Results of the Healthy Body Healthy Spirit Trial
10
Results of the Healthy Body Healthy Spirit Trial Ken Resnicow, Alice Jackson, Dhana Blissett, Terry Wang, Frances McCarty, Simone Rahotep, and Santhi Periasamy Emory University Healthy Body Healthy Spirit was a multicomponent intervention to increase fruit and vegetable (F & V) consumption and physical activity (PA) delivered through Black churches. Sixteen churches were randomly assigned to 3 intervention conditions. At baseline, 1,056 individuals were recruited across the 16 churches, of which 906 (86%) were assessed at 1-year follow-up. Group 1 received standard educational materials, Group 2 received culturally targeted self-help nutrition and PA materials, and Group 3 received the same intervention as did Group 2 as well as 4 telephone counseling calls based on motivational interviewing (MI) delivered over the course of 1 year. At 1-year follow-up, Groups 2 and 3 showed significant changes in both F & V intake and PA. Changes were somewhat larger for F & V. For F & V, but not PA, there was a clear additive effect for the MI intervention. Keywords: motivational interviewing, health promotion, African Americans Poor dietary patterns and sedentary lifestyle together account for between 300,000 and 500,000 deaths each year, ranking second only to tobacco use as causes of preventable deaths (McGinnis & Foege, 1993). Diets high in fruit and vegetable (F & V) intake have been shown to be protective for several cancers, stroke, heart disease, and age-related blindness (Gillman et al., 1995; Wargov- ich, 1997; Witte et al., 1996). Likewise, a sedentary lifestyle has been associated with higher mortality rates due to heart disease, stroke, cancer, and diabetes (U.S. Department of Health and Hu- man Services, 1996). Increasing the proportion of Americans who consume at least five servings of F & V per day as well as the proportion who engage in moderate to vigorous physical activity (PA) for 30 min most days of the week are national health priorities (U.S. Department of Health and Human Services, 2000). The present study had two primary aims: (a) to test the effec- tiveness of a culturally targeted (i.e., group-tailored) self-help diet and PA intervention versus standard health education materials not tailored for an African American church population and (b) to test the effectiveness of motivational interviewing (MI) delivered by telephone on F & V intake and PA. Another aim of this study, and the larger initiative through which it was funded (Nigg, Allegrante, & Ory, 2002; Ory, Jordan, & Bazzarre, 2002), was to examine the pattern of change among individuals being asked to modify more than one health behavior. Whereas there have been numerous interventions targeting diet or PA in healthy populations, little is known about the impact of interventions that simultaneously ad- dress both behaviors (Nigg et al., 2002; Ory et al., 2002). The present article reports the results of the Healthy Body Healthy Spirit intervention and includes an analysis of simultaneous change. Theoretical Background The first aim of the study was to test the effectiveness of a culturally targeted self-help intervention compared with standard educational materials (i.e., Group 1 vs. Group 2). Although it is virtually self-evident, at least in a general sense, that health pro- motion programs should be tailored to the social and cultural characteristics of the target population, what such group “tailor- ing” entails, how to achieve it, and its impact on treatment out- comes has not been adequately examined. (Braithwaite & Resni- cow, 2002; Resnicow, Braithwaite, Ahluwalia, & Baranowski, 1999; Resnicow, Soler, Ahluwalia, Butler, & Braithwaite, 2000). Cultural sensitivity has been operationalized in two primary dimensions (Resnicow et al., 1999; Resnicow, Braithwaite, Ahlu- walia, & DiIorio, 2001): surface structure and deep structure. Surface structure involves matching intervention materials and messages to observable social and behavioral characteristics of a target population. For audiovisual materials, surface structure may involve using people, places, language, music, foods, brand names, esthetics, and locations familiar to, and preferred by, the target audience. Surface structure conveys how well interventions fit within the culture, experience, and behavioral patterns of the audience. The second dimension, deep structure, reflects how cultural, social, psychological, environmental, political, economic, and his- torical factors influence health behaviors differently across racial/ ethnic populations (Marin et al., 1995; Resnicow et al., 1999; Resnicow, Braithwaite, et al., 2001; Sabogal, Otero-Sabogal, Pa- sick, Jenkins, & Perez-Stable, 1996). The second primary aim of this study was to test the effective- ness of telephone-based MI to improve diet and PA behaviors (Group 3 vs. Group 2). MI is a client-centered counseling approach designed to enhance intrinsic motivation for behavior change by Ken Resnicow, Alice Jackson, Dhana Blissett, Terry Wang, Frances McCarty, Simone Rahotep, and Santhi Periasamy, School of Public Health, Emory University. This project was supported by a grant from the National Heart Lung Blood Institute, awarded to Ken Resnicow. Correspondence concerning this article should be addressed to Ken Resnicow, who is now at the School of Public Health, University of Michigan, 1420 Washington Heights, Room 5009, Ann Arbor, MI 48109. E-mail: [email protected] Health Psychology Copyright 2005 by the American Psychological Association 2005, Vol. 24, No. 4, 339 –348 0278-6133/05/$12.00 DOI: 10.1037/0278-6133.24.4.339 339
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Results of the Healthy Body Healthy Spirit Trial

Results of the Healthy Body Healthy Spirit Trial
Ken Resnicow, Alice Jackson, Dhana Blissett, Terry Wang, Frances McCarty,Simone Rahotep, and Santhi Periasamy
Emory University
Healthy Body Healthy Spirit was a multicomponent intervention to increase fruit and vegetable (F & V)consumption and physical activity (PA) delivered through Black churches. Sixteen churches wererandomly assigned to 3 intervention conditions. At baseline, 1,056 individuals were recruited across the16 churches, of which 906 (86%) were assessed at 1-year follow-up. Group 1 received standardeducational materials, Group 2 received culturally targeted self-help nutrition and PA materials, andGroup 3 received the same intervention as did Group 2 as well as 4 telephone counseling calls based onmotivational interviewing (MI) delivered over the course of 1 year. At 1-year follow-up, Groups 2 and3 showed significant changes in both F & V intake and PA. Changes were somewhat larger for F & V.For F & V, but not PA, there was a clear additive effect for the MI intervention.
Keywords: motivational interviewing, health promotion, African Americans
Poor dietary patterns and sedentary lifestyle together account forbetween 300,000 and 500,000 deaths each year, ranking secondonly to tobacco use as causes of preventable deaths (McGinnis &Foege, 1993). Diets high in fruit and vegetable (F & V) intake havebeen shown to be protective for several cancers, stroke, heartdisease, and age-related blindness (Gillman et al., 1995; Wargov-ich, 1997; Witte et al., 1996). Likewise, a sedentary lifestyle hasbeen associated with higher mortality rates due to heart disease,stroke, cancer, and diabetes (U.S. Department of Health and Hu-man Services, 1996). Increasing the proportion of Americans whoconsume at least five servings of F & V per day as well as theproportion who engage in moderate to vigorous physical activity(PA) for 30 min most days of the week are national healthpriorities (U.S. Department of Health and Human Services, 2000).
The present study had two primary aims: (a) to test the effec-tiveness of a culturally targeted (i.e., group-tailored) self-help dietand PA intervention versus standard health education materials nottailored for an African American church population and (b) to testthe effectiveness of motivational interviewing (MI) delivered bytelephone on F & V intake and PA. Another aim of this study, andthe larger initiative through which it was funded (Nigg, Allegrante,& Ory, 2002; Ory, Jordan, & Bazzarre, 2002), was to examine thepattern of change among individuals being asked to modify morethan one health behavior. Whereas there have been numerousinterventions targeting diet or PA in healthy populations, little isknown about the impact of interventions that simultaneously ad-dress both behaviors (Nigg et al., 2002; Ory et al., 2002). The
present article reports the results of the Healthy Body HealthySpirit intervention and includes an analysis of simultaneouschange.
Theoretical Background
The first aim of the study was to test the effectiveness of aculturally targeted self-help intervention compared with standardeducational materials (i.e., Group 1 vs. Group 2). Although it isvirtually self-evident, at least in a general sense, that health pro-motion programs should be tailored to the social and culturalcharacteristics of the target population, what such group “tailor-ing” entails, how to achieve it, and its impact on treatment out-comes has not been adequately examined. (Braithwaite & Resni-cow, 2002; Resnicow, Braithwaite, Ahluwalia, & Baranowski,1999; Resnicow, Soler, Ahluwalia, Butler, & Braithwaite, 2000).
