATION
To keep pace with the expanding global eradicationprogramme, e very effort has been made during 1962to provide the best available technical services.Without an adequate number of well- trained advisorypersonnel it is not possible to give the requiredassistance in planning and carrying -out, at the neces-sary high standard, the wide range of activities thatcollectively comprise an eradication programme
Besides the advisory services at country level, theOrganization maintains technical personnel at theregional offices and at headquarters. These threeechelons are interdependent, the responsibility foradvising the Director -General on over -all planningand co- ordination resting with the Division of MalariaEradication at Geneva. In a similar manner themalaria staff at regional offices assist their regionaldirectors in the provision of technical advice togovernments and in the promotion of country co-ordination.
The staffing of regional office malaria units duringthe year has reflected the progress of the programmein individual regions. In two regions additionalmedical officers have been assigned to assist in theepidemiological evaluation and assessment of pro-grammes. In the Regional Office for Africa the increasein the number of programmes to be initiated hasjustified the establishment of a third malariologist's
post to maintain adequate liaison with the WHOcountry malaria advisers, and a meeting was held ofall these advisers, together with the regional officeand country WHO public health advisory staff whoare intimately concerned with development of thehealth infrastructure for the pre- eradication pro-gramme -the principal item discussed at the meeting.
During the year, eleven of the more senior fieldproject staff from different regions visited otheroperating projects under the programme of studytours for advisers.
The serious shortage of sufficiently experiencedpersonnel available for recruitment has made itnecessary for the Organization to continue its pro-gramme of selecting staff as trainees and arrangingspecific intensive training courses for them. Theneeds of pre- eradication programmes in terms ofdeveloping a basic rural health infrastructure havemade it desirable wherever possible to select medicalofficers with public health experience, adding to thisfoundation training in malaria eradication techniques.
The numbers and categories of the Organization'stechnical staff engaged in the malaria programme inDecember 1962 are shown in Table F, with thecorresponding figures for 1958.
The increase in the number of medical officers,engineers, entomologists and sanitarians reflects the

100 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
increase in programme activities, and that of admin-istrative officers the necessity of providing advice togovernments on the administrative aspects of theirmalaria eradication programmes. Rapid training ofnational technicians has enabled the Organizationto reduce its staff in this category in some regions.
TABLE F. COMPARATIVE FIGURES FOR WHOCOUNTRY ADVISORY STAFF, 1958 AND 1962
Category December1958
December1962
Medical officers 74 117Public health advisers - 1
Engineers 19 40Entomologists 31 57Sanitarians 68 108Technicians 31 30Administrative officers - 26Others * 21 32
Total 244 411
* Assistant malariologists, parasitologists, statisticians, health educators,etc.
The posts are financed from the regular budget, the Expanded Programmeof Technical Assistance, the Malaria Eradication Special Account, and theSpecial Malaria Fund of the Pan American Health Organization.
The Organization has continued to supply workersin all fields of malaria with up -to -date information
on the various advances of techniques, new discoveriesand fresh approaches in malaria eradication. Inaddition to the Organization's regular publications -such as reports of the Expert Committee on Malaria,monographs and special issues of the Bulletin devotedto malaria and insecticides -mimeographed documentsare issued for limited circulation. These documents,issued in over 1500 copies in English and French,are circulated to national institutes, senior officials ofnational malaria eradication programmes and publichealth and research workers who have a particularinterest in malaria. During 1962, forty -four suchpapers were produced, four on general aspects ofmalaria, five on chemotherapy, fifteen on entomology,eight on insecticides, eight on parasitology and fouron other aspects of malaria eradication. The regionaloffices similarly issue documents and newsletters ofregional interest.
A further activity, already referred to in chapter 2,is the preparation of manuals and guides on variousaspects of the malaria eradication programme. In1962 a Manual on Epidemiological Evaluation andSurveillance in Malaria Eradication was issued byWHO in Geneva and a Practical Guide for MalariaEntomologists in the African Region of WHO wasissued by the Regional Office for Africa. A furthermanual on entomology covering the broader globalaspects was in preparation at headquarters for issuein 1963. Regional manuals on geographical recon-naissance have been produced by the Regional Officesfor Africa and for the Eastern Mediterranean.
4. GENERAL HEALTH SERVICES AND MALARIA ERADICATION PROGRAMMES
One of the requirements for the satisfactory oper-ation of a malaria eradication programme is theformation in the country of a national malaria eradi-cation service. The director of such a service shouldhave direct access to the chief officer of the ministryof health and, if necessary, to the minister, andshould have complete administrative control over thestaff of the eradication service and over the expenditureof the funds allotted to the programme.
In some countries there has been a tendency forthe national malaria eradication service to take tooliterally the recommendation that the service shouldhave " operational autonomy " and thus there hasdeveloped a segregation, with the result that themalaria eradication service has divorced itself fromother branches of the ministry of health, causing theofficials of the general public health service to loseall contact with it and, what is worse, to lose interestin a campaign which generally has the first priorityamongst the country's public health endeavours. Such
a state of affairs leads to an expensive and sometimesruinous dispersion and misuse of effort and resources,which could be avoided by proper understanding andco- ordination. The Organization is doing its utmostto correct this deviation and is trying to ensure thatmalaria eradication programmes have the full supportand participation of the general health service of thecountry from the beginning of the campaign, becauseit is of the utmost importance that such support andparticipation be forthcoming unstintingly during theconsolidation phase and that the general publichealth service should be prepared to accept the fullresponsibility for the maintenance phase of theprogramme when the national malaria eradicationservice, having fulfilled its function, is disbanded.
But good understanding, close collaboration andperhaps " integration " will solve the problem, atleast in those places where the population is actually" covered " by public health services. In areas wheresuch services are deficient or non -existent, the lacunae
ANNEX 8 101
should be filled by the establishment of new healthposts, especially in vulnerable areas, which are thosehaving a high potential for transmission and at thesame time a liability to the reintroduction of thedisease. Unfortunately, almost all the rural areas ofthe countries in the tropics fall into this category.It must be understood, therefore, that when the term" public health services " is used in connexion withmalaria eradication, " rural health services " aremeant, and these should be spread with more emphasison geographical coverage than on high technicalstandards. A few model health centres will be ofvery little help to the malaria eradication campaign.
In its ninth report 1, the Expert Committee onMalaria made a number of suggestions to ensureadequate co- ordination at all stages in the developmentof the malaria eradication programme. They include
the following : that a proper mental attitude shouldbe created throughout the entire health organizationtowards the malaria eradication programme; thatpublic health planning groups and malaria eradicationboards should be established for policy guidance andshould be attended by staff of both the generalhealth services and the malaria eradication service,and that at all levels the chiefs of the respectiveservices should maintain co- ordination of theiractivities through frequent and close contact untiltheir services were merged. The Organization isimplementing these recommendations. With thisaim, a seminar for advisers at country level was heldin Ibadan, Nigeria, in October 1962, and otherseminars are being planned for the benefit of respon-sible national authorities.
5. OPERATIONAL ASPECTS
5.1 Eradication Programmes
5.1.1 Planning, Organization and Management
Most governments with malaria eradication pro-grammes in operation have continued during 1962to recognize the importance of realistic and detailedplanning. It has to be noted, however, that in severalmajor programmes the execution of plans of actionand the organization of operations have been ham-pered in varying degrees by defective managementpractices, particularly with regard to the nationalfinancing of these programmes. In many instancesthroughout the year, malaria operations failed toreach planned targets because national funds werediverted to other government programmes, despitethe fact that governments had agreed upon andappropriated the funds estimated as required in theplans for the malaria eradication programme. Failureto achieve total coverage in spraying and surveillanceoperations may prolong the time needed to reacheradication and may therefore entail greater financialoutlays by the government and by participatingagencies.
There has been a growing recognition on the partof governments during the year under review thatthe practicability of reaching and maintaining eradi-cation depends on the existence in their countries ofessential basic health structures and services, and thatwithout such services success is unlikely. This isparticularly relevant in relation to the extent ofcoverage by the basic health services needed tosupport surveillance and vigilance operations. All too
Wld Hlth Org. techn. Rep. Ser., 1962, 243.
often there has been insufficient effort in the prepar-ation and planning of these basic health services, sothat their necessary full and effective participation inthe relevant activities of the malaria eradicationprogrammes has been lacking.
Having reviewed the situation in the light of thesefactors, some governments have decided to aim ateradication by way of a pre- eradication programme,which will enable them gradually to build up theessential health infrastructure and train personnel forthe future national malaria eradication service. Thishas resulted in some cases in the conversion of pre -eradication surveys and pilot projects into pre -eradication programmes which will enhance theprospects for eventual success of the future pro-grammes of malaria eradication.
5.1.2 Spraying OperationsAlthough there has been no important change
during the year in the methodology of sprayingoperations, there has been increasing acceptance ofthe need for greater field supervision. There are still,however, large programmes in which the sprayingoperations are not the responsibility of special officers,and the desirability of employing engineers for theseoperations is not universally appreciated.
The following figures indicate the vast scale ofthese spraying operations. More than 50 000 tonsof insecticide are used annually in malaria program-mes. This material is distributed in nearly a milliondrums to 25 000 spraying squads. It is mixed with200 million gallons of water (occasionally with kero-sene) and sprayed on the inside walls and ceilingsof 100 million houses at intervals of six to twelve

102 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
months. The insecticide used annually costs some$30 million and the transport and spraying equipmentused -a quarter of which needs to be replaced everyyear- represent an investment of another $30 million.
The value of sound geographical reconnaissance isreceiving ever -increasing recognition; it is not onlya necessity for malaria programmes in the attackphase, but is vital if the consolidation phase is to beimplemented successfully. As a help in tackling thisdifficult problem effectively and economically, espe-cially in areas with scattered and impermanenthabitations, a manual is being prepared, on the basisof the field experience of engineers and sanitarians inall regions.
New and temporary houses, replastered walls andnew roofs, rooms inaccessible for spraying becauseof grain storage, silk -worm culture, or simple refusalto permit spraying, and seasonal and nomadic popu-lation movements, make the achievement of totalcoverage often difficult and sometimes impossible.These problems are tackled in various ways, dependingon the local situation, but with a degree of successthat enables most programmes to adhere to a plannedschedule.
The insecticide used in by far the greatest numberof projects is a suspension of DDT water -dispersiblepowder. Special circumstances necessitate the use ofdieldrin in some projects. Kerosene solutions orwater emulsions of these insecticides are sometimesrequired. No convincing evidence has been forth-coming to warrant widespread changes in the existingdosages and frequency of application of the insecti-cides in use. In addition to small -scale insecticidetrials in the Americas, a full -scale field trial of mala-thion has been organized in Uganda and the initialoperations, begun at the end of 1962, will continuethrough 1963. The WHO insecticide testing team inLagos, Nigeria, had completed its investigations withdichlorvos (DDVP) (2, 2- dichlorovinyl dimethylphosphate) with promising results, and a field trialwith this fumigant insecticide is being undertaken inNorthern Nigeria in 1963.
There is considerable interest in improvements inspraying equipment. The rubber disc flow regulator,which had undergone extensive field tests, has beenadopted in a number of programmes; when certaintechnical improvements are completed, a wide useof this device is expected. An expert committee oninsecticides to meet in 1963 will consider, inter alia,the revision and extension of specifications for vectorcontrol equipment used in malaria programmes.
5.1.3 Drug Administration
There have been no important changes in the use ofantimalarial drugs during 1962. Chemotherapy has
continued to be used as the main antimalarial measurein the consolidation phase of eradication programmes,with the purpose of eliminating all residual or impor-ted infections and thus ensuring eventual completeeradication of the disease. As a precautionary measure,a single -dose treatment is usually given to all suspectedmalaria cases, followed by radical treatment aftermicroscopical confirmation of the infection. Theserious difficulties that are encountered in manyprogrammes in providing for prompt and completeradical treatment of all confirmed cases have oncemore emphasized the need for an efficient ruralhealth service as an essential condition for implement-ing the consolidation phase. The building -up ofsuch a service is one of the main aims of pre- eradi-cation programmes, which are now being adopted byan increasing number of countries.
Mass drug administration, either direct, by tablets,or indirect, by medicated salt, has its main applicationin the attack phase of an eradication programme. Itmay be used as an adjuvant measure to house -sprayingin areas where insecticides alone are fully effectivein interrupting transmission. In this case, drug admin-istration is not strictly necessary, but even if it isgiven only at the time of the spraying round, it willcontribute to reducing the parasite reservoir andthereby hasten the interruption of transmission.Moreover, a single -dose treatment given at the timewhen house spraying is carried out is often helpful inpromoting co- operation of the inhabitants with thespray teams.
Much more important is the use of mass drugadministration as a complementary method to housespraying in areas where, owing to the habits of thevector or of man, complete interruption of trans-mission cannot be achieved with insecticides alone.As more and more programmes are approaching theend of the attack phase, a certain number of areashave been found where, despite several years of totalcoverage with insecticides, transmission is still goingon. With the disclosure of these " problem areas ",where for various reasons malaria is refractory toinsecticides, the need for mass drug administrationas a complementary method to house spraying hasbeen accentuated and an increased use of this measureis to be expected during the next few years. In certainproblem areas in the central part of the Americas(Mexico, Guatemala, Nicaragua and El Salvador)regular mass drug treatment as a complementarymethod of attack has been introduced.
In areas where house spraying is either ineffectiveor impracticable and where mass drug administrationappears to be the sole possible method of attack,interruption of transmission by the use of drugsalone cannot be expected unless complete coverage
ANNEX 8 103
is achieved. Experience has shown that, howeverefficient the distribution system, it is practicallyimpossible to ensure that a hundred per cent. of apopulation will take a certain number of antimalarialtablets at regular, short intervals over a prolongedperiod. With the drugs at present in use, direct massdrug administration as the sole method of attackcannot be recommended, except where malariaincidence is at a very low level, or where the trans-mission season is very short.
In those areas where salt is used as a regular foodadditive by the entire population, indirect mass drugadministration in the form of medicated salt distri-bution may be the method of choice, provided thatinfants and children, whose normal diet containslittle or no salt, are covered by a simultaneous pro-gramme of direct drug administration.
Medicated salt projects have been carried out inlimited areas in a number of countries. In Brazil,distribution of chloroquinized salt was continued inthe Amazon Basin until the end of 1961, and wasthen suspended pending the results of a special studyof the effectiveness of the project and of the possibleoccurrence of chloroquine tolerance or resistance inthe local strains of P. falciparum. In British Guiana,a chloroquinized salt programme covering the wholeof the interior was started early in 1961 as the onlysuitable method of attack in this difficult part of thecountry; the results have been most promising, exceptin one area where non -medicated salt was available.In Tanganyika a small field trial, in which chloro-quinized salt is used, is being carried out; its initialresults are excellent, as shown by the reduction ofparasite rates to a very low level, except in childrenbelow the age of two years (see section 8.2, page 118).In Iran, following encouraging results of a preliminarytrial with medicated salt among two small tribalgroups, it is planned to implement this method ona larger scale among a predominantly nomadic popu-lation in the Jareh area of Kazerun. In Ghana,distribution of medicated salt exclusively throughthe existing commercial channels could not preventthe entrance of non -medicated salt into the projectarea. A new arrangement, in which the normalcommercial channels are superseded by government -sponsored distribution, was introduced during thelast quarter of 1962, and the duration of the projecthas been extended until the end of 1963.
From a purely technical point of view, there is nodoubt that medicated salt is highly effective. Never-theless, the results of medicated salt projects havefrequently not come up to expectations, mainlybecause of the complexity of the operation on alarge scale. Public health officials have supervisiononly at each end of the operation -at the beginning,
during the incorporation of the drug into the commonsalt, and at the end, for the evaluation of the pro-gramme, when it is necessary to ascertain whetherthe medicated salt is actually being consumed by thewhole population and what are the results. Betweenthese two technical aspects of the programme liesthe whole process of the distribution and marketingof the product, which is carried out under the controlof other government agencies not necessarily deeplyconcerned with the objectives of the programme.Other social factors also complicate the operation. It isfor these reasons that the projects in Cambodia andWest New Guinea (West Irian) have been terminated.
Nevertheless, these projects have been of consider-able value in providing much useful information;they have revealed and clarified various practicalproblems connected with the use of medicated saltin under -developed rural areas, so that this methodcan now be applied much more judiciously andefficiently than before.
One of the objectives of pre- eradication program-mes is the distribution of antimalarial drugs for thegeneral protection of inhabitants of malarious areas.In its ninth report 1 the Expert Committee on Malariasuggested that in pre- eradication programmes anti-malarial drugs should be used mainly as follows :drug treatment should be readily available to allclinical malaria cases through the network of ruralhealth units and any other suitable distributioncentres; where regular mass drug administrationaiming at the prevention of clinical symptoms ofmalaria is feasible, priority should be given to (a) par-ticularly vulnerable population groups such aspregnant and nursing women, infants and smallchildren, and (b) groups of epidemiological andsocio- economic importance.
5.1.4 Epidemiological Evaluation and SurveillanceOperations
The methodology adopted in epidemiological eval-uation and surveillance operations, which is basedon the experience gained since the implementation ofthe global malaria eradication programme, has nowbeen presented in the Manual on EpidemiologicalEvaluation and Surveillance in Malaria Eradicationand given a wide circulation.
With the application of the methodology in differentprogrammes, field malariologists have taken theinitiative in developing certain techniques and pro-cedures to bring about a high quality performance.These have included improvements in samplingtechniques for conducting malariometric surveys,and in the training and supervision of microscopists;the development of practical schedules for surveil-
1 Wld Hlth Org. techn. Rep. Ser., 1962, 243.

104 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
lance agents and of concomitant and consecutivesupervisory techniques; improvements in logistics tolessen the time -lag between the taking of slides andthe relay of results; and, last but not least, the deve-lopment of an effective reporting system on the basisof the WHO- promoted quarterly surveillance reports.All these factors have contributed to the improvementnoted in the quality of the work and have made forgreater confidence in the reliability of the epidemio-logical data.
The realization, by those responsible for nationalmalaria eradication programmes, of the need tostrengthen national epidemiological sections, includingthe units dealing with surveillance operations, labo-ratory services and entomological activities, has ledto the organization of specialized courses for bothprofessional and auxiliary personnel. Units havebeen reorganized so that the results of their workcan be co- ordinated and focused on interruptingmalaria transmission and eliminating the reservoirof infection -a major activity of malaria eradicationprogrammes at the consolidation phase. In theSouth -East Asia Region, a regional blood examinationcentre has been established to provide independentcross -checking for blood films from countries in theRegion.
During the year, the development of independentassessments by teams not directly connected with theexecutive part of the malaria eradication programmein the respective units or zones, and with the participa-tion of members of the public health service (as inIndia) has resulted in greater adherence to the WHOepidemiological criteria regarding the interruption oftransmission and withdrawal of spraying.
From the point of view of quantitative assessment,the increase in the annual blood examination ratecan be seen in all programmes in the consolidationphase, and even during the last year of the attackphase. The fact that the annual parasite incidencein areas projected for withdrawal of spraying fallsbelow the permissible rate of 0.5 per thousand inthe presence of an active case -detection mechanismin the last year of the attack phase is a favourablesign. Unfortunately, the qualitative aspect of the work-the achievements in covering the total populationwith an effective case -detection mechanism, bothactive and passive; the progressive participationof all medical institutions; and the improvements insupervisory arrangements- although outstanding,cannot be presented statistically.
As a result of the emphasis placed on adequatecoverage by rural health services and on their participa-tion in case -detection and in the administration
of radical cure, there has been a very noticeablerise in the number of slides taken, under passivecase -detection, by medical institutions. The co-operation of these health services has been activatedin two ways, by attaching some personnel fromthe malaria service to the hospitals and dispensarieson certain days to take blood films from fever cases,and also by arranging for the malaria service toexamine slides submitted by hospitals and dispensariesand relay the results within forty -eight hours. It isgratifying to note that the public health servicesare showing greater interest in and awareness of theachievements of malaria eradication and their ownrole in such a gigantic public health undertaking.
The concept of a problem area is now accepted,as is the necessity for detecting such areas early,during the attack phase. The same applies to theconcept of a malaria focus, its epidemiologicalsignificance and dynamics, the methodology ofinvestigation and the machinery for applying remedialmeasures quickly. Very commendable work has beenrecorded in many countries in these respects.
In view of the value of entomological contributionsto the overall epidemiological evaluation, a reorienta-tion of the malaria entomologist's work has beeneffected through regional refresher courses for ento-mologists and the development of a manual on ento-mological techniques. The gearing of the work ofentomologists to the needs of an eradication pro-gramme, has resulted in valuable contributions beingmade in investigations into the persistence of malariatransmission, both in limited foci and in problemareas.
5.2 Pre -eradication Programmes
The Expert Committee on Malaria in its eighthreport,2 in considering the approach which shouldbe made to malaria eradication in developing coun-tries, noted that :
The criteria necessary for the establishment ofa malaria eradication programme are that eradica-tion should be technically, administratively andpractically feasible, and that the programme shouldbe planned with the object of eradication on acountry -wide scale.
Technical feasibility implies the possibility ofindicating the processes that would result in anabsolute interruption of transmission in anyepidemiological circumstances that might beencountered.
1 Wld Hlth Org. techn. Rep. Ser., 1961, 205.
ANNEX 8 105
Administrative feasibility implies the possibilityof creating an organization that would deploy theskills and resources necessary to secure and maintainthe interruption of transmission over a sufficientarea and with sufficient uniformity for a sufficientlylong period of time.
Practical feasibility implies that the mechanismrequired for these processes is within the financialand material resources available to the governmentconcerned, and that open communications, freedomof movement, and the co- operation of the publicwill be sufficient to make it possible to ensuretotal coverage in the application of insecticides andto secure adequate country -wide surveillance andmaintenance in due course.Taking into account these criteria, which need to
be met before a country can reasonably undertake amalaria eradication programme, the Expert Com-mittee considered that, from the malaria eradicationpoint of view, a developing country should be definedas one " in which the general administration andhealth services have not yet reached a level thatwould enable it to undertake a malaria eradicationprogramme, and in which, therefore, the necessaryfoundations for this kind of closely co- ordinated,thorough, and time -limited activity have first to belaid ".
The Expert Committee, therefore, proposed a newtype of assistance that would be required as a preludeto malaria eradication and would enable a countryto make good the deficiencies mentioned above. Thecomplex of preliminary operations has been termed a" pre- eradication programme " which was defined inthe report to the Fourteenth World Health Assembly 1as follows :
... a preliminary operation undertaken in acountry whose general administration and healthservices have not yet reached a level which wouldenable it to undertake a malaria eradication pro-gramme and in which, therefore, the necessarybasic foundations for this kind of co- ordinated,thorough and time -limited activity have first to be laid.
The main purposes of a pre- eradication programmeare the stimulation and concurrent development ofthe " necessary basic foundations ", usually referredto as " the two main objectives ", namely (a) thehealth infrastructure, and (b) the national malariaservice.
The health infrastructure may be defined as thenetwork of rural public health services which, by theend of the attack phase and through the whole ofthe consolidation phase, should be able to provideefficient collaboration in the detection of malaria
1 Mimeographed document A14 /P &B /2, December 1960.
cases and their adequate treatment and which, duringthe maintenance phase, should be prepared to assumeresponsibility for keeping a watch over the area andmaintaining it permanently free from a re- establish-ment of the disease. At the present stage reached bymany of the newly developing countries, such arural network could be staffed entirely by auxiliarypersonnel.
The national malaria service is the organizationwhich, in due course, will become the national malariaeradication service, with all the skill and resourcesnecessary to secure the interruption of transmissionand maintain it until eradication is achieved.
5.2.1 Planning
A pre- eradication programme is not a " time -limitedoperation " which must adhere to a strict schedulefrom month to month and year to year, as is a malariaeradication programme, with its several definite phasesleading to a specific goal. It is rather a programmeof orderly and purposeful growth and development,aiming at the eventual full preparedness of a countryto undertake the very exigent malaria eradicationprogramme which is expected to follow. Whateverthe level of development in a country, both elementsof the pre- eradication programme, namely the healthinfrastructure and the malaria service, need to growuntil they reach the minimum organizational levelrequired. The great variation in the initial level ofpreparedness of different countries makes it impossibleto lay down any standard plan for pre- eradicationprogrammes or to indicate any strict schedule ofachievements for the years to come. Plans should,therefore, be made for two years at a time, the situa-tion being carefully reviewed as each renewal isprepared. The first task during the initial period isthe investigation and preparation of an inventory ofall available facilities related to " the two mainobjectives ". As it is expected that this will take somesix months, the first plan of operations should providefor the preparation of an addendum at the end ofthis period containing the inventory of availablefacilities and setting out the detailed plan of actionfor the remainder of the first two years, with anindication of the intermediate targets to be aimed atand the steps to be taken to this end. These willinclude : the establishment of adequate facilities fortraining personnel of the various categories needed;the assessment of the malaria situation and the furtherstudy of epidemiological conditions; the organizationof medical aid consisting of diagnostic services andthe distribution of drugs to people living in malariousareas; and the study and development of the mostsuitable approach to ensure the fullest collaboration ofthe public in the future malaria eradication programme.

106 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
The keynote of the development of the rural healthinfrastructure in a pre- eradication programme is
" total coverage "; but the type of health networkrequired for the support of the malaria eradicationprogramme which is to follow is of the simplest, forit is not the concern of a pre- eradication programmeto promote the development of administrative andhealth services to the level required to meet a country'sover -all health needs. At the same time it cannotbe expected that any country will remain content withthe elementary, though total coverage, service requiredin connexion with malaria eradication, and in thisway a pre- eradication programme should always belooked upon as a true public health promotionalactivity.
Although there is no rigid limit to the duration ofa pre- eradication programme, the relative timing ofthe achievement of " the two main objectives " isof importance. The national malaria service must befully ready to carry out its specialized role, at leastin the first operational zone of the country, beforea malaria eradication programme can be launched;and it is essential that the development of the healthinfrastructure be planned so that it will reach theminimum level required for the support of surveil-lance activities not later than the beginning of thethird year of the attack phase. Both in the interestsof economy and for the sake of the morale of thestaff, the malaria service should not be brought tooperational strength until the development of thehealth infrastructure by the required time can bedefinitely assured.
5.2.2 Health InfrastructureThe importance of the support given by a country's
general health services to its malaria eradicationprogramme and of its participation in that programmehas already been stressed earlier in this report(chapter 4 - General Health Services and MalariaEradication Programmes), and in paragraph 5.2.1above the essential elements of the developmentof the rural health infrastructure as the first mainobjective of a pre- eradication programme have beenmentioned.
In a malaria eradication programme, the respon-sibilities to be discharged by the health services areconnected, for the most part, with surveillanceoperations, and for this purpose the building -up ofthe peripheral services or " infrastructure " is essential.Such an infrastructure is a network of health postscapable of providing certain basic health services andplanned in such a way that an area is totally andevenly covered by it. It will form the permanentfoundation on which the health services can laterexpand according to needs and available resources.
A health post is a basic constituent of the infra-structure, and may serve a population of from 2500to 20 000. The size of the area served dependslargely on the prevailing local conditions and 5000to 10 000 is not an unreasonable average figure forplanning purposes. The primary responsibilities of ahealth post are described by the Expert Committeeon Malaria in its ninth report 1 as simple medicalcare, detection and prevention of certain communi-cable diseases, collection of information on vitalstatistics, maternal and child health work, basicenvironmental sanitation, and health education.
A health post should always have two distinctelements, one stationary and the other mobile, bothstaffed with auxiliary personnel. The stationaryelement should have a dispenser or nurse with ele-mentary training in simple medical care, functioningat the health post; the mobile element should havea health auxiliary to make routine visits covering theentire area assigned to the post, carrying out case -finding, reporting and simple preventive proceduresfor certain communicable diseases. The training ofsuch health auxiliaries is very elementary; in theMoroccan programme, for example, it takes eightmonths.
A health post should be able to perform, as oneof its normal functions, case -detection for malaria
both (by -house visits) andpassive (at the stationary health posts). Eventually,additional functions such as radical treatment, someelementary epidemiological investigations, etc., canalso be delegated to the post. The development ofthe infrastructure should be planned so that the healthposts reach the minimum standard required not laterthan the third year of the attack phase of a malariaeradication programme, in order to be able to carryout case -detection at the beginning of that activity.
The health infrastructure must be developed toinclude an effective supervision of the health posts.The first echelon of field supervisors can consist ofhealth auxiliaries, although they will need to bebetter qualified by training and experience than thoseworking at the health posts. A higher echelon ofprofessional supervision must also be assured.
5.2.3 National Malaria Service and AntimalariaActivities
The second basic objective of a pre- eradicationprogramme is to develop the national malaria service,which will become, in due course, the " nationalmalaria eradication service ", able to deploy theskill and resources necessary to secure and to maintainthe interruption of transmission until eradication isachieved.
1 Wld Hlth Org. techn. Rep. Ser., 1962, 243.

ANNEX 8 107
The national malaria service needs to grow graduallybut steadily, gathering information about the extentand nature of the malaria problem of the country,gaining knowledge and experience of its present andfuture responsibilities and developing the ability tomanage country -wide operations.
The first country -wide active antimalaria measurewhich needs to be implemented from the beginningof a pre- eradication programme is the organizationof a reliable system for the microscopic diagnosis ofmalaria and the distribution of antimalarial drugs,mainly for curative purposes, through existing healthunits, schools, post offices and any other suitablemethod of distribution. These activities should helpto create a " malaria consciousness " and must goalong with a health education campaign to stimulateand promote the maximum co- operation of the public,as well as of private and government agencies. Thedirection for such action must come initially fromthe highest government level, but the continued driveand supervision to ensure that the supply of drugsis adequate and that the diagnostic service is satis-factorily developed will be the duty of the nationalmalaria service in co- operation with the general healthservice. The Organization may assist with the labo-ratory equipment and drugs necessary for this basicantimalaria activity in cases where they are not pro-vided from other sources.
The next important function of the malaria serviceis to collect and study all pre- existing data on theepidemiology of malaria in the country and to carryout the surveys necessary to fill any gaps in knowledge,so that the extent of the malarious areas may beaccurately demarcated and the level of endemicity indifferent parts of the country determined Theresources for carrying out such duties, both parasito-logical and entomological, may be limited at thebeginning, but will certainly increase step by step.These investigations will comprise malariometricsurveys (both spleen and parasite) in randomlyselected areas. In areas in which the impact of era-dication measures is to be tested, priority has to begiven to parasite rates, especially infant parasite rates,as these are the most sensitive. It is also of importanceto have information on the distribution of the differentparasite species in the country.
For the planning of the future eradication pro-gramme, the study of the transmission season orseasons is essential, and it is here that entomologyhas a vital role to play. In the past it has all toofrequently happened that pressure to initiate sprayingoperations urgently has drastically reduced the timeavailable for basic entomological survey during thepreparatory phase of an eradication programme.The pre- eradication programme, however, provides
adequate opportunities to assemble the necessarybasic entomological data during complete cycles ofseasons, preferably covering two years. The mainvectors have to be determined, as well as their seasonalincidence in different parts of the malarious area.A full geographical and topographical study toobtain this information is important for the eventualdrawing -up of a sound plan of operations and willenable the entomologist to suggest the most appro-priate techniques from the wide range now available.
In order to ensure the gradual growth of the nationalmalaria service mentioned .earlier, practical fieldexperience has to be provided for its increasingnumber of technical personnel. For this purpose,demonstration and training areas are selected wherethe organizational requirements for spraying andsurveillance operations and other malaria eradicationprocedures, and their administrative implications, canbe demonstrated. These operational areas are limitedto the size required for demonstration and trainingpurposes and do not normally cover a populationgreater than 100 000, though in large countries, whereconditions may vary considerably from one part toanother and where these different conditions necessi-tate the trial of several organizational requirements, mo-re than one such operational area may need to be selec-ted and organized. These demonstration areas will alsoserve to collect preliminary data on the impact ofattack measures on malaria transmission under localconditions. Where necessary, and within the limitsof its available resources, the Organization is preparedto provide operational supplies and other assistance.
5.2.4 Progress in Pre -eradication Programmes
The progress achieved in the development of pre -eradication programmes is indicated by the fact thatby the end of 1962 programmes had started or werein the planning stage in twenty -three countries : ten inthe African Region - Cameroon, Ghana, Liberia,Madagascar, Mauritania, Mozambique, Nigeria, Sene-gal, Togo and Uganda; two in the South -East AsiaRegion- Indonesia (outer islands) and Nepal (in areasnot easily accessible); two in the European Region -Algeria and Morocco; four in the Eastern Mediter-ranean Region - Ethiopia, Saudi Arabia, Somalia andSudan; and five in the Western Pacific Region -Brunei, Cambodia, Republic of Korea, Republic ofViet -Nam, and West New Guinea (West Irian).
The approach to malaria eradication by way of thepre- eradication programme was fully discussed at theThird African Malaria Conference held at Yaoundéin July 1962, at which ministers of health, directorsof health and directors of malaria services met withsenior officials of the Organization. The technicalpolicies and prospects for development of the pre-

108 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
eradication programmes were fully endorsed by theparticipants and the majority of national represent-atives were anxious to begin planning for pre- eradica-tion programmes at an early date. An orientationseminar for WHO public health and malaria advisersof the African Region was held in October, at whichparticular attention was given to the implementationof a pre- eradication programme and the developmentof the rural health infrastructure as an integral part ofsuch a programme.
In Togo a detailed assessment has been made of theexisting basic public health services to permit the pre-paration of a plan for the development of the necessaryhealth infrastructure. Similar action will now beundertaken in other countries in the African Region.Considerable progress has, however, been made inthe collection of basic data on the epidemiology ofmalaria in a number of countries of the Region.
In South -East Asia, before the actual implement-ation of a pre- eradication programme in the outerislands of Indonesia, the national malaria eradicationservice has already been collecting demographic dataand studying the communications and facilitiesavailable in the area.
In the Eastern Mediterranean, the pre- eradicationprogrammes already in operation in Ethiopia andSomalia have facilities for training of health per-sonnel, and attention is being given to the develop-ment of the health infrastructure. Antimalaria demon-stration and training areas are also in operation.There are WHO- assisted malaria eradication trainingcentres in Ethiopia and Sudan. In Sudan, where thegeneral health services have been already well de-veloped, both in quality and extent, malaria eradicationis expected to be undertaken as part of the generalhealth programme once sufficient specialized personnelhave been trained.
In the European Region a very large trainingscheme for auxiliary health workers is already wellunder way in Morocco in twenty -four schools andcentres. All the personnel needed to staff the infra-structure at the required level are expected to beavailable not later than the beginning of 1965. Asthese personnel become available they are beingdeployed to carry out basic surveys and geographicalreconnaissance, and to make domiciliary visits forgeneral health purposes. The training of micro-scopists has been practically completed. Althoughthe pre- eradication programme proper is still in theplanning stage in Algeria, the training of auxiliaryhealth workers and microscopists has already started.
All five pre- eradication programmes in operation inthe Western Pacific Region have followed on otherantimalaria operations in these countries so that,except in Brunei, the basic structure of the nationalmalaria service exists, and extensive field operationshave already been undertaken. Particular attentionis, therefore, being given to the development ofadequate health infrastructures.
While there has been general acceptance by govern-ments of the soundness of the pre- eradication approachto eventual malaria eradication programmes, somehave hesitated to shoulder the large commitment thatseems to be involved in undertaking the developmentof country -wide rural health services, even of the mostelementary kind. In view of the determination ofthe World Health Assembly to reach the accepted goalof the global eradication of malaria, and the funda-mental role which the health infrastructure plays inmalaria eradication as well as in other health pro-grammes, it is hoped that enough financial assistancewill be obtainable to enable governments to developthese necessary services.
6. REGISTRATION OF AREAS WHERE MALARIA HAS BEEN ERADICATED,AND MAINTENANCE OF ACHIEVED ERADICATION
The official register of areas from which malaria hasbeen eradicated was established by the- Director -General at the request of the Thirteenth World HealthAssembly (resolution WHA13.55). During 1962, nofurther country or territory was entered in thisregister; thus Venezuela is so far the only countrylisted in the register as having achieved malariaeradication in large parts of the national territory.
However, in addition to various requests for futurecertification and registration already received, pri-marily from countries of the European continent,Cyprus, Grenada and St Lucia have, during the pastyear, asked to be included in the register after the
necessary certification. Cyprus has been under main-tenance since eradication was achieved in 1950 andno indigenous malaria cases have been reported sincethen. In Grenada and St Lucia malaria has beeneliminated after execution of a normal malaria era-dication programme. In both islands no malariacases have been found for several years, in spite ofelaborate case -detection activities. The island ofGrenada is considered to have been under maintenancesince July 1962, while St Lucia terminated its consoli-dation phase at the end of December 1962.
Consideration was given during the year to im-proving the methodology of certification. In anti-

ANNEX 8 109
cipation of the final certification of malaria eradicationin the near future in a number of Greek islands andin Spain, officials of the WHO Regional Office forEurope visited Greece and Spain to advise the Govern-ments on the methodology for carrying out the certi-fication during 1963. This includes the provision ofevidence that the epidemiological criteria for theachievement of eradication have been met, and ofinformation on the adequacy of the coverage by therural health services and their proficiency in malariacase -detection and investigation.
In view of the increase in the number of countriesapproaching the end of the consolidation phase,
7.1 Problem Areas
especially in the European continent, considerableattention was given during 1962 to the preparation ofthe health services to undertake vigilance responsi-bilities.
A major concern in maintenance areas is to preventthe reintroduction of malaria. In order to assistnational public health services in this task, the Organ-ization began in 1962 periodical dissemination ofinformation on the epidemiological status of malariain the world through the Weekly EpidemiologicalRecord. This will allow health authorities to appraisethe degree of danger of reintroduction of malaria fromother parts of the world.
7. PROBLEMS FACING MALARIA ERADICATION
The drive towards malaria eradication in the worldhas brought to light a number of new technicalproblems, some of them of very definite operationalsignificance. For some time physiological resistanceto insecticides has been recognized as an importanttechnical problem in malaria eradication, but duringthe last two or three years it has been realized thatother technical problems may account for the persist-ence of transmission in what are commonly referredto as problem areas, that is, areas in which transmis-sion has not been interrupted in spite of regularspraying and good coverage.
In Mexico, after four years of attack phase, it wasfound that transmission had been interrupted in 77 percent. of the originally malarious territory. In approx-imately 10 per cent. of the remaining areas, the persist-ence of transmission could be attributed to opera-tional problems and administrative shortcomings,but in about 13 per cent. of the originally malariousterritory, with a population of approximately2 600 000,
transmission persisted for technical reasons -in thePacific coastal area, where the vector is Anophelesalbimanus, and in inland areas where malaria is carriedby A. pseudopunctipennis. Reasons for the persist-ence of transmission in a country of such variedtopography and climate as Mexico may differ fromone problem area to another, but from the studiesundertaken jointly by the Mexican malaria eradica-tion service and the WHO team for special epidemio-logical studies, it appears that in the State of Oaxacacontinued transmission is probably due to the behav-iour of A. albimanus and A. pseudopunctipennis andnot to physiological resistance to DDT -at least inthe case of A. pseudopunctipennis, the main vector inthe area. Human ecology, on the other hand, seemsa comparatively unimportant factor. The local in-
habitants seldom sleep out -of- doors, and labourmigrations and other population movements are rarein the area. The type of houses, however, may beof importance. A survey of housing conditions in thearea indicated that positive cases tended to occur inisolated or peripheral dwellings of poor construction,with lack of walls or discontinuity of walls. In themore solidly built houses in the centre of the villagespositive cases were rare, but they occurred neverthe-less, indicating that housing conditions alone could notexplain the persistence of transmission. The abilityof the vectors to enter sprayed houses at night, bitethe inhabitants inside and escape after little or nocontact with the sprayed walls, seemed to be the maincause of the persistence of transmission.
An incipient development of DDT resistance inA. albimanus appeared to exist in some of the localitiesstudied in Oaxaca, but this was not considered themain reason for the persistence of transmission. InEl Salvador, where aerial spraying against cottonpests has produced a very marked DDT resistance inA. albimanus, a research team from the RegionalOffice for the Americas found that the degree ofresistance was not correlated with the amount oftransmission, and that causes other than physiologicalresistance were at play.
In Venezuela, in what are called areas of " refractorymalaria," which are in fact " problem areas ", thelocal vector, A. nuñez- tovari, seems to avoid the actionof DDT, probably because of its exophilic habits.The use of other insecticides and the increase in thenumber of DDT spraying cycles, combined withvigorous mass treatment there, has not resulted in thecomplete interruption of transmission, probablybecause of the continuous influx of fresh infectionsbrought by imported labour from neighbouringColombia, where the same thorough eradication meas-ures have not yet been undertaken.

110 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Mass distribution of drugs has been used withsuccess in Trinidad to overcome the problem of out-door biting A. (Kertezia) bellator. Monthly treat-ment with chloroquine and primaquine resulted in arapid interruption of transmission, no autochthonouscases having been found in the island since September1960.
Larviciding from the ground on a small scale hasbeen tried in Mexico and El Salvador as a supplemen-tary measure to DDT spraying without clear success,but the more promising large -scale larviciding from theair is now being tried in El Salvador. In this and otherCentral American countries the possibility of usingfor residual spraying insecticides other than chlori-nated hydrocarbons is being considered. In El Sal-vador and Nicaragua malathion was tried recently,without conclusive results, perhaps because the sprayedareas were too small.
Outside the Region of the Americas the delimitationand study of problem areas is less advanced, probablybecause the eradication programmes have not pro-gressed at the same pace as in the Americas. Thereare nevertheless some well -known problem areas, suchas the A. stephensi areas in Iran, where this vectorhas developed insecticide resistance to both the DDTand dieldrin groups of chlorinated hydrocarbons.Also in the area of distribution of A. 1. balabacensis,particularly in Thailand, Cambodia and Viet -Nam,problems of behaviour rather than physiologicalresistance seem to account for the failure to interrupttransmission, but here it has not yet been possible toseparate entirely the technical problems from admin-istrative and operational shortcomings, the two oftenoverlapping.
To face the threat posed by the persistence of trans-mission in problem areas, the Organization has in thefirst place encouraged the investigation of the factorsthat may account for this failure. A team for specialepidemiological studies was set up to help in investi-gating some of the problem areas of the world and alsoin developing an adequate methodology. The Organ-ization has also established a scheme for screening andvetting new insecticides that could be used againstmalaria and other insect -borne diseases; with theco- operation of the Governments of Uganda andNigeria it is now carrying out field trials in Africawith malathion and DDVP, which represent the laststage in this screening and testing scheme.
7.2 Resistance of Malaria Parasites to DrugsTo date, drug resistance had nowhere become a
grave problem in malaria eradication. The onlydrugs to which definite resistance of malaria parasiteshas occurred on a significant scale are proguanil andpyrimethamine. Proguanil, on account of its short-
lived action, is not recommended in eradication pro-grammes, and resistance to pyrimethamine can beavoided if this drug is not used alone for treatment ofestablished blood infections. Pyrimethamine shouldbe used only for its prophylactic and sporontocidalaction and always in association with adequate dosesof chloroquine or amodiaquine.
Since October 1960, drug resistance has attractedrenewed attention, following reports of the occurrenceof a" Plasmodium falciparum strain with a highdegree of tolerance to chloroquine. This strain,which seems to have originated in Colombia, wasisolated from a non -immune patient who had workedin Colombia and had suffered from frequent malariaattacks in spite of repeated treatment with chloroquine.The strain was investigated in the National Institutesof Health in the United States of America and wasfound to have a high tolerance, not only to chloro-quine, but also to other 4- aminoquinolines. In viewof these findings, a number of field epidemiologicalsurveys have been carried out in the areas of the pos-sible origin of this strain, as well as in various areasof Brazil from which "chloroquine- resistant" P. falci-parum infections had been reported. These surveys,which began in early 1961, are still continuing, but sofar no evidence has been found of any occurrence ofchloroquine- resistant strains in these areas. Theresistant strain from Colombia thus appears to be anisolated case and has probably not spread in the field.
More recently, observations have been reportedthat falciparum infections in non -immune patients,who had acquired the infection in Thailand, Cambodiaor Malaya, did not respond " normally " to the usualstandard treatment with chloroquine, or that earlyrelapses occurred. These cases are still under investi-gation.
Since chloroquine is at present the most widelyused drug in eradication programmes, it is obviousthat widespread resistance to this and similar drugswould present a serious problem in malaria eradication.It is therefore necessary to maintain a close watchon the situation and to analyse carefully any reportsof alleged drug resistance in the field. The occur-rence of drug resistance should be considered onlyafter all possibilities of inadequate treatment or of drugfailure have been ruled out.
Drug failure, which is a much more common eventthan drug resistance, may be due to many causes, andmost often to the fact that the prescribed doses of thedrug have not actually been taken.
7.3 Vector Reactions to InsecticidesWhen the original concept of malaria eradication,
based primarily on the use of insecticides against thevector, was formulated it was realized that physio-
ANNEX 8 lIl
logical resistance to DDT and other residual insecti-cides might develop and constitute a serious obstacleto the malaria eradication programme. The fact thatresistance to DDT had already been reported in oneor two countries in the course of malaria controloperations provided an added incentive to establisha world -wide information service about the suscepti-bility status of all major vectors of malaria. By meansof the WHO susceptibility test, all this informationhas been obtained and recorded in a standardizedmanner, the results being summarized periodically bythe Organization and widely circulated. From theconsiderable information now available certain factsare emerging which are of some importance, in thatthey indicate that the practical significance of resistanceto insecticides depends largely on which of the twomain insecticides -DDT or dieldrin -is implicated.
As far as dieldrin resistance is concerned, the situa-tion is fairly well defined. When dieldrin resistancedevelops it usually progresses rapidly to the pointwhere a highly resistant mosquito population isselected out, and the insecticide ceases to be of furtheroperational value. In this connexion the dieldrinsusceptibility test data can provide a valuable earlywarning about impending breakdowns in the field.
The position with regard to DDT resistance ofvectors is very different, and there is increasing evi-dence that DDT may still be of operational value inseveral of the species which have developed " resist-ance ", or " increased tolerance " to DDT, forexample, A. sachavori, A. culicifacies and, possibly,A. pharoensis.
In contrast to the cases mentioned above, whereDDT has continued to be of operational value despitethe development of resistance, there are now severalwell established instances where DDT after severalyears of application is still failing to interrupt malariatransmission completely, despite the fact that thestandard physiological tests show that the vectorshave not developed any resistance or tolerance. Anoutstanding example of this is provided by A. gambiaein the savannah areas of West Africa, where dieldrinis contra -indicated because of established resistance,and where DDT, now being used, has failed to bringabout complete interruption of transmission, despitethe continued normal susceptibility of the vector.
It now appears that the explanation of this apparentanomaly must lie in the behaviour characteristics ofthe vectors concerned, particularly their reactions tothe well -known irritant quality of DDT deposits.Some vector species can continue to enter treatedhouses and feed on the occupants, but leave the housewithout having settled long enough on the irritantinsecticide deposits to absorb a lethal dose. In othercases the irritant effect of DDT may discourage the
vectors from entering treated houses, or may drivethem out of the house before they have had on oppor-tunity to feed. In the latter event the vital contactwith man may be disrupted to such an extent thatinterruption of transmission is achieved.
With the increasing attention being paid to problemareas (see section 7.1), it is clear that, when DDT isthe insecticide concerned, this behaviour aspect maybe the principal factor involved, even in some of theareas where recorded resistance to DDT might appearto offer the obvious explanation for failure to achievecontrol. The study of these behaviour reactions of thevector in the presence of insecticide is still at an earlystage, and further investigations may reveal thatirritability is not the only aspect to be considered. Thepossibility that other aspects of vector behaviour mayplay a major role in determining the success or other-wise of insecticide treatment is being kept in mind,particularly with regard to the new organophosphorusand carbamate insecticides now becoming availablefor field use.
With regard to the information on the resistancestatus of vectors, summarized in Table G, the fol-lowing features call for special comment. The con-siderable amount of information now available aboutthe susceptibility or resistance of the main malariavectors to the two principal insecticides in use -DDTand dieldrin- indicates that the general situation isbecoming more stabilized. In many countries inwhich physiological resistance to dieldrin was pre-viously reported, the switch -over to DDT has beenaccomplished without giving rise to new problems ofdual resistance. The comparatively few new recordsof resistance to dieldrin may be attributed in part tothe fact that the use of this insecticide is promptlysuspended as soon as resistance is detected, and inpart to a general decrease in the use of dieldrin inmalaria eradication programmes wherever there is apossibility of resistance developing.
The wide -scale use of the WHO susceptibility testhas confirmed that dieldrin resistance on the part ofA. gambiae is fairly widespread over the westerncountries of tropical Africa between a northern limitof Upper Volta and Northern Nigeria, and a southernlimit of the Congo (Brazzaville). In the countries ofeastern and south -eastern Africa, however, no dieldrinresistance has been recorded despite the use of insecti-cides of the dieldrin /BHC group for many years inparts of Tanganyika, Southern Rhodesia and Swazi-land. Throughout the whole of its area of distribu-tion A. gambiae continues to be susceptible to DDT.
With regard to the recently reported resistance ofA. minimus flavirostris to dieldrin in East Java, it isstill too early to judge its significance. The importanceof this species as a malaria vector in the Philippines
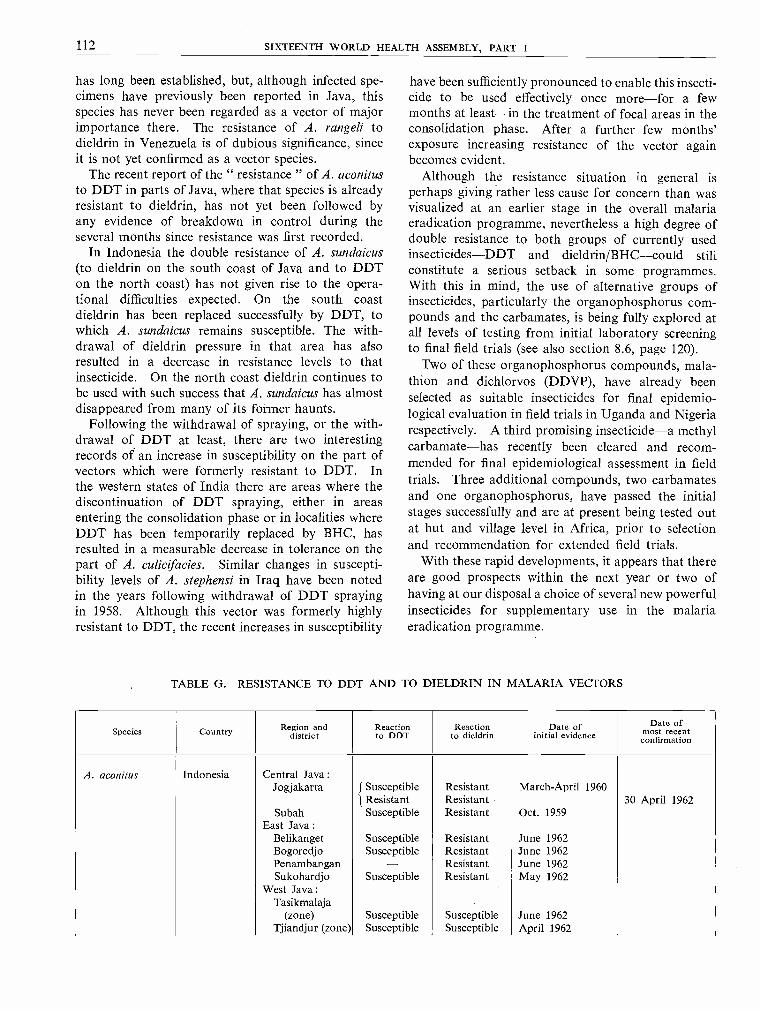
112 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
has long been established, but, although infected spe-cimens have previously been reported in Java, thisspecies has never been regarded as a vector of majorimportance there. The resistance of A. rangeli todieldrin in Venezuela is of dubious significance, sinceit is not yet confirmed as a vector species.
The recent report of the " resistance " of A. aconitusto DDT in parts of Java, where that species is alreadyresistant to dieldrin, has not yet been followed byany evidence of breakdown in control during theseveral months since resistance was first recorded.
In Indonesia the double resistance of A. sundaicus(to dieldrin on the south coast of Java and to DDTon the north coast) has not given rise to the opera-tional difficulties expected. On the south coastdieldrin has been replaced successfully by DDT, towhich A. sundaicus remains susceptible. The with-drawal of dieldrin pressure in that area has alsoresulted in a decrease in resistance levels to thatinsecticide. On the north coast dieldrin continues tobe used with such success that A. sundaicus has almostdisappeared from many of its former haunts.
Following the withdrawal of spraying, or the with-drawal of DDT at least, there are two interestingrecords of an increase in susceptibility on the part ofvectors which were formerly resistant to DDT. Inthe western states of India there are areas where thediscontinuation of DDT spraying, either in areasentering the consolidation phase or in localities whereDDT has been temporarily replaced by BHC, hasresulted in a measurable decrease in tolerance on thepart of A. culicifacies. Similar changes in suscepti-bility levels of A. stephensi in Iraq have been notedin the years following withdrawal of DDT sprayingin 1958. Although this vector was formerly highlyresistant to DDT, the recent increases in susceptibility
have been sufficiently pronounced to enable this insecti-cide to be used effectively once more -for a fewmonths at least -in the treatment of focal areas in theconsolidation phase. After a further few months'exposure increasing resistance of the vector againbecomes evident.
Although the resistance situation in general isperhaps giving rather less cause for concern than wasvisualized at an earlier stage in the overall malariaeradication programme, nevertheless a high degree ofdouble resistance to both groups of currently usedinsecticides -DDT and dieldrin /BHC -could stillconstitute a serious setback in some programmes.With this in mind, the use of alternative groups ofinsecticides, particularly the organophosphorus com-pounds and the carbamates, is being fully explored atall levels of testing from initial laboratory screeningto final field trials (see also section 8.6, page 120).
Two of these organophosphorus compounds, mala-thion and dichlorvos (DDVP), have already beenselected as suitable insecticides for final epidemio-logical evaluation in field trials in Uganda and Nigeriarespectively. A third promising insecticide -a methylcarbamate -has recently been cleared and recom-mended for final epidemiological assessment in fieldtrials. Three additional compounds, two carbamatesand one organophosphorus, have passed the initialstages successfully and are at present being tested outat hut and village level in Africa, prior to selectionand recommendation for extended field trials.
With these rapid developments, it appears that thereare good prospects within the next year or two ofhaving at our disposal a choice of several new powerfulinsecticides for supplementary use in the malariaeradication programme.
TABLE G. RESISTANCE TO DDT AND TO DIELDRIN IN MALARIA VECTORS
Species Country Region anddistrict
Reactionto DDT
Reactionto dieldrin
Date ofinitial evidence
Date ofmost recent
confirmation
A. aconitus Indonesia Central Java :Jogjakarta Susceptible Resistant March -April 1960
J Resistant Resistant 30 April 1962Subah Susceptible Resistant Oct. 1959
East Java :Belikanget Susceptible Resistant June 1962Bogoredjo Susceptible Resistant June 1962Penambangan - Resistant June 1962Sukohardjo Susceptible Resistant May 1962
West Java :Tasikmalaja
(zone) Susceptible Susceptible June 1962Tjiandjur (zone) Susceptible Susceptible April 1962
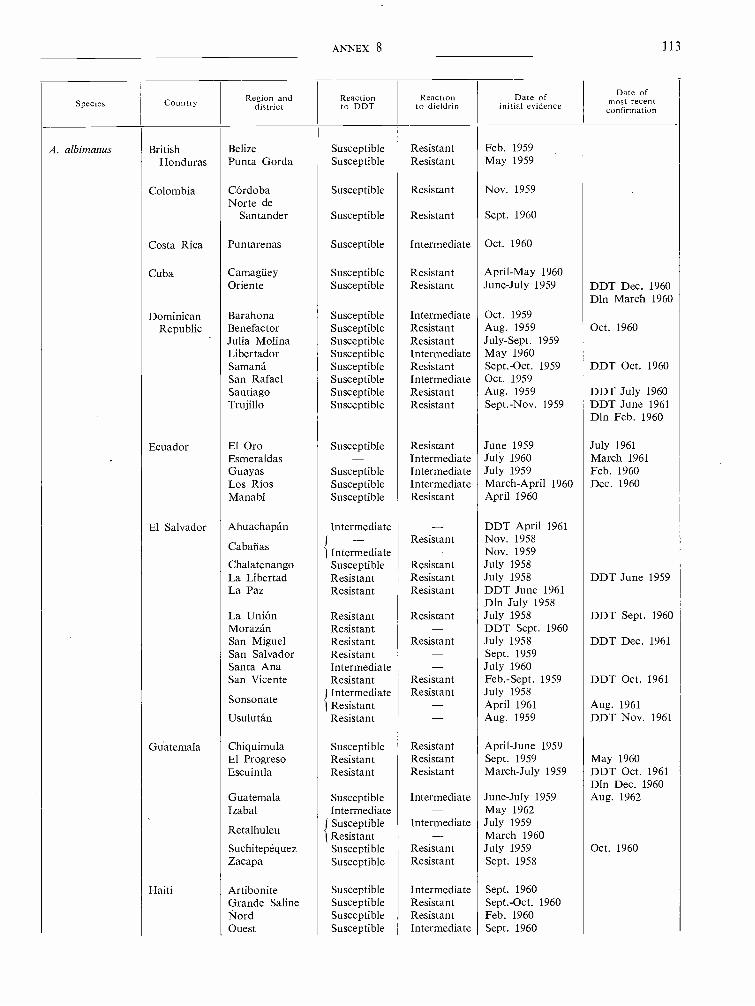
ANNEX 8 113
Species CountryRegion and
districtReactionto DDT
Reactionto dieldrin
Date ofinitial evidence
Date ofmost recent
confirmation
A. albimanus British Belize Susceptible Resistant Feb. 1959Honduras Punta Gorda Susceptible Resistant May 1959
Colombia Córdoba Susceptible Resistant Nov. 1959Norte de
Santander Susceptible Resistant Sept. 1960
Costa Rica Puntarenas Susceptible Intermediate Oct. 1960
Cuba Camagüey Susceptible Resistant April -May 1960Oriente Susceptible Resistant June -July 1959 DDT Dec. 1960
DIn March 1960
Dominican Barahona Susceptible Intermediate Oct. 1959Republic Benefactor Susceptible Resistant Aug. 1959 Oct. 1960
Julia Molina Susceptible Resistant July -Sept. 1959Libertador Susceptible Intermediate May 1960Samaná Susceptible Resistant Sept. -Oct. 1959 DDT Oct. 1960San Rafael Susceptible Intermediate Oct. 1959Santiago Susceptible Resistant Aug. 1959 DDT July 1960Trujillo Susceptible Resistant Sept. -Nov. 1959 DDT June 1961
Din Feb. 1960
Ecuador El Oro Susceptible Resistant June 1959 July 1961Esmeraldas Intermediate July 1960 March 1961Guayas Susceptible Intermediate July 1959 Feb. 1960Los Ríos Susceptible Intermediate March -April 1960 Dec. 1960Manabí Susceptible Resistant April 1960
El Salvador Ahuachapán Intermediate DDT April 1961Resistant Nov. 1958
Cabañas { Intermediate Nov. 1959Chalatenango Susceptible Resistant July 1958La Libertad Resistant Resistant July 1958 DDT June 1959La Paz Resistant Resistant DDT June 1961
Din July 1958La Unión Resistant Resistant July 1958 DDT Sept. 1960Morazán Resistant DDT Sept. 1960San Miguel Resistant Resistant July 1958 DDT Dec. 1961San Salvador Resistant Sept. 1959Santa Ana Intermediate July 1960San Vicente Resistant Resistant Feb. -Sept. 1959 DDT Oct. 1961
Sonsonate/Intermediatel Resistant
Resistant July 1958April 1961 Aug. 1961
Usulután Resistant Aug. 1959 DDT Nov. 1961
Guatemala Chiquimula Susceptible Resistant April -June 1959El Progreso Resistant Resistant Sept. 1959 May 1960Escuintla Resistant Resistant March -July 1959 DDT Oct. 1961
Dln Dec. 1960Guatemala Susceptible Intermediate June -July 1959 Aug. 1962Izabal Intermediate May 1962
Retalhuleu {SusceptibleResistant
Intermediate July 1959March 1960
Suchitepéquez Susceptible Resistant July 1959 Oct. 1960Zacapa Susceptible Resistant Sept. 1958
Haiti Artibonite Susceptible Intermediate Sept. 1960Grande Saline Susceptible Resistant Sept. -Oct. 1960Nord Susceptible Resistant Feb. 1960Ouest Susceptible Intermediate Sept. 1960

