
(Un?)Healthy Politics: The Political Determinants of Subnational Health Systems in Brazil
34
(Un?)Healthy Politics: The Political Determinants of Subnational Health Systems in Brazil Jorge Antonio Alves Department of Political Science Queens College, City University of New York [email protected] Forthcoming in Latin American Politics and Society. **Please do not cite without permission.** Abstract How does political competition shape institutions that govern the expansion of social policy subnationally? Brazilian states have shown a surprising variation in the design of their public health institutions, which regulate the distribution of health resources and citizen access to public health care. While many states have experienced fragmentation, some have remained highly centralized and discretionary, and only a select few have established a coordinated system based on power-sharing and rules-based distribution. Accounts that link public health care expansion to federal government imposition, presence of the public health care movement and leftist parties cannot fully explain this variation. Instead, in the three Brazilian states examined here, the nature of subnational political competition triggered different institution-building strategies. The findings indicate plural political competition yielded incentives for limiting state-level discretion and sharing power with municipal governments, while political concentration reinforced the attraction to centralized and discretionary policy-making. Acknowledgements An earlier version of this article was presented at the Conference on Subnational Research in Comparative Politics hosted by the Center for Latin American and Caribbean Studies at the Watson Institute for International Studies, Brown University, May 9-10, 2013. I appreciate helpful feedback from John Bowman, Tulia Falleti, Julie George, Patrick Heller, Wendy Hunter, Pauline Jones-Luong, Eduardo Moncada, Alfred Montero, Lorena Moscovich, Celina Souza, and three anonymous LAPS reviewers. I am especially grateful to Richard Snyder for ongoing advice and support. Support for field research was provided by the National Science Foundation under Grant No. 0819267 and Brown University.
Transcript of (Un?)Healthy Politics: The Political Determinants of Subnational Health Systems in Brazil

(Un?)Healthy Politics: The Political Determinants of Subnational Health Systems in Brazil
Jorge Antonio Alves Department of Political Science Queens College, City University of New York [email protected]
Forthcoming in Latin American Politics and Society.
**Please do not cite without permission.**
Abstract
How does political competition shape institutions that govern the expansion of social policy
subnationally? Brazilian states have shown a surprising variation in the design of their public health
institutions, which regulate the distribution of health resources and citizen access to public health care.
While many states have experienced fragmentation, some have remained highly centralized and
discretionary, and only a select few have established a coordinated system based on power-sharing and
rules-based distribution. Accounts that link public health care expansion to federal government
imposition, presence of the public health care movement and leftist parties cannot fully explain this
variation. Instead, in the three Brazilian states examined here, the nature of subnational political
competition triggered different institution-building strategies. The findings indicate plural political
competition yielded incentives for limiting state-level discretion and sharing power with municipal
governments, while political concentration reinforced the attraction to centralized and discretionary
policy-making.
Acknowledgements
An earlier version of this article was presented at the Conference on Subnational Research in
Comparative Politics hosted by the Center for Latin American and Caribbean Studies at the Watson
Institute for International Studies, Brown University, May 9-10, 2013. I appreciate helpful feedback from
John Bowman, Tulia Falleti, Julie George, Patrick Heller, Wendy Hunter, Pauline Jones-Luong, Eduardo
Moncada, Alfred Montero, Lorena Moscovich, Celina Souza, and three anonymous LAPS reviewers. I am
especially grateful to Richard Snyder for ongoing advice and support. Support for field research was
provided by the National Science Foundation under Grant No. 0819267 and Brown University.
Alves – (Un?)Healthy Politics
2
Brazil’s redemocratization process ushered important developments for expanded citizenship
such as greater responsibilities for social policies by the state—of specific interest, the determination
that health was a right, leading to the foundation of a universal health system (Sistema Único de Saúde,
henceforth SUS)—along with expanded mandates for the provision of public services by subnational
governments.1 But degrading macro and socio-economic conditions resulting from endemic corruption,
bureaucratic gridlock, and the predatory behavior of resurgent state-level political elites (Weyland 1996;
Abrúcio 1998; Hagopian 1996; Samuels 2003; Souza and Dantas Neto 2006) tempered these
developments. National democracy has since become increasingly consolidated (Power and Zucco
2012), as the federal government has implemented important reforms, including macroeconomic
stabilization and inducing programmatic social policies on subnational governments. This has had
important socio-economic and political impacts, including the increasing, though uneven, level of
political competition in Brazilian states (Souza 1997, 2009; Borges 2007, 2011). In some cases the
political competition has led to leftist party victories in former conservative strongholds (Montero 2012;
Zucco and Samuels 2014). But while existing research explains these important shifts in the nature of
political competition in Brazil, this literature says little about the impact of shifting competition on
subnational institutions and public policies.
This article argues that equitable social service expansion at the subnational level in Brazil is
determined by the nature of state-level political competition. The equitable distribution and expansion
of public health services obtain when state-level governments limit their own discretion over health
policy by building governance institutions that include municipal governments in decisions of policy
design and resource allocation, especially when those institutions govern the distribution of state as well
1 Brazil is a three-tiered federal system with 26 states, a Federal District, and 5,570 municipalities. Each level has
elected executives, legislatures, and a bureaucracy composed by career civil servants and political appointees.
Alves – (Un?)Healthy Politics
3
as federal resources. But actors2 shape health governance not only with an eye on health policy, but as
part of broader strategies to engage shifting electoral scenarios both nationally and subnationally.
National institutional blueprints are not fully implemented in the majority of states, but especially in
those where political competition is concentrated. Equitable governance institutions result where
political competition is plural. The argument is based on evidence from a comparative study of health
care governance using data collected during fieldwork in the states of Bahia, Minas Gerais and São
Paulo.3
These findings supplement and challenge existing studies of the political determinants of public
health and social policies. Past research emphasizes the importance of leftist partisanship (Navarro and
Shi 2001; Cameron and Hershberg 2010; Pribble et al. 2009; Levitsky and Roberts 2011; Pribble 2013),
programmatic networks (e.g. Hassenteufel et al. 2010), institutional factors such as concentration of
executive power (Immergut 1992), or policy legacies (Haggard and Kaufman 2008; Pribble 2013). In
Brazil, social and health service expansion has been linked to either national or local-level factors, such
as the infiltration of the state by programmatic actors of the Movimento Sanitário (Escorel 1998; Paim
2008; Falleti 2010), proliferation of leftist ideology and rule (Pimenta 2007; Sugiyama 2008), and the
spread of participatory governance institutions (Dagnino 2002; Coelho 2006; Avritzer 2009). While
important, these factors do not fully account for how patterns of political competition at the subnational
level shape the governance structures in which local health policies are derived and implemented. A
focus on subnational political competition strengthens our understanding of the conditions under which
2 The main agents in this study are political elites (incumbents or challengers for state and municipal governments) and their immediate political circles, especially the cabinet-level appointments such as public health managers (Secretários Estaduais e Municipais de Saúde) and the main lower-tier appointments that make policy decisions. 3 Data was collected during hundreds of hours of participant observation in 61 public meetings, over 80 semi-structured elite interviews—ranging from elected officials, appointed health managers, career civil-servants and public health specialists—as well as archival research, in two years of field research in three Brazilian states and the national capital between August 2008 and June 2010. Due to space restrictions, I cite the most relevant source, but most claims presented have been corroborated by multiple actors.
Alves – (Un?)Healthy Politics
4
equitable social policy expansion is more likely to take place.
Institutions, Political Competition and Social Policy
The public health policy literature considers a wide variety of determinants of equitable health
policy, ranging from global actors (e.g. Ruger 2004) down to local managerial and technical capacities
(e.g. Arretche and Marques 2002), epidemiological or social-economic determinants of health (e.g. WHO
2008). An important subsection of the public health and comparative literature has focused on the link
between political institutions, especially democracy and expanded health and other social services
(Brown and Hunter 1999; Sen 199; Franco et al. 2004; Ruger 2005; Huber et al. 2008; Haggard and
Kaufman 2008; McGuire 2010). However, the variation in approaches to health policy across both
established and third-wave democracies points to the importance of contextual factors shaping health
policy, ranging from social features such as ethnic composition (Gauri and Lieberman 2006) or the
prevalence of interest groups such as doctors or programmatic networks (Falleti 2010; Hassenteufel et
al. 2010), public support (Schlesinger and Lau 2000), to political and ideological aspects such as Leftist
rule (Navarro and Shi 2001; Cameron and Hershberg 2010; Levitsky and Roberts 2011; Pribble 2013).
An important subset of this broader literature focuses on how institutional features within the
state determine social policies, such as concentration of power in the executive and the proliferation of
veto points (Immergut 1992; Castiglioni 2005; Huber et al. 2008), the legacies of pre-existing policies
(Haggard and Kaufman 2008; Pribble 2013), and participatory governance (Dagnino 2002; Coelho 2006;
Avritzer 2009). Such institutions—formal legal or organizational constructs that constrain actors by
laying out rules or expectations of behavior—make outcomes more or less likely in part by regulating
participation in the policy discussion, what powers participants are granted, and how interests are
funneled into the decision-making process.
