Upregulation of REG Iα accelerates tumor progression in pancreatic cancer with diabetes
9
Upregulation of REG Ia accelerates tumor progression in pancreatic cancer with diabetes Lin Zhou 1 , Ruifeng Zhang 2 , Lishun Wang 3 , Shaoming Shen 3 , Hiroshi Okamoto 4 , Akira Sugawara 4 , Li Xia 3 , Xiaoling Wang 3 , Naoya Noguchi 4 , Takeo Yoshikawa 4 , Akira Uruno 4 , Weiyan Yao 1 and Yaozong Yuan 1 1 Department of Gastroenterology, Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China 2 Department of Respiratory medicine, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, China 3 Institute of Health Science, Shanghai Institutes for Biological Sciences, Chinese Academy of Sciences/Shanghai Jiaotong University School of Medicine, Shanghai, China 4 Department of Advanced Biological Sciences for Regeneration, Tohoku University Graduate School of Medicine, Sendai, Japan Diabetes is now generally accepted as a crucial event in the process of pancreatic cancer (PaC). However, molecular mechanisms underlying the relationship between diabetes and PaC are not fully understood. Regenerating gene (REG)Ia is a growth factor affecting pancreatic islet beta cells, and it has been shown to be involved in the carcinogenesis in gastrointestinal tract. It is rational to speculate that REG Ia plays a potential role in the pathogenesis of PaC with diabetes. The aim of this study was to evaluate the REG Ia protein expression profile in PaC with and without diabetes, and define the contribution of REG Ia on PaC development. We found that REG Ia protein preferentially expressed in cancerous tissues of PaC patients with diabetes by Western blot. REG Ia positive cancer cells in PaC with diabetes (n 5 38) was significantly higher than that in subjects without diabetes (n 5 42, p < 0.05) by immunohistochemical analysis. Furthermore, we found that overexpression of REG Ia protein in PaC cell lines resulted in accelerated cell proliferation and consequently tumor growth, both in vitro and in vivo. The findings suggest that REG Ia may act as one of the tumor promoter and contribute to the aggressive nature of PaC, especially in the subpopulation with diabetes. This study would shed new insights for understanding the molecular mechanisms underlying the link between diabetes and PaC. Pancreatic cancer (PaC), one of the most aggressive human cancers, with the 5-year survival rate of 5%. 1 The disease is characterized by rapid tumor spread and dismal prognosis. Most PaC patients are diagnosed at an advanced stage, and only up to 9% of patients undergo a potentially curative pro- cedure. 2 Based on human epidemiologic and animal studies, diabetes is now generally accepted as a crucial event in the development of PaC. A recent population-based study showed that diabetes has a high (40%) prevalence in PaC and frequently is new onset. 3 Another observation showed that PaC patients with diabetes tend to present a more advanced stage of the disease and a shorter survival period than their nondiabetic counterparts. 4 Therefore, it is impera- tive to better understand the biological influence of diabetes on PaC. Previous studies have shown that several kinds of growth factors, such as insulin and insulin-like growth fac- tors, have been found to stimulate the PaC cells prolifera- tion 5,6 ; however, more molecular mechanisms underlying the relationship between diabetes and PaC remain to be elucidated. The Regenerating gene (REG), an epithelial growth factor, 7 was originally isolated from a complementary DNA (cDNA) library derived from regenerating rat pancreatic islets, and its human homologue was named REG Ia. 8 REG Ia is a known growth factor affecting pancreatic islet beta cells, which enco- des a 166-amino acid protein with a 22-amino acid signal sequence. 8 Reg I gene has been previously associated with di- abetes. For examples, overexpression of Reg I in the pancreas of nonobese diabetic mice at various degrees of diabetogene- sis has been found. 9,10 Recently, REG Ia was suggested to be involved not only in inflammatory diseases but also in carci- nogenesis in various gastroenterological tissues, such as the stomach, 11,12 colon 13 and bile duct. 14 Therefore, it is rational to speculate that pancreatic REG Ia level may be different in PaC patients with and without diabetes, and REG Ia may play an important role in the development of PaC. Key words: REG Ia, pancreatic cancer, diabetes Abbreviations: IFN: interferon; IL: interleukin; PaC: pancreatic cancer; PCNA: proliferating cell nuclear antigen; REG: regenerating gene; WST-8: 2-methoxy-4-nitrophenyl-3-(4-nitrophenyl)-5-(2,4- disulfophenyl)-2H-tetrazolium, monosodium salt. Additional Supporting Information may be found in the online version of this article. Grant sponsor: Key Program of Science and Technology Committee of Shanghai, China; Grant number: 06JC14055 DOI: 10.1002/ijc.25188 History: Received 14 Apr 2009; Accepted 28 Dec 2009; Online 22 Jan 2010 Correspondence to: Yaozong Yuan, Department of Gastroenterology, Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai 200025, China, Tel/Fax: þ[86-21-64150773], E-mail: [email protected] Cancer Cell Biology Int. J. Cancer: 127, 1795–1803 (2010) V C 2010 UICC International Journal of Cancer IJC
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Upregulation of REG Iα accelerates tumor progression in pancreatic cancer with diabetes

Upregulation of REG Ia accelerates tumor progressionin pancreatic cancer with diabetes
Lin Zhou1, Ruifeng Zhang2, Lishun Wang3, Shaoming Shen3, Hiroshi Okamoto4, Akira Sugawara4, Li Xia3, Xiaoling Wang3,
Naoya Noguchi4, Takeo Yoshikawa4, Akira Uruno4, Weiyan Yao1 and Yaozong Yuan1
1 Department of Gastroenterology, Ruijin Hospital, Shanghai Jiaotong University School of Medicine, Shanghai, China2 Department of Respiratory medicine, Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, Hangzhou, China3 Institute of Health Science, Shanghai Institutes for Biological Sciences, Chinese Academy of Sciences/Shanghai Jiaotong University School of Medicine,
Shanghai, China4 Department of Advanced Biological Sciences for Regeneration, Tohoku University Graduate School of Medicine, Sendai, Japan
Diabetes is now generally accepted as a crucial event in the process of pancreatic cancer (PaC). However, molecular
mechanisms underlying the relationship between diabetes and PaC are not fully understood. Regenerating gene (REG) Ia is a
growth factor affecting pancreatic islet beta cells, and it has been shown to be involved in the carcinogenesis in
gastrointestinal tract. It is rational to speculate that REG Ia plays a potential role in the pathogenesis of PaC with diabetes.