Cultural sensitivity has been operationalized in two primarydimensions (Resnicow et al., 1999; Resnicow, Braithwaite, Ahlu-walia, & DiIorio, 2001): surface structure and deep structure.Surface structure involves matching intervention materials andmessages to observable social and behavioral characteristics of atarget population. For audiovisual materials, surface structure mayinvolve using people, places, language, music, foods, brand names,esthetics, and locations familiar to, and preferred by, the targetaudience. Surface structure conveys how well interventions fitwithin the culture, experience, and behavioral patterns of theaudience.
The second dimension, deep structure, reflects how cultural,social, psychological, environmental, political, economic, and his-torical factors influence health behaviors differently across racial/ethnic populations (Marin et al., 1995; Resnicow et al., 1999;Resnicow, Braithwaite, et al., 2001; Sabogal, Otero-Sabogal, Pa-sick, Jenkins, & Perez-Stable, 1996).
The second primary aim of this study was to test the effective-ness of telephone-based MI to improve diet and PA behaviors(Group 3 vs. Group 2). MI is a client-centered counseling approachdesigned to enhance intrinsic motivation for behavior change by
Ken Resnicow, Alice Jackson, Dhana Blissett, Terry Wang, FrancesMcCarty, Simone Rahotep, and Santhi Periasamy, School of Public Health,Emory University.
This project was supported by a grant from the National Heart LungBlood Institute, awarded to Ken Resnicow.
Correspondence concerning this article should be addressed to KenResnicow, who is now at the School of Public Health, University ofMichigan, 1420 Washington Heights, Room 5009, Ann Arbor, MI 48109.E-mail: [email protected]
Health Psychology Copyright 2005 by the American Psychological Association2005, Vol. 24, No. 4, 339–348 0278-6133/05/$12.00 DOI: 10.1037/0278-6133.24.4.339
339

exploring and resolving ambivalence (Miller & Rollnick, 2002).Originally developed for the treatment of addictions, public healthprofessionals have increasingly begun to apply this approach toencourage change in chronic disease behaviors such as diet, PA,cancer screening, and medical adherence (Emmons & Rollnick,2001; Resnicow, DiIorio, Soet, Borrelli, Ernst, & Hecht, 2002).Several reviews of MI-based interventions have been reported,with most studies showing positive effects (Burke, Arkowitz, &Menchola, 2003; Dunn, Deroo, & Rivara, 2001; Resnicow, Di-Iorio, Soet, Borrelli, Ernst, & Hecht, 2002; Resnicow, DiIorio,Soet, Borrelli, Ernst, Hecht, et al., 2002).
The MI counselor tailors the encounter to match the partici-pant’s needs, experiences, barriers, fears, readiness, and reasonsfor change. Clients are encouraged to think about and verballyexpress their own reasons for and against change and how theircurrent health behavior may conflict with their health goals or theirability to achieve their broader life goals or core values. MIcounselors avoid argumentation; they “roll with resistance” asopposed to contesting it (Rollnick, Mason, & Butler, 1999). MIcounselors rely heavily on reflective listening rather than on directquestioning, persuasion, or advice giving.
The primary study hypotheses are outlined below:
Hypothesis 1: Individuals receiving a culturally sensitivemulticomponent intervention will show significantly greaterimprovement in F & V intake and PA patterns than thosereceiving standard exercise and nutrition education materials.
Hypothesis 2: Individuals receiving a culturally sensitive in-tervention plus four telephone counseling calls using MItechniques will show greater improvement in F & V intakeand PA than those receiving a culturally sensitive self-helpintervention without telephone counseling.
Method
Setting
The study was conducted in a set of socioeconomically diverse churchesin the Atlanta metropolitan area. The Black church has been the site ofnumerous health promotion initiatives (Baskin, Resnicow, & Campbell,2001; Resnicow, Coleman-Wallace, et al., 2000; Resnicow, Jackson,Wang, Dudley, & Baranowski, 2001; Thomas, Quinn, Billingsley, &Caldwell, 1994). Many Black churches consider health to be part of theiroverall mission, offering health services and programs through specialcommittees and ministries (Lasater, Becker, Hill, & Gans, 1997; Thomas etal., 1994; U.S. Department of Health and Human Services & NationalInstitutes of Health, 1989) that can greatly facilitate the implementation ofresearch programs in this setting. Churches often provide excellent infra-structure for participant recruitment and tracking and, in particular, accessto middle and upper socioeconomic African Americans, a group oftenunderrepresented in health promotion studies.
Design
Sixteen churches were randomly assigned to three intervention condi-tions. Group 1 (5 churches) received standard nutrition and PA interventionmaterials, Group 2 (6 churches) received culturally targeted self-helpnutrition and PA intervention materials, and Group 3 (5 churches) receivedthe same intervention as Group 2 and four telephone counseling calls basedon MI (Miller & Rollnick, 1991).
Intervention Materials (Groups 2 and 3)
In designing the culturally targeted materials for this project, we used aframework developed by our group, described in more detail elsewhere(Resnicow et al., 1999; Resnicow, Braithwaite, et al., 2001), to determinethe most acceptable and salient messages for an African American southernchurch population (Resnicow et al., 1999; Resnicow, Braithwaite, et al.,2001). The process included a series of focus groups (four addressingF & V and four addressing PA) with members of local Black churches notparticipating in this project. This “diagnostic” research yielded numerouselements for surface structure tailoring, including food preferences, cook-ing practices, and exercise patterns relevant to this population (Resnicow,Braithwaite, et al., 2001). Deep structure issues that emerged includeunique attitudes regarding body image, concerns among many womenregarding the effort to redo their hair after exercising, safety concerns insome neighborhoods, and lack of time for exercise due to extensive churchand family commitments. Other deep structure issues included the potentialuse of scripture and religious themes as well as a focus on improving thehealth of the larger community (as opposed to the health of individuals) asmotivations for behavior change (Resnicow, Jackson, et al., 2002).
After an iterative process of pretesting and revision, we developed thefollowing core materials for participants in Groups 2 and 3. The F & Vvideo and cookbook were designed for a prior trial (Eat for Life), whichalso was conducted in Black churches (Resnicow, Coleman-Wallace, et al.,2000; Resnicow, Jackson, et al., 2001). The process used to develop thesematerials was similar to that used for this project (Resnicow, Jackson, etal., 2002).
Overview of Intervention Materials
Nutrition video. Forgotten Miracles is an 18-min video developed forour prior Eat for Life study, which uses biblical and spiritual themes tomotivate healthy eating (Resnicow, Coleman-Wallace, et al., 2000). Thestory centers around two families who are introduced preparing for churchon a Sunday morning. One family exhibits healthy habits (e.g., fruit forbreakfast), whereas the other family is shown eating candy and soda forbreakfast. During Sunday services, while the pastor lectures on the “down-fall of the glutton,” the father of the “unhealthy” family nods off anddreams he has a heart attack while eating a large after-church meal. Duringthe remainder of the video, this character transforms his eating patterns toinclude more F & V. Woven into the story line is information about thehealth benefits of F & V, analysis of costs, recipes, and cooking tips. Keymessages are conveyed with biblical themes and passages. For example,the pastor relates the story of Daniel (Daniel 1:8–16), who rejects the“kings diet” high in fat for his “natural diet” high in F & V. Other biblicalmessages used include “whatever you do, whatever you eat, do for theglory of God” and “your body is God’s temple.”
Cookbook. The Eat for Life cookbook contains recipes submitted bymembers of the participating churches. Qualifying recipes were required tocontain at least one fourth a serving of fruit or vegetable per serving and tobe low in fat (� 30% of total calories). Recipes were analyzed in theNutrient Data System software (University of Minnesota) to determinewhether they met these requirements. Qualifying recipes were taste tested,and the 60 most preferred recipes were included in the book. The cookbookalso contains information about the health benefits of F & V, tips forshopping and storing F & V, and cooking techniques.
