Translational imaging studies of cortical spreading depression in experimental models for migraine...
10
Perspective 10.1586/14737175.8.5.759 © 2008 Expert Reviews Ltd ISSN 1473-7175 759 www.expert-reviews.com Translational imaging studies of cortical spreading depression in experimental models for migraine aura Expert Rev. Neurotherapeutics. 8(5), 759–768 (2008) Justin M Smith, Michael F James, James A Fraser and Christopher L-H Huang † † Author for correspondence Physiological Laboratory, University of Cambridge, Downing Street, Cambridge CB2 3EG, UK Tel.: +44 1223 333 822 Fax: +44 1223 333 840 [email protected] This perspective discusses cortical spreading depression (CSD) phenomena and their translational significance for human migraine aura and the peri-infarct events following cerebral ischemia and injury. They begin with interstitial K + release and accumulation following neuronal stimulation, and a buffering astrocytic K + influx and remote liberation propagating waves of neuronal hyperexcitability and depression. Diffusion-weighted echoplanar MRI demonstrates CSD features in gyrencephalic brains recapitulating human migraine aura, spatial and temporal features of single primary events and multiple secondary events, their stimulus dependence, pharmacological properties, and their relationship to blood oxygenation level-dependant signals and late cerebrovascular changes. The article finally explores prospects for physiological studies of CSD gaining fuller insights both into mechanisms underlying the pathology of the corresponding human condition and possible approaches to management. KEYWORDS: cerebral ischemia • cortical spreading depression • head injury • migraine • MRI The pathophysiological phenomenon of corti- cal spreading depression (CSD) was first identi- fied in the cerebral cortex of rabbits [1–3] as a propagating wave of neuronal excitation fol- lowed by transient quiescence. It has since been implicated in a wide range of clinical situations [4]. For example, the distinct aura of classical migraine follows a prodromal phase and accom- panies disturbances in visual, general sensory and/or motor function [5–9]. This is followed by neurovascular events that produce a generalized headache that lasts for minutes or hours; addi- tionally there may be 1–3 s episodes of sharp scalp or orbital pain. Recent reports associate the clinical findings occurring during the aura phase of migraine and CSD [10–14]. They sug- gest a hyperexcitability in widespread regions throughout the occipital cortex providing the site for a potential CSD to be triggered in migraine, and describe CSD-like activity during migrainous aura [15–19]. Direct current magneto- encephalography (DC-MEG), used to non- invasively map magnetic fields from different areas of cortical electrical activity during spon- taneous and visually-induced migraine with aura, demonstrated multiple areas of hyper- excitability in the right primary visual cortex and occipital parietal regions during the aura [20]. Neurophysiological studies between attacks suggest that migrainous brains show a lack of habituation of evoked responses for a number of different sensory modalities; this could reflect an increased cortical hyperexcitability, or alter- natively an abnormal responsivity owing to decreased preactivation levels [21]. CSD-like phenomena in the form of peri-infarct depolari- zation (PID) may also occur with the cerebral pathology following ischemia or head trauma [22–24]. Depolarization-like events in post- operative neurosurgical patients affected by traumatic or ischemic neocortical injury have recently been directly demonstrated and quanti- tatively characterized using neurophysiological methods [25]. Such depolarization events might contribute to tissue pathology in acute clinical disorders in the brain [24,26].
-
Upload
ninevehtrust -
Category
Documents
-
view
0 -
download
0
Transcript of Translational imaging studies of cortical spreading depression in experimental models for migraine...

Perspective
10.1586/14737175.8.5.759 © 2008 Expert Reviews Ltd ISSN 1473-7175 759www.expert-reviews.com
Translational imaging studies of cortical spreading depression in experimental models for migraine auraExpert Rev. Neurotherapeutics. 8(5), 759–768 (2008)
Justin M Smith, Michael F James, James A Fraser and Christopher L-H Huang†
†Author for correspondencePhysiological Laboratory, University of Cambridge, Downing Street, Cambridge CB2 3EG, UKTel.: +44 1223 333 822Fax: +44 1223 333 [email protected]
This perspective discusses cortical spreading depression (CSD) phenomena and theirtranslational significance for human migraine aura and the peri-infarct events followingcerebral ischemia and injury. They begin with interstitial K+ release and accumulationfollowing neuronal stimulation, and a buffering astrocytic K+ influx and remote liberationpropagating waves of neuronal hyperexcitability and depression. Diffusion-weightedechoplanar MRI demonstrates CSD features in gyrencephalic brains recapitulating humanmigraine aura, spatial and temporal features of single primary events and multiple secondaryevents, their stimulus dependence, pharmacological properties, and their relationship toblood oxygenation level-dependant signals and late cerebrovascular changes. The articlefinally explores prospects for physiological studies of CSD gaining fuller insights both intomechanisms underlying the pathology of the corresponding human condition and possibleapproaches to management.
KEYWORDS: cerebral ischemia • cortical spreading depression • head injury • migraine • MRI
The pathophysiological phenomenon of corti-cal spreading depression (CSD) was first identi-fied in the cerebral cortex of rabbits [1–3] as apropagating wave of neuronal excitation fol-lowed by transient quiescence. It has since beenimplicated in a wide range of clinical situations[4]. For example, the distinct aura of classicalmigraine follows a prodromal phase and accom-panies disturbances in visual, general sensoryand/or motor function [5–9]. This is followed byneurovascular events that produce a generalizedheadache that lasts for minutes or hours; addi-tionally there may be 1–3 s episodes of sharpscalp or orbital pain. Recent reports associatethe clinical findings occurring during the auraphase of migraine and CSD [10–14]. They sug-gest a hyperexcitability in widespread regionsthroughout the occipital cortex providing thesite for a potential CSD to be triggered inmigraine, and describe CSD-like activity duringmigrainous aura [15–19]. Direct current magneto-encephalography (DC-MEG), used to non-invasively map magnetic fields from different
areas of cortical electrical activity during spon-taneous and visually-induced migraine withaura, demonstrated multiple areas of hyper-excitability in the right primary visual cortexand occipital parietal regions during the aura[20]. Neurophysiological studies between attackssuggest that migrainous brains show a lack ofhabituation of evoked responses for a numberof different sensory modalities; this could reflectan increased cortical hyperexcitability, or alter-natively an abnormal responsivity owing todecreased preactivation levels [21]. CSD-likephenomena in the form of peri-infarct depolari-zation (PID) may also occur with the cerebralpathology following ischemia or head trauma[22–24]. Depolarization-like events in post-operative neurosurgical patients affected bytraumatic or ischemic neocortical injury haverecently been directly demonstrated and quanti-tatively characterized using neurophysiologicalmethods [25]. Such depolarization events mightcontribute to tissue pathology in acute clinicaldisorders in the brain [24,26].

