Use of complementary and alternative medicine among people living with diabetes: literature review
13
Use of complementary and alternative medicine among people living with diabetes: literature review Hsiao-yun Chang, Marianne Wallis & Evelin Tiralongo Accepted for publication 1 February 2007 Hsiao-yun Chang BN MN RN PhD Candidate School of Nursing and Midwifery, Griffith University, Gold Coast, Queensland, Australia Marianne Wallis BSc PhD RN Professor of Clinical Nursing Research Griffith University Research Centre for Clinical Practice Innovation and Gold Coast Health Service District, Queensland, Australia Evelin Tiralongo BPharmSc PhD Lecturer School of Pharmacy, Griffith University Gold Coast, Queensland, Australia Correspondence to Hsiao-yun Chang: e-mail: [email protected] CHANG H.-Y., WALLIS M. & TIRALONGO E (2007) CHANG H.-Y., WALLIS M. & TIRALONGO E (2007) Use of complementary and alternative medicine among people living with diabetes: literature review. Journal of Advanced Nursing 58(4), 307–319 doi: 10.1111/j.1365-2648.2007.04291.x Abstract Title. Use of complementary and alternative medicine among people living with diabetes: literature review Aim. This paper is a report of a literature review to explore the prevalence of complementary and alternative medicine use amongst people with diabetes to in- form nursing practice, education and research. Background. Diabetes mellitus affects the entirety of a person’s being and increas- ingly people use complementary and alternative medicine in conjunction with other medical treatments and lifestyle modifications to manage their condition and improve well-being. Methods. The CINAHL, Medline, ProQuest nursing journals and Psych INFO databases were searched for the period 1990–2006 using identified keywords. Results. A total of 18 studies from nine countries were found. The results suggest that the prevalence of complementary and alternative medicine use among people with diabetes ranges from 17% to 72 8%. The most widely used therapies among diabetic populations are nutritional supplements, herbal medicines, nutritional advice, spiritual healing and relaxation techniques. The characteristics which influence complementary and alternative medicine use are age, duration of diabetes, degree of complications and self-monitoring of blood glucose. Conclusion. Although inconsistency in the definition of complementary and alter- native medicine and varying research designs make estimation of usage prevalence difficult, evidence suggests that a high proportion of people with diabetes use these therapies concurrently with conventional healthcare services. Healthcare profes- sionals need to be aware of this issue and may need to incorporate complementary and alternative medicine information into patient assessment and intervention. Keywords: alternative medicine, complementary medicine, diabetes mellitus, literature review, nursing, prevalence Introduction Interest in and use of complementary and alternative medicine (CAM) has recently expanded in many countries around the world. Population-based studies in countries in the developed world, such as Australia, Scotland, UK, Taiwan, Singapore and the United States of America (USA), report that one-half to two-thirds of adults use CAM (Emslie et al. 1996, REVIEW PAPER JAN Ó 2007 The Authors. Journal compilation Ó 2007 Blackwell Publishing Ltd 307
-
Upload
independent -
Category
Documents
-
view
5 -
download
0
Transcript of Use of complementary and alternative medicine among people living with diabetes: literature review

Use of complementary and alternative medicine among people living
with diabetes: literature review
Hsiao-yun Chang, Marianne Wallis & Evelin Tiralongo
Accepted for publication 1 February 2007
Hsiao-yun Chang BN MN RN
PhD Candidate
School of Nursing and Midwifery, Griffith
University, Gold Coast, Queensland,
Australia
Marianne Wallis BSc PhD RN
Professor of Clinical Nursing Research
Griffith University Research Centre for
Clinical Practice Innovation and Gold Coast
Health Service District, Queensland,
Australia
Evelin Tiralongo BPharmSc PhD
Lecturer
School of Pharmacy, Griffith University Gold
Coast, Queensland, Australia
Correspondence to Hsiao-yun Chang:
e-mail: [email protected]
CHANG H.-Y. , WALLIS M. & TIRALONGO E (2007)CHANG H.-Y. , WALLIS M. & TIRALONGO E (2007) Use of complementary and
alternative medicine among people living with diabetes: literature review. Journal of
Advanced Nursing 58(4), 307–319
doi: 10.1111/j.1365-2648.2007.04291.x
AbstractTitle. Use of complementary and alternative medicine among people living with
diabetes: literature review
Aim. This paper is a report of a literature review to explore the prevalence of
complementary and alternative medicine use amongst people with diabetes to in-
form nursing practice, education and research.
Background. Diabetes mellitus affects the entirety of a person’s being and increas-
ingly people use complementary and alternative medicine in conjunction with other
medical treatments and lifestyle modifications to manage their condition and
improve well-being.
Methods. The CINAHL, Medline, ProQuest nursing journals and Psych INFO
databases were searched for the period 1990–2006 using identified keywords.
Results. A total of 18 studies from nine countries were found. The results suggest
that the prevalence of complementary and alternative medicine use among people
with diabetes ranges from 17% to 72Æ8%. The most widely used therapies among
diabetic populations are nutritional supplements, herbal medicines, nutritional
advice, spiritual healing and relaxation techniques. The characteristics which
influence complementary and alternative medicine use are age, duration of diabetes,
degree of complications and self-monitoring of blood glucose.
Conclusion. Although inconsistency in the definition of complementary and alter-
native medicine and varying research designs make estimation of usage prevalence
difficult, evidence suggests that a high proportion of people with diabetes use these
therapies concurrently with conventional healthcare services. Healthcare profes-
sionals need to be aware of this issue and may need to incorporate complementary
and alternative medicine information into patient assessment and intervention.
Keywords: alternative medicine, complementary medicine, diabetes mellitus,
literature review, nursing, prevalence
Introduction
Interest in and use of complementary and alternative medicine
(CAM) has recently expanded in many countries around the
world. Population-based studies in countries in the developed
world, such as Australia, Scotland, UK, Taiwan, Singapore
and the United States of America (USA), report that one-half
to two-thirds of adults use CAM (Emslie et al. 1996,
REVIEW PAPERJAN
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 307

MacLennan et al. 2002, Lew-Ting 2003, Lim et al. 2005,
Tindle et al. 2005). This significant CAM usage in the general
population can be expected to lead to a demand for informa-
tion on CAM usage by the clients of health professionals.
The presence of chronic, debilitating or painful illness has
consistently been found to be a reason people seek out CAM
(Eisenberg et al. 1998). Diabetes mellitus (DM) is one such
disease which is highly prevalent worldwide. The mortality
associated with diabetes is significant, and primarily arises
from complications of long-standing hyperglycaemia.
Around 3Æ2 million deaths every year worldwide are attrib-
utable to complications of diabetes, which equates to six
deaths every minute (World Health Organization 2004).
Conventional medicine for diabetes has been geared toward
regulating blood glucose with a combination of dietary
modification, insulin and/or oral agents, maintaining ideal
body weight, exercising regularly and self-monitoring blood
sugar. Good glucose control can, however, be difficult for
many people with diabetes, because these conventional
treatment plans require changes to behaviour and lifestyle
(Dunning 2003). Due to the chronic course of the disease, the
debilitation of complications and threat of death, as well as
the complexities of treatment plans, people with diabetes
often work proactively to manage their condition, optimize
their health and alleviate complications through the use of
CAM (Yeh et al. 2002, Dunning 2003, Bell et al. 2006).
Complementary and alternative medicine refers to prac-
tices, approaches, knowledge and beliefs incorporating plant,
animal and mineral-based medicines, spiritual therapies,
manual techniques and exercises (World Health Organization
2003). A variety of definitions and descriptions are used to
explain CAM. The most broadly used functional definition of
CAM has been developed by the National Centre for
Complementary and Alternative Medicine (NCCAM) in the
USA. This definition states that ‘CAM is a group of diverse
medical and healthcare systems, practices and products that
are not presently considered to be part of orthodox medicine’
(NCCAM 2002, p. 1). CAM is a categorical term that
encompasses a broad spectrum of medicines, therapies and
practices. The NCCAM categorized CAM into five major
domains:
(1) Alternative medical systems: these are built upon com-
plete systems of theory and practice, such as homeopathic
medicine and traditional Chinese medicine.