Exercise video. The 20-min video is hosted by well known AfricanAmerican celebrities from the Atlanta area. One was a local female newsanchor, and the other was a former Mister Olympia and owner of severallocal fitness facilities. Approximately 10 families, recruited from Blackchurches, were provided with a video camera, and a designated person,usually an adolescent living in that home, was trained in its use. Thisperson was asked to document the efforts of one of his or her parents asthey attempted to increase or maintain (if they were high at baseline) theiractivity level over a 4-week period. Participants included both low and high
340 RESNICOW ET AL.

exercisers as well as two pastors. The goal of this “documentary” compo-nent was to provide real-world role models to whom our participants couldrelate. The documentary footage is linked by narration and instruction fromthe two hosts. The two pastors were also filmed giving sermons on theimportance of exercise and maintaining a healthy body, and clips from theirpreaching are spliced throughout the video, along with biblical scripturesthat relate to health.
Exercise guide. The 37-page, four-color manual was developed toaccompany the Healthy Body Healthy Spirit video. Whereas the video wasintended to increase motivation, the written guide contains more back-ground information, instruction, and skills-building information. Most ofthe models shown in the guide also appear in the video, and again, biblicalthemes and scripture are woven throughout. The guide includes the fol-lowing core messages: (a) Obtain 30 min of PA on most days of the week;and (b) activity of greater intensity and duration will result in added healthbenefits (Pate et al., 1995; U.S. Department of Health and Human Services,1996).
The guide provides an activity program for three levels: beginner,intermediate, and advanced. It emphasizes walking as a core strategy,particularly for those at initially lower levels of activity. To encouragewalking, all participants in Groups 2 and 3 were provided with a pedometer(Yamax, Digiwalker; Tokyo, Japan) at the beginning of the program(baseline health fair). The guide also addresses other forms of activity,ranging from low to high intensity, as well as strength and flexibilityexercises.
Audiocassette. Participants received an audiocassette containing gos-pel music. Songs were sequenced so that their tempo matched a three-phaseworkout: warm up, aerobic activity, and cool down. Biblical quotes andbrief sound bytes of pastor sermons relating to health are spliced betweensongs.
Comparison group materials. To maximize internal validity of thecomparison between Groups 1 and 2, it was important that these groupsdiffer by the intervention content rather than the format or dose. Therefore,participants in the comparison group received an intervention of approxi-mately equal intensity and type. They received the same health fair andindividualized results letter as did the intervention group, the projectnewsletter, a commercial aerobics video (no F & V video could beidentified), and numerous health education brochures drawn from govern-ment sources and health voluntary agencies (e.g., Down Home HealthCooking; National Cancer Institute #96–3408). After the final posttest, thecomparison group received all the culturally targeted materials (Resnicow,Jackson, et al., 2002).
MI Intervention (Group 3)
The MI intervention was delivered by telephone by master’s- ordoctoral-level psychologists who received approximately 16 hr of initialtraining and 12 hr of ongoing individual/group supervision. Counselorswere provided with a semistructured protocol that outlined the basic flowof each call while still allowing for spontaneous discussion and reflectivelistening. The four MI calls were delivered at approximately weeks 4, 12,26, and 40. Each call had a 6-week window, after which the participant wasconsidered as having missed that call.
The protocol focused on eliciting change talk (CT) through severaldiscrete strategies. First, using the method developed by Rollnick (Butler etal., 1999; Rollnick, Butler, & Stott, 1997), we asked participants thefollowing two questions: (a) “On a scale of 0 to 10 (with 10 being thehighest), how motivated/interested are you in increasing your fruit/vege-table consumption (or increasing PA)?” and (b) “On a scale of 0 to 10 (with10 being the highest), assuming you wanted to, how confident are you thatyou could increase your fruit/vegetable consumption (or increase yourPA)?”
After the client’s response, the counselor asked two probes: (a) “Whydid you not choose a lower number, like a 1 or 2?” (this is used to elicit
positive motivating statements) and (b) “Why did you not choose a highernumber?” and/or “What would it take to get you to a higher number?” (thisis used to elicit barriers). If barriers were presented, counselors promptedparticipants to solve their own barriers.
A second strategy to elicit CT involved the use of a values clarificationstrategy, based on the work of Miller (Wagner & Sanchez, 2002). Clientswere asked to choose from a list of approximately 20 values the top 3 or4 that were most important to them. Then they were asked to explore whatconnection, if any, they saw between their current health behavior and theirability to achieve these goals or live out these values. Alternatively, thecounselor may have asked how changing their health behavior may berelated to these goals or values.
Two of the four MI calls addressed F & V intake, and two addressed PA.During the first and third calls, participants chose which topic they wouldlike to address. If they elected to address F & V during their first call, PAwas addressed in the second call. This choice was repeated during the thirdcall.
For the first and second calls (depending on whether the participantpreviously reported materials use), the use of key intervention components(i.e., video and cookbook) was briefly reviewed. At the end of the call,participants were asked to restate what was agreed on, and a verbal contractwas secured. Additional details regarding the MI intervention can be foundelsewhere (Resnicow, Jackson, et al., 2002).
In each church, a liaison was hired to assist in participant recruitmentand retention as well as in coordination of the health fairs. A quotasampling framework was used. At baseline, the liaison was asked toprovide at least 45 names and telephone numbers of participants and todistribute questionnaires approximately 3 weeks before the health fair.Churches were provided with a $10 donation for each adult participant (upto 60 per church) who completed the baseline assessment. Participantswere requested to complete their questionnaires prior to the health fair, butif they did not, they were allowed to complete them at the health fair.Pastors were asked to encourage congregants to attend the health fairs,which were generally conducted immediately after Sunday services. Flyerswere posted, and announcements were placed in church bulletins.
To assist members who may have limited literacy skills, at health fairs,staff asked all participants whether they would like to have someone fromthe program read the questionnaire with them. At posttest, liaisons wereasked to assist in encouraging baseline participants to attend the follow-uphealth fair. Churches received an incentive that increased from $250 to$2,000 on the basis of the proportion of baseline participants who attendedthe posttest health fair.
Health fairs at baseline and at 1-year follow-up were set up with various“stations,” which included registration, height/weight, blood pressure, cho-lesterol (finger stick), “blood draw” (venapuncture for carotenoids sample),fitness test, optional diabetes test (random nonfasting glucose), individu-alized printed results, and buffet. Total cholesterol and blood glucose wereoffered to increase participation. Because they were not target outcomes ofthe trial, the values are not reported here.
Measures
Diet. Multiple measures of dietary intake were obtained to provide aconverging (i.e., triangulated) estimate of true intake. All participantscompleted the recently developed National Cancer Institute 19-item F & Vfood frequency questionnaire (FFQ), which assesses intake in the pastmonth (Thompson et al., 2000). A 2-item measure was used to assess usualF & V intake (1 item each for F & V consumed “each day”; Resnicow,Odom, et al., 2000), and the third instrument was a 36-item F & V FFQbased on the Health Habits and History Questionnaire (HHHQ; Resnicow,Odom, et al., 2000), originally developed for the Eat for Life study. Thethree measures were averaged to yield a composite F & V variable. The19-item and 36-item measures included an item that assessed intake offrench fries and fried potatoes. These items were excluded from thecomputation of F & V servings.
341HEALTHY BODY HEALTHY SPIRIT

Validity of the 2-item and 36-item measures, using serum carotenoids,has been reported previously (Resnicow, Odom, et al., 2000). For thisstudy, the three FFQ methods were again validated against serum totalcarotenoids (sum of lutein, cryptoxanthin, � carotene, and � carotene),which were obtained at baseline from approximately 79% of the partici-pants as well as three 24-hr recalls (20% of the participants). The corre-lation of F & V servings by FFQ and serum carotenoids was .37, .17, and.28, for the 2-item, 19-item, and 36-item measures, respectively. Thecorrelation of F & V servings by FFQ and three 24-hr recalls, was .28, .31,and .35, for the 2-item, 19-item, and 36-item measures respectively.Though small to moderate in magnitude, these correlations are in the rangeof validity coefficients for other self-report dietary measures (Campbell etal., 1994; Coates et al., 1991; Resnicow, Odom, et al., 2000).