The aim of this study was to evaluate the REG Ia protein expression profile in PaC with and without diabetes, and define the
contribution of REG Ia on PaC development. We found that REG Ia protein preferentially expressed in cancerous tissues of PaC
patients with diabetes by Western blot. REG Ia positive cancer cells in PaC with diabetes (n 5 38) was significantly higher
than that in subjects without diabetes (n 5 42, p < 0.05) by immunohistochemical analysis. Furthermore, we found that
overexpression of REG Ia protein in PaC cell lines resulted in accelerated cell proliferation and consequently tumor growth,
both in vitro and in vivo. The findings suggest that REG Ia may act as one of the tumor promoter and contribute to the
aggressive nature of PaC, especially in the subpopulation with diabetes. This study would shed new insights for
understanding the molecular mechanisms underlying the link between diabetes and PaC.
Pancreatic cancer (PaC), one of the most aggressive humancancers, with the 5-year survival rate of �5%.1 The disease ischaracterized by rapid tumor spread and dismal prognosis.Most PaC patients are diagnosed at an advanced stage, andonly up to 9% of patients undergo a potentially curative pro-cedure.2 Based on human epidemiologic and animal studies,diabetes is now generally accepted as a crucial event in thedevelopment of PaC. A recent population-based studyshowed that diabetes has a high (40%) prevalence in PaCand frequently is new onset.3 Another observation showed
that PaC patients with diabetes tend to present a moreadvanced stage of the disease and a shorter survival periodthan their nondiabetic counterparts.4 Therefore, it is impera-tive to better understand the biological influence of diabeteson PaC. Previous studies have shown that several kinds ofgrowth factors, such as insulin and insulin-like growth fac-tors, have been found to stimulate the PaC cells prolifera-tion5,6; however, more molecular mechanisms underlying therelationship between diabetes and PaC remain to beelucidated.
The Regenerating gene (REG), an epithelial growth factor,7
was originally isolated from a complementary DNA (cDNA)library derived from regenerating rat pancreatic islets, and itshuman homologue was named REG Ia.8 REG Ia is a knowngrowth factor affecting pancreatic islet beta cells, which enco-des a 166-amino acid protein with a 22-amino acid signalsequence.8 Reg I gene has been previously associated with di-abetes. For examples, overexpression of Reg I in the pancreasof nonobese diabetic mice at various degrees of diabetogene-sis has been found.9,10 Recently, REG Ia was suggested to beinvolved not only in inflammatory diseases but also in carci-nogenesis in various gastroenterological tissues, such as thestomach,11,12 colon13 and bile duct.14 Therefore, it is rationalto speculate that pancreatic REG Ia level may be different inPaC patients with and without diabetes, and REG Ia mayplay an important role in the development of PaC.
Key words: REG Ia, pancreatic cancer, diabetes
Abbreviations: IFN: interferon; IL: interleukin; PaC: pancreatic
cancer; PCNA: proliferating cell nuclear antigen; REG: regenerating
gene; WST-8: 2-methoxy-4-nitrophenyl-3-(4-nitrophenyl)-5-(2,4-
disulfophenyl)-2H-tetrazolium, monosodium salt.
Additional Supporting Information may be found in the online
version of this article.
Grant sponsor: Key Program of Science and Technology Committee
of Shanghai, China; Grant number: 06JC14055
DOI: 10.1002/ijc.25188
History: Received 14 Apr 2009; Accepted 28 Dec 2009; Online 22
Jan 2010
Correspondence to: Yaozong Yuan, Department of
Gastroenterology, Ruijin Hospital, Shanghai Jiaotong University
School of Medicine, Shanghai 200025, China, Tel/Fax:
þ[86-21-64150773], E-mail: [email protected]
Can
cerCellBiology
Int. J. Cancer: 127, 1795–1803 (2010) VC 2010 UICC
International Journal of Cancer
IJC

In this study, we investigated the expression of REG Ia inhuman PaC tissues, with and without diabetes. Further, weexamined the effects of REG Ia on proliferation and tumori-genicity of PaC cells, in vitro and in vivo. These findings maycontribute to understanding the molecular mechanismsunderlying the relationship between diabetes and PaC.
Material and MethodsPatients and specimens
Seven PaC patients (five males, two females; age range 48–77years) with diabetes and seven stage-matched PaC patients(four males, three females; age range 43–75 years) without dia-betes underwent pancreatectomy at the Department of Surgery,Ruijin Hospital, between April 2007 and September 2007 werestudied. Pancreatic tissues including tumor and adjacent tu-mor-free regions from each subject were collected for Westernblot analysis. In addition, paraffin-embedded tissue blocks con-taining 80 PaC tissues, 10 adjacent tumor-free tissues and 5normal pancreatic tissues from trauma cases, obtained frompatients who underwent pancreatectomy between 2001 and2007, were subjected to immunohistochemical analysis. Thestudy was approved by the Ethics Committee of Ruijin Hospi-tal, Shanghai Jiaotong University School of Medicine, andinformed consent was obtained from all patients.
