Uneven advance of knowledge, uneven distribution of benefits: the world public health at a crossroad
27
1 Draft: needs English improvement Draft: needs English improvement Uneven advance of knowledge, uneven distribution of benefits: the world public health at a crossroad Guillermo Foladori 1 Introduction The turn of the millennium reveals an apparent paradox: the intensification of the globalization process, which constitutes a sure path for poor countries to overcome their historical socio-economic delay according to spokesmen from the World Bank, the World Trade Organization, and the World Health Organization, and the resurgence of several infectious diseases, which place many countries in a catastrophic situation characterized by declining populations and medieval life expectancy levels. This paradox is expressed in the crisis of the medicine production by the market. The major actors are the transnational pharmaceutical companies and the organizations that defend patients’ interests. Though the interests of these two groups are expressed through the positions of countries and international organizations, it is evident that health has become, in the last decade, one of the clearest expressions of social struggle. In this article, I will review the health crisis on an international level, and discuss two trends which are emerging: first, the privatization of the world public health system, through Private-Public-Partnerships (PPPs); and, second, greater autonomy of countries in the satisfaction of their needs through public health and against the pressure imposed by international institutions. 1. The mistaken hypothesis of the “epidemiological transition” In the last fifty years, life expectancy in the less developed countries has increased from 44 to 64 years. However, due to pandemics such as AIDS, tuberculosis, and other infectious diseases, this gain may be reversed in a few years in many countries. In sub- Sahara Africa, for example, life expectancy is expected to fall from 62 to 43 years during the next decade (Geffen, 2001). In Mozambique, life expectancy by 2010 will be about 36 years (GFRH, 2002). During the last decade, humanity has seen the rapid growth of economic and social integration and of infectious diseases. Some of these diseases are newly researched, or “emergent”, such as HIV/AIDS and the Brazilian purple fever; other diseases have been known for years, such as hantavirus, malaria, dengue, and ebola fever. Finally, others result from changes in the microbes with an antropic pressure on the ecosystem, such as tuberculosis resistant to multidrugs (Farmer, 1996). 1 Research Scholar. Center for Science, Policy, & Outcomes. Columbia University. www.cspo.org
Transcript of Uneven advance of knowledge, uneven distribution of benefits: the world public health at a crossroad
1
Draft: needs English improvementDraft: needs English improvement
Uneven advance of knowledge, uneven distribution of benefits: the world public health at a crossroad
Guillermo Foladori1
Introduction The turn of the millennium reveals an apparent paradox: the intensification of the globalization process, which constitutes a sure path for poor countries to overcome their historical socio-economic delay according to spokesmen from the World Bank, the World Trade Organization, and the World Health Organization, and the resurgence of several infectious diseases, which place many countries in a catastrophic situation characterized by declining populations and medieval life expectancy levels. This paradox is expressed in the crisis of the medicine production by the market. The major actors are the transnational pharmaceutical companies and the organizations that defend patients’ interests. Though the interests of these two groups are expressed through the positions of countries and international organizations, it is evident that health has become, in the last decade, one of the clearest expressions of social struggle. In this article, I will review the health crisis on an international level, and discuss two trends which are emerging: first, the privatization of the world public health system, through Private-Public-Partnerships (PPPs); and, second, greater autonomy of countries in the satisfaction of their needs through public health and against the pressure imposed by international institutions. 1. The mistaken hypothesis of the “epidemiological transition” In the last fifty years, life expectancy in the less developed countries has increased from 44 to 64 years. However, due to pandemics such as AIDS, tuberculosis, and other infectious diseases, this gain may be reversed in a few years in many countries. In sub-Sahara Africa, for example, life expectancy is expected to fall from 62 to 43 years during the next decade (Geffen, 2001). In Mozambique, life expectancy by 2010 will be about 36 years (GFRH, 2002). During the last decade, humanity has seen the rapid growth of economic and social integration and of infectious diseases. Some of these diseases are newly researched, or “emergent”, such as HIV/AIDS and the Brazilian purple fever; other diseases have been known for years, such as hantavirus, malaria, dengue, and ebola fever. Finally, others result from changes in the microbes with an antropic pressure on the ecosystem, such as tuberculosis resistant to multidrugs (Farmer, 1996).
1 Research Scholar. Center for Science, Policy, & Outcomes. Columbia University. www.cspo.org
2
During the second half of the twentieth century, the developed countries experienced the so called “epidemiological transition” where infectious diseases stopped being important causes of death, and cardiovascular diseases and cancer became the main concerns.2 Accompanying that process, biomedical research within the developed countries concentrated on cancer, circulatory diseases, skin problems, and other diseases associated with high living standards (Lewontin and Levins, 1996). By 2001, for instance, 10% of R&D expenditures were for cancer, 1.1 % for all vaccines, and 5% for AIDS (only 0.6% for AIDS vaccines) (Kettler & Towse, 2001). In the meantime, poor countries continued suffering from infectious diseases as important causes of mortality; even though cancer and heart disease were also major causes. Brazil is a typical example of that hybrid, and, in 2001, 32% of the total causes of death was due to problems in the circulatory system, while infectious diseases accounted for a 6% (RIPSA, 2002). Several challenges lie in the assumption that developed countries have already gone beyond the infectious diseases phase and poor countries are following the same path. In fact, infectious diseases do not recognize political borders. Their nonexistence in developed countries does not guarantee immunity, as long as they exist in other countries. A good example is HIV/AIDS, but other infectious diseases are becoming serious threats in the developed world, like Nile fever which accounted for 216 deaths in 2002 in the United States,3 or the 403 000 cases of patients with cryptosporidiosis in Milwaukee in 1993; the estimated 8 000 to 18 000 people that get legionnaires' disease annually in the United States, and others (CDC, 2002). The possibility of a premeditated introduction of infectious diseases could be a direct mechanism of terrorism. During the Korean War (1951) the United States created the Intelligence Service of Epidemics as a preventive mechanism to address that possibility. Currently, the United States government is aiming to vaccinate the population against smallpox in the next two years in fear of a terrorist attack (Connolly, 2002). Nonexistence of an infectious disease in a country does not keep it free if the disease still exists in other countries, unless ecological conditions prevent it, and these too can also change as indicated by global warming.4 Secondly, infectious diseases are strongly associated with poverty. It is not certain that the economic growth of the last decades brought a greater equality in the distribution of income.5 Several studies, on the relation between poverty, social status and diseases show a complex, but constant correlation among them. Evans, et. al. (1994) show that not only is poverty associated with disease but an equality in income distribution is correlated with
2 The concept of epidemio logical transition hides the fact that within those developed countries poor people continue suffering from other type of diseases (Farmer, 1996), or experiencing new diseases poorly investigated, like obesity in the United States (Townsend, M., et al., 2002). 3 Also thousands of wild animals, dozens of exotic species in zoos, and possibly extensive amounts of farm animals died the same year (Weiss, 2002). 4 According to the Inter-governmental Panel of the Climatic Change and the World-Health Organization, the global warming could cause the expansion of diseases transmitted between people by the bite of insects, like malaria, encephalitis and yellow fever (Theo, J.; Dana, F., 1998). 5 Although the World Bank informs that poverty stagnated in absolute terms in the last ten years, and that this would be the favorable result of globalization, other studies show that the methodology used by the World Bank, based in averages by countries, hides the inequality generated within the countries, and argue that, as a whole, inequality grew, instead of diminishing (Wade, 2001).
3
a healthy population, instead of a high income average as considered by most statistics. They also show that a spirit of progress, derived from a period of economic development and an improved society in relation to other countries is important in ameliorating its population’s life expectancy. Evans, et. al. (1994) also elaborate that under conditions of poverty a disease can fill the space of another previously eradicated disease, which questions the efficacy of unilateral policies against some diseases without accounting for the socioeconomic context.6 In the United States, Auerbach & Krimgold (2001) show that correlation between poverty and disease is also present.7 It is evident that the increase of poverty and inequality in the world or, as the World Bank argues, the constant amount of poor people in the last decade (1 200 million) with an increasing expansion of several epidemic diseases, does not bode well for Third World’s populations. It is also indicative of the correlation between poverty, inequality and disease that, in many cases, an increase on the living standard significantly reduces the presence of diseases even without health policies specifically addressed. The historical research on diseases in the eighteenth and nineteenth centuries by McKeown, for instance, shows that the incidence of the main infectious diseases in Europe and the United States was declining several decades before the introduction of vaccines and antibiotics, as a result of the increase on the living standard (Tesh, 1996). Tuberculosis, for example, being the main cause of death among young adult people, declined considerably in the industrialized countries even before the streptomycin treatment was discovered in 1943, and as a possible consequence of the general improvement of the population’s living standard. In the case of the malaria epidemic within the United States in the nineteenth century, diminishment in the following century was not a result of specific health policies, but of changes in economic structure and land use (Farmer, 1996). Thirdly, infectious diseases require a surveillance system, forecasting and continual attention. During the 1980s and 90s, economic crisis and failed health policies of the World Health Organization and several governments led to the dismantling of national health systems, and the consequent resurgence of previously controlled diseases. In 1990, UNICEF declared that 80% of the world’s children were immunized against the six main childhood diseases (diphtheria, tetanus, whooping cough, polio, measles and tuberculosis ). One decade later, the cover fell to 75%, and in 19 African countries there was a drop by 50%. In Nigeria, for example, the general coverage fell from 80% (1990) to 27% (1998); in Togo, it dropped from 100% to 54% during the same period of time. As a consequence, 3 million additional deaths were accounted per year, by diseases for which there were existing vaccines (Hardon, 2001). Fourth, globalization by its economic power changes ecosystems, allowing the substitution of some diseases by others. Rural depopulation, an outcome of agricultural
6 During 2002, Brazil had a dengue epidemic. Considering that the vector is the same for yellow fever, and that vaccination against this disease is not compulsory, Brazil is now facing the possibility of a yellow fever epidemic. By January 2003, 24 cases were reported, with 5 deaths (WHO, 2003b). 7 “income inequality and socioeconomic status are the most significant factors affecting health in this country too” (After, GFRH, 2002).

