One hundred human pancreatic islet isolations at Baylor Research Institute
8
341 The effectiveness of pancreatic islet isolation must be maximized to make islet cell transplantation (ICT) a standard therapy. We have performed 100 human islet isolations at Baylor Research Institute including islet isolations for research, for clinical allogeneic transplantation, and for autologous islet transplantation. In this study, we analyzed the results of these isola- tions. First, we assessed 79 islet isolations using brain-dead donors to determine variables associated with successful islet isolation. Univariate logistic regression analysis revealed that seven variables influenced the success of islet isolation for allogeneic ICT: cause of death, mechanism of death, techniques for pancreas procurement and preservation, heavy fatty infiltration, collagenase type, dilution time, and islet purification method. Multivariate regression analysis revealed that only the current isolation protocol, the Baylor Islet Isolation Method (BIIM)—with its four required elements of pancreas procurement by the team, pancreatic ductal injection, the two-layer method with perfluorocarbon, and density- adjusted density gradient purification—had a significant positive impact on successful islet isolation (P = 0.02). Second, we compared allogeneic and autologous ICT using the BIIM. There were no significant differences in islet yields between allogeneic and autologous ICT using the BIIM; total islet yield after purification was 628 ± 84 × 10 3 IE in allogeneic ICT vs. 576 ± 49 × 10 3 IE in autologous ICT (P = 0.59). This retrospective study revealed that the BIIM provided favorable outcomes for both autologous and allogeneic ICT. slet cell transplantation (ICT) is a promising treatment for type 1 diabetic patients who have damaged insulin secretory capacity due to autoimmunity (1, 2). It was reported that islet recipients could achieve insulin independence, improve glycemic control and quality of life, and prevent chronic diabetic complications, although these findings were based on a limited number of study cohorts (3–6). Recently our survey revealed that >85% of type 1 diabetic patients wanted to become insulin independent, and >75% believed that transplantation should replace insulin injection therapy (7). However, several issues remain before ICT can be a standard treatment, including the use of multiple donors to achieve and/or maintain long-term insulin independence and the adverse effects of immunosup- pressants (3, 5, 8, 9). e modification of islet isolation has helped improve the amount and quality of isolated islets, which is one factor for successful ICT. Since February 2007, we have implemented a modified islet isolation method based on the Kyoto islet isolation method (KIIM), a method developed for non–heart-beating donors in Japan (10, 11), to improve the efficacy of ICT. ICT using the recipient’s own islets is also useful to maintain excellent glycemic control in patients with chronic pancreatitis who undergo a total pancreatectomy (autologous ICT) (12, 13). A cytoprotective strategy during islet isolation might be more im- portant in autologous ICT, which uses pancreata with chronic in- flammation. Baylor Regional Transplant Institute has performed autologous ICT since October 2006 and has used a modified islet isolation method, called the Baylor Islet Isolation Method (BIIM), since December 2007. We have already reported 17 cases of autologous ICT and demonstrated excellent graft function and improvement of intractable abdominal pain (14). In February 2010, the total number of islet isolations per- formed by Baylor Research Institute reached 100. Herein, we review all islet isolations with two objectives: 1) to determine variables associated with successful islet isolation for allogeneic ICT and 2) to investigate the differences in donor character- istics and the islet isolation outcome between allogeneic and autologous ICT. METHODS Study overview All records of pancreatic islet isolations performed at Baylor Research Institute (Dallas, TX) from January 2005 to February 2010 were reviewed on the basis of previous reports (15–19). First, we conducted univariate logistic regression analysis fol- lowed by multivariate analysis using data from islet isolations From Baylor Research Institute, Fort Worth Campus, Fort Worth, Texas (Takita, Matsumoto, Noguchi, Sugimoto, Itoh); the Department of Internal Medicine (Shimoda), Department of Surgery (Lamont), and Division of Gastroenterology (Lara), Baylor University Medical Center at Dallas; Baylor Institute for Immunology Research, Dallas, Texas (Chujo); and Baylor Regional Transplant Institute, Dallas, Texas (Onaca, Naziruddin, Klintmalm, Levy). This work was supported in part by the Baylor All Saints Health Foundation and the Baylor Health Care System Foundation. Dr. Chujo has been supported by the W. W. Caruth Jr. Chair for Organ Transplantation Immunology to J. Banchereau, PhD. Corresponding author: Shinichi Matsumoto, MD, PhD, Baylor All Saints Islet Cell Laboratory, 1400 8th Avenue, Fort Worth, Texas 76104 (e-mail: ShinichM@ BaylorHealth.edu). One hundred human pancreatic islet isolations at Baylor Research Institute Morihito Takita, MD, Shinichi Matsumoto, MD, PhD, Hirofumi Noguchi, MD, PhD, Masayuki Shimoda, MD, PhD, Daisuke Chujo, MD, PhD, Koji Sugimoto, MD, PhD, Takeshi Itoh, MD, PhD, Jeffrey P. Lamont, MD, Luis F. Lara, MD, Nicholas Onaca, MD, Bashoo Naziruddin, PhD, Goran B. Klintmalm, MD, PhD, and Marlon F. Levy, MD I Proc (Bayl Univ Med Cent) 2010;23(4):341–348
-
Upload
baylorhealth -
Category
Documents
-
view
1 -
download
0
Transcript of One hundred human pancreatic islet isolations at Baylor Research Institute

341
The effectiveness of pancreatic islet isolation must be maximized to make
islet cell transplantation (ICT) a standard therapy. We have performed 100
human islet isolations at Baylor Research Institute including islet isolations
for research, for clinical allogeneic transplantation, and for autologous
islet transplantation. In this study, we analyzed the results of these isola-
tions. First, we assessed 79 islet isolations using brain-dead donors to
determine variables associated with successful islet isolation. Univariate
logistic regression analysis revealed that seven variables influenced the
success of islet isolation for allogeneic ICT: cause of death, mechanism
of death, techniques for pancreas procurement and preservation, heavy
fatty infiltration, collagenase type, dilution time, and islet purification
method. Multivariate regression analysis revealed that only the current
isolation protocol, the Baylor Islet Isolation Method (BIIM)—with its four
required elements of pancreas procurement by the team, pancreatic
ductal injection, the two-layer method with perfluorocarbon, and density-
adjusted density gradient purification—had a significant positive impact
on successful islet isolation (P = 0.02). Second, we compared allogeneic
and autologous ICT using the BIIM. There were no significant differences
in islet yields between allogeneic and autologous ICT using the BIIM; total
islet yield after purification was 628 ± 84 × 103 IE in allogeneic ICT vs.
