Visual outcome of Phacoemulsification
49
Sudanese Journal of Ophthalmology July 2009 - Volume 1, Issue 2
Transcript of Visual outcome of Phacoemulsification

SSuuddaanneessee JJoouurrnnaall ooff OOpphhtthhaallmmoollooggyy
July 2009 - Volume 1, Issue 2

49
Sudanese Journal of Ophthalmology
Published by Sudan Eye Centre in collaboration with Sudanese Eye Research Group.
Editor-in-Chief
Dr. Nadir A M Ali
Associate Editor
Dr. Ismail Abdalla Al Fadul
Production Editor
Optom. Khalid Mohamed Ahmed
Editorial Board (National)
Professor A. Salim Al Hakeem
Dr. Abdel Gadir Al Hassan Al Saori
Dr. Abdalla Al Siddig
Dr. Awad Hassan
Dr. Kamal Hashim Binnawi Assoc. Prof. Mahgoub Saleem
Professor Mamoun M. A. Homeida
Professor Osman Bakheet
Assoc. Prof. Samira Mohamed Ibrahim
Editorial Board (International)
Professor Clare Gilbert
Dr. Paul Courtright
Professor Jia-quan Shen
Professor Lina Hao
Professor S C Reddy Dr. Tajunisah Iqbal
Assoc. Prof. Visvaraja Subarayan
Professor Asad Aslam Khan
Dr. Muhammad Zahid Jadoon
Professor Ahmed Abdel-kareem Mohamed El
Massry
Correspondence:
Sudan Eye Center
Street No. 41, Amarat,
11111 Khartoum
Tel: +249-919-519-413 Email: [email protected]
Website: www.sudaneyecenter.com/sjo
Enquiries related to advertising and
subscriptions: Email: [email protected]
Copyrights:
Sudanese Journal of Ophthalmology (SJO) is
published biannually (January and July) by
Sudan Eye Center. All rights reserved; no part of
this publication may be translated, reproduced,
stored in a retrieval system or transmitted in any
form or by any means without prior written
permission from the publisher. Submitted
manuscripts must not have been published in
other journals or submitted simultaneously to other journals. With the acceptance of the
manuscript for publication, SJO acquires full and
exclusive rights.
Disclaimer:
All articles published in SJO represent the
opinion of the authors and do not reflect the
official policy of the journal, sponsors or
publishers unless it is clearly specified. SJO and the publishers do not endorse or guarantee,
directly or indirectly, the quality or efficacy of
any product described in the advertisements.
Although every effort has been made to ensure
the completeness and accuracy of information
published in this journal, editors and publishers
cannot be held responsible for any errors that
may have inadvertently occurred during
publication and shall not be liable under any
circumstances what-so-ever for any damages as a
result of any errors or omissions or changes.
Because of rapid advances in medical sciences, the method of diagnosis and drug dosages should
be verified.
Aims and Scope
Sudanese Journal of Ophthalmology (SJO) publishes original, peer-reviewed reports of research in
ophthalmology, including basic scientific papers, clinical studies and interesting case reports. Topics include
new diagnostic and surgical techniques, treatment methods and outcome, instrument updates, the latest drug
findings, results of clinical trials and other research findings. The journal also publishes major reviews of
specific topics by acknowledged authorities.

50 Sudanese Journal of Ophthalmology
Instructions to authors
Sudanese Journal of Ophthalmology (SJO) is the
official publication of the Sudan Eye Center in
collaboration with Sudanese Ophthalmological
Research Group. It is a peer-reviewed biannual
publication in January and July. All manuscripts,
written in English language, must be submitted
on-line through the website. First time users will
have to register at this site. Registered authors can
keep track of their articles after logging into the
site using their user name and password. If you
experience any problem, please contact our editorial office by e-mail to the following address:
Submitted manuscripts should adhere to the stated
format. Otherwise they will be returned by editor
without review. A covering letter along with
authors‟ declaration form and signed copyright
form should be included. The receipt of
submissions will be acknowledged.
Manuscripts are sent to two expert reviewers without revealing the identity of the contributors
to the reviewers. Based on the comments from the
reviewers, Editor takes a final decision on the
acceptance of manuscript for publication. The
contributors will be informed about the reviewers' comments and acceptance/rejection of manuscript.
All accepted papers become the permanent
property of Sudan Journal of Ophthalmology and
may not be published elsewhere without written
permission from the editor. Page proofs will be
sent to the corresponding author, just before the
publication of article in the journal, which has to
be returned within three days. Correction received
after that period may not be included.
Types of manuscript
Editorials - Should not exceed 1000 words.
Original Articles - Should not exceed 3000
words; the total number of Tables and Figures
should not be more than 6, and references not
more than 30. Headings of the paper should
include Abstract; Keywords; Introduction;
Material and methods; Results; Discussion and
References. Acknowledgement should be written
before the references whenever required. Clinical studies of screening and diagnostic test, outcome
studies, randomized controlled trials, intervention
studies, case-control series, and surveys with high
response rate come in this category.
Review Articles - Should not exceed 4000 words;
the total number of Tables and Figures should not
be more than 10, and references not more than 50.
Method of literature search should be mentioned
in the introduction section.
Case Reports - Should not exceed 1500 words;
the total number of Tables and Figures should not
be more than 4, and references not more than 10. Case should be highly unusual, very rare, under
reported in the literature. Cases with clinical
educational value will be given priority. Letters to the Editor - Communications on all
aspects of ophthalmology are encouraged. Length
should not exceed more than 500 words, and
references should not be more than 5. They should
not be preliminary observations that need a later
paper for validation.
Manuscript Preparation:
The manuscript should be typed in double spacing
with margins 2.5 cm from all four sides, and
arranged as follows: Title Page - The title page should contain the title
of the article, which should be concise but
informative; a short running title of fewer than 40
characters (including spaces); the first name,
middle initials, and last name of all authors; the
name of the department(s) and institution(s) to
which each author is affiliated; the full name,
address, telephone and fax numbers, and e-mail
address of the corresponding author.
Abstract and Keywords - The abstract for
original articles must be structured with the
following sub-headings: Aims, Material and Methods, Results, and Conclusion. Abstracts for
case reports must be unstructured, but should
include the key points discussed in the paper.
Abstracts should be no longer than 250 words.
The key words must not be more than 6 and
should fit into Medline/ Index Medicus.
Text of the manuscript - For original articles, the
following sections should be included:
Introduction - The rationale for the study should
be mentioned with relevant background material.
Material and methods - This section should describe all the methods used in the study in
detail. Manuscripts that contain the results of
human or animal studies should make clear that a
high standard of ethics was applied. Invasive
studies of humans should state that the research
protocol was approved by the local ethics
committee.
Results - The results should be presented in
logical sequence in the text, Tables, and Figures;

51
repetitive presentation of the same data in
different forms should be avoided. When data are
summarized in the Results section, give numeric
results not only as derivatives (for example,
percentages) but also as the absolute numbers
from which the derivatives were calculated, Results must be statistically analysed where
appropriate.
Discussion - Data given in the Results section
should not be repeated here. The Discussion may
include key findings and their relationship to the
existing body of knowledge in the field; effects on
patient care and health policy, possible
mechanisms. Contributors should avoid making
statements on economic benefits and costs unless
their manuscript includes economic data and
analyses. This section should present the
implications and limitations of the study. Conclusions should be incorporated into the final
paragraph and should be consistent with and
completely supported by data in the text.
Acknowledgements - Acknowledgements can be
made to people who have offered assistance in the
research or preparation of the manuscript and who
do not fulfill authorship criteria. Research or
project support should also be stated.
References – References should be numbered
serially in the order of appearance in the text (not
in alphabetic order). Identify references in text and tables by Arabic numerals in superscript
without bracket after the punctuation marks.
References cited only in tables should be
numbered in accordance with the sequence
established in the text or table. The titles of
journals should be abbreviated according to the
style used in Index Medicus. Use complete name
of the journal for non-indexed journals. Avoid
citing a "personal communication" unless it
provides essential information not available from
a public source, in which case the name of the
person and date of communication should be cited in parentheses in the text. The commonly cited
types of references are shown here.
Journals
1. Wright KW, Erikscn KJ, Shors TJ et al.
Recording pattern visual evoked potential under
chloralhydrate sedation. Arch Ophthalmol.
1986;104:718-72. List first 3 authors followed
by et al.
2. Carney RJ. Incontinentia pigmenti – A world
statistical analysis. Arch Dermatol.
1976;112:535-542.
Books and Other Monographs 1. Sagerman RH, Alberti WE. Radiotherapy of
intraocular and orbital tumours. 2nd ed. Vol 1.
New York, Springer, 2003:1-295.
2. American Medical Association Department of
Drugs. AMA drug evaluation (3rd ed.).
Littleton, Publishing Sciences Group, 1977.
Chapter in Book:
Weinstein L, Swartz MN. Pathogenic properties of invading micro-organisms. In : Sodeman
WAJr, Sodeman WA (eds). Pathogenic
physiology : mechanisms of disease. Philadelphia,
WB Saunders, 1974 : 457-72.
Tables – Tables should be self-explanatory and
should not duplicate textual material. Number
tables, in Arabic numerals, consecutively in the
order of their first citation in the text and supply a
brief title for each. Place explanatory matter in
footnotes, not in the heading. Explain in footnotes
all non-standard abbreviations that are used in
each table. For footnotes use symbols. Figures (illustrations) - Figures should be
numbered in Arabic numerical consecutively
according to the order in which they have been
first cited in the text. It should be in JPEG or TIFF
format (300 dpi). File should be within 500kb
size, 8cm width and 6-9 cm height depending on
the type of photo. The colour photos are free in
online version. However, their cost will be
charged to the corresponding author for printed
version; if not they will be printed black and white
free of cost. Symbols, arrows, or letters used in photos should contrast with the background and
should be visible clearly. Legends for figures
should be written on a separate paper. If
photographs of people are used, either the subjects
must not be identifiable or their pictures must be
accompanied by written permission to use the
photograph. The Journal reserves the right to
crop, rotate, reduce, or enlarge the photographs to
an acceptable size. The magnification and the
staining method should be written for
photomicrographs.
Reprints - Journal provides no free printed reprints, but a free copy of the issue in which the
paper is published will be sent to the
corresponding author. If the author wants
reprints, it is mandatory to purchase minimum
number of reprints; payment for which should be
done at the time of submitting the proofs.
Check list for corresponding author
1. Manuscript written in the format of SJO.
2. Author‟s declaration form signed by all authors.
3.Copyright form signed by corresponding author.

