Vol. 36, No. 3 September 2019
134
Vol. 36, No. 3 September 2019 eISSN 2384-0293 https://yujm.yu.ac.kr Yeungnam University College of Medicine Yeungnam University Institute of Medical Science
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Vol. 36, No. 3 September 2019

Vol. 36, No. 3 September 2019eISSN 2384-0293
https://yujm.yu.ac.kr
Yeungnam University College of Medicine Yeungnam University Institute of Medical Science

Vol. 36 · No. 3 · September 2019
Aims and scopeYeungnam University Journal of Medicine (Yeungnam Univ J Med, YUJM, eISSN 2384-0293, https://yujm.yu.ac.kr), the official publication of the Yeungnam University College of Medicine, is an international, peer-reviewed, and open access journal in the medical field.
YUJM aims to communicate new medical information to medical personnel, and to facilitate the development of medicine and the propagation of medical knowledge by publishing high quality evidence-based articles. It covers all fields of medical science, including clinical research and basic medical science.
YUJM publishes original articles, case reports, review articles, and editorials. All manuscripts should be creative, informative, and helpful for the diagnosis and treatment of medical diseases and for the communication of valuable information about all fields of medicine.
The first volume was published in December 1984. YUJM is published in English, three times a year (January 31, May 31, and September 30).
YUJM is indexed/tracked/covered by DOAJ, KoreaMed, Korea Citation Index, KoMCI, WPRIM, DOI/CrossRef, and Google Scholar.
Open accessThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
PublisherSung Su Yun, Dean of Yeungnam University College of Medicine
Editor-in-chief Joon Hyuk Choi, Yeungnam University College of Medicine
Editorial office Yeungnam University College of Medicine170, Hyeonchung-ro, Nam-gu, Daegu 42415, KoreaTel: +82-53-640-6832 Fax: +82-53-651-0394 E-mail: [email protected]
Printing office M2community Co.8th FL, DreamTower, 66 Seongsui-ro, Seongdong-gu, Seoul 04784, KoreaTel: +82-2-2190-7300 Fax: +82-2-2190-7333 E-mail: [email protected]
Published on September 30, 2019
Copyright © 2019 Yeungnam University College of Medicine This paper meets the requirements of KS X ISO 9706, ISO 9706-1994 and ANSI/NISO Z39. 48-1992 (Permanence of paper)
yujm.yu.ac.kreISSN 2384-0293

Editor-in-chief Joon Hyuk Choi Yeungnam University College of Medicine, Korea
Associate editor Tae Gon Kim Yeungnam University College of Medicine, Korea
Editorial board Kiwon Ban City University of Hong Kong, Hong Kong
Min Cheol Chang Yeungnam University College of Medicine, Korea
Du-Hyong Cho Yeungnam University College of Medicine, Korea
Kyu Hyang Cho Yeungnam University College of Medicine, Korea
Kwang Hae Choi Yeungnam University College of Medicine, Korea
Jinmyoung Dan CHA University College of Medicine, Korea
Kyung-Oh Doh Yeungnam University College of Medicine, Korea
Jong Ryul Eun Hanyang University College of Medicine, Korea
Mi Jin Gu Yeungnam University College of Medicine, Korea
Geu-Ru Hong Yonsei University College of Medicine, Korea
Ming-Yen Hsiao National Taiwan University College of Medicine, Taiwan
Insoo Kang Yale University School of Medicine, USA
Jae Woon Kim Yeungnam University College of Medicine, Korea
Ung Kim Yeungnam University College of Medicine, Korea
Shaw Hua Anthony Kueh Auckland City Hospital, New Zealand
Dong Shik Lee Yeungnam University College of Medicine, Korea
Jae-Lyun Lee Ulsan University College of Medicine, Korea
Keun Mi Lee Yeungnam University College of Medicine, Korea
Yong Su Lim Gachon University College of Medicine, Korea
Chul Hyun Park Yeungnam University College of Medicine, Korea
Hosun Park Yeungnam University College of Medicine, Korea
Jeong Hyun Park Kangwon National University College of Medicine, Korea
So-young Park Yeungnam University College of Medicine, Korea
Joon Sakong Yeungnam University College of Medicine, Korea
In Hwan Song Yeungnam University College of Medicine, Korea
Hoon-Ki Sung University of Toronto, Canada
Kyu Chang Won Yeungnam University College of Medicine, Korea
Wan-Hee Yoo Chonbuk National University College of Medicine, Korea
Statistical editor Sang Won Kim Yeungnam University, Korea
Keun Jung Ryu Yonsei Kim & Jung Hospital, Korea
Manuscript editor Eun-il Lee Yeungnam University College of Medicine, Korea
Editorial board

Vol. 36 · No. 3 · September 2019
Contents
Review articles
163 Intraoperative consultation for ovarian tumors Insun Kim
183 Cognitive dysfunctions in individuals with diabetes mellitus Hye-Geum Kim
192 Current status of stereotactic body radiotherapy for the treatment of hepatocellular carcinoma Jongmoo Park, Jae Won Park, Min Kyu Kang
201 Prepectoral breast reconstruction Sung-Eun Kim
Original articles
208 Feasibility and efficacy of coil embolization for middle cerebral artery aneurysms Jae Young Choi, Chang Hwa Choi, Jun Kyeung Ko, Jae Il Lee, Chae Wook Huh, Tae Hong Lee
219 Factors that determine WAI of street cleaners Jung Won Kim, Seonhee Yang, Insung Chung, Mi-Young Lee
225 Computer-based clinical coding activity analysis for neurosurgical terms Jong Hyuk Lee, Jung Hwan Lee, Wooseok Ryu, Byung Kwan Choi, In Ho Han, Chang Min Lee
231 Assessment of solid components of borderline ovarian tumor and stage I carcinoma: added value of combined diffusion- and perfusion-weighted magnetic resonance imaging See Hyung Kim
241 Determining the correlation between outdoor heatstroke incidence and climate elements in Daegu metropolitan city Jung Ho Kim, Hyun Wook Ryoo, Sungbae Moon, Tae Chang Jang, Sang Chan Jin, You Ho Mun, Byung Soo Do, Sam Beom Lee, Jong-yeon Kim
Case reports
249 Apathy syndrome in a patient previously treated with selective serotonin reuptake inhibitors for depression Hye-Geum Kim, Bon-Hoon Koo, Seung Woo Lee, Eun-Jin Cheon
254 Catastrophic catecholamine-induced cardiomyopathy rescued by extracorporeal membrane oxygenation in recurrent malignant pheochromocytoma Daniel Min

Vol. 36 · No. 3 · September 2019
260 Late complication of the Nuss procedure: recurrent cardiac tamponade Won Jong Park, Jang Won Son, Kyu Hwan Park, You Min Kim, Jong Ho Nam, Kang Un Choi, Jung Ho Kim
265 Incidentally found cystic lymphangioma of the adrenal gland in an elderly male cadaver Hee Cheol Kim, Yunji Kang, Young Hee Maeng, Jinu Kim, Sang-Pil Yoon
269 Isolated hemorrhage in the cerebellar vermis with vertigo and body lateropulsion to the contralesional side Dong Hyun Lee, Se-Jin Lee
273 Massive cerebral venous sinus thrombosis secondary to Graves’ disease Hye-Min Son

The primary function of intraoperative frozen consultation is to provide an as accurate and prompt diagnosis as possible during surgery and to guide the surgeon in further management. However, the evaluation of frozen section (FS) is sometimes difficult because of suboptimal tissue quality and frozen artifacts compared with routinely processed tissue section. The pathologist re-sponsible for the FS diagnosis requires experience and good judgment. Ovarian tumors are a het-erogeneous group of tumors including primary surface epithelial tumors, germ cell tumors and sex cord-stromal tumors, secondary tumors, and other groups of tumors of uncertain histogene-sis or nonspecific stroma. Intraoperative FS is a very important and reliable tool that guides the surgical management of ovarian tumors. In this review, the diagnostic key points for the patholo-gist and the implication of the FS diagnosis on the operator’s decisions are discussed.
Keywords: Frozen section; Intraoperative consultation; Ovarian tumors
Intraoperative consultation for ovarian tumors Insun Kim Department of Pathology, Jinju Korea Hospital, Jinju, Korea
Introduction
Intraoperative frozen consultation is one of the most important and difficult tasks of pathologists. Frozen section (FS) is per-formed during surgery, from which the pathologist provides a preliminary diagnosis, hence guiding the surgeon in further man-agement. The three main purposes of FS are to establish the presence and nature of a lesion, to determine the adequacy of the surgical margins, and to establish whether the obtained tissue contains diagnostic material or whether additional sampling is needed [1]. The indications and limitations of FS vary from or-gan to organ. However, this procedure should not be used by sur-geons to satisfy their curiosity, to recognize normal anatomic structures, or to communicate immediately with the patient’s rel-atives. The pathologist responsible for the FS diagnosis requires experience, knowledge of clinical medicine and pathology, good judgment, and an awareness of the limitation of the FS method. To effectively obtain the result, the pathologist should review the patient’s clinical history and ideally have a discussion with the surgeon before the operation.
Review articleeISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):163-182https://doi.org/10.12701/yujm.2019.00227
Received: April 23, 2019 Revised: May 30, 2019 Accepted: May 31, 2019
Corresponding author: Insun KimDepartment of Pathology, Jinju Korea Hospital, 2, Dongjin-ro, Jinju 52726, Korea Tel: +82-55-750-2570Fax: +82-55-757-4705E-mail: [email protected]
When the fresh tissue is received, the pathologist should select the best area from the specimen according to the purpose of the FS. The tissue is quickly frozen using liquid nitrogen, sectioned with cryostat, stained with hematoxylin-eosin, and evaluated un-der the microscope by the pathologist. Special stains and immu-nostains as well as cytologic smears obtained through touch preparation can be added [2]. Compared with routine pathologic diagnosis of formalin-fixed paraffin-embedded tissue prepara-tions, FS evaluation is limited by suboptimal tissue quality, frozen artifacts, time limitation, and lack of ancillary studies. It is also af-fected by the pathologist’s experience, supportive persons, avail-ability of a subspecialty pathologist, concurrent multiple FS specimens, and technical problems such as issues related to the instruments or the skill of the technician [3].
Gynecologic tumors are one of the most frequently encountered FS specimens in pathology laboratories. However, the evaluation of these lesions is often difficult because of the numerous disease entities and morphologic diversities, as well as their variants. Espe-cially, ovarian tumors are a heterogeneous group of tumors includ-ing primary surface epithelial tumors, germ cell tumors and sex
163https://doi.org/10.12701/yujm.2019.00227
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

cord-stromal tumors, secondary tumors, and other groups of tu-mors of uncertain histogenesis or nonspecific stroma [4].
Helpful information for the FS diagnosis of an ovarian tumor includes the patient’s age; relevant clinical and familial history; history of malignancy; serum markers such as alpha-fetoprotein, carcinoembryonic antigen, carcinoma antigen 125, carbohydrate antigen 19.9, and human chorionic gonadotropin; hormone lev-els (estrogen, androgen); and imaging studies. A high concor-dance between FS diagnosis and final permanent section diagno-sis has been reported, and the overall accuracy of FS diagnosis ranges between 80.7% and 97.1% for primary ovarian tumors [5,6]. However, the ultimate aim of FS in ovarian lesions is pro-viding the surgeon with helpful information for the next step of the operation, rather than providing a specific pathologic diagno-sis. If the tumor is benign, no further surgery is indicated. In bor-derline tumors, total abdominal hysterectomy and bilateral salp-ingo-oophorectomy (TAH-BSO) and staging procedure are indi-cated in postmenopausal women; however, unilateral salpin-go-oophorectomy (SO) and staging operation are indicated in young patients. In patients with ovarian carcinoma, TAH-BSO and debulking with staging procedure are recommended, where-as young patients with malignant sex cord-stromal tumors and germ cell tumors are suggested to undergo unilateral SO and staging procedure. Intraoperative FS is very important for guid-ing the surgical management of ovarian tumors.
In this review, the clinicopathologic, gross, and microscopic features of ovarian tumors are discussed, with special emphasis on the diagnostic key points and the implication of the FS diag-nosis on the operator’s decision during surgery. The materials and data collected from four university hospitals (Korea Anam, Inje Busan Paik, Gyeongsang, and Dankook Cheil) between 2016 and 2017 were reviewed, and the classification of ovarian tumors followed the 2014 World Health Organization classifica-tion of tumors of the female reproductive organs [4].
General categories of ovarian tumors
A total of 491 cases were submitted for frozen diagnosis of ovari-an tumors. Excluding nonneoplastic and nonovarian lesions, 446 tumors were primary ovarian tumors (95.5%) and 21 tumors were metastatic (4.5%) on permanent diagnosis. Among the pri-mary tumors, 372 were surface epithelial tumors (83.4%), 43 were sex cord-stromal tumors (9.6%), and the remaining 31 were germ cell tumors (7.0%).
Surface epithelial tumors were classified into 166 mucinous tu-mors (44.6%), 120 serous tumors (32.3%), 43 endometrioid tu-mors (11.6%), 16 clear cell tumors (4.3%), 15 seromucinous tu-
mors (4.0%), and 2 Brenner tumors (0.5%). The remaining 10 cases (2.7%) comprised 4 mixed carcinomas, 4 malignant mixed Mullerian carcinomas, 1 undifferentiated carcinoma, and 1 endo-metrial stromal sarcoma. Sex cord-stromal tumors were classified into 30 fibroma-thecoma tumors (69.8%) (19 fibromas, 6 cellu-lar fibromas, 4 thecofibromas, and 1 thecoma), 11 granulosa cell tumors (GCTs) (25.6%), and 2 Sertoli-Leydig cell tumors (SLCTs) (4.6%). Germ cell tumors were classified into 23 ma-ture cystic teratomas (74.2%), 3 dysgerminomas (9.7%), 2 im-mature teratomas (6.5%), 1 yolk sac tumor (3.2%), 1 choriocar-cinoma (3.2%), and 1 mixed tumor (3.2%). The metastatic tu-mors comprised 17 adenocarcinomas, 2 malignant lymphomas, 1 squamous cell carcinoma, and 1 atypical carcinoid.
Thirty-six tumors reported as “benign” on FS were finally diag-nosed as mucinous cystadenoma in 12 cases, endometriosis in 10 cases, serous cystadenoma in 9 cases, teratoma in 3 cases, mu-cinous borderline tumor (MBT) in 1 case, and seromucinous tu-mor in 1 case. Twenty-eight tumors reported as “adenocarcino-ma” or “carcinoma” were finally diagnosed as serous carcinoma in 15 cases, endometrioid carcinoma (EC) in 4 cases, clear cell carcinoma in 2 cases, mucinous carcinoma in 2 cases, carcinosar-coma in 2 cases, and metastatic tumor in 2 cases.
Surface epithelial tumors
Tumors of surface epithelial origin are the most commonly en-countered group in ovarian FS. Intraoperative FS evaluation is very important for determining the extent of surgery. In malig-nant tumors, staging laparotomy including total abdominal hys-terectomy with bilateral SO, lymphadenectomy, peritoneal sam-pling, and omentectomy should be done, whereas limited cystec-tomy or unilateral SO is done for benign tumors, especially in young patients who want to preserve their fertility. Misinterpre-tation of FS may lead to unnecessary extensive surgery or a risk for a second operation. The distinction between borderline tu-mors and invasive cancers is sometimes difficult. A conservative approach may be appropriate, especially in young patients. The findings of careful gross examination, bilaterality, clinical history of a previous malignancy, and the patient’s age and reproductive status are important in intraoperative consultation. In addition, the differential diagnosis of surface epithelial tumors may include other primary ovarian neoplasms.
1. Mucinous tumors Mucinous tumors are classified into benign cystadenoma/cysta-denofibroma/adenofibroma, MBT/atypical proliferative muci-nous tumor (APMT), and mucinous carcinoma. Mucinous tu-
https://doi.org/10.12701/yujm.2019.00227164
Kim I. Ovarian tumors

mors are characterized by cyst and glands lined by epithelial cells containing intracytoplasmic mucin. They tend to be the largest of all ovarian tumors, with many of them being 15–30 cm in di-ameter and are typically unilateral. Approximately 75% are be-nign, 10% are borderline, and 15% are carcinomas. In the review of 166 frozen diagnosis of mucinous tumors, 67.5% were benign, 22.3% were borderline, and 10.2% were malignant.
1) Mucinous cystadenoma/cystadenofibroma/adenofibroma Benign mucinous tumors are cystic, unilocular or multilocular, and contain viscous, mucoid material. If the tumor is partly or entirely solid, cystadenofibroma or adenofibroma is considered. The important point in intraoperative consultation is the distinc-tion from other benign cysts, if possible, because a metastatic mucinous tumor from the appendix may sometimes mimic a pri-mary benign mucinous cystic tumor. The surgeon may explore the appendix and perform appendectomy to exclude the possi-bility of an appendix origin. An additional FS or additional sam-pling for permanent section may be indicated in mucinous cysta-denoma with focal epithelial proliferation and atypia.
Among 93 tumors diagnosed as mucinous cystadenoma on FS, 11 tumors were diagnosed as borderline, 8 as focally prolifer-ative, and 2 as teratomas (1 mature and 1 immature) on perma-nent diagnosis. Twenty-two tumors diagnosed as cystadenoma with focal proliferation were diagnosed as borderline in 6 cases, cystadenoma in 4 cases, and seromucinous tumor in 1 case. Up-grading to a borderline tumor was seen in cases of cystadenoma (Fig. 1) and cystadenoma with focal proliferation. The distinc-
tion from a seromucinous tumor is not crucial on FS. Because mucinous ovarian tumors are commonly heterogeneous with a morphologic spectrum from benign to borderline to malignant areas, adequate sampling from the most solid area is very import-ant for a correct diagnosis.
2) Mucinous borderline tumors/atypical proliferative mucinous tumors Multilocular cystic tumors contain viscous mucoid material. A solid component is uncommon; however, if it is present, carcino-ma or mural nodule should be considered. Because the tumor is heterogeneous in morphology, multiple areas should be sampled for FS. Epithelial proliferation is seen in > 10% of tumors, but no stromal invasion is noted.
MBT/APMT with intraepithelial carcinoma represents muci-nous tumors showing areas of stratification to 4 or more layers or a cribriform pattern with severe nuclear atypia, but no stromal invasion. MBT/APMT with microinvasion indicates MBT with stromal invasion of < 5 mm.
Four tumors among 18 MBTs/APMTs and 2 of 4 MBTs/AP-MTs with microinvasion were diagnosed as mucinous carcino-mas on permanent section (Fig. 2). Five of 6 tumors reported as MBTs/APMTs rather than mucinous carcinomas were finally di-agnosed as mucinous carcinomas.
A definite diagnosis of intraepithelial carcinoma or microinva-sion, and the distinction from seromucinous borderline tumor (SMBT) are not necessary in FS. The frozen diagnosis of MBT/APMT is adequate. If the distinction from a mucinous carcinoma
Fig. 1. On frozen section, the multilocular cyst is lined by single layer of tall columnar cells (A), but the epithelial cells are stratified and show papillary growth indicating mucinous borderline tumor on permanent section (B).
A B
165https://doi.org/10.12701/yujm.2019.00227
Yeungnam Univ J Med 2019;36(3):163-182

is difficult, a frozen diagnosis of “at least MBT” can be made. Because of the excellent prognosis, even with intraepithelial
carcinoma or microinvasion, fertility-sparing surgery is adequate for young patients with MBT/APMT [7].
3) Mucinous carcinomas Mucinous carcinoma is a relatively rare histologic subtype and presents with a large, unilateral mass ( > 10 cm). The tumor is complex and multicystic with solid areas. Necrosis and hemor-rhage may be present. Two patterns of stromal invasion ( > 5 mm), expansile (confluent) and destructive (infiltrative), should be identified (Fig. 3). The tumor may have areas resembling a benign cystadenoma or a borderline tumor (Fig. 4). Multiple ad-
equate samplings from solid areas and areas near necrosis are key for the intraoperative FS diagnosis of MBT/APMT and muci-nous carcinoma, because of the heterogeneous morphologic continuum from benign to borderline to malignant areas.
Among 7 tumors that were diagnosed as mucinous carcinoma on FS, 1 tumor was a clear cell carcinoma and 1 tumor was a met-astatic carcinoma. The distinction from metastatic carcinoma is very important, because surgical staging should be done for a pri-mary ovarian tumor but not for a metastatic carcinoma. Bilateral-ity, small tumor size ( < 10 cm), and the patient’s clinical history of a prior malignancy indicate a metastatic carcinoma rather than a primary tumor [8]. The presence of a teratomatous component suggests a primary ovarian tumor.
Fig. 2. On frozen section, the tumor was diagnosed as mucinous borderline tumor (A), but permanent histologic section shows expansile type of mucinous carcinoma (B).
Fig. 3. Two patterns of invasion in mucinous carcinoma: expansile (A) and infiltrative (B).
A
A
B
B
https://doi.org/10.12701/yujm.2019.00227166
Kim I. Ovarian tumors

4) Mucinous tumors with mural nodules Reactive sarcoma-like mural nodules and malignant mural nod-ules are rarely associated with benign, borderline, or malignant mucinous tumors. A reactive mural nodule typically occurs in younger patients and does not alter the prognosis, whereas a ma-lignant mural nodule characterized by anaplastic carcinoma or sarcoma is usually seen in older patients and has a poor prognosis (Fig. 5) [9,10]. High-grade carcinoma/sarcoma associated with a mucinous tumor may be enough for frozen diagnosis, and the final diagnosis can be deferred for permanent sections.
2. Serous tumors Serous tumors are classified as benign cystadenoma/cystadeno-fibroma/adenofibroma, serous borderline tumor (SBT)/ atypi-cal proliferative serous tumor (APST), SBT/APST micropapil-lary variant/noninvasive low-grade serous carcinoma (LGSC),
Fig. 4. Goss finding of mucinous carcinoma is cystic, with polypoid mass (A). On section, the solid mass is sponge-like with hemorrhage and necrosis (B). The cystic area is mucinous borderline tumor (C), but solid portion is mucinous carcinoma (D).
A
C
B
D
Fig. 5. Mucinous borderline tumor shows mural nodule composed of anaplastic carcinoma.
167https://doi.org/10.12701/yujm.2019.00227
Yeungnam Univ J Med 2019;36(3):163-182
invasive LGSC, and high-grade serous carcinoma (HGSC). Ap-proximately 70% of serous tumors are benign, 10% are border-line, and 20% are carcinomas. However, among 120 serous tu-mors on FS, borderline and malignant tumors accounted for 22.5% and 43.3%, respectively, and benign tumors comprised only 24.2%.
1) Serous cystadenoma/cystadenofibroma/adenofibroma Benign serous tumors usually occur in adults, and bilaterality is observed in about 20%. The tumor is a unilocular or an oligoloc-ular cyst containing clear watery fluid. In cystadenofibroma, the tumor is cystic and solid and shows firm papillary projection, whereas the tumor is solid and firm with small spaces in adenofi-broma. Epithelial proliferation involves < 10% of the epithelial lining [11]. If the frozen diagnosis is cystadenoma with focal epi-thelial proliferation, additional frozen sampling is recommended; however, no staging is required. The distinction from benign, nonneoplastic cyst is not important, but mucinous tumor should be ruled out because appendectomy may be done to exclude me-tastasis from a primary appendix tumor.
Among 22 benign serous tumors on frozen diagnosis, 1 tumor was borderline and 2 tumors were mucinous tumors. Among 4 benign versus borderline tumors, 1 was benign and the other was SMBT.
The distinction from a mucinous tumor should be based on the histologic cell type, not on the cystic content. The papillary projection in benign tumors is typically firm and small in num-ber, whereas papillary growth in SBT/APST is soft, friable, and large in number.
2) Serous borderline tumor/atypical proliferative serous tumor SBT/APST is bilateral in up to 55% of cases, and typically cystic. Abundant friable papillary projections are present on the inner lining of the cyst and/or a cauliflower-like mass may be present on the ovarian surface without a cystic component (serous sur-face papillary borderline tumor). Microscopically, epithelial pro-liferation is seen in at least 10% of tumors (Fig. 6). A micropapil-lary or cribriform pattern may also be seen ( < 5 mm). Psammo-matous calcification, which may be observed in benign and ma-lignant serous tumors, is found in approximately one-fourth of the cases. Microinvasion ( < 5 mm in greatest dimension) may be present. The distinction from serous cystadenoma with or with-out focal epithelial proliferation ( < 10%) is sometimes difficult on FS. A conservative approach is recommended, especially in young patients. If the stromal invasion is > 5 mm, it should be classified as invasive LGSC. If the micropapillary pattern is > 5 mm, it should be classified as noninvasive LGSC, micropapillary variant [11,12]. However, the distinction from noninvasive or in-vasive low-grade carcinoma is not crucial at the time of FS. “At least SBT” or “SBT with micropapillary features” is an appropri-ate FS diagnosis. HGSC requiring complete surgical staging should be ruled out on FS.
SBT/APST is associated with peritoneal implants in about 30–40% of the cases. The implants are classified into the nonin-vasive and invasive types, and the noninvasive type is subdivided into the epithelial and desmoplastic subtypes [13]. Invasive im-plants behave like LGSC [4]. The distinction between noninva-sive implants of SBT/APST and LGSC may not be crucial at the time of FS, especially in older patients. Additional sampling from
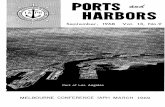
Fig. 6. Serous borderline tumor on frozen section (A) and on permanent section (B). Epithelial proliferation is characterized by hierarchical branching papillae with budding and tufting, and stratification of the cells.
A B
https://doi.org/10.12701/yujm.2019.00227168
Kim I. Ovarian tumors

the peritoneum or ovary may be helpful for a specific diagnosis. Among 17 SBTs/APSTs on FS, 1 tumor was SMBT. Among 6
borderline versus malignant tumors, 3 tumors were malignant and 1 was SMBT. The distinction from SMBT has no impact on the surgical management at the time of FS.
3) Noninvasive low-grade serous carcinoma The clinical and gross findings of noninvasive LGSC (SBT/APST micropapillary variant) are similar to those of SBT/APST.
Microscopically, it is characterized by a nonhierarchical branching micropapillary or cribriform architecture in at least 1 confluent area measuring 5 mm [6]. Micropapillae are defined as at least 5 times taller than wide, with scant or no fibrovascular cores. The distinction from SBT/APST may not be crucial at the time of FS. “At least SBT” or “SBT with micropapillary features” may be enough for the frozen diagnosis, and fertility-sparing sur-gery may be done in young patients.
4) Low-grade serous carcinoma LGSC is relatively rare and commonly advanced at the time of presentation. It is often bilateral and solid or partly cystic, with papillary growth. Microscopically, it is characterized by relatively uniform nuclei with mild to moderate atypia, and mitotic figures < 12/10 high-power fields (HPFs) [14]. Psammoma bodies may be abundant. Destructive stromal invasion ( > 5 mm) is present. The distinction from SBT/APST may not be crucial at the time of FS. Additional biopsy from extraovarian lesions or implants may be helpful in identifying destructive stromal invasion. The value of fertility-sparing surgery is not well documented in this group, and the prognosis is dependent on the disease stage.
Pelvic or para-aortic lymph nodes are not infrequently in-volved by the papillary or glandular structures, similar to primary ovarian SBT/APST or LGSC. The distinction between primary nodal proliferation and metastasis from the ovary may be diffi-cult. However, both findings do not change the prognosis and do not influence the treatment. Occasionally, extensive lymph node involvement in patients with invasive peritoneal implants is asso-ciated with a poor prognosis.
The distinction from HGSC should be done on FS. High-grade carcinoma characterized by marked nuclear atypia, numer-ous mitotic figures, and necrosis is different from low-grade car-cinoma [14]. Unfortunately, most of the cases were not ade-quately diagnosed as LGSC or HGSC in this review.
5) High-grade serous carcinoma HGSC is the most common type of ovarian carcinoma. It occurs in older age groups, presents at an advanced stage, and is bilateral
in the majority of the cases. Grossly, the tumor is solid or solid and cystic with frequent involvement of the ovarian surface. Hemorrhage and necrosis are common. Histologically, the tumor is characterized by an admixture of solid, complex glandular growth with slit-like spaces, cribriform, and papillary patterns (Fig. 7). Marked nuclear atypia with prominent nucleoli, pleo-morphism, and numerous mitotic figures ( > 12/10 HPFs) with atypical forms are present [14]. Stromal invasion is present. A tu-mor with an intracystic papillary pattern showing marked nucle-ar atypia and numerous mitotic figures, but without stromal in-vasion, is also classified as HGSC. The important issue in FS is the recognition of high-grade epithelial malignancy. The distinc-tion from LGSC is the presence of marked nuclear atypia and numerous mitotic figures ( > 12/10 HPFs). The differential diag-nosis from other high-grade carcinomas of Mullerian origin, en-dometrioid, clear cell carcinoma, and malignant Brenner tumor is not important. “High-grade carcinoma, consistent with a Mul-lerian origin” may be adequate in difficult cases. HGSC may arise from the fallopian tube or peritoneum and metastasizes from en-dometrial serous carcinoma. The distinction from these primary sites is not crucial on FS.
3. Endometrioid tumors Endometrioid tumors include benign endometriotic cyst and cystadenoma/adenofibroma, endometrioid borderline tumor (EBT)/atypical proliferative tumor (APET), and malignant car-cinoma. In the review of 43 frozen diagnoses, endometriotic cysts accounted for 70%, malignant tumors accounted for 25%, and borderline tumors accounted for 5.0%.
1) Endometriotic cyst/cystadenoma/adenofibroma Endometriotic cyst is a cystic form of endometriosis. Histologi-cally, the cyst is lined by endometrial epithelium and underlying endometrial stroma, but cystadenoma/adenofibroma is lacking the endometrial stroma. The distinction from other benign le-sions is not crucial on frozen diagnosis. Endometriosis with cyto-logic atypia or atypical hyperplasia should be managed conserva-tively. However, adequate sampling is important because it may be associated with borderline and malignant endometrioid, clear cell, and seromucinous tumors.
In the review of 20 benign endometriotic lesions, 1 case was associated with clear cell carcinoma and the other was a muci-nous cystadenoma. Sampling from a polypoid or solid lesion of an endometriotic cyst is considered important.
2) Endometrioid borderline tumor/atypical proliferative tumor EBT/APET is an uncommon tumor that is predominantly solid
169https://doi.org/10.12701/yujm.2019.00227
Yeungnam Univ J Med 2019;36(3):163-182

but shows a focally cystic or sponge-like cut surface. Histologi-cally, the tumor shows complex, crowded glandular structures in a fibromatous or intracystic pattern. Squamous metaplasia is common. Mild to moderate nuclear atypia, but without stromal invasion, is present. EBT/APET with intraepithelial carcinoma is defined as marked cytologic atypia but without stromal invasion, whereas EBT/APET with microinvasion is defined as confluent glandular growth or stromal invasion of < 5 mm dimension.
Complete surgical staging is the standard surgical management for EBT/APET, but fertility-sparing surgery may be an option for young patients because of their excellent prognosis. The pres-ence of intraepithelial carcinoma or microinvasion does not change the surgical management, but adequate sampling is rec-ommended to confirm unequivocal invasion [15,16]. EC may arise in the background of EBT/APET or endometriosis. Six en-dometrioid tumors were interpreted as borderline versus malig-nant on FS, and 3 of them were finally diagnosed as EC.
3) Endometrioid carcinoma ECs occur in older age groups, and bilaterality is observed in up to 17% of the cases [4]. The tumor is a solid or blood-filled cyst with intraluminal soft mass or polypoid nodule. Histologically, the tumor resembles endometrial EC. The stromal invasion should be > 5 mm. Squamous differentiation is often present, in up to 30–50% of the cases (Fig. 8) [17]. Adequate sampling from solid and necrotic areas is important to rule out EC in the case of EBT/APET.
The distinction from other primary ovarian serous, clear cell, and seromucinous carcinomas is not crucial; however, mucinous
differentiation should be ruled out because of the possibility of a metastatic carcinoma. Metastatic carcinoma from a primary col-orectal and endocervical tumor may mimic EC. Squamous dif-ferentiation and an association with EBT/APET or endometrio-sis in the background are the most helpful features indicating a primary ovarian origin. The “garland” pattern with intraluminal dirty necrosis is the feature indicative of metastasis. Information on the patient’s history of prior malignancies or concurrent le-sions should be obtained from the surgeon. Simultaneous ovari-an and endometrial ECs are present in 15–20% of the cases [18]. Whether the ovarian tumor is a primary tumor or a metastasis from the endometrium is not important on frozen diagnosis. Among 9 ECs, only 1 case was correctly diagnosed on FS and the others were serous carcinoma (5 cases), seromucinous carcino-ma (1 case), mixed MC and EC (1 case), and metastatic carcino-ma (1 case).
4. Clear cell tumors Benign tumors are exceptionally rare, and borderline tumors ac-count for < 1%. Most tumors are clear cell carcinomas. Clear cell tumors arise as a solid adenofibromatous or a cystic endometri-otic type [19,20]. In the solid type, the cut surface is sponge-like with numerous small cysts (Fig. 9A). A benign tumor is micro-scopically characterized by benign-appearing glandular epitheli-um, whereas a borderline tumor shows atypical or malignant epi-thelium without invasion or microinvasion. A frankly invasive component ( > 5 mm in size) is present in a malignant tumor. A cystic tumor is unilocular or multilocular, with protruding polyp-oid masses in the lumens (Fig. 9B). The lining of the cyst rep-
Fig. 7. High grade serous carcinoma shows solid and complex glandular growth patterns and psammomatous calcification on frozen section (A), and slit-like spaces of tumor cells with marked nuclear atypia (B).
A B
https://doi.org/10.12701/yujm.2019.00227170
Kim I. Ovarian tumors

Fig. 9. Clear cell carcinoma may have a solid cut surface (A) or may show a predominantly cystic appearance with intraluminal solid growth (B). On frozen section, the tumor has solid and papillary growth patterns and psammomatous calcification (C). The tumor cells are large and pleomorphic. Hyaline bodies are found (D).
A
C
B
D
Fig. 8. Endometrioid adenocarcinoma shows confluent, back-to back glandular proliferation with loss of intervening stroma (A), and squamous component (B).
A B
171https://doi.org/10.12701/yujm.2019.00227
Yeungnam Univ J Med 2019;36(3):163-182

resents benign or atypical endometriosis. The tumors are charac-terized by various cell types and histologic patterns (Fig. 9C). The most diagnostic features include dense hyalinized cores of papillae and hyaline bodies, which are present in 25% of the cases (Fig. 9D). Because a benign or borderline clear cell tumor is ex-ceedingly rare, multiple additional sections should be taken to rule out carcinoma. Marked nuclear atypia is helpful in the differ-entiation of intracystic papillary clear cell carcinoma from SBT/APST. The distinction from primary ovarian HGSC and EC as well as the distinction between metastatic clear cell carcinoma and Mullerian clear cell carcinoma are not crucial on FS. Yolk sac tumor and dysgerminoma should be ruled out, because fertili-ty-sparing surgery is an option for young patients. Germ cell tu-mors typically occur in younger age groups (2nd and 3rd decades) than clear cell carcinoma. All 11 clear cell carcinomas diagnosed
on FS were correct; however, 3 tumors were diagnosed as adeno-carcinoma and 1 as mucinous carcinoma. The other 1 case aris-ing in association with endometriosis was misdiagnosed as endo-metriosis.
5. Seromucinous tumors Seromucinous tumor is a mixed epithelial neoplasm with 2 or more Mullerian cell types, all accounting for at least 10% of the epithelium. The tumors are unilocular or paucilocular with pap-illary excrescences (Fig. 10A). Seromucinous tumors are associ-ated with endometriosis in 30% of the cases (Fig. 10B) [4]. The most predominant epithelial cell types are serous and endocervi-cal-type mucinous epithelium (Fig. 10C). The tumors are classi-fied into benign seromucinous cystadenoma/ adenofibroma, borderline seromucinous tumor/atypical proliferative seromuci-
Fig. 10. Seromucinous borderline tumor is grossly cystic and shows intraluminal papillary growth (A). Histologically papillary growth is similar to serous borderline tumor (B). Frozen (C) and permanent (D) sections show complex glands composed of serous and mucin-secreting cells infiltrated with neutrophils.
A
C
B
D
https://doi.org/10.12701/yujm.2019.00227172
Kim I. Ovarian tumors
nous tumor, and malignant seromucinous carcinoma. Benign and malignant tumors are rather uncommon, and most tumors belong to the borderline category. These tumors are architectur-ally similar to SBT/APST, but larger papillae have edematous stroma containing neutrophils (Fig. 10D). Microinvasion, in-traepithelial carcinoma, and a micropapillary pattern may occur.
On FS, the distinction from SBT/APST may be difficult; how-ever, it is not important at the time of FS.
Seromucinous tumors were frequently diagnosed as serous tu-mors, but also as mucinous or endometrioid tumors in this review.
Sex cord-stromal tumors
Sex cord-stromal tumors account for approximately 5–10% of all ovarian tumors and are commonly associated with estrogenic or androgenic manifestations. The tumors are classified into pure stromal tumors, pure sex cord tumors, and mixed sex cord-stro-mal tumors, and present a variety of histologic types [6]. Because the biologic behavior of sex cord-stromal tumors differs accord-ing to the histologic type, recognition of the specific entity may guide the intraoperative management.
1. Fibroma-thecoma Fibroma is the most common type of stromal tumor. The tumor is solid, firm, white or tan, or hemorrhagic because of torsion (Fig. 11A). Microscopically, the tumor is composed of intersect-ing bundles and fascicles of spindle cells with hyalinization, colla-gen bands, or plaque (Fig. 11B). Cellular fibroma accounts for about 10% and is densely cellular with scant collagen. The num-ber of mitosis is ≤ 3/10 HPFs, and nuclear atypia is absent or
mild. A cellular tumor with mitotic activity of ≥ 4/10 HPFs and no more than mild nuclear atypia is defined as mitotically active cellular fibroma, whereas a tumor with at least moderate nuclear atypia and increased mitotic activity of ≥ 4/10 HPFs, often with atypical form, is termed as fibrosarcoma [21].
Thecomas are relatively uncommon tumors that typically oc-cur in postmenopausal women with symptoms of estrogen pro-duction. The tumors are unilateral, and the cut surface is solid and yellow. The tumor is microscopically composed of sheets of oval or round cells with moderate to abundant pale eosinophilic cytoplasm. The tumor is designated as a fibrothecoma when an area resembling a fibroma is present.
On FS, the distinction of fibroma from thecoma is not import-ant. However, the distinction from metastatic carcinoma with re-active stromal proliferation (Krukenberg tumor) is important. Bilaterality should raise a suspicion for metastasis, and careful microscopic examination to search for scattered tumor cells with a signet ring or breast lobular carcinoma should be done. Thor-ough sampling is recommended when minor sex cord elements are present, to rule out GCT or SLCT. Luteinized cells in theco-mas may suggest the possibility of Leydig cell tumor or SLCT. Distinction from Leydig cell tumor is not crucial, but identifica-tion of a Sertoli cell component is important because surgical staging is required for SLCT [22].
Among 30 tumors, 1 fibrothecoma was suggested to be a met-astatic poorly differentiated carcinoma and 3 cellular fibromas were diagnosed on permanent section.
2. Granulosa cell tumors GCT is a low-grade malignant tumor composed of granulosa
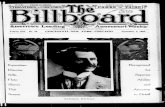
Fig. 11. Cut surface of fibroma is solid, firm, tan white and yellow (A). Histologically, the tumor is hypercellular and hypocellular with interlacing fascicles of spindle tumor cells (B).
A B
173https://doi.org/10.12701/yujm.2019.00227
Yeungnam Univ J Med 2019;36(3):163-182

cells often with a variable number of fibroblasts and theca cells. The tumors comprise of two different clinicopathologic sub-types: adult and juvenile. The adult type more often occurs in postmenopausal patients, whereas the juvenile type mainly oc-curs in children and younger women. The patients may present abnormal vaginal bleeding associated with estrogenic manifesta-tions. Patients with adult GCT have concurrent endometrial hy-perplasia (25%) or adenocarcinoma (5%), and younger patients may present isosexual precocity [23]. The tumors are commonly unilateral, typically solid and cystic, and tan-yellow or white. Mi-croscopically, the adult form is characterized by a mixture of vari-ous morphologic patterns, and the tumor cells are uniform with scanty cytoplasm and pale grooved nuclei (Figs. 12A, 12B). The juvenile form typically shows macrofollicles filled with basophil-ic secretions, as well as cells with moderate to abundant cyto-plasm and darker nuclei usually without grooves [24].
The surgical treatment of GCT in postmenopausal patients in-
cludes total hysterectomy and bilateral SO as part of the complete surgical staging procedure, whereas fertility-sparing surgery includ-ing unilateral SO and staging procedure may be done in younger patients with unilateral tumor without surface involvement [25,26].
On FS, the distinction between the adult and juvenile forms is not crucial. The distinction of the adult type from benign sex cord-stromal tumors and metastatic carcinoma is the most im-portant, because these lesions do not require surgical staging. Clinical history, bilaterality, and marked nuclear atypia with nu-merous mitotic figures should raise suspicion for a metastatic car-cinoma. An adult-type tumor with a microfollicular pattern can mimic a metastatic or primary typical or atypical carcinoid tumor. Carcinoid tumors have round nuclei with smooth nuclear mem-brane and stippled chromatin, in contrast to oval nuclei and nucle-ar groove in GCT (Figs. 12C, 12D). In the distinction of the sar-comatoid type from cellular fibroma/fibrosarcoma, the character-istic nuclear features and identification of other morphologic pat-
Fig. 12. Adult granulosa cell tumor typically shows microfollicular pattern with Call-Exner bodies (A), and the tumor cells are oval and have angular nucleus with groove (B). Metastatic atypical carcinoid may show microfollicular structure, but the nuclei of the tumor cells are different from those of granulosa cell tumor.
A
C
B
D
https://doi.org/10.12701/yujm.2019.00227174
Kim I. Ovarian tumors

terns of GCT can be helpful. If the frozen diagnosis is adult GCT, evaluation of the endometrium is also recommended.
One SLCT and 1 metastatic atypical carcinoid were diagnosed as adult GCT on FS.
3. Sertoli-Leydig cell tumors SLCT is a rare tumor that commonly occurs in young patients and presents androgenic symptoms. Most of the tumors are uni-lateral, solid, and tan-yellow, or partly cystic in tumors with a reti-form pattern or a mucinous heterologous component. Micro-scopically, the tumor is characterized by open or solid tubules, cords and diffuse sheets of primitive stromal appearance of Ser-toli cells, and a variable degree of Leydig cells (Fig. 13A). The tu-mors are classified into well, moderately, and poorly differentiat-ed groups, according to the differentiation of Sertoli cells. Ap-proximately 20% of the tumors have heterologous components such as mucinous epithelium, cartilage, or skeletal muscle, and approximately 15% of SLCTs show a retiform pattern [4,27]. The prognosis of patients depends on the differentiation and on the presence of retiform and heterologous components [28]. Conservative fertility-sparing surgery in young patients with stage 1 tumor includes unilateral SO and staging procedure; however, bilateral SO, total hysterectomy, and complete surgical staging are performed in patients who do not wish to preserve fertility [22].
The differential diagnosis between moderately and poorly dif-ferentiated SLCT and adult GCT is not easy on FS, but the surgi-cal management is basically similar (Fig. 13B). In distinguishing from ovarian primary sertoliform EC, the presence of unilaterali-
ty, younger age, absence of squamous differentiation, and pres-ence of Leydig cells can be helpful in the diagnosis of SLCT. Sur-gical staging is more extensive in ovarian epithelial malignancy. Among 2 SLCTs, 1 tumor was diagnosed as adult GCT on FS.
Germ cell tumors
Germ cell tumors comprise the second most common type of tumors; however, the majority of tumors are benign mature cys-tic teratomas. Malignant germ cell tumors are relatively rare, but the recognition of these tumors and their distinction from ag-gressive epithelial carcinomas are crucial. Because most malig-nant germ cell tumors occur in young patients, fertility-sparing surgery is important. Fortunately, adjuvant chemotherapy is now the standard management for these tumors. The patient’s age, hormonal manifestations such as precocious puberty, and serum tumor markers can provide the diagnostic clues for the FS diag-nosis. Mixed germ cell tumors of 2 or more types of malignant germ cell tumors may occur. Identification of different histologi-cal components is important for the treatment and prognosis. However, it is not crucial on FS. “Malignant germ cell tumor, probably mixed components” is sufficient for the FS diagnosis.
1. Mature and immature teratoma Teratoma is a very common ovarian tumor. Mature teratomas ac-count for > 95% of all teratoma and most commonly occur during the reproductive ages. On the other hand, immature tera-tomas are relatively rare, representing 1–3% of all teratomas, and most commonly occur during the first 2 decades of life. Bilateral-
Fig. 13. Sertoli-Leydig cell tumor (A) has sex cord component similar to adult granulosa cell tumor (B), but Leydig cell component is present in Sertoli-Leydig cell tumor (circle in A).
A B
175https://doi.org/10.12701/yujm.2019.00227
Yeungnam Univ J Med 2019;36(3):163-182

ity is observed in 10–15% of the cases. Mature teratoma is almost always cystic, but rarely solid. Immature teratoma is solid and cystic. Microscopically, the neural elements in mature teratoma may mimic the primitive immature neuroepithelial tissue of im-mature teratoma [29]. Immature mesenchymal and endodermal elements are sometimes difficult to detect on FS. The diagnosis of immature teratoma should rely on the identification of imma-ture neuroepithelial tissue (Fig. 14A). Carcinosarcoma, com-posed of carcinomatous and sarcomatous components, may be considered in the differential diagnosis, but it most often occurs in the postmenopausal ages (Fig. 14B). Monodermal teratomas include struma ovarii and carcinoid tumor. Malignant transfor-mation of mature teratoma rarely occurs, most often in post-menopausal patients; however, when it occurs, full surgical stag-ing is required [30]. The FS diagnosis of mature cystic teratoma is straightforward, but adequate sampling from solid areas in-cluding the Rokitansky protuberance should be done.
2. Dysgerminoma Dysgerminoma is the most common malignant germ cell tumor, occurring most often during the 2nd and 3rd decades of life. It is a rapidly growing tumor and may arise in dysgenetic gonads with gonadoblastoma. The tumor is unilateral in 80–90% of the cases, and is large, solid, and flesh and tan-yellow in color (Fig. 15A). Microscopically, the tumor is characterized by solid nests, sheets, or cords of relatively uniform polygonal cells with abundant clear or eosinophilic cytoplasm and prominent nucleoli, with inter-secting fibrous septae infiltrated with lymphocytes (Fig. 15B).
On FS, contralateral ovarian biopsy should be performed to
rule out bilateral tumor or underlying dysgenetic gonads and/or gonadoblastoma, for which bilateral oophorectomy is indicated. However, fertility-sparing surgery (unilateral SO with peritoneal biopsy and lymph node sampling) is adequate for unilateral dys-germinoma [31]. The distinction from other malignant germ cell tumors, yolk sac tumor and embryonal carcinoma is not crucial on FS. The surgical management is essentially identical. The most important issue concerning dysgerminoma on FS is its dif-ferentiation from diffuse large cell lymphoma, because the man-agement of lymphoma is basically nonsurgical (Figs. 15C, 15D).
One of 2 dysgerminomas was diagnosed as metastatic carcino-ma, whereas 1 malignant lymphoma was interpreted as dysger-minoma on FS in this review.
3. Yolk sac tumor Yolk sac tumor accounts for 20% of malignant germ cell tumors and occurs during the 2nd and 3rd decades of life. This tumor may be a component of a mixed germ cell tumor and rarely occurs in association with a surface epithelial tumor, usually endometrioid [32,33]. The serum alpha-fetoprotein level is elevated. The tu-mor is nearly always unilateral, large, solid, and tan-yellow, with areas of necrosis, hemorrhage, and cyst formation. Microscopi-cally, various growth patterns, such as reticular pattern, endoder-mal sinus pattern with Schiller-Duval bodies, solid pattern, alveo-lar glandular pattern, and other rare polyvesicular vitelline or hepatoid patterns, are present within the same tumor (Fig. 16).
The distinction from other malignant germ cell tumors is not crucial on FS, because the surgical management is similar. The most important entity in the differential diagnosis is clear cell
Fig. 14. Immature teratoma shows primitive neuroepithelial component, in addition to immature epithelial and mesenchymal tissues including immature cartilage (A), whereas carcinosarcoma is composed of carcinomatous (B, left) and sarcomatous components with malignant-looking cartilage (B, right).
A B B(left) (right)
https://doi.org/10.12701/yujm.2019.00227176
Kim I. Ovarian tumors
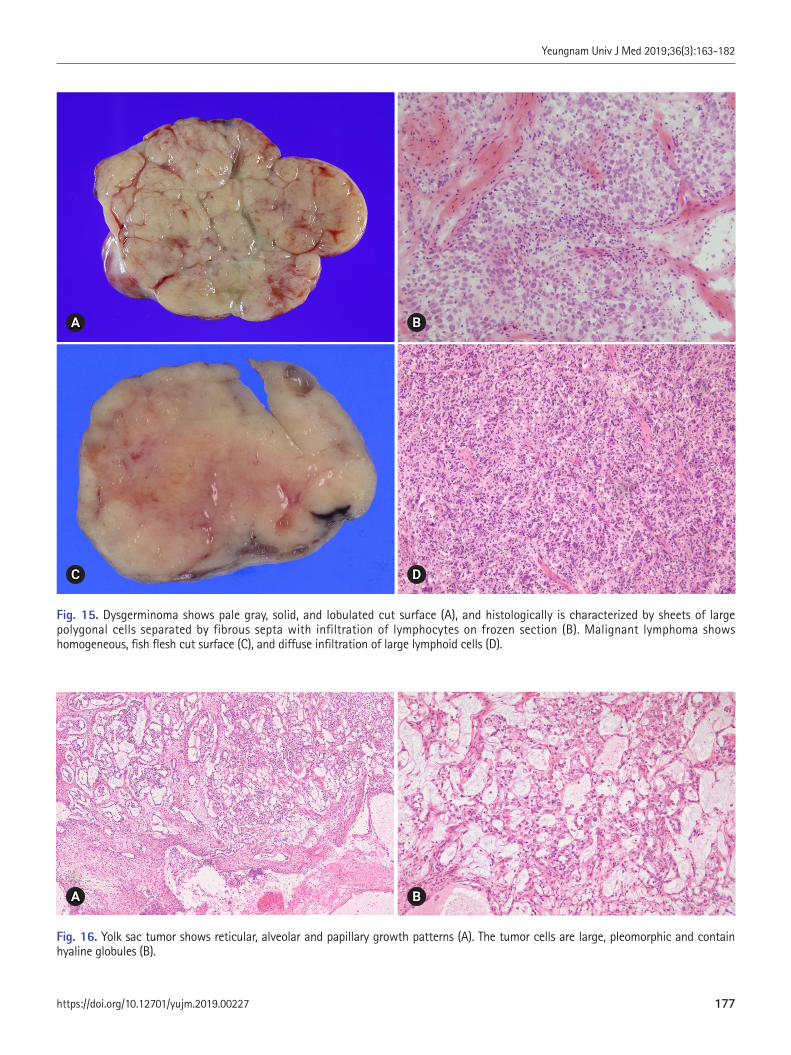
Fig. 15. Dysgerminoma shows pale gray, solid, and lobulated cut surface (A), and histologically is characterized by sheets of large polygonal cells separated by fibrous septa with infiltration of lymphocytes on frozen section (B). Malignant lymphoma shows homogeneous, fish flesh cut surface (C), and diffuse infiltration of large lymphoid cells (D).
A
C
B
D
Fig. 16. Yolk sac tumor shows reticular, alveolar and papillary growth patterns (A). The tumor cells are large, pleomorphic and contain hyaline globules (B).
A B
177https://doi.org/10.12701/yujm.2019.00227
Yeungnam Univ J Med 2019;36(3):163-182

carcinoma, which requires more extensive staging. Clear cell car-cinoma usually occurs in older ages and is commonly associated with endometriosis.
4. Choriocarcinoma Choriocarcinoma is a rare type of malignant germ cell tumor. Nongestational choriocarcinoma occurs in children and young adults and may be mixed with other malignant germ cell tumor components, whereas gestational choriocarcinoma occurs in old-er age groups. Elevated serum beta-human chorionic gonadotro-pin level and isosexual pseudoprecocity may be present. The tu-mor is typically large and solid and cystic, often with hemorrhage and necrosis. Microscopically, a biphasic pattern of cytotropho-blasts and multinucleated syncytiotrophoblasts is typically pres-ent (Fig. 17). Other malignant germ cell tumors may show isolat-ed syncytiotrophoblastic giant cells, but the distinction on FS is not crucial. However, poorly differentiated surface epithelial car-cinoma with trophoblastic differentiation, typically occurring in postmenopausal patients, should be differentiated because it re-quires more aggressive surgery [34]. One choriocarcinoma in this review was interpreted as torsion because of the presence of extensive hemorrhagic necrosis.
Metastatic tumors
Metastatic tumors account for about 15% of ovarian malignan-cies and 6–7% of all adnexal masses [35]. Among 467 cases of ovarian tumors, 21 (4.5%) cases were metastatic tumors. Ovari-an metastasis most commonly originates from the gastrointesti-nal tract (colon, appendix, stomach, and pancreatobiliary tract).
The breast is the most frequent primary site among the nongas-trointestinal origins [36]. Endometrial and cervical carcinoma may metastasize to the ovary. Metastatic ovarian tumor can be present synchronously or metachronously with the primary neo-plasm, but an ovarian tumor may represent the first manifesta-tion of an occult nonovarian primary neoplasm. Metastatic tu-mors are bilateral in approximately 70% of the cases, are small in size ( < 10 cm), and show superficial surface involvement and multinodular growth; however, they can be unilateral, large, and cystic, resembling a primary ovarian neoplasm [37]. Microscopi-cally, metastatic tumors are characterized by surface implants, multinodularity, lymphovascular invasion, and extensive extrao-varian spread. However, the microscopic appearance of the me-tastasis is variable depending on the primary tumor, although the histologic features of metastatic tumors are not always identical to those of the primary tumors.
Among 19 metastatic tumors excluding 2 malignant lympho-mas, 17 tumors were adenocarcinomas, 1 tumor was a squamous cell carcinoma, and 1 was an atypical carcinoid. The primary sites were the stomach in 8 cases, the colon in 4 cases, the uterine cervix in 3 cases, and unknown in 3 cases. The 3 tumors among 19 metastatic tumors were misinterpreted as 1 mucinous carci-noma, 1 EC, and 1 GCT.
1. Colorectal adenocarcinoma Metastatic adenocarcinoma from the colorectum is often bilateral and solid or solid and cystic with a tan-yellow or gray cut surface (Fig. 18A). Ovarian surface involvement and multinodular growth pattern are commonly seen. Histologically, the tumor shows variable-sized, often cystic, irregular glands. A cribriform
Fig. 17. Choriocarcinoma shows extensive hemorrhagic necrosis (A). Viable tumor nest is composed of two cell pattern of cytotrophoblasts and syncytiotrophoblasts (B).
A B
https://doi.org/10.12701/yujm.2019.00227178
Kim I. Ovarian tumors

architecture with dirty necrosis is called a garland pattern. The differential diagnosis from primary ovarian mucinous and endo-metrioid adenocarcinoma is important (Fig. 18B). Bilaterality, size < 10 cm, ovarian surface involvement, and a multinodular growth pattern suggest metastasis rather than a primary ovarian tumor [37]. If the tumor shows mucinous differentiation, intraop-erative surgical evaluation of the abdominal cavity is recommend-ed to find the possible primary lesion of the metastasis. Squamous differentiation in adenocarcinoma indicates primary ovarian EC rather than metastasis from a primary colorectal tumor.
2. Signet ring cell carcinoma The primary site of metastatic signet ring cell carcinoma is most commonly the stomach (70%), but less commonly the colorec-
tum, appendix, breast, and pancreaticobiliary system [38,39]. The tumor is bilateral, grossly solid, and tan-yellow or white, but may also be firm or soft, and gelatinous (Fig. 19A). Histological-ly, the tumor shows a pseudo-lobular pattern with hypercellular and hypocellular areas or diffusely cellular dense stroma (Fig. 19B). Signet ring cells individually infiltrate or form small clus-ters or tubules. Extracellular mucin may be present. On FS, signet ring cells may be missed and misinterpreted as fibroma or fi-brothecoma. Primary ovarian sex cord-stromal tumors are usual-ly unilateral.
3. Appendiceal tumors The most common appendiceal tumor with ovarian involvement is low-grade mucinous neoplasm. Less commonly, intestinal-type
Fig. 18. Multilocular cystic metastasis from colon cancer with multifocal yellow necrotic foci (A). Garland pattern with central necrosis simulates endometrioid carcinoma on frozen section (B).
Fig. 19. Metastatic signet ring cell carcinoma involving both ovaries (A). Fibrous stroma is infiltrated with nests and cords of small tumor cells on frozen section (B).
A
A
B
B
179https://doi.org/10.12701/yujm.2019.00227
Yeungnam Univ J Med 2019;36(3):163-182
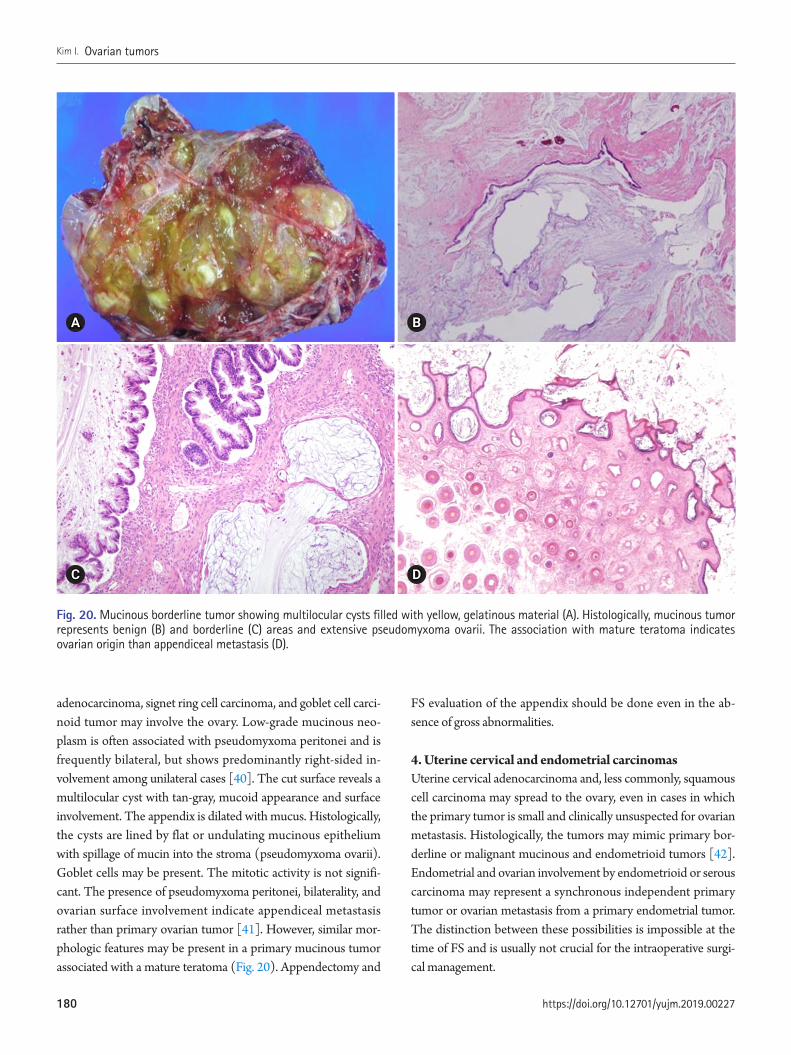
adenocarcinoma, signet ring cell carcinoma, and goblet cell carci-noid tumor may involve the ovary. Low-grade mucinous neo-plasm is often associated with pseudomyxoma peritonei and is frequently bilateral, but shows predominantly right-sided in-volvement among unilateral cases [40]. The cut surface reveals a multilocular cyst with tan-gray, mucoid appearance and surface involvement. The appendix is dilated with mucus. Histologically, the cysts are lined by flat or undulating mucinous epithelium with spillage of mucin into the stroma (pseudomyxoma ovarii). Goblet cells may be present. The mitotic activity is not signifi-cant. The presence of pseudomyxoma peritonei, bilaterality, and ovarian surface involvement indicate appendiceal metastasis rather than primary ovarian tumor [41]. However, similar mor-phologic features may be present in a primary mucinous tumor associated with a mature teratoma (Fig. 20). Appendectomy and
FS evaluation of the appendix should be done even in the ab-sence of gross abnormalities.
4. Uterine cervical and endometrial carcinomas Uterine cervical adenocarcinoma and, less commonly, squamous cell carcinoma may spread to the ovary, even in cases in which the primary tumor is small and clinically unsuspected for ovarian metastasis. Histologically, the tumors may mimic primary bor-derline or malignant mucinous and endometrioid tumors [42]. Endometrial and ovarian involvement by endometrioid or serous carcinoma may represent a synchronous independent primary tumor or ovarian metastasis from a primary endometrial tumor. The distinction between these possibilities is impossible at the time of FS and is usually not crucial for the intraoperative surgi-cal management.
Fig. 20. Mucinous borderline tumor showing multilocular cysts filled with yellow, gelatinous material (A). Histologically, mucinous tumor represents benign (B) and borderline (C) areas and extensive pseudomyxoma ovarii. The association with mature teratoma indicates ovarian origin than appendiceal metastasis (D).
A
C
B
D
https://doi.org/10.12701/yujm.2019.00227180
Kim I. Ovarian tumors