I argue that two main institutional features shape subnational health care systems in Brazil. First
is how state-level officials approach health governance institutions within the state, especially the
Alves – (Un?)Healthy Politics
5
Intergovernmental Joint-Management Commissions (Comissões Intergestores Bipartite, CIBs) that are
tasked with coordinating health policy among state and municipal managers (Levcovitz et al 2001; Lima
and Viana 2011). Though these institutions are nationally mandated, the subnational approach applied
here identifies and structures the explanation of local variation in how state-level governments
approach their CIBs or, more broadly, these institutions’ “process of becoming” (Abers and Keck 2013).
While some states included many facets of policy, negotiating and at times even jointly deliberating
policy with municipal governments, others included some but not all aspects of policy, and others
avoided them all but entirely. The face of state systems also depends on the extent of municipal
independence; therefore I also examine the extent to which state-level governments acquiesced to
further decentralization of health resources that granted municipalities control over higher-complexity
services.
Existing literature provides limited leverage in understanding the context in which decisions
shaping such governance structures take place. Due to the existing theoretical link between leftist rule,
programmatic governance and social service expansion (Navarro and Shi 2001; Sugiyama 2008; Pribble
et al. 2009; Cameron and Hershberg 2010; Levitsky and Roberts 2011; Pribble 2013), one leading
hypothesis is that health governance institutions will be strengthened in those states or municipalities
where leftist parties take office. In Brazil, scholars have classified the PT as the relevant case of
programmatic party in the left (Keck 1992; Hunter 2010), and linked PT-led administrations with the
local adoption of participatory governance (Abers 2000; Avritzer 2009; Baiocchi 2005) and of municipal
health reform (Pimenta 2007). Yet, these studies have a harder time explaining why subnational PT
governments do not equally pursue the creation or strengthening of participatory institutions, nor the
way in which they pursue the implementation or expansion of particular policies, such as public health
care, championed by sector-specific interests within the party.
Analysis of Brazilian health politics also highlight the role of the public health movement known
Alves – (Un?)Healthy Politics
6
as the Movimento Sanitário, or Sanitaristas, in driving national-level universal health reform (Weyland
1996; Escorel 1998; Arretche 2004; Paim 2008; Falleti 2010; McGuire 2010), or local-level reforms (e.g.
Gibson 2012). The importance of the Movimento Sanitário in expanding the concept of citizenship
during Brazilian redemocratization and in particular to health reform cannot be overstated.
Nonetheless, accounts that attempt to capture its salience in shaping public health in democratic Brazil
tend to ignore its fractious nature, especially as disagreements broke out during the process of
implementation of the SUS,4 and do not focus on the inherent tensions generated by the often
conflicting interests of state and municipal governments—despite the fact that many managers share
Sanitarista credentials and values. Finally, they cannot properly account for the proliferation of
Sanitaristas serving as career civil servants in even the most dysfunctional state health offices.
To build and extend on these studies I unpack subnational electoral competition to establish the
factors that shape the behavior of a broader set of political and bureaucratic actors. One strand of
scholarship predicts association between increased and/or more plural competition and implementation
of state and policy reforms, such as expanded public goods (Borges 2008; Diaz-Cayeros 2008; Arvate
2013), decentralization (O’Neill 2003), transparency (Berliner & Erlich 2015), or building strengthened
oversight institutions (Grzymala-Busse 2007). Other studies, however, argue that the relationship
between political competition, uncertainty, and reforms might be curvilinear (Sartori 1976; Geddes
1994; Montero 2001; Grzymala-Busse 2007; Alston et al. 2008): when competition is too heated, actors
revert to short-term and centralizing strategies to win political support. Only when political forces—and
therefore the costs of reform—are fairly balanced, are incumbents likely to build capacity in a way that
limits discretion.
I find that the nature of subnational political competition, more so than political party label or
4 See for example the discussion about the best way to decentralize the national social security health network in
MS/SGEP (2006). Arretche (2004) is an exception.
Alves – (Un?)Healthy Politics
7
ideology, determines how state-level governments shape healthcare governance institutions. In
politically concentrated settings, incumbents face few incentives to shed centralized and discretionary
control over policy, since the bulk of the costs would be imposed on the group currently in control. In
such an environment, opposition forces are less able to challenge the status quo because the
incumbents have a strong grasp over the state and continued exclusion from resources makes co-
optation ever more tempting to opposition mayors and legislators. Incumbents therefore seek to build
weak institutions, ensuring continued control over policy and greater discretion in how they allocate
resources. Similarly, the longer the continuity (incumbency) of the executive, the more likely that one
group will penetrate further into the state apparatus. And while this might generate further probability
of corruption and malfeasance, it also creates strong disincentives for policy experimentation or risk-
taking.
Conversely, settings with plural political competition generate incentives for building institutions
that contain executive discretion and share power, even if not directly. This is partly linked to a more
balanced division of political power, which implies that opposition forces are more viable in challenging
and constraining the incumbent’s discretion. Facing a greater number of viable political actors, both in
terms of a wider distribution of political power but also greater turnover at the state executive, provides
incentives for building institutions that distribute resources based on a clearer set of rules. Incumbents
do so to claim credit with voters who live in municipalities controlled by competitors or placate other
relevant political groups, while preventing future exclusion in the case of electoral defeat. A greater
division of political forces not only spreads the costs of reform (by the loss of spoils of discretion) but
turnover—especially repeated turnover—creates incentives for taking risks; risks which very well might
be introducing good-governance policies and trying to rise to the top of state politics by giving up a bit
(discretion) to get a lot (continued control over the state).
Variation in State-Level Health Systems
Alves – (Un?)Healthy Politics
8
Universal health care in Brazil envisioned not only an expansion of service provision, but also an
ontological shift in the system by emphasizing local-level governance, cost-effective primary care, and
civil society participation and oversight (Paim et al. 2011). Fulfilling this expansive mandate continues to
be a major challenge for Brazilian states and municipalities. Expanding care entailed overcoming
perverse institutional legacies, including fragmentation, geographic concentration, and the reliance on
an expensive, overly-curative network of private providers generated under one of the most centralized,
corrupt and unresponsive bureaucracies under the military regime (Weyland 1996; Falleti 2010).
The initial centrality of local governments to the SUS project also created unforeseen problems.
As municipal governments absorbed the provision of basic care services, they committed a growing
proportion of their revenues (16% in 2000-03, and almost 20% during 2004-2010)—vastly exceeding
their legal share (SIOPS 2013).5 Shortages in physical and human capital led to a scramble to build
expensive facilities, further atomizing health care investments in small, inefficient and low-quality
hospitals (La Forgia and Couttolenc 2008) and a bidding war to hire a limited number of existing medical
personnel. Predatory behavior, including free-riding by sending patients to receive care in other
municipalities with no compensation and municipalities accepting compensation and then failing to
provide services (PPI-BA 2009; PPI-SP 2009), became commonplace. Such issues proliferated in the
absence of intermediary organization between federal policy design and municipal service delivery. Seen
by national reformers as part of the problem, state-level governments were in some instances left out
and at times actively cut out of the public health system. Unsure of their mandate and losing access to
health resources, state-level health offices lost purpose and prestige (Government officials, SES-SP 2009;
SES-MG 2010).
5 Legal public health commitments increased in this same period from 7% of municipal revenues in 2000 to 15% after 2004. The extra municipal burden is partly due to a relative decrease in federal funding, but also to state-level governments shirking their required commitment (12% of revenues) by using a series of well-documented accounting tricks, such as including expenditures on corporatist health plans for civil servants or military, with the acquiescence of legislative and judicial branches.
Alves – (Un?)Healthy Politics
9
National public health activists had sought to ensure the continued growth of public health in
Brazil and to coordinate this expansion by developing a governance infrastructure that ingrained
technocratic expertise and grassroots participation. National legislation required that all health policies
and budgets be deliberated and approved in participatory institutions that included public health
professionals and organized civil society (the aforementioned Conselhos de Saúde, or health councils),
and that technical commissions facilitate horizontal and vertical coordination across levels of
government—the Comissões Intergestores, or intergovernmental joint-management commissions
(Levcovitz et al. 2001, Lima and Viana 2011). By governing the flow of policy and implementation
discussions in such a system, SUS designers hoped to ensure a high quality policy discussion within the
health sector, and therefore minimize political discretion. But what SUS designers did not envision was
that state-level governments might reject or co-opt the SUS project by how they chose to implement
these institutions.