4
mechanization in some cases or of the land degradation in others, increased the rural-urban migration and the overcrowding of cities without adequate sanitary conditions and water distribution, processes that were deepened remarkably in the Third World during the 1980s and 90s. In addition, the rural landscape changed via ample zones of monoculture, drying of wetlands, docks and irrigation channels, substitution of agriculture by cattle raising, deforestation or forest expansion in replacement of agricultural lands or pasturing areas. Also, global warming can facilitate the expansion of certain tropical diseases to temperate countries. Fifth, the growth of international migration due to economic causes or wars helped the displacement of diseases.8 The commerce of merchandise increased during the last decades, giving rise to the involuntary transport of associate microbes. Air transportation carried virus and bacteria inadvertently along with its passengers and objects.9 2. Market oriented science and technology (S&T) in health A S&T policy in health must address and analyze all previously mentioned tendencies and changes, in order to orient research and development (R&D) towards social needs. But the present structure of R&D in the production of medicine is not oriented in this direction. Biomedical research is decentralized in the world. While the pharmaceutical industry does some basic research, universities, hospitals and public research centers, are conducting much of basic research. From the total R&D expenditure in 1992, more than 50% corresponds to government expenditure, while pharmaceutical industry accounts for 44% (Kettler & Towse, 2001).10 Since the 1970s, technological advances have allowed the entry of small companies into the market with two major scientific developments: the discovery of the mechanism by means of which part of a gene can be inserted into another (changing its characteristics (rDNA) and allowing the production of vaccines and medicine) and the development of techniques to fuse and multiply cells (hybridomas).
8 “The net result is that much of the TB seen in developed countries today is in immigrants. Overall 36% of TB cases in developed countries (DC) are in the foreign born, and the percentage is increasing. As expected, immigrants from countries where TB incidence is high have an increased risk of developing active TB, especially if they immigrated after age 5 when latent infection has generally been established” (Coberly, 2000). 9 “the recent U.S. invasion by Asian long horned beetles, which arrived in wood packaging from China, is expected to cost the nation as much as $ 669 billion in insect-destroyed trees in urban areas alone in coming decades” (Weis, 2002). 10 Although the data is controversial, some authors argue the strong presence of public funds in the developing of new drugs by pharmaceutical industry. “In Cockburn and Henderson (1997) the authors noted a study by Maxwell and Eckhardt (1990) of 32 innovative drugs introduced prior to 1990 which found that 62 per cent of drugs would not have been discovered or would have been much delayed without public sector input. To explore the links Cockburn and Henderson look at 21 drugs identified by two experts as ‘having had the most impact upon therapeutic practice’ between 1965 and 1992. they found that only 24 per cent (six) were developed with no public sector input into basic or applied research that was necessary to bring the product to the market place —a lower share than in the earlier paper, suggesting public sector research has become more important over time” (Kettler & Towse, 2001:16).
5
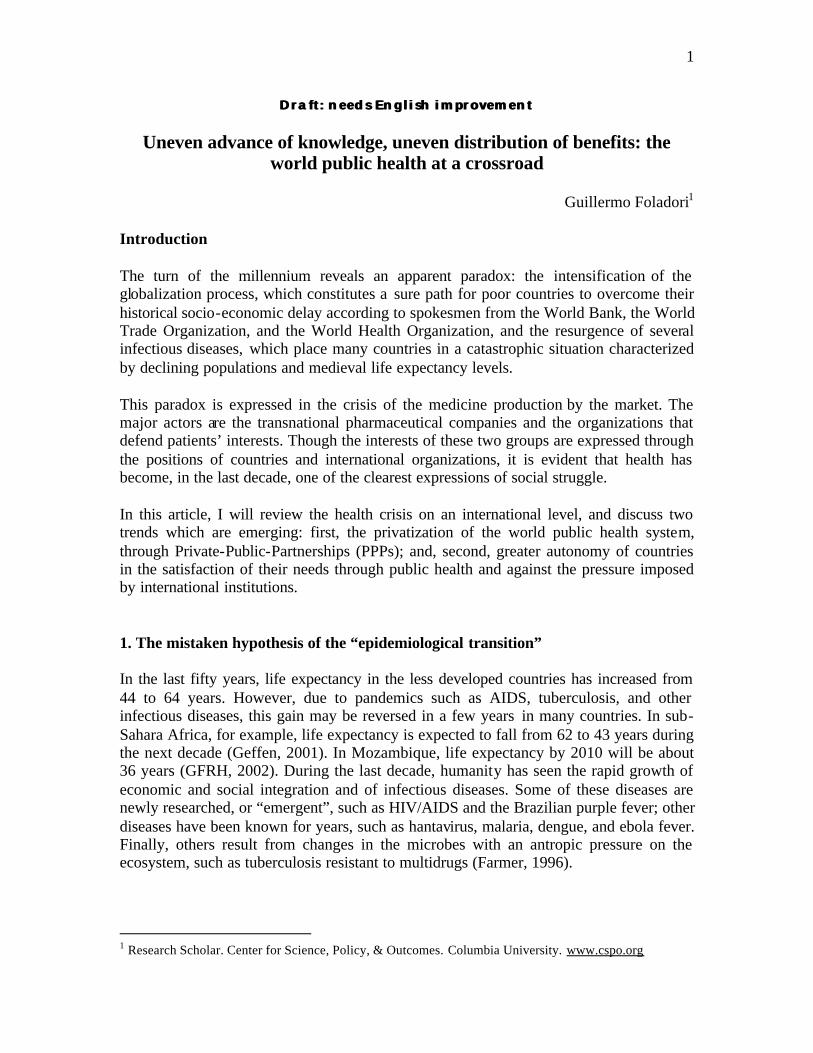
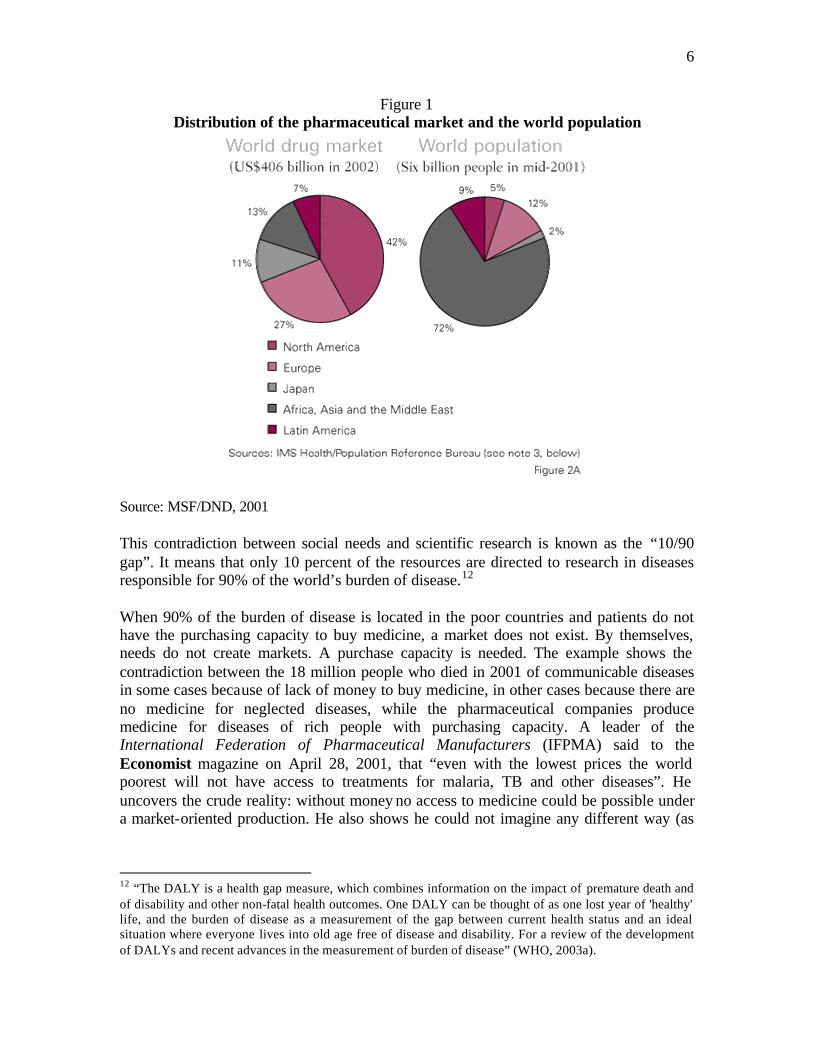
New biotechnology companies of small size arose, as the necessary capital scale for the drug’s discovery reduced (Simpson, 2002; Kettler, 2002c). New Biotechnology Firms (companies or universities) registered 41% of patents at the European Patent Office between 1987 and 1993 (Kettler & Towse, 2001:20). To discover a new drug is not the same as to develop (tests, trials, etc.) or commercialize it. Therefore, small biotechnology companies have no other alternative than to become suppliers to big multinational pharmaceutical companies (Sussex & Marchant, 2002; Kettler, 2002c; Kettler & Towse, 2001). The same is generally true with public institutions. Where the first steps in the development of a new drug were performed does not matter. The main concern is its launching to the market as a patented medicine made by large pharmaceutical corporations.11 Of a total of 196 new drugs (new chemical entities —NCE) approved by the Food & Drug Administration of the United States between 1981 and 1990, 92% were developed by the pharmaceutical industry (Montaner, et al, 2001). This does not mean investments are entirely private, or that these private companies do not use previous information developed by public institutions. Many antiretroviral AIDS drugs were invented in the United States with public funds. It is well known that the pharmaceutical industry uses direct public funds, in the form of subsidies or trials made by public institutions or indirect resources such as tax reduction, to make profits at the expense of the consumer (Love, 2000). The aim of any business is profit. The pharmaceutical industry does not escape this motive. If the production of medicine does not offer a rate of return equal to or great than that of other economic sectors, the stakeholders will sell their actions and production will fall; the greater rate of return, the more attractive the business. Figure 1 shows how the pharmaceutical market is heavily concentrated in the developed countries. North America, Japan and Europe, which have 23% of the world’s population, account for 80% of the drug market, leaving most of the low income countries practically without medical coverage.
11 “While basic science research takes place in the university or government laboratories, drug development is done almost exclusively by the pharmaceutical industry (“pharma”). The selection of promising candidate drugs by pharma is based on potential profits for the company and its shareholders, not global public health concerns. This system obviously fails the needs of poor countries” (Zumla, 2002:393).
