Spatial methods for analysing large-scale artefact inventories (2012)

Correspondence: Paul R. Barach, Kjell Arholms Hus, Faculty of Social Sciences, Department of Health Studies, University of Stavanger, 4036 Stavanger, Norway. Tel: 51831534. E-mail: [email protected]
(Received 30 March 2013 ; accepted 23 June 2013 )
Background Paper Series on European collaborative projects
What can artefact analysis tell us about patient transitions between the hospital and primary care? Lessons from the HANDOVER project
Julie K. Johnson 1 , Vineet M. Arora 2 & Paul R. Barach 3 , on behalf of the European HANDOVER Research Collaborative
1 Centre for Clinical Governance Research, University of New South Wales, Sydney, Australia, 2 Department of Medicine, University of Chicago, USA, and 3 Faculty of Social Sciences, Department of Health Studies, University of Stavanger, Stavanger, Norway
ABSTRACT Background: Hospital discharge often faces breakdowns in information, communication, and coordination. The European Union FP7 Health Research Programme commissioned the European HANDOVER Project in 2008, a three year, 3.5 million Euro programme to examine transitions of patient care from the hospital to the community care settings. Six European countries — Italy, the Netherlands, Poland, United Kingdom, Spain, and Sweden — participated in this collaborative study. Objectives: This paper highlights a multi-centre, multi-national research programme. We describe how HANDOVER participants conducted an ‘ artefact analysis ’ as one element of the mixed methods study to inform opportunities to make patient handovers between hospital and community care more e! ective. Methods: The artefact analysis consisted of a four-step process to assess di! erent tools used in communication and treatment and their e! ects on the communication processes between the hospital and general practice settings. Results: Four themes emerged from our analysis: (a) The inpatient care of a patient is ‘ hospital centric ’ whereby the hospital ‘ pulls ’ information regarding a patient ’ s family physician (b) There are rich cognitive artefacts that support the patient clinician encounter; c) The use of information technology does not necessarily improve the communication process; and (d) There is a role for the patient, albeit not particularly well-defi ned or explicit, as a conduit for essential information communication.
Conclusion: Cognitive artefact analysis is an innovative method to provide insights into transitions of patient care. It may be most useful to think about interventions at both the individual patient and the system levels that more fully address and overcome the system issues at work.
Keywords: patient safety , transitions of care , handovers , cognitive artefacts , artefact analysis
European Journal of General Practice, 2013; 19: 185–193
ISSN 1381-4788 print/ISSN 1751-1402 online © 2013 Informa HealthcareDOI: 10.3109/13814788.2013.819850
KEY MESSAGE:
• The European HANDOVER Research Collaborative is a multi-centre, multi-national ‘ community of practice ’ for conducting research on transitions of care. • Establishing a community of practice is a way to achieve the research aims while supporting the researchers as a learning community. • Artefact analysis is an innovative health services research method to gain insights into the patient and care provider experience.
INTRODUCTION
Transitions between primary and secondary care
Healthcare reform is increasing pressure on health care organizations to improve quality while reducing costs. Over the past decade, awareness has grown that transitions
of care are particularly vulnerable and costly periods in the patient journey. Evidence suggests that during these transitions vital information often is lost, distorted or misinterpreted (1 – 3). Often, the transitions between the primary care setting and the inpatient hospital are less than optimal, and the repercussions can be
Eur J
Gen
Pra
ct D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y U
nive
rsity
New
Sou
th W
ales
on
09/1
6/13
For p
erso
nal u
se o
nly.

186 J. K. Johnson et al.
far-reaching — including as much as 20% of patients suf-fer a hospital re-admission, and signifi cant morbidity and mortality (4). Hospitals are often held accountable for a re-admission, but the hospital stay is only part of the patient journey; the care in the community, and more importantly, the communication around the transition of the patient ’ s care from the hospital to the community care setting may reveal successful interventions to atten-uate harm.
The HANDOVER Project
The authors have had a unique opportunity to explore these issues internationally. In 2007, the Agency for Healthcare Research and Quality in the United States (US) funded a study to explore a model for e! ective communication for patient transitions from inpatient to community care settings (5,6). In 2008, the European Union FP7 Health Programme commissioned a three-year grant — the European HANDOVER Project — to examine transitions of patient care and the growing concerns over patient readmissions across six European countries (7 – 10). Academic centres in Italy, the Neth-erlands, Poland, the UK, Spain, and Sweden partici-pated in HANDOVER (see Box 1). The countries were specifi cally selected to represent di! erent European healthcare funding systems with variable organization models. The participating researchers in this interna-tional multi-centre project studied how to best opti-mize the continuum of clinical care between primary care and the hospital to reduce unnecessary treatment, medical errors, and avoidable harm. The specifi c objectives included identifying and studying best prac-tices, creating standardized approaches to handover
communication, and measuring the e! ectiveness in terms of impacts on patients and health care costs. The project was organized into seven work packages and 12 deliverables (9).
