What are the appropriate indicators of surgical difficulty during ...
15
ORIGINAL ARTICLE What are the appropriate indicators of surgical difficulty during laparoscopic cholecystectomy? Results from a Japan-Korea-Taiwan multinational survey Yukio Iwashita · Tetsuji Ohyama · Goro Honda · Taizo Hibi · Masahiro Yoshida · Fumihiko Miura · Tadahiro Takada · Ho-Seong Han · Tsann-Long Hwang · Satoshi Shinya · Kenji Suzuki · Akiko Umezawa · Yoo-Seok Yoon · In-Seok Choi · Wayne Shih-Wei Huang · Kuo-Hsin Chen · Manabu Watanabe · Yuta Abe · Takeyuki Misawa · Yuichi Nagakawa · Dong-Sup Yoon · Jin-Young Jang · Hee Chul Yu · Keun Soo Ahn · Song Cheol Kim · In Sang Song · Ji Hoon Kim · Sung Su Yun · Seong Ho Choi · Yi-Yin Jan · Shyr-Ming Sheen-Chen · Yan-Shen Shan · Chen-Guo Ker · De-Chuan Chan · King-Teh Lee · Naoyuki Toyota · Ryota Higuchi · Yoshiharu Nakamura · Yoshiaki Mizuguchi · Yutaka Takeda · Masahiro Ito · Shinji Norimizu · Shigetoshi Yamada · Naoki Matsumura · Junichi Shindoh · Hiroki Sunagawa · Hiroshi Hasegawa · Toshiki Rikiyama · Naohiro Sata · Nobuyasu Kano · Seigo Kitano · Hiromi Tokumura · Yuichi Yamashita · Goro Watanabe · Kunitoshi Nakagawa · Taizo Kimura · Tatsuo Yamakawa · Go Wakabayashi · Itaru Endo · Masaru Miyazaki · Masakazu Yamamoto Published online: 5 September 2016 © 2016 Japanese Society of Hepato-Biliary-Pancreatic Surgery The author’s affiliations are listed in the Appendix. Correspondence to: Tadahiro Takada, Department of Surgery, Teikyo University School of Med- icine, 2-11-1 Kaga, Itabashi-ku, Tokyo 173-8605, Japan. e-mail:[email protected] DOI: 10.1002/jhbp.375 Abstract Background Serious complications continue to occur in laparoscopic cholecystectomy (LC). The commonly used indicators of surgical difficulty such as the duration of surgery are insufficient because they are surgeon and institution dependent. We aimed to identify ap- propriate indicators of surgical difficulty during LC. Methods A total of 26 Japanese expert LC surgeons discussed using the nominal group technique (NGT) to generate a list of intraoperative findings that contribute to surgical diffi- culty. Thereafter, a survey was circulated to 61 experts in Japan, Korea, and Taiwan. The questionnaire addressed LC experience, surgical strategy, and perceptions of 30 intraopera- tive findings listed by the NGT. Results The response rate of the survey was 100%. There was a statistically significant dif- ference among nations regarding the duration of surgery and adoption rate of safety mea- sures and recognition of landmarks. The criteria for conversion to an open or subtotal cholecystectomy were at the discretion of each surgeon. In contrast, perceptions of the im- pact of 30 intraoperative findings on surgical difficulty (categorized by factors related to in- flammation and additional findings of the gallbladder and other intra-abdominal factors) were consistent among surgeons. Conclusions Intraoperative findings are objective and considered to be appropriate indica- tors of surgical difficulty during LC. Keywords Critical view of safety · Laparoscopic cholecystectomy · Nominal group technique · SS-Inner theory · Surgical difficulty Introduction Laparoscopic cholecystectomy (LC) is undoubtedly the most widely accepted laparoscopic procedure across the world and has been frequently used to treat acute cholecystitis [1–3]. However, severe inflammation of the gallbladder and its surroundings is known to be J Hepatobiliary Pancreat Sci (2016) 23:533–547 DOI: 10.1002/jhbp.375
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of What are the appropriate indicators of surgical difficulty during ...

ORIGINAL ARTICLE
What are the appropriate indicators of surgical difficulty duringlaparoscopic cholecystectomy? Results from a Japan-Korea-Taiwanmultinational survey
Yukio Iwashita · Tetsuji Ohyama · Goro Honda · Taizo Hibi · Masahiro Yoshida · Fumihiko Miura · Tadahiro Takada ·Ho-Seong Han · Tsann-Long Hwang · Satoshi Shinya · Kenji Suzuki · Akiko Umezawa · Yoo-Seok Yoon · In-Seok Choi ·Wayne Shih-Wei Huang · Kuo-Hsin Chen · Manabu Watanabe · Yuta Abe · Takeyuki Misawa · Yuichi Nagakawa ·Dong-Sup Yoon · Jin-Young Jang · Hee Chul Yu · Keun Soo Ahn · Song Cheol Kim · In Sang Song · Ji Hoon Kim ·Sung Su Yun · SeongHoChoi · Yi-Yin Jan · Shyr-Ming Sheen-Chen · Yan-Shen Shan · Chen-GuoKer · De-Chuan Chan ·King-Teh Lee · Naoyuki Toyota · Ryota Higuchi · Yoshiharu Nakamura · Yoshiaki Mizuguchi · Yutaka Takeda ·Masahiro Ito · Shinji Norimizu · Shigetoshi Yamada · Naoki Matsumura · Junichi Shindoh · Hiroki Sunagawa ·Hiroshi Hasegawa · Toshiki Rikiyama · Naohiro Sata · Nobuyasu Kano · Seigo Kitano · Hiromi Tokumura ·Yuichi Yamashita · Goro Watanabe · Kunitoshi Nakagawa · Taizo Kimura · Tatsuo Yamakawa · Go Wakabayashi ·Itaru Endo · Masaru Miyazaki · Masakazu Yamamoto
Published online: 5 September 2016
© 2016 Japanese Society of Hepato-Biliary-Pancreatic Surgery
The author’s affiliations are listedin the Appendix.
Correspondence to: TadahiroTakada, Department of Surgery,Teikyo University School of Med-icine, 2-11-1 Kaga, Itabashi-ku,Tokyo 173-8605, Japan.e-mail: [email protected]
DOI: 10.1002/jhbp.375
AbstractBackground Serious complications continue to occur in laparoscopic cholecystectomy(LC). The commonly used indicators of surgical difficulty such as the duration of surgeryare insufficient because they are surgeon and institution dependent. We aimed to identify ap-propriate indicators of surgical difficulty during LC.Methods A total of 26 Japanese expert LC surgeons discussed using the nominal grouptechnique (NGT) to generate a list of intraoperative findings that contribute to surgical diffi-culty. Thereafter, a survey was circulated to 61 experts in Japan, Korea, and Taiwan. Thequestionnaire addressed LC experience, surgical strategy, and perceptions of 30 intraopera-tive findings listed by the NGT.Results The response rate of the survey was 100%. There was a statistically significant dif-ference among nations regarding the duration of surgery and adoption rate of safety mea-sures and recognition of landmarks. The criteria for conversion to an open or subtotalcholecystectomy were at the discretion of each surgeon. In contrast, perceptions of the im-pact of 30 intraoperative findings on surgical difficulty (categorized by factors related to in-flammation and additional findings of the gallbladder and other intra-abdominal factors)were consistent among surgeons.Conclusions Intraoperative findings are objective and considered to be appropriate indica-tors of surgical difficulty during LC.
Keywords Critical view of safety · Laparoscopic cholecystectomy · Nominal grouptechnique · SS-Inner theory · Surgical difficulty
Introduction
Laparoscopic cholecystectomy (LC) is undoubtedly the most widely accepted laparoscopicprocedure across the world and has been frequently used to treat acute cholecystitis [1–3].However, severe inflammation of the gallbladder and its surroundings is known to be
J Hepatobiliary Pancreat Sci (2016) 23:533–547DOI: 10.1002/jhbp.375