6
Figure 1 Distribution of the pharmaceutical market and the world population
Source: MSF/DND, 2001 This contradiction between social needs and scientific research is known as the “10/90 gap”. It means that only 10 percent of the resources are directed to research in diseases responsible for 90% of the world’s burden of disease.12 When 90% of the burden of disease is located in the poor countries and patients do not have the purchasing capacity to buy medicine, a market does not exist. By themselves, needs do not create markets. A purchase capacity is needed. The example shows the contradiction between the 18 million people who died in 2001 of communicable diseases in some cases because of lack of money to buy medicine, in other cases because there are no medicine for neglected diseases, while the pharmaceutical companies produce medicine for diseases of rich people with purchasing capacity. A leader of the International Federation of Pharmaceutical Manufacturers (IFPMA) said to the Economist magazine on April 28, 2001, that “even with the lowest prices the world poorest will not have access to treatments for malaria, TB and other diseases”. He uncovers the crude reality: without money no access to medicine could be possible under a market-oriented production. He also shows he could not imagine any different way (as
12 “The DALY is a health gap measure, which combines information on the impact of premature death and of disability and other non-fatal health outcomes. One DALY can be thought of as one lost year of 'healthy' life, and the burden of disease as a measurement of the gap between current health status and an ideal situation where everyone lives into old age free of disease and disability. For a review of the development of DALYs and recent advances in the measurement of burden of disease” (WHO, 2003a).

7
the tax system and public health works in many countries) for patients with no resources to access medicine.
An indicator of the existence of neglected diseases is the results of R&D in drugs. According to a report from Doctors without Borders, between 1972 and 1997, nearly 1450 new drugs (NCE) were commercialized. But only 13 of them responded to communicable and tropical diseases and are considered as essential drugs according to the World Health Organization. Two of those 13 drugs were updated versions of pre-existing ones; two came out of military research, five from veterinary research, and one from the Chinese pharmacopoeias. So, only three drugs can be considered as genuine products of R&D from the western pharmaceutical companies (Trouiller, et al., 1999).
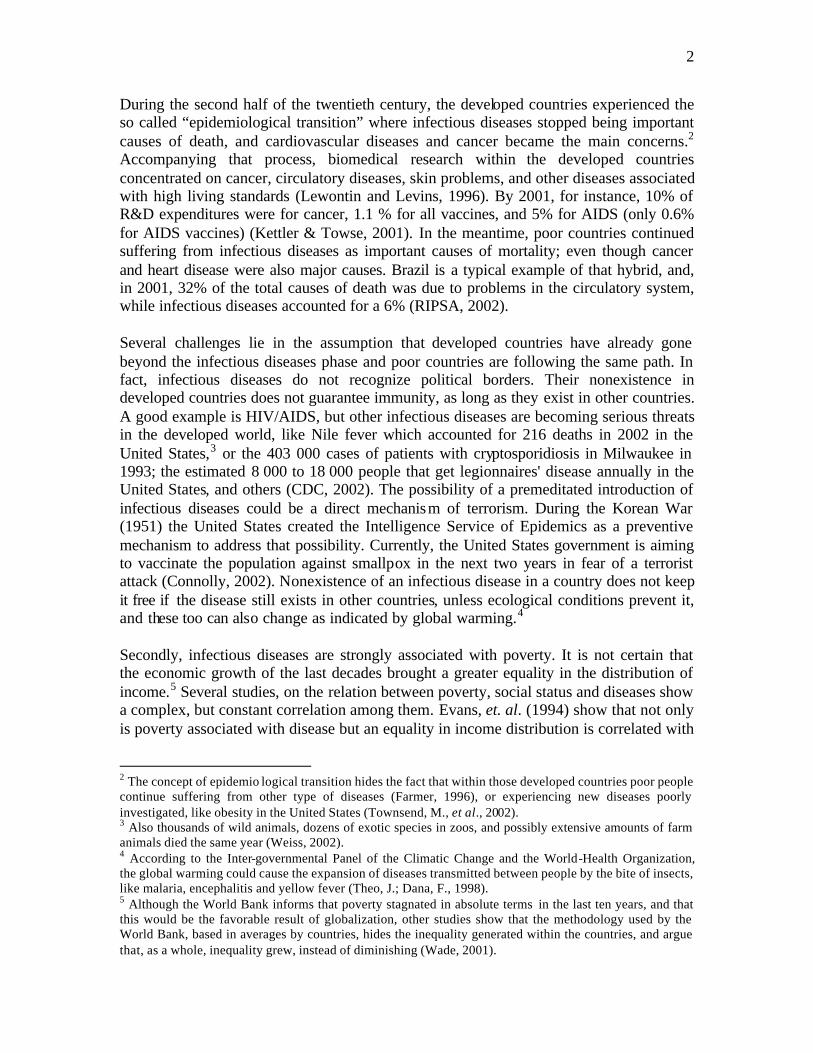
But, is it possible to blame the pharmaceutical industry for not researching and developing medicine, which does not offer profit or offers a lower profit as compared to others? During the last decades, research has tried to determine the margins of profit by the pharmaceutical industry. Although this seems simple, it is extremely complicated. The accounting can easily hide part of the profits on the wages of executives, confuse donations and subsidies with costs, not properly consider the tax benefits, the profits derived from the licenses borrowed from other industries or the contributions from public institutions, or can also not properly consider the capital’s cycle. Grabowski & Vernon (1994) concluded that only the biggest selling drugs in circulation allow recovery in costs and profits, and that many others by themselves, would yield losses. This shows that for a pharmaceutical industry, as for any company of another sector of production, the cost-benefit relation must be based on all the products, not one by one. In addition, the new drugs (NCE) take between 10 to 12 years to recover their investments and corresponding profit. The pharmaceutical industry argues that the costs of R&D are high, and that the prescribed barriers extend the time between the development of the drug and its commercialization between 8 to 10 years. The time of development, trials, tests results, and the administrative procedure of certification should be considered. They also argue, against their own interests, that property rights (which last twenty years) complicate the entrance into the market by other companies, and this increases the “wait” costs. Against the previous economic difficulties, other studies show that the pharmaceutical industry is one of the most profitable industries. Fortune magazine illustrated that in 2001 the most profitable industry was the pharmaceutical with 16.2 % return, followed by the financial sector with 11.6% (Fortune ). The industry has also been concentrated in a few multinationals in the past years, which could be an indicator of its financial strength. Kettler (2000a) compiles research on the amount of money needed to send a new drug (NCE) to the market and the increase in this cost over time (table 1). According to Zeneca, Lehman Brothers, the total cost of R&D of a new drug in the second half of the nineties reached 635 million dollars.

8
Table 1 Estimated cost to bring a “new chemical entity” into the market
Source: taken from Kettler (2002a). Note: "Years" refer to the years a product under study enters trial phase. But this information can be interpreted as a sign of vitality or weakness by the pharmaceutical industry. It is certain that the greater volume of capital invested for each new drug means a concentration of capital. The cost of production rises too, forcing more sales and more medicine to recover capital. Five hundred million dollars or more required by the pharmaceutical industry to develop a new drug can seem exaggerated if compared with public institutions (Geffen, 2001). In 1988, the National Cancer Institute of the United States spent between 2.3 and 6 million for R&D for developing new drugs.13 The PPP Global Alliance for TB Drug Development calculates that they need between 115 and 240 million dollars to develop a new drug, again far from the estimations of the pharmaceutical industry (Henry & Lexchin, 2002). Another critic of the pharmaceutical industry says that the expenses in publicity are greater than in R&D, and this is what elevates the final price (Angell, 2000). Even advertising the beneficial effects of the drug to the public and professionals is a small part of all the publicity costs.14 Those companies that participate in the Pharmaceutical Price Regulation Scheme in the United Kingdom spend five pounds for promotion for each pound spent in information (Collier & Iheanacho, 2002). But, aren’t the expenses on publicity part of the production costs for any company? The same could be said of the costs of publicity in the price of cars or cleaning products. Against the pharmaceutical industry it is also argued that much R&D is duplicative. The most striking example is the “me too drugs” or medicine that are copies of the prototypes, sent to the market by competitive companies. These medical copies have similar active principles and look forward to gain a parcel of the clients who consume the prototype. It means a waste of time and materials that could be used in the research of new prototypes 13 “It is interesting that in 1988, the US National Cancer Institute estimated that it spent on average between 2.3 and 6 million US dollars to research and develop a new drug through to the end of Phase III trials. This does not include adjustments for inflation, the opportunity costs of capital or risk adjustments for failed drugs. But even taking these into account, drug company estimates for R&D of a new drug of over US$500 million imply either massive inefficiency or exaggeration” (Geffen, 2001:15). 14 Pharmaceutical companies argue that a great part of the expenses on marketing are in education, since they have to inform doctors and health personnel about the characteristics of the medicine.
