ULTRASOUND OF THE ABDOMEN IN THE ADULT HORSE
11
ULTRASOUND OF THE ABDOMEN IN THE ADULT HORSE Kate Chope, VMD Tufts University Cummings School of Veterinary Medicine 200 Westboro Road, North Grafton, MA, USA 01536 INTRODUCTION: Ultrasound of the abdomen in large animals is performed for a variety of indications and can provide valuable diagnostic information. However, it is important to remember that due to the size of the large animal abdomen and the presence of normally gas filled viscera, only a portion of the entire abdomen is visualized. General indications for abdominal ultrasound include acute or chronic colic, chronic weight loss, diarrhea, fever of unknown origin, abnormal mass on rectal examination, hyperfibrinoginemia, abnormalities of specific organ profiles, and search for abdominal metastasis. Text framed with **** is FYI only. TECHNIQUE AND PREPARATION: The abdomen of the horse is evaluated transcutaneously from the paralumbar fossa to about the sixth intercostal space bilaterally, and along ventral midline. Examination from the rectal window is also performed when indicated. Proper patient preparation is essential to obtaining a diagnostic quality scan. Whenever possible, the animal should be clipped with a number 40 blade (surgical) clipper, the skin cleaned and gel applied. Large animals are not generally fasted for sonographic evaluation. Fig 1: Area for abdominal scan A variety of probes should be used if available, with the majority of the abdomen best evaluated with a lower frequency abdominal probe (3.5-5.0 MHz sector or convex) and a slightly higher (5.0-8.0 MHz sector/convex/microconvex) probe. Care should be taken to change, depth, frequency and probes when necessary to obtain both a high detail and complete view of the abdomen. Organs typically seen on examination of the right side of the abdomen include: cecum, right dorsal colon, right ventral colon, right kidney, liver, and duodenum. Small intestine and spleen may be seen infrequently. Organs typically seen on the left side of the abdomen include left kidney, left dorsal colon, left ventral colon, spleen, stomach, and liver. The ventral colon,
Transcript of ULTRASOUND OF THE ABDOMEN IN THE ADULT HORSE

ULTRASOUND OF THE ABDOMEN IN THE ADULT HORSE
Kate Chope, VMD Tufts University Cummings School of Veterinary Medicine
200 Westboro Road, North Grafton, MA, USA 01536 INTRODUCTION: Ultrasound of the abdomen in large animals is performed for a variety of indications and can provide valuable diagnostic information. However, it is important to remember that due to the size of the large animal abdomen and the presence of normally gas filled viscera, only a portion of the entire abdomen is visualized. General indications for abdominal ultrasound include acute or chronic colic, chronic weight loss, diarrhea, fever of unknown origin, abnormal mass on rectal examination, hyperfibrinoginemia, abnormalities of specific organ profiles, and search for abdominal metastasis.
Text framed with **** is FYI only.
TECHNIQUE AND PREPARATION:
The abdomen of the horse is evaluated transcutaneously from the paralumbar fossa to about the
sixth intercostal space bilaterally, and along ventral midline. Examination from the rectal window is also performed when indicated. Proper patient preparation is essential to obtaining a diagnostic
quality scan. Whenever possible, the animal should be clipped with a number 40 blade (surgical)
clipper, the skin cleaned and gel applied. Large animals are not generally fasted for sonographic evaluation.
Fig 1: Area for abdominal scan
A variety of probes should be used if available, with the majority of the abdomen best evaluated
with a lower frequency abdominal probe (3.5-5.0 MHz sector or convex) and a slightly higher (5.0-8.0 MHz sector/convex/microconvex) probe. Care should be taken to change, depth,
frequency and probes when necessary to obtain both a high detail and complete view of the abdomen.
Organs typically seen on examination of the right side of the abdomen include: cecum, right dorsal colon, right ventral colon, right kidney, liver, and duodenum. Small intestine and spleen
may be seen infrequently. Organs typically seen on the left side of the abdomen include left kidney, left dorsal colon, left ventral colon, spleen, stomach, and liver. The ventral colon,
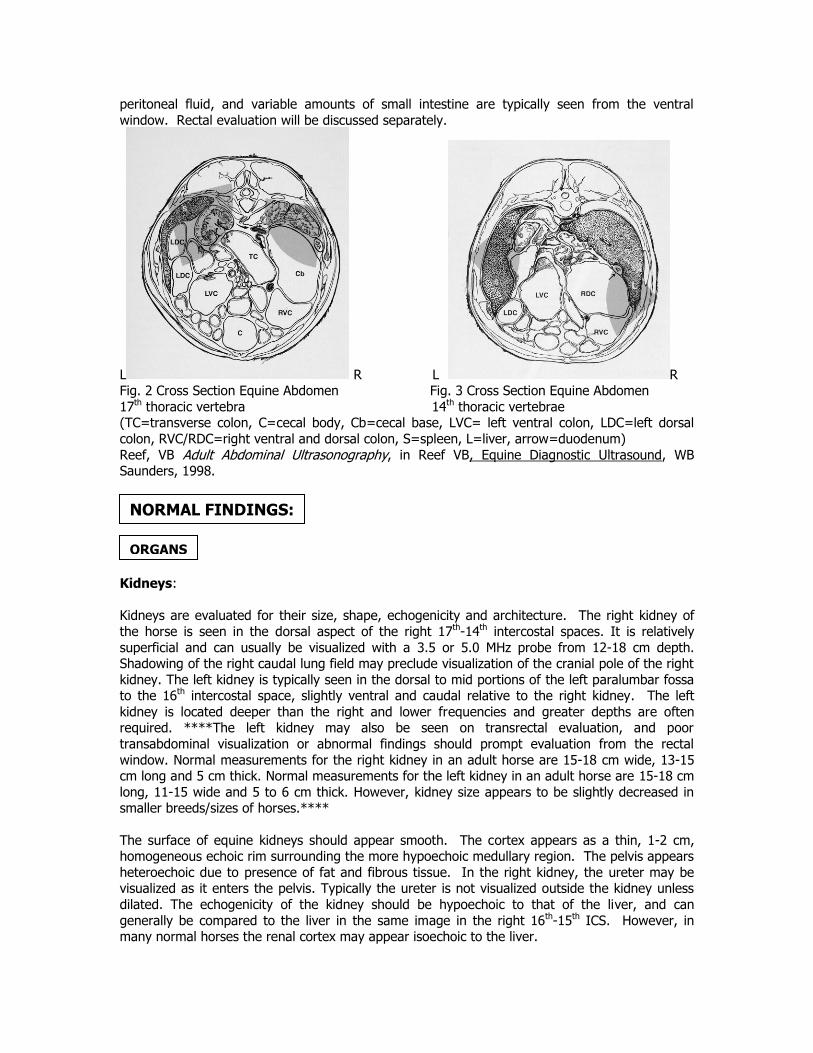
peritoneal fluid, and variable amounts of small intestine are typically seen from the ventral
window. Rectal evaluation will be discussed separately.
