
Influence of vitrification on mouse metaphase II oocyte spindle dynamics and chromatin alignment
Upload
independentCategory
view
0download
0
ARTICLE IN PRESS
0142-9612/$ - se
doi:10.1016/j.bi
$Editor’s N
instituted series
opinions on to
have some featu
and some fea
comprehensive.
Chief and revie�Correspond
fax: +6567735
E-mail addr
(L.L. Kuleshov
(D.W. Hutmac
Biomaterials 28 (2007) 1585–1596
www.elsevier.com/locate/biomaterials
Leading Opinion
Vitrification as a prospect for cryopreservation oftissue-engineered constructs$
L.L. Kuleshovaa,�, S.S. Gouka, D.W. Hutmacherb
aLow Temperature Preservation Unit, National University Medical Institutes, Yong Loo Lin School of Medicine, National University of Singapore,
#03-01C Block MD11, 10 Medical Drive, Singapore 117597, SingaporebFaculty Division of Bioengineering, Faculty of Engineering, National University of Singapore, Engineering Drive 1, Singapore 119260, Singapore
Received 6 September 2006; accepted 29 November 2006
Available online 18 December 2006
Abstract
Cryopreservation plays a significant function in tissue banking and will presume yet larger value when more and more tissue-
engineered products will routinely enter the clinical arena. The most common concept underlying tissue engineering is to combine a
scaffold (cellular solids) or matrix (hydrogels) with living cells to form a tissue-engineered construct (TEC) to promote the repair and
regeneration of tissues. The scaffold and matrix are expected to support cell colonization, migration, growth and differentiation, and to
guide the development of the required tissue. The promises of tissue engineering, however, depend on the ability to physically distribute
the products to patients in need. For this reason, the ability to cryogenically preserve not only cells, but also TECs, and one day even
whole laboratory-produced organs, may be indispensable. Cryopreservation can be achieved by conventional freezing and vitrification
(ice-free cryopreservation). In this publication we try to define the needs versus the desires of vitrifying TECs, with particular emphasis
on the cryoprotectant properties, suitable materials and morphology. It is concluded that the formation of ice, through both direct and
indirect effects, is probably fundamental to these difficulties, and this is why vitrification seems to be the most promising modality of
cryopreservation.
r 2006 Elsevier Ltd. All rights reserved.
Keywords: Tissue-engineered constructs; Vitrification; Freezing; Cryopreservation
1. Introduction
The more recently coined term ‘‘regenerative medicine’’represents a shift in emphasis from current methods toreplace tissues with medical devices and artificial organs tomore biological approaches which focus on regenerationrather than replacement or repair. Regenerative medicine
e front matter r 2006 Elsevier Ltd. All rights reserved.
omaterials.2006.11.047
ote: Leading Opinions: This paper is one of a newly
of scientific articles that provide evidence-based scientific
pical and important issues in biomaterials science. They
res of an invited editorial but are based on scientific facts,
tures of a review paper, without attempting to be
These papers have been commissioned by the Editor-in-
wed for factual, scientific content by referees.
ing author. Tel.: +6565163359, lab: +65 65163767;
461.
esses: [email protected], [email protected]
a), [email protected] (S.S. Gouk), [email protected]
her).
has many components; however it can be argued that celltherapy and tissue engineering are currently the flagshipareas [1]. This technology has the potential to developtherapies for previously untreatable diseases and condi-tions. Examples of disease or trauma that regenerativemedicine might alleviate one day include diabetes, heartdisease, renal failure, osteoporosis and spinal cord injuries.The current generation of baby boomers would almostcertainly rally behind the rationale to advance intoregenerative medicine as it offers them the greatest hopefor the most effective medical treatment and quality of lifein their senior years. Beyond the obvious health benefits ofregenerative medicine from a patient point of view, thistechnology is desperately needed to challenge risinghealthcare costs around the globe.Unfortunately, to the disappointment of everyone
involved, today we must recognize the fact that cell-basedtherapies and tissue engineering have not lived up to the

ARTICLE IN PRESSL.L. Kuleshova et al. / Biomaterials 28 (2007) 1585–15961586
promises communicated 10 years ago. Although there havebeen some successes, it is widely recognized that tissueengineering is not yet delivering significant progress interms of clinical outcomes and commercialization. Part ofthe problem has been that we have failed to fullyunderstand what regenerative medicine really means andto appreciate that regeneration here is synonymous withcreation [2]. More importantly, cell transplantation orscaffold-based tissue-engineering processes, for example,involve many different phases and substantially differentscientific inputs, as such, there has been insufficientintegration of these phases within any holistic regenerativemedicine technology platform.
In the future, commercially successful companies willhave a broad product spectrum comprising diverse productsegments such as ‘‘off-the-shelf’’ and patient specificproducts as well as innovative cell-based services. Thispromise, however, depends on the ability to physicallydistribute the products to patients in need and to producethese products ‘‘off-the-shelf’’. For this reason, the abilityto cryogenically preserve not only cells, but also tissue-engineered constructs (TECs), and eventually wholelaboratory-produced organs, is an important part of aholistic technology platform.
Until recently, the cryopreservation of TECs seemed as aremote prospect to most observers, but developments overthe past few years are rapidly changing the scientific basisfor preserving even the most difficult and delicate organsfor unlimited periods of time. The majority of organs havebeen shown not to accommodate freezing protocols due totheir high vascularization. Only animal intestines andovaries have been frozen, thawed, and shown to functionafter transplantation. The preservation of TECs and vitalorgans will most likely require vitrification.
Based on the above-mentioned background it is clearthat vitrification might play a central role in the develop-ment of modern tissue-engineering technology platforms,and is thus the focus of this article. In addition toconsiderations of performance based on a holistic vitrifica-tion strategy, practical considerations of manufacture arise.For realistic and practical clinical applications, manufac-ture must be achievable in a reproducible, controlled, costand time-effective fashion [3]. The manufacturing processmust accommodate the presence of a large number of cells(1 million cells per millilitre) in the construct, and it may benecessary to allow vitrification of large neo-tissue volumes(bigger than 5 cm3).
In this article, we make an attempt to provide a broadpicture of cryopreservation by vitrification. Following anintroduction to the concept of cryopreservation, theoreticalexplanations are given to support the use of vitrificationrather than ‘‘freezing’’. Supporting these concepts, numer-ous studies are reviewed to demonstrate superiority ofvitrification versus freezing. We believe that vitrification, asan approach to cryopreservation of TECs, will becomeeven more important with progress in regenerativemedicine.
2. Freezing
The conservative methods used for cryopreservation ofcells/tissues are based on the slow cooling approach. Itshould be admitted that certain non-sensitive cells may bepreserved in liquid nitrogen with little damage by the slowcooling method. For this, they are usually cooled in thepresence of a cryoprotectant, at a selected cooling rate, andin a programmable freezing device where they becomesurrounded by ice crystals. The slow cooling rate allows thecells to dehydrate by maintaining equilibrium with thepartially frozen extra-cellular solution [4]. The success ofthis method requires freezing with low cooling rates toallow the efflux of water from cells during extra-cellular iceformation. The slow cooling technique is very well under-stood as it was established many years ago, and it iscompatible with straightforward warming. However, thismethod is not economical as it requires a controlled ratefreezer. More importantly, it is extremely difficult topreserve the intactness of biomaterials and the integrityof neo-tissues during the liquid-ice phase transition.Uncontrolled freezing, e.g. cooling in two subsequent stepsin common freezers (at �20 1C and �80/86 1C) could beeven more detrimental for fragile 3-D constructs seededwith sensitive cells, such as the majority of mammalian cellsused in tissue engineering. It is not advisable to use thislatter method, which is a simplified adaptation of acontrolled-rate freezing device, for cryopreservation pur-poses. Perspectives on the freezing approach are not asubject of consideration in this paper.
3. Cryoprotectants
Cryoprotectants were formulated with the purpose toreplace water in cells/tissues. This minimizes damagecaused by ice formation and encourages formation of anamorphous state in cells, rather than ice crystals, during thecooling–cryostorage–warming cycle. Cryoprotectants canbe divided by their role in cryopreservation into two maingroups, namely penetrating and non-penetrating agents.Classification of cryoprotectants is presented in Table 1.Although the cryoprotective properties of the first pene-
trating agent (glycerol) were discovered almost 60 years ago[5], the role of component selection in the formulation ofeffective cryoprotectants became crucial only with thedevelopment of vitrification technology since this methodrequires the employment of a high concentration of chemicals.A variety of agents have been tested and new formulationshave been developed for the application of vitrification.
