238 00 hundred and forty-third 'tinting general conference ...
Upload
independentCategory
view
0download
0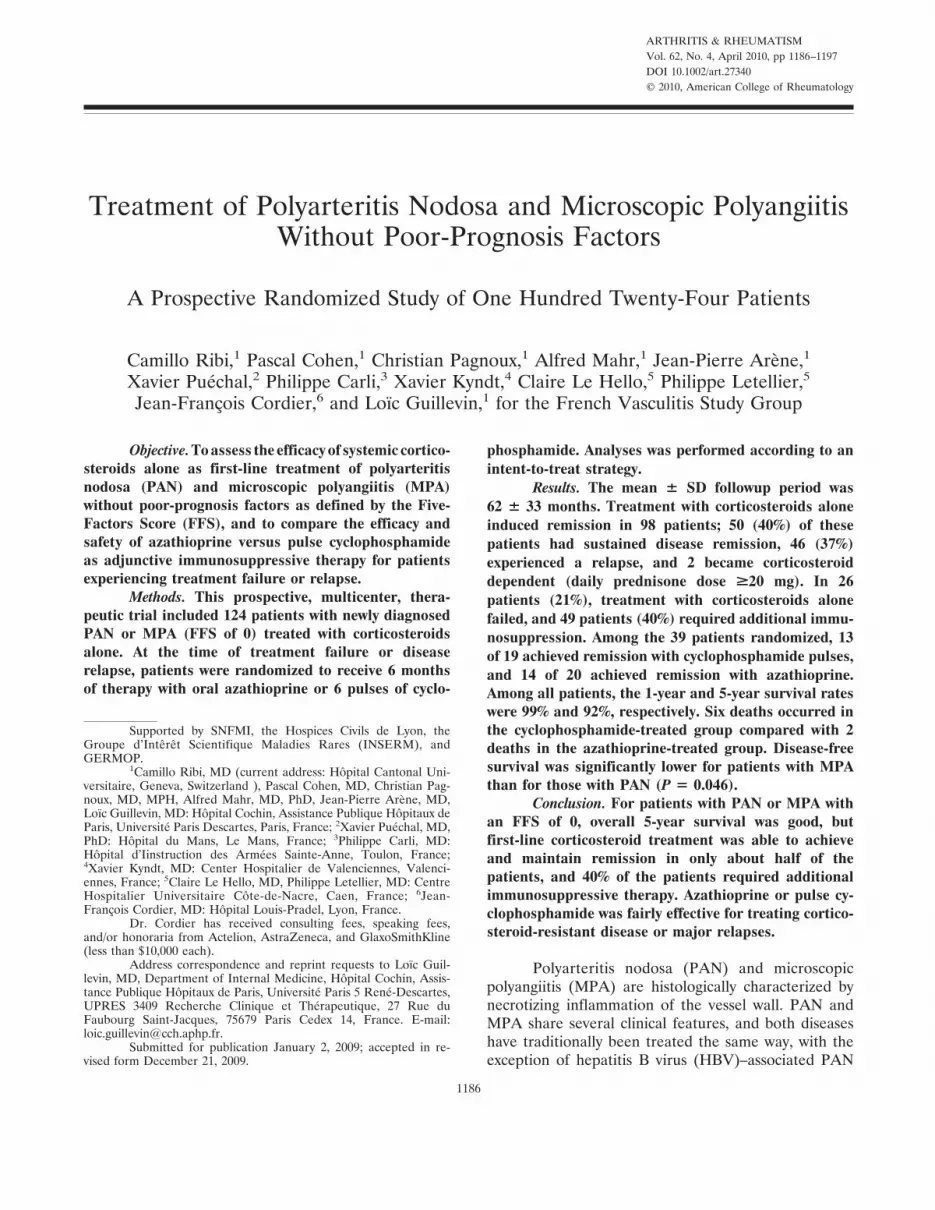
ARTHRITIS & RHEUMATISMVol. 62, No. 4, April 2010, pp 1186–1197DOI 10.1002/art.27340© 2010, American College of Rheumatology
Treatment of Polyarteritis Nodosa and Microscopic PolyangiitisWithout Poor-Prognosis Factors
A Prospective Randomized Study of One Hundred Twenty-Four Patients
Camillo Ribi,1 Pascal Cohen,1 Christian Pagnoux,1 Alfred Mahr,1 Jean-Pierre Arène,1
Xavier Puéchal,2 Philippe Carli,3 Xavier Kyndt,4 Claire Le Hello,5 Philippe Letellier,5
Jean-François Cordier,6 and Loïc Guillevin,1 for the French Vasculitis Study Group
Objective. To assess the efficacy of systemic cortico-steroids alone as first-line treatment of polyarteritisnodosa (PAN) and microscopic polyangiitis (MPA)without poor-prognosis factors as defined by the Five-Factors Score (FFS), and to compare the efficacy andsafety of azathioprine versus pulse cyclophosphamideas adjunctive immunosuppressive therapy for patientsexperiencing treatment failure or relapse.
Methods. This prospective, multicenter, thera-peutic trial included 124 patients with newly diagnosedPAN or MPA (FFS of 0) treated with corticosteroidsalone. At the time of treatment failure or diseaserelapse, patients were randomized to receive 6 monthsof therapy with oral azathioprine or 6 pulses of cyclo-
phosphamide. Analyses was performed according to anintent-to-treat strategy.
Results. The mean � SD followup period was62 � 33 months. Treatment with corticosteroids aloneinduced remission in 98 patients; 50 (40%) of thesepatients had sustained disease remission, 46 (37%)experienced a relapse, and 2 became corticosteroiddependent (daily prednisone dose >20 mg). In 26patients (21%), treatment with corticosteroids alonefailed, and 49 patients (40%) required additional immu-nosuppression. Among the 39 patients randomized, 13of 19 achieved remission with cyclophosphamide pulses,and 14 of 20 achieved remission with azathioprine.Among all patients, the 1-year and 5-year survival rateswere 99% and 92%, respectively. Six deaths occurred inthe cyclophosphamide-treated group compared with 2deaths in the azathioprine-treated group. Disease-freesurvival was significantly lower for patients with MPAthan for those with PAN (P � 0.046).
Conclusion. For patients with PAN or MPA withan FFS of 0, overall 5-year survival was good, butfirst-line corticosteroid treatment was able to achieveand maintain remission in only about half of thepatients, and 40% of the patients required additionalimmunosuppressive therapy. Azathioprine or pulse cy-clophosphamide was fairly effective for treating cortico-steroid-resistant disease or major relapses.
Polyarteritis nodosa (PAN) and microscopicpolyangiitis (MPA) are histologically characterized bynecrotizing inflammation of the vessel wall. PAN andMPA share several clinical features, and both diseaseshave traditionally been treated the same way, with theexception of hepatitis B virus (HBV)–associated PAN
Supported by SNFMI, the Hospices Civils de Lyon, theGroupe d’Interet Scientifique Maladies Rares (INSERM), andGERMOP.
1Camillo Ribi, MD (current address: Hopital Cantonal Uni-versitaire, Geneva, Switzerland ), Pascal Cohen, MD, Christian Pag-noux, MD, MPH, Alfred Mahr, MD, PhD, Jean-Pierre Arene, MD,Loıc Guillevin, MD: Hopital Cochin, Assistance Publique Hopitaux deParis, Universite Paris Descartes, Paris, France; 2Xavier Puechal, MD,PhD: Hopital du Mans, Le Mans, France; 3Philippe Carli, MD:Hopital d’Iinstruction des Armees Sainte-Anne, Toulon, France;4Xavier Kyndt, MD: Center Hospitalier de Valenciennes, Valenci-ennes, France; 5Claire Le Hello, MD, Philippe Letellier, MD: CentreHospitalier Universitaire Cote-de-Nacre, Caen, France; 6Jean-Francois Cordier, MD: Hopital Louis-Pradel, Lyon, France.
Dr. Cordier has received consulting fees, speaking fees,and/or honoraria from Actelion, AstraZeneca, and GlaxoSmithKline(less than $10,000 each).
Address correspondence and reprint requests to Loıc Guil-levin, MD, Department of Internal Medicine, Hopital Cochin, Assis-tance Publique Hopitaux de Paris, Universite Paris 5 Rene-Descartes,UPRES 3409 Recherche Clinique et Therapeutique, 27 Rue duFaubourg Saint-Jacques, 75679 Paris Cedex 14, France. E-mail:[email protected].
Submitted for publication January 2, 2009; accepted in re-vised form December 21, 2009.