associated with increased complication rates. In particular, theincidence of serious morbidities such as vasculobiliary inju-ries is reported as 0.2–1.1% [4–6] and is speculated to be 2–5-fold higher than in open cholecystectomy [7, 8]. BecauseLC is extensively practiced worldwide for benign disease ofthe gallbladder, the total number of patients suffering severecomplications is considerably high despite its low incidencerate, making it a “rare but common” problem. To mitigatethese complications, various attempts have been made to clar-ify predictive factors (e.g. preoperative radiological findings)[9–11] of surgical difficulty during LC. Moreover, in patientswith acute cholecystitis, the optimal timing for LC [3, 12] andindications of other preoperative interventions (e.g. percuta-neous transhepatic gallbladder drainage) [13, 14] has alsobeen vigorously studied to standardize treatment strategy.However, none of the previous multicenter trials havesucceeded in providing high-level evidence on surgicaldifficulty during LC. Most of the publications have used
either the duration of surgery [9–11] or open conversion rate[15–19] as surrogate markers of surgical difficulty.Nevertheless, these factors are highly dependent on surgicalskill and institutional policies, precluding head-to-head com-parison among surgeons and centers. To overcome these ma-jor limitations, objective assessment of the inflammatorystatus of the gallbladder is one option. Preoperative radiolog-ical findings and blood tests are readily accessible and enableaccurate comparison among individuals and studies; however,they do not necessarily correlate with the actual difficulty ofthe operation. In theory, postoperative histopathological diag-nosis is another alternative. However, practically speaking, aprecise microscopic evaluation of the dissection margin, themajor determinant of surgical difficulty during LC, is very dif-ficult because of thermal injury due to energy devices or evenimpossible because subtotal cholecystectomy is performed inpatients with severe inflammation and scaring. Therefore, wehypothesized that objective findings during LC that directly
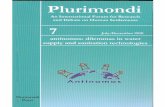
Fig. 1 The sequence of events fromthe manifestation of the initial idea tothe inauguration of a Japan–Korea–Taiwan multinational collaborativeproject and the thought process thatled to the present study
J Hepatobiliary Pancreat Sci (2016) 23:533–547534