760 Expert Rev. Neurotherapeutics 8(5), (2008)
Perspective Smith, James, Fraser & Huang
Initiation & cellular mechanisms
Normal neuronal tissue is continually active with action poten-tial firing increasing extracellular K+ concentration ([K+]o) andconsuming metabolic energy. Astroglia reverse this process byrecycling glutamate and K+, and mediating substrate and waterfluxes between neurons and vasculature [27]. CSD may reflect aperturbation of this normal, static, localized and essentially ran-dom picture of tissue ion, water and energy transfer, which isdependent on local cerebral needs and occurs throughout thebrain, by a focal insult that results in a coherent, regenerativeand amplified state. This description of signal propagationbreaking through a noisy environment is reminiscent of thephenomenon of stochastic resonance, which has proven usefulin the analysis of a wide range of biological phenomena (seelater) [28,29]. Such events might be more likely in hyperexcitablesituations [15,30,31] that would alter the noise level towards acritical threshold following triggering stimuli.
A range of mechanical, faradic and chemical stimuli have thusinitiated CSD phenomena in different in vivo and in vitro experi-mental systems. Stimuli using KCl have proven to lead to themost reproducible events in both nonimaging [32–35] and imag-ing studies [35–44]. Indeed, alterations in [K+]o might be involvedin the pathophysiological process itself [22,27,45]. It has been sug-gested that K+ accumulation in the extracellular space, releasedby hyperexcitable cortical neurons undergoing repetitive andfrequent cycles of depolarization and repolarization, is what ini-tiates CSD [23]. This released K+ accumulates in the restrictedinterstitial space of brain tissue and further depolarizes the verycells that released it. There is consequently a massive extra-cellular release of K+ which leads to local [K+]o levels as high as60 mM. A rise in [K+]o will cause an inward movement of K+
into glia. This causes a transient cellular swelling accompaniedby a transient fall in neuronal cytoplasmic pH and an increase inglial cytoplasmic and extracellular pH [46]. Imaging studies usingin vitro neocortical and hippocampal slices suggest that it islikely that neurons also undergo swelling and show an accompa-nying dendritic beading similar to changes observed followingcortical damage previously described in vivo [47].
Thus, astrocytes may initially buffer the increases in [K+]oboth through this K+ uptake and its transfer to spatially distantcells through gap junction connectivity and thereby dampenspreading depression (SD). Astrocytes can thus remove K+ fromthe extracellular space through: active transport via Na+/K+-ATPase; carrier-mediated Na+/K+/2Cl- cotransport; H+/K+
exchange; carrier-mediated K+/Cl- cotransport; inwardly rectify-ing K+ channels; and K+ Cl- uptake by Donnan forces [48,49].Neurons can be cultured without their glial satellites and sur-vive in hippocampal slices immediately after glial poisoningin vitro [50], but resting levels of [K+]o can then rise to more than20 mM with consequent spontaneous SD activity [51].
Changes in Ca2+ homeostasis, possibly involving Ca2+-acti-vated K+ channels, have been implicated in the mechanismsthat might trigger this K+ release into the extracellular space.
First, cortical excitability resulting in repetitive CSD in ratcortex is markedly reduced by pharmacological inhibition ofN- and P/Q-type and less so by block of L-type voltage-gatedCa2+ channels [52]. Second, there is the possibility that glial Ca2+
waves are critical for initiation or propagation of SD. Ca2+ waveshave been observed propagating through cultures of astrocytes[53–56], neurons [53,57] and from astrocytes to neurons [58]. Astro-cytic Ca2+ waves, which propagate at rates similar to CSD, arepreceded by local Ca2+ elevations [58–60], but propagation of thesubsequent Ca2+ wave is critically dependent on couplingbetween astrocytes by functional gap junctions [58,60–65].
However, in the event of [K+]o rising above a physiologicalceiling (>15–20 mM) astrocytes may then contribute to thepropagation of CSD through their gap junction connectivityand reversal of membrane transporters, thereby amplifying SDpropagation. Such regenerative activity may account for boththe relatively long duration of the aura phase in some patientsand the multiple focal regions of activity. Subsequent restora-tion of ionic homeostasis is energy dependent, with increases inmetabolic indices during and briefly following the extracellularDC change associated with CSD. The effect is to create a coher-ent wave of increased then decreased [K+]o associated with atriphasic slow potential change and a period of cortical electricalsilence [66,67]. Dendritic NMDA receptor activation may alsocontribute to CSD initiation and propagation. Glutamatetransporters are highly concentrated in glial cell membranes thatface nerve terminals and axons, although such contributionsmay vary between the types of CSD initiated [68].
Genetic evidence is consistent with migraine aura likely toreflect similarly abnormal ion fluxes with consequent altera-tions in the distribution of water, detectable by MRI methods[69]. Familial hemiplegic migraine has been associated with anumber of gene abnormalities involving molecules bearing ontransmembrane ionic transport. These include mutations inthe CACNA1A gene coding for the pore-forming α1A trans-membrane subunit of a Ca2+ channel with P/Q-type proper-ties [70–75]. There is also an association with haploinsufficien-cies in ATP1A2 encoding a Na+-K+-ATPase subunit [76] andwith a gain-of-function mutation in SCN1A, which encodesthe neuronal voltage-gated Na+ channel [77].
Studies in intact brain
Whole-animal studies of CSD initiation and propagation innormal animal systems have been performed for both smooth,lissencephalic and convoluted, gyrencephalic brain types underdifferent experimental and stimulus conditions [33,78,79]. In par-ticular, MRI together with MEG have recently proven to be use-ful complementary noninvasive translational tools in the in vivocharacterization of CSD owing to their high temporal and spa-tial resolution, and its applicability to both experimental andhuman clinical studies, in mapping changes that can be anatom-ically and functionally linked with migraine aura symptoms [80].They thus add to electrophysiological and other techniques,

Cortical spreading depression Perspective
www.expert-reviews.com 761
such as laser Doppler flow, in unraveling some of the patho-physiological mechanisms of migraine [21,81]. Different MRItechniques can be used to investigate specific aspects of theCSD phenomenon. Thus:
• Functional (blood oxygenation level-dependent [BOLD])MRI detects alterations in the deoxyhemoglobin content ofvenous blood and has demonstrated physiological changes ina time scale of seconds, during activation of human visual ormotor cortex [82,83].
• Gradient echo sequences are particularly sensitive to changesin cerebral blood flow (CBF) and metabolism that occurduring CSD wave propagation. They successfully demon-strated propagating waves of CSD initiated by KCl in anes-thetized lissencephalic brains of rats as zones of increased sig-nal intensity (3–15%) lasting approximately 1 min, whichpropagated away from the initiation site at a mean velocityof 2.90 mm min-1 [40].
• In addition diffusion-weighted (DW-)MRI detects reducedtissue water diffusibility, which follows with increased meta-bolic demand during depolarization and water movementfrom extracellular to intracellular compartments to give riseto the cellular swelling characteristic of CSD [84]. Thus, stim-uli known to elicit electrophysiologically measurable CSDalso produced rapid dips and recoveries in apparent diffusioncoefficients (ADC) [44,85].
• A further introduction of DW and fast echoplanar imaging(EPI) after KCl stimuli revealed transient propagated ADCthat appeared simultaneously with the DC shift and relativecerebral blood volume increases that followed with a delay ofapproximately 16.5 s [38]. The regions of decreased ADCoccurred within 1 min after cortical stimulation and propa-gated across the ipsilateral cortex at a speed of approximately3.5 mm min-1 [41].
