The spatial pattern of health facilities in Saudi Arabia: Development and planning
11
GeoJournal 25.4 423-433 1991 (Dec) by Kluwer Academic Publishers 423 The Spatial Pattern of Health Facilities in Saudi Arabia: Development and Planning Al-Kahtani, Mohammed M. Sh., Ass. Prof. Dr., King Saud University, Department of Geography, Abha Branch, PO Box 917, Abha, Saudi Arabia Introduction Developing health facilities has always been an important feature of the national development plans in Saudi Arabia, particularly since the launching of the Kingdom's first development plan in 1970. The main aim of this paper is to evaluate the pattern of regional distribution of health facilities in Saudi Arabia. The national policy objectives of health services have been to improve access to facilities and personnel by distributing them equally according to population and to eliminate the differences between rural and urban areas in health provision (Fourth Plan 1985). Thus, this paper attempts to determine how far these objectives have been accomplished and to identify the problems that may exist in the distribution of health facilities in various regions in the country. Therefore, an attempt is made in this paper to study this problem by examining and evaluating in some detail the existing pattern of health facilitiy provision in Saudi Arabia. By correlating various techniques, especially population/health facilities ratios, Chi-square test and standard deviations, it was possible to identify some of the problems of health service provision at the regional level. Because of this some important policy objectives have to be developed to improve the distribution of regional facilities in order to bridge the existing gap between regions. Geographical Setting The Kingdom of Saudi Arabia comprises about 80 % of the Arabian peninsula or a land area of about 2.15 million km 2. Geographically the Kingdom can be divided into six parts from west to east (Fig 1). The W coastal plains known as Tihama, along the Red Sea coast, runs from the N to the S, a distance of about 1,800 km. Its width varies from 40 to 80 kin. To the E of these plains are the western highlands which run parallel to the coastal plain and are broken here and there by a series of fertile valleys which allow for settlements between the mountains. In the Asir region in the S, the highest peaks rise to more than 3000 m and form the highest mountain in the country, but they are lower to about 1,200 m in the N. To the E of the mountains in the N is the northern steppeland which joins the Jordanian and Iraqi borders to the N. The Najd plateau lies-directly to the E of the mountains in the central part of the Kingdom, which has an averange elevation ranging from 600 to 1,200 m. The E lowland which lies east of the Najd plateau has an average height of about 300 m and declines down to the Arabian Gulf. This area includes all the major oil fields in the country. Finally, occupying the S part of the country is the Empty Quarter (AI Rub A1 Khali) a vast area of sand covering about 25 % of the total area of the country. This desert is virtually uninhabited.
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of The spatial pattern of health facilities in Saudi Arabia: Development and planning

GeoJournal 25.4 4 2 3 - 4 3 3
�9 1991 (Dec) by Kluwer Academic Publishers
423
The Spatial Pattern of Health Facilities in Saudi Arabia: Development and Planning
Al-Kahtani, Mohammed M. Sh., Ass. Prof. Dr., King Saud University, Department of Geography, Abha Branch, PO Box 917, Abha, Saudi Arabia
Introduction
Developing health facilities has always been an important feature of the national development plans in Saudi Arabia, particularly since the launching of the Kingdom's first development plan in 1970. The main aim of this paper is to evaluate the pattern of regional distribution of health facilities in Saudi Arabia. The national policy objectives of health services have been to improve access to facilities and personnel by distributing them equally according to population and to eliminate the differences between rural and urban areas in health provision (Fourth Plan 1985).
Thus, this paper attempts to determine how far these objectives have been accomplished and to identify the problems that may exist in the distribution of health facilities in various regions in the country.
Therefore, an attempt is made in this paper to study this problem by examining and evaluating in some detail the existing pattern of health facilitiy provision in Saudi Arabia. By correlating various techniques, especially population/health facilities ratios, Chi-square test and standard deviations, it was possible to identify some of the problems of health service provision at the regional level. Because of this some important policy objectives have to be developed to improve the distribution of regional facilities in order to bridge the existing gap between regions.
