Water accessibility and child health: Use of the leave-out strategy of instruments
11
Journal of Health Economics 30 (2011) 1000–1010 Contents lists available at ScienceDirect Journal of Health Economics jo u rn al hom epage : www.elsevier.com/locate/econbase Water accessibility and child health: Use of the leave-out strategy of instruments Dirga Kumar Lamichhane a,∗ , Eiji Mangyo b a Graduate School of International Relations, International University of Japan (IDP 2009), Japan b Graduate School of International Relations, International University of Japan, Japan a r t i c l e i n f o Article history: Received 6 September 2009 Received in revised form 29 June 2011 Accepted 5 July 2011 Available online 12 July 2011 JEL classification: C31 I12 O10 Keywords: Fetching water time Leave-out strategy Endogenous project placement Child health a b s t r a c t This paper investigates the leave-out strategy of instruments by using the leave-out community ratio of household access to in-yard water sources and community water infrastructure as instruments for hours in fetching water time, and the data on disease symptoms. The results show that community-level access to clean water is significantly associated with both water-relevant and irrelevant disease symptoms, which suggests that the correlation between community-level access to clean water and child health is at least partially due to endogenous project placement potentially with respect to unobserved community wealth. The paper concludes that the OLS estimates have a potential endogeneity bias problem and that IV estimates under this strategy is subject to endogenous project placement and is not valid. A policy implication of this study is that careful attention should be paid to both self-selection and endogenous project placement in studying the effect of water accessibility on child health. © 2011 Elsevier B.V. All rights reserved. 1. Introduction Studies in the economic literature have commonly used the leave-out strategy of instruments 1 to address the potential endo- geneity and possible measurement error of water accessibility on child health (see, for example, Ilahi and Grimard, 2000; Glick et al., 2004; Mangyo, 2007). It is therefore important to examine the conditions that determine the validity of the leave-out strategy of instruments. In this paper, we look at the potential weakness of this instrumentation strategy in examining the effect of water accessibility on child health. The idea behind this instrument is that community-level access to clean water reflects past infrastructure projects conducted by government or non-governmental organizations (NGOs) rather than individual choice of water access by individual household. Thus, this instrumenting strategy is effective against self-selection of household into better access to clean water but is potentially subject to endogenous project placement. For example, unob- ∗ Corresponding author. Current address: AHTCS, P.O. Box 419, Ramghat, Pokhara, Nepal. Tel.: +977 98560 27083; fax: +977 61 535807. E-mail address: dirga [email protected] (D.K. Lamichhane). 1 The use of community-level access to water as the instrument for household- level access to water by calculating the ratio of sample households with water access for each sample community but excluding the self-household both from numerator and denominator. served community wealth may be positively correlated with both community-level access to clean water and child health, leading to an upward bias. For another example, unobserved pollution level of community may be positively correlated with community-level access to clean water (more urbanized areas may have better access to clean water) and negatively associated with child health, leading to a negative bias. Ilahi and Grimard (2000) address the potential endogeneity of the availability of in-yard water by using the leave-out community ratio of households with in-house access to water in cross-sectional data from Pakistan. The focus of the study was on the relation- ship between access to water and time allocation of women, who had primary responsibility for water collection. They show that improvement in water-supply infrastructure would lower the total time women spend in all activities including hours in water col- lection. The examination of hours in water collection using the leave-out strategy in Madagascar and Uganda finds that feasible public investment would not lead to large reduction in water col- lection times or change the relative burden of overall work in men and women (Glick et al., 2004). They also find that an investment in water does not necessarily have a dramatic effect on female time use. In a panel data study, one of the limited studies in the economic literature, the use of leave-out community ratio as the instrument for change in in-yard water source finds that the access to in-yard water sources improved child health of well-educated mothers in China (Mangyo, 2007). 0167-6296/$ – see front matter © 2011 Elsevier B.V. All rights reserved. doi:10.1016/j.jhealeco.2011.07.001
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Water accessibility and child health: Use of the leave-out strategy of instruments

W
Da
b
a
ARRAA
JCIO
KFLEC
1
lgc2cooa
tgtTos
N
lfa
0d
Journal of Health Economics 30 (2011) 1000– 1010
Contents lists available at ScienceDirect
Journal of Health Economics
jo u rn al hom epage : www.elsev ier .com/ locate /econbase
ater accessibility and child health: Use of the leave-out strategy of instruments
irga Kumar Lamichhanea,∗, Eiji Mangyob
Graduate School of International Relations, International University of Japan (IDP 2009), JapanGraduate School of International Relations, International University of Japan, Japan
r t i c l e i n f o
rticle history:eceived 6 September 2009eceived in revised form 29 June 2011ccepted 5 July 2011vailable online 12 July 2011
EL classification:31
12
a b s t r a c t
This paper investigates the leave-out strategy of instruments by using the leave-out community ratio ofhousehold access to in-yard water sources and community water infrastructure as instruments for hoursin fetching water time, and the data on disease symptoms. The results show that community-level accessto clean water is significantly associated with both water-relevant and irrelevant disease symptoms,which suggests that the correlation between community-level access to clean water and child health is atleast partially due to endogenous project placement potentially with respect to unobserved communitywealth. The paper concludes that the OLS estimates have a potential endogeneity bias problem and thatIV estimates under this strategy is subject to endogenous project placement and is not valid. A policy
10
eywords:etching water timeeave-out strategyndogenous project placement
implication of this study is that careful attention should be paid to both self-selection and endogenousproject placement in studying the effect of water accessibility on child health.
© 2011 Elsevier B.V. All rights reserved.
scaoatt
trdshit
hild health
. Introduction
Studies in the economic literature have commonly used theeave-out strategy of instruments1 to address the potential endo-eneity and possible measurement error of water accessibility onhild health (see, for example, Ilahi and Grimard, 2000; Glick et al.,004; Mangyo, 2007). It is therefore important to examine theonditions that determine the validity of the leave-out strategyf instruments. In this paper, we look at the potential weaknessf this instrumentation strategy in examining the effect of waterccessibility on child health.
The idea behind this instrument is that community-level accesso clean water reflects past infrastructure projects conducted byovernment or non-governmental organizations (NGOs) ratherhan individual choice of water access by individual household.
hus, this instrumenting strategy is effective against self-selectionf household into better access to clean water but is potentiallyubject to endogenous project placement. For example, unob-∗ Corresponding author. Current address: AHTCS, P.O. Box 419, Ramghat, Pokhara,epal. Tel.: +977 98560 27083; fax: +977 61 535807.
E-mail address: dirga [email protected] (D.K. Lamichhane).1 The use of community-level access to water as the instrument for household-
evel access to water by calculating the ratio of sample households with water accessor each sample community but excluding the self-household both from numeratornd denominator.
llplaiulfwC
167-6296/$ – see front matter © 2011 Elsevier B.V. All rights reserved.oi:10.1016/j.jhealeco.2011.07.001
erved community wealth may be positively correlated with bothommunity-level access to clean water and child health, leading ton upward bias. For another example, unobserved pollution levelf community may be positively correlated with community-levelccess to clean water (more urbanized areas may have better accesso clean water) and negatively associated with child health, leadingo a negative bias.
Ilahi and Grimard (2000) address the potential endogeneity ofhe availability of in-yard water by using the leave-out communityatio of households with in-house access to water in cross-sectionalata from Pakistan. The focus of the study was on the relation-hip between access to water and time allocation of women, whoad primary responsibility for water collection. They show that
mprovement in water-supply infrastructure would lower the totalime women spend in all activities including hours in water col-ection. The examination of hours in water collection using theeave-out strategy in Madagascar and Uganda finds that feasibleublic investment would not lead to large reduction in water col-
ection times or change the relative burden of overall work in mennd women (Glick et al., 2004). They also find that an investmentn water does not necessarily have a dramatic effect on female timese. In a panel data study, one of the limited studies in the economic
iterature, the use of leave-out community ratio as the instrumentor change in in-yard water source finds that the access to in-yardater sources improved child health of well-educated mothers inhina (Mangyo, 2007).

of Hea
guTidAca
asoaT(hbwzsodabyrtoac(cwwiIb
cwiudhaomloiwipoanSoofdnna
Hwpies4wSd
cdadaatfud
luicwtcaomhahsjg
tdrc
2
2
iwlayears in 8707 households included in the survey. The DHS samplingdesign2 allowed for community level estimates in 260 clusters (pri-mary sampling units) for 5 development regions in the country.
