
Transversus abdominis muscle release: Technique, indication ...
8
© 2018 International Journal of Abdominal Wall and Hernia Surgery | Published by Wolters Kluwer - Medknow 79 Transversus abdominis muscle release: Technique, indication, and results Wolfgang Reinpold Abstract: Component separation technique (CST) allows the mobilization of large musculofascial flaps of the abdominal wall and was developed for the treatment of very large, primary and incisional abdominal wall hernias. The classic open anterior CST first published by Albanese and later by Ramirez is associated with high complication rates. According to a recent literature review, CST without mesh should no longer be performed because of high recurrence rates. Classic anterior CST is associated with high rates of surgical-site occurrences and infections and should only be performed as endoscopic- and perforator-sparing anterior CST. The unfavorable results of classic CST resulted in the development of numerous new anterior and posterior CST modifications, several of them were minimally invasive. The posterior CST with transversus abdominis muscle (TAM) release (TAR) published by Novitsky et al. is an extension of the original retrorectus Rives operation and Stoppa procedure. The technique avoids vast skin flaps and allows the closure of large abdominal wall defects and insertion of very large retromuscular alloplastic standard sublay meshes without damaging the vessels and intercostal nerves. The TAR procedure is one of the major advances of abdominal wall surgery of the last decades. Several new promising minimally invasive modifications including robotic-assisted TAR have been published recently. The indications and technique of the TAM (TAR) procedure and its minimally invasive modifications are described. Keywords: Component separation technique, endoscopic component separation technique, perforator-sparing component separation technique, robotic transversus abdominis release, transversus abdominis release Introduction T he concept of component separation technique (CST) for the treatment of very large primary and incisional abdominal wall hernias was developed because the traditional suture and mesh techniques without relaxing the musculofascial flaps lead to unfavorable results. [1‑6] The classic open anterior CST was first published by Albanese [3,4] and decades later popularized by Ramirez. [5,6] The open anterior CST was developed for the reconstruction of a functional abdominal wall with autologous tissue repair. [3‑6] The key steps of their classic anterior open CST include vast skin flap of the rectus compartment; longitudinal division of the external oblique aponeurosis immediately lateral of the rectus compartment; vast dissection of the almost avascular space between external and internal oblique muscles; complete separation of the rectus abdominis muscle from its posterior rectus sheath; and then mobilizing the myofascial flap consisting of the rectus, internal oblique, and transversus abdominis muscle (TAM) medially. [3‑6] The classic CST without mesh augmentation is associated with high recurrence rates. [1,2] Moreover, due to the vast skin mobilization and destruction of the perforating vessels of the rectus compartment, there are frequent wound‑healing problems and infections. [1,2] The high complication rates of the traditional open CST resulted in the development of numerous open and Address for correspondence: Dr. Wolfgang Reinpold, Department of Surgery and Reference Hernia Center, Gross Sand Hospital, Gross Sand 3, D 21107 Hamburg, Germany. E-mail: w.reinpold@ gross-sand.de Submission: 24-10-2018 Accepted: 28-10-2018 Department of Surgery and Reference Hernia Center, Gross Sand Hospital, Hamburg, Germany Review Article Access this article online Quick Response Code: Website: www.herniasurgeryjournal.org DOI: 10.4103/ijawhs.ijawhs_27_18 How to cite this article: Reinpold W. Transversus abdominis muscle release: Technique, indication, and results. Int J Abdom Wall Hernia Surg 2018;1:79-86. This is an open access journal, and articles are distributed under the terms of the Creative Commons Aribuon‑NonCommercial‑ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given and the new creaons are licensed under the idencal terms. For reprints contact: [email protected] [Downloaded free from http://www.herniasurgeryjournal.org on Monday, November 4, 2019, IP: 10.232.74.26]
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Transversus abdominis muscle release: Technique, indication ...