Geographical Setting
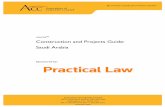
The Kingdom of Saudi Arabia comprises about 80 % of the Arabian peninsula or a land area of about 2.15 million km 2. Geographically the Kingdom can be divided into six parts from west to east (Fig 1). The W coastal plains known as Tihama, along the Red Sea coast, runs from the N to the S, a distance of about 1,800 km. Its width varies from 40 to 80 kin. To the E of these plains are the western highlands which run parallel to the coastal plain and are broken here and there by a series of fertile valleys which allow for settlements between the mountains. In the Asir region in the S, the highest peaks rise to more than 3000 m and form the highest mountain in the country, but they are lower to about 1,200 m in the N.
To the E of the mountains in the N is the northern steppeland which joins the Jordanian and Iraqi borders to the N. The Najd plateau lies-directly to the E of the mountains in the central part of the Kingdom, which has an averange elevation ranging from 600 to 1,200 m. The E lowland which lies east of the Najd plateau has an average height of about 300 m and declines down to the Arabian Gulf. This area includes all the major oil fields in the country. Finally, occupying the S part of the country is the Empty Quarter (AI Rub A1 Khali) a vast area of sand covering about 25 % of the total area of the country. This desert is virtually uninhabited.
424 GeoJournal 25.4/1991
Fig 1 Physical features of Saudi Arabia
Most of Saudi Arabia has a dry climate, except for the SW region. The N and central areas enjoy a more continental dry climate, hot in summer and cool in winter. All seasons are "dry, but an average rainfall of about 100 mm is recorded. On the coastal areas, humidity is higher and there is rather more rainfall, particularly in the SW. The mountainous areas in the SW enjoy a distinctly milder climate than the rest of the country, as well as more abundant rainfall of 250-500 ram.
Since Saudi Arabia has no overland free-flowing fresh water, the country has to depend on underground reservoirs for irrigation and other purposes. The Ministry of Agriculture and Water has recently developed another water resource by desalinating seawater to help meet the increased demand of industrial and urban areas. At present, Saudi Arabia leads the world in the amount of desalinated water with more than 500 million US gallons (1,908 million litres) per day in 1987 (Ministry of Planning 1989).
Because Saudi Arabia is geographically divided into several areas, each different in its climate, physical environment and way of life, each can be expected to display different common health problems. But there is
little information on common health problems in the country or differences that exist across the Kingdom's regions.
In general terms, malaria is a prevailing disease in Saudi Arabia particularly in the Tihama areas (Sebai 1987). In 1988 a total of 569,560 persons were examined for malaria, and a total of 7802 were found positive, 51% of them were found in Jizan region (Ministry of Health 1989).
Bilharzia is also endemic all over the country, especially in the Tihama and Central areas. During 1988 a total of 9422 cases of bilharzia were diagnosed in the Kingdom, 47 % of them were found in the SW part of the country. Leishmaniasis is also widespread in the country, especially in Baha, Asir, Riyadh, Gasim, Jawf and Eastern regions. According to the 1989 Annual Health Report of the Ministry of Health, 14,642 cases of contagious leishmaniasis were diagnosed in the Kingdom, about 29 % of them were reported in Eastern region.
Infectious diseases are still widespread in the country. During 1985 a total of 127, 932 infectious diseases were reported in the country, 31% of them were found in Jizan and Asir regions. In fact, the Ministry of Health has

GeoJournal 25.4/1991 425
Tab 1 Regional distribution of population in Saudi Arabia, 1988"
Health region Population % oftotat Area km 2
Medina Jizan Gasim Hail Tabuk Baha Najran Northern Frontier Jawf Qurrayyat National Total
949.944 77 140,868 6.7 7671706 6.2 15,517 49.5 598~93 4.8 53,922 tl, 1 �9 174,853 3.8 118,332 ~.0 362,387 2,9 95;202 3.8 368,435 3.0 101690 34.5 275,958 2.2 139.858 2.0 237,426 1.9 120,744 2.0 174,961 1.4 64,758 2.7 92,480 0.7 49,794 1.9
12.396.073 10010 2,156.753 5.7
given much attention to preventive medicine in recent years. By 1988 nine malaria stations and 27 substations were already established in the country. In 1988, there were also 14 bilharzia and 14 leishmaniasis stations in the Kingdom. All of these stations were created to carry out preventive health programmes to try to control the spread of these widespread diseases, and there efforts have paid off. A major immunization programme has also been conducted in the Kingdom. During 1988, a total of 5,418,985 vaccines were given by the hospitals and the health centres in the country. These included vaccines against poliomyelitis, measles, tuberculosis, tetanus, diphtheria and others.