576 ± 49 × 103 IE in autologous ICT (P = 0.59). This retrospective study
revealed that the BIIM provided favorable outcomes for both autologous
and allogeneic ICT.
slet cell transplantation (ICT) is a promising treatment for type 1 diabetic patients who have damaged insulin secretory capacity due to autoimmunity (1, 2). It was reported that islet recipients could achieve insulin independence, improve
glycemic control and quality of life, and prevent chronic diabetic complications, although these fi ndings were based on a limited number of study cohorts (3–6). Recently our survey revealed that >85% of type 1 diabetic patients wanted to become insulin independent, and >75% believed that transplantation should replace insulin injection therapy (7). However, several issues remain before ICT can be a standard treatment, including the use of multiple donors to achieve and/or maintain long-term insulin independence and the adverse eff ects of immunosup-pressants (3, 5, 8, 9). Th e modifi cation of islet isolation has helped improve the amount and quality of isolated islets, which is one factor for successful ICT. Since February 2007, we have
implemented a modifi ed islet isolation method based on the Kyoto islet isolation method (KIIM), a method developed for non–heart-beating donors in Japan (10, 11), to improve the effi cacy of ICT.
ICT using the recipient’s own islets is also useful to maintain excellent glycemic control in patients with chronic pancreatitis who undergo a total pancreatectomy (autologous ICT) (12, 13). A cytoprotective strategy during islet isolation might be more im-portant in autologous ICT, which uses pancreata with chronic in-fl ammation. Baylor Regional Transplant Institute has performed autologous ICT since October 2006 and has used a modifi ed islet isolation method, called the Baylor Islet Isolation Method (BIIM), since December 2007. We have already reported 17 cases of autologous ICT and demonstrated excellent graft function and improvement of intractable abdominal pain (14).
In February 2010, the total number of islet isolations per-formed by Baylor Research Institute reached 100. Herein, we review all islet isolations with two objectives: 1) to determine variables associated with successful islet isolation for allogeneic ICT and 2) to investigate the diff erences in donor character-istics and the islet isolation outcome between allogeneic and autologous ICT.
METHODSStudy overview
All records of pancreatic islet isolations performed at Baylor Research Institute (Dallas, TX) from January 2005 to February 2010 were reviewed on the basis of previous reports (15–19). First, we conducted univariate logistic regression analysis fol-lowed by multivariate analysis using data from islet isolations
From Baylor Research Institute, Fort Worth Campus, Fort Worth, Texas (Takita,
Matsumoto, Noguchi, Sugimoto, Itoh); the Department of Internal Medicine
(Shimoda), Department of Surgery (Lamont), and Division of Gastroenterology
(Lara), Baylor University Medical Center at Dallas; Baylor Institute for Immunology
Research, Dallas, Texas (Chujo); and Baylor Regional Transplant Institute, Dallas,
Texas (Onaca, Naziruddin, Klintmalm, Levy).
This work was supported in part by the Baylor All Saints Health Foundation and the
Baylor Health Care System Foundation. Dr. Chujo has been supported by the W. W.
Caruth Jr. Chair for Organ Transplantation Immunology to J. Banchereau, PhD.
Corresponding author: Shinichi Matsumoto, MD, PhD, Baylor All Saints Islet
Cell Laboratory, 1400 8th Avenue, Fort Worth, Texas 76104 (e-mail: ShinichM@
BaylorHealth.edu).
One hundred human pancreatic islet isolations at Baylor Research InstituteMorihito Takita, MD, Shinichi Matsumoto, MD, PhD, Hirofumi Noguchi, MD, PhD, Masayuki Shimoda, MD, PhD, Daisuke Chujo, MD, PhD, Koji Sugimoto, MD, PhD, Takeshi Itoh, MD, PhD, Jeffrey P. Lamont, MD, Luis F. Lara, MD, Nicholas Onaca, MD, Bashoo Naziruddin, PhD, Goran B. Klintmalm, MD, PhD, and Marlon F. Levy, MD
I
Proc (Bayl Univ Med Cent) 2010;23(4):341–348

Baylor University Medical Center Proceedings Volume 23, Number 4342
with brain-dead donors in order to identify factors that in-fl uence the success of islet isolation. Successful islet isolations were defi ned as islet yields >300,000 islet equivalents (IEs). Th is amount allows approximately 5000 IE per kg of body weight, since the average body weight of islet recipients is ap-proximately 60 kg, according to the latest annual report of the Collaborative Islet Transplant Registry (20). Four isolations using brain-dead donors were excluded from this analysis due to technical failures of islet isolation. Second, we compared donor characteristics and outcomes of islet isolations using the same method between autologous and allogeneic transplanta-tions (Figure). Th e institutional review board of Baylor Research Institute approved this study.
Pancreas donor characteristicsData on characteristics of pancreas donors were obtained
from donor charts provided by organ procurement organizations (LifeGift, Fort Worth; Southwest Transplant Alliance, Dallas) or from patient records for autologous ICT. Categories of do-nor characteristics were defi ned based on the United Network for Organ Sharing/Organ Procurement and Transplantation Network data collection system (21). For donor cause of death, three groups were used for statistical analysis: cerebrovascular/stroke, head trauma, and other. Similarly, for mechanism of death, three categories were used: blunt injury, intracranial hemorrhage/stroke, and other. Donor body mass index (BMI) was calculated using the formula of kg/m2, and body surface area was calculated using Mosteller’s formula of √[height (cm) × weight (kg)/3600] (22).