All the specimens in the study were pancreatic ductal ade-nocarcinoma by histologic examination. Diabetes was diag-nosed following the American Diabetes Association criteria15:study subjects were defined as having diabetes if at least onefasting glucose value was 126 mg/dL or greater. Other clinicalinformation was obtained by chart review.
Protein extraction and Western blot analysis
Tissue samples were obtained immediately after surgery andtransported in liquid nitrogen. The frozen tissues were pulv-erized and mixed with 1.5 mL 10% TCA in cold (�20�C) ac-etone. The samples were kept at �20�C overnight to allowcomplete precipitation. The samples were then centrifugedfor 30 min at 15,000g and washed twice with 1.5 mL acetone.The deposit was then homogenized in 10 volumes of lysisbuffer containing 7 M urea, 2 M thiourea, 4% CHAPS, 30mM Tris (base), and 1� Complete protease inhibitor cocktailtablets (Roche, Indianapolis, IN), followed by centrifuge at40,000g for 60 min at 4�C. The soluble fraction was used forprotein analysis. The protein concentration was determinedusing the RC-DC method (Bio-Rad, Hercules, CA). Proteinlysates were loaded onto 12% SDS-PAGE, and electrophoreti-cally transferred to NC membrane (Bio-Rad, Hercules, CA).The membranes were blotted with antibodies against REG Ia(Santa Cruz, Santa Cruz, CA), proliferating cell nuclear anti-gen (PCNA; Cell Signal, Boston, MA), and b-actin (Onco-gene, San Diego, CA), followed by incubation with horserad-ish peroxidase-conjugated secondary antibody (DakoCytomation, Glostrup, Denmark). The protein signal wasdetected by luminal detection reagent (Santa Cruz).
Immunohistochemistry
Immunohistochemical staining for REG Ia protein andPCNA protein were performed with an LSAB kit (DAKOCytomation, Marseille, France), using anti-human REG Iaantibody (1:50) and anti-PCNA antibody (1:500). The sec-tions were incubated in 3, 30-diaminobenzide tetrahydro-chloride with 0.05% H2O2 for 3 min and then counterstainedwith Mayer’s hematoxylin. To evaluate the immunoreactivityof REG Ia protein, at least 500 tumor cells were counted infive different visual fields for each sample of cancerous speci-men. The REG Ia protein labeling index in each sample wascalculated as the percentage of positive tumor cells. A humanpancreatic cancerous specimen was considered positive forREG Ia when more than 20% of the tumor cells were posi-tively stained.11 As a control for antibody specificity, goatanti-REG Ia polyclonal antibody was mixed with an excessof the REG Ia blocking peptide (Santa Cruz) and incubatedovernight at 4�C before application to tissue sections asdescribed above. Buffer constituents in both control andblocked antibody preparations were identical. Additionally,the percentage of PCNA-positive cells was calculated from500 cells in nude mice xenografts sections.
Cell lines and cultures
Human pancreatic ductal cancer cell lines BxPC3 andSW1990 were originally obtained from the American TypeCulture Collection (Rockville, MD). All cells were routinelymaintained in DMEM medium (Invitrogen, Grand Island,NY) containing 10% fetal bovine serum (Invitrogen) in ahumidified incubator at 37�C with an atmosphere of 5%CO2.
Human REG Ia cDNA transfection and selection
of BxPC3 stable transfectants
The full length of human REG Ia cDNA was cloned into thepReceiver-M02 vector containing cytomegalovirus promoter(Genecopoeia, Germantown, MD). After cloning and verify-ing the nucleotides of the human REG Ia cDNA by sequenc-ing, the construct was named pReceiver-M02-REG Ia, andpReceiver-M02 vector without insert was used as a control.Plasmids were transfected into BxPC3 and SW1990 cellsusing Polyfect transfection reagent (QIAGEN, Valencia, CA),as protocol described. Additional transfected cells to selectpReceiver-M02-REG Ia and pReceiver-M02 vector-stabletransfected cells (BxPC3-REG Ia and BxPC3-vector) werecultured for 4 weeks in medium containing G418 (Gibco,800–1,000 lg/mL), and surviving colonies were pooled.
Preparation of conditioned medium
To prepare conditioned medium, we cultured human embry-onic kidney 293T cells in DMEM supplemented with 10% fe-tal bovine serum. The 293T cells were transfected with 10 lgof pReceiver-M02-REG Ia or control plasmid using Polyfecttransfection reagent. The conditioned medium was then
Can
cerCellBiology
1796 REG Ia in pancreatic cancer with diabetes
Int. J. Cancer: 127, 1795–1803 (2010) VC 2010 UICC
collected as a source of recombinant REG Ia protein after a36-h incubation period.
Cell growth assay
Cell growth was evaluated by WST-8 (2-methoxy-4-nitro-phenyl-3-(4-nitrophenyl)-5-(2,4-disulfophenyl)-2H-tetrazo-lium, monosodium salt) cleavage assays (Cell CountingKit-8; Dojindo, Kumamoto, Japan). BxPC3 and SW1990cells (5 � 103) transfected with pReceiver-M02-REG Ia orcontrol plasmid were plated in 96-well microplates. Twelvehours later, cells were incubated in serum-free DMEM me-dium for 24, 48 and 72 h. After addition of 10 lL of theCell Counting Kit-8 reagent followed by 3 h incubation,the plates were read at 450 nm in a spectrophotometer(Tecan Safire2, San Jose, CA).