We excluded from the analysis any participant who was missing morethan half of the vegetable (10 items) or fruit items (8 items) from the36-item FFQ. At baseline, 17 cases were excluded, and at posttest, 15 caseswere excluded. Cases missing fewer than one half of the fruit or vegetableitems were assigned a frequency of 0 for those missing items. In addition,13 and 12 additional cases were excluded at baseline and posttest becauseof extreme values (� 3 SDs). The proportion of excluded cases based onthe above criteria was different across the three treatment groups, �2(2) �6.6, p � .04. The percentage of excluded cases was 3.3%, 3.4%, and 1.4%for the comparison, self-help, and self-help � MI groups, respectively.
PA. The primary PA measure was an adaptation of the CommunityHealthy Activities Model Program for Seniors (CHAMPS) PA recall(Harada, Chiu, King, & Stewart, 2001; Stewart et al., 2001), a self-administered instrument developed for underactive populations and testedprimarily among older adults. The frequency of activity is assessed in timesper week, and duration is classified using six categories ranging from “lessthan 1 hr per week” to “9 or more hours per week.” On the basis of focusgroups and pilot testing of the instrument, some modifications were made.First, items from the social activities and recreation/hobbies sections (e.g.,use a computer and woodworking) were excluded to reduce responseburden and because these activity domains were not targets of our inter-vention. Second, we modified the recall time frame from the past month tothe past 2 weeks, as formative work indicated that individuals may bebetter able to accurately recall activity during this more proximal recallperiod. Finally, a single item assessing the frequency of dancing duringchurch was added with the following wording: “How often in the past twoweeks did you dance during church services or sway to the music of thechoir?” The original measure included 41 items, and the final version usedin the study comprised 31 items.
The modified CHAMPS instrument was scored to yield three indices ofactivity: total minutes per week; minutes of moderate to vigorous PA(MVPA), defined as those with a metabolic equivalent task (MET) value �
3.0; and “intentional exercise activities,” comprised of 20 exercise orsports-related activities that were not part of daily functioning. The activ-ities included in this index were fast walking, jog/run, biking, aerobicmachines, stair/step machine, swimming (gently or moderate/fast), waterexercises, stretching, yoga/tai-chi, aerobics, dance, strength training (light,moderate/heavy), general conditioning, basketball, soccer, racquetball, golf(cart and walking), and tennis (singles and doubles).
Excluded from the analyses were 89 individuals at baseline, and 36 at1-year posttest, who failed to respond to at least 2 items (frequency orduration) on at least two pages of the modified CHAMPS questionnaire orwhose value for weekly minutes for all activities exceeded 3 SDs. Valuesgreater than 3 SDs would be equivalent to more than 8 hr of daily PA. Forthose responding to at least 2 items on different pages of the questionnaire,missing values were coded as 0. These criteria were invoked to excludethose respondents who either did not completely attend to the questionnaireor who may have misunderstood the instructions and overestimated theiractivity levels. Again, the proportion of excluded cases based on the abovecriteria was different across the three treatment groups, �2(2) � 6.3, p �
.04. The percentage of excluded cases was 5.2%, 8.8%, and 7.1% for thecomparison, self-help, and self-help � MI groups, respectively.
The CHAMPS instrument was validated against submaximal treadmilltest (n � 138) and three 24-hr recalls (n � 210) conducted in a subsampleof participants. Correlations between the CHAMPS indices and predictedVO2 maximum ranged from .17 for total activity to .32 for the sports index.Correlations between the CHAMPS indices and 24-hr recall indices (hoursper day for all activities, activities � 3 METs, and recreational activities)ranged from .16 for all activities to .41 for intentional exercise activities.These validity coefficients are similar to those observed for other similarself-report PA measures (Harada et al., 2001; Stewart et al., 2001). Addi-tional details about the validity study can be found elsewhere (Resnicow etal., 2003).
Other variables assessed. Income was assessed with an eight-categoryordinal item, with answers ranging from � $10,000 to � $149,999. For thepresent analyses, responses were collapsed into four categories: � $20,000,$20–39,999, $40–79,000, and � $80,000. Education was categorized as“high school/vocational school or less,” “some college,” and “completedcollege or higher.”
Process measures and dose–response analyses. At 1-year posttest,participants in Groups 2 and 3 were asked to report their usage of thevarious intervention elements. Usage was assessed with single forced-choice items for each main intervention component. For purposes ofconducting “dose–response” analyses, individuals reporting watching mostor all of the F & V video or activity video were coded as having used thesematerials. Individuals reporting using at least one recipe from the cookbookor having read most of the activity guide were coded as having used thematerials. Individuals reporting using their pedometers at least a few daysper week over the past year were considered “pedometer users.”
Statistical Analyses
Outcomes were analyzed with a mixed model repeated measures anal-ysis of variance program, SAS PROC MIXED, that allows for adjustmentof subject nonindependence within churches (Murray, 1998). The intra-class correlations for the main outcomes of F & V and PA (i.e., those listedin Table 1) ranged from .005 (2-item F & V) to .02 (exercise index on theCHAMPS).
The initial multivariate model included fixed effect terms for experi-mental condition and the covariates age, gender, income, and education aswell as random effect terms for church, nested in treatment condition, andindividual nested within church. Because the treatment groups did notdiffer on these covariates and because they were not significantly associ-ated with our main outcomes, they were not included in the final model. Allprimary outcome analyses (excluding dose–response analyses) are basedon an intention to treat analysis, with individuals included in each conditionregardless of how much of the intervention they received or used.
Approximately 230 individuals (generally spouses) from the samehousehold (2 individuals from 115 households) participated in the study.Because the majority of “family” units comprised a single individual (77%of the sample), individuals were not nested within families within therepeated measures model (Murray, Hannan, & Baker, 1996). Analyseswere also conducted including only one randomly selected member perhousehold, and the results were not appreciably altered by the exclusion ofthe second household member.
Models were also run including three-way Group � Time � “___”interaction terms for age, gender, income, and education. These interactionterms were selected because they have been shown to be effect modifiersin prior interventions. The primary test of intervention effects was theGroup � Time interaction. When omnibus differences were obtained,contrasts were run to determine which groups differed as well as the patternof change. Servings of F & V from the FFQs were transformed by naturallog to better normalize their distribution, and CHAMPS index scores weretransformed by square root to better normalize their distribution. Tables
342 RESNICOW ET AL.
present untransformed values, whereas p values are based on analysesusing transformed values.
Examination of Simultaneous Change
To examine the pattern of simultaneous change, each participant wasclassified into one of three exclusive categories of change: (a) little or nochange, defined as a pretest–posttest difference of .25 SDs or less; (b)moderate change, defined as a pretest–posttest difference of .26 to .5 SDs;and (c) large change, defined as a pretest–posttest difference of greaterthan .5 SDs. We report the percentage of individuals who fell into each ofthese categories for the two primary behaviors of interest.
Results
Sample Description
At baseline, 1,056 individuals were recruited across the 16churches. The number of participants per church averaged 66
(range � 44–88). Although children and adolescents were al-lowed to participate in the health fairs, the study sample includedonly individuals 18 years of age and older. Of the initial sample,906 (86%) were assessed at 1-year follow-up. Follow-up rates inthe three intervention groups were 89%, 90%, and 82%,respectively.
Dropouts did not differ from cohort members with regard togender, marital status, F & V intake, or PA. Dropouts were,however, significantly younger and more likely to be from lowereducation and income brackets. With regard to differential attri-tion, dropouts across the three groups did not differ for any of thevariables listed in Table 1 (data not shown).
