Thornton Carmody chapter from Carlstedt Handbook
46
This chapter has two goals: to provide the reader with a general awareness of traumatic brain injury (TBI), mild in particular, and the multiple complex issues involved in this area, and to offer a detailed understanding of the role of quantitative electroencephalography (qEEG) in the assessment and treatment of the cognitive deficits of the TBI patient. Sections I–IV address the first goal. Sec- tion I discusses definitions, sports, vulnerable groups, the concept of spontaneous cure, and roles of loss of consciousness and post-traumatic amnesia criteria. Sec- tion II addresses the biomechanics of a TBI. Section III discusses the physical damage to the brain caused by the TBI as measured by modern medical imaging. Sec- tion IV reviews the neuropsychological and emotional results of a TBI that may be clinically manifested in a patient. The second goal is addressed in section V, which discusses the scientific basics of qEEG technology, de- velopment of the technology over the past two decades, and its application in the assessment of the TBI patient. The coordinated allocation of resources (CAR) model of brain functioning, which employs a cognitive chal- lenge or activation method, is discussed in the context of how a TBI specifically affects brain and cognitive functioning. An example of the differences between the normative and the TBI response patterns are presented in detail for the cognitive task of auditory memory. We review the results of rehabilitation efforts employing the CAR model, which have proved to be dramatically superior to the minimal results of traditional cognitive rehabilitation models. SECTION I Definition, Measurement and Incidence/ Prevalence of TBI TBI is a major medical, social, and financial problem in the United States. The annual cost of 1.5 million cases is $60 billion dollars. Causes of TBI include motor vehi- cle accidents, assaults, sports activities, falls, and blast injuries in the Iraq war. The most prevalent type of TBI is mild TBI, which doesn’t involve prolonged periods of coma. 18 Quantitative Electro- encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury Kirtley E. Thornton Dennis P. Carmody Copyright Springer Publishing Company
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Thornton Carmody chapter from Carlstedt Handbook

This chapter has two goals: to provide the reader with a general awareness of traumatic brain injury (TBI), mild in particular, and the multiple complex issues involved in this area, and to offer a detailed understanding of the role of quantitative electroencephalography (qEEG) in the assessment and treatment of the cognitive defi cits of the TBI patient. Sections I–IV address the fi rst goal. Sec-tion I discusses defi nitions, sports, vulnerable groups, the concept of spontaneous cure, and roles of loss of consciousness and post-traumatic amnesia criteria. Sec-tion II addresses the biomechanics of a TBI. Section III discusses the physical damage to the brain caused by the TBI as measured by modern medical imaging. Sec-tion IV reviews the neuropsychological and emotional results of a TBI that may be clinically manifested in a patient.
The second goal is addressed in section V, which discusses the scientifi c basics of qEEG technology, de-velopment of the technology over the past two decades, and its application in the assessment of the TBI patient. The coordinated allocation of resources (CAR) model of brain functioning, which employs a cognitive chal-lenge or activation method, is discussed in the context
of how a TBI specifi cally affects brain and cognitive functioning. An example of the differences between the normative and the TBI response patterns are presented in detail for the cognitive task of auditory memory. We review the results of rehabilitation efforts employing the CAR model, which have proved to be dramatically superior to the minimal results of traditional cognitive rehabilitation models.
SECTION I
Defi nition, Measurement and Incidence/Prevalence of TBI TBI is a major medical, social, and fi nancial problem in the United States. The annual cost of 1.5 million cases is $60 billion dollars. Causes of TBI include motor vehi-cle accidents, assaults, sports activities, falls, and blast injuries in the Iraq war. The most prevalent type of TBI is mild TBI, which doesn’t involve prolonged periods of coma.
18 Quantitative Electro-encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury Kirtley E. Thornton Dennis P. Carmody
Copyright Springer Publishing Company

464 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
Defi nition of TBI The Centers for Disease Control and Prevention (2008) defi nes traumatic brain injury (TBI) as a blow or jolt to the head or a penetrating head injury that disrupts the normal function of the brain, which results in concus-sion (functional defi cits) or contusion (bruising). The blow or jolt can be a direct impact or non-impact event, such as whiplash. The severity of a TBI may range from mild to severe. The signs can be subtle, and symp-toms may not appear for days or weeks or may even be missed, as individuals may look fi ne even though they act or feel differently (Centers for Disease Control and Prevention, 2008). The World Health Organization (1992) codes the injury in the International Statistical Classifi cation of Diseases and Related Health Problems as ICD-S06, intracranial injury.
The most prevalent fi nding of TBI is mild TBI (MTBI), which is estimated to constitute 70%–90% cases of TBI (Torg, 1991). The Centers for Disease Con-trol and Prevention (2008) indicated that MTBI is an injury to the head as a result of blunt trauma or accelera-tion or deceleration forces that result in either observed or self-reported conditions of confusion, disorientation, memory dysfunction, or loss of consciousness (LOC). Recent defi nitions of MTBI formulated by the Depart-ment of Defense and the Department of Veterans Affairs (Helmick et al., 2006) are consistent with national defi -nitions (Borg et al., 2004; Centers for Disease Control and Prevention, 2003).
The clinical diagnosis and classifi cation of mild TBI are based on several factors, including whether the length of the LOC is less than 30 minutes and whether post-traumatic amnesia (PTA) is greater than 24 hours, in addition to physical and neurological examinations (Borg et al., 2004). As we discuss, the criteria of LOC and PTA present some problems in diagnosis of TBI and are not always useful or clear indicators of possible cog-nitive effects of a MTBI. The classifi cation of compli-cated MTBI has been used in cases with neurological defi cits that are evident on neuroimaging procedures.
Measurement of TBI Severity Scales have been developed for use in rapid assessment of TBI, such as the Rancho Los Amigos Scale and the Glasgow Coma Scale (GCS). The better known is the GCS, which is used in emergency departments to evaluate the likelihood of coma and to assess loss of consciousness (Teasdale & Jennett, 1974). It is simple to administer, has a high degree of interobserver reliability (Teasdale, Knill-Jones, & van der Sande, 1978), and correlates well with outcome following severe brain injury (Teasdale &
Jennett, 1976). The GCS provides rating scales for best motor response (obeys commands fully to no response), best verbal response (alert and oriented to no sounds), and best eye opening (spontaneous eye opening to no eye opening) in order to generate a severity score rang-ing from 3 to 15. Three grades of severity are recognized: severe (8 or less), moderate (9–12), and mild (13–15; Jennett, 2005). Lower scores are associated with poorer functioning. While the GCS is useful in evaluating coma, there are questions about the predictive power of scores that are higher than the cutoff score of 8 for coma. The original studies required that coma be present for at least 6 hours in order to use the GCS score as a tool for as-sessing outcome (Teasdale & Jennett, 1974, 1976). The scale was not designed to diagnose patients with mild or even moderate TBI, nor was it intended to be used in place of a neurological examination. Instead, the GCS was designed to provide an easy-to-use assessment tool for serial evaluations by relatively inexperienced care providers, and to facilitate communication between care providers on rotating shifts. While single, isolated GCS scores are of limited value, serial scores are more predic-tive. Some 13% of patients who eventually enter into coma had initial GCS scores of 15 (Jennett et al., 1977). A GCS score of 15 is of no help in determining whether brain injury has occurred.
Critics of the use of the GCS point to problems in di-agnosing TBI (Laureys, Piret, & Ledoux, 2005), predicting long-term outcome (Waxman, Sundine, & Young, 1991), and predicting death versus vegetative coma (Braak-man, 1992). GCS scores in the mild range (13 – 14 vs. 15) are not associated with the outcome measures of neurobehavioral symptoms and signs, psychological is-sues, psychiatric diagnosis, functional and psychosocial outcome, frequency of somatic complaints, or return-to-work rates (McCullagh, Oucherlony, Protzner, Blair, & Feinstein, 2001), despite the fact that the 13–14 group has more CT abnormalities and longer PTA duration. The criteria for MTBI examines the behavior at the time of the event but not the typical symptoms that follow MTBI, which include problems in memory, concentra-tion, and decision making; slowness; headache; fatiga-bility; confusion; mood vacillations; sleep problems; dizziness; balance problems; increased sensitivity to light or sound; changes in vision, smell, taste; nausea; and ringing in the ears (Centers for Disease Control and Prevention, 2003).
Incidence and Prevalence of TBI TBI is a major cause of death and disability in the United States, with a yearly incidence of 1.5 million; 1.1 million presently live with a disability related to the TBI (Thur-
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 465
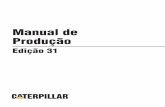
man, Alverson, Dunn, Guerrero, & Sniezek, 1999). As a result of these injuries, 50,000 die, 230,000 are hos-pitalized and survive, and an estimated 80,000–90,000 experience the onset of long-term disability (Thurman et al., 1999). Table 18.1 indicates the breakdown of the causes of TBI (Centers for Disease Control and Preven-tion, 2008).
Gender and age are related to the relative risk for TBI. Males are about twice as likely as females to sus-tain a TBI. The two age groups at highest risk for TBI are infants and children up to 4 years of age and teenag-ers between the ages of 15 and 19. Adults age 75 years and older have the highest rates of TBI-related hospi-talization and death (Centers for Disease Control and Prevention, 2008). Some of the TBI estimates in the lit-erature are based upon emergency room records. How-ever, there is a tendency to underreport, as is evident in one study in which 56% of MTBI patients identifi ed by interview did not have an emergency department record of a MTBI (J. M. Powell, Ferraro, Dikmen, Tem-kin, & Bell, 2008). Interestingly, the highest emergency department identifi cation occurred when there was a LOC and the lowest when the symptom was confusion. This phenomenon of underreporting casts suspicion on all estimates of MTBI based on emergency department records. The economic impact of MTBI is substantial, accounting for about 44% of the $56 billion annual cost of TBI in the United States (Thurman, 2001). It is es-timated that the cost in the United States in 2000 was $60 billion, which takes into consideration both the di-rect medical cost and the indirect cost, such as lost pro-ductivity caused by TBI (Finkelstein, Corso, & Miller, 2006).
Events Including Sports The third major cause of TBI is events; this includes sports TBI. Investigators of sports TBI have developed their own body of research literature, including return-to-play criteria. The Centers for Disease Control and Prevention (2008) estimates that there are 1.6–3.8 mil-lion sports- and recreation-related concussions in the United States each year.
Breakdown by Sports Activities
TBI in sports is of particular concern given that children and adolescents compete in sports. For example, one report estimates that some 1.25 million athletes com-pete in contact sports at the high school level (Lovell et al., 2003). Another report examined TBI occurring in 10 sports at 235 high schools and found football ac-counting for 63% and wrestling for 10% of TBI (J. W. Powell & Barber-Foss, 1999). Data for the years 1985–2000 indicate that ice hockey and rugby had the highest incidence of concussion for high school, college, and amateur athletes (Koh, Cassidy, & Watkinson, 2003). At the recreational level, female taekwondo participants and male boxers had the highest frequency of concus-sion (Koh & Cassidy, 2004).
However, the estimates of TBI in high school sports are probably on the low side. For example, a survey of high school football players found that only 47% of the athletes reported a concussion at the time of injury (Mc-Crea, Hammeke, Olsen, Leo, & Guskiewicz, 2004). The reasons the students gave for not reporting the concus-sion were belief that the injury was not serious enough to merit medical attention (66%), desire to stay in the game (41%), failure to recognize the occurrence of a concussion (36%), and desire not to disappoint their teammates (22%).
Criteria for Return to Play
While MTBI is seen frequently in athletes, severity grading and management remain controversial (Gebke, 2002). Evaluation of the concussed athlete is essential before a recommendation to return to play can be made (Putukian, 2006). Often these decisions are made by the certifi ed athletic trainer either on the fi eld or sideline during the game or at post-game follow-up. As such, these decisions frequently do not involve the clinician. While MTBI occurs in athletes of all ages, many inju-ries are unreported, particularly among recreational athletes. Younger athletes are less likely than collegiate athlete to have access to on-fi eld medical care (Lovell, Collins, Iverson, Johnston, & Bradley, 2004).
18.1 Causes of Traumatic Brain Injury
CAUSE INCIDENCE
Falls28%
Motor vehicle accidents 20%
Struck by/against events 19%
Assaults 11%
From What Is Traumatic Brain Injury ? by Centers for Disease Control and Prevention, 2008. Retrieved from http://www.cdc.gov/ncipc/tbi/tbi.htm.
Copyright Springer Publishing Company

466 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
Premature return to play exposes athletes to addi-tional risk of more serious brain injury and leads to a worsening of symptoms and lowered threshold for re-injury, as well as the possibility of second impact syn-drome. Second impact syndrome is defi ned as a second injury following incomplete recovery from an initial in-jury (Lovell et al., 2004) and represents a serious issue as one consequence is death. The decision to return the athlete to play resolves around the identifi cation of a concussion. Concussion is typically associated with grossly normal structural neuroimaging studies. The cornerstone of concussion management is rest until all symptoms resolve, then a graded program of exer-tion before the athlete returns to sport (McCrory et al., 2005). A research area that has been gaining attention is balance control. The clinician may run across these measures in clinical reports in the future. The Balance Error Scoring System for evaluation of postural insta-bility has been recommended (Guskiewicz, 2001). This balance measure typically resolves in 3–5 days post-injury (McCrea et al., 2003).
An international meeting of professionals involved in TBI resulted in the Prague guidelines (McCrory et al., 2005). One of the guidelines involves a distinction be-tween simple and complex concussions. In the simple concussion diagnosis, the LOC is less than 1 minute and the symptoms resolve within 7–10 days without complications. In the complex concussion diagnosis, there is a prolonged LOC and the symptoms last longer than 7–10 days or there is a history of multiple concus-sions. The 7-day recovery time frame is consistent with animal research models demonstrating neurometabolic irregularities for 7–10 days after injury (Hovda, Prins, & Becker, 1999).
Other Prague guideline recommendations are that players should not be allowed to return to play in the current game or practice and should not be left alone, and regular monitoring for deterioration of function is essential during the initial few hours after injury. Return to play must follow a medically supervised se-ries of steps involving a graded program of exertion, and players should not return to play while symptoms persist. However, the determination of a concussion is fraught with lack of precision. LOC has proved to be of limited value, however, in return-to-play decisions, as LOC is reported for only 9% of those sustaining a concussion (Guskiewicz, Weaver, Padua, & Garrett, 2000). In addition, the presence and duration of LOC and PTA are not used to differentiate between the symptomatic and asymptomatic sports-related MTBI groups (Collie, Makdissi, Maruff, Bennell, & McCrory, 2006). However, a MTBI group with LOC of 15 minutes
experienced more depression than a severe TBI group (Alexander, 1992). Mental status changes have proved to be useful in return-to-play decisions. Athletes with duration of on-fi eld mental status changes lasting less than 5 minutes demonstrated a return to baseline within 4 days. Athletes with post-injury anterograde amnesia, retrograde amnesia, or disorientation lasting longer than 5 minutes, as a group, did not fully recover in 7 days (Lovell et al., 2003). Resolution of the clinical and cognitive symptoms typically follows a sequential course.
TBI Sequelae in Vulnerable Groups: Pediatric, Repeat Concussions, the Elderly, and Females When a clinician determines that his or her patient has a history of a TBI, it is important to know more than just the severity of the injury, but also the age, sex, and previous head injury history of the person who experi-enced the injury. The research reviewed in this section indicates that some individuals are more susceptible to the negative effects of a TBI than others.
Pediatric
Children and adolescent athletes represent a distinct group in that conservative management of concussion is required (Lovell & Fazio, 2008). For example, high school athletes with concussion had prolonged memory dysfunction compared with college athletes with con-cussion (Field, Collins, Lovell, & Maroon, 2003). Head injuries account for a large portion of school related injuries (Di Scala, Gallagher, & Schneps, 1997). Chil-dren with preexisting disabilities are at increased risk of head injury (Limbos, Ramirez, Park, Peek-Asa, & Kraus, 2004; Max et al., 2004), while those with specifi c pre-existing learning disabilities are more susceptible to the effects of a TBI (Collins et al., 1999)
TBI in children is related to defi cits in cognitive functioning, personality (Max et al., 2004), and emo-tional processing. For example, TBI affects immediate and short-term memory (Catroppa & Anderson, 2002), working memory (Levin et al., 2004; Roncadin, Guger, Archibald, Barnes, & Dennis, 2004), and attention (Cat-roppa & Anderson, 1999; Goldacre, Abisgold, Yeates, & Seagroatt, 2006). Associations have been found between TBI and diagnoses of attention-defi cit/hyperactivity dis-order (Max et al., 2004; Scheibel et al., 2007). Intel-ligence is affected for up to a few years (Ewing-Cobbs, Fletcher, Levin, Francis, Davidson, & Miner, 1997; Ewing-
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 467
Cobbs et al., 2006) and attention can be defi cient up to 5 years post-injury (Catroppa, Anderson, Morse, Hari-tou, & Rosenfeld, 2007). In addition, functional defi cits in executive function and inhibitory control (Leblanc et al., 2005) last at least 2 years in severe TBI cases (An-derson & Catroppa, 2005; Ewing-Cobbs et al., 1998). Long-term defi cits (20 years post-injury) in children with complicated MTBI indicate that children are prob-ably more vulnerable to neuropsychological dysfunction than adults sustaining similar head injuries (Hessen, Nestvold, & Anderson, 2007).
It has also been argued that children “grow into the defi cits” as the specifi c cognitive defi cits become ap-parent years after the injury (Fletcher, Miner, & Ewing-Cobbs, 1987; Middleton, 2001). In section V we will discuss how the phenomenon might be manifested in the qEEG variables. Development of specifi c long-term learning disabilities is associated with multiple concus-sions in youth (Iverson, Gaetz, Lovell, & Collins, 2004; Kirkwood, Yeates, & Wilson, 2006). A younger brain may have longer recovery time because of its imma-turity (Field et al., 2003). One study indicated that TBI in children results in low self-esteem, loneliness, an-tisocial behavior, and prolonged memory defi cits (An-drews, Rose, & Johnson, 1998).
Repeat Concussions
Some 20% of college football players have two or more concussions during their career (Collins, Lovell, Iver-son, Cantu, Maroon, & Field, 2002). A history of previ-ous concussions is associated with decreased memory performance. For example, athletes who had a previous history of three or more concussions were 9 times more likely to demonstrate LOC and greater anterograde and retrograde amnesias (PTA) following a concussion than those without such a history, thus refl ecting a linger-ing vulnerability (Collins & Hawn, 2002; Collins et al., 2002). Athletes with a prior history of concussion were 7 times more likely to show decreased memory perfor-mance than matched cohorts (Iverson et al., 2004).
In a study of retired professional athletes with a history of concussions, more than 50% reported expe-riencing LOC or memory loss from at least one of their concussive episodes (Guskiewicz et al., 2007). Of those with one or two previous concussions, 12% reported that the injuries have had a permanent effect on their thinking and memory skills as they have gotten older. This incidence increased to 31% in retirees with three or more previous concussions, indicating a positive as-sociation between a higher number of concussions and the perception that those concussions negatively affect
cognitive functioning. There are studies of the outcomes of TBI in the professional football player showing the association between recurrent sport-related concussion and increased risk of both dementia-related syndromes and clinical depression (Guskiewicz et al., 2007). The dementia related syndromes are probably mediated by the E4 variant of the ApoE gene (Emmerling et al., 2000).
The Elderly and Females
The elderly are more negatively affected by TBI, as they show greater decline in the 5-year post-accident period than younger groups (Marquez de la Plata et al., 2008), are more likely to be hospitalized (2.5 times greater than those under 65), have poorer functional outcomes than younger TBI patients (Ashman et al., 2008), and have twice the mortality rates of younger TBI patients (under 64 years) in both mild and moderate TBI cases (Mosenthal et al., 2002).
According to a meta-analytic review of outcome literature, outcomes are worse in women than in men (Farace & Alves, 2000). Female high school and uni-versity athletes have signifi cantly greater declines than males in reaction times (simple and complex) within 7 days after their concussion (Broshek, Kaushik, Free-man, Erlanger, Webbe, & Barth, 2005). Furthermore, high school and college female soccer players are 1.2 to 2.5 times more likely to suffer a TBI than male soccer players (Ellemberg, Leclerc, Couture, & Daigle, 2007). In terms of cognitive functions, TBI female athletes dem-onstrated signifi cantly lower visual memory scores than male athletes (Covassin, Schatz, & Swanik, 2007).
From these research fi ndings, we suggest that the cognitive, personality, and social defi cits and prob-lems that are found in these groups may have as their source the TBI, whether the injury was reported or not (Thornton & Carmody, 2005). As such, many psycho-logical interventions that are successful with children without a history of TBI may not be helpful until the TBI defi cits in brain functioning have been successfully treated, especially if memory functioning was affected. The problem, however, is that cognitive rehabilitation interventions have not been found to be particularly effective (Thornton & Carmody, 2008). Section V will review the effectiveness of present cognitive rehabilita-tion models and discuss an intervention that has proved to be particularly effective, the CAR model for EEG bio-feedback. In order to understand the alterations in brain structure and functioning that occur as a result of TBI, in sections III and V we address the neuroimaging and qEEG studies of brain structure and function.
Copyright Springer Publishing Company

