
Using a Hybrid Electronic Medical Record System for the Surveillance of Adverse Surgical Events and...
10
ORIGINAL SCIENTIFIC REPORT Using a Hybrid Electronic Medical Record System for the Surveillance of Adverse Surgical Events and Human Error in A Developing World Surgical Service Grant Laing • John Bruce • David Skinner • Nikki Allorto • Colleen Aldous • Sandie Thomson • Damian Clarke Ó Socie ´te ´ Internationale de Chirurgie 2014 Abstract Introduction The quantification and analysis of adverse events is essential to benchmark surgical outcomes and establish a foundation for quality improvement interventions. We developed a hybrid electronic medical record (HEMR) system for the accurate collection and integration of data into a structured morbidity and mortality (M&M) meeting. Methodology The HEMR system was implemented on January 1, 2013. It included a mechanism to capture and classify adverse events using the ICD-10 coding system. This was achieved by both prospective reporting by clients and by retrospective sentinel-event-trawling performed by administrators. Results From January 1, 2013 to March 20, 2014, 6,217 patients were admitted within the tertiary surgical service of Greys Hospital. A total of 1,314 (21.1 %) adverse events and 315 (5.1 %) deaths were recorded. The adverse events were divided into 875 ‘‘pathology-related’’ morbidities and 439 ‘‘error-related’’ morbidities. Pathology-related morbidities included 725 systemic complications and 150 operative complications. Error-related morbidities included 257 cognitive errors, 158 (2.5 %) iatrogenic injuries, and 24 (1.3 %) missed injuries. Error accounted for 439 (33 %) of the total number of adverse events. A total of 938 (71.4 %) adverse events were captured prospectively, whereas the remaining 376 (28.6 %) were captured retrospectively. The ICD-10 coding system was found to have some limitations in its classification of adverse events. Conclusions The HEMR system has provided the necessary platform within our service to benchmark the incidence of adverse events. The use of the international ICD-10 coding system has identified some limitations in its ability to classify and categorise adverse events in surgery. G. Laing (&) Surgery, UKZN, Durban, South Africa e-mail: [email protected] J. Bruce Á N. Allorto Á D. Clarke General Surgery, Greys Hospital, Pietermaritzburg, South Africa D. Skinner Critical Care and Anaesthesia, King Edward VIII Hospital, Durban, South Africa C. Aldous School of Clinical Medicine, King Edward VIII Hospital, Durban, South Africa S. Thomson Gastrointestinal Unit University of Cape Town, Groote Schuur Hospital, Cape Town, South Africa 123 World J Surg DOI 10.1007/s00268-014-2766-x
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Using a Hybrid Electronic Medical Record System for the Surveillance of Adverse Surgical Events and...

ORIGINAL SCIENTIFIC REPORT
Using a Hybrid Electronic Medical Record Systemfor the Surveillance of Adverse Surgical Events and Human Errorin A Developing World Surgical Service
Grant Laing • John Bruce • David Skinner •
Nikki Allorto • Colleen Aldous • Sandie Thomson •
Damian Clarke
� Societe Internationale de Chirurgie 2014
Abstract
Introduction The quantification and analysis of adverse events is essential to benchmark surgical outcomes and
establish a foundation for quality improvement interventions. We developed a hybrid electronic medical record
(HEMR) system for the accurate collection and integration of data into a structured morbidity and mortality (M&M)
meeting.
Methodology The HEMR system was implemented on January 1, 2013. It included a mechanism to capture and
classify adverse events using the ICD-10 coding system. This was achieved by both prospective reporting by clients
and by retrospective sentinel-event-trawling performed by administrators.
