
Differential item functioning detection with logistic regression

Brain and Cognition 83 (2013) 34–44
Contents lists available at SciVerse ScienceDirect
Brain and Cognition
journal homepage: www.elsevier .com/locate /b&c
Regional cortical volume and cognitive functioning following traumaticbrain injury
0278-2626/$ - see front matter � 2013 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.bandc.2013.06.007
⇑ Corresponding author. Address: School of Psychology and Psychiatry, MonashUniversity, Clayton, VIC 3800, Australia.
E-mail address: [email protected] (G. Spitz).
Gershon Spitz a,b,⇑, Erin D. Bigler c,d, Tracy Abildskov e, Jerome J. Maller f,g, Richard O’Sullivan h,Jennie L Ponsford a,b
a School of Psychology and Psychiatry, Monash University, Melbourne, Australiab Monash-Epworth Rehabilitation Research Centre, Epworth Hospital, Melbourne, Australiac Department of Psychology and Neuroscience Center, Brigham Young University, Provo, UT 84602, United Statesd Department of Psychiatry, University of Utah, Salt Lake City, UT 84132, United Statese Department of Psychological Science, Brigham Young University, Provo, UT 84602, United Statesf Central Clinical School, Monash University, Melbourne, Australiag Monash Alfred Psychiatry Research Centre, Alfred Hospital, Melbourne, Australiah Healthcare Imaging Services, Epworth Hospital, Melbourne, Australia
a r t i c l e i n f o a b s t r a c t
Article history:Accepted 18 June 2013
Keywords:Traumatic brain injuryMRINeuropsychologyCognition
There has been limited examination of the effect of brain pathology on subsequent function. The currentstudy examined the relationships between regional variation in grey matter volume, age and cognitiveimpairment using a semi-automated image analysis tool. This study included 69 individuals withmild-to-severe TBI, 41 of whom also completed neuropsychological tests of attention, working memory,processing speed, memory and executive functions. A widespread reduction in grey matter volume wasassociated with increasing age. Regional volumes that were affected also related to the severity of injury,whereby the most severe TBI participants displayed the most significant pathology. Poorer retention ofnewly learned material was associated with reduced cortical volume in frontal, parietal, and occipitalbrain regions. In addition, poorer working memory and executive control performance was found forindividuals with lower cortical volume in temporal, parietal, and occipital regions. These findings are lar-gely in line with previous literature, which suggests that frontal, temporal, and parietal regions are inte-gral for the encoding of memories into long-term storage, memory retrieval, and working memory. Thepresent study suggests that automated image analysis methods may be used to explore the relationshipsbetween regional variation in grey matter volume and cognitive function following TBI.
� 2013 Elsevier Inc. All rights reserved.
1. Introduction
Traumatic brain injury (TBI) is a leading cause of disability andlife-long impairment, resulting in significant financial burden tothe individual and health service providers (Access Economics,2009). Sequelae are often multifaceted, affecting individuals’ social,behavioural, emotional, and cognitive functioning (Novack, Bush,Meythaler, & Canupp, 2001; Ponsford, Olver, & Curran, 1995). Ofthese, impairments in memory, processing speed, and executivefunctions continue to be some of the most common complaints fol-lowing TBI, significantly influencing individuals’ rehabilitation ef-forts and community reintegration (Dikmen, Machamer, Winn, &Temkin, 1995; Draper & Ponsford, 2008). Although deficits in cog-nition have been consistently demonstrated in neuropsychological
outcome studies (Spitz, Ponsford, Rudzki, & Maller, 2012), theirneuropathological basis is less clear. However, gradual develop-ments and utilisation of neuroimaging modalities have allowedfor a better understanding of the ways in which pathologicalchanges in the brain result in cognitive impairments followinginjury.
Initial neuroimaging investigations of brain pathology followingTBI required the use of time-consuming manual, tracing tech-niques to better characterise atrophic changes. Nevertheless, theseinitial studies demonstrated that significant atrophy occurs in greyand white matter brain regions following injury (Anderson & Big-ler, 1995; Anderson, Wood, Bigler, & Blatter, 1996; Thatcheret al., 1997). The role of ventricular dilation as an indirect measureof atrophy in white and grey matter regions was also highlighted,in part because of the relative ease of tracing the ventricular out-line on either computed tomography (CT) or magnetic resonanceimaging (MRI) scans (Anderson & Bigler, 1994; Bigler, 2001; Bigler,Kurth, Blatter, & Abildskov, 1992). In addition, any distinct region

G. Spitz et al. / Brain and Cognition 83 (2013) 34–44 35
of interest (ROI) or identifiable brain structure could be handtraced and either its volume and/or surface area determined. Suchtechniques were applied to a variety of ROIs, particularly the thal-amus, basal ganglia, corpus callosum and fornix, along with lobularand whole brain volume.
Although earlier studies cemented the idea that structural brainchanges following injury are related to subsequent loss in function,use of manual techniques to assess the extent of atrophy is not fea-sible on a daily basis in the clinical environment. Fortunately, theadvent of newer, semi-automated image analysis tools has allowedfor greater flexibility in investigating different structural brainchanges following TBI (Burgess & Shallice, 1997; Dale, Fischl, &Sereno, 1999; Fischl, Sereno, & Dale, 1999a), with the most widelyused automated neuroimage analysis tool being Freesurfer (Destri-eux, Fischl, Dale, & Halgren, 2010; Fischl, 2012). Instead of manu-ally tracing ROIs, new methods utilise semi-automated tissuesegmentation, largely based on the contrast and intensity of differ-ent tissue types. Studies using these newer methods have vali-dated earlier investigations that demonstrated significantventricular enlargement as well as loss in volume of white andgrey matter regions (Bigler, Anderson, & Blatter, 2002; MacKenzieet al., 2002; Ng et al., 2008). For example, in the same TBI subjectsBigler et al. (2010) demonstrated that operator-controlled hand-tracing ROI volumes adequately corresponded to automatedmethods.
Studies of non-TBI patients have also shown that automatedmethods approximate those of operator-controlled ROI tracingmethods, demonstrating the practical use of these methods (De-wey et al., 2010; Morey et al., 2009; Shen et al., 2010). In addition,the association between regional structural changes and clinicalvariables, such as injury severity and cognitive functioning havealso been reproduced (Bigler et al., 1997, 2002; Trivedi et al.,2007). A major limitation of past research using operator-con-trolled methods was that a priori decisions governed which ROIswere examined. However, such a priori constraints are not arequirement of automated methods, which depend on the neuro-imaging analysis method used and permit simultaneous compari-sons of cortical and subcortical structures. FreeSurfer is the mostcommon method with demonstrated applicability to automatedimage analysis in TBI (Hudak et al., 2011; McCauley et al., 2010;Wilde et al., 2011; Yurgelun-Todd et al., 2011).
Several previous studies have used Freesurfer and other semi-automated image analysis tools in adult TBI populations. However,many of these previous studies have only included severe (Sidaroset al., 2009; Tomaiuolo et al., 2005; Turken et al., 2009) or moder-ate-to-severe (Bendlin et al., 2008; Salmond, Chatfield, Menon, Pic-kard, & Sahakian, 2005; Warner et al., 2010) TBI participants, withall TBI participants included in analyses. Moreover, many of theprevious studies have had relatively small sample sizes. Therefore,specific comparisons between injury severity groups have beenlacking. The Glasgow Coma Scale (GCS) has been used almostexclusively to classify injury severity. Recent studies have sug-gested that post-traumatic amnesia (PTA) duration may be morestrongly associated with cognitive and functional outcome thanGCS (Brown et al., 2005). Few of these studies have reported onthe association between neuropsychological performance and vol-umetric loss in specific brain areas. Those that have conductedsuch analyses have noted an association between poorer cognitivefunctioning—in the domains of working memory, attention, execu-tive functions, and memory—and reduced regional volume inwhite and grey matter structures (Bendlin et al., 2008; Gale, Baxter,Roundy, & Johnson, 2005; Vannorsdall et al., 2010). Volumetric lossin subcortical regions, such as the thalamus, amygdala, and hippo-campus has also shown a relationship with reduced processingspeed and memory functions (Strangman et al., 2010; Warneret al., 2010).
1.1. Present study objective and aims
The objective of the current study was to a use semi-automatedimage analysis tool to examine the relationship between regionalvariation in grey matter volume, injury severity, and performanceon tests of attention, working memory, information processingspeed, memory, and executive function following TBI. This studycomplements, and extends previous studies by applying awhole-brain voxel-based morphometry analysis to a sample ofmild-to-severe participants, using duration of PTA, rather thanGCS, to classify injury severity.