Pancreas preservation and islet isolationFor the standard method, a donated pancreas was procured
and shipped by a remote center team. Th e harvested pancreas was preserved in chilled University of Wisconsin (UW) solution. Th e following modifi cations were recorded: “pancreas procure-ment by islet team” when surgeons who belonged to our team procured the pancreas, “ductal injection” when approximately 1 mL/g of chilled preservation solution (ET-Kyoto solution,
Otsuka Pharm Fact Inc., Naruto, Japan, or similar solution) was injected into the main pancreatic duct (10, 11, 23, 24), and “oxygen-charged static two-layer method (TLM)” when oxy-genated perfl uorocarbon (PFC) and preservation solution (25) were used for pancreas preservation. Cold ischemia time was defi ned as the time from cross-clamp to the start of perfusion.
All isolations were performed based on the modifi ed Ricordi method (26). Islets were purifi ed with the COBE 2991 cell pro-cessor (CaridianBCT, Inc., Lakewood, CO) with a continuous density gradient using Ficoll, iodixanol, or both (27). Islet vi-ability after purifi cation was evaluated with fl uorescein diacetate (10 μmol/L) and propidium iodide (15 μmol/L) staining (28). Th e average viability of 50 islets was calculated. Islet yield was assessed using dithizone staining (Sigma Chemical Co., St. Louis, MO) (2 mg/mL) and converted into a standard number of islet equivalents (IE, diameter standardizing to 150 μm) (29).
Baylor Islet Isolation MethodSince the KIIM was originally developed for non–heart-beat-
ing donors, we modifi ed the method for brain-dead donors (Ta-ble 1). Th e modifi ed method consists of four factors—pancreas procurement by the islet team, ductal injection with preservation solution, the TLM with oxygenated PFC, and density-adjusted continuous gradient purifi cation with iodixanol—which together defi ne the BIIM. Th e BIIM has also been applied for autologous ICT (14). When comparing isolations for allogeneic ICT and those for autologous ICT, we included only cases that met all four criteria for the BIIM to avoid confounding eff ects due to diff er-ences of pancreas preservation and islet isolation methods.
Statistical analysisNumbers and percentages were reported for categorical varia-
bles, while means and standard errors were calculated for continuous
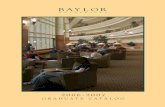
Figure 1. Study flow chart. *Purification was not performed due to technical
failures. **Analysis among this cohort was reported in a previous publication
(14).
100 islet isolations at Baylor Research Institute
17 isolations forauto-ICT**12 isolations for
allo-ICT71 isolations for
research
83 pancreata from brain-dead donors
11 isolationsStudy 2: Comparison between isolations for allo and auto ICT
79 isolationsStudy 1: Variables associated
with isolation success
4 cases excluded*
BIIM was performed for 5 cases for allo and 6 for auto ICT
Table 1. Comparison of islet isolation methods
Standard Kyoto Baylor
Donor Brain-deadNon–heart-
beatingBrain-dead
In-situ cooling system No Yes No
Pancreas
procurement team
Multiorgan
procurement
team
Kidney procure-
ment with islet
team
Islet team
Ductal preservation NoUlinastatin +
Kyoto solution
Kyoto solution or
similar solution
Pancreas storage
Two-layer
method or
University of
Wisconsin
solution
Two-layer
method
Two-layer
method
Pancreas digestionRicordi
methodRicordi method Ricordi method
Islet purificationDensity
gradient
Density-
adjusted density
gradient
Density-adjusted
density gradient

October 2010 343
variables. P values < 0.05 were considered statistically signifi -cant. All statistical analyses were performed by JMP (version 8.0; SAS Institute).
To fi nd possible factors associated with successful islet isola-tion of brain-dead donors, univariate logistic regression analysis was performed preliminarily, calculating odds ratios (OR) and P values for each variable. For continuous variables, OR and P values were calculated using variables above the 75th percen-tile and below the 25th percentile. Afterwards, selected factors with statistical signifi cance (P < 0.05) in the univariate logistic regression model were evaluated by multivariate logistic regres-sion analysis, which allows correction of covariates as predictors of islet isolation success. Hosmer-Lemeshow statistics were used to assess the goodness of fi t to islet isolation success (30).
Allogeneic and autologous ICT were compared by evaluating continuous variables by Student’s t test and categorical data by Fisher’s exact test.
RESULTSVariables associated with islet isolation success—preliminary univariate analysis
Characteristics of brain-dead donors. In all 79 cases, pancreata were obtained from brain-dead donors who had no past history of diabetes mellitus. Cerebrovascular/stroke as cause of death and intracranial hemorrhage/stroke as mechanism of death were signifi cantly associated with unsuccessful islet isolation (OR = 0.29, P = 0.01 and OR = 0.36, P = 0.04, respectively) (Table 2). Since 88% (30/34) of cases of cerebrovascular/stroke also had intracranial hemorrhage as mechanism of death (Fisher’s exact test P < 0.0001), cerebrovascular/stroke was in-put for further multivariate regression analysis. Gender had a marginally signifi cant correlation with islet isolation success (OR of women = 2.64, P = 0.053).
Variables for pancreas procurement, preservation, and is-let isolation. Pancreas procurement by the islet team had a significant positive impact on successful islet isolation (OR = 7.14, P = 0.0001) (Table 3). Both ductal injection and the TLM at pancreas preservation were also found to be statisti-cally signifi cant (OR = 8.57, P < 0.0001 and OR = 4.20, P = 0.03, respectively). All pancreata were intact and not edematous. When heavy fat infi ltration was observed, the islet isolation was more likely to be unsuccessful (OR = 0.35, P = 0.04).
For digestion, Liberase HI and Collagenase NB were found to be signifi cant variables (P = 0.001 and P = 0.04, respectively), although Liberase HI was only used before March 2007 and Collagenase NB was only used after May 2007 (Table 4). A long dilution time signifi cantly correlated with success (OR = 5.82, P = 0.03). Continuous gradient purifi cation was performed at all islet isolations. For density gradient of purifi cation, density-adjusted iodixanol was signifi cantly associated with success (OR = 3.24, P = 0.02), while Ficoll was less successful (OR = 0.36, P = 0.03).
