
Thesis - Research Explorer
202
UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl) UvA-DARE (Digital Academic Repository) Development and evaluation of a patient-centered cardiovascular health education program among insured primary care patients with hypertension in rural Nigeria: The QUICK-II study Odusola, A.O. Publication date 2015 Document Version Final published version Link to publication Citation for published version (APA): Odusola, A. O. (2015). Development and evaluation of a patient-centered cardiovascular health education program among insured primary care patients with hypertension in rural Nigeria: The QUICK-II study. General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. Download date:10 Jan 2022
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of Thesis - Research Explorer

UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Development and evaluation of a patient-centered cardiovascular healtheducation program among insured primary care patients with hypertension inrural Nigeria: The QUICK-II study
Odusola, A.O.
Publication date2015Document VersionFinal published version
Link to publication
Citation for published version (APA):Odusola, A. O. (2015). Development and evaluation of a patient-centered cardiovascularhealth education program among insured primary care patients with hypertension in ruralNigeria: The QUICK-II study.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s)and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an opencontent license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, pleaselet the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the materialinaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letterto: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. Youwill be contacted as soon as possible.
Download date:10 Jan 2022

InvitationYou are invited to attend the public defense of the thesis
Development and evaluation of a
patient-centered cardiovascular health
education program among insured
primary care patients with hypertension
in rural Nigeria
The QUICK-II study
~Aina Olufemi Odusola
Wednesday December 16, 2015at 16.00 hours
AgnietenkapelOudezijds Voorburgwal 231
1012 EZ Amsterdam
Aina Olufemi [email protected]
Development and evaluationof a patient-centered cardiovascular healtheducation program among insured primary
care patients with hypertensionin rural Nigeria
The QUICK-II study
Aina Olufemi Odusola
Development and evaluation of a patient-centered cardiovascular health education program
among insured prim
ary care patients with hypertension in rural N
igeria The QU
ICK-II study ~ Aina Olufem
i Odusola

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development and evaluation of a patient-centered cardiovascular health education program among insured primary
care patients with hypertension in rural Nigeria
The QUICK-II study
Aina Olufemi Odusola

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development and evaluation of a patient-centered cardiovascular health education program among insured primary care patients with hypertension in rural Nigeria. The QUICK-II study. Academic thesis, University of Amsterdam, The Netherlands
Cover design: Adolphus OparaLay-out: Legatron Electronic Publishing, Rotterdam, the Netherlands
Copyright: A.O. Odusola, 2015, Lagos, Nigeria
All rights reserved. No part of this publication may be reproduced, stored or transmitted in any form or by any means, electronically or mechanically, including photocopy, recording or otherwise without the written permission of the author.
The research described in this PhD thesis was funded by the Health Insurance Fund.Additional financial support was obtained from NUFFIC through a grant (# CF7536/2011).

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development and evaluation of a patient-centered cardiovascular health education program among insured primary care patients with hypertension in rural Nigeria
The QUICK-II study
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctor
aan de Universiteit van Amsterdam
op gezag van de Rector Magnificus
prof. dr. D.C. van den Boom
ten overstaan van een door het College voor Promoties ingestelde commissie,
in het openbaar te verdedigen in de Agnietenkapel
op 16 december 2015, te 16.00 uur
door
Aina Olufemi Odusola
geboren te Lagos, Nigeria

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Promotiecommissie
Promotores: Prof. dr. K. Stronks Universiteit van Amsterdam Prof. dr. A. Osibogun Lagos University Teaching Hospital Co-promotores: Dr. J.A. Haafkens Universiteit van Amsterdam Dr. C. Schultsz Universiteit van Amsterdam Overige leden: Prof. dr. A.P. Verhoeff Universiteit van Amsterdam Prof. dr. F.J. Snoek Universiteit van Amsterdam Prof. dr. R. Reis Leids Universitair Medisch Centrum Prof. dr. M.L. Essink- Bot Universiteit van Amsterdam Prof. dr. P.J.E. Bindels Erasmus Universiteit Rotterdam
Faculteit der Geneeskunde

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Table of content
List of abbreviations 7
Chapter 1 General introduction 9
Chapter 2 Development and evaluation of a patient centered cardiovascular health 25 education program for insured patients in rural Nigeria (QUICK-II)
Chapter 3 Perceptions of inhibitors and facilitators for adhering to hypertension 39 treatment among insured patients in rural Nigeria: a qualitative study
Chapter 4 Enablers and barriers for implementing high-quality hypertension care in a 67 rural primary care setting in Nigeria: perspectives of primary care staff and health insurance managers
Chapter 5 Development of cardiovascular health education for Nigerian primary care 105 patients with hypertension
Chapter 6 How group-based cardiovascular health education affects treatment 127 adherence and blood pressure control among insured hypertensive Nigerians: A pre-test, post-test study
Chapter 7 General discussion 153
Appendix Summary 173 Summary in Dutch (Nederlandse samenvatting) 177 Images from Cardiovascular Health Education Program (CHEP) sessions 181 Acknowledgements 187 List of publications 193 PhD Portfolio 195 Curriculum Vitae 199

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
List of abbreviations
AIGHD Amsterdam Institute for Global Health and DevelopmentAMC Academic Medical CenterBMI Body mass indexBMQ Beliefs about Medicines QuestionnaireBP Blood PressureCAC Christ Apostolic ChurchCAHE Culturally Adapted Hypertension EducationCBHI Community Based Health Insurance CHEP Cardiovascular Health Education ProgramCI Confidence IntervalCVD Cardiovascular DiseasesDBP Diastolic Blood PressureDM Diabetes MellitusHCHC Hygeia Community Health CareHCHP Hygeia Community Health PlanHCP Health Care ProfessionalsHIF Health Insurance FundHMO Health Maintenance OrganizationHTN HypertensionID IdentityIPQ-R Revised Illness Perception QuestionnaireIQR Inter Quartile Range ISH International Society of HypertensionJCI Joint Commission InternationalLMIC Low and Middle Income CountriesKSHI Kwara State Health InsuranceNCD Non-Communicable DiseasesNGN Nigerian NairaNHIS National Health Insurance Scheme MAXQDA MAX Qualitative Data AnalysisMASES-R Revised Medication Adherence Self Efficacy ScaleMMAS Morisky Medication Adherence ScaleMSG Monosodium GlutamateNUFFIC Netherlands organization for international cooperation in higher educationOOH Ogo Oluwa Hospital

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
OR Odds RatioQUICK Quality Improvement Cardiovascular Care KwaraSBP Systolic Blood PressureSD Standard DeviationSSA Sub Saharan AfricaTICD Tailored Implementation of Chronic DiseasesTOD Target Organ DamageUITH University of Ilorin Teaching HospitalUSD United States DollarWHO World health organization

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Chapter 1
General introduction
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 10 —
Chapter 1
BACKGROUND
Cardiovascular diseases in Nigeria and sub Saharan AfricaGlobally cardiovascular diseases (CVD) are a major cause of premature mortality and disability. In 2012 alone CVD caused an estimated 17.3 million (31%) of total deaths worldwide. Over three quarters of these deaths occurred in low and middle income countries (LMIC) including sub Saharan Africa (SSA) where equitable access to primary healthcare services is currently a challenge [1-3]. In recent decades the incidence of CVD has risen steadily in the African region [4]. The increasing incidence of CVD and associated risk factors had resulted partly from the combined effects of poverty, globalization, urbanization and westernization [5-7]. In Nigeria CVD has increased steadily over the past decades [8] and this was responsible for 7% of the 24% premature mortality attributable to Non Communicable Diseases (NCD) in 2012 [9]. Utilizing a global response plan WHO in 2013 set the year 2020 as deadline to reduce the burden of CVD through the following strategies: 1) a reduction by 25% in the global prevalence of hypertension (Blood pressure ≥ 140/90 mmHg in individuals aged ≥ 18 years); and 2) an increase to at least 50% in the number of eligible people that should receive drug therapy and counseling to prevent heart attacks and strokes [1].
Prevalence, treatment and control of Hypertension in Nigeria and sub Saharan AfricaHypertension, an important risk factor for CVD has been classified as a global public health challenge and is infamously described as a ‘silent killer’ due to its ability to silently inflict significant damage to vital body organs (heart, kidneys, brain, eyes, blood vessels) oftentimes before symptoms or signs manifests. In 2008 the prevalence rate for hypertension was 40% globally, 35% for high income countries, and 46% for Africa and LMIC [10]. In the African region the burden of hypertension and other cardiovascular risk factors has increased steadily [11-17]. In Nigeria the age standardized prevalence of hypertension (BP ≥ 140/90 mmHg) for individuals aged ≥ 18 years was 27.8% (28.1% males, 27.5% females) in 2014 [9]. The increasing prevalence of hypertension in Nigeria is attributable to poor access to primary care services and sub-optimal prevention and control efforts. Several studies from Nigeria have reported an increasing incidence and a high prevalence, poor awareness, low treatment coverage and poor control of hypertension and other CVD risk factors [15, 18-30]. Researchers involved in these studies have urged urgent interventions to prevent epidemics of CVD in future.
Prevention of cardiovascular diseases in sub Saharan Africa To limit CVD in SSA preventive and integrated health promoting measures must be implemented urgently [31]. Fortunately important CVD risk factors hypertension and diabetes have been shown to have causal links to other predisposing factors that are largely modifiable or amenable to behavior change using health counseling. However to be effective and acceptable to end-users such counseling programs should be well focused and developed tailoring their contents, materials and messages to the views, beliefs, norms and practices of the patients who are diagnosed with

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General introduction
— 11 —
the risk factors themselves. This is important especially in rural Africa where deep rooted cultural beliefs and practices may exert substantial influence on people’s lives and actions including health behaviors. In Africa investigative research into how people’s cultural beliefs and practices may affect their health actions is currently limited but quite important. But equally important is the translation of findings from such research efforts into clinical practice in order to transfer benefits therein to affected populations. Efforts targeted at translating research findings from implementation of cardiovascular health education into clinical practice for improved patient outcomes have potential to help limit CVD. To be specific, such efforts may include the development of education programs that can empower hypertensive patients and others at risk of CVD to adhere to dictates of prescribed treatments. In the current effort we aim to develop and test a culturally sensitive cardiovascular health education program among insured hypertensive primary care patients from rural Nigeria [32]. Modifiable risk factors for hypertension and cardiovascular diseases To prevent CVD traditional risk factors e.g., hypertension, diabetes and dyslipidemia must be controlled effectively. This is achievable if medications (where necessary) are taken as prescribed and modifiable risks factors for the traditional CVD risk factors themselves (e.g., stress, physical inactivity, overweight/obesity, tobacco use, salt use, alcohol and inadequate consumption of fruits and vegetables) are addressed effectively. Whilst most studies have been performed in high income countries, available data suggest that also in the black African population, modification of these traditional risk factors is likely to be effective in controlling cardiovascular disease development. In the following sections we provide insights into how these modifiable risk factors may influence traditional CVD risk factors among Nigerians and SSA populations.
Dieting Ideally for an adult, a healthy diet should on a daily basis contain at least 400 grams of fruits and vegetables (approximately five servings), less than 5 grams of salt, less than 10% of total calorie intake as free sugars (e.g., less than 50g or 12 level teaspoons of sugar) and less than 30% of total energy intake as fats, preferably unsaturated fats (e.g., as found in fish, sunflower oil, nuts, olive oil) as against saturated fats (e.g., as found in meat, butter, margarine, palm oil) [33-35].
SaltBlack Africans who overuse salt are particularly at greater risk for hypertension and CVD. Yet many are ignorant of the relationship between salt and hypertension. A study found no relationship between hypertension awareness and treatment, and sodium and potassium intake levels among urban South Africans [36]. Findings from some Nigerian studies suggest that increased salt sensitivity and high salt taste threshold may predispose individuals to development of hypertension [37,38]. But a reduced salt use has health benefits on CVD and risk factor prevention [39,40]. Reducing salt use effectively translates to a substantial reduction in the amount of salt used during food preparation

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 12 —
Chapter 1
and avoidance of extra use (table salt) when eating meals. To achieve this it is equally important to limit consumption of snacks and processed foods with high salt contents.
Fatty foods, fruits, vegetablesThere is no doubt that increasing urbanization drives may have exposed populations in rural African communities to certain diets that may be relatively unhealthy for cardiovascular health. Even though many rural African communities are endowed with local possibilities that promote healthy dieting e.g., arable lands for fruits and vegetable farming and rivers for fishing, but undesirably also these communities have other possibilities that may encourage unhealthy dieting e.g., easy access to meat from rampant goat breeding practice and fat laden unhealthy oils from groundnut and palm tree farming. In such a contrasting scenario, access to culturally relevant health education to enlighten and inform people of the right dietary choices is desirable and important. A recent Nigerian study reported high prevalence of unhealthy dietary habits, overweight, obesity and hypertension among traders suggesting further that educational interventions are needed to promote healthy dietary habits [41]. But inadequate healthy dieting was also reported from other parts of SSA as another study reported inadequate consumption of fruits and vegetables among black South Africans and therefore suggested educational intervention to promote adequate consumption of fruits and vegetables [42]. In support of suppositions that healthy dieting promotes cardiovascular health, evidence from several other studies have shown that healthy dietary habits that include fruits and vegetables have beneficial effects on hypertension and reduction of CVD risk [43-45].
Physical inactivity Insufficient physical activity is a significant risk factor for CVD and a leading global cause of death, currently causing 3.2 million annual deaths. Globally 25% of adults and 80% of adolescents are not sufficiently active physically [46]. In 2010, 22.3% of Nigerians (20.6% males, 24% females) were insufficiently active physically [46]. Some studies carried out among Nigerians reported a high prevalence of physical inactivity [47], and a significant association between insufficient physical activity and CVD risk factors [48]. World Health Organization (WHO) defines physical activity as ‘any bodily movement produced by skeletal muscles that require energy expenditure – including activities undertaken while working, playing, carrying out household chores, travelling, and engaging in recreational pursuits’ [46]. The broad scope of this definition implies that even activities consciously or unconsciously engaged as part of everyday life including work-related activities could contribute towards physical fitness particularly if performed in accordance with recommendations (e.g., physical activity of light or moderate intensity for at least 30 minutes daily in mid-life or old age).
Obesity and overweightSomewhat linked to the challenge of physical inactivity is the problem of obesity and overweight as related to cardiovascular health. Currently classified as a global epidemic, obesity is a significant

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General introduction
— 13 —
risk factor for CVD. Obesity which is predisposed to by increasing urbanization is mainly caused by physical inactivity, sedentary lifestyle, and increased consumption of fat-laden and calorie-based foods. WHO defined obesity which is an abnormal or excessive accumulation of fat that presents a risk to health, as a body mass index (BMI) ≥ 30 k/m2, and overweight as a BMI ≥ 25 k/m2. In 2014, 33.3% (26% males, 40.9% females) of Nigerians aged 18 years or over were classified overweight and 11% (5.9% males, 16.3% females) were obese [35]. Some recent studies have similarly reported a high prevalence of obesity and overweight among Nigerians [15,19,28,49]. But because in many parts of Africa including Nigeria certain cultural orientations and perceptions encourage people to increase body size for social reasons [50], using culturally targeted education, it is important to positively influence those cultural perceptions and practices that can compromise cardiovascular health. These include among others the perception that “the bigger one is, the more affluent, the more comfortable or the more beautiful one would be, and that slim people are either sick or suffer from some serious internal disease [50].
Tobacco useGlobally the smoking of tobacco and its derivatives kill nearly 6 million people each year, and close to 80% of the world’s one billion smokers live in LMIC. Second hand exposure to tobacco smoke is equally a threat to non-smokers killing almost 600,000 each year [51]. Tobacco kills gradually after several years of smoking by causing serious cardiovascular and respiratory diseases. WHO estimates that in 2011 6% (10% males, 2% females) of Nigerians aged 15 years or over were current smokers of tobacco products [51]. These figures are expected to increase if non-smoking use of tobacco e.g., snuff (fine ground tobacco) is considered. A population based study in south-west Nigeria in 2011 reported a prevalence of 8.7% for current smokers [52]. Measures e.g., behavioral counseling which can help smokers to quit smoking and prevent secondary exposure to non-smokers will certainly save millions of lives each year. But in parts of Africa in particular rural settings, including rural Nigeria, the use of smokeless tobacco (taba, snuff) by licking or sniffing is commonly practiced. Interestingly these non-smoking but equally dangerous forms of exposure to tobacco are perceived useful and more culturally acceptable than actual smoking. This may imply that some hypertensive patients who may also perceive usefulness in these forms of tobacco may see no harm in using them. Furthermore, there is a gender-based perspective to the problem as once reported in a Nigerian study that male smoking is comparatively more culturally permissible than female use of tobacco in Nigerian societies [53]. It is therefore important to inform people, in particular patients about dangers of tobacco using culturally sensitive health education.
Use of Alcohol The harmful use of alcohol which kills 3.3 million people annually [54] is a threat to individuals with cardiovascular health challenges. A recent study in SSA reported a significant association between self reported harmful use of alcohol, and development of hypertension and CVD related mortality [55]. In 2010 WHO estimated that the prevalence of heavy episodic drinking (consumption of more

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 14 —
Chapter 1
than 60 grams of pure alcohol in the previous 30 days) was as high as 6.7% (11.3% males, 2.0% females) among Nigerians [54]. To prevent CVD hypertensive patients who currently use more than 3 units of alcohol daily must be advised to reduce intake [(one unit (drink) = half pint of beer/lager (5% alcohol), 100 ml of wine (10% alcohol), 25 ml of spirits (40% alcohol)]. In several parts of Africa including the region of the current study, aside conventional or popular alcohol brands (e.g. beer/lager), various other forms of local alcoholic beverages (palm wine, ogogoro, burukutu, kainkain, gin) with varying alcohol contents are perceived useful and used [50]. Therefore behavioral counseling must of necessity be deployed to inform people about the health risks of some apparently harmless cultural perceptions and practices. Furthermore, with the recent penetration of the global alcohol industry into Africa and the weak alcohol control policies in African countries [56, 57], there is an urgent need to devise and develop newer, more effective strategies or innovations to empower populations at risk of CVD using culturally tailored cardiovascular education programs to protect such vulnerable groups e.g., hypertensive patients in Africa.
StressAlthough certain psycho-social factors (stress, anxiety, depression and insufficient social support) may predispose vulnerable individuals to CVD and risk factors, these may not have featured prominently among the population represented in the current study. However considering the potential implications of physical or mental stress on cardiovascular health and of insufficient social or family support on adherence efforts of patients, it is nonetheless important to address psychosocial factors in the counseling of hypertensive patients as was done in the current study.
Cardiovascular health education programs among hypertensive patients in SSATo our knowledge not much information is currently available with regards to past efforts in the implementation of tailored or specially developed cardiovascular health education programs for use among hypertensive patients in SSA. While few studies may have demonstrated the usefulness of educational interventions in managing hypertension, and some others may have tested the effects of some informal forms of education e.g., educational counseling for patients, increased risk factor awareness and knowledge [58,59], most of such efforts were implemented among general populations with no diagnoses of hypertension or other CVD risk factors. None of the previous studies made specific attempt to develop or test a tailored cardiovascular health education program among hypertensive patients and certainly not among hypertensive patients with access to affordable quality hypertension care as in the current Kwara State Health Insurance (KSHI) program. The current study may therefore just have marked the advent of regional efforts to produce such highly desirable and focused CVD preventing interventions among hypertensive patients. The potential reproducibility of this or similar studies in other regions will certainly help to address challenges of poor hypertension control and enhance quality of life among hypertensive patients. To achieve this, affected patients must be empowered to build personal self-management capabilities to attain and sustain risk factor control. We hypothesize that such self-management

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General introduction
— 15 —
capacity building is achievable using well developed, attractive, acceptable and implementable culturally tailored educational programs. Therefore in the current study we aimed to achieve this by designing, developing and testing for effectiveness a tailored cardiovascular health education program (CHEP) among Nigerian hypertensive patients with access to affordable care in a rural primary care hospital.
Access to affordable careFinancial health protection in Nigeria Nigeria has a huge population 178.5 million (2014) but most of her citizens currently live below poverty line (less than USD2 per day). In 2012 the total expenditure on health as % of GDP was 6.1%, and the general government expenditure on health as % of total government expenditure was quite low 6.7% [60]. Majority of Nigerians particularly those living in the rural regions (approximately 54%) currently do not have access to affordable primary care and certainly not to one with high quality input as the KSHI program offers. The state of development of financial protection schemes is poor, rather rudimentary and currently incapable of providing affordable care to many. As a result, irrespective of socioeconomic status most Nigerians currently pay out-of-pocket for the most basic health care needs including primary care. In 2012 the out-of-pocket expenditure as a % of private expenditure on health was huge 95.7% [61]. This huge out-of-pocket health expenditures further impoverishes the people and predispose them to poorer health status. Even the recently introduced National Health Insurance Scheme currently grapples with teething problems and has not offered sustainable solution to the problem as the scheme currently caters for only government employees and those employed in the formal sector leaving out the substantial others engaged in the informal sector. Furthermore although most private sector employees resort to prepaid private schemes that are managed by private Health Maintenance Organizations (HMOs), private prepaid plans as a % of private expenditure on health has been abysmally low (3.1% in 2012). In recent times, to increase access to primary care community based health insurance schemes are being introduced and are increasingly popular. One of such schemes is the KSHI initiative co-funded by the Kwara State government and the international development organization Health Insurance Fund (HIF).
Kwara State Health Insurance Program The Kwara State Health Insurance program is a community based health insurance scheme implemented in Nigeria by the local Health Maintenance Organization (HMO) Hygeia. Co-financed by HIF and the Kwara State Government KSHI was launched in Kwara in 2007 to provide subsidized health insurance for low- and middle income groups in Africa. The program commenced in Nigeria in early 2007 with the farming population in Kwara. At that time the Dutch organization PharmAccess International performed quality monitoring and evaluation into the operations of the scheme. This function is currently performed by SafeCare a member of the PharmAccess group. SafeCare is a tripartite healthcare quality monitoring and accreditation partnership between the

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 16 —
Chapter 1
Dutch organization PharmAccess International, Joint Commission International of United States and the Council for Health Services Accreditation of Southern Africa. As part of the KSHI quality assurance program, international guidelines for CVD prevention were implemented during the QUICK program which commenced in June 2010 in the participating clinic Ogo Oluwa Hospital (OOH). To improve quality of care OOH was provided with facilities and new equipment for diagnostic testing, treatment protocols and quarterly staff trainings with feedback on guideline adherence and organizational support. Furthermore to promote affordable care KSHI offers individual enrolment to farmers and their family members using highly subsidized annual insurance premiums. In 2010 each enrollee paid NGN 200/300 (about 8 percent of the annual premium) for basic primary and limited secondary care including hypertension management. The remaining part of the annual premium was covered by a subsidy from HIF previously unilaterally but later through joint contribution from both HIF and Kwara State Government. The insurance benefit package covers consultations, drugs and diagnostic tests for basic primary care and limited secondary care including care for hypertension and other CVD risk factors. Reimbursement of cost of care to providers was implemented mainly through capitation payments. At the start of this study about 400 patients diagnosed with hypertension were enrolled in KSHI at Ogo Oluwa Hospital.
Poor hypertension control in high-quality primary care in NigeriaNigeria currently has an underdeveloped health systems and low primary health care coverage. At the same time because financial health protection policy is mostly lacking or poorly implemented primary health care is currently hardly affordable for majority of those affected with hypertension. This may have contributed to the poor hypertension treatment and control rates in the country. A recent community household survey conducted in rural Kwara, Nigeria reported 3%, 5% and 8% respectively as the hypertension control, treatment and awareness rates [62]. However the control of hypertension requires more than ‘just’ affordable care; patients’ ability to comply with prescribed treatment is equally important. For example the KSHI program offered high quality hypertension primary care and implemented substantial quality improvement inputs. Despite this almost 50% of the 349 hypertensive patients who accessed high quality CVD prevention care in the Quality Improvement Cardiovascular care Kwara (QUICK-I) study [63] had uncontrolled BP and/or were not adherent to prescribed medication and/or healthy behavior at the end of a 12-month study period. This suggests there may yet be some other factor apart from access to high quality hypertension care that is likely to be relevant in achieving BP control target. We thought this may relate to the form, mode, content or relevance of the education given. Because the almost 50% participants referred to above had access to standard guideline-based hypertension education offered in usual care we felt implementing a well developed, structured and tailored hypertension education program may help improve medication adherence and hypertension control among the studied population. We therefore hypothesized that the missing link in the usual care that was being accessed could be poor adherence to prescribed medicines and/or healthy behavior. To investigate this we developed a structured cardiovascular health education program and designed

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General introduction
— 17 —
a pre/post observational 6 months follow-up study QUICK-II to test the program for its effects on adherence to prescribed treatment and BP control among affected patients.
Reasons for and how we addressed poor hypertension control within the QUICK programAt the end of QUICK-I study we observed that almost 50% of about 350 participants who were included in that study had uncontrolled BP and/or low/medium medication adherence. Reasons for this observation may not be far-fetched considering that only guideline-based patient education of usual care was offered in QUICK-I. This may have been insufficient to achieve and sustain optimal BP control. But QUICK-I had implemented high quality hypertension care that included all aspects of care lacking only in the application of a structured education program that is made culturally relevant by tailoring contents to patients’ views. More so the usual care education contents of QUICK-I did not address patients’ cultural perspectives and therefore may not have been patient-centered or culturally sensitive. To address the challenges (low medication adherence and poor BP control) we implemented QUICK-II study which had the aim to develop a patient-centered and culturally sensitive cardiovascular health education program and to test it for effectiveness.
STUDy SETTING AND POPULATION
Nigeria and Kwara StateNigeria is the most populous African country. Currently the biggest oil exporter and with the largest Natural gas reserves in the continent Nigeria recorded a GDP of USD568.5 billion (2014), an inflation rate of 8.1% (2014) and poverty rate of 64.2% (majority being in the rural areas) [63]. The country has a poorly developed and underfunded healthcare delivery system. Her economy which is currently one of the most rapidly growing in the continent is however heavily dependent on oil-revenue. Although earning substantially from Petroleum and Natural gas resources the fact that her wealth is inequitably distributed among her mostly poor population has placed her in lower middle income class among other nations. However if her retinue of human and natural resources is fiscally managed and well harnessed she could be better positioned for greater economic growth, poverty reduction, infrastructural development and affordable access to quality healthcare for her people. Nigeria has diverse ethnic and cultural identities, two major religions (Islam and Christianity) and several variants of traditional African religions. With almost 500 indigenous languages, her population is comprised of over 200 ethnic groups the three largest being Hausa-Fulani (north), Yoruba (southwest) and Ibo (southeast). For administrative purposes, the country has been divided into 6 geopolitical zones of which Kwara State (host to the current study) is located in the north-central zone.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 18 —
Chapter 1
Kwara State is populated by 3 major ethnic groups Yoruba, Nupe and Baruba. In 2009-2010 World Bank estimates rated Kwara as the 4th poorest among Nigeria’s 36 states. The predominant occupations practiced in the State are farming, trading, artisanship and services. In the 1990s Bacita (Kwara north) where the current project is implemented was a busy commercial center. The original population of Bacita is Nupe but her commercial vibrancy at that time attracted Nigerians of various ethnic nationalities particularly the Yoruba. Bacita later lost its economic vibrancy and is currently considered a poor community with farming, petty trading, artisanship, hunting and fishing now constituting the predominant livelihood activities of inhabitants of the town. Eventually a substantial majority of the economic migrants of that time settled permanently in Bacita. Therefore Yoruba language is also widely spoken alongside the native Nupe. At the time of this study roughly two-thirds of the about 400 hypertensive patients who enrolled in the insurance program at Ogo Oluwa Hospital resided within Bacita; the remaining third lived in some distantly located surrounding villages.
THE CHEP STUDy
Cardiovascular health education program The cardiovascular health education program(CHEP) was developed to help hypertensive patients enrolled in a community based health insurance program in rural Nigeria adhere adequately to prescribed treatment. The study consists of 2 parts (part 1 – development of program, part 2 – evaluation of program).
DevelopmentIn part 1, we used the results of the qualitative interviews held with 40 hypertensive patients who had accessed hypertension care for at least one year in the Kwara State Health Insurance (KSHI) program in a primary care hospital – Ogo Oluwa Hospital (OOH) to develop the education program. In addition, using qualitative interviews held with 11 healthcare professionals of OOH and 4 health insurance managers of KSHI we similarly explored for the optimal strategies required for a successful implementation of CHEP in clinical practice.
The Intervention Briefly, the Intervention consists of 3 group educational sessions spread 4-6 weeks apart and delivered to groups of 12-15 participants using interactive teaching over a period of 6 months. The first session CHEP 1 focused on increasing patients’ knowledge and awareness about hypertension with regards to the cause, course, consequences, nature, presentations and prevention. The second education session CHEP 2 focused on assisting patients to overcome hypertension self-management difficulties encountered daily and to live positively or cope well with their hypertension. Furthermore, dietary materials collected from the local market were used to guide

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General introduction
— 19 —
participants on healthy cooking methods and hypertension friendly diet. In addition to contents of CHEP 2, the third education session CHEP 3 incorporated a practical (physical fitness) exercise session. The training materials used include audiovisuals, information leaflets and pictorial posters. While CHEP 1 lasted 2 hours, CHEP 2 and CHEP 3 each lasted 2 hours, 30 minutes.
EvaluationBased on eligibility criteria of having uncontrolled BP and/or being non-adherent to prescribed medication and/or behavioral advice after accessing affordable, quality hypertension care for 12 months in a previous CVD prevention quality improvement program QUICK-I study [63], 149 out of 349 participants qualified and were included into the CHEP evaluation study QUICK-II. Details of the evaluation and results are available elsewhere [64] but briefly this involved initial baseline assessments including physical anthropometric measures and medication and behavioral adherence scores of participants followed by three educational sessions delivered over a period of 6 months at the end of which final measurements as exact as the baseline were taken to assess impact of the education program. Primary outcomes were improvements in medication and/or behavioral adherence while secondary outcomes were improvements in blood pressure control and/or body mass index.
THE THESIS
Aim of the thesisTo prevent CVD effectively it is important to attain and sustain optimal control of CVD risk factors. But risk factor control would be difficult if affordable and quality primary care is lacking. The combined effect of affordable health insurance and high quality hypertension care can help overcome these challenges. However in the current study we observed that although patients had opportunity to access affordable high quality hypertension care, many performed poorly still with respect to treatment goals. Potentially these patients could benefit from tailored educational counseling assistance. This assumption formed the basis of the two main objectives formulated for this thesis which are:• To develop a patient-centered education program targeted to help insured hypertensive
patients increase their adherence capacities towards achieving and sustaining prescribed treatment goals.
• To test the developed education program with respect to effectiveness in practice.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 20 —
Chapter 1
OUTLINE OF THE THESIS
The first research objective which was to develop a patient-centered education program targeted to help insured hypertensive patients increase adherence capacities towards achieving and sustaining prescribed treatment goals is addressed in chapters 3, 4 and 5 while the second research objective which was to test the developed education program with respect to effectiveness in practice is addressed in chapter 6. In chapter 2 we describe the design of the study which has the primary goal to develop and evaluate a patient-centered cardiovascular health education program for hypertensive patients insured in a community based health insurance program in rural Nigeria. Chapter 3 was used to describe the results of the first qualitative interview study conducted to assess the perceptions of inhibitors and enablers for adhering to hypertension treatment among insured primary care patients in rural Nigeria. Findings from this study were used to develop the educational intervention that was later used to assist patients with uncontrolled hypertension to increase adherence and improve on their blood pressure targets. Chapter 4 describes the results of the second qualitative interview study held with healthcare professionals of the participating hospital and health insurance managers of the implementing insurance company to identify the resources required for implementing high quality hypertension care within the insurance program. Findings from this interview study were further used to identify optimal strategies required for a successful implementation in practice of the educational intervention that would be developed later. In chapter 5 we describe the development of the educational intervention cardiovascular health education program (CHEP) including the formative research undertaken to develop the program and how information from the two qualitative studies conducted earlier are linked to produce the education protocol. Chapter 6 was used to describe the quantitative pretest/posttest study that was used to evaluate the effect of the developed educational intervention CHEP with regards to its effectiveness on treatment outcomes. Finally in chapter 7 we write a general discussion of the main findings of the thesis, the clinical importance and implications for future research and offer recommendations for practical application of the results. The potential usefulness of the education program in other settings was highlighted and the necessity and possibility to further test its impact using a control study was noted.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General introduction
— 21 —
REFERENCES
1. WHO | Cardiovascular diseases (CVDs). 2014 [http://www.who.int/topics/cardiovascular_diseases/en/] 2. Ayinde H, Gillum RF: Cardiovascular disease mortality in Sub-Saharan Africa and the Caribbean. Ethn
Dis 2014, 24:495–501.3. Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY,
others: Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet 2013, 380:2095–2128.
4. Alwan A, World Health Organization: Global status report on noncommunicable diseases 2010. 2011:176 pp.
5. Schram A, Labonté R, Sanders D: Urbanization and international trade and investment policies as determinants of noncommunicable diseases in Sub-Saharan Africa. Prog Cardiovasc Dis 2013, 56:281–301.
6. Yarahmadi S, Etemad K, Hazaveh AM, Azhang N: Urbanization and non-communicable risk factors in the capital city of 6 big provinces of iran. Iran J Public Health 2013, 42:113–118.
7. Oyebode O, Pape UJ, Laverty AA, Lee JT, Bhan N, Millett C: Rural, urban and migrant differences in non-communicable disease risk-factors in middle income countries: a cross-sectional study of WHO-SAGE data. PloS One 2015, 10:e0122747.
8. Ao M, U M: Incidence and patterns of cardiovascular disease in north western Nigeria. Niger Med J 2009, 50:55.
9. WHO | Cardiovascular diseases. 2014 [http://apps.who.int/gho/data/node.country.country-NGA]10. WHO | Cardiovascular diseases.2014 [http://www.who.int/topics/cardiovascular_diseases/en/]11. Hamer M, von Känel R, Reimann M, Malan NT, Schutte AE, Huisman HW, Malan L: Progression of
cardiovascular risk factors in black Africans: 3 year follow up of the SABPA cohort study. Atherosclerosis 2015, 238:52–54.
12. Caleyachetty R, Echouffo-Tcheugui JB, Tait CA, Schilsky S, Forrester T, Kengne AP: Prevalence of behavioural risk factors for cardiovascular disease in adolescents in low-income and middle-income countries: an individual participant data meta-analysis. Lancet Diabetes Endocrinol 2015.
13. Ataklte F, Erqou S, Kaptoge S, Taye B, Echouffo-Tcheugui JB, Kengne AP: Burden of undiagnosed hypertension in sub-saharan Africa: a systematic review and meta-analysis. Hypertension 2015, 65:291–298.
14. Iwelunmor J, Airhihenbuwa CO, Cooper R, Tayo B, Plange-Rhule J, Adanu R, Ogedegbe G: Prevalence, determinants and systems-thinking approaches to optimal hypertension control in West Africa. Glob Health 2014, 10:42.
15. Commodore-Mensah Y, Samuel LJ, Dennison-Himmelfarb CR, Agyemang C: Hypertension and overweight/obesity in Ghanaians and Nigerians living in West Africa and industrialized countries: a systematic review. J Hypertens 2014, 32:464–472.
16. Alsheikh-Ali AA, Omar MI, Raal FJ, Rashed W, Hamoui O, Kane A, Alami M, Abreu P, Mashhoud WM: Cardiovascular risk factor burden in Africa and the Middle East: the Africa Middle East Cardiovascular Epidemiological (ACE) study. PloS One 2014, 9:e102830.
17. Capingana DP, Magalhães P, Silva ABT, Gonçalves MAA, Baldo MP, Rodrigues SL, Simões CCF, Ferreira AVL, Mill JG: Prevalence of cardiovascular risk factors and socioeconomic level among public-sector workers in Angola. BMC Public Health 2013, 13:732.
18. Ogah OS, Okpechi I, Chukwuonye II, Akinyemi JO, Onwubere BJ, Falase AO, Stewart S, Sliwa K: Blood pressure, prevalence of hypertension and hypertension related complications in Nigerian Africans: A review. World J Cardiol 2012, 4:327–340.
19. Olatunbosun ST, Kaufman JS, Bella AF: Prevalence of obesity and overweight in urban adult Nigerians. Obes Rev Off J Int Assoc Study Obes 2011, 12:233–241.
20. Ibekwe R: Modifiable Risk factors of Hypertension and Socio-demographic Profile in Oghara, Delta State; Prevalence and Correlates. Ann Med Health Sci Res 2015, 5:71–77.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 22 —
Chapter 1
21. Obembe AO, Olaogun MO, Bamikole AA, Komolafe MA, Odetunde MO: Awareness of risk factors and warning signs of stroke in a Nigeria university. J Stroke Cerebrovasc Dis Off J Natl Stroke Assoc 2014, 23:749–758.
22. Adeloye D, Basquill C: Estimating the prevalence and awareness rates of hypertension in Africa: a systematic analysis. PloS One 2014, 9:e104300.
23. Adebayo RA, Balogun MO, Adedoyin RA, Obashoro-John OA, Bisiriyu LA, Abiodun OO: Prevalence of hypertension in three rural communities of Ife north local Government area of Osun state, south West nigeria. Int J Gen Med 2013, 6:863.
24. Adebayo RA, Balogun MO, Adedoyin RA, Obashoro-John OA, Bisiriyu LA, Abiodun OO: Prevalence and pattern of overweight and obesity in three rural communities in southwest Nigeria. Diabetes Metab Syndr Obes Targets Ther 2014, 7:153–158.
25. Ogunmola OJ, Olaifa AO, Oladapo OO, Babatunde OA: Prevalence of cardiovascular risk factors among adults without obvious cardiovascular disease in a rural community in Ekiti State, Southwest Nigeria. BMC Cardiovasc Disord 2013, 13:89.
26. Oguoma VM, Nwose EU, Skinner TC, Digban KA, Onyia IC, Richards RS: Prevalence of cardiovascular disease risk factors among a Nigerian adult population: relationship with income level and accessibility to CVD risks screening. BMC Public Health 2015, 15:397.
27. Makusidi MA, Liman HM, Yakubu A, Isah MDA, Jega RM, Adamu H, Chijioke A: Prevalence of non-communicable diseases and its awareness among inhabitants of Sokoto metropolis: outcome of a screening program for hypertension, obesity, diabetes mellitus and overt proteinuria. Arab J Nephrol Transplant 2013, 6:189–191.
28. Chukwuonye II, Chuku A, John C, Ohagwu KA, Imoh ME, Isa SE, Ogah OS, Oviasu E: Prevalence of overweight and obesity in adult Nigerians-a systematic review. Diabetes Metab Syndr Obes Targets Ther 2013, 6:43–47.
29. Amole OI, Olaolorun DA, Odeigah OL: Body size and abnormal lipids among adult patients at the Baptist Medical centre, Ogbomoso, Nigeria. Afr Health Sci 2013, 13:32–37.
30. Sani MU, Wahab KW, Yusuf BO, Gbadamosi M, Johnson OV, Gbadamosi A: Modifiable cardiovascular risk factors among apparently healthy adult Nigerian population-a cross sectional study. BMC Res Notes 2010, 3:11.
31. Sampson UKA, Amuyunzu-Nyamongo M, Mensah GA: Health promotion and cardiovascular disease prevention in sub-Saharan Africa. Prog Cardiovasc Dis 2013, 56:344–355.
32. Odusola AO, Hendriks M, Schultsz C, Stronks K, Lange J, Osibogun A, Akande T, Alli S, Adenusi P, Agbede K: Development and evaluation of a patient centered cardiovascular health education program for insured patients in rural Nigeria (QUICK-II). BMC Public Health 2011, 11:171.
33. WHO | Healthy diet [http://www.who.int/mediacentre/factsheets/fs394/en/]34. WHO | Salt reduction [http://www.who.int/mediacentre/factsheets/fs393/en/]35. WHO | Obesity and overweight [http://www.who.int/mediacentre/factsheets/fs311/en/]36. Maseko MJ, Majane HO, Milne J, Norton GR, Woodiwiss AJ: Salt intake in an urban, developing South
African community. Cardiovasc J South Afr Off J South Afr Card Soc South Afr Soc Card Pract 2006, 17:186–191.
37. Azinge EC, Sofola OA, Silva BO: Relationship between salt intake, salt-taste threshold and blood pressure in Nigerians. West Afr J Med 2011, 30:373–376.
38. Elias SO, Azinge EC, Umoren GA, Jaja SI, Sofola OA: Salt-sensitivity in normotensive and hypertensive Nigerians. Niger Q J Hosp Med 2011, 21:85–91.
39. Bibbins-Domingo K, Chertow GM, Coxson PG, Moran A, Lightwood JM, Pletcher MJ, Goldman L: Projected effect of dietary salt reductions on future cardiovascular disease. N Engl J Med 2010, 362:590–599.
40. He FJ, Li J, Macgregor GA: Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ 2013, 346:f1325.
41. Awosan KJ, Ibrahim MTO, Essien E, Yusuf AA, Okolo AC: Dietary pattern, lifestyle, nutrition status and prevalence of hypertension among traders in Sokoto Central market, Sokoto, Nigeria. Int J 2014, 6:9–17.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General introduction
— 23 —
42. Peltzer K, Phaswana-Mafuya N: Fruit and vegetable intake and associated factors in older adults in South Africa. Glob Health Action 2012, 5:1–8.
43. Johnsen SP, Overvad K, Stripp C, Tjønneland A, Husted SE, Sørensen HT: Intake of fruit and vegetables and the risk of ischemic stroke in a cohort of Danish men and women. Am J Clin Nutr 2003, 78:57–64.
44. He FJ, Nowson CA, MacGregor GA: Fruit and vegetable consumption and stroke: meta-analysis of cohort studies. Lancet 2006, 367:320–326.
45. Ovesen LF: [Increased consumption of fruits and vegetables reduces the risk of ischemic heart disease]. Ugeskr Laeger 2005, 167:2742–2747.
46. WHO | Physical activity [http://www.who.int/mediacentre/factsheets/fs385/en/]47. Akarolo-Anthony SN, Adebamowo CA: Prevalence and correlates of leisure-time physical activity among
Nigerians. BMC Public Health 2014, 14:529.48. Oyeyemi AL, Adeyemi O: Relationship of physical activity to cardiovascular risk factors in an urban
population of Nigerian adults. Arch Public Health 2013, 71:1–9.49. Akarolo-Anthony SN, Willett WC, Spiegelman D, Adebamowo CA: Obesity epidemic has emerged among
Nigerians. BMC Public Health 2014, 14:455.50. Odusola AO, Hendriks M, Schultsz C, Bolarinwa OA, Akande T, Osibogun A, Agyemang C, Ogedegbe G,
Agbede K, Adenusi P, others: Perceptions of inhibitors and facilitators for adhering to hypertension treatment among insured patients in rural Nigeria: a qualitative study. BMC Health Serv Res 2014, 14:624.
51. WHO | Tobacco [http://www.who.int/topics/tobacco/en/]52. Adepoju EG, Olowookere SA, Adeleke NA, Afolabi OT, Olajide FO, Aluko OO: A population based study on
the prevalence of cigarette smoking and smokers’ characteristics at osogbo, Nigeria. Tob Use Insights 2013, 6:1–5.
53. Egbe CO, Meyer-Weitz A, Asante KO, Petersen I: “A Woman is not Supposed To Smoke”: Exploring Gendered Stereotypes in Smoking Patterns in a Nigerian Setting. J Psychol 2014, 5 (1):1–7.
54. WHO | Global information system on alcohol and health [http://www.who.int/gho/alcohol/en/]55. Zatu MC, Van Rooyen JM, Kruger A, Schutte AE: Alcohol intake, hypertension development and mortality
in black South Africans. Eur J Prev Cardiol 2014.56. Jernigan DH, Babor TF: The concentration of the global alcohol industry and its penetration in the
African region. Addict Abingdon Engl 2015, 110:551–560.57. Ferreira-Borges C, Esser MB, Dias S, Babor T, Parry CDH: Alcohol Control Policies in 46 African Countries:
Opportunities for Improvement. Alcohol Alcohol Oxf Oxfs 2015.58. Cappuccio FP, Kerry SM, Micah FB, Plange-Rhule J, Eastwood JB: A community programme to reduce salt
intake and blood pressure in Ghana [ISRCTN88789643]. BMC Public Health 2006, 6:13.59. 59. Salaudeen A, Musa O, Akande T, Bolarinwa O: Effects of health education on cigarette smoking
habits of young adults in tertiary institutions in a northern Nigerian state. Health Sci J 2011, 5:216–228.60. Nigeria | Data [http://data.worldbank.org/country/nigeria]61. Global Health Observatory Data Repository [http://apps.who.int/gho/data/node.country.country-NGA]62. Hendriks ME, Wit FW, Roos MT, Brewster LM, Akande TM, de Beer IH, Mfinanga SG, Kahwa AM, Gatongi
P, Van Rooy G: Hypertension in sub-Saharan Africa: cross-sectional surveys in four rural and urban communities. PloS One 2012, 7:e32638.
63. Hendriks M, Brewster L, Wit F, Bolarinwa OA, Odusola AO, Redekop W, Bindraban N, Vollaard A, Alli S, Adenusi P, others: Cardiovascular disease prevention in rural Nigeria in the context of a community based health insurance scheme: QUality Improvement Cardiovascular care Kwara-I (QUICK-I). BMC Public Health 2011, 11:186.
64. Odusola AO, Nelissen H, Hendriks M, Schultsz C, Wit F, Bolarinwa OA, Akande T, Agyemang C, Ogedegbe G, Agbede K, others: How Group-Based Cardiovascular Health Education Affects Treatment Adherence and Blood Pressure Control among Insured Hypertensive Nigerians: A Pre-Test, Post-Test Study. World J Cardiovasc Dis 2015, 5:181.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Chapter 2
Development and evaluation of a patient centered cardiovascular health education program for insured patients in rural Nigeria (QUICK-II)
Odusola AOHendriks MSchultsz CStronks KLange JOsibogun AAkande TAlli SAdenusi PAgbede KHaafkens J
BMC Public Health. 2011 Mar 21;11:171.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 26 —
Chapter 2
ABSTRACT
BackgroundIn Sub Saharan Africa, the incidence of hypertension and other modifiable cardiovascular risk factors is growing rapidly. Poor adherence to prescribed prevention and treatment regimens by patients can compromise treatment outcomes. Patient-centered cardiovascular health education is likely to improve shortcomings in adherence. This paper describes a study that aims to develop a cardiovascular health education program for patients participating in a subsidized insurance plan in Nigeria and to evaluate the applicability and effectiveness in patients at increased risk for cardiovascular disease.
Methods/Design Design: The study has two parts. Part 1 will develop a cardiovascular health education program, using qualitative interviews with stakeholders. Part 2 will evaluate the effectiveness of the program in patients, using a prospective (pre-post) observational design. Setting: A rural primary health center in Kwara State, Nigeria.Population: For part 1: 40 patients, 10 healthcare professionals, and 5 insurance managers. For part 2: 150 patients with uncontrolled hypertension or other cardiovascular risk factors after one year of treatment. Intervention: Part 2: patient-centered cardiovascular health education program.Measurements: Part 1: Semi-structured interviews to identify stakeholder perspectives. Part 2: Pre- and post-intervention assessments including patients’ demographic and socioeconomic data, blood pressure, body mass index and self-reporting measures on medication adherence and perception of care. Feasibility of the intervention will be measured using process data.Outcomes: For program development (part 1): overview of healthcare professionals’ perceptions on barriers and facilitators to care, protocol for patient education, and protocol implementation plan.For program evaluation (part 2): changes in patients’ scores on adherence to medication and life style changes, blood pressure, and other physiological and self-reporting measures at six months past baseline. Analysis: Part 1: content analytic technique utilizing MAXQDA software. Part 2: univariate and multilevel analysis to assess outcomes of intervention.
DiscussionDiligent implementation of patient-centered education should enhance adherence to cardio-vascular disease prevention and management programs in low income countries.
Trial RegistrationISRCTN47894401

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Design of the development and evaluation of education program
— 27 —
BACKGROUND
Sub Saharan African (SSA) countries are currently experiencing a rapid increase in the incidence of cardiovascular diseases (CVD) [1,2]. Hypertension is an important risk factor for CVD. Poor adherence to prescribed medication regimens or lifestyle advices can severely compromise the effectiveness of CVD prevention and treatment [3]. For that reason, the World Health Organization (WHO) emphasized in a recent report that any attempt to improve cardiovascular care should also address the issue on non-adherence [3]. The views and beliefs of patients regarding disease conditions and treatment may differ from medical perceptions, and it is well documented that patients do have significant roles to play in adherence to medications and lifestyle measures [4-6]. Evidence to date indicates that patient education is one of the most successful interventions to improve adherence and patient self-management of chronic diseases, especially if the education addresses patients’ beliefs and concerns about the condition and treatment, identifies social cultural and individual barriers to adherence and enhances patients’ confidence in their ability to overcome those barriers [7]. In this paper, we describe the design of a study that has the aim to develop and test a program for cardiovascular health education for patients who are enrolled in a subsidized, community-based health insurance program in Nigeria and are at an increased risk of developing CVD. This study is part of the project “QUality Improvement for Cardiovascular care Kwara (QUICK)”. The project will be evaluated by two studies: QUICK-I and QUICK-II. This paper describes the design of the ‘Development and evaluation of a patient centered cardiovascular health education program for insured patients in rural Nigeria’ (QUICK-II) study that focuses on patient education. A detailed description of the insurance program and the QUICK-I study can be found elsewhere [8].
AIM OF THE STUDy
The World Health Organization/International Society of Hypertension (WHO/ISH) guidelines recommend patient education as part of CVD prevention care [9], but they do not provide clear recommendations on how this education should be delivered and tailored to the specific target groups in the region. We hypothesize that tailored patient education will improve adherence to cardiovascular care among patients.
For that reason, the main aims of QUality Improvement Cardiovascular care Kwara II (QUICK-II) are: 1. To develop and implement a targeted cardiovascular health education program (CHEP) for
patients participating in the Hygeia Community Health Plan (HCHP).2. To evaluate the newly developed program with respect to its applicability and effectiveness in
patients at an increased risk for CVD.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 28 —
Chapter 2
METHODS
Project designQUICK-II consist of two consecutive parts. In part 1 of the study, we will develop a stakeholder based Cardiovascular Health Education Program (CHEP) that is to be used to educate patients at risk of CVD who are enrolled in a private health insurance plan in rural Nigeria. To develop CHEP, we will use the following step-wise approach: (i) open qualitative interviews will be conducted with key stakeholders in CVD care to explore their perceptions on CVD, CVD risk factor management and CVD prevention and care. These stakeholders include patients at risks for CVD, healthcare providers (HCP), and health insurance managers of HCHP; (ii) on the basis of the outcomes of interviews with patients, CHEP will be developed; (iii) supportive strategies needed to implement CHEP successfully will be identified on the basis of the outcomes of the interviews with HCP and health insurance managers. In Part 2 of the study we aim to evaluate the effect of CHEP through a prospective hospital-based study, using a pre-post intervention design. Measurements will be conducted in a subset of patients included in QUICK-I: those who have uncontrolled hypertension or other CVD risk factors, or are non adherent to medication after 12 months of treatment. In addition, case file data will be reviewed and interviews with health care professionals in the participating clinic will be held and analyzed to evaluate the feasibility of the application of CHEP in practice.
SettingOgo Oluwa Hospital (OOH) in Bacita (Kwara State). A detailed description of this setting can be found in the accompanying paper describing the QUICK-I study design [8]. Because part 1 and part 2 of this study have different designs, we will describe the study procedures in different sections.
PART 1: DEVELOPMENT OF CHEP
Study PopulationThe study population for Part 1 will consist of four groups: Group 1: A purposeful sample of 20 patients with ‘controlled hypertension’ equally distributed by gender (50% male and female), and age (18-35yrs, 36-55yrs, 56yrs and over) who were included in the QUICK-I study; Group 2: A purposeful sample of 20 patients with ‘uncontrolled hypertension’ equally distributed by gender (50% male and female), and age (18-35yrs, 36-55yrs, 56yrs and over) who were included in QUICK-I study; Group 3: Eight to ten healthcare professionals treating patients with hypertension (HTN), diabetes mellitus (DM) or CVD at OOH; and Group 4: Five to ten managers and doctors of the Health Maintenance Organization (HMO) Hygeia.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Design of the development and evaluation of education program
— 29 —
Sample size and RecruitmentSample sizeFor qualitative interviews, data saturation is a criterion for calculation of the sample size. In general, about 20 interviews are required until saturation is reached and no new information on the major themes is collected [10,11]. For that reason we decided to interview 40 patients (20 with controlled and 20 with uncontrolled hypertension). The number of interviews for HCP is less because the number of health care professionals working in the region is limited. The same accounts for health insurance managers and doctors of Hygeia HMO.
Patient recruitmentThe patients in Groups 1 and 2 will be recruited among participants in the QUICK-I study in the first month after their inclusion. Health care professionals (Group 3); and managers and doctors working for Hygeia HMO (Group 4) will be included in the first 3 months of QUICK-I. Eligible respondents will be adequately informed of the objectives of the qualitative study. Permission for the interview and written or tape-recorded informed consents will be taken.
OutcomesThe outcomes envisaged for part 1 include: (i) an overview of patients’ perceptions on CVD, CVD risk factors and inhibiting or facilitating factors for CVD prevention and care; (ii) an overview of perceptions of HCP, and health insurance managers and doctors of Hygeia HMO on barriers and facilitators to implementation of CVD prevention and care; (iii) a protocol for CHEP; and (iv) a plan of supportive strategies for implementation of CHEP, including training for HCP.
MATERIALS AND MEASUREMENTS
In part one, patients allocated to Groups 1 and 2 will be interviewed using a semi-structured questionnaire that is based on a topic list used in a similar study by Beune et al. [12], but modified to suit the Nigerian setting. Healthcare professionals from Groups 3 and 4 will similarly be interviewed using semi structured questionnaires based on topic lists specifically designed to address the particular concerns of these groups. A researcher who speaks English and Yoruba fluently, assisted by interpreters in Nupe, the other dominant local language, will conduct interviews. CHEP will be developed based on a systematic review of literature on similar past patient education programs, and analysis of the interview data.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 30 —
Chapter 2
Data management and analysisData entry and cleaningThe researcher will transcribe the semi-structured interviews conducted in part 1 and check unclear passages with respondents, if needed.
Data analysisThe transcribed qualitative interview data will be analyzed using content analytical techniques: fragments containing the respondents’ ideas about major themes, for example inhibitors or facilitators of cardiovascular diseases care, will be identified from each interview and coded. Similar codes will be assigned to related statements, resulting in a code list for each interview. Code lists will be compared to identify common and unique themes, leading to a thematic matrix for each group of respondents. Similarities, variations and patterns between groups will be compared, using these matrices. Data entry and analysis will be supported by MAXQDA software (www.maxqda.com). MAXQDA facilitates data management, the assignment of labels, codes and themes to text fragments and the generation of thematic matrices containing these elements. In the past, MAXQDA software has been successfully used in similar studies [13].
PART 2: EVALUATION OF CHEP
Study populationTo be included in the evaluation study of the effect of CHEP (part 2), patients have to meet the following inclusion criteria. They must: (i) be enrolled in HCHP; (ii) be registered as a patient in OOH; (iii) be included in the QUICK-I study for at least 12 months; (iv) have a diagnosis of hypertension; (v) have uncontrolled BP (≥ 140 mmHg systolic or ≥ 90 mmHg diastolic) or be non adherent to prescribed medication or any other recommended life style changes according to their score on the Morisky scale [14]; and (vi) be ≥ 18 years of age. Patients who meet these inclusion criteria will be excluded if their treating health care professional judges them unfit for participation (e.g. due to co morbidity) or if they are not capable or unwilling to give informed consent. Female patients who are pregnant or lactating will be excluded from the entire study because the etiology, prognosis and treatment regimes of gestational diabetes and pregnancy-induced hypertension are different compared to hypertension and diabetes in non-pregnant women. To be included in the qualitative interviews for the feasibility analysis, healthcare professionals must: (i) be a HCP in OOH who participated in the implementation of CHEP, or be managers and doctors of HCHP; and (ii) give informed consent. Table 1 shows an overview of the inclusion and exclusion criteria for CHEP study. For an overview of the inclusion and exclusion criteria of QUICK-I, see the article of the QUICK-I study design [8].