Although, the efforts of the Ministry of Health have already shown success in controlling these diseases many of the peoples in the SW regions continue to be inflicted by one or more diseases.
Population
According to the most recent national census taken in 1974, the Kingdom of Saudi Arabia had a population of about 7 millions. About 47 % of the population lived in towns and cities with 5,000 inhabitants or more. About one quarter of the population is described as nomadic. About 28% (or about 2 millions) of the country's population are considered rural who are living in villages with less than 5,000 persons in 1974. However, estimates for 1988 put the figure at 12.4 millions giving rise to a 77 % increase during the 14 year period (Tab 1). This rapid growth of population is to be expected because of the high birth rate and the declining death rate as well as immigration. The population of Saudi Arabia is characterized by a large youthful element. Persons under 20 years of age constitute about 56% of the total population. This means that the authorities have to focus,
heavily in various public services, especially in education and health facilities.
The Kingdom's regions vary greatly in their respective area, population densities and the number of the inhabitants (Tab 1 shows some of these variations). The Makkah region is the most populated with about 26 % of the total population, followed by Riyadh region with 18%. The Eastern and Asir regions come in third and forth with 11% and 10% of the national population respectively. In fact, these four regions account for more than 65 % of the country's population.
Because over half of Saudi Arabia is occupied by desert and semi-desert, population densities are generally low. On the basis of the estimated population in 1988, overall density was only 5.7 persons per km 2. The Southwestern regions (Jizan, Baha and Asir) are the most densely populated regions (49.5/km 2, 34.5/km 2 and 16.3/ km 2) in the country. In fact, this greater density is almost entirely the result of a very large number of rural settlements rather than urban centres. These regions have more than 50% of the Kingdom's 10,365 villages (Ministry of Municipal and Rural Affairs 1984). The Makkah region is the third most densely populated region in the country, with an average density of about 24 persons per km 2. This higher density has resulted mainly from the large urban centres of Jeddah, Makkah and Tail which together account for about 32 % of the total urban population in the country (Al Shawl 1988). The average density in the orther regions is low because of their extensive desert areas, particularly in the E and N regions.
There have been major changes in the socio-economic structure and standard of living of the Kingdom's population in the last 15 years. One result of these changes is the substantial increase in urban population and a decline in the nomadic population. The urban population is estimated to have increased from 47% in

426 GeoJournal 25.4/1991
o
~ - - - Afar ",. .c'l " - ' - . \_.
WF ./ I . . ~ , "~ NORTHERN
_{ FRONTIER ' " - - . T . . . . .\
7--, ,, % eHal l " . . . t
i HAIL / - . I i . ~,
I " "" - t . aama % .< GAS~M_~' "F
! j
--'#,*-.,a " " % ' L NA , t " Riyadh
, "L~ r /~
�9 [
,.~ RIYADH
~IAKKAH / EASTERN PROVINCE kkah
~RA~/"' ", _, AS/R j . . . . . . . -~ ' J I ~,.
bha / / NAJRAN
:AIZAN ~'- ~ ""~ ,ao . -
J a i ~ n T ) ~ , . . . . . . . . . . . . . . . . . . . . "
J �9 . t . / ~
, , 3 0km k - - - -
g r o g i o n
i !
I I i I !
! . , I
, , . , . , / .
. s ' ' f f
S ea
Fig 2 Health regions of Saudi Arabia
1974 to more than 67% in 1987 (AI-Shawf 1988). The nomadic population had declined from 27 % in 1974 to less than 10% in 1985 (E1-Bushra 1989). In fact, the majority of the Kingdom's population lives either in the 102 towns or scattered among the 10,365 villages.
Health Facility D e v e l o p m e n t
In spite of the relatively early unification of Saudi Arabia in 1932, no coordinated national health programme was formulated until after the establishment of the Ministry of Health in 1950. Since then the Ministry became the main responsible and supervising body for the health service development in the country. The development of health facilities in Saudi Arabia occurred slowly until very recently due to the fact that the national economy was not of sufficient size to be able to support an effective health service provision.
All the facility and health infrastructures that were developed before the 1970's was confined on curative health care service through hospitals in the main urban centres, e.g. Riyadh, Makkah, Dammam and Jeddah. In
fact, the health facilities that were in existence before the 1970's were physically out of reach of the rural populations, which is to say that health facilities were not accessible to the majority of the Kingdom's inhabitants.
