The Relationship Between Fhysical Function ing and Mood State ...
90
The Relationship Between Fhysical Function ing and Mood State in Fersons with Cancer by Wendy W. Crabbe THESIS Submitted in partial satisfaction of the requirements for the degree of MºSTER OF SCIENCE in NURSING in the GRADUATE DIVISION Of the UNIVERSITY OF CALI FORNIA San Francisco
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of The Relationship Between Fhysical Function ing and Mood State ...
The Relationship Between Fhysical Function ing and Mood State
in Fersons with Cancer
by
Wendy W. Crabbe
THESIS
Submitted in partial satisfaction of the requirements for
the degree of
MºSTER OF SCIENCE
in
NURSING
in the
GRADUATE DIVISION
Of the
UNIVERSITY OF CALI FORNIA
San Francisco
copyright (1992)
by
Wendy W. Crabbe
ii
Acknowl edgements
I would like to thank my husband Matt for re-doing my
tables and for his unfail ing love and support , and to my
son, Christopher for my inspiration . I would al sc l i ke to
thank my mother Sharon for her typing skills, love , and
support , and my friends Jeff and Mary for their computer in
my time of need .
Thanks also go to Drs. Fatricia Larson , Christine
Mi ask owsk: i , and Suzanne Dibble for their many hours of
expertise and support. Special thanks go to Dr. Maryl in
Dodd for the use of the data from the NCI funded study
"Self-Care to Decrease Chemotherapy Morbidity".
iii
The Relationship Between Physical Function ing and Mood State
in Fersons with Cancer by Wendy W. Crabbe
Abstract
The in it i at ion of chemotherapy of ten causes a literationsin physical and emotional health ; which places the burden ofmanaging the effects of chemotherapy on the patient at home ,on their own . The purpose of this study was to determinethe relationship between physical function in g and mood stateof cancer patients receiving four consecutive cycles ofchemotherapy. The larger study, where the data weregenerated by Lodd et al . ( 1988) Lised the Stress and Cop ingtheory of Lazarus & Fol k man ( 1984) as back ground to assessthe experience of chemotherapy related treatment morb 1 d 1 tyin persons with cancer. The conceptual framework for thisreport focuses on how physical function ing and mood stateare related to the way individual s eval uate and cope withthe stresses of ill ness and of everyday l l ving . Themajority of the participants (N = 1.27) were caucasian (89%) ,middle-aged (mean age of 52) , female (68.5%) ,married/partnered (61%) , with two years of collegeeducation . The most common cancer diagnosis was breastcancer (42.5%) , foll owed by lung cancer (15%) . Fhysicalfunction ing was measured using the Karnofsky FerformanceScore (KF5) and Fhysical Health Status (FHS) duest icnnaires.Higher scores indicate better physical function ing. Moodstate was measured L1s ing the Frofile of Mood States (FON15) -Higher scores of the FOMS subscales reflected more anger ,depression , f at i gue , and mood disturbance . All threeinstruments were administered as self-report questionnairesbefore chemotherapy was in it i ated (T 1) , and every cycle(T2-T4) for four months. The relationship between KFS , FHS,and FOMS were tested using Fearson 's Correl at i conCoefficients. Sign if i cant correl at 1 ons were found betweenK.FS and Total Mood List Lurbance (TMD) and between FHS and TMDat all four cycles, indicating that a decreased abil it y tofunction physical 1 y was associated with greater mooddisturbance. Fatigue, Vigor, and TMD were highly correl atedwith KFS and FHS at all 4 cycles of chemotherapy. ResultsOf this study emphasize the need for health professional s,especial 1 y nurses to make ongoing assessments of physicalfunction ing and mood state of patients receivingchemotherapy. Further research is needed to determine thespecific factors that contribute to alterations in physicalf Lunction in g and mood state .
iv.
Chapter I :
Chapter II :
Chapter I I I :
Chapter IV:
Ühapter V:
Chapter VI :
Table c + Contents
Introduct i On to the Froblem
Purpose
Assumptions
Lief in it i on cyf Terms
Concept Llal Framework
Literature Review
Fhysical Function ing and Mood State
Functional Status and Performance
Modd State
Methods
Research Iles ign
Sample
Research Setting
Instruments
Frocedures
Data Analysis
Results
Sample Lemographics
St Ludy Furpose 1
Study Furpose 2
Study Furpose 3
L. 1 scussion
Sign if i cance
Limitations
Impl i cat i Ons for Fract ice
2
33
36
37
Table of Contents ( continued )
References
Tables 1
through 7
Figures 1
through 1 Q
Appendix A Demographic Questionnaire
Appendix B Karnofsky Ferformance Score
Appendix C Fhysical Health Status Questionnaire
Appendix II Frofil e Of Mood State
E -,--|--
71
*,*-
.