468 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
The Invalid Spontaneous Cure Concept There has been an implicit assumption and sometimes as well as explicit statements in the MTBI fi eld that somehow these brain problems spontaneously resolve or recover over time (Jay, 2000; Wood & McMillan, 2002). What is problematic about this concept is that it is unclear whether the word “recover” implies a spon-taneous cure or a compensation. A second assumption is that patients who still report symptoms after a certain period of time are most likely malingering or the symp-toms have psychological causes. The concept of resolu-tion implies either a spontaneous cure or a successful compensation by the brain. Despite the research we will present later in this chapter, some reports continue to assert that symptom persistence beyond 3 months after MTBI is psychogenic in nature (Binder, Rohling, & Lar-rabee, 1997; Kashluba, Hanks, Casey, & Millis, 2008). The concept of spontaneous cure is no longer an ap-propriate, viable, or even a valid concept, and a better model is one that involves compensation, although not necessarily a successful compensation, as some TBI pa-tients live with the cognitive consequences for the rest of their lives.
Initial Estimates
Initially it was thought that 50% of MTBI cases ex-perience recovery by 3 months post-injury, albeit in-complete in some cases (Dikmen, McLean, Temkin, & Wyler, 1986). Other research supports this general time frame in that post-concussive symptoms persisting be-tween 3 and 6 months post-injury occur in about 40% of persons with mild TBI (Ingebrigtsen, Waterloo, Mar-up-Jensen, Attner, & Romner, 1998; McCullagh et al., 2001). Some reports indicate a range of 1% to 20% of MTBI for long-term negative effects 6 months post-injury (Beetar, Guilmette, & Sparadeo, 1996; Deb, Lyons, Koutzoukis, Ali, & McCarthy, 1999; Leininger, Gram-ling, Farrell, Kreutzer, & Peck, 1990; Levin & Eisenberg, 1991). Factors that contribute to the long-term effect in-clude a previous history of TBI (Rimel, Giordani, Barth, Boll, & Jane, 1981), alcohol use at the time of accident (Ashman, Schwartz, Cantor, Hibbard, & Gordon, 2004), and female sex (Emerson, Headrick, & Vink, 1993). However, the long-term negative effect estimate of 20% of MTBI has come under increasing challenge by re-searchers who have indicated that there are symptoms at 6 months, with 50% of their MTBI patients reporting dizziness and headache, and about 75% reporting fa-tigue (McCullagh et al., 2001).
Estimates from Physical Measurement
Long-term effects have also been documented in physi-cal measurements, such as the protein S-100B serum. The serum S-100B is a peripheral biochemical marker of neural injury, including reactive gliosis, astrocytic death, and/or blood-brain barrier dysfunction (Wong, Rooney, & Bonser, 1999). Associations have been found between MTBI and S-100B (De Kruijk, Leffers, Men-heere, Meerhoff, Rutten, & Twijnstra, 2002). Neuropsy-chological defi cits were found in 74% ( N = 36) of MTBI cases at the 2-week testing point and 67% ( N = 29) at the 6-month testing point, even though all the pa-tients were fully functional on the Functional Indepen-dence Measure in terms of activities of daily living. At 6 months since accident, the MTBI group did not show any signs of intracranial pathology or EEG abnormality (no qEEG data). However, the MTBI group did show signifi cant neuropsychological defi cits in the individu-als with raised S-100B serum concentrations (about 50% of sample of 79 patients) at 6 months since the accident. In those patients with increased S-100B levels there was a twofold increase in severity of dizziness, headache, and memory problems. All the patients with normal S-100B levels 6 hours after the injury who were not reporting dizziness, nausea, or headaches were fully recovered at the 6-month time period. The S-100b level would indicate that about 50% of the MTBI pa-tients were still experiencing problems 6 months after the accident.
TBI Diagnosis Problems with Use of Loss-of-Consciousness and Post -Traumatic Amnesia Criteria There are negative and positive arguments for the use of LOC as a diagnostic criterion for TBI. On the positive side, the Prague guidelines (McCrory et al., 2005) make a distinction between simple and complex concussions. In the simple concussion diagnosis, the LOC is less than 1 minute and the symptoms resolve within 7–10 days without complications. It has also been reported that athletes who had a previous history of three concus-sions were 9.3 times more likely to demonstrate LOC and greater anterograde and retrograde amnesias fol-lowing a concussion than those without such a history (Collins & Hawn, 2002; Collins et al., 2002), refl ecting a lingering vulnerability. A MTBI group (LOC 15 min) experienced a signifi cantly higher proportion of cases
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 469
involving depression than a severe TBI group (Alexan-der, 1992).
On the negative side, when the patient comes into the ER there is a tendency for the diagnosis of TBI to be rendered when the patient reports an LOC (J. M. Powell et al., 2008), which may refl ect a diagnostic bias. LOC has also proved to be of limited value in return-to-play decisions, as LOC is reported for only 9% of those sustaining a concussion (Guskiewicz et al., 2000). In addition, the presence and duration of LOC do not dif-ferentiate between the symptomatic and asymptomatic sports-related MTBI groups (Collie et al., 2006). There are studies of the outcomes of TBI in professional foot-ball players showing the association between recurrent sport-related concussion and increased risk of demen-tia-related syndromes such as Alzheimer’s irregardless of the presence of LOC (Guskiewicz et al., 2005).
There are also arguments both for and against the usefulness of the PTA criteria for estimating severity. On the pro side, the GCS 13–14 group had more CT abnor-malities and longer PTA duration (McCullagh et al., 2001) than the group with a GCS of 15. On the negative side, there was no association between the GCS rating and outcome measures such as return to work, neurobehav-ioral symptoms, and frequency of somatic complaints. In addition, the presence and duration of PTA did not differentiate between the symptomatic and asymptom-atic sports-related MTBI groups (Collie et al., 2006).
SECTION II
The Biomechanics of a TBI The following description of the biomechanical, bio-physical, and biological forces that are produced by a TBI is provided to enable the reader to appreciate the complexity of a TBI. The TBI fi eld was unfortunately hampered initially, and to this day by the use of the term “mild,” which implies a minimal event. The somewhat detailed physical explanations that follow are intended, in part, to provide the reader with an appreciation of the physical dynamics that affect the human brain dur-ing a TBI.
There are six distinct biomechanical processes that have been described as likely to be involved in the in-duction of a concussive (loss of function) state (Shaw, 2002). Table 18.2 shows the processes in the both brain stem effects and non–brain stem effects. We provide a broad overview of the brain’s physical properties and the effects of physical forces involved in a TBI on the biology and neuroanatomy of the brain.
18.2 Biomechanical Processes in the Induction of a Concussive State
BRAIN STEM EFFECTS NON-BRAIN STEM EFFECTS
Hemispheres pivot on base
Impact between brain’s surface and skull—shearing/tearing of neurons
Head accelerates with respect to neck
Skull bone is depressed
Acceleration of head about axis of neck
Propagation of intracranial pressure waves
Adapted from “The Neurophysiology of Concussion,” by N. A. Shaw, 2002. Progress in Neurobiology, 67(4), 281–344.
Brain Neuroanatomy and Anatomy The human brain weighs about 3 pounds, has a jelly- or gelatin-like quality, and lies within the skull, surrounded by cerebral spinal fl uid (5.1 ounces). There are gender differences in the number of neocortical neurons; males (23 billion) have more neurons than females (19 billion) (Pakkenberg & Gundersen, 1997; Pakkenberg et al., 2003). Estimates of the number of synapses in the ce-rebral cortex are as high as 240 trillion (Koch, 1999). Just beneath the skull resides the cortical gray matter, a thin (.14–.20 inch) layer mainly composed of neurons, glia cells, axons, dendrites, and capillaries. From within the 6 layers of the gray matter the white matter bundles originate and send information to the other parts of the brain. About 5% of myelinated fi bers have their origin in the subcortex (the deeper structures in the brain) and connect the two hemispheres, while about 95% of the myelinated axons that are in the cortical white matter are located within the same hemisphere (Braitenberg, 1972, 1978). There are two important structural facts that are relevant to the TBI patient: (1) the white matter fi bers reside just beneath the gray matter and the inter-section of these two masses provides an opportunity for shearing forces to operate and (2) in the skull behind the eyes and in front of the temporal lobes are sets of jagged boney structures, including such structures as the sphenoid and ethmoid bones. These boney struc-tures are frequent points of impact for the brain.
The brain is composed of two main hemispheres (left/right) each of which has fi ve cortical lobes (frontal,
Copyright Springer Publishing Company

470 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
temporal, sensorimotor, parietal, and occipital). The functions of these lobes can be described very simplis-tically thusly: the frontal lobe controls executive func-tion, the temporal lobe controls memory and verbal functions, the sensorimotor lobe controls reception of sensory information and execution of motor impulses, the parietal lobe controls association areas, and the oc-cipital lobe controls visual processing. However, these broadly described functions do not do justice to the complexity of the system and multiple interactions in-volved in any specifi c cognitive task. This is apparent in the qEEG analysis of auditory memory presented in section V. The cerebellum and subcortical structures are also strongly involved in cognitive function.
Effects of Physical Forces on Biology in TBI Extensive analyses of the physical forces occurring during a TBI reveal the resultant biological effects. We present a brief overview of these non–brain stem forces and their effects. The classic biological effect of a TBI is diffuse axonal injury (DAI), which was fi rst described by Holbourn (1943) in examination of the mechani-cal forces of a TBI. His focus was on non–brain stem effects of the impact between the brain’s surface and skull (2a), resulting in the shearing or tearing of the neurons; this work helped explain that shear injury is caused by rotational forces and not by linear or trans-lational forces, in which all of an object moves in a straight line in unison.
Acceleration-deceleration forces can produce rota-tional movements in the brain. Two-thirds of DAI le-sions (damaged tissue) occur at the gray-white matter junction, where the density differences are the great-est. The research supports the following magnitude and direction (vector) concepts: “centripetal” force vector, where the pressure is highest at the outer cortex with a gradient to the subcortex and brain stem (Ommaya, Goldsmith, & Thibault, 2002), a rotational vector (Hol-bourn, 1943, 1945; Lee & Advani, 1970), and a shear vector (Advani, Ommaya, & Yang, 1982; Ommaya, Thi-bault, & Bandak, 1994). Most injuries occur in the gray matter of the frontal and temporal lobes, independent of the direction of impact to the skull (Ommaya, 1995; Sano, Nakamura, & Hirakaws, 1967). This refl ects the additional effect of the brain impacting on the jagged sphenoid and ethmoid bones. The second non–brain stem effect (2b) involves a deformation caused by a de-pressed skull bone and has not received much attention in the literature. The third non–brain stem effect (2c) is
the percussion shock wave that moves from the impact point and makes contact with the opposite side of the skull in less than 200 ms. The shock wave can result in a “coup contra-coup” injury (Ommaya, 1995; Sano et al., 1967).
A neurochemical cascade involving a multitude of cellular changes develops immediately following the biomechanical trauma to the brain. The biomechanical effects are on the stretching and tearing of the axons. As a result of the physical trauma, edema (fl uid) and leakage occur in the axon. This effect is most intense during the fi rst 2 weeks following injury. The resulting lesions (damage) generally involve small areas (.04–.60 inches diameter). Neuronal membranes are negatively affected. The axonal stretching leads to an increase in extracellular potassium, followed by subsequent depo-larization and then a release of excitatory neurotransmit-ters. This has been termed a “neurotransmitter storm” (Mendez, Corbett, Macias, & Laptook, 2005). This se-quence involves a loss of ionic gradients, apoptosis (cell death), cell depolarization, cytotoxic edema (swelling of the cell elements), glutamate release, and other bio-chemical effects. As a result of these events, the neuron breaks down, the axon splits into two sections, a retrac-tion ball (collection of cytoplasm) is formed at the end of the axon, and Wallerian degeneration occurs, which results in axonal collapse and resultant disconnection effects (Povlishock & Katz, 2005).
Non–Brain Stem Neuroanatomical Effects in TBI When the brain moves suffi ciently enough to have an impact with the bone, a contusion (bruising) can occur. The bruising typically affects the superfi cial gray matter of the inferior, lateral, and anterior aspects of the frontal and temporal lobes. The occipital poles and cerebellum are less involved. A subdural hemorrhage can occur when the movements of the brain are suffi cient to tear the bridging veins on the surface. These veins bridge the brain surface to the dural venous sinus. Generally, these subdural hemorrhages are found in parietal and frontal contours. In a whiplash-type injury there is a sudden acceleration and no direct impact. In this situation, the brain’s movement lags behind that of the skull. The forces effect the connections between the brain and the bridging veins as well as the brain tissue. Resultant ruptures of the bridging veins can result in subdural he-matomas, axonal damage, and bleeding. When the skull stops moving, the brain is thrown against the skull and simultaneously pulls away from the posterior skull. Op-
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 471
posite the internal contact a contra-coup can result from the negative pressure, which may cause the formation of cavitation bubbles. The brain is then thrown back-wards (deceleration) and a similar dynamic occurs. The reader is referred to Taber, Warden, and Hurley (2006), who illustrate nonpenetrating TBI injury locations for diffuse axonal injury, contusion, and subdural hemor-rhages. The illustrations indicate that DAI affects the following locations: the gray matter–white matter (cor-ticomedullary) junction (particularly frontal-temporal), internal capsule, deep gray matter, upper brain stem, and corpus callosum (CC).
SECTION III
Modern Medical Imaging Research with TBI The past 20 years have seen an enormous growth in the medical diagnostic imaging technology area; these new techniques have been applied to TBI patients. The research has focused on the effects of TBI on cortical structures and functions as well as the differences in the response patterns between a normal group and TBI pa-tients. The imaging techniques vary in their intrusive-ness and in the types of information they provide to the clinician. Among the more intrusive techniques that are used for both clinical and research purposes are SPECT (single-photon emission tomography) and PET (positron emission tomography), which require injections of a ra-diopharmaceutical (SPECT) or radionuclide (PET). The images that are produced reveal the metabolism of the brain (SPECT) or the regional blood fl ow (PET). The tech-niques are often combined in clinical applications with other forms of imaging in order to obtain high-resolution anatomic images of brain structures. Computed tomogra-phy (CT), also called computed axial tomography (CAT), has been used clinically to reveal brain structure; how-ever, to produce the images, the patient must be exposed to ionizing radiation. A technique that is less intrusive is MRI (magnetic resonance imaging), which uses a power-ful magnetic fi eld to produce images of the structure of the brain. MRI requires patients to enter a scanner and remain motionless as the scans are obtained. The advan-tages of MRI are the lower degree of invasiveness and lack of radiation exposure. A recently developed form of MRI is DTI (diffusion tensor imaging), which is used to visualize the white matter fi bers of the brain.
Several techniques for visualizing the function of the brain are available to the clinician. One technique
that requires use of a MRI scanner is functional mag-netic resonance imaging (fMRI). Often, for research pur-poses, the patient’s fMRI scans are collected following a structural MRI procedure. The use of fMRI in clinical applications is not common. The fMRI images are used to measure the hemodynamic response of the activity of the brain; one measure of the activity is the BOLD signal, which is the blood oxygen level dependent sig-nal. Typically, the BOLD signal is fi rst measured while the patient is at rest; then the patient is given tasks to perform, with intermittent rest periods. The BOLD sig-nals of the at-rest periods and the task are compared. In this way, the activity of the brain when involved in a task is quantifi ed. It is possible to look at the activity of individual patients and also to combine the activity of groups of patients to identify brain regions involved in tasks. Such tasks might involve attention, memory, and problem solving, which are the processes that are affected by a TBI. While brain function attributed to a task is determined by comparison to function at rest, there are concerns that brain regions active in the rest-ing state are, at times, more active and are active in different ways than when involved in cognitive tasks (Gusnard, Akbudak, Shulman, & Raichle, 2001; Gus-nard & Raichle, 2001; Raichle et al., 2001). To manage this concern, some fMRI studies have used a different comparison to identify differential brain function. For example, one study examined the patient’s brain acti-vation after hearing his or her own fi rst name in con-trast to hearing the names of others (Carmody & Lewis, 2006).
There are techniques that are less invasive than SPECT, PET, CT, and MRI. They measure the electrical activity of the brain, rather than metabolic or hemody-namic processes. These techniques include EEG, ERP, and qEEG. These techniques require patients to wear electrodes on their heads in order to assess brain ac-tivity. The number of electrodes varies from as few as one in the clinical setting to 256 or more electrodes in research studies.
While there is support for the use of neuroimag-ing to identify the structural and functional changes as-sociated with TBI (Levine et al., 2006), some feel that caution is necessary. For example, Erin Bigler (2001), in his Distinguished Psychologist Award lecture, identi-fi ed the relationships between TBI and structural brain changes. In contrast, others have indicated that there is little evidence of such damage in MTBI (Lees-Haley, Green, Rohling, Fox, & Allen, 2003). While this disagree-ment, as well as others, is based on neuroimaging using structural MRI, there is evidence from DTI that subtle alterations in brain structure are associated with TBI as
Copyright Springer Publishing Company

472 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
well as with lower performance on neuropsychological testing (Kraus, Susmaras, Caughlin, Walker, Sweeney, & Little, 2007). These associations between DTI image results and neuropsychological testing have also been found in pediatric studies of TBI (Levin et al., 2008). We examine this issue in the next section.
SPECT imaging shows that regional cerebral blood fl ow is reduced in symptomatic patients with long-standing MTBI, but with unremarkable structural brain imaging (Bonne et al., 2003). Although the group analy-sis shows statistically signifi cant differences, the clinical application of brain SPECT imaging in MTBI to associate clinical examination, neuropsychological assessment, and cerebral perfusion at the individual patient level is not available. Therefore, caution should be exercised in using neuroimaging at the individual level of analysis. An additional concern that the TBI damage may alter blood perfusion, thus changing the basis of the BOLD signal in fMRI, has also been raised (Ricker, Hillary, & DeLuca, 2001).
Structure and Function Normal Participants
Imaging research during the past several decades have attempted to localize functions to different locations, often fi nding that the brain has a multiple-location ac-tivation response pattern to different tasks. It has been possible to localize specifi c functions to locations or combinations of locations with the different medical technologies. One should keep in mind, however, that the imaging method determines the nature of the re-sults. For example, an fMRI study of verbal memory indicated a temporal lobe (predominantly left) and left frontal lobe activation response pattern in adults (Ma-zoyer et al., 1993). However, from the CAR perspective, adult verbal memory is a function of broadly activated SCC alpha activity in adults, which involves the left temporal lobe, left hemisphere, and right frontal lobe (Thornton, 2006). The fMRI approach does not examine coherence or SCC relationships. The fi nal understand-ing will come from a melding of these points of view.
TBI Patients
After experiencing a TBI, the patient’s brain function can be altered relative to noninjured brains: this may involve low levels of activation (SPECT studies), greater activation (than normal group) of different regions in response to a task, or activation of different locations (such as the right hemisphere) as well as more loca-
tions. However, these different response patterns do not necessarily lead to lowered functional levels on neurop-sychological measures nor have the increased activa-tions necessarily always been tied to success at the task. Specifi c locations, such as the CC, appear particularly susceptible to white matter damage and DAI. This is discussed separately in this section and in section V.
SPECT/PET Studies The studies with SPECT/PET technology have generally indicated lowered blood fl ow (frontal, temporal) under at-rest conditions, increased blood fl ow under cognitive activation conditions, greater impairment in the TBI patient on more diffi cult cognitive tasks, greater right hemisphere involvement, failed activations (compared to normative group), and a more dispersed response. TBI patients show decreased blood fl ow in the frontal cortex (PET studies) or hypometabolism (SPECT; Ricker et al., 2001). Contrary to most SPECT studies, one study actually demonstrated increased blood fl ow during a cognitive task in the same brain regions that, at rest, demonstrated signifi cant hypometabolism (Duara, Barker, Chang, Yoshii, Loewenstein, & Pascal, 1992). Blood fl ow (rCBF), however, is not the same as cerebral metabolism. It has been shown that in the TBI patient there is a decoupling of these two measures, which nor-mally function together (Obrist, Langfi tt, Jaggi, Cruz, & Gennarelli, 1984), rendering interpretation of results somewhat problematic and refl ective of the breakdown of the system in the TBI patient.
MTBI patients are more impaired than controls on the more diffi cult free-recall measure (Thornton, 2003) and have lower left frontal lobe and increased poste-rior rCBF, relative to controls, during free and cued retrieval (Ricker et al., 2001). The MTBI patients does not show decreased verbal working memory but does show greater right hemisphere activation and more dis-persed activity. Thus the TBI patient appears to activate posterior and right hemisphere locations in response to a verbal memory task, a fi nding that is echoed in the qEEG results discussed in section V. The increased activations, failed activations (compared to normative group), and right hemisphere involvement are similar to the fi ndings from fMRI (Maruishi, Miyatani, Nakao, & Muranaka, 2007; McAllister et al., 1999) and PET (Christodoulou et al., 2001).
Most SPECT studies, when conducted within the fi rst few weeks post-injury, reveal hypoperfusion asso-ciated with MTBI. There is a consistent pattern of hy-poperfusion in the frontal and temporal regions across studies (Belanger, Vanderploeg, Curtiss, & Warden,
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 473
2007). In one study, however, there were no differences in the resting condition between MTBI and a normal control group in frontal and temporal locations, while there were differences under cognitive challenge (S. H. Chen, Kareken, Fastenau, Trexler, & Hutchins, 2003). When spatial working memory was assessed, the TBI group failed to activate the right frontal location as much as the control group did, although their perfor-mance was equal to that of the control group, suggest-ing a compensatory activity by the TBI group to achieve the same results.
The MTBI patient has also been shown to exhibit hyper-metabolism (vs. controls) in midtemporal and frontal subcortical locations during a continuous per-formance test (1–5 years post-injury, PET study; Gross, Kling, Henry, Herndon, & Lavretsky, 1996). Retrieval was compared to the input condition. The retrieval con-dition normally elicits a greater right frontal/temporal pattern of retrieval in the functional neuroimaging lit-erature (Christodoulou et al., 2001). Although the TBI activation pattern was similar to normals; that is, there were more diffusely activated regions, higher levels of activation, and less lateralization. The TBI group dis-played greater right frontal lobe activation (superior and middle frontal gyrus) and more errors, whereas controls displayed greater left hemispheric activation in these same regions. There is a consistent pattern in the TBI literature of more diffuse activation in the TBI pa-tient. In summary, the MTBI patient shows changes in rCBF that can differ from the normative group, and the differences are task dependent.
Functional Magnetic Resonance Imaging (fMRI) The fMRI studies of concussion offer a somewhat con-fusing picture of the MTBI response pattern compared to control groups with an overall pattern of increased activations in frontal temporal and right frontal areas and increased right hemisphere activation, depending on the task. The increased activations were not related to more successful performance. Diffuse brain activa-tion was found in athletes on memory and sensorimo-tor tasks relative to pre-concussion baseline (Jantzen, Anderson, Steinberg, & Kelso, 2004). The increased ac-tivations on the sensorimotor task were mostly in the frontal/temporal areas, while the level of performance was unchanged. Concussed athletes demonstrated in-creased left frontal (dorsolateral) activation during a Go-NoGo task, which usually requires the patient to re-spond to a certain stimulus and not respond to a differ-
ent stimulus (Easdon, Levine, O’Connor, Tisserand, & Hevenor, 2004). In another study, concussed athletes showed reduced activity in the right frontal dorsolateral area during a working memory task, and less activation in the mid-dorsolateral prefrontal cortex, which is a re-gion important for working memory (J. K. Chen, John-ston, Frey, Petrides, Worsley, & Ptito, 2004). In addition, there was a negative correlation between right frontal dorsolateral activation and severity of symptoms. Simi-larly, hyperactivation in a group of high school athletes assessed 1 week after injury predicted a longer recovery period than for those athletes without fMRI hyperacti-vation (Lovell et al., 2007).
The effects of MTBI on working memory and simple reaction time were examined by an fMRI study of MTBI patients and controls (McAllister et al., 1999). While the MTBI group did not differ from controls in working memory ability, their brain activation patterns differed. The different brain activation patterns refl ect the brain’s attempt to provide other resources to accomplish the task, in this case resulting in equal performance to the normative group. The MTBI signifi cantly increased ac-tivation compared to the normative group during the high working memory load condition, particularly in the right parietal and right frontal (dorsolateral) regions. The MTBI group’s performance was slower in response speed on both the simple reaction time and distractibil-ity tasks of the Continuous Performance Test (CPT). The MTBI patients also reported signifi cantly more symp-toms, especially with memory. What is particularly in-teresting about this study is that researchers attempted to link task success to the activation patterns. The cor-relation coeffi cients indicated a signifi cant positive re-lationship, in the normal group, between left frontal activation and accuracy on the working memory task as well as accuracy on the CPT distractibility subtest. However, in a normal population the CPT task elicits a right frontal activation pattern (Fallgatter & Strik, 1997) thus suggesting that the MTBI patient has adapted a dif-ferent approach to solving the problem.
The effects of MTBI on reaction time were assessed in an fMRI paradigm (Maruishi et al., 2007). The MTBI patients had confi rmed DAI on the basis of MRI lesions. Although the patients did not differ from the controls in the measures of reaction time, their brain activation pat-terns did differ. While the controls showed activations in the left frontal gyrus, left parietal gyrus, and right inferior parietal gyrus, the DAI patients showed activa-tions in the left inferior frontal gyrus, right inferior fron-tal gyrus, and right middle frontal gyrus. Analysis of the differences on the reaction time task demonstrated that the DAI patient had signifi cantly greater activation of
Copyright Springer Publishing Company