Study Years1 Total costs (millions $ 1997)
Hansen, 1979 1963-75 138
Wiggins, 1987 1963-75 156
DiMasi et. al., 1991 1970-82 312
OTA, 1993 1970-82 431
Myers and Howe, 1997 1970-82 459

9
or in the reduction on the price of existing medicine (Garanttini, 1997). Again, although it is an argument of great ethical weight, it is of little practical utility. In any branch of the economy, competitors exist who have to develop independently what other industries have already done. The duplication of efforts or “waste” of materials and human energy in researching what is already known, or in introducing small variations to existing merchandise or in changing the form and appearance for a same content is the essence of the capitalist production and economic growth. Without that, there would not be competition or market freedom. An argument against the pharmaceutical industry is also the policy of “archiving” of scientific knowledge, which does not promise clear economic results. This is the case of multidrugs resistant tuberculosis, where there have been important scientific advances since 1970, with no treatment due to the lack of expected profit (Farmer, 1999). Or, also, the legal and bureaucratic ties that companies establish with competitors in order to “win time”, or to prevent detrimental information from being made public by their own researchers or associate researchers of independent centers (Collier & Iheanacho, 2002).15 Or the mechanisms for “evergreening” patents (extending the patent’s life) by means of registering the same drug for different treatments, legal claims for actions upon undergoing patents that can extend the period for a month or more. (Henry & Lexchin, 2002; Barret, 2001; Angell, 2000). Or, also, mechanisms to extend an already approved medicine for different treatments without the necessary new bureaucratic procedure, helped by loopholes within the law (Armstrong & Forelle, 2002). In order to try to solve this contradiction between ethical principles and economic logic, some authors argue that we are dealing with a failure of the market. A market failure occurs when a majority of the patients do not have enough money to buy medicine or the pharmaceutical industry does not research medicine for neglected diseases. (Brundtland, 2001). But, this argument can be easily criticized. If the problem is of market failure, no sector of the economy would exist where markets do not fail, since there are 1 200 million indigents who practically cannot afford buying anything. In fact, it is not the failure of the market, but its successful operation, that results in those inequalities. In the case of medicine, contradiction acquires an ethical frame because it shows that the market-driven medicine production cannot translate its advances in S&T to address the main world health problems.16
15 The information on drug research is a pharmaceutical’s secret. Even when the drug is presented for government’s certification, the information offered is only part of the existing one, so researchers of other companies do not have access to all the information available. “Occasionally, in attempts to ensure a positive bias, companies have threatened legal action to stop nominally independent researchers from publishing negative material…Moreover, researchers who communicate negative results have faced intimidation, efforts to discredit them professionally, and threats of legal action to recover the value of lost sales. Often, the potential for such comp any intervention is written into the researcher's contract. For example, in a sample of US research centers, around 30% of contracts with researchers allowed the sponsoring company to delete information from the report and to delay publication” (Collier & Iheanacho, 2002). 16 This does not imply that market failures do not exist. They do exist. A report of the Federal Trade Commission’s Bureau of Competition (2001) contains detailed data from three companies that incurred, at the end of the nineties, in illegal monopolistic actions to avoid competition. Abbott Laboratories paid US$ 4.5 million each month during the litigation period of the patent to Geneva Pharmaceuticals in order not to

10
Beyond the discussion of the pharmaceutical industries’ profit or the trends in medicine production, the pharmaceutical industry is going through a phase of capital concentration, centralization, and space relocation. During the 1990s, a corridor has been formed in the Northeast of the United States, from Boston to the District of Columbia, where 15 headquarters of the 20 leader pharmaceutical and biotechnology industries of the world are located. While all the industries of that area have lost 220 000 jobs during the first two years of the twenty first century, the health activities have increased jobs by 50 000. Several elements justify this relocation in an area where for a century a strong base of hospitals and pharmaceutical industries already existed. The proximity of Washington DC is of importance for political lobbying. The health sector spent 209 million dollars in lobbying in 2000. It was the third lobbyist spending sector after finance (229 million) and Misc. Business (224 million). During the last presidential campaign, pharmaceutical and health products made contributions for nearly 25 million dollars, ranking in the ninth place of industries’ contributions, and in third if we summed up health professionals (CRP, 2003). In Maryland, the National Institute of Health uses public funds for basic research, which is later used by private companies. Sixteen of the main 50 U.S. medical hospitals and institutes are located in the area. Important university centers like Harvard Medicine School, Johns Hopkins, University of Pennsylvania, Massachusetts General Hospital, Center for Drug Development of the Tufts University, all contribute to the pool of necessary talent the industry needs. Pharmacia, for example, moved from London to New Jersey at the end of the 1990s and was soon bought by Pfizer. Novartis with its base in Switzerland is installing a research center in Cambridge, Massachusetts; Altana from Germany, recently opened an office in New Jersey (Leonhardt, 2002). The biggest medicine market is also in the United States with the highest prices on medicine and a health system completely privatized, constituting paradise for the pharmaceutical industry and pain for the patients. 3. Recent changes in the crisis of the health market The developed countries began to explicitly worry about the diseases of the poor people as these diseases expanded to the first world or as the poor people of the developed countries organized themselves to protest for health care. A combination of both causes is the case of HIV/AIDS where, after its introduction in the United States and Europe and the demands of its patients, the pharmaceutical industry obtained important advances in a
produce the generic competitive with her drug Hytrin. Hoechst Marion Roussel (Aventis) paid to Andrx Corporation more than 80 million dollars during the litigation period of the patent, to avoid that company from entering with the competitive generic to her Cardizem CD. Schering-Plough Corporation paid 30 million dollars to Upsher-Smith Laboratories and to ESI Lederle, Inc. in order not to enter with generic versions of his product K-Dur and for the license of products of ESI. Mylan Laboratories, Inc., raised the price as a consequence of an agreement with the providers of the main active ingredients. In 1998 they raised the wholesale price of clorazepate from 11.36 to 377 dollars the bottle of 500 pills, and also of lorazepam that went from 7.3 to 190 dollars per bottle of 500 pills. The American consumers had to pay 120 millions more (Federal Trade Commission, 2001).
11
relatively short time, producing the cocktail that improves and extends life.17 But, where the diseases are restricted mainly to the Third World countries, the advances are not so fast. There are still neglected diseases with little research such as tuberculosis and malaria, and even “most neglected diseases” as Chagas disease, sleeping sickness and leishmaniasis. However, infectious diseases and parasites are responsible for more than 40% of the total burden of disease (WHO, 2002). This situation is changing for several reasons. First, patients’ organizations and NGOs that defend their interests are increasingly mobilized. This mobilization has made explicit the contradiction between the millions of patients with infectious diseases that do not have cures, or whose medicine prices are not affordable, and the representatives of the transnational pharmaceutical industry and their defenders like the World Trade Organization or the governments of the United States and other developed countries, who value profits more than humanitarian interests (Love, 2001; Angell, 2000). During the last decade, these mobilizations have made important advances, although not definitive, in their favor, damaging the economic interests of the transnational pharmaceutical corporations. Civic mobilizations have pressured countries like Brazil to produce generic medicine for HIV/AIDS treatment, thereby surpassing the regulations of intellectual property rights (TRIPS) defended by the World Trade Organization. 18 They have forced the pharmaceutical industry to lower the prices of HIV/AIDS medicine sold in some Third World countries.19 They have forced the World Trade Organization produce the Doha declaration (2001) that establishes a relaxation of its patents’ regulation, allowing countries with epidemics to produce generic medicine, competitive with name brand medicine, recognizing formally what was already going on by practical means.20 The European Parliament went further, approving in 2002, that generic medicine can be sold to Third World countries under compulsory licenses, favoring those poor countries that cannot use the right to produce generics under
17 The first 14 antiretroviral drugs for the treatment of AIDS took an average of 4 to 5 years for their development, whereas the average for a new drug is of approximately 12 years. 18 In 2001, after not reaching an agreement with Roche —producer of the drug nelfinavir— Brazil began to produce generic medicine, failing to fulfill with the agreements of the intellectual property rights(TRIP) of the World Trade Organization (Donnelly, 2001). 19 As a result of the pressure that the production of generic medicine caused, Brazil was able to negotiate with Merck a reduction of 65% in the price of Indinavir and 59% in the price of Efavirenz (part of the cocktail to fight AIDS) (Ministério da Saúde, 2002). “Pharmaceutical giants —including U.S.-based Merck, Pfizer and Bristol-Myers Squibb— admit they could sell AIDS drugs in the developing world at discounts of up to 90 percent and still turn a profit” (Galeria, 2001). 20 Some paragraphs of the Doha declaration say: “We recognize that under WTO rules no country should be prevented from taking measures for the protection of human, animal, or plant life or health… We stress the importance we attach to implementation and interpretation of the Agreement on Trade’s Related Aspects of Intellectual Property Rights (TRIPS Agreement) in a manner supportive of public health, by promoting both access to existing medicine and research and development into new medicine”. “During a national emergency such as “HIV/AIDS, tuberculosis, malaria and other epidemics” —it is permissible for a country to grant a compulsory license to a local “third party” manufacturer to supply a drug for domestic use despite the drug being under patent.” But, despite this apparent advance, actually there have been no results in the regulation of this declaration, and the United States and other developed countries insist on the position of the pharmaceutical transnational companies to limit the countries and the diseases that are included in the declaration (Loff, 2002b).
12
epidemic conditions because of the lack of domestic pharmaceutical development (Loff, 2000a). The mobilization of patients also creates great alarm. As a way to answer these claims, several organizations that try to negotiate with transnational pharmaceutical industry, public institutions and international institutions, have arisen during the last decade. They are called Public-Private Partnerships (PPPs) and have the humanitarian intention to give a solution to the problem by means of donations, and the political intention of containing mobilizations within property right rules.21 It is the case, for example, of the Global Forum for Health Research, an independent international foundation established in 1998 with the aim of narrowing the “10/90 gap” through R&D. By itself, the goal is a recognition that the market is not the best way to allocate the resources of S&T in the most vital area of humanity. But these negotiations are difficult, and in its annual report 2001-2002, the Global Forum for Health Research recognizes that eleven years after the Commission on Health Research for Development recommended the creation of the Global Forum the problems are almost at the same stage (Ramsay, 2001). The Global Alliance for Vaccines and Immunization is another example; or Medicine for Malaria Venture (Kettler, 2002b). The administrative facilities granted by the European Parliament and the government of the United States in 2002, (Rogers, 2002) so that generic medicine could enter the market once the patents expire, must be seen as a result of those social struggles, and the search to guarantee property rights making slight modifications that make market driven production of medicine more efficient. Because of the possibility of the expansion of epidemics to the developed countries, infectious diseases have become a global problem due to migrations, an increase in tourism, and also the wider international trade. Less than a century ago when there was an epidemic, all the passengers and crew were retained for quarantine in islands or isolated in establishments in ports. This is no longer possible due to the most individual, diverse and decentralized movement of international tourism. Sixteen million people die annually by infectious diseases, and although 90% of those cases occur in Third World countries, the possibility of epidemics in developed countries cannot be discarded. The crisis of the public health systems in developed countries also constitutes a threat that forced changes. Since the 1990s, the health systems of many developed countries entered in crisis, as a result of the ageing of their population and the increase in medicine’s costs (Evans, et. al., 1994). The result is that budgets are less able to maintain decent coverage for all the population. 22 In case an epidemic of a tropical disease happens, the response
21 The claims of patients are seen as expressions of political instability that could foment social revolts. A speech of the director of the World Health Organization is eloquent on this: “A world in which the divide between the rich and the poor continues to deepen; a world in which only a privileged few have access to the fruits of the technological revolution, is a world which will become ever more insecure. In the past, desperate conditions on another continent might cynically be written out of one's memory. The process of globalization has already made such an option impossible” (Brundtland, 2001). 22 The European Federation of Pharmaceutical Industries and Associations (EFPIA) considers that the expenses in drugs by the European health services in 2001 doubled the expenses of the previous decade (Rogers, 2002). The medicine expenses are, between all the health expenses, the ones that grow faster in the United States (Angell, 2000).
