
Time discrimination in traumatic brain injury patients
14
This article was downloaded by: [Universita di Padova] On: 27 December 2012, At: 11:01 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of Clinical and Experimental Neuropsychology Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/ncen20 Time discrimination in traumatic brain injury patients Giovanna Mioni a , Franca Stablum a & Anna Cantagallo b a Dipartimento di Psicologia Generale, Università di Padova, Padua, Italy b BrainCare, srl, Padua, Italy Version of record first published: 24 Dec 2012. To cite this article: Giovanna Mioni , Franca Stablum & Anna Cantagallo (2012): Time discrimination in traumatic brain injury patients, Journal of Clinical and Experimental Neuropsychology, DOI:10.1080/13803395.2012.755151 To link to this article: http://dx.doi.org/10.1080/13803395.2012.755151 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript of Time discrimination in traumatic brain injury patients

This article was downloaded by: [Universita di Padova]On: 27 December 2012, At: 11:01Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: MortimerHouse, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Clinical and ExperimentalNeuropsychologyPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/ncen20
Time discrimination in traumatic brain injurypatientsGiovanna Mioni a , Franca Stablum a & Anna Cantagallo ba Dipartimento di Psicologia Generale, Università di Padova, Padua, Italyb BrainCare, srl, Padua, ItalyVersion of record first published: 24 Dec 2012.
To cite this article: Giovanna Mioni , Franca Stablum & Anna Cantagallo (2012): Time discrimination in traumaticbrain injury patients, Journal of Clinical and Experimental Neuropsychology, DOI:10.1080/13803395.2012.755151
To link to this article: http://dx.doi.org/10.1080/13803395.2012.755151
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Any substantial orsystematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distributionin any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that thecontents will be complete or accurate or up to date. The accuracy of any instructions, formulae, anddrug doses should be independently verified with primary sources. The publisher shall not be liable forany loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever causedarising directly or indirectly in connection with or arising out of the use of this material.

JOURNAL OF CLINICAL AND EXPERIMENTAL NEUROPSYCHOLOGY2012, iFirst, 1–13
Time discrimination in traumatic brain injury patients
Giovanna Mioni1, Franca Stablum1, and Anna Cantagallo2
1Dipartimento di Psicologia Generale, Università di Padova, Padua, Italy2BrainCare, srl, Padua, Italy
Time management skills are required for most daily activities. Traumatic brain injury (TBI) patients often presentwith cognitive dysfunction, but few studies have investigated temporal impairment. The aim of the present studywas to assess temporal abilities in TBI patients using a time discrimination task. Twenty-seven TBI patients (ages=18–60 years) and 27 controls (ages = 20–60 years) were asked to discriminate between two time intervals presentedsequentially. The standard intervals were 500 ms or 1,300 ms long followed by a comparison stimulus that was25% shorter or longer than the standard one. Participants were also asked to perform two tasks to assess attention,speed-of-processing (the Stroop task), and working memory (the n-back task) abilities. The TBI patients were lessaccurate than the controls on the time discrimination task and showed greater time-order error effects. In fact, TBIpatients pressed the “short” key more times when the standard time interval was 500 ms and the “long” key moretimes when the standard interval was 1,300 ms. Significant correlations were found between time discrimination,working memory, and speed of processing in both TBI and controls when the standard time interval was 1,300 ms.Attention appeared to be involved in different ways in the two groups. Working memory and speed of processingwere involved in time processing only in TBI patients when the standard time interval was 500 ms. These data lendadditional support to the notion that two different systems are responsible for elaborating time durations shorteror longer than a second.
Keywords: Traumatic brain injury; Time discrimination; Attention; Working memory; Speed of processing.
INTRODUCTION
The ability to estimate the passage of time is a keyelement involved in most daily activities; neverthe-less how individuals perceive time is still not entirelyunderstood. Good temporal skills are essential fornormal daily activities such as crossing a busystreet, preparing a meal, or organizing the day’sschedule.
A dominant theory with respect to time per-ception explains temporal judgments made on thebasis of a clock stage, memory stores, and deci-sion mechanisms (scalar-timing model; Church,1984; Gibbon, 1991; Treisman, 1963). The clock
The information in this manuscript and the manuscript itself have never been published either electronically or in print. There areno financial or other relationships that could be interpreted as a conflict of interest affecting this manuscript. This research received nospecific grant from any funding agency, or commercial or not-for-profit organizations. The authors gratefully acknowledge the staff ofthe Modulo di Neuropsicologia Riabilitativa (Azienda Ospedaliero–Universitaria Ferrara, Italy) and the participants and their familiesand friends who cooperated in this study. The authors are grateful to Linda Inverso Moretti for her assistance in editing the Englishversion of this manuscript.
Address correspondence to Giovanna Mioni, Dipartimento di Psicologia Generale, Università di Padova, Via Venezia 8, 35131Padova, Italy (E-mail: [email protected]).
stage consists of a pacemaker (an internal clock), aswitch, and an accumulator. The pacemaker emitspulses at a regular rate. When a temporal dura-tion must be estimated, the switch is turned on,and the accumulator counts the total number ofpulses emitted during that time period. The dura-tion perceived represents the total number of pulsesthat are transferred to a working memory store-house where a comparison with the contents ofthe reference memory is made. The reference mem-ory stores long-term memory representations ofpast temporal information. More recent researchemphasizes the mediation of attention and memoryprocesses involved in temporal judgments. Block
© 2012 Taylor & Francis
http://www.tandfonline.com http://dx.doi.org/10.1080/13803395.2012.755151
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12

2 MIONI, STABLUM, CANTAGALLO
and Zakay’s (1996, 2006) proposal is based on thescalar-timing model but also incorporates a cog-nitive module in the form of an attentional gate,which explains the influence of attentional resourceallocation on temporal judgments. The model pre-dicts that participants with attention and workingmemory problems should make more timing errorswith respect to those with more efficient controlfunctions (Pouthas & Perbal, 2004; Zakay & Block,1996, 2004).
There are four major experimental methods forassessing the accuracy of temporal processing:time reproduction, time production, verbal estima-tion, and method of comparison (Block, Zakay,& Hancock, 1998; Grondin, 2010; Zakay, 1990).In time reproduction tasks, participants must repro-duce the duration of a previously presented stimu-lus. The time interval presented needs to be encodedand stored in the reference memory from whichit will subsequently be retrieved and reproduced(Block & Zakay, 2006; Buhusi & Meck, 2005;Grondin, 2010). In time production tasks, partici-pants are required to produce a time interval and totranslate it from an objectively labeled duration toa subjectively experienced one. In verbal estimationtasks, participants are exposed to a time intervaland are then required to translate it (objective dura-tion) into clock units (subjective duration; Buhusi &Meck, 2005; Grondin, 2010). Time production andverbal estimation are suitable methods to investi-gate the rate of the internal pacemaker (Block et al.,1998; Meck, 1996; Rammsayer, Hennig, Haag, &Lange, 2001).
A time discrimination task, one of the most fre-quently used temporal comparison tasks (Grondin,2010; Rubia, Taylor, Taylor, & Sergeant, 1999), wasemployed in the present study. In time discrimina-tion tasks, participants are asked to judge the rela-tive duration of two sequentially presented intervals(a standard time interval and a comparison one)and to indicate whether the second stimulus isshorter or longer than the first one (Grondin, 2010).Temporal performance is modulated by stimulusduration and by the magnitude of the time dif-ference between the two stimuli; the greater thedifference between the two stimuli the higher theaccuracy tends to be (Grondin, 2010). Temporalperformance is, moreover, modulated by the orderin which the standard and comparison stimuli arepresented (Le Dantec et al., 2007; Paul, Le Dantec,Bernard, Lalonde, & Rebaï, 2003). Order of presen-tation of standard and comparison stimuli can varyfrom trial to trial (roving method; Grondin, 2010;Macmillan & Creelman, 2005) or can always be pre-sented in the same order with the standard stimulusbeing presented first followed by the comparison
one (reminder method; Grondin, 2010; Grondin &McAuley, 2009). In both methods, presenting twointervals one after the other induces a bias in per-ceiving the duration, often called time-order error(TOE; Hellström, 1985; Hellström & Rammsayer,2004). Generally, when standard time intervals varywithin the same session, TOE has been found tobe negative for longer durations (the comparisonintervals are perceived as being longer than thestandard intervals) and positive for shorter ones(the comparison intervals are perceived shorterthan the standard ones; Hellström & Rammsayer,2004).