Multi-methods research. The HANDOVER project built on and extended the multi-methods approach that was developed and tested in the US to explore and describe the handovers, including key stakeholder interviews with patients/carers and care providers, focus groups, process mapping, and artefact analysis (6). The study design required a mixed-methods approach in which researchers conducted semi-struc-tured interviews with key stakeholders (patients and their care providers) and focus groups with patients, patient representatives, and hospital-based and com-munity-based providers (e.g. physicians and nurses, etc.). While the overall focus was on the hospital to primary care interface, each country had a unique clinical focus that represented the interest areas of the researchers: general medicine patients in the Nether-lands, under-represented minority patients in Spain, emergency department patients in Italy and Sweden, and geriatric patients in Poland. Our research plan extended beyond the traditional set of qualitative methods to develop and apply quality improvement tools (specifi cally Ishikawa diagrams, process mapping, narrative analyses of near misses and patient stories, and review of artefacts) to enhance participants ’ understanding of the complexity of patient handover processes as well as explore facilitators and barriers to e! ective handovers (6,8). We also used a series of quantitative methods to assess the cost e! ectiveness of handover training (11,12).
Italy Azienda Sanitaria Firenze: F. Venneri and A. Molisso. Clinical Risk Management and Patient Safety Centre, Tuscany Region: S. Albolino and G. Toccafondi.
The Netherlands Patient Safety Centre, University Medical Centre Utrecht, Utrecht: P. Gademan, B. G ö bel, C. Kalkman, L. Pijnenborg, P. Barach, J. Johnson. Scientifi c Institute for Quality of Healthcare, Radboud University Nijmegen Medical Centre, Nijmegen: H. Wollersheim, G. Hesselink,
L. Schoonhoven, M. Zegers. Centre for Learning Sciences and Technologies, Open University, Heerlen: E. Boshuizen, H. Drachsler, W. Kicken, M. van der Klink,
S. Stoyanov.
Poland National Centre for Quality Assessment in Health Care, Krakow: B. Kutryba, E. Dudzik-Urbaniak, M. Kalinowski, H. Kutaj-Wasikowska.
Spain Avedis Donabedian Institute, Universidad Aut ó noma de Barcelona, Barcelona: R. Su ñ ol, O. Groene, C. Orrego.
Sweden Karolinska University Hospital, Stockholm: G. Ö hl é n, F. Airosa, S. Bergenbrant, M. Flink, H. Hansagi, M. Olsson.
United Kingdom University of Birmingham, Birmingham: R. Lilford, Y.-F. Chen, N. Novielli, S. Manaseki-Holland.
Box 1. The European HANDOVER research collaborative.
Eur J
Gen
Pra
ct D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y U
nive
rsity
New
Sou
th W
ales
on
09/1
6/13
For p
erso
nal u
se o
nly.

Communication between the hospital and general practice 187
Results of the HANDOVER project
The handovers we studied were often characterized by communication failures, environmental barriers and adverse care (13). Signifi cant di! erences were seen in the patient discharge, transfer, and rehabilitation pro-cesses in each participating country. We identifi ed the cultural barriers and facilitators in the medical and social contexts where patient handover takes place (14). We found that current interventions aimed at improving handovers at the hospital-primary care interface fall short in addressing these barriers and facilitators as they tend to overlook the essential role of the patient (15,16).
Patient experience. Patient ’ s beliefs and experiences can infl uence patient participation in handovers between primary and secondary care (13) and that immigrants to healthcare systems are particularly vulnerable to handover procedure shortcomings (17).
Microsystems, professional roles, and communication. E! ective handover interventions are mostly aimed at improving organizational and technical aspects of the handover process and ignore the clinical microsystem (18). The lack of awareness of di! erent professional per-spectives, inherent to primary and secondary profes-sional domains, seems to infl uence the roles and responsibilities in patient diagnosis and treatment. We demonstrated that it is common for the general practi-tioner to play an essential part in the coordination of patient care (19) . Multiple factors, such as the lack of direct contact between professionals, involvement of multiple professionals and the lack of feedback, make it di" cult for the general practitioner to fulfi l this role e! ectively and to be accountable.
Predicting costs of interventions. Using Bayesian meth-ods, we were able to demonstrate that the costs related to the service delivery handover interventions can be e! ectively predicted before they are imple-mented (20). Implementing the use of discharge nurses in the Stockholm County Council, with a one year fol-low up of 268 patients improved SF36 evaluations in all eight parameters and the total health care expen-diture was reduced by 46% (21). The HANDOVER model supported the notion that a full time discharge nurse can reduce health care expenditure by 540 000 Euros a year.
Training and education. Finally, the project developed a standardized training toolkit for improving hando! care and processes that can be tailored to meet local and/or institutional needs (22).