Conclusion
The discrepancies between frozen diagnosis and permanent di-agnosis are mainly due to sampling errors and misinterpretation by pathologists but may also be due to suboptimal quality of the FS. If the diagnosis is doubtful, the gross specimen should be re-examined and additional sections should be taken, a second opinion from an experienced pathologist should be obtained, and promptly discuss with the surgeon to obtain more history in-formation and to discuss about a difficult diagnostic interpreta-tion.
Conflicts of interest
No potential conflicts of interest relevant to this article was re-ported.
Acknowledgements
I would express many thanks to Dr. Cho, Hwa Jin (Inje Universi-ty Busan Paik Hospital), Dr. Lee, Jeong Hyeon (Korea University Anam Hospital), Dr. Kim, Hye Sun (Dankuk University Cheil Hospital), Dr. Lee, Jeong Hee (Gyeongsang National University Hospital) for collecting the cases.
ORCID
Insun Kim, https://orcid.org/0000-0002-1924-7893
References
1. Gal AA, Cagle PT. The 100-year anniversary of the description of the frozen section procedure. JAMA 2005;294:3135–7.
2. Krishnamurthy S, Meric-Bernstam F, Lucci A, Hwang RF, Kuerer HM, Babiera G, et al. A prospective study comparing touch im-print cytology, frozen section analysis, and rapid cytokeratin im-munostain for intraoperative evaluation of axillary sentinel lymph nodes in breast cancer. Cancer 2009;115:1555–62.
3. Novis DA, Zarbo RJ. Interinstitutional comparison of frozen sec-tion turnaround time. A College of American Pathologists Q-Probes study of 32868 frozen sections in 700 hospitals. Arch Pathol Lab Med 1997;121:559–67.
4. Kurman RJ; International Agency for Research on Cancer (IARC). WHO classification of tumours of female reproductive organs. 4th ed. Lyon: International Agency for Research on Can-cer; 2014.
5. Bige O, Demir A, Saygili U, Gode F, Uslu T, Koyuncuoglu M.
Frozen section diagnoses of 578 ovarian tumors made by pathol-ogists with and without expertise on gynecologic pathology. Gy-necol Oncol 2011;123:43–6.
6. Malipatil R, Crasta JA. How accurate is intraoperative frozen sec-tion in the diagnosis of ovarian tumors? J Obstet Gynaecol Res 2013;39:710–3.
7. Rodríguez IM, Prat J. Mucinous tumors of the ovary: a clinico-pathologic analysis of 75 borderline tumors (of intestinal type) and carcinomas. Am J Surg Pathol 2002;26:139–52.
8. Lee KR, Young RH. The distinction between primary and meta-static mucinous carcinomas of the ovary: gross and histologic findings in 50 cases. Am J Surg Pathol 2003;27:281–92.
9. Bagué S, Rodríguez IM, Prat J. Sarcoma-like mural nodules in mu-cinous cystic tumors of the ovary revisited: a clinicopathologic analysis of 10 additional cases. Am J Surg Pathol 2002;26:1467–76.
10. Provenza C, Young RH, Prat J. Anaplastic carcinoma in muci-nous ovarian tumors: a clinicopathologic study of 34 cases em-phasizing the crucial impact of stage on prognosis, their histo-logic spectrum, and overlap with sarcomalike mural nodules. Am J Surg Pathol 2008;32:383–9.
11. Seidman JD, Soslow RA, Vang R, Berman JJ, Stoler MH, Sher-man ME, et al. Borderline ovarian tumors: diverse contempo-rary viewpoints on terminology and diagnostic criteria with il-lustrative images. Hum Pathol 2004;35:918–33.
12. McKenney JK, Balzer BL, Longacre TA. Patterns of stromal in-vasion in ovarian serous tumors of low malignant potential (borderline tumors): a reevaluation of the concept of stromal microinvasion. Am J Surg Pathol 2006;30:1209–21.
13. Bell DA, Weinstock MA, Scully RE. Peritoneal implants of ovar-ian serous borderline tumors. Histologic features and prognosis. Cancer 1988;62:2212–22.
14. Malpica A, Deavers MT, Lu K, Bodurka DC, Atkinson EN, Ger-shenson DM, et al. Grading ovarian serous carcinoma using a two-tier system. Am J Surg Pathol 2004;28:496–504.
15. Roth LM, Emerson RE, Ulbright TM. Ovarian endometrioid tumors of low malignant potential: a clinicopathologic study of 30 cases with comparison to well-differentiated endometrioid adenocarcinoma. Am J Surg Pathol 2003;27:1253–9.
16. Bell KA, Kurman RJ. A clinicopathologic analysis of atypical proliferative (borderline) tumors and well-differentiated endo-metrioid adenocarcinomas of the ovary. Am J Surg Pathol 2000;24:1465–79.
17. Brescia RJ, Dubin N, Demopoulos RI. Endometrioid and clear cell carcinoma of the ovary. Factors affecting survival. Int J Gy-necol Pathol 1989;8:132–8.
18. Zaino RJ, Unger ER, Whitney C. Synchronous carcinomas of the uterine corpus and ovary. Gynecol Oncol 1984;19:329–35.
181https://doi.org/10.12701/yujm.2019.00227
Yeungnam Univ J Med 2019;36(3):163-182

19. Roth LM, Langley FA, Fox H, Wheeler JE, Czernobilsky B. Ovarian clear cell adenofibromatous tumors. Benign, of low malignant potential, and associated with invasive clear cell carci-noma. Cancer 1984;53:1156–63.
20. Scarfone G, Bergamini A, Noli S, Villa A, Cipriani S, Taccagni G, et al. Characteristics of clear cell ovarian cancer arising from en-dometriosis: a two center cohort study. Gynecol Oncol 2014;133:480–4.
21. Irving JA, Alkushi A, Young RH, Clement PB. Cellular fibromas of the ovary: a study of 75 cases including 40 mitotically active tumors emphasizing their distinction from fibrosarcoma. Am J Surg Pathol 2006;30:929–38.
22. Bhat RA, Lim YK, Chia YN, Yam KL. Sertoli-Leydig cell tumor of the ovary: analysis of a single institution database. J Obstet Gynaecol Res 2013;39:305–10.
23. van Meurs HS, Bleeker MC, van der Velden J, Overbeek LI, Kenter GG, Buist MR. The incidence of endometrial hyperpla-sia and cancer in 1031 patients with a granulosa cell tumor of the ovary: long-term follow-up in a population-based cohort study. Int J Gynecol Cancer 2013;23:1417–22.
24. Young RH, Dickersin GR, Scully RE. Juvenile granulosa cell tu-mor of the ovary. A clinicopathological analysis of 125 cases. Am J Surg Pathol 1984;8:575–96.
25. Schumer ST, Cannistra SA. Granulosa cell tumor of the ovary. J Clin Oncol 2003;21:1180–9.
26. Iavazzo C, Gkegkes ID, Vrachnis N. Fertility sparing manage-ment and pregnancy in patients with granulosa cell tumour of the ovaries. J Obstet Gynaecol 2015;35:331–5.
27. Young RH, Scully RE. Ovarian Sertoli-Leydig cell tumors. A clinicopathological analysis of 207 cases. Am J Surg Pathol 1985;9:543–69.
28. Gui T, Cao D, Shen K, Yang J, Zhang Y, Yu Q, et al. A clinico-pathological analysis of 40 cases of ovarian Sertoli-Leydig cell tumors. Gynecol Oncol 2012;127:384–9.
29. Norris HJ, Zirkin HJ, Benson WL. Immature (malignant) tera-toma of the ovary: a clinical and pathologic study of 58 cases. Cancer 1976;37:2359–72.
30. Stamp GW, McConnell EM. Malignancy arising in cystic ovari-an teratomas. A report of 24 cases. Br J Obstet Gynaecol 1983;90:671–5.
31. Eskander RN, Randall LM, Berman ML, Tewari KS, Disaia PJ, Bristow RE. Fertility preserving options in patients with gyne-cologic malignancies. Am J Obstet Gynecol 2011;205:103–10.
32. Nogales FF, Preda O, Nicolae A. Yolk sac tumours revisited. A review of their many faces and names. Histopathology 2012;60:1023–33.
33. Roth LM, Talerman A, Levy T, Sukmanov O, Czernobilsky B. Ovarian yolk sac tumors in older women arising from epithelial ovarian tumors or with no detectable epithelial component. Int J Gynecol Pathol 2011;30:442–51.
34. Oliva E, Andrada E, Pezzica E, Prat J. Ovarian carcinomas with choriocarcinomatous differentiation. Cancer 1993;72:2441–6.
35. Ulbright TM, Roth LM, Stehman FB. Secondary ovarian neo-plasia. A clinicopathologic study of 35 cases. Cancer 1984;53:1164–74.
36. Mazur MT, Hsueh S, Gersell DJ. Metastases to the female geni-tal tract. Analysis of 325 cases. Cancer 1984;53:1978–84.
37. Yemelyanova AV, Vang R, Judson K, Wu LS, Ronnett BM. Dis-tinction of primary and metastatic mucinous tumors involving the ovary: analysis of size and laterality data by primary site with reevaluation of an algorithm for tumor classification. Am J Surg Pathol 2008;32:128–38.
38. Young RH. From krukenberg to today: the ever present prob-lems posed by metastatic tumors in the ovary: part I. Historical perspective, general principles, mucinous tumors including the krukenberg tumor. Adv Anat Pathol 2006;13:205–27.
39. Kiyokawa T, Young RH, Scully RE. Krukenberg tumors of the ovary: a clinicopathologic analysis of 120 cases with emphasis on their variable pathologic manifestations. Am J Surg Pathol 2006;30:277–99.
40. Young RH, Gilks CB, Scully RE. Mucinous tumors of the ap-pendix associated with mucinous tumors of the ovary and pseu-domyxoma peritonei. A clinicopathological analysis of 22 cases supporting an origin in the appendix. Am J Surg Pathol 1991;15:415–29.
41. Stewart CJ, Ardakani NM, Doherty DA, Young RH. An evalua-tion of the morphologic features of low-grade mucinous neo-plasms of the appendix metastatic in the ovary, and comparison with primary ovarian mucinous tumors. Int J Gynecol Pathol 2014;33:1–10.
42. Ronnett BM, Yemelyanova AV, Vang R, Gilks CB, Miller D, Grav-itt PE, et al. Endocervical adenocarcinomas with ovarian metasta-ses: analysis of 29 cases with emphasis on minimally invasive cer-vical tumors and the ability of the metastases to simulate primary ovarian neoplasms. Am J Surg Pathol 2008;32:1835–53.
https://doi.org/10.12701/yujm.2019.00227182
Kim I. Ovarian tumors
Cognitive dysfunctions in individuals with diabetes mellitus Hye-Geum Kim Department of Psychiatry, Yeungnam University College of Medicine, Daegu, Korea
Some patients with type 1 and type 2 diabetes mellitus (DM) present with cognitive dysfunctions. The pathophysiology underlying this complication is not well understood. Type 1 DM has been associated with a decrease in the speed of information processing, psychomotor efficiency, at-tention, mental flexibility, and visual perception. Longitudinal epidemiological studies of type 1 DM have indicated that chronic hyperglycemia and microvascular disease, rather than repeated severe hypoglycemia, are associated with the pathogenesis of DM-related cognitive dysfunction. However, severe hypoglycemic episodes may contribute to cognitive dysfunction in high-risk pa-tients with DM. Type 2 DM has been associated with memory deficits, decreased psychomotor speed, and reduced frontal lobe/executive function. In type 2 DM, chronic hyperglycemia, long duration of DM, presence of vascular risk factors (e.g., hypertension and obesity), and microvas-cular and macrovascular complications are associated with the increased risk of developing cog-nitive dysfunction. The pathophysiology of cognitive dysfunction in individuals with DM include the following: (1) role of hyperglycemia, (2) role of vascular disease, (3) role of hypoglycemia, and (4) role of insulin resistance and amyloid. Recently, some investigators have proposed that type 3 DM is correlated to sporadic Alzheimer’s disease. The molecular and biochemical consequences of insulin and insulin-like growth factor resistance in the brain compromise neuronal survival, ener-gy production, gene expression, plasticity, and white matter integrity. If patients claim that their performance is worsening or if they ask about the effects of DM on functioning, screening and assessment are recommended.
Keywords: Alzheimer’s disease; Cognition; Dementia; Diabetes
Introduction
Diabetes mellitus (DM) is a metabolic disease that can cause complications in the peripheral nervous system and several or-gans in the body, including the kidney, eyes, and brain [1]. Among the complications of DM, cognitive dysfunctions are rel-atively less addressed. Some patients with type 1 and 2 DM pres-ent with cognitive dysfunctions. Both hypoglycemia and hyper-glycemia are known to cause cognitive dysfunctions. However, the underlying pathophysiology is not well understood [2]. Re-
Received: June 10, 2019 Revised: July 9, 2019 Accepted: July 10, 2019
Corresponding author: Hye-Geum KimDepartment of Psychiatry, Yeungnam University College of Medicine, 170, Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-3340Fax: +82-53-629-0256E-mail: [email protected]
search results about one hypothesis are conflicting, and studies with consistent results are not available. In addition, the most ap-propriate method for diagnosing, treating, and preventing cogni-tive dysfunctions in DM is not yet identified [2]. Although the mechanisms and results remain inconsistent, some patients with DM present with cognitive dysfunctions, and the decline in cog-nitive function has a significant impact on activities of daily liv-ing. Therefore, cognitive dysfunctions in patients with DM must be reviewed and summarized to obtain useful information. The
Review articleeISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):183-191https://doi.org/10.12701/yujm.2019.00255
183https://doi.org/10.12701/yujm.2019.00255
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

present study aimed to review the characteristics of cognitive dysfunctions in patients with DM to summarize the factors af-fecting cognitive functions and the hypotheses about the mecha-nisms of cognitive dysfunctions.
Cognitive dysfunctions in type 1 diabetes mellitus
In a recent meta-analysis [3] that included 33 studies, the authors have analyzed the result of the cognitive function assessment performed during normal blood glucose state in adults with type 1 DM. Results showed that some cognitive domains, including speed of information processing, psychomotor efficiency, visual and sustained attention, mental flexibility, and visual perception, were significantly impaired in patients with type 1 DM compared with those of the controls. However, the cognitive domains of patients with type 1 DM were not significantly different from those of the controls, which include memory, motor speed, selec-tive attention, and language. A recent systematic review [2] has shown that cognitive dysfunctions commonly observed in pa-tients with type 1 DM are associated with the decreased speed of information processing, psychomotor efficiency, attention, memory, learning, problem solving skills, motor speed, vocabu-lary, visuoconstruction, visual perception, somatosensory exam-ination, motor strength, mental flexibility, and executive func-tion. Among these areas, decreased speed of information pro-cessing, psychomotor efficiency, attention, visuoconstruction, and mental flexibility have strong supporting data (Table 1).
In the early 1990s, cognitive dysfunctions in type 1 DM were more prominent in individuals who repeatedly presented with severe hypoglycemia. This finding is consistent with those of an-ecdotal reports of severe hypoglycemia that leads to cortical changes in the frontal lobe and in other regions of the brain, such as the temporal lobe, basal ganglia, and hippocampus [4,5]. However, a more recent evidence indicated that hypoglycemic episodes may not cause cognitive dysfunctions. The results of longitudinal epidemiological studies have indicated that chronic
hyperglycemia and microvascular complications cause DM-relat-ed cognitive dysfunctions. The Diabetes Control and Complica-tions Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications is a 18.5-year longitudinal epidemiological study with 1,144 participants. Of these participants, 40% had ex-perienced one or more severe hypoglycemic episodes (blood glucose concentration < 2.8 mmol/L accompanied by seizure or coma) during the study period. However, hypoglycemic episodes and cognitive dysfunctions were not significantly associated [6]. Rather, the 5 independent variables predicting the decrease in psychomotor speed over a follow-up period of 18.5 years were as follows: old age, low education, high lifetime hemoglobin A1c (HbA1c) concentrations, proliferative diabetic retinopathy, and renal complications [7]. In addition, an increase in carotid inti-ma-media thickness was slightly associated with a decline in cog-nitive performance. In particular, retinopathy was most closely associated with cognitive dysfunctions in this study [6]. A limita-tion of this study is that only younger participants (aged < 50 years) were included; thus, the study might have been conducted before the onset of cognitive dysfunctions due to hypoglycemia. However, this study showed that the risk of cognitive dysfunc-tions is lower, and the progression is also slower in young patients with DM who have good glycemic control. Systematic meta-anal-yses with similar results have reported that repeated hypoglyce-mia and cognitive decline were not correlated [3]. Several other studies have reported that microvascular complications are asso-ciated with an increased risk of cognitive decline [8].
However, hypoglycemia is associated with decreased cognitive function in the high-risk group, which was diagnosed early with-in the first few years of life [9,10]. Moreover, diagnosis at a younger age in patients with type 1 DM is associated with an in-creased risk of cognitive dysfunctions. Those who developed type 1 DM before the age of 4 years had impaired executive skills, attention, and processing speed compared to those diagnosed af-ter the age of 4 years [11].
Appropriate glycemic control plays an important role in the cognitive functions of patients with type 1 DM. Better glycemic control improves functions, such as psychomotor efficiency, at-tention, motor speed, memory, and academic achievement [2]. In a DCCT study, patients with type 1 DM with a mean glycated hemoglobin (HbA1c) of 7.4% had significantly better motor speed and psychomotor efficiency than those with a mean HbA1c of 8.8% [6].
Cognitive function was worse in patients with type 1 DM who presented with DM complications. One study has reported that deficits in fluid intelligence, information processing, attention, and concentration are correlated to the presence of background
Table 1. Cognitive dysfunction domains frequently reported by diabetes mellitus types
Type 1 DM Type 2 DMSpeed of information processing MemoryPsychomotor efficiency Psychomotor speedAttention Frontal lobe/executive functionMental flexibilityVisual perception
DM, diabetes mellitus.
https://doi.org/10.12701/yujm.2019.00255184
Kim HG. Cognitive dysfunctions in diabetes
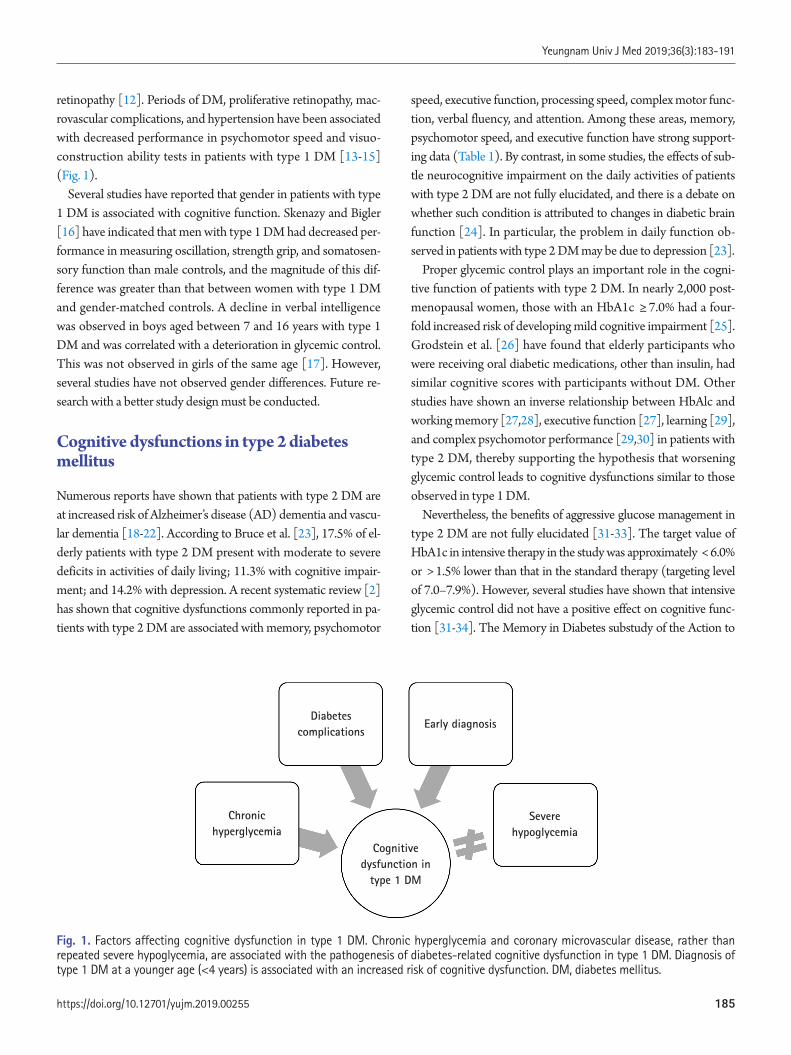
retinopathy [12]. Periods of DM, proliferative retinopathy, mac-rovascular complications, and hypertension have been associated with decreased performance in psychomotor speed and visuo-construction ability tests in patients with type 1 DM [13-15] (Fig. 1).
Several studies have reported that gender in patients with type 1 DM is associated with cognitive function. Skenazy and Bigler [16] have indicated that men with type 1 DM had decreased per-formance in measuring oscillation, strength grip, and somatosen-sory function than male controls, and the magnitude of this dif-ference was greater than that between women with type 1 DM and gender-matched controls. A decline in verbal intelligence was observed in boys aged between 7 and 16 years with type 1 DM and was correlated with a deterioration in glycemic control. This was not observed in girls of the same age [17]. However, several studies have not observed gender differences. Future re-search with a better study design must be conducted.
Cognitive dysfunctions in type 2 diabetes mellitus
Numerous reports have shown that patients with type 2 DM are at increased risk of Alzheimer’s disease (AD) dementia and vascu-lar dementia [18-22]. According to Bruce et al. [23], 17.5% of el-derly patients with type 2 DM present with moderate to severe deficits in activities of daily living; 11.3% with cognitive impair-ment; and 14.2% with depression. A recent systematic review [2] has shown that cognitive dysfunctions commonly reported in pa-tients with type 2 DM are associated with memory, psychomotor
speed, executive function, processing speed, complex motor func-tion, verbal fluency, and attention. Among these areas, memory, psychomotor speed, and executive function have strong support-ing data (Table 1). By contrast, in some studies, the effects of sub-tle neurocognitive impairment on the daily activities of patients with type 2 DM are not fully elucidated, and there is a debate on whether such condition is attributed to changes in diabetic brain function [24]. In particular, the problem in daily function ob-served in patients with type 2 DM may be due to depression [23].
Proper glycemic control plays an important role in the cogni-tive function of patients with type 2 DM. In nearly 2,000 post-menopausal women, those with an HbA1c ≥ 7.0% had a four-fold increased risk of developing mild cognitive impairment [25]. Grodstein et al. [26] have found that elderly participants who were receiving oral diabetic medications, other than insulin, had similar cognitive scores with participants without DM. Other studies have shown an inverse relationship between HbAlc and working memory [27,28], executive function [27], learning [29], and complex psychomotor performance [29,30] in patients with type 2 DM, thereby supporting the hypothesis that worsening glycemic control leads to cognitive dysfunctions similar to those observed in type 1 DM.
Nevertheless, the benefits of aggressive glucose management in type 2 DM are not fully elucidated [31-33]. The target value of HbA1c in intensive therapy in the study was approximately < 6.0% or > 1.5% lower than that in the standard therapy (targeting level of 7.0–7.9%). However, several studies have shown that intensive glycemic control did not have a positive effect on cognitive func-tion [31-34]. The Memory in Diabetes substudy of the Action to
Fig. 1. Factors affecting cognitive dysfunction in type 1 DM. Chronic hyperglycemia and coronary microvascular disease, rather than repeated severe hypoglycemia, are associated with the pathogenesis of diabetes-related cognitive dysfunction in type 1 DM. Diagnosis of type 1 DM at a younger age (<4 years) is associated with an increased risk of cognitive dysfunction. DM, diabetes mellitus.
Severe hypoglycemia
Early diagnosisDiabetes
complications
Chronic hyperglycemia
Cognitive dysfunction in
type 1 DM
185https://doi.org/10.12701/yujm.2019.00255
Yeungnam Univ J Med 2019;36(3):183-191

Control Cardiovascular Risk in Diabetes trial has reported that ag-gressive glucose-lowering therapy did not have positive effects on not only cognitive function but also total brain volume during the 40-month follow-up in patients with type 2 DM [34].
Similar to type 1 DM, type 2 DM is associated with deficits in cognitive function when accompanied by diabetic complications, such as peripheral neuropathy [28,35]. One study has reported that diabetic retinopathy in men, but not in women, was associat-ed with a decrease in cognitive performance [28]. The duration of type 2 DM and chronic hyperglycemia were associated with changes in cognitive function [8,36] (Fig. 2).
Some reports have shown that impaired glucose tolerance be-fore DM was a risk factor of cognitive decline [37]. Numerous studies have shown that patients with impaired glucose tolerance had lower Mini-Mental State Examination and long-term memo-ry scores [36], decreased verbal fluency [38], and worse Alzhei-mer’s dementia [20] and vascular dementia [19] than control subjects. However, not all studies obtained similar results.
Pathophysiology of cognitive dysfunction in diabetes mellitus
Thus far, the underlying pathophysiology of cognitive dysfunc-tions in DM is not well understood. However, several hypotheses have been proposed, and research results that validate such hy-potheses have been published.
First, there is a hypothesis that cognitive dysfunction is cor-
related to hyperglycemia. Although hyperglycemia may be asso-ciated with decreased cognitive function in type 1 and 2 DM, the mechanism by which hyperglycemia mediates is still unclear. In other organs, hyperglycemia affects function by the following mechanism: polyol pathway activation, increased formation of advanced glycation end products, diacylglycerol activation of protein kinase C, and increased glucose shunting in the hexosamine pathway [39-42]. Several studies have indicated that the same mechanisms may work in the brain.
Second, there is a hypothesis that vascular disease plays an im-portant role. Patients with DM are 2–6 times more likely at risk of thrombosis, which contributes to cognitive dysfunction [43-45]. Thickening of capillary basement membranes (the hallmark of diabetic microangiopathy) is also found in the brain of patients with DM [46]. The duration of illness was associated with the decreased global rates of cerebral blood flow in patients with DM. Interestingly, the cerebral blood flow rate of patients with DM is similar to that observed in patients with AD [47]. The co-existence of ischemia and hyperglycemia was considered detri-mental to the brain. One potential mechanism by which hyper-glycemia may enhance ischemic damage is lactate accumulation [48]. Hyperglycemia produces more substrate for the formation of lactic acid, causing cellular acidosis and exacerbated damage. Another mechanism is glutamate accumulation in the context of hyperglycemia and ischemia [49,50].
Third, whether hypoglycemic episodes contribute to cognitive impairment is controversial, and it may depend on the patient’s
Fig. 2. Factors affecting cognitive dysfunction in type 2 DM. Chronic hyperglycemia, long duration of diabetes, presence of vascular risk factors (e.g., hypertension and obesity), and microvascular and macrovascular complications are associated with an increased risk of developing cognitive dysfunction in type 2 DM. Some authors have claimed that AD is type 3 DM with a combination of insulin deficiency and insulin resistance, particularly in patients with sporadic AD without the APOE e4 allele. DM, diabetes milletus; AD, Alzheimer’s disease; APOE, apolipoprotein E.
Brain insulindeficiency
and resistance without APOE-e4
Cognitive dysfunction in
type 2 DM
Vascular risk factors
Diabetes durations
Diabetes complications
Type 3 DM ?
Chronic hyperglycemia
https://doi.org/10.12701/yujm.2019.00255186
Kim HG. Cognitive dysfunctions in diabetes

age. However, extremely long-term severe hypoglycemia causes brain damage and even death [45]. In animal models, blood glu-cose levels of 0.12–1.36 mmol/L for 30–60 min lead to increased extracellular aspartate levels, alkalemia, and nerve necrosis with nerve energy damage, thereby resulting in a flat electroencepha-lograph result [51]. The cortex, basal ganglia, and hippocampus may be most vulnerable to hypoglycemia, and autopsies per-formed in human patients who died from hypoglycemia showed lamellar necrosis and gliosis in these areas [52]. Other human autopsy studies conducted after death secondary to hypoglyce-mia have shown multifocal or diffuse necrosis of the cerebral cor-tex and chromatolysis of ganglion cells [53]. Some researchers have hypothesized that hypoglycemia-induced neuronal damage occurs due to the overactivation of the excitatory neurotransmit-ter subtypes of the N-methyl-D-aspartate receptor (NMDA) re-ceptor [54]. Interestingly, NMDA receptor antagonists prevent neuronal necrosis, indicating a potential treatment for hypogly-cemia-induced brain injury [55].
Fourth, in recent studies, insulin resistance has been consid-ered a mechanism of cognitive decline in patients with DM. In fact, historically, the brain was believed to be an insulin-indepen-dent organ. However, recent studies have questioned such con-cept. There is a growing body of evidence showing that insulin resistance can play an important role in the pathogenesis of AD. Since glucose is the main fuel of the brain, the brain is starved due to the lack of glucose uptake and utilization. Insulin stimu-lates brain glucose uptake and utilization, metabolism, memory, and cognition. Insulin resistance/deficiency induces impair-ments in glucose metabolism and disrupts brain energy balance, thereby increasing oxidative stress, production of reactive oxygen species, deoxyribonucleic acid damage, and mitochondrial dys-function, all of which drive pro-apoptosis, pro-inflammatory, and pro-amyloid-beta (Aβ) cascades [56]. Therefore, insulin and in-sulin-like growth factor (IGF) signaling pathways play critical roles in brain functions, such as cognitive functions in the central nervous system (CNS). Insulin, IGF-1 and IGF-2 polypeptides, and receptor genes are expressed in neuronal and glial cells throughout the brain. Their highest levels are in structures that are strongly targeted by neurodegeneration, particularly in AD [56-58]. Correspondingly, experimental depletion or suppres-sion of brain insulin receptor expression and function causes cognitive dysfunction and the molecular and biochemical abnor-malities observed in AD [59]. In this context, it is argued that AD is considered a brain disease with complex features of type 1 (insulin deficiency) and type 2 (insulin resistance) DM. To con-solidate this concept, numerous investigators have proposed that AD should be referred to as type 3 DM [60,61].
Evidence of type 3 diabetes mellitus in Alzheimer’s disease
Sporadic AD as the cause of Aβ accumulation, which accounts for more than 90% of AD cases, is not yet well understood. Recent evidence has indicated that insulin/IGF resistance in the brain as both a cause and outcome. Insulin stimulation promotes the transport of Aβ from the trans-Golgi network from which it is de-rived to the plasma membrane for extracellular secretion [62]. Furthermore, insulin inhibits intracellular accumulation of Aβ and degradation by insulin-degrading enzymes [63,64]. Impaired in-sulin signaling disrupts amyloid-beta precursor protein peptides (AβPP) processing and AβPP-Aβ clearance in the brain [65].
The tau pathology is a representative neuropathological finding of AD along with Aβ. Moreover, studies have shown that insulin resistance affects tau expression and phosphorylation. Tau expres-sion and phosphorylation are regulated by insulin and IGF [66,67]. In AD, brain insulin and IGF resistance impair signaling through phosphoinositol-3-kinase (PI3K), Akt, and Wnt/β-caten-in and promote glycogen synthase kinase-3 beta (GSK-3β) activa-tion. Overactivation of GSK-3β is responsible for tau hyperphos-phorylation, which promotes tau misfolding and fibril aggregation.
The strongest evidence supporting the notion of type 3 DM in AD was from an experimental study of rats that received strepto-zotocin, a pro-diabetic drug, via intracerebroventricular injection. Streptozotocin-treated rats develop cognitive dysfunctions as characterized by lack of spatial learning and memory, brain insu-lin resistance and deficiency, and AD-like neurodegeneration [68,69]. Targeted exposure to pro-diabetic agents can cause neu-rodegeneration with structural, molecular, biochemical, and functional abnormalities that closely mimic the pathology of AD in humans. In particular, streptozotocin is a nitrosamine-related compound that can be found in processed and preserved foods, and it causes cognitive impairment, AD-type neurodegeneration, and brain insulin resistance with experimental exposures to low, sub-mutagenic doses. Some authors have shown that over the last few decades, western populations have been constantly pre-senting with increasing levels of exposure to nitrosamines due to constant and gradual contact with nitrates and nitrites in the en-vironment, agriculture, and food resources, and this has recently been linked to the increased incidence of dementia [68,69].
Some studies have indicated that insulin resistance affects neu-rotransmission and memory formation. Streptozotocin-induced diabetic rats have reduced acetylcholine production and release as compared to control rats [70]. A mouse model in which cho-linergic activity is blocked by scopolamine experienced memory loss and hyperactivity, a deficit that may be reversed by glucose
187https://doi.org/10.12701/yujm.2019.00255
Yeungnam Univ J Med 2019;36(3):183-191

administration [71]. Moreover, glucose administration with ele-vated endogenous insulin levels or insulin administration to pa-tients with AD has also been shown to cause changes in behavior, possibly by enhancing cholinergic activity [72]. DM and insulin may affect long-term potentiation in the opposite way. Long-term potentiation is important for memory formation and is in-duced by NMDA receptor activation, a process that is upregulat-ed in the presence of insulin. However, rats presumed to have DM and relative insulin deficiency has reduced long-term poten-tiation in the hippocampus as measured via electrophysiology [73,74]. Thus, brain insulin resistance in AD may require a high-er level of insulin to stimulate memory [75]. However, it is un-clear whether the direct effect of insulin is directly or indirectly influenced by other mediators [76].
Recently, a noteworthy report has indicated that the relation-ship between insulin resistance and cognitive impairment in AD is dependent on the presence or absence of the apolipoprotein E (APOE)-e4 allele. The presence of the APOE-e4 allele itself in-creases the risk of AD by a factor of 2–8, which plays a rather op-posite role in the development of AD associated with insulin re-sistance. Insulin resistance is only an important risk factor of AD in patients without the APOE-e4 allele [20]. Participants with AD without the APOE-e4 allele also had improved memory scores in the hyperinsulinemic setting, which was not the case for APOE-e4 allele-positive participants [77] (Fig. 2).
One of the important reasons for the active research in these fields may be the anticipation that antidiabetic drugs may play a preventive or therapeutic role in AD, which is known to have no cure. It has been hypothesized that neurodegeneration and cog-nitive dysfunctions in AD may be reduced or prevented with the early treatment of insulin-sensitizer antidiabetic agents, such as peroxisome proliferator-activated receptor (PPAR) agonists. Studies have reported that the PPAR agonist treatments prevent cerebral atrophy, preserve insulin and IGF-2 receptor-bearing CNS neurons, and specifically prevent it from ic-streptozoto-cin-induced deficits in learning and memory [78]. Some trials have shown that rosiglitazone, a PPAR-gamma, have a beneficial effect on memory in patients with AD. In a small randomized study published by Watson et al. [79] in 2005, patients with mild AD who were treated with rosiglitazone for 6 months had better memory and selective attention than the controls. A larger study published in 2006 has shown improvement in cognitive function after the administration of rosiglitazone for 6 months in patients with AD without the APOE-e4 allele. However, no improve-ments were observed in patients with AD with the APOE-e4 al-lele [80]. Similar studies have been conducted. However, the re-sults remained inconsistent reports. The results of the systematic
review and network meta-analysis [81] in 2018 have shown the significant effects of antidiabetic agents on AD and mild cogni-tive impairment, and pioglitazone 15–30 mg was more effective than placebo in a network meta-analysis.
Conclusion
Several studies about cognitive dysfunctions in patients with type 1 and type 2 DM have been conducted, and the results were inconsistent. Although some studies obtained conclusions, lim-itations were still observed. Type 1 DM has been associated with a decrease in the speed of information processing, psychomotor efficiency, attention, mental flexibility, and visual perception, and type 2 DM has been associated with memory deficits, a decrease in psychomotor speed, and reduced frontal lobe/executive func-tion. Improved glycemic control and decreased diabetic compli-cations may be associated with the prevention of cognitive dys-function. However, the benefits of intensive glucose control in type 2 DM remain unclear. Severe hypoglycemic episodes may not have a long-term cognitive impact. However, it may cause cognitive impairment in high-risk patients diagnosed with DM ( < 4 years). The underlying pathophysiology is not well under-stood. Some authors have claimed that AD is type 3 DM with a combination of insulin deficiency and resistance particularly in patients with sporadic AD without the APOEe4 allele. However, results of previous studies remained inconsistent, and more con-sistent results must be obtained. If a patient reports that their performance is worsening or if they ask about the effects of DM on functioning, screening and assessment are recommended.
Conflicts of interest
No potential conflicts of interest relevant to this article was re-ported.
ORCID
Hye-Guem Kim, https://orcid.org/0000-0002-9677-7011
References
1. McCrimmon RJ, Ryan CM, Frier BM. Diabetes and cognitive dysfunction. Lancet 2012;379:2291–9.
2. Kodl CT, Seaquist ER. Cognitive dysfunction and diabetes melli-tus. Endocr Rev 2008;29:494–511.
3. Brands AM, Biessels GJ, de Haan EH, Kappelle LJ, Kessels RP. The effects of type 1 diabetes on cognitive performance: a me-
https://doi.org/10.12701/yujm.2019.00255188
Kim HG. Cognitive dysfunctions in diabetes

ta-analysis. Diabetes Care 2005;28:726–35.4. Feinkohl I, Aung PP, Keller M, Robertson CM, Morling JR, Mc-
Lachlan S, et al. Severe hypoglycemia and cognitive decline in older people with type 2 diabetes: the Edinburgh type 2 diabetes study. Diabetes Care 2014;37:507–15.
5. Gold AE, Deary IJ, Frier BM. Recurrent severe hypoglycaemia and cognitive function in type 1 diabetes. Diabet Med 1993; 10:503–8.
6. Diabetes Control and Complications Trial/Epidemiology of Dia-betes Interventions and Complications Study Research Group; Jacobson AM, Musen G, Ryan CM, Silvers N, Cleary P, et al. Long-term effect of diabetes and its treatment on cognitive func-tion. N Engl J Med 2007;356:1842–52.
7. Jacobson AM, Ryan CM, Cleary PA, Waberski BH, Weinger K, Musen G, et al. Biomedical risk factors for decreased cognitive functioning in type 1 diabetes: an 18 year follow-up of the Diabe-tes Control and Complications Trial (DCCT) cohort. Diabetolo-gia 2011;54:245–55.
8. Wessels AM, Scheltens P, Barkhof F, Heine RJ. Hyperglycaemia as a determinant of cognitive decline in patients with type 1 dia-betes. Eur J Pharmacol 2008;585:88–96.
9. Asvold BO, Sand T, Hestad K, Bjørgaas MR. Cognitive function in type 1 diabetic adults with early exposure to severe hypoglyce-mia: a 16-year follow-up study. Diabetes Care 2010;33:1945–7.
10. Aye T, Reiss AL, Kesler S, Hoang S, Drobny J, Park Y, et al. The feasibility of detecting neuropsychologic and neuroanatomic ef-fects of type 1 diabetes in young children. Diabetes Care 2011;34:1458–62.
11. Northam EA, Anderson PJ, Jacobs R, Hughes M, Warne GL, Werther GA. Neuropsychological profiles of children with type 1 diabetes 6 years after disease onset. Diabetes Care 2001; 24:1541–6.
12. Ferguson SC, Blane A, Perros P, McCrimmon RJ, Best JJ, Ward-law J, et al. Cognitive ability and brain structure in type 1 diabe-tes: relation to microangiopathy and preceding severe hypogly-cemia. Diabetes 2003;52:149–56.
13. Ryan CM, Geckle MO, Orchard TJ. Cognitive efficiency declines over time in adults with Type 1 diabetes: effects of micro- and macrovascular complications. Diabetologia 2003;46:940–8.
14. Ryan CM, Williams TM, Finegold DN, Orchard TJ. Cognitive dysfunction in adults with type 1 (insulin-dependent) diabetes mellitus of long duration: effects of recurrent hypoglycaemia and other chronic complications. Diabetologia 1993;36:329–34.
15. Wessels AM, Rombouts SA, Remijnse PL, Boom Y, Scheltens P, Barkhof F, et al. Cognitive performance in type 1 diabetes pa-tients is associated with cerebral white matter volume. Diabeto-logia 2007;50:1763–9.
16. Skenazy JA, Bigler ED. Neuropsychological findings in diabetes mellitus. J Clin Psychol 1984;40:246–58.
17. Schoenle EJ, Schoenle D, Molinari L, Largo RH. Impaired intel-lectual development in children with Type I diabetes: associa-tion with HbA(1c), age at diagnosis and sex. Diabetologia 2002;45:108–14.
18. Cukierman T, Gerstein HC, Williamson JD. Cognitive decline and dementia in diabetes--systematic overview of prospective observational studies. Diabetologia 2005;48:2460–9.
19. Curb JD, Rodriguez BL, Abbott RD, Petrovitch H, Ross GW, Masaki KH, et al. Longitudinal association of vascular and Alz-heimer’s dementias, diabetes, and glucose tolerance. Neurology 1999;52:971–5.
20. Kuusisto J, Koivisto K, Mykkänen L, Helkala EL, Vanhanen M, Hänninen T, et al. Association between features of the insulin resistance syndrome and Alzheimer’s disease independently of apolipoprotein E4 phenotype: cross sectional population based study. BMJ 1997;315:1045–9.
21. Leibson CL, Rocca WA, Hanson VA, Cha R, Kokmen E, O’Brien PC, et al. Risk of dementia among persons with diabe-tes mellitus: a population-based cohort study. Am J Epidemiol 1997;145:301–8.
22. Luchsinger JA, Tang MX, Stern Y, Shea S, Mayeux R. Diabetes mellitus and risk of Alzheimer’s disease and dementia with stroke in a multiethnic cohort. Am J Epidemiol 2001;154:635–41.
23. Bruce DG, Casey GP, Grange V, Clarnette RC, Almeida OP, Foster JK, et al. Cognitive impairment, physical disability and depressive symptoms in older diabetic patients: the Fremantle Cognition in Diabetes Study. Diabetes Res Clin Pract 2003; 61:59–67.
24. Gregg EW, Brown A. Cognitive and physical disabilities and aging-related complications of diabetes. Clin Diabetes 2003; 21:113–8.
25. Yaffe K, Blackwell T, Whitmer RA, Krueger K, Barrett Connor E. Glycosylated hemoglobin level and development of mild cognitive impairment or dementia in older women. J Nutr Health Aging 2006;10:293–5.
26. Grodstein F, Chen J, Wilson RS, Manson JE; Nurses’ Health Study. Type 2 diabetes and cognitive function in communi-ty-dwelling elderly women. Diabetes Care 2001;24:1060–5.
27. Munshi M, Grande L, Hayes M, Ayres D, Suhl E, Capelson R, et al. Cognitive dysfunction is associated with poor diabetes con-trol in older adults. Diabetes Care 2006;29:1794–9.
28. Perlmuter LC, Hakami MK, Hodgson-Harrington C, Ginsberg J, Katz J, Singer DE, et al. Decreased cognitive function in aging non-insulin-dependent diabetic patients. Am J Med 1984;
189https://doi.org/10.12701/yujm.2019.00255
Yeungnam Univ J Med 2019;36(3):183-191

77:1043–8. 29. Reaven GM, Thompson LW, Nahum D, Haskins E. Relation-
ship between hyperglycemia and cognitive function in older NIDDM patients. Diabetes Care 1990;13:16–21.
30. Ryan CM, Geckle MO. Circumscribed cognitive dysfunction in middle-aged adults with type 2 diabetes. Diabetes Care 2000;23:1486–93.
31. Effects of intensive diabetes therapy on neuropsychological function in adults in the Diabetes Control and Complications Trial. Ann Intern Med 1996;124:379–88.
32. Duckworth W, Abraira C, Moritz T, Reda D, Emanuele N, Reav-en PD, et al. Glucose control and vascular complications in vet-erans with type 2 diabetes. N Engl J Med 2009;360:129–39.
33. Action to Control Cardiovascular Risk in Diabetes Study Group; Gerstein HC, Miller ME, Byington RP, Goff DC Jr, Big-ger JT, et al. Effects of intensive glucose lowering in type 2 dia-betes. N Engl J Med 2008;358:2545–59.
34. Williamson JD, Miller ME, Bryan RN, Lazar RM, Coker LH, Johnson J, et al. The Action to Control Cardiovascular Risk in Diabetes Memory in Diabetes Study (ACCORD-MIND): ra-tionale, design, and methods. Am J Cardiol 2007;99:112i-22i.
35. Ding J, Strachan MW, Reynolds RM, Frier BM, Deary IJ, Fowkes FG, et al. Diabetic retinopathy and cognitive decline in older people with type 2 diabetes: the Edinburgh Type 2 Dia-betes Study. Diabetes 2010;59:2883–9.
36. Reijmer YD, van den Berg E, Ruis C, Kappelle LJ, Biessels GJ. Cognitive dysfunction in patients with type 2 diabetes. Diabetes Metab Res Rev 2010;26:507–19.
37. Vanhanen M, Koivisto K, Kuusisto J, Mykkänen L, Helkala EL, Hänninen T, et al. Cognitive function in an elderly population with persistent impaired glucose tolerance. Diabetes Care 1998; 21:398–402.
38. Kanaya AM, Barrett-Connor E, Gildengorin G, Yaffe K. Change in cognitive function by glucose tolerance status in older adults: a 4-year prospective study of the Rancho Bernardo study co-hort. Arch Intern Med 2004;164:1327–33.
39. Biessels GJ, van der Heide LP, Kamal A, Bleys RL, Gispen WH. Ageing and diabetes: implications for brain function. Eur J Pharmacol 2002;441:1–14.
40. Brownlee M. The pathobiology of diabetic complications: a unifying mechanism. Diabetes 2005;54:1615–25.
41. Klein JP, Waxman SG. The brain in diabetes: molecular changes in neurons and their implications for end-organ damage. Lancet Neurol 2003;2:548–54.
42. Toth C, Schmidt AM, Tuor UI, Francis G, Foniok T, Brussee V, et al. Diabetes, leukoencephalopathy and rage. Neurobiol Dis 2006;23:445–61.
43. Reske-Nielsen E, Lundbaek K. Pathological changes in the cen-tral and peripheral nervous system of young long-term diabet-ics. II. The spinal cord and peripheral nerves. Diabetologia 1968;4:34–43.
44. Reske-Nielsen E, Lundbæk K, Rafaelsen OJ. Pathological changes in the central and peripheral nervous system of young long-term diabetics: i. diabetic encephalopathy. Diabetologia 1966;1:233–41.
45. McCall AL. The impact of diabetes on the CNS. Diabetes 1992;41:557–70.
46. Johnson PC, Brendel K, Meezan E. Thickened cerebral cortical capillary basement membranes in diabetics. Arch Pathol Lab Med 1982;106:214–7.
47. Biessels GJ, Kappelle AC, Bravenboer B, Erkelens DW, Gispen WH. Cerebral function in diabetes mellitus. Diabetologia 1994;37:643–50.
48. Kushner M, Nencini P, Reivich M, Rango M, Jamieson D, Faze-kas F, et al. Relation of hyperglycemia early in ischemic brain in-farction to cerebral anatomy, metabolism, and clinical outcome. Ann Neurol 1990;28:129–35.
49. Coyle JT, Puttfarcken P. Oxidative stress, glutamate, and neuro-degenerative disorders. Science 1993;262:689–95.
50. Li PA, Shuaib A, Miyashita H, He QP, Siesjö BK, Warner DS. Hyperglycemia enhances extracellular glutamate accumulation in rats subjected to forebrain ischemia. Stroke 2000;31:183–92.
51. Auer RN. Hypoglycemic brain damage. Forensic Sci Int 2004; 146:105–10.
52. Patrick AW, Campbell IW. Fatal hypoglycaemia in insulin-treat-ed diabetes mellitus: clinical features and neuropathological changes. Diabet Med 1990;7:349–54.
53. Comi G. Evoked potentials in diabetes mellitus. Clin Neurosci 1997;4:374–9.
54. Siesjö BK, Bengtsson F. Calcium fluxes, calcium antagonists, and calcium-related pathology in brain ischemia, hypoglycemia, and spreading depression: a unifying hypothesis. J Cereb Blood Flow Metab 1989;9:127–40.
55. Wieloch T. Hypoglycemia-induced neuronal damage prevented by an N-methyl-D-aspartate antagonist. Science 1985;230: 681–3.
56. de la Monte SM, Wands JR. Review of insulin and insulin-like growth factor expression, signaling, and malfunction in the cen-tral nervous system: relevance to Alzheimer’s disease. J Alzhei-mers Dis 2005;7:45–61.
57. de la Monte SM, Longato L, Tong M, Wands JR. Insulin resis-tance and neurodegeneration: roles of obesity, type 2 diabetes mellitus and non-alcoholic steatohepatitis. Curr Opin Investig Drugs 2009;10:1049–60.
https://doi.org/10.12701/yujm.2019.00255190
Kim HG. Cognitive dysfunctions in diabetes

58. Broughton SK, Chen H, Riddle A, Kuhn SE, Nagalla S, Roberts CT Jr, et al. Large-scale generation of highly enriched neural stem-cell-derived oligodendroglial cultures: maturation-depen-dent differences in insulin-like growth factor-mediated signal transduction. J Neurochem 2007;100:628–38.
59. de la Monte SM. Contributions of brain insulin resistance and deficiency in amyloid-related neurodegeneration in Alzheimer’s disease. Drugs 2012;72:49–66.
60. Steen E, Terry BM, Rivera EJ, Cannon JL, Neely TR, Tavares R, et al. Impaired insulin and insulin-like growth factor expression and signaling mechanisms in Alzheimer’s disease--is this type 3 diabetes? J Alzheimers Dis 2005;7:63–80.
61. Rivera EJ, Goldin A, Fulmer N, Tavares R, Wands JR, de la Monte SM. Insulin and insulin-like growth factor expression and function deteriorate with progression of Alzheimer’s dis-ease: link to brain reductions in acetylcholine. J Alzheimers Dis 2005;8:247–68.
62. Watson GS, Peskind ER, Asthana S, Purganan K, Wait C, Chap-man D, et al. Insulin increases CSF Abeta42 levels in normal older adults. Neurology 2003;60:1899–903.
63. Gasparini L, Gouras GK, Wang R, Gross RS, Beal MF, Green-gard P, et al. Stimulation of beta-amyloid precursor protein traf-ficking by insulin reduces intraneuronal beta-amyloid and re-quires mitogen-activated protein kinase signaling. J Neurosci 2001;21:2561–70.
64. Gasparini L, Netzer WJ, Greengard P, Xu H. Does insulin dys-function play a role in Alzheimer’s disease? Trends Pharmacol Sci 2002;23:288–93.
65. Messier C, Teutenberg K. The role of insulin, insulin growth factor, and insulin-degrading enzyme in brain aging and Alzhei-mer’s disease. Neural Plast 2005;12:311–28.
66. Schubert M, Brazil DP, Burks DJ, Kushner JA, Ye J, Flint CL, et al. Insulin receptor substrate-2 deficiency impairs brain growth and promotes tau phosphorylation. J Neurosci 2003;23:7084–92.
67. Schubert M, Gautam D, Surjo D, Ueki K, Baudler S, Schubert D, et al. Role for neuronal insulin resistance in neurodegenerative diseases. Proc Natl Acad Sci U S A 2004;101:3100–5.
68. Lester-Coll N, Rivera EJ, Soscia SJ, Doiron K, Wands JR, de la Monte SM. Intracerebral streptozotocin model of type 3 diabe-tes: relevance to sporadic Alzheimer’s disease. J Alzheimers Dis 2006;9:13–33.
69. Weinstock M, Shoham S. Rat models of dementia based on re-ductions in regional glucose metabolism, cerebral blood flow and cytochrome oxidase activity. J Neural Transm (Vienna) 2004;111:347–66.
70. Welsh B, Wecker L. Effects of streptozotocin-induced diabetes
on acetylcholine metabolism in rat brain. Neurochem Res 1991;16:453–60.
71. Stone WS, Cottrill KL, Walker DL, Gold PE. Blood glucose and brain function: interactions with CNS cholinergic systems. Be-hav Neural Biol 1988;50:325–34.
72. Craft S, Newcomer J, Kanne S, Dagogo-Jack S, Cryer P, Sheline Y, et al. Memory improvement following induced hyperinsulin-emia in Alzheimer’s disease. Neurobiol Aging 1996;17:123–30.
73. Kamal A, Biessels GJ, Urban IJ, Gispen WH. Hippocampal syn-aptic plasticity in streptozotocin-diabetic rats: impairment of long-term potentiation and facilitation of long-term depression. Neuroscience 1999;90:737–45.
74. Palovcik RA, Phillips MI, Kappy MS, Raizada MK. Insulin inhib-its pyramidal neurons in hippocampal slices. Brain Res 1984; 309:187–91.
75. Craft S, Asthana S, Cook DG, Baker LD, Cherrier M, Purganan K, et al. Insulin dose-response effects on memory and plasma amyloid precursor protein in Alzheimer’s disease: interactions with apolipoprotein E genotype. Psychoneuroendocrinology 2003;28:809–22.
76. Kálmán J, Palotás A, Bódi N, Kincses TZ, Benedek G, Janka Z, et al. Lactate infusion fails to improve semantic categorization in Alzheimer’s disease. Brain Res Bull 2005;65:533–9.
77. Craft S, Asthana S, Schellenberg G, Cherrier M, Baker LD, New-comer J, et al. Insulin metabolism in Alzheimer’s disease differs according to apolipoprotein E genotype and gender. Neuroen-docrinology 1999;70:146–52.
78. de la Monte SM, Tong M, Lester-Coll N, Plater M Jr, Wands JR. Therapeutic rescue of neurodegeneration in experimental type 3 diabetes: relevance to Alzheimer’s disease. J Alzheimers Dis 2006;10:89–109.
79. Watson GS, Cholerton BA, Reger MA, Baker LD, Plymate SR, Asthana S, et al. Preserved cognition in patients with early Alz-heimer disease and amnestic mild cognitive impairment during treatment with rosiglitazone: a preliminary study. Am J Geriatr Psychiatry 2005;13:950–8.
80. Risner ME, Saunders AM, Altman JF, Ormandy GC, Craft S, Foley IM, et al. Efficacy of rosiglitazone in a genetically defined population with mild-to-moderate Alzheimer’s disease. Phar-macogenomics J 2006;6:246–54.
81. Cao B, Rosenblat JD, Brietzke E, Park C, Lee Y, Musial N, et al. Comparative efficacy and acceptability of antidiabetic agents for Alzheimer’s disease and mild cognitive impairment: a systemat-ic review and network meta-analysis. Diabetes Obes Metab 2018;20:2467–71.
191https://doi.org/10.12701/yujm.2019.00255
Yeungnam Univ J Med 2019;36(3):183-191

Current status of stereotactic body radiotherapy for the treatment of hepatocellular carcinoma Jongmoo Park1, Jae Won Park2, Min Kyu Kang1
1Department of Radiation Oncology, School of Medicine, Kyungpook National University, Daegu, Korea 2Department of Radiation Oncology, Yeungnam University College of Medicine, Daegu, Korea
Stereotactic body radiotherapy (SBRT) is an advanced form of radiotherapy (RT) with a grow-ing interest on its application in the treatment of hepatocellular carcinoma (HCC). It can de-liver ablative radiation doses to tumors in a few fractions without excessive doses to normal tissues, with the help of advanced modern RT and imaging technologies. Currently, SBRT is recommended as an alternative to curative treatments, such as surgery and radiofrequency ablation. This review discusses the current status of SBRT to aid in the decision making on how it is incorporated into the HCC management.
Keywords: Hepatocellular carcinoma; Image-guided radiotherapy; Radiotherapy; Stereotactic body radiotherapy
Introduction
Liver cancer is the sixth most common cancer and the second leading cause of cancer-related mortality in Korea [1]. Hepato-cellular carcinoma (HCC) is the major histologic type of prima-ry liver cancers, accounting for 70–85% [2], and has the highest mortality rate among major cancers in Korea [3]. Current treat-ment guidelines for HCC recommend surgical resection, liver transplantation, and radiofrequency ablation (RFA) as standard treatment options for small HCCs [4,5]. However, hepatic resec-tion is possible in only < 30% of patients due to multifocal dis-ease, unfavorable location, or inadequate functional hepatic re-serve, and liver transplantation is associated with many hurdles such as donor availability [6]. RFA is not always safe or effective depending on the tumor size or locations [7].
Stereotactic body radiotherapy (SBRT), or stereotactic abla-tive radiotherapy, is an advanced form of radiotherapy (RT) that can deliver ablative radiation doses to tumors in a few fractions
Review articleeISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):192-200https://doi.org/10.12701/yujm.2019.00269
Received: July 3, 2019 Revised: July 22, 2019 Accepted: July 30, 2019
Corresponding author: Min Kyu KangDepartment of Radiation Oncology, Kyungpook National University Chilgok Hospital, 807, Hoguk-ro, Buk-gu, Daegu 41404, Korea Tel: +82-53-200-2653Fax: +82-53-200-2029E-mail: [email protected]
without excessive doses to normal tissues with the help of ad-vanced modern RT and imaging technologies [8]. Several case series on SBRT have reported high local control rates of over 80% [9]. Current treatment guidelines for HCC recommend SBRT when other liver-directed therapies have failed or are con-traindicated [4,5,10]. In addition, it is tried to be combined with other locoregional or systemic therapies.
However, radiation-induced complications in the liver and gas-trointestinal (GI) tract prevent the use of SBRT. Patients with HCC often have cirrhotic liver with poor baseline liver function or less recovery ability, which could be related to a higher inci-dence of radiation-induced liver disease (RILD). The GI tract near the tumors often prevents high-dose irradiation from being delivered to the tumors. Respiratory movement of the liver con-taining tumors prevents the safe use of SBRT. For these reasons, various efforts have been implemented to understand the risk of toxicities and determine solutions.
This review discusses the current status of SBRT for HCCs in
https://doi.org/10.12701/yujm.2019.00269192
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

terms of technical and clinical aspects to help in the decision making of using SBRT while treating patients with HCC.
Radiotherapeutic considerations
1. Process of stereotactic body radiotherapy The first step of treatment planning is acquisition of planning computed tomography (CT) images in the treatment position. Immobilization devices, such as stereotactic body frame and vac-uum cushions, are usually used to improve the positional repro-ducibility and reduce the possible movement during the long treatment time of SBRT. Four-dimensional CT (4D-CT) scan with intravenous contrast media is usually used to identify tumor and normal organ movements during respiration. Depending on methods used for tumor localization and respiratory control during treatment, planning CT scans can be performed in vari-ous settings: free breathing or breath-hold with or without ab-dominal compression.
After transferring CT images to the RT treatment planning system, target volumes and normal organs are delineated. Gross tumor volume (GTV) is defined as the tumor(s) seen on imag-ing studies. In cases of invisible tumor(s) or unclear tumor mar-gin on planning CT images, rigid or deformable registration with diagnostic CT or magnetic resonance imaging (MRI) can be used. The clinical target volume for SBRT is usually the same as for GTV, even though microscopic tumor extension might exist up to several millimeters. The internal target volume (ITV) is the sum of GTVs in all respiratory phases (or some predefined phases for respiratory gating). Planning target volume (PTV) is generated by adding a margin of about 5 mm (up to 10 mm) to ITV [11]. Thereafter, treatment plans are generated while con-sidering tolerance doses of normal organs, especially for the nor-mal liver and GI tract. Typically, 40–50 Gy in 3–5 fractions is prescribed to encompass the edge of PTV [11-14].
Immediately before treatment, the patient and tumor position are verified with orthogonal radiographs or cone-beam CT scans using various surrogate markers, such as the diaphragm, surgical clips, residual lipiodol after transarterial chemoembolization (TACE) or fiducial markers inserted a few days before planning CT. Recently, the MRI device integrated into the RT machine can be used for real-time tumor tracking during treatment. Final-ly, treatment starts with respiratory motion management such as active breathing control [15], abdominal compression [16], re-spiratory gating, and real-time tumor tracking. Respiratory gating is a technique that can treat tumors only at predefined respiratory phases. Tumor-tracking technique is thought to be an ideal meth-od to treat moving targets, which can treat the tumors with the
smallest PTV compared to other methods. With the proper use of these techniques, SBRT-related toxicities in the liver and GI tract can be minimized while ensuring enough doses to tumors.
Various imaging tools described above are used to maximize the accuracy and precision throughout the whole process, which is called image-guided radiotherapy (IGRT). The technical aspects of RT for HCC are discussed in detail elsewhere [17,18]. Fig. 1 shows an example of SBRT using tracking intensity-modulated beams.
2. Tumor dose Radiation oncologists have used various dose fractionation sched-ules and investigated the impact of total dose and tumor size. For small tumors of < 3 cm (or < 5 cm), a high local control of > 90% has been achieved with a biologically effective dose (BED) of ≥ 100 Gy10 (e.g., 50 Gy in 5 fractions or 45 Gy in 3 fractions), which is considered as an ablative dose [12,19,20]. BED, using a conventional linear-quadratic model assuming α/β of 10 Gy, was calculated as follows: BED = nd (1+d/[α/β]), where n is the num-ber of fractions and d is the fraction size. In a retrospective study that escalated the radiation dose from 45 Gy in 3 fractions to 60 Gy in 3 fractions for HCCs of < 3 cm, no difference in local con-trol was found between the 2 dose groups [20]. In contrast, sever-al studies have reported lower local control rates in larger tumors [12,19,21]. Although Jang et al. [21] revealed that large tumors needed a higher radiation dose for the same tumor control proba-bility of 90% as small tumors (51.1 Gy in 3 fractions for tumors of ≤ 5 cm vs. 62.1 Gy in 3 fractions for tumors of > 5–7 cm), higher radiation doses would inevitably increase the liver dose related to liver toxicity. Sanuki et al. [13] achieved a high 3-year local control rate of 91% with relatively low doses (40 Gy in 5 fractions in Child–Pugh [CP] A and 35 Gy in 5 fractions in CP B). A pooled analysis of 25 studies on SBRT revealed that overall survival was not different according to radiation doses (equivalent dose in 2 Gy per fractions [EQD2] using the α/β ratio of 10 Gy: < 80 Gy vs. ≥ 80 Gy), where all available median EQD2 estimates ranged from 47.9 Gy to 100 Gy with a median of 83.3 Gy (equal to 100 Gy10 in BED) [9]. Therefore, considering that higher radiation dose and/or larger tumor volume could increase hepatic and/or GI toxicities, the risk adaptive dose–fractionation regimens would be useful to balance both tumor control and toxicities, especially in patients with poor liver function.
3. Charged particle therapy Charged particles such as proton or carbon ions have a unique beam profile known as Bragg peak, which can prevent irradiation of normal tissues beyond the tumor. Treatment outcomes in pa-tients with HCC treated with proton or carbon ions are promis-
193https://doi.org/10.12701/yujm.2019.00269
Yeungnam Univ J Med 2019;36(3):192-200