I focus on two features of the institutional choices by state-level governments that shaped the
character of health care policy. The first is the level of municipal independence, most readily visible in
the extent of decentralization of health resources. Since the bulk of public health actions is
constitutionally allocated to municipalities, further decentralization is visible by state governments’
willingness to share responsibility and resources over higher-complexity procedures that entail
increased visibility, greater funding, and where the division of responsibilities between state and local
governments are not clearly defined. Municipal governments could expand their control over these
resources by applying for different levels of certification. While the specific extent of responsibilities
increased over time for each type of certification, the highest level of certification gave municipal
governments “Full Management” (Gestão Plena) of the municipal system, including the right to choose
providers and especially access to the full cadre of per-capita funding to finance medium and high-
complexity services transferred by federal Ministry of Health (otherwise controlled by the state health
Alves – (Un?)Healthy Politics
10
office). As Table 1 illustrates, state governments took noticeably different approaches in response to
municipal interest in further decentralization. In Bahia the state health office vocally rejected and
bureaucratically delayed municipal applications for certification. By contrast, state officials in São Paulo
eagerly embraced decentralization, shedding primary care facilities and personnel to municipalities and
encouraging municipalities to apply for higher certification. As a result, São Paulo’s municipalities
became, as a group, the most independent from the state level—independence that would later
increase the operational and political costs of coordinating state and municipal action. State-level
response in Minas Gerais was intermediate; it supported certification for a small number of larger,
higher-capacity municipalities, but the state office’s skepticism to additional decentralization is visible by
the slow expansion of certifications over time.
[Table 1 about here].
The second institutional feature is the extent to which state offices favor rules-based distribution
strategies for capacity and financial resources by empowering their joint management commissions
(CIBs). This requires examining how health institutions actually functioned in local settings. By bringing
together state and municipal health managers and requiring consensus to approve policies before they
could access federal funding, CIBs sought to guarantee participation by municipal governments –
including those in the political opposition. State-level officials did not always approach these institutions
willingly. In Bahia, ruling elites favored having state health officials guard central control over policy by
perpetuating lack of institutional controls; hence state-level leaders stunted and co-opted participatory
institutions. In São Paulo, state and municipal agents developed robust joint management institutions
that were highly capable of equitably negotiating the distribution of federal resources, but that lacked
power over important policy areas and the ability to coordinate state and municipal action. The CIB in
Minas Gerais matched São Paulo’s capacity to allocate federal resources, but also counted on additional
powers because state officials gave municipal managers a greater role in policy design and governance
Alves – (Un?)Healthy Politics
11
of health resource allocation within the state. Using the rules jointly developed within the CIB gave the
state health office in Minas Gerais the power to coordinate municipal action in a way São Paulo’s system
could not achieve.
Table 2 shows a summary of three distinct state-level systems that challenges the vision among
SUS founders and national-level designers of a fully functioning, cooperative governance of subnational
health care policy based on clear rules and power-sharing institutions. Only in Minas Gerais did plural
political competition enable such an outcome, whereas low political competition in Bahia and São Paulo
led governance institutions to be either coopted or realize limited success.
[Table 2 about here.]
Analysis of a few critical cases, especially within one country, is an established strategy to
examine internal variation while accounting for confounding national phenomena. The ability to
generalize hinges on careful case selection. While the cases are not strictly representative of the
population of 27 Brazilian states, they do fall contiguously along the fault-lines of “three Brazils,” a
developed and economically dynamic one to the south (São Paulo), a historically undeveloped and
stagnant north and northeast (Bahia), and an intermediate region that shares some features with each
extreme (Minas Gerais). Despite the socio-economic disadvantage of poorer states like Bahia, it is
important to study these distinct environments in conjunction exactly because national blueprints were
disseminated uniformly with the expectation that these institutions would function in similar fashion.
Yet, as the next section shows, the distinct political environments in these states generated sharply
contrasting institutional outcomes.
The Impact of Political Competition on State-Level Health Systems
Identifying Key Differences in State-Level Politics
Because differences in electoral environments are central to my argument, I first illustrate the
differences in political competition in Bahia, Minas Gerais and São Paulo using a disaggregated set of
Alves – (Un?)Healthy Politics
12
indicators to capture the distinct though inter-related facets of political contestation. First, I measure
political continuity at the state executive by calculating the proportion of gubernatorial elections that
resulted in either the reelection of an incumbent or a victory by a member of the governor’s party, out
of the overall number of elections. I also include the electoral margin of victory in first-round
gubernatorial elections, since high electoral margins have also been associated with lower quality
democracy. Next, I measure the executive’s legislative support. There are three legislative arenas where
the governor can have influence: the state-level Assembly (Assembléia Legislativa), the national
Chamber of Deputies (Câmara dos Deputados) and the national Senate (Senado). I calculate the
governor’s party share in each legislative body, and present them as a simple average. This measure
therefore captures not only the legislative control at the state level, but also incorporates a governor’s
political importance at the national stage.6 Finally, I also measure a governor’s clout over municipal
governments by the share of mayors held by the governor’s political party. Together these measures
provide a comprehensive and nuanced picture of state-level patterns of political competition.7 All
measures are averages for seven electoral cycles for governor and legislators between 1982 and 2006,
as well as four municipal elections between 1996 and 2008, from the Brazilian electoral authority.8 Table
3 provides a panorama of state-level politics in Bahia, Minas Gerais and São Paulo that shows sharp
differences in political environments.9
[Table 3 about here.]
For most of the period since redemocratization, politics in Bahia have been highly concentrated.
6 Some scholars challenge the notion that governors influence national-level legislators (e.g. Figueiredo and Limongi 2000). While conceding that governors are not the only actors shaping legislator behavior, I nevertheless follow Samuels’ (2003) insight that they do have extensive sources of influence over state delegations. 7 Though operationalized differently, these indicators are in line with other studies of subnational political
competition, such as Borges’ (2007) and Giraudy (2010). 8 There is no electronic access to the municipal electoral data prior to 1996. 9 These findings are similar to those in Borges’s (2007, 2010) studies of electoral competition in Brazil’s states, where Minas Gerais scored in the most competitive quartile, São Paulo in the second highest, and Bahia in the lowest.
Alves – (Un?)Healthy Politics
13
Most elections in this period were controlled by the right-wing Partido da Frente Liberal (Party of the
Liberal Front, PFL), led by charismatic state political boss Antonio Carlos Magalhães (nationally known by
his initials, ACM).10 ACM’s political group, known as Carlistas, won five of the seven gubernatorial
elections in Bahia since 1982, generally with sizable margins. The PFL singlehandedly held a majority of
the state’s legislative seats, an uncommon feat in Brazil’s highly fragmented system of proportional
representation. High as they may seem, the average results presented in Table 3 actually understate the
extent of Carlista dominance throughout most of the period. For one, the values are lowered by the lack
of political dominance when the PT’s Jacques Wagner surprisingly won the state gubernatorial election
in 2006. During the Carlista peak (1990-2005), the PFL held on average 57% of Bahia’s national and
state-level legislative seats. Furthermore, the focus on the PFL alone misses a unique feature of Carlista
political control in Bahia. Magalhães used a series of small parties in the state as de facto satellites to
the PFL to accommodate intra-alliance political disputes (Souza 1997; Dantas Neto 2006a). Incorporating
these colonized parties expands Carlista legislative dominance to 63%, with a peak of 73% during the
1998-2001 term. The weight of political dominance is even stronger at the municipal level, as the
broader Carlista alliance controlled an average of 71% of municipalities in the same period.
And yet, politics in Bahia was more volatile than such control would predict. Magalhães
experienced two embarrassing political defeats during this period. In 1986 Waldir Pires, from the
centrist Partido do Movimento Democrático Brasileiro (Brazilian Democratic Movement Party, PMDB),
united oppositions and soundly defeated Carlistas, backed by similar shares of legislatures and
municipalities. Benefitting from support from President Luis Inácio ‘Lula’ da Silva, the PT was also able to
edge out the favored Carlista candidate in 2006. The memory and risk of losing elections made ACM
renew efforts in exclusionary and clientelistic practices (Dantas Neto 2006a), with important
10
In 2007, the PFL officially changed its name to Democratas (DEM). Since the study mostly focuses in the period pre-dating the change, I use the old party label.
Alves – (Un?)Healthy Politics
14
implications for institution-building and the relationship with municipal governments in health policy.
Table 3 provides evidence of the competitive nature of politics in Minas Gerais. The greatest
discrepancy between Minas and the other two states is the lack of continuity in the state executive,
where turnover occurred twice as often as continuity, and winners carried relatively thin margins.
Executive control was also weathered by a plural distribution of legislative seats. The party of the
governor of Minas Gerais never controlled more than one of three national senators, and failed to gain
the most seats for the Chamber of Deputies or the State Assembly between 1990 and 2006. Unlike
Bahia, governors in Minas Gerais could not count on long coattails and had to interact with strong
political opponents from distinct groups and with legislative bases spread across the state. The
precarious hold on state-level office generated a high level of political and administrative instability.