4. Vitrification
4.1. General principles and fundamental approaches of
vitrification
Vitrification is defined as glass-like solidification and/orcomplete avoidance of ice crystal formation during cooling

ARTICLE IN PRESS
Table 1
Classification of cryoprotectant agents by their molecular weights and other properties
A. Penetrating cryoprotectants (PCs) B. Non-penetrating cryoprotectants (NPCs)
Low-molecular weight agents: MWo100Da Sugars: 180oMWo 594Da High-molecular weight agents: MW41000Da
Polyalcohols (PVAs): Ficoll
Dextran
Ethylene glycol (EG) Monosaccharides: Polyvinyl pyrrolidone (PVP)
Dimethyl sulphoxide (DMSO) Fructose, glucose, Polyethylene glycol (PEG)
Propylene glycol Lactose, maltose Polyvinyl alcohol (PVA)
Glycerol PVA-derived ice blocking agents
Hydroxyethyl starch (HES)
Butandiols: 1,2-/2,3-butandiol Disaccharides: sucrose, trehalose
Formamide, acetamide Polysaccharides: raffinose
L.L. Kuleshova et al. / Biomaterials 28 (2007) 1585–1596 1587
and warming. It is understandable that cryopreservation ofTECs is more efficient when the cryopreservation solutionsenclosed in constructs and cells are ice-free during theentire procedure. Vitrification is typically achieved bypartial replacement of water via penetrating agents whichare easy glass formers and by accompanying dehydrationof the biological materials via non-penetrating cryoprotec-tants. In practice, such a brief procedure is usuallyperformed at room temperature. Afterwards, TECs areintroduced to the temperature of cryostorage, typically byimmersion into liquid nitrogen. The TECs are usuallywarmed rapidly and cryoprotectants removed graduallywithin a short period of time. It is apparent that the role ofnon-penetrating cryoprotectants is especially significant invitrification protocols, since samples require fast dehydra-tion before immersion into liquid nitrogen.
In order to create conditions for vitrification, certainknowledge concerning the physical properties of thecryoprotective solutions employed is required. To achievecryopreservation free from ice damage it is necessary tocool rapidly through the temperature region of potentialcrystallization and to reach the amorphous glassy statebefore ice crystals have the opportunity to form. Similarlyduring the warming phase, the process needs to be rapidenough to avoid ice crystal formation. To achieve theseconditions, it is necessary to determine the lowest totalsolute concentration for each of the vitrification solutioncandidates at given cooling and warming rates. Soluteconcentration is crucial in the stability of the supercooledstate, since it is known that dilute aqueous solutions areextremely difficult to vitrify. On the other hand, it isadequate to evaluate the ‘‘critical’’ warming and coolingrates at which a chosen solution remains in a stableamorphous state.
4.1.1. Choice of cryoprotectants
Systematic studies of non-equilibrium ice or hydratecrystallization on cooling and warming have been done ona variety of aqueous solutions, with the aim to find moreefficient solutes and to determine conditions for vitrifica-tion [6–12]. We have established how the molecular weightand type of sugars/polymers influence the vitrification
properties of polyalcohols and designed a number of sugar/polymer-based vitrification solutions with the lowestpossible solute concentration [13,14].To inhibit ice nucleation and growth by non-colligative
mechanisms in vitrification solutions, an additional class ofcompounds such as natural antifreeze proteins (discovered incold-hardy fish and insects) has been employed. However, theusage of antifreeze proteins is not cost effective. It appearsthat synthetic ice blockers (polyvinyl alcohol (PVA)-derivedice-blocking agents) are able to bind and inactivate hetero-geneous nucleators and emerging ice crystals in a mannersimilar to that of natural antifreeze proteins. Unlikeconventional cryoprotectants that inhibit freezing by inter-acting with water, ice blockers are believed to act by directmolecular recognition of ice nucleators [15] or perhaps iceitself [16–18]. This selective attraction to surfaces of icegrowth permits ice blockers to exert significant effects evenwith very low concentrations [15,19]. Small quantities of iceblocker can reduce the requirements for conventionalcryoprotectants while maintaining vitrification tendency,and therefore it is effective in reducing toxicity [20].It has been demonstrated that PVA copolymer strongly
suppresses the devitrification of aqueous cryoprotectantsolutions of ethylene glycol (EG) [19]. PVA blocks iceprimarily by inhibition of heterogeneous rather thanhomogeneous nucleation on cooling as suggested by visualobservation and differential scanning calorimeter data [19].New prospects for improvement of vitreous cryopreserva-tion by natural antifreeze proteins and, in particular, by theimplementation of PVA-derived ice-blocking agents, areemerging [21].
4.1.2. Importance of component selection
Another issue to consider in developing cryopreservationprocedures is the avoidance of the potential toxicity ofcryopreservation solutions. An important goal is to applyvitrification solutions that are not only stable, but are alsonon-toxic to cells seeded on scaffolds and neo-tissues, evenafter prolonged exposure. Comparative toxicity of pene-trating cryoprotectants is a subject of thorough investiga-tion [22], since all low-molecular weight agents arepotentially toxic to cells. In cryobiology, a way to assess

ARTICLE IN PRESSL.L. Kuleshova et al. / Biomaterials 28 (2007) 1585–15961588
the effects of a cryoprotectant on cell viability is wellestablished. This assessment is usually performed byvariable evaluation of the following parameters: type ofcryoprotectant, cryoprotectant concentration, and time ofexposure to the cryoprotectant. One comprehensive study[22] demonstrated that, at a high concentration (30%), EGwas dramatically less toxic than its counterparts; the cellviability was three fold higher than the second bestcryoprotectant studied, which was DMSO. Additionally,they also reported that, at constant concentration (20%),the adverse effects of exposure became more pronounced inbutanediols than in polyalcohols as the time of exposurewas doubled; however, within the polyalcohol group itself,glycerol was more toxic than EG. In addition, the impacton cell viability of ten vitrification solutions consisting of30 or 40% penetrating cryoprotectants, Ficoll and sucrosewas compared following short- and long-term exposures atdifferent temperatures. It was found that the highestsurvival rates were obtained from EG-based vitrificationsolutions (490%) [23].
Generally, careful component selection is a vital strategyto avoid toxic effects of vitrification solutions. Incorpora-tion of sugars (mono-, di-, and polysaccharides) andpolymers in the vitrification solutions appears to be themost prominent direction of such strategy. Our laboratory[13,14,24] and other groups [25,26] have engaged in thestudy of the impact of non-penetrating cryoprotectants byexposing sensitive cells to a range of sugars/polymersduring long-term culture, as well as briefly exposing cells tohigh concentrations of these additives. Assessment wasperformed systematically to screen a wide range ofpolymers for the application of cryopreservation, and themost suitable polymer was selected for biological applica-tions [27]. To reduce the toxicity of vitrification solutions,the amount of penetrating cryoprotectant was system-atically replaced by mono-, di-, or polysaccharides [13]. Inthe vitrification of human oocytes toxic effect of vitrifica-tion solution was eliminated by replacing a partial amountof polyalcohol with disaccharide [24,28].
Retrospectively, since the early 1990s, the benefits ofreplacing penetrating cryoprotectants with non-penetratingadditives (polymers and/or sugars) for vitrification ofbiological materials [23,29,30] were identified. Currently,effective vitrification solutions commonly consist of aminimum of 2 (penetrating cryoprotectant+sugar/poly-mer) [31] or 3 components (penetrating cryoprotectant+sugar+polymer) [23,32]. With regards to vitrification,non-penetrating cryoprotectants could completely replacepenetrating cryoprotectants in certain effective cryopreser-vation protocols, e.g., in the comparative study of thecryopreservation of red blood cells in 30% dextran versus35.5% glycerol [33] and hydroxyethyl starch (HES) [34].