• More recently T1 (i.e., spin-lattice relaxation time)-weighted,manganese-enhanced MRI indicated that the rat brainappears to contain little barrier to CSD spread once it hasbeen initiated [86].
• N-acetyl aspartate and lactate proton imaging shows promisein characterization of CSD-like activity [87].
Diffusion-weighted MRI studies in gyrencephalic brain
By contrast, gyrencephalic cortices (e.g., cat and macaque mon-key) have proven less susceptible to the induction and propaga-tion of CSD events. This could reflect their larger ratio of glia toneurons, which might protect against SD. Their clearer differen-tiation of cerebral cortex into gray and white matter, and theformation of gyri and sulci provide a partial degree of protectionto an area of cortex bounded by a sulcus. CSD propagationdecelerates from 8 to 6 mm min-1 on gyri and to 1–2 mm min-1
in sulci of gyrencephalic porcine brain [20]. Vascular events asso-ciated with CSD similarly failed to traverse prominent sulci dur-ing human migrainous aura [8]. By contrast, SD events in the
lissencephalic rabbit brain propagated with a constant velocityof 3.5 mm min-1 [20]. Feline gyrencephalic, rather than rodentlissencephalic, brains accordingly provide CSD models moreclosely comparable to human cerebral cortex [36,39]. DW-EPIof CSD events in feline brain permits a close investigation ofthe detailed features of individual CSD events [33,35,39]. Hori-zontal imaging planes selectively capture the gray matter ofindividual gyri and can detect CSD along the entire length ofeach gyrus. This also facilitates studies of CSD propagationbetween two neighboring gyri, as well as comparisons withactivity on the control contralateral side [88]. To detect CSDpropagation, horizontal DW-EPI images have been acquiredusing a repeated single-shot spin-echo imaging sequence.Weakly (low-b) and strongly (high-b) DW images, acquiredalternately [89], were recorded for approximately 30 min priorto and after stimulus application.
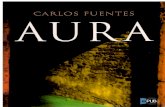
A single sustained KCl stimulus applied to the suprasylviangyrus elicited multiple CSD events [36]. FIGURE 1 and the supple-mentary movie illustrate the initial CSD or primary eventspreading across the entire hemisphere. It is followed by sec-ondary events whose ADC deflections were of similar ampli-tude, but had lower propagation velocities; the spread andtimescale of these phenomena are compared in FIGURES 2A & 2B.Both types of events altered ADC by approximately 20%, wereconfined to a single hemisphere and were most common in thegyrus where the activity was initiated [39]. Primary events cov-ered approximately 26 mm2 of cortical surface (FIGURE 2A) andpropagated relatively rapidly at approximately 3.5 mm min-1.Secondary events were multiple, more spatially restricted, cov-ering approximately 7.6 mm2, of brain surface (FIGURE 2B), oftenconfined to the originating gyrus and slower in propagation(2.3 mm min-1) [36]. Transient KCl stimuli produced fewernumbers of events (∼3.8 events per animal) than did sustainedstimuli (∼7.4 events per animal) [43]. Furthermore, their pri-mary CSD events showed peak deflections that declined byapproximately 30% as they propagated from their initiation siteto the interhemispheric boundary. Their secondary events pro-duced successively smaller ADC deflections separated by pro-gressively longer time intervals. These changes paralleledhuman migraine aura [7,8,15,17,90]. Thus, the waves propagatedwith velocities similar to classical clinical and laser Dopplerobservations of visual cortical disturbances associated withmigraine [3,79]. In addition, CSD activity could be maintainedfor long periods (>2 h) after the initiating stimulus wasremoved. Finally, inhibitory boundaries appeared to exist in thegyrencephalic brain, which limits the spread of CSD activity,perhaps reflecting inhibitory anatomical influences in the morecomplex human brain [39].
The novel antimigraine compound tonabersat (SB220453)inhibits the duration of CSD activity and the number of CSDevents [42,91,92], in parallel with electrical measurements of corti-cal DC potential and pial artery dilatation [33]. It also reducesthe cortical area involved in CSD episodes, but increases thevelocity of primary event propagation. By contrast, sumatriptan

762 Expert Rev. Neurotherapeutics 8(5), (2008)
Perspective Smith, James, Fraser & Huang
has no effect on the number of CSD events initiated [42].Indeed, it increases the propagation of events across gyri, whichnormally appear to block CSD propagation [36].
Vascular changes associated with CSD
CSD is associated with the vascular changes that in turn can becorrelated with similar alterations actually observed duringmigraine. CSD is directly accompanied by transient increases(∼3 min) in CBF initially detected using autoradiography,laser-Doppler velocimetry [33,93,94] and MRI measurements ofcerebral blood volume [38]. FIGURE 3 illustrates findings fromrecent MRI studies in feline brain that interleaved the acquisi-tion of ADC, BOLD images and DC potential [39]. It
demonstrates a clear reciprocal correlation between the wave-forms shown by the ADC and BOLD signals, in agreementwith studies in localized areas using NO measurement [95] oroptical changes [96]. BOLD-MRI has successfully detected sim-ilar physiological alterations in human migraine aura [7,8,90].Prolonged reductions in CBF last minutes to hours and there-fore persist well after CSD waves have passed [97]. These experi-mental findings correlate well with the period of decreased CBFduring the headache stage of human migraine [90]. This maythen be followed by an approximate 10-min hyperperfusionphase [94].
Experimental CSD has also been associated with even latercerebrovascular changes. Application of independent compo-nent analysis (ICA) applied to experimental BOLD data sets
Figure 1. Cortical spreading depression propagation across the surface of the cat brain. (A) Control, horizontal, gradient-echo anatomical image depicting the s.g. and m.g. (B–L) Colored overlays, shown at 60, 80, 90, 100, 110, 120, 140, 160, 200, 220 and 240 s after KCl application, represent elliptical regions of reduced diffusion traveling away from the KCl application site with a velocity of approximately 3.2 mm/min. Over the first five frames (B–F) the wave travels both rostrally and caudally along the suprasylvian gyrus; when it reaches the caudal junction of the two gyri (F–H) it appears to pass into the marginal gyrus (H–K); likewise, rostrally, the wave passes into the ectosylvian gyrus before it dissipates (K–L). Waves were never detected in the contralateral hemisphere. Overlays were obtained by subtracting a baseline image from the high-b images obtained in the diffusion-weighted echoplanar sequence and transforming the signal difference into a percentage change (blue 5%, red 25%). A: Anterior; L: Left; m.g.: Marginal gyrus; P: Posterior; R: Right; s.g.: Suprasylvian gyrus.
15 mm
R
PA
Lm.g.
s.g.25%
5
I
BA C D
E F H
I J K L
G
Sig
nal d
iffer
ence

Cortical spreading depression Perspective
www.expert-reviews.com 763
successfully extracted biphasic waveforms that arose up to 20min after the primary CSD event localized to specific sites ipsi-lateral to the stimulus [98]. A similar biphasic response has beendescribed in humans: this was attributed to a hypoperfusion fol-lowed by a reactive hyperperfusion [7]. The antimigraine agentsumatriptan completely blocks this biphasic vascular response.