HANDOVER as a community of practice. In addition to achieving the research aims, HANDOVER addressed and demonstrated e! ective ways to overcome the challenges of creating a robust, multi-centre, multi-national ‘ community of practice ’ for conducting research (8). This learning collaborative was designed to assist the researchers to defi ne a common purpose, build research teams and engage researchers further in the larger set of research topics, while engendering trust among the team members. HANDOVER fostered adoption of good practices and collaboration via Euro-pean clinical, educational and regulatory as well as patient advocacy bodies (7). The project fi ndings were incorporated into the WHO 2013 report on patient empowerment (23).
ARTEFACT ANALYSIS
The aim of this paper is to present the artefact analyses of patient handover processes from several countries as an example of a collaborative research e! ort that was part of the European HANDOVER Research Collabora-tive. First, we defi ne artefact analysis, and then discuss the role of artefact analysis in the HANDOVER project; second, we provide results of the artefact analysis; and, fi nally we discuss the challenges of conducting a multi-national research collaborative. We defi ne artefacts as the implements, notes, or materials that are used in the daily workfl ow of patient care. Artefact analysis is the study of these implements. It has been suggested that artefacts can be used to more fully describe a social-technical phenomenon when used with self-reported experience and satisfaction data (24).
What is ‘ artefact analysis ’ ?
Cognitive artefacts may be defi ned as ‘ those artifi cial devices that maintain, display, or operate upon infor-mation to serve a representational function and that a! ect human cognitive performance (25). ’ Cognitive artefacts are, in other words, man-made implements that seem to aid or enhance our cognitive abilities. Some examples include calendars, to-do lists, electronic mails, phone texts, phone messages, computer screen printouts, or simply ‘ tying a string around your fi nger as a reminder (24). ’
Cognitive artefacts are widely used in healthcare and include items such as an operating theatre whiteboard, end-of-shift sign-out sheet, surgery schedule or a written sign-out that are used as reminders of what needs to be completed for patient care (26). We chose to study arte-facts as they help one better understand how clinicians perceive and actually do their work. We outlined the role of the artefact in helping clinicians achieve the planned work of patient transitions. Cognitive artefacts can be
Eur J
Gen
Pra
ct D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y U
nive
rsity
New
Sou
th W
ales
on
09/1
6/13
For p
erso
nal u
se o
nly.

188 J. K. Johnson et al.
collection in the UK included an analysis of potential interventions and cost e! ective analyses (20).
The artefact analysis was a multi-step process (see Box 3). The fi rst step was to map the process of care to depict the inpatient journey. This was developed at a level that captures most of the major steps for the aver-age patient, and at a minimum included the stages of patient admission, inpatient stay, discharge, and fol-low-up care in the community. The second step was to draw upon existing resources (i.e. informal discussions, patient records, etc.) to identify relevant artefacts. The teams chose to either conduct the analysis on an indi-vidual patient or to conduct the analysis at a systems level taking into account the care of multiple patients. The patient level analysis looks at the artefacts that were generated for a specifi c patient, while the systems level analysis looked at the artefacts that were used to support patient care processes.
Choosing a patient that would be the focus of the artefact analysis required ‘ sleuthing work ’ to identify an appropriate case where either the transition was effective or where there were multiple failures at communication opportunities. The key stakeholder interviews of the providers involved in the handover process provided a mechanism to identify a specific case that would serve as an example of inefficiencies related to the handover process. A systems level anal-ysis, in contrast to the patient level analysis, looked at the artefacts that were used to support patient care processes, in general, and not related to a specific patient encounter.
The next step was to look for clues within the arte-facts that provided information or insight into the care process. The fi nal step was to link the relevant docu-ments containing pertinent information about the pro-cess of care to create a visual representation of the process. Figure 1 shows the visual representation that was created in the pilot phase and which served as the base for the methods deployed in the European HAN-DOVER study sites. Figure 1 illustrates how the artefact analysis pieces together the inpatient team plans to communicate with the patient ’ s primary care physician (PCP). For example, at hospital admission there are reminders to contact the PCP along with mechanisms to record the PCPs contact information. The patient ’ s
especially helpful in communication research of health-care teams when direct observation of communication is not always feasible due to its variable nature, quality and untimeliness. The study of cognitive artefacts yields insights into the nature of work and the socio-technical relationships that are supported by the artefact (27).
Box 2 lists potential cognitive artefacts related to care transitions that describe the process of events sur-rounding the patient care pathway. Examining the arte-facts associated with patient handovers may help to give a more realistic understanding of the challenges and human factors that clinicians face when transitioning patients, what tools are available to support their work, and insights into how we help clinicians redesign their work fl ow around patient transitions. It also might help explicate why much handover research has had limited impact on reducing patient re-admissions and prevent-ing patient harm (14).
While healthcare providers do their best to provide cohesive care across inpatient and community settings, the healthcare system does not adequately support their e! orts. Healthcare providers often work in isola-tion, not taking advantage of the ‘ virtual microsystem ’ and web of connections that exist between the inpa-tient and community care settings (18). Proven care processes can fail when production pressures do not allow su" cient time and e! ort to be attentive to the system (28). Clinicians become very skilled at using a rich tapestry of data, cues, and heuristics to navigate the healthcare system to mitigate and attenuate harm to patients.