(2) Mind–body interventions: these use a variety of tech-
niques designed to enhance the mind’s ability, such as
meditation, prayer and art therapies.
(3) Biologically based therapies: these use substances found
in nature, such as dietary supplements, herbal products
and botanical products.
(4) Manipulative and body-based methods: these are based
on the movement of one or more body parts, such as
chiropractic, osteopathic and massage.
(5) Energy therapies: these involve the use of energy fields
that are believed to surround and penetrate the human
body, such as biofield therapies (Gi Gong and Thera-
peutic Touch); and bioelectromagnetic-based therapies
(pulse fields and magnetic fields).
Despite the diverse ways in which these systems and
therapies have developed, they share common themes, such
as the use of complex interventions; individual diagnosis;
belief in the healing power of nature; union of mind, body
and spirit; and more holistic and integrative approaches to
individualized treatment plans. Several comprehensive
reviews have been written on the evidence that CAM
therapies can be beneficial for the management of diabetes
(Goguen & Leiter 2001, Shane-McWhorter 2001, Dey et al.
2002, Liu et al. 2002, Yeh et al. 2003). For example, a
number of herbal medicines and nutritional supplements have
been shown to decrease blood glucose level through various
mechanisms, and if used correctly, these effects can help
people with diabetes to manage their disease and to improve
their quality of life (see Table 1). However, while evidence is
mounting in support of the use of various CAMs to treat
diabetes and its complications, it is unclear how many people
with diabetes use CAM and whether they use the CAMs that
are beneficial for diabetes management.
Aim
The aim of the review was to explore the prevalence of CAM
use amongst diabetic populations in order to inform nursing
practice, education and research.
Search methods
Databases and keywords
The following databases were searched for the period 1990
to October 2006: CINAHL, Medline, ProQuest nursing
journals and Psych INFO. The keywords used were com-
plementary and alternative medicine, complementary medi-
cine, complementary therapy and alternative medicine (and
related terms such as traditional medicine, folk medicine
and unconventional/non-conventional medicine), prevalence
and DM. Some papers were found through tracking citations
from other publications. Inclusion criteria were prevalence
studies of CAM use by people with diabetes and other
research reports of studies exploring CAM use by people
with diabetes. Exclusion criteria were: publication in a
H.-Y. Chang et al.
308 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

language other than English; not available by inter-library
loan service in Australia; and publication dates before 1990
as this was when the increasing use of CAM began to be
reported.
Review limitations
This review included research-based studies focusing on
CAM use among people with diabetes. As this was not a
systematic review of efficacy, expert judgement rather a
formal quality appraisal was used to determine which studies
were included. Some studies which demonstrated design,
selection and measurement bias were included because they
provided useful insights into either the problems in definition
of terms or because they included information about disclo-
sure to healthcare professionals.
Results
The search produced 232 abstracts. This number was further
reduced by selecting research-based papers, specifically those
studies related to the prevalence of CAM use and those
related to the types of CAM commonly used by people with
diabetes. This resulted in 18 papers being selected for
inclusion in the review. Thirteen reported quantitative studies
that related to prevalence of CAM use and type of CAM used
by people with diabetes. Five reported qualitative studies
related to the type of CAM used by people with diabetes. The
Table 1 Overview of herbal medicine and nutritional supplements used in the treatment of diabetes
Herbal medicines Effects
Potential interactions and
contraindications References
Bitter melon
(Momordica charantia)
Hypoglycaemic activity Hypoglycaemic agents
Pregnancy
Basch et al. (2003)
Fenugreek
(Trigonella foenum graecum)
Hypoglycaemic activity
Lipid-lowering effects
Increased HDL cholesterol
Hypoglycaemic agents
Pregnancy
Anticoagulant drugs.
MAO inhibitors
Yeh et al. (2003)
Ginseng (Panax ginseng) Hypoglycaemic activity
Improved psycho-physiological
performance
Immune stimulant effects
Hypoglycaemic agents
Corticosteroids
Oral contraceptives
Anticoagulant drugs
Digoxin
MAO inhibitors and tricyclic
antidepressants
Diuretics
Sievenpiper et al. (2004)
Ginkgo (Ginkgo biloba) Antioxidant, Neuroprotective
Beneficial in cerebrovascular
insufficiency and peripheral
vascular disease
Anticoagulant drugs
SSRI
MAO inhibitors
Herbs: ginger, garlic and feverfew
Shane-McWhorter (2001)
Supplements
Chromium Increased insulin sensitivity
Lipid-lowering effects
N/A Guerrero-Romero and
Rodriguez-Moran (2005)
Fish oil Triglyceride-lowering effects
Anti-inflammatory
Anti-platelet
Hypotensive
Pregnant or breastfeeding
Anticoagulant drugs
Anti-hypertension drugs
Farmer et al. (2001),
Pittler and Ernst (2005)
Magnesium Essential in glucose metabolism
Prevent diabetic complications
Antibiotics
Drugs to prevent osteoporosis
Calcium channel blockers
Muscle relaxants
Diuretics
Guerrero-Romero and
Rodriguez-Moran (2005)
Zinc Metalloenzyme activitor
Immune function
Improved insulin levels
Lipid-lowering effects
Improved weight loss
Reduce absorption folic acid,
tetracyclines, copper
Reduce the effect of therapies that rely on
dopamine receptor antagonists
Vitamin A
Franz et al. (2002)
JAN: REVIEW PAPER Use of complementary and alternative medicine people with diabetes
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 309

remaining papers were either not research-based studies or
not related to the purpose of this literature review. All the
included studies were reviewed and compared, then sum-
marized in a matrix form, in terms of the aims of the review.
The key data from the 18 publications covered in this
review are summarized in Tables 2 and 3. Most of the studies
were published between 2000 and 2006 with only one study
published during the 1990s. Publications were based on
studies conducted in nine countries. The majority of papers
were derived from the USA (nine studies) and Australia (two
studies). Most of the studies were conducted in developed
countries with respondents recruited from conventional
hospitals. Unfortunately, data from Europe were limited,
because there were either none reported in English or no
studies conducted. Although this is a limitation, the present
review summarizes the available data on the prevalence of
CAM use among people with diabetes worldwide.
Challenges in interpreting the published literature
The papers reviewed report a high level of CAM use in people
with diabetes attending conventional healthcare services in
different countries and regions. The comparison of CAM use
prevalence data between these studies is difficult, however,
because these studies differ markedly in their definitions of
CAM, research design, methods of data collection, time-
frames and response rates.
Defining the term CAM is not an easy task. Murphy et al.
(2003) searched biomedical databases on CAM to estimate
the degree to which the literature displays the use of
controlled vocabulary among authors, indexers, and inves-
tigators, and concluded that validity of the definition of
CAM was the most difficult search concept, largely due to
inconsistent use of terminology between studies. As Table 2
demonstrates, the reviewed research studies provided limited
information about the instruments used. Each study had its
own operational definition of CAM and there were differ-
ences between the specific types of therapy included as
CAM, which therapies were classified into which subcate-
gory and how many CAMs were investigated. For example,
the studies of Ryan et al. (2001), Yeh et al. (2002), Garrow
and Egede (2006) and Bell et al. (2006) used different
criteria to determine whether vitamins or mineral supple-
mentation were defined as a form of CAM and thus,
included in the survey. If some studies had included all types
of vitamins not just mega-vitamins, the reported CAM use
could be much higher than the original data. In comparison
with these studies, electrotherapy, exercise, special diet
control and psychotherapy seldom came under the umbrella
of CAM.
The second problem regarding the operational definition of
CAM is the manner in which different researchers categorize
CAM. Rather than using the NCCAM’s domains, some
researchers use other conceptual models; for example, in the
Lee et al. (2004) study, biologically based therapies were
further categorized in terms of the origin of the CAM
product, such as plant-derived, animal materials and miscel-
laneous.
