Upcoming tactile events and body ownership in schizophrenia
7
Upcoming tactile events and body ownership in schizophrenia Francesca Ferri a,b,c, ⁎, Marcello Costantini b,c, ⁎⁎, Anatolia Salone b,c , Giuseppe Di Iorio b,c,e , Giovanni Martinotti b,c , Antonio Chiarelli b,c , Arcangelo Merla b,c , Massimo Di Giannantonio b,c,e , Vittorio Gallese a,d a Department of Neuroscience, University of Parma, Italy b Department of Neuroscience and Imaging, University G. d'Annunzio, Chieti, Italy c Institute for Advanced Biomedical Technologies — ITAB, Foundation University G. d'Annunzio, Chieti, Italy d IIT (Italian Institute of Technology) Brain Center for Social and Motor Cognition, Parma, Italy e Psychiatric Clinic “Villa Jolanda”, Jesi, Italy abstract article info Article history: Received 18 February 2013 Received in revised form 7 June 2013 Accepted 10 June 2013 Available online xxxx Keywords: Schizophrenia Body ownership Rubber hand illusion Tactile expectation Multisensory integration Ipseity Schizophrenic patients may report unusual perception of their own body. Studies using the rubber hand illu- sion (RHI) proposed that they exhibit a distorted sense of body ownership. However, since the RHI is mostly achieved with the contribution of visuo-tactile integration, the stronger RHI observed in schizophrenic pa- tients could reflect either a general increase of the response to multisensory stimuli or a larger influence of visual cues on the tactile sensory experience. The purpose of the present study is to investigate patients' per- ception of their own body by means of a behavioral paradigm that measures their proneness to the RHI with- out relying on multisensory integration occurring during actual experience of touch. In a previous study we demonstrated in healthy participants that expectation of touch experience arising at the sight of a human hand approaching a rubber hand is enough to induce a sense of ownership over the same hand. Here we take advantage of the same paradigm to investigate body ownership in schizophrenia. Patients observed the experimenter's hand while approaching – without touching – either a rubber hand or a piece of wood placed in front of them. The seen object could be either aligned to participant's hand or rotated by 180°. Phenomenology of the illusion revealed that schizophrenic patients exhibited sense of ownership over the rubber hand, but more weakly than healthy controls. The present study sheds new light on the experience of body ownership in schizophrenic patients, corroborating the notion that alterations of bodily self- awareness play an important role in schizophrenia. © 2013 Elsevier B.V. All rights reserved. 1. Introduction Schizophrenia-spectrum disorders have been described as psychiat- ric conditions critically associated with anomalies of self-experiences. Schizophrenic patients can suffer from deficits in self-recognition and self-attribution of thoughts and actions (Schneider, 1950). Unrevealing the processes that underlie these symptoms might shed some light on the human ability to make a distinction between self and non-self and on the origin of its disruption in schizophrenia. Accordingly, from the phenomenological perspective, recent investigations suggest that dis- turbances of basic self-experience are predictive of psychosis onset in the ultra high risk for psychosis prodromal population (Nelson et al., 2012). Empirical research on self-recognition processes in schizophrenia mainly refer to a disruption of the sense of ownership, defined as the feeling that something is part of one's own body, and agency of action, defined as the subjective awareness that one is controlling one's own volitional actions in the world (for reviews see, for example, Cermolacce et al., 2007; Jeannerod, 2009; Moore and Fletcher, 2012). As highlighted by Waters and Badcock (2010), in general, studies on sense of body ownership and sense of agency examine specific cues contributing in their own unique way to the sense of self-recognition, such as sensory integration and body schema (body ownership process- es), efferent motor signal processing and psychological binding experi- ences (action representation processes). In particular, previous studies investigating body ownership in schizophrenic patients used the rubber hand illusion (RHI, Botvinick and Cohen, 1998). To elicit this illusion, the participant's real hand is hidden from view while a rubber hand is placed in front of her. The experimenter generally uses two paint- brushes to stroke synchronously the rubber hand and the participant's hidden hand. After a short period (about 30 s), people have the Schizophrenia Research xxx (2013) xxx–xxx ⁎ Correspondence to: F. Ferri, Department of Neuroscience—Section of Physiology, University of Parma, Via Volturno 39, I-43100 Parma, Italy. Tel.: +39 0521 903881; fax: + 39 0521 903900. ⁎⁎ Correspondence to: M. Costantini, Department of Neuroscience and Imaging, University of Chieti, Via dei Vestini 33, 66013 Chieti, Italy. Tel.: +39 0871 3556945; fax: + 39 0871 3556930. E-mail addresses: [email protected] (F. Ferri), [email protected] (M. Costantini). SCHRES-05470; No of Pages 7 0920-9964/$ – see front matter © 2013 Elsevier B.V. All rights reserved. http://dx.doi.org/10.1016/j.schres.2013.06.026 Contents lists available at SciVerse ScienceDirect Schizophrenia Research journal homepage: www.elsevier.com/locate/schres Please cite this article as: Ferri, F., et al., Upcoming tactile events and body ownership in schizophrenia, Schizophr. Res. (2013), http://dx.doi.org/ 10.1016/j.schres.2013.06.026
Transcript of Upcoming tactile events and body ownership in schizophrenia

Schizophrenia Research xxx (2013) xxx–xxx
SCHRES-05470; No of Pages 7
Contents lists available at SciVerse ScienceDirect
Schizophrenia Research
j ourna l homepage: www.e lsev ie r .com/ locate /schres
Upcoming tactile events and body ownership in schizophrenia
Francesca Ferri a,b,c,⁎, Marcello Costantini b,c,⁎⁎, Anatolia Salone b,c, Giuseppe Di Iorio b,c,e,Giovanni Martinotti b,c, Antonio Chiarelli b,c, Arcangelo Merla b,c,Massimo Di Giannantonio b,c,e, Vittorio Gallese a,d
a Department of Neuroscience, University of Parma, Italyb Department of Neuroscience and Imaging, University G. d'Annunzio, Chieti, Italyc Institute for Advanced Biomedical Technologies — ITAB, Foundation University G. d'Annunzio, Chieti, Italyd IIT (Italian Institute of Technology) Brain Center for Social and Motor Cognition, Parma, Italye Psychiatric Clinic “Villa Jolanda”, Jesi, Italy
⁎ Correspondence to: F. Ferri, Department of NeurosUniversity of Parma, Via Volturno 39, I-43100 Parma,fax: +39 0521 903900.⁎⁎ Correspondence to: M. Costantini, Department oUniversity of Chieti, Via dei Vestini 33, 66013 Chieti, Itfax: +39 0871 3556930.
E-mail addresses: [email protected] (F. [email protected] (M. Costantini).