A
C
E
D
B
Fig. 1. An example of stereotactic body radiotherapy using tracking intensity-modulated beams for a 20-mm-sized lesion in segment 1 that occurred after right hepatectomy and 5 times of radiofrequency ablation. (A) Gold fiducial markers are inserted before the simulation for patient/tumor position verification and real-time tumor tracking. (B, C) Target volumes and normal tissues are delineated in breath-hold images, and then treatment plan using 9 intensity-modulated beams is generated (gross tumor volume in red, planning target volume in cyan, and the intestine in green). (D) In the treatment room, locations of fiducial markers are verified using cone-beam computed tomography. (E) The treatment beams are delivered while monitoring the movement of the fiducial markers in real time. Electronic portal imaging device shows the movement of each beamlet during tracking treatment. Images in B, C, and E are from this patient, and images in A and D are from other patients for demonstration.
https://doi.org/10.12701/yujm.2019.00269194
Park J et al. Current status of SBRT for HCC
ing with high local control rates of 87–90% at 3 years [22,23]. Based on dosimetric studies comparing the proton and photon, proton SBRT was preferred for larger tumors in terms of liver toxicity and could meet liver dose constraints even when photon SBRT could not [24,25]. Despite the limited number of particle therapy facilities, charged particle therapy is a promising modali-ty for the treatment of HCC.
Clinical considerations
1. Clinical outcomes of stereotactic body radiotherapy Many institutions have reported their clinical outcomes after SBRT for HCC after the first report by Blomgren et al. [26]. Even though dose schedules and patient/tumor characteristics were heterogeneous, clinical outcomes were promising in terms of tu-mor control and toxicities. Recently, Rim et al. [9] conducted a meta-analysis on the results of 32 studies, including 1,950 pa-tients, published in between 2010 and 2018. The median propor-tion of CP A was 82.3% (range, 47.9–100%). The median of the median tumor sizes was 3.3 cm (range, 1.6–8.6 cm). The median of the median EQD2 estimates was 83.3 Gy (range, 48.0–114.8 Gy). Pooled 1-, 2-, and 3-year overall survival rates were 72.6% (95% confidence interval [CI], 65.7–78.6), 57.8% (95% CI, 50.9–64.4), and 48.3% (95% CI, 40.3–56.5), respectively. Pooled 1-, 2-, and 3-year local control rates were 85.7% (95% CI, 80.1-90.0), 83.6% (95% CI, 77.4–88.3), and 83.9% (95% CI, 77.6–88.6), respectively. Larger tumor size of ≥ 5 cm was a significant factor for worse local control and overall survival rates. Hepatic and GI complication rates of grade ≥ 3 were 4.7% (95% CI, 3.4–6.5) and 3.9% (95% CI, 2.6–5.6), respectively. Overall, these re-sults imply that SBRT is a safe and effective local ablative therapy.
2. Selection of local modalities Tumors unsuitable for ablation or surgical resection or with failed treatments have usually been treated with SBRT; however, deciding whether a patient is a proper candidate for SBRT or which is the best modality is difficult. Data below would help the multidisciplinary team to recommend SBRT for a given patient, even though the evidence level is low.
Overall local control rates of SBRT and RFA have been report-ed to be comparably high [27,28]. SBRT was notably achieved a higher local control rate than RFA for tumors of ≥ 2 cm in Wahl et al.’s study [28], which may be related to the better radiation dose coverage of SBRT and limited heat transfer to long distanc-es from the heat source of RFA. In addition, tumor control was not influenced by the tumor size after SBRT in two studies with a median tumor size of 2.2 cm (range, 0–10.0 cm) and 7.2 cm
(range, 1.4–23.1 cm) [28,29], which implies that SBRT could be a preferred treatment option for large tumors.
RFA is less effective or contraindicated in the following situa-tions: tumors close to the major vessels (due to the heat sink ef-fect); tumors abutting the diaphragm (due to the risk of dia-phragmatic injury); tumors on the liver capsule (due to the risk of rupture or track seeding); centrally located tumors (due to the risk of bile duct injury); and invisible tumors on ultrasonography [30]. Instead, SBRT is less influenced by tumor location, except its distance from the GI tract.
An important difference between RFA and SBRT is repeatabili-ty. In contrast to RFA, repeated use of SBRT is limited for new HCC lesions due to the decreased liver function after SBRT [31]. Considering that frequent intrahepatic recurrences of HCC re-quire repeated treatments, SBRT might be spared for lesions un-suitable for other liver-directed treatments. In contrast, Lee et al. [32] reported the treatment outcomes after a repeated SBRT for recurrent HCCs with a median tumor size of 1.7 cm (interquartile range, 1.4–2.2 cm) in 85 patients. The 3-year local control rates were not different between the first and second SBRT (94.9% vs. 90.4%, p = 0.667). None of the 73 patients with CP A experienced RILD after the second SBRT, whereas 2 of the 12 patients with CP B experienced irreversible liver function deterioration. Although the use of repeated SBRT has been limited so far, SBRT can be re-applied to highly selected patients with good liver function.
The superiority in the survival aspect between SBRT and oth-er treatments has been controversial. RFA showed superior sur-vival compared to SBRT in a study based on a large number of patients from the National Cancer Database [33]. When com-paring SBRT with surgical resection, survival was comparable or superior in the surgery group, depending on the studies [34,35]. However, a firm conclusion cannot be made because of both the retrospective design and potential selection bias in these studies.
Toxicities after stereotactic body radiotherapy
1. Liver Liver toxicities, or RILD, is the most important dose-limiting factor for the treatment of liver tumors [36]. Patients with HCC are more vulnerable to the development RILD, because HCC frequently occurs in a cirrhotic liver susceptible to radiation inju-ry. Non-classic RILD (elevation of liver transaminases or decline of CP score) is usually reported after SBRT, rather than classic RILD (anicteric hepatomegaly and ascites or elevation of alkaline phosphatase). The RILD rate of grade ≥ 3 was as low as 4.7% (95% CI, 3.4–6.5) in a pooled analysis of 23 studies, which was
195https://doi.org/10.12701/yujm.2019.00269
Yeungnam Univ J Med 2019;36(3):192-200

generally transient [9]. Since worse baseline liver function is cor-related with higher risk of severe RILD [13,37-40], caution is warranted in deciding the treatment and SBRT planning in pa-tients with poor liver function. Although no definite guidelines were available for liver constraints, the following guidelines have been used: limiting SBRT to CP A or B7 patients [5]; adjusting prescription dose using the normal tissue complication probabil-ity of the liver [39]; limiting the normal liver dose (e.g., mean normal liver dose: < 13–18 Gy in 3–6 fractions for CP A vs. < 6 Gy in 4–6 fractions for CP B) [36]; or sparing the critical residu-al liver volume (e.g., ≥ 700 mL of normal liver receives ≤15 Gy in 3–5 fractions) [36].
2. Gastrointestinal tract Because tolerance doses of luminal structures such as the esopha-gus, stomach, or intestine are much lower than ablative doses used for SBRT, special concerns are required for lesions close to lumi-nal structures. In one case series, all 5 patients who experienced grade 3 or 4 GI toxicities had lesions within 0–0.4 cm from the GI tract [21]. Radiation oncologists generally recommend SBRT for lesions with enough distance from GI tract (e.g., > 1–2 cm) [14,41]. To overcome this limitation, various techniques are at-tempted, including 4D-CT, abdominal compression, gated RT, tracking RT, or intensity-modulated beam. Real-time tumor track-ing, using fiducial markers (Fig. 1A) or MRI images, is the current most advanced method used to avoid the GI tract close to tumors. Fig. 1 shows an example of a patient undergoing follow-up with-out GI complication at 33 months after receiving tracking SBRT for a tumor at 5 mm from the bowel. Tolerance doses of luminal structures are discussed in detail elsewhere [42-45].
3. Bile duct Biliary stricture has been occasionally reported at the rate of 0–3% [12,28,32,46-48]. Eriguchi et al. [49] found biliary stenosis in 2 out of 50 patients irradiated with over 20 Gy to the central biliary system; 1 patient experienced biliary stricture at the area irradiat-ed with > 80 Gy after the second SBRT and the stenotic site of the other patient was outside the area irradiated with > 20 Gy. In ad-dition, even in a study that investigated the relationship between the central hepatobiliary tract dose and hepatobiliary toxicity rate (not only for biliary tract complications), no biliary stricture was observed in 20 patients with HCC unlike the intrahepatic cholan-giocarcinoma with high rate of biliary stricture (38.8% of 26 pa-tients) [50]. Therefore, SBRT seems to be a feasible modality for centrally located tumors unsuitable for other treatments.
Additional indications of stereotactic body radiotherapy
1. As a bridge therapy Bridge therapies can be used to prevent tumor progression while waiting for transplantation or to downstage tumors into the Mi-lan criteria. SBRT as a bridge therapy has also been reported as safe and effective. O’Connor et al. [51] and Andolino et al. [52] reported that SBRT did not increase surgical complications. Sap-isochin et al. [53] revealed that drop-out, post-transplant surviv-al, and HCC recurrence rates after liver transplantation were sim-ilar among SBRT, TACE, and RFA. Mohamed et al. [54] showed that acute toxicities of SBRT and yttrium-90 radioembolization were lower than those of TACE or RFA. These results suggest that SBRT is a viable option as bridge to transplantation.
2. In advanced hepatocellular carcinoma HCC with portal vein tumor thrombosis (PVTT) has poor prognosis; however, the standard treatment strategy remains to be established. RT has been used to restore the portal flow and facilitate subsequent treatments such as surgery or TACE. The response rate was 39–57% with conventional RT using a small fraction size of 1.8–3 Gy, which requires a long treatment period (e.g., 45–50 Gy in 25 fractions over 5 weeks) [55]. Advanced RT techniques such as intensity-modulated RT or IGRT facilitate giving higher radiation doses without increasing GI toxicities, with which higher tumor response and better survival would be expected [56]. Although advanced tumor characteristics related to PVTT, poor liver function, or close distance to GI tract often limit the use of SBRT for PVTT [57], recent studies have report-ed high PVTT response rates (70–76%) after SBRT using rela-tively low dose regimens (e.g., 40 Gy in 5–6 fractions over 1–2 weeks) [58-60]. Therefore, SBRT, which ends in a short treat-ment period, is worth of future investigation for the treatment of PVTT, especially in combination with recently developed sys-temic agents.
Large or multiple HCCs not suitable for curative treatments are often treated with TACE with or without RT [4,5]. A me-ta-analysis by Meng at al. [61], comparing TACE plus RT to TACE alone, revealed that the adding RT to TACE improved the tumor response and survival, where small doses per fraction or lower total doses were usually used for fear of toxicities in the liv-er and GI tract. As SBRT has a higher capability of sparing nor-mal tissues as compared to RT techniques used before, SBRT could be assumed to increase the clinical outcomes when com-bined with TACE for large HCCs. Jacob et al. [62] reported that TACE plus SBRT (45 Gy in 3 fractions) achieved better local
https://doi.org/10.12701/yujm.2019.00269196
Park J et al. Current status of SBRT for HCC

control and survival rates than TACE alone in HCCs of ≥ 3 cm. Paik et al. [63] confirmed the comparable survival outcomes among the three treatment groups (complete TACE alone, in-complete TACE followed by curative treatments, and incomplete TACE followed by SBRT [46–60 Gy in 3–5 fractions]). These results imply that SBRT is an effective adjuvant treatment for HCCs showing an incomplete response to TACE.
3. In combination with systemic therapies Despite the high local control rates of SBRT, there is a demand to combine SBRT with systemic agents due to frequent intrahepatic or extrahepatic recurrences after SBRT. Sorafenib, a multikinase inhibitor, was attempted to be combined with SBRT based on improved overall survival in patients with advanced HCC treated with sorafenib (vs. best supportive care group) in SHARP phase III trial [64] and in vitro and in vivo radiosensitizing effect of sorafenib in HCC cell lines [65]. However, the addition of sorafenib to SBRT is not currently recommended due to in-creased risk of GI toxicities [66,67].
Recently, immunotherapy has been successfully employed for the treatment of solid tumors such as melanoma and non-small cell lung cancer, and the combination of immunotherapy with RT is an active field of clinical investigation [68]. SBRT using a high radiation dose per fraction is known to have an immunomodula-tory effect, which can potentially improve tumor response and survival outcomes of immunotherapy [69]. Notably, abscopal ef-fect, or tumor regression outside the RT field, has been increas-ingly reported when RT was combined with immunotherapy, even though it was a rare phenomenon before the era of cancer immunotherapy. Mechanisms of abscopal effect, related to sys-temic effect of radiation, are also being revealed [70,71]. In 2017 and 2018, 2 immune checkpoint antibodies, nivolumab and pem-brolizumab, have been approved to be used as a second-line thera-py for HCC by the Food and Drug Administration. Preclinical data showed that the combination of programmed death ligand 1 blockade and RT significantly suppressed the tumor growth in a murine HCC model compared with single treatments [72]. And, there are several ongoing phase I or II trials combining immuno-therapy and SBRT for patients with HCC (NCT03203304, NCT03316872, NCT03482102, and NCT03817736). With this new strategy, the prognosis of both early and advanced HCCs is anticipated to improve via enhanced local and systemic effects.
Conclusion
Current evidences support the use of SBRT as an alternative or complement to curative treatments based on its high local con-
trol rates and low toxicity profiles. There is also an emerging in-terest in combining SBRT with other locoregional or systemic therapies to potentially maximize treatment outcomes. Clinical uses of SBRT are summarized in Table 1. However, optimal dose–fractionation regimens balancing tumor control and toxicities and methods to overcome the current limitations of SBRT should be determined. Given that clinical presentations of patients with HCC are significantly heterogeneous, a multidisciplinary team approach could determine the best candidates who would bene-fit from SBRT with or without combined treatments.
Conflicts of interest
No potential conflicts of interest relevant to this article was reported.
ORCID
Jongmoo Park, https://orcid.org/0000-0002-7004-8128 Jae Won Park, https://orcid.org/0000-0003-1100-5301 Min Kyu Kang, https://orcid.org/0000-0002-7962-7054
References
1. Jung KW, Won YJ, Kong HJ, Lee ES; Community of Popula-tion-Based Regional Cancer Registries. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2015. Cancer Res Treat 2018;50:303–16.
2. Perz JF, Armstrong GL, Farrington LA, Hutin YJ, Bell BP. The contributions of hepatitis B virus and hepatitis C virus infections to cirrhosis and primary liver cancer worldwide. J Hepatol 2006;45:529–38.
3. Ock M, Choi WJ, Jo MW. Trend analysis of major cancer statis-
Table 1. Clinical uses of stereotactic body radiotherapy for hepatocellular carcinoma
1. Recommended by major guidelines for HCC management- As an alternative to curative treatment options for single tumors or
multiple small lesions with a limited number (BCLC stage 0-A)2. Based on small case series
- As a bridge therapy to prevent tumor progression or to downstage tumors into the Milan criteria
- As an adjuvant therapy after incomplete transarterial chemoemboli-zation for large tumors (BCLC stage A) or multiple lesions (BCLC stage B)
- As palliative therapy to restore the portal flow and facilitate subse-quent treatments in HCC with portal vein thrombosis (BCLC stage C)
3. Promising- In combination with immunotherapy with the potential to enhance
local and systemic control
HCC, hepatocelluar carcinoma; BCLC, Barcelona Clinic Liver Cancer.
197https://doi.org/10.12701/yujm.2019.00269
Yeungnam Univ J Med 2019;36(3):192-200

tics according to sex and severity levels in Korea. PLoS One 2018;13:e0203110
4. European Association for the Study of the Liver. EASL clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol 2018;69:182–236.
5. Korean Liver Cancer Association; National Cancer Center. 2018 Korean Liver Cancer Association-National Cancer Center Korea Practice Guidelines for the management of hepatocellular Carci-noma. Gut Liver 2019;13:227–99.
6. Delis SG, Dervenis C. Selection criteria for liver resection in pa-tients with hepatocellular carcinoma and chronic liver disease. World J Gastroenterol 2008;14:3452–60.
7. Tiong L, Maddern GJ. Systematic review and meta-analysis of survival and disease recurrence after radiofrequency ablation for hepatocellular carcinoma. Br J Surg 2011;98:1210–24.
8. Benedict SH, Yenice KM, Followill D, Galvin JM, Hinson W, Ka-vanagh B, et al. Stereotactic body radiation therapy: the report of AAPM Task Group 101. Med Phys 2010;37:4078–101.
9. Rim CH, Kim HJ, Seong J. Clinical feasibility and efficacy of ste-reotactic body radiotherapy for hepatocellular carcinoma: a sys-tematic review and meta-analysis of observational studies. Radio-ther Oncol 2019;131:135–44.
10. Vogel A, Cervantes A, Chau I, Daniele B, Llovet J, Meyer T, et al. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2018;29(Suppl 4):iv238–55.
11. Murray LJ, Dawson LA. Advances in stereotactic body radiation therapy for hepatocellular carcinoma. Semin Radiat Oncol 2017;27:247–55.
12. Yoon SM, Lim YS, Park MJ, Kim SY, Cho B, Shim JH, et al. Ste-reotactic body radiation therapy as an alternative treatment for small hepatocellular carcinoma. PLoS One 2013;8:e79854
13. Sanuki N, Takeda A, Oku Y, Mizuno T, Aoki Y, Eriguchi T, et al. Stereotactic body radiotherapy for small hepatocellular carcino-ma: a retrospective outcome analysis in 185 patients. Acta On-col 2014;53:399–404.
14. Sanuki N, Takeda A, Kunieda E. Role of stereotactic body radia-tion therapy for hepatocellular carcinoma. World J Gastroenter-ol 2014;20:3100–11.
15. Dawson LA, Brock KK, Kazanjian S, Fitch D, McGinn CJ, Law-rence TS, et al. The reproducibility of organ position using ac-tive breathing control (ABC) during liver radiotherapy. Int J Ra-diat Oncol Biol Phys 2001;51:1410–21.
16. Herfarth KK, Debus J, Lohr F, Bahner ML, Fritz P, Höss A, et al. Extracranial stereotactic radiation therapy: set-up accuracy of patients treated for liver metastases. Int J Radiat Oncol Biol Phys 2000;46:329–35.
17. Brock KK. Imaging and image-guided radiation therapy in liver cancer. Semin Radiat Oncol 2011;21:247–55.
18. Park SH, Kim JC, Kang MK. Technical advances in external ra-diotherapy for hepatocellular carcinoma. World J Gastroenterol 2016;22:7311–21.
19. Scorsetti M, Comito T, Cozzi L, Clerici E, Tozzi A, Franzese C, et al. The challenge of inoperable hepatocellular carcinoma (HCC): results of a single-institutional experience on stereotac-tic body radiation therapy (SBRT). J Cancer Res Clin Oncol 2015;141:1301–9.
20. Lee KH, Yu JI, Park HC, Park SY, Shin JS, Shin EH, et al. Is high-er dose always the right answer in stereotactic body radiation therapy for small hepatocellular carcinoma? Radiat Oncol J 2018;36:129–38.
21. Jang WI, Kim MS, Bae SH, Cho CK, Yoo HJ, Seo YS, et al. High-dose stereotactic body radiotherapy correlates increased local control and overall survival in patients with inoperable he-patocellular carcinoma. Radiat Oncol 2013;8:250.
22. Mizumoto M, Okumura T, Hashimoto T, Fukuda K, Oshiro Y, Fukumitsu N, et al. Proton beam therapy for hepatocellular car-cinoma: a comparison of three treatment protocols. Int J Radiat Oncol Biol Phys 2011;81:1039–45.
23. Kasuya G, Kato H, Yasuda S, Tsuji H, Yamada S, Haruyama Y, et al. Progressive hypofractionated carbon-ion radiotherapy for hepatocellular carcinoma: combined analyses of 2 prospective trials. Cancer 2017;123:3955–65.
24. Toramatsu C, Katoh N, Shimizu S, Nihongi H, Matsuura T, Takao S, et al. What is the appropriate size criterion for proton radiotherapy for hepatocellular carcinoma? A dosimetric com-parison of spot-scanning proton therapy versus intensity-modu-lated radiation therapy. Radiat Oncol 2013;8:48.
25. Gandhi SJ, Liang X, Ding X, Zhu TC, Ben-Josef E, Plastaras JP, et al. Clinical decision tool for optimal delivery of liver stereo-tactic body radiation therapy: Photons versus protons. Pract Radiat Oncol 2015;5:209–18.
26. Blomgren H, Lax I, Näslund I, Svanström R. Stereotactic high dose fraction radiation therapy of extracranial tumors using an accelerator. Clinical experience of the first thirty-one patients. Acta Oncol 1995;34:861–70.
27. Shiozawa K, Watanabe M, Ikehara T, Matsukiyo Y, Kogame M, Kishimoto Y, et al. Comparison of percutaneous radiofrequency ablation and CyberKnife® for initial solitary hepatocellular carci-noma: A pilot study. World J Gastroenterol 2015;21:13490–9.
28. Wahl DR, Stenmark MH, Tao Y, Pollom EL, Caoili EM, Law-rence TS, et al. Outcomes after stereotactic body radiotherapy or radiofrequency ablation for hepatocellular carcinoma. J Clin Oncol 2016;34:452–9.
https://doi.org/10.12701/yujm.2019.00269198
Park J et al. Current status of SBRT for HCC

29. Bujold A, Massey CA, Kim JJ, Brierley J, Cho C, Wong RK, et al. Sequential phase I and II trials of stereotactic body radiotherapy for locally advanced hepatocellular carcinoma. J Clin Oncol 2013;31:1631–9.
30. Rhim H, Yoon KH, Lee JM, Cho Y, Cho JS, Kim SH, et al. Ma-jor complications after radio-frequency thermal ablation of he-patic tumors: spectrum of imaging findings. Radiographics 2003;23:123–34.
31. Rice SL, Bale R, Breen DJ, de Baere T, Denys A, Guiu B, et al. The management of colorectal cancer liver metastases: the in-terventional radiology viewpoint. Int J Radiat Oncol Biol Phys 2019;103:537–9.
32. Lee S, Kim H, Ji Y, Cho B, Kim SS, Jung J, et al. Evaluation of he-patic toxicity after repeated stereotactic body radiation therapy for recurrent hepatocellular carcinoma using deformable image registration. Sci Rep 2018;8:16224.
33. Rajyaguru DJ, Borgert AJ, Smith AL, Thomes RM, Conway PD, Halfdanarson TR, et al. Radiofrequency ablation versus stereo-tactic body radiotherapy for localized hepatocellular carcinoma in nonsurgically managed patients: analysis of the national can-cer database. J Clin Oncol 2018;36:600–8.
34. Nakano R, Ohira M, Kobayashi T, Ide K, Tahara H, Kuroda S, et al. Hepatectomy versus stereotactic body radiotherapy for primary early hepatocellular carcinoma: a propensity-matched analysis in a single institution. Surgery 2018;164:219–26.
35. Su TS, Liang P, Liang J, Lu HZ, Jiang HY, Cheng T, et al. Long-term survival analysis of stereotactic ablative radiotherapy ver-sus liver resection for small hepatocellular carcinoma. Int J Radi-at Oncol Biol Phys 2017;98:639–46.
36. Pan CC, Kavanagh BD, Dawson LA, Li XA, Das SK, Miften M, et al. Radiation-associated liver injury. Int J Radiat Oncol Biol Phys 2010;76(3 Suppl):S94–100.
37. Liang SX, Zhu XD, Xu ZY, Zhu J, Zhao JD, Lu HJ, et al. Radia-tion-induced liver disease in three-dimensional conformal radi-ation therapy for primary liver carcinoma: the risk factors and hepatic radiation tolerance. Int J Radiat Oncol Biol Phys 2006;65:426–34.
38. Jung J, Yoon SM, Kim SY, Cho B, Park JH, Kim SS, et al. Radia-tion-induced liver disease after stereotactic body radiotherapy for small hepatocellular carcinoma: clinical and dose-volumetric parameters. Radiat Oncol 2013;8:249.
39. Culleton S, Jiang H, Haddad CR, Kim J, Brierley J, Brade A, et al. Outcomes following definitive stereotactic body radiotherapy for patients with Child-Pugh B or C hepatocellular carcinoma. Radiother Oncol 2014;111:412–7.
40. Su TS, Liang P, Lu HZ, Liang J, Gao YC, Zhou Y, et al. Stereotac-tic body radiation therapy for small primary or recurrent hepa-
tocellular carcinoma in 132 Chinese patients. J Surg Oncol 2016;113:181–7.
41. Dawson LA. Overview: where does radiation therapy fit in the spectrum of liver cancer local-regional therapies? Semin Radiat Oncol 2011;21:241–6.
42. Kavanagh BD, Pan CC, Dawson LA, Das SK, Li XA, Ten Haken RK, et al. Radiation dose-volume effects in the stomach and small bowel. Int J Radiat Oncol Biol Phys 2010;76(3 Sup-pl):S101–7.
43. Bae SH, Kim MS, Kim SY, Jang WI, Cho CK, Yoo HJ, et al. Se-vere intestinal toxicity after stereotactic ablative radiotherapy for abdominopelvic malignancies. Int J Colorectal Dis 2013; 28:1707–13.
44. LaCouture TA, Xue J, Subedi G, Xu Q, Lee JT, Kubicek G, et al. Small bowel dose tolerance for stereotactic body radiation ther-apy. Semin Radiat Oncol 2016;26:157–64.
45. Goldsmith C, Price P, Cross T, Loughlin S, Cowley I, Plowman N. Dose-volume histogram analysis of stereotactic body radio-therapy treatment of pancreatic cancer: a focus on duodenal dose constraints. Semin Radiat Oncol 2016;26:149–56.
46. Yamashita H, Onishi H, Murakami N, Matsumoto Y, Matsuo Y, Nomiya T, et al. Survival outcomes after stereotactic body ra-diotherapy for 79 Japanese patients with hepatocellular carcino-ma. J Radiat Res 2015;56:561–7.
47. Sapir E, Tao Y, Schipper MJ, Bazzi L, Novelli PM, Devlin P, et al. Stereotactic body radiation therapy as an alternative to transar-terial chemoembolization for hepatocellular carcinoma. Int J Radiat Oncol Biol Phys 2018;100:122–30.
48. Jeong Y, Jung J, Cho B, Kwak J, Jeong C, Kim JH, et al. Stereotac-tic body radiation therapy using a respiratory-gated volumet-ric-modulated arc therapy technique for small hepatocellular carcinoma. BMC Cancer 2018;18:416.
49. Eriguchi T, Takeda A, Sanuki N, Oku Y, Aoki Y, Shigematsu N, et al. Acceptable toxicity after stereotactic body radiation thera-py for liver tumors adjacent to the central biliary system. Int J Radiat Oncol Biol Phys 2013;85:1006–11.
50. Toesca DA, Osmundson EC, Eyben RV, Shaffer JL, Lu P, Koong AC, et al. Central liver toxicity after SBRT: an expanded analysis and predictive nomogram. Radiother Oncol 2017;122:130–6.
51. O’Connor JK, Trotter J, Davis GL, Dempster J, Klintmalm GB, Goldstein RM. Long-term outcomes of stereotactic body radia-tion therapy in the treatment of hepatocellular cancer as a bridge to transplantation. Liver Transpl 2012;18:949–54.
52. Andolino DL, Johnson CS, Maluccio M, Kwo P, Tector AJ, Zook J, et al. Stereotactic body radiotherapy for primary hepato-cellular carcinoma. Int J Radiat Oncol Biol Phys 2011;81:e447–53.
199https://doi.org/10.12701/yujm.2019.00269
Yeungnam Univ J Med 2019;36(3):192-200

53. Sapisochin G, Barry A, Doherty M, Fischer S, Goldaracena N, Rosales R, et al. Stereotactic body radiotherapy vs. TACE or RFA as a bridge to transplant in patients with hepatocellular car-cinoma. An intention-to-treat analysis. J Hepatol 2017;67:92–9.
54. Mohamed M, Katz AW, Tejani MA, Sharma AK, Kashyap R, Noel MS, et al. Comparison of outcomes between SBRT, yttri-um-90 radioembolization, transarterial chemoembolization, and radiofrequency ablation as bridge to transplant for hepato-cellular carcinoma. Adv Radiat Oncol 2015;1:35–42.
55. Kim JY, Chung SM, Choi BO, Kay CS. Hepatocellular carcino-ma with portal vein tumor thrombosis: Improved treatment outcomes with external beam radiation therapy. Hepatol Res 2011;41:813–24.
56. Im JH, Yoon SM, Park HC, Kim JH, Yu JI, Kim TH, et al. Ra-diotherapeutic strategies for hepatocellular carcinoma with por-tal vein tumour thrombosis in a hepatitis B endemic area. Liver Int 2017;37:90–100.
57. Bae SH, Kim MS, Jang WI, Kim JH, Kim WC, Kim JH, et al. Multicenter planning comparison of stereotactic body radio-therapy for hepatocellular carcinoma with major portal vein tu-mor thrombosis (KROG 16-17). J Liver Cancer 2018;18:130–41.
58. Xi M, Zhang L, Zhao L, Li QQ, Guo SP, Feng ZZ, et al. Effective-ness of stereotactic body radiotherapy for hepatocellular carcino-ma with portal vein and/or inferior vena cava tumor thrombosis. PLoS One 2013;8:e63864
59. Kang J, Nie Q, DU R, Zhang L, Zhang J, Li Q, et al. Stereotactic body radiotherapy combined with transarterial chemoemboli-zation for hepatocellular carcinoma with portal vein tumor thrombosis. Mol Clin Oncol 2014;2:43–50.
60. Shui Y, Yu W, Ren X, Guo Y, Xu J, Ma T, et al. Stereotactic body radiotherapy based treatment for hepatocellular carcinoma with extensive portal vein tumor thrombosis. Radiat Oncol 2018; 13:188.
61. Meng MB, Cui YL, Lu Y, She B, Chen Y, Guan YS, et al. Tran-scatheter arterial chemoembolization in combination with ra-diotherapy for unresectable hepatocellular carcinoma: a system-atic review and meta-analysis. Radiother Oncol 2009;92:184–94.
62. Jacob R, Turley F, Redden DT, Saddekni S, Aal AK, Keene K, et
al. Adjuvant stereotactic body radiotherapy following transarte-rial chemoembolization in patients with non-resectable hepato-cellular carcinoma tumours of ≥ 3 cm. HPB (Oxford) 2015;17:140–9.
63. Paik EK, Kim MS, Jang WI, Seo YS, Cho CK, Yoo HJ, et al. Ben-efits of stereotactic ablative radiotherapy combined with incom-plete transcatheter arterial chemoembolization in hepatocellular carcinoma. Radiat Oncol 2016;11:22.
64. Llovet JM, Ricci S, Mazzaferro V, Hilgard P, Gane E, Blanc JF, et al. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 2008;359:378–90.
65. Yu W, Gu K, Yu Z, Yuan D, He M, Ma N, et al. Sorafenib poten-tiates irradiation effect in hepatocellular carcinoma in vitro and in vivo. Cancer Lett 2013;329:109–17.
66. Barney BM, Markovic SN, Laack NN, Miller RC, Sarkaria JN, Macdonald OK, et al. Increased bowel toxicity in patients treat-ed with a vascular endothelial growth factor inhibitor (VEGFI) after stereotactic body radiation therapy (SBRT). Int J Radiat Oncol Biol Phys 2013;87:73–80.
67. Brade AM, Ng S, Brierley J, Kim J, Dinniwell R, Ringash J, et al. Phase 1 trial of sorafenib and stereotactic body radiation thera-py for hepatocellular carcinoma. Int J Radiat Oncol Biol Phys 2016;94:580–7.
68. Kang J, Demaria S, Formenti S. Current clinical trials testing the combination of immunotherapy with radiotherapy. J Immuno-ther Cancer 2016;4:51.
69. Bernstein MB, Krishnan S, Hodge JW, Chang JY. Immunother-apy and stereotactic ablative radiotherapy (ISABR): a curative approach? Nat Rev Clin Oncol 2016;13:516–24.
70. Formenti SC. Optimizing dose per fraction: a new chapter in the story of the abscopal effect? Int J Radiat Oncol Biol Phys 2017;99:677–9.
71. Vanpouille-Box C, Formenti SC, Demaria S. Toward precision radiotherapy for use with immune checkpoint blockers. Clin Cancer Res 2018;24:259–65.
72. Kim KJ, Kim JH, Lee SJ, Lee EJ, Shin EC, Seong J. Radiation improves antitumor effect of immune checkpoint inhibitor in murine hepatocellular carcinoma model. Oncotarget 2017;8: 41242–55.
https://doi.org/10.12701/yujm.2019.00269200
Park J et al. Current status of SBRT for HCC

Implant-based breast reconstruction is the most commonly used reconstruction technique after mastectomy. This is because skin-sparing mastectomy has become possible with advancements in oncology. In addition, the development of breast implants and the advent of acellular dermal matrices have reduced postoperative complications and resulted in superior cosmetic results. The most frequently performed surgical breast reconstruction procedure for the past 20 years was the insertion of an implant under the pectoralis major muscle by means of the dual plane approach. However, some patients suffered from pain and animation deformity caused by muscle manipu-lation. Recently, a prepectoral approach has been used to solve the above problems in select pa-tients, and the results are similar to subpectoral results. However, this technique is not always chosen due to the number of considerations for successful surgery. In this article, we will discuss the emergence of prepectoral breast reconstruction, indications and contraindications, surgical procedures, and outcomes.
Keywords: Acellular dermal matrix; Breast implants; Mastectomy; Prepectoral breast reconstruc-tion
Prepectoral breast reconstruction Sung-Eun Kim Department of Plastic and Reconstructive Surgery, Catholic University of Daegu School of Medicine, Daegu, Korea
Introduction
Breast reconstruction is increasing every year alongside increases in breast cancer. According to American Society of Plastic Sur-geons statistical report, the numbers of breast reconstructions in the United States in 2000 and 2018 were 78,832 and 101,657, re-spectively [1]. The most frequently used reconstructive method is an implant-based reconstruction. In 2018 in the United States, 83,216 implant-based reconstructions were performed, while 18,441 autologous tissue reconstructions were done [1]. Pros-thetic breast reconstruction is the number one procedure because advancements in implants and improvements in mastectomy techniques have resulted in better aesthetic outcomes. Recently, an issue has arisen regarding which plane implants should be placed in. In other words, a reverse shift from submuscular to prepectoral placement has occurred.
Review articleeISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):201-207https://doi.org/10.12701/yujm.2019.00283
Received: June 28, 2019 Revised: August 12, 2019 Accepted: August 14, 2019
Corresponding author: Sung-Eun KimDepartment of Plastic and Reconstructive Surgery, Catholic University of Daegu School of Medicine, 33, Duryugongwon-ro 17-gil, Nam-gu, Daegu 42472, Korea Tel: +82-53-650-4578Fax: +82-53-650-4584Email: [email protected]
History
The ideal location for implants was once thought to be under the skin where the original breast tissue was, above the pectoralis major muscle. Silicone or saline implants were inserted subcuta-neously until the introduction of the tissue expander. This ap-proach was simple and able to preserve muscles, but typically, the mastectomy flap was too thin, and the subcutaneous tissue was deficient, resulting in many complications associated with this method. Implants that became exposed through the skin in-creased the risk of infection of the implants. Ultimately, removal of the implants occurred frequently, and capsular contracture, in particular, was a common complication [2]. These led to a sub-muscular approach where the implants were completely covered by the pectoralis major and serratus anterior muscles using a prepectoral approach. Gruber et al. reported a comparison of submuscular and subcutaneous techniques for breast reconstruc-
201https://doi.org/10.12701/yujm.2019.00283
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

tion following mastectomy [3] and concluded that submuscular implants are clearly superior to subcutaneous ones and that the subserratus techniques provided the lowest incidence of capsular contracture. Augmentation case studies have also concluded that the subpectoral approach is superior, especially in regard to cap-sular contracture [4,5].
However, the full muscle coverage technique has some prob-lems. It could not expand the lower pole and natural ptotic breasts. In addition, implants were not covered by only the pectoralis ma-jor muscle, and the recruitment of other muscle flaps, such as the serratus muscle or the rectus abdominis sheath, was needed. To solve these problems, the partial muscle coverage, or dual plane, technique was introduced. This technique enabled expansion of the lower pole, but the pectoralis major muscle was not fixed to the chest wall, so it often migrated superiorly, resulting in so-called window shading [6-8].
These problems were addressed by the advent of acellular der-mal matrices (ADMs). An ADM is a biotechnologically designed human tissue of bovine or porcine origin that has served numer-ous purposes across surgical subsectors. Tissue processing re-moves cellular antigens that can generate an immunological re-sponse while maintaining a structural matrix that promotes angio-genesis and tissue regeneration. In 1995, for the first time, ADM was used to treat full-thickness burns [9]. Then, in 2006, Salzberg published his experience using ADM in immediate breast recon-struction, and ADM became an important ingredient in breast re-construction [10].
Afterward, the dual plane approach of ADM and covering the implant with the pectoralis major muscle was commonly per-formed. In this procedure, the ADM was sutured to the inferior margin of the pectoralis major muscle, which enabled not only ex-pansion of the lower pole but also a decreased incidence of win-dow shading. In addition, the ADM defines the lateral inframam-mary fold and supports the inferolateral portion, resulting to min-imize migration of the implant caused by muscle contraction.
However, there still remain problems of animation deformity due to muscle contraction, as well as pain caused by the dissection of the muscle. Ultimately, plastic surgeons were reminded of the idea of inserting an implant in the site of the original breast tissue without operating again on the muscle. Notably, capsular contrac-ture, which was the main complication of previous subcutaneous breast reconstruction procedures, has been reduced with the use of ADMs. Kim et al. reported that the levels of myofibroblasts were significantly lower in ADM capsules than in submuscular capsules [11]. Now, with advances in oncology such as the skin-sparing mastectomy with optimal skin flap, improved implants, and ADMs, prepectoral breast reconstruction has become feasible.
Patient selection
Prepectoral breast reconstruction has obvious advantages. In addi-tion to the surgical technique being simple and less invasive, the operation time is short, and the muscle is left intact, reducing bleeding, pain, and recovery time after surgery. The biggest advan-tage is that it significantly reduces the occurrence of animation de-formities. Because the contraction of the muscle does not affect the implant, there is less implant migration. Despite these advantages, the use of this method is limited because the appropriateness of the mastectomy skin flap after oncologic resection determines the via-bility of the operation. In other words, good vascularity and suffi-cient subcutaneous fat tissue should remain (Table 1) [12]. If the skin flap is too thin, it can cause rippling and palpability problems. If the vascularity is poor, skin necrosis, infection, and other compli-cations may occur. Therefore, for successful surgery, it is important to select appropriate patients through close cooperation between the breast surgeon and the plastic surgeon.
Prepectoral breast reconstruction is especially recommended for athletes, who require extensive use of the pectoralis major muscle, or for those whose shoulder function should be preserved. Howev-er, this lifestyle alone cannot determine the operation. There are two major factors in play, one of which is adequate vascularization of the mastectomy skin flap, which can be assessed before and during surgery, and the other is the oncologic consideration.
Patient factors that may affect the vascularity of the skin flap be-fore surgery should be considered (Table 2) [13,14]. Poorly con-trolled blood glucose, obesity, and recent smokers are contraindi-
Table 1. Indications of prepectoral reconstruction
Good perfusion of the mastectomy skin flapsAthletes who require extensive pectoralis major useGrade 1 or 2 ptosis, or volume of mastectomy specimen <500 gLow BMI (<35 kg/m2)Non- or ex-smokers
BMI, body mass index.
Table 2. Contraindications of prepectoral reconstruction
Poorly vascularized mastectomy skin flapActive smokers/recent smokersBMI >40 kg/m2
Immunocompromised patientsHbA1c >7.5%Large tumors (>5 cm)Tumors within 0.5 cm of the pectoralis major muscleChest wall involvementGrossly positive axillary involvement
BMI, body mass index; HbA1c, hemoglobin A1c.
https://doi.org/10.12701/yujm.2019.00283202
Kim SE. Prepectoral breast reconstruction

cations. Large breasts require large implants, resulting in a de-crease of the perfusion of skin, so they are a contraindication. In addition, immunocompromised patients are at increased risk in general and are not suitable for this procedure. Another important factor is the irradiated status of the breast. Preoperative radiation therapy affects wound healing and increases rates of infection, skin necrosis, capsular contracture, and more. Instead of prepectoral breast reconstruction, it is recommended that these patients un-dergo autologous tissue reconstruction [15]. Although there are few studies related to prepectoral reconstruction and postmastec-tomy radiation therapy (PMRT), there are arguments that the prepectoral approach may be a more appropriate choice for pa-tients receiving adjuvant radiation therapy than the dual plane ap-proach. Sigalove et al. studied 33 patients who underwent 52 breast reconstructions via the prepectoral approach and the short-term outcomes. They concluded that an immediate implant-based prepectoral breast reconstruction followed by PMRT appeared to be well tolerated, with no excess risk of adverse outcomes [16]. According to Sinnott et al., patients undergoing submuscular breast reconstruction who received PMRT had a capsular con-tracture rate three times greater, with more severe contractures (Baker grade III or IV) than did patients receiving PMRT who underwent prepectoral breast reconstruction [17]. Sbitany et al. studied 26 breasts that underwent immediate prepectoral recon-struction and 31 breasts that underwent immediate submuscular/dual plane reconstruction in the setting of PMRT and found no significant differences in complication rates between the two re-constructive groups [18].
It is important to evaluate the condition of the skin flap intraop-eratively, and there is a method for clinically or objectively evaluat-ing whether the perfusion of a mastectomy skin flap is good or bad, which will be discussed in detail in the surgical technique section.
Another concern with prepectoral breast reconstruction is the problem associated with the detection of cancer recurrence. If the tumor is located close to the pectoralis muscle, with a subpectoral implant placement, a recurring tumor can be detected by palpa-tion. However, with a prepectoral implant placement, tumor re-currence may be detected later. Therefore, the location of the tu-mor should be taken into consideration during prepectoral recon-struction.
Surgical technique
1. Assessment of mastectomy skin flap Clinical examination is important for evaluating the vascularity of skin flaps (Fig. 1), and bleeding on the incision edge should be seen. Any subcutaneous fat should also be preserved because if there is only dermis and no fat, blood flow will be inadequate. In those cases, it is necessary to consider a dual plane placement or staged reconstruction rather than an immediate prepectoral place-ment. However, skin thinning is not necessarily contraindicated. Even with thin skin, if the subdermal plexus is preserved, prepec-toral breast reconstruction is possible.
Another method of assessing tissue perfusion is the use of indo-cyanine green angiography. This can evaluate the blood flow of arterial and venous vasculature in real time and helps to confirm
Fig. 1. The mastectomy skin flap has good vascularity (A), and a moderate amount of fat tissue is preserved (B).
A B
203https://doi.org/10.12701/yujm.2019.00283
Yeungnam Univ J Med 2019;36(3):201-207

the clinical examination. It is helpful to predict the viability of the skin flap, especially if the skin is expanded when the implant is placed, and it allows the surgeon to ensure that any skin flap ex-pected to become necrotizing is removed.
2. Choice of implant and acellular dermal matrix The implant in a prepectoral reconstruction should be carefully selected to prevent rippling. To do so, the selected implant must have a base width dimension that is correct for the pocket of the ADM or skin flap. The cohesiveness of the implant is determined by the thickness of the skin [19]. The thinner the flap, the better it is to choose a highly cohesive gel implant. Less cohesive gel im-plants are more prone to wrinkling but could be selected for better projection because there is more collapse at the upper pole and descent to the lower pole. However, whether round or smooth can be selected dependent on the operator’s preference and the patient’s desire.
With two-stage surgery, it is important to underfill the tissue ex-pander to make the tight pocket in the second stage. The height of the expander is chosen depending on whether the implant is ana-tomic or round. Typically, short to medium height expanders are used in the first stage for planned round implants, and full height expanders are used for planned anatomical implants.
The ADM is typically used in prepectoral breast reconstruction, but it is not necessarily used [20]. It has been reported that there was no difference in complication rates between groups where an ADM was used and groups where it was not, but it is clear that the incidence of capsular contracture is significantly lower in the ADM group [21–26]. The selected ADM is usually 2–3 mm thick. If a perforated ADM is used, fluid can flow in both directions, mini-mizing sticking between the ADM and the skin flap. In addition, the perforations create an adhesive area between the ADM and the skin flap, thereby promoting incorporation [27].
3. Acellular dermal matrix coverage There are various methods for covering an implant with an ADM [28], and there is some controversy whether it is better to use 1 large ADM sheet or to sew 2 or more sheets together. There is also controversy as to whether it is better to cover the implant only anteriorly or both anteriorly and posteriorly. The latter idea of total ADM coverage of the device has been assessed to demon-strate the lower incidence of capsular contracture [22,29]. Be-cause ADMs are shaped in flat sheets and there are various sizes, there are more ways to cover the three-dimensional shape of im-plants. For example, Braxon (DECO med s.r.l., Marcon, Venice, Italy) is a preshaped, porcine, non-cross-linked ADM that can be wrapped around an implant.
There are two main ways to place an ADM in the prepectoral space, according to US Food and Drug Administration (FDA) la-beling. The FDA requires that an ADM for breast reconstruction is used for tissue support. Therefore, with the on-label method, a trimmed ADM is inserted into the prepectoral space, and after in-sertion of the implant, the edges of the ADM are sutured to the inframammary fold along the chest wall, leaving a 3–4 cm cuff along the pectoralis major muscle. With this method, an inferior “gutter” is created to support the lower pole. In contrast, with the off-label technique, the ADM supports the implant. The implant is wrapped with the ADM on the back table, making a peripheral “cuff,” and then the device with the ADM is inserted in the prepectoral space. In this method, the implant is either partially (Fig. 2) or completely (Fig. 3) wrapped with ADM. Whichever option the operator chooses, it is important for a permanent im-plant to align the ADM to the shape of the implant without laxity. For an expander, it is possible to make an ADM pocket with a lit-tle laxity. After insertion of the device into the mastectomy pock-et, the ADM is fixated to the underlying pectoralis major muscle circumferentially using absorbable sutures. In cases where a tissue expander is used, it is fixed to the pectoralis to anchor the expand-er tabs.
Outcomes
There is a lack of long-term outcomes for prepectoral breast re-construction. However, several authors have reported on the safe-ty, functional and aesthetic outcomes, and complications. Sigalove et al. published preliminary results from over 350 prepectoral breast reconstructions using ADMs [30]. Complications such as infection, seroma, and flap necrosis occurred at rates of less than 5%, and there were no capsular contractures. Patients with prior radiation therapy had higher rates of complications (5 out of 10). In contrast, patients with PMRT had no complications. Zhu et al. reported on comparative studies of prepectoral and total muscle coverage breast reconstruction [31] where they demonstrated similar morbidity rates with regard to infection, superficial skin necrosis, and seroma in both groups but decreased rates of capsu-lar contracture in the prepectoral group. Bernini et al. examined the surgical and aesthetic results of 34 subpectoral and 39 subcu-taneous techniques using titanium-coated polypropylene mesh [32]. Although there were no significant differences between the groups, the subcutaneous group had an implant failure rate of 5.1%, while the subpectoral group had a 0% failure rate. The sub-cutaneous group also had significantly better aesthetic outcomes.
Schaeffer et al. reported early functional outcomes following prepectoral breast reconstruction in comparison with subpectoral
https://doi.org/10.12701/yujm.2019.00283204
Kim SE. Prepectoral breast reconstruction

Fig. 2. Two sheets of fenestrated acellular dermal matrices are sewn together and draped over the implant (A). On the back, the implant is partially covered (B).
A B
Fig. 3. The device is fully covered by 2 sheets of acellular dermal matrices (A). On the back, the implant is fully covered (B).
breast reconstruction [33]. They showed that the prepectoral groups had significantly lower inpatient pain scores. In addition, the range of shoulder motion in the prepectoral group had fully returned in half the number days as in the subpectoral group.
Rippling and wrinkling are commonly seen in the setting of
prepectoral reconstruction. There is also a clear step-off between the chest wall and the prepectoral implant. Although there are very few studies about the effect of autologous fat grafting on patient re-ported outcomes following prepectoral breast reconstruction, many authors have argued that the primary means for correcting
A B
205https://doi.org/10.12701/yujm.2019.00283
Yeungnam Univ J Med 2019;36(3):201-207

these deformities is autologous fat grafting [13,30,34,35]. Advanc-es in fat grafting techniques have made fat grafting a routine proce-dure in breast surgery [30]. In fact, in 2018 in the United States, nearly 30% of all breast reconstruction cases utilized autologous fat grafts [1]. This allows the soft tissue volume between the implant and the mastectomy flap to be supported and augmented.
The cost of ADM is an issue in the setting of prepectoral recon-struction. Two or 4 times the size of ADM that is used for subpec-toral breast reconstruction is needed for this procedure, which will certainly result in incurring additional costs in a range of $5,000 to $20,000 per breast. However, some authors have claimed that prepectoral breast reconstruction is economically advantageous, but more studies should be performed [25,36]. For cost-savings, other authors have noted the use of alternative mate-rials such as Vicryl mesh [21], porcine mesh [22], or titani-um-coated polypropylene mesh [32]. All have demonstrated suc-cess in the prepectoral setting and may have cost-saving benefits.
Conclusion
Prepectoral breast reconstruction is a simple muscle-sparing tech-nique that reduces pain and recovery time after surgery. Above all, the occurrence rate of animation deformities can be reduced. In addition, aesthetically superior outcomes have been demonstrat-ed. A successful prepectoral approach is possible with appropriate patient selection, availability of ADM, and improved fat grafting techniques. However, more long-term outcomes of prepectoral breast reconstructions, especially with PMRT, are required, along with studies of the mechanisms allowing for decreases in capsular contracture with ADMs.
Conflicts of interest
No potential conflicts of interest relevant to this article was re-ported.
Patient consent
Patient provided written consent for the use of her images.
ORCID
Sung-Eun Kim, https://orcid.org/0000-0002-3413-7094
References
1. American Society of Plastic Surgeons. 2018 Plastic surgery statis-
tics report [Internet]. Arlington Heights: American Society of Plastic Surgeons; 2019 [cited 2019 Jun 27]. https://www.plas-ticsurgery.org/documents/News/Statistics/2018/plastic-sur-gery-statistics-full-report-2018.pdf
2. Schlenker JD, Bueno RA, Ricketson G, Lynch JB. Loss of silicone implants after subcutaneous mastectomy and reconstruction. Plast Reconstr Surg 1978;62:853–61.
3. Gruber RP, Kahn RA, Lash H, Maser MR, Apfelberg DB, Laub DR. Breast reconstruction following mastectomy: a comparison of submuscular and subcutaneous techniques. Plast Reconstr Surg 1981;67:312–7.
4. Puckett CL, Croll GH, Reichel CA, Concannon MJ. A critical look at capsule contracture in subglandular versus subpectoral mammary augmentation. Aesthetic Plast Surg 1987;11:23–8.
5. Biggs TM, Yarish RS. Augmentation mammaplasty: a compara-tive analysis. Plast Reconstr Surg 1990;85:368–72.
6. Spear SL, Pelletiere CV. Immediate breast reconstruction in two stages using textured, integrated-valve tissue expanders and breast implants. Plast Reconstr Surg 2004;113:2098–103.
7. Serra-Renom JM, Fontdevila J, Monner J, Benito J. Mammary re-construction using tissue expander and partial detachment of the pectoralis major muscle to expand the lower breast quadrants. Ann Plast Surg 2004;53:317–21.
8. Hammond DC, Capraro PA, Ozolins EB, Arnold JF. Use of a skin-sparing reduction pattern to create a combination skin-mus-cle flap pocket in immediate breast reconstruction. Plast Reconstr Surg 2002;110:206–11.
9. Wainwright DJ. Use of an acellular allograft dermal matrix (Allo-Derm) in the management of full-thickness burns. Burns 1995; 21:243–8.
10. Salzberg CA. Nonexpansive immediate breast reconstruction using human acellular tissue matrix graft (AlloDerm). Ann Plast Surg 2006;57:1–5.
11. Kim IK, Park SO, Chang H, Jin US. Inhibition mechanism of acellular dermal matrix on capsule formation in expander-im-plant breast reconstruction after postmastectomy radiotherapy. Ann Surg Oncol 2018;25:2279–87.
12. Vidya R, Iqbal FM. A guide to prepectoral breast reconstruc-tion: a new dimension to implant-based breast reconstruction. Clin Breast Cancer 2017;17:266–71.
13. Ter Louw RP, Nahabedian MY. Prepectoral breast reconstruc-tion. Plast Reconstr Surg 2017;140(5 Suppl):51S–9S.
14. Storm-Dickerson T, Sigalove N. Prepectoral breast reconstruc-tion: the breast surgeon’s perspective. Plast Reconstr Surg 2017;140(6 Suppl):43S–8S.
15. Spear SL, Boehmler JH, Bogue DP, Mafi AA. Options in recon-structing the irradiated breast. Plast Reconstr Surg 2008;122:
https://doi.org/10.12701/yujm.2019.00283206
Kim SE. Prepectoral breast reconstruction