Results From January 1, 2013 to March 20, 2014, 6,217 patients were admitted within the tertiary surgical service
of Greys Hospital. A total of 1,314 (21.1 %) adverse events and 315 (5.1 %) deaths were recorded. The adverse
events were divided into 875 ‘‘pathology-related’’ morbidities and 439 ‘‘error-related’’ morbidities. Pathology-related
morbidities included 725 systemic complications and 150 operative complications. Error-related morbidities included
257 cognitive errors, 158 (2.5 %) iatrogenic injuries, and 24 (1.3 %) missed injuries. Error accounted for 439 (33 %)
of the total number of adverse events. A total of 938 (71.4 %) adverse events were captured prospectively, whereas
the remaining 376 (28.6 %) were captured retrospectively. The ICD-10 coding system was found to have some
limitations in its classification of adverse events.
Conclusions The HEMR system has provided the necessary platform within our service to benchmark the incidence
of adverse events. The use of the international ICD-10 coding system has identified some limitations in its ability to
classify and categorise adverse events in surgery.
G. Laing (&)
Surgery, UKZN, Durban, South Africa
e-mail: [email protected]
J. Bruce � N. Allorto � D. Clarke
General Surgery, Greys Hospital, Pietermaritzburg, South Africa
D. Skinner
Critical Care and Anaesthesia, King Edward VIII Hospital,
Durban, South Africa
C. Aldous
School of Clinical Medicine, King Edward VIII Hospital,
Durban, South Africa
S. Thomson
Gastrointestinal Unit University of Cape Town, Groote Schuur
Hospital, Cape Town, South Africa
123
World J Surg
DOI 10.1007/s00268-014-2766-x

Introduction
The realisation that human error contributes significantly to
surgical adverse events has fostered interest in quality
improvement (QI) initiatives, which directly target human
error [1–3]. The traditional forum for the identification and
discussion of surgical adverse events has been the Mor-
bidity and Mortality (M&M) meeting. The M&M meeting,
however, has not always been an effective driver of
improved patient safety. The two most apparent reasons for
this failure include the lack of structures to facilitate an
understanding of the contribution of error to adverse events
and the lack of robust systems to capture both the incidence
and type(s) of adverse events and errors. We have
attempted to address the first deficiency by introducing
taxonomy of error into a structured M&M to analyse the
contribution of error to adverse events [4]. However,
underreporting of errors and adverse events has remained a
challenge and this is not unique to our institution. Most
adverse-events-surveillance-systems rely upon self-report-
ing and hence fail to capture the true incidence of both
adverse events and errors [5]. We have previously pub-
lished on the design, construction, and implementation of a
hybrid electronic medical record (HEMR) system within a
developing world tertiary surgical service [6]. This cost-
effective information system captured data at multiple
points in time (admission, operative intervention, endo-
scopic intervention, adverse events, and discharge). The
HEMR system combined handwritten documents and
printed medical records, hence its description as a hybrid
system, and merged the functions of a registry and an
electronic medical record (EMR). It was intended that the
HEMR system not only capture data for research purposes
but act as a driver of QI projects by facilitating work flow,
record keeping, and assist clinical management by the
inclusion of an integrated clinical decision support system
(CDSS). Careful attention was paid to integrating the
HEMR system into the ergonomic structure of the service,
by using it to replace or simplify preexisting tasks and to
support current educational initiatives. This study reviews
the use of the HEMR system to capture and aggregate data
pertaining to adverse events for analysis and discussion
within a structured weekly M&M meeting. It also quanti-
fies and classifies adverse events and errors within our
service with the intention of using these data to drive
ongoing QI programs.
Methodology
Ethical approval to construct and implement the HEMR
system was obtained before any development (ethics
number BCA221/13 BREC UKZN). The following terms
are defined for the purpose of clarity. An information
system, which combines an electronic registry with an
EMR system and a traditional paper-based record system,
can be referred to as a HEMR system. Clinical decision
support systems (CDSS) attempt to use information tech-
nology to improve the quality of care by supporting deci-
sion-making and directing staff down appropriate
management algorithms. The efficacy of self-reporting of
adverse events is dependent on the compliance of indi-
vidual clients. A sentinel event is an event in the process of
patient care, which is typically closely associated with
adverse events and as such, needs to be reviewed. Adverse
events have been classified into cases of ‘‘pathology-rela-
ted’’ morbidity and ‘‘error-related’’ morbidity for the pur-
poses of this study. Sentinel-event-trawling refers to the
independent retrospective review of all patients who have
experienced an adverse event, with the purpose of identi-
fying unreported cases of morbidity and error.