4.2. Advantages of vitrification
In contrast to the conventional slow cooling (freezing)procedure, vitrification commonly employs direct immer-
sion of cells in sealed containers into liquid nitrogen[27,29,30]. This provides high cooling rates and therefore itis believed that the success of vitrification does not rely onserum and proteins for supporting cells. Regarding liquidnitrogen immersion, a user friendly procedure for cryopre-servation was designed by Kuleshova and Shaw [35]. Thismethod was effectively applied for cryopreservation ofTECs [36,37], animal and human embryos [35,38], andneural stem or precursor cells (NSCs) [39]. This incombination with protein/serum-free of cryopreservationsolutions provides a simple and effective strategy forreducing or eliminating risk of contamination duringcooling, storage and warming.In addition to the above-mentioned concern, addition of
serum and proteins, mainly from animal sources, may exertadditional adverse effects if they are used for therapeutictransplantation. Recent scientific publications have demon-strated that all existing embryonic stem cell (ESC) lines arecontaminated with a mouse protein containing sialic acidand mutated [40]. Sialic acids are a family of acidic sugarsdisplayed on the surfaces of all cell types, and on manysecreted proteins. The two most common mammalian sialicacids are N-glycolylneuraminic acid (Neu5Gc) and N-acetylneuraminic acid (Neu5Ac), with Neu5Ac being themetabolic precursor of Neu5Gc. Humans are geneticallyunable to produce Neu5Gc from Neu5Ac [41], howeverhuman ESCs can incorporate non-human sialic acidNeu5Gc from the mouse feeder layer and/or the medium,leading to an immune response upon transplantation,which would result in cell death in vivo [40]. Hence, thesestem cell (SC) lines are neither safe nor suitable for therapy.Suppression of ice crystallization in vitrification elim-
inates the risk of fractures in assembled tissue equivalentsand TECs. In addition, chilling injury, which occurs duringslow cooling, that is detrimental to sensitive cells such asstem cells, is also prevented using this approach. Cells/tissues are usually introduced to a vitrification solution in astepwise manner during 10–15min prior to introducingthem to the temperature of cryostorage. Vitrificationmakes it possible to maintain cells and tissues at a heatedstage or at room temperature during equilibration/dilutionsteps; at physiological temperature, extensive cellularinterference with the cryoprotectant is avoided. In conclu-sion, vitrification procedure is effective, less time consum-ing and economical since no expensive controlled-ratefreezer is required; this approach can be easily incorporatedin virtually any laboratory. This is an important advantageto propel the progress in the quest for an effectivepreservation method for TECs.The application of vitrification in cryopreservation of
cells/tissues/TECs, no doubt, has its problem and limita-tions too. One major problem lies in the toxicity of highconcentrations of penetrating cryoprotectants required inthe vitrification protocol and the osmotic damage duringaddition and removal of cryoprotectants. The toxicity of ahigh concentration of penetrating cryoprotectants waspreviously minimized by conducting the experiments at
ARTICLE IN PRESSL.L. Kuleshova et al. / Biomaterials 28 (2007) 1585–1596 1589
lower temperatures, such as at 4 1C. Nevertheless, up to 1 hstepwise exposure to vitrification solution was required toachieve high viability of cells upon warming [42,43];however such long exposure is not ideal.
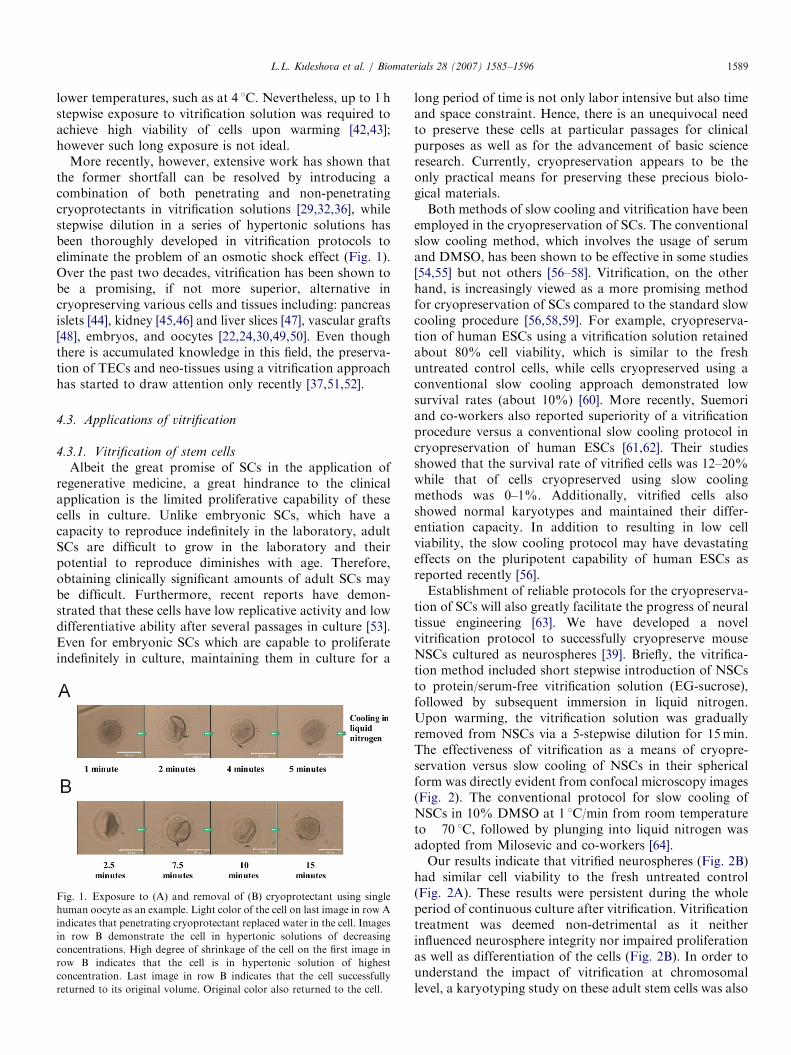
More recently, however, extensive work has shown thatthe former shortfall can be resolved by introducing acombination of both penetrating and non-penetratingcryoprotectants in vitrification solutions [29,32,36], whilestepwise dilution in a series of hypertonic solutions hasbeen thoroughly developed in vitrification protocols toeliminate the problem of an osmotic shock effect (Fig. 1).Over the past two decades, vitrification has been shown tobe a promising, if not more superior, alternative incryopreserving various cells and tissues including: pancreasislets [44], kidney [45,46] and liver slices [47], vascular grafts[48], embryos, and oocytes [22,24,30,49,50]. Even thoughthere is accumulated knowledge in this field, the preserva-tion of TECs and neo-tissues using a vitrification approachhas started to draw attention only recently [37,51,52].
4.3. Applications of vitrification
4.3.1. Vitrification of stem cells
Albeit the great promise of SCs in the application ofregenerative medicine, a great hindrance to the clinicalapplication is the limited proliferative capability of thesecells in culture. Unlike embryonic SCs, which have acapacity to reproduce indefinitely in the laboratory, adultSCs are difficult to grow in the laboratory and theirpotential to reproduce diminishes with age. Therefore,obtaining clinically significant amounts of adult SCs maybe difficult. Furthermore, recent reports have demon-strated that these cells have low replicative activity and lowdifferentiative ability after several passages in culture [53].Even for embryonic SCs which are capable to proliferateindefinitely in culture, maintaining them in culture for a
Fig. 1. Exposure to (A) and removal of (B) cryoprotectant using single
human oocyte as an example. Light color of the cell on last image in row A
indicates that penetrating cryoprotectant replaced water in the cell. Images
in row B demonstrate the cell in hypertonic solutions of decreasing
concentrations. High degree of shrinkage of the cell on the first image in
row B indicates that the cell is in hypertonic solution of highest
concentration. Last image in row B indicates that the cell successfully
returned to its original volume. Original color also returned to the cell.