Artefact analysis in the HANDOVER project
Research teams in Italy, the Netherlands, Poland, Spain, and Sweden conducted comprehensive artefact analyses to assess the di! erent tools and cognitive aids used in communication and patient treatment and their impact on the e! ectiveness of communication processes between inpatient and community care settings (data
• Reminder written by the inpatient physician to contact the patient ’ s general practitioner or family medicine physician
• Handwritten note scribbled as personal reminder of what needs to be communicated about a patient during the handover to the next shift
• Physician progress notes documenting contact with the patient ’ s general practitioner
• The discharge summary, requesting follow-up appointments with the general practitioner
• The general practitioner ’ s notes for a recently hospitalized patient
• Recovery room whiteboard • Pharmacy prescription • Electronic mail between hospital and community clinicians
Box 2. Cognitive artefacts related to care transitions.
1. Map the process of care. 2. Collect artefacts that support each step in the process of
care (If conducting an analysis of a specifi c patient, identify the case.)
3. Search artefacts for relevant information or clues that provide insight into the process.
4. Create a visual display of the artefacts and patient care process.
Box 3. Developing the artefact analysis.
Eur J
Gen
Pra
ct D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y U
nive
rsity
New
Sou
th W
ales
on
09/1
6/13
For p
erso
nal u
se o
nly.

Communication between the hospital and general practice 189
Figure 1. Artefact analysis - from the pilot study site in the United States.
history and physical hospital form includes a check box for the attending physician to attest ‘ I counselled the resident [physician] to inform the patient ’ s primary care physician of this admission. ’ During the inpatient stay, patient progress notes include handwritten notes
to follow up with the PCP and the handover documents between resident physicians including a personal note as a reminder, for example, ‘ Don ’ t forget to call the PCP about lung cancer follow up. ’ During the patient dis-charge, the physician orders includes a note to the
Eur J
Gen
Pra
ct D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y U
nive
rsity
New
Sou
th W
ales
on
09/1
6/13
For p
erso
nal u
se o
nly.
190 J. K. Johnson et al.
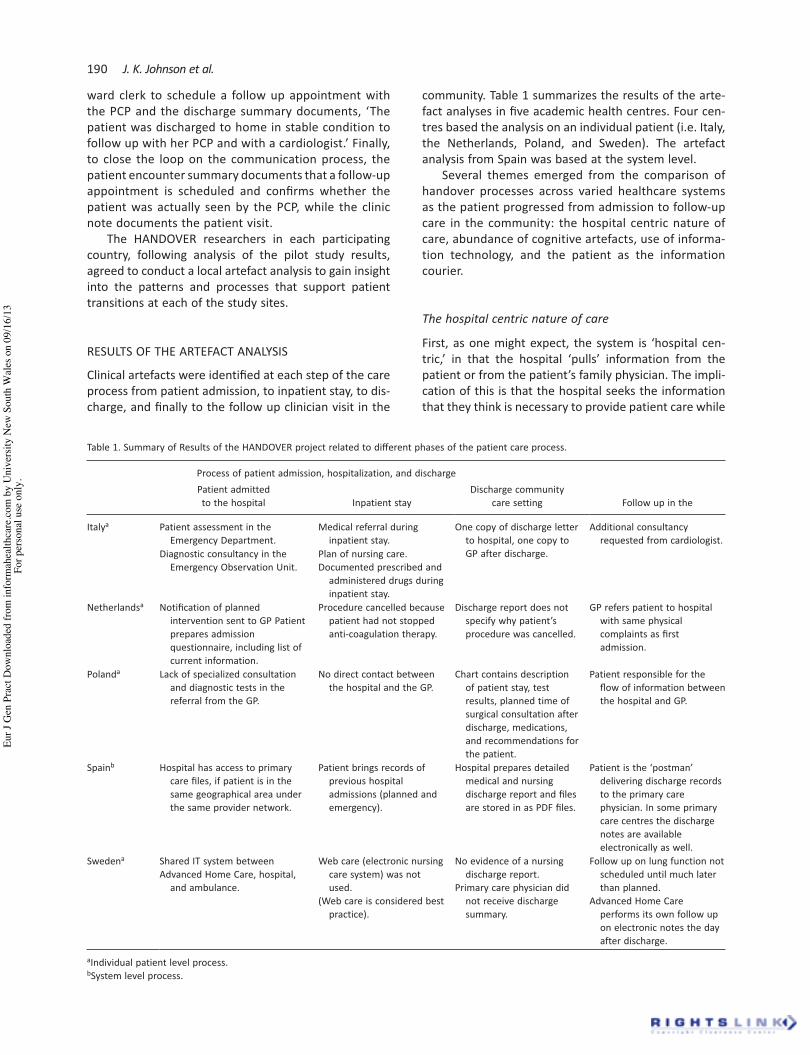
community. Table 1 summarizes the results of the arte-fact analyses in fi ve academic health centres. Four cen-tres based the analysis on an individual patient (i.e. Italy, the Netherlands, Poland, and Sweden). The artefact analysis from Spain was based at the system level.