The third problem that arose when attempting to compare
the selection of CAM therapies used in studies, was the lack
of consistency with which CAMs were included in the
investigation. For example, some studies focus only on the
usage of the ‘biologically based therapies’ such as vitamins,
nutritional supplements and herbal medicine, whereas a
number of surveys included the whole spectrum of CAM
therapies. Only one study (Lind et al. 2006) reported
consultation with CAM practitioners by people with diabe-
tes. All these differences and inconsistencies can be seen in the
Table 2, under ‘research question’ and ‘popular therapies
list’. Because of a lack of consistency in categorization of
CAM therapies and a lack of consensus about which type and
how many therapies should be examined, it is difficult to
make an accurate evaluation of the frequency with which
CAM therapies are used.
A variety of research designs have been used in an attempt
to assess CAM use among people with diabetes. When
reviewing the literature on the prevalence of CAM use, a
number of important caveats have to be considered, such as
the fact that each survey covers a slightly different timeframe,
selection criteria vary and the methods of recruitment vary
(Ernst 1999). Some surveys were aimed at determining
lifetime prevalence of CAM use, while others used 1 year
or current use data. These differences may be seen in the
column of ‘timeframe’ in Table 2. Some researchers, such as
Leese et al. (1997), Al-Saeedi et al. (2003), Argaez-Lopez
et al. (2003) and Ryan et al. (2001) did not mention the
timeframe at all. In the studies that investigated lifetime
prevalence of CAM use there was limited reporting of the
measures taken to minimize recall bias.
Another issue of considerable importance in comparing
and contrasting previous studies is the difference in meth-
odological approaches undertaken by researchers. To enable
high response rates, survey questions are necessarily short
and uncomplicated (Harris & Rees 2000). Self-reported
questionnaires and telephone interviews, in particular, are
dependent for accuracy, upon respondents’ knowledge of
CAM therapies, and/or their willingness to report that use. As
a consequence, the quality of data related to the prevalence of
CAM use may be influenced by these factors. Additionally,
most studies had selection biases as a result of high
H.-Y. Chang et al.
310 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

Table
2Q
uan
tita
tive
rese
arc
hre
port
sre
late
dto
com
ple
men
tary
and
alt
ernati
ve
med
icin
e(C
AM
)th
erapie
suse
dby
peo
ple
wit
hdia
bet
esm
elli
tus
(DM
)
Auth
or
Countr
yn
(RR
)D
esig
nsa
mpli
ng
Res
earc
hques
tion
Tim
efra
me
Use
rate
Popula
rth
erapie
slist
(%)
Lee
seet
al.
(1997),
UK
246
DM
(75%
)
Conven
ience
sam
ple
wit
hper
sonal
inte
rvie
w
Pati
ents
att
endin
gth
e
dia
bet
escl
inic
ass
esse
d
the
uti
liza
tion
of
CA
M
NM
17%
Acu
punct
ure
(n¼
18)
Hom
eopath
y(n¼
11)
Her
bal
ther
apy
(n¼
7)
Refl
exolo
gy(n¼
4)
Aro
mat
her
apy
(n¼
4)
Hypnoth
erap
y
(n¼
3)
Cel
luar
nutr
itio
n
(n¼
2)
Chir
opra
ctor
(n¼
2)
Oth
ers
(n¼
5)
Ryan
etal
.(2
001),
Canada
703
DM¼
502
Non-D
M¼
201
(NM
)
Non-r
andom
sam
ple
52%
per
sonal
inte
rvie
w
48%
tele
phone
inte
rvie
w
What
kin
dof
med
icati
on
pre
sentl
yin
use
of
over
-the-
counte
r
supple
men
ts(O
TC
S)and
anoth
erm
edic
ati
on
(AM
)?
NM
AM
31%
OT
CS
44%
OT
Csu
pple
men
ts
Mult
ivit
am
ins
(27Æ5
)
Vit
am
inE
(18Æ9
)
Vit
am
inC
(18Æ7
)
Calc
ium
(16Æ0
)
Asp
irin
(13Æ9
)
Vit
am
inB
Com
ple
x
(6Æ5
)
Alt
ernati
ve
med
icin
es
Gar
lic
(11Æ6
)
Ech
inace
a(8
Æ9)
Her
bal
mix
ture
s
(8Æ5
)
Glu
cosa
min
e(5
Æ8)
Chro
miu
m(5
Æ8)
Gin
kgo
bil
oba
(4Æ9
)
Eged
eet
al.
(2002),
USA
21,5
71
DM¼
825
(77Æ7
%)
Nati
onally
repre
senta
tive
sam
ple
wit
hhouse
hold
inte
rvie
w
Have
you
seen
an
alt
ernati
ve
hea
lthca
re
pro
vid
ersu
chas
those
list
ed?
12
Ms
NM
Fiv
eco
mm
on
type
of
CA
M
Nutr
itio
nal
advi
ce
(n¼
37)
Her
bal
rem
edie
s
(n¼
20)
Spir
itual
hea
ling
(n¼
21)
Mass
age
ther
apy
(n¼
19)
Med
iati
on
train
ing
(n¼
14)
Pro
vid
erof
CA
M
Cle
rgy/s
pir
itualist
(n¼
18)
Mass
age
ther
apis
t
(n¼
16)
Nurs
e(n¼
13)
Acu
punct
uri
st
(n¼
9)
Yeh
etal
.(2
002),
USA
2055
DM¼
96
(NM
)
Nati
onally
repre
senta
tive
sam
ple
wit
hte
lephone
inte
rvie
w
Have
you
ever
use
dany
of
the
follow
ing
16
ther
apie
s?
Ifso
,have
you
done
so
wit
hin
the
last
12
month
s?
12
Ms
57%
Pra
yer
/spir
itual
(45Æ9
)
Her
bal
med
icin
e(1
6Æ2
)
Rel
axati
on
tech
niq
ues
(11Æ7
)
Chir
opra
ctic
(8Æ1
)
Folk
rem
edie
s(5
Æ1)
Mass
age
(6Æ9
)
Spec
ial
die
t(6
Æ8)
Meg
avit
am
ins
(5Æ9
)
Aro
mat
her
apy
(2Æ2
)
Sel
f-hel
pgro
up
(2Æ0
)
Cli
fford
etal
.(2
003),
Aust
rali
a
351
DM
(NM
)
Conven
ience
sam
ple
wit
hper
sonal
inte
rvie
w
Whic
hof
the
follow
ing
have
you
use
din
the
past
yea
r?(t
he
list
of
pro
duct
s
consi
der
edto
be
Com
ple
men
tary
med
icin
es)
12
Ms
23Æ6
%V
itam
inC
(18Æ0
)
Garl
ic(1
7Æ0
)
Fis
hoil
(14Æ0
)
Mult
ivit
am
ins
(12Æ0
)
Vit
am
inB
(11Æ0
)
Calc
ium
(8Æ0
)
Glu
cosa
min
e(1
0Æ0
)
Chro
miu
m(7
Æ0)
Gin
kgo
bil
oba
(6Æ0
)
JAN: REVIEW PAPER Use of complementary and alternative medicine people with diabetes
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 311

Table
2(C
onti
nued
)
Auth
or
Countr
yn
(RR
)D
esig
nsa
mpling
Res
earc
hques
tion
Tim
efra
me
Use
rate
Popula
rth
erapie
sli
st(%
)
Al-
Sae
edi
etal
.(2
003),
Ara
bia
1039
DM
(89Æ4
%)
Random
sam
ple
wit
h
per
sonal
inte
rvie
w
Do
not
men
tion
(her
bal
rem
edie
s)
NM
30Æ1
%Fen
ugre
ek(6
Æ1)
Chin
aber
ryle
ave
s–
Nee
m
(5Æ1
)and
Ham
al
(4Æ8
)
Yel
low
wood
sorr
el
(1Æ9
)
Oli
ve
leave
s(1
Æ6)
Bit
ter
apple
(1Æ3
)
Radis
h(1
Æ0)
Arg
aez
-Lopez
etal
.
(2003),
Mex
ico
353
Typ
e2
dia
bet
es
(NM
)
Do
not
men
tion
Have
you
ever
use
dany
of
the
follow
ing
nin
e
ther
apie
s?
