
Live birth after artificial insemination using cryopreserved ...
ORIGINAL ARTICLE Psychology and counselling
To continue or discontinue storageof cryopreserved embryos? Patients’decisions in view of their child wishV. Provoost1,*, G. Pennings1, P. De Sutter2, J. Gerris2,A. Van de Velde2, and M. Dhont2
1Bioethics Institute Ghent, Ghent University, Blandijnberg 2, B-9000 Ghent, Belgium 2Department of Reproductive Medicine,Ghent University Hospital, De Pintelaan 185, 9000 Ghent, Belgium
*Correspondence address. E-mail: [email protected]
Submitted on August 19, 2010; resubmitted on November 23, 2010; accepted on December 3, 2010
objective: Cryopreservation of supernumerary embryos resulting from IVF treatment offers extra chances to conceive. The objective ofthis study is to describe patients’ decisions to continue or discontinue storage of their embryos after a minimum storage period of 2 years.
methods: Female patients who had embryos stored at the Infertility Centre of the Ghent University Hospital (Belgium) were sent a mailquestionnaire to be completed anonymously.
results: The questionnaire had a response rate of 79% (326/412). After an embryo storage period of at least 2 years, 40% of thecouples who were still together wished to continue storage of their embryos. Half of these had no concrete plans for a transferand wanted to postpone the decision or keep all options open. For those who decided to discontinue storage (60%), the main reasonwas the completion of their families. Despite the fact that the patients’ child wish was the main factor in their storage decision,two groups of patients with distinct profiles made decisions that were inconsistent with their child wish: those who wanted tocontinue storage while not wanting a(nother) child (7% of those with no child wish), and those who wanted a(nother) child but decidedto discontinue storage (25% of those with a child wish). Overall, these patients more often expressed emotional difficulties regarding thisdecision.
conclusions: This study demonstrates the importance of gaining more insight into patients’ embryo storage decisions (along with theirembryo disposition decisions) and into the emotional factors playing a role in patients’ decision-making.
Key words: embryo disposition / decision-making / ethics / IVF
IntroductionCryopreservation of supernumerary embryos offers patients whoundergo IVF/ICSI extra chances to conceive without the need toundergo a new stimulation cycle. However, along with this possibility,the couples need to make a number of decisions, such as whetherthey want to use these embryos for future transfers. When theanswer to that question is no, they need to make an embryo disposi-tion decision (EDD). Over the last decennium, various empiricalstudies have examined patients’ EDDs. Some studies focused ondecisions about fresh embryos (Choudhary et al., 2004; Haimes andTaylor, 2009) while other (both quantitative and qualitative) studiesfocused on EDD-making regarding cryopreserved embryos. Theselatter studies concentrated on either one (Newton et al., 2003;McMahon and Saunders, 2009), two (Bangsbøll et al., 2004,Newton et al., 2007; Mohler-Kuo et al., 2009) or all three
(Hammarberg and Oke, 2000; McMahon et al., 2000; de Lacey,2005; Hammarberg and Tinney, 2006, Fuscaldo et al., 2007; Provoostet al., 2009) disposition options: donation to another couple forreproductive reasons, donation for science and discarding.
In Belgium, since the 2007 law on medically assisted reproductionand the disposition of supernumerary embryos and gametes, bothpartners have to make a choice on the disposition of frozenembryos in a written contract before starting their first IVF/ICSIcycle (Pennings, 2007). By stipulating a maximum storage period of5 years for all embryos from the moment of cryopreservation, thislaw intends to prevent an accumulation of stored embryos belongingto couples who no longer present themselves for further treatmentbut who fail to make an EDD.
Next to providing an account of patients’ disposition preferences,several empirical studies on EDDs have elucidated the emotional dif-ficulties and stress patients’ experience when faced with decisions
& The Author 2011. Published by Oxford University Press on behalf of the European Society of Human Reproduction and Embryology. All rights reserved.For Permissions, please email: [email protected]
Human Reproduction, Vol.26, No.4 pp. 861–872, 2011
Advanced Access publication on January 18, 2011 doi:10.1093/humrep/deq392
at Ghent U
niversity on August 22, 2012
http://humrep.oxfordjournals.org/
Dow
nloaded from

about their stored embryos (Oke et al., 1998; Newton et al., 2003;Hammarberg and Tinney, 2006). Moreover, some patients seem towant to postpone the EDD, even ad infinitum (McMahon et al.,2000). In order to fully comprehend these difficulties, it is necessaryto scrutinize the larger context of patients’ EDD-making. This includeslooking into their perception of cryopreserved embryos and the use ofthese embryos for their own fertility treatment.
The focal point of the majority of studies on patients’ decision-making about cryopreserved embryos is the EDD. In the chronologyof decision-making, though, this decision is preceded by severalother decisions. First, a cryopreservation decision allows the medicalteam to freeze and store supernumerary embryos. Secondly, patientshave to decide whether (and when) they want to use these embryosfor their own treatment. This decision can be called the transferdecision. Thirdly, patients can decide about the continuation ofstorage of the embryos in a storage decision. In principle, there is arelation between the storage decision and the transfer decision(which is the main reason for which embryos are stored) and patientsare expected to opt for continued storage of their embryos in antici-pation of the transfer. However, this link is no prerequisite. Patientscould perceive their cryopreserved embryos as a reproductivereserve or an ‘insurance policy’ they want to hold on to (until theymake a transfer decision) but for which they have no concrete inten-tion at the time of the storage decision or they may find it difficult tomake a storage decision even though they no longer want a transfer(Lyerly et al., 2010; Nachtigall et al., 2010). Both the transfer decisionand the storage decision can be made at any time following cryopre-servation of embryos, as long as there are embryos in storage.Fourthly, when patients have decided not to use their embryos anddiscontinue storage, they have to make an EDD. Essential to thewhole decision-making process up to this stage is the desire to havea child. At the stage of the EDD, this desire no longer plays acentral role and another disposition will have to be chosen. Thisdoes not imply that at that stage there is no child wish. It is possiblethat one of the partners still has a child wish but will not attempt tofulfil this wish in an agreement with their partner. Moreover, in separ-ated couples, the ex-partners’ child wishes no longer have to bematched in order to reach a joint decision. In this study, we mainlyfocus on couples who are still together and have to make a decisiontogether, or at least a decision on which both partners can agree.
A recent multi-institutional US survey found that 4 in 10 patientswith frozen embryos who had said that they either did not wanta(nother) baby or were undecided about their child wish were reluc-tant towards both further preservation and the EDD (Lyerly et al.,2010). A recent qualitative study shows that patients often knowlittle about the cryopreservation procedure and that their perceptionof cryopreserved embryos often contains misconceptions such as thebelief that the quality of the embryo diminishes during the storageperiod (Provoost et al., 2010). Findings such as these demonstratethe importance of including the patients’ other decisions regardingcryopreserved embryos instead of only looking at the outcome ofthe EDD. Data on other decisions, such as the storage decision,could provide information to clarify the context of decision-making.
Most empirical studies in this domain focus on patients who havealready made a transfer decision and a storage decision or whoseanswers start from that hypothetical situation, and therefore do nottake into account the prior phases in the EDD-making process.
Overall, empirical studies about the transfer decision or aboutpatients’ attitudes towards the use of cryopreserved embryos fortheir own treatment are rare and up till now few studies have beendedicated to the storage decision as such (Provoost et al., 2010).
The aim of this study is to describe patients’ decisions about con-tinuing or discontinuing storage of their cryopreserved embryos inthe light of their treatment goal.