Several themes emerged from the comparison of handover processes across varied healthcare systems as the patient progressed from admission to follow-up care in the community: the hospital centric nature of care, abundance of cognitive artefacts, use of informa-tion technology, and the patient as the information courier.
The hospital centric nature of care
First, as one might expect, the system is ‘ hospital cen-tric, ’ in that the hospital ‘ pulls ’ information from the patient or from the patient ’ s family physician. The impli-cation of this is that the hospital seeks the information that they think is necessary to provide patient care while
ward clerk to schedule a follow up appointment with the PCP and the discharge summary documents, ‘ The patient was discharged to home in stable condition to follow up with her PCP and with a cardiologist. ’ Finally, to close the loop on the communication process, the patient encounter summary documents that a follow-up appointment is scheduled and confi rms whether the patient was actually seen by the PCP, while the clinic note documents the patient visit.
The HANDOVER researchers in each participating country, following analysis of the pilot study results, agreed to conduct a local artefact analysis to gain insight into the patterns and processes that support patient transitions at each of the study sites.
RESULTS OF THE ARTEFACT ANALYSIS
Clinical artefacts were identifi ed at each step of the care process from patient admission, to inpatient stay, to dis-charge, and fi nally to the follow up clinician visit in the
Table 1. Summary of Results of the HANDOVER project related to di! erent phases of the patient care process.
Process of patient admission, hospitalization, and dischargePatient admitted to the hospital Inpatient stay
Discharge community care setting Follow up in the
Italy a Patient assessment in the Emergency Department.
Medical referral during inpatient stay.
One copy of discharge letter to hospital, one copy to GP after discharge.
Additional consultancy requested from cardiologist.
Diagnostic consultancy in the Emergency Observation Unit.
Plan of nursing care.Documented prescribed and
administered drugs during inpatient stay.
Netherlands a Notifi cation of planned intervention sent to GP Patient prepares admission questionnaire, including list of current information.
Procedure cancelled because patient had not stopped anti-coagulation therapy.
Discharge report does not specify why patient ’ s procedure was cancelled.
GP refers patient to hospital with same physical complaints as fi rst admission.
Poland a Lack of specialized consultation and diagnostic tests in the referral from the GP.
No direct contact between the hospital and the GP.
Chart contains description of patient stay, test results, planned time of surgical consultation after discharge, medications, and recommendations for the patient.
Patient responsible for the fl ow of information between the hospital and GP.
Spain b Hospital has access to primary care fi les, if patient is in the same geographical area under the same provider network.
Patient brings records of previous hospital admissions (planned and emergency).
Hospital prepares detailed medical and nursing discharge report and fi les are stored in as PDF fi les.
Patient is the ‘ postman ’ delivering discharge records to the primary care physician. In some primary care centres the discharge notes are available electronically as well.
Sweden a Shared IT system betweenAdvanced Home Care, hospital,
and ambulance.
Web care (electronic nursing care system) was not used.
(Web care is considered best practice).
No evidence of a nursing discharge report.
Primary care physician did not receive discharge summary.
Follow up on lung function not scheduled until much later than planned.
Advanced Home Care performs its own follow up on electronic notes the day after discharge.
a Individual patient level process. b System level process.
Eur J
Gen
Pra
ct D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y U
nive
rsity
New
Sou
th W
ales
on
09/1
6/13
For p
erso
nal u
se o
nly.
Communication between the hospital and general practice 191
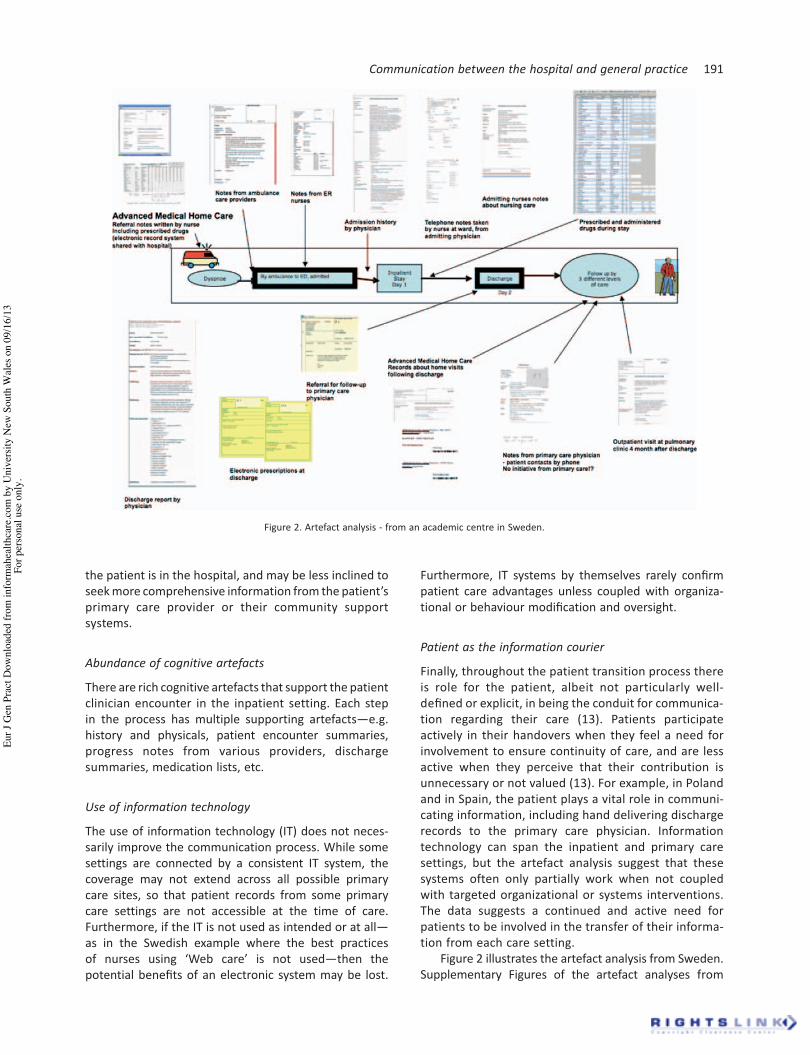
Figure 2. Artefact analysis - from an academic centre in Sweden.