Some authors have speculated that time dis-crimination is the purest measure of time per-ception (Rubia et al., 1999) and, compared totime reproduction and time production, it appearsto be the best method to detect temporal dif-ferences when short intervals (from hundreds ofmilliseconds to a few seconds) are employed(Rammsayer, 2001). Time discrimination perfor-mance predominately relies upon working mem-ory abilities, as participants must bear in mindthe initial time interval while simultaneously pro-cessing another comparison one. Adequate atten-tion and speed-of-processing capacities are, more-over, required to accurately discriminate betweentwo temporal stimuli and to rapidly respond afterthe second stimulus has been presented (Grondin,2010).
Time perception relies on various cognitive pro-cesses such as attention, working memory, andspeed of processing (Block & Zakay, 1996), allconnected to frontal lobe functioning (Moscovitch,1995; Shimamura, 1995). Given the vulnerabil-ity of the frontal lobes to damage as a resultof traumatic brain injury (TBI; Aharon Peretz &Tomer, 2007; Bigler, 2001, 2007) and in view of thefact that cognitive dysfunction commonly followsTBI (Boelen, Spikman, Rietveld, & Fasotti, 2009;Hartikainen et al., 2010), it would seem reason-able to expect time perception alteration in thesepatients. Temporal dysfunctions have, in fact, beendocumented in patients with focal frontal lesions(Casini & Ivry, 1999; Harrington, Haaland, &Knight, 1998; Mangels, Ivry, & Shimizu, 1998;Nichelli, Clark, Hollnagel, & Grafman, 1995;Picton, Stuss, Shallice, Alexander, & Gillingham,2006; Rubia & Smith, 2004).
To our knowledge, only five studies have inves-tigated time perception abilities in TBI patients(Anderson & Schmitter-Edgecombe, 2011; Meyers& Levin, 1992; Mioni, Stablum, McClintock, &Cantagallo, 2012; Perbal, Couillet, Azouzi, &Pouthas, 2003; Schmitter-Edgecombe & Rueda,2008; Table 1).
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12

TIME DISCRIMINATION AFTER TBI 3
TAB
LE
1S
umm
ary
tabl
eof
stud
ies
that
have
prev
ious
lyin
vest
igat
edtim
epe
rcep
tion
inT
BIp
atie
nts
Aut
hor
Yea
rP
atie
nts
Clin
ical
char
acte
rist
ics
Tas
ksC
ondi
tion
Dur
atio
ns(s
)E
ffec
tsi
zea
Res
ults
Mey
ers
&L
evin
1992
Dis
orie
nted
TB
I=
10O
rien
ted
TB
I=
24C
ontr
ols=
12
18se
vere
,5m
oder
ate,
11m
ild;P
TA=
16da
ys;m
ean
tim
epo
stin
jury=
37da
ys
Tim
ere
prod
ucti
onV
erba
lest
imat
ion
Sim
ple
5,10
,and
15T
ime
repr
oduc
tion
d=
0.23
a
Ver
bale
stim
atio
nd=
0.42
b
TB
Ipa
tien
tsw
ere
asac
cura
teas
cont
rols
onti
me
repr
oduc
tion
and
verb
ales
tim
atio
n.In
the
tim
ere
prod
ucti
onta
sk,5
-an
d10
-sin
terv
als
wer
ere
late
dw
ith
atte
ntio
nsp
an,
and
15-s
inte
rval
was
rela
ted
wit
hor
ient
atio
nle
vel.
Per
bale
tal
.20
03T
BI
pati
ents=
15C
ontr
ols=
15G
CS=
6.4;
PT
A=
88da
ys;
mea
nti
me
post
inju
ry=
11m
onth
s
Tim
ere
prod
ucti
onT
ime
prod
ucti
onC
oncu
rren
tre
adin
gC
ontr
olco
unti
ng
5,14
,and
38N
AT
BI
pati
ents
wer
eas
accu
rate
but
mor
eva
riab
leth
anco
ntro
ls.
Schm
itte
r-E
dgec
ombe
&R
ueda
2008
TB
Ipa
tien
ts=
27C
ontr
ols=
2714
seve
rean
d13
mod
erat
eT
BI;
PT
A=
24.1
1da
ys;
mea
nti
me
post
inju
ry=
41.9
3da
ys
Ver
bale
stim
atio
nC
oncu
rren
tre
adin
g10
,25,
45,a
nd60
Bri
efdu
rati
onb
d=
0.46
Lon
gdu
rati
onc
d=
1.03
Sign
ifica
ntdi
ffer
ence
sw
ere
foun
dbe
twee
ngr
oups
whe
nte
sted
wit
hdu
rati
ons
exce
edin
gth
eir
wor
king
mem
ory
capa
city
.A
nder
son
&Sc
hmit
ter-
Edg
ecom
be
2011
TB
Ipa
tien
ts=
15C
ontr
ols=
158
seve
rean
d7
mod
erat
e;P
TA=
23.2
7;m
ean
tim
epo
stin
jury=
432.
13da
ys
Ver
bale
stim
atio
nC
oncu
rren
tre
adin
g10
,25,
45,a
nd60
Gro
upη
2=
.18
Des
pite
cont
inue
dep
isod
icm
emor
yim
pair
men
t,T
BI’
ste
mpo
ralp
erfo
rman
cew
assi
mila
rto
that
ofco
ntro
ls.
Mio
niet
al.
2012
TB
Ipa
tien
ts=
18C
ontr
ols=
1818
seve
re;G
CS=
6.77
;P
TA=
11.7
8;m
ean
tim
epo
stin
jury=
24.5
0m
onth
s
Tim
ere
prod
ucti
onC
oncu
rren
tre
adin
g4,
9,an
d14
Gro
upη
2=
.01
TB
Ipa
tien
tsw
ere
asac
cura
tebu
tm
ore
vari
able
than
cont
rols
.Si
gnifi
cant
corr
elat
ions
wer
efo
und
betw
een
tim
epe
rcep
tion
and
wor
king
mem
ory.
Not
e.T
BI=
trau
mat
icbr
ain
inju
ry;P
TA=
post
trau
mat
icam
nesi
a(d
ays)
;GC
S=
Gla
sgow
Com
aSc
ale
(Tea
sdal
e&
Jenn
ett,
1974
);N
A=
not
avai
labl
e.aA
naly
ses
wer
eco
nduc
ted
onra
wda
ta.b
Ana
lyse
sw
ere
cond
ucte
dbe
twee
nT
BI
pati
ents
(ori
ente
dan
ddi
sori
ente
dT
BI
toge
ther
)an
dco
ntro
ls.c B
rief
dura
tion
refe
rto
10-
and
25-s
inte
rval
sw
hile
long
dura
tion
sre
fer
to45
-an
d60
-sin
terv
als.
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12

4 MIONI, STABLUM, CANTAGALLO
Three of these were conducted using time repro-duction tasks (Meyers & Levin, 1992; Mioni et al.,2012; Perbal, Couillet, Azouzi, & Pouthas, 2003),one (Perbal et al., 2003) also utilized a time produc-tion task, while three used time verbal estimationtasks (Anderson & Schmitter-Edgecombe, 2011;Meyers & Levin, 1992; Schmitter-Edgecombe &Rueda, 2008). All five studies used time durationsfalling within a range between 4 and 60 s, andall found temporal dysfunction when TBI patientswere tested using long intervals, which probablyexceed the episodic memory span (Meyers & Levin,1992; Schmitter-Edgecombe & Rueda, 2008). TBIpatients were, moreover, more variable in their per-formance with respect to healthy controls, and thishas been linked to working memory and atten-tional dysfunction (Mioni et al., 2012; Perbal et al.,2003).