379–88. 16. Sigalove S, Maxwell GP, Sigalove NM, Storm-Dickerson TL,
Pope N, Rice J, et al. Prepectoral implant-based breast recon-struction and postmastectomy radiotherapy: short-term out-comes. Plast Reconstr Surg Glob Open 2017;5:e1631.
17. Sinnott CJ, Persing SM, Pronovost M, Hodyl C, McConnell D, Ott Young A. Impact of postmastectomy radiation therapy in prepectoral versus subpectoral implant-based breast reconstruc-tion. Ann Surg Oncol 2018;25:2899–908.
18. Sbitany H, Gomez-Sanchez C, Piper M, Lentz R. Prepectoral breast reconstruction in the setting of postmastectomy radiation therapy: an assessment of clinical outcomes and benefits. Plast Reconstr Surg 2019;143:10–20.
19. Gabriel A, Maxwell GP. Implant selection in the setting of prepectoral breast reconstruction. Gland Surg 2019;8:36–42.
20. Salibian AH, Harness JK, Mowlds DS. Staged suprapectoral ex-pander/implant reconstruction without acellular dermal matrix following nipple-sparing mastectomy. Plast Reconstr Surg 2017;139:30–9.
21. Kobraei EM, Cauley R, Gadd M, Austen WG Jr, Liao EC. Avoid-ing breast animation deformity with pectoralis-sparing subcuta-neous direct-to-implant breast reconstruction. Plast Reconstr Surg Glob Open 2016;4:e708.
22. Reitsamer R, Peintinger F. Prepectoral implant placement and complete coverage with porcine acellular dermal matrix: a new technique for direct-to-implant breast reconstruction after nip-ple-sparing mastectomy. J Plast Reconstr Aesthet Surg 2015; 68:162–7.
23. Woo A, Harless C, Jacobson SR. Revisiting an old place: sin-gle-surgeon experience on post-mastectomy subcutaneous im-plant-based breast reconstruction. Breast J 2017;23:545–53.
24. Eskenazi LB. New options for immediate reconstruction: achieving optimal results with adjustable implants in a single stage. Plast Reconstr Surg 2007;119:28–37.
25. Glasberg SB. The economics of prepectoral breast reconstruc-tion. Plast Reconstr Surg 2017;140(6 Suppl):49S–52S.
26. Radovan C. Breast reconstruction after mastectomy using the temporary expander. Plast Reconstr Surg 1982;69:195–208.
27. Frey JD, Alperovich M, Weichman KE, Wilson SC, Hazen A, Saadeh PB, et al. Breast reconstruction using contour fenestrat-ed alloderm: does improvement in design translate to improved outcomes? Plast Reconstr Surg Glob Open 2015;3:e505.
28. Sigalove S. Options in acellular dermal matrix-device assembly. Plast Reconstr Surg 2017;140(6 Suppl):39S–42S.
29. Macadam SA, Lennox PA. Acellular dermal matrices: use in re-constructive and aesthetic breast surgery. Can J Plast Surg 2012; 20:75–89.
30. Sigalove S, Maxwell GP, Sigalove NM, Storm-Dickerson TL, Pope N, Rice J, et al. Prepectoral implant-based breast recon-struction: rationale, indications, and preliminary results. Plast Reconstr Surg 2017;139:287–94.
31. Zhu L, Mohan AT, Abdelsattar JM, Wang Z, Vijayasekaran A, Hwang SM, et al. Comparison of subcutaneous versus submus-cular expander placement in the first stage of immediate breast reconstruction. J Plast Reconstr Aesthet Surg 2016;69:e77–86.
32. Bernini M, Calabrese C, Cecconi L, Santi C, Gjondedaj U, Roselli J, et al. Subcutaneous direct-to-implant breast recon-struction: surgical, functional, and aesthetic results after long-term follow-up. Plast Reconstr Surg Glob Open 2016;3:e574.
33. Schaeffer CV, Dassoulas KR, Thuman J, Campbell CA. Early functional outcomes after prepectoral breast reconstruction: a case-matched cohort study. Ann Plast Surg 2019;82(6S Suppl 5):S399–403.
34. Darrach H, Kraenzlin F, Khavanin N, Chopra K, Sacks JM. The role of fat grafting in prepectoral breast reconstruction. Gland Surg 2019;8:61–6.
35. Sbitany H, Piper M, Lentz R. Prepectoral breast reconstruction: a safe alternative to submuscular prosthetic reconstruction fol-lowing nipple-sparing mastectomy. Plast Reconstr Surg 2017; 140:432–43.
36. Cattelani L, Polotto S, Arcuri MF, Pedrazzi G, Linguadoca C, Bonati E. One-step prepectoral breast reconstruction with der-mal matrix-covered implant compared to submuscular implan-tation: functional and cost evaluation. Clin Breast Cancer 2018;18:e703–11.
207https://doi.org/10.12701/yujm.2019.00283
Yeungnam Univ J Med 2019;36(3):201-207
Background: The anatomy of middle cerebral artery (MCA) aneurysms has been noted to be un-favorable for endovascular treatment. The purpose of this study was to assess the feasibility and efficacy of coiling for MCA aneurysms. Methods: From January 2004 to December 2015, 72 MCA aneurysms (38 unruptured and 34 rup-tured) in 67 patients were treated with coils. Treatment-related complications, clinical outcomes, and immediate and follow-up angiographic outcomes were retrospectively analyzed. Results: Aneurysms were located at the MCA bifurcation (n=60), 1st segment (M1, n=8), and 2nd segment (M2, n=4). Sixty-nine aneurysms (95.8%) were treated by neck remodeling techniques using multi-catheter (n=44), balloon (n=14), stent (n=8), or combination of these (n=3). Only 3 aneurysms were treated by single-catheter technique. Angiographic results were 66 (91.7%) complete, 5 (6.9%) remnant neck, and 1 (1.4%) incomplete occlusion. Procedural complications included aneurysm rupture (n=1), asymptomatic coil migration to the distal vessel (n=1), and acute thromboembolism (n=10) consisting of 8 asymptomatic and 2 symptomatic events. Treat-ment-related permanent morbidity and mortality rates were 4.5% and 3.0%, respectively. There was no bleeding on clinical follow-up (mean, 29 months; range, 6-108 months). Follow-up an-giographic results (mean, 26 months; range, 6-96 months) in patients included 1 major and 3 minor recanalizations. Conclusion: Coiling of MCA aneurysms could be a technically feasible and clinically effective treatment strategy with acceptable angiographic and clinical outcomes. However, the safety and efficacy of this technique as compared to surgical clipping remains to be ascertained.
Keywords: Coil embolization; Intracranial aneurysm; Middle cerebral artery
Feasibility and efficacy of coil embolization for middle cerebral artery aneurysms Jae Young Choi1, Chang Hwa Choi2, Jun Kyeung Ko2, Jae Il Lee2, Chae Wook Huh2, Tae Hong Lee3
1Department of Neurosurgery, Kosin University Gospel Hospital, Busan, Korea 2Department of Neurosurgery, Pusan National University Hospital, Busan, Korea 3Department of Diagnostic Radiology, Pusan National University Hospital, Busan, Korea
Original articleeISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):208-218https://doi.org/10.12701/yujm.2019.00192
Received: January 9, 2019 Revised: February 19, 2019 Accepted: April 10, 2019
Corresponding author: Chang Hwa ChoiDepartment of Neurosurgery, Pusan National University Hospital, 179, Gudeok-ro, Seo-gu, Busan 49241, Korea Tel: +82-51-240-7547Fax: +82-51-244-0282E-mail: [email protected]
Introduction
The International Subarachnoid Aneurysm Trial (ISAT) data in 2002 led to a significant change in the treatment of intracranial aneurysms. Although the ISAT study had exclusively addressed ruptured intracra-nial aneurysms, their results were rapidly assimilated into the treat-ment of unruptured intracranial aneurysms [1].
However, there is still controversy about the treatment strategy for middle cerebral artery (MCA) aneurysms and surgical clip-ping is the preferred strategy, because MCA aneurysms are proxi-mal to the cerebral surface and require less brain retraction to ac-cess and expose [2-4]. Moreover, endovascular coil embolization was likely to be unfavorable because MCA aneurysms often have wide necks and incorporate branches. Although some recent
https://doi.org/10.12701/yujm.2019.00192208
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

studies have demonstrated that endovascular embolization is equivalent to surgical clipping for the treatment of selected MCA aneurysms, coiling of wide-necked MCA aneurysm still remains technically challenging [5-9].
However, newly developed devices and advanced neck-remod-eling techniques using multi-catheter, balloon, stent, or a combi-nation of these permit endovascular treatment (EVT) of complex aneurysms [9-12].
The aim of this study was to retrospectively analyze the feasibil-ity and efficacy of EVT for ruptured and unruptured MCA aneu-rysms at a center where coiling is the first option considered.
Materials and methods
From January 2004 to December 2015, EVT was performed on 72 MCA aneurysms in 67 patients. Informed written consent was obtained from all patients in this retrospective study and approved by the Institutional Review Board of Kosin University Gospel Hospital (KUGH 2019-03-009).
Patient and aneurysm characteristics, angiographic and clinical outcomes, and follow-up were evaluated by the referring neuro-surgeons and an interventional neuroradiologist. Decision regard-ing treatment type (clipping versus coiling) was made by a neuro-vascular team involving neurosurgeons and an interventional neu-roradiologist after completion of initial digital subtraction angiog-raphy (DSA). In agreement with our neurovascular team, coiling was the first-line treatment for MCA aneurysms, unless associated with compressive hematoma requiring immediate surgical evacu-ation. An experienced interventional neuroradiologist determined the possibility of coil embolization for MCA aneurysms, taking into consideration their shape, size, length of the neck, and com-plexity. Wide-neck aneurysms were defined as having a large neck (more than 4 mm) or a dome-to-neck ratio less than 1.5. Complex MCA aneurysms were defined by using particular anatomic fea-tures, including a branch vessel arising from the aneurysm sac and wide neck aneurysm with parent vessel incorporation.
Inclusion criteria for this study were (1) ruptured MCA aneu-rysm, (2) unruptured MCA aneurysm ≥ 7 mm in size, (3) unrup-tured MCA aneurysm < 7 mm in size with risk factors for aneu-rysm rupture such as previous or family history of subarachnoid hemorrhage (SAH), presence of lobulation or daughter sac, in-creased size on follow-up study, or multiple intracranial aneu-rysms, (4) patient criteria including young age, long life expectan-cy, and patients’ preferred treatment modality, or (5) recurred MCA aneurysm after coiling or clipping. The ruptured patients group was classified according to the Hunt and Hess grading scale (HHGS) to determine the clinical severity of the SAH. The mod-
ified Rankin scale (mRS) score was used to assess the clinical re-sults recorded at each patient’s last follow-up consultation.
1. Endovascular treatment Antiplatelet premedication was not routinely prescribed in the early study period. Most patients with unruptured aneurysms were pre-medicated with dual antiplatelet therapy (aspirin 100 mg, clopidogrel 75 mg once a day) for at least 5 days prior to the procedure according to the patients’ medical condition. But, we did not use prophylactic antiplatelet pre-medication for patients with acutely ruptured aneurysms.
SAH patients were treated within 24 hours after aneurysm rup-ture. In all patients with unruptured aneurysm, the therapeutic procedures were performed during a second angiography session. Local anesthesia was administered to all of the patients and elec-trocardiogram, arterial oxygen saturation, and blood pressure were appropriately monitored. A percutaneous intra-arterial ap-proach was used after a standard Seldinger method and a 6 F in-troducer sheath was placed in the femoral artery. The baseline ac-tivated clotting time (ACT) was obtained before the procedure. Then patients received systemic heparinization and a bolus injec-tion of 3,000 to 5,000 IU heparin just before starting the thera-peutic procedure. A booster of 1,000 IU heparin was administered every hour to provide an ACT of longer than 250 seconds or twice the baseline ACT during the procedure.
A 6 F guiding catheter (Envoy; Cordis Endovascular, Miami Lakes, FL, USA) was positioned in the internal carotid artery (ICA). A 6 F Shuttle sheath was used in patients with tortuous aortic arch and carotid artery anatomy or in cases in which com-plex endovascular techniques were anticipated.
In most cases, coiling was tried first with the conventional sin-gle-catheter technique. When a single-catheter technique failed to make a stable coil mesh or was not suitable due to aneurysm geom-etry, aneurysm neck remodeling techniques using a multi-catheter, balloon, stent, or a combination of these were used.
Immediate angiographic results were classified according to the Raymond classification [13]. Complete occlusion was defined as occlusion of the entire aneurysm sac; neck remnant occlusion, as the minimal portion of the aneurysm neck region filled with con-trast media; and incomplete occlusion, as the aneurysm dome filled with contrast media.
Immediate clinical outcome was evaluated according to the mRS by the neurosurgeons and the interventional neuroradiologist. All patients underwent non-enhanced brain computed tomography (CT) for evaluation of possible hemorrhagic complications and were monitored postoperatively at the intensive care unit.
After the procedure, 2,850 IU of low molecular weight heparin
209https://doi.org/10.12701/yujm.2019.00192
Yeungnam Univ J Med 2019;36(3):208-218
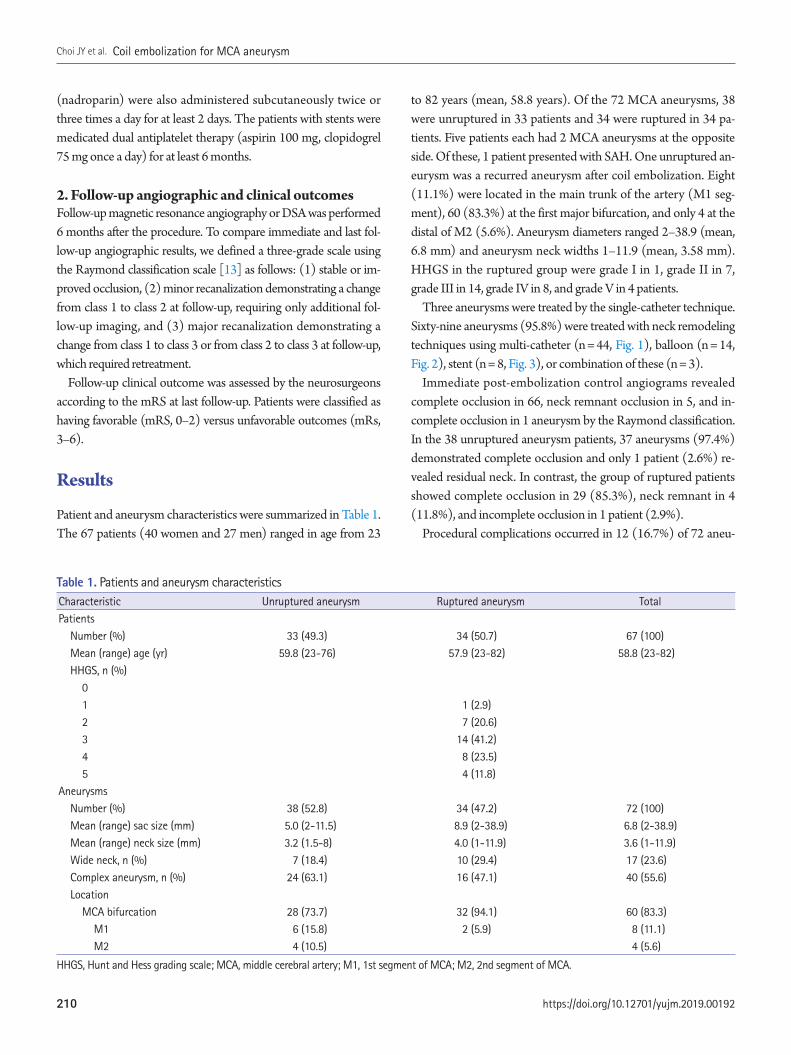
(nadroparin) were also administered subcutaneously twice or three times a day for at least 2 days. The patients with stents were medicated dual antiplatelet therapy (aspirin 100 mg, clopidogrel 75 mg once a day) for at least 6 months.
2. Follow-up angiographic and clinical outcomes Follow-up magnetic resonance angiography or DSA was performed 6 months after the procedure. To compare immediate and last fol-low-up angiographic results, we defined a three-grade scale using the Raymond classification scale [13] as follows: (1) stable or im-proved occlusion, (2) minor recanalization demonstrating a change from class 1 to class 2 at follow-up, requiring only additional fol-low-up imaging, and (3) major recanalization demonstrating a change from class 1 to class 3 or from class 2 to class 3 at follow-up, which required retreatment.
Follow-up clinical outcome was assessed by the neurosurgeons according to the mRS at last follow-up. Patients were classified as having favorable (mRS, 0–2) versus unfavorable outcomes (mRs, 3–6).
Results
Patient and aneurysm characteristics were summarized in Table 1. The 67 patients (40 women and 27 men) ranged in age from 23
to 82 years (mean, 58.8 years). Of the 72 MCA aneurysms, 38 were unruptured in 33 patients and 34 were ruptured in 34 pa-tients. Five patients each had 2 MCA aneurysms at the opposite side. Of these, 1 patient presented with SAH. One unruptured an-eurysm was a recurred aneurysm after coil embolization. Eight (11.1%) were located in the main trunk of the artery (M1 seg-ment), 60 (83.3%) at the first major bifurcation, and only 4 at the distal of M2 (5.6%). Aneurysm diameters ranged 2–38.9 (mean, 6.8 mm) and aneurysm neck widths 1–11.9 (mean, 3.58 mm). HHGS in the ruptured group were grade I in 1, grade II in 7, grade III in 14, grade IV in 8, and grade V in 4 patients.
Three aneurysms were treated by the single-catheter technique. Sixty-nine aneurysms (95.8%) were treated with neck remodeling techniques using multi-catheter (n = 44, Fig. 1), balloon (n = 14, Fig. 2), stent (n = 8, Fig. 3), or combination of these (n = 3).
Immediate post-embolization control angiograms revealed complete occlusion in 66, neck remnant occlusion in 5, and in-complete occlusion in 1 aneurysm by the Raymond classification. In the 38 unruptured aneurysm patients, 37 aneurysms (97.4%) demonstrated complete occlusion and only 1 patient (2.6%) re-vealed residual neck. In contrast, the group of ruptured patients showed complete occlusion in 29 (85.3%), neck remnant in 4 (11.8%), and incomplete occlusion in 1 patient (2.9%).
Procedural complications occurred in 12 (16.7%) of 72 aneu-
Table 1. Patients and aneurysm characteristicsCharacteristic Unruptured aneurysm Ruptured aneurysm TotalPatients Number (%) 33 (49.3) 34 (50.7) 67 (100) Mean (range) age (yr) 59.8 (23-76) 57.9 (23-82) 58.8 (23-82) HHGS, n (%) 0 1 1 (2.9) 2 7 (20.6) 3 14 (41.2) 4 8 (23.5) 5 4 (11.8)Aneurysms Number (%) 38 (52.8) 34 (47.2) 72 (100) Mean (range) sac size (mm) 5.0 (2-11.5) 8.9 (2-38.9) 6.8 (2-38.9) Mean (range) neck size (mm) 3.2 (1.5-8) 4.0 (1-11.9) 3.6 (1-11.9) Wide neck, n (%) 7 (18.4) 10 (29.4) 17 (23.6) Complex aneurysm, n (%) 24 (63.1) 16 (47.1) 40 (55.6) Location MCA bifurcation 28 (73.7) 32 (94.1) 60 (83.3) M1 6 (15.8) 2 (5.9) 8 (11.1) M2 4 (10.5) 4 (5.6)
HHGS, Hunt and Hess grading scale; MCA, middle cerebral artery; M1, 1st segment of MCA; M2, 2nd segment of MCA.
https://doi.org/10.12701/yujm.2019.00192210
Choi JY et al. Coil embolization for MCA aneurysm

rysms. Six of 38 unruptured aneurysms experienced complications, including procedural aneurysm rupture (n=1) and acute thrombo-embolism without neurological deterioration (n =5). Two of 5 acute thromboembolic patients experienced symptomatic acute stroke at 6 and 10 days after treatment. Six of 34 ruptured aneurysm patients experienced complications, including asymptomatic coil migration to the distal vessel (n =1) and acute thromboembolism (n=5) which consisted of 3 asymptomatic embolic infarctions and 2 symptomatic acute strokes.
One unruptured wide-necked aneurysm (5 mm in diameter) was ruptured during stent-assisted coil embolization. The M2
branch was occluded after temporary balloon occlusion of the distal M1 and additional coil embolization for bleeding control. The final angiogram revealed nearly complete occlusion of the an-eurysm sac and no flow compromise. This patient had severe neu-rological deficits after embolization and SAH revealed on post-procedural CT. A follow-up CT the next day revealed SAH and severe brain swelling due to cerebral infarction requiring de-compressive craniectomy. This patient experienced progressive infarction with hemorrhagic transformation and eventually died after 7 days.
Procedural coil migration occurred in one patient with a tiny
Fig. 1. A 43-year-old man presented with a subarachnoid hemorrhage. (A) Anteroposterior oblique view of left internal carotid angiogram shows a wide-necked aneurysm (arrow) at the right middle cerebral artery bifurcation. (B) The aneurysm is treated with two catheter technique (arrowheads). (C) Final control angiogram reveals complete occlusion of the aneurysm (arrow) without flow compromise of the parent artery. (D) Eighteen-month follow-up angiogram shows stable, complete occlusion of the aneurysm (arrow).
A
C
B
D
211https://doi.org/10.12701/yujm.2019.00192
Yeungnam Univ J Med 2019;36(3):208-218

Fig. 2. A 73-year-old woman with a ruptured aneurysm at the left middle cerebral artery bifurcation. (A) Anteroposterior oblique view of left internal carotid angiogram shows an elongated aneurysm (arrows). (B) The aneurysm is treated with balloon-assisted technique (arrow) due to coil protrusion into the parent artery at coil insertion into the neck portion. Immediate post-procedural radiograph (C) and angiogram (D) reveal complete occlusion of the aneurysm (arrow) without coil protrusion into parent artery. Follow-up 18-month angiogram (E) and 41-month magnetic resonance angiogram (F) show stable, complete occlusion of the aneurysm (arrow).
A
C
E
B
D
F
https://doi.org/10.12701/yujm.2019.00192212
Choi JY et al. Coil embolization for MCA aneurysm
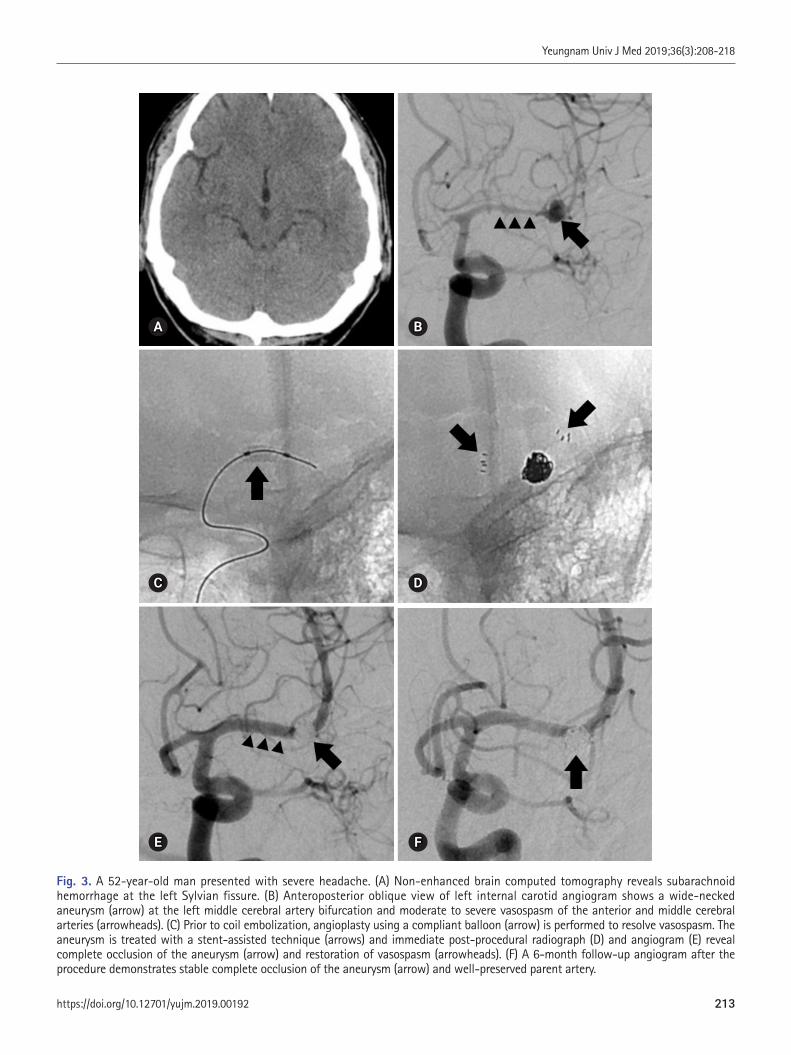
Fig. 3. A 52-year-old man presented with severe headache. (A) Non-enhanced brain computed tomography reveals subarachnoid hemorrhage at the left Sylvian fissure. (B) Anteroposterior oblique view of left internal carotid angiogram shows a wide-necked aneurysm (arrow) at the left middle cerebral artery bifurcation and moderate to severe vasospasm of the anterior and middle cerebral arteries (arrowheads). (C) Prior to coil embolization, angioplasty using a compliant balloon (arrow) is performed to resolve vasospasm. The aneurysm is treated with a stent-assisted technique (arrows) and immediate post-procedural radiograph (D) and angiogram (E) reveal complete occlusion of the aneurysm (arrow) and restoration of vasospasm (arrowheads). (F) A 6-month follow-up angiogram after the procedure demonstrates stable complete occlusion of the aneurysm (arrow) and well-preserved parent artery.
A
C
E
B
D
F
213https://doi.org/10.12701/yujm.2019.00192
Yeungnam Univ J Med 2019;36(3):208-218

ruptured aneurysm (2 mm in diameter) during a balloon-assisted embolization. The detached coil migrated into the distal M2 branch and on post-procedural angiogram, thrombotic occlusion was seen. After intra-arterial administration of a glycoprotein IIb/IIIa inhibitor (abciximab), acute thrombosis was lysed and the distal MCA flow was improved. At the immediate post-procedur-al neurological examination, patients did not show neurological differences compared to before the procedure; long-term fol-low-up DSA showed no flow compromise at the coil migrated distal MCA branch.
Acute thromboembolic complications occurred in 5 unrup-tured and 5 ruptured aneurysms in 10 patients. After intra-arterial administration of a glycoprotein IIb/IIIa inhibitor, acute throm-boembolism was completely lysed in 9 patients, except for one pa-tient with a ruptured aneurysm. One patient without recanaliza-tion after a glycoprotein IIb/IIIa inhibitor injection experienced major cerebral infarction and deterioration of consciousness level after the procedure and finally expired after 3 weeks. One patient with a ruptured aneurysm and recanalization after a glycoprotein IIb/IIIa inhibitor injection presented with progressive infarction within a day and was discharged at mRS2. Two of 5 acute throm-
boembolic patients with unruptured aneurysm presented with symptomatic acute stroke at 6 and 10 days after treatment even though no neurological deterioration was revealed on immediate post-procedural neurologic examination. The patients were dis-charged without neurologic deficit. But, the patients visited the emergency room for acute stroke and were discharged at mRS 1 and 4.
The rate of early post-procedural morbidity and mortality was 6.1% and 3.0% for unruptured aneurysms compared to 2.9% and 2.9% for ruptured aneurysms. As a result, over-all procedure-relat-ed permanent morbidity and mortality rates were 4.5% and 3.0% for unruptured and ruptured aneurysms, respectively. These data are summarized in Table 2.
In the final clinical grading of 33 unruptured aneurysm patients, 2 symptomatic acute stroke patients were discharged at mRS 1 and 4 respectively. One patient improved to mRS 3. None of the surviving patients had any deterioration of functional neurologi-cal outcomes (mRS, 0-2).
Thirty-four patients with ruptured aneurysm were discharged with mRS 0 in 7 patients, mRS 1 in 10 patients, mRS 2 in 3 pa-tients, mRS 3 in 2 patients, mRS 4 in 1 patient, mRS 5 in 4 pa-
Table 2. Endovascular treatment, complications, and angiographic and clinical outcomesUnruptured Ruptured Total
Treatment methods, n (%) Single catheter 1 (2.6) 2 (5.9) 3 (4.2) Multicatheter 23 (60.5) 21 (61.8) 44 (61.1) Balloon-assisted 8 (21.1) 6 (17.6) 14 (19.4) Stent-assisted 4 (10.5) 4 (11.8) 8 (11.1) Combined 2 (5.3) 1 (2.9) 3 (4.2)Procedure-related complications, n (%) Coil migration 1 (2.9) 1 (1.4) Thromboembolism 5 (13.5) 5 (14.3) 10 (13.9) Recanalization with ReoPro 5 (100) 4 (80) 9 (90) Aneurysm rupture 1 (2.7) 1 (1.4)Procedure-related permanent morbidity (%) 6.1 2.9 4.5Procedure-related permanent mortality (%) 3 2.9 3Clinical outcomes, n (%) Favorable (mRS, 0-2) 32 (97.0) 20 (58.8) 52 (77.6) Unfavorable (mRS, 3-6) 1 (3.0) 14 (41.2) 15 (22.4)Immediate angiographic results, n (%) Complete 37 (97.4) 29 (85.3) 66 (91.7) Neck remnant 1 (2.6) 4 (11.8) 5 (6.9) Incomplete 1 (2.9) 1 (1.4)Follow-up angiographic results, n (%) Stable or improved 18 (90.0) 10 (83.3) 28 (87.5) Major recanalization 1 (5.0) 1 (3.1) Minor recanalization 1 (5.0) 2 (16.7) 3 (9.4)
mRS, modified Rankin scale.
https://doi.org/10.12701/yujm.2019.00192214
Choi JY et al. Coil embolization for MCA aneurysm
tients, and mRS 6 in 7 patients. Therefore, there were 20 patients in the favorable outcome group (mRS, 0–2) and 14 patients in the unfavorable outcome group (mRS, 3–6). Seven patients were hospitalized with HHGS IV or V and severe cerebral hemorrhage at the time of visit. They were mostly elderly and expired with se-vere cerebral hemorrhage and other systemic complications in-cluding pneumonia and multiple organ damage.
Clinical follow-up was available only in 12 of 34 ruptured pa-tients because 22 patients were transferred to another hospital, died or outpatient visits were impossible. Thirty-two aneurysms in 31of the 45 patients who could visit as outpatients at least once at 6–24 months (mean, 26 months; range, 6–96 months) received follow-up angiography. Follow-up angiographic results revealed 1 major and 3 minor recanalizations. One major recanalization an-eurysm was re-treated by coiling with no complications.
Discussion
Ausman was the first neurosurgeon to advocate EVT of cerebral aneurysms as a first option treatment in 1997. In his experience, 50% of aneurysms were suitable for EVT [14]. Unlike coiling of other cerebral aneurysm locations, the success rate of MCA coil-ing was initially low at the beginning. In 1999, Regli et al. [2] re-ported on a consecutive series of 30 patients with 34 unruptured MCA aneurysms. Of the 34 aneurysms evaluated, only 2 (6%) were successfully obliterated with endovascular coil embolization. In 32% of the cases, EVT was attempted but abandoned, and in the remaining 62%, surgery was considered the best therapeutic choice. In this series, 94% of the unruptured MCA aneurysms were treated with surgical clipping. Until recently, EVT for MCA aneurysms showed a higher procedural failure rate and inconsis-tent results compared with EVT application to aneurysms at oth-er sites [2,6-8,15,16].
MCA aneurysms have been traditionally considered not ideal for coiling because of their unfavorable anatomic features, includ-ing a wide neck and partial incorporation of 1 or both M2 branch-es [17]. Although the ISAT and some reports [18,19] have con-firmed that EVT was equal or superior to clipping for all aneu-rysms regardless of their location, the treatment of MCA aneu-rysms, which accounted for 14% of aneurysms, is still controver-sial [20]. Recently, with the development of interventional devic-es and technologies, various neck remodeling endovascular tech-niques have attempted to treat MCA aneurysms with complex morphologic features. Even if EVT technology has advanced re-cently, neurovascular surgeons still seem to prefer clipping to coil-ing for MCA aneurysms. Suzuki et al. [15] reported a consecutive series of 115 patients with MCA aneurysms in which only 40% of
patients were treated with coiling. Similarly, another recent study of 152 MCA aneurysms reported that 32.6% of the MCA aneu-rysms were either not considered for EVT or sent to surgery after EVT was attempted [16].
However, the selection rate for EVT of MCA aneurysms did not appear to be due to the difficulty of treating aneurysms via this technique. It seems that the difference is between medical in-stitutions that consider MCA aneurysm embolization to be the first treatment modality and institutions that still believe surgery is the predominant treatment modality for MCA aneurysms. For example, there are some centers where embolization is the first treatment option considered [7,10]. In contrast, some institutions have applied very stringent criteria to select MCA aneurysm pa-tients who will be treated with EVT. Raftopoulos et al. [4] chose EVT only when the ratio of neck to sac was less than 1:3. Our neurovascular team considered EVT as the first treatment modal-ity for MCA aneurysms. Although almost all MCA aneurysms (95.8%) were treated with neck remodeling techniques, the tech-nical success rate of EVT was 100% in this study. EVT for MCA aneurysms could be a technically feasible treatment strategy.
One major concern about EVT for MCA aneurysms is proce-dure-related complications. Choi et al. [21] compared the out-comes of clipping and coiling and evaluated the benefits of clip-ping for 178 ruptured and unruptured MCA aneurysms. Inclu-sion criteria for coiling were very strict and only 25 of 178 MCA aneurysms were treated by coiling. In their study, a multidisci-plinary neurovascular team decided the treatment strategy (obser-vation, clip, or coil) after discussion. If they expected there would be no definite benefits between the 2 treatment options (clip or coil) in terms of patient outcome and perioperative complica-tions, they primarily chose microsurgical clipping. EVTs were considered in some selected cases that lacked complexity such as a relatively small neck ( ≤ 4 mm), large dome-to-neck ratio ( > 1.5), no incorporated branches in angiographic findings, clini-cally ruptured aneurysms with a high Hunt-Hess grade and/or use of medications such as warfarin. In the surgical group, periop-erative complications occurred in 17 patients (11.1%). However, in the strictly selected EVT group, 8 patients (32%) experienced procedural complications (25% in the ruptured group and 35% in the unruptured group). Therefore, the complication rate for MCA embolization may seem to be high. However, most of the compli-cations included 5 asymptomatic embolic infarctions observed on diffusion magnetic resonance (MR) imaging and 1 asymptomatic intraprocedural aneurysm rupture. Furthermore, there were no cases of procedure-related morbidity and mortality in the EVT group. Their results suggested that EVT for MCA aneurysms in selected patients can be effectively performed but the complica-
215https://doi.org/10.12701/yujm.2019.00192
Yeungnam Univ J Med 2019;36(3):208-218

tion rate is not negligible. Generally, complications during EVT were stratified into three
groups: (1) thromboembolic complications, (2) parent artery oc-clusion, and (3) aneurysm perforation [22]. But, it is not easy to analyze EVT complications compared to the complications of surgery. Because complications were determined by the neuroint-erventionalist who performed the procedure, there are many oth-er factors that can or cannot be classified as complications.
The first reason is that EVT cases have not been analyzed yet and there are not enough to compare to clipping cases. The next reason is that the definition of EVT complications is vague and unclear. In the case of asymptomatic embolic infarction, institu-tions which perform MR diffusion after the procedure report it as a complication. But, it is not a complication at institutions that do not perform MR diffusion after the procedure.
In addition, aneurysm rupture during clipping is not classified as a complication. This is probably because most of them are con-trollable in the surgical field and do not cause other serious symp-toms. Unlike clipping, aneurysm ruptures during embolization may cause serious symptoms and may lead to death or disability. However, many cases of intraprocedural rupture can be treated as-ymptomatically. Therefore, it is unclear if asymptomatic rupture should be classified as a complication.
Most of the complications in this study were thromboembo-lism. We thought at first this was related to antiplatelet premedi-cation. Thromboembolic complications occurred mainly in pa-tients who did not receive premedication. In the early days of at-tempting unruptured MCA coiling, premedication was not ad-ministrated.
The second cause of thromboembolism was related to selection criteria and the endovascular technique. We performed EVT as a first treatment for MCA aneurysms regardless of their morpho-logical complexity. Most cases (95.8%) could by treated by neck-remodeling techniques using multiple catheters, balloon, or stent. These complex procedures using multiple intravascular de-vices were known to be a cause of thromboembolic complications [23].
Lastly, we performed the procedure with the goal of complete occlusion. Therefore, immediate angiographic outcomes revealed complete occlusion in 66 cases (91.7%) by the Raymond classifi-cation. Trying complete occlusion of an aneurysm may be likely to increase the incidence of thromboembolic complications during the procedure. Quadros et al. [7] prioritized prevention of thromboembolic complications during MCA aneurysm coiling. They did not treat with a complex, neck-remodeling technique in many cases and left the neck portion of the aneurysms to reduce the rate of thromboembolic complications.
Fortunately, thromboembolism could be prevented or resolved with administration of antiplatelet premedication or glycoprotein IIb/IIIa inhibitors. In this study, thromboembolism occurred in 10 patients. Although 2 patients experienced immediate post-pro-cedural symptomatic ischemic events, procedural thromboembo-lism was completely lysed with intra-arterial administration of gly-coprotein IIb/IIIa inhibitor. Therefore, like intraprocedural aneu-rysm rupture, it is unclear that the asymptomatic procedural thromboembolism should be classified as a complication.
Another major concern is the recurrence rate after coiling for MCA aneurysms [7]. Immediate angiographic complete occlu-sion was known to an important factor for decreasing recurrence rate after coiling [24]. Brinjikji at al. [22] reported in a review arti-cle of 12 series that post-operative complete occlusion was 82.4% and follow-up results of 758 aneurysms demonstrated that 70 (9.3%) had a minor recurrence not requiring re-treatment and 73 (9.6%) had major recanalization requiring retreatment. Overall angiographic stability or progression to better obliteration was re-ported in 81% of patients undergoing follow-up angiography. However, in our series, immediate angiographic outcomes were 91.7% complete occlusion; only 1 major recanalization (3.1%) was detected on follow-up angiography. We thought that this fol-low-up angiographic outcome might be related to complete occlu-sion immediately after the procedure.
There are some limitations in this study. First, this is a retro-spective study and included a small number of MCA aneurysm cases at only 1 institution. Second is patient selection bias. As mentioned above, EVT is a first treatment option for MCA aneu-rysms in this study regardless of aneurysm morphological com-plexity. Considering improved operator experience and devices, our result may not represent the general situation of MCA coiling in this era because our cases were collected over 10 years.
Coil embolization of MCA aneurysms could be a technically feasible and clinically effective treatment strategy with acceptable angiographic and clinical outcomes. In the future, increased oper-ator experience, improved new devices, and various neck-remod-eling techniques might greatly increase the feasibility and efficacy of MCA aneurysm coiling.
However, the safety and efficacy of this technique as compared to surgical clipping remains to be determined.
Acknowledgements
This work was supported by a 2-Year Research Grant of Pusan National University.
https://doi.org/10.12701/yujm.2019.00192216
Choi JY et al. Coil embolization for MCA aneurysm

Conflicts of interest
No potential conflicts of interest relevant to this article was report-ed.
ORCID
Jae Young Choi, https://orcid.org/0000-0002-2227-3216Chang Hwa Choi, https://orcid.org/0000-0001-6430-1396Jun Kyeung Ko, https://orcid.org/0000-0002-5652-7659Jae Il Lee, https://orcid.org/0000-0003-1412-4146Chae Wook Huh, https://orcid.org/0000-0002-7020-0468Tae Hong Lee, https://orcid.org/0000-0002-6176-8086
References
1. Molyneux A, Kerr R, Stratton I, Sandercock P, Clarke M, Shrimp-ton J, et al. International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 pa-tients with ruptured intracranial aneurysms: a randomised trial. Lancet 2002;360:1267–74.
2. Regli L, Uske A, de Tribolet N. Endovascular coil placement compared with surgical clipping for the treatment of unruptured middle cerebral artery aneurysms: a consecutive series. J Neuro-surg 1999;90:1025–30.
3. Regli L, Dehdashti AR, Uske A, de Tribolet N. Endovascular coil-ing compared with surgical clipping for the treatment of unrup-tured middle cerebral artery aneurysms: an update. Acta Neuro-chir Suppl 2002;82:41–6.
4. Raftopoulos C, Mathurin P, Boscherini D, Billa RF, van Boven M, Hantson P. Prospective analysis of aneurysm treatment in a se-ries of 103 consecutive patients when endovascular emboliza-tion is considered the first option. J Neurosurg 2000;93:175–82.
5. Iijima A, Piotin M, Mounayer C, Spelle L, Weill A, Moret J. Endo-vascular treatment with coils of 149 middle cerebral artery berry aneurysms. Radiology 2005;237:611–9.
6. Doerfler A, Wanke I, Goericke SL, Wiedemayer H, Engelhorn T, Gizewski ER, et al. Endovascular treatment of middle cerebral artery aneurysms with electrolytically detachable coils. AJNR Am J Neuroradiol 2006;27:513–20.
7. Quadros RS, Gallas S, Noudel R, Rousseaux P, Pierot L. Endo-vascular treatment of middle cerebral artery aneurysms as first option: a single center experience of 92 aneurysms. AJNR Am J Neuroradiol 2007;28:1567–72.
8. Horowitz M, Gupta R, Gologorsky Y, Jovin T, Genevro J, Levy E, et al. Clinical and anatomic outcomes after endovascular coiling of middle cerebral artery aneurysms: report on 30 treated aneu-
rysms and review of the literature. Surg Neurol 2006;66:167–71.9. Kim J, Chang C, Jung Y. Feasibility and midterm outcomes of en-
dovascular coil embolization of an unruptured middle cerebral artery aneurysm with an incorporated branch. World Neurosurg 2018;118:e745–52.
10. Kim BM, Park SI, Kim DJ, Kim DI, Suh SH, Kwon TH, et al. Endovascular coil embolization of aneurysms with a branch in-corporated into the sac. AJNR Am J Neuroradiol 2010;31:145–51.
11. Lubicz B, Leclerc X, Gauvrit JY, Lejeune JP, Pruvo JP. Hyper-Form remodeling-balloon for endovascular treatment of wide-neck intracranial aneurysms. AJNR Am J Neuroradiol 2004;25:1381–3.
12. Lubicz B, Lefranc F, Levivier M, Dewitte O, Pirotte B, Brotchi J, et al. Endovascular treatment of intracranial aneurysms with a branch arising from the sac. AJNR Am J Neuroradiol 2006; 27:142–7.
13. Roy D, Milot G, Raymond J. Endovascular treatment of unrup-tured aneurysms. Stroke 2001;32:1998–2004.
14. Ausman JI. The future of neurovascular surgery. Part I: intracra-nial aneurysms. Surg Neurol 1997;48:98–100.
15. Suzuki S, Tateshima S, Jahan R, Duckwiler GR, Murayama Y, Gonzalez NR, et al. Endovascular treatment of middle cerebral artery aneurysms with detachable coils: angiographic and clini-cal outcomes in 115 consecutive patients. Neurosurgery 2009; 64:876–88.
16. Bracard S, Abdel-Kerim A, Thuillier L, Klein O, Anxionnat R, Finitsis S, et al. Endovascular coil occlusion of 152 middle cere-bral artery aneurysms: initial and midterm angiographic and clinical results. J Neurosurg 2010;112:703–8.
17. Jayaraman MV, Do HM, Versnick EJ, Steinberg GK, Marks MP. Morphologic assessment of middle cerebral artery aneurysms for endovascular treatment. J Stroke Cerebrovasc Dis 2007; 16:52–6.
18. Higashida RT, Lahue BJ, Torbey MT, Hopkins LN, Leip E, Han-ley DF. Treatment of unruptured intracranial aneurysms: a na-tionwide assessment of effectiveness. AJNR Am J Neuroradiol 2007;28:146–51.
19. van Rooij WJ, Sluzewski M. Procedural morbidity and mortality of elective coil treatment of unruptured intracranial aneurysms. AJNR Am J Neuroradiol 2006;27:1678–80.
20. Molyneux AJ, Kerr RS, Yu LM, Clarke M, Sneade M, Yarnold JA, et al. International subarachnoid aneurysm trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 pa-tients with ruptured intracranial aneurysms: a randomised comparison of effects on survival, dependency, seizures, re-bleeding, subgroups, and aneurysm occlusion. Lancet 2005;
217https://doi.org/10.12701/yujm.2019.00192
Yeungnam Univ J Med 2019;36(3):208-218

366:809–17. 21. Choi JH, Park JE, Kim MJ, Kim BS, Shin YS. Aneurysmal neck
clipping as the primary treatment option for both ruptured and unruptured middle cerebral artery aneurysms. J Korean Neuro-surg Soc 2016;59:269–75.
22. Brinjikji W, Lanzino G, Cloft HJ, Rabinstein A, Kallmes DF. En-dovascular treatment of middle cerebral artery aneurysms: a systematic review and single-center series. Neurosurgery 2011; 68:397–402.
23. Kim SR, Vora N, Jovin TG, Gupta R, Thomas A, Kassam A, et al. Anatomic results and complications of stent-assisted coil em-bolization of intracranial aneurysms. Interv Neuroradiol 2008; 14:267–84.
24. Nishido H, Piotin M, Bartolini B, Pistocchi S, Redjem H, Blanc R. Analysis of complications and recurrences of aneurysm coil-ing with special emphasis on the stent-assisted technique. AJNR Am J Neuroradiol 2014;35:339–44.
https://doi.org/10.12701/yujm.2019.00192218
Choi JY et al. Coil embolization for MCA aneurysm

Background: Korea has shown a rapid pace of aging and has become an aged society in a shorter period than Western countries. Therefore, it is important that middle-aged workers maintain their ability to work in the industrial field at the maximum level while maintaining their health. The purpose of this study was to analyze the factors affecting work ability and to use this data to maintain the working ability of middle-aged workers in the future. Methods: From 2015 to 2017, we surveyed 371 street cleaners who visited a health center for health promotion in a metropolitan city. The relationship between the general characteristics of the survey subjects and the Work Ability Index (WAI) was confirmed by a univariate analysis. Sta-tistically significant (p<0.2) factors were selected and a multiple linear regression analysis was conducted with WAI scores as a dependent variable. Results: Age, body mass index, body fat percentage, the Alcohol Use Disorders Identification Test-Korea (AUDIT-K) scores, the Psychosocial Well-Being Index-Short Form (PWI-SF) scores, maximal oxygen consumption (VO2max), and hypertension showed statistically significant correla-tions with the WAI in the univariate analysis. In the multivariate analysis, the VO2max, AUDIT-K scores, and PWI-SF scores were included in the regression equation. VO2max had the greatest ef-fect on the standardization coefficient indicating the relative contribution of independent vari-ables, followed by the AUDIT-K scores and the PWI-SF scores. Conclusion: Programs to increase workers’ physical work ability and alleviate psychosocial stress and drinking habits should be developed and implemented in the future.
Keywords: Middle aged; Oxygen consumption; Physical endurance; Work ability evaluation
Factors that determine the Work Ability Index of street cleaners Jung Won Kim1, Seonhee Yang1, Insung Chung1,2, Mi-Young Lee1,2
1Department of Occupational and Environment Medicine, Keimyung University Donsan Medical Center, Daegu, Korea 2Department of Preventive Medicine, Keimyung University School of Medicine, Daegu, Korea
Original articleeISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):219-224https://doi.org/10.12701/yujm.2019.00199
Received: October 30, 2018 Revised: April 11, 2019 Accepted: April 23, 2019
Corresponding author: Mi-Young LeeDepartment of Preventive Medicine, Keimyung University School of Medicine, 1095, Dalgubeol-daero, Dalseo-gu, Daegu 42601, Korea Tel: +82-53-250-7874Fax: +82-53-250-7850E-mail: [email protected]
Introduction
According to the Korea National Statistical Office, most street cleaners are over 50 years old; the mean age of street cleaners is 58.4 years, which is higher than the average ages of other work-ers—for instance, 50.4 years for managers, 38.5 years for profes-sional workers, 39.6 years for office workers, 45.5 years for ser-vice workers, 39.1 years for sales workers, and 44.0 years for agri-cultural workers [1]. As of August 2018, the labor force partici-
pation rate of the elderly is 69.1%, and the employment rate of the elderly is 66.9% [2]. It is therefore important that mid-dle-aged workers be able to maintain their health in the industrial setting and exercise their maximum work ability.
Work ability is the ability to carry out a given job well and to maintain physical and mental health. In Europe, a number of studies have indicated that increasing age reduces working ability [3-5]. Decreases in the youth population due to aging and in-creases in the mean age of the workforce are associated with re-
219https://doi.org/10.12701/yujm.2019.00199
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

duced work productivity owing to reduced working ability [6]. As workers age, disability and illness increase due to reduced working ability and declining physical and mental abilities [7]. According to the U.S. Bureau of Labor Statistics, the number of major accidents among street cleaners in 2016 was 5.7 per 1,000 workers, with 439 being industrial accidents, making it the fourth most dangerous job in the US [8].
Working ability largely involves power of the muscles and re-spiratory system to determine how much work can be done in a given amount of time and how long one can last at the same strength. Therefore, we used maximal oxygen consumption (VO2max) as an indicator of aerobic work ability. VO2max is highly correlated with total endurance including cardiopulmonary abili-ty, oxygen transport ability of the blood, and oxygen utilization ability of tissues [9].
In addition to age and aerobic work ability, work performance, body mass index, personal health status, and psychosocial stress have been reported to affect Work Ability Index (WAI) [10-13]. The relationship between age and WAI is controversial. While there are studies reporting negative correlations between age and WAI due to decreased physical ability, cognitive ability, and reac-tion rates in elderly people, there is also a study reporting a posi-tive correlation owing to increasing work proficiency [10]. Addi-tionally, there are studies reporting no correlation between age and WAI [13].
A few reports indicate other factors affecting the WAI besides psychosocial stress, age, work type, and aerobic work ability, and there are also a few regarding drinking habits and WAI. There-fore, it is important to understand the relationship between age and WAI and to identify other factors that affect WAI, including drinking habits.
The purpose of this study was to identify the factors affecting the WAIs of street cleaners and to use these data for the evalua-tion and management of working ability among middle-aged workers in the future.
Materials and methods
The study population comprised 411 street cleaners who visited occupational health facilities in Daegu from 2015 to 2017. Of these, 371 people were included in the final study population af-ter excluding 28 cases including a small percentage of female cas-es, 10 cases of individuals with existing cerebral cardiovascular disease or pulmonary disease, and two cases of incomplete re-sponses to the questionnaire.
Body fat and skeletal muscle percentage rate were measured using an Inbody 770 (InBody Korea [HQ], Seoul, Korea). The
Alcohol Use Disorders Identification Test-Korea (AUDIT-K) was conducted with scores ranging from 0 to 27. Higher scores indicated a higher risk of a drinking habit. Drinking status was categorized as "low" if the score was below 11 and otherwise "high" [14]. The Psychosocial Well-Being Index-Short Form (PWI-SF) questionnaire was used to assess psychosocial stress on 4-point scale; each item was assigned a score of 0-1-2-3 and the scores were added up. On a scale of 0 to 54, scores lower than 27 were classified as "low," meaning low stress, and higher scores were classified as "high" [15].
Work ability was assessed using the WAI questionnaire. The WAI questionnaire [16]: consists of seven items on physical, mental, and social competence. Each item has a range of 0 to 10, and on item 1, current work ability is measured on a 10-point scale as compared to most active work ability. On item 2, physical and mental conditions related to job performance are measured on a 5-point scale. The weight for each item is given differently depending on whether the worker has a blue-collar or white-col-lar occupation. On item 3, a score is given based on the number of diseases diagnosed by a doctor (1 point for more than 5 dis-eases, 7 points for no disease). On item 4, the degree of occupa-tional disability due to disease is measured on a 6-point scale. Item 5 is measured on a 5-point scale assessing the number of days of absence or illness, and item 6 is measured on a 7-point scale measuring the extent to which the respondent expects to be able to continue working after 2 years. On item 7, the mental health status of workers is further divided and the results are summed to obtain a score. The total score is evaluated from a minimum of 7 points to a maximum of 49 points.
The VO2max was calculated using the Bruce equation (85.42–13.73 × sex–0.409 × age [yr]) –3.24–0.114 × weight (kg).
In this study, an independent t-test and a correlation test were performed to investigate the variables that affect WAI. The ad-justment variables, which showed p-values ≤ 0.2 in the univariate analysis, were included in the multiple logistic regression as inde-pendent variables. WAI was the dependent variable. All statistical analyses were performed using IBM SPSS version 25.0 (IBM Co., Armonk, NY, USA). This study was approved by the Institu-tional Review Board of Keimyung University Hospital (2019-03-047-001).
Results
The ages of the 371 subjects ranged from 21 to 70 years, and the mean age was 48.6 years (Table 1). There was a statistically sig-nificant negative correlation between age and WAI (Table 2). As age increased, WAI tended to decrease (Table 3).
https://doi.org/10.12701/yujm.2019.00199220
Kim JW et al. Factors that determine Work Ability Index
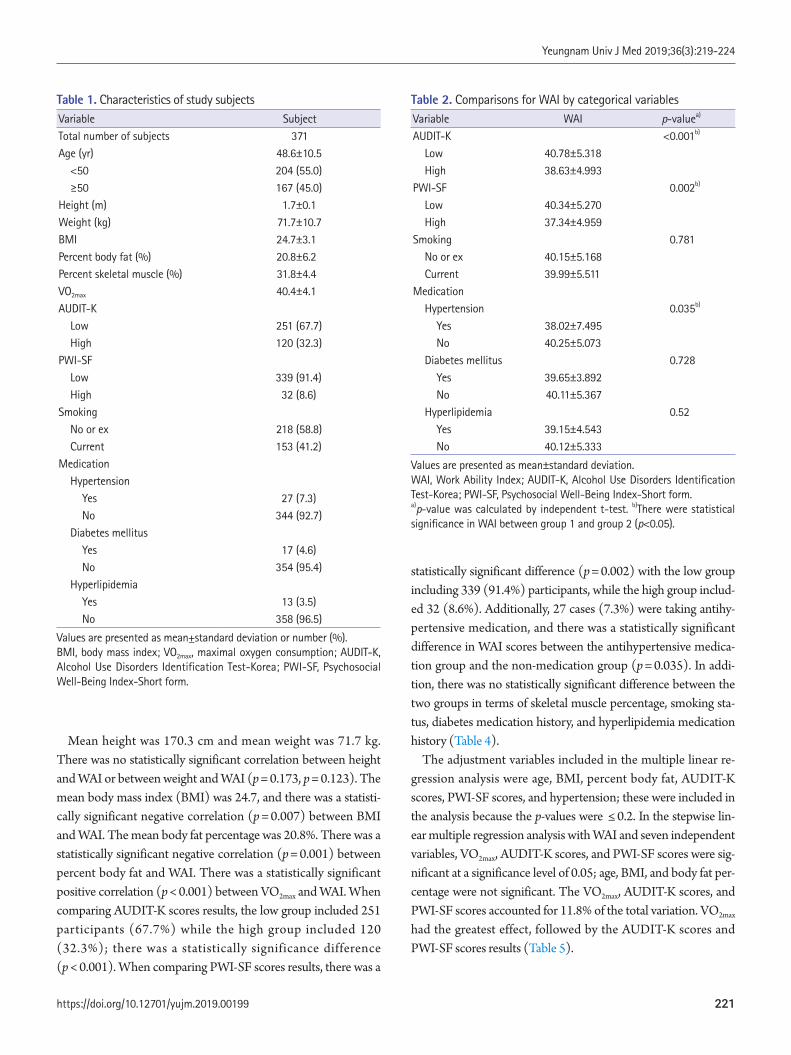
Table 1. Characteristics of study subjectsVariable SubjectTotal number of subjects 371Age (yr) 48.6±10.5 <50 204 (55.0) ≥50 167 (45.0)Height (m) 1.7±0.1Weight (kg) 71.7±10.7BMI 24.7±3.1Percent body fat (%) 20.8±6.2Percent skeletal muscle (%) 31.8±4.4VO2max 40.4±4.1AUDIT-K Low 251 (67.7) High 120 (32.3)PWI-SF Low 339 (91.4) High 32 (8.6)Smoking No or ex 218 (58.8) Current 153 (41.2)Medication Hypertension Yes 27 (7.3) No 344 (92.7) Diabetes mellitus Yes 17 (4.6) No 354 (95.4) Hyperlipidemia Yes 13 (3.5) No 358 (96.5)
Values are presented as mean±standard deviation or number (%).BMI, body mass index; VO2max, maximal oxygen consumption; AUDIT-K, Alcohol Use Disorders Identification Test-Korea; PWI-SF, Psychosocial Well-Being Index-Short form.
Table 2. Comparisons for WAI by categorical variablesVariable WAI p-valuea)
AUDIT-K <0.001b)
Low 40.78±5.318 High 38.63±4.993PWI-SF 0.002b)
Low 40.34±5.270 High 37.34±4.959Smoking 0.781 No or ex 40.15±5.168 Current 39.99±5.511Medication Hypertension 0.035b)
Yes 38.02±7.495 No 40.25±5.073 Diabetes mellitus 0.728 Yes 39.65±3.892 No 40.11±5.367 Hyperlipidemia 0.52 Yes 39.15±4.543 No 40.12±5.333
Values are presented as mean±standard deviation.WAI, Work Ability Index; AUDIT-K, Alcohol Use Disorders Identification Test-Korea; PWI-SF, Psychosocial Well-Being Index-Short form.a)p-value was calculated by independent t-test. b)There were statistical significance in WAI between group 1 and group 2 (p<0.05).
Mean height was 170.3 cm and mean weight was 71.7 kg. There was no statistically significant correlation between height and WAI or between weight and WAI (p = 0.173, p = 0.123). The mean body mass index (BMI) was 24.7, and there was a statisti-cally significant negative correlation (p = 0.007) between BMI and WAI. The mean body fat percentage was 20.8%. There was a statistically significant negative correlation (p = 0.001) between percent body fat and WAI. There was a statistically significant positive correlation (p < 0.001) between VO2max and WAI. When comparing AUDIT-K scores results, the low group included 251 participants (67.7%) while the high group included 120 (32.3%); there was a statistically significance difference (p < 0.001). When comparing PWI-SF scores results, there was a
statistically significant difference (p = 0.002) with the low group including 339 (91.4%) participants, while the high group includ-ed 32 (8.6%). Additionally, 27 cases (7.3%) were taking antihy-pertensive medication, and there was a statistically significant difference in WAI scores between the antihypertensive medica-tion group and the non-medication group (p = 0.035). In addi-tion, there was no statistically significant difference between the two groups in terms of skeletal muscle percentage, smoking sta-tus, diabetes medication history, and hyperlipidemia medication history (Table 4).
The adjustment variables included in the multiple linear re-gression analysis were age, BMI, percent body fat, AUDIT-K scores, PWI-SF scores, and hypertension; these were included in the analysis because the p-values were ≤ 0.2. In the stepwise lin-ear multiple regression analysis with WAI and seven independent variables, VO2max, AUDIT-K scores, and PWI-SF scores were sig-nificant at a significance level of 0.05; age, BMI, and body fat per-centage were not significant. The VO2max, AUDIT-K scores, and PWI-SF scores accounted for 11.8% of the total variation. VO2max had the greatest effect, followed by the AUDIT-K scores and PWI-SF scores results (Table 5).
221https://doi.org/10.12701/yujm.2019.00199
Yeungnam Univ J Med 2019;36(3):219-224
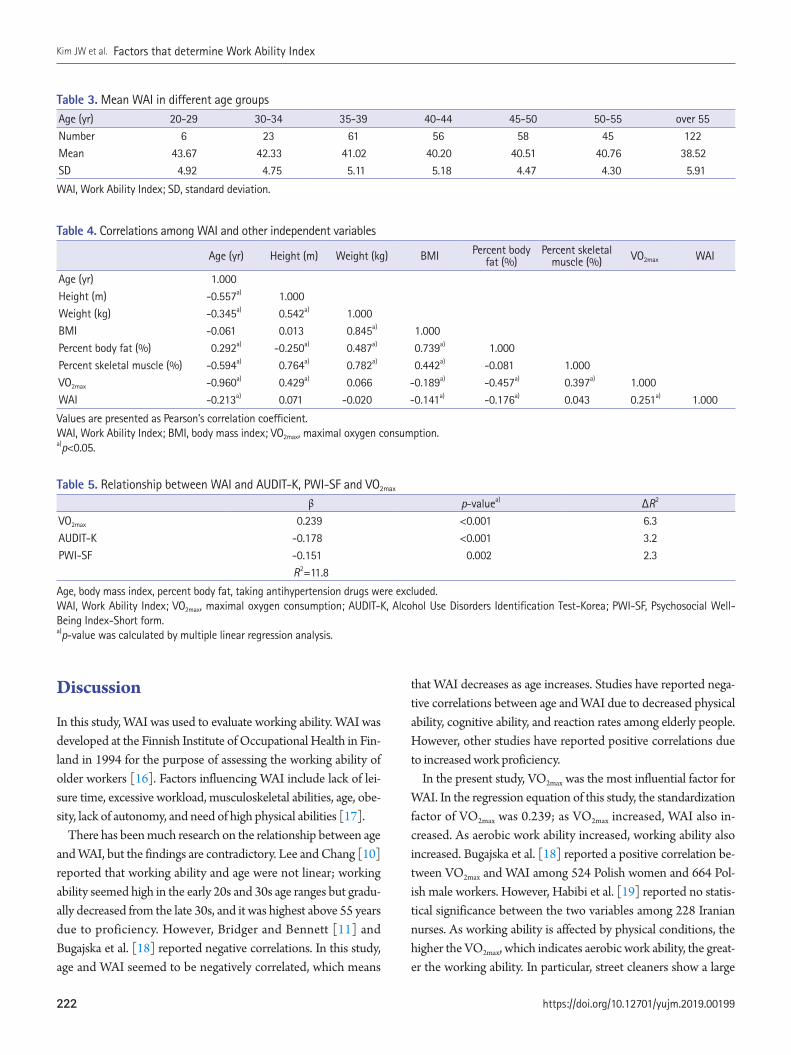
Discussion
In this study, WAI was used to evaluate working ability. WAI was developed at the Finnish Institute of Occupational Health in Fin-land in 1994 for the purpose of assessing the working ability of older workers [16]. Factors influencing WAI include lack of lei-sure time, excessive workload, musculoskeletal abilities, age, obe-sity, lack of autonomy, and need of high physical abilities [17].
There has been much research on the relationship between age and WAI, but the findings are contradictory. Lee and Chang [10] reported that working ability and age were not linear; working ability seemed high in the early 20s and 30s age ranges but gradu-ally decreased from the late 30s, and it was highest above 55 years due to proficiency. However, Bridger and Bennett [11] and Bugajska et al. [18] reported negative correlations. In this study, age and WAI seemed to be negatively correlated, which means
that WAI decreases as age increases. Studies have reported nega-tive correlations between age and WAI due to decreased physical ability, cognitive ability, and reaction rates among elderly people. However, other studies have reported positive correlations due to increased work proficiency.
In the present study, VO2max was the most influential factor for WAI. In the regression equation of this study, the standardization factor of VO2max was 0.239; as VO2max increased, WAI also in-creased. As aerobic work ability increased, working ability also increased. Bugajska et al. [18] reported a positive correlation be-tween VO2max and WAI among 524 Polish women and 664 Pol-ish male workers. However, Habibi et al. [19] reported no statis-tical significance between the two variables among 228 Iranian nurses. As working ability is affected by physical conditions, the higher the VO2max, which indicates aerobic work ability, the great-er the working ability. In particular, street cleaners show a large
Table 4. Correlations among WAI and other independent variables
Age (yr) Height (m) Weight (kg) BMI Percent body fat (%)
Percent skeletal muscle (%) VO2max WAI
Age (yr) 1.000Height (m) -0.557a) 1.000Weight (kg) -0.345a) 0.542a) 1.000BMI -0.061 0.013 0.845a) 1.000Percent body fat (%) 0.292a) -0.250a) 0.487a) 0.739a) 1.000Percent skeletal muscle (%) -0.594a) 0.764a) 0.782a) 0.442a) -0.081 1.000VO2max -0.960a) 0.429a) 0.066 -0.189a) -0.457a) 0.397a) 1.000WAI -0.213a) 0.071 -0.020 -0.141a) -0.176a) 0.043 0.251a) 1.000
Values are presented as Pearson’s correlation coefficient.WAI, Work Ability Index; BMI, body mass index; VO2max, maximal oxygen consumption.a)p<0.05.
Table 5. Relationship between WAI and AUDIT-K, PWI-SF and VO2max
β p-valuea) ΔR2
VO2max 0.239 <0.001 6.3AUDIT-K -0.178 <0.001 3.2PWI-SF -0.151 0.002 2.3
R2=11.8
Age, body mass index, percent body fat, taking antihypertension drugs were excluded.WAI, Work Ability Index; VO2max, maximal oxygen consumption; AUDIT-K, Alcohol Use Disorders Identification Test-Korea; PWI-SF, Psychosocial Well-Being Index-Short form.a)p-value was calculated by multiple linear regression analysis.
Table 3. Mean WAI in different age groupsAge (yr) 20-29 30-34 35-39 40-44 45-50 50-55 over 55Number 6 23 61 56 58 45 122Mean 43.67 42.33 41.02 40.20 40.51 40.76 38.52SD 4.92 4.75 5.11 5.18 4.47 4.30 5.91
WAI, Work Ability Index; SD, standard deviation.
https://doi.org/10.12701/yujm.2019.00199222
Kim JW et al. Factors that determine Work Ability Index

correlation between VO2max and WAI because they engage in many outdoor activities.
The standardization factor of the AUDIT-K scores was -0.178, and the standardization factor of the PWI-SF scores was -0.151. In this study, the groups with good drinking habits and low psy-chosocial stress had great working ability. Hur et al. [15] reported that there was no statistically significant relationship between drinking habits and work ability, but reported that working abili-ty decreased with increasing psychosocial stress. Ye et al. [20] re-ported that the higher the level of psychosocial stress, the lower the working ability. Kim and Kim [13] and Lee et al. [14] also re-ported that stress and WAI were negatively correlated. It is sug-gested that stress management is helpful for improving work ability. The relationship between drinking habits and working ability were unknown in previous studies. In the present study, the group with good drinking habits showed higher WAI. Alco-hol weakens attentiveness, motor coordination abilities, and re-sponse speed to external stimuli; thus, post-drinking tasks show reduced job accuracy and efficiency. There is also the possibility of reducing working ability by increasing impulsive behavior and weakening temperance. Therefore, proper drinking habits should improve work ability.
In this study we used the WAI, which can visually evaluate the abstract concept of working ability, to increase the reliability of the study. Age and also body fat percentage, alcohol status, and psychosocial stress were included as independent factors.
The present study has several limitations. It is difficult to gen-eralize the findings because it investigated mostly male street cleaners in only one area. Factors such as job stress or shift work may also affect work ability, but these factors are not reflected. In addition, there is a limitation in that VO2max cannot be obtained directly but was estimated using an indirect formula.
The significant findings of this study showed that aerobic physical ability, drinking habits, and psychosocial stress were cor-related with working ability. Experimental evaluation of working ability, such as oxygen consumption and maximum heart rate, has the advantage of obtaining accurate results under constrained conditions, but it is difficult to apply at the worksite, and there are also time and cost constraints. On the other hand, work per-formance evaluation using the WAI questionnaire is subjective. Reliability is not high compared with the experiment, but this evaluation method is simple, time and cost effective, and easy to apply at the actual work site. Therefore, middle-aged workers will be able to utilize WAI as an indicator of their working ability in programs that can then easily evaluate and maintain their physi-cal ability.
ORCID
Jung Won Kim, https://orcid.org/0000-0002-7090-5687Seon Hee Yang, https://orcid.org/0000-0002-2487-1324In Sung Jung, https://orcid.org/0000-0001-8532-1070Mi Young Lee, https://orcid.org/0000-0002-2210-3890
Conflicts of interest
No potential conflicts of interest relevant to this article was re-ported.
References
1. Statistics Korea. [ Job, gender, salary and working conditions] [Internet]. Daejeon: Statistics Korea; 2018 [cited 2018 October 5]. http://kosis.kr/statHtml/statHtml.do?orgId = 118&t-blId= DT_118N_PAYM31&conn_path= I2
2. Statistics Korea. [Employment trends for the elderly] [Internet]. Daejeon: Statistics Korea; 2018 [cited 2018 October 5]. http://www.index.go.kr/potal/main/EachDtlPageDetail.do?idx_cd= 1496
3. Ilmarinen J, Tuomi K, Klockars M. Changes in the work ability of active employees over an 11-year period. Scand J Work Environ Health 1997;23(Suppl 1):49–57.
4. Tuomi K, Huuhtanen P, Nykyri E, Ilmarinen J. Promotion of work ability, the quality of work and retirement. Occup Med (Lond) 2001;51:318–24.
5. Liira J, Matikainen E, Leino-Arjas P, Malmivaara A, Mutanen P, Rytkönen H, et al. Work ability of middle-aged Finnish construc-tion workers - a follow-up study in 1991-1995. Int J Ind Ergon 2000;25:477–81.
6. de Zwart BC, Frings-Dresen MH, van Dijk FJ. Physical workload and the aging worker: a review of the literature. Int Arch Occup Environ Health 1995;68:1–12.
7. Kim YU, Kim JG. The evaluation of work ability and job stress for subway worker. J Korean Soc Saf 2008;23:85–9.
8. U.S. Bureau of Labor Statistics. 2016 Census of Fatal Occupation-al Injuries (final data) [Internet]. Washinton, DC: U.S. Bureau of Labor Statistics; 2017 [cited 2018 October 5]. https://www.bls.gov/iif/oshcfoi1.htm#2016
9. Wagner PD. New ideas on limitations to VO2max. Exerc Sport Sci Rev 2000;28:10–4.
10. Lee YJ, Chang SR. A study on the Work Ability Index by the type of business, age and job. J Ergon Soc Korea 2010;29:101–5.
11. Bridger RS, Bennett AI. Age and BMI interact to determine work ability in seafarers. Occup Med (Lond) 2011;61:157–62.
223https://doi.org/10.12701/yujm.2019.00199
Yeungnam Univ J Med 2019;36(3):219-224
12. Lee YJ, Chang SR. A study on the job stress and the work ability of workers in the shipbuilding industry. J Korean Soc Saf 2010;25:71–7.
13. Kim YC, Kim JK. A study on evaluation of work ability and job stress for doctor. J Ergon Soc Korea 2008;27:9–14.
14. Lee BO, Lee CH, Lee PG, Choi MJ, Namkoong K. Develop-ment of Korean version of Alcohol Use Disorder Identification Test (AUDIT-K): its reliability and validity. J Korean Acad Ad-dict Psychiatry 2000;4:83–92.
15. Hur SO, Chang SS, Koo JW, Park CY. The assessment of stress between white and blue collar workers by using Psychosocial Well-being Index. Korean J Prev Med 1996;29:609–16.
16. Ilmarinen J. The work ability index (WAI). Occup Med 2007;57:160.
17. van den Berg TI, Elders LA, de Zwart BC, Burdorf A. The effects of work-related and individual factors on the Work Ability Index: a systematic review. Occup Environ Med 2009;66:211–20.
18. Bugajska J, Makowiec-Dąbrowska T, Jegier A, Marszałek A. Physical work capacity (VO2 max) and work ability (WAI) of active employees (men and women) in Poland. Int Congr Ser 2005;1280:156–60.
19. Habibi E, Dehghan H, Zeinodini M, Yousefi H, Hasanzadeh A. A study on Work Ability Index and physical work capacity on the base of fax equation VO(2) max in male nursing hospital staff in Isfahan, Iran. Int J Prev Med 2012;3:776–82.
20. Ye S, Kang D, Kim Y, Son M, Kim J, Park S. The relationship be-tween work ability and job stress factors in manufacturing in-dustries. Ann Occup Environ Med 2008;20:260–71.
https://doi.org/10.12701/yujm.2019.00199224
Kim JW et al. Factors that determine Work Ability Index

