
Smeenk bw - Research Explorer
137
UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl) UvA-DARE (Digital Academic Repository) Combined modality treatment of pseudomyxoma peritonei Smeenk, R.M. Publication date 2007 Document Version Final published version Link to publication Citation for published version (APA): Smeenk, R. M. (2007). Combined modality treatment of pseudomyxoma peritonei. General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. Download date:24 Jul 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Smeenk bw - Research Explorer

UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Combined modality treatment of pseudomyxoma peritonei
Smeenk, R.M.
Publication date2007Document VersionFinal published version
Link to publication
Citation for published version (APA):Smeenk, R. M. (2007). Combined modality treatment of pseudomyxoma peritonei.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s)and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an opencontent license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, pleaselet the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the materialinaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letterto: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. Youwill be contacted as soon as possible.
Download date:24 Jul 2022
Combined modality treatmentof pseudomyxoma peritonei
Combined modality treatment of pseudomyxoma peritoneiBy Robert M. Smeenk
This study has been performed inThe Netherlands Cancer Institute – Antoni van Leeuwenhoek HospitalAmsterdam, the Netherlands.
The Netherlands Cancer Institute – Antoni van Leeuwenhoek HospitalStichting Bevordering Kanker onderzoekUniversiteit van AmsterdamNutricia B.V.Dansac NederlandThermoSolutionsNovartis Oncology
AstraZeneca B.V.Johnson and Johnson Medical B.V.Tyco Healthcare B.V.
ISBN-13: 978-90-9021441-2
Cover design: Dustin RemméLay-out: Chris BorPrinted by: Printing Partners Ipskamp
Combined modality treatmentof pseudomyxoma peritonei
ACADEMISCH PROEFSCHRIFT
ter verkrijging van de graad van doctor aan de Universiteit van Amsterdam
prof. mr. P.F. van der Heijdenten overstaan van een door het college voor promoties ingestelde commissie,
in het openbaar te verdedigen in de Aula der Universiteitop 2 februari 2007, te 10.00 uur
door
Robert Matthijs Smeenk
geboren te Moshi (Tanzania)
vrijdag
Promotiecommissie:Promotor: Prof. dr. B.B.R. Kroon
Co-promotores: Dr. F.A.N. Zoetmulder Dr. V.J. Verwaal
Overige leden: Prof. dr. J.J.B. van Lanschot Prof. drs. J.F.W.M. Bartelsman Prof. dr. D.J. Richel Prof. dr. T. Wiggers Dr. H. Boot Dr. M.J. van de Vijver
Faculteit der Geneeskunde

ContentsChapter 1Introduction and outline of the thesis
Chapter 2 Pseudomyxoma peritonei and appendiceal neoplasms: a population based studySubmitted
Chapter 3Pseudomyxoma peritonei: three illustrating case histories Ned Tijdschr Geneesk, in press.
Chapter 4Toxicity and mortality of cytoreduction and intraoperative hyperthermic intraperitoneal chemotherapy in pseudomyxoma peritonei - a report of 103 proceduresEur J Surg Oncol 2006; 32(2):186-90
Chapter 5Survival analysis of pseudomyxoma peritonei patients treated by cytoreductive surgery and hyperthermic intraperitoneal chemotherapyAnn Surg, in press
Chapter 6Learning curve of combined modality treatment in patients with peritoneal surface diseaseSubmitted
Chapter 7 Progressive pseudomyxoma peritonei after combined modality treatment: management and outcomeAnn Surg Oncol, in press
Chapter 8Pseudomyxoma peritonei and the urinary tract: involvement and treatment related complicationsJ Surg Oncol 2006; 93(1):20-3
7
13
27
37
47
59
71
83

Chapter 9Pseudomyxoma peritonei and pregnancy: a report of two casesSubmitted
Chapter 10Pseudomyxoma peritonei: a comprehensive reviewCanc Treat Rev, in press
Chapter 11General discussion
Chapter 12Summary, Nederlandse samenvatting
Dankwoord
Curriculum vitae
91
97
113
121
131
135
1c h a p t e r
Introduction and outline of the thesis


9
Introduction and outline of the thesis
Pseudomyxoma peritonei (PMP) is a rare disease with an incidence of approximate-ly one per million, characterized by diffuse collections of gelatinous material in the abdomen and pelvis, and mucinous implants on the peritoneal surfaces. If literately translated, PMP implies a false mucinous tumour of the peritoneum as the tumour is
in 1884 as a peculiar reaction of the peritoneum to jelly like material, related to an ovar-ian neoplasm.1was reported.2 Since then, there has been a considerable number of reports about this disease.
The term PMP was originally applied to intraperitoneal mucinous spread originat-ing from a cystadenoma of the appendix. When this tumour grows and occludes the lumen, mucous accumulates and the appendix ruptures. The peritoneum is then seeded with mucous-producing cells, which continue to proliferate and produce progressive
have obtained evidence that PMP is a disease of intestinal goblet cells with mucin-secreting proteins that account for the high mucin/cell ratio which can exceed 10:1.3,4
gravity.5 Finally, this results in the characteristic abdominal distension or so-called “jelly belly”.6 Inevitably, this condition progresses to intestinal obstruction, which with-out treatment is fatal.Although the site of the primary tumour is mainly reported as the appendix, also pan-creas, urachus, colon and especially the ovaries have been described as primaries of PMP.7,8 There has been a huge controversy regarding the frequent ovarian involvement in women with PMP: the ovaries have been proposed as both the primary tumour and metastases from an appendiceal primary.6,9-16
In addition, there has been some debate regarding the histopathology of PMP. It has
to apply the term PMP only to a pathologically and prognostic homogeneous group of cases. These cases are characterized by histological benign peritoneal tumours that are frequently associated with an appendiceal mucinous adenoma and have an indolent clinical course.17 Clinicopathological studies have supplied growing evidence that this mucinous cystadenoma of the appendix as the common primary of PMP.14,18 Important
-mas of gastro-intestinal and ovarian origin. These tumours have a completely different biological and prognostic behaviour, and should be treated in a different way.6,9

Chapter 1
10
-thology, and diagnostic signs. PMP is still mistaken for mucinous carcinomatosis and ovarian involvement is regularly incorrectly diagnosed as an ovarian mucinous tumour
treated by inappropriate regimens. Knowledge of disease characteristics will facilitate
patients.
Originally, treatment of PMP involved surgery but other modalities such as mucolytic agents, phototherapy and radiotherapy have been applied.19-21 Surgical debulking with appendectomy, ovariectomy and omentectomy has been the mainstay of treatment for a long period but survival after this treatment strategy is not satisfactory and disease recurrence or progression is imminent.22-24 In the last 20 years PMP treatment has how-
was introduced and combined modality treatment for peritoneal surface disease such as peritoneal carcinomatosis and PMP became available.25-31 This treatment scheme con-sists of a loco regional approach with cytoreductive surgery and intraperitoneal lavage with chemotherapy. The goal of this treatment strategy is two-fold: surgery for complete removal of macroscopic tumour and intraperitoneal chemotherapy to erase microscopic residue. Nowadays, the intraperitoneal chemotherapy is performed intraoperatively and optimized by hyperthermia to improve tissue penetration and cytotoxic properties of the chemotherapeutic agent.32
The Netherlands Cancer Institute – Antoni van Leeuwenhoek Hospital (NKI-AvL) ini-tiated this treatment scheme in 1995 and PMP patients are now treated standard with cytoreductive surgery and intraoperative hyperthermic intraperitoneal chemotherapy (HIPEC). The HIPEC-procedure includes 90 minutes of peritoneal lavage with a heated
has proved to be an effective chemotherapeutic agent for PMP.28 In the NKI-AvL, this procedure is performed by the open coliseum technique with the aid of a homemade perfusion machine.27
This thesis provides an overview of current understanding of and recent developments in PMP pathogenesis, diagnosis, and treatment. It contains a population based study (Chapter 2), three illustrative case histories (Chapter 3), the results on morbidity, mor-tality, survival and learning curve of this combined modality treatment at the NKI-AvL (Chapter 4 to 6) and a discussion of management and outcome of progressive disease (Chapter 7). In addition, the rare involvement of the retroperitoneal urinary tract by PMP (Chapter 8), two cases of PMP in pregnant women (Chapter 9), and a review of

11
Introduction and outline of the thesis
recent literature (Chapter 10) is presented. This dissertation closes with a general discus-sion (Chapter 11) and a summary (Chapter 12).
References1. Werth R. Klinische und anatomische untersuchungen zur lehre von den bauchgeschwuelsten und der
laparotomie. Arch Gynaecol Obstet 1884; 24:100-118.2. Frankel E. Uber das sogenannte pseudomyxoma peritonei. Med Wochenschr 1901;965-970.3. O’Connell JT, Tomlinson JS, Roberts AA et al. Pseudomyxoma peritonei is a disease of MUC2-
expressing goblet cells. Am J Pathol 2002; 161:551-564.4. Heiskala K, Giles-Komar J, Heiskala M et al. High expression of RELP (Reg IV) in neoplastic goblet
cells of appendiceal mucinous cystadenoma and pseudomyxoma peritonei. Virchows Arch 2006; 448:295-300.
5. Sugarbaker PH. Pseudomyxoma peritonei. A cancer whose biology is characterized by a redistribution phenomenon. Ann Surg 1994; 219:109-111.
6. Sugarbaker PH, Ronnett BM, Archer A et al. Pseudomyxoma peritonei syndrome. Adv Surg 1996; 30:233-280.
7. de Bree E, Witkamp A, Van De Vijver M et al. Unusual origins of Pseudomyxoma peritonei. J Surg Oncol 2000; 75:270-274.
8. Smeenk RM, Bex A, Verwaal VJ et al. Pseudomyxoma peritonei and the urinary tract: involvement and treatment related complications. J Surg Oncol 2006; 93:20-23.
9. Young RH, Gilks CB, Scully RE. Mucinous tumors of the appendix associated with mucinous tumors of the ovary and pseudomyxoma peritonei. A clinicopathological analysis of 22 cases supporting an origin in the appendix. Am J Surg Pathol 1991; 15:415-429.
10. Prayson RA, Hart WR, Petras RE. Pseudomyxoma peritonei. A clinicopathologic study of 19 cases with emphasis on site of origin and nature of associated ovarian tumors. Am J Surg Pathol 1994; 18:591-603.
11. Seidman JD, Elsayed AM, Sobin LH et al. Association of mucinous tumors of the ovary and appen-dix. A clinicopathologic study of 25 cases. Am J Surg Pathol 1993; 17:22-34.
12. Cuatrecasas M, Matias-Guiu X, Prat J. Synchronous mucinous tumors of the appendix and the ovary associated with pseudomyxoma peritonei. A clinicopathologic study of six cases with comparative analysis of c-Ki-ras mutations. Am J Surg Pathol 1996; 20:739-746.
13. Guerrieri C, Franlund B, Fristedt S et al. Mucinous tumors of the vermiform appendix and ovary, and pseudomyxoma peritonei: histogenetic implications of cytokeratin 7 expression. Hum Pathol 1997; 28:1039-1045.
14. Ronnett BM, Shmookler BM, Diener-West M et al. Immunohistochemical evidence supporting the appendiceal origin of pseudomyxoma peritonei in women. Int J Gynecol Pathol 1997; 16:1-9.
15. Szych C, Staebler A, Connolly DC et al. Molecular genetic evidence supporting the clonality and appendiceal origin of Pseudomyxoma peritonei in women. Am J Pathol 1999; 154:1849-1855.
16. Ronnett BM, Kurman RJ, Zahn CM et al. Pseudomyxoma peritonei in women: a clinicopathologic analysis of 30 cases with emphasis on site of origin, prognosis, and relationship to ovarian mucinous tumors of low malignant potential. Hum Pathol 1995; 26:509-524.
17. Ronnett BM, Zahn CM, Kurman RJ et al. Disseminated peritoneal adenomucinosis and peritoneal mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol 1995; 19:1390-1408.
18. Young RH. Pseudomyxoma peritonei and selected other aspects of the spread of appendiceal neoplasms. Semin Diagn Pathol 2004; 21:134-150.
Chapter 1
12
19. Green N, Gancedo H, Smith R et al. Pseudomyxoma peritonei-nonoperative management and
20. Piver MS, Lele SB, Patsner B. Pseudomyxoma peritonei: possible prevention of mucinous ascites by peritoneal lavage. Obstet Gynecol 1984; 64:95S-96S.
21. El Sayed S. Pseudomyxoma peritonei treated by radiotherapy. Clin Oncol (R Coll Radiol) 1990; 2:120-122.
22. Gough DB, Donohue JH, Schutt AJ et al. Pseudomyxoma peritonei. Long-term patient survival with an aggressive regional approach. Ann Surg 1994; 219:112-119.
23. Smith JW, Kemeny N, Caldwell C et al. Pseudomyxoma peritonei of appendiceal origin. The Memo-rial Sloan-Kettering Cancer Center experience. Cancer 1992; 70:396-401.
24. Miner TJ, Shia J, Jaques DP et al. Long-term survival following treatment of pseudomyxoma perito-nei: an analysis of surgical therapy. Ann Surg 2005; 241:300-308.
25. Sugarbaker PH, Gianola FJ, Speyer JC et al. Prospective, randomized trial of intravenous versus
98:414-422.26. Mann WJ, Jr., Wagner J, Chumas J et al. The management of pseudomyxoma peritonei. Cancer 1990;
66:1636-1640.27. Zoetmulder FA, van der Vange N, Witkamp AJ et al. [Hyperthermic intra-peritoneal chemotherapy
(HIPEC) in patients with peritoneal pseudomyxoma or peritoneal metastases of colorectal carcino-ma; good preliminary results from the Netherlands Cancer Institute]. Ned Tijdschr Geneeskd 1999; 143:1863-1868.
28. Sugarbaker PH, Landy D, Jaffe G et al. Histologic changes induced by intraperitoneal chemotherapy -
noma of the colon or appendix. Cancer 1990; 65:1495-1501.29. Sugarbaker PH. Cytoreductive surgery and peri-operative intraperitoneal chemotherapy as a curative
approach to pseudomyxoma peritonei syndrome. Eur J Surg Oncol 2001; 27:239-243.30. Sugarbaker PH. Cytoreductive surgery and intraperitoneal chemotherapy with peritoneal spread of
cystadenocarcinoma. Eur J Surg Suppl 1991;75-82.31. Sugarbaker PH, Zhu BW, Sese GB et al. Peritoneal carcinomatosis from appendiceal cancer: results
in 69 patients treated by cytoreductive surgery and intraperitoneal chemotherapy. Dis Colon Rectum 1993; 36:323-329.
32. Witkamp AJ, de Bree E, Van Goethem R et al. Rationale and techniques of intra-operative hyperther-mic intraperitoneal chemotherapy. Cancer Treat Rev 2001; 27:365-374.

2c h a p t e r
Pseudomyxoma peritonei and appendicealneoplasms: a population based study
R.M. Smeenk MD1; M.L.F. van Velthuysen MD PhD2;V.J. Verwaal MD PhD1; F.A.N. Zoetmulder MD PhD1
Department of Surgery1, Department of Pathology2
The Netherlands Cancer Institute - Antoni van Leeuwenhoek HospitalAmsterdam, the Netherlands

Background: Pseudomyxoma peritonei (PMP) is a rare disease, which is thought to originate from an appendiceal mucinous epithelial neoplasm, but the primary tumour is
dominance. Aim of this study is to evaluate epidemiology of PMP in a nationwide data-base and substantiate the primary origin of this disease.Methods: The nationwide pathology database of the Netherlands was searched for both primary appendiceal lesions and PMP between 1995 and 2005 to determine incidence, patient characteristics, and histopathological features. In addition, the relation between appendiceal lesions and PMP was investigated.Results: Annually approximately 17.000 appendectomies are performed in the Neth-
malignant) and twenty percent (20%) of these patients developed PMP. Thirteen per-cent of patients with an appendiceal epithelial neoplasm had an additional epithelial lesion in the colon. From the nationwide database 267 patients (62 men and 205 women)
dominated by the appendix (82%). Although mucinous epithelial neoplasms were more common in women (M:F=1:1.8), the development of PMP in these women was more common than in men with similar lesions (22 vs. 15%). For mucocele and non-muci-nous neoplasm the association with PMP was only 2% and 3%, respectively.Conclusions: Patients with an epithelial neoplasm at appendectomy should undergo colonoscopy for additional colonic epithelial neoplasms. Patients with a mucinous epithelial neoplasm of the appendix, especially women, should be followed for develop-ment of PMP.
Submitted

15
Population based study of PMP
Introduction-
eration.1 A few decennia later in 1884 Werth introduced the term pseudomyxoma peritonei (PMP), literally translated as an untrue mucinous tumour of the peritoneum.2He described it as a peculiar reaction of the peritoneum to a jelly-like substance in the
-
appendiceal mucinous cyst.3 Since then there have been numerous reports on origin, histopathology, and epidemiology of PMP.
Currently PMP is thought to be associated with appendiceal mucinous epithelial neo-plasms.4-8 These tumours tend to form progressive amounts of mucous, which eventually results in the blow-out of the appendix and the release of mucous producing tumour cells in the peritoneal cavity. Free tumour cells are spread throughout the peritoneal
and gravity.9 Ultimately, progressive peritoneal implants and mucinous ascites arise, the characteristic clinical features of PMP.PMP is often characterized as a benign peritoneal surface disease because tumour cells hardly show any invasive properties, lymphatic metastases are found in only few cases, and there is no hematogenic dissemination. Analysis of tumour specimen has how-
described a categorization into three pathological subtypes with increasing malignancy grade.10 Disseminated peritoneal adenomucinosis (DPAM) is the subtype with benign characteristics. It is characterized by pools of mucous with only few well-differentiated epithelial tumour cells (high mucus/cell ratio) with no or hardly any atypia. Perito-neal mucinous carcinomatosis (PMCA), the other end of the spectrum, is characterized by larger amounts of moderately or poorly differentiated tumour cells with consider-able atypia (and sometimes invasive properties). PMCA is the subtype with malignant features, histopathologically comparable with peritoneal mucinous carcinomatosis of colorectal origin, and a grim prognosis.6,10 Finally, an intermediate subtype PMCA-I is characterized predominantly by features of DPAM but focal characteristics of PMCA. Notwithstanding its convenience, especially regarding the assessment of prognosis, this
malignancy grade.11-13
Because ovarian involvement is seen in the majority of female patients, an ovarian pri-mary has long been suggested the cause of PMP.14-18 However, results of several clinical, histopathological, immunohistochemical and molecular genetic studies strongly suggest

Chapter 2
16
that in PMP ovarian tumour deposits are almost always metastases of an appendiceal primary.7,11,19-22
The main purpose of this study was to evaluate PMP epidemiology in the Netherlands and associated appendiceal neoplasms. Furthermore, patients treated at The Netherlands Cancer Institute were evaluated for their representation of the Dutch PMP population.
MethodsDatabasesThis study is based on a search in the nationwide pathology database of the Netherlands (Pathologic Anatomic National Automated Archive or PALGA). This database con-tains anonymous patient characteristics such as age, gender, and conclusions and coded summaries of all pathology reports in the Netherlands since 1992.To relate the number of primary appendiceal neoplasms resulting in PMP to the inci-dence of these neoplasms, three queries were performed. First the database was searched for all patients with a primary appendiceal epithelial neoplasm or mucocele mentioned in the coded summary. The second query was limited to pathology reports mentioning PMP either in the conclusion or in the coded summary. A third query was performed to search for all appendectomies performed in the Netherlands. All searches regarded the 10-year period from 1995 to 2005. The search on PMP included the entire pathological history of the patients.To investigate whether the patient group of the national cancer institute of the Nether-lands is representative for the Dutch PMP patient population, the results of the queries in the nationwide database were compared with a prospective PMP database built at this institute. Both databases obviously display an overlap of patients.
Database analysis and inclusion criteriaPrimary appendiceal lesionsThe diagnosis appendiceal lesion was based on the conclusion of pathology reports from the PALGA database. Appendiceal lesions were categorized into 3 groups: muco-celes; mucinous epithelial neoplasms, consisting of mucinous cystadenoma (MCA) or mucinous adenocarcinoma (MAC); non-mucinous epithelial neoplasms, consisting of villous-, tubular-, serrated adenoma or adenocarcinoma. Metastases in the appendix and carcinoid tumours were excluded from analysis.

17
Population based study of PMP
PMPThe diagnosis PMP was based on the descriptive conclusion of pathology reports from the PALGA database, which had to mention tumour specimen with abundant extra cellular mucus and/or peritoneal mucinous deposits containing no or few (well dif-ferentiated) epithelial cells with no or very little cytological atypia. Pathology reports concluding PMP but only mentioning extra cellular mucin were excluded from analysis as the other criteria were not met. Pathology reports concluding PMP but describing an overt mucinous adenocarcinoma were excluded as well.
-ing PMP and a primary appendiceal epithelial neoplasm or a mucocele. In case of
-nite primary origin, the site of origin was diagnosed as consistent with the appendix. This was based on previous criteria formulated after comparing ovarian and appendi-ceal origins of PMP.11,23
two ovaries and a normal appendix in the pathologic history.
The difference between the number of PMP patients with an appendiceal primary found in the PMP search (n=148), and the number of PMP patients found in the search for appendiceal neoplasms (n=138) is partly caused by the fact that, in cases of extensive surgery, the appendix is mentioned in the conclusion of the report but not in the coded summary, and partly due to metachronous presentation of the appendiceal lesion.
StatisticsStatistical analysis of difference between variables was performed using the Pearson Chi-Square test. Patients with missing data were excluded from analysis. Statistical sig-
Package for Social Sciences (SPSS Inc., Chicago, IL), version 11.5, and SAS version 8.2.
ResultsPrimary appendiceal lesionsApproximately 170.000 appendectomies were performed in the Netherlands between
patients (608 men and 874 women), which translates to an incidence of 9 per million per year. The median age of these patients was 61 years (range 7-93) for men and 64 years (range 11-97) for women.A mucocele was found in approximately 1 out of every 300 appendices. One out of every 165 resected appendices contained an epithelial neoplasm, 50% mucinous and 50% non-mucinous. The mucinous epithelial neoplasms were benign in 73% and malig-
Chapter 2
18
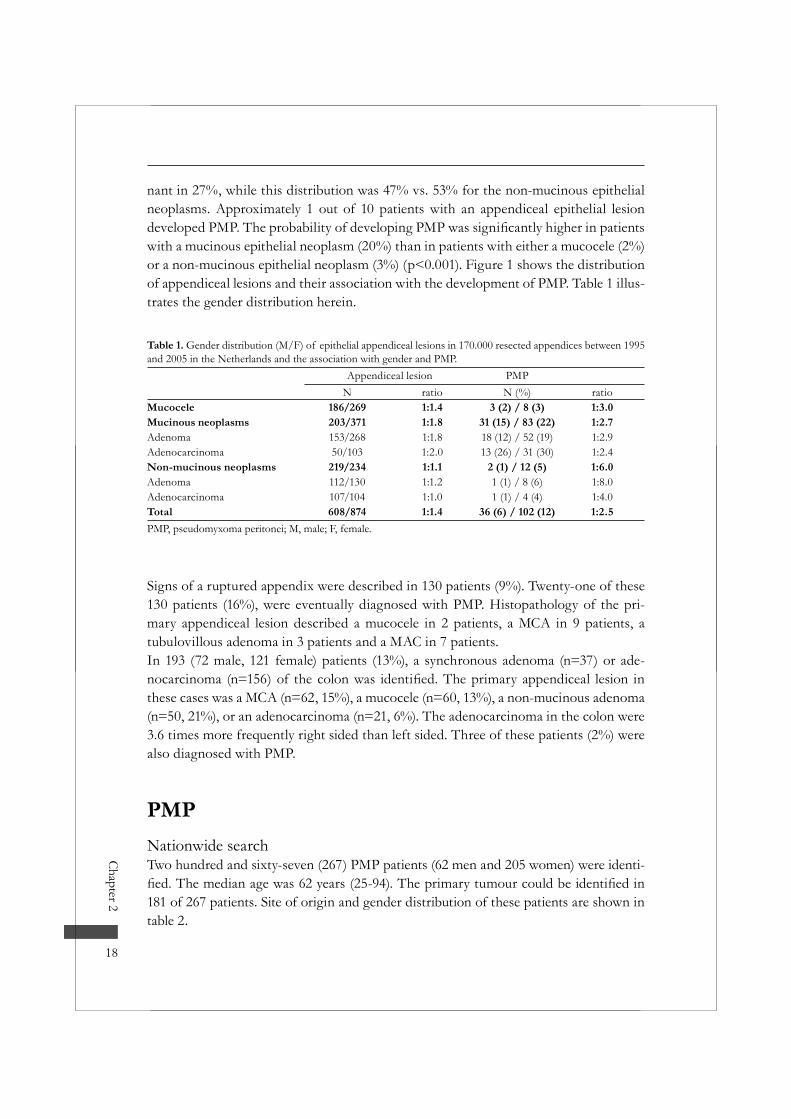
nant in 27%, while this distribution was 47% vs. 53% for the non-mucinous epithelial neoplasms. Approximately 1 out of 10 patients with an appendiceal epithelial lesion
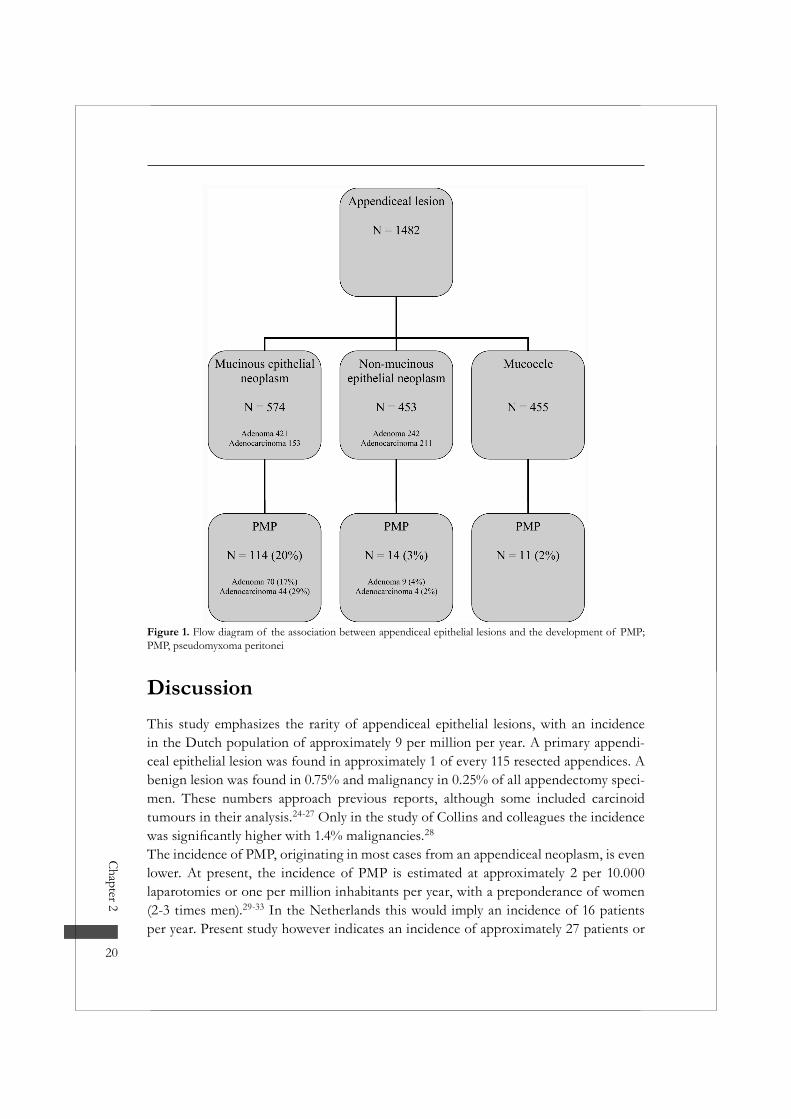
with a mucinous epithelial neoplasm (20%) than in patients with either a mucocele (2%) or a non-mucinous epithelial neoplasm (3%) (p<0.001). Figure 1 shows the distribution of appendiceal lesions and their association with the development of PMP. Table 1 illus-trates the gender distribution herein.
Table 1. Gender distribution (M/F) of epithelial appendiceal lesions in 170.000 resected appendices between 1995 and 2005 in the Netherlands and the association with gender and PMP.
Appendiceal lesion PMPN ratio N (%) ratio
Mucocele 186/269 1:1.4 3 (2) / 8 (3) 1:3.0Mucinous neoplasms 203/371 1:1.8 31 (15) / 83 (22) 1:2.7Adenoma 153/268 1:1.8 18 (12) / 52 (19) 1:2.9Adenocarcinoma 50/103 1:2.0 13 (26) / 31 (30) 1:2.4Non-mucinous neoplasms 219/234 1:1.1 2 (1) / 12 (5) 1:6.0Adenoma 112/130 1:1.2 1 (1) / 8 (6) 1:8.0Adenocarcinoma 107/104 1:1.0 1 (1) / 4 (4) 1:4.0Total 608/874 1:1.4 36 (6) / 102 (12) 1:2.5PMP, pseudomyxoma peritonei; M, male; F, female.
Signs of a ruptured appendix were described in 130 patients (9%). Twenty-one of these 130 patients (16%), were eventually diagnosed with PMP. Histopathology of the pri-mary appendiceal lesion described a mucocele in 2 patients, a MCA in 9 patients, a tubulovillous adenoma in 3 patients and a MAC in 7 patients.In 193 (72 male, 121 female) patients (13%), a synchronous adenoma (n=37) or ade-
these cases was a MCA (n=62, 15%), a mucocele (n=60, 13%), a non-mucinous adenoma (n=50, 21%), or an adenocarcinoma (n=21, 6%). The adenocarcinoma in the colon were 3.6 times more frequently right sided than left sided. Three of these patients (2%) were also diagnosed with PMP.
PMPNationwide searchTwo hundred and sixty-seven (267) PMP patients (62 men and 205 women) were identi-
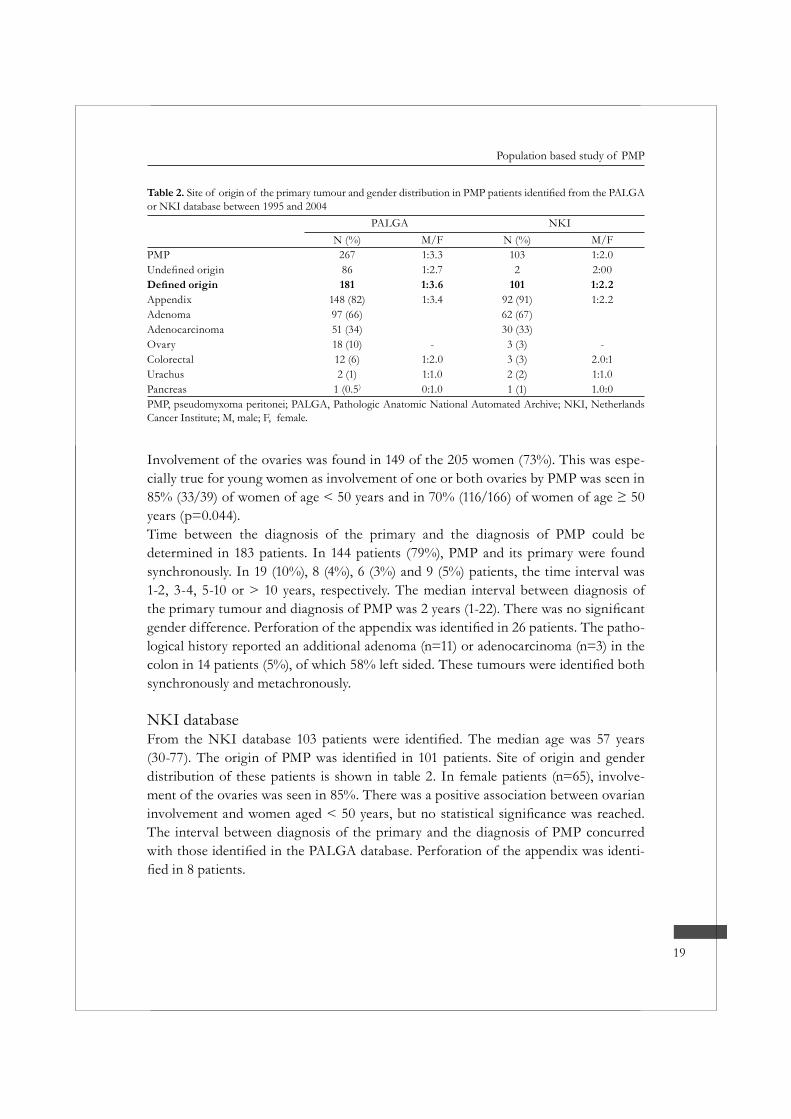
181 of 267 patients. Site of origin and gender distribution of these patients are shown in table 2.
19
Population based study of PMP
Involvement of the ovaries was found in 149 of the 205 women (73%). This was espe-cially true for young women as involvement of one or both ovaries by PMP was seen in
years (p=0.044).Time between the diagnosis of the primary and the diagnosis of PMP could be determined in 183 patients. In 144 patients (79%), PMP and its primary were found synchronously. In 19 (10%), 8 (4%), 6 (3%) and 9 (5%) patients, the time interval was 1-2, 3-4, 5-10 or > 10 years, respectively. The median interval between diagnosis of
patients. The patho-logical history reported an additional adenoma (n=11) or adenocarcinoma (n=3) in the
synchronously and metachronously.
NKI database
distribution of these patients is shown in table 2. In female patients (n=65), involve-ment of the ovaries was seen in 85%. There was a positive association between ovarian
The interval between diagnosis of the primary and the diagnosis of PMP concurred -
Table 2.or NKI database between 1995 and 2004
PALGA NKIN (%) M/F N (%) M/F
PMP 267 1:3.3 103 1:2.086 1:2.7 2 2:00181 1:3.6 101 1:2.2
Appendix 148 (82) 1:3.4 92 (91) 1:2.2Adenoma 97 (66) 62 (67)Adenocarcinoma 51 (34) 30 (33)Ovary 18 (10) - 3 (3) -Colorectal 12 (6) 1:2.0 3 (3) 2.0:1Urachus 2 (1) 1:1.0 2 (2) 1:1.0Pancreas 1 (0.5) 0:1.0 1 (1) 1.0:0PMP, pseudomyxoma peritonei; PALGA, Pathologic Anatomic National Automated Archive; NKI, Netherlands Cancer Institute; M, male; F, female.
Chapter 2
20
DiscussionThis study emphasizes the rarity of appendiceal epithelial lesions, with an incidence in the Dutch population of approximately 9 per million per year. A primary appendi-ceal epithelial lesion was found in approximately 1 of every 115 resected appendices. A benign lesion was found in 0.75% and malignancy in 0.25% of all appendectomy speci-men. These numbers approach previous reports, although some included carcinoid tumours in their analysis.24-27 Only in the study of Collins and colleagues the incidence
28
The incidence of PMP, originating in most cases from an appendiceal neoplasm, is even lower. At present, the incidence of PMP is estimated at approximately 2 per 10.000 laparotomies or one per million inhabitants per year, with a preponderance of women (2-3 times men).29-33 In the Netherlands this would imply an incidence of 16 patients per year. Present study however indicates an incidence of approximately 27 patients or
Figure 1. Flow diagram of the association between appendiceal epithelial lesions and the development of PMP; PMP, pseudomyxoma peritonei