long period of time is not only labor intensive but also timeand space constraint. Hence, there is an unequivocal needto preserve these cells at particular passages for clinicalpurposes as well as for the advancement of basic scienceresearch. Currently, cryopreservation appears to be theonly practical means for preserving these precious biolo-gical materials.Both methods of slow cooling and vitrification have been
employed in the cryopreservation of SCs. The conventionalslow cooling method, which involves the usage of serumand DMSO, has been shown to be effective in some studies[54,55] but not others [56–58]. Vitrification, on the otherhand, is increasingly viewed as a more promising methodfor cryopreservation of SCs compared to the standard slowcooling procedure [56,58,59]. For example, cryopreserva-tion of human ESCs using a vitrification solution retainedabout 80% cell viability, which is similar to the freshuntreated control cells, while cells cryopreserved using aconventional slow cooling approach demonstrated lowsurvival rates (about 10%) [60]. More recently, Suemoriand co-workers also reported superiority of a vitrificationprocedure versus a conventional slow cooling protocol incryopreservation of human ESCs [61,62]. Their studiesshowed that the survival rate of vitrified cells was 12–20%while that of cells cryopreserved using slow coolingmethods was 0–1%. Additionally, vitrified cells alsoshowed normal karyotypes and maintained their differ-entiation capacity. In addition to resulting in low cellviability, the slow cooling protocol may have devastatingeffects on the pluripotent capability of human ESCs asreported recently [56].Establishment of reliable protocols for the cryopreserva-
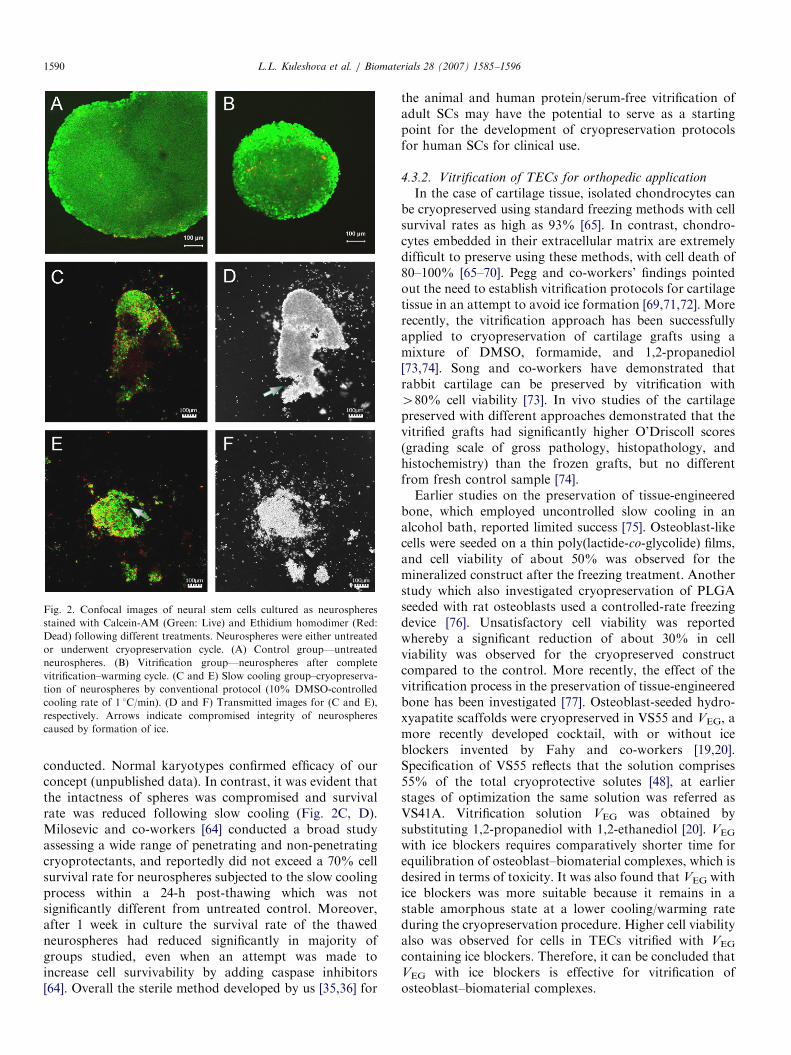
tion of SCs will also greatly facilitate the progress of neuraltissue engineering [63]. We have developed a novelvitrification protocol to successfully cryopreserve mouseNSCs cultured as neurospheres [39]. Briefly, the vitrifica-tion method included short stepwise introduction of NSCsto protein/serum-free vitrification solution (EG-sucrose),followed by subsequent immersion in liquid nitrogen.Upon warming, the vitrification solution was graduallyremoved from NSCs via a 5-stepwise dilution for 15min.The effectiveness of vitrification as a means of cryopre-servation versus slow cooling of NSCs in their sphericalform was directly evident from confocal microscopy images(Fig. 2). The conventional protocol for slow cooling ofNSCs in 10% DMSO at 1 1C/min from room temperatureto �70 1C, followed by plunging into liquid nitrogen wasadopted from Milosevic and co-workers [64].Our results indicate that vitrified neurospheres (Fig. 2B)
had similar cell viability to the fresh untreated control(Fig. 2A). These results were persistent during the wholeperiod of continuous culture after vitrification. Vitrificationtreatment was deemed non-detrimental as it neitherinfluenced neurosphere integrity nor impaired proliferationas well as differentiation of the cells (Fig. 2B). In order tounderstand the impact of vitrification at chromosomallevel, a karyotyping study on these adult stem cells was also
ARTICLE IN PRESS
Fig. 2. Confocal images of neural stem cells cultured as neurospheres
stained with Calcein-AM (Green: Live) and Ethidium homodimer (Red:
Dead) following different treatments. Neurospheres were either untreated
or underwent cryopreservation cycle. (A) Control group—untreated
neurospheres. (B) Vitrification group—neurospheres after complete
vitrification–warming cycle. (C and E) Slow cooling group–cryopreserva-
tion of neurospheres by conventional protocol (10% DMSO-controlled
cooling rate of 1 1C/min). (D and F) Transmitted images for (C and E),
respectively. Arrows indicate compromised integrity of neurospheres
caused by formation of ice.
L.L. Kuleshova et al. / Biomaterials 28 (2007) 1585–15961590
conducted. Normal karyotypes confirmed efficacy of ourconcept (unpublished data). In contrast, it was evident thatthe intactness of spheres was compromised and survivalrate was reduced following slow cooling (Fig. 2C, D).Milosevic and co-workers [64] conducted a broad studyassessing a wide range of penetrating and non-penetratingcryoprotectants, and reportedly did not exceed a 70% cellsurvival rate for neurospheres subjected to the slow coolingprocess within a 24-h post-thawing which was notsignificantly different from untreated control. Moreover,after 1 week in culture the survival rate of the thawedneurospheres had reduced significantly in majority ofgroups studied, even when an attempt was made toincrease cell survivability by adding caspase inhibitors[64]. Overall the sterile method developed by us [35,36] for
the animal and human protein/serum-free vitrification ofadult SCs may have the potential to serve as a startingpoint for the development of cryopreservation protocolsfor human SCs for clinical use.
4.3.2. Vitrification of TECs for orthopedic application
In the case of cartilage tissue, isolated chondrocytes canbe cryopreserved using standard freezing methods with cellsurvival rates as high as 93% [65]. In contrast, chondro-cytes embedded in their extracellular matrix are extremelydifficult to preserve using these methods, with cell death of80–100% [65–70]. Pegg and co-workers’ findings pointedout the need to establish vitrification protocols for cartilagetissue in an attempt to avoid ice formation [69,71,72]. Morerecently, the vitrification approach has been successfullyapplied to cryopreservation of cartilage grafts using amixture of DMSO, formamide, and 1,2-propanediol[73,74]. Song and co-workers have demonstrated thatrabbit cartilage can be preserved by vitrification with480% cell viability [73]. In vivo studies of the cartilagepreserved with different approaches demonstrated that thevitrified grafts had significantly higher O’Driscoll scores(grading scale of gross pathology, histopathology, andhistochemistry) than the frozen grafts, but no differentfrom fresh control sample [74].Earlier studies on the preservation of tissue-engineered
bone, which employed uncontrolled slow cooling in analcohol bath, reported limited success [75]. Osteoblast-likecells were seeded on a thin poly(lactide-co-glycolide) films,and cell viability of about 50% was observed for themineralized construct after the freezing treatment. Anotherstudy which also investigated cryopreservation of PLGAseeded with rat osteoblasts used a controlled-rate freezingdevice [76]. Unsatisfactory cell viability was reportedwhereby a significant reduction of about 30% in cellviability was observed for the cryopreserved constructcompared to the control. More recently, the effect of thevitrification process in the preservation of tissue-engineeredbone has been investigated [77]. Osteoblast-seeded hydro-xyapatite scaffolds were cryopreserved in VS55 and VEG, amore recently developed cocktail, with or without iceblockers invented by Fahy and co-workers [19,20].Specification of VS55 reflects that the solution comprises55% of the total cryoprotective solutes [48], at earlierstages of optimization the same solution was referred asVS41A. Vitrification solution VEG was obtained bysubstituting 1,2-propanediol with 1,2-ethanediol [20]. VEG
with ice blockers requires comparatively shorter time forequilibration of osteoblast–biomaterial complexes, which isdesired in terms of toxicity. It was also found that VEG withice blockers was more suitable because it remains in astable amorphous state at a lower cooling/warming rateduring the cryopreservation procedure. Higher cell viabilityalso was observed for cells in TECs vitrified with VEG
containing ice blockers. Therefore, it can be concluded thatVEG with ice blockers is effective for vitrification ofosteoblast–biomaterial complexes.

ARTICLE IN PRESS
Fig. 4. SEM images of osteogenically induced pig bone marrow cells
cultured on nanofiber scaffolds. (A and C) Control group, (B and D)
vitrification group. Intactness of cells and absence of scaffold rupture are
observed in vitrification group when compared to controls. Extensive cell
bridging and proliferation are clearly evident in vitrified constructs (B and
D) indicating the efficiency of the vitrification protocol used. The
uniformity of the nanostructure in the scaffold (A) provides good support
to robust cell growth (B–D). Scale bars represent 10 mm (A and B), 500mm(C), and 50 mm (D), respectively.