Computer-based clinical coding activity analysis for neurosurgical terms Jong Hyuk Lee1, Jung Hwan Lee2, Wooseok Ryu3, Byung Kwan Choi2, In Ho Han2, Chang Min Lee1
1Convergence Medical Institute of Technology, Pusan National University Hospital, Busan, Korea 2Department of Neurosurgery, Pusan National University Hospital, Busan, Korea 3Department of Healthcare Information Management, Catholic University of Pusan, Busan, Korea
Background: It is not possible to measure how much activity is required to understand and code a medical data. We introduce an assessment method in clinical coding, and applied this method to neurosurgical terms. Methods: Coding activity consists of two stages. At first, the coders need to understand a pre-sented medical term (informational activity). The second coding stage is about a navigating ter-minology browser to find a code that matches the concept (code-matching activity). System-atized Nomenclature of Medicine – Clinical Terms (SNOMED CT) was used for the coding system. A new computer application to record the trajectory of the computer mouse and record the us-age time was programmed. Using this application, we measured the time that was spent. A se-nior neurosurgeon who has studied SNOMED CT has analyzed the accuracy of the input coding. This method was tested by five neurosurgical residents (NSRs) and five medical record adminis-trators (MRAs), and 20 neurosurgical terms were used. Results: The mean accuracy of the NSR group was 89.33%, and the mean accuracy of the MRA group was 80% (p=0.024). The mean duration for total coding of the NSR group was 158.47 sec-onds, and the mean duration for total coding of the MRA group was 271.75 seconds (p=0.003). Conclusion: We proposed a method to analyze the clinical coding process. Through this method, it was possible to accurately calculate the time required for the coding. In neurosurgical terms, NSRs had shorter time to complete the coding and higher accuracy than MRAs.
Keywords: Clinical coding; Medical informatics; Systematized nomenclature of medicine
Original articleeISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):225-230https://doi.org/10.12701/yujm.2019.00220
Received: April 1, 2019 Revised: May 21, 2019 Accepted: May 24, 2019
Corresponding author: Jung Hwan Lee Department of Neurosurgery, Pusan National University Hospital, 179, Gudeok-ro Seo-gu, Busan 49241, Korea Tel: +82-51-240-7257 Fax: +82-51-244-8373E-mail: [email protected]
Introduction
Recently, the ability to collect and analyze data has developed, and researches using so-called "big data" have been actively con-ducted in various fields [1]. In the medical area, various studies using big data also have been attempted. However, differences in clinical coding systems and data structures are major barriers to such researches [2]. Therefore, researches on data standardization
using a tool such as a common data model is being carried out [3]. In our country, researches on standardizing medical data are also conducted by the government [2].
However, maintaining such standardized medical data requires human and financial resources in hospitals, and there have been challenges regarding accuracy, coding variation, quality assurance and so on [4-6]. Recently, the adoption and use of electronic health records (EHRs) system has been increasing worldwide.
225https://doi.org/10.12701/yujm.2019.00220
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

Thus, it has become easier to collect medical data. However, most EHRs are not interchangeable [7]. In the neurosurgical fields, the incidence of diseases is relatively low, and there are many surgical techniques that have relatively low frequency. Thus, medical data before EHRs is also very important in the neurosurgical field.
It is not possible to measure how much activity is required for individuals to understand a medical data objectively or how much time is needed to search codes when they already know the mean-ing of medical data. Such information will be very important in predicting the costs of future research. We will also be able to identify problems with clinical coding. The purpose of this study is to propose a clinical coding activity analysis method using the computer mouse, and to analyze the results after coding of neuro-surgical terms using this method.
Material and methods
1. Collection of neurosurgical data We selected 1,071 patients who was admitted to the neurosurgical department for a year at our institute. We reviewed the name of the surgery and the diagnosis. From this pool of terms, we ran-domly selected 10 names of the diagnosis and 10 names of the surgery using “Rand function” of Microsoft Office Excel 2013 (Microsoft Co., Redmond, WA, USA). Selected terms are listed in Table 1.
2. Systematized Nomenclature of Medicine – Clinical Terms The Systematized Nomenclature of Medicine – Clinical Terms (SNOMED CT) is an international clinical terminology that can facilitate interoperability by capturing clinical data in a standard-ized manner. The International Health Terminology Standards
Development Organization was established to maintain and pro-mote SNOMED CT as a clinical reference terminology. Many countries have designated SNOMED CT as the preferred clinical reference terminology for use in EHRs [8]. However, it is not used in our country. We used SNOMED CT, which coders partic-ipating in this study have never used.
3. Clinical coding activity In this study, clinical coding activity consists of two stages. In the first stage, the coders need to understand a presented medical term (informational activity). They use the internet search engine to understand the meaning of terms or abbreviations during infor-mation activity. The second stage is about navigating the termi-nology browser to find a code that matches the concept (code-matching activity). In order to evaluate the accuracy of these activities, a senior neurosurgeon who has studied SNOMED CT has analyzed the accuracy of input coding.
This coding activity was carried out by five neurosurgical resi-dents (NSRs) as domain experts and five medical record adminis-trators (MRAs) as coding experts. The NSRs consisted of two fourth-year residents, two third-year residents, and a second-year resident. And, the career of MRAs was at least 5 years. However, both of the groups had very limited experience with SNOMED CT and CliniClueXplore, which was used as the browser of SNOMED CT. Before the experiment, we briefly gave instruction on how to use CliniClueXplore and SNOMED CT in general to each test subject. The time required for introduction was about 20 minutes. During the test, there was no more explanation or in-struction for understanding the meaning of given terms. The ran-domly collected diagnosis and surgery terms were presented to each participant to perform the clinical coding activity.
Table 1. The list of randomly selected neurosurgical diagnosis and surgery names
No Diagnosis name No Surgery name1 Spinal stenosis with foraminal stenosis L4/5 L5/S1 11 Nerve root block L2 Lt2 HNP L4/5 Lt sequestrated 12 OLM L4/5 Rt3 Brain tumor (R/O atypical meningioma) 13 ACDF C4/5 with allogenic bone filled zero-p PEEK cage4 Unruputured aneurysm MCA aneurysm 14 Clipping of aneurysm5 Hydrocephalus 15 Osteoplastic craniotomy for removal of acute SDH Lt F-T-P6 Fracture of odontoid process (Type II) 16 Transcorporeal approach C6/7 Rt7 Mature teratoma at middle cranial fossa with extracranial extension 17 Transsylvian approach for removal of ICH Rt basal ganglia8 Posthemorrhage hydrocephalus 18 Percutaneous endoscopic laminectomy9 Spinal intradural tumor T9/10 Rt (R/O Schwannoma) 19 UBL L3/4 Rt10 Suprasellar cystic tumor with optic neuropathy 20 IPG insertion
HNP, herniated nucleus pulposus; Lt, left; R/O, rule out; MCA, middle cerebral artery; Rt, right; OLM, open laminectomy and microdisectomy; ACDF, anterior cervical decompression and fusion; PEEK, polyestherestherketone; SDH, subdural hematoma; F-T-P, frontotemporoparietal; ICH, intracerebral hematoma; UBL, unilateral approach and bilateral laminectomy; IPG, implanted pulse generator.
https://doi.org/10.12701/yujm.2019.00220226
Lee JH et al. Clinical coding activity analysis
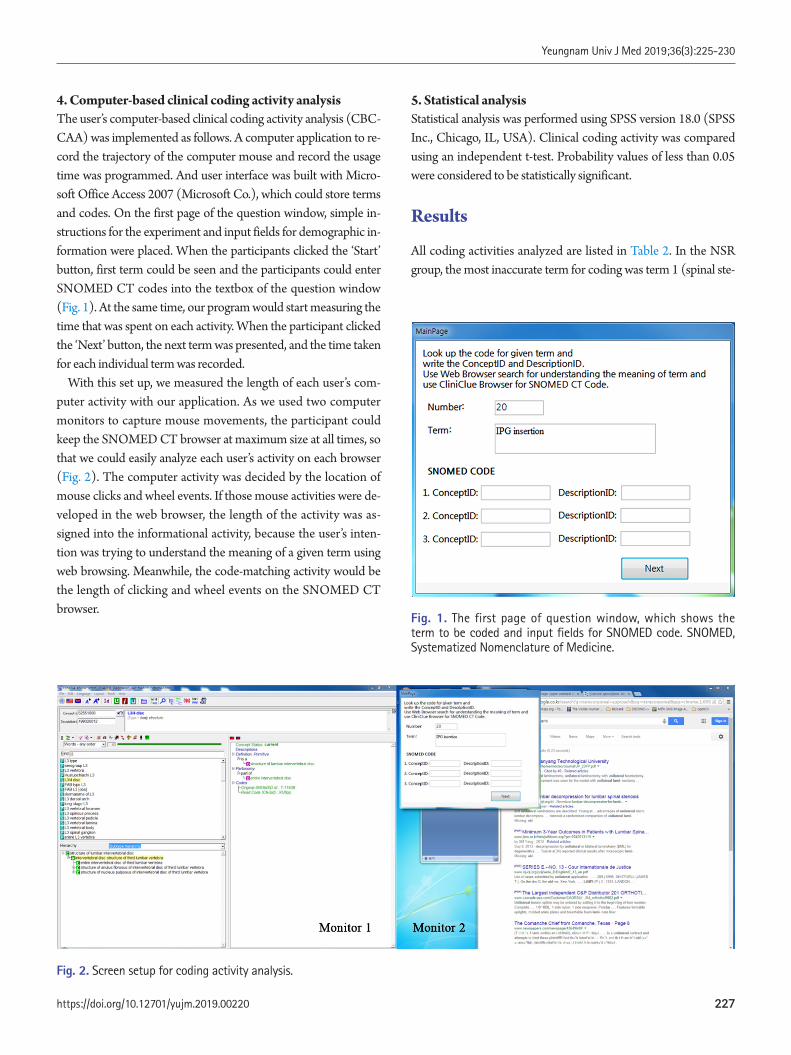
4. Computer-based clinical coding activity analysis The user’s computer-based clinical coding activity analysis (CBC-CAA) was implemented as follows. A computer application to re-cord the trajectory of the computer mouse and record the usage time was programmed. And user interface was built with Micro-soft Office Access 2007 (Microsoft Co.), which could store terms and codes. On the first page of the question window, simple in-structions for the experiment and input fields for demographic in-formation were placed. When the participants clicked the ‘Start’ button, first term could be seen and the participants could enter SNOMED CT codes into the textbox of the question window (Fig. 1). At the same time, our program would start measuring the time that was spent on each activity. When the participant clicked the ‘Next’ button, the next term was presented, and the time taken for each individual term was recorded.
With this set up, we measured the length of each user’s com-puter activity with our application. As we used two computer monitors to capture mouse movements, the participant could keep the SNOMED CT browser at maximum size at all times, so that we could easily analyze each user’s activity on each browser (Fig. 2). The computer activity was decided by the location of mouse clicks and wheel events. If those mouse activities were de-veloped in the web browser, the length of the activity was as-signed into the informational activity, because the user’s inten-tion was trying to understand the meaning of a given term using web browsing. Meanwhile, the code-matching activity would be the length of clicking and wheel events on the SNOMED CT browser.
5. Statistical analysis Statistical analysis was performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). Clinical coding activity was compared using an independent t-test. Probability values of less than 0.05 were considered to be statistically significant.
Results
All coding activities analyzed are listed in Table 2. In the NSR group, the most inaccurate term for coding was term 1 (spinal ste-
Fig. 2. Screen setup for coding activity analysis.
Fig. 1. The first page of question window, which shows the term to be coded and input fields for SNOMED code. SNOMED, Systematized Nomenclature of Medicine.
227https://doi.org/10.12701/yujm.2019.00220
Yeungnam Univ J Med 2019;36(3):225-230
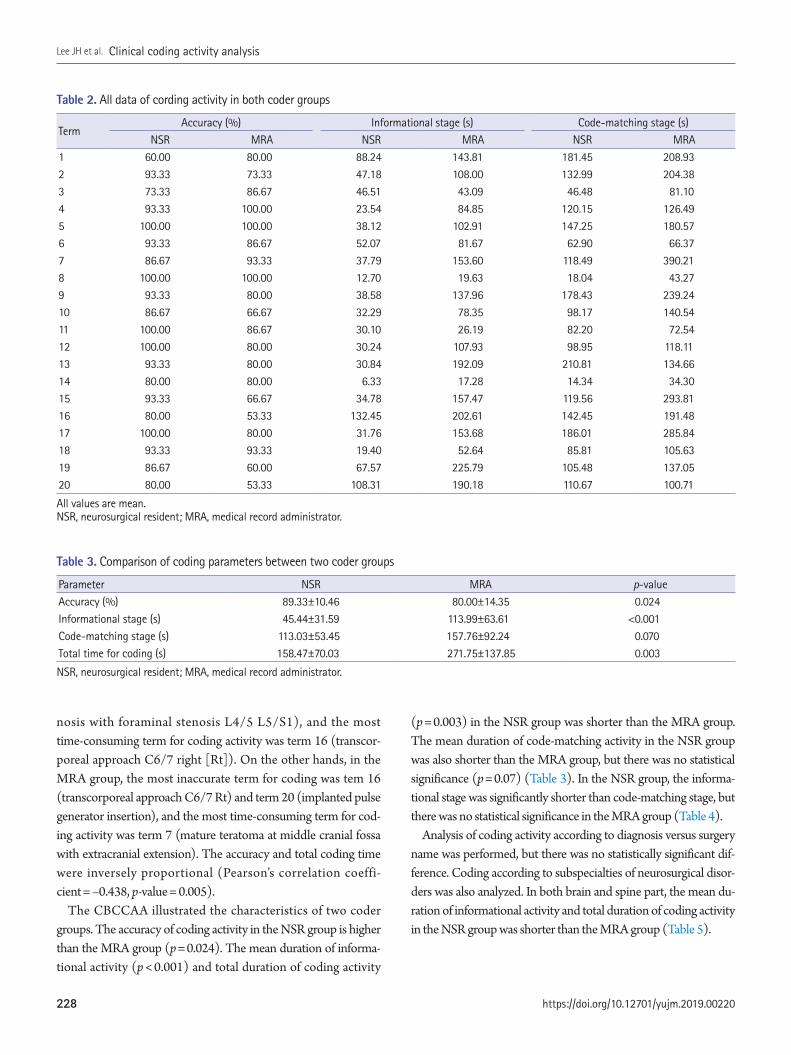
nosis with foraminal stenosis L4/5 L5/S1), and the most time-consuming term for coding activity was term 16 (transcor-poreal approach C6/7 right [Rt]). On the other hands, in the MRA group, the most inaccurate term for coding was tem 16 (transcorporeal approach C6/7 Rt) and term 20 (implanted pulse generator insertion), and the most time-consuming term for cod-ing activity was term 7 (mature teratoma at middle cranial fossa with extracranial extension). The accuracy and total coding time were inversely proportional (Pearson’s correlation coeffi-cient = –0.438, p-value = 0.005).
The CBCCAA illustrated the characteristics of two coder groups. The accuracy of coding activity in the NSR group is higher than the MRA group (p = 0.024). The mean duration of informa-tional activity (p < 0.001) and total duration of coding activity
(p = 0.003) in the NSR group was shorter than the MRA group. The mean duration of code-matching activity in the NSR group was also shorter than the MRA group, but there was no statistical significance (p = 0.07) (Table 3). In the NSR group, the informa-tional stage was significantly shorter than code-matching stage, but there was no statistical significance in the MRA group (Table 4).
Analysis of coding activity according to diagnosis versus surgery name was performed, but there was no statistically significant dif-ference. Coding according to subspecialties of neurosurgical disor-ders was also analyzed. In both brain and spine part, the mean du-ration of informational activity and total duration of coding activity in the NSR group was shorter than the MRA group (Table 5).
Table 2. All data of cording activity in both coder groups
TermAccuracy (%) Informational stage (s) Code-matching stage (s)
NSR MRA NSR MRA NSR MRA1 60.00 80.00 88.24 143.81 181.45 208.932 93.33 73.33 47.18 108.00 132.99 204.383 73.33 86.67 46.51 43.09 46.48 81.104 93.33 100.00 23.54 84.85 120.15 126.495 100.00 100.00 38.12 102.91 147.25 180.576 93.33 86.67 52.07 81.67 62.90 66.377 86.67 93.33 37.79 153.60 118.49 390.218 100.00 100.00 12.70 19.63 18.04 43.279 93.33 80.00 38.58 137.96 178.43 239.2410 86.67 66.67 32.29 78.35 98.17 140.5411 100.00 86.67 30.10 26.19 82.20 72.5412 100.00 80.00 30.24 107.93 98.95 118.1113 93.33 80.00 30.84 192.09 210.81 134.6614 80.00 80.00 6.33 17.28 14.34 34.3015 93.33 66.67 34.78 157.47 119.56 293.8116 80.00 53.33 132.45 202.61 142.45 191.4817 100.00 80.00 31.76 153.68 186.01 285.8418 93.33 93.33 19.40 52.64 85.81 105.6319 86.67 60.00 67.57 225.79 105.48 137.0520 80.00 53.33 108.31 190.18 110.67 100.71
All values are mean.NSR, neurosurgical resident; MRA, medical record administrator.
Table 3. Comparison of coding parameters between two coder groups
Parameter NSR MRA p-valueAccuracy (%) 89.33±10.46 80.00±14.35 0.024Informational stage (s) 45.44±31.59 113.99±63.61 <0.001Code-matching stage (s) 113.03±53.45 157.76±92.24 0.070Total time for coding (s) 158.47±70.03 271.75±137.85 0.003
NSR, neurosurgical resident; MRA, medical record administrator.
https://doi.org/10.12701/yujm.2019.00220228
Lee JH et al. Clinical coding activity analysis

Discussion
Recently, as interest in big data, deep learning, and artificial intelli-gence has increased, interest in data collection has increased. In order to receive compensation, the code related to the health in-surance had to be continuously input, and many studies using this data have been performed [9]. However, such data are limited, and new data collection is required depending on the content of the study. For clinical data collection and standardization, coding the data at each hospital is very important. Understanding and code-searching are the two main stages of medical coding. We tried to use these two particular concepts to analyze clinical cod-ing activity.
In this study, we provided a method to evaluate coding activity in an objective way. A benefit of this method is that the parame-ters are produced with numeric values that can be measured by computers. Thus, we can compare parametric results quantitative-ly, and can analyze the efficiency according to the coder and kinds of terminology. When we reviewed the data in this study, coding activities were very varied greatly, depending on the coders. The NRS group did more efficient coding than the MRA group. The coding time was significantly shorter in the information stage, and thus the total time was shortened (Table 3). The accuracy of cod-ing was higher in NSR group, probably because they understood neurosurgical terms better than the MRAs did. We expected that the MRA group would take less time for code-matching, because they specialized in coding. However, there was no significant dif-ference in the code-matching time between the NSR group and the MRA group. In the healthcare field, there are various type of occupations (physicians, dentist, nurses, MRA, clinical laboratory technologists, radiologic technologists, etc.) and costs are differ-
ent. Using the method presented in this study, it can be expected which job group will be efficiently at clinical coding data.
We also analyzed coding processes by each stages. In the NSR group, the informational stage was shorter than code-matching stage. As mentioned previously, a short informational activity means that the coder has no difficulty with understanding the terms. On the other hands, long code-matching activity refers to problems matching concepts to codes in the terminology browser. Inefficient browsers can be more time-consuming in code-match-ing activity. Thus, if this phenomenon persists, the browser used for coding should be improved. We also analyzed the coding ac-tivity according to the kind of terminology. Neurosurgical diseases and surgery were classified into brain and spine. In both brain and spine part, coding activity of the NSR group was effective than the MRA group.
In this study, we can confirm that the coding time was longer for terms that had low coding accuracy, because less-understood terms took longer to find. For example, a term that was difficult to code in both groups was “transcorporeal approach C6/7, Rt,” be-cause this is that this surgery has been proposed relatively recently, and is called by various names [10].
Although the coders could start the test by pressing a button, the coder’s activity was measured by the length of activity on the designated window. Because the computer mouse logging func-tion automatically evaluates the coding process, there is no manu-al evaluation to categorize the coder’s activity which may lead to subjective results. Since we are heading towards a computerized coding environment, those parameters need to be evaluated by computer-based tools as well [11]. As far as we know, this is the first study to analyze the clinical coding process by means of com-puter activity. By this approach, we can clarify practical problems
Table 4. Comparison of coding activities between information and code-matching stages
Coder group Informational stage (s) Code-matching stage (s) p-valueNSR 45.44±31.59 113.03±53.45 <0.001MRA 113.99±63.61 157.76±92.24 0.089
NSR, neurosurgical resident; MRA, medical record administrator.
Table 5. Comparison of coding activities between spine and brain part
Brain SpineNSR MRA p-value NSR MRA p-value
Accuracy (%) 89.33±9.53 82.67±16.39 0.281 89.33±11.84 77.33±12.25 0.039Informational stage (s) 37.21±27.78 100.1±61.86 0.012 53.67±34.43 127.87±65.47 0.005Code-matching stage (s) 97.92±55.53 167.68±118.90 0.117 128.15±49.39 147.84±60.05 0.434Total time for coding (s) 135.13±69.18 267.79±168.34 0.040 181.81±66.01 275.71±108.36 0.034
NSR, neurosurgical resident; MRA, medical record administrator.
229https://doi.org/10.12701/yujm.2019.00220
Yeungnam Univ J Med 2019;36(3):225-230

with coding activity and analyze proper solutions to such issues.
Conflicts of interest
No potential conflicts of interest relevant to this article were reported.
ORCID
Jong Hyuk Lee, https://orcid.org/0000-0003-3134-8029Jung Hwan Lee, https://orcid.org/0000-0002-1393-7105Wooseok Ryu, https://orcid.org/0000-0002-3893-6184Byung Kwan Choi, https://orcid.org/0000-0001-5244-4592In Ho Han, https://orcid.org/0000-0001-7193-6533Chang Min Lee, https://orcid.org/0000-0002-9884-2024
References
1. Nishimura A, Nishimura K, Kada A, Iihara K; J-ASPECT Study GROUP. Status and future perspectives of utilizing big data in neurosurgical and stroke research. Neurol Med Chir (Tokyo) 2016;56:655–63.
2. Yoon D, Ahn EK, Park MY, Cho SY, Ryan P, Schuemie MJ, et al. Conversion and data quality assessment of electronic health re-cord data at a Korean tertiary teaching hospital to a common data model for distributed network research. Healthc Inform Res 2016;22:54–8.
3. Popovic JR. Distributed data networks: a blueprint for Big Data sharing and healthcare analytics. Ann N Y Acad Sci 2017;1387:105–11.
4. Carter KJ, Rinehart S, Kessler E, Caccamo LP, Ritchey NP, Erick-son BA, et al. Quality assurance in anatomic pathology: automat-ed SNOMED coding. J Am Med Inform Assoc 1996;3:270–2.
5. Wasserman H, Wang J. An applied evaluation of SNOMED CT as a clinical vocabulary for the computerized diagnosis and prob-lem list. AMIA Annu Symp Proc 2003:699–703.
6. Haliasos N, Rezajooi K, O’neill KS, Van Dellen J, Hudovsky A, Nouraei S. Financial and clinical governance implications of clini-cal coding accuracy in neurosurgery: a multidisciplinary audit. Br J Neurosurg 2010;24:191–5.
7. Yoon D, Chang BC, Kang SW, Bae H, Park RW. Adoption of elec-tronic health records in Korean tertiary teaching and general hos-pitals. Int J Med Inform 2012;81:196–203.
8. Lee D, de Keizer N, Lau F, Cornet R. Literature review of SNOMED CT use. J Am Med Inform Assoc 2014;21:e11–9.
9. Sohn S, Kim J, Chung CK, Lee NR, Sohn MJ, Kim SH. A na-tion-wide epidemiological study of newly diagnosed primary spine tumor in the adult Korean population, 2009-2011. J Kore-an Neurosurg Soc 2017;60:195–204.
10. Choi BK, Han IH, Cho WH, Cha SH. Inferiorly migrated disc fragment at t1 body treated by t1 transcorporeal approach. J Ko-rean Neurosurg Soc 2011;49:61–4.
11. de Lusignan S. The barriers to clinical coding in general practice: a literature review. Med Inform Internet Med 2005;30:89–97.
https://doi.org/10.12701/yujm.2019.00220230
Lee JH et al. Clinical coding activity analysis

Assessment of solid components of borderline ovarian tumor and stage I carcinoma: added value of combined diffusion- and perfusion-weighted magnetic resonance imagingSee Hyung Kim Department of Radiology, School of Medicine, Kyungpook National University, Daegu, Korea
Background: We sought to determine the value of combining diffusion-weighted (DW) and per-fusion-weighted (PW) sequences with a conventional magnetic resonance (MR) sequence to as-sess solid components of borderline ovarian tumors (BOTs) and stage I carcinomas. Methods: Conventional, DW, and PW sequences in the tumor imaging studies of 70 patients (BOTs, n=38; stage I carcinomas, n=32) who underwent surgery with pathologic correlation were assessed. Two independent radiologists calculated the parameters apparent diffusion coefficient (ADC), Ktrans (vessel permeability), and Ve (cell density) for the solid components. The distribution on conventional MR sequence and mean, standard deviation, and 95% confidence interval of each DW and PW parameter were calculated. The inter-observer agreement among the two ra-diologists was assessed. Area under the receiver operating characteristic curve (AUC) and multi-variate logistic regression were performed to compare the effectiveness of DW and PW sequenc-es for average values and to characterize the diagnostic performance of combined DW and PW sequences. Results: There were excellent agreements for DW and PW parameters between radiologists. The distributions of ADC, Ktrans, and Ve values were significantly different between BOTs and stage I carcinomas, yielding AUCs of 0.58 and 0.68, 0.78 and 0.82, and 0.70 and 0.72, respectively, with ADC yielding the lowest diagnostic performance. The AUCs of the DW, PW, and combined PW and DW sequences were 0.71±0.05, 0.80±0.05, and 0.85±0.05, respectively. Conclusion: Combining PW and DW sequences to a conventional sequence potentially improves the diagnostic accuracy in the differentiation of BOTs and stage I carcinomas.
Keywords: Borderline ovarian tumor; Diagnosis; Magnetic resonance imaging; Stage I ovarian carcinoma
Received: May 8, 2019 Revised: June 4, 2019 Accepted: June 6, 2019 Corresponding author: See Hyung KimDepartment of Radiology, School of Medicine, Kyungpook National University, 130, Dongdeok-ro, Jung-gu, Daegu 41944, Korea Tel: +82-53-200-5390Fax: +82-53-422-2677E-mail: [email protected]
Introduction
The presence of solid components in ovarian tumors strongly suggests carcinoma, but solid components can also be seen in
borderline ovarian tumors (BOTs). BOTs are a class of epithelial tumors; histologically, they show atypical nuclei without cell pro-liferation and epileptic involvement. Resection is considered to be sufficient treatment for BOTs; adjuvant chemotherapy after
Original articleeISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):231-240https://doi.org/10.12701/yujm.2019.00234
231https://doi.org/10.12701/yujm.2019.00234
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

surgery has no significant correlation with the recurrence rate. BOTs have been shown to have a low recurrence rate and a high survival rate [1-5].
The preoperative diagnosis of BOTs and stage I carcinomas re-mains difficult, despite the development of various imaging tech-niques. Ultrasonography is generally used to assess ovarian tu-mors, but its accuracy is not high because of the overlapping fea-tures of different tumor types. Magnetic resonance imaging (MRI) is superior to ultrasound or computed tomography in the evaluation of tissue components and easily identifies solid com-ponents. Therefore, MRI is often used to diagnose ovarian can-cers, focusing on detection of solid areas, among other features, in distinguishing tumor types. However, even with conventional MRI, it is difficult to distinguish between BOTs with solid com-ponents and primary carcinomas [5-7].
Recent advances in MRI have improved the preoperative diag-nosis of ovarian tumors. The usefulness of diffusion-weighted (DW) and perfusion-weighted (PW) sequences has been report-ed in several studies; these imaging sequences have been used to assess the density of tumor cells and evaluate neovasculature and microvasculature [7-9]. Solid components in BOTs and stage I carcinomas are characterized by high signal intensity, reflecting long tumor relaxation time with prolonged T2 relaxation time on DW images, and early dynamic enhancement reflecting tu-mor angiogenesis associated with microvessel densities [9-12]. It has already been shown that combining DW or PW imaging with a conventional magnetic resonance (MR) sequence is effective in discriminating benign and malignant ovarian tumors [11-13]. However, no reports have been published to date that demon-strate the contribution of DW and PW sequences to the differen-tial diagnosis of BOTs and stage I carcinomas. Therefore, the purpose of this study is to assess the combination of PW and DW sequences with a conventional MR sequence to potentially improve diagnostic accuracy in the differentiation of BOTs and stage I carcinomas.
Materials and methods
This study was approved by the Kyungpook National Universi-
ty Hospital Institutional Review Board (Approval No. S-201221) with waiver of informed consent. We reviewed the medical re-cords dating from December 2015 to May 2017 of 118 patients with BOTs or stage I carcinomas treated in our institution. Of these patients, 70 with solid tumors on MRI were included (BOTs, 38 patients; stage I carcinomas, 32 patients). All tumor di-agnoses were confirmed histopathologically. MRI, including con-ventional, DW, and PW sequences, was performed in 57 of the 70 patients. DW sequences were excluded in 7 patients (T1-weight-ed high-intensity mass, 3 patients; artifact shadow, 4 patients), and 9 patients (contrasted myometrial defects, 4 patients; technical problems such as artificial shadowing, 5 patients). Table 1 sum-marizes the results of the exponential test in the patient groups that underwent imaging with DW and PW sequences in combi-nation with conventional MRI. Of the patients with tumors iden-tified as BOTs, 12 had mucinous tumors and 26 had serous tu-mors, whereas 11 of the patients with stage I carcinoma had muci-nous tumors and 21 had serous tumors. The ages of the patients with BOTs ranged from 19 to 62 years (mean, 40.8 ± 14.2 years). The ages of the patients with stage I carcinoma ranged from 25 to 71 years (mean, 43.2 ± 13.2 years). Thirteen patients had under-gone unilateral or bilateral salpingo-oophorectomy (BSO) due to clinical conditions such as fertility problems. The remaining pa-tients had undergone hysterectomy, BSO, and lymphadenectomy for a clinical diagnosis of carcinoma.
MRI was performed with a 1.5-T scanner (Avanto; Siemens, Erlangen, Germany) using a pelvic phased array coil. Patients were given 1 mg of glucagon into the muscle just before the test to reduce intestinal peristalsis. Table 2 summarizes the MR se-quence parameters. First, conventional T1-weighted turbo spin-echo imaging with both axial and sagittal T2-weighted turbo spin-echo images and fat suppression and fat suppression exclu-sion was performed. Next, DW sequences were obtained from the axial plane using a single-shot echo plane image using the sensitivity coding technique. The b values corresponding to the diffusion detection gradient were 0 and 1,000 mm2/sec. T1- and T2-weighted and DW images were acquired with a cut thickness of 5 mm and a cutoff interval of 1 mm. The motion search gradi-ent pulses were arranged in 3 orthogonal directions. Finally, PW
Table 1. Patient population and index test results
Conv MR (n=70)Conv MR+DW (n=63) Conv MR+PW (n=61) Conv MR+DW+PW (n=57)
BOT Stage I carcinoma BOT Stage I carcinoma BOT Stage I carcinoman=33 n=30 n=33 n=28 n=32 n=25
BOT, borderline ovarian tumor; n, number of patients; Conv MR, conventional magnetic resonance sequence; DW, diffusion-weighted sequence; PW, perfusion-weighted sequence.
https://doi.org/10.12701/yujm.2019.00234232
Kim SH. Borderline ovarian tumor and stage I carcinoma

sequences were performed on all tumors, with emphasis on the area of the solid component in the non-enhanced MRI. The im-ages were acquired on an axial plane including the myometrium adjacent to the tumor on the optimal plane. Three-dimentional (3D), radiofrequency, and time resolved angiography stochastic trajectories (TWISTs) images (GRAPPA factor 2; Simens Healthcare, Erlangen, Germany) were used. Conventional dy-namic contrast enhancement images were obtained using the TWIST technique. Gadolinium chelate (Gadovist; Bayer, Ger-many) was intravenously injected at a concentration of 0.1 mmol per/kg. Injection was performed with a high-pressure automatic injector (Medrad Spectris, Polkhach, Germany). The flow rate of 2 mL/sec was equivalent to 5 seconds of transient injection up to 120 mL. Then, 20 mL isotonic saline was immediately injected at the same flow rate.
Two experienced radiologists (10 and 12 years of abdominal imaging) analyzed the masses according to the following crite-ria: size, bilaterality, presence of multiple locules with various signal intensities, multiseptation, presence of solid component, presence of multiple, peritoneal seeding, and lymphadenopathy. Solid portions in cystic tumors refers to the proliferation, solid portion, and thickened septum of the wall or septum of the mass, as defined by Timmerman et al. [14]. All of the solid com-ponents showed enhancement after contrast injection. On T2-weighted image (T2WI), the signal intensity in the solid component was low or intermediate compared with myometri-um. Two radiologists referenced the region of interest (ROI) (average, 10.2 mm; range, 8.8–12.8 mm in the largest dimen-sion) with reference to a T2WI. The ROI was selected for each of the 3 regions with relatively low signal intensities in the solid phase, and then the mean value was calculated as the representa-
tive value for the calculated values of the diffusivity in each ROI. In order not to include the edge of the solid portion, the ROI is mainly included in the center portion. Similar to the method of calculating the current apparent diffusion coefficient (ADC), a ROI average of 10.0 mm (range, 8.0–12.0 mm in the largest di-mension) was set for the same region to derive the time course enhancement pattern of the solid component. Perfusion coeffi-cients were determined using commercial perfusion analysis software (Syngo Tissue 4D; Siemens Medical Solutions, Erlan-gen, Germany). In addition, color maps were fused to T2WIs. To calculate the contrast ratio (Ktrans) and the extracellular and extracellular fraction (Ve) between the vessels and the tissues, a known Tofts model was applied. When using the Tofts model, we used the estimated mean values from various clinical perfu-sion imaging studies to evaluate the contrast injection function that is always applied together.
To determine whether the distribution of BOT and stage I carcinomas differs statistically from their distribution on con-ventional MRI, we used Mann-Whitney and Fisher's exact tests for each criterion for continuous and categorical criteria, respec-tively. The mean, standard deviation, and 95% confidence inter-val range of each DW and PW sequence parameter were then calculated. The quadratic k coefficients were calculated to evalu-ate the agreement between the 2 radiologist observers (k-value, 0–0.19; poor, 0.20–0.39; fair, 0.40–0.59; moderate, 0.60–0.79; substantial, 0.80–1.00; excellent). A linear mixture model with both p-values was used to verify whether the differences be-tween the distributions of each parameter were statistically sig-nificant. We also performed a receiver operating characteristic (ROC) curve analysis to evaluate the efficacy of conventional MRI, DW, and PW sequences in discriminating BOTs and stage
Table 2. Magnetic resonance imaging protocols
ParameterT2-weighted turbo spin-echo Axial T1-weighted turbo
spin-echo Axial DW echo-plana Axial PW time resolved angiog-raphy stochastic trajectoriesAxial Sagittal
Repetition time (msec) 3,100.0 3,700.0 500.0 5,500.0 12.0Echo time (msec) 100.0 110.0 9.4 87.0 4.2Echo train length 23 25 3 1 1Flip angle (degree) 150.0 150.0 149.0 90.0 12.0Sectional thickness (mm) 5 5 5 5 3.5Intersection gap (mm) 1 1 1 1 1Field of view (mm) 260×260 250×250 260×260 260×220 300×200Matrix 380×260 380×260 320×250 160×80 190×80Number of acquired signals 2 2 1 3 1Number of sections 25 30 25 35 4Acquisition time (sec) 150 165 25 110 60
DW, diffusion-weighted; PW, perfusion-weighted.
233https://doi.org/10.12701/yujm.2019.00234
Yeungnam Univ J Med 2019;36(3):231-240

I carcinoma. The area under the ROC curve (AUC) was used to determine diagnostic performance and the sensitivity and speci-ficity were calculated from this curve analysis. Multivariate logis-tic regression analysis was performed to determine whether the combination of conventional MRI findings and the associated parameters such as ADC, Ktrans, and Ve improved the differentia-tion between BOTs and stage I carcinomas. All statistical analy-ses were performed using SAS 9.2 software (SAS Institute, Cary, NC, USA), and p < 0.05 was considered statistically significant.
Results
Table 3 summarizes the features of conventional MR sequence for BOTs and stage I carcinomas. The most prevalent features of
stage I carcinoma were bilaterality (17 of 53 patients, 53%), peritoneal implants (9 of 14, 64%), and lymphadenopathy (4 of 8 patients, 50%). There was no statistically significant difference in size, multilocularity, the presence of loculi with various signal intensities, the presence of multiple septa, and distributions of solid components. Table 4 summarizes the 2 radiologists’ mea-surement results of the prevalence of the ADC, Ktrans, and Ve val-ues for BOTs and stage I carcinomas. A case of BOTs and stage 1 carcinoma is presented (Figs. 1, 2).
There was good consensus between the radiologists for the values (BOT, k = 0.850; stage I carcinoma, k = 0.890). The linear composite model of dispersion showed that the distribution of the ADC was significantly different between BOTs and stage I carcinomas (p < 0.03). In this analysis, multiple lesions of a giv-
Table 3. Conventional MR sequence characteristics of borderline tumors and stage I carcinomas
Characteristic No. of findings Borderline tumors (n=38) Stage I carcinomas (n=32) p-valueMean patient age (yr) 70 40.8±14.2 43.2±13.2 0.58a)
Mean lesion size (cm) 70 12.5±4.4 14.1±5.2 0.42a)
Bilaterality 70 16 (6/38) 53 (17/32) 0.005b)
Multilocularity 48 59 (13/22) 69 (18/26) 0.01b)
Loculi with different signal intensity 25 50 (5/10) 47 (7/15) 0.38b)
Multiseptation 50 71 (20/28) 64 (14/22) 0.08b)
Solid components 70 - -Vegetation 32 58 (7/12) 65 (13/20) 0.08a)
Solid portion 20 57 (4/7) 62 (8/13) 0.10a)
Thickened septa 18 62 (5/8) 70 (7/10) 0.08a)
Ascites 31 40 (4/10) 43 (9/21) 0.07a)
Peritoneal implants 20 33 (2/6) 64 (9/14) 0.03b)
Lymphadenopathy 8 0 50 (4/8) 0.001b)
Signal intensity of solid component on T2 70 - -Low signal intensity 25 43 (6/14) 45 (5/11) 0.10b)
Intermediate signal intensity 45 54 (15/28) 64 (11/17) 0.09b)
Values are presented as mean±standard deviation or number. Numbers in parentheses are numbers of lesions.a)Calculated with the Mann-Whitney test. b)Calculated with the Fisher exact test.
Table 4. Results of the comparison of ADC, Ktrans, and Ve values for borderline tumors and stage I carcinomas between 2 radiologists
ParameterRadiologist 1 Radiologist 2
k-valueMean SD 95% CI Mean SD 95% CI
Borderline tumors 0.850 ADC (×10-3 mm2/sec) 1.151 0.282 1.201-1.335 1.132 0.301 1.094-1.412 Ktrans (/min) 0.236 0.054 0.201-0.284 0.258 0.051 0.214-0.291 Ve 0.148 0.053 0.132-0.197 0.156 0.056 0.125-0.207Stage I carcinomas 0.890 ADC (×10-3 mm2/sec) 1.053 0.214 0.924-1.103 1.087 0.195 0.956-1.102 Ktrans (/min) 0.309 0.053 0.291-0.359 0.326 0.038 0.279-0.346 Ve 0.305 0.041 0.288-0.374 0.318 0.046 0.288-0.356
SD, standard deviation; CI, confidence interval; ADC, apparent diffusion coefficient.
https://doi.org/10.12701/yujm.2019.00234234
Kim SH. Borderline ovarian tumor and stage I carcinoma

en patient were randomly selected to ensure that one lesion of a certain type was correctly included in the analysis. Therefore, it is necessary to correct the analysis by the fixation effect, and the distribution of ADC is significantly different between the BOT and the stage I carcinoma (p = 0.02). Fig. 3 shows the distribu-tion of individual ADCs. Although the mean ADCs differ sig-nificantly, the distribution of some values overlap. The mixed model analysis of variance showed that Ktrans and Ve values were
significantly different between BOTs and stage I carcinomas (p < 0.01). In this analysis, multiple lesions in a given patient were randomly selected. Estimates of the fixation effect indicate that the distribution of Ktrans and Ve values is significantly differ-ent between BOTs and stage I carcinomas (p = 0.009 and p = 0.02, respectively). The ROC of the ADC yielded AUCs of 0.58 and 0.68 for differentiation between BOTs and stage I car-cinomas. The ROC of the ADC yielded AUCs of 0.58 and 0.68
Fig. 1. Images of a serous cystadenoma borderline tumor in a 46-year-old woman. (A) T2-weighted fast spin-echo axial MR image shows a right ovarian tumor with cystic and solid components as solid portions (arrows) with low signal intensity. Ascites (arrowhead) is shown. (B) ADC map obtained at b=1,000 mm2/sec shows restricted diffusion in the solid portions (arrows, measured mean ADC map=1.12×10-3 mm2/sec). (C) Ktrans and Ve map color overlain on a T2-weighted MR image shows increased Ktrans and Ve values throughout the solid portions (measured Ktrans and Ve of the ROI2=0.254/min and 0.150). (D) Relative enhancement time fitting curve of the solid component of the borderline tumor is shown. MR, magnetic resonance; ADC, apparent diffusion coefficient; ROI, region of interest.
A
C
B
D
235https://doi.org/10.12701/yujm.2019.00234
Yeungnam Univ J Med 2019;36(3):231-240

for differentiation between BOTs and stage I carcinomas. The AUCs of Ktrans were 0.78 and 0.82, and those of Ve were 0.70 and 0.72 (Fig. 4). DW sequences of BOTs and stage I carcinomas showed relatively low diagnostic performance, while PW se-quences showed slightly higher diagnostic performance. Fig. 5 shows the AUC of the ADC, Ktrans, and Ve parameters.
Discussion
The results of this study demonstrate the diagnostic value of DW and PW sequence techniques in discriminating between BOTs and stage I carcinomas. In this study, all of the solid components on T2WIs showed low or intermediate signal intensity and could not be used as a reference for discrimination. Previous studies have suggested that bilaterality, peritoneal implants, and lymph-
Fig. 2. Images of a stage I serous adenocarcinoma in a 42-year-old woman. (A) T2-weighted fast spin-echo axial MR image shows a right ovarian tumor with predominant solid portions (arrows) with low to intermediate signal intensity. (B) ADC map obtained at b=1,000 mm2/sec shows restricted diffusion in the solid portions (arrows, measured mean ADC map=1.07×10-3 mm2/sec). (C) Ktrans and Ve map color overlain on a T2-weighted MR image shows increased Ktrans and Ve values over the area corresponding to the carcinoma (measured Ktrans and Ve of the ROI1=0.323/min and 0.332). (D) Relative enhancement time fitting curve of the solid component of the carcinoma is shown. MR, magnetic resonance; ADC, apparent diffusion coefficient; ROI, region of interest.
A
C
B
D
https://doi.org/10.12701/yujm.2019.00234236
Kim SH. Borderline ovarian tumor and stage I carcinoma
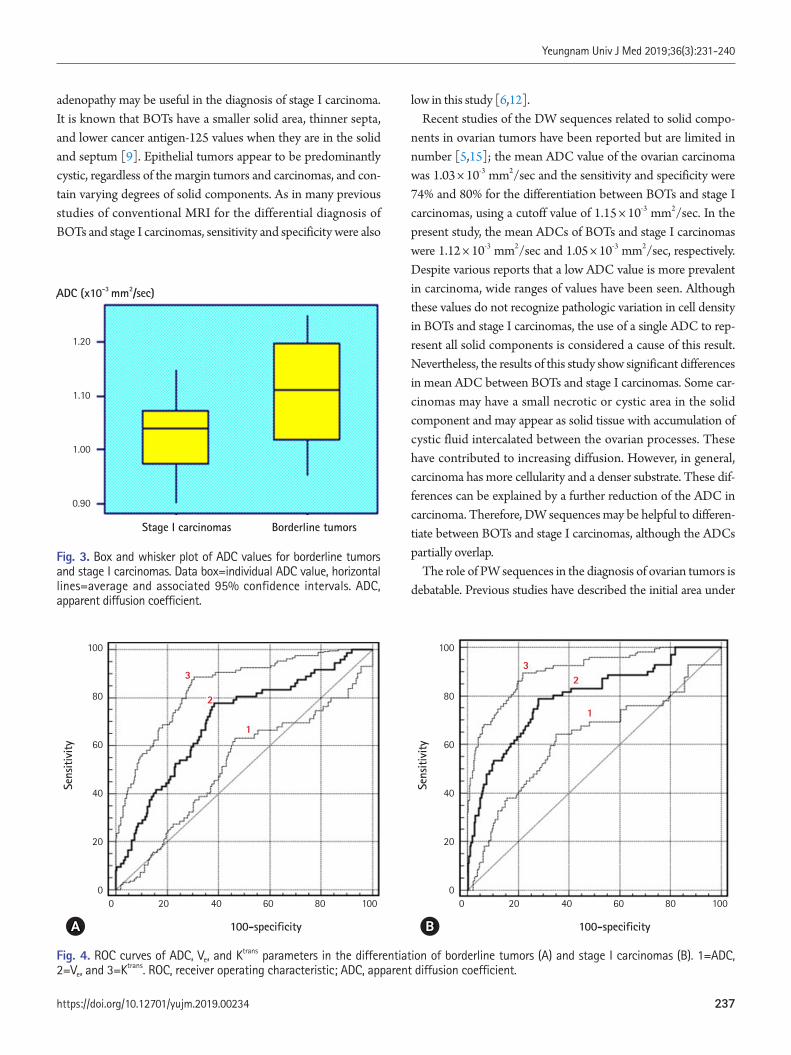
low in this study [6,12]. Recent studies of the DW sequences related to solid compo-
nents in ovarian tumors have been reported but are limited in number [5,15]; the mean ADC value of the ovarian carcinoma was 1.03 × 10-3 mm2/sec and the sensitivity and specificity were 74% and 80% for the differentiation between BOTs and stage I carcinomas, using a cutoff value of 1.15 × 10-3 mm2/sec. In the present study, the mean ADCs of BOTs and stage I carcinomas were 1.12 × 10-3 mm2/sec and 1.05 × 10-3 mm2/sec, respectively. Despite various reports that a low ADC value is more prevalent in carcinoma, wide ranges of values have been seen. Although these values do not recognize pathologic variation in cell density in BOTs and stage I carcinomas, the use of a single ADC to rep-resent all solid components is considered a cause of this result. Nevertheless, the results of this study show significant differences in mean ADC between BOTs and stage I carcinomas. Some car-cinomas may have a small necrotic or cystic area in the solid component and may appear as solid tissue with accumulation of cystic fluid intercalated between the ovarian processes. These have contributed to increasing diffusion. However, in general, carcinoma has more cellularity and a denser substrate. These dif-ferences can be explained by a further reduction of the ADC in carcinoma. Therefore, DW sequences may be helpful to differen-tiate between BOTs and stage I carcinomas, although the ADCs partially overlap.
The role of PW sequences in the diagnosis of ovarian tumors is debatable. Previous studies have described the initial area under
Fig. 3. Box and whisker plot of ADC values for borderline tumors and stage I carcinomas. Data box=individual ADC value, horizontal lines=average and associated 95% confidence intervals. ADC, apparent diffusion coefficient.
Fig. 4. ROC curves of ADC, Ve, and Ktrans parameters in the differentiation of borderline tumors (A) and stage I carcinomas (B). 1=ADC, 2=Ve, and 3=Ktrans. ROC, receiver operating characteristic; ADC, apparent diffusion coefficient.
adenopathy may be useful in the diagnosis of stage I carcinoma. It is known that BOTs have a smaller solid area, thinner septa, and lower cancer antigen-125 values when they are in the solid and septum [9]. Epithelial tumors appear to be predominantly cystic, regardless of the margin tumors and carcinomas, and con-tain varying degrees of solid components. As in many previous studies of conventional MRI for the differential diagnosis of BOTs and stage I carcinomas, sensitivity and specificity were also
Stage I carcinomas
ADC (x10-3 mm2/sec)
Borderline tumors
1.20
1.10
1.00
0.90
Sens
itivi
ty
100-specificity
0 20 40 60 80 100
100
80
60
40
20
0
1
3
2
A 100-specificity
Sens
itivi
ty
0 20 40 60 80 100
100
80
60
40
20
0
1
23
B
237https://doi.org/10.12701/yujm.2019.00234
Yeungnam Univ J Med 2019;36(3):231-240

the curve of time intensity curve as the most important factor for carcinoma differentiation. Therefore, to accurately perform the discrimination decision of a mass with high accuracy, the maxi-mum slope ratio and the initial area under the time intensity curve must be considered together. Furthermore, a type 3 time-weight-ed curve, which defines a steeper initial rise in signal intensity of solid tissue compared to the normal myometrial signal, appears unusual in carcinoma [16-18]. In contrast, in this study, quantita-tive analysis of PW sequences was conducted to differentiate BOTs and stage I carcinomas. Recent studies have shown that the presence of vulnerable neovasculature, initially incompletely formed, acts as an optimal mediator, as the malignant tumor pro-gresses more rapidly than the BOTs or benign tumors, and that enhancement and detachment may occur [19-23]. In carcinoma, blood vessel formation occurs due to the synthesis and secretion of angiogenic factors. The number of blood vessels is increased and the integrity of the blood vessel wall is low, so that the per-meability of the tumor wall increases and the interstitial space is increased. Because of these differences, carcinomas with angio-genic neovasculature have prominent enhancement [24-26]. Thus, quantitative physiological parameters such as perfusion volume, blood volume, capillary permeability, and fraction vol-ume contribute to this enhancement. In this study, contrast en-
hancement characteristics were different between BOTs and stage I carcinomas, and quantitative perfusion imaging parameters such as Ktrans and Ve were helpful in differentiating between BOTs and stage I carcinomas. In brain, prostate, and breast tumors, diagnos-tic information from multiple parameters, including DW and PW sequences, is obtained and provides better accuracy than is possi-ble with the use of a single parameter [21-26].
In this study, the ADC has low statistical significance in the lo-gistic regression model analysis and the AUCis only 0.71. Fur-ther, ADC is less effective than Ktrans and Ve in differentiating be-tween BOTs and stage I carcinomas, but diagnostic accuracy when combined with Ktrans and Ve increases sensitivity with a low false positive rate. Prospective study of the association of DW and PW sequences is needed to evaluate the clinical usefulness of this approach to discriminate between BOTs and stage I carcinomas.
This study has some limitations. First, histopathologically proven cases involving only solid components are considered. This might have introduced selection and verification bias. In ad-dition, there were few cases of BOTs and it was difficult to per-form precise analysis to distinguish them from stage I carcino-mas. Second, the current implementation plan for MRI has lim-itations with respect to planar resolution and image sharpness. These can affect the computation of quantitative parameters of the DW and PW sequences. In cases where the amount of solid content is small, the accuracy of DW and PW sequences may de-crease due to the increase in motion artifacts. However, recent techniques such as multi-shot DW and volume isotropic turbo spin-echo acquisition segmented 3D sequences have enabled im-proved quantification of tissue components and dynamic signal time course features. Third, only 57 patients underwent imaging with both DW and PW sequences. Larger populations are need-ed to verify whether there is a meaningful difference between conventional MRI with both DW and PW sequences compared with the respective ones. In addition, in this study, the diagnosis could not be corrected for the same tumor misdiagnosed on DW and PW sequences. In some cases, the PW sequence was useful for diagnosis and the DW sequence was irrelevant, and in other cases, the opposite occurred. Finally, these techniques require ex-ternal validation, such as establishing a firm cutoff value for the standardized ADC, Ktrans, and Ve for universal use. Because the accuracy of this study was based on thresholds set from the same population, performance may have been overestimated. Im-provement of DW and PW techniques enables evaluation of the overall solid content, thereby reducing the possibility of overlap-ping parameters. Therefore, the sensitivity and specificity for predicting the solidity of a solid component can be improved.
In conclusion, the parameters of DW and PW sequences were
Fig. 5. ROC curves of diagnostic performance for PW sequence, DW sequence, and combining PW and DW sequences to a conventional sequence in the differentiation of borderline tumors and stage I carcinomas. 1=DW sequence only, 2=PW sequence only, and 3=combined PW+DW sequences. ROC, receiver operating characteristic; PW, perfusion-weighted; DW, diffusion-weighted.
Sens
itivi
ty
100-specificity
0 20 40 60 80 100
100
80
60
40
20
0
2
3
1
https://doi.org/10.12701/yujm.2019.00234238
Kim SH. Borderline ovarian tumor and stage I carcinoma