NM
62Æ0
%H
erbal
rem
edie
s(9
4Æ2
)
Opunti
a(7
3Æ1
)
Oth
ers
(5Æ8
)
Lee
etal
.(2
004),
Kore
an
223
DM
(87Æ8
%–97Æ1
%)
dif
fere
nt
sett
ing
Conven
ience
sam
ple
wit
h
self
-rep
ort
Have
you
ever
use
d
alt
ernati
ve
ther
apie
s?
Ali
stof
CA
Mw
asuse
d
for
furt
her
ques
tion
Lif
e-ti
me
65Æ0
%Pla
nt
der
ived
(63Æ7
)
Cer
eal
and
seed
(21Æ0
)
Ste
am
and
leave
s(2
1Æ0
)
Root
(15Æ8
)Fru
it(6
Æ7)
Flo
wer
(4)
Sea
wee
d(0
Æ8)
Anim
al
mate
rials
(21Æ6
)
Mea
t(1
6Æ4
)
Mari
ne
pro
duct
(5Æ2
)
Mis
cell
aneo
us
(14Æ7
)
Mix
edm
ate
rial
(8Æ5
)
Moola
sarn
etal
.(2
005),
Thail
and
159
DM
(98Æ1
%)
Conven
ience
sam
ple
wit
h
per
sonal
inte
rvie
w
Have
you
use
dC
AM
duri
ng
the
past
3m
onth
s?
3M
s47Æ0
%Y
oga/e
xer
cise
(46Æ0
)
Unch
anged
form
of
her
bal
med
icin
e(4
2Æ1
)
Changed
form
of
her
bal
med
icin
e(2
5Æ0
)
Acu
punct
ure
/
acu
pre
ssure
(10Æ5
)
Men
tal
ther
apy
(7Æ9
)
Die
tsu
pple
men
t(5
Æ3)
Oil
mass
age
(2Æ6
)
Oth
ers
(1Æ3
)
Arc
ury
etal
.(2
006),
rura
lU
SA
701
Eld
erly
wit
hdia
bet
es
(89%
)
Random
sam
ple
wit
h
per
sonal
inte
rvie
w
Have
you
use
dat
least
one
ther
apy
inea
chof
the
eight
CA
Mca
tegori
esin
the
past
yea
r?
12
Ms
NM
For
gen
eral
reaso
n
Oth
erhom
ere
med
ies
(56Æ0
)
Food
hom
ere
med
ies
(52Æ0
)
Vit
am
ins
(44Æ8
)
Min
erals
(17Æ3
)
CA
Mth
erapie
s(9
Æ9)
CA
Mpra
ctit
ioner
s(8
Æ4)
For
dia
bet
esre
aso
n
Food
hom
ere
med
ies
(11Æ9
)
Oth
erhom
ere
med
ies
(10Æ5
)
Vit
am
ins
(5Æ7
)
CA
Mth
erapie
s(2
Æ5)
Min
erals
(2Æ 4
)
Her
bs
(2Æ4
)
Lin
det
al.
(2006),
USA
20,7
22
DM
(NM
)
Cla
ims
data
from
two
larg
ein
sure
rs
CA
Mpra
ctit
ioner
use
by
insu
red
pati
ents
wit
h
dia
bet
es
12
Ms
17Æ4
%C
hir
opra
ctors
(14Æ6
)
Lic
ense
dm
ass
age
ther
apis
t(3
Æ4)
Acu
punct
uri
sts
(1Æ4
)
Natu
ropath
y
physi
cians
(1Æ1
)
Kum
aret
al.
(2006),
India
493
DM
(NM
)
Syst
emat
icsa
mpli
ng
wit
h
per
sonal
inte
rvie
w
New
case
sin
clin
ics
by
ass
essi
ng
thei
ruse
of
CA
M
india
bet
es
Curr
ent
67Æ7
%N
atu
ropath
y(9
7Æ3
)
Ayurv
eda
(16Æ2
)
Hom
eopath
y(1
2Æ9
)
Acu
pre
ssure
(2Æ7
)
Oth
ers
(3Æ0
)
H.-Y. Chang et al.
312 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

non-response rates and the choice of study sample (six of 13
studies used convenience sampling) (see Table 2). In addition,
recall bias may have occurred in retrospective studies. The
other problem that hinders comparison of studies of CAM
use is the size of the sample. For example, the sample sizes in
two US studies, while large overall, only included small
numbers of people living with diabetes and using CAM. In
Yeh et al.’s (2002) study there were only 53 people with
diabetes and only 62 people in Egede et al.’s (2002) study. It
would be very difficult to extrapolate an expected prevalence
within the larger population from these samples.
Due to the inconsistency in the definition of CAM and the
inconsistency of research design, considerable uncertainties
exist in regard to demonstrating the true prevalence of CAM
use by people with diabetes. Despite these limitations, several
interesting characteristics and consistent trends emerged
within this review that may inform nurse and patient
education, clinical practice and clinical research.
Prevalence of CAM use among people with diabetes
worldwide
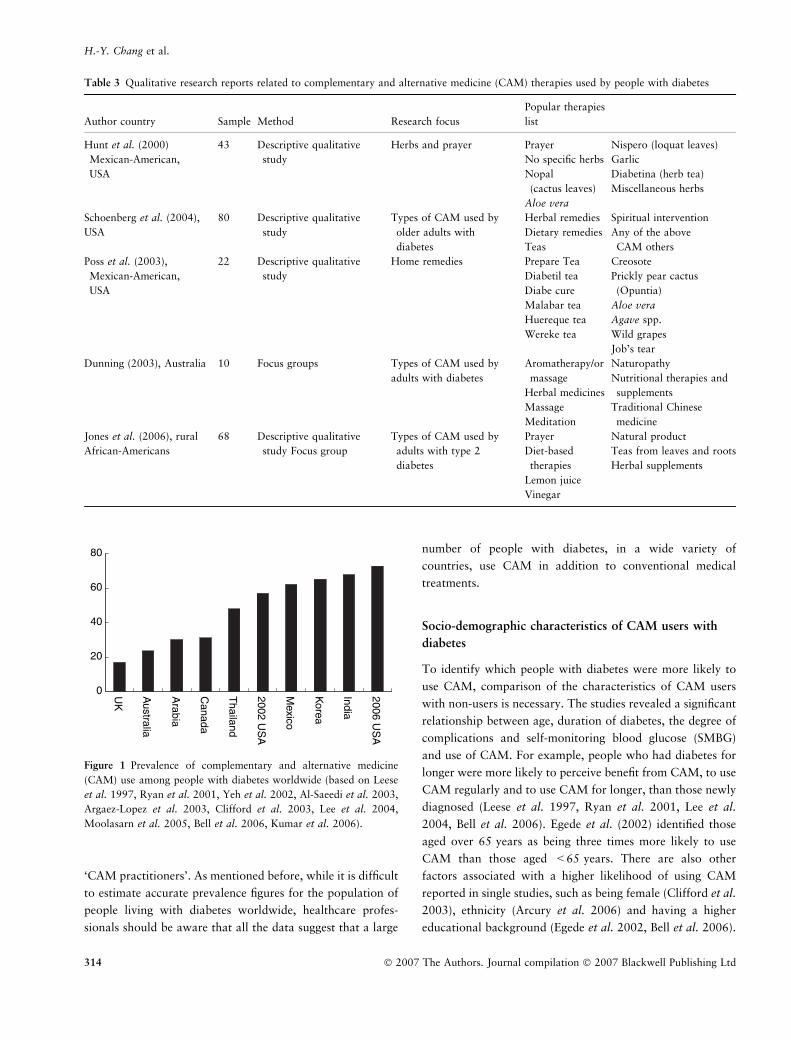
The results of this literature review illustrate that prevalence
estimates vary widely, depending on the definition of CAM
and survey design used by researchers. Figure 1 shows the
prevalence of CAM use among people with diabetes outlined
in each of the studies. The results range from a low of 17% in
a study conducted in United Kingdom (UK) to a high of
72Æ8% in the newest data from the USA. The average
percentage of CAM use across populations living with
diabetes (45Æ53%) suggests that nearly half of people with
diabetes have used some form of CAM in conjunction
with conventional medicines.