21
Population based study of PMP
1.7 per million per year, which is slightly higher.31 Actually, the incidence could even be 2 per million because we believe not all PMP patients have not been included in our analysis. In these cases PMP has not been recognized as such and was therefore not reported in the pathology reports.
In the present study we found that approximately 10% of patients with an epitheli-al appendiceal lesion will develop PMP, which means 1 case of PMP in every 1000 appendectomy specimen. Especially patients with an appendiceal mucinous epithelial neoplasm are prone to develop PMP, particularly if the neoplasm is interpreted as an adenocarcinoma. In contrast, there is no clear relation of PMP with the appendiceal mucocele. This suggests that a mucocele should not be regarded as a neoplastic lesion, although the accumulation of mucous in the appendiceal lumen might suggest oth-erwise. The non-mucinous epithelial appendiceal neoplasms are not related to PMP either. These observations are in accordance with previous studies that have reported on the dominance of mucinous neoplasms in the appendix and right-sided colon, and the different behaviour in contrast to non-mucinous neoplasms.34-38 In this series the proportion of mucinous adenocarcinomas (40%) of the appendix is even higher than in previous series.39 Apparently, mucinous neoplasms of the appendix are more likely to develop PMP than non-mucinous appendiceal or mucinous colonic neoplasms. In our understanding, this can be explained by the ability to produce mucous, with consequent rising intraluminal pressure, rupture of the appendiceal wall, and tumour spill into the peritoneal cavity.Our study shows that the median evolution time from an appendiceal neoplasm to PMP is 2 years, but the interval can be more than 10 years. This is in accordance with the literature where spontaneous evolution of PMP from mucinous lesions has been described to be approximately 21 months, but extremely long intervals have been report-ed as well.40,41 Such indolent tumour behaviour suggests that these patients should be followed for life to detect PMP at an early stage. However, this is debatable as most (79%) of appendiceal lesions were detected synchronously. Regarding the aspects of PMP behaviour discussed, we recommend a follow-up of 5 years in patients with a mucinous epithelial appendiceal neoplasm, consisting of a computed tomography scan once a year or when indicated.
The patient group of the NKI seems representative for the patient group found in the national database as patient and pathological features largely comply. The appendix was
6,7 However, in the NKI the primary site,
in 22% of cases in the query of the national database. Bulky PMP deposits, especially

Chapter 2
22
site in these cases.Despite the appendiceal dominance, 10% of patients in the national database were clas-
NKI database. In these cases the appendix was explicitly reported as normal and a rup-tured primary ovarian cystadenoma or cystadenocarcinoma is suggested as the cause of tumour cell dissemination. In fact, ovarian tumours (of low-malignant potential) have been reported as the site of origin of PMP, but they present with distinctive features: in contrast to ovaries with PMP localization, the size of these primary ovarian tumours is usually bigger, the presentation unilaterally with multiloculated cysts and the tumour found in the stroma instead of at the surface.23,42 Still to exclude a primary appendiceal lesion, appendectomy should be routine in patients with a mucinous ovarian tumour.
Some other observations in this study are remarkable. First, this study demonstrates
reports.33,43-45 It is therefore tempting to attribute a role to the ovaries in the patho-genesis of PMP, strengthened by the favoured ovarian involvement in premenopausal
stepping stone for tumour cell deposits. Besides this pure mechanical aspect one might think of hormonal micro environmental factors. It can however also not be excluded that some male PMP patients are in fact diagnosed as adenocarcinoma of unknown primary.Secondly, the additional neoplasm in the colon in 13% of patients with an appendiceal
Connor and colleagues, who reported a high incidence of synchronous and metachronous colorectal cancer.24 Also, the dominant right sided location of adenocarcinoma of the colon concurs with previous reports.46-48
-plasm in case of ileocoecal resection for a right-sided colonic carcinoma, in our opinion the alleged multifocality in colorectal tumours still warrants colonoscopy in patients with an epithelial neoplasm at appendectomy.
In a practical sense, based on this study, we recommend colonoscopy in all patients with an appendiceal neoplasm in appendectomy specimen. Patients with a mucinous epithelial neoplasm of the appendix at appendectomy should be monitored for the development of PMP.
23
Population based study of PMP
References1. Weaver C.H. Mucocele of the appendix with pseudomucinous degeneration. Am J Surg 1937;
36:523.2. Werth R. Klinische und anatomische untersuchungen zur lehre von den bauchgeschwuelsten und der
laparotomie. Arch Gynaecol Obstet 1884; 24:100-118.3. Frankel E. Uber das sogenannte pseudomyxoma peritonei. Med Wochenschr 1901;965-970.4. Lamps LW, Gray GF, Jr., Dilday BR et al. The coexistence of low-grade mucinous neoplasms of the
appendix and appendiceal diverticula: a possible role in the pathogenesis of pseudomyxoma peritonei. Mod Pathol 2000; 13:495-501.
5. Carr NJ, Emory TS, Sobin LH. Epithelial neoplasms of the appendix and colorectum: an analysis of cell proliferation, apoptosis, and expression of p53, CD44, bcl-2. Arch Pathol Lab Med 2002; 126:837-841.
6. Bradley RF, Stewart JH, Russell GB et al. Pseudomyxoma peritonei of appendiceal origin: a clinico-pathologic analysis of 101 patients uniformly treated at a single institution, with literature review. Am J Surg Pathol 2006; 30:551-559.
7. Young RH. Pseudomyxoma peritonei and selected other aspects of the spread of appendiceal neoplasms. Semin Diagn Pathol 2004; 21:134-150.
8. Byron RL, Jr., Yonemoto RH, King RM et al. The management of pseudomyxoma peritonei second-ary to ruptured mucocele of the appendix. Surg Gynecol Obstet 1966; 122:509-512.
9. Sugarbaker PH. Pseudomyxoma peritonei. A cancer whose biology is characterized by a redistribution phenomenon. Ann Surg 1994; 219:109-111.
10. Ronnett BM, Zahn CM, Kurman RJ et al. Disseminated peritoneal adenomucinosis and peritoneal mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol 1995; 19:1390-1408.
11. Prayson RA, Hart WR, Petras RE. Pseudomyxoma peritonei. A clinicopathologic study of 19 cases with emphasis on site of origin and nature of associated ovarian tumors. Am J Surg Pathol 1994; 18:591-603.
12. Loungnarath R, Causeret S, Bossard N et al. Cytoreductive surgery with intraperitoneal chemohyper-thermia for the treatment of pseudomyxoma peritonei: a prospective study. Dis Colon Rectum 2005; 48:1372-1379.
13. Elias D, Laurent S, Antoun S et al. [Pseudomyxoma peritonei treated with complete resection and immediate intraperitoneal chemotherapy]. Gastroenterol Clin Biol 2003; 27:407-412.
14. Seidman JD, Elsayed AM, Sobin LH et al. Association of mucinous tumors of the ovary and appen-dix. A clinicopathologic study of 25 cases. Am J Surg Pathol 1993; 17:22-34.
15. Wertheim I, Fleischhacker D, McLachlin CM et al. Pseudomyxoma peritonei: a review of 23 cases. Obstet Gynecol 1994; 84:17-21.
16. Cuatrecasas M, Matias-Guiu X, Prat J. Synchronous mucinous tumors of the appendix and the ovary associated with pseudomyxoma peritonei. A clinicopathologic study of six cases with comparative analysis of c-Ki-ras mutations. Am J Surg Pathol 1996; 20:739-746.
17. Chuaqui RF, Zhuang Z, Emmert-Buck MR et al. Genetic analysis of synchronous mucinous tumors of the ovary and appendix. Hum Pathol 1996; 27:165-171.
18. Campbell JS, Lou P, Ferguson JP et al. Pseudomyxoma peritonei et ovarii with occult neoplasms of appendix. Obstet Gynecol 1973; 42:897-902.
19. Szych C, Staebler A, Connolly DC et al. Molecular genetic evidence supporting the clonality and appendiceal origin of Pseudomyxoma peritonei in women. Am J Pathol 1999; 154:1849-1855.
20. Guerrieri C, Franlund B, Fristedt S et al. Mucinous tumors of the vermiform appendix and ovary, and pseudomyxoma peritonei: histogenetic implications of cytokeratin 7 expression. Hum Pathol 1997; 28:1039-1045.
Chapter 2
24
21. Ronnett BM, Shmookler BM, Diener-West M et al. Immunohistochemical evidence supporting the appendiceal origin of pseudomyxoma peritonei in women. Int J Gynecol Pathol 1997; 16:1-9.
22. Young RH, Gilks CB, Scully RE. Mucinous tumors of the appendix associated with mucinous tumors of the ovary and pseudomyxoma peritonei. A clinicopathological analysis of 22 cases supporting an origin in the appendix. Am J Surg Pathol 1991; 15:415-429.
23. Ronnett BM, Kurman RJ, Zahn CM et al. Pseudomyxoma peritonei in women: a clinicopathologic analysis of 30 cases with emphasis on site of origin, prognosis, and relationship to ovarian mucinous tumors of low malignant potential. Hum Pathol 1995; 26:509-524.
24. Connor SJ, Hanna GB, Frizelle FA. Appendiceal tumors: retrospective clinicopathologic analysis of appendiceal tumors from 7,970 appendectomies. Dis Colon Rectum 1998; 41:75-80.
25. Marudanayagam R, Williams GT, Rees BI. Review of the pathological results of 2660 appendicec-tomy specimens. J Gastroenterol 2006; 41:745-749.
26. Burgess P, Done HJ. Adenocarcinoma of the appendix. J R Soc Med 1989; 82:28-29.27. Schmutzer KJ, Bayar M, Zaki AE et al. Tumors of the appendix. Dis Colon Rectum 1975; 18:324-
331.
Am J Proctol 1963; 14:265-281.29. Mann WJ, Jr., Wagner J, Chumas J et al. The management of pseudomyxoma peritonei. Cancer 1990;
66:1636-1640.30. Moran BJ. Establishment of a peritoneal malignancy treatment centre in the United Kingdom. Eur J
Surg Oncol 2006; 32:614-618.31. Mukherjee A, Parvaiz A, Cecil TD et al. Pseudomyxoma peritonei usually originates from the appen-
dix: a review of the evidence. Eur J Gynaecol Oncol 2004; 25:411-414.32. Smith JW, Kemeny N, Caldwell C et al. Pseudomyxoma peritonei of appendiceal origin. The Memo-
rial Sloan-Kettering Cancer Center experience. Cancer 1992; 70:396-401.
Obstet Invest 2001; 51:73-80.34. Carr NJ, McCarthy WF, Sobin LH. Epithelial noncarcinoid tumors and tumor-like lesions of the
appendix. A clinicopathologic study of 184 patients with a multivariate analysis of prognostic factors. Cancer 1995; 75:757-768.
35. Green JB, Timmcke AE, Mitchell WT et al. Mucinous carcinoma--just another colon cancer? Dis Colon Rectum 1993; 36:49-54.
36. Nozoe T, Anai H, Nasu S et al. Clinicopathological characteristics of mucinous carcinoma of the colon and rectum. J Surg Oncol 2000; 75:103-107.
37. Kang H, O’Connell JB, Maggard MA et al. A 10-year outcomes evaluation of mucinous and signet-ring cell carcinoma of the colon and rectum. Dis Colon Rectum 2005; 48:1161-1168.
38. Kabbani W, Houlihan PS, Luthra R et al. Mucinous and nonmucinous appendiceal adenocarcinomas: different clinicopathological features but similar genetic alterations. Mod Pathol 2002; 15:599-605.
39. Du W, Mah JT, Lee J et al. Incidence and survival of mucinous adenocarcinoma of the colorectum: a population-based study from an Asian country. Dis Colon Rectum 2004; 47:78-85.
40. Darnis E, Ronceray J, Grosieux P et al. [Pseudomyxoma peritonei in females. 13 personal cases. Prac-tical deductions from a review of 420 cases in the literature]. J Gynecol Obstet Biol Reprod (Paris) 1987; 16:343-353.
41. Solkar MH, Akhtar NM, Khan Z et al. Pseudomyxoma extraperitonei occurring 35 years after appen-dicectomy: a case report and review of literature. World J Surg Oncol 2004; 2:19.
42. Ronnett BM, Shmookler BM, Sugarbaker PH et al. Pseudomyxoma peritonei: new concepts in diag-nosis, origin, nomenclature, and relationship to mucinous borderline (low malignant potential) tumors of the ovary. Anat Pathol 1997; 2:197-226.
43. Hananel N, Powsner E, Wolloch Y. Adenocarcinoma of the appendix: an unusual disease. Eur J Surg 1998; 164:859-862.
25
Population based study of PMP
44. Deliniere F, Arnaud JP, Casa C et al. [Pseudomyxoma peritonei. Apropos of 19 cases]. J Chir (Paris) 1993; 130:141-145.
45. Landen S, Bertrand C, Maddern GJ et al. Appendiceal mucoceles and pseudomyxoma peritonei. Surg Gynecol Obstet 1992; 175:401-404.
in colorectal carcinoma. Tech Coloproctol 2004; 8 Suppl 1:s123-s125.47. King-Yin LA, Ong K, Ho YH. Colorectal mucinous adenocarcinoma: the clinicopathologic features
48. Zhang H, Evertsson S, Sun X. Clinicopathological and genetic characteristics of mucinous carcino-mas in the colorectum. Int J Oncol 1999; 14:1057-1061.

3c h a p t e r
Pseudomyxoma peritonei: three illustrating case histories
R.M. Smeenk, V.J. Verwaal, F.A.N. Zoetmulder
Department of SurgeryThe Netherlands Cancer Institute - Antoni van Leeuwenhoek Hospital
Amsterdam, the Netherlands

Cytoreductive surgery and intraoperative hyperthermic intraperitoneal chemo-therapy as treatment for pseudomyxoma peritonei – Three patients, aged 30, 47 and 48 years, were diagnosed with pseudomyxoma peritonei (PMP). They presented with appendicitis-like symptoms, progressive abdominal distension, and an ovarian mass, respectively. Treatment consisted of cytoreductive surgery (CRS) followed by hyper-thermic intraperitoneal chemotherapy (HIPEC). After a mean follow-up of 64 months (19-89) after initial treatment, one patient had died of progression, and two patients were alive without disease.PMP is a rare disease, characterised by progressive intraperitoneal accumulation of mucous, produced by peritoneal mucinous implants, mostly originating from an appen-diceal mucinous adenoma. Treatment by CRS and HIPEC results in a 5-years survival probability of > 60%, depending on pathological subtype and completeness of CRS. Recognising PMP patients in an early stage, in which complete cytoreduction is still achievable, can result in a considerable survival improvement.
Ned Tijdschr Geneesk, in press

29
Three illustrating case histories
Pseudomyxoma peritonei (PMP) is a disease that is characterized by the presence of mucinous tumour deposits on the peritoneal surface and omentum with a progressive quantity of mucinous ascites. PMP is a rare disease with an incidence of approximately 1 per million per year. Since 1995, the Netherlands Cancer Institute – Antoni van Leeu-wenhoek Hospital (NKI – AVL) has developed into a treatment centre for patients with PMP in the Netherlands.1,2 We want to bring attention to this rare disease, which sometimes is not recognized as such, by presenting three case histories.
Case historiesPatient A, a 47-year old man, was admitted elsewhere for appendectomy due to a sus-
appendix revealed a cystadenoma. The patient was seen again 4 years later with vague
5). A computed tomography (CT) scan and a biopsy suggested PMP. Laparotomy was performed in our hospital, during which a massive amount of mucinous ascites was removed, the peritoneal surface was stripped and a distal gastrectomy, transverse colon resection, ileocoecum resection, partial small bowel resection, rectum resection, cho-lecystectomy, peritonectomy, and omentectomy were performed. Unfortunately, the entire tumour mass could not be removed: some small PMP deposits were left behind on the small bowel surface and in the sub hepatic region. Then the abdominal cavity
-mic intraperitoneal chemotherapy or HIPEC), after which necessary bowel anastomoses were made. The postoperative period was uncomplicated and the patient was released 18 days after operation. Pathological examination showed PMP specimen with few epithelial cells and very little atypia. Because of the latter, systemic chemotherapy (5-Fluorouracil/Leucovorin) was given. In the next years, there was slow progression of disease and 69 months after the primary treatment a second procedure of CRS and HIPEC was performed. This time a macroscopic complete cytoreduction could be accomplished. The postoperative period was uncomplicated. At a recent follow-up, 19 months after the second procedure, there was no evidence of disease.
Patient B, a 30-years old man from Portugal, was referred to our institute due to progres-sive abdominal distension and suspicion of PMP. A laparoscopy and intra-abdominal
and extensive peritoneal tumour growth. Four litres of mucinous ascites were drained. The peritoneum was stripped and an ileocoecum resection, a rectosigmoid resec-tion, a subtotal gastrectomy, a splenectomie, a cholecystectomy, an omentectomy, and peritonectomy were performed, by which a macroscopic complete cytoreduction was

Chapter 3
30
accomplished. After this, the lavage with HIPEC was performed. The postoperative period was uncomplicated and the patient could be discharged 14 days after opera-tion. Pathological examination showed a primary villous adenoma of the appendix and PMP with only few epithelial cells without atypia. Additional systemic chemotherapy was therefore withdrawn. Nine months after treatment there was mass recurrence with ascites. Histology showed a well-differentiated adenocarcinoma, demonstrating dedif-ferentiation of tumour cells. Despite treatment with 5-Fluorouracil, Leucovorin and Oxaliplatin, progressive disease developed and the patient died ten months after the diagnosis of recurrence.
Patient C, a 48-year old woman, was admitted to a hospital elsewhere for the treatment of an ovarian neoplasm. At laparotomy the uterus, ovaries and omentum were resect-ed. Pathological examination showed PMP originating from a mucinous cystadenoma of the appendix with ovarian metastases. Initially no treatment was started, but after a rise in tumour marker CA-125 systemic chemotherapy (Endoxan/Carboplatin) was given. Despite this, recurrence developed and she was referred to our institute. CEA
and a subtotal gastrectomy, a subtotal colectomy, a splenectomy, a cholecystectomy, and an omentectomy were performed. A complete cytoreduction could however not be achieved and tumour residues of less than 2.5mm thick remained around the liver and
colostomy was constructed. Pathological examination revealed extra cellular mucus with few epithelial cells with no atypia. This resulted in abandoning systemic chemotherapy. The postoperative period was initially uncomplicated and the patient was released after
surgery of the bladder was performed. The colostomy was removed 3 years after initial treatment. At last follow-up, 7 years and 5 months after initial treatment there was no evidence of disease.
DiscussionPathogenesisIn PMP the primary tumour is usually a mucinous (cyst)adenoma of the appendix.3Progressive intraluminal mucous production and obstruction eventually results in a mucocele. When this mucocele perforates, mucous producing tumour cells are released in the abdominal cavity, where they do not grow in the vicinity of the perforation to multiply locally like as in a carcinoma, but are spread throughout the peritoneal cav-ity conforming to the redistribution phenomenon.4 This pattern of dissemination is

31
Three illustrating case histories
is produced, and passes the paracolic gutters towards omentum and diaphragm, where
addition, gravity transports tumour cells and mucous to the pelvis, where in women a large ovarian tumour mass can develop. Finally, tumour cells may accumulate at sticky surgical wound surfaces. Altogether, this explains the characteristic distribution of PMP with limited tumour at the primary appendix site and often massive tumour on the ova-ries, omentum and sub diaphragmatic space.3 The small bowel is, because of its mobility in contrast to other intraperitoneal viscera, usually free from tumour until a late stage.
Histopathologically, PMP is essentially a benign tumour. Histology shows adenomatous epithelial cells that are of GI tract origin on immunohistochemistry, show little mitosis, and show no tendency of invasive growth or systemic metastasis. There is however a gradual transition from pure benign PMP to PMP with more malignant features. Ron-nett and colleagues divided PMP in 3 pathological subtypes with different pathological characteristics (grade of malignancy) and prognosis.5 -tion is found in the determination of prognosis and evaluation of additional treatment. Dedifferentiation from low to high malignancy grade has been observed at time of
6
Presenting symptomsPMP is actually a clinical diagnosis. The median age of PMP patients is 57 years. The classic presentation sign (in 23% of patients) is increasing abdominal girth, the so-called
an ovarian mass. These patients are usually in a late stage of disease. In some cases (14%),
is acute appendicitis. In contrast, these patients are in the early stage of the disease.
Figure 1. Omental cake of PMP.
Chapter 3
32
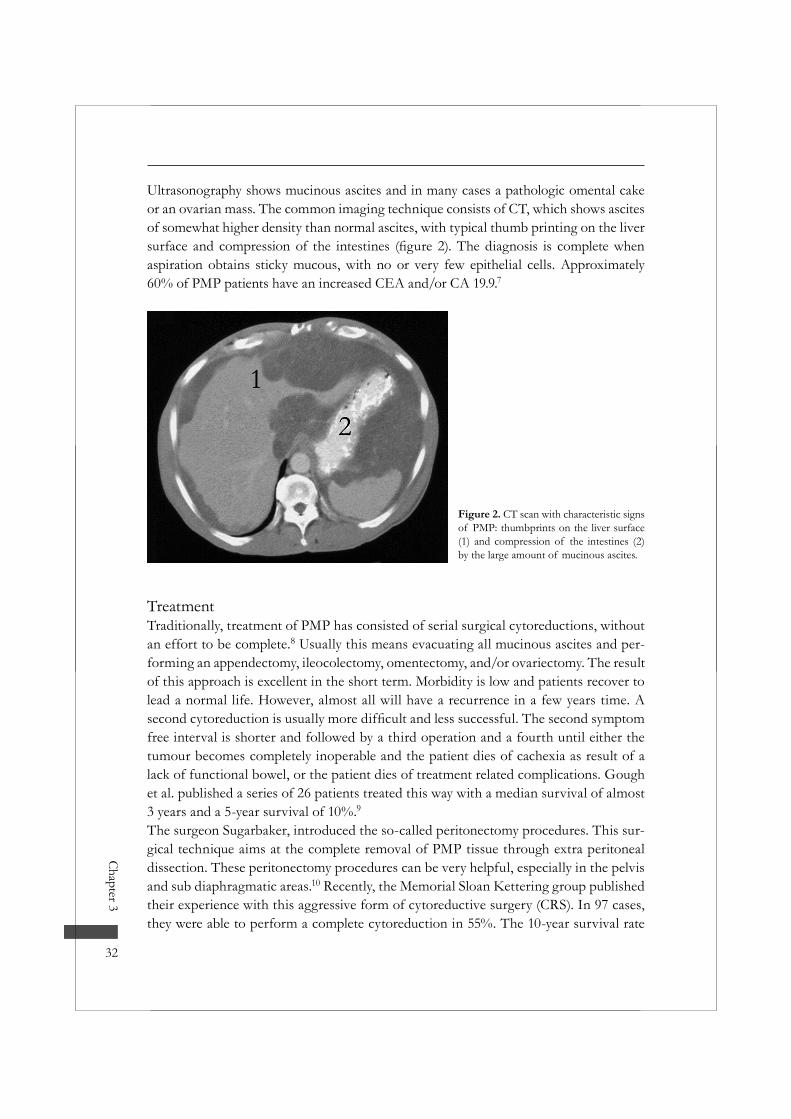
Ultrasonography shows mucinous ascites and in many cases a pathologic omental cake or an ovarian mass. The common imaging technique consists of CT, which shows ascites of somewhat higher density than normal ascites, with typical thumb printing on the liver
aspiration obtains sticky mucous, with no or very few epithelial cells. Approximately 60% of PMP patients have an increased CEA and/or CA 19.9.7
Figure 2. CT scan with characteristic signs of PMP: thumbprints on the liver surface (1) and compression of the intestines (2) by the large amount of mucinous ascites.
TreatmentTraditionally, treatment of PMP has consisted of serial surgical cytoreductions, without an effort to be complete.8 Usually this means evacuating all mucinous ascites and per-forming an appendectomy, ileocolectomy, omentectomy, and/or ovariectomy. The result of this approach is excellent in the short term. Morbidity is low and patients recover to lead a normal life. However, almost all will have a recurrence in a few years time. A
free interval is shorter and followed by a third operation and a fourth until either the tumour becomes completely inoperable and the patient dies of cachexia as result of a lack of functional bowel, or the patient dies of treatment related complications. Gough et al. published a series of 26 patients treated this way with a median survival of almost 3 years and a 5-year survival of 10%.9The surgeon Sugarbaker, introduced the so-called peritonectomy procedures. This sur-gical technique aims at the complete removal of PMP tissue through extra peritoneal dissection. These peritonectomy procedures can be very helpful, especially in the pelvis and sub diaphragmatic areas.10 Recently, the Memorial Sloan Kettering group published their experience with this aggressive form of cytoreductive surgery (CRS). In 97 cases, they were able to perform a complete cytoreduction in 55%. The 10-year survival rate
33
Three illustrating case histories
was 21%, but only 12% of patient was free of disease. Completeness of cytoreduction and histology were strong prognostic indicators.11
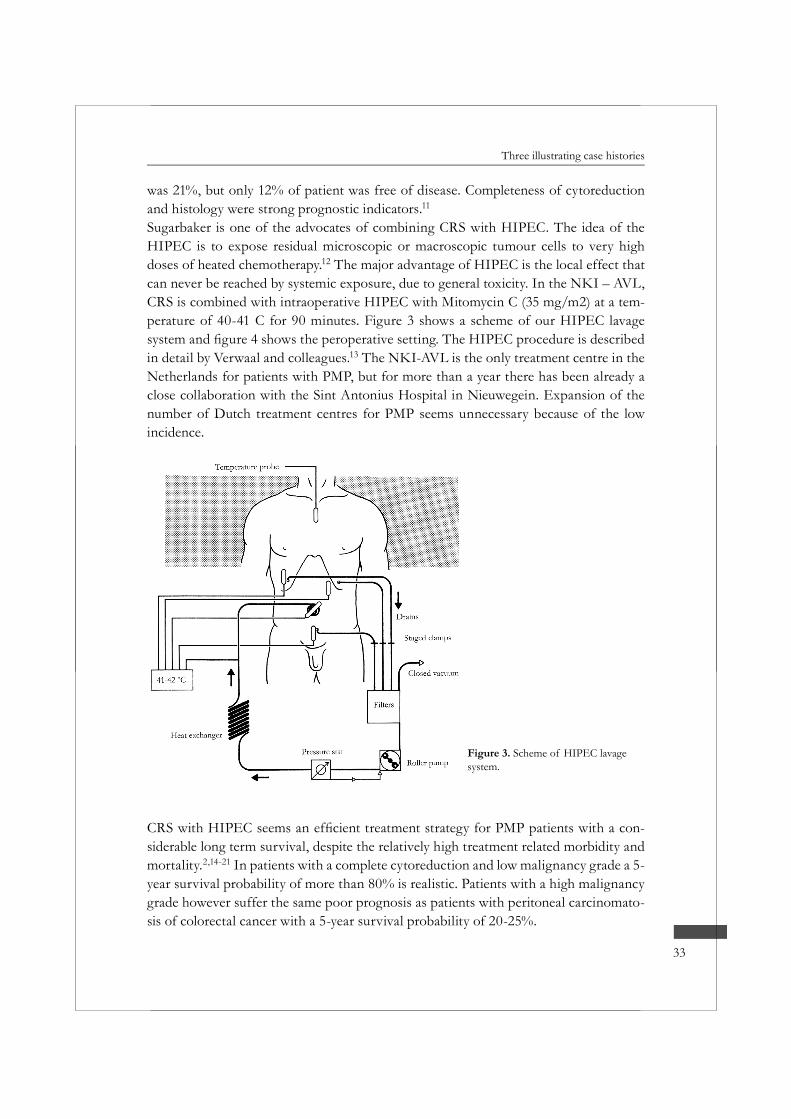
Sugarbaker is one of the advocates of combining CRS with HIPEC. The idea of the HIPEC is to expose residual microscopic or macroscopic tumour cells to very high doses of heated chemotherapy.12 The major advantage of HIPEC is the local effect that can never be reached by systemic exposure, due to general toxicity. In the NKI – AVL, CRS is combined with intraoperative HIPEC with Mitomycin C (35 mg/m2) at a tem-perature of 40-41 C for 90 minutes. Figure 3 shows a scheme of our HIPEC lavage
in detail by Verwaal and colleagues.13 The NKI-AVL is the only treatment centre in the Netherlands for patients with PMP, but for more than a year there has been already a close collaboration with the Sint Antonius Hospital in Nieuwegein. Expansion of the number of Dutch treatment centres for PMP seems unnecessary because of the low incidence.
-siderable long term survival, despite the relatively high treatment related morbidity and mortality.2,14-21 In patients with a complete cytoreduction and low malignancy grade a 5-year survival probability of more than 80% is realistic. Patients with a high malignancy grade however suffer the same poor prognosis as patients with peritoneal carcinomato-sis of colorectal cancer with a 5-year survival probability of 20-25%.
Figure 3. Scheme of HIPEC lavage system.

Chapter 3
34
The use of additional systemic chemotherapy for PMP with malignant features is based on the employment of systemic therapy in patients with peritoneal carcinomatosis of colorectal cancer origin. The value of systemic therapy in such a loco regional disease as PMP is however questionable, as the history of patient B and C illustrates.6,15 In our institute we have currently changed our regimen for PMP patients with high malig-nancy grade from 5-Fluorouracil and Leucovorin to Xeloda. The future must reveal the additional value of this treatment approach.
ConclusionPseudomyxoma peritonei is a rare disease that originates in most cases from a mucinous adenoma of the appendix. With CT scan and a histological biopsy, one can usually ascertain the right diagnosis. As PMP is restricted to the peritoneal cavity, it is very suit-able for a loco regional approach such as CRS plus HIPEC.
References1. Zoetmulder FA, van der Vange N, Witkamp AJ et al. [Hyperthermic intra-peritoneal chemotherapy
(HIPEC) in patients with peritoneal pseudomyxoma or peritoneal metastases of colorectal carcino-ma; good preliminary results from the Netherlands Cancer Institute]. Ned Tijdschr Geneeskd 1999; 143:1863-1868.
2. Smeenk RM, Verwaal VJ, Zoetmulder FA. Toxicity and mortality of cytoreduction and intraoperative hyperthermic intraperitoneal chemotherapy in pseudomyxoma peritonei-a report of 103 procedures. Eur J Surg Oncol 2005.
3. Sugarbaker PH, Ronnett BM, Archer A et al. Pseudomyxoma peritonei syndrome. Adv Surg 1996; 30:233-280.
4. Sugarbaker PH. Pseudomyxoma peritonei. A cancer whose biology is characterized by a redistribution phenomenon. Ann Surg 1994; 219:109-111.
Figure 4. Peroperative setting of the
drain; 2: temperature probe; 3: clamp for

35
Three illustrating case histories
5. Ronnett BM, Zahn CM, Kurman RJ et al. Disseminated peritoneal adenomucinosis and peritoneal mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol 1995; 19:1390-1408.
6. Smeenk RM, Verwaal VJ, Antonini N, Zoetmulder FA. Progressive pseudomyxoma peritonei after combined modality treatment: management and outcome. Ann Surg Oncol . 2006. Ref Type: In Press
7. Carmignani CP, Hampton R, Sugarbaker CE et al. Utility of CEA and CA 19-9 tumor markers in diagnosis and prognostic assessment of mucinous epithelial cancers of the appendix. J Surg Oncol 2004; 87:162-166.
8. Dejong CH, Booster MH, Theunissen PH et al. [Pseudomyxoma peritonei]. Ned Tijdschr Geneeskd 1997; 141:1196-1198.
9. Gough DB, Donohue JH, Schutt AJ et al. Pseudomyxoma peritonei. Long-term patient survival with an aggressive regional approach. Ann Surg 1994; 219:112-119.
10. Sugarbaker PH. Peritonectomy procedures. Surg Oncol Clin N Am 2003; 12:703-27, xiii.11. Miner TJ, Shia J, Jaques DP et al. Long-term survival following treatment of pseudomyxoma peri-
tonei: an analysis of surgical therapy. Ann Surg 2005; 241:300-308.12. Witkamp AJ, de Bree E, Van Goethem R et al. Rationale and techniques of intra-operative hyperther-
mic intraperitoneal chemotherapy. Cancer Treat Rev 2001; 27:365-374.13. Verwaal VJ, van Ruth S, de Bree E et al. Randomized trial of cytoreduction and hyperthermic intra-
peritoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with perito-neal carcinomatosis of colorectal cancer. J Clin Oncol 2003; 21:3737-3743.
14. Sugarbaker PH. New standard of care for appendiceal epithelial neoplasms and pseudomyxoma peri-tonei syndrome? Lancet Oncol 2006; 7:69-76.
15. Smeenk RM, Verwaal VJ, Zoetmulder FA. Survival analysis of pseudomyxoma peritonei treated by cytoreductive surgery in combination with intraoperative hyperthermic intraperitoneal chemotherapy. Ann Surg . 2006. Ref Type: In Press
16. Guner Z, Schmidt U, Dahlke MH et al. Cytoreductive surgery and intraperitoneal chemotherapy for pseudomyxoma peritonei. Int J Colorectal Dis 2005; 20:155-160.
17. Deraco M, Baratti D, Inglese MG et al. Peritonectomy and intraperitoneal hyperthermic perfusion
Oncol 2004; 11:393-398.18. Elias D, Laurent S, Antoun S et al. [Pseudomyxoma peritonei treated with complete resection and
immediate intraperitoneal chemotherapy]. Gastroenterol Clin Biol 2003; 27:407-412.19. Loungnarath R, Causeret S, Bossard N et al. Cytoreductive surgery with intraperitoneal chemohyper-
thermia for the treatment of pseudomyxoma peritonei: a prospective study. Dis Colon Rectum 2005; 48:1372-1379.
20. Moran BJ. Establishment of a peritoneal malignancy treatment centre in the United Kingdom. Eur J Surg Oncol 2006; 32:614-618.
21. Bryant J, Clegg AJ, Sidhu MK et al. Systematic review of the Sugarbaker procedure for pseudomyxo-ma peritonei. Br J Surg 2005; 92:153-158.
4c h a p t e r
Toxicity and mortality of cytoreduction and intra-operative hyperthermic intraperitoneal chemotherapy in pseudomyxoma peritonei
- A report of 103 procedures -
R. M. Smeenk., V. J. Verwaal, F.A.N. Zoetmulder
Department of SurgeryThe Netherlands Cancer Institute - Antoni van Leeuwenhoek Hospital
Amsterdam, the Netherlands

Aims: To report on treatment related toxicity and mortality in patients with pseudo-myxoma peritonei (PMP) treated by cytoreduction in combination with intraoperative hyperthermic intraperitoneal chemotherapy (HIPEC) and to identify prognostic fac-tors. Methods: A review was performed of 103 procedures of cytoreduction and intraopera-tive HIPEC for PMP between 1996 and 2004. Toxicity was graded according to the
-
Pre and peroperative factors were studied on their relationship to toxicity and mortal-ity. Results: The median hospital stay was 21 days (4-149) with a treatment related toxicity of 54% and a 30 days mortality of 3%. In univariate analysis, toxicity was associated with abdominal tumour load (p<0.01), completeness of cytoreduction (p<0.01), and age (p=0.05). Surgical complications, mainly small bowel perforations/suture leaks, were the main cause of toxicity. A favourable pathology decreased mortality. Conclusion: Cytoreduction in combination with intraoperative HIPEC in PMP patients is a treatment with a relatively high toxicity, but a considerable long-term survival in selected patients. Toxicity is mainly surgery related. Concentration of cases to acquire
essential to reduce treatment related toxicity and mortality.
Eur J Surg Oncol 2006 Mar;32(2):186-90

39
Toxicity and mortality
IntroductionPseudomyxoma peritonei (PMP) is a rare disease. The incidence is approximately 1/1.000.000 a year1. It is characterised by disseminated intraperitoneal mucous, asso-ciated with mucinous implants on the peritoneal surfaces, the omentum and in the sub diaphragmatic spaces. These tumour deposits contain mucous producing epithelial cells2-4. PMP is often described as a syndrome that produces its symptoms by abundant intraperitoneal mucous accumulation that causes abdominal distension.PMP has been divided into 3 pathological subtypes by Ronnett et al.: disseminated peritoneal adenomucinosis (DPAM), peritoneal mucinous carcinomatosis (PMCA) and an intermediate group (PMCA-I)5. The histological architecture of DPAM shows low-grade adenomatous mucinous epithelium with minimal cytological atypia or mitotic activity. PMCA is a form of PMP in which cells show features of a well differentiated mucinous carcinoma. In the intermediate group, peritoneal lesions demonstrate pre-dominantly features of DPAM, but focally also of PMCA.The origin of PMP is usually an adenoma (or a well-differentiated adenocarcinoma) of the appendix, and sometimes of the ovary6-9. Other primary tumour sites are rare and include pancreas7,9,10, stomach9, colon7,9, urachus7, and small bowel9. Solitary lesions are also described11.The anatomy of abdomen and pelvis yields predictable sites where mucous secreting neoplasm will accumulate4,12. The most important factor that determines these locali-sations is the lack of adhesive properties of the tumour cells. This restricts seeding
-nism whereby the tumour cells are distributed in the peritoneal cavity. Due to these intraperitoneal seeding mechanisms, and its most common primary site of origin, PMP occurs at predictable abdominal sites: the vesicorectal space, the left abdominal gutter, the right sub diaphragmatic space, and omentum. Another important factor that deter-mines PMP localization is the presence of sticky surfaces. Tumour cells may seed on the ovary in young women or on surgical surfaces caused by prior surgery.
The cornerstone of successful treatment of PMP is extensive cytoreductive surgery. -
thermic intraperitoneal chemotherapy (HIPEC). Since 1995, this has been the standard treatment for PMP at the Netherlands Cancer Institute. The aim of this study is to report on toxicity and mortality of this treatment strategy in patients affected by PMP, and to identify clinical factors that predispose to toxicity and mortality.