114 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Species Country Region anddistrict
Reactionto DDT
Reactionto dieldrin
Date ofinitial evidence
Date ofmost recentconfirmation
A. albimanus Honduras Atlántida Intermediate Oct. 1960(continued) Choluteca Resistant - Nov. 1959 Sept. 1961
Comayagua Resistant Resistant Nov. 1958 DDT Nov. 1960Cortés Susceptible Resistant Jan. 1959El Paraíso Intermediate - July 1960Francisco Mora -
zán Resistant Resistant Jan. -April 1959 Oct. 1962Valle Resistant - Nov. 1961
Jamaica Susceptible Resistant Nov. 1958 Feb. 1959
Mexico Chiapas Susceptible Resistant Dec. 1959 Din Sept. 1960Guerrero Susceptible Intermediate May 1960Michoacán Resistant May 1959Puebla Susceptible Intermediate Oct. 1960
Nicaragua Carazo Intermediate Resistant Nov. 1959
Chinandega 1 Resistant- ResistantOct. 1959Oct. 1958
Nov. 1961May 1960
Chontales Resistant - May 1961Estelí Resistant Resistant Feb. 1960Granada Intermediate Resistant Oct. -Nov. 1959León Resistant Resistant April -Sept. 1959 DDT March 1961Madriz Resistant - Feb. -March 1961Managua Resistant Resistant Oct. 1958 Dec., 1960Masaya Intermediate - July 1959Nueva Segovia Susceptible Resistant Oct. 1958Rivas Susceptible Resistant April 1959
A. albitarsis * Colombia Tolima Resistant Resistant April 1961
Venezuela Barinas Susceptible Resistant Sept. 1961
A. aquasalis Brazil Pará Susceptible Resistant March -May 1959
Trinidad andTobago Trinidad Susceptible Resistant Aug. 1958 Feb. -July 1959
Venezuela Sucre Susceptible Resistant Aug. 1959 Sept. 1961
A. culicifacies India Andhra Pradesh :Krishna Susceptible Intermediate Nov. 1960
Gujarat :Ahmedabad Intermediate May 1961Ahwa Intermediate - 1961
Baroda Intermediate Susceptible Sept. 1959 1961Broach Intermediate Susceptible 1961Dangs Intermediate - 1961
Kaira Intermediate Susceptible Dec. 1959 April 1961Resistant Susceptible Sept. 1959 April 1961
Panch Mahals 1 Resistant - May 1962Surat Intermediate 1961
Madhya PradeshBetul Intermediate Jan. 1961 Jan. 1962
Maharashtra : Intermediate 1961Chanda 1 Resistant Feb. 1962
East Khandesh Resistant Jan. 1961 July and Sept.(Jalgaon) 1962
Thana Susceptible Intermediate Oct. 1958
* Vector status not established.
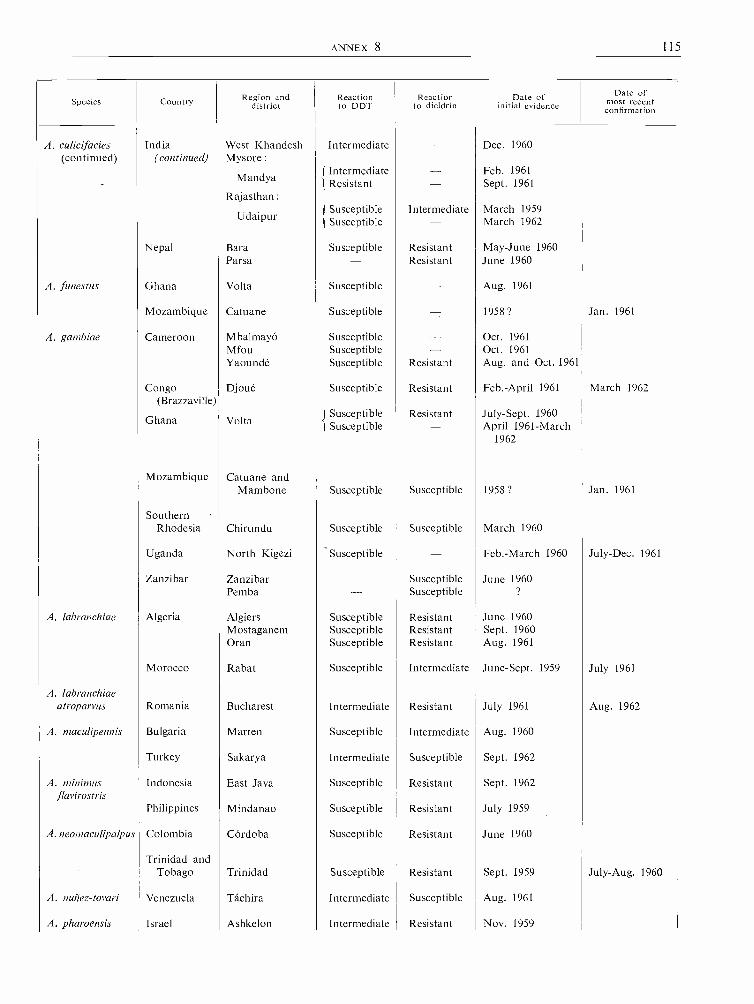
ANNEX 8 115
Species Country Region anddistrict
Reactionto DDT
Reactionto dieldrin
Date ofinitial evidence
Date ofmost recent
confirmation
A. culicifacies India West Khandesh Intermediate - Dec. 1960(continued) (continued) Mysore :
MandyaIntermediate - Feb. 1961
Î Resistant - Sept. 1961Rajasthan :
Udaipur 1 Susceptiblet Susceptible
Intermediate- March 1959March 1962
Nepal Bara Susceptible Resistant May -June 1960Parsa - Resistant June 1960
A. funestus Ghana Volta Susceptible - Aug. 1961
Mozambique Catuane Susceptible - 1958 ? Jan. 1961
A. gambiae Cameroon Mbalmayó Susceptible - Oct. 1961Mfou Susceptible - Oct. 1961Yaoundé Susceptible Resistant Aug. and Oct. 1961
Congo Djoué Susceptible Resistant Feb. -April 1961 March 1962(Brazzaville)
Ghana Volta( Susceptible
SusceptibleResistant- July -Sept. 1960
April 1961 -March1962
Mozambique Catuane andMambone Susceptible Susceptible 1958 ? Jan. 1961
SouthernRhodesia Chirundu Susceptible Susceptible March 1960
Uganda North Kigezi ' Susceptible - Feb. -March 1960 July -Dec. 1961
Zanzibar Zanzibar - Susceptible June 1960Pemba - Susceptible ?
A. labranchiae Algeria Algiers Susceptible Resistant June 1960Mostaganem Susceptible Resistant Sept. 1960Oran Susceptible Resistant Aug. 1961
Morocco Rabat Susceptible Intermediate June -Sept. 1959 July 1961
A. labranchiaeatroparvus Romania Bucharest Intermediate Resistant July 1961 Aug. 1962
A. maculipennis Bulgaria Marten Susceptible Intermediate Aug. 1960
Turkey Sakarya Intermediate Susceptible Sept. 1962
A. minimsflavirostris
Indonesia East Java Susceptible Resistant Sept. 1962
Philippines Mindanao Susceptible Resistant July 1959
A. neomaculipalpus Colombia Córdoba Susceptible Resistant June 1960
Trinidad andTobago Trinidad Susceptible Resistant Sept. 1959 July -Aug. 1960
A. nuñez- tovari Venezuela Táchira Intermediate Susceptible Aug. 1961
A. pharoensis Israel Ashkelon Intermediate Resistant Nov. 1959
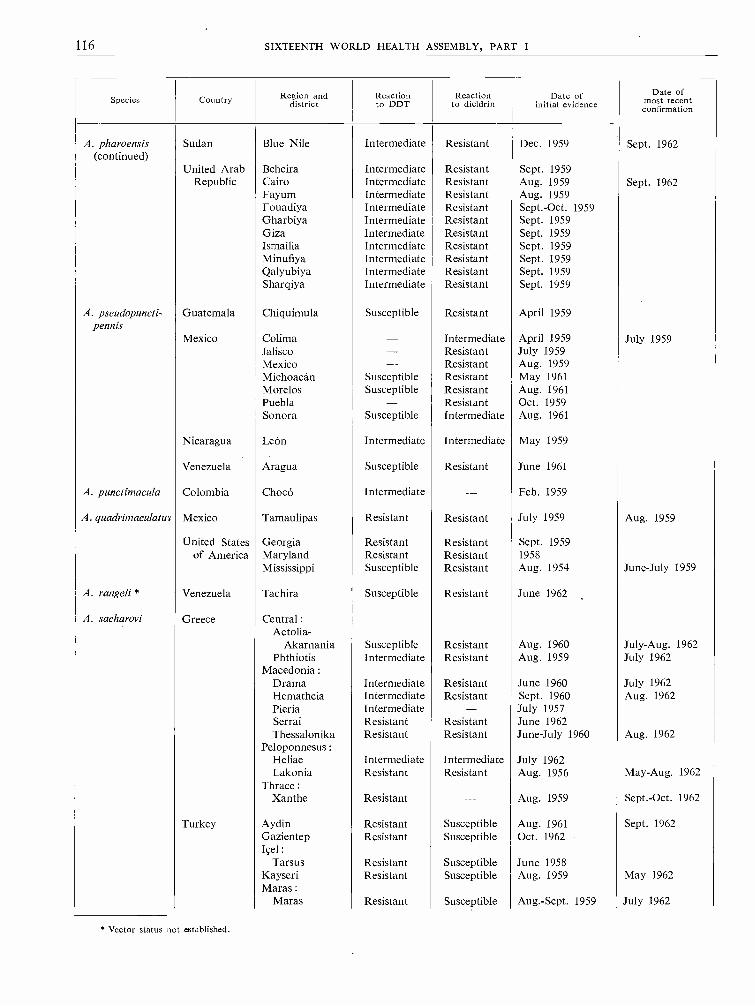
116 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Species Country Region anddistrict
Reactionto DDT
Reactionto dieldrin
Date ofinitial evidence
Date ofmost recent
confirmation
A. pharoensis(continued)
Sudan Blue Nile Intermediate Resistant Dec. 1959 Sept. 1962
United Arab Beheira Intermediate Resistant Sept. 1959Republic Cairo Intermediate Resistant Aug. 1959 Sept. 1962
Fayum Intermediate Resistant Aug. 1959Fouadiya Intermediate Resistant Sept. -Oct. 1959Gharbiya Intermediate Resistant Sept. 1959Giza Intermediate Resistant Sept. 1959Ismailia Intermediate Resistant Sept. 1959Minufiya Intermediate Resistant Sept. 1959Qalyubiya Intermediate Resistant Sept. 1959Sharqiya Intermediate Resistant Sept. 1959
A. pseudopuncti-pennis
Guatemala Chiquimula Susceptible Resistant April 1959
Mexico Colima - Intermediate April 1959 July 1959Jalisco - Resistant July 1959Mexico - Resistant Aug. 1959Michoacán Susceptible Resistant May 1961Morelos Susceptible Resistant Aug. 1961Puebla - Resistant Oct. 1959Sonora Susceptible Intermediate Aug. 1961
Nicaragua León Intermediate Intermediate May 1959
Venezuela Aragua Susceptible Resistant June 1961
A. punctimacula Colombia Chocó Intermediate - Feb. 1959
A. quadrirnaculatus Mexico Tamaulipas Resistant Resistant July 1959 Aug. 1959
United States Georgia Resistant Resistant Sept. 1959of America Maryland Resistant Resistant 1958
Mississippi Susceptible Resistant Aug. 1954 June -July 1959
A. rangeli * Venezuela Tachira Susceptible Resistant June 1962
A. sacharovi Greece Central:Aetolia-
Akarnania Susceptible Resistant Aug. 1960 July -Aug. 1962Phthiotis Intermediate Resistant Aug. 1959 July 1962
Macedonia :Drama Intermediate Resistant June 1960 July 1962Hematheia Intermediate Resistant Sept. 1960 Aug. 1962Pieria Intermediate - July 1957Serrai Resistant Resistant June 1962Thessalonika Resistant Resistant June -July 1960 Aug. 1962
Peloponnesus:Heliae Intermediate Intermediate July 1962Lakonia Resistant Resistant Aug. 1956 May -Aug. 1962
Thrace :Xanthe Resistant - Aug. 1959 Sept. -Oct. 1962
Turkey Aydin Resistant Susceptible Aug. 1961 Sept. 1962Gazientep Resistant Susceptible Oct. 1962Içel:
Tarsus Resistant Susceptible June 1958Kayseri Resistant Susceptible Aug. 1959 May 1962Maras :
Maras Resistant Susceptible Aug. -Sept. 1959 July 1962
* Vector status not established.
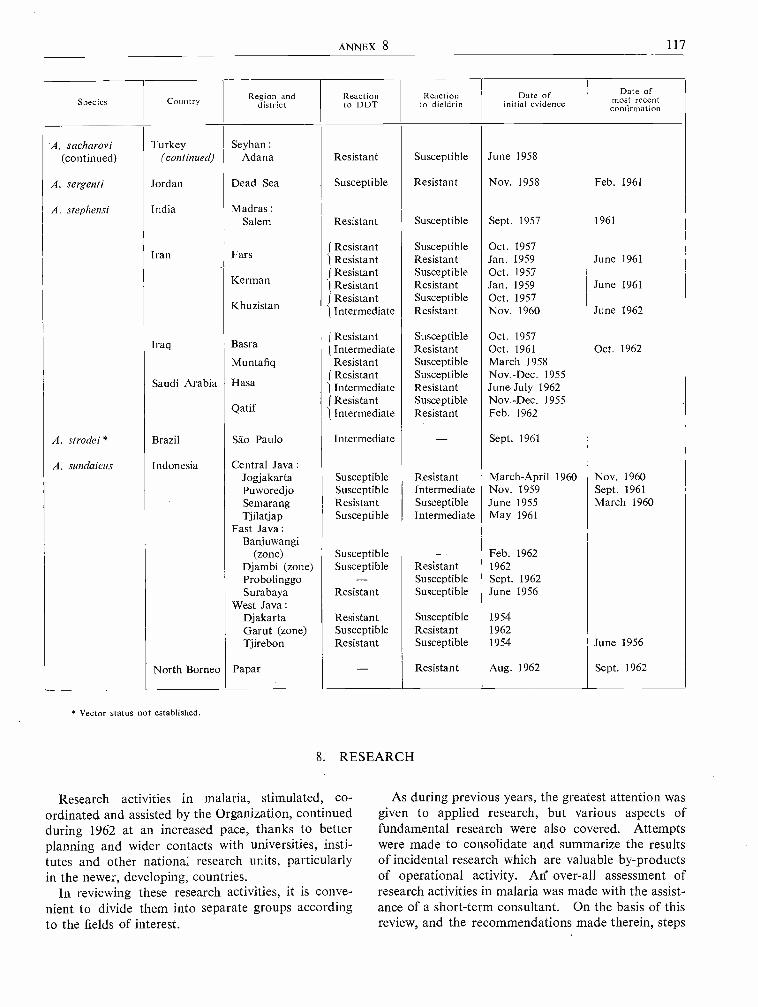
ANNEX 8 117
Species Country Region anddistrict
Reactionto DDT
Reactionto dieldrin
Date ofinitial evidence
Date ofmost recent
confirmation
A. sacharovi Turkey Seyhan :(continued) (continued) Adana Resistant Susceptible June 1958
A. setgenti Jordan Dead Sea Susceptible Resistant Nov. 1958 Feb. 1961
A. stephensi India MadrasSalem Resistant Susceptible Sept. 1957 1961
Iran FarsJ ResistantI Resistant
SusceptibleResistant
Oct. 1957Jan. 1959 June 1961
KermanJ Resistantl Resistant
SusceptibleResistant
Oct. 1957Jan. 1959 June 1961
Resistant Susceptible Oct. 1957Khuzistan Intermediate Resistant Nov. 1960 June 1962
Iraq Basra f Resistantl Intermediate
SusceptibleResistant
Oct. 1957Oct. 1961 Oct. 1962
Muntafiq Resistant Susceptible March 1958
Saudi Arabia Hasa J ResistantIntermediate
SusceptibleResistant
Nov, -Dec. 1955June -July 1962
J Resistant Susceptible Nov. -Dec. 1955Qatif IIntermediate Resistant Feb. 1962
A. strodei * Brazil Sao Paulo Intermediate - Sept. 1961
A. sundaicus Indonesia Central Java :Jogjakarta Susceptible Resistant March -April 1960 Nov. 1960Puworedjo Susceptible Intermediate Nov. 1959 Sept. 1961Semarang Resistant Susceptible June 1955 March 1960Tjilatjap Susceptible Intermediate May 1961
East Java :Banjuwangi
(zone) Susceptible - Feb. 1962Djambi (zone) Susceptible Resistant 1962Probolinggo - Susceptible Sept. 1962Surabaya Resistant Susceptible June 1956
West Java :Djakarta Resistant Susceptible 1954Garut (zone) Susceptible Resistant 1962Tjirebon Resistant Susceptible 1954 June 1956
North Borneo Papar - Resistant Aug. 1962 Sept. 1962
* Vector status not established.
8. RESEARCH
Research activities in malaria, stimulated, co-ordinated and assisted by the Organization, continuedduring 1962 at an increased pace, thanks to betterplanning and wider contacts with universities, insti-tutes and other national research units, particularlyin the newer, developing, countries.
In reviewing these research activities, it is conve-nient to divide them into separate groups accordingto the fields of interest.
As during previous years, the greatest attention wasgiven to applied research, but various aspects offundamental research were also covered. Attemptswere made to consolidate and summarize the resultsof incidental research which are valuable by- productsof operational activity. Alf over -all assessment ofresearch activities in malaria was made with the assist-ance of a short -term consultant. On the basis of thisreview, and the recommendations made therein, steps
118 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
are being taken to channel research efforts along themost fruitful lines.
8.1 Parasitology of Malaria
An investigation is in progress on the growth of exo-erythrocytic forms of P. gallinaceum in vitro andattempts are being made to infect erythrocytes fromsuch cultures in vitro. It may be possible to use thecultures of exo- erythrocytic forms as sources ofinfection of erythrocytes in vitro and as a known andconstant parasite material for chemotherapeutic assayand for the investigation of metabolic pathways ofmalaria parasites generally and in relation to somespecific drugs.
A study of the development of the peritrophic mem-brane of A. atroparvus, A. gambiae, A. stephensi andAedes aegypti is in progress; the behaviour of theookinete of P. gallinaceum and P. cynomolgi in rela-tion to peritrophic membrane development is beinginvestigated. It has been found that the peritrophicmembrane is quickly secreted and its developmentcompleted in thirty hours after the taking of a bloodmeal in Aedes aegypti and Anopheles gambiae and inforty -eight hours after taking a blood meal in A. atro-parvus. Ookinetes of P. gallinaceum adherent to iso-lated peritrophic membranes of Aedes aegypti have beenstudied and seen to change position very slowly.
As a result of an observation made in the field,which may be of some importance, the Organizationhas supported experimental work on the possibleinteraction between Semliki Forest virus and P. galli-naceum in Aedes aegypti.
An important field for research in parasitology todayis the study of simian malarias. The discovery of apossible zoonosis involving P. cynomolgi bastianelliihas stimulated interest in this field.
Investigations on simian malaria are at present beingcarried out by a joint research group of the UnitedStates Public Health Service and a national researchinstitute. A number of new species of simian malariaparasites have been discovered and their natural ano-pheline vectors traced in some cases. However, noevidence of natural transmission of monkey malariato man has been established. As many parallels maybe drawn from the study of the parasitological, ento-mological and epidemiological aspects of simian mala-ria and those of human malaria, the Organization hassigned an agreement with a research institute to under-take a study which may assist in explaining some ofthe puzzling epidemiological situations which occurat times.
The identification of plasmodial infections found insome species of Anopheles in the field is of particularimportance in areas where human malaria and animal
malaria occur. A research project is being carriedout on the identification of the species of sporozoitesfound in the salivary glands of mosquitos.
8.2 Chemotherapy
A small -scale trial of medicated salt has been set upin Africa, covering a population of some 3000 livingin a reasonably isolated area. The salt sources andintake have been carefully studied and on this basismedicated salt containing 0.3 per cent. chloroquinebase has been supplied. The medicated salt is soldat the same rate as normal salt and is extremelypopular. The results thus far obtained in this holo-endemic area have been encouraging.
For the preparation of medicated salt, compoundsof low water solubility, such as chloroquine hydroxy-naphthoate and chloroquine tannate, would be ofadvantage because they are not subject to " leachingout " as are the very soluble chloroquine diphosphateand sulfate. When given to children in large singledoses, choloroquine hydroxynaphthoate and tannatewere found to be poorly absorbed and thereforerelatively ineffective. It was thought, however, thatsmall daily amounts of these drugs, such as could beingested with medicated salt, might be completelyabsorbed. It was found on investigation that smalldaily doses of the hydroxynaphthoate, correspondingto 38 mg of the base and given to children for sevendays, cleared asexual parasitaemia due to P. falci-parum. Similar doses of chloroquine tannate provedless satisfactory.
At the annual meeting in November 1962 of theAmerican Society of Tropical Medicine, a new develop-ment in the field of malaria chemotherapy was reportedwhich may provide a valuable addition to the presentrange of therapeutic agents. This is a long- acting,injectable drug at present called CI -501 and chemicallyconsisting of the pamoic acid salt of 4,6- diamino -l-(p-chlorophenyl ) -1,2- dihydro -2,2- dimethyl -s- triazine.It is reported that a single dose of CI -501 protectedmonkeys from severe challenges with malaria parasitesfor an average of thirty -four weeks and that somewere protected for up to fifty weeks. None of thedoses caused local irritation or was systematicallytoxic. Similar results, though not so long lasting,were obtained in human volunteers. If further trialswith this drug give results as promising as those alreadyobtained, its employment may be considered in certainsituations in malaria eradication programmes, but itshould not be expected to solve all the problems. Asthe time has come when a field trial of this drug shouldbe carried out, a research project is being set up bythe Organization for the purpose. This project willalso serve for the testing of other potential anti-malarial drugs under development.

ANNEX S 119
A study of the mechanism and dynamics of drugresistance was undertaken; P. bastianellii and P. cyno-molgi were used for this work.
Consideration of the chemical structure of meta-bolites of some drugs may foretell the occurrence ofcross -resistance between these drugs. Nevertheless,the appearance of cross -resistance is not always pre-dictable; thus some proguanil- resistant strains of mala-ria parasite seem to be resistant to pyrimethamine,whereas others are not; but strains made resistant topyrimethamine by treatment with that drug appear tobe resistant to proguanil. This problem has not beenfully investigated under controlled conditions, and astudy of it has just begun.
A research project was started to study metabolicpathways of chloroquine- resistant and chloroquine-susceptible strains of rodent and primate malaria para-sites, using various substrates labelled with radioactivecarbon. The aim of these studies is to assess the pos-sible relationship between the phenomenon of drugresistance and the permeability barrier.
Research covering the synthesis of a series of deriv-atives of phenyl -diamidine -urea in order to assess theirpotential value as antimalarial drugs is being stimul-ated and supported.
Investigations devoted to the synthesis of compoundsof 6- aminoquinolines and of pyrocatechols and to theassessment of their value as antimalarials are now inprogress, and the first results obtained in avian andsimian malaria are encouraging.
A comparative study of the haemolytic effect ofprimaquine and quinocide in individuals with glucose -6- phosphate dehydrogenase (G- 6 -P.D.) deficiency isbeing carried out. For this investigation, a prelimi-nary survey of a group of West African males wascompleted and it was found that 20 per cent. weredeficient in this enzyme. All the G- 6 -P.D. deficientindividuals exhibited low blood -cell oxygen consump-tion but neither G- 6 -P.D. deficiency nor the presenceof abnormal haemoglobins appears to affect the hae-moglobin concentration. The investigation continues.
8.3 Immunology
One of the problems of practical importance in theimmunology of malaria concerns the development ofbetter techniques for detection of malaria infectionand for quantitative measurement of the degree ofacquired immunity to it. A research project toinvestigate these possibilities is being carried out inEurope, and another, with a slightly different experi-mental approach, in Africa. The methods used forthese investigations are fluorescent antibody tracing(direct and indirect) and gel diffusion technique forprecipitating antibodies.
An exceptionally (interesting application of themethod of fluorescent protein tracing has been deve-loped for the measurement of circulating antibody toplasmodial infections in the African population livingin holoendemic areas. Here the antigen was P. falci-parum, the conjugated serum was anti -human -globulinserum and the sera under test were from local in-habitants; these sera were serially diluted to obtaintitres at which the test gave a threshold staining re-action. The results showed that the technique can beused satisfactorily as a serological test for malariaimmunity.
The work on fluorescent protein tracing carried outunder semi -laboratory conditions is now ready forextension to the field and for assessment of the value ofthe test for malaria case -detection. This fieldproject on epidemiology is being carried out in WestAfrica, where a new phase in the development ofimmunology applied to malaria was started with thediscovery by a research team of a causal relationshipbetween the gamma -globulin level in the blood andacquired immunity to malaria. Purified gamma -globulin fractions were found to have a definite effecton the course of malaria infection.
Among the methods fot the assessment of immuneresponse to infection with blood protozoa, the respiro-metric test showed much promise, and research on itspractical value in mammalian malaria was stimulatedand assisted by WHO. The test is based on the factthat the energy of the malaria parasite is obtainedthrough oxydative glycolysis, the oxygen beingobtained from the oxyhaemoglobin. Parasitized redblood cells show a considerably increased oxygenconsumption, and it was necessary to determinewhether the antibody acts against the whole infectedred blood cell or only against the parasite itself.An alternative test, the tanned red cell haemagglutina-tion test, was developed and proved to be a sensitivetechnique for measuring antibodies developed againsta wide variety of antigens. Recently a modificationof this test, employing formolized tanned sheep cells,was used to determine its value for plasmodial infec-tions of primates.
8.4 Epidemiology
Knowledge of the duration of P. falciparum infec-tion in subjects with various degrees of acquired im-munity in the absence of transmission is of obviousimportance, and a research project aimed at the col-lection of some reliable data is now being carried outin Europe. At the present time only a small sampleof suitable subjects is being investigated and theinformation gathered is of limited value, but moreprogress is expected before long.

120 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
It has been recognized that a study of this kindwould be easier to carry out in an area closer to thesource of infection, where suitable subjects would beavailable in larger numbers. A second investigationhas therefore been sponsored by the Organization inan area where there is an influx of workers from mala-rious areas to a non -malarious area. These workersshould prove to be most suitable subjects, as they arelikely to remain in the non -malarious area for up tofive years before returning to their homes. The aimof this project is to study over a period of years theparasitology and symptomatology of P. falciparummalaria and effect of treatment in immune and semi -immune mine -workers transferred to a malaria -freearea.
An investigation of the frequency and character ofmalaria infections connected with blood transfusionhas been started.
A study of the relationship between malaria infec-tion of the placenta and prematurity and perinataldeath is taking place in East Africa.
An investigation of the relationship between theincidence of cerebral malaria and degree of parasi-taemia and the presence of abnormal haemoglobin inWest Africans was completed. The results showedthat all cases of fatal cerebral malaria occurred incarriers of AA haemoglobin and not one in carriers ofAS haemoglobin. The mean density of parasitaemiawas lower in subjects with the sickle -cell trait. Thepresence of AC haemoglobin and the presence of theglucose -6- phosphate dehydrogenase deficiency trait didnot seem to have a protective action in malaria infec-tion with P. falciparum.
8.5 Entomology
Research activities supported by WHO have beenmainly concerned with two important aspects of vectorreaction to insecticide treatment : first, the fact thatcertain vector species readily develop resistance toinsecticides while other species do not; secondly, thefact that different vectors may show different beha-viour in the presence of insecticide, this behavioursometimes playing a major role in determining thesuccess or otherwise of spraying operations.
With regard to the first aspect, a considerableamount of work is being carried but on the geneticsof resistance in order to study the mode of inheritanceand the factors causing the selection of resistant strainsin populations repeatedly exposed to insecticidepressure. This type of work, under an agreementwith WHO, has been particularly actively pursuedover the last four years. The most important fieldsof study are on the dieldrin- resistant strain of A. gam -biae from various parts of West Africa and the DDT -resistant strain of A. sundaicus from Indonesia. In
addition, strains of A. quadrimaculatus from the UnitedStates of America, A. pharoensis from the UnitedArab Republic, A. albimanus from El Salvador, andA. stephensi from India, are also being investigated.
Field investigations closely linked with these inten-sive laboratory studies have been carried out in Indo-nesia, in association with the national staff, to findout the effect of different insecticides and combina-tions of insecticides in delaying or suppressing theselection of vector strains resistant to dieldrin or toDDT. Those studies, primarily concerned with assist-ing in the long -term planning of the Indonesian pro-gramme, have already yielded information which maybe of great significance in the context of malariaeradication as a whole.
With regard to the behaviour of vectors whenexposed to insecticide, support is being given to studieson different aspects of this increasingly importantsubject. Field investigations are being carried out inSouthern Rhodesia and in Swaziland to explain whyinsecticide treatment -with BHC -in those countriesappears to have eradicated a man -biting strain of thevector A. gambiae, leaving behind a strain of thisvector which is mainly attracted to cattle and haslittle, if any, malarial significance. Supplementarystudies on the behaviour of vectors are also beingcarried out in West Africa, Europe and the Levant.
Closely concerned with the problems both of resist-ance and of behaviour is the increasing emphasisplaced on the existence of different strains of vectors,particularly A. gambiae in Africa. The existence ofsuch strains has long been suspected, in view of thefact that the same vector species may differ in reactionto insecticides, or differ in behaviour in different partsof Africa. Recent work supported by WHO andbased primarily on a careful analysis of crossingexperiments involving mosquito colonies of differentorigin has confirmed the existence of such strains, inA. gambiae at least. Two main groups of differingbehaviour have been defined so far. These groups orpopulations are isolated by a sterility barrier and cantherefore remain distinct even when they exist side byside in the same area. This work is being continuedon a collaborative basis -supported by WHO -byscientists in Africa and in Europe. It is expected thatthese investigations will have an increasingly importantbearing on the question of interpreting the effect onthe vector of different malaria eradication measures,as well as providing guidance on the choice of insecti-cide in long -term programmes.
8.6 Developments in Insecticides
The Organization's programme of research, evalua-tion and testing of insecticides provides, in the laststage, for the assessment under field conditions of any

ANNEX 8 121
new insecticide of potential value, as an alternative orotherwise, to the chlorinated hydrocarbons used inmalaria eradication. Following tests of restrictedeffectiveness and toxicological investigations, twoproducts -malathion and dichlorvos (DDVP) -are atpresent being tested in large -scale field trials. Bothare organophosphorus insecticides, but the first isapplied as a residual contact insecticide, while thesecond is strictly a fumigant, producing its effect onmosquitos by vapour concentration.
In order to assess their practical value in malariaeradication programmes, these insecticides are testedas regards their capacity to interrupt malaria trans-mission in areas with high or moderate endemicityand a long transmission season, with, if possible, littlepopulation movement, minimal outdoor sleepinghabits of the local population and one or, at the most,two vectors known to transmit malaria indoors.These technical requirements are a sine qua non for asound epidemiological evaluation in which malario-metric and entomological indices may be relied upon.Two areas responding to the above conditions havebeen found, in each of which 20 000 people will beunder protection of the insecticide and another 10 000
will be studied in a check area. For malathion, thefield trial area is located in Uganda, in the Masakadistrict; malathion is applied at a dosage of 2 g /m2,at intervals of three to four months. For dichlorvos,the project area is in Northern Nigeria, in the vicinityof Kankiya; in this latter trial two types of dispensers,one with solid and one with liquid 20 per cent. for -mulation, will be under test, each type being used forhalf the population in the field trial area. The resultsof the village scale trials out so far indicate that on theaverage one dispenser per 21 m3 is effective for tenweeks -a cycle and dosage which will be tried initiallyin the project. Both the malathion and dichlorvosfield research projects will be staffed by WHO teamscomposed of a malariologist, an entomologist, a sani-tarian and a technician.
Fenthion, another organophosphorus insecticide,which in preliminary and village scale trials has shownto be promising, requires further investigation on thetoxicological side.
Amongst other products tested in the WHO scheme,a carbamate insecticide has successfully passed throughall the preliminary stages and is ready for trial infield conditions.
9. CO- ORDINATION
Malaria eradication demands the closest possibleco- operation and the most effective co- ordination atall levels. Within a country, co- operation and co-ordination are required among the general medicaland health services, the malaria service, the publicservices as a whole and the general public. At thegovernmental level, interministerial and interdepart-mental co- ordination must be assured, and for thispurpose stress has been laid on the importance ofnational co- ordination committees in order to establishthe concurrent responsibilities of the various minis-tries, departments and agencies involved. Inter -country co- ordination is required between neigh-bouring countries in order that operations in borderareas may be carried out in the most effective andeconomical manner; and wider inter -country co-ordination between larger groups of neighbouringcountries is needed in order that they may movetogether towards the goal of eradication and thusreduce the risk of reimportation of the disease.
At this inter -country level, considerable progresshas been made during the year; in the Eastern Mediter-ranean Region, Iraq, Jordan, Lebanon and Syriahave agreed to develop a co- ordinated plan similarto that previously adopted by the European Region.This plan indicates the expected timing of the end
of the consolidation phase in the various areas andprovides for the periodic exchange of epidemiologicalinformation.
In addition to the meetings of directors of nationalmalaria eradication services which take place withinregions, there have been several important inter-regional conferences bringing together representativesof countries with common borders. During 1962,for example, there were the Second European Con-ference on Malaria Eradication. in Tangier in March,the Inter -regional Technical Meeting on MalariaEradication in Teheran in May, the Third AfricanMalaria Conference in Yaoundé in July, and theFourth Asian Malaria Conference in Manila inSeptember. Another form of international co- ordina-tion is reflected in the visits by senior personnel ofnational programmes to other malaria eradicationservices under the scheme for the exchange of scientificworkers.
Every effort has been made to maintain the closestcollaboration with the different international andbilateral agencies which are assisting countries inmalaria eradication. During the year, UNICEFco- operated with WHO in furnishing material assist-ance to thirty -three malaria eradication programmes,

122 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
of which twenty -one were in the Region of the Ameri-cas. UNICEF also gave assistance to the pre- eradi-cation survey in Sudan. The United States Agencyfor International Development (AID) assisted inseventeen malaria programmes (ten in the Americas)and co- operated with WHO /PAHO in the operation
of the malaria eradication training centre at Kingston,Jamaica. In line with past practice, as a means ofensuring the greatest possible collaboration betweenAID, UNICEF and WHO, a fifth meeting of aninformal co- ordinating committee of these agenciestook place in Washington in December 1962.
10. STATUS OF MALARIA ERADICATION BY REGIONS
10.1 African Region
10.1.1 General Progress and Prospects
In the concept of malaria eradication in the AfricanRegion, two basic facts must be considered of para-mount importance. First, the newly emerged countriesof Africa, with their urgent need of manpower foreconomic and social development, can ill afford tocontinue to pay the heavy toll which malaria mortalityimposes on the young age -groups of the population.Secondly, the campaign in this region forms partof the global malaria eradication programme; it is,therefore, imperative that the Region participate inthis collective effort in order to eliminate the dangerof reintroducing the disease from tropical Africa toother continents -a danger which becomes a realitywith present -day travel facilities.
The only eradication programmes in the region arethose on the islands of Mauritius and the ZanzibarProtectorate, and in Swaziland and the Republicof South Africa. In Mauritius, steady progress hasbeen made towards eradication : in 1961, 955 positivecases were recorded, as compared with only 226 casesin 1962. The case -detection mechanism was streng-thened by the reorganization of the malaria eradicationproject during April 1962. This included a reorganiza-tion of the epidemiological zones on the island,together with improved supervision of active case -detection and promotion of a better participationof the existing network of rural health service posts.In the Zanzibar programme, critical evaluation ofthe spraying operations has shown that total coveragehad not been attained in the past -which may explainthe failure to secure the complete interruption oftransmission. Geographical reconnaissance has,therefore, been instituted and the revised plan ofaction includes the spraying of all sprayable surfaces.
At its twelfth session the Regional Committee forAfrica endorsed a regional co- ordinated plan forinitiating pre- eradication programmes, envisaging theimplementation of seven new projects in 1962, ten in1963, and seventeen in 1964. Pre -eradication pro-grammes meet, first, the universal desire of newMember States to provide as rapidly as possible,
within their financial resources, a basic health servicefor their respective populations and, secondly, theirwish, as expressed during the deliberations of theWorld Health Assembly, to embark upon a pro-gramme for malaria eradication.
It is fully appreciated that there exist among MemberStates in the African Region different levels of pre-paredness for malaria eradication programmes, andalso differences in the time -schedules that those Statescan set themselves to reach full preparedness. Theco- ordination of effort by the several countriesincluded in the regional co- ordinated plan is cal-culated to ensure that no one country or group ofcountries in the African Region will be lagging too farbehind in the general progress towards the minimumpreparedness necessary for launching a full -scalemalaria eradication programme.
10.1.2 Training of National Malaria EradicationStiff
The training of the professional and auxiliarypersonnel in techniques of malaria eradication hasshown steady progress. The WHO malaria eradicationtraining centre at Lagos, Nigeria, for English- speakingstudents, held its first course from October to Decem-ber 1962; it was attended by fifteen non -professionaltrainees from the following countries : Gambia, Ghana,Liberia, Mauritius, Nigeria and Sierra Leone. Thefollowing courses were planned for 1963: a seniorcourse for professional staff, 7 January to 3 May;a course for senior national laboratory technicians,27 May to 28 August; and a junior course for auxiliarypersonnel, 1 October to 17 December.
A second WHO malaria eradication training centrehas been planned for French -speaking students atLomé, Togo. A preliminary agreement has beennegotiated with the Government, and constructionof the instructional block is due to be completed inMay 1963. The first course at this malaria eradicationtraining centre is expected to be organized before theend of 1963.
In addition to these training facilities which arebeing developed in the Region, twenty fellowshipswere awarded to nationals of various countries for

ANNEx 8 123
attendance at malaria eradication training courses atBelgrade, Kingston, Moscow and Sáo Paulo. Atcountry level, training of more junior categories ofnational staff destined to serve in the national malariaservice is undertaken in Cameroon, the Federationof Rhodesia and Nyasaland, Ghana, Mozambique,Togo, Uganda and Zanzibar.
10.1.3 Operational Aspects
In Mauritius, which has the most advanced WHO-assisted eradication programme in the Region, acritical reappraisal has resulted in the preparationof a new plan of operation ; this was signed by theGovernment and WHO in August 1962. For purposesof planning the programme, the island was dividedinto three operational zones, delimited on the basisof the existing malaria situation -a central main-tenance zone, an intermediary consolidation zone anda coastal attack zone. Since the beginning of sur-veillance operations in 1960, active case -detectionhas been the principal method used and has produced70 per cent. of the slides collected. Results during1962 showed steady progress, the total number ofpositive cases on the island having dropped from 955in 1961 to 226 in 1962, of which 932 and 207 res-pectively were in the coastal areas. Of the 207 casesin the coastal areas in 1962, 119 were in the district ofPort Louis. Here, active surveillance was not suffi-ciently developed and, despite the number of medicalunits situated in the suburban area, it has beenconsidered necessary to establish total coverage byactive case -detection.
In the programme in Zanzibar Protectorate, stepswere taken in 1962 to deal with several inherentdifficulties. The main defect discovered was that totalcoverage had not been attained in the past because theextremely high roofs in parts of the islands had notbeen treated. Furthermore, preliminary geographicalreconnaissance has demonstrated the need to bringthe existing maps up to date and to complete a full -scale geographical operation. For this purpose a firstgroup of twenty -four mappers has been trained.Provision has been made to combine the twice -yearlyspraying cycles with mass drug administration, usingcombined 4- aminoquiline /primaquine therapy, withthe aim of reducing the apparent asymptomaticparasite reservoir; however, the full impact of thismeasure will be assessed only in 1963.
In Southern Rhodesia, in the eastern sector of theproject area, where some spraying operations havebeen carried out during the past years, residualspraying was discontinued from May 1962 in orderto allow a complete geographical reconnaissanceto be undertaken before the resumption of sprayingin 1963. Under the terms of a new plan of operations,
which is under negotiation, this sector will serve asan area for demonstration and training and for costanalysis of spraying operations in typical areas ofvarying population density. In the western sector ofthe malaria eradication pilot project, the area has beenused to develop surveillance activities. Here trans-mission . has been interrupted, following residualspraying for some three years.
Spraying operations were carried out in theYaoundé pilot project of Cameroon from 1954 andwere discontinued in February 1960 after an assess-ment which proved that transmission of malaria hadbeen interrupted. Surveillance activities were there-fore initiated; however, by the second half of 1961,and especially during 1962, a high incidence ofmalaria started to reappear in the entire former pilotarea. This was also confirmed by data from clinicsin the project area which, inquiries revealed, werebeing attended by a continually increasing numberof patients with fever symptoms typical of malaria,although in the years up to mid -1961 malaria caseswere rarely seen there. The failure to keep the projectarea free from malaria was due not only to the factthat the area is completely surrounded by districtswith hyper- endemic malaria and that it has at itscentre the capital, Yaoundé, which attracts a con-siderable movement of population, but also todeficiencies in the surveillance operations.
Following the acceptance of the policy for pre -eradication programmes in the less developed newlyemerging countries, the Regional Office for Africa wasengaged in 1962, at the request of the Governmentsconcerned, in converting malaria eradication pilotprojects into pre- eradication programmes in Came-roon, Ghana, Mozambique, Northern Nigeria, Togoand Uganda, and initiating new pre -eradicationprogrammes in Liberia, Madagascar, Mauritania,Nigeria (two) and Senegal. Notification of acceptancehas been received from the Ivory Coast, while requestsfor additional information have been submitted bythe Governments of Dahomey and Tanganyika.There is little doubt that, as a principle on which toplan for the general development of health servicesin countries, the pre- eradication programme hasfound general acceptance in the countries of theRegion.
As regards the pre- eradication programmes whichhave already been started, demonstration and trainingareas are in operation in Ghana covering a populationof approximately 80 000. The northern section of thearea has been used primarily for the field trainingof national auxiliary personnel who are to serve in asupervisory capacity in the eventual malaria eradi-cation programme. In Cameroon, the results ofepidemiological surveys have made it essential for
124 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
the entire previous Yaoundé pilot project area to beused as the demonstration and training area for thepre- eradication programme. In Northern Nigeria,the demonstration and training area has yet to bedelineated but provisions have been made in the planof operation for it to be within the Western Sokotomass malaria control area where the Government iscommitted to maintaining field activities at least atexisting levels. In Togo, it was previously plannedthat the demonstration and training area under thepre- eradication programme would be in the northernpart of the country; however, that area does notappear to be suitable for all purposes and anotheris being considered. For this programme a short -termconsultant carried out, in co- operation with theTogolese and WHO country advisory staff, a surveyof the existing health resources of the country, witha view to drawing up a plan for the development ofthe rural health infrastructure, including the phasedtraining of the personnel required.
As in Cameroon, the epidemiological situation inthe Kigezi pilot project area in Uganda has made itnecessary to retain that project area for trainingpurposes in the pre- eradication programme in Uganda.
In Northern Ghana a field trial of medicated saltwas continued during the year. Distribution ofmedicated salt was started in July 1961 in the projectarea and within two months encouraging results wererecorded, as shown by a rapid reduction of over -allparasite rates from 80 to 6 per cent. However, therate of turnover of medicated salt started to declinein October 1961, and by December 1961 the dailyconsumption of medicated salt per person had fallenfrom the 5 g originally estimated to about 1 g. Investi-gations showed that the actual rate of salt consumptionhad not changed from the original estimates, and itwas proved that unmedicated salt was being madeavailable for sale surreptitiously. Following discus-sions with the Government, it was decided to amendthe method of salt distribution so that wholesalerswould be by- passed, and the retail sale would beundertaken by government- nominated agents. Inaddition, provisions were made for pre -packagingthe medicated salt in pennyworth plastic bags in aneffort to standardize the cost to the consumer. Thesenew measures became effective from 12 September1962.
Field trials with malathion are being undertaken inUganda, and with dichlorvos (DDVP) in NorthernNigeria.
10.1.4 Co- ordination
The Third African Malaria Conference was held inYaoundé, Cameroon, from 3 to 13 July 1962 under
the joint auspices of the Organization and the Com-mission for Technical Co- operation in Africa (CCTA).It was attended by representatives of 25 countriesin the African Region, by observers from CCTA andthe United States Agency for International Develop-ment, and by WHO staff of the African and EasternMediterranean Regions and headquarters.
As a sequel to the Yaoundé Conference, a meetingof WHO malariologists was held in Ibadan, Nigeria,in October 1962. This meeting was attended by WHOpublic health and malaria advisers of the Region,headquarters and regional office staff, and malariaadvisers of the Eastern Mediterranean Region fromprojects in the north -eastern part of Africa.
10.2 Region of the Americas
10.2.1 General Progress and Prospects
The malaria eradication programme progressedsteadily in 1962. During the year the attack phasewas completed throughout British Honduras, Jamaicaand Trinidad and Tobago, and these areas enteredthe consolidation phase. In parts of Argentina,Bolivia, Colombia, Costa Rica, Guadeloupe, Gua-temala, Honduras, Nicaragua, Panama Canal Zone,Peru, Surinam and Venezuela, further areas were alsoplaced in the consolidation phase. Some twelve anda half million more people than in 1961 are nowliving in areas in the consolidation phase.
Haiti began total coverage early in January and bythe end of the year had completed two cycles ofspraying without encountering serious problems. InBrazil new areas entered the attack phase and, ifthere is no setback in government support, the entiremalarious area of the country will be in the attackphase by the end of 1964. In addition to areas ofVenezuela, the islands of Carriacou, Grenada andSt Lucia entered the maintenance phase. These islandsare being registered as areas where malaria has beeneradicated.
A summary of the progress made towards eradica-tion is given below :
Population in areaswhere malaria
eradicationclaimed
in consolidationphase
1959 53 251 000 2 156 0001960 54 365 000 10 010 0001961 56 279 000 17 879 0001962 59 326 000 30 436 000
In addition, out of a total population of 153 891 000in the originally malarious areas, 49 386 000 are in
ANNEX 8 125
areas in the attack phase and 13 753 000 in areas inthe preparatory phase.
However, progress was not uniform throughoutthe Region. Administrative and financial deficiencieswere responsible for setbacks in some areas, and fornear stagnation in others. A serious economic crisisprevented extension of spraying operations to theprovinces of Chaco and Formosa in Argentina.This part of the campaign, therefore, will have to beconsidered as again in the preparatory phase, althoughgreat achievements have been accomplished in thepast. On the other hand, some countries (Colombia,El Salvador, Mexico, Nicaragua and Peru, amongothers) require additional funds to supplement theirprogrammes in order to interrupt transmission inproblem areas.
With the progress of the attack phase and theimprovement of epidemiological operations it hasbeen possible to delimit, with some precision, theareas with definite persistence of transmission incertain countries. In these areas, in addition to housespraying with insecticides, relatively expensive sup-plementary methods of attack must be applied.
Experience gained in 1962 shows that eradicationof malaria in the Americas within the present decadewill depend upon the will of the governments to giveit top priority in planning economic development.
At the end of 1962 the islands of Grenada andCarriacou and St Lucia were in the process of regis-tration as having achieved malaria eradication.
In Bolivia, British Honduras, Costa Rica, Domi-nica, Guadeloupe, Guatemala, Honduras, Jamaica,Panama Canal Zone, Surinam, Trinidad and Tobagoand Venezuela, progress has been maintained andcomplete eradication of malaria seems assured.
In a number of countries the prospects for eradi-cation appear good, but technical or administrativedifficulties have still to be overcome. For instance,inadequate financial support by the Government ofArgentina has slowed down the campaign in thatcountry. In British Guiana, transmission has beenalmost interrupted in the interior, except in part ofthe border with Brazil, where the population is usingnon -medicated salt which can be obtained morecheaply from over the border. Plans are being madeto begin spraying operations in this area. Totalcoverage has not yet been achieved throughout theentire malarious areas in Colombia, where a reorgani-zation of the administration of the campaign is necessary.In the Dominican Republic administrative reorganiza-tion is also required. In El Salvador and Nicaragua,technical difficulties are being encountered in theinterruption of transmission, and additional measures,
such as the use of organophosphorus insecticides,mass drug administration and larviciding, are beingtried out. In Mexico, additional financial supportis being sought to cover the cost of the supplementarymeasures needed to achieve interruption of transmis-sion in the problem areas. Financial difficulties arealso being encountered in Paraguay and Peru.
In Brazil, the attack phase began by stages in 1961and it is planned to achieve total coverage by the endof 1964. The prospects of success seem assuredin the State of Sao Paulo, where the attack phase isproceeding well. Cuba is still at the very beginningof the attack phase; by the end of 1962, sprayingoperations had covered only a small area of thecountry. In Ecuador, DDT has been employed forless than two years but there was a substantial reduc-tion of P. falciparum cases during 1962. Total coverageof the malarious areas of French Guiana is plannedfor 1963. In Haiti, total coverage started in January1962 and there is a good prospect of success of thisprogramme, which is adequately administered andfinanced. In Panama, total coverage with DDTtwice a year began in May 1962; however, there arefinancial difficulties with this programme.
10.2.2 Training and Staffing for National MalariaEradication Projects
During 1962 three training centres continued tooffer regular courses on techniques of malaria era-dication. The XVIII International Course on Malariaand Metaxenic Diseases was given in Maracay,Venezuela; three courses for senior and one for juniorofficers were given by the malaria eradication trainingcentre in Kingston, Jamaica, and two courses forsenior officers and one for entomologists were givenby the Faculty of Hygiene and Public Health of theUniversity of Sao Paulo, Brazil. No formal coursewas given in Mexico.
Each national malaria eradication service continuedto provide training for its own staff. Every campaignin the attack phase retrains the spraying personnelin the interval between the spraying cycles andorganizes training courses for auxiliary personnel forepidemiological operations according to needs.
10.2.3 Operational Aspects
Revised plans for malaria eradication were com-pleted in Brazil, the Dominican Republic and Panama.In addition, administrative reorganization was necess-ary in Guatemala, Haiti, Honduras and Nicaragua,where the programmes until then were administeredby the Inter -American Co- operative Service ofPublic Health (SCISP) which has since been closed.

126 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
In Paraguay, as further epidemiological studieswere required to redefine the total malarious area,the country has reverted to the preparatory phase.
To improve case -detection activities, Mexicoadopted in 1961 a new organizational system. It wasagreed that the department of spraying operationswas better equipped than the epidemiological depart-ment to carry out the case -detection activities; thus theengineers were made responsible for both the sprayingand case -detection operations. As a result, insteadof having two competing operations, one of sprayingand another of epidemiology, each working inde-pendently under the supervision of one inspector notinterested in the other's activities, each inspector ofa sector of field operations was made responsible forall basic malaria eradication activities in his area.The association of attack and evaluation kept thepersonnel more interested in the battle they arefighting and gave them more hope for their ownfuture employment. At the Tenth Meeting of Directorsof Central America, Panama and Mexico, the par-ticipating countries agreed to adopt the system.
In order to improve the participation of the localhealth services in case -detection, especially during theconsolidation and maintenance phases, two seminarsare planned for the Americas in 1963, one for theSouth American and the other for the Central Ame-rican countries. They will be attended by the nationaldirectors of health, the directors of local healthservices and the directors of the national malariaeradication services.
In 1962 the Communicable Disease Center of theUnited States Public Health Service, and the Govern-ments of Guatemala and Nicaragua with the assistanceof UNICEF and the Organization jointly conductedfield trials on the usefulness of a pressure regulatordisc in the nozzle tip of spray pumps. Results wereconsidered satisfactory enough to justify the adoptionof the disc in most house spraying operations withwettable powder insecticides. Experience has shownthat, in addition to 10 per cent. savings in insecticides,the device has contributed to an increased output perman -day of operation. The device cannot, at present,be used for spraying emulsion or solutions of DDT ordieldrin because the chemicals used in these formula-tions attack the synthetic rubber disc that regulatesthe pressure.
There was a considerable increase in the use ofdrugs in 1962. This was due to expansion of case -detection activities, an increase in the number ofthose given radical treatment, and mass drug treat-ment in pilot areas. With few exceptions, in all areasin the attack and consolidation phases a " presump-tive " treatment of chloroquine was administered tothe patients who gave a blood sample. The dose
consisted of 600 mg (base) for adults with more than60 kg of body weight, and 450 mg (base) for adultsand children over twelve years with a body weightbetween 40 and 60 kg. Children of nine to twelve years(25 -40 kg) received 300 mg, those between four andeight (15 -25 kg) 150 mg, and between six months andfour years (7 -15 kg) 75 mg.
In Mexico, presumptive cases in areas in the con-solidation phase were treated with pyrimethamine.The dose was two tablets of 25 mg (base) for indivi-duals over fifteen years of age and one tablet for thoseof fifteen years or less.
Malaria was eradicated from areas in Trinidadinfested by A. (Kertezia) bellator, an outdoor daylightbiter, by mass drug treatment of the populationinvolved. In order further to observe methods ofdrug distribution and costs, the Organization spon-sored, during 1962, pilot projects of mass treatmentin some of the problem areas of Costa Rica, ElSalvador, Guatemala, Mexico and Nicaragua. Afterpreliminary observation of a small trial carried out inEl Salvador in 1961, it was established that a combinedtablet of chloroquine and primaquine would be used.The success of this method of mass medicationdepends a great deal upon the effectiveness of the workduring the preparatory phase. Health educators mustsurvey the area to explain the programme and thereasons for it to the population. Simultaneously itis necessary to study the population's habits principallyto determine where people stay during the varioushours of the day - for example, old persons and veryyoung children are generally found at home, teenagersat school and adults at their place of work.
The distribution of chloroquinized salt in theinterior of British Guiana began in January 1961.The programme has been well received by the public,and the co- operation of the salt dealers has beenexcellent. Medicated salt had reached more than96 per cent. of the houses in the interior by the endof 1962. Malaria transmission has been virtuallyinterrupted in the entire population of 35 000 in theinterior, except in those living in the Lethem area,which borders upon Brazil. The problem in this areahas been insufficient coverage of the 1400 inhabitantswith chloroquinized salt, because non -medicated salthas been readily available on the Brazilian side athalf the price of the chloroquinized salt. In addition,it has been suspected that there may be a strain ofP. falciparum resistant to chloroquine in this area. It isplanned to make a careful study of the possibilityof drug resistance in the area. It is also planned tospray the houses in the Lethem area as a supplementarymeasure and at the same time to request the Brazilianauthorities to intensify their malaria eradication effortsalong the border.