© 2018 International Journal of Abdominal Wall and Hernia Surgery | Published by Wolters Kluwer - Medknow 79
Transversus abdominis muscle release: Technique, indication, and resultsWolfgang Reinpold
Abstract:Component separation technique (CST) allows the mobilization of large musculofascial flaps of the abdominal wall and was developed for the treatment of very large, primary and incisional abdominal wall hernias. The classic open anterior CST first published by Albanese and later by Ramirez is associated with high complication rates. According to a recent literature review, CST without mesh should no longer be performed because of high recurrence rates. Classic anterior CST is associated with high rates of surgical-site occurrences and infections and should only be performed as endoscopic- and perforator-sparing anterior CST. The unfavorable results of classic CST resulted in the development of numerous new anterior and posterior CST modifications, several of them were minimally invasive. The posterior CST with transversus abdominis muscle (TAM) release (TAR) published by Novitsky et al. is an extension of the original retrorectus Rives operation and Stoppa procedure. The technique avoids vast skin flaps and allows the closure of large abdominal wall defects and insertion of very large retromuscular alloplastic standard sublay meshes without damaging the vessels and intercostal nerves. The TAR procedure is one of the major advances of abdominal wall surgery of the last decades. Several new promising minimally invasive modifications including robotic-assisted TAR have been published recently. The indications and technique of the TAM (TAR) procedure and its minimally invasive modifications are described.Keywords:Component separation technique, endoscopic component separation technique, perforator-sparing component separation technique, robotic transversus abdominis release, transversus abdominis release
Introduction
The concept of component separation technique (CST) for the treatment of
very large primary and incisional abdominal wall hernias was developed because the traditional suture and mesh techniques without relaxing the musculofascial flaps lead to unfavorable results.[1‑6] The classic open anterior CST was first published by Albanese[3,4] and decades later popularized by Ramirez.[5,6] The open anterior CST was developed for the reconstruction of a functional abdominal wall with autologous tissue repair.[3‑6] The key steps of their classic anterior open CST include vast
skin flap of the rectus compartment; longitudinal division of the external oblique aponeurosis immediately lateral of the rectus compartment; vast dissection of the almost avascular space between external and internal oblique muscles; complete separation of the rectus abdominis muscle from its posterior rectus sheath; and then mobilizing the myofascial flap consisting of the rectus, internal oblique, and transversus abdominis muscle (TAM) medially.[3‑6] The classic CST without mesh augmentation is associated with high recurrence rates.[1,2] Moreover, due to the vast skin mobilization and destruction of the perforating vessels of the rectus compartment, there are frequent wound‑healing problems and infections.[1,2] The high complication rates of the traditional open CST resulted in the development of numerous open and
Address for correspondence:
Dr. Wolfgang Reinpold, Department of Surgery and Reference Hernia
Center, Gross Sand Hospital, Gross
Sand 3, D 21107 Hamburg, Germany. E-mail: w.reinpold@
gross-sand.de
Submission: 24-10-2018Accepted: 28-10-2018
Department of Surgery and Reference Hernia
Center, Gross Sand Hospital, Hamburg,
Germany
Review Article
Access this article onlineQuick Response Code:
Website:www.herniasurgeryjournal.org
DOI:10.4103/ijawhs.ijawhs_27_18
How to cite this article: Reinpold W. Transversus abdominis muscle release: Technique, indication, and results. Int J Abdom Wall Hernia Surg 2018;1:79-86.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
[Downloaded free from http://www.herniasurgeryjournal.org on Monday, November 4, 2019, IP: 10.232.74.26]

Reinpold: Transversus abdominis muscle release
80 International Journal of Abdominal Wall and Hernia Surgery - Volume 1, Issue 3, October-December 2018
minimally invasive modifications and new techniques of CST. The endoscopic anterior CST was first popularized by Rosen et al.[7] Meanwhile, several modifications have been published.[8,9] The first posterior CST was published by Milburn et al.[10] in 2007 who performed a cadaver trial comparing laparoscopic transperitoneal medial longitudinal release of the TAMs with classic open CST. Both techniques resulted in comparable release of the abdominal wall.
Development of Technique
The most suitable position for mesh placement is the retromuscular/preperitoneal (= sublay) plane.[1,11] One major disadvantage of the traditional retromuscular rives mesh operation is its limitation to the rectus compartment. In very large hernias and abdominal wall defects, confining the mesh to the rectus compartment often comes along with insufficient mesh overlap and defect bridging, which results in a high risk of recurrence. Before the advent of the posterior CST with TAM release (TAR), extension of the operation to the lateral compartment resulted in sacrificing the segmental nerves of the rectus abdominis muscle. In 2008, Carbonell et al. published a posterior CST technique[12] which was later coined “classic” posterior component separation:” the technical details of the procedure are as follows: (1) midline laparotomy (MLL) with complete lysis of adhesions, (2) incision of the posterior rectus sheath and its complete separation from the rectus muscle, (3) the posterior rectus sheath is incised at its most lateral edge, thus dividing the posterior aponeurotic sheath of the internal oblique muscle. This allows access to the plane between the internal oblique and TAM, (4) dissection is carried out as far lateral, inferior, and superior as desired, allowing for a large mesh underlay, (5) the posterior rectus sheath is then reapproximated in the midline with a running suture, (6) the mesh is placed in the retromuscular space and secured with sutures, and (7) the anterior rectus sheath is then reapproximated in the midline to cover the mesh.[12] The major disadvantages of this technique are as follows: longitudinal incision of the posterior rectus sheath at the lateral border of the rectus compartment is not possible without cutting the intercostal nerves, which may result in complete or partial paralysis of the rectus muscle. The plane between the internal oblique and TAM is least suitable for dissection and mesh placement since nerves and blood vessels are located in this space. Due to the unsolved problem of segmental nerve damage, the “classic posterior CST” cannot be recommended.
