The use of acellular dermis in the prevention of Frey's syndrome
6
The Laryngoscope Lippincott Williams & Wilkins, Inc., Philadelphia © 2001 The American Laryngological, Rhinological and Otological Society, Inc. The Use of Acellular Dermis in the Prevention of Frey’s Syndrome Satish Govindaraj, MD; Michael Cohen, MD; Eric M. Genden, MD; Peter D. Costantino, MD, FACS; Mark L. Urken, MD, FACS Educational Objective: At the conclusion of this presentation, the participant should be able to discuss the indications and advantages of using acellular der- mis in the prevention of post-parotidectomy gustatory sweating (Frey’s Syndrome). Introduction: Gustatory sweating is a common postoperative problem and a challenge to treat. The purpose of this study was to evaluate the role of acellular dermis in preventing post- parotidectomy gustatory sweating. Methods: Sixty-four patients were randomly assigned to two groups. Group I consisted of 32 patients who underwent a superficial lobe parotidectomy. Group II consisted of 32 patients who underwent a superficial lobe parotidectomy and underwent intraoperative placement of acellular der- mis within the parotid bed, between the skin flap and the remaining parotid tissue. The implanted volume of acellular dermis was determined by the amount re- quired to aesthetically restore lateral facial contour. All 64 patients were evaluated for gustatory sweating by identical phone and mail questionnaires. Thirty ran- domly chosen patients (group I 15, group II 15) were evaluated using a modified Minor’s Starch-Iodine Test (MSIT). In all 30 patients, the MSIT was administered to both sides of the face. Results: The responses to ques- tionnaires (N 64) demonstrated the subjective pres- ence of gustatory sweating in 3 of 32 patients (9.3%) in group I, whereas group II demonstrated a subjective incidence in 1 of 32 patients (3.1%). The objective inci- dence determined by those who underwent the MSIT (n 30) revealed a 40% (6) and 0% incidence of Frey’s Syndrome in groups I and II, respectively. The compli- cation rate in group I was 9% (3 seromas) and in group II it was 25% (7 seromas and 1 wound infection). Con- clusions: Acellular dermis appears to be an effective method for preventing post-parotidectomy gustatory sweating, despite its higher complication rate. Key Words: Frey’s Syndrome, acellular dermis, gustatory sweating. Laryngoscope, 111:1993–1998, 2001 INTRODUCTION Frey’s Syndrome is a long-term complication of pa- rotid excision that is characterized by two main symp- toms: gustatory sweating and gustatory flushing. Diag- nostic testing and clinical familiarity have traditionally focused on the “sweating” component of the syndrome; however, clinicians need to be cognizant of difficulties with gustatory flushing as well, which can result in sig- nificant discomfort from cosmetic embarrassment and pain from local vascular engorgement. The incidence of Frey’s Syndrome has been studied in numerous articles with variable percentages (Table I). Some reasons for this variability are that incidence rates are reported based on the presence of clinical symptoms, whereas others report results obtained from objective test- ing (i.e., starch-iodine test). Perhaps the first article to bring Frey’s Syndrome to the forefront as a common post- parotidectomy entity was Laage-Hellman’s in 1957. 1 In his study of 123 patients, he used the Minor’s Starch- Iodine Test to determine an objective incidence of Frey’s Syndrome in nearly 100% of patients. This number has been difficult to duplicate in subse- quent studies; however, the overall average is 38% for subjective (clinical symptoms) presence of Frey’s Syn- drome and 86% when objective testing is performed with Minor’s Starch-Iodine Test. 2 Ten percent of patients re- port having distressing symptoms. Botulinum toxin A has been used in the treatment of Frey’s Syndrome with reported success 3,4 ; however, ther- apeutic modalities are rarely permanent in efficacy and those that are surgical in nature place the facial nerve at significant risk as a result of prior excision of the overlying superficial parotid lobe. Because of the limited efficacy of therapeutic modalities, preventive measures that protect against the future development of Frey’s Syndrome and add minimal risk and operative time are needed. A recent study by Dulguerov et al. reviewed the effi- cacy of synthetic and semisynthetic barriers in the pre- vention of Frey’s Syndrome. 2 It is thought that by the interposition of a barrier (i.e., dermal graft, synthetic ma- terials, adipose tissue), the severed postganglionic auto- nomic fibers of the parotid gland will be prevented from aberrant outgrowth to the overlying sweat glands. In ad- dition, the interposition techniques have the added benefit From the Departments of Otolaryngology (S.G., M.C., E.M.G., M.L.U.) and Otolaryngology (M.L.U.), Mount Sinai Medical Center, New York, NY; and the Center for Cranial Base Surgery, Department of Otolaryngology (P.D.C.), St. Luke’s-Roosevelt Hospital Center, New York, NY, U.S.A. Editor’s Note: This Manuscript was accepted for publication July 16, 2001. Send Correspondence to Satish Govindaraj, MD, Department of Oto- laryngology, Mount Sinai Medical Center, One Gustave L. Levy Place, Box 1189, New York, NY 10029, U.S.A. Laryngoscope 111: November 2001 Govindaraj et al.: Frey’s Syndrome 1993
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of The use of acellular dermis in the prevention of Frey's syndrome
The LaryngoscopeLippincott Williams & Wilkins, Inc., Philadelphia© 2001 The American Laryngological,Rhinological and Otological Society, Inc.