Materials and MethodsBefore cryopreservation, all patients of the Department of ReproductiveMedicine of the Ghent University Hospital (Belgium) signed a form(after receiving information) allowing medical staff to freeze and storetheir supernumerary embryos when the quality of these embryos is con-sidered sufficient to allow cryopreservation. Since 1992 and up to 2008(when the 5-year storage limit was introduced), all patients whoseembryos have been cryopreserved at the department received an EDDform by mail every 2 years following the year in which the embryoswere frozen. The EDD form provides four options: continued storagefor 2 more years and three options for a final EDD: donation toother(s) for reproductive purposes, donation for research or discarding.A mail questionnaire was sent together with the EDD form to all patientswith embryos in storage that were frozen in the years 1998, 2000, 2002and 2004.
ParticipantsAll patients whose embryos were cryopreserved at the Department ofReproductive Medicine of the Ghent University Hospital between 1996and 2004 and were still in storage in January 2007 were included. Datawere gathered between January 2007 and July 2007.
Excluded from the study were four patients whose embryos werecreated with donor gametes and eight patients who did not speakDutch. Another six patients who had all their stored embryos transferredbefore responding were excluded during the study period. The generalpractitioners of all patients for whom no current address was available(because the patient moved without notifying the clinic) were asked forthe current address. At the start of the procedure, 448 patients wereincluded. In 36 cases (8%), the patients moved without notifying theclinic and could not be reached. The remaining 412 patients received aquestionnaire along with an EDD form that was sent by the clinic every2 years following cryopreservation to ask patients to make or renewtheir EDD.
ProcedureData were collected using an anonymous questionnaire based on a quan-titative methodology addressing a large enough sample of patients tocompare their decision-making with other characteristics and to identifytypes of decision-making (in light of their treatment goal) that are onlymade by a minority of people. The mailing procedure was based on thetotal design method to increase response (Dillman, 1991). The question-naire was addressed to the female patient and was aimed at describingpatients’ decisions to continue or discontinue storage of their cryopre-served embryos, the grounds for their decisions, their intentions at thetime of cryopreservation and their and their partners’ desire to havechildren.
Patients were also asked to rate the moral status they attached to anembryo on a seven-point semantic differential scale. The labels ‘collectionof cells’ and ‘child’ were used for the end-points of the scale. Attitudestatements, to be scored on a five-point Likert-type scale (stronglyagree, agree, neutral point, disagree and strongly disagree), were
862 Provoost et al.
at Ghent U
niversity on August 22, 2012
http://humrep.oxfordjournals.org/
Dow
nloaded from

presented to explore several aspects of the patients’ attitude towardscryopreserved embryos, their use for fertility treatment and the decisionsregarding these embryos (with a special focus on the transfer decision andthe storage decision). The statements were placed in a random order tooptimize task performance and to reduce unintended order effects.
A final part of the questionnaire was designed to measure the patients’socio-demographics (having children resulting from fertility treatments, levelof education and life stance) and treatment history (time since the last treat-ment, outcome and assessment of treatment burden). The Ethics Committeeof the Ghent University Hospital approved this procedure.
AnalysisPatients were divided into two groups based on their storage decisions: con-tinue or discontinue storage. Data were analysed using Predictive AnalyticsSoftware (PASW version 18) and StatXact (version 8). Fisher’s exact testwas used to compare the distribution of unordered variables andKruskal–Wallis exact test was used for single-order categories. One-wayanalysis of variance was used for continuous data normally distributed(age) and the Wilcoxon test was used for data not normally distributed(number of embryos). P , 0.05 was considered statistically significant.
The storage decision (continue versus discontinue storage) was treatedas a dependent variable in a binary logistic regression in which socio-demographic and treatment characteristics as well as patients’ scores onattitude statements were used as covariates.
Results
Patient characteristicsThe questionnaire had a response rate of 79% (326/412). For threequarters of the patients (75.0%, n ¼ 228), the last treatment cyclewas .2 years ago (Table I). The high number of patients who hadtheir embryos stored for .2 years is a result of the policy of thecentre to send patients a decision form after 2 years of storage. Forless than one in four, the outcome of the last treatment cycle wasnegative. Most patients with a negative outcome who had cryopre-served embryos opted for a transfer of these embryos in themonths following the unsuccesful treatment cycle and thereby didnot fulfil the criteria to be included in the EDD mailing programme:having cryopreserved embryos for .2 years. Nearly, 6 in 10 patientsdescribed their last treatment cycle as burdensome.
The patients had on average 4.7 embryos stored at the fertilitycentre. More than 90% of all patients had children, with 88.2%
........................................................................................
Table I Demographic and treatment characteristics(all respondents, n 5 326).
n %
Last treatment cycle
Time until the present
,2 years ago 81 25.0
Between 2 and 3 years ago 178 54.9
.3 years ago 65 20.1
Outcome
No pregnancy (or later miscarriage) 73 22.6
(Ongoing) pregnancy (and birth) 250 77.4
Patient assessment of treatment burden
Bearable 132 41.0
Physically burdensome 17 5.3
Emotionally burdensome 67 20.8
Physically and emotionally burdensome 106 32.9
Number of embryos in storage
Range 1–21
Mean 4.69
Median 4
Age of the female patient
Range 27–48
Mean 36.15
Median 36
Children
Currently pregnant
No 308 94.8
Yes 17 5.2
Childrena
No children 31 9.6
Children, but none were conceived through IVF 36 11.1
At least one child was conceived through IVF 257 79.3
Level of education of the female patient
No upper secondary education 22 6.8
Upper secondary education 109 33.7
Tertiary education, short 103 31.9
Tertiary education, long 89 27.6
Life stance and religion
Christian overall 183 56.3
Catholic 108 33.2
Protestant 7 2.2
Christian 68 20.9
Muslim 10 3.1
No denomination 129 38.7
Other 13 4.0
Continued
........................................................................................
Table I Continued
n %
Relationship between gamete providers for possible cryopreservedembryos
Still together 308 95.1
Separated 16 4.9
Data missing for one case for ‘Currently pregnant’ and ‘Life stance and religion’; for 2cases for ‘Children’, ‘Timing of last treatment cycle’ and for ‘Relationship betweengamete providers’; for 3 cases for ‘Level of education of the female patient’ and‘Outcome of last treatment cycle’; for 4 cases for ‘Patient assessment of treatmentburden’ and for 25 cases for ‘Number of embryos in storage’.aCurrent pregnancy not included.
To continue or discontinue the storage of embryos? 863
at Ghent U
niversity on August 22, 2012
http://humrep.oxfordjournals.org/
Dow
nloaded from

having genetically related children (not shown). About 80% of thepatients had at least one child resulting from an IVF/ICSI treatment.
More than half of the patients adhered to a Christian denomination,whereas 38.7% were not religious or did not adhere to a specific reli-gion. Four in 10 respondents (41.5%) stated that their life stance orreligion was important in making decisions about their embryos,whereas for one-third of the respondents (33.2%), life stance andreligion were unimportant in this context.
Sixteen patients (4.9%) were separated from their partner who wasthe male gamete provider for the embryos and all those couples haddecided to discontinue storage of their embryo(s). Patients who wereseparated from their partner or who provided no information aboutthe partner relationship (n ¼ 2) were excluded from most further ana-lyses, as were patients who were undecided about the storagedecision (n ¼ 3). This brought the total number of patients to 305,that is, all patients who were able to make a storage decision andwho were still in a (partner) relationship with the other gamete pro-vider for the embryos.
Intention at the time of cryopreservationAt the time of cryopreservation, three quarters of all patients (n ¼326) intended to use their cryopreserved embryos in a subsequenttransfer while one in four patients had no clear intention to do so(Table II). Moreover, 5.9% of patients had no intention to cryopre-serve. They either had acted upon the suggestion of the medicalstaff (5.3%) or were even unaware of the cryopreservation of theirembryos (0.6%) despite having signed a consent form at the time ofthe cryopreservation decision.