CSD-type events in cerebral ischemia
CSD-like phenomena are associated with a wide range of addi-tional clinical situations that include stroke [99], cortical trauma[7,22,25], models of cerebral ischemia [87], status epilepticus [100]
and subarachnoid hemorrhage [101]. These PIDs have beenimplicated in the progression of the injury. In rodents, middlecerebral artery occlusion produces a core of severe ischemia sur-rounded by a region of reduced cerebral perfusion. SD-likeevents, radiated from this penumbra at a similar velocity as CSD[102] and caused diffusional changes detectable by MRI [85].
Comparison of CSD and PID suggests that the detailed fea-tures of CSD phenomena might vary according to the nature oftheir initiating pathology. As indicated earlier, CSD activity fromtransient KCl stimuli parallel features shown by migraine aura[33,43], with primary CSD events formingorderly, slowly propagating wave frontsinvolving extensive ipsilateral cortical areasand ADC deflections that decrease inamplitude with propagation distance. Sub-sequent secondary events affect smaller cor-tical areas with smaller ADC deflectionswith each event separated by progressivelylarger time intervals. These persist well afterstimulus withdrawal, consistent with theduration of migraine aura (40–60 min).
By contrast, persistent KCl stimuli giveprimary and secondary events similar tothe more sustained PID phenomenon. Alocalized T2-weighted hyperintensity sur-rounded by sustained ADC changes thattriggered repeated activity develops at thestimulus site. Amplitudes of primary andsecondary ADC deflections are similar andare maintained with propagation. Succes-sive secondary events propagate with lowervelocities and recur, separated by similartime intervals [43]. Halothane-anesthetizedrats demonstrate two populations of PIDafter middle cerebral artery occlusion [102].Extracellular DC potentials associatedwith PIDs form events of long and shortduration, of which the latter resembleCSD. The frequency of such PIDscorrelates with final lesion volume [102].Thus, the reduction in oxygen and glu-cose, as occurs in the ischemic penumbra,
depresses the tissue’s capacity to recover after PID invasion drop-out and predisposes it to necrosis [103]. CSD accordingly con-tributes to ischemic brain injury. A large increase in [K+]o occurswithin the ischemic core and it has been suggested that thislarge [K+]o diffuses into the penumbra and triggers PID [104].
Figure 2. Time course of typical (A) primary and (B) secondary event. False-color provides spectrum (red to magenta) adjusted to the overall time course, (A) 375 s (B) 450 s, of typical events mapped onto a diffusion-weighted image of a cortical section of feline brain.
A B
Figure 3. Detailed correlations between changes in the DC potential, ADC and blood oxygenation level-dependent (BOLD) signals. (A) DC potential recorded at the brain surface, (B) alterations in the BOLD signal measuring haemoglobin oxygenation and (C) ADC, within a single region of interest close to the DC recording electrode, following application of KCl. (B & C) demonstrate an inverse correlation between apparent diffusion coefficients and blood oxygenation level-dependent signals in any cortical region.ADC: Apparent diffusion coefficient; DC: Direct current.Reproduced with permission from [39].
7.00 10 20 30 40 50 60 70
1.000
1.025
1.075
1.100
1.125
1.050
7.5
8.0
8.5
9.0
9.5
-8.0
0.0
+8.0
AD
C (
10-4
mm
2 s-1)
Time (min)
Sig
nal
Inte
nsi
ty (
×105 )
Ch
ang
e in
DC
(m
V)
A
B
C

764 Expert Rev. Neurotherapeutics 8(5), (2008)
Perspective Smith, James, Fraser & Huang
A full description of the cellular and biochemical basis forCSD and related phenomena thus remains elusive. Neverthe-less, there is increasing evidence for its relevance to conditionssuch as migraine, stroke and brain injury [7,8,24,25]. Imagingmay offer a physiological technique that could be translatedinto noninvasive human CSD investigations to make the studyof the corresponding human disease less difficult to approach.
Expert commentary
Even 60 years after its first observation, a full description of thecellular and biochemical basis for CSD and related phenome-non remains elusive. Nevertheless, this field of CSD and its pos-sible analysis by imaging methods is an exciting one. The imag-ing approach owes itself to a systems-oriented analysis of thestrikingly coherent outward spreading primary and secondaryevents from an initiating focus and its inducibility from a singlebrain locus that involves an integration of insights from individ-ual cellular mechanisms. It complements approaches based onelectrophysiological analysis at the cellular level [21,80,81].
CSD thus emerges as the result of complex interactionsbetween certain key cellular participants in this drama. On theone hand, neuronal dendrites may form a substrate for CSDpropagation, possibly mediated by synaptic NMDA receptoractivity, for which there has been recent exploration for thera-peutic possibilities (see [105]). On the other hand, astrogliamight dissipate the local increases in [K+]o, but then release itfurther away to propagate a traveling wave. The releases ofextracellular K+ are then rapidly cleared with a co-uptake ofextracellular water and Ca2+. These events represent an amplifi-cation of the physiological processes normally supportingaction potential firing, associated with a recycling of glutamate,K+ and water involving astroglia [27]. Yet, this normal, static,localized and essentially random picture of tissue ion, waterand energy transfer, dependent on local cerebral needs, at thecellular level breaks into a coherent, regenerative and amplifiedCSD state. At the systems level, this is strongly suggestive of aclass of physical event undergoing a nonlinear cooperative sto-chastic resonance between a critical level of background noiseand a weak periodic stimulus, as described in a number ofother biological examples [28,29].
It will similarly be analysis at the systems and not only thecellular level that resolves how normally localized dendritic-astroglial interactions transform into a magnified, coherent andwidely propagating cascade. This will likely involve at leastthree fundamental essential components. First, there is the sup-porting matrix needed for the intimate interactions betweenelectrically excitable neuronal dendrites and their supportingastroglia. Second, the noise component would be representedby the background exchange of ions, water, metabolic sub-strates and neurotransmitters between dendrites and astroglia.Third, in the context of the present article the initiating signalwould result from experimental perturbations variously takingthe form of focally increased [K+]o and cell swelling, mechanical
injury, ischemia, increased electrical discharge or metabolicinsufficiency. In such a situation, alterations in either the noiseor the stimulus level could ignite the cooperative interactionnecessary to trigger the CSD process.
There is considerable evidence that pathogenesis of migrainedepends upon a hyperexcitable condition of abnormal sensoryprocessing detectable interictally [15,18,30,31,106]. Increasedinterictal excitability then would alter the noise level towardsthe threshold critical for initiating stochastic resonance orCSD. The clinical triggering stimuli for the migraine attackitself are often sensory, often visual, but they may also be chem-ical, such as substances in red wine or chocolate, or metabolic,involving physical exercise [107]. Thus, the idea of CSD as sto-chastic resonance might be relevant to human conditions suchas migraine at the translational level.