correlate with inflammatory changes of the gallbladder areideal indices to evaluate surgical difficulty. The sequence ofevents from the manifestation of the initial idea to the inaugu-ration of a Japan–Korea–Taiwan multinational collaborativeproject and the thought process that led to the present studyis succinctly presented in Figure 1. At this stage, all the coremembers of this project agreed that it is of paramount impor-tance to elucidate the difference in current LC practice and in-sights into potential factors contributing to surgical difficultyamong expert LC surgeons of Japan, Korea, and Taiwan. Inthe present study, we conducted a meeting using a nominalgroup technique (NGT) [20], followed by a questionnairesurvey to develop a universal standard of surgical difficultyduring LC, which would become the foundation of futureLC studies to provide a high level of evidence.
Materials and methods
A total of 26 attending surgeons in Japanese specialized cen-ters of hepatobiliary and pancreatic surgery held a round tablediscussion to exhaustively identify objective findings duringLC that correlate with surgical difficulty. The NGT was thenused to prioritize items brought up in the discussion and gen-erate a list of important intraoperative findings to be includedin the web-based multinational survey. The questionnaire ad-dressed each respondent’s surgical experience in LC, surgicalstrategy for LC (maximum duration of surgery and estimatedblood loss tolerated by each surgeon, safetymeasures, recogni-tion of landmarks and gallbladder anatomy, etc.), rationale foropen conversion or subtotal cholecystectomy, and perceptionsof 30 intraoperative findings that were listed by the NGT. Thequestionnaire was distributed online to 61 attending surgeonsin specialized centers of hepatobiliary and pancreatic surgeryin Japan, Korea, and Taiwan. As shown in Figure 1, the con-cept of the project originated in Japan and eventually spreadtoKorea andTaiwan; therefore, the selection criteria of “expertLC surgeons” to be invited to the surveywas dependent on thechairperson of each nation (T. T., H. H. S., and T. L. H.). Thelanguage used was English, and the web-based survey wasconducted in August 2015 (Korea and Taiwan) and inFebruary 2016 (Japan). In brief, 12 questions included in thequestionnaire were as follows (Fig. 2):
1 Workplace;2 Experience in cholecystectomy (both LC and open
cholecystectomy);3 Experience in LC;4 Maximum duration of surgery accepted for LC;5 Maximum estimated blood loss tolerable for LC;6 Performance rate of LC-related procedures (i.e. intraoper-
ative cholangiogram, “Critical view of safety” technique[21], and identification of Rouvière’s sulcus [22]);
7 Recognition of the subserosal (SS)-Inner layer (the SSlayer which consists of an abundant vasculature thatappears after removing the fat-rich tissue layer, i.e.SS-Outer layer, beneath the serosa of the gallbladder wall)theory [23];
8 Exposure of the SS-Inner layer during dissection of thegallbladder bed;
9 Intraoperative clinical scenarios to abandon conventionalLC and convert to open cholecystectomy, laparoscopicpartial cholecystectomy, etc.;
10 Whether the respondent considers changing to open sur-gery would make the operation much easier in difficultLC cases;
11 Grading of 30 potential factors contributing to surgicaldifficulty that can be identified at the time of operationon a seven-stage scale ranging from 0 (easiest) to 6 (mostdifficult);
12 Description of any other intraoperative findings consid-ered to correlate with surgical difficulty (free answer).
Data were presented as number (%) of respondents. InQuestion 11, data were presented as median and interquartilerange (IQR) using box-and-whisker plots because the re-sponses were collected as ordinal variables and showed anon-normal distribution [24]. χ2 test or Fisher’s exact proba-bility test was used for comparisons among different LC expe-rience level and nations. A P-value of <0.05 was defined asstatistically significant. All statistical analyses were performedusing R software (http://cran.r-project.org). This survey wasconducted after approval from the Institutional Review Boardof Oita University (Approval No. 818).
Results
List of objective findings that can be evaluated during theoperation generated by the NGT
A total of 30 items were listed and categorized intothree groups: (1) Factors related to inflammation of the gall-bladder; (2) Additional findings of the gallbladder and its sur-roundings; and (3) Intra-abdominal factors unrelated toinflammation of the gallbladder (Fig. 3).
Demographics of the respondents (Questions 1–3)
All 61 participants (Japan, n = 32; Korea, n = 12; Taiwan, n =17) replied to the survey (response rate, 100%). Table 1 showsthe distribution of respondents’ experience of LC based on na-tions. In theKorean group, 10 out of 12 (83%) had experienced≥1,000 cases of LC,whichwas significantly higher than that inthe Japanese (38%) or Taiwanese (35%) groups (P = 0.003).
J Hepatobiliary Pancreat Sci (2016) 23:533–547 535

Fig. 2 Full version of the Japan–Korea–Taiwan multinational web-based survey on the surgical difficulty of laparoscopic cholecystectomy
J Hepatobiliary Pancreat Sci (2016) 23:533–547536

Fig. 2 (Continued)
J Hepatobiliary Pancreat Sci (2016) 23:533–547 537

Fig. 2 (Continued)
J Hepatobiliary Pancreat Sci (2016) 23:533–547538

Fig. 2 (Continued)
J Hepatobiliary Pancreat Sci (2016) 23:533–547 539

Maximum duration of surgery and estimated blood loss forLC (Questions 4–5)
The most common answer was “≤180 min” (41%), followedby “No limits” (26%). The distribution did not show
significant differences when categorized based on LC experi-ence (P = 0.09); although when categorized based on nations,the Korean (33%) and Taiwanese (35%) groups replied “Nolimits”more often than the Japanese group (19%) (P = 0.004,Table 1). A total of 38% of respondents answered “≤500 ml”
Fig. 2 (Continued)
J Hepatobiliary Pancreat Sci (2016) 23:533–547540

Fig. 3 A total of 26 expert LC surgeons in Japan generated a list of important objective findings that potentially correlate with surgical difficulty duringlaparoscopic cholecystectomy by the nominal group technique. A total of 30 items were categorized into three groups (see left). The box-and-whiskerdiagrams on the right indicate the grading of each item on a seven-stage scale ranging from 0 (easiest) to 6 (most difficult) by a total of 61 expert LCsurgeons in Japan, Korea, and Taiwan who participated in the web-based survey. The left and right ends of the whiskers represent the minimum andmaximum of all the responses, respectively. The width of each box indicates the interquartile range (IQR), which consists of the middle 50% of the data
J Hepatobiliary Pancreat Sci (2016) 23:533–547 541