The problem of extending the dissection from the rectus abdominis muscle compartment to the lateral compartment and vice versa was solved by Novitsky et al.[13] Their working group published a modification of
the posterior CST with TAR. For the understanding of the TAR procedure, detailed knowledge of the abdominal wall anatomy is mandatory [Figure 1]. In the lateral compartment, the segmental intercostal nerves run between the transversus abdominis and internal oblique muscles. The nerves enter the rectus abdominis muscle compartment laterally and run approximately 1 cm on the anterior surface of the posterior rectus sheath. There they turn ventrally to enter the rectus abdominis muscle. Often, the segmental nerves are accompanied by segmental blood vessels. The posterior rectus sheath has to be incised medially to the segmental nerves [Figures 2‑4].
Transversus Abdominis Muscle Release in Large Midline Defects
TAR is an extension of the traditional Rives operation. (1) the operation usually starts with a midline incision; (2) the hernial sac is identified and dissected to the fascial border of the hernial ring; (3) the hernial sac and peritoneum are mobilized from the fascial hernial ring, posterior rectus sheath bilaterally, and cephalad and caudal of the hernial defect from the linea alba; (4) the posterior rectus sheath is medially incised longitudinally; and (5) the rectus abdominis muscle is completely separated from the posterior rectus sheath to the lateral edge of the rectus muscle compartment; the retromuscular plane in the rectus muscle compartment is developed toward the junction between the posterior and anterior rectus sheaths. The perforators to the rectus muscle (branches of the thoracoabdominal segmental nerves, penetrating the lateral edge of the posterior rectus sheath and their accompanying blood vessels) [Figure 10] are identified and preserved.[13] Usually, the dissection extends cranially to the costal margin and approximately 4 cm dorsal to the xiphoid. Caudal to the arcuate line,
Figure 1: Anatomy of the abdominal wall: The linea semilunaris depicts the medial end points of transversus abdominis muscle fibers
[Downloaded free from http://www.herniasurgeryjournal.org on Monday, November 4, 2019, IP: 10.232.74.26]

Reinpold: Transversus abdominis muscle release
International Journal of Abdominal Wall and Hernia Surgery - Volume 1, Issue 3, October-December 2018 81
the fascia transversalis (FT) and peritoneum which are often firmly attached to each other are separated from the rectus muscles. In the space of Retzius, the urinary bladder is identified and carefully detached from the abdominal wall. Like in total extraperitoneal (TEP) and transabdominal preperitoneal (TAPP) repairs, the dissection extends approximately 4 cm dorsal to the symphysis and 3 cm caudal to the Cooper’s ligament.
In the original publication by Novitsky et al.,[13] the TAR procedure starts cephalad (top‑down dissection): at the costal margin, the posterior rectus sheath is longitudinally incised medial to the segmental intercostal nerves, 1.5–2 cm medial to the lateral border of the rectus compartment with electrocautery, alternatively with a scalpel [Figures 2 and 3]. The linea semilunaris which describes the medial end points of the TAM fibers [Figure 1] is exposed after incision of the posterior rectus sheath. In the upper third to the upper half of the abdominal wall, the linea semilunaris runs medial to the lateral border of the rectus muscle compartment:
the medial end points of the TAM are encountered dorsal to the posterior rectus sheath [Figures 1 and 3‑6]. After complete division of the TAM fibers at the level of the incision of the posterior rectus sheath, the FT is exposed [Figures 3b, 4‑6 and 9c]. The TAM is bluntly detached from the FT which is located ventral to the peritoneum [Figures 4‑7]. FT and peritoneum form a double layer. Especially in the lower abdomen, the FT is sometimes very thin. The dissection in the lateral compartment can be extended to the spine and central diaphragm, allowing a wide retromuscular mesh overlap cranial to the costal margin [Figures 5‑7]. Below the arcuate line, the dissection is performed in the preperitoneal plane like in TEP or TAPP inguinal hernia repairs. Once the dissection in the lateral compartments is completed, the abdominal cavity is inspected for intestinal lesions and hemorrhage. After a wide release of FT is performed on both sides, the posterior rectus sheaths are reapproximated in the midline with a
Figure 4: Transversus abdominis muscle release incision completed. The fascia transversalis is partly separated from the transversus abdomins muscle. Classic
transversus abdominis muscle release incision (red dotted line) and Madrid modification (green dotted line), open cadaver operation
Figure 2: The right rectus muscle completely separated from the posterior rectus sheath: planned “bottom‑up” transversus abdominis muscle release incision of the
posterior rectus sheath starting at the arcuate line (open cadaver operation)
Figure 5: Open transversus abdominis muscle release: Blunt separation of the fascia transversalis from transversus abdomins muscle with dissecting sponge
Figure 3: (a‑d) Transversus abdominis muscle release incision of the posterior rectus sheath: (a) “Bottom‑up” incision starting at arcuate line; (b) classic