Storage decisionOf all patients who made a storage decision and were still togetherwith their partner, 40.0% (n ¼ 122) wanted to continue while 60.0%(n ¼ 183) wanted to discontinue the storage of their embryos. The fol-lowing paragraphs will describe first the storage decisions in general(along with the reasons for the decision and also in relation topatient or treatment characteristics, patients’ attitudes towards cryo-preserved embryos and the moral status they attach to them) andthen the types of inconsistencies between the storage decision andthe patients’ desire to have a child will be described.
Reasons to continue or discontinue storageOnly 27.3% of the patients who wanted to continue storage had madeplans for a transfer within the year (Table III). Half of the patients eitherwanted to keep all options open or postpone the decision. Three patients(2.5%) wanted to continue storage because there was a difference ofopinion between the partners about what to do with the embryos.
The most common reason (70.4%) for patients to want to discon-tinue the storage of their embryos was that they considered theirfamilies to be complete. In addition, some wanted another child butfound the treatment too burdensome. One in four of the patientsstated another reason. In 8.9% of the patients, age and/or medicalreasons were mentioned. Alternatively, 6.5% had achieved naturalpregnancy and 1.8% were in the process of adoption. Four patients(2.4%) merely mentioned that they had given up on further treatmentand five patients (3.0%) indicated that they did not want these cryo-preserved embryos.
Storage decision according to patient or treatment characteristicsAs could be expected, the child wish of both partners was positivelylinked to the couples’ storage decision: patients who still had a childwish more often decided to hold on to their embryos (Table IV).There was no association between patients’ storage decision andtheir age or their intention at the time of cryopreservation (data notshown). However, the moral status patients attached to theirembryo(s) was related to the decision to continue or discontinuestorage (P . 0.001): patients who wanted to continue the storageof their embryos attached a higher moral status to them than those
........................................................................................
Table II The patients’ intention at the time ofcryopreservation (n 5 326).
n %
To use in subsequent treatment (transfer) 244 75.5
To keep in order to decide later 60 18.6
No intentions, cryopreservation because it had beensuggested
17 5.3
I did not know at the time that the embryos were goingto be cryopreserved
2 0.6
........................................................................................
Table III Patients’ reasons to (dis)continue storage(n 5 305).
n %
Reasons to continue storage (n ¼ 122)a
I want to transfer the embryos within the year 33 27.3
I think about transferring the embryos but I have noconcrete plans
24 19.8
I don’t know whether I want to transfer them, I want tokeep all options open
49 40.5
I want to postpone the decision 11 9.1
My partner and I have a difference of opinion 3 2.5
Other reason 1 0.8
Reasons to discontinue storage (more than one answerpossible) (n ¼ 183)b
At this moment, my family is completed 119 70.4
I want another child but the treatment is tooburdensome physically
11 6.5
I want another child but the treatment is tooburdensome emotionally
15 8.9
Other reasons: 42 24.9
Age and/or medical reasons 15 8.9
Achieved natural pregnancy in the mean time 11 6.5
I give up 4 2.4
I am in the process of adoption 3 1.8
I do not want (these) cryopreserved embryos 5 3.0
Other 6 3.6
aData missing for one case.bData missing for 14 cases. Patients could choose more than one answer.
864 Provoost et al.
at Ghent U
niversity on August 22, 2012
http://humrep.oxfordjournals.org/
Dow
nloaded from

who wanted to discontinue storage. However, this link does not showa causal relation. Patients could want to further store their embryosbecause they attached a higher moral status to them but it is also poss-ible that patients who decided to hold on to their embryos (and whoconsider having them transferred) tended to attach higher moral statusto these embryos. Religion was not associated with their storagedecisions (data not shown).
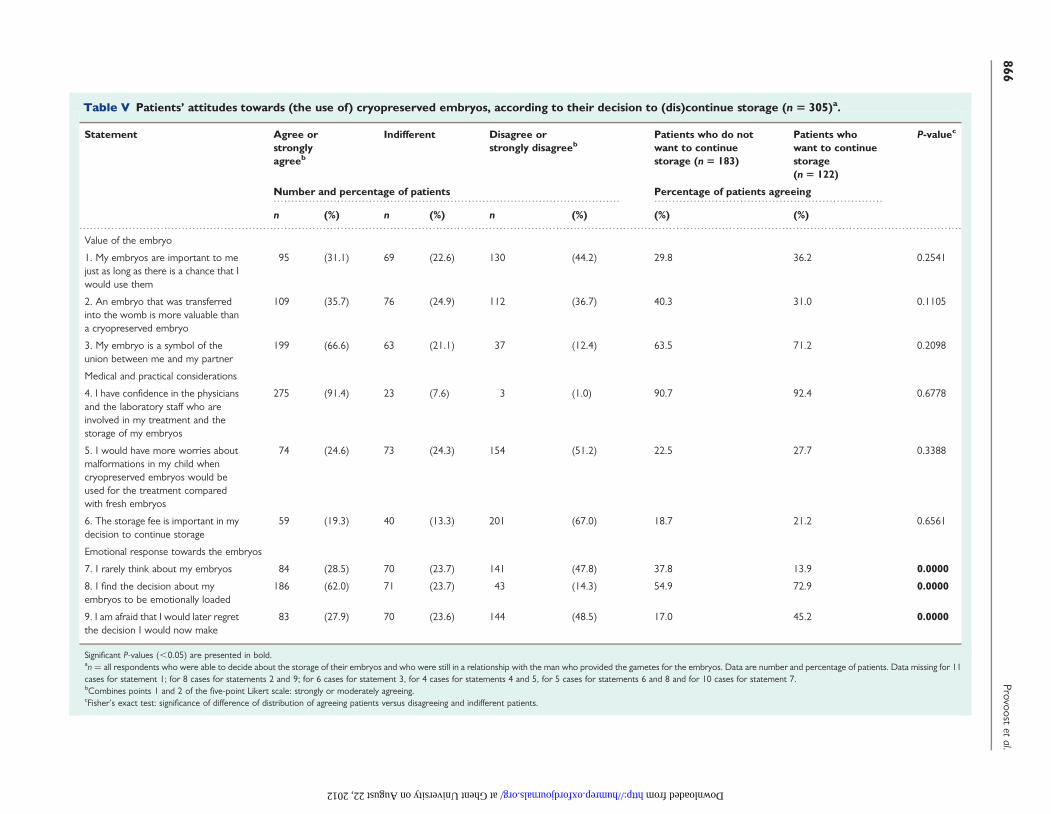
Patients’ attitudes towards (the use of) cryopreserved embryosWith respect to the value of the embryo, about one in three agreedthat an embryo is important to them as long as there is a chance thatthey would use it, while 44.2% thought their embryos were importantto them regardless of use (Table V). Two-thirds (66.6%) of thepatients considered their embryo as a symbol of the relationshipbetween them and their partner.
One in four patients had worries about malformations in the futurechild in relation to the cryopreservation. For two-thirds, the storagefee was not at all important in their storage decision.
There were no statistically significant differences between patientswanting to continue and those choosing to discontinue the storageof their embryos with regard to statements on the value of theembryo or the medical and practical considerations about treatmentwith cryopreserved embryos. However, there was a clear linkbetween patients’ emotional attitudes and their storage decisions.More than 60% of the patients agreed that the decision about theirembryos was emotionally loaded and more than one in four wereafraid that they would later regret the decision. Patients whowanted to continue storage significantly more often had an emotionalapproach towards their embryo (on all three emotional statements)compared with those who wanted to discontinue storage, with
.......................... .......................... ..........................