ANNEX 8 127
Preparations were made for a screening centre forthe detection of strains of human plasmodia resistant,or highly tolerant to, chloroquine and other anti-malarial drugs to be opened in the State of Sáo Paulo,Brazil, with the support of the Organization, earlyin 1963.
The countries with malaria eradication programmesand that have areas where eradication is claimed orhas been registered have maintained adequate sur-veillance operations in such areas. All cases detectedhave been investigated and classified as recommendedby the Organization. The only country which reportedindigenous cases in its area in the maintenance phasewas British Guiana. Areas in Venezuela registeredas areas where malaria has been eradicated continuedunder heavy pressure owing to the arrival of malariacases imported from abroad. Argentina also reportednine introduced cases and three imported from itsown malarious area in the attack phase. From thecountries in which malaria was eradicated before 1957information is scarce, except from the United Statesof America. Every year the United States PublicHealth Service publishes a report indicating all casesof malaria that have been detected in the country.During 1962, sixty -six cases were reported, of whichsix were classified as indigenous, four as relapses,forty -six as imported from abroad, and two as induced;and eight were not classified.
As the attack phase advanced, epidemiologicalactivities increased; an increase in the number of slidesexamined, as compared with 1961, was reported fromevery campaign. An indication of the developmentof case -detection methods over the past four years isgiven in Table H.
TABLE H. DEVELOPMENT OF CASE -DETECTIONMETHODS, 1959 -1962: REGION OF THE AMERICAS
Number and source of slides
Year
Active detection Passive detection Total
1959 1 815 845 869 774 2 685 6191960 2 533 709 1 306 936 3 840 6451961 2 844 099 2 032 953 4 877 0521962 3 446 735 2 166 353 5 613 088
The trend in 1962 has been towards an increase in theuse of active case -detection compared with passive;however, 3.4 per cent. of the slides taken duringpassive case -detection were reported positive, com-pared with only 0.9 per cent. during active case -detection.
No indigenous cases were found in nine of theseventeen countries that reported case -finding activitiesin areas in the consolidation phase.
Entomological work was greatly intensified in theproblem areas. During 1962 an epidemiological studyteam continued to work in El Salvador in order toinvestigate the causes of persistence of transmissionin the coastal area. The team found that the vector,A. albimanus, in addition to being resistant to dieldrinand DDT, in certain areas has also acquired a highlysensitive repellency to DDT. This excito- repellencyis sometimes so high that the mosquitos do not reston the sprayed walls long enough to absorb a lethaldose of the insecticide. Populations that are suscepti-ble and resistant to DDT sometimes behave in thesame manner.
A device called the " Excito- Repellency Test Box(Model PAHO) " was developed during 1962 by thepersonnel of the epidemiological study team for thestudy of Anopheles mosquitos in relation to wallsurfaces that have been sprayed with DDT. Whilethe potentialities of the device have not been fullyexplored, it has already given some very interestinginformation about the variation in excito- repellencyof the populations of A. albimanus in different localitiesin Central America.
An insecticide testing programme has been operatingduring 1962 in both El Salvador and Bolivia. Inaddition to testing insecticides sprayed indoors, theteam began operational research on larviciding, tobe used in certain areas where house spraying doesnot halt transmission ; hand spraying or liquid anddusting larvicides, as well as aerial dusting, weretested. Studies of malathion were carried out duringthe year in El Salvador and Nicaragua. A project toevaluate the fumigant insecticide DDVP in the fieldwas started in Haiti, and other trials of Sevin andBayer 39007 will be conducted in that country.
10.2.4 Co- ordination
Close co- ordination has continued with the multi-lateral and bilateral agencies collaborating in themalaria eradication programme in the Region of theAmericas. Some formal meetings were held by theagencies during the year, and in addition frequentexchanges of views have taken place.
In May 1962 the Tenth Meeting of the Directorsof the National Malaria Service of Central America,Panama and Mexico was held in Honduras. Thefinal report, in Spanish, was mimeographed anddistributed to all malaria projects of the Region.
A seminar was held in Paramaribo, Surinam, from25 to 28 September 1962, with the participation ofthe health authorities of Brazil, British Guiana, FrenchGuiana and Surinam, to discuss the problem of

128 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
malaria eradication in the rural population of thisarea. This seminar not only resulted in a betterunderstanding of common problems, but also set apattern for future border meetings on the details ofjoint activities in these difficult operational areas.As a consequence of this seminar, border meetingsbetween Brazil and British Guiana, and Brazil andFrench Guiana, took place on 25 November and10 December 1962 respectively. The final report ofthe seminar, issued in English, Spanish and Portu-guese, was distributed to all countries of the Region.
Other border meetings held in 1962 were : Gua-temala and Mexico, 8 -10 February; Brazil andParaguay, 21 -23 June; and Colombia and Venezuela,24 -26 October.
10.3 South -East Asia Region
10.3.1 General Progress and ProspectsWith the exception of the programmes in Burma
and Thailand, there has been an overall improvementin the malaria eradication programmes in South -EastAsia.
In Afghanistan, the total population of the malariousareas is 4 501 000, of which 312 000 are in areas in thepreparatory phase, 4 102 000 in the attack phase,and 87 000 in the consolidation phase. About aquarter of a million more people have been broughtunder protection by DDT spraying during the year.Antilarval measures protecting a population of 500 000in urban areas have been continued. In Nangarharit is hoped that areas with a population of 445 000will be brought into the consolidation phase during1963 and areas with a population of just over onemillion in the province of Kataghan will be includedin the consolidation phase in 1964 -1965. There appearto be no technical problems to impede the programmein Afghanistan.
In Burma, following an assessment of the pro-gramme carried out in 1961, new plans have beendrawn up, reducing the area of operations to a sizecommensurate with the resources available. Theassessment emphasized the need for more effectivesupervision of operations and recommended delayingactivities in areas where such supervision was imprac-ticable on account of insecurity. The Government hasplanned to continue the programme on the generallines suggested in the assessment but without theassistance of WHO field staff, who were withdrawnat the Government's request by October 1962. Outof a population of approximately 19 million undermalaria risk, 10.14 million were protected by residualinsecticide spraying. Another 4.5 million were undersurveillance. Efforts are being made to secure theco- operation of the general health services and
voluntary agencies in the implementation of theoperations. It has been planned to continue thespraying operations in 1963 by employing voluntarylabour. Although this programme has no obvioustechnical problems, there are operational difficultiesin the way of its successful implementation. Thefuture of the programme is difficult to assess under theexisting conditions.
Ceylon has the most advanced malaria eradicationprogramme in South -East Asia. Thirty -one malariacases were recorded during the year and only twobetween July and December; both of these had comefrom the Maldive Islands.
The national malaria eradication programme ofIndia entered the fifth year of operations in 1962.There has been an all -round improvement in theperformance of the programme. Altogether 390 units,each covering a population of over a million, were inoperation. Both in quality and in coverage, thespraying operations and surveillance activities haveshown a remarkable improvement. In the 140 units,covering a population of 153 million, from whichspraying was withdrawn during the year, 1632 positiveslides were found during surveillance up to the end ofSeptember. The majority of these cases were dis-tributed in a few foci and prompt remedial measureshave been taken. It was noted that not a single casehas been recorded from fifty -six units out of 140 unitsnow in consolidation. The blood examination rateof the population under surveillance during the yearvaried from 4 to 12 per cent. Up to the end of Sep-tember a total of 13.6 million slides had been examinedthroughout the country. It is expected that during1963 additional areas with a population of approxi-mately 90 million will pass into the consolidationphase. One of the major problems that will face thisprogramme is the inadequacy of rural health servicesfor meeting the needs of the maintenance phase. TheGovernment of India is fully aware of this problemand concerted efforts are being made to plan the futurecourse of action for augmenting and expanding ruralhealth services.
The programme in Indonesia has shown a markedimprovement, particularly in operational efficiency.During the year, out of forty -two zones in the centralislands complex of Java, Bali and South Sumatra, allexcept three have entered the attack phase, and thesethree should also become fully operational duringthe first half of 1963. This programme was assessedby a special WHO /AID evaluation team during thelast quarter of 1962. The assessment report stressedthe operational efficiency of the programme; the chiefweakness found was the failure to undertake systematicinvestigation and follow -up of positive cases. Thenational malaria eradication headquarters is fully

ANNEX 8 129
alive to these problems and a further nineteen medicalofficers are being trained for work in the malariaeradication service. It is considered that the pro-gramme in the present operational areas will achieveits goal of eradication, but for the maintenance oferadication in these areas it will be necessary toeliminate the possibility of reintroduction of malariafrom the neighbouring outer islands.
In Nepal, the malaria eradication programme isstill confined to the central zone, in which a populationof 2 169 000 is being protected by DDT spraying.There has been very little improvement in the per-formance of spraying operations and supervisionstill leaves much to be desired in some areas. On theother hand, there appears to be a general improvementin case -finding and in entomological activities. Withcertain exceptions, transmission has been interruptedin all areas in the attack phase. The urgent need ofthe programme is the development of surveillancethroughout the central zone, where the malariometricindices have already reached low levels. The activitiesof the programme have to be concentrated in this zoneand expansion to the outer zones should be under-taken only after stabilizing the operations there.
There has been very little progress in the malariaeradication programme in Thailand during 1962. Adraft plan of operations has been prepared, envisagingthe development of the programme by stages. During1963, it is planned to protect an area with a populationof 12.8 million, for which insecticides have beenprovided by AID. Surveillance activities have shownthe prevalence of malaria cases in areas where sprayingceased over five years ago and these areas are scheduledfor spraying again during 1963. The central organiza-tion of the national malaria eradication service, whichwas reorganized during the latter part of 1961, hasnot proved very effective and the Government hasrecently effected further changes with a view toimproving its efficiency.
10.3.2 Training of National Malaria EradicationStaff
Except in India and Indonesia, the senior personnelof the national malaria eradication services in theRegion are trained in international training centres.For example, Afghanistan received five WHO fellow-ships for the training of medical officers, and threestudy tours were arranged by the Organization. Nepalreceived three WHO and four AID fellowships forthe training of its senior staff abroad.
The training of paramedical personnel in Afghan-istan is carried out at the Malaria Institute, Kabul,and at regional centres. A total of 226 inspectors,microscopists and entomological assistants attended
courses during 1962. Similarly, in Burma, trainingis carried out both at the Malaria Institute, Rangoon,and at regional centres. In Ceylon, training was givenat the malaria headquarters at Colombo and at thefour regional centres to 129 trainees in the malariaeradication services, and in addition lectures anddemonstrations were given to 100 staff of the generalhealth service. India has a Central Institute forCommunicable Diseases at Delhi for the training ofall senior categories, both for its own programmesand for the training of candidates from other countriesin the Region. There are six regional co- ordinatingorganizations which provide training for laboratorytechnicians and some of the larger states have separatetraining centres of their own. During 1962, fourteencourses were held at the Central Institute for Com-municable Diseases, the state training centres andregional co- ordination organizations, and 330 personsreceived training. In addition, eight seminars wereheld -four for consolidation areas, attended by192 medical officers; and four for pre -consolidationareas, attended by 182 medical officers.
In Indonesia, training continues to be provided inheadquarters, provincial, zonal and sector trainingcentres. The Tjiloto training centre has been con-siderably expanded and new laboratories, classroomsand dormitories, etc. have been installed. The WHOand AID staff assigned to the programme assist thenational director in conducting the courses. Seventeenqualified doctors entered the national malaria eradi-cation service on 12 Noyember 1962 (Malaria Day)and at present are receiving special training in epi-demiology at the Tjiloto training centre.
In Nepal, the national malaria eradication organiza-tion trained various paramedical personnel in sur-veillance, evaluation, entomology, parasitology, healtheducation operations, administration, cartographyand transport. A total of 2259 persons, including1730 spraymen, were trained.
In Thailand, two training centres were established,one in Chiengmai, in Northern Thailand, and theother in Prabhudhabad in Central Thailand, underthe direction of the Deputy Director of HealthEducation and Training. Forty technicians completeda one - and -a -half years' course in public health withemphasis on malaria eradication. Twenty micro-scopists also received training for two months inBangkok. In- service training of forty -four zonechiefs, 218 sector chiefs, 896 squad chiefs, eighty -fivemicroscopists, 1540 house visitors and twenty -ninespraymen was carried out at regional and head-quarters centres. During the year, sixteen medicalofficers received further training on AID fellowships.

130 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
10.3.3 Operational Aspects
The malaria eradication programme in Afghanistanis under a semi -autonomous body with full authorityfor technical and administrative direction of theprogramme and for incurring all expenditure necessaryfor it out of the funds provided for the purpose.
The national malaria eradication programme inIndia is an integral part of the normal health organiza-tion of the country. The direction of the programmeis vested in the Director, National Malaria EradicationProgramme, who functions under the Director -General of Health Services of India. The responsibilityfor implementation of the programme rests with thestate governments. In each state the programme iscontrolled by the Director of Health Services, throughthe state malariologist. There is, however, completeco- ordination between the centre and the state and theorganization is considered adequate and satisfactory.A high -powered special working committee exists atthe central level under the chairmanship of theDirector -General of Health Services, and this com-mittee decides all important matters. The Director,National Malaria Eradication Programme, is secretaryto this committee. The country is divided into sixregions, and for purposes of co- ordination of eradi-cation activities and for rendering advisory assistance,each region is provided with a regional co- ordinationorganization which functions directly under theDirector, National Malaria Eradication Programme.
The Indian programme is massive; over 41 millionhouses were sprayed in 1962 and over 40 000 spraymenwere utilized for spraying operations. In some states,diazinon has been incorporated with DDT in orderto overcome refusals to permit spraying because ofthe prevalence of bed -bugs which have becomeresistant to DDT.
Existing hospitals, dispensaries and health unitsparticipate in the passive detection of cases. Inhospitals and dispensaries with large out -patientattendance, the malaria eradication programme pro-vides a blood -taker for collecting blood slides fromall fever cases. The participation of the generalhealth services in passive case -detection has showna great improvement during 1962.
In certain areas in India, A. culicifacies, which hasfor some years shown resistance to dieldrin, is alsoshowing resistance to DDT. In one district of GujaratState, although such double resistance occurs, thereis no evidence of any indigenous transmission ofmalaria, but in other areas a low -grade transmissionis taking place and BHC has been substituted forDDT, with an immediate improvement in the trans-mission rates. In Indonesia, during the year, bothvectors, A. sundaicus and A. aconitus, have presented
fresh instances of resistance to the insecticides, thelatter for the first time showing an intermediateresistance to DDT.
Routine mass drug administration is not practisedin any of the countries in the Region. In a few areasin Thailand and in Indonesia, mass drug administra-tion, using 600 mg chloroquine base and 50 mgpyrimethamine (adult dose), was employed forcombating localized outbreaks of malaria. In Afgha-nistan, Burma, Ceylon, India, Indonesia and Nepal,presumptive treatment was given as part of surveillanceactivities to fever cases and to those with a historyof fever. For this purpose, one of the 4- aminoquinolinedrugs together with pyrimethamine was used. In pre -
consolidation and consolidation areas this wasfollowed with primaquine for the radical treatmentof P. vivax and P. malariae infections. In India, thestandard radical treatment consists of 600 mg chloro-quine and a five -day course of primaquine. InIndonesia the more commonly accepted fourteen -daycourse of primaquine is employed.
In Burma, during 1962, a population of 5.86 millionwas under surveillance, each house being visited oncea month. In this programme epidemiological investi-gation and follow -up of cases and the supervision ofsurveillance activities need considerable improvement.
Out of the 390 units in India, 364.5 undertake sur-veillance activities, domiciliary visits for case -detectionbeing carried out at fortnightly intervals. The remain-ing 25.5 are either border areas or are units wherethe parasite prevalence is still high. In the 140 units(153 million population) from which spraying hasbeen withdrawn, the annual parasite incidence worksout at 0.01 per thousand. In the earlier stages of theprogramme, there was a gross under -estimate of thenumber of blood slides that would be collected duringsurveillance. Originally, therefore, only two micro-scopists per unit were provided. Since then, thenumber of microscopists per unit has been raised toeight. There was also an acute shortage of micro-scopes, resulting in the microscopists working indouble shifts to deal with the work load; but theGovernment has arranged to procure 800 microscopesand WHO has agreed to supply an additional 600.
In Indonesia, voluntary collaborators have beenengaged, with varying results ; in one area over athousand such workers have been reported as workingwell, whereas in another all the 380 voluntary workersengaged had to be discharged because of inefficiency.Attempts will continue to be made to enlist theservices of voluntary workers. During 1962 the mainepidemiological problems consisted of importationof cases from unsprayed into sprayed areas.
Surveillance operations only started in Nepal in1962. Until July 1962, epidemiological evaluation

ANNEX 8 131
was carried out by assessment of infant and childparasite rates in index villages, and entomologicalassessment by routine checking in fixed observationposts. In the second half of 1962, it became apparentthat the infant and child parasite rates were no longersensitive indices, and these were replaced by massblood surveys. There was more emphasis in 1962 onepidemiological evaluation.
Ceylon is expected to request certification of era-dication of malaria at the end of the maintenanceperiod in 1966.
10.3.4 Co- ordination
Five countries in the Region receive substantialassistance from AID - Ceylon, India, Indonesia, Nepaland Thailand; and UNICEF provides supplies toAfghanistan.
The unequal development of programmes inadjacent countries has presented problems caused byimported cases of malaria. This applies to the bordersbetween India and Pakistan, India and Nepal, andAfghanistan and Pakistan. There is also the problemof export of malaria from Kalimantan to Sarawakand North Borneo. An inter -country antimalariaco- ordination meeting was held in Lahore in Novem-ber 1962 with participants from Burma, India andPakistan. A similar conference between India andNepal had to be postponed to 1963. An inter -regionaltechnical conference was held in Teheran, in whichIndia and Afghanistan participated.
The Fourth Asian Malaria Conference was heldin Manila from 27 September to 3 October 1962.
During this conference, WHO and AID advisers andIndonesian officials discussed border malaria problemswith malariologists and government officials fromBrunei, North Borneo, Sarawak and West NewGuinea (West Irían). Discussions were also held withparticipants from Cambodia, Laos, the Federation ofMalaya, the Republic of Viet -Nam, and Thailand onproblems affecting inter -country co- ordination ofantimalaria activities.
10.4 European Region
10.4.1 General Progress and Prospects
Noteworthy progress towards malaria eradicationhas been reported in 1962 in the European Region.In continental Europe, the eight countries (Albania,Bulgaria, Greece, Portugal, Romania, Spain, theUnion of Soviet Socialist Republics and Yugoslavia)covered by the " Co- ordinated Plan establishingPriority for the Eradication of Malaria in ContinentalEurope " have achieved the objectives laid down inthe plan, i.e., the last areas in the attack phase whichstill existed in those countries moved into the conso-lidation phase at the end of 1962, except in the USSR,where there is a zone with a population of 40 000inhabitants still in the attack phase. As much of theactual change from consolidation to maintenanceand from attack to consolidation did not take placeuntil 1 January 1963, the detailed statement inAppendix 1 (page 149) does not fully show the presentsituation in continental Europe. This is summarizedin Table 1, together with the figures for 1961 and 1962.
TABLE I. SUMMARY OF GENERAL DEVELOPMENT OF THE MALARIA ERADICATIONPROGRAMME IN CONTINENTAL EUROPE
Areas
End of 1961 End of 1962 Beginning of 1963
Population(in thousands)
% of populationof originally
malariousareas
Population(in thousands)
% of populationof originally
malariousareas
Population(in thousands)
% of populationof originally
malariousareas
In which eradication achieved * . . .
In consolidation phaseIn attack phaseWithout eradication programme . .
24019612 208
3 349-93.9
4.81.3-
245 74411 7582 948-
94.44.51.1
252 4517 959
40
96.903.080.02-
100.0 100.0 100.0
Originally malarious 255 753 260 450 260 450
* Including the Byelorussian SSR, Czechoslovakia, France (Corsica), Hungary, Italy, the Netherlands, Poland and the Ukrainian SSR, which havealready achieved eradication throughout the national territory.

132 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
There are no technical or administrative problemsin any of these countries that are likely to preventelimination of the residual foci. All these countriespossess an excellent public health infrastructure whichpromises well for the quality of vigilance operations.It can be assumed without undue optimism that themaintenance phase will be achieved everywhere bythe end of 1966.
In Albania by the end of 1962 all zones were in theconsolidation phase and the whole of the formerlymalarious area should move into the maintenancephase at the end of 1965. In Bulgaria the last zonepassed into the maintenance phase at the end of 1962.In Greece it is expected that all the originally malariousareas will have passed into the maintenance phase bythe end of 1965. In Romania the attack phase opera-tions were completed by the end of 1962 and the wholecountry should, by the end of 1965, have passed intothe maintenance phase. In the USSR 99.4 per cent.of the population of the originally malarious areashad moved into the maintenance phase by the end of1962, only 0.57 per cent. were still in the consolidationphase and 0.03 per cent. in the attack phase. InPortugal, only one indigenous case was detectedduring 1962. Several other imported cases (mainlyfrom Africa) were detected and treated by the epi-demiological vigilance service. There has been nochange in the population of the zones in the consoli-dation phase in 1962 compared with 1961, except forthe normal demographic increase. In Yugoslaviaattack phase operations ended in the last zone (Mace-donia) in 1962. At the beginning of 1963, nearlytwo -fifths of the population of the originally malariouszones were in areas in the consolidation phase, theremainder being in the maintenance phase, and thelast areas of the country should reach this final phaseby the end of 1965.
There are, in the Region, three countries where theeradication programme is less advanced : Algeria,Morocco and Turkey. In Turkey the attack phaseoperations still covered 35.5 per cent. of the populationin the originally malarious zones at the end of 1962,but all the originally malarious areas should havemoved into the consolidation phase by the end of1965 and into the maintenance phase by the end of1968. In Morocco the pre- eradication programmelaunched in 1961 was continued in 1962. During 1962the emphasis was laid on the training and assignmentto posts of the staff of the rural health infrastructure.It is planned to establish three demonstration andtraining areas in 1963, covering a total of 300 000persons. It is thought that the preparatory phasecould begin in 1964 and the attack phase in 1965. InAlgeria, discussions with the Government are still inprogress on methods of meeting the dangers of
epidemics that may arise in 1963 and on the launchingof a pre- eradication programme with WHO assistance.As part of the pre- eradication programme, twodemonstration and training areas are envisaged,but these will not be developed before the end of 1963.It is hoped to start the eradication programme in1967.
The implementation of the Co- ordinated Planestablishing Priority for the Eradication of Malariain Continental Europe has given a powerful impetusto the exchange of epidemiological information.The WHO system of quarterly reports on surveillanceoperations has been adopted by almost all countries.Of the eight countries participating in the plan,transmission has practically ceased throughout thearea, except for a few scattered residual foci in Greeceand the USSR. The reduction in the size of theparasite reservoir in these zones in the consolidationphase is demonstrated by the fall in the annualparasite rate and its low level by the end of 1962 (seeTable J).
TABLE J. PARASITE RATE IN CONTINENTALEUROPE, 1961 AND 1962
Country
Annual parasite rateper thousand of the population
End of 1961 End of 1962
Albania 0.052 ...Bulgaria 0 0Greece 0.05 0.046Portugal 0.018 0.014Romania 0.002 0.001Spain ........... 0.08 0.003Union of Soviet Socialist
Republics 0.032 0.013Yugoslavia 0.05 0.01
In Turkey, which is not in continental Europe, theannual parasite rate fell from 0.06 per thousand in1961 to 0.055 per thousand at the end of 1962 in theareas in the consolidation phase. Relatively numerousfoci of transmission have been discovered in thoseareas. None of these foci is really critical, and theyare eliminated as they are discovered. Their discoveryis usually due to an improvement in the surveillancesystem, and their existence either to operationalshortcomings or to problems of human ecology.
10.4.2 Training of National Malaria EradicationStaff
At the national level, the countries in the Regionthat still need to train personnel for their malariaeradication campaigns have organized courses with
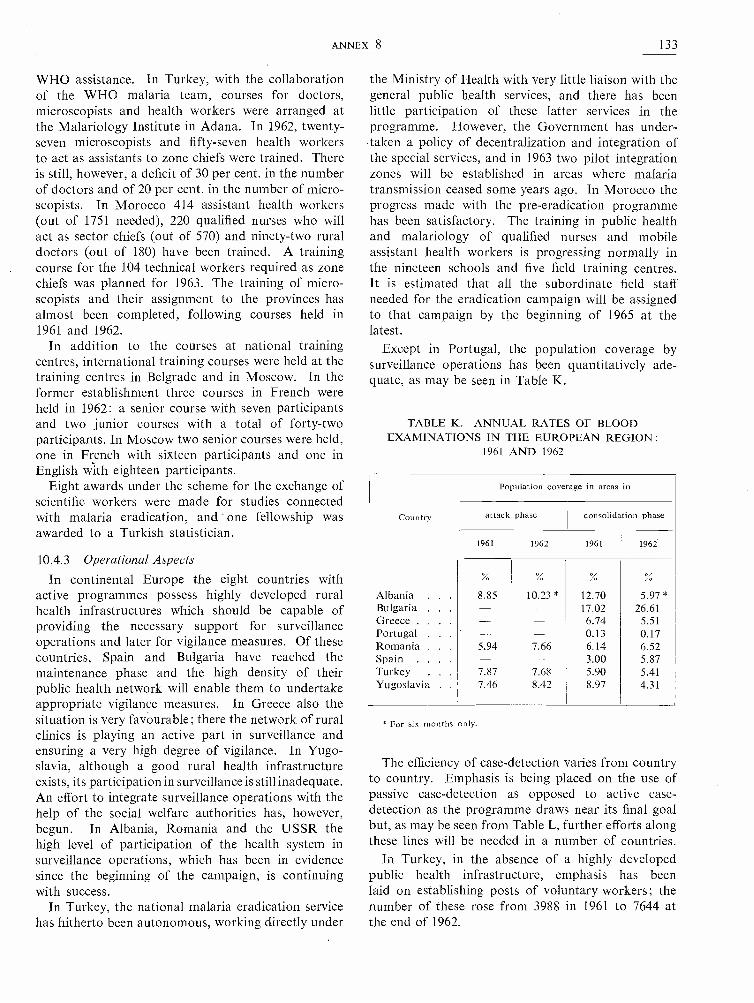
ANNEX 8 133
WHO assistance. In Turkey, with the collaborationof the WHO malaria team, courses for doctors,microscopists and health workers were arranged atthe Malariology Institute in Adana. In 1962, twenty -seven microscopists and fifty -seven health workersto act as assistants to zone chiefs were trained. Thereis still, however, a deficit of 30 per cent. in the numberof doctors and of 20 per cent. in the number of micro-scopists. In Morocco 414 assistant health workers(out of 1751 needed), 220 qualified nurses who willact as sector chiefs (out of 570) and ninety -two ruraldoctors (out of 180) have been trained. A trainingcourse for the 104 technical workers required as zonechiefs was planned for 1963. The training of micro-scopists and their assignment to the provinces hasalmost been completed, following courses held in1961 and 1962.
In addition to the courses at national trainingcentres, international training courses were held at thetraining centres in Belgrade and in Moscow. In theformer establishment three courses in French wereheld in 1962: a senior course with seven participantsand two junior courses with a total of forty -twoparticipants. In Moscow two senior courses were held,one in French with sixteen participants and one inEnglish with eighteen participants.
Eight awards under the scheme for the exchange ofscientific workers were made for studies connectedwith malaria eradication, and one fellowship wasawarded to a Turkish statistician.
10.4.3 Operational Aspects
In continental Europe the eight countries withactive programmes possess highly developed ruralhealth infrastructures which should be capable ofproviding the necessary support for surveillanceoperations and later for vigilance measures. Of thesecountries, Spain and Bulgaria have reached themaintenance phase and the high density of theirpublic health network will enable them to undertakeappropriate vigilance measures. In Greece also thesituation is very favourable; there the network of ruralclinics is playing an active part in surveillance andensuring a very high degree of vigilance. In Yugo-slavia, although a good rural health infrastructureexists, its participation in surveillance is still inadequate.An effort to integrate surveillance operations with thehelp of the social welfare authorities has, however,begun. In Albania, Romania and the USSR thehigh level of participation of the health system insurveillance operations, which has been in evidencesince the beginning of the campaign, is continuingwith success.
In Turkey, the national malaria eradication servicehas hitherto been autonomous, working directly under
the Ministry of Health with very little liaison with thegeneral public health services, and there has beenlittle participation of these latter services in theprogramme. However, the Government has under-taken a policy of decentralization and integration ofthe special services, and in 1963 two pilot integrationzones will be established in areas where malariatransmission ceased some years ago. In Morocco theprogress made with the pre- eradication programmehas been satisfactory. The training in public healthand malariology of qualified nurses and mobileassistant health workers is progressing normally inthe nineteen schools and five field training centres.It is estimated that all the subordinate field staffneeded for the eradication campaign will be assignedto that campaign by the beginning of 1965 at thelatest.
Except in Portugal, the population coverage bysurveillance operations has been quantitatively ade-quate, as may be seen in Table K.
TABLE K. ANNUAL RATES OF BLOODEXAMINATIONS IN THE EUROPEAN REGION:
1961 AND 1962
Country
Population coverage in areas in
attack phase consolidation phase
1961 1962 1961 1962
Albania . . . 8.85 10.23 * 12.70 5.97 *Bulgaria . . . - - 17.02 26.61Greece . . . . - - 6.74 5.51Portugal . . . 0.13 0.17Romania . . . 5.94 7.66 6.14 6.52Spain . . . . - - 3.00 5.87Turkey . . 7.87 7.68 5.90 5.41Yugoslavia . . 7.46 8.42 8.97 4.31
* For six months only.
The efficiency of case -detection varies from countryto country. Emphasis is being placed on the use ofpassive case -detection as opposed to active case -detection as the programme draws near its final goalbut, as may be seen from Table L, further efforts alongthese lines will be needed in a number of countries.
In Turkey, in the absence of a highly developedpublic health infrastructure, emphasis has beenlaid on establishing posts of voluntary workers; thenumber of these rose from 3988 in 1961 to 7644 atthe end of 1962.

134 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
TABLE L. CASE -DETECTION IN AREAS IN THECONSOLIDATION PHASE IN THE EUROPEAN REGION
IN 1962
Country
Passive case -detection Active case -detection
Slides Positivefindings Slides Positive
findings
/ %
Albania . . . 66.35 0.02 33.65 0.02Bulgaria . . . 33.24 0 6.47 0Greece . . . 41.61 0.10 34.90 0.11Portugal . . . 99.13 0.37 0 0Romania . . . 56.31 0 38.82 0Spain . . . . 15.95 0.03 79.75 0Turkey . . . . 2.56 0.18 88.16 0.12Yugoslavia . . 3.57 0.007 80.32 0
One problem is the persistence of a few cases due toP. malariae, which occur mainly as a result of bloodtransfusions. A study on this subject is in progress inRomania and Yugoslavia. On the basis of a samplesurvey, it has been calculated, for example, that inYugoslavia, in the Macedonian Republic alone, thereare probably some 550 cases of symptomless P. mala-riae carriers among a population of 1 400 000. As aresult of this situation, an indigenous but isolatedcase due to P. malariae occurs from time to time incertain countries in the Region.
Difficulties have been encountered in eradicatingresidual foci in Greece, the Soviet Union and Turkey.In Greece, three small foci of transmission still existin the districts of Elis, Pieria and Serrai. In the SovietUnion, the two foci of transmission in Azerbaidzanand Tadzikistan are disappearing as a result of themeasures taken after the occurrence of a local epidemicin 1961. In Turkey, epidemiological problems havegiven rise to special inquiries. In a sector in the eastof Turkey, an entomological team has elucidated thepart played by A. claviger, an exophilic biting species,in the persistence of transmission. In certain zonesin the west of the country (Denizli, Aydin, Antalyaand Kutahya) there is now every reason to supposethat the persistence of transmission in certain foci ismainly due to the exophilic habits of A. superpictus.
The Second European Conference on MalariaEradication discussed ways of transferring the re-sponsibility for malaria eradication to the generalhealth services of a country moving into the main-tenance phase, and the organization and improvementof services intended to prevent the reintroduction ofmalaria into areas from which it had been eliminated.A questionnaire has been sent out to countries in theRegion with a view to assessing the number ofimported cases of malaria and the danger which they
represent of a re- establishment of malaria trans-mission.
Greece has requested the certification of eradicationof malaria in respect of Crete, the Dodecanese andthe Cyclades, where eradication was achieved before1957, and also the certification of the islands ofLesbos, Chios, Samos and Euboea. Spain has askedfor certification of eradication in 1963 for the wholenational territory. Steps have been taken for anevaluation team in 1963 to meet these requests andany others that may be made later.
Despite the very real danger of malaria beingimported, so far no instance of re- establishment oftransmission following importation of a case ofmalaria has been reported from the countries ofcontinental Europe which have eradicated malaria.
10.4.4 Co- ordination
The success of the Co- ordinated Plan establishingPriority for the Eradication of Malaria in ContinentalEurope provides an excellent example of inter -countryco- ordination in Europe.
The Second European Conference on MalariaEradication was held in Tangier from 1 to 8 March1962. The following countries took part : Bulgaria,France, Greece, Italy, Morocco, the Nétherlands,Portugal, Romania, Spain, Turkey, USSR andYugoslavia. Turkey and the USSR took part in aninter -regional technical meeting held at Teheran(Iran) in May 1962. A technical conference of thecountries of North Africa is planned for 1963.
In countries in the Region a number of meetingsof the staff of the national malaria eradication serviceshave been held; for example, in Turkey quarterlyconferences have brought together the professionalpersonnel responsible for malaria eradication opera-tions; in Yugoslavia there was a meeting of the annualconference of the medical personnel directing theantimalaria operations in each of the republics; andin Morocco the doctors from the health districtshave been invited to " information days " on malariaeradication. The annual border meeting betweenPortugal and Spain was held in 1962.
UNICEF continued to give assistance to the pro-gramme in Turkey in 1962.
The Regional Office has continued to issue everysix months an information bulletin on the develop-ment of malaria eradication programmes in theEuropean Region; this bulletin, issued in French inover 300 copies, has a wide distribution.
10.5 Eastern Mediterranean Region
10.5.1 General Progress and ProspectsOf the twenty -five countries or territories in the
Region, one -Kuwait -is naturally free from malaria;
ANNEX 8 135
four -Aden Colony, Cyprus, French Somaliland andthe Gaza Strip -have reached the maintenancephase; Israel has areas in both the maintenance andthe consolidation phases, Lebanon is in the phase ofadvanced consolidation; five -Iran, Iraq, Jordan,Libya and Syria -are in the consolidation and attackphases; and one -Pakistan -is in the attack phaseonly; two countries -Ethiopia and Somalia -havepre- eradication programmes in operation and threeothers -Saudi Arabia, Sudan and Yemen -are devel-oping similar programmes, following, in the casesof Saudi Arabia and Sudan, completion of pre -eradication surveys; and Tunisia and the United ArabRepublic are conducting extensive control pro-grammes and are meanwhile developing their basichealth infrastructure with a view to implementingmalaria eradication through these services.
On the whole, the progress made during 1962 isvery encouraging and strengthens the conviction thatthe eradication of malaria is very near in manycountries of the Region and that, although in othercountries it will take longer, they are also expectedto achieve eradication within the planned time.
Aden Colony, Cyprus, French Somaliland andGaza Strip will shortly be eligible for certificationthat malaria has been eradicated, after the necessaryassessment has been made. Of these countries,agreement has been reached with the Governmentof Cyprus for an assessment of the malaria situationin 1963 with a view to certifying that malaria eradi-cation has been achieved.
One -third of the total population of Israel is inareas in the maintenance phase and the remainingtwo -thirds in areas in the advanced consolidationphase. Only five indigenous cases were discoveredin 1962 in the consolidation area. Thanks to thecountry's comprehensive health services and to thedevelopment of an efficient passive surveillancesystem in the areas in the consolidation phase, theprospects of achieving eradication in the remainingareas in the near future are extremely bright.
In Lebanon, the transfer of the entire area to themaintenance phase is expected to take place in 1964.A small outbreak of malaria at the end of 1962, whichwas promptly discovered, was caused by the arrival ofcarriers from abroad. The planning and the imple-mentation of measures to prevent the reintroductionof malaria from abroad are, in fact, the only majorproblems to be solved before final success is achieved.
In Iran, about five per cent. of the total populationunder malaria risk are now at the end of the consol-idation phase, but the rural health infrastructure hasnot yet been sufficiently developed to take overvigilance responsibilities. Almost 40 per cent. (includ-ing the above five per cent.) are in areas in the con-
solidation phase altogether, mostly in northern andwestern provinces; 49 per cent. are under attackand 11 per cent. in the preparatory phase in the extremesouth. The programme in the north is progressingsatisfactorily and solutions to the special problems ofthe south are being sought through pilot projects;measures such as drug distribution and spraying withnewer insecticides, etc., are being tried out singly orin combination, to find the best approach. At thesame time, the development of health services is beingaccelerated through the new health development planand operational facilities are being built up by themalaria eradication service as fundamental stepstowards the ultimate eradication of malaria fromthese areas.
The programme in Iraq is at an advanced stage.During 1962, 90.5 per cent. of the total populationunder malaria risk were in areas in the consolidationphase and only 9.5 per cent. in areas in the attackphase -riverain tracts and valleys in the north. In thelatter areas, total coverage spraying was not achievedowing to administrative difficulties, and consequentlytransmission continued to persist. In the southernregion, the doubly resistant vector, A. stephensi, longabsent, has reappeared. However, in this region,in addition to active surveillance, a system of passivesurveillance has been organized which functionedquite efficiently during 1962. Steps are being takento prevent malaria from being reintroduced into thefree areas from the part of Iraq still in the attack phaseand from neighbouring countries; an importantpart is played by the co- ordination of programmesalong the borders with Iran through periodic meetings.No reduction in the present area under attack isplanned for 1963.
In Jordan, steady progress was maintained in 1962.The areas under consolidation were extended to coveralmost 94 per cent. of the total population at risk;the areas inhabited by the remainder -the JordanValley and parts of the east of the country -werestill in the attack phase. Some of these will be shiftedto consolidation in 1963, whereas part of the areas atpresent in consolidation will be put in the maintenancephase. With the completion of an extensive geo-graphical reconnaissance, the surveillance operationscoverage achieved a highly satisfactory level.
Although the programme in Libya clearly made someprogress during the year, administrative shortcomings,caused by the mistaken assumption that malaria hadbecome a minor problem, have considerably sloweddown the advance.
In Syria, four -fifths of the total population undermalaria risk are now in areas in the consolidationphase; the remaining one -fifth is still in areas coveredby attack operations, but these will move into the
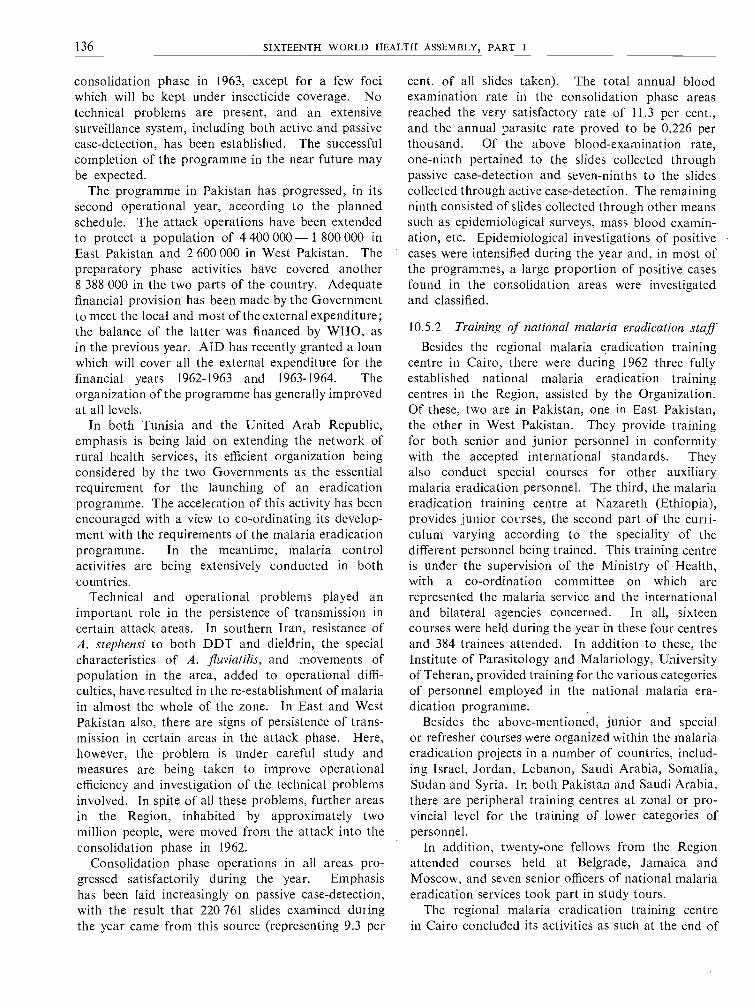
136 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
consolidation phase in 1963, except for a few fociwhich will be kept under insecticide coverage. Notechnical problems are present, and an extensivesurveillance system, including both active and passivecase -detection, has been established. The successfulcompletion of the programme in the near future maybe expected.
The programme in Pakistan has progressed, in itssecond operational year, according to the plannedschedule. The attack operations have been extendedto protect a population of 4 400 000 - 1 800 000 inEast Pakistan and 2 600 000 in West Pakistan. Thepreparatory phase activities have covered another8 388 000 in the two parts of the country. Adequatefinancial provision has been made by the Governmentto meet the local and most of the external expenditure;the balance of the latter was financed by WHO, asin the previous year. AID has recently granted a loanwhich will cover all the external expenditure for thefinancial years 1962 -1963 and 1963 -1964. Theorganization of the programme has generally improvedat all levels.
In both Tunisia and the United Arab Republic,emphasis is being laid on extending the network ofrural health services, its efficient organization beingconsidered by the two Governments as the essentialrequirement for the launching of an eradicationprogramme. The acceleration of this activity has beenencouraged with a view to co- ordinating its develop-ment with the requirements of the malaria eradicationprogramme. In the meantime, malaria controlactivities are being extensively conducted in bothcountries.
Technical and operational problems played animportant role in the persistence of transmission incertain attack areas. In southern Iran, resistance ofA. stephensi to both DDT and dieldrin, the specialcharacteristics of A. fluviatilis, and movements ofpopulation in the area, added to operational diffi-culties, have resulted in the re- establishment of malariain almost the whole of the zone. In East and WestPakistan also, there are signs of persistence of trans-mission in certain areas in the attack phase. Here,however, the problem is under careful study andmeasures are being taken to improve operationalefficiency and investigation of the technical problemsinvolved. In spite of all these problems, further areasin the Region, inhabited by approximately twomillion people, were moved from the attack into theconsolidation phase in 1962.
Consolidation phase operations in all areas pro-gressed satisfactorily during the year. Emphasishas been laid increasingly on passive case -detection,with the result that 220 761 slides examined duringthe year came from this source (representing 9.3 per
cent. of all slides taken). The total annual bloodexamination rate in the consolidation phase areasreached the very satisfactory rate of 11.3 per cent.,and the annual parasite rate proved to be 0.226 perthousand. Of the above blood -examination rate,one -ninth pertained to the slides collected throughpassive case -detection and seven -ninths to the slidescollected through active case -detection. The remainingninth consisted of slides collected through other meanssuch as epidemiological surveys, mass blood examin-ation, etc. Epidemiological investigations of positivecases were intensified during the year and, in most ofthe programmes, a large proportion of positive casesfound in the consolidation areas were investigatedand classified.
10.5.2 Training of national malaria eradication staffBesides the regional malaria eradication training
centre in Cairo, there were during 1962 three fullyestablished national malaria eradication trainingcentres in the Region, assisted by the Organization.Of these, two are in Pakistan, one in East Pakistan,the other in West Pakistan. They provide trainingfor both senior and junior personnel in conformitywith the accepted international standards. Theyalso conduct special courses for other auxiliarymalaria eradication personnel. The third, the malariaeradication training centre at Nazareth (Ethiopia),provides junior courses, the second part of the curri-culum varying according to the speciality of thedifferent personnel being trained. This training centreis under the supervision of the Ministry of Health,with a co- ordination committee on which arerepresented the malaria service and the internationaland bilateral agencies concerned. In all, sixteencourses were held during the year in these four centresand 384 trainees attended. In addition to these, theInstitute of Parasitology and Malariology, Universityof Teheran, provided training for the various categoriesof personnel employed in the national malaria era-dication programme.
Besides the above -mentioned, junior and specialor refresher courses were organized within the malariaeradication projects in a number of countries, includ-ing Israel, Jordan, Lebanon, Saudi Arabia, Somalia,Sudan and Syria. In both Pakistan and Saudi Arabia,there are peripheral training centres at zonal or pro-vincial level for the training of lower categories ofpersonnel.
In addition, twenty -one fellows from the Regionattended courses held at Belgrade, Jamaica andMoscow, and seven senior officers of national malariaeradication services took part in study tours.
The regional malaria eradication training centrein Cairo concluded its activities as such at the end of

ANNEX 8 137
1962 after four years of existence, during whichperiod it provided training to 135 professional and173 auxiliary staff, in four senior and seven juniorcourses respectively. 'However, the Cairo trainingcentre is to continue during the coming years as anational centre providing training for the malariaworkers of the future malaria eradication programmeof the United Arab Republic.
10.5.3 Operational Aspects
In the Iran programme a planning and evaluationsub -committee was set up, attached to the ScientificCouncil and consisting of staff of the malaria erad-ication service and of the Institute of Parasitologyand Malariology. From its inception the sub- commit-tee has made a considerable contribution to the workand has proved most valuable. It meets periodicallyand reviews the progress made in the field and adviseson any changes that may be needed in the operationof the programme Its main function is to reviewat the end of the year the plans of action prepared byzone offices and to draw up a master plan coveringthe entire country for consideration and approvalby the Scientific Council.
In a number of programmes, such as those in Iraq,Jordan and Syria, where attack operations have beennearly concluded or greatly reduced, measures arebeing taken to simplify field operations and sprayingto a minimum required for emergencies. Thisreorganization will be carried out gradually as theareas enter into the consolidation phase, and care willbe taken to use the malaria eradication staff tostrengthen and develop the health services of theseareas.
It should be mentioned that in some countries,where programmes are far advanced, governmentstend to integrate the malaria eradication services pre-maturely and too suddenly into the general healthservices. Efforts were made to dissuade them fromtaking such precipitate action and instead a gradualintegration process was advised.
In Pakistan, .where full autonomous status has beengiven to the national malaria eradication service, therewere a number of problems in the early stages, suchas difficulties in establishing salary and allowancescales and in formulating financial rules and regulations.However, these have now mostly been straightenedout and the autonomy is showing its full benefits.In Iran, the malaria eradication service has beenseparated from that dealing with environmentalsanitation and its responsibilities are now confinedto malaria eradication alone.
The financial situation in most of the programmeshas up to now been satisfactory, although occasionaldelays have occurred in making sufficient funds
available in time for the operation of the project. InWest Pakistan, delay in the provision of the budgetresulted in a postponement of expansion of operationsin 1963.
Health education was given serious attention duringthe year. Iran now has a section of health educationat the headquarters division of operations, with twohealth educators, and a further eleven health educatorsin the provinces, fully equipped with audiovisualmobile units and other necessary equipment andtransport. Main activities were 598 film shows withan attendance of 322 000 persons in the villages, 241village conferences for 191 000 persons, and twenty -sixhealth education training courses, totalling seventyhours of lectures, for 150 000 village teachers, fieldworkers and agriculture extension agents. In Pakistan,health education was carried out by the zone eval-uators, but the results hoped for were not fullyobtained because of the lack of professional healtheducators. The necessary staff have now been recruitedand are being trained. In other programmes, healtheducation is carried out by the malaria eradicationstaff as part of the routine work.
Efforts were made, with little success, to recruitmore engineers for malaria eradication programmesin the attack phase. In Pakistan, although coverageby attack operations is increasing impressively, nonational engineer has so far been appointed to thestaff of the malaria eradication service. Two inter-nationally- recruited engineers and two sanitariansare at present serving in this programme. The situationis very much the same in other programmes, exceptin Iran and Saudi Arabia. In Iran, twenty -sevenengineers are at present working in the field operationdivision at headquarters, regional and zone levels.
Mass drug administration has been practised insome countries of the Region as a supplementarymeasure in areas where spraying operations alonewere not enough to interrupt the transmission ofmalaria. Thus, in Iran mass drug administration hasbeen carried out by two methods. In the Sarakhsarea of Khorassan, where transmission persists dueto the exophily of A. superpictus, the fortnightlydistribution of drugs was carried out by surveillanceagents during the transmission season (mid -June tomid -September). In the area where persistence oftransmission is caused by double resistance of A. ste-phensi, single -dose treatment has been carried out byclinics, dispensaries and hospitals. In the Sarakhsarea, the adequacy of the drugs used, their dosageand frequency of distribution, has been proved by theabsence of positive cases. In the other area, the drugdistribution was irregular and contributed only tokeeping down the level of endemicity. In Iraq, 5000inhabitants were protected by mass drug administra-

138 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
tion in three communities in which malaria epidemicsoccurred in 1962. The drugs were administeredfortnightly from September to November and asevidenced by active case -detection were successful instopping transmission. In Syria, 236 inhabitantsalong the Yarmuk river and the military personnelof Kuneitra area were protected by weekly adminis-tration of 25 mg of pyrimethamine for adults.
A medicated salt pilot project was organized by theInstitute of Parasitology and Malariology, Iran,covering a small tribal population in the Bagdeli sectof the Ghashgai tribe. The experiment has givensatisfactory results and it is intended to continue theexperiment on a larger scale in 1963, to protect apopulation of 22 000 by chloroquinized salt.
Surveillance operations have been systematicallyimplemented in a number of countries of the Region(in some countries as early as from the second year ofattack phase). Both active and passive methods ofcase -detection, as well as epidemiological surveys,follow -up and other surveys, were carried out. Acomparison of the data on surveillance activities for1962 with those for 1961 shows clearly, by the increasein the number of slides collected, that there has beena remarkable improvement in population coverage.In 1962, 2 358 165 slides were taken and examined,as compared with only 1 663 125 in 1961. The numberof positive cases found by passive case -detection issmall compared with the number of positives detectedby active case -detection, owing to the insufficientcoverage of rural areas by the health services in mostof the countries of the Region.
On the other hand, the number of positive casesdetected by epidemiological and other surveys ishigh in relation to the positives detected by activecase -detection, which shows that the quality ofactive case -detection has not reached the requiredlevel, even though there was a substantial improve-ment in 1962. A certain number of cases have beendetected by follow -up of previously confirmed cases,such cases presumably being the consequence ofincomplete radical treatment.
During 1962, small epidemics were observed in somecountries in which malaria eradication programmesare in an advanced stage. Thus, in Syria, in theKuneitra area, there was an outbreak of malariamainly involving military personnel, and althoughthe total number of cases detected was small, it showeda typical epidemic trend. In the same country, anotherfocus of fresh transmission with some sixty indigenouscases was detected in the Al- Rashid district. Bothepidemics were caused by P. vivax. In Lebanon, asmall epidemic, also caused by P. vivax, occurred latein 1962 in the Nahr -Beirut district; eighty -six indi-genous cases were detected. In Jordan, more than
two -thirds of all cases detected during 1962 occurredin the Balqa district. Out of 217 cases in that district,214 have been proved to be P. vivax infections.
Table M shows that there aire defects in the presentcase -detection systems in certain countries in theRegion.
TABLE M. CASE DETECTION IN THE EASTERNMEDITERRANEAN REGION
Country
Positive cases found by
passivecase-
detection
active
case-detection
a p loio-idemgical
survey andfollow -up
othersurveys
(includingmass blood
survey)
IranIraqIsrael . . .
Jordan . . .
Lebanon . .
Syria
28.937.152.539.425.039.7
54.119.345.026.58.0
29.1
17.015.7
2.510.719.018.2
-27.9-23.448.013.0
10.5.4 Co- ordination
To develop and maintain co- ordination among theworkers engaged in the field of malaria eradication -innational services as well as in those of WHO and ofbilateral organizations- various meetings were organ-ized in the Region, which afforded opportunitiesfor an exchange of information.
An Inter -regional Technical Meeting on MalariaEradication was held at Teheran (Iran) from 1 to6 May 1962, with participants from Afghanistan,India, Iran, Iraq, Pakistan, Syria, Turkey and theUSSR. In addition, there were observers fromUNICEF, AID and the United Nations TechnicalAssistance Bureau.
The Third Burma /India /Pakistan Border MalariaEradication Co- ordination Meeting was held atLahore (Pakistan) from 28 to 30 November.
The Second and Third Iran /Iraq Border MalariaEradication Co- ordination Meetings were held atBasra (Iraq) and at Hamadan (Iran) from 28 to 29March and 28 to 30 October 1962, respectively. Thereis a proposal to broaden the scope of these meetingsto include two bordering States -Turkey and Syria.
The Second Jordan /Syria Border Malaria Eradi-cation Co- ordination Meeting was held in Irbed duringMarch 1962. The main subject discussed was theco- ordination of the plan of action for 1962 along theYarmuk Valley and information was exchangedregarding the malaria situation on both sides of theborder.