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Design of the development and evaluation of education program
— 31 —
Table 1: Inclusion and exclusion criteria for CHEP study.
Inclusion Criteria Exclusion Criteria
Patients: • Enrollment in HCHP• Registered and accessing care in OOH• Inclusion in QUICK-I for at least 12 months• Diagnosis of hypertension• Uncontrolled hypertension or non adherence to
prescribed medication or lifestyle changes after 12 months in QUICK-I
• Age of 18 years and over• Give informed consent
Patients: • Unwillingness to give informed consent• Unfit for participation (e.g. due to co morbidity)• Pregnant or lactating females
Healthcare Professionals for interviews on feasibility of CHEP:• HCP of OOH who participated in the implementation
of CHEP, or• Managers and Doctors of HCHP• Give informed consent
Figure 1 describes the project populations for QUICK-II and their relationship to the QUICK-I study.
Figure 1: Project populations and relationship between QUICK-I and CHEP study in QUICK-II.
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 32 —
Chapter 2
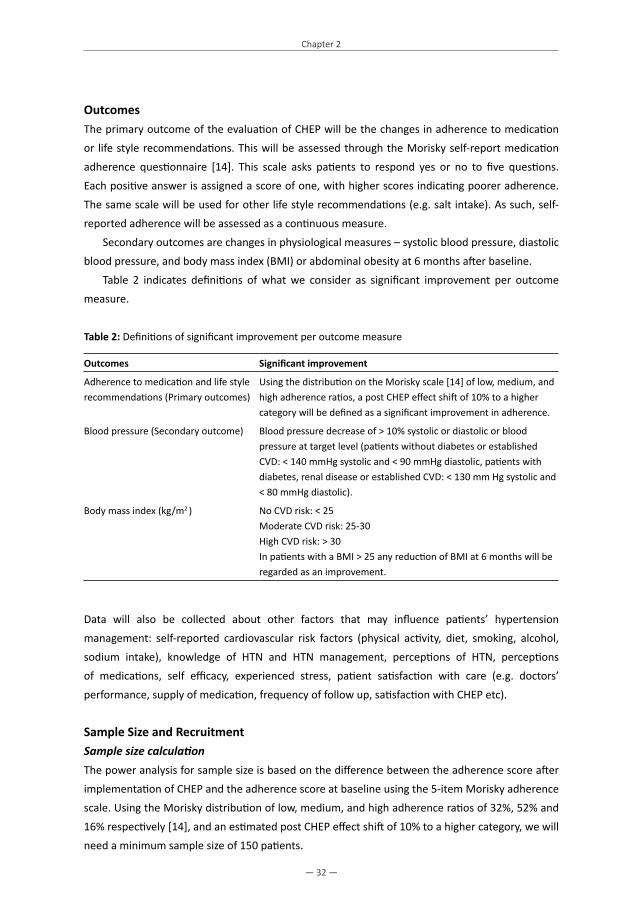
OutcomesThe primary outcome of the evaluation of CHEP will be the changes in adherence to medication or life style recommendations. This will be assessed through the Morisky self-report medication adherence questionnaire [14]. This scale asks patients to respond yes or no to five questions. Each positive answer is assigned a score of one, with higher scores indicating poorer adherence. The same scale will be used for other life style recommendations (e.g. salt intake). As such, self-reported adherence will be assessed as a continuous measure. Secondary outcomes are changes in physiological measures – systolic blood pressure, diastolic blood pressure, and body mass index (BMI) or abdominal obesity at 6 months after baseline. Table 2 indicates definitions of what we consider as significant improvement per outcome measure.
Table 2: Definitions of significant improvement per outcome measure
Outcomes Significant improvement
Adherence to medication and life style recommendations (Primary outcomes)
Using the distribution on the Morisky scale [14] of low, medium, and high adherence ratios, a post CHEP effect shift of 10% to a higher category will be defined as a significant improvement in adherence.
Blood pressure (Secondary outcome) Blood pressure decrease of > 10% systolic or diastolic or blood pressure at target level (patients without diabetes or established CVD: < 140 mmHg systolic and < 90 mmHg diastolic, patients with diabetes, renal disease or established CVD: < 130 mm Hg systolic and < 80 mmHg diastolic).
Body mass index (kg/m2 ) No CVD risk: < 25 Moderate CVD risk: 25-30High CVD risk: > 30 In patients with a BMI > 25 any reduction of BMI at 6 months will be regarded as an improvement.
Data will also be collected about other factors that may influence patients’ hypertension management: self-reported cardiovascular risk factors (physical activity, diet, smoking, alcohol, sodium intake), knowledge of HTN and HTN management, perceptions of HTN, perceptions of medications, self efficacy, experienced stress, patient satisfaction with care (e.g. doctors’ performance, supply of medication, frequency of follow up, satisfaction with CHEP etc).
Sample Size and RecruitmentSample size calculationThe power analysis for sample size is based on the difference between the adherence score after implementation of CHEP and the adherence score at baseline using the 5-item Morisky adherence scale. Using the Morisky distribution of low, medium, and high adherence ratios of 32%, 52% and 16% respectively [14], and an estimated post CHEP effect shift of 10% to a higher category, we will need a minimum sample size of 150 patients.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Design of the development and evaluation of education program
— 33 —
Patient recruitmentThe following steps will be applied in recruiting patients for the CHEP study:1. Researchers will use the records of the QUICK-I study to identify all patients with uncontrolled
hypertension or with low or medium adherence scores for medication or other life style measures on the Morisky Scale at 12 months after inclusion into the study.
2. Eligible patients will be informed about QUICK-II and invited for participation through a written invitation.
3. A research assistant will assess patients who are interested in participating for eligibility criteria and eligible patients will be asked to give informed consent.
4. Patients who give informed consent will be invited to a one-hour baseline assessment session.5. Included patients who have completed baseline assessments will be invited to have three CHEP
sessions spaced over a period of 4 months and one final assessment interview six months after baseline.
To encourage participation, all included patients will be reimbursed for extra travel costs incurred in visiting for assessments and CHEP sessions outside their normal clinic days.
InterventionThe intervention (CHEP) will be developed in part 1 of this project. Subsequently, patients will be given (i) three CHEP sessions over a period of four months conducted by a trained nurse; (ii) audio-visual or written educational materials containing specific information for the target group and (iii) if necessary, referrals to regional facilities or initiatives that may help patients to adopt healthier lifestyles.
SessionsThe first session will take place two weeks after the baseline assessment interview, and the next two sessions will occur one and three months thereafter. Clinical guidelines generally recommend a patient centered approach as the preferred strategy for supporting patients in achieving CVD treatment goals, such as adherence to prescribed medication, dietary changes, and weight reduction, reduced sodium intake, increased physical activity and moderate use of alcohol [3]. While CHEP will use this framework, it will have the additional aim of eliciting and discussing culturally and socially specific aspects of patients’ perceptions of cardiovascular risk factors and treatment. This method is based on the work of Arthur Kleinman [15], as well as more recent approaches to improving adherence in hypertensive patients of various ethnic and geographical background, such as those recently developed in The Netherlands [16]. In short, after identifying potential communication barriers and establishing a rapport with the patient, it is expected that the first session will focus on the patient’s beliefs about hypertension. The next two sessions will deal with the daily challenges they face in achieving hypertension treatment goals within the broader context of their lives. Education will take place in group training sessions.
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 34 —
Chapter 2
Educational materialsPatients will also be given information leaflets or audio visual materials that provide answers to frequently asked questions about hypertension. These will be designed to address the specific languages, customs, habits, norms and dietary cultures that characterize the communities of the patients participating in the program.
Supporting healthier lifestylesIf necessary, patients will be referred to initiatives offering healthier lifestyle support that is tailored to the target group, based on a referral list that will be established for this purpose in the first part of this study.
The nursesIn order to ensure treatment fidelity and to avoid organizational- and healthcare-related obstacles to implementation, the nurses who will provide CHEP will be given clear guidelines and extensive training in implementing these guidelines.
MATERIALS AND MEASUREMENTS
We will use the following measurements and materials to evaluate the effects of CHEP: patients’ adherence to medication and other life style recommendations will be measured by using the five point Morisky Scale; and patients’ blood pressure will be measured using pre validated OMRON M6 Comfort electronic equipment. The blood pressure will be measured on 3 occasions with the patient seated comfortably for 5 minutes, and the last two values averaged. All other physiological measures will be performed according standardized procedures using standard equipment. Other self-reporting measures (see Table 3) will be measured using the questionnaire of the OHD 2 trial in the Netherlands [16]. Aspects of this questionnaire will be adapted to the Nigerian specifics where necessary. All assessments will take place at baseline and 6 months after. A trained nurse will perform all physiological assessments. A trained interviewer will perform pre- and post CHEP assessment interviews. The researcher will be responsible for the training of the nurses and the interviewers. Table 3 presents all the measurements that will be used in the study.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Design of the development and evaluation of education program
— 35 —
Table 3: Timelines and measures used in CHEP study.
Measures Baseline Final
Physiological measures• Clinic BP measurements, Heart rate • Height, weight, Body Mass Index• Hip and waist circumference
XXX
XXX
Self-reporting measures• Patient demographics• Additional cardiovascular risk factors (physical activity, diet,
smoking, alcohol, sodium intake) • Medication adherence• Adherence to lifestyle recommendations• Knowledge of HTN• Perceptions of HTN• Perceptions of medication• Self efficacy • Satisfaction with care• Perception of stress
XX
XXXXXXXX
X
XXXXXXXX
Case file data• Prescribed medication• Prescribed lifestyle measures• Co-morbidity
XXX
XXX
Process data• Records office visits, patient drop-out data etc • HCP interviews
X XX
Data AnalysisStatistical methodsThe rate of adherence will be examined according to the intention to treat principle. Primary and secondary outcome measures will be calculated for every patient at baseline and 6 months thereafter to assess possible improvements. Furthermore, univariate and multi-level analyses will be performed to evaluate the modifying effect of the outcome measures (see above) on adherence or blood pressure. If the N is sufficient, we will perform separate subgroup analyses for gender. While a p value of 0.05 will be the critical value for all analysis, the p value will be adjusted for subgroup analysis according to standard procedures. Data from interviews with HCP will be analyzed and used to identify potential barriers to the implementation of CHEP in practice.
Ethical approvalEthical approval was obtained for both QUICK studies [8].

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 36 —
Chapter 2
DISCUSSION
Recent prevalence data from National Surveys indicate that many risk factors for CVD are highly prevalent in Nigeria: alcohol abuser/dependant – 4.4% (M – 8.1%, F – 0%); overweight/obesity (BMI ≥ 30 kg/m2) – 13.9% (M – 5.5%, F – 21.1%); physical inactivity – 6.8%; tobacco use – 9.9% (M – 19.3%, F – 1.8%); raised cholesterol – (M – 10.4%, F – 21.6%); raised blood pressure (systolic ≥ 160 mmHg or diastolic ≥ 95 mmHg) – 12.4% (M – 12.1%, F – 12.7%); and diabetes – 2.8% (M – 2.7%, F – 3%). There are no data on dietary intake such as fruits and vegetables (https://apps.who.int/infobase/Indicators.aspx). A substantial majority of CVD are preventable or treatable if patients at risk have access to quality CVD prevention and care programs. Quality care is, however, mostly inaccessible in resource-limited settings. Even where such care may be available and accessible, strict compliance and adherence to the dictates of therapy regimes becomes paramount for the successful control of CVD risk factors, and prevention of CVD in the affected populations. A recent study in Kwara state, Nigeria where QUICK is being implemented concluded that control of hypertension is unacceptably poor because of poor knowledge of hypertension and adverse practices by patients [17]. In a similar vein, another Nigerian study suggested that physicians should allocate special time for health education, having concluded that lack of time by physicians and inadequate knowledge about hypertension by patients are some of the potent barriers to effective CVD prevention and care [18]. Furthermore, with particular reference to SSA where deep routed cultural practices still play prominent roles in people’s lives, health education to prevent CVD must be patient centered, and developed with due consideration for socio-cultural relevance in order for the intervention to be successful. By researching into the most optimal methods to implement an appropriately developed cardiovascular health education program, our expectation is that the present study will provide insight into, and contribute substantially to the improvement in CVD management and outcomes. We hope that the envisaged intervention, CHEP, will become productively applicable not only in Nigeria, but also in other similar settings in SSA and across the globe.
The study has one notable limitationThe design of our evaluation of CHEP could have been improved by using a control group and a randomized design. However, the study is conducted in a very specific context, where it is impossible to avoid contamination. For example, patients have generally long waiting hours and may communicate about their condition or the treatment with each other. Moreover, the number of health care professionals in the clinic is limited such that it would be impossible to randomize them into a control and experimental condition. In addition, given the context of the community health insurance program, other clinics that provide standard cardiovascular care are difficult to find in the region. Nevertheless, to address this limitation, we consider analyzing the data collected during QUICK-I study for the patients included in QUICK-II to further compare and evaluate the effects of CHEP.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Design of the development and evaluation of education program
— 37 —
Acknowledgements We are grateful to the following persons for their immense support and productive collaboration in the preparation, planning and implementation of this project: the staff of Ogo Oluwa Hospital, Bacita for their cooperation in the preparation and implementation; the entire QUICK staff at the project site; Dr Ayorinde of Oluseyi Hospital for his cooperation; Dr O. Opowoye and the staff of HCHP in Kwara for their cooperation and logistics support; Dr Bolarinwa of University of Ilorin Teaching Hospital for significant inputs to project supervision and monitoring support; Prof. A. Elebute and Mrs. F. Laoye, Hygeia Nigeria Ltd, Lagos; Dr A. Vollaard and Dr M. Van Vugt of Pharmaccess Foundation, Amsterdam; Mrs. E. Coles of the Health Insurance Fund.
The QUICK-I and QUICK-II studies are funded by the Health Insurance Fund (HIF). HIF is not involved in the study design; in the collection, analysis, and interpretation of data; in the writing of the manuscript nor in the decision to submit the manuscript for publication.
Authors’ contributionsAOO drafted the manuscript, conducts the study and contributed to the design. MH, JH, CS, KS, and JL designed the study and they are members of the supervising board. AO, TA, SA, PA, KA were involved in the design of the study. JH revised several early drafts of the paper and KS, CS and MH commented on the final draft. All authors read and approved the final manuscript.
Competing interestsThe authors declare that they have no competing interests.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 38 —
Chapter 2
REFERENCES
1. Kengne AP, Awah PK, Fezeu L, Mbanya JC: The burden of high blood pressure and related risk factors in urban sub-Saharan Africa: evidences from Douala in Cameroon. African health sciences 2007, 7:38-44.
2. Kengne AP, Dzudie A, Sobngwi E: Heart failure in sub-Saharan Africa: a literature review with emphasis on individuals with diabetes. Vascular health and risk management 2008, 4:123-130.
3. De Geest S, Sabate E: Adherence to long-term therapies: evidence for action. Eur J Cardiovasc Nurs 2003, 2:323.
4. Ike SO, Aniebue PN, Aniebue UU: Knowledge, perceptions and practices of lifestyle-modification measures among adult hypertensives in Nigeria. Transactions of the Royal Society of Tropical Medicine and Hygiene, 104:55-60.
5. Boulware LE, Daumit GL, Frick KD, Minkovitz CS, Lawrence RS, Powe NR: An evidence-based review of patient-centered behavioral interventions for hypertension. American journal of preventive medicine 2001, 21:221-232.
6. Krousel-Wood M, Hyre A, Muntner P, Morisky D: Methods to improve medication adherence in patients with hypertension: current status and future directions. Current opinion in cardiology 2005, 20:296-300.
7. Bodenheimer T, Lorig K, Holman H, Grumbach K: Patient self-management of chronic disease in primary care. Jama 2002, 288:2469-2475.
8. Hendriks M, Brewster L, Wit F, Bolarinwa AO, Odusola AO, Redekop W, Bindraban N, Vollaard A, Alli S, Adenusi P, Agbede K, Akande T, Lange J, Schultsz C: Cardiovascular disease prevention in rural Nigeria in the context of a community based health insurance scheme: QUality Improvement Cardiovascular care Kwara-I (QUICK-I). BMC Public Health, in press.
9. Mendis S, Lindholm LH, Mancia G, Whitworth J, Alderman M, Lim S, Heagerty T: World Health Organization (WHO) and International Society of Hypertension (ISH) risk prediction charts: assessment of cardiovascular risk for prevention and control of cardiovascular disease in low and middle-income countries. Journal of hypertension 2007, 25:1578-1582.
10. Britten N: Qualitative interviews in medical research. BMJ (Clinical research ed 1995, 311:251-253.11. Mays N, Pope C: Rigour and qualitative research. BMJ (Clinical research ed 1995, 311:109-112.12. Beune EJ, Haafkens JA, Agyemang C, Schuster JS, Willems DL: How Ghanaian, African-Surinamese and
Dutch patients perceive and manage antihypertensive drug treatment: a qualitative study. Journal of hypertension 2008, 26:648-656.
13. Kronenwetter C, Weidner G, Pettengill E, Marlin R, Crutchfield L, McCormac P, Raisin CJ, Ornish D: A qualitative analysis of interviews of men with early stage prostate cancer: the Prostate Cancer Lifestyle Trial. Cancer nursing 2005, 28:99-107.
14. Morisky DE, Green LW, Levine DM: Concurrent and predictive validity of a self-reported measure of medication adherence. Medical care 1986, 24:67-74.
15. Pappas G: Some implications for the study of the doctor-patient interaction: power, structure, and agency in the works of Howard Waitzkin and Arthur Kleinman. Social science & medicine (1982) 1990, 30:199-204.
16. Haafkens JA, Beune EJ, van Charante EP, Agyemang CO: A cluster-randomized controlled trial evaluating the effect of culturally-appropriate hypertension education among Afro-Surinamese and Ghanaian patients in Dutch general practice: study protocol. BMC health services research 2009, 9:193.
17. Katibi IA, Olarinoye JK, Kuranga SA: Knowledge and practice of hypertensive patients as seen in a tertiary hospital in the middle belt of Nigeria. Nigerian journal of clinical practice, 13:159-162.
18. Familoni BO, Ogun SA, Aina AO: Knowledge and awareness of hypertension among patients with systemic hypertension. Journal of the National Medical Association 2004, 96:620-624.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Chapter 3
Perceptions of inhibitors and facilitators for adhering to hypertension treatment among insured patients in rural Nigeria: a qualitative study
Odusola AOHendriks MSchultsz CBolarinwa OAAkande TOsibogun AAgyemang COgedegbe GAgbede KAdenusi PLange Jvan Weert HStronks KHaafkens JA
BMC Health Serv Res. 2014; 14: 624

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 40 —
Chapter 3
ABSTRACT
BackgroundUniversal health care coverage has been identified as a promising strategy for improving hypertension treatment and control rates in sub Saharan Africa (SSA). Yet, even when quality care is accessible, poor adherence can compromise treatment outcomes. To provide information for adherence support interventions, this study explored what low income patients who received hypertension care in the context of a community based health insurance program in Nigeria perceive as inhibitors and facilitators for adhering to pharmacotherapy and healthy behaviors.
MethodsWe conducted a qualitative interview study with 40 insured hypertensive patients who had received hypertension care for > 1 year in a rural primary care hospital in Kwara state, Nigeria. Supported by MAXQDA software, interview transcripts were inductively coded. Codes were then grouped into concepts and thematic categories, leading to matrices for inhibitors and facilitators of treatment adherence.
ResultsImportant patient-identified facilitators of medication adherence included: affordability of care (through health insurance); trust in orthodox “western” medicines; trust in Doctor; dreaded dangers of hypertension; and use of prayer to support efficacy of pills. Inhibitors of medication adherence included: inconvenient clinic operating hours; long waiting times; under-dispensing of prescriptions; side-effects of pills; faith motivated changes of medication regimen; herbal supplementation/substitution of pills; and ignorance that regular use is needed. Local practices and norms were identified as important inhibitors to the uptake of healthier behaviors (e.g. use of salt for food preservation; negative cultural images associated with decreased body size and physical activity). Important factors facilitating such behaviors were the awareness that salt substitutes and products for composing healthier meals were cheaply available at local markets and that exercise could be integrated in people’s daily activities(e.g. farming, yam pounding, and household chores).
ConclusionsWith a better understanding of patient perceived inhibitors and facilitators of adherence to hypertension treatment, this study provides information for patient education and health system level interventions that can be designed to improve compliance.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 41 —
BACKGROUND
Cardiovascular disease (CVD) is a leading cause of death globally [1,2]. Hypertension is a major risk factor for CVD [3]. Once rare in SSA, hypertension and its related complications are increasingly common in the region [4]. Treatment with medication and behavioral changes (reduction in dietary salt intake, weight reduction, moderation of alcohol intake and increased physical activity) can greatly reduce blood pressure (BP) and the risk of CVD-related mortality among people with hypertension [5]. In SSA, CVD prevention is a recent development [6], and hypertension detection, treatment and control rates are generally low [7]. The absence of affordable community based primary care services has been identified as a major obstacle to effective hypertension treatment in the region [8]. But several countries in SSA are now developing programs that provide such services [9,10]. Hypertension is a chronic condition that requires lifelong adherence to pharmacotherapy and healthy behaviors. For many patients, long-time adherence to hypertension treatment is a problem [11-16]. There is evidence that hypertension care is more effective if it includes educational interventions that address barriers to adherence [12,17,18]. Theoretical frameworks underlying various models for patient education propose that, in order to be effective, education should be patient-centered, and tailored to patients’ (cultural) views about the condition and the treatment [17-19]. In high income countries, where access to affordable care is generally available, many (mostly qualitative) studies have investigated patients’ perspectives on adherence to hypertension treatment in different populations [13,20-22]. A recent systematic review of 53 of those studies indicated that common patient-related factors for non-adherence to antihypertensive medication across countries and ethnic groups include patients’ beliefs that medication is unnecessary when symptoms of hypertension or stress disappear, a dislike of medications, fear of addiction, and the experience of side effects [22]. Data from such studies have provided content for educational interventions to improve adherence and health outcomes in patients with hypertension in the USA and Europe [23-25]. Non-adherence to hypertension treatment can have serious consequences for the patients, in terms of lost opportunities for health improvements, and for the health care systems, in terms of wasted financial and human resources. New programs that provide universal primary care coverage are emerging in SSA [26]. So far, few studies in the region have investigated perceptions of hypertension treatment among patients who are covered by health insurance [27]. Hence, it is important to fill this gap [28]. Nigeria is one of the countries in SSA where initiatives are being taken to introduce private or public community based health insurance plans [29]. The estimated prevalence rates of hypertension in Nigeria are 19.3% for rural areas, 36.6% for semi-urban areas, 42% for urban areas, and from 12.4%-to-34.8% for the country as a whole [29-32]. Studies of patients’ perceptions of hypertension treatment have been carried out in several settings and communities in Nigeria [15,16,33-36], but not among patients who were covered by health insurance. Understandably, many of these studies concluded that patients perceived

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 42 —
Chapter 3
financial constraints as the major reason for not adhering to treatment [16,37,38]. The present study was conducted in the context a subsidized community based health insurance program that covers the costs of primary and limited secondary health care and medications, for low income residents of rural communities in Kwara state, the 9th poorest among Nigeria’s 36 states. A recent population-based study that was conducted in Kwara reported hypertension awareness, treatment and control rates of 8%, 5% and 3%, respectively [29]. As a first stage of a larger project [39], we conducted a qualitative study among hypertensive patients who participated in the community based health insurance program in Kwara state to explore their views on hypertension management. The specific research questions of the study were as follows: 1) what are patients’ views on factors that may inhibit or facilitate adherence to prescribed medications?; and 2) what are patients’ views on factors that may inhibit or facilitate adherence to behavioral recommendations?
METHODS
We used a qualitative research design and individual interviews with open-ended questions to explore patients’ perceptions on inhibitors and facilitators for adhering to hypertension treatment [40].
Setting and participantsFor this study we recruited patients who had enrolled in the Hygeia Health Care Plan and were treated for hypertension at Ogo Oluwa Hospital, which is located in Bacita, a small rural town in Kwara state, Nigeria. The Hygeia Community Health Care Plan, now called the Kwara State Health Program, is financed by an international development organization – the Health Insurance Fund (HIF) [41,42]. This health care plan was launched in 2007 to provide subsidized community based health insurance for low- and middle income groups in Lagos state (western) Nigeria and Kwara state (north-central) Nigeria. The insurance package covers primary and limited secondary care, including hypertension treatment. Ogo Oluwa Hospital is one of the first clinics in Kwara state that joined the Hygeia Community Health Care Plan. It is a large, busy private hospital that has offered primary and secondary care to people from the Bacita area for over 25 years. In the 1990s, Bacita was a busy commercial center that hosted the then thriving but later moribund state-owned Nigeria Sugar Company. The original population of Bacita is Nupe, but the Sugar Company attracted other Nigerians of various ethnic origins, particularly the Yoruba. Although the Sugar Company went out of business, a substantial majority of the economic migrants of the time settled permanently in the Bacita area. Therefore, Yoruba is now widely spoken alongside the native

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 43 —
Nupe. Currently considered a poor community, the predominant livelihood activities of the inhabitants are farming, petty trading, artisanship, hunting and fishing. Ogo Oluwa Hospital is owned and managed by an experienced General Practitioner, assisted at that time by about 2 other doctors, 10 nurses, 3 pharmacy staff, 4 laboratory staff and 4 records staff. At the start of this study, about 400 of the hospital’s patients were treated for hypertension and attended clinics on a monthly or bi-monthly basis. Most of them had joined the Hygeia Community Health Care Plan. About two-thirds resided within the town at an average distance of 10 to 20 minutes travel time to the hospital; the remaining third were living in some distantly located surrounding villages. The inclusion criteria for this study were as follows: having Hygeia Community Health Care Plan; diagnosed with hypertension (systolic BP ≥ 140 mmHg and/or diastolic BP ≥ 90 mmHg); in treatment for hypertension at Ogo Oluwa Hospital for ≥ 12 months; having been prescribed antihypertensive medication for ≥ 12 months; aged 18 years or over; and being prepared to give verbal (recorded) informed consent. Since pregnancy induced hypertension has a different course and etiology, pregnant or lactating hypertensive females were excluded from participation in this study. We also sought equal participation of men and women. In qualitative interview studies, data or thematic saturation is a criterion for determining sample size [43,44]. This means that the number of respondents is sufficient if interviews with new respondents do not yield new themes. Fifteen interviews is generally enough to achieve saturation [43,44]. On the basis of these considerations and the inclusion criteria, we selected a purposeful sample of 40 patients from the case file records of Ogo Oluwa Hospital and invited them to the study. None of the invited patients declined. Patients who agreed to participate were reminded about the appointment some days prior to date of interview. At the beginning of each interview session, patients were asked to give audio-recorded informed consent and were assured of confidentiality. Travel expenses incurred for study visits outside usual clinic days were reimbursed.
Interview guide and data collectionTo explore patients’ perceptions of hypertension treatment we developed a semi-structured interview guide. The guide built on instruments that were used in previous qualitative interview studies of patient perceptions of hypertension [13,45] and it was adapted to the specific context and purpose of this study. The interview guide was edited in English and translated into Yoruba and Nupe by native speakers. Eight main topic areas of the interview guide that referred to hypertension treatment were: knowledge and personal views about hypertension; access to care; the role of health insurance; sources of information about hypertension; views on (prescribed) medications; views on behavioral adaptations; satisfaction with care; and general views on CVD prevention (Additional file 1). Information on the socio-demographic characteristics of the participants was collected through close-ended questions. Information on the participants’ recent health related outcomes, (blood pressure, co-morbidities), was

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 44 —
Chapter 3
collected from the respondents’ case file records. Data collection and analysis are continuous and simultaneous iterative processes in qualitative studies [46]. In this study, we held a first set of 30 interviews between July and October 2010 and a second set of 10 interviews between November and December 2010. The specific aim of the last set of interviews was to explore a number of emerging themes that were identified through the analysis of the first 30 interviews. The researcher (AOO) conducted the interviews at Ogo Oluwa Hospital. He is not from the study area and he did not know the participants, prior to the interview. He made his profession, researcher with a medical background (MD), known to the participants. Each of the first set of interviews lasted 120 minutes on average, and the second set lasted about 60 minutes each. All interviews were recorded, transcribed and translated into English by the researcher and an assistant.
Data analysisThe interview transcripts were analyzed, using steps and coding procedures of the method of qualitative data analysis that was developed by Strauss and colleagues (grounded theory) [47]. Briefly, this inductive method begins with the assignment of a series of open codes to the transcripts of individual interviews, which are then grouped into clusters (concepts) in order to make them more workable. From these concepts, broader categories and subcategories are generated, through a process of constant comparison or verification. The ultimate outcome is a data-based matrix of concepts and (sub-) categories, which serve as an input for developing theoretical or conceptual frameworks. We imported all interview transcripts into MAXQDA and we used this qualitative data analysis software to support consistent data analysis, processing, ordering and comparison of the results at different stages [48]. Underneath we provide some more detail about the process of data analysis that was adopted in the present study. First, in each of the interview transcripts, sections containing information on respondents’ ideas on hypertension and hypertension treatment (medications and behavioral changes) were identified, and inductively coded. Similar codes were assigned to text fragments that reflected the same idea. These coding activities yielded a codebook that included all the codes that were created during the analysis of the individual interview transcripts. To conclude this stage we reviewed the code book to eliminate duplicates and to inspect if the remaining codes captured similar concepts so that they could be grouped together. The goal was to establish a smaller set of mutually exclusive conceptual codes that expressed the meaning of the underlying codes without loss of the original content. The identified “concepts”, and underlying text fragments were then scrutinized and grouped under four major themes referring to our research questions; inhibitors and facilitators of adherence to medication and behavioral recommendations. Subsequently, thematic coding procedures were used to group the concepts under each of the four major themes into categories and sub-categories. Results
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 45 —
of these multi-level coding procedures were summarized into matrices. (See Additional file 2 for an example).
TrustworthinessThe researcher (AOO) selected the sections of the interview transcripts that served as an input for the data analysis. To increase reliability and trustworthiness of the analysis, the following steps were taken:1. To establish a consistent open coding procedure, two members of the research team (AOO
and JAH) coded fragments of 15 interviews independently. Results were compared and if differences occurred (for instance with respect to the most plausible naming of a code) they were resolved through discussion and by going back to the original data.
2. To establish the (short) list of conceptual codes, two members of the team (AOO and JAH) independently reviewed the code book and created relevant concepts. Differences of opinion with respect to the clustering of codes or the naming of concepts were resolved by discussion and by going back to the original data.
3. The categorization of concepts under the main themes (inhibitors and facilitators of adherence) was done by AOO and supervised by JAH, who made sure that every decision was plausible and could be justified.
4. The preliminary results of the data analysis were based on 30 interviews. Overlooking these results, AOO and JAH acknowledged that some additional interviews (10) were needed to further confirm or explore some of the themes and concepts that had emerged from this preliminary analysis, so that thematic saturation could be reached. Examples of such themes were related to the perceived role of religion on (non) adherence to medication and patients’ ideas about “local practices” that can inhibit or enhance healthy eating habits and physical exercise.
5. Based on the analysis of the last set of interviews some new conceptual codes were added to the original list, where appropriate. The researcher returned to the transcripts of the first set of interviews to check if any of these new codes could also be applied here.
6. Thematic coding was done by AOO and JAH. They reviewed the conceptual coding trees for each of the four major themes (research questions) and independently categorized those concepts into categories and subcategories. Differences in opinion were resolved by discussions and by checking the underlying data. At several occasions other members of the research team (KS, CS) asked critical questions as regards the categorization of the concepts, and this led to some adaptations in the final ordering and presentation of the categories and sub categories and consequently the results.
7. The final results of the analyses that are presented in the Tables in this paper were reviewed by all authors.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 46 —
Chapter 3
EthicsThis study is part of a larger project that aims to develop and evaluate cardiovascular health education program for insured patients with hypertension in rural Nigeria [39]. Ethical approval was obtained on 30th March, 2010 from University of Ilorin Teaching Hospital prior to the start of the study in July. Guidelines for quality assurance of qualitative research in health from the Academic Medical Center were used to ensure appropriate conduct of the study [49]. COREQ criteria for reporting qualitative interviews were used as a guideline for reporting this study [50].
RESULTS
We interviewed 40 patients. Half of them had controlled BP – systolic BP < 140 mmHg and diastolic BP < 90 mmHg, and the other half uncontrolled BP – systolic BP ≥ 140 mmHg and/or diastolic BP ≥ 90 mmHg (Table 1). Most were older than 50 years. All were rural dwellers, 80% earned less than 5 USD per day, and 70% had none or only primary school education, almost all (92%) lived in poor housing conditions and most (75%) were farmers, artisans or traders. All were religious, 62.5% practiced Christianity and 37.5% practiced Islam.
Table 1: Socio-demographic and clinical characteristics of respondents (n = 40).
Characteristics N (%)
Age group (years)
• 30-50 9 (22.5%)
• 50-70 26 (65%)
• 70-90 5 (12.5%)
Gender
• Male 16 (40%)
• Female 24 (60%)
Educational level
• None or primary education 28 (70%)
• Secondary education 9 (22.5%)
• Tertiary education 3 (7.5%)
Ethnicity
• Nupe 6 (15%)
• Yoruba 31 (77.5%)
• Others 3 (7.5%)

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 47 —
Table 1: (Continued)
Characteristics N (%)
Religion
• Christianity 25 (62.5%)
• Islam 15 (37.5%)
Marital status
• Married 38 (95%)
• Widowed 2 (5%)
Employment status
• Unemployed 1 (2.5%)
• Self-employed* 39 (97.5%)
Income level (USD per day)
• Less than 2 23 (57.5%)• 2-4 9 (22.5%)• More than 5 8 (20%)
Health insurance status
• Insured (Hygeia Community Health Care Plan) 40 (100%)
Hypertension control status
• Controlled 20 (50%)
• Uncontrolled 20 (50%)
Duration of hypertension history (years)
• 1-5 28 (70%)
• 5-10 7 (17.5%)
• Above 10 5 (12.5%)
Co-morbid conditions
• Diabetes 7 (17.5%)
• Others (osteoarthritis, peptic ulcer disease) 7 (17.5%)
• None 26 (65%)
*Most frequent employment types: artisanship/farming/trading/hunting/fishing.
Factors inhibiting and facilitating medication adherence Some patients said they did not always take their medications according to prescription. Frequently mentioned patterns of “self-regulation” included reducing the daily dosage, skipping medications under specific circumstances and discontinuing medications for several days or weeks. None had stopped using medications all together. Patients’ accounts of factors that inhibited them from using their pills as prescribed could be classified into five main categories (Table 2):1. Healthcare related factors: The way in which hypertension care was organized was
perceived as one inhibitory factor for medication adherence. In general patients at Ogo

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 48 —
Chapter 3
Oluwa hospital are required to attend hypertension clinic once a month for follow-up and medication refills. The hypertension clinic is always held at fixed hours on Fridays. Other obligations such as attending Muslim praying hours (Fridays), work, household chores or being on a trip out of town will sometimes prevent patients from meeting their appointments at these fixed hours. The distance to the clinic was also mentioned as a reason for missing appointments. Highlighting the resultant financial challenge, a 50 year old woman with uncontrolled hypertension [ID6] said – visiting [regularly] is problematic for me in the sense that the clinic is far from my residence and travel cost is prohibitive; I spend 500 naira (3USD) to get here and another 500 naira to go back home. Long waiting times at the clinic were also cited as a reason for missing appointments. Asked how regularly he attends clinic, a 72 year old man with uncontrolled hypertension [ID27] replied – visiting is difficult for me because of the many hours spent in clinic, which could be used on my business; in fact I once stopped coming for about 2 months when I realized my hypertension was ‘under control’. Sometimes, the pharmacy is out of stock for particular drugs and not all prescribed medications can be dispensed. A 50 year old woman with controlled hypertension [ID11] responded – sometimes, the pharmacy doesn’t have all the drugs prescribed so they write it in paper for me to buy or come back to collect them oftentimes days after being without pills to use.
2. Patient related factors: patients’ own views such as the idea that hypertension is a transient, curable condition also emerged as a consideration for deviating from the prescribed medication. Responding to a question on how long she expects to continue to use hypertension medication, a 64 year old woman with uncontrolled hypertension [ID13] replied – surely, hypertension can be cured, one cannot continue to use drugs all days of one’s life; with prayers, in no time it will go.
3. Medication related factors: side-effects experienced and the complexity of prescribed regimens also emerged as adherence inhibitors. A 55 year old woman with uncontrolled hypertension [ID38] responded – I am okay with everything but the helplessness of the doctor about the serious side-effects that I experience with my drugs; I sometimes miss my clinic appointments because of these side-effects. A 50 year old woman with uncontrolled hypertension [ID6] responded – if the pills can be formulated such that fewer pills will do the work of the 8 pills that I currently take daily perfectly; then fewer pills are preferred as they are easier for me to manage. Some patients mentioned incompatibility between religious fasting and regular pills use, and some others unilaterally substituted or supplemented prescribed pills with herbal remedies without recourse to their doctor. A participant [ID11] responded – in order to observe my religious obligation (Ramadan fast), I usually skip my afternoon dose for the pills I normally take three times a day although I do not inform my doctor about this. Asked what other treatments she uses, a 55 year old female participant with uncontrolled hypertension [ID16] responded – apart from the pills given to me by my doctor, I also take ‘bitter leaf water’; it is said to be good for hypertension.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 49 —
Table 2: Factors inhibiting adherence to medications: thematic matrix of categories, subcategories and concepts (n = 40).
Category Sub-category Concepts
1. Healthcare related factors
Inflexible clinic hours • Clinic visits always coincide with religious worship time [n = 3]*
• Works/farm during clinic hours [n = 10]
• Difficult to refill drugs for longer periods when travelling out of town [n = 6]
Long waiting time • Less time available for business or other important activities [n = 31]
Logistics/ travel costs constraints • Residence too far from clinic [n = 4]
Medications out of stock • Under dispensed prescriptions [n = 11]
• Prescribed pills not dispensed [n = 3]
2. Patient related factors
Poor knowledge about hypertension • Hypertension is curable, transient [n = 23]
• Feels well, no symptoms, so don’t use pills [n = 3]
3. Medication related factors
Adverse effects, side effects • Abandon pills to avoid intolerable effects [n = 7]
Complexity of prescription regimes • Too many pills prescribed, too frequent dosing to follow [n = 6]
Substitution/supplementation of prescribed medicines
• Takes herbal drugs alongside prescribed pills [n = 5]
• Takes herbal drugs in place of prescribed pills [n = 2]
4. Religion related factors
Medication use discouraged by faith practice
• Believes in faith healing [n = 2]
• Dosing frequency incompatible with faith practice (fasting) [n =13]
5. Social factors None or poor social support • Wife lacks husband’s approval (which is) mandatory for outings – clinic visits [n = 1]
*n refers to the number of respondents whose perceptions contribute to the corresponding concepts.
4. Religious factors: the potential inhibitory influence of religion on adherence manifested in the accounts of some patients who strongly believe in faith healing. A woman with controlled hypertension [ID37] stated – I use only the drugs prescribed to me, but ordinarily, as a member of Christ Apostolic Church Christian faith, I really do not use drugs if not that this is really important; I believe in faith healing.
5. Social support: sometimes, lack of social support was an inhibitory factor for hypertension clinic visits. For instance, a husband (family head) may sometime disapprove his wife’s outings for reasons that may be personal. The wife of a religious leader (an Imam), with uncontrolled hypertension [ID6] responded – I usually get a month’s supply of drugs from

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 50 —
Chapter 3
the pharmacy, but for reasons best known to him my husband would sometimes not allow me to come to the clinic and I cannot come without his permission.
Table 3 shows respondents’ perceptions of factors that can facilitate medication adherence in five main categories:1. Health care related factors: four sub-categories emerged from this category namely:
affordability of care; appreciation of healthcare provider; trust in orthodox medicines; and availability of prescribed pills. Some patients view the virtually free Hygeia Community Health Care Plan, previously unavailable in that community as a good and timely blessing from God. This encouraged them to adhere to their medications. A 61 year old man with controlled hypertension [ID22] stated – this Hygeia insurance program is very useful for me and I do pray regularly for success for the operators of the program; the program manages my hypertension well and makes me healthier and stronger to work for my ‘daily bread’.The easy approachability of the doctor was also perceived as facilitating factor for medication adherence. A female participant with uncontrolled hypertension [ID3] responded – last January when I was about to travel, I approached my Doctor and told him that I will be away for 2 months requesting enough drugs stock to last the period; this he willingly did, so I always take my drugs whether traveling or not. Another, a 61 year old man with controlled hypertension [ID22] responded – during the last fasting season, I approached my doctor 2 weeks earlier to seek advice on how to use my drugs, he decided to withdraw my ‘thrice a day’ pill and replace this with a ‘twice a day’ pill, and later reverted back to the ‘thrice a day’ drug after the month-long fasting.
2. Patient related factors: responses grouped under this category show that knowledge and fear of complications of hypertension may motivate patients to comply with their medications. A 60 year old man with controlled hypertension [ID24] stated – hypertension is something that brings death in different forms; one can be working and suddenly fall down and slump or become paralyzed. It is called ‘kosibale okan‘in Yoruba meaning ‘there’s no peace of mind’. Another patient [ID29] similarly alluded to the danger of hypertension thus – hypertension is dangerous and can kill suddenly; it shows no mercy.
3. Medication related factors: many patients said they comply with their medications because they firmly believe orthodox ‘western’ medicines are effective, especially when compared with alternative ‘traditional’ medicines. A 70 year old man with uncontrolled hypertension [ID29] responded – I am into herbs and I have used them severally in the past but they did not work like the white man’s medicine.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 51 —
Table 3: Factors facilitating adherence to medications: thematic matrix of categories, subcategories and concepts (n = 40).
Category Sub-category Concepts
1. Healthcare related factors
Affordability of quality ‘Hygeia Community Health Care’ Plan
• Free access to ‘good’ Hygeia community health care “obliges” and encourages compliance with pills [n = 30]*
• Free Hygeia community health care is timely blessing from God and conscientious pill use maximizes this blessing [n = 5]
Appreciation of healthcare provider • Impressive professional and social reputation of Doctor stimulates compliance [n = 12]
Approachability of healthcare provider
• The listening, concerned doctor [n = 29]
• Doctor’s willingness to dose pills relevant to circumstances (e.g. fasting period) [n = 10]
Availability of medication • Pills free and always available [n = 30]
2. Patient related factors
Perceived dreaded nature of hypertension
• Hypertension is dangerous and can kill [n = 38]
3. Medication related factors
Perceived efficacy of orthodox (western) medicines
• White man’s pills work better than traditional medicines (herbs) [n = 20]
4. Religion related factors
Faith related support • Prayer makes pills work well [n = 19]
• Motivation from health counseling at faith meetings/services [n = 6]
5. Social support factors
Supportive and concerned family • Family members remind patient and monitor pill use [n = 10]
Peer support • Motivation from other ‘positive living’ hypertensive patients [n = 4]
* n refers to the number of respondents whose perceptions contribute to the corresponding concepts.
4. Social support: some patients view reminders and monitoring by family members and support from peers with same condition as important factors that motivate compliance. Asked how carefully she uses her medicines, a 56 year old woman with controlled hypertension [ID37] replied – I don’t miss my pills; if I do, my children will be annoyed with me, they monitor me closely to be sure I take my drugs regularly every day.
5. Religious factors: many patients said prayer supported them in using and in improving the beneficial effect of their medications. Moreover, additional health education from religious leaders was also deemed important by some. A 62 year old man with controlled hypertension [ID25] said – I have received enlightenment about hypertension from some radio programs and from my church too; they are useful advices and I usually followed them.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 52 —
Chapter 3
Factors inhibiting and facilitating adherence to behavioral recommendationsManaging hypertension requires a healthy behavior, including limited use of salt, weight reduction or maintenance, exercise, cessation of smoking and limited use of alcohol and other stimulants. Table 4 illustrates factors which inhibit achieving such healthy behaviors, in the eyes of our respondents.1. Salt: while most participants said they had been informed by their doctor that they need
to be prudent with the use of salt, our data also suggest that some patients were aware of the impact of salt on their BP. Local food practices may inhibit salt reduction; in some communities, salt is used to preserve food, particularly meat and fish against microbial decomposition over time. When asked what local customs encourage salt use, a 70 year old man with controlled hypertension [ID19] replied – in some parts of the north where I come from, we use salt to preserve food and meat. Food preparation practices can also inhibit compliance with advice to reduce salt. In the study region, adding salt and salt substitutes/seasoning agents like maggi (salt plus hydrogenated oil plus monosodium glutamate – MSG), ajinomoto (an MSG product) etc. has become standard practice while cooking. The consumption of canned (processed) foods, often salty is also increasingly common in the region. The previously fairly common cultural habit of drinking salted water in attempts to treat ‘undiagnosed’ abdominal discomfort of all sorts was practiced by some respondents. A 50 year old woman with uncontrolled hypertension [ID6] stated – it is more or less customary for people to cook food with salt in this region,… and for some people who may sometimes have stomach upset, tradition demands that one should pour salt into a cup of water and drink to treat the ailment; I used to do this too but being better aware, have now stopped the practice.
2. Weight control: participants mentioned a number of local or cultural practices that may prevent people from losing weight including the cultural perceptions; that large body sizes are associated with wealth, comfort or beauty; that weight loss is associated with disease; and that weight (fatness) is an unchangeable family trait. A 50 year old woman with uncontrolled hypertension [ID3] responded – people often see being fat as synonymous with affluence, comfort and peace of mind; they also sometimes associate fatness in a woman with beauty. Some of us women prefer to be fat or robust believing that by so doing; we will be more attractive to our husbands and men generally. Some men too prefer to be plump so they will be liked by women. A 63 year old man with controlled hypertension [ID30] said – in this region, people often link weight loss to disease particularly if the slimming down is getting too much, suggesting that such might be due to disease; at other times they suggest that slim people are very miserly and would rather not spend money to eat well and get robust. Highlighting the perceived link with inheritance, a 55 year old woman with uncontrolled hypertension [ID16] responded – my friends and neighbors often say I was too fat, but I’m not bothered about such comments as I believe I inherited the trait from my mother; we are usually fat in my family. Local food practices may also inhibit
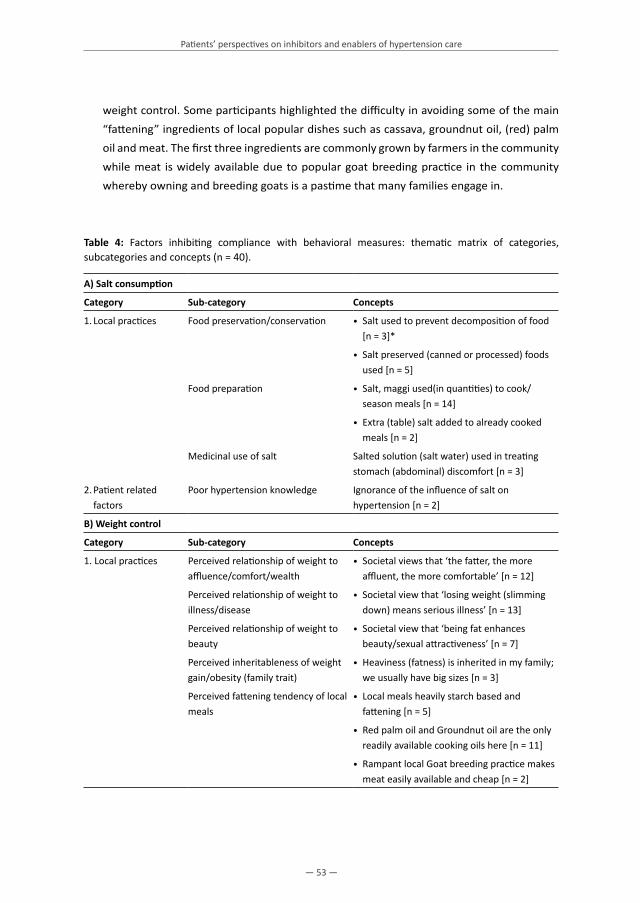
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 53 —
weight control. Some participants highlighted the difficulty in avoiding some of the main “fattening” ingredients of local popular dishes such as cassava, groundnut oil, (red) palm oil and meat. The first three ingredients are commonly grown by farmers in the community while meat is widely available due to popular goat breeding practice in the community whereby owning and breeding goats is a pastime that many families engage in.
Table 4: Factors inhibiting compliance with behavioral measures: thematic matrix of categories, subcategories and concepts (n = 40).
A) Salt consumption
Category Sub-category Concepts
1. Local practices Food preservation/conservation • Salt used to prevent decomposition of food [n = 3]*
• Salt preserved (canned or processed) foods used [n = 5]
Food preparation • Salt, maggi used(in quantities) to cook/season meals [n = 14]
• Extra (table) salt added to already cooked meals [n = 2]
Medicinal use of salt Salted solution (salt water) used in treating stomach (abdominal) discomfort [n = 3]
2. Patient related factors
Poor hypertension knowledge Ignorance of the influence of salt on hypertension [n = 2]
B) Weight control
Category Sub-category Concepts
1. Local practices Perceived relationship of weight to affluence/comfort/wealth
• Societal views that ‘the fatter, the more affluent, the more comfortable’ [n = 12]
Perceived relationship of weight to illness/disease
• Societal view that ‘losing weight (slimming down) means serious illness’ [n = 13]
Perceived relationship of weight to beauty
• Societal view that ‘being fat enhances beauty/sexual attractiveness’ [n = 7]
Perceived inheritableness of weight gain/obesity (family trait)
• Heaviness (fatness) is inherited in my family; we usually have big sizes [n = 3]
Perceived fattening tendency of local meals
• Local meals heavily starch based and fattening [n = 5]
• Red palm oil and Groundnut oil are the only readily available cooking oils here [n = 11]
• Rampant local Goat breeding practice makes meat easily available and cheap [n = 2]