2. Materials and methods
2.1. Participants
This study included 69 individuals with mild-to-severe TBI re-cruited consecutively from a head injury rehabilitation program.Study ethics approval was received from human research and ethicscommittees. Participants provided informed consent prior toassessment. The MR imaging took place on average 19.64 months(SD = 15.56, range = 2.76–64.59) post-injury. Participants with TBIhad no history of other neurological or psychiatric disturbance,nor were they taking medication at the time of assessment thatcould affect cognitive abilities. In addition, participants were con-sidered eligible for testing once they were confirmed by their treat-ing neuropsychologist to have emerged from PTA—measuredprospectively on a daily basis using the Westmead PTA scale—andto have sufficient cognitive, communication and physical abilitiesto perform assessment. A subsample of the individuals with TBI alsocompleted the neuropsychological tests. This subsample did notdiffer significantly from the individuals with TBI that did not haveneuropsychological assessment in regards to age (t(67) = 1.92,p = .06), education (t(61.66) = 0.94, p = .35), PTA duration(t(66) = �0.25, p = .81), or gender (v2 (1, N = 69) = 0.03, p = .86).
A healthy control group was also assessed, comprising 25healthy individuals. They had no previous history of any neurolog-ical or psychiatric disorder, nor were they on any medication or il-licit drugs that might impair their performance on cognitive tests.Control participants completed both an MRI scan and a neuropsy-chological assessment. Table 1 presents descriptive statistics forcontrol participants and classifies TBI participants according to in-jury severity. In addition, analyses were undertaken to comparethe control group with each TBI injury severity group, adjustingfor multiple comparisons using Bonferroni correction. No signifi-cant differences were found between control participants andany of the TBI severity groups in terms of age or years of education.Although no difference in the distribution of gender was found be-tween the control and the mild TBI group (v2 (1, N = 33) = 2.33,p = .13), the moderate (v2 (1, N = 41) = 7.76, p = .005) and severe(v2 (1, N = 69) = 9.06, p = .003) groups had a higher proportion ofmales compared to controls.
2.2. Materials
Participants completed neuropsychological tests assessingattention, working memory, information processing speed, mem-ory and executive functions, which have been shown to be sensi-tive to cognitive impairments following TBI (Draper & Ponsford,2008).
2.2.1. BIRT memory and information processing battery-list learningsubtest
The BIRT list learning test (Coughhlan, Oddy, & Crawford, 2007)assesses verbal recall. Participants recalled a list of words over five

Table 1Descriptive statistics for control participants as well as individuals with TBI categorised by injury severity.
Total TBI sample(n = 69)
Mild TBI (n = 8) Moderate TBI(n = 16)
Severe TBI(n = 45)
TBI cognitive subsample(n = 41)
Control (n = 25)
N (%) N (%) N (%) N (%) N (%) N (%)
Gender (male) Cause ofinjury
56 (81.2) 6 (75) 14 (87.5)a 35 (79.5)a 33 (80.5) 11 (44)
Car accident 37 (54.4) 3 (37.5) 6 (37.5) 28 (63.6) 20 (50)Motorcycle 11 (16.2) 1 (12.5) 2 (12.5) 8 (18.2) 5 (12.5)Pedestrian 8 (11.8) 1 (12.5) 3 (18.8) 4 (9.1) 7 (17.5)Bicycle 5 (7.4) 1 (12.5) 3 (18.8) 1 (2.3) 5 (12.5)Fall 3 (4.4) 1 (12.5) 0 (0) 2 (4.5) 1 (2.5)Other 4 (6.0) 1 (12.5) 2 (12.6) 1 (2.3) 2 (5)
PTA categoriesMild (0–1 day) 8 (11.8) 3 (7.3)Moderate (>1 to 67 days) 16 (23.5) 13 (31.7)Severe (>7 days) 45 (64.7) 25 (61)
Abnormal CT Scan 58 (84.1) 8 (100) 10 (62.5) 40 (88.9) 33 (80.5)Contusion 30 (42.9) 4 (50) 2 (12.5) 24 (53.3) 14 (34.1)DAI 10 (14.3) 0 (0) 3 (18.8) 21 (46.7) 9 (22)SAH 28 (40) 4 (50) 3 (18.8) 21 (46.7) 15 (36.6)SDH 15 (21.4) 3 (37.5) 4 (25) 8 (17.8) 9 (22)EDH 7 (10) 2 (25) 2 (12.5) 3 (6.7) 2 (4.9)ICH 11 (15.7) 2 (25) 1 (6.3) 8 (17.8) 6 (14.6)IVH 3 (4.3) 0 (0) 0 (0) 3 (6.7) 0 (0)
M (SD) range M (SD) range M (SD) range M (SD) range M (SD) range M (SD) range
Age 34.74 (12.41) 38.73 (12.58) 32.68 (13.42) 34.21 (11.69) 37.07 (12.76) 30.26 (12.48)17–69 23–52 20–69 17–57 17–69 18–69
Education 12.97 (2.75) 12.63 (2.97) 12.75 (1.94) 13.03 (2.97) 13.21 (3.09) 14.68 (1.51)10.22.5 10–18 10–16 10–22 10–22.5 12–17
PTA (days) 18.92 (20.72) 18.41 (21.76)0.5–05 0.5–105
TICV (mm3) 1,538,570 (163,348) 1,566,190(122,165)
1,512,065(187,244)
1,543,083(162,772)
1,549,953 (168,945) 1,565,662(146,350)
Brain volumes (cc3)Total grey matter 692.73 (70.12) 700.14 (70.52) 703.52 (81.11) 687.57 (66.97) 695.88 (73.22) 724.08 (53.97)Total white matter 492.66 (61.08) 510.46 (49.90) 491.60 (61.87) 489.87 (63.23) 508.36 (60.70) 508.28 (61.84)Total CSF 25.92 (12.80) 19.83 (10.71) 18.80 (5.98) 29.54 (13.57) 24.42 (10.09) 16.70 (10.52)Total brain volume 1,083.91 (112.56) 1,105.43 (102.92) 1,085.68 (128.91) 1,079.46 (110.11) 1,100.77 (111.74) 1,123.99 (105.44)
Note: Group comparisons were undertaken using post hoc test with Bonferroni correction. Brain volumes are present in cubic centimeters.a Statistically significant chi-square test between control participants and the respective TBI group. DAI = Diffuse axonal injury; SAH = Subarachnoid haemorrhage;
SDH = Subdural haemorrhage; EDH = Epidural haemorrhage; ICH = Intracerebral haemorrhage; IVH = Intraventricular haemorrhage.
36 G. Spitz et al. / Brain and Cognition 83 (2013) 34–44
trials. Total correctly recalled words over the five learning trialswere used as a measure of ‘Total Recall’. The BIRT list learning taskhas demonstrated a test–retest reliability coefficient of .68. Listlearning tests have shown to be sensitive to impairments followingTBI, compared to healthy controls (Draper & Ponsford, 2008; Spitzet al., 2012).
2.2.2. The Doors Test from the Doors and People TestThe Doors Test (Baddeley, Emslie, & Nimmo-Smith, 1994) is de-
signed to assess visual memory. This test required participants torecognise a target door they have previously seen among threeother distractor doors not seen before. There were two trials, of12 target doors, with the second trial using more similar distrac-tors. The score for each trial ranges from 0 to 12 with an overallscore for the test ranging from 0 to 24. The two trials were aggre-gated to form a measure of ‘Visual Memory’. The Doors and PeopleTest has been found to differentiate between individuals with TBIand healthy controls (Draper & Ponsford, 2008).
2.2.3. The Hayling Sentence Completion Test from the Hayling andBrixton Tests
The Hayling Sentence Completion Test (Burgess & Shallice,1997) assesses participants’ speed of initiation and response inhi-bition abilities. This test comprises two sections, each comprising15 sentences with the last word missing. In the first section
(Hayling A) participants were required to finish the sentence witha word that logically completed the sentence as quickly as possible.In the second section (Hayling B) participants were asked to com-plete the sentences with an unrelated word. The overall scaledscore—which incorporates the total time taken in parts A and Bof the test, as well as the number of errors—was used in the currentstudy. The first and second sections exhibit test–retest reliabilitiesof .62 and .78, respectively. The Hayling Sentence Completion Testhas also been found to differentiate individuals with TBI fromhealthy controls (Draper & Ponsford, 2008).
2.2.4. Controlled Oral Word Association TestsThe COWAT (Benton, Hamsher, & Rey, 1994) is a measure of
verbal fluency and idea generation. Participants were required togenerate as many words as they could, beginning with a specificletter, within a time span of 1 min. The total number of words gen-erated was recorded for the letters C, F and L. Test–retest reliabilityhas been found to be .88 in a sample of adults. The COWAT hasbeen shown to differentiate individuals with TBI from healthy con-trol participants (Spitz et al., 2012).
2.2.5. Trail Making Test – Parts A and BThe TMT (Reitan & Wolfson, 1988) measures processing speed,
attention, mental flexibility, and working memory, requiringparticipants to join numbers in sequence (Trails A) and to switch

G. Spitz et al. / Brain and Cognition 83 (2013) 34–44 37
between numbers and letters in sequence (Trails B) as quickly aspossible. To further focus on the executive control component ofthe TMT, a third variable was computed by subtracting Trails Afrom Trails B time (Trails B – Trails A). Trails A has demonstrateda test–retest correlation of .75 and Part B a test–retest correlationof .85 in a sample with no history of neurological or psychiatricsymptoms (Giovagnoli et al., 1996). The TMT has been shown todifferentiate individuals with TBI from healthy control participants(Spitz et al., 2012).