as the tolerable maximum estimated blood loss during LC. Nosignificant difference based on LC experience or nations wasobserved (P = 0.14, Table 1).
Safety measures and recognition of landmarks andgallbladder anatomy during LC (Questions 6–8)
Among the three major procedures to secure safety during LC(intraoperative cholangiogram, “Critical view of safety” tech-nique, and identification of Rouvière’s sulcus), intraoperativecholangiogram was performed “Always” and in the “Majorityof cases” only in 35% of all respondents, whereas the other twotechniques were practiced in the 90% range of cases. No signif-icant difference was found in any of these procedures based onLC experience. Although 40%–50% of the Japanese andTaiwanese groups performed intraoperative cholangiogram(“Always” and in the “Majority of cases” combined), none ofthe Korean group answered that they employed this procedure.All respondents from Japan applied the “Critical view ofsafety” technique (“Always” and in the “Majority of cases”combined); however, the Korean (83%) and Taiwanese(88%) groups used this technique less frequently. Similar re-sults were obtained for the identification of Rouvière’s sulcus(Japan, 100%; Korea, 83%; and Taiwan, 65%). The differencesin the adoption rate of these three procedures among the threenations were statistically significant (all P < 0.05, Table 2).
A total of 89% of respondents were familiar with the articleon the “SS-Inner Layer” theory and the standard procedure to
continuously expose the SS-Inner Layer (data not shown).Over 80% of respondents replied that they use this techniqueat the time of dissection at the gallbladder bed (“Always” andin the “Majority of cases” combined, Table 2).
Intraoperative clinical scenarios to abandon conventional LC(Question 9)
In all, 87% of respondents answered that they wouldabandon conventional LC if “Damage to adjacent organsor biliary tract injury” occurs. Majority of the surgeonswould stop when they encounter “Extensive blood loss”and “Severe fibrosis and/or scarring in the Calot’s trianglearea or the gallbladder bed due to inflammation.” Thenumber reduced to 36% if they only suffer “Extensive op-erative time” (Table 2). None of the items showed a sig-nificant difference when categorized based on LCexperience and or nations.
Whether open conversion would make the operation mucheasier in difficult LC cases (Question 10)
Although approximately 80% of respondents answered “Yes”and “Depends on cases,” the remaining considered that openconversion would not change the situation (20%) or may evenmake it worse (2%). No significant difference was observedamong nations (P = 0.26, Table 3).
Table 1 Experience in laparoscopic cholecystectomy and acceptable maximum duration of surgery and estimated blood loss
Overalln = 61
Japann = 32
Korean = 12
Taiwann = 17
P-value
Number of cases performed as an operator or instructor
1–199 9 (15%) 3 (9%) 1 (8%) 5 (29%) 0.003
200–499 13 (21%) 7 (22%) 0 (0%) 6 (35%)
500–999 11 (18%) 10 (31%) 1 (8%) 0 (0%)
≥1,000 28 (46%) 12 (38%) 10 (83%) 6 (35%)
Maximum duration of surgery
≤60 min 0 (0%) 0 (0%) 0 (0%) 0 (0%) 0.004
≤90 min 5 (8%) 1 (3%) 2 (17%) 2 (12%)
≤120 min 7 (12%) 0 (0%) 3 (25%) 4 (24%)
≤180 min 25 (41%) 19 (59%) 2 (17%) 4 (24%)
≤240 min 8 (13%) 6 (19%) 1 (8%) 1 (6%)
No limits 16 (26%) 6 (19%) 4 (33%) 6 (35%)
Maximum estimated blood loss
≤100 ml 2 (3%) 2 (6%) 0 (0%) 0 (0%) 0.14
≤200 ml 9 (15%) 4 (13%) 2 (17%) 3 (18%)
≤300 ml 13 (21%) 11 (34%) 1 (8%) 1 (6%)
≤400 ml 7 (12%) 3 (9%) 3 (25%) 1 (6%)
≤500 ml 23 (38%) 9 (28%) 6 (50%) 8 (47%)
No limits 7 (12%) 3 (9%) 0 (0%) 4 (24%)
J Hepatobiliary Pancreat Sci (2016) 23:533–547542

Intraoperative findings correlated with surgical difficultyduring LC (Questions 11 and 12)
Overall, the perceptions of 30 items generated by the NGTwere consistent among surgeons, regardless of LC experi-ence or nation (Fig. 3): All responses fell within a narrow
IQR of ≤2 with the majority of items (18/30) showing evenhigher degree of convergence (IQR ≤1). In the itemsgrouped under the heading of “Factors related to inflamma-tion of the gallbladder,” edematous change either around thegallbladder, in the area of Calot’s triangle, or in the gall-bladder bed had a minimal impact on surgical difficulty.
Table 2 Safety measures and recognition of landmarks during laparoscopic cholecystectomy and criteria for conversion to an open or subtotalcholecystectomy
Overalln = 61
Japann = 32
Korean = 12
Taiwann = 17
P-value
Adoption rate of laparoscopic cholecystectomy related procedures
Intraoperative cholangiogram
Always 14 (23%) 7 (22%) 0 (0%) 7 (41%) 0.03
Majority of cases 7 (12%) 5 (16%) 0 (0%) 2 (12%)
Exceptional cases 31 (51%) 17 (53%) 7 (58%) 7 (41%)
Never 9 (15%) 3 (9%) 5 (42%) 1 (6%)
“Critical view of safety” technique
Always 32 (53%) 21 (66%) 3 (25%) 8 (47%) 0.04
Majority of cases 25 (41%) 11 (34%) 7 (58%) 7 (41%)
Exceptional cases 3 (5%) 0 (0%) 1 (8%) 2 (12%)
Never 1 (2%) 0 (0%) 1 (8%) 0 (0%)
Identification of Rouvière’s sulcus
Always 31 (51%) 22 (69%) 3 (25%) 6 (35%) 0.002
Majority of cases 22 (36%) 10 (33%) 7 (58%) 5 (29%)
Exceptional cases 6 (10%) 0 (0%) 2 (17%) 4 (24%)
Never 2 (3%) 0 (0%) 0 (0%) 2 (12%)
Exposure of the SS-Inner layer
Always 15 (25%) 10 (31%) 0 (0%) 5 (29%) 0.09
Majority of cases 34 (56%) 19 (59%) 8 (67%) 7 (41%)
Exceptional cases 8 (13%) 2 (6%) 3 (25%) 3 (18%)
Never 4 (7%) 1 (3%) 1 (8%) 2 (12%)
Intraoperative clinical scenarios to abandon conventional laparoscopic cholecystectomy
Extensive operative time 22 (36%) 15 (47%) 4 (33%) 3 (18%) 0.11
Extensive blood loss 44 (72%) 25 (78%) 8 (67%) 11 (65%) 0.56
Damage to adjacent organs or biliary tract injury 53 (87%) 29 (91%) 10 (83%) 14 (82%) 0.60
Extensive and dense adhesion to surroundingorgans and/or greater omentum
28 (46%) 17 (53%) 4 (33%) 7 (41%) 0.46
Severe fibrosis and scarring in Calot’s triangle or gallbladderbed due to inflammation
40 (66%) 22 (69%) 6 (50%) 12 (71%) 0.49
Table 3 When you encounter difficult LC cases, do you think open conversion would make the operation much easier?
Overalln = 61
Japann = 32
Korean = 12
Taiwann = 17
P-value
Yes 14 (23%) 8 (25%) 3 (25%) 3 (18%) 0.26
Depends on cases 34 (56%) 17 (53%) 8 (67%) 9 (53%)
No 12 (20%) 7 (22%) 0 (0%) 5 (29%)
Make it more difficult 1 (2%) 0 (0%) 1 (8%) 0 (0%)
J Hepatobiliary Pancreat Sci (2016) 23:533–547 543