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 54 —
Chapter 3
Table 4: (Continued)
C) Exercise
Category Sub-category Concepts
1. Local practices Perceived needlessness of exercise • Societal view that ‘exercise is meant for the unengaged, unserious and greedy persons that rather walk to avoid travel costs’ [n = 5]
Perceived danger of exercise for the aged
• Societal view that ‘exercise is dangerous’ for older adults and the elderly [n = 7]
2. Patient related factors
Poor knowledge of relationship between exercise and hypertension
• Perception that ‘exercise is dangerous’, makes hypertension worse [n = 5]
Poor awareness on ‘how to exercise’ • Ignorance about available and easy everyday exercise activities [n = 11]
D) Tobacco, alcohol, stimulants
Category Sub-category Concepts
1. Local practices Perceived benefits of tobacco (smoking)
• Alcohol used in relieving stress/tension [n = 2]
Perceived benefits of alcohol (local palm wine)
• Palm wine makes vision clearer [n = 1]
Perceived benefits of snuff (Nicotine powder)
• Snuff useful in relieving stress and tension [n = 1]
Perceived benefits of Kola nut consumption
• Normal for older adults and the elderly to chew ‘Kola’ regularly; Kola nuts stimulate work [n = 2]
*n refers to the number of respondents whose perceptions contribute to the corresponding concepts.
3. Exercise: perceived inhibitors of exercising include ‘local practices’ and lack of information. Prevailing local or cultural views that exercise is “needless or useless’, dangerous, or incompatible with advancing age, may prevent people from being physically active. Exercise is sometimes regarded by people as an activity for unserious fellows, the unengaged or the miserly that rather walk habitually than pay for transportation costs to destinations. An elderly male patient with controlled hypertension [ID30] responded – when people see me ‘walking to exercise’ they often slight me and make derogatory comments that one is greedy and would rather walk long distances than spend money on transportation. Asked further how people see exercising or sporting activities, he replied – some people see those who exercise as unserious people. Sports like playing football are only engaged by youths not elderly people like me.Several respondents said they were not aware or informed about positive effects of exercise on BP or easy ways to exercise. Insufficient knowledge makes some patients view exercise as dangerous for their hypertension. Some others are simply unfamiliar with practicable exercises.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 55 —
4. Tobacco and stimulants: besides cigarettes and alcohol, other locally accessible stimulants like snuff (fine-ground tobacco) and kola (caffeine-containing) nuts are also used by some people in the region. Some patients perceive positive effects from using these substances, as illustrated in the following expressed views: cigarette is useful in relieving stress/tension; palm wine (local alcoholic beverage) and Ogogoro (distilled palm wine) make vision clearer; snuff stimulates work; and chewing kola nuts is ideal norm for elders. A 65 year old man with controlled hypertension [ID23] responded – our fore fathers used to say palm wine makes one to see very well, but it is glaring to me now that such thing is not good. Another elderly (70 year old) man with uncontrolled hypertension [ID29] said – in this environment, we believe kola nuts and snuff aid work, though I personally don’t use any of them. A 60 year old woman with controlled hypertension [ID33] said – I still chew Kola nuts although I have reduced the quantity I consume since I became hypertensive. Such views make it difficult to quit using these substances. Another 64 year old man with controlled hypertension [ID25] highlighted the social consequences of giving up smoking and drinking thus – the people and friends I used to drink and smoke with had to separate from me gradually after I stopped these habits, but this is fine with me as my health is more important.
Table 5 shows perceived facilitators for implementing behavioral measures.
1. Salt: some patients mentioned that ‘health education’ had facilitated the reduction of their use of salt. Respondents highlighted the usefulness of getting health education from multiple ‘channels’ such as churches and mosques, besides the doctor, and of getting information about suitable local substitutes for salt and maggi. Iru (African locust bean paste) is a harmless locally available substitute for salt; it has similar taste as salt, is natural and normally contains no added sodium. A 49 year old female respondent with controlled hypertension [ID14] stated – I got useful advices and was able to apply them though with little difficulty; I later (…) replaced salt and maggi with Iru which serves same purpose although I have also been using Iru together with salt before now. The availability of substitutes for salt in local markets was similarly viewed as a facilitator. Finally ‘social support’ particularly the family’s willingness to eat low salt meals was identified as an important motivator for reducing salt. As one respondent, a 50 year old woman with controlled hypertension [ID11] puts it – yes, I was able to make use of the advice; we now reduce the quantity of salt added to common ‘family pot’ food generally; thereafter those in the family that desire more salt in their food can add extra salt to their portion after dishing.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 56 —
Chapter 3
Table 5: Factors facilitating compliance with behavioral measures: thematic matrix of categories, subcategories and concepts (n = 40).
A) Salt reduction
Category Sub-category Concepts
1. Health education Multiple educational channels • Information from extra channels (radio, church, mosque) reinforces Doctor’s effort [n = 9]*
Relevance and local content of education messages
• Counseling on available suitable local substitutes for salt, maggi – Iru ‘Locust beans’ paste [n = 9]
• Counseling on ‘saltiness’ of meals not self-prepared – (food from canteens, social ‘parties) [n = 4]
2. Local practices Compliance easy with substitutes • ‘Iru’ cheap, easy to find [n = 9]
3. Social support factors
Family cooperation • Readiness of other family members to adjust to meals prepared with less salt [n = 26]
B) Weight control
Category Sub-category Concepts
1. Local practices Perception of body size; weight and beauty
• Societal view that being too fat means ugliness, sexual unattractiveness [n = 5]
Perception of body size; weight and body smartness
• Perception that being too fat leads to physical unfitness (can’t lift body) [n = 3]
Vegetable gardening and farming practice
• Vegetables cheaply available and easily grown [n = 4]
Possibility and practice of fishing (from local rivers)
• Fish easily available and more consumed than meat [n = 7]
C) Exercising
Category Sub-category Concepts
1. Social support factors
Awareness that exercise requires not much extra effort such as:
• Possible to exercise using everyday activities [n = 11]
• using household chores to exercise • Sweeping, washing clothes, Pulling water from well [n = 10]
• farming to exercise • Hoeing, shoveling, clearing bush, harvesting, gardening [n = 4]
• transporting to exercise • Canoe paddling, bicycling, walking [n = 23]
• preparing food to exercise • Mortar grinding/pounding, wood axing [n = 11]
• exercising during religious worship practice/meetings
• Clapping, dancing, singing, jumping, bending & rising [n = 5]
• using leisure to exercise • Drumming, cultural dancing [n = 11]

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 57 —
Table 5: (Continued)
C) Exercising
Category Sub-category Concepts
2. Patient related factors
Perceived influence of exercise on hypertension
• Exercising makes body light and good for BP control [n = 27]
3. Health education Reinforcement through education • Exposure to regular counseling on need to exercise [n = 19]
D) Quitting/not using tobacco, alcohol, stimulants
Category Sub-category Concepts
Religion related factors Faith based support (health counseling)
Abhorrence of ‘ungodly’ (unhealthy) social habits (smoking, alcohol use) by Islam and Christianity [n = 2]
Social support factors Gender based support (societal view) African society frowns at the habit of women
smoking or using alcohol [n = 2]
*n refers to the number of respondents whose perceptions contribute to the corresponding concepts.
2. Weight control: the perceived facilitators of weight control related mostly to local practices. Some people said the changing local and cultural perceptions on linkages between: ‘weight, wealth, beauty and health’ are an important condition to facilitate weight control. Being too fat is sometimes viewed as being tantamount to ugliness and physical unfitness or sluggishness. When asked what people’s comments on fatness are, a 65 year old man with controlled hypertension [ID23] replied – people will say, look at him, ‘big for nothing’, yet he will not be able to enjoy breathing, worse still, his bigness really has nothing to do with wealth. Another respondent [ID26] said – beauty is a good thing that sometimes goes with bigness but some people are ugly looking when fat. The ample availability of affordable healthy foods from local vegetable farmers and fishermen was equally seen as an important motivator for changing one’s diet and for weight control.
3. Exercise: some respondents saw their regular daily activities as good and socially acceptable ways for getting enough exercise without much extra effort. A 63 year old man with controlled hypertension [ID30] said – exercise is generally good but the only ways I exercise is to walk to the farm, work on the farm and walk back home. I do walk regularly where I sometimes can otherwise use transportation.Another woman [ID33] said – exercising is good for hypertension; although I can’t farm, I exercise by washing clothes in the river and axing woods to make fire for cooking. A 55 year old woman with uncontrolled hypertension [ID16] said – I was told to do some exercise every morning like doing some domestic chores, walking (…); also, dancing and clapping in church are other kinds of exercise although we don’t normally clap in my church but we dance and sweat in the process. Alluding further to the usefulness of household chores in exercising, an elderly

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 58 —
Chapter 3
male respondent with controlled hypertension [ID21] said – in my community, women pound yam using mortar to prepare pounded yam, a popular local delicacy; this is also a form of exercise because they sweat a lot when they grind the mortar. Another respondent, a 57 year old man with uncontrolled hypertension [ID26] said – I get some fitness while paddling my canoe on the river in the mornings while fishing or transporting; this can also serve as exercise. I don’t have time for extra activities.
4. Tobacco and stimulants: social support was perceived as the most important facilitator for cessation of smoking and reduction of the use of alcohol and other local stimulants. This category is sub-divided into supports people get from ‘faith-based’, and ‘gender-based’ social norms. These habits are seriously frowned upon and discouraged by the two major religions – Islam and Christianity. A 56 year old female respondent with controlled hypertension [ID37] stated – I have been advised about the danger of all these things (smoking, alcohol, snuff, kola nut) but I don’t even do them before; my religion does not allow me to use them. Similarly, there exists a prevailing gender-based perception or norm in most African societies that a woman should not smoke cigarette or drink alcohol, although this has become less stringent nowadays.
DISCUSSION
In this study we explored perspectives on treatment adherence among patients who received hypertension care in the context of a community based health insurance program in rural Nigeria. Results suggest that, having free access to previously unaffordable high quality care, from a healthcare center headed by a physician who was highly respected in the community, and to Western medication, were perceived as important facilitators for being adherent to medications, as was the perception that hypertension is a serious condition. Similarly, the performance of prayers, support from family members and other patients with hypertension and counseling from religious institutions were seen as factors reinforcing adequate medication use. Interestingly, compared to results from similar qualitative studies on hypertension in Western countries [22] the patients in this study regarded modern “white man’s” medications more positively and seemed to be less likely to alter the prescription according to their own insights. This finding seems credible in the light of a number of other Nigerian studies. In a qualitative study of explanatory models of hypertension among patients in a Lagos hospital, it was found that patients lacked “the desire to be active participants in their health care decisions” while they believed that “the doctor knew what was best for their care” [33]. Another study from urban Western Nigeria also found that patients were motivated to comply with treatment because they had access to Western prescription medications [36]. The Nigerian antihypertensive adherence trial demonstrated that medication adherence was very high among those participants who did not drop out of the study. The authors concluded

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 59 —
that this is in line with the general experience that patients with “no or little prior contact with organized modern medical care will readily adhere to recommended therapy” [38]. At the same time, however, certain characteristics of the way care was organized could still hinder medication adherence, the most important being travel costs associated with clinic visits for those patients living far from the clinic, clinic operating hours, waiting times and the under-dispensing of prescribed medications. In addition, patients’ idea that hypertension is a temporary condition for which medications may no longer be required once symptoms disappear, was an inhibiting factor for taking medications regularly, or a reason for omitting clinic visits. While the practice of faith healing or the use of herbal drugs might inhibit the use of prescription drugs, in their own case, participants said they would use these remedies only to supplement antihypertensive medications and not as a substitute. Interestingly, lack of social support from the patient’s immediate environment was rarely mentioned as an inhibitor for using medications. These findings are plausible in the light of other studies that have also identified travel costs, long waiting times, clinic operating hours and limited knowledge by patients as factors limiting medication use [16,33]. While most respondents said they were aware that healthy behaviors could have a positive influence on their health and BP, adopting a healthy lifestyle seemed to be a greater challenge to them than taking their medications. Local practices and norms held by people in the community were identified as important inhibiting factors for behavioral changes including: use of salt for food preservation; negative cultural images associated with decreased body size and physical activity; and perceived (social) benefits of using palm wine, kola nuts, tobacco and snuff. Anthropologists have noted that a resistance to change (traditional) local food and eating practices and body images is common among people throughout the world, as these are often seen as an important component of an individual’s cultural identity [51]. Yet, our study offers also some insight into the factors that may facilitate healthier behaviors, and tackle the inhibitors. These include sufficient knowledge or understanding of how healthy behaviors may affect hypertension, and support from family or religion, but most importantly the awareness that healthier behaviors will not require profound changes of one’s usual daily life. By using open interviews, the strength of this study is that it builds on direct experiences of the patients. We interviewed a sufficient number of patients to achieve thematic saturation, which is a criterion for sample size and internal validity in qualitative studies [43]. The iterative approach taken in this study [44] and specifically the decision to collect additional data on the basis of themes that were unclear from the preliminary analysis of data from the first set of interviews, added value to the results. We learned from these additional interviews that our informants attached significant importance to a traditional rural African way of life. And, when probed, they were readily able to describe how this way of life, not only provides inhibitors, but also opportunities for adhering to the behavioral recommendations they were given by their doctor. For example, the interviews provided much detail on what affordable food products are

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 60 —
Chapter 3
available in local markets to compose healthy meals (certain types of fruits, salt substitutes, vegetables and fish), and how people’s normal daily activities (e.g. farming, household chores, yam pounding, walking, drawing water from well) offer ample opportunities for getting exercise. The additional interviews also provided further insight into reasons for medication adherence. It became clear that some patients felt particularly motivated or obliged to adhere to their medications because they perceived their health insurance and, consequently, their access to good treatment as blessings from God. But at the same time, religious practices (e.g., fasting) could sometimes pose practical barriers to medication adherence. In line with quality criteria of qualitative research [50], we undertook several efforts to reduce individual biases in the analysis and to strengthen the trustworthiness and credibility of the findings: e.g., by using MAXQDA software to ensure consistency of analytic procedures, and by involving two or more members of the research team at crucial stages of the analysis. The study also has limitations. The participants consisted of insured hypertensive rural dwelling low income Nigerians reachable through telephone, who had continued to visit the clinic for treatment for at least one year. Consequently, our findings do not capture ideas from other groups of patients. For example, within the context of a community based health insurance program, it would also be relevant to further investigate views on treatment adherence among patients who dropped out of treatment, despite the fact that they had access to good care. In terms of data collection and analysis, our possibility to verify what patients told us against other sources (triangulation) was limited: ethical considerations prevented us from interviewing significant others to crosscheck information from participants. Similarly, since the interviews were conducted in local languages and transcribed in English, it is not impossible that some deeper meanings participants’ intended to convey might be lost in the process of translation. Poor adherence to treatment has been identified as one of the most important modifiable barriers to BP control in patients with hypertension [14,19,52]. Overlooking the accounts of the patients who participated in this study, it becomes clear that adherence can be affected by multiple spheres of influence including public policy (e.g., health insurance), institutional and organizational factors (e.g., health care system), environmental factors (e.g., availability of healthy foods), social and cultural norms and practices (e.g., food conservation and preparation practices), social networks (e.g., interactions with other patients, family members) and intrapersonal factors (e.g., patients’ knowledge and awareness level). This provides support for social ecological approaches to health promotion [53]. These approaches assume that single interventions, such as the provision of free access to care are generally not sufficient to promote healthier behaviors and that a mixture of interventions aimed at different levels is needed to accomplish this. The framework of inhibitors and facilitators to adherence that emerged from this study (see Figure 1) suggests that, in the case of the community based health insurance program

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 61 —
in Kwara state, a number of additional interventions may be needed to remove barriers that patients face in adhering to their treatment.
Figure 1: Summary of factors related to hypertension treatment adherence.
First, more attention could be paid to patient education. The findings suggest that patients with difficulty in managing their medications may benefit from further counseling or education about the nature of hypertension, why medications need to be taken regularly, what they may discuss with their doctor to make regular medication use easier (e.g., side effects, dosing, alternative medications, frequency of clinic visits), how they may deal with specific social, cultural or religious impediments encountered in taking their medications, and with the logistic challenges faced in getting refills on time. In addition, patients who experience challenges in managing behavioral changes may benefit from further counseling or education about the positive influence of salt reduction,

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 62 —
Chapter 3
weight control, healthy diet and exercise on BP and health, and on how existing dietary and physical activity-related local practices may help them in implementing behavioral changes. Community education may be one possible solution to avoid limited human resources and financial problems which patient education can pose to the already charged health care clinics. This type of education has been effectively used in the USA [54]. It can be delivered to groups of patients at the health care center or in other community settings the patients are familiar with, such as schools, churches or mosques. The education must be delivered by people who are known, trusted, culturally competent, and fluent in the language of the target community. These educators need not be health professionals, but they do need to be prepared for their role. Such preparation can be provided through careful training programs which can be offered by the health care center. Secondly, it must be acknowledged that not all the patient-perceived barriers to adherence that were identified in this study can be tackled by education alone. Solutions will also have to be found at the level of the health care facility or the insurance program, for instance in order to address some of the logistic obstacles patients face with the monthly clinic visits.
ConclusionThis qualitative study of patients’ perspectives on adherence to prescribed treatment reveals that hypertensive patients in an SSA setting who receive affordable care may still face challenges in adhering effectively to their prescribed hypertension treatment. More than just ‘health insurance’ is required to enable adherence to treatment. Local communities in rural Africa may present specific barriers but also opportunities for adhering to medications and to healthier behaviors. With more insight into the specific inhibitors and facilitators perceived or experienced by patients, actionable community based educational interventions can be designed to strengthen adherence. However, some barriers cannot be tackled through patient education alone and should be addressed by interventions at the level of health care services and payment systems.
KEy MESSAGES
1. Despite ‘affordability of care’ – a feature of community based health insurance programs and insured care in general, hypertensive patients in SSA settings may still face other challenges in adhering effectively to prescribed treatment. More than ‘just’ health insurance is required to improve adherence and treatment outcomes.
2. Using information from exploration of patients’ perspectives on adherence to prescribed treatment this study suggests that local communities in low resource settings may offer specific barriers but also opportunities for adhering to medications and to healthier behaviors.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 63 —
3. Adherence counseling and education for patients may benefit from addressing the identified specific inhibitors and facilitators perceived or experienced by patients.
Competing interestsThe authors declare that they have no competing interests.
Authors’ contributionsAOO drafted the manuscript, conducts the study and participated in the design, reporting, analysis and revision. JAH, JL, KS and MH participated in the original designing of the study. JAH revised, commented and made substantial input to several drafts of the manuscript. AO, CA, CS, GO, HW, JAH, JL, KS, MH, OAB and TA reviewed the manuscript. JAH and KS participated in data quality improvement and analysis. CS, HW, JAH and KS participated in review of the data, procedures and content of the study. KA, PA and TA provided logistic supports. AO, CS, JAH, JL and KS are members of the supervisory board. All authors read and approved the final manuscript.
AcknowledgementsSpecial tributes and profound gratitude go to late Prof. Joep Lange who originated, promoted and created the enabling environment for this study and related projects. Authors are grateful to the Medical Director of Ogo Oluwa hospital – Dr K. Agbede and his staff for facilitating an enabling environment for successful data collection during the study. We are grateful to all the participants for collaborating in the study. We thank Yemi Adegboye who participated in transcription of the interview data. We are grateful to PharmAccess Foundation and Hygeia Community Health Care for supports in facilitating the study. This study was funded by Health Insurance Fund. The Fund was not involved in the study design, data collection, analysis, and interpretation or reporting of the data. A.O. Odusola received additional funding from NUFFIC (grant nr. CF7536/2011).

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 64 —
Chapter 3
REFERENCES
1. Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, Ezzati M, Shibuya K, Salomon JA, Abdalla S: Disability-adjusted life years (DALys) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2013, 380:2197–2223.
2. WHO | Cardiovascular diseases. [http://www.who.int/topics/ cardiovascular_diseases/en/]3. Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, Amann M, Anderson HR, Andrews KG,
Aryee M: A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2013, 380:2224–2260.
4. Ibrahim MM, Damasceno A: Hypertension in developing countries. Lancet 2012, 380:611–619.5. Lewington S: Prospective studies collaboration: age-specific relevance of usual blood pressure to vascular
mortality: a meta-analysis of individual data for one million adults in 61 prospective studies (vol 360, pg 1903, 2002). Lancet 2003, 361:1060.
6. Arogundade FA, Barsoum RS: CKD prevention in Sub-Saharan Africa: a call for governmental, nongovernmental, and community support. Am J Kidney Dis 2008, 51:515–523.
7. Addo J, Smeeth L, Leon DA: Hypertension in sub-Saharan Africa: a systematic review. Hypertension 2007, 50:1012–1018.
8. Mayosi BM: The 10 “Best Buys” to combat heart disease, diabetes and stroke in Africa. Heart 2013, 99:973–974.
9. Van de Vijver S, Oti S, Addo J, de Graft-Aikins A, Agyemang C: Review of community-based interventions for prevention of cardiovascular diseases in low-and middle-income countries. Ethn Health 2012, 17:651–676.
10. Lim SS, Gaziano TA, Gakidou E, Reddy KS, Farzadfar F, Lozano R, Rodgers A: Prevention of cardiovascular disease in high-risk individuals in low-income and middle-income countries: health effects and costs. Lancet 2007, 370:2054–2062.
11. Krousel-Wood M, Thomas S, Muntner P, Morisky D: Medication adherence: a key factor in achieving blood pressure control and good clinical outcomes in hypertensive patients. Curr Opin Cardiol 2004, 19:357–362.
12. Harmon G, Lefante J, Krousel-Wood M: Overcoming barriers: the role of providers in improving patient adherence to antihypertensive medications. Curr Opin Cardiol 2006, 21:310–315.
13. Ogedegbe G, Harrison M, Robbins L, Mancuso CA, Allegrante JP: Barriers and facilitators of medication adherence in hypertensive African Americans: a qualitative study. Ethn Dis 2004, 14:3–12.
14. Odedosu T, Schoenthaler A, Vieira DL, Agyemang C, Ogedegbe G: Overcoming barriers to hypertension control in African Americans. Cleve Clin J Med 2012, 79:46–56.
15. Akpa MR, Agomuoh DI, Odia OJ: Drug compliance among hypertensive patients in Port Harcourt, Nigeria. Niger J Med 2005, 14:55–57.
16. Amira CO, Okubadejo NU: Factors influencing non-compliance with anti-hypertensive drug therapy in Nigerians. Niger Postgrad Med J 2007, 14:325–329.
17. Boulware LE, Daumit GL, Frick KD, Minkovitz CS, Lawrence RS, Powe NR: An evidence-based review of patient-centered behavioral interventions for hypertension. Am J Prev Med 2001, 21:221–232.
18. Krousel-Wood M, Hyre A, Muntner P, Morisky D: Methods to improve medication adherence in patients with hypertension: current status and future directions. Curr Opin Cardiol 2005, 20:296–300.
19. Fongwa MN, Evangelista LS, Hays RD, Martins DS, Elashoff D, Cowan MJ, Morisky DE: Adherence treatment factors in hypertensive African American women. Vasc Health Risk Manag 2008, 4:157–166.
20. Khatib R, Schwalm J-D, Yusuf S, Haynes RB, McKee M, Khan M, Nieuwlaat R: Patient and healthcare provider barriers to hypertension awareness: treatment and follow Up: a systematic review and meta-analysis of qualitative and quantitative studies. PLoS ONE 2014, 9:e84238.
21. Beune EJ, Haafkens JA, Agyemang C, Schuster JS, Willems DL: How Ghanaian, African-Surinamese and Dutch patients perceive and manage antihypertensive drug treatment: a qualitative study. J Hypertens 2008, 26:648–656.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Patients’ perspectives on inhibitors and enablers of hypertension care
— 65 —
22. Marshall IJ, Wolfe CD, McKevitt C: Lay perspectives on hypertension and drug adherence: systematic review of qualitative research. BMJ 2012, 345:e3953.
23. Haafkens JA, Beune EJ, van Charante EP M, Agyemang CO: A cluster- randomized controlled trial evaluating the effect of culturally-appropriate hypertension education among Afro-Surinamese and Ghanaian patients in Dutch general practice: study protocol. BMC Health Serv Res 2009, 9:193.
24. Ogedegbe G, Tobin JN, Fernandez S, Gerin W, Diaz-Gloster M, Cassells A, Khalida C, Pickering T, Schoenthaler A, Ravenell J: Counseling African Americans to Control Hypertension (CAATCH) trial: a multi-level intervention to improve blood pressure control in hypertensive blacks. Circ Cardiovasc Qual Outcomes 2009, 2:249–256.
25. Fernandez S, Scales KL, Pineiro JM, Schoenthaler AM, Ogedegbe G: A senior center-based pilot trial of the effect of lifestyle intervention on blood pressure in minority elderly people with hypertension. J Am Geriatr Soc 2008, 56:1860–1866.
26. Carapinha JL, Ross-Degnan D, Desta AT, Wagner AK: Health insurance systems in five Sub-Saharan African countries: medicine benefits and data for decision making. Health Policy 2011, 99:193–202.
27. Salako BL, Ajose FA, Lawani E: Blood pressure control in a population where antihypertensives are given free. East Afr Med J 2003, 80:529–531.
28. Ogah OS, Rayner BL: Recent advances in hypertension in sub-Saharan Africa. Heart 2013, 99:1390–1397.29. Hendriks ME, Wit FW, Roos MT, Brewster LM, Akande TM, de Beer IH, Mfinanga SG, Kahwa AM, Gatongi P,
Van Rooy G: Hypertension in sub-Saharan Africa: cross-sectional surveys in four rural and urban communities. PLoS ONE 2012, 7:e32638.
30. Ekwunife OI, Aguwa CN: A meta-analysis of prevalence rate of hypertension in Nigerian populations. J Public Health Epidemiol 2011, 3:604–607.
31. Adedoyin RA, Mbada CE, Balogun MO, Martins T, Adebayo RA, Akintomide A, Akinwusi PO: Prevalence and pattern of hypertension in a semiurban community in Nigeria. Eur J Cardiovasc Prev Rehabil 2008, 15:683–687.
32. Ulasi II, Ijoma CK, Onwubere BJC, Arodiwe E, Onodugo O, Okafor C: High prevalence and low awareness of hypertension in a market population in Enugu, Nigeria. Int J Hypertens 2011, 2011:869675.
33. Taylor KD, Adedokun A, Awobusuyi O, Adeniran P, Onyia E, Ogedegbe G: Explanatory models of hypertension among Nigerian patients at a University Teaching Hospital. Ethn Health 2012, 17:615–629.
34. Ike SO, Aniebue PN, Aniebue UU: Knowledge, perceptions and practices of lifestyle-modification measures among adult hypertensives in Nigeria. Trans R Soc Trop Med Hyg 2010, 104:55–60.
35. Iyalomhe GB, Iyalomhe SI: Hypertension-related knowledge, attitudes and life-style practices among hypertensive patients in a sub-urban Nigerian community. J Public Health Epidemiol 2010, 2:71–77.
36. Osamor PE, Owumi BE: Factors associated with treatment compliance in hypertension in southwest Nigeria. J Health Popul Nutr 2011, 29:619–628.
37. Okoro RN, Ngong CK: Assessment of patient’s antihypertensive medication adherence level in non-comorbid hypertension in a tertiary hospital in Nigeria. Int J Pharm Biomed Sci 2012, 3:47–54.
38. Adeyemo A, Tayo BO, Luke A, Ogedegbe O, Durazo-Arvizu R, Cooper RS: The Nigerian Anti-Hypertensive Adherence Trial (NA-HAT): a community-based randomized trial. J Hypertens 2013, 31:201–207.
39. Odusola AO, Hendriks M, Schultsz C, Stronks K, Lange J, Osibogun A, Akande T, Alli S, Adenusi P, Agbede K: Development and evaluation of a patient centered cardiovascular health education program for insured patients in rural Nigeria (QUICK-II). BMC Public Health 2011, 11:171.
40. Britten N: Qualitative research: qualitative interviews in medical research. BMJ 1995, 311:251–253.41. Health Insurance Fund. [http://www.hifund.org/]42. Gustafsson-Wright E, Van der Gaag J, Tanovic Z: A Short-Term Impact Evaluation of the Health Insurance
Fund Program in Central Kwara State, Nigeria. Amsterdam, Netherlands: Pharm Access Foundation; 2013.43. Francis JJ, Johnston M, Robertson C, Glidewell L, Entwistle V, Eccles MP, Grimshaw JM: What is an
adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health 2010, 25:1229–1245.
44. Mason M: Sample Size and Saturation in PhD Studies Using Qualitative Interviews. In Forum Qual SozialforschungForum Qual Soc Res, Volume 11; 2010.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 66 —
Chapter 3
45. Beune EJ, Haafkens JA, Schuster JS, Bindels PJ: “Under pressure”: how Ghanaian, African-Surinamese and Dutch patients explain hypertension. J Hum Hypertens 2006, 20:946–955.
46. Pope C, Ziebland S, Mays N: Qualitative research in health care: analysing qualitative data. BMJ 2000, 320:114–116.
47. Corbin J, Strauss A: Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory. Sage Publications; 2008.
48. Kuckartz U: MAXQDA: Qualitative Data Analysis. In Berl VERBI Softw; 2007.49. Plochg T, Zwieten MV: Guidelines for Quality Assurance in Health and Health Care Research: Qualitative Research
Academic Medical Centre. Amsterdam: University of Amsterdam; 2002.50. Tong A, Sainsbury P, Craig J: Consolidated criteria for reporting qualitative research (COREQ): a 32-item
checklist for interviews and focus groups. Int J Qual Health Care 2007, 19:349–357.51. Helman CG: Culture Health and Illness: an Introduction for Health Professionals. Butterworth-Heinemann;
2014.52. Ogedegbe G: Barriers to optimal hypertension control. J Clin Hypertens Greenwich 2008, 10:644–646.53. Golden SD, Earp JAL: Social ecological approaches to individuals and their contexts twenty years of health
education & behavior health promotion interventions. Health Educ Behav 2012, 39:364–372.54. Stanford Patient Education Research Center. [http://patienteducation. stanford.edu/]

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Chapter 4
Enablers and barriers for implementing high-quality hypertension care in a rural primary care setting in Nigeria: perspectives of primary care staff and health insurance managers
Odusola AOStronks KHendriks MESchultsz CAkande TOsibogun Avan Weert HHaafkens JA
Glob Health Action, Submitted 2015

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 68 —
Chapter 4
ABSTRACT
BackgroundThe implementation of affordable hypertension treatment in primary care settings is crucial for the prevention of cardiovascular diseases in Sub Saharan Africa. This requires innovations in primary care systems. Such innovations are more likely to succeed if stakeholder perspectives on context specific factors that can enable or hinder implementation are recognized.
ObjectiveTo explore and compare what staff members of a primary healthcare centre and a health insurance company perceived as inhibitors and enablers for the delivery of quality hypertension care in primary care clinics in rural Kwara State Nigeria.
Design Qualitative study, using semi-structured in-depth interviews with professional and administrative staff of a healthcare clinic (n = 11) and managers from a health insurance company (n = 4). Data were analysed using standard qualitative techniques.
ResultsBoth groups considered the availability of health insurance as a crucial incentive for the delivery of high-quality hypertension treatment. In addition, other resources and incentives that were perceived to be essential include trust in the sustainability of care, treatment guidelines, tools for patient education, human resources, capacity building, (diagnostic) equipment and drugs, an adequate care administration infrastructure, quality assurance monitoring, adequate provider payments benchmarking and good provider/insurer relationships. Observed differences between both groups as regards to factors that foster effective implementation of high-quality care were related to perceptions of how the health insurance system operates and serves the needs of the population and contracted providers.
ConclusionOur study suggests that a health insurance programme can take away some barriers for implementing high-quality hypertension care, but that other resources and incentives for quality care also need attention (e.g., trust in sustainability of care, treatment guidelines, human resources challenges, administrative infrastructure for care, provider payments, teamwork between providers and insurers). The data can be useful for developing CVD prevention programs in low resource primary care settings in Africa.
Key wordsHypertension management, Primary Care, Community Based Health Insurance, Sub Saharan Africa, Stakeholder perspectives, Qualitative study

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 69 —
INTRODUCTION
Hypertension is the leading global risk factor for cardiovascular disease (CVD) and premature mortality among adults [1]. In 2014, the global hypertension prevalence in adults aged 18 years and over (defined as systolic and/or diastolic blood pressure equal to or above 140/90 mmHg) was 22%. The highest prevalence rates were found in countries in Sub Saharan Africa (SSA) [2]. For Nigeria, the most populous country in SSA, the most recent estimate of the overall hypertension prevalence is 28.9% [3]. Reduction of the blood pressure through timely and sustained treatment reduces mortality due to CVD [4-6]. International guidelines for the management of hypertension with specific recommendations for the African region have been available since 2002 [7-9]. Yet, in most SSA countries the level of anti-hypertensive treatment coverage is poor [10,11]. This is a major contributor to the growing CVD burden in SSA [1]. Many of the reasons for the low hypertension treatment coverage in SSA countries are related to their weak health systems. At the primary care level, the quality of hypertension care is often insufficient due to a lack of trained staff, essential drugs and supplies, and organizational capacity to deliver chronic care [12-15]. Moreover, for many patients in SSA care is not affordable [15,16]. The World Health Organization (WHO) advocates the upgrading of hypertension management and control in primary care as one of the “best bets” by which low and middle income countries can curb the growing burden of CVD, because costs are relatively low- and health benefits accrue in a relatively short time [17,18]. In response to this, in a number of SSA countries new programs have been introduced to strengthen CVD prevention and hypertension management in primary care settings [19,20]. The implementation of such program can be conceived of as an innovation of healthcare practice. Implementation science research has demonstrated that many context specific factors may either limit or enable the uptake of innovations in practice [21-26]. Collectively, these factors are known as “determinants of practice” [26]. Systematic review evidence suggests that innovation in healthcare is more likely to succeed if implementation strategies are tailored to context specific determinants of practice [27,28]. To date, research on factors that may prevent or facilitate the implementation of high-quality hypertension care has mainly been conducted in healthcare settings in high income countries [29,30]. Given the context-specific character of determinants of practice, comparable studies are needed in low- and middleincome countries as well [31]. With the broader objective to inform strategies for the implementation of CVD prevention programs in primary care settings in SSA, in this qualitative study we explored perspectives of informants from two different stakeholder groups, namely a health insurance company and a primary care facility, on factors that might inhibit or facilitate the implementation of high-quality hypertension care in practice. As, respectively, purchasers/payers and providers of care, both stakeholder groups were involved in the implementation of a program that aimed to improve quality of CVD prevention care in Kwara State, Nigeria.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 70 —
Chapter 4
METHODS
This study took place between July and December 2010 [31]. Qualitative methods – semi-structured in-depth interviews were used to explore perspectives of stakeholders. We followed the consolidated criteria for reporting qualitative research guideline (COREQ) for reporting the study [32]. (Additional file 1).
Context and setting The study was conducted among informants who were staff members of a rural primary care clinic in Kwara State1 and the Kwara State Health Insurance (KSHI) program. A detailed description of the KSHI program can be found elsewhere [33,34], (additional file 2). Briefly, the Dutch organization Health Insurance Fund (HIF) [35], in partnership with PharmAccess Foundation and the Nigerian insurance company Hygeia Health Maintenance Organization introduced the “subsidized” health insurance program in 2007 to ensure affordable care for the population. The program is financially supported by the Dutch government and the Kwara State Government. In 2014 the Kwara State Government carried 60% of the premium subsidy and had pledged to take over the full funding of the program and its future scale up to 600,000 enrollees in the State. KSHI provides access to all primary- and limited secondary care for enrollees and supports the improvement of the quality of care in contracted clinics. As part of its quality assurance program, the KSHI program had introduced WHO- [36] and other international guidelines [4] for hypertension and CVD prevention care in a number of contracted clinics and provided them with new equipment, organizational support and staff trainings to facilitate implementation [20]during 2010, followed by the implementation of the SafeCare quality improvement program. At that time, enrollees in KHSI paid an annual premium of 300 Nigerian Naira (NGN) (2 US dollars), about 12% of the annual premium. The remaining part of the premium was subsidized by HIF and the Kwara State Government [35]. Provider clinics received a “capitation fee” for all patients who were registered at KSHI, irrespective of their care utilization. In addition, providers received a fixed monthly extra fee of 2000 NGN (USD 12.50) per hypertension patient, if the patient had visited their clinic that month. The combination of the revenue from capitation fees and the additional fee for hypertensive patients was supposed to cover all out-patient hypertension care, including consultations, diagnostic tests and drug treatments. The insurance covered in-patient hospital care for a maximum of five nights, irrespective of the patient’s condition. The primary care clinic where we recruited staff members for this study was contracted by KHSI. During the time of the study the clinic had about 400 insured patients who were treated for hypertension and 24 staff members, including 3 primary care doctors, 10 staff nurses and midwives and 3 pharmacy technicians, 4 laboratory technicians and 4 administrative staff.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 71 —
Study participantsWe used purposive sampling [37] to identify study participants. Within the clinic we sampled professionals and administrative staff who had participated in hypertension care for at least one year. At the insurance company we sampled insurance managers who had liaised with contracted clinics about standards of CVD prevention care for at least one year. We aimed to recruit 15 informants. This is generally an adequate sample size for qualitative studies [38].
Data collectionData were collected through in-depth individual interviews, guided by a topic list. Topic lists were structured around the following leading aspects: 1) what is your opinion about the current way in which hypertension care is provided?; 2) are there barriers that can make it difficult to provide high-quality hypertension care?; and 3) in your experience, what can facilitate the provision of (consistent) high-quality hypertension care? For each question various probes were used. The topic lists contained one section with questions about hypertension care in general and specific sections with questions that are relevant for the functions of each participating respondent group (additional file 3 – example of a topic list). The first author (AOO) conducted the interviews, using a voice recorder, after informed consent was taken. Interviews with all respondents were held in their own workplace. The researcher transcribed and explored each interview immediately after it was held. Additional interviews were held with 3 participants to further explore some of the emerging themes. The first set of 15 interviews lasted about 90 minutes each and the 3 additional interviews 25 minutes each.
Data analysis Data were analyzed for thematic content using an inductive method described by Strauss et al, (grounded theory) [39]. We used qualitative data management software, MAXQDA, to support consistent analysis, processing, ordering and comparison of the data [40]. Additional file 4 provides a detailed description of the data analysis and procedures that were used to ensure trustworthiness. Briefly, the process of data analysis began with the assignment of a series of open codes to the interview transcripts, which were then grouped into clusters (concepts) in order to make them more workable. From these concepts, broader categories and subcategories were generated, through a process of constant comparison or verification. The final outcomes were represented in data-based matrices of (sub-) categories and concepts. Further analysis and ordering of the data was informed by the comprehensive theory- and research-based framework that describes factors (determinants of practice) that may inhibit or enable the uptake of innovation in primary care practices. This framework was recently developed by the European “Tailored Implementation for Chronic Diseases (TICD)” network [26]. The TICD framework comprises 7 broad domains (guideline factors, health professional factors, patient factors, professional interactions, incentives and resources, capacity for organizational change, and social, political, and legal factors), each of which is divided into a range of sub-domains. We
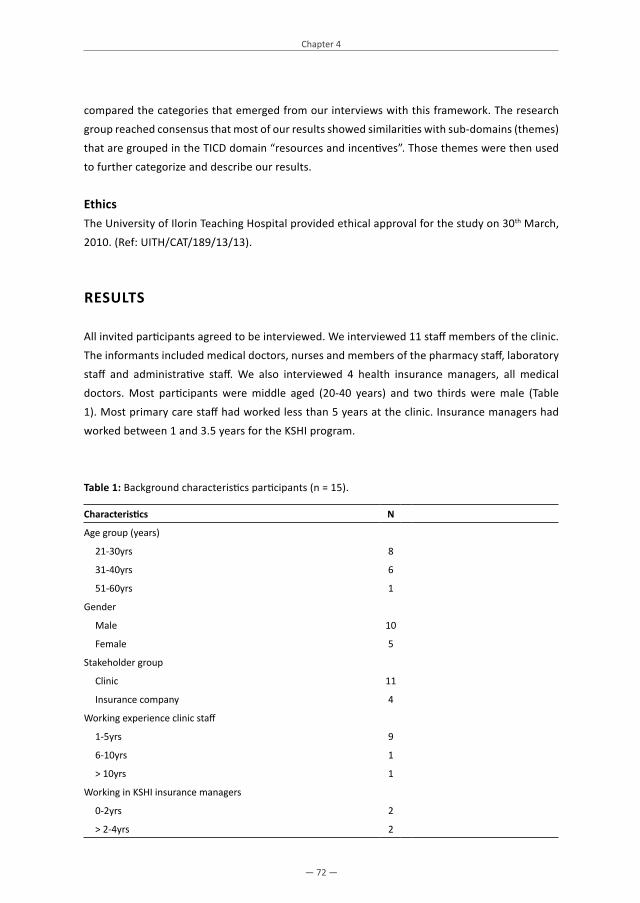
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 72 —
Chapter 4
compared the categories that emerged from our interviews with this framework. The research group reached consensus that most of our results showed similarities with sub-domains (themes) that are grouped in the TICD domain “resources and incentives”. Those themes were then used to further categorize and describe our results.
EthicsThe University of Ilorin Teaching Hospital provided ethical approval for the study on 30th March, 2010. (Ref: UITH/CAT/189/13/13).
RESULTS
All invited participants agreed to be interviewed. We interviewed 11 staff members of the clinic. The informants included medical doctors, nurses and members of the pharmacy staff, laboratory staff and administrative staff. We also interviewed 4 health insurance managers, all medical doctors. Most participants were middle aged (20-40 years) and two thirds were male (Table 1). Most primary care staff had worked less than 5 years at the clinic. Insurance managers had worked between 1 and 3.5 years for the KSHI program.
Table 1: Background characteristics participants (n = 15).
Characteristics N
Age group (years)
21-30yrs 8
31-40yrs 6
51-60yrs 1
Gender
Male 10
Female 5
Stakeholder group
Clinic 11
Insurance company 4
Working experience clinic staff
1-5yrs 9
6-10yrs 1
> 10yrs 1
Working in KSHI insurance managers
0-2yrs 2
> 2-4yrs 2

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 73 —
Perceived enablers and barriers for implementing high-quality hypertension care: clinic staff Analysis of the interviews with clinic staff yielded 12 major categories referring to enablers or inhibitors for providing high-quality hypertension care (Table 2). These categories could be grouped under the following sub-domains (themes) that are part of the aforementioned domain “incentives and resources” of the TICD framework: 1) necessary resources; 2) financial incentives and disincentives; 3) nonfinancial incentives and disincentives; 4) information systems; 5) quality assurance and patient safety systems; and 6) continuing education system.
1: Availability of necessary resources 1.1: The clinic staff described the availability of affordable health insurance as one of the most important resources that had made it possible to provide high-quality hypertension care to the local, mostly poor, population:
“This health insurance has been the main driver that enabled people to now access quality care which they did not have before; by paying just 200/300 naira a whole year, and the insurance pays the rest for them... ....I used to think before now that hypertension and diabetes were not common... In fact, most of our adult consultations now are due to hypertension apart from the obstetric and gynecologic care” (R2).“The insured patients are better compliant with visits, drugs and advices and are better controlled. This has a lot to do with the fact that barriers to access care have been removed by the insurance” (R1).
Yet, some clinic staff also viewed “the dependency of the poor” on “subsidized” health insurance as a potential threat to the sustainability of quality hypertension care:
“I will be very honest with you. If the insurance subsidy stops, the program will simply collapse unless there is an alternative subsidy.” (R2).
Secondly, clinic staff perceived the support from the insurance company for equipment upgrades and the development of quality improvement plans at their clinic also as an incentive for improving hypertension care. Nevertheless, despite this support, some staff members still experienced certain inhibitors to the delivery of quality hypertension care. They pointed out that high-quality care requires regular diagnostic and screening tests to prevent or detect CVD (e.g., lipid profile, electrocardiogram, electrolytes, urea, creatinine, microalbuminuria, glycosylated hemoglobin). In the perception of some clinic staff, the costs of these services were not fully covered by the insurance reimbursement system. In addition, it was noted that the actual implementation of clinic upgrades was challenged by the limited availability of trained personnel:
“Since KSHI program came and upgraded our laboratory for us, we can do many additional tests... But the success of doing all CVD related tests [...] depends on availability of qualified personnel” (R2).

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 74 —
Chapter 4
1.2: The guidelines and protocols that have been introduced as part of the insurance program were seen as a relevant incentive for improving quality of hypertension care in the clinic. But some clinic staff noted that international (clinical) guidelines do not always provide sufficient information to make them applicable in local contexts:
“If we use the (WHO) guideline [which recommends three monthly clinic visits] many patients would end up not using drugs appropriately; they will mismanage drug stocks because of longer times between appointments; storage becomes difficult also... For now I think the once monthly arrangement should be appropriate for the literacy level of the patients we see here” (R1).
In addition to guidelines, the clinic staff emphasized that instruments are needed to encourage patients’ adherence to guideline-based care. They emphasized the need for tools that allow for good communication between providers and patients, particularly in a context where the local population speaks many different languages:
“Language barriers with patients are also sometimes a limitation during consultation in a setting such as ours (where people speak different languages) because even the interpreter (if you have one) can sometimes inadvertently give wrong information” (R1).
They also felt there was a need for educational tools that make it possible to address the specific cultural and local understandings of “health” among the patient population in the area.
1.3: All clinical staff perceived the consistent availability of qualified healthcare personnel (human resources) as a vital resource for implementing high-quality hypertension care and education. Since the introduction of the health insurance program, the number of patients who sought hypertension care at the clinic had increased significantly. The increased patient load had brought the issue of acute personnel shortages to light, which was viewed as a barrier to quality care.
“I see on average 45 patients per (hypertension) clinic day. This number is too much. (…) Consulting time is 10 to 15 minutes, but the ideal time for our level of development should be 30-40 minutes. Especially if the patient is coming for the first time we spend almost an hour including educating them” (R1).
1.4: Since the introduction of the program, diagnostic equipment, drugs and laboratory consumables for the provision of quality care were more readily available. Clinic staff emphasized, however, that the facility also needed to take additional measures to ensure the proper use of these materials such as the implementation of an “equipment maintenance plan” to address “the poor equipment maintenance culture” and an “alert system” to forestall supplies shortages (see also 5.2).