2.2.6. Digit Span subtest of the Wechsler Memory Scale – Third andFourth Editions
The Forwards and Backwards Digit Span (Wechsler, 1997;Wechsler, 2008) was used to assess participants’ immediate atten-tion span and working memory capacity. The number of correct tri-als was recorded for the Forward and Backward conditions. Thistest has been found to have a reliability coefficient of .86 and theBackwards condition has specifically been shown to discriminatebetween head injured and control participants (Chan, 2000; Kinsel-la et al., 1996).
2.2.7. Symbol Digit Modalities Test – Oral version (SDMT)The SDMT (Smith, 1973) assesses processing speed. Participants
are provided with 90 s to verbalise to the experimenter the correctnumber that belongs under a specific symbol, based on the waythey are paired in an index at the top of the page. Total numberof correct entries was used in the current study. Repeated admin-istrations have not been found to significantly affect the reliabilityof this test in a sample of mildly head-injured participants and dis-plays a test–retest coefficient of .72 (Hinton-Bayre, Geffen, &McFarland, 1997). The SDMT has also found to differentiate indi-viduals with TBI from healthy controls (Draper & Ponsford, 2008).
2.3. Neuroimaging acquisition
Neuroimaging was performed on a Siemens Magnetom Verio 3Tesla MRI scanner (Siemens Medical Imaging, Erlangen, Germany).After a scout scan, an AC-PC aligned axial FLAIR sequence was ac-quired (TR = 8500, TE = 81, slice thickness = 3.0 mm, FOV = 240 mm,matrix = 192 � 256, in-plane = 0.94 mm � 0.94 mm). In addition, a3D T1-weighted sequence was acquired in the sagittal orientation(TI = 1100 ms, TR = 1930 ms TE = 2.48 ms, resolution = 256 � 256� 160, flip angle = 12�, FOV = 256 mm, slice thickness = 1.00 mm(160slices)).
3. Data analysis
Cortical reconstruction and segmentation was performed withthe Freesurfer image analysis suite (http://surfer.nmr.mgh.har-vard.edu/). This comprised several stages, of which the technicaldetails can be found in the cited publications. The initial step com-prised the reconstruction of the cortical surface (Dale et al., 1999).Normalised intensity images are created, corrected for the varia-tions in intensity due to magnetic field inhomogeneity. Voxels be-yond the cerebral cortex, namely the skull, are then removedbefore segmentation is initiated. Segmentation is based on the geo-metric structure where grey and white matter interface, and subse-quently separates the left and right hemispheres as well as corticalfrom subcortical structures. The resulting cortical volume is cov-ered in a triangular tessellation and deformed to more accuratelyrepresent grey and white matter interface as well as the pial sur-face. Once the cortex has been reconstructed this volume may be‘inflated’ or ‘flattened’ to better visualise the sulci, but also regis-tered to a spherical atlas (Fischl, Sereno, Tootell, & Dale, 1999b; Fis-chl et al., 1999a) and parcellated into regions based on the sulcal
and gyral structures (Desikan et al., 2006; Fischl et al., 2004). Usingthe distance between the grey/white and pial surface, measures ofcortical thickness may then be undertaken (Fischl & Dale, 2000).
Prior to analyses being undertaken, quality assurance of theFreesurfer registration and segmentation was undertaken by visualinspection to insure that proper classification had occurred. Addi-tionally, scatterplots of various FreeSurfer output (i.e., total intra-cranial volume, hippocampal volume, etc.) variables were run, asa check on whether the outlier reflected misclassification. All outli-ers detected were not deemed to be due to misclassification of tis-sue or to other alignment issues. After all of the individuals’ imageswere reconstructed using the processes described above, corticalvolume group analysis was undertaken within Qdec, a GraphicalUser Interface tool for Freesurfer. Qdec was used to model the datausing the General Linear Model (GLM) as well as for permutationtesting to correct for multiple comparisons. Analyses were under-taken in a number of steps. Firstly, the associations between demo-graphic and injury-related variables were examined for the full TBIsample. One goal of this step was to reveal confounding variablesthat may need to be partialled out of subsequent analyses. Sec-ondly, group comparisons were conducted between the healthycontrols and mild, moderate, and severe TBI samples. Thirdly, theassociation between neuropsychological measures and cortical vol-ume was examined in the TBI subsample for which neuropsycho-logical data were obtained. The subsequent parameters withinQdec were used for all of the analyses: Measure = Volume,Smoothing = 10, Monte Carlo simulation used to correct for multi-ple comparisons using a Threshold of 1.3 (p < .05) and the appropri-ate one-tailed test—either positive or negative—was applied.
4. Results
4.1. Demographic, injury severity variables and cortical volume
The relationships between age, years of education, time post in-jury, and gender were initially assessed in relation to cortical vol-ume for the full TBI sample. Of these variables, only age and timepost injury were found to be associated with volume of both theleft and right hemispheres. Reduced cortical volume was associ-ated with older age and shorter time post-injury. As can be seenin Fig. 1, the effect of age was found to be widespread, affectingmuch of the cerebral cortex. The largest clusters of difference werefound in the temporal and parietal regions. In addition, time postinjury was found to have a widespread effect on cortical volume.Individuals scanned at longer times post injury were found to havehigher cortical volume. A strong association was found in frontal,occipital, parietal and temporal lobe regions.
Conversely, a relatively weak association was found betweenage and cortical volume for the control group. That is, for controlparticipants regional variation in cortical volume was only associ-ated with a restricted region in the left hemisphere. The cluster ofhighest significance was found in the insula. Interestingly, an ageby cortical volume interaction was found between TBI and controlparticipants in the right hemisphere. The clusters of highest signif-icance were found in the superiorparietal and superiortemporal re-gions. That is, with increasing age these regions displayedsignificantly lower volume for TBI participants compared tohealthy controls. These findings are illustrated in Fig. 1A–D, andmore specific cluster-related details included in Tables 3 and 4.
4.2. Injury severity and regional cortical volume
Group comparisons were made between control participantsand the full TBI sample. In addition, TBI participants were catego-rised into mild, moderate, and severe injury based on days of PTA.

(A) (B)
(C) (D)
(E) (F)
Fig. 1. Illustrative results of Freesurfer analysis, examining correlations between age and time post injury. (A) Regions displaying reduced cortical volume with older age forthe left hemisphere for TBI participants. (B) Regions displaying reduced cortical volume with older age for the right hemisphere for TBI participants. (C) Regions displayingreduced cortical volume with older age for the left hemisphere for Control participants. (D) Regions displaying the age x group interaction for cortical volume in the righthemisphere. (E) Regions displaying reduced cortical volume with less time post injury for the left hemisphere of TBI participants. (F) Regions displaying reduced corticalvolume with less time post injury for the right hemisphere of TBI participants. Note: Cortical surfaces have been inflated. The colour bar was generated following the MonteCarlo simulation to correct for multiple comparisons. Clusters are thresholded at ±2.5 to indicate p < .05.
38 G. Spitz et al. / Brain and Cognition 83 (2013) 34–44
Controls were compared to each TBI subgroup, and the TBI sub-groups with one another. All of the group comparisons controlledfor age, years of education, and total intracranial volume. The TBIgroup as a whole displayed reduced cortical volume in both the left
Table 2Cognitive test performance comparisons between TBI and control participants.