The HEMR system was designed to capture data at
admission, operation, endoscopy, and at discharge, trans-
fer, or death. At discharge, an ICD-10 diagnostic code was
assigned to each patient. Data relating to adverse events
were captured using both free-text descriptions and an
ICD-10 (Version 2010) classification. The identity of the
data capturer was documented as either a client or the
administrator, as well as whether it was prospectively or
retrospectively captured. The categories of data were
designed as a relational database, with the ability to create
unique, one-to-many relationships. Patients entered into the
HEMR system were automatically assigned a reference
identification (ID) number and their demographic details
were entered into the primary table. A number of second-
ary tables were related to the primary table, including
general, paediatric, and trauma surgery tables for admis-
sions and discharges, an operative table, an endoscopy
table, and a table for adverse events. The data model was
expanded into a series of digital layouts, which constitute
the system interface, where data pertaining to adverse
events would be entered using a combination of free-text
and predesigned dropdown menus with ICD-10 codes.
Fifteen desktop computers were positioned within the
hospital and local network connectivity enabled multiple
client access to the registry. The HEMR file was uploaded
via a host computer onto a secure server. Separate user-
names and passwords were created for the administrators
and clients. Automated hourly backups of the HEMR
system file were integrated into the design for data pro-
tection. The HEMR system was implemented at Greys
Hospital, Pietermaritzburg, Kwa-Zulu Natal, South Africa
on January 1, 2013. The estimated costs required for the
computer hardware and software for this project were
*150,000 South African rands ($15,720). No further fees
were required for external technologic support or added
World J Surg
123
human resources. A training program was initiated for
clients involved in the use of the HEMR system and
included an introductory lecture with personal training
within a computer laboratory. As a quality assurance
measure the data entered into the HEMR system were
analysed and validated by the administrators on a weekly
basis.
Adverse event reporting mechanism
The interface for the adverse event reporting is illustrated
in Appendices in Figs. 4 and 6. This component relies on
prospective self-reporting by clients. The department
adopted and implemented a local policy, including a pre-
printed document for the conduct of morning and afternoon
ward rounds. This document includes a tick-box for the
presence or absence of new adverse events. Adverse events
identified by members of the surgical team were then
documented using the tick-box and thereafter prospectively
entered by the client onto the HEMR system. The design of
the HEMR system included automated reports for the
purpose of weekly departmental M&M meetings (Appen-
dix in Fig. 6). Data and statistics within these reports
included the total number of surgical admissions and dis-
charges, operations performed, adverse events, and deaths.
Sentinel-event-trawling
To complement the prospective self-reporting arm of the
system, an exercise of independent retrospective sentinel-
event-trawling was instituted. Administrators of the HEMR
system performed a retrospective analysis of patient
records to identify the incidence of unreported surgical
adverse events. Sentinel markers based on The American
College of Surgeons National Surgical Quality Improve-
ment Program (ACS-NSQIP) definitions of what consti-
tutes a complication and what should be reported to the
Northwestern Online Surgical Quality Improvement
(NOSQI) were used to identify unreported morbidity and
error. These included all complications (within 30 days of
surgery or at any time if related to the surgery), morbidities
in nonoperative patients, deaths, readmissions, unantici-
pated reoperations, admissions to ICU, prolonged hospital
stay, and specific complications, such a hospital-acquired
pneumonias, drug-related adverse reactions, and decubitus
pressure ulcers.