The Use of Acellular Dermis in thePrevention of Frey’s Syndrome
Satish Govindaraj, MD; Michael Cohen, MD; Eric M. Genden, MD; Peter D. Costantino, MD, FACS;Mark L. Urken, MD, FACS
Educational Objective: At the conclusion of thispresentation, the participant should be able to discussthe indications and advantages of using acellular der-mis in the prevention of post-parotidectomy gustatorysweating (Frey’s Syndrome). Introduction: Gustatorysweating is a common postoperative problem and achallenge to treat. The purpose of this study was toevaluate the role of acellular dermis in preventing post-parotidectomy gustatory sweating. Methods: Sixty-fourpatients were randomly assigned to two groups. GroupI consisted of 32 patients who underwent a superficiallobe parotidectomy. Group II consisted of 32 patientswho underwent a superficial lobe parotidectomy andunderwent intraoperative placement of acellular der-mis within the parotid bed, between the skin flap andthe remaining parotid tissue. The implanted volume ofacellular dermis was determined by the amount re-quired to aesthetically restore lateral facial contour. All64 patients were evaluated for gustatory sweating byidentical phone and mail questionnaires. Thirty ran-domly chosen patients (group I � 15, group II � 15) wereevaluated using a modified Minor’s Starch-Iodine Test(MSIT). In all 30 patients, the MSIT was administered toboth sides of the face. Results: The responses to ques-tionnaires (N � 64) demonstrated the subjective pres-ence of gustatory sweating in 3 of 32 patients (9.3%) ingroup I, whereas group II demonstrated a subjectiveincidence in 1 of 32 patients (3.1%). The objective inci-dence determined by those who underwent the MSIT (n� 30) revealed a 40% (6) and 0% incidence of Frey’sSyndrome in groups I and II, respectively. The compli-cation rate in group I was 9% (3 seromas) and in groupII it was 25% (7 seromas and 1 wound infection). Con-clusions: Acellular dermis appears to be an effectivemethod for preventing post-parotidectomy gustatorysweating, despite its higher complication rate. KeyWords: Frey’s Syndrome, acellular dermis, gustatorysweating.
Laryngoscope, 111:1993–1998, 2001
INTRODUCTIONFrey’s Syndrome is a long-term complication of pa-
rotid excision that is characterized by two main symp-toms: gustatory sweating and gustatory flushing. Diag-nostic testing and clinical familiarity have traditionallyfocused on the “sweating” component of the syndrome;however, clinicians need to be cognizant of difficultieswith gustatory flushing as well, which can result in sig-nificant discomfort from cosmetic embarrassment andpain from local vascular engorgement.
The incidence of Frey’s Syndrome has been studied innumerous articles with variable percentages (Table I).Some reasons for this variability are that incidence ratesare reported based on the presence of clinical symptoms,whereas others report results obtained from objective test-ing (i.e., starch-iodine test). Perhaps the first article tobring Frey’s Syndrome to the forefront as a common post-parotidectomy entity was Laage-Hellman’s in 1957.1 Inhis study of 123 patients, he used the Minor’s Starch-Iodine Test to determine an objective incidence of Frey’sSyndrome in nearly 100% of patients.
This number has been difficult to duplicate in subse-quent studies; however, the overall average is 38% forsubjective (clinical symptoms) presence of Frey’s Syn-drome and 86% when objective testing is performed withMinor’s Starch-Iodine Test.2 Ten percent of patients re-port having distressing symptoms.
Botulinum toxin A has been used in the treatment ofFrey’s Syndrome with reported success3,4; however, ther-apeutic modalities are rarely permanent in efficacy andthose that are surgical in nature place the facial nerve atsignificant risk as a result of prior excision of the overlyingsuperficial parotid lobe. Because of the limited efficacy oftherapeutic modalities, preventive measures that protectagainst the future development of Frey’s Syndrome andadd minimal risk and operative time are needed.
A recent study by Dulguerov et al. reviewed the effi-cacy of synthetic and semisynthetic barriers in the pre-vention of Frey’s Syndrome.2 It is thought that by theinterposition of a barrier (i.e., dermal graft, synthetic ma-terials, adipose tissue), the severed postganglionic auto-nomic fibers of the parotid gland will be prevented fromaberrant outgrowth to the overlying sweat glands. In ad-dition, the interposition techniques have the added benefit
From the Departments of Otolaryngology (S.G., M.C., E.M.G., M.L.U.)and Otolaryngology (M.L.U.), Mount Sinai Medical Center, New York, NY;and the Center for Cranial Base Surgery, Department of Otolaryngology(P.D.C.), St. Luke’s-Roosevelt Hospital Center, New York, NY, U.S.A.
Editor’s Note: This Manuscript was accepted for publication July 16,2001.
Send Correspondence to Satish Govindaraj, MD, Department of Oto-laryngology, Mount Sinai Medical Center, One Gustave L. Levy Place, Box1189, New York, NY 10029, U.S.A.
Laryngoscope 111: November 2001 Govindaraj et al.: Frey’s Syndrome
1993
of potential cosmetic enhancement by providing soft tissuereplacement. However, these surgical management op-tions are limited by at least one of the following factors:the need for a second operation (with its associated poten-tial morbidity), the need for an additional donor site, theprolonged time under general anesthesia, and a higherrate of postoperative complications.