Measure TBI total cognitive subsample N = 41 TBI mild N = 3 TMean (SD) Mean (SD) M
Total recall 44.83 (10.53) 40.33 (14.43) 4Visual memory 16.37 (4.04) 19.33 (3.06) 1Hayling—Time A 15.05 (18.45) 9.33 (3.06) 1Hayling—Time B 39.22 (52.66) 16.67 (15.54) 4Hayling—Scaled 5.76 (1.62) 5 (1.41)Hayling—errors 4.03 (5.45) 6.33 (10.11)COWAT 38.03 (13.07) 40.33 (3.06) 3Trails A time 29.25 (11.24) 27.61 (4.40) 3Trails B time 71.99 (37.23) 69.44 (53.90) 7Trails B – Trails A 42.75 (31.56) 41.83 (50.34) 4Digit Span: Forward 10.18 (3.04) 9.00 (1.00) 1Digit Span: backwards 8.21 (3.08) 6.33 (2.31)SDMT 51.17 (11.85) 57.00 (4.00) 5
SDMT = Symbol Digits Modalities Test, Hayling = Hayling overall scaled score.* p < .05.** p < .01.*** p < .001.
and right hemispheres (Fig. 2A and B). Clusters of maximum signif-icance were present in the cuneus of the left hemisphere and theinferior parietal and frontal regions of the right hemisphere. Indi-viduals with mild TBI, categorised as individuals with PTA of 24 h
BI moderate N = 13 TBI severe N = 25 Control N = 25 Total TBI vs controlean (SD) Mean (SD) Mean (SD) t
7.38 (9.32) 44.04 (10.83) 55.36 (8.12) 4.56***
5.38 (4.52) 16.52 (3.81) 19.00 (2.53) 3.26**
8.00 (16.51) 14.39 (20.56) 7.54 (5.18) �2.07*
6.73 (79.20) 38.57 (39.57) 19.17 (11.48) �2.24*
6.33 (1.97) 5.65 (1.54) 6.13 (0.61) 1.052.18 (3.03) 4.61 (5.70) 2.92 (1.93) �1.119.33 (15.54) 37.12 (12.80) 42.52 (9.33) 1.501.71 (13.16) 28.18 (10.92) 23.47 (9.00) �2.12*
2.75 (46.14) 71.93 (31.64) 55.99 (23.74) �2.07*
7.17 (36.26) 43.76 (24.89) 32.53 (18.45) �1.610.00 (3.86) 10.42 (2.80) 11.24 (2.45) 1.468.67 (3.75) 8.21 (2.81) 9.68 (2.21) �2.07*
1.46 (14.90) 50.32 (10.80) 62.84 (9.21) 4.21***
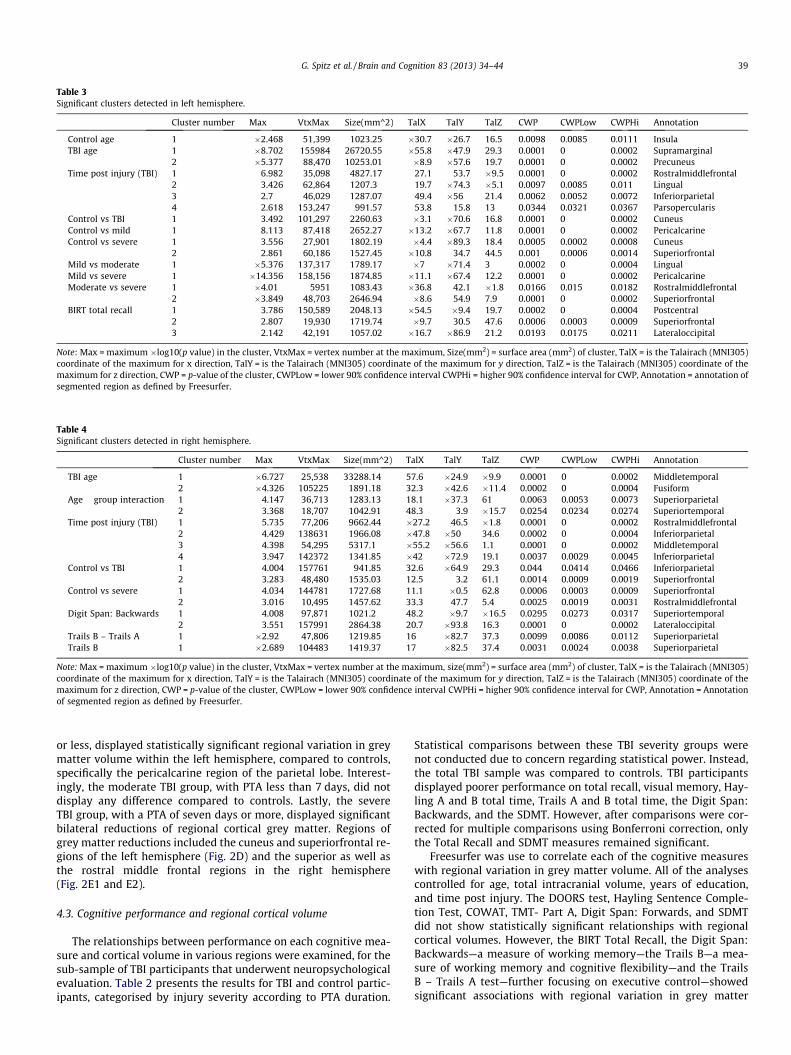
Table 3Significant clusters detected in left hemisphere.
Cluster number Max VtxMax Size(mm^2) TalX TalY TalZ CWP CWPLow CWPHi Annotation
Control age 1 �2.468 51,399 1023.25 �30.7 �26.7 16.5 0.0098 0.0085 0.0111 InsulaTBI age 1 �8.702 155984 26720.55 �55.8 �47.9 29.3 0.0001 0 0.0002 Supramarginal
2 �5.377 88,470 10253.01 �8.9 �57.6 19.7 0.0001 0 0.0002 PrecuneusTime post injury (TBI) 1 6.982 35,098 4827.17 27.1 53.7 �9.5 0.0001 0 0.0002 Rostralmiddlefrontal
2 3.426 62,864 1207.3 19.7 �74.3 �5.1 0.0097 0.0085 0.011 Lingual3 2.7 46,029 1287.07 49.4 �56 21.4 0.0062 0.0052 0.0072 Inferiorparietal4 2.618 153,247 991.57 53.8 15.8 13 0.0344 0.0321 0.0367 Parsopercularis
Control vs TBI 1 3.492 101,297 2260.63 �3.1 �70.6 16.8 0.0001 0 0.0002 CuneusControl vs mild 1 8.113 87,418 2652.27 �13.2 �67.7 11.8 0.0001 0 0.0002 PericalcarineControl vs severe 1 3.556 27,901 1802.19 �4.4 �89.3 18.4 0.0005 0.0002 0.0008 Cuneus
2 2.861 60,186 1527.45 �10.8 34.7 44.5 0.001 0.0006 0.0014 SuperiorfrontalMild vs moderate 1 �5.376 137,317 1789.17 �7 �71.4 3 0.0002 0 0.0004 LingualMild vs severe 1 �14.356 158,156 1874.85 �11.1 �67.4 12.2 0.0001 0 0.0002 PericalcarineModerate vs severe 1 �4.01 5951 1083.43 �36.8 42.1 �1.8 0.0166 0.015 0.0182 Rostralmiddlefrontal
2 �3.849 48,703 2646.94 �8.6 54.9 7.9 0.0001 0 0.0002 SuperiorfrontalBIRT total recall 1 3.786 150,589 2048.13 �54.5 �9.4 19.7 0.0002 0 0.0004 Postcentral
2 2.807 19,930 1719.74 �9.7 30.5 47.6 0.0006 0.0003 0.0009 Superiorfrontal3 2.142 42,191 1057.02 �16.7 �86.9 21.2 0.0193 0.0175 0.0211 Lateraloccipital
Note: Max = maximum �log10(p value) in the cluster, VtxMax = vertex number at the maximum, Size(mm2) = surface area (mm2) of cluster, TalX = is the Talairach (MNI305)coordinate of the maximum for x direction, TalY = is the Talairach (MNI305) coordinate of the maximum for y direction, TalZ = is the Talairach (MNI305) coordinate of themaximum for z direction, CWP = p-value of the cluster, CWPLow = lower 90% confidence interval CWPHi = higher 90% confidence interval for CWP, Annotation = annotation ofsegmented region as defined by Freesurfer.
Table 4Significant clusters detected in right hemisphere.
Cluster number Max VtxMax Size(mm^2) TalX TalY TalZ CWP CWPLow CWPHi Annotation
TBI age 1 �6.727 25,538 33288.14 57.6 �24.9 �9.9 0.0001 0 0.0002 Middletemporal2 �4.326 105225 1891.18 32.3 �42.6 �11.4 0.0002 0 0.0004 Fusiform
Age � group interaction 1 4.147 36,713 1283.13 18.1 �37.3 61 0.0063 0.0053 0.0073 Superiorparietal2 3.368 18,707 1042.91 48.3 3.9 �15.7 0.0254 0.0234 0.0274 Superiortemporal
Time post injury (TBI) 1 5.735 77,206 9662.44 �27.2 46.5 �1.8 0.0001 0 0.0002 Rostralmiddlefrontal2 4.429 138631 1966.08 �47.8 �50 34.6 0.0002 0 0.0004 Inferiorparietal3 4.398 54,295 5317.1 �55.2 �56.6 1.1 0.0001 0 0.0002 Middletemporal4 3.947 142372 1341.85 �42 �72.9 19.1 0.0037 0.0029 0.0045 Inferiorparietal
Control vs TBI 1 4.004 157761 941.85 32.6 �64.9 29.3 0.044 0.0414 0.0466 Inferiorparietal2 3.283 48,480 1535.03 12.5 3.2 61.1 0.0014 0.0009 0.0019 Superiorfrontal
Control vs severe 1 4.034 144781 1727.68 11.1 �0.5 62.8 0.0006 0.0003 0.0009 Superiorfrontal2 3.016 10,495 1457.62 33.3 47.7 5.4 0.0025 0.0019 0.0031 Rostralmiddlefrontal
Digit Span: Backwards 1 4.008 97,871 1021.2 48.2 �9.7 �16.5 0.0295 0.0273 0.0317 Superiortemporal2 3.551 157991 2864.38 20.7 �93.8 16.3 0.0001 0 0.0002 Lateraloccipital
Trails B – Trails A 1 �2.92 47,806 1219.85 16 �82.7 37.3 0.0099 0.0086 0.0112 SuperiorparietalTrails B 1 �2.689 104483 1419.37 17 �82.5 37.4 0.0031 0.0024 0.0038 Superiorparietal
Note: Max = maximum �log10(p value) in the cluster, VtxMax = vertex number at the maximum, size(mm2) = surface area (mm2) of cluster, TalX = is the Talairach (MNI305)coordinate of the maximum for x direction, TalY = is the Talairach (MNI305) coordinate of the maximum for y direction, TalZ = is the Talairach (MNI305) coordinate of themaximum for z direction, CWP = p-value of the cluster, CWPLow = lower 90% confidence interval CWPHi = higher 90% confidence interval for CWP, Annotation = Annotationof segmented region as defined by Freesurfer.