L.L. Kuleshova et al. / Biomaterials 28 (2007) 1585–1596 1591
Hutmacher’s group has engaged in engineering of boneand cartilage grafts over the last 7 years [78]. The firstgeneration of these products has received FDA approval inthe area of oral and maxillofacial surgery [79]. However, asmost of current TEC applications these strategies are basedon using autologous cells. As stated above it is a conditionsine qua non to develop an ‘‘off-the-shelf ‘‘strategy to assurea wide clinical application. Hence, the authors of thisarticle started a collaboration which aims at the vitrifica-tion of adult stem cells and/or TECs for bone and cartilagegrafts using adiposed-derived and bone marrow cells.Adipose-derived SCs have been recently shown to becapable of differentiating into bone, cartilage, and fat [80].In our preliminary study, we have obtained encouragingresults on the vitrification of adipose-derived SCs encapsu-lated in alginate/fibrin glue beads (Fig. 3) as well asosteogenically induced pig bone marrow cells cultured onnanofiber scaffolds (Fig. 4). The vitrification protocolwhich we used in the study of NSC preservation (Fig. 2)was employed here too. Confocal images showed that thevitrified TEC (Fig. 3B, C; row I) maintained 95% cellviability, identical to that of the control group (Fig. 3A;row I). Additionally, the transmission images indicate thatthe preservation of integrity in the vitrified beads (Fig. 3B,C; row II) is comparable to that of the control specimen.The success of this procedure will provide a strongfoundation to extend the application for the preservationof larger TECs. Currently, we are investigating if tissue-engineered tubular bone constructs (Fig. 5) can becryopreserved by vitrification. If we will be successful incryopreserving TECs of larger volume it will have highimpact on the clinical application as it will be possible todevelop products ‘‘off-the-shelf’’.
Fig. 3. Confocal images of adipose derived stem cells cultured in alginate/
fibrin glue beads: (A) control group and (B and C) vitrification group.
(Row I) Fluorescence images of cells stained with Calcein-AM (Green: live
cells) and Ethidium Homodimer (Red: dead cells) show that the cell
viability was maintained in the vitrification group. (Row II) Transmitted
images of cells on alginate beads. The transmitted images of the alginate
beads indicate that the integrity of the beads has not been compromised.
4.3.3. Vitrification of encapsulated rat and pig hepatocytes
Kuleshova’s group were the first who studied differentvitrification solutions and techniques involving a range ofcooling and warming rates of matrix–cell complexes usingmicroencapsulated hepatocytes as a model [36,81]. Vitrifiedrat hepatocytes entrapped at different cell densities wereassessed in continuous culture to confirm efficacy of theproposed approach (Fig. 6). Two types of engineeredcollagen matrices were studied: methylated collagen, whichhas a superior mechanical property [82], and galactosylatedcollagen [83], which has enhanced chemical propertiesallowing specific interaction with the asialoglycoproteinreceptor on hepatocytes. The nature of collagens causeddifferences in the size of capsules. The optimal methodincluded rapid stepwise introduction of microencapsulatedhepatocytes to an EG-sucrose vitrification solution. Therewere no broken capsules or free cells observed aftervitrification in all experiments (Fig. 6). Thus, it was foundthat microcapsules with a different nature of biomaterialscan be completely preserved without evident damage totheir integrity. It was also observed that hepatocyte naturalmigration and aggregation in capsules formed by galacto-sylated collagen were not affected by vitrification. Micro-encapsulated cells exhibited similar trends to untreatedcontrols in the rate of cell death and the decline of theirfunctions during continuous culture. Maximum relativechanges of cell functions in microcapsule configurationentrapped at different cell densities after vitrificationcompared to those of non-treated hepatocytes ranged from7% to 16%, which is non-significantly different for allmicroencapsulated systems studied (Fig. 7A, B).

ARTICLE IN PRESS
Fig. 6. Optical microscopy images of microencapsulated rat hepatocytes
entrapped at high (Row I) and low (Row II) densities. Control group (A).
Vitrification group (B). Scale bar represents 100mm.
Fig. 7. Confocal images of encapsulated hepatocytes for rat (A and B)
and pig (C and D). Microcapsules were stained with resorufin for P450
activity, which assessed the functional ability of hepatocytes. (A and C)
Control group. (B and D) Vitrification group.
Fig. 5. Process of engineering tubular bone in vitro. Dynamic culturing of
constructs in spinner flask at 15 rounds per minute. (A) Assembly of a
hMSC cell sheet–nanofiber mesh construct through wrapping of cell sheet
around the nanofiber mesh and a segment of syringe as supporter. (B)
Confocal laser microscopy showed that cells are viable in cell sheet. Scale
bar represents 100mm. (C) MicroCT analysis showed a highly mineralized
tubular structure with an outer diameter of 13.86mm, and this result was
confirmed by SEM; scale bar represents 50mm (D).
L.L. Kuleshova et al. / Biomaterials 28 (2007) 1585–15961592
Previous study aimed at examining the efficacy ofvarious freezing protocols has confirmed low efficiency ofthe freezing approach for cryopreservation of microencap-sulated cells. In this study, freezing of microcapsules byconventional methods (10% DMSO) resulted in 89% lossof microcapsule integrity even for capsules with superiormechanical properties [84]. During microcapsule forma-tion, a weaker shell is formed when galactosylated collagenbinds to the polymer providing less mechanical support
and a higher risk for damage by ice during conventional‘‘freezing’’.Pigs are from a physiological point of view similar to
humans and are proposed as an alternative to humansource of hepatocytes for tissue engineering applications[85]. Although porcine hepatocytes are smaller and moresensitive compared to rat-derived hepatocytes, vitrificationcould also be effectively applied for cryopreservation ofporcine hepatocytes (Fig. 7C, D). The developed vitrifica-tion approach can be applied to other TECs withcomparable sizes, various cell numbers and properties ofthe biomaterials involved.
4.3.4. Vitrification of encapsulated tissue-engineered
pancreatic substitutes
Diabetes has been a leading cause of death in manycountries. Implantation of functional islet cells is poten-tially a curative treatment for diabetes; however long-termimmune rejection of the tissues [86] remains the mainproblem to this treatment. Implantation of encapsulated,immunoprotected, insulin-secreting constructs appears as apromising alternative to conventional insulin injections[87]. Nevertheless, long-term storage for ‘‘off-the-shelf’’availability still remains an issue, which can be addressedby cryopreservation. Cryopreservation of a model TEPS bytwo vitrification solutions designated VS55 and PEG400(mixture of propanediol, DMSO and PEG400) in compar-ison to a conventional freezing protocol was investigated[52]. The model substitute consisted of insulin-secretingmouse insulinoma beta TC3 cells entrapped in calciumalginate/poly-L-lysine/alginate beads. Cell viability andstatic insulin secretion from the thawed cryopreservedgroups were compared against fresh controls. Cell viability

ARTICLE IN PRESSL.L. Kuleshova et al. / Biomaterials 28 (2007) 1585–1596 1593
tests showed that, compared to the fresh groups, the VS55had the highest viability followed by both the PEG400 andthe frozen groups. In addition, the static insulin secretiondata showed that the VS55 and PEG400 groups had similarinduction levels against the fresh group, whereas the frozengroup had the poorest secretion rate. Cryosubstitution ofcapsules showed ice formation in the frozen group but noice in the vitrified groups. Microscopic observationsrevealed holes and/or tears within beads subjected tofreezing, whereas no such abnormalities were detected inthe vitrified samples. Overall, vitrification was found to bea promising preservation procedure for this encapsulatedcell system.
4.3.5. Vitrification of tissue-engineered blood vessels
Generally, the conventional methods used for nativeblood vessel cryopreservation has produced unsatisfactoryresults [88]. The major challenge in cryopreservation ofnative tissues is to minimize or diminish cryoinjury, whichis predominantly associated with ice formation uponfreezing and thawing. Hence, fractures in blood vesselsduring cryopreservation have been a great concern andwere observed even in vitrification solution alone [89,90]. Itwas concluded that fractures were associated with thecooling rate and thermal uniformity across the specimens[90]. Pegg and co-workers [91] successfully preventedfracturing in vascular tissues during cryopreservation byrelatively slow warming (at less than 50 1C/min) to�100 1C, at which temperature the vitreous material hassoftened. Subsequent thawing should be carried out rapidlyto avoid devitrification. With the advancement of vitrifica-tion formulations, vitreous cryopreservation has beenshown to be effectively applied to the preservation of veins[48,92]. Improved tissue functions in vascular tissuescryopreserved using a vitrification approach were observedcompared to a standard freezing method [48]. Themaximum contractions achieved in vitrified vessels were480% of fresh matched controls with similar drugsensitivities, whereas frozen vessels exhibited maximalcontractions below 30% of controls and significantdecrease in drug sensitivity [48]. In vivo studies of vitrifiedvessel segments in an autologous transplant model showedno adverse effect of vitrification compared to fresh tissuegrafts [92].