ANNEX 8 139
A meeting of malaria personnel of Lebanon andSyria was held in May 1962, at a border site in Syrianterritory.
Close liaison and co- ordination have been main-tained with AID and UNICEF, in the field and at theregional level. The projects assisted by AID in thefield of malaria in the Region are in Ethiopia, Iran,Jordan, Libya and Pakistan. UNICEF assistancewas given to the malaria eradication programmes inIran, Iraq, Jordan, Lebanon and Syria.
10.6 Western Pacific Region
10.6.1 General Progress and Prospects
In the Western Pacific Region, about one -thirdof the 78 million people in the originally malariousareas (excluding China (mainland), North Koreaand North Viet -Nam) are now covered by the erad-ication programme.
The WHO -assisted malaria projects in the Regionmay be classified as follows :
(a) There are five countries, namely, China(Taiwan), North Borneo, the Ryukyu Islands, Sara-wak and the Philippines, with full eradication pro-grammes.
The eradication programme in China (Taiwan) isthe most advanced in the Region. However, three welldefined small foci of transmission were discoveredduring 1962 and also the reactivation of transmissionwas found in an old focus. Nevertheless, the totalincidence of malaria remained low during the year;of nearly one million persons examined during thisperiod, through various case -detection measures, onlysixty -seven parasite carriers were found. Reappraisalof the surveillance system is now being undertakenwith a view to strengthening the passive case -detectionsystem throughout the country, in order that informa-tion may be obtained for the certification of eradica-tion. Reintroduction of malaria cases, mainly throughmass immigration from abroad, is a threat to thesuccess of malaria eradication. However, well plannedcounter -measures have been implemented to copewith the problem.
In the programme in North Borneo, spraying wascarried out in 1962 in all malarious areas, and a smallsector is in the consolidation phase. The programmehas good operational facilities, including staff andlogistic support. Periodical assessment was carriedout and results so far indicate good prospects ofachieving eradication, provided that the developmentof the rural health infrastructure and its participationin the eradication efforts are expeditiously implementedas planned.
In the Ryukyu Islands efforts were made to improvethe surveillance activities and epidemiological assess-
ment. The previous shortcomings in these respectswere due mainly to the lack of adequately trainedpersonnel. WHO provided a short -term consultantin 1962 to assist in this project, and also five WHOfellowships were granted to the national workers forstudy in China (Taiwan). With the implementationof the reorganized programme, the prospects ofachieving eradication soon are good.
In Sarawak the eradication programme is in anadvanced stage and, of the 660 000 people in theoriginally malarious areas, 505 000 were in areas inthe consolidation phase and 155 000 in areas in theattack phase in 1962. However, the campaign hasmet with the difficult problem of the importation ofmalaria from the unsprayed areas of Kalimantanacross the border. Nearly half of Sarawak is affectedby this problem, which requires intensive surveillanceoperations in areas in both the attack and theconsolidation phases and the spraying of a band ofcountry about ten miles wide along the border mustbe carried out until a spraying programme starts inKalimantan.
Some progress was made in the malaria eradicationprogramme in the Philippines. In addition to theadministrative difficulties resulting from the change-over from a centralized to a decentralized scheme,certain technical problems, including the developmentof resistance to dieldrin in A. minimus flavirostris andpopulation movement from the malaria -free coastalplains to the hinterlands, have favoured continuationof transmission. A new comprehensive plan ofoperation has been completed recently. It is expectedthat an extensive reorganization of the project willbe carried out from 1963 in line with the new plan.
All these five malaria eradication programmes haveadopted the WHO quarterly surveillance reportingsystem. The calculation of the annual parasiteincidence in most of these countries is based on anadequate number of blood samples collected throughroutine case -detection procedures; the annual parasiteincidence is well below 0.5 per thousand in China(Taiwan), North Borneo and the Ryukyu Islands; inSarawak it is just below this figure; but in the Phi-lippines the incidence in the area in the consolidationphase is still above the maximum permissible level.In North Borneo, as a result of epidemiologicalassessment, the plans of action of the programme wererevised and the premature advancement of areas fromthe attack phase to the consolidation phase wasprevented.
(b) In two countries, the Federation of Malayaand the British Solomon Islands Protectorate, malariaeradication pilot projects are in operation. In Malaya,the pilot project entered its third year of operation in
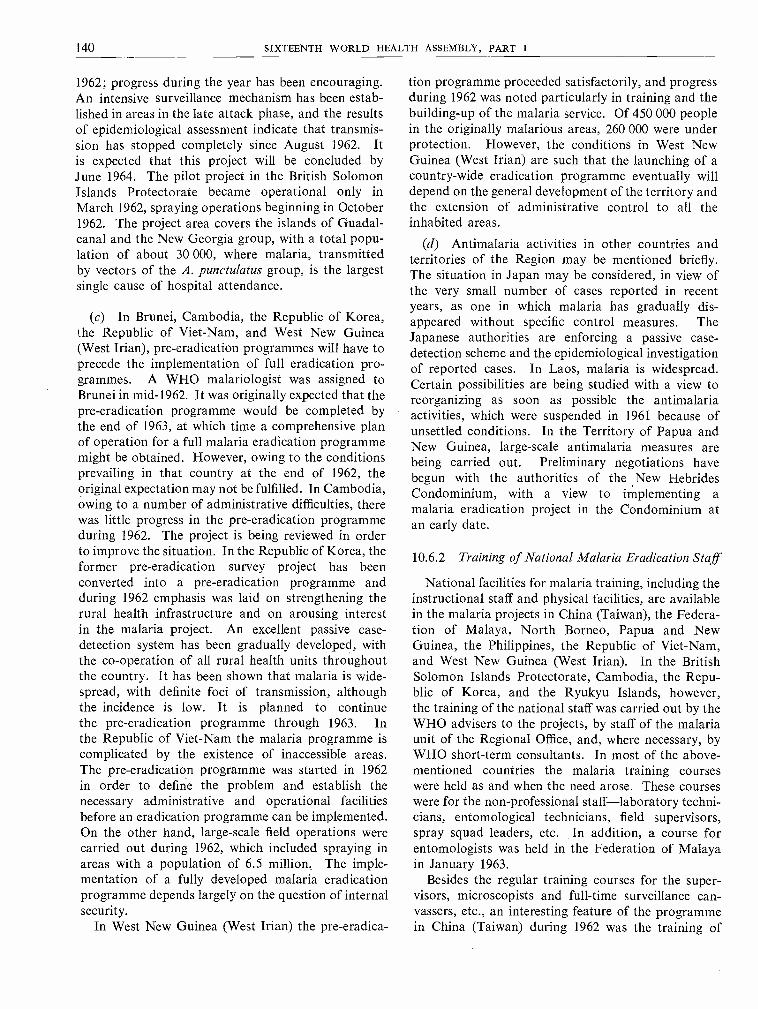
140 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
1962; progress during the year has been encouraging.An intensive surveillance mechanism has been estab-lished in areas in the late attack phase, and the resultsof epidemiological assessment indicate that transmis-sion has stopped completely since August 1962. Itis expected that this project will be concluded byJune 1964. The pilot project in the British SolomonIslands Protectorate became operational only inMarch 1962, spraying operations beginning in October1962. The project area covers the islands of Guadal-canal and the New Georgia group, with a total popu-lation of about 30 000, where malaria, transmittedby vectors of the A. punctulatus group, is the largestsingle cause of hospital attendance.
(c) In Brunei, Cambodia, the Republic of Korea,the Republic of Viet -Nam, and West New Guinea(West Irian), pre- eradication programmes will have toprecede the implementation of full eradication pro-grammes. A WHO malariologist was assigned toBrunei in mid -1962. It was originally expected that thepre -eradication programme would be completed bythe end of 1963, at which time a comprehensive planof operation for a full malaria eradication programmemight be obtained. However, owing to the conditionsprevailing in that country at the end of 1962, theoriginal expectation may not be fulfilled In Cambodia,owing to a number of administrative difficulties, therewas little progress in the pre- eradication programmeduring 1962. The project is being reviewed in orderto improve the situation. In the Republic of Korea, theformer pre- eradication survey project has beenconverted into a pre- eradication programme andduring 1962 emphasis was laid on strengthening therural health infrastructure and on arousing interestin the malaria project. An excellent passive case -detection system has been gradually developed, withthe co- operation of all rural health units throughoutthe country. It has been shown that malaria is wide-spread, with definite foci of transmission, althoughthe incidence is low. It is planned to continuethe pre- eradication programme through 1963. Inthe Republic of Viet -Nam the malaria programme iscomplicated by the existence of inaccessible areas.The pre- eradication programme was started in 1962in order to define the problem and establish thenecessary administrative and operational facilitiesbefore an eradication programme can be implemented.On the other hand, large -scale field operations werecarried out during 1962, which included spraying inareas with a population of 6.5 million The imple-mentation of a fully developed malaria eradicationprogramme depends largely on the question of internalsecurity.
In West New Guinea (West Irian) the pre-eradica-
tion programme proceeded satisfactorily, and progressduring 1962 was noted particularly in training and thebuilding -up of the malaria service. Of 450 000 peoplein the originally malarious areas, 260 000 were underprotection. However, the conditions in West NewGuinea (West Irian) are such that the launching of acountry -wide eradication programme eventually willdepend on the general development of the territory andthe extension of administrative control to all theinhabited areas.
(d) Antimalaria activities in other countries andterritories of the Region may be mentioned briefly.The situation in Japan may be considered, in view ofthe very small number of cases reported in recentyears, as one in which malaria has gradually dis-appeared without specific control measures. TheJapanese authorities are enforcing a passive case -detection scheme and the epidemiological investigationof reported cases. In Laos, malaria is widespread.Certain possibilities are being studied with a view toreorganizing as soon as possible the antimalariaactivities, which were suspended in 1961 because ofunsettled conditions. In the Territory of Papua andNew Guinea, large -scale antimalaria measures arebeing carried out. Preliminary negotiations havebegun with the authorities of the New HebridesCondominium, with a view to implementing amalaria eradication project in the Condominium atan early date.
10.6.2 Training of National Malaria Eradication Staff
National facilities for malaria training, including theinstructional staff and physical facilities, are availablein the malaria projects in China (Taiwan), the Federa-tion of Malaya, North Borneo, Papua and NewGuinea, the Philippines, the Republic of Viet -Nam,and West New Guinea (West Irian). In the BritishSolomon Islands Protectorate, Cambodia, the Repu-blic of Korea, and the Ryukyu Islands, however,the training of the national staff was carried out by theWHO advisers to the projects, by staff of the malariaunit of the Regional Office, and, where necessary, byWHO short -term consultants. In most of the above -mentioned countries the malaria training courseswere held as and when the need arose. These courseswere for the non -professional staff -laboratory techni-cians, entomological technicians, field supervisors,spray squad leaders, etc. In addition, a course forentomologists was held in the Federation of Malayain January 1963.
Besides the regular training courses for the super-visors, microscopists and full -time surveillance can-vassers, etc., an interesting feature of the programmein China (Taiwan) during 1962 was the training of

ANNEX 8 141
2390 school nurses and teachers and 1920 voluntarycollaborators in clinical symptoms and treatmentof malaria, as well as in the techniques of blood -slidetaking and mailing procedures. All of them haveparticipated in passive case -detection, since theirtraining.
Efforts to re- establish a training centre in Manilahave been made in collaboration with the Govern-ment of the Philippines and AID. It is planned toopen the new centre in 1963.
During 1962, WHO fellowships were awarded tonineteen national staff from the Region (two fromNorth Borneo, two from the Philippines, seven fromthe Republic of Korea, four from the Republic ofViet -Nam, three from the Ryukyu Islands and onefrom Sarawak) to attend regular or special coursesin malaria eradication. Grants of limited durationwere also made to four senior officers of nationalprogrammes (one from the British Solomon IslandsProtectorate, one from China (Taiwan), one fromNorth Borneo and one from Sarawak) for observationtours in selected malaria eradication programmes.
10.6.3 Operational Aspects
There has been a growing realization on the partof governments during the year under review that thepossibility of reaching eradication and the maintenanceof areas from which malaria- has been eradicateddepend on the existence in the country of essentialbasic health structures and services, and that withoutthem success is unlikely. This is particularly relevantin relation to the extent of coverage by the basic healthservices necessary to support surveillance and vigilanceoperations.
The eradication programme of Sarawak is prac-tically integrated into the general health services,while in the Philippines the implementation of malariaeradication is now the responsibility of the regionalhealth directors, each of whom is responsible for themedical and health administration in one of the eightregions into which the whole country is divided. InChina (Taiwan), a specialized malaria service is incharge of the eradication programme, but there isalso a well developed network of rural health servicesreaching all parts of the island. This excellent ruralhealth service system, which comprises a networkof twenty -two county health centres, 360 townshipor district health stations and 197 health sub -stations,has rendered indispensable assistance to the malariaeradication programme. At each health centrecounty health supervisors, and at each health stationor sub -station health technicians spend seven to tendays each month on malaria surveillance activities -active case -detection, radical treatment of the con-firmed cases, follow -up investigations, etc.
Mass drug administration is employed in the elim-ination of small residual foci of infection found inthe consolidation phase areas in China (Taiwan).Radical treatment is given to confirmed cases and,whenever thought necessary, weekly single doses ofchloroquine and primaquine (adult dose 300 mg and30 mg respectively) for eight weeks are also distributedto the population in the focus. In the areas of NorthBorneo in the attack phase drugs are given as anadjuvant measure to house spraying; a single dosetreatment (adult dose 600 mg of chloroquine baseand 50 mg of pyrimethamine) is given to the wholepopulation when house spraying is carried out. Insome parts of West New Guinea (West Irian), massdrug administration is used as a complementarymethod to house spraying. Two medicated saltprojects were in operation during 1962 -in Cambodiaand West New Guinea (West Irian); both wereterminated by the end of the year (see section 5.1.3,page 103).
The surveillance operations in areas in the con-solidation phase in the malaria eradication pro-grammes in China (Taiwan), North Borneo andSarawak have made further progress in 1962, bothqualitatively and quantitatively. The collection ofdata in the field by active and passive case -detectionmeasures, the assessment of the data, and the initiationof consequent remedial action, have been improved.The surveillance operations in the other two eradica-tion programmes, in the Philippines and the RyukyuIslands, however, need to be strengthened; for thatreason the services of a short -term consultant wereprovided to the latter project, and in the Philippinesthe plan of action has been completely reviewed anda new one has been established.
The annual blood examination rate in 1962 showedsatisfactory coverage of the population concernedin the programmes in China (Taiwan), North Borneo,Ryukyu Islands and Sarawak. The annual bloodexamination rate for the five eradication programmesin 1962 is shown in Table N.
TABLE N. ANNUAL BLOOD EXAMINATION RATE INTHE WESTERN PACIFIC REGION IN 1962
CountryPopulation inareas in con-
solidation phase
Number ofslides
examined
Annual bloodexamination
rate
China .
(Taiwan) . . 941 000 963 000 102North Borneo . 13 000 22 600 174Philippines . . 3 261 000 184 000 5.6Ryukyu Islands 42 000 8 000 19.0Sarawak . . . 505 000 172 300 34.1

142 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
During 1962 considerable progress was made inChina (Taiwan) in the development of the passivecase -detection scheme. At present there are 2390school nurses and teachers, 4611 private clinics,761 public health units, 257 military medical unitsand 2197 voluntary collaborators, organized intoseveral hundred malaria working groups, participat-ing in passive case -detection. In Sarawak a newexperiment is under way to utilize the " home helps "(village people with first -aid training) in passive case -detection.
The prevention of introduced infection from importedmalaria has become of growing importance in themalaria eradication programme in China (Taiwan),North Borneo and Sarawak. In China (Taiwan),among 4392 persons from the Sino- Burmese borderwho were evacuated to Taiwan in March 1961,seventy -two cases of relapsing vivax infection werefound during 1962 through follow -up investigations,while at least one transmission focus was suspected tooriginate from these imported parasite carriers. Also,a number of refugee groups from China (mainland)arrived in Taiwan during 1962 and there was theconstant danger of parasite carriers being introducedinto the malaria -free areas of Taiwan. Similar prob-lems faced Sarawak and North Borneo, where theimportation of malaria from neighbouring unsprayedKalimantan is a constant threat to the success of thetwo programmes. In Sarawak nearly half of thecountry is constantly exposed to the danger of import-ed malaria from any part of the 700 -kilometre -longborder with Kalimantan.
In August 1962, A. sundaicus, one of the malariavectors in North Borneo, was discovered to be resist-ant to dieldrin in the Papar area, where dieldrin wassprayed once in July 1961. Fortunately, a plan wasmade at the beginning of 1962 to replace this insecticidewith DDT, the first spraying of which was undertakenin July 1962. A. balabacensis in Cambodia (andprobably also in the Republic of Viet -Nam) causes atechnical problem. The interruption of malaria trans-mission by DDT spraying has not been achieved sofar, owing to the exophilic habits of A. balabacensis andalso on account of the primitive construction of farmhuts, which usually have no walls. A plan is beingconsidered to carry out studies on this problem inCambodia. Field trials on the optimum number ofcycles and dosage of insecticide were undertaken inNorth Borneo and West New Guinea (West Irian).Results so far obtained indicate that it is necessaryto spray DDT at 2 g per square metre twice a yearagainst A. balabacensis, A. barbirostris and A. sundaicusin the former country, and against A. farauti and A.koliensis in the latter. The damage to attap (thatch)roofing by insecticide resistant caterpillars is causing
concern in some eradication projects, particularlyin the Federation of Malaya and in North Borneo.The attap roofs are generally infested with variouscaterpillars (Herculia nigrivitta, Simplicia caemen-salis) ; in Malaya, Herculia is naturally kept undercontrol by the chalcid fly. But this fly is susceptible toDDT, and the caterpillar is resistant; therefore, afterspraying the caterpillars vastly increase in numberand destroy the roof. This gives rise to refusals toallow house spraying.
The five pre- eradication programmes started in 1962in the Western Pacific Region -in Brunei, Cambodia,the Republic of Korea, the Republic of Viet -Nam, andWest New Guinea (West Irian) were all convertedfrom previous antimalaria projects, some of whichwere assisted by WHO. Consideration is being given toestablishing a demonstration and training area in thepre- eradication programme in the Republic of Korea,where spraying will also be carried out. The ruralhealth infrastructure is being developed and strength-ened. At present, 182 county health centres and 672district medical units are established. The mobilizationof this health network to participate in the pre -
eradication programme has been undertaken. In theRepublic of Viet -Nam the backbone of the rural healthprogramme is the village health station, of whichthere are more than 7000, and it is anticipated that thegoal of 10 000 will be realized by the end of 1963.Supplementing and supervising the village level healthfacilities there are, at the present time, 210 districthealth centres. Close co- operation between the ruralhealth infrastructure and the malaria service has beengradually established. In West New Guinea (WestIrian) considerable progress has been made in recentyears in establishing a network of the rural healthservices throughout the territory.
It is expected that the certification and registrationof malaria eradication from China (Taiwan) may berequested by the Government in 1964. Towards thisobjective the surveillance operations in the areas inthe consolidation and maintenance phases are beingstrengthened to obtain adequate data. Prospects ofregistration of the achievement of eradication in thenear future in Japan and the Ryukyu Islands are good.
10.6.4 Co- ordination
Most of the malarious countries in the Region holdregular meetings for the purpose of co- ordination andco- operation; these include the meetings of the Anti -malaria Co- ordination Board serving Cambodia, theFederation of Malaya, Laos and the Republic of Viet -Nam, together with Burma and Thailand from theSouth -East Asia Region; the Inter -territorial MalariaConferences for the South -West Pacific, grouping

ANNEX 8 143
West New Guinea (West Irian), the Territory ofPapua and New Guinea, the British Solomon IslandsProtectorate and the New Hebrides Condominium;and the Borneo Malaria Conferences, serving Brunei,Indonesia, North Borneo and Sarawak.
Participants at the Fourth Asian Malaria Con-ference, which took place in Manila from 27 Septemberto 3 October 1962, included representatives fromcountries and territories of the South -East Asia and
Western Pacific Regions, as well as from Pakistan inthe Eastern Mediterranean Region.
Close co- ordination is being maintained with theUnited States Agency for International Development(AID) which supports malaria eradication programmesin Cambodia, China (Taiwan), Laos, the Philippinesand the Republic of Viet -Nam, and with UNICEF,which supports programmes in North Borneo andWest New Guinea (West Irian).
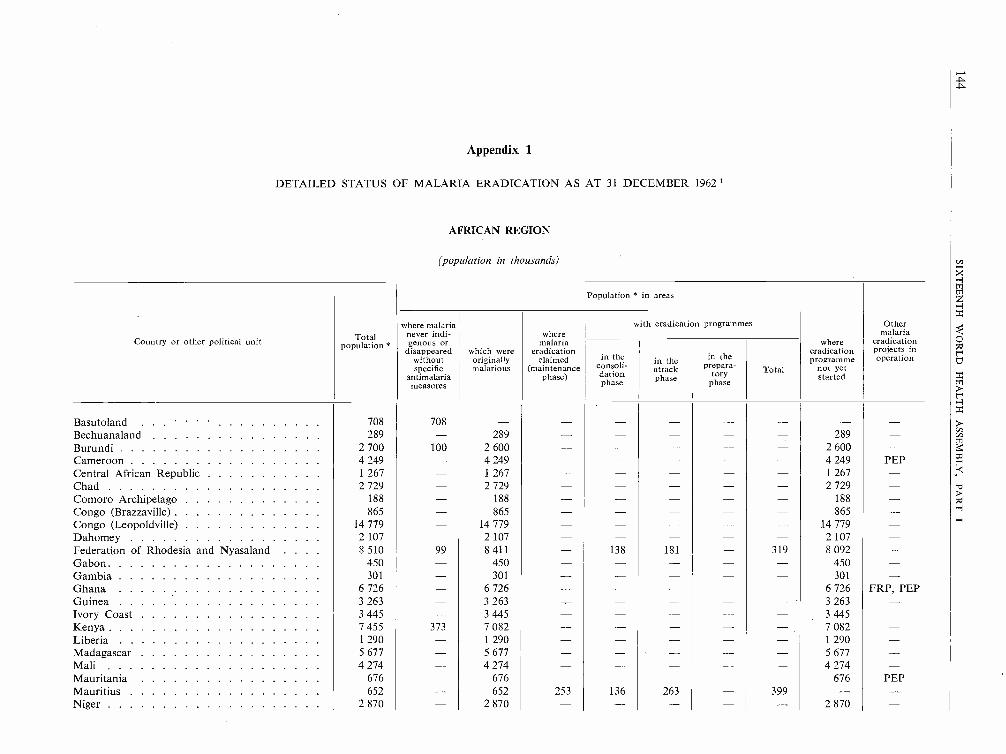
Appendix 1
DETAILED STATUS OF MALARIA ERADICATION AS AT 31 DECEMBER 1962
AFRICAN REGION
(population in thousands)
Population * in areas
where malaria with eradication programmes Other
Country or other political unit Total*
never indi-genous or
disappeared which were
wheremalaria
eradicationwhere
eradication
malariaeradicationprojects in
without originally claimed in the in the in the programme operationspecificP malarious (maintenance consoli- attack prepara- Total not yetY
antimalariameasures
phase) dationphase
phase toryphase
started
Basutoland . . . 708 708 - - - - - - - -Bechuanaland 289 - 289 - - - - - 289 -Burundi 2 700 100 2 600 - - - - - 2 600 -Cameroon 4 249 - 4 249 - - - 4 249 PEPCentral African Republic 1 267 - 1 267 - - - - - 1 267 -Chad 2 729 - 2 729 - - - - - 2 729 -Comoro Archipelago 188 - 188 - - - - - 188 -Congo (Brazzaville) 865 - 865 - - - - - 865 -Congo (Leopoldville) 14 779 - 14 779 - - - - - 14 779 -Dahomey 2 107 - 2 107 - - - - - 2 107 -Federation of Rhodesia and Nyasaland . . . . 8 510 99 8 411 - 138 181 - 319 8 092 -Gabon 450 - 450 - - - - - 450 -Gambia 301 - 301 - - - - - 301 -Ghana 6 726 - 6 726 - - - - - 6 726 FRP, PEPGuinea 3 263 - 3 263 - 3 263Ivory Coast 3 445 - 3 445 - - - - - 3 445 -Kenya 7 455 373 7 082 - - - 7 082 -Liberia 1 290 - 1 290 - - - - - 1 290 -Madagascar 5 677 - 5 677 - - - - - 5 677 -Mali 4 274 - 4 274 - - - - - 4 274 -Mauritania 676 - 676 - 676 PEPMauritius 652 - 652 253 136 263 - 399 - -Niger 2 870 - 2 870 - - - - - 2 870 -

Nigeria 36 431 36 431 36 431 PEP
Portugal :Angola 4 753 4 753 4 753
Cape Verde Islands 208 208 24 94 94 90
Mozambique 6 665 6 665 6 665 PEP
Portuguese Guinea 584 584 584
São Tomé and Principe 66 66 66
Réunion 359 359 359
Rwanda 2 201 180 2 021 2 021
Senegal 2 980 2 980 2 980
Seychelles 42 42
Sierra Leone 2 450 2 450 2 450
South Africa 16 122 11 931 4 191 2 886 1 012 293 1 305
South West Africa 522 320 202 202
Spain :Sidi Ifni 54 54
Spanish Guinea 246 246 246
Spanish Sahara 146 127 19 19
St Helena 5 5
Swaziland 274 274 115 149 10 159
Tanganyika 9 573 876 8 697 8 697
Togo 1 553 1 553 1 553 PEP
Uganda 7 016 7 016 7 016 PEP
Upper Volta 4 400 4 400 4 400
Zanzibar 314 314 314 314
TOTALS 172 434 14 815 157 619 3 278 1 435 ' 1 155 2 590 151 751
' Latest available figures. FRP Field research project.
- Not applicable or none. PEP Pre- eradication programme.
1 Since the terms " preparatory ", " attack " and " consolidation " are applied specifically to malaria eradication programmes, the figures shown in the relevantparts of this table do not include the antimalaria activities, often considerable, of countries and other political units in which eradication programmes as such have notyet been implemented. -
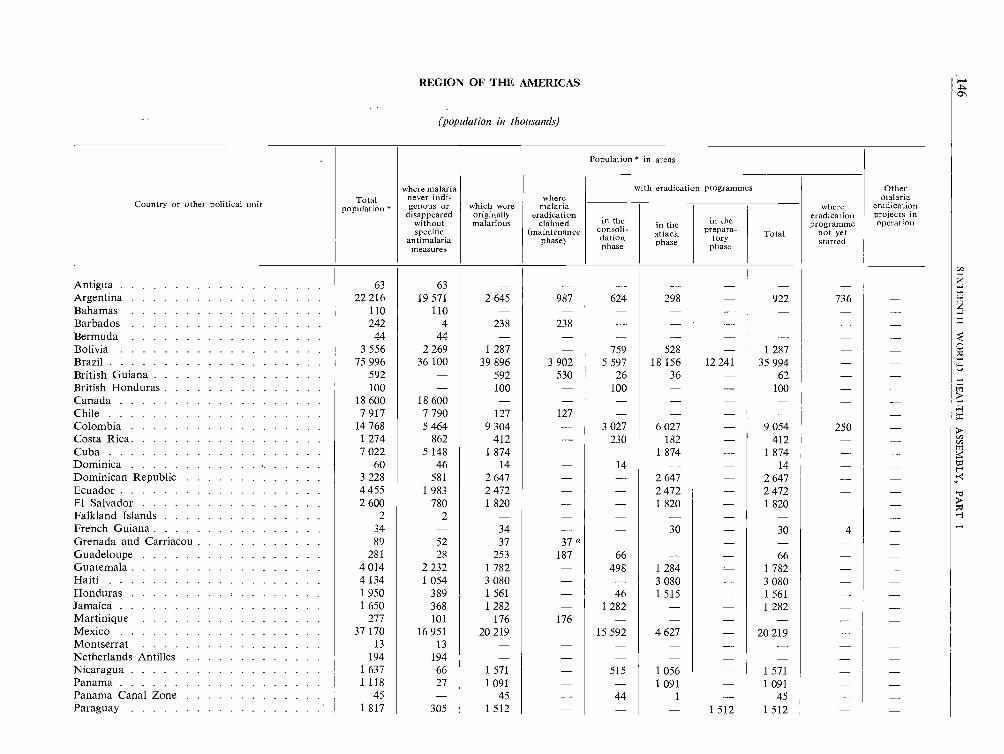
REGION OF THE AMERICAS
(population in thousands)
. Population * in areas
where malaria with eradication programmes Other
Country or other political unit Total*
never indi-genous or which were
wheremalaria where
malariaeradicationpopulation
disappeared originally eradication eradication projects inwithout malarious claimed in the in the in the programme operationspecific (maintenance consoli- attack prepara- Total not yet
antimalariameasures
phase) dationphase
phase toryphase started
Antigua 63 63 - - - - - -Argentina 22 216 19 571 2 645 987 624 298 - 922 736 -Bahamas 110 110 - - - - - -Barbados 242 4 238 238 - - - - - -Bermuda 44 44 - - - - - -Bolivia 3 556 2 269 1 287 - 759 528 - 1 287 - -Brazil 75 996 36 100 39 896 3 902 5 597 18 156 12 241 35 994British Guiana 592 - 592 530 26 36 - 62 - -British Honduras 100 - 100 - 100 - - 100 - -CanadaChile
18 6007 917
18 6007 790
-127 127 - - -- -- -- -
Colombia 14 768 5 464 9 304 - 3 027 6 027 - 9 054 250 -Costa Rica 1 274 862 412 - 230 182 - 412 - -Cuba 7 022 5 148 1 874 - - 1 874 - 1 874 - -Dominica 60 46 14 - 14 - - 14 - -Dominican Republic 3 228 581 2 647 - - 2 647 - 2 647 - -Ecuador 4 455 1 983 2 472 - - 2 472 - 2 472 - -El Salvador 2 600 780 1 820 - - 1 820 - 1 820 - -Falkland Islands 2 2 - - - -French Guiana 34 - 34 - - 30 - 30 4 -Grenada and Carriacou 89 52 37 37 a - - - - - -Guadeloupe 281 28 253 187 66 - - 66Guatemala 4 014 2 232 1 782 - 498 1 284 - 1 782 - -Haiti 4 134 1 054 3 080 - - 3 080 - 3 080 - -Honduras 1950 389 1 561 - 46 1 515 - 1 561 - -Jamaica 1 650 368 1 282 - 1 282 - - 1 282 - -Martinique 277 101 176 176 - - - - - -Mexico 37 170 16 951 20 219 - 15 592 4 627 - 20 219 - -Montserrat 13 13 - - - - - -Netherlands Antilles 194 194 - - - - - - - -Nicaragua 1 637 66 1 571 - 515 1 056 - 1 571Panama 1118 27 1091 - - 1091 - 1091 - -Panama Canal Zone 45 - 45 - 44 1 - 45 - -Paraguay 1 817 305 1 512 - - - 1 512 1 512 - -
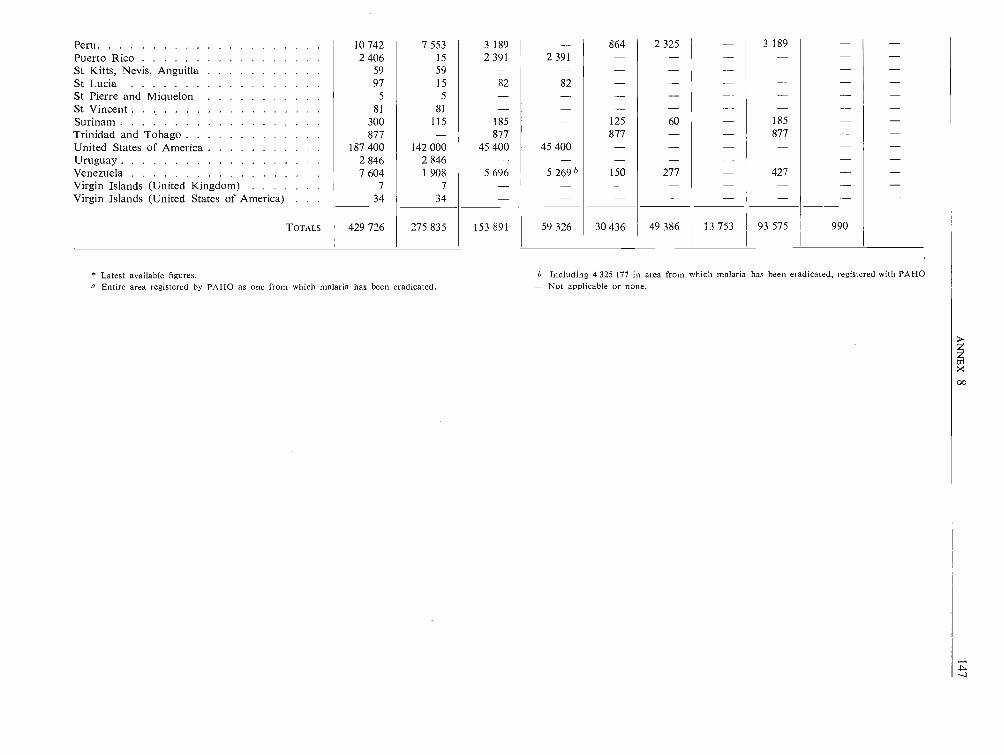
Peru 10 742 7 553 3 189 864 2 325 3 189
Puerto Rico 2 406 15 2 391 2 391
St Kitts, Nevis, Anguilla 59 59 -St Lucia 97 15 82 82St Pierre and Miquelon 5 5 -St Vincent 81 81 -Surinam 300 115 185 125 60 185
Trinidad and Tobago 877 - 877 877 877United States of America 187 400 142 000 45 400 45 400Uruguay 2 846 2 846 --Venezuela 7 604 1 908 5 696 5 269 b 150 277 427Virgin Islands (United Kingdom) 7 7 -Virgin Islands (United States of America) 34 34
TOTALS 429 726 275 835 153 891 59 326 30 436 49 386 13 753 93 575 990
* Latest available figures. b Including 4 325 177 in area from which malaria has been eradicated, registered with PAHOa Entire area registered by PAHO as one from which malaria has been eradicated. - Not applicable or none.

SOUTH -EAST ASIA REGION
(population in thousands)
Country or other political unit Totalo *population
Population * in areas
Oth-malaria
eradicationprojects inoperation
where malarianever indi-genous or
disappearedwithoutspecific
antimalariameasures
which wereoriginallymalarious
wheremalaria
eradicationclaimed
(maintenancephase)
with eradication programmes'where
eradicationprogramme
not yetstarted
in theconsoli-dationphase
in theattackphase
in theP re ara-tory
phaseTotal
AfghanistanBhutanBurmaCeylonIndiaIndonesiaMaldive IslandsMongoliaNepalThailand
TOTALS
14 380670
21 64010 061
453 04597 085
891 0009 407
27 301
9 879560
1 0533 518
14 465-12
1 0004 751-
4 501110
20 5876 543
438 58097 085
77-4 656
27 301
---1 447
20-----
87-4 1001 294
154 887----1 660
4 102-10 1553 802
283 57964 253--2 169
13 000 a
312-------1 7397 140
4 501-14 2555 096
438 46664 253--
3 90821 800
-110
6 332-94
32 83277-
7485 501
----------
634 678 35 238 599 440 1 467 162 028 381 060 9 191 552 279 45 694
* Latest available figures.a Including 3000 in municipal areas not sprayed.
- Not applicable or none.

EUROPEAN REGION
(population in thousands)
Population * in areas
where malaria with eradication programmes Other
Country or other political unit Totalpopulation *
never indi-genous or
disappearedwithout
which wereoriginallymalarious
wheremalaria
eradicationclaimed
whereeradicationprogrammenot yet
malariaeradicationprojects inoperationin the in the in the
specific
antimalariameasures
(maintenancephase)
consoli-dationphase
attack
phaseprepara-
toryphase
Total started
Albania 1 625 225 1 400 300 1 053 47 - 1 100 - -Algeria 11 020 1 301 9 719 - - - - - 9 719 -Andorra 8 8 - - - -Austria 7 067 7 067 - - - - -Belgium 9 153 9 153 - - - - - - - -Bulgaria 7 867 6 143 1 724 1 676 48 - - 48
Byelorussian SSR 8 316 10 8 306 8 306 - - - - - -Czechoslovakia 13 776 13 626 150 150 - - - - - -Denmark 4 581 4 581 - - - - - - -Finland 4 467 4 467 - -France 45 960 45 815 145 145 - - - - - -Germany, Democratic Republic 18 368 18 368 - - - - - - -Germany, Federal Republic 54 450 54 450 - - - - - - - -Gibraltar 27 27 - - - - - -Greece 8 389 3 918 4 471 2 304 2 167 - - 2 167 - -Hungary 10 028 8 528 1 500 1 500 -Iceland 176 176 - - - - - - - -Ireland 2 815 2 815 - - - - - -Italy 49 549 45 549 4 000 4 000 - - -Liechtenstein 16 16 - - - - - - - -Luxembourg 314 314 - - - - - -Malta and Gozo 329 329 - - - - -Monaco 22 22 - - - - - -Morocco 11 626 3 178 8 448 - - - - - 8 448 PEPNetherlands 11 637 9 790 1 847 1 847 - - - - - -Norway 3 611 3 611 - - - - - - - -Poland 29 965 29 860 105 105 - - - - - -Portugal 9 196 6 958 2 238 1 560 678 - - 678 - -Romania 18 680 11 202 7 478 - 6 326 1 152 7 478 - -San Marino 17 17 - - - - - - - -Spain 31 500 9 400 22 100 21 802 298 - - 298 - -Sweden 7 520 7 520 - - - - - - - -Switzerland 5 470 5 470 - -- - - - .

Country or other political unit Totalpopulation *
Population * in areas
Othermalaria
eradicationprojects inoperation
where malarianever indi-genous or
disappearedwithoutspecific
antimalariameasures
which wereoriginallymalarious
wheremalaria
eradicationclaimed
(maintenancephase)
with eradication programmes
whereeradicationprogramme
not yetstarted
in theconsoli-dationphase
in theattackphase
in the
prepara-tory
phaseTotal
TurkeyUkrainian SSRUnion of Soviet Socialist RepublicsUnited Kingdom of Great Britain and Northern
IrelandYugoslavia
TOTALS
28 30743 527
167 902
52 92518 655
-3
11 621
52 92513 474
28 30743 524
156 281
-5 181
-43 524
155 351
-3 174
18 268-890
-298
10 039-40
-1 709
-----
28 307-930
-2 007
-----
-----
698 861 391 937 306 924 245 744 30 026 12 987 - 43 013 18 167
Latest available figures.- Not applicable or none.
PEP Pre -eradication programme.
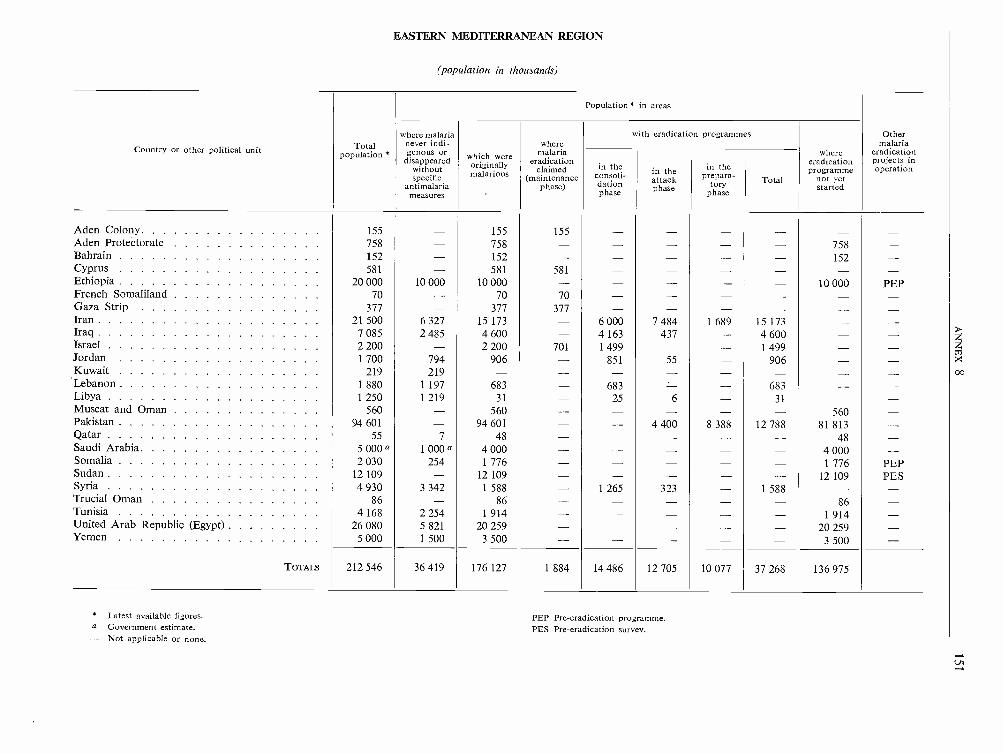
EASTERN MEDITERRANEAN REGION
(population in thousands)
Population' in areas
where malaria with eradication programmes Other
Country or other political unit Total never indi-enous or
wheremalaria where
malariaeradicationpopulation * g
disappeared which were eradication eradication projects inwithout
originallyclaimed in the in the in the programme operation
specificmalarious (maintenance( consoli- attack prepara- Total not yetY
antimalariameasures
phase) dationphase
phase toryphase
started
Aden Colony 155 - 155 155 - - - - - -Aden Protectorate 758 - 758 - - - - - 758 -Bahrain 152 - 152 - - - - - 152 -Cyprus 581 - 581 581 - - - - - -Ethiopia 20 000 10 000 10 000 - - - - - 10 000 PEPFrench Somaliland 70 - 70 70 - - - - - -Gaza Strip 377 - 377 377 - - - - - -Iran 21 500 6 327 15 173 - 6 000 7 484 1 689 15 173 - -Iraq 7 085 2 485 4 600 4 163 437 - 4 600 - -Israel 2 200 - 2 200 701 1 499 - - 1 499 - -Jordan 1 700 794 906 - 851 55 - 906 - -Kuwait 219 219 - - - - - - -Lebanon 1 880 1 197 683 - 683 - - 683 - -Libya 1 250 1 219 31 - 25 6 - 31 - -Muscat and Oman 560 - 560 - - - - - 560 -Pakistan 94 601 - 94 601 - - 4 400 8 388 12 788 81 813 -Qatar 55 7 48 - - - - - 48 -Saudi Arabia 5 000 a 1 000 a 4 000 - - - - - 4 000 -Somalia 2 030 254 1 776 - - - - - 1 776 PEPSudan 12 109 - 12 109 - - - - - 12 109 PESSyria 4 930 3 342 1 588 - 1 265 323 - 1 588 - -Trucial Oman 86 - 86 - - - - - 86 -Tunisia 4 168 2 254 1 914 - - - - - 1 914 -United Arab Republic (Egypt) 26 080 5 821 20 259 - - - - - 20 259 -Yemen 5 000 1 500 3 500 - - - - - 3 500 -
TOTALS 212 546 36 419 176 127 1 884 14 486 12 705 10 077 37 268 136 975
Latest available figures.a Government estimate.- Not applicable or none.
PEP Pre -eradication programme.PES Pre- eradication survey.

WESTERN PACIFIC REGION
(population in thousands)
Population * in areas
where malaria with eradication programmes Other
Country or other political unit Totalpopulation *
never indi-genous or
disappearedwithoutspecific
antimalariameasures
which wereoriginally
wheremalaria
eradicationclaimed
(maintenancephase)
whereeradicationprogrammenot yetstarted
malariaeradicationprojects inoperationin the
consoli-dationphase
in theattackphase
in theprepara-
toryphase
Total
American Samoa 21 21 - - - - - - - -Australia 11292 11 282 10 - - - - - 10 -Bonin Islands ** ** - - - -British Solomon Islands Protectorate 135 - 135 - 135 PPBrunei 90 30 60 - - - 60 PEPCambodia 5 197 4 147 1 050 - - - - - 1 050 PEP, FRPCanton and Enderbury Islands ** ** - - - - - - - -China (Taiwan) 11 171 - 11 171 10 226 945 - - 945 - -Christmas Island 3 3 - - - - - - - -Cocos Islands 1 1 - - - - - - -Cook Islands 18 18 - - - - - - - -Fiji 394 394 - - - - - -French Polynesia 80 80 - - - - - - - -Gilbert and Ellice Islands 46 46 - - - - - - -Guam 67 67 - - - - - -Hawaii 613 613 - - - - - - - -Hong Kong 3 128 - 3 128 2 728 - - - - 400 -Japan 94 285 94 285 - - - - - - - -Korea, Republic of 24 994 - 24 994 - - - - - 24 994 PEPLaos 1 850 - 1 850 - - - - - 1850 -Macao 207 7 200 - - - - - 200 -Malaya, Federation of 7 271 - 7 271 - - - - - 7 271 PPMidway Islands 2 2 - - - - - - - --Nauru 4 4 - - - - -New Caledonia 77 77 - - - - - - - -New Hebrides 61 - 61 - - - 61 -New Zealand 2 420 2 420 - - - - - -Niue 5 5 - - - - - - - -Norfolk Island 1 1 - - - - -- - -North Borneo 487 70 417 - 13 404 - 417 - -Pacific Islands 78 78 - - - - - - - -Papua and New Guinea 2 000 - 2 000 - - - - - 2 000 -Philippines 29 578 20 402 9 176 1 967 3 261 3 250 280 6 791 418 -Pitcairn Island ** ** - - - - - - - -

Portuguese Timor 502 100 402 402
Ryukyu Islands 904 103 801 759 42 42
Sarawak 782 122 660 505 155 660
Singapore 1687 - 1687 1 687
Tokelau Islands 2 2 -Tonga 63 63 -Viet -Nam, Republic of 15 197 2 267 12 930 12 930 PEP
Wake Island ** **
West New Guinea (West Irian) 750 300 450 450 PEP
Western Samoa 110 110 -
TOTALS 215 573 137 120 78 453 17 367 4 766 3 809 280 8 855 52 231
China (mainland) 669 000North Korea 10 197 No information available.North Viet -Nam 15 915
TOTALS 910 685
* Latest available figures.** Under 500.- Not applicable or none.
FRP Field research project.PEP Pre- eradication programme.PP Pilot project.

154 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Appendix 2
PROFESSIONAL STAFF EMPLOYED IN NATIONAL MALARIA ERADICATION SERVICESAS AT 31 DECEMBER 1962
AFRICAN REGION
Country or otherpolitical unit
Totalprofessional
personnelPhysicians Engineers Entomologists Other
CameroonFederation of Rhodesia and
NyasalandGhanaMauritiusPortuguese African Provinces :
MozambiqueSouth AfricaTogoUgandaZanzibar
TOTAL
2 -3 (I)I -1 -3 -3 -1 (1)
(1)- (1)
1 (1)
1 -1
2 -1 (1)
(1)(1)
1
1 Parasitologist1 Health education officer
14 (4) 7 (4) 1 4 2
Figures in brackets indicate number of staff employed part -time.
REGION OF THE AMERICAS
TotalCountry or other professional Physicianspolitical unit personnelEngineers Entomologists Other
Argentina
Bolivia
Brazil (excluding Sao Paulo). .
Brazil (Sao Paulo)British GuianaBritish Honduras
Colombia
Costa RicaCubaDominicaDominican Republic
Ecuador
El SalvadorFrench GuianaGrenadaGuadeloupe
Guatemala
Haiti
Honduras
11
21
82
28--48
3
10
6
20
7
2
9
16
7
(4)
(2)(2)
(2)
(1)
(4)(1)--
6
9
40
12--32
1
8
3
10
3
1
3
8
2
(2)
---
(1)(1)
---
(1)--
(4)(1)
--
2 -5 -
23
8
-
7
1
1
-3
7
1-
2 -5
5
8
1-
1
1
1
1
1
1
--
(1)
1 - StatisticianI 1 (2) Biochemists
1 - Statistician1 - Health education officer
( 6 - Health education officers1 3 - Pharmacists
2 - Veterinarians7 (2) Health education officers-
- (1) Health education officer4 - Health education officers
t 4 - Statisticians1 - Bacteriologist
f 1 - Health education officerl 1 - Veterinarian
3 - Statisticians
J 1 - Health education officer2 - Statisticians1 - Statistician
1 1 - Health education officer4 - Statisticians
Figures in brackets indicate number of staff employed part -time.
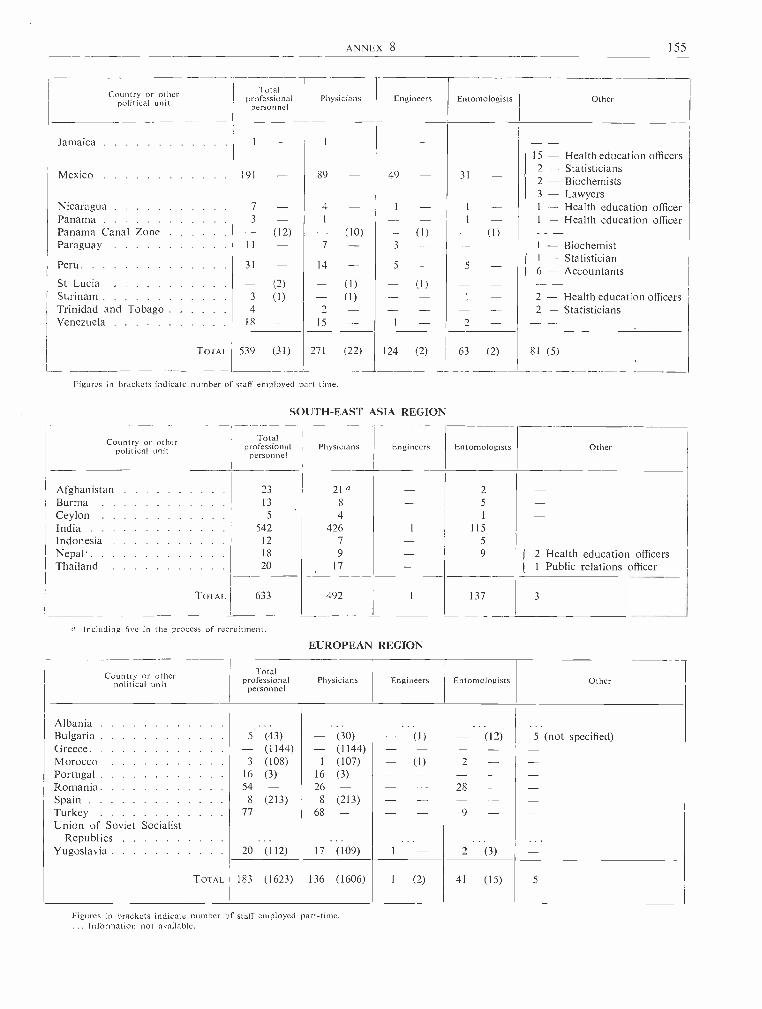
ANNEX 8 155
Country or otherpolitical unit
Totalprofessional Physicians
personnelEngineers Entomologists Other
Jamaica 1
15 - Health education officers2 - Statisticians
Mexico 191 89 - 49 31 2 - Biochemists3 - Lawyers
Nicaragua 7 4 l - 1 -- Health education officerPanama 3 1 1 - 1 - Health education officerPanama Canal Zone (12) (10) - (1) - (1)Paraguay II 7 3 - I - Biochemist
1 - StatisticianPeru 31 14 5 - 5 - 6 - AccountantsSt Lucia (2) (1) - (1)Surinam 3 (1) (1) 1 2 - Health education officersTrinidad and Tobago 4 2 2 - StatisticiansVenezuela 18 15 1 2
TOTAL 539 (31) 271 (22) 124 (2) 63 (2) 81 (5)
Figures in brackets indicate number of staff employed part -time.
SOUTH -EAST ASIA REGION
Country or otherpolitical unit
Totalprofessional
personnelPhysicians Engineers Entomologists Other
Afghanistan 23 21 a - 2Burma 13 8 - 5
Ceylon 5 4 - 1
India 542 426 I 115
Indonesia 12 7 - 5
Nepal' 18 9 - 9 I 2 Health education officersThailand 20 17 - I 1 Public relations officer
TOTAL 633 492 1 137 3
a Including five in the process of recruitment.
EUROPEAN REGION
Country or otherpolitical unit
Totalprofessional Physicians
personnelEngineers Entomologists Other
AlbaniaBulgaria 5 (43) (30) - (1) - (12) 5 (not specified)Greece - (1144) (1144)Morocco 3 (108) 1 (107) - (1) 2Portugal 16 (3) 16 (3)Romania 54 - 26 - 28Spain 8 (213) 8 (213)Turkey 77 - 68 - 9
Union of Soviet SocialistRepublics
Yugoslavia 20 (112) 17 (109) 1 2 (3)
TOTAL 183 (1623) 136 (1606) 1 (2) 41 (15) 5
Figures in brackets indicate number of staff employed part -time.... Information not available.

156 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
EASTERN MEDITERRANEAN REGION
Country or otherpolitical unit
Totalprofessional
personnelPhysicians Engineers Entomologists Other
Ethiopia 2 - 1 - - 1 -Iran 73 - 38 - 27 8 -Iraq 2 (7) 1 (7) - 1 -Israel 2 (16) 1 (16) - 1 -Jordan 1 - 1 - - - -Lebanon 2 - - - 1 1 -Libya - - - - - - -Pakistan 28 - 28 - - - -Saudi Arabia 15 - 5 - 6 4 -Somalia - - - - - - -Sudan 2 - 1 - - 1
Syria 5 - 4 - - 1
Tunisia ... . .
United Arab Republic ' 22 - 18 - - 4 -TOTAL 154 (23) 98 (23) 34 22 -
Figures in brackets indicate number of staff employed part -time.... Information not available.
WESTERN PACIFIC REGION
Country or otherpolitical unit
Totalprofessional
personnelPhysicians Engineers Entomologists Other
British Solomon Islands . . . . 1 (1) - (1) - 1 Health education officerBrunei - (1) - (1) - - - -Cambodia 5 - 5 - - - - -China (Taiwan) 9 - 4 - 1 2 - i 1 Biologist
1 Health education officerHong Kong 1 - 1 - - - - -Korea, Republic of 3 (1) 2 (1) - 1 - -Laos 4 - 4 - - -Malaya, Federation of 4 - 1 - 1 1 - 1 Health education officerNorth Borneo 1 (1) 1 (1) - - - -Papua and New Guinea 5 (1) 3 - - 2 (1) -Philippines 65 - 38 - 12 15 - -Ryukyu Islands 1 - 1 - - - - -Sarawak - (5) - (5) - - - -Viet-Nam, Republic of 14 - 13 - - 1 - -West New Guinea (West Irian) 4 - 3 - - 1 - -
TOTAL 117 (10) 76 (9) 14 23 (1) 4
Figures in brackets indicate number of staff employed part -time.
ANNEX 9 157
Annex 9
REVIEW AND APPROVAL OF THE PROGRAMME AND BUDGET ESTIMATES FOR 1964 1
1. REPORT OF THE AD Hoc COMMITTEE OF THE EXECUTIVE BOARD
1. The Executive Board, at its thirty -first session," having examined in detail the programme andbudget estimates for 1964 2 prepared and submittedby the Director -General in accordance with theprovisions of Article 55 of the Constitution " recom-mended " to the Health Assembly that it approvean effective working budget for 1964 in the amountof $33 716 000, as proposed by the Director -General "
" subject to minor adjustments in cost estimates,to be reported by the Director -General to the SixteenthWorld Health Assembly, through the Ad Hoc Com-mittee of the Executive Board ".3
2. In accordance with resolution EB31.R52, theAd Hoc Committee established by the ExecutiveBoard and consisting of Dr M. K. Afridi, ProfessorE. Aujaleu and Dr A. Nabulsi, met on 6 May 1963in the Palais des Nations, Geneva. Dr Afridi waselected Chairman.
3. In considering the adjustments in the cost estimatesof the proposed programme and budget estimates for1964 reported by the Director -General (see part 2 ofthis annex), the Committee noted that these werein part consequential to and in part in line with theadditional requirements included in the supplementarybudget estimates for 1963 and recommended by theExecutive Board for approval by the Sixteenth WorldHealth Assembly.4
4. Thus the Committee found that the continuingcosts of the increases relating to the salary scalesfor general services staff (in Geneva, Copenhagen andNew Delhi) and in the payments to the pensionersof the Office International d'Hygiène Publique(OIHP) amounting to $192 100 (see part 2 of thisannex, paragraph 5) were of a mandatory nature,and as a result of its examination the Committee wasof the opinion that these estimates were satisfactory.
See resolution WHA16.28.2 Off. Rec. Wld Huth Org. 121.
3 Resolution EB31.R30 and footnote, OJf. Rec. Wld HuthOrg. 124, 18.
See Annex 3, part 2.
[A16 /P &B /12 Add.1, A16 /AFL /9 Add.1 Rev.l - 9 May 1963]
5. With regard to the continuing costs of a discretion-ary nature, the Committee noted that the Director -General proposed the inclusion of the same minimalamount of $40 000 as in the supplementary budgetestimates for 1963 for the purpose of meeting requestsfor services from new Members and Associate Mem-bers as well as from Members resuming active parti-cipation in the work of the Organization (see part 2,paragraph 4).
6. The steps which the Director- General proposesbe taken in 1964 to assist in meeting some of theadditional costs of the headquarters building andwhich are similar to those proposed in the supplement-ary estimates for 1963 (see part 2, paragraph 2) wereconsidered by the Committee to be sounds
7. In its report to the Sixteenth World HealthAssembly on accommodation for the Regional Officefor Africa, the Committee endorsed the Director -General's view that no adjustment need be madewith regard to Appropriation Section 12 " Reimburse-ment of the Working Capital Fund ", in the proposedprogramme and budget estimates for 1964.8
8. As a result of its examination of the proposedadjustments to the programme and budget estimatesfor 1964, the Committee, on behalf of the Board,recommends to the Sixteenth World Health Assemblythat it approve the inclusion of the following pro-visions :
(a) Increases in the salary scales for general servicesus s
staff and in the payments of OIHP pensioners
(b) Provision for services to new Members and
192 100
Members resuming active participation . . .
(c) Headquarters Building Fund (apart from revisingthe title of Appropriation Section 10 to read" Headquarters Building Fund ")
40
117
000
000
349 100
5 See also Annex 3, part 1.6 See Annex 4.
158 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
9. In considering the manner of financing theadditional expenditure of $349 100 proposed to beadded to the effective working budget level, as recom-mended by the Executive Board, the Committee fullyendorses the Director -General's proposal to useavailable casual income to meet this additionalexpenditure. The Committee calls the attention ofthe Sixteenth World Health Assembly to the fact that,
1. Introduction
by using $849 100 of casual income to help financethe proposed adjusted effective working budget of$34 065 100 for 1964, no increase in the total assess-ments on Members will be necessary as compared tothe total assessments for the effective working budgetlevel of $33 716 000 proposed by the Executive Boardat its thirty -first session (see part 2, Appendix 2).
2. REPORT BY THE DIRECTOR- GENERAL
1.1 The Executive Board, at its thirty -first session," having examined in detail the programme andbudget estimates for 19641 prepared and submittedby the Director -General in accordance with theprovisions of Article 55 of the Constitution ", recom-mended to the Sixteenth World Health Assembly" that it approve an effective working budget for 1964in the amount of $33 716 000, as proposed by theDirector -General " ... " subject to minor adjust-ments in cost estimates, to be reported by the Director -General to the Sixteenth World Health Assembly,through the Ad Hoc Committee of the ExecutiveBoard ",2 meeting on 6 May 1963.
1.2 When the Executive Board examined the estim-ates it was informed that adjustments might becomenecessary, specifically in the amounts included underAppropriation Sections 10 " Headquarters Building :Repayment of Loans " and 12 " Reimbursement ofthe Working Capital Fund ". Accordingly, as statedin paragraphs 204 and 206 of Chapter IV of its report 3on its examination of the proposed programme andbudget estimates for 1964, the Board decided thatthese provisions should be referred to its Ad HocCommittee for review. Since the session of the Board,developments have occurred which make necessaryadjustments in the estimates (i) to provide servicesto new Members and Associate Members and toMembers resuming active participation in the workof the Organization (see paragraph 4 below), (ii) tomeet increases in the salary scales for general servicesstaff in certain locations (see paragraph 5) and (iii) tomeet increases in the payments to pensioners of theOffice International d'Hygiène Publique (OIHP) (seeparagraph 5); none of these increased costs wasforeseen at the time.
1 Off Rec. Wld H1th Org. 121.2 Resolution EB31.R30 and footnote, Off Rec. Wld Hlth Org.
124, 18.3 Off. Rec. Wld Huth Org. 125, 58.
[A16 /P &B /12, A16 /AFL /9 - 3 May 1963]
2. Appropriation Section 10 : Headquarters Building :Repayment of Loans
2.1 Under agenda item 3.11, the Director -Generalis submitting a progress report on headquartersaccommodation,4 and as explained in the Director -General's report on the supplementary budget estim-ates for 1963 5 (agenda item 3.3), the Director - Generalconsiders that the increase in cost of the headquartersbuilding will require a number of steps to be taken.Of the two steps which he believes can now be taken,the first envisages that the amount of US $387 000appropriated by the Fifteenth World Health Assemblyunder Appropriation Section 10 " HeadquartersBuilding : Repayment of Loans ", of the Appropria-tion Resolution for the financial year 1963(WHA15.42), be used for a credit to the HeadquartersBuilding Fund, the title of Appropriation Section 10being changed to read " Headquarters BuildingFund "; and the second envisages that the amountof US $387 000 be increased to US $500 000 by theinclusion in the supplementary estimates for 1963 ofan additional amount of US $113 000.
2.2 The Director -General proposes, as he did for1963, that the amount of US $383 000 included in theproposed estimates for 1964 under AppropriationSection 10 " Headquarters Building : Repayment ofLoans " be increased by US $117 000 to US $500 000,to be credited to the Headquarters Building Fund;and that the title of Appropriation Section 10 bechanged accordingly.
3. Appropriation Section 12: Reimbursement of theWorking Capital Fund
For the reasons explained in the Director -General'sreport on accommodation for the Regional Office forAfrica 6 (agenda item 3.12), the Director- General
4 See Annex 7, part 2.5 See Annex 3, part 2.6 See Annex 4, part 2.
ANNEX 9 159
does not consider any adjustment necessary in theamount provided under this appropriation section.
4. Provision for Services to New Members andMembers resuming Active Participation
As explained in the Director -General's report onthe supplementary budget estimates for 1963,' theDirector -General proposed that an amount ofUS $40 000 be included in the supplementary estimatesfor 1963 for the purpose of meeting requests from newMembers and Associate Members as well as fromMembers resuming active participation in the workof the Organization. The Director -General proposesthat a similar amount of US $40 000 be added to theproposed programme and budget estimates for 1964for the same purpose.
5. Increases in the Salary Scales for General ServicesStaff and in the Payments to OIHP Pensioners
As explained in the Director -General's report onthe supplementary budget estimates for 1963,1 theDirector -General has found it necessary to includeprovision in the supplementary estimates for 1963to meet additional expenditure resulting from increasesin (a) the salary scales for general services staff inGeneva, Copenhagen and New Delhi, and (b) thepayments to OIHP pensioners. At the time theproposed programme and budget estimates for 1964were prepared these increases were not foreseen andthe Director -General now reports that the additionalexpenditure for 1964 in respect of these requirementstotals US $192 100, as follows :
(a) Increased costs resulting from increases in thesalary scales for general services staff in Geneva,Copenhagen and New Delhi
(b) increased payments to OIHP pensioners . . .
6. Total Adjusted Estimates for 1964
US
1964 as presented in Official Records No. 121, theamounts required to be added, and the resulting totalestimates proposed for 1964. The two statementsalso reflect the adjustments required to be made asbetween Appropriation Sections 6 (Expert Com-mittees) and 4 (Programme Activities) should theSixteenth World Health Assembly adopt the Director -General's recommendation that a study group ratherthan an expert committee be convened on specialcourses for national staff with higher administrativeresponsibilities in the health services.
7. Method of Financing the Additional Requirements
As indicated in the Summary of Budget Estimates 3and in the Summary Table showing Total Budget,Income, Assessments and Effective Working Budget,4the Director -General recommended that casual incomeavailable in the amount of US $500 000 be used tohelp finance the proposed programme and budgetestimates for 1964 as presented in Official RecordsNo. 121. This recommendation was endorsed by theExecutive Board in its report on its examination ofthe proposed programme and budget estimatesfor 1964.5
As sufficient casual income is available, over andabove the amount of US $438 100 recommended tobe used to help finance the supplementary budgetestimates for 1963,' to cover the increased require-ments for 1964 as described in paragraphs 2, 4 and 5above, the Director -General recommends that theseadditional requirements be financed by using availablecasual income in the amount of US $349 100. Thetotal amount of casual income which the Director -
General recommends be used to help finance the 1964budget is therefore US $849 100, made up as follows :
189
2
700
400Assessments on new Members from previous yearsMiscellaneous incomeAvailable by transfer from the cash portion of the
Assembly Suspense Account
uss98 860
454 733
295 507
192 100
849 100
The Director -General submits a statement 2 showing,by appropriation section and by purpose-of- expendi-ture code, the amounts required to be added to theestimates for 1964 to take account of the above -mentioned increased requirements. He also submitsa statement (see Appendix 1, page 160 (showing,by appropriation section, the proposed estimates for
1 See Annex 3, part 2.Unpublished.
The adjustments that will have to be made to the1964 column of the Summary Table on page 11 ofOfficial Records No. 121 in order to reflect the aboveproposals are shown in Appendix 2.
3 Off. Rec. Wld HIM Org. 121, 9.' Off. Rec. Wud HO Org. 121, 11.5 Off Rec. Wld Huth Org. 125, 84.