13
capacity of these institutions will be quite weak, because of financial reasons as well as the ignorance and lack of experience in those diseases by health personnel. This is a possibility, if we consider that many of those diseases are not exclusive of tropical countries, like malaria, that was an important cause of death in many states of the United States during the middle of the nineteenth century. Although the ecosystems have since changed, other diseases can take their place, as in the case of the tuberculosis resistant to multidrugs (Farmer, 1996). The possibility of a virus or bacteria used by terrorist is another cause of forced changes. The possibility of a war headed by the United States on Iraq has as explicit justification bio-terrorists attacks. In the United States, it is considered a national security problem, as indicated by the existence of a task force group at the Central Intelligence Agency (CIA, 2000). This possibility forces the mobilization of information, infrastructure and materials to combat possible infectious diseases. As an example, the government of the United States is planning to vaccinate all the population against smallpox, a disease supposedly eradicated. The deterioration of the work force due to epidemics also argues in favor of changes. The South African’s employers are worried about their workers contracting AIDS. The Economist (10/05/2002) writes that several mining companies began, by the year 2002, paying for medicine needed by their infected workers. Although it can mean an increase of more than 5% in the production costs, it is cheaper than to instruct new workers, without knowing how long they will be healthy. 23 Not only are the companies in operation worried about epidemics, new investments have higher risks in epidemic areas. India, a promising market for the computer industry, can see its population at risk as a result of the advance of AIDS. It is estimated that in 2010, between 20 and 25 million people will be infected. Microsoft had recently donated, through the Gate’s Foundation, 100 million dollars for AIDS treatment. But the company is also interested in economic benefits, and will invest 400 million dollars in the next three years, being the greatest investment of the company outside the United States. Market interests can sometimes subsume humanitarians’ interests (Lancet, 2002). In Holland, the non-profit organization Lange’s International Antiviral Therapy Evaluation Center is looking forward for agreements between employers and the pharmaceutical companies to deal with the cost of the worker’s illness in some countries as South Africa (Gellman, 2000b).24 This situation generates a strong contradiction between the pharmaceutical industry and other industries that consider that the government must assume its public health responsibility, even
23 Firms are beginning to see a loss of productivity, low morale, absenteeism, and the death of workers aged between 20 and 40. As skilled and experienced workers die, their firms face rising retraining costs and the loss of valuable know-how, as well as the need to deal with grief-stricken colleagues. Even for unskilled workers, there are extra hiring costs and sick-leave payments. AngloGold, for example, estimates that the virus adds as much as $6 to the $170-180 cost of producing an ounce of gold…Providing drugs, educating workers and treating infections may sometimes be a firm’s cheapest option” (Economist, 2002). 24 “after selecting simple treatment protocols, the Dutch group approached large employers in Africa. Lange reasoned that corporations facing ‘the loss of half their skilled work force’ might be better motivated, finances and organized to subsidize AIDS treatment than many host governments…” (Gellman, 2000b).
14
producing generics or find ways to reduce the price of medicine, even against the pharmaceutical industry’s interests. The general result of these changes is still unclear. Two poles seem to compete as “attractors” of the possible paths: the command of national and international pub lic funds by multinational pharmaceutical corporations through Public-Private Partnerships; or the control of the health system by the public sector. On one hand, due to the last triumph of several countries in producing generics antiretroviral for AIDS, it seems as though the pharmaceutical industry is withdrawing, and organizations that defend patients have won important victories, even though each step has lasted years during which millions have died. But that triumph is not definitive. On the other hand, governments and international organizations are pressuring the pharmaceutical industry to “come to reason” and lower their prices. This will have the advantage of guaranteeing intellectual property rights and the market oriented production of medicine. Once again, the health problem is between public and private health care institutions. 4. The rise of an innovative policy: The Public-Private Partnerships (PPPs) In 1993, during the Forty Sixth World Health Assembly, the organization decided to call for support of partnerships with the private sector and NGOs (Buse & Waxman, 2001). In 1997, a private meeting supported by the World Business Council on Sustainable Development and the presidency of the General Assembly of the UN was held where 37 participants, the majority from corporations, were invited to discuss the possibilities of multi party agreements for orienting funds.25 A year later, the World Bank and the World Health Organization announced a call for this type of agreement (Reich, 2002). PPPs are non-profit organizations that aim to integrate NGOs, members of the civil society like academics, philanthropic institutions, national and international public institutions, and the pharmaceutical companies. It is a mechanism of coordination and R&D, as well as for funding purposes. The goal is to reduce health inequality, stimulating research in the less lucrative areas, and facilitating the access for vaccines and medicine for people without the purchasing capacity. PPPs also aim to administer public funds from countries, WHO, UNICEF, World Bank or other organizations. At first sight they are humanitarian alternatives based on mutual confidence. PPPs can not be identified as a unique policy, since there are a wide variety with different management and administrative procedures. Nevertheless, the most important ones in capital and public presence (e.g. GAVI, IAVI, MMV) show the main trends. Why are these agreements necessary? Globalization brings with it a strong concentration of wealth. Several transnational corporations have annual sales superior to the domestic product of hundreds of countries. The five main pharmaceutical corporations have sales higher than the national income of the less developed 100 countries. The pressure of these corporations on the governments of the developed countries, especially on the United States has resulted in a delay in the contributions to the United Nations, and the
25 “to examine steps toward establishing terms of reference for business sector participation in the policy setting process of the UN and partnering in the uses of UN development assistance funds” (Korten, 1997).
15
resulting financial crisis. Once created, the problem, the support from the great companies becomes a question of survival for UN’s institutions. The PPP Global Alliance for Vaccines and Immunization (GAVI), created in 1999 could not have arisen without the initial contribution of the Gates Foundation with 750 million dollars, which was greater than the contributions made later by WHO and other countries and foundations. There is also one particular dogma, which considers the market as being the only way to solve allocation difficulties. So, a market failure appears when something does not correspond with expectation. To solve it, orthodox economists find but two alternatives: pull or push. The first consists on stimulating private production, the second on stimulating purchase capacity. 26 These alternatives are by means of subsidies, tax instruments, or donations that can only come from those who have money (i.e. corporations). In addition, if international public institutions do not participate, they will be out of the game, since corporations can easily sign multilateral agreements with governments and between companies, with greater impacts than the whole programs of these international institutions. But, on the other hand, it is of interest to the corporations to have the United Nations and the World Bank as partners that give an image of impartiality. Another argument considers the diseases as the cause of the lack of development (Sachs, n/d). It says that in the case of Sub-Saharan countries, epidemics as AIDS or malaria are an impediment for development, and that its immediate treatment would propel these countries on the path to development. This interpretation rests on three related ideas. First, there is a lineal causal relation between disease and poverty, so the cure of the disease will also overcome poverty. Second, the only way to solve the problem is through market mechanisms that respect patent rights. As the pharmaceutical industry has or could produce the necessary medicine and vaccines, the problem is not of push mechanisms but of the lack of internal market, this could be replaced by donations coming from PPPs. Third, these PPPs would not have the bureaucratic ties of the international institutions and could be more effective in addressing the problems for which they were created. Although the negotiations between the World Health Organization and the pharmaceutical companies for collaboration for inexpensive medicine for AIDS began in 1991, only a few small African countries reached an agreement to get subsidies medicine by the end of 2002; in the meantime, countries such as Thailand, India, China, Brazil, and others, developed their own generic medicine, a faster way than negotiating with pharmaceutical companies —highly competitive among them, and so with great internal contradictions— and the international institutions that try to command, at least in appearance, the PPPs. Many of these PPPs in the health area arose from the intellectual property rights struggle. As part of the Free Trade Agreement of the World Trade Organization (WTO), 123
26 Push mechanisms are: R&D tax credits, R&D grants, social venture capital funds, investments in clinical trial infrastructure in LDCs, or speed up the approval process. Pull mechanisms are: improve intellectual property protection for LDC medicines Reaming market exclusivity, purchase funds, price guarantees, tax credit on sales, creating functioning markets in LDCs (Kettler & Towse, 2001).