Classification and taxonomy
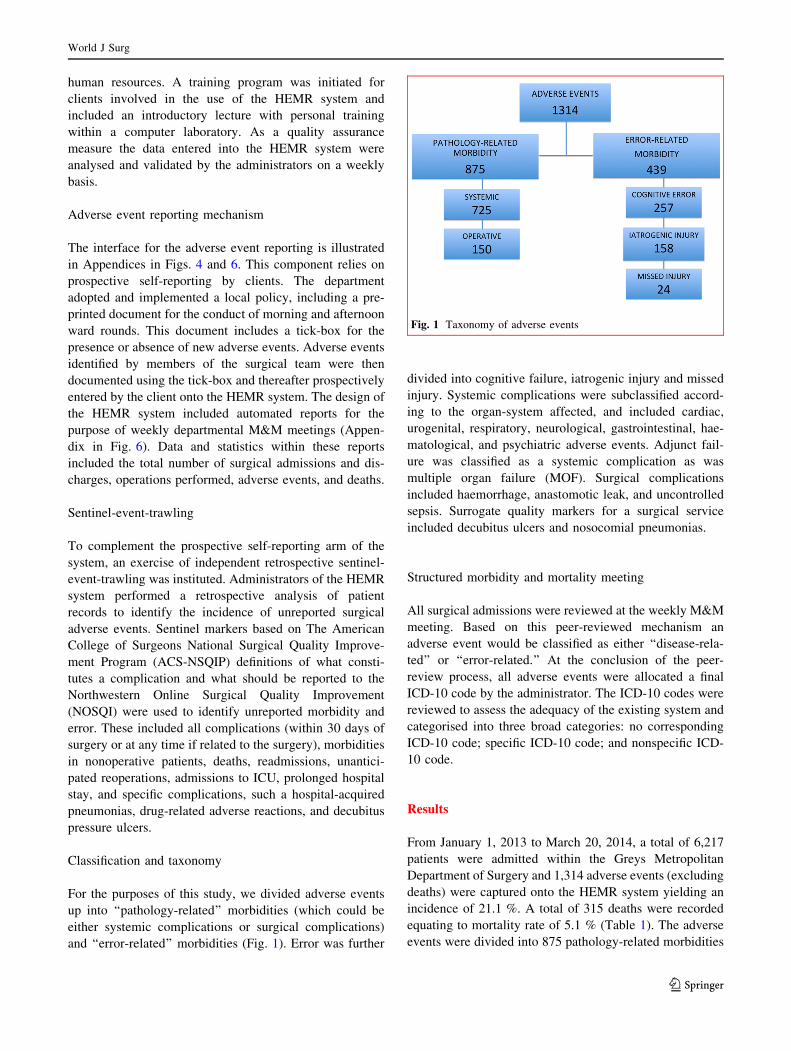
For the purposes of this study, we divided adverse events
up into ‘‘pathology-related’’ morbidities (which could be
either systemic complications or surgical complications)
and ‘‘error-related’’ morbidities (Fig. 1). Error was further
divided into cognitive failure, iatrogenic injury and missed
injury. Systemic complications were subclassified accord-
ing to the organ-system affected, and included cardiac,
urogenital, respiratory, neurological, gastrointestinal, hae-
matological, and psychiatric adverse events. Adjunct fail-
ure was classified as a systemic complication as was
multiple organ failure (MOF). Surgical complications
included haemorrhage, anastomotic leak, and uncontrolled
sepsis. Surrogate quality markers for a surgical service
included decubitus ulcers and nosocomial pneumonias.
Structured morbidity and mortality meeting
All surgical admissions were reviewed at the weekly M&M
meeting. Based on this peer-reviewed mechanism an
adverse event would be classified as either ‘‘disease-rela-
ted’’ or ‘‘error-related.’’ At the conclusion of the peer-
review process, all adverse events were allocated a final
ICD-10 code by the administrator. The ICD-10 codes were
reviewed to assess the adequacy of the existing system and
categorised into three broad categories: no corresponding
ICD-10 code; specific ICD-10 code; and nonspecific ICD-
10 code.