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 75 —
1.5: Both medical and administrative officers felt that adequate health records and patient-follow up are essential for quality care:
“We have recently improved our (manual) documentation system. The folders have columns and rows for every patient, so we don’t miss things, and we document drugs, treatment and follow-up appointment” (R1).
Linked to this, the clinic was setting up a patient recall/reminder system to help track patients and identify those who don’t show up at appointments, so as to encourage adherence:
“We have a recording book for patients’ visits and appointments. We know if patients don’t turn up for appointment. We then make phone calls to recall them. If necessary, we use their contact addresses to go and search physically for them in their villages“(R9).
But the administrative officers noted the limitations of this contact tracing system as it only works if patients have traceable addresses.
2: Financial incentives and disincentives2.1: In the interviews, the clinical staff pointed at problems in the management of health insurance claims, such as late payments. In addition, the combination of capitation payment and a monthly fixed additional fee per patient for hypertension care utilization was perceived as not always sufficient for covering all the costs of care that are recommended by hypertension guidelines e.g. specific laboratory investigations.
2.2: Most healthcare staff felt an enhanced salary and welfare package is essential to attract, retain and motivate healthcare personnel in rural communities and to ensure high-quality care:
“The current salary package is a limitation to us and one wouldn’t mind seeking government employment [elsewhere] in order to get better package than now; the hospital is trying its best though, but will need assistance on this” (R6).
3: Non financial incentives and disincentives3.1: The managerial staff felt that constructive dialoguing and fostering of a good provider- insurer working relationship is essential in order to prevent and remove prevailing organizational and administrative obstacles to quality care:
“One major challenge now is that we have not really had time to sit down as stakeholders to dialogue over practical realities of implementing some of the program recommendations in our own setting here. There is communication gap. We need to have a stakeholder session for others to also see what we experience in implementing this program” (R2).
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 76 —
Chapter 4
4: Information systems 4.1: As typical for facilities in remote areas, at the clinic also, to one of the respondents the information and communication technology system was poor. Computers were out-dated and internet connections often dysfunctional. The clinic staff strongly believed that the availability of better hardware and management software would motivate better care and management:
“For over a year now, the internet service has not worked. This contributes to our own financial loss because we do many things that cannot immediately be mailed out or communicated to the insurance company and this has affected our revenue negatively while our services and wage bills are rising” (R2).
5: Quality assurance and patient safety systems 5.1: Efficient internal and external quality control systems were considered essential to ensure quality of care, such as in the case of laboratory results:
“We have recently commenced internal quality control for our spectrophotometer and if the control is out of range during a quality control test, the result will not be issued out. (…) Quality control determines the quality of our laboratory results” (R5).
5.2: The availability of a protocol to ensure that vital supplies like drugs and laboratory consumables are potent and unexpired when used was also viewed as an essential condition for quality CVD prevention care. Not oblivious of the potential ease with which fake drugs and medical supplies can be acquired in Nigeria, health professionals mentioned that reliable “test”- and ‘near expiry alert’ systems and quality-certification of suppliers of medical consumables was important.
6: Continuing education system6.1: Regular capacity building for staff was perceived as pivotal for implementing high-quality hypertension and CVD prevention care. KSHI’s training program was considered very relevant and the clinic staff would appreciate opportunities for further specialization in CVD care:
“If given the opportunity, I will be very happy to specialize as a cardiovascular nurse as this will also help to reduce the mortality and morbidity associated with these diseases. It is not good to stay without increasing knowledge” (R3).
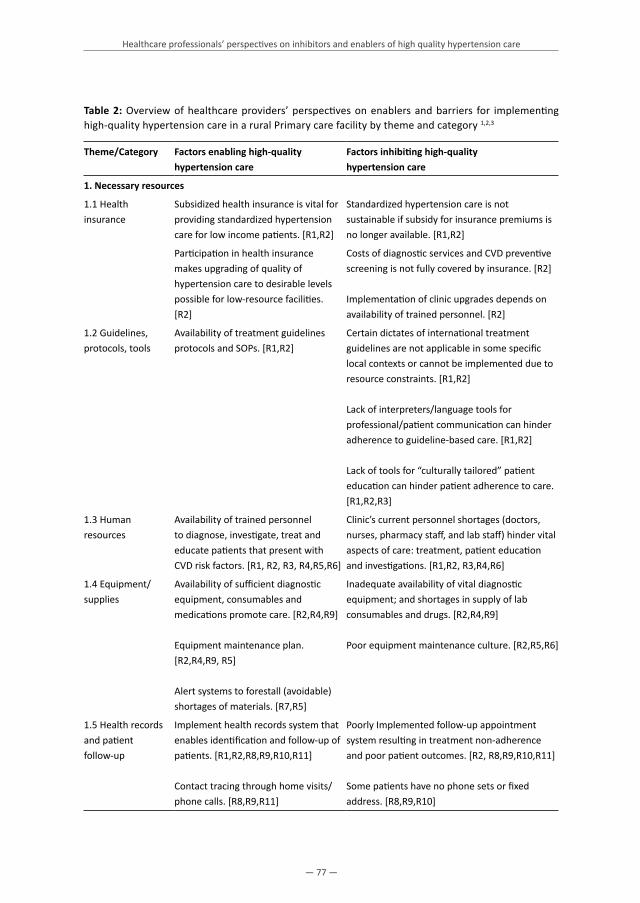
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 77 —
Table 2: Overview of healthcare providers’ perspectives on enablers and barriers for implementing high-quality hypertension care in a rural Primary care facility by theme and category 1,2,3
Theme/Category Factors enabling high-quality hypertension care
Factors inhibiting high-quality hypertension care
1. Necessary resources
1.1 Health insurance
Subsidized health insurance is vital for providing standardized hypertension care for low income patients. [R1,R2]
Standardized hypertension care is not sustainable if subsidy for insurance premiums is no longer available. [R1,R2]
Participation in health insurance makes upgrading of quality of hypertension care to desirable levels possible for low-resource facilities. [R2]
Costs of diagnostic services and CVD preventive screening is not fully covered by insurance. [R2]
Implementation of clinic upgrades depends on availability of trained personnel. [R2]
1.2 Guidelines, protocols, tools
Availability of treatment guidelines protocols and SOPs. [R1,R2]
Certain dictates of international treatment guidelines are not applicable in some specific local contexts or cannot be implemented due to resource constraints. [R1,R2]
Lack of interpreters/language tools for professional/patient communication can hinder adherence to guideline-based care. [R1,R2]
Lack of tools for “culturally tailored” patient education can hinder patient adherence to care. [R1,R2,R3]
1.3 Human resources
Availability of trained personnel to diagnose, investigate, treat and educate patients that present with CVD risk factors. [R1, R2, R3, R4,R5,R6]
Clinic’s current personnel shortages (doctors, nurses, pharmacy staff, and lab staff) hinder vital aspects of care: treatment, patient education and investigations. [R1,R2, R3,R4,R6]
1.4 Equipment/ supplies
Availability of sufficient diagnostic equipment, consumables and medications promote care. [R2,R4,R9]
Equipment maintenance plan. [R2,R4,R9, R5]
Alert systems to forestall (avoidable) shortages of materials. [R7,R5]
Inadequate availability of vital diagnostic equipment; and shortages in supply of lab consumables and drugs. [R2,R4,R9]
Poor equipment maintenance culture. [R2,R5,R6]
1.5 Health records and patient follow-up
Implement health records system that enables identification and follow-up of patients. [R1,R2,R8,R9,R10,R11]
Contact tracing through home visits/ phone calls. [R8,R9,R11]
Poorly Implemented follow-up appointment system resulting in treatment non-adherence and poor patient outcomes. [R2, R8,R9,R10,R11]
Some patients have no phone sets or fixed address. [R8,R9,R10]

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 78 —
Chapter 4
Table 2: (Continued)
Theme/Category Factors enabling high-quality hypertension care
Factors inhibiting high-quality hypertension care
2. Financial incentives and disincentives
2.1 Insurance claims management system
Remuneration system
Adequate and timely compensation by the insurance company for all care services duly rendered by the provider. [R2 ]
In addition to “capitation” payments, ‘fee for service’ remuneration will enable screening and early preventive treatment where needed. [R2]
Recurrent delays and inconsistencies in settlements of verifiable claims. [R2]
Reimbursement of CVD prevention through current remuneration system de-motivates providers and underfunds certain aspects of care. [R2 ]
2.2 Benefits package of rural workers
Enhanced salary/benefits package will motivate and retain rural healthcare personnel. [R1, R3,R5, R6,R9,R10,R11]
Poor remuneration and poor living conditions dampens moral of rural healthcare workers. [R5, R1]
3. Non- financial incentives and disincentives
3.1 Provider – Insurer working relationship
Constructive dialoguing between provider and insurer. [R2]
Insufficient communication with insurer can hinder administrative processes and the quality of CVD prevention care. [R2]
4. Information systems
4.1 Information technology systems
Implement electronic health management information system to facilitate and optimize administration of care. [R1,R2]
Dysfunctional computers/ internet connections negatively impact quality and output of care. [R2]
5. Quality assurance and patient safety systems
5.1 Reliability of laboratory results
Implement internal and external quality control processes for laboratory investigations to assure quality and reliability of laboratory results. [R5,R6]
Lack of credible quality assurance system creates doubt in the laboratory results used for monitoring progress of care. [R5]
5.2 Reliability of vital consumables
Ensure potency of vital consumables using certified, credible suppliers and a ‘near expiry’ alert system for drugs / laboratory consumables. [R2,R4]
Uncertainty about potency of vital consumables used for CVD care may lead to poor patient outcomes. [R2]
6. Continuing education system
6.1 Capacity building for staff
Consistent skills update trainings for healthcare workers through continuous medical education to promote quality of CVD prevention care. [R1,R2 R3,R4, R5,R6]
Lack of institutionalized system of continuous knowledge renewal through refresher trainings on CVD prevention care can hinder the quality of care. [R1,R5,R6]
NB:1. Theme refers to specific themes grouped under the TICD domain “resources and incentives” [26]. 2. Category refers to categories found in this study3. R refers to ID numbers given to respondents

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 79 —
Perceived enablers and barriers for implementing high-quality hypertension care: health insurance staffTable 3 provides an overview of categories and themes that emerged from the interviews with health insurance staff. Many of them are similar to those found in the interviews with the clinic staff. But the health insurance staff reflected on enablers and barriers for implementing high-quality hypertension care from a different perspective, given their specific position in the system:
“I see myself as a catalyst in ensuring quality care from providers to the enrollees. I try to maintain a cordial relationship with every one, so that the providers don’t see me as a threat while I satisfy the insurance company’s monitoring expectations and strike a balance to benefit the patient”(IR1).
1: Availability of necessary resources 1.1: Health insurance staff stated that health insurance and “risk pooling” are essential to improve the quality of life of the local population. They argued that people with chronic conditions, like hypertension, are the greatest “beneficiaries” of health insurance schemes.
“Health insurance benefits chronically ill patients with hypertension and diabetes since it increases access to care and alleviates costs of managing these conditions” (IR4)
One informant noted, however, that additional (travel) costs might still hamper access to care for patients. Overall, managers were more optimistic than healthcare providers about the financial sustainability of the insurance program:
“Even if external funding stops later as expected, people would have experienced the benefits of the program and would be willing to pay fully by themselves thus driving feasibility and sustainability” (IR2).
All interviewees emphasized that it is the insurance company’s policy to promote a “proactive” approach to CVD risk factors and hypertension management, to prevent CVD in the first place:
“Proactive management is currently not well done in provider settings. Ideally it should involve the healthcare provider marshalling all resources at its disposal to treat, inform and educate patients in attempts to prevent CVD” (IR4).
One important consideration for promoting a proactive approach is that it benefits patients and the population as a whole:
“When CVD is prevented in a patient you promote good quality of life in him, make him more useful to his family and the society, reduce costs on the insurance company, reduce the workload in provider hospital, and for the country at large you reduce morbidity and mortality burden” (IR3).

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 80 —
Chapter 4
The interviewees viewed the insurance company’s quality improvement program also as an important resource for the improvement of hypertension care in contracted clinics. But they observed that financial constraints at local clinics could still hinder implementation:
“Some providers find it difficult to implement the upgrade plan that we recommended to them, because of lack of funds on their part” (IR4).
More specifically, personnel shortages and the concomitant long waiting time for patients were seen as one of the main challenges to delivery of high-quality care in rural primary care settings. Some informants feared, however, that ‘quality upgrades’ provided by the insurance company could make providers “overly-dependent” on external support, failing to implement (complimentary) upgrades plan of their own.
1.2: Like the clinic staff, health insurance staff saw the introduction of international guidelines as one of the key instruments that could help improve the quality of care by providers and the monitoring of care by the insurance company.
1.3: According to the health insurance staff, the KSHI program’s monitoring activities support clinics to minimize shortages and maximize the quality of vital equipment, supplies and drugs needed for high-quality care.
2: Financial incentives and disincentives2.1: Even though insurance managers agreed with providers that the “prompt settlement of claims” would motivate quality care, they emphasized that for an insurance company the proper verification of claims is crucial and time consuming:
“The process of verifying claims and removing errors takes quite some time. We visit hospitals, sometimes to audit their case files and see whether the claimed care was actually delivered” (IR3).
2.2: The health insurance staff agreed with the opinion of the clinic staff that adequate provider remuneration acts as an incentive for quality care. They differed, however, in their perception on the adequate system for remuneration. They pointed out that KSHI program offers a fixed ‘extra’ fee on top of the ‘standard capitation fee’ to assist providers in reducing the financial burden of chronic CVD prevention and hypertension care:
“Our company’s administrative policy compensates chronic disease care under ‘capitation’ payments”. However, for CVD prevention care we offer them an additional NGN 2000 (USD 13.3) per month for each hypertension patient who utilizes care that month” (IR2).

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 81 —
They pointed out that this administrative policy is built on the view that the current remuneration system is developed with a focus on what the patient in a low-resource setting truly needs, namely preventive CVD care and a low premium for health insurance.
2.3: Most managers recognized that the poor benefits package for rural health workers could negatively impact care:
“Rapid employee turnover and low moral from the staff because of issues related to employee wellbeing are some of the limitations encountered by providers” (IR1).
3: Nonfinancial incentives and disincentives 3.1: In the perspective of health insurance staff, monitoring and evaluation of contracted provider hospitals is a vital strategy for ensuring high-quality (hypertension) care. But they observed that this could disrupt a good provider-insurer relationship, whereas some providers see monitoring activities as a threat. In order to improve “teamwork” between stakeholders, insurance managers said they were using several strategies, such as the provision of feedback to clinics on how they are improving, staff training and the establishment of cordial relations with hospital directors.
“We give feedback to the hospital and dialogue with the staff and try to find amicable solutions to problems” (IR2).
4: Information systems 4.1: Like the clinic staff, health insurance staff perceived the availability of a functional and effective information technology system as being critical for an efficient administration and implementation of the CVD prevention program
5: Quality assurance and patient safety systems 5.1: The KSHI program conducts regular pharmacy and laboratory checks in contracted clinics and ensures that suppliers of drugs and other materials are certified. In the eyes of health insurance staff, external quality assessment is not only necessary for materials and consumables but also for real aspects of treatment:
“We use (patients’) case file data to verify prescribed/dispensed drugs, behavioral advice, improvements in BP, other disease data and target organ screening” (IR3).
Moreover, they highlighted the importance of monitoring patients’ experiences with care:“We do mystery shopping once in a while, and carry out regular ‘patient satisfaction surveys’ on providers” (IR3).

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 82 —
Chapter 4
6: Continuous professional education6.1: Like the clinic staff, health insurance staff attributed great value to the implementation of a professional development program for the contracted clinics, even though they observed that they may not get lasting benefits from the capacity building, due to the high turn-over of health workers.
Table 3: Overview of health insurance managers’ perspectives on enablers and barriers for implementing high-quality hypertension care in a rural primary care facility, by theme and category 1,2,3
Theme/Category
Factors enabling high-quality hypertension care
Factors inhibiting high-quality hypertension care
1. Necessary resources
1.1 Health insurance
Health insurance makes CVD prevention and hypertension management affordable for enrollees. [IR1, IR2, IR3, IR4]
If subsidy stops, resources in community will be found to sustain the program. [IR1,IR2, IR4]
Patients spend more than the annual premium on transport to clinic. [IR2]
Proactive care approach by insurance benefits population health and insurance. [IR1, IR2, IR3, IR4]
The insurance program’s quality improvement and education policy facilitates delivery of standardized CVD prevention care in contracted hospitals. [IR1, IR2, IR3]
Resource constraints experienced by healthcare providers hinder implementation of recommended improvements. [IR3,IR2]
1.2 Guideline and Protocols
Insurance company’s use of guidelines to monitor and ensure high-quality care. [IR1,IR2,IR4]
Inconsistent and inadequate use of guidelines by healthcare professionals hinders care. [IR2,IR4]
1.3 Equipment and supplies
Clinic upgrades and monitoring activities substantially minimized shortages of essential drugs, diagnostic tools and materials. [IR3,IR2]
Some providers lack capacity/will to fund complementary acquisition of diagnostic tools and materials. [IR4,IR2]
2. Financial incentives and disincentives
2.1 Insurance claims management system
Quick claim settlement motivates providers. [IR1, IR2, IR3, IR4]
Claim verification process is time consuming and intensive for insurance company. [IR2, IR1,IR4]
2.2 Remuneration
A ‘fixed extra fee’ on top of regular monthly “capitation fee” per patient promotes quality of CVD prevention care. [IR2]
Providers want ‘capitation’ and ‘fee for service’ payments. [IR2,IR1]
2.3 Benefits package of rural workers
Government and provider must Improve welfare of rural health workers. [IR1]
Rural-based providers have no funds to improve welfare of health workers unilaterally. [IR1]

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 83 —
Table 3: (Continued)
Theme/Category
Factors enabling high-quality hypertension care
Factors inhibiting high-quality hypertension care
3. Non-financial incentives and disincentives
3.1 Provider – Insurer relationship
Monitoring and evaluation (M&E) essential to ensure that hypertension/CVD prevention care is delivered according to standard. [IR1, IR2,IR2, IR4]
Feedback, training and teamwork will minimize credibility issues arising from monitoring of quality of care. [IR1]
Some providers see M&E as a threat. [IR1,IR3]
4. Information systems
4.1 Information Technology Systems
A functional ICT system will facilitate efficient administration and promote quality of care. [IR1,IR2,IR3,IR4]
Dysfunctional information technology (IT) infrastructure hinders provider-insurer communication, leads to inefficient administration and diminishes quality of care. [IR1,IR2,IR3,IR4]
5. Quality assurance and patient safety systems
5.1 Monitoring all aspects of treatment including patient satisfaction
Patient file checks to verify drugs, lifestyle advise, other treatment, BP outcomes, Pharmacy stock and quality reviews. [IR1,IR3,IR4]
Laboratory checks. Certification of suppliers of drugs, laboratory reagents and other materials. [IR1,IR2,IR2, IR4]
Mystery shopping and surveys to investigate patient satisfaction. [IR1,IR2,IR4]
6. Continuing professional education system
6.1 Professional development for providers
Continuous skills improvement update trainings made available for health professionals. [IR1,IR2,IR4]
High attrition of rural health workers means limited benefits of training on patients. [IR4]
1. Theme refers to specific themes grouped under the TICD domain “resources and incentives” [26]2. Category refers to categories found in interviews with health insurance managers in this study3. IR1, IR2, IR3 and IR4 refers to ID number informants

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 84 —
Chapter 4
DISCUSSION
This study explored perceptions of healthcare staff and health insurance staff on enablers and inhibitors for implementing high-quality hypertension care in a rural primary care setting in Nigeria. Our study is different from previous studies describing stakeholder perspectives on barriers to hypertension care in low-and middle-income countries [12,13,29,41], in that it was conducted in the context of a health insurance program, and provides insights in the perspectives of both providers and purchasers/financers of care. The health insurance program was designed to address some of the previously identified health system related barriers to quality care, including financial barriers to care for patients and financial and logistic barriers to the delivery of care for participating clinics [19,20]. We found that, in addition to health insurance, healthcare staff and health insurance managers mentioned a range of other resources and incentives that are required to enable the delivery of high-quality care in a low-resource primary care setting in rural Africa: international guidelines, sufficient staff, equipment and medication, an adequate (electronic) patient registration and management system, quality assurance and patient safety monitoring, a good provider/insurer relationship, adequate reimbursement of provider services, capacity building possibilities for staff and tools to support patient adherence. Both stakeholder groups acknowledged that health insurance had removed part of the financial barriers to care for patients and part of the logistic and financial barriers to the provision of high-quality care for clinics. Nevertheless, our study also showed that a number of implementation challenges were not resolved in the perspective of the study participants. First, we observed a gap between the perceptions of the clinic staff on one hand and of health insurance staff on the other as to how the health insurance system and its provider payment system work. For example, whereas the reimbursement of fees were perceived by health care staff as insufficient to cover all costs related to activities that are recommended by guidelines, the health insurance staff argued that this system fitted the needs of the population. A recent systematic review of literature on provider payment methods used by community based health insurance (CBHI) programs in developing countries found initial evidence that the level of provider participation in designing CBHI payment methods has a direct impact on the participation and buy-in of local health workers, as well as on their general satisfaction to work with the CBHI management, once the scheme became operational [42]. This underscores the importance of establishing a good collaboration between providers and financers of care. In other words, in order to promote the effective implementation of a health insurance system in a context where such a system was previously unknown, specific attention should be given to making the different stakeholders familiar with the rationales behind and the principles of the insurance system, including the ideas about risk pooling, promoting preventive care by specific reimbursements arrangements etc. In fact, the relevance of good communication between medical and health insurance staff on issue of claims management was also emphasized by stakeholders in our study. Second, both groups of stakeholders emphasized that a health insurance program does not provide a solution for all the

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 85 —
problems care providers in rural Africa are faced with. Problems such as shortages of qualified personnel, power outages or dysfunctional information technology systems were considered a threat to high-quality care by healthcare staff and insurance staff alike. Interestingly, it was noted that these problems became more visible after more people in the community had joined the KSHI program so that the demand for high-quality services increased. Third, while informants from both stakeholder groups agreed that high-quality hypertension care is not financially feasible for non-insured patients, they had diverging opinions about the sustainability of the KSHI program. Some clinic staff believed that patients would drop out of care if the Kwara State Government and third parties would diminish the subsidy for the insurance premium. Similar concerns were observed in previous studies that were conducted in Nigeria and Kenya [43,44]. Health insurance staff had a different expectation, as they envisioned that insurance enrolment rates would increase in the future and that the local population would be willing to contribute more to their health insurance, after having experienced the benefits. Fourth, our data show that the administrative part of the healthcare system (e.g. patient filing systems, billing and claims settlement procedures, quality assurance mechanisms) was seen as an essential factor that could either enable or inhibit high-quality hypertension care. These administrative issues are certainly not specific for low income countries, but our data show that the limited availability of material and human resources in these contexts, such as information systems or qualified personnel, can hinder the development of adequate administrative procedures. In fact, as a previous systematic review of studies on provider perspective on barriers to hypertension treatment indicated that providers from low- and middle income countries seem to perceive factors such as shortage of equipment, medication, staff, specialists and time as the most important barriers to care [29]. Finally, the implementation of treatment-guidelines has been widely advocated as a strategy for removing health system constraints to quality care in primary care settings [9,17]. Our results underline, however, that these guidelines should be adapted to the local context. For instance, it was noted that tools were needed to adapt general treatment recommendations to the level of health literacy and cultural understandings and languages of the local patient population. The strength of this study is that we were able to elicit information about perspectives on enablers and inhibitors to hypertension care from two stakeholder groups that have not been studied together previously: clinical and health insurance staff from rural Africa. Information from qualitative studies on stakeholder perspectives on enablers and inhibitors for the uptake of innovations in health care has been found to be particularly useful for the development of interventions that aim to remove barriers to implementation [25-27,29,30]. However, this study collected information from healthcare providers from one single site and insurance managers from one single health insurance program. Moreover, we interviewed only a limited number of informants. Even though we applied recommended procedures for ensuring the quality of data collection, analysis and verification in qualitative research (additional file 4), results of qualitative studies are always context specific and cannot be automatically generalized to other contexts.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 86 —
Chapter 4
Nevertheless, we saw that our results are plausible in the light of the previously developed theoretical TICD framework of determinants of practice that can either inhibit or facilitate the uptake of innovations in the primary care for patients with chronic conditions [26]. Our results showed many similarities with all sub-domains of one of the seven domains of this framework.
Conclusion Implementation of innovations in health care is possible if context specific barriers are taken away. In the perception of respondents in this study a range of incentives and resources needs to be available to facilitate the implementation of high-quality hypertension care in rural primary care facilities in Nigeria. Many of these incentives and resources have also been identified as “determinants of practice” that can influence the uptake of innovations in primary care practice in high income countries [26]. Others are context specific. Our study suggests that a health insurance programme can take some financial and material barriers to high-quality care away, but that other factors also need attention (e.g., the human, material and administrative resources that are needed for delivering quality care). Our data also illustrate that teamwork and a common understanding between providers and insurers as regards to the way health insurance operates and serves the needs of the insured population and contracted providers are important to facilitate quality care.
Implications for practiceThe implementation of any innovation in health care requires the development of an evidence based implementation plan describing the potential barriers that may be expected during implementation and how they may be addressed [23]. The barriers and enablers identified in this study (Table 2 and 3) provide useful data for developing an implementation plan for interventions to stimulate the implementation of CVD prevention and hypertension management programs in low resource primary care settings in Africa.
Authors’ contributionsAOO drafted the manuscript, conducted the study and participated in the design of the study. JH, KS, CS and MH originally designed the study. JH and KS provided substantial input and critically revised several drafts of the manuscript. AO, CS, HvW, JH, KS, MH, and TA reviewed the manuscript. AOO, JH and KS advised in the data collection. CS, HvW, JH and KS reviewed the data, and advised in the data analysis. AOO, JH and KS participated in the data analysis. AO, CS, JH, KS and TA are members of the supervisory board. All authors read and approved the final draft.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 87 —
AcknowledgementsSpecial tributes go to late Prof. Joep Lange, who tragically passed away before the manuscript had been finished. He initiated and promoted an enabling environment for the study and related projects. Authors are grateful to the Medical Director and staff of the participating hospital for facilitating an enabling environment for a successful data collection. We are grateful to the health insurance staff that collaborated in the study. We thank Health Insurance Fund, PharmAccess Foundation, KSHI and NUFFIC for supporting the study.
List of additional filesAdditional file 1: Consolidated criteria for reporting qualitative studies (COREQ) used in this studyAdditional file 2: Description of the Kwara State Health Insurance program and the study setting Additional file 3: An example of a topic list that was used to interview healthcare professionals (Doctors)Additional file 4: Qualitative analysis and trustworthiness: specific steps taken in this study
Conflicts of Interest and Source of Funding A.O. Odusola had received a grant (# CF7536/2011) from NUFFIC. The study was funded by Health Insurance Fund. Health Insurance Fund was not involved in the study design, data collection, analysis, and interpretation or reporting of the data. For the remaining authors none were declared.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 88 —
Chapter 4
REFERENCES
1. Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet, 2012; 380(9859):2224-2260.
2. World Health Organization. Global status report on noncommunicable diseases 2014. Geneva: World Health Organization; 2015. 298 p. Available from: http://www.who.int/nmh/publications/ncd-status-report-2014/en/
3. Adeloye D, Basquill C, Aderemi AV, Thompson JY, Obi FA. An estimate of the prevalence of hypertension in Nigeria: a systematic review and meta-analysis. J Hypertens. 2015 Feb;33(2):230-42.
4. Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, et al. 2007 ESH-ESC practice guidelines for the management of arterial hypertension: ESH-ESC task force on the management of arterial hypertension. J Hypertens. 2007;25(9):1751–62.
5. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo Jr JL, et al. The seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. Jama. 2003;289(19):2560–71.
6. Lewington S. Prospective studies collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies (vol 360, pg 1903, 2002). Lancet. 2003;361(9362):1060–1060.
7. Mendis S, Lindholm LH, Mancia G, Whitworth J, Alderman M, Lim S, et al. World Health Organization (WHO) and International Society of Hypertension (ISH) risk prediction charts: assessment of cardiovascular risk for prevention and control of cardiovascular disease in low and middle-income countries. J Hypertens. 2007;25(8):1578–82.
8. World Health Organization. CVD–Risk Management Package for Low and Medium-Resource Settings. Geneva: WHO, 2002.
9. Lemogoum D, Seedat YK, Mabadeje AFB, Mendis S, Bovet P, Onwubere B, et al. International Forum for Hypertension control and prevention in Africa: Recommendations for prevention, diagnosis and management of hypertension and cardiovascular risk factors in sub-Saharan Africa. J Hypertens. 2003;21(11):1993–2000.
10. Pereira M, Lunet N, Azevedo A, Barros H. Differences in prevalence, awareness, treatment and control of hypertension between developing and developed countries. J Hypertens. 2009;27(5):963–75.
11. Kayima J, Wanyenze RK, Katamba A, Leontsini E, Nuwaha F. Hypertension awareness, treatment and control in Africa: a systematic review. BMC Cardiovasc Disord. 2013;13(1):1–11.
12. Peck R, Mghamba J, Vanobberghen F, Kavishe B, Rugarabamu V, Smeeth L, et al. Preparedness of Tanzanian health facilities for outpatient primary care of hypertension and diabetes: a cross-sectional survey. Lancet Glob Health. 2014;2(5):e285–92.
13. Mendis S, Abegunde D, Oladapo O, Celletti F, Nordet P. Barriers to management of cardiovascular risk in a low-resource setting using hypertension as an entry point. J Hypertens. 2004;22(1):59–64.
14. Van de Vijver S, Oti S, Addo J, de Graft-Aikins A, Agyemang C. Review of community-based interventions for prevention of cardiovascular diseases in low-and middle-income countries. Ethn Health. 2012;17(6):651–76.
15. Lim SS, Gaziano TA, Gakidou E, Reddy KS, Farzadfar F, Lozano R, et al. Prevention of cardiovascular disease in high-risk individuals in low-income and middle-income countries: health effects and costs. The Lancet. 2007;370(9604):2054–62.
16. Reidpath DD, Allotey P. The burden is great and the money little: Changing chronic disease management in low- and middle-income countries. J Glob Health. 2012 Dec;2(2):020301.
17. Beaglehole R, Epping-Jordan J, Patel V, Chopra M, Ebrahim S, Kidd M, et al. Improving the prevention and management of chronic disease in low-income and middle-income countries: a priority for primary healthcare. Lancet 2008; 372:940–949.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 89 —
18. World Health Organization. Prevention and control of non-communicable diseases: implementation of the global strategy. 2008. [http://www who int/nmh/NCD%20Action%20Plan%20Resolution pdf].
19. Hendriks M, Brewster L, Wit F, Bolarinwa OA, Odusola AO, Redekop W, et al. Cardiovascular disease prevention in rural Nigeria in the context of a community based health insurance scheme: QUality Improvement Cardiovascular care Kwara-I (QUICK-I). BMC Public Health. 2011;11(1):186.
20. Hendriks ME, Bolarinwa OA, Wit FW, Brewster LM, Odusola AO, Rosendaal NT, et al. Feasibility and quality of cardiovascular disease prevention within a community-based health insurance program in rural Nigeria: an operational cohort study. J Hypertens. 2014;32:000–000.
21. Grimshaw JM, Eccles MP, Lavis JN, Hill SJ, Squires JE. Knowledge translation of research findings. Implement Sci. 2012;7(1):50.
22. Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O. Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q. 2004;82(4):581–629.
23. Grol RP, Bosch MC, Hulscher ME, Eccles MP, Wensing M. Planning and studying improvement in patient care: the use of theoretical perspectives. Milbank Q. 2007;85(1):93–138.
24. Wensing M, van der Weijden T, Grol R. Implementing guidelines and innovations in general practice: which interventions are effective? Br J Gen Pract. 1998;48(427):991–7.
25. Grimshaw J, Eccles M, Thomas R, MacLennan G, Ramsay C, Fraser C, et al. Toward Evidence-Based Quality Improvement. J Gen Intern Med. 2006;21(S2):S14–20.
26. Flottorp SA, Oxman AD, Krause J, Musila NR, Wensing M, Godycki-Cwirko M, et al. A checklist for identifying determinants of practice: a systematic review and synthesis of frameworks and taxonomies of factors that prevent or enable improvements in healthcare professional practice. Implement Sci. 2013;8(1):35.
27. Baker R, Camosso-Stefinovic J, Gillies C, Shaw EJ, Cheater F, Flottorp S, et al. Tailored interventions to overcome identified barriers to change: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2010;(3):CD005470.
28. Nieuwlaat R, Schwalm J-D, Khatib R, Yusuf S. Why are we failing to implement effective therapies in cardiovascular disease? Eur Heart J. 2013;34(17):1262–9.
29. Khatib R, Schwalm J-D, Yusuf S, Haynes RB, McKee M, Khan M, et al. Patient and Healthcare Provider Barriers to Hypertension Awareness, Treatment and Follow Up: A Systematic Review and Meta-Analysis of Qualitative and Quantitative Studies. PloS One. 2014;9(1):e84238.
30. Wensing M, Huntink E, van Lieshout J, Godycki-Cwirko M, Kowalczyk A, Jäger C, et al. Tailored implementation of evidence-based practice for patients with chronic diseases. PLoS One. 2014 Jul 8;9(7):e101981.
31. Odusola AO, Hendriks M, Schultsz C, Stronks K, Lange J, Osibogun A, et al. Development and evaluation of a patient centered cardiovascular health education program for insured patients in rural Nigeria (QUICK-II). BMC Public Health. 2011;11(1):171.
32. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–57.
33. Gustafsson-Wright E, Schellekens OP. Achieving Universal Health Coverage in Nigeria One State at a Time: A Public-Private Partnership Community-Based Health Insurance Model. Washington D.C.: Brookings Institution; 2013. Available at: http://www.brookings.edu/research/papers/2013/06/achievinguniversal-health-coverage-nigeria-gustafsson-wright.
34. Humphreys G, Saraki AB. Nigerian farmers rejoice in pilot insurance plan. Bull World Health Organ. 2010;88:329–30.
35. Health Insurance Fund. HIF. Available from: http://www.hifund.org/ [cited 2014 Mar 22]36. World Health Organization. Prevention of cardiovascular disease: pocket guidelines for assessment
and management of cardiovascular risk: (WH. 2007); Available from: http://apps.who.int/iris/handle/10665/43784. [cited 2015 May 21]
37. Dahlgren L, Emmelin M, Winkvist A. Qualitative methodology for international public health Umeå: Epidemiology and Public Health Sciences, Umeå University, 2007.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 90 —
Chapter 4
38. Francis JJ, Johnston M, Robertson C, Glidewell L, Entwistle V, Eccles MP, et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health. 2010;25(10):1229–45.
39. Corbin, J., & Strauss, A. (2008). Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory (3rd ed.). Thousand Oaks, CA: Sage
40. http://www.maxqda.com/41. Parker WA, Steyn NP, Levitt NS, Lombard CJ. Health promotion services for patients having non-
comminicable diseases: Feedback from patients and health care providers in Cape Town, South Africa. BMC Public Health. 2012; 4;12:503.
42. Robyn PJ, Sauerborn R, Bärnighausen T. Provider payment in community-based health insurance schemes in developing countries: a systematic review. Health Policy Plan. 2013 Mar;28(2):111-22.
43. Onwujekwe O, Okereke E, Onoka C, Uzochukwu B, Kirigia J, Petu A. Willingness to pay for community-based health insurance in Nigeria: do economic status and place of residence matter? Health Policy Plan. 2010 Mar;25(2):155–61.
44. Mwaura JW, Pongpanich S. Access to health care: the role of a community based health insurance in Kenya. Pan Afr Med J. 2012;12:35.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 91 —
ADDITIONAL FILE 1: CONSOLIDATED CRITERIA FOR REPORTING QUALITATIVE STUDIES (COREQ): 32-ITEM CHECKLIST
Developed from:Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. International Journal for Quality in Health Care. 2007. Volume 19, Number 6: pp. 349 – 357
yOU MUST PROVIDE A RESPONSE FOR ALL ITEMS. ENTER N/A IF NOT APPLICABLE
No. Item Guide questions/description Reported on Page #
Domain 1: Research team and reflexivity
Personal Characteristics
1. Interviewer/facilitator Which author/s conducted the interview or focus group?
First author: AO Odusola (Page 9)
2. Credentials What were the researcher’s credentials? E.g. PhD, MD MD, MPH
3. Occupation What was their occupation at the time of the study? Researcher/PhD candidate
4. Gender Was the researcher male or female? Male
5. Experience and training What experience or training did the researcher have? Research methodology
Relationship with participants
6. Relationship established Was a relationship established prior to study commencement?
Yes
7. Participant knowledge of the interviewer
What did the participants know about the researcher? e.g. personal goals, reasons for doing the research
Reasons for doing the research
8. Interviewer characteristics
What characteristics were reported about the interviewer/facilitator? e.g. Bias, assumptions, reasons and interests in the research topic
Reasons and interests in the research topic
Domain 2: study design
Theoretical framework
9. Methodological orientation and Theory
What methodological orientation was stated to underpin the study? e.g. grounded theory, discourse analysis, ethnography, phenomenology, content analysis
Grounded theory(Page 9)
Participant selection
10. Sampling How were participants selected? e.g. purposive, convenience, consecutive, snowball
Purposive sampling (Page 8)
11. Method of approach How were participants approached? e.g. face-to-face, telephone, mail, email
Face-to-face (Page 9)
12. Sample size How many participants were in the study? 15 (Page 8)

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 92 —
Chapter 4
No. Item Guide questions/description Reported on Page #
Domain 2: study design
Participant selection
13. Non-participation How many people refused to participate or dropped out? Reasons?
None (Page 8)
Setting
14. Setting of data collection
Where was the data collected? e.g. home, clinic, workplace
Clinic and workplace (Page 9)
15. Presence of non-participants
Was anyone else present besides the participants and researchers?
No
16. Description of sample What are the important characteristics of the sample? e.g. demographic data, date
Age group: 21-40yrs (93.3%); Gender: Males (66.7%);Work experience: 1-5yrs (86.6%)6-10yrs (6.7%)>10yrs (6.7%)(Table 1)
Data collection
17. Interview guide Were questions, prompts, guides provided by the authors? Was it pilot tested?
Yes, also pilot tested (Add. File 3)
18. Repeat interviews Were repeat interviews carried out? If yes, how many? Yes, 3(Page 9)
19. Audio/visual recording Did the research use audio or visual recording to collect the data?
Yes, audio recording(Page 9)
20. Field notes Were field notes made during and/or after the inter view or focus group?
Yes, field notes taken (Page 9)
21. Duration What was the duration of the interviews or focus group?
90 minutes each(Page 9)
22. Data saturation Was data saturation discussed? Yes (Page 9)
23. Transcripts returned Were transcripts returned to participants for comment and/or correction?
Yes, for clarification of some themes (Page 9)
Domain 3: analysis and findings
Data analysis
24. Number of data coders How many data coders coded the data? 2 (Page 9)
25. Description of the coding tree
Did authors provide a description of the coding tree? Yes(Add File 4)(Page 9)
26. Derivation of themes Were themes identified in advance or derived from the data?
Themes were derived from data(Add File 3)(Page 9)
27. Software What software, if applicable, was used to manage the data?
MAXQDA(Page 9)
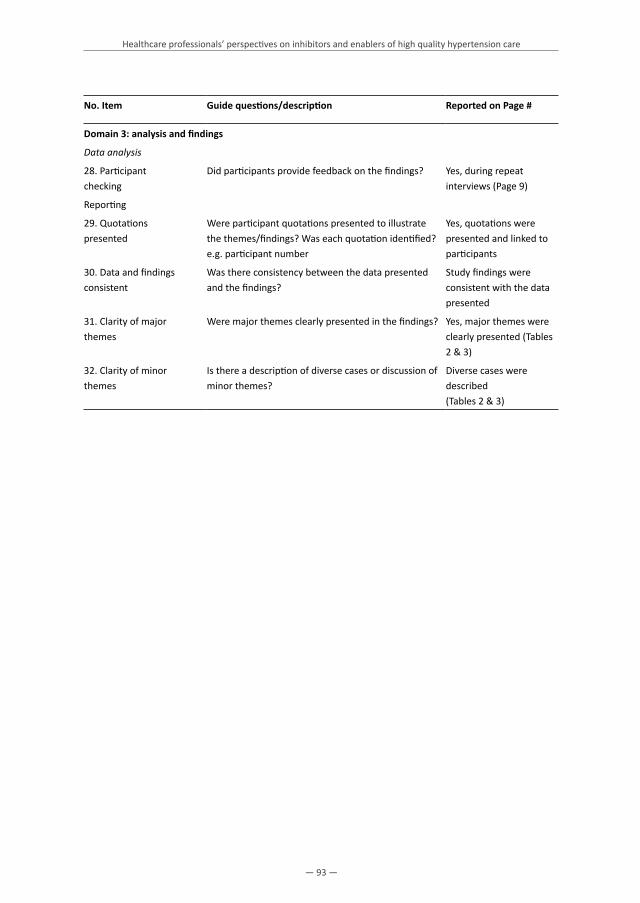
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 93 —
No. Item Guide questions/description Reported on Page #
Domain 3: analysis and findings
Data analysis
28. Participant checking
Did participants provide feedback on the findings? Yes, during repeat interviews (Page 9)
Reporting
29. Quotations presented
Were participant quotations presented to illustrate the themes/findings? Was each quotation identified? e.g. participant number
Yes, quotations were presented and linked to participants
30. Data and findings consistent
Was there consistency between the data presented and the findings?
Study findings were consistent with the data presented
31. Clarity of major themes
Were major themes clearly presented in the findings? Yes, major themes were clearly presented (Tables 2 & 3)
32. Clarity of minor themes
Is there a description of diverse cases or discussion of minor themes?
Diverse cases were described(Tables 2 & 3)

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 94 —
Chapter 4
ADDITIONAL FILE 2: DESCRIPTION OF THE KWARA STATE HEALTH INSURANCE PROGRAM AND THE STUDy SETTING
The Kwara State Health Insurance program (previously Hygeia Community Health Care program)The Health Insurance Fund (HIF) was initiated in 2006 by the international development organization PharmAccess, with a grant from the Dutch government. The PharmAccess Group is committed to providing access to quality healthcare for low- and middle income groups in several African countries through innovative financing mechanisms and improvement of the quality of healthcare [1-5]. From the onset, HIF has been working towards the following objectives: • To increase access to quality basic health care for currently uninsured groups, mainly through
private health facilities.• To evaluate different private healthcare delivery models based on a demand-driven and
results-oriented approach.• To directly support Millennium Development Goals (MDG) 1 and 6: reducing poverty and
halting the spread of HIV/AIDS, tuberculosis, malaria and other major diseases.• To lower the threshold for investment in private healthcare infrastructure.• To build sustainable medical and financial-administrative capacity in the health sector
To achieve these objectives, the Health Insurance Fund initiated, implemented and evaluated a variety of health insurance, healthcare quality and financial health care delivery models for low-income target groups and providers in sub Saharan Africa. Key elements on the demand side of the HIF program include the focus on organized groups in the informal sector and their dependents, for example communities of farmers; the provision of subsidized insurance premiums; co-payment of the premium by enrolees to encourage the groups to demand quality care; and voluntary enrolment. On the supply side, the key elements include capacity building, quality assurance, involvement of the private and public sector, focus on performance-based financing and management [6]. The HIF program uses a public-private partnership model and is implemented by PharmAccess and private African Health Maintenance Organizations (HMOs) or health insurance companies. The HMOs are responsible for execution of the program and for contracting a network of healthcare providers to provide the care for the enrolees [6]. Donor money – from both international and local sources – is used to develop and set up the insurance program and to upgrade the medical and administrative capacity of the HMOs and healthcare providers contracted under the program. The payment of healthcare providers is related to their performance. The program started in Lagos and Kwara State in Nigeria in 2007 in collaboration with the HMO Hygeia Limited under the name of Hygeia Community Health Care [6], which later changed to the Kwara State Health Insurance (KSHI) program.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 95 —
Quality assurance within KSHI programQuality and efficiency of care are monitored through independent audits of an international quality improvement and assessment body called SafeCare [3], a partnership of PharmAccess International, the American Joint Commission International, and the South-African Council for Health Services Accreditation of Southern Africa. When a healthcare provider is contracted by the HMO, a baseline assessment in the clinic is conducted by SafeCare and a quality improvement plan is formulated. The provider specific improvement plans consist of specific targets in 13 different domains including management and leadership, human resource management, patients’ rights and access to care, management of information, risk management, primary healthcare services, inpatient care, operating theatre, laboratory, diagnostic imaging, medication management, facility management and support services. The improvement plans are implemented by the healthcare providers with technical and financial support from the HMO. SafeCare monitors the progress on quality improvement through annual follow-up assessments with the SafeCare Quality Standards. Examples of quality improvement interventions include implementation of treatment guidelines (for example for hypertension), training of staff in guideline-based care, upgrading of laboratory equipment and training of laboratory staff to enable basic laboratory testing, assurance of continuous essential drug supplies, adequate medical file keeping, waste management protocols and hospital infection control protocols [6].
The KSHI program in KwaraSince 2007, the KSHI program has been rolled out in 3 regions in Kwara Sate, Nigeria: Kwara North (Kwara Edu), Kwara Central (Kwara Asa), and Kwara South (Kwara Oyun). In January 2015, 85,100 people were enrolled in the KSHI program in the 3 regions in Kwara State. The details and advantages of the health insurance program were communicated by the HMO through several channels. Activities included face-to-face information sharing (through outreach activities to the communities, house-to-house visits by enrolment officers, health education and advocacy visits to community opinion leaders) and large-scale communication and marketing activities in the target communities (through billboards, comics, brochures, flyers and elaborate announcements and information sharing on the radio). All households living in the districts in which the program is operational are eligible for enrolment. There is no pre-enrolment screening for chronic diseases [6]. Beneficiaries are enrolled individually (as opposed to household enrolment) on an annual basis and pay a co-premium of 300 NAIRA or approximately US$2 per person per year. Currently, individuals are responsible for about 12% of the premium. The Health Insurance Fund and the Kwara State Government subsidize the remaining part of the premium. The Kwara State Government started contributing to the premium subsidies in 2009 and its contribution has increased from 20% to 60% over the past years and it plans to eventually take over all costs of the premium subsidy. Prior to 2009, the HIF paid the greater part of the premium subsidy through a grant from the Dutch Ministry of Foreign Affairs. The co-premium ranges from 0.96% of the

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 96 —
Chapter 4
average annual per capita consumption for the lowest wealth quintile to 0.16% for the highest wealth quintile (data from baseline survey 2009). The scheme’s beneficiaries do not incur out-of-pocket costs for the services covered since the clinics are paid directly by the insurance scheme [6]. The HMO has contracted 25 health facilities, 4 small health posts and 2 referral clinics to provide the care for their enrolees. Most health facilities are primary and secondary care clinics that provide outpatient services and have admission capacity. Tertiary care can be provided in the 2 referral clinics in Ilorin (the Kwara State capital) if needed.
Coverage within the KSHI program in KwaraThe insurance package provides coverage for consultations, diagnostic tests, and medication for all disease categories, including hypertension and diabetes, that can be managed at a primary care level and limited coverage of secondary care services. Secondary care services provided include radiological and more complex laboratory diagnostic tests and hospital admissions for different disease categories, minor and intermediate surgery, antenatal care and delivery care, neonatal care, immunizations, annual check-ups and HIV/AIDS treatment care and support. Excluded from the program are high technology investigations (computed tomography and magnetic resonance imaging), major surgeries and complex eye surgeries, family planning commodities, treatment for substance abuse/addiction, cancer care requiring chemotherapy and radiation therapy, provision of spectacles, contact lenses and hearing aids, dental care, intensive care treatment and dialyses [6]. Management of acute cardiovascular events such as thrombolysis for stroke or for myocardial infarction is excluded. In case of an acute cardiovascular event, admission to a hospital for supportive care is covered including for example treatment with intravenous fluids, and antibiotics for infectious complications. The healthcare provider can claim a maximum of 12 clinic visits related to hypertension per patient. Furthermore, since a large share of the payment from the insurer to the healthcare provider is paid trough capitation, providers are encouraged to prevent overutilization of services.
Study area and populationKwara State is located in western Nigeria and is the fourth poorest state of the country [7]. The majority of the population lives in rural areas. The baseline survey conducted in 2009 demonstrated that Yoruba was the dominant ethnic group in both the program (67.8%) and control (89.2%) area. Nupe was another large ethnic group in the program area (9.9%). Islam and Christianity were the main religions, trading and farming the main occupations. The baseline survey showed that 20% of the population lived below the poverty line of US $2 (PPP adjusted) per day. Similar to the rest of the country, Kwara State has a weak health system with inadequate government funding for health, weak governance and legislation, inadequate health infrastructure and poor service quality. Kwara State is participating in the federally funded National Health Insurance Scheme (NHIS). The majority of its enrolees, however, are individuals

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 97 —
working in the formal sector. But most people in Kwara work in the informal sector and are thus not covered by the NHIS. In the 1990s, Bacita in Kwara north where the current project is located was a busy commercial center that hosted the then thriving State owned Nigerian Sugar Company. The original population of Bacita is Nupe, but the Sugar Company (which later closed) at that time attracted Nigerians of various ethnic nationalities particularly the Yoruba. Therefore, Yoruba language is also widely spoken alongside the native Nupe.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 98 —
Chapter 4
REFERENCES
1. Health Insurance Fund. Health Insurance Fund Website. 2014. http://hifund.org/. Accessed October 8, 2014.
2. PharmAccess Foundation. PharmAccess Foundation website. http://pharmaccess.org/RunScript.asp?p=ASP\Pg0.asp. Accessed March 13, 2015.
3. SafeCare. SafeCare Website. 2014. http://www.safe-care.org/. Accessed October 8, 2014.4. IFHA. Investment Fund for Health in Africa (IFHA) website. http://www.ifhafund.com/. Accessed March
13, 2015.5. Medical Credit Fund. Medical Credit Fund website. http://www.medicalcreditfund.org/. Accessed
March 13, 2015.6. Hendriks ME, Wit FWNM, Akande TM, et al. Effect of Health Insurance and Facility Quality
Improvement on Blood Pressure in Adults with Hypertension in Nigeria: A Population-Based Study. JAMA Intern Med. 2014;174(4):555-563. doi:10.1001/jamainternmed.2013.14458.
7. Gustafsson-Wright E, Schellekens O. Achieving Universal Health Coverage in Nigeria One State at a Time: A Public-Private Partnership Community-Based Health Insurance Model. Washington, DC; 2013. http://www.brookings.edu/~/media/research/files/papers/2013/06/achieving%20universal%20health%20coverage%20nigeria%20gustafsson%20wright/achieving%20universal%20health%20coverage%20in%20nigeria.pdf. Accessed October 8, 2014.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 99 —
ADDITIONAL FILE 3: AN EXAMPLE OF THE TOPIC LIST USED TO INTERVIEW HEALTHCARE PROFESSIONALS (DOCTORS)
Preparation• Greetings• Explain the purpose of the interview and obtain audio-recorded informed consent • Ask participant for permission to audio-record the interview.• Make and document brief assessment of socio-demographic data (age, gender, qualifications,
professional background, length of professional practice, religion, nationality).
Introduction In sub Saharan Africa, incidence of hypertension is increasing rapidly. If not managed effectively, hypertension often leads to poor patient outcomes, poor quality of life and an increased burden of cardiovascular diseases. Yet many hypertensive patients in Africa lack affordable access to care. To improve this situation, many African countries now adopt and implement affordable health insurance programs. However, the quality of hypertension care also contributes to treatment outcomes. For these reasons, we would like to know your views and experiences regarding the barriers and facilitators of hypertension care in your capacity as a health care professional or health insurance manager in the ongoing community health insurance program: what is currently being done rightly; what is wrongly done and should be implemented in better ways. Please feel free to air your views in your own words. All you say will remain confidential. If we report on the interviews, this will only serve as feedback to improve the system; we will not use your name or any other information by which you can be identified. We also seek your permission to audio-record the interview for ease of transcription and analysis.
(A) How do you regard the current way in which hypertension care is provided?1. How do you diagnose hypertension?• What cut off points do you use?• What signs / symptoms do you look out for?• Which other health conditions should be screened for in managing hypertension? What
investigations should be performed and how often should these be done during ongoing care? (N.B – Responses should be assessed in the light of current National guidelines on treatment of hypertension)
2. How do you document details of hypertension treatment encounters – history taking, physical examination, laboratory investigations: 1) on first visit; 2) during follow up visits?

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 100 —
Chapter 4
Quality of hypertension care3. Did you attend any refresher trainings or continuous medical education on management of
hypertension? If yes, how does it affect your work?4. Do you encounter any challenges in prescribing medication (availability, out of stock, quality
of drugs, credibility suppliers)? How do you handle the situation when there are issues with medication?
5. What is your view about the screening of hypertensive patients (e.g., periodic target organ screening)?
6. Are you using clinical guidelines and standard operating procedures when providing hypertension care? What is your experience with guidelines?
7. What barriers or facilitators do you encounter if you want to implement clinical guidelines?8. How do you assess treatment outcomes in your patients – for out-patients? For in-patients?
What do you do if your patient is not making expected clinical improvement on their hypertension control?
Organization of hypertension care9. In your opinion, how frequently should outpatient hypertension follow up clinic be organized?
What are the reasons for your answers? How compliant are the patients with the current visit schedule (once monthly)?
10. What do you do when patients fail to turn up for follow-up appointments or become lost to follow up? If and when such return to clinic, how do you rate their hypertension control status? How can we improve hypertension clinic follow up compliance by patients?
11. On a typical hypertension clinic day, how many patients do you see on the average? Is this number okay? Too much? Too few? Explain your answer?
12. What is the average consulting time you spend on each patient? Is this okay? Too long? Too short? What should be the ideal consulting time for good healthcare delivery? How much of the consulting time do you spend on health education? How do you view the time spent on health education?
13. How should hypertension care be organized for effectiveness?
Sustainability of (affordable) hypertension care14. What is your view about health insurance and its role in the management of hypertension?
Positive impact? Potential negative impacts? 15. What influence if any does access to affordable healthcare through health insurance has on
compliance with prescribed hypertension treatment?
Administration of (insured) hypertension care16. What are your experiences working with the insurance company? How does it impact your
work? What are currently done well and what should change for the better?