“top‑down” incision with division of transversus abdominis muscle fibers starting at the costal margin. (c and d) Madrid modification: medial incision of posterior rectus
sheath without division of muscle fibers (open cadaver operation)
dc
ba
[Downloaded free from http://www.herniasurgeryjournal.org on Monday, November 4, 2019, IP: 10.232.74.26]

Reinpold: Transversus abdominis muscle release
82 International Journal of Abdominal Wall and Hernia Surgery - Volume 1, Issue 3, October-December 2018
running long‑term absorbable monofilament 2–0 or 0 suture. All tears and holes of the peritoneum are closed with absorbable 2–0 sutures. The TAR procedure allows the retromuscular/preperitoneal sublay implantation of very large uncoated standard alloplastic meshes which may cover the complete medial and lateral compartments. If the hernial defect and anterior fascia can be closed with low tension ventral to the large mesh, there is no need for mesh fixation. The hernial defect is closed and the linea alba is restored by re‑approximation of the anterior fascia in the midline using a nonabsorbable or long‑term absorbable running suture (0) in small‑stitch small‑bite technique.[13]
Transversus Abdominis Muscle Release after Transverse Laparotomies and Stoma
Reversal
Scar tissue and adhesions may impede the dissection between the posterior rectus sheath and transversalis fascia. It is advisable to start the TAR dissection cephalad and caudal of the scar zone in the right plane of virgin territory. Coming from the right plane, the scar is dissected with scissors or scalpel. Electrocautery should only be used if bowel adhesions to the scar field are ruled out.
Transversus Abdominis Muscle Release for the Treatment of Parastomal Hernias
The TAR procedure is indispensable for the retromuscular (sublay) mesh repair of parastomal hernias (PSHs). TAR allows wide dissection of the retromuscular plane around the PSH, key hole, and Sugarbaker sublay mesh repair of PSH. However, scar tissue around the stoma site may lead to firm adhesions between the FT and posterior rectus sheath, making the dissection of the right plane difficult.
Reversed transversus abdominis muscle release for the treatment of large lateral and flank herniasLateral and flank hernias should be treated with retromuscular (sublay) mesh repair. Especially in large hernias, a sufficient mesh overlap of at least 5–7 cm can only be achieved by a reversed TAR procedure. Starting the dissection in the lateral compartment, the FT and peritoneum are separated from the TAM and the posterior rectus sheath up to a line 3 cm medial to the lateral border of the rectus compartment and approximately 1 cm medial to the TAR incision line of the posterior rectus sheath and there, the posterior rectus sheath is incised longitudinally. Thus, the segmental nerves are preserved, and the retromuscular dissection (RMD) can be continued to the medial border of the rectus muscle compartment.
Transversus Abdominis Muscle Release Modifications
Several recent publications reported on minimally invasive TAR repair.[14‑20] Belyansky et al.[14] have published the laparoscopic transperitoneal and endoscopic extraperitoneal TEP TAR technique:[20] the technical steps are bilateral placement of three ports, reduction of the hernial content, and adhesiolysis. The posterior rectus sheath is incised 1 cm lateral to the edge of the defect and linea alba. The posterior rectus sheath is incised along its whole length from cephalad to caudal direction with hook electrocautery or laparoscopic scissors. The technical steps are analogous to the open procedure. Unilateral laparoscopic TAR can achieve up to 7 cm of fascial medial mobilization. After closure of the posterior rectus sheath in a running fashion, the mesh is placed behind the muscles and fixed. The anterior fascial defect is then sutured “upside down.”[14]
Reinpold et al. have developed an endoscopic‑assisted mini or less open (MILOS) TAR approach.[21] Through a
Figure 6: Vast medialization of the posterior rectus sheath beyond midline (open transversus abdominis muscle release operation)
Figure 7: Vast separation of the fascia transversalis/peritoneum from the abdominal wall and right diaphragm to the level of the spine and falciform ligament
(open cadaver operation)
[Downloaded free from http://www.herniasurgeryjournal.org on Monday, November 4, 2019, IP: 10.232.74.26]

Reinpold: Transversus abdominis muscle release
International Journal of Abdominal Wall and Hernia Surgery - Volume 1, Issue 3, October-December 2018 83
5‑cm incision (mini open) or 6–12‑cm incision (less open) directly above the center of the main hernial defect, the operation is performed with light‑armed laparoscopic instruments using the Endotorch™ [ Richard Wolf, Knittlingen, Germany; Figure 8], while the abdominal wall is elevated with retractors by the assistant. After the transhernial insertion of a flexible monoport (Alexis™, Applied Medical, Rancho Santa Margarita, CA, USA) and standard working ports [Figure 9a], the operation can be performed endoscopically [Figure 9b‑d]. The incision of the posterior rectus sheath is performed with hook electrocautery [Figure 9b and c]. The operational steps and the extension of the dissection are the same as in open TAR.