Results
From January 1, 2013 to March 20, 2014, a total of 6,217
patients were admitted within the Greys Metropolitan
Department of Surgery and 1,314 adverse events (excluding
deaths) were captured onto the HEMR system yielding an
incidence of 21.1 %. A total of 315 deaths were recorded
equating to mortality rate of 5.1 % (Table 1). The adverse
events were divided into 875 pathology-related morbidities
Fig. 1 Taxonomy of adverse events
World J Surg
123

and 439 error-related morbidities (Fig. 1). Error accounted
for 33 % (439) of the surgical adverse events. The cases of
error-related morbidities included 257 cognitive errors
(Table 2), 158 (2.5 %) iatrogenic injuries (Table 3), and 24
(1.3 %) missed injuries. Pneumothorax following central
line insertion accounted for 25 % (n = 27) of iatrogenic
injuries (Table 3; Fig. 2). The pathology-related morbidi-
ties included 725 systemic complications and 150 surgical
complications (Table 4). Sepsis accounted for 34 %
(n = 301) of the pathology-related morbidities. Nosocomial
pneumonia (n = 100) and surgical site infection (n = 96)
collectively accounted for 65 % of all septic complications
(Fig. 3). Considering the total series numeric, our results
quantified an incidence of septic complications of 4.5 %
(301/6217). Of the adverse events, 938 (71.4 %) were
captured prospectively through client entry, whereas the
remaining 376 (28.6 %) were captured retrospectively
through the process of sentinel-event-trawling. The ICD-10
(version 2010) coding system was found to have limitations
in the classification of adverse events; 56 % had a highly
specific corresponding ICD-10 code, 25 % have a loosely
associated ICD-10 code, and 19 % of adverse events had no
identifiable ICD-10 code. This was particularly noticeable
with regards to the classification of medical error (Table 5),
missed, and iatrogenic injuries.
Discussion
Since the turn of the millennium when the Institute of
Medicine (IOM) published the monograph, ‘‘To Err is
Table 1 Total number of surgical admissions, adverse events, and
mortality rate
Admissions 6217
General surgery 3374
Trauma surgery 1792
Paediatric surgery 1051
Adverse events 1314 21.1 %
Pathology-related morbidities 875
Error-related morbidities 439
Deaths 315 5.1 %
Table 2 Cognitive error-related complications (subdivision of error-
related morbidities)
Cognitive errors 257
Error of omission 126
Error of commission 73
Cancellation OT 23
Error of assessment 22
Delay treatment 6
Error system failure 3
Error of planning 2
Error of assessment 1
Failed SNOM 1
SNOM selective nonoperative management
Table 3 Iatrogenic injury (subdivision of error-related morbidities)
Iatrogenic 158
Cardiac arrest 1
Adverse drug reaction 4
Warfarin toxicity 4
Fall (from stretcher) 6
Anaphylaxis 8
Unplanned adjunct removal 27
Anatomical injuries 108
Fig. 2 Iatrogenic injuries (N = 108)
Table 4 Pathology-related morbidities
Systemic 725
Sepsis 301
CVSa 106
Urogenital 81
Respiratory 77
Neurological 41
GITb 40
Metabolic 27
Systemic 26
Adjunct failure 13
HPBc 6
Hematological 4
Psychiatric 3
Operative 150
Total 875
a Cardiovascular systemb Gastrointestinal tract systemc Hepato-pancreatico-biliary system
World J Surg
123

Human,’’ there has been a great deal of interest in error in
health care and in improving patient safety [1, 7–15]. The
ACS-NSQIP is the prototype of a surgically driven pro-
gram to improve quality of care and the central feature of
this initiative is the need for accurate data on adverse
events. MediBank is a South African software solution,
which has predominantly been utilised within the private
healthcare sector with approximately 36 participating
hospitals across four provinces [16]. The objectives of
MediBank have focused on performance improvement, the
optimisation of hospital operations, injury and disease
prevention, and medical research. The design, develop-
ment, and implementation of the HEMR system aimed to
pursue a comparable vision to MediBank. The HEMR
system has proven to be a simple, cost-effective informa-
tion solution, which can be implemented and maintained
within the service delivery of a government healthcare
institution—without requirements for additional research
assistants and information technology (IT) staff. The
HEMR system has enabled us to quantify the incidence and
spectrum of adverse events within our service by incor-
porating both a prospective self-reporting mechanism and
retrospective sentinel-event-trawling. Our results compare
with similar studies, which reported adverse event inci-
dences of 30–42 % [1, 4, 7, 8, 14].