474 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
the right inferior frontal gyrus, and right middle frontal gyrus than the control participants.
Diffusion Tensor Imaging Diffusion tensor imaging (DTI) examines the align-ment of water molecules in determining white mat-ter tracks. Factional anisotropy (FA) is a measure of the directional diffusivity of water made through the use of diffusion tensor imaging. A low FA refl ects a breakdown in the white matter organization. Further technical explanation is available elsewhere (Le Bihan et al., 2001). The research has very consistent fi ndings in that a low FA is uniformly associated with poorer cognitive abilities.
A striking research fi nding was reported in a DTI study of MTBI cases. Multiple white matter regions with reduced FA, predominantly involving cerebral lobar white matter, cingulum, and CC were recorded in patients 5.5 months post-injury (Rutgers, Toulgoat, Cazejust, Fillard, Lasjaunias, & Ducreux, 2008). The white matter bundles mostly involved the supratento-rial projection fi ber bundles, callosal fi bers, and fronto-temporo-occipital association fi ber bundles. The report indicated that 19% (of 249 white matter fi ber bundles) had discontinuity on fi ber tracking; in addition, and most importantly, there was no signifi cant relationship between the time interval after injury and the DTI fi ber tracking fi ndings. This last fi nding indicates that the brain does not spontaneously cure itself. A similar fi nd-ing was observed in qEEG research (Thatcher, Biver, McAlaster, & Salazar, 1998; Thornton, 1999), which is discussed in section V.
DTI studies have not always been consistent in their results, but the overall pattern is one of a strong relationship between DTI FA measures and cogni-tion. For example, while decreased FA was found in 13 studied regions for the moderate to severe TBI group, reduced FA was restricted to the cortico-spinal tract, sagittal stratum, and superior longitudinal fascic-ulus (bundle of fi bers) for the mild TBI group (Kraus et al., 2007).
Reduced FA is associated with impaired learning and memory in moderate and severe TBI (Salmond et al., 2006). Diffusely reduced FA had higher negative correla-tions with the neuropsychological measures (executive and memory function) than FA measures at individual locations, refl ecting the integrative nature of cognition. There are confl icting reports in recent studies of the as-sociation of FA and recovery. While one study reported that low white matter FA values at the time of injury were predictive of impaired performance in execu-
tive functioning ability at 6 months post-injury (Miles, Grossman, Johnson, Babb, Diller, & Inglese, 2008), an-other study concludes that the lower FA in the total CC did indicate higher levels of post-concussion symptoms and emotional distress (Wilde et al., 2008).
However, it has also been shown that specifi c lo-cations are relevant to specifi c cognitive abilities, as research shows that there is signifi cant dissociation be-tween cognitive impairments in TBI individuals whose predominant pathology is in the anterior corona radi-ata or uncinate fasciculus (Ghajar & Ivry, 2008). The anterior corona radiata connects the lateral prefrontal cortex (PFC) with areas such as the thalamus and cer-ebellum; the uncinate fasciculus is a primary pathway between the lateral PFC and parahippocampal cortex. The TBI patients with shearing in the uncinate fascic-ulus exhibited defi cits in working memory tasks. TBI patients with shearing in the anterior corona radiata exhibited defi cits in executive attention (Niogi et al., 2008).
Event-Related Potentials Electrophysiological measurements of the brain have also proved very sensitive to the effects of a TBI. The qEEG and ERP technologies have improved our scien-tifi c understanding of the brain’s response to a TBI. Event-related potentials involve the measurement of the magnitude of brain’s electrical response pattern within milliseconds of a stimulus (some ERPs go up to 700–800 msec following stimulation). The response can involve several waves of different amplitudes and at different time delays from the stimulus. Each wave has been named and classifi ed as to the proposed process-ing occurring. The ERP research offers an additional perspective on the TBI patient’s cognitive problem and appears to be useful and predictive of cognitive issues. Both the magnitude of the response and the response time were affected negatively in the TBI patient, as we discuss below.
The P300 has been shown in several studies to be a viable indicator of the negative effect of a TBI on the electrophysiology of the brain, mostly in terms of its lower amplitude but also increased time delay from stimulus onset (latency). The P300 (P3) wave is re-corded via the EEG as a positive defl ection in voltage at a latency of 300 ms from the onset of the stimulus. It is mostly observed in the parietal lobes and is considered involved in cognitive functioning.
Longer reaction times, which are negative fi nd-ings, were exhibited by symptomatic athletes compared to asymptomatic athletes (Lavoie, Dupuis, Johnston,
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 475
Leclerc, & Lassonde, 2004). This effect was not infl u-enced by the length of time since injury. This fi nding is further support for the hypothesis that there is no spontaneous cure in the TBI patient. There was an in-verse relationship between severity of post-concussion symptoms and P300 amplitude. Similar results were found for amplitude of ERPs following MTBI in col-lege athletes (Dupuis, Johnston, Lavoie, Lepore, & Las-sonde, 2000). The MTBI patients showed a signifi cant decrease in the amplitude of the waveform around 300 msec (P300), which was negatively related to the severity of post-concussive symptoms; specifi cally, lower amplitude was associated with more symptoms. MTBI patients with persistent attention and memory impairments have been shown to demonstrate abnor-malities in the hippocampally mediated P50 evoked re-sponse (Arciniegas et al., 1999; Arciniegas & Topkoff, 2004) and the frontocentral P300 response (Arciniegas, Anderson, Topkoff, & McAllister, 2005; Pratap-Chand, Sinniah, & Salem, 1988; Schatz & Zillmer, 2003).
Reduction in the amplitude of N1, P2, and P3 components, which indicate the early and late stages of auditory processing, were found in symptomatic and asymptomatic athletes with TBI in comparison to control athletes on an auditory oddball task (Gosselin, Theriault, Leclerc, Montplaisir, & Lassonde, 2006). An oddball task generally requires the patient to respond differently when a specifi c rare stimulus is presented. There were no group differences in the reaction times or in latency of the ERP components, except for P3 latency, in which the controls showed a shorter latency than the MTBI group. Headaches and concentration problems were both negatively correlated with the amplitude of the P3 component. These results, as the researchers amply suggest, challenge the practice of returning the non-symptomatic athlete to competition.
The effects of multiple concussions in athletes were examined in a visual oddball task (De Beaumont, Bris-son, Lassonde, & Jolicoeur, 2007). Three groups were compared on neuropsychological measures as well as P300: athletes with no history of concussion, those with one concussion (mean time of 59 months since inci-dent), and those with more than one concussion (mean time since of 31 months since last concussion). While there were no differences on neuropsychological mea-sures between the three groups, the multiple-concussion group showed reduced P3 amplitudes compared to the other two groups some 2.5 years after the injury. In conclusion, the P300 appears to be a viable measure of the brain’s response to the trauma in that reduced amplitudes and longer delays are associated with brain dysfunction.
Corpus Callosum Much of the research has implicated the CC, which con-nects the two hemispheres, as one of the major sites of injury. This discussion focuses on the CC while ac-knowledging that there is evidence in the literature of ef-fects of TBI on other brain structures. The other affected areas include the gray-white matter interface, dorsolat-eral aspect of brain stem, subcortical white matter, basal ganglia, and body and posterior (splenium) section of the CC and cerebellum (Parizel et al., 1998).
The CC is the largest white matter tract in the brain and has long been considered to be vulnerable to TBI (Gorrie, Dufl ou, Brown, Gibson, & Waite, 2001). Shear-strain mechanisms are common in the splenium (Gennarelli et al., 1982; Gentry, Thompson, & Godersky, 1988; Mendelsohn, Levin, Harward, & Bruce, 1992). Autopsy studies of MTBI patients who died of unrelated causes showed that the CC was the most frequent site of DAI, which is followed by the brain stem and then white matter in the lobes (Belanger et al., 2007). Thus, even in MTBI cases, DAI effects have been found. Atrophy of the CC is found in the TBI patient for both adults (An-derson, Bigler, & Blatter, 1995; Gale, Johnson, Bigler, & Blatter, 1995; Levin et al., 2000) and children (Levin et al., 2000). Interestingly, the longer the coma lasts, the more the callosal volume reduction (Tomaiuolo et al., 2004). Measures of memory were positively associated with volume of selected structures. For example, immediate free recall of word lists positively correlated with the volume of the fornix and the CC. Delayed recall of word lists and immediate recall of the Rey fi gure both posi-tively correlated with the volume of the fornix. Delayed recall of the Rey fi gure positively correlated with the volume of the fornix and the right hippocampus. Thus differential cognitive effects are found with damage to different structures. MTBI is associated with reduced FA in the white matter, compared to controls, most notably in the internal capsule and CC, despite normal-appear-ing white matter on MRI (Arfanakis, Hermann, Rogers, Carew, Seidenberg, & Meyerand, 2002). The FA reduc-tion was often less evident 1 month after injury. How-ever, even if the time frame is extended to 18 months, reductions in CC FA have been reported in adults with TBI (Rugg-Gunn, Symms, Barker, Greenwood, & Dun-can, 2001).
Pediatric TBI patients exhibited decreased mean FA in the splenium of the CC, compared to matched controls, irrespective of the presence or location of spe-cifi c callosal or extra-callosal focal injury (Wilde et al., 2008). This pattern was also present in anterior regions of the CC despite the absence of focal lesions. Lesions
Copyright Springer Publishing Company

476 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
in the splenium were found in only 25% of the children despite decreased mean FA. Higher FA was related to increased cognitive processing speed and faster interfer-ence resolution on an inhibition task. In the pediatric TBI patients, higher FA was related to better functional outcome as measured by the dichotomized Glasgow Outcome Scale. In conclusion, the CC shows evidence of dysfunction immediately after a MTBI, 18 months later, and at autopsy.
Inconsistencies in Anterior Corpus Callosum Response The Stroop task elicited the normal fMRI response pattern (frontal, occipital, parietal) in fi ve recovering severe TBI patients, except for a decrease in activation of the ante-rior CC (ACC) (Soeda, Nakashima, Okumura, Kuwata, Shinoda, & Iwama, 2005). The TBI patients (1–7 years post-injury) generally did as well as the control partici-pants on the Stoop but manifested poor memory for recent events and had trouble with their jobs. In a func-tional PET study, TBI patients increased their activity in the ACC and in frontal and occipital lobe activity dur-ing working memory tasks (Levine, Cabeza, McIntosh, Black, Grady, & Stuss, 2002).
Greater Effort in the TBI patient One hypothesis that has arisen as a result of the re-search is that the TBI patient engages in greater sub-jective “cognitive effort” to attain the same objective level of cognitive performance as controls (Braver et al., 1997) on the same tasks. TBI patients often report that they must now “work harder” to perform previously simple tasks. How this “effort” is translated to medical imaging measures and qEEG measures is undetermined at this point, although subjective and objective greater cognitive load may involve greater frontal lobe involve-ment, which may refl ect “greater effort” (Braver et al., 1997). Data presented in section V indicate that greater levels of beta activity in the frontal lobe are character-istic of the TBI patient’s response pattern to cognitive tasks and thus may refl ect the subjective experience of greater effort.
A comparison of patients with orthopedic injury (OI) to TBI patients (moderate to severe at 3 months post-injury) found that the frontal (cingulate, medial frontal, middle frontal, and superior frontal gyrus re-gions) brain activation during a stimulus-response in-compatibility task is greater in TBI patients than in OI patients and is positively related to TBI severity (Schei-
bel et al., 2007). The number of lesions in the TBI group do not relate to the degree of activation elicited. In ad-dition, the more severe TBI patients (i.e., lower GCS) have greater activation within deeper structures that include the basal ganglia, thalamus, anterior cingulate gyrus, and CC. The researchers had speculated that DAI, rather than contusions and other focal pathology, may be responsible for the increased activation. The report also indicated a positive relationship between activa-tion (anterior cingulate gyrus, medial frontal, parietal regions, as well as brain stem) and response accuracy during a stimulus-response incompatibility task for the OI, but not the TBI patients, indicating increases in acti-vation results in performance benefi ts for the OI patient but not the TBI group. The task involved a stimulus-and-response feature that involved either the same side of the body (e.g., right-hand response to a visual stimu-lus presented on the right side) or a different side of the body (e.g., right-hand response to a left-sided visual stimulus).
Another fMRI study of working memory showed greater activation for patients with moderate and se-vere TBI with DAI (Turner & Levine, 2008). The patients had greater activation than controls in frontal lobe (left middle frontal, right inferior) as well as bilateral pari-etal and left temporo-occipital areas. The TBI patients showed these brain activation differences despite per-formance equal to that of the control group.
In conclusion, the medical imaging literature has provided evidence of damage to the TBI brain in the MTBI cases. The pattern is one of increased arousal (compared to the normative group) on relatively sim-ple tasks, breakdown on more diffi cult tasks, discon-nection between regions, and increased employment of frontal and right hemisphere locations. The possible clinical implications are that the TBI patient is (1) trying harder to deal with simple tasks, (2) cognitively breaks down under complex situations, (3) is not employing the more verbally oriented left hemisphere, and (4) is employing the more emotional/spatially oriented right hemisphere.
SECTION IV
Neuropsychological Testing The clinician needs to know the cognitive, behavioral, and emotional issues of the TBI patient to develop a treatment plan. This section addresses what science knows and the problem of the limitations of science in understanding the cognitive and emotional effects of a
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 477
TBI. Neuropsychological tests have been the standard for assessing cognitive functioning following TBI. Surpris-ingly, up to 90% of the “recovered” cases of moderate TBI continue to have cognitive defi cits on neuropsycho-logical testing (Rimel et al., 1981). The clinician should be aware that neuropsychological measures have suf-fered from problems in interpretation, which include such issues as:
( 1) A valid pre-trauma baseline ( 2) Possibility of malingering ( 3) Relationship to medical imaging results ( 4) Psychometric issues: retesting effects, availability of
valid and reliable parallel forms of measures, dis-criminate sensitivity to other conditions (such as preexisting learning disabilities)
(5) Differential diagnosis in relation to preexisting conditions
(6) Relationship to outcome measures (job, etc.) (7) Relationship to depression and other emotional and
behavioral conditions.
These topics lead to questions concerning the valid-ity of interpretation of results, which should alert the clinician to be cautious in blindly accepting conclusions in reports. However, some valid assumptions regard-ing baseline functioning can be made in the absence of pre-incident data and give validity to neuropsycho-logical conclusions. For example, a patient who was a straight-A student throughout his academic career and, following a TBI, is performing two standard deviations below the normative group on a particular test cannot be considered unaffected by the TBI in the absence of other possible causes. In addition, without evidence to the contrary, most individuals (68%) can be expected to fall within one standard deviation range on a test, and about 95% within two standard deviations, pro-viding a basis for some reasonable interpretations of defi cits on tests. Therefore a neuropsychologist can, on occasion, correctly infer that an individual’s preexist-ing condition was above his presently tested functional level on measures and thus accurately infer the pres-ence of brain damage.
Pre-Trauma Baseline In both the military and sports the problem of pre-trauma baseline testing is understood and is beginning to be addressed. The pre-trauma baseline problem re-fers to the problem of determining if there is a defi cit in functioning based on post-trauma testing performance. If a subject is performing at a normal level, it doesn’t
necessarily mean that the TBI has had no effect, as the subject may have been performing well above the nor-mal range prior the injury. To establish an effect of a TBI, the evaluator needs to have some measure or es-timate of what the pre-morbid level of functioning was on a particular measure.
In sports and military studies involving computer-ized cognitive batteries such as the ImPACT instrument (Iverson, Lovell, & Collins, 2003), the Concussion Sen-tinel (Erlanger, 2002), and Automated Neuropsycho-logical Assessment Matrices (Reeves, Culligan, LaCour, Raynsford, Elsmore, & Winter, 2001) are being employed to establish baselines. However, pre-trauma baseline data are typically unavailable in injuries resulting from motor vehicle accidents, falls, and assault, and the best that can be obtained is school records, which are far from an ideal baseline. Even with the availability of pre-trauma neuropsychological data, there are problems of retesting within short time frames, even on alternate forms. There is the additional problem of the brain’s physical adaptation, which can result in normal scores despite evidence of physical damage. In addition, it has been demonstrated at a 4-month retest interval that im-provements on assessment measures (ANAM) can sig-nifi cantly improve in noninjured athletes (Daniel et al., 1999). So if the practice effect or cognitive improvement can occur at 4 months, then how can we rely upon mea-sures that use return to preexisting level as the criterion of recovery? We should, rather, use improvement from baseline as the guideline.
Neuropsychological testing is especially useful when baseline studies are obtained and compared with post-injury examinations (Echemendia, Putukian, Mackin, Julian, & Shoss, 2001). For example, neurop-sychological testing was useful in detecting cognitive impairment in college athletes following MTBI and was more effective than subjective report in differentiating injured from non-injured athletes (Echemendia et al., 2001). The addition of the ImPACT computerized bat-tery to the subjective report increased diagnostic accu-racy by 19% (van Kampen, Lovell, Pardini, Collins, & Fu, 2006).
This research challenges the assumption that the patient is the best judge of the cognitive effects of his or her own injury. However, not everyone favors a widespread adoption of neuropsychological testing. For example, one view is that due to time/fi nancial costs of testing, the lack of validation in determining recovery, the limited validation and utility of diagnos-ing concussion, and numerous logistical concerns, the widespread use of such testing is not viable (Grindel, 2006).
Copyright Springer Publishing Company

478 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
Malingering The clinician needs to monitor the athlete’s motivation for performance in the post-concussion evaluation (Bai-ley, Echemendia, & Arnett, 2006). In the sports arena the tendency is to minimize/deny effects. In the per-sonal injury realm the tendency is to exaggerate/fabri-cate effects. The possibility of malingering has been a major focus in neuropsychological testing for a number of years, and assessment of malingering is presently rec-ommended by the National Academy of Neuropsychol-ogy as part of a neuropsychological assessment (Bush et al., 2005). In most neuropsychological evaluations the goal is to determine the presence of exaggeration, not minimization, of cognitive defi cits. However, in-terpretations of the results of the malingering batteries face problems in validity. Many of the research reports appear to implicitly assume that because someone is litigating the case, the patient must be malingering, and then proceed to show data of “exaggerated” complaints. However, it is equally plausible that the patient who is experiencing more symptoms is more likely to litigate. Historically, judgments were based solely upon clinical testing data, as medical imaging technology (CT, MRI) was not able to provide suffi cient basis to provide vi-able alternate data. In addition, in most situations the patient has not even undergone relevant physical assess-ment. The imaging studies using DTI, ERP, and qEEG have proved to be the most sensitive and relevant to the underlying physical damage caused by the trauma and thus offer a more valid and useful assessment approach to malingering than paper-and-pencil or computerized neuropsychological measures. The most valid medically diagnostic instruments (qEEG, DTI) are seldom used to address the question of malingering. The qEEG results are discussed in section V.
Empirical studies of malingering in litigation offer perspectives in contrast to the assumption that all pa-tients with symptoms persisting months after TBI are malingerers. For example, one study estimates that while 57% of TBI patients complained of symptoms at the time of the medicolegal report (mean interval 9–12 months), 39% had symptoms at the time of settle-ment (mean interval 22–1 months) and 34% had symp-toms 1 year after litigation (Fee & Rutherford, 1988). If litigants were all malingerers, then the question that can be raised is why there was any reduction in symp-toms from the report time period to the settlement and why was there only a 5% decrease in symptoms after the settlement. The possible counterargument is that the claimant was just continuing to present malingered symptoms to avoid the possible reopening of the case.
However, it would be unlikely that a case would be re-opened once the patient claimed the symptoms were gone. A meta-analytic review of 18 studies of 2,353 individuals with TBI of varying severity was used to explore the relationship between litigation and symp-toms (Binder & Rohling, 1996). The conclusion of the review was that fi nancial incentives may account for 20%–25% of the persistent signs and symptoms. How-ever, in the absence of a clear physical defi nition of TBI, any estimate is suspect. Other studies have failed to fi nd associations between compensation or litigation and frequency or severity of post-concussive symptoms (Keshavan, Channabasavanna, & Reddy, 1981; Merskey & Woodforde, 1972; Rimel et al., 1981). Although base rates of the concussion symptoms are an important consideration, it is perhaps more valid to establish the pre-accident symptom base rate for the individual TBI patient, which is problematic.
In conclusion, while it most certainly is the case that malingering exists, neuropsychological or psycho-logical reports which that statements on a patient’s mo-tivational state and infer malingering need to be taken with caution. Frequently relevant physical (DTI, qEEG) diagnostic tests are not available to confi rm or deny as-sertions of malingering. In addition, lack of structural damage on the CT and MRI instruments is not evidence of malingering due to the low frequency of structural defi cits in MTBI cases. Two decades ago, many symp-tomatic patients had normal MRI scans (Levin et al., 1987). More recent estimates continue to indicate that 43%–68% of mild TBI patients have normal structural MRI scans (Hofman, Stapert, van Kroonenburgh, Jolles, de Kruijk, & Wilmink, 2001; D. G. Hughes, Jackson, Mason, Berry, Hollis, & Yates, 2004).
Relationship Between Neuropsychology and Medical Imaging Technologies Neuropsychological measures and medical imaging techniques have not reached a level of sophistication that always allows us to identify the relationship be-tween specifi c neuropsychological defi cits and a lesion in a particular locations, or sets of lesions in different locations. Part of this problem resides in our present understanding of the mind-body problem. The follow-ing results provide some research information on the complexity of the problem facing this fi eld.
In a group of TBI patients, neuropsychological func-tioning improved while DTI fractional anisotropy (FA), mean diffusivity (MD) from the DTI images, and vox-el-based analyses of the gray matter (GM) and white
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 479
matter (WM) probability maps revealed signifi cantly greater negative gray and white matter change over time (2 months vs. 12.7 months post-injury) in patients compared to controls (Bendlin et al., 2008). This line of evidence supports Thornton’s (2000) assertion that there is no spontaneous cure of the underlying physical damage in the TBI patient, and in this case, the under-lying physical damage worsened. The TBI affected all the major fi ber bundles in the brain, which include CC, cingulum, superior and inferior longitudinal fascicules, uncinate fasciculus, and brain stem fi ber tracts. Thus improved neuropsychological testing doesn’t necessar-ily mean that the brain has repaired itself. In this ex-ample, it would appear that the brain found some way to change its physical response, as it couldn’t rely upon the injured white matter tracts to function as well. The neuropsychological testing may not have been sensi-tive enough to reveal the underlying physical damage. The counterargument to this interpretation is that the brain has found a different and equally effective way to solve the problem due to its adaptive nature, albeit with limitations with more complex and demanding tasks (Thornton, 2003).
Psychometric Issues: Retest Effects, Alternate Forms The additional issues of retest effects have availability of valid alternate forms have been traditional areas of concern in psychological assessment and are not spe-cifi c to the TBI literature.
In the sports arena, the problem has drawn consid-erable attention. The ImPACT test is a popular screening measure for sports concussion (Schatz, Pardini, Lovell, Collins, & Podell, 2006). Test-retest reliability values of the ImPACT test range from .15 to .61 in a group of 115 normal participants retested at 45 and 50 days follow-ing original evaluation (Broglio, Macciocchi, & Ferrara, 2007). These low reliability values render the test sta-tistically unacceptable for these time periods. The other measures assessed by Schatz et al. (2006) included the Concussion Sentinel and the Headminder Concus-sion Resolution Index. The researchers concluded that these instruments also demonstrated similar low reli-ability values. The false positive rate, which identifi es a normal individual as a concussed patient, was 38% at 45 days for the ImPACT tests, 19% for the Headminder Concussion Resolution Index and 33% for the Concus-sion Sentinel. Other researchers have reported higher reliabilities for shorter periods of time. For example, there are no signifi cant practice effects in normals on
the ImPACT measure when tested within several days (Iverson et al., 2003). The ImPACT test has also been shown to correctly identify mildly concussed athletes (Schatz et al., 2006). However, Broglio et al. (2007) con-cluded that currently no assessment test could be rec-ommended. In addition, without equivalent alternate forms, the “improvements” on these measures taken within days of each other are susceptible to practice ef-fects. Similar conclusions were reached regarding com-puterized testing in the sports concussion area based upon cost, validity, and reliability issues (Grindel, 2006; Randolph, McCrea, & Barr, 2005). Even with equivalent forms the validity of repeat testing within a short period of time opens up the potential effect of practice on the results. Other researchers have argued that following a single repetition of a test there is no further evidence of a practice effect on computerized tasks (Collie et al., 2006). For example, in one study the researchers stud-ied three groups of athletes (control, symptomatic con-cussed athletes, and asymptomatic concussed athletes) and conducted repeated computerized testing. Follow-ing the TBI, the asymptomatic athletes had diffi culty with only the divided attention task, not the motor or attentional tasks. In contrast, the symptomatic group demonstrated large and signifi cant defi cits on almost all the measures of reaction time and attention, espe-cially on tasks assessing speed. Both the control and asymptomatic groups signifi cantly improved on repeat computerized testing, from pre-season baseline to post-injury for asymptomatic group. This demonstrates the problem of repeat testing. However, the symptomatic group’s performance on paper-and-pencil tests did not deteriorate despite signifi cant defi cits on the computer-ized battery, calling into question the validity of paper and pencil neuropsychological testing instruments. The presence and duration of LOC and PTA did not differ-entiate between the symptomatic and asymptomatic groups. Erlanger et al. (2001) addressed the complexity of this problem with respect to a Web-based neurop-sychological test protocol and reported that the Con-cussion Resolution Index showed resistance to practice effects. Researchers have argued that a .90 test-retest reliability measure is the appropriate statistical criteria for clinical and research use of a test (Randolph et al., 2005).
The reliability problem relates to the underlying true value of a variable. Confi dence intervals employ high and low values that refl ect different probability values (95%, 98%, etc.) of the true value within the assigned range. As the reliability decreases, the con-fi dence interval of a test score becomes larger, thus compromising the ability to make defi nitive probability
Copyright Springer Publishing Company