However, considerable improvement and expansion of the infrastructure of health facilities has occurred after the launching of the First National Development Plan in 1970, following the rapidly rising flow of oil revenues. Government revenues from oil have increased from just SR 4,936 million in 1970 to SR 312,819 million in 1980, an increase of 63 fold. This rapid increase has greatly enabled the Saudi government to implement ambitions development plans to develop the health facilities both in quantity and quality.
The Kingdom has successfully implemented four five- year plans of socio-economic development (1970-1990), and the Fifth Plan (1990-1995) is already through implementation period. All these plans have emphasized the importance of health services in the socio-economic development of the country. For example, the main objective for the nation's health development in the Fourth Plan (1985-1990) was: "The provision of high quality health services and facilities in all regions of the

GeoJoumal 25.4/1991 427
Tab 2 The development of health facilities in Saudi Arabia over the period 1970-1988
Kingdom, so that the population can have access to the required health care services" (p. 61).
The Saudi government has allocated a vast amount of money to health service provisions during the implementation of the National Development Plans in line with the government policy objective to make health facilities accessible to all population free of charge. In the First Development Plan (1970-1975), the financial allocation for the Ministry of Health was SR 1,297 million or 3.1% of public sector investment under the Plan. However, the allocation for health services increased to SR 43,593 million under the Third Plan (1980-1985), an increase of 30 folds, representing about 6 % of the public sector investment under the Plan. In fact, the health service provision continues to be a high priority in the Fourth Plan (1985-1990), receiving the second highest single allocation of SR 62,239 million.
Tab 2 shows the remarkable improvement and expansion of health facilities in Saudi Arabia during the period 1970-1988. The table shows that the number of hospitals increased from only 74 in 1970 to 248 in 1988 and the number of beds in these hospitals increased from 9,039 in 1970 to 38,848 in 1988, an increase of 329.8 %. The number of health centres rose from 519 in 1970 to 2,087 in 1988. Large increases occurred in the number of medical staff. For instance, the number of physicians rose from 1,172 in 1970 to 21,144 in 1988, an increase of 17 fold. The number of nursing staff increased from 3,261 in 1970 to 43,963 in 1988, an increase of 12 fold.
As a result of these impressive rates of growth the infant mortality rate per 1000 live births dropped from 148 in 1965 to 61 in 1985. The average life expectancy for males increased from 47 years in 1965 to 60 years in 1985, and for females increased from 50 years in 1965 to 64 in 1985 (Ministry of Planning 1989). The physician population ratio improved from 1 : 4, 266 in 1970 to 1 : 586 in 1988. Also, the ratio of population per bed improved from 1:553 in 1970 to 1:319 in 1988, although not all of these were Ministry of Health facilities.