To assess the effect of REG Ia in the medium, we addedanti-REG Ia antibody11,12 (50 lg/mL, provided by Dr AkiraSugawara) to serum-free DMEM medium, and cells incu-bated for 72 h were also evaluated in the same procedure.Normal mouse IgG (Santa Cruz) was used as a negative con-trol to investigate the nonspecific biological effects of theneutralizing antibody. Cell growth assay was also performedto examine the effect of REG Ia protein on PaC cells. Briefly,BxPC3 cells (5 � 103) were cultured in 96-well microplatesfor 24 h. Then, the medium was changed to conditioned
medium containing human recombinant REG Ia or controlmedium with different dilution ratio, and cells incubated for48 h were also evaluated in the same procedure.
Colony formation assay
Cells (3 � 103) were trypsinized to single-cell suspension andthen plated in triplicate onto six-well plates in complete cul-ture medium containing 0.3% agar on top of 0.6% agar inthe same medium. The plates were incubated at 37�C in 5%CO2 for 16 days. Colonies were fixed with 70% ethanol andstained with 0.2% crystal violet. The colonies containing atleast 50 cells were counted.
In vivo experiments
Balb/c nude mice were maintained under specific pathogen freecondition in Shanghai Experimental Animals Centre of Chi-nese Academy of Sciences. BxPC3, BxPC3-vector and BxPC3-REG Ia cells were harvested and resuspended in PBS, respec-tively, then 5 � 106 cells in 100 lL PBS were subcutaneouslyinjected into the right flank of a 4-wk-old Balb/c nude mouse.Six mice were included in each group. The tumor size wasmeasured using a caliper and was calculated according to theformula AB2/2, where A is the longest diameter and B is theshortest diameter of the tumor. Animals were sacrificed 6 wkafter tumor cell implantation. The tumor weight was measuredat Wk 6. Protocols were approved by the Shanghai JiaotongUniversity Institutional Animal Care and Use Committee.
Statistical analysis
All values were expressed as the mean 6 SD. Statistical dif-ferences between the two groups were assessed by the t test.Chi-squared analyses were performed to test the significanceof the difference between various pathological parameters. Ap value of <0.05 was considered to be statistical significance.
ResultsREG Ia expression in human pancreatic cancer tissues
by Western blot analysis
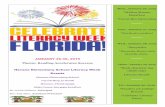
Western blot was performed for assessment of REG Ia proteinin PaC tissues with and without diabetes, with representativeresults shown in Figure 1a. Semiquantitative analysis (Fig. 1b)of all samples showed a significant increase of REG Ia proteinexpression in diabetic PaC specimens compared with nondia-betic PaC tissues. Moreover, the expression level of REG Iaprotein was higher in adjacent tumor-free tissues than PaC tis-sues in both diabetic and nondiabetic groups. Additionally, themRNA level of REG Ia in pancreatic cancer tissues with diabe-tes was also significantly higher than that without diabetes(Supplemental Fig. 1a and Supplemental materials).
REG Ia expression and localization in human pancreatic
cancer tissues by immunohistochemistry
To confirm the specificity of the anti-REG Ia polyclonal anti-body for immunohistochemical staining, we performed aimmunizing peptide blocking experiment. Preincubating the
Figure 1. Expression of REG Ia protein in human pancreatic
tissues. (a) Representative results of Western blot for REG Ia
protein expression in human pancreatic tissues, with b-actin as a
loading control. (b) Data in the graph represent the densitometric
ratios of REG Ia protein to b-actin (n ¼ 7 in each group). PaC:
pancreatic cancer; TF:adjacent tumor-free tissues of PaC; DMPaC:
pancreatic cancer tissues with diabetes; DMTF: adjacent tumor-free
tissues of DMPaC. Values in panel (b) represented means 6 SD.
*p < 0.05, #p < 0.05, vs. PaC group; and &p < 0.05, vs. DMPaC
group.
Can
cerCellBiology
Zhou et al. 1797
Int. J. Cancer: 127, 1795–1803 (2010) VC 2010 UICC

blocking protein with REG Ia antibody removed the REG Iasignal in all immunopositive cells (Fig. 2a). We analyzed REGIa expression in 80 PaC tissues, 10 adjacent tumor-free tissuesand 5 normal pancreatic tissues by immunohistochemistry(Fig. 2b).The immunoreactive pattern of REG Ia was predomi-nantly positive identified in the cytoplasm, scattered through-out the neoplasm. Compared with adjacent tumor-free tissues,acinar cells and ductal cells were relatively slight labeled or notlabeled for REG Ia in normal pancreas (The image was alsoshown in Supplemental Fig. 2). In most PaC tissues withoutdiabetes, REG Ia was not detected in ductal cancer cells. Con-versely, REG Ia-immunoreactive signals were detected in can-cer cells in most PaC tissues with diabetes. Further, semiquanti-tative expression (positive cell percentage) of REG Ia proteinwas significantly higher in diabetic PaC patients (36.4 6 17.9,38 patients) than in nondiabetic PaC subjects (14.9 6 11.8, 42patients, p< 0.05; Fig. 2c).