significantly different between BOTs and stage I carcinomas. Al-though the use of a quantitative DW sequence alone is not effective for discrimination, combination of the ADC, Ktrans, and Ve can im-prove the differentiation compared to the use of the ADC alone.
Conflicts of interest
No potential conflicts of interest relevant to this article were reported.
ORCID
See Hyung Kim, https://orcid.org/0000-0002-3268-3091
References
1. Aref M, Handbury JD, Xiuquan Ji J, Aref S, Wiener EC. Spatial and temporal resolution effects on dynamic contrast-enhanced magnetic resonance mammography. Magn Reson Imaging 2007;25:14–34.
2. Cuenod CA, Fournier L, Balvay D, Guinebretière JM. Tumor an-giogenesis: pathophysiology and implications for contrast-en-hanced MRI and CT assessment. Abdom Imaging 2006;31:188–93.
3. deSouza NM, O’Neill R, McIndoe GA, Dina R, Soutter WP. Borderline tumors of the ovary: CT and MRI features and tumor markers in differentiation from stage I disease. AJR Am J Roent-genol 2005;184:999–1003.
4. Emoto M, Iwasaki H, Mimura K, Kawarabayashi T, Kikuchi M. Differences in the angiogenesis of benign and malignant ovarian tumors, demonstrated by analyses of color Doppler ultrasound, immunohistochemistry, and microvessel density. Cancer 1997;80:899–907.
5. Fujii S, Kakite S, Nishihara K, Kanasaki Y, Harada T, Kigawa J, et al. Diagnostic accuracy of diffusion-weighted imaging in differen-tiating benign from malignant ovarian lesions. J Magn Reson Im-aging 2008;28:1149–56.
6. Hricak H, Chen M, Coakley FV, Kinkel K, Yu KK, Sica G, et al. Complex adnexal masses: detection and characterization with MR imaging--multivariate analysis. Radiology 2000;214:39–46.
7. Kozlowski P, Chang SD, Jones EC, Berean KW, Chen H, Golden-berg SL. Combined diffusion-weighted and dynamic contrast-en-hanced MRI for prostate cancer diagnosis--correlation with biop-sy and histopathology. J Magn Reson Imaging 2006;24:108–13.
8. Landis JR, Koch GG. An application of hierarchical kappa-type statistics in the assessment of majority agreement among multiple
observers. Biometrics 1977;33:363–74.9. Lee EJ, Kim SH, Kim YH, Lee HJ. Is CA-125 an additional help
to radiologic findings for differentiation borderline ovarian tumor from stage I carcinoma? Acta Radiol 2011;52:458–62.
10. Metz CE, Shen JH. Gains in accuracy from replicated readings of diagnostic images: prediction and assessment in terms of ROC analysis. Med Decis Making 1992;12:60–75.
11. Metz CE, Pan X. “Proper” binormal ROC curves: theory and maximum-likelihood estimation. J Math Psychol 1999;43:1–33.
12. Moore RG, Bast RC Jr. How do you distinguish a malignant pel-vic mass from a benign pelvic mass? Imaging, biomarkers, or none of the above. J Clin Oncol 2007;25:4159–61.
13. Nakayama T, Yoshimitsu K, Irie H, Aibe H, Tajima T, Nishie A, et al. Diffusion-weighted echo-planar MR imaging and ADC mapping in the differential diagnosis of ovarian cystic masses: usefulness of detecting keratinoid substances in mature cystic teratomas. J Magn Reson Imaging 2005;22:271–8.
14. Timmerman D, Valentin L, Bourne TH, Collins WP, Verrelst H, Vergote I, et al. Terms, definitions and measurements to de-scribe the sonographic features of adnexal tumors: a consensus opinion from the International Ovarian Tumor Analysis (IOTA) Group. Ultrasound Obstet Gynecol 2000;16:500–5.
15. Sohaib SA, Sahdev A, Van Trappen P, Jacobs IJ, Reznek RH. Characterization of adnexal mass lesions on MR imaging. AJR Am J Roentgenol 2003;180:1297–304.
16. Thomassin-Naggara I, Daraï E, Cuenod CA, Rouzier R, Callard P, Bazot M. Dynamic contrast-enhanced magnetic resonance imaging: a useful tool for characterizing ovarian epithelial tu-mors. J Magn Reson Imaging 2008;28:111–20.
17. Thomassin-Naggara I, Bazot M, Daraï E, Callard P, Thomassin J, Cuenod CA. Epithelial ovarian tumors: value of dynamic con-trast-enhanced MR imaging and correlation with tumor angio-genesis. Radiology 2008;248:148–59.
18. Thomassin-Naggara I, Daraï E, Cuenod CA, Fournier L, Tous-saint I, Marsault C, et al. Contribution of diffusion-weighted MR imaging for predicting benignity of complex adnexal mass-es. Eur Radiol 2009;19:1544–52.
19. Nishida N, Yano H, Komai K, Nishida T, Kamura T, Kojiro M. Vascular endothelial growth factor C and vascular endothelial growth factor receptor 2 are related closely to the prognosis of patients with ovarian carcinoma. Cancer 2004;101:1364–74.
20. Orre M, Lotfi-Miri M, Mamers P, Rogers PA. Increased mi-crovessel density in mucinous compared with malignant serous and benign tumours of the ovary. Br J Cancer 1998;77:2204–9.
21. Oto A, Kayhan A, Jiang Y, Tretiakova M, Yang C, Antic T, et al. Prostate cancer: differentiation of central gland cancer from
239https://doi.org/10.12701/yujm.2019.00234
Yeungnam Univ J Med 2019;36(3):231-240

benign prostatic hyperplasia by using diffusion-weighted and dynamic contrast-enhanced MR imaging. Radiology 2010; 257:715–23.
22. Padhani AR, Dzik-Jurasz A. Perfusion MR imaging of extracra-nial tumor angiogenesis. Top Magn Reson Imaging 2004; 15:41–57.
23. Song T, Laine AF, Chen Q, Rusinek H, Bokacheva L, Lim RP, et al. Optimal k-space sampling for dynamic contrast-enhanced MRI with an application to MR renography. Magn Reson Med 2009;61:1242–8.
24. Takemori M, Nishimura R, Hasegawa K. Clinical evaluation of
MRI in the diagnosis of borderline ovarian tumors. Acta Obstet Gynecol Scand 2002;81:157–61.
25. Takeuchi M, Matsuzaki K, Nishitani H. Diffusion-weighted magnetic resonance imaging of ovarian tumors: differentiation of benign and malignant solid components of ovarian masses. J Comput Assist Tomogr 2010;34:173–6.
26. Yankeelov TE, Lepage M, Chakravarthy A, Broome EE, Nier-mann KJ, Kelley MC, et al. Integration of quantitative DCE-MRI and ADC mapping to monitor treatment response in hu-man breast cancer: initial results. Magn Reson Imaging 2007; 25:1–13.
https://doi.org/10.12701/yujm.2019.00234240
Kim SH. Borderline ovarian tumor and stage I carcinoma
Determining the correlation between outdoor heatstroke incidence and climate elements in Daegu metropolitan city Jung Ho Kim1, Hyun Wook Ryoo2, Sungbae Moon2, Tae Chang Jang3, Sang Chan Jin4, You Ho Mun1, Byung Soo Do1, Sam Beom Lee1, Jong-yeon Kim5
1Department of Emergency Medicine, Yeungnam University College of Medicine, Daegu, Korea 2Department of Emergency Medicine, School of Medicine, Kyungpook National University, Daegu, Korea 3Department of Emergency Medicine, Catholic University of Daegu School of Medicine, Daegu, Korea 4Department of Emergency Medicine, Keimyung University School of Medicine, Daegu, Korea 5Department of Preventive Medicine, Catholic University of Daegu School of Medicine, Daegu, Korea
Background: Heatstroke is one of the most serious heat-related illnesses. However, establishing public policies to prevent heatstroke remains a challenge. This study aimed to investigate the most relevant climate elements and their warning criteria to prevent outdoor heatstroke (OHS). Methods: We investigated heatstroke patients from five major hospitals in Daegu metropolitan city, Korea, from June 1 to August 31, 2011 to 2016. We also collected the corresponding regional climate data from Korea Meteorological Administration. We analyzed the relationship between the climate elements and OHS occurrence by logistic regression. Results: Of 70 patients who had heatstroke, 45 (64.3%) experienced it while outdoors. Consider-ing all climate elements, only mean heat index (MHI) was related with OHS occurrence (p=0.019). Therefore, the higher the MHI, the higher the risk for OHS (adjusted odds ratio, 1.824; 95% con-fidence interval, 1.102–3.017). The most suitable cutoff point for MHI by Youden’s index was 30.0°C (sensitivity, 77.4%; specificity, 73.7%). Conclusion: Among the climate elements, MHI was significantly associated with OHS occurrence. The optimal MHI cutoff point for OHS prevention was 30.0°C.
Keywords: Climate; Heatstroke; Incidence; Meteorology; Policy
Received: April 25, 2019 Revised: June 20, 2019 Accepted: June 24, 2019
Corresponding author: Jong-yeon KimDepartment of Preventive Medicine, Catholic University of Daegu School of Medicine, 33, Dooryugongwon-ro 17-gil, Nam-gu, Daegu 42472, Korea Tel: +82-53-650-4494Fax: +82-53-2675-4752E-mail: [email protected]
Introduction
Increasing greenhouse gas emissions and consequent global warming continue to be major environmental issues. The average global temperature in July 2016 was 0.82°C higher than the mean temperatures from 1951 to 1980 [1]. Global warming may cause previously unobserved weather patterns, including extreme heat
and cold. Prolonged exposure to high temperatures can cause various heat-related illnesses, such as edema, cramps, syncope, exhaustion, and heatstroke, which can lead to death in severe cas-es [1-6]. For example, heatwaves, excessively hot weather lasting for days or weeks, claimed 14,800 lives in France in 2003 and 55,000 lives in Russia in 2010. In 2009, Australia reported a 14-fold increase in hospitalizations due to heat-related illnesses
Original articleeISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):241-248https://doi.org/10.12701/yujm.2019.00248
241https://doi.org/10.12701/yujm.2019.00248
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
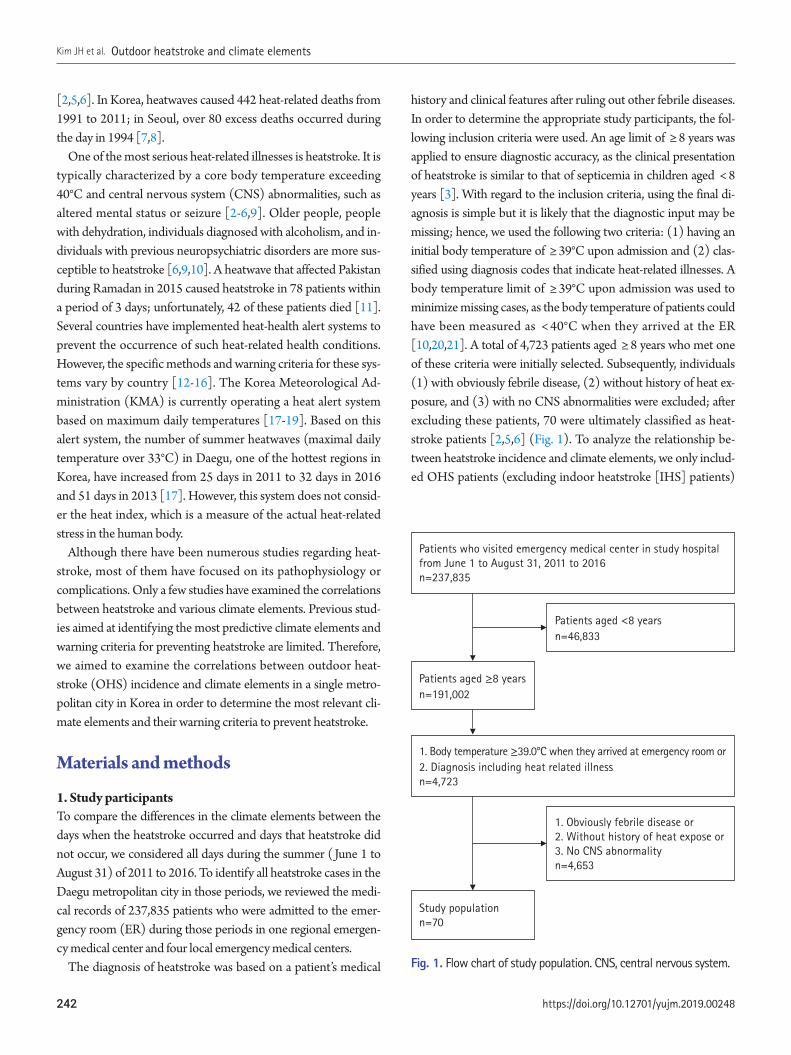
[2,5,6]. In Korea, heatwaves caused 442 heat-related deaths from 1991 to 2011; in Seoul, over 80 excess deaths occurred during the day in 1994 [7,8].
One of the most serious heat-related illnesses is heatstroke. It is typically characterized by a core body temperature exceeding 40°C and central nervous system (CNS) abnormalities, such as altered mental status or seizure [2-6,9]. Older people, people with dehydration, individuals diagnosed with alcoholism, and in-dividuals with previous neuropsychiatric disorders are more sus-ceptible to heatstroke [6,9,10]. A heatwave that affected Pakistan during Ramadan in 2015 caused heatstroke in 78 patients within a period of 3 days; unfortunately, 42 of these patients died [11]. Several countries have implemented heat-health alert systems to prevent the occurrence of such heat-related health conditions. However, the specific methods and warning criteria for these sys-tems vary by country [12-16]. The Korea Meteorological Ad-ministration (KMA) is currently operating a heat alert system based on maximum daily temperatures [17-19]. Based on this alert system, the number of summer heatwaves (maximal daily temperature over 33°C) in Daegu, one of the hottest regions in Korea, have increased from 25 days in 2011 to 32 days in 2016 and 51 days in 2013 [17]. However, this system does not consid-er the heat index, which is a measure of the actual heat-related stress in the human body.
Although there have been numerous studies regarding heat-stroke, most of them have focused on its pathophysiology or complications. Only a few studies have examined the correlations between heatstroke and various climate elements. Previous stud-ies aimed at identifying the most predictive climate elements and warning criteria for preventing heatstroke are limited. Therefore, we aimed to examine the correlations between outdoor heat-stroke (OHS) incidence and climate elements in a single metro-politan city in Korea in order to determine the most relevant cli-mate elements and their warning criteria to prevent heatstroke.
Materials and methods
1. Study participants To compare the differences in the climate elements between the days when the heatstroke occurred and days that heatstroke did not occur, we considered all days during the summer (June 1 to August 31) of 2011 to 2016. To identify all heatstroke cases in the Daegu metropolitan city in those periods, we reviewed the medi-cal records of 237,835 patients who were admitted to the emer-gency room (ER) during those periods in one regional emergen-cy medical center and four local emergency medical centers.
The diagnosis of heatstroke was based on a patient’s medical
history and clinical features after ruling out other febrile diseases. In order to determine the appropriate study participants, the fol-lowing inclusion criteria were used. An age limit of ≥ 8 years was applied to ensure diagnostic accuracy, as the clinical presentation of heatstroke is similar to that of septicemia in children aged < 8 years [3]. With regard to the inclusion criteria, using the final di-agnosis is simple but it is likely that the diagnostic input may be missing; hence, we used the following two criteria: (1) having an initial body temperature of ≥ 39°C upon admission and (2) clas-sified using diagnosis codes that indicate heat-related illnesses. A body temperature limit of ≥ 39°C upon admission was used to minimize missing cases, as the body temperature of patients could have been measured as < 40°C when they arrived at the ER [10,20,21]. A total of 4,723 patients aged ≥ 8 years who met one of these criteria were initially selected. Subsequently, individuals (1) with obviously febrile disease, (2) without history of heat ex-posure, and (3) with no CNS abnormalities were excluded; after excluding these patients, 70 were ultimately classified as heat-stroke patients [2,5,6] (Fig. 1). To analyze the relationship be-tween heatstroke incidence and climate elements, we only includ-ed OHS patients (excluding indoor heatstroke [IHS] patients)
Patients who visited emergency medical center in study hospital from June 1 to August 31, 2011 to 2016n=237,835
1. Body temperature ≥39.0°C when they arrived at emergency room or 2. Diagnosis including heat related illnessn=4,723
Patients aged <8 yearsn=46,833
1. Obviously febrile disease or2. Without history of heat expose or 3. No CNS abnormality n=4,653
Patients aged ≥8 yearsn=191,002
Study populationn=70
Fig. 1. Flow chart of study population. CNS, central nervous system.
https://doi.org/10.12701/yujm.2019.00248242
Kim JH et al. Outdoor heatstroke and climate elements
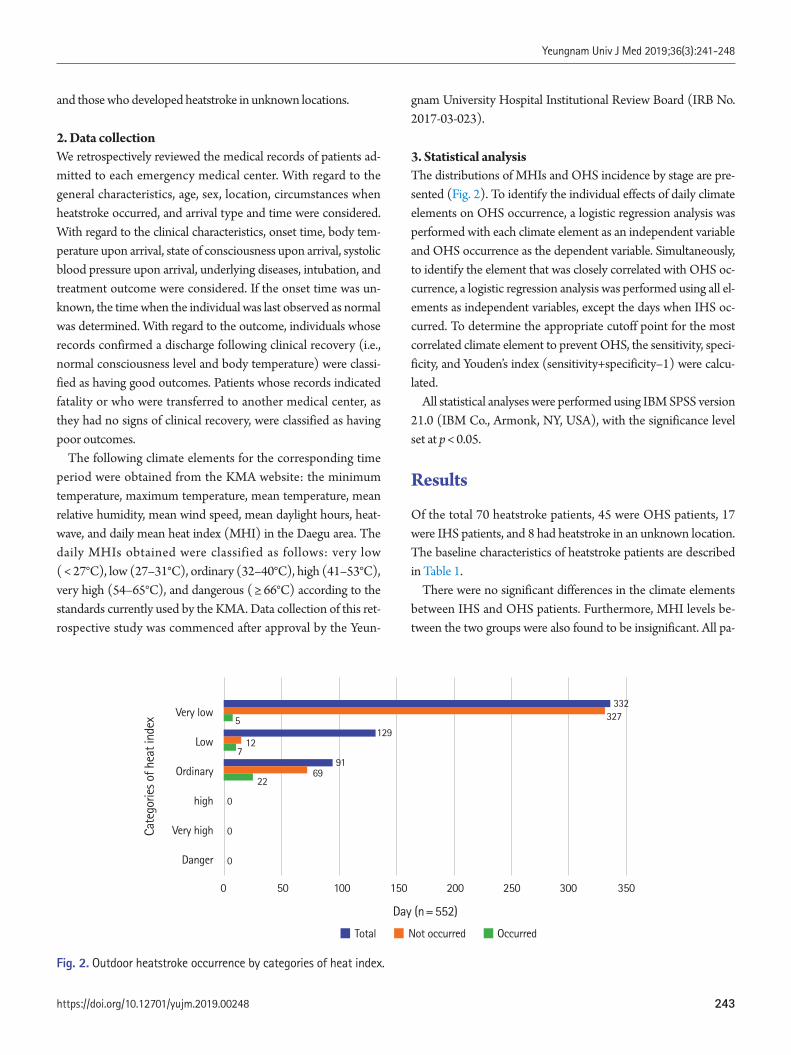
and those who developed heatstroke in unknown locations.
2. Data collection We retrospectively reviewed the medical records of patients ad-mitted to each emergency medical center. With regard to the general characteristics, age, sex, location, circumstances when heatstroke occurred, and arrival type and time were considered. With regard to the clinical characteristics, onset time, body tem-perature upon arrival, state of consciousness upon arrival, systolic blood pressure upon arrival, underlying diseases, intubation, and treatment outcome were considered. If the onset time was un-known, the time when the individual was last observed as normal was determined. With regard to the outcome, individuals whose records confirmed a discharge following clinical recovery (i.e., normal consciousness level and body temperature) were classi-fied as having good outcomes. Patients whose records indicated fatality or who were transferred to another medical center, as they had no signs of clinical recovery, were classified as having poor outcomes.
The following climate elements for the corresponding time period were obtained from the KMA website: the minimum temperature, maximum temperature, mean temperature, mean relative humidity, mean wind speed, mean daylight hours, heat-wave, and daily mean heat index (MHI) in the Daegu area. The daily MHIs obtained were classified as follows: very low ( < 27°C), low (27–31°C), ordinary (32–40°C), high (41–53°C), very high (54–65°C), and dangerous ( ≥ 66°C) according to the standards currently used by the KMA. Data collection of this ret-rospective study was commenced after approval by the Yeun-
gnam University Hospital Institutional Review Board (IRB No. 2017-03-023).
3. Statistical analysis The distributions of MHIs and OHS incidence by stage are pre-sented (Fig. 2). To identify the individual effects of daily climate elements on OHS occurrence, a logistic regression analysis was performed with each climate element as an independent variable and OHS occurrence as the dependent variable. Simultaneously, to identify the element that was closely correlated with OHS oc-currence, a logistic regression analysis was performed using all el-ements as independent variables, except the days when IHS oc-curred. To determine the appropriate cutoff point for the most correlated climate element to prevent OHS, the sensitivity, speci-ficity, and Youden’s index (sensitivity+specificity–1) were calcu-lated.
All statistical analyses were performed using IBM SPSS version 21.0 (IBM Co., Armonk, NY, USA), with the significance level set at p < 0.05.
Results
Of the total 70 heatstroke patients, 45 were OHS patients, 17 were IHS patients, and 8 had heatstroke in an unknown location. The baseline characteristics of heatstroke patients are described in Table 1.
There were no significant differences in the climate elements between IHS and OHS patients. Furthermore, MHI levels be-tween the two groups were also found to be insignificant. All pa-
Fig. 2. Outdoor heatstroke occurrence by categories of heat index.
Day (n=552)
■ Total ■ Not occurred ■ Occurred
0 50 100 150 200 250 300 350
Very low
Low
Ordinary
high
Very high
Danger
Cate
gorie
s of h
eat i
ndex
3323275
129
9169
22
0
0
0
127
243https://doi.org/10.12701/yujm.2019.00248
Yeungnam Univ J Med 2019;36(3):241-248

tients developed heatstroke at an MHI level below “ordinary” (Table 2).
During the study period (552 days), the day of heatstroke oc-curred was 47 days, including the 34 days in which OHS oc-curred. The MHI of the 34 days in which OHS occurred were higher than that of the other 518 days (32.1 ± 4.5°C and 26.1 ± 4.2°C, respectively). A 1°C increase in the MHI was sig-nificantly associated with a 1.393-fold increase in the risk for OHS (95% confidence interval [CI], 1.255–1.546). The mean,
maximum, and minimum daily temperatures and diurnal tem-perature range of OHS occurred days were also greater than those of the other days. A 1°C increase in the mean, maximum, and minimum daily temperatures and diurnal temperature range was significantly associated with a 1.710-fold (95% CI, 1.436–2.036), 1.787-fold (95% CI, 1.489–2.145), 1.450-fold (95% CI, 1.246–1.688), and 1.352-fold (95% CI, 1.175–1.557) increase in the risk for OHS, respectively. Similarly, a 1-hr increase in day-light hours was significantly associated with a 1.397-fold increase
Table 2. Climate elements and location of heatstroke
Variable Outdoor (n=45) Indoor (n=17) Unidentified (n=8) Total (n=70) p-valuea)
Climate element Mean heat index (°C) 32.6±4.6 33.7±2.4 34.5±1.4 33.1±4.0 0.228 Mean air temperature (°C) 29.4±2.9 30.4±1.8 30.8±0.9 29.8±2.5 0.106 Maximal air temperature (°C) 35.2±2.5 36.0±1.8 36.2±0.9 35.5±2.2 0.252 Minimum air temperature (°C) 24.3±3.3 25.5±2.1 25.8±1.4 24.7±3.0 0.100 Daily temperature range (°C) 11.0±1.9 10.5±1.5 10.3±1.9 10.8±1.8 0.394 Mean relatively humidity (%) 62.7±8.6 60.2±6.9 61.5±6.8 61.9±8.0 0.301 Mean wind speed (m/sec) 1.7±0.4 1.9±0.5 1.8±0.4 1.8±0.4 0.155 Amount of sunshine (hr) 9.7±2.4 10.0±3.5 9.5±2.6 9.8±2.7 0.722Heat index stage 0.302 Very low 7 (15.6) 0 (0.0) 0 (0.0) 7 (10.0) Low 9 (20.0) 4 (23.5) 0 (0.0) 13 (18.6) Ordinary 29 (64.4) 13 (76.5) 8 (100.0) 50 (71.4)
Values are presented as mean±standard deviation or number (%).a)Analysis between outdoor and indoor cases by t-test and Fisher`s exact test.
Table 1. Baseline characteristics of heatstroke patients according to the place
Variable Total (n=70) Outdoor (n=45) Indoor (n=17) Unknown (n=8)Age (yr) 64.2±21.0 62.1±22.8 71.7±16.6 60.4±16.8Male 50 36 (80.0) 7 (41.2) 7 (87.5)Type of arrival Public EMS 44 24 (53.3) 17 (100.0) 3 (37.5) From other hospital 24 19 (42.2) 0 (0.0) 5 (62.5) Others 2 2 (4.4) 0 (0.0) 0 (0.0)BT when arrival at hospital (°C) 39.5±1.7 39.0±1.7 41.0±0.7 39.6±1.8SBP when arrival at hospital (mmHg) 118.0±31.0 115.6±29.9 130.6±33.9 103.8±24.4Mental status when arrival at hospital Alert 21 14 (31.1) 5 (29.4) 2 (25.0) Drowsy 25 16 (35.6) 4 (23.5) 5 (62.5) Stupor 7 5 (11.1) 1 (5.9) 1 (12.5) Coma 17 10 (22.2) 7 (41.2) 0 (0.0)Underlying disease Hypertension 25 13 (28.9) 12 (70.6) 0 (0.0) Diabetics mellitus 11 7 (15.6) 4 (23.5) 0 (0.0) Cerebrovascular disease 8 4 (8.9) 3 (17.6) 1 (12.5)
Values are presented as mean±standard deviation or number (%).EMS, emergency medical service; BT, body temperature; SBP, systolic blood pressure.
https://doi.org/10.12701/yujm.2019.00248244
Kim JH et al. Outdoor heatstroke and climate elements

risk for OHS (95% CI, 1.227–1.589). A 1% increase in mean humidity was significantly associated
with a 0.938-fold reduction in the risk for OHS (95% CI, 0.909– 0.969). A 1 m/sec increase in the mean wind speed was also sig-nificantly associated with a 0.371-fold reduction in the risk of OHS (95% CI, 0.199–0.694). However, when all climate ele-ments were considered simultaneously, only the daily MHI was found to significantly increase OHS risk: a 1°C increase in the daily MHI resulted in a 1.824-fold (95% CI, 1.102–3.017) in-crease in OHS risk (Table 3).
The sensitivity, specificity, and Youden’s index, with exception of the days when heatstroke occurred indoors, were calculated to determine the warning criteria for OHS. The most suitable cutoff point was confirmed to be a daily MHI of 30.0°C (Youden’s in-dex, 0.511; sensitivity, 77.4%; specificity, 73.7%; Table 4).
Discussion
Extreme weather phenomena due to global warming continue to occur worldwide, with a significant impact on human life [22-26]. Heatwaves are one of the most concerning meteorological conditions expected to cause damage as climate change progress-es [7,27-29]. An individual affected by heatstroke loses the abili-ty to regulate body temperature due to damage to the hypotha-lamic thermoregulatory system following prolonged exposure to high temperatures [30,31]. A sustained elevated core tempera-ture can damage a number of internal organs, which can lead to a life-threatening situation [2-4,21]. Thus, many countries have been making efforts to reduce the disease burden associated with heat-related illnesses, including the implementation of effective heat alert systems [15,16,32-37]. An effective alert system re-quires the selection of the most appropriate climate elements and their warning criteria to predict heatstroke occurrence [38].
In the literature, there are conflicting findings regarding which elements are most predictive of heatstroke occurrence. Some studies have reported that heat index is strongly correlated with the number of patients admitted to the ER due to heat-related ill-nesses, which suggests the application of the heat index as a pre-dictor of heat-related illness [19,39,40]. Other studies have re-ported that the daily maximum temperature is a more appropri-ate predictor of heatstroke occurrence than the heat index [8,28,41]. Heat index is the biometeorological indicator used by the United States National Weather Service [19]. It is calculated by measuring the dry-bulb Fahrenheit temperature and relative humidity to estimate the heat burden according to outdoor con-ditions.
Based on our study, various climate elements, including the mean, maximum, and minimum daily temperatures; diurnal temperature variations; daylight hours; and the MHI, were sig-nificant risk factors for OHS occurrence, whereas mean humidity and mean wind speed were significant protective factors. This finding is congruent to the fact that, aside from prolonged expo-sure to high heat, dry conditions and poor ventilation increase the risk of heatstroke. However, after simultaneously considering these climate elements, we found that the MHI was the only ef-fective predictor of OHS incidence. The risk of OHS increased significantly by 1.82-fold for each 1°C increase in the MHI. The finding that the MHI was the only significant predictor of OHS may be attributed to the fact that the MHI is a biometeorological index that incorporates both dry bulb temperature and relative humidity for measuring climate-related heat stress in the human body. Thus, the heat index, which reflects both air temperature and humidity, may be more useful for predicting OHS incidence than the maximum daily temperature, which only reflects air temperature.
In South Korea, the KMA has been operating heatwave alerts
Table 3. Association between climate elements and days of outdoor heatstroke by logistic regression analysis
Outdoor heatstroke day Yes (n=34 days) Noa) (n=508 days) OR [95% CI] aORb) [95% CI]Mean heat index (°C) 32.1±4.5 [22-39] 26.0±4.2 [18-39] 1.353 [1.217-1.504] 1.708 [1.131-2.828]Mean air temperature (°C) 28.9±2.7 [22-32] 25.0±2.9 [17-32] 1.654 [1.375-1.988] 0.776 [0.315-1.913]Maximal air temperature (°C) 34.8±2.4 [28-38] 29.9±3.6 [19-37] 1.713 [1.418-2.069] 0.671 [0.265-1.669]Minimum air temperature (°C) 24.0±3.1 [16-27] 21.3±2.9 [12-28] 1.384 [1.182-1.622] 1.492 [0.572-3.892]Daily temperature range (°C) 10.4±1.9 [7-15] 8.2±2.8 [1-16] 1.356 [1.166-1.578] 1.770 [0.732-4.282]Mean relatively humidity (%) 60.7±8.8 [36-76] 69.1±11.6 [32-97] 0.941 [0.909-0.973] 0.950 [0.879-1.027]Mean wind speed (m/sec) 1.2±0.5 [1-3] 1.7±0.8 [0-5] 0.392 [0.201-0.764] 0.440 [0.180-1.078]Amount of sunshine (hr) 9.4±2.5 [2-12] 5.1±4.0 [0-13] 1.396 [1.212-1.608] 1.220 [0.958-1.553]
Values are presented as mean±standard deviation [minimum, maximum].OR, odds ratio; CI, confidence interval; aOR, adjusted OR.a)Excepted 10 days of indoor heatstroke only. b)Calculated considering all climates elements together.
245https://doi.org/10.12701/yujm.2019.00248
Yeungnam Univ J Med 2019;36(3):241-248
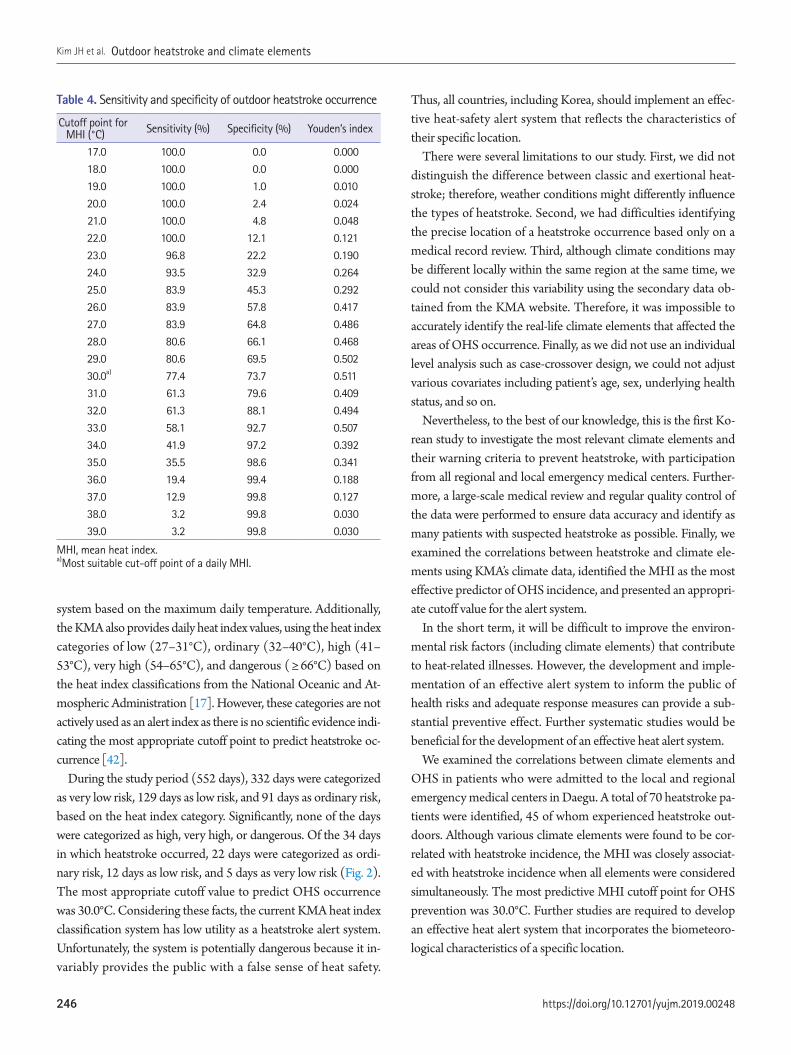
system based on the maximum daily temperature. Additionally, the KMA also provides daily heat index values, using the heat index categories of low (27–31°C), ordinary (32–40°C), high (41–53°C), very high (54–65°C), and dangerous ( ≥ 66°C) based on the heat index classifications from the National Oceanic and At-mospheric Administration [17]. However, these categories are not actively used as an alert index as there is no scientific evidence indi-cating the most appropriate cutoff point to predict heatstroke oc-currence [42].
During the study period (552 days), 332 days were categorized as very low risk, 129 days as low risk, and 91 days as ordinary risk, based on the heat index category. Significantly, none of the days were categorized as high, very high, or dangerous. Of the 34 days in which heatstroke occurred, 22 days were categorized as ordi-nary risk, 12 days as low risk, and 5 days as very low risk (Fig. 2). The most appropriate cutoff value to predict OHS occurrence was 30.0°C. Considering these facts, the current KMA heat index classification system has low utility as a heatstroke alert system. Unfortunately, the system is potentially dangerous because it in-variably provides the public with a false sense of heat safety.
Thus, all countries, including Korea, should implement an effec-tive heat-safety alert system that reflects the characteristics of their specific location.
There were several limitations to our study. First, we did not distinguish the difference between classic and exertional heat-stroke; therefore, weather conditions might differently influence the types of heatstroke. Second, we had difficulties identifying the precise location of a heatstroke occurrence based only on a medical record review. Third, although climate conditions may be different locally within the same region at the same time, we could not consider this variability using the secondary data ob-tained from the KMA website. Therefore, it was impossible to accurately identify the real-life climate elements that affected the areas of OHS occurrence. Finally, as we did not use an individual level analysis such as case-crossover design, we could not adjust various covariates including patient’s age, sex, underlying health status, and so on.
Nevertheless, to the best of our knowledge, this is the first Ko-rean study to investigate the most relevant climate elements and their warning criteria to prevent heatstroke, with participation from all regional and local emergency medical centers. Further-more, a large-scale medical review and regular quality control of the data were performed to ensure data accuracy and identify as many patients with suspected heatstroke as possible. Finally, we examined the correlations between heatstroke and climate ele-ments using KMA’s climate data, identified the MHI as the most effective predictor of OHS incidence, and presented an appropri-ate cutoff value for the alert system.
In the short term, it will be difficult to improve the environ-mental risk factors (including climate elements) that contribute to heat-related illnesses. However, the development and imple-mentation of an effective alert system to inform the public of health risks and adequate response measures can provide a sub-stantial preventive effect. Further systematic studies would be beneficial for the development of an effective heat alert system.
We examined the correlations between climate elements and OHS in patients who were admitted to the local and regional emergency medical centers in Daegu. A total of 70 heatstroke pa-tients were identified, 45 of whom experienced heatstroke out-doors. Although various climate elements were found to be cor-related with heatstroke incidence, the MHI was closely associat-ed with heatstroke incidence when all elements were considered simultaneously. The most predictive MHI cutoff point for OHS prevention was 30.0°C. Further studies are required to develop an effective heat alert system that incorporates the biometeoro-logical characteristics of a specific location.
Table 4. Sensitivity and specificity of outdoor heatstroke occurrence
Cutoff point for MHI (°C) Sensitivity (%) Specificity (%) Youden’s index
17.0 100.0 0.0 0.00018.0 100.0 0.0 0.00019.0 100.0 1.0 0.01020.0 100.0 2.4 0.02421.0 100.0 4.8 0.04822.0 100.0 12.1 0.12123.0 96.8 22.2 0.19024.0 93.5 32.9 0.26425.0 83.9 45.3 0.29226.0 83.9 57.8 0.41727.0 83.9 64.8 0.48628.0 80.6 66.1 0.46829.0 80.6 69.5 0.50230.0a) 77.4 73.7 0.51131.0 61.3 79.6 0.40932.0 61.3 88.1 0.49433.0 58.1 92.7 0.50734.0 41.9 97.2 0.39235.0 35.5 98.6 0.34136.0 19.4 99.4 0.18837.0 12.9 99.8 0.12738.0 3.2 99.8 0.03039.0 3.2 99.8 0.030
MHI, mean heat index.a)Most suitable cut-off point of a daily MHI.
https://doi.org/10.12701/yujm.2019.00248246
Kim JH et al. Outdoor heatstroke and climate elements

Conflicts of interest
No potential conflicts of interest relevant to this article was re-ported.
ORCID
Jung Ho Kim, https://orcid.org/0000-0002-3215-4640Hyun Wook Ryoo, https://orcid.org/0000-0002-1361-9887Sungbae Moon, https://orcid.org/0000-0001-6928-8573Tae Chang Jang, https://orcid.org/0000-0002-0895-5990Sang Chan Jin, https://orcid.org/0000-0002-4347-0171You Ho Mun, https://orcid.org/0000-0003-0585-8674Sam Beom Lee, https://orcid.org/0000-0002-1236-2629Jong-yeon Kim, https://orcid.org/0000-0002-4478-6127
References
1. NASA’s Goddard Institute for Space Studies. July 2017 equaled record July 2016 [Internet]. Pasadena: Earth Science Communi-cations Team at NASA’s Jet Propulsion Laboratory; 2017 [cited 2018 Dec 20]. https://climate.nasa.gov/news/2618/july-2017-equaled-record-july-2016/
2. Bouchama A, Knochel JP. Heat stroke. N Engl J Med 2002;346:1978–88.
3. Jardine DS. Heat illness and heat stroke. Pediatr Rev 2007; 28:249–58.
4. Wang Y, Bobb JF, Papi B, Wang Y, Kosheleva A, Di Q, et al. Heat stroke admissions during heat waves in 1,916 US counties for the period from 1999 to 2010 and their effect modifiers. Environ Health 2016;15:83.
5. Yan YE, Zhao YQ, Wang H, Fan M. Pathophysiological factors underlying heatstroke. Med Hypotheses 2006;67:609–17.
6. Yaqub B, Al Deeb S. Heat strokes: aetiopathogenesis, neurological characteristics, treatment and outcome. J Neurol Sci 1998; 156:144–51.
7. Kim DW, Chung JH, Lee JS, Lee JS. Characteristics of heat wave mortality in Korea. Atmosphere 2014;24:225–34.
8. Kim J, Lee DG, Park IS, Choi BC, Kim JS. Influences of heat waves on daily mortality in South Korea. Atmosphere 2006;16:269–78.
9. Pryor RR, Bennett BL, O’Connor FG, Young JM, Asplund CA. Medical evaluation for exposure extremes: heat. Wilderness Envi-ron Med 2015;26(4 Suppl):S69–75.
10. Kim SH, Jo SN, Myung HN, Jang JY. The effect of pre-existing medical conditions on heat stroke during hot weather in South Korea. Environ Res 2014;133:246–52.
11. Ghumman U, Horney J. Characterizing the impact of extreme
heat on mortality, Karachi, Pakistan, June 2015. Prehosp Disas-ter Med 2016;31:263–6.
12. Alberini A, Gans W, Alhassan M. Individual and public-program adaptation: coping with heat waves in five cities in Canada. Int J Environ Res Public Health 2011;8:4679–701.
13. Anderson GB, Bell ML, Peng RD. Methods to calculate the heat index as an exposure metric in environmental health research. Environ Health Perspect 2013;121:1111–9.
14. Hajat S, Sheridan SC, Allen MJ, Pascal M, Laaidi K, Yagouti A, et al. Heat-health warning systems: a comparison of the predic-tive capacity of different approaches to identifying dangerously hot days. Am J Public Health 2010;100:1137–44.
15. Kovats RS, Kristie LE. Heatwaves and public health in Europe. Eur J Public Health 2006;16:592–9.
16. Toloo G, FitzGerald G, Aitken P, Verrall K, Tong S. Evaluating the effectiveness of heat warning systems: systematic review of epidemiological evidence. Int J Public Health 2013;58:667–81.
17. Korea Meteorological Administration. [Korean climate resourc-es] [Internet]. Seoul: Korea Meteorological Administration; 2019 [cited 2018 Dec 20]. http://www.kma.go.kr/weather/cli-mate/average_south.jsp
18. National Centers for Environmental Information. Climate change and variability [Internet]. Asheville: National Centers for Envi-ronmental Information; 2018 [cited 2018 Dec 20]. https://www.ncdc.noaa.gov/climate-information/climate-change-and-vari-ability
19. Sung TI, Wu PC, Lung SC, Lin CY, Chen MJ, Su HJ. Relation-ship between heat index and mortality of 6 major cities in Tai-wan. Sci Total Environ 2013;442:275–81.
20. Jo YH, Shin SD, Kim DH, Jo IJ, Rhee JE, Suh GJ, et al. Descrip-tive study of prognostic factors of exertional heat stroke in mili-tary personnel. J Korean Soc Emerg Med 2003;14:409–14.
21. LoVecchio F. Heat emergencies. In: Tintinalli JE, Stapczynski JS, MA OJ, Cline DM, Meckler GD, Yealy DM, editors. Tintinalli’s emergency medicine: a comprehensive study guide. 8th ed. New York: McGraw-Hill Education; 2016. p. 1365–71.
22. Harlan SL, Ruddell DM. Climate change and health in cities: im-pacts of heat and air pollution and potential co-benefits from miti-gation and adaptation. Curr Opin Environ Sustain 2011;3:126–34.
23. Marchetti E, Capone P, Freda D. Climate change impact on mi-croclimate of work environment related to occupational health and productivity. Ann Ist Super Sanita 2016;52:338–42.
24. Murakami S, Miyatake N, Sakano N. Changes in air temperature and its relation to ambulance transports due to heat stroke in all 47 prefectures of Japan. J Prev Med Public Health 2012;45:309–15.
247https://doi.org/10.12701/yujm.2019.00248
Yeungnam Univ J Med 2019;36(3):241-248
25. Schmeltz MT, Petkova EP, Gamble JL. Economic burden of hospitalizations for heat-related illnesses in the United States, 2001-2010. Int J Environ Res Public Health 2016;13:pii:E894.
26. Zhang Y, Nitschke M, Bi P. Risk factors for direct heat-related hospitalization during the 2009 Adelaide heatwave: a case crossover study. Sci Total Environ 2013;442:1–5.
27. Kravchenko J, Abernethy AP, Fawzy M, Lyerly HK. Minimiza-tion of heatwave morbidity and mortality. Am J Prev Med 2013; 44:274–82.
28. Li Y, Li C, Luo S, He J, Cheng Y, Jin Y. Impacts of extremely high temperature and heatwave on heatstroke in Chongqing, China. Environ Sci Pollut Res Int 2017;24:8534–40.
29. Williams S, Nitschke M, Weinstein P, Pisaniello DL, Parton KA, Bi P. The impact of summer temperatures and heatwaves on mortality and morbidity in Perth, Australia 1994-2008. Environ Int 2012;40:33–8.
30. Kenney WL, DeGroot DW, Alexander LM. Extremes of human heat tolerance: life at the precipice of thermoregulatory failure. J Therm Biol 2004;29:479–85.
31. Kosaka M, Yamane M, Ogai R, Kato T, Ohnishi N, Simon E. Human body temperature regulation in extremely stressful en-vironment: epidemiology and pathophysiology of heat stroke. J Therm Biol 2004;29:495–501.
32. Canada. Health Canada. Health Environments and Consumer Safety. Heat alert and response systems to protect health: best practices guidebook. Ottawa-Ontario: Health Canada; 2012.
33. Josseran L, Fouillet A, Caillère N, Brun-Ney D, Ilef D, Brucker G, et al. Assessment of a syndromic surveillance system based on morbidity data: results from the Oscour network during a heat wave. PLoS One 2010;5:e11984.
34. Li T, Ding F, Sun Q, Zhang Y, Kinney PL. Heat stroke internet searches can be a new heatwave health warning surveillance in-
dicator. Sci Rep 2016;6:37294.35. Méndez-Lázaro P, Muller-Karger FE, Otis D, McCarthy MJ,
Rodríguez E. A heat vulnerability index to improve urban pub-lic health management in San Juan, Puerto Rico. Int J Biomete-orol 2018;62:709–22.
36. Nitschke M, Tucker GR, Hansen AL, Williams S, Zhang Y, Bi P. Impact of two recent extreme heat episodes on morbidity and mortality in Adelaide, South Australia: a case-series analysis. Environ Health 2011;10:42.
37. Sheridan SC, Kalkstein LS. Progress in heat watch–warning sys-tem technology. Bull Am Meteorol Soc 2004;85:1931–42.
38. O’Neill MS, Carter R, Kish JK, Gronlund CJ, White-Newsome JL, Manarolla X, et al. Preventing heat-related morbidity and mortality: new approaches in a changing climate. Maturitas 2009;64:98–103.
39. Harlan SL, Chowell G, Yang S, Petitti DB, Morales Butler EJ, Ruddell BL, et al. Heat-related deaths in hot cities: estimates of human tolerance to high temperature thresholds. Int J Environ Res Public Health 2014;11:3304–26.
40. Lee MS, Hong KJ, Shin SD, Song KJ, Ryoo HW, Song SW, et al. Development and implementation of emergency department based heat related illness active surveillance system: effect of heat index on daily emergency department visits due to heat re-lated illness. J Korean Soc Emerg Med 2014;25:595–601.
41. Bai L, Ding G, Gu S, Bi P, Su B, Qin D, et al. The effects of sum-mer temperature and heat waves on heat-related illness in a coastal city of China, 2011-2013. Environ Res 2014;132:212–9.
42. Kalkstein AJ, Sheridan SC. The social impacts of the heat-health watch/warning system in Phoenix, Arizona: assessing the per-ceived risk and response of the public. Int J Biometeorol 2007;52:43–55.
https://doi.org/10.12701/yujm.2019.00248248
Kim JH et al. Outdoor heatstroke and climate elements

There is considerable overlap in the clinical presentations of apathy and depression. However, differential diagnosis between apathy and other psychiatric conditions, including depression and dementia, is important. In this report, we present the case of a 67-year-old woman with a history of receiving selective serotonin reuptake inhibitor (SSRI) treatment for depression. Dif-ferential diagnosis between treatment-resistant depression and SSRI-induced apathy syn-drome was required. The symptoms of her apathy syndrome were relieved after the discontin-uation of SSRIs and the addition of olanzapine, methylphenidate, and modafinil. Furthermore, we briefly review related literature in this article.
Keywords: Apathy; Depression; Serotonin reuptake inhibitor
Apathy syndrome in a patient previously treated with selective serotonin reuptake inhibitors for depression Hye-Geum Kim, Bon-Hoon Koo, Seung Woo Lee, Eun-Jin Cheon Department of Psychiatry, Yeungnam University College of Medicine, Daegu, Korea
Introduction
Apathy is a behavioral syndrome characterized by a decrease in interest, motivation, or initiation of action. Apathy may present in a similar manner as depression. However, Marin [1] emphasized the importance of differentiating between apathy and other psy-chiatric conditions, including depression, dementia, delirium, abulia, akinesia, despair, and demoralization. He proposed the fol-lowing definition of apathy: a syndrome in which there is a prima-ry absence of motivation that is not attributable to cognitive im-pairment, emotional distress, or diminished level of consciousness [1]. Many patients with apathy syndrome reported that “this feel-ing was unlike the lack of motivation they had sometimes experi-enced during prior episodes of depression,” or that “their feelings of apathy bore no relationship to depression.”
One reason for the importance of differentiating apathy syn-drome from depression is that apathy syndrome has been report-ed in a number of patients receiving selective serotonin reuptake inhibitor (SSRI) treatment over the last decade [2]. Apathy also
Case reporteISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):249-253https://doi.org/10.12701/yujm.2019.00150
Received: January 25, 2019 Revised: March 5, 2019 Accepted: March 6, 2019
Corresponding author: Eun-Jin Cheon Department of Psychiatry, Yeungnam University College of Medicine, 170, Hyeonchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-3340 Fax: +82-53-629-0256 E-mail: [email protected]
serves as a behavioral marker for rapidly progressing dementia, with a greater decline in cognitive, functional, and emotional im-pairment [3]. The presence of apathy is linked to deficits in the performance of activities of daily living and a functional decline [4]. Thus, the prompt recognition and treatment of apathy are crucial [4].
Here, we report the case of a patient who experienced apathy syndrome that was difficult to differentiate from depression and dementia. Written informed consent for the publication of this case report, approved by the institutional review board (YUMC 2017-12-022), was obtained from the patient.
Case
A 67-year-old woman with a remote history of depression was re-ferred to our clinic due to the presentation of resistant depressive symptoms despite being treated with multiple antidepressant drugs, including escitalopram, paroxetine, duloxetine, and mir-tazapine. She was admitted to the psychiatric clinic for approxi-
249https://doi.org/10.12701/yujm.2019.00150
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

mately a month with depression diagnosed about 2 years previ-ously. Subsequently, her symptoms had improved. About 3 months previously, she relapsed and was admitted to the same clinic again, where she received medications including duloxetine 60 mg, mirtazapine 30 mg, escitalopram 20 mg, aripiprazole 1 mg, and quetiapine 75 mg for 2 months. However, her symptoms did not improve with the medication, and she was referred to our clinic. The depression symptoms included diminished interest, loss of energy, psychomotor agitation, weight loss, and insomnia. She reported that she was lethargic and did not want to do any-thing but she was not particularly depressed and had not experi-enced any increase in stress recently. She was admitted to our de-partment of psychiatry for accurate assessment and treatment. The patient received a score of 26 on the Hamilton Depression Rating Scale. In addition to depressive symptoms, she had experi-enced cognitive impairment with gradual onset. She had a score of 22/30 on the Korean-Mini Mental State Examination, 1 on the Clinical Dementia Rating, and 4 on the Global Deterioration Scale. Her cognitive functions, including memory, executive func-tion, and language function, were particularly impaired. In a struc-tural brain imaging study, no degenerative changes other than a small aneurysm and internal carotid artery stenosis that had al-ready been diagnosed were observed (Fig. 1). The results of the brain single-photon emission computed tomography for the eval-uation of brain function indicated reduced perfusion in both ante-rior cingulate gyri (Fig. 2). She had no other medical history.
During the evaluation, we prescribed antidepressants such as fluoxetine 60 mg, venlafaxine 225 mg, mirtazapine 30 mg, and ar-ipiprazole 5 mg, because the patient’s symptoms for depression required immediate treatment. She continued to take the medica-tions for more than a month, but the symptoms did not improve, and she appeared to be deteriorating. In a reassessment of the pa-tient's medical history we focused on her apathy symptoms in-stead of her depression symptoms. At that point, the patient was evaluated and received a score of 72 on the Apathy Evaluation Scale (AES). This 18-item scale assesses apathy in behavioral, cognitive, and emotional domains over the previous 4 weeks. Scores range from 18 to 72, with higher scores indicating greater apathy. Subsequently, we first reduced and then discontinued all antidepressants, including SSRIs. Olanzapine and sleeping pills were continued to control her insomnia and agitation. Subse-quently, she became slightly more active but this change was not sufficient. We prescribed methylphenidate and gradually in-creased its dosage to 25 mg. We then added modafinil 200 mg to her treatment regime. Following these changes of medication, her score on the AES improved to 35, and she continued performing her daily activities after discharge. The drugs she was taking at dis-
charge were: methylphenidate 25 mg, modafinil 200 mg, olanzap-ine 10 mg, donepezil 10 mg, and aripiprazole 5 mg. As her activity levels increased a little, her daily life function improved slightly but her subjective cognitive decline continued. We will keep track of the changes in her cognitive function in the future.
Discussion
Apathy is a common behavioral problem that often goes undiag-nosed and untreated [4]. There is considerable overlap in the clinical presentations of apathy and depression. Furthermore, apa-thy may be part of a cluster of negative symptoms in patients with illnesses such as schizophrenia or Alzheimer’s disease [5]. How-ever, apathy has been demonstrated to relate, independently of these other psychiatric symptoms, to a variety of outcomes [5]. The presence of apathy is linked to deficits in the performance of activities of daily living and functional decline and can be of con-siderable clinical significance [4].
A common feature of many of the conditions in which apathy is prominent is the presence of lesions or other abnormalities in the frontal lobe-subcortical circuitry. Neuroimaging studies of various clinical populations have reported correlations between apathy and structural and functional changes within the frontal lobe, par-ticularly the anterior cingulate gyrus and subregions of the basal
Fig. 1. No degenerative changes on T2-flair image. RPF, right posterior feet.
https://doi.org/10.12701/yujm.2019.00150250
Kim HG et al. Apathy syndrome in a patient previously treated with SSRIs

ganglia. Neuropsychological studies have reported a relationship between apathy and poorer performance on tests of executive functions [6]. Indeed, in the present case, the patient displayed decreased function of the anterior cingulate gyri as well as deteri-oration of executive functions.
A recent case-control study [7] reported that apathy appeared to be greater in patients who were treated with SSRI than in pa-
tients who were not. Currently, we do not have enough data to understand how altering of serotonergic signaling might cause ap-athy. It is biologically possible that frontal lobe dysfunction, in-duced by SSRIs, may be responsible for the apathy [7]. Condi-tions that can induce frontal lobe dysfunctions are often caused by imbalances of neurotransmitters in the brain. Prolonged and ex-cessive serotonin in the synapse may lead to a decrease in the
Fig. 2. Mild reduction of perfusion in anterior cingulate gyrus on brain single-photon emission computed tomography.
251https://doi.org/10.12701/yujm.2019.00150
Yeungnam Univ J Med 2019;36(3):249-253
transmission of dopamine in the frontal lobe. High serotonin lev-els may also cause a decrease in acetylcholine which can induce an increase in dopamine function. A relationship between serotonin and noradrenaline is another possible mechanism [8].
If SSRI-induced apathy is detected, reduction of SSRI dose or discontinuation of SSRIs is required. When discontinuation of the SSRI is not successful, augmentation or switching to a differ-ent class of medications is helpful [2]. Apathy has been emerging as a target for pharmacotherapeutic interventions, and new trials have recently been completed [9]. Methylphenidate for the treat-ment of apathy has been investigated in double-blind, place-bo-controlled randomized trials (RCTs), and an effect on apathy was reported [10]. The findings of these studies were consistent with other findings supporting dopaminergic dysfunction in apa-thy. Other catecholamine agonists that can treat the symptoms of apathy include amantadine [11], bromocriptine [12], levodopa [13], selegiline [14], and bupropion [15]. RCTs have provided evidence of the efficacy of cholinesterase inhibitors [16] and me-mantine [17] in the treatment of apathy in Alzheimer’s disease. Modafinil is a multimodal stimulant that increases the activity of histamine, norepinephrine, serotonin, dopamine, and orexin sys-tems in the brain [18]. Two recent case reports [4,19] suggested its effectiveness in the treatment of apathy. Additionally, several studies have investigated the effects of olanzapine on negative symptoms, including apathy. Apathetic patients with major de-pressive disorder may benefit from treatment with olanzapine. In an open-label study [20] with nonpsychotic, major depressive disorder patients who were treated with SSRIs and displayed sig-nificant apathy, the addition of olanzapine in the treatment regime yielded a significant decrease on the AES.
In the present case, the apathy symptoms improved slightly but the patient continued to experience cognitive impairment. Apathy is the most common behavioral problem associated with Alzhei-mer’s dementia, affecting 70–90% of patients, and the presence of apathy is linked to deficits in the performance of activities of daily living and functional decline [4]. In one study, minor cognitive impairment (MCI) patients with apathy symptoms, not depres-sive symptoms, were diagnosed with Alzheimer’s dementia al-most seven times more frequently than MCI patients without ap-athy symptoms. Patients with apathy should keep track of their cognitive function, taking into consideration the risk of dementia.
The growing body of empirical investigations on the neurobi-ology of apathy will likely prove helpful in providing a sound theoretical basis for the application of currently available treat-ments, as well as for the development of novel therapeutic inter-ventions [5].
Conflicts of interest
No potential conflicts of interest relevant to this article was re-ported.
ORCID
Hye-Guem Kim, https://orcid.org/0000-0002-9677-7011Bon-Hoon Koo, https://orcid.org/0000-0001-9633-3835Seung Woo Lee, https://orcid.org/0000-0002-3730-066XEun-Jin Cheon, https://orcid.org/0000-0002-6986-0768
References
1. Marin RS. Apathy: a neuropsychiatric syndrome. J Neuropsychi-atry Clin Neurosci 1991;3:243–54.
2. Barnhart WJ, Makela EH, Latocha MJ. SSRI-induced apathy syn-drome: a clinical review. J Psychiatr Pract 2004;10:196–9.
3. Starkstein SE, Jorge R, Mizrahi R, Robinson RG. A prospective longitudinal study of apathy in Alzheimer's disease. J Neurol Neu-rosurg Psychiatry 2006;77:8–11.
4. Padala PR, Burke WJ, Bhatia SC. Modafinil therapy for apathy in an elderly patient. Ann Pharmacother 2007;41:346–9.
5. Roth RM, Flashman LA, McAllister TW. Apathy and its treat-ment. Curr Treat Options Neurol 2007;9:363–70.
6. McPherson S, Fairbanks L, Tiken S, Cummings JL, Back-Madru-ga C. Apathy and executive function in Alzheimer's disease. J Int Neuropsychol Soc 2002;8:373–81.
7. Wongpakaran N, van Reekum R, Wongpakaran T, Clarke D. Se-lective serotonin reuptake inhibitor use associates with apathy among depressed elderly: a case-control study. Ann Gen Psychia-try 2007;6:7.
8. Dubini A, Bosc M, Polin V. Do noradrenaline and serotonin dif-ferentially affect social motivation and behaviour? Eur Neuropsy-chopharmacol 1997;7(Suppl 1): S49–55.
9. Lanctôt KL, Agüera-Ortiz L, Brodaty H, Francis PT, Geda YE, Is-mail Z, et al. Apathy associated with neurocognitive disorders: Recent progress and future directions. Alzheimers Dement 2017;13:84–100.
10. Galynker I, Ieronimo C, Miner C, Rosenblum J, Vilkas N, Rosenthal R. Methylphenidate treatment of negative symptoms in patients with dementia. J Neuropsychiatry Clin Neurosci 1997;9:231–9.
11. van Reekum R, Bayley M, Garner S, Burke IM, Fawcett S, Hart A, et al. N of 1 study: amantadine for the amotivational syndrome in a patient with traumatic brain injury. Brain Inj 1995;9:49–53.
12. Marin RS, Fogel BS, Hawkins J, Duffy J, Krupp B. Apathy: a treat-
https://doi.org/10.12701/yujm.2019.00150252
Kim HG et al. Apathy syndrome in a patient previously treated with SSRIs

able syndrome. J Neuropsychiatry Clin Neurosci 1995;7:23–30.13. Debette S, Kozlowski O, Steinling M, Rousseaux M. Levodopa
and bromocriptine in hypoxic brain injury. J Neurol 2002; 249:1678–82.
14. Newburn G, Newburn D. Selegiline in the management of apathy following traumatic brain injury. Brain Inj 2005;19:149–54.
15. Corcoran C, Wong ML, O'Keane V. Bupropion in the manage-ment of apathy. J Psychopharmacol 2004;18:133–5.
16. Holmes C, Wilkinson D, Dean C, Vethanayagam S, Olivieri S, Langley A, et al. The efficacy of donepezil in the treatment of neuropsychiatric symptoms in Alzheimer disease. Neurology 2004;63:214–9.
17. Zhang N, Wei C, Du H, Shi FD, Cheng Y. The effect of meman-
tine on cognitive function and behavioral and psychological symptoms in mild-to-moderate Alzheimer's disease patients. Dement Geriatr Cogn Disord 2015;40:85–93.
18. Gerrard P, Malcolm R. Mechanisms of modafinil: a review of current research. Neuropsychiatr Dis Treat 2007;3:349–64.
19. Camargos EF, Quintas JL. Apathy syndrome treated successfully with modafinil. BMJ Case Rep 2011;2011:pii: bcr0820114652.
20. Marangell LB, Johnson CR, Kertz B, Zboyan HA, Martinez JM. Olanzapine in the treatment of apathy in previously depressed participants maintained with selective serotonin reuptake inhib-itors: an open-label, flexible-dose study. J Clin Psychiatry 2002;63:391–5.
253https://doi.org/10.12701/yujm.2019.00150
Yeungnam Univ J Med 2019;36(3):249-253