Efforts by Minas’ executives to emulate ACM’s strategies failed to co-opt or exclude the other powerful
political groups in the state and lost power in subsequent elections. Observing this trend, Aécio Neves,
heir to a prominent traditional elite in Minas Gerais and up-and-coming leader in the PSDB, gambled on
good governance to change the nature of political competition in his state. To do so, he tasked
technocrats with institution-building while seeking support from opposition groups by sharing power.
Finally, São Paulo displayed a political stalemate. Three of the four measures in Table 3 show a
plural political environment in São Paulo, with power being fairly dispersed in the legislatures and
among municipal executives. The state’s voters consistently elected a plural delegation to the national
congress, including leading figures in both the national government and opposition. There is a
multifaceted balance of municipal forces, with larger cities surrounding the capital supporting leftist
administrations, while important medium-sized wealthy municipalities from centrist and center-right
parties. Electoral margins for gubernatorial elections were also relatively thin. The dissonance is the
continuous hold that one party, the PSDB, has enjoyed over the governorship of the state for most of
the democratic period. As we shall see, this created dual sets of political incentives within the state.
Alves – (Un?)Healthy Politics
15
First, the plural environment yielded some incentives to build rules-based institutions both due to higher
contestation by viable political opposition forces but also as a hedge in case national or local
connections strengthened the opposition. In fact, a temporally disaggregated measure would exhibit a
decreasing hold of the governor’s party on São Paulo’s legislative seats, in part due to the legislative and
local strengthening of the PT following the party’s rise to the presidency. The PSDB’s share of legislative
seats consistently shrunk between 1998 (25%) and 2006 (17%). But second, uninterrupted control over
the most powerful gubernatorial seat in the country also made state-level officials impervious to
opposition and municipal forces, leading to a substantial degree of discretion in formulating some state
policies.
Political competition was thus concentrated in Bahia, plural in Minas Gerais, and configured in a
stalemate resulting from plural competition and executive continuity in São Paulo. How did these
distinct configurations impact the design of public health institutions in each state?
Concentrated Politics and Discretionary Health in Bahia
Concentrated politics in Bahia led to the construction of a state health system that was similarly
concentrated, with discretionary policies derived to serve state-level political incumbents’ policy
preferences and by distributing health capacity and funding as pork and patronage. Concentrated
control over the state-level government allowed Carlista incumbents to distribute public health
resources as one more spoil of political victory in order to control local allies and punish opposition
forces. As a result, Carlista elites resisted the SUS’s expansive agenda and the pluralizing effects of
national democratization for over two decades.
A prominent force in Bahia’s politics dating back to Brazil’s bureaucratic-authoritarian regime,
Magalhães maintained political control through a combination of clientelistic strategies and exploiting
links to the national government and media (Motter 1994). Despite initial concern with the
Alves – (Un?)Healthy Politics
16
modernization of Bahia, he became increasingly focused on establishing tight political control over the
state (Dantas Neto 2006a). As specialists in Bahia’s politics have shown (Souza 1997; Dantas Neto 2006a,
b), ACM’s large electoral margins diminish when one considers the large abstention rates in Bahia’s
elections. These studies show that while Magalhães could control a steady 30% of Bahia’s total
electorate, mostly in the state’s poor interior, electoral defeat was a threat if the opposition could unite
and tap this large share of alienated voters, as with Pires’ election in 1986. Dantas Neto argues that
Magalhães regrouped from electoral defeat in José Sarney’s national cabinet, strengthening his pre-
disposition for personalistic and centralized control when he once again took control of Bahia’s state-
level government in 1990.
The concentrated nature of political competition in Bahia not only shaped ACM’s policy
preferences but also translated into a highly centralized, discretionary and ultimately exclusionary
health care system in Bahia. The state government strongly defended centralized government despite
substantial coaxing by the federal Ministry of Health. One such strategy by the Ministry tied resources to
the development of a series of technical and planning instruments that ensure equitable and consistent
distribution among municipalities. Bahia’s state health office (known by the acronym SESAB) under the
Magalhães government centralized and insulated this process, drafting a state health plan with no input
from municipal managers, purposefully omitting programs that would bring federal funding for
municipalities, delaying an influx of health resources that would in practice make them less dependent
on the state government.11 It was an unofficial but widely known SESAB policy to delay municipal
applications for service accreditation, withholding even the most basic form of certification for 85% of
municipalities until 1997 (Guimarães 2003), while holding more advanced certifications to a minimum.
11 A telling example is that Bahia’s state health plan, does not make use of the term municipalização (decentralization to the municipal level), a ubiquitous term during this period of heavy emphasis on local health governance (see for example the final report of the 1993’s 9
th National Health Conference, titled “Municipalization
Is The Way” (Municipalização É o Caminho)).
Alves – (Un?)Healthy Politics
17
Centralization was also visible in other institutional decisions: As municipalities in Bahia were relatively
weak compared to the financial and technical capacities of the state government, this generally meant
that health services had historically been provided either by publicly-funded non-profits or directly
owned and operated by the SESAB. The health office in Bahia maintained control of these facilities,
distributing the appointment of their managerial posts to political allies who could in turn use them as
local sources of patronage (Civil servant, SESAB, 2009).12 While subsequent governments have since
decentralized more basic units such as local clinics, the state office still controls a disproportionate part
of the facilities in Bahia.
Discretionary control over the health system was reinforced by the concurrent undermining and
co-optation of health support institutions. Bahia was a laggard in national terms in the implementation
of each of the legally-mandated institutions, begrudgingly founding them only when they became
requisites for accessing federal funding. Delay was followed by co-optation, ensuring the rubber-
stamping of top-down decisions (Members of CIB-BA, 2008-2009). The institutions were populated with
allies from within the coalition, mostly managers from small municipalities, at the expense of larger
cities controlled by the opposition.13 Even then, co-optation was paired with an emptying of actual
power. Within the coalition, intergovernmental negotiations consistently took place outside of
participatory institutions and quite often sidestepped the state health office altogether (Government
official, SESAB, 2008). Likewise, the main policy decision of the Carlista period—to outsource the
expansion of hospital capacity to nonprofits—was introduced as a bill to the acquiescent State Assembly
before it was ever considered by the CIB or the state health council, inverting the legal decision-flow.
12
This has clear implications for the nature of care locally. In municipalities within the coalition, the mayor or legislator can direct services to their clients. In opposition municipalities, hospital managers can deny or complicate service, practicing de facto opposition within their territory. 13 Records from the municipal health managers’ association (COSEMS-BA) from this period reveal that leadership and seats in the CIB were occupied by managers from at times remote municipalities governed by the governor’s party, while opposition municipalities were virtually absent.
Alves – (Un?)Healthy Politics
18
Unpopular among the public health sector and highly contested in other states’ participatory
institutions, the policy was quickly approved due to state-level influence (Members of CES-BA, 2008-
2010).
The Carlista group also made use of centralized control and co-opted participatory institutions
to punish the few municipal governments openly in the opposition. One such municipality was Vitória da
Conquista, the state’s third largest, and an important first-mover on public health due to historical ties
to the Sanitarista movement. Despite being a net provider of services to neighboring municipalities,
Conquista’s PT government did not receive proper compensation for those patients, since the system of
compensation that governs financial allocations across municipalities (Programação Pactuada e
Integrada, PPI), led by the SESAB, directed funding to other municipalities from within the Carlista
coalition. Likewise, access to federal funding for basic care programs was prevented by red tape and
bureaucratic foot-dragging by the SESAB (SMS-BA 2010). The opposition-controlled capital city of
Salvador was similarly denied accreditations, even in a situation when a SESAB technical memorandum
recommended that the CIB approve at least partial certification (Government official, SESAB, 2009).
When Carlistas won Salvador’s municipal election in 1995, the municipal health office under the PFL
dropped certification applications, focusing on running basic care facilities and acquiesced to the state-
level office running the city’s hospital network (Mayor 2009). Salvador’s isolation made it the last among
state capitals to receive full-management rights (CIT 2008).
The result is that health institutions in Bahia during the ACM years failed to meet the SUS’s
aspirations for equitable expansion of care. The state network continues to be disproportionately
owned and controlled by the state health office. Health expansion was limited and targeted; plans
commissioned to health experts that would be based on rules and health needs were ultimately shelved
(Government official, SES-MG, 2010). To access health funding, municipalities could fall in line, such as
the small town of São Félix that was rewarded with an expensive Neonatal Intensive Care Unit, go at it
Alves – (Un?)Healthy Politics
19
alone and risk limited success, such as Vitória da Conquista, or face abject failure, as in Salvador. All this
was tied to the Carlista response to Bahia’s politically concentrated environment.
Competition Breeding Health Care Coordination in Minas Gerais
In Minas Gerais a competitive and plural political environment produced a rules-based and
highly participatory system to govern public health; a system that limited the discretion of the state-
level government but in return granted it substantial power as coordinator of municipal action. Building
rules-based institutions and sharing policy design with municipal and opposition forces in Minas’ CIB was
the result of a gamble by a political incumbent and his agents in the state health office given the
constant turnover faced by his predecessors and the plurality of viable political forces controlling parts
of the state’s legislative representation and municipal governments.