480 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
statements regarding the signifi cance of the difference between two administrations of a measure. For example, the Wechsler IQ measures have a mean of 100, an SD of 15, and reliability of .90. When 95% confi dence inter-vals are used, a 7-point drop is statistically signifi cant (Randolph et al., 2005). As the reliability of a measure decreases, there is more uncertainty regarding the true value, and thus a wider confi dence interval to enable a similar probability value. If the reliability of the IQ test was .70, it would require a 20-point drop in IQ to be signifi cant. It is relevant for the clinician to under-stand these issues when presented with reports of lack of progress in a treatment program.
Differential Diagnosis Differentiating the effects of a TBI from a preexisting learn-ing disability, a previous TBI, or other CNS-damaging events has always been extremely problematic. The availability of academic records (grades, SAT scores) is only occasionally useful, due to the lack of equivalence of these measures to neuropsychological measures. High schools do not generally administer neuropsycho-logical batteries. On occasion, a previous child study team evaluation can be useful.
Relationship Between Neuropsychological Measures and Real-World Outcome The association between neuropsychological status and functional impairment was examined with equa-tion modeling in 87 patients with moderate to severe TBI studied longitudinally (Rassovsky et al., 2006). The results of the modeling showed that only neuropsycho-logical status, not emotional or behavioral diffi culties, consistently mediated the relationship between TBI severity and functional outcome at 12 months post-injury. No direct effect of injury severity on functional outcome was found. Rather, it was the indirect effect that was found to be signifi cant, suggesting that other intervening variables mediate the relationship between injury severity and functional outcome. Some studies of MTBI show support for a relationship between sever-ity of neuropsychological defi cits and various outcome measures, including employment status (Ross, Millis, & Rosenthal, 1997). However, concerning the relationship between injury severity and neuropsychological status, research studies have found only a weak relationship between these parameters (Binder et al., 1997). Other researchers have found that other factors, such as pre-morbid IQ, emotional functioning, and fi nancial incen-
tives, may exert a larger effect on outcome than injury severity (Binder & Rohling, 1996). A review of the lit-erature concludes that many neuropsychological tests have a moderate level of ecological validity predicting everyday cognitive functioning (Chaytor & Schmitter-Edgecombe, 2003). Specifi cally, high scores on tests predicted full-time employment 62% of the time, while low scores predicted unemployment 67% of the time (Fabiano & Crewe, 1995).
Depression, Brain Structures, Cognition, and Personality Changes in TBI Depression
There is a large body of evidence indicating that depres-sion is a common complication of TBI, with a preva-lence of 16%–61% meeting criteria for major depressive disorder. This high variability suggests problems in the diagnostic methods used, or variability in sampling methods, such as randomization versus self-selection, and recruitment patterns (Kim et al., 2007). Depres-sion is the most cited psychological disturbance after TBI, with prevalence rates ranging from 6% in cases of mild traumatic brain injury to 77% in more severe TBI within the fi rst year after injury (Jorge, Robinson, Stark-stein, & Arndt, 1993). For example, 91 consecutive TBI patients admitted to a general hospital at 3, 6, 9, and 12 months post-injury were compared for depression with 27 patients admitted for multiple traumas without TBI (Jorge et al., 1993). In the TBI sample, 52% met DSM-IV criteria for mood disorder due to TBI, 33% had major depressive features, 10% had depressive features, and 9% had either manic or mixed features. In the com-parison group, 7% had major depression, and 15% had depression without major depressive features. Retired professional football players ( N = 2,552) with an av-erage age of 53.8 years and an average professional football-playing career of 6.6 years were administered a general health questionnaire that included questions about prior injuries, the SF-36 (Short Form 36), and other markers for depression (Guskiewicz et al., 2007). Eleven percent of 2,434 athletes reported having prior or current diagnosis of clinical depression.
There was an association between recurrent con-cussion and diagnosis of lifetime depression, suggesting that the depression prevalence increases with increas-ing concussion history. Compared with retired players with no history of concussion, retired players report-ing three or more previous concussions (24%) were 3 times more likely to be diagnosed with depression; those with a history of one or two previous concussions
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 481
(36%), were 1.5 times more likely to be diagnosed with depression. An MTBI group with LOC of 15 minutes experienced more depression than a severe TBI group (Alexander, 1992). World War II veterans were assessed for prevalence of depression several decades after the initial injury (Holsinger et al., 2002). After age, edu-cation, and health conditions were accounted for, an 18% lifetime prevalence of depression was observed in veterans who suffered a head injury in their 20s, which was signifi cantly higher than the observed 13% lifetime prevalence for those without a history of head injury.
Depression and Brain Structure Relationship
The following discussion provides evidence of the oc-currence of emotional and personality changes in the TBI patient. However, it should be kept in mind that there is an implicit confusion in this type of literature. The fact that we are able to indicate a certain percent-age of TBI patients are depressed doesn’t mean that we can state unequivocally that the TBI is the cause of the depression. The problem resides in our inability to state whether the causal link is the physical effect on the brain or the sequelae of the TBI on psychological, cognitive, social, and economic functioning. For exam-ple, has the patient become depressed because recall of events is poor, or because life has changed since the TBI, or because as a consequence of the TBI the patient cannot pay bills and has lost employment?
The alternate to the environmental or psychologi-cal cause of the depression is a physical one, which is that the TBI results in a brain response pattern that is present in depressed individuals, and thus the patient is physiologically depressed. Patients with major depres-sion alone tend to have left anterior hemisphere lesions, while depression with anxiety is associated with right hemisphere lesions (Jorge et al., 1993). qEEG measures of prefrontal activation asymmetry at rest showed that patients with greater relative left prefrontal activation report more positive and less negative moods (David-son, Coe, Dolski, & Donzella, 1999). In addition, acutely depressed patients as well as remitted depressed pa-tients exhibit decreased left prefrontal activation com-pared with never-depressed controls. There is evidence suggesting that damage to the basal ganglia or fronto-striatal tracts may play a role in depression following head injury. One study found that head trauma resulting in frontal (left dorsolateral frontal) and/or subcortical (left basal ganglia) lesions was associated with the high-est rates of depressive episodes (Fedoroff et al., 1992). In other samples with prior head injury, there is evidence for involvement of subcortical (basal ganglia) (Steffens,
Helms, Krishnan, & Burke, 1999) and frontal (ventrome-dial orbitofrontal area) locations in depression (Elliott et al., 1997). As this chapter has elucidated, it is well known that a TBI affects frontal lobe functioning.
TBI patients with MRI identifi ed lateral lesions dem-onstrate, at 3 months post-injury, more intense depres-sion, greater problems in social skills and daily living, and more apathy than patients with medial lesions (Par-adiso, Chemerinski, Yazici, Tartaro, & Robinson, 1999). Major depression in TBI is also associated with reported smaller hippocampal and amygdala volumes, structural and morphological changes in the prefrontal and orbito-frontal cortex, and basal ganglia structures (Guskiewicz et al., 2007). Studies that fail to address the issue of brain-based versus environmentally based depression or anxiety will not offer clarity to this problem.
Depression and Cognition
Given the above qualifi cations it remains relevant to the clinician to know about the possible role of a TBI in his or her patient’s history as a possible contributory factor to depression. The large presence of depression in the TBI group also raises the question of whether depression could be affecting the cognitive measures associated with mild and moderate TBI. TBI patients with major depression (28%), relative to nondepressed TBI, were found to have signifi cantly lower scores on measures of working memory, processing speed, ver-bal memory, and executive function (Rapoport, Mc-Cullagh, Shammi, & Feinstein, 2005). The differences averaged about .45 SD advantage for nondepressed. This is similar to the defi cit of .50 SD on the California Verbal Learning test (CVLT) found in major depression patients in a psychiatric hospital (Otto, Bruder, Fava, Delis, Quitkin, & Rosenbaum, J 1994). TBI patients (200 days post-injury and 28% with major depression) were found to have signifi cantly lower scores on measures of working memory, verbal memory, executive function, and processing speed than the control group (Rapoport et al., 2005). This study demonstrated that at 6 months following mild and moderate TBI, major depression is associated with worse performance across an array of cognitive domains, including attention, memory, and executive functioning. While more than -half of the pa-tients without major depression were unimpaired on any cognitive test, this was true for only 15% of the pa-tients with major depression. The literature has gener-ally been reporting negative or confl icting results in this area, leaving the question of the infl uence of depression on memory functioning in the TBI patient unresolved, although suggestive of a negative infl uence.
Copyright Springer Publishing Company

482 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
Post-Traumatic Stress Disorder and Brain Structures
The physical measurement of PTSD offers an inconsis-tent set of results. An fMRI evaluation of PTSD showed signifi cantly less activation of the thalamus, the anterior cingulate gyrus (Brodmann’s area 32), and the medial frontal gyrus (Brodmann’s area 10/11) than a com-parison group (Lanius et al., 2001). However, contrary to that fi nding is the observation that combat-related PTSD soldiers had increased beta power over frontal regions relative to veterans without PTSD (Begic, Ho-tujac, & Jokic-Begic, 2001). Risk of PTSD was directly associated with the volume of left temporal lesions in MRI scans in 95 pediatric patients with TBI (Vasa et al., 2004). Left orbitofrontal lesions were associated with decreased risk of hyperarousal symptoms, while diffuse brain lesions were related to increased risk of avoidant symptoms.
In MTBI, depression, and PTSD, the frontal lobes are affected, as well as other structures. The task of dif-ferentiating between these diagnostic categories based upon frontal lobe problems is challenging. Defi nitive statements regarding the causality of neuropsychologi-cal problems in these groups becomes extremely prob-lematic, as we have only (1) a limited understanding of how some of these neuropsychological tasks function with respect to brain structures and (2) a limited un-derstanding of how PTSD and MTBI affect brain struc-tures and functions. To render a defi nitive statement that the depression, not MTBI or PTSD, is affecting the memory system would require knowledge that a spe-cifi c brain structure is involved in memory and is not affected structurally or functionally by PTSD or MTBI. The qEEG appears to be particularly well suited, once research has discovered the different qEEG patterns for PTSD and MTBI, to address simultaneously both cogni-tion and emotional states.
Personality Changes
A study of children ages 5–14 with TBI found person-ality changes in 22% of participants between 6 and 12 months after injury, and 12%–13% in the second year after injury (Max et al., 2006). The severity of in-jury consistently predicted personality change, and pre-injury adaptive function predicted personality change only in the second year post-injury. Superior frontal gyrus lesions were associated with personality change between 6 and 12 months following injury, after sever-ity of injury and the presence of other brain lesions were controlled for. Only lesions in the frontal lobe white matter were signifi cantly related to personality change
in the second year after injury. Emotional instability was the most common subtype of the disorder, followed by the aggressive subtype and then the disinhibited sub-type. The other two personality changes described were the rare and generally resolving apathetic and paranoid subtypes. A review of the literature from 1978 to 2006 found a large prevalence of psychiatric disorders fol-lowing nonpenetrating TBI (Kim et al., 2007). The dis-orders were psychosis (20%), depression (18%–61%); PTSD (3%–59%), mania (83%–22%), and aggression (20%–40%). However, as indicated by the authors of the study, the prevalence needs to be confi rmed in con-trolled studies.
SECTION V
The Role of the Quantitative EEG in the Assessment and Rehabilitation of the TBI Patient This section provides (1) a basic understanding of the qEEG in terms of the frequencies, variables and locations employed; (2) information on what is presently known about the relationship between the qEEG variables and TBI; (3) a brief history of the relationship between the qEEG and the fi eld of EEG biofeedback; (4) a descrip-tion of the activation qEEG model of evaluation and the resultant Coordinated Allocation of Resource model of brain function; (5) a discussion of the qEEG correlates of auditory and reading functioning; (6) principles of intervention and results with the TBI patient; (7) a com-parison of the TBI and normal response pattern in the auditory processing task with particular attention to the CC; and (8) information on the rehabilitation of the TBI patient with specifi c examples.
The 10–20 System The brain produces electrical signals in the range of 40–100 microvolts, which are detected by the electrodes. Due to differences in skull thickness, the microvolt lev-els can vary in that thicker skulls don’t allow the electri-cal energy to be transmitted as easily, resulting in lower microvolt levels than thinner skulls. The EEG data, once collected, need to undergo an artifacting analysis. Arti-facts are signals that are not due to brain activity are but mostly due to eye movements, muscle activity, or other non-brain events. Software programs typically allow the evaluator to mark the epoch (a period of time) as deleted due to artifact presence. The data are then analyzed by
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 483
software and compared to an available database. Pres-ently almost all databases are eyes closed. None have evaluated the relationship between the qEEG variables and task success and most do not extend the frequency range above 21 Hz (sine waves per second).
Figure 18.1 presents the standard nomenclature of the 10–20 system. The 10–20 system standardizes the electrode location to similar anatomical locations de-spite the differences in head size among patients. Nylon caps that have the electrodes located in the 10–20 sys-tem are typically employed; caps are available in differ-ent sizes to fi t the age span from infants to adults. The letter F refers to frontal, T to temporal, C to central, P to parietal, and O to occipital locations. Left hemi-sphere locations are indicated by odd numbers, and right hemisphere locations by even numbers. Typically what occurs in a qEEG recording is that the electro-cap is placed on the head, and ear reference electrodes are attached to the ear lobes. The nylon caps have tin plates that are separated from the scalp by a small space, which is fi lled with electro-gel to enable conductance of the electrical energy from the scalp to the tin plate. Figure 18.2 presents a visual representation of the dif-ferent frequencies.
The following discussion provides a description of the qEEG measures. Not all the measures have proved to be correlated with cognitive performance. The descrip-tions are provided, as other researchers have reported
signifi cant fi ndings with these variables. From Thorn-ton’s (2001) viewpoint and data with the TBI popula-tion, learning disabilities, and attention defi cit disorders, there are two classes of critical variables, each of which has two critical variables. The fi rst general class involves what is happening at a specifi c location and measures the different frequencies in terms of their relative power and microvolt values. The second class involves the similarity of the waveforms between different locations with such measures as the Spectral Correlation Coeffi -cient (SCC) or coherence and phase. The phase measure is a more time-sensitive measure of the SCC. The second measures are refl ective of the activity in the long myeli-nated fi bers connecting the locations. The connection issues have been addressed with several different con-ceptual (coherence, co-modulation, spectral correlation, phase) and mathematical defi nitions (Collura, 2008). It is empirically unclear, at this point, how these different methods of calculating these relationships interrelate, as well as how they relate to cognition. The exception to this statement is the Thornton (2001) research that employed the Lexicor Spectral Correlation Coeffi cient measure and correlated the qEEG measures with cogni-tive measures. Thornton’s research has found that three variables (relative power, SCC, and phase values) are the most useful in predicting cognitive effectiveness and understanding the effect of a TBI on the brain’s electro-physiology. The reports by other researchers on coher-ence employ their own specifi c defi nitions.
Defi nitions of Measures Microvolt. The average strength in absolute microvolts of the signal of a band during an epoch. This measure merely refl ects how strong the signal is in terms of mi-crovolts.
Relative power. The microvolts of the particular band divided by the total microvolts generated by all bands at a location, averaged over the epoch time pe-riod. This measure is insensitive to skull thickness, as it measures the total microvolts at a location and de-termines the percentage of the total microvolts that are within a particular frequency range.
Peak frequency. The peak frequency of a band dur-ing an epoch (defi ned in frequency)
Peak amplitude. The peak amplitude (measured in microvolts) of a band during an epoch.
Symmetry. The peak amplitude symmetry between two locations in a particular bandwidth—defi ned as (location A minus location B)/(location A plus location B), where A and B represent two locations of the 10–20 system.
Figure 18.1 Standard 10-20 system and nomenclature for locations.
Copyright Springer Publishing Company

484 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
0.0 0.2 0.4 0.6 0.8 1.0
0.0 0.2 0.4 0.6 0.8 1.0
0.0 0.2 0.4 0.6 0.8 1.0
0.0 0.2 0.4 0.6 0.8 1.0
Delta 0–4 Hz
Theta 4–8 Hz
Alpha 8–13 Hz
Beta1 13–32 Hz
Beta2 32–64 Hz
0.0 0.2 0.4 0.6 0.8 1.0
Figure 18.2 The different frequencies.
Spectral correlation coeffi cient. The average ampli-tude similarity between the waveforms of a particular band in two locations over an epoch. This variable is defi ned within a particular frequency range.
Phase. The time lag between two locations (A and B), in the 10–20 system, of a particular band as defi ned by how soon after the beginning of an epoch a particu-lar waveform at location A is matched in amplitude at location B. The measurement time period for this vari-able is considerably less than for the SCC variable and can occur over a period of milliseconds.
The qEEG and TBI The qEEG has been shown to have higher discriminant function rates than other standard EEG or MRI technolo-gies in differentiating TBI from normal participants. For example, researchers in the TBI fi eld have argued that routine EEG and MRI measures are not useful in TBI
identifi cation due to their low sensitivity and reliability in discerning mild to moderate TBI (e.g., under 20% accuracy; Thatcher et al., 1998). qEEG has been used to differentiate between 608 MTBI adult patients and 108 age-matched controls with an accuracy rate of about 90% (Thatcher, Walker, Gerson, & Geisler, 1989). Mod-erate to severe cases were not included in the analysis. The useful qEEG measures included increased frontal theta coherence (Fp1-F3), decreased frontal beta (13–22 Hz) phase (Fp2-F4, F3-F4), increased coherence beta (T3-T5, C3-P3), and reduced posterior relative power alpha (P3, P4, T5, T6, O1, O2, T4). Three independent cross validations resulted in accuracy rates of 84%, 93%, and 90%. The prognostic effi cacy of qEEG was compared to that of GCS, brain stem auditory evoked potentials, and CT in 162 TBI coma patients recorded 1–21 days after injury (Thatcher, Cantor, McAlaster, Geisler, & Krause, 1991). The EEG results and the GCS score at the time proved to be an effective discriminant
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 485
(96% accuracy) between good outcome and death, with EEG phase measurements accounting for 44% of the variance in outcome, followed by EEG coherence values. The researchers suggested that the phase and coherence values may refl ect DAI severity issues. Signif-icantly higher power in the delta band and lower power in the alpha band were found for a TBI group compared with matched controls in an eyes-closed task (Korn, Golan, Melamed, Pascual-Marqui, & Friedman, 2005). Changes in spectral EEG recordings were superior to the GCS and brain stem evoked potentials in determin-ing outcome in a group of 29 comatose patients (Alster, Pratt, & Feinsod, 1993). Improvement on spectral EEG recordings in the alpha and beta bands were related to improvements on GCS measures over time, while the delta frequency positively correlated with the depth of coma. In either case, the EEG and ERP information is providing useful information in the TBI situation.
qEEG techniques were integrated with conventional MRI to explore the shift in the water proton relaxation times in moderate to severe TBI (Thatcher et al., 1998). Nuclear magnetic resonance of brain water proton T2 relaxation times, determined by the proton density within various tissue compartments, and absolute mi-crovolt measures of the qEEG were obtained from 19 moderate to severe TBI (1.7 years post-accident) pa-tients. The results were interpreted as providing some support to the hypothesis that there is either a disrup-tion in the integrity of the protein-lipid membranes of neurons or neuronal death resulting in reduced EEG mi-crovolts. Associations were found between the locations of lesions and the EEG measures. While gray matter lesions were related to decreased microvolts on alpha and beta bandwidths, white matter lesions were associ-ated with increased microvolts in the delta bandwidth. Gray matter atrophy in TBI cases has also been docu-mented (Cohen, Inglese, Rusinek, Babb, Grossman, & Gonen, 2007). Neuropsychological defi cits within this TBI group also were correlated positively with an in-crease in the delta microvolts, and negatively with a de-crease in alpha and beta EEG amplitudes. These qEEG effects were not correlated with the interval of time between injury and MRI test nor with edema or acute injury effects, refl ecting lack of spontaneous curing of the underlying physical problem (cross-sectional data). Thatcher was the fi rst to indicate a lack of spontaneous cure in the TBI group (Thatcher et al., 1998). Thornton (2000) supported Thatcher’s qEEG data and initiated the hypothesis that time does not heal in the TBI case.
Several measures of the changes in qEEG in TBI have been replicated in other studies. A discriminant analy-sis employing the qEEG variables to distinguish MTBI
from cerebral vascular accidents and normals showed 100% accuracy in separating TBI versus cerebral vascu-lar accidents (Leon-Carrion, Martin-Rodriguez, Damas-Lopez, Martin, & Dominguez-Morales Mdel, 2008). The results with eyes-closed data indicated that the higher delta (1–3.5 Hz) microvolts were associated with lower the functionality measures (Functional Independence Measure) and Functional Assessment Measure). In addition the lower the beta (12–30 Hz) coherence val-ues the lower the functionality measures. qEEG differ-ences were reported between asymptomatic concussed athletes (89 days post-concussion) patients and con-trol participants under the postural task conditions of standing up (J. Thompson, Sebastianelli, & Slobounov, 2005). Concussed athletes showed decreases in EEG mi-crovolts in all frequencies under the standing condition when their eyes were closed.
One review of the research in the traumatic brain injury area indicated that numerous eyes-closed EEG and qEEG studies of severe head injury (GCS score of 4–8) and moderate injury (GCS score of 9–12) have agreed that increased theta and decreased alpha power (microvolts) and/or decreased coherence and symme-try deviations from normal groups often characterize such patients (J. R. Hughes & John, 1999). Changes in these measures provide the best predictors of long-term outcome. Other studies have reported that similar qEEG abnormalities are correlated with the numbers of bouts or knockouts in boxers (Ross, Cole, Thompson, & Kim, 1983) and with professional soccer players who frequently used their heads to affect the soccer ball’s tra-jectory (“headers”; Tysvaer, Storli, & Bachen, 1989). The qEEG has also proven useful in discriminating between soldiers who experienced a blast injury and normals. The Thatcher discriminant function (Thatcher et al., 1989) correctly identifi ed 88% of the soldiers with a blast injury history and 75% with no blast injury his-tory (Trudeau et al., 1998).
There is additionally the problem of determining if the reductions in coherence or SCC values are the re-sult of damage to the myelinated fi bers (as indicated in DTI research) or damage to the gray matter, which is involved in the generation of the signal. In theory, the lowered coherence or SCC values could be attributable to either or both, as lowered coherence or SCC values could be due to lowered ability of the gray matter to gen-erate a signal or transmit the signal to the white matter. However, the discussion that follows indicates that the gray matter still retains the ability to generate activity, as it is generating more beta activity than the normative group and is defi cient in the SCC values. Whether the problem resides additionally in the gray matter’s ability
Copyright Springer Publishing Company