the patient is in the hospital, and may be less inclined to seek more comprehensive information from the patient ’ s primary care provider or their community support systems.
Abundance of cognitive artefacts
There are rich cognitive artefacts that support the patient clinician encounter in the inpatient setting. Each step in the process has multiple supporting artefacts — e.g. history and physicals, patient encounter summaries, progress notes from various providers, discharge summaries, medication lists, etc.
Use of information technology
The use of information technology (IT) does not neces-sarily improve the communication process. While some settings are connected by a consistent IT system, the coverage may not extend across all possible primary care sites, so that patient records from some primary care settings are not accessible at the time of care. Furthermore, if the IT is not used as intended or at all — as in the Swedish example where the best practices of nurses using ‘ Web care ’ is not used — then the potential benefi ts of an electronic system may be lost.
Furthermore, IT systems by themselves rarely confi rm patient care advantages unless coupled with organiza-tional or behaviour modifi cation and oversight.
Patient as the information courier
Finally, throughout the patient transition process there is role for the patient, albeit not particularly well-defi ned or explicit, in being the conduit for communica-tion regarding their care (13). Patients participate actively in their handovers when they feel a need for involvement to ensure continuity of care, and are less active when they perceive that their contribution is unnecessary or not valued (13). For example, in Poland and in Spain, the patient plays a vital role in communi-cating information, including hand delivering discharge records to the primary care physician. Information technology can span the inpatient and primary care settings, but the artefact analysis suggest that these systems often only partially work when not coupled with targeted organizational or systems interventions. The data suggests a continued and active need for patients to be involved in the transfer of their informa-tion from each care setting.
Figure 2 illustrates the artefact analysis from Sweden. Supplementary Figures of the artefact analyses from
Eur J
Gen
Pra
ct D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y U
nive
rsity
New
Sou
th W
ales
on
09/1
6/13
For p
erso
nal u
se o
nly.

192 J. K. Johnson et al.
Italy, the Netherlands, Poland, and Spain are available online only, at http//www.informahealthcare.com/doi/abs/10.3109/13814788.2013.819850.
DISCUSSION
Main fi ndings
We conducted artefact analyses in the fi ve countries participating in project HANDOVER to document, visu-alize, and explain what happens during a patient tran-sition. The artefacts collected in each hospital highlight the complexities in optimizing patient transitions from inpatient care to ambulatory care. The study o! ers clear insights and clarifi cation on how easy it is for communication acts between the hospital care and primary care to degrade in quality and lead to patient harm. It may be most useful to think about artefacts at both the individual patient and the system levels to more fully describe the system issues at work. Similarly, identifying e! ective and problematic transi-tions or system failures provides additional learning opp ortunities about how to meaningfully change and improve the processes of patient care. Our study linking tangible artefacts to the patient care process reveals opportunities for improving workfl ow, work implements, and patient transitions.
Implications for practice
The research described here invites providers and healthcare institutions to becoming increasingly accountable for what happens to their patients after hospital discharge. The need for an active patient role in the handover between the hospital and primary care was emphasized by most patients and healthcare professionals participating in surveys, interviews and focus groups that explored the patient ’ s role in the handover. Flink et al., found that patients preferred a transition process where responsibility was clear and unambiguous, regardless of whether it rested with the healthcare professional or was shared with the patient (13). Patients expressed a need for healthcare organi-zations to have a clear system of responsibility for the handover that takes into account the patients ’ need for clarity, and tailored support in relation to their own resources. Artefacts highlight how work implements can support e! ective communication as well as to illuminate the evidence about what could be improved when systems fail and allow errors to propagate to harm.