A “barrier” that would demonstrate efficacy with regardto prevention of gustatory sweating, while at the same timeaddressing the above four factors, was needed. It was hy-pothesized that acellular dermis AlloDerm® (LifeCell Corp.,The Woodlands, Texas) would serve as an ideal barrier be-cause it undergoes fibrous tissue ingrowth, thus serving asan obstruction to aberrant nerve growth into overlying sweatglands. In addition, parotid tumors affect patients in all agegroups and after tumor removal with generous margins, asmall soft tissue defect is commonly present in the parotidbed, between the sternocleidomastoid muscle and the man-dible.5 This is especially true in large superficial lobe tumors.Acellular dermis, in addition to serving as a nerve barrier,would serve as an effective soft tissue augmentation devicein the head and neck.6,7
METHODSThis study was conducted in a tertiary care medical center
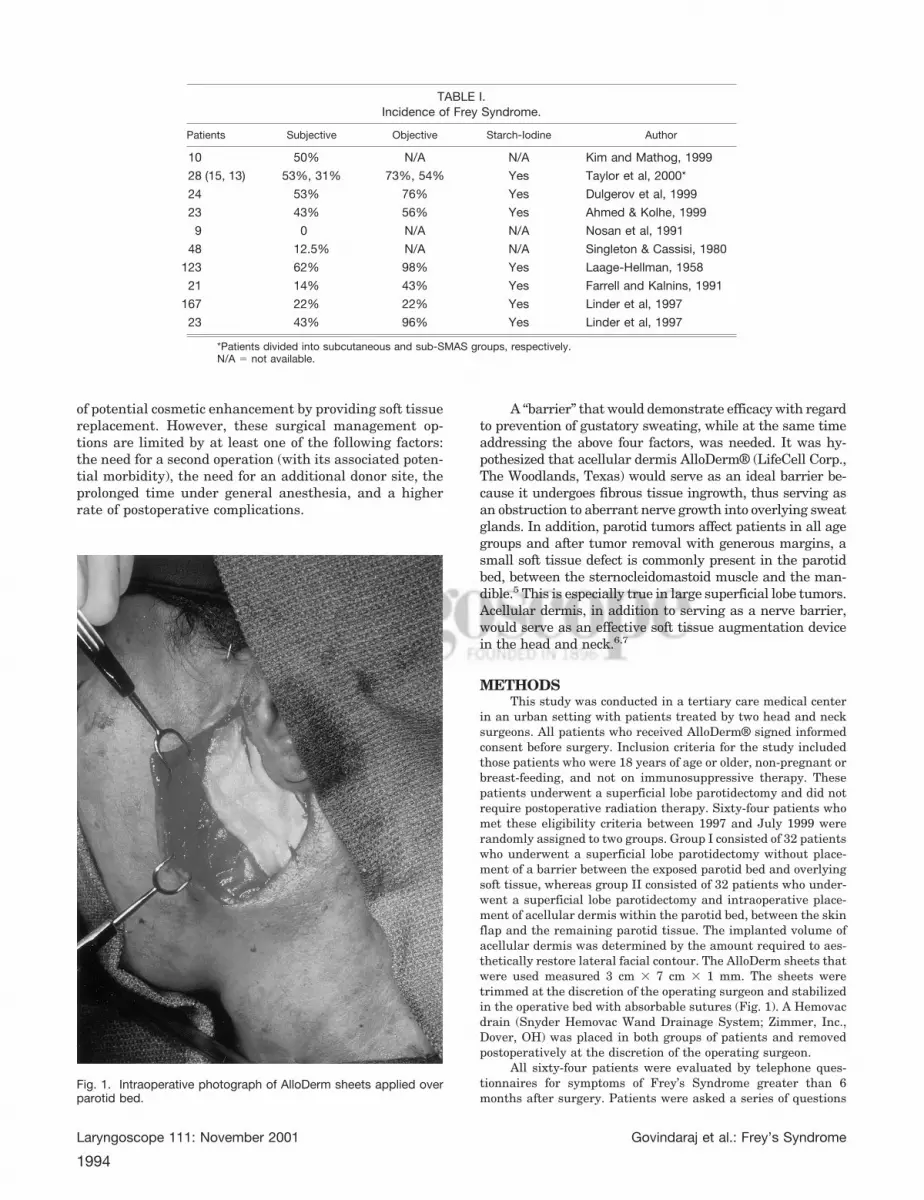
in an urban setting with patients treated by two head and necksurgeons. All patients who received AlloDerm® signed informedconsent before surgery. Inclusion criteria for the study includedthose patients who were 18 years of age or older, non-pregnant orbreast-feeding, and not on immunosuppressive therapy. Thesepatients underwent a superficial lobe parotidectomy and did notrequire postoperative radiation therapy. Sixty-four patients whomet these eligibility criteria between 1997 and July 1999 wererandomly assigned to two groups. Group I consisted of 32 patientswho underwent a superficial lobe parotidectomy without place-ment of a barrier between the exposed parotid bed and overlyingsoft tissue, whereas group II consisted of 32 patients who under-went a superficial lobe parotidectomy and intraoperative place-ment of acellular dermis within the parotid bed, between the skinflap and the remaining parotid tissue. The implanted volume ofacellular dermis was determined by the amount required to aes-thetically restore lateral facial contour. The AlloDerm sheets thatwere used measured 3 cm � 7 cm � 1 mm. The sheets weretrimmed at the discretion of the operating surgeon and stabilizedin the operative bed with absorbable sutures (Fig. 1). A Hemovacdrain (Snyder Hemovac Wand Drainage System; Zimmer, Inc.,Dover, OH) was placed in both groups of patients and removedpostoperatively at the discretion of the operating surgeon.