Table 2. Donor characteristics affecting islet isolation success
N (%) or mean (±1 SE)
Variable
<300,000 IEs(n = 27, 34.2%)
≥300,000 IEs(n = 52, 65.8%)
Oddsratio*
Age (years)‡ 44.4 ± 2.4 41.3 ± 1.9 0.61
Gender
Women 7 (21.9) 25 (78.1) 2.64
Men 20 (42.6) 27 (57.5) 0.38
Weight (kg)‡ 89.6 ± 3.8 90.5 ± 3.3 0.78
Body mass index (kg/m2)‡ 29.5 ± 1.3 30.4 ± 1.0 1.38
Body surface area (m2)‡ 2.08 ± 0.0 2.07 ± 0.0 0.93
Race/ethnicity
White/Caucasian 22 (38.6) 35 (61.4) 0.47
African American 1 (11.1) 8 (88.9) 4.73
Hispanic 4 (33.3) 8 (66.7) 1.04
Cause of death
Cerebrovascular/stroke† 17 (50.0) 17 (50.0) 0.29
Head trauma 9 (26.5) 25 (73.5) 1.85
Other 1 (9.1) 10 (90.9) 6.19
Mechanism of death
Blunt injury 6 (28.6) 15 (71.4) 1.41
Intracranial hemorrhage/
stroke† 16 (47.1) 18 (52.9) 0.36
Other 5 (20.8) 19 (79.2) 2.53
Past history
Hypertension 8 (30.8) 18 (69.2) 1.25
Smoking 15 (31.3) 33 (68.8) 1.39
Duration of the last
hospitalization (days)‡3.6 ± 0.5 4.0 ± 0.4 1.04
*Calculated using univariate logistic regression.
†P < 0.05.
‡Odds ratios, 95% confidence intervals, and P values were reported between 75th
and 25th percentiles.
Table 3. Variables for pancreas procurement and preservation
N (%) or mean (±1 SE)
Variable<300,000 IEs
(n = 27, 34.2%)≥300,000 IEs
(n = 52, 65.8%)Oddsratio*
Pancreas procurement
by islet team† 10 (19.2) 42 (80.8) 7.14
Ductal injection† 7 (15.2) 39 (84.8) 8.57
Two-layer method† 20 (29.4) 48 (70.6) 4.20
Cold ischemia time‡
(min)410.7 ± 56.5 271.3 ± 24.1 0.39
*Calculated using univariate logistic regression.
†P < 0.05.
‡Odds ratios, 95% confidence intervals, and P values were reported between 75th
and 25th percentiles.
One hundred human pancreatic islet isolations at Baylor Research Institute

Baylor University Medical Center Proceedings Volume 23, Number 4344
In May 2007, we started to implement the BIIM. Cases that involved the BIIM were associated with successful islet isolation (OR = 8.64, P = 0.0002). To avoid colinearity among the modifi ed techniques, the BIIM was used for further mul-tivariate analysis instead of the following variables: pancreas procurement by the islet team, ductal injection, the TLM, and density-adjusted density gradient for purifi cation. Success rates were signifi cantly higher for the BIIM than for other isola-tion methods: 27/30 (90.0%) and 25/49 (51.0%), respectively (P = 0.0005, Fisher’s exact test).
Variables associated with islet isolation success—multivariate analysis
Based on results of univariate logistic regression analysis (Tables 2–4) and considerations about colinearity as mentioned above, several variables were included for further multivariate analysis: cerebrovascular/stroke as cause of death, heavy fatty
infi ltration in the pancreas, Roche Liberase HI and Serva Collagenase NB as collagenase, dilution time, and the BIIM. Based on the Hosmer-Lemeshow statistic, the fi nal model had a good fi t (P = 0.25). Only the BIIM was a signifi cant variable among the selected items (OR = 5.91, P = 0.02) (Table 5).
Comparison of allogeneic and autologous ICT using the BIIMTh is part of the study compared the fi ve cases of allogeneic
ICT and the six cases of autologous ICT that employed the BIIM. Th e six autologous ICT patients had had symptoms of chronic pancreatitis for 5.6 ± 0.7 years. Before autologous ICT, all had regularly used narcotics for pain management
Table 4. Variables for islet isolation
N (%) or mean (±1 SE)
Variable<300,000 IEs
(n = 27, 34.2%)≥300,000 IEs
(n = 52, 65.8%)Oddsratio*
Pancreas status and
distension
Predistention pancreas
weight‡ (g)105.7 ± 6.3 103.5 ± 4.4 0.75
Heavy fatty infiltration† 11 (52.4) 10 (47.6) 0.35
Predistention pancreas
temperature‡ (°C)11.8 ± 1.0 10.4 ± 0.5 0.37
Postdistention pancreas
temperature‡ (°C)14.2 ± 1.1 11.7 ± 0.6 0.26
Collagenase provider
and type
Roche Liberase HI† 17 (56.7) 13 (43.3) 0.20
Roche Liberase MTF 2 (15.4) 11 (84.6) 3.35
Serva Collagenase NB† 7 (21.2) 25 (78.1) 2.65
Sigma Vitacyte LLC 1 (25.0) 3 (75.0) 1.59
Digestion and dilution
Digestion time‡ (min) 19.0 ± 1.1 16.0 ± 0.6 0.36
Dilution time†‡ (min) 45.5 ± 2.5 52.7 ± 2.1 5.82
Total (digestion and
dilution)‡ (min)64.2 ± 3.1 68.3 ± 2.1 2.40
Type of gradient for
continuous purification
Ficoll† 15 (48.4) 16 (51.6) 0.36
Iodixanol† 8 (21.1) 30 (78.9) 3.24
Both 4 (40.0) 6 (60.0) 0.75
*Calculated using univariate logistic regression.
†P < 0.05.
‡Odds ratios, 95% confidence intervals, and P values were reported between 75th
and 25th percentiles.
Table 5. Multivariate logistic regression model for successful islet isolation
Variable Odds ratio*
Cause of death
Cerebrovascular/stroke 0.32
Pancreas status
Heavy fatty infiltration 1.08
Collagenase provider and type
Roche Liberase HI 0.64
Serva Collagenase NB 0.93
Dilution
Dilution time‡ (min) 1.03
Baylor Islet Isolation Method† 5.91
*Calculated using multivariate logistic regression.
†P < 0.05.
‡Odds ratios and P values were reported between 75th and 25th percentiles.