Catastrophic catecholamine-induced cardiomyopathy rescued by extracorporeal membrane oxygenation in recurrent malignant pheochromocytoma Daniel Min Department of Cardiology, G SAM Hospital, Gunpo, Korea
Pheochromocytoma (PCC) is a rare catecholamine-producing tumor with the incidence in hyper-tension of 0.1-0.6%. PCC crisis is an endocrine emergency that can lead to hemodynamic distur-bance and organ failure such as catecholamine-induced cardiomyopathy. The circulatory collapse caused by it often requires mechanical support. The author reports an unusual case in which a patient who previously underwent surgery for malignant PCC developed catecholamine-induced cardiomyopathy, and successfully recovered using extracorporeal membrane oxygenation.
Keywords: Cardiogenic shock; Cardiomyopathy; Extracorporeal membrane oxygenation; Pheo-chromocytoma
Introduction
Pheochromocytoma (PCC) is a rare catecholamine-producing neuroendocrine tumor derived from chromaffin cells of the sym-pathetic nervous system. Because it can present with various clinical symptoms other than the classical triad of headache, pal-pitation and sweating, early diagnosis is not easy [1,2]. PCC cri-sis is a situation in which the secretion of catecholamine abruptly increases, caused by some spontaneous or specific stimuli. This is an endocrine emergency that can lead to hemodynamic distur-bance and organ failure associated with significant mortality [3,4]. This situation often requires mechanical support, and some cases of effective recovery using extracorporeal membrane oxygenation (ECMO) are reported [5,6]. In a considerable num-ber of cases, PCC is initially diagnosed due to the outbreak of a PCC crisis [3]. However, there are very few cases in which pa-tients who have undergone surgical treatment for PCC are later diagnosed with a recurrence due to PCC crisis. Here, the author
Case reporteISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):254-259https://doi.org/10.12701/yujm.2019.00213
Received: March 27, 2019 Revised: April 30, 2019 Accepted: May 8, 2019
Corresponding author: Daniel Min Department of Cardiology, G SAM Hospital, 591, Gunpo-ro, Gunpo 15839, Korea Tel: +82-31-389-3634Fax: +82-31-389-3787E-mail: [email protected]
reports an unusual case in which a patient who previously under-went surgery for malignant PCC developed catecholamine in-duced cardiomyopathy after taking glucocorticoids, and success-fully recovered using ECMO.
Case
A 44-year-old Asian female visited the emergency room com-plaining of a headache, nausea and vomiting. She had visited the hospital 11 years earlier for gestational hypertension. She had been diagnosed with PCC in the right adrenal gland (Fig. 1A) and successfully treated with a right adrenalectomy. PCC of the adrenal gland scaled score had been 7, so the tumor had been di-agnosed as malignant. For the first 5 years of follow-up, no signs of recurrence had been found, and she had not visited the hospi-tal since then. Four hours before her visiting the present hospital, she took 4 mg of methylprednisolone due to urticaria.
Her blood pressure (BP) was 180/100 mmHg, and other vital
https://doi.org/10.12701/yujm.2019.00213254
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

signs were stable. An electrocardiogram and a chest X-ray showed normal findings. She had no history of diabetes, but her glucose level was 330 mg/dL, and bicarbonate level was reduced at 13.5 mmol/L. Other blood tests showed no abnormal findings, and urine dipstick analysis showed ketone 1+. Hydration was per-formed with normal saline due to the possibility of early phase diabetic ketoacidosis. Abdomen-pelvis computed tomography (CT) was performed, and there was no evidence of local recur-rence of PCC (Fig. 1B).
Four hours after visiting the hospital, she complained of severe dyspnea. She showed tachycardia with a pulse of 130 beats/min, severe tachypnea with a respiratory rate of over 35 breaths/min, and a fever of 38°C. Rale was heard from both lung fields, and a chest X-ray revealed a rapidly developed bilateral consolidation (Fig. 2). Intubation and mechanical ventilation were performed because of severe hypoxemia. According to echocardiography conducted at bedside, although the cardiac chamber size was normal, there was severe global hypokinesia of the left and right ventricles. The left ventricular ejection fraction was approximate-ly 20% and the tricuspid annular peak velocity had decreased to 6cm/s, indicating severe ventricular dysfunction of both ventri-cles. Antibiotics and diuretics were used, considering the possi-bility of acute respiratory distress syndrome due to atypical pneumonia or acute pulmonary edema caused by heart failure. She was moved to the intensive care unit from the emergency
Fig. 1. (A) Abdomen-pelvis CT of 11 years ago shows a 9x7 cm sized pheochromocytoma (arrow) in the right adrenal gland. (B) There is no evidence of local recurrence on abdomen-pelvis CT at admission. CT, computed tomography.
A B
Table 1. Plasma levels of catecholaminesCatecholamine Level Normal range (×108/kg)Epinephrine 19,752.5 0-140 pg/mLNorepinephrine 5,641.0 70-1,700 pg/mLMetanephrine 46.1 0-0.5 nmol/LNormetanephrine 23.5 0-0.9 nmol/L
room. Five hours after intubation, her BP was dropped to 60/30 mmHg and pulse gradually slowed. One mg of epinephrine and 1 mg of atropine were injected immediately, but asystole oc-curred. Cardiopulmonary resuscitation was performed immedi-ately and venoarterial ECMO was prepared. ECMO was initiated 15 minutes after arrest. Asystole and return of circulation were repeated 3 times for 42 minutes. After that, the patient’s rhythm was restored and no further cardiac arrest occurred. She was treated for 5 days with support of ECMO, mechanical ventila-tion, and inotropic agents. She recovered consciousness and ECMO was removed when her vital signs became stable without inotropics. After 10 days, ventilator weaning and extubation were performed.
The results of hormone tests performed at the time of hospi-talization showed an overall increase in catecholamine (Table 1), and catecholamine-induced cardiomyopathy due to PCC was strongly suspected. In order to confirm the recurrence of PCC, a 131I-metaiodobenzylguanidine (MIBG) scan was performed, but
255https://doi.org/10.12701/yujm.2019.00213
Yeungnam Univ J Med 2019;36(3):254-259

Fig. 2. (A) No abnormality is seen on chest X-ray at admission. (B) Chest X-ray after 4 hours of admission reveals a rapidly developed bilateral consolidation.
A B
no focal radioactive uptake lesion was shown. The patient’s CT was reviewed closely, and a faint mass-like lesion was detected on her right sacrum. Sacrum magnetic resonance imaging was per-formed, and a 2.7 × 2.9 × 2.8 cm sized well-defined, lobulated, and slightly expansile mass with mainly T1 low T2 high signal in-tensity and heterogeneous enhancement at right upper sacral ala was seen (Fig. 3). Other small lesions, which are assumed to be metastasis, were also found at the S2 level of the sacrum, right ili-ac bone, and lower L4 vertebral body. A positron emission to-mography scan showed an increase of uptake in the same regions (Fig. 4). For a histological verification, an open bone biopsy was performed. Atypical spindle-shaped tumor cells showing synap-tophysin and chromogranin positivity were found upon histo-pathologic examination (Fig. 5). These results demonstrated that the lesions on the sacrum were recurrent metastatic PCC.
In the patient’s follow-up, the cardiac functions, including left and right ventricles, were found to be completely recovered, with 65% of ejection fraction. Coronary angiography performed after ventilator weaning showed no abnormal findings. Currently, her BP is being successfully regulated with an α-blocker (doxazocin) and β-blocker (carvedilol) and treatment for the recurrent PCC is planned.
Fig. 3. Sacrum magnetic resonance imaging shows a 2.7x2.9x2.8 cm sized well-defined, lobulated, and slightly expansile mass (arrow) at right upper sacral ala.
https://doi.org/10.12701/yujm.2019.00213256
Mim D. Pheochromocytoma crisis rescued by ECMO

Fig. 4. Positron emission tomography scan shows an increase of uptake in the mass of sacrum.
gressive mechanical support should be considered during the un-stable period of PCC crisis. It can save the patients from the vi-cious cycle and increases their chances for cardiac function recov-ery, which would ultimately increase the survival rate [8].
Causes of PCC crisis include trauma, surgery, and anesthesia, as well as drugs such as glucagon, radiocontrast agent, tyramine, tricyclic antidepressant, and metoclopramide [3]. Cases occur-ring after glucocorticoid administration are very rare, with only about 20 cases reported to date [9-11]. In this case, methylpred-nisolone taken prior to admission was suspicious of the cause of PCC crisis. Although it was a low dose, no other possible causes were found, and since PCC crisis also occurred in another case when 2 mg of dexamethasone was administered during dexa-methasone suppression test [9], the possibility of 4 mg dose of methylprednisolone being the cause was believed to be sufficient enough.
Two possible mechanisms by which glucocorticoid causes PCC crisis can be considered. First, glucocorticoid promotes the production and release of catecholamines. In normal adrenal gland, the adrenal medulla is already exposed to excessive amount of glucocorticoid secreted from nearby adrenal cortex, and thus, it is not significantly affected by introduction of exter-nal glucocorticoid. However, PCC is not surrounded by the ad-renal cortex and has a modified vascular structure, and as a result, it has lost the ability to regulate external steroids and overreacts to them [12]. Glucocorticoid activates enzymes involved in cate-cholamine metabolism, production, and secretion in PCC, there-by promoting catecholamine secretion [13]. Second, glucocorti-coid reinforces the actions of catecholamines in the peripheral vascular tissues by suppressing the formation of endothelial-de-rived vasodilators such as nitric oxide and prostacyclin [14].
The point of interest in this case is that PCC crisis occurred in a patient who was already being treated for malignant PCC and recurrence was confirmed through such event, as well as this cri-sis was induced by steroids. PCC itself is not a common disease, and recurrences are very rare with only 4.6–6.5% [15]. The prog-nosis of malignant PCC is poor and the 5-year survival rate is re-ported to be 20–50% [16]. Poor prognosis is associated with lo-cal recurrence or distant metastasis, which often appear within the first 2 years from the initial diagnosis, but such occurrence even after 40 years has also been reported [17]. In this case, bone metastasis might had proceeded 5 years after surgery. In the meantime, catecholamine was not being secreted in excessive amounts to cause symptoms, but catecholamine secretion did in-crease suddenly when steroids were taken, which is believed to have caused the PCC crisis.
In this case, we could not easily find the lesion, because there
Discussion
Classic symptoms of PCC are headache, palpitation and sweat-ing. However, many patients show atypical symptoms and it is not difficult to find cases with PCC crisis as the first symptom [1,2]. PCC crisis involves suddenly released cathecholamines that act on α-adrenergic receptors to cause arterial contraction, along with reduction in intravascular effective volume, which ul-timately causes cellular ischemia to have a systemic effect [3]. It often causes cardiovascular emergencies, such as myocardial in-farction, catecholamine-induced cardiomyopathy, and acute myocarditis, which eventually lead to progression of circulatory collapse. The mechanism of cardiac injury includes direct cardiac myocyte damage of catecholamine, increased myocardial oxygen demand and decreased oxygen supply due to coronary artery spasm [4].
The key to treat PCC crisis is to recognize early and stabilize the patient’s vital sign until the causes are corrected, but medical treatment alone is not enough in some cases. There have been re-ports of using mechanical support, such as intraaortic balloon pump or ECMO, in effectively treating such cases [5,6]. In this case, the patient was effectively rescued with timely use of ECMO even though the patient had suffered a cardiac arrest. Fortunately, most catecholamine induced cardiac injuries are reversible, and as such, many cases including this case show recovery of damaged cardiac functions later on [7]. Therefore, if necessary, more ag-
257https://doi.org/10.12701/yujm.2019.00213
Yeungnam Univ J Med 2019;36(3):254-259

was no focal recurrence on CT and no focal radioactive uptake lesion showing on the 131I-MIBG scan. The MIBG scan is an ef-fective functional imaging procedure for detecting PCC. Its spec-ificity is quite high (95–100%), but the sensitivity is relatively low (approximately 77–90%). The false-negative of the MIBG scan can be affected by tumor size, drugs that interfere with io-dine uptake, amount of iodine isotope used, imaging time etc. Several studies have reported that the sensitivity of the MIBG scan is higher for adrenal PCC than for extra-adrenal PCC indi-cating that tumor location also affects sensitivity [18]. In this case, because the recurrent lesion was a sacrum, extra-adrenal le-sion, it would not have been found with an MIBG scan.
In conclusion, PCC crisis is a very serious condition that can often be life threatening, and as such, the patient needs to be treated carefully; and if necessary, mechanical support should be
considered without hesitation. In addition, it can be caused by various medications, and since steroids that are commonly pre-scribed can also be a cause, although rare, caution should be tak-en when prescribing steroids. Attention should be paid not only to patients that are currently suspected of having PCC, but also patients with prior treatment history as well.
Conflicts of interest
No potential conflicts of interest relevant to this article was re-ported.
ORCID
Daniel Min, https://orcid.org/0000-0003-0573-6351
A
C
B
D
Fig. 5. Histopathologic findings of the sacral mass. There are atypical spindle-shaped tumor cells (hematoxylin and eosin stain, ×100 [A] and ×200 [B]) show synaptophysin (C) and chromogranin (D) positivity (×100).
https://doi.org/10.12701/yujm.2019.00213258
Mim D. Pheochromocytoma crisis rescued by ECMO

References
1. Lenders JW, Eisenhofer G, Mannelli M, Pacak K. Phaeochromo-cytoma. Lancet 2005;366:665–75.
2. Lenders JW, Duh QY, Eisenhofer G, Gimenez-Roqueplo AP, Grebe SK, Murad MH, et al. Pheochromocytoma and paragan-glioma: an endocrine society clinical practice guideline. J Clin Endocrinol Metab 2014;99:1915–42.
3. Whitelaw BC, Prague JK, Mustafa OG, Schulte KM, Hopkins PA, Gilbert JA, et al. Phaeochromocytoma crisis. Clin Endocri-nol (Oxf) 2014;80:13–22.
4. Prejbisz A, Lenders JW, Eisenhofer G, Januszewicz A. Cardiovas-cular manifestations of phaeochromocytoma. J Hypertens 2011;29:2049–60.
5. Suh IW, Lee CW, Kim YH, Hong MK, Lee JW, Kim JJ, et al. Cat-astrophic catecholamine-induced cardiomyopathy mimicking acute myocardial infarction, rescued by extracorporeal membrane oxygenation (ECMO) in pheochromocytoma. J Korean Med Sci 2008;23:350–4.
6. Sojod G, Diana M, Wall J, D’Agostino J, Mutter D, Marescaux J. Successful extracorporeal membrane oxygenation treatment for pheochromocytoma-induced acute cardiac failure. Am J Emerg Med 2012;30:1017.e1-3.
7. Giavarini A, Chedid A, Bobrie G, Plouin PF, Hagège A, Amar L. Acute catecholamine cardiomyopathy in patients with phaeochromocytoma or functional paraganglioma. Heart 2013;99:1438–44.
8. Otusanya O, Goraya H, Iyer P, Landi K, Tibb A, Msaouel P. A vi-cious cycle of acute catecholamine cardiomyopathy and circula-tory collapse secondary to pheochromocytoma. Oxf Med Case Reports 2015;2015:343–5.
9. Yi DW, Kim SY, Shin DH, Kang YH, Son SM. Pheochromocyto-
ma crisis after a dexamethasone suppression test for adrenal inci-dentaloma. Endocrine 2010;37:213–9.
10. An JY, Kim DR, Oh JY, Han YC, Lee IS, Kown TJ, et al. A case of recurrent glucocorticoid-induced pheochromocytoma crisis during the treatment of urticarial. Korean J Med 2015;88:564–9.
11. Barrett C, van Uum SH, Lenders JW. Risk of catecholaminergic crisis following glucocorticoid administration in patients with an adrenal mass: a literature review. Clin Endocrinol (Oxf) 2015;83:622–8.
12. Tischler AS, Perlman RL, Morse GM, Sheard BE. Glucocorti-coids increase catecholamine synthesis and storage in PC12 pheochromocytoma cell cultures. J Neurochem 1983;40:364–70.
13. McMahon A, Sabban EL. Regulation of expression of dopamine beta-hydroxylase in PC12 cells by glucocorticoids and cyclic AMP analogues. J Neurochem 1992;59:2040–7.
14. Yang S, Zhang L. Glucocorticoids and vascular reactivity. Curr Vasc Pharmacol 2004;2:1–12.
15. Harari A, Inabnet WB 3rd. Malignant pheochromocytoma: a review. Am J Surg 2011;201:700–8.
16. Baudin E, Habra MA, Deschamps F, Cote G, Dumont F, Caba-nillas M, et al. Therapy of endocrine disease: treatment of ma-lignant pheochromocytoma and paraganglioma. Eur J Endocri-nol 2014;171:R111–22.
17. Tanaka S, Ito T, Tomoda J, Higashi T, Yamada G, Tsuji T. Malig-nant pheochromocytoma with hepatic metastasis diagnosed 20 years after resection of the primary adrenal lesion. Intern Med 1993;32:789–94.
18. Ilias I, Divgi C, Pacak K. Current role of metaiodobenzylguani-dine in the diagnosis of pheochromocytoma and medullary thyroid cancer. Semin Nucl Med 2011;41:364–8.
259https://doi.org/10.12701/yujm.2019.00213
Yeungnam Univ J Med 2019;36(3):254-259

Late complication of the Nuss procedure: recurrent cardiac tamponade Won Jong Park1, Jang Won Son2, Kyu Hwan Park3, You Min Kim4, Jong Ho Nam2, Kang Un Choi5, Jung Ho Kim6
1Division of Cardiology, Department of Internal Medicine, Dong-Eui Medical Center, Busan, Korea 2Division of Cardiology, Department of Internal Medicine, Yeungnam University College of Medicine, Daegu, Korea 3Division of Cardiology, Department of Internal Medicine, Daegu Veterans Hospital, Daegu, Korea 4Division of Cardiology, Department of Internal Medicine, Pohang SM Christianity Hospital, Pohang, Korea 5Division of Cardiology, Department of Internal Medicine, Dongguk University Gyeongju Hospital, Gyeongju, Korea 6Department of Emergency Medicine, Yeungnam University Medical Center, Daegu, Korea
Pectus excavatum (PE) is known as one of the most common congenital deformities of the an-terior chest wall. The Nuss procedure is an effective surgical therapy to correct PE. Here, we re-port a case of recurrent cardiac tamponade due to hemopericardium that occurred after 16 months following the Nuss procedure. The cause of recurrent hemopericardium was thought to be local, repetitive irritation of the pericardium by the Nuss steel bar. We should keep in mind that this serious complication can occur after the Nuss procedure, even in the late phase.
Keywords: Cardiac tamponade; Complication; Nuss procedure; Pectus excavatum
Introduction
Pectus excavatum (PE) is one of the most common congenital chest wall deformities, occurring in approximately 1:400 births and affecting males 5 times more often than females [1]. Patients with PE may have a variety of symptoms, such as nonspecific chest pain, shortness of breath on exertion, and psychological distress, which are the indications of surgical treatment.
There are two standard surgical therapies of PE: the Ravich procedure, corrective osteotomy, and the Nuss procedure, mini-mally invasive repair of PE using the Nuss bar. The Nuss proce-dure has become a widely used method correcting PE since Dr.
Received: May 20, 2019 Revised: June 6, 2019 Accepted: June 10, 2019
Corresponding author: Jang Won SonDivision of Cardiology, Department of Internal Medicine, Yeungnam University College of Medicine, 170, Hyunchung-ro, Nam-gu, Daegu 42415, Korea Tel: +82-53-620-3314Fax: +82-53-621-3310E-mail: [email protected]
Donald Nuss introduced it in 1998, with benefits including being a minimally invasive technique and having a short operative du-ration [2]. This procedure elevates the depressed sternum by passing a suitably shaped, concave steel bar beneath the sternum, resting on the outer aspects of the ribs on each side under thora-coscopic guidance [3]. Pericarditis or pericardial effusions as one of the postoperative complications have been reported in 1.6–2.4% of cases [4-6], but progression to cardiac tamponade is very rare.
Here, we introduce an instructive case which gives us mean-ingful messages that cardiac tamponade can occur as a late com-plication of the Nuss procedure.
Case reporteISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):260-264https://doi.org/10.12701/yujm.2019.00241
https://doi.org/10.12701/yujm.2019.00241260
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
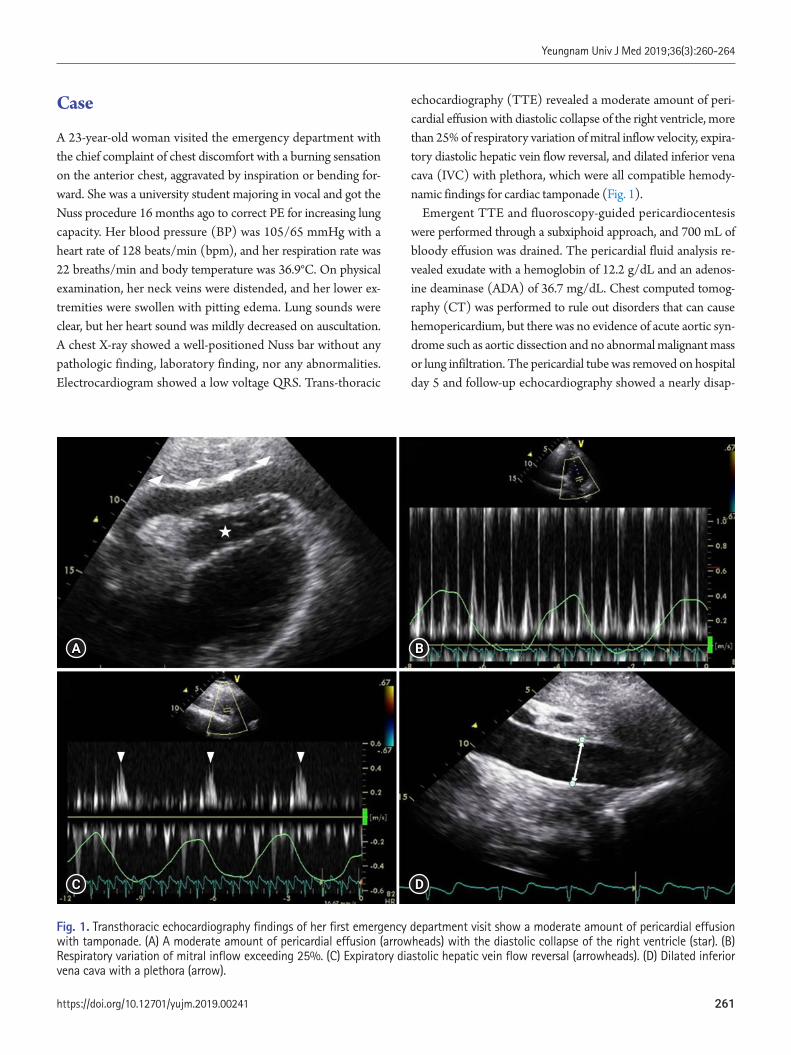
Case
A 23-year-old woman visited the emergency department with the chief complaint of chest discomfort with a burning sensation on the anterior chest, aggravated by inspiration or bending for-ward. She was a university student majoring in vocal and got the Nuss procedure 16 months ago to correct PE for increasing lung capacity. Her blood pressure (BP) was 105/65 mmHg with a heart rate of 128 beats/min (bpm), and her respiration rate was 22 breaths/min and body temperature was 36.9°C. On physical examination, her neck veins were distended, and her lower ex-tremities were swollen with pitting edema. Lung sounds were clear, but her heart sound was mildly decreased on auscultation. A chest X-ray showed a well-positioned Nuss bar without any pathologic finding, laboratory finding, nor any abnormalities. Electrocardiogram showed a low voltage QRS. Trans-thoracic
echocardiography (TTE) revealed a moderate amount of peri-cardial effusion with diastolic collapse of the right ventricle, more than 25% of respiratory variation of mitral inflow velocity, expira-tory diastolic hepatic vein flow reversal, and dilated inferior vena cava (IVC) with plethora, which were all compatible hemody-namic findings for cardiac tamponade (Fig. 1).
Emergent TTE and fluoroscopy-guided pericardiocentesis were performed through a subxiphoid approach, and 700 mL of bloody effusion was drained. The pericardial fluid analysis re-vealed exudate with a hemoglobin of 12.2 g/dL and an adenos-ine deaminase (ADA) of 36.7 mg/dL. Chest computed tomog-raphy (CT) was performed to rule out disorders that can cause hemopericardium, but there was no evidence of acute aortic syn-drome such as aortic dissection and no abnormal malignant mass or lung infiltration. The pericardial tube was removed on hospital day 5 and follow-up echocardiography showed a nearly disap-
Fig. 1. Transthoracic echocardiography findings of her first emergency department visit show a moderate amount of pericardial effusion with tamponade. (A) A moderate amount of pericardial effusion (arrowheads) with the diastolic collapse of the right ventricle (star). (B) Respiratory variation of mitral inflow exceeding 25%. (C) Expiratory diastolic hepatic vein flow reversal (arrowheads). (D) Dilated inferior vena cava with a plethora (arrow).
A
C
B
D
261https://doi.org/10.12701/yujm.2019.00241
Yeungnam Univ J Med 2019;36(3):260-264
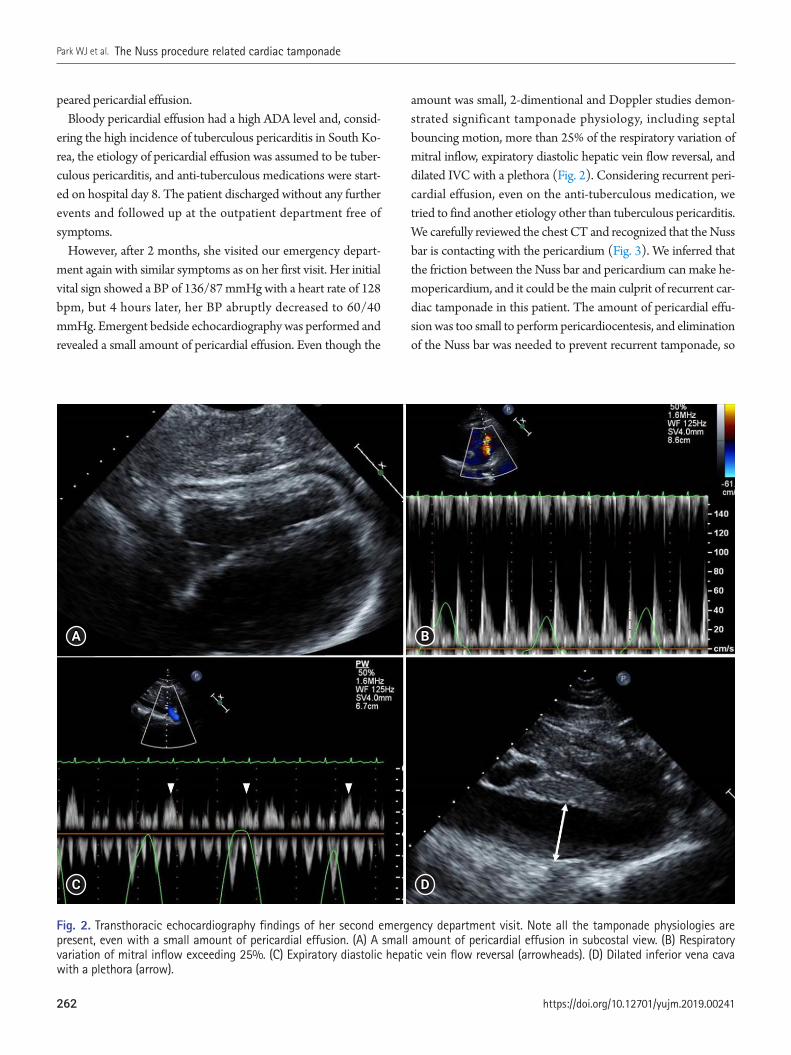
peared pericardial effusion. Bloody pericardial effusion had a high ADA level and, consid-
ering the high incidence of tuberculous pericarditis in South Ko-rea, the etiology of pericardial effusion was assumed to be tuber-culous pericarditis, and anti-tuberculous medications were start-ed on hospital day 8. The patient discharged without any further events and followed up at the outpatient department free of symptoms.
However, after 2 months, she visited our emergency depart-ment again with similar symptoms as on her first visit. Her initial vital sign showed a BP of 136/87 mmHg with a heart rate of 128 bpm, but 4 hours later, her BP abruptly decreased to 60/40 mmHg. Emergent bedside echocardiography was performed and revealed a small amount of pericardial effusion. Even though the
amount was small, 2-dimentional and Doppler studies demon-strated significant tamponade physiology, including septal bouncing motion, more than 25% of the respiratory variation of mitral inflow, expiratory diastolic hepatic vein flow reversal, and dilated IVC with a plethora (Fig. 2). Considering recurrent peri-cardial effusion, even on the anti-tuberculous medication, we tried to find another etiology other than tuberculous pericarditis. We carefully reviewed the chest CT and recognized that the Nuss bar is contacting with the pericardium (Fig. 3). We inferred that the friction between the Nuss bar and pericardium can make he-mopericardium, and it could be the main culprit of recurrent car-diac tamponade in this patient. The amount of pericardial effu-sion was too small to perform pericardiocentesis, and elimination of the Nuss bar was needed to prevent recurrent tamponade, so
Fig. 2. Transthoracic echocardiography findings of her second emergency department visit. Note all the tamponade physiologies are present, even with a small amount of pericardial effusion. (A) A small amount of pericardial effusion in subcostal view. (B) Respiratory variation of mitral inflow exceeding 25%. (C) Expiratory diastolic hepatic vein flow reversal (arrowheads). (D) Dilated inferior vena cava with a plethora (arrow).
A
C
B
D
https://doi.org/10.12701/yujm.2019.00241262
Park WJ et al. The Nuss procedure related cardiac tamponade
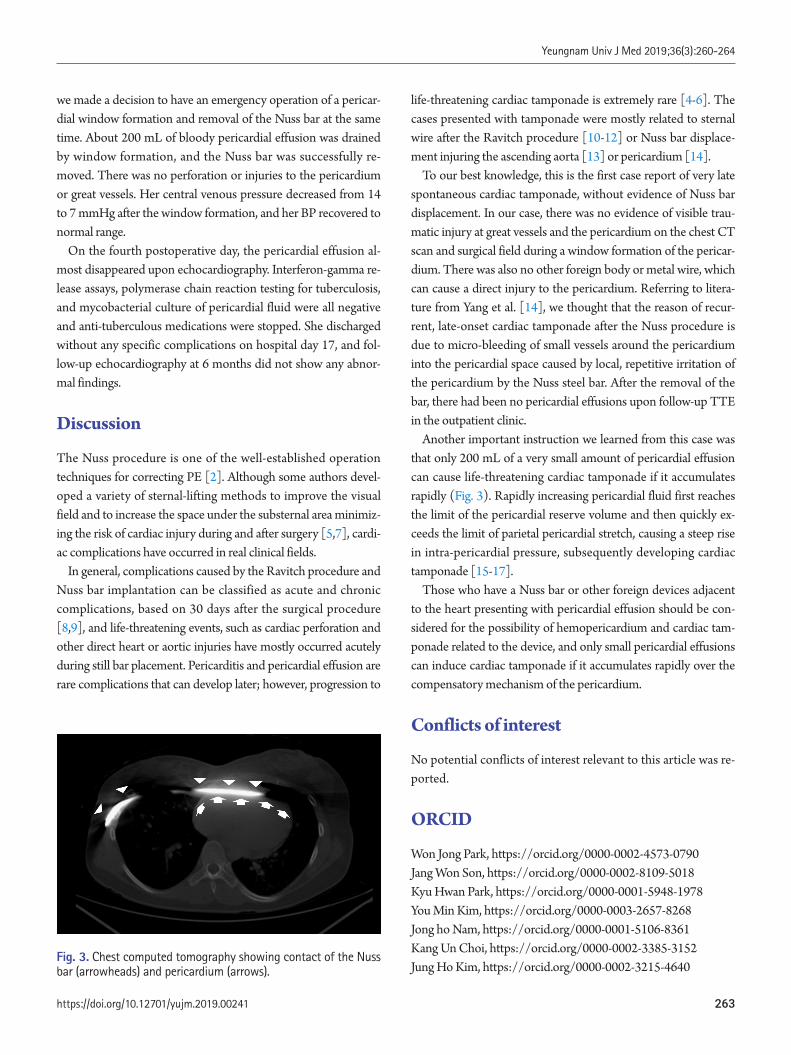
we made a decision to have an emergency operation of a pericar-dial window formation and removal of the Nuss bar at the same time. About 200 mL of bloody pericardial effusion was drained by window formation, and the Nuss bar was successfully re-moved. There was no perforation or injuries to the pericardium or great vessels. Her central venous pressure decreased from 14 to 7 mmHg after the window formation, and her BP recovered to normal range.
On the fourth postoperative day, the pericardial effusion al-most disappeared upon echocardiography. Interferon-gamma re-lease assays, polymerase chain reaction testing for tuberculosis, and mycobacterial culture of pericardial fluid were all negative and anti-tuberculous medications were stopped. She discharged without any specific complications on hospital day 17, and fol-low-up echocardiography at 6 months did not show any abnor-mal findings.
Discussion
The Nuss procedure is one of the well-established operation techniques for correcting PE [2]. Although some authors devel-oped a variety of sternal-lifting methods to improve the visual field and to increase the space under the substernal area minimiz-ing the risk of cardiac injury during and after surgery [5,7], cardi-ac complications have occurred in real clinical fields.
In general, complications caused by the Ravitch procedure and Nuss bar implantation can be classified as acute and chronic complications, based on 30 days after the surgical procedure [8,9], and life-threatening events, such as cardiac perforation and other direct heart or aortic injuries have mostly occurred acutely during still bar placement. Pericarditis and pericardial effusion are rare complications that can develop later; however, progression to
life-threatening cardiac tamponade is extremely rare [4-6]. The cases presented with tamponade were mostly related to sternal wire after the Ravitch procedure [10-12] or Nuss bar displace-ment injuring the ascending aorta [13] or pericardium [14].
To our best knowledge, this is the first case report of very late spontaneous cardiac tamponade, without evidence of Nuss bar displacement. In our case, there was no evidence of visible trau-matic injury at great vessels and the pericardium on the chest CT scan and surgical field during a window formation of the pericar-dium. There was also no other foreign body or metal wire, which can cause a direct injury to the pericardium. Referring to litera-ture from Yang et al. [14], we thought that the reason of recur-rent, late-onset cardiac tamponade after the Nuss procedure is due to micro-bleeding of small vessels around the pericardium into the pericardial space caused by local, repetitive irritation of the pericardium by the Nuss steel bar. After the removal of the bar, there had been no pericardial effusions upon follow-up TTE in the outpatient clinic.
Another important instruction we learned from this case was that only 200 mL of a very small amount of pericardial effusion can cause life-threatening cardiac tamponade if it accumulates rapidly (Fig. 3). Rapidly increasing pericardial fluid first reaches the limit of the pericardial reserve volume and then quickly ex-ceeds the limit of parietal pericardial stretch, causing a steep rise in intra-pericardial pressure, subsequently developing cardiac tamponade [15-17].
Those who have a Nuss bar or other foreign devices adjacent to the heart presenting with pericardial effusion should be con-sidered for the possibility of hemopericardium and cardiac tam-ponade related to the device, and only small pericardial effusions can induce cardiac tamponade if it accumulates rapidly over the compensatory mechanism of the pericardium.
Conflicts of interest
No potential conflicts of interest relevant to this article was re-ported.
ORCID
Won Jong Park, https://orcid.org/0000-0002-4573-0790Jang Won Son, https://orcid.org/0000-0002-8109-5018Kyu Hwan Park, https://orcid.org/0000-0001-5948-1978You Min Kim, https://orcid.org/0000-0003-2657-8268Jong ho Nam, https://orcid.org/0000-0001-5106-8361Kang Un Choi, https://orcid.org/0000-0002-3385-3152Jung Ho Kim, https://orcid.org/0000-0002-3215-4640
Fig. 3. Chest computed tomography showing contact of the Nuss bar (arrowheads) and pericardium (arrows).
263https://doi.org/10.12701/yujm.2019.00241
Yeungnam Univ J Med 2019;36(3):260-264

References
1. Jaroszewski DE, Fonkalsrud EW. Repair of pectus chest deformi-ties in 320 adult patients: 21 year experience. Ann Thorac Surg 2007;84:429–33.
2. Nuss D, Kelly RE Jr, Croitoru DP, Katz ME. A 10-year review of a minimally invasive technique for the correction of pectus excava-tum. J Pediatr Surg 1998;33:545–52.
3. Krasopoulos G, Goldstraw P. Minimally invasive repair of pectus excavatum deformity. Eur J Cardiothorac Surg 2011;39:149–58.
4. Žganjer M, Žganjer V. Surgical correction of the funnel chest de-formity in children. Int Orthop 2011;35:1043–8.
5. Yoon YS, Kim HK, Choi YS, Kim K, Shim YM, Kim J. A modi-fied Nuss procedure for late adolescent and adult pectus excava-tum. World J Surg 2010;34:1475–80.
6. Park HJ, Lee SY, Lee CS, Youm W, Lee KR. The Nuss procedure for pectus excavatum: evolution of techniques and early results on 322 patients. Ann Thorac Surg 2004;77:289–95.
7. Johnson WR, Fedor D, Singhal S. A novel approach to eliminate cardiac perforation in the Nuss procedure. Ann Thorac Surg 2013;95:1109–11.
8. Kelly RE Jr, Mellins RB, Shamberger RC, Mitchell KK, Lawson ML, Oldham KT, et al. Multicenter study of pectus excavatum, fi-nal report: complications, static/exercise pulmonary function, and anatomic outcomes. J Am Coll Surg 2013;217:1080–9.
9. Fallon SC, Slater BJ, Nuchtern JG, Cass DL, Kim ES, Lopez ME, et al. Complications related to the Nuss procedure: minimizing
risk with operative technique. J Pediatr Surg 2013;48:1044–8.10. Barakat MJ, Morgan JA. Haemopericardium causing cardiac
tamponade: a late complication of pectus excavatum repair. Heart 2004;90:e22.
11. Cope SA, Rodda J. Cardiac tamponade presenting to the emer-gency department after sternal wire disruption. Emerg Med J 2004;21:389–90.
12. Lee SH, Cho BS, Kim SJ, Lee SY, Kang MH, Han GS, et al. Car-diac tamponade caused by broken sternal wire after pectus exca-vatum repair: a case report. Ann Thorac Cardiovasc Surg 2013;19:52–4.
13. Hoel TN, Rein KA, Svennevig JL. A life-threatening complica-tion of the Nuss procedure for pectus excavatum. Ann Thorac Surg 2006;81:370–2.
14. Yang MH, Cheng YL, Tsai CS, Li CY. Delayed cardiac tampon-ade after the Nuss procedure for pectus excavatum: a case re-port and simple management. Heart Surg Forum 2008;11: E129–31.
15. Spodick DH. Acute cardiac tamponade. N Engl J Med 2003;349:684–90.
16. Gascho JA, Martins JB, Marcus ML, Kerber RE. Effects of vol-ume expansion and vasodilators in acute pericardial tamponade. Am J Physiol 1981;240:H49–53.
17. Spodick DH. The normal and diseased pericardium: current concepts of pericardial physiology, diagnosis and treatment. J Am Coll Cardiol 1983;1:240–51.
https://doi.org/10.12701/yujm.2019.00241264
Park WJ et al. The Nuss procedure related cardiac tamponade
Incidentally found cystic lymphangioma of the adrenal gland in an elderly male cadaver Hee Cheol Kim1, Yunji Kang1, Young Hee Maeng2, Jinu Kim3, Sang-Pil Yoon3,4
1Medical Course, Jeju National University School of Medicine, Jeju, Korea 2Department of Pathology, Jeju National University School of Medicine, Jeju, Korea 3Department of Anatomy, Jeju National University School of Medicine, Jeju, Korea 4Institute for Medical Science, Jeju National University, Jeju, Korea
Adrenal cystic lymphangiomas are extremely rare entities that are often identified incidentally, with less than 60 cases reported to date. We found a protruding ovoid mass consisting of a mul-tiloculated cystic lesion within right adrenal gland in the cadaver of a 75-year-old Korean man. The epithelial cells lining the adrenal cyst were diffusely positive for cluster of differentiation 31 and podoplanin, and negative for pan-cytokeratin. The histopathological diagnosis confirmed a cystic lymphangioma arising from the adrenal gland. Post-mortem findings of the present case are discussed based on the clinicopathological features of adrenal cystic lymphangiomas.
Keywords: Adrenal cyst; Cadaver; Lymphangioma; Male
Introduction
Benign adrenal vascular pathologies, including tumors, cysts, and pseudocysts, are relatively rare entities that are mostly right-sided and predominantly observed in females [1]. These lesions may oc-cur concomitantly with other adrenal tumors associated with hor-mone secretion. Cysts of the adrenal glands are rare and often de-tected incidentally during radiological examinations or at autopsy. Their reported incidence ranges 0.06–0.18% [2-4].
Adrenal cysts are classified into the following four main groups: endothelial cysts (45%), pseudocyst (39%), epithelial cysts (9%), and parasitic cysts (7%) [5]. Endothelial cysts include hemangio-ma and lymphangioma [6]. Adrenal cystic lymphangiomas do not exhibit pathognomonic clinical or radiological presentation. Certain features of these entities raise the suspicion of malignancy, including a heterogeneous appearance in imaging analyses, the
Received: May 31, 2019 Revised: July 7, 2019 Accepted: July 11, 2019
Corresponding author: Sang-Pil Yoon Department of Anatomy, Jeju National University School of Medicine, 102, Jejudaehak-ro, Jeju 63243, Korea Tel: +82-64-754-3823Fax: +82-64-725-2593E-mail: [email protected]
presence of necrosis in the center of the mass accompanied by cal-cification, and the size of the adrenal mass [7].
We present a case of a cystic lesion on the right adrenal gland in an elderly man and discuss its common and distinct features.
Case
We found multiloculated cysts on the right adrenal gland in the cadaver of a 75-year-old Korean man, whose cause of death was pneumonia, during routine educational dissection.
An ovoid cystic mass protruded from the outer surface of the adrenal gland (Fig. 1A). Dissection revealed a multilocular cystic lesion measuring 3.3 × 3.0 cm (longest and transverse diameters in external dimension, respectively) within the adrenal gland. The cystic walls were thin, and the cavities contained a pale to tan-colored gelatinous material (Fig. 1B).
Case reporteISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):265-268https://doi.org/10.12701/yujm.2019.00262
265https://doi.org/10.12701/yujm.2019.00262
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

Microscopy analysis revealed that the cystic structures were surrounded by flattened adrenal parenchyma (Figs. 2A, 2B) and the inner surfaces were lined by a single layer of flattened cells with bland nuclei (Fig. 2C). The lining cells were diffusely posi-tive for cluster of differentiation 31 (CD31) (Fig. 2D) and podo-planin (D2-40) (Fig. 2E), and negative for pan-cytokeratin (Fig. 2F). The pathological diagnosis confirmed a cystic lymphangio-ma arising from the adrenal gland.
Discussion
Lymphangiomas, benign malformations of lymphatic vessels, are most frequently noted in children aged less than 2 years [8,9]. Although the exact cause has not been established yet, these enti-ties are generally regarded as congenital malformations in which obstruction or agenesis of lymphatic tissue results in lymphangi-ectasia due to a lack of normal communication within the lym-phatic system [8,10]. The majority of lymphangiomas are detect-ed in the neck, axillary region and mediastinum (95%), and the remaining 5% are found in the abdominal cavity [8,11]. Adrenal lymphangiomas account for less than 1% of all abdominal lymphangiomas [12]. To date, less than 60 adrenal lymphangio-ma cases have been described [13], with only 7 cases reported in Korean [14].
While lymphangiomas are typically detected in childhood and are rare in adults, adrenal lymphangiomas are predominantly
noted in women in aged approximately 40 years, mostly right-sid-ed, and unilateral (mean size 8.9 cm; range 2.0–35.0 cm). Histo-logically, all adrenal lymphangiomas show a typical multicystic lesion composed of irregular dilated spaces that are lined by flat-tened bland simple endothelial cells [12] and have potential ma-lignancy incidence of about 4.1% [10,15]. Adrenal cystic lymph-angiomas are usually asymptomatic because of their size and lo-cation [8]. The most common complaint is pain, which is local-ized in back, the right upper quadrant of abdomen, or is general-ized as abdominal pain [10]. Transabdominal adrenalectomy is the treatment of choice. Recent recommendations entail the as-piration of material from the adrenal cysts instead of their surgi-cal excision both for diagnosis and management, in cases where malignancy is not suspected or the lesion is non-functional and asymptomatic [6,8,10,12,16].
In conclusion, small asymptomatic adrenal cystic lymphangio-mas without malignant transformation were incidentally detect-ed in an elderly Korean male cadaver and the diagnosis was con-firmed by histopathological staining for CD31 and D2-40. Un-like other adrenal cystic lymphangiomas, the adrenal lymphangi-oma in the present case was detected in an elderly male cadaver due to their size during postmortem investigation. Therefore, careful inspection of the adrenal cysts by clinicians and anato-mists is warranted, despite the patient’s age and sex.
Fig. 1. Gross findings of the right-sided adrenal cystic mass. (A) The protruding mass (asterisk) shows smooth outer surface. (B) The multilocular cystic structures (asterisks) are surrounded by flattened adrenal parenchyma (arrows) on the section surface.
A B
https://doi.org/10.12701/yujm.2019.00262266
Kim HC et al. Adrenal cystic lymphangioma in an elderly male
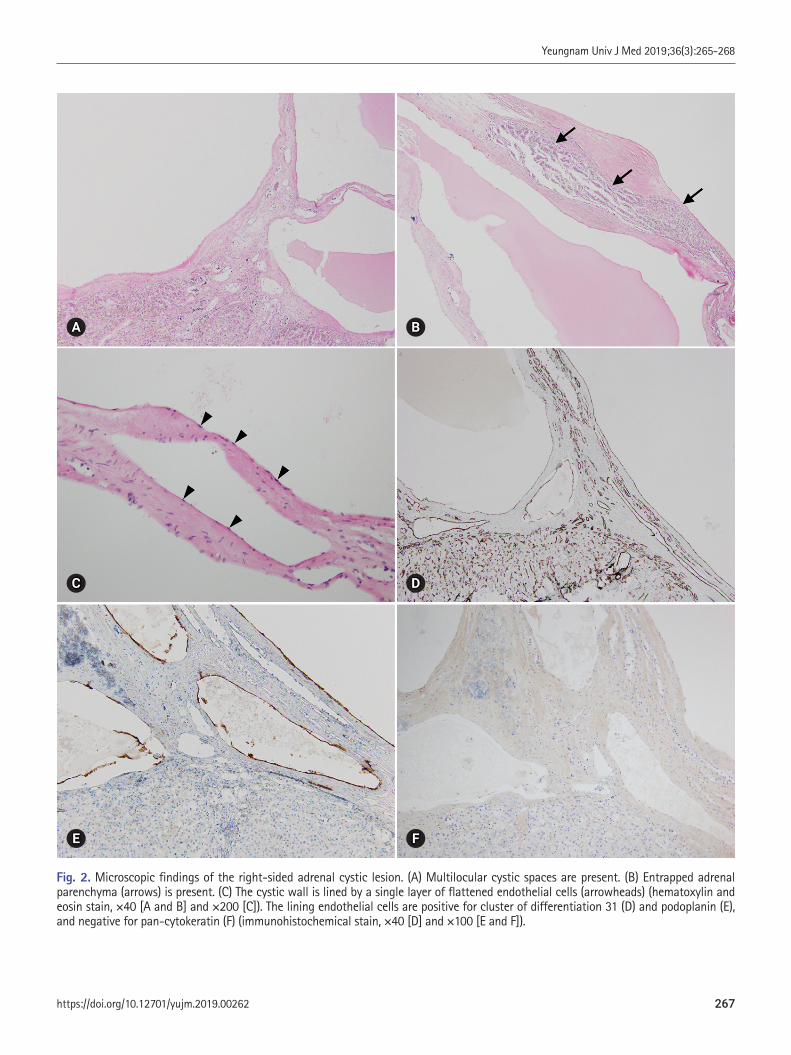
Fig. 2. Microscopic findings of the right-sided adrenal cystic lesion. (A) Multilocular cystic spaces are present. (B) Entrapped adrenal parenchyma (arrows) is present. (C) The cystic wall is lined by a single layer of flattened endothelial cells (arrowheads) (hematoxylin and eosin stain, ×40 [A and B] and ×200 [C]). The lining endothelial cells are positive for cluster of differentiation 31 (D) and podoplanin (E), and negative for pan-cytokeratin (F) (immunohistochemical stain, ×40 [D] and ×100 [E and F]).
A
C
E
B
D
F
267https://doi.org/10.12701/yujm.2019.00262
Yeungnam Univ J Med 2019;36(3):265-268

Acknowledgements
This work was supported by the 2019 education, research and student guidance grant funded by Jeju National University.
Conflicts of interest
No potential conflicts of interest relevant to this article was re-ported.
ORCID
Hee Cheol Kim, https://orcid.org/0000-0002-1820-1543Yunji Kang, https://orcid.org/0000-0001-9082-4107Young Hee Maeng, https://orcid.org/0000-0003-3168-6482Jinu Kim, https://orcid.org/0000-0002-1313-4791Sang-Pil Yoon, https://orcid.org/0000-0003-1350-3582
References
1. Zheng W, Fung KM, Cheng L, Osunkoya AO. Benign vascular tumors, cysts, and pseudocysts of the adrenal gland: a contempo-rary multi-institutional clinicopathological analysis of 55 cases. Hum Pathol 2018;82:95–102.
2. Pollack HM. Miscellaneous conditions of the adrenals and adre-nal pseudotumors. Clin Urogr 1990;3:2403–5.
3. Rozenblit A, Morehouse HT, Amis ES Jr. Cystic adrenal lesions: CT features. Radiology 1996;201:541–8.
4. Tagge DU, Baron PL. Giant adrenal cyst: management and re-view of the literature. Am Surg 1997;63:744–6.
5. Foster DG. Adrenal cysts. Review of literature and report of case.
Arch Surg 1966;92:131–43.6. Longo JM, Jafri SZ, Bis KB. Adrenal lymphangioma: a case re-
port. Clin Imaging 2000;24:104–6.7. Rowe SP, Bishop JA, Prescott JD, Salvatori R, Fishman EK. CT
appearance of adrenal cystic lymphangioma: radiologic-patho-logic correlation. AJR Am J Roentgenol 2016;206:81–5.
8. Ates LE, Kapran Y, Erbil Y, Barbaros U, Dizdaroglu F. Cystic lymphangioma of the right adrenal gland. Pathol Oncol Res 2005;11:242–4.
9. Kafadar MT, Özyuvalı E, Miryaguboğlu AM, Çaviş T, İnan A. In-cidental giant adrenal lymphangioma presenting as nonfunction-al cystic mass. Turk J Surg 2018;1–3. [Epub ahead of print].
10. Michalopoulos N, Laskou S, Karayannopoulou G, Pavlidis L, Kanellos I. Adrenal gland lymphangiomas. Indian J Surg 2015;77(Suppl 3):1334–42.
11. Poncelet V. Retroperitoneal cystic lymphangioma. J Belge Radi-ol 1998;81:245.
12. Ellis CL, Banerjee P, Carney E, Sharma R, Netto GJ. Adrenal lymphangioma: clinicopathologic and immunohistochemical characteristics of a rare lesion. Hum Pathol 2011;42:1013–8.
13. Bibi M, Sellami A, Taktak T, Chelly B, Ghorbel Z, Zouari H, et al. Giant cystic lymphangioma of adrenal gland: a case report and review of the literature. Urol Case Rep 2018;22:6–7.
14. Kim KH, Lee JI, Bae JM. Significant growth of adrenal lymph-angioma: a case report and review of the literature. Int J Surg Case Rep 2015;17:48–50.
15. Tanuma Y, Kimura M, Sakai S. Adrenal cyst: a review of the Jap-anese literature and report of a case. Int J Urol 2001;8:500–3.
16. Satou T, Uesugi T, Nakai Y, Hayashi Y, Imano M, Hashimoto S. Case of adrenal lymphangioma with atypical lymphocytes in aspirate cytology. Diagn Cytopathol 2003;29:87–90.
https://doi.org/10.12701/yujm.2019.00262268
Kim HC et al. Adrenal cystic lymphangioma in an elderly male