All sixty-four patients were evaluated by telephone ques-tionnaires for symptoms of Frey’s Syndrome greater than 6months after surgery. Patients were asked a series of questions
Fig. 1. Intraoperative photograph of AlloDerm sheets applied overparotid bed.
TABLE I.Incidence of Frey Syndrome.
Patients Subjective Objective Starch-Iodine Author
10 50% N/A N/A Kim and Mathog, 1999
28 (15, 13) 53%, 31% 73%, 54% Yes Taylor et al, 2000*
24 53% 76% Yes Dulgerov et al, 1999
23 43% 56% Yes Ahmed & Kolhe, 1999
9 0 N/A N/A Nosan et al, 1991
48 12.5% N/A N/A Singleton & Cassisi, 1980
123 62% 98% Yes Laage-Hellman, 1958
21 14% 43% Yes Farrell and Kalnins, 1991
167 22% 22% Yes Linder et al, 1997
23 43% 96% Yes Linder et al, 1997
*Patients divided into subcutaneous and sub-SMAS groups, respectively.N/A � not available.
Laryngoscope 111: November 2001 Govindaraj et al.: Frey’s Syndrome
1994
regarding the presence of Frey’s Syndrome symptoms as well astheir perception of cosmetic appearance and facial symmetry. Inaddition, patients were mailed questionnaires with identicalquestions and asked to mail completed forms back to investiga-tors. Institutional Review Board approval was obtained beforeinitiating any research study procedures.
Fifteen patients from each group were randomly selected toundergo a Modified Minor’s Starch-Iodine Test to both sides of theface so that the non-operative side could serve as an internalcontrol. Photographs were taken after 5 minutes of observationand two blinded evaluators were used to review the presence ofcolor change. Of note, one patient refused photographs to betaken at time of starch-iodine testing. A grading system of mild,moderate, and severe was used8 (Table II).
In the control patients, drain removal was on postoperativeday 1 if output was minimal. At the outset of the study, AlloDermpatients underwent identical postoperative drain management;however, because of the higher incidence of seroma/sialocele for-mation postoperatively, patients were discharged with drains inplace and removal was performed in office on postoperative days5 through 7.
RESULTSDuring the 3-year study period, 64 patients were en-
rolled with 15 patients from each group randomly assignedto undergo objective testing. Group I, the control group,consisted of 18 females and 14 males with a mean age of 49.8years (range, 19–85 y). Group II, the AlloDerm group, con-sisted of 20 females and 12 males with a mean age of 51.7years (range, 19–79 y). All patients underwent superficiallobe parotidectomies. Radical neck dissections and deep lobeparotidectomies were not performed in either group.