The exclusive reliance on self-reporting of adverse events
results in underreporting and a consequent underestimation
of its incidence. Previous studies have estimated that
approximately one-third of adverse events and deaths are
never discussed at M&M meetings. There are many reasons
for the reluctance of doctors to report adverse events. The
culture of some M&M meetings may make full disclosure
less palatable. Cognitive dissonance may cause staff to
suppress poor outcomes. This is most apparent when staff
use the terms ‘‘nature of disease’’ or the ‘‘disease process’’
when discussing and accounting for complications. There is
a lack of appreciation of the systematic failures associated
with adverse outcomes. Staff members generally demon-
strate a tendency to defensiveness and anxiety concerning
the presentation of information relating to adverse events
and errors. In an attempt to improve this situation, North
Western University developed and implemented the NOS-
QI—a web-based, self-reporting system, which allowed for
the anonymous reporting of adverse events [5]. The authors
used a sentinel-event-trawling mechanism to compare
morbidity reported on the NOSQI with actual morbidity and
mortality rates by reviewing all readmissions and all hos-
pital recorded deaths on the preexisting hospital adminis-
trators North Western Event Tracking System (NETS).
They estimated that less than one-third of adverse events
were self-reported. Our results identified an improved
compliance rate with an incidence of underreporting of
28.6 %. This statistic illustrates that despite the implemen-
tation of a well-structured, planned, and executed depart-
mental program, underreporting is inevitable and suggests
retrospective sentinel-event-trawling systems and prospec-
tive self-reporting systems must work in conjunction to
obtain a more accurate estimate of adverse events.
Fig. 3 Sepsis-related morbidities (N = 301)
Table 5 ICD-10 limitations in the classification of error(s)
Adverse event N ICD-10 CODE
Error-related 439 Y60–Y69 Misadventures to patients during
surgical and medical care
Iatrogenic 158 Y60–Y69 Misadventures to patients during
surgical and medical care
Error of
omission
126 Y66 Nonadministration of surgical and
medical care
Error of
commission
73 No ICD-10 code
Missed injury 24 No ICD-10 code
Cancellation
OT
23 Z53.8 Procedure not carried out for other
reasons
Error of
assessment
22 No ICD-10 code
Delay
treatment
6 No ICD-10 code
Error system
failure
3 No ICD-10 code
Error of
planning
2 No ICD-10 code
Error of
assessment
1 No ICD-10 code
Failed
SNOM
1 No ICD-10 code
World J Surg
123

The HEMR system has enabled us to quantify accurately
the impact of error on surgical adverse events and it would
appear that that 30–40 % of surgical adverse events could
be attributed to error. We describe a missed injury rate of
1.3 % amongst trauma patients and an iatrogenic injury
rate of 2.5 %. This compares with our previously reported
incidence of missed injuries of 2.5 %, which was estimated
during a 6-month period [9]. The ICD-10 coding system
appears to have limitations with regards to its classification
of human error, missed injury, and iatrogenic injury. With
the current focus on limiting the incidence of error in
surgical care, it is hoped that future versions of the ICD-10
coding system develop taxonomy for error-related adverse
events.