Five-year view
There is every prospect that imaging methods will become trans-latable to studies of important human diseases such as migraine,stroke and brain injury to which CSD may be related, and thatthese will circumvent some of the difficulties of performing suchresearch in humans [7,8,24,25]. Admittedly, they will need to dealwith the essentially stochastic overall nature of CSD, the lack ofnoninvasive initiating methods and the reliability of the few thatare available [15]. Nevertheless, they could potentially not onlyhelp assess use of agents with potential or established therapeuticapplications in management of migraine, but in doing so alsoyield insights into the underlying pathophysiology itself. A sys-tems approach need not exclude empirical use of agents whoseprecise cellular mechanisms may be complex. For example, testsof a hypothesis that established migraine prophylactic agents sup-press CSD as a common mechanism of action might investigatethe effects of chronic, and not only acute, daily administration ofthe widely prescribed prophylactic drugs topiramate, valproate,propranolol, amitriptyline and methysergide thereby comple-menting electrophysiological studies in the lissencephalic brainsof rats [81]. In experimental studies, the adrenergic agonists nore-pinephrine and clonidine, the β-antagonist propranolol and theα-2-antagonist yohimbine dose-dependently diminish migrationvelocity or propagation of CSD without altering regional CBF orsystemic arterial blood pressure [108]. In clinical situations, long-term clinical lamotrigine treatment reduces both migraine auraand headache frequency consistent with possible roles of aura-like events and CSD in triggering trigeminal vascular activationleading to development of migraine headaches, and of possiblepharmacological management using anticonvulsant therapy [109].
Such studies may also offer insights into background condi-tions predisposing to migraine [17]. Migraine patients displayincreased α-band phase synchronization as an effect of stimulusfrequency. Some antiepileptic drugs, as exemplified for lamot-rigine above, appear effective in migraine prophylaxis, increas-ing the threshold for its excitation [110]. Normal individualscontrastingly display a desynchronization with comparable

Cortical spreading depression Perspective
www.expert-reviews.com 765
stimuli. Such synchronization is reversed by preventative leveti-racetam and topiramate treatment [111]. Levetiracetam antago-nizes neuronal hypersynchronization in the seizure-prone CA3area of rat hippocampal slices [112]. Topiramate similarly inhib-its electrophysiological manifestations of CSD in cat and ratmodels relevant to migraine [91]. Both agents also decreasedmigraine frequency [113].
A final example of translational investigation might considermigraine-related side effects of other commonly usedpharmacological agents. For example, gender differences in theincidence of migraine with aura may be related to high circulat-ing levels of ovarian hormones, such as estradiol and progester-one; these correlate with physiological studies that report dose-dependent increases in repetition rate and amplitude of SD inrat neocortical slices induced by KCl microinjection [114].
Information resources: supplementary film
A time-lapse movie (7 s/frame) illustrating CSD propagationacross the surface of the cat brain, as demonstrated by regionsof reduced diffusion traveling away from the KCl applicationsite with a velocity of approximately 3.2 mm/min, is available
at www.expert-reviews.com. Overlays were obtained by sub-tracting a baseline image from the high-b images obtained inthe diffusion-weighted echoplanar sequence and transformingthe signal difference into a percentage change as represented inthe color map in FIGURE 1. Note the initial propagation of thewave both rostrally and caudally along the suprasylvian gyrus.When the wave reaches the caudal junction of the two gyri, itthen passes into the marginal gyrus, and rostrally into theectosylvian gyrus before dissipating. Waves never occur in thecontralateral hemisphere.
Financial and competing interests disclosure
We thank GlaxoSmithKline, the Biotechnology and Biological SciencesResearch Council (BBSRC), the University of Cambridge, the HerchelSmith Endowment, the Medical Research Council (MRC) and the RoyalSociety and Wellcome Trust for funding support of our research.
The authors have no other relevant affiliations or financial involvementwith any organization or entity with a financial interest in or financialconflict with the subject matter or materials discussed in the manuscriptapart from those disclosed.
No writing assistance was utilized in the production of this manuscript.
Key issues
• Cortical spreading depression (CSD) phenomena have a translational significance for human migraine aura as well as peri-infarct events following cerebral ischemia and injury.
• They begin with a K+ release into and accumulation in the cerebral interstitial space following neuronal stimulation in turn producing further depolarization. A buffering K+ influx into astrocytes followed by its liberation from remote interconnected astrocytes then propagates a wave of transient neuronal hyperexcitability followed by depression.
• Following MRI studies in intact lissencephalic brains, diffusion-weighted echoplanar imaging in gyrencephalic brains demonstrate features of CSD recapitulating classical human migraine aura amenable to study by pharmacological agents.
• They go on to demonstrate single primary and multiple secondary events varying reciprocally with blood oxygenation level-dependant signals, and followed by late cerebrovascular changes blocked by the antimigraine agent sumatriptan and whose features depend upon their originating stimuli.
• Experimental studies of CSD for which MRI provides a powerful method of characterization and quantification thus offer important insights into both mechanisms underlying the pathology of the corresponding human condition.
• The article concludes with prospects for further experimental and theoretical studies of CSD gaining full insights into both mechanisms underlying the pathology of the corresponding human condition, and an approach to the testing of current and future therapeutic agents with a view to possible approaches to management, and further understanding of its related clinical conditions.
References
1 Somjen G. Aristides Leão’s discovery of cortical spreading depression. J. Neurophysiol. 94, 2–4 (2005).
2 Leão AAP. Spreading depression activity in the cerebral cortex. J. Neurophysiol. 7, 359–390 (1944).
3 Lashley KS. Patterns of cerebral integration indicated by the scotomas of migraine. Arch. Neurol. Psychiatry 46, 331–339 (1941).
4 Gorji A. Spreading depression: a review of the clinical relevance. Brain Res. Rev. 38, 33–60 (2001).
5 Lauritzen M. Pathophysiology of migraine aura: the spreading depression theory. Brain 117, 199–210 (1994).
6 Flippen C, Welch KM. Imaging the brain of migraine sufferers. Curr. Opin. Neurol. 10, 226–230 (1997).
7 Cao Y, Welch KMA, Aurora S, Vikingstad EM. Functional MRI-BOLD of visually triggered headache in patients with migraine. Arch. Neurol. 56, 548–554 (1999).
8 Hadjikhani N, del Rio MS, Wu O et al. Mechanisms of migraine aura revealed by functional MRI in human visual cortex. Proc. Natl Acad. Sci. USA 98, 4687–4692 (2001).
9 Bramanti P, Grugno R, Vitetta A et al. Migraine with and without aura: electrophysiological and functional neuroimaging evidence. Funct. Neurol. 20, 29–32 (2005).
10 Lauritzen M. Long lasting reduction of cortical blood flow of the rat brain after spreading depression with preserved autoregulation and impaired CO2 response. J. Cereb. Blood Flow Metab. 4, 546–554 (1984).
11 Milner PM. Note on a possible correspondence between the scotomas of migraine and spreading depression of Leão. Electroencephalogr. Clin. Neurophysiol. 10, 705 (1958).

766 Expert Rev. Neurotherapeutics 8(5), (2008)
Perspective Smith, James, Fraser & Huang
12 Parsons AA. Recent advances in mechanisms of spreading depression. Curr. Opin. Neurol. 11, 227–233 (1998).
13 Parsons AA, Raval P, Smith MI, Read SJ, Bingham S. Cortical spreading depression and migraine: A missing link? In: Development in Neurology (12th Edition). Clifford Rose (Ed.). Elsevier, Amsterdam, The Netherlands, 153–161 (1996).