52 Sudanese Journal of Ophthalmology
Table of Contents
Editorial Can H1N1 virus (Swine flu) affect the eye? 53
Ali NA
Review Article HIV-related eye diseases -Current updates 54
Tajunisah I
Original Articles Sudan test (ST), a design of simple reading chart in Arabic language with predicted 65
magnification for low vision
Ali AB, Elawad ME, Elsheikh EA
Toxic effects of antiglaucoma topical medications on the conjunctiva – a histological study 71
Hayet M, Soraya M, Abdenacer T, Myriam O
Laser-assisted in situ keratomileusis (LASIK) surgery in the management of anisometropic 76
amblyopia in Sudanese Children
Binnawi KH, Ali NA
Visual Outcome of Phacoemulsification in Al Walidain Charity Eye Hospital – 81
The first 120 cases
Ali MA, Binnawi KH, Ali NA
Chemical injuries of the eye – Clinical study of 40 cases 86
Reddy SC, Reddy PR
Case Reports
Unilateral Isolated Ocular Tuberculosis with no systemic involvement 91 Chan UT , Choo MM , Reddy SC
Letter to Editor 95
Sudan Test (ST) for near vision test
Ali AB
Announcements 96
53
EDITORIAL
Can H1N1 virus (Swine flu) affect the eye?
Welcome to the second issue of Sudanese
Journal of Ophthalmology! I am proud to
announce that we are now indexed in
African Index Medicus (AIM/Hinari),1
and our inclusion in African Journals
Online (AJOL) is also in process. We are
aware that indexing is an important issue
for any peer-reviewed journal to ensure
maximum spread. Thus, one of our
priorities is to get the journal indexed in
all relevant indexing bodies.
One of my anxious patients, who had
common cold and red eyes, asked me
„Doctor, Can this be Swine flu? Can the
virus affect my eyes?!‟ In fact, ocular
involvement in human influenza A virus
diseases (e.g. seasonal influenza) is
common but usually limited to mild
conjunctivitis. Avian Influenza virus
(H5N1), was reported to cause
inflammation of the choriocapillaris and
atrophy of the retinal pigment
epithelium.2
The current outbreak of H1N1 influenza
(formerly known as Swine flu) has
caused global terror. This pandemic was
first reported in Mexico in March 2009
with rapid global spread in a geometric
progression.3 In May, 2009 there was
10,243 confirmed cases worldwide,
including 80 deaths, in 41 countries.4
These figures increased to more than
134,500 affected people in more than 100
countries, including more than 800
deaths, by end of July, 2009.5 Sudan
reported its first two cases of the H1N1
flu virus on 16th of July, with no deaths so
far.6
In view of the rapid spread and the
virulence of this new mutation of H1N1
virus, further clinical studies are needed
to determine its behavior in human eyes.
References
1. African index medicus/Hinari website.
Available at http://indexmedicus.afro.who.int/Journals/Index
j.htm (Accessed on 15th July, 2009)
2. Michaelis M, Geiler J, Klassert D, et al.
Infection of human retinal pigment epithelial
cells with influenza A viruses. Invest
Ophthalmol Vis Sci. 2009 Jun 24. [Epub ahead
of print]
3. Center for Infectious disease research and
policy, University of Minnesota.
http://www.cidrap.umn.edu/cidrap/content/influ
enza/swineflu/news/may0109mexico.html (Accessed on 30/7/2009)
4. WHO. Weekly epidemiological record 2009;
84:185–196
5. WHO. Influenza A (H1N1): Special Highlights.
World Health Organization. Available at
http://www.who.int/csr/don/2009_07_27/en/ind
ex.html (Accessed on 30/7/2009)
6. Reuters News agency.
http://www.reuters.com/article/africaCrisis/idU
SHEA670400 (Accessed on 23/7/2009)
Dr. Nadir A M Ali Editor-In-Chief
54 Sudanese Journal of Ophthalmology
REVIEW
HIV-related eye diseases - Current updates Tajunisah Begam Iqbal
Dept. of Ophthalmology, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia
Correspondence to: Dr. Tajunisah Iqbal, Dept. of Ophthalmology, Faculty of Medicine, University of Malaya, 50603 Kuala Lumpur, Malaysia, Email: [email protected], Tel. No. +60192189510.
Abstract
This review is to describe the most common HIV-related eye diseases and to summarize current
updates and recent literature regarding the clinical manifestations, ocular complications and the current treatment strategies of the various diseases.
This review was written based on the search of the Medline, using PubMed, specifically for words
that included current updates of HIV-related eye diseases, AIDS, retinal microvasculopathy, herpes
zoster ophthalmicus, molluscum contagiosum, cytomegalovirus retinitis, acute retinal necrosis, opportunistic infections, Kaposi sarcoma, treatment of retinitis and immune recovery uveitis.
Articles were selected based on clinical importance and references of key articles were included.
Non-English abstracts were not included in this review.
Keywords: HIV-related eye diseases; herpes zoster ophthalmicus; cytomegalovirus retinitis;
toxoplasmic retinochoroiditis; Kaposi sarcoma; immune recovery uveitis.
There are estimated 40 million people worldwide living with HIV/AIDS and 90% of
them are living in developing countries,
particularly those in sub-Saharan Africa and Southeast Asia.
1 The incidence rate for new
HIV infections is still highest in the world in
sub-Saharan Africa and the life expectancy in
these countries has decreased as a result of AIDS complications. These complications,
affecting virtually all organ systems, have
been the principal cause of morbidity and mortality in patients with AIDS.
2
The first report of the ocular manifestations
of AIDS has been reported by Holland et al3
in 1982 and since then, it has been
recognized that 70-80% of adult AIDS
patients will experience an ocular
complication at some point in their illness. A broad range of ocular complications can
occur involving the ocular adnexa and orbit,
anterior segment and posterior segment
manifestations. All patients with HIV disease should undergo routine ophthalmologic
examination since some retinal opportunistic
infections may have a rapid and devastating course leading to blindness in these patients.
The pattern of ocular involvement in HIV
infection has changed over the years with the advent of highly active antiretroviral therapy
(HAART) era.4 Previously ocular
opportunistic infections, especially cytomegalovirus (CMV) retinitis, was a
notorious sign of poor survival but with the
increased use of HAART treatment and the improved survival of patients with better
immune system, ocular infections became
more manageable. In general, CD4+ T-
lymphocyte count has been used to predict the onset of certain ocular infections in
patients who are HIV positive (Table 1).
55
Table 1: Ocular complications of HIV infection versus degree of immunodeficiency as indicated by CD4+ Tcell
count.
Patient’s
CD4+ T cell
count
Type of ocular complications
Vascular Infection Tumor
Any Large-vessel vaso-occlusion Disseminated molluscum contagiosum Ocular surface squamous neoplasia
≤500 cells/µ Herpes zoster ophthalmicus Kaposi sarcoma Lymphoma
≤200 cells/µl Ocular tuberculosis Pneumocystosis
≤100 cells/µl HIV retinopathy Toxoplasmic retinitis Progressive outer retinal necrosis Cryptococcal chroiditis
≤ 50 cells/µl CMV retinitis
CLINICAL PRESENTATIONS
Orbital and adnexal manifestations
Orbital manifestations of HIV infection are not seen very often and some reported cases
include orbital cellulites and primary non-
Hodgkin‟s lymphoma.5 The more common
ocular adnexa lesions in patients who are HIV positive include herpes zoster
ophthalmicus (HZO), Kaposi sarcoma,
molluscum contagiosum and ocular surface squamous neoplasia.
Herpes Zoster Ophthalmicus (HZO)
Herpes zoster ophthalmicus (HZO) is a
painful vesicular dermatitis over the
forehead, which results from the reactivation of latent varicella zoster virus in the
ophthalmic division of the trigeminal nerve
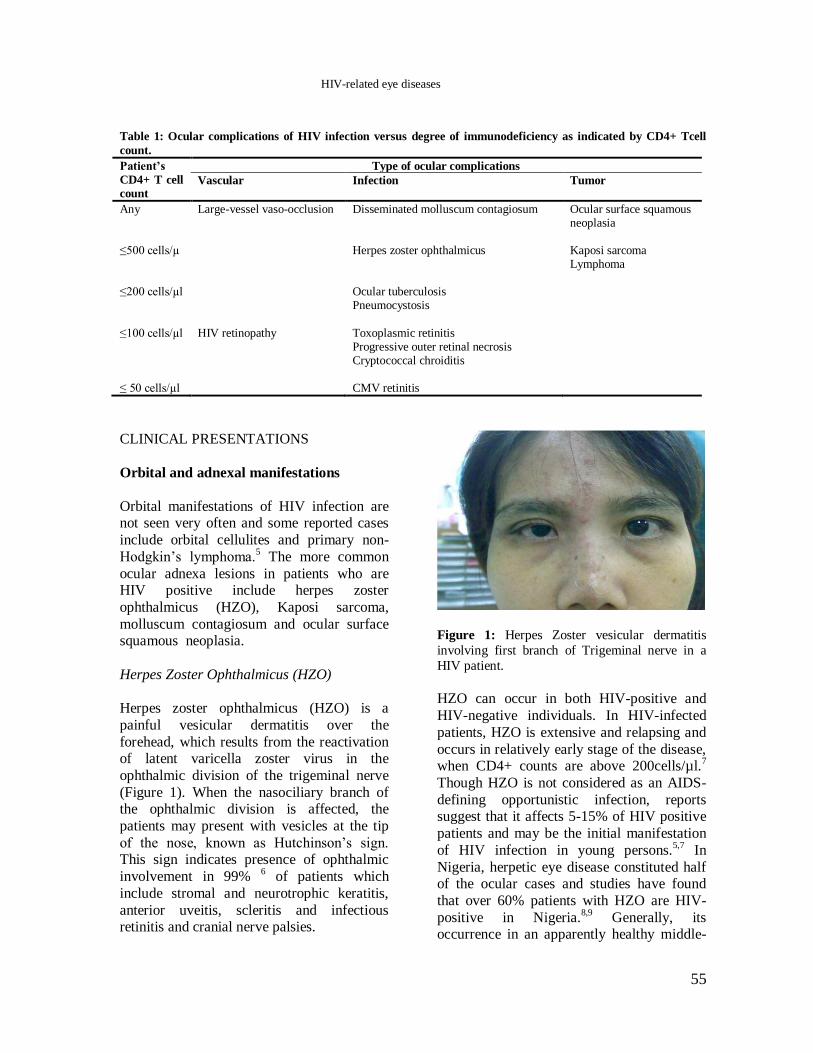
(Figure 1). When the nasociliary branch of the ophthalmic division is affected, the
patients may present with vesicles at the tip
of the nose, known as Hutchinson‟s sign. This sign indicates presence of ophthalmic
involvement in 99% 6 of patients which
include stromal and neurotrophic keratitis,
anterior uveitis, scleritis and infectious retinitis and cranial nerve palsies.
Figure 1: Herpes Zoster vesicular dermatitis
involving first branch of Trigeminal nerve in a
HIV patient.
HZO can occur in both HIV-positive and
HIV-negative individuals. In HIV-infected
patients, HZO is extensive and relapsing and
occurs in relatively early stage of the disease, when CD4+ counts are above 200cells/µl.
7
Though HZO is not considered as an AIDS-
defining opportunistic infection, reports suggest that it affects 5-15% of HIV positive
patients and may be the initial manifestation
of HIV infection in young persons.5,7
In
Nigeria, herpetic eye disease constituted half of the ocular cases and studies have found
that over 60% patients with HZO are HIV-
positive in Nigeria.8,9
Generally, its occurrence in an apparently healthy middle-
HIV-related eye diseases
56 Sudanese Journal of Ophthalmology
aged or younger person is an indication for
HIV testing. 10
Ocular complications result from
inflammation, nerve damage and tissue
scarring. The severity of the skin rash is an
important prognostic parameter of subsequent ocular involvement.
11 HIV infection also
appeared to correlate with more severe
corneal involvement and post-herpetic neuralgia.
6, 12
Patients with skin rashes near the eye may be
treated with oral acyclovir, bacitracin skin ointment for the skin lesions and acyclovir
eye ointment for conjunctival or corneal
involvement. In cases of acute retinal
necrosis (ARN) or cranial nerve involvement, intravenous acyclovir (10mg/kg body weight
three times a day for seven days) followed by
an oral maintenance regimen (800mg 3-5 times a day with slow taper over a month or
more) are indicated. Other options include
oral therapy with famciclovir or valaciclovir which are more expensive.
6,13
Kaposi Sarcoma
Kaposi sarcoma (KS), a vascular tumour
caused by human herpesvirus 8 (HHV-8), is
one of the earliest identified complications of AIDS and can be considered as an AIDS-
related illness.14
About 20% of HIV patients
have asymptomatic Kaposi sarcoma of the
eyelids, conjunctiva and rarely the orbit.15
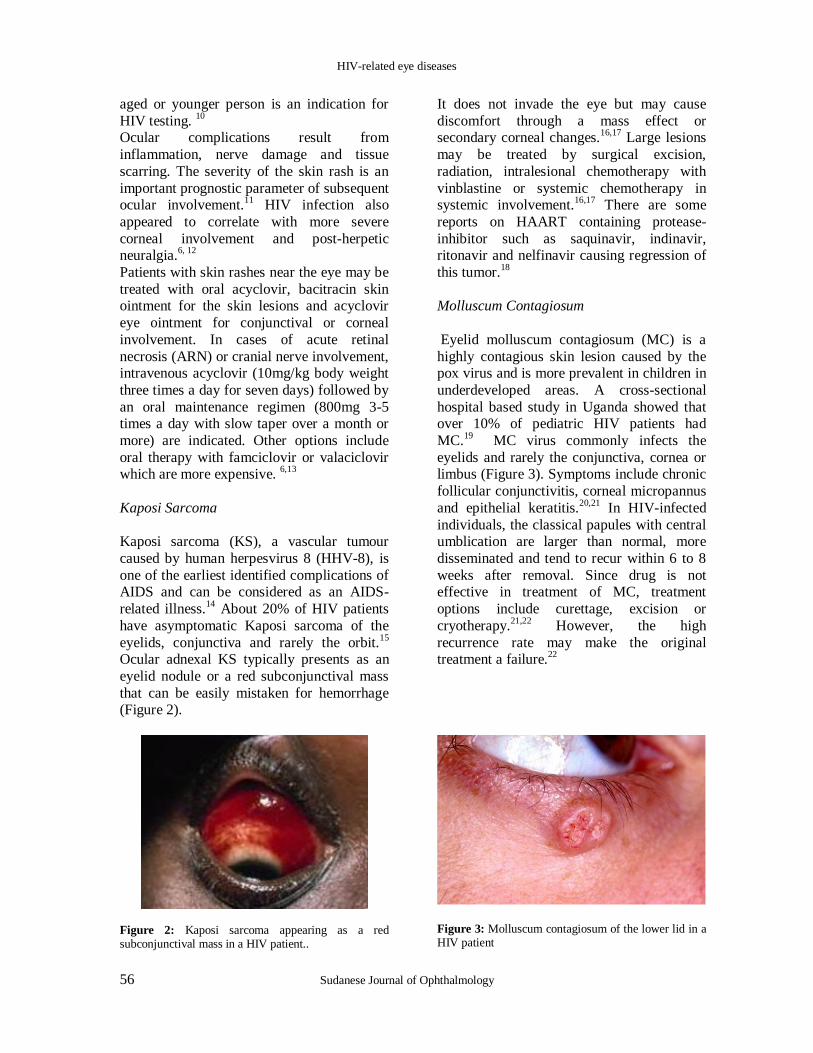
Ocular adnexal KS typically presents as an
eyelid nodule or a red subconjunctival mass
that can be easily mistaken for hemorrhage (Figure 2).
Figure 2: Kaposi sarcoma appearing as a red subconjunctival mass in a HIV patient..
It does not invade the eye but may cause
discomfort through a mass effect or secondary corneal changes.
16,17 Large lesions
may be treated by surgical excision,
radiation, intralesional chemotherapy with
vinblastine or systemic chemotherapy in systemic involvement.
16,17 There are some
reports on HAART containing protease-
inhibitor such as saquinavir, indinavir, ritonavir and nelfinavir causing regression of
this tumor.18
Molluscum Contagiosum
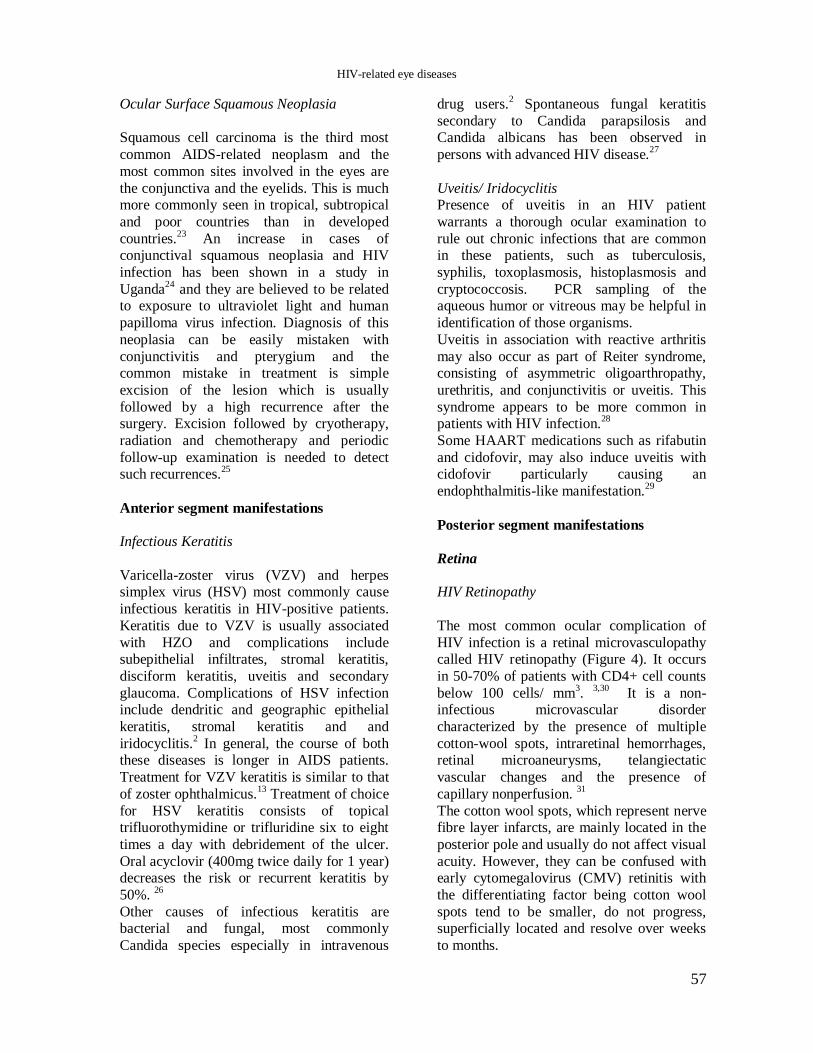
Eyelid molluscum contagiosum (MC) is a
highly contagious skin lesion caused by the pox virus and is more prevalent in children in
underdeveloped areas. A cross-sectional
hospital based study in Uganda showed that over 10% of pediatric HIV patients had
MC.19
MC virus commonly infects the
eyelids and rarely the conjunctiva, cornea or limbus (Figure 3). Symptoms include chronic
follicular conjunctivitis, corneal micropannus
and epithelial keratitis.20,21
In HIV-infected
individuals, the classical papules with central umblication are larger than normal, more
disseminated and tend to recur within 6 to 8
weeks after removal. Since drug is not effective in treatment of MC, treatment
options include curettage, excision or
cryotherapy.21,22
However, the high
recurrence rate may make the original treatment a failure.
22
Figure 3: Molluscum contagiosum of the lower lid in a HIV patient
HIV-related eye diseases
57
Ocular Surface Squamous Neoplasia
Squamous cell carcinoma is the third most
common AIDS-related neoplasm and the
most common sites involved in the eyes are
the conjunctiva and the eyelids. This is much more commonly seen in tropical, subtropical
and poor countries than in developed
countries.23
An increase in cases of conjunctival squamous neoplasia and HIV
infection has been shown in a study in
Uganda24
and they are believed to be related to exposure to ultraviolet light and human
papilloma virus infection. Diagnosis of this
neoplasia can be easily mistaken with
conjunctivitis and pterygium and the common mistake in treatment is simple
excision of the lesion which is usually
followed by a high recurrence after the surgery. Excision followed by cryotherapy,
radiation and chemotherapy and periodic
follow-up examination is needed to detect such recurrences.
25
Anterior segment manifestations
Infectious Keratitis
Varicella-zoster virus (VZV) and herpes simplex virus (HSV) most commonly cause
infectious keratitis in HIV-positive patients.
Keratitis due to VZV is usually associated
with HZO and complications include subepithelial infiltrates, stromal keratitis,
disciform keratitis, uveitis and secondary
glaucoma. Complications of HSV infection include dendritic and geographic epithelial
keratitis, stromal keratitis and and
iridocyclitis.2 In general, the course of both
these diseases is longer in AIDS patients.
Treatment for VZV keratitis is similar to that
of zoster ophthalmicus.13
Treatment of choice
for HSV keratitis consists of topical trifluorothymidine or trifluridine six to eight
times a day with debridement of the ulcer.
Oral acyclovir (400mg twice daily for 1 year) decreases the risk or recurrent keratitis by
50%. 26
Other causes of infectious keratitis are bacterial and fungal, most commonly
Candida species especially in intravenous
drug users.2 Spontaneous fungal keratitis
secondary to Candida parapsilosis and Candida albicans has been observed in
persons with advanced HIV disease.27
Uveitis/ Iridocyclitis Presence of uveitis in an HIV patient
warrants a thorough ocular examination to
rule out chronic infections that are common in these patients, such as tuberculosis,
syphilis, toxoplasmosis, histoplasmosis and
cryptococcosis. PCR sampling of the aqueous humor or vitreous may be helpful in
identification of those organisms.
Uveitis in association with reactive arthritis
may also occur as part of Reiter syndrome, consisting of asymmetric oligoarthropathy,
urethritis, and conjunctivitis or uveitis. This
syndrome appears to be more common in patients with HIV infection.
28
Some HAART medications such as rifabutin
and cidofovir, may also induce uveitis with cidofovir particularly causing an
endophthalmitis-like manifestation.29
Posterior segment manifestations
Retina
HIV Retinopathy
The most common ocular complication of
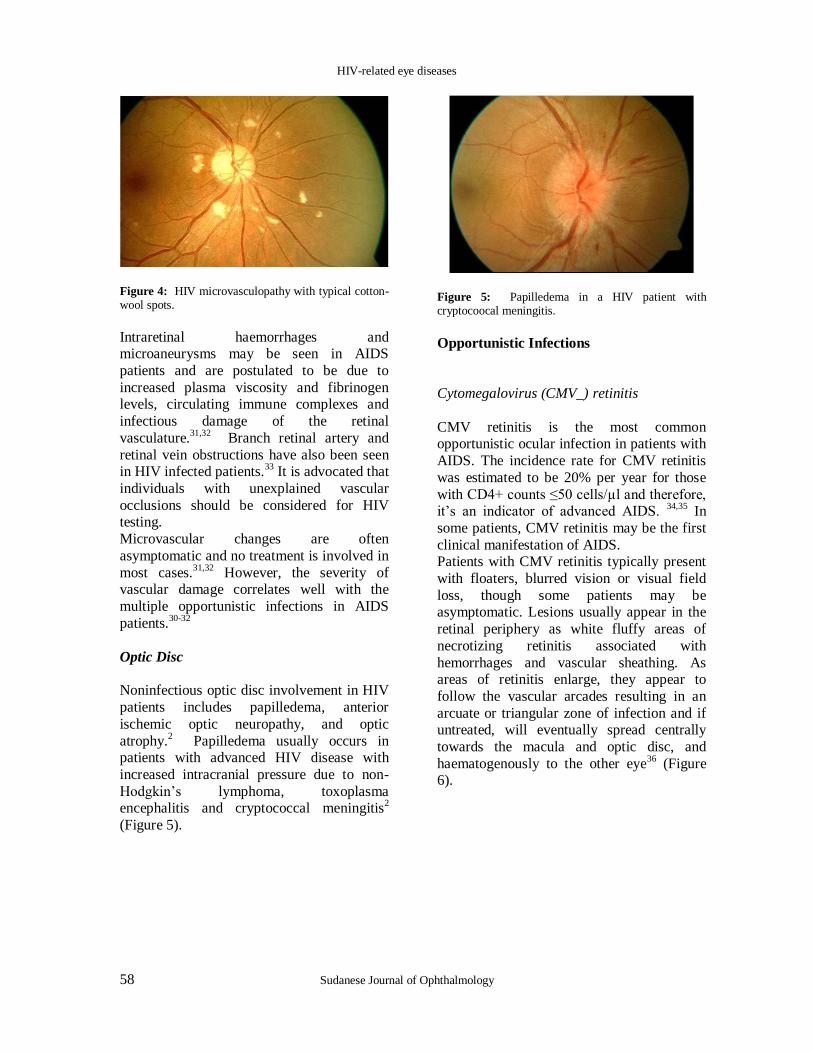
HIV infection is a retinal microvasculopathy called HIV retinopathy (Figure 4). It occurs
in 50-70% of patients with CD4+ cell counts
below 100 cells/ mm3.
3,30 It is a non-
infectious microvascular disorder
characterized by the presence of multiple
cotton-wool spots, intraretinal hemorrhages, retinal microaneurysms, telangiectatic
vascular changes and the presence of
capillary nonperfusion. 31
The cotton wool spots, which represent nerve fibre layer infarcts, are mainly located in the
posterior pole and usually do not affect visual
acuity. However, they can be confused with early cytomegalovirus (CMV) retinitis with
the differentiating factor being cotton wool
spots tend to be smaller, do not progress, superficially located and resolve over weeks
to months.
HIV-related eye diseases
58 Sudanese Journal of Ophthalmology
Figure 4: HIV microvasculopathy with typical cotton-wool spots.
Intraretinal haemorrhages and microaneurysms may be seen in AIDS
patients and are postulated to be due to
increased plasma viscosity and fibrinogen levels, circulating immune complexes and
infectious damage of the retinal
vasculature.31,32
Branch retinal artery and
retinal vein obstructions have also been seen in HIV infected patients.
33 It is advocated that
individuals with unexplained vascular
occlusions should be considered for HIV testing.
Microvascular changes are often
asymptomatic and no treatment is involved in
most cases.31,32
However, the severity of vascular damage correlates well with the
multiple opportunistic infections in AIDS
patients.30-32
Optic Disc
Noninfectious optic disc involvement in HIV
patients includes papilledema, anterior
ischemic optic neuropathy, and optic
atrophy.2 Papilledema usually occurs in
patients with advanced HIV disease with
increased intracranial pressure due to non-
Hodgkin‟s lymphoma, toxoplasma encephalitis and cryptococcal meningitis
2
(Figure 5).
Figure 5: Papilledema in a HIV patient with cryptocoocal meningitis.
Opportunistic Infections
Cytomegalovirus (CMV_) retinitis
CMV retinitis is the most common opportunistic ocular infection in patients with
AIDS. The incidence rate for CMV retinitis
was estimated to be 20% per year for those
with CD4+ counts ≤50 cells/µl and therefore, it‟s an indicator of advanced AIDS.
34,35 In
some patients, CMV retinitis may be the first
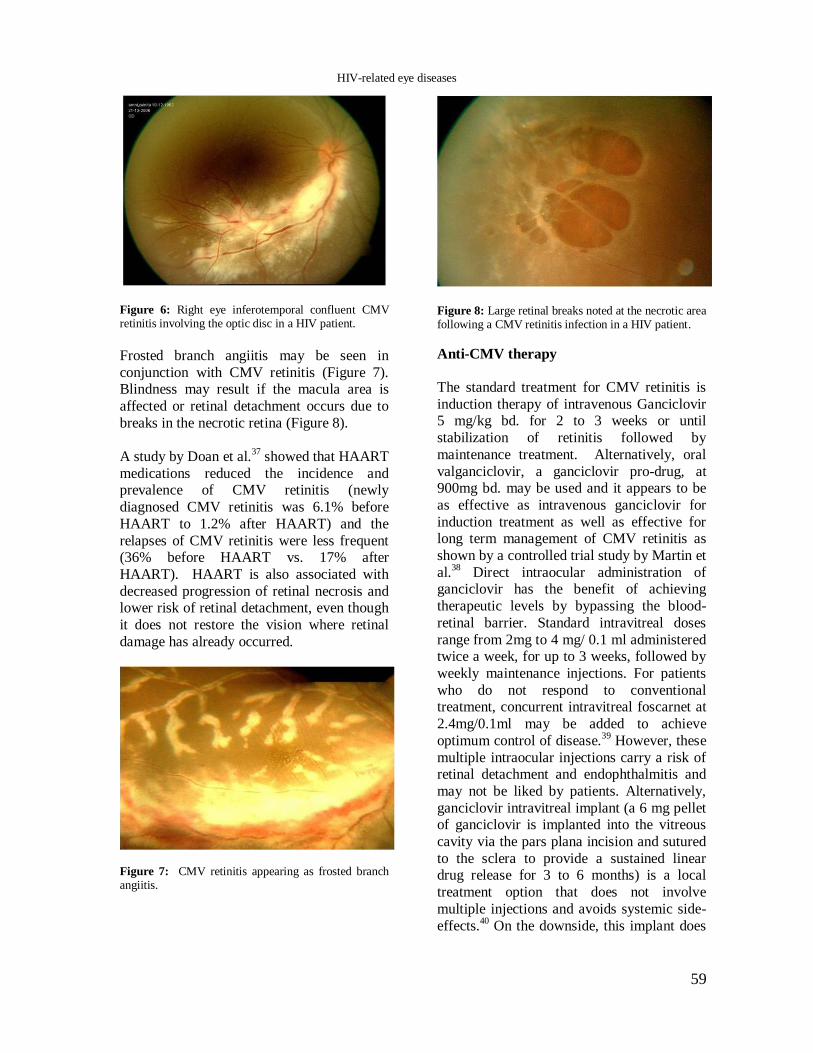
clinical manifestation of AIDS. Patients with CMV retinitis typically present
with floaters, blurred vision or visual field
loss, though some patients may be asymptomatic. Lesions usually appear in the
retinal periphery as white fluffy areas of
necrotizing retinitis associated with
hemorrhages and vascular sheathing. As areas of retinitis enlarge, they appear to
follow the vascular arcades resulting in an
arcuate or triangular zone of infection and if untreated, will eventually spread centrally
towards the macula and optic disc, and
haematogenously to the other eye36
(Figure 6).
HIV-related eye diseases
59
Figure 6: Right eye inferotemporal confluent CMV retinitis involving the optic disc in a HIV patient.
Frosted branch angiitis may be seen in
conjunction with CMV retinitis (Figure 7). Blindness may result if the macula area is
affected or retinal detachment occurs due to
breaks in the necrotic retina (Figure 8).
A study by Doan et al.37
showed that HAART
medications reduced the incidence and prevalence of CMV retinitis (newly
diagnosed CMV retinitis was 6.1% before
HAART to 1.2% after HAART) and the
relapses of CMV retinitis were less frequent (36% before HAART vs. 17% after
HAART). HAART is also associated with
decreased progression of retinal necrosis and lower risk of retinal detachment, even though
it does not restore the vision where retinal
damage has already occurred.
Figure 7: CMV retinitis appearing as frosted branch angiitis.
Figure 8: Large retinal breaks noted at the necrotic area following a CMV retinitis infection in a HIV patient.
Anti-CMV therapy
The standard treatment for CMV retinitis is
induction therapy of intravenous Ganciclovir 5 mg/kg bd. for 2 to 3 weeks or until
stabilization of retinitis followed by
maintenance treatment. Alternatively, oral
valganciclovir, a ganciclovir pro-drug, at 900mg bd. may be used and it appears to be
as effective as intravenous ganciclovir for
induction treatment as well as effective for long term management of CMV retinitis as
shown by a controlled trial study by Martin et
al.38
Direct intraocular administration of ganciclovir has the benefit of achieving
therapeutic levels by bypassing the blood-
retinal barrier. Standard intravitreal doses
range from 2mg to 4 mg/ 0.1 ml administered twice a week, for up to 3 weeks, followed by
weekly maintenance injections. For patients
who do not respond to conventional treatment, concurrent intravitreal foscarnet at
2.4mg/0.1ml may be added to achieve
optimum control of disease.39
However, these
multiple intraocular injections carry a risk of retinal detachment and endophthalmitis and
may not be liked by patients. Alternatively,
ganciclovir intravitreal implant (a 6 mg pellet of ganciclovir is implanted into the vitreous
cavity via the pars plana incision and sutured
to the sclera to provide a sustained linear drug release for 3 to 6 months) is a local
treatment option that does not involve
multiple injections and avoids systemic side-
effects.40
On the downside, this implant does
HIV-related eye diseases
60 Sudanese Journal of Ophthalmology
not protect the fellow eye or protect against
systemic CMV infections. Other treatment options are intravenous
foscarnet that is associated with renal
insufficiency, and cidofovir therapy that has
ben associated with uveitis and hypotonia and has the potential for nephrotoxicity,
particularly in patients with kidney disease.29
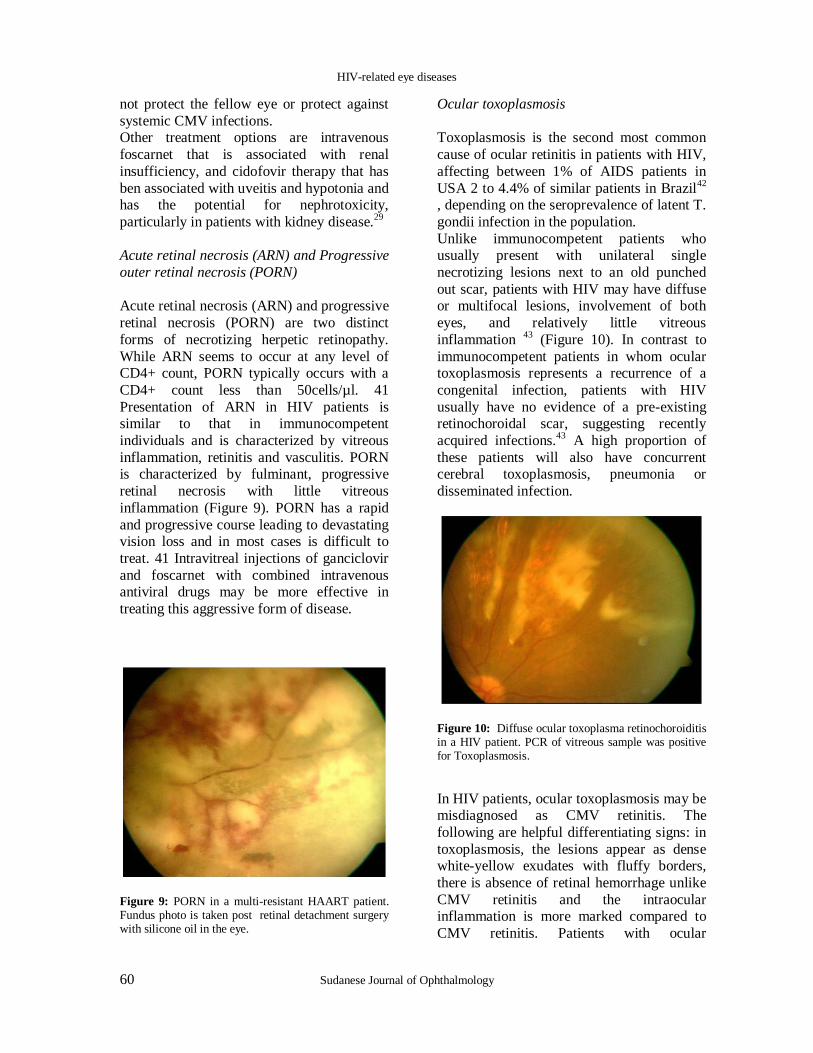
Acute retinal necrosis (ARN) and Progressive
outer retinal necrosis (PORN)
Acute retinal necrosis (ARN) and progressive
retinal necrosis (PORN) are two distinct
forms of necrotizing herpetic retinopathy.
While ARN seems to occur at any level of CD4+ count, PORN typically occurs with a
CD4+ count less than 50cells/µl. 41
Presentation of ARN in HIV patients is similar to that in immunocompetent
individuals and is characterized by vitreous
inflammation, retinitis and vasculitis. PORN is characterized by fulminant, progressive
retinal necrosis with little vitreous
inflammation (Figure 9). PORN has a rapid
and progressive course leading to devastating vision loss and in most cases is difficult to
treat. 41 Intravitreal injections of ganciclovir
and foscarnet with combined intravenous antiviral drugs may be more effective in
treating this aggressive form of disease.
Figure 9: PORN in a multi-resistant HAART patient. Fundus photo is taken post retinal detachment surgery with silicone oil in the eye.
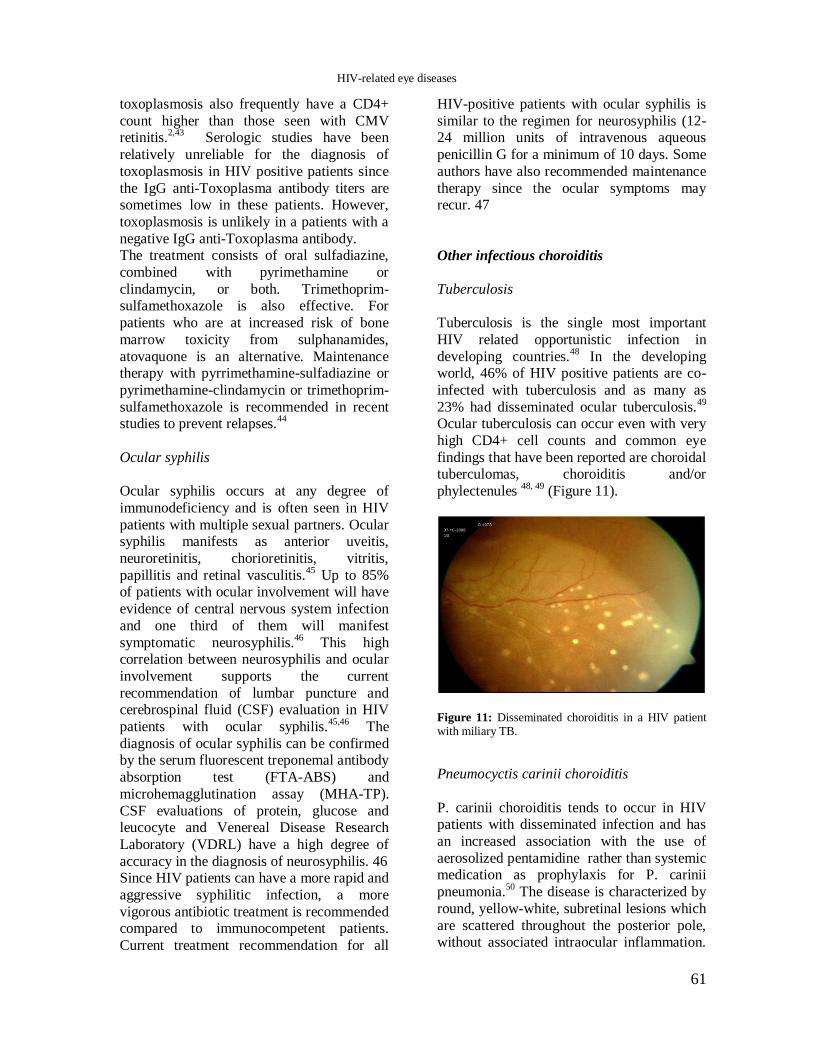
Ocular toxoplasmosis
Toxoplasmosis is the second most common
cause of ocular retinitis in patients with HIV,
affecting between 1% of AIDS patients in
USA 2 to 4.4% of similar patients in Brazil42
, depending on the seroprevalence of latent T.
gondii infection in the population.
Unlike immunocompetent patients who usually present with unilateral single
necrotizing lesions next to an old punched
out scar, patients with HIV may have diffuse or multifocal lesions, involvement of both
eyes, and relatively little vitreous
inflammation 43
(Figure 10). In contrast to
immunocompetent patients in whom ocular toxoplasmosis represents a recurrence of a
congenital infection, patients with HIV
usually have no evidence of a pre-existing retinochoroidal scar, suggesting recently
acquired infections.43
A high proportion of
these patients will also have concurrent cerebral toxoplasmosis, pneumonia or
disseminated infection.
Figure 10: Diffuse ocular toxoplasma retinochoroiditis in a HIV patient. PCR of vitreous sample was positive for Toxoplasmosis.
In HIV patients, ocular toxoplasmosis may be misdiagnosed as CMV retinitis. The
following are helpful differentiating signs: in
toxoplasmosis, the lesions appear as dense white-yellow exudates with fluffy borders,
there is absence of retinal hemorrhage unlike
CMV retinitis and the intraocular inflammation is more marked compared to
CMV retinitis. Patients with ocular
HIV-related eye diseases
61
toxoplasmosis also frequently have a CD4+
count higher than those seen with CMV retinitis.
2,43 Serologic studies have been
relatively unreliable for the diagnosis of
toxoplasmosis in HIV positive patients since
the IgG anti-Toxoplasma antibody titers are sometimes low in these patients. However,
toxoplasmosis is unlikely in a patients with a
negative IgG anti-Toxoplasma antibody. The treatment consists of oral sulfadiazine,
combined with pyrimethamine or
clindamycin, or both. Trimethoprim-sulfamethoxazole is also effective. For
patients who are at increased risk of bone
marrow toxicity from sulphanamides,
atovaquone is an alternative. Maintenance therapy with pyrrimethamine-sulfadiazine or
pyrimethamine-clindamycin or trimethoprim-
sulfamethoxazole is recommended in recent studies to prevent relapses.
44
Ocular syphilis
Ocular syphilis occurs at any degree of
immunodeficiency and is often seen in HIV
patients with multiple sexual partners. Ocular syphilis manifests as anterior uveitis,
neuroretinitis, chorioretinitis, vitritis,
papillitis and retinal vasculitis.45
Up to 85% of patients with ocular involvement will have
evidence of central nervous system infection
and one third of them will manifest
symptomatic neurosyphilis.46
This high correlation between neurosyphilis and ocular
involvement supports the current
recommendation of lumbar puncture and cerebrospinal fluid (CSF) evaluation in HIV
patients with ocular syphilis.45,46
The
diagnosis of ocular syphilis can be confirmed by the serum fluorescent treponemal antibody
absorption test (FTA-ABS) and
microhemagglutination assay (MHA-TP).
CSF evaluations of protein, glucose and leucocyte and Venereal Disease Research
Laboratory (VDRL) have a high degree of
accuracy in the diagnosis of neurosyphilis. 46 Since HIV patients can have a more rapid and
aggressive syphilitic infection, a more
vigorous antibiotic treatment is recommended compared to immunocompetent patients.
Current treatment recommendation for all
HIV-positive patients with ocular syphilis is
similar to the regimen for neurosyphilis (12-24 million units of intravenous aqueous
penicillin G for a minimum of 10 days. Some
authors have also recommended maintenance
therapy since the ocular symptoms may recur. 47
Other infectious choroiditis
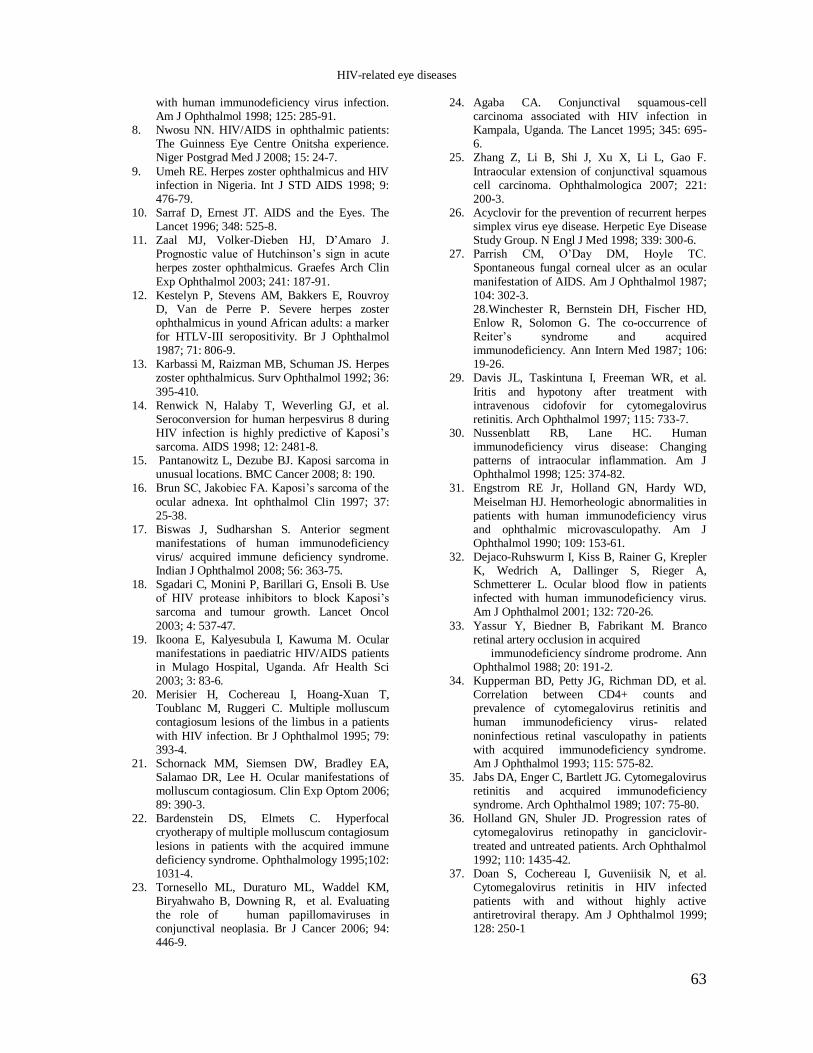
Tuberculosis
Tuberculosis is the single most important
HIV related opportunistic infection in
developing countries.48
In the developing world, 46% of HIV positive patients are co-
infected with tuberculosis and as many as
23% had disseminated ocular tuberculosis.49
Ocular tuberculosis can occur even with very
high CD4+ cell counts and common eye
findings that have been reported are choroidal tuberculomas, choroiditis and/or
phylectenules 48, 49
(Figure 11).
Figure 11: Disseminated choroiditis in a HIV patient with miliary TB.
Pneumocyctis carinii choroiditis
P. carinii choroiditis tends to occur in HIV patients with disseminated infection and has
an increased association with the use of
aerosolized pentamidine rather than systemic medication as prophylaxis for P. carinii
pneumonia.50
The disease is characterized by
round, yellow-white, subretinal lesions which
are scattered throughout the posterior pole, without associated intraocular inflammation.
HIV-related eye diseases