L R L R Fig. 2 Cross Section Equine Abdomen Fig. 3 Cross Section Equine Abdomen
17th thoracic vertebra 14th thoracic vertebrae (TC=transverse colon, C=cecal body, Cb=cecal base, LVC= left ventral colon, LDC=left dorsal
colon, RVC/RDC=right ventral and dorsal colon, S=spleen, L=liver, arrow=duodenum)
Reef, VB Adult Abdominal Ultrasonography, in Reef VB, Equine Diagnostic Ultrasound, WB Saunders, 1998.
Kidneys:
Kidneys are evaluated for their size, shape, echogenicity and architecture. The right kidney of
the horse is seen in the dorsal aspect of the right 17th-14th intercostal spaces. It is relatively
superficial and can usually be visualized with a 3.5 or 5.0 MHz probe from 12-18 cm depth. Shadowing of the right caudal lung field may preclude visualization of the cranial pole of the right
kidney. The left kidney is typically seen in the dorsal to mid portions of the left paralumbar fossa to the 16th intercostal space, slightly ventral and caudal relative to the right kidney. The left
kidney is located deeper than the right and lower frequencies and greater depths are often required. ****The left kidney may also be seen on transrectal evaluation, and poor
transabdominal visualization or abnormal findings should prompt evaluation from the rectal
window. Normal measurements for the right kidney in an adult horse are 15-18 cm wide, 13-15 cm long and 5 cm thick. Normal measurements for the left kidney in an adult horse are 15-18 cm
long, 11-15 wide and 5 to 6 cm thick. However, kidney size appears to be slightly decreased in smaller breeds/sizes of horses.****
The surface of equine kidneys should appear smooth. The cortex appears as a thin, 1-2 cm, homogeneous echoic rim surrounding the more hypoechoic medullary region. The pelvis appears
heteroechoic due to presence of fat and fibrous tissue. In the right kidney, the ureter may be visualized as it enters the pelvis. Typically the ureter is not visualized outside the kidney unless
dilated. The echogenicity of the kidney should be hypoechoic to that of the liver, and can
generally be compared to the liver in the same image in the right 16th-15th ICS. However, in many normal horses the renal cortex may appear isoechoic to the liver.
ORGANS
NORMAL FINDINGS:
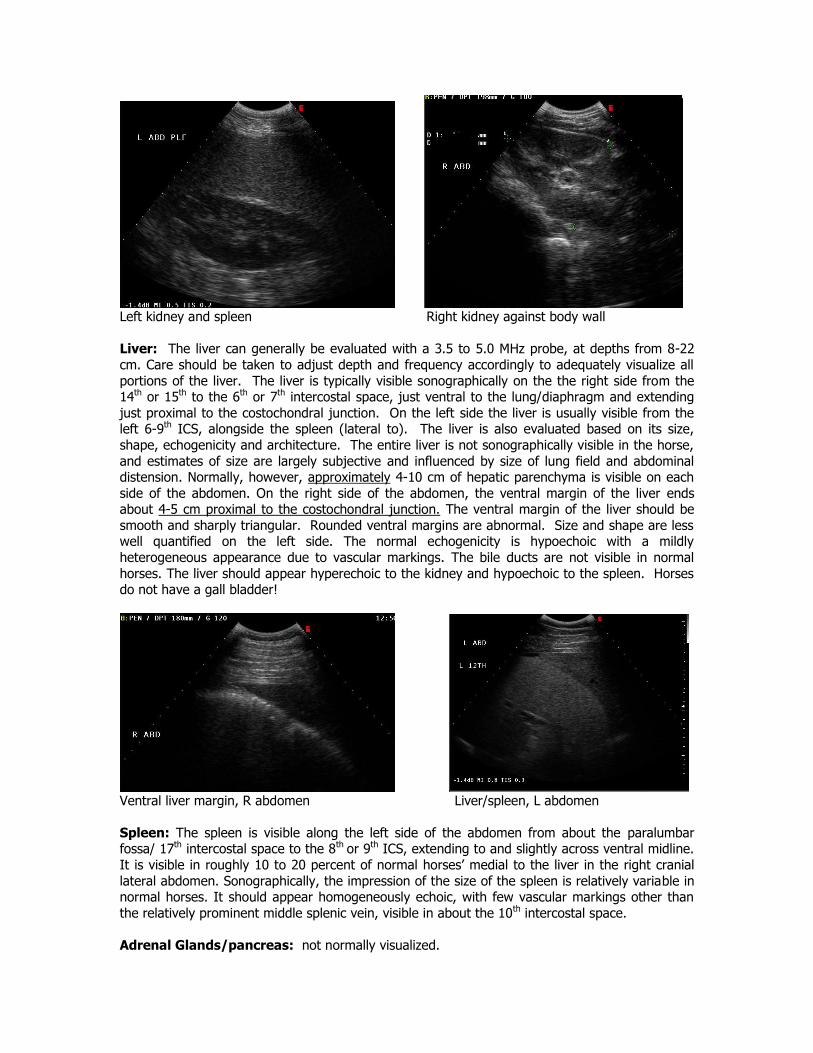
Left kidney and spleen Right kidney against body wall
Liver: The liver can generally be evaluated with a 3.5 to 5.0 MHz probe, at depths from 8-22
cm. Care should be taken to adjust depth and frequency accordingly to adequately visualize all
portions of the liver. The liver is typically visible sonographically on the the right side from the 14th or 15th to the 6th or 7th intercostal space, just ventral to the lung/diaphragm and extending
just proximal to the costochondral junction. On the left side the liver is usually visible from the left 6-9th ICS, alongside the spleen (lateral to). The liver is also evaluated based on its size,
shape, echogenicity and architecture. The entire liver is not sonographically visible in the horse,
and estimates of size are largely subjective and influenced by size of lung field and abdominal distension. Normally, however, approximately 4-10 cm of hepatic parenchyma is visible on each
side of the abdomen. On the right side of the abdomen, the ventral margin of the liver ends about 4-5 cm proximal to the costochondral junction. The ventral margin of the liver should be
smooth and sharply triangular. Rounded ventral margins are abnormal. Size and shape are less well quantified on the left side. The normal echogenicity is hypoechoic with a mildly
heterogeneous appearance due to vascular markings. The bile ducts are not visible in normal
horses. The liver should appear hyperechoic to the kidney and hypoechoic to the spleen. Horses do not have a gall bladder!