It should be noted that the literature on timeperception in frontal lobe patients shows tempo-ral dysfunction even when they are exposed totime intervals in the seconds and milliseconds range(Casini & Ivry, 1999; Harrington et al., 1998;Nichelli et al., 1995; Picton et al., 2006; Rubia &Smith, 2004;). As TBI and frontal patients maypresent lesions in similar brain regions and havesimilar cognitive dysfunctions (Knight, Harnett, &Titov, 2005), we expected to find temporal dysfunc-tion even when TBI patients are tested using timedurations falling in the milliseconds and secondsrange.
To date, despite the fact that numerous every-day activities fall within a time range of millisec-onds to a few seconds (Block, 1990; Buhusi &Meck, 2005; Fraisse, 1984), no studies have inves-tigated temporal abilities in TBI patients usingthose intervals. We predicted that TBI patientswill present temporal dysfunction even when testedusing durations ranging from hundreds of millisec-onds to few seconds. A difference in temporal per-formance, with reference to time intervals shorteror longer than 1 second, is another important sub-ject needing investigation. In accordance with thehypothesis that there are two distinct timing mech-anisms (more automatic for the milliseconds rangevs. more controlled for the seconds range; Lewis& Miall, 2003a, 2003b), we predicted higher cogni-tive involvement when participants are required todiscriminate longer time intervals.
One of the novelties about this research liesin the attempt to further investigate the relation-ship between standard and comparison intervalsby analyzing the number of keys pressed. Thisdependent variable makes it possible to quantifythe response bias. If only accuracy had been takeninto consideration, information concerning the type
of errors made by the participants would havegone unnoticed. Participants in the present studywere required to discriminate between two tempo-ral intervals by pressing two distinct keys. As anequal number of accurate responses are connectedto each key, a larger number of key presses oneither side could indicate a response bias, whichis often observed (Hellström, 1985; Hellström &Rammsayer, 2004) but has never been investigatedin TBI patients.
METHOD
Participants
Twenty-seven TBI patients (8 females and 19 males)took part in the study. The patients’ demographicand clinical features are outlined in Table 2.The TBI patients were all right-handed, weretested at least 6 months after their injury, andhad a score equal to or above 6 on the Levelof Cognitive Functioning (LCF) scale (Hagen,Malkmus, Durham, & Bowman, 1979). The LCFscale is used to assess cognitive functioning inpostcoma patients (a score = 6 is the prerequi-site for TBI patients to be tested and indicatesthat patient gives appropriate responses in famil-iar contexts but may still have memory problems).All the patients were able to provide neuroimaginginformation (computed tomography or magneticresonance imaging) showing damage to a varietyof cortical areas, and the majority had frontallesions. According to available clinical records, theparticipants were not densely amnesic or aphasic.Patients who had preexisting neurological, psychi-atric, or developmental disorders, a history of sub-stance or alcohol abuse, or previous head injurywere excluded. This study was conducted in accor-dance with the principles of the Declaration ofHelsinki, and all the patients and participants gaveinformed consent (59th WMA General Assembly,Seoul, 2008).
The control group was made up of 27 par-ticipants matched for gender, age, and level ofeducation (8 females and 19 males; mean age =36.37 years, SD = 9.20, range = 20–60; mean levelof education = 11.74 years, SD = 4.11, range =8–18). All were recruited through the University ofPadua or the community, the controls were right-handed, had never suffered from TBI, and hadno neuropsychiatric disorders or history of drug-alcohol abuse. The differences in age, t(52) = 0.229,p = .820, d = 0.06, or level of education, t(52) =−0.89, p = .375, d = –0.24, between the TBI andthe control group were not significant.
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12
TIME DISCRIMINATION AFTER TBI 5
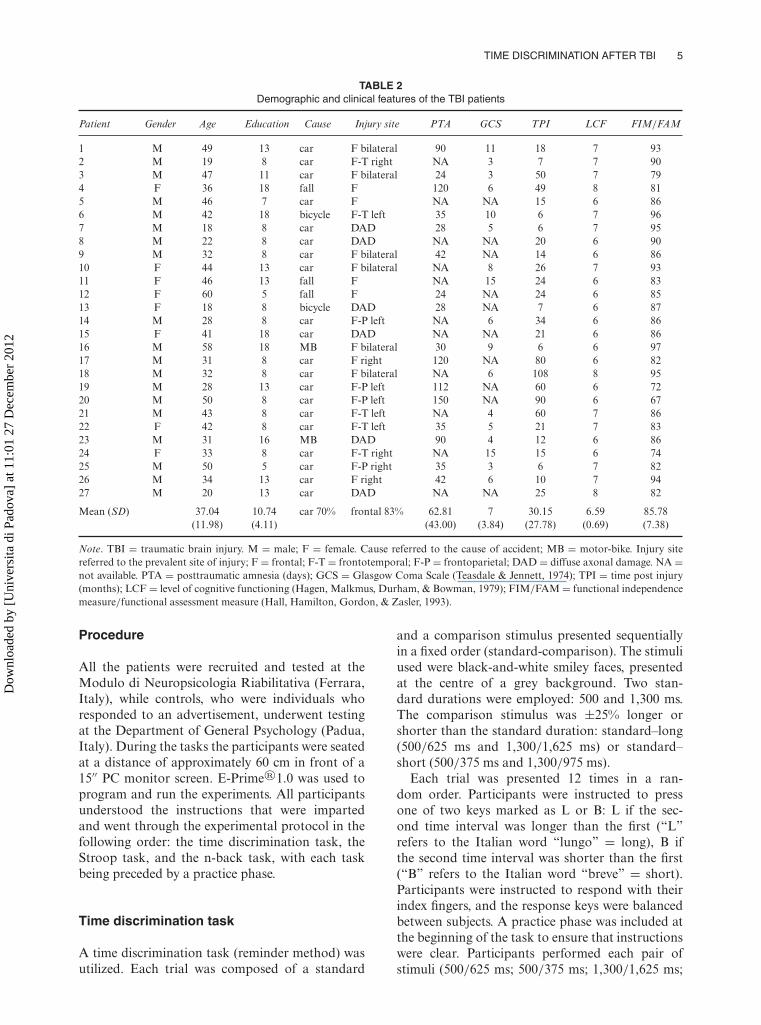
TABLE 2Demographic and clinical features of the TBI patients
Patient Gender Age Education Cause Injury site PTA GCS TPI LCF FIM/FAM
1 M 49 13 car F bilateral 90 11 18 7 932 M 19 8 car F-T right NA 3 7 7 903 M 47 11 car F bilateral 24 3 50 7 794 F 36 18 fall F 120 6 49 8 815 M 46 7 car F NA NA 15 6 866 M 42 18 bicycle F-T left 35 10 6 7 967 M 18 8 car DAD 28 5 6 7 958 M 22 8 car DAD NA NA 20 6 909 M 32 8 car F bilateral 42 NA 14 6 8610 F 44 13 car F bilateral NA 8 26 7 9311 F 46 13 fall F NA 15 24 6 8312 F 60 5 fall F 24 NA 24 6 8513 F 18 8 bicycle DAD 28 NA 7 6 8714 M 28 8 car F-P left NA 6 34 6 8615 F 41 18 car DAD NA NA 21 6 8616 M 58 18 MB F bilateral 30 9 6 6 9717 M 31 8 car F right 120 NA 80 6 8218 M 32 8 car F bilateral NA 6 108 8 9519 M 28 13 car F-P left 112 NA 60 6 7220 M 50 8 car F-P left 150 NA 90 6 6721 M 43 8 car F-T left NA 4 60 7 8622 F 42 8 car F-T left 35 5 21 7 8323 M 31 16 MB DAD 90 4 12 6 8624 F 33 8 car F-T right NA 15 15 6 7425 M 50 5 car F-P right 35 3 6 7 8226 M 34 13 car F right 42 6 10 7 9427 M 20 13 car DAD NA NA 25 8 82
Mean (SD) 37.04 10.74 car 70% frontal 83% 62.81 7 30.15 6.59 85.78(11.98) (4.11) (43.00) (3.84) (27.78) (0.69) (7.38)
Note. TBI = traumatic brain injury. M = male; F = female. Cause referred to the cause of accident; MB = motor-bike. Injury sitereferred to the prevalent site of injury; F = frontal; F-T = frontotemporal; F-P = frontoparietal; DAD = diffuse axonal damage. NA =not available. PTA = posttraumatic amnesia (days); GCS = Glasgow Coma Scale (Teasdale & Jennett, 1974); TPI = time post injury(months); LCF = level of cognitive functioning (Hagen, Malkmus, Durham, & Bowman, 1979); FIM/FAM = functional independencemeasure/functional assessment measure (Hall, Hamilton, Gordon, & Zasler, 1993).