0920-9964/$ – see front matter © 2013 Elsevier B.V. Allhttp://dx.doi.org/10.1016/j.schres.2013.06.026
Please cite this article as: Ferri, F., et al., Upco10.1016/j.schres.2013.06.026
a b s t r a c t
a r t i c l e i n f oArticle history:Received 18 February 2013Received in revised form 7 June 2013Accepted 10 June 2013Available online xxxx
Keywords:SchizophreniaBody ownershipRubber hand illusionTactile expectationMultisensory integrationIpseity
Schizophrenic patients may report unusual perception of their own body. Studies using the rubber hand illu-sion (RHI) proposed that they exhibit a distorted sense of body ownership. However, since the RHI is mostlyachieved with the contribution of visuo-tactile integration, the stronger RHI observed in schizophrenic pa-tients could reflect either a general increase of the response to multisensory stimuli or a larger influence ofvisual cues on the tactile sensory experience. The purpose of the present study is to investigate patients' per-ception of their own body by means of a behavioral paradigm that measures their proneness to the RHI with-out relying on multisensory integration occurring during actual experience of touch. In a previous study wedemonstrated in healthy participants that expectation of touch experience arising at the sight of a humanhand approaching a rubber hand is enough to induce a sense of ownership over the same hand. Here wetake advantage of the same paradigm to investigate body ownership in schizophrenia. Patients observedthe experimenter's hand while approaching – without touching – either a rubber hand or a piece of woodplaced in front of them. The seen object could be either aligned to participant's hand or rotated by 180°.Phenomenology of the illusion revealed that schizophrenic patients exhibited sense of ownership over therubber hand, but more weakly than healthy controls. The present study sheds new light on the experienceof body ownership in schizophrenic patients, corroborating the notion that alterations of bodily self-awareness play an important role in schizophrenia.
© 2013 Elsevier B.V. All rights reserved.
1. Introduction
Schizophrenia-spectrum disorders have been described as psychiat-ric conditions critically associated with anomalies of self-experiences.Schizophrenic patients can suffer from deficits in self-recognition andself-attribution of thoughts and actions (Schneider, 1950). Unrevealingthe processes that underlie these symptoms might shed some light onthe human ability to make a distinction between self and non-self andon the origin of its disruption in schizophrenia. Accordingly, from thephenomenological perspective, recent investigations suggest that dis-turbances of basic self-experience are predictive of psychosis onset in
cience—Section of Physiology,Italy. Tel.: +39 0521 903881;
f Neuroscience and Imaging,aly. Tel.: +39 0871 3556945;
erri),
rights reserved.
ming tactile events and body
the ultra high risk for psychosis prodromal population (Nelson et al.,2012).
Empirical research on self-recognition processes in schizophreniamainly refer to a disruption of the sense of ownership, defined as thefeeling that something is part of one's own body, and agency of action,defined as the subjective awareness that one is controlling one's ownvolitional actions in the world (for reviews see, for example,Cermolacce et al., 2007; Jeannerod, 2009; Moore and Fletcher, 2012).As highlighted by Waters and Badcock (2010), in general, studies onsense of body ownership and sense of agency examine specific cuescontributing in their own unique way to the sense of self-recognition,such as sensory integration and body schema (bodyownership process-es), efferent motor signal processing and psychological binding experi-ences (action representation processes). In particular, previous studiesinvestigating body ownership in schizophrenic patients used the rubberhand illusion (RHI, Botvinick and Cohen, 1998). To elicit this illusion, theparticipant's real hand is hidden from view while a rubber hand isplaced in front of her. The experimenter generally uses two paint-brushes to stroke synchronously the rubber hand and the participant'shidden hand. After a short period (about 30 s), people have the
ownership in schizophrenia, Schizophr. Res. (2013), http://dx.doi.org/

2 F. Ferri et al. / Schizophrenia Research xxx (2013) xxx–xxx
experience that the rubber hand is their own hand and that it is the rub-ber hand that senses the touch of the paintbrush. The experience of theillusion can be quantified by means of the proprioceptive drift. In thistest participants verbally report, before and after the synchronousvisuo-tactile stimulation, the perceived location of their hand (Tsakirisand Haggard, 2005). After synchronous visuo-tactile stimulation, peo-ple consider their hand to be closer to the rubber hand than it reallywas.
According to limited current knowledge, schizophrenia patientsshow higher sensitivity to the illusion as compared to healthy controls(Peled et al., 2000; Peled et al., 2003; Thakkar et al., 2011). Moreover,in patients, vividness of the illusion seems to be associated with elevat-ed positive symptoms (Peled et al., 2000, 2003; Thakkar et al., 2011).However, sense of body ownership and its experimental proxy, that isthe RHI, rely on the integration of sensory signals from differentmodal-ities (Botvinick and Cohen, 1998; Botvinick, 2004; Tsakiris andHaggard,2005; Tsakiris, 2010; Ehrsson, 2012). Thus, when the visual andspatio-temporal signals received from a limb all match, a feeling ofownership then arises for that limb (Ehrsson, 2012).
Such constitutive role of the integration of actual multisensory sig-nals in the RHI makes its use problematic to investigate sense of bodyownership in schizophrenic patients. There is, indeed, enough evi-dence suggesting that multisensory integration is altered in schizo-phrenia (Foucher et al., 2007; de Jong et al., 2009; Seubert et al.,2010; Ebisch et al., 2013). For example, it has been demonstratedthat schizophrenia patients show reduced McGurk effects (Pearl etal., 2009). The McGurk effect is a phenomenon where an auditory syl-lable is presented simultaneously with a silent video showing a modelarticulating an incongruent syllable which results in fused or com-bined syllable perception (McGurk and MacDonald, 1976). Schizo-phrenia patients also show reduced interference effects whendetecting the emotional content of voices paired with facial expres-sions of a different emotion (de Jong et al., 2009), and patients benefitless from seeing the visual articulation of words when combined withnoisy vocal presentations of the same words (Ross et al., 2007). It wassuggested that these deficits result from impairments in higher-orderspeech processing and biological motion perception networks (Rosset al., 2007; Szycik et al., 2009); however, a more general disturbanceof multisensory integration may also contribute to the phenomena.Accordingly, Williams, Light, Braff, and Ramachandran (Williams etal., 2010) recently revealed that schizophrenia patients show impair-ments in basic audio–visual integration. This observation was madeby using a simple target detection task without a speech component.
We think that multisensory integration deficits should be carefullyconsidered before reaching the conclusion that schizophrenic patients“might have a weaker or more flexible internal model of their body,making themmore susceptible to the illusion” (Thakkar et al., 2011). In-deed, the stronger RHI observed in these patients (Peled et al., 2000;Peled et al., 2003; Thakkar et al., 2011) could reflect either a general in-crease of the response to multisensory stimuli (e.g., Stone et al., 2011),or a larger influence of visual cues on tactile sensory experience, com-pared to healthy participants. This would be also consistent with possi-ble alterations of proprioception and somatosensory processing (Changand Lenzenweger, 2005).