1186

(1). A better understanding of pathophysiologic mecha-nisms, along with the availability of antineutrophil cyto-plasmic antibody (ANCA) testing in the 1980s, led toeasier distinction of MPA, which is frequently associatedwith ANCAs and is classically characterized by crescen-tic glomerulonephritis and alveolar hemorrhage. TheAmerican College of Rheumatology (ACR) establishedclassification criteria for PAN (2) but did not considerMPA to be a separate disease. It was not until the 1992Chapel Hill Consensus Conference (CHCC) nomencla-ture of vasculitides was published in 1994 that MPA wasclearly separated from PAN (3).
In a previous study of 342 patients with systemicnecrotizing vasculitis (SNV) (4), the French VasculitisStudy Group (FVSG) identified 5 factors that are sig-nificantly associated with a poor outcome (the Five-Factors Score [FFS]), as follows: elevated serum creati-nine levels (�140 �moles/liter or 1.58 mg/dl),proteinuria (�1 gm/day), severe gastrointestinal tractinvolvement, cardiomyopathy, and/or central nervoussystem (CNS) involvement. According to that analysis,when 1 factor was present at the time of disease onset,the 5-year mortality rate was 25.9%, when �2 factorswere present, the 5-year mortality rate increased to 46%,and when no factors were present, the 5-year mortalityrate was 11.9%.
The aim of this study was to treat patients withPAN or MPA who have no poor-prognosis factors withcorticosteroids alone as first-line therapy and to identifythe subgroup of patients requiring additional immuno-suppression. This multicenter, prospective, open-labelstudy was also designed to compare, for nonresponse tocorticosteroids or relapse during or after their tapering,the efficacies and safety profiles of 2 immunosuppressiveregimens, by randomizing patients to receive azathio-prine or pulse intravenous (IV) cyclophosphamide.MPA and PAN were considered together in this studybecause their comparable prognoses and outcomes hadpreviously been demonstrated (4), and because theprotocol had been established before the CHCC nomen-clature was published (3).
PATIENTS AND METHODS
Study design. We conducted a multicenter, prospec-tive, randomized, open-label trial in France and the UK underthe auspices of the FVSG and the European Vasculitis StudyGroup (EUVAS). The institutional review board (ComiteConsultatif pour la Protection des Personnes Participant a uneRecherche Biomedicale) of the Hospices Civils de Lyon ap-proved the protocol. The study was conducted in accordance
with the Declaration of Helsinski, and each participant gavesigned informed consent.
Patients. From 1993 to 2005, 157 patients with newlydiagnosed PAN or MPA were screened by the coordinatingcenter for inclusion in the study (Figure 1), and 124 wereincluded. Only patients with a baseline FFS of 0 were included.Patients with other systemic vasculitides, e.g., Wegener’s gran-ulomatosis, rheumatoid vasculitis, Henoch-Schonlein purpura,or cryoglobulinemia, were excluded. The results obtained froma cohort of patients with Churg-Strauss syndrome and an FFSof 0 who were treated according to the same protocol werepreviously published (5). Other exclusion criteria were asfollows: age younger than 15 years, previously treated SNV,history of cancer, women who were pregnant or breast-feeding,psychiatric disorders that might compromise compliance withtherapy, contraindications for the study drug, participation inanother ongoing therapeutic trial, and the concomitant pres-ence of HBV infection, HCV infection, or human immunode-ficiency virus infection.
Ninety-six patients (77%) fulfilled at least 3 of theACR 1990 classification criteria for PAN (2). Because patientswithout HBV or severe renal impairment were selected, 2 ofthe criteria for PAN were nonapplicable. The remaining 28patients, despite having �3 ACR criteria, had other clinicalfeatures characteristic of PAN or MPA, were antimyeloperoxi-dase (anti-MPO) antibody positive, or had histologicallyproven SNV. Although no distinction was made between PANand MPA at the time of inclusion, the 2 entities were separatedretrospectively based on biopsy reports, and histologic slideswere reviewed by a pathologist when necessary. For patientswith inconclusive results of histologic analysis, selection wasbased on the ANCA status and clinical features.
One hundred twenty-three patients were recruited inFrance, and 1 patient was recruited in the UK. Patientsoriginated from the departments of internal medicine (n � 77),rheumatology (n � 21), neurology (n � 5), dermatology (n �5), vascular medicine (n � 4), nephrology (n � 4), respiratorydiseases (n � 3), infectious diseases (n � 3), and geriatrics(n � 2).
Sera obtained from the study patients were tested forthe presence of ANCAs by indirect immunofluorescence (IIF)according to EUVAS recommendations (6). For every patientin whom ANCAs were detected by IIF, proteinase 3 and MPOspecificities were assessed by enzyme-linked immunosorbentassay (ELISA). A serum ELISA was recommended but notcompulsory when IIF findings were negative.
Treatment regimen. All patients were initially treatedwith corticosteroids (prednisone) alone. One IV methylpred-nisolone pulse (15 mg/kg) at the initiation of treatment wasallowed. Oral prednisone at a dosage of 1 mg/kg/day wasprescribed for 3 weeks before being tapered by 5 mg every 10days to a dosage of 0.5 mg/kg/day, then by 2.5 mg every 10 daysuntil a dosage of 15 mg/day was obtained and, finally, by 1 mgevery 10 days to the minimal effective dose or, when possible,until definitive withdrawal. The following adjuvant treatmentswere compulsory: potassium, calcium, vitamin D3, andbisphosphonates. The latter agents have been recommendedsince 1998 to prevent corticosteroid-induced osteoporosis.
The treating physicians were allowed to treat minorrelapses with corticosteroids without referring the patients for
TREATMENT OF PAN AND MPA WITHOUT POOR-PROGNOSIS FACTORS 1187

randomization, provided that the dosage did not exceed 0.5mg/kg/day for 1 month.
Patients with persistent clinical manifestations of activevasculitis because of either the initial failure of corticosteroidsor the impossibility of tapering corticosteroid dosages below 20mg/day, those with major relapses, and those with minorrelapses that were recurrent or refractory to treatment wererandomized to receive either 6 months of oral azathioprine (2mg/kg) or 6 IV cyclophosphamide pulses (600 mg/m2). IVcyclophosphamide pulses were administered every 2 weeks for1 month, then every 4 weeks; mesna was systematically coad-ministered to prevent hemorrhagic cystitis. Monthly hemato-logic monitoring was required throughout cyclophosphamidetherapy. For patients with a CD4� lymphocyte count of�300/mm3, cotrimoxazole prophylaxis against Pneumocystisjiroveci pneumonia was given.
When patients failed to respond to the assigned immu-nosuppressant or subsequently experienced a relapse, thetreating physician was free to modify the treatment and chooseanother immunosuppressant or switch from IV to oral cyclo-phosphamide.
Definitions and assessment. The primary end pointswere the occurrence of a major or minor relapse, treatmentfailure or death, and adverse events. Overall survival wasdefined as the percentage of survivors since treatment onset.Complete remission was defined as the absence of clinical andbiologic manifestations of active vasculitis for �3 months.Treatment failure was defined as the absence of clinicalremission, the appearance of new vasculitis manifestations, ordeath while receiving treatment. Relapses were defined as therecurrence of at least 1 vasculitis manifestation. Major relapseswere defined as the emergence of major organ involvement,alveolar hemorrhage, abdominal pain, and/or neuropathy.Minor relapses were defined as the recurrence of vasculitismanifestations without evidence of major organ involvement.Recurrence of nonspecific inflammatory symptoms, e.g., ar-thralgias or fever, was considered a minor relapse, afterexclusion of other causes. Adverse events were defined asobjective findings that necessitated treatment interruption,dose modifications, additional medication, or hospitalization.
We also retrospectively applied the Birmingham Vas-culitis Activity Score (BVAS) at baseline (7). The BVAS is aclinical index of disease activity based on symptoms and signsin 9 separate organ categories (systemic signs, skin, mucousmembranes and eyes, ear-nose-throat, chest, heart and vessels,gastrointestinal, kidney, nervous system). According to thenumber and severity of clinical and biologic symptoms, apredefined number of points are accorded to each category;then, the individual category scores are added to yield amaximum possible score of 63. Disease features are consideredonly when they are attributable to active vasculitis. Because theBVAS had not been validated when the therapeutic protocolwas designed, it was not used to select patients for inclusion orto assess outcome.