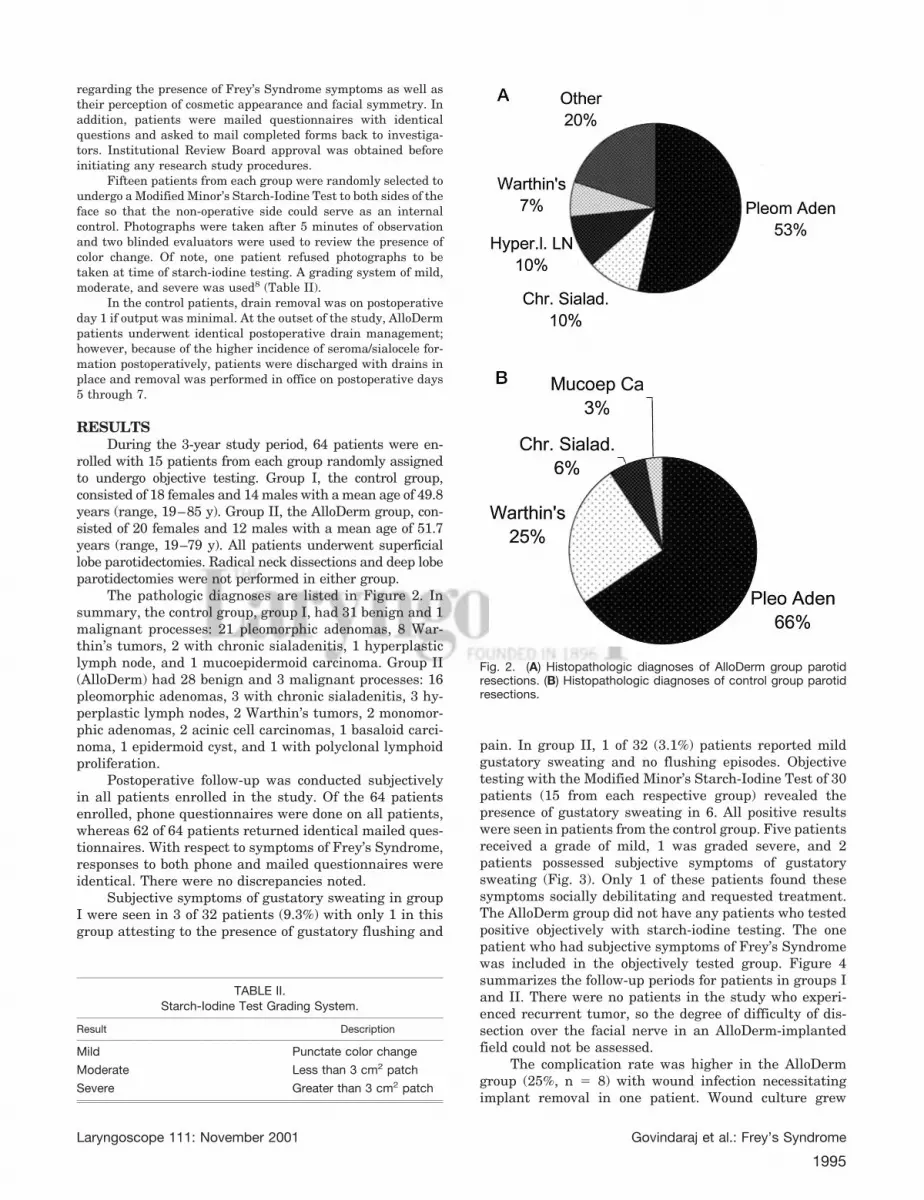
The pathologic diagnoses are listed in Figure 2. Insummary, the control group, group I, had 31 benign and 1malignant processes: 21 pleomorphic adenomas, 8 War-thin’s tumors, 2 with chronic sialadenitis, 1 hyperplasticlymph node, and 1 mucoepidermoid carcinoma. Group II(AlloDerm) had 28 benign and 3 malignant processes: 16pleomorphic adenomas, 3 with chronic sialadenitis, 3 hy-perplastic lymph nodes, 2 Warthin’s tumors, 2 monomor-phic adenomas, 2 acinic cell carcinomas, 1 basaloid carci-noma, 1 epidermoid cyst, and 1 with polyclonal lymphoidproliferation.
Postoperative follow-up was conducted subjectivelyin all patients enrolled in the study. Of the 64 patientsenrolled, phone questionnaires were done on all patients,whereas 62 of 64 patients returned identical mailed ques-tionnaires. With respect to symptoms of Frey’s Syndrome,responses to both phone and mailed questionnaires wereidentical. There were no discrepancies noted.
Subjective symptoms of gustatory sweating in groupI were seen in 3 of 32 patients (9.3%) with only 1 in thisgroup attesting to the presence of gustatory flushing and
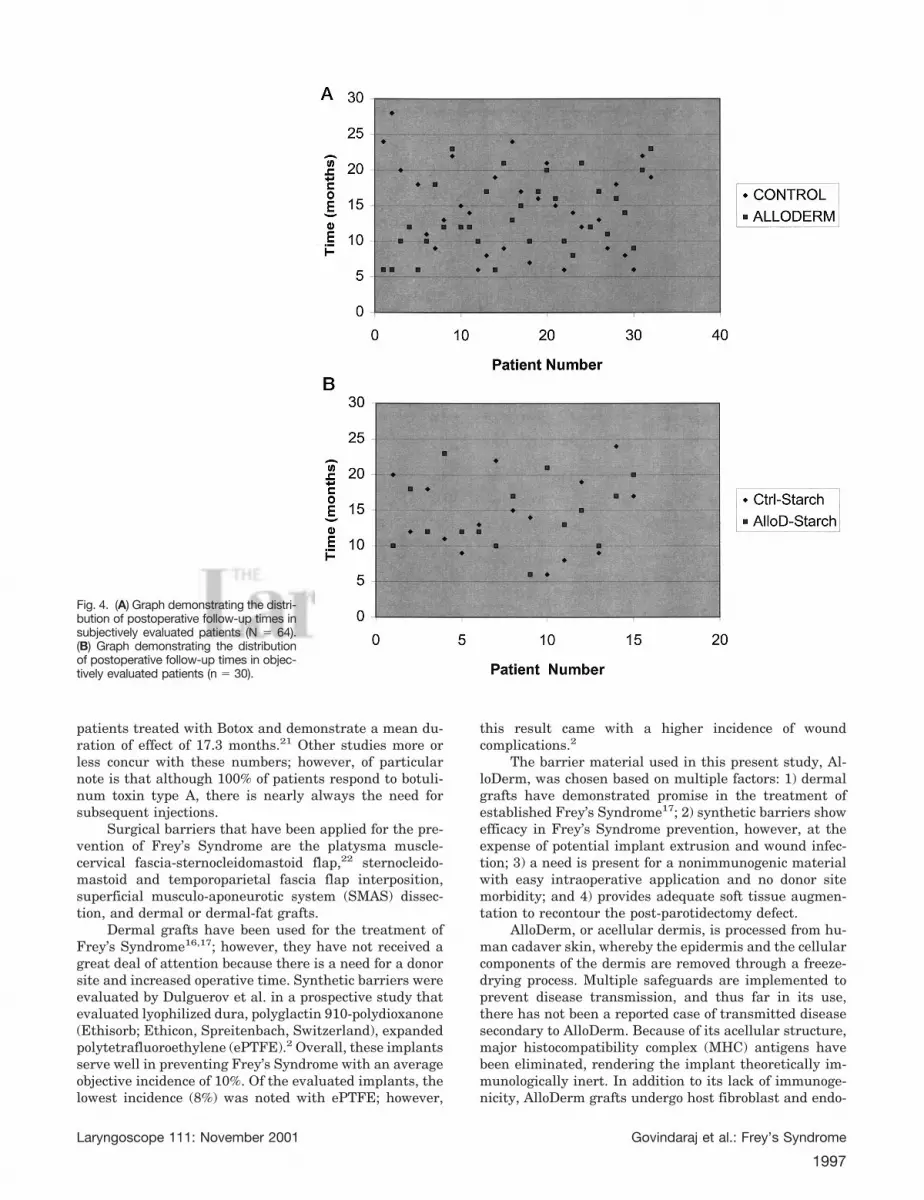
pain. In group II, 1 of 32 (3.1%) patients reported mildgustatory sweating and no flushing episodes. Objectivetesting with the Modified Minor’s Starch-Iodine Test of 30patients (15 from each respective group) revealed thepresence of gustatory sweating in 6. All positive resultswere seen in patients from the control group. Five patientsreceived a grade of mild, 1 was graded severe, and 2patients possessed subjective symptoms of gustatorysweating (Fig. 3). Only 1 of these patients found thesesymptoms socially debilitating and requested treatment.The AlloDerm group did not have any patients who testedpositive objectively with starch-iodine testing. The onepatient who had subjective symptoms of Frey’s Syndromewas included in the objectively tested group. Figure 4summarizes the follow-up periods for patients in groups Iand II. There were no patients in the study who experi-enced recurrent tumor, so the degree of difficulty of dis-section over the facial nerve in an AlloDerm-implantedfield could not be assessed.