The studies related to prevalence of biologically based
CAM use came from three studies conducted in Australia,
Arabia and Canada (Ryan et al. 2001, Al-Saeedi et al. 2003,
Clifford et al. 2003). These studies showed similar usage rates
ranging from 23Æ6% to 31% (see Figure 1). The remaining
studies from Thailand, the USA, Mexico, Korea, and India
investigated the whole spectrum of CAM use among people
with diabetes and demonstrated not surprisingly a higher
prevalence of CAM use with a range between 47Æ8% and
72Æ8% (Leese et al. 1997, Yeh et al. 2002, Argaez-Lopez et al.
2003, Lee et al. 2004, Moolasarn et al. 2005, Bell et al. 2006,
Garrow & Egede 2006, Kumar et al. 2006) (see Figure 1).
Only in one study (Lind et al. 2006), a survey of the use of
CAM practitioners, did the prevalence remain low (17Æ4%)
(see Table 2). On the basis of the data outlined in this review,
the prevalence of the whole spectrum of CAM use is clearly
greater than that of only ‘biologically based therapies’ orTable
2(C
onti
nued
)
Auth
or
Countr
yn
(RR
)D
esig
nsa
mpli
ng
Res
earc
hques
tion
Tim
efra
me
Use
rate
Popula
rth
erapie
slist
(%)
Garr
ow
and
Eged
e
(2006),
USA
>31,0
00
DM¼
2474
(NM
)
2002
Nati
onal
inte
rvie
w
surv
ey
Coll
ecte
dover
17
dif
fere
nt
types
of
CA
M
inth
epast
yea
r?
12
Ms
48Æ0
%V
itam
ins
(67Æ0
)
Pra
yer
(67Æ0
)
Her
bal
rem
edy
(22Æ0
)
Chir
opra
ctic
care
(21Æ0
)
Rel
axati
on
tech
niq
ues
(17Æ0
)
Oth
erC
AM
s(1
4Æ0
)
Die
t-base
dth
erapie
s
(7Æ0
)
Yoga
(4Æ0
)
Bel
let
al.
(2006),
USA
30,7
85
DM
(99Æ2
%)
2002
Nati
onal
Inte
rvie
w
Surv
ey
Have
you
use
dth
e
foll
ow
ing
20
CA
M
ther
apie
sin
the
past
yea
r?
12
Ms
72Æ8
%Sel
f-pra
yer
(61Æ2
)
Oth
erpra
yer
(39)
Pra
yer
gro
up
(16Æ2
)
Natu
ral
pro
duct
(non-v
itam
in,
non-m
iner
al)
(15Æ7
)
Rel
axati
on
tech
niq
ues
(12Æ7
)
Acu
punct
uri
sts
(1Æ4
)
Chir
opra
ctic
care
(6Æ8
)
Hea
ling
ritu
al
(4Æ2
)
Die
t-base
dth
erapie
s
(3Æ2
)
Meg
avit
am
in(3
Æ1)
CA
M,
com
ple
met
ary
and
alt
ernati
ve
med
icin
e;D
M,
dia
bet
esm
elli
tus;
Ms,
month
s;n,
num
ber
of
sam
ple
;N
M,
not
men
tioned
;R
R,
resp
onse
rate
.
JAN: REVIEW PAPER Use of complementary and alternative medicine people with diabetes
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 313
‘CAM practitioners’. As mentioned before, while it is difficult
to estimate accurate prevalence figures for the population of
people living with diabetes worldwide, healthcare profes-
sionals should be aware that all the data suggest that a large
number of people with diabetes, in a wide variety of
countries, use CAM in addition to conventional medical
treatments.
Socio-demographic characteristics of CAM users with
diabetes
To identify which people with diabetes were more likely to
use CAM, comparison of the characteristics of CAM users
with non-users is necessary. The studies revealed a significant
relationship between age, duration of diabetes, the degree of
complications and self-monitoring blood glucose (SMBG)
and use of CAM. For example, people who had diabetes for
longer were more likely to perceive benefit from CAM, to use
CAM regularly and to use CAM for longer, than those newly
diagnosed (Leese et al. 1997, Ryan et al. 2001, Lee et al.
2004, Bell et al. 2006). Egede et al. (2002) identified those
aged over 65 years as being three times more likely to use
CAM than those aged <65 years. There are also other
factors associated with a higher likelihood of using CAM
reported in single studies, such as being female (Clifford et al.
2003), ethnicity (Arcury et al. 2006) and having a higher
educational background (Egede et al. 2002, Bell et al. 2006).
Table 3 Qualitative research reports related to complementary and alternative medicine (CAM) therapies used by people with diabetes
Author country Sample Method Research focus
Popular therapies
list
Hunt et al. (2000)
Mexican-American,
USA
43 Descriptive qualitative
study
Herbs and prayer Prayer
No specific herbs
Nopal
(cactus leaves)
Aloe vera
Nispero (loquat leaves)
Garlic
Diabetina (herb tea)
Miscellaneous herbs
Schoenberg et al. (2004),
USA
80 Descriptive qualitative
study
Types of CAM used by
older adults with
diabetes
Herbal remedies
Dietary remedies
Teas
Spiritual intervention
Any of the above
CAM others
Poss et al. (2003),
Mexican-American,
USA
22 Descriptive qualitative
study
Home remedies Prepare Tea
Diabetil tea
Diabe cure
Malabar tea
Huereque tea
Wereke tea
Creosote
Prickly pear cactus
(Opuntia)
Aloe vera
Agave spp.
Wild grapes
Job’s tear
Dunning (2003), Australia 10 Focus groups Types of CAM used by
adults with diabetes
Aromatherapy/or
massage
Herbal medicines
Massage
Meditation
Naturopathy
Nutritional therapies and
supplements
Traditional Chinese
medicine
Jones et al. (2006), rural
African-Americans
68 Descriptive qualitative
study Focus group
Types of CAM used by
adults with type 2
diabetes
Prayer
Diet-based
therapies
Lemon juice
Vinegar
Natural product
Teas from leaves and roots
Herbal supplements
0
20
40
60
80
UK
Australia
Arabia
Canada
Thailand
2002 US
A
Mexico
Korea
India
2006 US
A
Figure 1 Prevalence of complementary and alternative medicine
(CAM) use among people with diabetes worldwide (based on Leese
et al. 1997, Ryan et al. 2001, Yeh et al. 2002, Al-Saeedi et al. 2003,
Argaez-Lopez et al. 2003, Clifford et al. 2003, Lee et al. 2004,
Moolasarn et al. 2005, Bell et al. 2006, Kumar et al. 2006).
H.-Y. Chang et al.
314 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

Interestingly, receiving a diabetes education programme
was associated with a higher use of CAM in Korea (Lee et al.
2004). Similarly, it was found in Australia that people
completing a home blood glucose monitoring diary are more
likely to use CAM (Clifford et al. 2003). Hunt et al. (2000)
explained this by indicating that people who are highly
motivated to control their diabetes usually engage in an
earnest effort to try all types of CAM available to them. It
also has been identified in scientific studies that people view
CAM as less authoritarian, more empowering and as offering
them more personal autonomy and control over their
healthcare decisions (Astin 1998, Thorne et al. 2002). The
findings indicate that people actively engage in the use of
CAM as a strategy for health self-management. Nowadays,
diabetes care focuses on self-management with patients and
healthcare professionals collaborating as equals. Therefore,
assisting patients in the assessment of potential benefits,
adverse effects and potential interactions of CAMs with
conventional medicine, when used concomitantly, is an
essential role of healthcare professionals.