Statistical analysis. Randomization was centralized atthe coordinating center and made by phone, fax, or e-mail. Inthe randomized part of the study, we expected a 50% adverseevent rate for the group receiving cyclophosphamide. Wehypothesized that in the azathioprine-treated group, 5% of thepatients would have side effects, and another 12% would havecorticosteroid-related bone events. Because no prospective
data were available on the use of azathioprine to treat PAN orMPA, the estimation was based on its use in patients withBehcet’s disease (8). For alpha and beta risks of 5%, weneeded to recruit 36 patients into each group (i.e., a total of 72randomized patients). The duration of the trial was notpredefined. In addition to the first 12 months of followuprequired by the protocol, investigators were asked to providelong-term updates. Because an interim analysis 12 years afterinclusion in the first study showed that only 39 patients hadbeen randomized, the goal of 72 randomizations within areasonable amount of time was considered beyond reach, andthe trial was stopped.
The time to events (treatment failure, minor and majorrelapses, and/or death) occurring in each group defined thedisease-free survival rate. The final analysis was performed 12years after the first patient was enrolled. For patients who werelost to followup, we made inquiries at the end of the study tolocal authorities who register the deaths of French citizens.
All data were analyzed according to an intent-to-treatstrategy using the SAS statistical package, version 8.12 (SASInstitute, Cary, NC) and the SPSS statistical package, version11 (SPSS, Chicago, IL). Quantitative variables, which wereexpressed as the mean � SD, were compared using Student’st-test or nonparametric tests. Categorical variables were com-pared using the chi-square test or, when appropriate, Fisher’sexact test.
Time to relapse and/or death was calculated from thetime of initiation of treatment. Kaplan-Meier survival curveswere plotted using GraphPad Prism software, version 4.00(GraphPad Software, San Diego, CA), and their differenceswere calculated using the log-rank method. P values less than0.05 were considered significant.
RESULTS
Baseline characteristics. Between November 4,1993 and January 1, 2005, a total of 124 patients wereincluded in the study. The baseline demographics, clin-ical characteristics, and biologic characteristics are sum-marized in Table 1. None of the patients had alveolarhemorrhage or severe renal impairment, and no renalbiopsy specimens were obtained.
ANCAs were detected in 36 patients (29%). Theresults of IIF and ELISA are summarized in Table 1.Among the 66 patients classified as having MPA, 32 hadANCAs, with perinuclear labeling and MPO specificitypredominating. Among the 58 patients classified ashaving PAN, 4 had ANCAs of unknown specificities.Percutaneous angiography led to a diagnosis of PAN in10 patients, 9 of whom had characteristic visceral angio-grams and 1 of whom had femoral artery vasculitis.
All patients underwent at least 1 biopsy. A totalof 204 tissue samples were obtained, 126 (62%) of whichwere positive. The biopsy specimens were predomi-nantly skin (n � 59), neuromuscular (sural; n � 53),muscle (n � 46), and temporal artery (n � 27), with
1188 RIBI ET AL

vasculitis observed in 71%, 81%, 67%, and 30% of thespecimens, respectively. Vasculitis was histologicallyconfirmed in 107 patients (86%).
Outcome. Inclusion and outcome data are sum-marized in Figure 1. Patients were followed up for amean � SD period of 62 � 33 months (range 3–135months). Seven patients were lost to followup after amean � SD time period of 74 � 44 months (range11–125 months).
Twenty-six patients (21%) failed to respond toinitial treatment, whereas corticosteroid treatment in-duced remission in the remaining patients. Of the 98patients with disease in remission, 2 became cortico-
steroid dependent (i.e., the dosage of prednisone couldnot be decreased below 20 mg/day), and the other 46patients experienced a relapse. Among the 74 patientswho experienced either corticosteroid failure or relapse,9 (12%) subsequently developed severe vasculitis (FFS�1), involving the CNS in 5 patients, the kidney in 2patients, the bowel in 1 patient, and the heart in 1patient. Fifty patients (40%) achieved sustained diseaseremission. Overall, second-line immunosuppressantswere prescribed for 49 (40%) of 124 patients.
Randomization. Among the 56 patients in whomvasculitis was not controlled by corticosteroids alone, 39were randomized (13 patients with PAN and 26 patients
Table 1. Demographic, clinical, and biologic features of the 124 patients with PAN or MPA*
ParameterAll patients(n � 124)
PAN(n � 58)
MPA(n � 66) P
Demographic featuresNo. men/no. women (male:female ratio) 72/52 (1.38) 36/22 (1.64) 36/30 (1.2) NSAge, mean � SD (range) years 56.5 � 16.6 (15.7–92) 55.5 � 17.6 (15.7–78.3) 57.4 � 15.8 (23–92) NSFollowup, mean � SD (range) months 62 � 33 (3–135) 66 � 35 (13–135) 58 � 32 (3–129) NSInitial BVAS, mean � SD (range) 12.6 � 5.4 (3–30) 12.3 � 6 (3–30) 12.8 � 4.9 (3–26) NS
Clinical presentationGeneral signs 118 (95) 54 (93) 64 (97) NS
Myalgias 86 (69) 40 (69) 46 (70) NSFever �38.5°C 72 (58) 34 (59) 38 (58) NSWeight loss �4 kg 70 (56) 31 (53) 39 (59) NSArthralgias 65 (52) 30 (52) 35 (53) NS
Skin lesions 79 (64) 38 (66) 41 (62) NSPurpura 34 (27) 14 (24) 20 (30) NSLivedo 33 (27) 14 (24) 19 (29) NSNodules 23 (19) 16 (28) 7 (11) 0.015
Eye involvement 6 (5) 3 (5) 3 (5) NSENT involvement 15 (12) 7 (12) 8 (12) NSPulmonary involvement 21 (17) 5 (9) 16 (24) 0.021Cardiovascular involvement 28 (23) 16 (28) 12 (18) NSAbdominal pain, not severe 18 (15) 9 (16) 9 (14) NSRenal and urogenital tract 38 (31) 15 (26) 23 (35) NS
Mild proteinuria 18 (15) 11 (19) 7 (11) NSMicrohematuria 11 (9) 4 (7) 7 (11) NSHypertension 9 (7) 8 (14) 1 (2) 0.009Testicular pain 10 (8) 7 (12) 3 (5) NS
Peripheral neuropathy 82 (66) 33 (57) 49 (74) 0.042Mononeuritis multiplex 69 (56) 28 (48) 41 (62) NSSymmetrical polyneuropathy 13 (10) 5 (9) 8 (12) NS
Headache 14 (11) 9 (16) 5 (8) NSBiologic parameters
ANCA positive by IIF 36 (29) 4 (7) 32 (48) �0.001Perinuclear pattern, no. IIF positive/no. assessed (%) 31/36 (86) 1/4 (25) 30/32 (94) �0.001Myeloperoxidase specificity by ELISA, no. positive/
no. assessed (%)24/36 (67) 0 24/32 (75) �0.001
ESR �30 mm/hour, no. positive/no. assessed (%) 92/121 (76) 44/56 (79) 48/65 (74) NSCRP, mean � SD (range) mg/dl 97 � 89 (0–480) 105 � 103 (2–480) 90 � 76 (0–250) NSSerum creatinine, mean � SD (range) �moles/liter 82 � 20 (35–141) 84 � 21 (35–141) 80 � 19 (52–140) NS
Angiographic features of vasculitis 10 (8) 10 (17) 0 �0.001Histologically proven vasculitis 107 (86) 45 (78) 62 (94) �0.001
* Except where indicated otherwise, values are the number (%). PAN � polyarteritis nodosa; MPA � microscopic polyangiitis; NS � not significant;BVAS � Birmingham Vasculitis Activity Score; ENT � ear, nose, and throat; ANCA � antineutrophil cytoplasmic antibodies; IIF � indirectimmunofluorescence; ELISA � enzyme-linked immunosorbent assay; ESR � erythrocyte sedimentation rate; CRP � C-reactive protein.
TREATMENT OF PAN AND MPA WITHOUT POOR-PROGNOSIS FACTORS 1189

with MPA). The reasons for randomization were asfollows: no remission (22 patients [11 receiving cyclo-phosphamide and 11 receiving azathioprine]), majorrelapses (13 patients [7 receiving cyclophosphamide and6 receiving azathioprine]), and corticosteroid depen-dence during induction or after minor relapses (4 pa-tients [2 receiving cyclophosphamide and 2 receivingazathioprine). Seven patients were randomized afterhaving experienced vasculitis flares, which in 5 patientshad been managed with corticosteroids according to theprotocol. Two patients received higher corticosteroiddoses and for longer durations than were foreseen by theprotocol before randomization, but these 2 patients wereretained for the final analysis.