;
vi
Table
Table
Table
Table
TAble
Table
Table
2
5
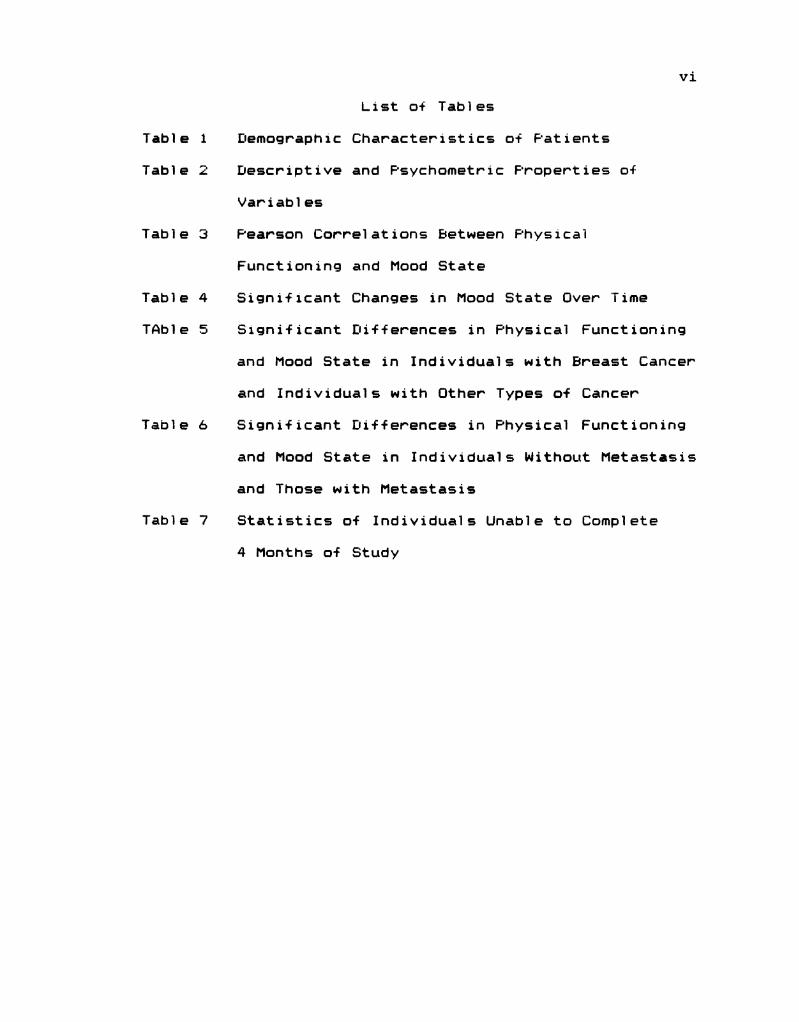
List of Tables
Demographic Characteristics of Fatients
Lescriptive and F'sychometric Froperties of
Variables
Fearson Correl at icºn's Between Physical
Function in g and Mood State
Sign i + 1 cant Changes in Mood State Over Time
Sign if i cant [.. if + erences in Fhysical Function ing
and Mood State in Individual s with Breast Cancer
and Individuals with Other Types of Cancer
Significant Differences in Physical Function ing
and Mood State in Individual s Without Metast as is
and Those with Metastasis
Statistics of Individual s Unable to Complete
4 Months of Study
vii
Figure
Figure
Figure
Figure
Figure
Figure
Figure
Figure
Figure
Figure
2
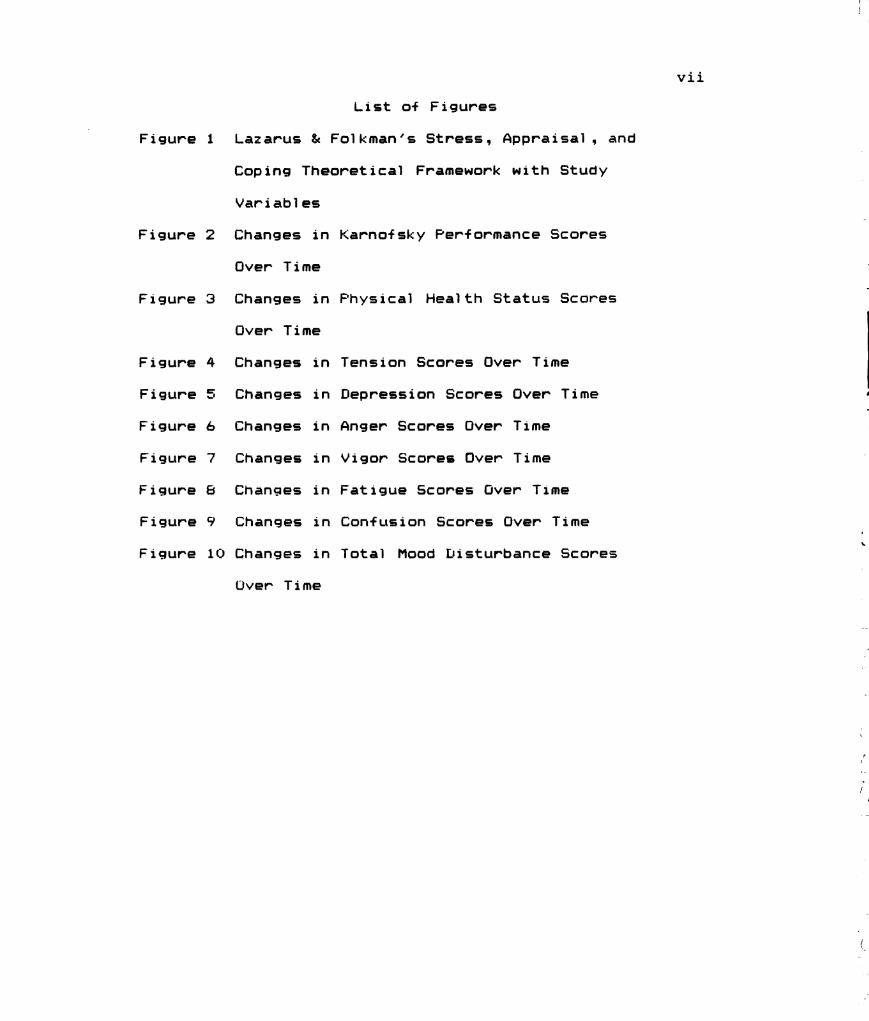
List of Figures
Lazarus & Folk man 's Stress, Appraisal , and
Coping Theoretical Framework with Study
Variables
Changes in
Over Time
Changes in
Over Time
Changes
Changes
Ühanges
Changes
Changes
Changes
Changes
in
in
in
in
in
in
in
Üver Time
Karnofsky Performance Scores
Fhysical Health Status Scores
Tension Scores Over Time
Depression Scores Over Time
Anger Scores Over Time
Vigor Scores Over Time
Fat i gue Scores Uver T 1 ■ he
Confusion Scores Over Time
Total Mood Listurbance Scores
|
.
-
2
Chapter I : Introduction to the Froblem
Many new antineoplastic drugs have been devel oped in
the last decade. As a result, many types of cancer can be
cured or control led with the administration of chemotherapy.
It is recognized cl i ni call y that the in it i at 1 on of
chemotherapy chal lenges the patient physica i l y and
emotional l y. However, the relationship between physical
function ing and emotional status of persons undergoing
chemotherapy has not been empirical l y described .
The physical health of persons undergoing chemotherapy
for their cancer is chal lenged by repeated episodes of
nausea, vomiting , and weakness, which can lead to major
disruptions in performance and functional capabil it i es at
work or at home (Schag, Heinrich , & Ganz , 1783; Freidenbergs
et al . , 1781-82; and Meyerowitz, Sparks, & Spears, 1777) .
Even though the Karnofsky Ferformance Score (KFS) is
frequently assessed by physicians during the course of
chemotherapy, l itt i e i = written about the specific changes
in physical function ing associated with treatment , and the
impact of these changes on the patient (Schag, Heinrich , &
Ganz , 1783; and Fre idenbergs et al . , 1981-82).