Recently, the vitreous cryopreservation of TEBVs wasimproved by optimization and modification of the meth-odology and solutions applied in the vitrification of nativeblood vessels. Collagen-based constructs were used in thefirst attempt to study feasibility of vitrification for TEBVs[93]. Rat aortic smooth muscle cells were mixed with type Ibovine collagen and injected into a test tube mold. After a3-week culture period, the constructs were subjected tovitrification-warming. The solution traditionally employedfor vitrification of vascular grafts consists of DMSO,formamide, and propylene glycol, with total soluteconcentration 55% as mentioned previously [94]. Cryosub-stitution studies [93] of frozen and vitrified constructs
showed extensive ice formation in frozen specimens butnegligible ice formation in the vitrified samples. However, areduction in viability was observed in both frozen andvitrified constructs (38% and 39%) compared to 63%viability of the fresh untreated control.In the subsequent study, TEBVs made of polymeric
scaffold was used [51]. Cellular TEBVs were engineered byseeding porcine smooth muscle cells in a polyglycolic acid(PGA) mesh which was sewn into a cylindrical constructand incubated for 7 weeks [51]. Similarly, cryosubstitutionmethod showed that ice formation was negligible (0% ofvessel area) in the vitrified specimens while extensive iceformation (68%) was evident in the extracellular matrix offrozen specimens. The metabolic assay and TUNELstaining results indicated that vitrified tissue had similarviability to fresh controls. The contractility of vitrifiedsamples was as high as 83%, against 11% of the frozensamples, when compared to fresh controls. These encoura-ging results on cellular physiological functions clearly favorthe vitrification approach to the cryopreservation of theseTEBVs.Another important issue to address in vitrification of
TEBVs is the preservation of biomechanical propertiessince it is these properties that influence blood flow throughorgans; sufficient mechanical strength would allow thevessels to withstand suturing and to resist dilatation in vivo[95]. It was demonstrated by uniaxial tensile testing thatboth the strength and stiffness of the specimen increasedafter the freezing as well as after the vitrification process[93]. They subsequently revealed, through passive mechan-ical testing, a significantly increased burst pressure in boththe vitrified and frozen specimens compared to the freshcontrol [51]. The enhanced mechanical properties might beattributed to an increased cross-linking of collagen fibrilsas a result of dehydration phenomenon. Dehydration hasbeen shown to increase crosslinking between collagenfibrils [96] and cause tissues to stiffen [97]. Water move-ment and bulk water redistribution have also beenimplicated in the changes of mechanical properties infreezing of arteries [98]. It is noteworthy that enhancedtensile strength in vitrified vessels might correspond to anincrease in stiffness of vessels which could be an unfavor-able outcome for particular types of vascular graft surgery.A recent comprehensive study on human native blood
vessels supports the superiority of vitrification to freezingin preserving biomechanical properties of blood vessels[99]. The study showed no significant difference inviscoelastic properties between vitrified specimens andfresh untreated controls, whereas cryopreservation usingconventional freezing method significantly increased theoverall tensile strength and elasticity of the vessels [99].Extracellular ice formation, which might disrupt the ECMin the vessel wall, could be the cause leading to the poorfunction of cryopreserved vessels [48,100].Though it has been shown in human native blood vessels
that vitrification is more superior to conventional freezingmethod in preserving biomechanical properties, similar

ARTICLE IN PRESSL.L. Kuleshova et al. / Biomaterials 28 (2007) 1585–15961594
results have yet to be demonstrated in TEBVs. Furtherinvestigation on this aspect is warranted.
5. Conclusion
Cryopreservation plays an important role in tissuebanking and will assume even greater importance whentissue engineering becomes an everyday reality. Theproblems in TEC cryopreservation are not typically dueto difficulties in preserving the living cells per se, but arisefrom the properties of the integrated scaffold/matrix neo-tissue construct. Some examples of such challenges invitrifying TECs are described in this article. It is concludedthat the formation of ice, through both direct and indirecteffects, is probably fundamental to these difficulties, andthis is why vitrification seems to be the most likely wayforward. However, two major problems still to be over-come are cryoprotectant toxicity and ice-formation thatarises due to the considerably big size of TECs. Moreobvious, and certainly better understood is damage causedby gradual reduction in temperature [101]; this mayhighlight furthermore the fundamental importance ofvitrification. More than ever, there is growing evidencedemonstrating the superior performance of vitrification forpreserving cells/tissues/TECs when compared to the tradi-tional ‘‘freezing’’ method.
Acknowledgments
This research was supported by a grant from theBiomedical Research Council of Singapore (Grant no.:04/1/21/19/317). Some of the work shown in this articlewas executed in collaboration with Prof. H. Yu and Dr.G.S. Dawe. We thank Ms. R Magalhaes and Mr. Lee KHfor their excellent technical support and help in preparingthe manuscript.
All animal experiments were approved by the Institu-tional Animal Care and Use Committee of the NationalUniversity of Singapore and were conducted in accordancewith the ‘‘Guide for the Care and Use of LaboratoryAnimals’’, National Institutes of Health, USA.
References
[1] Hutmacher DW. Regenerative medicine will impact, but not replace,
the medical device industry. Expert Rev Med Devices
2006;3(4):409–12.
[2] Williams DF. To engineer is to create: the link between engineering
and regeneration. Trends Biotechnol 2006;24(1):4–8.
[3] Mason C. Regenerative medicine: revolution in the making. Med
Device Technol 2005;16(9):22.
[4] Mazur P. Kinetics of water loss from cells from subzero
temperatures and the likehood of intracellular freezing. J Gen
Physiol 1963;47:347–69.
[5] Polge C, Smith AY, Parkes AS. Revival of spermatozoa after
vitrification and de-hydration at low temperatures. Nature
1949;164:666.
[6] Kroener C, Luyet B. Discontinuous change in expansion coefficient
at the glass transition temperature in aqueous solutions of glycerol.
Biodynamica 1966;10:41–5.
[7] Luyet B, Rasmussen D. Study by differential thermal analysis of
temperature instability of rapidly cooled solutions of glycerol,
ethylene glycol, sucrose and glucose. Biodynamica 1967;10:167–91.
[8] Rapatz G, Luyet B. Patterns of ice formation in aqueous solution of
glycerol. Biodynamica 1966;10:69–80.
[9] Rapatz G, Luyet B. Patterns of ice formation in aqueous solution of
polyvinyl-pyrrolidone and temperatures of instability of the frozen
solution. Biodynamica 1968;10:149–66.
[10] Rasmussen D, Luyet BJ. Complementary study of some none-
qulibrium phase transmitions in frozen solution of glycerol, ethylene
glycol, glucose and sucrose. Biodynamica 1969;10:319–31.
[11] Rasmussen DH, Mackenzie AP. Phase diagram for the system
water-dimethylsulphoxide. Nature 1968;220(174):1315–7.
[12] Sutton RL. Critical cooling rates for aqueous cryoprotectants in the
presence of sugars and polysaccharides. Cryobiology 1992;29:
585–98.
[13] Kuleshova LL, MacFarlane DR, Trounson AO, Shaw JM. Sugars
exert a major influence on the vitrification properties of ethylene
glycol-based solutions and have low toxicity to embryos and
oocytes. Cryobiology 1999;38:119–30.
[14] Shaw JM, Kuleshova LL, MacFarlane DR, Trounson AO.
Vitrification properties of solutions of ethylene glycol in saline
containing PVP, Ficoll or Dextran. Cryobiology 1997;35:219–29.
[15] Wowk B, Fahy GM. Inhibition of bacterial ice nucleation by
polyglycerol polymers. Cryobiology 2002;44(1):14–23.
[16] Taylor MJ, Song YC, Brockbank KGM. Vitrification in tissue
preservation: new developments. In: Fuller BJ, Lane N, Benson EE,
editors. Life in the frozen state. Boca Raton, FL: CRC Press; 2004.
p. 604–41.
[17] Walsh JR, Taylor MJ, Brockbank KGM. Molecular ice control for
avoidance of ice. Cryobiology 2002;45(3):237 [Abstract].
[18] Wowk B, Leitl E, Kersh K, Fahy GM. Molecular mechanisms of
ice control by polyvinyl alcohol. Cryobiology 2002;41(4):352–3
[Abstract].
[19] Wowk B, Leitl E, Rasch CM, Mesbah-Karimi N, Harris SB, Fahy
GM. Vitrification enhancement by synthetic ice blocking agents.
Cryobiology 2000;40(3):228–36.
[20] Fahy GM, Wowk B, Wu J, Paynter S. Improved vitrification
solutions based on the predictability of vitrification solution toxicity.
Cryobiology 2004;48(1):22–35.
[21] Wowk B. Use of synthetic ice blockers in vitrification protocol.
Cryobiology 2005;50(3):325–31.
[22] Valdez CA, Mazni OA, Takahashi Y, Fujikawa S, Kanagawa H.