In the present study we explore the extent to which visuo-tactileintegration contributes to susceptibility to the RHI in schizophrenia,by using a procedure in which no tactile stimulation is applied andmultisensory integration is elicited only by anticipation of touch ex-perience. Indeed, we want to rule out the possibility that the strongerRHI observed in schizophrenic patients, compared to controls, is dueto an imbalanced contribution of vision and experience of touch. Tothis aim we take advantage of a new induction procedure of the RHI(Ferri et al., in 2013), that is, without delivering synchronizedvisuo-tactile stimuli. In this new induction procedure, participantsobserve a rubber hand being approached but not touched, whiletheir own hand is out of sight. Obtaining the same results as with
Please cite this article as: Ferri, F., et al., Upcoming tactile events and body10.1016/j.schres.2013.06.026
the classic RHI induction procedure would mean that higher suscep-tibility to “classic” RHI in patients does not rely either on actual stim-ulation nor on the overweighting of visual over tactile information,but it likely reflects a more flexible internal model (Thakkar et al.,2011). However, one could also hypothesize different scenarios. 1)Patients might experience RHI as much as control participants,which would indicate that higher susceptibility to “classic” RHI in pa-tients does rely on actual stimulation and overweighting visual infor-mation so that when actual stimulation is absent, visuo-tactileintegration seems generally unimpaired. 2) Patients might experi-ence RHI less than control participants, which would indicate thathigher susceptibility to “classic” RHI in patients does rely on actualstimulation and that anticipation, rather than actual experience oftouch, is not sufficient to create ownership over the rubber hand inschizophrenic patients. In this case, it would be also possible that al-tered self experiences, that is, disturbed body ownership manifestingitself as lower susceptibility to RHI, could be differently related tosymptomatology. In particular, it could be associated with negativesymptoms, whereas higher susceptibility to RHI could be associatedwith positive symptoms.
2. Methods
2.1. Participants
21 schizophrenic patients (SCZ; 11 inpatients, 10 outpatients) and17 control participants (HC) were included in the present study(Table 1). Patients were diagnosed according to the structured clinicalinterview for DSM-IV. Exclusion criteria for all participants comprisedsignificant medical or neurological illness, substance abuse or depen-dence in the previous six months, IQ b 85, and, for the HC group, apersonal history of Axis I/II disorders or a history of psychosis infirst-degree relatives. SCZ and HC groups were matched for age, gen-der and education. SCZ patients were recruited from outpatient ser-vices at Chieti mental health department and from inpatients at thepsychiatric clinic “Villa Jolanda”. The mean illness duration was12,16 ± 9,33 years. The SCZ group had intellectual capacities in therange of the average healthy population (IQ mean scores =104.7 ± 6.5). Chlorpromazine equivalents were calculated (Woods,2003) for antipsychotics (Table 1). The study was approved by theEthics Committee of Chieti University. Written informed consentwas obtained from all participants after full explanation of the proce-dure of the study, in line with the Declaration of Helsinki.
2.2. Evaluation scales
SCZ patients were evaluated by the structured clinical interviewfor DSM-IV Axis I disorders (SCID-I) (First et al., 1996b) to establishaxis I diagnoses. They were rated for symptom severity using thebrief psychiatric rating scale (BPRS; Overall and Gorham, 1962), thescale for assessment of positive symptom (SAPS) and the scale for as-sessment of negative symptom (SANS; Andreasen, 1984a, b)(Table 1). Patients' intelligence quotient (IQ) was evaluated bymeans of the Raven standard progressive matrices (SPM).
HC participants were evaluated by means of the structured clinicalinterview for DSM-IV for Axis II personality disorders (SCID-II) (Firstet al., 1996a). All the evaluation scales were administered by trainedpsychiatrists.
2.3. Procedure
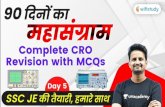
Participants sat in front of a table. The right arm was placed on thetable in a relaxed position at a fixed point inside a frame. A smallertable, measuring 80 by 30 cm and 20 cm in height, was positionedover the table where the real hand was placed (see Fig. 1). This tablewas used to both hide participants' hand and to support the object
ownership in schizophrenia, Schizophr. Res. (2013), http://dx.doi.org/

Table 1Demographic information about schizophrenia group (SCZ) and healthy control group(HC).
SCZ(n° = 21)
HC(n° = 17)
DSM-IV schizophrenia typeParanoid, no (%) 10 (47.6%) n.a.Disorganized, n° (%) 6 (29%) n.a.Catatonic, n° (%) 0 (0%) n.a.Undifferentiated, n° (%) 4 (19.05%) n.a.Residual, n° (%) 1 (4.7%) n.a.
Age (mean ± SD) 41.1 ± 11.4 46.6 ± 13.9Female sex (n°) 0 0Handedness
Right, n° (%) 21 (100%) 17 (100%)Left, n° (%) 0 (0%) 0 (0%)
Education (mean ± SD) 11.5 ± 3.5 12.0 ± 3.3Illness duration (mean ± SD) 12.2 ± 9.3 n.a.SCID-II n.a. NegativeBPRS (mean ± SD) 42.7 ± 9.2 n.a.SAPS (mean ± SD)
Hallucinations 4.7 ± 5.4 n.a.Delusions 8.0 ± 7.3 n.a.Bizarre behavior 2.6 ± 3.4 n.a.Formal thought disorders 7.0 ± 6.8 n.a.
SANS (mean ± SD)Affective flattening 10.9 ± 8.2 n.a.
Alogia 4.5 ± 4.7 n.a.Avolition–apathy 6.3 ±3.3 n.a.Anhedonia–asociality 10.6 ± 4.4 n.a.Attention 3.2 ± 2.7 n.a.
Chlorpromazine equivalent (mg/die) 404.0 ± 268.2 n.a.Typical antipsychotic, n° (%) 2 (9.5%) n.a.
Haloperidol 1 (4.8%)Levopromazine 1 (4.8%)
Atypical antipsychotic, n° (%) 13 (61.9%) n.a.Clozapine 1 (4.8%)Risperidone 8 (38.1%)Quetiapine 3 (14.3%)
Atypical + typical antipsychotic, n° (%) 6 (28.6%) n.a.Quetiapine + haloperidol 3 (14.3%)Risperidone + haloperidol 2 (9,5%)Risperidone + chlorpromazine 1 (4.8%)
3F. Ferri et al. / Schizophrenia Research xxx (2013) xxx–xxx
(i.e. the rubber hand or the piece of wood, see the Experimental designsection). The participants' hand and the viewed object were aligned onthe vertical axis and were positioned at 20 cm from each other. The ex-perimenter stood at the participant's right side, hidden behind a blackcurtain. She moved her hand towards the viewed object (which variedaccording to the experimental condition, see the Experimental designsection) with a velocity of 0.02 m/s, starting from a distance of 70 cmfrom the viewed object and stopping at 15 cm away from the viewedobject. The experimenter's hand never touched the viewed object. Theexperimenter, previously trained, followed audio instructions byearphones to perform controlled movements during the experiment.The consistency of movement direction and speed across trials wasallowed by four pairs of switches fixed onto two vertical rods 70 cmin height, enabling to record experimenter'smovements, speed and po-sition. The 4 switches were positioned on each rod at 60, 45, 30, 15 cmfrom the object, respectively. A further switch was positioned at thestarting point (70 cm). Each switch fed a signal to the PowerLab(ADinstrument), thus allowing post-hoc validation of experimenter'shand movements.