There was a consensus that the level of surgical difficultybecomes increasingly high as fibrotic changes and scarringworsens, particularly in the area of Calot’s triangle. In “Ad-ditional findings of the gallbladder and its surroundings,”necrotic changes and abscess formation were considered tohave a moderately detrimental effect on surgical difficulty,but the development of a cholecysto-enteric fistula was re-vealed to be the most aggravating factor. Among items in“Intra-abdominal factors unrelated to inflammation of thegallbladder,” inversion of the gallbladder and collateral veinformation due to liver cirrhosis were recognized as contrib-uting factors in surgical difficulty. In Question 12 (free an-swer), the following five intraoperative findings wereproposed: “Atrophic gallbladder with no lumen due to se-vere contraction,” “Cholecysto-choledocal fistula,” “MirizziSyndrome,” and “Non-inflammatory (physiological) adhe-sion around the gallbladder.”
Discussion
We found that there is a significant difference among nationsin the performance rate of major safety measures in LC (intra-operative cholangiogram, “Critical view of safety” technique,and identification of Rouvière’s sulcus). The difference in“standard” LC procedure may affect the duration of surgery,complication rates, etc., and it is paramount to standardizethe surgical procedure and set an acceptable range of technicalvariance in a multinational collaborative study.
The duration of surgery [9–11], one of the most commonlyused indices of surgical difficulty, is highly dependent on sur-geons’ skill and experience. In this study, most of the sur-geons (87%) chose “Damage to adjacent organs or biliarytract injury,” i.e. when complication occurs, as the clinicalscenario to consider changing from conventional LC to opencholecystectomy, laparoscopic subtotal cholecystectomy,
Table 4 A total of 25 key intraoperative findings that contribute to surgical difficulty during laparoscopic cholecystectomy
A. Factors related to inflammation of the gallbladder
(a) Appearance around the gallbladder
1. Fibrotic adhesions around the gallbladder due to inflammation
2. Partial scarring adhesions around the gallbladder
3. Diffuse scarring adhesions around the gallbladder
(b) Appearance of the Calot’s triangle area
4. Sparse fibrotic change in the Calot’s triangle area
5. Dense fibrotic change but no scarring in the Calot’s triangle area
6. Partial scarring in the Calot’s triangle area
7. Diffuse scarring in the Calot’s triangle area
(c) Appearance of the gallbladder bed
8. Sparse fibrotic change in the gallbladder bed
9. Dense fibrotic change but no scarring in the gallbladder bed
10. Partial scarring in the gallbladder bed
11. Diffuse scarring in the gallbladder bed (includes atrophic gallbladder with no lumen due to severe contraction)
(d) Additional findings of the gallbladder and its surroundings
12. Edematous change around the gallbladder/in the Calot’s triangle area/in the gallbladder bed
13. Easy bleeding at dissection around the gallbladder/in the Calot’s triangle area/in the gallbladder bed
14. Necrotic changes around the gallbladder/in the Calot’s triangle area/in the gallbladder bed
15. Non-iatrogenic, perforated gallbladder wall and/or abscess formation towards the abdominal cavity noted during adhesiolysis around the gallbladder
16. Abscess formation towards the liver parenchyma
17. Cholecysto-enteric fistula
18. Cholecysto-choledochal fistula (included in the expanded classification of Mirizzi syndrome)
19. Impacted gallstone in the confluence of the cystic, common hepatic, and common bile duct (included in the expanded classification ofMirizzi syndrome)
B. Intra-abdominal factors unrelated to inflammation
20. Excessive visceral fat
21. Inversion of the gallbladder in the gallbladder bed due to liver cirrhosis
22. Collateral vein formation due to liver cirrhosis
23. Non-inflammatory (physiological) adhesion around the gallbladder
24. Anomalous bile duct
25. Gallbladder neck mounting on the common bile duct
J Hepatobiliary Pancreat Sci (2016) 23:533–547544