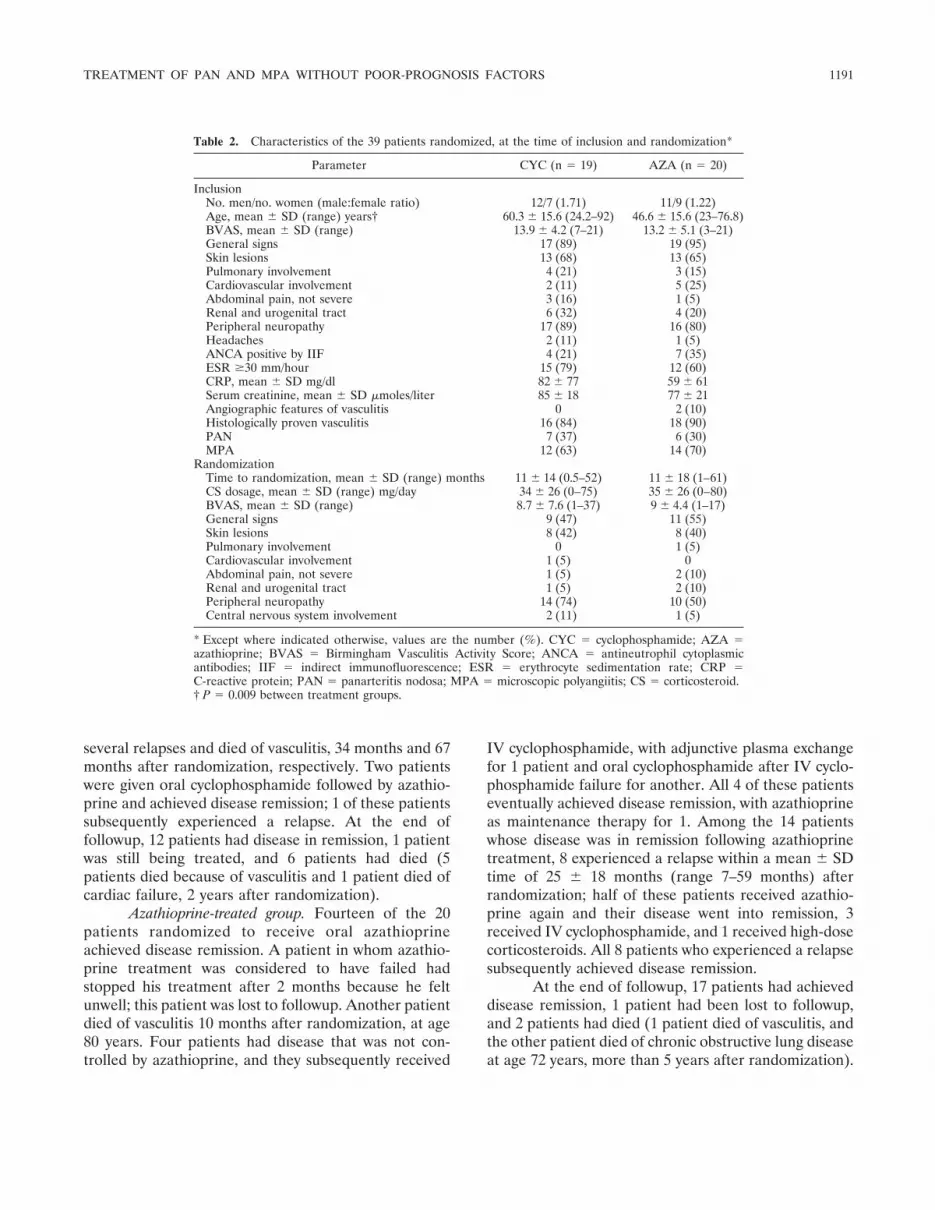
The characteristics of the 2 groups at the time ofinclusion are summarized in Table 2. The only signifi-cant between-group difference was the older age of thecyclophosphamide-assigned patients at the time of inclu-sion and randomization. The treatment responses of the39 randomized patients are detailed in Figure 2.
Cyclophosphamide-treated group. Thirteen of the19 patients randomized to receive pulse cyclo-phosphamide achieved disease remission. One patientdied of bowel infarction after the first cyclophosphamidepulse, and bowel infarction had not been an initial PANfeature. The 5 cyclophosphamide nonresponders were
subsequently treated according to local practice. One27-year-old patient with biopsy-proven MPA who wasrandomized because of a major relapse, with CNS, renal,and pancreatic involvement, underwent plasma ex-changes after 2 cyclophosphamide pulses; she died ofthrombotic microangiopathy and sepsis 3 months afterrandomization. Another patient with mononeuropathyand biopsy-proven PAN was randomized after nonre-sponse to first-line corticosteroids and steadily deterio-rated despite receiving pulse and then oral cyclo-phosphamide, plasma exchange, IV immunoglobulin,and cyclosporine; he died at age 66 years of possibleCNS involvement. No autopsy was performed. In 3patients, disease eventually went into remission, but 2 ofthem experienced major relapses 7 months and 46months after randomization, respectively; both of thesepatients had CNS involvement (cerebrovascular dam-age, pachymeningitis). Both of these patients receivedIV cyclophosphamide, and disease was in remission in 1patient, and the other patient was still receiving treat-ment at study end.
Of the 13 patients with disease in remission afterreceiving the allocated treatment, 4 experienced a re-lapse 8 months, 19 months, 32 months, and 63 monthsafter randomization, respectively. Despite having re-ceived IV cyclophosphamide, 2 of them experienced
Figure 1. Flow chart showing the distribution of 124 patients with polyarteritis nodosa (PAN) ormicroscopic polyangiitis (MPA), from inclusion in the study through outcome and randomization foradditional immunosuppressive treatment. The reasons for noninclusion were as follows: no definitePAN or MPA (n � 17), factors of poor prognosis (n � 8), refusal (n � 3), contraindication to study drug(n � 2), or other (n � 3). CS � corticosteroids.
1190 RIBI ET AL
several relapses and died of vasculitis, 34 months and 67months after randomization, respectively. Two patientswere given oral cyclophosphamide followed by azathio-prine and achieved disease remission; 1 of these patientssubsequently experienced a relapse. At the end offollowup, 12 patients had disease in remission, 1 patientwas still being treated, and 6 patients had died (5patients died because of vasculitis and 1 patient died ofcardiac failure, 2 years after randomization).
Azathioprine-treated group. Fourteen of the 20patients randomized to receive oral azathioprineachieved disease remission. A patient in whom azathio-prine treatment was considered to have failed hadstopped his treatment after 2 months because he feltunwell; this patient was lost to followup. Another patientdied of vasculitis 10 months after randomization, at age80 years. Four patients had disease that was not con-trolled by azathioprine, and they subsequently received
IV cyclophosphamide, with adjunctive plasma exchangefor 1 patient and oral cyclophosphamide after IV cyclo-phosphamide failure for another. All 4 of these patientseventually achieved disease remission, with azathioprineas maintenance therapy for 1. Among the 14 patientswhose disease was in remission following azathioprinetreatment, 8 experienced a relapse within a mean � SDtime of 25 � 18 months (range 7–59 months) afterrandomization; half of these patients received azathio-prine again and their disease went into remission, 3received IV cyclophosphamide, and 1 received high-dosecorticosteroids. All 8 patients who experienced a relapsesubsequently achieved disease remission.
At the end of followup, 17 patients had achieveddisease remission, 1 patient had been lost to followup,and 2 patients had died (1 patient died of vasculitis, andthe other patient died of chronic obstructive lung diseaseat age 72 years, more than 5 years after randomization).