Table 6. Pancreas donor characteristics between allogeneic and autologous transplantation
Variable
Isolations for allogeneic
transplant (n = 5)
Isolations for autologous
transplant (n = 6)
Age* (years) 49.2 ± 3.7 39.2 ± 2.3
Gender: female/male 4/1 5/1
Weight (kg) 83.8 ± 9.8 70.9 ± 4.1
Body mass index (kg/m2) 28.5 ± 2.5 26.3 ± 1.3
Body surface area (m2) 1.98 ± 0.1 1.79 ± 0.1
Race/ethnicity
White/Caucasian 4 (80.0) 5 (83.3)
Hispanic 1 (20.0) 1 (16.7)
Past history
Hypertension 2 (40.0) 0 (0)
Smoking 3 (60.0) 3 (50.0)
*P < 0.05.

October 2010 345
(morphine equivalent dose [31]: 339 ± 96 mg/day) and had undergone endoscopic sphincterotomy or endoscopic stent replacement while complaining of severe abdominal pain of 7.3 ± 0.8 on a visual analog scale (with 0 indicating no pain and 10
indicating severe pain) (31). None had had surgical operations for chronic pancreatitis or had a history of diabetes mellitus. Four cases of chronic pancreatitis were idiopathic, one was related to pancreatic divisum, and one was related to alcohol.
Donor characteristics. Th ere were no signifi cant diff erences between allogeneic and autologous ICT in donor characteris-tics, except for age. Th e ages of donors for allogeneic ICT were signifi cantly higher than those for autologous ICT (P = 0.04, Table 6).
Outcomes of islet isolation. Th ere was no signifi cant diff er-ence in pancreas weight between allogeneic and autologous ICT, but cold ischemia time in allogeneic ICT was signifi cantly longer than that in autologous ICT (P = 0.0002, Table 7). Th ere were no signifi cant diff erences between the two groups in islet yield after digestion or after purifi cation. Th e purity of alloge-neic ICT was signifi cantly higher than that of autologous ICT (P = 0.0004). In addition, tissue volume after purifi cation for autologous ICT was signifi cantly higher than that for allogeneic ICT (P < 0.0001).
Size of isolated islets. Smaller-sized islets were observed more frequently in isolations for autologous ICT than in those for allogeneic ICT, which was evidenced by the signifi cantly higher ratio of 100 to 149 μm islets for autologous ICT (P = 0.03) (Table 8).
DISCUSSIONTh is report analyzed the fi rst 100 human pancreatic islet
isolations completed at Baylor Research Institute. Markmann et al indicated that approximately 100 human islet isolations were necessary before initiating clinical islet transplantation (32). We initiated clinical islet transplantation at Baylor Re-gional Transplant Institute before performing 50 human islet isolations. In addition, we have had a high success rate of clini-cal islet isolation and achieving insulin independence after islet transplantation (23). Th ose excellent results were mainly due to adaptation of the KIIM (10, 11, 23, 24).
In modifying the KIIM (10, 11), we eliminated the in situ cooling system (33) because it was designed to minimize warm ischemic injury after cardiac arrest, and the BIIM was developed for brain-dead donors without warm ischemic injury. We also eliminated ulinastatin for ductal preservation because ulinastatin was not available in the United States and the eff ect of trypsin inhibitors on islet isolation was controversial (34, 35). Th erefore, we used Kyoto solution or a similar solution without ulinastatin for ductal preservation in the BIIM. To perform ductal preserva-tion, at least one surgeon from the islet team was involved in the pancreas procurement. We used the oxygen-charged static TLM and the standard Ricordi method for both the KIIM and the BIIM; those elements were both stable and reliable and required no modifi cation. Density-adjusted density gradient was originally developed for islet purifi cation using brain-dead donors (36), and it was also benefi cial for non–heart-beating donors (10, 11). Th erefore, density-adjusted density gradients were used for both the KIIM and the BIIM.
In the fi rst part of the study, variables associated with successful isolation were investigated because one important
Table 8. Distribution of islet size between allogeneic and autologous islet transplants*
Islet size (μm)Isolations for allogeneic
transplant (n = 6)Isolations for autologous
transplant (n = 5)
50–99 27.1 ± 4.0 33.7 ± 2.7
100–149† 23.2 ± 3.2 33.7 ± 2.4
150–199 20.9 ± 2.0 14.5 ± 2.8
200–249 12.0 ± 2.1 7.7 ± 0.8
250–299 5.6 ± 1.2 3.4 ± 0.6
300–349 3.9 ± 0.4 2.6 ± 0.8
≥350 7.3 ± 1.3 4.2 ± 1.6
*The percentages of categorized size/total islets.
†P < 0.05.
Table 7. Outcomes of islet isolations between allogeneic and autologous islet transplant
Variable
Isolations for allogeneic
transplant (n = 6)
Isolations for autologous
transplant (n = 5)
Pancreas weight (g) 106.8 ± 10.4 93.4 ± 7.6
Cold ischemia time* (min) 224.6 ± 32.8 38.3 ± 6.9
Collagenase
Liberase MTF (n) 2 3
Collagenase NB (n) 3 3
Digestion time (min) 15.2 ± 2.4 12.7 ± 2.5
Digested pancreas
weight (%)89.6 ± 1.6 92.3 ± 1.5
Dilution time (min) 58.2 ± 5.5 49.7 ± 5.1
Postdigestion count
Islet yield (103 IE) 798 ± 107 659 ± 41
Islet yield/pancreas
weight (IE/g)7510 ± 700 7283 ± 735
Tissue volume (mL) 55.2 ± 14.4 36.7 ± 4.6
Postpurification count
Total islet yield (103 IE) 628 ± 84 576 ± 49
Total islet yield/pancreas
weight (IE/g)5900 ± 513 6351 ± 770
Total islet yield/recipient
body weight (IE/kg)10,589 ± 867 8255 ± 864
Purity* (%) 56.1 ± 2.5 37.3 ± 2.4
Viability (%) 97.7 ± 0.5 98.0 ± 0.4
Product volume* (mL) 5.7 ± 0.8 15.1 ± 0.5
*P < 0.05.
One hundred human pancreatic islet isolations at Baylor Research Institute

Baylor University Medical Center Proceedings Volume 23, Number 4346
element of successful ICT is maximization of islet yields (15–19, 24). In the second part, diff erences between allogeneic and autologous ICT were investigated using cases that implemented the BIIM.