486 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
to transmit the signal to the white matter is unresolved at this point. We delve into these distinctions and their respective values in more detail in the following discus-sion of the activation qEEG evaluation.
In conclusion, the research attests to the viability of the use of the qEEG in the determination of a TBI, along with other clinical information. It should be noted, however, that all of the research reported relationships were based upon eyes-closed data with the frequency range generally 21 Hz and lower. Although this line of research has proven productive in many clinical areas, there are inherent limitations to these types of data in two areas: (1) the limitation of the frequency range and (2) the inability to relate qEEG variables under task conditions directly to task performance.
Brief History of Field Earlier studies of EEG biofeedback located the electrodes along the sensorimotor strip (see Figure 18.1, C3-Cz-C4) and employed a protocol that inhibited theta microvolts and augmented/rewarded beta (frequency range defi ned by authors) microvolts in a operant (rewarding of spon-taneous behavior) EEG biofeedback session (Carmody, Radvanski, Wadhwani, Sabo, & Vergara, 2001; Linden, Habib, & Radojevic, 1996; Lubar, 1985; Othmer, Othmer, & Kaiser, 1999; Tansey, 1991; L. Thompson & Thompson, 1998). Positive clinical results of increases on IQ mea-sures (average of 15 points across 4 studies; Linden et al., 1996; Othmer et al., 1999; Tansey, 1991; L. Thompson & Thompson, 1998), �.50 SD improvements in attentional abilities (Kaiser & Othmer, 2000), and a reduction in inat-tention as measured by the Test of Variables of Attention (Carmody et al., 2001) were documented. While the goal of this protocol is a reduction in theta microvolts and an increase in beat microvolts, the results of the training are not necessarily in that direction. For example, in a study conducted on site in an elementary school setting, children with the lowest initial microvolts of beta had signifi cant increases over session, while those with the higher initial levels of beta show decreases in microvolts (Carmody, Quintela, Radvanski, Sabo, & Giorgi, 1999; Carmody et al., 2001). The differences in the fi ndings of this study and that of others may be in the selection of subjects. Specifi cally, while the children in the Carmody studies were selected for ADHD based on the DSM-IV cri-teria, earlier studies selected children through the use of DSM-III criteria. The larger set of criteria used by DSM-IV may result in children who do not necessarily follow the “high-theta” and “low-beta” profi le.
The next development in the fi eld was the employ-ment of eyes-closed databases, which could examine an
individual on a host of qEEG variables in comparison to an appropriate normative group. Protocol interven-tions were geared toward normalizing the qEEG. While normalizing theta and beta levels might seem to be a self-evident positive intervention, the normalizing of SCC and coherence and phase values is problematic. Under the assumption that coherence/SCC and phase values refl ect white matter structure and functional ability, why would it be desirable to lower these val-ues? In addition, in what frequency is it desirable to lower SCC or coherence values? The only way to an-swer these questions, and others, satisfactorily is to examine the brain under activation conditions and ex-amine the correlations between cognitive success and the qEEG variables, thus the development of the acti-vation qEEG evaluation. The employment of a higher frequency range in the activation database (32–64 Hz) has proven to be an important frequency, especially in the TBI situation (Thornton, 1999, 2000, 2003). In ad-dition, the clarifi cation of SCC values, which are nega-tively related to performance, was addressed with the fi nding that SCC theta generally is a negative correlate of effective cognition, especially in children under the age of 14. The SCC values in the higher frequencies (alpha to beta2) were usually related to more effective cognitive performance.
The Activation/Cognitive Challenge qEEG Evaluation Pribram (2009) has commented that the “combination of recording EEG during problem solving behavior has led to and continues to lead to exciting breakthroughs in our understanding of the brain/behavior relationship.” In order to understand the nature of what is under-taken in the activation qEEG evaluation, the following description is provided. The preparation of the patient for the evaluation is the same as with obtaining eyes-closed data. The acquisition of data takes about 1 ½–2 hours, including preparing the patient and administer-ing the tasks. The bandwidths are divided according to the following division: delta = 0–4 Hz, theta = 4–8 Hz, alpha = 8–13 Hz, beta1 = 13–32 Hz, beta2 = 32–64 Hz. The standard 10–20 system (linked ears reference) is employed.
The following is the sequence of task administration.
(1) Baseline—A sample of 300 seconds of eyes-closed data for baseline purpose is obtained. This phase allows the participant to accommodate to the test-ing situation in addition to gathering data.
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 487
(2) Auditory recall task—This task is conducted with eyes closed. The participant listens to four stories in sequence. After hearing the story the partici-pant recalls the story silently for 40–50 seconds. The recording is then paused and the participant is asked to tell the examiner all the information the participant was able to recall during the quiet recall period.
(3) Reading task—The participant is presented with one printed stories. They are asked to read the ma-terial quietly to themselves and reminded that they will be asked to recall the material. The recording lasts for 100 seconds. After the 100 seconds of read-ing, the participant is asked to close their eyes and silently recall for 50 seconds as much as they can about the story. After the quiet recall period, the recording is paused and the participant is asked to verbally recall as much as they can recall about the material that was just read.
(4) Problem solving task—The participant is presented with the selected problems (series D and E) from the Raven’s matrices. One of the items is employed as a sample to demonstrate the logic of the Raven’s and discussed until the participant understands the purpose of the task. The participant then silently analyzes the problems and verbalizes his solution (providing a number). Due to the probability of in-creased artifacts in this task, data is collected for 400–500 epochs. This task also allows for a delay period with different cognitive activity intervening.
(5) Delayed auditory recall task—The participant is asked to recall quietly for 60 seconds all of the sto-ries that were read previously. Following the quiet recall period, the participant is asked to tell the ex-aminer all of the information that was recalled dur-ing the quiet period.
(6) Reading recall (delayed) task 5—The participant is asked, with eyes closed, to recall the story that they read. The participant is allowed 60 seconds of quiet recall time (eyes closed). The participant then informs the examiner out loud of all of the recall information.
After data collection, the artifacting process is ap-plied to eliminate non-EEG signals in the data. The arti-facting process involves visual inspection of each of the epochs and marking (via software) which epochs are affected by artifact (eye movements, muscle activity, etc.). The analyzed data is then run through analysis software that calculates means and SD s of the partici-pant’s response pattern across the nine cognitive tasks (not including eyes closed) on all the qEEG variables
available (microvolts, relative power, peak amplitudes, peak frequency, symmetry measures, SCC and phase). The software also averages the response pattern of the normative group across the nine cognitive activation tasks (excluding the eyes-closed task); this allows a comparison of the participant’s overall response pattern to the overall normative response pattern. This type of analysis allows for the unique evaluation of consistent patterns of defi cits in each task.
There are many measures of brain activity that are available from the qEEG. A specifi c location generates 18 values for the SCC value in a particular frequency. The 19 locations generate 171 SCC values for one fre-quency, and similarly for the phase values. When the fi ve frequencies are combined for all locations across the phase and SCC values, the number of variables becomes 1710. To address the statistical problem resulting from these large numbers a fl ashlight metaphor is employed. We assume that each location is capable of generating a signal within a frequency range and that signal can be sent to every other location, thus reducing the statistical problem by a factor of eight. The concept of generator has been used (Schreckenberger et al., 2004) in the qEEG fi eld and is thus a natural extension of the concept.
However, it should be noted that many theorists and empirical evidence point to subcortical locations as the possible origin of certain frequencies, nota-bly the alpha rhythm originating from the thalamus. A mathematical technology called LORETA that, theo-retically, enables specifi cation of the location of the subcortical generator is currently being developed (Pas-cual-Marqui, 2002; Pascual-Marqui, Esslen, Kochi, & Lehmann, 2002). There are controversies concerning the ability of this technology, however, to fi x accu-rately the origin of the signal. From a practical point of view the present 10–20 system combined with the high frequency activation database appears to be suffi cient to obtain useful enough information to understand electrophysiological defi cits and effectively direct re-habilitation efforts.
The Coordinated Allocation of Resources Model of Brain Functioning Thornton and Carmody (2009a) proposed the coor-dinated allocation of resources (CAR) model of brain functioning. The model states that performance on any particular cognitive skill (auditory memory, read-ing memory, problem solving, etc.) is a function of the use of different electrophysiological variables (rela-tive power, SCC, etc.) and locations. While different
Copyright Springer Publishing Company

488 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
cognitive skills may employ similar qEEG variables and locations as other skills, each skill operates differently than another skill. This model is somewhat implicit in fMRI and PET studies, which report location activation during cognitive tasks. A model of brain functioning that asserts not just what the brain does in response to a task but elucidates the necessary variables and their values or directions is a critical step in any theory of brain functioning. The CAR model is an initial attempt to provide the identifi cation of these functions in terms of qEEG variables. In the case of MTBI it is a question of how the system is affected and what the effects are on the different cognitive tasks. If the CC is damaged in TBI cases, what does that mean for auditory or read-ing memory skills or what skill does it affect and to what degree? One method of answering the effect issue is to combine normals with a TBI group and correlate performance across the two groups with the qEEG vari-ables. This was done in the case of auditory memory (Thornton, 2003) and the results will be discussed in this section.
The qEEG offers a viable technology for establish-ing the correlates of effective cognitive functioning as well as providing a rehabilitation method (Thornton & Carmody, 2009b). Most of the TBI research reports have employed an eyes-closed database. The research has shown that the TBI has elevated microvolt values in the lower frequencies (delta, theta) and decreased microvolt values in the upper frequencies (alpha, beta). These qEEG patterns have been assumed to be tied to cognitive problems in the TBI patient, as assessed dur-ing a different time period. In addition, problems in co-herence in the TBI patient have also been documented in terms of increased frontal theta coherence, decreased frontal beta phase and increased left hemisphere beta coherence (Thatcher et al., 1989) and reduced beta SCCs (Thornton, 1999, 2000, 2003). The SCC and phase values are tied to white matter activity. The assumption is that lowered coherence/SCC and phase values refl ect damage to the cortical-cortical white matter and/or the cortical-subcortical white matter (Destexhe, Contreras, & Steriade, 1998). While resting coherence and SCC val-ues may be sensitive to white matter damage, a more demanding activation approach would more likely elicit where the weaknesses are in the white matter, which has been demonstrated in the Thornton (1999, 2000, 2003) studies.
The CAR model was built upon the idea that activa-tion conditions are required for a thorough understand-ing of what is involved in the brain’s electrophysiological functioning. The CAR model examines the qEEG vari-ables on three levels: (1) what are the differences in qEEG
patterns between different brain states (Thornton & Carmody, 2008) such as auditory attention to listening to paragraphs; (2) what variables are being activated that relate to success at the task (Thornton, 2001) and (3) what are the relationship between task success and the absolute level of the specifi c qEEG variables that are positively and negatively correlated with success (Thornton, 2001). SPECT, fMRI and DTI studies (and others) have traditionally focused on identifying which variables are activated and then made the assumption that the activation relates to success at the task. While intuitively appealing, the assumption hasn’t always been confi rmed or examined. Thornton and Carmody (2008) investigated whether that assumption is valid in qEEG research by looking at the activation patterns of the different relevant conditions. For example, a partici-pant engages in an auditory attention task (pen tapping on a table) and then an auditory memory task (listening to paragraphs). Success in the auditory memory task is related to specifi c qEEG variables (i.e., variables X, Y, Z). It would be a natural assumption that the participant would increase the values of the X, Y, Z variables from the auditory attention task. As an analogy an individ-ual would engage certain muscle groups when lifting weights and other muscles when running, as each task requires activations of specifi c muscle groups to be suc-cessful. However, this is not what happens. The ineffi -ciency hypothesis proposed by Thornton and Carmody (2009b) asserts that the normal (individuals with no history of learning disability, ADHD, psychiatric his-tory) human brain does not increase the relevant qEEG values from the comparison condition (i.e., auditory at-tention vs. listening to paragraphs). For example, the coherence alpha relationships are critical to success in the listening to paragraph task yet the normal group does not increase these coherence alpha values from the auditory attention condition. Modern medical im-aging technology needs to address this problem if the research results are to have relevance.
The CAR Model With Auditory and Reading Memory
The CAR model was developed on a number of cogni-tive skills (Thornton, 2001). We review two cognitive tasks—auditory memory for paragraphs and memory for reading material. Based on the results of a standard neuropsychological battery, only the logical memory subtest (paragraph recall) of the Wechsler Memory Scale–Revised predicted return to work at one year in a group of MTBI patients (Cifu et al., 1997). Based on this outcome, the logical memory (paragraph recall) was the task employed in the development of the activation
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 489
database. We present the effective qEEG response pat-tern in normal individuals for both auditory and read-ing memory and then examine one TBI individual’s TBI response pattern for these tasks. The effective normal response pattern results have been previously pub-lished (Thornton, 2000, 2002). Figure 18.3 presents the correlates of effective auditory memory. The fi gure dis-plays the reanalysis of the Thornton (2000) data with the fl ashlight metaphor. Circles with stars represent origin of the metaphorical fl ashlight beam of coherence alpha.
For auditory memory, in Thornton’s (2001) norma-tive sample of individuals (ages 14–70), these SCC alpha fl ashlights (F7, F8, C3, T3, P3) during the input stage (listening to paragraphs) are also the predictors during the subsequent recall period. The SCC alpha fl ashlights (F7, F8, C3, T3, P3) during the input stage of listening are predictors during of auditory memory the subsequent recall period in the normative sample. The predictors during the quiet recall stage are F7, F8, C3, T3, P3, and F4. The predictors for long-term recall (20 minutes later) remain the SCC alpha fl ashlights from T3, F7 and F8. Thus across three auditory recall tasks the SCC alpha re-lationships are the critical ones for success. Figure 18.4 presents an example of the effect of a TBI on SCC alpha relationships during the auditory input stage.
Stars represent the origin of the fl ashlight beam. Values in circles represent the differences of the subject from the normative database in standard deviations. The white circles represent values that are within .50 SD units of the normal mean (i.e., between −.50 SD and �.50 SD ). The light gray enclosed circles represent values between −.50 SD and −1.50 SD . The darker gray enclosed circles represent values below −1.50 SD . The numbers in the circles show the SD value.
Figure 18.5 presents the qEEG correlates of reading memory. There was also a negative predictor from the
right posterior (T6-PB1). As the fi gure indicates the F7 fl ashlight SCC and phase activity in the beta frequen-cies (13–64 Hz) as well as T5 SCC alpha activity are the determinants of reading recall in a normal population.
Figure 18.6 represents the SD values for SCC and phase qEEG variables in a TBI participant during the reading task. As Figure 18.6 demonstrates, this TBI par-ticipant has signifi cant defi cits in SCC and phase beta2 values from the left frontal (F7) location. The star rep-resents the origin of the fl ashlight. The light gray rep-resents values between −.50 SD and −1.50 SD while the dark gray circles represent values below −1.50 SD . Stars represent origin of fl ashlight beam. Values in cir-cles represent standard deviation difference of subject from normative database.
Figure 18.7 presents the fl ashlights of posterior origin for the same TBI participant. The SCC beta2 relationships have experienced signifi cant defi cits in functioning as a result of the TBI. The star represents the origin of the fl ashlight. The light gray represents values between −.50 SD and −1.50 SD while the dark gray circles represent values below −1.50 SD . Values in circles represent standard deviation difference of sub-ject from normative database.
Intervention Rationale In the CAR approach the selection of locations and pro-tocols is determined by the results of the comparison of the patient’s response pattern to Thornton’s (2001) normative database for auditory input tasks (paragraph recall and auditory attention) and visual input tasks (reading, problem solving and visual attention). The total results are examined initially to localize weak-nesses in the system. Then the individual tasks are ex-amined, until a pattern of defi cits becomes apparent. A specifi c task is approached fi rst for treatment. The
Figure 18.3 SCC alpha fl ashlight correlates of auditory memory.From NCLB Goals (and More) Are Attainable with Neurocognitive Approach (Vol. 1), by K. Thornton, 2006, Charleston, SC: Booksurge.
Copyright Springer Publishing Company

490 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
0.1
0.0
0.3
–0.4
–0.4
–1.2
–0.2
–0.4
–0.6
–0.8–0.8
–0.9
–2.6
–2.6
–2.5
–1.0
–1.0
–1.7
–1.7
–1.2
–2.2 –2.8
–2.6–2.8
–0.5
–1.3–0.9
–1.7
–0.5 –0.4–0.4
–2.3 –1.7 –1.5
–0.8
–0.7 –3.5 –4.1
–2.9–3.2–4.3–3.8
–2.6
–1.4–2.3–3.0–1.3–1.4
–0.7–1.1 –1.0
–0.7–1.0 0.6
–1.2
–1.4–1.0–1.2–1.2
–0.6
–0.5 –0.9 –0.1
–0.4 –0.3–0.2–0.2
–0.6–1.5
–0.4
0.3
–3.5–3.5 –3.5–0.7–0.6 –0.6
–0.5
–1.1–1.6–1.9–2.9
–2.0–3.5 –2.0
–0.5–0.6
–1.4 –2.8 –0.7
Paragraph Listening (Average)Spectral Correlation
Alpha Z-ScoresP3
Paragraph Listening (Average)Spectral Correlation
Alpha Z-ScoresT3
Paragraph Listening (Average)Spectral Correlation
Alpha Z-ScoresC3
Paragraph Listening (Average)Spectral Correlation
Alpha Z-ScoresF8
Paragraph Listening (Average)Spectral Correlation
Alpha Z-ScoresF7
Figure 18.4 TBI example: Auditory memory.
fi rst task addressed is usually auditory memory due to its importance in activities of daily life. When defi cits are found in auditory memory, then the left temporal (T3) location is addressed fi rst. The reasoning behind this decision resides in the PET and fMRI research data that indicate the importance of the left temporal lobe in auditory and verbal processing. A similar type of rea-soning is applied to the selection of the protocols as the participant responds to the treatment and improves
their qEEG values. The SCC values are generally very responsive to the interventions. However, sometimes increases in SCC are diffi cult to obtain. In this situation, a different set of connection locations are selected.
Intervention Results
Most reviewers in the area of cognitive rehabilitation have not been encouraging of the approaches that have
Figure 18.5 Correlates of reading in normal population.
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 491
–0.6 –1.7
–1.7–1.7–1.3
–2.0
–1.0 –1.7 –1.8 –1.8 –0.7
–1.2 –0.7
–0.8–1.6
–1.8 –1.7 –2.1
–2.3–2.3 –1.9–0.4
–1.5–2.1
–2.2
–1.7
–1.7–2.7
–1.4
–2.1 –1.4 –2.3 –2.2
–1.5–1.7
–1.9–2.0 –2.1
–1.7
–1.1
–1.1 –0.8
–1.7–1.5–1.7 –1.2
–0.7
–2.9 –2.5 –2.2 –1.7 –0.5
–1.9 –1.3
–1.3
–0.9–0.8
–1.1 –05
–2.0 –2.2–2.2
–0.1–1.1
0.3
–1.3–1.2–1.3
–1.1–1.1
–1.6
–1.6
–1.4
–1.2–1.8–1.8 –2.4
–0.9–1.2–2.1–2.2–1.1
–1.7–2.1
–0.6 –1.00.1
–2.1–1.1
–1.8
Silent ReadingSpectral Correlation
Beta 1 Z-ScoresF7
Silent ReadingSpectral Correlation
Beta 2 Z-ScoresF7
Silent ReadingSpectral Correlation
Alpha Z-ScoresF5
Silent ReadingPhase
Beta 1 Z-ScoresF7
Silent ReadingPhase
Beta 2 Z-ScoresF7
Figure 18.6 TBI frontal response pattern: Reading.
–0.5
–1.3–2.6 –2.1
–0.2
–1.9–0.5
–0.6–1.5–1.9–3.6–0.6
–3.1 –2.2–2.1
–2.2 –2.1
–0.9 –3.1
–1.8
–1.8
–2.0
–0.9 –2.6
–0.4 –0.9
–1.1–2.1 –2.1
–0.6 –0.4
–1.9
–1.9 –0.1 –1.0 –2.6
–2.2–1.6
–2.1–2.0
–2.2
–2.1
–1.8
–3.2–2.0
–1.6 –1.5
–1.5
–1.6–2.5–2.4
–2.9 –2.0 –0.5
–0.3
–0.3
–0.4
–0.4
–0.0
–2.6–2.1
–2.5
–2.9 –3.2
–0.1
–0.1
–0.1–0.6
–2.0 –0.9
–1.3–2.2
–2.2–2.9
–1.7–2.9
–1.8–2.0
–0.9
–1.8–1.7–6.1–1.0
–1.3–1.9–2.7 –1.8
–0.5
–0.2–1.1
Silent ReadingSpectral Correlation
Beta2 Z-ScoresT5
Silent ReadingSpectral Correlation
Beta2 Z-ScoresP3
Silent ReadingSpectral Correlation
Beta2 Z-Scores01
Silent ReadingSpectral Correlation
Beta2 Z-Scores02
Silent ReadingSpectral Correlation
Beta2 Z-ScoresP4
Figure 18.7 TBI posterior response pattern: Reading.
been employed to date, due to lackluster research re-sults (Thornton & Carmody, 2008). One study indicated there was no conclusive evidence for the effi cacy of cognitive rehabilitation for children with acquired brain injury (Limond & Leeke, 2005). The Veteran’s Adminis-tration concluded that there are no evidence-based clin-ical practice guidelines that address treatment of mild TBI. A report from the Rand Corporation emphasized the need to develop evidence based effective interven-tions for the cognitive problems of the TBI participant (Tanielian, Jaycox, Schell, Marshall, & Burnam, 2008). The evidence that follows will hopefully begin to change these opinions.
Employing the CAR model, the following EEG bio-feedback intervention results have been reported with the LD/ADHD and TBI populations. Thornton and Car-mody (2005) reported improvement in auditory memory function in a group of 20 LD/ADHD children that aver-aged 3 SDs for reading memory and 3.33 SD (or 296%) for auditory memory. Traditional tutoring methods with the LD/ADHD child average �.49 SD (Thornton, 2006) on the different measures employed by the respective
researchers. For example, the measures might assess comprehension, pronunciation, or vocabulary skills. Similarly, a group of 19 TBI patients improved audi-tory memory by an average of �2.61 SD s or 185 per-cent (Thornton & Carmody, 2008). In TBI intervention research, the cognitive rehabilitation methods using computers and strategies have low levels of improve-ment with an average of �.41 SD for paragraph recall. Thornton and Carmody (2008) employed SD effect size and confi dence intervals to determine recommendation levels. The only recommendation obtained for the strat-egy and computer intervention approach was for word lists with computer interventions. Computers and strat-egies approaches obtained a ‘not recommended’ deci-sion by the authors for paragraph recall, attention, and problem-solving skills. The only moderate recommen-dation obtained was for the activation qEEG approach to paragraph recall.
It is of some value to note that for both clinical groups (LD/ADHD and TBI) the EEG treatment group’s performance at the end of the treatment was above that of the respective normative control group, a result that
Copyright Springer Publishing Company

492 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
could be considered a cure for the memory problems of these groups. For the LD/ADHD group, the initial mean was 8.4 ( SD = 5.5) and the post mean was 21.8 ( SD = 6.6). The comparison to the normative control group indicated that the treatment group was 1.53 SD above the control group at the end of the treatment. For the TBI group, the control group’s mean average was 18 ( SD = 2.45). The treatment group started at a mean of 8.6 ( SD = 4.31) and ended at a mean of 24.5 ( SD = 7.25) or 1.92 SD above the control group (employing means and SD of both groups). It would appear from these results with two different patient populations that EEG biofeedback intervention based upon an activation qEEG evaluation and guided by the CAR model is an effective intervention approach.
Specifi c Effects With TBI
The high frequency range (32–64 Hz) SCC effect of a TBI was originally reported in the Thornton (1999, 2000, 2003) studies that employed the high frequency activation data-base. The results indicated a specifi c defi cit in the higher frequency (32–64 Hz) range in the SCC and phase rela-tionships, under eyes closed, simple activation tasks, and paragraph recall tasks. These papers began to explicate what the connection between white matter damage and the qEEG variables might be under the assumption that the SCC values are determined by white matter function-ing. The results for the TBI patient involved lower values in the SCC values of the beta2 frequency (32–64 Hz) for reasons biologically unclear at this point.
This discussion is relevant to the previously pre-sented issue of children “growing into the defi cit” caused by a TBI during youth. Thornton (2001) estab-lished that the predominant effective qEEG variable of children resides in relative power and microvolt lev-els of beta1 (13–32 Hz) and reduced relative power of theta. As the brain passes through adolescence and into adulthood these variables are no longer the dominant effective electrophysiological parameters during cogni-tive tasks. The predictors of cognitive effectiveness then predominantly reside in SCC and phase relationships. As these variables are the ones most affected by the TBI, the damage done to a young brain won’t be ap-parent until early adolescence has passed and the need to employ SCC relationships becomes paramount. If, however, the damaged white matter connections have not spontaneously healed themselves then cognitive problems will become apparent, whereas previously they were not. Of particular relevance to this problem is the observation that “time does not heal” (Thornton, 2000). In the group of 32 mild to moderate TBI patients
the defi cit pattern in the SCC and phase beta2 relation-ship was not a function of time since injury. In other words, the time distance between injury and assessment (cross sectional, not longitudinal data) had no effect on the defi cit pattern. Thus, time did not result in sponta-neous cure of the problem. This fi nding echoes those of previous reports (Lavoie et al., 2004; Rutgers et al., 2008; Thatcher et al., 1998).
The fi nding has signifi cant implications for the fi eld as it indicates that the presumed spontaneous cure does not fi nd a correlate in the electrophysiology of the brain. Compensation then becomes the possible mechanism of return to normal functioning as determined by neu-ropsychological assessment. The Thornton (2003) study also indicated a change (compensation) in response functioning in the TBI patient as performance on audi-tory memory tasks was positively correlated with right temporal (T4) phase beta1 and left frontal (F7) phase beta2. In Thornton’s (2001) normative sample auditory memory is partly determined by left temporal (T3) and left frontal (F7) SCC alpha (Figure 18.8).
Thus, there was a change to a higher frequency and a partial shift to the right hemisphere, characteristic of a compensatory mechanism. However it needs to be noted that the shift did not result in equal performance to the normal group. Thus the compensation pattern was inef-fective in matching the performance of the normative group, a result contrary to other reported research in the area when simple tasks are employed. This result may be due to the high cognitive demands of free recall as well as the problems with high task demand tasks in the TBI patient. In fact, the performance of the TBI group was 1.28 SD below the normal group (employ-ing means and SD of both groups) (TBI = 85, normal = 54) with an average of 3.2 years since time of acci-dent. In addition, the Shipley Institute of Living Verbal IQ estimate for the TBI group was some 9 points below the normative group, while the education level differ-ence was essentially the same (TBI-13.7 years of edu-cation; normative group 13.8 years of education). The nine point drop in IQ was also found with another TBI group using with the Wechsler Adult Intelligence Scale–Revised (Matarazzo & Herman, 1984). The abstraction scale of the Shipley revealed a seven point drop for the TBI group (Paulson & Lin, 1970). This particular group of TBI patients could be the 20% (or greater) who are hypothesized in the literature to experience signifi cant and long lasting problems as a result of the TBI. There was a signifi cant positive correlation between the Ship-ley verbal IQ measure (eyes closed) and time since ac-cident (�.32) indicating some resolution over time of verbal abilities. However, neither the Shipley abstrac-
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 493
Figure 18.9 Listening to paragraphs (N = 85). Arrows indicated decreased SCC values for TBI group at p <.005.
tion IQ measure nor the auditory memory score corre-lated positively with time since accident, indicating no spontaneous resolution of these problems.
The MTBI defi cits do not affect SCC alpha fl ash-light activity to a signifi cant degree. However, analyses of individual SCC alpha relationships do fi nd signifi cant defi cits for the MTBI group when compared to the nor-mative group. When the MTBI and normative group are combined and the relationships between qEEG vari-ables and task success are examined, the defi cit pattern
of SCC and phase beta2 relationships becomes predic-tive of success and failure on the task. The lowered SCC and phase beta2 relationships are negatively related to auditory memory performance, indicating that these variables are relevant to auditory memory (Thornton, 2002). As previously discussed, this type of data begins to answer how the defi cits caused by a TBI affect spe-cifi c abilities. In this example, the negative effect is on the normal predictors of auditory recall (SCC alpha rela-tionships) and decreased SCC and phase beta2 relation-
Figure 18.8 Stars represent origin of fl ashlight indicating the positive relations to total recall—within MTBI group.
Copyright Springer Publishing Company