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 101 —
(B) Can you think of any barriers that can make it difficult to provide high-quality hypertension care?General: barriers of hypertension care17. Generally, what in your opinion and experience are the limitations of delivering high-quality
hypertension care?18. In particular, what limitations have you encountered in the course of treating hypertensive
patients in the ongoing insurance program in this hospital? What issues if any have you had regarding any of the following:
• Availability and functionality of equipment • Adequacy of hospital (laboratory) investigative capacity• Providing health education to patients • Communication with patients during consultations (e.g. language barrier) • Workload / adequacy of healthcare personnel• Availability of motivational incentives / management support• Availability of opportunities for refresher trainings / continuous education• Use of clinical guidelines and standard operating procedures• Organization/division of tasks within the healthcare team.• Relationship with Health Insurance Company (C) In your experience, what can help ensure the provision of (consistent) high-quality hypertension care?General: enablers of hypertension care19. Generally, what in your opinion and experience are the enablers of delivering high-quality
hypertension care?20. In particular, what facilitations have you encountered in the course of treating hypertensive
patients in the ongoing insurance program in this hospital? What issues if any have you had regarding any of the following:
• Availability and functionality of equipment • Adequacy of hospital (laboratory) investigative capacity• Providing health education to patients • Communication with patients during consultations (E.g. language barrier) • Workload / adequacy of healthcare personnel• Availability of motivational incentives / management support• Availability of opportunities for refresher trainings / continuous education• Use of clinical guidelines and standard operating procedures• Organization/division of tasks within the healthcare team.• Relationship with Health Insurance Company

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 102 —
Chapter 4
ADDITIONAL FILE 4: QUALITATIVE ANALySIS AND TRUSTWORTHINESS: SPECIFIC STEPS TAKEN IN THIS STUDy
Data analysisAll transcribed interviews were uploaded in MAXQDA. After each interview, the researcher (AOO) wrote a memo in which he provided a summary of respondents’ answers to the interview questions, what they had identified as inhibitors or enablers for high-quality hypertension care and suggestions for further questions that needed to be explored in follow-up interviews. After all interviews were held, all sections from the interview transcripts that contained information about respondents’ perceptions on inhibitors and enablers were selected and inductively coded. Similar codes were assigned to text fragments that reflected the same idea. These coding activities yielded a codebook that included all the codes that were created during the analysis of the individual interview transcripts. To conclude this stage we reviewed the code book to eliminate duplicates and to inspect if the remaining codes captured similar concepts, so that they could be grouped together. The goal was to establish a smaller set of mutually exclusive conceptual codes that expressed the meaning of the underlying codes without loss of the original content. The identified “concepts”, and underlying text fragments were then scrutinized and grouped under the two major themes referring to our research questions; inhibitors and facilitators of high-quality hypertension and CVD prevention care. Subsequently, thematic coding procedures were used to group the concepts under these two major themes into categories and sub-categories. For each professional group (health care providers and insurance managers), results of these multilevel coding procedures were summarized into matrices (See below for an example). After these procedures were finished, we conducted a literature search that had the aim to identify if and how the inductively created categories that emerged from the interviews corresponded with existing conceptual frameworks of determinants that influence the uptake of best practices in health care. The research group reached consensus that the categories we had found in our study could be grouped under one of the seven dimensions of the TICD checklist that was developed by Flottorp et al (26), namely the dimension “resources and incentives”. To make our findings more comparable with those from other implementation studies, we report the findings of this study according to the sub-categories of “resources and incentives” dimension suggested by the TICD.
TrustworthinessTo ensure a rigorous research process and the credibility and trustworthiness of the findings, the following steps were taken. 1. To establish questions that required further attention in follow-up interviews the researcher
discussed the memos describing the results of the first fifteen interviews with a senior researcher (JH) and they discussed together what additional information would be needed to substantiate the initial themes that emerged from the data. Based on this, three additional follow-up interviews were held at a later stage.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Healthcare professionals’ perspectives on inhibitors and enablers of high quality hypertension care
— 103 —
2. The researcher selected the interview fragments that were used in this study and performed the initial open coding procedure which resulted in a codebook. Another researcher (JH) reviewed the final codebook and checked if codes were workable and reflected the underlying content.
3. Two researchers (AOO and JH) categorized the codes into broader concepts independently in three rounds. At each round they discussed whether the broader concepts reflected the codes and the underlying data and they reached consensus about the final list of broader concepts.
4. The researcher categorized the concepts (and underlying content) under the two main research questions, and JH checked this to ensure that this categorization was plausible and could be justified.
5. The next step of coding, where concepts were organized under major themes, was done by AOO and JH separately in several rounds. The thematic matrixes that emerged from these exercises were discussed and differences in opinion were resolved through consensus. The final matrices were discussed in the core research group (KS, HvW, CS).
6. Even though thematic matrices that emerge from analytic approaches based on grounded theory are informative and useful as such, the research group decided that it would be relevant to conduct a literature search to explore if the findings were consistent with other conceptual frameworks. Through a consensus procedure KS, AOO, and JH agreed that there was a good fit between some of the categories and sub-categories of the TICD and the categories and sub-categories that emerged from our study.
7. The final results of the analyses that are presented in the Tables 2 and 3 in this paper were reviewed by all authors.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 104 —
Chapter 4
MATRIX (CODING TREE)
Example of thematic matrix on what is needed to implement high-quality hypertension care based on perceptions of inhibitors and facilitators by healthcare providers and health insurance managers
Theme Sub-theme Concept
Improving efficiency of organized care in limited resource settings
Diversifying functions of limited personnel more efficiently
Implement task shifting: to free more time for optimal care, doctors can train and delegate simple tasks to nurses, other paramedics [R2,R3,R4]
To reduce patients’ waiting time and doctors’ workload, some nurses expressed willingness to take up additional tasks (e.g. health education) delegated by doctors [R3,R4]
Redeploying limited care time more productively
Engage patients with group health educational audio-visuals productively during (unavoidably long) waiting times [IR2]
Addressing procedural constraints
Resolve issues of: long waiting time; inadequate personnel; work overload; high personnel attrition rate; dysfunctional/insufficient equipment/tools and communication infrastructure. Implement contact tracing arrangement for defaulting clinic patients [R2,R1,R3,R8,R9,R5,IR1,IR2]
Addressing drugs availability constraints
Eliminate drugs stock outs, failed drug refill occurrences [R7,IR1,IR3]

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Chapter 5
Development of cardiovascular health education for Nigerian primary care patients with hypertension
Odusola AOStronks KSchultsz CHendriks MEAkande TOsibogun ABeune EHaafkens JA
Health Promotion Practice, Submitted 2015

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 106 —
Chapter 5
ABSTRACT
The project described in this paper aimed to develop a culturally-sensitive cardiovascular health education program (CHEP) for primary care patients with hypertension in rural Nigeria, in the context of a health insurance program. Inspired by a previous patient-centered and culturally-sensitive hypertension education program from Europe, CHEP was developed through a formative process, using a literature review and qualitative interviews with 15 health professionals and 40 patients from the program area. Themes that emerged from qualitative studies and the literature were used to develop the educational tools and the specific content for CHEP. The developed program consists of three educational modules, which aim to strengthen patients’ understanding of hypertension and their knowledge and ability for managing hypertension in their daily life. The first module focuses on hypertension and the next modules on aspects of medication use, reduction of salt intake and weight, healthy diets and physical exercise. Educational tools used in CHEP include group counseling and supportive posters and audiovisuals with information adapted to the target group. The educational program developed in this study offers a practical and effective framework for educating primary care patients about blood pressure control in a low resource setting in Africa.
Keywords: Hypertension, Patient education program, Cultural adaptation, Primary care, Nigerians

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development of cardiovascular health education program
— 107 —
INTRODUCTION
Hypertension is highly prevalent in sub Saharan Africa (SSA) (World Health Organization, 2015) and raised blood pressure is the leading risk factor for cardiovascular disease (CVD) and related premature death in this region (Lim et al., 2013). In Nigeria, the estimated hypertension prevalence (systolic blood pressure (BP) ≥ 140 mmHg or diastolic BP ≥ 90 mmHg) is 28.9% among people aged 15 years and older (Adeloye, Basquill, Aderemi, Thompson, & Obi, 2015). It is well established that long-term treatment, which includes behavioral adaptations (e.g., weight control, reduced salt intake, regular exercise, smoking cessation and moderate alcohol use) and pharmacotherapy if needed, reduces the BP and, concomitantly, the risk of developing CVD and other hypertension-related complications (Murray et al., 2003). However, BP control rates are low in SSA (Kayima, Wanyenze, Katamba, Leontsini, & Nuwaha, 2013). Unfortunately, many people in the region have no access to affordable hypertension care in their communities. In addition, in settings where affordable care is available, poor compliance can compromise treatment outcomes (De Geest & Sabate, 2003; Mendis, Abegunde, Oladapo, Celletti, & Nordet, 2004; van de Vijver, Oti, Addo, de Graft-Aikins, & Agyemang, 2012). Indeed, adequate hypertension management is challenging in SSA and multiple interventions are needed to improve both access to- and compliance with quality care (Brown & Bussell, 2011). A review of community-based interventions for CVD prevention in low- and middle income countries suggests that patient education can have a positive effect on treatment adherence and BP control among patients with hypertension (van de Vijver et al., 2012). The literature provides ample information on health education programs to support hypertension self-management for patients living in high income countries (Whitlock, Orleans, Pender, & Allan, 2002). However, information on suitable educational programs for patients with hypertension in low resource countries is not available (Hubley, 2006; http://www.hubley.co.uk/listing.htm). To fill the gap, in this paper we describe the formative phases by which we developed a cardiovascular health education program (CHEP) that is designed for insured primary care patients with hypertension in Kwara State, Nigeria. By positively influencing patients’ perceptions of hypertension and medication, the developed program has been shown to strengthen medication adherence, and consequently BP reduction among the affected population (Odusola et al., 2015).
BACKGROUND
ContextKwara State was the fourth poorest State in Nigeria in 2010 (World Bank Report). The majority of the population lives in rural areas and works in agriculture, fishery or (petty) trading. About one third of the population is illiterate. The main ethnic groups in the State are Yoruba and Nupe. Islam and Christianity are the main religions. In 2007, a subsidized health insurance program,

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 108 —
Chapter 5
the Kwara State Health Insurance (KSHI), was introduced in three rural regions in Kwara, where about 20% of the population lives below the poverty line of 2 USD per day (Gustafsson-Wright & Schellekens, 2013). KSHI provides coverage for consultations, diagnostic tests and drugs for all conditions, that can be managed at a primary care level, including hypertension, and limited coverage for secondary care services. In December 2014, about 67,000 people were enrolled in KSHI. In 2010 enrollees paid approximately 8% of the yearly premium of 30 USD themselves, while the Kwara State Government and the Health Insurance Fund subsidized the remaining 92% (‘Health Insurance Fund’). In 2010, hypertension was identified as the most important risk factor for CVD in rural Kwara, with a prevalence of 21% among the population aged ≥ 18 years and low levels of awareness (8%), antihypertensive treatment coverage (5%), and BP control (3%) among those with hypertension (Hendriks et al., 2012). As part of its quality improvement program KSHI introduced WHO guidelines for CVD risk management, including hypertension care, (World Health Organization, 2007) in contracted primary care clinics and offered them new equipment, organizational support and training to facilitate implementation (Hendriks et al., 2011). Because clinical guidelines offer little guidance on methods for patient education, CHEP was developed to support KSHI’s initiative to improve the quality of CVD prevention care in Kwara (Odusola et al., 2011).
Concepts underlying the development of CHEPAccording to common sense models of health behaviour [(Leventhal, Diefenbach, & Leventhal, 1992) and (Kleinman, Eisenberg, & Good, 2006)], patients’ perceptions of a health problem (e.g., hypertension) and its treatment are an important determinant of treatment adherence. These perceptions can be rooted in individual experiences but also in the broader social, cultural, economic or environmental context of patients’ lives. This was also highlighted in recent reviews of studies of patient perspectives on hypertension (Khatib et al., 2014; Marshall, Wolfe, & McKevitt, 2012). It is well recognized that “patient-centred” health education can play an important role in promoting adequate hypertension self-management, and particularly education that addresses patient perceptions on hypertension (e.g., its causes, symptoms, duration, severity, consequences), the recommended treatment and their own ability to use medication and implement the recommended behavioural changes (Boulware et al., 2001; Whitlock et al., 2002). The five A’s approach (Ask, Advise, Assess, Assist, and Arrange) is an example of a widely used “patient-centered” approach for supporting hypertension self-management (Whitlock et al., 2002). However, several authors have emphasized it is also vital that educational interventions are “culturally sensitive” and that deep-rooted cultural norms (e.g., beliefs and traditions) and structural factors (e.g., socioeconomic status, health literacy) influencing behaviours of target groups are considered when developing such interventions (Greenhalgh & Meadows, 1999; Netto, Bhopal, Lederle, Khatoon, & Jackson, 2010; Resnicow, Baranowski, Ahluwalia, & Braithwaite, 1998). In doing so, intervention developers must ensure

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development of cardiovascular health education program
— 109 —
that both the form in which health promotion interventions are delivered (the surface structure) and their content (deep structure) acknowledge customs, socio-demographic characteristics, and social, cultural and environmental values of the targeted population groups (Netto et al., 2010; Resnicow et al., 1998). Our work drew upon a practical protocol for hypertension education developed by Beune et al. (2014) to support treatment adherence and BP control among Afro-Surinamese and Ghanaian primary care patients with hypertension in the Netherlands. This protocol includes a generic “patient-centred” part, based on the method of the five A’s (Whitlock et al., 2002) and a “culturally adapted” part, based on a framework proposed by Kleinman. The protocol allows educators to address both individual and cultural specific perspectives on hypertension self-management.
METHODS
CHEP was developed in two phases: a formative phase and a construction phase. The goal of the formative phase was to collect information from the literature and qualitative interviews with 40 primary care patients with hypertension and 11 health care professionals and 4 health insurance managers from Kwara on themes that require attention in developing the form and the content of CHEP. For the literature review a narrative approach was used. The methods employed in the interview studies are reported elsewhere (Odusola et al., 2015, submitted; Odusola et al., 2014). The goal of the construction phase was to review information that emerged in the formative phase and to supplement the protocol and materials developed by Beune et al. (2014) with information collected during the formative phase, so as to make the program and educational materials relevant to patients in Nigeria.
RESULTS
Formative phaseSurface structureThe information gleaned from the literature provided little information about the best form of educational programs for the priority group of CHEP. However, interviews with health care professionals provided some relevant insights. They suggested various educational forms or strategies for enhancing patients’ hypertension self-management capacities that are suitable within rural contexts in Africa where financial resources and health care personnel are limited: periodic group education led by trained nurses or paramedics (in addition to individual consulting room education); cardiovascular health clubs for patients to stimulate regular exercise and a healthy diet; the use of well known “positively living” community figures and peers as educators; involvement of patients’ family members in education to ensure necessary social

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 110 —
Chapter 5
support for hypertension management; the use of local languages or interpreters in education; the use of pictorial and audiovisual materials (audiovisuals, posters, pictures, pamphlets) to reinforce learning, especially for illiterate patients. Moreover, professionals emphasized that the organization of educational events during religious holidays, Muslim prayer hours and market days should be avoided. They also viewed the use of a “contact tracing system” to remind patients of their scheduled clinic visits as an educational tool.
Deep structureIn order to develop the content of CHEP we sought “in-depth” information on how patients’ “explanatory models” of hypertension (understandings of the causes, mechanisms or pathophysiology, course of illness, symptoms) and its treatment relate to their daily hypertension self-management behaviours. To this end we conducted a qualitative interview study to investigate perceptions on hypertension and its management among primary care patients with hypertension in Kwara State (Odusola et al., 2014) and reviewed similar studies from Nigeria on this topic (Osamor & Owumi, 2011; Taylor et al., 2012). Table 1 summarizes some of the main themes that emerged from the study and the literature. These themes illustrate that poor knowledge, cultural beliefs and customs and contextual factors may hamper adherence to treatment among patients, but that the local context also provides specific possibilities for harnessing adherence.
Table 1: Explanatory models of hypertension, treatment recommendations and corresponding hypertension self-management behaviors; examples of themes derived from qualitative interviews with primary care patients with hypertension in Kwara
Explanatory model Hypertension self-management
Perceptions of hypertension
Cause
• Thinking too much/stress • Staying calm (through cigarettes, snuff and alcohol)
• The stressful living conditions in Nigeria • Praying things will change
Course of hypertension
• Hypertension comes and goes • Take medication/treatment when BP is perceived to be high
• Hypertension is not present when you feel well • Stop medication when feels well
• Hypertension is curable • With prayer and treatment hypertension will stop soon
• Only doctors know • Follow treatment as long as doctor tells you so
Symptoms
• Not always noticeable • Did not inform doctor, unilaterally stop treatment
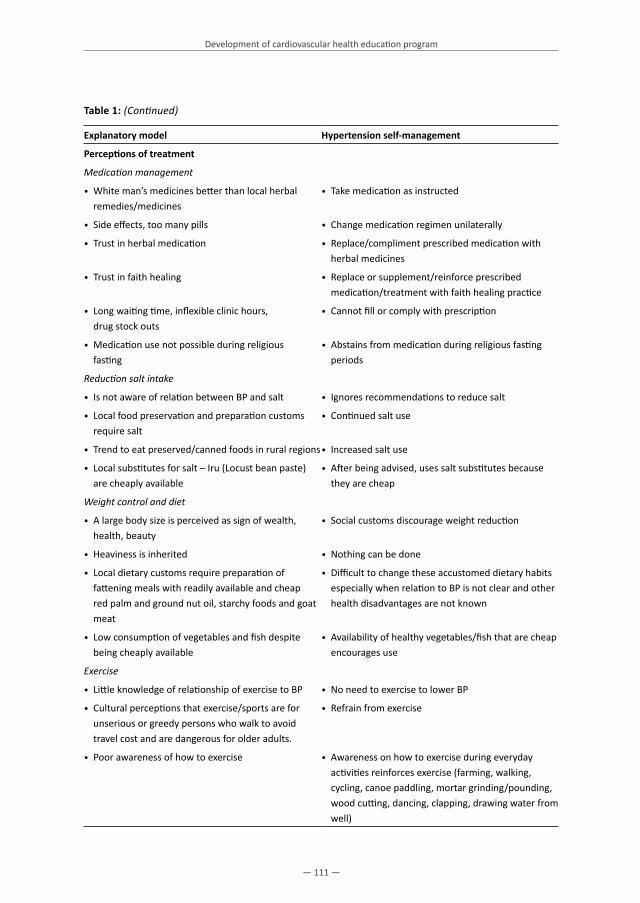
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development of cardiovascular health education program
— 111 —
Table 1: (Continued)
Explanatory model Hypertension self-management
Perceptions of treatment
Medication management
• White man’s medicines better than local herbal remedies/medicines
• Take medication as instructed
• Side effects, too many pills • Change medication regimen unilaterally
• Trust in herbal medication • Replace/compliment prescribed medication with herbal medicines
• Trust in faith healing • Replace or supplement/reinforce prescribed medication/treatment with faith healing practice
• Long waiting time, inflexible clinic hours, drug stock outs
• Cannot fill or comply with prescription
• Medication use not possible during religious fasting
• Abstains from medication during religious fasting periods
Reduction salt intake
• Is not aware of relation between BP and salt • Ignores recommendations to reduce salt
• Local food preservation and preparation customs require salt
• Continued salt use
• Trend to eat preserved/canned foods in rural regions• Increased salt use
• Local substitutes for salt – Iru (Locust bean paste) are cheaply available
• After being advised, uses salt substitutes because they are cheap
Weight control and diet
• A large body size is perceived as sign of wealth, health, beauty
• Social customs discourage weight reduction
• Heaviness is inherited • Nothing can be done
• Local dietary customs require preparation of fattening meals with readily available and cheap red palm and ground nut oil, starchy foods and goat meat
• Difficult to change these accustomed dietary habits especially when relation to BP is not clear and other health disadvantages are not known
• Low consumption of vegetables and fish despite being cheaply available
• Availability of healthy vegetables/fish that are cheap encourages use
Exercise
• Little knowledge of relationship of exercise to BP • No need to exercise to lower BP
• Cultural perceptions that exercise/sports are for unserious or greedy persons who walk to avoid travel cost and are dangerous for older adults.
• Refrain from exercise
• Poor awareness of how to exercise • Awareness on how to exercise during everyday activities reinforces exercise (farming, walking, cycling, canoe paddling, mortar grinding/pounding, wood cutting, dancing, clapping, drawing water from well)

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 112 —
Chapter 5
Table 1: (Continued)
Explanatory model Hypertension self-management
Alcohol, tobacco, stimulants
• Increasingly available, sometimes culturally permissible
• Exploits religious- and gender based social disapproval to discourage use of tobacco products and alcoholic beverages, particularly in women
• Support for hypertension management • Support (additional counseling) from family and other sources can help overcome challenges with medication use and weight control
• Family, peers, local leaders, media
Construction phase CHEP Based on the formative phase, we developed a final protocol for CHEP with the following overall objectives: 1. To enhance patients’ understanding of hypertension and its treatment/management2. To raise patients’ awareness and confidence on how they can manage hypertension in their
daily lives3. To raise patients’ awareness and confidence on how they can cope with the challenges in
managing hypertension in the long run
In order to achieve these objectives we developed a final protocol of cardiovascular health education program that consists of three sequential modules for group-based educational sessions. Table 2 provides an overview of the specific objectives and the proposed content and educational tools for each of these sessions.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development of cardiovascular health education program
— 113 —
Tabl
e 2:
Ove
rvie
w o
f gro
up-b
ased
Car
diov
ascu
lar H
ealth
Edu
catio
n Pr
ogra
m (C
HEP
)
Inte
rven
tion
Sess
ions
Gro
up se
ssio
n 1
(CHE
P-1)
(wee
k 3)
Gro
up se
ssio
n 2
(CHE
P-2)
(wee
k 7)
Gro
up se
ssio
n 3
(CHE
P-3)
(wee
k 15
)
Ove
rall
obje
ctive
sTo
enh
ance
pati
ents
’ und
erst
andi
ng o
f hy
pert
ensio
n an
d its
trea
tmen
t/m
anag
emen
tTo
raise
pati
ents
’ aw
aren
ess a
nd c
onfid
ence
on
how
they
can
man
age
hype
rten
sion
in th
eir d
aily
liv
es
To ra
ise p
atien
ts’ a
war
enes
s and
con
fiden
ce o
n ho
w th
ey c
an c
ope
with
the
chal
leng
es in
man
agin
g hy
pert
ensio
n (in
the
long
run)
Sess
ion
obje
ctive
sTo
elic
it pa
rtici
pant
s’ id
eas a
bout
hyp
erte
nsio
n an
d tr
eatm
ent;
info
rm th
em a
bout
med
ical
pe
rspe
ctive
; rea
ch c
onse
nsus
; and
est
ablis
h tr
eatm
ent o
bjec
tives
for n
ext s
essio
n –
CHEP
-2
To e
xplo
re d
aily
cha
lleng
es p
artic
ipan
ts fa
ce
in m
anag
ing
hype
rten
sion;
how
they
cur
rent
ly
cope
with
the
iden
tified
cha
lleng
es; i
nfor
m th
em
on h
ow th
ey m
ay c
ope
bette
r; an
d es
tabl
ish
obje
ctive
s for
nex
t ses
sion
– CH
EP-3
To e
xplo
re d
aily
cha
lleng
es p
artic
ipan
ts fa
ce in
m
anag
ing
hype
rten
sion;
how
they
cur
rent
ly c
ope
with
the
iden
tified
cha
lleng
es, i
nfor
m th
em o
n ho
w
they
may
cop
e be
tter;
and
esta
blish
how
they
can
co
ntinu
e to
dea
l with
the
chal
leng
es in
futu
re
Sess
ion
dura
tion
Educ
ation
al
tool
s
2 ho
urs
2 ho
urs,
30
min
utes
2 h
ours
, 30
min
utes
Grou
p di
scus
sion/
inst
ructi
on le
d by
trai
ners
, in
divi
dual
ass
ignm
ent
Disc
ussio
n of
resu
lts o
f ind
ivid
ual a
ssig
nmen
t, gr
oup
disc
ussio
n, in
stru
ction
led
by tr
aine
rs,
supp
orte
d by
pos
ters
and
vid
eo, i
ndiv
idua
l as
signm
ent
Disc
ussio
n of
resu
lts o
f ind
ivid
ual a
ssig
nmen
t, gr
oup
disc
ussio
n/ in
stru
ction
by
trai
ners
, su
ppor
ted
by p
oste
rs a
nd v
ideo
Prog
ram
in
stru
ction
s1.
1: H
yper
tens
ion
and
its m
anag
emen
t: gr
oup
disc
ussi
on (
30 m
inut
es)
2.1:
Med
icati
on u
se: g
roup
dis
cuss
ion
(1
5 m
inut
es)
3.1:
Med
icati
on u
se: g
roup
dis
cuss
ion
(1
5 m
inut
es)
• W
hat i
s hyp
erte
nsio
n?
• W
hat c
halle
nges
do
you
face
?•
Wha
t cha
lleng
es d
o yo
u fa
ce?
• Is
hyp
erte
nsio
n a
dise
ase?
•
How
did
you
cop
e?•
How
did
you
cop
e?
• W
hat a
re y
our v
iew
s abo
ut h
yper
tens
ion?
2.2:
Die
tary
adv
ice/
salt:
gro
up d
iscu
ssio
n
(15
min
utes
)3.
2: D
ieta
ry a
dvic
e/sa
lt: g
roup
dis
cuss
ion
(1
5 m
inut
es)
• W
hat c
ause
s hyp
erte
nsio
n?
• W
hat c
halle
nges
do
you
face
?•
Wha
t cha
lleng
es d
o yo
u fa
ce?
• W
ho c
an g
et h
yper
tens
ion?
• Ho
w d
id y
ou c
ope?
• Ho
w d
id y
ou c
ope?

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 114 —
Chapter 5
Tabl
e 2:
(Con
tinue
d)
Inte
rven
tion
Sess
ions
Gro
up se
ssio
n 1
(CHE
P-1)
(wee
k 3)
Gro
up se
ssio
n 2
(CHE
P-2)
(wee
k 7)
Gro
up se
ssio
n 3
(CHE
P-3)
(wee
k 15
)
•Is
hyp
erte
nsio
n da
nger
ous,
If so
, how
dan
gero
us
is it?
2.3:
Wei
ght r
educ
tion/
exer
cise
gro
up d
iscu
ssio
n (1
5 m
inut
es)
3.3:
Wei
ght r
educ
tion/
exer
cise
gro
up d
iscu
ssio
n (1
5 m
inut
es)
•Is
hyp
erte
nsio
n cu
rabl
e?
• W
hat c
halle
nges
do
you
face
?•
Wha
t cha
lleng
es d
o yo
u fa
ce?
•Ho
w lo
ng d
oes h
yper
tens
ion
last
? •
How
did
you
cop
e?•
How
did
you
cop
e?
•Ho
w d
oes h
yper
tens
ion
pres
ent?
2.
4: A
tten
ding
you
r fol
low
-up
appo
intm
ents
re
gula
rly a
s adv
ised
gro
up d
iscu
ssio
n
(15
min
utes
)
3.4:
Att
endi
ng y
our f
ollo
w-u
p ap
poin
tmen
ts
regu
larly
as a
dvis
ed g
roup
dis
cuss
ion
(1
5 m
inut
es)
•Ho
w d
id y
ou g
et y
our h
yper
tens
ion?
•
Wha
t cha
lleng
es d
o yo
u fa
ce?
•W
hat c
halle
nges
do
you
face
?
•W
hat c
an y
ou d
o to
pre
vent
hyp
erte
nsio
n?
• Ho
w d
id y
ou c
ope?
•Ho
w d
id y
ou c
ope?
•Ho
w c
an h
yper
tens
ion
be tr
eate
d?2.
5 Au
diov
isua
l ‘Li
ving
pos
itive
ly w
ith
hype
rten
sion
’: In
stru
ction
(25
min
utes
)3.
5: A
udio
visu
al ‘L
ivin
g po
sitiv
ely
with
hy
pert
ensi
on’:
Inst
ructi
on (2
5 m
inut
es)
•Ho
w is
hyp
erte
nsio
n re
late
d to
you
r life
styl
e an
d w
hat y
ou e
at?
• Vi
ew a
nd d
iscus
s vid
eo “
livin
g po
sitive
ly w
ith
hype
rten
sion”
and
som
e pa
tient
-cen
tred
ex
erci
se re
gim
es to
hel
p co
ping
(35
min
utes
)
•Vi
ew a
nd d
iscus
s vid
eo “
livin
g po
sitive
ly w
ith
hype
rten
sion”
and
som
e pa
tient
-cen
tere
d ex
erci
se re
gim
es to
hel
p co
ping
(35
min
utes
)
1.2:
Wha
t pati
ents
can
do
to m
anag
e hy
pert
ensi
on: i
nter
activ
e in
stru
ction
(3
0 m
inut
es) *
2.6:
Sim
ple
exer
cise
s you
can
do
at h
ome
(2
0 m
inut
es)
•Ta
ke y
our m
edic
ation
s reg
ular
ly a
s pre
scrib
ed•
Post
er te
achi
ng se
ssio
n (5
min
utes
)3.
6: S
impl
e ex
erci
ses y
ou c
an d
o at
hom
e
(20
min
utes
)
•Se
ek su
ppor
t fro
m y
our f
amily
/frie
nds o
n re
min
ders
in ta
king
you
r dru
gs re
gula
rly a
nd in
re
duci
ng sa
lt in
take
• Pr
actic
al e
xerc
ise se
ssio
n (1
5 m
inut
es)
•Pa
tient
frie
ndly
exe
rcise
pra
ctice
sess
ions
usin
g:
loca
l acti
vitie
s suc
h as
woo
d cu
tting
, gar
deni
ng,
mor
tar g
rindi
ng, d
raw
ing
wat
er fr
om w
ell,
othe
r ho
useh
old
chor
es, f
arm
ing,
bik
ing,
bris
k w
alki
ng,
leisu
re a
ctivi
ties e
.g. d
rum
min
g, d
anci
ng.
acboers
Sticky Note
Unmarked set by acboers
acboers
Sticky Note
Unmarked set by acboers

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development of cardiovascular health education program
— 115 —
Tabl
e 2:
(Con
tinue
d)
Inte
rven
tion
Sess
ions
Gro
up se
ssio
n 1
(CHE
P-1)
(wee
k 3)
Gro
up se
ssio
n 2
(CHE
P-2)
(wee
k 7)
Gro
up se
ssio
n 3
(CHE
P-3)
(wee
k 15
)
•Ad
opt h
ealth
y di
et (d
escr
ibed
)•
2.7:
Indi
vidu
al a
ssig
nmen
t (10
min
utes
): 3.
7: F
inal
clo
sing
sess
ion
(Inst
ructi
ons)
, 10
min
utes
•De
crea
se a
mou
nt o
f sod
ium
/sal
t in
your
die
t•
Set 3
goa
ls o
n w
hat y
ou w
ant t
o ac
hiev
e be
fore
you
r nex
t CHE
P vi
sit t
o ke
ep y
our
bloo
d pr
essu
re c
ontr
olle
d (e
.g. r
educ
e sa
lt co
nsum
ption
, inc
reas
e ph
ysic
al a
ctivi
ty
thro
ugh
exer
cise
)
In m
ovin
g fo
rwar
d:
•St
ay p
hysic
ally
acti
ve /
exer
cise
regu
larly
•
Mak
e th
e le
sson
s lea
rnt f
rom
this
prog
ram
you
r da
ily ro
utine
for l
ife
•Lo
se e
xces
s wei
ght
•Ta
ke y
our d
rugs
regu
larly
•Q
uit s
mok
ing
•Ex
erci
se d
aily,
regu
larly
•Q
uit/
redu
ce a
lcoh
ol in
take
•Re
duce
salt
inta
ke a
nd a
dopt
hea
lthy
diet
•Q
uit s
nuff,
Kol
a nu
ts
•Att
end
your
follo
w-u
p cl
inic
regu
larly
•Li
mit
expo
sure
to p
hysic
al/e
moti
onal
stre
ss•
Get n
eede
d su
ppor
t fro
m fa
mily
mem
bers
/fr
iend
s in
your
hyp
erte
nsio
n se
lf-m
anag
emen
t eff
orts
•1.
3: A
ddre
ssin
g w
hat c
an m
ake
hype
rten
sion
man
agem
ent d
ifficu
lt fo
r pati
ents
: gro
up
disc
ussio
n (3
0 m
inut
es)
•Re
ad/c
onsu
lt yo
ur h
yper
tens
ion
info
rmati
on
leafl
et/p
amph
let r
egul
arly
for a
dditi
onal
supp
ort
•Ta
king
you
r pill
s reg
ular
ly•
View
atte
ntive
ly th
e au
diov
isual
s tha
t will
be
mad
e av
aila
ble
to y
ou d
urin
g w
aitin
g tim
e in
cl
inic
•Re
duci
ng sa
lt in
take
• Ad
optin
g a
heal
thy
diet
•Re
ad/c
onsu
lt yo
ur h
yper
tens
ion
info
rmati
on
leafl
et/p
amph
let r
egul
arly
for a
dditi
onal
supp
ort
•St
ayin
g ph
ysic
ally
acti
ve
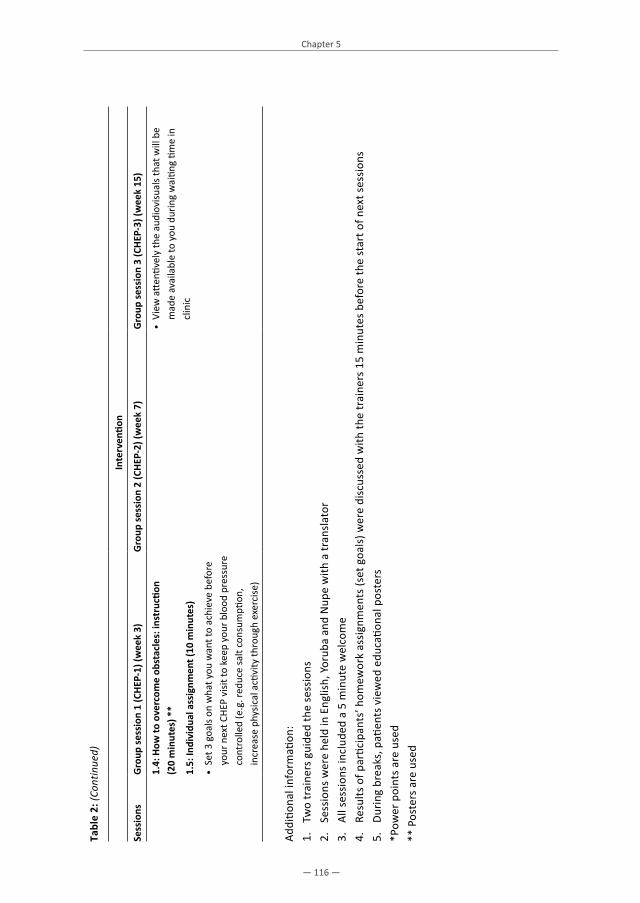
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 116 —
Chapter 5
Tabl
e 2:
(Con
tinue
d)
Inte
rven
tion
Sess
ions
Gro
up se
ssio
n 1
(CHE
P-1)
(wee
k 3)
Gro
up se
ssio
n 2
(CHE
P-2)
(wee
k 7)
Gro
up se
ssio
n 3
(CHE
P-3)
(wee
k 15
)
1.4:
How
to o
verc
ome
obst
acle
s: in
stru
ction
(2
0 m
inut
es) *
*•
View
atte
ntive
ly th
e au
diov
isual
s tha
t will
be
mad
e av
aila
ble
to y
ou d
urin
g w
aitin
g tim
e in
cl
inic
1.5:
Indi
vidu
al a
ssig
nmen
t (10
min
utes
)
• Se
t 3 g
oals
on w
hat y
ou w
ant t
o ac
hiev
e be
fore
yo
ur n
ext C
HEP
visit
to k
eep
your
blo
od p
ress
ure
cont
rolle
d (e
.g. r
educ
e sa
lt co
nsum
ption
, in
crea
se p
hysic
al a
ctivi
ty th
roug
h ex
erci
se)
Addi
tiona
l inf
orm
ation
:1.
Tw
o tr
aine
rs g
uide
d th
e se
ssio
ns2.
Se
ssio
ns w
ere
held
in E
nglis
h, Y
orub
a an
d N
upe
with
a tr
ansl
ator
3.
All s
essi
ons
incl
uded
a 5
min
ute
wel
com
e4.
Re
sults
of p
artic
ipan
ts’ h
omew
ork
assi
gnm
ents
(set
goa
ls) w
ere
disc
usse
d w
ith th
e tr
aine
rs 1
5 m
inut
es b
efor
e th
e st
art o
f nex
t ses
sion
s5.
Du
ring
brea
ks, p
atien
ts v
iew
ed e
duca
tiona
l pos
ters
*Pow
er p
oint
s ar
e us
ed**
Pos
ters
are
use
d

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development of cardiovascular health education program
— 117 —
Translation of findings from formative phase into CHEPCHEP was inspired by the three modules of the culturally adapted hypertension education (CAHE) program developed by Beune et al. (2014). The overall- and specific objectives of the educational sessions of CHEP as listed above, are similar to those of CAHE. In brief CHEP consists of 3 group educational sessions spread 4-6 weeks apart and delivered to groups of 12-15 participants using interactive teaching over a period of 6 months. The first session CHEP 1 focused on increasing patients’ knowledge and awareness about hypertension with regards to the cause, course, consequences, nature, presentations and prevention. The second education session CHEP 2 focused on assisting patients to overcome hypertension self-management difficulties encountered daily and to live positively or cope well with their hypertension. Furthermore, dietary materials collected from the local market were used to guide participants on healthy cooking methods and hypertension friendly diet. In addition to contents of CHEP 2, the third education session CHEP 3 incorporated a practical (physical fitness) exercise session. The training materials used include audiovisuals, information leaflets and pictorial posters. While CHEP 1 lasted 2 hours, CHEP 2 and CHEP 3 each lasted 2 hours, 30 minutes. However, based on information from the formative phase, several changes were made to components of CAHE, so as to adapt the program to the Nigerian socio-cultural context (details in Table 3). Firstly, rather than individual counseling, which was used in CAHE, CHEP used group-interviewing, group-discussions and group-education as the main educational tools. Secondly, to reinforce education about medication use and lifestyle adaptations, CHEP used posters with images, a video film and physical exercise sessions at the clinic’s compound. Instead, CAHE used a booklet containing written information. Given the low literacy level of the priority groups of CHEP, pictorial information and practical exercises were deemed more appropriate. Finally, in order to ensure cultural sensitivity, we designed the form (surface structure) and the specific content (deep structure) of CHEP by using findings from the interviews held during formative phase as illustrated in Table 3. Table 4 provides an overview of the key information that was provided to CHEP trainers about commonly held patient perspectives that may either hinder or enable adherence to treatment. This information was used by the educators to facilitate training on specific topics such as what hypertension is, or what can encourage appropriate medication, dietary or behavioral adaptations.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 118 —
Chapter 5
Tabl
e 3:
Ada
pted
com
pone
nts
of th
e Ca
rdio
vasc
ular
Hea
lth E
duca
tion
prot
ocol
.
Aim
Spec
ific
aim
sEd
ucati
onal
tool
s C
ultu
ral a
dapt
ation
s
Form
Cont
ent
Enha
nce
patie
nts
unde
rsta
ndin
g of
hyp
erte
nsio
n /t
reat
men
t
Expl
ore
patie
nt p
ersp
ectiv
es
on h
yper
tens
ion
and
trea
tmen
t
Grou
p in
terv
iew
ing
to e
licit
vario
us e
xpla
nato
ry m
odel
s,
usin
g op
en q
uesti
ons
Educ
ation
offe
red
in lo
cal
lang
uage
s by
trai
ned
doct
ors/
nurs
es fa
mili
ar w
ith th
e lo
cal
cont
ext
Educ
ator
s are
fam
iliar
with
info
rmati
on o
n w
ays i
n w
hich
pati
ents
in lo
cal s
etting
per
ceiv
e hy
pert
ensio
n an
d tr
eatm
ent,
elic
it ad
ditio
nal
info
rmati
on fr
om tr
aine
es
Info
rm p
atien
ts o
n m
edic
al
pers
pecti
ve o
n hy
pert
ensio
n an
d tr
eatm
ent
Grou
p ed
ucati
on to
info
rm
patie
nts a
bout
med
ical
m
odel
s
Idem
Inst
ructi
on u
ses a
pplic
able
pati
ent
perc
eptio
ns to
ena
ble
educ
ation
to re
-orie
nt
misu
nder
stan
ding
s of h
yper
tens
ion
Agre
e on
key
issu
es a
s re
gard
s to
hype
rten
sion
and
trea
tmen
t
Grou
p di
scus
sion
Idem
Set f
easib
le tr
eatm
ent g
oals
Fill
out p
erso
nal p
atien
t bo
okle
tAs
sist i
llite
rate
pati
ents
to
note
trea
tmen
t goa
ls
Raise
pati
ents
’ aw
aren
ess a
nd
confi
denc
e on
how
they
can
m
anag
e hy
pert
ensio
n in
thei
r da
ily li
ves
Expl
ore
daily
cha
lleng
es
with
med
icati
on u
se, w
eigh
t co
ntro
l, sa
lt us
e an
d ex
erci
se
Grou
p in
terv
iew
sEd
ucati
on o
ffere
d in
loca
l la
ngua
ges b
y tr
aine
d do
ctor
s/nu
rses
fam
iliar
with
the
loca
l co
ntex
t
Educ
ator
s are
fam
iliar
with
and
use
in
form
ation
on
inhi
bito
rs o
f tre
atm
ent
adhe
renc
e in
loca
l setti
ng; i
nfor
mati
on fr
om
trai
nees
is u
sed

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development of cardiovascular health education program
— 119 —
Tabl
e 3:
(Co
ntinu
ed)
Aim
Spec
ific
aim
sEd
ucati
onal
tool
s C
ultu
ral a
dapt
ation
s
Form
Cont
ent
Expl
ore/
prov
ide
exam
ples
of
adeq
uate
way
s to
cope
with
ch
alle
nges
with
med
icati
on
use,
wei
ght c
ontr
ol, s
alt u
se
and
exer
cise
Grou
p in
terv
iew
sid
emEd
ucat
ors a
re fa
mili
ar w
ith in
form
ation
on
way
s for
cop
ing
with
hyp
erte
nsio
n tr
eatm
ent
in lo
cal s
ituati
on; T
rain
ees p
rovi
de a
dditi
onal
in
form
ation
Prov
ide
exam
ples
of
adeq
uate
/fea
sible
way
s fo
r fac
ing
chal
leng
es w
ith
med
icati
on u
se, w
eigh
t co
ntro
l, sa
lt us
e an
d ex
erci
se
Post
ers
Post
ers p
rovi
de p
ictu
res t
o m
ake
them
acc
essib
le to
ill
itera
te p
atien
ts
Post
ers u
se e
xam
ples
of w
ays o
f cop
ing
sugg
este
d by
pati
ents
in fo
rmati
ve p
hase
Vide
o ab
out c
opin
g w
ith li
fe
styl
e m
odifi
catio
nCo
mm
unity
mem
bers
use
d as
ac
tors
/scr
ipt w
riter
s to
allo
w
iden
tifica
tion
Vide
o us
es e
xam
ples
fam
ily si
tuati
ons t
hat
inhi
bit/
faci
litat
e lif
esty
le a
dapt
ation
s
Skill
s dev
elop
men
t for
ad
here
nce
Grou
p ed
ucati
onEd
ucati
onal
sess
ion
refe
rrin
g to
com
mon
ly e
ncou
nter
ed
obst
acle
s
How
to fi
nd su
ppor
t for
con
tinue
d m
edic
ation
ad
here
nce
from
doc
tor a
nd fa
mily
; wha
t are
ch
eap,
loca
lly a
vaila
ble
food
s for
subs
tituti
ng
salt
and
com
posin
g a
heal
thy
diet
; wha
t are
fe
asib
le w
ays f
or d
aily
exe
rcise
; w
hat a
re w
ays f
or u
sing
fam
ily m
embe
rs,
com
mun
ity/r
elig
ious
gro
ups t
o su
ppor
t he
alth
y ea
ting
prac
tices
and
exe
rcise
Exer
cise
cla
sses
at h
ealth
fa
cilit
yU
se o
f com
mon
dai
ly a
ctivi
ties a
s for
ms o
f ex
erci
se
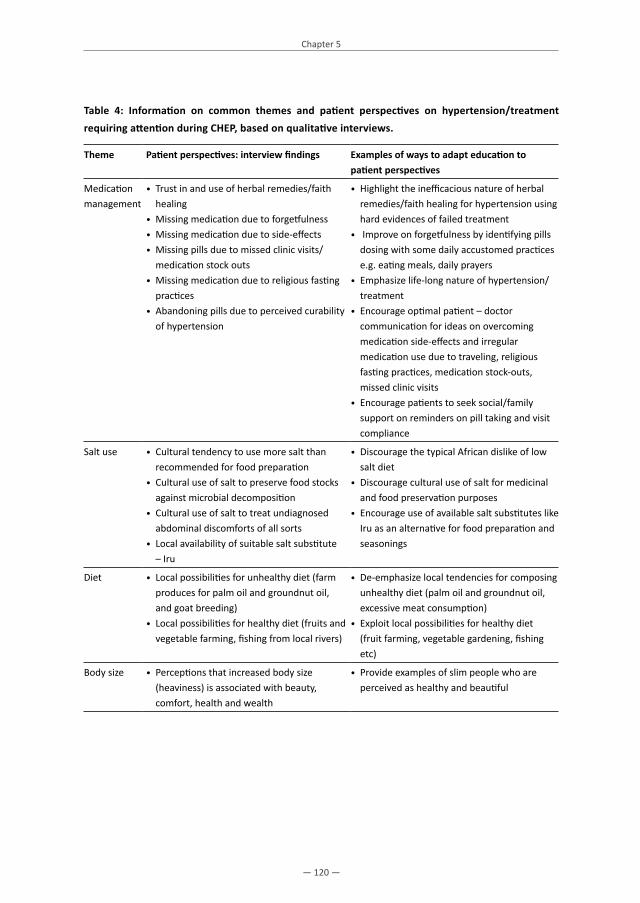
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 120 —
Chapter 5
Table 4: Information on common themes and patient perspectives on hypertension/treatment requiring attention during CHEP, based on qualitative interviews.
Theme Patient perspectives: interview findings Examples of ways to adapt education to patient perspectives
Medication management
• Trust in and use of herbal remedies/faith healing
• Missing medication due to forgetfulness• Missing medication due to side-effects• Missing pills due to missed clinic visits/
medication stock outs• Missing medication due to religious fasting
practices• Abandoning pills due to perceived curability
of hypertension
• Highlight the inefficacious nature of herbal remedies/faith healing for hypertension using hard evidences of failed treatment
• Improve on forgetfulness by identifying pills dosing with some daily accustomed practices e.g. eating meals, daily prayers
• Emphasize life-long nature of hypertension/treatment
• Encourage optimal patient – doctor communication for ideas on overcoming medication side-effects and irregular medication use due to traveling, religious fasting practices, medication stock-outs, missed clinic visits
• Encourage patients to seek social/family support on reminders on pill taking and visit compliance
Salt use • Cultural tendency to use more salt than recommended for food preparation
• Cultural use of salt to preserve food stocks against microbial decomposition
• Cultural use of salt to treat undiagnosed abdominal discomforts of all sorts
• Local availability of suitable salt substitute – Iru
• Discourage the typical African dislike of low salt diet
• Discourage cultural use of salt for medicinal and food preservation purposes
• Encourage use of available salt substitutes like Iru as an alternative for food preparation and seasonings
Diet • Local possibilities for unhealthy diet (farm produces for palm oil and groundnut oil, and goat breeding)
• Local possibilities for healthy diet (fruits and vegetable farming, fishing from local rivers)
• De-emphasize local tendencies for composing unhealthy diet (palm oil and groundnut oil, excessive meat consumption)
• Exploit local possibilities for healthy diet (fruit farming, vegetable gardening, fishing etc)
Body size • Perceptions that increased body size (heaviness) is associated with beauty, comfort, health and wealth
• Provide examples of slim people who are perceived as healthy and beautiful

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development of cardiovascular health education program
— 121 —
Table 4: (Continued)
Theme Patient perspectives: interview findings Examples of ways to adapt education to patient perspectives
Physical fitness
• Lack of interest in conventional physical fitness activities
• Possibility to achieve some level of physical fitness through usual daily physical activities
• Perceived age- and health related barriers for exercise activities
• Preference for simple, practicable, user-friendly exercise regimes
• Enlighten participants on potential positive effect of exercise on blood pressure
• De-emphasize need for conventional regimented physical exercise activities (sports)
• Exploit possibility to achieve physical fitness with usual everyday activities (household chores; religious activities, e.g., clapping, dancing; leisurely activities, e.g. singing, drumming, dancing; work-related activities, e.g., farming, gardening; food preparation activities, e.g. wood axing, yam pounding
• Encourage only practicable and patient-friendly preferred forms of moderate conventional exercise activities such as on the spot jogging, brisk walking and cycling to and from work/farm
• Organize physical fitness sessions at clinic compound
Social and family support
• Inadequate family support from family and environment hampers clinic visits, regular medication use and lifestyle changes
• Good family support with regards to cooperation on dietary prescriptions like low salt diet
• Ample room to improve upon current social support from community leaders and religious organizations in reinforcing regular pills use and healthy behavioral counseling
• Encourage participants to get adequate support from family members in following prescribed treatments
• Invite family members of patients and solicit their supports and cooperation to help patients achieve treatment adherence
• Exploit the possibilities presented through potential roles of community leaders and religious organizations in further spreading the message of hypertension treatment adherence
EvaluationCHEP was implemented for a group of 150 primary care patients who were not sufficiently adherent to treatment recommendations or had a BP above target after they had received guideline-based treatment for at least one year in the context of KSHI. In a previous published report of a pretest/posttest study, we have shown that the developed program was able to strengthen medication adherence, in particular by positively influencing patients’ perceptions of medications (Odusola et al., 2015).