Procedure
All the patients were recruited and tested at theModulo di Neuropsicologia Riabilitativa (Ferrara,Italy), while controls, who were individuals whoresponded to an advertisement, underwent testingat the Department of General Psychology (Padua,Italy). During the tasks the participants were seatedat a distance of approximately 60 cm in front of a15′′ PC monitor screen. E-Prime®1.0 was used toprogram and run the experiments. All participantsunderstood the instructions that were impartedand went through the experimental protocol in thefollowing order: the time discrimination task, theStroop task, and the n-back task, with each taskbeing preceded by a practice phase.
Time discrimination task
A time discrimination task (reminder method) wasutilized. Each trial was composed of a standard
and a comparison stimulus presented sequentiallyin a fixed order (standard-comparison). The stimuliused were black-and-white smiley faces, presentedat the centre of a grey background. Two stan-dard durations were employed: 500 and 1,300 ms.The comparison stimulus was ±25% longer orshorter than the standard duration: standard–long(500/625 ms and 1,300/1,625 ms) or standard–short (500/375 ms and 1,300/975 ms).
Each trial was presented 12 times in a ran-dom order. Participants were instructed to pressone of two keys marked as L or B: L if the sec-ond time interval was longer than the first (“L”refers to the Italian word “lungo” = long), B ifthe second time interval was shorter than the first(“B” refers to the Italian word “breve” = short).Participants were instructed to respond with theirindex fingers, and the response keys were balancedbetween subjects. A practice phase was included atthe beginning of the task to ensure that instructionswere clear. Participants performed each pair ofstimuli (500/625 ms; 500/375 ms; 1,300/1,625 ms;
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12

6 MIONI, STABLUM, CANTAGALLO
1,300/975 ms) one time, the stimuli were the sameas those used in the task. No feedback on perfor-mance was provided.
Attention, working memory, andspeed-of-processing tasks
A Stroop task was employed to study the attentionand speed-of-processing components. Each trialwas composed of three colored words displayed atthe centre of the computer screen for 2 s. The wordsat the centre (variably RED, YELLOW, GREEN,and BLUE) were presented in 20-point-size Arialfont and were colored in red, yellow, green, orblue, while the words to the right and left werealways in black. The central word was the targetstimulus, whereas the two black lateral words werethe possible responses (i.e., GREEN RED RED).Participants were instructed to judge the color ofthe central word by pressing a key on the keyboardmarked with an arrow pointing either right (→) orleft (←), depending on the position of the correctresponse. Whenever the answer was on the left, the(←) key had to be pressed with the left index finger,and whenever the answer was on the right, the (→)key had to be pressed with the right index finger.Two possible conditions were randomly presented:congruent and incongruent. In the congruent con-dition, the color of the central word correspondedto the written word (the word “RED” written withred ink). In the incongruent condition, the colordid not match the written word (the word “RED”written with green ink). Forty-eight stimuli werepresented in each condition (for a total of 96 stim-uli), and an equal number of correct responseswere presented on the right or left of the centralword (see Del Missier, Mäntylä, & Bruine de Bruin,2010). A practice phase was included at the begin-ning of the task to clarify the instructions and tofamiliarize with the task: Participants performed10 trials, 5 in the congruent and 5 in the incongruentcondition.
The n-back task was employed to study the work-ing memory component (for a review see Owen,McMillan, Laird, & Bullmore, 2005). The stim-uli were common two-syllable words presented atthe centre of the computer screen and written in36-point size Courier New font in white ink on ablack background. Participants were instructed toindicate, by pressing the left mouse key, when theword that appeared was the same as the one pre-sented 2 words back. The task comprised 48 targetstimuli (24 different stimuli presented 2 times) and48 nontarget stimuli; 12 nontarget stimuli were pre-sented only once, 12 stimuli were 3-back, 12 stimuli
were 4-back, and 12 stimuli were 5-back. A practicephase was made at the beginning of the task to clar-ify the instructions and to familiarize with the task.Five target words and 10 nontarget words were pre-sented during the practice phase; no feedback onperformance was provided.
RESULTS
Time discrimination task
The time discrimination task was analyzed interms of response accuracy reflecting the percent-age of correct responses. Data were analyzed viaa mixed-model analysis of variance (ANOVA) withgroup (TBI vs. control) as a between-group factor,and within factors of standard duration (500 vs.1,300 ms) and comparison duration (short vs. long).The significance level for this and all the subsequentanalyses was p < .05. The post hoc analyses wereperformed with the Bonferroni correction.
The main effect of group, F(1, 52) = 27.60,MSE = 0.957, p < .001, η2
p = .347, and standardduration, F(1, 52) = 6.34, MSE = 0.125, p < .05,η2
p = .109, were significant, whereas the main effectof the comparison duration did not reach the signif-icance level, F(1, 52)= 0.22, MSE = 0.011, p= .64,η2
p = .004. The TBI patients were less accurate thanthe controls (70% vs. 83%). The participants weremore accurate when discriminating the 1,300-msduration than when discriminating the 500-msduration (79% vs. 74%). The Group × StandardDuration, F(1, 52) = 4.34, MSE = 0.086, p < .05,η2
p = .077, and Standard Duration × ComparisonDuration, F(1, 52) = 79.02, MSE = 1.938, p <
.001, η2p = .603, interactions were significant.
These interactions were qualified by the signifi-cant Group × Standard Duration × ComparisonDuration interaction, F(1, 52) = 14.22, MSE =.349, p < .0001, η2
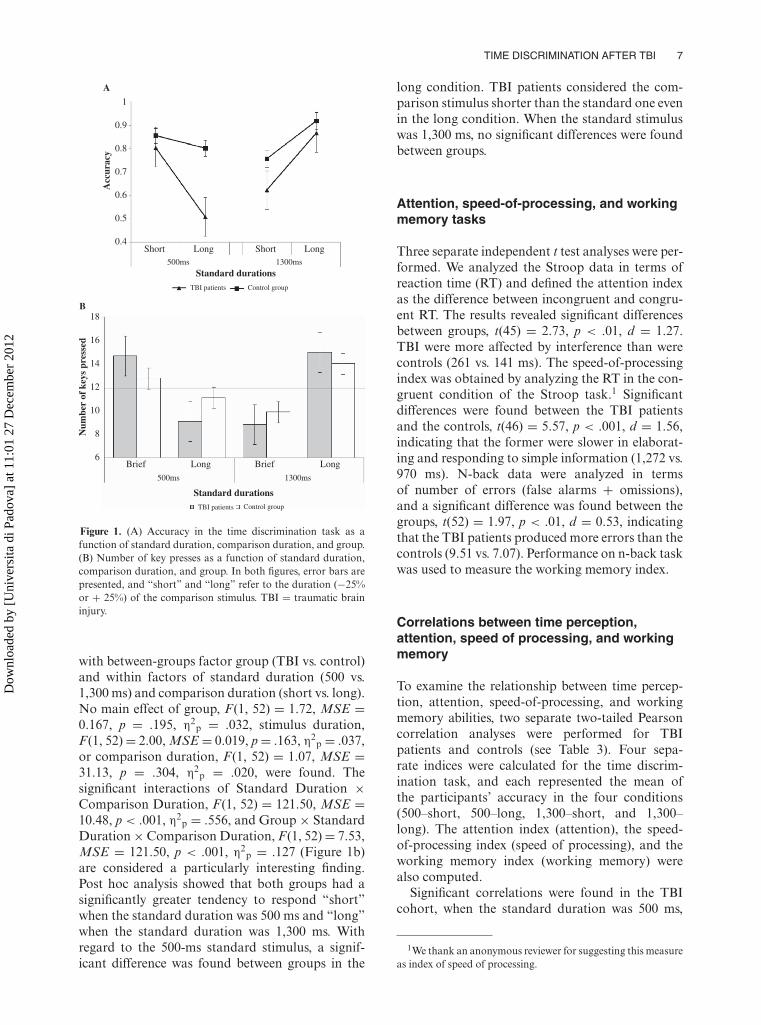
p = .215 (Figure 1a). Post hocanalyses indicated significant differences betweengroups when the standard interval was 500 ms, andthe comparison condition was long (500–625 ms).The pattern was reversed when the standard inter-val was 1,300 ms. In fact, TBI patients were signifi-cantly less accurate in the short comparison condi-tion (1,300–975 ms). No significant differences werefound between groups in the short condition whenthe standard interval was 500 ms (p = .241) or inthe long condition when the standard interval was1,300 ms (p = .201).