Despite its recent history of good governance (Montero 2001, Borges 2008), political
competition in Minas Gerais did not always have such beneficial effects. Historical accounts point to the
oligarchic and conservative nature of its politics and the survival of its pragmatic and risk-avoiding
traditional elites (Hagopian 1996; Bates 1997). The electoral free-for-all following redemocratization
initially eroded the quality of public services, including the proliferation of patronage appointments that
threatened fiscal insolvency by the late 1990s. Aécio Neves, a rising political figure in national politics,
thus sought not only to win power in Minas Gerais, but also to keep power by building institutions that
would deliver a modicum of good governance. In doing so Neves would break Minas Gerais’ political
deadlock and emerge as the fulcrum of its new balance.
Neves tasked reformist technocrats to design and implement a “management shock” reform
program, streamline government institutions, invest in human capital, and emphasize governance
through close monitoring of performance indicators. Top positions at the state health office (SES-MG)
were staffed with a tandem of a political insider and a respected public health expert that together
Alves – (Un?)Healthy Politics
20
structured a strategic role for the state office as a manager and coordinator of municipal action. The
state office shed its health care network and supported municipal governments when they applied for
basic certifications and federal funding for basic care. Support for decentralization was limited, as the
SES-MG discouraged all but larger municipal governments from applying for certification of more
complex and expensive services. State-level managers sought to recentralize the strategic management
of the state system by structuring the territorial allocation of resources to maximize regional impact
irrespective of individual municipal interests (Civil Servants, SES-MG, 2010). Creating and strengthening
regional hubs entailed a de facto concentration of investments on fewer providers but also host
municipalities. While it is politically costly for a state incumbent to announce hospital closures, the state
health office revealed this intention by designing a program (Pro-Hosp) that tackled the prevalence of
small inefficient hospitals by targeting a select few (136 out of existing 600) that received strategic
support in order to build regional scale in the hospital sector.
There should have been significant resistance from municipal and private sector providers who
would individually stand to lose from the concentration of resource allocation in such a way. And yet,
programs such as hospital support continue to be very popular among the majority of municipal
managers interviewed and observed for this study. This outcome was the result of the state-level
strategies of creating rules-based allocation criteria for such programs. Rules that would govern the
state’s major health programs were determined in participatory forums such as Minas Gerais’ CIB,
where policy design was shared with municipalities. Municipal representatives from each of the state’s
regions were guaranteed a place at the negotiating table, which ensured that recipients were picked in
territorially equitable fashion and that recipients would have continued incentives to incorporate the
Alves – (Un?)Healthy Politics
21
needs not only of their home municipality, but also of their neighbors.14 The consistent enforcement of
those rules once programs were implemented meant that eligible municipalities, irrespective of political
allegiance, had a fair chance of receiving state support (Opposition SMS-MG, 2009).
A strengthened CIB and the enforcement of deliberated policies yielded re-centralization as the
state health office gained the authority to coordinate municipal action. In addition to including
municipalities in the policy design process, the SES-MG spurred coordination by shouldering the costs of
development and implementation of coordination tools such as the state’s medical referral system
(SUSFácil), generating financial inducements for municipal participation, and by acting as a funder-of-
last-resort by creating a revolving fund (câmara de compensação) that would square away any
discrepancies between predicted and actual patient flows in order to get the system up and running.
Since these incentives were rolled out concurrently with rules-based and deliberated processes and
regulations, municipalities of different political groups nonetheless had incentives to join. Once local
governments experienced the financial and operational relief of cooperative action, the state’s system
became increasingly popular among municipal managers (SMS-MG, 2009b).
As a result of risk-taking in light of high competition and the constraints imposed by a plural
division of political power, Minas Gerais’ state government surrendered complete discretion of state
health policy design in exchange for a de facto degree of centralization. By following allocation rules
devised jointly with both political allies and opponents, the state health office built a coordinated health
system that decreased inefficient investments and increased patient access to existing health capacity.
This system is popular with managers across the political spectrum, despite the fact that the state
government in Minas Gerais is one of only two states that underinvests in health based on minimal
investment requirements. Neves’ government thus harnessed health politics to become a key political
14 For example, one of the eligibility criteria for hospital support was the proportion of patients from other municipalities brought in through the state’s patient referral network (see for example CIB-MG resolution 427/2008).
Alves – (Un?)Healthy Politics
22
broker in an otherwise balanced political scenario.
Stalemate and Fragmentation in São Paulo
In São Paulo, state executive continuity in an otherwise plural environment produced a
fragmented health system. Plural municipal forces pushed for a robust system of participatory
institutions that strongly contest state action and equitably distribute federal funding. However,
continuity at the state-level led to the exclusion of municipal and opposition forces from shaping the
state health office’s (SES-SP) extensive health network, yielding a system that is fragmented both
vertically (in the interface between state and municipalities) but also horizontally, among municipalities.
In this system, municipal governments atomized health investments, duplicated health capacity in
response to local political incentives and continued to prop up low-quality small hospitals. Municipal
systems also do not interface with the state’s hospital network, causing problems for patient access to
São Paulo’s unparalleled health capacity. While higher financial and human resource endowments
certainly play a role in this outcome, it cannot be properly understood without comprehending the
state’s political environment; in particular the state incumbent’s disincentives to risk a powerful position
with reforms that potentially empower municipal opposition.
The coexistence of prominent opposition forces with a steady stronghold on the state
government by the PSDB has peculiar impacts on health policies in São Paulo. Prominent Sanitaristas
permeate the state’s health sector, and their participation in health care institution-building is
disproportionate even to the left’s increasing political representation.15 As leaders of the national
Sanitarista movement, São Paulo’s local health managers mobilized early to demand decentralization
15 While the PT controlled an average of 9% of São Paulo’s municipal governments in the state of São Paulo in the period 2003-2008, representatives from PT-led municipalities accounted for an average of 39% of leadership seats in the municipal health managers’ association (COSEMS-SP), including its presidency. Despite heavy Sanitarista presence in both other states, the PT block of municipalities did not achieve such levels of representation. (Author’s calculation based on COSEMS-BA, MG and SP records and electoral data from TSE).
Alves – (Un?)Healthy Politics
23
from the state government (Pimenta 2007), and found willing partners in the Sanitaristas within the SES-
SP. The state office yielded an extensive network of primary care facilities to municipal governments,
along with fully-funded personnel to staff them. State officials also encouraged municipalities to apply
for certification to take over responsibilities beyond primary care, allowing virtually all interested actors
to receive them (Civil servants, SES-SP, 2009). A quarter of all municipalities applied and received
certification in the first year of eligibility alone, meaning that almost half of the state’s citizens lived in
municipalities who had full responsibility over health care service provision.
Despite the agreement on decentralization, the SES-SP retained significant control over the
extensive and high-capacity public hospital network. Owned and operated by the state-level
government since the later 19th century (Hochman 1998; Mendes and Oliveira 2009), this system
demands large financial and managerial commitments from the SES-SP, adding impetus for state health
officials to shed what it considered to be its non-essential network of basic health services. This focus
generates a series of conflicts between state and municipal managers. First is a lack of institutional
attention to local problems—abandoning municipalities with unequal capacities to solve collective
action problems. The SES-SP has kept control over its network by making strategic decisions about its
expansion and operation outside the CIB. Exclusion from the management of such an important
component of the state’s health system frustrates local managers, who commonly voiced their
displeasure in meetings of the municipal health managers association (COSEMS-SP), especially those
from PT-led municipalities (SMS-SP 2009). Finally, despite having the resources to finance most of its
own actions, São Paulo still looks to the Ministry of Health for funding whenever possible. This produces
some conflict of interest in the distribution of new federal resources in joint institutions because the
state office functions as both a mediator between municipal governments and a competitor seeking
Alves – (Un?)Healthy Politics
24
resources.16
As a result of these processes, São Paulo’s robust health governance institutions nevertheless
exhibit a confluence of rules-based distribution with a consistently exercised right to self-determination.
The equitable distribution of federal resources is extensively deliberated. Yet both municipal and state-
level health officials are willing and able to hold onto entrenched positions to respect their freedom of
action in the running of their existing systems. Municipal managers equally defend the freedom to
expand local capacity as they see fit, while opposition managers further toughen the deal for the state
to pay the administrative and financial costs of coordination. Comfortable in its political position and
with a large network of health services to manage, the state office has no incentive to engage the
coordination battle. A telling example is that state and municipal officials failed to agree on a formula
for the system that governs financial allocations between municipalities (PPI) until 2007, years after
poorer and less developed states had theirs in operation (Civil servant, SMS-SP 2009; CGR-SP 2009).