Table 2. Characteristics of the 39 patients randomized, at the time of inclusion and randomization*
Parameter CYC (n � 19) AZA (n � 20)
InclusionNo. men/no. women (male:female ratio) 12/7 (1.71) 11/9 (1.22)Age, mean � SD (range) years† 60.3 � 15.6 (24.2–92) 46.6 � 15.6 (23–76.8)BVAS, mean � SD (range) 13.9 � 4.2 (7–21) 13.2 � 5.1 (3–21)General signs 17 (89) 19 (95)Skin lesions 13 (68) 13 (65)Pulmonary involvement 4 (21) 3 (15)Cardiovascular involvement 2 (11) 5 (25)Abdominal pain, not severe 3 (16) 1 (5)Renal and urogenital tract 6 (32) 4 (20)Peripheral neuropathy 17 (89) 16 (80)Headaches 2 (11) 1 (5)ANCA positive by IIF 4 (21) 7 (35)ESR �30 mm/hour 15 (79) 12 (60)CRP, mean � SD mg/dl 82 � 77 59 � 61Serum creatinine, mean � SD �moles/liter 85 � 18 77 � 21Angiographic features of vasculitis 0 2 (10)Histologically proven vasculitis 16 (84) 18 (90)PAN 7 (37) 6 (30)MPA 12 (63) 14 (70)
RandomizationTime to randomization, mean � SD (range) months 11 � 14 (0.5–52) 11 � 18 (1–61)CS dosage, mean � SD (range) mg/day 34 � 26 (0–75) 35 � 26 (0–80)BVAS, mean � SD (range) 8.7 � 7.6 (1–37) 9 � 4.4 (1–17)General signs 9 (47) 11 (55)Skin lesions 8 (42) 8 (40)Pulmonary involvement 0 1 (5)Cardiovascular involvement 1 (5) 0Abdominal pain, not severe 1 (5) 2 (10)Renal and urogenital tract 1 (5) 2 (10)Peripheral neuropathy 14 (74) 10 (50)Central nervous system involvement 2 (11) 1 (5)
* Except where indicated otherwise, values are the number (%). CYC � cyclophosphamide; AZA �azathioprine; BVAS � Birmingham Vasculitis Activity Score; ANCA � antineutrophil cytoplasmicantibodies; IIF � indirect immunofluorescence; ESR � erythrocyte sedimentation rate; CRP �C-reactive protein; PAN � panarteritis nodosa; MPA � microscopic polyangiitis; CS � corticosteroid.† P � 0.009 between treatment groups.
TREATMENT OF PAN AND MPA WITHOUT POOR-PROGNOSIS FACTORS 1191
Patients not randomized. Eighteen patients whohad achieved remission while receiving first-line cortico-steroid treatment experienced minor relapses, whichwere managed with corticosteroids according to theprotocol; all achieved disease remission. One patientdied of heart failure at age 83 years due to a preexistingvalvulopathy that was not related to vasculitis, 17 monthsafter the last vasculitis flare.
Seventeen of the 56 patients eligible for random-ization were not randomized; 6 of these patients refusedadditional immunosuppression, whereas the reasons fornonreferral of 11 patients for randomization remainunknown. For these 17 patients, the reasons for second-line treatment were as follows: nonresponse to cortico-steroids (n � 4), major relapse (n � 12), and cortico-steroid dependency (n � 1). Seven patients receivedhigh-dose corticosteroids alone: 3 of these patientsexperienced disease remission, 2 patients (both of whomwere age 80 years) died while receiving treatment, 2 and9 months after relapsing, respectively, and 2 patientswere still being treated at the end of the study. Tenpatients were prescribed additional immunosuppres-sants; all of these patients achieved remission, but 2subsequently experienced a disease relapse, and 1 be-came corticosteroid dependent.
Adverse events. Adverse events occurred in 67patients (54%); these adverse events are shown in Table3. Corticosteroid-related bone and joint complications
(osteoporotic fractures and osteonecrosis of the femoralhead) occurred in 10 patients (8%); subclinical osteo-porosis was observed in another 4 patients. Bone densityscans were not routinely performed, and, thus, theasymptomatic osteoporosis rate is probably higher. Six-teen patients (13%) experienced infectious complica-tions requiring hospitalization, including 2 fatalities; 1patient died of septic shock–complicated uncontrolledvasculitis, and the other died of pneumonia 8 years afterinclusion in the study. Other potentially corticosteroid-related adverse events included cataract and intraocularhypertension, arterial hypertension, diabetes mellitus,psychiatric disorder, and adrenal insufficiency. Amongthe 6 reported thromboembolic events, 4 occurredwithin the first 6 months of treatment, and 2 occurredafter 1 year. One patient who had previously received IVcyclophosphamide was treated with oral cyclo-phosphamide following a major relapse; hemorrhagiccystitis developed, which subsided after treatment wasswitched back to pulse cyclophosphamide. No hypersen-sitivity reaction to or hepatic toxicity with azathioprinewas reported. Cytopenia developed in 1 patient who wasbeing treated concomitantly with allopurinol.
Malignancies developed in 5 patients. Two non-randomized patients had received second-line immuno-suppressants following relapses. In 1 of these patients,who had PAN and received azathioprine, Hodgkin’slymphoma developed at age 24 years, 19 months after
Figure 2. Flow chart showing the outcomes of the 39 randomized patients. � � One patient died due to ongoingvasculitis. † � One patient died due to ongoing vasculitis, and 1 patient stopped treatment with azathioprine andwas lost to followup. ‡ � Two patients died due to vasculitis, and 1 patient received ongoing treatment.
1192 RIBI ET AL

inclusion and 17 months after starting azathioprine; heunderwent chemotherapy and was alive more than 8years after lymphoma was diagnosed. In the otherpatient, who had MPA and received cyclophosphamideand methotrexate, breast cancer was diagnosed at age 68years, 39 months after inclusion and 32 months afterstarting cyclophosphamide; this patient underwent suc-cessful surgery and chemotherapy and was alive 3 yearsafter cancer was diagnosed. The other 3 patients withmalignancies had been treated with corticosteroidsalone, and their disease was in remission. In 1 of thesepatients, who had PAN, colon cancer was diagnosed atage 68 years, 4 years after inclusion; colon cancer wassuccessfully treated with surgery and 5-fluorouracil, andthe patient was alive 45 months after cancer was diag-nosed. In a patient with MPA, metastatic colon cancerwas diagnosed at age 78 years, 32 months after inclusion,and this patient died 4 months later. Finally, in a patientwith PAN, an in situ colon cancer was removed at age 78years, 10 months after inclusion, and this patient wasalive 18 months later.
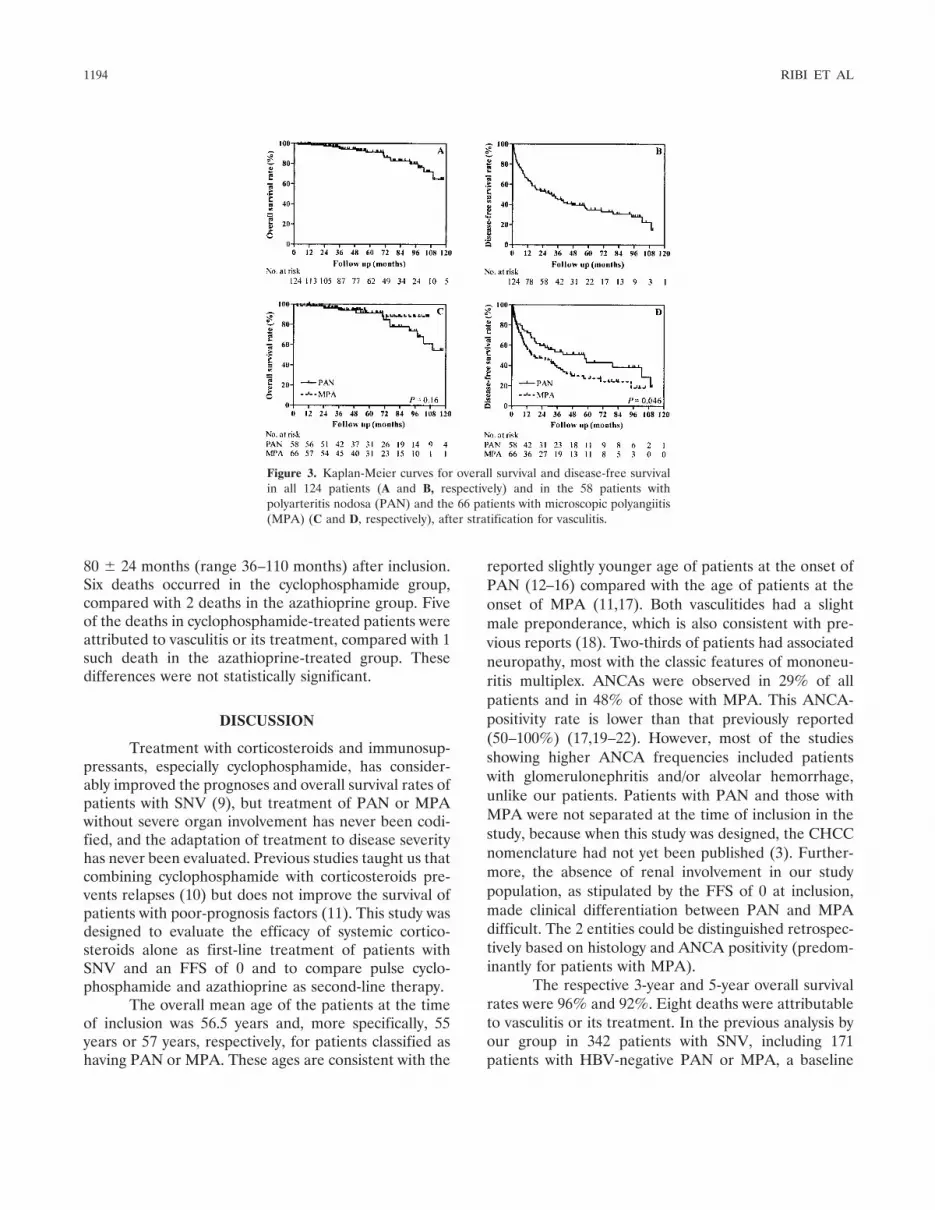
Survival. Overall survival is shown in Figure 3A.The 1-year and 5-year survival estimates were 99% and92%, respectively. Disease-free survival is shown inFigure 3B. Five-year survival estimates indicated that65% of patients either failed treatment with cortico-steroids, experienced a relapse, or were dead. Theoverall survival of patients with PAN and those withMPA did not differ significantly (Figure 3C), butdisease-free survival was lower for the patients withMPA (Figure 3D).