In add it i con 1 ittle is known about the effect
chemotherapy has cyn the emotional status of an individual .
Mood is one indi cat cor of an individual 's emotional status .
Mood changes could affect an individual 's ability to
function or v i sa versa, but the exact nature of this
rel at i onship is unclear . Depending on the patient 's
perception of the severity of the physical and emotional
effects of chemotherapy, patients may exhib it ineffective
coping behaviors, which may interfere with the treatment
plan and support from others (Mages & Mendol sohn , 1777 ;
Holmes, 1789; Love, Leventhal , Easterling , & Nerenz , 1989) .
Purpose
1. The primary purpose of this study was to determine the
rel at ionship between physical function i ng and mood state of
cancer patients receiving four consecutive cycles of
chemotherapy.
2. A second purpose was to determine if a relationship
existed between the demographic variable ( i.e. , age) and
physical function ing and mood state.
3. A third purpose was to determine if there was a
difference in physical f Lunction ing and mood state between
individual s with breast cancer and those with other types of
cancer ; between men and women ; and between individual s with
no evidence of metast as is and those with evidence of
metast as is .
fassumption=
The Lunderlying assumptions used in this study were as
+ C) l l ows :
1 . The experience of receiving chemotherapy is stressful to
the cancer patient , especial l y as reflected by the
individual ‘s perception of their physical + Lunction in G and
mood state during the + our cycles of chemotherapy.
2. A component of physical health includes phys 1 cal
function i ng of an individual .
3. A component of emotional health is mood state .
4. Cognitive appraisal of the person toward his/her cancer
and its treatment can affect the individual ‘s perception of
physical function ing and mood state. Fhysical function ing
and mood are related to the way individual 5 evaluate and
cope with the stresses of ill ness and everyday living
(Lazarus & Folk man, 1984) .
Lief in it i Cºn D+ Terms
1 . Fhysical function i ng - is defined as performance and
functional status, or one 's abil it y to take care of onesel f ,
or perform in the multiple role capacities at work or at
home, as measured by the Karnofsky Performance Score (KFS)
and the Fhysical Health Status Quest i connaire (FHS)
(Karnofsky & Burchenal , 1947; and Stewart, Ware, Brook: , &
Davies-Avery, 1978) . Fhysical function i ng also refers to
the patient 's ability to carry out normal activities such as
driving , walk i ng , bending , c 1 imb in g stairs, bath in g : eat in g .
dress l ng , and to il et . (Schag , Heinrich , & Ganz , 1984; and
Stewart, Ware, Brook: , & Davies–Avery, 1778) .
2 . Mood state - is the psychol og i cal traits and reactions
an individual has to a situation (Gottschal k. , 1784) , as
measured by the Frofile of Mood State (FDMS) (McNair, Lorr,
& Dropp 1 eman, 1971 ) .
3. Cancer - is uncontrol led cell proliferation which , when
left untreated , can be fatal (Holl eb , 1786) .
5
4. Metastasis - patients with documented evidence of
metastatic disease ; and with breast cancer patients,
evidence of one or more positive lymph nodes.
5. Four consecutive cycles of chemotherapy - In it i at i on of
chemotherapy is cycle 1 (Time 1 ) , the second cycle begins
approximately one month or 4 weeks after the first cycle
(Time 2) through the fourth cycle (Time 4) .
Chapter II : Conceptual Framework.
The theoretical framework for this study was guided by
the larger study (Dodd et al . , 1988) which used the stress,
coping , and adaptation theory of Lazarus & Folk man ( 1984) .
Coping is defined as "constantly changing cognitive and
behavioral efforts that are appraised as tax i ng or exceeding
the resources of the person" (Lazarus & Folkman, 1984, p.
141 ) . The importance of the cognitive process of appraisal
is to distinguish a potential l y stressful / harmful situation ,
such as the changes in physical function ing and mood state
as a result of chemotherapy, from potentially beneficial or
irrel evant stimul i . The presumed stressful stimul Lus in this
study is the chemotherapy experience.
Appraisal processes are also influenced by the
characteristics of the individual . The characteristics of
the individual of interest in this study were the perceived
physical function ing and mood state of the person during the
cancer chemotherapy experience . How a person appraises and
copes with the stressful situation of chemotherapy can be
influenced by physical function ing and mood state.