.............................................................................................................................................................................................
Table IV The storage decision according to patient and treatment characteristics (n 5 305)a.
Continue(n 5 122)
Discontinue(n 5 183)
Total P-valuec
n % n % n %
The desire to have a(nother) child
Woman’s desire
Child wish 69 58.5 27 14.9 96 32.1 0.0000
Undecided 36 30.5 37 20.4 73 24.4
No child wish 13 11.0 117 64.6 130 43.5
Man’s desirea
Child wish 61 53.0 22 12.3 83 28.2 0.0000
Undecided 32 27.8 26 14.5 58 19.7
No child wish 22 19.1 131 73.2 153 52.0
Last treatment cycle
Time until the present
,2 years ago 36 29.7 40 21.9 76 25.0 0.0542
Between 2 and 3 years ago 57 47.1 112 61.2 169 55.6
.3 years ago 28 23.1 31 16.9 59 19.4
Level of education of the female patient
No upper secondary education 11 9.1 10 5.5 21 6.9 0.0049
Upper secondary education 37 30.6 69 37.9 106 35.0
Tertiary education, short 27 22.3 63 34.6 90 29.7
Tertiary education, long 46 38.0 40 22.0 86 28.4
Children conceived by IVF treatmentb
No children 9 7.4 18 9.9 27 8.9 0.1780
Children, but none conceived by IVF 7 5.7 20 11.0 27 8.9
At least one child conceived by IVF 106 86.9 143 79.0 249 82.2
Moral status attached to the embryos on a scale of 1 (collection of cells)–7 (person/child)
Mean 4.25 3.31 3.69 0.0000
Median 4 3 4
Significant P-values (,0.05) are presented in bold. Column percentages.Data missing for: 1 case for ‘time until the present’ and ‘children’; 2 cases for ‘level of education of the female patient’ and for ‘children conceived by IVF treatment’; 9 cases for ‘moralstatus attached to the embryo’; 6 cases for ‘woman’s desire’ and 11 cases for ‘man’s desire’ to have a(nother) child.aAccording to the female patient to whom the questionnaire was addressed.bCurrent pregnancy not included.cKruskall–Wallis exact test was used for ‘Last treatment cycle: time until the present’, ‘Moral status attached to the embryos’ (singly ordered: scale 1–7) and ‘Level of education of thefemale patient’. Fisher’s exact test was used for the other variables.
To continue or discontinue the storage of embryos? 865
at Ghent U
niversity on August 22, 2012
http://humrep.oxfordjournals.org/
Dow
nloaded from
.................................................................................................. ................................................................
..........................................................................................................................................................................................................................................................
Table V Patients’ attitudes towards (the use of) cryopreserved embryos, according to their decision to (dis)continue storage (n 5 305)a.
Statement Agree orstronglyagreeb
Indifferent Disagree orstrongly disagreeb
Patients who do notwant to continuestorage (n 5 183)
Patients whowant to continuestorage(n 5 122)
P-valuec
Number and percentage of patients Percentage of patients agreeing
n (%) n (%) n (%) (%) (%)
Value of the embryo
1. My embryos are important to mejust as long as there is a chance that Iwould use them
95 (31.1) 69 (22.6) 130 (44.2) 29.8 36.2 0.2541
2. An embryo that was transferredinto the womb is more valuable thana cryopreserved embryo
109 (35.7) 76 (24.9) 112 (36.7) 40.3 31.0 0.1105
3. My embryo is a symbol of theunion between me and my partner
199 (66.6) 63 (21.1) 37 (12.4) 63.5 71.2 0.2098
Medical and practical considerations
4. I have confidence in the physiciansand the laboratory staff who areinvolved in my treatment and thestorage of my embryos
275 (91.4) 23 (7.6) 3 (1.0) 90.7 92.4 0.6778
5. I would have more worries aboutmalformations in my child whencryopreserved embryos would beused for the treatment comparedwith fresh embryos
74 (24.6) 73 (24.3) 154 (51.2) 22.5 27.7 0.3388
6. The storage fee is important in mydecision to continue storage
59 (19.3) 40 (13.3) 201 (67.0) 18.7 21.2 0.6561
Emotional response towards the embryos
7. I rarely think about my embryos 84 (28.5) 70 (23.7) 141 (47.8) 37.8 13.9 0.0000
8. I find the decision about myembryos to be emotionally loaded
186 (62.0) 71 (23.7) 43 (14.3) 54.9 72.9 0.0000
9. I am afraid that I would later regretthe decision I would now make
83 (27.9) 70 (23.6) 144 (48.5) 17.0 45.2 0.0000
Significant P-values (,0.05) are presented in bold.an ¼ all respondents who were able to decide about the storage of their embryos and who were still in a relationship with the man who provided the gametes for the embryos. Data are number and percentage of patients. Data missing for 11cases for statement 1; for 8 cases for statements 2 and 9; for 6 cases for statement 3, for 4 cases for statements 4 and 5, for 5 cases for statements 6 and 8 and for 10 cases for statement 7.bCombines points 1 and 2 of the five-point Likert scale: strongly or moderately agreeing.cFisher’s exact test: significance of difference of distribution of agreeing patients versus disagreeing and indifferent patients.
866Provoost
etal.
at Ghent University on August 22, 2012 http://humrep.oxfordjournals.org/ Downloaded from

nearly three times as many patients reporting feelings of anticipatedregret among the first group compared with the latter (P ¼ 0.0000).
Moral status of the embryoThe lower side of the seven-point semantic differential scale on themoral status of the embryo, representing a status approximating a col-lection of cells, was chosen by 43.9% while the upper end of the scale,representing the moral status of a child or person, was chosen by30.9%. The moral status attached to the embryo was related to edu-cational level, with patients who had at most a secondary degree (orhigh school) scoring higher on the scale (more towards personhood)than those with a tertiary degree (college or university) (3.93 versus3.51; P ¼ 0.047). Furthermore, there was a difference betweenpatients who did not have children and those who had children(mean embryo status 2.88 and 3.76, respectively; P ¼ 0.010). Conver-sely, years passed since the last treatment cycle, being pregnant at thetime of the questionnaire or having children with IVF/ICSI was notrelated to the moral status. Interestingly, while the moral status waslinked to their storage decision and religion was not, religion waslinked with the moral status: religious patients tended to attach ahigher moral status (more towards the scale point of person/child)compared with other patients (P ¼ 0.012; data not shown).
Modelling analysisLogistic regression analysis showed that couples, in which neitherpartner still had a child wish, were more likely to discontinue thestorage of their embryos. The proportions of variance explained bya model with these two variables (child wish of the female partner
and of the male partner) were 77.4%. Adding the variables ‘anticipatedregret’, ‘children’ (no children, children without IVF/CSI treatment,children resulting from IVF/ICSI treatment), ‘thinking about theembryos’ and ‘level of education of the female patient’ only increasedthe proportion of the explained variance by 2.1%.
Inconsistencies between patients’ storagedecisions and their desire for a childOverall, the partners’ individual desires to have a child are excellent predic-tors for the couples decision to (dis)continue storage. Table VI comparesthe couples’ combined desire to have a(nother) child to their storagedecisions. For 11 patients (3.6% of all couples who were still together),we did not have the data on the desire to have a child for both partners.For all other patients, the combination was made. Interestingly, for 48patients (16.2% of all couples who were still together), two types ofdecisions were documented that were inconsistent with their child wish.