62 Sudanese Journal of Ophthalmology
Patients with P. carinii choroiditis are often
asymptomatic.50
Treatment is the same as that for pneumocystis pneumonia.
Cryptococcus chorioretinitis
Cryptococcosis is the most common fungal
infection occurring in 5-10% of all AIDS
patients. Central nervous system involvement with Cryptococcus neoforman in HIV
patients is relatively common and often
results in meningitis with secondary ocular findings.
2 A Sub-Sahara African study
showed that in Zimbabwe, 45% of meningitis
in adults is cryptococcal, and cryptococcal
meningitis is the third leading cause of death in HIV patients in rural Uganda. In Rwanda,
9% of patients with cryptococcal meningitis
developed visual loss and sixth nerve palsy.51
Cryptococcal infection may present as
papilledema due to increased intracranial
pressure from meningitis, optic atrophy with visual loss and multifocal choroiditis that
appears as multiple, discrete yellowish spots
with accompanying vitritis.52
Candida endophthalmitis
This infection is more likely in HIV patients with intravenous sources of infection
including indwelling catheters. Fungal
lesions appear as fluffy white infiltrates in the
choroid and may break through into the vitreous. It is usually accompanied by dense
vitritis and may form vitreous abscesses.
Treatment is with intravenous amphotericin.10
HAART and the eye
The use of highly active antiretroviral therapy
(HAART), which consists of a combination
of nucleoside reverse transcriptase inhibitors,
HIV protease inhibitors and non nucleoside reverse transcriptase inhibitors has decreased
plasma HIV viral load and increased CD4+ T
lymphocytes counts, improving the immune function of patients with HIV infection. 53,54
However, adverse side effects, drug
resistance and the emergence of immune reconstitution disease are the universal
problems associated with the usage of
HAART in HIV patients. Long-term use of
zidovudine may induce a mutation in the mitochondrial DNA that may account for the
late complication of Leber hereditary optic
neuropathy in patients with family history of
the disease.55
Zidovudine and protease inhibitors used alone can induce endothelial
cell proliferation and dysregulation of
angiogenesis which may make HIV patients more prone to hemangiomas such as KS.
56
Immune recovery uveitis is an inflammatory
condition in AIDS patients receiving HAART who had prior CMV retinitis.
57 It is
characterized by anterior uveitis, vitritis,
optic disc and macula edema. Complications
may include cataract, epiretinal membrane formation and cystoid macula edema. The
exact mechanism of this condition remains
unclear. It is generally believed to be caused by an increase in the immune response of the
host upon starting HAART treatment against
the persistence of CMV antigen in the host‟s eye. There are some reports showing that
protease inhibitors may be associated with
increased cytomegalovirus-specific
lymphocyte proliferation and production of inflammatory cytokines.
58 Another study
showed that the use of cidofovir as anti-CMV
therapy increased the risk of immune recovery uveitis.
59
References
1. UNAIDS/WHO report on the global HIV/AIDS
epidemic. Geneva: World Health Organization, December 2003.
2. Jabs DA. Ocular manifestations of HIV infection. Trans Am Ophthalmol Soc 1995; 93: 623-83.
3. Holland GN, Gottlieb MS, Yee RD, Schanker HM, Pettit TH. Ocular disorders associated with a new severe acquired cellular immunodeficiency syndrome. Am J Ophthalmol 1982; 93: 393-402.
4. Ng WT, Versace P. Ocular association of HIV infection in the era of highly active antiretroviral therapy and the global perspective. Clin Experiment Ophthalmol 2005; 33: 317-29.
5. Mansour AM. Adnexal findings in AIDS. Ophthal Plast Reconstr Surg 1993; 9: 273-79.
6. Looney BD. Herpes zoster ophthalmicus. Clinical Eye and Vision Care 1997; 9: 203-11.
7. Margolis TP, Milner MS, Shama A, Hodge W, Seiff S. Herpes zoster ophthalmicus in patients
HIV-related eye diseases
63
with human immunodeficiency virus infection. Am J Ophthalmol 1998; 125: 285-91.
8. Nwosu NN. HIV/AIDS in ophthalmic patients: The Guinness Eye Centre Onitsha experience. Niger Postgrad Med J 2008; 15: 24-7.
9. Umeh RE. Herpes zoster ophthalmicus and HIV infection in Nigeria. Int J STD AIDS 1998; 9: 476-79.
10. Sarraf D, Ernest JT. AIDS and the Eyes. The Lancet 1996; 348: 525-8.
11. Zaal MJ, Volker-Dieben HJ, D‟Amaro J. Prognostic value of Hutchinson‟s sign in acute herpes zoster ophthalmicus. Graefes Arch Clin
Exp Ophthalmol 2003; 241: 187-91. 12. Kestelyn P, Stevens AM, Bakkers E, Rouvroy
D, Van de Perre P. Severe herpes zoster ophthalmicus in yound African adults: a marker for HTLV-III seropositivity. Br J Ophthalmol 1987; 71: 806-9.
13. Karbassi M, Raizman MB, Schuman JS. Herpes zoster ophthalmicus. Surv Ophthalmol 1992; 36:
395-410. 14. Renwick N, Halaby T, Weverling GJ, et al.
Seroconversion for human herpesvirus 8 during HIV infection is highly predictive of Kaposi‟s sarcoma. AIDS 1998; 12: 2481-8.
15. Pantanowitz L, Dezube BJ. Kaposi sarcoma in unusual locations. BMC Cancer 2008; 8: 190.
16. Brun SC, Jakobiec FA. Kaposi‟s sarcoma of the
ocular adnexa. Int ophthalmol Clin 1997; 37: 25-38.
17. Biswas J, Sudharshan S. Anterior segment manifestations of human immunodeficiency virus/ acquired immune deficiency syndrome. Indian J Ophthalmol 2008; 56: 363-75.
18. Sgadari C, Monini P, Barillari G, Ensoli B. Use of HIV protease inhibitors to block Kaposi‟s sarcoma and tumour growth. Lancet Oncol
2003; 4: 537-47. 19. Ikoona E, Kalyesubula I, Kawuma M. Ocular
manifestations in paediatric HIV/AIDS patients in Mulago Hospital, Uganda. Afr Health Sci 2003; 3: 83-6.
20. Merisier H, Cochereau I, Hoang-Xuan T, Toublanc M, Ruggeri C. Multiple molluscum contagiosum lesions of the limbus in a patients
with HIV infection. Br J Ophthalmol 1995; 79: 393-4.
21. Schornack MM, Siemsen DW, Bradley EA, Salamao DR, Lee H. Ocular manifestations of molluscum contagiosum. Clin Exp Optom 2006; 89: 390-3.
22. Bardenstein DS, Elmets C. Hyperfocal cryotherapy of multiple molluscum contagiosum
lesions in patients with the acquired immune deficiency syndrome. Ophthalmology 1995;102: 1031-4.
23. Tornesello ML, Duraturo ML, Waddel KM, Biryahwaho B, Downing R, et al. Evaluating the role of human papillomaviruses in conjunctival neoplasia. Br J Cancer 2006; 94: 446-9.
24. Agaba CA. Conjunctival squamous-cell carcinoma associated with HIV infection in Kampala, Uganda. The Lancet 1995; 345: 695-6.
25. Zhang Z, Li B, Shi J, Xu X, Li L, Gao F.
Intraocular extension of conjunctival squamous cell carcinoma. Ophthalmologica 2007; 221: 200-3.
26. Acyclovir for the prevention of recurrent herpes simplex virus eye disease. Herpetic Eye Disease Study Group. N Engl J Med 1998; 339: 300-6.
27. Parrish CM, O‟Day DM, Hoyle TC. Spontaneous fungal corneal ulcer as an ocular
manifestation of AIDS. Am J Ophthalmol 1987; 104: 302-3. 28.Winchester R, Bernstein DH, Fischer HD, Enlow R, Solomon G. The co-occurrence of Reiter‟s syndrome and acquired immunodeficiency. Ann Intern Med 1987; 106: 19-26.
29. Davis JL, Taskintuna I, Freeman WR, et al.
Iritis and hypotony after treatment with intravenous cidofovir for cytomegalovirus retinitis. Arch Ophthalmol 1997; 115: 733-7.
30. Nussenblatt RB, Lane HC. Human immunodeficiency virus disease: Changing patterns of intraocular inflammation. Am J Ophthalmol 1998; 125: 374-82.
31. Engstrom RE Jr, Holland GN, Hardy WD,
Meiselman HJ. Hemorheologic abnormalities in patients with human immunodeficiency virus and ophthalmic microvasculopathy. Am J Ophthalmol 1990; 109: 153-61.
32. Dejaco-Ruhswurm I, Kiss B, Rainer G, Krepler K, Wedrich A, Dallinger S, Rieger A, Schmetterer L. Ocular blood flow in patients infected with human immunodeficiency virus. Am J Ophthalmol 2001; 132: 720-26.
33. Yassur Y, Biedner B, Fabrikant M. Branco retinal artery occlusion in acquired immunodeficiency síndrome prodrome. Ann Ophthalmol 1988; 20: 191-2.
34. Kupperman BD, Petty JG, Richman DD, et al. Correlation between CD4+ counts and prevalence of cytomegalovirus retinitis and human immunodeficiency virus- related
noninfectious retinal vasculopathy in patients with acquired immunodeficiency syndrome. Am J Ophthalmol 1993; 115: 575-82.
35. Jabs DA, Enger C, Bartlett JG. Cytomegalovirus retinitis and acquired immunodeficiency syndrome. Arch Ophthalmol 1989; 107: 75-80.
36. Holland GN, Shuler JD. Progression rates of cytomegalovirus retinopathy in ganciclovir-
treated and untreated patients. Arch Ophthalmol 1992; 110: 1435-42.
37. Doan S, Cochereau I, Guveniisik N, et al. Cytomegalovirus retinitis in HIV infected patients with and without highly active antiretroviral therapy. Am J Ophthalmol 1999; 128: 250-1
HIV-related eye diseases
64 Sudanese Journal of Ophthalmology
38. Martin DF, Sierra-Madero J, Walmsley S, et al. A controlled trial of valganciclovir as induction therapy for cytomegalovirus retinitis. N Engl J Med 2002; 346: 1119-26.
39. Velez G, Roy CE, Whitcup SM, et al. High-dose
Intravitreal ganciclovir and foscarnet for cytomegalovirus retinitis. Am J Ophthalmol 2001; 131: 396-7.
40. Kunou N, Ogura Y, Yasukawa T,et al. Long-term sustained release of ganciclovir from biodegradable scleral implant for the treatment of cytomegalovirus retinitis. J Control Release 2000; 68: 263-71.
41. Yin PD, Kurup SK, Fischer SH, et al. Progressive outer retinal necrosis in the era of highly active antiretroviral therapy: successful management with Intravitreal injections and monitoring with quantitative PCR. J Clin Virol 2007; 38: 254-9.
42. Matos KT, Santos MC, Muccioli C. Ocular manifestations in HIV infected patients
attending the department of ophthalmology of Universidade Federal de Sao Paolo. Rev Assoc Med Bras 1999; 45: 323-6.
43. Holland GN, Engstrom RE, Jr, Glasgow BJ, et al. Ocular toxoplasmosis in patients with the acquired immunodeficiency syndrome. Am J Ophthalmol 1988; 106: 653-67.
44. Moraes HV. Ocular manifestations of
HIV/AIDS. Curr Opin Ophthalmol 2002; 13: 397-403.
45. Margo CE, Hamed LM. Ocular syphilis. Surv Ophthalmol 1992; 37: 203-20.
46. Feraru ER, Aronow HA, Lipton RB. Neurosyphilis in AIDS patients: initial CSF VDRL may be negative. Neurology 1990; 40: 541-3.
47. Browning DJ. Posterior segment manifestations
of active ocular syphilis, their response to a neurosyphilis regimen of penicillin therapy, and the influence of human immunodeficiency virus status on response. Ophthalmology 2000; 107: 2015-23.
48. Havlir DV, Barnes PF. Tuberculosis in patients with human immunodeficiency virus infection. New England J Med 1999; 340: 367-73.
49. DeCock KM, Soro B, Lucas SB. Tuberculosis and HIV infection in sub-Saharan Africa. J Amer Med Assoc 1992; 268: 1581-7.
50. Dugel PU, Rao NA, Forster DJ,et al. Pneumocystis carinii choroiditis after long-term aerosolized pentamidine therapy. Am J Ophthalmol 1990; 110: 113-7.
51. Nikomazana O, Tshitswana D. Ocular
complications of HIV infection in sub-Sahara Africa. Curr HIV/ AIDS Rep 2008; 5: 120-5.
52. Andreola C, Ribeiro MP, de Carli CR, Gouvea AL, Curi AL. Multifocal choroiditis in disseminated Crptococcus neoformans infection. Am J Ophthalmol 2006; 142: 346-8.
53. Collier AC, Coombs RW, Schoenfeld DA, et al. Treatment of human immunodeficiency virus
infection with saquinavir, zidovudine, and zalcitabine: AIDS Clinical Trials Group. N Engl J Med 1996; 334: 1011-7.
54. Hammer SM, Squires KE, Hughes MD, et al. A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency virus infection and CD4 cell counts of 200 per cubic millimeter or less: AIDS
Clinical Trial Group 320 Study Team. N Engl J Med 1997; 337: 725-33.
55. Shaikh S, Ta C, Basham AA, Mansour S. Leber hereditary optic neuropathy associated with antiretroviral therapy for human immunodeficiency virus infection. Am J Ophthalmol 2001; 131: 143-5.
56. Di Simone N, De Santis M, Tamburrini E, Di
Nicuolo F, Lucia MB, Riccardi P, D‟Ippolito S, Cauda R, Caruso A. Effects of antiretroviral therapy on tube-like network formation of human endotelial cells. Biol Pharm Bull 2007; 30: 982-4.
57. Robinson MR, Csaky KG, Lee SS, et al. Fibrovascular changes misdiagnosed as cytomegalovirus retinitis reactivation in a patient with immune recovery. Clin Infect Dis
2004; 38: 139-41. 58. Song MK, Azen SP, Buley A, et al. Effect of
anti-cytomegalovirus therapy on the incidence of immune recovery uveitis in AIDS patients with healed cytomegalovirus retinitis. Am J Ophthalmol 2003; 136: 696-702.
59. Martinez de la Casa JM, Matilla Rodero M, Castillo A, Gracia Feijoo J, Gracia Sanchez J.
Ocular complications after treatment with intravenous cidofovir for cytomegalovirus retinitis. Arch Soc Esp Oftalmol 2001; 76: 213-20.
HIV-related eye diseases
65
ORIGINAL ARTICLE
Sudan test (ST), a design of simple reading chart in
Arabic language with predicted magnification for low
vision
Atif B. Mohamed Ali1, Mohamed Elhassan A. Elawad
1, Elhadi A. Elsheikh
2
1Faculty of Optometry, Alneelain Univeristy, Khartoum, Sudan 2Ophthalmology department, Faculty of Medicine, University of Khartoum, Sudan
Correspondence to: Dr. Atif Babikir, Faculty of optometry; University of Alneelain, P.O 12702, Khartoum, Sudan. E-mail: atfbm@ yahoo.com. Tel: +249911371556.
Abstract AIMS: To assess near vision for subjects with low vision and to provide a quick method for
predicting magnification. MATERIAL AND METHODS: A reading test chart in Arabic language
using continuous meaningful text was designed for assessing low vision subjects. The Sudan test
(ST) uses fifteen paragraphs with 2 or 3 lines of related words in each paragraph. The font print size (horizontal case of word or font-thickness) decreases in a log MAR progression denominated
(ST.170 the largest size to ST.30 the smallest size) which equivalent to (15 M and 0.63 M) of meter
system. The reading ability at standard distances was taken to measure the resolution of acuity with ST and Bailey-Lovie near vision reading chart in 30 university subjects. RESULTS: There was
significant correlation in reading acuity between ST and Bailey-Lovie near vision reading chart in
each compared size. CONCLUSION: ST offers a reading acuity measurement for low vision Arabic
readers at 25 cm distance and quick calculated magnification for common reading.
Keywords: Arabic font, chart, low vision.
INTRODUCTION
There is a strong advocacy in favor of a geometrical progression of letter sizes used in
vision testing. Since Snellen′s original test,
which has been found to be close to a regular geometrical progression (a mathematical
series in which each number bears a constant
ratio to the previous one) this ratio is about 6√10 or a multiplier of 1.468. Bennett
1
pointed out, a constant ratio of 10√10 or
(1.2589 multiplier or 0.1 log unit) was
suggested as a geometrical progression of
letter size. This progression was chosen by
the Australian optometrists Bailey and Lovie2
to express visual acuity in terms of the
logarithm of the angular limb width (in min
of arc) of the smallest letters recognized at 6m (meter). This notation was termed log
MAR (minimum angle of resolution).
Relative magnification: Magnification is the ratio of the size of the image (formed by lens
system) to the size of the original object. This
ratio can be quantified by comparing the
transverse height of the image to that of the