Common types of CAM used by people with diabetes
When examining which CAM are most frequently used by
people with diabetes, there are two major kinds of surveys:
those that include the whole spectrum of CAM and those that
include only ‘biologically based therapies’. The studies that
focus only on biologically based CAMs were conducted in
Canada and Australia. They display similar results, for
example, the most frequently used biologically based CAM
were: vitamins (most frequently used were multivitamins and
vitamins B and C); nutritional supplements (fish oil, glucosa-
mine and calcium); and herbal medicines (garlic, echinacea
and ginkgo) (Ryan et al. 2001, Clifford et al. 2003). The other
surveys included the whole spectrum of CAM therapies used
in countries such as the USA and Thailand and those most
frequently used for diabetes were prayer/spiritual practice,
herbal medicines, relaxation techniques, chiropractic, nutri-
tional advice and massage (Egede et al. 2002, Moolasarn et al.
2005, Arcury et al. 2006, Bell et al. 2006). However, countries
with a long tradition of alternative health systems such as
Arabia, Mexico and Korea reported regimens ranging widely
from plant derived to animal materials, such as fenugreek,
opuntia, and silk worm (Argaez-Lopez et al. 2003, Lee et al.
2004, Moolasarn et al. 2005). This phenomenon may occur
because when people choose a particular CAM, they are
usually attracted to options congruent with their values,
culture and world view (Vincent & Furnham 1996, Astin
1998, Dunning 2003). All the popular CAM therapies
outlined in each study are presented in Tables 2 and 3.
Even though the common types of CAM may differ from
country to country, the distribution among diabetic popula-
tions seems to follow a common pattern. The most frequently
used CAMs have been identified as: nutritional supplements,
herbal medicines, nutritional advice, spiritual healing, and
relaxation techniques. Reflecting on these common patterns,
it seems that living with the continual burden of blood
glucose testing, following particular eating habits, injecting
insulin, feeling different from normal, facing complications
and coming to terms with their own mortality has a
significant effect on the patient’s quality of life; often
engendering fear and powerlessness; and can compromise
physical and psychological functioning (Dunning 2003).
Importantly, since providing people with appropriate recom-
mendations, so they can make informed decisions is a
significant aspect of nursing care; nurses need to seek
evidence-based information regarding CAM for the manage-
ment of diabetes in order to assist people with diabetes to use
CAMs safely and to plan a suitable approach to achieve
maximal blood glucose control.
Disclosure of CAM use to healthcare professionals
Safety of CAM use is an important issue from the point of
view of people using these medicines and healthcare profes-
sionals, particularly because of the growing popularity of
CAM use among people with diabetes. Although CAM is not
presently considered as part of conventional medicine, the
majority of patients use CAM along with conventional
medicine rather than in place of it. Problematically, the
extent to which people disclose their use of CAM to their
physicians actually remains low. However, only four out of
the 13 studies included in this review reported on the issue of
the disclosure of CAM use to healthcare professionals. In the
USA, the non-disclosure rate (43%) (Egede et al. 2002) is
lower than in countries such as Mexico (64%) (Argaez-Lopez
et al. 2003) and Thailand (64Æ4%) (Moolasarn et al. 2005).
In one qualitative study, conducted by Dunning (2003) in
Australia (see Table 3), only one of 10 participants had
informed conventional health professionals of CAM use;
however, all participants had informed their CAM therapist
that they had diabetes, and detailed the medications they
were taking. There is an opportunity for nursing staff to
make a difference by taking time in patient assessment and
displaying an attitude that encourages people to disclose their
CAM use.
Patients usually expressed the attitude that CAM may not
help much, but will probably not hurt, provided they
continue with the conventional treatments recommended by
their physicians (Hunt et al. 2000). Contrary to this popular
JAN: REVIEW PAPER Use of complementary and alternative medicine people with diabetes
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 315

belief, several case reports indicated that the use of both
herbal medicine and conventional medicine resulted in the
adverse effects from herb–drug interaction (Gill et al. 1994,
Dunning et al. 2001, Goudie & Kaye 2001, Wood et al.
2004). For example, Clifford et al. (2003) reported that, of
people with diabetes, >43% who used CAM had the
potential for herb–drug interaction, and required extra
monitoring for the adverse effects. Therefore, a responsible
healthcare approach is that patients should receive evidence-
based CAM information about efficacy, effectiveness, adverse
effects and possible interactions, to inform their decision-
making related to CAM use.
Implications for nursing
The high levels of CAM use, reported in the studies
summarized in Tables 2 and 3, highlight the need for an
evidence-based assessment of CAM. This is necessary because
all of these therapies and medicines have their own potential
benefits and potential interactions with conventional treat-
ments and should be evaluated for quality, safety and efficacy
before use. Common herbal medicines used by people with
diabetes include ginseng, bitter melon, fenugreek and nutri-
tional supplements such as chromium, magnesium and fish oil
(Ezzo et al. 2001, Yeh et al. 2003, Manyam 2004). Table 1
presents an overview of commonly used medicinal herbs and
nutritional supplements; however, this list is not a complete
review of CAMs used in diabetes. More than 1000 traditional
plants have been claimed to benefit treatment of diabetes
worldwide (Day 2005), but not all of these have been
thoroughly investigated. Several comprehensive reviews sum-
marize the evidence for the use of numerous plants and
supplements such as fish oil in the treatment of diabetes
(Farmer et al. 2001, Shane-McWhorter 2001, Yeh et al.
2003). CAM therapies commonly used for the treatment of
diabetes include traditional Chinese medicine, yoga and
massage. However, no recent reviews of the evidence of
some CAM therapies such as acupuncture exist, although
initial studies suggest beneficial effects, for example in
diabetes related peripheral neuritis (Jiang et al. 2006).
This literature review not only assists nurses and other
healthcare professionals to understand the prevalence of
CAM use among people with diabetes, but also to raise the
issue of non-disclosure of CAM use to healthcare profession-
als and the resultant potential risks. Nurses need to be aware
of the possibility that their patients are using CAM therapies;
particularly, as they are often the patient’s first point of
contact within the healthcare system, and thus may under-
take the first assessment of the patient’s healthcare practices.
Essentially, nurses need knowledge about CAM in order to
undertake a complete health assessment, to identify which
CAMs have benefit for people with diabetes and potential
CAM–drug interactions, and to be able to inform physicians
and other healthcare professionals about their patients’ CAM
use (Cuellar et al. 2003).
The increased presence of CAM-related courses in medical
and nursing curricula is apparent in the USA and Canada, as
well as other countries (Haramati & Lumpkin 2004);
however, most CAM courses in a curriculum are electives
(Dutta et al. 2003) and few are offered in the baccalaureate
level programmes (Burke et al. 2004). Several research studies
indicated that the majority of healthcare professionals still
consider their knowledge insufficient to meet current needs
regarding answering their patients’ questions and appro-
priately referring them to reputable CAM practitioners
(DeKeyser et al. 2001, Fearson 2003, Wetzel et al. 2003).
Thus, up-to-date education on CAM within undergraduate
and postgraduate programmes and ongoing professional
development is imperative. For example, future nursing
curricula should include content on the efficacy and effect-
iveness of CAMs used by people with diabetes, possible toxic
effects and potential interactions with other medicines.
In future CAM surveys it is imperative that definitions and
methods are employed consistently to enable clinicians and
researchers to compare results across a number of studies. It
is important for researchers to use the most common
definition of CAM and the categories of CAM as defined
by NCCAM. It would also be helpful if researchers were to
survey and report separately on CAM therapist consultations
and the use of CAMs, as well as on point prevalence and
lifetime prevalence of use.
Most of the studies included in this review did not question
participants about their reasons for using CAM (Leese et al.
1997, Ryan et al. 2001, Argaez-Lopez et al. 2003, Clifford
et al. 2003). Ninety-one per cent, however, of participants in
Leese et al.’s (1997) study used CAM for non-diabetes-related
problems, while only 35% reported use specifically for
diabetes in Yeh et al.’s (2002) study. Future research needs
to include questions about reason for use of as well as type of
CAM used and frequency.
In order to assist healthcare professionals in the under-
standing of the culture of diabetes care, future studies might
benefit from using cultural frameworks such as the explan-
atory model of illness to explore the illness experience and the
role of CAM use in coping with chronic illness. While there is
currently some information available about which CAMs are
used by people with diabetes, further research needs to focus
on the patterns of use, the predictors of use, the factors
affecting communication with health professionals and the
efficacy and effectiveness of commonly used CAMs.