We analyzed how many times the key waspressed to investigate how the relative durationof the two stimuli affects temporal performance.Data were analyzed via a mixed-model ANOVA
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12
TIME DISCRIMINATION AFTER TBI 7
A
1
0.9
0.8
0.7
0.6
0.5
0.4
Acc
urac
y
Short ShortLong Long500ms 1300ms
Standard durationsTBI patients Control group
B
Brief Brief LongLong
500ms 1300ms
Standard durationsTBI patients Control group
18
16
14
12
10
8
6
Num
ber
of k
eys
pres
sed
Figure 1. (A) Accuracy in the time discrimination task as afunction of standard duration, comparison duration, and group.(B) Number of key presses as a function of standard duration,comparison duration, and group. In both figures, error bars arepresented, and “short” and “long” refer to the duration (−25%or + 25%) of the comparison stimulus. TBI = traumatic braininjury.
with between-groups factor group (TBI vs. control)and within factors of standard duration (500 vs.1,300 ms) and comparison duration (short vs. long).No main effect of group, F(1, 52) = 1.72, MSE =0.167, p = .195, η2
p = .032, stimulus duration,F(1, 52)= 2.00, MSE = 0.019, p= .163, η2
p = .037,or comparison duration, F(1, 52) = 1.07, MSE =31.13, p = .304, η2
p = .020, were found. Thesignificant interactions of Standard Duration ×Comparison Duration, F(1, 52) = 121.50, MSE =10.48, p < .001, η2
p = .556, and Group × StandardDuration×Comparison Duration, F(1, 52)= 7.53,MSE = 121.50, p < .001, η2
p = .127 (Figure 1b)are considered a particularly interesting finding.Post hoc analysis showed that both groups had asignificantly greater tendency to respond “short”when the standard duration was 500 ms and “long”when the standard duration was 1,300 ms. Withregard to the 500-ms standard stimulus, a signif-icant difference was found between groups in the
long condition. TBI patients considered the com-parison stimulus shorter than the standard one evenin the long condition. When the standard stimuluswas 1,300 ms, no significant differences were foundbetween groups.
Attention, speed-of-processing, and workingmemory tasks
Three separate independent t test analyses were per-formed. We analyzed the Stroop data in terms ofreaction time (RT) and defined the attention indexas the difference between incongruent and congru-ent RT. The results revealed significant differencesbetween groups, t(45) = 2.73, p < .01, d = 1.27.TBI were more affected by interference than werecontrols (261 vs. 141 ms). The speed-of-processingindex was obtained by analyzing the RT in the con-gruent condition of the Stroop task.1 Significantdifferences were found between the TBI patientsand the controls, t(46) = 5.57, p < .001, d = 1.56,indicating that the former were slower in elaborat-ing and responding to simple information (1,272 vs.970 ms). N-back data were analyzed in termsof number of errors (false alarms + omissions),and a significant difference was found between thegroups, t(52) = 1.97, p < .01, d = 0.53, indicatingthat the TBI patients produced more errors than thecontrols (9.51 vs. 7.07). Performance on n-back taskwas used to measure the working memory index.
Correlations between time perception,attention, speed of processing, and workingmemory
To examine the relationship between time percep-tion, attention, speed-of-processing, and workingmemory abilities, two separate two-tailed Pearsoncorrelation analyses were performed for TBIpatients and controls (see Table 3). Four sepa-rate indices were calculated for the time discrim-ination task, and each represented the mean ofthe participants’ accuracy in the four conditions(500–short, 500–long, 1,300–short, and 1,300–long). The attention index (attention), the speed-of-processing index (speed of processing), and theworking memory index (working memory) werealso computed.
Significant correlations were found in the TBIcohort, when the standard duration was 500 ms,
1We thank an anonymous reviewer for suggesting this measureas index of speed of processing.
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12

8 MIONI, STABLUM, CANTAGALLO
TABLE 3Pearson’s correlations between time discrimination, attention, working memory, and speed-of-processing indices separately for
TBI patients and controls
TBI patients Control group
Standard 500 ms Standard 1,300 ms Standard 500 ms Standard 1,300 ms
Index Short Long Short Long Short Long Short Long
Attention −.113 −.163 −.472∗ −.242 −.201 −.209 −.024 −.578∗∗Working memory −.394∗ −.226 −.331∗ −.567∗∗ .005 .211 −.350∗ −.332∗Speed of processing −.386∗ −.121 −.376∗ −.336∗ −.313 −.147 −.348∗ −.361∗
Note. TBI= traumatic brain injury. “Short” referred to the –25% duration of the comparison stimulus, and “long” referred to the+25%duration of the comparison stimulus. Attention = difference between the reaction times (RTs) in incongruent and congruent trials inthe Stroop task. Working memory = number of errors in the n-back task. Speed of processing = RT in the congruent condition of theStroop task. The analysis has been conducted separately on TBI patients and controls.∗p < .05. ∗∗p < .01.
and the comparison was short, with working mem-ory and speed-of-processing indices. It was foundthat TBI patients with better working memory andspeed-of-processing abilities were also more accu-rate at discriminating between the two intervals.No other significant correlations were found withregard to the 500-ms standard duration (with eitherthe short or long comparison duration) and atten-tion, working memory, and speed of processing inthe TBI or controls.
Interestingly, significant correlations were foundbetween time discrimination, when the standardduration was 1,300 ms, and the comparison dura-tion was short or long, with working memory andspeed of processing in both TBI patients and con-trols. Attention was involved differently in the twogroups. Taken together, the results indicate that par-ticipants with better cognitive resources have bettertemporal abilities and that cognitive involvementis differentiated depending on the standard andcomparison durations utilized.
Correlations between number of key presses,attention, working memory, and speed ofprocessing
Two separate two-tailed Pearson correlation anal-yses were performed for TBI patients and con-trols. Four separate indices were calculated forthe time discrimination task: Each represented thenumber of key presses for the four conditions(500–short, 500–long, 1,300–short, and 1,300–long). The attention index, the speed-of-processingindex, and the working memory index were alsocomputed.
The only significant correlation was found incontrol patients when the standard duration was500 ms, and the comparison duration was shorter,
with the index of speed of processing, r(52)= –.357,p < .05. Attention and working memory indiceswere not correlated with the number of key presses.
DISCUSSION
How different brain regions encode and elabo-rate temporal information and what cognitive pro-cesses are involved in time perception are intriguingsubjects. In the present study, TBI patients andhealthy controls were asked to undertake a dis-crimination task. Involvement of attention, work-ing memory, and processing speed in discriminat-ing time intervals shorter or longer than 1 sec-ond was also evaluated. Previous studies on TBIpatients have described higher variability (Mioniet al., 2012; Perbal et al., 2003) and less accuracywhen TBI patients were tested with time inter-vals exceeding the working memory span (above30 s; Anderson & Schmitter-Edgecombe, 2011;Schmitter-Edgecombe & Rueda, 2008). The liter-ature on time perception in frontal lobe patientshas, however, outlined temporal dysfunction evenwhen those patients are tested using shorter inter-vals in the milliseconds range (Casini & Ivry, 1999;Harrington et al., 1998; Mangels et al., 1998;Nichelli et al., 1995; Picton et al., 2006; Rubia &Smith, 2004).
The innovative aspect of the present work wasusing a time discrimination task to investigatethe temporal ability of TBI patients and to testdurations longer and shorter than 1 second. Ourresults showed temporal dysfunction in TBI. In par-ticular, TBI patients were found to be significantlyless accurate when discriminating 500 ms than whendiscriminating 1,300 ms, while no significant differ-ences were found between durations in the controlgroup. Discriminating 500-ms durations seems to
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12

TIME DISCRIMINATION AFTER TBI 9
be extremely challenging for TBI patients, whencompared to controls, presumably because of theadditional cognitive functions involved in time dis-crimination tasks.