160 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Appendix 1
PROPOSED ESTIMATES OF EXPENDITURE FOR 1964 UNDER THE REGULAR BUDGET
Appropriation Purpose of AppropriationSection
PART I: ORGANIZATIONAL MEETINGS
Proposedestimates ofexpenditure,as shown in
OfficialRecordsNo. 121US$
Proposedadjustments
US$
Totaladjusted
estimates ofexpenditure
US$
1. World Health Assembly 317 210 317 2102. Executive Board and its Committees 189 090 189 0903. Regional Committees 100 530 100 530
Total - Part I 606 830 606 830
PART II : OPERATING PROGRAMME4. Programme Activities 16 299 369 140 450 16 439 8195. Regional Offices 2 639 006 24 700 2 663 7066. Expert Committees 236 500 (9 900) 226 6007. Other Statutory Staff Costs 5 501 580 19 700 5 521 280
Total - Part II 24 676 455 174 950 24 851 405
PART III: ADMINISTRATIVE SERVICES
8. Administrative Services 1 876 632 48 550 1 925 1829. Other Statutory Staff Costs 610 083 8 600 618 683
Total - Part III 2 486 715 57 150 2 543 865
PART IV: OTHER PURPOSES10. Headquarters Building Fund 383 000 117 000 500 00011. Transfer to the Malaria Eradication Special Account 5 363 000 - 5 363 00012. Reimbursement of the Working Capital Fund 200 000 - 200 000
Total - Part IV 5 946 000 117 000 6 063 000
Sub -total - Parts I, II, III and IV 33 716 000 349 100 34 065 100
PART V : RESERVE13. Undistributed Reserve 2 230 540 - 2 230 540
Total - Part V 2 230 540 2 230 540
TOTAL - ALL PARTS 35 946 540 349 100 36 295 640
Appendix 2
SUMMARY TABLE SHOWING TOTAL BUDGET, INCOME, ASSESSMENTSAND EFFECTIVE WORKING BUDGET FOR 1964
As perOfficial Records
No. 121page 11
US$
Adjustments
US$
asTotal
adjusted
US$
Total budget 35 946 540 a 349 100 36 295 640 aDeductions 1 256 990 349 100 1 606 090
Assessments on Members 34 689 550 a 34 689 550 aLess: Amount of Undistributed Reserve 2 230 540 a, b 2 230 540 a, b
Assessments on Members for the effective working budget 32 459 010 - 32 459 010
a These amounts will be subject to adjustment if one or more Members resume active participation in the work of WHO, or ifthe membership of WHO increases by the time of the Sixteenth World Health Assembly.
b Equalling the assessments on inactive Members (at the time these estimates were prepared, the Byelorussian SSR and theUkrainian SSR) and on China.
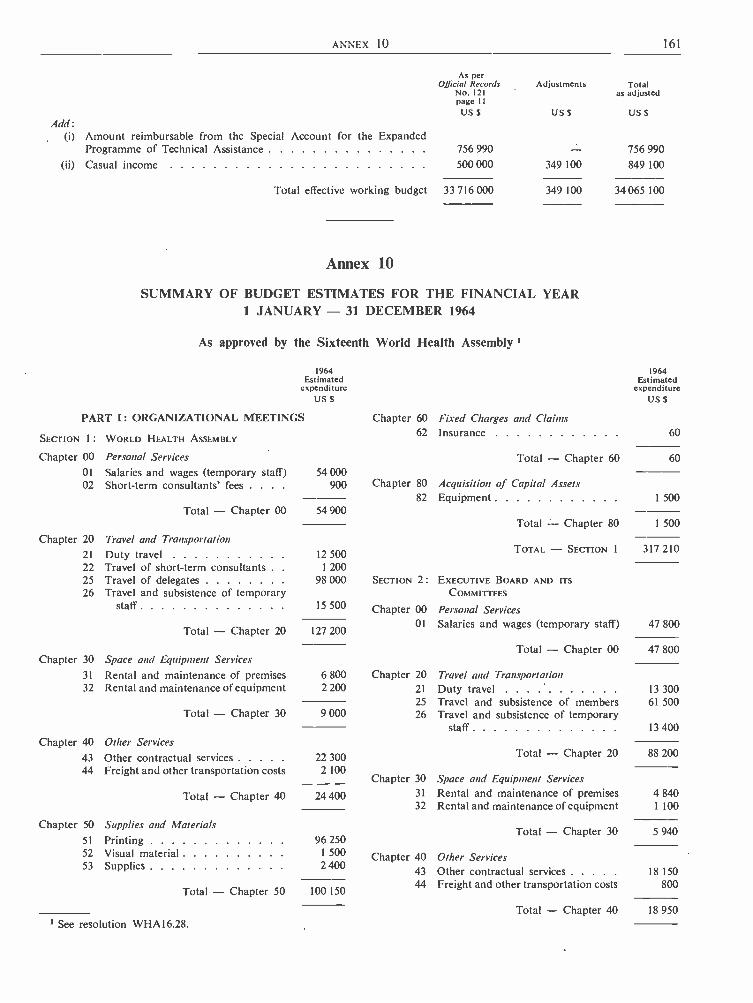
ANNEX 10 161
Add:
As perOfficial Records
No. 121page IIUS$
Adjustments
US$
Totalas adjusted
US $
(i) Amount reimbursable from the Special Account for the ExpandedProgramme of Technical Assistance 756 990 756 990
(ii) Casual income 500 000 349 100 849 100
Total effective working budget 33 716 000 349 100 34 065 100
Annex 10
SUMMARY OF BUDGET ESTIMATES FOR THE FINANCIAL YEAR1 JANUARY - 31 DECEMBER 1964
As approved by the Sixteenth World Health Assembly 1
1964Estimated
expenditureUS S
PART I: ORGANIZATIONAL MEETINGS Chapter 60 Fixed Charges and Claims
1964Estimated
expenditureUS $
62 Insurance 60SECTION 1 : WORLD HEALTH ASSEMBLY
Chapter 00 Personal Services Total - Chapter 60 60
01 Salaries and wages (temporary staff) 54 00002 Short -term consultants' fees . . . . 900 Chapter 80 Acquisition of Capital Assets
82 Equipment 1 50054 900Total - Chapter 00
1 500Total - Chapter 80Chapter 20 Travel and Transportation
21 Duty travel 12 500TOTAL - SECTION 1 317 210
22 Travel of short -term consultants . 1 20025 Travel of delegates 98000 SECTION 2: EXECUTIVE BOARD AND ITS26 Travel and subsistence of temporary COMMITTEES
staff 15 500 Chapter 00 Personal Services
Total - Chapter 20 127 20001 Salaries and wages (temporary staff) 47 800
Total - Chapter 00 47 800Chapter 30 Space and Equipment Services
31 Rental and maintenance of premises 6 800 Chapter 20 Travel and Transportation32 Rental and maintenance of equipment 2200 21 Duty travel 13 300
25 Travel and subsistence of members 61 5009 000Total - Chapter 30 26 Travel and subsistence of temporary
staff 13 400
Chapter 40 Other Services88 20043 Other contractual services 22 300 Total - Chapter 20
44 Freight and other transportation costs 2 100Chapter 30 Space and Equipment Services
Total - Chapter 40 24 400 31 Rental and maintenance of premises 4 84032 Rental and maintenance of equipment 1 100
Chapter 50 Supplies and Materials Total - Chapter 30 5 94051 Printing 96 25052 Visual material 1 500 Chapter 40 Other Services53 Supplies 2 400
43 Other contractual services 18 150
Total - Chapter 50 100 15044 Freight and other transportation costs 800
Total - Chapter 40 18 950
1 See resolution WHA16.28.
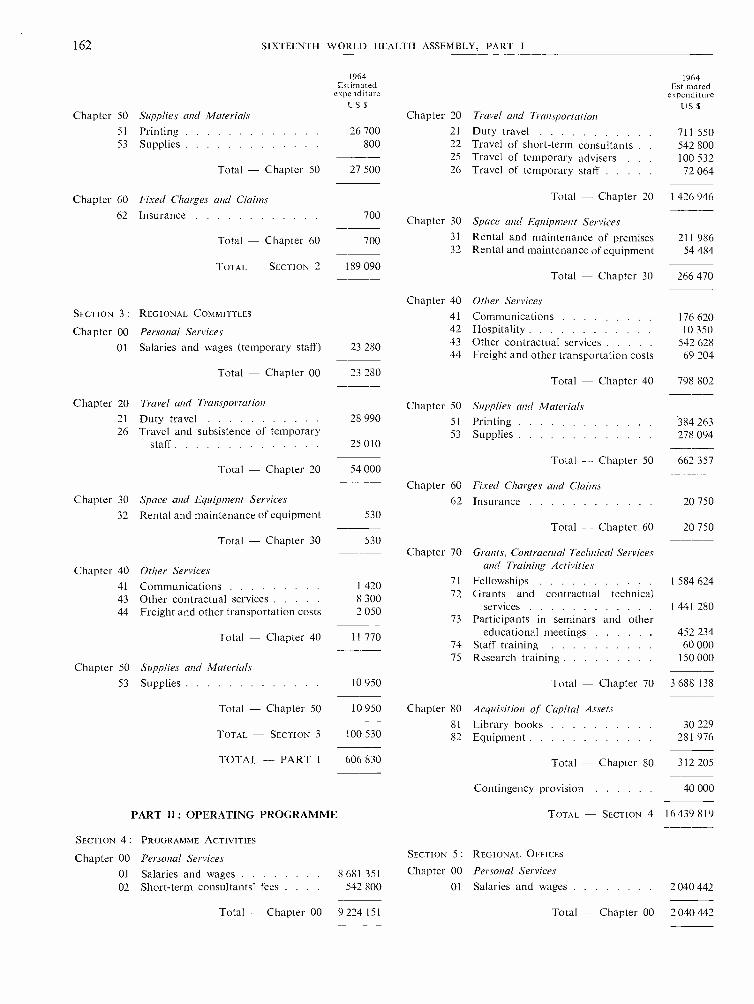
162 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Chapter 50
1964Estimated
expenditureUS $
Supplies and Materials Chapter 20 Travel and Transportation
1964Estimated
expenditureUS $
51 Printing 26 700 21 Duty travel 711 55053 Supplies 800 22 Travel of short -term consultants 542 800
25 Travel of temporary advisers . 100 532Total - Chapter 50 27 500 26 Travel of temporary staff 72 064
Chapter 60 Fixed Charges and Claims Total - Chapter 20 1 426 946
62 Insurance 700 Chapter 30 Space and Equipment Services
Total - Chapter 60 700 31 Rental and maintenance of premises 211 98632 Rental and maintenance of equipment 54 484
TOTAL - SECTION 2 189 090Total Chapter 30 266 470
Chapter 40 Other ServicesSECTION 3: REGIONAL COMMITTEES 41 Communications 176 620Chapter 00 Personal Services 42 Hospitality 10 350
01 Salaries and wages (temporary staff) 23 280 43 Other contractual services 542 62844 Freight and other transportation costs 69 204
Total - Chapter 00 23 280Total - Chapter 40 798 802
Chapter 20 Travel and Transportation Chapter 50 Supplies and Materials21 Duty travel 28 990 51 Printing 384 26326 Travel and subsistence of temporary 53 Supplies 278 094
staff 25 010
Total - Chapter 50 662 357Total - Chapter 20 54 000
Chapter 60 Fixed Charges and ClaimsChapter 30 Space and Equipment Services 62 Insurance 20 750
32 Rental and maintenance of equipment 53020 750Total - Chapter 60
Total - Chapter 30 530
Chapter 40
Chapter 70 Grants, Contractual Technical Servicesand Training ActivitiesOther Services
41 Communications 1 420 71 Fellowships 1 584 624
43 Other contractual services 8 300 72 Grants and contractual technical
44 Freight and other transportation costs 2 050 services 1 441 28073 Participants in seminars and other
Total - Chapter 40 11 770 educational meetings 452 23474 Staff training 60 00075 Research training 150 000
Chapter 50 Supplies and Materials53 Supplies 10 950 Total - Chapter 70 3 688 138
Total - Chapter 50 10 950 Chapter 80 Acquisition of Capital Assets81 Library books 30 229
TOTAL - SECTION 3 100 530 82 Equipment 281 976
TOTAL - PART I 606 830 Total - Chapter 80 312 205
Contingency provision 40 000
PART H : OPERATING PROGRAMME TOTAL - SECTION 4 16 439 819
SECTION 4: PROGRAMME ACTIVITIES
Chapter 00 Personal Services SECTION 5: REGIONAL OFFICES
01 Salaries and wages 8 681 351 Chapter 00 Personal Services02 Short -term consultants' fees . . . . 542 800 01 Salaries and wages 2 040 442
Total - Chapter 00 9 224 151 Total - Chapter 00 2 040 442
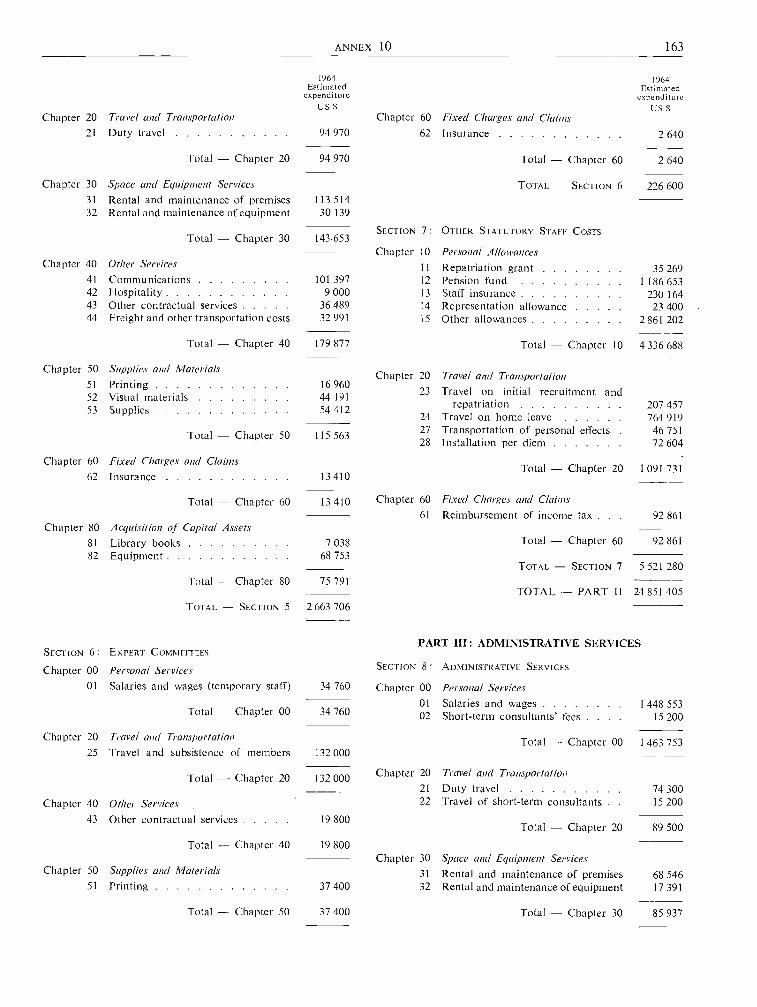
ANNEX 10 163
Chapter 20 Travel and Transportation
1964Estimated
expenditureUSs
1964Estimated
expenditureUS s
Chapter 60 Fixed Charges and Claims21 Duty travel 94 970 62 Insurance 2 640
Total - Chapter 20 94 970 Total - Chapter 60 2 640
Chapter 30 Space and Equipment Services TOTAL - SECTION 6 226 60031 Rental and maintenance of premises 113 51432 Rental and maintenance of equipment 30 139
SECTION 7: OTHER STATUTORY STAFF COSTSTotal - Chapter 30 143.653
Chapter 10 Personal AllowancesChapter 40 Other Services 11 Repatriation grant 35 269
41 Communications 101 397 12 Pension fund 1 186 65342 Hospitality 9 000 13 Staff insurance 230 16443 Other contractual services 36 489 14 Representation allowance 23 40044 Freight and other transportation costs 32 991 15 Other allowances 2 861 202
Total - Chapter 40 179 877 Total - Chapter 10 4 336 688
Chapter 50 Supplies and MaterialsChapter 20 Travel and Transportation
51
5253
PrintingVisual materialsSupplies
16 96044 19154 412
23 Travel on initial recruitment andrepatriation
24 Travel on home leave207764
457919
Total - Chapter 50 115 56327 Transportation of personal effects28 Installation per diem
4672
751
604
Chapter 60 Fixed Charges and Claims Total - Chapter 20 1 091 73162 Insurance 13410
Total - Chapter 60 Chapter 60 Fixed Charges and Claims13 41061 Reimbursement of income tax . . . 92 861
Chapter 80 Acquisition of Capital Assets81 Library books 7 038 Total - Chapter 60 92 861
82 Equipment 68 753TOTAL -- SECTION 7 5 521 280
Total -- Chapter 80 75 791TOTAL - PART I I 24 851 405
TOTAL - SECTION 5 2 663 706
PART III: ADMINISTRATIVE SERVICESSECTION 6: EXPERT COMMITTEES
Chapter 00 Personal Services SECTION 8: ADMINISTRATIVE SERVICES
01 Salaries and wages (temporary staff) 34 760 Chapter 00 Personal Services01 Salaries and wages 1 448 553
Total - Chapter 00 34 760 02 Short -term consultants' fees . . . 15 200
Chapter 20 Travel and Transportation Total - Chapter 00 1 463 75325 Travel and subsistence of members 132 000
Total - Chapter 20 1.32 000Chapter 20 Travel and Transportation
21 Duty travel 74 300
Chapter 40 Other Services 22 Travel of short -term consultants . 15 200
43 Other contractual services 19 800Total - Chapter 20 89 500
Total - Chapter 40 19 800
Chapter 30 Space and Equipment ServicesChapter 50 Supplies and Materials 31 Rental and maintenance of premises 68 546
51 Printing 37 400 32 Rental and maintenance of equipment 17 391
Total - Chapter 50 37 400 Total - Chapter 30 85 937
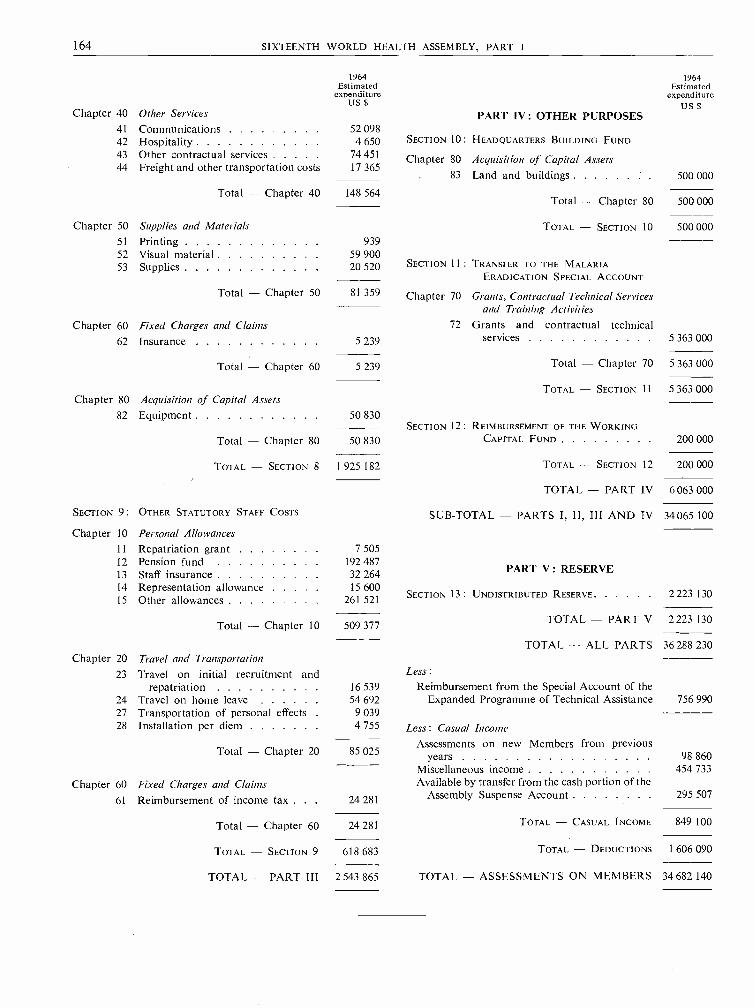
164 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
1964Estimated
expenditureUS $
1964Estimated
expenditureUS $
Chapter 40 Other Services PART IV : OTHER PURPOSES41 Communications 52 09842 Hospitality 4 650 SECTION 10: HEADQUARTERS BUILDING FUND
43 Other contractual services 74 451 Chapter 80 Acquisition of Capital Assets44 Freight and other transportation costs 17 365
83 Land and buildings 500 000
Total - Chapter 40 148 564Total - Chapter 80 500 000
Chapter 50 Supplies and Materials TOTAL - SECTION 10 500 00051 Printing 93952 Visual material 59 90053 Supplies 20 520 SECTION 11 : TRANSFER TO THE MALARIA
ERADICATION SPECIAL ACCOUNT
Total - Chapter 50 81 359 Chapter 70 Grants, Contractual Technical Servicesand Training Activities
Chapter 60 Fixed Charges and Claims 72 Grants and contractual technical
62 Insurance 5 239 services 5 363 000
Total - Chapter 60 5 239 Total - Chapter 70 5 363 000
TOTAL - SECTION 11. 5 363 000Chapter 80 Acquisition of Capital Assets
82 Equipment 50 830SECTION 12: REIMBURSEMENT OF THE WORKING
Total - Chapter 80 50 830 CAPITAL FUND 200 000
TOTAL - SECTION 8 1 925 182 TOTAL - SECTION 12 200 000
TOTAL - PART IV 6063 000
SECTION 9: OTHER STATUTORY STAFF COSTS SUB -TOTAL -- PARTS I, 11, III AND IV 34065 100
Chapter 10 Personal Allowances
11 Repatriation grant 7 50512 Pension fund13 Staff insurance
192 48732 264 PART V : RESERVE
14 Representation allowance 15 60015 Other allowances 261 521
SECTION 13: UNDISTRIBUTED RESERVE 2223 130
Total - Chapter 10 TOTAL - PART V 2 223 130509 377
TOTAL - ALL PARTS 36 288 230Chapter 20 Travel and Transportation
23 Travel on initial recruitment and Less:
repatriation 16 539 Reimbursement from the Special Account of the24 Travel on home leave 54 692 Expanded Programme of Technical Assistance 756 99027 Transportation of personal effects 9 03928 Installation per diem 4 755 Less: Casual Income
Assessments on new Members from previousTotal - Chapter 20 85 025 years 98 860Miscellaneous income 454 733
Chapter 60 Fixed Charges and Claims Available by transfer from the cash portion of the
61 Reimbursement of income tax . . . 24 281 Assembly Suspense Account 295 507
Total - Chapter 60 TOTAL - CASUAL INCOME 849 10024 281
TOTAL - SECTION 9 618 683 TOTAL - DEDUCTIONS 1 606 090
TOTAL - PART III 2 543 865 TOTAL - ASSESSMENTS ON MEMBERS 34 682 140

ANNEX 11 165
Annex 11
DECISIONS OF THE UNITED NATIONS, SPECIALIZED AGENCIES AND THEINTERNATIONAL ATOMIC ENERGY AGENCY AFFECTING WHO'S ACTIVITIES
(ADMINISTRATIVE, BUDGETARY AND FINANCIAL MATTERS) 1
REPORT BY THE DIRECTOR -GENERAL
1. The Director -General reported to the ExecutiveBoard at its thirty -first session on decisions of theUnited Nations, specialized agencies and the Interna-tional Atomic Energy Agency affecting WHO'sactivities in administrative, budgetary and financialmatters.2 The Executive Board, in its resolutionEB31.R43, noted the report and noted " with approvalthe position taken by the Director -General when theAdministrative Committee on Co- ordination con-sidered the extension of central and independentfacilities for dealing with salary and allowance ques-tions ". The Board also confirmed " its continuingconfidence in the International Civil Service AdvisoryBoard as a body of independent experts in publicadministration whose competence and objectivity havebeen amply demonstrated " and expressed " thehope that the Director -General will pursue thismatter in the Administrative Committee on Co-ordination and that an early and definitive conclusionwill be reached ".
2. The Administrative Committee on Co- ordination(ACC), at its meeting on 2 and 3 May 1963, agreedupon the basis on which, subject to the views of theBoard itself, the International Civil Service AdvisoryBoard might serve as an independent inter- organiza-tion body to make recommendations, through ACC,to all organizations on problems arising in the admin-istration of the common system of salaries andallowances. The Committee's intention to consultthe International Civil Service Advisory Board onthis matter was reported to the General Assembly inOctober 1962, and noted with approval by the GeneralAssembly in resolution 1869 (XVII). Primarily, thechange would mean broadening the terms of referenceof the Board to include responsibility for reviewing(when necessary) conditions of service and divergenciesas between organizations in the application of thecommon system. Final authority would, for constitu-tional reasons, remain with the appropriate authoritiesof each organization. The Board would retain its
1 See resolutions WHA16.32 and WHA16.33.2 Off. Rec. Wid Hlth Org. 124, Annex 20.
[A16 /AFL /21 - 15 May 1963]
present responsibility for advising on recruitment andpersonnel policies, the importance of which wouldnot be diminished by the additional functions. Work-ing arrangements, and the size of the Board, mayneed to be modified, both to enable it to verify thefacts on particular questions and to deal with urgentmatters which might arise between its regular sessions.The Board's views, with ACC's definitive proposals,will be reported to legislative bodies in due course.
3. Revised terms of reference have been suggestedby ACC for consideration by the International CivilService Advisory Board, when it meets on 20 May1963. The Director -General believes that if the newterms of reference and authorities are approved byall concerned, this step will become one of the mostimportant yet taken to improve co- ordination onadministrative matters.
4. ACC has also revised and amplified the inter -organization agreement on the transfer, secondmentor loan of staff from one organization to another;the new agreement will enter into force on 1 January1964.
5. ACC has agreed to continue for a further year,to 31 December 1964, the present cost -sharing arrange-ments by which the various organizations meet theexpenditures on certain joint administrative activities,such as those relating to the International CivilService Advisory Board, the Expert Committee onPost Adjustments and the Consultative Committeeon Administrative Questions.
6. ACC has also agreed upon arrangements tofacilitate the exchange of information regarding thescheduling of conferences by the various organizations.There is, however, a limit to the usefulness of suchinter- secretariat attempts to co- ordinate conferenceschedules, unless the government representatives inthe various bodies are prepared to take account ofestablished, recurring requirements of other bodies.In this connexion, the physical accommodation inthe Palais des Nations is becoming increasinglyinadequate. In fact, statutory meetings, particularly
166 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
the World Health Assembly and the Conference ofthe International Labour Organisation, are nowjeopardized by the scheduling of ad hoc and othermeetings in the Palais des Nations which conflictwith traditional, long- established dates. The timingof such statutory meetings is extremely important togovernments and determines the whole cycle of
operations of the organizations concerned. Further-more, the costs of dislocating the meetings of estab-lished bodies result in an unnecessary expense to govern-ments. In view of some of the impending decisions bythe Economic and Social Council and others, forexample, on the 1964 Trade Conference, this is amatter of immediate and urgent concern.
Annex 12
CLINICAL AND PHARMACOLOGICAL EVALUATION OF DRUGS 1
[A16 /P &B /4 - 3 April 1963]
REPORT BY THE DIRECTOR - GENERAL
1. Previous Resolutions of the Health Assembly andthe Executive Board
1.1 The Fifteenth World Health Assembly, inresolution WHA15.41, requested :
1. ... the Director -General to pursue, with theassistance of the Advisory Committee on MedicalResearch, the study of the scientific aspects of theclinical and pharmacological evaluation of phar-maceutical preparations;
2. ... the Executive Board and the Director -Generalto study the feasibility or otherwise, on the partof WHO, of
(a) establishing minimum basic requirementsand recommending standard methods for theclinical and pharmacological evaluation of phar-maceutical preparations;
(b) securing regular exchange of information onthe safety and efficacy of pharmaceutical prepara-tions; and, in particular,
(c) securing prompt transmission to nationalhealth authorities of new information on seriousside- effects of pharmaceutical preparations;
and to report to the Sixteenth World HealthAssembly on the progress of this study.
1.2 In resolution EB31.R6, adopted at its thirty -firstsession, the Executive Board emphasized the needfor early action in regard to rapid dissemination ofinformation on adverse drug reactions and consideredthat international co- operation was essential toachieve the objectives of the above -mentioned World
1 See resolution WHA16.36.
Health Assembly resolution; the Executive Boardthen requested the Director -General:
(i) to report to the Sixteenth World HealthAssembly on the outcome of the discussions in theforthcoming meeting of the scientific group [onthe evaluation of the safety and efficacy of drugs];(ii) to explore meanwhile ways and means ofcompiling information on serious adverse drugreactions and of supplying this information tonational health administrations in order to enablethem to take appropriate action ;
Further, in paragraph 2 of resolution EB31.R6, theExecutive Board recommended to the Sixteenth WorldHealth Assembly to invite Member States :
(i) to seek agreement, in co- operation with WHO,on basic principles and minimum requirementsapplicable to the toxicological, pharmacological andclinical evaluation of drugs; and(ii) to make available to WHO, for rapid dissem-ination to Member States, information of anyaction taken to prohibit or limit the use of a drugas a result of adverse reactions and of the evidencewhich led to this action.
2. Observations by the Director - General
2.1 As a first step towards the implementation ofthese resolutions, a Scientific Group on the Evaluationof the Safety and Efficacy of Drugs was convened.It was composed of thirteen clinicians and pharma-cologists from nine countries, many of them havingalso great experience in the administrative aspects ofthe problem. The mandate of this group, which metfrom 4 to 8 March 1963, in Geneva, was to advise theDirector -General on the way in which the Organiza-
ANNEX 12 167
tion could develop a programme related to thetoxicological, pharmacological and clinical evaluationof drugs.
Considering that the problems in this new field ofactivity for WHO were urgent and important fromthe point of view of the protection of public health,the Group held that the programme as outlined bythe Fifteenth World Health Assembly and specifiedby the Executive Board was within the Organization'stechnical capacity. The Group discussed, on thebasis of present scientific knowledge and taking intoaccount relevant activities being planned or pursuedin several countries, the feasibility of several contribu-tions that WHO might make towards an improvement,where desirable, of the present situation in regard tothe assessment of the safety and the efficacy of drugs.The report of the Scientific Group will be submittedto the Advisory Committee on Medical Research atits fifth session in June 1963.
A summary is given below of the Group's sugges-tions and recommendations as they refer to theobjectives of resolutions WHA15.41 and EB31.R6.
2.2 The feasibility of formulating basic principlesand requirements applicable to the evaluation ofdrugs at the various stages was explored carefully bythe Scientific Group. It considered that the preclinicalstudies (i.e. toxicological and pharmacological animalexperiments) as well as large -scale clinical trials are nowsufficiently advanced, as regards the methods appliedand experience gained, to allow essential criteria fortheir proper conduct to be formulated. The Group,therefore, recommended that such criteria be estab-lished by WHO for preclinical studies as well as forclinical trials, with a view to obtaining internationalagreement thereon.
It would be for further scientific groups to studythe matter, with the guidance of the Advisory Com-mittee on Medical Research, and to formulate adequatecriteria and requirements.
2.3 The question of securing regular exchange ofinformation on the safety and efficacy of drugs, asrecommended by the Fifteenth World Health Assemblyfor the study by the Executive Board and the Director -General, was also examined by the Scientific Group.The Group suggested that, in view of the vast amountof relevant evidence continuously being produced,the collection of such information from, and dissemi-nation to, national health authorities should belimited to data which WHO receives from MemberStates in relation to drugs approved or rejected, orfor which approval has been withdrawn. An invitationto Member States to furnish such data to the Organiza-tion might be appropriate. It will be noted that the
question of withdrawal (prohibition) of drugs isdealt with also in section 2.4 below.
The Group recognized that information in connexionwith rejection, though very valuable, would notalways be available. As for information on approveddrugs, the Group realized that the criteria used forapproval vary greatly from country to country -anadditional reason why it is desirable for WHO topromote generally agreed criteria for drug evalua-tion, as suggested in section 2.2 above.
2.4 A service of information on serious adverse drugreactions was, in the opinion of the Scientific Groupon the Evaluation of the Safety and Efficacy of Drugs,a matter of urgency. The Group considered that therapid exchange of information, through WHO, onaction taken to prohibit or limit the use of a drug asa result of adverse reactions was essential as a firststep, but that such a service should be extended asindicated below so as to allow for preventive measuresto be taken as early as possible.
The Group considered the practical implicationsof the inclusion of cases of " limitation of use " insuch an information service. It found that the questionof " limitation of use " of a drug or a group of drugswas so complex, and was dealt with so differently inthe various countries, that it could not formulategeneral conclusions as to the opportuneness of includ-ing relevant data in a regular system of information.
It should be possible for WHO to organize a morecomprehensive service of information on adverse drugreactions, having due regard to the need for preven-tion; but this would be feasible only if a sufficientnumber of Member States undertook to supply WHOwith the necessary information. To this end, MemberStates might be encouraged to devise a system forcollecting such information, in particular, after thegeneral release of new drugs. It would be for WHOto classify and assess the incoming information witha view to (a) publishing regularly a survey togetherwith a critical analysis; and (b) in severe cases ofgreat urgency, issuing immediately a warning tonational health authorities, or a cautionary statement,after having sought and obtained appropriate expertadvice in both instances.
2.5 A programme for action as outlined in thepreceding sections 2.2 to 2.4 might well be supple-mented by contributions in the form of researchgrants, fellowships, lectureships, and seminars for thepurpose of improving the methodology of drug testingand its proper application. Furthermore, the ScientificGroup recommended a number of relevant problemsfor study by meetings of groups of specialists, whichwould be arranged under the medical research pro-gramme of WHO.

168 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
3. Conclusions
3.1 It is the intention of the Director- General tostudy the technical and administrative aspects of thesuggestions and recommendations of the ScientificGroup, as reported in sections 2.2 to 2.5 above.In planning and implementing relevant activities hewill take into consideration the advice of the AdvisoryCommittee on Medical Research. Possible implica-tions of a legal nature may have to be studied in
connexion with the dissemination by WHO of certaintypes of information referred to in sections 2.3 and 2.4of this report.
3.2 For further action, the Assembly may wish totake into account the observations formulated in thelight of the report of the Scientific Group on theEvaluation of the Safety and Efficacy of Drugs andsubmitted herewith for its consideration.
Annex 13
UNITED NATIONS DEVELOPMENT DECADE[A16 /P &B /6 and Add. 1 -
5 April and 20 May 1963]
REPORT BY THE DIRECTOR -GENERAL
The Director -General has the honour to transmit to the Sixteenth World HealthAssembly the report on the United Nations Development Decade which he submittedto the Executive Board at its thirty -first session. (See report below, with Appendices 1 to 5.)
After considering this report, the Executive Board adopted resolution EB31.R50.2
The Special Committee on Co- ordination, referred to in paragraph 4 of the ExecutiveBoard's resolution, held its first meeting in New York from 25 to 28 February 1963.It decided to consider at its next meetings, beginning on 13 May 1963, its preliminaryfindings as regards priority areas relating to the objectives of the United Nations Develop-ment Decade and to prepare, in consultation with the agencies concerned, recommenda-tions thereon, which would be submitted to the Economic and Social Council.
To complete the information contained in his report to the Executive Board at itsthirty -first session on the United Nations Development Decade, the Director - Generalalso transmits to the Health Assembly an excerpt from the twenty- eighth report of theAdministrative Committee on Co- ordination to the Economic and Social Council (seeAppendix 6, page 179).
REPORT TO THE EXECUTIVE BOARD AT ITS THIRTY -FIRST SESSION, JANUARY 1963
1. The Director - General reported to the ExecutiveBoard, at its twenty -ninth session, on GeneralAssembly resolution 1710 (XVI) which designatedthe current decade as the United Nations DevelopmentDecade. In May 1962, he reported to the FifteenthWorld Health Assembly 3 on the action taken by the
1 See resolution WHA16.40.2 Off. Rec. Wld Hlth Org. 124, 27.
3 Off. Rec. Wld Huth Org. 118, Annex 3.
[EB31/28 - 12 Dec. 1962]
Executive Board, at its twenty -ninth session in itsresolution EB29.R44. The Fifteenth World HealthAssembly, in its resolution WHA15.57, endorsed theExecutive Board's recommendation that governmentsundertake a ten -year public health programme, withthe assistance of WHO, if they so wish, with certainspecific objectives and targets designed to raise thestandards of the health of the peoples, such as thepreparation of national plans for the development ofpublic health programmes; concentration on the
ANNEX 13 169
education and training of professional and auxiliarystaff for strengthening their health services; theestablishment as baselines of certain indices of theircurrent health situation; and the devotion of increasednational resources to the control of disease and theimprovement of health. This resolution was broughtto the attention of the United Nations GeneralAssembly, the Economic and Social Council, theTechnical Assistance Committee and the GoverningCouncil of the Special Fund.
2. The Secretary -General of the United Nationsconsulted the specialized agencies regarding hisproposals for action during the Decade, which hehad been requested in resolution 1710 (XVI) to submitto the Economic and Social Council at its thirty -fourth session in July 1962. The programme whichwas approved by the Executive Board, at its twenty -ninth session, and by the Fifteenth World HealthAssembly, was summarized in the document containingthe Secretary -General's proposals and set out infull in an addendum to that document.2 In presentinghis report to the Council, the Secretary -Generalspecifically referred to the fight against malnutritionand disease and suggested that expenditure on healthservices might be doubled. The Director- Generalof WHO also took part in the debate of the Economicand Social Council on the Development Decade, andinformed it of the action taken by WHO. His state-ment to the Council is reproduced in Appendix 1 tothis report.
3. The Economic and Social Council adoptedresolution 916 (XXXIV) (see Appendix 2), furtherdefining the objectives of the Decade, most of whichrelate to trade. However, one area of work to whichthe Council called particular attention was " thedevelopment of human resources through adequateprogrammes for education and vocational training,nutrition, health, sound public administration, hous-ing, urban and rural development ... and effectiveland reform, with particular emphasis on their contri-bution to overall development objectives and withthe co- operation where appropriate of trade unionsand other non -governmental organizations in con-sultative status ". This . resolution requested theSecretary- General, in co- operation with the specializedagencies and others, to submit in July 1963 " a pro-gramme consisting of detailed phased proposals foraction ".4. In compliance with this request, the Administra-tive Committee on Co- ordination, in October 1962,
i United Nations (1962) The United Nations DevelopmentDecade: proposals for action, New York. (United Nationsdocument E/3613).
2 United Nations document E/3613 Add. 1.
made arrangements for the preparation of detailedproposals. The contribution of WHO to the UnitedNations paper on " A programme consisting of detailedphased proposals for action with respect to the basicfacts of economic growth ", for presentation to thethirty -sixth session of the Economic and SocialCouncil, is given in Appendix 3.
5. Following the review of programme developmentand co- ordination, the Economic and Social Councildecided, in its resolution 920 (XXXIV), reproducedin Appendix 4, to set up a Special Committee onCo- ordination, with particular emphasis on theUnited Nations Development Decade, consisting ofrepresentatives of eleven States members of theCouncil or the Technical Assistance Committee.The Special Committee is to keep under review theactivities of the United Nations and its agencies in theeconomic, social, human rights and related fields;to consider, wherever appropriate, in consultationwith the agencies concerned, priority areas or projectsrelating to the objectives of the Decade, and to submitrecommendations on these matters to the Council.It will also assume certain functions of the ad hocWorking Group on Co- ordination, established byEconomic and Social Council resolution 798 (XXX),and will submit to the Council, for consideration, aconcise statement of the issues and problems in thefield of co- ordination, which call for special attention.The first meeting of the Special Committee is to beheld in February 1963.
6. The Director -General of WHO took part in thedebate on this proposal in the Economic and SocialCouncil and all specialized agencies agreed that nonew machinery for co- ordination was required. TheEconomic and Social Council underlined the factthat the new Committee was a subordinate body ofthe Council and should' not be regarded as a newpiece of machinery since it continued the work of theCouncil's ad hoc Working Group on Co- ordination.The Council invited ACC to express its views, and theACC, at its thirty -fifth session, agreed to a statement(reproduced in Appendix 5), drawing attention to theimportance of the participation by the representativesof the specialized agencies in the deliberations of theCouncil and its committees. It hoped that the existinginstruments at the disposal of the agencies for assistingdeveloping countries in making the Decade a successwould be fully utilized. On the basis of the statementand reservations made by ACC, the executive headsof agencies expressed their willingness to recommendco- operation with the Special Committee on Co-ordination to their governing bodies. The ACC alsosuggested that the budgets of the Expanded Pro-gramme of Technical Assistance, the Special Fund

170 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
and the World Food Programme, as well as theregular budgets of the specialized agencies, should beadjusted to the targets of the Development Decade.
7. In a further resolution on trade and the Develop-ment Decade, the Economic and Social Councilapproved the convening of a United Nations Con-ference on Trade and Development and called atten-tion to the importance of economic development,
particularly of the less developed countries, for thestability of the world economy and the maintenanceof international peace and security.'
8. The General Assembly of the United Nations isconsidering at its seventeenth session the report of theEconomic and Social Council on the DevelopmentDecade. Such decisions as it may make will bereported to the Executive Board.
Appendix 1
ADDRESS BY THE DIRECTOR -GENERAL OF THE WORLD HEALTH ORGANIZATIONTO THE ECONOMIC AND SOCIAL COUNCIL AT ITS THIRTY -FOURTH SESSION
Geneva, 11 July 1962
The spirit in which the General Assembly initiated the UnitedNations Development Decade and the goals it formulated led theWorld Health Assembly to adopt its resolution WHA15.57,which is before this Council in document E/3611, Addendum 1.The Health Assembly, " Cognizant of the profound effecthealth standards of families, communities and nations have ontheir social advancement and economic progress, particularlyin the developing areas of the world " and " aware of thebenefits accruing to health from the accelerated national pro-grammes for general socio- economic development ", recom-mended that " in so far as the health aspects of acceleratedeconomic and social development are concerned, governmentsparticipate in these programmes, with the assistance of theWorld Health Organization if they so wish, by undertaking aten -year public health programme with the objective of raisingthe standards of the health of the peoples " by a few closelyrelated actions.
The Development Decade gives the World Health Organiza-tion an opportunity and a responsibility to expand healthprogrammes and to review their focus as part of the commoneffort to speed the pace of development during these ten years.I appreciate this opportunity to bring to this Council some ofthe details of the contribution which my organization hopesto make in this co- operative effort. In this effort, health isimportant not only for its own sake, but because it is essentialfor economic development. For the newly independent countries,independence may mean a breakdown of the barest minimumof health services. The absence of health is one of the mostimportant contributing factors to instability of the individual,the family and of the entire community. The health problemsof newly independent and emerging countries must be faced.Indeed, economic values are not fully applicable to the savingof human life and the alleviation of suffering of people, forthese cannot wait and are not determined by economic factorsalone.
The Acting Secretary -General, in his statement the day beforeyesterday, emphasized clearly the overriding importance of thehuman factor in the entire development process. In the introduc-tion to his report, which is before this Council, containing hisproposals for action in the United Nations Development Decade,he also stated, " The widening of man's horizons througheducation and training and the lifting of his vitality throughbetter health, are not only essential pre -conditions for develop-
ment, they are also among its major objectives ". We mustbear constantly in mind that economic and social developmentis required for man, that human beings are the means of achievingthat development and that they are to be its beneficiaries.
Health means more than individual care for the sick, morethan the nation -wide or even international attacks on the causesof disease in which most countries are now engaged. It means,in every country, heightening the vitality of the people so thatthey have fewer casualties to care for, their work becomes moreproductive and -what is just as important -they have theenergy to learn the new skills and to adjust to the new patternsof living that constitute economic and social progress. Thus,improvement of the people's health contributes to progress inpractically every other sector of the development programme,just as advances in these other sectors can bring importantbenefits to health.
It is clear, too, that economic and social development is notsomething which can be given to people -it is, instead, somethingwhich they can only achieve for themselves. And the strengthof people to produce, their receptiveness to training, their willto work for their own betterment, require a healthy mind in ahealthy body.
When the Fifteenth World Health Assembly considered theGeneral Assembly's resolution, one of its main conclusionswas that " in developing countries, the creation of a networkof minimum basic health services must be regarded as an essentialpre- investment operation, without which agricultural andindustrial development would be hazardous, slow and un-economic ".2 It is axiomatic that, if a country is to achieve self -sustaining development, it must have an adequate infrastructure.It is also obvious that the infrastructure, to be complete, mustinclude a sufficient health component to provide the minimumhealth services for the country. These health services must becompetent to identify problems, to provide the minimumpreventive and curative services, to plan the further developmentof health services in the context of economic and social develop-ment and to avoid the health hazards which too often are theconcomitant of economic development. Thus, training forthe provision of the minimum health services is an essentialpre- investment activity.
ECOSOC resolution 917 (XXXIV).2 Resolution WHA15.57.