etc. In addition, the majority of the surgeons chose two othersituations considered unable to maintain safety, i.e. “Exten-sive blood loss” and “Severe fibrosis and/or scarring in theCalot’s triangle area or gallbladder bed due to inflammation.”On the contrary, “Extensive operative time” had the least im-pact on altering the surgical strategy (only 36% of surgeonsagreed), implying that there is a tendency of many surgeonsto adhere to a laparoscopic approach as long as safety is main-tained, regardless of time constraints. In addition, there was asignificant difference in the maximum duration of surgeryallowed among nations, suggesting that whether a surgeoncan continue a laparoscopic approach in a difficult case is de-pendent on socio-economical and/or institutional factorsrather than factors related to the patient or the surgeon. Theduration of surgery is therefore an inappropriate index of sur-gical difficulty in a multicenter study because there is no stan-dardized, objective scale to include only surgeons with anequivalent level of LC technique.
The open conversion rate is another alternative indexfrequently used to evaluate surgical difficulty during LC[14–18]. However, our study revealed that there is a widevariation in clinical scenarios that a surgeon would considerconversion to open cholecystectomy. Moreover, the decision-making process was not influenced either by LC experienceor by nations, indicating that the criteria for open conversionare at thediscretionof eachsurgeon. InaUKstudybasedonna-tional registry data, Ballal et al. reported that non-patient riskfactors of open conversion in LC include surgeons’ experienceand open conversion rate of the institution in the past, alongwith typical patient risk factors such as male gender, emergentLC, and elderly patients [25]. Similar observations have beendescribed by U.S.-based studies [26]. Therefore, open conver-sion is not a pertinent marker of surgical difficulty in a multi-center study.
If the duration of surgery and open conversion rate are in-valid, what could be the appropriate parameters of surgicaldifficulty? In the present study, we agreed with the NGT thatintraoperative findings are appropriate evaluation items tograde surgical difficulty during LC, which is in line with sev-eral other publications [27–29]. However, none of the previ-ous grading systems have evolved to a multicenter study onLC to establish a high level of evidence. We noticed that ex-pressions such as “Unable to…” and “Difficult dissectionof…” in these grading systems are essentially subjective andcan be easily biased by the operator. Thus, the 30 items inQuestion 11 were listed by the NGT with the intention toeliminate ambiguity and provide clarity. After the survey,the 26 attending surgeons in Japan who were engaged in theinitial meeting (to come up with a list of 30 items) held an-other discussion using the NGT to develop appropriate indica-tors of surgical difficulty based on the replies to Questions 11and 12. A “Short cystic duct”was considered less important in
determining difficulty and was removed from the list. Like-wise, phrases “edematous,” “easy bleeding,” and “necroticchanges” were grouped as “Additional findings.” At the end,25 items were listed as key intraoperative findings that con-tribute to surgical difficulty (Table 4). By weighting each itemaccording to its impact, a gold standard will be established touniversally grade surgical difficulty during LC. Thereafter,this gold standard would become the foundation of all typesof studies related to LC (e.g. the optimal timing for LC inacute cholecystitis, indications of percutaneous transhepaticgallbladder drainage, etc.).
The limitations of this study include the small number ofrespondents and the considerable difference in LC experienceamong nations because the initial concept evolved to a multi-national collaborative project in a stepwise fashion (Fig. 1)and the term “expert LC surgeon” remained ill defined (pleasesee Materials and Methods). We are currently preparing alarge-scale, multinational survey involving many expert LCsurgeons under a clear definition that enables us to performworkplace- and LC experience-based stratified analyses.Thereafter, an effective Delphi study is warranted to build anovel grading system of surgical difficulty during LC basedon intraoperative findings.
In conclusion, the duration of surgery and open conversionrate are invalid indices to evaluate surgical difficulty duringLC. Instead, objective findings during the operation are con-sidered to be appropriate indicators of surgical difficulty andshould be universally used in multicenter studies to providea high level of evidence. Investigations are underway to accu-rately weigh the intraoperative findings and integrate them toestablish a novel grading system of surgical difficulty.
Acknowledgments This survey was conducted as part of a Japan–Korea–TaiwanCollaborative Project: Defining the surgical difficulty dur-ing laparoscopic cholecystectomy based solely on intraoperative findings.
We express our sincere gratitude to Rintaro Mori, MD, PhD, MSc,FRCPCH (Director, Department of Health Policy and Department ofClinical Epidemiology, National Center for Child Health and Develop-ment, Tokyo, Japan; Director, Cochrane Japan), Masafumi Inomata,MD, PhD (Professor, Department of Gastroenterological and PediatricSurgery, Oita University Faculty of Medicine, Oita, Japan), and StevenM. Strasberg, MD, FACS (Pruett Professor of Surgery, Division of Gen-eral Surgery, Hepatobiliary-Pancreatic and Gastrointestinal Surgery Sec-tion, Washington University School of Medicine in St. Louis, Missouri,USA) for their professional guidance.
The content of this article was presented to some extent at the follow-ing meetings: The 42nd Congress of the Korean Association of Hepato-Biliary-Pancreatic Surgery (Gyeongju, Korea; April 24, 2015), the 27thMeeting of Japanese Society of Hepato-Biliary-Pancreatic Surgery(Tokyo, Japan; June 12, 2015), Symposium: “Defining the SurgicalDifficulties of Laparoscopic Cholecystectomy Based Solely on Intra-operative Findings” hosted by the Taiwan Surgical Society of Gas-troenterology (Taipei, Taiwan; July 11, 2015), and the 28th
Meeting of the Japanese Society of Hepato-Biliary-PancreaticSurgery (Osaka, Japan; June 2, 2016).
This project was supported by the Japanese Society of Hepato-Biliary-Pancreatic Surgery.
J Hepatobiliary Pancreat Sci (2016) 23:533–547 545