Ventral liver margin, R abdomen Liver/spleen, L abdomen
Spleen: The spleen is visible along the left side of the abdomen from about the paralumbar fossa/ 17th intercostal space to the 8th or 9th ICS, extending to and slightly across ventral midline.
It is visible in roughly 10 to 20 percent of normal horses’ medial to the liver in the right cranial
lateral abdomen. Sonographically, the impression of the size of the spleen is relatively variable in normal horses. It should appear homogeneously echoic, with few vascular markings other than
the relatively prominent middle splenic vein, visible in about the 10th intercostal space.
Adrenal Glands/pancreas: not normally visualized.
The gastrointestinal viscera are evaluated for normality of location, wall thickness and
appearance, luminal contents and motility With the exception of stomach and ileum, the wall thickness of all of the gastrointestinal viscera should not exceed .3 cm. All five layers of the
bowel wall are not often visualized transabdominally. Sedation will alter intestinal motility, and should be avoided unless necessary. Mucus, fluid and gas patterns have been described for the
lumen of equine bowel.
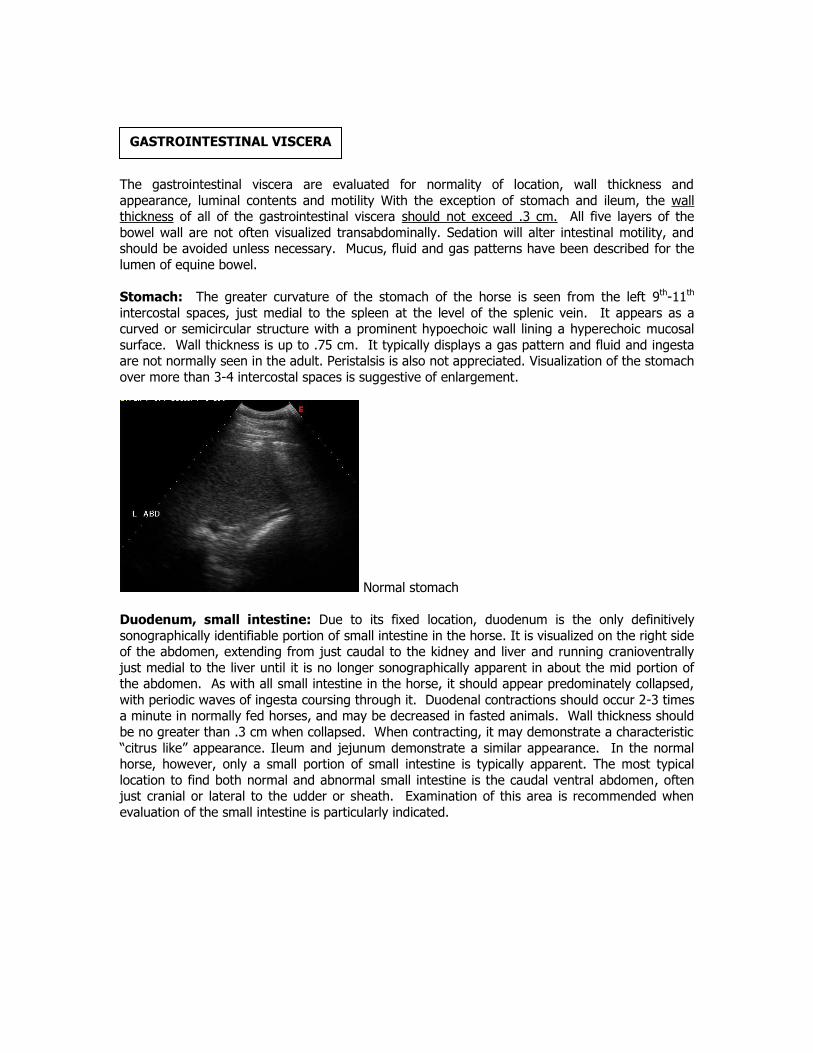
Stomach: The greater curvature of the stomach of the horse is seen from the left 9th-11th
intercostal spaces, just medial to the spleen at the level of the splenic vein. It appears as a curved or semicircular structure with a prominent hypoechoic wall lining a hyperechoic mucosal
surface. Wall thickness is up to .75 cm. It typically displays a gas pattern and fluid and ingesta are not normally seen in the adult. Peristalsis is also not appreciated. Visualization of the stomach
over more than 3-4 intercostal spaces is suggestive of enlargement.