The results concerning the number of keyspressed can be considered a particularly interest-ing outcome of this study. While previous stud-ies on time perception had already described thepresence of a time-order error (the interactionbetween standard duration and comparison dura-tion; Hellström, 1985; Hellström & Rammsayer,2004; Wiener, Turkeltaub, & Coslett, 2010), it hasoften been neglected and has never been investi-gated in TBI patients. Comprehending the interac-tion between standard and comparison durations,via the number of times the keys were pressed,also adds further depth to the study, providingadditional information on the cognitive processesinvolved in time discrimination in TBI patients.
If only accuracy had been taken into consid-eration, the conclusion would have been, on thebasis of those data, that TBI patients present tem-poral impairment only when the 500-ms standardduration was followed by the longer comparisonduration and when the 1,300-ms standard durationwas followed by the shorter comparison duration.However, the similar performance noted in TBIpatients and controls, when the 500-ms standardduration was followed by the shorter comparisonduration and when the 1,300-ms standard durationwas followed by the longer comparison duration,may have been obscured by a response bias (numberof keys pressed). Bearing in mind that the cor-rect number of times the keys should have beenpressed for each condition (500–long, 500–short,1,300–long, and 1,300–short) was 12, analyzing thenumber of times keys were really pressed shoulduncover the response bias. When the 500-ms stan-dard duration was presented, patients with TBIpressed the “short” key significantly more timesthan the controls did, whereas when the 1,300-msstandard duration was presented, patients with TBIpressed the “long” key significantly more times.It should be pointed out that both groups had agreater tendency to respond “short” when the stan-dard duration was 500 ms and “long” when thestandard duration was 1,300 ms, but this tendency(response bias) was greater in TBI patients when500-ms duration was presented.
The number of times the keys were pressed didnot correlate with attention or working memoryindices for either the TBI patients or the con-trols, confirming that this aspect was not cognitivelycontrolled but is more likely to be subcortically con-trolled and represent a response bias. Our findingsare consistent with previous studies that indicate a
significant interaction between standard and com-parison durations in healthy adults (Gontier et al.,2007; Gontier et al., 2009; Le Dantec et al., 2007;Paul et al., 2003), and now data concerning TBIpatients showing a greater response bias can beadded to the literature.
Various explanations may account for the pat-tern described. One could be linked to a memoryinterference in which the representation of any stim-ulus in memory decays after a certain time limit(Baddeley, 1992). Memory interference may havemade the first stimulus appear shorter than thesecond one especially with reference to the 1,300-ms standard duration when the long comparisoncondition was characterized by better performance.It is possible that the standard stimulus appearedshorter due to memory interference, and the dif-ference between the standard and the comparisonseemed more detectable (Paul et al., 2003). But thiswas not the case for the 500-ms standard dura-tion, in which case the better performances werenoted in the reverse condition (in the short compar-ison condition). For durations shorter than 1 s, atthe limit of the memory span, the “short” responsemay be activated automatically (Le Dantec et al.,2007; Paul et al., 2003). Lewis and Miall (2003b)reported that shorter intervals are generally pro-cessed in a less controlled manner than longer ones,with the former relying more on subcortical regions(Mangels et al., 1998).
A wider interpretation that takes into accountshort and long durations was provided by Gontieret al. (2007), who suggested that participants createan “anchor” stimulus in their memory and clas-sify stimuli approximately as below the “anchor”when short and above the “anchor” when long(see also Oshio, Chiba, & Inase, 2006). This couldalso be the case in our study: The participantscreated a memory representation of “anchor” dura-tion by averaging out the shorter (375 ms) and thelonger (1,625 ms) durations presented and classi-fied stimuli in relation to the “anchor.” Workingmemory is required to create and maintain the rep-resentation of the “anchor” duration active, anda working memory dysfunction may have alteredthe representation of the “anchor” duration andsubsequently affected temporal performance in TBIpatients.
Previous studies showed that different systemsare involved in perceiving duration in the millisec-onds and seconds rage (Lewis & Miall, 2003a,2003b; Mangels et al., 1998; Nichelli, Always, &Grafman, 1996; Nichelli et al., 1995; Rubia, 2006;Rubia & Smith, 2004). Our results seem to supportprevious studies confirming that a more cognitivelycontrolled system is involved when longer durations
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12

10 MIONI, STABLUM, CANTAGALLO
(longer than 1 second) are being assessed (Buhusi& Meck, 2005; Handy, Gazzaniga, & Ivry, 2003;Lewis & Miall, 2003a, 2003b). In fact, there weresignificant correlations in both groups, when thestandard duration was 1,300 ms, with attention,working memory and speed-of-processing indices.Participants with better cognitive abilities shouldalso present better temporal abilities (Block &Zakay, 2006). During time discrimination tasks,working memory resources seem to be involvedwhen participants are required to bear in mind arepresentation of the standard intervals to make thesubsequent decision, but a disruption in attentionhas also been shown to affect temporal perception(Casini, Macar, & Grondin, 1992; Grondin, 2010;Grondin & Macar, 1992; Mangels et al., 1998).Finally, at the decision stage, adequate speed-of-processing abilities are required to accurately per-ceive the two intervals and to judge their relativeduration. The fact that there were no significantcorrelations between the 500-ms standard dura-tion and attention, working memory, or speed-of-processing indices in the controls seems to supportthe hypothesis that temporal intervals shorter than1 s are processed in a more automatic mannerand require less involvement of high cognitive pro-cesses (Lewis & Miall, 2003a, 2003b). Interestingly,significant correlations were found only in TBIpatients, when the standard duration was 500 ms,and the comparison duration was short, with work-ing memory and speed-of-processing indices. TBIpatients seem to require additional cognitive abili-ties to discriminate temporal intervals shorter than1 second.
Neuroimaging (Gontier et al., 2007; Ivry &Spencer, 2004; Lewis & Miall, 2003b; Macar et al.,2002; Paul et al., 2003; Smith, Taylor, Lidzba, &Rubia, 2003) and patient studies (Ivry & Spencer,2004; Mangels et al., 1998; Nichelli et al., 1996;Nichelli et al., 1995) have identified different brainregions involved in the time perception networkconfirming the distinction between automatic andcognitively controlled temporal systems (Rubia,2006; Rubia & Smith 2004). Some have hypoth-esized that the cerebellum is the locus of theinternal clock, which is involved when milliseconddurations are being considered (Ivry & Spencer,2004; Rubia, 2006). The prefrontal cortex, thoughtto be the locus of counting mechanisms and storageand retrieval of temporal information, is involvedin perceiving longer temporal intervals (Mangelset al., 1998; Nichelli et al., 1995; Rubia, 2006).
Mangels et al. (1998) showed temporal impair-ment in neocerebellar patients in both milliseconds
(400 ms) and seconds (4 s) ranges, whereas frontalpatients presented temporal impairment only inrelation to longer durations, mainly due to work-ing memory dysfunction. Nichelli et al. (1995),instead, showed temporal impairment in frontalpatients with reference to both short (100–900 ms)and long time intervals (8–32 s). In accordancewith Nichelli et al.’s findings, our data demon-strated that TBI patients present temporal dysfunc-tion even when tested with intervals falling in themilliseconds range. The nature of the group dif-ferences on this task indicates a disruption at thedecisional level, with TBI patients utilizing a dif-ferent processing system when they are forced tomake rapid decisions. Attention, working mem-ory, and speed of processing were involved intime perception particularly when participants wererequired to discriminate durations longer than asecond, but TBI patients also required workingmemory and speed-of-processing abilities to dis-criminate intervals shorter than a second. The dif-ferent pattern noted in the involvement of atten-tion, working memory, and speed of processingin TBI patients and controls gives additional sup-port to the hypothesis that there are two differentsystems that govern the perception of intervalsshorter or longer than 1 s (Lewis & Miall, 2003a,2003b).