The provision of public health services in Saudi Arabia is the main responsibility of the Ministry of Health which provides the majority of health facilities in the country. However, a total of 13 other government agencies, in addition to the private sector, offer health services for their employees and segments of the general population. These other agencies include the military, the Red Crescent society, School health units and the Universities Medical Schools. The distribution of health facilities by sector is shown in Tab 3. It can be seen that the most important provider is the Health Ministry which provides 63 % of hospitals, 68 % of hospital beds, 71% of health centres, 56 % of physicians and 62 % of nursing staff. The other public agencies is the second largest provider of health facilities which provide about 17 % of the total hospital beds in the country, 20 % of physicians and 21% of nursing staff. Another significant provider of health facilities is the private sector. This sector plays an important role and has rapidly expanded in the last few
Tab 3 The distribution of health facilities by sector, 1988
Sector Hospitals Hospital beds No. % No. %
Ministry of Health 162 65.3 26.315 67.8 Private sector 55 22.2 5.956 15.3 Other public agencies 3] 12.4 5.577 16.9 National total 248 100.0 38.848 100.0
Sources: Ministry of Health (1989)o Annual Health Report, 1988, Riyadh
Physicians Nursingstaff Health centres No. % No % No. %
11.940 56.4 27.169 61.8 1.477 70.8 4.990 23.6 7.594 17.3 313 15.0 4.214 20.0 9.200 20.9 297 14.2
21.144 100.0 43.963 100.0 2 .087 100.0
428 GeoJournal 25.4/1991
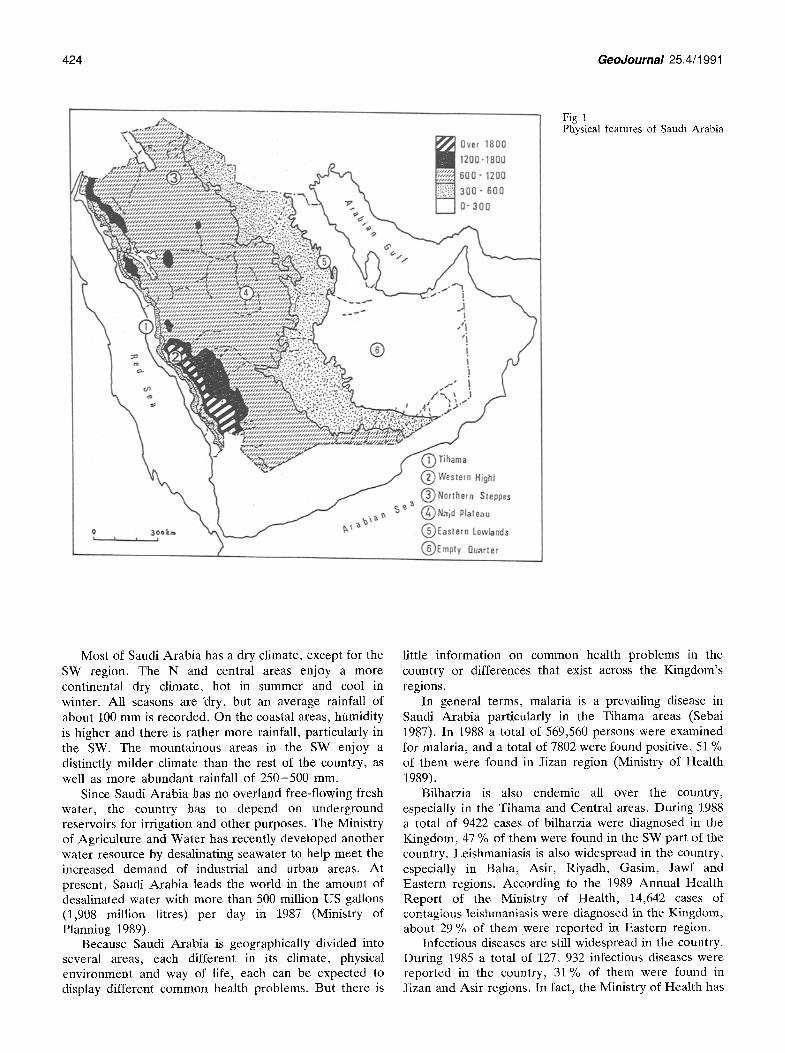
Tab 4 Regional distribution of health facilities in Saudi Arabia, 1988
Regional Distribution of Health Facilities
Before discussing the regional pattern of health facilities in Saudi Arabia, it is important to mention that the regional health data used in this paper are the official figures for the Ministry of Health and the private sector. Detailed data for the other public agencies are not available at the regional level so that this sector has been excluded from the following discussion.
The distribution of health facilities is based mainly on Regional Health Areas which coincided with the provincial divisions of the Ministry of Interior, and so these administrative units will be the spatial framework for much of the discussion that follows. There are 14
years as a result of the considerable government subsidies, such as interest-free 20 year loans for up to 50 % of the total cost of any private health project. This sector provides 22 % of hospitals, 15 % of hospital beds, 24 % of physicians and 17 % of the nursing staff.
With so many different agencies providing health care services in the country, the responsibility for equitable distribution of health facilities between the various regions of the country and between rural and urban areas rests on the Ministry of Health. Therefore, the main regional goal of the Ministry of Health is to provide the population in every region with a fully integrated and comprehensive system of free health facilities (Ministry of Health 1987).
Tab 5 Regional distribution of health service personnel and bed per population, 1988"

GeoJournal 25.4/1991 429
Fig 3 Population and health facilities by region (1988)
Health Regions in the Kingdom (Fig 2 and Tab 1) and they vary in areal size from 10,690 to 778,478 km 2 and in population, from 92,480 persons to 3,189,942 persons. These variations are also reflected in variations in the distribution of health services.