Lazarus & Folk man ( 1984) proposed that a person who
appraises a situation as a chal lenge may have a higher level
of physical function ing and a different physic] og i cal stress
response, than the person who appraises a situation as a
threat . Fhysical function ing has been reported to change
during chemotherapy treatment (Schag, Heinrich , & Ganz ,
1984; Fre idenbergs et al., 1981-82; and Meyerowitz , Sparks,
7
& Spears, 1%.7%) . Cl in i cally it is known that an individual
may devel op chemotherapy-induced nausea, vomiting , and/or
diarrhea that makes them so weak , they may need assistance
to use the commode; or may require them to take time off
from work ; or require them to seek assistance with household
activities and child care.
Chall enge appraisal s are also characterized by positive
emotions such as eagerness, excitement , and better mood. In
contrast , threat appraisal is characterized by negative
emotions such as anxiety, fear , and anger (Lazarus &
Folk man , 1984) . Fatients receiving outpatient chemotherapy
usual l y devel op and manage the side effects from their
chemotherapy at home. The chemotherapy treatment regimen
occurs over cycles, usual l y every four weeks for 4 to 6
months. Cl in i call y and from a study by Lodd et al . . ( 1990 ) ,
it is recognized that the first four cycles of therapy are
crial l enging . The emotional react i cºn to this stress may
el ic it feel ings of anxiety, depression , f at i gue , confusion ,
and mood changes. The patient has to appraise the stressful
situation and determine whether the situation presents as
harmful , a threat , or a chal lenge. The variables and time
points of interest in this study are presented in Figure 1 .
The cut come of this appraisal process impacts on the
patient 's physical function ing and mood state. For example,
if the individual appraises the side effects of chemotherapy
or even the chemotherapy itsel f as harmful , they may decide
not to continue with the chemotherapy treatments. This
B
decision could result in disease progression , which impacts
the patient physical l y and emotional l y. Fhysical ly, the
individual may experience more discomfort and l Cse their
ability to function as they move from an active treatment
state to the terminal stage of the ill ness. Emotional ly,
the person may become anxious , depressed , or confused about
his/her decision and situation , which may impact on his/her
Qual it y of 1 if e.
On the other hand , l if the person appraises chemotherapy
and the resultant side effects as a chal lenge , the person
will seek out as much informat i cri as possible and en l ist the
help of others to help manage the side effects (Lazarus &
Folk man, 1784) . If the individual is vomiting in excess,
s/he may try to manage on his/her own symptoms in it i al ly,
and if not successful may call the physician for more
effective relief . If successful , the individual 's
performance, functional status, and mood will increase to an
acceptable level . The person may then feel less anxious and
depressed because they are taking control of the situation.
In conclusion , the appraisal of a situation as
stressful and cop in g efforts to deal with this stress are
influenced by the interrel at i on ship between the person and
the environment or situation (Lazarus, Dunkel –Schettor,
Del ong is , & Gruen, 1986) . Fhysical function ing and mood
(positive and negative feel ings ) are related to the way
individual s eval uate and cope with the stresses of ill ness
and of everyday living (Lazarus & Folk man , 1984) .
Chapter I I I : Literature Review
This review emphasizes studies that eval uated physical
function ing and mood state of cancer patients using the
Karnofsky Performance Score (KFS) , the Fhysical Health
Status Questionnaire (FHS) , and the Profile of Mood States
(FDMS) . Research on physical function ing and mood state in
cancer patients have examined relationships between disease
status, age , depression , self-care abil it i es , and survival .
Few studies have directly eval uated the relationship between
the physical and emotional status of cancer patients
receiving chemotherapy. Only one study focused specifical ly
on both the physical function ing and mood state of cancer
patients (Cell a , Drofilamma , & Holl and , et al . , 1787) .
However , all the studies reported on here include some
measure of either physical function ing or emotional status.
Physical Functioning and Mood state
The studies reviewed in this section examined the
relationship between disease, treatment, physical
function ing, adjustment, and psychol og 1 cal distress referred
to as mood in this study. The relationship between extent
of disease, performance status, and psychol og ical distress
was studied in lung cancer patients receiving chemotherapy
for limited (n = 304) versus extensive disease (n = 151 )
(Cell a , Drofiamma, & Holl and , et al., 1987) . Ferformance
status (ECOG scale) was measured using a 5-point scale (C) =
no impairment to 4 = bedridden) . Fsychol og ical distress was
assessed Lising the Frofile of Mood States (FDMS) - Based on
1 (I)
correl at i on and regression anal yses, the data from th l =
study suggest that patients with more extensive d 1 sease and
poorer performance status had increased mood disturbance
(overal l regression , p < .. QQ1 ) .