Transversus Abdominis Muscle Release Operation Results of Reference Hernia
Center at Gross Sand Hospital, Hamburg
From January 2012 to September 2018, 178 TAR procedures were performed. The average defect size and mesh size were 242 and 1096 cm2, respectively. The mean operation time was 192 min. There were 54 cases of MILOS TAR and 35 cases of endoscopic MILOS TAR. There were three infections with one mesh removal, four hematomas with reoperation, one bowel obstruction, and one bowel injury which was immediately treated with a suture repair. One‑year questionnaire follow‑up revealed the following four recurrences: one central mesh rupture (lightweight mesh), one subxiphoidal, and two suprapubic recurrences. Chronic pain rate after 1 year was 5.2%.
Robotic Transversus Abdominis Muscle Release
Robotic‑assisted TAR is another recent innovation of CST.[15‑20] Warren et al.[16] compared 103 standard laparoscopic ventral hernial repairs with 53 robotic TARs. The width of the hernia defect was small in both cohorts (6.9 cm vs. 6.5 cm, P = 0.5). Fascial closure was achieved more often with the robotic technique (96.2% vs. 50.5%; P < 0.001). However, the operative time was longer with the robot (245 min vs. 122 min; P < 0.001). Seroma was more common after robotic TAR (47.2% vs. 16.5%; P < 0.001), but surgical‑site infections (SSIs) were similar (3.8% vs. 1%; P = 0.592). The median length of stay was shorter after robotic TAR (1 vs. 2 days; P = 0.004).
Bittner et al.[17] compared 76 open TARs and 26 robotic‑assisted TARs. Patient demographics and hernial defect sizes were comparable (260 ± 209 vs. 235 ± 107 cm2; P = 0.55). Robotic TAR lasted longer (287 ± 121 vs. 365 ± 78 min; P < 0.01) but trended toward lower morbidity (39.2% vs. 19.2%; P = 0.09) and less severe
Figure 8: Less open mini or less open transversus abdominis muscle release with light‑armed laparoscopic instruments using the Endotorch™ and direct
vision
Figure 10: Robotic retromuscular ventral hernia mesh repair: intercostal segmental nerves with accompanying blood vessel
Figure 9: Endoscopic mini‑open transversus abdominis muscle release: (a) port positions: mini incision over the large hernial defect sealed with transhernial flexible port; (b) endoscopic “bottom‑up” incision of the left posterior rectus
sheath; (c) division of posterior rectus sheath and medial fibers of the transversus abdomins muscle in the upper left abdomen. (d) endoscopic dissection of the fascia
transversalis from transversus abdomins muscle
dc
ba
[Downloaded free from http://www.herniasurgeryjournal.org on Monday, November 4, 2019, IP: 10.232.74.26]
Reinpold: Transversus abdominis muscle release
84 International Journal of Abdominal Wall and Hernia Surgery - Volume 1, Issue 3, October-December 2018
complications. Surgical‑site occurrences (SSOs) and readmission were comparable (6.6% vs. 7.7%; P = 1.00). Hospital stay was significantly shorter after robotic TAR (3 days, 95% confidence interval [CI]: 3.2–4.3 vs. 6 days, 95% CI: 5.9–8.3).
Comparable results were reported by Martin‑del‑Campo et al.[18]
In recent publications of laparoendoscopic or robotic TAR repair, a “bottom‑up” approach is described which starts at the arcuate line [Figures 2, 3a, c and d]. Another recent modification of the TAR procedure, coined “Madrid TAR modification,” has been published by Robin‑Lersundi et al.:[22] the FT is incised medial to the linea semilunaris, thus avoiding division of any TAM fibers [Figures 3a, c, d and 4].
How Much Medialization of the Abdominal Wall Does the Transversus Abdominis
Muscle Release Procedure Give?