Conflict of interest Itaru Endo has received research funding fromYakult Honsha Co., Ltd and Chugai Pharmaceutical Co., Ltd, and has re-ceived honoraria from Asahi Lase Pharma Corporation.
Appendix: author’s affiliations
Yukio Iwashita, Department of Gastroenterological and Pedi-atric Surgery, Oita University Faculty of Medicine, Oita,Japan; Tetsuji Ohyama, Department of Clinical Statisticsand Data Management, Oita University Faculty of Medicine,Oita, Japan; Goro Honda, Department of Surgery, TokyoMetropolitan Komagome Hospital, Tokyo, Japan; Taizo Hibiand Yuta Abe, Department of Surgery, Keio UniversitySchool of Medicine, Tokyo, Japan; Masahiro Yoshida, De-partment of Hemodialysis and Surgery, Chemotherapy Re-search Institute, International University of Health andWelfare, Chiba, Japan; Fumihiko Miura and TadahiroTakada, Department of Surgery, Teikyo University Schoolof Medicine, Tokyo, Japan; Ho-Seong Han and Yoo-SeokYoon, Department of Surgery, Seoul National UniversityBundangHospital, Seongnam-si, Korea; Tsann-LongHwang,Division of General Surgery, Lin-Kou Chang GungMemorialHospital, Tauyuan, Taiwan; Satoshi Shinya, Department ofSurgery, Tokyo Metropolitan Komagome Hospital, Tokyo,Japan; Kenji Suzuki, Department of Surgery, Fujinomiya CityGeneral Hospital, Shizuoka, Japan; Akiko Umezawa,Minimally Invasive Surgery Center, Yotsuya Medical Cube,Tokyo, Japan; In-Seok Choi, Department of Surgery,Konyang University Hospital, Daejeon, Korea; Wayne Shih-Wei Huang, Department of Surgery, Show Chwan MemorialHospital, Changhua, Taiwan; Kuo-Hsin Chen, Department ofSurgery and Department of Electrical Engineering,Far-Eastern Memorial Hospital and Yuan Ze University,New Taipei City, Taoyuan, Taiwan; Manabu Watanabe,Department of Surgery, Toho University Ohashi MedicalCenter, Tokyo, Japan, Takeyuki Misawa, Department ofSurgery, The Jikei University Kashiwa Hospital, Chiba,Japan; Yuichi Nagakawa, Department of Gastrointestinaland Pediatric Surgery, Tokyo Medical University, Tokyo,Japan; Dong-Sup Yoon, Department of Surgery, YonseiUniversity Gangnam Severance Hospital, Seoul, Korea;Jin-Young Jang, Department of Surgery, Seoul NationalUniversity Hospital, Seoul, Korea; Hee Chul Yu, Departmentof Surgery, Chonbuk National University Hospital, Jeonju,Korea; Keun Soo Ahn, Department of Surgery, KeimyungUniversity Dongsan Medical Center, Daegu, Korea; SongCheol Kim, Department of Surgery, University of UlsanCollege of Medicine and AsanMedical Center, Seoul, Korea;In Sang Song, Department of Surgery, Chungnam NationalUniversity Hospital, Daejeon, Korea; Ji Hoon Kim, Depart-ment of Surgery, Eulji University Hospital, Daejeon, Korea;Sung Su Yun, Department of Surgery, YeungnamUniversity,Daegu, Korea; Seong Ho Choi, Department of Surgery,
Sungkyunkwan University, Seoul, Korea; Yi-Yin Jan, Divi-sion of General Surgery, Lin-Kou Chang Gung MemorialHospital, Taoyuan, Taiwan; Shyr-Ming Sheen-Chen, Divisionof General Surgery, Kaohsiung ChangGungMemorial Hospi-tal, Kaohsiung, Taiwan; Yan-Shen Shan, Department ofSurgery, National Cheng Kung University Hospital, Tainan,Taiwan; Chen-Guo Ker, Department of Surgery, Yuan’s Gen-eral Hospital, Kaohsiung, Taiwan; De-Chuan Chan, Divisionof General Surgery, Tri-Service General Hospital, NationalDefense Medical Center, Taipei, Taiwan; King-Teh Lee,Department of Surgery, Kaohsiung Medical UniversityHospital, Kaohsiung, Taiwan; Naoyuki Toyota, Departmentof Surgery, Musashino Tokushukai Hospital, Tokyo, Japan;Ryota Higuchi andMasakazu Yamamoto, Department of Sur-gery, Institute of Gastroenterology, Tokyo Women’s MedicalUniversity, Tokyo, Japan; Yoshiharu Nakamura, Departmentof Gastrointestinal and Hepato-Biliary-Pancreatic Surgery,Nippon Medical School, Tokyo, Japan; Yoshiaki Mizuguchi,Department of Surgery, Nippon Medical School, Tokyo,Japan; Yutaka Takeda, Department of Surgery, Kansai RosaiHospital, Hyogo, Japan; Masahiro Ito, Department of Generaland Pancreatic Surgery, Quality and safety in healthcare,Fujita Health University, Aichi, Japan; Shinji Norimizu, De-partment of Surgery, NagoyaDaini Red CrossHospital, Aichi,Japan; Shigetoshi Yamada, Department of Surgery, KamedaMedical Center, Chiba, Japan; Naoki Matsumura and HiromiTokumura, Department of Surgery, Tohoku Rosai Hospital,Miyagi, Japan; Junichi Shindoh, Department of DigestiveSurgery, Toranomon Hospital, Tokyo, Japan; HirokiSunagawa, Department of Surgery, Nakagami Hospital,Okinawa, Japan; Hiroshi Hasegawa, Laparoscopic SurgeryCenter, Tokai Hospital, Aichi, Japan; Toshiki Rikiyama,Department of Surgery, Saitama Medical Center, Jichi Medi-cal University, Saitama, Japan; Naohiro Sata, Department ofSurgery, Jichi Medical University, Tochigi, Japan; NobuyasuKano, Director, Chiba Tokushukai Hospital, Chiba, Japan;Seigo Kitano, President, Oita University, Oita, Japan; YuichiYamashita, Department of Gastroenterological Surgery,Fukuoka University School of Medicine, Fukuoka, Japan;Goro Watanabe, Department of Surgery, Sanno Hospital,International University of Health and Welfare, Tokyo,Japan; Kunitoshi Nakagawa, Japanese Red Cross MiyagiBlood Center, Miyagi, Japan; Taizo Kimura, Department ofSurgery, Fujinomiya City General Hospital, Shizuoka, Japan;Tatsuo Yamakawa, Department of Surgery, Teikyo UniversitySchool of Medicine, University Hospital, Mizonokuchi,Kanagawa, Japan; Go Wakabayashi, Department of Surgery,Ageo Central General Hospital, Saitama, Japan; Itaru Endo,Department of Gastroenterological Surgery, Yokohama CityUniversity Graduate School of Medicine, Kanagawa, Japan;Masaru Miyazaki, Emeritus Professor, Graduate School ofMedicine, Chiba University, Chiba, Japan.
J Hepatobiliary Pancreat Sci (2016) 23:533–547546