As mentioned earlier, great improvement and expansion of health facilities have occurred during the implementation of the national development plans. However, these facilities are unequally distributed across the regions of the country. Tab 4 shows the regional distribution of health facilities under the authority of the Ministry of Health and the private sector. It indicates the extent to which the health services are unevenly provided. On most indicators including number of hospitals, hospital beds, physicians, nurses and health centres, the Makkah, Riyadh and Eastern regions enjoy a greater share of facilities and staff than the other regions. Together the Makkah, Riyadh and Eastern regions with 55 % of the country's population have 64 % of physicians and 62% of nursing staff. The concentration of health facilities along this axis of population distribution has been particularly emphasised because of urban primacy in these regions. Together
these regions have more than 71% of the total urban population in the country in 1987 (Al-Shawaf 1988).
In Makkah region, the most populated region in the country, religion has played a major role in the growth of the holy city of Makkah, while Jeddah has acted as the main commercial centre of this important region and Tail is the main summer resort. It is because of these functions that the government has made a special effort to expand health facilities in Makkah region. Riyadh region has become the focus of various expansive urbanization projects, especially metropolitan Riyadh, the capital city, which has come to exert a powerful pull on health as well as other facilities and activities that need to be at the centre of decision making body. In the Eastern region the growth of the oil industry has been responsible for the development of health facilities which resulted in high standard of health services.
Asir region with a population of 1,349,147 (10.3 %), is the fourth largest in population size, yet it has only 8 % of the total hospitals in the country, 6 % of hospital beds, 7 % of physicians and 8 % of nursing staff. Jizan region is by far the largest in population density and the 6th largest in population size, but it merely has 5 % of total

4 3 0 GeoJoumal 2 5 . 4 / 1 9 9 1
. .s"'/
, , :3~o k., , A~ a~ian
% x.,
J/N ~
Se a
~ +2 SD (3.5)
~ +1 S0(2.9) 2.6 Average ~ - 1 sD (2,3)
[~ - 2 SD ( 1 . 6 )
Fig 4 Standard deviations for hospital beds (per 10013 population), i988
hospitals, 4 % of hospital beds, 5 % of physicians and 5 % of nursing staff. Gasim region with a population of about 600,000 (5%), has as much as Asir region's share of health facilities.
It is obvious from a close examination of Tab 4 and Fig 3 that there are discrepancies between the distribution of population and the distribution of health facilities. Also it appears that those regions that have a few hospital facilities seem to have many more lower order health facilities like health centres. For instance, Asir region has only 8 % of the total hospitals in the country but has more than 13% of the total health centres. This is largely due to the fact that those regions have a greater proportion of rural population which is difficult to serve with hospital facilities. Even though health centres still play quite a minor role in health provision.
A Chi-square test (X 2) on the regional distribution of health facilities was used (Shaw and Wheeler 1985). The results for X 2 test (Tab 4) confirm clearly the real differences between the various regions in the provision of health services. These differences are statistically significant at the 95 % confidence level so that regional
variations in medical services could not be explained by chance distribution.
These inequalities in the regional distribution of health facilities imply considerable differences in the quality of health facilities provided by different types of hospitals and health centres. Generally, it is believed that the hospitals and health centres found in the major urban centres of Riyadh, Makkah and the Dammam-Dhahran- Khubar conurbation are much larger and better equipped and better staffed compared with those in small towns and villages in Asir or Hail region.
The unevenness of the regional distribution of health facilities is further aggravated by the fact that many major health services of other public agencies in the country which are not under the authority of the Ministry of Health are mostly found in the major urban centres of Makkah, Riyadh and the towns of the Eastern region (A1-Kahtani 1988). They include facilities such as King FaisaI Specialist Hospital (459 beds), the King Khaled Specialist Eye Hospital (263 beds), the various hospitals of the Ministry of Defense (794 beds), the National Guard Hospital (273 beds) and the National Security Hospital (120 beds), all in Riyadh City. Also, in Riyadh

GeoJournal 25.4/1991 431
Fig 5 Standard deviations for physicians (per 1000 population), 1988
U~
OL~ 300km m , �9
D ('X~~
. ~ g
,f~Hf/(t,.