66 Sudanese Journal of Ophthalmology
original object. The type known as relative
magnification compares the size of the retinal image produced by the magnifier to the
retinal image size produced by the object,
when viewed at a standard distance without
the magnifier. Most of manufacturers assume a reference distance of 25cm (or 4D) for
calculation of the magnification value given
for their instruments; this value is equivalent to M=F/4 (M is the magnification and F is the
power of the lens). Specifically, relative
magnification can be used to predict the magnification required, and it is assumed to
be equal to the actual magnification only
when certain conditions are met; (a) the
patient is emmetropic or corrected for any ametropia, (b) the object is in the anterior
focal plane of the magnifier (image formed at
infinity), and (c) the reference object size (with which the magnified image is
compared) corresponds to a distance of
25cm.3
However, magnification required can be defined as the ratio of the present acuity
level over desired acuity level (enlargement
ratio) or letter size can read over letter size
wants to read. For this to be valid, both acuities must be referenced to the same
distance.4
MATERIAL AND METHODS
The chart described here is based on a
geometric progression of sizes and aimed to provide the clinicians with text for testing
near vision reading and the predicted
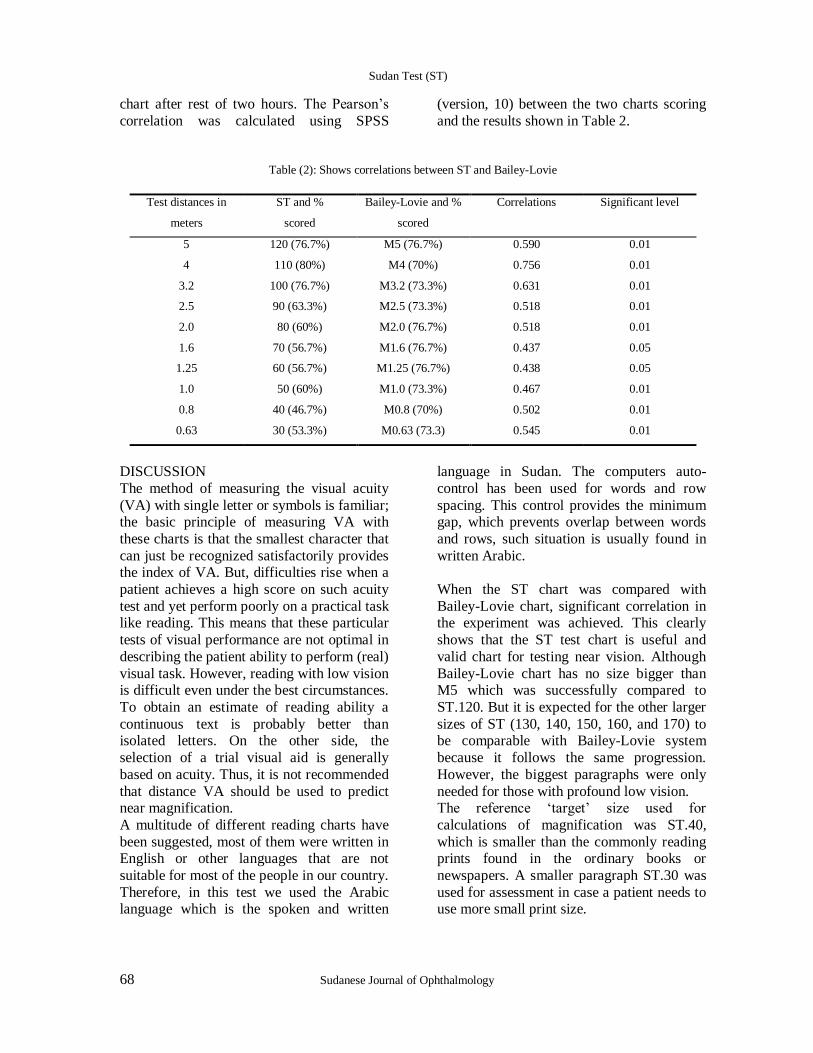
magnification for low vision persons. An example of this chart is shown in Figure 1. It
has the following design features.
Legibility: The text passages selected closely
resemble „normal every day reading‟ and
have simple linguistic content of continuous
paragraphs used from the common Arabic language.
Font-thickness: This term used to indicate the size (in mm) of the tool by which we can
write the Arabic words for example, tip of
pen (or the Nip size used in old writing of classical Arabic). For Latin alphabets the
height of a lower case letter such as “x” or
“o” should be used for measurement of visual
angle. For non-Latin alphabets the height of common, well known character should be
used. However, most of Arabic letters when
used for writing a word their shapes and
dimensions will change according to letter position in the word. Therefore in this design
the reference of calculation were based on the
measurement of font-thickness of words rather than height of letters. The
measurement reference was taken from any
part of the word that lies horizontally in the line. In other words, any part of the word
above or below the horizontal line excluded
from the measurement.
Font-thickness hypothesis: In design of this
test the font-thickness of the Arabic word
was assumed to be equal to one third (⅓) the height of the lower case of Latin alphabet in
each equivalent size.
Calculation of font-thickness: In the standard
Snellen chart letter height 8.73 mm seen at 6
m were defined 6/6 or equal to 0.0 log MAR,
and each gap of that letter subtend 1 min of arc 1. Consequently the height of a letter in a
standard distance 25 cm, which will be (0.25
X 8.73/6), equal to 0.36 mm. Therefore, from the font-thickness hypothesis the expected
font-thickness of word equivalent to (6/6) or
0.0 log MAR is equal to ⅓ X 0.36= 0.12 mm.
Font-thickness progression: The progression
of font-thickness used in this chart has a
constant ratio 10√10 and each step (paragraph) equal to exact multiplication
factor of 1.2589. Thus, the successive
increase of font size has a thickness 1.2589 times greater than that of the preceding size .
The first two decimal digits were written
without approximation (Table 1).
Printers′ type: The size of prints′ type was
selected carefully from the computer to be as
far as possible equal to the font-thickness calculated for each paragraph. A transparent
ruler and closed circuit television "CCTV"
were used to facilitate measure the font-thickness size.
Sudan Test (ST)
67
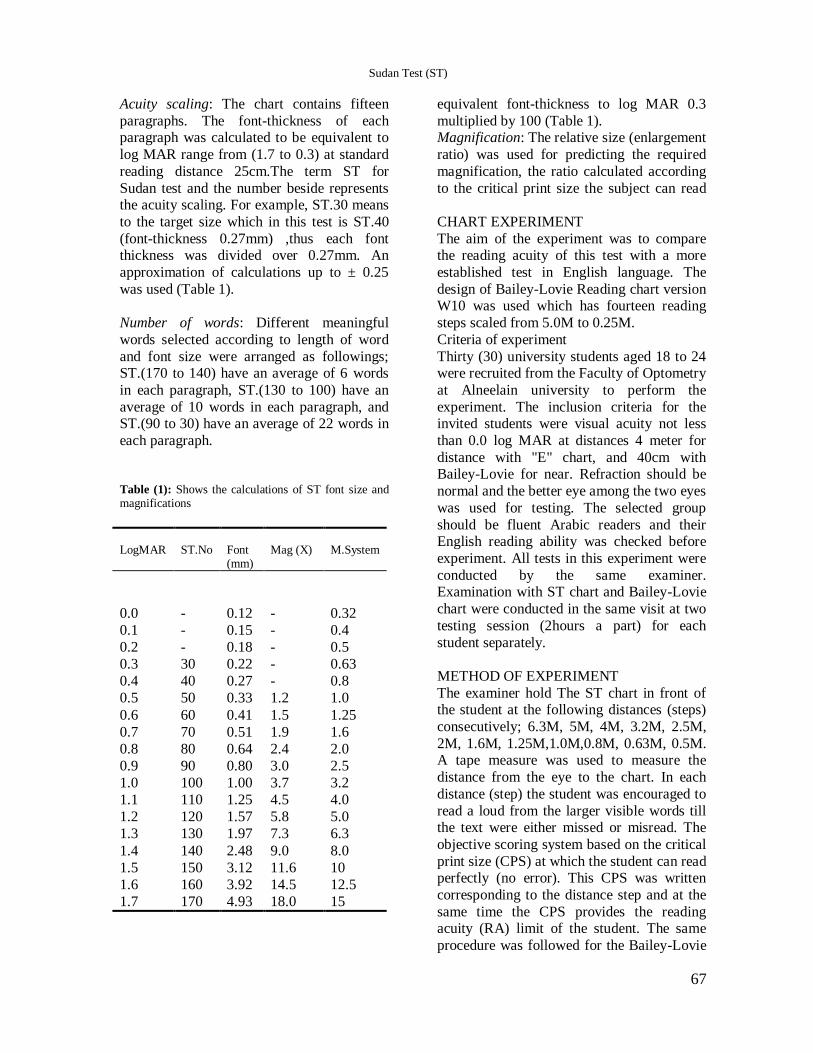
Acuity scaling: The chart contains fifteen
paragraphs. The font-thickness of each paragraph was calculated to be equivalent to
log MAR range from (1.7 to 0.3) at standard
reading distance 25cm.The term ST for
Sudan test and the number beside represents the acuity scaling. For example, ST.30 means
equivalent font-thickness to log MAR 0.3
multiplied by 100 (Table 1). Magnification: The relative size (enlargement
ratio) was used for predicting the required
magnification, the ratio calculated according
to the critical print size the subject can read
to the target size which in this test is ST.40
(font-thickness 0.27mm) ,thus each font thickness was divided over 0.27mm. An
approximation of calculations up to ± 0.25
was used (Table 1).
Number of words: Different meaningful
words selected according to length of word
and font size were arranged as followings; ST.(170 to 140) have an average of 6 words
in each paragraph, ST.(130 to 100) have an
average of 10 words in each paragraph, and ST.(90 to 30) have an average of 22 words in
each paragraph.
Table (1): Shows the calculations of ST font size and magnifications
M.System
Mag (X)
Font (mm)
ST.No
LogMAR
0.32
-
0.12
-
0.0
0.4 - 0.15 - 0.1
0.5 - 0.18 - 0.2
0.63 - 0.22 30 0.3
0.8 - 0.27 40 0.4
1.0 1.2 0.33 50 0.5
1.25 1.5 0.41 60 0.6
1.6 1.9 0.51 70 0.7
2.0 2.4 0.64 80 0.8
2.5 3.0 0.80 90 0.9
3.2 3.7 1.00 100 1.0
4.0 4.5 1.25 110 1.1
5.0 5.8 1.57 120 1.2
6.3 7.3 1.97 130 1.3
8.0 9.0 2.48 140 1.4
10 11.6 3.12 150 1.5
12.5 14.5 3.92 160 1.6
15 18.0 4.93 170 1.7
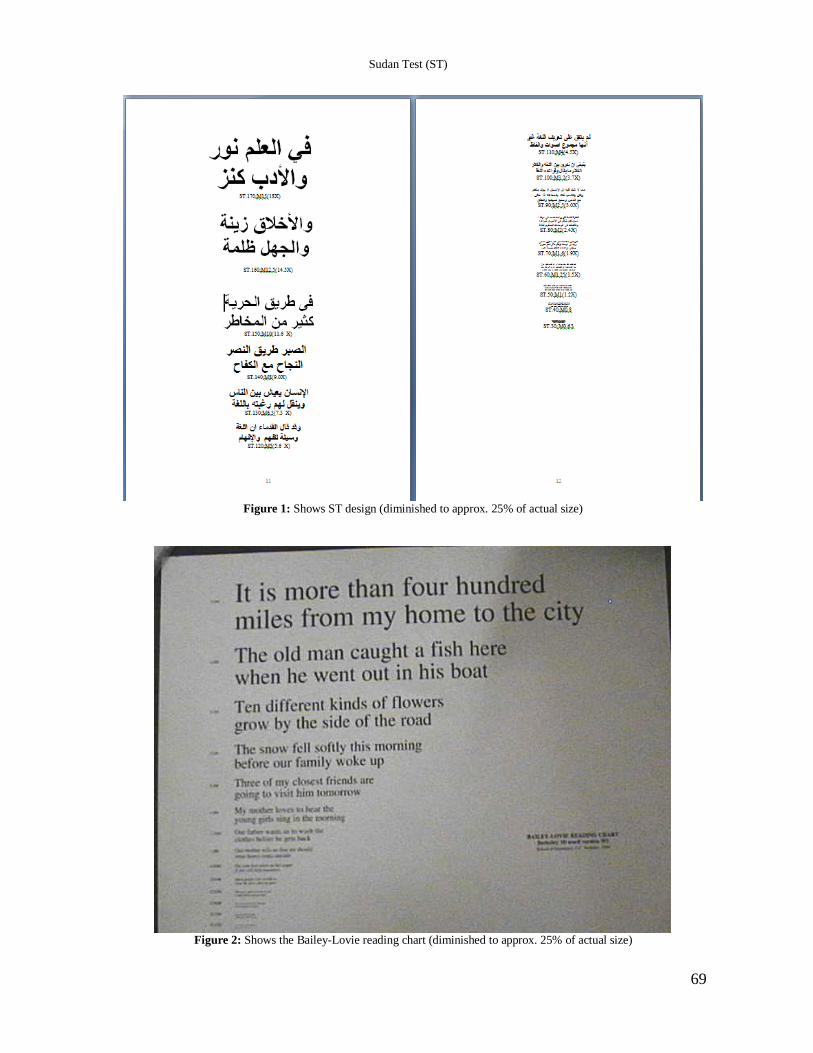
CHART EXPERIMENT
The aim of the experiment was to compare the reading acuity of this test with a more
established test in English language. The
design of Bailey-Lovie Reading chart version W10 was used which has fourteen reading
steps scaled from 5.0M to 0.25M.
Criteria of experiment
Thirty (30) university students aged 18 to 24 were recruited from the Faculty of Optometry
at Alneelain university to perform the
experiment. The inclusion criteria for the invited students were visual acuity not less
than 0.0 log MAR at distances 4 meter for
distance with "E" chart, and 40cm with Bailey-Lovie for near. Refraction should be
normal and the better eye among the two eyes
was used for testing. The selected group
should be fluent Arabic readers and their English reading ability was checked before
experiment. All tests in this experiment were
conducted by the same examiner. Examination with ST chart and Bailey-Lovie
chart were conducted in the same visit at two
testing session (2hours a part) for each
student separately.
METHOD OF EXPERIMENT
The examiner hold The ST chart in front of the student at the following distances (steps)
consecutively; 6.3M, 5M, 4M, 3.2M, 2.5M,
2M, 1.6M, 1.25M,1.0M,0.8M, 0.63M, 0.5M. A tape measure was used to measure the
distance from the eye to the chart. In each
distance (step) the student was encouraged to
read a loud from the larger visible words till the text were either missed or misread. The
objective scoring system based on the critical
print size (CPS) at which the student can read perfectly (no error). This CPS was written
corresponding to the distance step and at the
same time the CPS provides the reading acuity (RA) limit of the student. The same
procedure was followed for the Bailey-Lovie
Sudan Test (ST)
68 Sudanese Journal of Ophthalmology
chart after rest of two hours. The Pearson‟s
correlation was calculated using SPSS
(version, 10) between the two charts scoring
and the results shown in Table 2.
Table (2): Shows correlations between ST and Bailey-Lovie
Significant level Correlations Bailey-Lovie and %
scored
ST and %
scored
Test distances in
meters
0.01 0.590 M5 (76.7%) 120 (76.7%) 5
0.01 0.756 M4 (70%) 110 (80%) 4
0.01 0.631 M3.2 (73.3%) 100 (76.7%) 3.2
0.01 0.518 M2.5 (73.3%) 90 (63.3%) 2.5
0.01 0.518 M2.0 (76.7%) 80 (60%) 2.0
0.05 0.437 M1.6 (76.7%) 70 (56.7%) 1.6
0.05 0.438 M1.25 (76.7%) 60 (56.7%) 1.25
0.01 0.467 M1.0 (73.3%) 50 (60%) 1.0
0.01 0.502 M0.8 (70%) 40 (46.7%) 0.8
0.01 0.545 M0.63 (73.3) 30 (53.3%) 0.63
DISCUSSION
The method of measuring the visual acuity
(VA) with single letter or symbols is familiar; the basic principle of measuring VA with
these charts is that the smallest character that
can just be recognized satisfactorily provides the index of VA. But, difficulties rise when a
patient achieves a high score on such acuity
test and yet perform poorly on a practical task like reading. This means that these particular
tests of visual performance are not optimal in
describing the patient ability to perform (real)
visual task. However, reading with low vision is difficult even under the best circumstances.
To obtain an estimate of reading ability a
continuous text is probably better than isolated letters. On the other side, the
selection of a trial visual aid is generally
based on acuity. Thus, it is not recommended
that distance VA should be used to predict near magnification.
A multitude of different reading charts have
been suggested, most of them were written in English or other languages that are not
suitable for most of the people in our country.
Therefore, in this test we used the Arabic language which is the spoken and written
language in Sudan. The computers auto-
control has been used for words and row
spacing. This control provides the minimum gap, which prevents overlap between words
and rows, such situation is usually found in
written Arabic.
When the ST chart was compared with
Bailey-Lovie chart, significant correlation in the experiment was achieved. This clearly
shows that the ST test chart is useful and
valid chart for testing near vision. Although
Bailey-Lovie chart has no size bigger than M5 which was successfully compared to
ST.120. But it is expected for the other larger
sizes of ST (130, 140, 150, 160, and 170) to be comparable with Bailey-Lovie system
because it follows the same progression.
However, the biggest paragraphs were only
needed for those with profound low vision. The reference „target‟ size used for
calculations of magnification was ST.40,
which is smaller than the commonly reading prints found in the ordinary books or
newspapers. A smaller paragraph ST.30 was
used for assessment in case a patient needs to use more small print size.
Sudan Test (ST)
69
Figure 1: Shows ST design (diminished to approx. 25% of actual size)
Figure 2: Shows the Bailey-Lovie reading chart (diminished to approx. 25% of actual size)
Sudan Test (ST)