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 122 —
Chapter 5
DISCUSSION
CHEP is an educational program that was designed specifically for primary care patients with hypertension in Nigeria, with the aim to enhance their understanding of hypertension and better disease management. The rationale for developing this program was based on research which has demonstrated that a poor understanding of hypertension or aspects of the treatment may hamper adequate BP control among patients with hypertension, even if they receive affordable guideline-based treatment (Odusola et al., 2015). Rather than relying solely on information from healthcare providers on what patients need to know to manage hypertension, CHEP was developed using a formative approach that also considered data from qualitative interview studies on patients’ perspectives on inhibitors and facilitators for managing hypertension. An existing educational program for patients in Europe, CAHE (Beune, 2014) that combines principles of patient-centeredness and cultural sensitivity, was taken as point of departure in developing CHEP. Notions from Resnicow (1998) on cultural adaptation of health education were employed to adapt the program to fit the patient population in the program area. CHEP provides a framework for cardiovascular health education for patients with hypertension in Nigeria. However, the majority of the population investigated in the formative interview study had health insurance (100%), a low level of education (92%), was of Nupe or Yoruba origin, practicing either Christianity or Islam and did not suffer from hypertension-related complications or co-morbidity (Odusola et al., 2014). Therefore, CHEP may not address concerns of all hypertensive patients in Nigeria, including those from other social strata and ethnic and linguistic groups or patients treated in tertiary care hospitals. Future formative studies are needed to develop and test the CHEP framework among larger populations. Our initial evaluation in a non-controlled study suggests that CHEP can be implemented in rural primary care practices in Nigeria and that it can lead to a decrease in patients’ concerns about medication use and an increase in medication self-efficacy, and, concomitantly, better medication adherence (Odusola et al., 2015). There is a potential to test the impact of CHEP on treatment adherence and BP control in future randomized studies.
ConclusionThis paper provides a detailed description of the development and design of a protocol for cardiovascular health education that is applicable to patients with hypertension in rural Nigeria. The strength of the program is that it was developed based on “patient-centered” and “culturally-sensitive” approaches to health promotion and qualitative interviews with stakeholders. The program and the formative process for developing CHEP we described in this paper offer a framework for developing or adapting similar educational programs for other patient populations with a high risk of CVD in Africa. Even though we have shown that the developed program was able to strengthen medication adherence (Odusola et al., 2015), in the next phase CHEP will need to be evaluated in rigorous controlled studies.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development of cardiovascular health education program
— 123 —
Practice implications Although CHEP was developed in the context of a specific program to improve the quality of cardiovascular care for insured primary care patients with hypertension in Kwara State Nigeria, both the described process for developing CHEP and the protocol itself can be used as a framework for developing and testing cardiovascular health education in other settings in SSA. As CHEP has shown to have a potential to improve hypertension management and adherence to treatment among a selected group of patients, wider implementation and further evaluation in other settings is recommended.
Authors’ Notes Corresponding author: Aina O Odusola, Department of Global Health, Academic Medical Center, University of Amsterdam, Amsterdam and Institute for Global Health and Development, Amsterdam, the Netherlands, Phone: +234(0)8033330214, Fax: +31(20)5669557, Email: [email protected]
AcknowledgementWe thank the Health Insurance Fund (HIF), PharmAccess Foundation, the Kwara State Health Insurance (KSHI) Program and the Netherlands Organization for International Cooperation in Higher Education NUFFIC for supporting the study. A.O. Odusola received a grant (# CF7536/2011) from NUFFIC. The study was funded by HIF. The Funders were not involved in the study design, data collection, analysis and interpretation or reporting. The remaining authors declare that they have no competing interests. Tributes go to late Prof. Joep Lange, who initiated and promoted the project but tragically passed away before the manuscript was completed. We are grateful to all participants for collaborating in the study.
Authors’ contributionsAOO drafted the manuscript, conducted the study and participated in its design. JH, KS, CS and MH originally designed the study. JH and KS provided substantial input and critically revised several drafts of the manuscript. AOO, CS, JH and KS advised in the data collection and analysis during the formative phase. AOO, JH and KS participated in the data analysis. AO, CS, JH, E.J.A.J.B, KS, MH, and TA reviewed the manuscript for intellectual completeness. AO, CS, JH, KS and TA are members of the supervisory board. All authors read and approved the final draft.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 124 —
Chapter 5
REFERENCES
Adeloye D, Basquill C, Aderemi AV, Thompson JY, & Obi FA. (2015). An estimate of the prevalence of hypertension in Nigeria: a systematic review and meta-analysis. Journal of Hypertension, 33(2), 230–242.
Boulware LE, Daumit G L, Frick KD, Minkovitz CS, Lawrence RS, & Powe NR. (2001). An evidence-based review of patient-centered behavioral interventions for hypertension. Am J Prev Med, 21(3), 221–232.
Brown MT, & Bussell JK. (2011). Medication adherence: WHO cares? In Mayo Clinic Proceedings (Vol. 86, pp. 304–314). Elsevier. Retrieved from http://www.sciencedirect.com/science/article/pii/S0025619611600074
De Geest S, & Sabate E. (2003). Adherence to long-term therapies: evidence for action. Eur J Cardiovasc Nurs, 2(4), 323.
Greenhalgh J, & Meadows K. (1999). The effectiveness of the use of patient-based measures of health in routine practice in improving the process and outcomes of patient care: A literature review. Journal of Evaluation in Clinical Practice, 5(4), 401–416.
Gustafsson-Wright E, & Schellekens O. (2013). Achieving universal health coverage in Nigeria one state at a time: a public-private partnership community-based health insurance model. Washington: Brookings Institution. Retrieved from http://www.brookings.edu/research/papers/2013/06/achieving-universal-health-coverage-nigeria-gustafsson-wright
Health Insurance Fund. (n.d.). Retrieved 22 March 2014, from http://www.hifund.org/Hendriks M, Brewster L, Wit F, Bolarinwa OA, Odusola AO, Redekop W. … others. (2011). Cardiovascular
disease prevention in rural Nigeria in the context of a community based health insurance scheme: QUality Improvement Cardiovascular care Kwara-I (QUICK-I). BMC Public Health, 11(1), 186.
Hendriks ME, Wit FW, Roos MT, Brewster LM, Akande TM, de Beer IH, … Van Rooy, G. (2012). Hypertension in sub-Saharan Africa: cross-sectional surveys in four rural and urban communities. PloS One, 7(3), e32638.
Hubley J. (2006). Patient education in the developing world – a discipline comes of age. Patient Education and Counseling, 61(1), 161–164.
Kayima J, Wanyenze RK, Katamba A, Leontsini E, & Nuwaha F. (2013). Hypertension awareness, treatment and control in Africa: a systematic review. BMC Cardiovascular Disorders, 13(1), 54. http://doi.org/10.1186/1471-2261-13-54
Khatib R, Schwalm J-D, Yusuf S, Haynes RB, McKee M, Khan M, & Nieuwlaat R. (2014). Patient and Healthcare Provider Barriers to Hypertension Awareness, Treatment and Follow Up: A Systematic Review and Meta-Analysis of Qualitative and Quantitative Studies. PloS One, 9(1), e84238.
Kleinman A, Eisenberg L, & Good B. (2006). Culture, illness, and care: clinical lessons from anthropologic and cross-cultural research. FOCUS: The Journal of Lifelong Learning in Psychiatry, 4(1), 140–149.
Leventhal H, Diefenbach M, & Leventhal EA. (1992). Illness cognition: using common sense to understand treatment adherence and affect cognition interactions. Cognitive Therapy and Research, 16(2), 143–163.
Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, … Aryee M. (2013). A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. The Lancet, 380(9859), 2224–2260.
Marshall IJ, Wolfe CD, & McKevitt C. (2012). Lay perspectives on hypertension and drug adherence: systematic review of qualitative research. BMJ: British Medical Journal, 345, e3953–e3953.
Mendis S, Abegunde D, Oladapo O, Celletti F, & Nordet P. (2004). Barriers to management of cardiovascular risk in a low-resource setting using hypertension as an entry point. J Hypertens, 22(1), 59–64.
Murray CJ, Lauer JA, Hutubessy RC, Niessen L, Tomijima N, Rodgers A, … Evans DB. (2003). Effectiveness and costs of interventions to lower systolic blood pressure and cholesterol: a global and regional analysis on reduction of cardiovascular-disease risk. The Lancet, 361(9359), 717–725.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Development of cardiovascular health education program
— 125 —
Netto G, Bhopal R, Lederle N, Khatoon J, & Jackson A. (2010). How can health promotion interventions be adapted for minority ethnic communities? Five principles for guiding the development of behavioural interventions. Health Promotion International, 25(2), 248–257.
Odusola AO, Hendriks M, Schultsz C, Bolarinwa OA, Akande T, Osibogun A, … others. (2014). Perceptions of inhibitors and facilitators for adhering to hypertension treatment among insured patients in rural Nigeria: a qualitative study. BMC Health Services Research, 14(1), 624.
Odusola AO, Hendriks M, Schultsz C, Stronks K, Lange J, Osibogun A, … Agbede K. (2011). Development and evaluation of a patient centered cardiovascular health education program for insured patients in rural Nigeria (QUICK-II). BMC Public Health, 11(1), 171.
Odusola AO, Nelissen H, Hendriks M, Schultsz C, Wit F, Bolarinwa OA, … others. (2015). How Group-Based Cardiovascular Health Education Affects Treatment Adherence and Blood Pressure Control among Insured Hypertensive Nigerians: A Pre-Test, Post-Test Study. World Journal of Cardiovascular Diseases, 5(07), 181.
Odusola A, Stronks K, Hendriks M, Schultz C, Akande T, Osibogun A, … Haafkens J. (2015). Enablers and barriers for implementing high-quality hypertension care in a rural primary care setting in Nigeria: perspectives of primary care staff and health insurance managers. Global Health Action, Submitted, 2015.
Osamor PE, & Owumi BE. (2011). Factors associated with treatment compliance in hypertension in southwest Nigeria. Journal of Health, Population, and Nutrition, 29(6), 619.
Resnicow K, Baranowski T, Ahluwalia JS, & Braithwaite RL. (1998). Cultural sensitivity in public health: defined and demystified. Ethnicity & Disease, 9(1), 10–21.
Taylor KD, Adedokun A, Awobusuyi O, Adeniran P, Onyia E, & Ogedegbe G. (2012). Explanatory models of hypertension among Nigerian patients at a University Teaching Hospital. Ethnicity & Health, 17(6), 615–629.
van de Vijver S, Oti S, Addo J, de Graft-Aikins A, & Agyemang C. (2012). Review of community-based interventions for prevention of cardiovascular diseases in low-and middle-income countries. Ethnicity & Health, 17(6), 651–676.
Whitlock EP, Orleans CT, Pender N, & Allan J. (2002). Evaluating primary care behavioral counseling interventions: An evidence-based approach 1 1 The full text of this article is available via AJPM Online at www. ajpm-online. net. American Journal of Preventive Medicine, 22(4), 267–284.
World Health Organization. (2007). Prevention of cardiovascular disease : pocket guidelines for assessment and management of cardiovascular risk : (WHO/ISH cardiovascular risk prediction charts for the African Region). WHO Press. Retrieved from http://apps.who.int/iris/handle/10665/43784
World Health Organization. (2015). WHO | Global status report on noncommunicable diseases 2014. Retrieved 2 August 2015, from http://www.who.int/nmh/publications/ncd-status-report-2014/en/

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Chapter 6
How group-based cardiovascular health education affects treatment adherence and blood pressure control among insured hypertensive Nigerians: A pre-test, post-test study
Odusola AONelissen HHendriks MSchultsz CWit FBolarinwa OAAkande TAgyemang COgedegbe GAgbede KAdenusi POsibogun AStronks KHaafkens J
World Journal of Cardiovascular Diseases, 2015, 5, 181-198

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 128 —
Chapter 6
ABSTRACT
In sub Saharan Africa (SSA), access to affordable hypertension care through health insurance is increasing. But due to poor adherence, hypertension treatment outcomes often remain poor. Patient-centered educational interventions may reverse this trend. Using a pre-test/post-test design, in this study we investigated the effects of a structured cardiovascular health education program (CHEP) on treatment adherence, blood pressure (BP) control and body mass index (BMI) among Nigerian hypertensive patients who received guideline-based care in a rural primary care facility, in the context of a community based health insurance program. Study participants included 149 insured patients with uncontrolled BP and/or poor self-reported medication adherence after 12 months of guideline-based care. All patients received three group-based educational sessions and usual primary care over 6 months. We evaluated changes in self-reported adherence to prescribed medications and behavioral advice (primary outcomes); systolic BP (SBP) and/or diastolic BP (DBP) and BMI (secondary outcomes); and beliefs about hypertension and medications (exploratory outcomes). Outcomes were analyzed with descriptive statistics and regression analysis. 140 patients completed the study (94%). At 6 months, more participants reported high adherence to medications and behavioral advice than at baseline: respectively, 101 (72%) versus 70 (50%), (p < 0.001) and 126 (90%) versus 106 (76%), (p < 0.001). Participants with controlled BP doubled from 34 (24%) to 65 (46%), (p = 0.001). The median SBP and DBP decreased from 129.0 to 122.0 mmHg, (p = 0.002) and from 80.0 to 73.5 mmHg, (p < 0.001), respectively. BMI did not change (p = 0.444). Improved medication adherence was associated with a decrease in medication concerns (p = 0.045) and improved medication self-efficacy (p < 0.001). By positively influencing patient perceptions of medications, CHEP strengthened medication adherence and, consequently, BP reduction among insured hypertensive Nigerians. This educational approach can support cardiovascular disease prevention programs for Africa’s growing hypertensive population.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Evaluation of cardiovascular health education program
— 129 —
INTRODUCTION
Hypertension is a major risk factor for cardiovascular disease (CVD) [1]. The highest prevalence of adults with hypertension has been found in SSA, where a quarter of all premature deaths are due to this condition [1,2]. In Nigeria, 49% of the adults, aged 25 years and older, had hypertension in 2008 [2]. Long-term treatment with behavioral interventions alone, or in combination with drugs can lower BP and, thereby, the risk of developing CVD [1,3-5]. However, as in many other African countries, in Nigeria anti-hypertensive treatment coverage is low and treatment outcomes are poor [6,7]. Previous research in Nigeria and other countries in SSA has indicated that health system interventions such as health insurance coverage, organizational support to facilities and the training of health professionals can facilitate the access to and delivery of high quality CVD prevention care in primary care settings [8-14]. But even if high quality care is available, there is evidence that many patients fail to adhere to the recommended treatment and do not meet their treatment goals [15-17]. For that reason, the World Health Organization has emphasized that any attempt to improve hypertension and cardiovascular care should also address barriers to treatment adherence [18]. Theoretical models of health behavior have proposed that patients and health professionals have different explanatory models or beliefs about health and illness and that beliefs held by patients are important determinants of treatment adherence [19,20]. This has been confirmed by empirical studies of treatment adherence among patients with hypertension [20,21]. Evidence suggests that patient education can be effective in supporting treatment adherence and hypertension self-management, especially if the educational programs pay attention to underlying barriers to adherence such as patients’ beliefs and concerns about the nature of hypertension and the prescribed treatment, medication self-efficacy and specific social, cultural and individual barriers to optimal hypertension management [22-25]. A systematic review of studies on various strategies for improving the quality of primary hypertension care in high income countries concludes that organizational health system changes and patient education have the biggest impact on blood pressure (BP) outcomes [26]. Some recent primary care studies from Nigeria also demonstrate that organizational quality improvement interventions can lead to improved clinical outcomes in hypertensive patients [14,27,28]. However, to date little information is available about the impact of patient education on hypertension management in low resource communities in Nigeria or other countries in SSA. We had the opportunity to investigate this issue in a rural primary care facility in Kwara State Nigeria, where clinical guidelines were introduced in 2010 in order to improve the quality of hypertension management for patients enrolled in a Community Based Health Insurance (CBHI) program. To strengthen this quality improvement program, we implemented a tailored community-based cardiovascular health education program (CHEP) for patients. CHEP was developed and structured on the basis of the theoretical frameworks of Kleinman and Leventhal [19,20], and the content was based on findings from a previous qualitative study on perspectives on hypertension and treatment adherence among hypertensive patients from the local community

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 130 —
Chapter 6
[29]. Because patients in this facility had been offered free guideline-based cardiovascular prevention care, in the context of their health insurance, the setting allowed for a focused analysis of the value of patient education. The aims of this study were to evaluate the effects of CHEP on treatment adherence, BP control and body mass index (BMI) and to explore to what extent the changes that occurred in medication adherence after patients had completed CHEP were related to changes in the underlying determinants of adherence behavior that were addressed during the training (i.e. patients’ perceptions of hypertension, medication, and self-efficacy).
METHODS
The study design has been published previously [30]. This section summarizes the main procedures.
Study Site and ContextThe study was conducted at Ogo Oluwa hospital (OOH) in Bacita, a rural low-income community in Kwara State. OOH was contracted by the Kwara State Health Insurance (KSHI) program to provide primary and limited secondary care to patients who are enrolled in the health insurance plan. Financed by an international organization – the Health Insurance Fund (HIF) [31], the KSHI program was launched in Kwara State in 2007 with the aim to provide subsidized health insurance for low and middle income groups. As part of the insurance company’s quality assurance program, OOH had implemented guidelines and treatment protocols for CVD prevention [4,32,33], and upgraded its diagnostic equipment and medical record system. In a previously reported study, Quality Improvement Cardiovascular care Kwara (QUICK)-I, we evaluated the feasibility and quality of this program [28,34]. The QUICK-I study included 349 insured patients with hypertension and/or diabetes from OOH between June 2010 and January 2011, followed these patients over a period of 12 months and assessed them for health-related and other outcomes, including medication adherence, systolic BP (SBP) and diastolic BP (DBP). Of the 349 included patients 323 completed the study at one year of follow up [28].
Study Design and ParticipantsThe present study, QUICK-II, was an observational one-group pre-test post-test study of 149 patients who had completed the QUICK-I study [30]. QUICK-I patients were recruited for QUICK-II if the following criteria were present at the one-year follow up assessment of QUICK-I: enrolled in KSHI program; registered at OOH; aged ≥ 18 years; diagnosed with hypertension; having uncontrolled BP (SBP ≥ 140 mmHg or DBP ≥ 90 mmHg without co-morbidity – diabetes, renal disease, cardiovascular diseases – or SBP ≥ 130 mmHg or DBP ≥ 80 mmHg with co-morbidity) and/or being non-adherent to behavioral recommendations or prescribed medications (score < 8 on the Morisky Medication Adherence Scale (MMAS-8) [35,36]; and willing to provide informed consent. Pregnant or lactating females were excluded from the study.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Evaluation of cardiovascular health education program
— 131 —
Baseline assessments for QUICK-II patients (T0) were conducted between November 2011 and March 2012, and six-month-follow up assessments (T1) were conducted between April 2012 and September 2012. Between T0 and T1, all included patients were offered cardiovascular health education program (CHEP) counseling, in addition to their regular hypertension care. Two trained research nurses, fluent in local languages, conducted baseline and follow-up assessments of physiological and self-report measures. Questionnaires for assessing self-report measures were designed and piloted in English, and translated into the two dominant local languages (Yoruba and Nupe). Patients received a reminder 2 days before the scheduled study visits. Incurred travel costs were reimbursed if study visits took place outside a patient’s usual clinic days.
Intervention—CHEPThe intervention, CHEP, consisted of: (i) three group-based educational sessions; and (ii) culturally tailored written and audio-visual educational materials (see table, Additional File 1). The content of CHEP was inspired by a hypertension education program that was developed by Beune et al. [23], and results of a previous interview study with hypertensive patients of OOH [29]. All patients were randomly assigned to a group of 12-15 “trainees” which held the same composition throughout the program. The CHEP training sessions took place at OOH, at respectively 2, 6 and 14 weeks after T0. The first session lasted 2 hours and the second and third sessions lasted 2.5 hours each. The training was given by the researcher (AOO) and a trained research nurse. Sessions were held in the languages of choice of the group and interactive training techniques were used in all sessions.
Outcome Measures and Data CollectionPrimary and Secondary OutcomesThe primary outcomes were the proportion of study participants who had improved self-reported adherence to medication and behavioral recommendations at six months past baseline. Medication adherence was assessed with the MMAS-8 [35,36]. The MMAS-8 asks participants 7 “yes” or “no” questions and 1 question that can be answered on a 5-point Likert scale. Low adherence is defined as MMAS-8 scores < 6; medium adherence as scores ranging from 6-to < 8, and high adherence as a score of 8 [36]. We defined improvement in medication adherence as a shift to a higher category of adherence between T0 and T1 (e.g. from low to medium adherence) or as ‘high adherence’ (MMAS-8 score of 8) at both points in time. Adherence to behavioral advice was measured with the question “to what extent do you follow the behavioral advice from your doctor about smoking/nutrition/drinking alcohol/losing weight/physical activity or something else”? Answers were provided on a 4-point Likert scale, (1) never, (2) sometimes, (3) usually or (4) always. We defined improvement in adherence to behavioral recommendations as a shift from lower to a higher category of adherence between T0 and T1 or as high adherence (category 4) at both points in time.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 132 —
Chapter 6
Secondary outcomes were: the proportion of patients who showed an improvement in BP between T0 and T1; and the proportion of patients who showed a decrease in body mass index (BMI) by ≥ 1 unit kg/m2 between T0 and T1. BP was measured three times, 5 minutes apart, with an automated BP monitor (Omron M6 Comfort, OMRON Corporation, Kyoto, Japan), after the patient had been seated for 5 minutes. The second and third readings were averaged to calculate the SBP and DBP. A controlled BP was defined as a SBP of < 140 mmHg and a DBP of < 90 mmHg for patients without co-morbidity, or as SBP < 130 mmHg and DBP < 80 mmHg for patients with co-morbidity. Improvement in BP was defined as a ≥ 10% decrease in SBP and/or DBP between T0 and T1 or having a controlled BP at both T0 and T1. BMI was calculated from measures of the patient’s height and weight. Weight was measured with validated Omron BF 400 weighing scale, and height with a validated Leicester Stadiometer SECA 217. Both measures were taken without the patient wearing shoes and/or heavy clothing. Measurements were recorded to the nearest 0.1 cm (height) and 0.1 kg (weight). Normal weight was defined as a BMI below 25 kg/m2, overweight as a BMI between 25 and 29.9 kg/m2, and obesity as a BMI ≥ 30 kg/m2. Improvement in BMI was defined as a ≥ 1 unit kg/m2 decrease in BMI between T0 and T1 for patients with a baseline BMI ≥ 25 kg/m2.
Other MeasuresThe intervention targeted some determinants of medication adherence: patients’ perceptions of hypertension, medication, and medication self-efficacy. We measured these variables in order to obtain a better understanding of the expected change in primary outcomes. Patients’ perceptions of hypertension were assessed with the well validated Revised Illness Perception Questionnaire (IPQ-R) [37]. The IPQ-R asks participants to provide answers to statements on a 5-point Likert scale (1 = “strongly disagree”, 5 = “strongly agree”) on 9 dimensions of illness (hypertension), 7 of which were used in this study. Scores are totaled and overall score represents the degree to which hypertension is perceived as threatening or benign. High scores on the dimensions 1) emotional representations, 2) timeline chronic, 3) consequences, 4) timeline cyclical represent strongly held beliefs about 1) number of symptoms attributed to hypertension, 2) its chronicity, 3) its negative consequences and 4) its cyclical nature. High scores on the personal control, treatment control and illness coherence dimensions represent positive beliefs about the controllability of hypertension and a personal understanding of the illness. Patients’ beliefs about medicines were assessed with the Beliefs about Medicines Questionnaire (BMQ) [38]. BMQ is a well validated 18-item tool that consists of two sections. In this study we used only section 1 (BMQ-specific) which consists of two 5-item subscales. The first scale (Specific-necessity) assesses hypertensive patients’ beliefs about how necessary it is to take medications in order to improve/maintain their health. The second scale (Specific-concern) assesses respondents’ “concerns” about potential adverse consequences from taking their medications. BMQ uses 5-point Likert questions ranging from 1 = “strongly disagree” to 5 = “strongly agree”. The respondents’

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Evaluation of cardiovascular health education program
— 133 —
scores on each item are totaled. Higher scores indicate stronger beliefs about the necessity of taking medicines and concerns about adverse effects of medications. Medication self-efficacy was measured with the shortened Medication Adherence Self-Efficacy Scale (MASES-R) [39,40]. This 13-item scale assesses the patients’ beliefs in their confidence to adhere to prescribed anti-hypertensive medications under a variety of challenging situations, such as when busy at home, when there are symptoms, while traveling etc. Items are scored using a 4-point Likert scale, (1 = “not at all sure”, 4 = “extremely sure”). The scores on all items are totaled. Higher scores indicate higher self-reported medication adherence self-efficacy. In order to collect additional information about self-reported health behaviors, participants were asked questions about physical activity, dietary salt intake, alcohol and tobacco use. Daily moderate physical activity was defined as performing sports or exercise (e.g. walking to the market, performing heavy work) in addition to one’s normal daily activities such as dressing, washing and walking. Salt use was defined as adding any salt (a little/a lot) when cooking or when eating food. Alcohol use was defined as any self-reported use of alcohol daily, weekly or monthly. Tobacco use is self-reported use of any tobacco products, such as cigarettes, cigars or pipes. Information about patients’ socio-demographic characteristics was obtained from the QUICK-I study.
Statistical AnalysisData were analyzed using STATA, version 12.0 (StataCorp LP, College Station, Texas, USA). Adherence to medications and behavioral advice, BP control and BMI were calculated using descriptive statistics. Changes between T0 and T1 were compared using the Wilcoxon signed rank test for categorical and continuous variables and the McNemar exact test for binary variables. Changes in illness perceptions, medication beliefs and self-efficacy between T0 and T1 were compared using the Wilcoxon signed rank test. A first multivariable logistic regression analysis was performed to evaluate the association between improvement in BP between T0 and T1 (secondary outcome) and medication and behavioral adherence (primary outcome). A second multivariable logistic regression analysis was performed to explore the associations between improvement in adherence to medications between T0 and T1 (primary outcome) and illness perceptions, medication beliefs, and self-efficacy. The illness perceptions, medication beliefs and self-efficacy variables showing a p-value below 0.2 in a univariate analysis were included in the multivariate model. In both models no control variables (i.e. age, gender, level of education, ethnicity, co-morbidities, etc.) were included since no substantial change was expected in these variables during the study period. The odds ratios (OR), 95% confidence interval (CI) and p-values were reported.To evaluate the association between change in SBP and DBP (between T0 and T1) and medication and behavioral adherence, two multivariable linear regression analyses were performed. Coefficients (in mmHg), 95% CI and p-values were reported and similar to the logistic regression models, no control variables were included in the analyses.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 134 —
Chapter 6
Endline measurements in QUICK-I were used to determine patients eligibility for QUICK-II (uncontrolled BP and/or non-adherence to medications). On average, there was a gap of 4.7 months between the endline QUICK-I assessment and the baseline QUICK-II assessment (T0). During this period, 33% (n = 49) of the eligible QUICK-II patients had improved in BP and/or medication adherence (see Additional file 2). The number of patients with a controlled BP at T0 was high (59.7%), resulting in a low power for the first multivariable regression analysis. In the original design of the study [30], our definitions of the secondary outcome measure, BP improvement was very strict (a ≥ 10% decrease in SBP and/or DBP between T0 and T1 or having a controlled BP at both T0 and T1). We believe, however, that any BP decrease can be favorable in the studied participants. For this reason, the research group decided to measure the secondary outcome also by assessing the BP improvement continuously as the delta of SBP and DBP between T0 and T1 and to perform the two multivariable linear regression analyses mentioned above.
EthicsEthical approval for the study was obtained on 30th March, 2010 from the Ethics committee of the University of Ilorin Teaching Hospital, Kwara State (Ref: UITH/CAT/189/13/13). Patients were adequately informed about the study and informed consents were taken prior to commencement of study by signature or fingerprint.
RESULTS
Patient CharacteristicsThe QUICK-II cohort consisted of 149 patients. Participant flow is shown in Figure 1. Out of 323 patients who completed QUICK-I study 156 were referred to QUICK-II, 7 of whom were excluded because they had diabetes but not hypertension. The remaining 149 patients were included in QUICK-II. For different reasons, nine patients (6%) were lost to follow-up. Of those who completed the study (n = 140), 132 (94%) attended all three CHEP sessions. Table 1 shows participants’ socio-demographic characteristics. The median age was 56.5 years (IQR: 49.4-65.5), 63 (42%) were males and 85 (57%) were not formally educated.
Changes in Adherence to Medication and Behavioral Recommendations, BP and BMIAs Table 2 shows, medication adherence improved during the study period (p < 0.001). As compared to T0, more patients reported a high level of medication adherence (MMAS-8 = 8) at a T1: N = 70 (50%) versus N = 101 (72%). A similar pattern was observed for adherence to behavioral

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Evaluation of cardiovascular health education program
— 135 —
Figure 1: Flow of QUICK-II study participants.
Table 1: Characteristics of study participants (N = 149).
Characteristics N (%)
Male, n (%) 63 (42.3)
Age in years, median (IQR) 56.5 (49.4-65.5)
Educational level attained, n (%)
No school at all 85 (57.0)
<Primary 3 (2.0)
Primary 33 (22.1)
Secondary 12 (8.1)
Tertiary 16 (10.7)
Employment status, n (%)
Farmer/fisherman 36 (24.2)
Trader 59 (39.6)
No paid job 23 (15.4)
Other 31 (20.8)

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 136 —
Chapter 6
Table 1: (Continued)
Characteristics N (%)
Marital status, n (%)
Married 133 (89.3)
Widowed 16 (10.7)
Religion, n (%)
Muslim 80 (53.7)
Christian 69 (46.3)
Ethnicity, n (%)
Nupe 60 (40.3)
Yoruba 67 (45.0)
Igbo 10 (6.7)
Other 12 (8.1)
Household size, median (IQR)* 5.0 (3.0-6.0)
Co-morbidities**, n (%)
None 121 (81.2)
Diabetes 19 (12.8)
CVD 4 (2.7)
Renal disease 1 (0.7)
Two or three co-morbidities 4 (2.7)
Start anti-hypertensive treatment, n (%)
< 1.5 year 49 (32.9)
> 1.5 year 100 (67.1)
Number of prescribed antihypertensive pills per day**, n (%)***
<= 4 pills 71 (50.8)
5-6 pills 34 (24.2)
>= 7 pills 35 (25.0)
Travel time to the clinic during hypertension visits (in minutes), median (IQR)
14.0 (9.8-29.0)
*n = 147; Note: Characteristics are taken at baseline QUICK-I. Age is newly calculated using the date of QUICK-II baseline assessment and the date of birth recorded in QUICK-I; **Based on end-line QUICK-I assessment; ***n = 140.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Evaluation of cardiovascular health education program
— 137 —
Table 2: Changes in adherence to medications and behavioral advice, BP and BMI between baseline and endline.
Measures Baseline (N = 140)
Endline (N = 140)
p-value (baseline vs endline)
Adherence to medication (Morisky), n (%) < 0.001
Low adherence (< 6) 31 (22.1) 16 (11.4)
Medium adherence (6-7.9) 39 (27.9) 23 (16.4)
High adherence (= 8) 70 (50.0) 101 (72.1)
Adherent to behavioral advices, n (%) 106 (75.7) 126 (90.0) < 0.001
Alcohol use, n (%) 8 (5.7) 3 (2.1) 0.063
Tobacco use, n (%) 6 (4.3) 1 (0.7) 0.125
Moderate physical activity, n (%) 98 (70.0) 124 (89.2)* < 0.001
Salt use, n (%) 72 (51.8)* 72 (51.4) 1.000
Fully adherent to medication and behavioral advice, n (%)
58 (41.4) 94 (67.1) < 0.001
Systolic BP, median (IQR) 129.0 (118.3-147.3) 122.0 (108.0-138.0) < 0.001
Diastolic BP, median (IQR) 80.0 (71.3-87.8) 73.5 (65.0-85.0) < 0.001
Hypertension classification (JNC7), n (%) <0.001
Normal (SBP < 120 and DBP < 80) 34 (24.3) 65 (46.4)
Pre-hypertension (SBP 120-139 or DBP 80- 89)
57 (40.7) 40 (28.6)
Stage 1 hypertension (SBP 140-159 or DBP 90-99)
30 (21.4) 24 (17.1)
Stage 2 hypertension (SBP ≥ 160 or DBP ≥ 100)
19 (13.6) 11 (7.9)
Body Mass Index, median (IQR) 25.1 (22.2-29.3) 24.9 (22.2-29.4) 0.444
Body Mass Index, n (%) 0.739
Normal weight (< 25) 69 (49.3) 71 (50.7)
Overweight (25-29.9) 43 (30.7) 40 (28.6)
Obesity (≥ 30) 28 (20.0) 29 (20.7)
BP, blood pressure; SBP, systolic blood pressure; DBP, diastolic blood pressure. *n = 139.
recommendations; the proportion of patients who reported to always adhere to behavioral advice increased from 106 (76%) at T0 to 126 (90%) at T1 (p < 0.001). Median SBP and DBP levels dropped significantly from 129.0 mmHg (IQR: 118.3-147.3) to 122.0 mmHg (IQR: 108.0-138.0) (p < 0.001) and from 80.0 mmHg (IQR: 71.3-87.8) to 73.5 mmHg (IQR: 65.0-85.0) (p < 0.001), respectively. No significant change was found for BMI (p = 0.444). However, more participants reported engaging in moderate physical activity for 30 or more minutes a day, on 3 or more days a week at T1: 124 (89%) versus 98 (70%) at T0 (p < 0.001). No statistically significant changes were observed in dietary salt intake, smoking or alcohol consumption between T0 and T1.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 138 —
Chapter 6
Improvement in Treatment Adherence Associated with Improvement in BPAlthough trends were positive, no statistically significant associations was observed between BP improvement and changes in medication adherence (OR = 1.55, p = 0.351) and adherence to behavioral recommendations (OR = 1.93, p = 0.327) during the study period (Table 3). But when using our second definition of BP improvement (Table 4), improvement in medication adherence during the study was associated with a 9.2 mmHg (p = 0.038) reduction in SBP and a 6.1 mmHg (p = 0.027) reduction in DBP. The improvement in adherence to behavioral recommendations was not associated with decrease in BP (SBP: p = 0.214; DBP: p = 0.318). Included in the definition of improvements in medication adherence are the patients that remained adherent at T0 and T1. In this subgroup we observed no association between medication adherence and decrease in SBP (p = 0.610) and DBP (p = 0.820) (results not shown).
Table 3: Association between treatment adherence and improvement in BP at six months; multivariable logistic regression models.
Measures Improvement in BP*, n (%) (N = 140)
OR (95% CI) p-value
Medication adherence**
Ref: Did not improve at six months 21 (15.0) 1.00
Improved at six months 87 (62.1) 1.55 (0.62-3.86) 0.351
Behavioral adherence
Ref: Did not improve at six months 7 (5.0) 1.00
Improved at six months 101 (72.1) 1.93 (0.52-7.15) 0.327
*Improvement in blood pressure (BP) is defined as having BP on target at endline or a > 10% decline in BP at endline compared to baseline; **Improvement in adherence to medication/behavioral advice is defined as having moved to a higher category of adherence between T0 and T1, or as having remained in the highest category of adherence at both time points.
Table 4: Association between treatment adherence and improvement in BP at six months; multivariable linear regression model.
Measures All respondents (N = 140)
Coef. (95% CI) p-value
1. Systolic BP change
Improved medication adherence* -9.2 (-17.9 to -0.5) 0.038
Improved behavioral adherence -8.4 (-21.6 to 4.9) 0.214
2. Diastolic BP change
Improved medication adherence -6.1 (-11.5 to -0.7) 0.027
Improved behavioral adherence -4.2 (-12.4 to 4.1) 0.318
*Improved adherence to medication/behavioral advice is defined as having moved to a higher category of adherence between T0 and T1, or as having remained in the highest category of adherence at both time points.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Evaluation of cardiovascular health education program
— 139 —
Illness Perceptions, Medication Beliefs and Self-Efficacy and Medication AdherenceAs intended by CHEP, statistically significant differences between T0 and T1 were observed in some of the illness perception variables, namely for the dimensions timeline chronic (p < 0.001), consequences (p < 0.001), timeline cyclical (p = 0.001) and emotional representations (p < 0.001) (Table 5). Similarly, statistically significant changes between T0 and T1 were observed with respect to participants’ medication self-efficacy (p < 0.001), beliefs about the necessity of medications (p < 0.001), and their concerns about adverse effects of medications (p = 0.002) (Table 5). An improvement in medication adherence during the study period was associated with an increase in medication self-efficacy (OR = 5.99, p < 0.001) and a decrease in patients’ concerns about adverse effects of medications (OR = 2.57, p = 0.045) (Table 6). The association between improved adherence to behavioral advice and illness perceptions, medication beliefs and self-efficacy could not be assessed because of the high number of participants who reported a high adherence to behavioral advice at T0 (76%) and T1 (89%), (Table 2). Furthermore, in the multivariate analysis, the most important determinants of the improvements in medication adherence (directly), and BP control (indirectly) were changes in perceived medication self-efficacy (OR = 5.99, p < 0.001); concerns about medications (OR = 2.57, p = 0.045); and personal control (OR = 0.45, p = 0.092), although the latter association was not statistically significant.
Table 5: Changes in illness perceptions, medication self-efficacy and beliefs about medicines between baseline and endline.
Measures Baseline (N = 140) median (IQR)
Endline (N = 140) median (IQR)
p-value (baseline vs endline)
Min-max
Illness perceptions (IPQ)
Timeline chronic 2.6 (2.3-3.0) 3.0 (2.5-4.0) <0.001 (1.0-5.0)
Consequences 2. (1.4-3.0) 1.4 (1.0-2.2) <0.001 (1.0-5.0)
Personal control 2.0 (1.7-2.7) 2.0 (1.7-3.0) 0.166 (1.0-5.0)
Treatment control 4.3 (4.0-4.7) 4.7 (4.0-5.0) 0.080 (1.0-5.0)
Illness coherence 3.0 (1.0-4.0)* 3.0 (1.0-4.0) 0.179 (1.0-5.0)
Timeline cyclical 3.0 (3.0-3.5) 3.5 (3.0-4.5) 0.001 (1.0-5.0)
Emotional representations 2.5(1.8-3.6) 1.8 (1.0-3.3) <0.001 (1.0-5.0)
Self-efficacy medication (MASES-R) 3.8 (3.4-4.0) 4.0 (3.8-4.0) <0.001 (1.0-4.0)
Beliefs about medication (BMQ)
Necessity 20.0 (17.0-23.0) 23.0 (20.0-25.0) <0.001 (5.0-25.0)
Concern 10.0 (9.0-14.0) 9.0 (7.0-13.0) 0.002 (5.0-25.0)
*n = 139.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 140 —
Chapter 6
Table 6: Associations between changes in IPQ, MASES-R, BMQ, and improvement in medication adherence; multivariable logistic regression models.
Improvement in medication adherence, n (%)
(N = 140)
OR 95% CI p-value
Illness perceptions (IPQ)
Consequences
Ref: decrease + no change (low + med) 84 (60.0) 1.00
Increase + no change (high) 26 (18.6) 0.83 (0.29-2.38) 0.728
Personal control
Ref: decrease + no change (low + med) 59 (42.1) 1.00
Increase + no change (high) 51 (36.4) 0.45 (0.17-1.14) 0.092
Emotional representations
Ref: Increase + no change (med + high) 31 (22.1) 1.00
Decrease + no change (low) 79 (56.4) 1.65 (0.60-4.55) 0.335
Self-efficacy medication (MASES-R)
Ref: decrease + no change (low + med) 13 (9.3) 1.00
Increase + no change (high) 97 (69.3) 5.99 (2.19-16.37) < 0.001
Beliefs about medicine (BMQ)
Concern
Ref: Increase + no change (med + high) 37 (26.4) 1.00
Decrease + no change (low) 73 (52.1) 2.57 (1.02-6.51) 0.045
DISCUSSION
Our study demonstrated that a tailored group-based cardiovascular health education program strengthened guideline-based CVD prevention care among hypertensive patients from primary care clinic in a rural community in Nigeria. The patients in question did not adhere to treatment recommendations or had a blood pressure outside the normal range after they had received guideline-based care alone for one year. We observed that 89% of the patients completed all educational sessions. Studies of similar educational interventions in primary care settings in Europe and the USA recorded lower attendance rates, namely 79% and 58% [23,41]. The high attendance rate in this study suggests that CHEP responded to patients’ needs, which is plausible in the light of a previous qualitative study that was conducted in the area [29]. Secondly, we observed that patients who attended CHEP showed improvements in adherence to medication and behavioral recommendations. These improvements may, of course, simply be explained by the fact that patients knew that their hypertension management and adherence was monitored in this study (Hawthorn effect). However, our study provides several indications that the

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Evaluation of cardiovascular health education program
— 141 —
intervention itself has contributed to the improvement in medication adherence. The education program was specifically designed to address previously identified contextual or behavioral barriers to treatment adherence, including patients’ perceptions about hypertension and the treatment (see Additional File 1). We found that improved medication adherence after CHEP was positively associated with improved medication self-efficacy (MASES-R) and with a reduction of concerns about medications as measured by the BMQ. It is unlikely that changes in these underlying determinants of adherence to hypertension treatment [42-49] would have occurred without the educational intervention. More patients had begun to engage in moderate physical activity during the study period. This improvement may be explained by the fact that CHEP addressed cultural barriers to physical exercise in the community and suggested opportunities for exercise that are part of people’s usual everyday activities, such as yam pounding, drawing water from the well, walking, dancing, clapping, fishing or farming. However, for salt use and other behavioral risk factors for CVD no improvements were observed despite the fact that possibilities for changing these behaviors were also specifically addressed during CHEP. Anthropological studies have indicated that dietary practices are particularly difficult to change as they are an important component of one’s culture and cultural identity [50]. Changes in dietary behaviour may need more specific approaches than CHEP could offer in three sessions [51-53]. Third, we did not find the expected > 10% decline in SBP/DBD. However, we observed that the median SBP declined with 9.2 mmHg (p < 0.001) and the median DBP with 6.1 mmHg (p < 0.001). Moreover, after the study period, more patients could be classified as having a BP within the normal range according to the JNC7 hypertension classification system. These results are, as such, clinically relevant [54]. Moreover, we found that the decline of the median BP levels was associated with an improvement in medication adherence. To our knowledge this is one of the first studies that analyzed the potential impact of hypertension education in the context of a CBHI program that aims to improve the quality of CVD prevention in low resource primary care setting in Africa. The study is also unique in its explicit description of the educational intervention and its potential replicability by healthcare providers and researchers in other settings (Additional File 1).
LimitationsYet, this study has several limitations, the most important being the lack of a control group. Although, we observed significant improvements in outcome measures, the lack of a control group limits the possibility of drawing firm conclusions as to the causality of the measured effects. The link between CHEP and behavioral and clinical outcomes should be further tested in randomized controlled trials or prospective studies. Medication adherence (MMAS-8) and behavioral adherence were measured through self-report scales, and answers could have been influenced by social desirability. Nevertheless, MMAS-8 is a validated, reliable, simple, and low-cost instrument that has been successfully used to estimate medication adherence in many previous studies involving hypertensive patients [55-59], including low-income patients of African origin [36]. Furthermore,

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 142 —
Chapter 6
due to the relatively small sample size, only a limited number of variables could be taken into consideration within our multivariate analysis. We have opted for the inclusion of variables that refer to behavioral determinants of adherence. The inclusion of additional variables such as the type or the number of medications used might have strengthened this study. In addition, the limited sample size also made it impossible to conduct sub-group analyses, for instance for patients with different levels of formal school education or for those with different levels of treatment adherence at the start of the study. Furthermore, to evaluate the long-term effect of CHEP longer follow-up studies are needed. Finally, a recent study from Nigeria reported that the adherence level was higher among hypertensive patients attending specialized clinics compared to those attending general outpatient clinics, despite the former’s use of more medications [60]. In future studies evaluating CHEP, attention should be given to the influence of the context in which care is provided and to the type and the number of medications patients are being prescribed. CHEP was designed to meet the specific needs of the study population. Some of the culturally specific issues that were addressed by CHEP may not be relevant to patients who live in other socio-cultural settings. Yet the description of CHEP provides general outlines for structuring and providing patient education, which makes it possible to adapt the specific contents to the needs of other patient populations. It should be realized, however, that the patients in our study had access to free primary care through health insurance. The findings might therefore not automatically be generalizable to the broader group of (mostly uninsured) hypertensive patients in the larger hypertensive population in Africa or to those who are treated at secondary and tertiary levels of care. Finally, the study was conducted in a health care facility that had participated in a CVD quality improvement program (for over a year) that was subsidized by a CBHI program. It is likely that the usual care that was being provided in this facility is better than that in other facilities. Consequently, the effects of CHEP might have been greater if we had conducted the study in a common primary care setting in Nigeria or elsewhere in Africa.
Implication for Practice and Further ResearchThis study found that CHEP responds to patients’ needs and that it can be a useful component of the primary care management of hypertension in low resource communities in SSA, if it is combined with appropriate pharmaceutical treatment. Further (controlled) studies are needed to confirm or refute these findings. This type of health education can be delivered (efficiently) by nurses and other trained health workers, and not just by physicians. The modules of the cardiovascular health education program (CHEP) are well described (Additional File 1) and can serve as a (useful) framework for further development and evaluation of educational interventions for patients who are at risk of developing CVD, and particularly for those living in disadvantaged communities in SSA.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Evaluation of cardiovascular health education program
— 143 —
ConclusionThis study suggests that the evaluated education program (CHEP) improved adherence to medications, followed by an increase in BP control among insured hypertensive patients in rural Nigeria. At the end of the study, more participants reported high adherence to medications and behavioral advice than at baseline: respectively, 101 (72%) versus 70 (50%), (p < 0.001) and 126 (90%) versus 106 (76%), (p < 0.001). Participants with controlled BP doubled from 34 (24%) to 65 (46%), (p = 0.001). The median SBP and DBP decreased from 129.0 to 122.0 mmHg, (p = 0.002) and from 80.0 to 73.5 mmHg, (p < 0.001), respectively. BMI did not change (p = 0.444). Improved medication adherence was associated with a decrease in medication concerns (p = 0.045) and improved medication self-efficacy (p < 0.001). Making such programs available to affected populations in SSA has the potential to help reduce burden of cardiovascular diseases and associated mortality.
Competing InterestsA.O.: Odusola received a grant (# CF7536/2011) from NUFFIC. The study was funded by Health Insurance Fund. The Fund was not involved in the study design, data collection, analysis, and interpretation or reporting of the data. The remaining authors declare that they have no competing interests.
Author ContributionsAOO drafted the manuscript, conducted the study and participated in the design, reporting, analysis and revision. JH, JL, KS and MH participated in the original study design. JH and KS made substantial revision of several drafts of the manuscript. HN conducted the statistical analyses with critical contributions from FW. AOO drafted the education program with critical contributions from JH. AO, CA, CS, FW, GO, HN, JH, KS, MH, OAB and TA reviewed the manuscript critically. KA and PA provided vital logistic supports. CS, JH and KS reviewed the data collection and management procedures. AO, TA, CS, JH, and KS are members of the supervisory board. All authors read and approved the final draft.
AcknowledgementsSpecial tributes go to late Prof. Joep Lange, who tragically passed away before the manuscript had been finished. He initiated and promoted an enabling environment for the study and related projects. We thank the Medical Director and staff of Ogo Oluwa hospital for facilitating a successful data collection. We are grateful to all participants for collaboration in the study. We thank HIF, Pharm Access Foundation, KSHI and NUFFIC for supporting the study.
Additional FilesAdditional File 1: (1) CSV; Table; Cardiovascular Health Education Program (CHEP); Overview of group-based Cardiovascular Health Education Program used in QUICK-II study; (2) CSV; Table; Changes in inclusion characteristics of QUICK-II participants between endline QUICK-I and baseline QUICK-II assessments.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 144 —
Chapter 6
REFERENCES
1. WHO (2011) Global Atlas on Cardiovascular Disease Prevention and Control. http://www.who.int/cardiovascular_diseases/publications/atlas_cvd/en/
2. Alwan, A. and WHO (2011) Global Status Report on Non-Communicable Diseases 2010. http://whqlibdoc.who.int/publications/2011/9789240
3. WHO and Others (2007) Prevention of Cardiovascular Disease: Pocket Guidelines for Assessment and Management of Cardiovascular Risk (WHO/ISH Cardiovascular Risk Prediction Charts for the European Region).
4. Mendis S, Lindholm LH, Mancia G, Whitworth J, Alderman M, Lim S, et al. (2007) World Health Organization (WHO) and International Society of Hypertension (ISH) Risk Prediction Charts: Assessment of Cardiovascular Risk for Prevention and Control of Cardiovascular Disease in Low and Middle-Income Countries. Journal of Hypertension, 25,1578-1582. http://dx.doi.org/10.1097/HJH.0b013e3282861fd3
5. Lewington S, Clarke R, Qizilbash N, Peto R. and Collins R. (2002) Prospective Studies Collaboration: Age-Spe- cific Relevance of Usual Blood Pressure to Vascular Mortality: A Meta-Analysis of Individual Data for One Million Adults in 61 Prospective Studies. Lancet, 360, 1903-1913. http://dx.doi.org/10.1016/S0140-6736(02)11911-8Kayima, J., Wanyenze, R.K., Katamba, A., Leontsini, E. and Nuwaha, F. (2013) Hypertension Awareness, Treatment and Control in Africa: A Systematic Review. BMC Cardiovascular Disorders, 13,1-11.
6. http://dx.doi.org/10.1186/1471-2261-13-547. Ogah OS, Okpechi I, Chukwuonye II, Akinyemi JO, Onwubere BJ, Falase AO, et al. (2012) Blood Pressure,
Prevalence of Hypertension and Hypertension Related Complications in Nigerian Africans: A Review. World Journal of Cardiology, 4,327-340. http://dx.doi.org/10.4330/wjc.v4.i12.327
8. Beaglehole R, Epping-Jordan J, Patel V, Chopra M, Ebrahim S, Kidd, M, et al. (2008) Improving the Prevention and Management of Chronic Disease in Low-Income and Middle-Income Countries: A Priority for Primary Health Care. The Lancet, 372,940-949. http://dx.doi.org/10.1016/S0140-6736(08)61404-X
9. Mendis S, Abegunde D, Oladapo O, Celletti F. and Nordet P. (2004) Barriers to Management of Cardiovascular Risk in a Low-Resource Setting Using Hypertension as an Entry Point. Journal of Hypertension, 22,59-64. http://dx.doi.org/10.1097/00004872-200401000-00013
10. Maimaris W, Paty J, Perel P, Legido-Quigley H, Balabanova D, Nieuwlaat R, et al. (2013) The Influence of Health Systems on Hypertension Awareness, Treatment, and Control: A Systematic Literature Review. PLoS Medicine, 10,e1001490. http://dx.doi.org/10.1371/journal.pmed.1001490
11. Adebisi OO and Samali A. (2013) Poverty and Hypertension in Nigerian Adults: A Barrier to Its Control and Treatment: A Review. Unique Research Journals, 1,013-014.
12. Mwaura JW and Pongpanich S. (2012) Access to Health Care: The Role of a Community Based Health Insurance in Kenya. The Pan African Medical Journal, 12,35.
13. Onoka C, Onwujekwe O, Uzochukwu B. and Ezumah N. (2013) Promoting Universal Financial Protection: Con- straints and Enabling Factors in Scaling-Up Coverage with Social Health Insurance in Nigeria. Health Research Policy and Systems, 11,20. http://dx.doi.org/10.1186/1478-4505-11-20
14. Hendriks ME, Wit FW, Akande TM, Kramer B, Osagbemi GK, Tanović Z, et al. (2014) Effect of Health Insurance and Facility Quality Improvement on Blood Pressure in Adults With Hypertension in Nigeria A Population-Based Study. JAMA Internal Medicine, 174,555-563. http://dx.doi.org/10.1001/jamainternmed.2013.14458
15. Krousel-Wood M, Thomas S, Muntner P. and Morisky D. (2004) Medication Adherence: A Key Factor
in Achieving Blood Pressure Control and Good Clinical Outcomes in Hypertensive Patients. Current
Opinion in Cardiology, 19,357-362. http://dx.doi.org/10.1097/01.hco.0000126978.03828.9e

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Evaluation of cardiovascular health education program
— 145 —
16. Bowry AD, Shrank WH, Lee JL, Stedman M. and Choudhry NK. (2011) A Systematic Review of Adherence to Cardiovascular Medications in Resource-Limited Settings. Journal of General Internal Medicine, 26, 1479-1491. http://dx.doi.org/10.1007/s11606-011-1825-3
17. AlGurair S, Hughes C, Simpson S. and Guirguis L. (2012) A Systematic Review of Patient Self-Reported Barriers of Adherence to Antihypertensive Medication Using the World Health Organization Multidimensional Adherence Model. The Journal of Clinical Hypertension, 14,877-886. http://dx.doi.org/10.1111/j.1751-7176.2012.00699.x
18. De Geest S. and Sabate E. (2003) Adherence to Long-Term Therapies: Evidence for Action. European Journal of Cardiovascular Nursing, 2,323. http://dx.doi.org/10.1016/S1474-5151(03)00091-4
19. Kleinman A, Eisenberg L. and Good B. (2006) Culture, Illness, and Care: Clinical Lessons from Anthropologic and Cross-Cultural Research. FOCS, 4,140-149. http://dx.doi.org/10.1176/foc.4.1.140
20. Leventhal H, Brissette I. and Leventhal EA. (2003) The Common-Sense Model of Self-Regulation of Health and Illness. The Self-Regulation of Health and Illness Behaviour, 1,42-65.
21. Marshall IJ, Wolfe CD. and McKevitt C. (2012) Lay Perspectives on Hypertension and Drug Adherence: Systematic Review of Qualitative Research. BMJ, 345,e3953-e3953. http://dx.doi.org/10.1136/bmj.e3953
22. Houston TK, Allison JJ, Sussman M, Horn W, Holt CL, Trobaugh J, et al. (2011) Culturally Appropriate Storytelling to Improve Blood Pressure: A Randomized Trial. Annals of Internal Medicine, 154,77-84. http://dx.doi.org/10.7326/0003-4819-154-2-201101180-00004
23. Beune EJ, van Charante EPM, Beem L, Mohrs J, Agyemang CO, Ogedegbe G, et al. (2014) Culturally Adapted Hypertension Education (CAHE) to Improve Blood Pressure Control and Treatment Adherence in Patients of African Origin with Uncontrolled Hypertension: Cluster-Randomized Trial. PloS ONE, 9,e90103. http://dx.doi.org/10.1371/journal.pone.0090103
24. González-fernández RA, Rivera M, Torres D, Quiles J. and Jackson A, (1990) Usefulness of a Systemic Hypertension In-Hospital Educational Program. American Journal of Cardiology, 65,1384-1386. http://dx.doi.org/10.1016/0002-9149(90)91332-Z
25. Warsi A, Wang PS, LaValley MP, Avorn J. and Solomon DH. (2004) Self-management Education Programs in Chronic Disease: A Systematic Review and Methodological Critique of the Literature. Archives of Internal Medicine, 164,1641-1649. http://dx.doi.org/10.1001/archinte.164.15.1641
26. Walsh JM, Sundaram V, McDonald K, Owens DK. and Goldstein MK. (2008) Implementing Effective Hypertension Quality Improvement Strategies: Barriers and Potential Solutions. The Journal of Clinical Hypertension, 10,311-316. http://dx.doi.org/10.1111/j.1751-7176.2008.07425.x
27. Mendis S, Johnston SC, Fan W, Oladapo O, Cameron A. and Faramawi MF, (2010) Cardiovascular Risk Management and Its Impact on Hypertension Control in Primary Care in Low-Resource Settings: A Cluster-Randomized Trial. Bulletin of the World Health Organization, 88,412-419. http://dx.doi.org/10.2471/BLT.08.062364
28. Hendriks ME, Bolarinwa OA, Wit FW, Brewster LM, Odusola AO, Rosendaal NT, et al. (2014) Feasibility and Quality of Cardiovascular Disease Prevention within a Community-Based Health Insurance Program in Rural Nigeria: An Operational Cohort Study. Journal of Hypertension, 33,366-375.
29. Odusola AO, Hendriks M, Schultsz C, Bolarinwa OA, Akande T, Osibogun A, et al. (2014) Perceptions of Inhibitors and Facilitators for Adhering to Hypertension Treatment among Insured Patients in Rural Nigeria: A Qualitative Study. BMC Health Services Research, 14,624. http://dx.doi.org/10.1186/s12913-014-0624-z
30. Odusola AO, Hendriks M, Schultsz C, Stronks K, Lange J, Osibogun A, et al. (2011) Development and Evalu- ation of a Patient Centered Cardiovascular Health Education Program for Insured Patients in Rural Nigeria (QUICK-II). BMC Public Health, 11,171. http://dx.doi.org/10.1186/1471-2458-11-171
31. Health Insurance Fund. http://www.hifund.org32. American Diabetes Association (2010) Standards of Medical Care in Diabetes – 2010. Diabetes Care,
33,S11-S61. http://dx.doi.org/10.2337/dc10-S011