Seventeen patients (14%) died during followup;their mean � SD age was 72 � 20 years (range 27–92years). Eight deaths were attributed to active vasculitisand occurred 37 � 25 months (range 3–71 months) afterstarting treatment. In 9 patients, the cause of death wasnot related to vasculitis; in these patients the causes ofdeath were as follows: cardiovascular event (n � 4),cancer (n � 1), hemorrhage (n � 1), dementia (n � 1),chronic obstructive lung disease (n � 1), and pneumonia(n � 1). The mean � SD age of these patients was 75 �6 years (range 65–83 years), and their deaths occurred
Table 3. Details of the adverse events recorded in 67 of 124 patients*
Adverse event
No. ofpatientsaffected
Patientsrandomized
to CYC(n � 10)
Patientsrandomized
to AZA(n � 12)
Mean � SD time ofoccurrence from CS
initiation, months
Infection† 16 4 5 24 � 30Ophthalmologic complications‡ 14 5 2 24 � 16Hypertension 11 1 1 9 � 5Osteoporotic fractures§ 9 2 3 28 � 25Diabetes mellitus 9 1 1 5 � 4CS-induced myopathy 8 0 2 9 � 9Thromboembolic events¶ 6 2 0 7 � 7Malignancy# 5 0 0 29 � 15Subclinical osteoporosis 4 0 1 58 � 33Cardiovascular damage** 4 0 1 19 � 17Cerebrovascular damage†† 3 1 1 27 � 25Hematologic toxicity‡‡ 3 1 2 29 � 36Adrenal insufficiency 2 0 1 15 � 9CS-induced psychiatric disorder 2 0 0 0.3 � 0.2Osteonecrosis of the femoral head 1 0 0 8Hepatotoxicity 1 0 1 6Iatrogenic aneurysm§§ 1 0 0 0.1CYC-induced cystitis 1 1 0 20
* CYC � cyclophosphamide; AZA � azathioprine; CS � corticosteroid.† Pneumonia (n � 4), shingles (n � 4), sepsis (n � 3), urinary tract infection (n � 3), Candida esophagitis(n � 1), lower respiratory tract infection (n � 1).‡ Cataract (n � 9), cataract and glaucoma (n � 3), glaucoma (n � 1), retinal detachment (n � 1).§ Vertebrae (n � 8), vertebrae and femoral head (n � 1).¶ Deep vein thrombosis (n � 5 [n � 3 bilateral]), pulmonary embolism (n � 1).# Colon cancer (n � 3), breast cancer (n � 1), Hodgkin’s lymphoma (n � 1).** Cardiac failure (n � 2), atrial fibrillation (n � 1), myocardial infarction (n � 1).†† Ischemic optic neuropathy (n � 1), ischemic stroke (n � 1), chronic subdural hematoma (n � 1).‡‡ Azathioprine–allopurinol interaction (n � 1), thrombocytopenia (n � 1), megaloblastic anemia (n � 1).§§ Aneurysm formation and psoas hemorrhage after arteriography.
TREATMENT OF PAN AND MPA WITHOUT POOR-PROGNOSIS FACTORS 1193
80 � 24 months (range 36–110 months) after inclusion.Six deaths occurred in the cyclophosphamide group,compared with 2 deaths in the azathioprine group. Fiveof the deaths in cyclophosphamide-treated patients wereattributed to vasculitis or its treatment, compared with 1such death in the azathioprine-treated group. Thesedifferences were not statistically significant.
DISCUSSION
Treatment with corticosteroids and immunosup-pressants, especially cyclophosphamide, has consider-ably improved the prognoses and overall survival rates ofpatients with SNV (9), but treatment of PAN or MPAwithout severe organ involvement has never been codi-fied, and the adaptation of treatment to disease severityhas never been evaluated. Previous studies taught us thatcombining cyclophosphamide with corticosteroids pre-vents relapses (10) but does not improve the survival ofpatients with poor-prognosis factors (11). This study wasdesigned to evaluate the efficacy of systemic cortico-steroids alone as first-line treatment of patients withSNV and an FFS of 0 and to compare pulse cyclo-phosphamide and azathioprine as second-line therapy.
The overall mean age of the patients at the timeof inclusion was 56.5 years and, more specifically, 55years or 57 years, respectively, for patients classified ashaving PAN or MPA. These ages are consistent with the
reported slightly younger age of patients at the onset ofPAN (12–16) compared with the age of patients at theonset of MPA (11,17). Both vasculitides had a slightmale preponderance, which is also consistent with pre-vious reports (18). Two-thirds of patients had associatedneuropathy, most with the classic features of mononeu-ritis multiplex. ANCAs were observed in 29% of allpatients and in 48% of those with MPA. This ANCA-positivity rate is lower than that previously reported(50–100%) (17,19–22). However, most of the studiesshowing higher ANCA frequencies included patientswith glomerulonephritis and/or alveolar hemorrhage,unlike our patients. Patients with PAN and those withMPA were not separated at the time of inclusion in thestudy, because when this study was designed, the CHCCnomenclature had not yet been published (3). Further-more, the absence of renal involvement in our studypopulation, as stipulated by the FFS of 0 at inclusion,made clinical differentiation between PAN and MPAdifficult. The 2 entities could be distinguished retrospec-tively based on histology and ANCA positivity (predom-inantly for patients with MPA).
The respective 3-year and 5-year overall survivalrates were 96% and 92%. Eight deaths were attributableto vasculitis or its treatment. In the previous analysis byour group in 342 patients with SNV, including 171patients with HBV-negative PAN or MPA, a baseline
Figure 3. Kaplan-Meier curves for overall survival and disease-free survivalin all 124 patients (A and B, respectively) and in the 58 patients withpolyarteritis nodosa (PAN) and the 66 patients with microscopic polyangiitis(MPA) (C and D, respectively), after stratification for vasculitis.
1194 RIBI ET AL

FFS of 0 was associated with 12% 5-year mortality (4).The very good survival rate in this study confirmed thepredictive value of the FFS for non-HBV–associatedPAN and MPA.
However, disease-free survival was limited; 65%of the patients did not respond to corticosteroids aloneor experienced a relapse or were dead at 5 years.Although corticosteroid treatment induced remission in79% of patients, vasculitis was not controlled in one-fifthof the patients, and only 40% of the patients withinitially corticosteroid-controlled vasculitides achievedsustained remission. The relapse rate in this trial washigher than those previously reported (20% for PANand 35% for MPA [23]). Relapses were more frequent inMPA, which is consistent with previous observations(17). As observed for patients with Churg-Strauss syn-drome who were included in a similar trial (5), anddespite differences between one SNV and another,corticosteroids alone failed to induce or maintain initialremission in a substantial patient population. Combiningcorticosteroids with an immunosuppressant at the startof treatment might have prevented treatment failure orrelapses in some of these patients.
The limited number of randomized patients pre-cludes the ability to make statistically valid comparisonsbetween groups. It should be noted, however, thatpatients given azathioprine had better outcomes thanthose given cyclophosphamide, with significantly fewerdeaths. The BVAS was comparable in the 2 groups, bothat baseline and at the time of randomization, and MPAand PAN were equally represented. Also, cyclo-phosphamide and azathioprine seemed equally effectiveat inducing remission, which was achieved in two-thirdsof patients. In contrast, the mean age of the cyclo-phosphamide group was significantly higher, whichcould account for some of the higher vasculitis- andtreatment-related mortality.