70 Sudanese Journal of Ophthalmology
Acknowledgements
The authors would like to acknowledge Professor Ian Bailey the inventor of Bailey-
Lovie chart for his knowledgeable guidance
to perform the experiment. Also we
acknowledge Dr. Christine Dickinson the editor of Ophthalmic and Physiological
Optics for her great advices. Also we
appreciate the encouragement given by Mr. Hassan Minto of Sight Savers international,
and Dr. Kamal Hashim the coordinator of the
National Programme for Prevention of Blindness in Sudan.
References 1. Rabbetts R B. Visual acuity and contrast sensitivity.
In: Bennett and Rabbetts′ Clinical visual optics, 3rd
edn, Butterworth- Heinemann, 2000; pp.20 – 29. 2. Bailey I L, Lovie J E. New design principles for
visual acuity letter charts. Am J Optom 1976; 53: 740 – 45.
3. Woo G C, Mah-Leung A. The term magnification. Clin.Exp.Optom 200); 84: 3: 113 – 19.
4. Rosenthal B P, Cole R G. Visual acuity and the predicted reading add. In: Functional assessment of
low vision, Mosby, London, 1996; pp.28.
Sudan Test (ST)
71
ORIGINAL ARTICLE
Toxic effects of antiglaucoma topical medications on
the conjunctiva – a histological study Mehida Hayet, Moulessehoul Soraya, Tou abdenacer, Ouadah Myriam 1 Biotoxicology laboratory, djillali liabes university, Algeria 2 Anatomo-pathology department, djillali liabes university, Algeria 3 Ophthalmology department, CHU Tlemcen, Algeria
Correspondence to: Mehida Hayet, Biotoxicology laboratory, djillali liabes university, Algeria. Tel:
+213775868249, email: [email protected]
Abstract
AIMS: To evaluate the extent of epithelial conjunctival changes associated with prolonged use of topical
glaucoma medications. MATERIAL AND METHODS: forty eye of glaucomatous patients treated with various
eye drops (Timolol, Trusopt, Pilocarpine and Xalatan) and for different lengths of time were selected and
classified in five groups: the first group received Timolol, second was treated with Timolol and Pilocarpine,
the third one with Timolol and Trusopt, the fourth with Timolol, Trusopt and Pilocarpine, finally the last
group with Xalatan. The Conjunctival inflammation was evaluated with light microscopy.
RESULTS: Examination of the conjunctival biopsies revealed profound changes on the histological
parameters, an inflammatory reaction on the connective fabric with a vascular congestion, oedema and a
leucocytic inflammatory infiltrate, a disappearance of caliciform cells, exulceration of the mucous membrane, abrasion and malpighien metaplasia on the epithelium. The frequency of appearance of these deteriorations
is according to the treatment and to its duration. CONCLUSION: Although the adverse effects of glaucoma
medications on the ocular surface are likely multifactorial. We noted that the use of only one drug, applied
for more than 10 months causes significant modifications concerning the histology of the connective tissue. In
addition, the application of a combined therapy revealed more conjunctival lesions than the mono therapy.
Keywords: Glaucoma; Eye drops; Conjunctiva; Toxic effect; Histology.
INTRODUCTION The chronic glaucoma with open angle poses
a major problem of public health; it is the
second leading cause of blindness in the world.
1 It is defined by the presence of
elevated Intraocular pressure.2 It touches
approximately 1 to 2% of the population
more than 40 years, its incidence increases with the age.
3 Its treatment requires a long
and prolonged therapy by eye medication.4
However the prolonged use of these eye drops can induce histological changes on the
ocular surface.
The local application of the antiglaucoma eye
medications is generally well accepted however various types of conjunctival
reactions can occur.5,6,7
The epithelial barriers
conjunctival and corneal are the principal
ways of entry of these eye medications in the ocular tissues,
8 but the majority of the actives
molecules pass with difficulty through these
barriers because of their hydro solubility. Therefore, wetting agents equipped with
detergent properties are needed to increase
their effectiveness, which also allow the
preservation and the sterility of the eye medications long duration. Prolonged use of
eye medications with preservatives presented
a certain risk to ocular surface,9, 10, 11
such as thickness of sub epithelial collagen of
conjunctiva,12
a chronic subclinical
inflammation as shown by the presence of
immunologic changes and inflammatory infiltrates.
13
In Algeria this is the first study realized in
this field it was undertaken to determine the
72 Sudanese Journal of Ophthalmology
histolocical changes in the conjunctiva in
patients who were treated with different types of antiglaucoma topical medications for
variable period of time.
MATERIAL AND METHODS This study was done in the ophthalmology
department of the CHU Tlemcen and the
CHU of Sidi Bel Abbes (west Algeria) over a period of 36 months.
Conjunctival biopsies were taken from 40
eyes of open angle glaucoma, aged 40 years and above, they were treated with different
types of eye medications for varying period
of time.
All patients who were presented to these departments during the period of study, and
planned for the cataract surgery or glaucoma
surgery was included; Biopsies were taken from the infero-temporal bulbar quadrant
with a biopsy forceps. The biopsies were
divides into 5 groupes according to the type of eye medication used, the first group (13
samples) from the patients treated with
Timolol alone, ( betabloquant); the second
group (7 samples) from patients treated with Timolol –trusopt (betblaoqant and inhibitor
of the carbonic anhydrase) combination, the
third group (05 samples) from patients treated with Timolol - pilocarpine
(betabloquant and myotic) combination the
fourth group (03 samples) from patients
treated with Timolol, Trusopt and Pilocarpine (betabloquant, inhibitor of the carbonic
anhydrase and myotic) combination, and the
fifth (12 samples) from patients treated with Xalatan (prostaglandin) alone. The durations
of treatment varied from 06 months to 18
years. Only two biopsies were taken from healthy
conjunctiva as controls, The specimens were
fixed and carried out according to usual
techniques' of light microscopy14
Hemalun – éosine stain was used in this study.
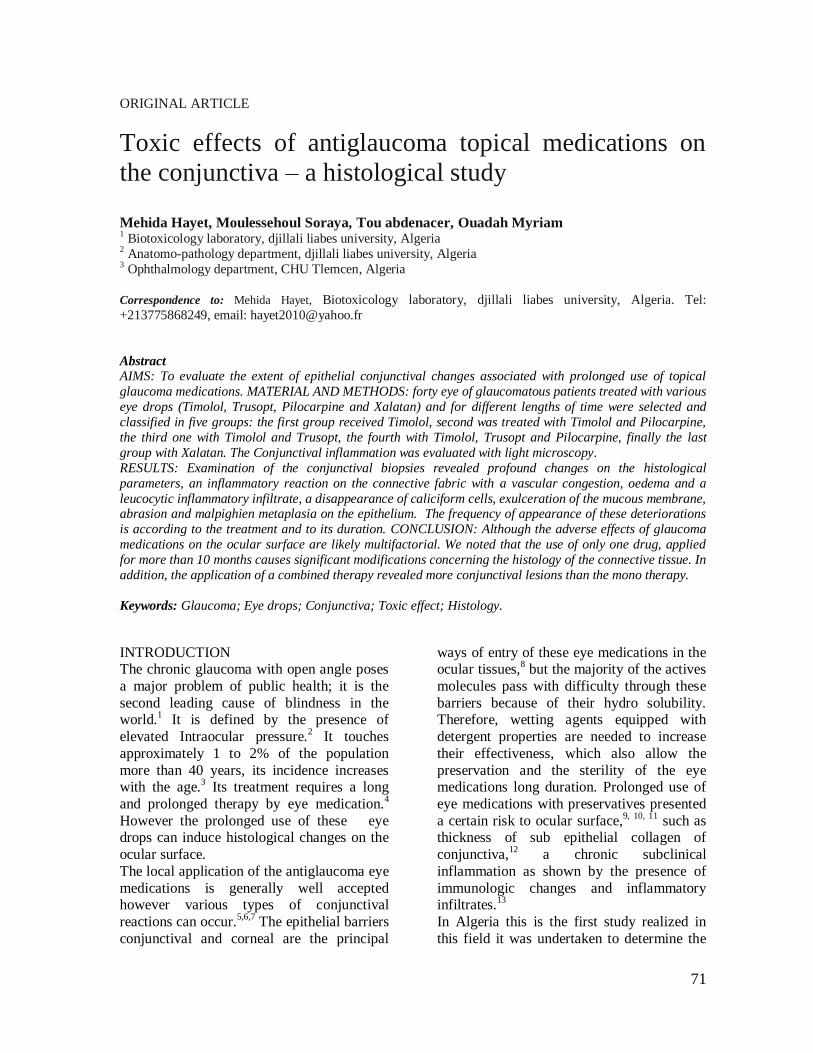
RESULTS: The histological features of healthy
conjunctiva showed a laminated prismatic
epithelium comprising caliciform mucous cells resting on its basal membrane of a
chorion of connective tissue (figure 1).
Figure 1: Histological cut of healthy conjunctiva Bar = 1.5cm = 100μ
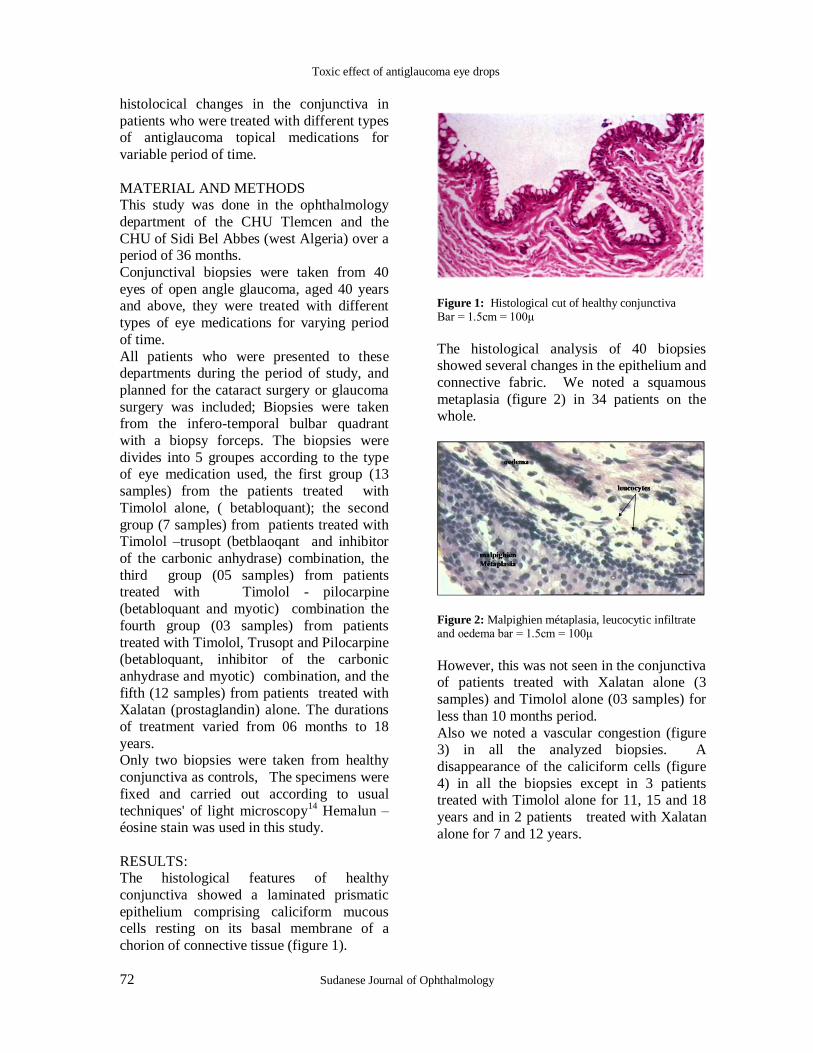
The histological analysis of 40 biopsies showed several changes in the epithelium and
connective fabric. We noted a squamous
metaplasia (figure 2) in 34 patients on the whole.
Figure 2: Malpighien métaplasia, leucocytic infiltrate and oedema bar = 1.5cm = 100μ
However, this was not seen in the conjunctiva of patients treated with Xalatan alone (3
samples) and Timolol alone (03 samples) for
less than 10 months period.
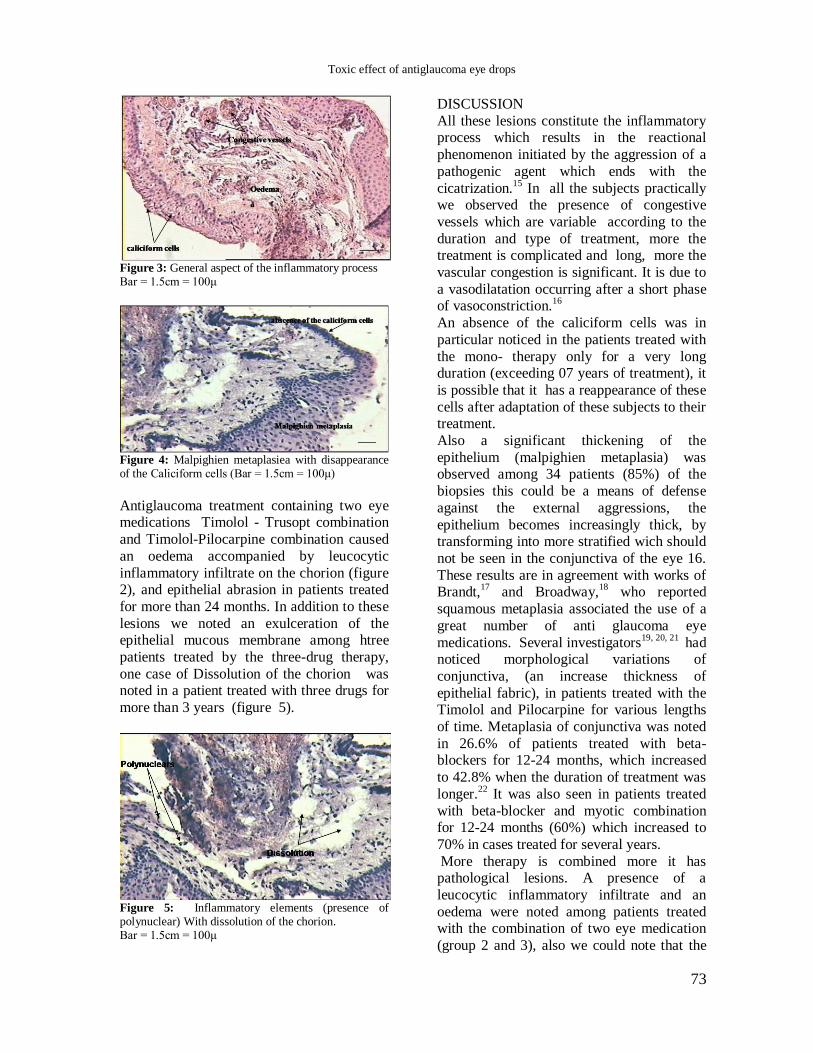
Also we noted a vascular congestion (figure 3) in all the analyzed biopsies. A
disappearance of the caliciform cells (figure
4) in all the biopsies except in 3 patients treated with Timolol alone for 11, 15 and 18
years and in 2 patients treated with Xalatan
alone for 7 and 12 years.
Toxic effect of antiglaucoma eye drops
73
Figure 3: General aspect of the inflammatory process Bar = 1.5cm = 100μ
Figure 4: Malpighien metaplasiea with disappearance of the Caliciform cells (Bar = 1.5cm = 100μ)
Antiglaucoma treatment containing two eye medications Timolol - Trusopt combination
and Timolol-Pilocarpine combination caused
an oedema accompanied by leucocytic
inflammatory infiltrate on the chorion (figure 2), and epithelial abrasion in patients treated
for more than 24 months. In addition to these
lesions we noted an exulceration of the epithelial mucous membrane among htree
patients treated by the three-drug therapy,
one case of Dissolution of the chorion was noted in a patient treated with three drugs for
more than 3 years (figure 5).
Figure 5: Inflammatory elements (presence of polynuclear) With dissolution of the chorion. Bar = 1.5cm = 100μ
DISCUSSION
All these lesions constitute the inflammatory process which results in the reactional
phenomenon initiated by the aggression of a
pathogenic agent which ends with the
cicatrization.15
In all the subjects practically we observed the presence of congestive
vessels which are variable according to the
duration and type of treatment, more the treatment is complicated and long, more the
vascular congestion is significant. It is due to
a vasodilatation occurring after a short phase of vasoconstriction.
16
An absence of the caliciform cells was in
particular noticed in the patients treated with
the mono- therapy only for a very long duration (exceeding 07 years of treatment), it
is possible that it has a reappearance of these
cells after adaptation of these subjects to their treatment.
Also a significant thickening of the
epithelium (malpighien metaplasia) was observed among 34 patients (85%) of the
biopsies this could be a means of defense
against the external aggressions, the
epithelium becomes increasingly thick, by transforming into more stratified wich should
not be seen in the conjunctiva of the eye 16.
These results are in agreement with works of Brandt,
17 and Broadway,
18 who reported
squamous metaplasia associated the use of a
great number of anti glaucoma eye
medications. Several investigators19, 20, 21
had noticed morphological variations of
conjunctiva, (an increase thickness of
epithelial fabric), in patients treated with the Timolol and Pilocarpine for various lengths
of time. Metaplasia of conjunctiva was noted
in 26.6% of patients treated with beta-blockers for 12-24 months, which increased
to 42.8% when the duration of treatment was
longer.22
It was also seen in patients treated
with beta-blocker and myotic combination for 12-24 months (60%) which increased to
70% in cases treated for several years.
More therapy is combined more it has pathological lesions. A presence of a
leucocytic inflammatory infiltrate and an
oedema were noted among patients treated with the combination of two eye medication
(group 2 and 3), also we could note that the
Toxic effect of antiglaucoma eye drops
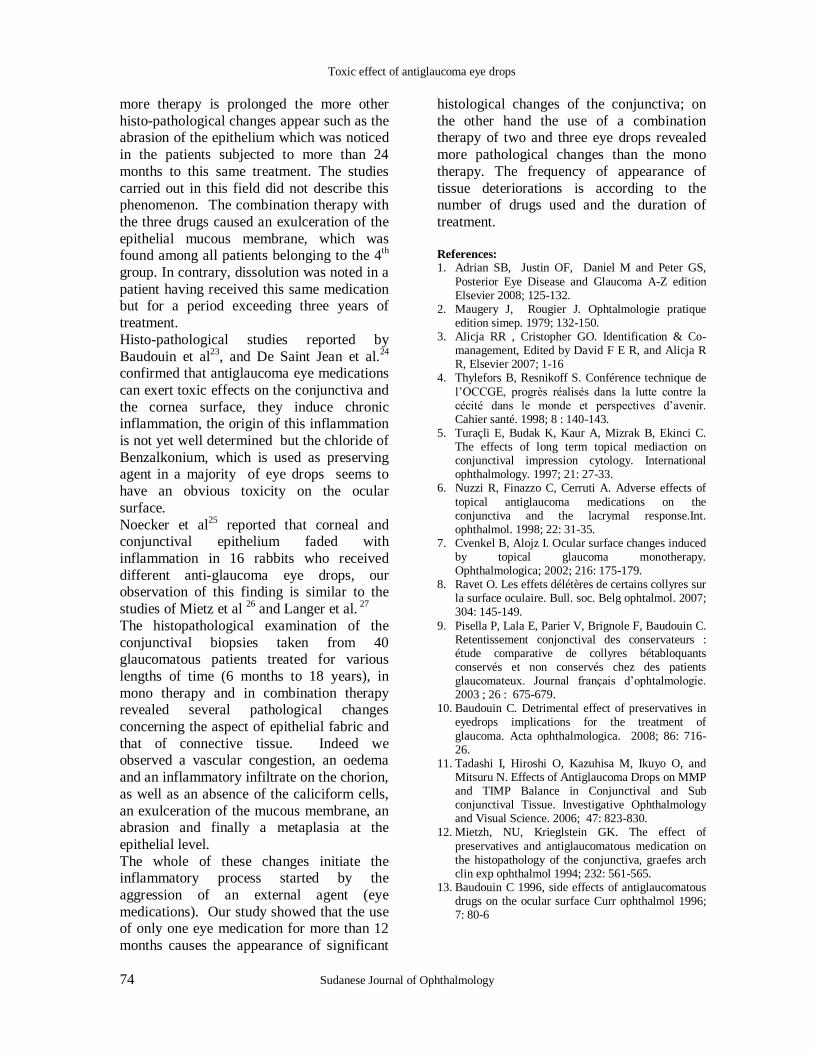
74 Sudanese Journal of Ophthalmology
more therapy is prolonged the more other
histo-pathological changes appear such as the abrasion of the epithelium which was noticed
in the patients subjected to more than 24
months to this same treatment. The studies
carried out in this field did not describe this phenomenon. The combination therapy with
the three drugs caused an exulceration of the
epithelial mucous membrane, which was found among all patients belonging to the 4
th
group. In contrary, dissolution was noted in a
patient having received this same medication but for a period exceeding three years of
treatment.
Histo-pathological studies reported by
Baudouin et al23
, and De Saint Jean et al.24
confirmed that antiglaucoma eye medications
can exert toxic effects on the conjunctiva and
the cornea surface, they induce chronic inflammation, the origin of this inflammation
is not yet well determined but the chloride of
Benzalkonium, which is used as preserving agent in a majority of eye drops seems to
have an obvious toxicity on the ocular
surface.
Noecker et al25
reported that corneal and conjunctival epithelium faded with
inflammation in 16 rabbits who received
different anti-glaucoma eye drops, our observation of this finding is similar to the
studies of Mietz et al 26
and Langer et al. 27
The histopathological examination of the
conjunctival biopsies taken from 40 glaucomatous patients treated for various
lengths of time (6 months to 18 years), in
mono therapy and in combination therapy revealed several pathological changes
concerning the aspect of epithelial fabric and
that of connective tissue. Indeed we observed a vascular congestion, an oedema
and an inflammatory infiltrate on the chorion,
as well as an absence of the caliciform cells,
an exulceration of the mucous membrane, an abrasion and finally a metaplasia at the
epithelial level.
The whole of these changes initiate the inflammatory process started by the
aggression of an external agent (eye
medications). Our study showed that the use of only one eye medication for more than 12
months causes the appearance of significant
histological changes of the conjunctiva; on
the other hand the use of a combination therapy of two and three eye drops revealed
more pathological changes than the mono
therapy. The frequency of appearance of
tissue deteriorations is according to the number of drugs used and the duration of
treatment.
References: 1. Adrian SB, Justin OF, Daniel M and Peter GS,
Posterior Eye Disease and Glaucoma A-Z edition Elsevier 2008; 125-132.
2. Maugery J, Rougier J. Ophtalmologie pratique edition simep. 1979; 132-150.
3. Alicja RR , Cristopher GO. Identification & Co-management, Edited by David F E R, and Alicja R R, Elsevier 2007; 1-16
4. Thylefors B, Resnikoff S. Conférence technique de
l‟OCCGE, progrès réalisés dans la lutte contre la cécité dans le monde et perspectives d‟avenir. Cahier santé. 1998; 8 : 140-143.
5. Turaçli E, Budak K, Kaur A, Mizrak B, Ekinci C. The effects of long term topical mediaction on conjunctival impression cytology. International ophthalmology. 1997; 21: 27-33.
6. Nuzzi R, Finazzo C, Cerruti A. Adverse effects of
topical antiglaucoma medications on the conjunctiva and the lacrymal response.Int. ophthalmol. 1998; 22: 31-35.
7. Cvenkel B, Alojz I. Ocular surface changes induced by topical glaucoma monotherapy. Ophthalmologica; 2002; 216: 175-179.
8. Ravet O. Les effets délétères de certains collyres sur la surface oculaire. Bull. soc. Belg ophtalmol. 2007; 304: 145-149.
9. Pisella P, Lala E, Parier V, Brignole F, Baudouin C. Retentissement conjonctival des conservateurs : étude comparative de collyres bétabloquants conservés et non conservés chez des patients glaucomateux. Journal français d‟ophtalmologie. 2003 ; 26 : 675-679.
10. Baudouin C. Detrimental effect of preservatives in eyedrops implications for the treatment of
glaucoma. Acta ophthalmologica. 2008; 86: 716-26.
11. Tadashi I, Hiroshi O, Kazuhisa M, Ikuyo O, and Mitsuru N. Effects of Antiglaucoma Drops on MMP and TIMP Balance in Conjunctival and Sub conjunctival Tissue. Investigative Ophthalmology and Visual Science. 2006; 47: 823-830.
12. Mietzh, NU, Krieglstein GK. The effect of
preservatives and antiglaucomatous medication on the histopathology of the conjunctiva, graefes arch clin exp ophthalmol 1994; 232: 561-565.
13. Baudouin C 1996, side effects of antiglaucomatous drugs on the ocular surface Curr ophthalmol 1996; 7: 80-6
Toxic effect of antiglaucoma eye drops