In addition , age , marital status, gender , and education
were also tested as predictor variables of psychol cq i cal
distress. Only female gender and decreased performance
status had a sign if i cant association with Total Mood
Listurbance (TMD) scores as measured by the FOMS, indicating
that women with a poorer performance status had greater mood
disturbance . Fearson correl at i Ons where done between
Ferformance Status Rat in g (FSR) and the 7 variables Cyf the
FUMS. All correl at ions were sign if i cant , but in the low
range : FSR to tension ( . 17) ; FSR to depression ( . 14) ; FSR
to anger ( .. Q6) ; FSR to vigor (- .34) ; FSR to fatigue (.35) ;
FSR to confusion (.25) ; and FSR to TMD ( .26) (Cell a ,
Ordif i amma , & Holl and , et al . , 1987) . No p values were
reported .
The role of i l l ness and treatment-related Factors as
predictors of psychosocial adjustment was evaluated in 78
breast cancer outpatients ( Tayl or , Lichtman , Wood, Bluming ,
Losik , & Leibowitz , 1985) . I l l ness and treatment-related
factors assessed included physical dysfunction , prognosis,
type of surgery, radiation , and chemotherapy. The FON15 .
Rosenberg Self-Esteem score , Campbe il , Converse, & Rodgers
Index of Wei l-Being , Lock-wall ace Scal e of Marita
Adjustment , and the Global Adjustment to I l l ness Scal e
11
(GAIS) along with open and close ended quest ions were used
to measure psychol og i cal adjustment . [I is abil it y , rated on a
1 to 5 scale for each dimension included assessment of
phantom l imb sensation , pain , and/or arm Luse difficulty.
The results of this study ( Tayl or et al . , 1985) suggest
that poorer prognosis was associated with poorer
psychol og i cal adjustment (r. = .26 , p < .. Q3) . Whether or not
the subject was currently receiving chemotherapy did predict
adjustment (r. = .30 , p & . QQ8) , showing that patients
receiving chemotherapy were having trouble with
psychol og i cal adjustment . However , when the same data was
control led for prognosis, the relationship declined (r. =
. 15, p < . 1 1 ) , suggesting that poorer prognosis rather than
chemotherapy-related disability was the reason for the poor
adjustment . FOMS was used as part of the measure of
psychol og i cal adjustment but results of this study cannot be
compared to cyther studies using the PDMS due to the lack of
reported scores.
Functional Status and Ferformance
The Karnofsky Ferformance Score (KFS) has been the
"gol d standard" + or eval Lating the changes in performance
status associated with chemotherapy since 174% (Schag,
Heinrich , & Ganz , 1984) . The KPS has been widel y used in
making cl in ical decisions about escal at i ng chemotherapy
doses ; as one of the evaluation criteria in cl in ical trial s :
in evaluating the impact of chemotherapy on a patient ‘s
qual it y of l if e : and in guiding the physician in the
12
individual ization of treatment plans. In addition , the KFS
has been a predictor of responses to therapy and survival
(Kennealey, & Mitchel 1 , 1777; Mor, LaLiberte, Morris, &
Wiemann , 1784; Conil 1, Verger, & Sal amero, 17%); and Schag,
Heinrich , & Ganz , 1984) .
To help define performance status further and improve
the validity of KFS ratings, multiple regression analyses
were Lused to compare the KFS and Cancer Inventory of Froblem
Situations (CIFS) in 2%.3 patients (Schag, Heinrich , & Ganz,
1984) . The four components of the KFS are evidence of
disease, daily activity, self-care abil it iss, and work . A
strong relationship was found between the four components of
the KFS and the performance activities of the CIFS using
multiple regression techniques: ability to work , drive a
car, energy level , grooming , and an increase or decrease in
weight (p & . Q.5) (Schag, Heinrich , & Ganz , 1784) . The
behavior components help define the KFS in terms of physical
Health and f Lunction i ng .