16
countries signed the agreement on intellectual property rights (TRIPS) that came into effect in 1995, although for Third World countries there is flexible deadline. That treaty forces the signatory countries to respect the period of twenty years of property rights for pharmaceutical products. During that time generic medicine, equivalent to brand patents cannot be produced and the brand has the monopoly. This advantage explains why pharmaceutical companies pressure countries to establish in their legislation intellectual property rights. Since 1993, the government of the United States, reflecting the interests of the multinational pharmaceutical industries, began to pressure the expansion of patents elsewhere (Gellman, 2000a). But several countries began producing generics. Even South Africa, after a debate in the Supreme Court, won the right to produce generic medicine, against the block formed by 39 transnational pharmaceutical companies. With this kind of action, the lucrative market of medicine came down. In the United States, AIDS treatment coasted up to 15 000 dollars per year. In other developed countries where patent rights are respected, it is not lower than 9 000 dollars annually. But Brazil is already producing the cocktail for less than 3 000 dollars and India offers it for 300 dollars. As the representative of the pharmaceutical industry of South Africa said, after the verdict against her cause, the problem is of precedent: “while South Africa may represent less than 1% of world drug sales, the precedent of allowing a government to step on drug company’s patent rights would have far-reaching effects, beyond the questions of cost and crises” (Block, 2001). A country’s declaration of health emergency and the possibility of granting compulsory licenses to produce generic medicine may expand like wild fire, causing pharmaceutical companies to lose millions of dollars. With this prospect, WHO and pharmaceutical corporations embarked on the creation of PPPs in order to resist such initiatives. As a journalist says, speaking of the licensing by Pharmacia of a drug to a nonprofit International Dispensary Association of the Netherlands, “The pact is an effort to make essential medicines available at reduced prices in the developing world while protecting the economic interests of brand-name drug markers in their profitable home markets” (Hensley, 2003). By the beginning of 2003, the data bank of the Initiative on Public-Private for Partnerships Health had registered 82 PPPs (IPPPH) that respond to diverse criteria of formation, participation and decision methods. The International AIDS Vaccine Initiative (IAVI), founded in 1996, is a PPP that tries to accelerate the development of a vaccine against HIV/AIDS. The Global Alliance for Vaccines and Immunization (GAVI), founded in 1999, has the commitment to facilitate the immunization of children from poor countries, as well as to stimulate the pharmaceutical industry to produce vaccines for neglected diseases. Another example is Medicine for Malaria Venture (MMV), also founded in 1999, as a result from conversations between the World Health Organization and the Federation of International Associations of Pharmaceutical Manufacturers (IFPMA) to develop vaccines against malaria. Through PPPs, multinational pharmaceutical companies will manage public funds. Public institutions addressing social needs through taxes seem to be a thing of the past. Nowadays social needs are becoming increasingly addressed through public funds and donations managed by private corporations. Although there is a wide diversity of
17
structures, and some PPPs could be “controlled” by the public sector, what large pharmaceutical companies try is to take control of them. This is the PPP trend. There are several doubts and criticisms of the effectiveness of PPPs (Richter, 2003; Horton, 2002; Boseley, 2002; Hardon, 2001; Hancock, 1998). Most of these could be grouped together under two considerations. One technical, the other social. From a technical point of view, PPPs extend the reductionist approach on health that the pharmaceutical industry represents. A reductionist approach on health is one that looks forward to cure a disease without considering the individual context (behavior patterns) and the ecological context (changes in the ecosystem and social relations). Facing a disease, the reductionist approach tries to develop the drug that can cure it, or the vaccine to prevent it. Nobody could negate that this approach has reached outstanding results that could be seen —at least partially— in the rise of life expectancy during the last 50 years. Nevertheless, the retreat of some health indicators in the last ten years show that a reductionist approach is not enough. An ecological approach considers that any change in the physical or social surroundings affect the pattern of exposure to a health threat, as well as the vulnerability to it (Levins, quoted by Lefkowitz, s/d); so, sometimes, positive changes in the socio-physical environment as well as preventive health policies could deal with diseases better than a medicine. This wider view of health is not in the interest of the pharmaceutical corporations, though, could not be a goal of PPPs where this industry participates. From a social point of view, PPPs reinforce the market driven production and distribution of medicine. Although it is the aim of PPPs to narrow the gap that the market failure creates, the mechanisms to reach it is by pull or push mechanisms that do not attempt to overcome market laws, but only to make them less aggressive. But it is not clear that a market driven medicine production is the best alternative. At least it has never been, since pharmaceutical industry has always been directly or indirectly subsidized by the public sector. If markets are the best way, the pharmaceutical industry should research and develop medicine alone in all stages, which has not been the case, even for rich countries’ health diseases as cancer. All PPPs are presented as win-win proposals. Everybody wins: patients, institutions, and pharmaceutical industries. But, this view hides the important differences between the actors. The interest of pharmaceutical industry is profit. This is obtained by producing medicine for ill people. Ill people with purchase capacity are, for profit purposes, better than healthy people. It is more profitable to produce medicine for long term treatments than for a vaccine applied a few times in the life of a person. This is why the vaccines market does not represent more than 1% of the pharmaceutical companies’ sales. The declaration by a leader of a pharmaceutical company is eloquent of the corporate interest: "the great thing about AIDS drugs is you have to keep taking them" (Gellman, 2000). On the contrary, the interest of public health is to have healthy people, who have a lower chance of becoming ill, need less medic ine, and less medical attention. It is evident that these are agents with opposed interests. How can these PPPs reach optimal results for all involved?
18
PPPs are agreements of stakeholders with enormous differences in power. Let’s consider that while WHO has an annually budget of approximately 1.7 billion dollars, the Bill and Melinda Gates Foundation donated more than 1 billion dollars for PPPs that take care of infectious diseases in the last three years (Gates Foundation). There are PPPs, like GAVI, that have a budget only slightly less than that of WHO. Thus, public institutions are pressed. It is evident that these PPPs do not have the same accountability as a government nor can they be questioned in the same form. Many of the ir decisions are internal. There is no transparency. Who will establish audit mechanisms to evaluate the relation between the goals and the outcomes? The beneficiaries rarely participate in the Board of Directors of the PPPs, discuss their agenda, nor have the possibility of auditing finances (Walt, 2000; Hayes, 2000). For corporations this is of great importance, not only because of the operational freedom, but also because they can use the highest drug prices to inflate the value of their participation. How, for instance, will the retroviral HIV/AIDS treatment be valued? At the US price or at the Indian value nearly 60% less? For public institutions it is a mechanism of cleaning accounts. Investment in a PPP is an expense, when investment in a public institution could be a debt. Publicity and social recognition play a fundamental role in PPPs’ interests. They raise the public image of pharmaceutical corporations, as well as of donors who will eventually use it as a platform to lobby other interests, but also for public institutions that are by this means legitimized with their people. For image concerns, PPPs prefer poor countries and diseases where an immediate and tangible improvement could be reached. But, as explained earlier, important evidence exist that show that in situations of extreme poverty and malnutrition one disease supplants another (Evans, et al, 1994). This is particularly significant in the case of vector born diseases like malaria, yellow fever, or dengue. It is possible that other diseases take the place or the eradicated one, with similar consequences on health, economics and demographics. Corporations are interested in PPPs working in selected countries, while they are guaranteed the high prices of medicine in developed countries and developing countries with large markets as in Brazil, Mexico or India. Prices of medicine in some selected African counties will diminish, propaganda will promote the brand name but, meanwhile, millions of patients in other countries, including poor people of developed countries that do not have access to cheap medicine, will be abandoned. Besides, several drugs do not give any profit in poor countries, so there is no profit risk for a large pharmaceutical company to participate in a PPP that sell cheap while maintaining high prices in developed countries. In fact, this could be an advantage. The case of Pharmacia licensing, at the beginning of 2003, the drug rescriptor to a nonprofit association will imply that several industries will start producing generics and paying 5% royalties to Pharmacia, where otherwise they would not receive anything. 27
27 “Generic makers would pay a royalty to the patent holder, 5% in the Pharmacia case, and would be encouraged to compete on price. Generics makers would be prohibited from selling against the patent holder in developed markets, however, thus preserving profit incentives for the branded drug industry… Sales on Rescriptor in the developing countries where Pharmacia kept its rights are so low the company hasn’t been required to disclose them and they aren’t immediately available…” (Hensley, 2003).
19
When relations of property maintain most of the population under misery, the eradication of a disease does not necessarily lead to development (Brown, after Muraskin, 2001).28 It is economic development that has normally lead to increases in health level and the disappearance of infectious diseases, even without health policies, as has been the case of tuberculosis and malaria in the United States and Europe (Farmer, 1996; Tesh, 1996). Large pharmaceutical companies are interested in treatment, not in prevention (Schulz-Asche, 2000). It is not accidental that several (22%) PPPs have, as a goal, HIV/AIDS treatment. Although it is the most terrible pandemic of our days, it has the great advantage, for corporate pharmaceutical industry, that the patents of many of their drugs are still effective and patients must take them for life. The epidemic also exists in rich countries. Pharmaceutical corporations participate in PPPs on new vaccines, as is the case of dengue, whose patent has Aventis-Pasteur and will be launched to market by 2004. But corporations are not willing to subsidize old infectious diseases without a patent. This creates the possibility of a country being immunized against a disease on which a new vaccine has been developed and not immunized from old diseases where vaccines have existed for a long time (Hardon, 2001). The spread of PPPs implies a dilution of health policies into several strategies, which drive to duplicate efforts or the abandonment of old health policies. Thus, while Boehringen Ingelheim through a PPP donates nevirapine to reduce the risks of mother-child HIV transmission, a food producer company, Nestlé presses WHO to lower the norms for the maternal breast- feeding period, arguing the possibility of HIV transmission, but incrementing their milk sales. A person from a seminar on PPPs once said, "while 1.7 million babies might have contracted HIV through breast milk in the last twenty years, almost certainly 30 million will have died from the replacement of breastfeeding by artificial feeding in the same time" (Rundall, 2000; Schulz-Asche, 2000). In this case, WHO as a world public institution gets tramped between a PPP in which it participates and an external corporation. Another characteristic of the participation of pharmaceutical corporations in PPPs is its “double face” policy. On one hand, they make agreements that appear in newspapers as
28 The anthropologist Brown tested the hypothesis that malaria is a barrier for development in Sardinia Island. After World War II the Rockefeller Foundation implemented a successful campaign to eradicate the mosquito vector of malaria. But the expected economic development did not come. Brown considered that malaria consumes 4.6 % of the victim’s calories while macro parasitism of the landowners consumes, in the form of rent, 62 % of the calories. With this he shows that the productive relations, and not the disease, are the determinants of poverty. And he adds: “When I first arrived ... in western Sardinia in 1976, I explained to some peasant farmers all about the “malaria Blocks Development” hypothesis and how I wanted to study about the positive economic effects of malaria eradication…. [M]ost [of the peasants] openly laughed at the argument. To them, the island’s economic problems,…were to be traced to problems of land ownership…From their perspective, malaria had been a consequence and not a cause of their poverty”…“discussions of the social and economic benefits of disease control fail to ask the question ‘development for whom?’”… [For example] the answer to this question in British Ceylon was clearly the owners of large tea plantations…[E]ven in the wake of World War III…the social and economic benefits of malaria control continued to serve the needs of [large private entrepreneurs]…with only limited advantages for impoverished rural farmers…”(Muraskin, 2001:107-108).
20
examples of their humanitarian interest. On the other hand, they continue pressing governments of developed countries to impose penalties on countries that grant compulsive licenses or produce generic medicine to treat epidemics. A report by Oxfam (2002) illustrates and quantifies this type of action on the part of the pharmaceutical companies so that the trade representative of the United States includes their demands in the agreements of the World Trade Organization or establishes bilateral sanctions with the accused countries. A letter signed on November 25, 2002, by twenty pharmaceutical companies and sent to the commercial representative of the United States is indicative of this type of threat: "An open-ended or unclear exception to the standards for patent protection would seriously undermine our interest and set back the long-term public objectives Doha was designed to achieve. We urge you to negotiate a solution that is specifically limited to the diseases that were the focus of the Doha Declaration, namely HIV/AIDS, TB and malaria and other epidemics of similar scale. In addition, it should be clear that only truly disadvantaged countries in sub-Saharan Africa be the recipient of the changed rules” (Loff, 2002). PPPs do not show any sign of sustainability. In all cases, the donations have fixed times: 2, 3, 5 years. This raises doubt as to who will finance them once the donor retires. And the question remains of whether public institutions of poor countries will be able to take care of the health administration after the PPP disappears and the administrative process becomes used to a different administrative path. Perhaps the dismantling of a PPP some years later will be, in the long term, a great advantage for pharmaceutical corporations. It is well known that specific infectious diseases can reappear after a short time of lack of surveillance, so new PPPs will be necessary, with the consequent increase of sales on the part of the pharmaceutical industry. At last there is a matter of technological path. For the pharmaceutical companies, there is no other technological alternative to treating diseases than the one they are currently researching, namely western drugs. Nevertheless, there are many other health treatments that are not main market cures, which could potentially be useful for countries with a different health tradition. PPPs, where big pharmaceutical companies participate, will not be willing to develop alternative medicine as natural cure, homeopathy, acupuncture, and others with popular acceptance in many Third World Countries; this could represent cheaper health treatments.