2 DHS data contains a household sample which was collected in a two stage. Atthe first-stage of sampling, 260 primary sampling units (PSU), 82 in urban areas
D.K. Lamichhane, E. Mangyo / Journal
Behrman and Lavy (1997) have extensively studied the endo-eneity of child health, measurement error, and the impact ofnobserved fixed and choice inputs on child schooling in Ghana.hey suggest that the true impact of child health on child school-ng success is not significant and that returns to scale are limitedespite the use of typical family and community instruments.lthough they have shown the relationship between schooling andhild health while addressing endogeneity, their study method canlso be applied to a similar study on child health and water access.
Previous studies found a positive relationship between waterccess and child health. Many of them have examined the relation-hip between access to piped water and child health, and somef them have also explored the interaction between safe waternd other household characteristics (see, for example, Cebu Studyeam, 1991; Jalan and Martin, 2003; Esrey, 1996). Galiani et al.2005), using panel data at the locality level, compare changes inealth over time across before and after changes in water accessi-ility. They control for locality and time fixed effects and exploitithin locality variability to identify the effect of water privati-
ation on child health. They find that the privatization of waterervices and subsequent improvements of water infrastructurenly affects water related deaths and not other non-water relatedeaths in Argentina. A study in Nigeria finds that water supplynd sanitation projects have helped to improve weight-for-heightut not for height-for-age for children under the age of threeears (Huttly et al., 1990). Thomas and Strauss (1992) examine theelationship between parental characteristics, community charac-eristics, and child height in Brazil. They find that the availabilityf modern sewerage, piped water, and electricity has significantlyffected child height, and the impact of mother’s education onhild height does not solely reflect resource availability. Esrey et al.1985) analyzes the impact of water access on child health in fiveountries. They find no impact of water availability on height oreight in Bangladesh, and water access has a minor impact oneight-for-age in the Philippines. On the contrary, water availabil-
ty has improved height-for-age and weight-for-age in Colombia.n Nigeria, improved water access has a positive impact on weightut adversely affected height.
The exploration of interaction of safe water and maternal edu-ation has found that height-for-age improved with improvedater supplies for less well-educated mothers when this variable is
nteracted with maternal education (Barrera, 1990). Esrey (1996),sing multivariate analysis with Demographic and Health Surveyata, concluded that improved water quality can improve childeight and weight only when sanitation is also improved. Esreynd Habicht (1988), using data from Malaysia, examine the impactf maternal literacy, piped water, and access to toilets on infantortality. They find a synergistic relationship between maternal
iteracy and piped water. Butz et al. (1984) measures the impactf improved water and sanitation together with breast-feeding onnfant mortality. They find that the presence of both improved
ater and sanitation has the biggest impact on reduced mortal-ty in Malaysia. Jalan and Martin (2003) estimate the impact ofiped water on child health in terms of the incidence and severityf diarrhoea in rural India. They find a lower incidence of diarrhoeamong children living in piped water households. Using longitudi-al data from household survey conducted in the Philippines, Cebutudy Team (1991) studies the impact of behavioral inputs withther exogenous factors on child health especially on diarrhoealutcomes. The authors used family specific fixed effects to controlor unobserved heterogeneity. The results show that population
ensity, child age, exposure to contaminated water, fecal contami-ation, and rainfall increased the incidence of diarrhoea. However,one of them have addressed the endogenous nature of child healthnd water accessibility.apaai
lth Economics 30 (2011) 1000– 1010 1001
In this paper, we use the data from the Nepal Demographic andealth Survey 2006. In Nepal, the supply of improved drinkingater has encouragingly increased since 1990. The water sup-ly coverage reached about 81 percent in 2005, which drastically
ncreased from the 46 percent reported in 1990 (NPC, 2005). How-ver, there is still a problem of physical accessibility to a waterource and sanitation. According to WaterAid Nepal (2004), only2 percent of rural communities of Nepal have access to improvedater supplies within return journey times of less than 15 min.
ome households in hills have to spend as much as five hours peray for collecting water.
We assess the extent to which the community-level access tolean water is subject to endogenous project placement by utilisingata on disease symptoms. If the correlation between child healthnd community-level access to clean water is at least partiallyue to endogenous project placement, such unobserved differencescross communities not only affect water-relevant symptoms butlso affect water-irrelevant symptoms. Here, water-relevant symp-oms include diarrhoea, while water-irrelevant symptoms includeever and cough. For example, there is no reason to expect thatnobserved community differences in wealth affect only the inci-ence of diarrhoea but not the incidence of fever and cough.
Our econometric results show that the leave-out community-evel access to clean water appears to be correlated withnobserved differences across communities, implying that our
nstrument is not valid. Our econometric results find thatommunity-level access to clean water is negatively correlatedith the incidence of both water-relevant and irrelevant symp-
oms. One plausible story behind this finding would be unobservedommunity wealth is positively correlated with community-levelccess to clean water and negatively correlated with the incidencef both water-relevant and irrelevant symptoms. Thus, our econo-etric estimates of the impact of fetching water time on child
ealth fails to pin down the true effect. However, our study presents potential weakness of the leave-out instrumenting strategy whichas been popular in the economic literature. Our study clearlyhows that the leave-out community-level instruments are sub-ect to endogenous project placement and could do more harm thanood.
The remainder of this paper is organized as follows. In Sec-ion 2, we describe the dataset, descriptive statistics, and variablesescription. Section 3 presents the empirical specification. Theesults and discussion are present in Section 4 and we close withonclusions and recommendations in Section 5.
. Data and variables
.1. Data description
Analysis of data was based on 5783 children aged 0–59 monthsncluded in the Nepal Demographic and Health Survey (DHS),
hich was carried out from February to August 2006. The DHS col-ected demographic, socioeconomic, and health data and formed
nationally representative sample of 10,793 women aged 15–49
nd 178 in rural areas, were selected using systematic sampling with probabilityroportional to size. The PSU includes a ward, sub ward, or group of wards in ruralreas, and sub wards in urban areas. While in the second-stage of sampling, theverage of 30 households per PSU in urban areas and average of 36 householdsn rural areas were selected by using systematic sampling. Urban area was over

1 of Health Economics 30 (2011) 1000– 1010
lTt2isTdran
2
mwiom(abn
thothoThoca(SHl
lcew
sw
w(wwa
csTcra
whwa
Table 1Description of main variables used in analysis.
Variable Description
Height-for-age (HAZ)and Weight-for-age(WAZ)
Z-scores of height-for-age and weight-for-agewhich are based on WHO international referencestandard.
Fetching water time Hours (per time) spent to get to the nearest watersources, get water and come back. 0 if water isavailable in-yard or plot.
Child age Child age in months ranging from 0 to 59.Mother height Height of mother in centimeters.Teenage mother Equals to 1 if mother at the time of first birth was
less than 19 years of age, 0 otherwise.Male Equals to 1 if child was male, 0 otherwise.Twin Equals to 1 if child was twin or multiple births, 0
otherwise.Wealth index Continuous variable of assets of the household.Mother/husband
primary educationEquals to 1 if mother/husband had primaryeducation, 0 otherwise.
Mother/husbandsecondary education
Equals to 1 if mother/husband had eithersecondary or higher education, 0 otherwise.
Mother education Equals to 1 if mother had either primary orsecondary education, 0 otherwise.
Mother no education Equals to 1 if mother had never attended school, 0otherwise.
Age difference to headof household
Equals to 1 if the gap between mother age andhead of household head was more than 20 years, 0otherwise.
Season Equals to 1 if month of interviews was February (2)or March (3) or April (4), 0 otherwise.
Household size Number of household member excluding visitors.In-yard water Non-self community ratio of household with
access to water sources on household premises tototal number of household within the community.
Public tap Non-self community ratio of household withaccess to stand pipe or public tap water to totalnumber of household within the community.
Tube well Non-self community ratio of household withaccess to tube well or borehole water to totalnumber of household within the community.
Piped water Non-self community ratio of household withaccess to piped water to total number of householdwithin the community.
Modern contraceptive Non-self community ratio of women who usedmodern contraceptive to total number ofhousehold within the community.
Basic vaccination Non-self community ratio of children whoreceived all the basic vaccines to total number ofhousehold within the community.