75
14. Beverlander G. Eléments d‟histologie. the C.V mostby company – St Louis, Sixième édition. Maloine S.A éditeur Paris 1973; 305-320.
15. Leeson T.S., Leeson R. C. (1980). Histologie. Deuxième édition Masson 1980; 258-269.
16. Hould R. Histologie descriptive. Decarie, éditeur Montréal; Maloine, éditeur Paris 1983 ; 563-588.
17. Brandt JD, Wittpen JR, Katz LJ, Steinmann WN, Spaeth GL. Conjunctival impression cytology in patients with glaucoma long-term topical medication. American Journal of Ophthalmology. 1991; 112: 297-301.
18. Broadway DC, Grierson I, Stürmer J, Hitchings RA.
Reversal of topical antiglaucoma medication effects on the conjunctiva. Archives ophthalmology. 1996; 114: 262-267.
19. Broadway DC, Grierson I, O‟brien C, Hitchings RA. Adverse effects of topical antiglaucoma medication. The conjonctival cell profile. Arch ophthalmol. 1994; 12: 1437-1445.
20. Baun O, Heegaard S, Keesing SV, Prause JU. The
morphology of conjunctiva after long-term topical antiglaucoma treatment. A quantitative analysis. Acta ophthalmologica scandinavica. 1995 ; 73: 242-245.
21. Mietz H, Schlötzer SU, Strassfeld C, Krieglstein GK. Effect of Latanoprost on the histopathology of
conjunctiva. Invest ophthalmol vis sci. 2001; 42: 679-687.
22. Wroblewska E. Squamous métaplasia of bulbar conjunctiva in the course of term topical antiglaucoma thérapy. Klin Oczna 1999; 101: 41-
43. 23. Baudouin C, Ettaiche M, Gastaud P. Experimental
study on corneo conjunctivalside effect of preservative solutions. Ophtalmologie. 1996;10: 376-379.
24. De Saint Jean M, Debbasch C, Brignol F, Rat P, Warnet JM, Baudouin C. Toxicity of preserved and unpreserved antiglaucoma topical drugs in an
invitro model of conjunctival cells. Current eye research. 2000; 20: 85-94.
25. Noeker R, Herrygers L, Anwaruddin R.. Corneal and Conjunctival Changes Caused by Commonly Used Glaucoma Medications. Cornea. 2004; 23: 490-496
26. Mietz H, Niesen U, Krieglstein GK. The effect of preservatives and antiglaucomatous medication
histopathology of the conjunctiva. Graefes Arch Clin Exp Ophthalmol. 1994; 232 :561-565.
27. Langer K, Mutschler E, Lambrecht G, Mayer D, Troschau G, Stieneker F, Evaluation as drug delivery system for ophthalmic applications. International journal of pharmaceutics. 1997; 158: 219-231.
Toxic effect of antiglaucoma eye drops

76 Sudanese Journal of Ophthalmology
ORIGINAL ARTICLE
Laser-assisted in situ keratomileusis (LASIK) surgery in
the management of anisometropic amblyopia in
Sudanese Children
Kamal H Binnawi 1
, Nadir A M Ali2
1Cornea department, Sudan Eye Center, Khartoum, Sudan 2Research department, Sudan eye Center, Khartoum, Sudan
Correspondence to: Dr. Kamal Hashim Binnawi, Cornea department, Sudan Eye Center, Khartoum, Sudan. E-mail: [email protected]. Tel: +249912309628
Abstract
AIM: To evaluate the use of LASIK followed by occlusion therapy for the management of
anisometropic amblyopia in children. MATERIAL AND METHODS: Twenty six children aged between 5 and 15 years with anisometropic ambyopia who failed conventional treatment with
optical correction and occlusion were included in the study. LASIK was done for the selected
patients, and they were followed up for one year after surgery. All patients continued postoperative
amblyopia therapy that included patching of the good eye according to the individual needs and wearing spectacles with the full cycloplegic refractive correction in both eyes. Pearson’s bivariate
correlational analysis was done to study possible associations between the different variables. A p-
value of 0.05 or less was considered statistically significant. RESULTS: Twenty six children were included in this study (16 females and 10 males). The mean age was 9.5 ± 3.5 years. All LASIK
procedures were uneventful under general anesthesia. All children had improved in terms of
UCVA, BCVA and refraction at one-year follow-up examination, and none of these children has
shown myopic regression after 12 months. There was no significant correlation between age/gender and postoperative UCVA, BCVA and Refraction. CONCLUSION: LASIK is a safe and effective
procedure for the treatment of myopic anisometric amblyopia.
Keywords: LASIK; anisometropic amblyopia; high myopia; Sudanese; Children.
INTRODUCTION
Amblyopia is the commonest cause of visual
impairment in children. The prevalence in
childhood is estimated worldwide to be around 1% to 4%. Laser-assisted in situ
keratomileusis (LASIK) is a well established
procedure used for the treatment of myopia, hypermetropia, and astigmatism in adults.
1
Photorefractive keratectomy (PRK) and
LASIK are reported to be beneficial in children with myopic anisometropia
associated with amblyopia.2,3
It has been
reported that visual acuity and binocular
vision outcomes were significantly better in
children who received permanent surgical
correction of anisometropia than in those who
were conventionally treated using contact
lenses.4,5
Davidorf et al6 and Medcedeva et
al7 have also suggested that refractive surgery
is indicated in the treatment of high
hyperopic anisometropic amblyopia in children. The visual outcomes of LASIK in
adolescents with anisometropic amblyopia
were previously studied among Sudanese population.
8 This study illustrates the effect
of LASIK procedure in lowering myopic
anisometropia in children, with one year of
follow-up, to assess its effect in the treatment

77
of high anisometropic amblyopia in 26
Sudanese children.
MATERIAL AND METHODS
Twenty six children aged between 5 and 15
years with anisometropic ambyopia due to myopia underwent LASIK in the amlyopic
eye. The target was decreasing the difference
in refraction (to eliminate anisometropia) or emmetropia of the operated eye and
refractive status of the other eye. Selection of
patients was on the basis of failed conventional amblyopia treatment with
optical correction and occlusion, or
intolerance to contact lenses and spectacles.
Informed consent for the procedure was obtained from the parents.
The patients received a full eye examination
preoperatively, including visual acuity, dilated funduscopy, refraction, corneal
topography and pachymetry. Visual acuity
was measured with Kays pictures or Snellen chart, according to age. Pilocarpine 1% was
instilled preoperatively to prevent distracting
hippos. All children underwent the surgery
under general anaesthetia. The eye was cleaned with 5% povidone iodine solution.
The surgical site was draped.
A flap measuring between 8.5 mm and 9.5 mm was created and hinged superiorly, using
Moria M2 microkeratome. Allegretto
excimer laser (Wavelight) was used. The eye
tracker was engaged during the surgery. The optic zone measured from 5.5–6.0 mm.
Postoperatively, a clear plastic shield was
applied. Postoperative topical medication included Maxitrol eye drops four times daily
for 5 days and Voltaren eye drops four times
daily for one week with Tears Naturale eye drops four times daily and Hypotears gel at
night time for one month. The shield was
advised to be used during sleep for 2 weeks.
All patients continued postoperative amblyopia therapy that included patching of
the good eye according to the individual
needs and wearing spectacles with the full cycloplegic refractive correction in both eyes.
A p-value of 0.05 or less was considered
statistically significant. Pearson‟s bivariate correlational analysis was done to study
possible associations between the different
variables.
RESULTS
Twenty six children were included in this
study. Sixteen were females and 10 were males. The mean age was 9.5 ± 3.5 years. All
children had improved in terms of UCVA,
BCVA and refraction (SE) at one-year follow-up examination (Figure 1, 2 and 3),
and none of these children has shown myopic
regression after 12 months. There was no significant correlation between
age and postoperative UCVA, BCVA and
Refraction (p=0.45, p=0.14, p=0.79
respectively). Similarly, no significant correlation was found between gender and
the above mentioned variables (p=0.48,
p=0.63, p=0.21 respectively). Those who had better BCVA preoperatively had better both
UCVA and BCVA postoperatively (p=0.03,
p<0.001 respectively). Similarly, higher preoperative value of spherical equivalent of
refraction was associated with higher
postoperative value (p<0.001).
None of the patients included in the study had any postoperative complications.
DISCUSSION Amblyopia is a major health problem among
children in Sudan. In a previous study done
among internally displaced people in
Khartoum state, the prevalence of amblyopia was found to be 32.5%, and it was the second
leading cause of blindness.9
The use of refractive surgery in the treatment of refractory cases of anisometropic
amblyopia is not new. Many studies proved
that excimer laser can safely and effectively correct anisometropia and improve
amblyopia in children.2-7 Payssee et al10
in
their case series of 11 children aged 2 to 11
years with refractory anisometropic amblyopia concluded that pediatric PRK can
be safely performed for anisometropia with
similar response of refractive error compared to adults; visual acuity and stereopsis
improved, so PRK may play a role in the
management of anisometropia in selected pediatric patients. On the other hand, Astle et
al11
assessed the refractive, visual acuity and
LASIK in management of anisometropic amblyopia
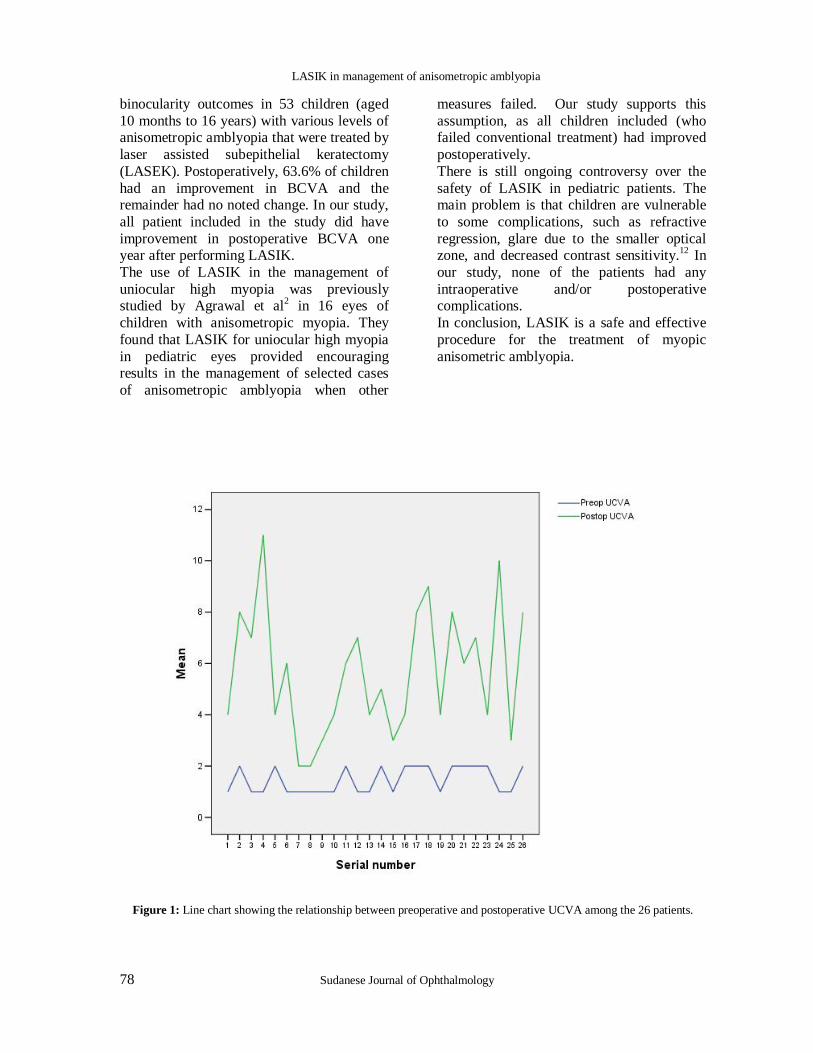
78 Sudanese Journal of Ophthalmology
binocularity outcomes in 53 children (aged
10 months to 16 years) with various levels of anisometropic amblyopia that were treated by
laser assisted subepithelial keratectomy
(LASEK). Postoperatively, 63.6% of children
had an improvement in BCVA and the remainder had no noted change. In our study,
all patient included in the study did have
improvement in postoperative BCVA one year after performing LASIK.
The use of LASIK in the management of
uniocular high myopia was previously studied by Agrawal et al
2 in 16 eyes of
children with anisometropic myopia. They
found that LASIK for uniocular high myopia
in pediatric eyes provided encouraging results in the management of selected cases
of anisometropic amblyopia when other
measures failed. Our study supports this
assumption, as all children included (who failed conventional treatment) had improved
postoperatively.
There is still ongoing controversy over the
safety of LASIK in pediatric patients. The main problem is that children are vulnerable
to some complications, such as refractive
regression, glare due to the smaller optical zone, and decreased contrast sensitivity.
12 In
our study, none of the patients had any
intraoperative and/or postoperative complications.
In conclusion, LASIK is a safe and effective
procedure for the treatment of myopic
anisometric amblyopia.
Figure 1: Line chart showing the relationship between preoperative and postoperative UCVA among the 26 patients.
LASIK in management of anisometropic amblyopia
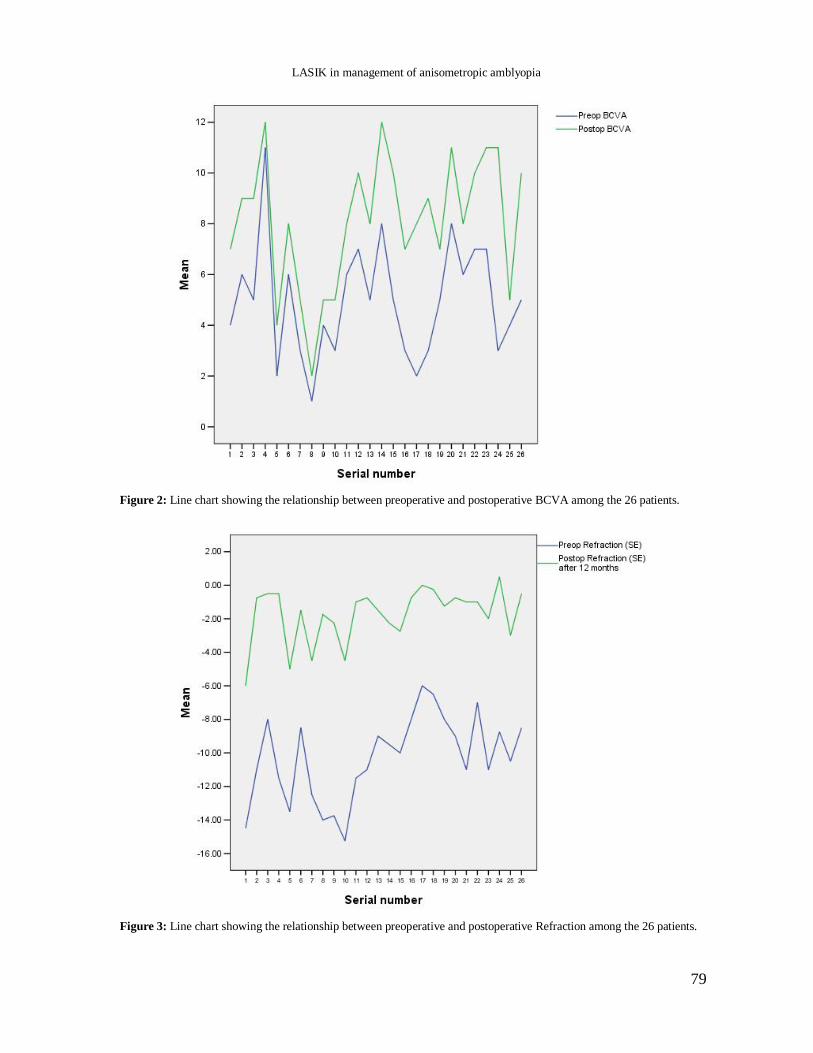
79
Figure 2: Line chart showing the relationship between preoperative and postoperative BCVA among the 26 patients.
Figure 3: Line chart showing the relationship between preoperative and postoperative Refraction among the 26 patients.
LASIK in management of anisometropic amblyopia