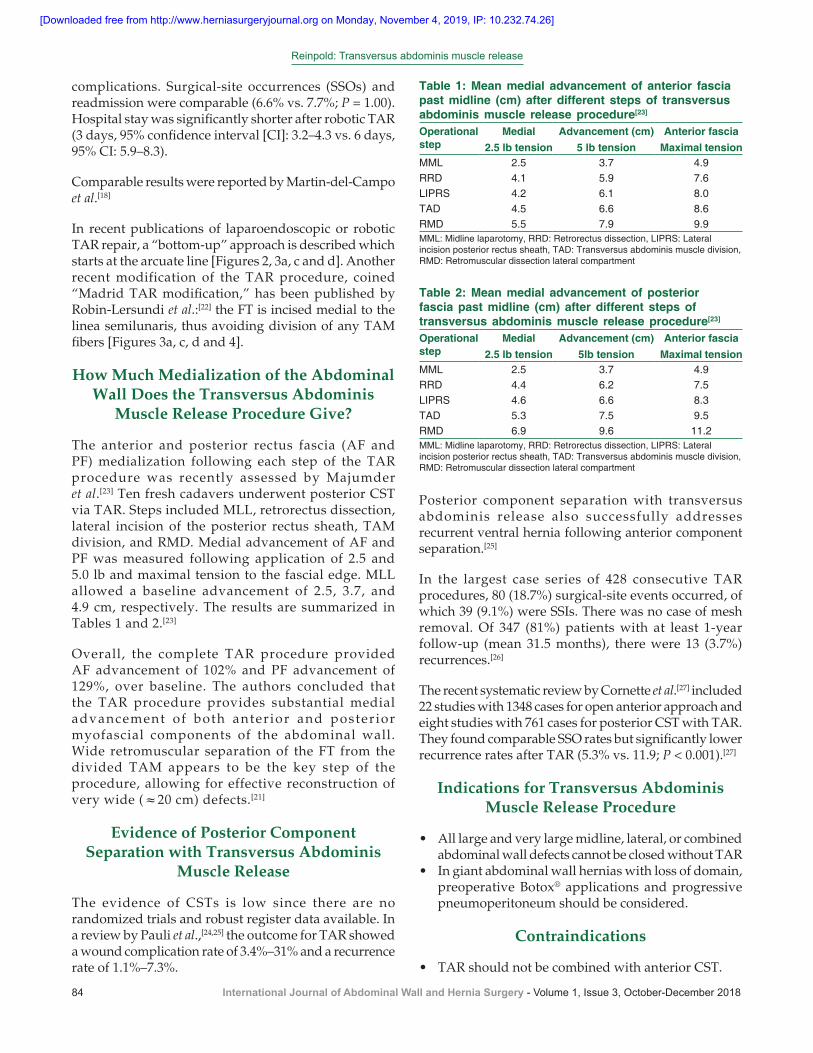
The anterior and posterior rectus fascia (AF and PF) medialization following each step of the TAR procedure was recently assessed by Majumder et al.[23] Ten fresh cadavers underwent posterior CST via TAR. Steps included MLL, retrorectus dissection, lateral incision of the posterior rectus sheath, TAM division, and RMD. Medial advancement of AF and PF was measured following application of 2.5 and 5.0 lb and maximal tension to the fascial edge. MLL allowed a baseline advancement of 2.5, 3.7, and 4.9 cm, respectively. The results are summarized in Tables 1 and 2.[23]
Overall, the complete TAR procedure provided AF advancement of 102% and PF advancement of 129%, over baseline. The authors concluded that the TAR procedure provides substantial medial advancement of both anterior and posterior myofascial components of the abdominal wall. Wide retromuscular separation of the FT from the divided TAM appears to be the key step of the procedure, allowing for effective reconstruction of very wide (≈20 cm) defects.[21]
Evidence of Posterior Component Separation with Transversus Abdominis
Muscle Release
The evidence of CSTs is low since there are no randomized trials and robust register data available. In a review by Pauli et al.,[24,25] the outcome for TAR showed a wound complication rate of 3.4%–31% and a recurrence rate of 1.1%–7.3%.
Posterior component separation with transversus abdominis release also successfully addresses recurrent ventral hernia following anterior component separation.[25]
In the largest case series of 428 consecutive TAR procedures, 80 (18.7%) surgical‑site events occurred, of which 39 (9.1%) were SSIs. There was no case of mesh removal. Of 347 (81%) patients with at least 1‑year follow‑up (mean 31.5 months), there were 13 (3.7%) recurrences.[26]
The recent systematic review by Cornette et al.[27] included 22 studies with 1348 cases for open anterior approach and eight studies with 761 cases for posterior CST with TAR. They found comparable SSO rates but significantly lower recurrence rates after TAR (5.3% vs. 11.9; P < 0.001).[27]
Indications for Transversus Abdominis Muscle Release Procedure
• All large and very large midline, lateral, or combined abdominal wall defects cannot be closed without TAR
• In giant abdominal wall hernias with loss of domain, preoperative Botox® applications and progressive pneumoperitoneum should be considered.
Contraindications
• TAR should not be combined with anterior CST.