Previous reports have demonstrated that deceased donor age, BMI, cause of death, and length of hospitalization aff ected islet isolation outcomes (15–19). In this study, cause of death had statistical signifi cance in univariate analysis, while the other donor characteristics did not reach statistical signifi cance. Th is might be explained by the fact that we accept obese donors for islet isolation. In fact, in our study, the average donor body weight, BMI, and body surface area in the unsuccessful isolation group were higher than in previous reports and close to that of others’ successful group.
In the fi rst part of the study using univariate regression analysis, it was found that the modifi ed techniques for pancreas preservation, including ductal injection with chilled preserva-tion solution and the TLM with oxygenated PFC, were associ-ated with islet isolation success. According to the latest annual reports of the Collaborative Islet Transplant Registry and Islet Cell Resource Centers, University of Wisconsin solution alone was used for approximately 50% to 60% of pancreas procure-ments (20, 37). Previous papers reported that the TLM as well as ductal injection signifi cantly improved the outcome of islet isolation (23, 25, 38, 39). Pancreas procurement by the is-let team made it possible to perform these special techniques smoothly.
Th e density-adjusted continuous density gradient purifi ca-tion with iodixanol, which reduces the force to islets during centrifugation by its low viscosity (10, 40, 41), signifi cantly improved islet isolation. Of note, the modifi ed techniques mentioned above were initiated in early 2007, and there was a possibility that these variables interact with each other in determining islet isolation success. To avoid confounding ef-fects with the other variables, multivariate logistic regression analysis was performed for selected variables on the basis of results of univariate analysis. Multivariate logistic regression analysis revealed that the BIIM, our current isolation protocol, was an independent predictor of success. Th e combination of multiple modifi ed techniques including procurement by the islet team, ductal injection, the TLM, and density-adjusted iodixanol-based continuous purifi cation could contribute to improve islet isolation.
Heavy fatty infi ltration was found to be a negative predic-tor of isolation success in univariate analysis. However, previ-ous studies demonstrated that fatty infi ltration of the pancreas was benefi cial for isolation success (15, 18). Th is discrepancy is most likely due to the association between fatty pancreas and high BMI. In our series, most pancreata were from high-BMI donors; therefore, the positive eff ect of high BMI was not ap-parent. On the contrary, although fatty infi ltration inhibited collagenase delivery and activity, the positive eff ect of high BMI might have overcome this disadvantage if pancreata from both low- and high-BMI donors were accepted.
In univariate analysis, collagenase type was associated with the outcome of islet isolation. However, as described in the
Results section, Liberase HI was used for old isolations and Collagenase NB was used for recent isolations, where modifi ed pancreas preservation techniques and islet isolation methods were implemented. Th erefore, careful interpretation is needed for univariate analysis of collagenase types, and in multivariate analysis no signifi cant eff ects were observed based on collagenase type.
A longer dilution time was also associated with islet isolation success. Earlier, it was shown that a short digestion time was associated with high islet yield due to avoidance of overdiges-tion (16). In this study, digestion time was shorter in the high islet yield group even though it did not reach statistical sig-nifi cance. A longer dilution time might refl ect underdigestion, which should increase islet yield due to avoidance of overdiges-tion as long as the amount of undigested pancreas is within an acceptable range.
Multivariate logistic regression analysis revealed that only the BIIM had a signifi cant impact on successful islet isolation with brain-dead donors. This suggests that the BIIM could overcome other factors to achieve successful islet isolation.
Next, we compared variables related to donor characteristics and islet isolation between allogeneic and autologous ICT where the BIIM was fully performed. Th is analysis can clarify the dif-ferences of donor variables and isolation outcomes between al-logeneic and autologous ICT, while avoiding eff ects of diff erent islet isolation methods. Th ere were no signifi cant diff erences in donor characteristics except for age. Th e diff erence of donor age between allogeneic and autologous ICT might be due to donor selection for allogeneic ICT. It should be noted that donors are selected for whole pancreas transplantation prior to ICT, and younger donors are favorable for whole pancreas transplanta-tion (42). In addition, there was a signifi cantly longer cold ischemia time for allogeneic ICT. On the other hand, pancreata for autologous islet isolation had inevitable chronic pancreati-tis. It was shown that chronic pancreatitis inhibited pancreas digestion, which resulted in poor islet yield (16). Older donor age and prolonged cold ischemia time were negative factors for allogeneic ICT, and chronic pancreatitis was a negative factor for autologous ICT. Interestingly, islet yields both after diges-tion and after purifi cation did not have signifi cant diff erences between the two groups when the BIIM was applied. Th erefore, the BIIM should be a favorable technique for both allogeneic and autologous ICT.
Final tissue volume was signifi cantly diff erent between the two groups, so purity also was signifi cantly diff erent. Th is re-sult can be explained by the diff erence of our protocols for maximum volume of fi nal product: 10 mL for allogeneic ICT and 15 mL for autologous ICT. All islet preparations for both allogeneic and autologous ICT were safely transplanted into the liver, except for one autologous ICT case where 602,709 IE was infused into the liver and 117,067 IE into the intraperitoneal cavity (14), and no portal vein thrombosis was observed in our cohort.
Interestingly, smaller islets were observed in isolation for autologous ICT compared with allogeneic ICT. Pancreata with

October 2010 347
chronic infl ammation would be easily overdigested since a pre-vious report suggested that overdigested islets became smaller compared with pre- and post-isolation islet sizes (18). Th erefore, careful digestion is necessary to avoid overdigestion, especially for autologous ICT.
In summary, we reviewed 100 pancreatic islet isolations at Baylor Research Institute. Th e BIIM was found to be a predic-tor of islet isolation success in multivariate logistic regression analysis. Comparison of allogeneic and autologous ICT revealed that the BIIM provided favorable outcomes for both.
ACKNOWLEDGMENTSTh e authors thank Ms. Sara Shah for the grammatical edit-
ing of the manuscript and Ms. Yoshiko Tamura and Mr. Greg S. Olsen for their technical support.