G. Spitz et al. / Brain and Cognition 83 (2013) 34–44 39
or less, displayed statistically significant regional variation in greymatter volume within the left hemisphere, compared to controls,specifically the pericalcarine region of the parietal lobe. Interest-ingly, the moderate TBI group, with PTA less than 7 days, did notdisplay any difference compared to controls. Lastly, the severeTBI group, with a PTA of seven days or more, displayed significantbilateral reductions of regional cortical grey matter. Regions ofgrey matter reductions included the cuneus and superiorfrontal re-gions of the left hemisphere (Fig. 2D) and the superior as well asthe rostral middle frontal regions in the right hemisphere(Fig. 2E1 and E2).
4.3. Cognitive performance and regional cortical volume
The relationships between performance on each cognitive mea-sure and cortical volume in various regions were examined, for thesub-sample of TBI participants that underwent neuropsychologicalevaluation. Table 2 presents the results for TBI and control partic-ipants, categorised by injury severity according to PTA duration.
Statistical comparisons between these TBI severity groups werenot conducted due to concern regarding statistical power. Instead,the total TBI sample was compared to controls. TBI participantsdisplayed poorer performance on total recall, visual memory, Hay-ling A and B total time, Trails A and B total time, the Digit Span:Backwards, and the SDMT. However, after comparisons were cor-rected for multiple comparisons using Bonferroni correction, onlythe Total Recall and SDMT measures remained significant.
Freesurfer was use to correlate each of the cognitive measureswith regional variation in grey matter volume. All of the analysescontrolled for age, total intracranial volume, years of education,and time post injury. The DOORS test, Hayling Sentence Comple-tion Test, COWAT, TMT- Part A, Digit Span: Forwards, and SDMTdid not show statistically significant relationships with regionalcortical volumes. However, the BIRT Total Recall, the Digit Span:Backwards—a measure of working memory—the Trails B—a mea-sure of working memory and cognitive flexibility—and the TrailsB – Trails A test—further focusing on executive control—showedsignificant associations with regional variation in grey matter

(A) (B)
(C) (D)
(E1) (E2)
(G)(F)
(H2)(H1)
Fig. 2. Illustrative results of Freesurfer analysis comparing healthy controls to TBI participants. (A) Regions displaying reduced cortical volume in the overall TBI groupcompared to healthy controls in the left hemisphere. (B) Regions displaying reduced cortical volume in the overall TBI group compared to healthy controls in the righthemisphere. (C) Regions displaying reduced cortical volume in the mild TBI group compared to healthy controls in the left hemisphere. (D) Regions displaying reducedcortical volume in the severe TBI group compared to healthy controls in the left hemisphere. (E1–E2) Regions displaying reduced cortical volume in the severe TBI groupcompared to healthy controls in the right hemisphere. (F) Regions displaying reduced cortical volume in the moderate TBI group compared to mild TBI group in the lefthemisphere. (G) Regions displaying reduced cortical volume in the severe TBI group compared to mild TBI group in the left hemisphere. (H1–H2) Regions displaying reducedcortical volume in the severe TBI group compared to moderate TBI group in the left hemisphere.
40 G. Spitz et al. / Brain and Cognition 83 (2013) 34–44
volume. Poorer performance on the BIRT Total Recall related to re-duced cortical volume in frontal and parietal regions in the lefthemisphere. Poorer performance on the Digit Span: Backwardswas related to reduced cortical grey matter in the right hemi-sphere, with the superior temporal and lateral occipital regionsdisplaying the greatest significance. Regions displaying reducedregional grey matter volume for the Trails B, as well as the TrailsB – Trails A, were also restricted to the right hemisphere, and dis-played very similar results. Poorer performance on the Trails B and
the Trails B – Trails A was associated with loss of regional corticalvolume in the superior parietal region (see Fig. 3).
5. Discussion
The current study used a semi-automated image analysis tool toexamine the association between demographic variables, TBIseverity, and regional variation in grey matter cortical volume. In

(A1) (A2)
(B2)(B1)
(C) (D)
Fig. 3. Illustrative results of Freesurfer analysis, correlating cognitive performance with regional variation in cortical volume. (A1–A2) Regions displaying greater corticalvolume with better Total Recall performance in the left hemisphere. (B1–B2) Regions displaying greater cortical volume with better performance on the Digit Span:Backwards task in the right hemisphere. (C) Regions displaying greater cortical volume with better performance on the Trail Making Test: Part B and cortical volume in theright hemisphere. (D) Regions displaying greater cortical volume with better performance on the TMT B-TMT A task in the right hemisphere. Note: Cortical surfaces have beeninflated. The colour bar was generated following the Monte Carlo simulation to correct for multiple comparisons. Clusters are thresholded at ±2.5 to indicate p < .05. (Forinterpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)
G. Spitz et al. / Brain and Cognition 83 (2013) 34–44 41
addition, the relationship between regional brain volume and cog-nitive performance was investigated. The results supported previ-ous studies that used operator controlled methods for imagequantification in highlighting the widespread impact of age on cor-tical volume, as well as the loss of cortical volume—compared tohealthy controls—following mild-to-severe TBI. However, findingsfrom the present study also showed that through the use ofsemi-automated image analysis tools, relationships between regio-nal loss in cortical volume and impairment of new learning, work-ing memory, and executive control could be observed followingTBI.
Whereas gender and years of education did not show a signifi-cant relationship with cortical volume, age was observed to havean effect over much of the cerebral cortex. That is, older individualsdisplayed reduced regional cortical volume in frontal, temporal,parietal, as well as occipital regions. However, the largest clustersof volume loss were present in the temporal and parietal regions.This large effect of age supports numerous previous studies, whichhave reported a consistent decline in cortical grey matter through-out the life span (Sullivan & Pfefferbaum, 2007). Interestingly, anage by cortical volume interaction was found between the TBIand healthy control groups. That is, with increasing age regionsin the superior temporal and superior parietal regions displayedsignificantly reduced volume for TBI participants compared to con-trols. Although this evidence is only cross-sectional—whereby indi-
viduals’ TBI-related changes were not followed-up over time—these findings support the idea that TBI may have disproportionateage-related effects. That is, older individuals may be more vulner-able to the initial impact, or to the sequealae of pathophysiologicalchanges that can occur for months following the initial injury. Forexample Schönberger, Ponsford, Reutens, Beare, and O’Sullivan(2009) found that older age was related to larger lesion volumesin grey and white matter brain regions. This increased vulnerabil-ity found in older individuals may, in part, help explain why olderindividuals display greater cognitive decline, compared to youngerTBI participants (de la Plata et al., 2008).
As expected, individuals with TBI displayed reduced corticalvolume compared to healthy controls. It is also not surprising thatsignificant loss in regional grey matter cortical volume was presentin frontal regions as these regions are especially susceptible todamage following TBI, due in part to the location of the brain inrelation to the sphenoid bone as well as the inner table of the skull(Bigler, 2007; Levine et al., 2008). However, reduced cortical vol-ume was also present in parietal and occipital sites. Mild TBI par-ticipants displayed reduced regional cortical volume in theparietal lobe compared to healthy controls. Interestingly, the mod-erate TBI group did not display significant differences compared tocontrols; however, the moderate TBI group displayed significantlyreduced cortical volume in the occipital lobe compared to mild TBIparticipants. Individuals with severe TBI displayed the most

42 G. Spitz et al. / Brain and Cognition 83 (2013) 34–44
widespread loss in regional cortical volume, compared to healthycontrols, mild, as well as moderate TBI participants.