Chapter 4
40
MethodsPatient populationPatients with PMP treated at the Netherlands Cancer Institute between 1996 and
abdominal mucous with characteristic distribution on computed tomography (CT) of the abdomen, and histology consistent with DPAM, PMCA, or PMCA-I. Both patients with primary and recurrent PMP were included. There was no evidence of liver or lung metastases on abdominal and chest CT scans.
TreatmentVerwaal describes the principles of cytoreduction and intra-operative HIPEC in detail13.
tumour deposits on parietal and/or visceral peritoneal surfaces, and if necessary resec-tion of involved viscera along. This is followed by heated intraperitoneal chemotherapy, with Mitomycin C 35 mg/m2 for 90 minutes at 40-41 0 Celsius, to erase microscopic residual tumour.At surgery, tumour load was recorded in seven distinctive abdominal regions: pelvis, ileocoecum, omentum/transverse colon, small bowel/mesentery, sub hepatic region, and sub phrenic left and right regions. Maximum diameter of tumour deposits was graded into 0 cm, 1-5 cm and >5 cm. Completeness of cytoreduction was recorded at the end of surgery: no residual macroscopic tumour (R1), residual macroscopic tumour smaller than 2.5 mm in any region (R2a) and tumour deposits larger than 2.5 mm in any region (R2b)13. The following additional factors were recorded: total operation time, blood loss, number of visceral resections, and number of suture lines.
Adjuvant chemotherapy and follow-upPatients, who showed evidence of PMCA and were in a good condition, were given systemic adjuvant chemotherapy for six months with 5-Fluorouracil (400 mg/m2)and Leucoverin (80 mg/m2) weekly. Long-term follow-up was performed by physical examination, assessment of tumour markers CEA and CA 19.9, and by CT scan of the abdomen every 6 months.
The following data were recorded by investigation of medical records: age, gender, pri-mary or recurrent presentation of PMP, previous surgery, the origin and histology of PMP, the postoperative treatment related toxicity, the length of stay in Intensive Care, the length of total hospital stay, time and cause of treatment related death. Treatment related (surgical) complications were graded in the form of toxicity according to the
41
Toxicity and mortality
Statistical methodsStatistical association between clinicopathological factors and toxicity was tested by the
less than 0.05. Survival was calculated by the Kaplan Meier method. Details of survival results will be presented in a different study.
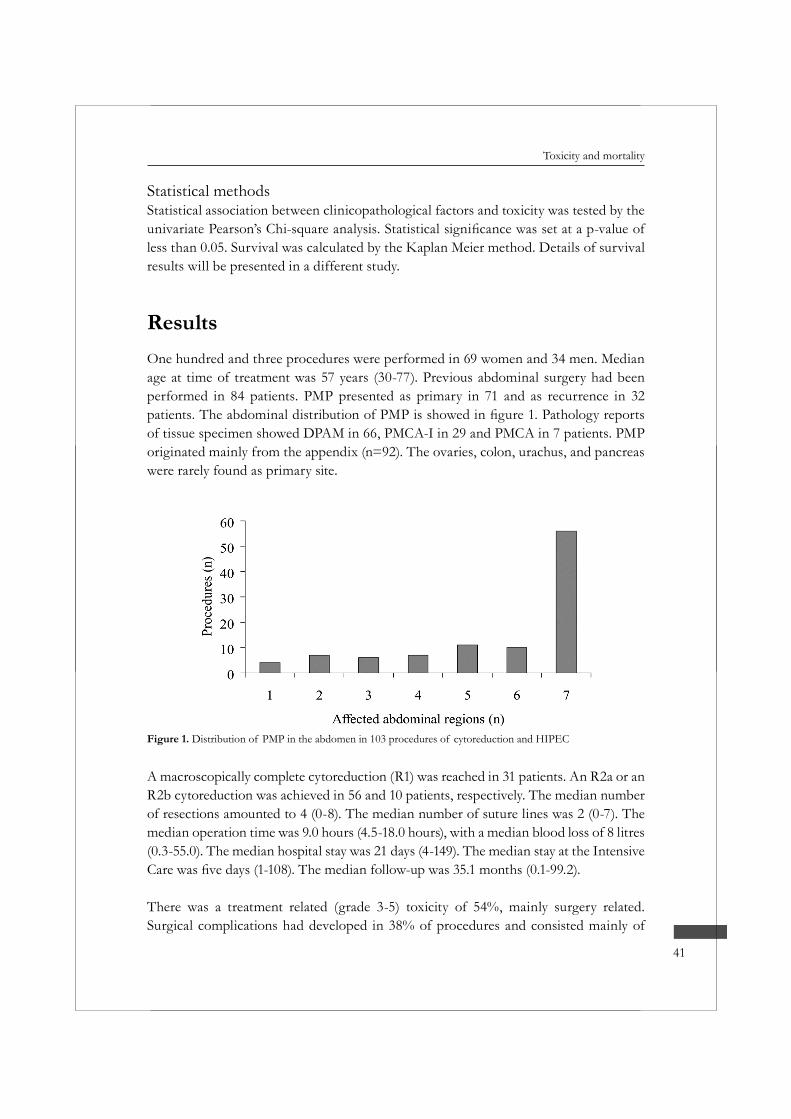
ResultsOne hundred and three procedures were performed in 69 women and 34 men. Median age at time of treatment was 57 years (30-77). Previous abdominal surgery had been performed in 84 patients. PMP presented as primary in 71 and as recurrence in 32
of tissue specimen showed DPAM in 66, PMCA-I in 29 and PMCA in 7 patients. PMP originated mainly from the appendix (n=92). The ovaries, colon, urachus, and pancreas were rarely found as primary site.
Figure 1. Distribution of PMP in the abdomen in 103 procedures of cytoreduction and HIPEC
A macroscopically complete cytoreduction (R1) was reached in 31 patients. An R2a or an R2b cytoreduction was achieved in 56 and 10 patients, respectively. The median number of resections amounted to 4 (0-8). The median number of suture lines was 2 (0-7). The median operation time was 9.0 hours (4.5-18.0 hours), with a median blood loss of 8 litres (0.3-55.0). The median hospital stay was 21 days (4-149). The median stay at the Intensive
There was a treatment related (grade 3-5) toxicity of 54%, mainly surgery related. Surgical complications had developed in 38% of procedures and consisted mainly of
Chapter 4
42
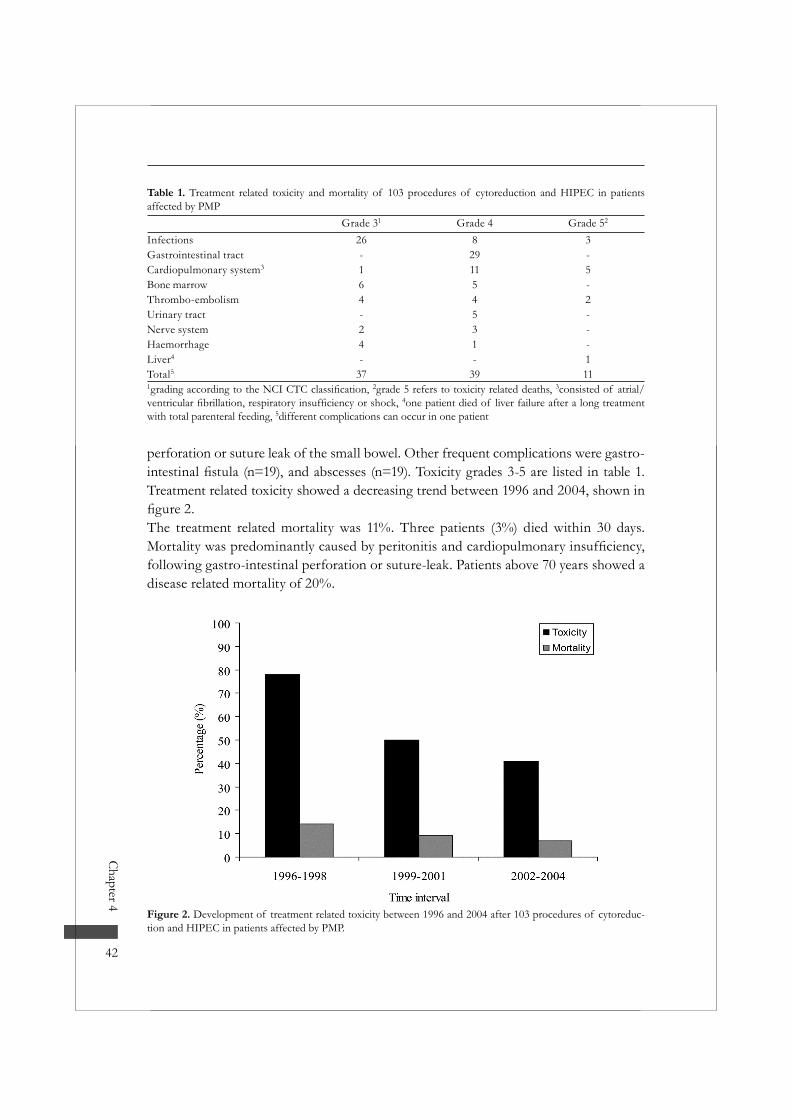
perforation or suture leak of the small bowel. Other frequent complications were gastro-
Treatment related toxicity showed a decreasing trend between 1996 and 2004, shown in
The treatment related mortality was 11%. Three patients (3%) died within 30 days.
following gastro-intestinal perforation or suture-leak. Patients above 70 years showed a disease related mortality of 20%.
Figure 2. Development of treatment related toxicity between 1996 and 2004 after 103 procedures of cytoreduc-tion and HIPEC in patients affected by PMP.
Table 1. Treatment related toxicity and mortality of 103 procedures of cytoreduction and HIPEC in patients affected by PMP
Grade 31 Grade 4 Grade 52
Infections 26 8 3Gastrointestinal tract - 29 -Cardiopulmonary system3 1 11 5Bone marrow 6 5 -Thrombo-embolism 4 4 2Urinary tract - 5 -Nerve system 2 3 -Haemorrhage 4 1 -Liver4 - - 1Total5 37 39 111 2grade 5 refers to toxicity related deaths, 3consisted of atrial/
4one patient died of liver failure after a long treatment with total parenteral feeding, 5different complications can occur in one patient
43
Toxicity and mortality
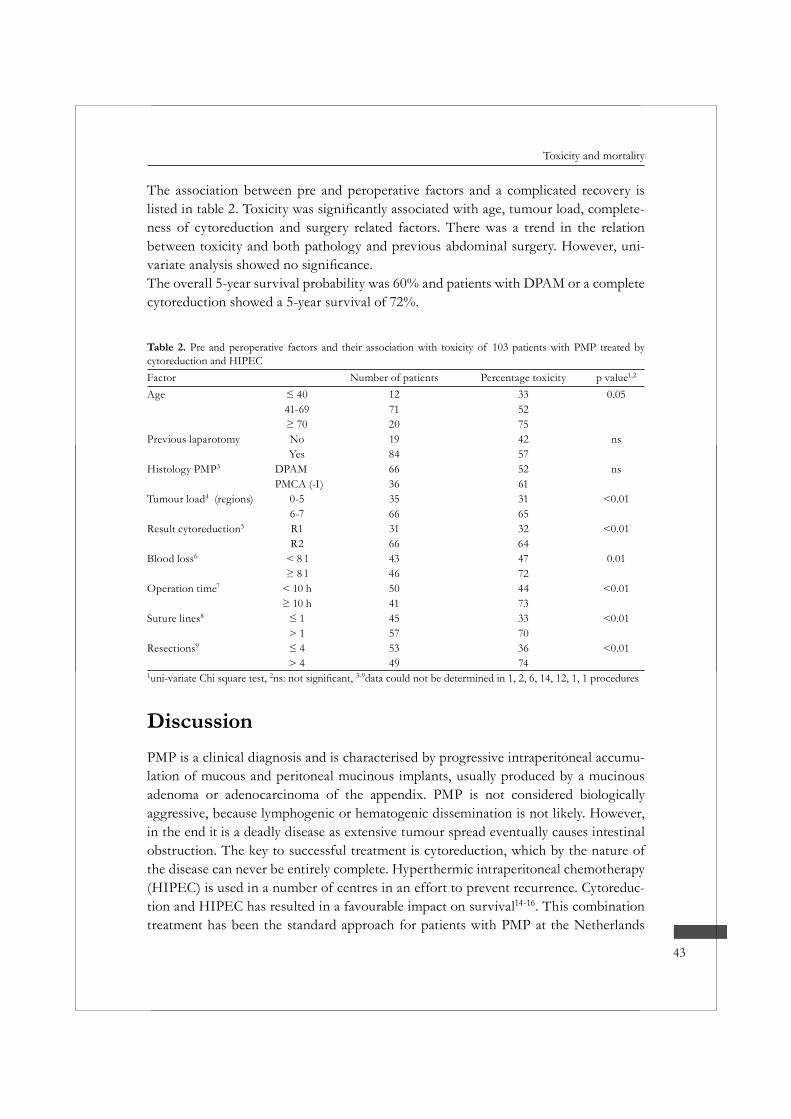
The association between pre and peroperative factors and a complicated recovery is -
ness of cytoreduction and surgery related factors. There was a trend in the relation between toxicity and both pathology and previous abdominal surgery. However, uni-
The overall 5-year survival probability was 60% and patients with DPAM or a complete cytoreduction showed a 5-year survival of 72%.
Table 2. Pre and peroperative factors and their association with toxicity of 103 patients with PMP treated by cytoreduction and HIPECFactor Number of patients Percentage toxicity p value1,2
Age 12 33 0.0541-69 71 52
20 75Previous laparotomy No 19 42 ns
Yes 84 57Histology PMP3 DPAM 66 52 ns
PMCA (-I) 36 61Tumour load4 (regions) 0-5 35 31 <0.01
6-7 66 65Result cytoreduction5 R1 31 32 <0.01
R2 66 64Blood loss6 < 8 l 43 47 0.01
46 72Operation time7 < 10 h 50 44 <0.01
41 73Suture lines8 45 33 <0.01
> 1 57 70Resections9 53 36 <0.01
> 4 49 741uni-variate Chi square test, 2 3-9data could not be determined in 1, 2, 6, 14, 12, 1, 1 procedures
DiscussionPMP is a clinical diagnosis and is characterised by progressive intraperitoneal accumu-lation of mucous and peritoneal mucinous implants, usually produced by a mucinous adenoma or adenocarcinoma of the appendix. PMP is not considered biologically aggressive, because lymphogenic or hematogenic dissemination is not likely. However, in the end it is a deadly disease as extensive tumour spread eventually causes intestinal obstruction. The key to successful treatment is cytoreduction, which by the nature of the disease can never be entirely complete. Hyperthermic intraperitoneal chemotherapy (HIPEC) is used in a number of centres in an effort to prevent recurrence. Cytoreduc-tion and HIPEC has resulted in a favourable impact on survival14-16. This combination treatment has been the standard approach for patients with PMP at the Netherlands

Chapter 4
44
Cancer Institute since 1995. In this series of 103 consecutive patients, survival has been very encouraging, with a 72% 5-year survival in patients with DPAM.Morbidity of this treatment strategy is high. In this study, we analyzed our data with the aim to identify means to improve the safety of this treatment in the future. Our high toxicity rate (54%) does not stand on its own. Toxicity rates of 18%-56% and a 30 days mortality of 3%-14% have been reported14,15,17-22. Differences in the method of grad-
we scored toxicity as strictly as possible, which certainly contributed to a high toxicity rate. Treatment related toxicity and mortality mainly consisted of surgical complica-tions. Most frequent serious complications were small bowel perforation and suture
extensive tumour load (64% of patients) were especially vulnerable. This was probably caused by extensive adhesions and small bowel involvement in recurrent PMP, leading to serosal damage during operation.In retrospect, it seems clear that we sometimes pushed our limits when trying to reach a complete cytoreduction. By doing so, we caused unrecognized injury to the small bowel, resulting in leakage usually by day 2 or 3. Whether the healing of small serosal damages was hampered by the HIPEC procedure cannot be concluded from this mate-
variations and the risk on surgical complications23. Although we used a high dose of 35 mg/m2 of Mitomycin-C, bone marrow toxicity was not a very important feature on itself. In combination with a surgical complication, a relatively minor leucocytopenia can become life threatening. As the nadir of the white blood cell count occurs around day 10 after HIPEC, we have learnt to be very active to correct any surgical problems before that time.It is encouraging that the toxicity and mortality rate decreased considerably in the sec-ond 50 cases. During the last three years, we have not had a post-operative death, so a clear learning curve can be observed. Part of this learning curve has clearly to do with selection. Extensive disease and age above 70 are important risk factors for complica-tions. The 20% disease related death we observed in elderly patients in this series is clearly too high. During the more recent years, we have used a two-step approach in these cases. We now start with a laparotomy to remove free mucous, perform an appen-dectomy and omentectomy, and remove ovarian metastases. It is often remarkable how easy even very cachectic patients will recover from such a limited operation, and what improvement of their general condition this allows. After 3 months we then go back to complete the cytoreduction and do the HIPEC procedure.In addition, selection has to include the pathological subtype. PMCA appears to behave as ordinary colon cancer. Patients with PMCA and extensive disease should probably be excluded from this approach, in the same way as extensive peritoneal carcinomatosis of colon cancer13

45
Toxicity and mortality
term prognosis is clearly less favourable in this intermediate group compared to DPAM, there should probably be some more restrained in accepting patients with extensive disease for this therapy.In conclusion, cytoreduction in combination with intra-operative HIPEC in PMP patients is a treatment with a relatively high toxicity but a considerable long–term sur-vival in selected patients. Treatment related toxicity and mortality is mainly surgery
age, pathology, and extent of disease is essential to reduce treatment related toxicity and mortality.
References1. Mukherjee A, Parvaiz A, Cecil TD et al. Pseudomyxoma peritonei usually originates from the appen-
dix: a review of the evidence. Eur J Gynaecol Oncol 2004; 25:411-414.2. Hinson FL, Ambrose NS. Pseudomyxoma peritonei. Br J Surg 1998; 85:1332-1339.3. Ronnett BM, Yan H, Kurman RJ et al. Patients with pseudomyxoma peritonei associated with dissem-
peritoneal mucinous carcinomatosis. Cancer 2001; 92:85-91.4. Sugarbaker PH. Pseudomyxoma peritonei. A cancer whose biology is characterized by a redistribution
phenomenon. Ann Surg 1994; 219:109-111.5. Ronnett BM, Zahn CM, Kurman RJ et al. Disseminated peritoneal adenomucinosis and peritoneal
mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol 1995; 19:1390-1408.
6. Prayson RA, Hart WR, Petras RE. Pseudomyxoma peritonei. A clinicopathologic study of 19 cases with emphasis on site of origin and nature of associated ovarian tumors. Am J Surg Pathol 1994; 18:591-603.
7. de Bree E, Witkamp A, Van De Vijver M et al. Unusual origins of Pseudomyxoma peritonei. J Surg Oncol 2000; 75:270-274.
8. Ronnett BM, Kurman RJ, Zahn CM et al. Pseudomyxoma peritonei in women: a clinicopathologic analysis of 30 cases with emphasis on site of origin, prognosis, and relationship to ovarian mucinous tumors of low malignant potential. Hum Pathol 1995; 26:509-524.
9. Costa MJ. Pseudomyxoma peritonei. Histologic predictors of patient survival. Arch Pathol Lab Med 1994; 118:1215-1219.
10. Chejfec G, Rieker WJ, Jablokow VR et al. Pseudomyxoma peritonei associated with colloid carcinoma of the pancreas. Gastroenterology 1986; 90:202-205.
11. Baker WC, Goldman LB, deVere White RW. Pseudomyxoma peritonei presenting as a scrotal mass. J Urol 1988; 139:821-822.
12. Sugarbaker PH, Ronnett BM, Archer A et al. Pseudomyxoma peritonei syndrome. Adv Surg 1996; 30:233-280.
13. Verwaal VJ, van Tinteren H, Ruth SV et al. Toxicity of cytoreductive surgery and hyperthermic intra-peritoneal chemotherapy. J Surg Oncol 2004; 85:61-67.
14. Deraco M, Baratti D, Inglese MG et al. Peritonectomy and intraperitoneal hyperthermic perfusion
Oncol 2004; 11:393-398.15. Elias D, Laurent S, Antoun S et al. [Pseudomyxoma peritonei treated with complete resection and
immediate intraperitoneal chemotherapy]. Gastroenterol Clin Biol 2003; 27:407-412.
Chapter 4
46
16. Sugarbaker PH. Cytoreductive surgery and peri-operative intraperitoneal chemotherapy as a curative approach to pseudomyxoma peritonei syndrome. Eur J Surg Oncol 2001; 27:239-243.
17. Deraco M, Gronchi A, Mazzaferro V et al. Feasibility of peritonectomy associated with intraperito-neal hyperthermic perfusion in patients with Pseudomyxoma peritonei. Tumori 2002; 88:370-375.
18. Deraco M, Kusamura S, Gronchi A. [Cytoreductive surgery (peritonectomy) and intraperitoneal hyperthermic chemotherapy: an innovative and effective approach to the treatment of pseudomyxo-ma peritonei]. Tumori 2003; 89:54-55.
19. Butterworth SA, Panton ON, Klaassen DJ et al. Morbidity and mortality associated with intraperito-neal chemotherapy for Pseudomyxoma peritonei. Am J Surg 2002; 183:529-532.
20. Scuderi S, Costamagna D, Vaira M et al. [Treatment of pseudomyxoma peritonei using cytoreduction and intraperitoneal hyperthermic chemotherapy]. Tumori 2003; 89:43-45.
21. van Ruth S, Acherman YI, van de Vijver MJ et al. Pseudomyxoma peritonei: a review of 62 cases. Eur J Surg Oncol 2003; 29:682-688.
22. Witkamp AJ, de Bree E, Kaag MM et al. Extensive surgical cytoreduction and intraoperative hyper-thermic intraperitoneal chemotherapy in patients with pseudomyxoma peritonei. Br J Surg 2001; 88:458-463.
23. van Ruth S, Mathot RA, Sparidans RW et al. Population pharmacokinetics and pharmacodynamics of mitomycin during intraoperative hyperthermic intraperitoneal chemotherapy. Clin Pharmacokinet 2004; 43:131-143.
5c h a p t e r
Survival analysis of pseudomyxoma peritonei patients treated by cytoreductive surgery and hyperthermic intraperitoneal chemotherapy
R.M. Smeenk1; V.J. Verwaal1; N. Antonini2; F.A.N. Zoetmulder1
Department of Surgery1, Department of Biometrics2
The Netherlands Cancer Institute - Antoni van Leeuwen-hoek Hospital Amsterdam, the Netherlands

Chapter 5
48
Objective: To evaluate the survival of patients with pseudomyxoma peritonei (PMP) treated by cytoreductive surgery and intraoperative hyperthermic intraperitoneal che-motherapy (HIPEC), and to identify factors with prognostic value.Summary Background Data: PMP is a clinical syndrome characterized by progressive intraperitoneal accumulation of mucous and mucinous implants, usually derived from a ruptured mucinous neoplasm of the appendix. Survival is dominated by pathology.Methods: One hundred and three patients (34 men and 69 women) treated at the Neth-
from date of initial treatment and corrected for a second procedure. PMP was patho-logically categorized into disseminated peritoneal adenomucinosis (DPAM), peritoneal mucinous carcinomatosis (PMCA) and an intermediate subtype (PMCA-I). Clinical and pathological factors were analyzed to identify their prognostic value for survival.Results: Median follow-up was 51.5 (0.1-99.5) months. Recurrence developed in 44%. A second procedure for recurrence was performed in 11 patients. The median disease free interval was 25.6 months (95% CI 14.8- 43.6). The 3-year and 5-year disease free survival probability was 43.6% (95% CI 34.4%- 55.2%) and 37.4% (95% CI 28.2%-
70.9% (95% CI 62.0%-81.2%) and 59.5% (95% CI 48.7%-72.5%), respectively. Factors associated with survival were pathological subtype, completeness of cytoreduction, and degree and location of tumor load (p<0.05). The main prognostic factor, independently associated with survival, was the pathological subtype (p<0.01).Conclusion: Cytoreductive surgery in combination with intraoperative HIPEC is a fea-sible treatment strategy for PMP in terms of survival. The pathological subtype remains the dominant factor in survival. Patients should be centralized to improve survival by a combination of surgical experience and adequate patient selection.
Ann Surg, in press

49
Survival analysis
IntroductionPseudomyxoma peritonei (PMP) is a rare disease with an incidence of approximately one per million a year.1 It is characterized by intraperitoneal disseminated mucous pro-duced by adenomucinous tumor cells in implants on peritoneal surfaces. These implants
located mucinous neoplasm.2 PMP is reported to originate from mucinous (cyst) adeno-ma, mucoceles and mucinous (cyst) adenocarcinoma of mostly appendix (or ovary).1,3-6
Incidental, PMP has unusual origins.7,8
Clinically, PMP is a slowly progressive disease. It mainly expresses as a so-called “jelly belly”, caused by the abundant intraperitoneal mucous. Sometimes patients present themselves with symptoms arising from the primary tumor, mimicking appendicitis. In other cases they present with an inguinal herniated sac or an ovarian mass.9-11 As PMP progresses, the excessive mucous accumulation causes compression of the intestines. Gastro-intestinal function is compromised and eventually obstruction is imminent. Consequently, PMP always results in the death of the patient unless radically treated.5
At the Netherlands Cancer Institute, aggressive cytoreductive surgery in combination with intraoperative hyperthermic intraperitoneal chemotherapy (HIPEC) is used as the treatment for PMP since 1995. The aim of this study is to evaluate this treatment strat-egy in terms of survival, and to identify clinical and pathological prognostic factors for survival.
MethodsPatient populationPatients were diagnosed PMP based on clinical symptoms, excessive abdominal mucous with characteristic distribution on computed tomography (CT) scans, and by pathologi-cal assessment. Both primary and recurrent PMP was included in the study. Patients with evidence of liver or lung metastases on CT scan were excluded from treatment.
Treatment scheduleThe principles of cytoreductive surgery and HIPEC have been described in detail elsewhere.12 -roscopic tumor deposits on parietal and/or visceral peritoneal surfaces, combined if necessary with resection of involved viscera. This is followed by intraoperative HIPEC with Mitomycin C 35 mg/m2 for 90 minutes at 40-410 Celsius to erase microscopic residual tumor. At the end of the procedure, the necessary anastomoses are made. A specialized surgical team performs the treatment.

Chapter 5
50
At surgery, tumor load is recorded in 7 distinctive abdominal regions: pelvis, ileocoe-cum, omentum/transverse colon, small bowel/mesentery, sub hepatic region, and sub phrenic left and right regions. Maximum diameter of tumor deposits are graded into 0 cm, 1-5 cm and >5 cm. Completeness of cytoreduction is recorded at the end of surgery: no residual macroscopic tumor (R1), residual macroscopic tumor smaller than 2.5 mm in any region (R2a) and tumor deposits larger than 2.5 mm in any region (R2b).
Additional treatment and follow upPMP patients with pathological evidence of malignant features at initial treatment were in addition treated with systemic chemotherapy conform hospital protocol. The hos-pital protocol consisted of 6 months 5-Fluorouracil (400 mg/m2) and Leucovorin (80 mg/m2) weekly. Patients had to be in a good condition. Long-term follow-up was per-formed by physical examination and assessment of tumor markers CEA and CA 19.9 every 3 months. A CT scan was performed every 6 months. Recurrence or progression was diagnosed in case of a profound raise of tumor marker(s) and/or evidence of relapse on CT scan, or during relaparotomy for any other cause.
Data collection and statistical analysisData were obtained from a prospective database of clinical records, surgical reports, reports of CT scans, laboratory and pathology reports, and contact with the patient’s
according to Ronnett’s criteria: disseminated peritoneal adenomucinosis (DPAM), peri-toneal mucinous carcinomatosis (PMCA), and an intermediate group (PMCA-I).13
The analyses were performed on patients treated for PMP between 1996 and 2004. In some patients, a second procedure was performed after recurrence or progression. A Cox-proportional hazard model was used to analyze the effect of several clinical
(DFS). Possible clinical and pathological prognostic factors for recurrence or death of disease that were investigated include age, gender, previous laparotomy, tumor load and involved regions, result of cytoreduction, pathology, and additional systemic chemo-therapy. The choice for independent factors in the multivariate model was based on the univariate results.
were analyzed using the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL), version 11.5, and SAS version 8.2.
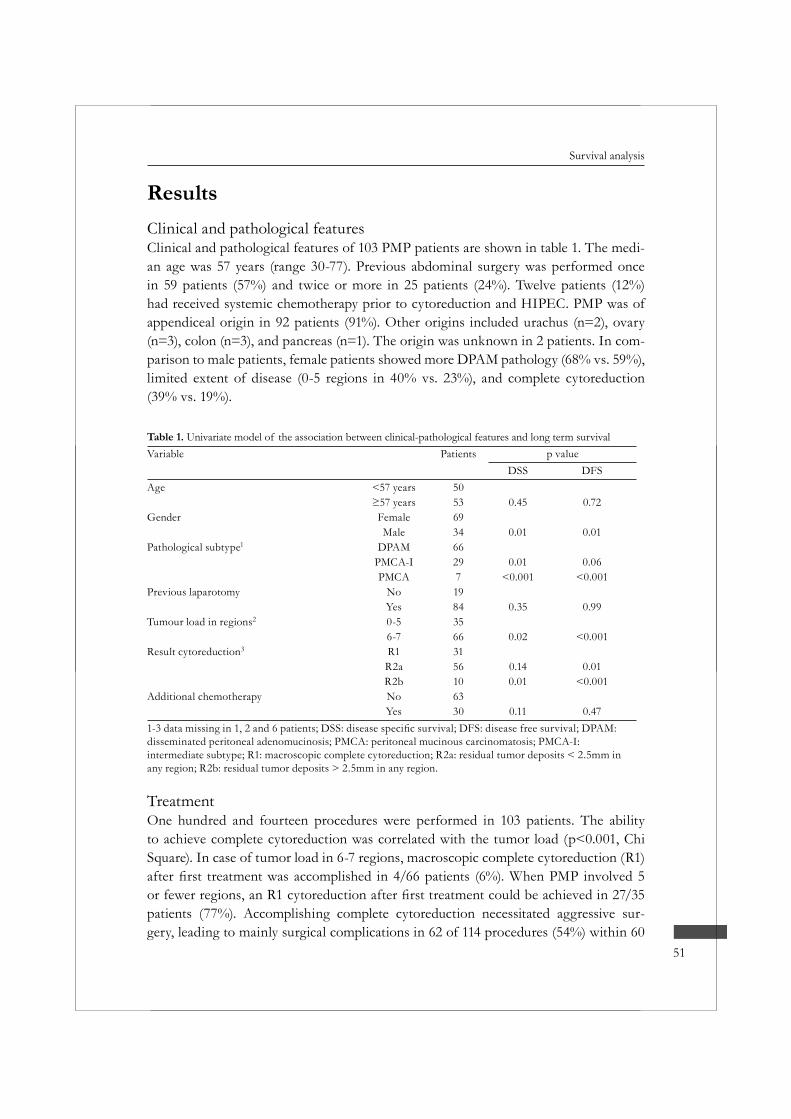
51
Survival analysis
ResultsClinical and pathological featuresClinical and pathological features of 103 PMP patients are shown in table 1. The medi-an age was 57 years (range 30-77). Previous abdominal surgery was performed once in 59 patients (57%) and twice or more in 25 patients (24%). Twelve patients (12%) had received systemic chemotherapy prior to cytoreduction and HIPEC. PMP was of appendiceal origin in 92 patients (91%). Other origins included urachus (n=2), ovary (n=3), colon (n=3), and pancreas (n=1). The origin was unknown in 2 patients. In com-parison to male patients, female patients showed more DPAM pathology (68% vs. 59%), limited extent of disease (0-5 regions in 40% vs. 23%), and complete cytoreduction (39% vs. 19%).
Table 1. Univariate model of the association between clinical-pathological features and long term survivalVariable Patients p value
DSS DFSAge <57 years 50
53 0.45 0.72Gender Female 69
Male 34 0.01 0.01Pathological subtype1 DPAM 66
PMCA-I 29 0.01 0.06PMCA 7 <0.001 <0.001
Previous laparotomy No 19Yes 84 0.35 0.99
Tumour load in regions2 0-5 356-7 66 0.02 <0.001
Result cytoreduction3 R1 31R2a 56 0.14 0.01R2b 10 0.01 <0.001
Additional chemotherapy No 63Yes 30 0.11 0.47
disseminated peritoneal adenomucinosis; PMCA: peritoneal mucinous carcinomatosis; PMCA-I: intermediate subtype; R1: macroscopic complete cytoreduction; R2a: residual tumor deposits < 2.5mm in any region; R2b: residual tumor deposits > 2.5mm in any region.
TreatmentOne hundred and fourteen procedures were performed in 103 patients. The ability to achieve complete cytoreduction was correlated with the tumor load (p<0.001, Chi Square). In case of tumor load in 6-7 regions, macroscopic complete cytoreduction (R1)
patients (77%). Accomplishing complete cytoreduction necessitated aggressive sur-gery, leading to mainly surgical complications in 62 of 114 procedures (54%) within 60
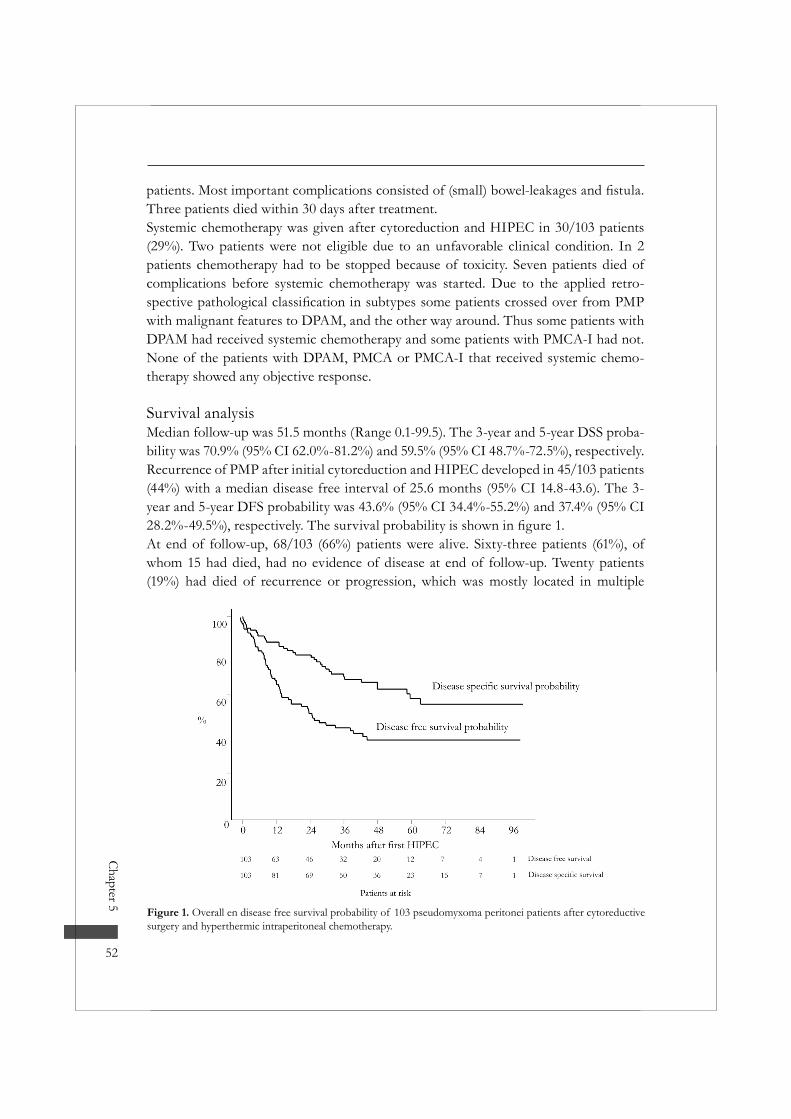
Chapter 5
52
Three patients died within 30 days after treatment.Systemic chemotherapy was given after cytoreduction and HIPEC in 30/103 patients (29%). Two patients were not eligible due to an unfavorable clinical condition. In 2 patients chemotherapy had to be stopped because of toxicity. Seven patients died of complications before systemic chemotherapy was started. Due to the applied retro-
with malignant features to DPAM, and the other way around. Thus some patients with DPAM had received systemic chemotherapy and some patients with PMCA-I had not. None of the patients with DPAM, PMCA or PMCA-I that received systemic chemo-therapy showed any objective response.
Survival analysisMedian follow-up was 51.5 months (Range 0.1-99.5). The 3-year and 5-year DSS proba-bility was 70.9% (95% CI 62.0%-81.2%) and 59.5% (95% CI 48.7%-72.5%), respectively. Recurrence of PMP after initial cytoreduction and HIPEC developed in 45/103 patients (44%) with a median disease free interval of 25.6 months (95% CI 14.8-43.6). The 3-year and 5-year DFS probability was 43.6% (95% CI 34.4%-55.2%) and 37.4% (95% CI
At end of follow-up, 68/103 (66%) patients were alive. Sixty-three patients (61%), of whom 15 had died, had no evidence of disease at end of follow-up. Twenty patients (19%) had died of recurrence or progression, which was mostly located in multiple
Figure 1. Overall en disease free survival probability of 103 pseudomyxoma peritonei patients after cytoreductive surgery and hyperthermic intraperitoneal chemotherapy.
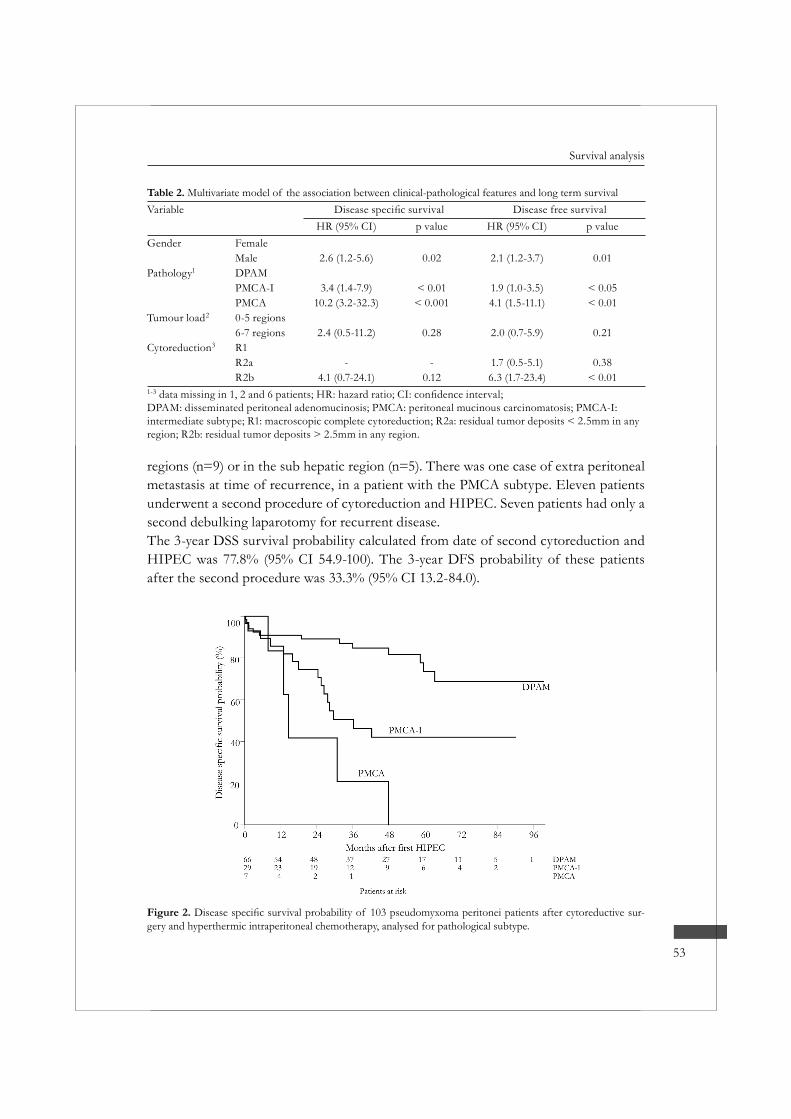
53
Survival analysis
regions (n=9) or in the sub hepatic region (n=5). There was one case of extra peritoneal metastasis at time of recurrence, in a patient with the PMCA subtype. Eleven patients underwent a second procedure of cytoreduction and HIPEC. Seven patients had only a second debulking laparotomy for recurrent disease. The 3-year DSS survival probability calculated from date of second cytoreduction and HIPEC was 77.8% (95% CI 54.9-100). The 3-year DFS probability of these patients after the second procedure was 33.3% (95% CI 13.2-84.0).
Table 2. Multivariate model of the association between clinical-pathological features and long term survivalVariable Disease free survival
HR (95% CI) p value HR (95% CI) p valueGender Female
Male 2.6 (1.2-5.6) 0.02 2.1 (1.2-3.7) 0.01Pathology1 DPAM
PMCA-I 3.4 (1.4-7.9) < 0.01 1.9 (1.0-3.5) < 0.05PMCA 10.2 (3.2-32.3) < 0.001 4.1 (1.5-11.1) < 0.01
Tumour load2 0-5 regions6-7 regions 2.4 (0.5-11.2) 0.28 2.0 (0.7-5.9) 0.21
Cytoreduction3 R1R2a - - 1.7 (0.5-5.1) 0.38R2b 4.1 (0.7-24.1) 0.12 6.3 (1.7-23.4) < 0.01
1-3
DPAM: disseminated peritoneal adenomucinosis; PMCA: peritoneal mucinous carcinomatosis; PMCA-I: intermediate subtype; R1: macroscopic complete cytoreduction; R2a: residual tumor deposits < 2.5mm in any region; R2b: residual tumor deposits > 2.5mm in any region.
Figure 2. -gery and hyperthermic intraperitoneal chemotherapy, analysed for pathological subtype.