The duration of second-line immunosuppres-sion in this trial had been limited to 6 months, forsafety considerations in patients with a priori goodprognoses. Most relapses occurred in the azathioprinegroup, which could mean that a 6-month course ofazathioprine was insufficient. Because most patientswith SNV that was refractory to corticosteroids sub-sequently had more severe disease courses, the ques-tion remains whether the adjunction of immunosup-pressants to corticosteroids at the start of treatmentmight lessen the need for and prolongation of second-line immunosuppression. In addition to cyclo-phosphamide and azathioprine, other second-linetreatments were prescribed for refractory or relapsing
SNV, but the patient numbers are too small to allowconclusions to be drawn. As for some of our patients,plasma exchange might be useful in the treatment ofSNV that is severe or refractory to treatment (24–26).Second-line therapy with IV immunoglobulin or bio-logic agents, e.g., tumor necrosis factor blockade andB cell depletion, might also be considered, becausepromising results were recently reported for rituximabefficacy in patients with MPA that is refractory toconventional treatment (27).
The majority of reported adverse events wereattributed to corticosteroids. The absence of systematicbone density scans (a test for which reimbursement wasnot provided by the French National Health Insuranceat that time) might have led to an underestimation of therate of asymptomatic corticosteroid-related osteo-porosis. Malignancies developed in 5 patients duringfollowup. Vasculitis is reported to occur during thecourse of malignancy in 2.4–8% of patients (28). Cancerwas diagnosed an average of 2 years after the time ofinclusion in the study, and vasculitis was controlled atthe time of a cancer diagnosis, which lowers the proba-bility of a paraneoplastic syndrome in those patients.There is also some concern about the carcinogenicpotential of immunosuppressive treatments. However,only 2 of the 5 patients had previously received immu-nosuppressants, and none of them experienced thedevelopment of a malignancy typically associated withimmunosuppressant agents. Infectious complications oc-curred in 13% of our patients, and 2 deaths wereattributed to infection.
To reduce relapse-related morbidity, differentstrategies might be applied as adjunctive therapies tocorticosteroids for the treatment of HBV-negative PANand MPA with limited organ involvement. Treatmentwith cyclophosphamide combined with corticosteroidshas been evaluated in a small number of these patientsand appears safer when cyclophosphamide is adminis-tered IV rather than in a daily oral formulation (29).Even though there are limited data on the efficacy ofcyclophosphamide in this setting, known safety issueslessen its potential as the first-line agent to treat PANand MPA without major organ involvement. To the bestof our knowledge, less toxic first-line alternatives, e.g.,azathioprine, methotrexate, and mycophenolate mofetil,have not yet been evaluated in a prospective and con-trolled manner. Given the impression that azathioprinedid at least as well as cyclophosphamide in this study, theFVSG is now undertaking a prospective, randomized,double-blind trial to evaluate azathioprine as a cortico-
TREATMENT OF PAN AND MPA WITHOUT POOR-PROGNOSIS FACTORS 1195

steroid-sparing agent and to improve control of PANand MPA in patients without poor-prognosis factors.
ACKNOWLEDGMENTS
We acknowledge our colleagues whose collaborationwas essential for this study: Michel Alcalay (Centre HospitalierUniversitaire, Poitiers), Christophe Arnal (Hopital Tenon,Paris), Jean-Paul Battesti (Hopital Avicenne, Bobigny), AlainBergere (Pole Sante Sarthe et Loir, La Fleche), ChristopheBernardeau (Hopital Lariboisiere, Paris), Nadine Boulanger(Centre Hospitalier, Le Mans), Anne Buu Sao (Hopital Avi-cenne, Bobigny), Jean-Jacques Buzon (Avesnes-les-Aubert),Jean Cabane (Hopital Saint-Antoine, Paris), Patrice Cacoub(Hopital Pitie–Salpetriere, Paris), Alain Cantagrel (HopitalRangueil, Toulouse), Ramiro Cevallos (Centre Hospitalier,Compiegne), Jacques Charbonneau (Centre Hospitalier,Montbeliard), Nathalie Costedoat (Hopital Pitie–Salpetriere,Paris), Alain Creange (Hopital Henri-Mondor, Creteil), Jol-anta Dadoniene (University Hospital, Vilnius, Lituania), Phil-ippe De Faucal (Nantes), Gilles Defuentes (Hopitald’Instruction des Armees Percy, Clamart), Jerome de Seze(Hopital Salengro, Lille), Claire Delaunay (Centre Hospi-talier, Niort), Louis Dubertret (Hopital Saint-Louis, Paris),Alain Dubois (CMC Beausoleil, Montpellier), Elisabeth Du-hamel (Centre Hospitalier, Saint-Brieuc), Didier Neau (Hopi-tal Pellegrin, Bordeaux), Eric Esteve (Centre Hospitalier,Orleans), Renato Fior (Hopital Antoine-Beclere, Clamart),Pierre Foullon (Centre Hospitalier Dracenie, Draguignan),Tsouria Gaida (Hopital Pellegrin, Bordeaux), Tatjana Galper-ine (Hopital Pellegrin, Bordeaux), Jean-Marie Garcin (Hopitald’Instruction des Armees Begin, Saint-Mande), Helder Gil(Centre Hospitalier Universitaire, Besancon), Brigitte Gilson(Centre Hospitalier, Verdun), Thomas Girard (HopitalAntoine-Beclere, Clamart), Bertrand Godeau (Hopital Henri-Mondor, Creteil), Pascal Godmer (Centre Hospitalier,Vannes), Isabelle Gueit (Centre Hospitalier Universitaire,Rouen), Mohamed Hamidou (Hopital Hotel-Dieu, Nantes),Dominique Israel-Biet (Hopital Europeen Georges-Pompidou, Paris), Anne-Sophie Labussiere (Hopital Jacques-Cœur, Bourges), Cedric Landron (Hopital La Mileterie, Poit-iers), Patricia Lanoux (Hopital Corvisart, Charleville-Mezieres), Pierre-Yves Le Berruyer (Hopital Robert-Debre,Reims), Francois Lhote (Centre Hospitalier Delafontaine,Saint-Denis), Olivier Lidove (Hopital Bichat, Paris),Veronique Loustaud-Ratti (Centre Hospitalier UniversitaireDupuytren, Limoges), Herve Maillard (Centre Hospitalier, LeMans), Othmane Mejjad (Centre Hospitalier Universitaire,Rouen), Pierre Miossec (Hopital Edouard-Herriot, Lyon),Jean-Francois Paris (Hopital d’Instruction des Armees Sainte-Anne, Toulon), Blaise Patri (Hopital Boucicault, Paris), Chris-tian Penalba (Hopital Corvisart, Charleville-Mezieres), Ed-ouard Pertuiset (Centre Hospitalier, Cergy-Pontoise), Jean-Michel Philippe (Centre Hospitalier, Montdidier), ThierryPonge (Hopital Hotel-Dieu, Nantes), Isabelle Quere (HopitalSaint-Eloi, Montpellier), Andry Randrianjohany (Hopital Avi-cenne, Bobigny), Elizabeth Rankin (University Hospital Bir-mingham, Birmingham, UK), Marielle Roux (Centre Hospi-talier, Bourgoin-Jallieu), Marc Ruivard (Hopital Gabriel-Montpied, Clermont-Ferrand), Jean-Luc Saraux (Centre
Hospitalier de Montmorency, Eaubonne), Annette Schaeffer(Hopital Henri-Mondor, Creteil), Claude Schmidt (CentreHospitalier Universitaire, Nancy), Stephane Schneebeli (Cen-tre Hospitalier, Lorient), Christian Seigneuric (Centre Hospi-talier, Montauban), Smail Amar (Centre Hospitalier Univer-sitaire, Amiens), Agnes Sparsa (Hopital Dupuytren, Limoges),Jerome Stirnemann (Hopital Jean-Verdier, Bondy), LaureSwiader (Hopital de la Timone, Marseille), Jean-Pierre Tail-landier (Hopital Paul-Brousse, Villejuif), Corinne Thevenot(Centre Hospitalier, Cayenne), Kiet-Phong Tiev (HopitalSaint-Antoine, Paris), Cecile Toledano (Hopital Saint-Louis,Paris), Nicolas Velmans (Centre Hospitalier, Lannion), Jean-Francois Viallard (Hopital Haut-Leveque, Bordeaux), Elisa-beth Vidal (Centre Hospitalier Universitaire Dupuytren, Li-moges), Marie-Josee Wahl (Centre Hospitalier Universitaire,Nancy), Marie-Jose Wattiaux (Hopital Saint-Antoine, Paris),Arnold Witte (Centre Hospitalier, Chartres), Jean-Marc Ziza(Hopital de la Croix–Saint-Simon, Paris), Abdelkader Zoulim(Centre Hospitalier Universitaire, Caen). We thank JanetJacobson for editorial assistance.