2.4. Experimental design
The experimental design was 2 × 2 factorial. The two factors were:the object (Rubber hand vs. Piece of wood) and the Position of the object(Congruent vs. Incongruent) relative to the participant's hidden arm. Therubber hand was a realistic prosthetic hand. The piece of wood was aplain wooden block, pale and beige in color, with a thumb-like featureand with one end tapered into a wrist-like shape. The four conditionswere: i) Rubber Hand Congruent — the rubber hand was aligned to theparticipant's own hand and the experimenter moved her hand towardsthe rubber hand; ii) Rubber Hand Incongruent— the rubber handwas ro-tated 180° relative the participant's own hand and the experimentermoved her hand towards the rubber hand; iii) Wood Congruent — thepiece of wood was aligned to the participant's own hand and the experi-mentermoved her hand towards thewood; and iv)Wood Incongruent—the piece of wood was rotated 180° relative the participant's own handand the experimenter moved her hand towards the wood. Stimuli hadcomparable overall size.
The experiment consisted of four blocks, one for each of the four ex-perimental conditions, whose presentation order was counterbalancedbetween participants. Each block lasted 2 min during which 4 ap-proaching movements were performed. At the beginning of the exper-imental session, participants were instructed to pay attention to theexperimenter's hand moving towards either a rubber hand or a pieceof wood placed in front of them. After receiving instructions partici-pants wore earphones through which white noise was delivered forthe entire duration of each block. After each block participants tookoff earphones and were required to complete the RHI questionnaire.
2.5. RHI questionnaire
We adopted a total of 15 questions from Longo et al. (Longo et al.,2008). The questions referred to two different components of the expe-rience of embodiment during the RHI paradigm: (a) Ten statements re-ferring to the embodiment of rubber hand. These comprised itemsrelating to the feelings that: the rubber hand belonged to the partici-pant, the participant had control over the rubber hand, the rubberhand and real hand were in the same location, and the rubber handhad taken on features of the actual hand. (b) Five statements referringto the experience of loss of one's hand. These comprised items relatingto the feelings of: being unable to move one's hand, one's handdisappearing, and one's hand being out of one's control. Participantscompleted four versions of the questionnaire, one for each experimen-tal condition. Participants answered each statement by choosing anumber from a 7-point Likert Scale, from “-3 being strongly in disagree-ment”, and “+3 being strongly in agreement”. The questions appeared
Please cite this article as: Ferri, F., et al., Upcoming tactile events and body10.1016/j.schres.2013.06.026
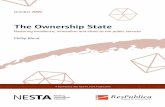
in random order. The mean ratings (see Fig. 2) for each component(Embodiment, Loss of own hand) of the experience of embodimentper condition were submitted to two separate multivariate ANOVA forrepeatedmeasureswith object (Rubber hand vs. Piece ofwood) and Po-sition of the object (Congruent vs. Incongruent), as within-subject fac-tors, and Group (SCZ vs. HC) as between-subject factor. In a furtheranalysis we focused on the two sub-components distinguished byLongo et al., (Longo et al., 2008) within the “embodiment of the rubberhand” general component, namely (a1) ownership and (a2) location, toassess whether they were equally involved during the induction of theRHI in both HC and SCZ. Post-hoc comparisons were performed usingthe Newman–Keuls methods when necessary.
Pearson's correlation coefficients were used to evaluate the associ-ation between the vividness of the illusion and the severity of positiveand negative symptoms in SCZ.
3. Results
(a) Embodiment questionsThe main effects of Object (F(1,36) = 41.0 p b 0.001; η2
p =0.53) and Position of the object (F(1,36) = 68.5 p b 0.001;η2
p = 0.65) were significant, as well as their interaction withthe group (object by Group: F(1,36) = 9.0 p b 0.01; η2
p =0.20; Position of the object by Group: F(1,36) = 5.1 p b 0.05;η2
p = 0.12). The interaction between the two within-subjectfactors was also significant (F(1,36) = 56.5, p b 0.001 η2
p =0.61). Post hoc comparisons showed higher mean rating forthe Hand Congruent (0.35) condition as compared to all the
ownership in schizophrenia, Schizophr. Res. (2013), http://dx.doi.org/

4 F. Ferri et al. / Schizophrenia Research xxx (2013) xxx–xxx
other conditions (−2.0, −1.6, and −2.1 for Hand Incongruent,Wood Congruent, and Wood incongruent, respectively; allp-values b 0.001; see Fig. 2). Importantly, there was also a sig-nificant Group by Object by Position of the object interaction(F(1,36) = 8.7, p b 0.01 η2
p = 0.20). Both groups showedhigher mean rating for the Hand Congruent condition as com-pared to all the other conditions (all p-values b 0.001), howeverHC (1.05) showed higher mean rating for the Hand Congruentcondition as compared to SCZ patients (−0.21; p b 0.01). Theother experimental conditions did not differ between HC andSCZ (all p-values > 0.40).
(b) Loss of one's hand questionsThe main effects of Object (F(1,36) = 17.4 p b 0.001; η2
p =0.33) and Position of the object (F(1,36) = 9.7 p b 0.001;η2
p = 0.21). The interaction between the two within-subjectfactors was also significant (F(1,36) = 4.8, p b 0.05 η2
p =0.12). Post hoc comparisons showed higher mean rating for theHand Congruent (−0.4) condition as compared to all the otherconditions (−1.21, −1.27, and −1.4 for Hand Incongruent,Wood Congruent, and Wood incongruent, respectively; allp-values b 0.01; see Fig. 2). Importantly, there was also a signif-icant Group by Object by Position of the object interaction(F(1,36) = 5.6, p b 0.05 η2
p = 0.14). The interaction wasexplained by the HC showing higher mean rating for the HandCongruent (−0.1; all p-values b 0.001) condition as comparedto all the other conditions (see Fig. 2). The same difference wasnot observed in SCZ patients (all p-values > 0.41).
Fig. 1. Experiment setup to evaluate rubber hand illusion. The experimenter moved herhand towards the viewed object (which varied according to the experimental condi-tion, see the Experimental design section) with a velocity of 0.02 m/s starting from adistance of 70 cm from the viewed object and stopping at 15 cm away from it. Theexperimenter's hand never touched the viewed object. White noise was deliveredthrough the headphones. EH: Experimenter's Hand; RH: Rubber Hand.