14 Zagami AS. Pathophysiology of migraine and tension-type headache. Curr. Opin. Neurol. 7, 272–277 (1994).
15 Aurora SK, Cao Y, Bowyer SM, Welch KMA. The occipital cortex is hyperexcitable in migraine: experimental evidence. Headache 39, 469–476 (1999).
16 Bowyer SM, Aurora SK, Moran JE, Tepley N, Welch KMA. Magnetoencephalographic fields from patients with spontaneous and induced migraine aura. Ann. Neurol. 50, 582–587 (2001).
17 Bowyer SM, Mason KM, Moran JE, Tepley N, Mitsias PD. Cortical hyperexcitability in migraine patients before and after sodium valproate treatment. J. Clin. Neurophysiol. 22, 65–67 (2005).
18 Schoenen J. Cortical electrophysiology in migraine and possible pathogenetic implications. Clin. Neurosci. 5, 10–17 (1998).
19 Welch KMA, Barkley GL, Ramadam NM, D’Andrea G. NMR spectroscopic and magnetoencephalographic studies in migraine with aura: supporting the spreading depression hypothesis. Pathol. Biol. 40, 349–350 (1992).
20 Bowyer SM, Tepley N, Papuashvili N et al. Analysis of MEG signals of spreading cortical depression with propagation constrained to a rectangular cortical strip II. Gyrencephalic swine model. Brain Res. 843, 79–86 (1999).
21 Ambrosini A, Schoenen J. The electrophysiology of migraine. Curr. Opin. Neurol. 16, 327–331 (2003).
22 Mayevsky A, Doron A, Manor T et al. Cortical spreading depression recorded from the human brain using a multiparametric monitoring system. Brain Res. 740, 268–274 (1996).
23 Strong AJ. Dr. Bernice Grafstein’s paper on the mechanism of spreading depression. J. Neurophysiol. 94, 5–7 (2005).
24 Strong AJ, Dardis R. Depolarisation phenomena in traumatic and ischaemic brain injury In: Advances and Technical Standards in Neurosurgery. Pickard JD (Ed.). Springer-Verlag, Wien, Austria, 3–49 (2005).
25 Strong AJ, Fabricius M, Boutelle MG et al. Spreading and synchronous depressions of cortical activity in acutely injured human brain. Stroke 33, 2738–2743 (2002).
26 Fabricius M, Fuhr S, Bhatia R et al. Cortical spreading depression and peri-infarct depolarization in acutely injured human cerebral cortex. Brain 129, 776–779 (2006).
27 Simard M, Nedergaard M. The neurobiology of glia in the context of water and ion homeostasis. Neuroscience 129, 877–896 (2004).
28 Collins JJ. Fishing for function in noise. Nature 402, 241–242 (1999).
29 Russell DF, Wilkens LA, Moss F. Use of behavioural stochastic resonance by paddle fish for feeding. Nature 402, 291–294 (1999).
30 Chronicle EP, Mulleners WM. Visual system dysfunction in migraine: a review of clinical and psychophysical findings. Cephalalgia 16, 525–535 (1996).
31 Mulleners WM, Chronicle EP, Palmer JE, Koehler PJ, Vredeveld JW. Suppression of perception in migraine: evidence for reduced inhibition in the visual cortex. Neurology 56, 178–183 (2001).
32 Smith MI, Evans M, Parsons AA, Benham CD. Relationship between cell volume and extracellular potential during spreading depression. Cephalalgia 18, 413 (1998).
33 Smith MI, Read SJ, Chan WN et al. Repetitive cortical spreading depression in a gyrencephalic feline brain: inhibition by the novel benzoylamino-benzopyran SB-220453. Cephalalgia 20, 546–553 (2000).
34 Martins-Ferreira H, Nedergaard M, Nicholson C. Perspectives on spreading depression. Brain Res. Rev. 32, 215–234 (2000).
35 Kuge Y, Hasegawa Y, Yokota C et al. Effects of single and repetitive spreading depression on cerebral blood flow and glucose metabolism in cats: a PET study. J. Neurol. Sci. 176, 114–123 (2000).
36 Bockhorst KHJ, Smith JM, Smith MI et al. A quantitative analysis of cortical spreading depression events in the feline brain characterized with diffusion weighted MRI. J. Magn. Reson. Imaging 12, 722–733 (2000).
37 de Crespigny A, Röther J, van Bruggen N, Beaulieu C. Mosely ME. Simultaneous measurement of diffusion, perfusion and direct current potential during cortical spreading depression. In: Fourth Scientific Meeting of the International Society of Magn. Reson. Med. John Wiley, NY, USA, 315 (1996).
38 de Crespigny A, Röther J, van Bruggen N, Beaulieu C, Moseley ME. Magnetic resonance imaging assessment of cerebral hemodynamics during spreading depression in rats. J. Cereb. Blood Flow Metab. 18, 1008–1017 (1998).
39 James MF, Smith MI, Bockhorst KHJ et al. Cortical spreading depression in the gyrencephalic feline brain studied by magnetic resonance imaging. J. Physiol. 519, 415–425 (1999).
40 Gardner-Medwin AR, van Bruggen N, Williams SR, Ahier RG. Magnetic resonance imaging of propagating waves of spreading depression in the anaesthetised rat. J. Cereb. Blood Flow Metab. 14, 7–11 (1994).
41 Hasegawa Y, Latour LL, Formato JE, Sotak CH, Fisher M. Spreading waves of reduced diffsuion coefficient of water in normal and ischaemic rat brain. J. Cereb. Blood Flow Metab. 15, 179–187 (1995).
42 Bradley DP, Smith MI, Netsiri C et al. Diffusion-weighted MRI used to detect in vivo modulation of cortical spreading depression: comparison of sumatriptan and tonabersat. Exp. Neurol. 172, 342–353 (2001).
43 Bradley DP, Smith JM, Smith MI et al. Cortical spreading depression in the feline brain following sustained and transient stimuli studied using diffusion-weighted imaging. J. Physiol. 544, 39–56 (2002).
44 Latour LL, Hasegawa Y, Formato JE, Fisher M, Sotak CH. Spreading waves of decreased diffusion-coefficient after cortical stimulation in the rat brain. Magn. Reson. Med. 32, 189–198 (1994).
45 Nicholson C, Syková E. Extra-cellular space analysis revealed by diffusion analysis. Trends Neurosci. 21, 207–215 (1998).
46 Chester M, Kraig RP. Intracellular pH transients of mammalian astrocytes. J. Neurosci. 9, 2011–2019 (1989).
47 Davies ML, Kirov SA, Andrew RD. Whole isolated neocortical and hippocampal preparations and their use in imaging studies. J. Neurosci. Methods 166, 203–216 (2007).
48 Orkand RK. Glial-interstitial fluid exchange. Ann. NY Acad. Sci. 481, 269–272 (1986).
49 Ransom BR, Sontheimer H. The neurophysiology of glial cells. J. Clin. Neurophysiol. 9, 224–251 (1992).
50 Keyser DO, Pellmar TC. Synaptic transmission in the hippocampus – critical role for glial-cells. Glia 10, 237–243 (1994).

Cortical spreading depression Perspective
www.expert-reviews.com 767
51 Largo C, Cuevas P, Somjen GG, Delrio RM, Herreras O. The effect of depressing glial function in rat brain in situ on ion homeostasis, synaptic transmission, and neuron survival. J. Neurosci. 16, 1219–1229 (1996).