Table 1: Mean medial advancement of anterior fascia past midline (cm) after different steps of transversus abdominis muscle release procedure[23]
Operational step
Medial Advancement (cm) Anterior fascia2.5 lb tension 5 lb tension Maximal tension
MML 2.5 3.7 4.9RRD 4.1 5.9 7.6LIPRS 4.2 6.1 8.0TAD 4.5 6.6 8.6RMD 5.5 7.9 9.9MML: Midline laparotomy, RRD: Retrorectus dissection, LIPRS: Lateral incision posterior rectus sheath, TAD: Transversus abdominis muscle division, RMD: Retromuscular dissection lateral compartment
Table 2: Mean medial advancement of posterior fascia past midline (cm) after different steps of transversus abdominis muscle release procedure[23]
Operational step
Medial Advancement (cm) Anterior fascia2.5 lb tension 5lb tension Maximal tension
MML 2.5 3.7 4.9RRD 4.4 6.2 7.5LIPRS 4.6 6.6 8.3TAD 5.3 7.5 9.5RMD 6.9 9.6 11.2MML: Midline laparotomy, RRD: Retrorectus dissection, LIPRS: Lateral incision posterior rectus sheath, TAD: Transversus abdominis muscle division, RMD: Retromuscular dissection lateral compartment
[Downloaded free from http://www.herniasurgeryjournal.org on Monday, November 4, 2019, IP: 10.232.74.26]

Reinpold: Transversus abdominis muscle release
International Journal of Abdominal Wall and Hernia Surgery - Volume 1, Issue 3, October-December 2018 85
Conclusions
• TAR avoids large skin flaps with damage of perforator vessels, thus reducing the risk of skin necrosis, SSOs, and SSIs
• TAR allows the closure of abdominal wall defects of up to 20 cm width
• TAR allows implantation of very large uncoated standard alloplastic meshes in the most suitable retromuscular sublay plane
• In most TAR cases, no mesh fixation is necessary• According to a recent systematic review, the SSO rates
after open anterior and open TAR are comparable, but the recurrence rate after open anterior CST is higher compared to that of open TAR[27]
• Today, no significant differences can be identified between the results of endoscopic anterior CST, perforator‑sparing anterior CST, and TAR[8,9,28‑32]
• The open anterior CST without mesh should no longer be performed because the risk of recurrence is too high[28‑30]
• At present, it is too early to evaluate the role of laparoscopic and robotic‑assisted TAR.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
References
1. Bittner R, Bingener‑Casey J, Dietz U, Fabian M, Ferzli GS, Fortelny RH, et al. Guidelines for laparoscopic treatment of ventral and incisional abdominal wall hernias (International Endohernia Society (IEHS)‑part 1. Surg Endosc 2014;28:2‑9.
2. Scheuerlein H, Thiessen A, Schug‑Pass C, Köckerling F. What do we know about component separation techniques for abdominal wall hernia repair? Front Surg 2018;5:24.
3. Albanese AR. Gigantic median xipho‑umbilical eventration; method for treatment. Rev Asoc Med Argent 1951;65:376‑8.
4. Albanese AR. Liberating incisions in the treatment of large supraumbilical eventrations. Prensa Med Argent 1966;53:2222‑7.
5. Ramirez OM, Ruas E, Dellon AL. “Components separation” method for closure of abdominal‑wall defects: An anatomic and clinical study. Plast Reconstr Surg 1990;86:519‑26.
6. Ramirez OM. Abdominoplasty and abdominal wall rehabilitation: A comprehensive approach. Plast Reconstr Surg 2000;105:425‑35.
7. Rosen MJ, Jin J, McGee MF, Williams C, Marks J, Ponsky JL, et al. Laparoscopic component separation in the single‑stage treatment of infected abdominal wall prosthetic removal. Hernia 2007;11:435‑40.
8. Ng N, Wampler M, Palladino H, Agullo F, Davis BR. Outcomes of laparoscopic versus open fascial component separation for complex ventral hernia repair. Am Surg 2015;81:714‑9.
9. Jensen KK, Henriksen NA, Jorgensen LN. Endoscopic component separation for ventral hernia causes fewer wound complications compared to open components separation: A systematic review and meta‑analysis. Surg Endosc 2014;28:3046‑52.
10. Milburn ML, Shah PK, Friedman EB, Roth JS, Bochicchio GV,
Gorbaty B, et al. Laparoscopically assisted components separation technique for ventral incisional hernia repair. Hernia 2007;11:157‑61.
11. Holihan JL, Nguyen DH, Nguyen MT, Mo J, Kao LS, Liang MK, et al. Mesh location in open ventral hernia repair: A systematic review and network meta‑analysis. World J Surg 2016;40:89‑99.
12. Carbonell AM, Cobb WS, Chen SM. Posterior components separation during retromuscular hernia repair. Hernia 2008;12:359‑62.
13. Novitsky YW, Elliott HL, Orenstein SB, Rosen MJ. Transversus abdominis muscle release: A novel approach to posterior component separation during complex abdominal wall reconstruction. Am J Surg 2012;204:709‑16.
14. Belyansky I, Zahiri HR, Park A. Laparoscopic transversus abdominis release, a novel minimally invasive approach to complex abdominal wall reconstruction. Surg Innov 2016;23:134‑41.