Please cite this article as: Ferri, F., et al., Upcoming tactile events and body10.1016/j.schres.2013.06.026
(a1) Ownership questionsThe main effects of Object (F(1,36) = 66.5 p b 0.001; η2
p =0.65) and Position of the object (F(1,36) = 71.4 p b 0.001;η2
p = 0.62) were significant, as well as their interaction withthe group (object by Group: F(1,36) = 10.7 p b 0.01; η2
p =0.23; Position of the object by Group: F(1,36) = 4.4 p b 0.05;η2
p = 0.11). The interaction between the two within-subjectfactors was also significant (F(1,36) = 49.5, p b 0.001 η2
p =0.58). Post hoc comparisons showed higher mean rating forthe Hand Congruent (0.28) condition as compared to all theother conditions (−2.1, −2.3, and −2.5 for Hand Incongruent,Wood Congruent, and Wood incongruent, respectively; allp-values b 0.001; see Fig. 2). Importantly, there was also a sig-nificant Group by Object by Position of the object interaction(F(1,36) = 6.7, p b 0.05 η2
p = 0.16). Both groups showedhigher mean rating for the Hand Congruent condition as com-pared to all the other conditions (all p-values b 0.001), howeverHC (1.08) showed higher mean rating for the Hand Congruentcondition as compared to SCZ patients (−0.37; p b 0.01). Theother experimental conditions did not differ between HC andSCZ (all p-values > 0.54).
(a2) Location questionsThe main effects of Object (F(1,36) = 6.8 p b 0.05; η2
p = 0.16)and Position of the object (F(1,36) = 77.3 p b 0.001; η2
p =0.68) were significant. The interaction between the twowithin-subject factors was also significant (F(1,36) = 13.0,p b 0.001 η2
p = 0.26). Post hoc comparisons showed highermean rating for the Hand Congruent (1.2) condition as com-pared to all the other conditions (−1.5, −0.12, and −1.4 forHand Incongruent, Wood Congruent, and Wood incongruent,respectively; all p-values b 0.001; see Fig. 2). The interactionGroup by Object by Position of the object was not significant(p > 0.1).
4. Correlation analysis
In patients, we explored the relationship between self-reported il-lusion vividness, as revealed by the ownership questions in each ex-perimental condition and subscales of the SAPS and SANS. Self-reported RHI strength in the rubber hand congruent, but not in allthe other experimental conditions was related to increased score onthe anhedonia subscale of the SANS (Pearson's r = 0.67, p =0.001,see Fig. 3).
5. Discussion
We investigated themalleability of body ownership in schizophren-ic patients by taking advantage of a new induction procedure of the RHIthat relies on tactile expectation rather than proper visuo-tactile stimu-lation (Ferri et al., in 2013). This paradigm allowed us to explore the ex-tent to which visuo-tactile integration contributes to susceptibility tothe RHI in schizophrenia.
Schizophrenic patients and healthy controls viewed theexperimenter's hand approaching either a rubber hand or a non cor-poreal object located just above their hidden real hand. Phenomenol-ogy of illusion was measured by questionnaires adapted from Longoet al. (Longo et al., 2008). Results indicated that both schizophrenicpatients and healthy participants experienced the illusion that theexperimenter's hand was about to touch their hidden hand ratherthan the rubber hand, as if the latter replaced their own hand. Thisdid not occur when the rubber hand was rotated by 180° with respectto their own hand or replaced by a piece of wood. Importantly,schizophrenic patients showed lower mean rating for the RubberHand Congruent condition, as revealed by the embodiment state-ments, compared to healthy controls. The mean rating for the otherconditions did not differ between groups.
ownership in schizophrenia, Schizophr. Res. (2013), http://dx.doi.org/
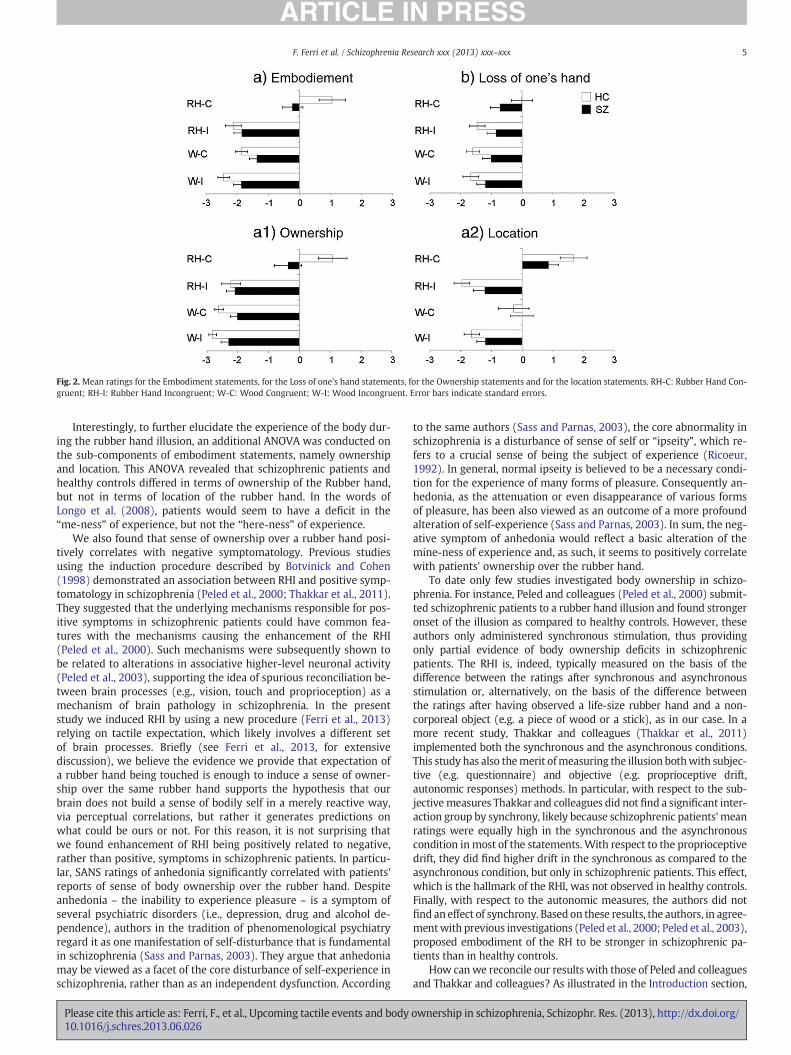
Fig. 2. Mean ratings for the Embodiment statements, for the Loss of one's hand statements, for the Ownership statements and for the location statements. RH-C: Rubber Hand Con-gruent; RH-I: Rubber Hand Incongruent; W-C: Wood Congruent; W-I: Wood Incongruent. Error bars indicate standard errors.