80 Sudanese Journal of Ophthalmology
References
1. Carones F, Vigo L, Scandola E. Laser in situ keratomileusis for hyperopia and hyperopic and mixed astigmatism With LADAR Vision Using 7-
to 10-mm ablation diameters. J Refract Surg 2003; 19: 548-554.
2. Agarwal A, Agarwal A, Agarwal T et al. Results of pediatric laser in situ keratomileusis. J Cataract Refract Surg 2000; 26: 684–689
3. Wang H, Yin ZQ, Chen L et al. LASIK for high myopia and high myopic astigmatism in children. Chinese J Strabismus Pediatr Ophthalmol 2003; 11:
229–233. 4. Autrata R, Rehurek J. Laser-assisted subepithelial
keratectomy and photorefractive keratectomy versus conventional treatment of myopic anisometropic amblyopia in children. J Cataract Refract Surg 2004; 30: 74–84.
5. Paysse EA, Coats DK, Hussein MAW, et al. Long-term outcomes of photorefractive keratectomy for
anisometropic amblyopia in children. Ophthalmology 2006; 113: 169–176
6. Davidorf JM. Pediatric refractive surgery. J Cataract Refract Surg 2000; 26: 1567–1568
7. N. I. Medcedeva and V. M. Sheludchenko. Choice of surgical correction method in hypermetropic anisometropia in children. Vestn-Oftalmol 2003; 119: 14-18
8. Binnawi KH, Mursi S, Ali NA. The use of laser in
situ keratomeleuisis in the management of refractory anisometropic amblyopia in Sudanese adolescents. Int J Ophthalmol 2009;1: 21-24
9. Zeidan Z, Hashim K, Muhit MA et al. Prevalence and causes of childhood blindness in camps for displaced persons in Khartoum: results of a household survey. East Mediterr Health J 2007;13:580-585
10. Paysse EA, Hamill MB, Hussein MA et al. Photorefractive keratectomy for pediatric anisometropia: safety and impact on refractive error, visual acuity, and stereopsis. Am J Ophthalmol 2004; 138:70-78.
11. Astle WF, Rahmat J, Ingram AD et al. Laser-assisted subepithelial keratectomy for anisometropic amblyopia in children: outcomes at 1
year. J Cataract Refract Surg 2007; 33:2028-2034. 12. Lin X, Yan X, Wang Z, et al. Long-term efficacy of
excimer laser in situ keratomileusis in the management of children with high anisometropic amblyopia. Chinese Med J 2009;122:813-817.
LASIK in management of anisometropic amblyopia
81
ORIGINAL ARTICLE
Visual Outcome of Phacoemulsification in Al Walidain
Charity Eye Hospital – the first 120 cases. Mustafa Abdu Ali
1, Kamal Hashim Binnawi
2, Nadir Ali Mohamed Ali
3
1Faculty of Optometry and Vision Sciences, University of Alneelain, Khartoum, Sudan 2Al Walidain Charity Eye Hospital, Omdurman, Sudan 3National Programme for Prevention of Blindness, Khartoum, Sudan
Correspondence to: Mustafa Abdu Ali, Faculty of Optometry and Vision Sciences, University of Alneelain, Khartoum, Sudan. Tel: +249122630711, Email: [email protected]
Abstract AIM: To study the visual outcome of phacoemulsification in Walidain Charity Eye hospital, Sudan
MATERIAL AND METHODS: The first 120 consecutive patients who underwent
phacoemulsification in Walidain Charity Eye hospital, Omdurman, Sudan were retrospectively
studied. Demographic data, best-corrected visual acuity (BCVA) preoperatively, keratometry readings, axial length, BCVA postoperatively and postoperative refraction after 6 months were the
main variables studied. Data analysis was done using SPSS version 13.0. Descriptive and bivariate
correlational analyses were the main statistical tests used. The p value < 0.05 was considered as significant. RESULTS: The mean age was 61.1 ± 10.58 years. Females comprised 45 (37.2%) of the
study population. Diabetes mellitus was prevalent in 15 cases (12.5%). Diabetics had worse
postoperative BCVA compared to non-diabetics (p=0.036). Furthermore, diabetic patients had
lesser K1 and K2 compared to non-diabetics (p<0.001. The mean BCVA preoperatively was 5/60 ± 3 lines, compared to a mean BCVA 6 months postoperatively of 6/9 ± 2 lines on Snellen’s chart,
with a mean improvement in BCVA of 5.87 ± 2.78 lines. Postoperative BCVA was 6/9 or better in
56.7%, 6/12 or better in 75.8% and 6/18 or better in 89.2% of the cases.Presence of astigmatism had no significant correlation with postoperative BCVA (p=0.257). The mean spherical equivalent
postoperatively was -0.80 ± 1.50 D. CONCLUSION: It can be anticipated that in the near future,
phacoemulsification will be the main cataract surgical procedure in Sudan in view of the better visual outcome and the patient’s satisfaction compared to the classical extracaspular cataract
surgery.
Keywords: Phacoemulsification; cataract; Visual outcome.
INTRODUCTION Cataract is the leading cause of blindness
world-wide as well as in Sudan. Due to the
environmental features of sub-Saharan Africa and poor Savannah regions, cataract
represents 60% of all cases of blindness in
the region.1 Cataract, with all its types, is
present in all regions of Sudan. The total number of cataract surgeries in year 2001
was 28,500 nation-wide. However, Only 55%
of those had intraocular lens implanted. Cataract surgical rate was estimated to be
950/million population/year.1
Likewise rest of the countries in the region, phacoemulsification is a new surgical
technique that was, until recently, not
performed in the region.2 Majority of cases
during the above period were extracapsular cataract surgeries. Phacoemulsification was
first done in Sudan in year 2001.1 Despite its
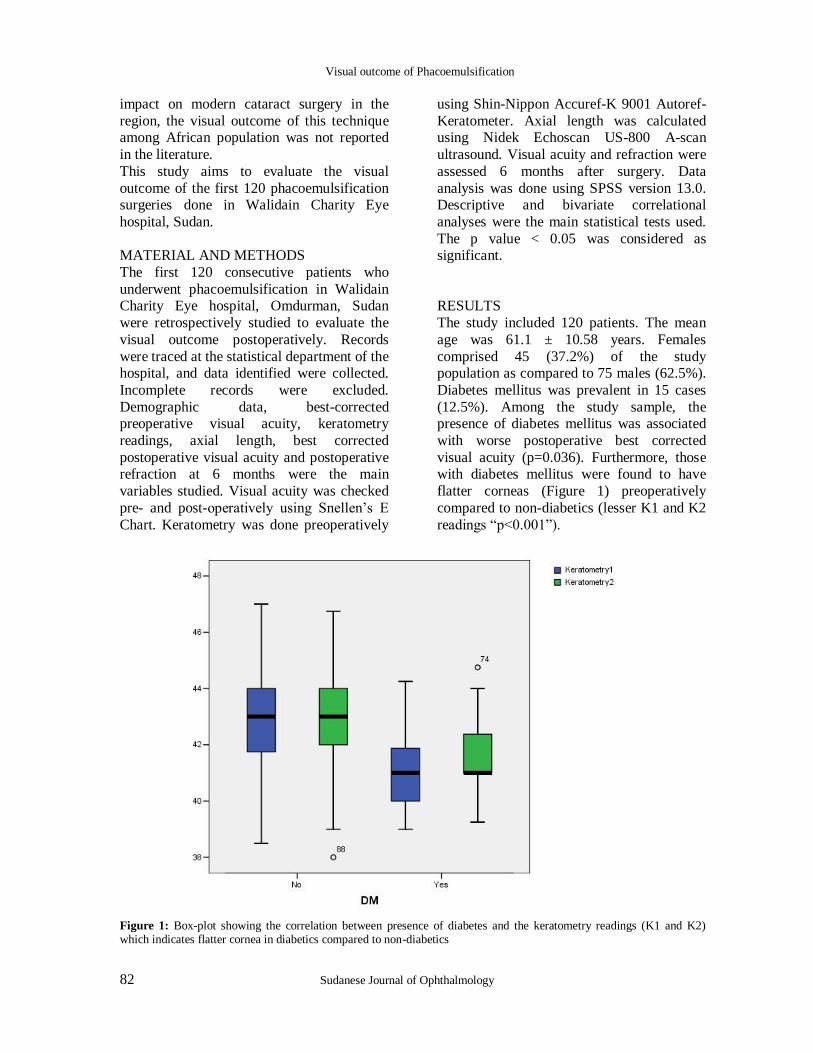
82 Sudanese Journal of Ophthalmology
impact on modern cataract surgery in the
region, the visual outcome of this technique among African population was not reported
in the literature.
This study aims to evaluate the visual
outcome of the first 120 phacoemulsification surgeries done in Walidain Charity Eye
hospital, Sudan.
MATERIAL AND METHODS
The first 120 consecutive patients who
underwent phacoemulsification in Walidain Charity Eye hospital, Omdurman, Sudan
were retrospectively studied to evaluate the
visual outcome postoperatively. Records
were traced at the statistical department of the hospital, and data identified were collected.
Incomplete records were excluded.
Demographic data, best-corrected preoperative visual acuity, keratometry
readings, axial length, best corrected
postoperative visual acuity and postoperative refraction at 6 months were the main
variables studied. Visual acuity was checked
pre- and post-operatively using Snellen‟s E
Chart. Keratometry was done preoperatively
using Shin-Nippon Accuref-K 9001 Autoref-
Keratometer. Axial length was calculated using Nidek Echoscan US-800 A-scan
ultrasound. Visual acuity and refraction were
assessed 6 months after surgery. Data
analysis was done using SPSS version 13.0. Descriptive and bivariate correlational
analyses were the main statistical tests used.
The p value < 0.05 was considered as significant.
RESULTS
The study included 120 patients. The mean
age was 61.1 ± 10.58 years. Females
comprised 45 (37.2%) of the study population as compared to 75 males (62.5%).
Diabetes mellitus was prevalent in 15 cases
(12.5%). Among the study sample, the presence of diabetes mellitus was associated
with worse postoperative best corrected
visual acuity (p=0.036). Furthermore, those with diabetes mellitus were found to have
flatter corneas (Figure 1) preoperatively
compared to non-diabetics (lesser K1 and K2
readings “p<0.001”).
Figure 1: Box-plot showing the correlation between presence of diabetes and the keratometry readings (K1 and K2) which indicates flatter cornea in diabetics compared to non-diabetics
Visual outcome of Phacoemulsification
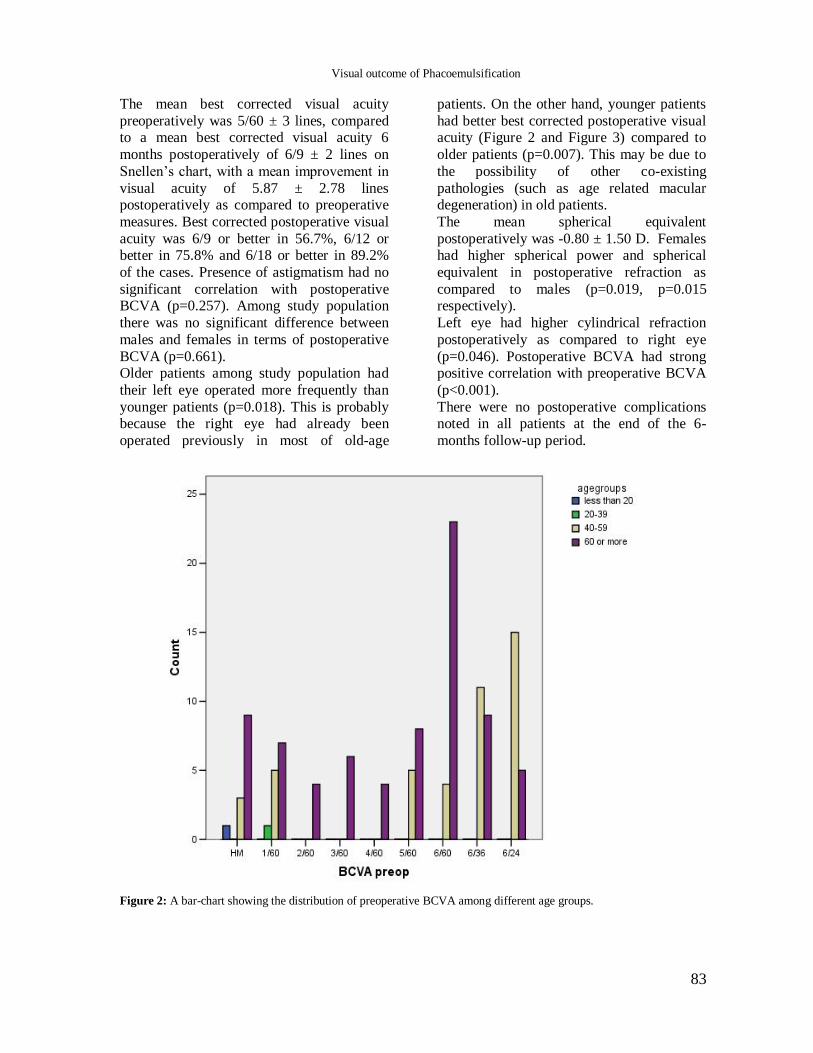
83
The mean best corrected visual acuity
preoperatively was 5/60 ± 3 lines, compared to a mean best corrected visual acuity 6
months postoperatively of 6/9 ± 2 lines on
Snellen‟s chart, with a mean improvement in
visual acuity of 5.87 ± 2.78 lines postoperatively as compared to preoperative
measures. Best corrected postoperative visual
acuity was 6/9 or better in 56.7%, 6/12 or better in 75.8% and 6/18 or better in 89.2%
of the cases. Presence of astigmatism had no
significant correlation with postoperative BCVA (p=0.257). Among study population
there was no significant difference between
males and females in terms of postoperative
BCVA (p=0.661). Older patients among study population had
their left eye operated more frequently than
younger patients (p=0.018). This is probably because the right eye had already been
operated previously in most of old-age
patients. On the other hand, younger patients
had better best corrected postoperative visual acuity (Figure 2 and Figure 3) compared to
older patients (p=0.007). This may be due to
the possibility of other co-existing
pathologies (such as age related macular degeneration) in old patients.
The mean spherical equivalent
postoperatively was -0.80 ± 1.50 D. Females had higher spherical power and spherical
equivalent in postoperative refraction as
compared to males (p=0.019, p=0.015 respectively).
Left eye had higher cylindrical refraction
postoperatively as compared to right eye
(p=0.046). Postoperative BCVA had strong positive correlation with preoperative BCVA
(p<0.001).
There were no postoperative complications noted in all patients at the end of the 6-
months follow-up period.
Figure 2: A bar-chart showing the distribution of preoperative BCVA among different age groups.
Visual outcome of Phacoemulsification
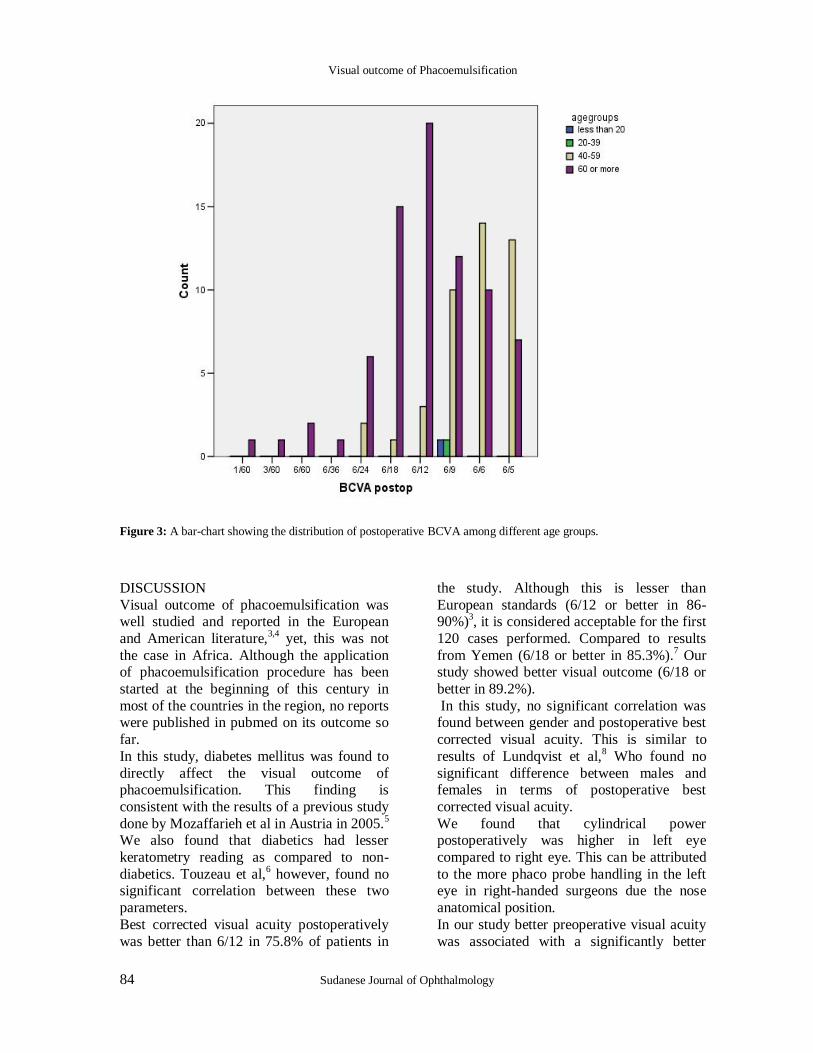
84 Sudanese Journal of Ophthalmology
Figure 3: A bar-chart showing the distribution of postoperative BCVA among different age groups.
DISCUSSION
Visual outcome of phacoemulsification was well studied and reported in the European
and American literature,3,4
yet, this was not
the case in Africa. Although the application of phacoemulsification procedure has been
started at the beginning of this century in
most of the countries in the region, no reports were published in pubmed on its outcome so
far.
In this study, diabetes mellitus was found to
directly affect the visual outcome of phacoemulsification. This finding is
consistent with the results of a previous study
done by Mozaffarieh et al in Austria in 2005.5
We also found that diabetics had lesser
keratometry reading as compared to non-
diabetics. Touzeau et al,6 however, found no
significant correlation between these two
parameters.
Best corrected visual acuity postoperatively
was better than 6/12 in 75.8% of patients in
the study. Although this is lesser than
European standards (6/12 or better in 86-90%)
3, it is considered acceptable for the first
120 cases performed. Compared to results
from Yemen (6/18 or better in 85.3%).7 Our
study showed better visual outcome (6/18 or
better in 89.2%).
In this study, no significant correlation was found between gender and postoperative best
corrected visual acuity. This is similar to
results of Lundqvist et al,8 Who found no
significant difference between males and females in terms of postoperative best
corrected visual acuity.
We found that cylindrical power postoperatively was higher in left eye
compared to right eye. This can be attributed
to the more phaco probe handling in the left eye in right-handed surgeons due the nose
anatomical position.
In our study better preoperative visual acuity
was associated with a significantly better
Visual outcome of Phacoemulsification

85
postoperative visual acuity. Hence, it is
recommended, in phacoemulsification, to go for surgery earlier, and not to wait until
cataract is hard enough to cause to
intraoperative and postoperative
complications. Currently, more eye surgeons are shifting to
phacoemulsification. It can be anticipated
that in the near future, phacoemulsification will be the main cataract surgical procedure
in Sudan in view of the better visual outcome
and the patient satisfaction compared to the classical extracaspular cataract surgery.
References 1. National plan for eye care in Sudan – A five-year
plan (2003 – 2007). Report by National Programme for Prevention of Blindness, Ministry of Health, Khartoum, Sudan, 2002.
2. Kaimbo wa Kaimbo D. Comparative study of
extracapsular and intracapsular cataract extraction
in Kinshasa (zaire) [Article in French]. Bull Soc Belge Ophtalmol. 1993;249:81-87
3. Slavíková A, Novák J, Krejzková T. European cataract outcome study--evaluation of 3 years in European study [Article in Czech]. Cesk Slov
Oftalmol. 2009;65:49-52. 4. Salomão SR, Soares FS, Berezovsky A, et al.
Prevalence and Outcomes of Cataract Surgery in Brazil: The São Paulo Eye Study. Am J Ophthalmol. 2009 Apr 29. [Epub ahead of print]
5. Mozaffarieh M, Heinzl H, Sacu S, et al. Clinical outcomes of phacoemulsification cataract surgery in diabetes patients: visual function (VF-14), visual
acuity and patient satisfaction. Acta Ophthalmol Scand. 2005;83:176-83.
6. Touzeau O, Levet L, Borderie V, et al. Anterior segment of the eye and diabetes mellitus [Article in French]. J Fr Ophtalmol. 2004;27:859-70.
7. Hameed AS, Alkhatib TK, Rageh MA, et al. Yemeni experience with phacoemulsification. Saudi Med J. 2009;30:687-92.
8. Lundqvist B, Mönestam E. Gender-related differences in cataract surgery outcome: a 5-year follow-up. Acta Ophthalmol. 2008;86:543-8.
Visual outcome of Phacoemulsification
86 Sudanese Journal of Ophthalmology
ORIGINAL ARTICLE
Chemical injuries of the eye – Clinical study of 40 cases S C Reddy, P R Reddy
Department of Ophthalmology, Osmania Medical College. Hyderabad, Andhra Pradesh, India
Correspondence to: Prof. Dr. S. C. Reddy. Dept. of Ophthalmology, UCSI School of Medicine, Bukit Khor,
mukim Rusila, 21600 Marang, Teremgganu, Malaysia. Email: [email protected]. Tel No: +6013-
6244532. Fax No: +609-6281885
Abstract AIM: To determine the type of chemical causing eye injury, occupation of patients, severity of
ocular injury, complications and visual outcome in patients who sustained chemical injuries of eye.
METHODS: Gender, age, occupation, nature of chemical, eye involved, vision at admission, severity of ocular injury, complications and visual outcome were noted from the case records of
patients who were treated for chemical injuries of eye over a period of one year. RESULTS: A total
number of 40 patients (53 eyes) were treated, of which 33 were males and 7 were females. There
were 13 patients with both eyes involved while 27 had one eye involvement. Industrial workers (32.5%) were the most commonly affected people. Injuries due to alkalis were more common than
acids. The vision at presentation was poor (< 6/60) in 43.4% of eyes. In majority of the patients
(73.6%) the severity of chemical injury was mild to moderate. Corneal opacity (45.2%) was the most common complication. Best corrected vision of 6/12 or better was achieved in 22.6% of eyes.
CONCLUSION: Public education and practice of protective measures for eyes at the work site will
help in reducing the severity of ocular injury due to chemicals. Thorough irrigation of eyes and appropriate immediate treatment will reduce the long term complications and sequelae in these
patients.
Keywords: Chemical injury of eye, acids, alkalies, complications..
INTRODUCTION Chemical injuries are potentially devastating
ocular surface injuries that can result in
permanent visual impairment or blindness. Acid injuries tend to remain confined to the
ocular surface and produce more superficial
damage, while alkalis penetrate easily into the eye and cause damage to the corneal
stroma, endothelium as well as other anterior
segment structures.1 Most victims of
chemical injuries are young with exposure occurring in industrial accidents, at home and
in personal assaults. Alkali injuries tend to
occur more commonly than acid injuries.2,3
Among the large number of reports available
from Western countries on chemical injuries
of eye in the Pubmed search, only few are from India.
4-8 Therefore, the present study
was undertaken to determine the
demographic and clinical profile,
87
complications and visual outcome of
chemical injuries in patients treated in a tertiary government eye hospital.
MATERIAL AND METHODS
The case records of all patients treated for chemical injuries of eye in Sarojini Devi Eye
Hospital, Osmania Medical College,
Hyderabad, Andhra Pradesh state, India, over a period of one year, were reviewed. Gender,
age, occupation of patients, nature of
chemical causing eye injury, visual acuity at admission, severity of ocular injury,
complications and visual outcome following
treatment were noted from the patients‟
records. When the patient was not sure about the type of chemical fallen into the eyes, its
nature was decided as acid or alkali based on
the litmus paper test which indicates the pH of tears. The chemical injuries were graded
according to Roper-Hall modification of the
Hughes classification system.9 All the patients were treated on the standard protocol
for chemical injury which included
immediate continuous irrigation of the eye
with normal saline until the pH of tears come to near neutral level, removal of foreign
particles from the eye, topical
dexamethasone, ciprofloxacin, homatropine, artificial tears, oral vitamin C, and oral
doxicycline. Timolol eye drops and Tab.
Acetazolamide were given whenever there
was increased intraocular pressure. Paching of the eye was done depending on the size of
corneal epithelial defect. Bandage soft
contact lens usage/tarsorrhaphy were done in eyes with persistent epithelial defect. The
complications during the follow up period
and visual outcome at the last follow up were noted. The results were analyzed using epi-
info programme.
RESULTS A total number of 40 patients (53 eyes) were
treated, of which 33 were males and 7 were
females. There were 13 patients with both eyes involved while 27 had one eye
involvement. The age of patients ranged from
8 years to 50 years; 5 were children below the age of 12 years. Majority of patients
(60%) were in the age group of 21-40 years.
More than half of the patients (23 out of 40,
57.5%) sustained injuries in factories, laboratories and/or workshops (Table 1).
Table 1: Occupation of the patients with chemical injuries of eye (n=40)
Occupation Number Percentage
Industrial worker 13 32.5% Pharmacy lab worker 8 20.0% Workshop mechanic 2 5.0% Student 7 17.5% Businessman 4 10.0% Housewife 3 7.5% Labourer 2 5.0%
Gold-smith 1 2.5%
The chemicals causing ocular injury were
alkalies (18), acids (16) and others (6);
the most common chemical being
hydrochloric acid (Table 2).
Table 2: Nature of chemicals causing ocular injury (n=40)
Nature of chemical Number Percentage
Alkalies Ammonia 5 12.5% Clacium hydroxide (Lime, cement)
8 20.0%
Sodium hydroxide
5 12.5%
Acid Hydrochloric acid 11 27.5% Sulphuric acid 4 10.0% Citric acid
1 2.5%
Others Dimethyl sulphate 2 5.0%
Dimethyl benzene 2 5.0% Copper sulphate 1 2.5% Sodium silicate 1 2.5%
Twenty patients (50%) came to the eye
hospital within 2 hours of the chemical injury to the eye; 10 patients (25%) came within 12
hours; 6 patients (15%) came within 24
hours; while 4 patients (10%) came after 24 hours. The probable delay in coming to the
hospital could be due to far distance from the
place of chemical injury and transportation time to come to the hospital. However, all the
patients gave history that their eyes were
washed with water immediately after the
chemical falling in the eyes. The visual acuity at admission ranged from
no perception of light (NPL) to 6/6. The
Chemical injuries of the eye
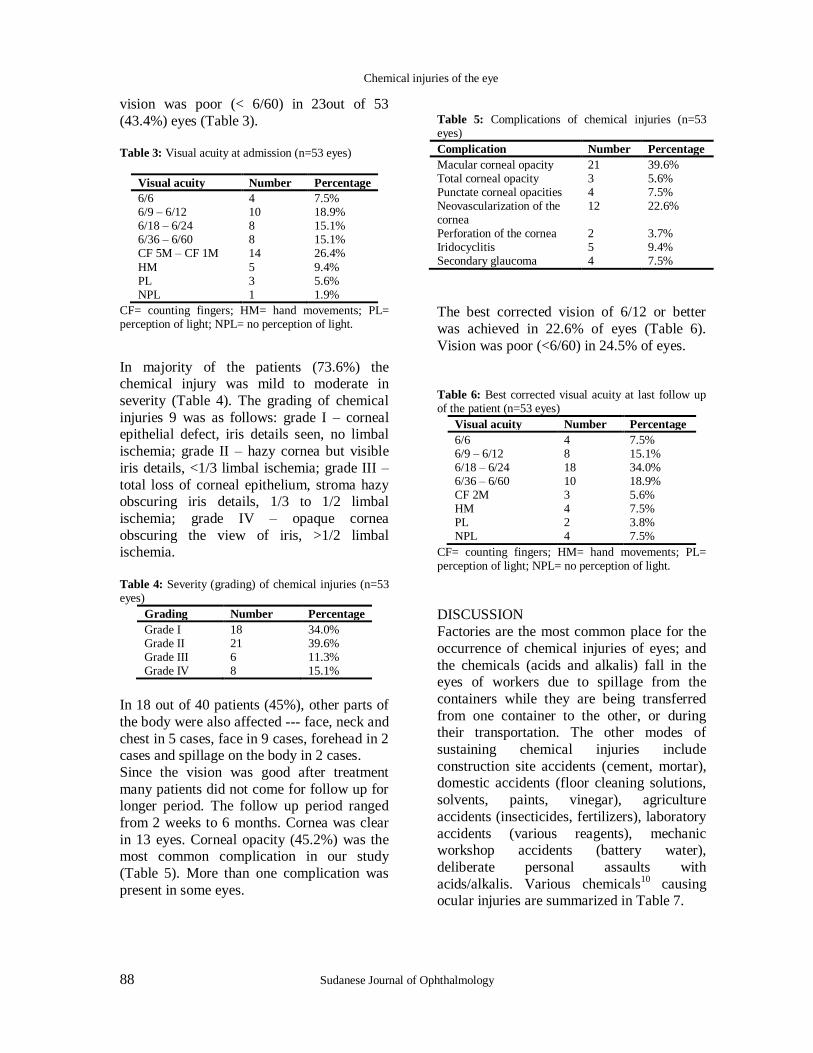
88 Sudanese Journal of Ophthalmology
vision was poor (< 6/60) in 23out of 53
(43.4%) eyes (Table 3). Table 3: Visual acuity at admission (n=53 eyes)
Visual acuity Number Percentage
6/6 4 7.5% 6/9 – 6/12 10 18.9% 6/18 – 6/24 8 15.1% 6/36 – 6/60 8 15.1% CF 5M – CF 1M 14 26.4%
HM 5 9.4% PL 3 5.6% NPL 1 1.9%
CF= counting fingers; HM= hand movements; PL= perception of light; NPL= no perception of light.
In majority of the patients (73.6%) the chemical injury was mild to moderate in
severity (Table 4). The grading of chemical
injuries 9 was as follows: grade I – corneal epithelial defect, iris details seen, no limbal
ischemia; grade II – hazy cornea but visible
iris details, <1/3 limbal ischemia; grade III –
total loss of corneal epithelium, stroma hazy obscuring iris details, 1/3 to 1/2 limbal
ischemia; grade IV – opaque cornea
obscuring the view of iris, >1/2 limbal ischemia.
Table 4: Severity (grading) of chemical injuries (n=53 eyes)
Grading Number Percentage
Grade I 18 34.0% Grade II 21 39.6% Grade III 6 11.3% Grade IV 8 15.1%
In 18 out of 40 patients (45%), other parts of
the body were also affected --- face, neck and
chest in 5 cases, face in 9 cases, forehead in 2 cases and spillage on the body in 2 cases.
Since the vision was good after treatment
many patients did not come for follow up for longer period. The follow up period ranged
from 2 weeks to 6 months. Cornea was clear
in 13 eyes. Corneal opacity (45.2%) was the most common complication in our study
(Table 5). More than one complication was
present in some eyes.
Table 5: Complications of chemical injuries (n=53 eyes)
Complication Number Percentage
Macular corneal opacity 21 39.6% Total corneal opacity 3 5.6% Punctate corneal opacities 4 7.5% Neovascularization of the cornea
12 22.6%
Perforation of the cornea 2 3.7% Iridocyclitis 5 9.4% Secondary glaucoma 4 7.5%
The best corrected vision of 6/12 or better
was achieved in 22.6% of eyes (Table 6).
Vision was poor (<6/60) in 24.5% of eyes.
Table 6: Best corrected visual acuity at last follow up of the patient (n=53 eyes)
Visual acuity Number Percentage
6/6 4 7.5% 6/9 – 6/12 8 15.1% 6/18 – 6/24 18 34.0% 6/36 – 6/60 10 18.9% CF 2M 3 5.6% HM 4 7.5% PL 2 3.8% NPL 4 7.5%
CF= counting fingers; HM= hand movements; PL= perception of light; NPL= no perception of light.
DISCUSSION
Factories are the most common place for the
occurrence of chemical injuries of eyes; and
the chemicals (acids and alkalis) fall in the eyes of workers due to spillage from the
containers while they are being transferred
from one container to the other, or during their transportation. The other modes of
sustaining chemical injuries include
construction site accidents (cement, mortar), domestic accidents (floor cleaning solutions,
solvents, paints, vinegar), agriculture
accidents (insecticides, fertilizers), laboratory
accidents (various reagents), mechanic workshop accidents (battery water),
deliberate personal assaults with
acids/alkalis. Various chemicals10
causing ocular injuries are summarized in Table 7.
Chemical injuries of the eye