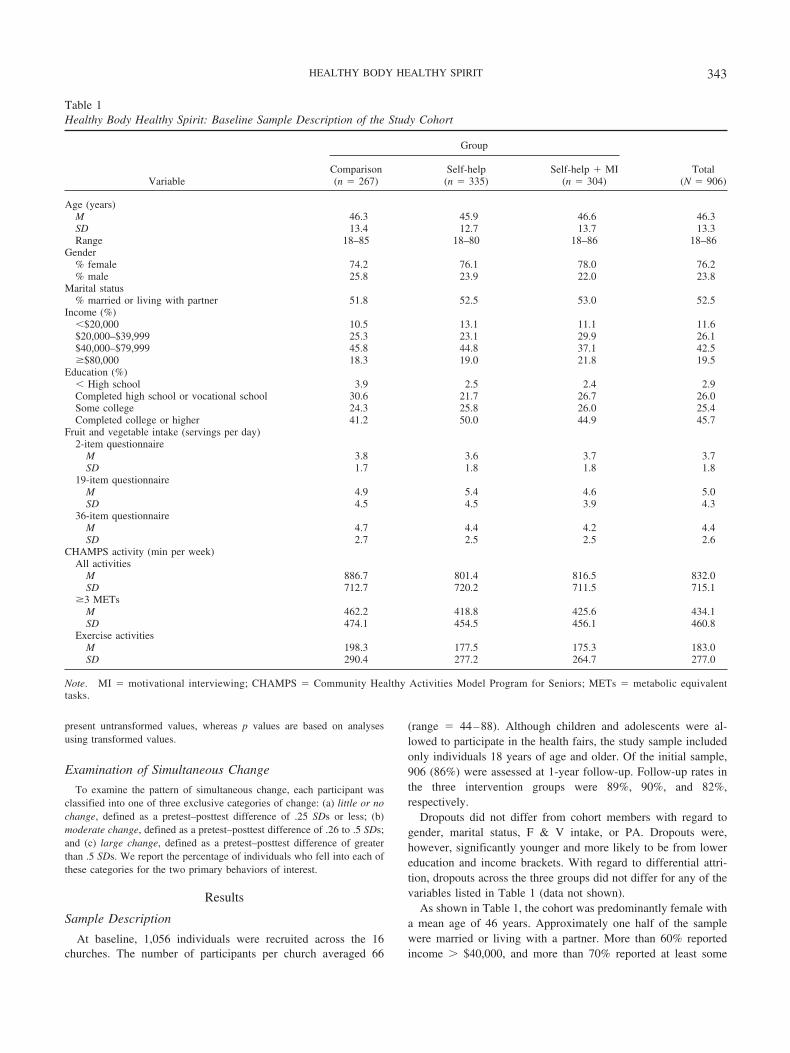
As shown in Table 1, the cohort was predominantly female witha mean age of 46 years. Approximately one half of the samplewere married or living with a partner. More than 60% reportedincome � $40,000, and more than 70% reported at least some
Table 1Healthy Body Healthy Spirit: Baseline Sample Description of the Study Cohort
Variable
Group
Total(N � 906)
Comparison(n � 267)
Self-help(n � 335)
Self-help � MI(n � 304)
Age (years)M 46.3 45.9 46.6 46.3SD 13.4 12.7 13.7 13.3Range 18–85 18–80 18–86 18–86
Gender% female 74.2 76.1 78.0 76.2% male 25.8 23.9 22.0 23.8
Marital status% married or living with partner 51.8 52.5 53.0 52.5
Income (%)�$20,000 10.5 13.1 11.1 11.6$20,000–$39,999 25.3 23.1 29.9 26.1$40,000–$79,999 45.8 44.8 37.1 42.5�$80,000 18.3 19.0 21.8 19.5
Education (%)� High school 3.9 2.5 2.4 2.9Completed high school or vocational school 30.6 21.7 26.7 26.0Some college 24.3 25.8 26.0 25.4Completed college or higher 41.2 50.0 44.9 45.7
Fruit and vegetable intake (servings per day)2-item questionnaire
M 3.8 3.6 3.7 3.7SD 1.7 1.8 1.8 1.8
19-item questionnaireM 4.9 5.4 4.6 5.0SD 4.5 4.5 3.9 4.3
36-item questionnaireM 4.7 4.4 4.2 4.4SD 2.7 2.5 2.5 2.6
CHAMPS activity (min per week)All activities
M 886.7 801.4 816.5 832.0SD 712.7 720.2 711.5 715.1
�3 METsM 462.2 418.8 425.6 434.1SD 474.1 454.5 456.1 460.8
Exercise activitiesM 198.3 177.5 175.3 183.0SD 290.4 277.2 264.7 277.0
Note. MI � motivational interviewing; CHAMPS � Community Healthy Activities Model Program for Seniors; METs � metabolic equivalenttasks.
343HEALTHY BODY HEALTHY SPIRIT

college education. At baseline, the three intervention groups didnot significantly differ for any of the variables listed in Table 1.
Completion of the MI Telephone Counseling
The MI calls for Group 3 participants were completed for 85%,79%, 74%, and 73% for Calls 1 through 4, respectively. Overall,in Group 3, 5.5% received 0 calls, 2.3% received one call, 9.4%received two calls, 9.7% received three calls, and 73.1% receivedall four calls. For Call 1, 62% of participants chose to work onF & V, and at Call 3, 57% chose to work on F & V.
Results on F & V intake. As shown in Table 2, across the threeFFQs, the change in F & V intake was largest in Group 3 andintermediate in Group 2. On the basis of the mean of the threeFFQs, the change (subtracting the pre-post change scores) was1.13 servings for Group 3, .44 servings for Group 2, and .17servings for Group 1. Using the composite FFQ and 19-itemvalues, the Group � Time effect was significant for Group 3compared with both Groups 1 and 2. For the 2-item and 36-itemvalues, Group 3 was significantly different than Group 1 but notGroup 2. On the basis of the 36-item measure, only the change inGroup 2 was significantly different than that in the control group.
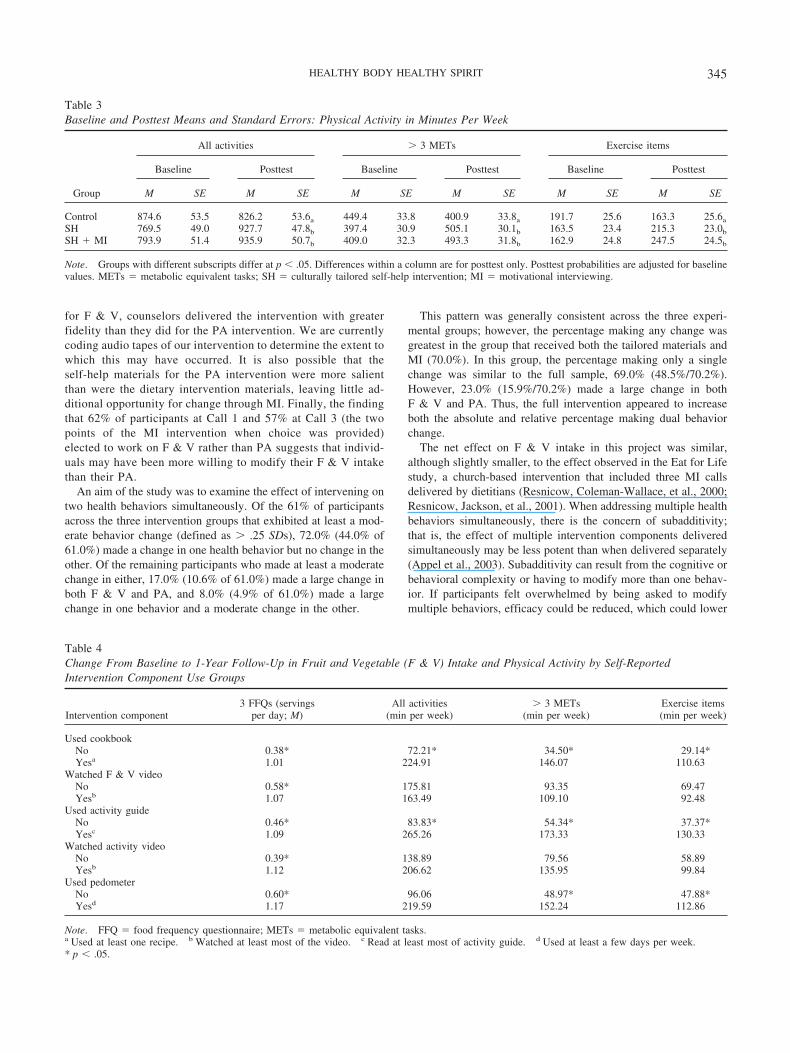
Results on PA. As shown in Table 3, the total minutes of PAbased on the CHAMPS measure increased significantly more inGroups 2 and 3 compared with Group 1 for each of the three indexscores; that is, all activities, � 3 METs, and exercise items. Groups2 and 3 did not differ on any of the three indices.