Challenges and success factors of international research collaboration
Multi-national, and even more so, multi-lingual research has a daunting task of ensuring consistency and assurance
of data collection methods, practices and analyses across multiple and geographically disparate sites and lan-guages (8). Our research spanned across fi ve countries and fi ve di! erent languages. Finding a ‘ common ground ’ around a specifi c research activity provided an opportu-nity was a challenge. Building trust and a common mental model, and growing the collaboration among the research teams was the key to reliably answering the research key questions around handovers and re-admission prevention (29).
Given the barriers created by distance between study sites, time zones and busy work schedules, we cannot over-emphasize the value of frequent face-to-face meet-ings in creating a shared understanding, support and mutual comfort despite the relative ease, and cost sav-ings, of relying only on electronic and virtual meetings. Although technology and cost containment e! orts sup-port a move toward virtual meetings, where participants attend a meeting without leaving their local settings, face-to-face meetings, supplemented with frequent tele-conferences, proved to be an invaluable component of building social capital and engendering trust among the project team. This procedure also stimulated and ensured a timely delivery of project milestones and deliverables.
Conclusion
Handovers at discharge from hospital are far from seam-less, ripe for improvement and redesign. Direct commu-nication between hospital physicians and primary care physicians occurs only in a small percentage of cases, and discharge summaries are frequently not available at the post-discharge visit or lack important information, with negative consequences for the quality of care and patient and provider satisfaction. Exploring cognitive artefacts is an innovative approach to under-standing how clinicians work and make sense (sense making) of their chaotic settings in supporting the care process. Artefact analysis is a useful mechanism to reconcile inconsistencies between the patient care process, the actual actions completed, and the out-comes that the systems achieved.
The HANDOVER project was designed to assist the researchers involved in the Project defi ne a common purpose, build research teams and engage researchers further in the larger set of research topics, while engen-dering trust among the team members.
Declaration of interest: The authors report no confl icts of interest. The authors alone are responsible for the content and writing of the paper.
Funding/support. The authors wish to acknowledge the two funding sources for these studies. The US study was supported by the Agency for Healthcare Research and
Eur J
Gen
Pra
ct D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y U
nive
rsity
New
Sou
th W
ales
on
09/1
6/13
For p
erso
nal u
se o
nly.

Communication between the hospital and general practice 193
Quality (AHRQ), 1 P20 HS017119 A model for e! ective communications for inpatient ambulatory transitions; the European study was supported by a grant from the European Union, the 7th Framework Programme of the European Commission (FP7-HEALTH-F2-2008-223409). The study sponsors had no role in the study design, col-lection, analysis, interpretation of the data, or any other contribution.
REFERENCES Kripalani S , LeFevre F , Phillips CO , Williams MV , Basaviah P , Baker 1. DW . Defi cits in communication and information transfer between hospital-based and primary care physicians: implications for patient safety and continuity of care . J Am Med Assoc. 2007 ; 831 – 41 . Jencks SF , Williams MV , Coleman EA . Rehospitalizations among 2. patients in the Medicare fee-for-service program . N Engl J Med. 2009 ; 1418 – 28. Horwitz LI , Meredith T , Schuur JD , Shah NR , Kulkarni RG , Jenq GY . 3. Dropping the baton: A qualitative analysis of failures during the transition from emergency department to inpatient care . Ann Emer Med. 2009 ; 701 – 10e4 . Forster AJ , Clark HD , Menard A , Dupuis N , Chernish R , Chandok 4. N , et al . Adverse events among medical patients after discharge from hospital . Can Med Assoc J. 2004 ; 345 – 9 . Arora VM , Prochaska ML , Farnan JM , D ’ Arcy MJt , Schwanz KJ , 5. Vinci LM , et al . Problems after discharge and understanding of communication with their primary care physicians among hospi-talized seniors: A mixed methods study . J Hosp Med. 2010 ; 385 – 91 . Johnson JK , Farnan JM , Barach P , Hesselink G , Wollersheim H , 6. Pijnenborg L , et al . Searching for the missing pieces between the hospital and primary care: Mapping the patient process during care transitions . Br Med J Q & S. 2012 ; 21(Suppl. 1) : i97 – 105 . Philibert I , Barach P . The European HANDOVER project: A multi-7. nation program to improve transitions at the primary care — inpatient interface . Br Med J Q & S. 2012 ; 21(Suppl. 1): i1 – 6 . Johnson JK , Barach P , Vernooij-Dassen M . Conducting a multicen-8. tre and multinational qualitative study on patient transitions . Br Med J Q & S. 2012 ; 21(Suppl. 1) : i22 – 8 . The European HANDOVER Research Collaborative . HANDOVER . 9. Available at: http://www.handover.eu (accessed 1 June 2013). Barach P , Gademan P , Kalkman C , Johnson J , Pijnenborg L . Identify 10. basic elements of e! ective communication . Utrecht, Nether-lands: The European HANDOVER Research Collaborativ e; 2010 . Lilford RJ , Chilton PJ , Hemming K , Girling AJ , Taylor CA , Barach P . 11. Evaluating policy and service interventions: Framework to guide selection and interpretation of study end points . Br Med J. 2010 ; 341 : c4413 . Stoyanov S , Boshuizen H , Groene O , van der Klink M , Kicken W , 12. Drachsler H , et al . Mapping and assessing clinical handover train-ing interventions . Br Med J Q & S. 2012 ; 21(Suppl. 1) : i50 – 7 . Flink M , Ohlen G , Hansagi H , Barach P , Olsson M . Beliefs and 13. experiences can infl uence patient participation in handover between primary and secondary care — a qualitative study of patient perspectives . Br Med J Q & S . 2012 ; 21(Suppl . 1): i76 – 83 .