Isolated hemorrhage in the cerebellar vermis with vertigo and body lateropulsion to the contralesional side Dong Hyun Lee, Se-Jin Lee Department of Neurology, Yeungnam University of College of Medicine, Daegu, Korea
There have been several reports of patients with isolated lesions of the cerebellar vermis present-ing with clinical features similar to those of peripheral vestibulopathy. We report a case of small, isolated hematoma in the cerebellar vermis in a patient who presented with vertigo, ipsilesional nystagmus, and body lateropulsion to the contralesional side without the usual signs or symp-toms of cerebellar dysfunction. Although they present with symptoms that mimic those of pe-ripheral vestibulopathy, and brain computed tomography shows no abnormality, as there may be a small, isolated hematoma or infarction in the cerebellar vermis. Thus, brain magnetic resonance imaging should be performed in elderly patients with vascular risk factors.
Keywords: Cerebellar vermis; Hemorrhage; Nystagmus; Vertigo; Vestibulopathy
Introduction
Hemorrhage in the cerebellar vermis represents only 5% of all cas-es of cerebellar hemorrhage [1], which can easily rupture into the fourth ventricle through its roof and frequently extends into the pontine tegmentum. Prognosis of patients with hemorrhage in the cerebellar vermis is worse than that for overall cerebellar hem-orrhages. Thus, cases of patients with a small hematoma in the cerebellar vermis, who present with clinical features of labyrin-thine disorder without any other additional neurological deficits suggestive of a cerebellar lesion, are extremely rare, with only few reported in the literature [2-4]. We report a case of isolated hema-toma in the vermis in a patient who presented with vertigo, ipsile-sional nystagmus, and body lateropulsion to the contralesional side as the sole clinical manifestation.
Case
A 64-year-old woman with hypertension and hypercholesterol-
Case reporteISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):269-272https://doi.org/10.12701/yujm.2019.00318
Received: June 22, 2019 Revised: August 20, 2019 Accepted: August 28, 2019
Corresponding author: Se-Jin LeeDepartment of Neurology, Yeungnam University College of Medicine, 170, Hyeonchung-ro Nam-gu, Daegu 42415, Korea Tel: +82-53-620-3683Fax: +82-53-627-1688E-mail: [email protected]
emia presented to the emergency department with acute onset of severe non-positional vertigo accompanied by nausea, vomiting, and postural imbalance. Three days before presentation, she had experienced mild vertigo with nausea after sauna bathing, which improved with bed rest. At first, the patient had rotational vertigo aggravated by head motion and change of position. The following morning, her vertigo gradually worsened and persisted regardless of posture, until she eventually lost the ability to maintain even a sitting posture due to severe vertigo and disequilibrium. She had no other posterior circulation symptoms, such as diplopia, slurred speech, limb clumsiness or weakness, sensory loss, tinnitus, or hearing loss. A bedside neurological examination revealed a spon-taneous right beating horizontal nystagmus with a torsional com-ponent in the primary position and upon gaze to the right or left. A bedside head impulse test was negative. There was no periodic alternating nystagmus. She had no skew deviation or head tilt and also showed no ophthalmoparesis, dysmetria, hypotonia, limb ataxia, or loss of proprioception. She fell to the left side when at-
269https://doi.org/10.12701/yujm.2019.00318
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
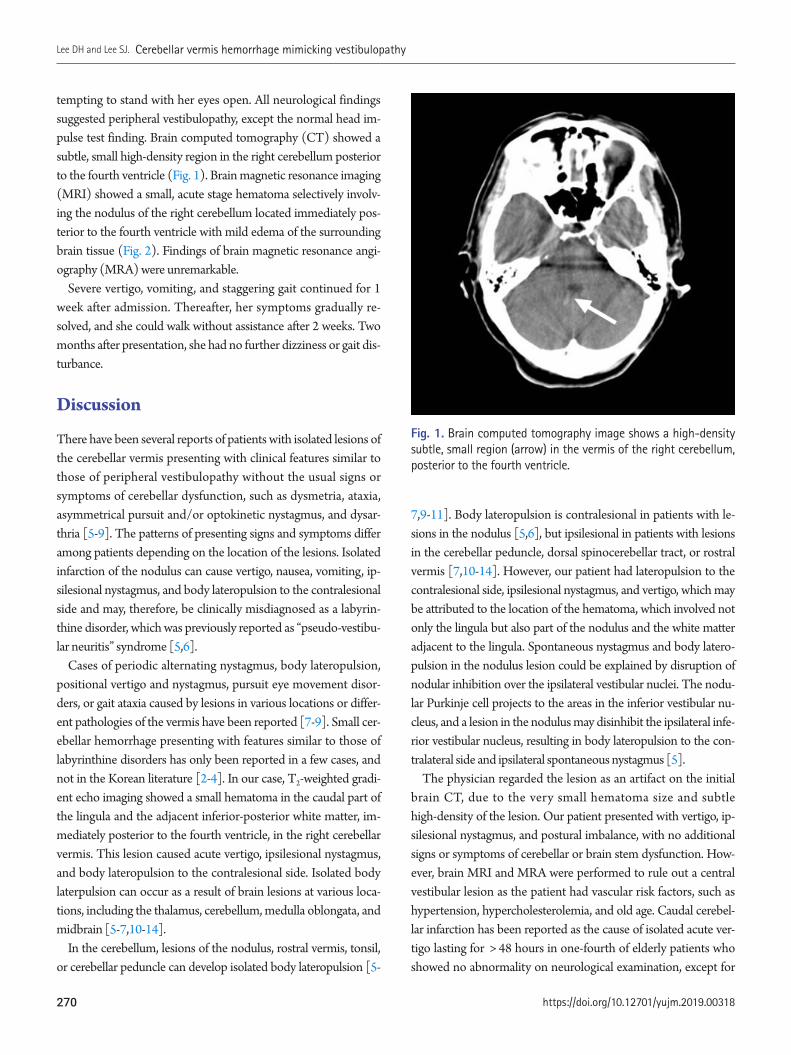
tempting to stand with her eyes open. All neurological findings suggested peripheral vestibulopathy, except the normal head im-pulse test finding. Brain computed tomography (CT) showed a subtle, small high-density region in the right cerebellum posterior to the fourth ventricle (Fig. 1). Brain magnetic resonance imaging (MRI) showed a small, acute stage hematoma selectively involv-ing the nodulus of the right cerebellum located immediately pos-terior to the fourth ventricle with mild edema of the surrounding brain tissue (Fig. 2). Findings of brain magnetic resonance angi-ography (MRA) were unremarkable.
Severe vertigo, vomiting, and staggering gait continued for 1 week after admission. Thereafter, her symptoms gradually re-solved, and she could walk without assistance after 2 weeks. Two months after presentation, she had no further dizziness or gait dis-turbance.
Discussion
There have been several reports of patients with isolated lesions of the cerebellar vermis presenting with clinical features similar to those of peripheral vestibulopathy without the usual signs or symptoms of cerebellar dysfunction, such as dysmetria, ataxia, asymmetrical pursuit and/or optokinetic nystagmus, and dysar-thria [5-9]. The patterns of presenting signs and symptoms differ among patients depending on the location of the lesions. Isolated infarction of the nodulus can cause vertigo, nausea, vomiting, ip-silesional nystagmus, and body lateropulsion to the contralesional side and may, therefore, be clinically misdiagnosed as a labyrin-thine disorder, which was previously reported as “pseudo-vestibu-lar neuritis” syndrome [5,6].
Cases of periodic alternating nystagmus, body lateropulsion, positional vertigo and nystagmus, pursuit eye movement disor-ders, or gait ataxia caused by lesions in various locations or differ-ent pathologies of the vermis have been reported [7-9]. Small cer-ebellar hemorrhage presenting with features similar to those of labyrinthine disorders has only been reported in a few cases, and not in the Korean literature [2-4]. In our case, T2-weighted gradi-ent echo imaging showed a small hematoma in the caudal part of the lingula and the adjacent inferior-posterior white matter, im-mediately posterior to the fourth ventricle, in the right cerebellar vermis. This lesion caused acute vertigo, ipsilesional nystagmus, and body lateropulsion to the contralesional side. Isolated body laterpulsion can occur as a result of brain lesions at various loca-tions, including the thalamus, cerebellum, medulla oblongata, and midbrain [5-7,10-14].
In the cerebellum, lesions of the nodulus, rostral vermis, tonsil, or cerebellar peduncle can develop isolated body lateropulsion [5-
Fig. 1. Brain computed tomography image shows a high-density subtle, small region (arrow) in the vermis of the right cerebellum, posterior to the fourth ventricle.
7,9-11]. Body lateropulsion is contralesional in patients with le-sions in the nodulus [5,6], but ipsilesional in patients with lesions in the cerebellar peduncle, dorsal spinocerebellar tract, or rostral vermis [7,10-14]. However, our patient had lateropulsion to the contralesional side, ipsilesional nystagmus, and vertigo, which may be attributed to the location of the hematoma, which involved not only the lingula but also part of the nodulus and the white matter adjacent to the lingula. Spontaneous nystagmus and body latero-pulsion in the nodulus lesion could be explained by disruption of nodular inhibition over the ipsilateral vestibular nuclei. The nodu-lar Purkinje cell projects to the areas in the inferior vestibular nu-cleus, and a lesion in the nodulus may disinhibit the ipsilateral infe-rior vestibular nucleus, resulting in body lateropulsion to the con-tralateral side and ipsilateral spontaneous nystagmus [5].
The physician regarded the lesion as an artifact on the initial brain CT, due to the very small hematoma size and subtle high-density of the lesion. Our patient presented with vertigo, ip-silesional nystagmus, and postural imbalance, with no additional signs or symptoms of cerebellar or brain stem dysfunction. How-ever, brain MRI and MRA were performed to rule out a central vestibular lesion as the patient had vascular risk factors, such as hypertension, hypercholesterolemia, and old age. Caudal cerebel-lar infarction has been reported as the cause of isolated acute ver-tigo lasting for > 48 hours in one-fourth of elderly patients who showed no abnormality on neurological examination, except for
https://doi.org/10.12701/yujm.2019.00318270
Lee DH and Lee SJ. Cerebellar vermis hemorrhage mimicking vestibulopathy

nystagmus. Therefore, brain MRI should be performed to differ-entiate cerebellar infarction from vestibular neuritis, especially in elderly patients with vascular risk factors [15]. Brain MRI clearly showed a small, acute stage hematoma in our case and is very helpful in patients with small hematomas restricted to the vermis, which may not be visible on brain CT. We concluded that the eti-
ology of the hemorrhage in our case was spontaneous and hyper-tensive because the patient had no history of recent head trauma and vascular anomaly on MRI and MRA, and furthermore, the coagulation system was normal.
In summary, we report the case of a patient with small, isolated hemorrhage in the cerebellar vermis who presented with acute
Fig. 2. Brain magnetic resonance imaging. Axial and sagittal fluid-attenuated inversion recovery imaging (A, B) and T2-weighted gradient echo imaging (C, D) show a small, isolated, acute stage hematoma (arrow) selectively involving the vermis of the right cerebellum located immediately posterior to the fourth ventricle, with mild edema of the surrounding brain tissue.
A
C
B
D
271https://doi.org/10.12701/yujm.2019.00318
Yeungnam Univ J Med 2019;36(3):269-272

vertigo and body lateropulsion to the contralesional side. We be-lieve that elderly patients, especially those with vascular risk fac-tors, need to be examined carefully and brain MRI should be per-formed to rule out the possibility of a cerebellar lesion, even though patients present with signs and symptoms suggestive of acute peripheral vestibulopathy. MRI allows for the accurate de-tection of even small, isolated hematomas or infarctions located in the cerebellar vermis.
Conflicts of interest
No potential conflicts of interest relevant to this article was re-ported.
ORCID
Dong Hyun Lee, https://orcid.org/0000-0002-4434-8901 Se-Jin Lee, https://orcid.org/0000-0001-7438-691X
References
1. Kase CS, Mohr JP, Caplan LR. Intracerebral hemorrhage. In: Mohr JP, Choi DW, Grotta JC, Weir B, Wolf PA, editors. Stroke: pathophysiology, diagnosis, and management. 4th ed. Philadel-phia: Churchill Livingstone; 2004. p. 327–76.
2. Kattah JC, Kolsky MP, Luessenhop AJ. Positional vertigo and the cerebellar vermis. Neurology 1984;34:527–9.
3. Huang CY, Yu YL. Small cerebellar strokes may mimic labyrin-thine lesions. J Neurol Neurosurg Psychiatry 1985;48:263–5.
4. Johkura K. Central paroxysmal positional vertigo: isolated dizzi-
ness caused by small cerebellar hemorrhage. Stroke 2007;38: e26–7.
5. Lee H, Yi HA, Cho YW, Sohn CH, Whitman GT, Ying S, et al. Nodulus infarction mimicking acute peripheral vestibulopathy. Neurology 2003;60:1700–2.
6. Lee H, Cho YW. A case of isolated nodulus infarction presenting as a vestibular neuritis. J Neurol Sci 2004;221:117–9.
7. Lee H. Isolated body lateropulsion caused by a lesion of the ros-tral vermis. J Neurol Sci 2006;249:172–4.
8. Oh YM, Choi KD, Oh SY, Kim JS. Periodic alternating nystagmus with circumscribed nodular lesion. Neurology 2006;67:399.
9. Muley SA, Bushara KO. Isolated gait ataxia due to cerebellar ver-mis infarct. Arch Neurol 2004;61:1461.
10. Shan DE, Wang V, Chen JT. Isolated lateropulsion of the trunk in cerebellar infarct. Clin Neurol Neurosurg 1995;97:195–8.
11. Bertholon P, Michel D, Convers P, Antoine JC, Barral FG. Isolat-ed body lateropulsion caused by a lesion of the cerebellar pe-duncles. J Neurol Neurosurg Psychiatry 1996;60:356–7.
12. Lee H, Sohn CH. Axial lateropulsion as a sole manifestation of lateral medullary infarction: a clinical variant related to ros-tral-dorsolateral lesion. Neurol Res 2002;24:773–4.
13. Kim SH, Cho J, Cho JH, Han SW, Kim SM, Park SC, et al. Iso-lated lateropulsion by a lesion of the dorsal spinocerebellar tract. Cerebrovasc Dis 2004;18:344–5.
14. Thömke F, Marx JJ, Iannetti GD, Cruccu G, Fitzek S, Urban PP, et al. A topodiagnostic investigation on body lateropulsion in medullary infarcts. Neurology 2005;64:716–8.
15. Norrving B, Magnusson M, Holtås S. Isolated acute vertigo in the elderly; vestibular or vascular disease? Acta Neurol Scand 1995;91:43–8.
https://doi.org/10.12701/yujm.2019.00318272
Lee DH and Lee SJ. Cerebellar vermis hemorrhage mimicking vestibulopathy

Cerebral venous sinus thrombosis (CVT) is a rare cerebrovascular condition accounting for 0.5–1% of all types of strokes in the general population. Hyperthyroidism is associated with proco-agulant and antifibrinolytic activity, thereby precipitating a hypercoagulable state that predis-poses to CVT. We report the case of a 31-year-old Korean man with massive CVT and diagnosis of concomitant Graves’ disease at admission. Early diagnosis and prompt treatment of CVT are important to improve prognosis; therefore, CVT should be considered in the differential diagno-sis in all patients with hyperthyroidism presenting with neurological symptoms.
Keywords: Graves’ disease; Hyperthyroidism; Intracranial thrombosis; Thyrotoxicosis
Received: August 6, 2019 Revised: September 9, 2019 Accepted: September 11, 2019
Corresponding author: Hye-Min SonDepartment of Radiology, Keimyung University Dongsan Hospital, 1035, Dalgubeol-daero, Dalseo-gu, Daegu 42601, KoreaTel: +82-53-250-4120Fax: +82-53-250-4153E-mail: [email protected]
Introduction
Cerebral venous sinus thrombosis (CVT) is often categorized as a distinct subgroup of cerebrovascular disease, showing an esti-mated incidence of 0.5–1% of all kinds of strokes in the general population [1]. CVT is associated with various conditions that result in a hypercoagulable state. Hyperthyroidism is a predispos-ing factor in approximately 1.7% of patients with CVT [2]. Nota-bly, 23 papers (including 11 case reports) have discussed the asso-ciation between thyrotoxicosis and CVT; however, few studies have investigated the pathophysiology of this condition or estab-lished a definitive association because of methodological limita-tions. We describe a patient who presented with massive CVT as-sociated with venous infarction in the right frontal lobe and diag-nosis of concomitant Graves’ disease.
Case
A 31-year-old Korean man visited the Emergency Department at Dongsan Hospital with fainting spells and convulsive movements.
Case reporteISSN 2384-0293
Yeungnam Univ J Med 2019;36(3):273-280https://doi.org/10.12701/yujm.2019.00339
Massive cerebral venous sinus thrombosis secondary to Graves’ diseaseHye-Min SonDepartment of Radiology, Keimyung University Dongsan Hospital, Daegu, Korea
He reported a several-day history of recurrent headaches with vomiting, as well as a several-month history of weight loss and heat intolerance. He also reported a history of appendectomy in 1994, short-term use of medications for suspected major depres-sive disorder in 2012, and surgery for shoulder fracture in 2014.
Initial laboratory investigations revealed normal blood counts, as well as kidney and liver function. Initial brain computed tomog-raphy (CT) revealed no definitive evidence of intracranial hemor-rhage or detectable low-density infarct-like lesions. Electrocardi-ography revealed sinus tachycardia. The patient’s symptoms worsened the day following his initial visit. Thyroid function tests revealed a serum thyroid-stimulating hormone (TSH) level < 0.01 µIU/mL, free thyroxine 4.73 ng/dL, and tri-iodothyronine 378.45 ng/dL. Laboratory tests performed for the assessment of a hypercoagulable state revealed the following results: anti-thyroid peroxidase (anti-TPO) 18.34 IU/mL, thyroglobulin antibody (Ab) within normal limits, TSH-receptor Ab 14.14 IU/L, d-dimer 5.74 µg/mL, fibrinogen 554.5 mg/dL, and factor VIII 210.6%.
Brain magnetic resonance imaging (MRI) was performed based on the emergency protocol followed at our hospital, includ-
273https://doi.org/10.12701/yujm.2019.00339
Copyright© 2019 Yeungnam University College of MedicineThis is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.

ing a sagittal T1-weighted image (T1WI), diffusion-weighted im-age (DWI), T2 fluid-attenuated inversion recovery (FLAIR) and T2* gradient recalled echo (GRE) sequences. It revealed focal hemorrhagic infarction in the right frontal lobe with venous thrombosis in the superior sagittal (Figs. 1A, 1B) and the right transverse (Fig. 1C) and sigmoid sinuses (not shown in the fig-ure). Indeed, the initial brain CT revealed a subtle hyperdensity lesion on non-enhanced CT images and filling defects in the af-fected venous sinuses on contrast-enhanced images, particularly partial CVT of the superior sagittal sinus with a contrast-outlined triangular filling defect (empty delta sign) (Figs. 1D–1F). Howev-er, these findings were missed during the initial evaluation of im-
ages. The patient developed left-sided weakness 3 days after his initial visit. Additional brain CT and MR venography revealed an increased thrombus burden, presenting as significant filling de-fects in the superior sagittal and the right transverse and sigmoid sinuses (Fig. 2). Previous focal hemorrhagic infarction remained stable without progression, and no additional infarct core or hem-orrhagic focus was identified. He received anticoagulation therapy with low-molecular-weight heparin (clexane 60 mg twice a day) on the same day. His left-sided weakness disappeared 3 days after treatment initiation, and headache and nausea also improved 2 days thereafter.
Work-up including thyroid ultrasonography, thyroid scan with
Fig. 1. Initial contrast-enhanced brain CT and MR scans. Focal hemorrhagic infarction is present in the right frontal lobe (asterisk) and a dark signal intensity representing a thrombus (blooming artifact) is present in the superior sagittal sinus (arrows) on the MR scan obtained the following day (A, FLAIR; B, T2* GRE sequences). A similar dark signal intensity representing a thrombus (arrow) is also present in the right transverse sinus (C, T2* GRE). These findings were neglected on the previous CT scan. The right transverse sinus shows a subtle hyperdensity (arrowhead) on a non-enhanced axial CT scan (D). Contrast-enhanced axial CT scans (E, F) show corresponding filling defect (arrowhead) at the same location and a partial empty delta sign (arrowhead) in the superior sagittal sinus, which were missed during evaluation of the initial brain CT scan. CT, computed tomography; MR, magnetic resonance; FLAIR, fluid-attenuated inversion recovery; GRE, gradient recalled echo.
A
D
B
E
C
F
https://doi.org/10.12701/yujm.2019.00339274
Son HM. Cerebral venous sinus thrombosis on Graves’ disease

Fig. 2. Brain CT and MR venography scans obtained on admission (3 days after the initial brain CT). Axial non-enhanced CT scan (A) shows a more prominent hyperdensity (HU 70) in the right transverse sinus (arrowhead), which shows the same density (HU 70) on contrast-enhanced brain CT scan (B). Absence of flow-related enhancement is present in the superior sagittal and right transverse to sigmoid sinuses, as opposed to normal flow-related enhancement observed in the left transverse sinus (arrowhead) on an MIP image (C). Sagittal reconstructed MR venography scan (D) shows the propagation of the filling defect along the superior sagittal sinus (arrows). CT, computed tomography; MR, magnetic resonance; HU, Hounsfield units; MIP, maximum intensity projection.
technetium-99m, and laboratory tests confirmed a diagnosis of Graves’ disease, and methimazole (antithyroid agent categorized as a TPO inhibitor) was administered at a dose of 12.5 mg twice a day along with indenol (beta blocker) at a dose of 10 mg three times a day. Normalization of thyroid function tests was observed following this treatment.
Follow-up contrast-enhanced CT and MR venography were performed with additional sequences (DWI, T2-FLAIR, T2* GRE) to evaluate residual venous thromboses, 27 days after the patient’s initial visit. These imaging studies revealed a significantly reduced thrombus burden in the cerebral deep venous sinuses and partially restored flow enhancement in the right transverse
A
C
B
D
275https://doi.org/10.12701/yujm.2019.00339
Yeungnam Univ J Med 2019;36(3):273-280
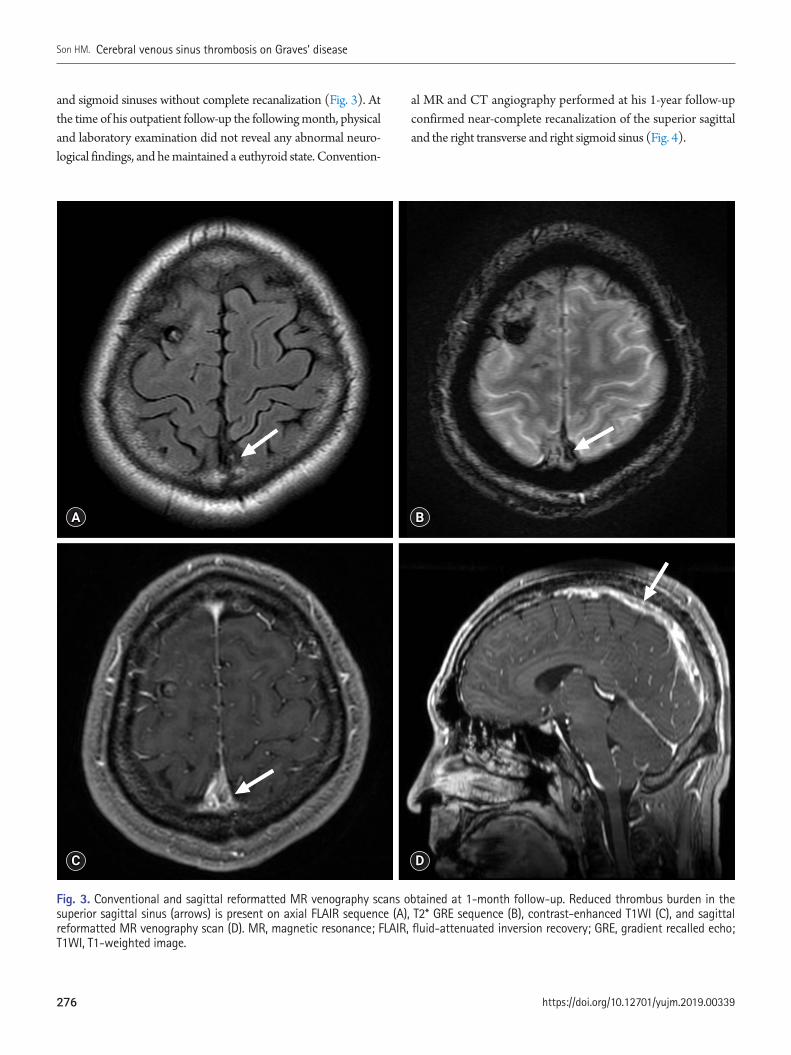
and sigmoid sinuses without complete recanalization (Fig. 3). At the time of his outpatient follow-up the following month, physical and laboratory examination did not reveal any abnormal neuro-logical findings, and he maintained a euthyroid state. Convention-
al MR and CT angiography performed at his 1-year follow-up confirmed near-complete recanalization of the superior sagittal and the right transverse and right sigmoid sinus (Fig. 4).
Fig. 3. Conventional and sagittal reformatted MR venography scans obtained at 1-month follow-up. Reduced thrombus burden in the superior sagittal sinus (arrows) is present on axial FLAIR sequence (A), T2* GRE sequence (B), contrast-enhanced T1WI (C), and sagittal reformatted MR venography scan (D). MR, magnetic resonance; FLAIR, fluid-attenuated inversion recovery; GRE, gradient recalled echo; T1WI, T1-weighted image.
A
C
B
D
https://doi.org/10.12701/yujm.2019.00339276
Son HM. Cerebral venous sinus thrombosis on Graves’ disease

Discussion
CVT is categorized as a distinct subgroup of cerebrovascular dis-ease, showing an incidence of approximately 0.5–1% of all kinds
of strokes in the general population [1]. CVT is associated with various conditions that result in a hypercoagulable state. Hyper-thyroidism is implicated as a predisposing factor for CVT because hyperthyroidism is known to cause elevated procoagulant levels
Fig. 4. Conventional MR and delayed-phase CT angiography scans obtained at the last follow-up showing near-complete recanalization of the cerebral venous sinuses. Conventional MR venography scan (A, FLAIR; B, T2* GRE; and C, contrast-enhanced T1WI) and delayed-phase CT angiography scan (D) obtained at 1-year follow-up shows near-complete recanalization of the superior sagittal and the right transverse and sigmoid sinuses (arrows). MR, magnetic resonance; CT, computed tomography; FLAIR, fluid-attenuated inversion recovery; GRE, gradient recalled echo; T1WI, T1-weighted image.
A
C
B
D
277https://doi.org/10.12701/yujm.2019.00339
Yeungnam Univ J Med 2019;36(3):273-280

in the vascular hemostatic system leading to a hypercoagulable state. However, to date only several small studies have directly in-vestigated the association between hyperthyroidism and CVT. Diagnostic radiological findings in patients with CVT include the following: venous sinus thrombosis can be identified as a hyper-density lesion of the affected sinus for the first 7–14 days on non-enhanced CT images. Following contrast administration, CVT presents as a filling defect in a sinus, and patients with in-volvement of the sagittal sinus typically show the ‘empty delta sign.’ Reportedly, CT venography shows a sensitivity of 95% in these cases. MRI can help in visualization of the clot as well as the sequelae. The clot shows variable signal intensity based on its stage (acute-to-chronic stage). During the acute stage, the clot ap-pears isointense on T1WI and hypointense on T2WI, and during the subacute stage the clot appears as a hyperintense lesion on T1WI. Notably, clots can be easily detected as a dark signal within areas of hemorrhage (typically described as blooming artifacts) on T2* GRE or susceptibility images. Venous infarction can be identified on DWI. Contrast-enhanced MR or MR venography shows greater sensitivity in detecting thrombosis, which presents as a venous filling defect in patients with CVT.
The patient described in this case report presented with mas-sive CVT without a medical history to support this diagnosis. Di-agnosis of Graves’ disease concomitant with CVT was established only at the time of his current admission. The association between CVT and thyrotoxicosis was first described by Kaliebe in 1913 [3] and by Doyle in 1927 [4]; 23 cases have been reported there-after [5-8]. A hypercoagulable state induced by high circulating levels of thyroid hormones is the likely mechanism contributing to the pathophysiology in these cases [9]. High levels of thyroid hormones increase blood levels of coagulation factors and inhibit fibrinolysis. Notably, increased levels of fibrinogen, von Wille-brand factor, coagulation factors VIII, IX and X, and plasminogen activator inhibitor-1 shorten the activated partial thromboplastin time and prolong the clot lysis time [10]. The combined effects of hyperthyroidism on procoagulant and fibrinolytic activity in-crease the risk of venous thrombosis. Bensalah et al. reported that increased Factor VIII levels were observed in 10 of 26 patients with CVT and concomitant thyrotoxicosis [9]. In our case, the factor VIII level was 210.6%. Currently, venous thrombosis is ac-cepted as a ‘multicausal’ disease because several genetic and envi-ronmental conditions work together [11].
Although initial laboratory investigations revealed poorly con-trolled thyroid hormone levels indicating thyrotoxicosis, the diag-nosis of CVT was delayed in this patient until confirmatory MR venography was performed, because we initially missed the partial empty delta sign in the affected cerebral venous sinuses. Any fur-
ther delay in diagnosis could have led to irreversible neurological injury even with optimal treatment. This case emphasizes the im-portance of careful evaluation for early diagnosis of venous throm-bosis in young adults with hyperthyroidism presenting with unex-plained neurological symptoms. Clinicians should be aware that further evaluation to confirm CVT should be considered with CT or MR angiography with venous phase and blood-sensitive MR sequences, such as T2* GRE or susceptibility weighted imag-ing in patients with a suspicious hyperdensity or the empty delta sign in the cerebral venous sinuses on brain CT.
In conclusion, previously published data strongly suggest that hyperthyroidism should be considered an important risk factor for CVT. Comprehensive evaluation is warranted for prompt di-agnosis of CVT in patients with hyperthyroidism presenting with unexplained neurological symptoms.
Conflicts of interest
No potential conflicts of interest relevant to this article was re-ported.
ORCID
Hye-Min Son, https://orcid.org/0000-0003-1748-0701
References
1. Einhäupl K, Bousser MG, de Bruijn SF, Ferro JM, Martinelli I, Masuhr F, et al. EFNS guideline on the treatment of cerebral ve-nous and sinus thrombosis. Eur J Neurol 2006;13:553–9.
2. Saposnik G, Barinagarrementeria F, Brown RD Jr, Bushnell CD, Cucchiara B, Cushman M, et al. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare profes-sionals from the American Heart Association/American Stroke Association. Stroke 2011;42:1158–92.
3. Kaliebe H. Autochthone sinusthrombose bei einem falle von morbus basedow und tabes. Med Klin 1913;9:1929–32.
4. Doyle JB. Obstruction of the longitudinal sinus. Arch Neurol Psy-chiatry 1927;18:374–82.
5. Hermans E, Mariën P, De Deyn PP. Sinus sigmoideus thrombosis secondary to graves’ disease: a case description. Case Rep Neurol 2011;3:203–9.
6. Hwang JU, Kwon KY, Hur JW, Lee JW, Lee HK. The role of hy-perthyroidism as the predisposing factor for superior sagittal si-nus thrombosis. J Cerebrovasc Endovasc Neurosurg 2012;14: 251–4.
7. Merino M, Guijarro MG, Iglesias P, Aladro Y, Montero P. Thyro-
https://doi.org/10.12701/yujm.2019.00339278
Son HM. Cerebral venous sinus thrombosis on Graves’ disease

toxicosis and cerebral venous sinus thrombosis, causality or chance alone? Endocrinol Nutr 2012;59:462–3.
8. Migeot M, Rutgers MP, Gille M. Puerperal cerebral sinus venous thrombosis and acute hyperthyroidism in Graves’ disease. Acta Neurol Belg 2013;113:331–3.
9. Bensalah M, Squizzato A, Ould Kablia S, Menia H, Kemali Z. Ce-rebral vein and sinus thrombosis and hyperthyrodism: a case re-
port and a systematic review of the literature. Thromb Res 2011;128:98–100.
10. Squizzato A, Romualdi E, Büller HR, Gerdes VE. Thyroid dys-function and effects on coagulation and fibrinolysis: a systemat-ic review. J Clin Endocrinol Metab 2007;92:2415–20.
11. Rosendaal FR. Venous thrombosis: a multicausal disease. Lan-cet 1999;353:1167–73.
279https://doi.org/10.12701/yujm.2019.00339
Yeungnam Univ J Med 2019;36(3):273-280

Yeungnam University Journal of Medicine (YUJM) is the official journal of College of Medicine Yeungnam University and is published three times a year (January 31, May 31, and September 30). The goal of the YUJM is to publish high quality manuscripts dedicated to clinical or basic research. Any authors affiliated with an accredited biomedical institution may submit manuscripts of editorials, review articles, original articles, and case reports. Manuscripts are received with the understanding that they are not under simultaneous consideration by any other publications, and that the authors realize that the identities of the reviewers are kept confidential. The editors reserve the right to make corrections, both literary and technical, to the papers. The agreement of copyright transfer from all the authors should be sent with the manuscript submission. A copyright transfer form is available at the journal homepage.
Editorial policy
The editor assumes that all authors listed in a manuscript have agreed with the following policy of the YUJM on submission of manuscript. Except for the negotiated secondary publication, manuscript submitted to the journal must be previously unpublished and not be under consideration for publication elsewhere.
The purpose of editing is to improve the quality of the paper and to make it possible to convey the topic to readers as briefly as possible. Appropriate peer reviewers are selected to evaluate the creativity and scientific basis of the paper. We also determines the appropriateness of charts and figures. Submitted papers are first reviewed by the editorial committee and rejected if the form is inappropriate or the contents are inadequate.
Anyone who would like to submit a manuscript is advised to carefully read the aims and scope section of this journal. Manuscripts should be prepared for submission according to the Introduction to Authors. For issues not addressed in these instructions, the author is referred to the International Committee of Medical Journal Editors (ICMJE) “Recommendations for the Conduct, Reporting, Editing and Publication of Scholarly Work
in Medical Journals” (http://www.icmje.org).Compliance with ICMJE Recommendations: The journal adheres
completely to the ethical guidelines and best practices published by professional organizations, including Recommendations for the Conduct, Reporting, Editing, and Publication of Scholarly Work in Medical Journals (http://www.icmje.org/icmje-recommendations.pdf) from ICMJE and Principles of Transparency and Best Practice in Scholarly Publishing (joint statement by COPE, DOAJ, WAME, and OASPA; (http://doaj.org/bestpractice).
Ethical considerations
Research ethicsAll of the manuscripts should be prepared based on strict observation of research and publication ethics guidelines recommended by the Council of Science Editors (http://www.councilscienceeditors.org), International Committee of Medical Journal Editors (ICMJE, http://www.icmje.org), World Association of Medical Editors (WAME, http://www.wame.org), and the Korean Association of Medical Journal Editors (KAMJE, https://www.kamje.or.kr/en/main_en). All studies involving human subjects or human data must be reviewed and approved by a responsible Institutional Review Board (IRB). Please refer to the principles embodied in the Declaration of Helsinki (https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/) for all investigations involving human materials. Animal experiments also should be reviewed by an appropriate committee (IACUC) for the care and use of animals. Also studies with pathogens requiring a high degree of biosafety should pass review of a relevant committee (IBC). The approval should be described in the Methods section. For studies of humans including case reports, state whether informed consents were obtained from the study participants. The editor of YUJM may request submission of copies of informed consents from human subjects in clinical studies or IRB approval documents. The YUJM will follow the guidelines by the Committee on Publication Ethics (COPE, http://publicationethics.org) for settlement of any misconduct.
Instructions to authorsEnactment December 30, 1984
First revision April 20, 2011Second revision May 22, 2012
Third revision July 17, 2013Fourth revision April 22, 2014
Fifth revised December 23, 2014Recently revised April 30, 2018
i

Conflicts of interestThe corresponding author of an article is asked to inform the Editor of the authors' potential conflicts of interest possibly influencing the research or interpretation of data. A potential conflicts of interest should be disclosed in the cover letter even when the authors are confident that their judgments have not been influenced in preparing the manuscript. Such conflicts may include financial support or private connections to pharmaceutical companies, political pressure from interest groups, or academic problems. Disclosure form shall be same with ICMJE Uniform Disclosure Form for Potential Conflicts of Interest (http://www.icmje.org/coi_disclosure.pdf). The Editor will decide whether the information on the conflicts should be included in the published paper. In particular, all sources of funding for a study should be explicitly stated. The YUJM asks referees to let its editor know of any conflicts of interest before reviewing a particular manuscript.
AuthorshipThe YUJM follows the recommendations for authorship by the ICMJE, 2017 (http://www.icmje.org/icmje-recommendations.pdf ) and Good Publication Practice Guidelines for Medical Journals 2nd Edition (KAMJE, 2013, https://www.kamje.or.kr/board/view?b_name=bo_publication&bo_id=7&per_page=).
Authorship credit should be based on (1) Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; (2) Drafting the work or revising it critically for important intellectual content; (3) Final approval of the version to be published; and (4) Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Authors should meet conditions of 1, 2, 3, and 4. In addition, an author should be accountable for the parts of the work he or she has done and should be able to identify which co-authors are responsible for specific other parts of the work. Authors should have confidence in the integrity of the contributions of their coauthors. All those designated as authors should meet all four criteria for authorship, and all who meet the four criteria should be identified as authors. Those who do not meet all four criteria should be acknowledged as contributors not be authors. These authorship criteria are intended to reserve the status of authorship for those who deserve credit and can take responsibility for the work. The criteria are not intended for use as a means to disqualify colleagues from authorship who otherwise meet authorship criteria by denying them the opportunity to meet criterion #2 or 3. Therefore, all individuals who meet the first criterion should have the opportunity to participate in the review, drafting, and final
approval of the manuscript.A corresponding author should be designated when there are
two or more authors. The corresponding author is primarily responsible for all issues to the editor and audience.
When a large, multicenter group has conducted the work, the group should identify the individuals who accept direct responsibility for the manuscript. When submitting a manuscript authored by a group, the corresponding author should clearly indicate the preferred citation and identify all individual authors as well as the group name. Journals generally list other members of the group in the Acknowledgements. Acquisition of funding, collection of data, or general supervision of the research group alone does not constitute authorship.
Redundant publication and plagiarismRedundant publication is defined as “reporting (publishing or attempting to publish) substantially the same work more than once, without attribution of the original source(s)”. Characteristics of reports that are substantially similar include the following: (a) “at least one of the authors must be common to all reports (if there are no common authors, it is more likely plagiarism than redundant publication),” (b) “the subjects or study populations are the same or overlapped,” (c) “the methodology is typically identical or nearly so,” and (d) “the results and their interpretation generally vary little, if at all.”
When submitting a manuscript, authors should include a letter informing the editor of any potential overlap with other already published material or material being evaluated for publication and should also state how the manuscript submitted to YUJM differs substantially from other materials. If all or part of your patient population was previously reported, this should be mentioned in the Methods, with citation of the appropriate reference(s).
The duplication will be checked through crosscheck (https://app.ithenticate.com) or eTBLAST (https://helioblast.heliotext.com) before submission. If duplicate publication related to the papers of this journal is detected, the manuscripts may be rejected, the authors will be announced in the journal, and their institutes will be informed. There will also be penalties for the authors.
Secondary publicationIt is possible to republish manuscripts if the manuscripts satisfy the condition of secondary publication of the Uniform Requirements for Manuscripts Submitted to Biomedical Journals by International Committee of Medical Journal Editors (ICMJE), available from http://www.icmje.org. These are:• The authors have received approval from the editors of both
journals (the editor concerned with the secondary publication must have access to the primary version).
ii

• The priority for the primary publication is respected by a publication interval negotiated by editors of both journals and the authors.
• The paper for secondary publication is intended for a different group of readers; an abbreviated version could be sufficient.
• The secondary version faithfully reflects the data and interpretations of the primary version.
• The secondary version informs readers, peers, and documenting agencies that the paper has been published in whole or in part elsewhere—for example, with a note that might read, "This article is based on a study first reported in the (journal title, with full reference)"—and the secondary version cites the primary reference.
• The title of the secondary publication should indicate that it is a secondary publication (complete or abridged republication or translation) of a primary publication. Of note, the United States National Library of Medicine (NLM) does not consider translations as "republications" and does not cite or index them when the original article was published in a journal that is indexed in MEDLINE.
Registration of the clinical trial researchClinical trial defined as “any research project that prospectively assigns human subjects to intervention and comparison groups to study the cause-and-effect relationship between a medical intervention and a health outcome” should be registered to the primary registry to be prior publication. YUJM accepts the registration in any of the primary registries that participate in the WHO International Clinical Trials Portal (http://www.who.int/ictrp/en/), NIH ClinicalTrials.gov (http://www.clinicaltrials.gov), ISRCTN Resister (www.ISRCTN.org), or the Clinical Research Information Service (CRIS), Korea CDC (https://cris.nih.go.kr/cris/index.jsp). The clinical trial registration number shall be published at the end of the abstract.
Data sharing statementYUJM accepts the ICMJE Recommendations for data sharing statement policy (http://icmje.org/icmje-recommendations.pdf ). All manuscripts reporting clinical trial results should submit a data sharing statement following the ICMJE guidelines from 1 July 2018. Authors may refer to the editorial, “Data Sharing statements for Clinical Trials: A Requirement of the International Committee of Medical Journal Editors,” in JKMS Vol. 32, No. 7:1051-1053 (http://crossmark.crossref.org/dialog/ ?doi=10.3346/jkms.2017.32.7.1051&domain=pdf&date_stamp=2017-06-05).
Process to manage the research and publication misconductW hen the Journal faces suspected cases of research and publication misconduct such as a redundant (duplicate) publication, plagiarism, fabricated data, changes in authorship, undisclosed conflicts of interest, an ethical problem discovered with the submitted manuscript, a reviewer who has appropriated an author’s idea or data, complaints against editors, and other issues, the resolving process will follow the flowchart provided by the Committee on Publication Ethics (http://publicationethics.org/resources/flowcharts). The Editorial Board of YUJM will discuss the suspected cases and reach a decision. YUJM will not hesitate to publish errata, corrigenda, clarifications, retractions, and apologies when needed.
For the policies on research and publication ethics not stated in the Instructions, Guidelines on Good Publication (http://publicationethics.org) or Good Publication Practice Guidelines for Medical Journals (http://kamje.or.kr) can be applied.
Categories of publications
YUJM publishes editorials, invited review articles, original articles, and case reports. Editorials are invited perspectives on an area of medical science, dealing with very active fields of research, current medical interests, fresh insights and debates. Review articles provide a concise review of a subject of importance to medical researchers written by an invited expert in medical science. Original articles are papers reporting the results of basic and clinical investigations that are sufficiently well documented to be acceptable to critical readers. Case reports deal with clinical cases of medical interest or innovation.
Manuscript submission
The main document with manuscript text and tables should be prepared with a Microsoft Word program. Authors should submit manuscripts via the online submission system (https://yujm.jams.or.kr). Please log in first as a member of the system and follow the directions. Manuscripts should be submitted by the corresponding author, who should indicate the address and phone number for correspondence in the title page of the manuscript. If available, a fax number and e-mail address would be helpful. The revised manuscript should be submitted through the same web system under the same identification numbers. Items pertaining to manuscripts submitted for publication, as well as letters or other forms of communication regarding the editorial management of YUJM, all correspondences and business communications should be sent to:
iii

Joon Hyuk Choi, M.D., Ph.D., Editor-in-ChiefYeungnam University Journal of MedicineYeungnam University College of Medicine170 Hyeonchung-ro, Nam-gu, Daegu 42415, KoreaTel: +82-53-640-6832, Fax: +82-53-651-0394E-mail: [email protected]: https://yujm.yu.ac.kr
Peer review process
YUJM reviews all manuscripts received. A manuscript is previewed for its format and academic relevancy, and then rejected or sent to the 2 (or more) relevant investigators available for review of the contents. The editor selects peer referees by recommendation of the editorial board members or from the board's specialist database. The identities of the reviewers and authors will not be revealed (double blinded review). All the radiologic images and pathologic (microscopic) images are reviewed by radiologist or pathologist for appropriateness. A manuscript containing statistical analysis will be reviewed by a statistical editor.
Upon completion of the review, authors will receive notification of the Editor's decision by e-mail with comments offered by the reviewers. Revised manuscripts must be submitted within 3 months of the date on the decision letter.
Acceptance of manuscripts is based on many factors, including the importance, originality, and priority of the research. Acceptance of the manuscript is decided based on the critiques and recommended decision of the referees. A referee may recommend "accept", "minor revision", "major revision," or "reject". If there is a marked discrepancy in the decisions between two referees or between the opinions of the author and referee(s), the editor may send the manuscript to another referee for additional comments and a recommended decision. The reviewed manuscripts are returned back to the corresponding author with comments and recommended revisions. Names and decisions of the referees are masked. A final editor's decision on acceptance or rejection for publication is forwarded to the corresponding author from the editorial office.
The usual reasons for rejection are topics that are too specific and target audience that is too limited, insufficient originality, serious scientific flaws, poor quality of illustrations, or absence of a message that might be important to readers. Rarity of a disease condition is itself not an acceptable justification for a case report. The peer review process takes usually 2–4 weeks after the manuscript submission.
Revisions are usually requested to take account of criticisms and comments made by referees. The revised manuscript should be resubmitted via the web system. Failure to resubmit
Manuscript preparation
Review articleReview articles are usually solicited by the Editor-in-Chief. However, unsolicited Reviews will be also considered. Authors should contact the Editor-in-Chief in advance to determine the appropriateness of their review articles for publication. All Review articles will undergo peer review. An abstract is required whereas Materials and methods section and a Results section are not required. The length of review articles is limited to 5,000-8,000 words with a maximum of 100 references. Also, there should be no more than 3 authors.
Original articleOriginal articles should begin with the title page followed by an abstract; a list of key words; an Introduction, Materials and methods, Results, Discussion, References (no more than 30), and tables and/or illustrations.
1) Title pageThe tile page should contain the following information: (1) title (less than 150 characters, including spaces); (2) author list (first name, middle name, and last name); (3)
the revised manuscript within 2 months without any notice from the corresponding author is regarded as a withdrawal. The corresponding author must indicate clearly what alterations have been made in response to the referee's comments point by point. Acceptable reasons should be given for noncompliance with any recommendation of the referees.
Copyrights and creative commons attribution license
The manuscript, when published, will become the property of the journal. All published papers become the permanent property of the Yeungnam University College of Medicine and must not be published elsewhere without written permission. Copyrights of all published materials are owned by the Yeungnam University College of Medicine. They also follow the Creative Commons Attribution Non-Commercial License (https://creativecommons.org/licenses/by-nc/4.0/).
iv

name of the institutions at which the work was performed; (4) acknowledgement of research support; (5) name, address, telephone, fax number, and e-mail address of the corresponding author; (6) running title (less than 50 characters, including spaces).
2) AbstractAbstract must be organized and formatted according to the following headings: Background, Methods, Results, and Conclusion. The abstract length is typically no more than 250 words.
3) KeywordsList 3-6 keywords from the list provided in Index Medicus under "Medical Subject Heading (MeSH)."
4) TextThe text of manuscripts must have the following sections: Introduction, Materials and methods, Results, and Discussion. The body of the manuscript should be written as concisely as possible. All pages of the manuscript should be numbered.
IntroductionThis should provide a context or background for the study and states the specific purpose or research objective of or hypothesis tested by the study. This may include mention of papers most closely related to the article, and of the problem.
Materials and methodsExplanation of the experimental methods should be concise but sufficient to allow other workers to reproduce the results. This provides the technical information, apparatus (the manufacturer's name and brief address) and procedures. Give references and brief descriptions for the methods that have been published. Describe statistical methods with enough detail to enable a reader with access to the original data to verify the reported results. Define statistical terms, abbreviations, and most symbols.
Ensure correct use of the terms sex (when reporting biological factors) and gender (identity, psychosocial or cultural factors), and, unless inappropriate, report the sex or gender of study participants, the sex of animals or cells, and describe the methods used to determine sex or gender. If the study was done involving an exclusive population, for example in only one sex, authors should justify why, except in obvious cases (e.g., prostate cancer). Authors should define how they determined race or ethnicity and justify their relevance.
ResultsThis should include a concise textual description of the data presented in tables and figures.
DiscussionThis section includes the new and important aspects of the study and the conclusions. The data should be interpreted concisely. Speculation is permitted, but it must be supported by the data presented by the authors.
ReferencesReferences should be numbered consecutively in the order in which they are first mentioned in the text, with numbers in square brackets before any closing punctuation. They should be listed on a separate document under the heading "References," and double-spaced. Reference format should conform to that set forth in "Uniform Requirements for Manuscripts Submitted to Biomedical Journals. 5th ed." ( JAMA 1997;277:927-34). Titles of journals should be abbreviated according to the Index Medicus style.
Reference style:
Journal articlesList all authors when six or less; when seven or more, list the first six and add et al.Vega KJ, Pina I. Heart transplantation is associated with an increased risk for pancreatobiliary disease. Ann Intern Med 1996;124:980-3.Verbalis JG. Renal physiology of nocturia. Neurourol Urodyn 2014;33(Suppl 1):S6-9.
BookRingsven MK, Bond D. Gerontology and leadership skills for nurses. 2nd ed. Albany (NY): Delmar Publishers; 1996. Luzikov VN. Mitochondrial biogenesis and breakdown. Galkin AV, translator; Roodyn DB, editor. New York: Consultants Bureau; 1985. p. 362
Book chapterPhillips SJ, Whisnant JP. Hypertension and stroke. In: Laragh JH, Brenner BM, editors. Hypertension: pathophysiology, diagnosis, and management. 2nd ed. New York: Raven Press; 1995. p. 465-78.
Web resourcesPolgreen PM, Diekema DJ, Vandeberg J, Wiblin RT, Chen YY, David S, et al. Risk factors for groin wound infection
v

after femoral artery catheterization: a case-control study. Infect Control Hosp Epidemiol [Internet]. 2006 [cited 2007 Jan 5];27:34-7. http://www.journals.uchicago.edu/ICHE/journal/issues/v27n1/2004069/2004069.web.pdfTesta J. The Thomson Reuters journal selection process [Internet]. Philadelphia: Thomson Reuters; 2012 [cited 2013 Sep 30]. http://wokinfo.com/essays/journal-selection-process
5) TablesTables should fit within a single page. The Table's legend may include any pertinent notes and must include definitions of all abbreviations and acronyms that have been used in the Table. For footnotes, the following symbols should be used in this sequence: a), b), c), d), e), f), g), h), etc. Authors are obligated to indicate the significance of their observations by appropriate statistical analysis.
6) IllustrationsFigures must be cited consecutively using Arabic numerals. Authors must submit illustrations as electronic files. Acceptable figure file formats are JPEG, TIFF, and PPT/PPTX. Each figure needs to be prepared in a resolution higher than 300 dpi with good contrast and sharpness. The file size of each submitted figure should not exceed 10 MB per figure. If the patient's photograph is presented in a paper, it should be manipulated to make it difficult to recognize. Patients introduced in the manuscripts should be informed and aware that their photographs, videotapes, and other images (imaging records) will be released by the authors, and the authors should attach the Authorization and Release Form available at the YUJM website (https://yujm.yu.ac.kr/authors/ethics.php) including each patient’s signature. If the patient is a minor, a written consent of the guardian must be submitted.
7) Legends for tables and illustrationsTyped legends that use double-spacing should start on a separate page with Arabic numerals corresponding to the Tables or Illustrations. When symbols, arrows, numbers, or letters are used to identify parts of the Tables or Illustrations, they should be individually identified and explained clearly in the legend.
8) AbbreviationsAuthors should limit the use of abbreviations to an absolute minimum. Abbreviations are not to be used in titles. Abstracts
may contain abbreviations for terms mentioned many times in the abstract section, but each term must be identified the first time it is mentioned.
9) Unit of measurementMeasurements of length, height, weight, and volume should be reported in metric units (meter, kilogram, or liter) or their decimal multiples. Temperature should be in degrees Celsius. Authors must consult the information for authors for the particular journal and should report laboratory information in both the local and International System of Units (SI).
Case reportCase reports should consist of an Abstract, Keywords, Introduction, Case, Discussion, and References (no more than 20). Case reports should have fewer than nine authors. The abstract should be concisely written (no more than 250 words).
Permission
If any portion of a manuscript has been previously published, the original source must be acknowledged, and the written permission from the copyright holder to reproduce the material must be submitted. It is the responsibility of the author to request permission from the publisher for any material that is being reproduced. This requirement applies to text, illustrations, and tables.
Article processing charges
Manuscripts that have accepted will be charged 200,000 won. The surcharge for color figures is none.
Author change
If the addition or deletion of authors or changes in the order of authorship is required, the correspondent author must complete the authorship change form and submit it to the editorial board with the signature of all existing authors and new authors. When there is a request for change by the author, the editorial committee convenes an ethics committee and judges whether it is appropriate. If a new author should be added or an author should be deleted after the submission, it is the responsibility of the corresponding author to ensure that all of the authors concerned are aware of and agree to the change in authorship. The YUJM has no responsibility for such changes.
vi

Research ethics
All of the manuscripts should be prepared based on strict observation of research and publication ethics guidelines recommended by the Council of Science Editors (http://www.councilscienceeditors.org), International Committee of Medical Journal Editors (ICMJE, http://www.icmje.org), World Association of Medical Editors (WAME, http://www.wame.org), and the Korean Association of Medical Journal Editors (KAMJE, https://www.kamje.or.kr/en/main_en). All studies involving human subjects or human data must be reviewed and approved by a responsible Institutional Review Board (IRB). Please refer to the principles embodied in the Declaration of Helsinki (https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/) for all investigations involving human materials. Animal experiments also should be reviewed by an appropriate committee (IACUC) for the care and use of animals. Also studies with pathogens requiring a high degree of biosafety should pass review of a relevant committee (IBC). The approval should be described in the Methods section. For studies of humans including case reports, state whether informed consents were obtained from the study participants. The editor of YUJM may request submission of copies of informed consents from human subjects in clinical studies or IRB approval documents. The YUJM will follow the guidelines by the Committee on Publication Ethics (COPE, http://publicationethics.org) for settlement of any misconduct.
Conflicts of interest
The corresponding author of an article is asked to inform the Editor of the authors' potential conflicts of interest possibly influencing the research or interpretation of data. A potential conflicts of interest should be disclosed in the cover letter even when the authors are confident that their judgments have not been influenced in preparing the manuscript. Such conflicts may include financial support or private connections to pharmaceutical companies, political pressure from interest groups, or academic problems. Disclosure form shall be same with ICMJE Uniform Disclosure Form for Potential Conflicts of Interest (http://www.icmje.org/coi_disclosure.pdf). The Editor will decide whether the information on the conflicts should be included in the published paper. In particular, all sources of funding for a study
should be explicitly stated. The YUJM asks referees to let its editor know of any conflicts of interest before reviewing a particular manuscript.
Authorship
The YUJM follows the recommendations for authorship by the ICMJE, 2017 (http://www.icmje.org/icmje-recommendations.pdf ) and Good Publication Practice Guidelines for Medical Journals 2nd Edition (KAMJE, 2013, https://www.kamje.or.kr/board/view?b_name=bo_publication&bo_id=7&per_page=).
Authorship credit should be based on (1) Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; (2) Drafting the work or revising it critically for important intellectual content; (3) Final approval of the version to be published; and (4) Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Authors should meet conditions of 1, 2, 3, and 4. In addition, an author should be accountable for the parts of the work he or she has done and should be able to identify which co-authors are responsible for specific other parts of the work. Authors should have confidence in the integrity of the contributions of their coauthors. All those designated as authors should meet all four criteria for authorship, and all who meet the four criteria should be identified as authors. Those who do not meet all four criteria should be acknowledged as contributors not be authors. These authorship criteria are intended to reserve the status of authorship for those who deserve credit and can take responsibility for the work. The criteria are not intended for use as a means to disqualify colleagues from authorship who otherwise meet authorship criteria by denying them the opportunity to meet criterion #2 or 3.Therefore, all individuals who meet the first criterion should have the opportunity to participate in the review, drafting, and final approval of the manuscript.
A corresponding author should be designated when there are two or more authors. The corresponding author is primarily responsible for all issues to the editor and audience.
When a large, multicenter group has conducted the work, the group should identify the individuals who accept direct responsibility for the manuscript. When submitting a manuscript authored by a group, the corresponding author should clearly
Research and publication ethics
vii

indicate the preferred citation and identify all individual authors as well as the group name. Journals generally list other members of the group in the Acknowledgements. Acquisition of funding, collection of data, or general supervision of the research group alone does not constitute authorship.
Redundant publication and plagiarism
Redundant publication is defined as “reporting (publishing or attempting to publish) substantially the same work more than once, without attribution of the original source(s)”. Characteristics of reports that are substantially similar include the following: (a) “at least one of the authors must be common to all reports (if there are no common authors, it is more likely plagiarism than redundant publication),” (b) “the subjects or study populations are the same or overlapped,” (c) “the methodology is typically identical or nearly so,” and (d) “the results and their interpretation generally vary little, if at all.”
When submitting a manuscript, authors should include a letter informing the editor of any potential overlap with other already published material or material being evaluated for publication and should also state how the manuscript submitted to YUJM differs substantially from other materials. If all or part of your patient population was previously reported, this should be mentioned in the Methods, with citation of the appropriate reference(s).
The duplication will be checked through crosscheck (https://app.ithenticate.com) or eTBLAST (https://helioblast.heliotext.com) before submission. If duplicate publication related to the papers of this journal is detected, the manuscripts may be rejected, the authors will be announced in the journal, and their institutes will be informed. There will also be penalties for the authors.
Secondary publication
It is possible to republish manuscripts if the manuscripts satisfy the condition of secondary publication of the Uniform Requirements for Manuscripts Submitted to Biomedical Journals by International Committee of Medical Journal Editors (ICMJE), available from http://www.icmje.org. These are:• The authors have received approval from the editors of both
journals (the editor concerned with the secondary publication must have access to the primary version).
• The priority for the primary publication is respected by a publication interval negotiated by editors of both journals and the authors.
• The paper for secondary publication is intended for a different group of readers; an abbreviated version could be sufficient.
• The secondary version faithfully reflects the data and
interpretations of the primary version. • The secondary version informs readers, peers, and documenting
agencies that the paper has been published in whole or in part elsewhere—for example, with a note that might read, "This article is based on a study first reported in the (journal title, with full reference)"—and the secondary version cites the primary reference.
• The title of the secondary publication should indicate that it is a secondary publication (complete or abridged republication or translation) of a primary publication. Of note, the United States National Library of Medicine (NLM) does not consider translations as "republications" and does not cite or index them when the original article was published in a journal that is indexed in MEDLINE.
Registration of the clinical trial research
Clinical trial defined as “any research project that prospectively assigns human subjects to intervention and comparison groups to study the cause-and-effect relationship between a medical intervention and a health outcome” should be registered to the primary registry to be prior publication. YUJM accepts the registration in any of the primary registries that participate in the WHO International Clinical Trials Portal (http://www.who.int/ictrp/en/), NIH ClinicalTrials.gov (http://www.clinicaltrials.gov), ISRCTN Resister (www.ISRCTN.org), or the Clinical Research Information Service (CRIS), Korea CDC (https://cris.nih.go.kr/cris/index.jsp). The clinical trial registration number shall be published at the end of the abstract.
Data sharing statement
YUJM accepts the ICMJE Recommendations for data sharing statement policy (http://icmje.org/icmje-recommendations.pdf ). All manuscripts reporting clinical trial results should submit a data sharing statement following the ICMJE guidelines from 1 July 2018. Authors may refer to the editorial, “Data Sharing statements for Clinical Trials: A Requirement of the International Committee of Medical Journal Editors,” in JKMS Vol. 32, No. 7:1051-1053 (http://crossmark.crossref.org/dialog/?doi=10.3346/jkms.2017.32.7.1051&domain=pdf&date_stamp=2017-06-05).
Process to manage the research and publication misconduct
When the Journal faces suspected cases of research and publication misconduct such as a redundant (duplicate) publication, plagiarism,
viii

fabricated data, changes in authorship, undisclosed conflicts of interest, an ethical problem discovered with the submitted manuscript, a reviewer who has appropriated an author’s idea or data, complaints against editors, and other issues, the resolving process will follow the flowchart provided by the Committee on Publication Ethics (http://publicationethics.org/resources/flowcharts). The Editorial Board of YUJM will discuss the
suspected cases and reach a decision. YUJM will not hesitate to publish errata, corrigenda, clarifications, retractions, and apologies when needed.
For the policies on research and publication ethics not stated in the Instructions, Guidelines on Good Publication (http://publicationethics.org) or Good Publication Practice Guidelines for Medical Journals (http://kamje.or.kr) can be applied.
ix
Affiliation:
Author’s name (please print):
Manuscript title:
All authors pledges that we follow the basic standards of research and publication ethics in the submission process to Yeungnam University Journal of Medicine
Check Yes ifResearch subject, research object and size, setting of controls, and the methods of data collection are suitable for the research ethics.
□ Yes □No
Check Yes ifAuthors should ensure that their submitted manuscripts are not against publication ethics such as fabrication, falsification or plagiarism.
□ Yes □No
Check Yes ifIn clinical research involving human, informed consent from patient should be conducted and written in the method section of the manuscript.
□ Yes □No
Check Yes ifAll clinical research involving human and animal subjects to be approved by the author’s Institutional Review Board (IRB) or equivalent committees.
□ Yes □No
Check Yes ifThis study is conducted in compliance with the Declaration of Helsinki and this comment is written in the method section of the manuscript.
□ Yes □No
Check Yes ifAll Authors must disclose all relationships that could be viewed as potential conflicts of interest. This relationship also includes any potential conflicts of interest with all material, products, and companies in the manuscript.
□ Yes □No
Check Yes ifAuthors should confirm that the submitted work is not under consideration or accepted for publications elsewhere, and would not be submitted in any other journals after acceptance.
□ Yes □No
Check Yes ifDuplicate publication, which includes ‘imalas publication’, ‘plagiarism’, and ‘salami publication’, is strictly not conducted.
□ Yes □No
If the rationale provided by the authors remains unsatisfactory in the judgment of the editors, the manuscript will be rejected or retracted. The authors will not be allowed to subsequently submit their research to Yeungnam University Journal of Medicine. The authors should keep the above mentioned disadvantages in mind.
Date:
Corresponding author’s name:
Research and publication ethics form
x

The author(s) submit manuscript with the following title
In consideration of editors and publisher’s effort in reviewing and editing our/my Article, the undersigned authors hereby transfer, convey, and assign all copyrights in the Article to the Editorial Board of the Yeungnam University Journal of Medicine (YUJM). The copyright transfer covers the right to print, publish, distribute and sell throughout the world the said contribution and parts thereof, including all revisions or versions and future editions, in all forms and media.
The authors certify that I have participated in the intellectual content, the analysis of data, and the writing of the Article, to take public responsibility for it The authors reviewed the final version of the Article, believe it represents valid work and approve it for publication The authors certify that none of the material in the manuscript has been published previously, is included in another manuscript The authors also certify that the Article has not been accepted for publication elsewhere, nor have they assigned any right or interest in the Article to any third party. The authors will obtain and include with the manuscript written permission from any respective copyright owners for the use of any text, figures, and tables that have been previously published. The authors agree that it is their responsibility to pay fees charged for permissions.
Copyright © Yeungnam University College of Medicine
This is an Open Access journal distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Author’s name
Signature
Copyright transfer agreement
xi

I am informed and aware of photographs, videotapes and other images (imaging records) taken by Dr. or his designee(s) of myself or any parts of my body regarding surgical procedures carried out by Dr. . I understand and consent that such imaging records may and will be used by Dr. as reference in diagnosing and treating other patients in the future. I further consent to the release and transfer of copyright ownership by Dr. to Yeungnam University Journal of Medicine of such imaging records.
I understand that by consenting on release of my imaging records, these may and will be used in upcoming issue or issues of the journal, as well as on the journal website, or any other print or electronic media for the purpose of informing medical professionals or other readers about surgical methods. I understand that when these imaging records are included in any articles, medical information regarding sex, age, operative date and treatment results may and will be included together. But I, nor any member of my family, will be identied by name in any publication, and any information that may aid in identifying me or my family will not be exposed. (In case of facial photographs, the photo is cropped to only necessary parts in order to make individual identication impossible.) I understand that whether I consent on this form or not, it bears no consequences whatsoever on any future actions, and that there will be no eect on the medical treatment I receive from Dr. or any subordinates.
I grant this consent as a voluntary contribution in the interest of public education, and certify that I have read the above Consent, Authorization and Release form and fully understand its terms. I understand that, if I do not revoke this authorization, it will expire ten years from the date written below.
20 . . .
I hereby transfer in above-mentioned terms, the copyright of my imaging records to
Dr. .
Name:
Hospital:
Designated Doctor:
Signature:
Department:
Signature:
Patient photographic and videographic consent,authorization and release form
xii