Type 1: continuing storage in the absence of a desire to havea(nother) childTen couples of which neither of the partners had a desire for a childopted for continued storage (eight) or were undecided about furtherstorage (two) (Table VI). In the latter cases, storage was continued inthe absence of a decision. Their reasons to continue storage were toleave all options open in four couples and postpone the decision infive couples. These reasons differed significantly from couples whodecided to continue storage while wanting another child (P ¼ 0.0019).Furthermore, several other differences were noticed (Table VII). In
..................... ..................... .. .... .... .... ...
.............................................................................................................................................................................................
Table VI Couples’ decisions to (dis)continue storage in light of their desire to have a child (n 5 308)a.
Continuestorage
Discontinuestorage
Undecided Total
n %c n %c n %c n
The couple’s desire to have a childb
No partner wants another child 8 7.0 105 91.3 2 1.7 115
Both partners are in doubt about whether they want another child 21 52.5 18 45.0 1 2.5 40
One doubts, the other does not want another child
Woman doubts, man does not want another child 7 26.9 19 73.1 0 0.0 26
Woman does not want another child, man doubts 0 0.0 4 100.0 0 0.0 4
One doubts, the other wants another child
Woman doubts, man wants another child 7 100.0 0 0.0 0 0.0 7
Woman wants another child, man doubts 11 73.3 4 26.7 0 0.0 15
One wants another child, the other does not want another child
Woman wants another child, man does not 7 50.0 7 50.0 0 0.0 14
Woman does not want another child, man does 5 45.5 6 54.5 0 0.0 11
Both partners want another child 49 75.4 16 24.6 0 0.0 65
Total 115 38.7 179 60.3 3 1.0 297
Bold print indicates the inconsistent categories.aSixteen respondents who were separated from the partner from whose gametes the embryos co-originated, and two respondents for whom information about the partnerrelationship was missing, were excluded from this analysis. Three patients who were undecided about the storage decision were included. For 11 other respondents, data were missingfor at least one of the variables.bThe variable ‘the couple’s desire to have a child’ was constructed as a combination of two questions: ‘Do you want a child at this moment?’ and ’Does your current partner want achild at this moment?’ These questions each had three possible answers: yes, no and ‘not certain about this yet’).cRow percentages.
To continue or discontinue the storage of embryos? 867
at Ghent U
niversity on August 22, 2012
http://humrep.oxfordjournals.org/
Dow
nloaded from

..................................................... .....................................................
............................ ..................... ..................... ............................
.............................................................................................................................................................................................
Table VII Factors associated with patients’ decisions to (dis)continue storage in patients who did not have a child wish(n 5 115) or in patients who either had a child wish or were in doubt about having another child (n 5 127)a,b.
No child wish Child wish
Continue storage Discontinuestorage
Continuestorage
Discontinuestorage
n (%)c P-valued n (%)c n (%)c n (%)c P-valued
Last treatment cycle
Time until the present 0.0103 0.0474
,2 years ago 2 20.0 15 14.3 29 33.0 16 42.1
Between 2 and 3 years ago 2 20.0 68 64.8 42 47.7 21 55.3
.3 years ago 6 60.0 22 21.0 17 19.3 1 2.6
Outcome 0.3551 0.0463
No pregnancy (or pregnancy and miscarriage) 0 0.0 15 14.3 19 21.6 15 40.5
(Ongoing) pregnancy (and birth) 10 100.0 90 85.7 69 78.4 22 59.5
Children 1.0000 0.0007
No children 0 0.0 6 5.8 7 7.9 10 26.3
Children (not conceived through IVF/ICSI) 0 0.0 6 5.8 5 5.6 7 18.4
Children (conceived through IVF/ICSI) 10 100.0 91 88.3 77 86.5 21 55.3
Level of education of the female patient 0.0106 0.0165
No upper secondary education 2 20.0 4 3.8 8 9.0 1 2.6
Upper secondary education 0 0.0 37 35.6 30 33.7 17 44.7
Tertiary education, short 2 20.0 37 35.6 17 19.1 14 36.8
Tertiary education, long 6 60.0 26 25.0 34 38.2 6 15.8
Attitude statements
Value of the embryo
1. My embryos are important to me just as long as there is a chancethat I would use them
0 0.0 0.1140 27 26.2 34 40.0 13 36.1 0.8386
2. An embryo that was transferred into the womb is more valuablethan a cryopreserved embryo
1 10.0 0.1698 34 33.0 29 34.5 21 55.3 0.0462
3. My embryo is a symbol of the union between me and my partner 7 70.0 1.7373 61 59.2 59 69.4 23 60.5 0.4084
Medical and practical considerations
4. I have confidence in the physicians and the laboratory staff whoare involved in my treatment and the storage of my embryos
9 90.0 1.0000 95 91.3 79 91.9 34 89.5 0.7353
5. I would have more worries about malformations in my childwhen cryopreserved embryos would be used for the treatmentcompared with fresh embryos
2 20.0 1.0000 19 18.3 24 27.9 12 31.6 0.6740
6. The storage fee is important in my decision to continue storage 1 10.0 1.0000 13 12.5 18 20.9 9 23.7 0.8143
Emotional response towards the embryos
7. I rarely think about my embryos 1 10.0 0.0409 49 47.1 11 13.3 11 30.6 0.0384
8. I find the decision about my embryos to be emotionally loaded 9 90.0 0.0179 51 49.0 60 69.8 20 52.6 0.0714
9. I am afraid that I would later regret the decision I would nowmake
9 90.0 0.0000 12 11.5 32 38.6 6 15.8 0.0183
Moral status attached to the embryo
Mean (median) 4.80 (4.5) 0.0428 3.14 (3.0) 4.34 (4.0) 3.41 (4.0) 0.1539
Significant P-values (,0.05) are presented in bold.aIncluding all respondents who are still in a relationship with the man from whose gametes the embryos co-originated (n ¼ 308). This includes three patients who were undecidedabout the storage decision. For 11 couples, information was missing about the child wish of at least one of both partners. Two types of couples were not included in this analysis:couples where one partner doubted while the other did not want another child (n ¼ 30) and couples where one partner wanted another child while the other did not (n ¼ 25).bData missing for one patient with a child wish for ‘Last treatment cycle: Time until the present’, for two patients without a child wish for ‘Children’, for three patients with a child wishand two patients without a child wish for ‘Moral status attached to the embryo’ and for one patient without a child wish for ‘Level of education of the female patient’. For the attitudestatements, data were missing for between zero and eight cases for patients with a child wish and between zero and two cases for patients without a child wish.cColumn percentages.dFisher’s exact test: significance of difference of distribution of patients who continued storage versus patients who discontinued storage for patients with and patients without a currentchild wish. Kruskal–Wallis exact test for ‘Last treatment cycle: Time until the present’, ‘Children’, ‘Level of education of the female patient’ and ‘Moral status attached to the embryo’.
868 Provoost et al.
at Ghent U
niversity on August 22, 2012
http://humrep.oxfordjournals.org/
Dow
nloaded from

patients who wanted to continue storage in the absence of a child wish,the last treatment was more often .3 years ago. These women morefrequently reported feelings of anticipated regret, compared withwomen who decided to continue storage in the presence of a childwish and they more often thought their embryos were important regard-less of use. In addition, all 10 women with this type of inconsistentstorage decision had children resulting from IVF/ICSI treatments.
The patients without a child wish who decided to continue storagewere compared with patients without a child wish who actually dis-continued the storage of their embryos (Table VII). This analysisshowed that the time gap between the questionnaire and the lasttreatment was significantly longer for patients who made the inconsist-ent storage decision. However, there was no relation with the age ofthe female patient. These women more often had a higher educationand attached a moral status to their embryos that was significantlyhigher. Finally, their emotional attitude towards their embryosshowed that they thought more often about the embryos instorage, that they found decisions about these embryos to beemotionally loaded and that they were more often afraid that theywould later regret their decisions.