Individuals’ memory recall abilities were directly related to re-gional grey matter cortical volume in frontal and parietal regions.The role of these regions in memory functions has been supportedin other studies. For example, Yonelinas, Otten, Shaw, and Rugg(2005) found that greater activation in frontal as well as parietalbrain regions were related to better recollection and familiarityof events. Todd and Marois (2004) also showed that the specificfunction of holding information in short-term memory was relatedto the posterior parietal region. Indeed, in their review Wagner,Shannon, Kahn, and Buckner (2005) reported that several parietalregions are heavily implicated in memory retrieval. Overall, theyconclude that greater activations in specific parietal regions arefound to be associated with better episodic memory retrieval, rec-ognition of old items, as well as familiarity of events. Furthermore,although the association between temporal lobe regions and mem-ory has been extensively investigated (Eichenbaum, Yonelinas, &Ranganath, 2007; Squire & Wixted, 2011), the frontal lobeshave—for some time now—also been established as regions inte-gral to the function of memory (Buckner, Kelley, & Petersen,1999; Kirchhoff, Wagner, Maril, & Stern, 2000). That is, increasedactivation of frontal regions is present during the encoding of infor-mation into long-term memory.
The Digit Span: Backwards task—regarded as a measure ofworking memory—was found to be associated with the volumeof superior temporal and occipital regions. On the other hand,the Trails B—a measure of working memory as well as cognitiveflexibility—and the Trails B – Trails A—an executive componentsof the TMT—were only associated with the right superior parietalregion. The superior temporal gyral region has been reported tobe a critical hub region for working memory maintenance (Parket al., 2011). Furthermore, important connections of the superiortemporal gyrus with frontal and parietal regions critical for atten-tion and regulation of the default mode network have been demon-strated (Beer, Plank, & Greenlee, 2011; Makris et al., 2012;Matsumoto et al., 2004). Previously, it has been shown the greateractivation in the prefontal cortex is related to better working mem-ory, though this relationship was not found in the current study(Desposito et al., 1995). However, Cohen et al. (1997) showed thatgreater activation in parietal regions as well as the prefrontal cor-tex were related to better maintenance of working memory andexecutive functions; these regions are critical for the default modenetwork and are likely disrupted in TBI, playing a role in reducedworking memory (Arenivas et al., 2012; Bonnelle et al., 2011;Bonnelle et al., 2012; Mayer et al., 2012). Moreover, studies showthat individuals with temporal lobe lesions also perform morepoorly on measure of working memory (Morris, Miotto, Feigen-baum, Bullock, & Polkey, 1997), though some have found this asso-ciation only with greater task difficulty (Owen, Morris, Sahakian,Polkey, & Robbins, 1996). Greater activation in medial temporallobe is also found during encoding and maintenance on a workingmemory task (Axmacher et al., 2007), and more specifically forworking memory concerning the conjunction of two unrelatedstimuli (Olson, Page, Moore, Chatterjee, & Verfaellie, 2006).
The relationship between regional variation in cortical vol-ume—in temporal as well as parietal regions—and neuropsycholog-ical functioning is well supported by previous studies that haveexamined these effects in clinical but also healthy populations.However, other more recent studies in the TBI field have not fo-cused on cortical grey matter; instead, these studies have investi-gated neuropsychological impairment in relation to theconnectivity of white matter tracts. For example, Bigler et al.(2010) examined the integrity of white matter tracts in the tempo-ral stem, finding the poorer integrity of these tracts was related toworse memory performance. It may be that a reduction in cortical
volume in particular areas acts as a marker for disruption in under-lying networks in which these particular cortical regions play arole. Disrupted connectivity is thought to be a key factor in TBI out-come (Caeyenberghs et al., 2012; Hillary et al., 2011; Kumar, Rao,Chandramouli, & Pillai, 2009; Marquez de la Plata et al., 2011). Fu-ture studies should combine the analysis of cortical volume withthe analysis of white matter integrity to further examine thisrelationship.
The results from the current study further support the idea thatautomated techniques can be used to aid in guiding prognosis fol-lowing TBI. Cortical regions expected to display impairment fol-lowing TBI were found to have reduced cortical volume relativeto controls, and this technique also seemed to display sufficientsensitivity to delineate between severity of TBI. Moreover, individ-uals’ neuropsychological abilities were found to relate to corticalvolume. As already suggested by Strangman et al. (2010) there isincreasing evidence that information regarding pathology as ac-quired using neuroimaging can inform subsequent rehabilitation.
5.1. Limitations
Although some of the TBI patients had lesions on CT and MRI,lesion masks were not used during the Freesurfer group analyses.With increasing injury severity following TBI there is also a con-comitant increase in the prevalence—as well as size—of lesions,causing such scans to be more distant from the template Freesurferapplies. Furthermore, shearing of the white matter is more com-monly found following severe TBI and separation of white and greymatter boundaries, which translates to ‘blurry’ white/grey matterboundaries on T1-weighted scans. Subsequently, white/grey mat-ter contrast is reduced—an aspect on which Freesurfer, and otherautomated techniques per se, rely in order to fit the scan into thesoftware’s template. Hence, it may be that when the severe TBIscans were warped into the normalized T1-weighted templatespace, the lesions, and other damaged regions, were displaced bystretched/warped matter surrounding those lesions to producethe impression of full (volumetrically speaking) regions of interest.Hence, our results may have underestimated the extent of damagefollowing severe TBI. Our future investigations will aim to incorpo-rate lesion masks to determine whether this is in fact the case.Moreover, the VBM method used in the current study differs fromtraditional VBM analyses, which count the grey matter voxel den-sity, instead of volume following brain tessellation. Although it hasbeen shown that these two methods are complimentary, tradi-tional VBM allows examination of both grey and white matter(Hutton, Draganski, Ashburner, & Weiskopf, 2009). Lastly, these re-sults may, in part, reflect unique spatial distribution of pathologyin the current TBI sample. Therefore, it is essential to examinehow these results generalise to other TBI samples.
6. Conclusion
This study demonstrates the utility of using FreeSurfer as anautomated method for assessing cortical volume and its relation-ship with age, injury severity and cognitive outcome in individualswith TBI. Volume changes detected with this method had a moreprominent frontotemporoparietal distribution in relationship tocognitive tasks involving memory, working memory, executivecontrol, and speed of processing.
Disclosure statement
The authors declare that they have no competing financialinterests. Erin Bigler co-directs the Neuropsychological Assessment

G. Spitz et al. / Brain and Cognition 83 (2013) 34–44 43
and Research Clinic at BYU that does perform forensic consultationin individuals who have sustained a TBI.’’ as in ms
Acknowledgments
We thank all the staff of Healthcare Imaging MRI facility at theEpworth Hospital, Melbourne, Victoria.
References
Access Economics (2009). The economic cost of spinal cord injury and traumaticbrain injury in Australia. Report for the Victorian Neurotrauma Initiative.
Anderson, C., & Bigler, E. D. (1994). The role of caudate nucleus and corpus callosumatrophy in trauma-induced anteior horn dilation. Brain Injury, 8, 565–569.
Anderson, C. V., & Bigler, E. D. (1995). Ventricular dilation, cortical atrophy, andneuropsychological outcome following traumatic brain injury. The Journal ofNeuropsychiatry and the Clinical Neurosciences, 7, 42–48.
Anderson, C. V., Wood, D. M. G., Bigler, E. D., & Blatter, D. D. (1996). Lesion volume,injury severity, and thalamic integrity following head injury. Journal ofNeurotrauma, 13, 59–65.
Arenivas, A., Diaz-Arrastia, R., Spence, J., Cullum, C. M., Krishnan, K., Bosworth, C.,et al. (2012). Three approaches to investigating functional compromise to thedefault mode network after traumatic axonal injury. Brain Imaging and Behavior,13, 1–13.
Axmacher, N., Mormann, F., Fernandez, G., Cohen, M. X., Elger, C. E., & Fell, J. (2007).Sustained neural activity patterns during working memory in the humanmedial temporal lobe. Journal of Neuroscience, 27, 7807–7816.
Baddeley, A., Emslie, H., & Nimmo-Smith, I. (1994). Doors and people. Bury StEdmunds: Thames Valley Test Company.
Beer, A. L., Plank, T., & Greenlee, M. W. (2011). Diffusion tensor imaging showswhite matter tracts between human auditory and visual cortex. ExperimentalBrain Research, 213, 299–308.
Bendlin, B. B., Ries, M. L., Lazar, M., Alexander, A. L., Dempsey, R. J., Rowley, H. A.,et al. (2008). Longitudinal changes in patients with traumatic brain injuryassessed with diffusion-tensor and volumetric imaging. Neuroimage, 42,503–514.
Benton, A. L., Hamsher, K., & Rey, G. J. (1994). Multilingual aphasia examination (3rded.). Iowa Cita, IA: AJA Associates.
Bigler, E. D. (2001). Quantitative magnetic resonance imaging in traumatic braininjury. The Journal of Head Trauma Rehabilitation, 16, 117–134.
Bigler, E. D. (2007). Anterior and middle cranial fossa in traumatic brain injury:Relevant neuroanatomy and neuropathology in the study of neuropsychologicaloutcome. Neuropsychology, 21, 515–531.