52 Richter F, Ebersberger A, Schaible HG. Blockade of voltage-gated calcium channels in rat inhibits repetitive cortical spreading depression. Neurosci. Lett. 334, 123–126 (2002).
53 Newman EA, Zahs KR. Calcium waves in retinal glial cells. Science 275, 844–847 (1997).
54 Venance L, Stella N, Glowinski J, Giaume C. Mechanism involved in initiation and propagation of receptor-induced intercellular calcium signaling in cultured rat astrocytes. J. Neurosci. 17, 1981–1992 (1997).
55 Wang Z, Tymianski M, Jones OT, Nedergaard M. Impact of cytoplasmic calcium buffering on the spatial and temporal characteristics of intercellular calcium signals in astrocytes. J. Neurosci. 17, 7359–7371 (1997).
56 Peters O, Schipke CG, Hashimoto Y, Kettenmann H. Different mechanisms promote astrocyte Ca2+ waves and spreading depression in the mouse neocortex. J. Neurosci. 23, 9888–9896 (2003).
57 Charles AC, Kodali SK, Tyndale RF. Intercellular calcium waves in neurons. Mol. Cell. Neurosci. 7, 337–353 (1996).
58 Nedergaard M. Direct signalling from astrocytes to neurons in cultures of mammalian brain cells. Science 263, 1768–1771 (1994).
59 Basarsky TA, Duffy SN, Andrew RD, MacVicar BA. Imaging spreading depression and associated intra-cellular calcium waves in brain slices. J. Neurosci. 18, 7189–7199 (1998).
60 Cornell-Bell AH, Finkbeiner SM. Ca2+ waves in astrocytes. Cell Calcium 12, 185–204 (1991).
61 Finkbeiner S. Calcium waves in astrocytes-filling in the gaps. Neuron 8, 1101–1108 (1992).
62 Hansen AJ. Effect of anoxia on ion distribution in the brain. Physiol. Rev. 65, 101–148 (1985).
63 Martins-Ferreira H, Ribeiro LJ. Biphasic effects of gap junctional uncoupling agents on the propagation of retinal spreading depression. Braz. J. Med. Biol. Res. 28, 991–994 (1995).
64 Nedergaard M, Cooper AJ, Goldman SA. Gap junctions are required for the propagation of spreading depression. J. Neurobiol. 28, 433–444 (1995).
65 Steinhardt RA, Bi G, Alderton JM. Cell membrane resealing by a vesicular mechanism similar to neurotransmitter release. Science 263, 390–393 (1994).
66 Canals S, Makarova I, Lopez-Aguado L et al. Longitudinal depolarization gradients along the somatodendritic axis of CA1 pyramidal cells: a novel feature of spreading depression. J. Neurophysiol. 94, 943–951 (2005).
67 Nicholson C, Kraig RP. The behaviour of extracellular ions during spreading depression In: The Application of Ion Selective Microelectrodes. Zeuthen T. (Ed.). Elsevier/North Holland Biomedical Press, 217–238 (1981).
68 Hansson E, Muyderman H, Leonova J et al. Astroglia and glutamate in physiology and pathology: aspects on glutamate transport, glutamate-induced cell swelling and gap-junction communication. Neurochem. Int. 37, 317–329 (2000).
69 Goadsby PJ, Kullmann DM. Another migraine gene. Lancet 366, 345–346 (2005).
70 Ophoff RA, Terwindt GM, Vergouwe MN et al. Familial hemiplegic migraine and episodic ataxia type-2 are caused by mutations in the Ca2+ channel gene CACNL1A4. Cell 87, 543–552 (1996).
71 Battistini S, Stenirri S, Piatti N et al. A new CACNA1A gene mutation in acetazoleamide-responsive familial hemiplegic migraine and ataxia. Neurology 53, 38–43 (1999).
72 Carrera P, Piatti M, Stenirri S et al. Genetic heterogeneity in Italian families with familial hemiplegic migraine. Neurology 53, 26–32 (1999).
73 Jen J, Yue Q, Nelson SF et al. A novel nonsense mutation in CACNA1A causes episodic ataxia and hemiplegia. Neurology 53, 34–37 (1999).
74 van den Maagdenberg AM, Pietrobon D, Pizzorusso T et al. A Cacna1a knockin migraine mouse model with increased susceptibility to cortical spreading depression. Neuron 41, 701–710 (2004).
75 Ayata C, Shimizu-Sasamata M, Lo EH, Noebels JL, Moskowitz MA. Impaired neurotransmitter release and elevated threshold for cortical spreading depression in mice with mutations in the α1A subunit of P/Q type calcium channels. Neuroscience 95, 639–645 (2000).
76 de Fusco M, Marconi R, Silvestri L et al. Haploinsufficiency of ATP1A2 encoding the Na+/K+ pump α2 subunit associated with familial hemiplegic migraine type 2. Nat. Genet. 33, 192–196 (2003).
77 Dichgans M, Freilinger T, Eckstein G et al. Mutation in the neuronal voltage-gated sodium channel SCN1A in familial hemiplegic migraine. Lancet 366, 371–377 (2005).
78 Ebersberger A, Schaible HG, Averbeck B, Richter F. Is there a correlation between spreading depression, neurogenic inflammation, and nociception that might cause migraine headache? Ann. Neurol. 49, 7–13 (2001).
79 Kaube H, Goadsby PJ. Anti-migraine compounds fail to modulate the propagation of cortical spreading depression in the cat. Eur. Neurol. 34, 30–35 (1994).
80 Welch KM. Brain hyperexcitability: the basis for antiepileptic drugs in migraine prevention. Headache 45(Suppl. 1), S25–S32 (2005).
81 Ayata C, Jin H, Kudo C, Dalkara T, Moskowitz MA. Suppression of cortical spreading depression in migraine prophylaxis. Ann. Neurol. 59, 652–661 (2006).
82 Kwong KK, Belliveau JW, Chesler DA et al. Dynamic magnetic resonance imaging of human brain activity during primary sensory stimulation. Proc. Natl Acad. Sci. USA 89, 5675–5679 (1992).
83 Ogawa S, Tank DW, Menon R et al. Intrinsic signal changes accompanying sensory stimulation: functional brain mapping with magnetic resonance imaging. Proc. Natl Acad. Sci. USA 89, 5951–5955 (1992).
84 Sotak CH. Nuclear magnetic resonance (NMR) measurement of the apparent diffusion coefficient (ADC) of tissue water and its relationship to cell volume changes in pathological states. Neurochem. Int. 45, 569–582 (2004).
85 Röther J, deCrespigny AJ, D’Arceuil H, Moseley ME. MR detection of cortical spreading depression immediately after focal ischemia in the rat. J. Cereb. Blood Flow Metab. 16, 214–220 (1996).
86 Henning EC, Meng X, Fisher M, Sotak CH. Visualization of cortical spreading depression using manganese-enhanced magnetic resonance imaging. Magn. Reson. Med. 53, 851–857 (2005).