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 146 —
Chapter 6
33. Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Böhm M, et al. (2013) 2013 ESH/ESC Guidelines for the Management of Arterial Hypertension. The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). European Heart Journal, 34,2159-2219. http://dx.doi.org/10.1093/eurheartj/eht151
34. Hendriks M, Brewster L, Wit F, Bolarinwa OA, Odusola AO, Redekop W, et al. (2011) Cardiovascular Disease Prevention in Rural Nigeria in the Context of a Community Based Health Insurance Scheme: Quality Improvement Cardiovascular Care Kwara-I (QUICK-I). BMC Public Health, 11,186. http://dx.doi.org/10.1186/1471-2458-11-186
35. Morisky DE, Green LW and Levine DM, (1986) Concurrent and Predictive Validity of a Self-Reported Measure of Medication Adherence. Medical Care, 24,67-74. http://dx.doi.org/10.1097/00005650-198601000-00007
36. Morisky DE, Ang A, Krousel-Wood M. and Ward HJ, (2008) Predictive Validity of a Medication Adherence Measure in an Outpatient Setting. The Journal of Clinical Hypertension, 10,348-354. http://dx.doi.org/10.1111/j.1751-7176.2008.07572.x
37. Moss-Morris R, Weinman J, Petrie K, Horne R, Cameron L. and Buick D, (2002) The Revised Illness Perception Questionnaire (IPQ-R). Psychology & Health, 17,1-16. http://dx.doi.org/10.1080 /08870440290001494
38. Horne R, Weinman J. and Hankins M, (1999) The Beliefs about Medicines Questionnaire: The Development and Evaluation of a New Method for Assessing the Cognitive Representation of Medication. Psychology & Health, 14,1- 24. http://dx.doi.org/10.1080/08870449908407311
39. Ogedegbe G, Mancuso CA, Allegrante JP. and Charlson ME, (2003) Development and Evaluation of a Medication Adherence Self-Efficacy Scale in Hypertensive African-American Patients. Journal of Clinical Epidemiology, 56 520-529. http://dx.doi.org/10.1016/S0895-4356(03)00053-2
40. Fernandez S, Chaplin W, Schoenthaler A. and Ogedegbe G, (2008) Revision and Validation of the Medication Adherence Self-Efficacy Scale (MASES) in Hypertensive African Americans. Journal of Behavioral Medicine, 31,453-462. http://dx.doi.org/10.1007/s10865-008-9170-7
41. Ogedegbe G, Tobin JN, Fernandez S, Cassells A, Diaz-Gloster M, Khalida C, et al. (2014) Counseling African Americans to Control Hypertension: Cluster-Randomized Clinical Trial Main Effects. Circulation, 129,2044-2051. http://dx.doi.org/10.1161/CIRCULATIONAHA.113.006650
42. Sweileh WM, Zyoud SH, Abu Nab’a RJ, Deleq MI, Enaia MI, Nassar SM, et al. (2014) Influence of Patients’ Disease Knowledge and Beliefs about Medicines on Medication Adherence: Findings from a Cross-Sectional Survey among Patients with Type 2 Diabetes Mellitus in Palestine. BMC Public Health, 14,94. http://dx.doi.org/10.1186/1471-2458-14-94
43. AlHewiti A. (2014) Adherence to Long-Term Therapies and Beliefs about Medications. International Journal of Family Medicine, 2014,Article ID: 479596.
44. Ruppar TM, Dobbels F. and De Geest S, (2012) Medication Beliefs and Antihypertensive Adherence among Older Adults: A Pilot Study. Geriatric Nursing, 33,89-95. http://dx.doi.org/10.1016/j.gerinurse.2012.01.006
45. Schoenthaler A, Ogedegbe G. and Allegrante JP, (2009) Self-Efficacy Mediates the Relationship Between Depressive Symptoms and Medication Adherence Among Hypertensive African Americans. Health Education & Behavior, 36,127-137. http://dx.doi.org/10.1177/1090198107309459
46. Gatti ME, Jacobson KL, Gazmararian JA, Schmotzer B. and Kripalani S, (2009) Relationships between Beliefs about Medications and Adherence. American Journal of Health-System Pharmacy, 66,657-664. http://dx.doi.org/10.2146/ajhp080064
47. Chen S-L, Tsai J-C. and Lee W-L, (2009) The Impact of Illness Perception on Adherence to Therapeutic Regimens of Patients with Hypertension in Taiwan. Journal of Clinical Nursing, 18,2234-2244. http://dx.doi.org/10.1111/j.1365-2702.2008.02706.x
48. Ross S, Walker A. and MacLeod MJ, (2004) Patient Compliance in Hypertension: Role of Illness Perceptions and Treatment Beliefs. Journal of Human Hypertension, 18,607-613. http://dx.doi.org/10.1038/sj.jhh.1001721
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Evaluation of cardiovascular health education program
— 147 —
49. Rajpura JR and Nayak R, (2014) Role of Illness Perceptions and Medication Beliefs on Medication Compliance of Elderly Hypertensive Cohorts. Journal of Pharmacy Practice, 27,19-24. http://dx.doi.org/10.1177/0897190013493806
50. Helman CG, (2014) Culture, Health and Illness: An Introduction for Health Professionals. Butterworth-Heinemann, Boston.
51. Campbell MK, DeVellis BM, Strecher VJ, Ammerman AS, DeVellis RF and Sandler RS, (1994) Improving Dietary Behavior: The Effectiveness of Tailored Messages in Primary Care Settings. American Journal of Public Health, 84,783-787. http://dx.doi.org/10.2105/AJPH.84.5.783
52. Campbell MK, Honess-Morreale L, Farrell D, Carbone E and Brasure M, (1999) A Tailored Multimedia Nutrition Education Pilot Program for Low-Income Women Receiving Food Assistance. Health Education Research, 14,257-267. http://dx.doi.org/10.1093/her/14.2.257
53. Abbott P, Davison J, Moore L and Rubinstein R, (2010) Barriers and Enhancers to Dietary Behaviour Change for Aboriginal People Attending a Diabetes Cooking Course. Health Promotion Journal of Australia, 21,33-38.
54. Staessen JA, Wang JG and Thijs L, (2001) Cardiovascular Protection and Blood Pressure Reduction: A Me-ta-Analysis. Lancet, 358,1305-1315. http://dx.doi.org/10.1016/S0140-6736(01)06411-X
55. Korb-Savoldelli V, Gillaizeau F, Pouchot J, Lenain E, Postel-Vinay N, Plouin P-F, et al. (2012) Validation of a French Version of the 8-Item Morisky Medication Adherence Scale in Hypertensive Adults. Journal of Clinical Hypertension, 14,429-434. http://dx.doi.org/10.1111/j.1751-7176.2012.00634.x
56. Oliveira-Filho AD, Barreto-Filho JA, Neves SJF and Lyra Jr DP, (2012) Association between the 8-Item Morisky Medication Adherence Scale (MMAS-8) and Blood Pressure Control. Arquivos Brasileiros De Cardiologia, 99,649-658. http://dx.doi.org/10.1590/S0066-782X2012005000053
57. Holt E, Joyce C, Dornelles A, Morisky D, Webber LS, Muntner P, et al. (2013) Sex Differences in Barriers to Antihypertensive Medication Adherence: Findings from the Cohort Study of Medication Adherence among Older Adults. Journal of the American Geriatrics Society, 61,558-564. http://dx.doi.org/10.1111/jgs.12171
58. Lee GKY, Wang HHX, Liu KQL, Cheung Y, Morisky DE and Wong MCS. (2013) Determinants of Medication Adherence to Antihypertensive Medications among a Chinese Population Using Morisky Medication Adherence Scale. PloS ONE, 8,e62775. http://dx.doi.org/10.1371/journal.pone.0062775
59. Sa’ed H, Al-Jab, SW, Sweileh WM and Morisky DE, (2013) Relationship of Treatment Satisfaction to Medication Adherence: Findings from a Cross-Sectional Survey among Hypertensive Patients in Palestine. Health and Quality of Life Outcomes, 11,191. http://dx.doi.org/10.1186/1477-7525-11-191
60. Akintunde AA and Akintunde TS, (2015) Antihypertensive Medications Adherence among Nigerian Hypertensive Subjects in a Specialist Clinic Compared to a General Outpatient Clinic. Annals of Medical and Health Sciences Re- search, 5, 73-178. http://dx.doi.org/10.4103/2141-9248.157492
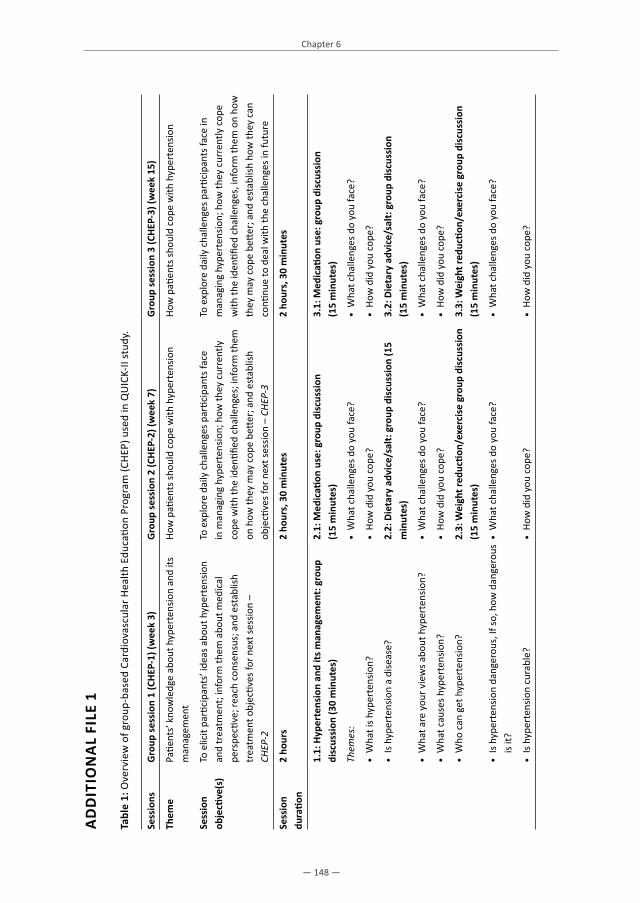
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 148 —
Chapter 6
AD
DIT
ION
AL
FILE
1
Tabl
e 1:
Ove
rvie
w o
f gro
up-b
ased
Car
diov
ascu
lar H
ealth
Edu
catio
n Pr
ogra
m (C
HEP
) use
d in
QU
ICK-
II st
udy.
Sess
ions
Gro
up se
ssio
n 1
(CHE
P-1)
(wee
k 3)
Gro
up se
ssio
n 2
(CHE
P-2)
(wee
k 7)
Gro
up se
ssio
n 3
(CHE
P-3)
(wee
k 15
)
Them
ePa
tient
s’ k
now
ledg
e ab
out h
yper
tens
ion
and
its
man
agem
ent
How
pati
ents
shou
ld c
ope
with
hyp
erte
nsio
nHo
w p
atien
ts sh
ould
cop
e w
ith h
yper
tens
ion
Sess
ion
obje
ctive
(s)
To e
licit
parti
cipa
nts’
idea
s abo
ut h
yper
tens
ion
and
trea
tmen
t; in
form
them
abo
ut m
edic
al
pers
pecti
ve; r
each
con
sens
us; a
nd e
stab
lish
trea
tmen
t obj
ectiv
es fo
r nex
t ses
sion
–
CHEP
-2
To e
xplo
re d
aily
cha
lleng
es p
artic
ipan
ts fa
ce
in m
anag
ing
hype
rten
sion;
how
they
cur
rent
ly
cope
with
the
iden
tified
cha
lleng
es; i
nfor
m th
em
on h
ow th
ey m
ay c
ope
bette
r; an
d es
tabl
ish
obje
ctive
s for
nex
t ses
sion
– CH
EP-3
To e
xplo
re d
aily
cha
lleng
es p
artic
ipan
ts fa
ce in
m
anag
ing
hype
rten
sion;
how
they
cur
rent
ly c
ope
with
the
iden
tified
cha
lleng
es, i
nfor
m th
em o
n ho
w
they
may
cop
e be
tter;
and
esta
blish
how
they
can
co
ntinu
e to
dea
l with
the
chal
leng
es in
futu
re
Sess
ion
dura
tion
2 ho
urs
2 ho
urs,
30
min
utes
2 ho
urs,
30
min
utes
1.1:
Hyp
erte
nsio
n an
d its
man
agem
ent:
grou
p di
scus
sion
(30
min
utes
)2.
1: M
edic
ation
use
: gro
up d
iscu
ssio
n
(15
min
utes
)3.
1: M
edic
ation
use
: gro
up d
iscu
ssio
n
(15
min
utes
)
Them
es:
• W
hat c
halle
nges
do
you
face
?•
Wha
t cha
lleng
es d
o yo
u fa
ce?
• W
hat i
s hyp
erte
nsio
n?•
How
did
you
cop
e?•
How
did
you
cop
e?
• Is
hyp
erte
nsio
n a
dise
ase?
2.2:
Die
tary
adv
ice/
salt:
gro
up d
iscu
ssio
n (1
5 m
inut
es)
3.2:
Die
tary
adv
ice/
salt:
gro
up d
iscu
ssio
n
(15
min
utes
)
• W
hat a
re y
our v
iew
s abo
ut h
yper
tens
ion?
• W
hat c
halle
nges
do
you
face
?•
Wha
t cha
lleng
es d
o yo
u fa
ce?
• W
hat c
ause
s hyp
erte
nsio
n?•
How
did
you
cop
e?•
How
did
you
cop
e?
• W
ho c
an g
et h
yper
tens
ion?
2.3:
Wei
ght r
educ
tion/
exer
cise
gro
up d
iscu
ssio
n (1
5 m
inut
es)
3.3:
Wei
ght r
educ
tion/
exer
cise
gro
up d
iscu
ssio
n (1
5 m
inut
es)
• Is
hyp
erte
nsio
n da
nger
ous,
If so
, how
dan
gero
us
is it?
• W
hat c
halle
nges
do
you
face
?•
Wha
t cha
lleng
es d
o yo
u fa
ce?
• Is
hyp
erte
nsio
n cu
rabl
e?•
How
did
you
cop
e?•
How
did
you
cop
e?

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Evaluation of cardiovascular health education program
— 149 —
Tabl
e 1:
(Con
tinue
d)
Sess
ions
Gro
up se
ssio
n 1
(CHE
P-1)
(wee
k 3)
Gro
up se
ssio
n 2
(CHE
P-2)
(wee
k 7)
Gro
up se
ssio
n 3
(CHE
P-3)
(wee
k 15
)
• Ho
w lo
ng d
oes h
yper
tens
ion
last
?2.
4: A
tten
ding
you
r fol
low
-up
appo
intm
ents
re
gula
rly a
s adv
ised
gro
up d
iscu
ssio
n
(15
min
utes
)
3.4:
Att
endi
ng y
our f
ollo
w-u
p ap
poin
tmen
ts
regu
larly
as a
dvis
ed g
roup
dis
cuss
ion
(1
5 m
inut
es)
• Ho
w d
oes h
yper
tens
ion
pres
ent?
• W
hat c
halle
nges
do
you
face
?•
Wha
t cha
lleng
es d
o yo
u fa
ce?
• Ho
w d
id y
ou g
et y
our h
yper
tens
ion?
• Ho
w d
id y
ou c
ope?
• Ho
w d
id y
ou c
ope?
• W
hat c
an y
ou d
o to
pre
vent
hyp
erte
nsio
n?2.
5: A
udio
visu
al ‘L
ivin
g po
sitiv
ely
with
hy
pert
ensi
on’:
Inst
ructi
on (2
5 m
inut
es)
3.5:
Aud
iovi
sual
‘Liv
ing
posi
tivel
y w
ith
hype
rten
sion
’: In
stru
ction
(25
min
utes
)
• Ho
w c
an h
yper
tens
ion
be tr
eate
d?•
View
and
disc
uss v
ideo
“liv
ing
positi
vely
with
hy
pert
ensio
n” a
nd so
me
patie
nt-c
entr
ed
exer
cise
regi
mes
to h
elp
copi
ng (3
5 m
inut
es)
• Vi
ew a
nd d
iscus
s vid
eo “
livin
g po
sitive
ly w
ith
hype
rten
sion”
and
som
e pa
tient
-cen
tere
d ex
erci
se re
gim
es to
hel
p co
ping
(35
min
utes
)
• Ho
w is
hyp
erte
nsio
n re
late
d to
you
r life
styl
e an
d w
hat y
ou e
at?
Prot
ocol
in
stru
ction
s1.
2: W
hat p
atien
ts c
an d
o to
man
age
hype
rten
sion
: int
erac
tive
inst
ructi
on
(30m
inut
es)*
2.6:
Sim
ple
exer
cise
s you
can
do
at h
ome
(20
min
utes
)3.
6: S
impl
e ex
erci
ses y
ou c
an d
o at
hom
e (2
0 m
inut
es)
Them
es:
• Po
ster
teac
hing
sess
ion
(5 m
inut
es)
• Pa
tient
frie
ndly
exe
rcise
pra
ctice
sess
ions
usin
g:
loca
l acti
vitie
s suc
h as
woo
d cu
tting
, gar
deni
ng,
mor
tar g
rindi
ng, d
raw
ing
wat
er fr
om w
ell,
othe
r ho
useh
old
chor
es, f
arm
ing,
bik
ing,
bris
k w
alki
ng,
leisu
re a
ctivi
ties e
.g. d
rum
min
g, d
anci
ng.
• Ta
ke y
our m
edic
ation
s reg
ular
ly a
s pre
scrib
ed•
Prac
tical
exe
rcise
sess
ion
(15
min
utes
)3.
7: F
inal
clo
sing
sess
ion
(Inst
ructi
ons)
, (10
m
inut
es)
• Se
ek su
ppor
t fro
m y
our f
amily
/frie
nds o
n re
min
ders
in ta
king
you
r dru
gs re
gula
rly a
nd in
re
duci
ng sa
lt in
take
2.7:
Indi
vidu
al a
ssig
nmen
t (10
min
utes
)In
mov
ing
forw
ard:

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 150 —
Chapter 6
Tabl
e 1:
(Con
tinue
d)
Sess
ions
Gro
up se
ssio
n 1
(CHE
P-1)
(wee
k 3)
Gro
up se
ssio
n 2
(CHE
P-2)
(wee
k 7)
Gro
up se
ssio
n 3
(CHE
P-3)
(wee
k 15
)
• Ad
opt h
ealth
y di
et (d
escr
ibed
)Se
t 3 g
oals
on w
hat y
ou w
ant t
o ac
hiev
e be
fore
yo
ur n
ext C
HEP
visit
to k
eep
your
blo
od p
ress
ure
cont
rolle
d (e
.g. r
educ
e sa
lt co
nsum
ption
, inc
reas
e ph
ysic
al a
ctivi
ty th
roug
h ex
erci
se)
• M
ake
the
less
ons l
earn
t fro
m th
is pr
ogra
m y
our
daily
routi
ne fo
r life
• De
crea
se a
mou
nt o
f sod
ium
/sal
t in
your
die
t•
Take
you
r dru
gs re
gula
rly
• St
ay p
hysic
ally
acti
ve/e
xerc
ise re
gula
rly•
Exer
cise
dai
ly, re
gula
rly
• Lo
se e
xces
s wei
ght
• Re
duce
salt
inta
ke a
nd a
dopt
hea
lthy
diet
• Q
uit s
mok
ing
• Att
end
your
follo
w-u
p cl
inic
regu
larly
• Q
uit/
redu
ce a
lcoh
ol in
take
• Ge
t nee
ded
supp
ort f
rom
fam
ily m
embe
rs/
frie
nds i
n yo
ur h
yper
tens
ion
self-
man
agem
ent
• Q
uit s
nuff,
Kol
a nu
ts
• Li
mit
expo
sure
to p
hysic
al/e
moti
onal
stre
ss
1.3:
Add
ress
ing
wha
t can
mak
e hy
pert
ensi
onm
anag
emen
t diffi
cult
for p
atien
ts:
grou
p di
scus
sion
(30
min
utes
)
• Re
ad/c
onsu
lt yo
ur h
yper
tens
ion
info
rmati
on
leafl
et/p
amph
let r
egul
arly
for a
dditi
onal
supp
ort
Them
es:
• Vi
ew a
ttenti
vely
the
audi
ovisu
als t
hat w
ill b
e m
ade
avai
labl
e to
you
dur
ing
wai
ting
time
in
clin
icTa
king
you
r pill
s reg
ular
ly
Redu
cing
salt
inta
ke
Adop
ting
a he
alth
y di
et
Stay
ing
phys
ical
ly a
ctive
1.4:
How
to o
verc
ome
obst
acle
s: in
stru
ction
(20
min
utes
) **

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Evaluation of cardiovascular health education program
— 151 —
Tabl
e 1:
(Con
tinue
d)
Sess
ions
Gro
up se
ssio
n 1
(CHE
P-1)
(wee
k 3)
Gro
up se
ssio
n 2
(CHE
P-2)
(wee
k 7)
Gro
up se
ssio
n 3
(CHE
P-3)
(wee
k 15
)
1.5:
Indi
vidu
al a
ssig
nmen
t (10
min
utes
)
• Se
t 3 g
oals
on w
hat y
ou w
ant t
o ac
hiev
e be
fore
yo
ur n
ext C
HEP
visit
to k
eep
your
blo
od p
ress
ure
cont
rolle
d (e
.g. r
educ
e sa
lt co
nsum
ption
, in
crea
se p
hysic
al a
ctivi
ty th
roug
h ex
erci
se)
Addi
tiona
l inf
orm
ation
:•
Two
inst
ruct
ors
guid
ed th
e se
ssio
ns•
Sess
ions
wer
e he
ld in
Eng
lish,
Yor
uba
and
Nup
e w
ith a
tran
slat
or•
All s
essi
ons
incl
uded
a 5
min
ute
wel
com
e•
Resu
lts o
f par
ticip
ants
’ hom
ewor
k as
sign
men
ts w
ere
disc
usse
d w
ith th
e tr
aine
rs 1
5 m
inut
es b
efor
e th
e st
art o
f nex
t ses
sion
s•
Durin
g br
eaks
, pati
ents
vie
wed
edu
catio
nal p
oste
rs*P
ower
poi
nts a
re u
sed;
**
Post
ers a
re u
sed.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 152 —
Chapter 6
Table 2: Changes in inclusion characteristics of QUICK-II participants between endline QUICK-I and baseline QUICK-II assessments.
Measurements Endline QUICK-I (N = 149)
Baseline QUICK-II (N = 149)
High BP no co-morbidities 36 (24.2) 15 (10.1)
High BP with co-morbidities 17 (11.4) 10 (6.7)
Low or medium adherence 61 (40.9) 40 (26.9)
High BP no co-morbidities AND low/med adherence 31 (20.8) 25 (16.8)
High BP with co-morbidities AND low/med adherence 4 (2.7) 10 (6.7)
Low BP and high adherence 0 (0.0) 49 (32.9)
LIST OF ABBREVIATIONS
BMQ: Beliefs about Medicines Questionnaire BP: Blood pressureCHEP: Cardiovascular Health Education Program DBP: Diastolic Blood PressureHIF: Health Insurance FundIPQ-R: Revised Illness Perception Questionnaire KSHI: Kwara State Health InsuranceMASES-R: Revised Medication Adherence Self Efficacy Scale MMAS: Morisky Medication Adherence ScaleNUFFIC: Netherlands organization for international cooperation in higher education OOH: Ogo Oluwa HospitalQUICK: Quality Improvement Cardiovascular Care Kwara SBP: Systolic Blood Pressure

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Chapter 7
General discussion

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 154 —
Chapter 7
This thesis had three specific objectives:1. To develop a patient-centered cardiovascular health education program for hypertensive
patients with access to affordable primary care in a community based health insuranceprogram implemented in a primary healthcare center in rural Nigeria.
2. To evaluate the developed education program with respect to impact on medication andbehavioral adherence, body mass index and blood pressure control.
3. To identify optimal strategies for a successful implementation of the education program inclinical practice.
To achieve these objectives we conducted four studies which aimed to develop and evaluate a cardiovascular health education program (CHEP) for primary care patients with hypertension, who were enrolled in the Kwara State Health Insurance (KSHI) program in rural Nigeria. In this chapter the main results are summarized and discussed. It starts with an overview of the main results of the three formative studies that were carried out to develop CHEP and of the fourth study that evaluated the effects of CHEP among primary care patients who were treated for hypertension. In the next part methodological considerations will be discussed. This is followed by a reflection on the process by which CHEP was developed and a discussion of its effectiveness on the target population in comparison with similar education programs within and outside Nigeria. In the last part, recommendations for clinical applications and future research are given and general conclusions are drawn.
SUMMARy OF KEy FINDINGS
A combination of qualitative, quantitative and descriptive designs was used to investigate the thesis objectives. A qualitative design was used to explore hypertensive patients’ and healthcare professionals’ perspectives on hypertension, care experience and self-management. Subsequently, a descriptive design was used to write the education program based on review of literature and exploratory findings from the qualitative studies. Finally, a quantitative design was used to evaluate the effectiveness of the program among patients.
Development of CHEPTo develop CHEP, we conducted a qualitative interview study (chapter 3) to explore the perspectives of 40 primary care patients who were treated for hypertension on what they perceived or experienced as inhibitors or facilitators for adhering to the recommended medications and healthy behaviors [1]. All patients were living in rural region of Kwara State and had enrolled in the KSHI program. The interview data yielded a rich mix of ideas and information some already known from previous studies, others unique to the current study. Highlighted below are factors perceived

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General discussion
— 155 —
or experienced by participants to inhibit or facilitate hypertension care that provided useful information for health behavior modification in the education program. Identified facilitators of medication adherence include: having affordable access to care; trust in orthodox “western” medicines; trust in Doctor; fear of hypertension; support from family and religion and use of prayer to support efficacy of pills. Inhibitors of medication adherence include: healthcare-related constraints (inconvenient clinic operating hours, long waiting times, under-dispensing of prescribed pills); side-effects of pills; faith motivated changes of medication regimen; herbal supplementation/substitution of pills; and not being aware that regular use of medication is needed. Certain local practices were perceived as inhibitors to healthier behaviors including: use of salt for food preservation; and the negative cultural images associated with decreased body size and physical activity. Facilitators of healthy behaviors include: awareness that salt substitutes and products for composing healthier meals were cheaply available in the community; and that patient-friendly exercises could be integrated in people’s daily activities (e.g. farming/gardening, household chores, leisure activities like drumming, dancing, clapping etc). Together these findings provided useful information for themes that require attention in an educational program designed to improve self-management and adherence capacities of hypertensive patients, particularly in the study area. In insured health care, aside patients other key stakeholders in the healthcare delivery partnership are the healthcare providers (professionals) and health insurance managers. Therefore to identify optimal strategies for the implementation of the education program, in Chapter 4 we conducted a second set of qualitative interviews to investigate views of 11 healthcare professionals and 4 health insurance managers on what they viewed as facilitators and inhibitors for delivering high-quality hypertension care for patients within the KSHI program. High-quality care for hypertension requires life-long treatment. We found that many of the factors mentioned by the informants referred to financial and organizational structures that need to be in place in order to provide long-term care in a low resource community. For example both groups considered the availability and access to affordable health insurance to be crucial for the delivery of high-quality hypertension care. Other resources or incentives perceived by both groups to be essential for high-quality hypertension care include: trust in the sustainability of care, treatment guidelines, tools for patient education, human resources, capacity building, (diagnostic) equipment and drugs, an adequate care administration infrastructure, quality assurance monitoring, adequate provider payments benchmarking and good provider/insurer relationships. However, both stakeholder groups also highlighted those patient-related factors such as poor adherence that might hamper the outcomes of care, including BP control. They suggest several mechanisms to stimulate adherence, including use of language interpreters where needed and patient education. In terms of patient education they provided suggestions for both the form in which it could be delivered (group education, pictorials, and audiovisuals) and the content (cultural relevance and patient-centeredness). In particular they suggested

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 156 —
Chapter 7
periodic group education model that could be implemented by other non-physician staff (nurses, other paramedics) specifically trained for the purpose as an optimal platform for delivery of the education program. Interestingly, since it has the added advantage of freeing valuable physicians’ time deployable for other aspects of clinical care this delivery model is particularly relevant in settings encountering significant healthcare personnel shortage as in the current setting. It is noteworthy also that this education delivery strategy is comparable in effect to the ‘task shifting’ strategy that has been deployed to address human resources shortage in similar settings as reported in a review [2]. The observed differences between both groups as regards to factors that foster effective implementation of high-quality care were mainly related to perceptions of how the health insurance system operates and serves the needs of the priority population and contracted providers. One of the main goals of this thesis was to develop a hypertension education program that is patient-centered and culturally sensitive because prior research had demonstrated that programs with these features are more likely to be accepted by patients. The cardiovascular health education program (CHEP) that was developed consisted of the following tools: 1) a face-to-face interactive group-based educational program; supported by 2) educational posters and leaflets; and 3) a video that used patients as actors. All educational tools used examples of potential barriers to hypertension self-management that were obtained during the formative phase of the research. Given the results from the interview studies during the formative phase it was assumed that a combination of these three tools would be most suited for the peculiar characteristics (e.g., low literacy level) of the patients in Kwara and the insufficiently available (human) resources. Briefly, CHEP protocol consisted of 3 group educational sessions spread 4-6 weeks apart over a period spanning 4 months and delivered to groups of 12 to 15 participants. The instructional methods were partly teaching and partly interactive. Procedurally, aspects of the people’s culture that are healthy were emphasized and encouraged and others that are unsafe for health were discouraged. Detailed content of the sessions is available in the CHEP protocol (chapter 6, Additional file 1, Table 1). Furthermore, a hypertension information leaflet written in English and local languages was used to teach participants what they need to know about hypertension self-management including the frequently asked questions about the presentations, causes, course, consequences, complications, prevention and control measures and treatment of hypertension. For the latter participants and other potential readers were advised to consult their doctors for appropriate diagnoses and care. To maximize adherence to prescribed care, the information that was delivered during the training sessions were also used to address patients’ self-management of prescribed medications and healthy behavior including physical fitness, diet and social habits.
Evaluation of CHEP The study reported in chapter 6 of this thesis makes a contribution to the evaluation of CHEP. In this pretest/posttest study three CHEP sessions were offered to 149 hypertensive patients of one

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General discussion
— 157 —
of the KSHI clinics which had implemented WHO guidelines for cardiovascular risk management and hypertension care [3]. The patients were selected because they had an uncontrolled blood pressure (BP) and/or poor self-reported medication adherence after they had received 12 months of guideline-based care. The study demonstrated that CHEP had several positive effects on patients. At 6 months, more participants reported high adherence to medications and behavioral advice than at baseline: respectively, 101 (72%) versus 70 (50%), (p < 0.001) and 126 (90%) versus 106 (76%), (p < 0.001). Participants with controlled BP doubled from 34 (24%) to 65 (46%), (p = 0.001). The median systolic BP (SBP) and diastolic BP (DBP) decreased from 129.0 to 122.0 mmHg, (p = 0.002) and from 80.0 to 73.5 mmHg, (p < 0.001), respectively. However body mass index (BMI) did not change (p = 0.444). Observable changes in BMI may require more than just the 6 months period during which CHEP was implemented. We however observed that the improvement in medication adherence was associated with a decrease in patients’ concerns about medication (p = 0.045) and an improvement in medication self-efficacy (p < 0.001). This was unsurprising as the latter topics were specifically targeted during CHEP trainings. Patient retention rates in CHEP were also very high in comparison with retention rates reported in similar hypertension education programs in other countries [4,5]. Consequently we concluded that by positively influencing patient perceptions of medications CHEP strengthened medication adherence and BP reduction among the study participants.
METHODOLOGICAL CONSIDERATIONS
Study participantsThis thesis is composed of a two-stage study (part 1 and part 2) involving qualitative and quantitative designs. In part 1 we conducted qualitative interviews with 40 hypertensive patients enrolled in the KSHI program and 11 healthcare professionals and 4 health insurance managers delivering/monitoring care in the KSHI program to respectively develop the intervention and identify optimal strategy for implementation in practice. In part 2 we used a pretest/posttest quantitative design on 149 hypertensive patients at risk of developing CVD to evaluate the education program with respect to effectiveness. Participating patients were low-income persons who had enrolled in the KSHI program for care. While the healthcare professionals included medical doctors, nurses, laboratory staff, pharmacy staff and health records staff who delivered hypertension care in the participating hospital, the health insurance managers consisted only of medical doctors who performed administrative and care monitoring functions in the insurance program. Having stated this, the methodical approach employed in this study has its strong points and weaknesses also. A key strength of the study is the qualitative design approach used in developing the education program. Among others, qualitative perception study design is well suited and clearly the best option available to answer our research questions as it allows us to deeply explore stakeholders’ views on the subjects and to discover how they view, experience

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 158 —
Chapter 7
or feel about issues at stake (hypertension care, self-management and quality of care). Second, in accordance with standard quality requirements in qualitative research we interviewed a sufficient number of participants to get the sample sizes after achieving data saturation [6,7] and we conducted additional interviews to collect additional information to clarify unclear themes from previous interviews. In following quality criteria for qualitative research [8], trustworthiness and credibility of our findings was promoted and assisted with appropriate data management and analytic tool. Third, our samples were representative of the target populations (insured hypertensive patients, healthcare professionals delivering insured hypertension care) as anticipated in the research questions. However for ethical considerations we were limited in our ability to crosscheck information provided by the participants with significant others (triangulation).
Study design While the multi method (qualitative and quantitative) designs employed in this study has potential to strengthen the results; the non-utilization of a control group in the evaluation of the education program obviously weakened the possibility of establishing a causal relationship between the intervention and results. However the lack of a control group was not accidental as this was inevitably included in the design due to realities met on ground within the KSHI program then. At the time when the study commenced there was no suitable comparable group of adequate sample size that can be used to control the study either within the KHSI system or elsewhere in the study region. However to improve the credibility of our results, the pretest/posttest design that was employed have been implemented in accordance with quality standards. Nevertheless the possibility of drawing firm conclusions as to the causality of the measured effects will certainly be strengthened in a randomized control trial.
Study context: affordable and quality careThe setting (insured high-quality care) where CHEP was implemented was contextually different from the usual care setting available in similar or other regions within or outside Nigeria. CHEP was implemented within a health insurance program in a primary care hospital in rural low-income community of Bacita, Edu local government area of Kwara State. At that time, Kwara State where about 20% of the population lives below poverty line of 2 USD per day was the fourth poorest in Nigeria. To underscore the poverty situation in Kwara, KSHI and Health Insurance Fund (HIF) subsidized about 92% of the annual insurance premium for each enrollee at the time of the study. Furthermore as part of KSHI’s quality improvements, the hospital implemented guidelines and treatment protocols for CVD prevention and upgraded its diagnostic equipment and medical record system. Therefore the potential for reproducibility of the kind of positive results obtained in CHEP should increase if hypertension care is delivered in similar contexts of insured high-quality care. Furthermore, the possibility that a less promising result than CHEP may be obtained in typical usual care setting (less affordable low-quality care) will certainly benefit from further

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General discussion
— 159 —
investigations. This therefore presents an opportunity to increase the generalizability of current CHEP results using the more conclusive randomized control trial design.
Contextual and local adaptability of CHEP, the study materials and procedures CHEP was specifically made to be culturally relevant to specific social context in both form and content based on findings from perceptual interview studies with representatives from the target population. Furthermore the CHEP trainings was implemented in a health insurance program setting with high-quality hypertension care using educational materials which consisted of the following in English and local languages: a) hypertension information leaflets for home use by participants; b) wall mounted pictorial posters to teach participants about self-management of medications, healthy diet and healthy behavior including locally available culturally relevant exercise regimes; c) a 20 minute audio-visual on how to live positively with hypertension starring some patients themselves; d) a 10 minute audio-visual introduction on hypertension, its nature, causes, course, symptoms, consequences, myths, realities, treatment and prevention of hypertension; and e) goal setting assessment forms. The message was delivered using interactive teachings in group educational sessions. The trainers consisted of the researcher (a medical doctor) and a nurse both of whom were familiar with the target population and had undergone appropriate training in CVD prevention prior to commencement of the studies. The first education session CHEP 1, the second CHEP 2 and the third CHEP 3 each used similar procedure although different contents. The process starts usually with an explanation of the day’s goals to the group e.g., to enlighten you about what you can do to keep your blood pressure under control. CHEP 3in addition had a 20 minutes practical exercise session. From the foregoing account, it becomes clear that although CHEP was implemented in specific contextual setting (insured high-quality hypertension care) the rather simplistic design of the protocol makes it easily reproducible and increases potential for adaptability to specific contexts in other local settings. This reproducibility and contextual adaptability of CHEP is an important characteristic that makes it relevant and useful to the needs of other populations including those with differing cultural backgrounds in different settings. However to get positive results that are better than or at least similar to what was already produced in CHEP, the context or setting of implementation may need to approximate to a similar scenario of affordable high-quality hypertension care.
REFLECTIONS ON THE DEVELOPMENT PROCESS
Theoretical and conceptual frameworkSome of the factors that may drive health behavior change in individuals include culture, attitude, beliefs, norms, social support and self-efficacy [9,10]. Findings from our CHEP evaluation study had revealed that patients could benefit from improvements in hypertension related knowledge with regards to the cause, course, nature, consequences and prevention [3].

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 160 —
Chapter 7
Therefore we selected a conceptual framework that considers patients’ culture and perceptions in the development of the education program. To produce the desired cultural content we adopted the theoretical model developed by Arthur Kleinman [11] regarding explanatory models of interactions between illness and health within socio-cultural contexts. This model which examines a patient’s health and health seeking behavior within cultural contexts explains illness within socio-cultural realities and has the capacity to influence how patients experience or perceive diseases. The model is used in health care to explore people’s views regarding what caused illness, how it manifests, in what ways it affects them and what makes them feel better. An opportunity to apply this framework was provided in the current study which took place in a rural setting where traditionally social and cultural beliefs and practices exert significant influence on the peoples’ attitudes including health behaviors. To further increase the cultural sensitivity of the education program, principles from another model developed by Resnicow et al was applied. Resnicow et al. (1999) defined cultural sensitivity as “the extent to which ethnic/cultural characteristics, experiences, norms, values, behavioral patterns and beliefs of a target population as well as relevant historical, environmental and social forces are incorporated in the design, delivery and evaluation of targeted health promotion interventions” [12]. The promising results so far obtained in the evaluation of CHEP [3] underscores the relevance of cultural contents in hypertension education messages that are implemented in specific socio-cultural settings. Therefore the current study clearly demonstrates the usefulness of including cultural considerations in educational messages formulated for the specific needs of patients diagnosed with hypertension as also partly demonstrated in a previous study [4].
Formative researchIn the current study CHEP was developed based on the results of a search of available literature on similar patient education programs as well as analysis of data from the qualitative interviews held with hypertensive patients, their treating healthcare professionals and health insurance managers of KSHI program. We conducted interviews with hypertensive patients to get an insight into how patients perceive the hypertension care they access. Analyzed data from the interviews yielded a rich mix of ideas/views on barriers and facilitators of prescribed hypertension treatment [1]. Inferences were drawn and used to write the CHEP protocol [3]. The best strategy for a successful implementation of CHEP was explored using results of similar interviews held with healthcare professionals and health insurance managers who deliver/administer care in the hospital [13]. But surprisingly a search of literature available in the field of development or implementation of formal cardiovascular health education programs revealed a rarity of such past efforts in Nigeria and SSA. This underscores the importance of increased efforts towards developing a structured cardiovascular health education program for the specific use of patients diagnosed with hypertension in Nigeria and SSA. Furthermore CHEP was developed and tested in specific contexts where participants had affordable access to high-quality hypertension care, a scenario which substantially differs from other contexts where usual hypertension care is offered.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General discussion
— 161 —
Interestingly the design and processes used in developing CHEP makes it reproducible and easily applicable to specific contexts in other settings although the pre-, post method employed to evaluate the program may be insufficient to firmly establish causal links between the intervention and the positive results until this is further tested using a design that involves a randomized controlled trial. This presents an indication and opportunity for future research in the field.
PERFORMANCE EFFECTIVENESS OF CHEP WITHIN KSHI PROGRAM (DESCRIPTIVE/GRAPHICAL ANALySIS)
The short-term effects of CHEPOne may wonder; what benefit or advantage might CHEP confer on treatment outcomes in the short run in typical clinical practice setting? Of the 149 patients included from QUICK-I into QUICK-II based on the criteria of uncontrolled BP and/or low or medium medication adherence scores using the 8 item Morisky Medication Adherence Scale (MMAS-8), 140 completed the evaluation study. (NB. The QUICK study comprises 2 studies QUICK-I and QUICK-II. While QUICK-I initially offered standard quality CVD prevention care according to international guidelines over a starting period of 12 months to 349 hypertensive patients enrolled in KSHI at the participating hospital, QUICK-II included a cohort of 149 patients from the 349; those whom at end of the 12 months yet had uncontrolled BP and/or low or medium medication adherence scores after exiting QUICK-I, and offered them CHEP in addition to the usual care of QUICK-I over a subsequent follow-up period of 6 months). The performance over time of the 140 patients that completed QUICK-II with regards to the study outcome measures (improvement in BP and / or medication/behavioral adherence) between baseline and endline of QUICK-II study is illustrated graphically in Figure 1. As shown, those participants included on the basis of different inclusion criteria: uncontrolled BP (n = 51), low/medium MMAS-8 (n = 56), both criteria (n = 33) and all (n = 140) gradually improved in the outcome measures SBP, DBP and MMAS-8 over time between baseline QUICK-I until the 9 months assessments of QUICK-I. However, an interesting scenario played out between the 9th month’s assessments of QUICK-I and the 12 months (endline QUICK-I) assessments, i.e. at the time participants were selected and invited for QUICK-II; with exception of the group that was included using uncontrolled BP as criterion, the medication adherence score MMAS-8 of other groups and in particular the total group (n = 140) got worse. Therefore the SBP control and DBP control also deteriorated generally during this period. But the blood pressure generally improved again between endline QUICK-I and baseline QUICK-II, a hitherto unanticipated 4.7 months period during which participants continued to access usual care only. Perhaps the observed improvements during this period may have resulted from the observation that among the total group (n = 140) MMAS-8 also improved and therefore influenced BP control positively. However it is unknown exactly what factors influenced the observed improvement in MMAS-8 of the total group (n=140) during the 4.7 months but a plausible explanation is as follows: procedurally patients that meet QUICK-II inclusion criteria are immediately informed

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 162 —
Chapter 7
of their potential inclusion and the reasons for this after exiting QUICK-I and indeed a red sticker is immediately stamped on their small personal follow-up visit biodata cards (which they usually take home and present in the clinic during every follow-up visits). It is not impossible that this information on poor performance and in particular the red sticker labeling might have sent danger signals to many of these potential QUICK-II participants who consequently may have made deliberate personal efforts to improve on their medication self-management and adherence capacities during the 4.7 months period. Furthermore, as expected with the introduction of CHEP during QUICK-II study, a prominent and significant improvement in the outcome parameters SBP, DBP, and MMAS-8 was observed. In particular, the MMAS-8 of all individual groups rose steeply during QUICK-II study. This is unsurprising as the CHEP sessions 1, 2 and 3 objectively addressed participants’ knowledge and perceptions on hypertension and self-management skills leading to an increase in medications self-efficacy and improvement in self-management capabilities. This development which reasonably resulted in improved BP control clearly demonstrates a positive effect of CHEP in the short-term during the evaluation study. Therefore to address the opening rider (question) asked above in the beginning of this section, the key message and indeed the implication for clinical practice in the short run could well be that CHEP may be a useful or important complement to standard guideline-based CVD prevention care for insured hypertensive patients.
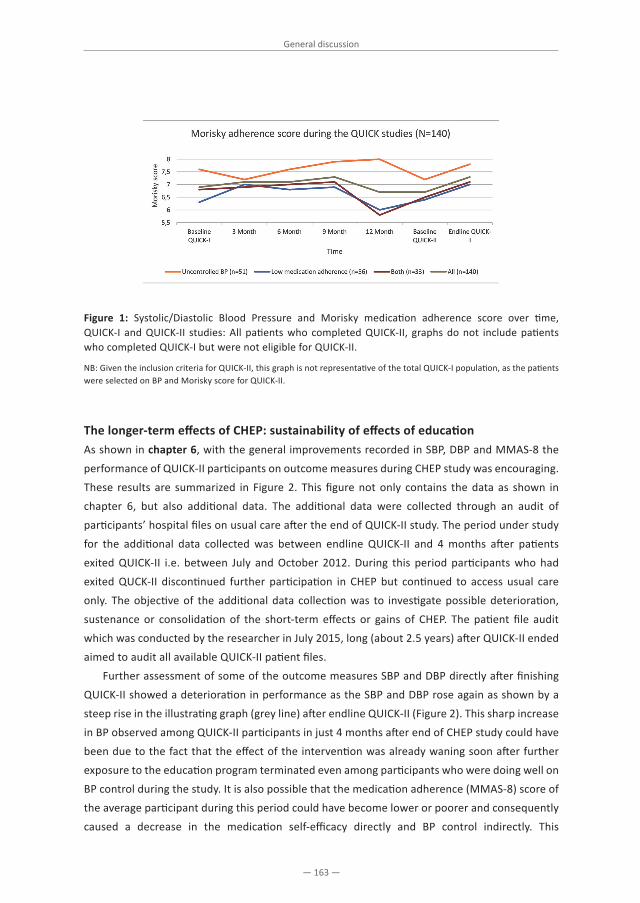
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General discussion
— 163 —
Figure 1: Systolic/Diastolic Blood Pressure and Morisky medication adherence score over time, QUICK-I and QUICK-II studies: All patients who completed QUICK-II, graphs do not include patients who completed QUICK-I but were not eligible for QUICK-II.
NB: Given the inclusion criteria for QUICK-II, this graph is not representative of the total QUICK-I population, as the patients were selected on BP and Morisky score for QUICK-II.
The longer-term effects of CHEP: sustainability of effects of education As shown in chapter 6, with the general improvements recorded in SBP, DBP and MMAS-8 the performance of QUICK-II participants on outcome measures during CHEP study was encouraging. These results are summarized in Figure 2. This figure not only contains the data as shown in chapter 6, but also additional data. The additional data were collected through an audit of participants’ hospital files on usual care after the end of QUICK-II study. The period under study for the additional data collected was between endline QUICK-II and 4 months after patients exited QUICK-II i.e. between July and October 2012. During this period participants who had exited QUCK-II discontinued further participation in CHEP but continued to access usual care only. The objective of the additional data collection was to investigate possible deterioration, sustenance or consolidation of the short-term effects or gains of CHEP. The patient file audit which was conducted by the researcher in July 2015, long (about 2.5 years) after QUICK-II ended aimed to audit all available QUICK-II patient files. Further assessment of some of the outcome measures SBP and DBP directly after finishing QUICK-II showed a deterioration in performance as the SBP and DBP rose again as shown by a steep rise in the illustrating graph (grey line) after endline QUICK-II (Figure 2). This sharp increase in BP observed among QUICK-II participants in just 4 months after end of CHEP study could have been due to the fact that the effect of the intervention was already waning soon after further exposure to the education program terminated even among participants who were doing well on BP control during the study. It is also possible that the medication adherence (MMAS-8) score of the average participant during this period could have become lower or poorer and consequently caused a decrease in the medication self-efficacy directly and BP control indirectly. This

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 164 —
Chapter 7
observation underscores the importance of a regular and sustained exposure to the educational intervention CHEP for the positive results obtained to be sustained long enough to manifest in improvement in treatment outcomes.
Comparative assessment of performance of QUICK-II and QUICK-I participants during CHEP study When compared to what is obtainable in a control trial, the positive results obtained from the evaluation of CHEP in the current study may not be conclusively attributed to a causal effect because of the relatively weak (pre-, post intervention) design employed in testing the effect. However, a comparative assessment of improvements or otherwise of key outcome measures (SBP and DBP) among QUICK-I and QUICK-II participants during the 6 months of the CHEP study presents an opportunity to assess the effect of CHEP in a scenario that mimics a control study. As shown in Figure 2, QUICK-II participants (grey line in graph) performed relatively better and achieved a better improved average BP control during the same time period when compared to the performance of the 160 patients who participated in QUICK-I (blue line in graph) but were not exposed to the intervention CHEP i.e. not included in QUICK-II. This apparent quasi control assessment indicating a positive effect of CHEP further strengthens the study results and may be cautiously used to interpret an approximate causal effect despite the lack of a control group. We should however note also that the data collection processes involved in this cautious interpretation was different: study file vs. patient standard care file.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General discussion
— 165 —
Figure 2: Systolic/Diastolic Blood Pressure over time, during QUICK-I and QUICK-II and around 3-4 months after QUICK-II (Population: All patients who completed QUICK-I or QUICK-II).
NB: The sample size indicates the number of patients who completed the study. It may be that some patients have missed visits. So, the N varies between the time points.
PERFORMANCE OF CHEP AS COMPARED TO OTHER PROGRAMS Comparison of CHEP with other cardiovascular health education programsAs mentioned earlier, a search of literature had revealed a general lack or insufficient implementation of specifically developed or formal hypertension education programs for persons with cardiovascular health challenges in the African sub continent. The tabular presentation (Table 1) below based on a search of available literature which compares CHEP (Nigeria) with similar education programs which were all outside Africa further supports this assertion and underscores the urgent need to implement such programs among Africa’s growing hypertensive population. Despite this, CHEP performed well and compared favorably with other similar education programs elsewhere [4-5,14-16] with regards to findings of remarkably significant improvements in study outcome measures and hypertension treatment outcomes. BP control and medication adherence or behavioral adherence either increased or are sustained with CHEP compared to few other programs where one or more of these outcome parameters may have stagnated, deteriorated, or were not assessed e.g., Park, et al. (2012) but shared substantial similarities with CHEP in development process, form and content. Furthermore perhaps because of its characteristics of patient-centeredness and cultural relevance, attractiveness and acceptability may have been higher with CHEP (94% uptake) compared to some of the programs from other settings which recorded moderate or lower uptake and poorer retention rate e.g., Houston et al. (2011) 77% uptake. CHEP’s group education and nurse-led delivery format was also an idea that could be quite relevant to address healthcare personnel shortages in regions with human resources challenge such as SSA. However, as indicated before, the positive results gotten from implementation of CHEP need to be interpreted cautiously because of the lack of a
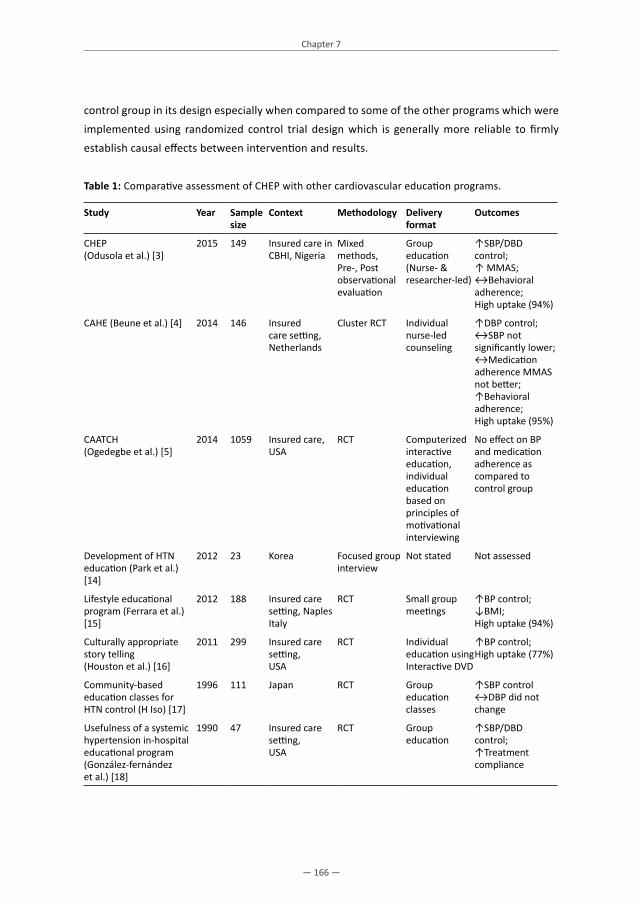
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 166 —
Chapter 7
control group in its design especially when compared to some of the other programs which were implemented using randomized control trial design which is generally more reliable to firmly establish causal effects between intervention and results.
Table 1: Comparative assessment of CHEP with other cardiovascular education programs.
Study year Sample size
Context Methodology Delivery format
Outcomes
CHEP(Odusola et al.) [3]
2015 149 Insured care in CBHI, Nigeria
Mixed methods,Pre-, Post observational evaluation
Group education(Nurse- & researcher-led)
↑SBP/DBD control; ↑ MMAS;↔Behavioral adherence;High uptake (94%)
CAHE (Beune et al.) [4] 2014 146 Insured care setting, Netherlands
Cluster RCT Individual nurse-led counseling
↑DBP control;↔SBP not significantly lower;↔Medication adherence MMAS not better; ↑Behavioral adherence;High uptake (95%)
CAATCH(Ogedegbe et al.) [5]
2014 1059 Insured care, USA
RCT Computerized interactive education, individual education based on principles of motivational interviewing
No effect on BP and medication adherence as compared to control group
Development of HTN education (Park et al.) [14]
2012 23 Korea Focused group interview
Not stated Not assessed
Lifestyle educational program (Ferrara et al.) [15]
2012 188 Insured care setting, Naples Italy
RCT Small group meetings
↑BP control;↓BMI;High uptake (94%)
Culturally appropriate story telling(Houston et al.) [16]
2011 299 Insured care setting,USA
RCT Individual education using Interactive DVD
↑BP control;High uptake (77%)
Community-based education classes for HTN control (H Iso) [17]
1996 111 Japan RCT Group education classes
↑SBP control↔DBP did not change
Usefulness of a systemic hypertension in-hospital educational program(González-fernández et al.) [18]
1990 47 Insured care setting,USA
RCT Group education
↑SBP/DBD control;↑Treatment compliance