Normal stomach
Duodenum, small intestine: Due to its fixed location, duodenum is the only definitively
sonographically identifiable portion of small intestine in the horse. It is visualized on the right side of the abdomen, extending from just caudal to the kidney and liver and running cranioventrally
just medial to the liver until it is no longer sonographically apparent in about the mid portion of the abdomen. As with all small intestine in the horse, it should appear predominately collapsed,
with periodic waves of ingesta coursing through it. Duodenal contractions should occur 2-3 times a minute in normally fed horses, and may be decreased in fasted animals. Wall thickness should
be no greater than .3 cm when collapsed. When contracting, it may demonstrate a characteristic
“citrus like” appearance. Ileum and jejunum demonstrate a similar appearance. In the normal horse, however, only a small portion of small intestine is typically apparent. The most typical
location to find both normal and abnormal small intestine is the caudal ventral abdomen, often just cranial or lateral to the udder or sheath. Examination of this area is recommended when
evaluation of the small intestine is particularly indicated.
GASTROINTESTINAL VISCERA
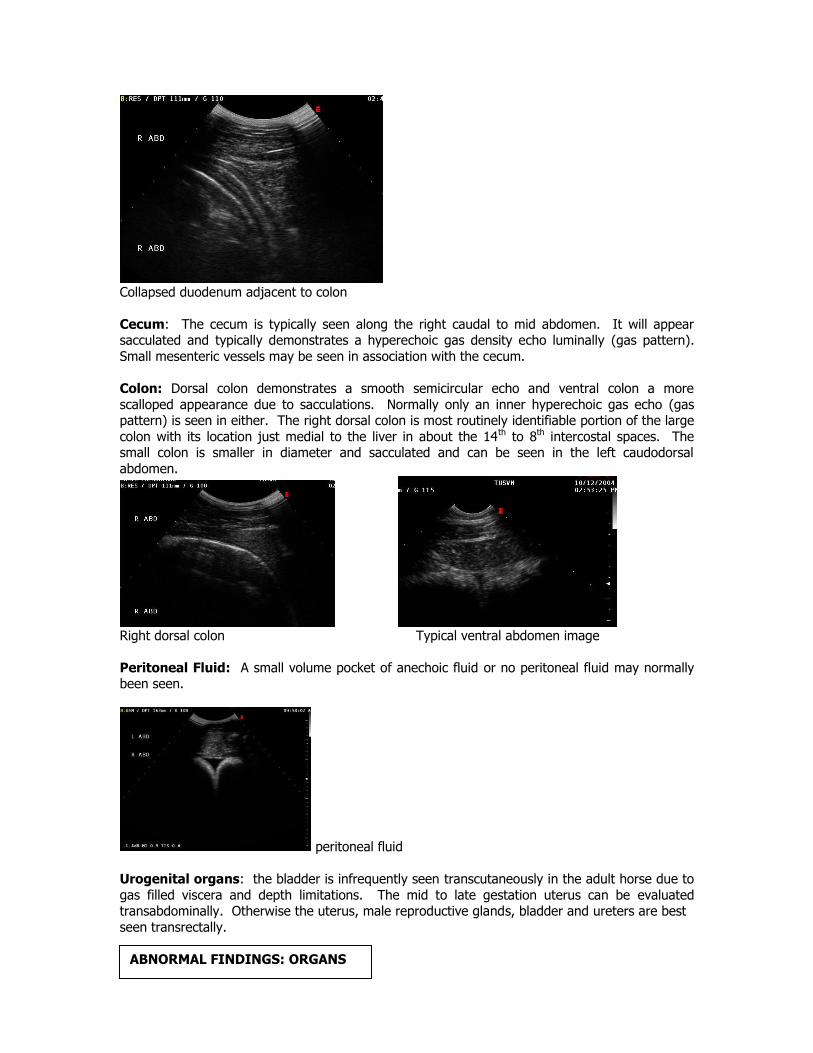
Collapsed duodenum adjacent to colon
Cecum: The cecum is typically seen along the right caudal to mid abdomen. It will appear sacculated and typically demonstrates a hyperechoic gas density echo luminally (gas pattern).
Small mesenteric vessels may be seen in association with the cecum.
Colon: Dorsal colon demonstrates a smooth semicircular echo and ventral colon a more
scalloped appearance due to sacculations. Normally only an inner hyperechoic gas echo (gas pattern) is seen in either. The right dorsal colon is most routinely identifiable portion of the large
colon with its location just medial to the liver in about the 14th to 8th intercostal spaces. The small colon is smaller in diameter and sacculated and can be seen in the left caudodorsal
abdomen.
Right dorsal colon Typical ventral abdomen image
Peritoneal Fluid: A small volume pocket of anechoic fluid or no peritoneal fluid may normally been seen.
peritoneal fluid
Urogenital organs: the bladder is infrequently seen transcutaneously in the adult horse due to
gas filled viscera and depth limitations. The mid to late gestation uterus can be evaluated transabdominally. Otherwise the uterus, male reproductive glands, bladder and ureters are best
seen transrectally.
ABNORMAL FINDINGS: ORGANS
Kidneys: The kidneys should evaluated for changes in size, shape, echogenicity and
architecture. Diffuse decreases in echogenicity are generally due to edema. Diffuse increases in echogenicity are generally due to cellular infiltrates (inflammatory, fibrotic, neoplastic). Specific
differentials for diffuse increases in echogenicity in large animals are similar to those in small.