Chapter 5
54
Table 1 shows a univariate model and table 2 shows a multivariate model of the asso-ciation between clinical-pathological factors and survival. Survival was dominated by
a decreased DSS probability were the sub diaphragmatic left and sub hepatic region
load > 5cm involving small bowel, diaphragm or liver, the DSS probability decreased
DiscussionPseudomyxoma peritonei is an indolent disease, and long-term survival up to 20 years has been described.14 Cytoreductive surgery is the key to successful treatment in PMP.
lacking, and there are three known approaches. The traditional approach consists of serial debulking surgery without the intention to be complete. The result of this strat-egy is excellent on a short term. Morbidity is low and patients recover to a normal life. However, almost all will recur in a few years time. A second debulking is usually more
by a third operation and a fourth. Eventually, either the tumor becomes inoperable and the patient dies of cachexia, or the patient dies of complications of the operation. Gough et al. published a series of 26 patients treated this way with an estimated 5-year survival of 53%.15 At end of follow-up only 3% were free of disease.Recently an analysis of 97 PMP patients treated at the Memorial Sloan-Kettering Can-cer Center was presented by Miner et al.16 An average of 2.2 debulking operations was
Table 3. Comparison of international survival results after treatment of pseudomyxoma peritoneiSeries (N) 5yr OS (%) 10yr OS (%) FU (Months) NED (%)Traditional treatment
Gough et al.15 (56) 53 32 144 3Miner et al.16 (97) 80A 21 57 12
Cytoreduction and (H)IPECDeraco et al.23 (33) 97A - 29 74Elias et al.20 (36) 66B > 60B,C 48 55Sugarbaker et al.24 (385) 86A > 80A,C 38 62Güner et al.25 (28) 80A - 51 -Loungnarath et al.22 (27) 52B - 23 -Moran et al.21 (100) 72A,C - 30 70
Present study (103) 60B >50B,C 51 56OS: overall survival; FU: follow-up (both mean and median are used); NED: no evidence of disease at end of follow-up.A Including only patients with complete cytoreduction and/or favorable pathology. B Including patients with both favorable and unfavorable pathology.C Estimated.

55
Survival analysis
performed and intraperitoneal chemotherapy was applied in 31%. They managed to reach complete cytoreduction in 53 patients (55%). Eventually, their treatment strategy resulted in a 10-years actuarial survival of 21%, calculated from date of diagnosis. The disease free rate at end of follow-up was 12%.Sugarbaker introduced an approach including extensive cytoreductive surgery with HIPEC.17 The surgical approach is based on extra peritoneal dissection, which allows the complete removal of peritoneal masses while dissecting in a tumor free plain. These peritonectomy procedures can be very helpful, especially in the pelvis and on the sub diaphragmatic areas.18 The idea of HIPEC is based on exposure of residual tumor cells on the peritoneal surface to very high doses of cytotoxic drugs potentiated by hyperther-mia.19 A local effect is hereby created that can never be reached by systemic exposure, due to general toxicity. In this way it may be assumed that at least the reseeding of surgical surfaces by free tumor cells, that are so widely present during these operations, can be prevented. Whether HIPEC also succeeds to sterilize tumor cells in remaining tumor deposits is uncertain. In several studies reporting on this aggressive treatment combination a large variation in survival rates is given, as shown in table 3.20-25 This wide range can be explained by the use of different treatment protocols and different
In our series, we report our results from the date of cytoreductive surgery and HIPEC. We feel that this represents more accurately the impact of treatment on the course of disease. Although the median follow-up was only 51 months, the Kaplan Meier survival curve (including patients with a poor prognosis) reached a plateau of 60% after 5 years. It seems therefore likely that the actuarial 10-year survival will be in the same range. At end of follow-up, 56% of patients were free of disease. Although 5-year survival for patients with DPAM/low grade pathology seems comparable, the 10-year and dis-ease free survival compare favorable to the Memorial Sloan Kettering Cancer Center
Though, it is clear that comparing these data produces some problems as differences
completeness of cytoreduction in the survival analysis.An important prognostic factor for long-term survival in PMP is pathology. Ronnett
-egories with different prognosis: disseminated peritoneal adenomucinosis (DPAM), peritoneal mucinous carcinomatosis (PMCA), and an intermediate/hybrid group. It is a
However, PMCA seems to behave like peritoneal carcinomatosis of ordinary colorectal adenocarcinoma origin. It has a very poor prognosis, shown in the Sugarbaker series
24 We agree with Sugarbaker and colleagues that PMCA

Chapter 5
56
as described by Verwaal et al.26
Completeness of cytoreduction is strongly associated with the extent of disease, and has prognostic value for survival as well.20,27 Our data show that in case of limited dis-ease (0-5 regions) a 5-year survival up to 82% is a realistic aim. Patients with extensive PMP are prone to incomplete cytoreduction and a complicated recovery. In addition, this series demonstrates that a large tumor load involving small bowel, diaphragm or sub hepatic region indicates a worse prognosis. We agree with Miner et al. that in these extensive PMP cases a planned two-step approach towards complete cytoreduction is preferable. We now resect the ileocoecum, the omentum and if necessary the ovaries in
the cytoreduction is completed and intraoperative HIPEC is given.
Our series presents some other interesting observations. Women had a better progno-sis, even after correction for pathology and extent of disease in the multivariate analysis. Maybe the dominance of ovarian involvement alters the behavior of PMP.
-temic 5-Fluorouracil based chemotherapy showed an objective response. This supports strongly the value of an aggressive loco-regional surgical approach in these cases.Cytoreduction and HIPEC has been quite a toxic treatment modality in our hands. Our data show however convincingly that a learning curve exists, with a reduced toxicity and mortality in the last 50 cases.28
In conclusion, cytoreductive surgery with intraoperative HIPEC is a treatment strategy with encouraging survival results for selected PMP patients. The pathological subtype remains the dominant factor for survival. Improvement of survival can be achieved by a combination of surgical experience and adequate patient selection. We feel that only by centralization of PMP patients the necessary expertise can be built up to improve the
57
Survival analysis
References1. Mukherjee A, Parvaiz A, Cecil TD et al. Pseudomyxoma peritonei usually originates from the appen-
dix: a review of the evidence. Eur J Gynaecol Oncol 2004; 25:411-414.2. Sugarbaker PH. Pseudomyxoma peritonei. A cancer whose biology is characterized by a redistribution
phenomenon. Ann Surg 1994; 219:109-111.3 Hinson FL, Ambrose NS. Pseudomyxoma peritonei. Br J Surg 1998; 85:1332-1339.4. Ronnett BM, Zahn CM, Kurman RJ et al. Disseminated peritoneal adenomucinosis and peritoneal
mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol 1995; 19:1390-1408.
5. Sugarbaker PH, Ronnett BM, Archer A et al. Pseudomyxoma peritonei syndrome. Adv Surg 1996; 30:233-280.
6. Wertheim I, Fleischhacker D, McLachlin CM et al. Pseudomyxoma peritonei: a review of 23 cases. Obstet Gynecol 1994; 84:17-21.
7. Chejfec G, Rieker WJ, Jablokow VR et al. Pseudomyxoma peritonei associated with colloid carcinoma of the pancreas. Gastroenterology 1986; 90:202-205.
8. de Bree E, Witkamp A, Van De Vijver M et al. Unusual origins of Pseudomyxoma peritonei. J Surg Oncol 2000; 75:270-274.
9. Baker WC, Goldman LB, deVere White RW. Pseudomyxoma peritonei presenting as a scrotal mass. J Urol 1988; 139:821-822.
10. Esquivel J, Sugarbaker PH. Pseudomyxoma peritonei in a hernia sac: analysis of 20 patients in whom
11. Ronnett BM, Kurman RJ, Zahn CM et al. Pseudomyxoma peritonei in women: a clinicopathologic analysis of 30 cases with emphasis on site of origin, prognosis, and relationship to ovarian mucinous tumors of low malignant potential. Hum Pathol 1995; 26:509-524.
12. Verwaal VJ, Van Tinteren H, Ruth SV et al. Toxicity of cytoreductive surgery and hyperthermic intra-peritoneal chemotherapy. J Surg Oncol 2004; 85:61-67.
13. Ronnett BM, Zahn CM, Kurman RJ et al. Disseminated peritoneal adenomucinosis and peritoneal mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol 1995; 19:1390-1408.
14. Lang H, Jahne J, Flemming P et al. Pseudomyxoma peritonei of appendiceal origin--a report of seven cases and a review of published reports. Eur J Surg 1995; 161:355-360.
15. Gough DB, Donohue JH, Schutt AJ et al. Pseudomyxoma peritonei. Long-term patient survival with an aggressive regional approach. Ann Surg 1994; 219:112-119.
16. Miner TJ, Shia J, Jaques DP et al. Long-term survival following treatment of pseudomyxoma perito-nei: an analysis of surgical therapy. Ann Surg 2005; 241:300-308.
17. Sugarbaker PH. Surgical treatment of peritoneal carcinomatosis: 1988 Du Pont lecture. Can J Surg 1989; 32:164-170.
18. Sugarbaker PH. Peritonectomy procedures. Ann Surg 1995; 221:29-42.19. Witkamp AJ, de Bree E, Van Goethem R et al. Rationale and techniques of intra-operative hyperther-
mic intraperitoneal chemotherapy. Cancer Treat Rev 2001; 27:365-374.20. Elias D, Laurent S, Antoun S et al. [Pseudomyxoma peritonei treated with complete resection and
immediate intraperitoneal chemotherapy]. Gastroenterol Clin Biol 2003; 27:407-412.21. Moran BJ, Mukherjee A, Sexton R. Operability and early outcome in 100 consecutive laparotomies for
peritoneal malignancy. Br J Surg 2005.22. Loungnarath R, Causeret S, Bossard N et al. Cytoreductive surgery with intraperitoneal chemohyper-
thermia for the treatment of pseudomyxoma peritonei: a prospective study. Dis Colon Rectum 2005; 48:1372-1379.
Chapter 5
58
23. Deraco M, Baratti D, Inglese MG et al. Peritonectomy and intraperitoneal hyperthermic perfusion
Oncol 2004; 11:393-398.24. Sugarbaker PH, Chang D. Results of treatment of 385 patients with peritoneal surface spread of
appendiceal malignancy. Ann Surg Oncol 1999; 6:727-731.25. Guner Z, Schmidt U, Dahlke MH et al. Cytoreductive surgery and intraperitoneal chemotherapy for
pseudomyxoma peritonei. Int J Colorectal Dis 2005; 20:155-160.26. Verwaal VJ, van Ruth S, de Bree E et al. Randomized trial of cytoreduction and hyperthermic intra-
peritoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with perito-neal carcinomatosis of colorectal cancer. J Clin Oncol 2003; 21:3737-3743.
27. Sugarbaker PH. Cytoreductive surgery and peri-operative intraperitoneal chemotherapy as a curative approach to pseudomyxoma peritonei syndrome. Eur J Surg Oncol 2001; 27:239-243.
28. Smeenk RM, Verwaal VJ, Zoetmulder FA. Toxicity and mortality of cytoreduction and intraoperative hyperthermic intraperitoneal chemotherapy in pseudomyxoma peritonei-a report of 103 procedures. Eur J Surg Oncol 2005.
6c h a p t e r
Learning curve of combined modality treatment in patients with peritoneal surface
disease
R.M. Smeenk1; V.J. Verwaal1; N. Antonini2; F.A.N. Zoetmulder1
Department of Surgery1, Department of Biometrics2
The Netherlands Cancer Institute - Antoni van Leeuwenhoek HospitalAmsterdam, the Netherlands

Background: Cytoreductive surgery with intraperitoneal chemotherapy has emerged as a new standard approach for peritoneal surface disease. Aim of this study was to investi-gate the learning curve of this combined modality treatment at a single institute.Methods: Investigated end-points regarding three consecutive treatment periods includ-
score (patient selection), result of cytoreduction, morbidity, in-hospital stay (treatment expertise), and survival.Results: From 1996 to 2006, 323 procedures were performed, 184 for peritoneal carci-nomatosis of colorectal cancer origin and 128 for pseudomyxoma peritonei. A second procedure was performed in 11 PMP patients. The mean SPCI score decreased signif-icantly (P<.0001), but the number of affected regions did not. The rate of complete cytoreductions increased from 35.6% to 65.1% (P=.012). Postoperative morbidity decreased from 71.2% to 34.1% (P<.0001). The median in-patient stay decreased from 24 to 17 days. Survival probability at 24 months showed a positive trend (P=.160) from 59.7% (95% CI 49.4%-72.2%) to 61.9% (95% CI 53.7%-71.3%) and 71.7% (95% CI 60.6%-84.7%).Conclusion: The learning curve of combined modality treatment for peritoneal surface
shows a positive trend for survival probability.
Submitted

61
Learning curve
IntroductionPeritoneal surface disease has in the past been a diagnosis with a poor prognosis. Sat-isfactory treatment options were not available until the introduction of cytoreductive surgery (CRS) in combination with chemotherapeutic lavage of the peritoneal cavity. This combined modality treatment was introduced by Sugarbaker in the previous decade.1The surgical modality consists of extensive surgical cytoreduction of tumour masses on visceral and/or parietal peritoneal surfaces with, if necessary, resection of the involved visceral organs. Surgery is at present mostly combined with hyperthermic intraperitoneal chemotherapy (HIPEC) in the same procedure. Techniques and materials differ between treatment centres, but overall treatment results are comparable and combined modality
-temic metastasis long-term overall and disease free survival can be accomplished.2-8,8-14
At this moment CRS with HIPEC has become the standard approach for pseudomyx-oma peritonei (PMP), peritoneal mesothelioma, and peritoneal carcinomatosis (PC) of colorectal cancer (CRC) origin.15-18
The counter side of this treatment approach is the considerable treatment related mor-bidity and mortality, mainly related to the surgical component.2,4,5,7-9,19-21 Previous studies however demonstrate a decrease of morbidity and mortality with increased experience with the procedure.19,20 At the Netherlands Cancer Institute, CRS and intraoperative HIPEC is performed for both PC of CRC origin and PMP since 1995. Aim of this study was to investigate the learning curve of this combined modality treatment at our insti-tute.
MethodsPatientsIn order to analyse factors associated with the learning curve of CRS and HIPEC, the study period was divided in three treatment periods. These periods are related to the
period (1996-1998) included part of a phase II trial. The second period (1999-2002) con-
major surgery and free of extra-peritoneal metastases.
TreatmentThe selection of patients and treatment procedure was performed by the same surgeon

Chapter 6
62
The medical team, including scrub nurses, a perfusionist, anaesthesiologists, radiologists,
the consecutive study periods. Treatment consisted of surgical resection of macroscopic tumour deposits on both parietal and visceral peritoneal surfaces, conforming to the peritonectomy procedures.22 In all patients surgical treatment aimed for complete cytore-duction. After surgery, lavage of the peritoneal cavity was performed in the same session by heated intraperitoneal chemotherapy with Mitomycin C 35 mg/m2 for 90 minutes at 40-410 Celsius. This combined modality treatment is described in detail elsewhere.14 In the phase II study the doses of Mitomycin C varied from 25 to 40 mg/m2. In the con-secutive periods Mitomycine C was used in a dosis of 35 mg/ m2.At the beginning of surgery, the volume and extent of disease was assessed by registering
23
For this purpose the abdomen was divided in 7 distinctive regions with anatomical sig-
hepatic region, and sub phrenic left and right region. The SPCI score was determined by the maximum tumour thickness in each of these 7 regions, using a grading system (0: no macroscopic tumour; 1: < 2 cm; 2: 2-5 cm; 3: > 5 cm). The SPCI score was calcu-lated by adding these numbers (range 0-21). The SPCI score could be hard to assess in
tumour and/or ascites in 6-7 involved regions were scored at maximum. In patients with less extensive disease it was feasible to record the affected regions and SPCI score con-forming to protocol.After surgery, the result of cytoreduction was recorded. No residual macroscopic tumour
in any region was categorized as an R2a cytoreduction; in case of tumour residue larger
Data and statistical analysisPrimary end-points of the learning curve were factors related to patient selection and treatment expertise. Survival was considered a secondary end-point. The learning effect regarding patient selection was evaluated by analysing the number of affected regions and SPCI score for each procedure per patient during the three treatment periods. Asso-ciation between treatment period and SPCI respectively affected regions was investigated
The gain of expertise in both the procedure and postoperative care was assessed by ana-lysing the result of cytoreduction, postoperative morbidity, and the duration of in-patient stay (days) for each procedure per patient during the three treatment periods. Morbidity was scored as toxicity conforming to the National Cancer Institute Common Toxicity
-

63
Learning curve
ity and necessitated minor (tube drainage, minor surgery) or major surgical intervention
treatment related mortality). The number of hospital days was calculated from day of treatment to date of discharge from the hospital. Multivariate logistic regression was conducted to investigate the correlation between treatment period and post operative morbidity respectively result of cytoreduction. A multivariate generalized linear model was conducted to investigate the correlation between treatment period and the number of days hospitalized (log transformed). All multivariate models included origin of dis-ease, number of affected regions and SPCI as covariates.The effect of the learning curve on treatment related mortality and probability of sur-vival was recorded by analyzing survival time related to treatment period. Survival time
treatment was used for grouping patients into the three periods. Because of the differ-ences in follow-up between treatment periods, survival probabilities were only estimated at 24 months, with the Kaplan Meier method. Multivariate Cox proportional hazards regression was conducted to investigate the difference between the three treatment peri-ods. The number of affected regions and SPCI score were considered as covariates, origin
plots. Patients were excluded from an analysis if data was missing related to a factor
ResultsPatient selectionFrom 1996 to 2006, 323 procedures of CRS and HIPEC were performed in 180 women and 143 men. Primary diagnosis was PC of CRC in 184 patients, PMP in 128. A sec-ond procedure after progression was performed in 11 PMP patients. The median age was 57 years (30-77) for PMP and 55 years (24-77) for PC of CRC. The distribution of
treatment periods, except for the malignant subtype, which increased from 3.6% and 6.5% to 12.5%. The number of procedures analysed per period and type of disease is shown in table 1. The median follow-up for the entire period was 42.0 months (0.1-119.5) for PC of CRC and 50.0 months (0.1-117.7) for PMP.The median number of affected regions and SPCI score could be determined in 311 pro-cedures. Table 1 shows the number of affected regions and SPCI score analysed for type of disease and treatment period. The mean SPCI score for the entire patient group decreased
(P<.0001), however the decrease in number of affected regions was not (P=.290).
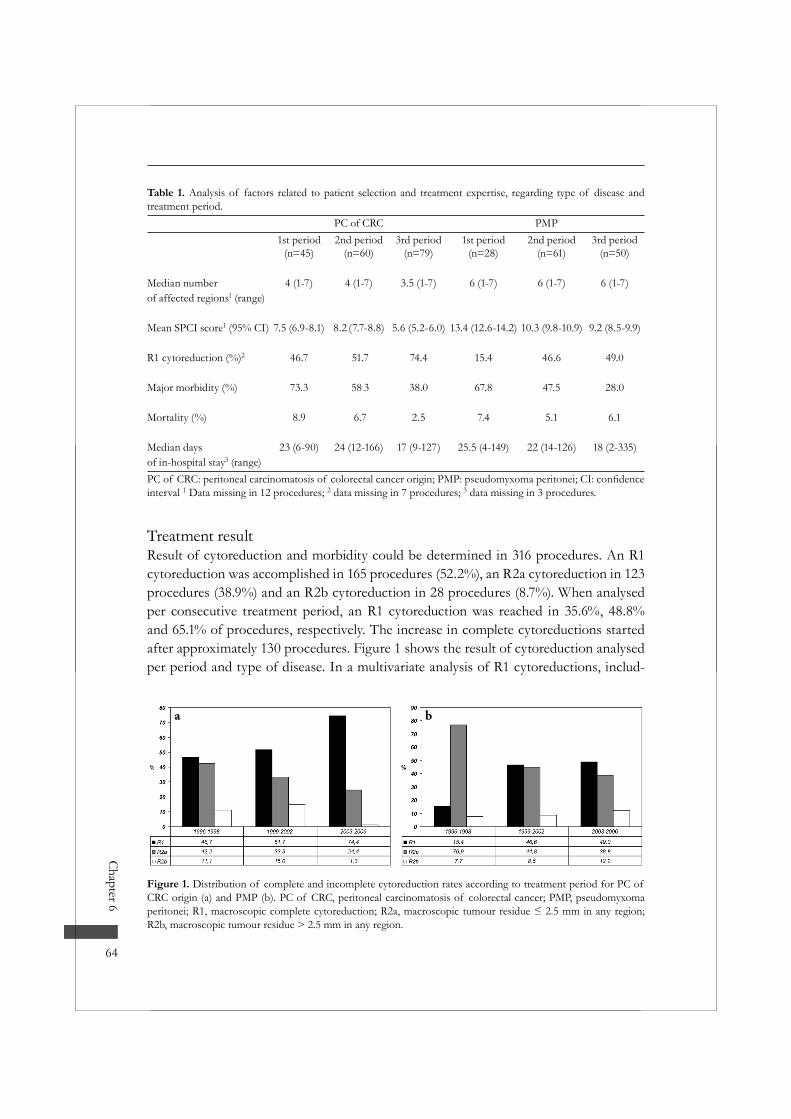
Chapter 6
64
Treatment resultResult of cytoreduction and morbidity could be determined in 316 procedures. An R1 cytoreduction was accomplished in 165 procedures (52.2%), an R2a cytoreduction in 123 procedures (38.9%) and an R2b cytoreduction in 28 procedures (8.7%). When analysed per consecutive treatment period, an R1 cytoreduction was reached in 35.6%, 48.8% and 65.1% of procedures, respectively. The increase in complete cytoreductions started after approximately 130 procedures. Figure 1 shows the result of cytoreduction analysed per period and type of disease. In a multivariate analysis of R1 cytoreductions, includ-
Table 1. Analysis of factors related to patient selection and treatment expertise, regarding type of disease and treatment period.
PC of CRC PMP1st period
(n=45)2nd period
(n=60)3rd period
(n=79)1st period
(n=28)2nd period
(n=61)3rd period
(n=50)
Median number 4 (1-7) 4 (1-7) 3.5 (1-7) 6 (1-7) 6 (1-7) 6 (1-7)of affected regions1 (range)
Mean SPCI score1 (95% CI) 7.5 (6.9-8.1) 8.2 (7.7-8.8) 5.6 (5.2-6.0) 13.4 (12.6-14.2) 10.3 (9.8-10.9) 9.2 (8.5-9.9)
R1 cytoreduction (%)2 46.7 51.7 74.4 15.4 46.6 49.0
Major morbidity (%) 73.3 58.3 38.0 67.8 47.5 28.0
Mortality (%) 8.9 6.7 2.5 7.4 5.1 6.1
Median days 23 (6-90) 24 (12-166) 17 (9-127) 25.5 (4-149) 22 (14-126) 18 (2-335)of in-hospital stay3 (range)
interval 1 Data missing in 12 procedures; 2 data missing in 7 procedures; 3 data missing in 3 procedures.
Figure 1. Distribution of complete and incomplete cytoreduction rates according to treatment period for PC of CRC origin (a) and PMP (b). PC of CRC, peritoneal carcinomatosis of colorectal cancer; PMP, pseudomyxoma
R2b, macroscopic tumour residue > 2.5 mm in any region.
a b
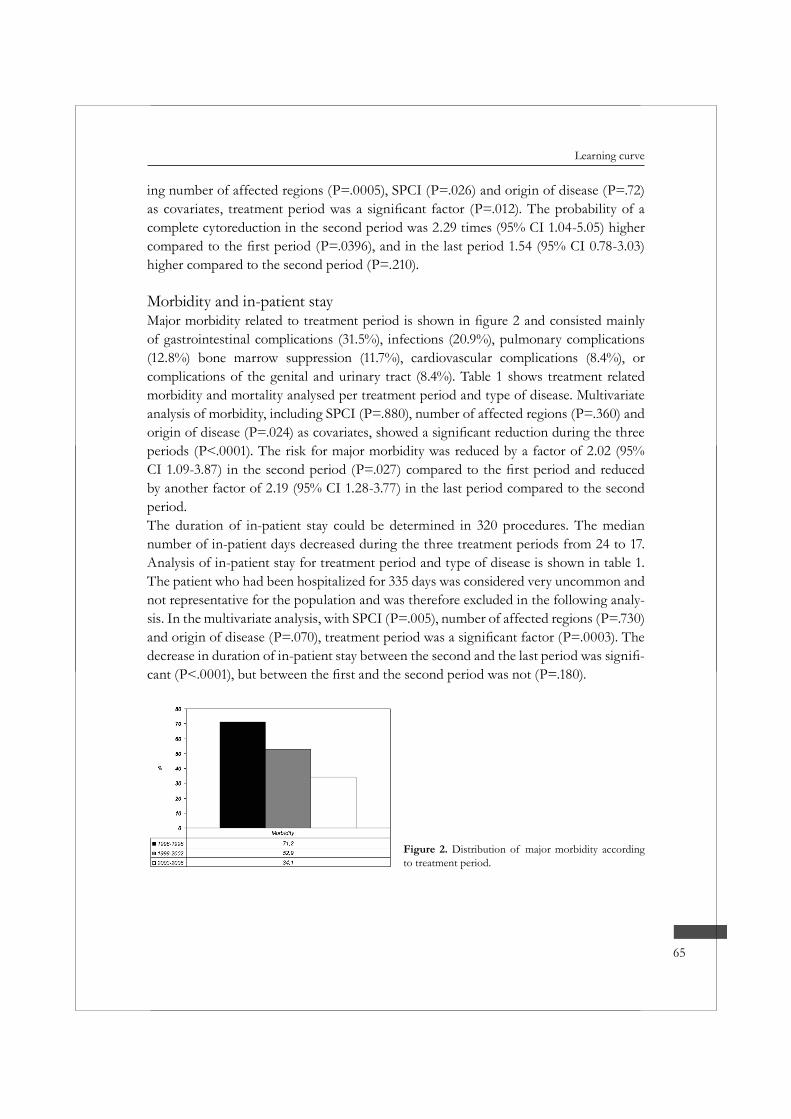
65
Learning curve
ing number of affected regions (P=.0005), SPCI (P=.026) and origin of disease (P=.72)
complete cytoreduction in the second period was 2.29 times (95% CI 1.04-5.05) higher
higher compared to the second period (P=.210).
Morbidity and in-patient stay
of gastrointestinal complications (31.5%), infections (20.9%), pulmonary complications (12.8%) bone marrow suppression (11.7%), cardiovascular complications (8.4%), or complications of the genital and urinary tract (8.4%). Table 1 shows treatment related morbidity and mortality analysed per treatment period and type of disease. Multivariate analysis of morbidity, including SPCI (P=.880), number of affected regions (P=.360) and
periods (P<.0001). The risk for major morbidity was reduced by a factor of 2.02 (95%
by another factor of 2.19 (95% CI 1.28-3.77) in the last period compared to the second period.The duration of in-patient stay could be determined in 320 procedures. The median number of in-patient days decreased during the three treatment periods from 24 to 17. Analysis of in-patient stay for treatment period and type of disease is shown in table 1. The patient who had been hospitalized for 335 days was considered very uncommon and not representative for the population and was therefore excluded in the following analy-sis. In the multivariate analysis, with SPCI (P=.005), number of affected regions (P=.730)
-
Figure 2. Distribution of major morbidity according to treatment period.
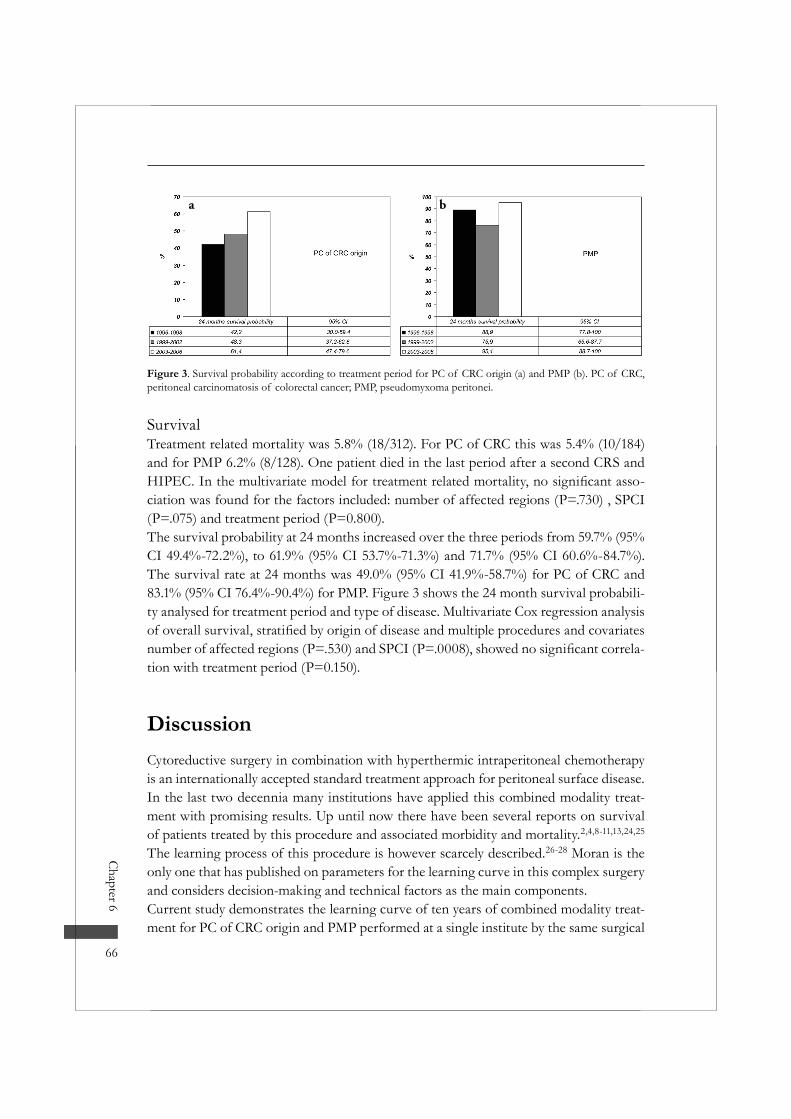
Chapter 6
66
SurvivalTreatment related mortality was 5.8% (18/312). For PC of CRC this was 5.4% (10/184) and for PMP 6.2% (8/128). One patient died in the last period after a second CRS and
-ciation was found for the factors included: number of affected regions (P=.730) , SPCI (P=.075) and treatment period (P=0.800).The survival probability at 24 months increased over the three periods from 59.7% (95% CI 49.4%-72.2%), to 61.9% (95% CI 53.7%-71.3%) and 71.7% (95% CI 60.6%-84.7%). The survival rate at 24 months was 49.0% (95% CI 41.9%-58.7%) for PC of CRC and 83.1% (95% CI 76.4%-90.4%) for PMP. Figure 3 shows the 24 month survival probabili-ty analysed for treatment period and type of disease. Multivariate Cox regression analysis
-tion with treatment period (P=0.150).
DiscussionCytoreductive surgery in combination with hyperthermic intraperitoneal chemotherapy is an internationally accepted standard treatment approach for peritoneal surface disease. In the last two decennia many institutions have applied this combined modality treat-ment with promising results. Up until now there have been several reports on survival of patients treated by this procedure and associated morbidity and mortality.2,4,8-11,13,24,25
The learning process of this procedure is however scarcely described.26-28 Moran is the only one that has published on parameters for the learning curve in this complex surgery and considers decision-making and technical factors as the main components.Current study demonstrates the learning curve of ten years of combined modality treat-ment for PC of CRC origin and PMP performed at a single institute by the same surgical
Figure 3. Survival probability according to treatment period for PC of CRC origin (a) and PMP (b). PC of CRC, peritoneal carcinomatosis of colorectal cancer; PMP, pseudomyxoma peritonei.
a b

67
Learning curve
team. Over the 3 treatment periods, the extent of disease diminished, together with the post-operative morbidity, while the percentage of complete cytoreductions and the prob-ability of 2 year survival increased. These observations are consistent with a learning curve with respect to patient selection and execution of this complicated treatment.
included for treatment regardless of tumour load. In these early years the surgical team strove for complete cytoreduction even in patients with extensive disease and/or small bowel involvement. Especially in patients with PC of CRC origin this resulted in a high
14,20 Consequently, selection criteria for PC -
involvement) on preoperative CT scan, are now excluded from treatment. The improved selection process has probably contributed to the improved treatment results in these patients. However, the rate of failed operations, in which patients deemed cytoreducible preoperatively but were inoperable at the moment of laparotomy, remained constant at 2 per year. In these patients small bowel involvement or liver metastases were not seen on preoperative CT scans. It seems that despite sensitive imaging techniques (CT scan) the extent of disease can still be underestimated. A recent study of de Bree and colleagues illustrates the limited value of preoperative CT scans in patient selection for PC of CRC origin, as the prognostic value is radiologist dependent.23 Besides further development of even more sensitive imaging techniques, improvement of experience in interpreting these images is necessary to improve this failure rate.Adjustment of patient selection has not been practised in patients with PMP as these patients are eligible for complete cytoreduction even with extensive disease and high SPCI scores. In contrast to PC of CRC origin, mucinous PMP deposits are usually non-invasive and can be carefully removed from all peritoneal surfaces. Exceptions herein might be tumour biology (malignant subtype) and tumour localisation in the sub hepatic or gastric region, which can be restricting factors for complete cytoreduction in PMP patients.29,30 In present study the increasing percentage of incomplete cytoreductions dur-ing the three treatment periods is mainly attributed to the increase of malignant subtypes alongside. The consequent logical suggestion to withdraw PMP patients with malignant subtype from combined modality treatment has already been raised in the past.29 As the pathological subtype is usually not available before surgery, such selection is however not feasible. Selection by localisation of disease seems unreasonable and unnecessary as most PMP patients have an indolent disease behaviour and progressive PMP after incomplete cytoreduction remains manageable in a considerable percentage of patients.31 At this moment the only treatment restriction for PMP patients is a moribund general health.