The complication rate was higher in the AlloDermgroup (25%, n � 8) with wound infection necessitatingimplant removal in one patient. Wound culture grew
TABLE II.Starch-Iodine Test Grading System.
Result Description
Mild Punctate color change
Moderate Less than 3 cm2 patch
Severe Greater than 3 cm2 patch
Fig. 2. (A) Histopathologic diagnoses of AlloDerm group parotidresections. (B) Histopathologic diagnoses of control group parotidresections.
Laryngoscope 111: November 2001 Govindaraj et al.: Frey’s Syndrome
1995

Streptococcus species, and infection responded adequatelyto oral antibiotics. In addition, 7 seromas/sialoceles(21.8%) were seen in the AlloDerm group. Five of theseoccurred before the initiation of prolonged Hemovac drainplacement. Two seromas occurred despite extended Hemo-vac drain placement. All fluid collections resolved sponta-neously with aspiration and local wound care. The controlgroup did not report any wound infections and seromas/sialoceles were seen in three patients that resolved withmeasures mentioned above. No patients in either groupexperienced permanent facial nerve paralysis and nocases of implant extrusion occurred in the AlloDermgroup. Of note, nonpurulent and non-bloody fluid collec-tions were considered seromas/sialoceles because labora-tory testing was not conducted on any aspirated fluid todetermine the presence of saliva.
DISCUSSIONThe first report of Frey’s Syndrome, which receives
its name from Polish neurologist, Lucie Frey, has beencommonly attributed to M. Duphenix in 1757.9 Althoughcited in multiple articles as the earliest described case ofFrey’s Syndrome, this belief has been appropriately chal-lenged by Dulguerov et al.,10 who comment that the casedescribed by Duphenix was in actuality a salivary fistula,and not gustatory sweating; thus the first case of Frey’sSyndrome should be accredited to Baillarger in 1853.
Lucie Frey is accredited with first describing the roleof the auriculotemporal nerve and its delivery of auto-nomic innervation to the parotid gland as the key playerin the development of Frey’s Syndrome.11 Shortly there-after, Andre Thomas proposed the aberrant regenerationtheory as the pathophysiological mechanism behind gus-tatory sweating and gustatory flushing.10 After parotidgland excision or injury, the postganglionic fibers thatinnervate the gland are severed and undergo aberrantregrowth and stimulate the overlying sweat glands andblood vessels. Thus, when the patient eats, parasympa-thetic stimulation results in gustatory sweating and/orflushing. Although never objectively demonstrated, thistheory represents the likely pathophysiological mecha-
nism because the neurotransmitter, acetylcholine (ACH),stimulates both postganglionic receptors.
The parasympathetic nerve fibers that innervate theparotid gland originate from the inferior salivatory nu-cleus and travel within the glossopharyngeal nerve, whichenters the middle ear as the Nerve of Jacobson then form-ing the tympanic plexus. The fibers reconstitute and leavethe plexus as the lesser petrosal nerve synapsing withinthe otic ganglion where the postganglionic parasympa-thetic fibers arise and travel through the auriculotempo-ral nerve to innervate the parotid gland. Because of theclose proximity of the chorda tympani, it is believed thatthere are intersecting fibers between the ninth and sev-enth cranial nerves, thus the chorda tympani suppliespartial parasympathetic innervation to the parotid gland.This anatomic relationship accounts for the partial re-sponse seen with tympanic neurectomy in the treatmentof Frey’s Syndrome.
Therapeutic and preventive measures for Frey’s Syn-drome can be subdivided into surgical and nonsurgicalmodalities. Surgical treatment is based on the presumedpathophysiology of aberrant parasympathetic nerve out-growth to the overlying sweat glands of the face, thuscausing autonomic symptoms of sweating and flushing inassociation with eating. The surgical methods mentionedin the literature either address the blockage of gland stim-ulation, such as tympanic neurectomy, or cause a severingof the nerve fibers by re-elevation of the overlying skinflap and placement of an interposition barrier between theparotid bed and overlying skin, such as the temporopari-etal fascia flap.12 More recently, established Frey’s Syn-drome is treated through the use of nonsurgical methods,such as topical glycopyrrolate13–15 and cutaneous injec-tions of botulinum toxin type A,3,4 and surgical methodshave been reserved for Frey’s Syndrome refractory to med-ical treatment,12 and more importantly for the preventionof Frey’s Syndrome using the concept of a barrier meth-od.8,16–20 Studies examining the efficacy of Botox (Aller-gan, Inc., Mougins, France) have demonstrated mean du-rations of effect from 12.1 months to 17.3 months3,4,21;however, Laskawi and Drobik have the largest group of
Fig. 3. Photograph demonstrating a pos-itive starch-iodine test with a grade of mildin a control group patient.