5F. Ferri et al. / Schizophrenia Research xxx (2013) xxx–xxx
Interestingly, to further elucidate the experience of the body dur-ing the rubber hand illusion, an additional ANOVA was conducted onthe sub-components of embodiment statements, namely ownershipand location. This ANOVA revealed that schizophrenic patients andhealthy controls differed in terms of ownership of the Rubber hand,but not in terms of location of the rubber hand. In the words ofLongo et al. (2008), patients would seem to have a deficit in the“me-ness” of experience, but not the “here-ness” of experience.
We also found that sense of ownership over a rubber hand posi-tively correlates with negative symptomatology. Previous studiesusing the induction procedure described by Botvinick and Cohen(1998) demonstrated an association between RHI and positive symp-tomatology in schizophrenia (Peled et al., 2000; Thakkar et al., 2011).They suggested that the underlying mechanisms responsible for pos-itive symptoms in schizophrenic patients could have common fea-tures with the mechanisms causing the enhancement of the RHI(Peled et al., 2000). Such mechanisms were subsequently shown tobe related to alterations in associative higher-level neuronal activity(Peled et al., 2003), supporting the idea of spurious reconciliation be-tween brain processes (e.g., vision, touch and proprioception) as amechanism of brain pathology in schizophrenia. In the presentstudy we induced RHI by using a new procedure (Ferri et al., 2013)relying on tactile expectation, which likely involves a different setof brain processes. Briefly (see Ferri et al., 2013, for extensivediscussion), we believe the evidence we provide that expectation ofa rubber hand being touched is enough to induce a sense of owner-ship over the same rubber hand supports the hypothesis that ourbrain does not build a sense of bodily self in a merely reactive way,via perceptual correlations, but rather it generates predictions onwhat could be ours or not. For this reason, it is not surprising thatwe found enhancement of RHI being positively related to negative,rather than positive, symptoms in schizophrenic patients. In particu-lar, SANS ratings of anhedonia significantly correlated with patients'reports of sense of body ownership over the rubber hand. Despiteanhedonia – the inability to experience pleasure – is a symptom ofseveral psychiatric disorders (i.e., depression, drug and alcohol de-pendence), authors in the tradition of phenomenological psychiatryregard it as one manifestation of self-disturbance that is fundamentalin schizophrenia (Sass and Parnas, 2003). They argue that anhedoniamay be viewed as a facet of the core disturbance of self-experience inschizophrenia, rather than as an independent dysfunction. According
Please cite this article as: Ferri, F., et al., Upcoming tactile events and body10.1016/j.schres.2013.06.026
to the same authors (Sass and Parnas, 2003), the core abnormality inschizophrenia is a disturbance of sense of self or “ipseity”, which re-fers to a crucial sense of being the subject of experience (Ricoeur,1992). In general, normal ipseity is believed to be a necessary condi-tion for the experience of many forms of pleasure. Consequently an-hedonia, as the attenuation or even disappearance of various formsof pleasure, has been also viewed as an outcome of a more profoundalteration of self-experience (Sass and Parnas, 2003). In sum, the neg-ative symptom of anhedonia would reflect a basic alteration of themine-ness of experience and, as such, it seems to positively correlatewith patients' ownership over the rubber hand.
To date only few studies investigated body ownership in schizo-phrenia. For instance, Peled and colleagues (Peled et al., 2000) submit-ted schizophrenic patients to a rubber hand illusion and found strongeronset of the illusion as compared to healthy controls. However, theseauthors only administered synchronous stimulation, thus providingonly partial evidence of body ownership deficits in schizophrenicpatients. The RHI is, indeed, typically measured on the basis of thedifference between the ratings after synchronous and asynchronousstimulation or, alternatively, on the basis of the difference betweenthe ratings after having observed a life-size rubber hand and a non-corporeal object (e.g. a piece of wood or a stick), as in our case. In amore recent study, Thakkar and colleagues (Thakkar et al., 2011)implemented both the synchronous and the asynchronous conditions.This study has also themerit ofmeasuring the illusion bothwith subjec-tive (e.g. questionnaire) and objective (e.g. proprioceptive drift,autonomic responses) methods. In particular, with respect to the sub-jectivemeasures Thakkar and colleagues did not find a significant inter-action group by synchrony, likely because schizophrenic patients' meanratings were equally high in the synchronous and the asynchronouscondition in most of the statements. With respect to the proprioceptivedrift, they did find higher drift in the synchronous as compared to theasynchronous condition, but only in schizophrenic patients. This effect,which is the hallmark of the RHI, was not observed in healthy controls.Finally, with respect to the autonomic measures, the authors did notfind an effect of synchrony. Based on these results, the authors, in agree-mentwith previous investigations (Peled et al., 2000; Peled et al., 2003),proposed embodiment of the RH to be stronger in schizophrenic pa-tients than in healthy controls.
How canwe reconcile our results with those of Peled and colleaguesand Thakkar and colleagues? As illustrated in the Introduction section,
ownership in schizophrenia, Schizophr. Res. (2013), http://dx.doi.org/

Fig. 3. Scatter plot of anhedonia scores against sense of ownership over the rubberhand.
6 F. Ferri et al. / Schizophrenia Research xxx (2013) xxx–xxx
“classic” RHI relies on the integration of actual sensory signals from dif-ferent modalities (Botvinick and Cohen, 1998; Tsakiris and Haggard,2005; Costantini and Haggard, 2007; Tsakiris et al., 2011), a processthat seems to be compromised in schizophrenic patients. The compari-son between results from the previous studies using the “classic” induc-tion procedure and from the present study suggests that highersusceptibility to “classic” RHI in patients does rely on actual stimulation,likely arising from a larger influence of visual cues on the tactile sensoryexperience, or from a general increase of the response to multisensorystimuli (e.g., Stone et al., 2011). Indeed, in absence of actual visuo-tactile signals, like in the present study, no higher susceptibility to RHIis observed in patients, even if multisensory integration is still elicited,but through anticipation mechanisms. Furthermore, the fact that pa-tients experience RHI less than control participants, when using thenew induction procedure, indicates that anticipation of touch is not suf-ficient for them to experience the RHI.
A possibility is that schizophrenic patients do not anticipate thetouch in the same way that controls do. Indeed, impairments in antic-ipating the position of a moving stimulus have been reported inschizophrenia–most extensively in the domain of smooth pursuiteye movements (Ross et al., 2000). Accordingly, investigation ofthe implicit processing of asynchrony by means of the Simon effect(i.e., the finding that manual responses are biased to the side of thestimulus) suggested that predictive mechanisms allowing anticipa-tion of upcoming events are impaired in patients, who would ratherrely on reactive mechanisms in order to perceive asynchrony. Indeed,patients appeared to process stimuli as if isolated rather than follow-ing each other (Lalanne et al., 2012).