Type 2: discontinuing storage while wanting a(nother) childAnother group of 38 couples (12.8%) decided to discontinue storagewhile they both still had a desire for a child, were both uncertain orwhere one partner wanted another child while the other was uncer-tain (Table VI). This decision is made by 45% of the couples inwhich both partners were in doubt about their child wish and by aquarter (24.6%) of the couples of which both partners actuallywanted another child. When asked about their reasons for thisdecision, 21 of the 38 respondents gave reasons in the category‘other’ in the provided set of responses.
Analysis of their written comments showed that 10 patients discon-tinued the storage of their embryos because they had shifted theirfocus to other family building methods such as adoption (three) orbecause they had conceived spontaneously (seven). Four patientsreferred to their age or to medical reasons to forego further treat-ment. Another five patients mentioned the psychological burden ofthe treatment or the fact that they stopped believing in a positiveoutcome, while two patients indicated that the treatment was tooburdensome physically. One respondent referred to a combinationof these reasons.
Additionally, for five patients, the reasons to discontinue the storageof their embryos were related to negative beliefs about cryopreservedembryos: they wanted further IVF/ICSI treatment, albeit not with(these) cryopreserved embryos. This is a higher number than thepatients who discontinued storage in the absence of a child wish(1/129 versus 5/36; P ¼ 0.0020). In their written comments, thesepatients referred to their preference for fresh embryos or ‘fresher’embryos (from a more recent cycle). The women pointed to thelow chance of success and their worries about unforeseen effects ofthe use of cryopreserved embryos. One patient indicated that aftera series of treatment cycles she wanted to take a break duringwhich she did not want to have embryos in storage. Moreover, com-parable doubts and uncertainties about the use of cryopreservedembryos for their treatment were found in the written answers oftwo other respondents who had no child wish and discontinuedstorage. In the margin of the question about whether they wanted
to (dis)continue storage of their embryos, one respondent mentionedher astonishment about the fact that her embryos had been kept forthat long.
The patients who made this type of seemingly inconsistent storagedecision more often had a more recent treatment history and a nega-tive outcome of their last treatment compared with patients whowanted to discontinue storage while they no longer had a desire fora child and also with patients who also still had a child wish and (there-fore) decided to hold on to their embryos (Table VII). Furthermore,patients who discontinued while still having a child wish also lessoften had children (conceived with IVF) and they more oftenthought that an embryo that was transferred into the womb wasmore valuable than a cryopreserved embryo. Finally, these patientsthought less often about their embryos and were less often afraidthat they would regret their decision compared with patients whoalso had a child wish and decided to continue storage.
DiscussionMore than 40% of the patients who had embryos stored for at least 2years thought that their embryos were important to them even whenthere would be no chance that they would use them for their ownreproductive treatment. More than one in four were afraid that theywould later regret their decision. For most patients, the storage feewas not an important factor in their storage decision. With respectto the use of cryopreserved embryos, one in four reported moreworries about malformations in the future child when theseembryos were used compared with ‘fresh’ ones. Worries like thesehave been described before (Skoog Svanberg et al., 2001a; Bangsbøllet al., 2004). On the whole, there was a clear link between thepatients’ emotional attitudes towards cryopreserved embryos andtheir storage decisions.
Of the couples who were still together and had embryos in storagefor at least 2 years, 40% wanted to hold on to their embryos. Of thosecouples, almost three-quarters had no concrete plans for a transferand up to half of them were not sure whether they ever wouldwant the embryos to be transferred. Conversely, 60% of coupleswho were still together wanted to discontinue the storage of theseembryos, with the completion of their families as the most importantreason for doing so. Overall, the desire to have a(nother) child was themost important factor in the storage decision, as has been describedelsewhere (Bangsbøll et al., 2004).
However, two groups of patients (16.2% of all couples who werestill together) with distinct profiles were found to make inconsistentdecisions: decisions that were not in line with their child wish. Forthese patients, the reasons for their decisions can be found infactors other than the child wish. Taking into account these otherfactors creates a more complete picture of their storage decisionand shows that decisions that are inconsistent with the child wishare not necessarily irrational. The first group wanted to continuestorage while they did not want a(nother) child. All of these coupleshad children resulting from IVF/ICSI. Furthermore, the time gapbetween the last treatment cycle of these patients was more oftenlarger and these women were more often positive about the valueof cryopreserved embryos, even those that would not be used bythem. They wanted to leave all options open or postpone thedecision. These patients were different in their emotional attitude
To continue or discontinue the storage of embryos? 869
at Ghent U
niversity on August 22, 2012
http://humrep.oxfordjournals.org/
Dow
nloaded from

(towards the embryos or the decision) from those who decided todiscontinue storage in the absence of a child wish. They more oftenthought about their embryos, had feelings of anticipated regret andperceived this decision as emotionally loaded. Interestingly, thesepatients had a higher education and attached a significantly highermoral status to their embryos than women who decided to discon-tinue storage in the absence of a child wish. The anticipated regretin this first group of patients offers a possible explanation for their puz-zling decision (holding on to something you do not need) and shouldbe addressed in counselling of patients who experience difficulties inEDD-making.
This type of storage decision that is inconsistent with the child wishpossibly explains part of the prolonged storage periods for cryopre-served embryos mentioned in literature reports worldwide, evenpast patient age limits for a transfer (Klock, 2004; Bankowski et al.,2005). Holding on to embryos for emotional reasons despite theabsence of a purpose could be a factor adding to the numbers ofpatients who extensively prolong the embryo storage period, wantto store indefinitely or do not make a disposition decision. Beside arecent study on the profile of women who still had embryos instorage after 5 years, there has been little knowledge on the charac-teristics of these patients (Stiel et al., 2010).
The second group of patients who were found to make a storagedecision that was inconsistent with their child wish has not yet beendescribed. This group consisted of nearly half of all couples in whichboth partners were in doubt about their child wish and a quarter ofall couples in which both partners actually wanted another child.These patients decided to discontinue the storage of their embryos.Part of this group were women who gave up on further treatment,sometimes referring to their age or to medical reasons, while otherwomen had conceived spontaneously or started an adoption pro-cedure. Five women, however, pointed out that they wanted furthertreatment, albeit not with (these) cryopreserved embryos. Most ofthe written information they provided to explain their puzzlingdecision was linked to misconceptions or an unfulfilled need for infor-mation. This finding confirms the results of our interview study whichshowed that, besides some worries for the health of the future child, anumber of patients believed that fresh embryos (or embryos cryopre-served at a later date compared with ‘older’ ones) offered a betterchance of treatment success (Provoost et al., 2010). From this inter-view study, it also appeared that patients who had doubts or mistrustsabout the use of cryopreserved embryos did not talk to the medicalstaff about their concerns, leaving them largely unaware of thisproblem. In terms of loss of treatment chances, additional treatmentburden and (society’s and patients’) increasing health care costs,these situations should be prevented. Hence, adequate informationfor patients is crucial. For instance, patients should know the differ-ences between a full stimulation cycle with an oocyte pick-up andthe transfer of cryopreserved embryos when they decide to foregothe transfer of their cryopreserved embryos because they perceivethe treatment as too burdensome.