Chapter 6
68
The learning curve with respect to the execution of treatment is demonstrated in the improvement of the result of cytoreduction, morbidity, and the duration of in-patient
-cacy of HIPEC and prognosis.4,6,14,29
may be found in the associated quality of life. Patients with previous abdominal surgery, extensive disease and, especially in case of PC of CRC origin, small bowel involvement have less chance of complete cytoreduction, a high chance of morbidity and consequent prolonged in-patient stay.2,7,19,20 Patient selection and treatment expertise seem closely related in their accountability for improvement of these aspects. The presented analysis however demonstrates that the effect of treatment expertise stands on its own, and may be attributed to improved surgical expertise of the surgical team and experience in han-dling complications by the entire medical team. An example of the acquired treatment expertise regards the changed treatment strategy in PMP patients with extensive tumour load (6-7 regions). In these patients cytoreduction is now performed in two stages to prevent high morbidity and mortality. First accessible tumour localisation is resected (ileocoecum, omentum and ovaries). A second operation is then performed after 4-6 months, when the patient has recovered, to complete the cytoreduction and to apply the HIPEC lavage.
Current analysis shows a positive trend of the learning curve on survival probability, espe-cially in patients with PC of CRC origin. This may be attributed to both improved patient selection and treatment expertise. In the PMP group survival probability increased as
treatment skill. The reason for the isolated fall in the second period remains unclear.Besides the surgical component of the treatment procedure, improved tumour expo-sure and perfusion technique during the HIPEC lavage might have contributed to the increased survival probability. In time several technical adjustments were made and the optimal dose of Mitomycin C was applied.
new diagnostic procedures, treatment techniques, complications and all other concomi-tant problems. In contrast, institutions that introduced combined modality treatment
during site visits or international congresses on peritoneal surface malignancy. This provides them with a head start in handling patient selection, treatment procedure and postoperative problems. Considering these arguments, this study also describes the aspect of the “world learning curve”, a curve that can not simply be applied on new-

69
Learning curve
restricting combined modality treatment to specialized institutes that treat these patients on a regular basis.
In conclusion, the learning curve of combined modality treatment for peritoneal surface
the learning curve for treatment expertise seems to be reached after approximately 130 procedures. The learning curve shows a positive effect on survival probability.
References1. Sugarbaker PH. Cytoreductive surgery and intraperitoneal chemotherapy with peritoneal spread of
cystadenocarcinoma. Eur J Surg Suppl 1991;75-82.2. Kusamura S, Younan R, Baratti D et al. Cytoreductive surgery followed by intraperitoneal hyperther-
mic perfusion: analysis of morbidity and mortality in 209 peritoneal surface malignancies treated with closed abdomen technique. Cancer 2006; 106:1144-1153.
3. Bryant J, Clegg AJ, Sidhu MK et al. Systematic review of the Sugarbaker procedure for pseudomyxo-ma peritonei. Br J Surg 2005; 92:153-158.
4. Glehen O, Kwiatkowski F, Sugarbaker PH et al. Cytoreductive surgery combined with periopera-tive intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study. J Clin Oncol 2004; 22:3284-3292.
5. Jacquet P, Stephens AD, Averbach AM et al. Analysis of morbidity and mortality in 60 patients with peritoneal carcinomatosis treated by cytoreductive surgery and heated intraoperative intraperitoneal chemotherapy. Cancer 1996; 77:2622-2629.
6. Sugarbaker PH. Cytoreductive surgery and peri-operative intraperitoneal chemotherapy as a curative approach to pseudomyxoma peritonei syndrome. Eur J Surg Oncol 2001; 27:239-243.
7. Stephens AD, Alderman R, Chang D et al. Morbidity and mortality analysis of 200 treatments with cytoreductive surgery and hyperthermic intraoperative intraperitoneal chemotherapy using the coli-seum technique. Ann Surg Oncol 1999; 6:790-796.
8. Butterworth SA, Panton ON, Klaassen DJ et al. Morbidity and mortality associated with intraperito-neal chemotherapy for Pseudomyxoma peritonei. Am J Surg 2002; 183:529-532.
9. Deraco M, Baratti D, Inglese MG et al. Peritonectomy and intraperitoneal hyperthermic perfusion
Oncol 2004; 11:393-398.10. Elias D, Laurent S, Antoun S et al. [Pseudomyxoma peritonei treated with complete resection and
immediate intraperitoneal chemotherapy]. Gastroenterol Clin Biol 2003; 27:407-412.11. Guner Z, Schmidt U, Dahlke MH et al. Cytoreductive surgery and intraperitoneal chemotherapy for
pseudomyxoma peritonei. Int J Colorectal Dis 2005; 20:155-160.12. Loungnarath R, Causeret S, Bossard N et al. Cytoreductive surgery with intraperitoneal chemohyper-
thermia for the treatment of pseudomyxoma peritonei: a prospective study. Dis Colon Rectum 2005; 48:1372-1379.
13. Moran BJ, Mukherjee A, Sexton R. Operability and early outcome in 100 consecutive laparotomies for peritoneal malignancy. Br J Surg 2005.
14. Verwaal VJ, van Ruth S, de Bree E et al. Randomized trial of cytoreduction and hyperthermic intra-peritoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with perito-neal carcinomatosis of colorectal cancer. J Clin Oncol 2003; 21:3737-3743.
15. Sugarbaker PH. New standard of care for appendiceal epithelial neoplasms and pseudomyxoma peri-tonei syndrome? Lancet Oncol 2006; 7:69-76.
Chapter 6
70
16. Brigand C, Monneuse O, Mohamed F et al. Peritoneal mesothelioma treated by cytoreductive surgery and intraperitoneal hyperthermic chemotherapy: results of a prospective study. Ann Surg Oncol 2006; 13:405-412.
17. Sugarbaker PH, Yan TD, Stuart OA et al. Comprehensive management of diffuse malignant perito-neal mesothelioma. Eur J Surg Oncol 2006.
18. Yan TD, Stuart OA, Yoo D et al. Perioperative intraperitoneal chemotherapy for peritoneal surface malignancy. J Transl Med 2006; 4:17.
19. Smeenk RM, Verwaal VJ, Zoetmulder FA. Toxicity and mortality of cytoreduction and intraoperative hyperthermic intraperitoneal chemotherapy in pseudomyxoma peritonei-a report of 103 procedures. Eur J Surg Oncol 2005.
20. Verwaal VJ, van Tinteren H, Ruth SV et al. Toxicity of cytoreductive surgery and hyperthermic intra-peritoneal chemotherapy. J Surg Oncol 2004; 85:61-67.
21. Sugarbaker PH, Alderman R, Edwards G et al. Prospective Morbidity and Mortality Assessment of Cytoreductive Surgery Plus Perioperative Intraperitoneal Chemotherapy To Treat Peritoneal Dissemi-nation of Appendiceal Mucinous Malignancy. Ann Surg Oncol 2006.
22. Sugarbaker PH. Peritonectomy procedures. Surg Oncol Clin N Am 2003; 12:703-27, xiii.23. de Bree E, Koops W, Kroger R et al. Preoperative computed tomography and selection of patients
with colorectal peritoneal carcinomatosis for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy. Eur J Surg Oncol 2006; 32:65-71.
24. Sugarbaker PH. Cytoreductive surgery and perioperative intraperitoneal chemotherapy as a curative approach to pseudomyxoma peritonei syndrome. Tumori 2001; 87:S3-S5.
25. Scuderi S, Costamagna D, Vaira M et al. [Treatment of pseudomyxoma peritonei using cytoreduction and intraperitoneal hyperthermic chemotherapy]. Tumori 2003; 89:43-45.
26. Cavaliere F, Valle M, De RB et al. [Peritonectomy and chemohyperthermia in the treatment of perito-neal carcinomatosis: learning curve]. Suppl Tumori 2005; 4:S119-S121.
27. Moran BJ. Establishment of a peritoneal malignancy treatment centre in the United Kingdom. Eur J Surg Oncol 2006; 32:614-618.
28. Moran BJ. Decision-making and technical factors account for the learning curve in complex surgery. J Public Health (Oxf) 2006.
29. Smeenk RM, Verwaal VJ, Zoetmulder FA. Survival analysis of pseudomyxoma peritonei treated by cytoreductive surgery in combination with intraoperative hyperthermic intraperitoneal chemotherapy. Ann Surg . 2006. Ref Type: In Press
30. Zoetmulder FA, Sugarbaker PH. Patterns of failure following treatment of pseudomyxoma peritonei of appendiceal origin. Eur J Cancer 1996; 32A:1727-1733.
31. Smeenk RM, Verwaal VJ, Antonini N, Zoetmulder FA. Progressive pseudomyxoma peritonei after combined modality treatment: management and outcome. Ann Surg Oncol . 2006. Ref Type: In Press

7c h a p t e r
Progression of pseudomyxoma peritonei after combined modality treatment: management
and outcome
Robert M. Smeenk 1; Vic J. Verwaal1; Ninja Antonini2; Frans A.N. Zoetmulder1
Department of Surgery1, Department of Biometrics2
The Netherlands Cancer Institute - Antoni van Leeuwenhoek HospitalAmsterdam, the Netherlands

Background: Cytoreductive surgery (CRS) with hyperthermic intraperitoneal che-motherapy (HIPEC) is a treatment strategy for pseudomyxoma peritonei (PMP) with curative intent. The aim of this study was to determine the patterns of failure in patients who underwent such a procedure and to evaluate management and outcome of progres-sive disease.Methods: After exclusion of patients with overt malignancy, progression was studied in 96 PMP patients treated primarily by CRS with HIPEC. Location, pathology, man-agement and outcome were recorded.Results: Median follow-up was 51.5 months (0.1-99.5). Median progression free surviv-al (PFS) was 28.2 months (95% CI 18.3->). Progressive disease was mainly located sub hepatic (38%) or in multiple regions (36%). Pathological dedifferentiation was observed in 8 patients (20%). The choice of treatment depended on pathology, extent of dis-ease and PFS. Seventeen patients were treated for progression by second CRS with (n=8) or without HIPEC (n=10). The 3-years overall survival (OS) probability after this treatment was 100% and 53.3% (95% CI 28.2%-100%), respectively. Fifteen patients with (slow) progression were observed. Three-years OS probability of these patients was 66.0% (95% CI 43.4%-100%). All patients treated for progression by systemic che-motherapy only (n=6) had died of disease after a median follow up of 14.8 (9.8-33.6) months. A longer PFS after primary treatment was associated with longer OS after progression (p=0.04).Conclusions: Progressive PMP after primary CRS with HIPEC is probably the result of technical failure and/or tumor biology. Management of progressive PMP can be valuable for selected patients and should depend primarily on the PFS.
Ann Surg Oncol, in press

73
Progressive PMP
IntroductionPseudomyxoma peritonei (PMP) is a rare disease characterized by peritoneal deposits of adenomucinous tumor cells producing a progressive amount of intraperitoneal muci-nous ascites. These intraperitoneal disseminated tumor cells usually originate from a ruptured appendiceal neoplasm. The process of dissemination throughout the perito-neal cavity is described as the redistribution phenomenon.1Aggressive cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemother-apy (HIPEC) is a treatment strategy for PMP with promising survival results.2-5 The peritonectomy procedures are a useful tool to optimize resection of macroscopic perito-
by the cytotoxic effect on (microscopic) tumor residue, especially in patients with low-grade pathology and complete cytoreduction.3,5-7 Recurrent or progressive disease after this combined modality treatment is however still a problem. Treatment approaches for recurrent or progressive PMP are not well described, although surgery seems to be the most common option.8-10
At the Netherlands Cancer Institute, the standard primary treatment of PMP patients consists of aggressive CRS by peritonectomy procedures in combination with intraop-erative HIPEC with Mitomycin C. Aim of this study is to determine the patterns of failure after this combined modality treatment and to evaluate the management and outcome of progressive PMP.
MethodsPrimary treatmentA prospective database of PMP patients treated at the Netherlands Cancer Institute has been maintained from 1996 onwards. Patients treated in the period 1996-2004 were retrospectively analyzed. All patients were primarily treated with aggressive CRS (peri-tonectomy procedures) with intraoperative HIPEC, a procedure described in detail elsewhere.11 The result (completeness) of cytoreduction was recorded at the end of sur-
2.5 mm in any region (R2a cytoreduction) and tumor deposits > 2.5 mm in any region (R2b cytoreduction).
Pathological subtypesFor analysis of this study, PMP was categorized into three pathological subtypes: dis-seminated peritoneal adenomucinosis (DPAM), peritoneal mucinous carcinomatosis (PMCA) and an intermediate subtype (PMCA-I).12 DPAM pathology shows charac-teristics of benign tumor containing no or very few epithelial cells with no or little

Chapter 7
74
atypia. PMCA pathology includes tumor containing epithelial cells with malignant phe-notype. PMCA-I is an intermediate subtype with mainly features of DPAM but focally characteristics of PMCA. Patients with PMCA pathology at primary presentation were excluded from this analysis as we feel that PMCA should be categorized as peritoneal carcinomatosis and not as PMP.
Follow upFollow up consisted of physical examination and assessment of tumor markers CEA
every 6 months. Abdominal computed tomography (CT) scan was performed 3 months after the primary treatment and after that at every 6 months follow up visit or when recurrence or progression was suspected.Policy towards recurrent or progressive disease in the period 1996-2004 was based on the following principles with important selection criteria consisting of the extent of disease (visualized on follow up CT scans), pathology and time to recurrent or progres-sive disease. Patients with limited (<3 regions) and resectable disease, both DPAM and PMCA-I subtype, were treated with local resection only. Patients with limited slowly progressive disease, especially DPAM but also PMCA-I subtype, were observed with-out therapy. Patients with early-developed diffuse disease of initial PMCA-I subtype or initial DPAM with signs of dedifferentiation at progression or with signs of extra-peritoneal disease were treated with 5-FU based systemic chemotherapy. Patients with late-developed diffuse disease of benign subtype (DPAM) were treated with second CRS plus HIPEC.
Data analysis and statistical methodsBoth recurrent PMP after an R1 cytoreduction and progressive disease after an R2
of primary treatment was analyzed in terms of progression free survival (PFS), calcu-
up. Progressive PMP was studied with regard to its location, pathology, management
(pelvis, small or large bowel and mesentery/omentum, sub hepatic region and right and left sub phrenic region), on surgical wound surfaces or extraperitoneal. When the site
treatment and progressive PMP from DPAM towards PMCA-I or PMCA. Patients with missing data were excluded.
-
up. The outcome of management for progressive PMP was analyzed in terms of PFS
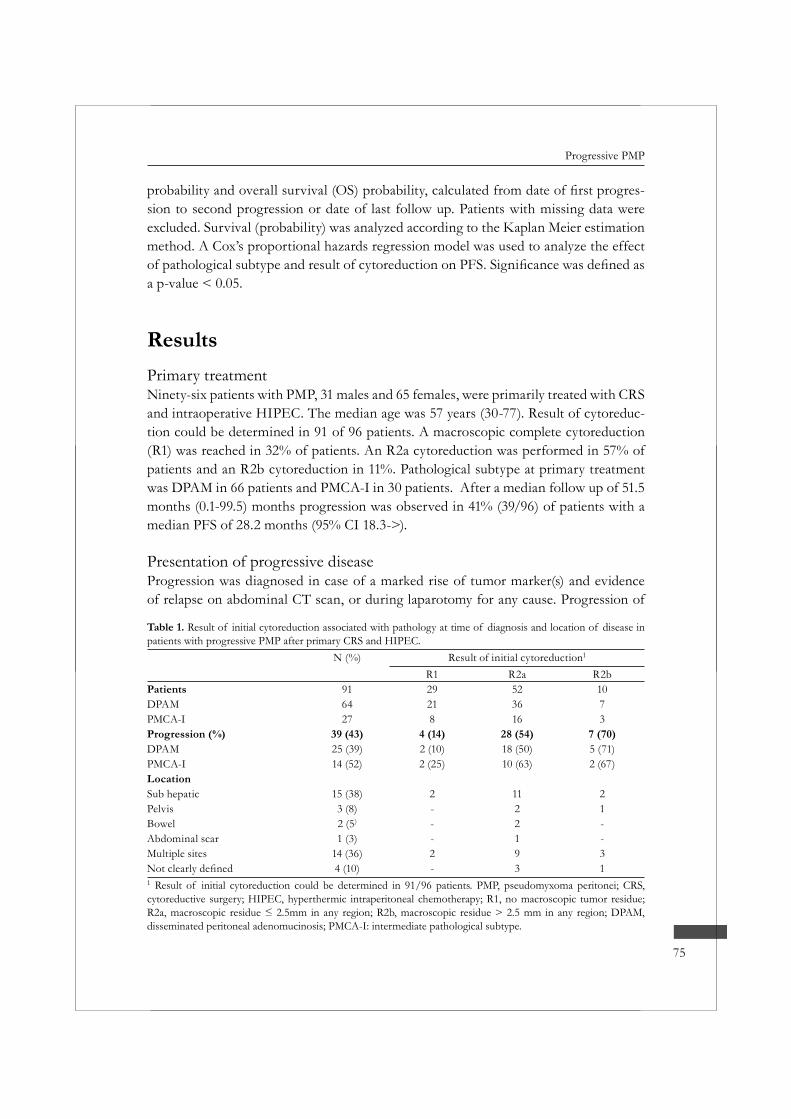
75
Progressive PMP
-sion to second progression or date of last follow up. Patients with missing data were excluded. Survival (probability) was analyzed according to the Kaplan Meier estimation method. A Cox’s proportional hazards regression model was used to analyze the effect
a p-value < 0.05.
ResultsPrimary treatmentNinety-six patients with PMP, 31 males and 65 females, were primarily treated with CRS and intraoperative HIPEC. The median age was 57 years (30-77). Result of cytoreduc-tion could be determined in 91 of 96 patients. A macroscopic complete cytoreduction (R1) was reached in 32% of patients. An R2a cytoreduction was performed in 57% of patients and an R2b cytoreduction in 11%. Pathological subtype at primary treatment was DPAM in 66 patients and PMCA-I in 30 patients. After a median follow up of 51.5 months (0.1-99.5) months progression was observed in 41% (39/96) of patients with a median PFS of 28.2 months (95% CI 18.3->).
Presentation of progressive diseaseProgression was diagnosed in case of a marked rise of tumor marker(s) and evidence of relapse on abdominal CT scan, or during laparotomy for any cause. Progression of
Table 1. Result of initial cytoreduction associated with pathology at time of diagnosis and location of disease in patients with progressive PMP after primary CRS and HIPEC.
N (%) Result of initial cytoreduction1
R1 R2a R2bPatients 91 29 52 10DPAM 64 21 36 7PMCA-I 27 8 16 3Progression (%) 39 (43) 4 (14) 28 (54) 7 (70)DPAM 25 (39) 2 (10) 18 (50) 5 (71)PMCA-I 14 (52) 2 (25) 10 (63) 2 (67)LocationSub hepatic 15 (38) 2 11 2Pelvis 3 (8) - 2 1Bowel 2 (5) - 2 -Abdominal scar 1 (3) - 1 -Multiple sites 14 (36) 2 9 3
4 (10) - 3 11 Result of initial cytoreduction could be determined in 91/96 patients. PMP, pseudomyxoma peritonei; CRS, cytoreductive surgery; HIPEC, hyperthermic intraperitoneal chemotherapy; R1, no macroscopic tumor residue;
disseminated peritoneal adenomucinosis; PMCA-I: intermediate pathological subtype.
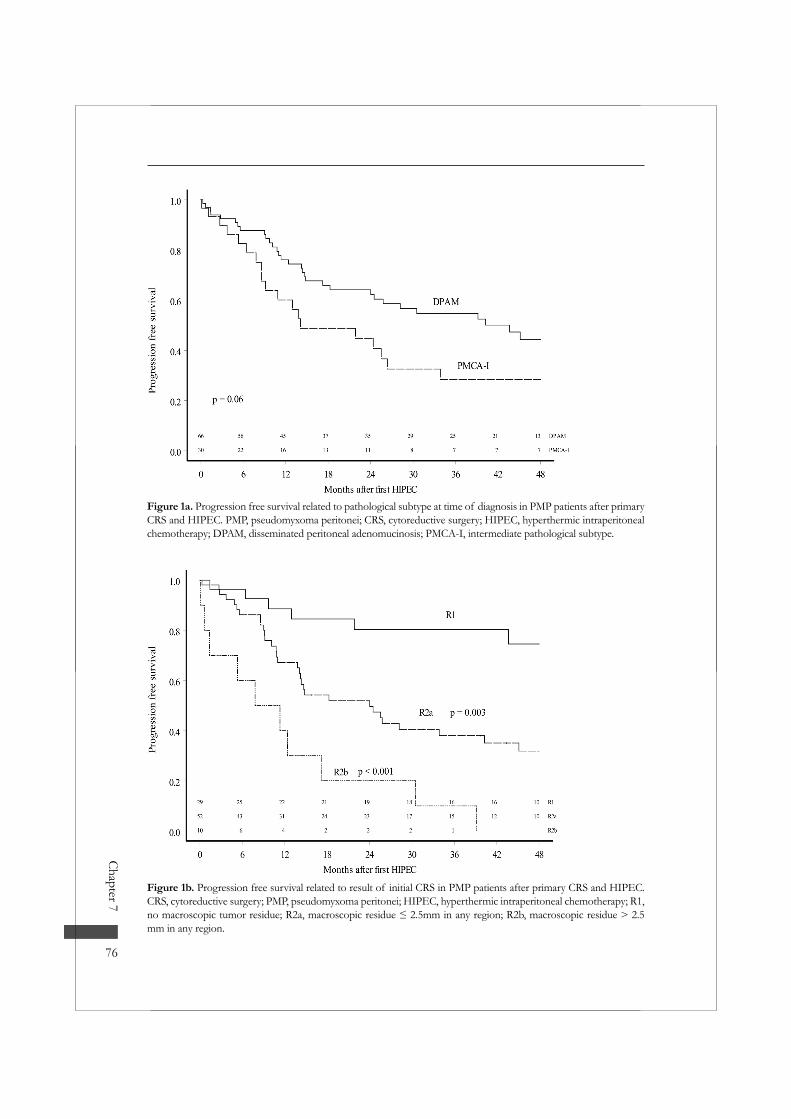
Chapter 7
76
Figure 1a. Progression free survival related to pathological subtype at time of diagnosis in PMP patients after primary CRS and HIPEC. PMP, pseudomyxoma peritonei; CRS, cytoreductive surgery; HIPEC, hyperthermic intraperitoneal chemotherapy; DPAM, disseminated peritoneal adenomucinosis; PMCA-I, intermediate pathological subtype.
Figure 1b. Progression free survival related to result of initial CRS in PMP patients after primary CRS and HIPEC. CRS, cytoreductive surgery; PMP, pseudomyxoma peritonei; HIPEC, hyperthermic intraperitoneal chemotherapy; R1,
mm in any region.
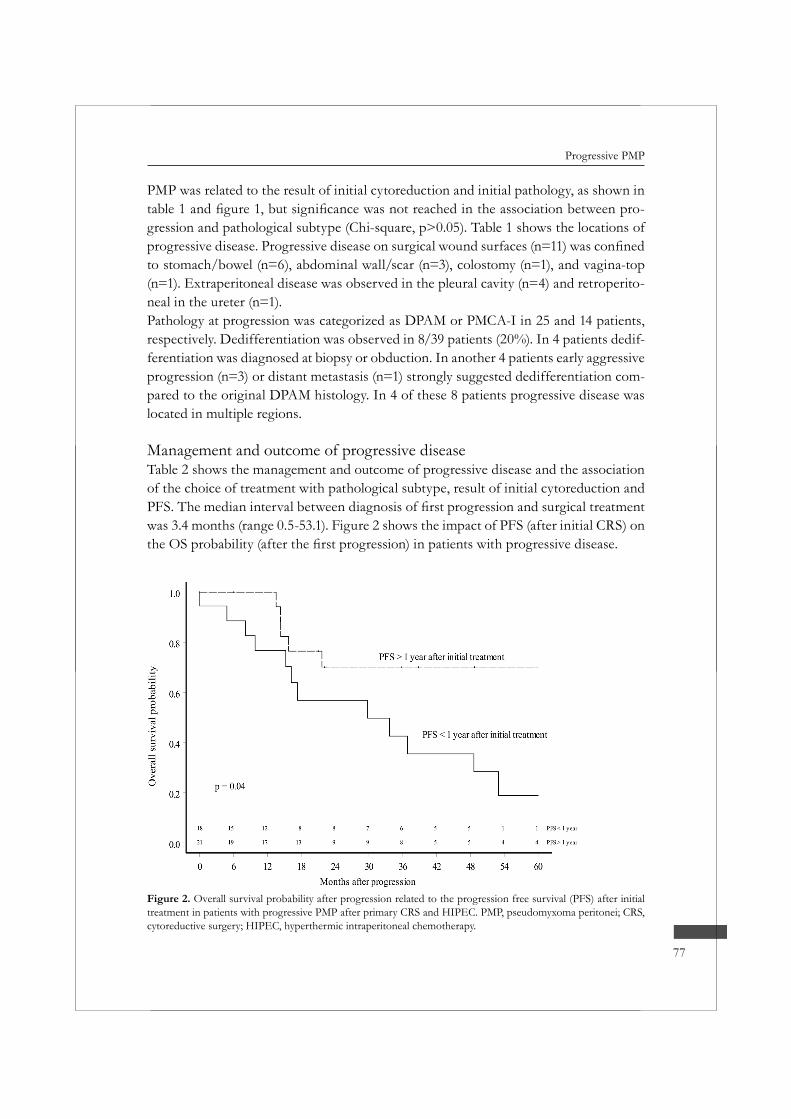
77
Progressive PMP
Figure 2. Overall survival probability after progression related to the progression free survival (PFS) after initial treatment in patients with progressive PMP after primary CRS and HIPEC. PMP, pseudomyxoma peritonei; CRS, cytoreductive surgery; HIPEC, hyperthermic intraperitoneal chemotherapy.
PMP was related to the result of initial cytoreduction and initial pathology, as shown in -
gression and pathological subtype (Chi-square, p>0.05). Table 1 shows the locations of
to stomach/bowel (n=6), abdominal wall/scar (n=3), colostomy (n=1), and vagina-top (n=1). Extraperitoneal disease was observed in the pleural cavity (n=4) and retroperito-neal in the ureter (n=1).Pathology at progression was categorized as DPAM or PMCA-I in 25 and 14 patients, respectively. Dedifferentiation was observed in 8/39 patients (20%). In 4 patients dedif-ferentiation was diagnosed at biopsy or obduction. In another 4 patients early aggressive progression (n=3) or distant metastasis (n=1) strongly suggested dedifferentiation com-pared to the original DPAM histology. In 4 of these 8 patients progressive disease was located in multiple regions.
Management and outcome of progressive diseaseTable 2 shows the management and outcome of progressive disease and the association of the choice of treatment with pathological subtype, result of initial cytoreduction and
was 3.4 months (range 0.5-53.1). Figure 2 shows the impact of PFS (after initial CRS) on

Chapter 7
78
The 3-year PFS probability and the 3-year OS probability after a second procedure of CRS and HIPEC (n=8) was 42.9% (95% CI 18.2%-100%) and 100%, respectively. In 2 of these patients systemic chemotherapy was given prior to the second procedure.In case of a surgical intervention only (n=10) 3-year PFS probability and 3-year OS probability was 22.2% (95% CI 6.5%-75.4%) and 53.3% (95% CI 28.2%-100%), respec-tively. In 2 of these patients, with DPAM subtype, a second procedure of CRS and
patients had no evidence of disease at end of follow up. One patient, with local pro-gression of DPAM in the abdominal scar, had been treated three times with a local resection. At end of follow up, 47.9 months after the primary treatment there was no evidence of disease.Fifteen patients with progression were observed and 42.9% of these patients (95% CI 18.2%-100%) showed no further progress during the 3 years after the diagnosis of pro-
was performed because of slowly diffuse progression. This patient was alive with dis-ease at end of follow up. Three-year OS probability of this treatment group was 66.0% (95% CI 43.4%-100%). All patients that had died of disease had the PMCA-I subtype.Six patients were treated for progressive disease with systemic chemotherapy. Three patients with initial DPAM subtype were treated this way as they had showed dediffer-entiation into PMCA-I at progression.
Table 2. Management and outcome of progressive PMP after primary CRS with HIPEC, associated with pathology at time of diagnosis, result of initial CRS and PFS after primary treatment.Extent Treatment for
progression (n)Initial
pathology (n)Result of
initial CRS (n)
Median PFS after initial CRS and
HIPEC,in months(95% CI)
Median FUafter treatment for
progression,in months
(range)
Outcome (n)
Limited Surgery only (10) DPAM (4) R1 (1) 21.7 (14.4-33.6) 18.1 (2.3-49.6) NED (6)PMCA-I (6) R2a (8) AWD (1)
R2b (1) DOD (3)Observation (15) DPAM (10) R1 (2) 64.4 (15.8,->) 16.8 (3.4-70.3) AWD (11)
PMCA-I (5) R2a (8) DOD (4)R2b (5)
Diffuse 2nd HIPEC (8) DPAM (8) R1 (1) 34.1 (13.8-68.3) 19.3 (8.8-56.6) NED (2)R2a (7) AWD (2)
DOD (4) Systemic chemo DPAM (3) R2a (5) 14.3 (12.8-17.3) 14.8 (9.8-33.6) DOD (6)
only (6) PMCA-I (3) R2b (1)PMP, pseudomyxoma peritonei; CRS, cytoreductive surgery; HIPEC, hyperthermic intraperitoneal
peritoneal adenomucinosis; PMCA-I: intermediate pathological subtype; R1, no macroscopic tumor residue;
evidence of disease; AWD, alive with disease; DOD, died of disease.