We next analyzed the relations between REG Ia proteinexpression and several clinicopathologic factors (Table.1). Itwas found that REG Ia expression was significantly associatedwith diabetes (p ¼ 0.001). In addition, a significant associationwas identified between tumor size and REG Ia staining. This
Table 1. Statistical analysis of REG Ia staining in pancreatic cancercells with clinical-pathologic parameter
Characteristics Total
REG Ia proteinexpression
pPositive Negative
Age at surgery (yr)
<55 52 29 23 0.906
�55 28 16 12
Gender
Male 59 33 26 0.923
Female 21 12 9
Diabetes
With 38 29 9 0.001
Without 42 16 26
Differentiation
Well 19 8 11 0.347
Moderate 32 20 12
Poor 29 17 12
Tumor size
<20 mm 23 7 16 0.003
�20 mm 57 38 19
Lymph node metastasis
Yes 35 21 14 0.551
No 45 24 21
Vascular invasion
Yes 42 26 16 0.284
No 38 19 19
Figure 2. Immunostaining for REG Ia protein in human pancreatic
tissues. (a) Immunohistochemical images of sequential sections from
a malignant pancreatic specimen, showing loss of staining after
blocking of REG Ia antibody with a REG Ia blocking peptide. (b)
Histopathologic sections of pancreas were stained with anti-REG Ia
antibody. Normal pancreas exhibited negative REG Ia staining in
acinar cells and ductal cells. Adjacent tumor-free tissues showed
strong staining. No immunostaining was detected in cancer cells of
most PaC without diabetes. Significantly staining of REG Ia was
observed in ductal cancer cells of most PaC with diabetes. (c)
Semiquantified results (percentage of REG Ia-positive cancer cells) of
immunohistochemistry for REG Ia protein expression in human PaC
samples. N: normal pancreas; TF: adjacent tumor-free tissues; PaC:
pancreatic cancer; DMPaC: pancreatic cancer with diabetes. Bars ¼50lm. *p < 0.05, vs. PaC group. [Color figure can be viewed in the
online issue, which is available at wileyonlinelibrary.com.]
Can
cerCellBiology
Int. J. Cancer: 127, 1795–1803 (2010) VC 2010 UICC
1798 REG Ia in pancreatic cancer with diabetes

was based on a classification of tumor size into groups of <20mm and �20 mm. No significant associations between REG Iaexpression and other parameters were observed.
Effects of REG Ia on cell proliferation and tumorigenicity
in pancreatic cancer cell lines
BxPC3 and SW1990 cells were transiently transfected withpReceiver-M02-REG Ia and pReceiver-M02 plasmids, respec-tively, and the expression of REG Ia protein was detected byWestern blot (Fig. 3a). BxPC3 and SW1990 cells transfectedwith pReceiver-M02-REG Ia showed significantly higher WST-8 cleavage levels than controls at the same time point (data notshown), and this phenomenon could be magnified by serumdeprivation (Fig. 3b). Next, we selected a clone derived fromstable transfectants (BxPC3-REG Ia) and control (BxPC3-vec-tor), respectively (Fig. 3c and Supplemental Fig. 1b). Soft agarcolony formation assay was done to evaluate the tumorigenicityof REG Ia overexpression cells in vitro. As shown in Fig 3d, col-
ony formation rates were 8.3 6 1.4%, 7.4 6 1.1% and 29.2 63.2% in parental BxPC3, BxPC3-vector and BxPC3-REG Ia cells,respectively. Compared with the controls, BxPC3-REGIa exhib-ited not only a more amount but also a bigger size of colonies.
Fashions of REG Ia on cell proliferation in BxPC3 cells
To confirm how REG Ia protein acts on PaC cells, we added tothe media-specific anti-REG Ia antibody (Fig. 4a). BxPC3-REG Ia cells showed significantly higher WST-8 cleavage levelsthan BxPC3-vector cells after 72 h incubation. Increased WST-8 cleavage in the BxPC3-REG Ia group was suppressed almostto control levels by addition of anti-REG Ia antibody. To con-firm that this effect was not because of a nonspecific compo-nent in our antibody source, normal mouse IgG was used as anegative control. WST-8 cleavage levels were unchanged inboth BxPC3-vector and BxPC3-REG Ia cells group when IgGwas added in the medium. Thus, we proposed that the secretedREG Ia protein could enhance BxPC3 cells growth.
Figure 3. Effects of REG Ia on cell growth in human pancreatic cancer cell lines. (a) BxPC3 and SW1990 transiently transfected with
pReceiver-M02-REG Ia were cultured for 24, 36, 48 and 72 h, with pReceiver-M02 plasmids as a control. REG Ia protein was detected by
Western blot with b-actin as a loading control. (b) Transiently transfected BxPC3, SW1990 cells and their controls were cultured for 24, 48
and 72 h. WST-8 cleavage in each group was measured (absorbance OD450). (c) REG Ia and PCNA proteins were detected in the stably
transfected BxPC3-REG Ia cells and controls (BxPC3 cells and BxPC3-vector cells) by Western blot with b-actin as a loading control. (d)
Colony formation rates of BxPC3-REG Ia, BxPC3-vector and BxPC3 were analyzed by soft agar assay. *p < 0.05, ** p < 0.01 compared with
controls. All the experiments were repeated for three times and with the similar results.
Can
cerCellBiology
Zhou et al. 1799
Int. J. Cancer: 127, 1795–1803 (2010) VC 2010 UICC

On the other hand, we found an abundant amount ofREG Ia protein in the medium of REG Ia-overexpressed293T cells (Fig. 4b), which significantly promoted BxPC3cells growth than control medium after 48 h incubation, andthis growth promotion was manifested in a dose-dependentmanner (Fig. 4c). Taken together, it is suggested that REG Iaprotein confers a trophic effect on PaC cells in a paracrineand/or autocrine fashion.