Successful cryopreservation of mouse blastocysts using a new
vitrification solution. J Reprod Fertil 1992;96(2):793–802.
[23] Mukaida T, Wada S, Takahashi K, Pedro PB, An TZ, Kasai M.
Vitrification of human embryos based on the assessment of suitable
conditions for 8-cell mouse embryos. Hum Reprod 1998;13(10):
2874–9.
[24] Kuleshova L, Gianoroli L, Magli C, Ferraretti A, Trounson A.
Birth following vitrification of small number of human oocytes.
Hum Rep 1999;14(12):3077–9.
[25] Fahy GM, MacFarlane DR, Angell CA, Meryman HT. Vitrification
as an approach to cryopreservation. Cryobiology 1984;21(4):407–26.
[26] Miyake T, Kasai M, Zhu SE, Sakurai T, Machida T. Vitrification of
mouse oocytes and embryos at various stages of development in
ethylene glycol-based solution by a simple method. Theriogenology
1993;40(1):121–34.
[27] Kuleshova LL, Shaw JM, Trounson AO. Studies on replacing most
of the penetrating cryoprotectant by polymers for embryo cryopre-
servation. Cryobiology 2001;43(1):21–31.
[28] Yoon TK, Kim TJ, Park SE, Hong SW, Ko JJ, Chung HM, et al.
Live births after vitrification of oocytes in a stimulated in vitro
fertilization—embryo transfer program. Fertil Steril 2003;79(6):
1323–6.
ARTICLE IN PRESSL.L. Kuleshova et al. / Biomaterials 28 (2007) 1585–1596 1595
[29] Saha S, Otoi T, Takagi M, Boediono A, Sumantri C, Suzuki T.
Normal calves obtained after direct transfer of vitrified bovine
embryos using ethylene glycol, trehalose, and polyvinylpyrrolidone.
Cryobiology 1996;33(3):291–9.
[30] Tada N, Sato M, Amann E, Ogawa S. A simple and rapid method
for cryopreservation of mouse 2-cell embryos by vitrification-
beneficial effect of sucrose and raffinose on their cryosurvival rate.
Theriogenology 1993;40(2):333–44.
[31] Al-Hasani S, Diedrich K, van der Ven H, Reinecke A, Hartje M,
Krebs D. Cryopreservation of human oocytes. Hum Reprod
1987;2(8):695–700.
[32] Kasai M, Komi JH, Takakamo A, Tsudera H, Sakurai T, Machida
T. A simple method for mouse embryo cryopreservation in low
toxicity vitrification solution, without appreciable loss of viability.
J Reprod Fertil 1990;89(1):91–9.
[33] Pellerin-Mendes C, Million L, Marchand-Arvier M, Labrude P,
Vigneron C. In vitro study of the protective effect of trehalose and
dextran during freezing of human red blood cells in liquid nitrogen.
Cryobiology 1997;35(2):173–86.
[34] Sputtek A, Singbartl G, Langer R, Schleinzer W, Henrich HA,
Kuhnl P. Cryopreservation of red-blood-cells with the nonpenetrat-
ing cryoprotectant hydroxyethyl starch. Cryo-Letters 1995;16:
283–8.
[35] Kuleshova LL, Shaw JM. A strategy for rapid cooling of embryos
within a double straw to eliminate risk of contamination during
cryopreservation and storage. Hum Rep 2000;15(12):2604–9.
[36] Kuleshova LL, Wang XW, Wu YN, Zhoi Y, Yu H. Vitrification of
encapsulated hepatocytes with reduced cooling/warming rates.
CryoLetters 2004;25(4):241–54.
[37] Wu Y, Yu H, Chang S, Magalhaes R, Kuleshova LL. Vitreous
cryopreservation of encapsulated hepatocytes. Tissue Eng 2006 (in
press).
[38] Kuleshova LL, Otani T, Takeda N, Odawara Y. The evolution and
current status in vitrification of oocytes and embryos. Cryobiology
2004;49(3):321.
[39] Kuleshova LL, Tan CKF, Dawe GS. Cryopreservation of adult
stem cells cultured as neurospheres. Cryobiology 2005;51(3):355–6.
[40] Martin MJ, Muotri A, Gage F, Varki A. Human embryonic stem
cells express an immunogenic nonhuman sialic acid. Nat Med
2005;11(2):228–32.
[41] Chou HH, Takematsu H, Diaz S, Iber J, Nickerson E, Wright KL,
et al. A mutation in human CMP-sialic acid hydroxylase occurred
after the Homo-Pan divergence. Proc Natl Acad Sci USA
1998;95(20):11751–6.
[42] Rall WF, Fahy GM. Ice free cryopreservation of mouse embryos at
196 1C by vitrification. Nature 1985;313(6003):573–5.
[43] Rall WF, Wood MJ, Kirby C, Whittingham DG. Development of
mouse embryos cryopreserved by vitrification. J Reprod Fertil
1987;80(2):499–504.
[44] Langer S, Lau D, Eckhardt T, Jahr H, Brandhorst H, Brandhorst
D, et al. Viability and recovery of frozen-thawed human islets and in
vivo quality control by xenotransplantation. J Mol Med 1999;77(1):
172–4.
[45] Fahy GM. Prospect for vitrification of whole organs. Cryobiology
1981;18(6):617–25.
[46] Fahy GM, Wowk B, Wu J, Phan J, Rasch C, Chang A, et al.
Cryopreservation of organs by vitrification: perspectives and recent
advances. Cryobiology 2004;48(2):157–78.
[47] Ekins S, Murray GI, Hawksworth GM. Ultrastructural and
metabolic effects after vitrification of precision-cut rat liver slices
with antifreeze proteins. Cryo-Letters 1996;17(3):157–64.
[48] Song YC, Khirabadi BS, Lightfoot F, Brockbank KG, Taylor MJ.
Vitreous cryopreservation maintains the function of vascular grafts.
Nat Biotechnol 2000;18(3):296–9.
[49] Kuleshova LL, Lopata A. Vitrification can be more favorable than
slow cooling. Fertil Steril 2002;78(5):449–54.
[50] Rall WF. Factors affecting the survival of mouse embryos
cryopreserved by vitrification. Cryobiology 1987;24(5):387–402.
[51] Dahl SL, Chen Z, Solan AK, Brockbank KG, Niklason LE, Song
YC. Feasibility of vitrification as a storage method for tissue-
engineered blood vessels. Tissue Eng 2006;12(2):291–300.
[52] Mukherjee N, Chen ZZ, Sambanis A, Song Y. Effects of
cryopreservation on cell viability and insulin secretion in a model
tissue-engineered pancreatic substitute (TEPS). Cell Transplant
2005;14(7):449–56.
[53] Paul G, Li JY, Brundin P. Stem cells: hype or hope? Drug Discov
Today 2002;7(5):295–302 [Review].
[54] Robertson EJ. Embryo derived stem cell lines. In: Robertson EJ,
editor. Teratocarcinomas and embryonic stem cell lines: a practical
approach. Oxford: IRL Press; 1987. p. 71–112.
[55] Shim H, GutierrezAdan A, Chen LR, BonDurant RH, Behboodi E,
Anderson GB. Isolation of pluripotent stem cells from cultured
porcine primordial germ cells. Biol Reprod 1997;57(5):1089–95.
[56] Katkov II, Isachenko V, Isachenko E, Kim MS, Lulat AGMI,
Mackay AM, et al. Low- and high-temperature vitrification as a new
approach to bio stabilization of reproductive and progenitor cells.
Int J Refrigerat 2006;29:346–57.
[57] Ji L, de Pablo JJ, Palecek SP. Cryopreservation of adherent human
embryonic stem cells. Biotechnol Bioeng 2004;88(3):299–312.
[58] Reubinoff BE, Pera MF, Vajta G, Trounson AO. Effective
cryopreservation of human embryonic stem cells by the open pulled
straw vitrification method. Hum Reprod 2001;16(10):2187–94.
[59] Heng BC, Ye CP, Liu H, Toh WS, Rufaihah AJ, Yang Z, et al. Loss
of viability during freeze-thaw of intact and adherent human
embryonic stem cells with conventional slow-cooling protocols is
predominantly due to apoptosis rather than cellular necrosis.
J Biomed Sci 2005;13(3):433–45.
[60] Richards M, Fong CY, Tan S, Chan WK, Bongso A. An efficient
and safe xeno-free cryopreservation method for the storage of
human embryonic stem cells. Stem Cells 2004;22(5):779–89.
[61] Fujioka T, Yasuchika K, Nakamura Y, Nakatsuji N, Suemori H. A
simple and efficient cryopreservation method for primate embryonic
stem cells. Int J Dev Biol 2004;48(10):1149–54.