ANNEX 13 171
The Health Assembly made specific recommendations togovernments in connexion with t he Development Decade.
Of basic importance is the establishment of a national healthplan for each country, co- ordinated with its plans for work inother sectors. A realistic and technically sound health planwould take epidemiological and other technical data intoconsideration, and would relate them directly to basic economicfacts, such as resources and costs, and also to the degree ofbenefit that can be expected.
Preparation of a sound plan will promote the establishmentand development of a basic health organization as the sine quanon for providing minimum health services to the people.
These plans must include provision for concentration oneducation and training, so that countries can staff their healthservices with their own professional and auxiliary workers,and can build up as early as possible their own training institu-tions for health staff. To this end, measurable targets must beset for expanding each category of staff according to the pre-determined needs.
It may help the Council in its deliberations to be aware ofthe order of magnitude of the problem. The minimum require-ments for basic health services are considered to be:
1 physician per 10 000 population,1 nurse per 5000 population,1 sanitarian per 15 000 population,1 sanitary engineer per 250 000 population.
The difficulties in achieving such a goal in the developingcountries will vary, for example, according to the proportion ofphysicians graduating in different areas of the world. Thus,according to estimates based on 1955 -1956 figures, while inEurope an average 6 or 7 physicians graduate every yearper 100 000 population, in the Americas and Oceania theproportion varies between 3.5 and 5 per 100 000 population,and those in Asia and in Africa are 0.8 and 0.5 per 100 000respectively.
We speak today of a Development Decade, but the man onwhom health work basically depends -the physician- requiresafter full secondary education six to seven years in which to betrained; in some countries without their own doctors, or with afew, the Decade will be two- thirds completed before even a verysmall part of the basic national staff can be graduated frommedical schools. This underlines the urgency to provide everypossible assistance to the developing countries not only intraining individuals as rapidly as possible, but also in the earlyestablishment of training institutions.
The Health Assembly also recommended that governmentsestablish as baselines certain indices of their current healthsituation, so that they can gauge progress towards their owntargets for the Decade.' Those targets, of course, would bedefined in the national health plans.
In many of the under- developed countries of the world today,
a high prevalence of communicable diseases represents a hazardwhich results in continued lower standards of living. Theexperience of the Organization has demonstrated that the circleof disease, low productivity and poverty, to which so manydelegations have referred, can successfully be broken by aconcentrated attack on its biological components throughsustained and mass campaigns against the most prevalentcommunicable diseases. As targets for the Decade, therefore,the World Health Assembly has proposed that certain of themost prevalent communicable diseases be attacked in a .moreconcentrated fashion with a view to achieving their eradication,or reduction to the point where they cease to be of seriouspublic health or economic importance. In the Decade increasedeffort must be made to prevent premature death and to increaselife expectancy, thereby achieving a more favourable age com-position. The infant mortality rate, the most sensitive of socialindicators, must be lowered during the Decade. Malnutrition,as has been pointed out by my colleague, Mr Sen, representsan immediate challenge during the Decade. In co- operationwith FAO and other organizations, WHO will intensify theprogramme in the health aspects of malnutrition. Finally, adirect attack on the environment through, in the first instance,a dynamic and intensified community water supply programme,will be undertaken.
The Health Assembly further recommended that countriesdevote increased resources to the control of disease and theimprovement of health. U Thant, in his speech the day beforeyesterday, stated that, in the less developed areas, expenditurefor public health services must double over the period, and wein WHO hope earnestly for the achievement of this modest goal.
During the past decade many new nations have obtainedtheir political freedom. They seek now their technical inde-pendence so that they will, themselves, be equipped to workeffectively for the emancipation of their peoples from thescourges of ill- health, poverty and ignorance. To these endsthe Development Decade can, as the words which created itare translated into action, make a crucial contribution.
Experience during the fourteen years of the existence of theWorld Health Organization, in providing assistance to govern-ments, at their request, to strengthen their health services, willbe invaluable in carrying our share of the responsibility of theDevelopment Decade. The Health Assembly has agreed upona programme of action which would enable the Organizationto become an active partner in this enterprise. We have thestructure, the machinery, the techniques. We need the additionalresources -human as well as financial -to carry out fully theobjectives of the Decade for the improvement of the well -beingof people everywhere.
Appendix 2
ECONOMIC AND SOCIAL COUNCIL RESOLUTION 916 (XXXIV)
United Nations Development DecadeThe Economic and Social Council,Recalling General Assembly resolution 1710 (XVI) of
19 December 1961 designating the current decade as the " United
1 Resolution WHA15.57.
Nations Development Decade ", in which Member States andtheir peoples will intensify their efforts to mobilize and tosustain support for the measures required on the part of bothdeveloped and developing countries in order to accelerateprogress towards self -sustaining growth of the economies ofthe individual nations and their social advancement so as to
172 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
attain in each under -developed country a substantial increasein the rate of growth, with each country setting its own target,taking as the objective a minimum annual rate of growth ofaggregate national income of 5 per cent. at the end of the Decade,
Considering that the economic and social development of theeconomically less developed countries is not only of primaryimportance to those countries, but is also basic to the attainmentof international peace and security and to a faster and mutuallybeneficial increase in world prosperity,
Recognizing that, in spite of a variety of efforts, policies, andmeasures designed to assist the developing countries in theirefforts to achieve economic growth through which much hasbeen accomplished, the rate of economic and social progressin these countries is still far from adequate,
Noting the essentiality of strengthening the economic inde-pendence of the less developed countries,
Bearing in mind that new problems affecting particularly thedeveloping countries and hampering and delaying their economicand social development, have arisen in international economicrelations in the course of the past years,
Having before it the report prepared by the Secretary- General 1presenting proposals for intensified national and internationalaction programmes during the present decade,
Noting:
(a) The views submitted by Governments concerningproposals for action in the Development Decade 2 and concerningthe role of the regional economic commissions in the Decade,3
(b) The proposals for action made by the related agencies,4and
(c) The views expressed during the Council's discussion ofthis subject,
1. Expresses appreciation to the Secretary -General for hiswork in producing the report and to the agencies and otherinstitutions which helped in its preparation;
2. Endorses the emphasis placed in the report on the develop-ment process as a many faceted one, based principally onindustrial development and a highly productive agricultureand requiring for success determined self -help and carefulplanning on the part of developing countries;
3. Calls upon the Governments of Member States, as wellas United Nations bodies and specialized agencies, to giveparticular consideration, in the first years of the implementationof the Development Decade, in addition to their endeavoursin other fields, to the following :
(a) Industrial development as a most important factor ineconomic diversification and general economic development;
(b) Improved access to the world markets in order to pro-mote export trade of the developing countries, taking intoaccount their foreign exchange needs for development and theeffects of deterioration in their terms of trade, including stepsfor early reduction or elimination of barriers to exports;
1 United Nations (1962) The United Nations Development_Decade: proposals for action, New York (United Nationsdocument E/3613).
2 United Nations document E/3613 Add. 2 and 3.3 Official Records of the Economic and Social Council, Thirty -
fourth Session, Annexes, agenda item 4, document E/3664.4 United Nations document E/3613 Add. 1.
(c) Appropriate measures, such as international commodityarrangements, to stabilize at remunerative levels the prices ofprimary commodities on international markets, and also soundcompensatory arrangements designed to mitigate excessivefluctuations in the export receipts of primary producing countriesand to compensate for the harmful effects thereof;
(d) The pursuance by regional and sub -regional economicgroupings of economic policies which avoid the introductionand facilitate the elimination of obstacles and restrictions whichmight hamper the necessary expansion of the trade of thedeveloping and under -developed countries or might discouragethe indispensable growth of their economies;
(e) A substantially increasing in -flow of long -term develop-ment capital, public and private, for financing their economicdevelopment programmes on terms which take into accountthe special requirements and conditions of the developingcountries so as to benefit them; and for this purpose the continuingneed for measures in both developing and developed countriesdesigned to facilitate and encourage its flow to the less developedcountries;
(f) The development of human resources through adequateprogrammes for education and vocational training, nutrition,health, sound public administration, housing, urban and ruraldevelopment, including community development and effectiveland reform, with particular emphasis on their contributionto overall development objectives and with the co- operationwhere appropriate of trade unions and other non- governmentalorganizations in consultative status;
(g) Exploration and exploitation of natural resources with aview to establishing a raw -material and energy basis for economicdevelopment ;
4. Recognizes the special significance of internationaleconomic relations and looks forward to the report of theworking group set up under Council resolution 875 (XXXIII)of 13 April 1962, on the question of a declaration on interna-tional economic co- operation;
5. Emphasizes that pre- investment activities should bedesigned to facilitate national efforts towards development;
6. Urges the prompt attainment of the present goal of$150 million for the Expanded Programme of Technical Assist-ance and the Special Fund in the interest of accelerating thedevelopment of human resources, natural resources and nationaland regional institutions, and requests the General Assemblyto consider, at an appropriate time, the establishment of newtargets, bearing in mind the observations of the Secretary -General in his report;
7. Urges further that participating Governments give fullsupport to the Freedom from Hunger Campaign of the Foodand Agriculture Organization of the United Nations and invitesthe Governments of States Members of the United Nations andmembers of the specialized agencies to take early steps toprepare for the Pledging Conference for the experimentalWorld Food Programme and, in determining their pledges,to bear in mind the necessity of attaining the goal of $100 millionin commodities, services and money;
8. Emphasizes the need for increased domestic savings andinvestment in the developing countries, through appropriatepolicies in the public and private sectors of the economy;

ANNEX 13 173
9. Stresses the increasingly important role envisaged in theSecretary -General's report for the United Nations, and expressesthe hope that resources commensurate with the task will bemade available;
10. Requests the Secretary- General to submit to the thirty -sixth session of the Council a report on the measures taken tosecure the full participation of the regional economic com-missions in the work called for in the United Nations Develop-ment Decade;
11. Requests the Secretary -General in co- operation withthe specialized agencies and the regional economic commissions,where appropriate, to provide on request assistance in thefield of planning to developing countries; looks forward to theestablishment and effective functioning of regional developmentinstitutes and the economic projections and programmingcentre, as provided in resolution 1708 II (XVI); and requeststhe Secretary -General to report to the Council at its thirty -sixthsession on progress made toward the goals envisaged therein;
Introduction
12. Looks forward to the results of the United NationsConference on the Application of Science and Technology forthe Benefit of the Less Developed Areas and requests theSecretary -General to make appropriate recommendations foraction resulting from the findings of the Conference;
13. Requests the Secretary -General to prepare, in co- opera-tion with the regional economic commissions and other bodiesand agencies of the United Nations family, and with suchexperts from outside as he may deem necessary, a programmeconsisting of detailed phased proposals for action with respectto the basic factors of economic growth in the light of theobjectives outlined above and a progress report setting forthachievements in the period ending 31 March, 1963;
14. Further requests the Secretary- General to acquaint allUnited Nations bodies and the specialized agencies with thepresent resolution and to transmit the aforementioned studiesand reports to the thirty -sixth session of the Council for con-sideration, wtien it will review the detailed programmes ofaction in order to adjust them to the changing situation.
1236th plenary meeting, 3 August 1962.
Appendix 3
WHO CONTRIBUTION TO THE UNITED NATIONS PAPER ON" A PROGRAMME CONSISTING OF DETAILED PHASED PROPOSALS FOR ACTION
WITH RESPECT TO THE BASIC FACTORS OF ECONOMIC GROWTH "
for Presentation to the Economic and Social Council at its Thirty -sixth Session, in July 1963
The aims and the nature of the United Nations DevelopmentDecade initiated by the General Assembly in its resolution1710 (XVI) led the World Health Assembly at its last sessionto adopt a resolution (WHA15.57) in which it stressed " theprofound effect health standards of families, communities andnations have on their social advancement and economic progress,particularly in the developing areas of the world ", and recom-mended that " in so far as the health aspects of acceleratedeconomic and social development are concerned, governmentsparticipate in these programmes, with the assistance of theWorld Health Organization, if they so wish, by undertaking aten -year public health programme with the objective of raisingthe standards of the health of the peoples ". Thus, the Assemblynot only approved WHO's participation in the Decade butalso recognized that this gives the Organization an opportunityand a responsibility to expand health programmes and toreview their focus as part of the common effort to speed up thepace of development during the forthcoming years.
In the development effort of newly- independent countrieshealth is important, not only per se, but as an essential factorfor economic development. For many such countries, inde-pendence may mean a suspension of even basic minimum healthservices. Poor health and illness are among the most importantcontributing factors to the instability of the individual and ofthe family; they affect the entire community and lead to itseconomic inefficiency. The health problems of newly- indepen-dent and emerging countries must, therefore, be faced; aconcentration of efforts is required to overcome the basic healthdeficiencies which still exist in many areas.
Economic values are only in part applicable to the saving ofhuman life, but it is not only for economic reasons that thealleviation of suffering is important. It is indeed now universallyrecognized that the human factor is essential to economicdevelopment and that human beings are not only the mostimportant and essential means for achieving that development,but that they are also to be its beneficiaries. Better individualhealth, eradication of epidemic and endemic diseases, a soundenvironment, better health consciousness and education, allcontribute to heightening the vitality of the people. This, inturn, means better productivity, fewer casualties to care forand new energies to learn the new skills and adjust to the newpatterns of living implicit in economic and social progress.Thus, improvement of the people's health contributes to theprogress in practically every sector of the development pro-gramme, just as advances in these other sectors can bringimportant benefits to health.
During its discussion on the Decade, the World HealthAssembly recognized the need for maintaining a balance in theactivities of the Organization, but it indicated certain areas ofaction which might be developed by governments in connexionwith the Development Decade.
Examples are given below of aspects of the programme whichcould be undertaken during the Decade by WHO, in conjunctionwith other sources of international assistance such as the Ex-panded Programme of Technical Assistance, UNICEF andthe Special Fund, on the basis of the activities already plannedfor 1963 -1964. The long -term figures are only indicative of theorder of magnitude of an international effort if some of thegoals of the Decade, as indicated, are to be achieved. Thefigures do not include the cost to governments, but an attempt

174 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
has been made to keep the proposals within the probable limitsof national absorptive capacity and within the boundariesof feasibility.
Planning
In its resolution on the Decade the World Health Assemblymade specific recommendations to governments for the establish-ment of a ten -year health programme to be based on detailedplanning. The establishment of a national health plan foreach country was recognized as being of primary importance.WHO is developing a programme of assistance in nationalhealth planning to countries. Such assistance would aim atgiving national health administrations technical support on along -term basis for the various steps which are needed inestablishing an overall health plan for a country as an essentialpart of general national social and economic planning. Sucha programme would involve preliminary fact -finding in orderto establish guidelines on which the further dévelopment ofservices and activities would be based. Detailed and co- ordinatedplans would then follow to determine priorities for health action,reorganize existing services, plan future trends and establishmachinery within the health services for application of theplan, training of personnel, both for general purposes and forthe implementation of the plan, and for co- ordination withother government services. Such a plan would involve investiga-tion of health needs in terms of personnel, building and supplies,and recurrent costs for salaries, maintenance, etc., with a viewto determining the most efficient ways of implementing the plan.Moreover, it would help international and other outside agenciesto concentrate their assistance on nationally -established andagreed priorities.
Planning is not considered as a static process, a one -phaseoperation. As recommended by the World Health Assembly,certain indices of health would be established as base -lineswhence to gauge the degrees of realization of the goals pre-determined as targets for the Decade. Progress would beevaluated by continuing operational research, which wouldalso give guidance for the periodic revision and adaptation ofthe plan to changes occurring in time and in scope for action.
The methods for implementing such national health planswill clearly have to be adapted to the needs and conditions ofeach country. It is envisaged that the formulation of a nationalhealth plan will require about one year, to be devoted to detailedsurvey to determine the needs, the type of health services thatbest suit local conditions and their pattern of development, aswell as to the preparation of the plan itself.
For the period 1963 -1964, if funds become available for thispurpose, it is WHO's hope to be in a position to make availableto ten countries interested in receiving assistance in this field,mainly in Africa, planning services of the type suggested. WHOwould provide a senior public health adviser and necessarystaff specialized in planning for each of the requesting countries.Such planning activities would be combined with a certainamount of local training for national personnel and financialprovision would be made for supplementing salaries and givingstipends for organizing courses in the countries. A certainamount of equipment and supplies would also be provided.Such assistance would be in addition to the advisory servicesalready provided at the ministerial level in a number of develop-ing countries. It is estimated that national health planningfora medium -sized country would require international assistancecosting around $50 000 and an additional $40 000 for training,bringing the total cost of assistance to national health planningto about $90 000 per year. The initial cost for WHO for 1963-1964 would therefore be about $900 000, and it is expectedthat, if the scheme is to be extended to some thirty countries
during the Decade, the total cost involved would be approxi-mately $2.7 million.
Education and Training
Education and training has long been recognized as one ofthe basic means for promoting the development of nationalhealth services. The guiding principles and methods of WHOin this field have repeatedly been outlined in documents submittedto the United Nations governing bodies. In developing countriesthe greatest need is for professional and auxiliary health staffto man the existing services, and further efforts are being madeto focus assistance on building up national or inter -countryinstitutions for the training of such staff.
WHO's budget shows that some $2 900 000 would be devotedin 1963 and 1964 to training activities under the regular budgetalone. In all, slightly more than $6 million is expected to beprovided for fellowships from all sources of financing (includingthe Pan American Health Organization) for the same period.
The immense need for health workers of professional andauxiliary categories makes it essential for developing countriesto establish new schools for health workers, and to extendexisting ones. Some figures are given below of the possibledevelopment of international assistance in this field duringthe Decade. The total needs for training programmes are fargreater than the figures suggested and in medical educationalone it is estimated that thirty to forty new medical schoolsare needed for African and Asian countries, but the proposalsmade here are considered as more realistic. The figures givenare in addition to the activities already undertaken by theOrganization in the various fields of education and training asindicated above.
(i) Establishment of new medical schools is an urgentnecessity in Africa and in some Asian countries. Some ofthese schools should be organized as inter -country institutionsfor the training of students with common cultural and socio-economic backgrounds, and those using a common languageas a medium of instruction. If four medical schools in Africaand four in Asia are to be started in the next two years, atotal amount of $120 million will be needed for this purposeduring the Decade, of which about 20 per cent. would beneeded in 1963 -1964.(ii) The establishment of post -basic and post -graduatetraining institutions to prepare teaching personnel for basicnursing and midwifery schools. Two schools in Africa andtwo in Asia could be set up within the Decade for an estimatedcost of $20 million, of which about one third would be neededin 1963 -1964.
(iii) Training of auxiliary health workers who are an essentialcomponent of the health services of developing countries.Taking into consideration the urgent needs for about 250 000health workers in this category to work in communicabledisease control and eradication programmes during theDecade, and on the other hand the relatively short period offormal training needed and the possibility of using alreadyexisting training institutions, an amount of about $10 millionis needed, of which about 60 per cent. could be used in 1963-1964.
Communicable Disease Control and Eradication
The prevalence of epidemic diseases is stillhigh in a numberof countries, notwithstanding the possibilities that now existfor eradicating certain of them or for controlling them so thatthey no longer form an important public health problem. It hasbeen amply demonstrated that community -wide efforts canlead to the practical eradication of malaria, smallpox,poliomyelitis and to the control of a number of viral, bacterial

ANNEX 13 175
and parasitic diseases such as trachoma, tuberculosis, leprosy,the venereal infectidns, a number of diseases common to manand animal, bilharziasis, cholera and plague. The problemhas now become more one of administrative and financialpossibilities than of scientific knowledge or medical technology.The experience of the Organization has demonstrated that thecircle of disease, low productivity and poverty can indeed besuccessfully broken by a concentrated attack on its biologicalcomponents, through organized and sustained mass campaigns,and that the elimination of such scourges in areas where pre-valence is still high has direct, positive repercussions in thefields of economic development, and particularly of agriculturaland industrial productivity.
As targets for the Decade, the World Health Assembly hasproposed that certain of the most prevalent communicablediseases be attacked in a more concentrated fashion with aview to achieving their eradication or control. Some examples,considered as being fully within the realm of feasibility, aregiven below.
MalariaOf the communicable diseases, malaria has the gravest effect
on the majority of countries in the tropical and sub -tropicalareas of the world. Approximately half the population of theworld lived in malarious areas in the first half of this centuryand the annual global number of deaths from malaria wasconsidered to be over three million. The number who sufferedfrom malaria each year was thought to be in the region of250 million. The global economic loss from this disease, notonly from human sickness and death but from aspects of landutilization, food production and industrial development, hasnever been assessed accurately, but already in 1935 in India itwas estimated at $400 million a year,' an estimate which waslater revised to over $500 million a year.
From its inception the World Health Organization has giventhe highest priority to the control of malaria, and since 1955the eradication of the disease from the world has been one ofthe primary aims of the Organization. By the end of 1962, onthe basis of information received from countries reporting toWHO, the disease had been eradicated in areas with a populationof 322 million and malaria eradication programmes covereda further 748 million people, but 377 million still lived in areaswhere eradication was not yet being undertaken.
This approach has been outstandingly successful in thecontinent of Europe and in many countries in the Americasand in Asia where the organization of the general health servicesof the countries has been sufficient to provide, or has beencapable of being rapidly built up to provide, an adequatemedical coverage of the population.
However, in countries where such general health servicesare as yet imperfect, eradication programmes have met withoperational difficulties; the Organization has therefore adopteda programme designated as a " pre- eradication programme "for these areas. In such a programme the initial emphasis isplaced on building up the infrastructure of health services toa level where the country can provide simple but adequatehealth coverage and, at the same time, developing the malariaservice of the country through intensive training of nationalstaff. Both aspects of the programme are aimed at preparationsfor a full malaria eradication programme in due time.
By 1970, and in the majority of cases far earlier, the countriesnow undertaking malaria eradication programmes (subject tofactors at present unpredictable) should have eradicated the
Sinton, J. A. (1935) What malaria costs India, nationally,socially and economically. In : Records of the malaria survey ofIndia, New Delhi, vol. 5.
disease and be in a final maintenance period, provided that thepresent level of assistance from the agencies of the UnitedNations, from bilateral agencies and from other sources ismaintained. These countries cover the whole of the continentsof Europe and the Americas and the greater part of the continentof Asia -except the Arabian Peninsula and the region east of900 longitude E.
But in virtually the whole continent of Africa and in severalcountries in the Arabian Peninsula, East Asia and Oceania,pre- eradication programmes will have to be adopted as apreparatory measure. It is anticipated that sixty such pro-grammes will be required (forty -two in Africa and eighteen inAsia and Oceania) phased over the next three years -ten com-mencing in 1962, twenty -six in 1963 and twenty -four in 1964.These pre -eradication programmes and their development indue time into full eradication programmes may be costed asrequiring on an average $100 000 each per year as supportfrom WHO. Thus in all, up to 1970 it is estimated that approxi.mately $50 million will be required for advisory services andsuch supplies and contributions to local costs as are normallyprovided by the Organization, of which about one -third for theperiod 1963 -1964.
For the total eradication programmes in the above -mentionedareas, most governments have been required to seek the assist-ance of other United Nations agencies, bilateral and othersources for the provision of types of assistance that the WorldHealth Organization is not able to provide. The figure forsuch a programme based on a population of 250 million overthe eight years to 1970 at $0.50 per head per year would approach$1000 million.
Yaws
This endemic infection by Treponema pertenue is prevalentin rural areas throughout the tropical belt. It is transmittedby direct contact with infectious skin lesions among childrenand sometimes adults. Yaws is a relapsing disease, destructivein its later stages : 10 per cent. of untreated infected childrenand adolescents end up as adult invalids with hands and feetaffected to such an extent that their working capacity isseriously or totally impaired.
Effective drugs and public health control methods are availableagainst yaws. WHO- assisted mass campaigns in high -prevalenceendemic areas in countries in the Western Pacific, South -EastAsia, and African Regions and the Region of the Americashave shown that the transmission of the disease can be interrup-ted, that the reservoir of infection can be effectively reduced,and that bringing disease under control will prevent incapacita-tion and invalidism. In a WHO /UNICEF- assisted programmeagainst yaws in Haiti, approximately 100 000 incapacitedpersons were returned to work, with a consequent increase inthe national production potential estimated at $5 million a year.2
The second International Conference on Yaws Control in 1955estimated that, among the 400 million people living in the ruralareas of the tropical belt, approximately one half are, duringtheir lifetime, exposed to the risk of infection with endemictreponematoses, particularly yaws. Between 1950 and 1960,approximately 125 million people had been examined and,when necessary, treated in WHO- assisted programmes in allregions. It is now estimated that some 75 million peopleremain in endemic areas not yet covered by surveys.
The WHO budget for 1963 -1964 shows that the cost oftechnical aid in this field, planned to be financed from fundsadministered by WHO, amounts to about $400 000 per year,
2 United States Department of State (1950) Point 4: co-operative program for aid in the development of economicallyunder -developed areas, Washington, D.C.

176 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
and that the estimated expenditure from other extra -budgetaryfunds (including UNICEF) is approximately the same -atotal of $800 000 per annum. A renewed impetus is requiredover the remaining years of the Decade to complete the objectiveof eliminating yaws in tropical countries as a serious public healthproblem, a goal which could be achieved at an estimated total.cost of $2 million per year for six years, beginning in 1965.
Bilharziasis
The transmission of bilharziasis is related to man's associationwith water and to the snail which is the intermediate host.Infection with the Schistosoma often leads to serious forms ofanaemia with consequent impairment of the physical andmental productive capacity of people so affected.
In sixteen countries recently surveyed by WHO in Africa andthe Middle East it was found that essentially all infectionsare acquired in natural habitats of the snail and in water con-servation ponds, while in four of them infection took placeprimarily in irrigation systems. These countries have undertakenor have plans for water and soil resource development whichcall for supplying an additional 19.71 million acres of landwith perennial irrigation and the construction of thousands ofponds within the next ten years. Similar developments arealso expected to take place in the endemic areas of SouthAmerica, South -East Asia and the Western Pacific. Realizationof these plans will cause the spread and enhance the intensity ofbilharziasis infection in agriculture development areas unlessproper control measures are instituted, and it is already apparentthat, notwithstanding some palliative measures undertakenlocally, the number of persons infected and the extent of theinfected areas are seriously increasing.
Methods for controlling this disease are known. They includewater management and agricultural practices, the use of mollusci-cides, and the treatment of infected persons. In countries inAsia it has been possible, by improved water management andagricultural methods, greatly to increase crop production andreduce the amount of molluscicide required.
Control activities can be developed according to an actionschedule which includes a survey of about one year's duration,a pilot control phase requiring about three years and thereaftera country or region -wide application of a prolonged duration.Such action requires close co- operation between the healthauthorities and those responsible for agricultural developmentschemes and water management from an early planning stageand throughout its execution.
In areas where general farming and cattle raising are dominant,with proper soil, water and crop management, snail controlcan be carried out for about $20 to $50 per 1000 acres. In areaswhere molluscicides alone are used, annual costs range upto $3 per irrigated acre.
WHO activities in this field for 1963 -1964 are of the order ofabout $400 000 each year for advisory services to governments,surveys and research. In Africa alone an additional $5 millionwould be needed during the Decade and $5 million more forother endemic areas in the world if the progressing trend of thisserious parasitic infection is to be arrested and measures foreffective control instituted.
Onchocerciasis
Onchocerciasis is transmitted to man by certain flies whichdevelop in many riverine areas of Africa and parts of theAmericas. In West Africa large areas bordering streams had
to be abandoned when the " river blindness " caused by thisparasite affected about 30 per cent. of the population, thusdepriving countries of crops from some of the most fertilelands in Africa, and also affecting fishing and the full use ofthe water resources.
Methods for controlling this disease are well known buttopographical and epidemiological data are still lacking formany endemic areas. WHO plans to spend some $150 000 in1963 -1964 on epidemiological studies and on research.
At the completion of this preliminary phase to investigate thedistribution of the disease, the practical application of controlmeasures under different conditions and the efficacy of newdrugs in infected populations, it should be possible to expandhealth action considerably towards a pre- eradication stage ofthe disease. It is estimated that such a goal could be achievedfor some eight countries in the Volta River area in Africawithin the Decade at a cost of about $1.5 million, and similaraction developed in the infected areas in Central and SouthAmerica with an additional $1.5 million.
Trypanosomiasis
This infection, better known as sleeping sickness, is highlyendemic in certain parts of Africa. The vector, the so- calledtsetse fly, favours savannah -type areas, affecting particularlyregions of agricultural economy, with little mineral wealth,no access to the sea and no bright prospects for industrialization.Trypanosomiasis creates a permanent danger for settlementof the areas where the tsetse fly is present because it infects notonly man but also his cattle, thus making the development ofmixed -type farming and often of agriculture altogetherimpossible. Other forms of trypanosomiasis with seriousdamaging influence on individual health and on the productivitypotential of nations also exist in the Americas.
Various control measures have been undertaken in differentAfrican areas, some with good and lasting success. More needsto be known, however, of the parasite, the vector, the distribu-tion of the infection and measures of control. WHO hasbudgeted for 1963 -1964 some $50 000 each year for researchand investigations; after such preliminary action has beencompleted, it should be possible to proceed to a broad controlaction in the infected areas. It is estimated that good progresscould be achieved in this direction during the Decade at a costwhich is tentatively considered of an order of about $2 millionfor the period.
Smallpox
The world incidence of smallpox is known : in 1961 therewere 24 140 cases in Africa, 1923 in the Americas, 52 342 inAsia, 25 in Europe, none in Oceania. Countries where smallpoxis prevalent are planning or applying eradication schemesthrough vaccination. A good, reliable vaccine exists and theproblem is essentially one of manpower, equipment and supplies.In the developing countries the main difficulties in developinga massive attack on the disease are the lack of vaccine,of means for refrigerated distribution, and of sufficient transport.
In 1959 cost estimates based on the world incidence of smallpoxduring the three preceding years showed that the average costthroughout the world for mass vaccination would be in theorder of $0.10 per person vaccinated. For about 1000 millioninhabitants living in areas where smallpox is still endemic,approximately $100 million from all sources, including the

ANNEX 13 177
governments concerned, would be required to achieve totalcoverage, divided as follows: Africa, $13 million; Americas,$11 million; Eastern Mediterranean, $17 million; South -EastAsia, $55 million; and Western Pacific, $4 million.
WHO has budgeted for some $350 000 in 1963 and 1964 toassist countries with advisory services, and by supplying vaccineand laboratory equipment. Plans for world -wide eradicationalready exist and an all -out attack could be undertaken in thenext four years of the Decade if an estimated $10 million couldbe made available to assist countries with such items as vehiclesand vaccine.
Community Water Supply
Community water supplies have a vital role in the economicdevelopment, and especially the industrial development ofurban areas in developing countries. The emergence of a nationfrom a less developed to a more advanced status is a step -by -stepprocess. There are certain stages of economic growth, some ofthem well defined in economic terms, that must be attainedconsecutively; at some of these stages the lack of safe andadequate supplies of piped water may retard or even be anactual bar to progress. Water supply is basic not only to healthbut to a wide variety of economic activities, and investmentin producing sufficient supplies of water in urban areas may-be a major factor in determining the rate at which industrialand commercial growth will proceed.
Today, about 320 million people live in urban communitiesin developing countries receiving assistance from WHO. It isestimated that this number will increase to about 415 millionat the close of the Development Decade. Of this urban popula-tion a recent study indicates that at least 70 per cent. have noaccess to piped water within reasonable distance of their homes.The need therefore exists to provide this essential service to asubstantial proportion of the urban population- estimated atmore then 200 million people -who have at present no pipedwater service, or an inadequate one. By the end of the Decade,the population increment will have raised this number to 300million.
WHO's programme of technical assistance to Membergovernments in promoting the creation or improvement ofcommunity water supplies is designed to provide assistanceat the rate of $1 million a year, if funds become available.This would require capital expenditure by the countries at therate of approximately $4 million a year.
It is anticipated, furthermore, that the United Nations SpecialFund will continue to support community water supply activitiesby projects of a pre- investment nature under which preliminaryengineering plans, feasibility reports and master plans forwater supplies for urban centres or urban complexes may beprepared.
An attainable goal within the Development Decade wouldbe approximately to double the proportion of urban populationwho have easy access to safe and adequate amounts of pipedwater. It is estimated that a programme of construction wouldcost approximately $400 million per year in order to attainthis goal in 1970. This annual capital investment in communitywater supplies would amount, on the average, to about 0.25per cent. of the gross national product of the investing nations.Of these annual expenditures a substantial part -perhapsone fourth of the total, or $100 million per year- should becomeavailable from foreign aid sources.
Strengthening of Basic Health Services
It cannot be too strongly emphasized that an essential pre-requisite for the implementation of any of the programmesalready described is the existence at the country or regionallevel of an adequate infrastructure both of health installationsand health personnel. With such a provision of staff andfacilities it should be possible in the majority of areas -subjectto difficulties of terrain, transportation and distance -to givea minimum coverage of preventive and curative health services,and wherever feasible to integrate them so that the wholepopulation, even in the rural areas, can benefit.
A notable contribution to the potential achievements of theDevelopment Decade can be made by the extension of theservice for maternal and child health. It is remarkable how,with better activities in health education and child care, advantagecan be taken of the recent developments in the control of thecommunicable diseases of the early years of life. The savingof life in these age -groups adds to the potential of educablechildren, who with appropriate training can become the techni-cians of the future, in whom the real wealth of a country lies.It is important too that maternal and child health servicesshould be integrated with the basic health services, thus attainingthe maximum of efficiency and availability.
Malnutrition also represents an immediate challenge to actionduring the Decade and the medical aspects of the problemcannot be ignored. In close co- operation with the Food andAgriculture Organization, other organizations, and particularlywith the activities of the United Nations /FAO World FoodProgramme, the World Health Organization will intensify itsactivities in this domain. Plans have already been made for1963 -1964 to assist countries to ascertain, through samplesurveys, the current nutrition problems and deficiencies oftheir populations, setting down standards for the developmentof nutrition conditions in subsequent years.
The strengthening of national health services has been andwill continue to be the goal of WHO's activities in the developingcountries for a number of years to come in accordance withthe guidance provided by its governing bodies in various resolu-tions and in the General Programme of Work covering a SpecificPeriod.
Most of the activities planned to be financed from fundsadministered by WHO in 1963 (at an estimated total cost ofalmost $50 million), and of those proposed for 1964 (at anestimated total cost of over $52 million) are aimed at the attain-ment of this goal.
Any accelerated health programme which might becomepossible during the remaining years of the Decade would haveconsiderable influence on the future programme activities ofthe Organization and on its financial requirements. It will bepossible to evaluate such repercussions after a more preciseprogramme for economic and social development as a wholehas been established, when the reactions of the governmentsconcerned have become known, and when the availability ofadditional financial means has been investigated and, if possible,established.
Summary
Certain health goals which could be fulfilled during theDecade have been indicated. While it is impossible to proposeat this time a complete phased programme for health develop-ment in the under -privileged areas of the world, broad areas
178 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
for action have been described where energetic interventionshould lead to progressive avenues and rapid improvement inthe living conditions of the people, and to a higher degree ofproductivity and of individual achievement.
The focus of immediate and local action will be in the countries
concerned, but WHO's structure, its close relationship tonational health agencies, and its existing programmes in thefield put it in a condition to meet any additional requirementswhich may emerge in connexion with the general programmeof international assistance for the Development Decade.
Appendix 4
ECONOMIC AND SOCIAL COUNCIL RESOLUTION 920 (XXXIV)
Special Committee on Co- ordination with Particular Emphasison the United Nations Development Decade
The Economic and Social Council,
Recalling General Assembly resolution 1710 (XVI) of19 December 1961,
Having considered the report of the Secretary -General TheUnited Nations Development Decade - Proposals for Action,'
Recognizing that the United Nations Development Decaderequires, for the fulfilment of its goals, concerted action withinthe United Nations family of organizations in the economic,social and human rights and related fields, in the UnitedNations Development Decade,
Believing that co- ordination of the activities of the UnitedNations and its related agencies would be facilitated if effortswere further concentrated upon selected areas of strategicimportance where the opportunities and needs for UnitedNations efforts are most apparent,
Believing further that the work of its ad hoc Working Groupon Co- ordination established by its resolution 798 (XXX) of3 August 1960 has greatly facilitated the discussion of co-ordination matters by the Council,
1. Decides to establish a special committee consisting ofrepresentatives of eleven States members of the Council or theTechnical Assistance Committee -to be elected annually atits resumed summer session on the basis of equitable geogra-phical distribution -who should be conversant with the pro-grammes and activities of the United Nations in the economic,social, human rights and related fields, and of the related agencies,as well as with the practice and procedures of co- ordinationamong these organizations;
2. Decides further that this special committee shall havethe following functions :
(a) (i) To keep under review the activities of the UnitedNations and its related agencies in the economic, social,human rights and related fields in the United NationsDevelopment Decade;
(ii) To consider, wherever appropriate, in consultation withthe agencies concerned, priority areas or projects relating tothe objectives of the United Nations Development Decadein accordance with its resolution 916 (XXXIV) of 3 August1962;
(iii) To submit recommendations on these matters to theCouncil;(b) To assume the functions of the ad hoc Working Groupon Co- ordination as follows :
(i) To study the reports of the Administrative Committeeon Co- ordination, appropriate reports of the United Nationsorgans, the annual reports of the specialized agencies and theInternational Atomic Energy Agency and other relevantdocuments;
(ii) To submit its conclusions to the Council, for considera-tion, in the form of a concise statement of the issues andproblems in the field of co- ordination arising from thesedocuments which call for special attention by the Council;3. Requests the Committee, in fulfilling its task under
paragraph 2 (a) above, to take into account any special observa-tions which the Administrative Committee on Co- ordinationmay deem it appropriate to submit;
4. Further requests the Committee to take into account theactivities of the ad hoc Committee of Ten on co- ordination oftechnical assistance activities;
5. Decides to convene the Special Committee in the firstinstance in February 1963.
Appendix 5
1236th plenary meeting, 3 August 1962.
EXCERPT FROM THE TWENTY- SEVENTH REPORT OF THE ADMINISTRATIVECOMMITTEE ON CO- ORDINATION
Ill. UNITED NATIONS DEVELOPMENT DECADE
10. The ACC has also considered resolution 920 (XXXIV)relating to the creation of a Special Committee on Co- ordinationwith particular emphasis on the United Nations Development
1 United Nations (1962) The United Nations DevelopmentDecade: proposals for action, New York (United Nationsdocument E/3613, and United Nations document E/3613Add. 1, 2 and 3).
[From United Nations doc. E/3695 - 10 Oct. 1962] 2
Decade, and has noted that this resolution requests the Com-mittee to take into account any special observations concerningthis resolution which the ACC may deem it appropriate tosubmit.
11. The Development Decade represents a new phase in thecontinuing process of ensuring proper co- ordination of thewide range of activities through which the members of theUnited Nations family are attempting, by a combination of
2 Mimeographed version.

ANNEX 13 179
concerted and mutually complementary action, to achieve thegeneral objectives set forth in the Charter; it embraces thetotality of all their activities and these can be adequately andeffectively co- ordinated only by the full use of all the resourcesof the Charter and the relationship agreements. The generalview of members of the ACC has been, and continues to be,that no new machinery for inter- agency co- ordination is requiredto implement the Development Decade. While holding theseviews, the members of the ACC have nevertheless consideredthe matter on the basis of the decision taken by the Councilat its thirty- fourth session.
12. The executive heads of the agencies, while willing to recom-mend to their respective governing bodies full and active co-operation with the Council through the Special Committeewhich the Council has established, feel it necessary to recall thebasis of such co- operation, as stated fully by the Council itselfas recently as 1958 when defining the basis on which the five -year appraisals were undertaken, and as recapitulated in para-graph 15 of the Appraisals Report.1 It is the understandingof the ACC that the principles so stated by the Council withreference to the appraisals continue to be applicable, and governthe whole implementation of plans for the Development Decade.It is on this understanding that the executive heads of theagencies will recommend co- operation with the Special Com-mittee to their governing bodies.
13. The executive heads of the agencies wish to draw specialattention to the importance of such co- operation being arrangedin a manner which carries out fully the spirit of the Charterand of the relationship agreements. They have been greatlyconcerned by certain recent cases in which committees appointedby the Council have, in effect, granted hearings to representativesof the specialized agencies and then proceeded to discuss, inthe absence of such representatives and with little or no furtherconsultation with them, the conclusions to be drawn from suchhearings. Such an approach is a major departure from the
manner in which co- operation within the United Nationsfamily has previously been arranged on the basis of the relevantprovisions of the Charter and the relationship agreements.The Charter provides for " participation " by the " repre-sentatives " of the specialized agencies in the " deliberations "of the Council and its commissions, and the agreements providefor such " participation " by " representatives " in " delibera-tions " as a matter of right; the inclusion of such a provision,which is reciprocal in its operation, was one of the basic condi-tions on which the agreements were concluded. The membersof the ACC assume that the co- operation of the agencies con-cerned with the Special Committee will take the form of theparticipation in the deliberations of the Committee by their repre-sentatives provided for in the Charter and the agreements.
14. The ACC is keenly aware of the primary importance ofwholehearted practical co- operation without undue emphasison matters of organization and procedure, in making a successof the Development Decade. It ventures to hope that theemphasis of future discussions will be essentially upon theproblem of securing a scale and continuity of effort, a wise andprudent use of the resources available, and an emphasis onmatching resources to needs, which will give real substance tothe hopes so widely entertained. If the Development Decadeis to result in an effective intensification of international action,the provision, in both the common programmes and the budgetsof the individual agencies, of resources adjusted to the targetswhich emerge as the Decade develops will be indispensable.
15. The peoples of the world will get out of the DevelopmentDecade what they and their Governments put into it and theessential role in the matter of the members of the United Nationsfamily is to serve as an instrument of co- operation throughwhich the determination of the peoples of the world to secure" better standards of life in larger freedom " can be sustainedand made effective. In fulfilling this role all members of theUnited Nations family will endeavour to play their full part.
Appendix 6
EXCERPT FROM THE TWENTY- EIGHTH REPORT OF THE ADMINISTRATIVECOMMITTEE ON CO- ORDINATION
II. UNITED NATIONS DEVELOPMENT DECADE
3. In later sections, reference will be made to some of themajor current international activities that are being undertaken-or expanded -within the framework of the United Nations
1 United Nations (1960) Five -year perspective, 1960 -1964,Geneva (United Nations document E/3347/Rev.1). The relevantpart of paragraph 15 reads :
(a) The appraisals are regarded as a step in the dynamicprocess of developing progressively the effectiveness of theUnited Nations and the specialized agencies as instrumentsfor assisting the countries of the world to develop economicallyand socially at a greatly accelerated rate.(b) The appraisals are a further step in the development ofco- ordination through which the respective programmes ofthe United Nations organizations have gained, over theyears, in purpose, depth and strength. Such co- ordinationhas been achieved not by way of centralization, not by direct-ives or orders, but by consultation and persuasion and by
[From United Nations doc. E/3765 - 6 May 1963] 2
Development Decade. At this point, the ACC wishes to recordthat the " programme of phased proposals for action withrespect to the basic factors of economic growth ", which isbeing submitted to the Council under the title "United NationsDevelopment Decade : Activities of the United Nations and
free co- operation in the efforts designed to improve the lotof men.(c) The appraisals are not to be understood as implyingthat the programmes and budgets of the " United Nations orthe specialized agencies should, or could, be determinedoutside the constitutional framework of each organization.They imply no attempt to interfere with the autonomy ofthe organizations within the United Nations family.(d) The appraisals do not require firm policy formulationlooking ahead for the five -year period, or any rigid commit-ment in regard to specific programmes. The appraisalsshould in no way interfere with the flexibility which theorganizations must have in determining their programmesfrom year to year.2 Mimeographed version.
180 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
related agencies in the immediate future " has been drawn up asa co- operative effort by the staffs of all the organizations con-cerned. It also wishes to express its appreciation for the mannerin which the Council's Special Committee on Co- ordinationreviewed a draft of the above report at its recent meetings, hassought the fullest participation of all agencies in its work andparticularly for providing the ACC the opportunity of com-menting on its own preliminary findings ... in the matter ofpriority areas relating to the objectives of the DevelopmentDecade.
4. As regards the priority areas referred to by the SpecialCommittee, the ACC feels that, while the preparations for theUnited Nations Conference on Trade and Development callfor special attention this year by the agencies directly concerned,this should not imply any lessening of efforts directed towardsthe development of human and natural resources, includingagricultural production, as well as industrial development.Nor should the emphasis placed on development planning be
understood as diminishing the importance of the programmesfor current assistance in those fields.
5. The ACC has noted the suggestion of the Special Com-mittee that a general framework of functional classificationsbe devised to include the activities of all members of the UnitedNations system under the Development Decade. Arrangementshave been made for the preparation of a draft framework ofthis kind, and the ACC hopes to be able to report on the matterlater.
6. It also noted that the Special Committee had mentioned inits preliminary findings a number of matters regarding whichthe ACC has already taken action; further progress on someof them is recorded in its present report : for example, sec-tion III (d) refers to co- ordination in the field and the role ofresident representatives; co- operation in regard to the regionaldevelopment planning institutes is mentioned in section IX,and some specific contributions that can be made to nationaldevelopment planning are suggested in sections V on educationand training and VI on rural development.
Annex 14
MEETINGS OF THE REGIONAL COMMITTEE FOR AFRICA
[A16 /AFL /6 -4 April 1963]
REPORT BY THE DIRECTOR- GENERAL
This item was placed on the agenda of the HealthAssembly by the Executive Board, in the light ofresolution AFR /RC12/R17 adopted by the RegionalCommittee for Africa at its twelfth session, the textof which reads as follows :
Reasons why the Regional Committee has met atthe WHO Headquarters in Geneva, and Measuresto be taken to avoid the Recurrence of similarCircumstances
The Regional Committee for Africa,
Considering that the Government of the Republicof South Africa, in spite of its long associationwith the World Health Organization, accepts andpractises the policy of apartheid, which policysubjects indigenous African citizens to racialdiscrimination to the detriment of their physical,mental and social well- being, in contravention ofthe principles, aims, and purposes of the Constitu-tion of the World Health Organization;
Considering the increasing trend on the part ofthe Member States of the Region to refuse to admiton their own territory the representatives of the
1 See resolution WHA16.43.
Government of South Africa or to sit side by sidewith them in regional meetings;
Considering that such a situation is liable in thenear future to paralyse the functioning of theRegional African Organization and to preventthe Regional Committee from fulfilling its constitu-tional functions;
Recognizing that the Constitution does notprovide for the cessation of the membership of aState;
Being conscious however of the needs of theSouth African population and of the necessity forthe World Health Organization to be able to assistthis population,1. REQUESTS the Director -General to draw theattention of the next World Health Assembly tothis situation; and2. REQUESTS the World Health Assembly to studythe appropriate measures to put an end to thissituation, but without prejudicing the health rightsof the South African population.
This resolution is therefore transmitted to the HealthAssembly for consideration.
For the information of the Health Assembly, thereis appended to this report the text of Part IV (a) ofthe report of the Regional Committee.

ANNEX 14 181
Appendix
EXTRACT FROM THE REPORT OF THE REGIONAL COMMITTEE FOR AFRICAON ITS TWELFTH SESSION, 24 SEPTEMBER - 2 OCTOBER 19621
IV (a) Reasons why the Regional Committee met at the WHOHeadquarters in Geneva and Measures to be taken to avoid theRecurrence of Similar Circumstances
The representative of Senegal summarized the reasons whythe twelfth session of the Regional Committee could not beheld in Dakar as had been decided. The addition of this newitem to the agenda had been agreed upon because it was by nomeans impossible that a similar case might occur again. If so,the logical answer would be to hold sessions in Brazzaville, theRegional Head Office, since the provisions of the agreementmade between WHO and the Congo (Brazzaville) in its capacityas host government, conferred the necessary privileges andimmunities on the Organization.
After a considerable debate the Regional Committee decidedto designate a sub -committee to draft a resolution. This resolu-tion was the subject of further discussion forty -eight hourslater.
1 Document AFR /RC12 /14 Rev.l.
The vote on the resolution (AFR /RCI2 /R17) was taken ina call -over giving the following results :
For the resolution: Cameroon, Congo (Brazzaville), Congo(Leopoldville), Dahomey, Guinea, IvoryCoast, Madagascar, Mali, Mauritania,Niger, Nigeria, Senegal, Tanganyika,Togo, United Kingdom, Upper Volta
Against the resolution: South AfricaAbstentions: France, Liberia, Sierra Leone, SpainAbsent : Central African Republic, Chad, Gabon,
GhanaNot taking part in
voting: Portugal
Number of Members present and voting 17Simple majority 9For the resolution 16Against the resolution 1
Abstentions 4

182 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Annex 15
ORGANIZATIONAL STUDY ON MEASURES FOR PROVIDING EFFECTIVE ASSISTANCEIN MEDICAL EDUCATION AND TRAINING TO MEET PRIORITY NEEDS
OF THE NEWLY INDEPENDENT AND EMERGING COUNTRIES 1
[A16 /P &B /10 - 19 April 1963]
The Fifteenth World Health Assembly,2 on the recommendation of the ExecutiveBoard,3 decided that the subject for the next organizational study of the Executive Boardshould be " Measures for providing effective assistance in medical education and trainingto meet priority needs of the newly independent and emerging countries ".
The Executive Board studied the subject at its thirtieth and thirty -first sessions, andthe draft report was circulated for final remarks to members of the Board in accordance withthe Board's decision.' The report of the Executive Board on its study is given below.
REPORT BY THE EXECUTIVE BOARD TO THE SIXTEENTH WORLD HEALTH ASSEMBLY
CONTENTS
Foreword
1. Introduction
2. Extent and Nature of Needs3. How to meet the Needs
3.1 Guiding Considerations3.2 Nature of Assistance Needed3.3 Some Special Considerations in
Teaching Institutions
4. Problems of Policy and Implementation4.1 Technical4.2 Organizational4.3 Financial
Concluding Note
establishing
Page
182
183
183
185
186
187
190190
190
191
Appendix 1 : Education and Training of Health Personnelin Africa (Extracts from a working papercontributed by WHO to the UNESCO /ECAConference of African States on theDevelopment of Education in Africa, AddisAbaba, May 1961)Table I - Medical and Paramedical Per-sonnel in Africa in 1960Table III - Estimated Health Personnel forAfrica for the Decade 1960 -1970 .
Table IV - Estimate of Number of Gra-duates in the Various Categories requiredto fill the Posts in 1970
Appendix 2: Some Information on Medical Schools inthe African Continent
Page
191
192
192
193
FOREWORD
On the recommendation of the Executive Board atits twenty -ninth session,3 the Fifteenth World HealthAssembly decided that the subject for the nextorganizational study of the Executive Board shouldbe " Measures for providing effective assistance inmedical education and training to meet priority needsof the newly independent and emerging countries ".2
At its thirtieth session the Executive Board con-sidered a preliminary outline for the organizationalstudy, and requested the Director -General to preparefor the thirty -first session of the Board a report on thesubject, taking into account the comments and
1 See resolution WHA16.29.2 Resolution WHA15.59.3 Resolution EB29.R53.4 Resolution EB31.R36.5 Resolution EB30.R18.
suggestions made by members of the Board at themeeting and after it.5
In addition, a note, based mainly on the findings ofthe surveys carried out in seventeen countries of Africa,was prepared for the twelfth session of the RegionalCommittee for Africa, which met in Geneva from24 September to 2 October 1962. An informal meetingwas devoted to obtaining the views of the members ofthe Regional Committee on the planning for healthpersonnel training in Africa.
The report requested by the Executive Board wasdiscussed at its thirty -first session, and amendmentsand clarifying elaborations have been incorporated inthe present text for presentation to the SixteenthWorld Health Assembly by the representatives of theExecutive Board, after circulation to the membersof the Board for their final remarks.'
In preparing this report the expression " medicaleducation and training " has not been taken literally
ANNEX 15 183
but has been used to cover medical education notonly at university standard but also at the auxiliarylevel, together with the education and training ofparamedical personnel, both professional and auxil-iary. The problem of training health and medicalpersonnel has to be faced as a whole, since the varioustypes and levels of such personnel are functionallyinterdependent.
1. Introduction
The attainment of independence by many countriesand their plans for rapid social and economic develop-ment encompass, naturally, the expansion of suchhealth services as exist and the establishment of others.World communications have made the peoples ofthose countries aware of standards of services existingin other countries and their demands are thereforeincreasing.
The expansion of services, however, depends on theavailability of the necessary trained personnel. Inmany instances trained personnel do not exist, ortheir numbers are inadequate. Furthermore, thedeparture of expatriate staff has, in many cases,aggravated the situation. At the same time, the gapsin trained personnel cannot be filled peremptorilyfrom outside sources.
There is therefore urgency for these countries tomake provision for the training of their own personnel,either at home or abroad or both. They need tobecome self-sufficient in personnel as soon as possible.Total self -sufficiency is perhaps a distant goal -especially as it depends upon a sufficient level ofgeneral education, which attainment is in itself a longprocess. But there are many steps that can be takentowards that goal, either by individual countries orby groups of countries with similar circumstances.
Although the process of attaining self -sufficiencymay be a gradual one, especially in the sense ofcountries developing the necessary institutions withintheir own territory, it could certainly be accelerated.The emerging countries would have the advantage ofa pool of experience from " older " countries andof a large fund of international goodwill and assistance.
This external assistance must be visualized as oflong duration, probably tapering in quantity as theyears go by. To be effective, the assistance may needto be considerably greater than that which is furnishedtoday as normal practice by WHO and other assistingagencies. It may in fact require joint action, ordistribution of tasks among more than one agency,and perhaps forms of assistance not now current.
It is the purpose of this study to explore the needsand the ways of meeting them, and in this process, todraw attention to possible orders of priority in meetingthese needs; and also to explore problems of policy
and implementation -technical, organizational orfinancial.
It is clearly understood that, in the meantime, theexisting programme of assistance to newly independentcountries will continue and will probably be expandedin certain directions, on the basis of surveys of needs,especially towards the establishment of trainingfacilities within the countries. In this regard, it isuseful to refer to the chapter on education and trainingof the report on continued assistance to newly inde-pendent States 1 submitted to the Fifteenth WorldHealth Assembly.
2. Extent and Nature of NeedsThe newly independent and emerging countries,
although they have many problems in common, areat very different stages of development. Some alreadyhave a substantial nucleus of trained personnel amongtheir nationals and a number of training institutions,including medical schools, though these are almostalways inadequate to meet the country's needs. Atthe other extreme there are countries where a beginninghas yet to be made in almost every field of medicaland allied education and training.
This study does not attempt to appraise the needsof each country. It is aimed at stating the commonelements among the needs of many emerging countriesfor the education and training of their medical andhealth personnel, and thus at providing a basis fordiscussions of policies and their implementation tomeet these needs on a broad scale. By " needs "is meant the gap between the trained personnelavailable and those reasonably required now and atcertain target dates in the future (e.g., five years,ten years), as well as the facilities necessary for theirtraining.
In order to permit such an over -all review, there hasbeen selected as an example the part of the worldwhere the largest number of newly independent andemerging countries is grouped -the continent ofAfrica. Fact -finding surveys, mostly by a teamconsisting of a doctor and a nurse specialized in educa-tion, covered seventeen of these countries in 1961 and1962 and have contributed to providing a generalview of the problem and of possible solutions.
Published data 9 on health personnel, hospital
1 Off. Rec. Wld Hlth Org. 118, Annex 4, Part 4.s World Health Organization (1962), Statistics of health
personnel and hospital establishments. In : Annual epidemio-logical and vital statistics, 1959, Geneva, p. 650;World Health Organization (1957) World directory of medicalschools, 2nd ed., Geneva;World Health Organization (1961) World directory of dentalschools, Geneva;World Health Organization (1963) World directory of veterinaryschools, Geneva;Second Report on the World Health Situation, 1957 -60 (Off.Rec. Wld Hlth Org. 1963, 122).