Bigler, E. D., Abildskov, T. J., Wilde, E. A., McCauley, S. R., Li, X. Q., Merkley, T. L., et al.(2010). Diffuse damage in pediatric traumatic brain injury: A comparison ofautomated versus operator-controlled quantification methods. Neuroimage, 50,1017–1026.
Bigler, E. D., Anderson, C. V., & Blatter, D. D. (2002). Temporal lobe morphology innormal aging and traumatic brain injury. American Journal of Neuroradiology, 23,255–266.
Bigler, E. D., Blatter, D. D., Anderson, C. V., Johnson, S. C., Gale, S. D., Hopkins, R. O.,et al. (1997). Hippocampal volume in normal aging and traumatic brain injury.American Journal of Neuroradiology, 18, 11–23.
Bigler, E. D., Kurth, S. M., Blatter, D., & Abildskov, T. J. (1992). Degenerative changesin traumatic brain injury – Postinjury magnetic-resonance identifiedventricular expansion compared to pre-injury levels. Brain Research Bulletin,28, 651–653.
Bonnelle, V., Ham, T. E., Leech, R., Kinnunen, K. M., Mehta, M. A., Greenwood, R. J.,et al. (2012). Salience network integrity predicts default mode network functionafter traumatic brain injury. Proceedings of the National Academy of Sciences ofThe United States of America, 109, 4690–4695.
Bonnelle, V., Leech, R., Kinnunen, K. M., Ham, T. E., Beckmann, C. F., De Boissezon, X.,et al. (2011). Default mode network connectivity predicts sustained attentiondeficits after traumatic brain injury. Journal of Neuroscience, 31, 13442–13451.
Brown, A. W., Malec, J. F., McClelland, R. L., Diehl, N. N., Englander, J., & Cifu, D. X.(2005). Clinical elements that predict outcome after traumatic brain injury: Aprospective multicentre recursive partitioning (decision-tree) analysis. Journalof Neurotrauma, 22, 1040–1051.
Buckner, R. L., Kelley, W. M., & Petersen, S. E. (1999). Frontal cortex contributes tohuman memory formation. Nature Neuroscience, 2, 311–314.
Burgess, P. W., & Shallice, T. (1997). The hayling and brixton tests. Bury St Edmunds:Thames Valley Test Company.
Caeyenberghs, K., Leemans, A., Heitger, M. H., Leunissen, I., Dhollander, T., Sunaert,S., et al. (2012). Graph analysis of functional brain networks for cognitivecontrol of action in traumatic brain injury. Brain, 135, 1293–1307.
Chan, R. C. (2000). Attentional deficits in patients with closed head injury: A furtherstudy to the discriminative validity of the test of everyday attention. BrainInjury, 14, 227–236.
Cohen, J. D., Perlstein, W. M., Braver, T. S., Nystrom, L. E., Noll, D. C., Jonides, J., et al.(1997). Temporal dynamics of brain activation during a working memory task.Nature, 386, 604–608.
Coughhlan, A. K., Oddy, M., Crawford, J. R. (2007). Birt memory and informationprocessing battery. London: Brain Injury Rehabilitation Trust.
Dale, A. M., Fischl, B., & Sereno, M. I. (1999). Cortical surface-based analysis – I.Segmentation and surface reconstruction. Neuroimage, 9, 179–194.
de la Plata, C. A. M., Hart, T., Hammond, F. H., Frol, A. B., Hudak, A., Harper, C. R., et al.(2008). Impact of age on long-term recovery from traumatic brain injury.Archives of Physical Medicine and Rehabilitation, 89, 896–903.
Desikan, R. S., Segonne, F., Fischl, B., Quinn, B. T., Dickerson, B. C., Blacker, D., et al.(2006). An automated labeling system for subdividing the human cerebralcortex on MRI scans into gyral based regions of interest. Neuroimage, 31,968–980.
Desposito, M., Detre, J. A., Alsop, D. C., Shin, R. K., Atlas, S., & Grossman, M. (1995).The neural basis of the central executive system of working-memory. Nature,378, 279–281.
Destrieux, C., Fischl, B., Dale, A., & Halgren, E. (2010). Automatic parcellation ofhuman cortical gyri and sulci using standard anatomical nomenclature.Neuroimage, 53, 1–15.
Dewey, J., Hana, G., Russell, T., Price, J., McCaffrey Harezlak, J., et al. (2010).Reliability and validity of MRI-based automated volumetry software relative toauto-assisted manual measurement of subcortical structures in HIV-infectedpatients from a multisite study. Neuroimage, 51, 1334–1344.
Dikmen, S. S., Machamer, J. E., Winn, H. R., & Temkin, N. R. (1995).Neuropsychological outcome at 1-year post head injury. Neuropsychology, 9,80–90.
Draper, K., & Ponsford, J. (2008). Cognitive functioning ten years following traumaticbrain injury and rehabilitation. Neuropsychology, 22, 618–625.
Eichenbaum, H., Yonelinas, A. P., & Ranganath, C. (2007). The medial temporallobe and recognition memory. Annual Review of Neuroscience, 302007,123–152.
Fischl, B. (2012). FreeSurfer. Neuroimage, 62, 774–781.Fischl, B., & Dale, A. M. (2000). Measuring the thickness of the human cerebral
cortex from magnetic resonance images. Proceedings of the National Academy ofSciences of the United States of America, 97, 11050–11055.
Fischl, B., Sereno, M. I., & Dale, A. M. (1999a). Cortical surface-based analysis – II:Inflation, flattening, and a surface-based coordinate system. Neuroimage, 9,195–207.
Fischl, B., Sereno, M. I., Tootell, R. B. H., & Dale, A. M. (1999b). High-resolutionintersubject averaging and a coordinate system for the cortical surface. HumanBrain Mapping, 8, 272–284.
Fischl, B., van der Kouwe, A., Destrieux, C., Halgren, E., Segonne, F., Salat, D. H., et al.(2004). Automatically parcellating the human cerebral cortex. Cerebral Cortex,14, 11–22.
Gale, S. D., Baxter, L., Roundy, N., & Johnson, S. C. (2005). Traumatic brain injury andgrey matter concentration: A preliminary voxel based morphometry study.Journal of Neurology, Neurosurgery, and Psychiatry, 76, 984–988.
Giovagnoli, A. R., Del Pesce, M., Mascheroni, S., Simoncelli, M., Laiacona, M., &Capitani, E. (1996). Trail Making Test: Normative values from 287 normal adultcontrols. Italian Journal of Neurological Sciences, 17, 305–309.
Hillary, F. G., Medaglia, J. D., Gates, K., Molenaar, P. C., Slocomb, J., Peechatka, A.,et al. (2011). Examining working memory task acquisition in a disrupted neuralnetwork. Brain, 134, 1555–1570.
Hinton-Bayre, A. D., Geffen, G., & McFarland, K. (1997). Mild head injury andspeed of information processing: A prosepctive study of professional rugbyleague players. Journal of Clinical and Experimental Neuropsychology, 19,275–289.
Hudak, A., Warner, M., de la Plata, C. M., Moore, C., Harper, C., & Diaz-Arrastia, R.(2011). Brain morphometry changes and depressive symptoms after traumaticbrain injury. Psychiatry Research: Neuroimaging, 191, 160–165.
Hutton, C., Draganski, B., Ashburner, J., & Weiskopf, N. (2009). A comparisonbetween voxel-based cortical thickness and voxel-based morphometry innormal aging. Neuroimage, 48, 371–380.
Kinsella, G., Murtagh, D., Landry, A., Homfray, K., Hammond, M., O’Beirne, L., et al.(1996). Everyday memory following traumatic brain injury. Brain Injury, 10,499–507.
Kirchhoff, B. A., Wagner, A. D., Maril, A., & Stern, C. E. (2000). Prefrontal-temporalcircuitry for episodic encoding and subsequent memory. Journal of Neuroscience,20, 6173–6180.
Kumar, S., Rao, S. L., Chandramouli, B. A., & Pillai, S. V. (2009). Reduction offunctional brain connectivity in mild traumatic brain injury during workingmemory. Journal of Neurotrauma, 26, 665–675.
Levine, B., Kovacevic, N., Nica, E., Cheung, G., Gao, F., Schwartz, M., et al. (2008). TheToronto traumatic brain injury study: Injury severity and quantified MRI.Neurology, 70, 771–778.
MacKenzie, J. D., Siddiqi, F., Babb, J. S., Bagley, L. J., Mannon, L. J., Sinson, G. P., et al.(2002). Brain atrophy in mild or moderate traumatic brain injury: Alongitudinal quantitative analysis. American Journal of Neuroradiology, 23,1509–1515.
Makris, N., Preti, M. G., Asami, T., Pelavin, P., Campbell, B., Papadimitriou, G. M., et al.(2012). Human middle longitudinal fascicle: Variations in patterns ofanatomical connections. Brain Structure and Function. http://dx.doi.org/10.1007/s00429-012-0441-2.