Future studies could recruit TBI patients accord-ing to the type of lesion (frontal or nonfrontal)to further investigate how the type of lesion isinvolved or differently affects temporal judgments.Although attention, working memory, and speed-of-processing deficits are well documented in TBIpatients (Knight et al., 2005), and the involvementof high cognitive abilities in time perception hasbeen described in the literature (Perbal et al., 2003;Zakay & Block, 2004), only a limited number ofstudies have attempted to investigate time percep-tion in TBI. As impaired time perception couldaffect the daily adaptive functioning of patientsrecovering from TBI (Fleming et al., 2008), thisstudy could have important clinical implicationsfor time perception rehabilitation, which shouldfocus not only on improving temporal abilities butalso on attention, working memory, and speed-of-processing components. Specific tasks utilizingboth time intervals (shorter or longer than 1 s)need, in fact, to be designed and developed to helprehabilitation projects.
Original manuscript received 22 March 2012Revised manuscript accepted 29 November 2012
First published online 24 December 2012
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12

TIME DISCRIMINATION AFTER TBI 11
REFERENCES
Aharon Peretz, J., & Tomer, R. (2007). Traumatic braininjury. In B. L. Miller & J. L. Cummings (Eds.),The human frontal lobes: Functions and disorders(2nd ed., pp. 540–551). New York, NY: GuilfordPress.
Anderson, J. W., & Schmitter-Edgecombe, M. (2011).Recovery of time estimation following moderate tosevere traumatic brain injury. Neuropsychology, 25,36–44. doi:10.1037/a0020333
Baddeley, A. D. (1992). Working memory. Science, 255,556–559. doi:10.1126/science.1736359
Bigler, E. D. (2001). The lesion(s) in traumatic braininjury: Implications for clinical neuropsychology.Archives of Clinical Neuropsychology, 16, 95–131.doi:10.1016/S0887-6177(00)00095-0
Bigler, E. D. (2007). Anterior and middle cranialfossa in traumatic brain injury: Relevant neu-roanatomy and neuropathology in the study ofneuropsychological outcome. Neuropsychology, 21,515–531. doi:10.1037/0894-4105.21.5.515
Block, R. A. (1990). Cognitive models of psychologicaltime. Hillsdale, NJ: Lawrence Erlbaum Associates.
Block, R. A., & Zakay, D. (1996). Models of psy-chological time revised. In H. Helfrich (Ed.), Timeand mind (pp. 171–195). Kirkland, WA: Hogrefe andHuber.
Block, R. A., & Zakay, D. (2006). Prospective remember-ing involves time estimation and memory processes.In J. Glickson & M. S. Myslobodsky (Eds.), Timingthe future: The case for a time-based prospective mem-ory (pp. 25–49). River Edge, NJ: World Scientific.doi:10.1142/9789812707123_0002
Block, R. A., Zakay, D., & Hancock, P. A. (1998).Human aging and duration judgments: A meta-analytic review. Psychology and Aging, 13, 584–596.doi:10.1037/0882-7974.13.4.584
Boelen, D. H. E., Spikman, J. M., Rietveld, A. C. M.,& Fasotti, L. (2009). Executive dysfunction in chronicbrain injured patients: Assessment in outpatientrehabilitation. Neuropsychological Rehabilitation, 19,625–644. doi:10.1080/09602010802613853
Buhusi, C. V., & Meck, W. H. (2005). What makes ustick? Functional and neural mechanisms of inter-val timing. Nature Reviews Neuroscience, 6, 755–765.doi:10.1038/nrn1764
Casini, L., & Ivry, R. B. (1999). Effects of divided atten-tion on temporal processing in patients with lesionsof cerebellum or frontal lobe. Neuropsychology, 13,10–21. doi:10.1037/0894-4105.13.1.10
Casini, L., Macar, F., & Grondin, S. (1992). Time estima-tion and attentional sharing. In F. Macar, V. Pouthas,& W. J. Friedman (Eds.), Time, action and cognition:Towards bridging the gap (pp. 177–180). Dordrecht,The Netherlands: Kluwer Academic.
Church, R. M. (1984). Properties of the internal clock.Annals of the New York Academy of Sciences, 423,566–582. doi:10.1111/j.1749-6632.1984.tb23459.x
Del Missier, F., Mäntylä, T., & Bruine de Bruin, W.(2010). Executive functions in decision making:An individual differences approach. Thinking andReasoning, 16, 69–97. doi:10.1080/13546781003630117
Fleming, J., Riley, L., Gill, H., Gullo, M. J., Strong, J.,& Shum, D. (2008). Predictors of prospective memory
in adults with traumatic brain injury. Journal of theInternational Neuropsychological Society, 14, 823–831.doi:10.1017/S1355617708080971
Fraisse, P. (1984). Perception and estimation of time.Annual Review of Psychology, 35, 1–36. doi:10.1146/annurev.ps.35.020184.000245
Gibbon, J. (1991). Origins of scalar timing. Learningand Motivation, 22, 3–38. doi:10.1016/0023-9690(91)90015-Z
Gontier, E., Le Dantec, C., Leleu, A., Paul, I.,Charvin, H., Bernard, C., . . . Rebaï, M. (2007).Frontal and parietal ERPs associated with durationdiscriminations with or without task interference.Brain Research, 1170, 79–89. doi:10.1016/j.brainres.2007.07.022
Gontier, E., Paul, I., Le Dantec, C., Pouthas, V., Jean-Marie, G., Bernard, C., . . . Rebaï, M. (2009). ERPs inanterior and posterior regions associated with dura-tion and size discriminations. Neuropsychology, 23,668–678. doi:10.1037/a0015757
Grondin, S. (2010). Timing and time perception: Areview of recent behavioural and neuroscience find-ings and theoretical directions. Attention, Perception,& Psychophysics, 72, 561–582. doi:10.3758/APP.72.3.561
Grondin, S., & Macar, F. (1992). Dividing attentionbetween temporal and non-temporal tasks: A perfor-mance operating characteristic—POC—analysis. InF. Macar, V. Pouthas, & W. J. Friedman (Eds.),Time, action and cognition: Towards bridging the gap(pp. 119–128). New York, NY: Kluwer Academic/Plenum.
Grondin, S., & McAuley, J. D. (2009). Duration dis-crimination in crossmodal sequences. Perception, 38,1542–1559. doi:10.1068/p6359
Hagen, C., Malkmus, D., Durham, P., & Bowman, K.(1979). Level of cognitive functioning. InRehabilitation of head injured adult: Comprehensivephysical management. Downey, CA: ProfessionalStaff Association of Rancho Los Amigos Hospital.
Hall, K. M., Hamilton, B. B., Gordon, W. A., &Zasler, N. D. (1993). Characteristic and compar-isons of functional assessment indices: Disabilityrating scale, functional independence measure andfunctional assessment measure. The Journal ofHead Trauma Rehabilitation, 8, 60–74. doi:10.1097/00001199-199308020-00008
Handy, T. C., Gazzaniga, M. S., & Ivry, R. B. (2003).Cortical and subcortical contributions to the repre-sentation of temporal information. Neuropsychologia,41, 1461–1473. doi:10.1016/S0028-3932%2803%2900093-9
Harrington, D. L., Haaland, K. Y., & Knight, R. T.(1998). Cortical networks underlying mechanisms oftime perception. The Journal of Neuroscience, 18,1035–1095.