184 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
establishments and certain training institutions,although lacking in precision, or not reflecting thelatest changes, illustrate sufficiently the shortage ofmedical and health personnel in some of the newlyindependent countries.
A summary of health personnel available, and theirratio to the population, was prepared in simplifiedform for the purposes of the UNESCO /ECA Con-ference of African States on the Development ofEducation in Africa, which was held in Addis Ababain May 1961. Tables I, III and IV, presented to theConference, are given as Appendix 1 to this report.Table IV especially emphasizes, if it were not alreadyknown, the nature and extent of the needs in trainedpersonnel. These figures take on added significancewhen it is remembered that facilities for trainingthese personnel are inadequate, and in some countriesnon -existent. Appendix 2, on medical schools in thecontinent of Africa, summarizes data made availableby the authorities concerned for the third edition ofthe World Directory of Medical Schools.
The magnitude of-the problem may be illustratedby some figures relating to medical graduates. Forthis illustration the field of medicine proper has beenselected, since it is more uniformly and generallyunderstood than that of auxiliary medical personnel,as regards both the training required and the functionsperformed. It is of crucial importance, because of theleadership role of medical personnel, and it can beconsidered as an indication of the problem as a whole.In the area covered by the WHO African Region(excepting the Republic of South Africa), the estimatedpopulation is 150 million, the total number of fullyqualified physicians little more than 7000. The pre-sent ratio of physicians to population is therefore lessthan 1 : 20 000, or one physician to over 21 thousandpeople. In order to bring the ratio even to 1 :10 000,it would be necessary over the next twenty years toproduce each year a minimum of -1200 medicalgraduates (350 per annum to meet wastage, plus350 to bring gradually the ratio to 1 :10 000 of existingpopulation, plus 500 to cover the estimated naturalincrease in population). The maximum potentialoutput of the existing medical schools in the area by1970 may be estimated at 450 medical graduates ayear. An output of 750 more graduates a year istherefore required. Assuming an average annualoutput per school of between fifty -five and sixtygraduates, thirteen new medical schools are neededin the area -and it should be borne in mind that on thebasis of this calculation these thirteen schools shouldbe starting to function now, but this is not realistic.
The problem is complicated by the fact that manycountries have available for professional medical orparamedical studies very few candidates who have
completed full secondary -school education. However,at a level lower than that required for professionaltraining there is a relatively large source of school-
leavers with primary or mid -secondary education.Three publications by UNESCO provide data on theexisting situation as to general education. Anotherpublication gives insight into the problem of highereducation in general, with specific reference to Africa.2Close contact should be maintained with UNESCO,since its assistance to countries may greatly contributeto the development of general education facilities -thus increasing the reservoir of suitable candidatesfor medical and allied education and for auxiliarytraining, as well as promoting all forms of highereducation.
A programme of health personnel training shouldcater for immediate needs and for the future. Inaddition to professional personnel in medical andparamedical categories, there are required trainedauxiliary 4 personnel in large numbers and in appro-priate numerical relation to the professionals whowill teach, lead and later supervise them. Auxiliarypersonnel, for whom the educational requirement islower (primary or elementary school for all but medicalassistants, in whose case a higher level is desirable)are normally produced after one or two years' training,mainly in specific skills and techniques, and thus areavailable for service earlier than the fully qualifiedprofessional groups in the same field.
It will therefore be necessary to rely on medical andparamedical auxiliary personnel to provide the bulkof the medical and health services for many years tocome. These auxiliaries (medical assistants -for thediagnosis and treatment of common diseases -assistantnurses, assistant midwives, assistant sanitarians,laboratory assistants, etc.) have a place of their ownin the health team, are especially trained for it, and
1 The educational situation in Africa today (UNESCO/EDAF /S /4, April 1961, mimeographed document);UNESCO (1961) Basic facts and figures, Paris;UNESCO (1961) World survey of education, III, Secondaryeducation, Paris.
2 UNESCO (1963) The development of higher education inAfrica (Conclusions and Recommendations of the Conferenceon the Development of Higher Education in Africa, Tananarive,3 -12 September 1962), Paris.
3 For the purpose of this paper, the term " paramedicalpersonnel " includes all the professions allied to medicinewhich together make up the team of health personnel, i.e.,nursing and midwifery, sanitation, dentistry, veterinary health,pharmacy, physiotherapy, statistics, microbiology, etc.
4 According to the definition accepted by all United Nationsagencies, an auxiliary worker is " a paid worker in a particularfield, with less than full professional qualifications in that fieldwho assists and is supervised by a professional worker ". Thus,these may be auxiliary personnel in medicine, nursing, sanitation,etc. Furthermore, there can be different levels within the broadcategory of auxiliaries, e.g., in nursing there are auxiliarynurses, nursing aides, etc.
ANNEX 15 185
should not be the product of a lower standard oftraining in the various professions to which theybelong. The importance of auxiliary personnelbecomes even more evident when it is recalled thatmuch of the population of the developing countriesis rural, lives in small scattered communities with fewmeans of communication, and has a low income level.
In the broadest terms, the situation as to healthpersonnel training in newly independent and emergingcountries, such as those in Africa, may be summarizedas follows :
(1) In all the countries there is an overwhelmingneed for the development of local training resources,which depend, however, on progress in generaleducation and the expansion of health services.Both these factors, in turn, depend on the economicconditions and potentialities of the several countries.
(2) International assistance will be necessary inpractically all instances. The full magnitude ofassistance will have to be studied in detail withinthe Region before a consolidated programme canbe formulated.(3) In many instances agreement between twoor more countries, or joint action, may also berequired to give the best results.
3. How to meet the Needs
3.1 Guiding Considerations
The following paragraphs set out guiding considera-tions for preparing an overall programme of medicaland allied education and training for countries in astage of rapid development.
3.1.1 Fact-finding and PlanningWhen essential information has been procured
concerning the existing assets, both of service personneland establishments and of the training potentialitiesto provide for replacement and expansion, plans basedon targets of personnel to be trained during statedperiods of years should be prepared. Though suchplans, if they are to be realistic, should be extremelyflexible, they should in their earlier stages attempt tomeet the immediate needs, and incorporate measuresfor the relief of those needs into the longer -termprogramme. The importance of avoiding expedientswhich might be sources of trouble in the future, suchas the creation of two grades of professional medicalpersonnel, should be noted.
3.1.2 Training in the Country ItselfEfforts to make available training facilities in the
country itself are clearly indicated when there is a
constant demand and a large enough number ofpersons available to be trained. Training underconditions prevailing in the country itself, withattention to its particular health problems, is necessaryfor the basic formation of all auxiliary personnel andhas advantages even for professional basic education.
3.1.3 Training at Home and Abroad: Professionaland Auxiliary
External assistance, including international assist-ance, is utilized for two parallel courses of action :(a) to develop teaching institutions within the countryfor the four main types of personnel (see 3.1.4), bothat the professional and at the auxiliary level; and(b) to provide basic professional training abroad (inmedicine, nursing, etc.), while facilities for suchtraining are not yet available within the country, andpost -basic or post -graduate training of key personnel,especially for leadership and teaching. Students sentabroad are usually accommodated within existingcourses. Special arrangements may, however, benecessary for special or for large groups. One instanceis the case of assistants médicaux from the Congo(Leopoldville) and other médecins africains com-plementing their medical education in Europe.Another instance is the organization of classes forEnglish -speaking students at the Hadassah MedicalSchool of the Hebrew University, Jerusalem, Israel.
The qualitative and quantitative needs in trainedpersonnel may be best met by two parallel pro-cedures- namely, the production of a small numberof fully qualified personnel in medicine and para-medical fields (such proportion of the secondary -school output as it is feasible to orient to healthprofessions), and the training of auxiliary personnel in'much larger numbers. The former would provide thesustaining and supervisory cadres, the leaders, theteachers; the latter would provide the manpowernecessary for increasing the coverage of direct servicesto the community.
Attention needs to be paid to wastage of candidatesadmitted to teaching institutions, especially medicalschools, at home or abroad. High failure rates callfor investigation of and possible improvement in theextent and level of prior general education, themethods of selection of candidates for medical schoolsand other teaching institutions for health personnel,and the methods of teaching and the provisions forstudent counselling in these institutions. At the sametime -since the number of candidates is usuallylimited -it is justifiable to try to retain for the healthservices students who have failed at some stage oftheir medical education by orienting them towardstraining for other types and levels of health work, forwhich they may be suitable and adequate.
186 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
3.1.4 Priority Types of Personnel
Training should aim at the production primarilyof four types of personnel, for whom there is a con-sistently large demand : medical practitioners, nurses,midwives and sanitarians, with their correspondingauxiliary grades. Provision should also be made,however, for training dentists, sanitary engineers,health statisticians, public health veterinarians, ento-mologists, laboratory technicians and others, againwith the corresponding auxiliary categories, to theextent that these personnel are necessary in the healthservices of the country.
A judicious distribution of functions between medi-cal and paramedical personnel on the one hand, andtheir respective auxiliaries on the other, should makefor economies in two ways : first, an economy oftrained staff, and secondly, an economy in the timeabsorbed on training, by reducing to a minimum thenumber of persons requiring the lengthiest and mostcomplex forms of higher training This calls for aserious planning effort by national health authoritiesin co- operation with educational authorities andnational planning bodies.
3.1.5 Patterns of Training
Training should, the patternswith which the countries are familiar and which haveproved useful elsewhere. It is not advisable to in-troduce totally new concepts likely to meet resistanceand to provoke contradictory advice. Furthermore,the presence of comparable types of personnel inseveral countries has many advantages, not the leastbeing that it increases the scope of assistance for bothbasic and advanced training, and makes easier inter -country co- operation in obtaining both operationaland teaching personnel.
3.1.6 Broad Basic Training
Basic training of a too specialized character shouldbe avoided as far as possible. A broad content ofinitial training provides a reservoir from whichpersons can be drawn for more specialized workaccording to their aptitudes and the changing needsof the services.
3.1.7 Opportunities for Existing Personnel
Persons employed in health services who havereceived only partial training, strictly specializedtraining, or training of a type likely to be abandoned,may be fitted into more complete and up -to -datecourses.
3.1.8 Advancement of Auxiliaries
For auxiliaries there should be opportunities foradvancement within their field by providing for train-ing, including refresher courses, to enable them tochange from single -purpose and specialized work togeneral multi -purpose work, and to assume responsibi-lities in the chain of supervision of auxiliaries withmore limited training, experience or range of activities.
3.1.9 Distribution ofResponsibilities among Countries
Where a country cannot embark upon its own full -range programme of personnel training at all levels,possibilities of training offered by neighbouringcountries should be considered. A group of countriesmight collaborate in providing a whole range oftraining facilities, each country assuming responsibilityfor one or more types of training and making themavailable to the other countries.
3.2 Nature of Assistance Needed
The following paragraphs are intended to give anindication of the types of assistance that may beneeded; the list is not exhaustive and is not limited toassistance that may be obtainable from WHO.
3.2.1 Indirect Assistance
3.2.1.1 Recommendations of expert committees onvarious aspects of medical, paramedical and auxiliaryeducation and training (including the report of theStudy Group on Internationally Acceptable MinimumStandards of Medical Education,' and the reporton the Use and Training of Auxiliary Personnel inMedicine, Nursing, Midwifery and Sanitation 2 bythe Expert Committee on Professional and TechnicalEducation of Medical and Auxiliary Personnel).
3.2.1.2 Information on medical and paramedicaleducation in the world, both published and otherwisecompiled and available from WHO (World Directoryof Medical Schools, World Directory of DentalSchools, World Directory of Veterinary Schools, etc.).
3.2.1.3 Recommendations of the present organi-zational study, of the previous organizational studyon the subject of education and training,3 of thetechnical discussions at the Fourth World HealthAssembly,4 and of resolutions of the Health Assemblyand Executive Board on education and training.
1 Wld Hlth Org. techn. Rep. Ser., 1962, 239.S Wld Hlth Org. techn. Rep. Ser., 1961, 212.3 Off: Rec. Wld Hlth Org. 46, 131.
4 Chron. Wld Hlth Org., 1951, 5, 287.
ANNEX 15 187
3.2.2 Direct Assistance
As the term " assistance " implies, and in accordancewith the normal practice of WHO, outside assistance,large or small, must supplement -not supplant -theefforts of the country itself in establishing needed andfeasible training facilities. The country's own materialand human contribution is basic to any undertaking.
3.2.2.1 Consultations with headquarters and regionalstaff for the following purposes : to enable the nationalauthorities concerned to obtain clarifications onpossible assistance; to enable them to benefit fromcumulating knowledge and experience in the solutionof similar problems in other countries; to enable themto obtain help in drawing up plans for developingpersonnel training and to avail themselves of WHO'sservices in any multi -national effort.
3.2.2.2 Consultants to help in fact -finding surveysand planning, as one means of assisting governments,if requested, to identify their needs and to developcomprehensive practical national plans to meet theseneeds. Once such plans are developed, any assistanceprovided by the international organizations would bedesigned to fulfil the requirements of some part ofthem.
3.2.2.3 Visiting professors, internationally recruited,to fill gaps in national teaching personnel, organizethe relevant departments, and increase the trainingqualifications of their counterparts or prepare youngerassistants for more responsibilities.
3.2.2.4 Fellowships to nationals : (a) for basicmedical education, where this is unobtainable locally;(b) for the training of teachers, organizers and leadingpersonnel; and (c) for attendance at educationalmeetings organized by WHO for the discussion ofspecific topics of medical and allied education,exchange of experience, and improvement of workthrough the cross -fertilization of ideas.
3.2.2.5 Maintenance and travel costs for studentsto attend internationally assisted teaching institutionsin their own countries, until such time as the countriescan make adequate budgetary provision for all theirstudents.'
3.2.2.6 Equipment and supplies : (a) for teachinginstitutions; and (b) for service institutions (such ashospitals, health centres) used for training.
3.2.2.7 Service staff, internationally recruited, to fillgaps in the key -personnel establishment of institutionsused for training (hospitals, health centres, etc.).
1 In accordance with resolution WHA6.35.
3.2.2.8 Salary or salary complements to nationalsavailable to hold key posts in teaching institutions,until such time as the country can make adequatebudgetary provisions. Need for caution was expressed,however, with regard to supplementation of localsalaries.
3.2.2.9 Buildings for teaching institutions.
3.3 Some Special Considerations in establishingTeaching Institutions
3.3.1 Training designed to meet Local Needs
It is of great importance that training should bedesigned to meet local needs and conditions. Thisshould present no great difficulty at the auxiliary leveland should also be relatively easy in the training ofprofessional nurses, midwives and sanitarians. Atthe level of professional medical training, however, theadjustments to meet local needs have to be madewithin the framework of the accepted patterns andstandards of education. Much of the teaching staffwill, in the beginning, come from abroad and thegraduates of the school must be able to receiverecognition abroad in order to be admitted to post-graduate studies.
3.3.2 Standards of TrainingThe scope and operations of training schools,
including schools of medicine, should be realistic andnot over- ambitious, at any rate in the early stages,until the capacity of students improves with higherstandards of general education and until the facultyis sufficiently well developed, qualitatively andquantitatively. On the other hand, there should be nodeliberate lowering of standards for purposes ofexpediency, such as haste to produce greater numbersof doctors and other qualified personnel. The pre-paration of future teachers and specialists enters intoall programmes of medical and paramedical education,and the basic diplomas obtainable in each countryshould be acceptable to higher institutions abroadwhere, as graduates, the students will need to studyat advanced levels.
As regards medical education, it is necessary todistinguish between the training of a lower " second "category of physicians, which is in general undesirable,and the training of a clearly distinct category ofauxiliaries in general medicine who, by their lowergeneral education and by their technical training,cannot be confused with fully qualified physicians andwho work under supervision and only within anorganized system of health services. This type ofauxiliary in general medicine will probably be neededin many countries, but the pattern of their trainingand utilization should be established in close relation-
188 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
ship to the plans for development of the country'shealth services.
The example may be given of a certain countrywhere abbreviated emergency training for doctorswas introduced twice under war conditions, but wassoon abandoned, and where the training of doctorsand auxiliaries in general medicine is being continued.In another country, where two categories of medicalschools originally existed, the situation has beenremedied by either up- grading or abandoning thelower category of training.
3.3.3 Preparation of Teaching StaffAs to the preparation of teachers of medical and
allied subjects, even in very recently opened trainingestablishments selected students might be assigned tojunior posts as demonstrators and instructors, thuspreparing them for future training for more responsibleposts and adding to the teaching potential of theinstitution. There might be added to the conditionsfor fellowships for post -graduate training abroadthe requirement that the fellow be given practice intutoring or class teaching in his subject.
3.3.4 Importing Teaching StaffWhen medical schools are established, staff are
usually recruited from other schools, if such exist inthe country. Where this movement has been wellprepared some years in advance, and where the futureteachers have been selected according to a plancovering their preparation for their new posts, theloss to the " giving " schools is not serious. Where,however, such procedures are impossible owing tothe absence of " giving " schools, almost total reliancehas to be placed on teachers from foreign countries.The practice of affiliation between a " new " medicalschool and an " old " one in a developed country hasconsiderable advantages from the staffing angle, asregards both the provision of personnel and thetraining of national graduates for future teachingposts. Fellowships programmes enter very largelyinto the training of teachers.
For schools of medicine there is today a world-wide lack of suitable teachers who are prepared totake posts outside their own countries for limitedperiods. This shortage of teachers is especially acutein the non -clinical subjects and in preventive and socialmedicine. Even contracts for five years are not oftenattractive to keen young teachers, who see theirchances of promotion in their own countries seriouslydiminished if they are away for one or more years.Career contracts of ten to fifteen years are more likelyto produce applicants.
Under the circumstances one may also consider asuggestion for the establishment of what may bedescribed as an " international nucleus faculty ", to
be assigned successively to newly established institu-tions until they develop their own staff. The recruit-ment of teachers from abroad may, however, besufficiently successful, with the normal contracts, tomake the consideration of measures of this kindunnecessary.
3.3.5 Establishing a New Medical SchoolThe establishment of a medical school of university
standard is the most difficult of the undertakings fortraining health personnel, and cannot be determinedsolely on the basis of the needs for education inmedicine. It entails a thorough review of the humanand material resources available for assuring that themedical school will function at a creditable level.
The following are among the matters for con-sideration :
(a) Location and teaching language of existingmedical schools within the country or' in neigh-bouring ones; possibilities for increasing the yearlynumber of admissions.(b) Output of secondary schools in the country andpossible number of candidates for medical studies;number of nationals with medical qualifications,from among whom a nucleus of teaching staff maybe gradually formed.Until both appear adequate, the only solution will
continue to be, for some time to come, to send studentsabroad to study.
3.3.5.1 When there is no immediate prospect ofestablishing a medical school, the possibility may beexplored of utilizing any available hospital for theclinical training of those who have carried out theirmedical studies abroad. If the hospital facilities-installation, equipment, medical, nursing and otherstaff -are adequate it may be possible to arrange forthe new graduates to take their internship yearthere, and perhaps even some of the clinical work inthe course of their studies. Arrangements would needto be made with the medical schools abroad. Sucharrangements, however difficult they may be, mightprepare the way for an increasing assumption ofresponsibilities and -if other conditions becamefavourable -might gradually lead to the establishmentof a full medical school, by adding facilities for basicmedical sciences.
A teaching institution is not only a device for pro-ducing trained personnel. Important as this trainingfunction certainly is, a new school of medicine isexpected to exert still other beneficial influences on thedevelopment of a community and of a country. Thisis particularly manifest in the case of the first schoolof this type in a country, where it provides a strongstimulus for setting up higher standards of medical

ANNEX 15 189
care in the community, compatible with modernscience and techniques. The school also provides anopportunity for advanced training in scientific andpractical areas of medicine. It further attracts thepotential scientists, teachers and leaders, and helpsthem to develop their potentialities. The medicalschool is also likely to accept some responsibilitiesin leading the health and social progress of the com-munity and the country, e.g., by providing the legis-lators and administrators with competent scientificinterpretation of the health phenomena and healthneeds of the society. Such a school keeps the countryaware of scientific progress in medicine and thusassists the medical profession and the service institu-tion in a continuing improvement of their per-formances.
3.3.5.2 In countries where the establishment of anundergraduate medical school is not precluded, thefollowing considerations are relevant :
(a) In ordinary circumstances an annual intake ofnot less than fifty students should be foreseen foran undergraduate medical school. This implies thatthe school serves a country or an area with a popu-lation of about two and a half to three million if thenumber of secondary -school graduates is reasonablylarge; not more than one -tenth of them can beexpected to take up medicine as a profession. Atthe beginning, the annual intake may have to beless than fifty and this would be better for thebeginning of their teaching. If it is foreseen,however, that the intake will remain small, carefulappraisal of the need for a medical school isindicated, in view of the high costs involved andthe scarcity of teaching staff. In appropriatecircumstances neighbouring countries sufficientlysimilar in culture and using the same language mightjoin to establish a school serving all of them.(b) One of the first steps to be taken would be toset up an organizing committee or a nucleusfaculty council with an executive officer, who wouldbe responsible for all the preparatory work (plan-ning, etc.) and with whom negotiations -in thefirst place -would be carried out as to the outsideassistance needed.(c) A period of four or five years should be allowedfor the development of the medical school to thestage of admitting students; during that time staffare prepared, buildings constructed and equippedand the programme of studies outlined. Wherelocal experience is not available external counselshould be used in planning. Later, teams of foreignteachers may initiate and conduct courses untilsuch time as their posts can be taken over bycounterpart nationals who have had special training
abroad and experience with their foreign advisersat home. Where there is no other source of potentialteaching personnel in a country or area, a lengthyperiod (ten to twenty years) must be expected toelapse before the medical school can be independentof foreign aid as regards the normal curriculum.(d) Attention needs to be paid, by local and visitingprofessors alike, to drawing up a curriculum whichwill primarily meet the minimum requirements foradequate medical education (see 3.2.2.1 and 3.3.1)with due regard to local needs and conditions. Itshould form a balanced whole, in which particularor specialized disciplines would not take pride ofplace, and in which the teaching of clinical scienceswould not be crowded out by basic sciences,teaching displaced by research or service, and socialand preventive medicine rejected in favour ofcurative medicine or vice versa.(e) Note might be taken of the order of magnitudeof the capital costs and maintenance charges(including staff) of a modern medical school. Thesenaturally vary greatly both within and betweencountries, but in general terms and within verywide approximations one might expect the buildingsand equipment of a medical school, catering for anannual intake of fifty to a hundred students, tobe around $10 000 000, and the annual cost perstudent to be between $1500 and $3000. Thesefigures do not include the cost of an ad hoc teachingor university college hospital nor the salaries ofclinical and laboratory hospital service staffs, muchof whose time may be given to teaching.
3.3.6 Training and Employment PossibilitiesThe production of both medical and paramedical
personnel depends on : (a) the government's personnelestablishment and its capacity to absorb all trainees asthey qualify; and (b) the attractiveness of these careers(chiefly in professional nursing, midwifery, and sanita-tion) compared with careers in commerce, in school -teaching, and in other government departments, allof which take their proportion of secondary schoolleavers.
The great length of full medical studies (a minimumof six years) may need to be compensated by specialadvantages during and after the studies in order toattract good and ambitious candidates now pre-ferring more immediate opportunities outside thehealth field.
On the other hand, there is seldom a lack ofapplicants for training for auxiliary grades requiringno more than elementary education.
It cannot be too strongly emphasized that thetraining of various types (medical, nursing, etc.) andlevels (the professional and the auxiliary) of health
190 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
personnel should be related to the plans and oppor-tunities for their employment. Special provisions maybe necessary to attract and retain professional per-sonnel, especially doctors, in key localities throughoutthe country and avoid their concentration in thecapital city. Satisfactory conditions of professionalwork should be secured by proper organization ofmedical facilities. Also, living conditions, and cir-cumstances such as facilities for education for thechildren, should be taken into consideration by thegovernments desirous of obtaining the services ofprofessional personnel in smaller towns or remoteplaces.
4. Problems of Policy and Implementation
4.1 Technical
Consideration of the various items under section 3," How to meet the needs ", afforded an opportunityof considering some of the technical issues involvedin providing assistance to newly independent andemerging countries in education and training. Theconclusions reached, together with established prac-tices based on resolutions of the World HealthAssembly and Executive Board, expert committeerecommendations, etc., provide the necessary technicalguidance. It is unnecessary to go over the sameground again.
4.2 Organizational
4.2.1 Inter -country Committee(s) on Medical andAllied Education
One of the basic considerations is how to approachthe situation in a particular group of countries witha view, on the one hand, to possible distribution offunctions among them and, on the other hand, to theassumption of responsibilities for assistance whichmay be given, in particular activities or in particularcountries, not only by WHO but also by other assistingorganizations.
There would seem to be advantages in developinga plan applicable to a whole area, if this werefeasible; not the least of these advantages would be thecentralization of resources and the co- ordination oftheir use, in contrast to uncoordinated expansionof services by individual countries, which would tendto perpetuate and extend existing inequalities.
For pursuing this aim, several possible methods ofprocedure were considered, including the following :
4.2.1.1 To take the opportunity of a regional com-mittee meeting (in the case of Africa, for example)and utilize its membership as a medical and alliededucation committee for the Region, with the additionof representatives of other agencies -international,
bilateral or private -who are available to giveassistance. The first aim of such a committee mightbe to discuss the broad lines of the problem and tolearn to what extent co- ordination of planning andimplementation would in principle be possible. Thecommittee itself might be subdivided into two or threesub -committees on a language -of- teaching basis.
4.2.1.2 To promote the establishment of medicaland allied education committees for groups of neigh..bouring countries using the same language for teachingpurposes. These committees, again, would consist ofgovernment representatives and representatives ofagencies.
The functions of a medical and allied educationcommittee would have to be carefully considered andagreement as to their range would have to be reached.
4.2.2 The following are subsidiary questions dis-cussed :
4.2.2.1 Pairing of teaching institutions. The valueof schemes whereby new teaching institutions are" paired " with old- established ones is not in doubt;among other things, they may help in overcomingdifficulties with the recruitment of teaching staff, espe-cially for university level education. In its consulta-tions with national authorities WHO may, therefore,take the initiative in promoting " pairing " betweenparticular institutions.
4.2.2.2 Associating bilateral agencies. There wouldbe advantages in WHO's inviting the co- operation ofcountries providing bilateral aid, with a view to asso-ciating them in any one long -term development plan.
4.3 Financial
4.3.1 Providing Effective Assistance
Providing effective assistance to meet the needs ofthe newly independent and emerging countries wouldrequire additional funds. Some indication of costsis given in the report submitted to the Fifteenth WorldHealth Assembly on continued assistance to newlyindependent States.'
4.3.2 Obtaining the Funds
The resolution of the Fifteenth World HealthAssembly on continued assistance to newly inde-pendent States refers to one source of funds for thisprogramme, the Special Account for AcceleratedAssistance to Newly Independent or Emerging States.2It is, however, unlikely that this account and theregular budget of WHO would suffice, and it would
1 Off. Rec. Wtd Hith Org. 118, Annex 4, Parts 3 and 4.2 Resolution WHA15.22, para. 8.

ANNEX 15 191
seem appropriate to consider other possible sources offinancing 1 such as the Expanded Programme ofTechnical Assistance, the United Nations SpecialFund, the International Bank for Reconstruction andDevelopment, the African Development Bank, theInternational Development Association, bilateral aid,and foundations and other private sources. In thisconnexion, it must be borne in mind that funds fromcertain sources are available for certain types ofexpenses only and not for others (e.g., personnel -international and local; equipment and supplies;buildings; fellowships).
4.3.2.1 Two suggestions with regard to financing havebeen considered as to their relative merits andfeasibility :
4.3.2.1.1 Establishing a single fund. While a singlefund, subscribed to by assisting agencies and admin-istered by one authority, has its attractions, it is notfeasible because of the regulations governing suchfunds. This does not exclude, however, considerationof establishing a fund to be devoted exclusively tomedical education and training, including the establish-ment of medical schools, where unrestricted voluntarycontributions might accrue.
4.3.2.1.2 Multiple financing of a programme. Morerealistic appears to be the seeking of contributors whowould finance, and in some instances assist in carryingout, specific aspects of an agreed comprehensiveprogramme.
4.3.3 With regard to the financing of internationallyrecruited service staff for institutions used for training(see 3.2.2.7), attention is called to the provisionsregarding operational staff in the resolution of theFifteenth World Health Assembly on continuedassistance to newly independent States.2 Stress hasalready been laid (see 3.2.2.8) on the need for cautionwith regard to the payment of salaries and salarycomplements of local personnel involved in teaching,even in those cases where the regulations governingassistance from international funds permit it. Anotherproblem, which needs to be worked out in each parti-cular case, is that of providing for and distributingamong countries costs for local personnel employedin inter -country projects.
CONCLUDING NOTE
This report, in its structure, has followed the threesteps which need to be taken when a study has to bemade -either for a number of countries or for one ofthem -of the measures for providing effective assist-
1 See resolution WHA15.22, para. 7.2 Resolution WHA15.22, especially paras 4 and 6 (a).
ance for the training of health personnel to meet thepriority needs of the newly independent countries :first, a study of the extent and nature of the needs;second, how these needs can be met; third, whatproblems of policy and implementation arise, in-cluding problems of financing, not only for theestablishment of the training facilities themselves, butalso for their annual running costs thereafter. Alsoto be taken into account is the cost of the salaries ofthe personnel available for employment after theirtraining has been successfully completed.
The whole process implies establishing an order ofpriority and a reasonable plan of development, forimmediate and long -term action, taking into accountsocio- economic, educational and other circumstances,including the nature and pattern of prevalent healthproblems and the outstanding needs of the populationand its component groups.
The report does not purport to embrace everyaspect of the extensive and complex problems itattempts to consider. We have reason to believe,however, that it will serve as a guide to the consider-ation of many facets of the problems of medical andallied education and training, whose solution is neces-sary for the maintenance and development of healthservices in all countries of the world, no matter whatstage of development they may have reached.
Appendix 1
EDUCATION AND TRAINING OF HEALTHPERSONNEL IN AFRICA
(Extracts from a working paper contributed by WHO to theUNESCO /ECA Conference of African States on the
Development of Education in Africa,' Addis Ababa, May 1961)
TABLE I. MEDICAL AND PARAMEDICAL PERSONNELIN AFRICA IN 1960 (EXCLUDING UNITED ARAB
REPUBLIC (PROVINCE OF EGYPT) ANDUNION OF SOUTH AFRICA 2)
Total Ratio toCategory number of popul-
personnel ation *
Physicians 9 869 1 : 20 204Dentists 1 167 1 : 170 860Pharmacists 2 647 1 : 75 300Nursing personnel ** . . 47 399 1 : 4 200Medical auxiliaries . . . . 1 377 1 : 144 800
1 Document UNESCO /EDAF /S /6, of 10 April 1961 (with figurescorrected).
2 Now Republic of South Africa.* Population estimate, 1960: 199 400 000.
** Includes nurses, assistant nurses, midwives and assistant midwives.
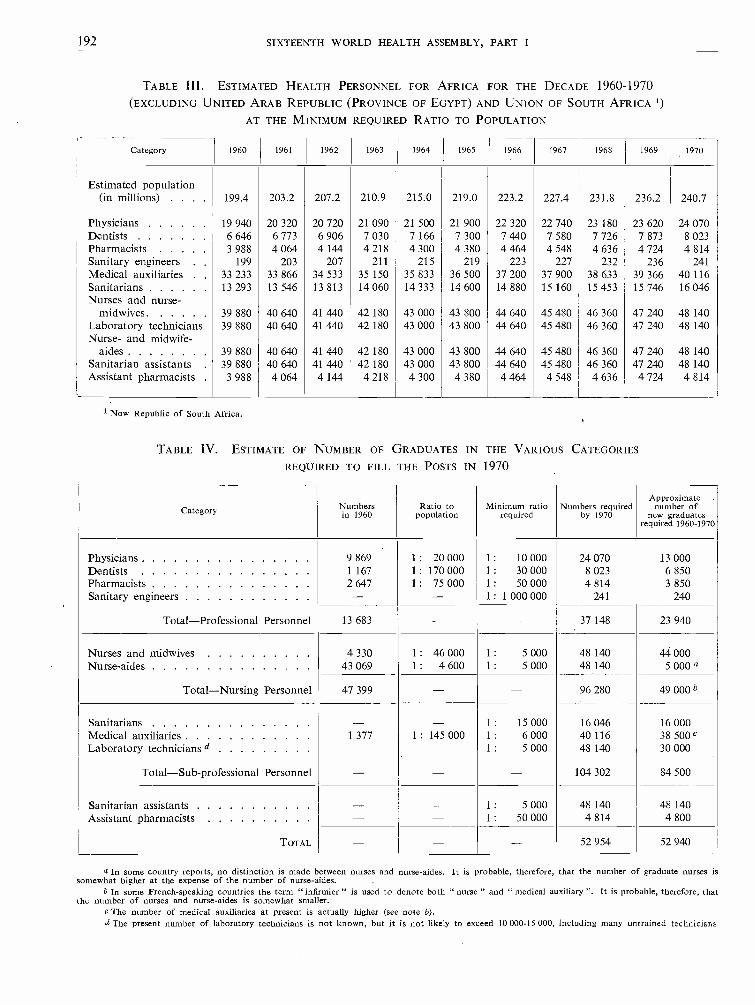
192 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
TABLE III. ESTIMATED HEALTH PERSONNEL FOR AFRICA FOR THE DECADE 1960 -1970
(EXCLUDING UNITED ARAB REPUBLIC PROVINCE OF EGYPT) AND UNION OF SOUTH AFRICA 1)
AT THE MINIMUM REQUIRED RATIO TO POPULATION
Category 1960 1961 1962 1963 1964 1965 1966 1967 1968 1969 1970
Estimated population(in millions) . . . . 199.4 203.2 207.2 210.9 215.0 219.0 223.2 227.4 231.8 236.2 240.7
Physicians 19 940 20 320 20 720 21 090 21 500 21 900 22 320 22 740 23 180 23 620 24 070Dentists 6 646 6 773 6 906 7 030 7 166 7 300 7 440 7 580 7 726 7 873 8 023Pharmacists 3 988 4 064 4 144 4 218 4 300 4 380 4 464 4 548 4 636 4 724 4 814Sanitary engineers . . 199 203 207 211 215 219 223 227 232 236 241Medical auxiliaries . 33 233 33 866 34 533 35 150 35 833 36 500 37 200 37 900 38 633 39 366 40 116Sanitarians 13 293 13 546 13 813 14 060 14 333 14 600 14 880 15 160 15 453 15 746 16 046Nurses and nurse -
midwives. 39 880 40 640 41 440 42 180 43 000 43 800 44 640 45 480 46 360 47 240 48 140Laboratory technicians 39 880 40 640 41 440 42 180 43 000 43 800 44 640 45 480 46 360 47 240 48 140Nurse- and midwife -
aides 39 880 40 640 41 440 42 180 43 000 43 800 44 640 45 480 46 360 47 240 48 140Sanitarian assistants . 39 880 40 640 41 440 42 180 43 000 43 800 44 640 45 480 46 360 47 240 48 140Assistant pharmacists . 3 988 4 064 4 144 4 218 4 300 4 380 4 464 4 548 4 636 4 724 4 814
1 Now Republic of South Africa.
TABLE IV. ESTIMATE OF NUMBER OF GRADUATES IN THE VARIOUS CATEGORIES
REQUIRED TO FILL THE POSTS IN 1970
Category Numbersin 1960
Ratio topopulation
Minimum ratiorequired
Numbers requiredby 1970
Approximatenumber of
new graduatesrequired 1960 -1970
Physicians 9 869 1 : 20 000 1 : 10 000 24 070 13 000Dentists 1 167 1 : 170 000 1 : 30 000 8 023 6 850Pharmacists 2 647 1 : 75 000 1 : 50 000 4 814 3 850Sanitary engineers - - 1 : 1 000 000 241 240
Total- Professional Personnel 13 683 - - 37 148 23 940
Nurses and midwives 4 330 1 : 46 000 1 : 5 000 48 140 44 000Nurse -aides 43 069 1 : 4 600 1 : 5 000 48 140 5 000 a
Total- Nursing Personnel 47 399 - - 96 280 49 000 b
Sanitarians - - 1 : 15 000 16 046 16 000Medical auxiliaries 1 377 1 : 145 000 1 : 6 000 40 116 38 500 C
Laboratory technicians d - - 1 : 5 000 48 140 30 000
Total- Sub -professional Personnel - - - 104 302 84 500
Sanitarian assistants - - 1 : 5 000 48 140 48 140Assistant pharmacists - - 1 : 50 000 4 814 4 800
TOTAL - - - 52 954 52 940
a In some country reports, no distinction is made between nurses and nurse -aides. It is probable, therefore, that the number of graduate nurses issomewhat higher at the expense of the number of nurse -aides.
b In some French -speaking countries the term "infirmier " is used to denote both " nurse " and " medical auxiliary ". It is probable, therefore, thatthe number of nurses and nurse -aides is somewhat smaller.
e The number of medical auxiliaries at present is actually higher (see note b).d The present number of laboratory technicians is not known, but it is not likely to exceed 10 000 -15 000, including many untrained technicians.

ANNEX 15 193
Appendix 2
SOME INFORMATION ON MEDICAL SCHOOLS IN THE AFRICAN CONTINENT 1
Year founded Teachingstaff in 1960E
Totalenrolmentin 1960
Admissionsin 1960 Graduates
Approximateannual
tuition fees
AlgeriaFaculté mixte de Médecine et de Pharmacie de 1857
l'Université d'Alger,ALGIERS
Congo
Faculté de Médecine de l'Université officielle 1956d'Elisabethville,
ELISABETHVILLE
Faculté de Médecine de l'Université Lovanium, 1954 6 80 5 * Fr. 2 000LEOPOLDVILLE
MadagascarEcole de Médecine et de Pharmacie, 1896 16 137 m 20 17 NoneTANANARIVE (6) 8 f
Ecole nationale de Médecine et de Pharmacie, 1961 5 Fr. CFA 3 825Université de Madagascar,TANANARIVE
NigeriaFaculty of Medicine, University College, 1948 50 213 60 19 £BWA 161 -261IBADAN
Medical School, University of Lagos, 1962 28 *LAGOS
Senegal
Faculté mixte de Médecine et de Pharmacie, 1950 44 160 60 Fr. CFA 2 400Université de Dakar,DAKAR
South AfricaFaculty of Medicine, 1956 20 257 106 Rand 112 -170University of Stellenbosch, (54)BELLVILLE, Cape Province
Faculty of Medicine, 1911 107 659m 188 81 Rand 232 -240University of Cape Town, (167) 114 fCAPE TOWN
Faculty of Medicine, 1951 38 190 m 41 16 Rand 121 -151University of Natal, (69) 23 fDURBAN
Medical School, 1919 87 502 m ** 138 ** 75 m Rand 242University of Witwatersrand, 96 f ** 9 fJOHANNESBURG
1 Unless otherwise indicated the information relates to 1960.2 Figures in brackets denote part -time teaching staff.
* 1962 data.** 1961 data.m Male.f Female.
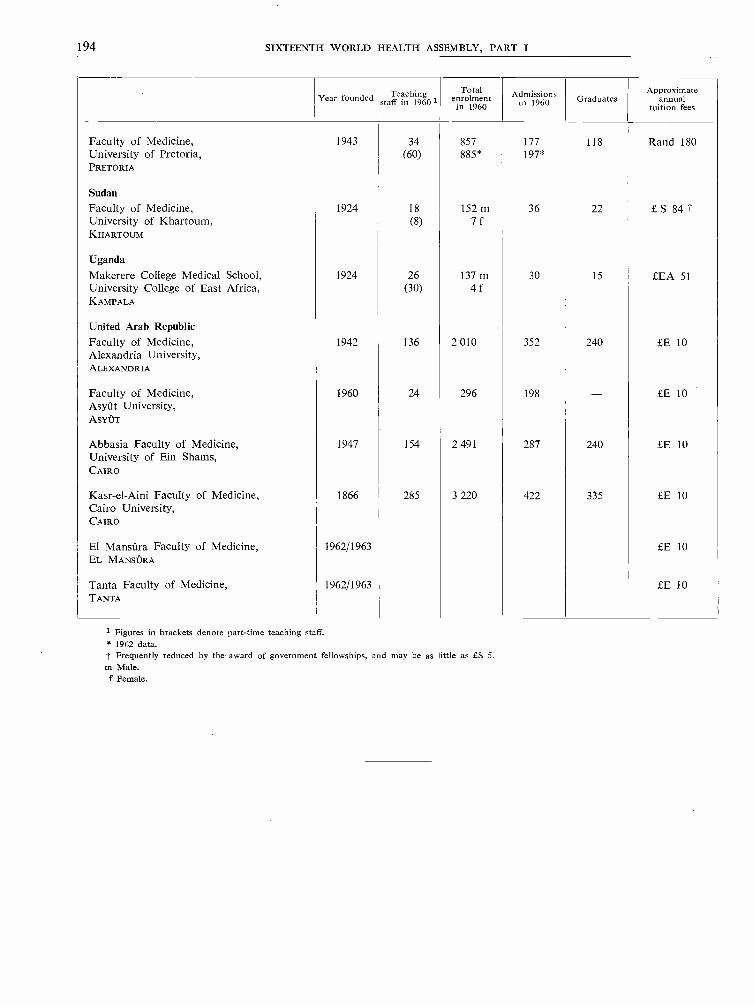
194 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Year founded Teachingstaff in 19601
Totalenrolment
in 1960Admissions
in 1960 GraduatesApproximate
annualtuition fees
Faculty of Medicine, 1943 34 857 177 118 Rand 180University of Pretoria, (60) 885* 197*PRETORIA
SudanFaculty of Medicine, 1924 18 152 m 36 22 £ S 84 tUniversity of Khartoum, (8) 7 fKHARTOUM
UgandaMakerere College Medical School, 1924 26 137 m 30 15 LEA 51University College of East Africa, (30) 4 fKAMPALA
United Arab RepublicFaculty of Medicine, 1942 136 2 010 352 240 LE 10Alexandria University,ALEXANDRIA
Faculty of Medicine, 1960 24 296 198 - LE 10Asyût University,ASYÛT
Abbasia Faculty of Medicine, 1947 154 2 491 287 240 LE 10University of Ein Shams,CAIRO
Kasr -el -Aini Faculty of Medicine, 1866 285 3 220 422 335 LE 10Cairo University,CAIRO
El Mansûra Faculty of Medicine, 1962/1963 LE 10EL MANSÛRA
Tanta Faculty of Medicine, 1962/1963 £E 10TANTA
1 Figures in brackets denote part -time teaching staff.* 1962 data.t Frequently reduced by the award of government fellowships, and may be as little as £S 5.m Male.f Female.

ANNEX 16 195
Annex 16
SMALLPDX ERADICATION PROGRAMME 1
[A16 /P &B/9 -18 April 1963]
REPORT BY THE DIRECTOR- GENERAL
CONTENTS
PART 1Page
Part IIPage
I. Introduction 195 A. Progress towards Smallpox Eradication 202
2. World Incidence of Smallpox 196
3. Study of Reported Incidence in relation to Endemicity 197 B. Progress in the Smallpox Eradication Programme4. Epidemiological and other Studies in Progress . . 199 in the WHO Regions with some Estimâtes of Financial5. Vaccine : Contributions to WHO 200 Needs 202
PART I
1. Introduction
This report has been prepared in two parts. In thefirst part an attempt is made to study the worldincidence of smallpox in relation to the endemic areas,as suggested by some members of the Executive Boardduring the discussion on the smallpox eradicationprogramme at the Board's thirty -first session. Thesecond part gives a summary of the present progressin the programme, as reported by Member States.
The number of reported cases of smallpox in 1962was 73 913, which is less than the number reported for1961 (78 325) and 1959 (77 555), but more than for1960 (59 221) (see Table I). The eradication pro-gramme, therefore, has not yet substantially reducedthe incidence of the disease and in the countries ofAfrica and Asia where it is endemic the rates havedeclined only slightly.
The persistence of endemic foci in Africa, Asia and,although on a smaller scale, in South America, con-tinues to be an important health problem to countriesin which smallpox is present, and a menace to theirneighbours and to all those countries throughout theworld that are now free from the disease.
In endemic areas, and particularly those that aredensely populated, epidemics are known to occur atregular intervals -usually in cycles of between five andseven years -owing to large accumulation of suscep-tibles. The epidemics of 1951 (489 922 cases) and of
1 See resolution WHA16.37.
1957 -1958 (154 446 and 245 978 cases respectively)are a warning of what may be expected in 1963 and1964 if eradication campaigns or vaccination controlmeasures are not intensified by immediate effort atboth national and international levels.
Effective eradication schemes are based on twofundamental elements, the ability of a public healthservice to organize -technically and administratively-a mass vaccination programme to cover at least80 per cent. of a country's population, and the avail-ability of a vaccine which is fully potent at the timeof inoculation. A few countries with relatively well-organized health services have been unable to eliminateendemic foci of smallpox after years of apparentlyintensive vaccination and revaccination, but whenall the factors involved in national control measuresare considered -vaccination coverage of the variousage -groups; potency of the vaccine used (particularlyof that used in remote rural areas); vaccinationtechnique; observation and recording of vaccinationresults -it has been found that one or more of thesemeasures has been incorrectly applied, and that thatcan account for the failure. In endemic areas notenough emphasis has ever been placed on the im-portance of evaluating vaccination campaigns and onthe efficient recording of vaccination and revaccinationresults.
A number of problems relating to the epidemiologyand virology of smallpox still require elucidation.The Organization (as will be seen later in this report)is closely associated with smallpox research efforts
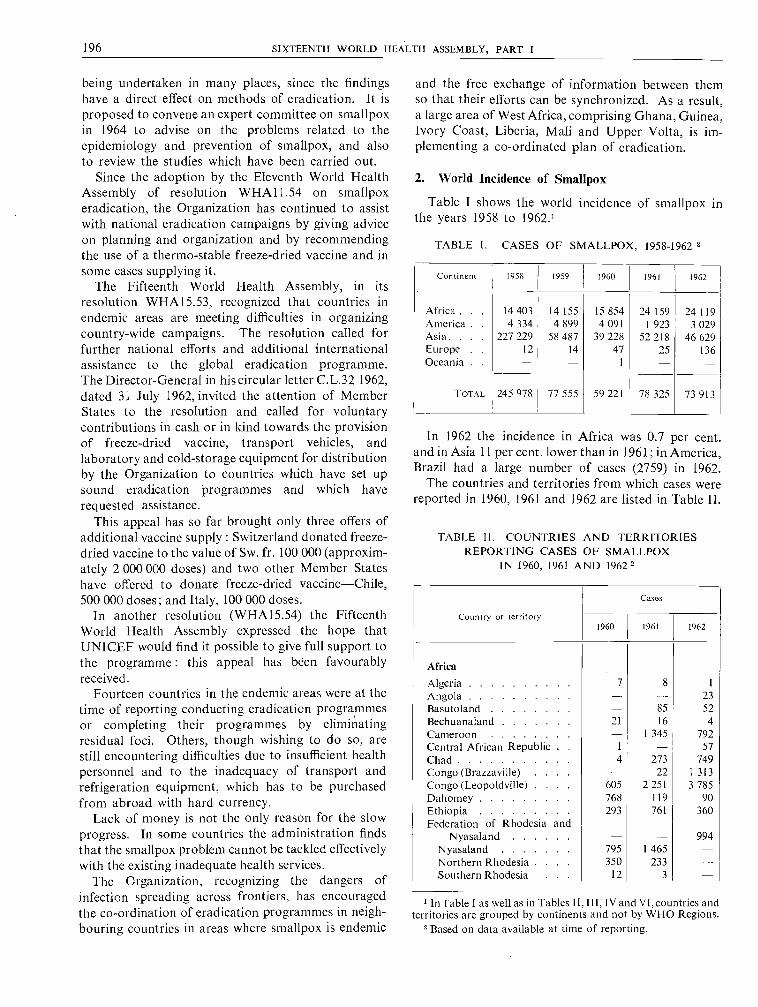
196 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
being undertaken in many places, since the findingshave a direct effect on methods of eradication. It isproposed to convene an expert committee on smallpoxin 1964 to advise on the problems related to theepidemiology and prevention of smallpox, and alsoto review the studies which have been carried out.
Since the adoption by the Eleventh World HealthAssembly of resolution WHA11.54 on smallpoxeradication, the Organization has continued to assistwith national eradication campaigns by giving adviceon planning and organization and by recommendingthe use of a thermo - stable freeze -dried vaccine and insome cases supplying it.
The Fifteenth World Health Assembly, in itsresolution WHA15.53, recognized that countries inendemic areas are meeting difficulties in organizingcountry -wide campaigns. The resolution called forfurther national efforts and additional internationalassistance to the global eradication programme.The Director -General in his circular letter C.L.32 1962,dated 31 July 1962, invited the attention of MemberStates to the resolution and called for voluntarycontributions in cash or in kind towards the provisionof freeze -dried vaccine, transport vehicles, andlaboratory and cold- storage equipment for distributionby the Organization to countries which have set upsound eradication programmes and which haverequested assistance.
This appeal has so far brought only three offers ofadditional vaccine supply : Switzerland donated freeze -dried vaccine to the value of Sw. fr. 100 000 (approxim-ately 2 000 000 doses) and two other Member Stateshave offered to donate freeze -dried vaccine -Chile,500 000 doses; and Italy, 100 000 doses.
In another resolution (WHA15.54) the FifteenthWorld Health Assembly expressed the hope thatUNICEF would find it possible to give full support tothe programme : this appeal has been favourablyreceived.
Fourteen countries in the endemic areas were at thetime of reporting conducting eradication programmesor completing their programmes by eliminatingresidual foci. Others, though wishing to do so, arestill encountering difficulties due to insufficient healthpersonnel and to the inadequacy of transport andrefrigeration equipment, which has to be purchasedfrom abroad with hard currency.
Lack of money is not the only reason for the slowprogress. In some countries the administration findsthat the smallpox problem cannot be tackled effectivelywith the existing inadequate health services.
The Organization, recognizing the dangers ofinfection spreading across frontiers, has encouragedthe co- ordination of eradication programmes in neigh-bouring countries in areas where smallpox is endemic
and the free exchange of information between themso that their efforts can be synchronized. As a result,a large area of West Africa, comprising Ghana, Guinea,Ivory Coast, Liberia, Mali and Upper Volta, is im-plementing a co- ordinated plan of eradication.
2. World Incidence of Smallpox
Table I shows the world incidence of smallpox inthe years 1958 to 1962.'
TABLE I. CASES OF SMALLPDX, 1958 -1962 8
Continent 1958 1959 1960 1961 1962
Africa . . . 14 403 14 155 15 854 24 159 24 119America . . 4 334 4 899 4 091 1 923 3 029Asia. . . . 227 229 58 487 39 228 52 218 46 629Europe . . I2 14 47 25 136Oceania . . - - I
TOTAL 245 978 77 555 59 221 78 325 73 913
In 1962 the incidence in Africa was 0.7 per cent.and in Asia 11 per cent. lower than in 1961; in America,Brazil had a large number of cases (2759) in 1962.
The countries and territories from which cases werereported in 1960, 1961 and 1962 are listed in Table II.
TABLE 11. COUNTRIES AND TERRITORIESREPORTING CASES OF SMALLPDX
IN 1960, 1961 AND 1962
Country or territory
Cases
1960 1961 1962
Africa
Algeria 7 8
Angola 23
Basutoland 85 52
Bechuanaland 21 16 4Cameroon 1 345 792Central African Republic . 1 57
Chad 4 273 749Congo (Brazzaville) 22 1 313Congo (Leopoldville) 605 2 251 3 785Dahomey 768 119 90Ethiopia 293 761 360Federation of Rhodesia and
Nyasaland 994Nyasaland 795 1 465Northern Rhodesia . 350 233Southern Rhodesia 12 3
i ln Table I as well as in Tables II, III, IV and VI, countries andterritories are grouped by continents and not by WHO Regions.
2 Based on data available at time of reporting.
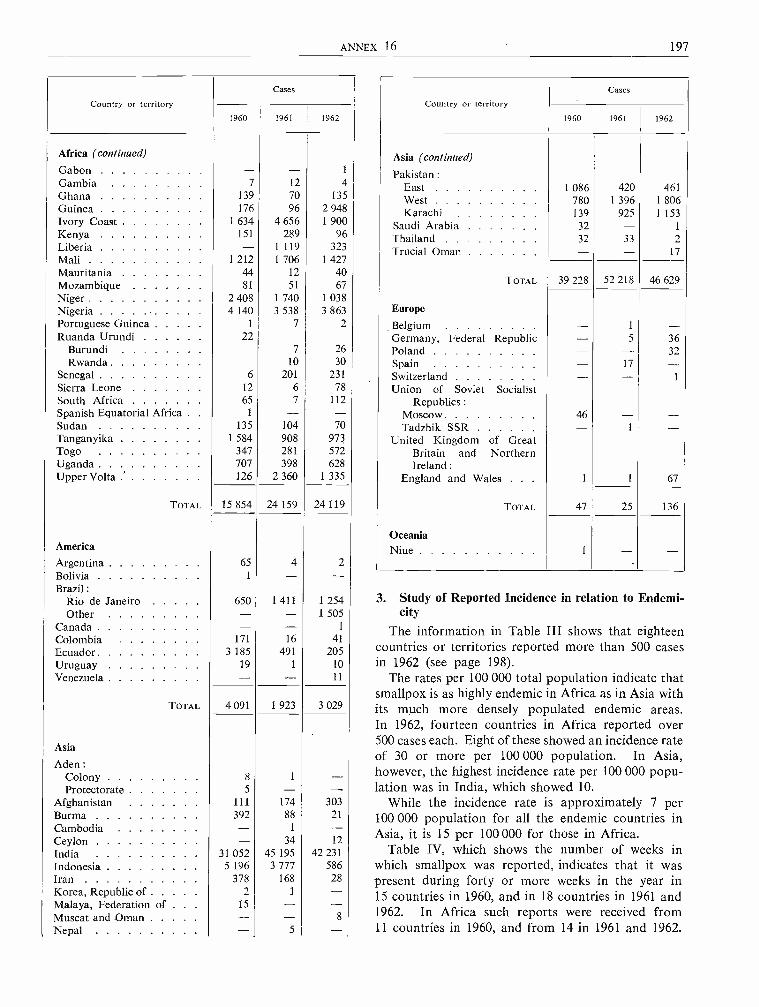
ANNEX 16 197
Country or territoryCases
1960 1961 1962
Africa (continued)
Gabon - - 1
Gambia 7 12 4Ghana 139 70 135Guinea 176 96 2 948Ivory Coast 1 634 4 656 1 900Kenya 151 289 96Liberia - 1119 323Mali 1 212 1 706 1 427Mauritania 44 12 40Mozambique 81 51 67Niger 2 408 1 740 1 038Nigeria 4 140 3 538 3 863Portuguese Guinea 1 7 2Ruanda Urundi 22
Burundi 7 26Rwanda 10 30
Senegal 6 201 231Sierra Leone 12 6 78South Africa 65 7 112Spanish Equatorial Africa . . 1 - -Sudan 135 104 70Tanganyika 1 584 908 973Togo 347 281 572Uganda 707 398 628Upper Volta ' 126 2 360 1 335
TOTAL 15 854 24 159 24 119
America
Argentina 65 4 2Bolivia 1 - -Brazil :
Rio de Janeiro 650 1 411 1 254Other - - 1 505
Canada - - 1
Colombia 171 16 41
Ecuador 3 185 491 205Uruguay 19 1 10
Venezuela - - 11
TOTAL 4 091 1 923 3 029
Asia
Aden :Colony 8 1 -Protectorate 5 - -
Afghanistan 111 174 303Burma 392 88 21
Cambodia - 1 -Ceylon - 34 12
India 31 052 45 195 42 231Indonesia 5 196 3 777 586Iran 378 168 28Korea, Republic of 2 1 -Malaya, Federation of . . . 15 - -Muscat and Oman - - 8
Nepal - 5 -
Country or territoryCases
1960 1961 1962
Asia (continued)
Pakistan :East 1 086 420 461West 780 1 396 1 806Karachi 139 925 1153
Saudi Arabia 32 - 1
Thailand 32 33 2Trucial Oman - - 17
TOTAL 39 228 52 218 46 629
Europe
Belgium - 1 -Germany, Federal Republic - 5 36Poland - - 32Spain - 17 -Switzerland - -Union of Soviet Socialist
Republics :Moscow 46 - -Tadzhik SSR - 1 -
United Kingdom of GreatBritain and NorthernIreland :
England and Wales . . 1 1 67
TOTAL 47 25 136
OceaniaNiue 1 - -
3. Study of Reported Incidence in relation to Endemi-city
The information in Table III shows that eighteencountries or territories reported more than 500 casesin 1962 (see page 198).
The rates per 100 000 total population indicate thatsmallpox is as highly endemic in Africa as in Asia withits much more densely populated endemic areas.In 1962, fourteen countries in Africa reported over500 cases each. Eight of these showed an incidence rateof 30 or more per 100 000 population. In Asia,however, the highest incidence rate per 100 000 popu-lation was in India, which showed 10.
While the incidence rate is approximately 7 per100 000 population for all the endemic countries inAsia, it is 15 per 100 000 for those in Africa.
Table IV, which shows the number of weeks inwhich smallpox was reported, indicates that it waspresent during forty or more weeks in the year in15 countries in 1960, and in 18 countries in 1961 and1962. In Africa such reports were received from11 countries in 1960, and from 14 in 1961 and 1962.