References
1. Barkun JS, Aronson JK, Feldman LS, Maddern GJ, Strasberg SM,Balliol Collaboration, et al. Evaluation and stages of surgical innova-tions. Lancet. 2009;374:1089–96.
2. Tucker JJ, Grim R, Bell T, Martin J, Ahuja V. Changing demo-graphics in laparoscopic cholecystectomy performed in the UnitedStates: hospitalizations from 1998 to 2010. Am Surg. 2014;80:652–8.
3. de Mestral C, Rotstein OD, Laupacis A, Hoch JS, Zagorski B, AlaliAS, et al. Comparative operative outcomes of early and delayed cho-lecystectomy for acute cholecystitis: a population-based propensityscore analysis. Ann Surg. 2014;259:10–5.
4. Giger UF, Michel JM, Opitz I, Th Inderbitzin D, Kocher T,Krähenbühl L, et al. Risk factors for perioperative complications in pa-tients undergoing laparoscopic cholecystectomy: analysis of 22,953consecutive cases from the Swiss Association of Laparoscopic andThoracoscopic Surgery database. J Am Coll Surg. 2006;203:723–8.
5. Harboe KM, Bardram L. The quality of cholecystectomy inDenmark: outcome and risk factors for 20,307 patients from the na-tional database. Surg Endosc. 2011;25:1630–41.
6. Navez B, Ungureanu F, Michiels M, Claeys D, Muysoms F, HubertC, et al. Surgical management of acute cholecystitis: results of a 2-year prospective multicenter survey in Belgium. Surg Endosc.2012;26:2436–45.
7. Morgenstern L, Wong L, Berci G. Twelve hundred open cholecys-tectomies before the laparoscopic era. A standard for comparison.Arch Surg. 1992;127:400–3.
8. Flum DR, Dellinger EP, Cheadle A, Chan L, Koepsell T. Intraoper-ative cholangiography and risk of common bile duct injury duringcholecystectomy. JAMA. 2003;289:1639–44.
9. Schrenk P, Woisetschläger R, Rieger R, Wayand WU. A diagnosticscore to predict the difficulty of a laparoscopic cholecystectomyfrom preoperative variables. Surg Endosc. 1998;12:148–50.
10. Sakuramoto S, Sato S, Okuri T, Sato K, Hiki Y, Kakita A. Preoper-ative evaluation to predict technical difficulties of laparoscopic cho-lecystectomy on the basis of histological inflammation findings onresected gallbladder. Am J Surg. 2000;179:114–21.
11. Hiromatsu T, Hasegawa H, Sakamoto E, Komatsu S, Kawai K,Tabata T, et al. Preoperative Evaluation ofDifficulty of LaparoscopicCholecystectomy. Jpn J Gastroenterol Surg. 2007;40:1449–55.
12. Li J, Frilling A, Nadalin S, Broelsch CE, Malago M. Timing and riskfactors of hepatectomy in the management of complications followinglaparoscopic cholecystectomy. J Gastrointest Surg. 2012;16:815–20.
13. Ito K, Fujita N, Noda Y, Kobayashi G, Kimura K, Sugawara T, et al.Percutaneous cholecystostomy versus gallbladder aspiration foracute cholecystitis: a prospective randomized controlled trial. AJRAm J Roentgenol. 2004;183:193–6.
14. Winbladh A, Gullstrand P, Svanvik J, Sandström P. Systematic re-view of cholecystostomy as a treatment option in acute cholecystitis.HPB (Oxford). 2009;11:183–93.
15. Lal P, Agarwal PN, Malik VK, Chakravarti AL. A difficult laparo-scopic cholecystectomy that requires conversion to open procedurecan be predicted by preoperative ultrasonography. JSLS.2002;6:59–63.
16. Kama NA, Kologlu M, Doganay M, Reis E, Atli M, Dolapci M. Arisk score for conversion from laparoscopic to open cholecystec-tomy. Am J Surg. 2001;181:520–5.
17. Lipman JM, Claridge JA, Haridas M, Martin MD, Yao DC, GrimesKL, et al. Preoperative findings predict conversion from laparo-scopic to open cholecystectomy. Surgery. 2007;142:556–65.
18. Rosen M, Brody F, Ponsky J. Predictive factors for conversion oflaparoscopic cholecystectomy. Am J Surg. 2002;184:254–8.
19. Simopoulos C, Botaitis S, Polychronidis A, Tripsianis G,Karayiannakis AJ. Risk factors for conversion of laparoscopic cho-lecystectomy to open cholecystectomy. Surg Endosc.2005;19:905–9.
20. GallagherM,Hares T, Spencer J, BradshawC,Webb I. The nominalgroup technique: a research tool for general practice ? Fam Pract.1993;10:76–8.
21. Strasberg SM, Hertl M, Soper NJ. An analysis of the problem of bil-iary injury during laparoscopic cholecystectomy. J Am Coll Surg.1995;180:101–25.
22. Hugh TB, Kelly MD, Mekisic A. Rouvière’s sulcus: a usefullandmark in laparoscopic cholecystectomy. Br J Surg. 1997;84:1253–4.
23. Honda G, Iwanaga T, Kurata M. Dissection of the gallbladder fromthe liver bed during laparoscopic cholecystectomy for acute or sub-acute cholecystitis. J Hepatobiliary Pancreat Surg. 2008;15:293–6.
24. Whitley E, Ball J. Statistics review 1: Presenting and summarisingdata. Crit Care. 2002;6:66–71.
25. Ballal M, David G, Willmott S, Corless DJ, Deakin M, Slavin JP.Conversion after laparoscopic cholecystectomy in England. SurgEndosc. 2009;2:2338–44.
26. Kaafarani HM, Smith TS, Neumayer L, Berger DH, Depalma RG,Itani KM. Trends, outcomes, and predictors of open and conversionto open cholecystectomy in Veterans Health Administration hospi-tals. Am J Surg. 2010;200:32–40.
27. Chang YC. A proposed inflammation grading system for laparo-scopic cholecystectomy. Hepatogastroenterology. 2005;52:33–6.
28. Cho KS, Baek SY, Kang BC, Choi HY, Han HS. Evaluation of pre-operative sonography in acute cholecystitis to predict technical diffi-culties during laparoscopic cholecystectomy. J Clin Ultrasound.2004;32:115–22.
29. Sugrue M, Sahebally SM, Ansaloni L, Zielinski MD. Grading oper-ative findings at laparoscopic cholecystectomy– a new scoring sys-tem. World J Emerg Surg. 2015;10:14.
30. Honda G, Iwanaga T, Kurata M, Watanabe F, Satoh H, Iwasaki K.The critical view of safety in laparoscopic cholecystectomy is opti-mized by exposing the inner layer of the subserosal layer. JHepatobiliary Pancreat Surg. 2009;16:445–9.
J Hepatobiliary Pancreat Sci (2016) 23:533–547 547