+2sa 11.91
~ + l S O {1.6) 1,4 Average ~ -ls0 (1.2)
~T-'~ -2SD (0.9)
there are two university hospitals with a capacity of 738 beds. In Makkah region there are six hospitals with a capacity of 1,112 beds. In fact, these hospitals are much larger and more sophisticated and better staffed than the hospitals of the Ministry of Health.
The ratios of medical staff and bed to population as shown in Tab 5 is a further proof of the regional variations in the quality of health service provision. Ratios of population per doctor of 1:732 and per bed of 1:384 and per nursing person of 1:357 for the whole country are indicative of a well-developed health facility compared to the situation in many developing countries. However, a close look at the situation at the regional level reveals that some regions are much better served than others. The table shows that the population in the Eastern province, Makkah, Riyadh and Gasim regions are much better served by health facilities than the other regions. The ratios for these regions are much better than the national average. The least served regions are, in fact, the predominantly rural regions like Hail, Asir, Tabuk and Jizan. These regions have ratios of population per physician of over 1 : 1000 and ratios of population per bed of over 1:500. It must also be pointed out however,
that these ratios are for large regions within which the rural areas will be much less served than the urban areas.
Some smaller regions like Baha and Jawf have more favourable ratios of population per bed, but come out unfavourable with the ratios of medical staff, particularly with the ratios of population per physician. The reason for this is the fact that some hospitals in these regions are newly established and numbers of beds are not used because of staff shortages. It is important to note that, one of the biggest problems facing the health service provision in Saudi Arabia is the near total reliance on expatriate medical staff. In 1988 only 7 % of physicians and about 8 % of nurses working with the Ministry of Health and the private sector were Saudis.
By using standard deviation it was possible to show clearly the marked variations between the different regions of the country in the standard of health facilities. The technique of standard score is calculated for each region so as to bring into focus the distribution of medical services in terms of standard deviations about the national average (Shaw and Wheeler 1985; and Levin 1978). The present study recognizes four levels of health facility provision. According to this study the standard of

432 GeoJournal 25,4/1991
U~
% oj"~ ,'t
OL I I 5ookm ~ x ~ \'~x
~ + 2 S D ~ 4 . 3 ,
~ + lSO (3.0) 2.8 Average ~ -lSO ~3.4)
~ - SO (1.6~
Fig 6 Standard deviations for nursing (per 1000 population), 1988
health services is considered "very good" if value is equal to +2 standard deviations away from the national average, "good" if value is equal to +1 standard deviation, "poor" if value is equal to - 1 standard deviation, and "very poor" if value is equal to - 2 standard deviation. The results for the regional distribution of hospital beds are shown in Fig 4 while the distribution of physicians and nurses are given in Fig 5 and 6.
It is interesting to see that these results for standard deviations confirm clearly the large regional inequality in the provision of health facilities. As is evident in Fig 4, 5 and 6, the Eastern region has the most advanced health facilities in Saudi Arabia. The standard of health facilities is considered good in four regions, namely, the Makkah, Riyadh, Gasim and Baha regions of which the standard is higher than the national average. The standard of health facilities is deemed poor in Qurayyat, Medina, Najran and Northern Frontier regions where health facilities fall short of the national average. In the regions of Hail, Asir, Tabuk, and Jizan, the standard of health facilities is considered very poor which is much lower than the national average (E1-Bushra 1989).
From the foregoing account, it is obvious that the spatial provision of health facilities in Saudi Arabia apparently follows an economic orientation. The best facilities are located in regions where economic and administrative power or opportunities lie. Within the large urban areas of the Eastern, Riyadh and Makkah regions, a spatial "hierarchy" of institutions is found from isolated private c l in ics to publicly administered large hospitals. In contrast the SW (Asir, Jizan and Najran) and N (Hail, Jawf, Tabuk, Qurayyat and Northern Frontier) regions are less developed economically and have the lowest levels of urbanization and are, therefore, receiving poor publicly owned and administered health facilities.
Conclusion
This study has shown that substantial progress in the provision of health care services in Saudi Arabia has been made during the last two decades. However, one aspect

Geodoumal 25.4/1991 433
of Saudi's health development that has not been seriously considered is lack of equitable distribution of health facilities. In spite of the stated policy objective of improving access for all population sectors, the distribution is still skewed in favour of the urban regions. This is a legacy from the launching of the country's First Development Plan in the early 1970's. The great achievements of health development plans were in terms of quantitative increases in facilities and medical personnel, but regional coverage has not improved significantly.