Hill Equals to 1 if people lived in hilly regions, 0otherwise.
002 D.K. Lamichhane, E. Mangyo / Journal
Survey regression analysis3 rather than non-survey ordinaryeast square (OLS) was used to control the DHS sampling design.he survey regression deals with three important sample charac-eristics: sampling weight, stratification, and clustering (Gutierrez,008). Failure to deal with sampling weight usually leads to bias
n standard errors and gives false statistical test results. In DHSampling, observations within a cluster were not independent.herefore, the OLS estimates will give a downward bias to its stan-ard errors. Further, in DHS, individuals were sampled in groupsather than individually; therefore, the standard errors should bedjusted for design effects. Hence, applying survey regression tech-ique produces correct standard errors.
.2. Variables description
Table 1 presents the variable definitions. Two anthropometriceasures (z-scores of height-for-age and weight-for-age), whichere standardized based on World Health Organization (WHO)
nternational reference standards,4 were used as health indicatorsf children. Child height-for-age and weight-for-age were used toeasure the longer-run child health in terms of nutritional status
MOHP, New ERA, and Macro International Inc., 2007). Weight-for-ge largely indicates the same aspect of health as height-for-age,ut it is influenced by a recent phenomenon. Height-for-age doesot vary according to recent dietary intake.
The physical accessibility of drinking water was defined inerms of fetching water time in hours5 (round-trip) which is ‘0′ ifousehold had water sources within premises (either piped waterr tube well water or public tap water); otherwise, it takes theime value up to 3 h, if water source was very far. The house-old physical accessibility of water is likely to be correlated withther socio-demographic factors that can also affect child health.herefore, the effects of hours in fetching water time on childealth were estimated after statistically controlling for the effectsf other potentially confounding factors. These factors included athild, household, and community level characteristics. The vari-bles included at the level of the child were child age in months0–59 months) in order to control for the age effect on child health.ex of the child and the status of being twins were also included.atkar and Bhide (1999) showed that the twin frequently gives
ower birth weight.The variables at the level of household are described as fol-
ows. As parental education is likely to be highly correlated with
hild health and water access, exclusion of education of either par-nt is likely to bias the coefficient estimate on hours in fetchingater time in the negative direction. Therefore, both mother’s andampled to obtain statistically reliable estimates of urban areas and total sample iseighted (MOPH, New ERA, and Macro International Inc., 2007).3 A survey design characteristic was set by Stata command: svyset. This commandas set for clustering (primary sampling unit), sample weight, and stratification
sample stratum number). The weighting factor was used after dividing the sampleeight by 1,000,000. Once the design characteristic was set, svy prefix was usedith supported estimation command. Except for the svy prefix, survey commands
re the same as non-survey commands.4 WHO released the new growth standard, in April 2006, and recommended new
ut-offs for data exclusion. The data were excluded if a child’s height-for-age z-core was below −6 or above +6 and weight-for-age z score below −6 or above +5.his cut-offs points were wider than those for the old cut-offs for the 1978. Z-scoreompares a child’s measurements with the measurements of similar children in theeference population from healthy population which has a z-score with mean zerond standard deviation one.5 To check the accuracy of reported time, a dummy variable for water accessibilityas also used for analysis. The dummy was equal to ‘1’ if water sources were withinousehold premises and equals to ‘0’ otherwise. The obtained results are consistentith the results presented in this paper. (The result with a dummy variable of water
ccess is not presented in this paper due to space limitation.)
Mountain Equals to 1 if people lived in mountain regions, 0otherwise.
Plain area (Terai) Equals to 1 if people lived in Terai region, 0otherwise.
Diarrhoea Equals to 1 if diarrhoea was prevalent in children,
hceawatth(
i
0 otherwise.Water-irrelevant Equals to 1 if either fever or cough was prevalent
in children, 0 otherwise.
usband’s education were included as categorical variables indi-ating whether the mother or husband had primary or secondaryducation, with no education as the reference group. Mother’sge at first birth was included as a dummy variable indicatinghether the mother was younger than 19 years of age6 or not
t the time of giving birth to the first child. Teenage motherypically found poor pregnancy outcome and is likely to be rela-
ively inexperienced in child rearing. Children of teenage mothersave also been typically found to suffer from lower birth weightMwabu, 2008). Age may not only reflect biological factor, but6 The cut-off point of below 19 year was chosen because the child height-for-agencreases with the age of mother at the time of birth up to approximately 18 years.

of Health Economics 30 (2011) 1000– 1010 1003
aiocdth
ciggh
ewPdwdHnocTno(is
rabwv(no
swem
2
rncla
ctabo
(
au
Table 2Descriptive statistics of main variables used in analysis.
Mean Standard deviation
Continuous variablesHAZ −1.960 1.336WAZ −1.717 1.061Fetching water time (h) 0.166 0.263Child age 29.975 17.345Wealth index −0.217 0.829Mother height 150.793 5.377Categorical variablesMale 0.506 0.500Twin 0.009 0.096Child age 0–5 months 0.087 0.282Child age 6–11 months 0.098 0.297Child age 12–23 months 0.199 0.399Child age 24–35 months 0.211 0.408Child age 36–47 months 0.198 0.398Child age 48–59 months 0.208 0.406Teenage mother 0.434 0.496Age difference to head of household 0.364 0.481Mother primary education 0.177 0.382Mother secondary education 0.208 0.406Husband primary education 0.294 0.456Husband secondary education 0.463 0.499Mother education 0.395 0.489Mother no education 0.605 0.489Diarrhoea 0.123 0.328Water-irrelevant 0.284 0.451Tube well 0.369 0.454Piped water 0.099 0.201In-yard water 0.417 0.323Public tap 0.249 0.313Modern contraceptive 0.343 0.199Basic vaccination 0.689 0.195Season 0.283 0.450Household size 6.667 3.182Hill 0.395 0.489
apcadasmeowtph
D.K. Lamichhane, E. Mangyo / Journal
lso can reflect socio-economic consideration. Maternal age cannfluence intra-household bargaining power of mothers relative tother household members (Smith et al., 2003). This possibility wasontrolled by including a dummy variable indicating a large ageifference (more than 20 years, which was imaginarily set) rela-ive to head of household, which was not necessarily the woman’susband.
Parental height reflects investments in health and other humanapital. Therefore, it may also serve as proxy for unobserved fam-ly background characteristics although it is partly influenced byenetics. As there is difference in racial composition in various geo-raphical locations of Nepal, in the absence of race control, mother’seight can be a good indicator for differing races.
DHS data does not have information on household income andxpenditure. Instead of income and expenditure, the wealth index7
as used to measure the long-run household wealth. Filmer andritchett (1996), using Nepal Living Standards Survey data, haveemonstrated that to use wealth index as a proxy for long-runealth was more reliable than conventional consumption expen-iture based measures. The effect of household size was included.owever, it is argued that household size may not be truly exoge-ous as there may be a trade-off between the quality and quantityf children. If women have access to modern contraceptive for birthontrol, household size could be determined by mother or family.8
he household size could be exogenous where family planning isot so widespread. However, it is possible that even in the absencef family planning, child mortality can influence household sizeLinnemayr et al., 2008). As it is difficult to find the acceptablenstruments to address this possible simultaneity, the householdize was included in our estimation.
The variables at the community-level included are geographicalegions (Mountain, Hill, and Terai), community water sources, and
community-level share of individual response on the use of all theasic vaccinations9 and the use of modern contraceptive methods,hich were used as a proxy for the availability of health care ser-
ices. According to Kabubo-Mariara et al. (2008) a community sharenon-self cluster ratio) of modern contraceptive methods is a sig-ificant variable in determining a proxy for the general availabilityf health care services.
Seasonal dummy was also included to control the effect of sea-on on child health. A dummy for season represents ‘1′ if childrenere interviewed at the end of dry season (February–April); oth-
rwise ‘0′ if children were interviewed at coming monsoon andonsoon season (May–August).