Laryngoscope 111: November 2001 Govindaraj et al.: Frey’s Syndrome
1996
patients treated with Botox and demonstrate a mean du-ration of effect of 17.3 months.21 Other studies more orless concur with these numbers; however, of particularnote is that although 100% of patients respond to botuli-num toxin type A, there is nearly always the need forsubsequent injections.
Surgical barriers that have been applied for the pre-vention of Frey’s Syndrome are the platysma muscle-cervical fascia-sternocleidomastoid flap,22 sternocleido-mastoid and temporoparietal fascia flap interposition,superficial musculo-aponeurotic system (SMAS) dissec-tion, and dermal or dermal-fat grafts.
Dermal grafts have been used for the treatment ofFrey’s Syndrome16,17; however, they have not received agreat deal of attention because there is a need for a donorsite and increased operative time. Synthetic barriers wereevaluated by Dulguerov et al. in a prospective study thatevaluated lyophilized dura, polyglactin 910-polydioxanone(Ethisorb; Ethicon, Spreitenbach, Switzerland), expandedpolytetrafluoroethylene (ePTFE).2 Overall, these implantsserve well in preventing Frey’s Syndrome with an averageobjective incidence of 10%. Of the evaluated implants, thelowest incidence (8%) was noted with ePTFE; however,
this result came with a higher incidence of woundcomplications.2
The barrier material used in this present study, Al-loDerm, was chosen based on multiple factors: 1) dermalgrafts have demonstrated promise in the treatment ofestablished Frey’s Syndrome17; 2) synthetic barriers showefficacy in Frey’s Syndrome prevention, however, at theexpense of potential implant extrusion and wound infec-tion; 3) a need is present for a nonimmunogenic materialwith easy intraoperative application and no donor sitemorbidity; and 4) provides adequate soft tissue augmen-tation to recontour the post-parotidectomy defect.
AlloDerm, or acellular dermis, is processed from hu-man cadaver skin, whereby the epidermis and the cellularcomponents of the dermis are removed through a freeze-drying process. Multiple safeguards are implemented toprevent disease transmission, and thus far in its use,there has not been a reported case of transmitted diseasesecondary to AlloDerm. Because of its acellular structure,major histocompatibility complex (MHC) antigens havebeen eliminated, rendering the implant theoretically im-munologically inert. In addition to its lack of immunoge-nicity, AlloDerm grafts undergo host fibroblast and endo-
Fig. 4. (A) Graph demonstrating the distri-bution of postoperative follow-up times insubjectively evaluated patients (N � 64).(B) Graph demonstrating the distributionof postoperative follow-up times in objec-tively evaluated patients (n � 30).
Laryngoscope 111: November 2001 Govindaraj et al.: Frey’s Syndrome
1997

thelial cell repopulation, thus resulting in an integratedgraft indistinguishable from host tissue. AlloDerm hasbeen used effectively in the augmentation of facial soft-tissue defects, such as lip augmentation, scar revisions,and nasolabial and glabellar furrow correction.6,7 Becausethe native structure of acellular dermis is extracellularmatrix that undergoes even further fibrovascular in-growth, AlloDerm should serve as an ideal choice for bar-rier prevention of Frey’s Syndrome.
The postoperative follow-up results from this studydemonstrate the efficacy of acellular dermis in the preven-tion of Frey’s Syndrome. The subjective and objective in-cidences of Frey’s Syndrome were significantly lower inthe AlloDerm group when compared with the patients inthe control group. Of note is the lower incidence of Frey’sSyndrome in our study when compared with other studies.Dulgerov et al. reviewed several studies that examinedthe incidence of both subjective and objective symptoms ofFrey’s Syndrome. Overall the subjective and objective in-cidences ranged from 0% to 62% and 43% to 98%, respec-tively.2 Our study population, AlloDerm patients as wellas control subjects, possessed a subjective incidence of9.3% and an objective incidence of 40%, numbers consid-erably less than that seen in other studies. The reason forthis discrepancy is unclear. Perhaps the Modified Starch-Iodine Test was not sufficiently sensitive to detect moresubclinical cases. Retesting after a 3- to 4-year intervalmay give us the actual incidence of Frey’s Syndrome.