Marquez de la Plata, C. D., Garces, J., Shokri Kojori, E., Grinnan, J., Krishnan, K.,Pidikiti, R., et al. (2011). Deficits in functional connectivity of hippocampal andfrontal lobe circuits after traumatic axonal injury. Archives of Neurology, 68,74–84.
Matsumoto, R., Nair, D. R., LaPresto, E., Najm, I., Bingaman, W., Shibasaki, H., et al.(2004). Functional connectivity in the human language system: A cortico-cortical evoked potential study. Brain, 127, 2316–2330.

44 G. Spitz et al. / Brain and Cognition 83 (2013) 34–44
Mayer, A. R., Yang, Z., Yeo, R. A., Pena, A., Ling, J. M., Mannell, M. V., et al. (2012). Afunctional MRI study of multimodal selective attention following mildtraumatic brain injury. Brain Imaging and Behavior, 6, 343–354.
McCauley, S. R., Wilde, E. A., Merkley, T. L., Schnelle, K. P., Bigler, E. D., Hunter, J. V.,et al. (2010). Patterns of cortical thinning in relation to event-based prospectivememory performance three months after moderate to severe traumatic braininjury in children. Journal of Head Trauma Rehabilitation, 35, 318–332.
Morey, R. A., Petty, C. M., Xu, Y., Hayes, J. P., Wagner, H. R., Lewis, D. V., et al. (2009).A comparison of automated segmentation and manual tracing for quantifyinghippocampal and amygdala volumes. Neuroimage, 45, 855–866.
Morris, R. G., Miotto, E. C., Feigenbaum, J. D., Bullock, P., & Polkey, C. E. (1997).Planning ability after frontal and temporal lobe lesions in humans: The effectsof selection equivocation and working memory load. Cognitive Neuropsychology,14, 1007–1027.
Ng, K., Mikulis, D. J., Glazer, J., Kabani, N., Till, C., Greenberg, G., et al. (2008).Magnetic resonance imaging evidence of progression of subacute brain atrophyin moderate to severe traumatic brain injury. Archives of Physical Medicine andRehabilitation, 89, S35–S44.
Novack, T. A., Bush, B. A., Meythaler, J. M., & Canupp, K. (2001). Outcome aftertraumatic brain injury: Pathway analysis of contributions from premorbid,injury severity, and recovery variables. Archives of Physical Medicine andRehabilitation, 82, 300–305.
Olson, I. R., Page, K., Moore, K. S., Chatterjee, A., & Verfaellie, M. (2006). Workingmemory for conjunctions relies on the medial temporal lobe. Journal ofNeuroscience, 26, 4596–4601.
Owen, A. M., Morris, R. G., Sahakian, B. J., Polkey, C. E., & Robbins, T. W. (1996).Double dissociations of memory and executive functions in working memorytasks following frontal lobe excisions, temporal lobe excisions or amygdalo-hippocampectomy in man. Brain, 119, 1597–1615.
Park, H., Kang, E., Kang, H., Kim, J. S., Jensen, O., Chung, C. K., et al. (2011). Cross-frequency power correlations reveal the right superior temporal gyrus as a hubregion during working memory maintenance. Brain Connectivity, 1, 460–472.
Ponsford, J., Olver, J. H., & Curran, C. (1995). A profile of outcome: 2 Years aftertraumatic brain injury. Brain Injury, 9, 1–10.
Reitan, R. M., & Wolfson, D. (1988). The halstead-reitan neuropsychological testbattery. Tucson, AZ: Neuropsychology Press.
Salmond, C. H., Chatfield, D. A., Menon, D. K., Pickard, J. D., & Sahakian, B. J. (2005).Cognitive sequelae of head injury: Involvement of basal forebrain andassociated structures. Brain, 128, 189–200.
Schönberger, M., Ponsford, J., Reutens, D., Beare, R., & O’Sullivan, R. (2009). Therelationship between age, injury severity, and MRI findings after traumaticbrain injury. Journal of Neurotrauma, 26, 2157–2167.
Shen, L., Saykin, A. J., Kim, S., Firpi, H. A., West, J. D., Risacher, S. L., et al. (2010).Comparison of manual and automated determination of hippocampal volumesin MCI and early AD. Brain Imaging and Behavior, 4, 86–95.
Sidaros, A., Skimminge, A., Liptrot, M. G., Sidaros, K., Engberg, A. W., Herning, M.,et al. (2009). Long-term global and regional brain volume changes followingsevere traumatic brain injury: A longitudinal study with clinical correlates.Neuroimage, 44, 1–8.
Smith, A. (1973). Symbol digit modalities test. Los Angeles: Western PsychologicalServices.
Spitz, G., Ponsford, J. L., Rudzki, D., & Maller, J. J. (2012). Association betweencognitive performance and functional outcome following traumatic braininjury: A longitudinal multilevel examination. Neuropsychology. http://dx.doi.org/10.1037/a0029239.
Squire, L. R., & Wixted, J. T. (2011). The cognitive neuroscience of human memorysince HM. Annual Review of Neuroscience, 342011, 259–288.
Strangman, G. E., O’Neil-Pirozzi, T. M., Supelana, C., Goldstein, R., Katz, D. I., & Glenn,M. B. (2010). Regional brain morphometry predicts memory rehabilitationoutcome after traumatic brain injury. Frontiers in Human Neuroscience, 4, 181.
Sullivan, E. V., & Pfefferbaum, A. (2007). Neuroradiological characterization ofnormal adult ageing. British Journal of Radiology, 80, S99–S108.
Thatcher, R. W., Camacho, M., Salazar, A., Linden, C., Biver, C., & Clarke, L. (1997).Quantitative MRI of the grey-white matter distribution in traumatic braininjury. Journal of Neurotrauma, 14, 1–14.
Todd, J. J., & Marois, R. (2004). Capacity limit of visual short-term memory in humanposterior parietal cortex. Nature, 428, 751–754.
Tomaiuolo, F., Worsely, K. J., Lerch, J., Di Paola, M., Carlesimo, G. A., Bonanni, R., et al.(2005). Changes in white matter in long-term survivors of severe non-missiletraumatic brain injury: A computational analysis of magnetic resonance images.Journal of Neurotrauma, 22, 76–82.
Trivedi, M. A., Ward, M. A., Hess, T. M., Gale, S. D., Dempsey, R. J., Rowley, H. A., et al.(2007). Longitudinal changes in global brain volume between 79 and 409 daysafter traumatic brain injury: Relationship with duration of coma. Journal ofNeurotrauma, 24, 766–771.
Turken, A. U., Herron, T. J., Kang, X., O’Connor, L. E., Sorenson, D. J., Baldo, J. V., et al.(2009). Multimodal surface-based morphometry reveals diffuse corticalatrophy in traumatic brain injury. BMC Medical Imaging, 9, 20.
Vannorsdall, T. D., Cascella, N. G., Rao, V., Pearlson, G. D., Gordon, B., & Schretlen, D. J.(2010). A morphometric analysis of neuroanatomic abnormalities in traumaticbrain injury. The Journal of Neuropsychiatry and Clinical Neurosciences, 22,173–181.
Wagner, A. D., Shannon, B. J., Kahn, I., & Buckner, R. L. (2005). Parietal lobecontributions to episodic memory retrieval. Trends in Cognitive Sciences, 9,445–453.
Warner, M. A., Marquez de la Plata, C., Spence, J., Wang, J. Y., Harper, C., et al. (2010).Assessing spatial relationships between axonal integrity, regional brainvolumes, and neuropsychological outcomes after traumatic axonal injury.Journal of Neurotrauma, 27, 2121–2130.
Wechsler, D. (1997). Wechsler memory scale (3rd ed.). San Antonio, TX: ThePsychological Corporation.
Wechsler, D. (2008). Wechsler adult intelligence scale (4th ed.). San Antonio, TX:Pearson.
Wilde, E. A., Newsome, M. R., Bigler, E. D., Pertab, J., Merkley, T. L., Hanten, G., et al.(2011). Brain imaging correlates of verbal working memory in children followingtraumatic brain injury. International Journal of Psychophysiology, 82, 86–96.
Yonelinas, A. P., Otten, L. J., Shaw, K. N., & Rugg, M. D. (2005). Separating the brainregions involved in recollection and familiarity in recognition memory. Journalof Neuroscience, 25, 3002–3008.
Yurgelun-Todd, D. A., Bueler, C. E., McGlade, E. C., Churchwell, J. C., Brenner, L. A., &Lopez-Larson, M. P. (2011). Neuroimaging correlates of traumatic brain injuryand suicidal behavior. The Journal of Head Trauma Rehabilitation, 26, 276–289.
Copyright © 2022 FDOKUMEN




![[Posterior cortical atrophy]](https://static.fdokumen.com/doc/165x107/6331b9d14e01430403005392/posterior-cortical-atrophy.jpg)