On the whole, there is little knowledge about why patients opt outof IVF/ICSI treatment while their child wish is still unfulfilled (Peddieet al., 2005; Eisenberg et al., 2010). From an ethical point of view,there are a number of requirements to the informed consent patientsgive at the start of a specific medical treatment. These decisionsshould be based on information and they should be made by a
competent person who freely consents with the treatment.However, especially in a context in which patients decide to foregofurther treatment, the decision could come years after their lastcontact with the clinic, and these decisions are concealed from theeyes of the medical staff. Consequently, it is difficult to assesswhether these decisions are made according to the recommendationsregarding informed consent. Usually in the IVF context, there will notbe a systematical enquiry into the reasons of patients who opt out‘during treatment’. Nevertheless, an awareness of the reasons thatplay a role in patients’ treatment decisions is needed to provide ade-quate assistance to patients in their decision-making and is thereforealso a prerequisite of good patient care. Identifying patients who areprone to make decisions that are possibly inconsistent with theirchild wish creates the opportunity to prevent them from unintention-ally disposing of vital chances to conceive.
Over the last years, milder stimulation protocols have beendescribed as an alternative to IVF/ICSI treatment with high dosagesof ovarian stimulation which aims to increase the number of retrieva-ble oocytes and as a consequence increase the number of embryos(Verberg et al., 2009). These protocols, also called ‘patient-friendlyprotocols’, prevent several negative effects of high-stimulation proto-cols such as ovarian hyperstimulation syndrome (Pennings andOmbelet, 2007; Raziel et al., 2009). The decrease in cryopreservedembryos following mild stimulation protocols has been described asa potential disadvantage. However, in patients who face emotional dif-ficulties in dealing with (decisions about) cryopreserved embryos, thiscould be an advantage. One should inform patients from the start ofthe existence of treatment options that give rise to fewer cryopre-served embryos. After counselling patients of the implications andpossibilities of cryopreserving embryos, they should be offered anexplicit choice of stimulation protocols. In this context, also the pro-gress in terms of cryopreservation of oocytes could bring acceptablealternatives for patients who find it difficult to deal with cryopreservedembryos (Bankowski et al., 2005; Jain and Paulson, 2006).
Two other aspects should be addressed in patient information andcounselling. The first is the success rate of frozen/thawed treatmentcycles since a lower success rate could be a reason for patients notto opt for cryopreservation. Second, the finding that there is no associ-ation between intention at the time of freezing and storage decisionshows that it is important to inform patients that their intentions atthe time of the cryopreservation (or in case of advanced directives,the decision) could change, possibly leaving patients with a situationthey did not foresee and would not have chosen if they had known.
In a multi-institutional US survey, a higher percentage (54%) ofrespondents wanted continuation of storage compared with thisstudy (Lyerly et al., 2010). Apart from differences in the culturalcontext, part of the difference can be explained by the fact that therespondents in this study had embryos stored for at least 2 years.The same explanation applies to the high proportion of patients inthis study whose last treatment cycle had a positive outcome. Patientswho had a negative outcome and who had embryos in storage couldhave had further transfers as long as their embryo supply allowed this.The participants in the US survey who wanted to continue storageindicated that they were very likely to use these embryos (Lyerlyet al., 2010). In our study, fewer patients had concrete plans regardingthe transfer of these embryos. In line with the above explanation,those with concrete plans have had the chance during the previous
870 Provoost et al.
at Ghent U
niversity on August 22, 2012
http://humrep.oxfordjournals.org/
Dow
nloaded from

years to return to the centre for the transfer of the embryos. It couldbe expected that when patients with lower success rates (of the lasttreatment cycle) were asked about their storage decision (or patientswho recently stored embryos instead of after 2 years), the percentageof decisions to continue storage would be considerably higher, inaccordance with these patients’ child wish.
Limited quantitative research has been done about the moral statuspatients attach to their embryos. Measuring a complex and still largelyunknown concept is difficult. The scale used in this study (with labelsfor the ends of the scale but not for the points in between) is designedin accordance with findings from our qualitative study (Provoost et al.,2009). In this study, we measured the moral status of the embryousing the classical continuum of statuses (as present in the ethical lit-erature) between a collection of cells and full personhood. We foundthat patients who wanted to continue storage attributed a highermoral status to their embryos. Moreover, patients who had a lowereducation level and those who had children attached a higher moralstatus to their embryos. In contrast, life stance and religion werenot linked to the storage decision, although it was linked to themoral status patients attached to their embryos in storage, which inturn had been linked to the storage decision. A possible explanationfor these puzzling results could be that the moral status patientsgive to the embryo (and possibly also patients’ perception ofembryos in general) is rather influenced by the decisions they makeabout them (such as the storage decision) than the other wayaround. The finding that patients thought their religion was not impor-tant in the context of embryo decisions is in line with our previousfindings based on the interview study and should also be situated ina cultural context in which mainstream Belgian Catholics are notactively committed (Provoost et al., 2009). Future research shouldfurther explore the concept of the moral status of embryos in laypeople such as infertility patients and search for instruments to deter-mine their views on embryo and EDDs.
Next to the patients’ child wish and their moral considerations, par-ticularly, their emotional attitude towards cryopreserved embryos wasclearly linked to the decision whether or not to continue storage. Thisis even more so in patients who continue storage without a tangiblepurpose. Emotional aspects as side-effects of EDD-making havebeen discussed. However, they are underreported in the literatureas potential factors determining the decision itself (Skoog Svanberget al., 2001b).
Our data were collected only through the female partners of thecouples. It would be ideal to gather data on some topics from bothpartners separately. However, studies that aimed at collecting datafrom both partners have a lower response rate in the male partner(Newton et al., 2003; McMahon and Saunders, 2009; Lyerly et al.,2010). Rather than risking an overall decrease of the response rateby addressing both partners, we opted to address one partner andask them for the other partners’ child wish. These data were usedfor analyses only in couples who were still together. Another limitationof this study is the fact that it dealt with small numbers, especiallyregarding specific types of decisions. However, despite being madeless frequently, these decisions are very interesting in the light of theproblem of abandoned embryos or postponed EDDs (which leadsto an accumulation of embryos in the infertility centres). In addition,sampling patients on the basis of their decisions (and their childwish) is very difficult because this type of information usually is only
revealed once the data collection has started. Therefore, a quantitativestudy, making an inventory of types of storage decisions in relation tothe treatment goal (fulfilment of child wish), offers a better opportu-nity to study these decisions and the factors related to them.
Further research should include an exploration of measures tosupport patients’ ability to make informed decisions regarding theircryopreserved embryos, including their need for information. More-over, the effects of the timing of decision-making and the way ofinforming patients on the types of decisions they make should bestudied. Further research on patients’ psychological profile, especiallythat of persons who are making seemingly inconsistent decisions, isneeded in order to facilitate an early detection of these patients andthe difficulties they encounter in their embryo decisions. A specialfocus should be given to misconceptions or negative beliefs aboutcryopreserved embryos. Insights from such studies could be usedfor setting up accurate counselling, especially regarding emotionalissues concerning having, using and deciding about cryopreservedembryos. In fact, lack of emotional support has been identified asone of the many weaknesses in fertility care in a recent study fromthe Netherlands (van Empel et al., 2010). Through accurate counsel-ling, infertility centres would be able to meet the expectations ofpatients who, according to another recent study, perceive their phys-icians and their clinics to be the mandatory assistance providers forembryo (disposition) decisions (Nachtigall et al., 2010).
In conclusion, despite the fact that the patients’ child wish was themain factor in their storage decision, two groups of patients with dis-tinct profiles were found to make two types of decisions that wereinconsistent with their child wish: patients who wanted to continuestorage while not wanting a(nother) child and those who wanteda(nother) child but decided to discontinue storage of their embryos.Overall, these patients expressed more often emotional difficultiesregarding their embryos and the decisions they needed to makeabout them. Misconceptions and negative beliefs about cryopreservedembryos played an important role in the decisions to discontinuestorage of patients who wanted further IVF/ICSI treatment. Thesebeliefs and misconceptions may not only be relevant to patients’storage decisions but also have an impact on their treatment decisions,specifically regarding the transfer of cryopreserved embryos. Finally,the results of this study show the importance of gaining more insightinto the storage decision as such.