In São Paulo, an unlikely stalemate of political features—plural competition in all arenas but the
state executive—has led to a fragmented state system, highly decentralized municipal health
governance but with centralized control of the state’s hospital network. While incremental development
occurs in São Paulo, the polarization of politics between its two most powerful political groups—the PT
and the PSDB—has made actors on both sides more intransigent in their intergovernmental relations.
Lessons from Comparing Health Institutions in Bahia, Minas Gerais and São Paulo
Comparing how the distinct political environments in these cases impacted institutional
outcomes reveals the importance of the governing strategies pursued by political elites to satisfy
political aspirations. Concentrated political control provided both the impetus and the permissive
16 The inherent conflict of interest when discussing distribution of federal funding (especially for hospital services, where the SES-SP is a major player) was brought up regularly by municipal managers in CIB-SP meetings, even during otherwise amicable deliberation.
Alves – (Un?)Healthy Politics
25
environment for a strategy of continued centralization and discretion in Bahia. Plural competition in
Minas Gerais led to repeated political failures until a suitor for state power attempted an inclusive
strategy that shared some power in policy design and catered to opposition forces by limiting state-level
discretion in the allocation of investments and resources. Finally, it was plural competition in São Paulo
that gave municipal and opposition actors enough clout to extract decentralization from the state office
and to ensure an equitable, rules-based division of federal funding. Yet, the PSDB’s entrenched control
over the state-level government gave it control over the state’s public hospital network, generating
incentives to guard centralized discretion, which in turn led to institutional and capacity fragmentation.
The application of these strategies had practical implications for the type of care offered in each
state as well as to broader political contestation. The political allocation of resources in Bahia limited
expansion in overall patient access while existing service capacity remained disproportionately in the
hands of the state government. This centralized discretion forced municipalities to fall in line while the
Carlista elite preserved the boundaries of state political power until losing their links to the federal
government. Health capacity in the capital city of Salvador, home to a fifth of the state’s residents,
remains stunted while the only public hospitals are run by the state government. Meanwhile,
coordinated care in Minas has boosted existing capacity and increased access to pooled resources
regardless of municipal size, location or political association. As a result, the health policies in Minas
Gerais are popular among elites as well as the population, part of the state government’s broader good
governance brand. This helped ensure a stronger political position that led to Neves’ emphatic
reelection (77% of votes), subsequently strengthening his technocratic and political managers to stay
the course while cementing his role as central power broker within a plurally divided political landscape.
Finally, the duality of political pluralization and executive continuity in São Paulo continued to yield a
political stalemate between state and municipal forces, leading to no compromise in the design of
coordination tools that would allow municipalities to pool resources and more credibly rely on each
Alves – (Un?)Healthy Politics
26
other’s capacity, as well as a disconnect between extensive primary care municipal networks and the
high-capacity secondary state network. The strengthening of the PT’s opposition in São Paulo, which is
historically overrepresented in public health circles, has further politicized the relationship between
state and municipal managers, increasing the stalemate and perpetuating fragmentation.
These findings suggest the importance of the form of political competition for the governing and
institution-building strategies pursued by subnational elites. They supplement the study of changing
national and regional patterns of political competition in Brazil by linking them to important and visible
differences in state-level governance structures in public health, which in turn affect the quality of care
provided to local citizens. These findings also have broader implications for the study of social policy in
increasingly competitive but still consolidating democracies. First, despite top-down pressures by an
overwhelmingly powerful national government and the empowering of municipal governments, state-
level governments still exercised wide latitude in how they implemented and expanded social policies.
Second, while institutions matter for the distribution and coordination of resources, they are designed
as strategic responses to local political environments, more so than national pressure, the presence of
local health movement actors (which was ubiquitous), or partisanship. Third, where institutions are
rules-based and equitable, they are built not only on technical expertise, but political viability. Finally,
despite increased political competition, subnational elites continue devising strategies to achieve and
maintain political power, potentially resisting and reversing these trends.
These lessons are tempered by the study’s limitations. While the comparative method allows for
closer examination of the processes and mechanisms within the cases, it cannot fully eliminate potential
alternative explanations or categorizations. Further study needs to test the hypotheses generated here
in the remaining Brazilian states. If the findings are robust, greater efforts need to be made to link them
with a broader comparative literature on health politics, but also to engage the broader conversation of
social policy and institutional reform in federal systems. Furthermore, the suggested connection
Alves – (Un?)Healthy Politics
27
between equitable governance structures and equitable health policies needs to be further explored,
both theoretically and empirically. Nevertheless, while the finding that subnational political competition
shapes governance institutions might appear focused, understanding the ways in which it does so locally
is of great significance for health care but also more broadly.
References
Abers, Rebecca Neaera. 2000. Inventing Local Democracy: Grassroots Politics in Brazil. Boulder, CO: Lynne Rienner.
Abers, Rebecca Neaera, and Margaret E. Keck. 2013. Practical Authority: Agency and Institutional Change in Brazilian Water Politics. New York: Oxford.
Abrúcio, Fernando. 1998. Os Barões da Federação: O Poder dos Governadores no Brasil Pós-Autoritário. São Paulo: Hucitec.
Alston, Lee, Marcus Melo, Bernardo Mueller, and Carlos Pereira. 2008. “The Predatory or Virtuous Choices Governors Make: Political Institutions and Economic Performance.” Available at: http://www.odi.org/events/docs/2071.pdf
Arretche, Marta. 2004."Toward a Unified and More Equitable Health System: Health Reform in Brazil." In Robert R. Kaufman, and Joan M. Nelson, Eds. Crucial Needs, Weak Incentives: Social Sector Reform, Democratization, and Globalization in Latin America. Baltimore, MD: Johns Hopkins.
Arretche, Marta, and Eduardo Marques. 2002. “Municipalização da Saúde no Brasil: Diferenças Regionais, Poder de Voto e Estratégias de Governo.” Ciência & Saúde Coletiva, 7(3):455-479.
Arvate, Paulo. 2013. “Electoral Competition and Local Government Responsiveness in Brazil.” World Development, 43(March): 67-83.
Avritzer, Leonardo. 2009. Participatory Institutions in Democratic Brazil. Baltimore: Johns Hopkins.
Baiocchi, Gianpaolo. 2005. Militants and Citizens: The Politics of Participatory Democracy in Porto Alegre. Stanford, CA: Stanford.
Bates, Robert. 1997. Open-Economy Politics: The Political Economy of the World Coffee Trade. Princeton: Princeton.
Berliner, Daniel and Aaron Erlich. 2015. “Competing for Transparency: Political Competition and Institutional Reform in Mexican States.” American Political Science Review, 109(1): 110-128.
Borges, André. 2007. “Rethinking State Politics: The Withering of State Dominant Machines in Brazil.” Brazilian Political Science Review, 1(2): 108-136.
_______. 2008. “State Government, Political Competition and Education Reform: Comparative Lessons from Brazil.” Bulletin of Latin American Research, 27(2): 235-254.
_______. 2011. “The Political Consequences of Center-Led Redistribution in Brazilian Federalism: The Fall of Subnational Party Machines.” Latin American Research Review, 46(3): 21-45.
Brown, David S., and Wendy Hunter. 1999. "Democracy and Social Spending in Latin America, 1980-92." American Political Science Review, 93(4): 779-790.
Alves – (Un?)Healthy Politics
28
Cameron, Maxwell A., and Eric Hershberg. 2010. Latin America's Left Turns: Politics, Policies, and Trajectories of Change. Boulder, CO: Lynne Rienner.
Castiglioni, Rossana. 2005. The Politics of Social Policy Change in Chile and Uruguay: Retrenchment versus Maintenance, 1973-1998. New York: Routledge.
CIT (Câmara Intergestores Tripartite). 2008. “Municípios Habilitados em Gestão Plena do Sistema Municipal de Saúde - Maio de 2006.”
Coelho, Vera Schattan. 2006. "Democratization of Brazilian Health Councils: The Paradox of Bringing the Other Side into the Tent." International Journal of Urban and Regional Research 30 (3):656-671.
Dagnino, Evelina. 2002. Sociedade Civil e Espaços Públicos no Brasil . São Paulo: Paz e Terra/ UNICAMP.
Dantas Neto, Paulo Fábio. 2006a. “Surf nas Ondas do Tempo: do Carlismo Histórico ao Carlismo Pós-Carlista”. Caderno CRH, 39: 213-235.
_______. 2006b. “O Carlismo Para Além de ACM: Estratégias Adaptativas de Uma Elite Política Estadual”. in: Celina Souza. and Paulo F. Dantas Neto (Eds.): Governo, Políticas Públicas e Elites Políticas nos Estados Brasileiros. Rio de Janeiro: Revan.
Diaz-Cayeros, Alberto. 2008. “Electoral Risk and Redistributive Politics in Mexico and the United States.” Studies in International Comparative Development, 43(2): 129-150.
Escorel, Sarah. 1998. Reviravolta na Saúde: Origem e Articulação do Movimento Sanitário. Rio de Janeiro: Fiocruz.