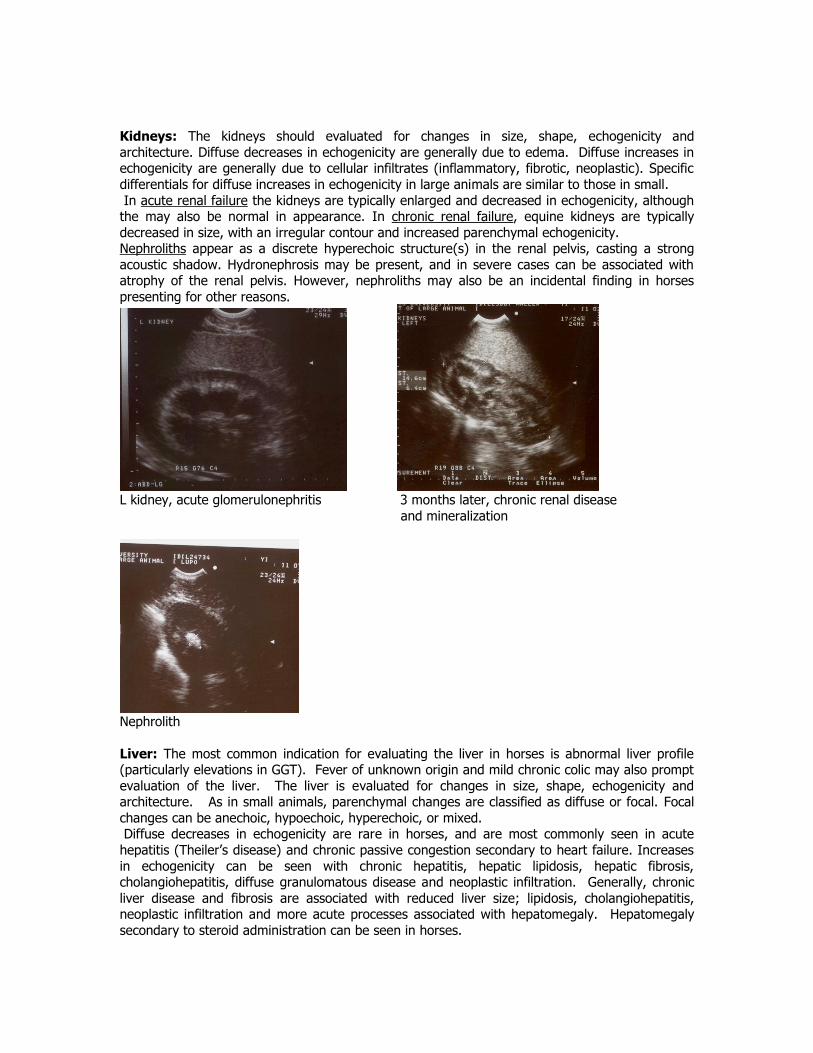
In acute renal failure the kidneys are typically enlarged and decreased in echogenicity, although the may also be normal in appearance. In chronic renal failure, equine kidneys are typically
decreased in size, with an irregular contour and increased parenchymal echogenicity. Nephroliths appear as a discrete hyperechoic structure(s) in the renal pelvis, casting a strong
acoustic shadow. Hydronephrosis may be present, and in severe cases can be associated with atrophy of the renal pelvis. However, nephroliths may also be an incidental finding in horses
presenting for other reasons.
L kidney, acute glomerulonephritis 3 months later, chronic renal disease
and mineralization
Nephrolith
Liver: The most common indication for evaluating the liver in horses is abnormal liver profile (particularly elevations in GGT). Fever of unknown origin and mild chronic colic may also prompt
evaluation of the liver. The liver is evaluated for changes in size, shape, echogenicity and architecture. As in small animals, parenchymal changes are classified as diffuse or focal. Focal
changes can be anechoic, hypoechoic, hyperechoic, or mixed. Diffuse decreases in echogenicity are rare in horses, and are most commonly seen in acute
hepatitis (Theiler’s disease) and chronic passive congestion secondary to heart failure. Increases
in echogenicity can be seen with chronic hepatitis, hepatic lipidosis, hepatic fibrosis, cholangiohepatitis, diffuse granulomatous disease and neoplastic infiltration. Generally, chronic
liver disease and fibrosis are associated with reduced liver size; lipidosis, cholangiohepatitis, neoplastic infiltration and more acute processes associated with hepatomegaly. Hepatomegaly
secondary to steroid administration can be seen in horses.
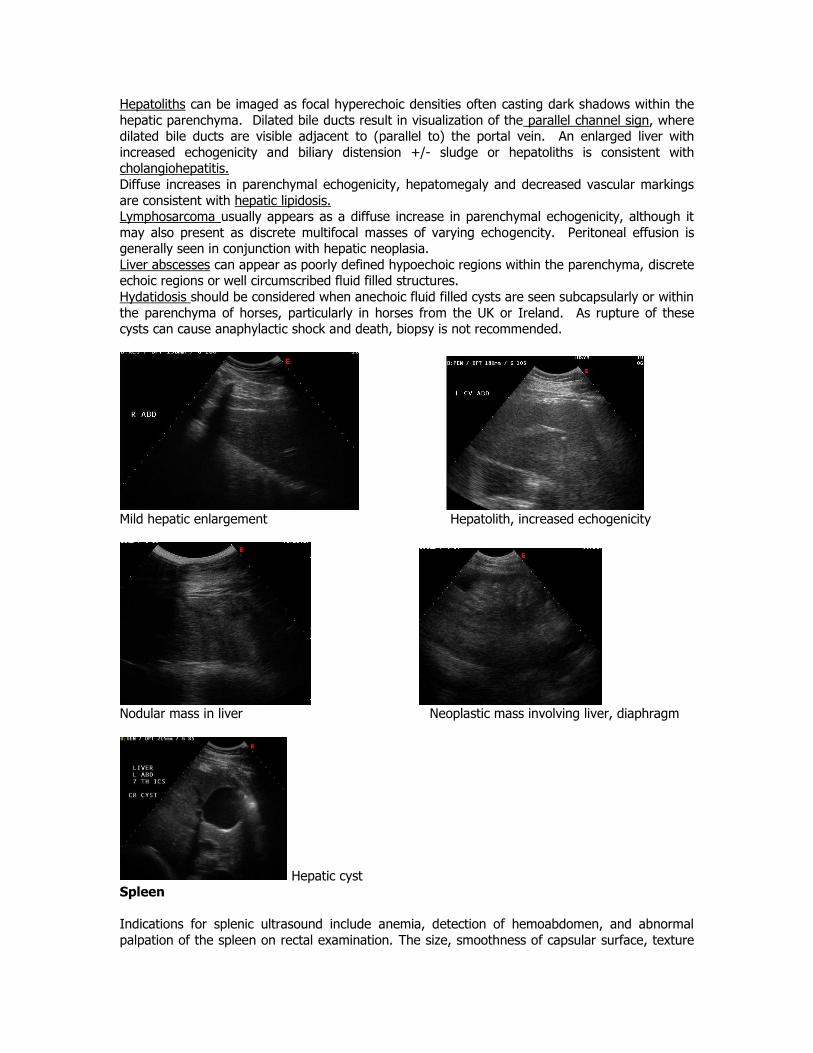
Hepatoliths can be imaged as focal hyperechoic densities often casting dark shadows within the
hepatic parenchyma. Dilated bile ducts result in visualization of the parallel channel sign, where dilated bile ducts are visible adjacent to (parallel to) the portal vein. An enlarged liver with
increased echogenicity and biliary distension +/- sludge or hepatoliths is consistent with cholangiohepatitis.