Effect of REG Ia overexpression on tumor growth in nude
mice
In vivo, heterotopic murine pancreatic carcinoma was suc-cessfully established in the flank of Balb/c nude mice. Injec-tion of BxPC3-REG Ia cells in nude mice resulted in acceler-ated tumor growth compared with the controls. Tumorvolumes of BxPC3-REG Ia group were significantly biggerthan those in BxPC3 and BxPC3-vector groups after 6 wk ofinjection (Fig. 5a). Tumor weight was also significantlyincreased in BxPC3-REG Ia groups compared with two con-trol groups (Fig. 5b). These are evidence that overexpressionof REG Ia accelerates tumor growth of PaC cells in vivo.
Immunohistochemical analysis of REG Ia and PCNA
proteins in excised tumor tissues from nude mice
The expression of REG Ia in excised tumors was analyzed byWestern blot (Fig. 6a) and immunostaining (Fig. 6c). Next,to confirm whether REG Ia overexpression impacts cell pro-liferation in vivo, we used immunostaining with anti-PCNAantibody to assess tumor cell proliferation in nude mice xen-ografts. BxPC3-REG Ia transfectants showed a more andstronger tumor cell positive staining for PCNA protein (Fig.6d) and a significantly higher PCNA index (Fig. 6e) thancontrols. These results suggested that REG Ia could acceleratetumor cells proliferation in nude mice.
DiscussionREG Ia is the product of REG I gene, which is a knowngrowth factor affecting pancreatic islet beta cells. The mainsource for REG Ia secretion in pancreas is acini. A previousstudy has reported that the presence of the REG protein inthe normal pancreas and its overexpression after a pancreaticaggression could be a key factor contributing to the physio-logically active defense mechanisms of the exocrine pan-creas.10 Moreover, another REG immunohistochemical studyof human pathologic pancreatic tissues has shown that theREG protein was expressed more broadly and densely inchronic pancreatitis with mild to moderate injury than innormal pancreas and very poorly in severely damaged pan-creata.16 Consistent with these findings, our results showedthat REG Ia protein was suppressed in PaC tissues duringthe development of PaC. The increased REG Ia levels in tu-mor-free tissues arise primarily from the host’s reaction topancreatic adenocarcinoma rather than the PaC itself. Moreintriguingly, we found that the local REG Ia protein levelwas significantly upregulated in tumor tissues of diabetic PaC
Figure 4. Effects of REG Ia gene induction or REG Ia conditioned
medium on the growth of pancreatic cancer cells. (a) Effects of
anti-REG Ia antibody on the cell growth of BxPC3-REG Ia and
BxPC3-vector. BxPC3-REG Ia and BxPC3-vector cells were incubated
with or without anti-REG Ia antibody (50 lg/mL) for 72 h, with
normal mouse IgG as a negative control. WST-8 cleavage in each
group was measured (absorbance OD450). (b) Source of REG Ia
protein. HEK293T cells were transfected with pReceiver-M02-REG Ia
plasmid or pReceiver-M02 plasmid as a control, and the REG Ia
protein conditioned and control medium were harvested after 36-h
incubation. Release of REG Ia protein into the medium of
pReceiver-M02-REG Ia transfected cells and controls were
confirmed by Western blot. (c) REG Ia protein conditioned and
control medium (36 h after transfection) were mixed with serum-
free fresh medium in different dilution ratio, and BxPC3 cells were
incubated with the mixed medium for 48 h. WST-8 cleavage in
each group was measured (absorbance OD450). All results were
expressed as the means 6 SD. (a) *p < 0.05, #p<0.05, vs. BxPC3-
REG Ia group, and &p < 0.05, vs. (BxPC3-REG Ia þ Ab) group.
(c) *p < 0.05, **p < 0.01 vs. control medium-treated cells at the
same dilution ratio.
Can
cerCellBiology
1800 REG Ia in pancreatic cancer with diabetes
Int. J. Cancer: 127, 1795–1803 (2010) VC 2010 UICC

Figure 5. Effects of REG Ia on tumor growth in nude mice. Xenografted pancreatic cancers were established by subcutaneous injection of
BxPC3, BxPC3-vector and BxPC3-REG Ia cells (5 � 106) into 4-wk-old Balb/c nude mice. (a) Tumor size was measured weekly for 6 wk.
(b)Tumor weights were measured at Wk 6. (n ¼ 6 in each group). All value in panels were represented as means 6 SD. *p < 0.05,
compared with controls.
Figure 6. Immunostaining for REG Ia and PCNA proteins in excised tumor tissues from nude mice. (a) The expression of REG Ia in excised
tumors was analyzed by Western blot, with b-actin as a loading control. (b) Histopathologic sections were stained with H&E. REG Ia (c) and
PCNA proteins (d) were detected by immunohistochemical staining in solid tumors derived from parental BxPC3 cells and stable
transfectants (BxPC3-REG Ia and BxPC3-vector). (e) Percentage of PCNA-positive cells was shown for each group. (n ¼ 6 in each group). All
value were represented as means 6 SD. **p < 0.01, compared with controls. [Color figure can be viewed in the online issue, which is
available at wileyonlinelibrary.com.]
Can
cerCellBiology
Zhou et al. 1801
Int. J. Cancer: 127, 1795–1803 (2010) VC 2010 UICC

patients compared with nondiabetic PaC subjects. Theseresults may suggest a possible link between REG Ia proteinexpression and PaC with diabetes.
PaC is characterized by intense desmoplastic stroma, andacinar cells are always injured by cancer cells aggression.Therefore, we used immunostaining to elucidate the locationof REG Ia in PaC tissues. We found that REG Ia expressednot only in acinar cells but also in malignant ductal cells.Furthermore, REG Ia was also detected in several PaC celllines. As REG Ia protein is reported to be mitogenic to gas-trointestinal epithelial cells,17 these findings further suggestedits potential influence on distinct physiologic and pathologicresponses in the PaC with diabetes.