494 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
ships. It has been hypothesized that this high frequency is intimately tied to memory processes (Lenz et al., 2008), refl ecting a conceptual link to these fi ndings.
Previously reported research with eyes-closed data (Leon-Carrion et al., 2008) had indicated defi cit coher-ence beta (13–20 Hz) problems related to function-ing problems. Thornton’s eyes-closed data did reveal differences between the TBI ( N = 92) and normative group ( N = 42) in the occipital locations (O1-O2) with higher values for the TBI group on relative power of beta2, peak amplitude of alpha, but lower microvolts alpha, similar to the Thatcher et al. (1989) report. The O1 position analysis revealed lower values of delta (peak amplitude delta, lower microvolt delta) & higher peak frequency delta values. The O2 location showed lower values of peak amplitude of beta1 but higher values of beta (peak frequency of beta1 and beta2) while the right frontal locations (F8, F4, Fp2) showed higher val-ues of peak frequency of beta2. The normal pattern of increased lower frequency (delta, theta) and decreased microvolts in the beta frequency range was not evident in our MTBI group, but were shown in previous reports in severe and moderate TBI (J. R. Hughes & John, 1999). In terms of SCC values the TBI group (eyes-closed data) had higher values of SCC theta fl ashlights from Fp1 and Fp2 while they had lower values of SCC alpha val-ues from mostly frontal and central locations (F3, F4, C3, C4, P4, Fz, and Cz). SCC beta2 values were lower for the TBI group from the C3, T5, and Fz locations. Lower frontal phase alpha values were lower for the TBI group (Fp1, Fp2, F7, T3 locations) and lower phase beta2 values from frontal (Fz) location. The increase in SCC theta from Fp1 was similar to the Thatcher (1989) result. In summary, the TBI appeared to have higher beta activation levels at the occipital locations and right frontal locations with increased frontal SCC theta and reduced SCC and phase values from the alpha to beta2 frequency.
In the Thornton (2003) research reports the major problems were evident in the beta2 frequency range and most dramatically evident under the listening condition. Although the alpha SCC values were also negatively affected, the effect was much more frequent in the beta2 frequency and considerably more evident in the listening task. For example, under listening conditions, there were signifi cant ( p value set at .05) lowered values in the TBI group ( N = 79) versus the normative group ( N = 45) in fl ashlight SCC alpha values ( N = 2), fl ashlight SCC beta2 (15), fl ashlight phase alpha (3), fl ashlight phase beta1 (3), fl ashlight phase beta2 ( N = 15). However, individual analysis (non-fl ashlight) of SCC relationships revealed negative
effects in all the frequencies, however, involving SCC and phase (delta, theta, alpha, beta1) mostly emanat-ing from frontal and temporal locations. This result is in line with previous reports of the effect of a TBI on frontal functioning.
qEEG Differences Between TBI and Normals During Auditory Memory Tasks We present the main activation differences between the TBI group and normals as the groups engage in the listening, immediate recall and delayed recall con-ditions. It is a critical point to understand that none of the following relative power differences, which dis-tinguish the TBI from the normal group, were evident under the commonly used eyes-closed condition while the SCC beta2 defi cit pattern was evident, albeit less so than in the cognitive tasks. Thus the eyes-closed database reports that the clinicians may come across are problematic in the identifi cation of a MTBI. Fig-ure 18.9 presents the signifi cant differences between the TBI and normative group during the listening task, with the p value set to .005. As can be seen in the fi gures the most prevalent results are the connection patterns across the hemispheres, implicating the role of the corpus callosum in the results. The fi gure also shows that the TBI group activated relative power of beta values in (right frontal relative power of beta2) frontal locations more than the normative group while decreasing relative power of delta values. This pattern was observed in the other measures of delta (peak am-plitude, microvolt) in frontal and other locations. Per-haps this frontal beta is the measure that refl ects the increased “effort” of the TBI group. However, it should also be repeated that the defi cits in Figure 18.9 were at the .005 level and below. When the individual rela-tionships are examined with respect to SD value dif-ferences, the homologous relationships generally (with some exceptions) had the greatest SD and raw score difference from Thornton’s (2001) normative group, indicating that the major effect in the relationships dis-played in Figure 18.9 were due to the CC effects, which are presented in Figure 18.10.
Figure 18.9 shows the breakdown of the homolo-gous (similar locations in opposite hemisphere) re-lationships and reveals that the signifi cant defi cits ( p value set at .05) involved these homologous loca-tions (except O1-O2) in SCC beta2 and phase beta2 (Fp1-Fp2, F7-F8, T3-T4) values. As homologous loca-tions are connected through the CC (Mildner, 2007), these results provide functional consistency with the
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 495
Figure 18.10 Relative power differences between TBI and normal in auditory memory task.
structural CC hypothesis evident in autopsy, DTI and other studies (Belanger et al., 2007; Taber et al., 2006; Wilde et al., 2008). In fi gure 18.10 the RDP indicates the relative power of Delta values lower for normals at p �.005, while RPB1 and RPB2 indicate the rela-tive power of beta1 and beta2 greater in TBI group at p �.05.
Corpus Callosum Effects
Figure 18.11 presents the signifi cant defi cits in homolo-gous relationships ( p = .05) for the SCC beta (CB2) and phase beta2 (PB2) values. The only other signifi -cant homologous patterns (with respect to frequency) that emerged were the T3-T4 lower phase relationships (delta, theta, alpha, beta1) and Fp1-Fp2 (SCC and phase delta) for the TBI group. It is unclear why these particu-lar locations and frequencies would be affected and not other homologous phase relationships.
The Thornton (2003) research report indicated that the relative power of beta1 values (12 locations of the 19 measured and involving fi ve of the seven frontal lo-cations) were negatively correlated with memory per-formance. A reasonable hypothesis would be that due to the damaged white matter in the TBI brain, the TBI patient activates beta activity (especially frontal) more than the normal group as a compensatory effort strategy, but this frontal activation is detrimental to the perfor-mance as memory performance, in adults, is predomi-nantly an issue of SCC activity. The TBI group was lower than the normative group on 27 individual SCC alpha relationships; only two alpha relationships in the right hemisphere were negatively affected (F8-T4, F4-C4) and
only one centrally (Fz-Cz). The remaining 24 defi cit SCC relationships involved left hemisphere locations. As left hemisphere SCC alpha relationships are the main cor-relates of auditory memory, these defi cits values can ex-plain the lowered memory performance in TBI. Thus, the defi cit pattern begins to elucidate the relationship between the effect of a TBI (defi cits in SCC beta2 and alpha values) on a specifi c cognitive task (auditory memory).
A similar pattern emerged for another auditory task (word list) both in terms of frontal beta activations and decreased values for the TBI group in the SCC and phase beta2 relationships (diffuse, but with greatest ef-fects from frontal locations). The homologous location defi cit was not as evident (although still signifi cant) in this task for the TBI group.
In terms of activation levels from auditory attention, the TBI group increased beta1 relative power at the T4 location 9.6 points while the normative group decreased this beta1 relative power value 8 points, confi rming a previous pattern noted of greater right hemisphere ac-tivation in the TBI group. In addition, an examination (Figure 18.9) of successful recall within the TBI group in-dicated there are positive correlations between T4 (phase beta1) and F7 (phase beta2) (Thornton, 2003). Thus the TBI group is increasing beta1 activity at a right hemi-sphere temporal location (T4) and increasing phase beta1 to obtain better memory scores while the normal subject is increasing coherence alpha from left hemisphere tem-poral locations (T3 and others) to obtain better memory scores. Thus the right hemisphere compensation argu-ment appears to have some weight with these results as the TBI patient is employing the right hemisphere tem-
Copyright Springer Publishing Company

496 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
poral location (T4) to improve performance while the normal group employs the left temporal (T3).
In a visually oriented task, a similar pattern (al-beit much weaker) was observed with respect to fron-tal beta activations and decreases in SCC and phase beta2 relationships from frontal locations. Of some interest to note, however, is that the frontal SCC and phase theta values were generally higher in the TBI group than the normative group. SCC theta values were negatively related to reading memory in the normative group. This type of analysis will begin to allow researchers to narrow in on the defi cient pat-terns that need to be addressed in the rehabilitation interventions.
As Figure 18.12 indicates, during the immediate re-call period the TBI values were similar to their relative values during the input stage, that is, lower levels of RPD (especially frontal), elevated levels of frontal beta (especially right frontal) and lowered levels of SCC alpha and beta2 as well as lower levels of phase beta2. The p value level was set to .05 for this analysis to display the broad effects on the SCC and phase beta2 relationships. If both the TBI and normative group are combined ( N = 114) and the recall performance is correlated with the qEEG variables, then the results indicate sev-eral positive relationships between RPD in frontal loca-
tions (Fp2, F7, F8, F3, F4) and MD at Fp2 and F4 and memory scores. Negative relationships with memory scores were evident with all frontal beta1 relative power values, beta1 relative power at T3 & C3, frontal beta2 relative power values (Fp2, F7, F8, F3, F4), and peak amplitude and microvolt beta2 (F7, F8, F3, F4).
Positive relationships between recall performance and SCC beta2 were evident from frontal locations (F7, F8, F3, F4, and F3) phase beta2. In other words, what the TBI group was doing differently from the norma-tive group (increased frontal beta activity, decreased frontal delta and decreased frontal SCC beta activity) was negatively related to success at recall. Within the TBI group ( N = 69) the following delta variables were positively related to recall (RPD-F7, F3, F4, T3, T4) with negative relationships for beta (RPB1-F7, F3; T4—peak amplitude and microvolt beta1 and beta2; and T3—microvolt beta1). Thus, within the TBI the same pattern of decreased frontal delta and increased beta activity was negatively related to recall.
Figure 18.13 presents the differences during the long-term recall part of the task. The delay period was about 20 minutes after the initial task.
As Table 18.2 indicates in the delayed recall condi-tion the TBI has higher activation levels of the frontal (especially right frontal) beta values but this time has
Figure 18.11 Homologous location SCC defi cits in TBI group.
CB2 PB2
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 497
Figure 18.12 Immediate recall period: TBI versus normative group.
higher beta2 levels in all posterior locations as well as right hemisphere beta2 variables (relative power, peak frequency). Almost all of the TBI group’s peak ampli-tude and microvolt delta values were below the norma-tive levels (not visually presented). As left hemisphere (T3) SCC alpha relationships are positively related to successful delayed recall, there is a physiological “ex-planation” of the reasons for the TBI poor performance. The delayed recall condition shows a similar pattern of decreased frontal delta and increased frontal beta in the TBI group compared to the normative group but with the addition of greater posterior beta activation in the TBI group, which was unrelated to memory perfor-mance. This posterior beta activation pattern is similar to the fi ndings of the Ricker et al. (2001) study, which found greater posterior rCBF (vs. controls) in the TBI group during free recall as well as greater right hemi-sphere activity and more dispersed activity (i.e., greater beta activations across diverse locations). In summary, the TBI patient’s response pattern (vs. normals) is very similar across all three auditory memory tasks. The TBI patient decreases frontal delta, increases frontal and
right hemisphere beta activity and decreases SCC levels, all of which contribute to lower memory scores.
TBI Rehabilitation Examples We provide some examples of how the qEEG activa-tion evaluation allows for useful understanding of the cognitive defi cits of the TBI patient and how the spe-cifi c qEEG information allows for effective rehabilita-tion of the cognitive problems associated with a TBI. Some of the issues facing rehabilitation in this area have been successfully addressed with the activation qEEG database. These issues include the effect of age, multiple TBIs, structural lesions (such as hemato-mas) time since injury and surgical intervention in anatomically important locations for memory. Single-case studies have been documented that indicate the ability of the approach to be successful in all of these situations.
Case study 1 was a 69-year-old female who had suffered a left frontal hematoma as a result of an
Copyright Springer Publishing Company

498 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
Figure 18.13 Delayed recall differences between TBI and normal group.
MVA. She was in a coma for several months. She en-tered treatment 2 years after the MVA. At the onset of the interventions she was able to recall 9.75 pieces of information from the paragraph recall task (im-mediate and delayed recall) and by the end of treat-ment she was recalling 32.5 pieces of information. A piece of information is a section of text that ex-presses an idea. For example, in a story that starts with “John Smith / went to the grocery store / on a Saturday” there are 3 pieces of information that are separated by the forward slashes. The interven-tions focused on the phase and SCC relationships be-tween Fp1 and F3 and Fp1 and T3, which showed signifi cant defi cits, presumable caused by the left frontal hematoma. She was able to substantially im-prove the values of the variables affected (Fp1-F3 phase beta2—from 35 to 70; Fp1-T3 phase alpha—from 52 to 66).
In case 2, the 34-year-old male patient underwent stereotaxic surgical removal of portions of his left an-terior temporal lobe, hippocampus and amygdala for seizures. He started with a total base memory of 11 and
was obtaining a total recall score of 19 by the end of the treatment. In case 3, the 48-year-old had experienced a TBI some 15 years prior to the evaluation. The patient’s initial recall score was 11.5 and by the end of the treat-ment he was obtaining a score of 31. A one year follow up assessment revealed that his memory had continued to improve as he obtained a score of 37.5. In case 4, there was a history of multiple mild head injuries as the patient was a 40-year-old stunt actress. The average SCC beta2 value from the right frontal location (F8) to the left posterior locations (T5, P3, O1) was 52. After 40 sessions she had improved this value to 74 (norma-tive group is 70) or 6.32 SD units. Her auditory memory improved from 16 to 37.5 and her reading memory im-proved from 25 to 43.
While it is important to demonstrate improvement on neuropsychological memory measures, it is also rel-evant to demonstrate that there are relevant changes in the qEEG values. In case 5, the individual was involved in a serious MVA during which his car fl ipped over twice resulting in the roof being caved in. The posterior and superior sections of his head impacted on different
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 499
structures of the car. He felt dazed, dizzy, had a “huge” bump on his head, and was in ICU for 5 days. Table 18.3 shows the initial Z score difference from the normative control group, the Z score difference following the treat-ment and the total Z score change. The values represent the average values across all 9 cognitive tasks involved in the evaluation (not including the eyes-closed con-dition). In the initial evaluation, the patient’s qEEG pattern showed excessive delta activity at T5 and P3. Treatment interventions were focused on this problem with the resultant changes shown in Table 18.3. The table presents the relative power values for the different frequencies in the left and right frontal and posterior locations, where the greatest changes occurred.
Of some interest to note is the increased beta activ-ity in the left frontal versus right frontal as well as left posterior versus right posterior. In both left hemisphere quadrants there was a greater decrease in delta and greater increase in beta activity. Table 18.4 presents the SCC beta changes at these respective locations.
As Table 18.3 indicates there was signifi cant im-provement in SCC beta activity. Overall (across all lo-cations) delta SCC values increased .24 SD , theta SCC values increased .72 SD , alpha SCC values increased .47 SD , beta1 SCC values increased 1.29 and SCC beta2 val-ues increased an average of 1.19 SD .
The cognitive changes included the following: a de-crease in errors on the Category test (77 to 56), Shipley IQ increase (99 to 113), improved total recall score on the CVLT (43 to 53) or standard score increase (25 to 41), decreased time (10 minutes to 7 minutes) and errors (13 to 5) on a visual scanning test developed by Thorn-ton, improvement in paragraph recall raw score value (22 to 36), improvement in raw reading recall scores from 5.5 to 18, no signifi cant change on the CALCAP reaction time test or Michigan Serial recall test of work-ing memory, and poorer performance on the Wisconsin Card Sorting Test. The CALCAP reaction time test is a series of 10 tasks requiring rapid responses (tapping a spacebar) based upon conceptual rules provided to the patient by the software. The focus of the treatment was on auditory recall.
In specifi c improvements in SCC alpha were ob-tained under the auditory recall condition. The SD change (post vs. pre) from the normative reference group averaged .72 SD across all locations and .69 SD on the fi ve predictors of auditory recall in Thornton’s (2001) normative sample (T3, F7, C3, F8, P3). The total SCC alpha relationships in the initial evaluation were −1.04 SD below the normative group and −.18 SD below normative group upon reevaluation. This change indicates that the intervention can return the TBI
18.3 Pre-Tx (Treatment) Versus Post-Tx SD Changes
LEFTHEMISPHERE
PRE-TX EVAL.
POST-TXEVAL.
SDCHANGE
RIGHTHEMISPHERE PRE–TX EVAL.
POST-TXEVAL.
SDCHANGE
F7: DeltaBeta1Beta2
�.521.8
�.13
�1.42.7.25
�.90.85.40
F8: DeltaBeta1Beta2
�.621.5.27
�1.22.2.22
�.56.67
�.05
F3: DeltaBeta1Beta2
�.311.5
�.40
�1.32.3.30
�1.0.85.69
F4: DeltaBeta1Beta2
�1.01.8
�.15
�1.21.90.0
�.20.08.15
T5: DeltaBeta1Beta2
.28
.90�.24
�.721.7.16
�1.0.84.43
T6: DeltaBeta1Beta2
�.47.61
1.3
�.85.95
1.4
�.38.34.16
P3: DeltaBeta1Beta2
.63
.91�.23
�.641.8.41
�1.3.91.65
P4: DeltaBeta1Beta2
�.701.2.69
�.911.5.87
�.21.28.18
Copyright Springer Publishing Company

500 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
18.4 Pre-Tx (Treatment) Versus Post-Tx SD Changes
LEFTHEMISPHERE
PRE-TXEVAL.
POST-TXEVAL.
SDCHANGE
RIGHTHEMISPHERE
PRE-TXEVAL.
POST-TXEVAL.
SDCHANGE
F7: Beta1Beta2
.29�.16
1.61.2
1.31.3
F8: Beta1Beta2
�.67�.62
.791.0
1.51.6
F3: Beta1Beta2
�.11�.22
1.21.1
1.31.3
F4: Beta1Beta2
�.35�.21
1.21.3
1.61.5
T5: Beta1Beta2
.16
.011.51.0
1.41.0
T6: Beta1Beta2
�.08�.25
1.0.26
1.1.51
P3: Beta1Beta2
�.35�.31
.88
.751.21.1
P4: Beta1Beta2
�.21�.31
.95
.781.21.1
individual to the normal effective response pattern and thus improve the underlying electrophysiological defi cit involved. This is the fi rst line of evidence that the cogni-tive defi cit in TBI can be returned to normal functioning both on a performance level as well as the electrophysi-ological level.
The conclusion from this above detailed analysis is that rehabilitation EEG biofeedback protocols need to be individualized, can be meaningfully related to specifi c cognitive skills, can be effectively addressed with EEG biofeedback employing the CAR model, can effectively address physical damage caused by a TBI, can obtain generalization of effects both in terms of cognitive abili-ties and qEEG variables, and can obtain signifi cantly better results than presently employed methods in the fi elds of rehabilitation of the learning disabled child and traumatic brain injured adult.
CONCLUSION AND RECOMMENDATIONS
The DTI, ERP, and qEEG approaches to the understand-ing the diagnostic issues of TBI appear to be the most productive. In providing useful rehabilitation informa-tion the qEEG appears to be the instrument of choice. Modern medical imaging technology has brought us forward with a better understanding (albeit still incom-plete) of what occurs in TBI. Rehabilitation efforts have been extremely limited in their effectiveness and lack-ing a sound empirical basis. The activation quantitative EEG offers a possible improved conceptual and empiri-
cal foundation to our understanding and rehabilitation efforts. The research results for qEEG interventions for auditory memory appear to be adequate for the TBI pa-tients at the present time.
REFERENCES Advani, S. H., Ommaya, A. K., & Yang, W. J. (1982). Head in-
jury mechanisms, characteristics and clinical evaluation. In D. Chista (Ed.), Human body dynamics (pp. 3–37). New York: Oxford University Press.
Alexander, M. P. (1992). Neuropsychiatric correlates of persistent postconcussive syndrome. Journal of Head Trauma Rehabilita-tion, 7, 60–69.
Alster, J., Pratt, H., & Feinsod, M. (1993). Density spectral array, evoked potentials, and temperature rhythms in the evalua-tion and prognosis of the comatose patient. Brain Injury, 7 (3), 191–208.
Anderson, C. V., Bigler, E. D., & Blatter, D. D. (1995). Frontal lobe lesions, diffuse damage, and neuropsychological functioning in traumatic brain-injured patients. Journal of Clinical and Ex-perimental Neuropsychology, 17 (6), 900–908.
Anderson, V., & Catroppa, C. (2005). Recovery of executive skills following paediatric traumatic brain injury (TBI): A 2 year follow-up. Brain Injury, 19 (6), 459–470.
Andrews, T. K., Rose, F. D., & Johnson, D. A. (1998). Social and behavioural effects of traumatic brain injury in children. Brain Injury, 12 (2), 133–138.
Arciniegas, D., Adler, L., Topkoff, J., Cawthra, E., Filley, C.M., & Reite, M. (1999). Attention and memory dysfunction after traumatic brain injury: Cholinergic mechanisms, sensory gat-ing, and a hypothesis for further investigation. /Brain Injury/, /13/, 1–13.
Arciniegas, D. B., Anderson, C. A., Topkoff, J., & McAllister, T. W. (2005). Mild traumatic brain injury: A neuropsychiatric ap-
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 501
proach to diagnosis, evaluation, and treatment. Neuropsychi-atric Disease and Treatment, 1 (4), 311–327.
Arciniegas, D. B., & Topkoff, J. L. (2004). Applications of the P50 evoked response to the evaluation of cognitive impairments after traumatic brain injury. American Journal of Physical Medicine & Rehabilitation, 15 (1), 177–203.
Arfanakis, K., Hermann, B. P., Rogers, B. P., Carew, J. D., Seiden-berg, M., & Meyerand, M. E. (2002). Diffusion tensor MRI in temporal lobe epilepsy. Magnetic Resonance Imaging, 20 (7), 511–519.
Ashman, T. A., Cantor, J. B., Gordon, W. A., Sacks, A., Spielman, L., Egan, M., et al. (2008). A comparison of cognitive function-ing in older adults with and without traumatic brain injury. Journal of Head Trauma Rehabilitation, 23 (3), 139–148.
Ashman, T. A., Schwartz, M. E., Cantor, J. B., Hibbard, M. R., & Gordon, W. A. (2004). Screening for substance abuse in in-dividuals with traumatic brain injury. Brain Injury, 18 (2), 191–202.
Bailey, C. M., Echemendia, R. J., & Arnett, P. A. (2006). The impact of motivation on neuropsychological performance in sports-related mild traumatic brain injury. Journal of the Inter-national Neuropsychological Society, 12 (4), 475–484.
Beetar, J. T., Guilmette, T. J., & Sparadeo, F. R. (1996). Sleep and pain complaints in symptomatic traumatic brain injury and neurologic populations. Archives of Physical Medicine and Re-habilitation, 77 (12), 1298–1302.
Begic, D., Hotujac, L., & Jokic-Begic, N. (2001). Electroencepha-lographic comparison of veterans with combat-related post-traumatic stress disorder and healthy subjects. International Journal of Psychophysiology, 40 (2), 167–172.
Belanger, H. G., Vanderploeg, R. D., Curtiss, G., & Warden, D. L. (2007). Recent neuroimaging techniques in mild traumatic brain injury. Journal of Neuropsychiatry & Clinical Neurosci-ences, 19 (1), 5–20.
Bendlin, B. B., Ries, M. L., Lazar, M., Alexander, A. L., Dempsey, R. J., Rowley, H. A., et al. (2008). Longitudinal changes in patients with traumatic brain injury assessed with diffusion-tensor and volumetric imaging. Neuroimage, 42 (2), 503–514.
Bigler, E. D. (2001). The lesion(s) in traumatic brain injury: Impli-cations for clinical neuropsychology. Archives of Clinical Neu-ropsychology, 16 (2), 95–131.
Binder, L. M., & Rohling, M. L. (1996). Money matters: A meta-analytic review of the effects of fi nancial incentives on recov-ery after closed-head injury. American Journal of Psychiatry, 153 (1), 7–10.
Binder, L. M., Rohling, M. L., & Larrabee, G. J. (1997). A review of mild head trauma. Part I: Meta-analytic review of neuropsy-chological studies. Journal of Clinical Experimental Neuropsy-chology, 19 (3), 421–431.
Bonne, O., Gilboa, A., Louzoun, Y., Kempf-Sherf, O., Katz, M., Fishman, Y., et al. (2003). Cerebral blood fl ow in chronic symptomatic mild traumatic brain injury. Psychiatry Research, 124 (3), 141–152.
Borg, J., Holm, L., Cassidy, J. D., Peloso, P. M., Carroll, L. J., von Holst, H., et al. (2004). Diagnostic procedures in mild trau-matic brain injury: Results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. Journal of Rehabili-tation Medicine (Suppl. 43), 61–75.
Braakman, R. (1992). Early prediction of outcome in severe head injury. Acta Neurochirurgica, 116 (2–4), 161–163.
Braitenberg, V. (1972). Comparison of different cortices as a basis for speculation on their functions. In H. Petsche & M. A. B. Brazier (Eds.), Synchronization of EEG activity in epilepsies (pp. 443–465). New York: Springer.
Braitenberg, V. (1978). Cortical architectonics: General and areal. In M. A. B. Brazier & H. Petsche (Eds.), Architectonics of the cerebral cortex (pp. 443–465). New York: Raven Press.
Braver, T. S., Cohen, J. D., Nystrom, L. E., Jonides, J., Smith, E. E., & Noll, D. C. (1997). A parametric study of prefrontal cortex involvement in human working memory. Neuroimage, 5 (1), 49–62.
Broglio, S. P., Macciocchi, S. N., & Ferrara, M. S. (2007). Sensitiv-ity of the concussion assessment battery. Neurosurgery, 60 (6), 1050–1057.
Broshek, D. K., Kaushik, T., Freeman, J. R., Erlanger, D., Webbe, F., & Barth, J. T. (2005). Sex differences in outcome follow-ing sports-related concussion. Journal of Neurosurgery, 102 (5), 856–863.
Bush, S. S., Ruff, R. M., Troster, A. I., Barth, J. T., Koffl er, S. P., Pliskin, N. H., et al. (2005). Symptom validity assessment: Practice issues and medical necessity NAN policy & plan-ning committee. Archives of Clinical Neuropsychology, 20 (4), 419–426.
Carmody, D. P., & Lewis, M. (2006). Brain activation when hear-ing one’s own and others’ names. Brain Research, 1116 (1), 153–158.
Carmody, D. P., Quintela, J., Radvanski, D. C., Sabo, M. J., & Giorgi, J. (1999). Neurofeedback training and attention disor-ders in an elementary school setting. Journal of Neurotherapy, 3 (4), 59.
Carmody, D. P., Radvanski, D. C., Wadhwani, S., Sabo, M. J., & Vergara, L. (2001). Neurofeedback training and attention defi cit hyperactivity disorder in an elementary school setting. Journal of Neurotherapy, 4 (3), 5–27.
Catroppa, C., & Anderson, V. (1999). Attentional skills in the acute phase following pediatric traumatic brain injury. Child Neuropsychology, 5 (4), 251–264.
Catroppa, C., & Anderson, V. (2002). Recovery in memory func-tion in the fi rst year following TBI in children. Brain Injury, 16 (5), 369–384.
Catroppa, C., Anderson, V. A., Morse, S. A., Haritou, F., & Rosen-feld, J. V. (2007). Children’s attentional skills 5 years post-TBI. Journal of Pediatric Psychology, 32 (3), 354–369.
Centers for Disease Control and Prevention. (2003). Heads up: Facts for physicians about mild traumatic brain injury (MTBI). Department of Health and Human Services: Centers for Dis-ease Control and Prevention.
Centers for Disease Control and Prevention. (2008). What is traumatic brain injury? Retrieved from http://www.cdc.gov/ncipc/tbi/tbi.htm
Chaytor, N., & Schmitter-Edgecombe, M. (2003). The ecological validity of neuropsychological tests: A review of the literature on everyday cognitive skills. Neuropsychology Review, 13 (4), 181–197.
Chen, J. K., Johnston, K. M., Frey, S., Petrides, M., Worsley, K., & Ptito, A. (2004). Functional abnormalities in symptomatic con-cussed athletes: An fMRI study. Neuroimage, 22 (1), 68–82.
Copyright Springer Publishing Company