15. Amaral MV, Guimarães JR, Volpe P, Oliveira FM, Domene CE, Roll S, et al. Robotic transversus abdominis release: Is it possible to offer minimally invasive surgery for abdominal wall complex defects? Rev Col Bras Cir 2017;44:216‑9.
16. Warren JA, Cobb WS, Ewing JA, Carbonell AM. Standard laparoscopic versus robotic retromuscular ventral hernia repair. Surg Endosc 2017;31:324‑32.
17. Bittner JG 4th, Alrefai S, Vy M, Mabe M, Del Prado PA, Clingempeel NL, et al. Comparative analysis of open and robotic transversus abdominis release for ventral hernia repair. Surg Endosc 2018;32:727‑34.
18. Martin‑Del‑Campo LA, Weltz AS, Belyansky I, Novitsky YW. Comparative analysis of perioperative outcomes of robotic versus open transversus abdominis release. Surg Endosc 2018;32:840‑5.
19. Carbonell AM, Warren JA, Prabhu AS, Ballecer CD, Janczyk RJ, Herrera J, et al. Reducing length of stay using a robotic‑assisted approach for retromuscular ventral hernia repair: A comparative analysis from the americas hernia society quality collaborative. Ann Surg 2018;267:210‑7.
20. Belyansky I, Daes J, Radu VG, Balasubramanian R, Reza Zahiri H, Weltz AS, et al. A novel approach using the enhanced‑view totally extraperitoneal (eTEP) technique for laparoscopic retromuscular hernia repair. Surg Endosc 2018;32:1525‑32.
21. Reinpold W, Schröder M, Berger C, Nehls J, Schröder A, Hukauf M, et al. Mini‑ or less‑open sublay operation: A new minimally invasive technique for the extraperitoneal mesh repair of incisional hernias. Ann Surg 2018. [Epub ahead of print].
22. Robin‑Lersundi A, Blazquez Hernando L, López‑Monclús J, Cruz Cidoncha A, San Miguel Méndez C, Jimenez Cubedo E, et al. How we do it: Down to up posterior components separation. Langenbecks Arch Surg 2018;403:539‑46.
23. Majumder A, Miller HJ, Del Campo LM, Soltanian H, Novitsky YW. Assessment of myofascial medialization following posterior component separation via transversus abdominis muscle release in a cadaveric model. Hernia 2018;22:637‑44.
24. Pauli EM, Rosen MJ. Open ventral hernia repair with component separation. Surg Clin North Am 2013;93:1111‑33.
25. Pauli EM, Wang J, Petro CC, Juza RM, Novitsky YW, Rosen MJ, et al. Posterior component separation with transversus abdominis release successfully addresses recurrent ventral hernias following anterior component separation. Hernia 2015;19:285‑91.
26. Novitsky YW, Fayezizadeh M, Majumder A, Neupane R, Elliott HL, Orenstein SB, et al. Outcomes of posterior component separation with transversus abdominis muscle release and synthetic mesh sublay reinforcement. Ann Surg 2016;264:226‑32.
27. Cornette B, de Bacquer D, Berrevoet F. Component separation technique for giant incisional hernia: A systematic review. Am J Surg 2017;215:1‑8.
28. Tong WM, Hope W, Overby DW, Hultman CS. Comparison of outcome after mesh‑only repair, laparoscopic component
[Downloaded free from http://www.herniasurgeryjournal.org on Monday, November 4, 2019, IP: 10.232.74.26]

Reinpold: Transversus abdominis muscle release
86 International Journal of Abdominal Wall and Hernia Surgery - Volume 1, Issue 3, October-December 2018
separation, and open component separation. Ann Plast Surg 2011;66:551‑6.
29. Slater NJ, van Goor H, Bleichrodt RP. Large and complex ventral hernia repair using “components separation technique” without mesh results in a high recurrence rate. Am J Surg 2015;209:170‑9.
30. Liang MK, Holihan JL, Itani K, Alawadi ZM, Gonzalez JR, Askenasy EP, et al. Ventral hernia management: Expert consensus
guided by systematic review. Ann Surg 2017;265:80‑9.31. Krpata DM, Blatnik JA, Novitsky YW, Rosen MJ. Posterior and
open anterior components separations: A comparative analysis. Am J Surg 2012;203:318‑22.
32. Petro CC, Orenstein SB, Criss CN, Sanchez EQ, Rosen MJ, Woodside KJ, et al. Transversus abdominis muscle release for repair of complex incisional hernias in kidney transplant recipients. Am J Surg 2015;210:334‑9.
[Downloaded free from http://www.herniasurgeryjournal.org on Monday, November 4, 2019, IP: 10.232.74.26]




