79
Progressive PMP
DiscussionPMP has been traditionally treated by limited CRS consisting of removal of the free mucus and resection of both the appendiceal primary and dominant metastatic sites such as the ovaries and omentum. In the short run this approach has been safe and successful in improving the patient’s well being. Recurrence or progression is however inevitable and leads to further surgery that is usually less successful. Intervals get short-er and eventually all surgical options are exhausted or patients die as consequence of surgical complications13. More aggressive surgery, which aims at complete removal of tumor in all affected areas, seems to prolong survival. Still in a recent series only 12% of patients remained free of disease at end of follow-up.14 The combination of complete CRS by the use of peritonectomy procedures and hyperthermic intraperitoneal chemo-therapy (HIPEC) aims to further reduce the percentage of recurrence and progression. A number of series using this approach has now been published, showing indeed that long-term disease free and progression free survival can be improved.3-6,15,16 Still, even after this combined modality treatment progression was observed in our series in 41% of cases. In other published series recurrence or progression rates of 40-70% have been reported.6,7,15 As in other series, we observed that pathological subtype and result of initial cytoreduction were the dominant factors related to progression.3,10,17
The diagnosis of progressive disease is not always easy. After extensive surgery CT
to make a baseline CT scan 3 months after primary CRS plus HIPEC and compare
tumor markers and/or progressive masses on CT scan.A dominant site of progressive disease has been the sub hepatic region. This is the
strongly suggests that incomplete resection is the dominant factor causing progression. Apparently HIPEC is not effective when large tumor residue is left behind. This is in accordance with our understanding of the action of HIPEC, which is probably only
one or two regions probably represents surgical failure, not HIPEC failure.In contrast, 36% of progressive disease was spread more diffuse in the abdomen, including areas that were left macroscopically free of disease. These patients seem to represent the failure of HIPEC to sterilize microscopic disease. Although this did not
-tiated DPAM) was overrepresented in this pattern of failure. It seems that these cases represent the pattern of failure caused by the biology of PMP itself.Laparotomy scar, top of the vagina and bowel suture lines were incidentally observed

Chapter 7
80
was probably the cause of progression. In 5 patients progressive disease was found out-side the abdominal cavity, especially in the thoracic cavity (n=4). Opening of routes to extra peritoneal spaces during CRS is probably the cause of this way of dissemina-tion.8,18 Since we leave the diaphragm open during perfusion after CRS in this area, so effectively including the involved pleural cavity in the perfusion, this has not been observed anymore. In one patient metastasis to the bones was observed. As PMP is a non-invasive neoplasm, this true metastatic disease is probably the result of dedifferen-tiation into PMCA.
-enced by our increasing experience. Consequently not always the same treatment choices
-ence. The progression free survival after initial CRS and HIPEC is the only statistically
This seems closely related to tumor biology. In patients with PMCA-I and in patients presenting with dedifferentiated progressive disease the progression free survival tend-ed to be short and the outcome of treatment of progressive disease poor. Based on our experience we now use the following algorithm.Patients with early progressive disease (short PFS) diffusely spread throughout the abdomen, usually PMCA-I subtype, are treated with (palliative) systemic chemotherapy, as prognosis in these patients is already very poor. However, the effect of chemotherapy is questionable as all patients in our series treated this way died within 3 years.Patients with early progressive disease limited to one or two regions are treated with simple resection. Such limited (residual) disease can easily be resected one more time. It seems obvious though, that patients with PMCA-I subtype have less chance of improved survival than DPAM patients as result of tumor biology.Patients with late progressive disease (long PFS) diffusely spread throughout the abdo-men or diffuse progression after simple resection, and in good general health, are
another curative attempt.Besides there is a group of patients with very indolent tumor behavior, with limited disease and hardly any progression over a long period of time, who are simply followed. In these cases it is probably worthwhile to observe before deciding to perform surgery with all its disadvantages.Because of the inherent differences in prognosis in these different patient groups it is impossible to judge the relative effectiveness of these different approaches. The excep-tion is the group that received systemic chemotherapy. We did not observe any objective response on 5 FU based chemotherapy in these patients. It is questionable whether mod-ern schedules including Capecitabin, Oxaliplatin and Bevacuzimab will do any better.
81
Progressive PMP
Notwithstanding the limitations of this study it is clear that management of progressive PMP after primary aggressive CRS and HIPEC is worthwhile and can result in long-term survival in a considerable percentage of patients. A second HIPEC is probably best restricted to patients with benign disease and progression free survival exceeding 1 year.
References1. Sugarbaker PH. Pseudomyxoma peritonei. A cancer whose biology is characterized by a redistribution
phenomenon. Ann Surg 1994; 219:109-111.2. Deraco M, Gronchi A, Mazzaferro V et al. Feasibility of peritonectomy associated with intraperito-
neal hyperthermic perfusion in patients with Pseudomyxoma peritonei. Tumori 2002; 88:370-375.3. Elias D, Laurent S, Antoun S et al. [Pseudomyxoma peritonei treated with complete resection and
immediate intraperitoneal chemotherapy]. Gastroenterol Clin Biol 2003; 27:407-412.4. Sugarbaker PH. Cytoreductive surgery and peri-operative intraperitoneal chemotherapy as a curative
approach to pseudomyxoma peritonei syndrome. Eur J Surg Oncol 2001; 27:239-243.5. Guner Z, Schmidt U, Dahlke MH et al. Cytoreductive surgery and intraperitoneal chemotherapy for
pseudomyxoma peritonei. Int J Colorectal Dis 2005; 20:155-160.6. Deraco M, Baratti D, Inglese MG et al. Peritonectomy and intraperitoneal hyperthermic perfusion
Oncol 2004; 11:393-398.7. Bryant J, Clegg AJ, Sidhu MK et al. Systematic review of the Sugarbaker procedure for pseudomyxo-
ma peritonei. Br J Surg 2005; 92:153-158.8. Zoetmulder FA, Sugarbaker PH. Patterns of failure following treatment of pseudomyxoma peritonei
of appendiceal origin. Eur J Cancer 1996; 32A:1727-1733.9. Gough DB, Donohue JH, Schutt AJ et al. Pseudomyxoma peritonei. Long-term patient survival with
an aggressive regional approach. Ann Surg 1994; 219:112-119.10. Sugarbaker PH, Fernandez-Trigo V, Shamsa F. Clinical determinants of treatment failure in patients
with pseudomyxoma peritonei. Cancer Treat Res 1996; 81:121-132.11. Verwaal VJ, van Tinteren H, Ruth SV et al. Toxicity of cytoreductive surgery and hyperthermic intra-
peritoneal chemotherapy. J Surg Oncol 2004; 85:61-67.12. Ronnett BM, Zahn CM, Kurman RJ et al. Disseminated peritoneal adenomucinosis and peritoneal
mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol 1995; 19:1390-1408.
13. Lang H, Jahne J, Flemming P et al. Pseudomyxoma peritonei of appendiceal origin--a report of seven cases and a review of published reports. Eur J Surg 1995; 161:355-360.
14. Miner TJ, Shia J, Jaques DP et al. Long-term survival following treatment of pseudomyxoma perito-nei: an analysis of surgical therapy. Ann Surg 2005; 241:300-308.
15. Moran BJ, Mukherjee A, Sexton R. Operability and early outcome in 100 consecutive laparotomies for peritoneal malignancy. Br J Surg 2005.
16. Loungnarath R, Causeret S, Bossard N et al. Cytoreductive surgery with intraperitoneal chemohyper-thermia for the treatment of pseudomyxoma peritonei: a prospective study. Dis Colon Rectum 2005; 48:1372-1379.
17. Yan H, Pestieau SR, Shmookler BM et al. Histopathologic analysis in 46 patients with pseudomyxoma peritonei syndrome: failure versus success with a second-look operation. Mod Pathol 2001; 14:164-171.
18. Smeenk RM, Bex A, Verwaal VJ et al. Pseudomyxoma peritonei and the urinary tract: involvement and treatment related complications. J Surg Oncol 2006; 93:20-23.

8c h a p t e r
Pseudomyxoma peritonei and the urinary tract: Involvement and treatment related
complications
R.M. Smeenk1, A. Bex2, V.J. Verwaal1,S. Horenblas2, F.A.N. Zoetmulder1
Department of Surgery1, Department of Urology2
The Netherlands Cancer Institute - Antoni van Leeuwenhoek HospitalAmsterdam, the Netherlands

Background: Pseudomyxoma peritonei (PMP) is a rare clinical syndrome characterized by intraperitoneal accumulation of mucus produced by neoplastic cells of mostly appen-diceal origin. The aim of this study was to analyze primary and secondary involvement and treatment related complications of the urinary tract in pseudomyxoma peritonei.Methods: A retrospective study of 92 patients with PMP, treated by cytoreduction and intraoperative hyperthermic intraperitoneal chemotherapy (HIPEC) at the Netherlands Cancer Institute between 1996 and 2004.Results: Seven patients presented with involvement of the urinary tract. Major urologic
urinary tract. Major urologic complications consisted predominantly of surgical compli-cations related to the bladder. All patients with secondary involvement and/or urologic complications had undergone previous pelvic surgery.Conclusions: The urinary tract is rarely involved in patients with PMP. Secondary involvement is mostly observed and may be a result of seeding of PMP of pelvic origin after prior pelvic surgery. There is a low urologic complication risk of treatment with cytoreduction and HIPEC. The combination of secondary involvement and previous pelvic surgery is an omen of treatment related urologic complications, necessitating (surgical) re-interventions and further management in close collaboration with urolo-gists.
J Surg Oncol 2006 Jan 1;93(1):20-3

85
PMP and the urinary tract
IntroductionPseudomyxoma peritonei (PMP) is a rare syndrome characterized by an extensive spread of intraperitoneal mucus and therefore patients mostly present with abdomi-nal distension. Adenomucinous epithelial cells along peritoneal surfaces and omentum, derived from a ruptured intra-abdominal neoplasm are responsible for the mucus pro-duction. Most commonly the pathological origin is an adenoma or well-differentiated adenocarcinoma of the appendix (or the ovaries)1-4. Other primary tumor sites are rare and include pancreas4-6, stomach4, colon4,7, small bowel4. In unusual cases the urinary tract may be the primary source of PMP and few cases of mucinous adenocarcinomas originating from the urachus4,8-12 have been described. Contrary to these exceptional primary urologic sites, little is known about the secondary involvement of the urinary tract related to PMP growth13-15. Due to intraperitoneal seeding and its most common primary site of origin, PMP occurs at predictable abdominal sites such as the vesicorec-tal space, right colic fossa, right hemi diaphragmatic space and omentum. As most parts of the urinary tract are anatomically either retroperitoneal or extraperitoneal, secondary involvement is not very likely.The cornerstone of treatment of PMP is extensive cytoreductive surgery in combination with intraoperative hyperthermic intraperitoneal chemotherapy (HIPEC). Complications of the urinary tract as a consequence of this aggressive management are not known.The aim of this study was to assess primary and secondary involvement of the urinary tract in PMP, and to analyze treatment related urologic complications.
Materials and methodsPatients were diagnosed with PMP based on excessive abdominal mucus with charac-teristic distribution and on histology consistent with DPAM (disseminated peritoneal adenomucinosis), PMCA (peritoneal mucinous carcinomatosis) or PMCA-I (interme-diate group), according to the criteria of Ronnett et al.16. There was no evidence of liver- or lung metastases on abdominal and chest computed tomography scans. Between 1996 and 2004, 92 patients were included. Eight patients underwent a second procedure because of recurrence. Each procedure was recorded as a single case. Patients were treated at the Netherlands Cancer Institute.The principles of cytoreduction and HIPEC are described in detail by Verwaal et al.17.
peritonectomy and resection of tumor-involved viscera. This is followed by intraopera-tive hyperthermic intraperitoneal chemotherapy with mitomycin C to erase microscopic residual tumor.

Chapter 8
86
To assess involvement of the urinary tract, medical records were analyzed for clini-cal, radiological and pathological evidence. Complications were registered as toxicity according to the NCI-CTC. Data from the medical history were collected with regard
-ment with cytoreduction and HIPEC. Urologic complications were analyzed, divided in minor and major complications. Treatment of these complications was recorded. Each recorded complication was matched to evidence of primary or secondary PMP involve-ment, histological subtypes of PMP and previous surgery. Involvement of the urinary
ResultsPatientsSeven patients (6 females, 1 male) with a median age of 54 years (30-71), presented with PMP involvement of the urinary tract. Two patients presented with the urachus as pri-mary source. One of these patients had also secondary involvement of the urinary tract
PMP in patients with urinary tract involvement included appendix (n=3), ovary (n=2) and urachus (n=2). In the entire patient population of this study PMP originated in 90% in the appendix, in 3% in the ovary, in 2% in the urachus and in 2% in the colon. The histopathological diagnosis in patients with involvement of the urinary tract con-sisted of DPAM, PMCA-I or PMCA in respectively 3, 2 and 2 patients.The pelvis was seriously affected in 6 of the 7 patients with urinary tract involvement. PMP was located mainly at the bladder (dome) and was mostly diagnosed by preopera-tive computed tomography (n=5). However, preoperative clinical presentation of urinary tract involvement by PMP was seen in 2 patients. Both patients presented with hydro-nephrosis due to ureter obstruction by massive PMP deposits. One of these patients presented with a combination of stress- and urge incontinence, and two-sided hydrone-phrosis due to massive PMP deposits on ureters and bladder. In the last patient, resection of the bladder with urinary deviation was assessed by urologists preoperatively.
SurgeryFifty-three patients had undergone previous surgery in the pelvis. This was due to
secondary involvement of the urinary tract by PMP had undergone prior pelvic surgery. Resection of a part of the urinary tract was performed in 7 patients.In 5 patients resection and re-implantation of a part of the ureter was performed during cytoreduction. Three of these patients were diagnosed with secondary involvement of DPAM (n=2) or PMCA-I (n=1). In the other 2 patients, with preoperative hydronephro-

87
PMP and the urinary tract
sis based on massive DPAM deposits, the distal ureter was resected (and re-implanted) due to surgical perforation at cytoreduction.In 2 patients with secondary involvement of DPAM, (part of) the bladder was resected at cytoreduction. Resection of the bladder dome with primary closure was performed in 1 patient. The other patient underwent cystectomy with a continent reservoir (Indiana pouch). Both patients with PMCA had undergone resection of both urachal tumor and bladder dome prior to treatment with cytoreduction and HIPEC.
Urologic complicationsThe median follow-up after treatment was 45 months (1-95). The median hospital stay was 22 days (range 12-149). Patients with no complications had a median hospital stay of 19 days (12-35). A total of 13 procedures were complicated by minor or major urologic com-plications (table 1). Median hospital stay of these patients was 25.5 days (range 15-72), in contrast to 33 days (range 15-149) for patients with complications other than urologic. All patients had undergone previous pelvic surgery. Secondary involvement of the uri-nary tract was observed in 3 of these 13 procedures. Two of these 3 procedures caused 4/7 of the major urologic complications: these patients, diagnosed with DPAM, devel-
procedures without involvement of the urinary tract were responsible for the remaining major urologic complications: these patients developed a suture leak of the bladder, a
with PMCA-I or PMCA did not develop urologic complications.Treatment of major urologic complications is shown in table 2. Surgical treatment was
Table 1. Distribution of minor and major urologic complicationsComplication Minor MajorSuture leak of bladder - 3
- 4Urinary retention 2 -Urinary tract infection 2 -Incontinence, stress 5 -Incontinence, urge 1 -Number of procedures1 8 51 in some procedures more than one kind of complication was scored
Table 2. Treatment of major urologic complicationsPatient Complication Treatment
1 Suture leak Relaparotomy2 Relaparotomy13 Transvaginal closure4 Relaparotomy5 Indwelling catheter
1 two relaparatomies were needed

Chapter 8
88
balloons. However, due to the severity of complications, in 1 patient a relaparotomy
2 patients a relaparotomy was eventually needed because of development of co-incident complications, such as an abscess or sepsis. Suture leaks of the bladder were repaired with a running suture of 3.0 Vicryl for the seromuscular layer, to be strengthened by a second suture line of single tied knots for the adventitia. A cystogram was performed routinely on day 7. In case of no extravasa-tions the transurethral catheter was removed. Ureter repairs were followed by urinary
imaging. Minor urologic complications were treated according to hospital protocols.
DiscussionThe urinary tract is rarely involved in patients with PMP. This explains the minimal description of urinary tract involvement in literature. In this series of 92 patients with PMP, only 7 patients showed involvement of the urinary tract. Over the entire patient population, PMP found its origin mostly in the appendix. PMP rarely originated from the urinary tract. This resembles results described in literature4,18. It was therefore remarkable that 4 out of 7 patients with involvement of the urinary tract were diag-nosed with PMP originating from an intrapelvic structure (urachus or ovary).The pelvis was seriously affected by PMP in all patients with secondary involvement of the urinary tract. Massive deposits of PMP were located at the vesicorectal space, the bladder dome or distal ureters. In addition, all patients with secondary involvement of the urinary tract had undergone prior surgery in the pelvis. It may be that prior pelvic surgery potentially compromises the integrity of the pelvic peritoneal lining. This may in turn explain the observed secondary involvement of the intrapelvic (but anatomi-cally extraperitoneal) urinary structures as the bladder dome or distal ureter by a non invasive peritoneal surface tumor like DPAM. Secondary involvement of the urinary tract would thus be either due to direct seeding on deperitonealized surfaces or due to extraperitoneal spread through peritoneal defects.Though the numbers are small, it is intriguing to argue that secondary involvement of the urinary tract may be a consequence of a combination of PMP of pelvic origin and an earlier surgical intervention in the pelvis. Assuming that developing a second-ary involvement is indeed associated with an earlier surgical intervention, the risk of developing it is not high. In this retrospective series, 53 patients had undergone pelvic surgery prior to cytoreduction and HIPEC. Among them were 6 patients with second-ary urinary tract involvement (14%). In contrast, we did not observe any secondary involvement in patients without previous surgery.

89
PMP and the urinary tract
As the urinary tract is rarely involved, major urologic complications occur infrequently. Minimal surgical manipulation or resection of (parts of) the urinary tract at cytoreduc-tion logically results in minimal urologic complications. In this study, an association between urologic complications and tumor involvement of the urinary tract was seen in 4 out of 7 patients with major urologic complications. All patients with urologic com-plications had a history of (multiple) previous pelvic surgery. It can therefore be argued that urologic complications in patients with secondary involvement of the urinary tract are simply the consequence of repeated surgery in the pelvic area. Major complications can be treated well, mostly surgically and in collaboration with urologists. Due to the low incidence of urinary tract involvement, we do not recommend preoperative evalu-ation of patients by urologists but in those cases that have actual involvement shown on CT scan. In those cases, urinary stents can in our opinion be introduced pre or peroperatively. As there are many different views on this, so we can not make a recom-mendation here.
ConclusionsThe urinary tract is rarely involved in patients with PMP and secondary tumor involve-ment is most frequently observed. This may be a result of seeding of PMP (of pelvic origin) after prior pelvic surgery. The urologic complication risk of current standard treatment for PMP is low and complications can be treated well. The combination of secondary involvement at cytoreduction and HIPEC, and previous pelvic surgery is an omen of treatment related urologic complications, necessitating (surgical) re-interven-tions and further management in close collaboration with urologists.
References1. Prayson RA, Hart WR, Petras RE. Pseudomyxoma peritonei. A clinicopathologic study of 19 cases
with emphasis on site of origin and nature of associated ovarian tumors. Am J Surg Pathol 1994; 18:591-603.
2. Ronnett BM, Zahn CM, Kurman RJ et al. Disseminated peritoneal adenomucinosis and peritoneal mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol 1995; 19:1390-1408.
3. de Bree E, Witkamp A, Van D, V et al. Unusual origins of Pseudomyxoma peritonei. J Surg Oncol 2000; 75:270-274.
4. Costa MJ. Pseudomyxoma peritonei. Histologic predictors of patient survival. Arch Pathol Lab Med 1994; 118:1215-1219.
5. de Bree E, Witkamp A, Van D, V et al. Unusual origins of Pseudomyxoma peritonei. J Surg Oncol 2000; 75:270-274.
Chapter 8
90
6. Chejfec G, Rieker WJ, Jablokow VR et al. Pseudomyxoma peritonei associated with colloid carcinoma of the pancreas. Gastroenterology 1986; 90:202-205.
7. de Bree E, Witkamp A, Van D, V et al. Unusual origins of Pseudomyxoma peritonei. J Surg Oncol 2000; 75:270-274.
8. Stenhouse G, McRae D, Pollock AM. Urachal adenocarcinoma in situ with pseudomyxoma peritonei: a case report. J Clin Pathol 2003; 56:152-153.
9. Sasano H, Shizawa S, Nagura H et al. Mucinous adenocarcinoma arising in a giant urachal cyst associ-ated with pseudomyxoma peritonei and stromal osseous metaplasia. Pathol Int 1997; 47:502-505.
10. Mendeloff J, McSwain NE, Jr. Pseudomyxoma peritonei due to mucinous adenocarcinoma of the urachus. South Med J 1971; 64:497-498.
11. de Bree E, Witkamp A, Van D, V et al. Unusual origins of Pseudomyxoma peritonei. J Surg Oncol 2000; 75:270-274.
12. Carr NJ, McLean AD. A mucinous tumour of the urachus: adenoma or low grade mucinous cystic tumour of uncertain malignant potential? Adv Clin Path 2001; 5:93-97.
13. Arly KS, Stephenson DV, Jr., Davis WC. Giant retroperitoneal mucocele simulating pseudomyxoma peritonei and mucinous adenocarcinoma. Am J Surg 1968; 116:439-443.
14. Moran CG, Morgan RH. Pseudomyxoma extraperitonei. J R Soc Med 1988; 81:668-669.15. Brady MB, Ewing RH, Robinson AE et al. Flank mass and pain in a 72-year-old man. Invest Radiol
1986; 21:419-423.16. Ronnett BM, Zahn CM, Kurman RJ et al. Disseminated peritoneal adenomucinosis and peritoneal
mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol 1995; 19:1390-1408.
17. Verwaal VJ, Van Tinteren H, Ruth SV et al. Toxicity of cytoreductive surgery and hyperthermic intra-peritoneal chemotherapy. J Surg Oncol 2004; 85:61-67.
18. de Bree E, Witkamp A, Van D, V et al. Unusual origins of Pseudomyxoma peritonei. J Surg Oncol 2000; 75:270-274.
9c h a p t e r
Pseudomyxoma peritonei and pregnancy- Report of two cases -
A. Koops1, R.M. Smeenk2, F.A.N. Zoetmulder2, A. Hoek1
1 Department of Obstetrics and Gynaecology, University Medical Centre Groningen, Groningen, the Netherlands
2 Department of Surgery, The Netherlands Cancer Institute- Antoni van Leeuwenhoek Hospital, Amsterdam, the Netherlands.

Background: Pseudomyxoma peritonei (PMP) is a rare disease that requires surgical debulking and hyperthermic intraperitoneal chemotherapy (HIPEC). A dilemma rises when young women with a child wish are diagnosed with PMP.Cases: Two young women with a child wish were diagnosed with PMP of benign pathology. Because of the infertility caused by chemotherapy and the assumed indolent benign character of their disease, both women had been treated by surgery only. Both patients had spontaneous pregnancies. One patient remained disease-free but the other patient had extensive progression with dedifferentiation of disease resulting in no fur-ther treatment options.Conclusion: Reserved surgical treatment instead of cytoreductive surgery with HIPEC in young women with PMP and a child wish can be founded when the disease shows signs of indolence and benign pathology. Any suspicion of progression strongly favours adequate combined modality treatment to improve survival.
Submitted
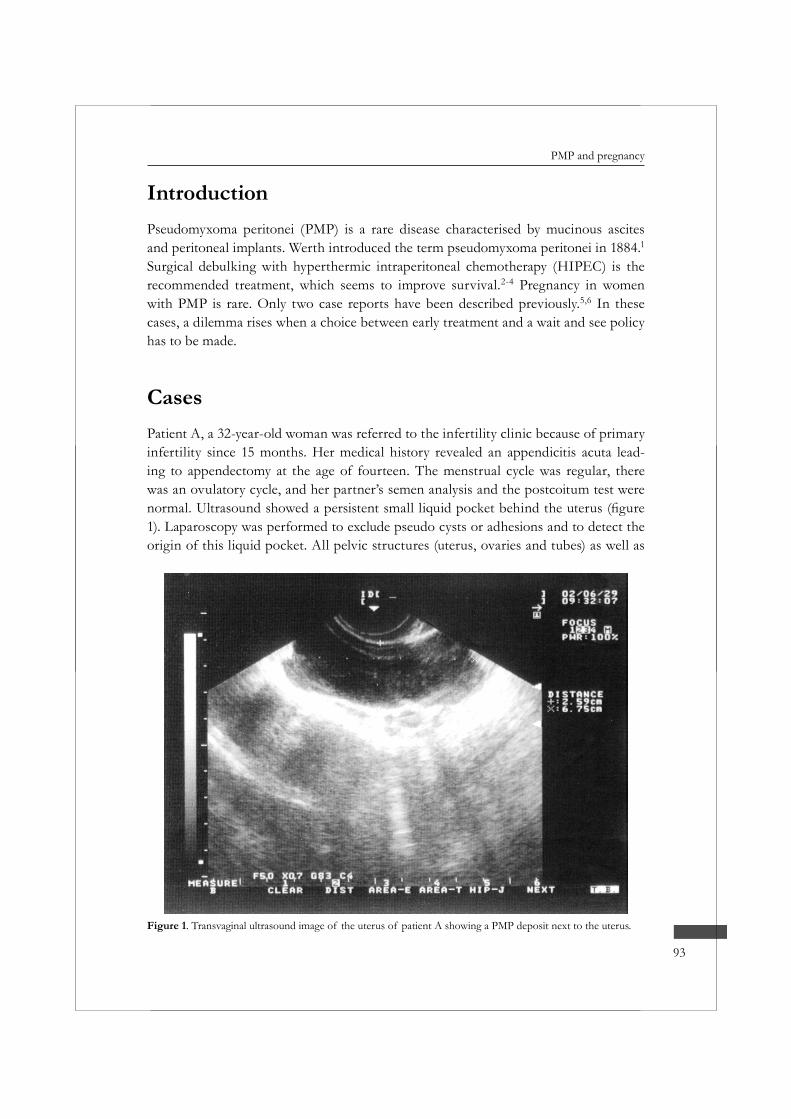
93
PMP and pregnancy
IntroductionPseudomyxoma peritonei (PMP) is a rare disease characterised by mucinous ascites and peritoneal implants. Werth introduced the term pseudomyxoma peritonei in 1884.1Surgical debulking with hyperthermic intraperitoneal chemotherapy (HIPEC) is the recommended treatment, which seems to improve survival.2-4 Pregnancy in women with PMP is rare. Only two case reports have been described previously.5,6 In these cases, a dilemma rises when a choice between early treatment and a wait and see policy has to be made.
CasesPatient A, a 32-year-old woman was referred to the infertility clinic because of primary infertility since 15 months. Her medical history revealed an appendicitis acuta lead-ing to appendectomy at the age of fourteen. The menstrual cycle was regular, there was an ovulatory cycle, and her partner’s semen analysis and the postcoitum test were
1). Laparoscopy was performed to exclude pseudo cysts or adhesions and to detect the origin of this liquid pocket. All pelvic structures (uterus, ovaries and tubes) as well as
Figure 1. Transvaginal ultrasound image of the uterus of patient A showing a PMP deposit next to the uterus.

Chapter 9
94
the cavum Douglasi were covered with a thick gelatinous liquid. A mucous-producing 4 cm long perforated appendix-stump was found and removed. The abdomen was rinsed thoroughly. Pathology showed a mucinous cystadenoma without evident atypia. Thus the diagnosis
made.7 A therapeutic dilemma arose since aggressive surgical therapy with HIPEC was indicated but would affect fertility. The decision was postponed because of patient’s concern about this. After 12 months observation and screening there was no tumour activity. A spontaneous pregnancy with a dichorial twin appeared, which was compli-cated by growth discordance. A caesarean section was performed at 37 weeks’ gestation and two dysmature boys of 2260 and 1050 grams were born and admitted at the child-ren’s ward. During the caesarean section the abdomen showed no signs of recurrence. There has been no evidence of recurrence until 40 months postoperative follow-up.
Patient B, a 36-year-old woman underwent a caesarean section and delivered a healthy son. During operation, a mucinous tumour of 5 x 7 cm behind the uterus was found and resected. Pathology revealed PMP of uncertain origin. After revalidation, an explorative laparotomy was performed, which showed no intra-abdominal pathology. The resected appendix showed no pathological abnormalities. After four years, when she became pregnant for the second time, she was in a good condition without evidence of recur-
2). By 28 weeks gestation the tumour was increased in size to 17 x 13 cm. The child was -
istration to enhance fetal lung maturation. A healthy boy of 2400 grams was born. The tumour was resected and exploration showed a PMP focus in the urachus. No other PMP deposits were found. A biopsy of the contra lateral ovary was normal. Therefore, the urachus as primary seemed most likely. Pathology was indifferent, but most suspi-cious for DPAM. At follow-up, 13 months after the second operation, there was a raise
the left ovary and omentum. During explorative laparotomy widespread involvement of all abdominal structures was observed. Histology revealed mucinous carcinomatosis (PMCA).7 Cytoreductive surgery and HIPEC was therefore not performed.
DiscussionPseudomyxoma peritonei is a rare and unpredictable disease. It follows a ruptured muci-nous epithelial neoplasm usually of the appendix but in rare cases also of ovary, pancreas or urachus.8,9 Mucous producing cells may implant on the peritoneal or omental surface resulting in PMP. Treatment by surgery alone results in long-term disease-free survival around 12%.10 Radical cytoreductive surgery in combination with heated intraperito-
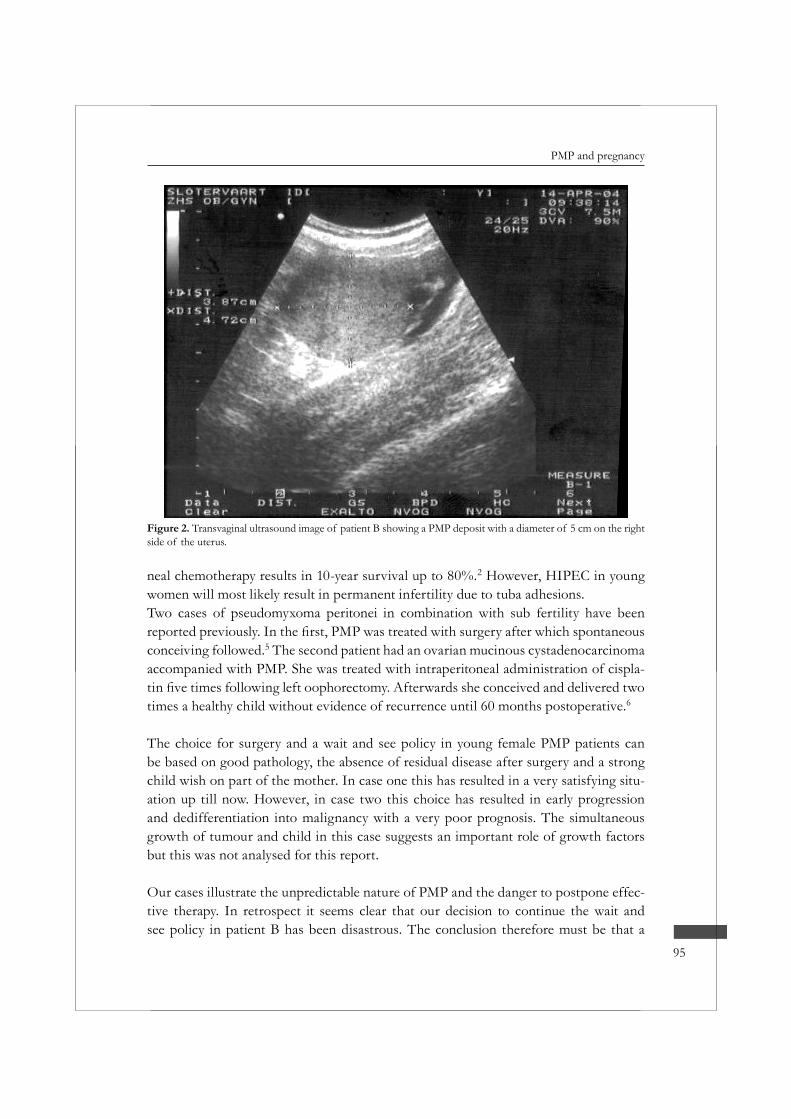
95
PMP and pregnancy
neal chemotherapy results in 10-year survival up to 80%.2 However, HIPEC in young women will most likely result in permanent infertility due to tuba adhesions.Two cases of pseudomyxoma peritonei in combination with sub fertility have been
conceiving followed.5 The second patient had an ovarian mucinous cystadenocarcinoma accompanied with PMP. She was treated with intraperitoneal administration of cispla-
times a healthy child without evidence of recurrence until 60 months postoperative.6
The choice for surgery and a wait and see policy in young female PMP patients can be based on good pathology, the absence of residual disease after surgery and a strong child wish on part of the mother. In case one this has resulted in a very satisfying situ-ation up till now. However, in case two this choice has resulted in early progression and dedifferentiation into malignancy with a very poor prognosis. The simultaneous growth of tumour and child in this case suggests an important role of growth factors but this was not analysed for this report.
Our cases illustrate the unpredictable nature of PMP and the danger to postpone effec-tive therapy. In retrospect it seems clear that our decision to continue the wait and see policy in patient B has been disastrous. The conclusion therefore must be that a
Figure 2. Transvaginal ultrasound image of patient B showing a PMP deposit with a diameter of 5 cm on the right side of the uterus.