Subgroup analyses and moderator effects. For the three indi-vidual and composite F & V measures, as well as the threeCHAMPS indices, interaction terms for age, gender, education,and income with Treatment Group � Time were all nonsignificant,indicating that the intervention did not have a differential impactacross these subgroups. Although intervention effects did notdiffer significantly by gender, women in Groups 2 and 3 weremore likely than men to report using each of the self-help in-tervention components (i.e., the two videos, exercise guide; seeTable 4).
Association between intervention exposure and outcomes. In-dividuals in Groups 2 and 3 who reported using the cookbook andwatching most or all of the F & V video showed a significantlygreater increase in F & V intake than did those not using thesematerials. Likewise, individuals who reported using the activityguide showed a significantly greater increase in PA than did thosenot using the guide. Although those who reported watching mostor all of the activity video showed a greater increase in activity
than did those not watching the activity video, these differenceswere not statistically significant. Regular use of the pedometer wasassociated with a greater increase in activity, and this differencewas statistically significant for moderate/vigorous activities andthe index of exercise items.
Simultaneous Change of Diet and Activity
Overall, 39% of the sample was classified as having made littleor no change for both F & V and PA, with the largest percentageoccurring in the control group (see Table 5). Approximately 45%of the participants reported making a moderate or large change inone health behavior but no change in the other. Specifically, thisincluded 21% who reported a large F & V change but no changein PA, 9% who reported a moderate F & V change but no PAchange, 10% who reported a large PA change and no F & Vchange, and 5% who reported moderate PA change but no F & Vchange. The remaining 17% of participants reported making mul-tiple changes. Across all three experimental groups, the mostcommon pattern of multiple change was a large change for bothF & V and PA. The other three possible change patterns, largechange in F & V and moderate change in PA, large change in PAand moderate change in F & V, and moderate change in bothF & V and PA were infrequent, in the range of 1%–3%.
Discussion
The two self-help interventions were generally successful ininducing change in F & V intake and PA, suggesting thatHypothesis 1 was confirmed. The effects were somewhatgreater for F & V than for PA. With regard to Hypothesis 2, theimpact of adding the MI component varied, depending on thehealth behavior. For F & V, there was a clear additive effect forthe MI component, whereas for PA, MI did not appreciablyenhance the impact of the self-help culturally targeted materi-als. There have been two previous MI interventions withhealthy populations that addressed either PA or F & V intake(Harland et al., 1999; Resnicow, Jackson, et al., 2001). Thestudy addressing PA did not show any significant 1-year effectson activity (Harland et al., 1999), whereas F & V intake wassignificantly improved in the Eat for Life study (Resnicow,Jackson, et al., 2001). It is possible that MI may be moreeffective in modifying diet than are PA behaviors. Anotherpossible explanation for the stronger effects of the MI inter-vention on F & V compared with PA in this study may be that,
Table 2Baseline and Posttest Means and Standard Errors: Fruit and Vegetable Intake in Servings Per Day
Group
2-item FFQ 19-item FFQ 36-item FFQ Composite of the 3 FFQs
Baseline Posttest Baseline Posttest Baseline Posttest Baseline Posttest
M SE M SE M SE M SE M SE M SE M SE M SE
Control 3.67 0.14 3.99 0.14a 4.46 0.31a 5.21 0.31a 4.66 0.27 4.50 0.28a 4.27 0.19 4.55 0.19a
SH 3.58 0.13 4.07 0.13 5.11 0.28 5.42 0.27a 4.26 0.25 4.92 0.25b 4.32 0.18 4.80 0.18b
SH � MI 3.70 0.13 4.63 0.13b 4.69 0.29 6.01 0.29b 4.31 0.27 5.23 0.27b 4.23 0.19 5.30 0.19b
Note. Groups with different subscripts differ at p � .05. Differences within a column are for posttest only. Posttest probabilities are adjusted for baselinevalues. FFQ � food frequency questionnaire; SH � culturally tailored self-help intervention; MI � motivational interviewing.
344 RESNICOW ET AL.
for F & V, counselors delivered the intervention with greaterfidelity than they did for the PA intervention. We are currentlycoding audio tapes of our intervention to determine the extent towhich this may have occurred. It is also possible that theself-help materials for the PA intervention were more salientthan were the dietary intervention materials, leaving little ad-ditional opportunity for change through MI. Finally, the findingthat 62% of participants at Call 1 and 57% at Call 3 (the twopoints of the MI intervention when choice was provided)elected to work on F & V rather than PA suggests that individ-uals may have been more willing to modify their F & V intakethan their PA.
An aim of the study was to examine the effect of intervening ontwo health behaviors simultaneously. Of the 61% of participantsacross the three intervention groups that exhibited at least a mod-erate behavior change (defined as � .25 SDs), 72.0% (44.0% of61.0%) made a change in one health behavior but no change in theother. Of the remaining participants who made at least a moderatechange in either, 17.0% (10.6% of 61.0%) made a large change inboth F & V and PA, and 8.0% (4.9% of 61.0%) made a largechange in one behavior and a moderate change in the other.
This pattern was generally consistent across the three experi-mental groups; however, the percentage making any change wasgreatest in the group that received both the tailored materials andMI (70.0%). In this group, the percentage making only a singlechange was similar to the full sample, 69.0% (48.5%/70.2%).However, 23.0% (15.9%/70.2%) made a large change in bothF & V and PA. Thus, the full intervention appeared to increaseboth the absolute and relative percentage making dual behaviorchange.
The net effect on F & V intake in this project was similar,although slightly smaller, to the effect observed in the Eat for Lifestudy, a church-based intervention that included three MI callsdelivered by dietitians (Resnicow, Coleman-Wallace, et al., 2000;Resnicow, Jackson, et al., 2001). When addressing multiple healthbehaviors simultaneously, there is the concern of subadditivity;that is, the effect of multiple intervention components deliveredsimultaneously may be less potent than when delivered separately(Appel et al., 2003). Subadditivity can result from the cognitive orbehavioral complexity or having to modify more than one behav-ior. If participants felt overwhelmed by being asked to modifymultiple behaviors, efficacy could be reduced, which could lower
Table 3Baseline and Posttest Means and Standard Errors: Physical Activity in Minutes Per Week
Group
All activities � 3 METs Exercise items
Baseline Posttest Baseline Posttest Baseline Posttest
M SE M SE M SE M SE M SE M SE
Control 874.6 53.5 826.2 53.6a 449.4 33.8 400.9 33.8a 191.7 25.6 163.3 25.6a
SH 769.5 49.0 927.7 47.8b 397.4 30.9 505.1 30.1b 163.5 23.4 215.3 23.0b
SH � MI 793.9 51.4 935.9 50.7b 409.0 32.3 493.3 31.8b 162.9 24.8 247.5 24.5b
Note. Groups with different subscripts differ at p � .05. Differences within a column are for posttest only. Posttest probabilities are adjusted for baselinevalues. METs � metabolic equivalent tasks; SH � culturally tailored self-help intervention; MI � motivational interviewing.
Table 4Change From Baseline to 1-Year Follow-Up in Fruit and Vegetable (F & V) Intake and Physical Activity by Self-ReportedIntervention Component Use Groups
Intervention component3 FFQs (servings
per day; M)All activities
(min per week)� 3 METs
(min per week)Exercise items(min per week)
Used cookbookNo 0.38* 72.21* 34.50* 29.14*Yesa 1.01 224.91 146.07 110.63
Watched F & V videoNo 0.58* 175.81 93.35 69.47Yesb 1.07 163.49 109.10 92.48
Used activity guideNo 0.46* 83.83* 54.34* 37.37*Yesc 1.09 265.26 173.33 130.33
Watched activity videoNo 0.39* 138.89 79.56 58.89Yesb 1.12 206.62 135.95 99.84
Used pedometerNo 0.60* 96.06 48.97* 47.88*Yesd 1.17 219.59 152.24 112.86
Note. FFQ � food frequency questionnaire; METs � metabolic equivalent tasks.a Used at least one recipe. b Watched at least most of the video. c Read at least most of activity guide. d Used at least a few days per week.* p � .05.