Falleti, Tulia G. 2010. “Infiltrating the State: The Evolution of Health Care Reforms in Brazil, 1964-1988.” In James Mahoney and Kathleen Thelen, Eds., Explaining Institutional Change: Ambiguity, Agency, and Power. New York: Cambridge.
Figueiredo, Argelina and Fernando Limongi. 2000. "Presidential Power, Legislative Organization, and Party Behavior in Brazil." Comparative Politics 32(2): 151-170.
Franco, Álvaro, Carlos Álvarez-Dardet, and Maria Teresa Ruiz. 2004. “Effect of Democracy on Health: Ecological Study.” BMJ, 329: 1421-1423.
Geddes, Barbara. 1994. Politician's Dilemma: Building State Capacity in Latin America. Berkeley: University of California.
Gauri, Varun, and Evan S. Lieberman. 2006. "Boundary institutions and HIV/AIDS policy in Brazil and South Africa." Studies in Comparative International Development, 41(3): 47-73.
Gibson, Christopher L. 2012. Civilizing the State: Civil Society and the Politics of Primary Public Health Care Provision in Urban Brazil. Ph.D. Dissertation.
Giraudy, Agustina. 2010. “The Politics of Subnational Undemocratic Regime Reproduction in Argentina and Mexico.” Journal of Politics in Latin America, 2(1): 53-84.
Grzymala-Busse, Anna. 2007. Rebuilding Leviathan: Party Competition and State Exploitation in Post-Communist Democracies. New York: Cambridge.
Guimarães, Maria do Carmo. 2003. “Processo Decisório e Conflitos de Interesse na Implementação da Descentralização da Saúde: Um Estudo das Instâncias Colegiadas na Bahia.” Caderno CRH, 39: 105-132.
Haggard, Stephan, and Robert R. Kaufman. 2008. Development, Democracy, and Welfare States: Latin America, East Asia, and Eastern Europe. Princeton: Princeton.
Hagopian, Frances. 1996. Traditional Politics and Regime Change in Brazil. New York: Cambridge.
Hall, Peter A., and Rosemary CR Taylor. 1996. "Political Science and the Three New
Alves – (Un?)Healthy Politics
29
Institutionalisms*." Political Studies, 44(5): 936-957.
Hassenteufel, Patrick, Marc Smyrl, William Genieys, and Francisco Javier Moreno-Fuentes. 2010. "Programmatic Actors and the Transformation of European Health Care States." Journal of Health Politics, Policy and Law, 35(4): 517-538.
Hochman, Gilberto. 1998. A Era do Saneamento: as Bases da Política de Saúde Pública no Brasil. São Paulo: Hucitec/ANPOCS.
Huber, Evelyne, Thomas Mustillo, and John D. Stephens. 2008. "Politics and Social Spending in Latin America." Journal of Politics, 70(2): 420-436.
Hunter, Wendy. 2010. The Transformation of the Workers’ Party in Brazil, 1989-2009. New York: Cambridge.
Immergut, Ellen M. 1992. Health Politics: Interests and Institutions in Western Europe. New York: Cambridge.
Keck, Margaret. 1992. The Workers’ Party and Democratization in Brazil. New Haven: Yale.
La Forgia, Gerard M., and Bernard F. Couttolenc. 2008. Hospital Performance in Brazil: The Search for Excellence. Washington, DC: World Bank.
Levcovitz, Eduardo, Luciana D. de Lima, and Cristiani V. Machado. 2001. "Política de Saúde nos Anos 90: Relações Intergovernamentais e o Papel das Normas Operacionais Básicas." Ciência e Saúde Coletiva, 6(2): 269-291.
Levitsky, Steven, and Kenneth M. Roberts. 2011.The Resurgence of the Latin American Left. Baltimore: Johns Hopkins.
Lima, Luciana Dias de, and Ana L. d'Ávila Viana. 2011."Descentralização, Regionalização e Instâncias Intergovermentais no Sistem Único De Saúde." In Ana L. d'Ávila Viana, Ed, Regionalização e Relações Federativas na Política de Saúde no Brasil. Rio de Janeiro: Contra Capa.
Mahoney, James, and Kathleen Thelen, Eds. 2010. Explaining Institutional Change: Ambiguity, Agency, and Power. New York: Cambridge.
McGuire, James W. 2010. Wealth, Health, and Democracy in East Asia and Latin America. New York: Cambridge.
Mendes, José D. and Vanessa E. de Oliveira. 2009. Saúde Pública Paulista: 60 Anos da Secretaria de Estado da Saúde. São Paulo: SES-SP.
Montero, Alfred P. 2001. Shifting States in Global Markets. Subnational Industrial Policy in Contemporary Brazil and Spain. University Park, PA: Pennsylvania.
_______. 2012. “A Reversal of Political Fortune: The Transitional Dynamics of Conservative Rule in the Brazilian Northeast.” Latin American Politics and Society, 54(1): 1-36.
Motter, Paulino. 1994. “O Uso das Concessões das Emissoras de Rádio e Televisão no Governo Sarney.” Comunicação and Política, 1(1): 89-115.
MS/SGEP (Ministério da Saúde/Secretaria de Gestão Estratégica e Participativa). 2006. A Construção do SUS: Histórias da Reforma Sanitária e do processo Participativo. Brasília: Ministério da Saúde.
Navarro, Vicente, and Leiyu Shi. 2001. “The Political Context of Social Inequalities and Health.” Social Science and Medicine, 52(3): 481-491.
O'Neill, Kathleen. 2003. "Decentralization as an Electoral Strategy." Comparative Political Studies, 36(9): 1068-1091.
Paim, Jairnilson. 2008. Reforma Sanitária Brasileira: Contribuição para a Compreensão e Crítica.
Alves – (Un?)Healthy Politics
30
Salvador, Brazil: EDUFBA.
Paim, Jairnilson, Claudia Travassos, Celia Almeida, Ligia Bahia and James Macinko. 2011. “The Brazilian Health System: History, Advances and Challenges.” Lancet, 377(9779): 1778-1797.
Pimenta, Aparecida L. 2007. A História do CONASEMS: da Fase Heróica da Década de 80 ao Desejo de Mudança do Modelo de Atenção e Gestão dos Anos 2000. Brasília: CONASEMS.
Power, Timothy J., and Cesar Zucco. 2012. “Elite Preferences in a Consolidating Democracy: The Brazilian Legislative Surveys, 1990-2009.” Latin American Politics and Society, 54(4): 1-27.
Pribble, Jennifer. 2013. Welfare and Party Politics in Latin America. New York: Cambridge.
Pribble, Jennifer, Evelyne Huber, and John D. Stephens. 2009. “Politics, Policies and Poverty in Latin America.” Comparative Politics, 41(4): 387-407.
Ruger, Jennifer P. 2004. "Health and social justice." The Lancet, 364(9439): 1075-1080.
Samuels, David. 2003. Ambition, Federalism, and Legislative Politics in Brazil. Cambridge: Cambridge.
Sartori, Giovanni. 1976. Parties and Party Systems: A Framework for Analysis. Cambridge, UK: Cambridge.
Schlesinger, Mark, and Richard R. Lau. 2000. The meaning and measure of policy metaphors. American Political Science Review, 94(03): 611-626.
Sen, Amartya. 1999. Development as Freedom. New York: Anchor Books.
Sistema de Informações Sobre Orçamentos Públicos Em Saúde (SIOPS). 2013. Available at: http://siops.datasus.gov.br/evolpercEC29.php.
Souza, Celina. 1997. Constitutional Engineering in Brazil: the Politics of Federalism and Decentralization. New York: St. Martin's.
Souza, Celina, and Paulo Fábio Dantas Neto, Eds. 2006. Governo, Políticas Públicas e Elites Políticas nos Estados Brasileiros. Rio de Janeiro: Revan.
Sugiyama, Natasha B. 2008. “Theories of Diffusion: Social Sector Reform in Brazil.” Comparative Political Studies, 41(2): 193-216.
Weyland, Kurt. 1996. Democracy Without Equity: Failures of Reform in Brazil. Pittsburgh, PA: University of Pittsburgh.
World Health Organization (WHO). 2008. Closing the Gap in a Generation: Health Equity Through Action on the Social Determinants of Health. Geneva: World Health Organization.
Zucco, Cesar, and David Samuels. 2014. “Crafting Mass Partisanship at the Grass Roots, from the Top Down.” British Journal of Political Science, available on CJO2014. doi:10.1017/S0007123413000549.
Author Interviews and Observations
CGR-SP. 2009. Observations. Campinas region, May 14 and October 14.
Civil servant at SESAB. 2009. Salvador, December 16.
Civil servants (two) at SES-MG. 2010. Belo Horizonte, February 23 and 25.
Civil servants (one career, one appointed) at SES-SP. 2009. São Paulo, 2009.