Chapter 9
96
wait and see policy in young women with PMP and a child wish can be founded if benign disease without recurrence after surgery is present. Any suspicion of PMP with malignant features or progressive disease strongly favours adequate combined modality treatment to improve survival.
References1. Werth R. Klinische und anatomische untersuchungen zur lehre von den bauchgeschwuelsten und der
laparotomie. Arch Gynaecol Obstet 1884; 24:100-118.2. Sugarbaker PH. Cytoreductive surgery and peri-operative intraperitoneal chemotherapy as a curative
approach to pseudomyxoma peritonei syndrome. Eur J Surg Oncol 2001; 27:239-243.3. Deraco M, Baratti D, Inglese MG et al. Peritonectomy and intraperitoneal hyperthermic perfusion
Oncol 2004; 11:393-398.4. Elias D, Laurent S, Antoun S et al. [Pseudomyxoma peritonei treated with complete resection and
immediate intraperitoneal chemotherapy]. Gastroenterol Clin Biol 2003; 27:407-412.5. Hales HA, Peterson CM, Jolles CJ et al. Pseudomyxoma peritonei associated with secondary infertility.
Fertil Steril 1992; 58:425-426.6. Niwa K, Morishita S, Murase T et al. Successful pregnancy in a patient with pseudomyxoma peri-
tonei arising from ovarian mucinous cystadenocarcinoma treated with cisplatin. Gynecol Oncol 1995; 59:398-400.
7. Ronnett BM, Zahn CM, Kurman RJ et al. Disseminated peritoneal adenomucinosis and peritoneal mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol 1995; 19:1390-1408.
8. van Ruth S, Acherman YI, van de Vijver MJ et al. Pseudomyxoma peritonei: a review of 62 cases. Eur J Surg Oncol 2003; 29:682-688.
9. Smeenk RM, Bex A, Verwaal VJ et al. Pseudomyxoma peritonei and the urinary tract: involvement and treatment related complications. J Surg Oncol 2006; 93:20-23.
10. Miner TJ, Shia J, Jaques DP et al. Long-term survival following treatment of pseudomyxoma peri-tonei: an analysis of surgical therapy. Ann Surg 2005; 241:300-308.
10c h a p t e r
Pseudomyxoma peritonei: a comprehensive review
R.M. Smeenk; V.J. Verwaal; F.A.N. Zoetmulder
Department of SurgeryThe Netherlands Cancer Institute - Antoni van Leeuwenhoek Hospital
Amsterdam, the Netherlands

AbstractPseudomyxoma peritonei (PMP) is a rare condition, which is known for its high mortal-
recognize this clinical syndrome preferably in an early stage. Knowledge of pathogene-sis and common diagnostic tools is essential in this regard. Treatment strategy for PMP should pursue complete cytoreduction and prevention of recurrence or progression. Combined modality treatment, consisting of cytoreductive surgery with hyperthermic
-rently carried out in many centers throughout the world with promising results and seems to win ground as the standard treatment approach.
Canc Treat Rev, in press

99
A comprehensive review
IntroductionPseudomyxoma peritonei (PMP) is a rare clinical syndrome with an estimated inci-dence of approximately one per million per year or 2 per 10.000 laparotomies, and a preponderance of women (2-3 times men).1-4 Literately, PMP implies an untrue muci-
1884 as a peculiar reaction of the peritoneum to jelly like material, produced by an ovar-ian neoplasm.5 In 1901 Frankel reported on the association of PMP with an appendiceal mucocele.6 Since then, there has been a considerable amount of reports on the patho-genesis, diagnosis, treatment and prognosis of PMP. This review is meant to provide a comprehensive outline of these facets of this intriguing disease.
PathogenesisEtiologyPMP is a loco regional disease within the abdomen characterized by mucinous tumor on peritoneal surfaces producing a progressive amount of mucinous ascites. The primary tumor is thought to be predominately a mucinous epithelial neoplasm of the appendix.7-
9 The development of PMP from a small mucinous epithelial tumor of the appendix is explained as follows. Multiplying adenomucinous tumor cells produce a large amount of intraluminal mucus and with progressive growth eventually cause obstruction of the appendiceal lumen. Consequently, rising intraluminal pressure results in the blow-out of the appendiceal mucocele with the slow leak of mucus containing mucinous epi-
development of PMP. The perforation of the appendix may reseal and become even invisible, while over the course of months or, in case of indolent behavior, years free epithelial cells in the peritoneal cavity continue to proliferate and produce mucinous ascites. In contrast to tumor cells of colorectal cancer origin, that implant in the vicin-ity of the primary tumor, tumor cells from the ruptured appendiceal neoplasm are
-ity. The absence of adhesive characteristics on the cell surface probably explains such
sites where tumor cells get entrapped in the small resorption channels. Gravity for its part draws tumor cells through the paracolic gutters towards the pelvis. Accumulation and reproduction of the free and implanted tumor cells leads to progressive perito-neal mucinous tumor and ascites, but invasion of the peritoneal surface usually remains absent. This process of characteristic spread of peritoneal masses and mucinous ascites is known as the redistribution phenomenon.10

Chapter 10
100
In established PMP, tumor deposits are found especially in the omentum, in the sub hepatic region, under the right diaphragm, in Douglas, around the rectum and sigmoid, and in women on the ovaries. Mobile peritoneal surfaces, such as the bowel surface, are spared in this stage of disease (visceral sparing), as tumor cells are not able to adhere.
as the ileocoecum, rectum and sigmoid. In late stage disease when PMP becomes gener-alized and mucinous ascites and tumor engulf the entire peritoneal cavity including the left diaphragm and the spleen, bowel movement becomes limited with eventually tumor involvement of all bowel surfaces. Patients with a history of previous abdominal surgery are prone to the invasion of surgical wound surfaces by PMP as well.
OriginsThe high incidence of simultaneous disease in appendix and ovaries in female PMP patients has led to confusion about the true origin. In clinicopathological, molecular genetic and immunohistochemical studies the origin of PMP has been studied inten-sively.2,11-16 The prominent hypothesis indicates ovarian tumor as metastatic disease from an appendiceal primary. Tumor cells spread to the pelvis conform the distribu-tion phenomenon tend to get entangled on the irregular surface of ovulating ovaries. It might be that the ovaries are acting as a stepping stone where free intraperitoneal
A contrasting theory designates a primary ovarian mucinous cystadenoma or cystade-nocarcinoma (with borderline or low malignant potential), which causes intraperitoneal tumor spread after rupture of the cystic tumor. These tumors present with distinctive features: their size is usually greater, their presentation unilaterally with multiloculated cysts and the tumor found in the stroma instead of at the surface.17,18 In these cases, an associated appendiceal tumor is not found. In rare cases two synchronous primary tumors (in the appendix and ovary) or a multifocal process might be associated with PMP.19,20
Despite this limited controversy, the appendix is still the alleged dominant origin asso-ciated with PMP.21 Origins other than appendix or ovary are rare and include pancreas, colon or urachus.22,23
Histopathology-
tures are inhomogeneous. PMP shows a wide range in the mucus/cell ratio and the amount, differentiation and grade of atypia of epithelial cells. A widely accepted and
as a clinical-pathological entity characterized by mucinous ascites and non-invasive mucinous implants with a typical distribution, containing histological benign muci-nous epithelium derived from an appendiceal mucinous adenoma and having a benign clinical course.24 Although they thus describe PMP as a benign disease, their catego-

101
A comprehensive review
characteristics (including malignant features) and associated with a different prognosis: disseminated peritoneal adenomucinosis (DPAM), peritoneal mucinous carcinomatosis (PMCA), and an intermediate subtype (PMCA-I). Histopathologically, DPAM is charac-terized by an abundance of mucus with focally adenomucinous epithelium with hardly any atypia or mitotic activity. DPAM has non-invasive properties, an indolent behavior and a good prognosis. PMCA in contrast is the pathological subtype with malignant features. Histopathologically, PMCA is characterized by peritoneal tumor composed of more abundant mucinous tumor cells with the architecture and cytological features of carcinoma. PMCA occasionally shows invasive properties, comparable with peritoneal carcinomatosis of colorectal origin, and has a grim prognosis. Finally, the intermediate subtype PMCA-I is characterized by an abundance of DPAM lesions but focal areas with PMCA lesions. The behavior and prognosis of PMCA-I subtype lies somewhere in between DPAM and PMCA.25-27
-tion separates PMP into low-grade or high-grade tumor. Recently Bradley et al. reviewed the pathology in 101 PMP patients and concluded that the low-grade histology of PMP included those cases referred to as DPAM in the same category as PMCA-I. PMCA
25
prognosis and the evaluation of further treatment strategy. Histopathological and sur-vival analysis of these different subtypes has shown that DPAM patients are most likely
a comparable prognosis.3,26,27
DiagnosisPresenting symptomsVery characteristic and essential in the diagnosis of PMP are the presenting symptoms, which can be categorized roughly into three groups. The most important symptom is increasing abdominal girth (50%), which characterizes the progressive stage of disease with peritoneal dissemination. Patients present with a typical “jelly belly” and com-plaints of intestinal obstruction, caused by the progressive amount of mucinous tumor and ascites.
location of the primary or metastatic tumor. Patients with symptoms mimicking an acute appendicitis (25%) will undergo an appendectomy, during which the surgeon

Chapter 10
102
step towards the development of PMP. Histopathological examination of the appendix
pelvic mass. The correct diagnosis is then awaited for until after surgery, when exami-nation of the mucinous ovarian tumor and the appendix reveals PMP metastases from an appendiceal primary or less frequently an ovarian primary. These patients are then referred to the surgeon.The last group of patients is diagnosed by coincidence (20%). During laparoscopy or laparotomy for whatever reason, or during hernia repair, the surgeon or gynecologist unexpectedly encounters mucus.28-31 Further analysis eventually discloses the true diag-nosis.
symptoms have not resulted in the correct diagnosis. These patients have had a vague right lower abdominal pain with no further treatment or a perforated appendix with
Figure 1. Perforated appendiceal mucocele with mucinous deposit on the outer surface. 1: coecum; 2: normal appendiceal lumen; 3: dilated lumen.
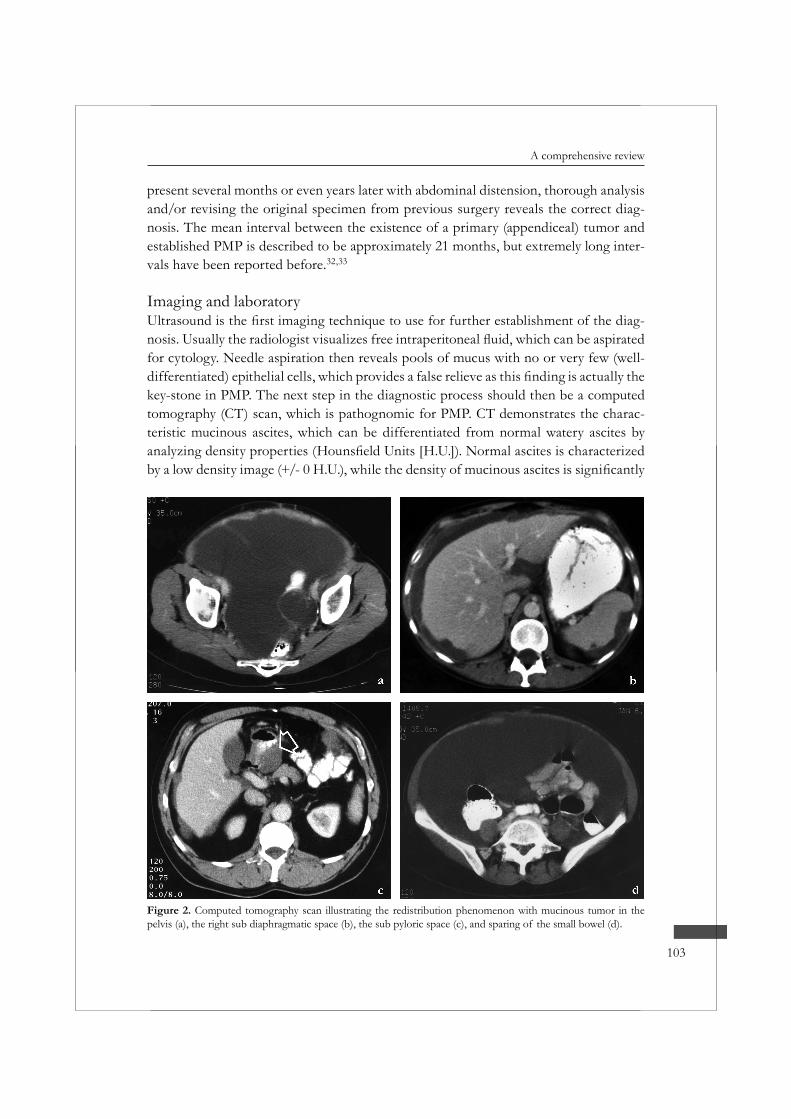
103
A comprehensive review
present several months or even years later with abdominal distension, thorough analysis and/or revising the original specimen from previous surgery reveals the correct diag-nosis. The mean interval between the existence of a primary (appendiceal) tumor and established PMP is described to be approximately 21 months, but extremely long inter-vals have been reported before.32,33
Imaging and laboratory-
for cytology. Needle aspiration then reveals pools of mucus with no or very few (well-
key-stone in PMP. The next step in the diagnostic process should then be a computed tomography (CT) scan, which is pathognomic for PMP. CT demonstrates the charac-teristic mucinous ascites, which can be differentiated from normal watery ascites by
Figure 2. Computed tomography scan illustrating the redistribution phenomenon with mucinous tumor in the pelvis (a), the right sub diaphragmatic space (b), the sub pyloric space (c), and sparing of the small bowel (d).
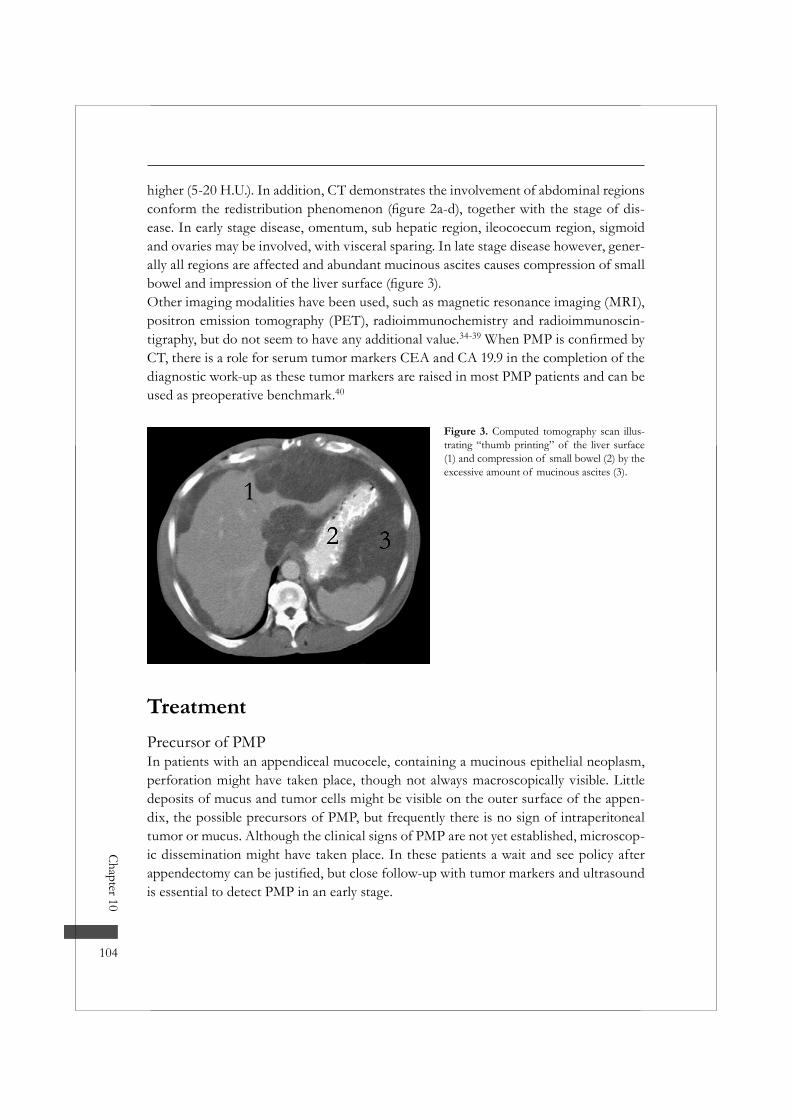
Chapter 10
104
higher (5-20 H.U.). In addition, CT demonstrates the involvement of abdominal regions -
ease. In early stage disease, omentum, sub hepatic region, ileocoecum region, sigmoid and ovaries may be involved, with visceral sparing. In late stage disease however, gener-ally all regions are affected and abundant mucinous ascites causes compression of small
Other imaging modalities have been used, such as magnetic resonance imaging (MRI), positron emission tomography (PET), radioimmunochemistry and radioimmunoscin-tigraphy, but do not seem to have any additional value.34-39
CT, there is a role for serum tumor markers CEA and CA 19.9 in the completion of the diagnostic work-up as these tumor markers are raised in most PMP patients and can be used as preoperative benchmark.40
Figure 3. Computed tomography scan illus-trating “thumb printing” of the liver surface (1) and compression of small bowel (2) by the excessive amount of mucinous ascites (3).
TreatmentPrecursor of PMPIn patients with an appendiceal mucocele, containing a mucinous epithelial neoplasm, perforation might have taken place, though not always macroscopically visible. Little deposits of mucus and tumor cells might be visible on the outer surface of the appen-dix, the possible precursors of PMP, but frequently there is no sign of intraperitoneal tumor or mucus. Although the clinical signs of PMP are not yet established, microscop-ic dissemination might have taken place. In these patients a wait and see policy after
is essential to detect PMP in an early stage.

105
A comprehensive review
Established PMPWhen mucinous tumor on peritoneal surface or mucinous ascites is visualized on CT or during abdominal surgery, adequate treatment of the established PMP should be pursued. The choice of treatment strategy in this case has varied much in the past. Advocators of a waiting policy felt that especially PMP with indolent behavior is not
41 These patients could be spared from surgery and its concomi-tant complications. However, although no survival data is available from large studies, untreated PMP patients will eventually suffer death through intestinal obstruction by massive mucinous ascites and large tumor deposits.7 Flimsy data has been presented on alternative non-surgical treatment, such as periodic symptomatic drainage of muci-nous ascites, mucolytic treatment, peritoneal washing with 5% dextrose and systemic chemotherapy.42-46 The major pitfall of these strategies is the limited number of only case-reports with limited follow-up.
Traditional surgical treatment is a moreover accepted and applied strategy. Early lit-erature on this approach consists mostly of reports from gynecologists, as in the past the assumed origin of PMP was ovarian.4,46-48
debulking with ovariectomy and omentectomy but recurrence is imminent and a second debulking with mechanical rinsing necessary. The third recurrence is usually accom-panied by intestinal obstruction, at which point the surgeon is consulted for bowel
by death through obstruction or complications of the treatment. Repetitive surgical debulking as treatment for PMP has been described mostly in case studies. The only large study was presented by the Mayo Clinic. They published a series of 26 patients treated this way with an estimated 5-year survival of 53%.49 At end of follow-up only 3% of patients was free of disease.
A more aggressive approach consists of aggressive cytoreductive surgery with the intent to obtain complete macroscopic cytoreduction in one or more operations. The Memo-rial Sloan Kettering Center reported on this treatment strategy in an analysis of 97 PMP patients.50 An average of 2.2 debulking operations was needed to reach complete cytoreduction in 55% of patients. Their treatment strategy resulted in a 10-years actu-arial survival of 21%, and a disease free rate at end of follow-up of 12%. The major disadvantage of repetitive surgical debulking seems the imminent recurrent or progres-sive disease as result of microscopic tumor residue.
A relatively new treatment approach, consisting of a surgical and chemotherapeutical modality, seems to win ground as standard treatment for peritoneal surface disease of all kinds of origin.51-56 For PMP patients this new treatment strategy was introduced in the early nineties by the surgeon P. Sugarbaker.57 The surgical modality, consist-

Chapter 10
106
aims at resection of peritoneal surfaces in a tumor-free plain, thus making it easier to accomplish a macroscopic complete cytoreduction.58 For the purpose of eradicating any macroscopic or microscopic tumor residue to prevent recurrence, surgery is combined with hyperthermic intraperitoneal chemotherapy (HIPEC). This combined modality
intent especially in PMP patients, because of the characteristic dissemination pattern and non-invasive character.
At present cytoreductive surgery with HIPEC is increasingly employed as treatment for PMP patients all over the world with promising results.59-66 Although no randomized trials are available because of the low incidence and ethical problems, results of various studies performed in the last 7 years show that combined modality treatment seems favorable compared to serial debulking surgery with unstandardized intraperitoneal chemotherapy (table 1). The observed inter-institutional variation is remarkable and is
Although there is a variety of techniques for performing the HIPEC lavage (table 1), it remains questionable whether these techniques differ in treatment outcome.The favorable outcome of combined modality treatment in comparison with traditional surgical treatment is probably related to the effort to accomplish not only macroscopic but also microscopic complete cytoreduction. HIPEC is thought to contribute to the prevention of recurrence or progression in patients with microscopic to minimal mac-roscopic tumor residue, as pharmacokinetic studies suggest a potential cytotoxic effect up to a tumor depth of 2.5mm.67
Figure 4. Peritonectomy procedure: en bloc resection of pseudomyxoma peritonei depos-its including colon (1) and peritoneum (2).
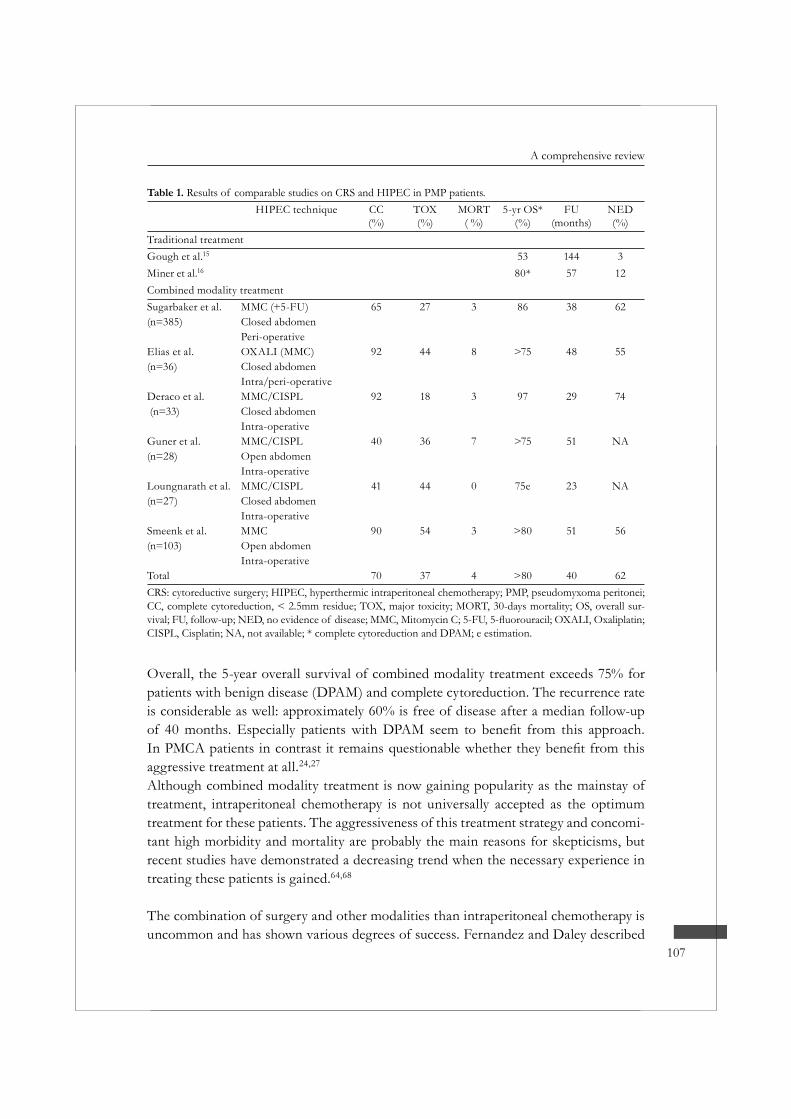
107
A comprehensive review
Overall, the 5-year overall survival of combined modality treatment exceeds 75% for patients with benign disease (DPAM) and complete cytoreduction. The recurrence rate is considerable as well: approximately 60% is free of disease after a median follow-up
aggressive treatment at all.24,27
Although combined modality treatment is now gaining popularity as the mainstay of treatment, intraperitoneal chemotherapy is not universally accepted as the optimum treatment for these patients. The aggressiveness of this treatment strategy and concomi-tant high morbidity and mortality are probably the main reasons for skepticisms, but recent studies have demonstrated a decreasing trend when the necessary experience in treating these patients is gained.64,68
The combination of surgery and other modalities than intraperitoneal chemotherapy is uncommon and has shown various degrees of success. Fernandez and Daley described
Table 1. Results of comparable studies on CRS and HIPEC in PMP patients.HIPEC technique CC
(%)TOX(%)
MORT( %)
5-yr OS*(%)
FU(months)
NED(%)
Traditional treatmentGough et al.15 53 144 3Miner et al.16 80* 57 12Combined modality treatmentSugarbaker et al. MMC (+5-FU) 65 27 3 86 38 62(n=385) Closed abdomen
Peri-operativeElias et al. OXALI (MMC) 92 44 8 >75 48 55(n=36) Closed abdomen
Intra/peri-operativeDeraco et al. MMC/CISPL 92 18 3 97 29 74 (n=33) Closed abdomen
Intra-operativeGuner et al. MMC/CISPL 40 36 7 >75 51 NA(n=28) Open abdomen
Intra-operativeLoungnarath et al. MMC/CISPL 41 44 0 75e 23 NA(n=27) Closed abdomen
Intra-operativeSmeenk et al. MMC 90 54 3 >80 51 56(n=103) Open abdomen
Intra-operativeTotal 70 37 4 >80 40 62CRS: cytoreductive surgery; HIPEC, hyperthermic intraperitoneal chemotherapy; PMP, pseudomyxoma peritonei; CC, complete cytoreduction, < 2.5mm residue; TOX, major toxicity; MORT, 30-days mortality; OS, overall sur-
CISPL, Cisplatin; NA, not available; * complete cytoreduction and DPAM; e estimation.

Chapter 10
108
with 44% for chemotherapy, but follow up was short and the number of treated patients was small. Gough et al. performed surgery in combination with intra cavitary isotope and external beam radiotherapy.49 -vival in case of adjuvant radiotherapy, but numbers were small (n=16) and there was no observed effect on overall survival. Photodynamic therapy combined with surgery has been applied widely in peritoneal surface disease other than PMP.69 It seems technically feasible, but the adjuvant effect for PMP has still to be evaluated.
The effect of systemic chemotherapy in PMP seems questionable. The loco regional spread of well-differentiated tumor with a poor blood supply greatly diminishes the
that describe a possibly cured case of PMP, secondary to an ovarian primary.44 Most studies question an objective response of PMP to systemic chemotherapy and consider systemic therapy to be reserved for a palliative setting in patients with recurrent or pro-gressive disease3,27,51
Late stage disease
-plete cytoreduction more common.27,64 Incomplete cytoreduction reduces the effect of HIPEC and inevitably results in progressive disease with an expected limited survival.70
However, it seems that further management of progressive disease is worthwhile in a considerable percentage of patients.71 To reduce morbidity and perhaps to increase the probability of complete cytoreduction, a two step procedure might be worthwhile in patients with extensive disease. First the most feasible resections (the ileocoecum, the omentum and if necessary the ovaries) are performed. In a second stage, when the patient has recovered, the cytoreduction can be completed with intraoperative HIPEC.
Follow-upAfter treatment, patients should be monitored for (recurrent or) progressive disease. A CT scan is a very important tool for detecting progressive disease and can be per-formed 3 months after treatment as basis for further follow-up.57,71,72 After that a CT
progression is suspected in the next years.Other useful servants in detecting disease in the post-surgical period are the tumor mark-ers CEA and CA 19.9, which also act as prognostic factors for survival.73,74 Together CT and tumor markers form a powerful combination for postoperative disease monitoring. Although progression occurs even after aggressive treatment, thorough management of

109
A comprehensive review
progressive disease seems worthwhile and can result in long-term survival.71 The choice of treatment for progressive disease should primarily depend on the disease free inter-val, but also on pathological subtype and extent of disease.
ConclusionPseudomyxoma peritonei (PMP) is a rare disease, with a grim prognosis when not
syndrome preferably in an early stage. Knowledge of pathogenesis and common diag-nostic tools is essential in this regard. CT imaging should be the choice of radiological assistance in the diagnostic process.Surgical debulking is the standard treatment for PMP, but combined modality treat-ment of aggressive peritonectomy with (intraoperative) HIPEC seems to win ground as new standard approach. Centralization of patients in centers that treat these patients on a regular basis is fundamental to prevent high morbidity and mortality.
References1. Mann WJ, Jr., Wagner J, Chumas J et al. The management of pseudomyxoma peritonei. Cancer 1990;
66:1636-1640.2. Mukherjee A, Parvaiz A, Cecil TD et al. Pseudomyxoma peritonei usually originates from the appen-
dix: a review of the evidence. Eur J Gynaecol Oncol 2004; 25:411-414.3. Smith JW, Kemeny N, Caldwell C et al. Pseudomyxoma peritonei of appendiceal origin. The Memo-
rial Sloan-Kettering Cancer Center experience. Cancer 1992; 70:396-401.
Obstet Invest 2001; 51:73-80.5. Werth R. Klinische und anatomische untersuchungen zur lehre von den bauchgeschwuelsten und der
laparotomie. Arch Gynaecol Obstet 1884; 24:100-118.6. Frankel E. Uber das sogenannte pseudomyxoma peritonei. Med Wochenschr 1901;965-970.7. Sugarbaker PH. Pseudomyxoma peritonei. Cancer Treat Res 1996; 81:105-119.8. Young RH. Pseudomyxoma peritonei and selected other aspects of the spread of appendiceal
neoplasms. Semin Diagn Pathol 2004; 21:134-150.9. Hinson FL, Ambrose NS. Pseudomyxoma peritonei. Br J Surg 1998; 85:1332-1339.
10. Sugarbaker PH. Pseudomyxoma peritonei. A cancer whose biology is characterized by a redistribution phenomenon. Ann Surg 1994; 219:109-111.
11. Prayson RA, Hart WR, Petras RE. Pseudomyxoma peritonei. A clinicopathologic study of 19 cases with emphasis on site of origin and nature of associated ovarian tumors. Am J Surg Pathol 1994; 18:591-603.
12. Young RH, Gilks CB, Scully RE. Mucinous tumors of the appendix associated with mucinous tumors of the ovary and pseudomyxoma peritonei. A clinicopathological analysis of 22 cases supporting an origin in the appendix. Am J Surg Pathol 1991; 15:415-429.
13. Lamps LW, Gray GF, Jr., Dilday BR et al. The coexistence of low-grade mucinous neoplasms of the appendix and appendiceal diverticula: a possible role in the pathogenesis of pseudomyxoma peritonei. Mod Pathol 2000; 13:495-501.
Chapter 10
110
14. Guerrieri C, Franlund B, Fristedt S et al. Mucinous tumors of the vermiform appendix and ovary, and pseudomyxoma peritonei: histogenetic implications of cytokeratin 7 expression. Hum Pathol 1997; 28:1039-1045.
15. Szych C, Staebler A, Connolly DC et al. Molecular genetic evidence supporting the clonality and appendiceal origin of Pseudomyxoma peritonei in women. Am J Pathol 1999; 154:1849-1855.
16. Ronnett BM, Shmookler BM, Diener-West M et al. Immunohistochemical evidence supporting the appendiceal origin of pseudomyxoma peritonei in women. Int J Gynecol Pathol 1997; 16:1-9.
17. Ronnett BM, Kurman RJ, Zahn CM et al. Pseudomyxoma peritonei in women: a clinicopathologic analysis of 30 cases with emphasis on site of origin, prognosis, and relationship to ovarian mucinous tumors of low malignant potential. Hum Pathol 1995; 26:509-524.
18. Ronnett BM, Shmookler BM, Sugarbaker PH et al. Pseudomyxoma peritonei: new concepts in diag-nosis, origin, nomenclature, and relationship to mucinous borderline (low malignant potential) tumors of the ovary. Anat Pathol 1997; 2:197-226.
19. Seidman JD, Elsayed AM, Sobin LH et al. Association of mucinous tumors of the ovary and appen-dix. A clinicopathologic study of 25 cases. Am J Surg Pathol 1993; 17:22-34.
20. Chuaqui RF, Zhuang Z, Emmert-Buck MR et al. Genetic analysis of synchronous mucinous tumors of the ovary and appendix. Hum Pathol 1996; 27:165-171.
21. Jacquemin G, Laloux P. Pseudomyxoma peritonei: review on a cluster of peritoneal mucinous diseas-es. Acta Chir Belg 2005; 105:127-133.
22. de Bree E, Witkamp A, Van De Vijver M et al. Unusual origins of Pseudomyxoma peritonei. J Surg Oncol 2000; 75:270-274.
23. Smeenk RM, Bex A, Verwaal VJ et al. Pseudomyxoma peritonei and the urinary tract: involvement and treatment related complications. J Surg Oncol 2006; 93:20-23.
24. Ronnett BM, Zahn CM, Kurman RJ et al. Disseminated peritoneal adenomucinosis and peritoneal mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol 1995; 19:1390-1408.
25. Bradley RF, Stewart JH, Russell GB et al. Pseudomyxoma peritonei of appendiceal origin: a clinico-pathologic analysis of 101 patients uniformly treated at a single institution, with literature review. Am J Surg Pathol 2006; 30:551-559.
26. Ronnett BM, Yan H, Kurman RJ et al. Patients with pseudomyxoma peritonei associated with dissem-
peritoneal mucinous carcinomatosis. Cancer 2001; 92:85-91.27. Smeenk RM, Verwaal VJ, Zoetmulder FA. Survival analysis of pseudomyxoma peritonei treated by
cytoreductive surgery in combination with intraoperative hyperthermic intraperitoneal chemotherapy. Ann Surg . 2006. Ref Type: In Press
28. Baker WC, Goldman LB, deVere White RW. Pseudomyxoma peritonei presenting as a scrotal mass. J Urol 1988; 139:821-822.
29. Young RH, Rosenberg AE, Clement PB. Mucin deposits within inguinal hernia sacs: a presenting
the literature. Mod Pathol 1997; 10:1228-1232.30. Kalu E, Croucher C. Appendiceal mucocele: a rare differential diagnosis of a cystic right adnexal
mass. Arch Gynecol Obstet 2005; 271:86-88.31. Khan S, Patel AG, Jurkovic D. Incidental ultrasound diagnosis of pseudomyxoma peritonei in an
asymptomatic woman. Ultrasound Obstet Gynecol 2002; 19:410-412.32. Darnis E, Ronceray J, Grosieux P et al. [Pseudomyxoma peritonei in females. 13 personal cases. Prac-
tical deductions from a review of 420 cases in the literature]. J Gynecol Obstet Biol Reprod (Paris) 1987; 16:343-353.
33. Solkar MH, Akhtar NM, Khan Z et al. Pseudomyxoma extraperitonei occurring 35 years after appen-dicectomy: a case report and review of literature. World J Surg Oncol 2004; 2:19.
111
A comprehensive review
34. Bechtold RE, Chen MY, Loggie BW et al. CT appearance of disseminated peritoneal adenomucinosis. Abdom Imaging 2001; 26:406-410.
35. Hanbidge AE, Lynch D, Wilson SR. US of the peritoneum. Radiographics 2003; 23:663-684.36. Tsai CJ. Ultrasound features of disseminated adenomucinosis (pseudomyxoma). Br J Radiol 1998;
71:564-566.37. Kairemo KJ, Jekunen AP, Bondestam S et al. Detection of pseudomyxoma peritonei by radioimmu-
nohistochemistry and radioimmunoscintigraphy. Cancer Biother Radiopharm 1996; 11:325-334.38. Buy JN, Malbec L, Ghossain MA et al. Magnetic resonance imaging of pseudomyxoma peritonei. Eur
J Radiol 1989; 9:115-118.39. Sulkin TV, O’Neill H, Amin AI et al. CT in pseudomyxoma peritonei: a review of 17 cases. Clin
Radiol 2002; 57:608-613.40. Carmignani CP, Hampton R, Sugarbaker CE et al. Utility of CEA and CA 19-9 tumor markers in
diagnosis and prognostic assessment of mucinous epithelial cancers of the appendix. J Surg Oncol 2004; 87:162-166.
41. Friedland JS, Allardice JT, Wyatt AP. Pseudomyxoma peritonei. J R Soc Med 1986; 79:480-482.42. Haid M, Bowie L, Kim D et al. Peritoneal washing therapy for pseudomyxoma peritonei. South Med
J 1981; 74:913-915.43. Green N, Gancedo H, Smith R et al. Pseudomyxoma peritonei-nonoperative management and
44. Jones CM, III, Homesley HD. Successful treatment of pseudomyxoma peritonei of ovarian origin with cis-platinum, doxorubicin, and cyclophosphamide. Gynecol Oncol 1985; 22:257-259.
45. Piver MS, Lele SB, Patsner B. Pseudomyxoma peritonei: possible prevention of mucinous ascites by peritoneal lavage. Obstet Gynecol 1984; 64:95S-96S.
46. Carter J, Moradi MM, Elg S et al. Pseudomyxoma peritonei--experience from a tertiary referral centre. Aust N Z J Obstet Gynaecol 1991; 31:177-178.
47. Wertheim I, Fleischhacker D, McLachlin CM et al. Pseudomyxoma peritonei: a review of 23 cases. Obstet Gynecol 1994; 84:17-21.
48. Galani E, Marx GM, Steer CB et al. Pseudomyxoma peritonei: the ‘controversial’ disease. Int J Gyne-col Cancer 2003; 13:413-418.
49. Gough DB, Donohue JH, Schutt AJ et al. Pseudomyxoma peritonei. Long-term patient survival with an aggressive regional approach. Ann Surg 1994; 219:112-119.
50. Miner TJ, Shia J, Jaques DP et al. Long-term survival following treatment of pseudomyxoma perito-nei: an analysis of surgical therapy. Ann Surg 2005; 241:300-308.
51. Sugarbaker PH. New standard of care for appendiceal epithelial neoplasms and pseudomyxoma peri-tonei syndrome? Lancet Oncol 2006; 7:69-76.
52. Kusamura S, Younan R, Baratti D et al. Cytoreductive surgery followed by intraperitoneal hyperther-mic perfusion: analysis of morbidity and mortality in 209 peritoneal surface malignancies treated with closed abdomen technique. Cancer 2006; 106:1144-1153.
53. Raspagliesi F, Kusamura S, Campos Torres JC et al. Cytoreduction combined with intraperitoneal hyperthermic perfusion chemotherapy in advanced/recurrent ovarian cancer patients: The experience of National Cancer Institute of Milan. Eur J Surg Oncol 2006.
54. Glehen O, Kwiatkowski F, Sugarbaker PH et al. Cytoreductive surgery combined with periopera-tive intraperitoneal chemotherapy for the management of peritoneal carcinomatosis from colorectal cancer: a multi-institutional study. J Clin Oncol 2004; 22:3284-3292.
55. Brigand C, Monneuse O, Mohamed F et al. Peritoneal mesothelioma treated by cytoreductive surgery and intraperitoneal hyperthermic chemotherapy: results of a prospective study. Ann Surg Oncol 2006; 13:405-412.
56. Verwaal VJ, van Ruth S, de Bree E et al. Randomized trial of cytoreduction and hyperthermic intra-peritoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with perito-neal carcinomatosis of colorectal cancer. J Clin Oncol 2003; 21:3737-3743.
Chapter 10
112
57. Sugarbaker PH, Ronnett BM, Archer A et al. Pseudomyxoma peritonei syndrome. Adv Surg 1996; 30:233-280.
58. Sugarbaker PH. Peritonectomy procedures. Surg Oncol Clin N Am 2003; 12:703-27, xiii.59. Sugarbaker PH. Cytoreductive surgery and peri-operative intraperitoneal chemotherapy as a curative
approach to pseudomyxoma peritonei syndrome. Eur J Surg Oncol 2001; 27:239-243.60. Butterworth SA, Panton ON, Klaassen DJ et al. Morbidity and mortality associated with intraperito-
neal chemotherapy for Pseudomyxoma peritonei. Am J Surg 2002; 183:529-532.61. Elias D, Laurent S, Antoun S et al. [Pseudomyxoma peritonei treated with complete resection and
immediate intraperitoneal chemotherapy]. Gastroenterol Clin Biol 2003; 27:407-412.62. Guner Z, Schmidt U, Dahlke MH et al. Cytoreductive surgery and intraperitoneal chemotherapy for
pseudomyxoma peritonei. Int J Colorectal Dis 2005; 20:155-160.63. Loungnarath R, Causeret S, Bossard N et al. Cytoreductive surgery with intraperitoneal chemohyper-
thermia for the treatment of pseudomyxoma peritonei: a prospective study. Dis Colon Rectum 2005; 48:1372-1379.
64. Smeenk RM, Verwaal VJ, Zoetmulder FA. Toxicity and mortality of cytoreduction and intraoperative hyperthermic intraperitoneal chemotherapy in pseudomyxoma peritonei-a report of 103 procedures. Eur J Surg Oncol 2005.
65. Scuderi S, Costamagna D, Vaira M et al. [Treatment of pseudomyxoma peritonei using cytoreduction and intraperitoneal hyperthermic chemotherapy]. Tumori 2003; 89:43-45.
66. Deraco M, Baratti D, Inglese MG et al. Peritonectomy and intraperitoneal hyperthermic perfusion
Oncol 2004; 11:393-398.67. Witkamp AJ, de Bree E, Van Goethem R et al. Rationale and techniques of intra-operative hyperther-
mic intraperitoneal chemotherapy. Cancer Treat Rev 2001; 27:365-374.68. Moran BJ. Establishment of a peritoneal malignancy treatment centre in the United Kingdom. Eur J
Surg Oncol 2006; 32:614-618.69. Sindelar WF, DeLaney TF, Tochner Z et al. Technique of photodynamic therapy for disseminated
intraperitoneal malignant neoplasms. Phase I study. Arch Surg 1991; 126:318-324.70. Glehen O, Mohamed F, Sugarbaker PH. Incomplete cytoreduction in 174 patients with peritoneal
carcinomatosis from appendiceal malignancy. Ann Surg 2004; 240:278-285.71. Smeenk RM, Verwaal VJ, Antonini N, Zoetmulder FA. Progressive pseudomyxoma perito-
nei after combined modality treatment: management and outcome. Ann Surg Oncol . 2006. Ref Type: In Press
72. Zoetmulder FA, Sugarbaker PH. Patterns of failure following treatment of pseudomyxoma peritonei of appendiceal origin. Eur J Cancer 1996; 32A:1727-1733.
73. van Ruth S, Hart AA, Bonfrer JM et al. Prognostic value of baseline and serial carcinoembryonic anti-gen and carbohydrate antigen 19.9 measurements in patients with pseudomyxoma peritonei treated with cytoreduction and hyperthermic intraperitoneal chemotherapy. Ann Surg Oncol 2002; 9:961-967.
74. Alexander-Sefre F, Chandrakumaran K, Banerjee S et al. Elevated tumour markers prior to complete tumour removal in patients with pseudomyxoma peritonei predict early recurrence. Colorectal Dis 2005; 7:382-386.
11c h a p t e r
General discussion