When we firstly reported our anticipation-based procedure to in-duce the RHI (Ferri et al., 2013), we also proposed that it likely recruitsactivity in the ventral premotor cortex (vPMC), specifically in a regionrepresenting the human homologue of monkey F4 (Bremmer et al.,2001). This brain region, indeed, has been described as having multi-sensory properties (Graziano, 1999; Graziano, 2001) and beinginvolved in the dynamic mapping of the peri-personal space(e.g., Rizzolatti et al., 1997), as well. Moreover, neuroimaging studieshave recently shown that human vPMC is activated during the implicitprocessing of one's own hand and face (Cardini et al., 2011; Ferri et al.,2012a). Given that the vPMC appears to be hypofunctional as well asnegatively correlated with self-experience disturbances in schizophre-nia (Ebisch et al., 2013), and since it has been demonstrated that pa-tients show a defective implicit sense of their bodily self (Ferri et al.,2012b), we hypothesize that the lack of anticipatory touch displayedby schizophrenic patients in the present study might share the samepremotor origin (see also Gallese and Ferri, in press).
In conclusion, schizophrenic patients seem to experience the RHIdifferently from control subjects. This happens both when actual tac-tile stimuli are actually delivered, as demonstrated by Thakkar et al.(2011) and Peled et al. (2000, 2003), as well as when touch is onlyexpected, as in the present study. However, the direction of the RHI
Please cite this article as: Ferri, F., et al., Upcoming tactile events and body10.1016/j.schres.2013.06.026
findings in schizophrenia, compared to control participants, seemsto be specifically associated with symptomatology in each case. Dis-turbed body ownership manifesting itself as higher susceptibility toRHI when actual multisensory stimuli are delivered has been sug-gested to contribute to psychotic symptoms (Thakkar et al., 2011).On the other hand, we suggest that disturbed body ownershipmanifesting itself as lower susceptibility to RHI when actual multi-sensory stimuli are absent might contribute to negative symptoms,such as anhedonia. In particular, in schizophrenic patients this couldbe associated with altered predictive processes allowing anticipationof touch experience.
Thus, RHI is able to highlight a specific difference between pa-tients and controls in the bodily self experience (Ferri et al., 2012b).However, to fully understand the outcome of the RHI, more systemat-ic investigations are required. Indeed, one major limitation of ourstudy is that only subjective reports were used and we have no indi-cation whether patients in this sample may have been less forthcom-ing with reporting the illusion or subject to response bias. Newinvestigations might help to understand under which conditions theRHI in patients is stronger or weaker than in healthy participantsand, in general, how environmental inputs and specific alterationsof their integration/processing differently affect the relation betweenself experience and symptomatology.
Role of funding sourceThe funders had no role in study design, data collection and analysis, decision to
publish, or preparation of the manuscript.
ContributorsFrancesca Ferri and Marcello Costantini conceived and designed the study, wrote
the protocol, collected the data, undertook the statistical analyses, managed the litera-ture searches and wrote the manuscript.
Vittorio Gallese conceived and designed the study.Anatolia Salone selected the patients and wrote the manuscript.Giuseppe Di Iorio, Giovanni Martinotti, Massimo Di Giannantonio selected the
patients.Antonio Chiarelli and Arcangelo Merla designed the experimental set up.All authors contributed to and have approved the final manuscript.
Conflict of interestThe authors have no financial or ethical conflict of interest to declare.
AcknowledgmentThis work was supported by the EU grant TESIS (Towards an Embodied Science of
InterSubjectivity).
References
Andreasen, N.C., 1984a. Scale for the Assessment of Negative Symptoms (SANS). Uni-versity of Iowa, Iowa City, Iowa.
Andreasen, N.C., 1984b. Scale for the Assessment of Positive Symptoms (SAPS). Univer-sity of Iowa, Iowa City, Iowa.
Botvinick, M., 2004. Probing the neural basis of body ownership. Science 305 (5685),782–783.
Botvinick, M., Cohen, J., 1998. Rubber hands ‘feel’ touch that eyes see. Nature 391(6669), 756.
Bremmer, F., Schlack, A., Shah, N.J., Zafiris, O., Kubischik, M., Hoffmann, K., Zilles, K.,Fink, G.R., 2001. Polymodal motion processing in posterior parietal and premotorcortex: a human fMRI study strongly implies equivalencies between humans andmonkeys. Neuron 29 (1), 287–296.
Cardini, F., Costantini, M., Galati, G., Romani, G.L., Ladavas, E., Serino, A., 2011. Viewingone's own face being touched modulates tactile perception: an fMRI study. J. Cogn.Neurosci. 23 (3), 503–513.
Cermolacce, M., Naudin, J., Parnas, J., 2007. The “minimal self” in psychopathology: re-examining the self-disorders in the schizophrenia spectrum. Conscious. Cogn. 16(3), 703–714.
Chang, B.P., Lenzenweger, M.F., 2005. Somatosensory processing and schizophrenialiability: proprioception, exteroceptive sensitivity, and graphesthesia performancein the biological relatives of schizophrenia patients. J. Abnorm. Psychol. 114 (1),85–95.
Costantini, M., Haggard, P., 2007. The rubber hand illusion: sensitivity and referenceframe for body ownership. Conscious. Cogn. 16 (2), 229–240.
de Jong, J.J., Hodiamont, P.P., Van den Stock, J., de Gelder, B., 2009. Audiovisual emotionrecognition in schizophrenia: reduced integration of facial and vocal affect.Schizophr. Res. 107 (2–3), 286–293.
ownership in schizophrenia, Schizophr. Res. (2013), http://dx.doi.org/

7F. Ferri et al. / Schizophrenia Research xxx (2013) xxx–xxx
Ebisch, S.J., Salone, A., Ferri, F., De Berardis, D., Romani, G.L., Ferro, F.M., Gallese, V.,2013. Out of touch with reality? Social perception in first-episode schizophrenia.Soc. Cogn. Affect. Neurosci. 8 (4), 394–403.
Ehrsson, H.H., 2012. The Concept of Body Ownership and Its Relation to MultisensoryIntegration. MIT Press, Cambridge, MA.
Ferri, F., Frassinetti, F., Ardizzi, M., Costantini, M., Gallese, V., 2012a. A sensorimotornetwork for the bodily self. J. Cogn. Neurosci. 24 (7), 1584–1595.
Ferri, F., Frassinetti, F., Mastrangelo, F., Salone, A., Ferro, F.M., Gallese, V., 2012b. Bodilyself and schizophrenia: the loss of implicit self-body knowledge. Conscious. Cogn.21 (3), 1365–1374.
Ferri, F., Chiarelli, A.M., Merla, A., Gallese, V., Costantini, M., 2013. The body beyond thebody: expectation of a sensory event is enough to induce ownership over a fakehand. Proc. R. Soc. B: Biol. Sci. 280 (1765).