89
Table 7: Common alkalis and acids causing ocular injury
Chemicals Common sources and uses
Alkalies Ammonia (NH3) fertilizers, refrigerants, cleaning agents (7%) Lye (NaOH) drain cleaners Potassium hydroxide (KOH) caustic potash Lime (CaOH2)
plaster, mortar, cement, whitewash
Acids
Sulfuric acid (H2SO4) industrial cleaner, battery acid Sulfurous acid (H2SO3) fruit and vegetable preservative, bleach, refrigerant Hydrofluoric acid (HF) glass polishing, glass frosting, mineral refining, gasoline alkylation, silicon
production Acetic acid (CH3COOH) vinegar (4-10%), essence of vinegar (80%), glacial acetic acid (90%) Chromic acid (Cr2O3) used in chromic plate industry Hydrochloric acid (HCl) Used as 32 – 38% solution
The frequency of chemical injuries in any
study depends on the number and variety of
industries present around the treating hospital, protective/preventive measures
practiced at the work site, and medical
facilities available around the site of accident. In the present study, males outnumbered the
females (4.5:1) which was similar to the
studies reported in the literature.2,3,7
Factory workers were more commonly involved
(32.5%) when compared to other
occupations. Kuckelkorn et al11
from
Germany reported 73.8% industrial accidents in their retrospective study of severe alkali
burns of the eyes. The occurrence of
domestic accidental chemical injuries in our study was 7.5% which is much lower than the
same reported from France12
(23%) and
Germany3 (37%).
Immediate irrigation of the eyes following
chemical injury is a very important step in the
management of these cases. Lesser extent of
ocular damage, better visual outcome and short duration of hospital stay has been
reported in patients treated with immediate
copious irrigation with tap water.13
In our series, grade III and IV injuries were noted in
14 out of 53 eyes (26.4%) which is less than
the percentage of the same reported from
Australia14
(27.6%) and one of the studies from India
7 (35.9%). The general observation
is that such severe injuries are more common
in personal assaults because the victim‟s face including the eyes are targeted usually in
such cases.15
The ultimate visual prognosis in chemical
injuries depends on the degree of severity of
the injury at initial presentation. In our study, the best corrected visual acuity at the last
follow up was 6/12 or better in 22.6% of
eyes, while the same vision was achieved in 76% of eyes in the study reported by Saini
and Sharma.7 Blindness (vision CF2M –
NPL) was noted in 24.4% of the eyes in our series, which is much lower than 57.4%
reported from China.16
The medical management of severe chemical
injuries of eye must be directed towards (1) promoting ocular surface epithelial recovery
and trans-differentiation with use of tear
substitutes, ointment at bed time, patching the eye, bandage soft contact lens, fibronectin,
epidermal growth factor, retinoic acid, and
viscoelastics; (2) augumenting corneal repair by supporting keratocyte collagen production
and minimizing ulceration related to
collagenase activity by using topical and
systemic ascorbate, tetracycline, and collagenase inhibitors; and (3) control of
inflammation with use of topical
corticosteroids, medroxyprogesteron 1%, nonsteroidal anti-inflammatory drugs,
andcitrate.17,18
In order to promote epithelial
wound healing, limbal stem cells
transplanataion19
, conjunctival transplantation
20, amniotic membrane
transplantation21
are performed in patients
with chemical injuries of eye. When the corneal opacity is developed, penetrating
keratoplasty for visual rehabilitation is done.
Chemical injuries of the eye
90 Sudanese Journal of Ophthalmology
The prognosis of its success depends on the
original severity of the ocular injury and its sequelae after the initial treatment such as
uncontrolled glaucoma, hypotony, anterior
chamber membrane formation and retinal
detachment.22
Keratoprosthesis procedure offers useful vision in hopeless bilateral
corneal blindness patients due to chemical
injuries, with good optic nerve and retinal function.
23
CONCLUSION Chemical injuries of the eyes are more
common in industrial workers. Public
education and practice of protective measures
for the eyes at the work site will help in reducing the severity of ocular injury due to
chemicals. Thorough irrigation of eyes at the
scene of accident and at hospital, and appropriate immediate treatment of severe
cases will reduce the long term complications
and visual impairment in these patients.
References 1. Wagoner MD, Kenyon KR. Chemical injuries of
eye. In: Albert DM, Jakobiec FE (eds). Principles and practice of Ophthalmology, Vol 2, 2nd ed, Philadelphia, WB Saunders Company. 2000; pp 943-59.
2. Morgan SJ. Chemical burns of the eye: causes and
management. Br J Ophthalmol 1987; 71:854-7. 3. Kuckelkorn R, Luft I, Kottek AA et al. Chemical
and thermal eye burns in residential area of RWTH Aachen: analysis of accidents in 1 year using a new automated documentation of findings. Kin Monatsbl Augenheilkd 1993; 203:39-42. (article in German)
4. Raizada JK, Dwivedi PC. Acute ocular lesions in Bhopal gas tragedy. Indian J Ophthalmol 1986;
34:324-7. 5. Maskati QB. Ophthalmic survey of Bhopal victims
– 100 days after the tragedy. Indian J ophthalmol 1986; 34:328-31.
6. Dada T, Sharma N, Kumar A. Chemical injury due to colours used at the festival of Holi. Natl Med J India 1997; 10: 256.
7. Saini JS, Sharma A. Ocular chemical burns –
Clinical and demographic profile. Burns 1993; 19:67-9.
8. Agarwal T, Vajpayee RB, Sharma N, Tandon R. Severe ocular injury resulting from chuna packets. Ophthalmology 2006; 113:961.
9. Roper-Hall MJ. Thermal and chemical burns. Trans ophthalmol Soc UK 1965; 85:631-53.
10. McCulley JP. Chemical injuries. In:Smolin g, Thoft RA (eds). The Cornea: Scientific Foundations and Clinical practice, 2nd ed. Boston, Little Brown 1987; pp 527-42.
11. Kuckelkorn R, Makropoulous W, Kottek a, Reim M. retrospective study of severe alkali burns of the eyes. Klin Monatsbl Augenheilkd 1993; 203: 397-402.9article in German)
12. Merle H, Donnio A, Ayeboua l, et al. Alkali ocular burns in Martinique (French West Indies) : evalauationof the use of an atmospheric solution as the rinsing product. Burns 2005; 31: 205-11.
13. Ikeda N, Hayasaka Y, Watanabe K. Alkali burns of the eye; effect of immediate copious irrigation with tap water on their severity. Ophthalmologica 2006; 220:225-8.
14. Brodovsky SC, Mccarty CA, Snibson G, et al. management of alkali burns: an 11 year retrospective review. Ophthalmology 200; 107: 1829-35.
15. Beare JD. Eye injuries from assault with chemicals. Br J Ophthalmol 1990; 74: 514-8.
16. Li GH. Clinical analysis of 107 cases with chemical burns. Zhonghua Zheng Xing Shao shang wai Ke
Za zhi 1990; 6; 34-35,76. (article in Chinese) 17. Wagoner MD. Chemical injuries of the ye. Surv
Ophthalmol 1997; 41: 275-313. 18. Kenyon KR. Decision making in the therapy of
external eye diseases: noninfected corneal ulcers. Ophthalmology 1982; 89: 44-51
19. Kenyon KR, Tseng SCG. Limbal autograft transplantation for ocular surface disorders. Ophthalmology 1989; 96: 709-22.
20. Thoft RA. Conjunctival transplantation. Arch ophthalmol 1977; 95: 1425-7.
21. Prabhasawat P, Tesavibul N, Prakairungthong N, Booranapong W. Efficacy of amniotic membrane patching for acute chemical and thermal ocular burns. J Med Assoc Thai 2007; 90: 319-26.
22. Brown SI, Bloomfield SE, Pearce DB. A follow-up report on transplantation of the alkali-burned
cornea. Am J Ophthalmol 1974; 77: 538-42. 23. Falcinelli G, Falsini B, Taloni M, et al. Modified
osteo-odonto-keratoprosthesis for treatment of corneal blindness: long term anatomical and functional outcomes of 118 cases. Arch Ophthalmol 2005; 123: 1319-29.
Chemical injuries of the eye
91
CASE REPORT
Unilateral Isolated Ocular Tuberculosis with no
systemic involvement
U T Chan , M M Choo , S C Reddy
Ophthalmology department, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia
Correspondence to: Dr.Chan U Teng. Dept. of Ophthalmology, Hospital Sultanah Nur Zahirah, Jalan Sultan Mahmud 20400 Kuala Terengganu, Terengganu, Malaysia. Email: [email protected], Tel No: +6012-9807009
Abstract
A case of tuberculous anterior uveitis in a 42 years old lady is reported. She presented with typical
signs of anterior uveitis in the left eye. There was no systemic tuberculosis in the body. The diagnosis was based on eye signs, raised ESR, positive tuberculin test and positive response to
isoniazid test. She regained normal vision with antituberculous treatment. This case highlights that
ocular tuberculosis may occur in the absence of systemic disease; early diagnosis and prompt
treatment may prevent ocular morbidity and blindness.
Keywords: Ocular Tuberculosis; Uveitis; Granulomatous; Koeppe nodule.
INTRODUCTION Ocular tuberculosis can manifest a myriad of
clinical presentation and the definitive
diagnosis can be daunting due to the
difficulty of getting ocular samples for microbiologic or histologic evaluation.
Granulomatous anterior uveitis may be a
primary manifestation of ocular tuberculosis. The disease may also present with severe
non-granulomatous anterior uveitis. Uveitis
may be acute relapsing, or chronic and
persistant. Tubercles may be seen on the iris, and more commonly in the choroid with
associated focal choroiditis.1 In a case
records study of 8759 cases of uveitis, Rathinam and Namperumalsamy
2 reported
that tuberculosis was found to be the cause in
5.6% of all types of uveitis (anterior, intermediate, posterior, diffuse).; and in 4%
of 5028 anterior uveitis patients. They
reviewed the pattern of uveitis of 15221 cases
reported from several countries over 35 years and found that tuberculosis comprised
between 0.2% and 10.5% as aetiology of uveitis. Literature search did not show any
data on the aetiology of uveitis in Malaysia.
We report a case of tuberculous anterior
uveitis, the diagnosis of which was based on typical signs of anterior uveitis, absence of
systemic tuberculosis in the body, raised
ESR, positive tuberculin test and positive response to isoniazid test.
CASE REPORT
A 42 years old Chinese lady presented to our eye clinic on 1/6/2005 with the complaints of
blurring of vision and redness of the left eye
for the past 2 months with worsening of condition over the past 3 weeks. She had no
history of chronic cough or fever, no
significant past medical history and no family history of tuberculosis. She was not on
immunosuppressive therapy. She saw a
general practitioner who gave eye drops with
no improvement.

92 Sudanese Journal of Ophthalmology
Ocular examination of the left eye showed a
visual acuity of 6/60, not improving with pinhole. There was circumcorneal injection.
Slit lamp examintion showed mutton fat
keratic precitpitates on the inferior half of the
corneal endothelium; +++ cells in the anterior chamber. A Koeppe nodule was noted
between 5 and 6 o‟clock position, and
posterior synechiae at 8 o‟clock (Figure 1).
Figure 1: showing Koeppe nodule between 5 and 6 o'clock position (white arrow) and posterior synechiae at 8 o'clock position (yellow arrow) in the left eye.
There was no hypopyon or rubeosis irides.
Intraocular pressure was 16 mm Hg. Fundus
examination revealed vitreous condensations. However, there was no evidence of active
vitritis. The optic disc was pink with a cup-
disc ratio of 0.3 and the retina was normal.
There was no perivascular sheathing or choroidal tubercle.
Examination of the right eye was normal,
with a 6/6 visual acuity. Intraocular pressure was 16 mmHg ; anterior and posterior
segments were normal.
Examination of the respiratory system
showed clear lungs with no palpable regional lymph nodes. The rest of systemic
examination was unremarkable.
A provisional diagnosis of anterior granulomatous uveitis was made. Gutt
dexamethasone 0.1% four hourly and gutt
homatropine 2% tds were started for the left eye. Blood investigations were carried out for
full blood count, renal profile, erythrocyte
sedimentation rate, connective tissue disease
screening, toxoplasma specific IgG and IgM,
VDRL, sputum for acid-fast bacilli and
Mantoux test. A chest radiograph was also done.
The patient was reviewed one week later.
Visual acuity of the left eye had improved to
6/18. Keratic precipitates were less in the size. The inflammatory reaction in the
anterior chamber was less (++ cells). Pupil
was irregular and dilated. All blood investigations were normal except raised
erythrocyte sedimentation rate (32mm/hour).
The Mantoux test was strongly positive with a blister measuring 25mm. The chest
radiograph was normal. A diagnosis of ocular
tuberculosis in the left eye was made and the
patient was started on anti-tuberculosis therapy which consisted of ethambutol
800mg once daily, isoniazid 300mg once
daily, rifampicin 600 mg once daily, pyrazinamide 1000 mg once daily and
pyridoxine 10 mg once daily.
On a review 2 weeks later, the visual acuity of the left eye had further improved to 6/12
and the anterior segment findings remained
the same. However, she developed vitritis
(+++ cells) with a hazy fundus view. Anti-tuberculosis therapy and topical steroids were
continued. Two weeks later, visual acuity of
the left eye had improved to 6/9 and the vitritis had reduced (+ cells). There was no
retinal vasculitis or choroidal tubercle.
On three successive follow up visits to the
clinic at two-weeks interval, the inflammatory cells in the anterior chamber
had reduced to occasional cells and there
were no cells in the vitreous; the topical steroids were reduced to a qid for 2 weeks,
tds for 2 weeks, bd for 2 weeks and od for 2
weeks in left eye; and then stopped. The intraocular pressure was 17-19 mm Hg
during the follow up period. On completion
of the 3-month intensive regime of the anti-
tuberculosis treatment, the visual acuity of the left eye was 6/12 with quiet anterior and
posterior segments. The left fundus was
normal. The intensive anti-tuberculosis treatment regime was subsequently switched
to a maintenance regime consisting of
isoniazid 300 mg daily and rifampicin 600 mg daily for six months. On the completion
of the regime, the visual acuity of the left eye
Ocular Tuberculosis

93
had improved to 6/6. The anterior and
posterior segments of the left eye were quiet. The intraocular pressure in left eye was
normal (18 mm Hg). The left eye remained
quiescent with a visual acuity of 6/6 on the
subsequent follow-up sessions in the next three months. The right eye remained
unaffected throughout the course of the
disease.
DISCUSSION
Endogenous Tuberculosis is a curable disease and it is one of the major causes of morbidity
and mortality worldwide. It is estimated to
affect 1.86 billion individuals with 8 million
new cases and 1.87 million deaths annually in the world.
3 Ocular tuberculosis is relatively
rare, comprising of 1% of all cases of
tuberculosis.4 It is often a result of
haematogenous spread or hypersensitivity
reaction to the Mycobacterium tuberculosis
antigen from a distant foci in the absence of any infectious agent in the eye.
Tuberculosis may affect any part of the eye,
the most common site being the choroid
because of its high level of blood supply and oxygenation. The infection may be primary
or secondary in nature. There is no systemic
lesion in primary ocular tuberculosis and the infection is usually restricted to the
conjunctiva and cornea and may present as an
ulcer, a tumour mass, phlyctenulosis or
interstitial keratitis. In secondary tuberculosis, the infection occurs as a result
of local spread from an adjacent structure or
haematogenous spread, mainly from the lungs.
5 Ocular tuberculosis is frequently
unilateral or asymmetric. The most common
manifestation is choroiditis followed by anterior uveitis and sclerokeratitis.
6 Ocular
tuberculosis may masquerade as ocular
neoplasm.7
Our patient presented with granulomatous anterior uveitis with the characteristic mutton
fat kerato-precipitates, iris nodules and
posterior synechiae but there was no choroidal involvement throughout the course
of the disease.
The definitive diagnosis of tuberculosis
requires a positive culture of Mycobacterium
tuberculosis from tissue samples. Ocular
tuberculosis is often difficult to diagnose owing to its similar clinical features of other
causes of uveitis, the invasiveness of
obtaining tissue samples and the limitations
of the available diagnostic tests. An initial work-up with negative results should not
eliminate tuberculosis from the differential
diagnosis. A thorough history and a complete physical examination are mandatory in
addition to the investigations. Sputum for
acid-fast bacilli is carried out to diagnose pulmonary tuberculosis as this method
detects the infectious cases of tuberculosis
and it is highly specific and inexpensive and
this was negative in this patient. Mantoux skin testing with purified protein
derivative of tuberculin is a widely used test
for screening but it is of limited value in the diagnosis because false negative reaction is
found in immunosuppressed patients and
false positive is observed in individuals vaccinated with bacilli Calmette-Guerin.
8 It
has been postulated that hypersensitivity to
mycobacterial antigens plays a role in the
pathogenesis of anterior uveitis.9 Mantoux
test was strongly positive in our patient with
a blister measuring 25 mm.
Polymerase chain reaction is a recent rapid diagnostic technique in which the
mycobacterial DNA is amplified and detected
with high sensitivity and specificity. This test
is of paramount importance in diagnosing primary ocular tuberculosis as only a small
amount of aqueous humour is needed.10
The detection of anti-cord factor antibody via enzyme-linked immunosorbent assay
(ELISA) is another new diagnostic method.
Cord factor (trehalose-6, 6‟dimycolate) is the most characteristic cell wall component of
the tubercle bacilli and the detection of
antibodies against the cord factor antigen
supports the diagnosis of tuberculosis.11
The isoniazid therapeutic trial, also known as
Schlagel test consists of a course of isoniazid
of 300 mg daily for 3 weeks. A positive test consists of a dramatic improvement in 1 to 3
weeks of treatment.12
The treatment of ocular tuberculosis is aimed at the infection and the inflammatory
reaction. Primary treatment for ocular
Ocular Tuberculosis

94 Sudanese Journal of Ophthalmology
tuberculosis should be systemic with a multi-
drug combination because pulmonary or other foci of infection may coexist. Multi-
drug therapy also avoids mycobacteria
resistance. An initial clinical response usually
occurs in 2 weeks.5 The American Thoracic
Society recommends a 2-month initial phase
of isoniazid, rifamipicin and pyrazinamide
followed by a 4-month maintenance phase of isoniazid and rifampicin.
13 The regime of this
patient differed (a 3-month initial phase and a
4-month maintenance phase) as it is tailored to this patient‟s clinical response.
Collaboration with the physician in the
management should be established to monitor
for the systemic toxic effects of the drugs. Ocular tuberculosis may occur in the absence
of systemic disease. The disease may mimic
several clinical entities. Early diagnosis and prompt treatment may prevent ocular
morbidity and blindness.
References 1. Massaro D, Katz S, Sachs M. Choroidal tubercles: a
clue to haematogenous tuberculosis. Ann Inten Med 1964; 60:231-41.
2. Rathinam SR, Namperumalsamy P. Global variation and pattern changes in epidemiology of uveitis. Indian J Ophthalmol 2007; 55:173-83.
3. Dye C, Schlee S, Dolin,P, Pathania V, Raviglione MC ; for the WHO Global Surveillance and
Monitoring Project. Global burden of tuberculosis:
estimated incidence, prevalence, and mortality by country. JAMA. 1999; 282:677-86.
4. Bouza E, Merino P, Munoz P. ocular tuberculosis. A prospective study in a general hospital. Medicine (Baltimore) 1997; 76:53-61.
5. Sheu SJ, Shyu JS, Chen LM, Chen YY, Chirn SC, Wang JS. Ocular manifestations of tuberculosis. Ophthalmology 2001; 108:1580-5.
6. Knox DL: syphilis and tuberculosis, in Ryan SJ (ed): Retina. St Louis, CV Mosby CO, 1989: 647-54.
7. Demirci H, Shields CL, Shields JA, Eagle RC. Oculat tuberculosis masquerading as ocular
tumours. Surv Ophthalmol 2004; 49:78-89. 8. Raviglione MC, O‟Brien RJ. Tuberculosis in
FauciAS, Braunwaid E, Isselbacher KJ: Harrison‟s Principle of Internal Medicine, 14th ed, New York, McGraw Hill, 1998;1004-14.
9. Kapoor AK, Gopal R, Lal B. Detection of anti-PPD IgG antibody and PPD-induced delayed type hypersensitivity in anterior uveitis patients. Indian J
Pathol Microbiol 1997; 40:303-7. 10. Arora SK, Gupta V, Gupta A, Bambery P, Kapoor
GS, Sehgel S. Diagnostic efficacy of polymerase chain reaction in granulomatous uveitis. Tubercle and Lung Disease 1999; 79:229-33.
11. Sakai J, Matsuzawa S, Usui M, Yano I. New diagnostic approach for ocular tuberculosis by ELISA using the cord factor as antigen. British J
Ophthalmol 2001; 85: 130-3. 12. Thompson MJ, Albert DM. Ocular tuberculosis.
Arch of Ophthalmol 2006; 123(6):844-49. 13. American Thoracic Society. Control of tuberculosis
in the United States. Am Rev Respir Dis 1992; 146:1623-33.
Ocular Tuberculosis
95
LETTER TO EDITOR
Sudan Test (ST) for near vision test
Dear Editor:
I would like to convey my congratulations for the launching of SJO as a first professional journal of
ophthalmology in Sudan concerning promotion of eye care.
I have a comment on the article titled “Causes of low vision and visual outcome after using of low
vision devices in Sudanese children” page 37 of the first issue. In that article it was mentioned that
near vision was performed by Jaeger test (ST).However, Jaeger test is different than ST. Jaeger was the first and oldest test for near vision acuity and in many countries was replaced by other
more standard tests like Meter and Point systems. ST is an abbreviation of Sudan Test which was
recently developed in Sudan (2005). Standard log MAR was used for progression of its letter size,
and it becomes commonly used in all low vision work and many clinics in Sudan.
Thank you
Sincerely
Dr. Atif B Mohamed Ali, PhD
96 Sudanese Journal of Ophthalmology
ANNOUNCEMENTS