.3. Descriptive statistics
Child data with missing information on 546 cases wereemoved. Similarly, 274 cases were removed because they wereot usually residents and observations were missing. Therefore, the
hildren sample size was narrowed down to 4963. The household-evel data were merged with child data. In Table 2, the meansnd standard deviations of key variables used in the regression7 The DHS data contains wealth index which was derived from using principalomponents analysis (PCA) procedure. This procedure first standardizes the indica-or variables (calculating z-scores); then the factor coefficient score (factor loadings)re calculated; and finally, for each household, the indicator values are multipliedy the loadings and summed to produce the household’s index value. In this process,nly the first of the factors produced is used to represent the wealth index.8 In Nepal, 44 percent of married women used modern contraceptive in 2006
MOHP, New ERA, and Marco International Inc., 2007).9 The basic vaccination was defined as children who received 3 doses of Polio
nd Diphtheria (DPT), and one dose of Tuberculosis (BCG) and Measles vaccinationsnder 5 years old.
ethOt
3
w
dp
Mountain 0.153 0.360Plain area (Terai) 0.452 0.498
re presented. Variations in child height and weight in the sam-le are approximate to normal distributions. About 39 percent ofhildren showed a weight-for-age z-score below −2 standard devi-tion and 11 percent of them showed a z-score below −3 standardeviation, which according to the WHO, is a sign of underweightnd severely underweight, respectively. Similarly, 50 percent weretunted and 21 percent were severely stunted.10 The mean age ofothers at first birth was 19.4 years and about 43 percent of moth-
rs gave birth under the age of 19 years. Approximately, 36 percentf women resided in the households where their age differencesere more than 20 years from their household heads. The educa-
ion status was lower for women with around 20 percent for bothrimary and secondary education while around 30 percent menad primary education and more than 45 percent had secondaryducation. Slightly less than 50 percent (47%) of the households inhe sample had access to water on premises and 45 percent house-olds had water source on round-trip journeys of less than 30 min.nly 8 percent of households needed to travel round-trips of more
han 30 min for water collection.
. Empirical specifications
The theoretical framework linking child health to access to cleanater is conceptually similar to that of Thomas and Strauss (1992).
10 According to WHO, children whose height-for-age z-scores are below −2 stan-ard deviations and −3 standard deviations from the median of the reference ofopulation are considered stunted and severely stunted, respectively.

1 of Health Economics 30 (2011) 1000– 1010
Tmts
mH
S
wtWia
H
wacwm
H
wg
H
wwacst
e
H
wtvc
swpumafpebif
tmbmhiwc
Table 3Summary of the endogeneity issues for different estimation strategies.
Model Self-selection ofwealthy household
Endogenous projectplacement
OLS X XCFE X No bias
pcptpepp
iuwwhmGripafriwt
mlsafbtmMlcjp
icats
dadent variables in probit analysis, the model is specified below:
Yi = f (Xj) (7)
004 D.K. Lamichhane, E. Mangyo / Journal
he model is based on Becker (1981) in which a household maxi-izes a utility function. In this case, a household may be assumed
o choose child health H, leisure L, and consumption of goods andervices C.
The problem is:
ax,C,LU = U(H, L, C; Xh, �) (1)
ubject to : I = PcC + WL + PY Y (2)
here Xh is a vector of household characteristics including educa-ional level; � unobserved heterogeneity; l is full income; and Pc,
, PY are price vectors of consumption goods, leisure, and healthnputs, respectively. Child health is generated by the followingnthropometric production function (constraint):
i = F(Yi, Xi, Xh, Xc, ωi) (3)
here Yi is a vector of health inputs; Xi is a vector of child char-cteristics which are age and sex; Xc is a vector of communityharacteristics; Xh is a vector of household characteristics includingater accessibility; and ωi is unobserved individual health endow-ents.In this framework, the reduced form function for child health is:
i = �(Xi, Xh, Xc, I, Pc, PY , �i) (4)
here � is particular functional form and � is unobserved hetero-eneity in health outcomes.
Assuming linearity, the estimation of Eq. (4) can be written as:
i = ˇ0 + ˇ1Wh + ˇ2Zi + ˇ3Zh + ˇ4Zc + εi (5)
here Hi is a vector of anthropometric measures of children; Wh isater access (fetching water time); Zi includes child specific char-
cteristics; Zh includes household characteristics; Zc is the set ofommunity characteristics which affect child health; s is the childpecific disturbance term. ˇ0, ˇ1, ˇ2, ˇ3 and ˇ4 are the coefficientso be estimated.
The effect of hours in fetching water time on child health wasstimated by the following community fixed effects model:
ic = ˛c + ˇ1Whc + ˇ2Xic + �c + εic (6)
here the subscripts i and c are individual and community indica-ors, respectively; Xic is the set of individual or household controlariables; �c is community-level fixed effects; and εic is the idiosyn-ratic disturbance.
Hours in fetching water time might be correlated with unob-ervable community wealth which, in turn, would be correlatedith child health; therefore, the OLS estimates of Eq. (5) wouldroduce a biased result. The direction of bias, moreover, may bepward or downward. Therefore, it is difficult to know the trueagnitude of the impact of fetching water time on child health
lthough it may be possible to establish an upper or lower boundor the true effect in Eq. (5). The community effects from the com-osite error can be purged by using community dummy in the fixedffects model (6). The use of community fixed effects remove anyias which arises from unobserved community-level heterogene-
ty that might be correlated with both child health and hours inetching water time.
Community fixed effects model might give bias results becausehe model is estimated only with cross-sectional data and this esti-
ator exploits within community variability. Hence the bias arisesecause of within community self-selection. Therefore, householdsight have control over convenient access to water and child
ealth within communities. However, this may not cause a biasf water accessibility is mostly determined by government or NGO
ater projects because, in this case, individual household has noontrol over access to clean water. Nevertheless, even if the water
yc
Leave-out (IV) No bias X or could be XX(aggravate)
roject is determined by NGO or government, one issue that stillauses a potential endogeneity is that water projects might belaced in the area where population health is getting worse or bet-er over time. If such water facilities were placed in the areas whereopulation health was poorest, the impact of the facilities wouldxhibit a downward bias. On the other hand, facilities might belaced in more accessible and prosperous areas, which leads to aositive bias.
To address the issue of endogeneity of water accessibility byndividual households, the leave-out strategy of instruments wassed in which the community shares of water infrastructure andater accessibility were used as instruments for household-levelater accessibility. Specially, the non-self community ratio11 ofouseholds with in-yard water access was used as the instru-ent for household-level hours in fetching water time (Ilahi andrimard, 2000; Mangyo, 2007). Similarly, the non-self community
atio of households with improved water sources was used as annstrument. As indicators of improved water sources, the share ofiped water into the dwelling, the share of stand pipe or public tap,nd the share of tube well water source were used as instrumentsor hours in fetching water time. The non-self community ratioseduced the endogeneity of household water access by exploit-ng variation in community-level difference in water infrastructure
hich reflects government or NGO projects in water access ratherhan individual demand by each household.
Table 3 summarizes the endogeneity issues of the different esti-ation strategies (OLS, community fixed effects (CFE), and the
eave-out strategy of instruments (IV)). The OLS is subject to bothelf-selection of wealthy households into access to clean waternd endogenous project placement at the community-level. CFE isree from endogenous project placement at the community-levelut subject to self-selection at the household level. Nonetheless,he CFE model with longitudinal data that exploits program place-
ent variability over time does not suffer from that source of bias.eanwhile, the IV would alleviate self-selection on the household-
evel but could suffer from endogenous project placement at theommunity-level. Thus, all available estimation strategies are sub-ect to either self-selection at the household-level or endogenousroject placement at the community-level, or both.
In Eq. (5), it was assumed that there was no observable variablesnteracting with regressors. However, it was argued that the edu-ation of mother had complementary relationship with convenientccess to water sources. This possibility was addressed by usingwo-stage least square (2SLS) regressions which were estimatedeparately for educated and less educated mothers.
To address the issue of endogenous project placement, data onisease symptoms categorized as water-relevant such as diarrhoeand water-irrelevant such as cough and fever were used as depen-
11 The non-self community ratio is calculated as the ratio of household with in-ard water source excluding self-household to the total number of household in theluster excluding the self-household.

D.K. Lamichhane, E. Mangyo / Journal of Health Economics 30 (2011) 1000– 1010 1005
Table 4Height-for-age with ordinary least square (OLS), community fixed effects (CFE), and instrumental variable (IV) regression results.