First, M.B., Spitzer, R.L., Gibbon, M., Williams, J.B.W., 1996a. Structured clinical inter-view for DSM-IV Axis I disorders, clinician version (SCID-CV). American PsychiatricPress, Washington, DC.
First, M.B., Gibbon, M., Spitzer, R.L., First, M.B., Gibbon, M., Spitzer, R.L., 1996b. Struc-tured clinical interview for DSM-IV Axis II personality disorders, (SCID-II, version2.0). Psychiatric Institute. New York: Biometric Research Department, New YorkState.
Foucher, J.R., Lacambre, M., Pham, B.T., Giersch, A., Elliott, M.A., 2007. Low time resolu-tion in schizophrenia Lengthened windows of simultaneity for visual, auditory andbimodal stimuli. Schizophr. Res. 97 (1–3), 118–127.
Gallese, V., Ferri, F., 2013. Jaspers, the body and Schizophrenia: the bodily self. Psycho-pathology (in press).
Graziano, M.S.A., 1999. Where is my arm? The relative role of vision and propriocep-tion in the neuronal representation of limb position. Proc. Natl. Acad. Sci. U. S. A.96 (18), 10418–10421.
Graziano, M.S.A., 2001. A system of multimodal areas in the primate brain. Neuron 29(1), 4–6.
Jeannerod, M., 2009. The sense of agency and its disturbances in schizophrenia: areappraisal. Exp. Brain Res. 192 (3), 527–532.
Lalanne, L., Van Assche, M., Wang, W., Giersch, A., 2012. Looking forward: an impairedability in patients with schizophrenia? Neuropsychologia 50 (12), 2736–2744.
Longo, M.R., Schüür, F., Kammers, M.P.M., Tsakiris, M., Haggard, P., 2008. What is em-bodiment? A psychometric approach. Cognition 107 (3), 978.
McGurk, H., MacDonald, J., 1976. Hearing lips and seeing voices. Nature 264 (5588),746–748.
Moore, J.W., Fletcher, P.C., 2012. Sense of agency in health and disease: a review of cueintegration approaches. Conscious. Cogn. 21 (1), 59–68.
Nelson, B., Thompson, A., Yung, A.R., 2012. Basic self-disturbance predicts psychosisonset in the ultra high risk for psychosis “prodromal” population. Schizophr. Bull.
Overall, J.E., Gorham, D.R., 1962. The brief psychiatric rating scale. Psychol. Rep. 10 (3),799–812.
Pearl, D., Yodashkin-Porat, D., Katz, N., Valevski, A., Aizenberg, D., Sigler, M., Weizman,A., Kikinzon, L., 2009. Differences in audiovisual integration, as measured byMcGurk phenomenon, among adult and adolescent patients with schizophreniaand age-matched healthy control groups. Compr. Psychiatry 50 (2), 186–192.
Please cite this article as: Ferri, F., et al., Upcoming tactile events and body10.1016/j.schres.2013.06.026
Peled, A., Ritsner, M., Hirschmann, S., Geva, A.B., Modai, I., 2000. Touch feel illusion inschizophrenic patients. Biol. Psychiatry 48 (11), 1105–1108.
Peled, A., Pressman, A., Geva, A.B., Modai, I., 2003. Somatosensory evoked potentialsduring a rubber-hand illusion in schizophrenia. Schizophr. Res. 64 (2–3), 157–163.
Ricoeur, P., 1992. Oneself as Another. The University of Chicago Press, Chicago.Rizzolatti, G., Fadiga, L., Fogassi, L., Gallese, V., 1997. The space around us. Science 277
(5323), 190–191.Ross, R.G., Olincy, A., Harris, J.G., Sullivan, B., Radant, A., 2000. Smooth pursuit eye
movements in schizophrenia and attentional dysfunction: adults with schizophre-nia, ADHD, and a normal comparison group. Biol. Psychiatry 48 (3), 197–203.
Ross, L.A., Saint-Amour, D., Leavitt, V.M., Molholm, S., Javitt, D.C., Foxe, J.J., 2007. Impairedmultisensory processing in schizophrenia: deficits in the visual enhancement ofspeech comprehension under noisy environmental conditions. Schizophr. Res. 97(1–3), 173–183.
Sass, L.A., Parnas, J., 2003. Schizophrenia, consciousness, and the self. Schizophr. Bull.29 (3), 427–444.
Schneider, K., 1950. Die psychopatischen Personlichkeiten (9th edn). Deuticke, Vienna.Seubert, J., Loughead, J., Kellermann, T., Boers, F., Brensinger, C.M., Habel, U., 2010. Mul-
tisensory integration of emotionally valenced olfactory–visual information in pa-tients with schizophrenia and healthy controls. J. Psychiatry Neurosci. 35 (3),185–194.
Stone, D.B., Urrea, L.J., Aine, C.J., Bustillo, J.R., Clark, V.P., Stephen, J.M., 2011. Unisensoryprocessing and multisensory integration in schizophrenia: a high-density electricalmapping study. Neuropsychologia 49 (12), 3178–3187.
Szycik, G.R., Munte, T.F., Dillo, W., Mohammadi, B., Samii, A., Emrich, H.M., Dietrich,D.E., 2009. Audiovisual integration of speech is disturbed in schizophrenia: anfMRI study. Schizophr. Res. 110 (1–3), 111–118.
Thakkar, K.N., Nichols, H.S., McIntosh, L.G., Park, S., 2011. Disturbances in body owner-ship in schizophrenia: evidence from the rubber hand illusion and case study of aspontaneous out-of-body experience. PLoS One 6 (10), e27089.
Tsakiris, M., 2010. My body in the brain: a neurocognitive model of body-ownership.Neuropsychologia 48 (3), 703.
Tsakiris, M., Haggard, P., 2005. The rubber hand illusion revisited: visuotactile integra-tion and self-attribution. J. Exp. Psychol. Hum. Percept. Perform. 31 (1), 80–91.
Tsakiris, M., Tajadura-Jiménez, A., Costantini, M., 2011. Just a heartbeat away from one'sbody: interoceptive sensitivity predicts malleability of body-representations. Proc.R. Soc. B Biol. Sci. 278 (1717), 2470–2476.
Waters, F.A., Badcock, J.C., 2010. First-rank symptoms in schizophrenia: reexaminingmechanisms of self-recognition. Schizophr. Bull. 36 (3), 510–517.
Williams, L.E., Light, G.A., Braff, D.L., Ramachandran, V.S., 2010. Reduced multisensory in-tegration in patients with schizophrenia on a target detection task. Neuropsychologia48 (10), 3128–3136.
Woods, S.W., 2003. Chlorpromazine equivalent doses for the newer atypical antipsy-chotics. J. Clin. Psychiatry 64 (6), 663–667.
ownership in schizophrenia, Schizophr. Res. (2013), http://dx.doi.org/