1. Shapiro AM, Ricordi C, Hering BJ, Auchincloss H, Lindblad R, Robertson RP, Secchi A, Brendel MD, Berney T, Brennan DC, Cagliero E, Alejandro R, Ryan EA, DiMercurio B, Morel P, Polonsky KS, Reems JA, Bretzel RG, Ber-tuzzi F, Froud T, Kandaswamy R, Sutherland DE, Eisenbarth G, Segal M, Preiksaitis J, Korbutt GS, Barton FB, Viviano L, Seyfert-Margolis V, Blue-stone J, Lakey JR. International trial of the Edmonton protocol for islet transplantation. N Engl J Med 2006;355(13):1318–1330.
2. Shapiro AM, Lakey JR, Ryan EA, Korbutt GS, Toth E, Warnock GL, Kneteman NM, Rajotte RV. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N Engl J Med 2000;343(4):230–238.
3. Fiorina P, Shapiro AM, Ricordi C, Secchi A. Th e clinical impact of islet transplantation. Am J Transplant 2008;8(10):1990–1997.
4. Th aravanij T, Betancourt A, Messinger S, Cure P, Leitao CB, Baidal DA, Froud T, Ricordi C, Alejandro R. Improved long-term health-related quality of life after islet transplantation. Transplantation 2008;86(9):1161–1167.
5. Ryan EA, Paty BW, Senior PA, Bigam D, Alfadhli E, Kneteman NM, Lakey JR, Shapiro AM. Five-year follow-up after clinical islet transplanta-tion. Diabetes 2005;54(7):2060–2069.
6. Fiorina P, Gremizzi C, Maffi P, Caldara R, Tavano D, Monti L, Socci C, Folli F, Fazio F, Astorri E, Del Maschio A, Secchi A. Islet transplantation is associated with an improvement of cardiovascular function in type 1 dia-betic kidney transplant patients. Diabetes Care 2005;28(6):1358–1365.
7. Hatanaka N, Takita M, Yamaguchi T, Kami M, Matsumoto S. Interests in beta-cell replacement therapies among Japanese patients with type 1 diabetes. Diabetes Res Clin Pract 2010;89(1):e5–e8.
8. Mineo D, Pileggi A, Alejandro R, Ricordi C. Point: steady progress and current challenges in clinical islet transplantation. Diabetes Care 2009;32(8):1563–1569.
9. Takita M, Matsumoto S, Noguchi H, Shimoda M, Ikemoto T, Chujo D, Tamura Y, Olsen SG, Naziruddin B, Purcell K, Onaca N, Levy MF. Ad-verse events in clinical islet transplantation: one institutional experience. Cell Transplant in press.
10. Matsumoto S, Okitsu T, Iwanaga Y, Noguchi H, Nagata H, Yonekawa Y, Ya-mada Y, Fukuda K, Shibata T, Kasai Y, Maekawa T, Wada H, Nakamura T, Tanaka K. Successful islet transplantation from nonheartbeating donor pancreata using modifi ed Ricordi islet isolation method. Transplantation 2006;82(4):460–465.
11. Matsumoto S, Tanaka K. Pancreatic islet cell transplantation using non–heart-beating donors (NHBDs). J Hepatobiliary Pancreat Surg 2005;12(3):227–230.
12. Blondet JJ, Carlson AM, Kobayashi T, Jie T, Bellin M, Hering BJ, Freeman ML, Beilman GJ, Sutherland DE. Th e role of total pancreatec-tomy and islet autotransplantation for chronic pancreatitis. Surg Clin North Am 2007;87(6):1477–1501.
13. Rodriguez Rilo HL, Ahmad SA, D’Alessio D, Iwanaga Y, Kim J, Choe KA, Moulton JS, Martin J, Pennington LJ, Soldano DA, Biliter J,
Martin SP, Ulrich CD, Somogyi L, Welge J, Matthews JB, Lowy AM. Total pancreatectomy and autologous islet cell transplantation as a means to treat severe chronic pancreatitis. J Gastrointest Surg 2003;7(8):978–989.
14. Takita M, Naziruddin B, Matsumoto S, Noguchi H, Shimoda M, Chujo D, Itoh T, Sugimoto K, Onaca N, Lamont JP, Lara LF, Levy MF. Variables as-sociated with islet yield in autologous islet cell transplantation for chronic pancreatitis. Proc (Bayl Univ Med Cent) 2010;23(2):115–120.
15. Kaddis JS, Danobeitia JS, Niland JC, Stiller T, Fernandez LA. Multicenter analysis of novel and established variables associated with successful human islet isolation outcomes. Am J Transplant 2010;10(3):646–656.
16. Liu X, Matsumoto S, Okitsu T, Iwanaga Y, Noguchi H, Yonekawa Y, Nagata H, Kamiya H, Ueda M, Hatanaka N, Miyakawa S, Kobayashi N, Song C. Analysis of donor- and isolation-related variables from non–heart-beating donors (NHBDs) using the Kyoto islet isolation method. Cell Transplant 2008;17(6):649–656.
17. Sakuma Y, Ricordi C, Miki A, Yamamoto T, Pileggi A, Khan A, Alejandro R, Inverardi L, Ichii H. Factors that aff ect human islet isolation. Transplant Proc 2008;40(2):343–345.
18. Hanley SC, Paraskevas S, Rosenberg L. Donor and isolation variables predict-ing human islet isolation success. Transplantation 2008;85(7):950–955.
19. Lakey JR, Warnock GL, Rajotte RV, Suarez-Alamazor ME, Ao Z, Shapiro AM, Kneteman NM. Variables in organ donors that aff ect the recovery of human islets of Langerhans. Transplantation 1996;61(7):1047–1053.
20. Collaborative Islet Transplant Registry. CITR annual report and supple-mentary materials. Rockville, MD: CITR, 2009. Available at http://www.citregistry.com; accessed June 30, 2010.
21. Th e US Organ Procurement and Transplantation Network and the Sci-entifi c Registry of Transplant Recipients. Th e 2008 OPTN/SRTR Annual Report: Transplant Data 1998–2007. Rockville, MD: US Department of Health and Human Services. Available at http://optn.transplant.hrsa.gov/ar2008/; accessed June 30, 2010.