345HEALTHY BODY HEALTHY SPIRIT

motivation and decrease behavioral persistence (Bandura, 1997).Given that the effects on F & V observed here were similar tothose observed when we intervened exclusively on F & V with asimilar intervention (Resnicow, Jackson, et al., 2001), it does notappear that subadditivity occurred to any substantial degree in thistrial.
The present project utilized trained master’s- or doctoral-levelpsychologists to deliver the MI intervention, whereas our priorstudy used trained dietitians. That both professional groups wereable to effect significant behavior change suggests that MI may bebroadly applicable, at least among health professions. Future stud-ies are needed to determine the feasibility and impact of usingother health professionals to deliver MI interventions. If provencost-effective, managed care or other health care delivery systemsmay be willing to provide similar services to effect chronic diseasebehaviors among their members.
MI researchers and practitioners have begun to distinguish full-blown MI from other permutations (Rollnick et al., 2002). Ourintervention, though deeply rooted in MI, should, on the basis ofthe criteria delineated by Rollnick et al., perhaps be more accu-rately labeled brief advice or behavior change counseling ratherthan classic MI, which entails greater training and supervision ofcounselors as well as more intensive client contact (Rollnick et al.,2002).
Diet and activity outcomes were not modified by income, edu-cation, age, or gender, indicating that the intervention workedsimilarly across these various sociodemographic groups. This find-ing is important, as it suggests that tailoring interventions by theseparameters may not be needed, and MI has broad applicability.
The study has several limitations and threats to validity. It ispossible that the reported increase in F & V intake and PA in theintervention groups was an artifact of social desirability bias.Intervention participants, particularly those in Group 3 who re-ceived the MI calls, may have overreported behavior change atposttest, due to the increased amount of interpersonal contact theyreceived. In addition to bias, the self-reported measures used maynot have been sensitive to change. Although self-reported F & Vintake and PA were significantly correlated at baseline with ob-
jective validity measures, that is, serum carotenoids and cardio-vascular fitness, and these validity coefficients were in the range ofother prior studies, the magnitude of the correlations were none-theless small to moderate. Low validity and reliability limits theability to detect change.
Participants were recruited by liaisons in each church using aquota sampling framework, for example, first come/first serve.Therefore, it is possible that study participants were not represen-tative of the entire church population. We do not have sufficientinformation from the participating churches to empirically exam-ine the issue of sampling bias, response rate, or representativeness,and external validity remains a concern.
A significant problem with the study is that the apparent effectsof MI on F & V intake (and to a lesser degree PA) may not havebeen due to MI per se but rather generic effects of attention orother elements of counseling not unique to MI. That is, becausethe additional MI intervention in Group 3 was not controlled forwith a similar amount of client contact in either Groups 1 or 2,the increased change in F & V intake observed in Group 3 canbe attributed to the added telephone contact rather than to MIin particular. To better determine the independent effects ofMI versus attention, it would be useful to test the effects ofan MI-based intervention to other counseling modalities holdingconstant client contact. In addition, to explore the potential con-tribution of MI to our intervention effects, we are currently codinga subset of audio-taped MI encounters to determine whethergreater fidelity to MI is related to greater changes in the targetbehaviors.
The study also has several strengths, including the relativelyhigh cohort retention rate, the large proportion of telephone callscompleted, and the inclusion of socioeconomically diverse AfricanAmericans. Consistent with several recent studies, churches appearto be an excellent setting to implement and evaluate health pro-motion programs for the African American community. The con-tinued refinement and evaluation of culturally targeted interven-tions and telephone counseling (and MI in particular) to modifychronic disease behaviors appears warranted.
Table 5Analysis of Behavior Change Patterns
Behavior change
Group
Total %Control % Self-help % Self-help � MI %
No changea F & V and PA 46.6 41.7 29.8 39.0One change groups
Large changeb F & V/no PA change 19.0 16.9 26.0 20.6Large change PA/no F & V change 8.1 9.6 9.0 8.9Moderate changec F & V/no PA change 11.3 9.9 9.3 10.1Moderate change PA/no F & V change 5.7 4.0 4.2 4.5
Dual change groupsLarge change F & V and PA 4.9 10.3 15.9 10.6Large F & V change/moderate PA change 2.8 3.0 3.5 3.1Large PA change/moderate F & V change 0.8 2.3 2.1 1.8Moderate change F & V and PA 0.8 2.3 0.3 1.2
Note. MI � motivational interviewing; F & V � the fruit and vegetable composite from three food frequency questionnaires; PA � minutes of physicalactivity on the basis of the Community Healthy Activities Model Program for Seniors.a Defined as pretest–posttest difference less than .25 standard deviation. b Defined as pretest–posttest difference greater than .50 standard deviation.c Defined as pretest–posttest difference of .25 to .50 standard deviation.
346 RESNICOW ET AL.

References
Appel, L. J., Champagne, C. M., Harsha, D. W., Cooper, L. S., Obarzanek,E., Elmer, P. J., et al. (2003). Effects of comprehensive lifestyle modi-fication on blood pressure control: Main results of the PREMIER clin-ical trial [Comment]. Journal of the American Medical Association, 289,2083–2093.
Bandura, A. (1997). Self efficacy: The exercise of control. New York:Freeman.
Baskin, M., Resnicow, K., & Campbell, M. (2001). Conducting healthinterventions in Black churches: A model for building effective partner-ships. Ethnicity and Disease, 11, 823–833.
Braithwaite, R., & Resnicow, K. (2002). Ethnicity and health: A case forcultural sensitivity. In G. L. Breslow, W. Keck, J. Last, L. Lave, & M.McGinnis (Eds.), Encyclopedia of public health (pp. 415–422). NewYork: Macmillan.
Burke, B. L., Arkowitz, H., & Menchola, M. (2003). The efficacy of MI:A meta-analysis of controlled clinical trials. Journal of Consulting andClinical Psychology, 71, 843–861.
Butler, C., Rollnick, S., Cohen, D., Bachman, M., Russell, I., & Stott, N.(1999). Motivational consulting versus brief advice for smokers ingeneral practice: A randomized trial. British Journal of General Prac-tice, 49, 611–616.
Campbell, D. R., Gross, M. D., Martini, M. C., Grandits, G. A., Slavin,J. L., & Potter, J. D. (1994). Plasma carotenoids as biomarkers ofvegetable and fruit intake. Cancer Epidemiology, Biomarkers & Pre-vention, 3, 493–500.
Coates, R., Eley, J., Block, G., Gunter, E., Sowell, A., Grossman, C., et al.(1991). An evaluation of a food frequency questionnaire for assessingdietary intake of specific carotenoids and vitamin E among low-incomeBlack women. American Journal of Epidemiology, 134, 658–671.
Dunn, C., Deroo, L., & Rivara, F. (2001). The use of brief interventionsadapted from MI across behavioral domains: A systematic review.Addiction, 96, 1725–1742.
Emmons, K., & Rollnick, S. (2001). Motivational interviewing in healthcare settings: Opportunities and limitations. American Journal of Pre-ventive Medicine, 20, 68–74.
Gillman, M. W., Cupples, L. A., Gagnon, D., Posner, B. M., Ellison, R. C.,Castelli, W. P., et al. (1995). Protective effect of fruits and vegetables ondevelopment of stroke in men. Journal of the American Medical Asso-ciation, 273, 1113–1117.
Harada, N., Chiu, V., King, A., & Stewart, A. (2001). An evaluation ofthree self-report PA instruments for older adults. Medicine and Sciencein Sports and Exercise, 33, 962–970.
Harland, J., White, M., Drinkwater, C., Chinn, D., Farr, L., & Howel, D.(1999). The Newcastle exercise project: A randomised controlled trial ofmethods to promote PA in primary care. British Medical Journal, 319,828–832.