Diffuse increases in parenchymal echogenicity, hepatomegaly and decreased vascular markings
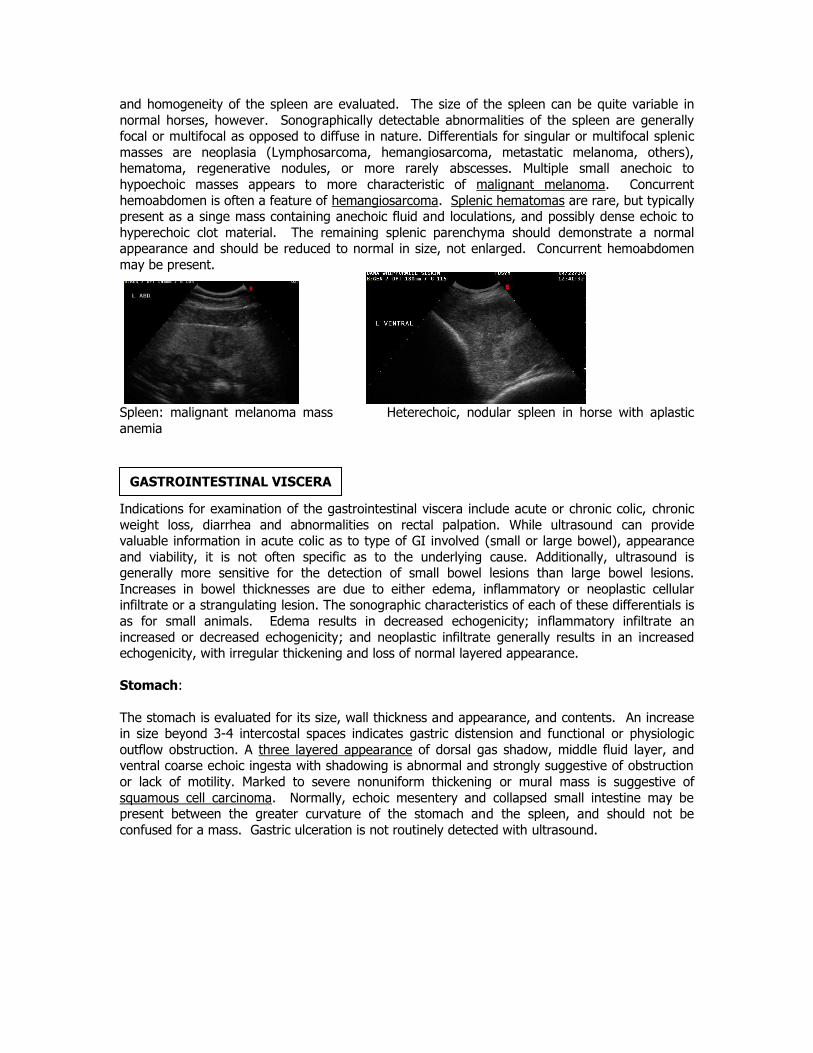
are consistent with hepatic lipidosis. Lymphosarcoma usually appears as a diffuse increase in parenchymal echogenicity, although it
may also present as discrete multifocal masses of varying echogencity. Peritoneal effusion is generally seen in conjunction with hepatic neoplasia.
Liver abscesses can appear as poorly defined hypoechoic regions within the parenchyma, discrete echoic regions or well circumscribed fluid filled structures.
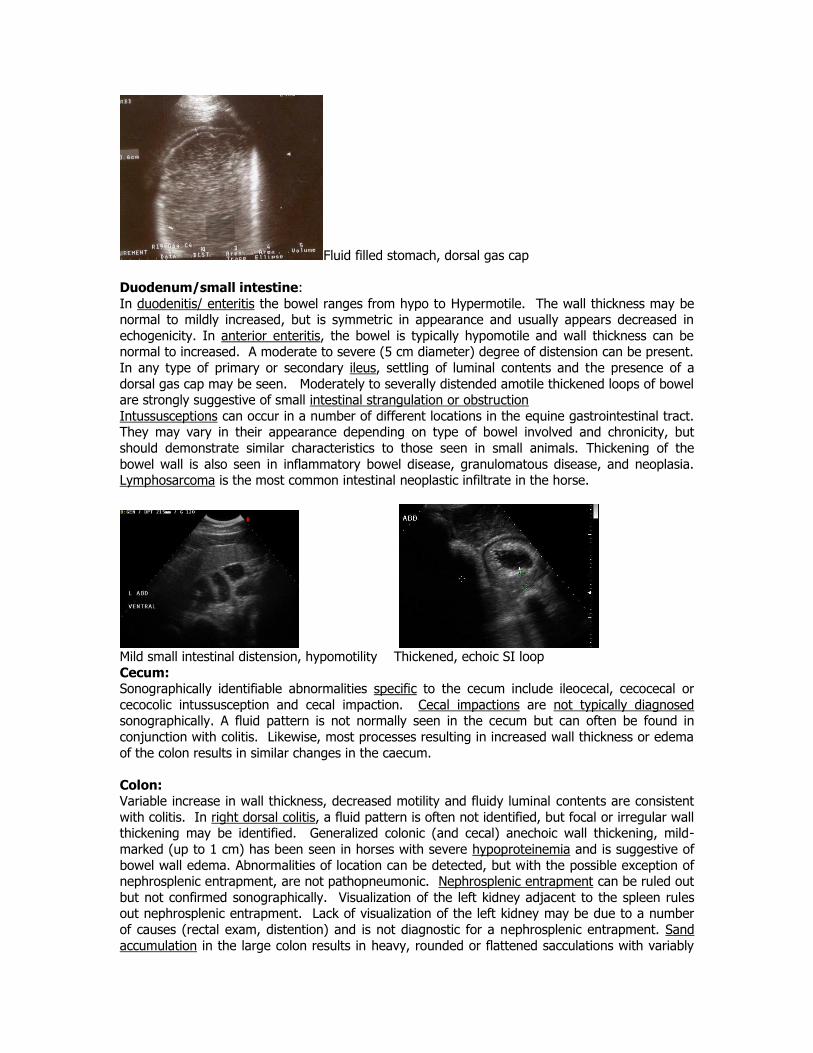
Hydatidosis should be considered when anechoic fluid filled cysts are seen subcapsularly or within
the parenchyma of horses, particularly in horses from the UK or Ireland. As rupture of these cysts can cause anaphylactic shock and death, biopsy is not recommended.