The quality of a surgical service is difficult to quantify
and requires the development of appropriate metrics for
benchmarking and measurement. As the quality of a health
care system is a multifaceted concept, obtaining an accu-
rate view of the efficiency of a system requires multiple
indicators [12–14]. Some of these indicators may be
qualitative as well as quantitative and must assess both the
process and the outcome of care. All quality markers are
dependent on accurate data collection for reliability, and
the HEMR system has functioned to meet these require-
ments. With these proven benchmarks, we hope to proceed
to develop and implement directed QI interventions to
improve outcomes and thereafter to accurately quantify the
impact of these programs.
Conclusions
The HEMR system has enabled us to capture accurately
and to analyse surgical adverse events. This was achieved
by combining a prospective electronic self-reporting
mechanism with a retrospective independent targeted
review system using sentinel-event-trawling. We have
integrated the HEMR system into the clinical workflow and
structure of our service. Although the study and interven-
tion cannot be proven to alter or improve patient outcomes,
it is hoped that that this will foster the development of
targeted QI programs to reduce the incidence and impact of
the most common adverse events identified through the
study. Targeted QI interventions to reduce the incidence of
nosocomial pneumonia, surgical site infection, and iatro-
genic pneumothorax (following central line insertion) are
the next priority based on our results. The ICD-10 coding
system was furthermore found to have some limitations
with regard to its classification of adverse events and it is
hoped that future editions will develop a mechanism to
improve its classification of error. It is possible that the
success of this system could be transferred to other clinical
disciplines.
Appendix
See Appendix Figs. 4, 5, and 6.
World J Surg
123

Fig. 4 HEMR system interface: ICD-10 search engine
World J Surg
123
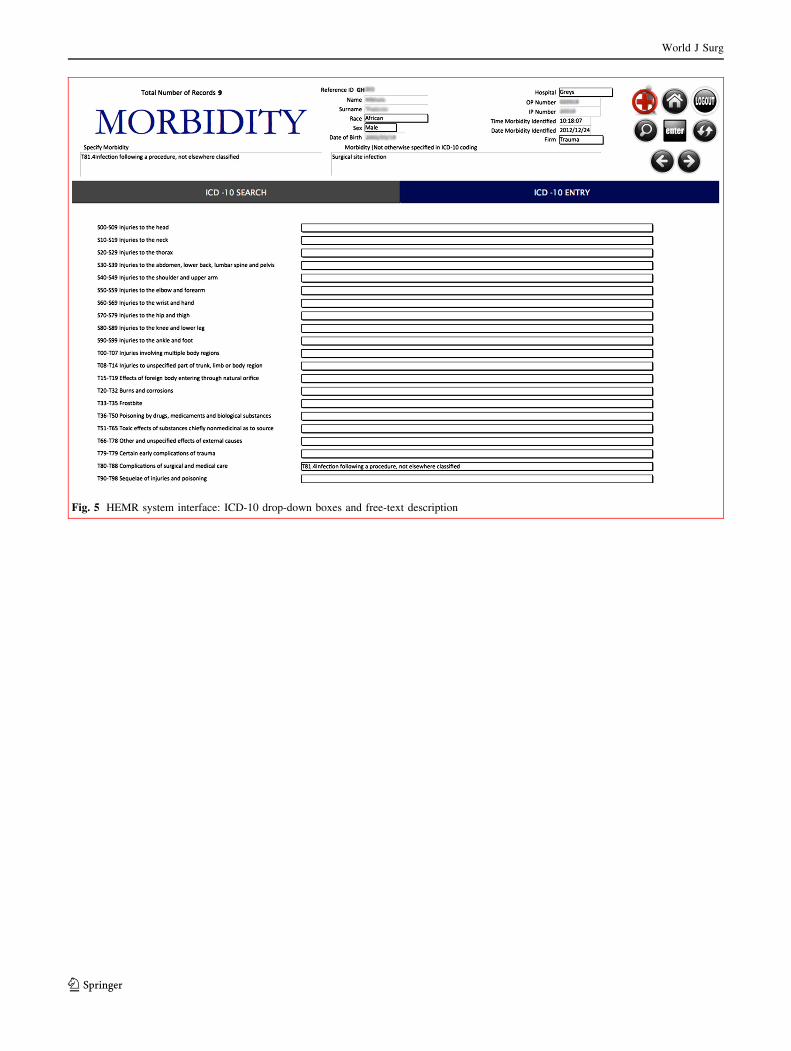
Fig. 5 HEMR system interface: ICD-10 drop-down boxes and free-text description
World J Surg
123