Variables OLS (1) CFE (2) IV (3) IV (4)
Fetching water time −0.179 (0.133) −0.100 (0.101) −0.759** (0.386) −0.701*** (0.181)Child age (6–11) −0.484 *** (0.094) −0.437*** (0.095) −0.478*** (0.092) −0.460*** (0.076)Child age (12–23) −1.286*** (0.085) −1.280*** (0.088) −1.277*** (0.084) −1.255*** (0.067)Child age (24–35) −1.577*** (0.081) −1.573*** (0.084) −1.573*** (0.082) −1.560*** (0.066)Child age (36–47) −1.608*** (0.082) −1.602*** (0.086) −1.601*** (0.083) −1.594*** (0.067)Child age (48–59) −1.501*** (0.083) −1.489*** (0.086) −1.502*** (0.085) −1.515*** (0.067)Male −0.009 (0.037) −0.041 (0.038) −0.020 (0.038) −0.036 (0.032)Twin −0.417* (0.230) −0.426** (0.191) −0.426** (0.219) −0.507*** (0.172)Wealth index 0.160*** (0.029) 0.227*** (0.046) 0.134*** (0.038) 0.168*** (0.027)Mother primary education 0.160*** (0.054) 0.059 (0.056) 0.162*** (0.052) 0.132*** (0.046)Mother secondary education 0.396*** (0.074) 0.282*** (0.067) 0.380*** (0.076) 0.338*** (0.052)Husband primary education 0.085 (0.059) 0.066 (0.057) 0.081 (0.061) 0.074* (0.045)Husband secondary education 0.083 (0.068) 0.047 (0.059) 0.067 (0.067) 0.066 (0.047)Mother height 0.054*** (0.004) 0.049*** (0.004) 0.055*** (0.004) 0.055*** (0.003)Season 0.162*** (0.059) −0.069 (0.426) 0.147*** (0.058) 0.074* (0.042)Age difference to head of household −0.004 (0.046) 0.008 (0.050) −0.004 (0.046) −0.029 (0.039)Teenage mother −0.07 (0.051) −0.046 (0.042) −0.075 (0.052) −0.072** (0.033)Household size −0.007 (0.006) −0.006 (0.009) −0.008 (0.007) −0.012** (0.006)Modern contraceptive 0.488*** (0.133) – 0.435*** (0.131) 0.476*** (0.096)Basic vaccination 0.009 (0.139) – 0.026 (0.134) 0.031 (0.094)Mountain −0.206*** (0.073) – −0.162** (0.081) −0.086 (0.055)Hill −0.027 (0.079) – 0.057 (0.101) 0.071 (0.049)Constant −9.089*** (0.623) −8.114*** (0.597) −9.114*** (0.627) −9.149*** (0.467)Observations 4914 4960 4914 4914R-squared 0.290 0.328 0.279 0.277First-stage R-squared – – 0.255 0.268F-statistics on excluded instruments – – F(25,119) = 23.12 F(4, 259) = 19.80Hausman (P-value) – – – 0.001Hansen (P-value) – – – 0.270RESET test (P-value) 0.213 – – 0.153
Note: Columns 1–3 are weighted regression, while column 4 is unweighted regression. Value of standard errors beneath the coefficient estimates in parenthesis. Non-surveystandard errors are robust to heteroskedasticity and clustering. The standard errors of cluster fixed effect are adjusted for heteroskedasticity.
wddtvh0m0spshwmcofa
t
Y
wa
dslt
hm
4
4e
tof(n(ecst
tsawcwe
* Indicates significance at 10% level.** Significance at 5% level.
*** Significant at 1% level of confidence.
here Yi is the presence of disease symptoms (water-relevantiseases symptoms or water-irrelevant disease); Xj is variablesetermining the disease symptoms, such as wealth index, educa-ion, hours in water fetching time, child age, sex, twin, season, basicaccination, use of modern contraceptive, prenatal care, mother’seight, and teenage mother. Child age was used as dummies of–5 months, 6–11 months, 12–23 months, 24–35 months, 36–47onths, and 48–59 months with the reference group being children
–5 months of age to capture more age-specific effects on diseaseymptoms. Additional variable used in this model compared to therevious one is the use of prenatal care. Prenatal care was repre-ented by a dummy variable if a woman received prenatal care forer last birth from professional medical workers (doctor or mid-ife or nurse). The use of modern contraceptive (‘1’ if woman usedodern contraceptive, ‘0’ otherwise) and basic vaccination (‘1’ if
hildren received all the required doses of basic vaccinations, ‘0’therwise) were also represented by dummy variables to controlor household-level effects on diseases symptoms (water-relevantnd irrelevant).
The econometric specification of the probit model can be writ-en as follows:
∗i = ̨ + ˇXj + ui (8)
here Y = 1, if Y∗i
> 0 or Y = 0 otherwise (in practice, Y∗i
is unobserv-ble).
The placement of water projects would mostly affect the inci-
ence of diarrhoea but would not affect water-irrelevant diseaseymptoms. Therefore, the correlation between the community-evel access to water relevant and irrelevant disease shows thathe community-level water access was correlated with unobservedtdnT
eterogeneity such as unobserved wealth difference across com-unities.
. Results and discussion
.1. General results for OLS, community fixed effects, and IVstimates
Tables 4 and 5 report the results of regressing child health onhe main variable of our interest, hours in fetching water time andther control variables. The z-scores of height-for-age and weight-or-age were used as health measures. Four regression models:i) weighted ordinary least square (OLS), (ii) weighted commu-ity fixed effects, (iii) weighted two-stage least square (2SLS), andiv) unweighted two-stage least square (2SLS) were computed forach health measure. The standard errors for weighted regressions,olumns 1 and 3, were adjusted for clustering and stratification. Thetandard errors for unweighted regression, column 4, were robusto heteroskedasticity and adjusted for clustering.
The OLS estimates of child height and weight for fetching waterime show the insignificant results with the expected negativeigns only for child height. Most of the control variables suchs child age, twin, mother’s height, mother’s education, season,ealth index, and mountain were significantly correlated with
hild height and weight. These variable effects on child healthere consistent with previous studies. Utilising community fixed
ffects made the estimated coefficient on hours in fetching water
ime smaller in magnitude for child height but did not make muchifference for child weight. This implies that unobserved determi-ants of child height may be swept out by community fixed effects.hus, community fixed effects eliminated any biases in the esti-
1006 D.K. Lamichhane, E. Mangyo / Journal of Health Economics 30 (2011) 1000– 1010
Table 5Weight-for-age with ordinary least square (OLS), community fixed effects (CFE), and instrumental variable (IV) regression results.
Variables OLS (1) CFE (2) IV (3) IV (4)
Fetching water time 0.032 (0.100) 0.038 (0.087) −0.165 (0.311) −0.306** (0.153)Child age (6–11) −0.553*** (0.083) −0.543*** (0.081) −0.550*** (0.081) −0.459*** (0.064)Child age (12–23) −0.853*** (0.073) −0.863*** (0.072) −850*** (0.073) −0.770*** (0.056)Child age (24–35) −0.889*** (0.060) −0.880*** (0.069) −0.887*** (0.060) −0.768*** (0.056)Child age (36–47) −0.908*** (0.072) −0.912*** (0.071) −0.906*** (0.072) −0.776*** (0.056)Child age (48–59) −0.884*** (0.066) −0.879*** (0.69) −0.885*** (0.067) −0.806*** (0.056)Male 0.054* (0.032) 0.037 (0.033) 0.050 (0.032) 0.032 (0.027)Twin −0.567*** (0.203) −0.593*** (0.169) −0.570*** (0.199) −0.534*** (0.145)Wealth index 0.210*** (0.024) 0.252*** (0.383) 0.202*** (0.028) 0.203*** (0.022)Mother primary education 0.255*** (0.043) 0.170*** (0.047) 0.255*** (0.043) 0.209*** (0.039)Mother secondary education 0.212*** (0.057) 0.149*** (0.059) 0.207*** (0.058) 0.195*** (0.044)Husband primary education 0.090* (0.053) 0.096** (0.046) 0.088* (0.052) 0.070* (0.038)Husband secondary education 0.106** (0.050) 0.079 (0.048) 0.099** (0.047) 0.079** (0.040)Mother height 0.033*** (0.003) 0.031*** (0.003) 0.033*** (0.003) 0.034*** (0.003)Season 0.217*** (0.051) −0.016 (0.412) 0.212*** (0.051) 0.223*** (0.035)Age difference to head of household 0.063* (0.039) 0.081 (0.044) 0.061 (0.039) 0.080** (0.033)Teenage mother −0.083** (0.034) −0.058* (0.034) −0.084** (0.034) −0.058** (0.028)Household size −0.017*** (0.005) −0.014* (0.008) −0.018*** (0.005) −0.019*** (0.005)Basic vaccination 0.006 (0.154) – 0.012 (0.152) 0.016 (0.079)Modern contraceptive 0.210* (0.110) – 0.192* (0.114) 0.167** (0.081)Mountain 0.202*** (0.068) – 0.217*** (0.072) 0.271*** (0.046)Hill 0.273*** (0.065) – 0.302*** (0.086) 0.309*** (0.041)Constant −6.234*** (0.494) −5.672*** (0.484) −6.242*** (0.492) −6.374*** (0.394)Observations 4914 4960 4914 4914R-squared 0.214 0.298 0.212 0.183First-stage R-squared – – 0.255 0.268F-statistics on excluded instruments – – F(25,119) = 23.12 F(4,259) = 19.80Hausman (P-value) – – – 0.037Hansen (P-value) – – – 0.149RESET Test (P-value) 0.209 – – 0.821
Note: Columns 1–3 are weighted regression, while column 4 is unweighted regression. Value of standard errors beneath the coefficient estimates in parenthesis. Non-surveystandard errors are robust to heteroskedasticity and clustering. The standard errors of cluster fixed effect are adjusted for heteroskedasticity.