Mild hepatic enlargement Hepatolith, increased echogenicity
Nodular mass in liver Neoplastic mass involving liver, diaphragm
Hepatic cyst Spleen
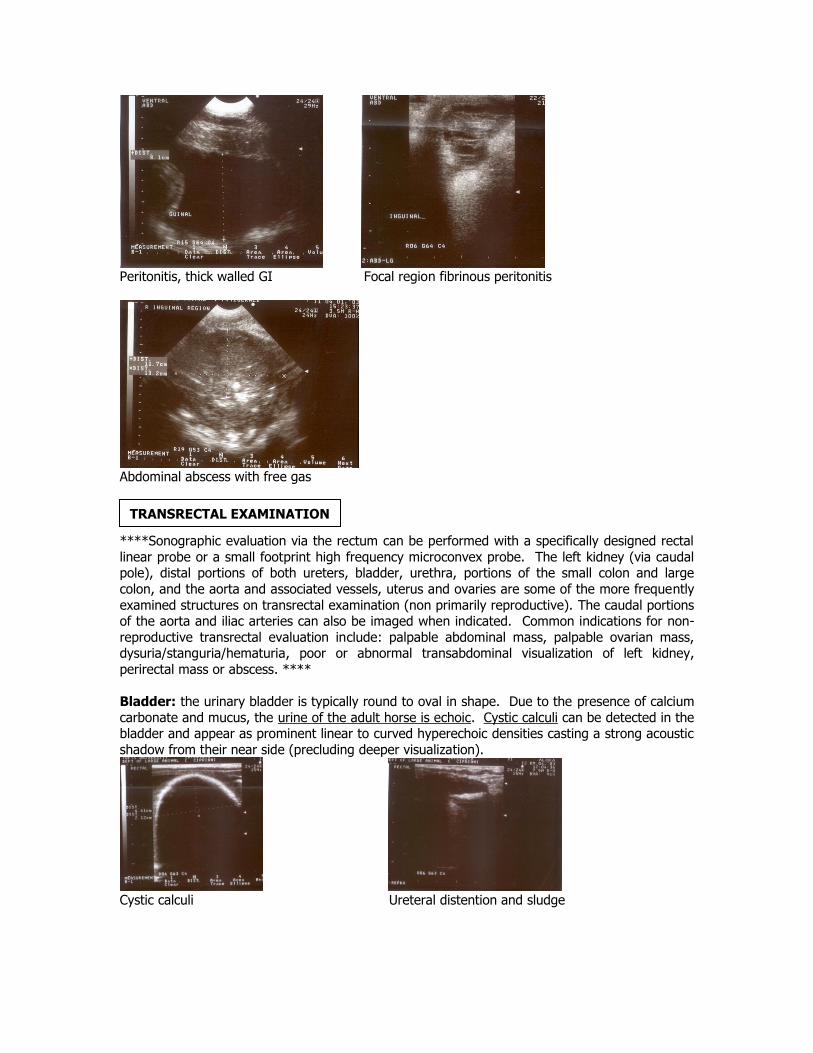
Indications for splenic ultrasound include anemia, detection of hemoabdomen, and abnormal
palpation of the spleen on rectal examination. The size, smoothness of capsular surface, texture
and homogeneity of the spleen are evaluated. The size of the spleen can be quite variable in
normal horses, however. Sonographically detectable abnormalities of the spleen are generally focal or multifocal as opposed to diffuse in nature. Differentials for singular or multifocal splenic
masses are neoplasia (Lymphosarcoma, hemangiosarcoma, metastatic melanoma, others), hematoma, regenerative nodules, or more rarely abscesses. Multiple small anechoic to
hypoechoic masses appears to more characteristic of malignant melanoma. Concurrent
hemoabdomen is often a feature of hemangiosarcoma. Splenic hematomas are rare, but typically present as a singe mass containing anechoic fluid and loculations, and possibly dense echoic to
hyperechoic clot material. The remaining splenic parenchyma should demonstrate a normal appearance and should be reduced to normal in size, not enlarged. Concurrent hemoabdomen
may be present.
Spleen: malignant melanoma mass Heterechoic, nodular spleen in horse with aplastic
anemia
Indications for examination of the gastrointestinal viscera include acute or chronic colic, chronic
weight loss, diarrhea and abnormalities on rectal palpation. While ultrasound can provide valuable information in acute colic as to type of GI involved (small or large bowel), appearance
and viability, it is not often specific as to the underlying cause. Additionally, ultrasound is generally more sensitive for the detection of small bowel lesions than large bowel lesions.