Given the evidence the trophic role for REG Ia in PaCcells, we used PaC cell lines with overexpression of REG Iato investigate whether it could contribute to the developmentof PaC. The in vitro results showed that REG Ia overexpres-sion resulted in the accelerated proliferation of BxPC3 andSW1990 cells. Consequently, we revealed that REG Ia con-tributed to the enhanced tumorigenicity of BxPC3 cells bothin vitro and in vivo. On the other hand, in vitro studies dem-onstrated that the addition of anti-REG Ia antibody to theincubation medium could abolish enhanced growth of REGIa-transfected cells. Similarly, culture medium containingrecombinant REG Ia significantly promoted PaC cells growththan control medium in a dose-dependent manner. Taken to-gether, REG Ia secreted from cancer cells exerts growth pro-moting action in a paracrine or autocrine fashion, which isimportant in the process of PaC with diabetes.
What factors could be responsible for the increase of REGIa expression in cancer cells from PaC patients with diabetes?Studies have shown that inflamed condition may conse-quently evoke REG Ia gene transcription via proinflamma-tory cytokines, such as interferon (IFN)-c, interleukin (IL)-6and IL-8, which are all known to transactivate REG Ia.13,18 Itis well known that diabetes shows a close correlation withinflammation and the expression of both IL-6 and IFN-c wasfound prominently increased in diabetic pancreas.19 Althoughwe did not measure levels of those cytokines in this study, itappears reasonable to speculate that increased levels ofinflammatory cytokines in the diabetic pancreas are at leastin part responsible for the enhanced expression of the REGIa gene in malignant ductal cells. Therefore, we speculate di-abetic tumor cells may exhibit a higher basal expression ofREG Ia compared with cancer cells of PaC only samples.
REG protein expression has been shown to correlate withfrequent vascular invasion, lymph node metastases and worse
prognosis in gastric cancers.12,20 In addition to tumor size, wefound no statistically significant correlations between REG Iaexpression and other parameters of invasion. The discrepan-cies between these results and our current data are not alto-gether surprising. First, carcinogenesis is a complicated eventin which many factors are involved. Further, we know thatmost PaC patients are diagnosed at an advanced stage, charac-terized by metastases at the time of diagnosis. Thus, the contri-bution of the protein to invasion in PaC can not only be meas-ured by examining associations in patients with resectablestage but also clearly other models are required. It should alsobe noted that although this study has focused on the growth-associated function of REG Ia, the precise role of REG Ia pro-tein in this cancer is still not fully understood. Recently, Fukuiand coworkers21 have reported that REG Ia protein was adownstream molecule of STAT3 signaling and gene abnormal-ities upstream of REG Ia led its upregulation, which in turnenhances expression of antiapoptotic proteins in gastric celllines. Further investigations should be carried out to under-stand the exact role of increased REG Ia protein in PaC.
Previous studies have reported a correlation between REGIa expression and survival of some kinds of cancer, such asstomach,12,20 colon,22,23 breast cancers24 and non-small celllung cancer.25 In this study, we have shown that the impor-tant role of REG Ia in PaC cell proliferation and conse-quently tumor growth. Although we did not investigatewhether REG Ia expression correlated with survival of PaCpatients, we presume that tumors expressing high levels ofREG Ia are related to poor prognosis of PaC, especially insubpopulation with diabetes. The relationship between REGIa expression and survival of PaC should be observed inlarge population-based study. We are currently enrollingpatients at our center for such a study.
In summary, this study is the first to demonstrate thatREG Ia protein is upregulated not only in cancerous tissuesbut also in malignant cells of most PaC with diabetes. More-over, overexpression of REG Ia protein in PaC cell linesresulted in accelerated cell proliferation and consequently tu-mor growth, in vitro and in vivo. These findings suggest thatREG Ia may act as one of the tumor promoter and contrib-ute to the aggressive nature of PaC, and would provide newinsights for understanding the molecular mechanisms basedon the closely link between diabetes and PaC.
AcknowledgementsWe thank grants from Science and Technology Committee of Shanghai(06JC14055) for supporting this work.
References
1. Berrino F, De Angelis R, Sant M, Rosso S,Bielska-Lasota M, Coebergh JW,Santaquilani M. Survival foreight major cancers and all cancerscombined for European adultsdiagnosed in 1995–99: results of the
EUROCARE-4 study. Lancet Oncol2007;8:773–83.
2. Sener SF, Fremgen A, Menck HR,Winchester DP. Pancreatic cancer: a reportof treatment and survival trends for100,313 patients diagnosed from 1985–
1995, using the National Cancer Database.J Am Coll Surg 1999;189:1–7.
3. Chari ST, Leibson CL, Rabe KG, TimmonsLJ, Ransom J, de Andrade M, PetersenGM. Pancreatic cancer-associateddiabetes mellitus: prevalence and
Can
cerCellBiology
1802 REG Ia in pancreatic cancer with diabetes
Int. J. Cancer: 127, 1795–1803 (2010) VC 2010 UICC

temporal association with diagnosisof cancer. Gastroenterology 2008;134:95–101.
4. Wakasugi H, Funakoshi A, Iguchi H.Clinical observations of pancreatic diabetescaused by pancreatic carcinoma, andsurvival period. Int J Clin Oncol 2001;6:50–4.
5. Fisher WE, Boros LG, Schirmer WJ.Insulin promotes pancreatic cancer:evidence for endocrine influence onexocrine pancreatic tumors. J Surg Res1996;63:310–3.