mhmirhos
soawTwTiaTswaaFi
o
h
Table 6First-stage regression results for instrumented regression in Tables 4 and 5.
Variables Coefficients
Tube welli −0.256*** (0.062)Piped wateri −0.129** (0.062)In-yard wateri −0.245*** (0.044)Public tapi −0.089*** (0.035)Child age (6–11) −0.005 (0.018)Child age (12–23) 0.009 (0.014)Child age (24–35) 0.004 (0.012)Child age (36–47) 0.008 (0.014)Child age (48–59) −0.007 (0.011)Male −0.015** (0.007)Twin 0.009 (0.030)Wealth index −0.009 (0.014)Mother primary education 0.003 (0.014)Mother secondary education −0.025* (0.014)Husband primary education −0.014 (0.014)Husband secondary education −0.035** (0.015)Season 0.000 (0.015)Age difference to head of household −0.012 (0.011)Teenage mother −0.004 (0.01)Household size −0.002 (0.001)Mother height 0.001 (0.001)
* Indicates significance at 10% level.** Significant at 5% level.
*** Significant at 1% level of confidence.
ated coefficients due to unobserved community factors such aseterogeneity in unobserved predetermined community endow-ents that affect hours in fetching water time and child health. The
mplication is that communities with favorable unobserved envi-onment for water access also have a favorable unobserved childeight environment. On the contrary, the coefficient estimatesn fetching water time in the child weight equation were notignificantly affected by the presence of community fixed effects.
Community fixed effects in column 2 perfectly control for unob-erved heterogeneity across communities. However, self-selectionf households into convenient access to clean water would cause
bias even after controlling for community fixed effects. To dealith this problem, we used instruments. The columns 3 and 4 in
ables 4 and 5 present the instrumental variable (IV) estimatesith fetching water time treated as endogenously determined.
hese columns display the results of using community-level waternfrastructure12 and community-level in-yard water accessibility13
s instruments for household-level hours in fetching water time.he first-stage regression results are reported in Table 6. The F-tatistics on the excluded instruments in the first-stage regressionsere more than 18 which showed that the endogenous variable
nd the excluded instruments were strongly correlated. The liter-
ture on instrumental variable regression argued that if first-stage-statistics on excluded instruments is more than 10, excludednstruments have a strong correlation with the endogenous vari-12 Non-self community ratios of household with access to piped water, stand piper public tap water, and tube well or borehole water sources.13 Non-self community ratio of household with access to water sources on house-old premises.
Mountain −0.140* (0.075)Hill −0.076 (0.075)Modern contraceptive 0.011 (0.027)Basic vaccination 0.015 (0.039)Constant 0.325**(0.137)
Note: Standard errors in the parenthesis. The set of community-level instruments isindicated by i.
* Indicates significance at 10% level.** Significance at 5% level.
*** Significant at 1% level of confidence.

D.K. Lamichhane, E. Mangyo / Journal of Health Economics 30 (2011) 1000– 1010 1007
Table 7Two-stage least square (2SLS) results for educated and less educated mothers.
Variable Educated Less educated
HAZ (1) WAZ (2) HAZ (3) WAZ (4)
Fetching water time −0.679* (0.400) 0.409 (0.390) −0.576 (0.399) 0.101 (0.339)Male −0.066 (0.077) 0.020 (0.062) −0.028 (0.075) 0.045 (0.059)Wealth index 0.152*** (0.040) 0.193*** (0.032) 0.277*** (0.059) 0.346*** (0.051)Husband primary education 0.186 (0.293) 0.264 (0.242) −0.083 (0.136) −0.065 (0.134)Husband secondary education 0.213 (0.292) 0.227 (0.215) −0.120 (0.117) −0.063 (0.133)Season 0.107 (0.092) 0.169** (0.078) 0.004 (0.118) 0.181* (0.104)Age difference to head of household 0.222** (0.094) 0.249*** (0.075) 0.041 (0.089) −0.093 (0.082)Teenage mother −0.186** (0.083) −0.159** (0.073) −0.106 (0.081) −0.101 (0.071)Mother height 0.047*** (0.009) 0.027*** (0.007) 0.051 (0.008) 0.037*** (0.007)Household size −0.019 (0.017) −0.033** (0.014) −0.013 (0.017) −0.039*** (0.011)Modern contraceptive 0.072 (0.241) −0.172 (0.167) 0.529** (0.250) 0.157 (0.219)Basic vaccination 0.230 (0.307) 0.139 (0.284) 0.299 (0.265) 0.087 (0.248)Constant −0.814*** (1.334) −5.730*** (1.052) −9.656*** (1.243) −6.933*** (1.152)Observations 1015 1015 867 867
Variable Educated Less educated
HAZ (1) WAZ (2) HAZ (4) WAZ (5)
R-squared 0.259 0.259 0.270 0.270F-statistics on excluded instruments F(4,209) = 20.36 F(4,209) = 20.36 F(4,226) = 25.59 F(4,226) = 25.59Hansen (P-value) 0.493 0.06 0.206 0.287RESET test (P-value) 0.938 0.063 0.534 0.292
Note: Value of standard errors below the coefficient estimates in parenthesis. Standard errors are robust to heteroskedasticity and clustering.
awTDagtHAHctftoeh
cewao
rTd
tewu
ent
(cctbcwanwmo
ptii
4a
* Indicates significance at 10% level.** Significance at 5% level.
*** Significant at 1% level of confidence.
ble (Bound et al., 1995). In addition to this result, other testsere also computed in unweighted IV regression in column 4.
he P-values of the Hansen test14 for overidentifying restriction,urbin–Wu–Hausman test15 for identifying the equality of the IVnd OLS estimates and RESET test16 for model misspecification areiven at the bottom of Tables 4 and 5. The Hansen test did not rejecthe null hypothesis of instruments being correctly excluded and theausman test rejected the null at the 5% level that OLS is consistent.lthough the economic literature is doubtful about the reliability ofausman test, in this case, the explanatory power of Hausman testould be considered higher because the excluded instruments fromhe leave-out strategy were very strongly correlated with hours inetching water time. Nakamura and Nakamura (1998) mentionedhat the power of an endogeneity test depends on the proportionf the variability of an endogenous variable that is explained by thexogenous variables. For these reasons, the main results for childeight and weight are presented based on IV estimates.