198 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
There seems, therefore, to be a clear indication of thepersistence of infection in the endemic areas, fromwhich the weekly reports of smallpox incidencehave been constant in 1961 and 1962.
It is of interest that while in some countries smallpoxcases are reported during a few weeks of the year only,in most countries cases occur almost all the yearround.
Though the degree of endemicity of smallpox in agiven country cannot be measured by the frequencyof the weekly reports of smallpox incidence, theinformation in Table IV clearly indicates -allowingfor unreliable and irregular reporting systems in somecountries -the areas of highest endemicity and theconstant exposure that neighbouring countries sufferfrom their contiguity to infected areas.
TABLE III. COUNTRIES AND TERRITORIESREPORTING OVER 500 CASES OF SMALLPDX IN 1962
Country or territoryApproximate
rate per100 000
population
Africa
Cameroon 20Chad 35
144Congo (Leopoldville) 29Federation of Rhodesia and Nyasaland . . 12Guinea 100Ivory Coast 58Mali 38Niger 34Nigeria 11
Tanganyika 10Togo 38Uganda 10Upper Volta 30
America
Brazil 4
Asia
India 10Indonesia 1
Pakistan 4
TABLE IV. NUMBER OF WEEKS IN WHICH CASESOF SMALLPDX WERE REPORTED, 1960, 1961 AND 1962
Country or territoryWeeks
1960 1961 1962
AfricaAlgeria 6 7 1
Basutoland 19 15Bechuanaland 7 9 2
Country or territoryWeeks
1960 1961 1962
Africa (continued)
Cameroon - 48 45Central African Republic . . . . 1 - 7Chad 4 26 44Congo (Brazzaville) - 7 39Congo (Leopoldville) 47 48 26Dahomey 39 26 33Ethiopia 51 45 47Federation of Rhodesia and Nyasa-
land :Nyasaland 52 52 52Northern Rhodesia 24 34 38Southern Rhodesia 8 2 10
Gambia 2 8 4Ghana 27 28 27Guinea 10 18 36Ivory Coast 51 52 51Kenya 41 47 48Liberia - 52 48Mali 41 50 45Mauritania 26 7 9Mozambique 8 18 25Niger 51 50 47Nigeria :
Eastern Region 20 9 32Northern Region 52 51 52Western Region 40 30 42
Portuguese Guinea 2 4 8Ruanda Urundi:
Burundi 8 4 7Rwanda 6 4 12
Senegal 4 28 13Sierra Leone 7 4 22Somalia (Northern Region) . . . 1 - -South Africa 12 4 11Spanish Guinea 1 - -Sudan 23 17 14Tanganyika 52 52 51Togo 42 44 51Uganda 51 50 49Upper Volta 24 47 50
Asia
Aden Protectorate 3 - -Afghanistan 44 51 52Burma 30 18 7Cambodia - 1 -Ceylon - 12 4India 52 52 52Indonesia 52 52 52Iran 26 9 8
Korea, Republic of 2 1 -Malaya, Federation of 4 - -Nepal - 2 -Pakistan :
East Pakistan 52 41 49West Pakistan 52 48 52
Saudi Arabia 14 5 1
Thailand 1 3 3

ANNEX 16 199
4. Epidemiological and other Studies in Progress
Epidemiological Investigations
An understanding of the epidemiology of smallpoxis the basis for the sound planning of eradicationcampaigns. It might be thought that all the necessaryinformation would be available in the literature whichextends over a century, but unfortunately on many ofthe points of particular importance to eradicationcampaigns information is either entirely absent orincomplete. It is necessary to know more of thebehaviour of the disease in densely populated areasas compared with that in the sparsely populated areas;in different age -groups; in persons in whom immunityhas partly waned because of long intervals betweenrevaccination or because of the use of vaccines which,though adequate for primary vaccination, are notsufficiently potent for revaccination. It is also necessaryto know if partially immune persons constitute areservoir of infection in the over -crowded parts of thelarger cities. If they do, would elimination of thereservoir by adequate vaccination result in a sub-stantial decrease in the general incidence of the disease?
Since definite answers to such questions are notavailable, inquiries are being made to find suitableareas for pilot studies and investigators to carry themout. If such studies fulfil their promise they will beextended.
Studies are also being made on methods of measuringthe level of protection of populations against smallpox.Vaccination and revaccination with a standard vaccineof high potency are being carried out on randomsamples of population to determine the percentage ofsusceptibles, by age and by the interval since thelast vaccination. This will give information on theoptimum intervals for the revaccination of persons ofdifferent ages.
Laboratory studies are being developed on thelevels of antibodies, in the blood of vaccinated persons,that afford protection against challenge with highlypotent vaccines. It is assumed that resistance tochallenge by vaccination runs parallel to resistanceto natural infection, and knowledge of the serumprotection level would permit serological surveys tobe carried out to determine the susceptibility ofpopulations to smallpox.
A Better Vaccine
One of the great difficulties in vaccination campaigns,especially those in tropical areas, has always beenthe rapid deterioration of glycerinated lymph vaccine.Attempts to surmount the difficulty have largelyresolved themselves into the production of driedvaccines, but laboratory experiments and fieldexperience have shown that desiccation alone does not
make smallpox vaccine stable and heat -resistant.Several campaigns carried out with dried vaccineshave failed because the vaccine deteriorated underfield conditions. Because of this, WHO organizedstudies of methods to ensure the regular production ofa suitable heat -resistant dried vaccine. Laboratorytests of vaccines produced by different methods indifferent laboratories were carried out in a comparativestudy in which laboratories from several countriesparticipated. These tests showed that vaccine produc-tion based on desiccation from the frozen state(lyophilization) gave 100 per cent. successful primaryvaccination rates after periods of storage of up to64 weeks at 37° C and 45° C, while other vaccines wereless satisfactory. Information about this method ofproduction and about subsequent technical improve-ments have been distributed to competent productionlaboratories and assistance has been given to some ofthem to produce the vaccine.
The importance of producing stable and highlypotent vaccines cannot be over -emphasized. It hasbeen established that a certain concentration of virusis necessary in order to obtain a high percentage of" takes ". Based on studies carried out under thesponsorship of WHO on persons previously vac-cinated,' the Study Group on Requirements forSmallpox Vaccine 2 established potency tests to ensureeffectivenéss in the field. More recent studies 3 haveshown that only vaccines of the highest potency willgive satisfactory revaccination " take " rates. With astandard vaccine the percentage of " takes " increaseswith the lapse of time from the previous vaccination.For example, after two years we may expect a revac-cination " take " rate of 33 per cent. After five yearsthe " take " rate will increase to about 70 per cent.
These findings are of obvious importance in relationto eradication campaigns. A vaccine producing ahigh percentage of " takes " in primary vaccinationsbut failing partially or completely in revaccinationsnot only dooms a campaign to failure, but also givesa dangerous false sense of security. Unfortunatelypractical examples of occurrences of this kind come tothe attention of the Organization not infrequently.
Methods of Administration of the VaccineThe successful utilization of jet injectors for the
rapid vaccination of large numbers of persons hasbeen reported.4 Comparative trials on the percentage
1 Cockburn, W. C. et aI. (1957) Bull. Wld Hlth Org. 16, 63.2 W/d Hlth Org. techn. Rep. Ser. 1959, 180, 19.3 Hobday, T. L. et al. (1961) Bull. Wld Hlth Org. 25, 69;
Mastyukova, Y. N. et al. (1961) Prob. Virol. 6, 207; Espmark,Espmark & Rabo cited by Dostal, V. (1962) Prog. med. Virol. 4,259.
4 Elisberg, B. L. et al. (1956) J. Immunol. 77, 340; Barclay,E. N. et al. (1962) Bull. Acad. Med. Cleveland.
200 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
of " takes " obtained by using jet injectors and byinoculation by the multiple -pressure method are inprogress in Liberia. In preliminary trials it has beenobserved that some persons inoculated with jetinjectors respond with induration without vesiculation,and the immunological significance of this response isalso being studied.
Passive Protection
The vaccination of contacts is not always successfulas a protective measure against smallpox. The chanceof failure increases as the interval between exposureand vaccination lengthens. Studies have been carriedout, with the support of WHO, on the use of vaccinalhyperimmune gamma -globulin in the prophylaxis ofsmallpox in contacts.' These studies showed theefficacy of gamma -globulin as a preventive agent.Because of the limited supply of this substance, itsprophylactic use has to be restricted to those at highestrisk. If an animal gamma -globulin could be used forthis purpose, larger quantities could be made available.It has been reported that gamma -globulin fromhyperimmune animals gives highly effective resultsin the prevention of experimental vaccinal infection.'WHO is supporting studies on the production andtesting of animal hyperimmune gamma- globulin witha view to its possible use in prevention and treatment.
Studies on the Infectiousness of Smallpox in the EarlyStages of the Disease and on the Dissemination of theVirus by Air
Epidemiological observations suggest that smallpoxis not highly infectious in the pre- eruptive period ofillness. The clarification of this point is of greatpractical importance for determining the periodduring which a patient might be infectious and forpurposes of isolation of contacts. Studies on thisproblem were carried out in Madras with the supportof WHO.3 No virus could be recovered from mouth -washings and garglings from patients in the first twodays of the disease. It was, however, frequently foundin specimens collected from the sixth and the ninthday of illness. This is further proof that most smallpoxpatients are not infective in the first days of fever,before the rash appears.
The question of the aerial spread of smallpox hasaroused great controversy for many years. It wastherefore thought of interest to obtain information onthe amount of virus disseminated in the air of a small-pox ward and in the immediate surroundings of small-
' Kempe, C. H. et al. (1961) Bull. Wld Hlth Org. 25, 41.2 Marennikova, S. S. (1962) Bull. Wld Hlth Org. 27, 325.3 Downie, A. W. et al. (1961) Bull. Wld Hlth Org. 25, 49.
pox patients at various stages of the disease.' Contraryto what was suspected, viruses were very difficult torecover, even when large volumes of air were collectedin the proximity of acutely ill patients. In order toexplore this matter further, new studies are beingcarried out, using more sensitive air -sampling methods.
Prevention of Complications
Smallpox vaccination is still unfortunately marredby the rare but serious complications of post -vaccinalencephalitis. Cases of post -vaccinal encephalitis areregularly reported from some countries, but never fromothers. The reasons for this are not clear. No modifica-tion introduced in the manufacture or administrationof the vaccine has yet been shown to be effective inpreventing the occurrence of post -vaccinal encephalitis.Recently the successful prophylactic effect of anti -vaccinal gamma -globulin administered at the same timeas the vaccination was reported.' Efforts, so far withoutgreat success, are also being made to develop inacti-vated vaccines. If an effective inactivated vaccine wereavailable its use might permit later vaccination witha live vaccine, and thus provide a satisfactory im-munity without the risk of post -vaccinal complications.In addition, it might be possible to combine such avaccine with other antigens, diminishing in this waythe number of inoculations, already quite large, thateach child has to receive during the first period of hislife.
5. Vaccine : Contributions to WHO
As reported to the Fifteenth World HealthAssembly,' the Organization continues to supplyMember States, on request, with freeze -dried vaccinefor use in their eradication programmes. The vaccineis drawn from the amounts donated by a numberof Member States.
One obstacle has been largely surmounted in thesmallpox eradication programme, namely the develop-ment of a potent and thermostable vaccine to meet therequirements of national mass vaccination campaigns.The main problem now is to ensure that vaccinesused in mass campaigns are of adequate potency atthe time when they are administered in the field, parti-cularly in remote rural areas, where storage andtransport facilities are deficient.
Before accepting any donated vaccine, the Organi-zation-as previously reported to the Fifteenth WorldHealth Assembly' - carries out tests on a sample of the
' Meiklejohn, G. et al. (1961) Bull. Wld Hlth Org. 25, 63.5 Nanning, W. (1962) Bull. Wld Hlth Org. 27, 317.6 Mimeographed document A15 /P &B /18 and A15 /P &B /18
(Corrs 1 & 2) May 1962.
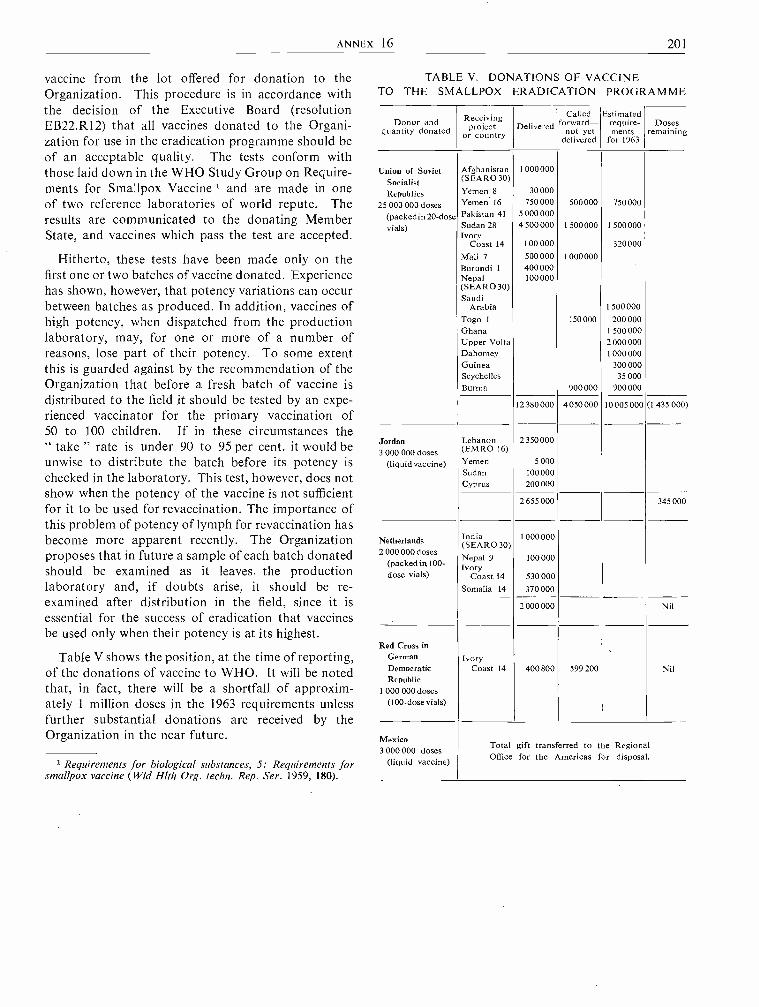
ANNEX 16 201
vaccine from the lot offered for donation to theOrganization. This procedure is in accordance withthe decision of the Executive Board (resolutionEB22.R12) that all vaccines donated to the Organi-zation for use in the eradication programme should beof an acceptable quality. The tests conform withthose laid down in the WHO Study Group on Require-ments for Smallpox Vaccine 1 and are made in oneof two reference laboratories of world repute. Theresults are communicated to the donating MemberState, and vaccines which pass the test are accepted.
Hitherto, these tests have been made only on thefirst one or two batches of vaccine donated. Experiencehas shown, however, that potency variations can occurbetween batches as produced. In addition, vaccines ofhigh potency, when dispatched from the productionlaboratory, may, for one or more of a number ofreasons, lose part of their potency. To some extentthis is guarded against by the recommendation of theOrganization that before a fresh batch of vaccine isdistributed to the field it should be tested by an expe-rienced vaccinator for the primary vaccination of50 to 100 children. If in these circumstances the" take " rate is under 90 to 95 per cent. it would beunwise to distribute the batch before its potency ischecked in the laboratory. This test, however, does notshow when the potency of the vaccine is not sufficientfor it to be used for revaccination. The importance ofthis problem of potency of lymph for revaccination hasbecome more apparent recently. The Organizationproposes that in future a sample of each batch donatedshould be examined as it leaves the productionlaboratory and, if doubts arise, it should be re-examined after distribution in the field, since it isessential for the success of eradication that vaccinesbe used only when their potency is at its highest.
Table V shows the position, at the time of reporting,of the donations of vaccine to WHO. It will be notedthat, in fact, there will be a shortfall of approxim-ately 1 million doses in the 1963 requirements unlessfurther substantial donations are received by theOrganization in the near future.
1 Requirements for biological substances, 5: Requirements forsmallpox vaccine (Wld Hlth Org. techn. Rep. Ser. 1959, 180).
TABLE V. DONATIONS OF VACCINETO THE SMALLPDX ERADICATION PROGRAMME
Donor andquantity donated
Receivingproject
or countryDelivered
Calledforward-
not yetdelivered
Estimatedrequire-ments
for 1963
Dosesremaining
Union of Soviet Afghanistan 1 000 000
Socialist (SEARO30)
Republics Yemen 8 30000
15 000 000 doses Yemen 16 750 000 500000 750 000
(packed in 20 -dose Pakistan 41 5 000 000
vials) Sudan 28 4 500000 I 500000 1 500000Ivory
Coast 14 100000 320000Mali 7 500000 1 000 000
Burundi 1 400000Nepal 100000(SEA RO 30)Saudi
Arabia 1 500 000
Togo 1 .150000 200000Ghana 1 500 000Upper Volta 2 000 000Dahomey 1 000 000Guinea 300000Seychelles 35 000Burma 900000 900000
12 380 000 4 050 000 10 005 000 (1 435 000)
Jordan Lebanon 2 350 000
3 000 000 doses (EMRO 16)
(liquid vaccine) Yemen 5 000Sudan 100000Cyprus 200000
2 655 000 345 000
Netherlands India(SEARO 30)
1 000 000
2 000 000 dosesNepal 9 100 000
(packed in 100- Ivorydose vials) Coast 14 530000
Somalia 14 370 000
2 000 000 Nil
Red Cross inGerman IvoryDemocratic Coast 14 400800 599200 NilRepublic
1 000 000 doses(100 -dose vials)
Mexico3 000 000 doses
Total gift transferred to the Regional
(liquid vaccine) Office for the Americas for disposal.
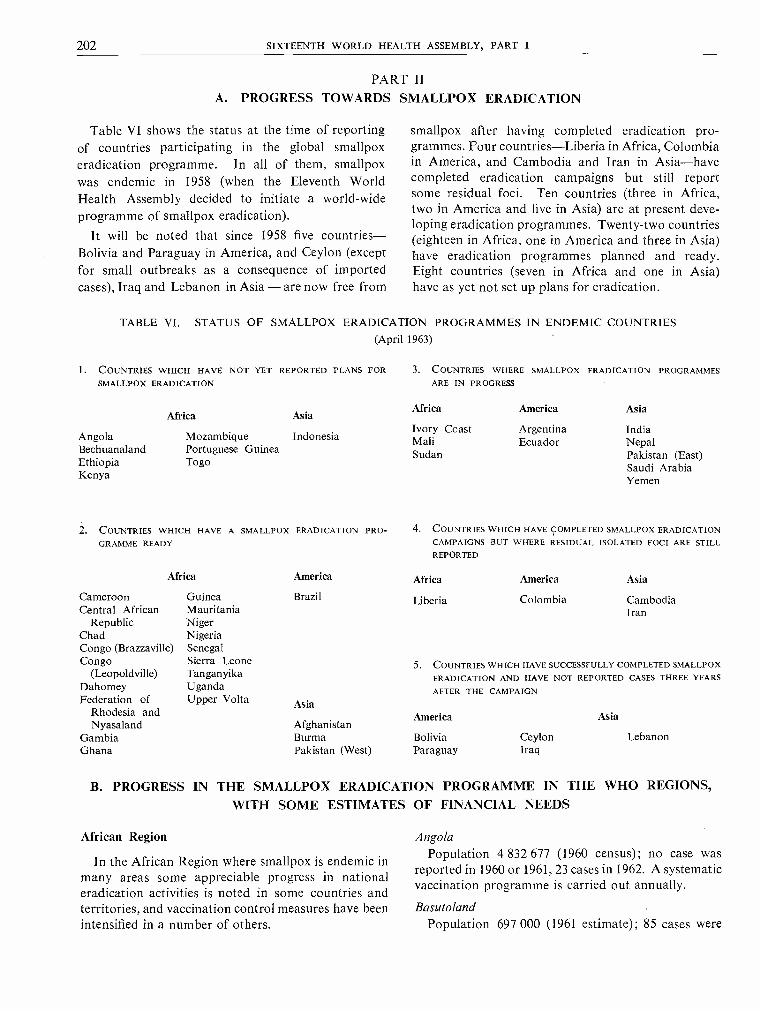
202 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
PART IIA. PROGRESS TOWARDS SMALLPDX ERADICATION
Table VI shows the status at the time of reportingof countries participating in the global smallpoxeradication programme. In all of them, smallpoxwas endemic in 1958 (when the Eleventh WorldHealth Assembly decided to initiate a world -wideprogramme of smallpox eradication).
It will be noted that since 1958 five countries -Bolivia and Paraguay in America, and Ceylon (exceptfor small outbreaks as a consequence of importedcases), Iraq and Lebanon in Asia - are now free from
smallpox after having completed eradication pro-grammes. Four countries -Liberia in Africa, Colombiain America, and Cambodia and Iran in Asia -havecompleted eradication campaigns but still reportsome residual foci. Ten countries (three in Africa,two in America and five in Asia) are at present deve-loping eradication programmes. Twenty -two countries(eighteen in Africa, one in America and three in Asia)have eradication programmes planned and ready.Eight countries (seven in Africa and one in Asia)have as yet not set up plans for eradication.
TABLE VI. STATUS OF SMALLPDX ERADICATION PROGRAMMES IN ENDEMIC COUNTRIES(April 1963)
1. COUNTRIES WHICH HAVE NOT YET REPORTED PLANS FORSMALLPDX ERADICATION
AngolaBechuanalandEthiopiaKenya
Africa Asia
MozambiquePortuguese GuineaTogo
Indonesia
3. COUNTRIES WHERE SMALLPDX ERADICATION PROGRAMMESARE IN PROGRESS
Africa America Asia
Ivory Coast ArgentinaMali EcuadorSudan
IndiaNepalPakistan (East)Saudi ArabiaYemen
2. COUNTRIES WHICH HAVE A SMALLPDX ERADICATION PRO-GRAMME READY
Africa America
Cameroon Guinea BrazilCentral African Mauritania
Republic NigerChad NigeriaCongo (Brazzaville) SenegalCongo Sierra Leone
(Leopoldville) TanganyikaDahomey UgandaFederation of Upper Volta Asia
Rhodesia andNyasaland Afghanistan
Gambia BurmaGhana Pakistan (West)
4. COUNTRIES WHICH HAVE COMPLETED SMALLPDX ERADICATION
CAMPAIGNS BUT WHERE RESIDUAL ISOLATED FOCI ARE STILLREPORTED
Africa America Asia
Liberia Colombia CambodiaIran
5. COUNTRIES WHICH HAVE SUCCESSFULLY COMPLETED SMALLPDX
ERADICATION AND HAVE NOT REPORTED CASES THREE YEARS
AFTER THE CAMPAIGN
America Asia
Bolivia Ceylon LebanonParaguay Iraq
B. PROGRESS IN THE SMALLPDX ERADICATION PROGRAMME IN THE WHO REGIONS,WITH SOME ESTIMATES OF FINANCIAL NEEDS
African Region
In the African Region where smallpox is endemic inmany areas some appreciable progress in nationaleradication activities is noted in some countries andterritories, and vaccination control measures have beenintensified in a number of others.
AngolaPopulation 4 832 677 (1960 census); no case was
reported in 1960 or 1961, 23 cases in 1962. A systematicvaccination programme is carried out annually.
BasutolandPopulation 697 000 (1961 estimate); 85 cases were
ANNEX 16 203
reported in 1961, 52 cases in 1962. Over 80 per cent.of the population is stated to have been successfullyvaccinated during the year and efforts are being madeto improve the standard of vaccination.
Burundi and RwandaPopulation 4 929 000 (Burundi 2 234 000, Rwanda
2 695 000 -1960 estimate); 22 cases were reported in1960, 7 in Burundi and 10 in Rwanda in 1961, and26 in Burundi and 30 in Rwanda in 1962. In 1961 andthe beginning of 1962 a mass vaccination campaignwas carried out in Rwanda.
CameroonPopulation 4 097 000 (1960 estimate); 1345 cases
were reported in 1961 (epidemic in North Cameroon),792 cases in 1962. A vaccination campaign has beenplanned to cover about 1.5 million inhabitants eachyear over three consecutive years. The total expend-iture necessary for the implementation of a smallpoxeradication campaign is estimated at US $163 000.If this were combined with other health activitiesin the field, the cost would be about US $57 000.
Central African RepublicPopulation 1 227 000 (1961 estimate); one case was
reported in 1960, none in 1961 and 57 cases in 1962.Smallpox vaccination is being carried out by the" Service de Lutte contre les Grandes Endémies "and will cover the total population in three years.The Government has requested assistance in obtaining1 200 000 doses of vaccine, supplies and equipment,the total cost of which would be approximatelyUS $10 000.
ChadPopulation 2 680 000 (1961 estimate); 4 cases were
reported in 1960, 273 in 1961 and 749 in 1962. TheGovernment's cost estimate for an eradication pro-gramme is US $163 265. In addition, one medicalofficer, 30 dressers and 60 auxiliaries, 15 vehicles,equipment and supplies, and three million doses ofdried vaccine are needed.
Congo (Brazzaville)Population 900 000 (1960 estimate); 22 cases were
reported in 1961, and 1313 in 1962. Smallpox vaccin-ation campaigns are carried out regularly each yearby the " Service des Grandes Endémies ". In Brazza-ville and Pointe- Noire, the Pasteur Institute and thegeneral health service help in the development of theannual vaccination programme. In 1962 the epidemicwhich broke out in Brazzaville was brought undercontrol as the Government had vaccine available. For1963, the Government requested assistance in the
provision of 150 000 doses of vaccine it would needfor its campaign.
Congo (Leopoldville)
Population 14 450 000 (1961 estimate); 605 caseswere reported in 1960, 2251 in 1961, and 3785 in 1962.An epidemic occurred in the early months of 1962 inLeopoldville and was brought under control througha mass vaccination campaign. Sporadic cases of small-pox and local outbreaks of varying severity are fre-quently reported from provincial areas. A WHOmedical officer from headquarters was sent to Leopold-ville in February 1962 to advise on the mass vaccinationcampaign which was implemented in the city and, inNovember 1962, he paid a second visit to advise onfuture activities in the control of smallpox and itsultimate eradication from the entire territory. A planfor a pilot eradication scheme in one province wasprepared and presented to the Government. TheOrganization will provide the vaccine needed for masseradication campaigns. Transport, equipment andsupplies will also be needed for the pilot scheme and themass vaccination campaign which follows.
Dahomey
Population 2 050 000 (1961 estimate); 768 cases werereported in 1960, 119 in 1961, and 90 in 1962. Noformal smallpox eradication programme has as yetbeen planned. At the twelfth session of the RegionalCommittee in 1962, the delegate of Dahomey expressedthe Government's desire to participate in the regionaleradication effort and accordingly an eradicationcampaign will soon be planned with WHO's assistance.Assistance needed would mainly consist of suppliesof vaccines -two million doses -and equipmentand other supplies.
Federation of Rhodesia and Nyasaland
Population 8 630 000 (1961 estimate); 1157 caseswere reported in 1960, 1701 in 1961, and 994 in 1962.The Government considers that, at present, it cancope with its programme, including the purchase ofvaccine lymph. The Government would welcome avisit from a WHO consultant to observe work donein the field of smallpox eradication in countries insouth -central Africa.
Gambia
Population 284 000 (1960 estimate); 7 cases werereported in 1960, 12 in 1961, and four in 1962. It isplanned that a smallpox eradication programme inGambia would last for three years. The principalneeds in this connexion would be a suitable vehicleand a supply of vaccine. The annual cost, estimated by
204 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
the Government, would be US $4200, and the totalcost of a three -year programme US $12 600.
Ghana
Population 6 943 000 (1961 estimate); 139 caseswere reported in 1960, 70 in 1961, and 135 in 1962.In view of the fact that the incidence of smallpoxin Ghana is low compared with that in some ofthe neighbouring countries, the Government hasdecided to intensify its existing smallpox controlmeasures rather than initiate a country -wide massvaccination campaign. This new programme willbe supported by legislative and administrative meas-ures to enforce vaccination and to give the vaccinatorsthe necessary authority for the effective vaccination ofthe population, since co- operation from the publicmay not always be forthcoming. The population ofthe rural areas will be vaccinated by the medicalfield units, whose sphere of activity has been enlargedin recent years. They will also be responsible forvaccination at frontier posts on the main highwaysnear the borders. Hospitals, maternal and childhealth clinics, health centres and dispensaries will alltake part in the intensified vaccination programmewhich, it is hoped, will cover infants, their mothersand the general public. The school population willbe vaccinated by school- teachers (600) who havealready been trained in vaccination techniques.These volunteers, it is hoped, will maintain an adequategroup immunity among school -age children.
Other groups, such as the army, police, factory andother specialized groups of workers, universitystudents, and the large number of people usuallyencountered at lorry parks, markets, etc., will bevaccinated through this strengthened vaccinationprogramme.
The estimated cost to the Government duringthe period of this intensified smallpox campaign willbe approximately US $548 800 per year. Ghana hasrequested assistance in the supply of six million dosesof freeze -dried vaccine for the four -year period of theintensified programme, and transport and refrigeratorswould also be needed.
Guinea
Population 3 000 000 (1960 estimate); 176 caseswere reported in 1960, 96 cases in 1961, and 2948 in1962. Wishing to participate in the regional smallpoxeradication effort, the Government is preparing avaccination programme to cover the whole populationof the country. A WHO medical officer from head-quarters recently visited Guinea and advised on theplanning of an eradication campaign. The Govern-ment would need assistance in obtaining the necessaryquantities of freeze -dried vaccine for the campaignand also transport vehicles for remote rural areas.
The Government has requested WHO's andUNICEF's assistance to develop a freeze -dried vaccineproduction centre at the Pasteur Institute at Kindia.Once this centre is established it could produce about20 million doses of freeze -dried vaccine to meet theneeds of neighbouring countries, in addition to thosefor smallpox control measures in Guinea.
Ivory CoastPopulation 3 300 000 (1961 estimate); 1634 cases
were reported in 1960, 4656 in 1961, and 1900 in 1962.A national smallpox eradication campaign was startedin July 1961 and is still in progress. Up to 31 December1962, a total of 3 109 943 vaccinations had been per-formed. The campaign, which started along thenorthern, eastern and western boundaries of thecountry, is now moving towards the southern areas.It is scheduled to be completed by the end of 1963,when it is expected to have covered the totalpopulation.
The Organization has provided freeze -dried vaccinefor the campaign and a supply of approximately600 000 doses has been called forward for 1963.
Kenya
Population 7 287 000 (1961 estimate); 151 caseswere reported in 1960, 289 in 1961, and 96 in 1962.No eradication campaign is planned for Kenya whichplaces reliance on a continuing programme to main-tain an 80 per cent. current vaccination status.
LiberiaPopulation 1 290 000 (1960 estimate); 1119 cases
were reported in 1961, and 323 in 1962. A WHO -assisted smallpox eradication project was due to startat the end of 1962. An amendment to the project hasrecently been agreed upon whereby the WHO seniormedical officer assigned to the campaign will conduct astudy to assess the immunity status of the inhabitantsin the light of the mass vaccination campaign whichcovered a large proportion of the population in 1961and the first five months of 1962. This assessmentcampaign, which started in December 1962, isscheduled to last six months.
WHO has provided one senior medical officer andhas agreed to provide the total amount of vaccine tocarry out a mass vaccination programme, but notthe vaccine required for maintenance of vaccination.WHO has also been requested to provide a fellowshipfor the training of a medical officer.
MaliPopulation 4 100 000 (1961 estimate); 1212 cases
were reported in 1960, 1706 in 1961, and 1427 in 1962.In 1961 a short -term consultant visited Mali to adviseon the smallpox situation there. Following his
ANNEX 16 205
report a WHO- assisted plan of operation for smallpoxeradication was agreed upon, whereby at least 80 percent. of the total population will be vaccinated within athree -year period. The Organization is providing thefreeze -dried vaccine for the campaign. Some 300 000inhabitants were vaccinated in early 1962 beforethe rainy season and the campaign was resumed inDecember. The Government has requested a WHOmedical officer to assist in the implementation of thecampaign.
MauritaniaPopulation 791 000 (1960 estimate); 44 cases were
reported in 1960, 12 in 1961, and 40 in 1962. Mauri-tania's health services have recently established four-teen health divisions. A doctor is in charge of themedical centre of each division and its dispensariesin the rural areas. Forty -eight such dispensariesserve the rural areas and a qualified dresser isresponsible for each dispensary. Since 1958, threeregional hospitals have been established in the im-portant centres of Atar, Aïon- el- Atrouss and Kaidi.In order to attend the nomadic population, fournomad squads and a special unit have been set up.The National Hospital of Nouakchott, with its schoolof nursing, will be the training centre for male andfemale nurses in Mauritania. When completed, it willhelp pilot schemes for eradication activities in Mauri-tania.
MozambiquePopulation 6 592 994 (1960 census); 81 cases were
reported in 1960, 51 in 1961, and 67 in 1962. Noeradication scheme is planned for Mozambique.However, a yearly vaccination programme is main-tained, whereby thousands of vaccinations are per-formed with a locally produced vaccine.
NigerPopulation 3 112 000 (1962 estimate); 2408 cases
were reported in 1960, 1740 in 1961, and 1038 in 1962.In Niger there is a programme for quadrennialvaccination against smallpox and yellow fever.Vaccination is carried out by (a) mobile teams fornomads -in west and east Niger; (b) mobile units inthe district; (c) school health services; and (d) maternaland child health services. In 1961, 124 000 personswere vaccinated. Coverage, however, is not more than56 per cent. In order to reach a high proportion of thepopulation and obtain at least an 80 per cent. vaccina-tion and revaccination coverage over a period of twoyears, five new mobile smallpox vaccination teamswould be necessary. The Government has requestedassistance as follows : transport (five vehicles), twomillion doses of vaccine and two refrigerators for the
storage of the vaccine at Niamey and Zinder; and alsovaccination equipment and supplies. The teams'sole duty would be to vaccinate the population invillages, market places and in scattered dwellings inthe rural areas. The Service des Grandes Endémieswill direct the programme and it is hoped that withthe new group of mobile teams the entire populationof the country will have been covered in two years.Special smallpox vaccination cards will be deliveredto those vaccinated.
Nigeria
Population 36 473 000 (1962 estimate); 4140 caseswere reported in 1960, 3538 in 1961, and 3863 in1962. The estimated needs, expressed as costs, toimplement a smallpox eradication programme in theregions of Nigeria are as follows :
(a) Northern Nigeria - over a three -year period :Labour, transport, vaccine equipment and
us $
permanent staff 1
(b) Eastern Nigeria :
680 000
Four boats, land transport and travelling,temporary staff, vaccine, equipment, etc.health education, contingencies 1
(c) Western Nigeria :
674 400
Wages, salaries, drivers, drugs and equipment,fuel and maintenance of transport, boatsfor creek areas 359 800
In addition, 16 million doses of freeze -driedvaccine.
(d) Federal Territory of Lagos :Additional staff and equipment for three years 28 000
RwandaSee Burundi and Rwanda.
SenegalPopulation 2 980 000 (1961 estimate); 6 cases were
reported in 1960, 201 in 1961, and 231 in 1962. Aquadrennial vaccination plan is in progress. Beginningin 1963 the Service des Grandes Endémies is startingvaccination of the whole population of the sevenregional areas. The Cape Vert region, however, willbe dealt with by the health service. The Governmenthas requested assistance in the form of freeze -driedvaccine (one million doses each year); and has alsoindicated that it will need additional personnel forthe vaccination campaign (US $12 898) and financialhelp for the operation and maintenance of existingtransport (US $8571).
Sierra LeonePopulation 2 450 000 (1961 estimate); 12 cases were
reported in 1960, 6 in 1961, and 78 in 1962. It is
206 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
estimated that four teams will be required for launch-ing a mass vaccination campaign in Sierra Leone.These teams will work simultaneously in each ofthe four provinces, the western area being regardedas a province, in order to cover the whole countrywithin a period of from nine to twelve months, takinginto consideration that very little can be done duringthe heavy rains. The composition of each team,equipment and estimated cost per province are : onehealth superintendent or senior health inspector,five vaccinators, and two drivers; two four -wheel -drivevehicles (long wheel- base), one portable refrigerator,two large vacuum flasks, five vaccination kits, one first -aid box with equipment to last nine months, travellingexpenses, fuel and oil, overtime fees (drivers), sta-tionery, 14 motor -cycles (350 cc) -US $31 088. Thecost for the four provinces is therefore estimated atUS $124 352.
South AfricaPopulation 16 236 000 (1961 estimate); 65 cases were
reported in 1960, 7 in 1961, and 112 in 1962. Measuresfor controlling and eventually eradicating smallpoxhave been in continuous operation for over fortyyears. These measures have recently been intensified.Sporadic outbreaks, which are frequently proved tohave been caused through infected persons fromother territories entering the Republic, still occur.Such outbreaks are, however, quickly brought undercontrol and localized, thus preventing the spread of thedisease to other areas. Adequately equipped to dealwith the situation in its territory, the Governmentconsequently does not require financial or otherassistance for the implementation of its smallpoxcampaign.
TanganyikaPopulation 9 560 000 (1962 estimate); 1584 cases
were reported in 1960, 908 in 1961, and 973 in 1962.The Government has prepared a smallpox eradicationscheme, the basis of which is the vaccinating unit,consisting of a vaccinator and a recorder whose dutiesare interchangeable. Each such unit is expected tovaccinate an average of 150 persons per day for 300days a year. These units will be organized in teams ofthree units, with one supervisor and one driver,travelling in a four- wheel -drive vehicle, and havingultra light- weight motor -cycles to enable them to reachsmall pockets of population groups inaccessible tofour -wheel transport. Ten vaccinating teams will besupervised by a sanitarian, travelling in a four- wheel-drive vehicle and accompanied by a clerk -interpreter.The whole scheme will be supervised by a medicalofficer, who will travel by four- wheel-drive vehicle,and have a clerk -interpreter. The Government hasindicated that it will require considerable assistance, as
follows : 1 medical officer; 3 sanitarians; 10 000 000doses of freeze -dried vaccine and insulated lymphcontainers; 34 four -wheel -drive vehicles; 60 ultralight- weight collapsible motor -cycles; 248 light- weightcamp beds; 596 blankets; 38 sets of camp equipment;34 pressure lamps; 100 hurricane lamps.
Togo
Population 1 500 000 (1962 estimate); 347 caseswere reported in 1960, 281 in 1961, and 572 in 1962.A smallpox vaccination programme, to be integratedwith a WHO- assisted yaws campaign, is being finalizedThe Organization will provide the freeze -dried vaccine.
Uganda
Population 6 845 000 (1961 estimate); 707 caseswere reported in 1960, 398 in 1961, and 628 in 1962.The average vaccination rate in Uganda over thepast five years is one million vaccinations per year.To carry out a mass vaccination campaign wouldpresent little difficulty from the point of view of staff.The Government's requirements have been indicatedas follows :
(a) Vaccine: depending on whether or not driedvaccine is to be used, financial provision is requiredfor the purchase of suitable insulated containersfor the transport and storage of lymph in ruralareas. Estimated cost US $1400. The estimatedcost of lymph is US $70 000.(b) Transport: vehicles. Estimated cost US $2800.
Upper VoltaPopulation 4 400 000 (1961 estimate); 126 cases
were reported in 1960, 2360 in 1961, and 1335 in 1962.The Government is eager to carry out a smallpoxeradication programme. During the visit of a medicalofficer from WHO headquarters in October 1962, ascheme was discussed with the health authorities andit was agreed that a formal eradication plan shouldbe sent to the Regional Office for Africa. The Govern-ment will need assistance in the form of supplies ofvaccine necessary for the mass campaign, vehicles andportable refrigerators. The mobile units of the Servicedes Grandes Endémies will be supported during thevaccination campaign by a large number of vaccin-ation centres to be established in dispensaries, healthcentres, etc.
Region of the AmericasThe smallpox eradication programme in the southern
hemisphere is progressing satisfactorily. Of the 1923cases of smallpox reported in 1961, 1411 occurred inRio de Janeiro, Brazil, 491 in Ecuador, 16 in Colombia,4 in Argentina and one (imported) in Uruguay. In1962 a total of 3029 cases was reported, of which 2759occurred in Brazil, 205 in Ecuador, 41 in Colombia,
ANNEX 16 207
11 in Venezuela and 10 in Uruguay. The highestincidence of smallpox is still in Brazil and Ecuador.
The smallpox eradication campaign in Colombia isa good example of proper planning, organization andoperation. The Organization collaborated with theGovernment of Colombia in the conduct of thisprogramme by furnishing a full -time consultant anda consultant specialized in dried -vaccine production,and by providing fellowships.
The Pan American Sanitary Bureau /RegionalOffice for the Americas signed an agreement withBolivia in February 1963 for a nation -wide campaignto vaccinate three million Bolivians against smallpox.The figure represents 86 per cent. of the nation's totalpopulation of 3.5 million. Following the vaccinationof almost 80 per cent. of the population in 1958, thereported number of smallpox cases dropped from theyearly average of 604 between 1946 and 1957, to7 in 1959. One case was reported in 1960; none in1961 and 1962.
The nation -wide campaign will be the country'sfirst since 1958. Its aim is to maintain in the populationa high level of immunity against smallpox.
BrazilPopulation 75 271 000 (1962 estimate); 650 cases
were reported in 1960, 1411 in 1961, and 2759 in 1962.The Government has recognized the need to eradicatethe disease and has decided to initiate a programmeexperimentally in some areas of Rio de Janeiro and ofthe state of Sergipe, and subsequently to extend it tothe state of Alagoas. Once the most suitable workingmethods have been established, the vaccinationcampaign will be extended to cover the entire country,unti180 per cent. of the population has been covered. TheOrganization has provided the equipment for pro-ducing freeze -dried vaccine; in addition a fellowshiphas been awarded to enable a medical officer to visitvarious centres producing dried vaccine on a largescale.
ColombiaPopulation 14 443 000 (1961 estimate); 171 cases
were reported in 1960, 16 in 1961, and 41 in 1962.The smallpox vaccination programme was initiatedin October 1955 and completed in April 1962. In all11 273 085 persons were vaccinated, of whom about4 484 000 were primary vaccinees.
EcuadorPopulation 4 579 000 (1962 estimate); 3185 cases
were reported in 1960, 491 in 1961 and 205 in 1962.The aim of the smallpox eradication programme inEcuador, which was initiated in 1958, is to vaccinate80 per cent. of the population within a period of fiveyears. Over 1.5 million persons, who live in remote
areas in the mountains and on the coast, still haveto be vaccinated. The Government request for materialassistance for vehicles for the transport of personnel,laboratory equipment to increase the production ofdried smallpox vaccine, field equipment, as well assanitary inspectors to co- operate with local personnelin the organization, development and supervision offield activities, amounting to approximately US $57 000has been met.
South -East Asia Region
Encountering many demographic, financial and, tosome extent, technical difficulties, this densely popul-ated and highly endemic region is, at the present,particularly active in the global eradication effort.The Indian national eradication programme, planningand implementation are being watched with greatinterest and hope.
AfghanistanPopulation 13 800 000 (1960 estimate); 111 cases
were reported in 1960, 174 in 1961, and 303 in 1962.In 1959 the Government adopted a country -widepre- eradication control programme, making vaccin-ation compulsory. Up to March 1962, four millionpeople had been vaccinated in Kabul and the provinces.WHO has provided a medical officer to advise on theorganization of the eradication programme. Assistanceneeded by the Government consists of transport,refrigerators, thermos flasks and 3 750 000 doses offreeze -dried vaccine to be supplied in instalmentsthrough 1962, 1963, 1964 and 1965. One million dosesof vaccine have already been supplied.
BurmaPopulation 22 342 000 (1962 estimate); 392 cases
were reported in 1960, 88 in 1961 and 21 in 1962.In recent years progress in reducing the incidence ofsmallpox has been achieved by a vaccination pro-gramme carried out by the network of rural healthcentres. In December 1961 a plan for a smallpoxeradication programme was prepared by the depart-ment of health and is being considered by the Govern-ment. Under this plan it is recommended that pilotareas representative of the prevailing conditions in thecountry should be selected in order to study the mostpractical approach and the requirements for a sub-sequent nation -wide mass vaccination campaign.The pilot eradication programme is expected to bestarted in May 1963. WHO assistance to the pilotprojects would consist of supplies of freeze -driedvaccine.
IndiaPopulation 441 631 000 (1961 estimate); 31 052
cases were reported in 1960, 45 195 in 1961, and
208 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
42 231 in 1962. After the conclusion on 31 March 1961of the pilot projects which were carried out in all16 states, and after much useful experience had beengained in the planning of an economical, practicaland effective eradication campaign, the Governmentreported on 25 April 1962 that the national eradicationprogramme had already been launched. By January1963 the smallpox eradication programme was com-pleted in 23 districts and is now in progress in 125others. 53.65 million vaccinations were performed.A committee was constituted to assess and evaluate thesmallpox eradication programme in the Union Terri-tory of Delhi in its attack phase. The assessment workstarted on 13 March 1963, and the results, whencompleted, could serve as a prototype for assessmentof the programmes elsewhere in India.
The Government of the USSR, under a bilateralassistance agreement, has undertaken to supply250 million doses of freeze -dried vaccine free of chargeto India in eight equal quarterly instalments, com-mencing in January 1962, to meet the additionalrequirements of smallpox vaccine for the nationalsmallpox eradication programme. The Governmentof India requires for its vaccine- producing institutesequipment such as deep- freeze cabinets for storingthe vaccine. In addition, it has considered the possibil-ity of starting to manufacture freeze -dried vaccine atBelgaum (Mysore) and Namkum (Bihar) to supplementthe existing WHO- and UNICEF -assisted producingcentres at Guindy (Madras) and Patwadangar(Uttar Pradesh). The Government also found itnecessary to plan a health education campaign as anessential part of the eradication programme.
The estimated cost of assistance needed from inter-national sources is US $2 549 412. The total costestimate for the national programme is approximately16 million dollars.
IndonesiaPopulation 96 750 000 (1961 estimate); 5196 cases
were reported in 1960, 3777 in 1961, and 586 in 1962.No formal smallpox eradication programme for thecountry has as yet been planned. A WHO epidemio-logist in Indonesia is helping the health authorities toestablish a network of provincial epidemiologicalservices. Epidemiological sections have now beenestablished in Djakarta, Semarang and Surabaya,and in the near future similar sections will beestablished in Medan (North Sumatra), Makassar(South Sulawesi) and in Palembang (South Sumatra).With this strengthening of the country's epidemio-logical organization a country -wide programme forsmallpox eradication would be developed. Outbreakshave been reported in 1962 from Serang and someregencies in Bandung (West Java) and the local health
authorities organized vaccination campaigns. Casesof smallpox were also reported from some areas inSouth Sumatra. In September and October 1962 anoutbreak occurred in Bandung and an intensifiedvaccination programme was immediately set up tocontrol the epidemic. In November 1962 a smallpoxepidemic occurred in Bekasi (about 50 kilometreseast of Djakarta) and a mass vaccination campaign hasbeen started by the epidemiological unit and the localhealth authorities. UNICEF has provided five jeeps.The UNICEF /WHO- assisted freeze -dried vaccinemanufacture unit in Bandung was, at the time ofreporting, in the experimental phase of production.
NepalPopulation 9 388 000 (1961 census); no cases were
reported in 1960, five in 1961, and no cases in 1962.The WHO- assisted smallpox control pilot projectwhich started in February 1962 is in progress. Plannedto cover a population group of approximately 450 000people in Kathmandu, the pilot project's short -termobjectives are :
(a) to train national health personnel in vaccina-tion techniques, care of vaccine, record -keeping,and generally in the organization and conduct ofthe vaccination programme, including health educa-tion aspects of the scheme;(b) to build up a nucleus of smallpox vaccinationactivities in a limited area in the first instance.
The long -term objectives of the pilot project aregradually to expand the smallpox control programmeas and when the situation permits, in order to build upthe group immunity of the population to a level atwhich smallpox is no longer a public health problem.The Organization's assistance consists of one publichealth nurse, and equipment and supplies whichinclude transport (one jeep station -wagon) and freeze -dried vaccine for the campaign. An estimate ofinternational assistance which may be required for aneradication campaign in Nepal will only be possiblesome time in 1964, after the results of the pilot projectover a period of two years have been assessed.
Thailand
Population 27 181 000 (1961 estimate); 32 cases in1960, 33 in 1961, and two in 1962. For the last fewyears, smallpox has not been a major problem inThailand. The smallpox eradication programme whichwas launched by the Government in 1961 is in progress.The objective of this programme is to vaccinate yearlyone -third, or about eight million people, of theestimated total population of 25 million A total of7 261 141 vaccinations was performed in 1961. Inter-national assistance requested consists of six vehicles
ANNEX 16 209
for supervisors of field work, and supplies of vaccinein 1962 and 1963 respectively. The UNICEF /WHO-assisted freeze -dried vaccine production unit inBangkok started production in 1960 and the outputis expected to increase in 1963 with additional equip-ment.
Eastern Mediterranean Region
In the Eastern Mediterranean Region almost allthe remaining endemic countries and territories arenow actively implementing eradication programmes.Pilot control projects, eradication campaigns andintensified vaccination control measures have shownsubstantial progress in 1962.
EthiopiaPopulation 20 000 000 (1960 estimate); 293 cases
were reported in 1960, 761 in 1961, and 360 in 1962.The Government is finding it difficult to undertake amass campaign against special diseases because ofthe very inadequate basic public health services. Atpresent, all efforts are being concentrated on thegradual development of these services, and the small-pox campaign is to be integrated with the over -allservices of the health centres and health stations.Since 1961 a department has been established in thecentral reference laboratory (at the Pasteur Institute)with the assistance of the Organization, for the pro-duction of lyophilized vaccine, the quality of whichhas been found to meet the recommended standards.This is a good step towards eventual undertaking ofmass vaccination in remote areas, using the local healthfacilities. A combined mass vaccination campaignagainst smallpox and yellow fever was carried out inthe south -western provinces of Ethiopia early in1961. About 800 000 persons were vaccinated andvaccination campaigns are being continued andsystematically expanded to cover large areas and moreof the population.
PakistanPopulation 93 720 613 (1961 census); 2005 cases
were reported in 1960, 2741 in 1961, and 3420 in1962.
East Pakistan. Population 50 840 235.Following the visit of a WHO consultant in 1960,
East Pakistan has planned a scheme aiming at theeradication of smallpox in that province. After apilot phase, which was carried out in the districts ofTipperah (population of approximately 4.4 millions)and Faridpur (population of approximately 3.2millions) from January to November 1961, a massvaccination campaign covering the whole province
was started in November 1961. The vaccination of thetotal population of East Pakistan will be achieved inthree phases from November 1961 through December1967. The first phase will be terminating at the endof 1963 and the two subsequent follow -up phases willbe conducted from 1964 through 1965, and from1966 through 1967. This programme has been madethe direct responsibility of an assistant director ofhealth services under the control of the director ofhealth services. In the 17 districts the chief medicalofficer of health or the district health officer is incharge of the implementation of the scheme. At thesub -divisional level, the health officers are responsiblefor the detailed planning, operation and supervisionof the vaccination campaign.
Vaccine. Since the middle of 1961 the Institute ofPublic Health in Dacca has ' produced freeze -driedsmallpox vaccine of satisfactory quality. The presentoutput is about 1.2 million doses a week which caneasily be raised to 2 million doses and which largelycovers the requirements for the planned province -widemass campaign. The Organization supplied theGovernment of East Pakistan with 5 million dosesof vaccine from the USSR donation, and that vaccinewas used in the pilot phases. Further requirements forthe campaign are indicated as transport and equipmentand supplies for freeze -dried vaccine production atan estimated cost of US $619 727.
West Pakistan. Population 42 880 378.The Government has decided to integrate a smallpox
vaccination campaign with the BCG campaign overa period of five years. Assistance required for thesmallpox eradication programme has been indicatedas 50 jeeps, 200 refrigerators and 4000 thermos flasks.In addition, equipment will be required for theincreased production of dried smallpox vaccine. Theestimated total cost of these requirements isUS $330 743.
Saudi ArabiaPopulation 6 036 000 (1956 estimate); 32 cases were
reported in 1960, but none in 1961, and one only in1962. The Government, being aware of the endemicityof smallpox, its periodic outbreaks in certain partsof the peninsula and the potential danger to thecountry of international traffic, has planned an eradica-tion programme with the assistance of the Organi-zation. The objective of the agreement is the eradica-tion of smallpox through the vaccination of the entirepopulation within three years. The Organization willprovide assistance in the form of ad hoc short -termconsultants as may be required in 1963, 1964. and1965, 4.5 million doses of freeze -dried vaccine to besupplied by instalments, and transport.

210 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Sudan
Population 12 650 000 (1962 estimate); 135 caseswere reported in 1960, 104 in 1961, and 70 in 1962.A plan of operation for a WHO- assisted smallpoxcontrol and eradication project in Sudan was agreed toin July 1962. The project aims at eradicating smallpoxby vaccinating the entire population in four years. Tothis end the country would be divided into fourdivisions, each to be covered in one full year of opera-tions. In the first year a pilot scheme will cover, inthe western zone of the country, the Kordofan andDarfur provinces with a total population of 3 417 000inhabitants. The Organization's assistance for thepilot scheme is one short -term consultant /epidemio-logist for a month in 1961, and a month in 1962;three million doses of freeze -dried vaccine to besupplied in instalments of one million doses, transport,sterilizers, refrigerators and thermos flasks.
Yemen
Population 5 000 000 (1960 estimate); no reportsare available on the incidence of cases. A plan ofoperation for a WHO -assisted smallpox control and
eradication project in Yemen was agreed to inDecember 1961. The aim of the project is to eradicatesmallpox by vaccinating the entire population withinthree years. The Organization has agreed to provideone short -term consultant for three months in 1962and three months in 1963, three million doses offreeze -dried vaccine to be provided in instalments,transport and all medical supplies needed for thecampaign. A decree for compulsory and free vaccina-tion of all the inhabitants of Yemen, including thenewly -born, was issued on 2 July 1962. On 10 Sep-tember 1962 the whole population of the city of Sanaa,the capital, was vaccinated.
Western Pacific Region
Countries in the Western Pacific Region are at thepresent time free from endemic smallpox. Vaccinationcontrol measures and intensified vaccination pro-grammes are, however, being undertaken by mostcountries in order to maintain a level of immunity bywhich serious outbreaks could be avoided when andwhere the disease is introduced.
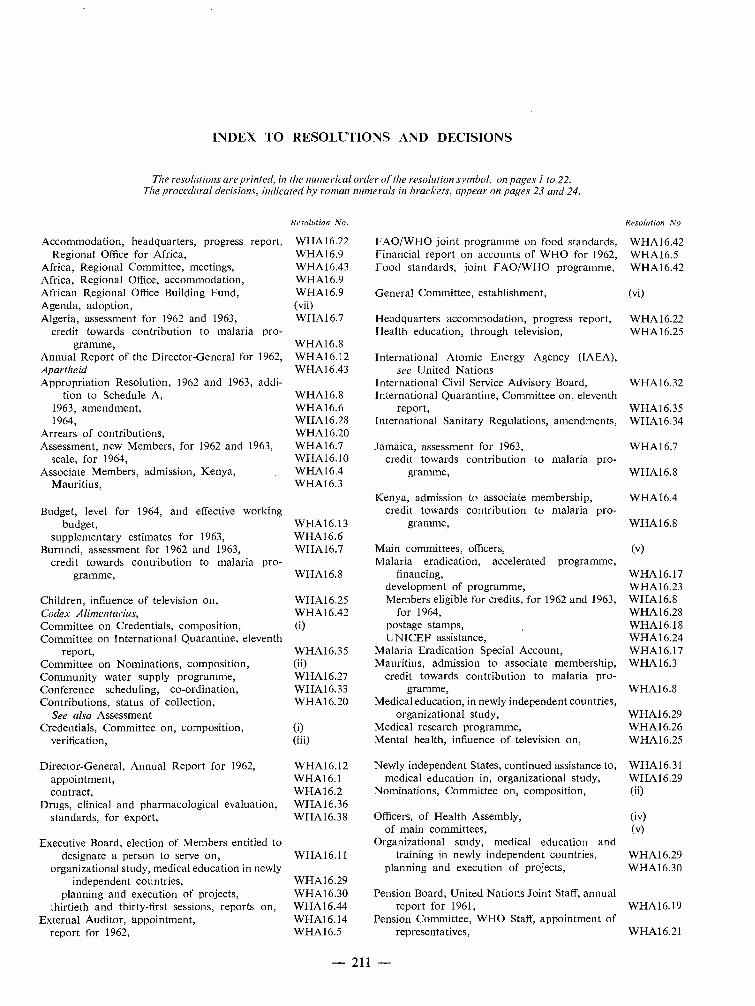
INDEX TO RESOLUTIONS AND DECISIONS
The resolutions are printed, in the numerical order of the resolution symbol, on pages Ito 22.The procedural decisions, indicated by roman numerals in brackets, appear on pages 23 and 24.
Resolution No. Resolution No
Accommodation, headquarters, progress report, W HA 16.22 FAO /WHO joint programme on food standards, WHA16.42Regional Office for Africa, WHA 16.9 Financial report on accounts of WHO for 1962, WHA16.5
Africa, Regional Committee, meetings,Africa, Regional Office, accommodation,African Regional Office Building Fund,Agenda, adoption,Algeria, assessment for 1962 and 1963,
credit towards contribution to malaria pro-gramme,
Annual Report of the Director -General for 1962,Apartheid
WHA 16.43WHA16.9WHA16.9(vii)WHA16.7
WHA16.8WHA16.12WHA16.43
Food standards, joint FAO /WHO programme,
General Committee, establishment,
Headquarters accommodation, progress report,Health education, through television,
International Atomic Energy Agency (IAEA),see United Nations
WHA16.42
(vi)
WHA16.22WHA16.25
Appropriation Resolution, 1962 and 1963, addi-tion to Schedule A,
1963, amendment,1964,
Arrears of contributions,Assessment, new Members, for 1962 and 1963,
scale, for 1964,Associate Members, admission, Kenya,
Mauritius,
Budget, level for 1964, and effective working
WHA16.8WHA16.6WHA16.28WHA16.20WHA1 6.7WHA16.10WHA16.4WHA 16.3
International Civil Service Advisory Board,International Quarantine, Committee on, eleventh
report,International Sanitary Regulations, amendments,
Jamaica, assessment for 1963,credit towards contribution to malaria pro-
gramme,
Kenya, admission to associate membership,credit towards contribution to malaria pro-
WHA16.32
WHA16.35WHA16.34
WHA16.7
WHA16.8
WHA16.4
budget,supplementary estimates for 1963,
Burundi, assessment for 1962 and 1963,credit towards contribution to malaria pro-
gramme,
Children, influence of television on,
WHA16.13WHA1 6.6WHA1 6.7
WHA1 6.8
WHA16.25
gramme,
Main committees, officers,Malaria eradication, accelerated programme,
financing,development of programme,Members eligible for credits, for 1962 and 1963,
WHA16.8
(v)
WHA16.17WHA16.23WHA16.8
Codex Alimentarius, WHA16.42 for 1964, WHA16.28Committee on Credentials, composition,Committee on International Quarantine, eleventh
report,
(i)
WHA16.35
postage stamps,UNICEF assistance,
Malaria Eradication Special Account,
WHA16.18WHA16.24WHA16.17
Committee on Nominations, composition,Community water supply programme,Conference scheduling, co- ordination,Contributions, status of collection,
See also AssessmentCredentials, Committee on, composition,
verification,
(ii)WHA16.27WHA16.33WHA16.20
(i)(iii)
Mauritius, admission to associate membership,credit towards contribution to malaria pro-
gramme,Medical education, in newly independent countries,
organizational study,Medical research programme,Mental health, influence of television on,
WHA16.3
WHA16.8
WHA16.29WHA16.26WHA16.25
Director -General, Annual Report for 1962,appointment,contract,
Drugs, clinical and pharmacological evaluation,standards, for export,
Executive Board, election of Members entitled to
WHA16.12WHA16.1WHA16.2WHA16.36WHA16.38
Newly independent States, continued assistance to,medical education in, organizational study,
Nominations, Committee on, composition,
Officers, of Health Assembly,of main committees,
Organizational study, medical education and
WHA16.31WHA16.29(ii)
(v)
designate a person to serve on,organizational study, medical education in newly
independent countries,planning and execution of projects,
thirtieth and thirty -first sessions, reports on,External Auditor, appointment,
report for 1962,
WHA16.11
WHA16.29WHA16.30WHA16.44WHA16.14WHA16.5
training in newly independent countries,planning and execution of projects,
Pension Board, United Nations Joint Staff, annualreport for 1961,
Pension Committee, WHO Staff, appointment ofrepresentatives,
WHA1 6.29WHA16.30
WHA16.19
WHA16.21
- 211 -
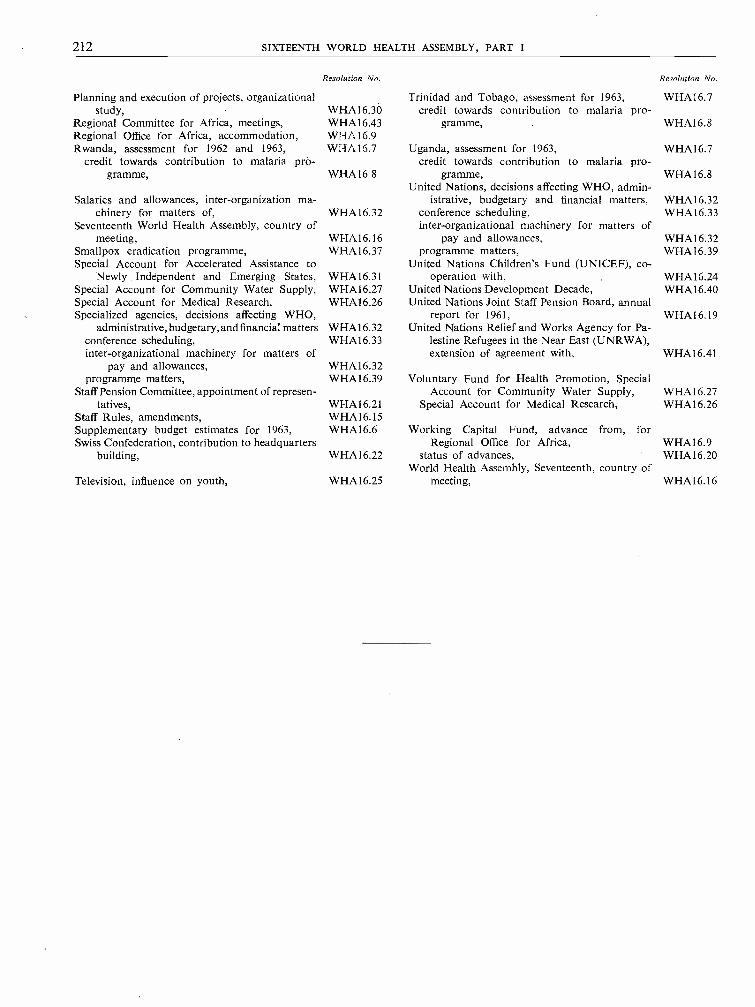
212 SIXTEENTH WORLD HEALTH ASSEMBLY, PART I
Planning and execution of projects, organizationalstudy,
Regional Committee for Africa, meetings,Regional Office for Africa, accommodation,Rwanda, assessment for 1962 and 1963,
credit towards contribution to malaria pro-gramme,
Salaries and allowances, inter -organization ma-chinery for matters of,
Seventeenth World Health Assembly, country ofmeeting,
Smallpox eradication programme,Special Account for Accelerated Assistance to
Newly . Independent and Emerging States,Special Account for Community Water Supply,Special Account for Medical Research,Specialized agencies, decisions affecting WHO,
administrative, budgetary, and financial mattersconference scheduling,inter -organizational machinery for matters of
pay and allowances,programme matters,
Staff Pension Committee, appointment of represen-tatives,
Staff Rules, amendments,Supplementary budget estimates for 1963,Swiss Confederation, contribution to headquarters
building,
Television, influence on youth,
Resolution No.
WHA16.30WHA16.43WHA 16.9WHA 16.7
WHA16 8
WHA16.32
WHA16.16WHA 16.37
WHA16.31WHA16.27WHA16.26
WHA16.32WHA16.33
WHA16.32WHA16.39
WHA16.21WHA16.15WHA16.6
WHAI6.22
WHA16.25
Trinidad and Tobago, assessment for 1963,credit towards contribution to malaria pro-
gramme,
Uganda, assessment for 1963,credit towards contribution to malaria pro-
gramme,United Nations, decisions affecting WHO, admin-
istrative, budgetary and financial matters,conference scheduling,inter -organizational machinery for matters of
pay and allowances,programme matters,
United Nations Children's Fund (UNICEF), co-operation with,
United Nations Development Decade,United Nations Joint Staff Pension Board, annual
report for 1961,United Nations Relief and Works Agency for Pa-
lestine Refugees in the Near East (UNRWA),extension of agreement with,
Voluntary Fund for Health Promotion, SpecialAccount for Community Water Supply,
Special Account for Medical Research,
Working Capital Fund, advance from, forRegional Office for Africa,
status of advances,World Health Assembly, Seventeenth, country of
meeting,
Resolution No.
WHA16.7
WHA 16.8
WHA16.7
WHA16.8
WHA16.32WHA16.33
WHA16.32WHA16.39
WHA16.24WHA 16.40
WHA16.19
WHA16.41
WHA16.27WHA16.26
WHA16.9WHA16.20
WHA16.16