The study of standard deviations has shown that the Eastern, Riyadh, Makkah and Gasim regions enjoy superior health facilities, whereas the SW and N regions are grossly underprovided. It is, therefore, recommended in this study that more attention should be devoted to develop health facilities in those lagging regions (E1- Bushra 1989). The rural-urban imbalance can be reduced by investing more in the rural health centres and by locating small hospitals in strategic village clusters that can maximize the accessibility of rural populations to health facilities.
I t is obvious that one of the basic problems of Saudi health care delivery system is the fragmentation of the administration of health services into several different agencies. There is, therefore, an urgent need for better cooperation and coordination between these various agencies in the regional development of health facilities. Another common weakness of health service provision is the near total reliance on expatriate medical personnel. This problem can be rectified by encouraging more Saudis to train in the medical profession. Another weakness of Saudi health care delivery system is the poor quality of the regional health data. Adequate data are essential both for identifying the regional health needs and for their subsequent analysis and planning. It is therefore important for the Ministry of Health to develop a wide range of spatial health data base as a first requirement of more accurate future of regional health development plans. Finally health service development in Saudi Arabia should be warranted not only in terms of health condition improvement, but also, in terms of the critical role of health in social and economic development projects.
References
A1-Kahtani, M.M.: Regional Development Planning in Saudi Arabia: An Evaluation of Public Service Provision in Asir Region. Unpublished PhD Thesis, Southampton University, England 1988.
A1-Shawaf, S.A.: Population and Urban Development Planning in Saudi Arabia (in Arabic). A1-Baladiyat 166, 42-59 (1988)
Daniels, P.W.: Some Perspective on the Geography of Services. Progress in Human Geography 13, 427-437 (1989)
Drury, P.: Some Spatial Aspects of Health Service Development: The British Experience. Progress in Human Geography 7, 60, 77 (1983)
E1-Bushra, EI-Sayed: Health Care Pattern and Planning in Saudi Arabia. GeoJournal 18, 4, 361-368 (1989)
Levin, R.I.: Statistics for Management. Prentice-Hall, Inc., Englewood Cliffs 1978.
Ministry of Health: Annual Health Report, 1988 (in Arabic). Riyadh, Saudi Arabia 1989.
Ministry of Health: Annual Health Report, 1985 (in Arabic). Riyadh, Saudi Arabia 1986.
Ministry of Health: Features of Health Care Development. Tihama, Jeddah, Saudi Arabia 1987.
Ministry of Municipal and Rural Affairs: Socio-economic Survey of Villages and Hijar in the Kingdom: General Report. Riyadh, Saudi Arabia 1984.
Ministry of Planning: The Second Development Plan, 1975-1980. Dar Okaz, Jeddah, Saudi Arabia 1976.
Ministry of Planning: The Third Development Plan, 1980-1985. Riyadh, Saudi Arabia 1980.
Ministry of Planning! The Fourth Development Plan, 1985-1990. Riyadh, Sandi Arabia 1985.
Ministry of Planning: Achievements of the Development Plans, 1970-1986. Facts and Figures. Riyadh, Saudi Arabia 1987.
Ministry of Planning: Achievements of the Development Plans, 1970-1987 (in Arabic). Riyadh, Saudi Arabia 1989.
Ministry of Planning: The Fifth Development Plan, 1990-1995. Riyadh, Saudi Arabia 1990.
Odone, T.: Saudi Arabia. The Middle East Review 14, 140-152 (1988)
Okafor, S.I.: Policy and Practice: The Case of Medical Facilities in Nigeria. Social Science and Medicine 16, 1971-1977 (1982)
Sebai, Z.A.: Health in Saudi Arabia, Volume Two. King Abdul Aziz City for Science and Technology, Riyadh, Saudi Arabia 1987.
Shaw, G.; Wheeler, D.: Statistical Techniques in Geographical Analysis. John Wiley and Sons, Chichester 1985.
Siddiqi, A.H.: Health Care Resources and Public Policy in Pakistan. Social Science and Medicine 14d, 291-298 (1980)
Whitelegg, J.: Inequalities in Health Care: Problems of Access and Provision. Straw and Barnes, Retford 1982