Lasater, T., Becker, D., Hill, M., & Gans, K. (1997). Synthesis of findingsand issues from religious-based cardiovascular disease prevention trials.Annals of Epidemiology, S7, S46–S53.
Marin, G., Burhansstipanov, L., Connell, C. M., Gielen, A. C., Helitzer-Allen, D., Lorig, K., et al. (1995). A research agenda for health educa-tion among underserved populations. Health Education Quarterly, 22,346–363.
McGinnis, J., & Foege, W. (1993). Actual causes of death in the UnitedStates. Journal of the American Medical Association, 270, 2207–2212.
Miller, W., & Rollnick, S. (1991). MI: Preparing people to change addic-tive behavior. New York: Guilford Press.
Miller, W. R., & Rollnick, S. (2002). MI: Preparing people for change(2nd ed.). New York: Guilford Press.
Murray, D. (1998). Design and analysis of group randomized trials (Vol.27). New York: Oxford University Press.
Murray, D., Hannan, P., & Baker, W. (1996). A Monte Carlo study ofalternative responses to intraclass correlation in community trials: Is it
ever possible to avoid Cornfield’s penalties? Evaluation Review, 20,313–337.
Nigg, C. R., Allegrante, J. P., & Ory, M. (2002). Theory-comparison andmultiple-behavior research: Common themes advancing health behaviorresearch. Health Education Research, 17, 670–679.
Ory, M. G., Jordan, P. J., & Bazzarre, T. (2002). The Behavior ChangeConsortium: Setting the stage for a new century of health behavior-change research. Health Education Research, 17, 500–511.
Pate, R. R., Pratt, M., Blair, S. N., Haskell, W. L., Macera, C. A.,Bouchard, C., et al. (1995). PA and public health. A recommendationfrom the Centers for Disease Control and Prevention and the AmericanCollege of Sports Medicine. Journal of the American Medical Associ-ation, 273, 402–407.
Resnicow, K., Braithwaite, R., Ahluwalia, J., & Baranowski, T. (1999).Cultural sensitivity in public health: Defined and demystified. Ethnicityand Disease, 9, 10–21.
Resnicow, K., Braithwaite, R., Ahluwalia, J., & DiIorio, C. (2001). Cul-tural sensitivity in public health. In R. Braithwaite & S. Taylor (Eds.),Health issues in the Black community (2nd ed., pp. 516–542). SanFrancisco: Jossey-Bass.
Resnicow, K., Coleman-Wallace, D., Jackson, A., DiGirolamo, A., Odom,E., Wang, T., et al. (2000). Dietary change through Black churches:Baseline results and program description of the Eat for Life trial. Journalof Cancer Education, 15, 156–163.
Resnicow, K., DiIorio, C., Soet, J., Borrelli, B., Ernst, D., & Hecht, J.(2002). Motivational interviewing in health promotion: It sounds likesomething is changing. Health Psychology, 21, 444–451.
Resnicow, K., DiIorio, C., Soet, J., Borrelli, B., Ernst, D., Hecht, J., &Thevos, A. (2002). Motivational interviewing in medical and publichealth settings. In W. Miller & S. Rollnick (Eds.), MI: Preparing peoplefor change (2nd ed., pp. 251–269). New York: Guilford Press.
Resnicow, K., Jackson, A., Braithwaite, R., DiIorio, C., Blissett, D.,Perisamy, S., & Rahotep, S. (2002). Healthy Body/Healthy Spirit: De-sign and evaluation of a church-based nutrition and PA interventionusing motivational interviewing. Health Education Research, 17, 562–573.
Resnicow, K., Jackson, A., Wang, T., Dudley, W., & Baranowski, T.(2001). A motivational interviewing intervention to increase fruit andvegetable intake through Black churches: Results of the Eat for Life trial.American Journal of Public Health, 91, 1686–1693.
Resnicow, K., McCarty, F., Blissett, D., Jackson, A., Heitzler, C., Wang,T., et al. (2003). Validity of a self-report physical activity questionnaireamong African Americans. Medicine & Science in Sports & Exercise,35, 1537–1545.
Resnicow, K., Odom, E., Wang, T., Dudley, W., Mitchell, D., Vaughan, R.,et al. (2000). Validation of three food frequency questionnaires andtwenty four hour recalls with serum carotenoids in a sample of AfricanAmerican adults. American Journal of Epidemiology, 152, 1072–1080.
Resnicow, K., Soler, R., Ahluwalia, J., Butler, J., & Braithwaite, R. (2000).Cultural sensitivity in substance use prevention. Journal of CommunityPsychology, 28, 271–290.
Rollnick, S., Allison, J., Ballasiotes, S., Barth, T., Butler, C., Rose, G., etal. (2002). Variations on a theme: Motivational interviewing and itsadaptations. In W. Miller & S. Rollnick (Eds.), Motivational interview-ing (2nd ed., pp. 270–283). New York: Guilford Press.
Rollnick, S., Butler, C. C., & Stott, N. (1997). Helping smokers makedecisions: The enhancement of brief intervention for general medicalpractice. Patient Education & Counseling, 31, 191–203.
Rollnick, S., Mason, P., & Butler, C. (1999). Health behavior change: Aguide for practitioners. London: Churchill Livingstone (Harcourt Brace,Inc.).
Sabogal, F., Otero-Sabogal, R., Pasick, R., Jenkins, C., & Perez-Stable, E.(1996). Printed health education materials for diverse communities:
347HEALTHY BODY HEALTHY SPIRIT

Suggestions learned from the field. Health Education Quarterly,23(Suppl.), S123–S141.
Stewart, A., Mills, K., King, A., Haskell, W., Gillis, D., & Ritter, P. (2001).CHAMPS PA questionnaire for older adults: Outcome for interventions.Medicine & Science in Sports & Exercise, 33, 1126–1141.
Thomas, S., Quinn, S., Billingsley, A., & Caldwell, C. (1994). The char-acteristics of northern Black churches with community health outreachprograms. American Journal of Public Health, 84, 575–580.
Thompson, F. E., Kipnis, V., Subar, A. F., Krebs-Smith, S. M., Kahle, L. L.,Midthune, D., et al. (2000). Evaluation of 2 brief instruments and a food-frequency questionnaire to estimate daily number of servings of fruit andvegetables. American Journal of Clinical Nutrition, 71, 1503–1510.
U.S. Department of Health and Human Services. (1996). Physical activityand health: A report of the Surgeon General. Atlanta, GA: Centers forDisease Control and Prevention, NCCDPHP.
U. S. Department of Health and Human Services. (2000). Healthy people2010. Washington, DC: Author.
U.S. Department of Health and Human Services & National Institutes ofHealth. (1989). Churches as an avenue to high blood pressure control(89–2725). Washington, DC: NIH.
Wagner, C., & Sanchez, F. (2002). The role of values in motivationalinterviewing. In W. Miller & S. Rollnick (Eds.), Motivational interview-ing: Preparing people for change (pp. 284–298). New York: GuilfordPress.
Wargovich, M. J. (1997). Experimental evidence for cancer preventiveelements in foods. Cancer Letters, 114(1–2), 11–17.
Witte, J. S., Longnecker, M. P., Bird, C. L., Lee, E. R., Frankl, H. D., &Haile, R. W. (1996). Relation of vegetable, fruit, and grain consumptionto colorectal adenomatous polyps. American Journal of Epidemiology,144, 1015–1025.
Correction to Pressman et al. (2005)
In the article “Loneliness, Social Network Size, and Immune Response to Influenza Vaccination inCollege Freshman,” by Sarah D. Pressman, Sheldon Cohen, Gregory E. Miller, Anita Barkin, BruceS. Rabin, and John J. Treanor (Health Psychology, 2005, Vol. 24, No. 3, pp. 297–306), Figure 3 onp. 303 was incorrect. The white bar in the “Medium Network” section of the graph (labeled“N � 13”) should be gray to represent “Medium Loneliness,” and the bar to its right (labeled“N � 4”) should be white to represent “High Loneliness.”
348 RESNICOW ET AL.