6. LeRoith D, Baserga R, Helman L, RobertsCT Jr. Insulin-like growth factors andcancer. Ann Intern Med 1995;122:54–9.
7. Okamoto H, Takasawa S. Recent advancesin the Okamoto model: the CD38-cyclicADP-ribose signal system and theregenerating gene protein (Reg)-Regreceptor system in beta-cells. Diabetes2002;51(suppl 3):S462–73.
8. Terazono K, Yamamoto H, Takasawa S,Shiga K, Yonemura Y, Tochino Y,Okamoto H. A novel gene activated inregenerating islets. J Biol Chem 1988;263:2111–4.
9. Baeza NJ, Moriscot CI, Renaud WP,Okamoto H, Figarella CG, Vialettes BH.Pancreatic regenerating geneoverexpression in the nonobese diabeticmouse during active diabetogenesis.Diabetes 1996;45:67–70.
10. Sanchez D, Baeza N, Blouin R, Devaux C,Grondin G, Mabrouk K, Guy-Crotte O,Figarella C. Overexpression of the reg genein non-obese diabetic mouse pancreasduring active diabetogenesis is restricted toexocrine tissue. J Histochem Cytochem2000;48:1401–10.
11. Fukui H, Fujii S, Takeda J, Kayahara T,Sekikawa A, Nanakin A, Suzuki K,Hisatsune H, Seno H, Sawada M, FujimoriT, Chiba T. Expression of reg I alpha
protein in human gastric cancers. Digestion2004;69:177–84.
12. Dhar DK, Udagawa J, Ishihara S, Otani H,Kinoshita Y, Takasawa S, Okamoto H,Kubota H, Fujii T, Tachibana M, NagasueN. Expression of regenerating gene I ingastric adenocarcinomas: correlation withtumor differentiation status and patientsurvival. Cancer 2004;100:1130–6.
13. Sekikawa A, Fukui H, Fujii S, Nanakin A,Kanda N, Uenoyama Y, Sawabu T,Hisatsune H, Kusaka T, Ueno S, Nakase H,Seno H, et al. Possible role of REG Ialphaprotein in ulcerative colitis and coliticcancer. Gut 2005;54:1437–44.
14. Harada K, Zen Y, Kanemori Y, Chen TC,Chen MF, Yeh TS, Jan YY, Masuda S,Nimura Y, Takasawa S, Okamoto H,Nakanuma Y. Human REG I gene is up-regulated in intrahepaticcholangiocarcinoma and its precursorlesions. Hepatology 2001;33:1036–42.
15. Report of the Expert Committee onthe Diagnosis and Classification ofDiabetes Mellitus. Diabetes care 1997;20:1183–97.
16. Satomura Y, Sawabu N, Ohta H, WatanabeH, Yamakawa O, Motoo Y, Okai T, ToyaD, Makino H, Okamoto H. Theimmunohistochemical evaluation of PSP/reg-protein in normal and diseased humanpancreatic tissues. Int J Pancreatol 1993;13:59–67.
17. Fukui H, Kinoshita Y, Maekawa T, OkadaA, Waki S, Hassan S, Okamoto H, ChibaT. Regenerating gene protein may mediategastric mucosal proliferation induced byhypergastrinemia in rats. Gastroenterology1998;115:1483–93.
18. Yoshino N, Ishihara S, Rumi MA, Ortega-Cava CF, Yuki T, Kazumori H, TakazawaS, Okamoto H, Kadowaki Y, Kinoshita Y.Interleukin-8 regulates expression of Regprotein in Helicobacter pylori-infected
gastric mucosa. Am J Gastroenterol 2005;100:2157–66.
19. Senn JJ, Klover PJ, Nowak IA, MooneyRA. Interleukin-6 induces cellular insulinresistance in hepatocytes. Diabetes 2002;51:3391–9.
20. Yonemura Y, Sakurai S, Yamamoto H,Endou Y, Kawamura T, Bandou E, ElnemrA, Sugiyama K, Sasaki T, Akiyama T,Takasawa S, Okamoto H. REG geneexpression is associated with the infiltratinggrowth of gastric carcinoma. Cancer 2003;98:1394–400.
21. Sekikawa A, Fukui H, Fujii S, Ichikawa K,Tomita S, Imura J, Chiba T, Fujimori T.REG Ialpha protein mediates an anti-apoptotic effect of STAT3 signaling ingastric cancer cells. Carcinogenesis 2008;29:76–83.
22. Macadam RC, Sarela AI, Farmery SM,Robinson PA, Markham AF, Guillou PJ.Death from early colorectal cancer ispredicted by the presence of transcripts ofthe REG gene family. Br J Cancer 2000;83:188–95.
23. Astrosini C, Roeefzaad C, Dai YY,Dieckgraefe BK, Jons T, Kemmner W.REG1A expression is a prognostic markerin colorectal cancer and associated withperitoneal carcinomatosis. Int J Cancer2008;123:409–13.
24. Sasaki Y, Minamiya Y, Takahashi N,Nakagawa T, Katayose Y, Ito A, Saito H,Motoyama S, Ogawa J. REG1A expressionis an independent factor predictive of poorprognosis in patients with breast cancer.Ann Surg Oncol 2008;15:3244–51.
25. Minamiya Y, Kawai H, Saito H, Ito M,Hosono Y, Motoyama S, Katayose Y,Takahashi N, Ogawa J. REG1A expressionis an independent factor predictive ofpoor prognosis in patients with non-smallcell lung cancer. Lung Cancer 2008;60:98–104.
Can
cerCellBiology
Zhou et al. 1803
Int. J. Cancer: 127, 1795–1803 (2010) VC 2010 UICC