The preval ence of clepressive states as well as the
rel at i Onship between medical and demographic variables and
depressive states were studied in 62 hosp it il ized cancer
patients (Bukberg , Fenman , & Hol l and , 1784) . The modified
LISM-III Depression Scale, Hamilton Rating for Depression ,
and KFS were Lused to measure depression . The majority of
depressed patients (18/26 or 70%) had a performance score of
60 or less, while the majority of patients without
depression (27/365 Cr 75% ) had a KFS C+ 6 () or greater. When
13
compared with other medical and demographic data , the extent
of physical disability (KFS scores) was the con l y variable
significantly related to depression (p & . QQ1 ) . The factor
most clearly associated with depression in cancer patients
in this study was a decreased KFS score (Buk berg , Fenman , &
Holl and , 1984) .
The relationship between psychol og i cal factors and
length of survival was studied in 35 women with metast at i c
breast cancer (Derogat is , Abel of f , & Mel i saratos, 1979) .
Patients were class i + i ed as short-term or long-term
survivors. Short-term survivors were those that died less
than one year from basel ine measurement and l ong-term
survivors lived for one year or longer. Instruments Lused
were the Global Adjustment to Ill ness Scale (GAIS) ; Fatient
Attitude , Information, and Expectancy Form (FAIE) which
measures accuracy of the patient 's appreciation of his/her
illness and treatment ; KFS ; Affect Balance Scale (ABS) which
measures patient 's mood in terms of positive and negative
mood dimensions ; SCLA-9QR measuring psychol og ical distress ;
and an open-ended interview concerning psychosocial
adjustment. The mean KFS scores for short-term survivors (n.
13) was 77, while the mean KFS for long-term survivors (n.
22) was 95. These differences while not statistical ly
sign if i cant , do demonstrate that long-term survivors had
better physical function ing. Fatients classified as
long-term survivors had more mood disturbance (as measured
by Affect Balance Scale, (p & . Ö5) . Short-term survivors had
14
more positive mood scores, but these d 1 fferences were not
statistical l y sign if i cant . The study find ings do not
suggest a relationship between physical function in G and mood
state. A limitation of this study was that short-term
survivors received significantly more chemotherapy (p &
. Q.5) , which may have influenced their survival and therefore
their performance status.
The efficacy of providing proactive information on
self-care was evaluated in 60 outpatients receiving
chemotherapy (Dodd , 1788) - Fatients were randomized to
receive standard patient teaching compared to the provision
Of specific side effect management (SEM) information . The
mean KFS scores in the control group pre and post
chemotherapy were 77.8 and 81 .3, respectively (p = . 14) .
KFS scores increased significantly from the pre to post
intervention interview for the experimental group (81.4 and
87.7, p = . QQ5) , who received the SEM information . The
results of this study indicate that proactive information
may positively affect performance status by enabling the
individual to manage the side effects of chemotherapy.
Previous studies (Bukberg, Fenman, & Holl and , 1984;
Derogat is , Abel of f, & Mel i saratos, 1979; and Lodd, 1988)
that have eval uated performance status using the KFS
demonstrated that cancer patients were in relatively good
physical health , with most mean KFS scores over 80 ,
indicating that the patient could participate in normal
activities with effort and that there were some signs and
symptoms of the disease (Karnofsky & Burchenal , 174%) .
The Fhysical Health Status Questionnaire (FHS) , was
selected to measure acute and chronic l imitations in
performance in four basic function ing categories: self-care
activities, mobil it y , physical activities, and role
activities. The FHS has only been used in studies of the
general population. Therefore, there are no studies to
critique in the cancer population Lising this instrument .
However , cancer patients do have both acute and chronic
l imitations, and it is important to ascerta in these
dimensions. The results of this study will provide
in format i on about the Lusef Ll ness of the FHS instrument in
patients with cancer .
Mood State
A multitude of studies have used the FON15 as a measure
of mood state , emotional distress and psychosocial status in
patients with cancer (Weisman & Worden , 1976-77; McCork le &
Benol i el , 1983; Cassil eth , Lusk , Brown , & Cross, 1986) .