AUTHOR CONTRIBUTIONS
All authors were involved in drafting the article or revising itcritically for important intellectual content, and all authors approvedthe final version to be published. Dr. Ribi had full access to all of thedata in the study and takes responsibility for the integrity of the dataand the accuracy of the data analysis.Study conception and design. Pagnoux, Arene, Puechal, Cordier,Guillevin.Acquisition of data. Ribi, Cohen, Pagnoux, Arene, Carli, Kyndt, LeHello, Letellier, Cordier, Guillevin.Analysis and interpretation of data. Ribi, Cohen, Pagnoux, Mahr,Puechal, Guillevin.
REFERENCES
1. Guillevin L, Mahr A, Callard P, Godmer P, Pagnoux C, Leray E,et al. Hepatitis B virus-associated polyarteritis nodosa: clinicalcharacteristics, outcome, and impact of treatment in 115 patients.Medicine (Baltimore) 2005;84:313–22.
2. Lightfoot RW Jr, Michel BA, Bloch DA, Hunder GG, Zvaifler NJ,McShane DJ, et al. The American College of Rheumatology 1990criteria for the classification of polyarteritis nodosa. ArthritisRheum 1990;33:1088–93.
3. Jennette JC, Falk RJ, Andrassy K, Bacon PA, Churg J, Gross WL,et al. Nomenclature of systemic vasculitides: proposal of aninternational consensus conference. Arthritis Rheum 1994;37:187–92.
4. Guillevin L, Lhote F, Gayraud M, Cohen P, Jarrousse B, Lortho-lary O, et al. Prognostic factors in polyarteritis nodosa andChurg-Strauss syndrome: a prospective study in 342 patients.Medicine (Baltimore) 1996;75:17–28.
5. Ribi C, Cohen P, Pagnoux C, Mahr A, Arene JP, Lauque D, et al,for the French Vasculitis Study Group. Treatment of Churg-Strauss syndrome without poor-prognosis factors: a multicenter,prospective, randomized, open-label study of seventy-two patients.Arthritis Rheum 2008;58:586–94.
6. Hagen EC, Daha MR, Hermans J, Andrassy K, Csernok E, GaskinG, et al. Diagnostic value of standardized assays for anti-neutrophil cytoplasmic antibodies in idiopathic systemic vasculi-tisa: EC/BCR project for ANCA assay standardization. Kidney Int1998;53:743–53.
7. Luqmani RA, Bacon PA, Moots RJ, Janssen BA, Pall A, Emery P,
1196 RIBI ET AL

et al. Birmingham Vasculitis Activity Score (BVAS) in systemicnecrotizing vasculitis. QJM 1994;87:671–8.
8. Yazici H, Pazarli H, Barnes CG, Tuzun Y, Ozyazgan Y, Silman A,et al. A controlled trial of azathioprine in Behcet’s syndrome.N Engl J Med 1990;322:281–5.
9. Fauci AS, Katz P, Haynes BF, Wolff SM. Cyclophosphamidetherapy of severe systemic necrotizing vasculitis. N Engl J Med1979;301:235–8.
10. Guillevin L, Jarrousse B, Lok C, Lhote F, Jais JP, Le Thi HuongD, et al, for the Cooperative Study Group for Polyarteritis Nodosa.Longterm followup after treatment of polyarteritis nodosa andChurg-Strauss angiitis with comparison of steroids, plasma ex-change and cyclophosphamide to steroids and plasma exchange: aprospective randomized trial of 71 patients. J Rheumatol 1991;18:567–74.
11. Gayraud M, Guillevin L, le Toumelin P, Cohen P, Lhote F,Casassus P, et al, for the French Vasculitis Study Group. Long-term followup of polyarteritis nodosa, microscopic polyangiitis,and Churg-Strauss syndrome: analysis of four prospective trialsincluding 278 patients. Arthritis Rheum 2001;44:666–75.
12. Leib ES, Restivo C, Paulus HE. Immunosuppressive and cortico-steroid therapy of polyarteritis nodosa. Am J Med 1979;67:941–7.
13. Cohen RD, Conn DL, Ilstrup DM. Clinical features, prognosis,and response to treatment in polyarteritis. Mayo Clin Proc 1980;55:146–55.
14. Guillevin L, Le Thi Huong D, Godeau P, Jais P, Wechsler B.Clinical findings and prognosis of polyarteritis nodosa and Churg-Strauss angiitis: a study in 165 patients. Br J Rheumatol 1988;27:258–64.
15. Guillevin L, Lhote F, Cohen P, Jarrousse B, Lortholary O,Genereau T, et al. Corticosteroids plus pulse cyclophosphamideand plasma exchanges versus corticosteroids plus pulse cyclo-phosphamide alone in the treatment of polyarteritis nodosa andChurg-Strauss syndrome patients with factors predicting poorprognosis: a prospective, randomized trial in sixty-two patients.Arthritis Rheum 1995;38:1638–45.
16. Fortin PR, Larson MG, Watters AK, Yeadon CA, Choquette D,Esdaile JM. Prognostic factors in systemic necrotizing vasculitis ofthe polyarteritis nodosa group: a review of 45 cases. J Rheumatol1995;22:78–84.
17. Guillevin L, Durand-Gasselin B, Cevallos R, Gayraud M, Lhote F,Callard P, et al. Microscopic polyangiitis: clinical and laboratoryfindings in eighty-five patients. Arthritis Rheum 1999;42:421–30.
18. Lhote F, Cohen P, Guillevin L. Polyarteritis nodosa, microscopicpolyangiitis and Churg-Strauss syndrome. Lupus 1998;7:238–58.
19. Pavone L, Grasselli C, Chierici E, Maggiore U, Garini G, RondaN, et al. Outcome and prognostic factors during the course ofprimary small-vessel vasculitides. J Rheumatol 2006;33:1299–306.
20. Gibson A, Stamp LK, Chapman PT, O’Donnell JL. The epidemi-ology of Wegener’s granulomatosis and microscopic polyangiitis ina southern hemisphere region. Rheumatology (Oxford) 2006;45:624–8.
21. Weidner S, Geuss S, Hafezi-Rachti S, Wonka A, Rupprecht HD.ANCA-associated vasculitis with renal involvement: an outcomeanalysis. Nephrol Dial Transplant 2004;19:1403–11.
22. Hauer HA, Bajema IM, Van Houwelingen HC, Ferrario F, NoelLH, Waldherr R, et al. Determinants of outcome in ANCA-associated glomerulonephritis: a prospective clinico-histopatho-logical analysis of 96 patients. Kidney Int 2002;62:1732–42.
23. Langford CA. Treatment of polyarteritis nodosa, microscopicpolyangiitis, and Churg-Strauss syndrome: where do we stand?[editorial]. Arthritis Rheum 2001;44:508–12.
24. Guillevin L, Fain O, Lhote F, Jarrousse B, Le Thi Huong D,Bussel A, et al. Lack of superiority of steroids plus plasmaexchange to steroids alone in the treatment of polyarteritis nodosaand Churg-Strauss syndrome: a prospective, randomized trial in 78patients. Arthritis Rheum 1992;35:208–15.
25. Pusey C, Rees A, Evans D, Peters DK, Lockwood CM. Plasmaexchange in focal necrotizing glomerulonephritis without anti-GBM antibodies. Kidney Int 1991;40:757–63.
26. Jayne DR, Gaskin G, Rasmussen N, Abramowicz D, Ferrario F,Guillevin L, et al, for the European Vasculitis Study Group.Randomized trial of plasma exchange or high-dosage methylpred-nisolone as adjunctive therapy for severe renal vasculitis. J Am SocNephrol 2007;18:2180–8.
27. Jones RB, Ferraro AJ, Chaudhry AN, Brogan P, Salama AD,Smith KG, et al. A multicenter survey of rituximab therapy forrefractory antineutrophil cytoplasmic antibody–associated vasculi-tis. Arthritis Rheum 2009;60:2156–68.
28. Fain O, Hamidou M, Cacoub P, Godeau B, Wechsler B, Paries J,et al. Vasculitides associated with malignancies: analysis of sixtypatients. Arthritis Rheum 2007;57:1473–80.
29. Gayraud M, Guillevin L, Cohen P, Lhote F, Cacoub P, Deblois P,et al. Treatment of good-prognosis polyarteritis nodosa andChurg-Strauss syndrome: comparison of steroids and oral or pulsecyclophosphamide in 25 patients. Br J Rheumatol 1997;36:1290–7.
TREATMENT OF PAN AND MPA WITHOUT POOR-PROGNOSIS FACTORS 1197
Copyright © 2022 FDOKUMEN