Hesselink G , Vernooij-Dassen M , Pijnenborg L , Barach P , 14. Gademan P , Dudzik-Urbaniak E , et al . Organizational culture: An important context for addressing and improving hospital to community patient discharge . Med Care 2013 ; 90 – 8 . Flink M , Hesselink G , Pijnenborg L , Wollersheim H , Vernooij-15. Dassen M , Dudzik-Urbaniak E , et al . The key actor: A qualitative study of patient participation in the handover process in Europe . Br Med J Q & S. 2012 ; 21(Suppl. 1) : i89 – 96 . Hesselink G , Schoonhoven L , Barach P , Spijker A , Gademan P , 16. Kalkman C , et al . Improving patient handovers from hospital to primary care: A systematic review . Ann Int Med. 2012 ; 417 – 28 . Groene RO , Orrego C , Sunol R , Barach P , Groene O . ‘ It’s like 17. two worlds apart ’ : an analysis of vulnerable patient handover practices at discharge from hospital . Br Med J Q & S. 2012 ; 21(Suppl. 1) : i67 – 75 . Gobel B , Zwart D , Hesselink G , Pijnenborg L , Barach P , 18. Kalkman C , et al . Stakeholder perspectives on handovers between hospital sta! and general practitioners: An evaluation through the microsystems lens . Br Med J Q & S. 2012 ; 21(Suppl. 1) : i106 – 13 . Hesselink G , Flink M , Olsson M , Barach P , Dudzik-Urbaniak E , 19. Orrego C , et al . Are patients discharged with care? A qualitative study of perceptions and experiences of patients, family members and care providers. Br Med J Q & S. 2012 ; 21(Suppl. 1) : i39 – 49 . Yao GL , Novielli N , Manaseki-Holland S , Chen YF , van der Klink M , 20. Barach P , et al . Evaluation of a predevelopment service delivery intervention: An application to improve clinical handovers . Br Med J Q & S. 2012 ; 21(Suppl. 1) : i29 – 38 . Reinius P , Johansson M , Fjellner A , Werr J , Ö hl é n G , Edgren G . A 21. telephone-based case-management intervention reduces healthcare utilization for frequent emergency department visitors . Eur J Emerg Med. 2012 . doi: 10.1097/MEJ.0b013 e328358bf5a Epublication date 2012/09/11. Drachsler H , Kicken W , van der Klink M , Stoyanov S , Boshuizen 22. HP , Barach P . The handover toolbox: A knowledge exchange and training platform for improving patient care . Br Med J Q & S. 2012 ; 21(Suppl. 1) : i114 – 20 . World Health Organisation . Exploring patient participation in 23. reducing health-care-related safety risks . Copenhagen, Denmark: WHO Regional O" ce for Europe ; 2013 . Wreathall J , Nemeth C . Assessing risk: The role of probabilistic 24. risk assessment (PRA) in patient safety improvement . Qual Saf Health Care 2004 ; 206 – 12 . Norman D . Cognitive artifacts. In: Carroll JM, editor. Designing 25. Interaction: Psychology at the human-computer interface . Cambridge: Cambridge University Press; 1991 . Nemeth C , O ’ Connor M , Klock A , Cook R . Discovering healthcare 26. cognition: The use of cognitive artifacts to reveal cognitive work . Organization Studies 2006 ; 27:1011 – 35 . Hutchins E . Cognition in the wild . Cambridge, MA: MIT Pres s; 27. 1995 . Hollnagel E . The ETTO principle: E" ciency – thoroughness trade-28. o! . Why things that go right sometimes go wrong. United Kingdom: Ashgate Publishing Limited ; 2009 . Toccafondi G , Albolino S , Tartaglia R , Guidi S , Molisso A , 29. Venneri F , et al . The collaborative communication model for patient handover at the interface between high-acuity and low-acuity care . Br Med J Q & S. 2012 ; 21(Suppl. )1 : i58 – 66 .
Supplementary material available online
Supplementary Figures 1–4 are available at http://www.informahealthcare.com/doi/abs/10.3109/13814788.2013.819850.
Eur J
Gen
Pra
ct D
ownl
oade
d fro
m in
form
ahea
lthca
re.c
om b
y U
nive
rsity
New
Sou
th W
ales
on
09/1
6/13
For p
erso
nal u
se o
nly.
Copyright © 2022 FDOKUMEN