Hartikainen, K. M., Wäljas, M., Isoviita, T., Dastidar, P.,Liimatainen, S., Solbakk, A. K., . . . Ohman, J. (2010).Persistent symptoms in mild to moderate traumaticbrain injury associated with executive dysfunction.Journal of Clinical and Experimental Neuropsychology,32, 767–774. doi:10.1080/13803390903521000
Hellström, Å. (1985). The time-order error and its rel-atives. Mirrors of cognitive processes in compar-ing. Psychological Bulletin, 97, 35–61. doi:10.1037/0033-2909.97.1.35
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12
12 MIONI, STABLUM, CANTAGALLO
Hellström, Å., & Rammsayer, T. H. (2004). Effectsof time-order, interstimulus interval, and feedbackin duration discrimination of noise bursts in the50- and 1000-ms ranges. Acta Psychologica, 116, 1–20.doi:10.1016/j.actpsy.2003.11.003
Ivry, R. B., & Spencer, R. M. C. (2004). The neural rep-resentation of time. Current Opinion in Neurobiology,14, 225–232. doi:10.1016/j.conb.2004.03.013
Knight, R. G., Harnett, M., & Titov, N. (2005). Theeffects of traumatic brain injury on the predictedand actual performance on a test of prospectiveremembering. Brain Injury, 19, 27–38. doi:10.1080/02699050410001720022
Le Dantec, C., Gontier, E., Paul, I., Charvin, H.,Bernard, C., Lalonde, R., & Rebaï, M. (2007). ERPsassociated with visual duration discriminations in pre-frontal and parietal cortex. Acta Psychologica, 125,85–98. doi:10.1016/j.actpsy.2006.07.003
Lewis, P. A., & Miall, R. C. (2003a). Brain activa-tion patterns during measurement of sub- and supra-second intervals. Neuropsychologia, 41, 1583–1592.doi:10.1016/S00283932(03)00118-0
Lewis, P. A., & Miall, R. C. (2003b). Distinct sys-tem from automatic and cognitively controlled timemeasurement: Evidence from neuroimaging. CurrentOpinion in Neurobiology, 13, 250–255. doi:10.1016/S0959-4388(03)00036-9
Macar, F., Lejeune, H., Bonnet, M., Ferrara, V., Pouthas,V., Vidal, F., & Maquet, P. (2002). Activation ofthe supplementary motor area and of attentionalnetworks during temporal processing. ExperimentalBrain Research, 142, 475–485.
Macmillan, N. A., & Creelman, C. D. (2005). Detectiontheory: A user’s guide (2nd ed.). Mahwah, NJ:Lawrence Erlbaum Associates.
Mangels, J. A., Ivry, R. B., & Shimizu, N. (1998).Dissociable contributions of the prefrontal andneocerebellar cortex to time perception. CognitiveBrain Research, 7, 15–39. doi:10.1016/S0926-6410(98)00005-6
Meck, W. H. (1996). Neuropharmacology of timing andtime perception. Cognitive Brain Research, 3, 227–242.doi:10.1016/0926-6410(96)00009-2
Meyers, C. A., & Levin, H. S. (1992). Temporal per-ception following closed head injury: Relationshipof orientation and attention span. Neuropsychiatry,Neuropsychology, and Behavioral Neurology, 5,28–32.
Mioni, G., Stablum, F., McClintock, S. M., &Cantagallo, A. (2012). Time-based prospectivememory in severe traumatic brain injury patients:The involvement of executive functions and timeperception. Journal of the International Neuro-psychological Society, 18, 697–705. doi:10.1017/S1355617712000306
Moscovitch, M. (1995). Models of consciousness andmemory. In M. S. Gazzaniga (Ed.), The cognitiveneuroscience (pp. 1341–1356). Cambridge, MA: TheMIT Press.
Nichelli, P., Always, D., & Grafman, J. (1996). Perceptualtiming in cerebellar degeneration. Neuropsychologia,34, 863–871. doi:10.1016/0028-3932(96)00001-2
Nichelli, P., Clark, K., Hollnagel, C., & Grafman, J.(1995). Duration processing after frontal lobe lesions.Annuals of the New York Academy of Sciences, 769,183–190. doi:10.1111/j.1749-6632.1995.tb38139.x
Oshio, K. I., Chiba, A., & Inase, M. (2006). Delayperiod activity of monkey prefrontal neurons dur-ing duration-discrimination task. European Journalof Neuroscience, 23, 2779–2790. doi:10.1111/j.1460-9568.2006.04781.x
Owen, A. M., McMillan, K. M., Laird, A. R.,& Bullmore, E. (2005). N-back working memoryparadigm: A meta-analysis of normative functionalneuroimaging studies. Human Brain Mapping, 25,46–59. doi:10.1002/hbm.20131
Paul, I., Le Dantec, C., Bernard, C., Lalonde, R.,& Rebaï, M. (2003). Event-related potentials inthe frontal lobe during performance of a visualduration discrimination task. Journal of ClinicalNeurophysiology, 20, 351–360.
Perbal, S., Couillet, J., Azouvi, P., & Pouthas, V. (2003).Relationship between time estimation, memory, atten-tion, and processing speed in patients with severe trau-matic brain injury. Neuropsychologia, 41, 1599–1610.doi:10.1016/S0028-3932(03)00110-6
Picton, T. W., Stuss, D. T., Shallice, T., Alexander, M. P.,& Gillingham, S. (2006). Keeping time: Effects of focalfrontal lesions. Neuropsychologia, 44, 1195–1209.doi:10.1016/j.neuropsychologia.2005.10.002
Pouthas, V., & Perbal, S. (2004). Time perception dependson accurate clock mechanisms as well as unimpairedattention and memory processes. Acta NeurobiologiaeExperimentalis, 64, 367–385.
Rammsayer, T. H. (2001). Ageing and temporalprocessing of durations within the psychologicalpresent. European Journal of Cognitive Psychology, 13,549–565. doi:10.1080/09541440125713
Rammsayer, T. H., Hennig, J., Haag, A., & Lange, N.(2001). Effects of noradrenergic activity on temporalinformation processing in humans. The QuarterlyJournal of Experimental Psychology, Section B:Comparative and Physiological Psychology, 54,247–258. doi:10.1080/713932756
Rubia, K. (2006). The neural correlates of timing func-tions. In J. Glickson & M. S. Myslobodsky (Eds.),Timing the future: The case for a time-based prospec-tive memory (pp. 213–238). River Edge, NJ: WorldScientific.
Rubia, K., & Smith, A. (2004). The neural corre-lates of cognitive time management: A review. ActaNeurobiologiae Experimentalis, 64, 329–340.
Rubia, K., Taylor, A., Taylor, E., & Sergeant, J. A.(1999). Synchronization, anticipation, and consis-tency in motor timing of children with dimensionalitydefined attention deficit hyperactivity behaviour.Perceptual and Motor Skills, 89, 1237–1258.doi:10.2466/pms.1999.89.3f.1237
Schmitter-Edgecombe, M., & Rueda, A. D. (2008).Time estimation and episodic memory follow-ing traumatic brain injury. Journal of Clinicaland Experimental Neuropsychology, 30, 212–223.doi:10.1080/13803390701363803
Shimamura, A. P. (1995). Memory and frontal lobefunction. In M. S. Gazzaniga (Ed.), The cognitiveneurosciences (pp. 803–814). Cambridge, MA: MITPress.
Smith, A., Taylor, E., Lidzba, K., & Rubia, K. (2003).A right hemispheric frontocerebellar network fortime discrimination of several hundreds of millisec-onds. NeuroImage, 20, 344–350. doi:10.1016/S1053-8119(03)00337-9
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12

TIME DISCRIMINATION AFTER TBI 13
Teasdale, G., & Jennett, B. (1974). Assessment of comaand impaired consciousness. A practical scale. Lancet,13, 81–84. doi:10.1016/S0140-6736(74)91639-0
Treisman, M. (1963). Temporal discrimination and theindifference interval: Implications for a model of the“internal clock.” Psychological Monographs, 77, 1–31.doi:10.1037/h0093864
Wiener, M., Turkeltaub, P. E., & Coslett, H. B.(2010). Implicit timing activates the left inferiorparietal cortex. Neuropsychologia, 48, 3967–3971.doi:10.1016/j.neuropsychologia.2010.09.014
Zakay, D. (1990). The evasive art of subjective timemeasurement: Some methodological dilemmas. In
R. A. Block (Ed.), Cognitive models of psychologicaltime (pp. 59–84). Hillsdale, NJ: Lawrence ErlbaumAssociates.
Zakay, D., & Block, R. A. (1996). The role of atten-tion in time estimation process. In M. A. Pastor& J. Artieda (Eds.), Time, internal clocks and move-ment (pp. 143–164). Amsterdam, The Netherlands:North-Holland/Elsevier Science. doi:10.1016/S0166-4115%2896%2980057-4
Zakay, D., & Block, R. A. (2004). Prospective and ret-rospective duration judgment: An executive-controlperspective. Acta Neurobiologiae Experimentalis, 64,319–328.
Dow
nloa
ded
by [
Uni
vers
ita d
i Pad
ova]
at 1
1:01
27
Dec
embe
r 20
12




