Increases in bowel thicknesses are due to either edema, inflammatory or neoplastic cellular infiltrate or a strangulating lesion. The sonographic characteristics of each of these differentials is
as for small animals. Edema results in decreased echogenicity; inflammatory infiltrate an
increased or decreased echogenicity; and neoplastic infiltrate generally results in an increased echogenicity, with irregular thickening and loss of normal layered appearance.
Stomach:
The stomach is evaluated for its size, wall thickness and appearance, and contents. An increase in size beyond 3-4 intercostal spaces indicates gastric distension and functional or physiologic
outflow obstruction. A three layered appearance of dorsal gas shadow, middle fluid layer, and ventral coarse echoic ingesta with shadowing is abnormal and strongly suggestive of obstruction
or lack of motility. Marked to severe nonuniform thickening or mural mass is suggestive of
squamous cell carcinoma. Normally, echoic mesentery and collapsed small intestine may be present between the greater curvature of the stomach and the spleen, and should not be
confused for a mass. Gastric ulceration is not routinely detected with ultrasound.
GASTROINTESTINAL VISCERA
Fluid filled stomach, dorsal gas cap
Duodenum/small intestine:
In duodenitis/ enteritis the bowel ranges from hypo to Hypermotile. The wall thickness may be normal to mildly increased, but is symmetric in appearance and usually appears decreased in
echogenicity. In anterior enteritis, the bowel is typically hypomotile and wall thickness can be normal to increased. A moderate to severe (5 cm diameter) degree of distension can be present.
In any type of primary or secondary ileus, settling of luminal contents and the presence of a
dorsal gas cap may be seen. Moderately to severally distended amotile thickened loops of bowel are strongly suggestive of small intestinal strangulation or obstruction
Intussusceptions can occur in a number of different locations in the equine gastrointestinal tract. They may vary in their appearance depending on type of bowel involved and chronicity, but
should demonstrate similar characteristics to those seen in small animals. Thickening of the
bowel wall is also seen in inflammatory bowel disease, granulomatous disease, and neoplasia. Lymphosarcoma is the most common intestinal neoplastic infiltrate in the horse.
Mild small intestinal distension, hypomotility Thickened, echoic SI loop
Cecum: Sonographically identifiable abnormalities specific to the cecum include ileocecal, cecocecal or
cecocolic intussusception and cecal impaction. Cecal impactions are not typically diagnosed sonographically. A fluid pattern is not normally seen in the cecum but can often be found in
conjunction with colitis. Likewise, most processes resulting in increased wall thickness or edema
of the colon results in similar changes in the caecum.
Colon: Variable increase in wall thickness, decreased motility and fluidy luminal contents are consistent
with colitis. In right dorsal colitis, a fluid pattern is often not identified, but focal or irregular wall thickening may be identified. Generalized colonic (and cecal) anechoic wall thickening, mild-
marked (up to 1 cm) has been seen in horses with severe hypoproteinemia and is suggestive of
bowel wall edema. Abnormalities of location can be detected, but with the possible exception of nephrosplenic entrapment, are not pathopneumonic. Nephrosplenic entrapment can be ruled out
but not confirmed sonographically. Visualization of the left kidney adjacent to the spleen rules out nephrosplenic entrapment. Lack of visualization of the left kidney may be due to a number
of causes (rectal exam, distention) and is not diagnostic for a nephrosplenic entrapment. Sand
accumulation in the large colon results in heavy, rounded or flattened sacculations with variably

increased wall thickness, decreased motility and hyperechoic to “glittery” lumen contents with an
acoustic shadow.
Thickened RDC with ingesta pattern
Thick colon and clot, cecocolic intussusception Cecocolic intussusception (same horse)
Peritoneal Cavity:
Anechoic fluid typically represents a transudate, and maybe secondary to congestive heart
failure, pericarditis, hypoproteinemia or uroperitoneum. Echoic fluid is usually an exudate, and complex fluid tends to be hemorrhagic, inflammatory or neoplastic. As in hemothorax, blood in
the peritoneal cavity appears as a swirling cellular fluid which may contain echoic clot material. Hemangiosarcoma should be strongly considered in nontraumatic hemoabdomen and the spleen
carefully evaluated. Peritonitis should be strongly considered when echoic or complex peritoneal fluid is seen. Fibrinous loculations and/or free gas may be present in septic peritonitis. Bowel
wall should be carefully evaluated for compromise in any suspected septic peritonitis. Large
volumes of anechoic to complex peritoneal fluid are often present in abdominal neoplasia.
Abdominal abscesses are typically found ventrally or at the root of the mesentery, and usually appear as circumscribed masses with an echoic outer rim, loculations, and cellular fluid or debris,
which may or may not demonstrate a fluid/gas line.
Peritonitis, thick walled GI Focal region fibrinous peritonitis
Abdominal abscess with free gas
****Sonographic evaluation via the rectum can be performed with a specifically designed rectal
linear probe or a small footprint high frequency microconvex probe. The left kidney (via caudal pole), distal portions of both ureters, bladder, urethra, portions of the small colon and large
colon, and the aorta and associated vessels, uterus and ovaries are some of the more frequently
examined structures on transrectal examination (non primarily reproductive). The caudal portions of the aorta and iliac arteries can also be imaged when indicated. Common indications for non-
reproductive transrectal evaluation include: palpable abdominal mass, palpable ovarian mass, dysuria/stanguria/hematuria, poor or abnormal transabdominal visualization of left kidney,
perirectal mass or abscess. ****
Bladder: the urinary bladder is typically round to oval in shape. Due to the presence of calcium
carbonate and mucus, the urine of the adult horse is echoic. Cystic calculi can be detected in the bladder and appear as prominent linear to curved hyperechoic densities casting a strong acoustic
shadow from their near side (precluding deeper visualization).
Cystic calculi Ureteral distention and sludge
TRANSRECTAL EXAMINATION