502 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
Chen, S. H., Kareken, D. A., Fastenau, P. S., Trexler, L. E., & Hutchins, G. D. (2003). A study of persistent post-concussion symptoms in mild head trauma using positron emission to-mography. Journal of Neurology, Neurosurgery and Psychiatry, 74 (3), 326–332.
Christodoulou, C., DeLuca, J., Ricker, J. H., Madigan, N. K., Bly, B. M., Lange, G., et al. (2001). Functional magnetic resonance imaging of working memory impairment after traumatic brain injury. Journal of Neurology, Neurosurgery and Psychiatry, 71 (2), 161–168.
Cifu, D. X., Keyser-Marcus, L., Lopez, E., Wehman, P., Kreutzer, J. S., Englander, J., et al. (1997). Acute predictors of successful return to work 1 year after traumatic brain injury: A multi-center analysis. Archives of Physical Medicine and Rehabilita-tion, 78 (2), 125–131.
Cohen, B. A., Inglese, M., Rusinek, H., Babb, J. S., Grossman, R. I., & Gonen, O. (2007). Proton MR spectroscopy and MRI-vol-umetry in mild traumatic brain injury. AJNR American Journal of Neuroradiology, 28 (5), 907–913.
Collie, A., Makdissi, M., Maruff, P., Bennell, K., & McCrory, P. (2006). Cognition in the days following concussion: Compari-son of symptomatic versus asymptomatic athletes. Journal of Neurology, Neurosurgery and Psychiatry, 77 (2), 241–245.
Collins, M. W., Grindel, S. H., Lovell, M. R., Dede, D. E., Mo-ser, D. J., Phalin, B. R., et al. (1999). Relationship between concussion and neuropsychological performance in college football players. Journal of the American Medical Association, 282 (10), 964–970.
Collins, M. W., & Hawn, K. L. (2002). The clinical management of sports concussion. Current Sports Medicine Reports, 1 (1), 12–22.
Collins, M. W., Lovell, M. R., Iverson, G. L., Cantu, R. C., Maroon, J. C., & Field, M. (2002). Cumulative effects of concussion in high school athletes. Neurosurgery, 51 (5), 1175–1179; discus-sion 1180–1171.
Collura, T. F. (2008). Towards a coherent view of brain connectiv-ity. Journal of Neurotherapy, 12 (2/3), 99–110.
Covassin, T., Schatz, P., & Swanik, C. B. (2007). Sex differences in neuropsychological function and post-concussion symptoms of concussed collegiate athletes. Neurosurgery, 61 (2), 345–350; discussion 350–341.
Daniel, J. C., Olesniewicz, M. H., Reeves, D. L., Tam, D., Bleiberg, J., Thatcher, R., et al. (1999). Repeated measures of cognitive processing effi ciency in adolescent athletes: Implications for monitoring recovery from concussion. Neuropsychiatry, Neu-ropsychology, and Behavioral Neurology, 12 (3), 167–169.
Davidson, R. J., Coe, C. C., Dolski, I., & Donzella, B. (1999). Indi-vidual differences in prefrontal activation asymmetry predict natural killer cell activity at rest and in response to challenge. Brain Behavior and Immunology, 13 (2), 93–108.
De Beaumont, L., Brisson, B., Lassonde, M., & Jolicoeur, P. (2007). Long-term electrophysiological changes in athletes with a history of multiple concussions. Brain Injury, 21 (6), 631–644.
De Kruijk, J. R., Leffers, P., Menheere, P. P., Meerhoff, S., Rutten, J., & Twijnstra, A. (2002). Prediction of post-traumatic com-plaints after mild traumatic brain injury: Early symptoms and biochemical markers. Journal of Neurology, Neurosurgery and Psychiatry, 73 (6), 727–732.
Deb, S., Lyons, I., Koutzoukis, C., Ali, I., & McCarthy, G. (1999). Rate of psychiatric illness 1 year after traumatic brain injury. American Journal of Psychiatry, 156 (3), 374–378.
Destexhe, A., Contreras, D., & Steriade, M. (1998). Mechanisms underlying the synchronizing action of corticothalamic feed-back through inhibition of thalamic relay cells. Journal of Neu-rophysiology, 79 (2), 999–1016.
Dikmen, S., McLean, A., Jr., Temkin, N. R., & Wyler, A. R. (1986). Neuropsychologic outcome at one-month postinjury. Archives of Physical Medicine and Rehabilitation, 67 (8), 507–513.
Di Scala, C., Gallagher, S. S., & Schneps, S. E. (1997). Causes and outcomes of pediatric injuries occurring at school. Journal of School Health, 67 (9), 384–389.
Duara, R., Barker, W. W., Chang, J., Yoshii, F., Loewenstein, D. A., & Pascal, S. (1992). Viability of neocortical function shown in behavioral activation state PET studies in Alzheimer disease. Journal of Cerebral Blood Flow and Metabolism, 12 (6), 927–934.
Dupuis, F., Johnston, K. M., Lavoie, M., Lepore, F., & Lassonde, M. (2000). Concussions in athletes produce brain dysfunction as revealed by event-related potentials. Neuroreport, 11 (18), 4087–4092.
Easdon, C., Levine, B., O’Connor, C., Tisserand, D., & Hevenor, S. (2004). Neural activity associated with response inhibition fol-lowing traumatic brain injury: An event-related fMRI investi-gation. Brain and Cognition, 54 (2), 136–138.
Echemendia, R. J., Putukian, M., Mackin, R. S., Julian, L., & Shoss, N. (2001). Neuropsychological test performance prior to and following sports-related mild traumatic brain injury. Clinical Journal of Sport Medicine, 11 (1), 23–31.
Ellemberg, D., Leclerc, S., Couture, S., & Daigle, C. (2007). Pro-longed neuropsychological impairments following a fi rst con-cussion in female university soccer athletes. Clinical Journal of Sport Medicine, 17 (5), 369–374.
Emerson, C. S., Headrick, J. P., & Vink, R. (1993). Estrogen im-proves biochemical and neurologic outcome following trau-matic brain injury in male rats, but not in females. Brain Research, 608 (1), 95–100.
Emmerling, M. R., Morganti-Kossmann, M. C., Kossmann, T., Sta-hel, P. F., Watson, M. D., Evans, L. M., et al. (2000). Traumatic brain injury elevates the Alzheimer’s amyloid peptide A beta 42 in human CSF. A possible role for nerve cell injury. Annals of the New York Academy of Sciences, 903 , 118–122.
Erlanger, D. (2002). HeadMinder Concussion Resolution Index (CRI): Professional manual. New York: HeadMinder.
Erlanger, D., Saliba, E., Barth, J., Almquist, J., Webright, W., & Freeman, J. (2001). Monitoring resolution of post-concussion symptoms in athletes: Preliminary results of a web-based neuropsychological test protocol. Journal of Athletic Training, 36 (3), 280–287.
Ewing-Cobbs, L., Fletcher, J. M., Levin, H. S., Francis, D. J., Da-vidson, K., & Miner, M. E. (1997). Longitudinal neuropsycho-logical outcome in infants and preschoolers with traumatic brain injury. Journal of the International Neuropsychological Society, 3 (6), 581–591.
Ewing-Cobbs, L., Prasad, M., Fletcher, J. M., Levin, H. S., Miner, M. E., & Eisenberg, H. M. (1998). Attention after pediatric traumatic brain injury: A multidimensional assessment. Child Neuropsychology, 4 (1), 35–48.
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 503
Ewing-Cobbs, L., Prasad, M. R., Kramer, L., Cox, C. S., Jr., Baumgartner, J., Fletcher, S., et al. (2006). Late intellectual and academic outcomes following traumatic brain injury sus-tained during early childhood. Journal of Neurosurgery, 105 (4 Suppl.), 287–296.
Fabiano, R. J., & Crewe, N. (1995). Variables associated with em-ployment following severe traumatic brain injury. Rehabilita-tion Psychology, 40, 223–231.
Fallgatter, A. J., & Strik, W. K. (1997). Right frontal activation during the continuous performance test assessed with near-infrared spectroscopy in healthy subjects. Neuroscience Let-ters, 223 (2), 89–92.
Farace, E., & Alves, W. M. (2000). Do women fare worse: A metaanalysis of gender differences in traumatic brain injury outcome. Journal of Neurosurgery, 93 (4), 539–545.
Fedoroff, J. P., Starkstein, S. E., Forrester, A. W., Geisler, F. H., Jorge, R. E., Arndt, S. V., et al. (1992). Depression in patients with acute traumatic brain injury. American Journal of Psy-chiatry, 149 (7), 918–923.
Fee, C. R., & Rutherford, W. H. (1988). A study of the effect of legal settlement on post-concussion symptoms. Archives of Emergency Medicine, 5 (1), 12–17.
Field, M., Collins, M. W., Lovell, M. R., & Maroon, J. (2003). Does age play a role in recovery from sports-related concussion? A comparison of high school and collegiate athletes. Journal of Pediatrics, 142 (5), 546–553.
Finkelstein, E., Corso, P., & Miller, T. (2006). Incidence and eco-nomic burden of injuries in the United States, 2000. New York: Oxford University Press.
Fletcher, J. M., Miner, M. E., & Ewing-Cobbs, L. (1987). Age and recovery from head injury in children: Developmental issues. In H. S. Levin, J. Grafman, & H. M. Eisenberg (Eds.), Neurobe-havioral recovery from head injury (pp. 279–291). New York: Oxford University Press.
Gale, S. D., Johnson, S. C., Bigler, E. D., & Blatter, D. D. (1995). Nonspecifi c white matter degeneration following traumatic brain injury. Journal of the International Neuropsychological Society, 1 (1), 17–28.
Gebke, K. B. (2002). Mild traumatic brain injury. Current Sports Medicine Reports, 1 (1), 23–27.
Gentry, L. R., Thompson, B., & Godersky, J. C. (1988). Trauma to the corpus callosum: MR features. AJNR American Journal of Neuroradiology, 9 (6), 1129–1138.
Ghajar, J., & Ivry, R. B. (2008). The predictive brain state: Timing defi ciency in traumatic brain injury? Neurorehabilitation and Neural Repair, 22 (3), 217–227.
Gennarelli, T. A., Thibault, L. E., Adams, J. H., Graham, D. I., Thompson, C. J., & Marcincin, R. P. (1982). Diffuse axonal injury and traumatic coma in the primate. Annals of Neurol-ogy, 12 (6), 564–574.
Goldacre, M. J., Abisgold, J. D., Yeates, D. G., & Seagroatt, V. (2006). Risk of multiple sclerosis after head injury: Record linkage study. Journal of Neurology, Neurosurgery and Psychia-try, 77 (3), 351–353.
Gorrie, C., Dufl ou, J., Brown, J., Gibson, T., & Waite, P. M. (2001). Extent and distribution of vascular brain injury in pediatric road fatalities. Journal of Neurotrauma, 18 (9), 849–860.
Gosselin, N., Theriault, M., Leclerc, S., Montplaisir, J., & Las-sonde, M. (2006). Neurophysiological anomalies in symp-
tomatic and asymptomatic concussed athletes. Neurosurgery, 58 (6), 1151–1161.
Grindel, S. H. (2006). The use, abuse, and future of neuropsy-chologic testing in mild traumatic brain injury. Current Sports Medicine Reports, 5 (1), 9–14.
Gross, H., Kling, A., Henry, G., Herndon, C., & Lavretsky, H. (1996). Local cerebral glucose metabolism in patients with long-term behavioral and cognitive defi cits following mild traumatic brain injury. Journal of Neuropsychiatry and Clini-cal Neurosciences, 8 (3), 324–334.
Guskiewicz, K. M. (2001). Postural stability assessment following concussion: One piece of the puzzle. Clinical Journal of Sport Medicine, 11 (3), 182–189.
Guskiewicz, K. M., Marshall, S. W., Bailes, J., McCrea, M., Cantu, R. C., Randolph, C., et al. (2005). Association between recur-rent concussion and late-life cognitive impairment in retired professional football players. Neurosurgery, 57 (4), 719–726.
Guskiewicz, K. M., Marshall, S. W., Bailes, J., McCrea, M., Hard-ing, H. P., Jr., Matthews, A., et al. (2007). Recurrent concus-sion and risk of depression in retired professional football players. Medicine & Science in Sports & Exercise, 39 (6), 903–909.
Guskiewicz, K. M., Weaver, N. L., Padua, D. A., & Garrett, W. E., Jr. (2000). Epidemiology of concussion in collegiate and high school football players. American Journal of Sports Medicine, 28 (5), 643–650.
Gusnard, D. A., Akbudak, E., Shulman, G. L., & Raichle, M. E. (2001). Medial prefrontal cortex and self-referential mental activity: Relation to a default mode of brain function. Proceed-ings of the National Academy of Sciences, USA, 98 (7), 4259–4264.
Gusnard, D. A., & Raichle, M. E. (2001). Searching for a baseline: Functional imaging and the resting human brain. Nature Re-views Neuroscience, 2 (10), 685–694.
Helmick, K., Guskiewicz, K., Barth, J., Cantu, R., Kelly, J. P., McDonald, E., et al. (2006). Defense and veterans brain in-jury center working group on the acute management of mild traumatic brain injury in military operational settings: Clinical practice guideline and recommendations. Retrieved Septem-ber 4, 2006, from http://www.pdhealth.mil/downloads/clinical_practice_guideline_recommendations.pdf
Hessen, E., Nestvold, K., & Anderson, V. (2007). Neuropsycho-logical function 23 years after mild traumatic brain injury: A comparison of outcome after paediatric and adult head inju-ries. Brain Injury, 21 (9), 963–979.
Hofman, P. A., Stapert, S. Z., van Kroonenburgh, M. J., Jolles, J., de Kruijk, J., & Wilmink, J. T. (2001). MR imaging, single-photon emission CT, and neurocognitive performance after mild trau-matic brain injury. American Journal of Neuroradiology, 22 (3), 441–449.
Holbourn, A.H.S. (1943). The mechanics of head injuries. Lancet, 2, 438–441.
Holbourn, A.H.S. (1945). The mechanics of brain injuries. British Medical Bulletin, 622, 147–149.
Holsinger, T., Steffens, D. C., Phillips, C., Helms, M. J., Havlik, R. J., Breitner, J. C., et al. (2002). Head injury in early adult-hood and the lifetime risk of depression. Archives of General Psychiatry, 59 (1), 17–22.
Copyright Springer Publishing Company

504 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
Hovda, D. A., Prins, M., & Becker, D. P. (1999). Neurobiology of concussion In J. E. Bailes, M. R. Lovell, & J. C. Maroon (Eds.), Sports-related concussion (pp. 12–51). St. Louis: Quality Medi-cal Publishing.
Hughes, D. G., Jackson, A., Mason, D. L., Berry, E., Hollis, S., & Yates, D. W. (2004). Abnormalities on magnetic resonance im-aging seen acutely following mild traumatic brain injury: Cor-relation with neuropsychological tests and delayed recovery. Neuroradiology, 46 (7), 550–558.
Hughes, J. R., & John, E. R. (1999). Conventional and quantita-tive electroencephalography in psychiatry. Journal of Neurop-sychiatry and Clinical Neuroscience, 11 (2), 190–208.
Ingebrigtsen, T., Waterloo, K., Marup-Jensen, S., Attner, E., & Romner, B. (1998). Quantifi cation of post-concussion symp-toms 3 months after minor head injury in 100 consecutive pa-tients. Journal of Neurology, 245 (9), 609–612.
Iverson, G. L., Gaetz, M., Lovell, M. R., & Collins, M. W. (2004). Cumulative effects of concussion in amateur athletes. Brain Injury, 18 (5), 433–443.
Iverson, G. L., Lovell, M. R., & Collins, M. W. (2003). Interpreting change on ImPACT following sport concussion. Clinical Neu-ropsychology, 17 (4), 460–467.
Jantzen, K. J., Anderson, B., Steinberg, F. L., & Kelso, J. A. (2004). A prospective functional MR imaging study of mild traumatic brain injury in college football players. AJNR American Jour-nal of Neuroradiology, 25 (5), 738–745.
Jay, G. W. (2000). Minor traumatic brain injury handbook: Diag-nosis and treatment. Boca Raton, FL: CRC Press.
Jennett, B. (2005). Development of Glasgow Coma and Outcome Scales. Nepal Journal of Neuroscience, 2, 24–28.
Jennett, B., Teasdale, G., Galbraith, S., Pickard, J., Grant, H., Braakman, R., et al. (1977). Severe head injuries in three countries. Journal of Neurology, Neurosurgery and Psychiatry, 40 (3), 291–298.
Jorge, R. E., Robinson, R. G., Starkstein, S. E., & Arndt, S. V. (1993). Depression and anxiety following traumatic brain in-jury. Journal of Neuropsychiatry and Clinical Neuroscience, 5 (4), 369–374.
Kaiser, D., & Othmer, S. (2000). Effect of neurofeedback on vari-ables of attention in a large multi-center trial. Journal of Neu-rotherapy, 4 (1), 5–17.
Kashluba, S., Hanks, R. A., Casey, J. E., & Millis, S. R. (2008). Neuropsychologic and functional outcome after complicated mild traumatic brain injury. Archives of Physical Medicine and Rehabilitation, 89 (5), 904–911.
Keshavan, M. S., Channabasavanna, S. M., & Reddy, G. N. (1981). Post-traumatic psychiatric disturbances: Patterns and predictors of outcome. British Journal of Psychiatry, 138 , 157–160.
Kim, E., Lauterbach, E. C., Reeve, A., Arciniegas, D. B., Coburn, K. L., Mendez, M. F., et al. (2007). Neuropsychiatric com-plications of traumatic brain injury: A critical review of the literature (a report by the ANPA Committee on Research). Journal of Neuropsychiatry & Clinical Neurosciences, 19 (2), 106–127.
Kirkwood, M. W., Yeates, K. O., & Wilson, P. E. (2006). Pediat-ric sport-related concussion: A review of the clinical man-agement of an oft-neglected population. Pediatrics, 117 (4), 1359–1371.
Koch, C. (1999). Biophysics of computation: Information process-ing in single neurons. New York: Oxford University Press.
Koh, J. O., & Cassidy, J. D. (2004). Incidence study of head blows and concussions in competition taekwondo. Clinical Journal of Sport Medicine, 14 (2), 72–79.
Koh, J. O., Cassidy, J. D., & Watkinson, E. J. (2003). Incidence of concussion in contact sports: A systematic review of the evidence. Brain Injury, 17 (10), 901–917.
Korn, A., Golan, H., Melamed, I., Pascual-Marqui, R., & Fried-man, A. (2005). Focal cortical dysfunction and blood-brain barrier disruption in patients with postconcussion syndrome. Journal of Clinical Neurophysiology, 22 (1), 1–9.
Kraus, M. F., Susmaras, T., Caughlin, B. P., Walker, C. J., Sweeney, J. A., & Little, D. M. (2007). White matter integrity and cogni-tion in chronic traumatic brain injury: A diffusion tensor imag-ing study. Brain, 130 (Pt. 10), 2508–2519.
Lanius, R. A., Williamson, P. C., Densmore, M., Boksman, K., Gupta, M. A., Neufeld, R. W., et al. (2001). Neural corre-lates of traumatic memories in posttraumatic stress disorder: A functional MRI investigation. American Journal of Psychia-try, 158 (11), 1920–1922.
Laureys, S., Piret, S., & Ledoux, D. (2005). Quantifying conscious-ness. Lancet Neurology, 4 (12), 789–790.
Lavoie, M. E., Dupuis, F., Johnston, K. M., Leclerc, S., & Las-sonde, M. (2004). Visual p300 effects beyond symptoms in concussed college athletes. Journal of Clinical and Experimen-tal Neuropsychology, 26 (1), 55–73.
Le Bihan, D., Mangin, J., Poupon, C., Clark, C., Pappata, S., Molko, N., et al. (2001). Diffusion tensor imaging: Concepts and applications. Journal of Magnetic Resonance Imaging, 13 (4), 534–546.
Leblanc, N., Chen, S., Swank, P. R., Ewing-Cobbs, L., Barnes, M., Dennis, M., et al. (2005). Response inhibition after traumatic brain injury (TBI) in children: Impairment and recovery. De-velopmental Neuropsychology, 28 (3), 829–848.
Lee, Y., & Advani, S. (1970). Transient response of a sphere to torsional loading: A head injury model. Mathematical Biosci-ences, 6, 473–487.
Lees-Haley, P. R., Green, P., Rohling, M. L., Fox, D. D., & Al-len, L. M., III. (2003). The lesion(s) in traumatic brain injury: Implications for clinical neuropsychology. Archives of Clinical Neuropsychology, 18 (6), 585–594.
Leininger, B. E., Gramling, S. E., Farrell, A. D., Kreutzer, J. S., & Peck, E. A., III. (1990). Neuropsychological defi cits in symp-tomatic minor head injury patients after concussion and mild concussion. Journal of Neurology Neurosurgery and Psychiatry, 53 (4), 293–296.
Lenz, D., Jeschke, M., Schadow, J., Naue, N., Ohl, F. W., & Her-rmann, C. S. (2008). Human EEG very high frequency oscilla-tions refl ect the number of matches with a template in audi-tory short-term memory. Brain Research, 1220 , 81–92.
Leon-Carrion, J., Martin-Rodriguez, J. F., Damas-Lopez, J., Mar-tin, J. M., & Dominguez-Morales Mdel, R. (2008). A QEEG index of level of functional dependence for people sustaining acquired brain injury: the Seville Independence Index (SINDI). Brain Injury, 22 (1), 61–74.
Levin, H. S., Amparo, E., Eisenberg, H. M., Williams, D. H., High, W. M., Jr., McArdle, C. B., et al. (1987). Magnetic resonance imaging and computerized tomography in relation to the neu-
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 505
robehavioral sequelae of mild and moderate head injuries. Journal of Neurosurgery, 66 (5), 706–713.
Levin, H. S., Benavidez, D. A., Verger-Maestre, K., Perachio, N., Song, J., Mendelsohn, D. B., et al. (2000). Reduction of corpus callosum growth after severe traumatic brain injury in chil-dren. Neurology, 54 (3), 647–653.
Levin, H. S., & Eisenberg, H. M. (1991). Neurobehavioral out-come. Neurosurgery Clinics of North America, 2 (2), 457–472.
Levin, H. S., Hanten, G., Zhang, L., Swank, P. R., Ewing-Cobbs, L., Dennis, M., et al. (2004). Changes in working memory after traumatic brain injury in children. Neuropsychology, 18 (2), 240–247.
Levin, H. S., Wilde, E. A., Chu, Z., Yallampalli, R., Hanten, G. R., Li, X., et al. (2008). Diffusion tensor imaging in relation to cognitive and functional outcome of traumatic brain injury in children. Journal of Head Trauma Rehabilitation, 23 (4), 197–208.
Levine, B., Cabeza, R., McIntosh, A. R., Black, S. E., Grady, C. L., & Stuss, D. T. (2002). Functional reorganisation of memory af-ter traumatic brain injury: A study with H(2)(15)0 positron emission tomography. Journal of Neurology, Neurosurgery and Psychiatry, 73 (2), 173–181.
Levine, B., Fujiwara, E., O’Connor, C., Richard, N., Kovacevic, N., Mandic, M., et al. (2006). In vivo characterization of traumatic brain injury neuropathology with structural and functional neuroimaging. Journal of Neurotrauma, 23 (10), 1396–1411.
Limbos, M. A., Ramirez, M., Park, L. S., Peek-Asa, C., & Kraus, J. F. (2004). Injuries to the head among children enrolled in spe-cial education. Archives of Pediatric and Adolescent Medicine, 158 (11), 1057–1061.
Limond, J., & Leeke, R. (2005). Practitioner review: Cognitive re-habilitation for children with acquired brain injury. Journal of Child Psychology and Psychiatry, 46 (4), 339–352.
Linden, M., Habib, T., & Radojevic, V. (1996). A controlled study of the effects of EEG biofeedback on cognition and behavior of children with attention defi cit disorder and learning disabili-ties. Biofeedback & Self Regulation, 21 (1), 35–49.
Lovell, M. R., Collins, M. W., Iverson, G. L., Field, M., Maroon, J. C., Cantu, R., et al. (2003). Recovery from mild concussion in high school athletes. Journal of Neurosurgery, 98 (2), 296–301.
Lovell, M. R., Collins, M. W., Iverson, G. L., Johnston, K. M., & Bradley, J. P. (2004). Grade 1 or “ding” concussions in high school athletes. American Journal of Sports Medicine, 32 (1), 47–54.
Lovell, M. R., & Fazio, V. (2008). Concussion management in the child and adolescent athlete. Current Sports Medicine Reports, 7 (1), 12–15.
Lovell, M. R., Pardini, J. E., Welling, J., Collins, M. W., Bakal, J., Lazar, N., et al. (2007). Functional brain abnormalities are re-lated to clinical recovery and time to return-to-play in athletes. Neurosurgery, 61 (2), 352–359.
Lubar, J. F. (1985). Changing EEG activity through biofeedback applications for the diagnosis and treatment of learning dis-abled children. Theory and Practice , 24, 106–111.
Marquez de la Plata, C. D., Hart, T., Hammond, F. M., Frol, A. B., Hudak, A., Harper, C. R., et al. (2008). Impact of age on long-term recovery from traumatic brain injury. Archives of Physical Medicine and Rehabilitation, 89 (5), 896–903.
Maruishi, M., Miyatani, M., Nakao, T., & Muranaka, H. (2007). Compensatory cortical activation during performance of an attention task by patients with diffuse axonal injury: A func-tional magnetic resonance imaging study. Journal of Neurol-ogy, Neurosurgery and Psychiatry, 78 (2), 168–173.
Matarazzo, J. D., & Herman, D. O. (1984). Relationship of edu-cation and IQ in WAIS-R standardization sample. Journal of Consulting and Clinical Psychology, 52 (4), 631–634.
Max, J. E., Lansing, A. E., Koele, S. L., Castillo, C. S., Bokura, H., Schachar, R., et al. (2004). Attention defi cit hyperactivity disorder in children and adolescents following traumatic brain injury. Developmental Neuropsychology, 25 (1–2), 159–177.
Max, J. E., Levin, H. S., Schachar, R. J., Landis, J., Saunders, A. E., Ewing-Cobbs, L., et al. (2006). Predictors of personality change due to traumatic brain injury in children and adolescents six to twenty-four months after injury. Journal of Neuropsychiatry and Clinical Neuroscience, 18 (1), 21–32.
Mazoyer, B. M., Tzourio, N., Frank, V., Syrota, A., Murayama, N., Levrier, O., et al. (1993). The cortical representation of speech. Journal of Cognitive Neuroscience, 5, 467–479.
McAllister, T. W., Saykin, A. J., Flashman, L. A., Sparling, M. B., Johnson, S. C., Guerin, S. J., et al. (1999). Brain activation during working memory 1 month after mild traumatic brain injury: A functional MRI study. Neurology, 53 (6), 1300–1308.
McCrea, M., Guskiewicz, K. M., Marshall, S. W., Barr, W., Ran-dolph, C., Cantu, R. C., et al. (2003). Acute effects and recov-ery time following concussion in collegiate football players: The NCAA Concussion Study. Journal of the American Medi-cal Association, 290 (19), 2556–2563.
McCrea, M., Hammeke, T., Olsen, G., Leo, P., & Guskiewicz, K. (2004). Unreported concussion in high school football players: Implications for prevention. Clinical Journal of Sport Medicine, 14 (1), 13–17.
McCrory, P., Johnston, K., Meeuwisse, W., Aubry, M., Cantu, R., Dvorak, J., et al. (2005). Summary and agreement statement of the 2nd International Conference on Concussion in Sport, Prague 2004. British Journal of Sports Medicine, 39 (4), 196–204.
McCullagh, S., Oucherlony, D., Protzner, A., Blair, N., & Fein-stein, A. (2001). Prediction of neuropsychiatric outcome following mild trauma brain injury: An examination of the Glasgow Coma Scale. Brain Injury, 15 (6), 489–497.
Mendelsohn, D. B., Levin, H. S., Harward, H., & Bruce, D. (1992). Corpus callosum lesions after closed head injury in children: MRI, clinical features and outcome. Neuroradiology, 34 (5), 384–388.
Mendez, D. R., Corbett, R., Macias, C., & Laptook, A. (2005). Total and ionized plasma magnesium concentrations in chil-dren after traumatic brain injury. Pediatric Research, 57 (3), 347–352.
Merskey, H., & Woodforde, J. M. (1972). Psychiatric sequelae of minor head injury. Brain, 95 (3), 521–528.
Middleton, J. A. (2001). Practitioner review: Psychological seque-lae of head injury in children and adolescents. Journal of Child Psychology and Psychiatry, 42 (2), 165–180.
Mildner, V. (2007). The cognitive neurosciene of human communi-cation Lawrence Erlbaum.
Miles, L., Grossman, R. I., Johnson, G., Babb, J. S., Diller, L., & Inglese, M. (2008). Short-term DTI predictors of cognitive
Copyright Springer Publishing Company