768 Expert Rev. Neurotherapeutics 8(5), (2008)
Perspective Smith, James, Fraser & Huang
87 Norris DG, Hoehn-Berlage M, Dreher W et al. Characterization of middle cerebral artery occlusion infarct development in the rat using fast nuclear magnetic resonance proton spectroscopic imaging and diffusion-weighted imaging. J. Cereb. Blood Flow Metab. 18, 749–757 (1998).
88 Smith JM, James MF, Bockhorst KHJ et al. Investigation of feline brain anatomy for the detection of cortical spreading depression with magnetic resonance imaging. J. Anat. 198, 537–554 (2001).
89 Xing D, Papadakis NG, Huang C-LH et al. Optimised diffusion-weighting for measurement of apparent diffusion coefficient (ADC) in human brain. Magn. Reson. Imaging 15, 771–784 (1997).
90 Cutrer FM, Sorensen AG, Weiskoff RM et al. Functional neuroimaging: enhanced understanding of migraine pathophysiology. Neurology 55(9 Suppl. 2), S36–S45 (2000).
91 Akerman S, Goadsby PJ. Topiramate inhibits cortical spreading depression in rat and cat: impact in migraine aura. Neuroreport 16, 1383–1387 (2005).
92 Tvedskov JF, Iversen HK, Olesen J. A double-blind study of SB-220453 (Tonerbasat) in the glyceryltrinitrate (GTN) model of migraine. Cephalalgia 24, 875–882 (2004).
93 Kaube H, Knight YE, Storer RJ et al. Vasodilator agents and supracollicular transection fail to inhibit cortical spreading depression in the cat. Cephalalgia 19, 592–597 (1999).
94 Windmuller O, Lindauer U, Foddis M et al. Ion changes in spreading ischaemia induce rat middle cerebral artery constriction in the absence of NO. Brain 128, 2042–2051 (2005).
95 Zhang ZG, Chopp M, Maynard KI, Moskowitz MA. Cerebral blood flow changes during cortical spreading depression are not altered by inhibition of nitric oxide synthesis. J. Cereb. Blood Flow Metab. 14, 939–943 (1994).
96 Wolf T, Lindauer U, Reuter U et al. Noninvasive near infrared spectroscopy monitoring of regional cerebral blood oxygenation changes during peri-infarct depolarizations in focal cerebral ischemia in the rat. J. Cereb. Blood Flow Metab. 17, 950–954 (1997).
97 Lacombe P, Sercombe R, Correze JL, Springhetti V, Seylaz J. Spreading depression induced prolonged reduction of cortical blood-flow reactivity in the rat. Exp. Neurol. 117, 278–286 (1992).
98 Netsiri C, Bradley DP, Takeda T et al. A delayed class of BOLD waveforms associated with spreading depression in the feline cerebral cortex can be detected and characterised using independent component analysis (ICA). Magn. Reson. Imaging 21, 1097–1110 (2003).
99 Kastrup A, Neumann-Haefelin T, Moseley ME, de Crespigny A. High speed diffusion magnetic resonance imaging of ischemia and spontaneous periinfarct spreading depression after thromboembolic stroke in the rat. J. Cereb. Blood Flow Metab. 20, 1636–1647 (2000).
100 Gorji A, Speckmann EJ. Spreading depression enhances the spontaneous epileptiform activity in human neocortical tissues. Eur. J. Neurosci. 19, 3371–3374 (2004).
101 Beaulieu C, Busch E, de Crespigny A, Moseley ME. Spreading waves of transient and prolonged decreases in water diffusion after subarachnoid hemorrhage in rats. Magn. Reson. Med. 44, 110–116 (2000).
102 Nallet H, MacKenzie ET, Roussel S. The nature of penumbral depolarizations following focal cerebral ischemia in the rat. Brain Res. 842, 148–158 (1999).
103 Back T, Kohono K, Hossman KA. Cortical negative DC deflections following middle cerebral artery occlusion and KCl-induced spreading depression: effect on blood flow, tissue oxygenation, and electroencephalogram. J. Cereb. Blood Flow Metab. 14, 9–12 (1994).
104 Gorji A, Scheller D, Straub H et al. Spreading depression in human neocortical slices. Brain Res. 906, 74–83 (2001).
105 Peeters M, Gunthorpe MJ, Strijbos PJ et al. Effects of pan- and subtype-selective N-methyl-D-aspartate receptor antagonists on cortical spreading depression in the rat: therapeutic potential for migraine. J. Pharmacol. Exp. Ther. 321, 564–572 (2007).
106 Marcus DA, Soso MJ. Migraine and stripe-induced visual discomfort. Arch. Neurol. 46, 1129–1132 (1989).
107 Blau JN. Migraine: clinical and research aspects In: Migraine (Ed.). The John Hopkins Universty Press, Baltimore, MD, USA, 3 (1987).
108 Richter F, Mikulik O, Ebersberger A, Schaible HG. Noradrenergic agonists and antagonists influence migration of cortical spreading depression in rat – a possible mechanism of migraine prophylaxis and prevention of postischemic neuronal damage. J Cereb. Blood Flow Metab. 25, 1225–1235 (2005).
109 Lampl C, Katsarava Z, Diener HC, Limmroth V. Lamotrigine reduces migraine aura and migraine attacks in patients with migraine with aura. J. Neurol. Neurosurg. Psychiatry 76, 1730–1732 (2005).
110 Ramadan NM, Buchanan TM. New and future migraine therapy. Pharmacol. Ther. 112, 199–212 (2006).
111 de Tommaso M, Marinazzo D, Nitti L et al. Effects of levetiracetam vs topiramate and placebo on visually evoked phase synchronization changes of α rhythm in migraine. Clin. Neurophysiol. 118, 2297–2304 (2007).
112 Margineanu DG, Klitgaard H. Inhibition of neuronal hypersynchrony in vitro differentiates levetiracetam from classical antiepileptic drugs. Pharmacol. Res. 42, 281–285 (2000).
113 Shank RP, Gardocki JF, Streeter AJ, Maryanoff BE. An overview of the preclinical aspects of topiramate: pharmacology, pharmacokinetics, and mechanism of action. Epilepsia 41(Suppl. 1), S3–S9 (2000).
114 Sachs M, Pape HC, Speckmann EJ, Gorji A. The effect of estrogen and progesterone on spreading depression in rat neocortical tissues. Neurobiol. Dis. 25, 27–34 (2007).
Affiliations
• Justin M Smith, PhDPhysiological Laboratory, University of Cambridge, Downing Street, Cambridge CB2 3EG, UKTel.: +44 122 333 3822Fax: +44 122 333 [email protected]
• Michael F James, PhDImmuno-Inflammation Centre of Excellence in Drug Discovery, GlaxoSmithKline, New Frontiers Science Park (North), Third Avenue, Harlow, Essex CM19 5AD, UKTel.: +44 127 962 [email protected]
• James A Fraser, BM BCh, PhDPhysiological Laboratory, University of Cambridge, Downing Street, Cambridge CB2 3EG, UK Tel.: +44 1223 333822Fax: +44 1223 333 [email protected]
• Christopher L-H Huang, DM, DScPhysiological Laboratory, University of Cambridge, Downing Street, Cambridge CB2 3EG, UKTel.: +44 122 333 3822Fax: +44 122 333 [email protected]