On the other hand, a current ideology pressures industries to improve their international image, especially in questions of environment, health at work, minorities, gender issues, etc. The donations, frequently made by transnational pharmaceutical companies to poor countries are part of this policy. The financial- investment company Calvert (2002), for example, bases its portfolio on social requirements the companies must fulfill including indigenous rights, environment, work place, and others. It is probable that in the near future, some aspects, specifically related to the commitment to public health could be added. International organizations such as the World Health Organization will argue that they can control the workings of those PPPs where they participate; this is doubtful. In
21
different procedures where the powerful pharmaceutical industry participate, such as administrative mechanisms of certification of medicine, registry or maintenance of patents, publication of articles in well known journals, international negotiations, etc., they lobby in their favor almost always winning. (Dukes, 2002; Henry & Lexchin, 2002; Montaner, et al., 2001; Barret, 2001; Galeria, 2001; Angell, 2000). Pharmaceutical and Food industries had also positioned its experts and expertise at FAO/WHO conferences, committees, publish in journals, etc., influencing WHO and FAO food and health policies (Boseley, 2003). In contrast with the PPPs path, when popular mobilizations have pressured governments for less market-oriented ways to take care the health issues, the result came faster, as in the production of generics against HIV/AIDS in Brazil, India, Thailand, China and other countries. Brazil is an eloquent example. Before 1996, medical inventions could not be patented. In 1996, under the pressure of the United States and as a result of the World Trade Organization Agreement, the Brazilian government approved the law of patents for pharmaceutical products. In 2001 under the pressure of the civil society, Brazil withdrew from the international agreement and released the production of competitive generic medicine for the treatment of HIV/AIDS (Donnelly, 2001; Harrington, 2000). Brazil started producing generics by 1998. By 2001 they were able to produce all of the components of the cocktail. The result has been multiple. The development of a national capacity to produce some drugs previously imported, with the consequent diminution of the technological dependency. There was also a strong reduction of prices, as much because generic ones are cheap (up to 5 or 6 times less) but also because transnational as Merck decided, as a consequence, to lower the price of its medicine up to 65% and 59% (Indinavir and Efavirenz respectively). From 1996 to 2001, the cost of AIDS treatment dropped 73%, according to the Ministry of Health (Vakhovskiy, 2001). Also, national production implied a reduction of the necessary budget and an economy of international currency. Besides, a reduction on prices extends the medical attention to more patients. Finally, Brazil can begin to sell its own medicine to third countries that do not have patent laws or compulsory licenses. Exactly the opposite of what the defenders of free market maintain occurred in Brazil. Instead of the regime of patents attracting capital to develop the industrial capacity to lower the price of products and to take a better care of the population, these were a consequence of abandoning the patent rules and starting generic medical production (Bermudez, et. al, 2002). This success must be compared with the suffering of South Africa that went through negotiation with the pharmaceutical transnational companies (Treatment Action Campaign). However, the effectiveness of a public production of medicine is also relative. The pressure of the transnational pharmaceutical companies on developed countries that produce generics is always present, and might have other commerce consequences. Finally, it is not the same to produce a medicine than to reach the consumer. Social controls and popular mechanisms are needed. Under strong mobilizations, significant advances are possible; however, once the civic reclamations diminish and the movements revert, it could also be expected from public policies. Third World governments under the pressure of the US could approve, in the near future, patents’ rights legislation,

22
withdrawing the advances made before. Or internal generic prices could rise as a consequence of inflation, becoming unaffordable for patients. This is why permanent mechanisms of surveillance from civil organizations are always needed. The environmental certifications performed by third parties are an attempt to control production by consumers. Similar mechanisms could arise in the health area. This could be part of a more advanced consciousness about health and globalization. Globalization processes do not have to be portrayed exclusively in terms of economic laws. Humanitarian agreements could represent a more solid way of solving some health issues. The pharmaceutical multinational companies and some developed countries consider globalization exclusively from an economic point of view. Currently, there is discussion about the implementation of the Doha declaration at the World Trade Organization. Developed countries, headed by the United States and the European Union, as well as with an active participation from Canada, Japan, Switzerland and others, defend the interests of the transnational pharmaceutical industry instead of the basic health rights of the poor. Any opposition to the agreements of the World Trade Organization is seen as an attack to globalization. However, several NGOs already express a broader view of how globalization should be considered. For example, the Treatment Action Campaign argues for globalization of human rights; in fact, an agreement signed in 1948 by more than 140 countries, should be considered superior to any agreement restricted to commerce. The declaration guarantees, among other things, medical attention. 29 The upcoming years will decide the realignment of political forces, which will have important impact on millions of sick people and future generations. Conclusions During the last years, humanity has undergone turmoil in world public health. Millions of patients, especially in the Third World, do not have access to medicine, either because they do not have the necessary purchasing capacity or because medicine for neglected diseases does not exist, and in many cases, both reasons prevail. The role of S&T is crucial in this struggle. All conflicting points of view recognize that either there is not enough research or that it does not culminate in available medicine. This is an evident demonstration that S&T in the area of medicine production is not addressed to solve the most urgent needs of the patients in the world, but only for the rich. This contradiction has led to popular mobilizations and to the formation of NGOs that defend the interests of patients. This has also led to a strong reaction from the pharmaceutical industry and the governments of the developed countries. The struggle transformed the dispute into a global matter between the rights of the rich and poor countries, as well as on a socioeconomic level within a country.
29 Article 25. 1.” (UN, 1948).

23
There is a need for an urgent solution because its strength has transformed it into a problem of public security, and the expansion of epidemics disables capital reproduction in some countries. In addition, globalization with more flow of persons and products, global warming, and the possibility of bio-terrorist attacks are worrying the health services of developed countries. These are all occurring in the context of bankruptcy of the health systems in developed countries. The United Nations, the World Health Organization, and the governments of the developed countries are looking for solutions that allow the main pharmaceutical transnational companies to maintain their control on S&T. This road will be reached if the transnational pharmaceutical companies, institutions such as the United Nations and World Bank, decide to create an important economic fund based on donations to produce drugs at cheap prices for the main neglected diseases and for selected countries. It would be a direct subsidy for the pharmaceutical industry, and it would guarantee intellectual property rights. This road is neither easy nor fast. Negotiations between the pharmaceutical industry and the World Health Organization started in 1991 for AIDS effects. Even after a decade, there have been no advancements, only grandiloquent declarations. The best way to reduce the gap between R&D for neglected diseases and social needs is the countries’ autonomy to produce or buy medicine thereby withdrawing intellectual property rights agreements. Several Third World countries already have an infrastructure, which allows them to produce medicine in huge quantities and to perform R&D on the needs of its population, if a public policy exists. International treaties between poor countries can easily update their requirements on S&T. The public sector must have, within this alterative, a fundamental weight. Everything seems to indicate that since the market is the cause of injustice, production and health care will fall into the hands of the public sector. Still this will not be enough. Organizations who respond to consumers should track and make permanent audits. References Armstrong, D.; Forelle, C. 2002. “Drugs officials may have broken rules on Neurontin”.
The Washington Post, 12/28/2002 Angell, M. 2000. “The pharmaceutical industry. To whom is it accountable?”. The New
England Journal of Medicine . Vol. 342(25). 22 June. P. 1902-1904. Auerbach, J.; Krimgold, B. 2001 Income. Socioeconomic Status and Health:
Exploring the relationships. National Policy Association. Barret, A. 2001. “Fifty Ways to Keep Your Patent” Business Week 12/07/2001
http://www.spancoalition.org/NewNews/MainNews/12.07.01M.htm [12/16/2002] Bermudez, J.; Epsztejn, R.; Oliveira, M.A.; Hasenclever, L. 2002. “Access to drugs, the
WTO TRIPS agreement, and patent protection in Brazil: trends, perspectives, and recommendations to help find our way”. MSF/DND Working Group.
Block, R. 2001. “AIDS Activists win skirmish in South Africa. Judge Widens scope of case to detriment of drug companies”. The Wall Street Journal, 03/07/2001.
24
Boseley, S. 2002. “Unhealthy influence”. The Guardian 02/06/2002. Boseley, S. 2003. “WHO ‘infilt rated by food industry’”. The Guardian 01/09/2003. Brundtland, Gro H. 2001. “Globalization as a force for better health”. 16 March
http://www.lse.ac.uk/collections/globalDimensions/lectures/globalisationAsAForceForBetterHealth/transcript.htm [12/03/2002].
Buse, K; Waxman, A. 2001. “Public-private health partnerships: a strategy for WHO”. Bulletin of the World Health Organization. 79 (8).
Calvert, 2002, www.carvertgroup.com [12/30/2002] Center for Disease, Control and Prevention (CDC). 2002.
http://www.cdc.gov/od/oc/media/wncount.htm [12/08/2002] Center for Responsive Politics (CRP). 2003. www.opensecrets.org [02/10/2003] Central Intelligence Agency (CIA). 2000. The Global Infectious Disease Threat and its
Implications for the United States. www.cia.gov/cia/publications/nie/report/nie99-17d.html [12/08/2002]
Coberly, J. 2000. "We Cannot Eliminate TB on One Continent. TB Crosses Borders". http://www.hopkins-tb.org/tb_conf/tb_conf_4.html [12/30/2002].
Collier, J. & Iheanacho, I. 2002. “The pharmaceutical industry as an informant” The Lancet, Volume 360, Issue 9343, November, 2. P. 1405-1409.
Connolly, C. 2002. “Homeland Bill Covers Smallpox Shot Liability”. U.S. Would Shield Firms, Health Workers”. The Washington Post, 11/16/2002, P. A13.
Donnelly, J. 2001. “Brazil to break AIDS drug patent”. Boston Globe 08/23/2001. www.globaltreatmentaccess.org/content/press_releases/a01/082301_BG_BRA_CL.html [12/05/2002].