H.-Y. Chang et al.
316 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

Conclusion
Diabetes mellitus is a chronic illness, and a leading cause of
death, disability and hospitalization. Since this chronic
disease affects the entirety of a person’s being, seeking
treatment through CAM approaches has become a strategy
used to improve well-being. Although there are considerable
uncertainties in regard to demonstrating the true prevalence
of CAM use among diabetic populations worldwide, due to
the inconsistency in the definition of CAM and the inconsis-
tency of research design, this literature review illustrates a
high level of CAM use among people with diabetes attending
conventional healthcare services in different countries and
regions. Additionally, a significant relationship between
CAM use and age, duration of DM, the degree of compli-
cations and SMBG has been revealed.
Although evidence supports the notion that people with
diabetes are using CAM as a supplementary means of
treating their disease, a substantial gap exists in their
attitudes related to communicating CAM use to healthcare
professionals. This may cause disease mismanagement when
healthcare professionals are unaware of CAM use.
Therefore, healthcare professionals must be aware of the
increase in the number of patients who use CAM while
under conventional care.
Through diabetes patient education programmes, nurses
are the members of healthcare team who work most closely
with people with diabetes in taking control of their disease,
especially in aiming to empower people to self-manage their
diabetes. However, if nurses do not consider the patient’s
background, health history, health beliefs and cultural
diversity, it would be difficult to address that patient’s health
problems and plan specific strategies designed to modify
lifestyle. Accepting that people with diabetes try CAM and
helping them sort through the many available choices are
important roles for nurses among other healthcare profes-
sionals. Therefore, understanding CAM therapies and their
integration into conventional medicine is needed in order to
ensure patient safety and optimize health care.
Author contributions
HC, MW and ET were responsible for the study conception
and design and the drafting of the manuscript. HC, MW and
ET made critical revisions to the paper. MW and ET
supervised the study.
References
Al-Saeedi M., Elzubier A.G., Bahnassi A.A. & Al-Dawood K.M.
(2003) Patterns of belief and use of traditional remedies by diabetic
patients in Mecca, Saudi Arabia. Eastern Mediterranean Health
Journal 9(1–2), 99–107.
Arcury T.A., Bell R.A., Snively B.M., Smith S.L., Skelly A.H., Wetmore
L.K. & Quandt S.A. (2006) Complementary and alternative medi-
cine use as health self-management: rural older adults with diabetes.
The Journals of Gerontology: Social Sciences 61B(2), S62–S70.
Argaez-Lopez N., Wacher N.H., Kumate-Rodriguez J., Cruz M.,
Talavera J., Rivera-Arce E. et al. (2003) The use of complementary
and alternative medicine therapies in type 2 diabetic patients in
Mexico. Diabetes Care 26(8), 2470.
Astin J.A. (1998) Why patients use alternative medicine: results of a
national study. JAMA: The Journal of the American Medical
Association 279(19), 1548–1553.
Basch E., Gabardi S. & Ulbricht C. (2003) Bitter melon (Momordica
charantia): a review of efficacy and safety. American Journal of
Health-System Pharmacy 60(4), 356–359.
Bell R.A., Suerken C.K., Grzywacz J.G., Lang W., Quandt S.A. &
Arcury T.A. (2006) Complementary and alternative medicine use
among adults with diabetes in the United States. Alternative
Therapies in Health and Medicine 12(5), 16–22.
Burke A., Peper E., Burrows K. & Kline B. (2004) Developing the
complementary and alternative medicine education infrastructure:
What is already known about this topic
• Diabetes mellitus is a chronic illness, and a leading
cause of death, disability and hospitalization.
• Complementary and alternative medicine use varies
from country to country and within different patient
populations.
• Diabetes mellitus affects the entirety of a person’s being
and increasingly people use complementary and alter-
native medicine in conjunction with other medical
treatments and lifestyle modifications to manage their
condition and improve well-being.
What this paper adds
• Review of the epidemiological studies related to com-
plementary and alternative medicine use is complicated
by inconsistency of definition and research design.
• Use of complementary and alternative medicine varies
among people with diabetes but nutritional supple-
ments, herbal medicines, nutritional advice, spiritual
healing and relaxation techniques are the most popular
therapies in this population.
• Because of the risk of interactions between conventional
and complementary medicines, healthcare professionals
need to include complementary and alternative medi-
cine use in patient assessment and there may be a need
to increase the focus on their use in nursing curricula.
JAN: REVIEW PAPER Use of complementary and alternative medicine people with diabetes
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 317

baccalaureate programs in the United States. Journal of Alternative
and Complementary Medicine 10(6), 1115–1121.
Clifford R.M., Batty K.T., Davis W. & Davis T.M. (2003) Prevalence
and predictors of complementary medicine usage in diabetes: Fre-
mantle Diabetes Study. Journal of Pharmacy Practice and Research
33(4), 260–264.
Cuellar N.G., Cahill B., Ford J. & Aycock T. (2003) The develop-
ment of an educational workshop on complementary and alter-
native medicine: what every nurse should know. Journal of
Continuing Education in Nursing 34(3), 128–135.
Day C. (2005) Are herbal remedies of use in diabetes? Diabetic
Medicine 22(Suppl. 1), 10–12.
DeKeyser F.G., Cohen B.B. & Wagner N. (2001) Knowledge levels
and attitudes of staff nurses in Israel towards complementary and
alternative medicine. Journal of Advanced Nursing 36(1), 41–48.
Dey L., Attele A.S. & Yuan C.S. (2002) Alternative therapies for type
2 diabetes. Alternative Medicine Review 7(1), 45–58.
Dunning T. (2003) Complementary therapies and diabetes. Com-
plementary Therapies in Nursing and Midwifery 9(2), 74–80.
Dunning T., Chan S.P., Hew F.L., Pendek R., Mohd M.A. & Ward G.
(2001) Transcultural therapy. A cautionary tale on the use of
complementary therapies. Diabetes Primary Care 3(2), 58–63.
Dutta A.P., Bwayo S., Xue Z., Akiyode O., Ayuk-Egbe P., Bernard D.
et al. (2003) Complementary and alternative medicine instruction
in nursing curricula. JNBNA: Journal of National Black Nurses’
Association 14(2), 30–33.
Egede L., Ye X., Zheng D. & Silverstein M. (2002) The prevalence
and pattern of complementary and alternative medicine use in
individuals with diabetes. Diabetes Care 25(2), 324–329.
Eisenberg D.M., Davis R.B., Ettner S.L., Appel S., Wilkey S., Van
Rompay M. et al. (1998) Trends in alternative medicine use in
the United States, 1990–1997: Results of a follow-up national
survey. JAMA: The Journal of the American Medical Association
280(18), 1569–1575.
Emslie M., Campbell M. & Walker K. (1996) Family Medicine
Complementary therapies in a local healthcare setting. Part 1: is
there real public demand? Complementary Therapies in Medicine
4(1), 39–42.
Ernst E. (1999) Prevalence of complementary/alternative medicine
for children: a systematic review. European Journal of Pediatrics
158(1), 7–11.
Ezzo J., Donner T., Nickols D. & Cox M. (2001) Is massage useful in
the management of diabetes? A systematic review. Diabetes Spec-
trum 14(4), 218–225.
Farmer A., Montori V.M., Dinneen S.F. & Clar C. (2001) Fish oil
in people with type 2 diabetes mellitus. Cochrane Database of
Systematic Reviews, Issue 3, 1–35, art. no.: CD003205. DOI:
10.1002/14651858. CD003205.
Fearson J. (2003) Complementary therapies: knowledge and attitudes
of health professionals. Paediatric Nursing 15(6), 31–35.
Franz M.J., Bantle J.P., Beebe C.A., Brunzell J.D., Chiasson J.-L.,
Garg A. et al. (2002) Evidence-based nutrition principles and rec-
ommendations for the treatment and prevention of diabetes and
related complications. Diabetes Care 25(1), 148–198.