Civil servant at one SMS-SP. 2009. Amparo, May 18.
Mayor of Salvador, BA (former). 2009. Salvador, December 9.
Alves – (Un?)Healthy Politics
31
Members of CES-BA. 2008-2010. Salvador, multiple interviews.
Members of CIB-BA (current and former). 2008-2009. Salvador, multiple interviews.
PPI-BA planning meetings. 2009. Observation. Salvador, December 3-11.
PPI-SP planning meetings. 2009. Observation. Campinas, March 14.
SMS-BA (Municipal Health Managers in Bahia) (two). 2010. Salvador, March 18 and 19.
SMS-MG (opposition municipality). 2009. Belo Horizonte, November 18.
SMS-MG (two). 2009b. Belo Horizonte, October 23.
SMS-SP. 2009. Amparo, May 6.
State government official (former) at SESAB. 2008. Salvador, December 18.
State government official (former) at SES-SP. 2009. São Paulo, May 20 and June 9.
State government official at SES-MG. 2010. Belo Horizonte, February 25.
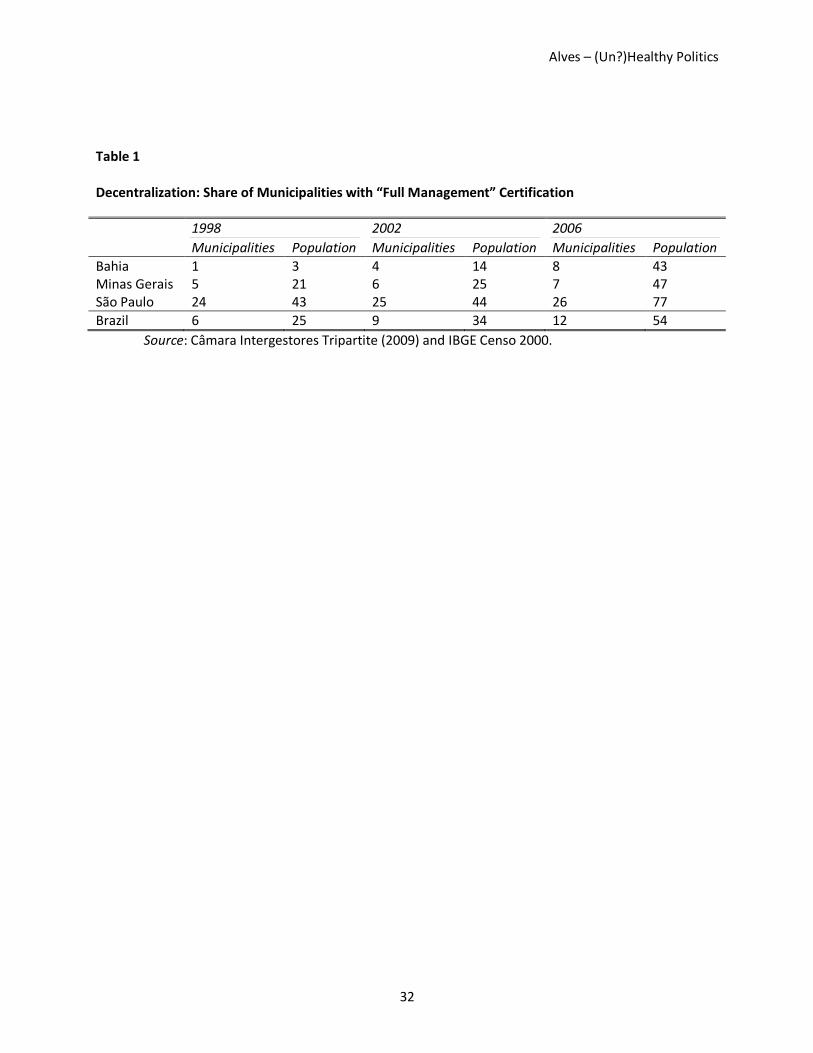
Alves – (Un?)Healthy Politics
32
Table 1
Decentralization: Share of Municipalities with “Full Management” Certification
1998 2002 2006
Municipalities Population Municipalities Population Municipalities Population
Bahia 1 3 4 14 8 43 Minas Gerais 5 21 6 25 7 47 São Paulo 24 43 25 44 26 77
Brazil 6 25 9 34 12 54
Source: Câmara Intergestores Tripartite (2009) and IBGE Censo 2000.

Alves – (Un?)Healthy Politics
33
Table 2
Political Competition and Health Systems in Bahia, Minas Gerais and São Paulo
Bahia Minas Gerais São Paulo
State Politics Concentrated Competitive and Plural
Stalemate (Competitive + Executive Continuity)
Health System Centralized and discretionary
Coordinated (Centralized and rules-based)
Fragmented (Decentralized and partly rules-based)
Implication for care
Service allocation is determined by central policy preferences and distribution of pork
Service is allocated based on a coordinated plan developed by state and local governments.
Dual and disconnected allocation of services by state and local governments.
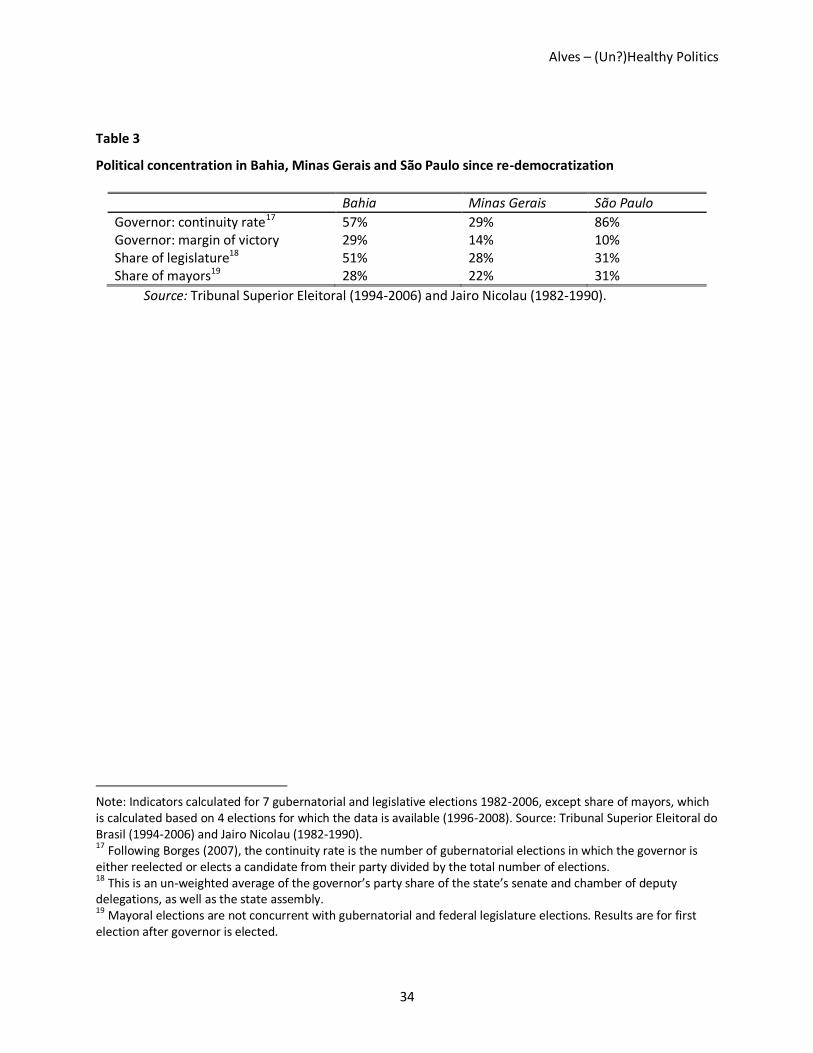
Alves – (Un?)Healthy Politics
34
Table 3
Political concentration in Bahia, Minas Gerais and São Paulo since re-democratization
Bahia Minas Gerais São Paulo
Governor: continuity rate17 57% 29% 86% Governor: margin of victory 29% 14% 10% Share of legislature18 51% 28% 31% Share of mayors19 28% 22% 31%
Source: Tribunal Superior Eleitoral (1994-2006) and Jairo Nicolau (1982-1990).
Note: Indicators calculated for 7 gubernatorial and legislative elections 1982-2006, except share of mayors, which is calculated based on 4 elections for which the data is available (1996-2008). Source: Tribunal Superior Eleitoral do Brasil (1994-2006) and Jairo Nicolau (1982-1990). 17
Following Borges (2007), the continuity rate is the number of gubernatorial elections in which the governor is either reelected or elects a candidate from their party divided by the total number of elections. 18 This is an un-weighted average of the governor’s party share of the state’s senate and chamber of deputy delegations, as well as the state assembly. 19
Mayoral elections are not concurrent with gubernatorial and federal legislature elections. Results are for first election after governor is elected.




