22. Mosteller RD. Simplifi ed calculation of body-surface area. N Engl J Med 1987;317(17):1098.
23. Matsumoto S, Noguchi H, Shimoda M, Ikemoto T, Naziruddin B, Jackson A, Tamura Y, Olson G, Fujita Y, Chujo D, Takita M, Kobayashi N, Onaca N, Levy M. Seven consecutive successful clinical islet isola-tions with pancreatic ductal injection. Cell Transplant 2010;19(3):291–297.
24. Matsumoto S, Noguchi H, Naziruddin B, Onaca N, Jackson A, Nobuyo H, Teru O, Naoya K, Klintmalm G, Levy M. Improvement of pancre-atic islet cell isolation for transplantation. Proc (Bayl Univ Med Cent) 2007;20(4):357–362.
25. Matsumoto S, Rigley TH, Qualley SA, Kuroda Y, Reems JA, Stevens RB. Effi cacy of the oxygen-charged static two-layer method for short-term pancreas preservation and islet isolation from nonhuman primate and human pancreata. Cell Transplant 2002;11(8):769–777.
26. Ricordi C, Lacy PE, Scharp DW. Automated islet isolation from human pancreas. Diabetes 1989;38(Suppl 1):140–142.
27. Lake SP, Bassett PD, Larkins A, Revell J, Walczak K, Chamberlain J, Rumford GM, London NJ, Veitch PS, Bell PR, et al. Large-scale purifi ca-tion of human islets utilizing discontinuous albumin gradient on IBM 2991 cell separator. Diabetes 1989;38(Suppl 1):143–145.
28. Bank HL. Rapid assessment of islet viability with acridine orange and propidium iodide. In Vitro Cell Dev Biol 1988;24(4):266–273.
29. Latif ZA, Noel J, Alejandro R. A simple method of staining fresh and cultured islets. Transplantation 1988;45(4):827–830.
30. Hosmer DW Jr, Lemeshow S. Applied logistic regression, 2nd ed. New York: John Wiley & Sons, 2000.
31. Loeser JD. Bonica’s Management of Pain, 3rd ed. Philadelphia: Lippincott Williams & Wilkins, 2001.
32. Markmann JF, Deng S, Huang X, Desai NM, Velidedeoglu EH, Lui C, Frank A, Markmann E, Palanjian M, Brayman K, Wolf B, Bell E, Vitamaniuk M, Doliba N, Matschinsky F, Barker CF, Naji A. Insulin independence following isolated islet transplantation and single islet infu-sions. Ann Surg 2003;237(6):741–749.
One hundred human pancreatic islet isolations at Baylor Research Institute

Baylor University Medical Center Proceedings Volume 23, Number 4348
33. Nagata H, Matsumoto S, Okitsu T, Iwanaga Y, Noguchi H, Yonekawa Y, Kinukawa T, Shimizu T, Miyakawa S, Shiraki R, Hoshinaga K, Tanaka K. Procurement of the human pancreas for pancreatic islet transplantation from marginal cadaver donors. Transplantation 2006;82(3):327–331.
34. Rose NL, Palcic MM, Helms LM, Lakey JR. Evaluation of Pefabloc as a serine protease inhibitor during human-islet isolation. Transplantation 2003;75(4):462–466.
35. Rose NL, Palcic MM, Shapiro AM, Lakey JR. Endogenous pancreatic enzyme activity levels show no signifi cant eff ect on human islet isolation yield. Cell Transplant 2004;13(2):153–160.
36. Phillips GO. Advances in Tissue Banking, vol. 6. Singapore: World Scien-tifi c Publishing, 2002.
37. National Islet Cell Resource Center Consortium. Annual Report 2008. Available at http://icr.coh.org/; accessed June 30, 2010.
38. Matsumoto S, Kuroda Y. Perfl uorocarbon for organ preservation before transplantation. Transplantation 2002;74(12):1804–1809.
39. Noguchi H, Ueda M, Hayashi S, Kobayashi N, Okitsu T, Iwanaga Y, Nagata H, Nakai Y, Matsumoto S. Ductal injection of preservation solu-tion increases islet yields in islet isolation and improves islet graft function. Cell Transplant 2008;17(1–2):69–81.
40. Okitsu T, Matsumoto S, Iwanaga Y, Noguchi H, Nagata H, Yonekawa Y, Maekawa T, Tanaka K. Kyoto islet isolation method: the optimized one for non–heart-beating donors with highly effi cient islet retrieval. Transplant Proc 2005;37(8):3391–3392.
41. Shintaku H, Okitsu T, Kawano S, Matsumoto S, Suzuki T, Kanno I, Kotera H. Eff ects of fl uid dynamic stress on fracturing of cell-aggregated tissue during purifi cation for islets of Langerhans transplantation. Journal of Physics D: Applied Physics 2008;41(11):115507.1–115507.9.
42. Stegall MD, Dean PG, Sung R, Guidinger MK, McBride MA, Sommers C, Basadonna G, Stock PG, Leichtman AB. Th e rationale for the new deceased donor pancreas allocation schema. Transplantation2007;83(9):1156–1161.
Sponsored byA. Webb Roberts Center for Continuing Medical Education
of Baylor Health Care System, Dallas
Th is activity has been approved for AMA PRA Category 1 credit.
To register, or for more information,see the conference website at
www.williamsburgheartconference.org or call 214-820-2317.
Program Director:William Cliff ord Roberts, MD
Faculty:December 5–7, 2010 December 5–7, 2010 at Williamsburg Conference Centerat Williamsburg Conference CenterWilliamsburg, VirginiaWilliamsburg, Virginia
Upcoming ConferenceUpcoming Conference 37th Annual 37th Annual Williamsburg Conference Williamsburg Conference on Heart Diseaseon Heart Disease
Upcoming Conference 37th Annual Williamsburg Conference on Heart Disease
December 5–7, 2010 at Williamsburg Conference CenterWilliamsburg, Virginia
William E. Boden, MD Barry J. Maron, MD Robert O. Bonow, MD Peter A. McCullough, MD Robert M. Doroghazi, MD Darren K. McGuire, MD Kenneth M. Kent, MD Joseph C. Piscatella Peter R. Kowey, MD Charles S. Roberts, MD James T. Willerson, MD