Dukes, M.N.G. 2002. “Accountability of the pharmaceutical industry”. The Lancet. Vol. 360 Nov.23 p. 1682-1684.
Economist. 2002. “Aids and South African Business. Tragic caring”. The Economist. October 11/05/2002. P. 64.
Evans, R; Barer, M; Marmor, T. (eds). 1994. Why are some people healthy and others not? The determinants of Health of Populations . Aldine de Gruyter. New York.
Farmer, P. 1999. “The consumption of the Poor: tuberculosis in the late twentieth century”. [Extract from the book Infections and Inequalities] www.pih.org/library/essays/consumption.html [12/02/2002].
Farmer, P. 1996. “Social Inequalities and Emerging Infectious Diseases”. Emerging Infectious Diseases. Vol. 2 No. 4. pp 259-269.
Federal Trade Commission on “Competition in the Pharmaceutical Marketplace: Antitrust Implications of Patent Settlements”. 2001. Report presented before the Committee on the Judiciary United States Senate. Washington DC. May 24. www.ftc.gov/os/2001/05/pharmtstmy.htm [12/02/2002].
Fortune. 2002. The 2002 global 500. The world's largest corporations. www.fortune.com [12/19/2002]
Galeria, J. 2001. “Patents Ignored. Brazil puts Aids care before drug profits”. www.americas.org/News/Features/200104_Brazil_AIDS_Drugs/20010401_index.asp [12/05/2002].
Garanttini, S. 1997. “Are me-too drugs justified?” Journal of Nephrology, 10:283-94. http://www.sin- italia.org/jnonline/vol10n6/garat/garat.htm [12/09/2002].
25
Gates Foundation. www.gatesfoundation.org Gellman, B. 2000a. “An unequal calculus of life and death: as millions perished in
pandemic, firms debated access to drugs; players in the debate over drug availability and pricing”. Washington Post. 12/27/2000.
Gellman, B. 2000b. “A turning point that left millions behind; drug discounts benefit few while protecting pharmaceutical companies’ profits series: death watch: aids, drugs and Africa 2/3. The Washington Post. 12/28/2000
Geffen, N. 2001. “Pharmaceutical Patents, Human Rights and the HIV/AIDS Epidemic”. TAC discussion document. www.tac.org.za [12/19/2002]
Global Forum for Research Health (GFRH). 2002. The 10/90 Report on Health Research 2001-2002. Global Forum for Health Research. www.globalforumhealth.org [12/04/2002].
Grabowski, H; Vernon, J. 1994. “Return to R&D on new drug introductions in the 1980s”. Journal of Health Economics 13:383-406.
Hancock, T. 1998. “Caveat partner: reflections on partnership with the private sector”. Health Promotion International. Vol. 13. No. 3. pp. 193-195. Oxford University Press.
Hardon, A. 2001. “Immunization for all? A critical look at the first GAVI partners meeting”. HAI-Lights. Hai Europe. Vol. 6, No. 1. www.haiweb.org/pubs/hailights/mar2001/mar01_lead.html [12/30/2002]
Harrington, M. 2000. “Brazil: What Went Right? The Global Challenge of Access to Treatment & the Issue of Compulsory Licensing”. 10th National Meeting of People Living with HIV and AIDS. Rio de Janeiro, Brazil. 3 November 2000. http://www.aidsinfonyc.org/tag/activism/brazil.html [12/10/2002].
Henry, D.; Lexchin, J. 2002. “The pharmaceutical industry as a medicine provider”. The Lancet. Vol. 360. Nov. 16. pp 1590-1595
Hensley, S. 2003 “Pharmacia nears generics deal on AIDS drug for poor nations”. The Wall Street Journal, 01/24/2003
Horton, R. 2002. “WHO: the casualties and compromises of renewal”. The Lancet. Vol. 359. May 4. P: 1605-1611.
Initiative on Public-Private Partnerships for Health (IPPPH). www.ippph.org Kettler, H. 2002a. “Updating the cost of a New Chemical Entity”. The Office of Health
Economics. www.ohe.org/updating.htm [11/30/2002]. Kettler, H. 2002b. “Narrowing the gap. Between provision and need for medicine in
developing countries”. The office of health economics. www.ohe.org/narrowing_the_gap.htm [12/05/2002].
Kettler, H. 2002c. “Consolidation and competition in the pharmaceutical industry”. The office of health economics. www.ohe.org/consolidation.htm [11/30/2002]
Kettler, H; Towse, A. 2001. “Public private partnerships”. CMH working paper series. No. WG2:21.
Korten, D. 1997. “The United Nations and the Corporate Agenda”. www.globalpolicy.org/reform/korten.htm [12/30/2002]
Lancet. 2002. “Editorial”. The Lancet, Vol. 360 N. 9346. Nov. 23. www.thelancet.com [12/01/2002].
Lefkowitz, B. S/d “Why human ecology is good for your health”. www.inequality.org/ecology2.html [interview to a Richard Levins] [02/10/2003].

26
Leonhardt, D. 2002. “Growing health care economy gives Northeast a needed boost”. The New York Times. 12/30/2002.
Lewontin, R.; Levins, R. 1996. “El regreso de las viejas enfermedades y el nacimiento de las nuevas”. Ecología Política. No. 12. Barcelona.
Loff, B. 2002a. “World Trade Organization wrestles with access to cheap drugs solution”. The Lancet. Vol. 360. Nov. 23. P. 1670.
Loff, B. 2002b. “No agreement reached in talks on access to cheap drugs”. The Lancet. Vol. 361. 12/14/2002.
Love, J. 2001. “US consumer groups respond to industry capitulation in South Africa Drug case”. www.cptech.org/ip/health/sa/CPTEA04192001.html [12/05/2002].
Love, J. 2000. “How much does it cost to develop a new drug”. www.cptech.org/up/health/econ/howmuch/html [12/05/2002].
Medecins Sans Frontiers (MSF)/Drugs for Neglected Diseases Working Group (DND). 2001. Fatal Imbalance. The crisis in research and development for drugs for neglected diseases. Geneva. www.msf.org
Ministerio da Saúde (Brasil). 2002. National STD/AIDS Program. Brazil. “Universal Access to Antiretroviral Therapy: The Brazilian Experience. Ministério da Saúde. Brasil.
Montaner, J.; O'Shaughnessy, M.; Schechter, M. 2001. “Industry-sponsored clinical research: a double-edged sword”. The Lancet, Volume 358, Issue 9296, P. 1893-1895.
Muraskin, W. 2001. Vaccines for developing Economies. Who will pay? The Albert B. Sabin Vaccines Institute. New Canaan, CT.
Oxfam. 2002. “US bullying on drug patents: one year after Doha”. Oxfam Briefing Paper 33. Washington D.C.
Ramsay, S. 2001. “No closure in sight for the 10/90 health-research gap”. The Lancet Vol. 358 issue 9290, Oct. 20, P. 1348.
Rede Interagencial de Informações para a saúde (RIPSA). 2002. “IDB 2001 Brasil. Indicadores Demográficos e Socioeconômicos”. Ministerio da Saúde. Brasilia. DF.
Reich, M. 2002. “Public-Private Partnerships for Public Health”. In: Reich, M. (ed). 2002. Public-Private Partnerships for Public Health. Harvard University Press. Cambridge, Massachusetts.
Richter, J. 2003. “’We the Peoples’ or ‘We the Corporations’? Critical reflections on UN-business ‘partnerships’”. IBFAN/GIFA. www.ibfan.org www.gifa.org [02/23/2003].
Rogers, A. 2002. “European Parliament approves pharma law overhaul”. The Lancet Vol. 360 issue 9343, Nov. 2. P. 1397-1398.
Sachs, J. n/d “Health spending and the poverty trap”. www.dse.de/ef/web02/sahcs.htm [12/19/2002].
Simpson, H. 2002. “Biotechnology and the Economics of Discovery in the Pharmaceutical Industry”. The office of Health economics. www.ohe.org/biotechn.htm [12/02/2002].
Sussex, J.; Marchant, N. 2002. “Risk and return in the Pharmaceutical Industry”. The Office of Health Economics. www.ohe.org/riskand.htm [12/30/2002]
27
Theo, J., Dana, F. 1998. “Changes in the distribution of dengue transmission under climate warming scenarios”. www.nal.usda.gov/ttic/tektran/data/000007/07/0000070756.html [08/12/2002].
Tesh, S. N. 1996. Hidden Arguments. Political Ideology and Disease Prevention Policy. Rutgers University Press. New Brunswick, New Jersey.
Treatment Action Campaign (TAC). www.tac.org.za Trouiller, P; Torreele, E.; Olliaro, P.; White, N.; Foster, S.; Wirth, D.; Pécoul, B. 2001.
“Drugs for neglected diseases: a failure of the market and a public health failure?” Tropical Medicine & International Health, 6 (11), 945-951.
Trouiller, P., Battistella, C., Pinel, J., Pecoul. 1999. “Is orphan drug status beneficial to tropical disease control? Comparison of the American and future European orphan drug acts”. Tropical Medicine and International Health. Vol. 4. No 6. June. P.412-420.
Townsend, M., Kaiser, L., Melgar-Quinonez, H., Crawford, P., Fujii, M., Feldman, N. 2002. “Food insecurity is differentially related to overweight among low-income Latina mothers and the ir children”. [Research Project not published. Department of Nutrition. University of California-Davis]
United Nations (UN). 1948. Declaración Universal de los Derechos Humanos. http://www.un.org/spanish/aboutun/hrights.htm [12/19/2002]
Vakhovskiy, A. 2001. “Winning the war on AIDS, Brazil Style”. 10/08/2001. Dartmouth Free Press. www.uwire.com/content/topops081001001.html [12/18/2002]
Wade, R. 2001. “The Rising Inequality of World Income Distribution”. Finance & Development. Vol. 38. No. 4. www.imf.org/external/pubs/ft/fandd/2001/12/wade.htm [12/08/2002]
Weiss, R. 2002. “West Nile’s Winding Toll”. The Washington Post, 12/28/2002 World Health Organization (WHO). 2002. World Health Report 2002. www.who.org World Health Organization (WHO) 2003a.
http://www.who.int/whr2001/2001/main/en/boxes/box2.2.htm [12/25/2002] World Health Organization (WHO) 2003b. “Weekly epidemiological record”. No. 4, 78.
www.who.int/wer [01/28/2003] Zumla, A. 2002. “Reflexion & Reaction” —correspondence— The Lancet. Vol. 2, July.