Garrow D. & Egede L.E. (2006) Association between com-
plementary and alternative medicine use, preventive care practices,
and use of conventional medical services among adults with dia-
betes. Diabetes Care 29(1), 15–19.
Gill G.V., Redmond S., Garratt F. & Paisey R. (1994) Diabetes and
alternative medicine: cause for concern. Diabetes Medicine 11(2),
210–213.
Goguen J.M. & Leiter L.A. (2001) Alternative therapy: the role of
selected mineral, vitamins, fiber, and herbs in treating hyperglyc-
ermia. In Evidence-Based Diabetes Care (Gerstein H.C. & Haynes
R.B., eds), BC Decker Inc., Hamilton, London, pp. 295–322.
Goudie A.M. & Kaye J.M. (2001) Contaminated medication pre-
cipitating hypoglycaemia. The Medical Journal of Australia
175(5), 256–257.
Guerrero-Romero F. & Rodriguez-Moran M. (2005) Complementary
therapies for diabetes: the case for chromium, magnesium, and
antioxidants. Archives of Medical Research 36(3), 250–257.
Haramati A. & Lumpkin M.D. (2004) Complementary and
alternative medicine: opportunities for education and research.
Experimental Biology and Medicine (Maywood, N.J.) 229(8),
695–697.
Harris P. & Rees R. (2000) The prevalence of complementary and
alternative medicine use among the general population: a sys-
tematic review of the literature. Complementary Therapies in
Medicine 8(2), 88–96.
Hunt L.M., Arar N.H. & Akana L.L. (2000) Herbs, prayer, and
insulin. Use of medical and alternative treatments by a group of
Mexican American diabetes patients. Journal of Family Practice
49(3), 216–223.
Jiang H., Shi K., Li X., Zhou W. & Cao Y. (2006) Clinical study on
the wrist-ankle acupucture threatment for 30 cases of diabetes
peripheral neuritis. Journal of Traditional Chinese Medicine 26(1),
8–12.
Jones R.A., Utz S., Wenzel J., Steeves R., Hinton I., Andrews D. et al.
(2006) Use of complementary and alternative therapies by rural
African Americans with type 2 diabetes. Alternative Therapies
Health and Medicine 12(5), 34–38.
Kumar D., Bajaj S. & Mehrotra R. (2006) Knowledge, attitude and
practice of complementary and alternative medicines for diabetes.
Public Health 120(8), 705–711.
Lee M.S., Lim H.J. & Moon S.R. (2004) Survey of the use of
complementary and alternative medicine among Korean diabetes
mellitus patients. Pharmacoepidemiology and Drug Safety 13(3),
167–171.
Leese G.P., Gill G.V. & Houghton G.M. (1997) Prevalence of
complementary medicine usage within a diabetes clinic. Practical
Diabetes International 14(7), 207–208.
Lew-Ting C.Y. (2003) Who uses non-biomedical, complement and
alternative health care? Sociodemographic undifferentiation and
the effects of health needs. Taiwan Journal Public Health 22(3),
155–166.
Lim M.K., Sadarangani P., Chan H.L. & Heng J.Y. (2005) Com-
plementary and alternative medicine use in multiracial Singapore.
Complementary Therapies in Medicine 13(1), 16–24.
Lind B.K., Lafferty W.E., Grembowski D.E. & Diehr P.K. (2006)
Complementary and alternative provider use by insured patients
with diabetes in Washington State. Journal of Alternative Com-
plement Medicine 12(1), 71–77.
Liu J.P., Zhang M., Wang W.Y. & Grimsgaard S. (2002) Chinese
herbal medicines for type 2 diabetes mellitus. Cochrane Database
of Systematic Reviews, Issue 3, 1–102, art. no.: CD003642. DOI:
10.1002/14651858.CD003642.pub2.
H.-Y. Chang et al.
318 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

MacLennan A.H., Wilson D.H. & Taylor A.W. (2002) The escalat-
ing cost and prevalence of alternative medicine. Preventive Medi-
cine 35(2), 166–173.
Manyam B.V. (2004) Diabetes mellitus, ayurveda, and yoga. Journal
of Alternative Complement Medicine 10(2), 223–225.
Moolasarn S., Sripa S., Kuessirikiet V., Sutawee K., Huasary J.,
Chaisila C. et al. (2005) Usage of and cost of complementary/
alternative medicine in diabetic patients. Journal of the Medical
Association of Thailand 88(11), 1630–1637.
Murphy L.S., Reinsch S., Najm W.I., Dickerson V.M., Seffinger
M.A., Adams A. et al. (2003) Searching biomedical databases on
complementary medicine: the use of controlled vocabulary among
authors, indexers and investigators. BMC Complementary and
Alternative Medicine 3(3), 1–13.
National Centre for Complementary and Alternative Medicine
(2002) NCCAM Publication No. D156 – What is Complementary
and Alternative Medicine? Retrieved from http://nccam.nih.gov/
health/whatiscam/ on 7 May 2005.
Pittler M.H. & Ernst E. (2005) Complementary therapies for
peripheral arterial disease: systematic review. Atherosclerosis
181(2005), 1–7.
Poss J.E., Jezewski M.A. & Stuart A.G. (2003) Home remedies for
type 2 diabetes used by Mexican Americans in El Paso, Texas.
Clinical Nursing Research 12(4), 304–323.
Ryan E.A., Pick M.E. & Marceau C. (2001) Use of alternative
medicines in diabetes mellitus. Diabetes Medicine 18(3), 242–
245.
Schoenberg N.E., Stoller E.P., Kart C.S., Perzynski A. & Chapleski
E.E. (2004) Complementary and alternative medicine use among a
multiethnic sample of older adults with diabetes. Journal of
Alternative and Complementary Medicine 10(6), 1061–1066.
Shane-McWhorter L. (2001) Biological complementary therapies: a
focus on botanical products in diabetes. Diabetes Spectrum 14(4),
199.
Sievenpiper J.L., Arnason J.T., Vidgen E., Leiter L.A. & Vuksan V.
(2004) A systematic quantitative analysis of the literature of the
high variability in ginseng (Panax spp.): should ginseng be trusted
in diabetes? Diabetes Care 27(3), 839–840.
Thorne S., Paterson B., Russell C. & Schultz A. (2002) Com-
plementary/alternative medicine in chronic illness as informed self-
care decision making. International Journal of Nursing Studies
39(7), 671–683.
Tindle H.A., Davis R.B., Phillips R.S. & Eisenberg D.M. (2005)
Trends in use of complementary and alternative medicine by US
adults: 1997–2002. Alternative Therapies in Health and Medicine
11(1), 42–49.
Vincent C. & Furnham A. (1996) Why do patients turn to com-
plementary medicine? An empirical study. British Journal of
Clinical Psychology 35(Pt 1), 37–48.
Wetzel M.S., Kaptchuk T.J., Haramati A. & Eisenberg D.M. (2003)
Complementary and alternative medical therapies: implications for
medical education. Annals of Internal Medicine 138(3), 191–196.
Wood D.M., Athwal S. & Panahloo A. (2004) The advantages and
disadvantages of a ‘herbal’ medicine in a patient with diabetes
mellitus: A case report. Diabetes Medicine 21(6), 625–627.
World Health Organization (2003) Fact Sheet No. 134 ‘‘Traditional
medicine’’. Retrieved from http://www.who.int/mediacentre/fact-
sheets/fs134/en/print.html on 16 September 2005.
World Health Organization (2004) Diabetes action now. Retrieved
from http://www.who.int/diabetes/actionnow/en/DANbooklet.pdf
on 16 November 2005.
Yeh G.Y., Eisenberg D.M., Davis R.B. & Phillips R.S. (2002) Use of
complementary and alternative medicine among persons with
diabetes mellitus: results of a national survey. American Journal of
Public Health 92(10), 1648–1652.
Yeh G.Y., Eisenberg D.M., Kaptchuk T.J. & Phillips R.S. (2003)
Systematic review of herbs and dietary supplements for glycemic
control in diabetes. Diabetes Care 26(4), 1277–1294.
JAN: REVIEW PAPER Use of complementary and alternative medicine people with diabetes
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 319