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General discussion
— 167 —
IMPLICATIONS FOR CLINICAL PRACTICE AND FUTURE RESEARCH AND RECOMMENDATIONS
As a result of the urgent need to limit CVD and the current scarcity of formally or specifically developed cardiovascular health education programs in the African sub-continent, the emergence of CHEP on the hypertension management landscape of Nigeria and SSA at large indicates a desirable development in efforts to prevent cardiovascular diseases and associated risk factors in the region. The positive results we got with implementation of CHEP underscores its usefulness in addressing this issue effectively and generally in clinical practice. However because CHEP was developed and implemented among patients who had affordable access to quality CVD prevention care in a community based health insurance setting in rural Nigeria, the practical application of CHEP in clinical practice in contexts essentially or substantially different from the specific community based health insurance scenario would require appropriate modification and adaptation of the contents to suit the differing specific contexts. For the future, implementing CHEP on a large scale in other settings with appropriate contextual modifications is indicated and highly recommended. Furthermore, studying the effect of the CHEP in its current form in a randomized control trial will improve the generalizability and increase the potential for a firm establishment of causal links to the positive results. In addition it is strongly recommended to further develop and improve CHEP in other settings and thereafter evaluate the effects of the adapted CHEP in a control trial. Such a result will further enhance its usefulness and reproducibility in specific settings. ConclusionThere is no doubt that the cardiovascular health education program that has been developed in this thesis is relevant for the needs of patients diagnosed with or at risk of developing cardiovascular diseases. CHEP has been developed using very rigorous and scientifically sound formative research approach that incorporates views of key stakeholders in particular patients in the design and implementation of the program. The intervention has been developed with careful consideration for patient-centeredness and cultural relevance. This development process may have contributed to attractiveness and user-acceptability of the intervention. In addition, this increases the potential for a sustainable application of the intervention among priority populations in future. Furthermore, the evaluation was scientifically implemented and produced positive results that have the potential to improve hypertension treatment outcomes. However, because CHEP has so far only been evaluated using a pre/post intervention design that is insufficient to draw a firm conclusion of causal effect of the intervention on results, it remains highly desirable and scientifically indicated to further test the effects of CHEP in future using the more conclusive randomized control trial. We hope that this thesis might serve as a source of inspiration for other people to further develop and test the program we have developed.
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 168 —
Chapter 7
REFERENCES
1. Odusola AO, Hendriks M, Schultsz C, Bolarinwa OA, Akande T, Osibogun A, Agyemang C, Ogedegbe G, Agbede K, Adenusi P, others: Perceptions of inhibitors and facilitators for adhering to hypertension treatment among insured patients in rural Nigeria: a qualitative study. BMC Health Serv Res 2014, 14:624.
2. Ogedegbe G, Gyamfi J, Plange-Rhule J, Surkis A, Rosenthal DM, Airhihenbuwa C, Iwelunmor J, Cooper R: Task shifting interventions for cardiovascular risk reduction in low-income and middle-income countries: a systematic review of randomised controlled trials. BMJ Open 2014, 4:e005983.
3. Odusola AO, Nelissen H, Hendriks M, Schultsz C, Wit F, Bolarinwa OA, Akande T, Agyemang C, Ogedegbe G, Agbede K, others: How Group-Based Cardiovascular Health Education Affects Treatment Adherence and Blood Pressure Control among Insured Hypertensive Nigerians: A Pre-Test, Post-Test Study. World J Cardiovasc Dis 2015, 5:181.
4. Beune EJ, van Charante EPM, Beem L, Mohrs J, Agyemang CO, Ogedegbe G, Haafkens JA: Culturally Adapted Hypertension Education (CAHE) to Improve Blood Pressure Control and Treatment Adherence in Patients of African Origin with Uncontrolled Hypertension: Cluster-Randomized Trial. PloS One 2014, 9:e90103.
5. Ogedegbe G, Tobin JN, Fernandez S, Cassells A, Diaz-Gloster M, Khalida C, Pickering T, Schwartz JE: Counseling African Americans to Control Hypertension: cluster-randomized clinical trial main effects. Circulation 2014, 129:2044–2051.
6. Francis JJ, Johnston M, Robertson C, Glidewell L, Entwistle V, Eccles MP, Grimshaw JM: What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health 2010, 25:1229–1245.
7. Mason M: Sample size and saturation in PhD studies using qualitative interviews. In Forum Qualitative Sozialforschung/Forum: Qualitative Social Research. Volume 11; 2010.
8. Tong A, Sainsbury P, Craig J: Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care J Int Soc Qual Health Care ISQua 2007, 19:349–357.
9. Airhihenbuwa CO, Ford CL, Iwelunmor JI: Why Culture Matters in Health Interventions Lessons From HIV/AIDS Stigma and NCDs. Health Educ Behav 2014, 41:78–84.
10. Strecher VJ, DeVellis BM, Becker MH, Rosenstock IM: The role of self-efficacy in achieving health behavior change. Health Educ Behav 1986, 13:73–92.
11. Kleinman A, Benson P: Anthropology in the Clinic: The Problem of Cultural Competency and How to Fix It. PLoS Med 2006, 3:e294.
12. Resnicow K, Baranowski T, Ahluwalia JS, Braithwaite RL: Cultural sensitivity in public health: defined and demystified. Ethn Dis 1998, 9:10–21.
13. Odusola A, Stronks K, Hendriks M, Schultz C, Akande T, Osibogun A, van Weert H, Haafkens J: Enablers and barriers for implementing high-quality hypertension care in a rural primary care setting in Nigeria: perspectives of primary care staff and health insurance managers. Glob Health Action, Submitted 2015.
14. Park S, Kwon J-S, Kim C, Lee Y, Kim H-K: Development of Nutrition Education Program for Hypertension Based on Health Belief Model, Applying Focus Group Interview. Korean J Community Nutr 2012, 17:623.
15. Ferrara AL, Pacioni D, Di Fronzo V, Russo BF, Staiano L, Speranza E, Gente R, Gargiulo F, Ferrara F: Lifestyle Educational Program Strongly Increases Compliance to Nonpharmacologic Intervention in Hypertensive Patients: A 2-year Follow-Up Study. J Clin Hypertens 2012, 14:767–772.
16. Houston TK, Allison JJ, Sussman M, Horn W, Holt CL, Trobaugh J, Salas M, Pisu M, Cuffee YL, Larkin D, others: Culturally Appropriate Storytelling to Improve Blood PressureA Randomized Trial. Ann Intern Med 2011, 154:77–84.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
General discussion
— 169 —
17. H Iso TS: Community-based education classes for hypertension control. A 1.5-year randomized controlled trial. Hypertension 1996, 27:968–74.
18. González-fernández RA, Rivera M, Torres D, Quiles J, Jackson A: Usefulness of a systemic hypertension in-hospital educational program. Am J Cardiol 1990, 65:1384–1386.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Appendix
Summary
Summary in Dutch (Nederlandse samenvatting)
Images from Cardiovascular Health Education Program (CHEP) sessions
Acknowledgements
List of publications
PhD portfolio
Curriculum Vitae

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Summary
— 173 —
Summary
Hypertension is a significant risk factor for the development of cardiovascular diseases. Cardiovascular diseases (CVD) themselves are a major cause of morbidity and premature mortality worldwide. In sub Saharan Africa (SSA) prevalence of hypertension is high but this is unfortunately currently not commensurate with the low treatment coverage and control. The most populous country in Africa, Nigeria is substantially affected with hypertension. To limit CVD and associated mortality and morbidity, mechanisms for effective health promoting, preventive and control measures are imperative. Furthermore sustainable access to affordable primary health care in the long run is both highly desirable and an indispensable complement to successful CVD control efforts. In addition, implementing quality hypertension care in accordance with international guidelines is equally important. But unfortunately in SSA including Nigeria where hypertension currently affect significant proportion of the population, health systems are rudimentary and poorly developed, poverty is rampant and endemic and sustainable access to affordable care is largely unavailable. This has negative effects on regional control efforts for these chronic conditions. One promising approach to address this issue is to focus CVD control efforts on interventions that have capacity to help hypertensive patients comply with the intricate details of prescribed treatment and thereby limit the potential to develop CVD. Such interventions among others include tailored educational counseling programs. But educational counseling has always been part of the usual primary care offered for hypertension in Nigeria in accordance with international guidelines. Yet hypertension control is poor and CVD frequently develops among hypertensive patients. This may imply that some key or important element is currently missing possibly the mode, form, content or delivery format of the educational counseling offered in usual hypertension care. What could this missing link be? Could it be that the offered usual care education was not attractive or acceptable enough to the target population because it did not address their specific needs with regards to cultural relevance? To answer these questions, in the current study first we attempted and successfully removed the two identified barriers to effective hypertension primary care namely: lack of access to affordable primary care using a health insurance model (Kwara State Health Insurance KSHHI program); and poor quality of hypertension care using a sustainable quality improvement program QUICK to deliver high-quality hypertension care in accordance with international guidelines. Second we developed a special cardiovascular health education program (CHEP) based on the care experience and cultural perceptions of hypertensive patients themselves, in one of the hospitals participating in the KSHI program. Moving on we exposed about 350 hypertensive patients at risk of developing CVD to the sustainable and affordable high-quality hypertension primary care in the KSHI program over a period of 12 months. To our surprise, almost half of this cohort was either yet uncontrolled with respect to blood pressure or non adherent to prescribed medication/healthy behavior at the end of the 12 month study period.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 174 —
Appendix
Based on this surprising observation we packaged a supposedly ideal prototype of ‘usual care’, which includes 3 key components: affordable access to care, high-quality hypertension care, and a specially developed culturally sensitive hypertension education program. Thereafter we exposed the almost 50% uncontrolled cohort to this prototype of usual care over a subsequent 6-month observational follow-up period (the difference being the added special education CHEP). Therefore in this thesis we conducted a research to develop and test a special cardiovascular health education program for insured Nigerian hypertensive patients who accessed high-quality CVD prevention care in the KSHI program at a primary health center in rural Nigeria based on the following specific research objectives:
1. To develop a patient-centered cardiovascular health education program for insured hypertensive patients in a primary care hospital in rural Nigeria
2. To evaluate the developed education program with respect to effectiveness3. To explore for an optimal strategy for a successful implementation of the program in practice
The first objective was addressed in chapter 3 and chapter 5, the second objective in chapter 6 and the third objective in chapter 4. In chapter 1 we introduced the subject under consideration by presenting available statistics to justify the submission or supposition that the issues at stake (hypertension and cardiovascular diseases) are of significant public health importance worldwide but also in SSA and in particular in Nigeria where the study took place. In the process we highlighted the problems of hypertension and cardiovascular diseases, their causes, prevention and control measures and how these may be inadequate to achieve expected results (desirable treatment outcomes) especially if the current health care delivery scenario (limited- or lack of access to quality hypertension primary care) are not effectively addressed. We discussed the modifiable risk factors for these conditions, highlighting the potential to modify these factors in an education program targeting hypertensive patients through improvement in capacity to adhere to prescribed treatment. Chapter 2 was used to describe the study design for the development and evaluation processes involved in the education program including the best strategies available for implementation in practice. In this chapter we outlined in a step by step approach the stages involved in the development process of the educational intervention including the formative phases during which perception based qualitative interview studies with hypertensive patients, healthcare professionals and health insurance managers were used to develop the education program in part 1 of the study. The chapter ended with a description of the pretest/posttest program evaluation design including how participants were to be selected, exposed to the intervention, monitored and assessed in part 2 of the study. The practical activities involved in the educational intervention development process were addressed in chapter 3. In this chapter we described how perception based qualitative interviews were held with a purposively selected sample of insured hypertensive patients to get insight into

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Summary
— 175 —
their views and experiences regarding factors that facilitate or inhibit hypertension care and self management efforts. Findings from the analyzed interview data would be used in a later chapter to develop the intervention. The results got include: having affordable access to care; trust in orthodox “western” medicines; trust in Doctor; fear of hypertension; support from family and religion and use of prayer to support efficacy of pills (as facilitators); inconvenient clinic operating hours; long waiting times; under-dispensing of prescribed pills; side-effects of pills; faith motivated changes of medication regimen; herbal supplementation/substitution of pills; and not being aware that regular use of medication is needed (as inhibitors). Others are use of salt for food preservation; and the negative cultural images associated with decreased body size and physical activity (as inhibitors) and the; awareness that salt substitutes and products for composing healthier meals were cheaply available in the community; and that patient-friendly exercises could be integrated in people’s daily activities (as facilitators). It was anticipated that incorporating these results from people’s local and cultural practices and believes in the development of the education program would make the intervention culturally relevant and therefore attractive and acceptable to the target population. To complete the program development process, in chapter 4 we conducted another set of qualitative interview studies, this time with healthcare professionals treating hypertensive patients and health insurance managers monitoring hypertension care within the KSHI program. The aim was to get insights into their perceptions regarding factors that may enable or inhibit high-quality hypertension care including an exploration for the optimal strategies deployable for the implementation of the cardiovascular health education program in practice. Our findings show that both stakeholder groups considered the availability and access to affordable health insurance to be crucial for the delivery of high-quality hypertension care including a hypertension education component. In particular periodic group education delivery model was suggested as an optimal delivery platform for the education program. Furthermore trust in the sustainability of care, treatment guidelines, tools for patient education, human resources, capacity building, (diagnostic) equipment and drugs, an adequate care administration infrastructure, quality assurance monitoring, adequate provider payments benchmarking and good provider/insurer relationships were identified by both groups as some of the key resources and incentives required for delivery of high-quality hypertension care. In chapter 5 we describe the practical steps and the processes carried out in developing the education program including a formative process phase that included a search of available literature regarding past hypertension education programs previously implemented in Nigeria and SSA, as well as the procedures undertaken to implement findings of the two perception based qualitative interview studies described in chapters 3 and 4 of this thesis. The literature search for education programs revealed that in contrast to efforts from other regions of the world, little or no past efforts were visible in the area of developing culturally tailored hypertension education programs in the African sub-continent. The themes that emerged from qualitative studies were used to develop the specific content of the education program. The program consists of three

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 176 —
Appendix
educational modules (sessions), which aimed to strengthen participants’ understanding of hypertension and their knowledge and ability to manage hypertension in their daily life. The first module focuses on hypertension and the next modules on aspects of medication use, reduction of salt intake and weight, healthy diets and physical exercise. Educational tools used in the intervention include group counseling and supportive posters and audiovisuals with information adapted to the target population. Chapter 6 was used to describe the process of evaluation of the intervention and the results obtained. In this chapter we gave a detailed description of the pretest/posttest study design including the participants recruitment process from an earlier quality improvement CVD prevention study (QUICK-I), baseline and final assessments, intervention exposure over a 6-month observation period, monitoring and implementation and limited process evaluation. In the end we got promising results with regards to treatment outcomes and outcome measures: more participants reported high adherence to medications and behavioral advice than at baseline: respectively, 101 (72%) versus 70 (50%), (p < 0.001) and 126 (90%) versus 106 (76%), (p < 0.001). Participants with controlled BP doubled from 34 (24%) to 65 (46%), (p = 0.001). The median SBP and DBP decreased from 129.0 to 122.0 mmHg, (p = 0.002) and from 80.0 to 73.5 mmHg, (p < 0.001), respectively. However Body mass index did not change (p = 0.444). We found that the improved medication adherence was associated with a decrease in medication concerns (p = 0.045) and improved medication self-efficacy (p < 0.001). Finally in chapter 7 we discussed the main findings of this thesis including the methodological considerations, study design, strengths and limitations and offer recommendations and suggest practical implications for future research and implementation in clinical practice. We presented a critical appraisal of the: overview of hypertensive patients’ perceptions on inhibitors/facilitators of hypertension care; healthcare professionals and health insurance managers perceptions on inhibitors/facilitators of high-quality hypertension care; the formative processes involved in the development of the educational intervention including the baseline theoretical and conceptual framework; the education program, its form, content and delivery process; evaluation of the educational intervention for effectiveness; and a description of the study context of affordable high-quality hypertension care. Finally we made a comparative assessment of performance effectiveness of the educational program both within and outside the Kwara State health insurance program setting in relation to other similar programs within and outside Africa. In the process we found that the intervention was effective in the short-term impact assessment but that for a longer-term sustenance of the positive results obtained there is need for a sustained exposure of participants to the intervention beyond the immediate study period. Furthermore we concluded that even though we got promising results using the pretest/posttest evaluation study design, the intervention will need to be further tested using a randomized controlled trial design in order to be able to draw a firm conclusion of existence of causal links between the promising results which we got and the education program.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Summary in Dutch (Nederlandse samenvatting)
— 177 —
Nederlandse samenvatting
Hart- en vaatziekten (HVZ) dragen wereldwijd in sterke mate bij aan morbiditeit en vroegtijdige sterfte. Hypertensie is een belangrijke risicofactor voor de ontwikkeling van HVZ. De prevalentie van hypertensie in Afrikaanse landen ten zuiden van de Sahara (sub-Sahara Afrika; SSA) is erg hoog terwijl slechts een relatief klein percentage van de patiënten wordt behandeld of een normale bloeddruk bereikt onder behandeling. Ook in Nigeria, het dichtstbevolkte land van Afrika, is de prevalentie van hypertensie aanzienlijk. Om invaliditeit en sterfte door HVZ te voorkomen zijn methoden ter bevordering van de gezondheid en het voorkómen van ziekte noodzakelijk. Bovendien is continue toegang tot betaalbare eerstelijns gezondheidszorg nodig voor een succesvolle behandeling van HVZ. Daarnaast is de implementatie van kwaliteitsrichtlijnen voor hypertensiezorg, in overeenstemming met internationale richtlijnen, van groot belang. Helaas is de gezondheidszorg in landen in SSA, waaronder ook Nigeria, vaak primitief en slecht ontwikkeld, er is veel armoede en continue toegang tot betaalbare zorg is vaak niet beschikbaar. Dit alles heeft een negatief effect op de regionale inspanningen om de ziektelast van deze chronische ziekten in te perken. Een veelbelovende benadering voor de bestrijding van HVZ is om patiënten met hypertensie te helpen met het naleven van de complexe voorgeschreven behandelingen, om daarmee de kans op het ontwikkelen van HVZ te verkleinen. Dergelijke interventies kunnen onder andere bestaan uit educatieve begeleidingsprogramma’s. Hoewel in Nigeria educatieve begeleiding, conform de internationale richtlijnen, altijd deel heeft uitgemaakt van de eerstelijns hypertensiezorg, wordt bloeddrukcontrole onvoldoende bereikt en ontwikkelen HVZ zich regelmatig bij patiënten met hypertensie. Dit kan betekenen dat een aantal belangrijke elementen ontbreken in de begeleiding zoals die wordt aangeboden in de hypertensiebehandeling. De vraag is welke deze elementen zouden kunnen zijn. Een van de mogelijkheden is dat de aangeboden educatie niet aantrekkelijk of acceptabel genoeg is voor de doelgroep omdat het niet voldoet aan hun specifieke behoeften met betrekking tot de culturele relevantie. Om deze vraag te beantwoorden hebben we allereerst geprobeerd twee belemmeringen voor effectieve eerstelijns hypertensiezorg te doorbreken: het gebrek aan toegang tot betaalbare eerstelijns gezondheidszorg met behulp van een ziektekostenverzekering (het Kwara State Health Insurance programma, KSHI) en het leveren van zorg van goede kwaliteit door middel van een kwaliteitsverbeteringsprogramma volgens internationale richtlijnen. Vervolgens hebben we een HVZ-educatieprogramma (CHEP) ontwikkeld in een van de klinieken in het KSHI programma, op basis van de ervaringen en culturele percepties van patiënten die behandeld werden voor hypertensie. Ongeveer 350 patiënten met hypertensie en een risico op het ontwikkelen van HVZ, die via het KSHI programma volgens internationale richtlijnen werden behandeld voor hun hypertensie, werden gedurende een periode van 12 maanden gevolgd. Tot onze verbazing bereikte de helft van deze groep na 12 maanden niet de gewenste bloeddrukdaling of leefde de

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 178 —
Appendix
voorgeschreven medicatie/leefstijl adviezen niet voldoende na. Op basis van deze verrassende waarneming hebben we een zogenaamd ideaal model van “standaard zorg” gecreëerd bestaande uit drie componenten: betaalbare toegang tot zorg, hypertensie behandeling van hoge kwaliteit en een hypertensie educatieprogramma dat rekening houdt met de lokale tradities en gewoonten. Vervolgens hebben we 50% van deze groep patiënten, die niet het gewenste bloeddruk niveau had bereikt of de voorgeschreven medicatie adviezen niet naleefde, deze aangepaste standaard zorg (met als verschil het hypertensie educatieprogramma, CHEP) aangeboden en geobserveerd gedurende een periode van 6 maanden. In dit proefschrift wordt het onderzoek beschreven naar het ontwikkelen en testen van een speciaal HVZ educatieprogramma voor via het KSHI verzekerde Nigeriaanse patiënten met hypertensie, met de volgende doelstellingen:1. Het ontwikkelen van een patiënt gericht HVZ educatieprogramma voor verzekerde patiënten
met hypertensie in een eerstelijns ziekenhuis in ruraal Nigeria2. Het evalueren van de effectiviteit van het ontwikkelde educatieprogramma 3. Het bepalen van de optimale strategie voor de succesvolle implementatie van het programma
in de praktijk.
De eerste doelstelling wordt behandeld in hoofdstuk 3 en hoofdstuk 5, de tweede doelstelling in hoofdstuk 6 en de derde doelstelling in hoofdstuk 4. In hoofdstuk 1 introduceren we het onderwerp van dit proefschrift en presenteren de beschikbare data die de omvang van het probleem dat hypertensie en HVZ vormen voor de wereldbevolking, inclusief SSA en in het bijzonder Nigeria waar het onderzoek plaatsvond, onderbouwen. We lichten de problemen van hypertensie en HVZ en de oorzaken hiervan toe, evenals mogelijke methoden voor preventie en controle en het feit dat deze methoden ontoereikend zijn om goede behandelresultaten te bereiken als het huidige gezondheidszorg systeem in SSA (geen of zeer beperkte toegang tot goede kwaliteit hypertensie behandeling) niet effectief wordt aangepakt. We bespreken de risicofactoren voor hypertensie en HVZ die beïnvloed kunnen worden en besteden aandacht aan de mogelijkheid om deze factoren te beïnvloeden door middel van een educatieprogramma voor patiënten met hypertensie dat de naleving van de voorgeschreven behandeling verbeterd. In hoofdstuk 2 beschrijven we de opzet van de studie voor de ontwikkeling en evaluatie van het educatieprogramma, inclusief optimale strategieën voor programma implementatie. We beschrijven stapsgewijs de verschillende fasen in de ontwikkeling van het educatieprogramma, inclusief de fasen waarin op basis van kwalitatieve interview studies onder hypertensie patiënten, gezondheidszorg medewerkers, en medewerkers van de ziektekostenverzekering het educatieprogramma werd opgezet (deel 1). Dit hoofdstuk eindigt met een beschrijving van de opzet van de evaluatie van het educatieprogramma volgens een voor- en na-test schema, inclusief selectie- en inclusiecriteria, de uitvoering van het educatieprogramma, het volgen van de patiënten en het effect op bloeddruk en naleven van medicatie en leefstijl adviezen (deel 2).

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Summary in Dutch (Nederlandse samenvatting)
— 179 —
In hoofdstuk 3 beschrijven we hoe het educatieprogramma werd opgebouwd. We beschrijven hoe met behulp van kwalitatieve interviews met een doelgerichte selectie van verzekerde patiënten met hypertensie, inzicht werd verkregen in hun ervaringen en meningen over de factoren die een goede behandeling van hypertensie en leefstijl aanpassingen in de weg staan of makkelijker maken. De uitkomsten van deze kwalitatieve studies werden gebruikt om het educatieprogramma te ontwerpen. De resultaten omvatten de volgende begrippen en denkbeelden: toegang tot betaalbare zorg; vertrouwen in conventionele “westerse” geneeskunde; vertrouwen in de dokter; angst voor hoge bloeddruk; ondersteuning van de familie en het geloof en van bidden om het effect van pillen te verbeteren; onhandige openingstijden van de kliniek; lange wachttijden; te weinig voorgeschreven medicatie uitgereikt krijgen; bijwerkingen van medicatie; op het geloof gebaseerde aanpassingen in medicatiegebruik; aanvullen of vervangen van medicatie met lokale kruiden; en het niet bewustzijn van de noodzaak om medicatie regelmatig in te nemen. Andere gebruiken of denkbeelden die genoemd werden, waren: gebruik van zout om voedsel te bewaren; negatieve culturele connotatie van een verminderde lichaamsomvang en lichaamsbeweging; kennis van het feit dat zout-vervangende producten en gezonde voeding in het algemeen voor een redelijke prijs beschikbaar zijn op de markt; en het feit dat lichamelijke inspanning geïntegreerd kan worden in de dagelijkse activiteiten. Het uitgangspunt voor de ontwikkeling van het educatieprogramma was dat wanneer de genoemde cultureel bepaalde denkbeelden en gebruiken onderdeel uitmaken van het programma, dit het programma aantrekkelijker zou maken en het programma beter geaccepteerd zou worden door de doelgroep. In hoofdstuk 4 beschrijven we aanvullende kwalitatieve interview studies, nu met gezond-heidszorg medewerkers die patiënten met hypertensie behandelen en met medewerkers van de ziektekostenverzekering die betrokken zijn bij de kwaliteitsverbetering binnen het KSHI programma. Het doel van deze studie was om inzicht te krijgen in hun beleving van en ervaring met factoren die kwalitatief goede hypertensie behandeling in de weg staan of bevorderen, inclusief factoren die van belang kunnen zijn voor de implementatie van een HVZ educatieprogramma. De resultaten van deze studie tonen aan dat beide groepen belanghebbenden de beschikbaarheid en toegang tot een betaalbare ziektekostenverzekering een cruciaal onderdeel beschouwen voor kwalitatieve HVZ preventie en hypertensiebehandeling inclusief hypertensie educatie. Met name een regelmatig terugkerende groepsgewijze methode werd gesuggereerd als een optimale vorm voor een educatieprogramma. Daarnaast werden vertrouwen in de duurzaamheid van de zorg, beschikbaarheid van richtlijnen voor behandeling, methoden voor educatie van patiënten, beschikbaarheid van human resources, capaciteitsopbouw, (diagnostische) apparatuur en medicatie, een adequaat administratiesysteem, kwaliteitsborging, adequate vergoedingssystemen, en een goede verhouding tussen zorgverlener en zorgverzekeraar genoemd als cruciale middelen en stimulansen voor het leveren van hoogwaardige HVZ zorg. In hoofdstuk 5 beschrijven we de praktijk van de ontwikkeling van het educatieprogramma. De ontwikkeling omvatte de samenstelling van een overzicht van de beschikbare literatuur over bestaande hypertensie educatieprogramma’s in SSA en Nigeria en het opzetten van de twee

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 180 —
Appendix
kwalitatieve interview studies waarvan de resultaten zijn beschreven in de hoofdstukken 3 en 4. De literatuurstudie toonde aan dat, in tegenstelling tot in andere regio’s in de wereld, nagenoeg geen initiatieven tot het ontwikkelen van lokaal geaccepteerde hypertensie educatieprogramma’s worden beschreven voor SSA. De thema’s die uit de kwalitatieve studies naar voren kwamen, werden gebruikt om de specifieke inhoud van het educatieprogramma te ontwikkelen. Het programma bestaat uit drie modules die beogen het begrip van hypertensie te verbeteren en de kennis en mogelijkheden om in het dagelijks leven met hypertensie om te gaan, te verhogen. De eerste module is gericht op hypertensie terwijl de twee volgende modules gericht zijn op medicatiegebruik, vermindering van zoutinname en van gewicht, gezonde voeding en lichamelijke inspanning. Groepseducatie en posters en audiovisuele informatiebronnen, aangepast aan de doelgroep, werden gebruikt als educatiemethoden. In hoofdstuk 6 beschrijven we de evaluatie van het educatieprogramma. Deze beschrijving omvat de opzet van de studie als een voor-na studie, de selectie- en inclusiecriteria op basis van de door de deelnemers behaalde resultaten in de QUICK-I studie, de uitkomstmaten en de implementatie en monitoring. De resultaten van deze studie kunnen bemoedigend genoemd worden voor wat betreft de belangrijkste uitkomstmaten: na deelname aan CHEP volgden meer patiënten medicatie- en levensstijl adviezen dan voorafgaand aan CHEP, respectievelijk 101 (72%) versus 70 (50%), (p<0.001) en 126 (90%) versus 106 (76%), (p<0.001). Het aantal patiënten met een genormaliseerde bloeddruk verdubbelde van 34 (24%) tot 65 (46%), (p=0.001). De mediane systolische en diastolische bloeddruk daalde van respectievelijk 129.0 tot 122.0 mmHg, (p=0.002) en van 80.0 tot 73.5 mmHg, (p<0.001). De Body Mass Index daalde echter niet significant (p=0.44). De verbeterde opvolging van medicatie adviezen was geassocieerd met een afname in zorgen of reserves over medicatie (p=0.045) en een verbetering van zelfredzaamheid voor wat betreft medicatiegebruik (p<0.001). Tenslotte worden in hoofdstuk 7 de belangrijkste bevindingen van dit onderzoek bediscussieerd, met inbegrip van methodologische afwegingen, studieopzet, de sterkte en zwakte van de gekozen opzet en aanbevelingen voor verder onderzoek en implementatie in de klinische praktijk. Daarnaast vergelijken we het effect van het educatieprogramma binnen het KSHI programma en daarbuiten met vergelijkbare programma in SSA en in andere geografische regio’s. CHEP lijkt effectief te zijn op de korte termijn maar voor een langere termijn effect is mogelijk een meer continue expositie aan een dergelijk programma nodig. Bovendien geven de resultaten van deze studie aanleiding om CHEP te testen in een gerandomiseerde gecontroleerde studie. Een dergelijke studie geeft beter inzicht in de causale relatie tussen CHEP en de belangrijkste uitkomstmaten dan een voor-na studie.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Images from Cardiovascular Health Education Program (CHEP) sessions
Images from Cardiovascular Health Education Program (CHEP) sessions

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 182 —
Appendix

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Images from Cardiovascular Health Education Program (CHEP) sessions
— 183 —

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 184 —
Appendix

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Images from Cardiovascular Health Education Program (CHEP) sessions
— 185 —

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Acknowledgements
— 187 —
Acknowledgements
This is the day that the Lord has made; therefore I will rejoice and be glad in it. And for this reason, first and foremost I want to give thanks to the Almighty One and only God who has seen us through a successful completion of this project. I can never thank him enough.
Following this I express my profound gratitude and appreciation to all who have been connected directly or indirectly, closely or remotely to the success of this laudable project. Passionately I submit that words of my mouth alone are inadequate to express my deep felt appreciation effectively to all. In particular, I give special thanks to all individuals, and organizations that have collaborated and contributed in one way or the other to the successful completion of this project including the Health Insurance Fund, PharmAccess Foundation, NUFFIC, Amsterdam Institute for Global Health and Development, University of Ilorin Teaching Hospital, Lagos University Teaching Hospital, Amsterdam Institute for International Development, Academic Medical Center (University of Amsterdam), Hygeia Community Health Care and Ogo Oluwa Hospital.
Particular thanks go to The Netherlands Organization for International Cooperation in Higher Education (NUFFIC) and the Health Insurance Fund. Both organizations provided valuable financial support for this research project.
Specifically, the following individuals have contributed substantially to this project and are hereby acknowledged:
Late Prof. Joep Lange. Although he is no longer with us now having tragically and painfully passed away recently in an avoidable plane crash (may his soul rest in peace), this great man, a teacher of teachers initiated, promoted and nurtured the idea that developed into the main project and other related projects including this PhD research project. A champion of Global Health reputed to have once made the famous statement (not quoted verbatim) that ‘if a bottle of Coke could find its way into the deepest forests in Africa, then antiretroviral drugs would too’ and he worked assiduously to achieve this until his untimely death creating cheap, affordable and virtually free access to healthcare including drugs for the poor and needy in Africa. If you do hear me I say thank you dear Joep Lange. Certainly your efforts in times past in improving healthcare delivery in Africa have not been in vain.
My Promotors Prof. Karien Stronks and Prof. Akin Osibogun.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 188 —
Appendix
Prof. Stronks, you represent a great source of inspiration and motivation for me on this project. As my supervisor your ever ready, patient and accommodating disposition towards critical and objective reviews of my works even sometimes at uncomfortable hours should not go without mention. You charted a course that was easy to follow, guiding me through the project in a way that allowed for development of independent research and analytic skills even while keeping a close watch to redirect me whenever I strayed off course. In my view you made my tasks easy with your supervisory style which gave me guided freedom to sharpen my reporting skills. It’s amazing that despite your very busy schedules, you were always able to do thorough reviews of stages of my work despite my being mostly far away in Nigeria. I thank you immensely. Prof. Osibogun, I will always be grateful to you sir. Even before the current PhD project you have always been there for me as a teacher and supervisor at virtually every developmental stage of my career through my undergraduate and postgraduate years at the University of Lagos. Once again providence has now placed you in strategic stead to contribute further and consolidate on your past efforts in building my capacity through my current PhD study. It is noteworthy that despite your very busy and highly demanding schedules as the Chief Medical Director of the Lagos University Teaching Hospital, you were able to find time to review some of my works. You represent a pillar of moral and academic support to me in Nigeria. Accept my sincere appreciation.
My co-promotors and daily supervisors Dr. Joke Haafkens and Dr. Constance Schultsz.Dr Haafkens, this PhD project will be incomplete without you as it will almost certainly have terminated without your indispensible inputs and strategic presence at critical times in the course of the study. Apart from being a pillar of vital academic support and daily guidance to me despite being thousands of miles away from you yet you were able to do a close supervision of all aspects of my work. It is noteworthy that you once stood up to and forestalled a distractive and unjustified potential disruption in the progress of this project. In your daily supervision and academic oversight on my work, you were very detailed and thorough and this has brought out the best in me. I have been lucky to have someone like you watch over me closely, instilling in me the needed research and analytic skills. You were never tired to regularly check on me even across great divides that often separate us. This was made possible with several supervisory phone calls, Skype sessions and telephone conferences to consolidate on the gains of our face-to-face interactions. Furthermore you were concerned about how I coped on the home front and how this might interfere with my study, including how my family was coping with my frequent study related short and long trips abroad. In a nut shell, you motivated me and you represent the engine room that sustained the project ultimately to a successful completion. I am extremely grateful. Dr Schultsz, I thank you for being there for me. Your supervision of my work especially whenever I am in the Netherlands no doubt contributed tremendously to the success of this project. You were always ready to offer suggestions and to advice on the right path for me.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Acknowledgements
— 189 —
You made inputs that no doubt contributed to the high quality output that has resulted from implementation of this project. Your contribution towards the successful acquisition of the NUFFIC grant for this study is noteworthy. You equally made numerous important and useful contributions to the success of this PhD project whenever it was discussed with you especially during the weekly research meetings at the AIGHD. You were sincerely concerned about the quality of output from this work. In the end this was achieved, I remain extremely grateful. Thank you.
Marleen Hendriks. I cannot reasonably gratify personalities that contributed to the successful completion of this project without a prominent reference to you Marleen. From the start we both were involved in the implementation of the cardiovascular diseases prevention project in the process obtaining our PhDs but I know also that you laid the foundation, and with others did the required ground work before I came on board. In the past I have had reasons to make recourse to you severally for useful and vital information and knowledge and you were always there. You started with implementation of QUICK-I and about a year later I followed with implementation of QUICK-II but you were also a resource for several useful examples that I followed in executing QUICK-II successfully. You were regularly available to offer useful suggestions that helped in moving the project forward. You were indeed a helpful companion. Thank you.
From the Cardiovascular Research Training (CaRT) Institute I thank Prof. Gbenga Ogedegbe and Prof. Charles Agyemang for the tremendous additional supervisory supports. The resources and trainings I received from you and the CaRT faculty no doubt contributed in no small measure to the success of this PhD research project. You both contributed in building my research capacity and refining my research skills. You facilitated an opportunity for me to participate in CaRT and this has contributed to my empowerment with highly desired research skills. Furthermore you both have been available to mentor, advice and supervise aspects of my works in the past. I am grateful for your supports.
To all my colleagues in PharmAccess Foundation the organization that facilitated this project I remain extremely grateful. To be specific I cannot but mention Dr Michelle van vugt and Hanneke Peeters both of whom were my immediate bosses in the Nigeria country office. From the very beginning you were both instrumental in motivating me greatly and in facilitating this capacity building opportunity to study for a PhD even while performing my primary project management functions at PharmAccess. Besides you both were compassionate superiors and motivated me towards this research project. I am grateful. To all my other colleagues at PharmAccess International office (Amsterdam) and PharmAccess Nigeria office including John Dekker, Nicole Spieker, Marijke Roos, Hans Peter Wiebing, Cees Hesp, Annedien Plantenga Ifeoma Philips, Florence Akinsete, Emeka Ajanwachuku, Dupsie Oludipe, Afolabi Osunbayo, Joseph, Emmanuel Aiyenigba and all others not mentioned (for space constraints) I say thank you for your supports,

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 190 —
Appendix
encouragements and cooperation. My interactions with you all have made this project a success and a reality. You were a wonderful team to have worked with and I am very grateful.To colleagues at AIGHD Amsterdam Ferdinand Wit, Alexander Boers, Heleen Nelissen, Nicole Rosendaal, Daniella Brals, Marijn van der List and all others I offer my profound gratitude for your collaborations and supports. You always contribute to making my stays in Amsterdam memorable, worthwhile and result oriented. Heleen your effort in the analysis of the project data was very significant and highly useful. Alex I thank you for an excellent financial administration of this project. Your usual timely logistic and material supports were very useful in facilitating my numerous trips abroad and between Lagos and Kwara-Bacita towards a successful completion of this project. Ferdinand you were a useful resource and I thank you for your helps and supervision in the analytic phase of this project.
A complete description of this PhD study and the facilitating QUICK research project cannot be achieved without giving due cognizance to great personalities within the Hygeia organization who collaborated and enabled a conducive atmosphere for the operational (QUICK) research and a successful data collection. My sincere thanks and appreciation go to the Chairperson of the Hygeia organization Mrs. Fola Laoye. Dr Peju Adenusi, I am immensely grateful for your supports. And to all the Doctors in the Kwara Hygeia team during the period of this research Olusegun Opowoye, Toyin Awofolajin, Emmanuel Aiyenigba and Bukola Shittu-Muideen your individual and collective efforts contributed to the success and completion of this project, I say thank you to you all.
And to that great and wonderful team in Kwara I remain ever grateful for your individual and collective contributions to the successful completion of this project. Indeed, I have benefited from the fruitful collaborations and excellent team spirit displayed while working together on various research projects (Household surveys, QUICK project). I have learnt many things from you all. Right from the head of the team Prof. Akande through others Drs Deji Aderibigbe, Akeem Bolarinwa, Kabir Durowade, Kayode Popoola, Busayo Agbana, Biodun Oladipo and Prof. Kayode Osagbemi. My sincere thanks go to Prof. Akande who had on several occasions in the past offered me logistics and supervisory supports. Dr Bolarinwa, your inputs into the quality control monitoring of the QUICK project is highly valued and greatly appreciated and you regularly gave advised me on many occasions, I appreciate this. I am very grateful to all others not mentioned above, for their valuable contributions at various stages of this project. Yemi Adegboye and Ezra Shalom I greatly appreciate your valuable contributions to the data entry and management for this project. I thank you all.
My special thanks and appreciation also goes to Dr Mrs. Elizabeth Oduwole (formerly Medical Director, General Hospital, Apapa) and now Permanent Secretary Lagos State Ministry of Wealth

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Acknowledgements
— 191 —
Creation and Employment for the tremendous moral and institutional support she gave me in the course of a successful completion of this PhD research project and data provision. The General Hospital Apapa, Lagos facilitated the acquisition of valuable data for the paper already published and the others awaiting publication in respect of the NIH-funded Cardiovascular Research Training in Accra, Ghana. Besides this, you have always been and remain a great source of inspiration, encouragement and motivation to me in my career. I am very grateful for your supports. Thank you.
In giving thanks to those who contributed to the success of this work, I cannot but highlight the roles played by the ‘ground force’ i.e. members of the core QUICK study research team namely Stephen, Esther, Samuel, Adisa, Dorcas and Abdulahi. With your dedication and exceptional performance during the field work and data collection stage of this project, we were able to achieve a successful completion. I am immensely grateful to you all.
Finally, without the wonderful cooperation, collaboration, supports and assistance rendered by the members of staff of Ogo Oluwa Hospital, Bacita we cannot realistically complete the documentation of the story of QUICK study. From the friendly and accommodating team of this hospital we got excellent cooperation both in terms of logistics and hospitality and this motivated and propelled us towards an efficient implementation of the QUICK research project. This ultimately culminated in the production of two PhD degrees. Dr and Mrs. Agbede, you both were very accommodating and supportive in this regard almost to a fault. Your cooperation and those of members of your team facilitated a conducive atmosphere for a successful data collection. We are grateful. Thank you.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
List of publications
— 193 —
List of publications
1. Odusola AO, Hendriks M, Schultsz C, Stronks K, Lange J, Osibogun A, Akande T, Alli S, Adenusi P, Agbede K: Development and evaluation of a patient centered cardiovascular health education program for insured patients in rural Nigeria (QUICK-II). BMC Public Health 2011, 11:171.
2. Odusola A, Stronks K, Hendriks M, Schultz C, Akande T, Osibogun A, van Weert H, Haafkens J: Enablers and barriers for implementing high-quality hypertension care in a rural primary care setting in Nigeria: perspectives of primary care staff and health insurance managers. Glob Health Action. Submitted 2015
3. Odusola AO, Nelissen H, Hendriks M, Schultsz C, Wit F, Bolarinwa OA, Akande T, Agyemang C, Ogedegbe G, Agbede K, others: How Group-Based Cardiovascular Health Education Affects Treatment Adherence and Blood Pressure Control among Insured Hypertensive Nigerians: A Pre-Test, Post-Test Study. World J Cardiovasc Dis 2015, 5:181.
4. Odusola AO, Hendriks M, Schultsz C, Bolarinwa OA, Akande T, Osibogun A, Agyemang C, Ogedegbe G, Agbede K, Adenusi P, others: Perceptions of inhibitors and facilitators for adhering to hypertension treatment among insured patients in rural Nigeria: a qualitative study. BMC Health Serv Res 2014, 14:624.
5. Hendriks M, Brewster L, Wit F, Bolarinwa OA, Odusola AO, Redekop W, Bindraban N, Vollaard A, Alli S, Adenusi P, others: Cardiovascular disease prevention in rural Nigeria in the context of a community based health insurance scheme: QUality Improvement Cardiovascular care Kwara-I (QUICK-I). BMC Public Health 2011, 11:186.
6. Hendriks ME, Bolarinwa OA, Wit FW, Brewster LM, Odusola AO, Rosendaal NT, Bindraban NR, Adenusi P, Agbede K, Lange JM, others: Feasibility and quality of cardiovascular disease prevention within a community-based health insurance program in rural Nigeria: an operational cohort study. J Hypertens 2014, 32:000–000.
7. Boima V, Ademola AD, Odusola AO, Agyekum F, Nwafor CE, Cole H, Salako BL, Ogedegbe G, Tayo BO: Factors Associated with Medication Nonadherence among Hypertensives in Ghana and Nigeria. Int J Hypertens 2015.

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
PhD portfolio
— 195 —
PhD Portfolio
PhD candidate: Aina Olufemi Odusola (Femi)PhD period: 2010-2015PhD supervisors: Prof. Karien Stronks, Prof. Akin OsibogunDaily supervisors: Dr. Joke Haafkens, Dr. Constance Schultsz
year Workload (ECTS)
1. PhD training
General courses
Department of community health, University of Lagos
Research methodology in Medicine 2010 2.6
MAXQDA online course
Introduction to qualitative data analysis 2011 0.5
MAXQDA 10 online tutorial (Basic and Advanced) 2011 0.5
MAXQDA 11 online tutorial (Update) 2011 0.5
AMC Graduate School
Reference Manager 2010 0.1
Reference Manager Advance 2011 0.2
PubMed Biomedical Sciences 2011 0.1
Other
Good clinical practice 2010 0.8
Lagos Health Service Commission – Stream/Pitman Training Institute Birmingham UK (in Lagos)
International and Local Protocols for Managing Cardiovascular Diseases 2010 1.0
Medical and Dental Council of Nigeria / BeyHealth MASTERCLASS
Primary and Secondary Prevention of Cardiovascular Diseases 2012 0.5
Differential Diagnoses and Management of Cardio-Respiratory Symptoms 2012 0.5
Primary Care and Public Health Implication of Cardio-Respiratory Disease 2012 0.5
ECG Made Easy, Artificial Ventilation 2012 0.5
Diabetes and Obesity in Primary and Secondary Care 2013 0.5
Cardiovascular Complications of Diabetic Disease 2013 0.5

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 196 —
Appendix
year Workload (ECTS)
Specific courses
National Institutes of Health – Cardiovascular Research Training Institute (CaRT), University of Ghana, Accra
Epidemiology: Measuring Morbidity 2012 0.5
Epidemiology: Measuring Mortality 2012 0.5
Epidemiology: Prognosis and Randomized Trials 2012 0.5
Epidemiology: Cohort Studies and Estimating Risk 2012 0.5
Epidemiology: Deriving Inferences from Cohort Studies; Bias; Confounding and Interaction
2012 0.5
Fundamentals of Research Methodology: Research Objective and Basic Research Architecture
2012 0.6
Fundamentals of Research Methodology: Components of Architecture – Definition of Outcomes
2012 0.6
Fundamentals of Research Methodology: Components of Architecture – Baseline or Initial State
2012 0.6
Fundamentals of Research Methodology: Components of Architecture – The Maneuver
2012 0.6
Bare Essentials of Biostatistics 2012 2.6
Advanced Biostatistics 2012 2.2
Health Psychology and Behavioral Models 2012 0.5
Culture, Health and Leadership 2012 0.3
Principles of Qualitative Research Methods 2012 0.6
Health Information Skills 2012 0.5
National Diabetes Program in Ghana 2012 0.2
Nutrition, Physical Activity and Obesity in Africa 2012 0.3
Epidemiological and Nutrition Transition in NCDs 2012 0.5
Stroke in Africa 2012 0.3
Survey Methodology 2012 1.0
Community-Based Intervention for Hypertension Prevention 2012 0.5
NIH-funded Project Task-Shifting: Hypertension Implementation Project 2012 1.5
H3 Africa Project funded by Welcome Trust Foundation and NIH 2012 0.2
METS NIH-funded Projects 2012 0.2
Career Paths: Faculty Round 2012 0.3
SPSS (Basics and Advance Courses) 2012 2.5
year Workload (ECTS)

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
PhD portfolio
— 197 —
Other
Getting started with STATA (Online course UCLA) 2012 0.5
Seminars and Workshops
Weekly Research Meetings AIGHD 2012-2014 1.5
Workshop on Quality Management and Upgrade Planning for Hospitals under the HCHC/KSHI Provider Network by PharmAccess International
2011 1.4
Presentations
Presentation on Quality Improvement Cardiovascular Care Kwara QUICK-II interim update in Bacita Kwara Nigeria
2012 0.2
Presentation on ‘Collection and Analysis of Panel Data on Health Outcomes in QUICK-II Study’ at the State-Supported Health Insurance Conference, Kwara State Nigeria
2015 0.2
Conferences
NIH funded Cardiovascular Research Training (CaRT) Institute Conference, Accra, Ghana
2015 0.5
State-Supported Health Insurance Conference (Organized by Kwara State Government, Hygeia, PharmAccess, University of Ilorin)
2015 0.5
2. Teaching
Facilitating / Lecturing / Supervising at Workshops/Surveys/Seminars
Lectured on ‘Good Clinical Practice’ to Researchers Implementing PASER Project (African Study on Antiretroviral Drug Resistance) at Lagos University Teaching Hospital, Lagos
2010 0.4
Trained QUICK Study Research Nurses on QUICK Study Research Methods and Introduction to Cardiovascular Diseases Prevention
2010, 2012 0.5
Supervised Research Assistants and Junior Researchers during series of HIF-funded Community Household Biomedical & Socioeconomic Surveys
2011-2013 2.2
Lectured on ‘Disaster Management and Emergency Preparedness’ (to Doctors and Dentists in a Continuous Medical Education series) at the Isolo General Hospital, Lagos.
2012 0.6

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
Curriculum Vitae
— 199 —
Curriculum Vitae
Aina Olufemi Odusola was born in Lagos Nigeria on 14, March 1965. He graduated from the College of Medicine, University of Lagos in 1992 obtaining his medical degree MBBS in the process. In 1993/94 session he had his internship at the Usman Dan Fodio University Teaching Hospital in Sokoto state northwest Nigeria. In 1994/95 he went through the mandatory one year National Youth Service Scheme and was during this time involved in primary health care services first at a rural General Hospital in Obubra (6 months) and later at an urban General Hospital in Calabar (6 months) both in Cross River State, southeast Nigeria. He followed this with another 6 months as a medical officer at the Nigerian Navy Medical Center, Calabar. On returning to Lagos in late 1995, he worked until 2000 in Internal Medicine in a series of private hospitals under direct supervision of renowned cardiologists. His experience and engagements in the latter hospitals no doubt contributed to his focused interest in the prevention of cardiovascular diseases, a desire which with the benefits of hindsight could now be said to have contributed to his focus for the current PhD research study. From 2000 to 2007 he was a senior medical officer with Lagos State Hospitals Management Board contributing to the delivery of primary and secondary healthcare in 2 of the state’s General Hospitals. In the early part of the latter period he studied on part time basis and obtained a Master’s degree in Humanitarian and Refugee Studies (MHRS) from the university of Lagos in 2001/2002, and later in 2004/2005 he took time off for a Masters in public health (MPH) degree also at the University of Lagos. With the acquisition of MPH his interests in public health practice developed further even while in clinical practice. In 2007 he took a ‘leave of absence’ from his Lagos State Hospital’s clinical job to join PharmAccess Foundation in the capacity of Project Medical Doctor for the organization’s Nigerian operations on the HIF-funded Hygeia Community Health Insurance program which commenced in Lagos and Kwara states. At PharmAccess the candidate had substantial exposure to public health practice locally and internationally, where he was involved in healthcare monitoring and evaluation activities in the insurance program, impact evaluation operational research activities in the insurance program, PharmAccess’s HIV/AIDS workplace program for foreign embassies and corporations and the PharmAccess African Studies to Evaluate Antiretroviral drugs Resistance (PASER) as project manager in Nigeria. His foray into public health was very productive and resulted in an opportunity to study for the current PhD in public health while engaged in the operational research activities of a member of the PharmAccess group Amsterdam Institute for Global Health and Development. In 2010 his proposed thesis won a NUFFIC grant (NFP-PhD.11/ 133) to embark on the current PhD study at the University of Amsterdam. His PhD research was conducted under the direct supervision of Promotors Prof. Karien Stronks and Prof. Akin Osibogun, and co-promotors Dr. Joke Haafkens and Dr. Constance Schultsz. The research which was carried out in the area of prevention of cardiovascular diseases focused on development of an educational intervention program to empower Nigerian hypertensive patients and others at risk of cardiovascular diseases to adhere

500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola500799-L-bw-Odusola
— 200 —
Appendix
to dictates of prescribed treatment towards optimization of treatment outcomes and limiting cardiovascular diseases. Currently back into clinical practice at the Lagos General Hospital supposedly temporarily, he keenly looks forward to new opportunities in public health practice to further contribute to empowerment of clinicians and promote a transformation of public health research findings into clinical practice for the ultimate benefits of patients and others affected in the population. Femi as the candidate is called is married to Tope (Topsy) and they have a boy David (Davido) aged 5 and two girls Oluwalayomi (Layomyte) aged 9 and Oluwalafe (Lafecious) aged 12.




