506 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
dysfunction in mild traumatic brain injury. Brain Injury, 22 (2), 115–122.
Mosenthal, A. C., Lavery, R. F., Addis, M., Kaul, S., Ross, S., Mar-burger, R., et al. (2002). Isolated traumatic brain injury: Age is an independent predictor of mortality and early outcome. Journal of Trauma, 52 (5), 907–911.
Niogi, S. N., Mukherjee, P., Ghajar, J., Johnson, C., Kolster, R. A., Sarkar, R., et al. (2008). Extent of microstructural white matter injury in postconcussive syndrome correlates with impaired cognitive reaction time: A 3T diffusion tensor imaging study of mild traumatic brain injury. American Journal of Neuroradiol-ogy, 29 (5), 967–973.
Obrist, W. D., Langfi tt, T. W., Jaggi, J. L., Cruz, J., & Gennarelli, T. A. (1984). Cerebral blood fl ow and metabolism in comatose patients with acute head injury. Relationship to intracranial hypertension. Journal of Neurosurgery, 61 (2), 241–253.
Ommaya, A. K. (1995). Head injury mechanisms and the concept of preventive management: A review and critical synthesis. Journal of Neurotrauma, 12 (4), 527–546.
Ommaya, A. K., Goldsmith, W., & Thibault, L. (2002). Biome-chanics and neuropathology of adult and paediatric head in-jury. British Journal of Neurosurgery, 16 (3), 220–242.
Ommaya, A. K., Thibault, L. E., & Bandak, F. A. (1994). Mecha-nisms of impact head injury. International Journal of Impact Engineering, 15 (4), 535–560.
Othmer, S., Othmer, S. F., & Kaiser, D. A. (1999). EEG Biofeed-back: Training for AD/HD and related disruptive behavior disorders. In J. A. Incorvaia, B. F. Mark-Goldstein & D. Tes-smer (Eds.), Understanding, diagnosing, and treating AD/HD in children and adolescents: An integrative approach (pp. 235–297). Northvale, NJ: Aronson.
Otto, M. W., Bruder, G. E., Fava, M., Delis, D. C., Quitkin, F. M., & Rosenbaum, J. F. (1994). Norms for depressed patients for the California verbal learning test: Associations with depression severity and self-report of cognitive diffi culties. Archives of Clinical Neuropsychology, 9 (1), 81–88.
Pakkenberg, B., & Gundersen, H. J. (1997). Neocortical neuron number in humans: Effect of sex and age. Journal of Compara-tive Neurology, 384 (2), 312–320.
Pakkenberg, B., Pelvig, D., Marner, L., Bundgaard, M. J., Gunder-sen, H. J., Nyengaard, J. R., et al. (2003). Aging and the hu-man neocortex. Experimental Gerontology, 38 (1–2), 95–99.
Paradiso, S., Chemerinski, E., Yazici, K. M., Tartaro, A., & Rob-inson, R. G. (1999). Frontal lobe syndrome reassessed: Com-parison of patients with lateral or medial frontal brain dam-age. Journal of Neurology Neurosurgery and Psychiatry, 67 (5), 664–667.
Parizel, P. M., Ozsarlak, Van Goethem, J. W., van den Hauwe, L., Dillen, C., Verlooy, J., et al. (1998). Imaging fi ndings in diffuse axonal injury after closed head trauma. European Radiology, 8 (6), 960–965.
Pascual-Marqui, R. D. (2002). Standardized low-resolution brain electromagnetic tomography (sLORETA): Technical details. Methods and Findings in Experimental and Clinical Pharma-cology, 24 (Suppl. D), 5–12.
Pascual-Marqui, R. D., Esslen, M., Kochi, K., & Lehmann, D. (2002). Functional imaging with low-resolution brain electromagnetic tomography (LORETA): A review. Methods and Findings in Ex-perimental and Clinical Pharmacology, 24 (Suppl. C), 91–95.
Paulson, M. J., & Lin, T. (1970). Predicting WAIS IQ from Shipley-Hartford scores. Journal of Clinical Psychology, 26 (4), 453–461.
Povlishock, J. T., & Katz, D. I. (2005). Update of neuropathology and neurological recovery after traumatic brain injury. Journal of Head Trauma Rehabilitation, 20 (1), 76–94.
Powell, J. M., Ferraro, J. V., Dikmen, S. S., Temkin, N. R., & Bell, K. R. (2008). Accuracy of mild traumatic brain injury diagno-sis. Archives of Physical Medicine and Rehabilitation, 89 (8), 1550–1555.
Powell, J. W., & Barber-Foss, K. D. (1999). Traumatic brain injury in high school athletes. Journal of the American Medical As-sociation, 282 (10), 958–963.
Pratap-Chand, R., Sinniah, M., & Salem, F. A. (1988). Cognitive evoked potential (P300): A metric for cerebral concussion. Acta Neurologica Scandinavica, 78 (3), 185–189.
Pribram, K. H. (2009). Some new horizons in recording the EEG. New Mathematics and Natural Computation, 5 (1), 7–17.
Putukian, M. (2006). Repeat mild traumatic brain injury: How to adjust return to play guidelines. Current Sports Medicine Reports, 5 (1), 15–22.
Raichle, M. E., MacLeod, A. M., Snyder, A. Z., Powers, W. J., Gusnard, D. A., & Shulman, G. L. (2001). A default mode of brain function. Proceedings of the National Academy of Sci-ences, USA, 98 (2), 676–682.
Randolph, C., McCrea, M., & Barr, W. B. (2005). Is neuropsycho-logical testing useful in the management of sport-related con-cussion? Journal of Athletic Training, 40 (3), 139–152.
Rapoport, M. J., McCullagh, S., Shammi, P., & Feinstein, A. (2005). Cognitive impairment associated with major depres-sion following mild and moderate traumatic brain injury. Jour-nal of Neuropsychiatry & Clinical Neurosciences, 17 (1), 61–65.
Rassovsky, Y., Satz, P., Alfano, M. S., Light, R. K., Zaucha, K., McArthur, D. L., et al. (2006). Functional outcome in TBI I: Neuropsychological, emotional, and behavioral mediators. Journal of Clinical and Experimental Neuropsychology, 28 (4), 567–580.
Reeves, D., Culligan, K., LaCour, S., Raynsford, K., Elsmore, T., & Winter, K. (2001). Automated neuropsychological assessment metrics (ANAM 2001). Pensacola, FL: Space and Naval War-fare Systems Command.
Ricker, J. H., Hillary, F. G., & DeLuca, J. (2001). Functionally ac-tivated brain imaging (O-15 PET and fMRI) in the study of learning and memory after traumatic brain injury. Journal of Head Trauma Rehabilitation, 16 (2), 191–205.
Rimel, R. W., Giordani, B., Barth, J. T., Boll, T. J., & Jane, J. A. (1981). Disability caused by minor head injury. Neurosurgery, 9 (3), 221–228.
Roncadin, C., Guger, S., Archibald, J., Barnes, M., & Dennis, M. (2004). Working memory after mild, moderate, or severe child-hood closed head injury. Developmental Neuropsychology, 25 (1–2), 21–36.
Ross, R. J., Cole, M., Thompson, J. S., & Kim, K. H. (1983). Boxers—computed tomography, EEG, and neurological evalu-ation. Journal of the American Medical Association, 249 (2), 211–213.
Ross, S. R., Millis, S. R., & Rosenthal, M. (1997). Neuropsycholog-ical prediction of psychosocial outcome after traumatic brain injury. Applied Neuropsychology, 4 (3), 165–170.
Copyright Springer Publishing Company

Quantitative Electro encephalography in the Assessment and Rehabilitation of Traumatic Brain Injury 507
Rugg-Gunn, F. J., Symms, M. R., Barker, G. J., Greenwood, R., & Duncan, J. S. (2001). Diffusion imaging shows abnormalities after blunt head trauma when conventional magnetic reso-nance imaging is normal. Journal of Neurology, Neurosurgery & Psychiatry, 70 (4), 530–533.
Rutgers, D. R., Toulgoat, F., Cazejust, J., Fillard, P., Lasjaunias, P., & Ducreux, D. (2008). White matter abnormalities in mild traumatic brain injury: A diffusion tensor imaging study. American Journal of Neuroradiology, 29 (3), 514–519.
Salmond, C. H., Menon, D. K., Chatfi eld, D. A., Williams, G. B., Pena, A., Sahakian, B. J., et al. (2006). Diffusion tensor imag-ing in chronic head injury survivors: Correlations with learn-ing and memory indices. Neuroimage, 29 (1), 117–124.
Sano, K., Nakamura, N., & Hirakawa, K. (1967). Mechanism of and dynamics of closed head injuries. Neurologia Medico-Chirurgica, 9 , 21–23.
Schatz, P., Pardini, J. E., Lovell, M. R., Collins, M. W., & Podell, K. (2006). Sensitivity and specifi city of the ImPACT Test Battery for concussion in athletes. Archives of Clinical Neuropsychol-ogy, 21 (1), 91–99.
Schatz, P., & Zillmer, E. A. (2003). Computer-based assessment of sports-related concussion. Applied Neuropsychology, 10 (1), 42–47.
Scheibel, R. S., Newsome, M. R., Steinberg, J. L., Pearson, D. A., Rauch, R. A., Mao, H., et al. (2007). Altered brain activation during cognitive control in patients with moderate to severe traumatic brain injury. Neurorehabilitation and Neural Repair, 21 (1), 36–45.
Schreckenberger, M., Lange-Asschenfeldt, C., Lochmann, M., Mann, K., Siessmeier, T., Buchholz, H. G., et al. (2004). The thalamus as the generator and modulator of EEG alpha rhythm: A combined PET/EEG study with lorazepam chal-lenge in humans. Neuroimage, 22 (2), 637–644.
Shaw, N. A. (2002). The neurophysiology of concussion. Progress in Neurobiology, 67 (4), 281–344.
Soeda, A., Nakashima, T., Okumura, A., Kuwata, K., Shinoda, J., & Iwama, T. (2005). Cognitive impairment after traumatic brain injury: A functional magnetic resonance imaging study using the Stroop task. Neuroradiology, 47 (7), 501–506.
Steffens, D. C., Helms, M. J., Krishnan, K. R., & Burke, G. L. (1999). Cerebrovascular disease and depression symptoms in the cardiovascular health study. Stroke, 30 (10), 2159–2166.
Taber, K. H., Warden, D. L., & Hurley, R. A. (2006). Blast-related traumatic brain injury: what is known? Journal of Neuropsy-chiatry & Clinical Neurosciences, 18 (2), 141–145.
Tanielian, T., Jaycox, L. H., Schell, T. L., Marshall, G. N., & Bur-nam, A. (2008). Invisible wounds of war: Psychological and cognitive injuries, their consequences, and services to assist re-covery. Santa Monica, CA: Rand.
Tansey, M. (1991). Wechsler (WISC-R) changes following treat-ment of learning disabilities via EEG biofeedback training in a private practice setting. Australian Journal of Psychology, 43, 147–153.
Teasdale, G., & Jennett, B. (1974). Assessment of coma and impaired consciousness. A practical scale. Lancet, 2 (7872), 81–84.
Teasdale, G., & Jennett, B. (1976). Assessment and prognosis of coma after head injury. Acta Neurochirurgica, 34 (1–4), 45–55.
Teasdale, G., Knill-Jones, R., & van der Sande, J. (1978). Observer variability in assessing impaired consciousness and coma. Journal of Neurology, Neurosurgery and Psychiatry, 41 (7), 603–610.
Thatcher, R. W., Biver, C., McAlaster, R., & Salazar, A. (1998). Biophysical linkage between MRI and EEG coherence in closed head injury. Neuroimage, 8 (4), 307–326.
Thatcher, R. W., Cantor, D. S., McAlaster, R., Geisler, F., & Krause, P. (1991). Comprehensive predictions of outcome in closed head-injured patients: The development of prognostic equations. An-nals of the New York Academy of Sciences 620, 82–101.
Thatcher, R. W., Walker, R. A., Gerson, I., & Geisler, F. H. (1989). EEG discriminant analyses of mild head trauma. Electroen-cephalography and Clinical Neurophysiology, 73 (2), 94–106.
Thompson, J., Sebastianelli, W., & Slobounov, S. (2005). EEG and postural correlates of mild traumatic brain injury in athletes. Neuroscience Letters, 377 (3), 158–163.
Thompson, L., & Thompson, M. (1998). Neurofeedback com-bined with training in metacognitive strategies: Effectiveness in students with ADD. Applied Psychophysiology and Biofeed-back, 23 (4), 243–263.
Thornton, K. (1999). Exploratory investigation into mild brain injury and discriminant analysis with high frequency bands (32–64 Hz). Brain Injury, 13 (7), 477–488.
Thornton, K. (2000). Exploratory analysis: Mild head injury, dis-criminant analysis with high frequency bands (32–64 Hz) un-der attentional activation conditions & does time heal? Journal of Neurotherapy, 3 (3/4), 1–10.
Thornton, K.. (2001). Method for improving memory by identify-ing and using qEEG parameters correlated to specifi c cognitive functioning.
Thornton, K. (2003). The electrophysiological effects of a brain injury on auditory memory functioning. The qEEG correlates of impaired memory. Archives of Clinical Neuropsychology, 18 (4), 363–378.
Thornton, K. (2006). NCLB goals (and more) are attainable with neurocognitive approach (Vol. 1). Charleston, SC: Booksurge.
Thornton, K. E., & Carmody, D. P. (2005). Electroencephalogram biofeedback for reading disability and traumatic brain injury. Child and Adolescent Psychiatric Clinics of North America, 14 (1), 137–162.
Thornton, K., & Carmody, D. P. (2008). Traumatic brain injury rehabilitation: Effi cacy review of computers, strategies, qEEG-guided biofeedback, and medications. Applied Psychophysiol-ogy and Biofeedback, 33 (2), 101–124.
Thornton, K. E., & Carmody, D. P. (2009a). Traumatic brain injury rehabilitation: QEEG biofeedback treatment protocols. Applied Psychophysiology and Biofeedback, 34 (1), 59–68.
Thornton, K., & Carmody, D. P. (2009b). Eyes-closed and acti-vation qEEG databases in predicting cognitive effectiveness and the ineffi ciency hypothesis. Journal of Neurotherapy, 13 , 1–21.
Thurman, D. (2001). The epidemiology and economics of head trauma. In L. Miller & R. Hayes (Eds.), Head trauma: Basic, pre-clinical, and clinical directions (pp. 327–347). New York: Wiley.
Thurman, D., Alverson, C., Dunn, K. A., Guerrero, J., & Sniezek, J. E. (1999). Traumatic brain injury in the United States: A public health perspective. Journal of Head Trauma Rehabili-tation, 14 (6), 602–615.
Copyright Springer Publishing Company

508 Handbook of Integrative Clinical Psychology, Psychiatry, and Behavioral Medicine
Tomaiuolo, F., Carlesimo, G. A., Di Paola, M., Petrides, M., Fera, F., Bonanni, R., et al. (2004). Gross morphology and morpho-metric sequelae in the hippocampus, fornix, and corpus callo-sum of patients with severe non-missile traumatic brain injury without macroscopically detectable lesions: A T1 weighted MRI study. Journal of Neurology, Neurosurgery and Psychiatry, 75 (9), 1314–1322.
Torg, J. S. (1991). Intracranial injuries. In J. S. Torg (Ed.), Athletic injuries to the head, neck, and face (pp. 272–274). St. Louis: Mosby-Year Book.
Trudeau, D. L., Anderson, J., Hansen, L. M., Shagalov, D. N., Schmoller, J., Nugent, S., et al. (1998). Findings of mild trau-matic brain injury in combat veterans with PTSD and a history of blast concussion. Journal of Neuropsychiatry and Clinical Neurosciences, 10 (3), 308–313.
Turner, G. R., & Levine, B. (2008). Augmented neural activity during executive control processing following diffuse axonal injury. Neurology, 71 (11), 812–818.
Tysvaer, A. T., Storli, O. V., & Bachen, N. I. (1989). Soccer inju-ries to the brain: A neurologic and electroencephalographic study of former players. Acta Neurologica Scandinavica 80 (2), 151–156.
Van Kampen, D. A., Lovell, M. R., Pardini, J. E., Collins, M. W., & Fu, F. H. (2006). The “value added” of neurocognitive test-
ing after sports-related concussion. American Journal of Sports Medicine, 34 (10), 1630–1635.
Vasa, R. A., Grados, M., Slomine, B., Herskovits, E. H., Thomp-son, R. E., Salorio, C., et al. (2004). Neuroimaging correlates of anxiety after pediatric traumatic brain injury. Biological Psy-chiatry, 55 (3), 208–216.
Waxman, K., Sundine, M. J., & Young, R. F. (1991). Is early pre-diction of outcome in severe head injury possible? Archives of Surgery, 126 (10), 1237–1241, 1242.
Wilde, E. A., McCauley, S. R., Hunter, J. V., Bigler, E. D., Chu, Z., Wang, Z. J., et al. (2008). Diffusion tensor imaging of acute mild traumatic brain injury in adolescents. Neurology, 70 (12), 948–955.
Wong, C. H., Rooney, S. J., & Bonser, R. S. (1999). S-100 beta re-lease in hypothermic circulatory arrest and coronary artery surgery. Annals of Thoracic Surgery, 67 (6), 1911–1914, 1919–1921.
World Health Organization. (1992). International statistical clas-sifi cation of diseases and related health problems (10th ed.). Geneva: Author.
Wood, R. L., & McMillan, T. (Eds.). (2002). Neurobehavioural dis-ability and social handicap following traumatic brain injury (brain damage, behaviour and cognition). Philadelphia: Psy-chology Press.
Copyright Springer Publishing Company