References
1. Kohn LT, Corrigan JM, Donaldson MS (eds) (2000) To err is
human Building a safer health system. National Academy Press,
Washington, DC
2. Reason J (1995) Understanding adverse events: human factors.
Qual Health Care 4:80–89
3. Reason J (2000) Human error: models and management. BMJ
320:768–770
4. Chang A, Schyve PM, Croteau RJ, O’Leary DS, Loeb JM (2005)
The JCAHO patient safety event taxonomy: a standardized ter-
minology and classification schema for near misses and adverse
events. Int J Qual Health Care 17(2):95–105
5. Bilimoria KY, Kmiecik TE, DaRosa DA, Halverson A, Eskandari
MK, Bell RH Jr, Soper NJ, Wayne JD (2009) Development of an
online morbidity, mortality, and near-miss reporting system to
identify patterns of adverse events in surgical patients. Arch Surg
144(4):305–311
6. Laing GL, Bruce JL, Skinner DL, Allorto NL, Clarke DL, Aldous
C (2013) Development, implementation and evaluation of a
hybrid electronic medical record system specifically designed for
a developing world surgical service. World J Surg Dec 31. [Epub
ahead of print] PMID: 24378554 [PubMed - as supplied by
publisher]
7. Leape LL (1994) Error in medicine. JAMA 272(23):1851–1857
8. Gruen RL, Jurkovich GJ, McIntyre LK, Foy HM, Maier RV
(2006) Patterns of errors contributing to trauma mortality: lessons
learned from 2,594 deaths. Ann Surg 244(3):371–380
9. Clarke DL, Gouveia J, Thomson SR et al (2008) Applying
modern error theory to the problem of missed injuries in trauma.
World J Surg 32(6):1176–1182. doi:10.1007/s00268-008-9543-7
10. Clarke DL, Furlong H, Laing GL, Aldous C, Thomson SR (2013)
Using a structured morbidity and mortality meeting to understand
the contribution of human error to adverse surgical events in a
South African regional hospital. S Afr J Surg 51(4):122–126.
doi:10.7196/sajs.1537
11. Pierluissi E, Fischer MA, Campbell AR, Landefeld CS (2003)
Discussion of medical errors in morbidity and mortality confer-
ences. JAMA 290(21):2838–2842
12. Mainz J (2003) Defining and classifying clinical indicators for
quality improvement. Int J Qual Health Care 15(6):523–530
13. Mainz J (2004) Quality indicators: essential for quality
improvement. Int J Qual Health Care 16:1–2
14. Mayer EK, Chow A, Vale JA et al (2009) Appraising the quality
of care in surgery. World J Surg 33(8):1584–1593. doi:10.1007/
s00268-009-0065-8
15. Laing GL, Skinner DL, Bruce JL, Aldous C, Oosthuizen GV,
Clarke DL (2014) Understanding the burden and outcome of
Fig. 6 HEMR system automated digital report
World J Surg
123

trauma care drives a new trauma systems model. World J Surg
38:1699–1706. doi:10.1007/s00268-014-2448-8 Jan 22. [Epub
ahead of print]
16. MediBank incorporates TraumaBank. A letter from the desk of
the president of the Trauma Society of South Africa (Professor
Ken Boffard). www.medibank.co.za/letterkentssa.pdf
World J Surg
123




