Although Taylor et al. and Linder et al. have reportedthe contrary,8,22 there are multiple studies that promotethe elevation of a thicker flap during surgery to serve asan added barrier to the aberrant growth of autonomicnerve fibers.18,19,23 Our study supports the findings ofTaylor et al. and Linder et al. in that the thickness ofstacked AlloDerm sheets did not play a role in preventingFrey’s Syndrome. A minimum of one sheet and a maxi-mum of four 1-mm thick sheets were used in this study.Tumor size also did not play a role in the occurrence ofFrey’s Syndrome. This finding is consistent withDulguerov et al. who noted no relationship between tumorsize and the presence of Frey’s Syndrome.2
CONCLUSIONTo justify any therapeutic modality, the benefits of
the proposed therapy should outweigh any potential risksassociated with its use. In the present study, AlloDermpatients experienced a higher rate of wound and seroma/sialocele formation when compared with control subjects.The one wound infection from the AlloDerm group oc-curred in a patient who had a predisposition to woundinfection, diabetes mellitus. The higher rate of seromaformation needed to be addressed during the course of thestudy by prolonged postoperative Hemovac drain place-ment. The increased seroma formation seen in the studygroup was possibly the result of the mechanical obstruc-tion of fluid absorption by the AlloDerm sheets. Prolongeddrain placement helped lower the degree of seroma forma-tion to a level similar to the control group.
A further long-term study on these patients is re-quired to find the true incidence of Frey’s Syndrome andits prevention using AlloDerm implantation.
BIBLIOGRAPHY1. Laage-Hellman JE. Treatment of gustatory sweating and
flushing. Acta Otolaryngol 1958;49:132–143.2. Dulguerov P, Quinodoz D, Cosendai G, Piletta P, Marchal F,
Lehman W. Prevention of Frey Syndrome during parotidec-tomy. Arch Otolaryngol Head Neck Surg 1999;125:833–839.
3. Laccourreye O, Akl E, Gutierrez-Fonseca R, Garcia D,Brasnu D, Bonan B. Recurrent gustatory sweating (FreySyndrome) after intracutaneous injection of botulinumtoxin type A. Arch Otolaryngol Head Neck Surg 1999;125:283–286.
4. Arad-Cohen A, Blitzer A. Botulinum toxin treatment forsymptomatic Frey’s Syndrome. Otolaryngol Head NeckSurg 2000;122:237–240.
5. Ahmed OA, Kolhe PS. Prevention of Frey’s Syndrome and vol-ume deficit after parotidectomy using the superficial tempo-ral artery fascial flap. Br J Plast Surg 1999;52:256–260.
6. Achauer BM, VanderKam VM, Celikoz B, et al. Augmenta-tion of facial soft-tissue defects with AlloDerm dermalgraft. Ann Plast Surg 1998;41:503–507.
7. Jones FR, Schwartz BM, Silverstein P. Use of a nonimmuno-genic acellular dermal allograft for soft tissue augmenta-tion: a preliminary report. Aesthetic Surgery Quarterly1996;16:196–201.
8. Taylor SM, Yoo J, Matthews W, Lampe HB, Trites JR. Frey’sSyndrome and parotidectomy flaps: a retrospective cohortstudy. Otolaryngol Head Neck Surg 2000;122:201–203.
9. Duphenix M. Observations sur les fistules du canal salivairede Stenon. I. Sure une playe complique a la joue ou le canalsalivaire fut dechine. Mémoires Académie Royale de Chi-rurgie 1757;3:431–439.
10. Dulguerov P, Marchal F, Gysin C. Frey Syndrome beforeFrey: the correct history. Laryngoscope 1999;109:1471–1473.
11. Frey L. Le syndrome du nerf auriculo-temporal. Rev Neurol1923;2:92–104.
12. Rubinstein RY, Rosen A, Leeman D. Frey Syndrome: treat-ment with temporoparietal fascia flap interposition. ArchOtolaryngol Head Neck Surg 1999;125:808–811.
13. Hays LL, Novack AJ, Worsham JC. The Frey Syndrome: asimple, effective treatment. Otolaryngol Head Neck Surg1982;90:419–425.
14. Urman JD, Bobrove AM. Diabetic gustatory sweating suc-cessfully treated with topical glycopyrrolate: report of acase and review of the literature. Arch Intern Med 1999;159:877–878.
15. May JS, McGuirt WF. Frey’s Syndrome: treatment with top-ical glycopyrrolate. Head Neck 1989;11:85–89.
16. Harada T, Inoue T, Harashina T, Hatoko M, Ueda K. dermis-fat graft after parotidectomy to prevent Frey’s Syndromeand the concave deformity. Ann Plast Surg 1993;31:450–452.
17. MacKinnon C, Lovie M. An alternative treatment for FreySyndrome. Plast Recontr Surg 1999;103:745–746.
18. Allison GR, Rappaport I. Prevention of Frey’s Syndrome withsuperficial musculoaponeurotic system interposition. Am JSurg 1993;166:407–410.
19. Casler JD, Conley J. Sternocleidomastoid muscle transferand superficial musculoaponeurotic system plication in theprevention of Frey’s Syndrome. Laryngoscope 1991;101:95–100.
20. Sultan MR, Wider TM, Hugo NE. Frey’s Syndrome: preven-tion with temporoparietal fascial flap interposition. AnnPlast Surg 1995;34:292–297.
21. Laskawi R, Drobik C, Schonebeck C. Up-to-date report ofbotulinum toxin type A treatment in patients with gusta-tory sweating (Frey’s Syndrome). Laryngoscope 1998;108:381–384.
22. Linder TE, Huber A, Schmid S. Frey’s Syndrome after paroti-dectomy: a retrospective and prospective analysis. Laryn-goscope 1997;107:1496–1501.
23. Singleton GT, Cassisi NJ. Frey’s Syndrome: incidence relatedto skin flap thickness in parotidectomy. Laryngoscope1980;90:1636–1639.
Laryngoscope 111: November 2001 Govindaraj et al.: Frey’s Syndrome
1998