115
General discussion
Pseudomyxoma peritonei (PMP) is an intriguing but sometimes confusing disease.
of the last century. Simultaneously, a new standard of care for PMP patients, consist-ing of cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy
very promising with a 3-year survival probability of 90%.1 These results have motivated many international oncology centres to apply this treatment strategy.2-6 This thesis pro-vides an outline of various aspects of this rare but fascinating disease, but focuses on combined modality treatment.
PathogenesisThe growing evidence that supports a dominant role of an appendiceal neoplasm as the origin of PMP is strengthened by this thesis. A population-based study demonstrates the obvious association between PMP and mucinous epithelial neoplasms of the appen-dix, and discusses the pathogenesis of the frequent ovarian involvement in female PMP patients. These ovarian tumour masses are probably the result of the intraperitoneal dissemination process of (appendiceal) tumour cells, but may in some cases consist of a true primary ovarian tumour. In addition, in this thesis we demonstrate the female dominance in PMP patients. An airtight explanation is however not at hand, but one might think of a pure mechanical factor, with the irregular surface of ovulating ovaries as stepping stone for tumour deposits, or hormonal environmental factors.
from benign to malignant properties of PMP tumour cells still contributes to confu-
presented by Ronnett and colleagues and seems useful in this regard.7 It can be used for preoperative patient selection, evaluation and adjustment of treatment strategy,
includes disseminated peritoneal adenomucinosis (DPAM), peritoneal mucinous car-cinomatosis (PMCA) and an intermediate subtype (PMCA-I). This thesis shows that PMCA resembles peritoneal carcinomatosis of colorectal origin in both histopathologi-cal features and prognosis, and should not be categorized as PMP.
DiagnosisVery important in recognizing PMP as such is knowledge of the presenting symptoms.
-tion of the appendix reveals an appendiceal mucinous neoplasm, patients should be

Chapter 11
116
monitored for the development of PMP. Patients also present with symptoms like an ovarian mucinous mass, mucinous deposits on the peritoneal surface, mucous found during hernia repair, or progressive abdominal distension. In these cases further analy-sis is necessary. The most important diagnostic tools in this analysis are ultrasound with needle biopsy (revealing mucous with no or very few epithelial cells), computed tomography (CT), and tumour markers CEA and CA 19.9. PMP is diagnosed prop-erly by recognizing the clinical presentation, the typical intraperitoneal distribution of mucous and peritoneal tumour on a CT scan, and the characteristic outcome of needle biopsy. The next step for patients with established PMP is treatment conforming to the current standard.
Combined modality treatmentTraditionally, treatment of PMP consists of surgical debulking, repetitive when neces-sary. Recurrence after this approach is however imminent and eventually patients die of progressive insensitive disease or treatment related complications. CRS with HIPEC is a relatively new treatment strategy for PMP, based on the loco regional behaviour of the disease.8 As PMP is a peritoneal surface disease with, in principle, no lymphatic or hae-matogenous dissemination, it is a suitable treatment strategy with curative intent. This combined modality treatment is based on two elements that complement each other.
-tomy procedures, is an attempt at complete resection of macroscopic tumour mass.9These peritonectomy procedures consist of one or more of the following resections: 1) Greater omentectomy with if necessary splenectomy; 2) Stripping of the left diaphragm; 3) Stripping of the right diaphragm; 4) Cholecystectomy and lesser omentectomy; 5) Distal gastrectomy (antrectomy); 6) Pelvic peritonectomy with resection of the rectosig-moid by anterior resection. The number of procedures depends on the localization of tumour involvement. Other involved viscera such as ovaries or colon are resected along when necessary. Over the years, several institutions throughout the world have gained considerable experience in this surgical technique.The second modality, hyperthermic intraperitoneal chemotherapy or HIPEC, is meant to eradicate any tumour residue. This follows the surgery in the same procedure, before anastomoses are made and peritoneal defects (e.g. diaphragm) are closed. Because of the peritoneal plasma barrier, chemotherapy (usually Mitomycin-C, sometimes cisplati-num) can be applied locally in a high concentration with relatively few systemic side effects: the so-called regional dose intensity.10,11 Chemotherapy enters tumour cells by simple diffusion and thereby probably has a limited penetration depth up to 2mm, so
-er, hyperthermia seems to enhance tumour penetration and to synergize the cytotoxic effect.8,12 Finally, intraoperative management with the open abdomen technique pro-

117
General discussion
vides the opportunity to optimize exposure by manual distribution and rinsing the bowel surface and surgical wound surfaces. Altogether, the main goal of HIPEC is the prevention of recurrent or, in case of irradical resection, progressive disease. Essential in the realisation of this goal is (near) complete cytoreduction.At this moment, we assume that (completeness of) the surgical cytoreduction plays a dominant role in the treatment effect of this combined modality treatment. It might
-duction only. However, randomized clinical trials that prove the superiority of CRS or
the subsequent ethical questions posed by such research.
Many studies, including those in this thesis, have shown that results of this combined modality treatment are promising.2-5,13,14 Long-term overall survival is achieved in a
is not seen within the 10 year follow-up. Those patients that sooner or later develop recurrent or (slow) progressive disease are not given up on. Instead, as demonstrated in this thesis, even for these patients treatment possibilities that prolong survival are at hand.15 Furthermore, this dissertation illustrates that the growing experience with com-bined modality treatment, as it has evolved to the standard treatment of PMP in many oncology centres, improves treatment results and long-term survival considerably.The counter side of combined modality treatment is the somewhat high morbidity, mainly related to the (aggressive) surgical modality.2-5,16,17 Especially PMP patients with extensive disease and a long surgical history, necessitating widespread adhesiolysis, do
abdomen is cytoreduced; after 4-6 months, when the patient is recovered, the cytore-duction is completed and the HIPEC is performed. This approach is applied at this moment in The Netherlands Cancer Institute, but results will not be available until a reasonable follow-up has been achieved.Perioperative additional nutrition to optimize the patient’s condition might result in a shortened and less complicated recovery.18,19 Preoperative nutrition is therefore recom-
aided in their recovery by enteral nutrition through a feeding tube in the jejunum or by total parenterale nutrition when enteral nutrition is impossible or contraindicated.The most important prognostic factors for morbidity and survival are pathology and completeness of cytoreduction.2-5,14,16,17 Patients with extensive tumour load and unfa-
is minimal, while there is a high chance of treatment related morbidity and mortality. These patients are probably better off when treated palliatively. Knowledge of these prognostic indicators has resulted in a change in patient selection, which is now based

Chapter 11
118
on pathological subtype and the probability of complete cytoreduction. Furthermore, the observed value of both adequate patient selection and surgical experience in dimin-ishing complications and improving survival has taught us the importance of patient centralization.
Future prospectsAlthough all facets of PMP have been analysed extensively, there is much research still to be done. A very important topic might be how to prevent the development of PMP. Of course, early resection of the primary tumour prevents tumour cell dissemination and thus the development of PMP. But can we develop measures (other than surgery)
cells are already released in the peritoneal cavity? Interference at this stage might pre-vent progressive production of mucinous ascites and tumour mass, with the consequent impact on survival.
the development of PMP. They suggest a correlation between this bacterium and the pathogenesis of PMP. The results of these analyses might further explore antibacterial treatment in PMP in addition to the known antibacterial effect of Mitomycin C. Studies on the pathogenesis of PMP on a molecular level are now undertaken and might pro-vide treatment techniques at a totally different level.
In conclusion, knowledge of pathogenesis and diagnosis might result in early detection of PMP and affects the prognosis. PMP patients should always be referred to oncology centres that have gained considerable experience in treating these patients. It seems that
from combined modality treatment.
References1. Sugarbaker PH, Zhu BW, Sese GB et al. Peritoneal carcinomatosis from appendiceal cancer: results
in 69 patients treated by cytoreductive surgery and intraperitoneal chemotherapy. Dis Colon Rectum 1993; 36:323-329.
2. Elias D, Laurent S, Antoun S et al. [Pseudomyxoma peritonei treated with complete resection and immediate intraperitoneal chemotherapy]. Gastroenterol Clin Biol 2003; 27:407-412.
3. Loungnarath R, Causeret S, Bossard N et al. Cytoreductive surgery with intraperitoneal chemohyper-thermia for the treatment of pseudomyxoma peritonei: a prospective study. Dis Colon Rectum 2005; 48:1372-1379.
4. Guner Z, Schmidt U, Dahlke MH et al. Cytoreductive surgery and intraperitoneal chemotherapy for pseudomyxoma peritonei. Int J Colorectal Dis 2005; 20:155-160.
119
General discussion
5. Deraco M, Baratti D, Inglese MG et al. Peritonectomy and intraperitoneal hyperthermic perfusion
Oncol 2004; 11:393-398.6. Moran BJ, Mukherjee A, Sexton R. Operability and early outcome in 100 consecutive laparotomies for
peritoneal malignancy. Br J Surg 2005.7. Ronnett BM, Zahn CM, Kurman RJ et al. Disseminated peritoneal adenomucinosis and peritoneal
mucinous carcinomatosis. A clinicopathologic analysis of 109 cases with emphasis on distinguishing pathologic features, site of origin, prognosis, and relationship to “pseudomyxoma peritonei”. Am J Surg Pathol 1995; 19:1390-1408.
8. Sugarbaker PH, Ronnett BM, Archer A et al. Pseudomyxoma peritonei syndrome. Adv Surg 1996; 30:233-280.
9. Sugarbaker PH. Peritonectomy procedures. Surg Oncol Clin N Am 2003; 12:703-27, xiii.10. van Ruth S, Verwaal VJ, Zoetmulder FA. Pharmacokinetics of intraperitoneal mitomycin C. Surg
Oncol Clin N Am 2003; 12:771-780.11. Jacquet P, Sugarbaker PH. Peritoneal-plasma barrier. Cancer Treat Res 1996; 82:53-63.12. Witkamp AJ, de Bree E, Van Goethem R et al. Rationale and techniques of intra-operative hyperther-
mic intraperitoneal chemotherapy. Cancer Treat Rev 2001; 27:365-374.13. Sugarbaker PH. Cytoreductive surgery and peri-operative intraperitoneal chemotherapy as a curative
approach to pseudomyxoma peritonei syndrome. Eur J Surg Oncol 2001; 27:239-243.14. Smeenk RM, Verwaal VJ, Zoetmulder FA. Survival analysis of pseudomyxoma peritonei treated by
cytoreductive surgery in combination with intraoperative hyperthermic intraperitoneal chemotherapy. Ann Surg . 2006. Ref Type: In Press
15. Smeenk RM, Verwaal VJ, Antonini N, Zoetmulder FA. Progressive pseudomyxoma peritonei after combined modality treatment: management and outcome. Ann Surg Oncol . 2006. Ref Type: In Press
16. Smeenk RM, Verwaal VJ, Zoetmulder FA. Toxicity and mortality of cytoreduction and intraoperative hyperthermic intraperitoneal chemotherapy in pseudomyxoma peritonei-a report of 103 procedures. Eur J Surg Oncol 2005.
17. Sugarbaker PH, Chang D. Results of treatment of 385 patients with peritoneal surface spread of appendiceal malignancy. Ann Surg Oncol 1999; 6:727-731.
18. Hensrud DD. Nutrition screening and assessment. Med Clin North Am 1999; 83:1525-1546.19. Hall JC. Nutritional assessment of surgery patients. J Am Coll Surg 2006; 202:837-843.
12c h a p t e r
SummaryIncluding Dutch summaryNederlandse samenvatting
123
Summary
Since 1995, pseudomyxoma peritonei (PMP) patients have been treated at The Neth-erlands Cancer Institute – Antoni van Leeuwenhoek Hospital (NKI – AVL) with cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC). This thesis focuses on aspects related to this combined modality treatment of PMP. In addition, pathogenesis and clinical features of this rare disease are discussed.Chapter 1 introduces PMP as a clinical entity and describes the current standard treat-ment approach for PMP. The end of this chapter contains the outline of the thesis.Chapter 2 provides a population based study of PMP in the Netherlands between 1995 and 2005. The main aim of this study was to evaluate PMP epidemiology in the Netherlands and associated appendiceal neoplasms. A mucinous epithelial neoplasm
20% of these patients developed PMP. Thirteen percent of patients had an additional epithelial lesion in the colon. From the nationwide database 267 patients (62 men and
appendix (82%). Especially mucinous epithelial neoplasms of the appendix were asso-ciated with PMP (20%). For mucocele and non-mucinous neoplasms the association with PMP was only 2% and 3%, respectively. In patients with an epithelial neoplasm at appendectomy colonoscopy is indicated and patients with a mucinous epithelial neo-plasm of the appendix should be followed for development of PMP.Chapter 3 illustrates clinical implications of PMP diagnosis and treatment. Symptoms, pathology, diagnosis, treatment, and follow up of three patients with PMP are dis-cussed. This chapter demonstrates how PMP is diagnosed with CT scan, biopsy, and serum tumour markers. The goal of these case histories is to contribute to the physi-cians’ familiarity with the disease as early recognition of PMP and referal of patients to a specialized institute improves the probability of long-term survival.
In Chapter 4 toxicity and mortality of CRS and HIPEC was studied in 103 consecutive procedures performed between 1996 and 2004. Treatment related toxicity was observed in 54% of procedures with a 30 days mortality of 3%. Small bowel perforations and suture leaks were the main cause of toxicity. In univariate analysis, toxicity was asso-ciated with abdominal tumour load and completeness of cytoreduction. A favourable pathology was associated with a lower mortality. These data suggest that CRS and HIPEC is a treatment with considerable toxicity but acceptable mortality, both mainly surgery related.Survival of PMP patients treated by CRS and HIPEC is discussed in Chapter 5. In total, 103 PMP patients (34 men and 69 women) treated at The NKI – AVL were identi-
3-year and 5-year survival probability was 70.9% and 59.5%, respectively. Factors associ-ated with survival were pathological subtype, completeness of cytoreduction, and degree

Chapter 12
124
and location of tumor load (p<0.05). The main prognostic factor, independently asso-ciated with survival, was the pathological subtype (p<0.01). These results suggest that
treatment. In contrast, PMP patients with overt malignant features and patients with grossly incomplete cytoreduction show hardly any improvement of survival in compari-son with untreated patients. Apparently CRS with intraoperative HIPEC appears to be a feasible treatment strategy for selected PMP patients.Chapter 6 illustrates the learning curve associated with CRS and HIPEC at The NKI-AvL. From 1996 to 2006, 323 HIPEC procedures were performed in 180 women and 143 men. Primary diagnosis was peritoneal carcinomatosis (PC) of colorectal cancer (CRC) origin in 184 patients and PMP in 128 patients. The learning effect was analysed
-
regions did not. The rate of complete cytoreductions increased from 35.6% to 65.1% (p=.012). Postoperative morbidity decreased from 71.2% to 34.1% (p<.0001). The median in-patient stay decreased from 24 to 17 days. Survival probability at 24 months showed a positive trend (p=.160) from 59.7% (95% CI 49.4%-72.2%) to 61.9% (95% CI 53.7%-71.3%) and 71.7% (95% CI 60.6%-84.7%). These results show that the learning
-ment expertise. The learning curve has a positive trend on survival probability.Progressive disease in PMP patients treated by combined modality treatment is evaluat-ed in Chapter 7. After exclusion of patients with overt malignancy, progressive disease was studied in 96 PMP patients treated primarily by CRS with HIPEC. With a median follow-up of 51.5 months (0.1-99.5) median progression free survival (PFS) was 28.2 months. The PFS was associated with the pathological subtype (p=0.06) and result of initial cytoreduction (p=0.03). Progressive disease was, in most cases, located sub hepatic (38%) or in multiple regions (36%). Patients with progression were treated by second CRS and HIPEC (n=8), surgical resection only (n=10), systemic chemotherapy only (n=6) or were merely observed (n=15). The 3-year overall survival (OS) probability of these patients was 100%, 53.3%, 0% and 66.0%, respectively. The choice of treat-ment depended on pathology, extent of disease and PFS. A longer PFS after primary treatment was associated with longer OS probability after progressive disease (p=0.04). This chapter demonstrates that management of progressive PMP after primary CRS and HIPEC is worthwhile and can result in long-term survival in a considerable per-centage of patients. It also stresses that the choice of treatment policy should depend primarily on the PFS.
In Chapter 8 the involvement of the urinary tract and urologic complications related to CRS and HIPEC are evaluated in PMP patients treated at The NKI - AVL. A ret-rospective study of 92 patients was performed. Seven patients with involvement of the

125
Summary
-
with involvement of the urinary tract and/or urologic complications had undergone previous pelvic surgery. It seems that the urinary tract is rarely involved in patients with PMP, as it is located outside the peritoneal cavity. It may be a result of seeding of PMP of pelvic origin after prior pelvic surgery. Our data also shows that the urologic com-plication risk of CRS and HIPEC is low. The combination of urinary tract involvement and previous pelvic surgery is an omen of treatment related urologic complications.Chapter 9 contains a report of two young women, wishing to bear children, that are
treatment has to be well considered. Reserved surgical treatment instead of CRS, includ-ing ovariectomy, with HIPEC in young women with PMP and a wish to bear children can be acceptable when the disease shows signs of indolence and benign pathology. Any suspicion of progression strongly favors combined modality treatment (CRS with HIPEC) to improve the probability of survival.Chapter 10 is a review on pathogenesis, diagnosis and treatment of PMP. It provides a short outline of PMP as a disease entity and describes the proper diagnostic procedure. In addition, all possible treatment strategies are discusses with emphasis on the current standard approach: combined modality treatment.


127
Sinds 1995 worden pseudomyxoma peritoneï (PMP) patiënten behandeld in het Ned-erlands Kanker Instituut – Antoni van Leeuwenhoek Ziekenhuis (NKI-AVL) middels cytoreductieve chirurgie (CRC) en hypertherme intraperitoneale chemotherapie (HIPEC). In dit proefschrift worden diverse aspecten belicht die gerelateerd zijn aan deze behandelingswijze. Daarnaast worden de pathogenese en klinische kenmerken van deze zeldzame ziekte besproken.Hoofdstuk 1 bevat een beschrijving van PMP als klinische entiteit en gaat in op de huidige benadering van deze ziekte. Aan het eind van dit hoofdstuk wordt het doel van dit proefschrift kort uiteen gezet.Hoofdstuk 2 bevat een op de populatie gebaseerde studie van PMP in Nederland in de periode 1995-2005. Het voornaamste doel van deze studie was het evalueren van de epidemiologie van PMP en de relatie met tumoren van de appendix. Hiervoor werd in de landelijke database van pathologie verslagen gezocht naar appendix tumoren en
en 27% maligne) van de appendectomieën, en 20% van deze patiënten ontwikkelde uit-eindelijk PMP. Dertien procent (13%) van de patiënten had daarbij ook een epitheliale
vrouwen, hetgeen betekent dat de incidentie de 2 per miljoen per jaar benadert. De primaire tumor werd herkend in 68% en was voornamelijk gelokaliseerd in de appendix (82%). Vooral slijmvormende epitheliale tumoren waren geassocieerd met PMP (20%). De relatie met PMP was minder voor mucoceles en niet slijmvormende tumoren, 2% and 3% respectievelijk. Van deze studie kan worden geconcludeerd dat bij patiënten met een epitheliale tumor bij appendectomie coloscopie is geïndiceerd, en dat patiënten met een slijmvormende epitheliale tumor van de appendix vervolgd moeten worden voor het ontwikkelen van PMP.In Hoofdstuk 3 worden de symptomen, histopathologie, diagnose, behandeling en fol-low-up van 3 patiënten met PMP besproken. PMP kan worden vastgesteld op basis van symptomen in combinatie met een CT scan, intra-abdominaal biopt en serum tumor markers. Het doel van deze casuïstische mededelingen is om bij te dragen aan de bekendheid van medici met deze ziekte, aangezien vroege herkenning van PMP en verwijzing van patiënten naar een gespecialiseerd instituut de kans op langetermijnover-leving aanzienlijk verbetert.
In Hoofdstuk 4 worden morbiditeit en mortaliteit van CRC en HIPEC bestudeerd in 103 opeenvolgende procedures tussen 1996 en 2004. Aan de behandeling gerelateerde complicaties werden gezien in 54% van de procedures en de 30 dagen mortaliteit was 3%. Perforaties en naadlekkages van de dunnedarm waren de voornaamste complica-ties. Uit een univariate analyse bleek dat morbiditeit vooral geassocieerd was met de uitgebreidheid van de ziekte (p<0,01) en de volledigheid van de resectie (p<0,01). Een benigne histopathologie was geassocieerd met een lagere sterfte. Uit deze gegevens kan
Nederlandse samenvatting

Chapter 12
128
worden afgeleid dat CRC in combinatie met HIPEC een behandeling is met aanzienli-jke morbiditeit (vooral chirurgische complicaties) maar acceptabele mortaliteit.De langetermijnoverleving van patiënten met PMP die behandeld zijn met CRC and HIPEC in het NKI-AVL wordt beschreven in Hoofdstuk 5. In totaal werden 103 PMP patiënten (34 mannen en 69 vrouwen) bestudeerd op overleving en factoren met voor-
respectievelijk. Factoren die gerelateerd waren aan de overleving waren het patholo-gische subtype, de volledigheid van resectie en de uitgebreidheid en locatie van tumor (p<0,05). De belangrijkste voorspellende factor die onafhankelijk geassocieerd was met de overleving was het pathologische subtype (p<0,01). Deze resultaten veronderstel-len dat vooral patiënten met het benigne subtype en een complete resectie voordeel ondervinden van deze behandeling. Daartegenover toonden patiënten met duidelijke maligne kenmerken en een grotendeels incomplete resectie nauwelijks een verbetering in de overleving in vergelijking met onbehandelde patiënten. CRC met HIPEC lijkt een aanwinst voor geselecteerde PMP patiënten.Hoofdstuk 6 beschrijft een studie van de leercurve geassocieerd met CRC en HIPEC. Tussen 1995 en 2005 werden in het NKI-AVL 323 HIPEC procedures verricht bij 180 vrouwen en 143 mannen. De primaire diagnose was peritonitis carcinomatosa (PC) van colorectale (CR) origine in 184 patiënten en pseudomyxoma peritonei (PMP) in 128 patiënten. De leercurve werd bestudeerd op het gebied van de patiëntenselectie, de
(p<0,0001), maar het aantal aangedane regio’s niet. Het aantal complete cytoreduc-ties steeg van 35,6% naar 65,1% (p = 0,012). De postoperatieve morbiditeit daalde van 71,2% naar 34,1% (p<0,0001). De mediane opnameduur verminderde van 24 naar 17 dagen. De overlevingskans na 24 maanden toonde een positieve trend (p=0,160) van 59,7% (95% CI 49,4%-72,2%) naar 61,9% (95% CI 53,7%-71,3%) en 71,7% (95% CI 60,6%-84,7%). Deze resultaten tonen dat de leercurve van deze gecombineerde behan-deling lang is en zich uit in zowel de patiëntenselectie als de behandelingsgerelateerde expertise. Daarnaast heeft de leercurve een positief effect op de overlevingskans.De behandeling en het beloop van progressieve ziekte bij 96 PMP patiënten die behan-deld waren middels CRC en HIPEC wordt geëvalueerd in Hoofdstuk 7. Patiënten met PMP van duidelijk maligne aard werden van deze studie uitgesloten. Met een mediane follow-up van 51,5 maanden (0,1-99,5) was de mediane progressievrije overleving (PVO) 28,2 maanden. De PVO was geassocieerd met het pathologische subtype (p=0,06) en de volledigheid van resectie (p=0,03). Progressieve ziekte werd vooral gezien in de sub-hepatische regio (38%) of in meerdere regio’s tegelijk (36%). Patiënten met progressie werden behandeld middels een tweede procedure (n=8), locale resectie (n=10), system-ische chemotherapie (n=6) of werden slechts geobserveerd (n=15). De 3-jaars overleving van deze patiënten was 100%, 53,3%, 0% en 66,0%, respectievelijk. De beleidskeuze bij

129
progressie hing af van de pathologische kenmerken, de uitgebreidheid van de ziekte en de PVO. Een langere PVO na de eerste procedure was geassocieerd met een langere overleving na progressie (p=0,04). Dit hoofdstuk demonstreert dat behandeling van progressief PMP na primaire CRC en HIPEC waardevol kan zijn en kan leiden tot langetermijnoverleving bij een aanzienlijk percentage van patiënten. Ook blijkt uit dit hoofdstuk dat de beleidskeuze voornamelijk afhangt van de PVO.
In Hoofdstuk 8 worden de betrokkenheid van de urinewegen en urologische compli-caties gerelateerd aan CRC en HIPEC geëvalueerd bij 92 PMP patiënten behandeld in het NKI-AVL. Bij 7 patiënten waren de urinewegen betrokken in het ziektepro-ces. Belangrijke urologische complicaties, voornamelijk chirurgisch en gerelateerd aan de blaas, werden gezien bij 5 patiënten. Het was opvallend dat alle patiënten met betrokkenheid van de urinewegen en/of urologische complicaties eerdere chirurgie in het bekken hadden ondergaan. Het lijkt erop dat de urinewegen zelden betrokken zijn bij PMP aangezien ze grotendeels buiten de peritoneaalholte liggen. De betrokkenheid is waarschijnlijk het gevolg van het uitzaaien van PMP vanuit het bekken na eerdere bekkenchirurgie. Deze studie laat ook zien dat de kans op urologische complicaties na CRC en HIPEC klein is. De combinatie van betrokkenheid van de urinewegen bij PMP en eerdere bekkenchirurgie is een voorteken voor urologische complicaties na CRC en HIPEC.Hoofdstuk 9 beschrijft 2 jonge vrouwen met PMP en een kinderwens. Terughoudende chirurgische behandeling in plaats van CRC met HIPEC (met vaak verwijdering van de ovaria) kan gerechtvaardigd zijn in deze gevallen mits er sprake is van een goedaardig en traag karakter van de ziekte. Enige verdenking op progressie vraagt om de combina-tie van CRC en HIPEC, om de kans op overleving te vergroten.Hoofdstuk 10 bevat een overzicht van de pathogenese, diagnose en behandeling van PMP. Het is bedoeld als een korte samenvatting van alle facetten van deze zeldzame en intrigerende ziekte. Daarbij worden alle mogelijke behandelingen besproken met de nad-ruk op de huidige meest toegepaste benadering: CRC met (intraoperatieve) HIPEC.
Nederlandse samenvatting

Dankwoord

133
Dankwoord
DankwoordHet tot stand komen van deze dissertatie heb ik te danken aan de mensen die mij gesteund en geholpen hebben in het hele proces van database tot proefschrift. Zonder hen was het me zeker niet gelukt dit resultaat te behalen. Ik wil deze personen dan ook persoonlijk bedanken.
Mijn hooggeleerde promotor, prof. dr. B.B.R. Kroon.Beste professor Kroon, u was voor mij een geweldige promotor. Uw beoordeling van mijn werk vond snel plaats en uw op- en aanmerkingen hebben me enorm geholpen in
en onmisbaar. Mede dankzij uw adequate medewerking is de promotie snel in zicht geko-men.
Mijn hooggeachte copromotor, dr. V.J. Verwaal.Beste Vic, jij was voor mij een ware copromotor. Jij hebt me uitstekend begeleid in mijn proces van vrijwilliger tot ervaren artsonderzoeker. Jouw adviezen en tips op velerlei gebieden, alsmede jouw ideeën op wetenschappelijk gebied, hebben er voor gezorgd dat dit proefschrift tot stand heeft kunnen komen. De avonden bij jouw thuis waren voor mij een teken van een goede en gezellige samenwerking. Briljant was ook het SSO congres in San Diego, waar we onze ooghandcoördinatie hebben getraind op de surfplank en velerlei inspiratie hebben opgedaan.
Mijn hooggeachte copromotor, dr. F.A.N. Zoetmulder.Beste Frans, jij bent een geweldige mentor en wetenschappelijk schrijver. Jouw ideeën en schrijverstalenten hebben mij aangespoord mijzelf steeds verder te ontwikkelen op weten-schappelijk gebied. Je hebt me enorm geholpen om mijn proefschrift te maken tot wat het nu is. Ik ken weinig mensen die zoveel ervaring hebben op het gebied van de wetenschap in zijn geheel als jij. Tenslotte zal ik de etentjes bij jou en je vrouw thuis nooit vergeten!
Dr. A. Bex, beste Axel, wij hebben vooral in het begin veel samengewerkt voor ons uro (logisch) stuk. Dit heeft tot een mooi resultaat geleid. Daarnaast gaven je verhalen en grappen tijdens de zaalvisite een extra cachet aan het werken in de kliniek.
Drs. N. Antonini, beste Ninja, jouw statistische inzichten en snelle analyses hebben -
cante bijdrage geleverd aan dit proefschrift.
Dr. M.L.F. van Velthuysen, beste Loes, ondanks dat we maar 1 artikel samen hebben geproduceerd heb ik veel geleerd van jouw kennis en inzichten op het gebied van de

134
pathologie. Ik ben je erg dankbaar voor het vele werk dat je hebt verricht om er een mooi en degelijk artikel van te maken. Het was een goedaardige samenwerking.
Zeer geachte leden van de promotiecommissie, Prof. dr. J.J.B. van Lanschot, Prof. drs. J.F.W.M. Bartelsman, Prof. dr. D.J. Richel, Prof. dr. T. Wiggers, Dr. H. Boot, Dr. M.J. van de Vijver, ik dank u allen voor de aandachtige en zorgvuldige beoordeling van dit proefschrift.
Hooggeleerde Prof dr. S. Rodenhuis, uw snelle beoordeling van mijn manuscripten heeft mede bijgedragen aan de snelle afronding van dit proefschrift. Bedankt voor uw kritische noten.
Beste paranimfen, Philip en Remko, het was een eer jullie als mijn paranimfen te hebben. Ik heb niet alleen genoten van jullie aanwezigheid, maar ook ben ik dankbaar voor jullie bijdrage aan het geheel. Jullie goede ideeën, humor en interesse waren kenmerkend voor onze samenwerking. Bedankt!
Beste collega artsonderzoekers, Bin, Jakko, Jimmy, Joost, Karel, Leonie, Maartje, Maya, Philip, Remco en Roelien, wetenschappelijk onderzoek verrichten in je eentje is saai, niet inspirerend, ongezellig en eigenlijk nagenoeg onmogelijk. Jullie tips & trics, verhalen,
Beste collega artsassistenten, Bas, Bart, Ingrid, Koen, Lisa, Marlou, Maurits, Remko, Ronald, Sanne, Simon, Thijs en Tom, ik heb met jullie allen een geweldige tijd gehad met briljante gezamenlijke momenten, herinneringen en ervaringen. Niet alleen samen werken op de afdelingen, maar vooral de borrels in die Rooie, Prins H, en het fantastische week-end in Friesland waren onvergetelijk.
Lieve verpleging van de 6e etage, ik heb een zeer gezellige tijd met jullie gehad en de sfeer op de afdeling is erg goed. De vrijdagmiddag borrel en overige uitstapjes zullen me altijd bijblijven. Bedankt voor de mooie tijd waardoor het werk automatisch plezierig werd. Dit heeft zeker bijgedragen aan mijn promotie.
Lieve ouders, lieve Charlotte, jullie onvoorwaardelijke en persisterende vertrouwen heb-ben er voor gezorgd dat ik me altijd voor de volle 100% heb kunnen inzetten voor dit proefschrift. Het is erg motiverend om te merken dat je emotioneel gesteund wordt. Lot, jij was in de eerste plaats mijn grote steun en toeverlaat. Jouw overweldigende enthousi-asme en geduld was vaak groter dan dat van mij zelf. Iemand die zo achter je staat kan alleen maar je grote liefde zijn!

135
Curriculum vitae
Curriculum vitaeRobert Matthijs Smeenk is geboren op 4 september 1977 te Moshi, Tanzania. Op 3-jari-ge leeftijd kwam hij in Nederland wonen. Na zijn jeugd deels te hebben doorgebracht in Zevenbergen, begon hij aan de kleuterschool en de lagere school in Breda. In 1989 vervolgde hij zijn opleiding op het Stedelijk Gymnasium te Breda. Na het eindexamen in 1995 zocht hij zijn heil in Amsterdam en begon aan de studie geneeskunde aan de Vrije Universiteit te Amsterdam. In 2001 begon hij na het behalen van zijn doctoraalbul aan zijn co-schappen. Tijdens deze periode heeft hij voor een keuze co-schap chirurgie 10 weken in Suriname doorgebracht. Eind 2003 behaalde hij zijn artsexamen.Hierna kreeg hij een baan als AGNIO chirurgie in het Flevo Ziekenhuis te Almere (onder leiding van dr. P.C.M. Verbeek), alwaar hij tot september 2004 heeft gewerkt. Toen kreeg hij in Het Nederlands Kanker Instituut – Antoni van Leeuwenhoek Zieken-huis te Amsterdam een gecombineerde aanstelling aangeboden. Deze aanstelling betrof een combinatie van AGNIO chirurgie en artsonderzoeker. Onder leiding van Prof. dr. B.B.R. Kroon heeft de onderzoeksperiode geleid tot de huidige dissertatie. Vanaf 01-07-2006 is hij in opleiding tot chirurg in het Amsterdams Medisch Centrum (onder leiding van Prof. dr. J.J.B. van Lanschot).





