The significant coefficient estimates on the control variables inolumns 1 and 3 in Tables 4 and 5 are not substantially differentxcept for the coefficient estimates for hours in fetching water time,
hich are almost 4 times larger for IV than for OLS for child heightnd around 6 times for IV than for OLS for child weight. The signf the coefficient on hours in fetching water time was as expected
14 The test value was obtained by using Stata command ivreg2 for unweighted IVegression with the null hypothesis of the instruments being correctly excluded.his command was used in non-survey regression as weighted survey regressionid not support the command ivreg2 in Stata.15 This was a general version of Hausman test where the null hypothesis was thathe OLS estimator was consistent. Wu–Hausman F-test also rejected the null hypoth-sis at the 5% level for both child height and weight. In these tests, standard errorsere not adjusted for heteroskedasticity and clustering since the tests do not applynder robust standard errors.16 The test statistics was generated by using Stata command ovtest after OLSstimation and by ivreset after 2SLS with the null that there were no neglectedonlinearities or no misspecification. We failed to reject null hypothesis saying thatest has not been able to detect any misspecification.
hremitcmfw
e
negatively correlated); however, only the coefficient estimate ofhild height (−0.759) was significant. Here, the estimated coeffi-ients on fetching water time were more negative for IV estimationhan for OLS for both child height and weight. This was unexpectedecause self-selection of households into convenient access tolean water implied a less negative coefficient estimate on fetchingater time with IV than with OLS. For example, unobserved wealth
cross households was positively correlated with child health andegatively correlated with water fetching time. Our instrumentsere effective against self-selection of households, thus, IV esti-ation should have produced less negative coefficient estimates
n fetching water time.However, our instruments are subject to endogenous project
lacement, which may be the main reason why our instrumentsurned out to produce more negative coefficient estimates on fetch-ng water time with IVs than with OLS. We will discuss this issuen the Section 4.3.
.2. Is maternal education a complement or substitute to waterccess?
Since mother’s education has a significant impact on childealth, it could also have either a complementary or substitutingelationship with convenient access to water. Such possibility wasxamined by using 2SLS separately for educated and less educatedothers. The 2SLS estimation finds the differential effects of fetch-
ng water time on child health by maternal education. The firstwo columns 1 and 2 in Table 7 present the 2SLS results for edu-ated mothers,17 and the last two columns 3 and 4 for less educated
others.18 The point estimate showed that the effect of hours inetching water time for educated mothers was −0.679 on height,hich was statistically significant at the 10% level and the sign was
17 Educated mother was defined as mother either having secondary or higherducation.18 Less educated mother was defined as mother who has primary education.

1008 D.K. Lamichhane, E. Mangyo / Journal of Health Economics 30 (2011) 1000– 1010
Table 8Probit analysis for diseases symptoms for mothers having education and no education.
Variables Education No education
Water-relevant (1) Water-irrelevant (2) Water-relevant (3) Water-irrelevant (4)
Fetching water time −0.485 (0.549) 0.131 (0.490) 0.658* (0.376) 0.728* (0.435)Child age (6–11) 0.276 (0.245) 0.159 (0.159) 0.545*** (0.172) 0.318** (0.140)Child age (12–23) 0.331 (0.207) 0.033 (0.203) 0.616*** (0.157) 0.350*** (0.108)Child age (24–35) −0.108 (0.208) −0.377* (0.192) 0.168 (0.164) 0.252** (0.115)Child age (36–47) −0.314 (0.245) −0.268 (0.222) −0.036 (0.187) 0.033 (0.115)Child age (48–59) −0.296 (0.264) −0.188 (0.260) −0.086 (0.199) 0.165 (0.137)Male 0.217*** (0.083) 0.072 (0.083) 0.103 (0.100) −0.001 (0.072)Twin 0.174 (0.587) −0.057 (0.545) −0.197 (0.384) 0.135 (0.384)Wealth index −0.059 (0.053) 0.034 (0.059) −0.041 (0.111) 0.154** (0.073)Season 0.093 (0.123) 0.290*** (0.115) 0.297*** (0.108) 0.290*** (0.097)Prenatal care 0.009 (0.122) −0.033 (0.102) −0.111 (0.095) 0.078 (0.072)Teenage mother 0.165* (0.113) 0.229** (0.096) −0.043 (0.088) 0.100 (0.067)Mother height 0.005 (0.009) 0.004 (0.007) −0.005 (0.009) 0.008 (0.006)Husband primary education −0.219 (0.263) 0.268 (0.207) 0.006 (0.100) 0.178** (0.088)Husband secondary education −0.164 (0.243) 0.213 (0.198) 0.052 (0.096) 0.059 (0.083)Household size −0.002 (0.015) −0.033** (0.014) −0.006 (0.011) −0.028** (0.012)Modern contraceptive 0.248*** (0.076) 0.009 (0.078) −0.158* (0.090) −0.023 (0.086)Basic vaccination −0.267* (0.145) −0.222 (0.158) −0.005 (0.096) −0.098 (0.074)Constant −1.805 (1.391) −1.299 (1.068) −0.704 (1.329) −2.078** (0.831)Observations 1473 1473 2167 2167Prob > F 0.00 0.00 0.00 0.001Instrumented Yes Yes Yes YesWald test (P-value) 0.378 0.790 0.082 0.102Fetching water time (Marginal effects) −0.104 (0.119) 0.046 (0.171) 0.135 (0.083) 0.227 (0.150)
Note: Weighted regression. Standard errors below the coefficient estimates in the parenthesis. Child age in months.
aclte
amdyswmfaw
hmt
4
whchAtwhnew
piwfi
eeTrwiwwwtto3icd
Table 8 presents the result of survey probit instrumentalvariable regression (SVY: IVPROBIT)21 in Eq. (7). The dependentvariable was a dummy variable indicating the incidence of either
19 Children data of DHS 2006 contain information about some diseases such ascough, diarrhoea, and fever. The data included information on: whether the childhad diarrhoea in the last 24 h or within the last two weeks; and whether the childrenhad fever or cough in the last two weeks.
* Indicates significance at 10% level.** Significance at 5% level.
*** Significant at 1% level of confidence.
s expected. On the other hand, the point estimate for less edu-ated mothers was not statistically significant at the conventionalevels. For child weight, the coefficient estimates on fetching waterime were not statistically significant for both educated and lessducated mothers.
These results were consistent with previous studies on waterccess and child health. Jalan and Martin (2003) found that whenothers were well educated, the impact of piped water on both the
uration and prevalence of diarrhoea among children below fiveears in rural India were significantly lower. They also argued thatkills and knowledge such as proper storing of water and boilingould be required to make water drinkable, so educated mothersay be able to adopt these skills more easily. Mangyo (2007) also
ound that access to in-yard water sources improved child healths measured by height and weight in China, only when mothersere relatively educated.
As this result supported that water accessibility and educationad a complementary relationship in producing child health aseasured by height, the benefit from water accessibility was biased
oward educated mothers.
.3. The effects of non-random water project placement
It has been argued that even if community-level water accessere exogenous to household demand, the water projects mightave been placed in areas that were purposely chosen by someriteria. Thus, some unobserved community characteristics couldave been correlated with both child health and water access.s previously discussed, our instruments produced more nega-
ive coefficient estimates on fetching water time in comparisonith OLS, which was unexpected because self-selection of wealthy
ouseholds into convenient access to clean water suggested lessegative coefficient estimates on fetching water time with IV. How-ver, endogenous project placement could be the main reason whye obtained the unexpected results with IV. For example, if waterh
og
rojects historically were mainly provided in rich areas rather thann poor areas, our instruments (community-level access to clean
ater) would have been positively correlated with unobserved dif-erences in wealth across communities, making our instrumentsnvalid. We discuss this issue in this section.
The issue of non-random placement of water project wasxplored by using the data on disease symptoms.19 The dis-ase symptoms included were child diarrhoea, fever, and cough.he disease symptoms were grouped into two categories. Diar-hoea was grouped into the water-relevant symptom category,hile the remaining two conditions were grouped into water-
rrelevant symptoms. To increase the reported number of theater-irrelevant disease symptoms, a dummy variable of theater-irrelevant diseases was equal to ‘1’ if either one of the twoater-irrelevant symptoms was reported or ‘0’ if neither of the
wo water-irrelevant symptoms was reported. The data showedhat about 26 percent of water-irrelevant diseases symptoms werebserved in the subsample20 where mothers had no education and3 percent were observed for mothers having education. Similarly,
n the case of the water-relevant disease symptom, 13 percent ofhildren reported the symptom in each sample of educated or une-ucated mothers.
20 The sample size for mother having education was 1912 and 3051 for motheraving no education.21 Stata command svy, subpsenop (): ivprobit was used for this regression. Theption subpop was used for sub-population analysis of education and no educationroups.

D.K. Lamichhane, E. Mangyo / Journal of Health Economics 30 (2011) 1000– 1010 1009
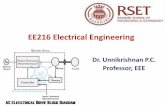
Note: + sign inside the polygon represents a positive correlation; and – sign represents a negative correlation.