Authors’ rolesAll authors take full responsibility for the reported research. Wewarrant that all authors have participated in the concept and design,analysis and interpretation of data, and drafting or revising of themanuscript and that they have approved of the manuscript assubmitted.
FundingV.P. and P.D.S. are holders of a Postdoctoral Mandate (V.P.) and aFundamental Clinical Research Mandate (P.D.S.) by the Flemish Foun-dation for Scientific Research (FWO-Vlaanderen).
To continue or discontinue the storage of embryos? 871
at Ghent U
niversity on August 22, 2012
http://humrep.oxfordjournals.org/
Dow
nloaded from

ReferencesBangsbøll S, Pinborg A, Yding Andersen C, Nyboe Andersen A. Patients’
attitudes towards donation of surplus cryopreserved embryos fortreatment or research. Hum Reprod 2004;19:2415–2419.
Bankowski BJ, Lyerly AD, Faden RR, Wallach EE. The social implications ofembryo cryopreservation. Fertil Steril 2005;84:823–832.
Choudhary M, Haimes E, Herbert M, Stojkovic M, Murdoch AP.Demographic and treatment characteristics associated with couples’decisions to donate fresh spare embryos for research. Hum Reprod2004;19:2091–2096.
de Lacey S. Parent identity and ‘virtual’ children: why patients discardrather than donate unused embryos. Hum Reprod 2005;20:1661–1669.
Dillman DA. The design and administration of mail surveys. Annu Rev Sociol1991;17:225–249.
Eisenberg ML, Smith JF, Millstein SG, Nachtigall RD, Adler NE, Pasch LA,Katz PP. Infertility outcomes program project group. Predictors of notpursuing infertility treatment after an infertility diagnosis: examinationof a prospective U.S. cohort. Fertil Steril 2010;94:2369–2371.
Fuscaldo G, Russell S, Gillam L. How to facilitate decisions about surplusembryos: patients’ views. Hum Reprod 2007;22:3129–3138.
Hammarberg K, Oke EK. The impact of changing legislation on coupleswith frozen embryos in excess of five years. In: 16th Annual Meeting ofthe European Society for Human Reproduction and Embryology, 25–28June 2000, Bologna, Italy. 2000 Abstract, p. 251.
Hammarberg K, Tinney L. Deciding the fate of supernumerary frozenembryos: a survey of couples’ decisions and the factors influencingtheir choice. Fertil Steril 2006;86:86–91.
Haimes E, Taylor K. Fresh embryo donation for human embryonic stemcell (hESC) research: the experiences and values of IVF couples askedto be embryo donors. Hum Reprod 2009;24:2142–2150.
Jain JK, Paulson RJ. Oocyte cryopreservation. Fertil Steril 2006;86:1037–1046.
Klock SC. Parents’ knowledge about the donors and their attitudes towarddisclosure in oocyte donation. Hum Reprod 2004;19:1575–1579.
Lyerly AD, Steinhauser K, Voils C, Namey E, Alexander C, Bankowski B,Cook-Deegan R, Dodson WC, Gates E, Jungheim ES et al. Fertilitypatients’ views about frozen embryo disposition: results of amulti-institutional U.S. survey. Fertil Steril 2010;93:499–509.
McMahon CA, Saunders DM. Attitudes of couples with stored frozenembryos toward conditional embryo donation. Fertil Steril 2009;91:140–147.
McMahon CA, Gibson F, Cohen J, Leslie G, Tennant C, Saunders D.Mothers conceiving through in vitro fertilization: siblings, setbacks, andembryo dilemmas after five years. Reprod Technol 2000;10:131–135.
Mohler-Kuo M, Zellweger U, Duran A, Hohl MK, Gutzwiller F, Mutsch M.Attitudes of couples towards the destination of surplus embryos: results
among couples with cryopreserved embryos in Switzerland. Hum Reprod2009;24:1930–1938.
Nachtigall RD, Dougall KM, Lee M, Harrington J, Becker G. What dopatients want? Expectations and perceptions of IVF clinic informationand support regarding frozen embryo disposition. Fertil Steril 2010;94:2069–2072.
Newton CR, McDermid A, Tekpetey F, Tummon IS. Embryo donation:attitudes toward donation procedures and factors predictingwillingness to donate. Hum Reprod 2003;18:878–884.
Newton CR, Fisher J, Feyles V, Tekpetey F, Hughes L, Isacsson D. Changesin patient preferences in the disposal of cryopreserved embryos. HumReprod 2007;22:3124–3128.
Oke K, Hammerberg K, Blood J. Frozen embryos—what decisions tomake? In: 17th Annual Scientific Meeting of the Fertility Society ofAustralia Hobart, Australia. 1998 Abstract, p. 30.
Peddie VL, Van Teijlingen E, Bhattacharya S. A qualitative study ofwomen’s decision-making at the end of IVF treatment. Hum Reprod2005;20:1944–1951.
Pennings G. Decision-making authority of patients and fertility specialists inBelgian law. Reprod Biomed Online 2007;15:19–23.
Pennings G, Ombelet W. Coming soon to your clinic: patient-friendlyART. Human Reprod 2007;22:2075–2079.
Provoost V, Pennings G, De Sutter P, Gerris J, Van de Velde A, DeLissnyder E, Dhont M. Infertility patients’ beliefs about theirembryos and their disposition preferences. Hum Reprod 2009;24:896–905.
Provoost V, Pennings G, De Sutter P, Gerris J, Van de Velde A, Dhont M.Patients’ conceptualization of cryopreserved embryos used in theirfertility treatment. Hum Reprod 2010;25:705–713.
Raziel A, Schachter M, Friedler S, Ron-El R. Outcome of IVF pregnanciesfollowing severe OHSS. Reprod Biomed Online 2009;19:61–65.
Skoog Svanberg A, Boivin J, Bergh B. Factors influencing the decision to useor discard cryopreserved embryos. Acta Obstet Gynaecol Scand 2001a;80:849–855.
Skoog Svanberg A, Boivin J, Hjelmstedt A, Andersson Bergh L, Collins A,Bergh T. The impact of frozen embryos on emotional reactions during invitro fertilization. Acta Obstet Gynaecol Scand 2001b;80:1110–1114.
Stiel M, McMahon CA, Elwyn G, Boivin J. Pre-birth characteristics and 5-year follow-up of women with cryopreserved embryos after successfulin vitro fertilisation treatment. J Psychosom Obstet Gynecol 2010;31:32–39.
Van Empel IWH, Nelen WLDM, Tepe ET, van Laarhoven EAP,Verhaak CM, Kremer JAM. Weaknesses, strengths and needs infertility care according to patients. Hum Reprod 2010;25:142–149.
Verberg MF, Macklon NS, Nargund G, Frydman R, Devroey P,Broekmans FJ, Fauser BC. Mild ovarian stimulation for IVF. HumReprod Update 2009;15:13–29.
872 Provoost et al.
at Ghent U
niversity on August 22, 2012
http://humrep.oxfordjournals.org/
Dow
nloaded from
Copyright © 2022 FDOKUMEN









![Uzdrawianie czy spełnianie życzeń? Spór o cele medycyny [Healing or wish-fulfilling? On the goals of medicine] - draft version](https://static.fdokumen.com/doc/165x107/633219f3f008040551044f2d/uzdrawianie-czy-spelnianie-zyczen-spor-o-cele-medycyny-healing-or-wish-fulfilling.jpg)