[62] Suemori H, Yasuchika K, Hasegawa K, Fujioka T, Tsuneyoshi N,
Nakatsuji N. Efficient establishment of human embryonic stem cell
lines and long-term maintenance with stable karyotype by enzymatic
bulk passage. Biochem Biophys Res Commun 2006;345(3):
926–32.
[63] Levenberg S, Burdick JA, Kraehenbuehl T, Langer R. Neurotro-
phin-induced differentiation of human embryonic stem cells on
three-dimensional polymeric scaffolds. Tissue Eng 2005;11(3–4):
506–12.
[64] Milosevic J, Storch A, Schwarz J. Cryopreservation does not affect
proliferation and multipotency of murine neural precursor cells.
Stem Cells 2005;23(5):681–8.
[65] Smith AU. Cartilage. In: Karow AM, Abouna GJM, Humphries
AL, editors. Organ preservation for transplantation. Boston: Little
Brown and Co; 1976. p. 214.
[66] Ohlendorf C, Tomford WW, Mankin HJ. Chondrocyte survival in
cryopreserved osteochondral articular cartilage. J Orthop Res
1996;14(3):413–6.
[67] Muldrew K, Hurtig M, Novak K, Schachar N, McGann LE.
Localization of freezing injury in articular cartilage. Cryobiology
1994;31(1):31–8.
[68] Wu FJ, Davisson TH, Pegg DE. Preservation of tissue-engineered
articular cartilage. Cryobiology 1998;37(4):410.
[69] Pegg DE, Wusteman MC, Wang L. Cryopreservation of articular
cartilage 1: conventional cryopreservation methods. Cryobiology
2006;52(3):335–46.
[70] Curran RC, Gibson T. The uptake of labelled sulphate by human
cartilage cells and its use as a test for viability. Proc R Soc B
1956;144:572–6.
[71] Pegg DE, Wang LH, Vaughan D, Hunt CJ. Cryopreservation of
articular cartilage. Part 2: mechanisms of cryoinjury. Cryobiology
2006;52(3):347–59.
ARTICLE IN PRESSL.L. Kuleshova et al. / Biomaterials 28 (2007) 1585–15961596
[72] Pegg DE, Wang LH, Vaughan D. Cryopreservation of articular
cartilage. Part 3: the liquidus-tracking method. Cryobiology
2006;52(3):360–8.
[73] Song YC, An YH, Kang QK, Li CY, Boggs JM, Chen ZZ, et al.
Vitreous preservation of articular cartilage grafts. J Invest Surg
2004;17(2):65–70.
[74] Song YC, Lightfoot FG, Chen Z, Taylor MJ, Brockbank KGM.
Vitreous preservation of rabbit articular cartilage. Cell Preserv
Technol 2004;2:67–74.
[75] Konfron MD, Opsitnick NC, Attawia MA, Laurencin CT.
Cryopreservation of tissue engineered constructs for bone. J Orthop
Res 2003;21(6):1005–10.
[76] Han DW, Park HK, Park YH, Kim TS, Yoon WS, Kim JK, et al.
Beneficial effects of freezing rate determined by indirect thermo-
physical calculation on cell viability in cryopreserved tissues. Artif
Cells Blood Substit Biotechnol 2006;34(2):205–21.
[77] Liu BL, McGrath J. Vitrification solutions for the cryopreservation
of tissue-engineered bone. Cell Preserv Technol 2004;2(2):133–43.
[78] Hutmacher DW, Sittinger M, Risbud MV. Scaffold-based tissue
engineering: rationale for computer-aided design and solid free-form
fabrication systems. Trends Biotechnol 2004;22(7):354–62 [Review].
[79] Schantz JT, Lim TC, Ning C, Teoh SH, Tan KC, Wang SC, et al.
Cranioplasty after trephination using a novel biodegradable burr
hole cover: technical case report. Neurosurgery 2006;58(Suppl. 1)
ONS-E176; discussion ONS-E176.
[80] Izadpanah R, Trygg C, Patel B, Kriedt C, Dufour J, Gimble JM, et
al. Biologic properties of mesenchymal stem cells derived from bone
marrow and adipose tissue. J Cell Biochem 2006 [Epub ahead of
print].
[81] Kuleshova LL, Hutmacher DW. Cryobiology. In: Van Blittersvijk
C, Lindahl A, Thomsen P, Williams DF, Hubbell J, Cancellah R,
editors. Textbook on tissue engineering. New Jersey: Wiley; in press.
[82] Chia SM, Leong KW, Li J, Yu H. Hepatocyte encapsulation for
enhanced cellular functions. Tissue Eng 2000;6(5):481–95.
[83] Ng S, Wu Y, Zhou Y, Toh YE, Ho ZZ, Chia SM, et al.
Optimization of 3-D hepatocyte culture by controlling the physical
and chemical properties of the extra-cellular matrices. Biomaterials
2005;26(16):3153–63.
[84] Chin Heng B, Yu H, Chye Ng S. Strategies for the cryopreservation
of microencapsulated cells. Biotechnol Bioeng 2004;85(2):202–13.
[85] Vilei MT, Granato A, Ferraresso C, Neri D, Carraro P, Gerunda G,
et al. Comparison of pig, human and rat hepatocytes as a source of
liver specific metabolic functions in culture systems-implications for
use in bioartificial liver devices. Int J Artif Organs 2001;24(6):392–6.
[86] Lanza RP, Butler DH, Borland KM, Staruk JE, Faustman DL,
Solomon BA, et al. Xenotransplantation of canine, bovine, and
porcine islets in diabetic rats without immunosuppression. Proc Natl
Acad Sci USA 1991;88(24):11100–4.
[87] Lim F, Sun AM. Microencapsulated islets as bioartificial endocrine
pancreas. Science 1980;210(4472):908–10.
[88] Gall KL, Smith SE, Willmette CA, O’Brien MF. Allograft heart
valve viability and valve-processing variables. Ann Thorac Surg
1998;65(4):1032–8.
[89] Kroener C, Luyet BJ. Formation of cracks during the vitrification of
glycerol solutions and disappearance of the cracks during rewarm-
ing. Biodynamica 1966;10(198):47–52.
[90] Fahy GM, Saur J, Williams RJ. Physical problems with the vitrification
of large biological systems. Cryobiology 1990;27(5):492–510.
[91] Pegg DE, Wusteman MC, Boylan S. Fractures in cryopreserved
elastic arteries. Cryobiology 1997;34(2):183–92.
[92] Song YC, Hagen PO, Lightfoot FG, Smith AC, Taylor MJ,
Brockbank KGM. In vivo evaluation of the effects of a new ice-free
cryopreservation process on autologous vascular grafts. J Invest
Surg 2000;13(5):279–88.
[93] Elder E, Chen Z, Ensley A, Nerem R, Brockbank K, Song Y.
Enhanced tissue strength in cryopreserved, collagen-based blood
vessel constructs. Transplant Proc 2005;37(10):4625–9.
[94] Fahy GM, da Mouta C, Tsonev L, Khirabadi BS, Mehl P,
Meryman HT. Cellular injury associated with organ cryopreserva-
tion: chemical toxicity and cooling injury. In: Lemasters JJ, Oliver
C, editors. Cell biology of trauma. Boca Raton, FL: CRC Press;
1995. p. 333–56.
[95] Mitchell SL, Niklason LE. Requirements for growing tissue
engineered vascular grafts. Cardiovasc Pathol 2003;12:59–64.
[96] Yannas I, Tobolsky AV. Cross-linking of gelatine by dehydration.
Nature 1967;215:509–10.
[97] Weadock K, Olson RM, Silver FH. Evaluation of collagen
crosslinking techniques. Biomater Med Devices Artif Org 1984;11:
293–318.
[98] Venkatasubramaniam RT, Grassl ED, Barocas VH, Lafontaine D,
Bischof JC. Effects of freezing and cryopreservation on the mechanical
properties of arteries. Anal Biomed Eng 2006;34(5):823–32.
[99] Thakrar RR, Patel VP, Hamilton G, Fuller BJ, Seifalian AM.
Vitreous cryopreservation maintains the viscoelastic property of
human vascular grafts. FASEB J 2006;20(7):874–81.
[100] Narine K, Ing EC, Cornelissen M, Desomer F, Beele H,
Vanlangenhove L, et al. Readily available porcine aortic valve
matrices for use in tissue valve engineering. Is cryopreservation an
option? Cryobiology 2006;53(2):169–81.
[101] Watson PF. Recent developments and concepts in the cryopreserva-
tion of spermatozoa and the assessment of their post-thawing
function. Reprod Fertil Dev 1995;7(4):871–91.
Copyright © 2022 FDOKUMEN




