Out instruments (community-level access to clean water)
Unobserved community
wealth
-
+
+
Child health Fetching water time
F omm−
tspmaTtwwotti
5
fohbuhmwgh
swpiic
iws
tfwaan
wwoccft
tctle
A
Scgai
R
ig. 1. The correlation among instruments, endogenous variable, and unobserved c sign represents a negative correlation.
he water-relevant or water-irrelevant diseases symptom. Table 8hows that the incidence of the water-irrelevant symptoms wasositively correlated with fetching water time22 with the instru-ents although the positive association was statistically significant
t the conventional level only for households having no education.his implied that endogenous placement of water projects wasoward wealthy areas. Our instruments were positively correlatedith unobserved community wealth and negatively correlatedith fetching water time (see Fig. 1). This story was consistent with
ur earlier finding that the coefficient estimate on fetching waterime was more negative with IV than with OLS. Of course, givenhe positive correlation with unobserved community wealth, ournstruments were invalid.
. Conclusions
This paper examined the effect of water accessibility in terms ofetching water time on child health, addressing the endogeneityf fetching water time. First, self-selection of wealthy house-olds into convenient access to clean water would be a source ofias if no measures were taken. To deal with this problem, wesed community-level access to clean water as instruments forousehold-level access to clean water. The idea behind this instru-ental variable strategy was that community-level access to cleanater reflected past water projects initiated by NGOs and/or local
overnments rather than individual choices by individual house-olds.
Although this IV strategy would be effective against self-election of wealthy households into convenient access to cleanater, community-level access to clean water may invite anotherroblem: endogenous project placement. To explore this possibil-
ty, we used data on disease symptoms. The idea here was thatf water projects were randomly placed across communities, noorrelation would have been expected between community access
22 In a separate 2SLS regression using in-yard water sources as a dummy (‘1’f water sources were on household premises, ‘0’ otherwise) instead of fetching
ater time showed the similar results as presented in Table 8 in terms of sign andignificance. (This result is not presented in this paper due to space limitation.)
B
B
B
B
unity wealth. Note: + sign inside the polygon represents a positive correlation and
o clean water and water-irrelevant symptoms such as cough andever. In contrast, if the historical allocation of water projectsere more toward richer areas, we would have expected a neg-
tive correlation between community-level access to clean waternd water-irrelevant symptoms because of unobserved commu-ity wealth.
We found that fetching water time was positively correlatedith water-irrelevant symptoms with community access to cleanater as instruments. This implied that the historical distribution
f water projects was more toward wealthy communities or thatommunity with unobserved factors was positively correlated withhild health. Thus, our instruments were invalid, implying that weailed to pin down the magnitude of the effect of fetching waterime on child health.
Our contribution in this paper is that we clearly showed a poten-ial weakness of the instrumenting strategy using the leave-outommunity ratio which is very popular in the economic litera-ure. Unless we paid due attention, the estimated effects using theeave-out community ratio as instruments could be biased due tondogenous project placement.
cknowledgements
We are grateful to Prof. Donghun Kim, Christopher Murphy,abina Shrestha, and two anonymous referees for their helpfulomments. We would also like to express our thanks to Demo-raphic and Health Survey data archive for providing us datand Noureddine Abderrahim for providing responses to our datanquiries.
eferences
arrera, A., 1990. The role of maternal schooling and its interaction with publichealth programs in child health production. Journal of Development Economics32 (1), 69–91.
ecker, G.S., 1981. A Treatise on the Family. Harvard University Press, Cambridge,MA.
ehrman, J.R., Lavy, V., 1997. Child health and schooling achievement: association,causality and household allocations. PIER working paper 97-023, Penn Institutefor Economic Research, University of Pennsylvania.
ound, J., Jaeger, D.A., Baker, R.M., 1995. Problems with instrumental variables esti-mation when the correlation between the instruments and the endogenous

1 of Hea
B
C
E
E
E
F
G
G
G
H
H
I
J
K
L
M
M
M
N
N
S
Thomas, D., Strauss, J., 1992. Price, infrastructure, household characteristics, and
010 D.K. Lamichhane, E. Mangyo / Journal
explanatory variable is weak. Journal of the American Statistical Association90 (430), 443–450.
utz, W., Habicht, J.P., Da Vanzo, J., 1984. Environmental factors in the relationshipbetween breast-feeding and infant mortality: the role of water and sanitationin Malaysia. American Journal of Epidemiology 119 (4), 516–525.
ebu Study Team, 1991. Underlying and proximate determinants of child health: theCebu longitudinal health and nutrition study. American Journal of Epidemiology133 (2), 185–201.
srey, S.A., 1996. Water, waste, and well-being: a multicountry study. AmericanJournal of Epidemiology 143 (6), 608–623.
srey, S.A., Feachem, R., Hughes, J., 1985. Interventions for the control of diarrhoealdiseases among young children: improving water supplies and excreta disposalfacilities. Bulletin of the World Health Organization 63 (4), 757–772.
srey, S.A., Habicht, J.P., 1988. Maternal literacy modifies the effect of toilets andpiped water on infant survival in Malaysia. American Journal of Epidemiology127 (5), 1079–1087.
ilmer, D., Pritchett, L., 1996. Estimating Wealth Effects Without Expenditure data-or tears: An Application to Educational Enrolments in States of India. The WorldBank, Washington, DC.
aliani, S., Gertler, P., Schargrodsky, E., 2005. Water for life: the impact of privatiza-tion of water services on child mortality. Journal of Political Economy 113 (1),83–120.
lick, P., Saha, R., Younger, S.D., 2004. Integrating Gender into Benefit Incidence andDemand Analysis. The World Bank, Washington, DC.
utierrez, R.G., 2008. Analyzing Survey Data using Stata 10. Summer NASUG,Chicago.
atkar, P., Bhide, A., 1999. Perinatal outcome of twins in relation to chorionicity.Journal of Postgraduate Medicine 45 (2), 33–37.
uttly, S., Blum, D., Kirkwood, B.R., Emeh, R.N., Okeke, N., Ajala, M., Smith, G.S.,Carson, D.C., Dosunmu, O., Feachem, G.R., 1990. The Imo state (Nigeria) drinkingwater supply and sanitation project, 2. Impact of drcunculiasis, diarrhoea andnutritional status. Transactions of the Royal Society of Tropical Medicine 84 (2),316–321.
W
lth Economics 30 (2011) 1000– 1010
lahi, N., Grimard, F., 2000. Public infrastructure and private cost: water supply andtime allocation of women in rural Pakistan. Economic Development and CulturalChange 49 (1), 45–75.
alan, J., Martin, R., 2003. Does piped water reduce diarrhoea for children in ruralIndia? Journal of Econometrics 112, 153–173.
abubo-Mariara, J., Godfrey, K.N., Domisiano, K.M., 2008. Determinants of children’snutritional status in Kenya: evidence from demographic and health surveys.Journal of African Economics, Advanced access published online on December3.
innemayr, S., Alderman, H., Ka, A., 2008. Determinants of malnutrition in Senegal:individual, household, and community variables, and their interaction. Eco-nomics and Human Biology 6, 252–263.
angyo, E., 2007. The effect of water accessibility on child health in China. Journalof Health Economics 27 (5), 1343–1356.
inistry of Health and Population (MOHP) [Nepal], New ERA, Macro InternationalInc., 2007. Nepal Demography and Health Survey 2006, Ministry of Health andPopulation, New ERA and Macro International Inc., Kathmandu, Nepal.
wabu, G., 2008. The production of child health in Kenya: a structural model ofbirth weight. Journal of African Economics 18 (2), 212–260.
akamura, A., Nakamura, M., 1998. Model specification and endogeneity. Journal ofEconometrics 83, 213–237.
PC, 2005. Nepal Millennium Development Goals: Progress Report. Governmentof Nepal/National Planning Commission and United Nations Country Team ofNepal.
mith, L., Ramakrishnan, U., Ndiaya, A., Haddad, L., Matrorell, R., 2003. The impor-tance of women’s status for child nutrition in developing countries. IFPRIResearch Report 131.
child height. Journal of Development Economics 39 (2), 301–331.aterAid Nepal, 2004. Water and Sanitation Millennium Development Targets in
Nepal: What Do They Mean? What Will They Cost? Can Nepal Meet Them?WaterAid Nepal, Kathmandu.