Several studies (Musc i & Dodd , 1990; Derogat is , Abel of f , &
Mel i saratos, 1979; Rogert ine, Van Kammen , & Fox , 1779;
Weisman & Worden , 1976–77: Morris, Greer, & White, 1977; and
Felton & Rever, son , 1984) also used the FDM15 to predict
cop i ng , self-care behaviors, and as one of a series of
measures to predict survival . Although all of these studies
used the FUMS, the terms Lused varied from emotional health
to d 1 stress to mood disturbance , making interpretation and
general ization of the study find ings difficult . Another
16
limitation, in analyzing studies using the FON15, is that
some researchers Lused the short form of the instrument
(Cell a , Jacobson , & Drav , et al . , 1987; and McCork le &
Benol iel , 1986) . Scores from the long form of the FDMS are
higher than those of the short form and cannot be compared .
Weisman & Worden ( 1776-77) studied the existential
pl ight of cancer in 120 patients with in the first 100 days
of diagnosis. Level s of emotional distress were eval Lated
at 4 to 6 week interval s by an Index of Vulnerabil i ty (VUL )
interview and a self-report scale (FOMS) . However, no VUL
or PDMS scores per se were reported from the study, but the
authors based their interpretations of emotional distress on
the FUM5 and VUL results - Fatients who were classi fied as
having high level s of emotional distress talked more about
health concerns and l isted more symptoms in the first 1 QQ
days after diagnosis. The patients with more advanced
disease (e. g . , 1 ung cancer) were indicated as having higher
TML and VUL scores. The study find ings suggest a positive
relationship between physical symptoms and emotional
di stress .
The level = of symptom d 1 stress, current concerns, and
mood disturbance were compared in 56 l Lung cancer patients
and 65 Myocardial Infarcticn (MI) patients one and two
months after d 1 agnosis (McCork le & Benol iel , 1783) .
Instruments used were the McCork le & Young Symptom Distress
Scal e (SDS) , the Weisman & Worden Inventory of Current
Concerns (ICC) , and the FDMS. The mean TMD score, one month
17
after diagnosis for lung cancer patients, was 32.3 and for
MI patients 17.8. Two months after diagnos 1 = the mean TML.
scores for cancer and MI patients was 22.2 and 14. 1 ,
respectively. The difference in TMD scores between the two
groups was significant (p = .05) with lung cancer patients
exhibiting more mood disturbance than MI patients at both
time periods. Cancer patients also had lower vigor and
higher fatigue scores than MI patients. The decrease in TMD
in both populations, from Time 1 to Time 2, might be
explained by the fact that patients felt relieved that the
symptoms associated with treatment were not as bad as they
had expected (McCork le & Benol i el , 1783) .
F'sychosocial status of 374 cancer patients and 378 next
of k in was measured Lusing the FON15 in a study addressing
normative data of the FOMS (Cassil eth , Lusk , Brown , & Cross,
1986) . The mean TML scores for cancer patients were 20.1
and family members 14.5, respectively . Ferformance status
was a 1 so measured by the ECOG scal e . Fall i at i ve care as
Opposed to active or foll ow-up care was assoc lated with
higher TML scores . A similar association was demonstrated
in an earl ier study with chronic ill nesses including cancer
(Cassil eth et a l . , 1784) . TNTLI scores from other studies
that used the FOMS (McCork le & Benol i el , 1983 : Spiegel ,
B1 ocm , & Gottheil , 1783; Worden, 1977; and McNair, Lorr, &
Dropp 1 eman , 1771 ) were compared to the 1986 study find ings
(Cassil eth et a . , 1986) . The mean TML scores of cancer
patients from previous studies (McCork; le & Benoi i e ] , 1783:
18
Spiegel , Bloom, & Gottheil , 1983; and Worden , 1777) ranged
from 1 1 - 8 to 25.6 , whereas psychotherapy patient E and
college students had mean TMD scores of 77.5 and 43.3 ,
respectively. Cassil eth et al . ( 1786) suggested that
psychiatric outpatients and college students were not
normative samples of the general put, l ic and a more suitable
control group would be large samples of patients with cancer
or normative samples of the general public .
Cop in g strategies and self-care behaviors were studied
in 1 QQ cancer famil ies receiving chemotherapy cºver six
months (Lodd, 1990) . The PDMS and KFS were measured at T 1
(i.e. , in it i at ion of chemotherapy) , T4 ( i.e. , 2 to 3 months
after chemotherapy was in it i ated ) , and T5 ( i .e. , 6 months
after chemotherapy began ) in patients with and without prior
chemotherapy. Although KFS and FOMS scores were considered
to be two of the causal antecedents and predictors of
self-care behaviors and coping strategies, neither the KFS
nor the FOMS scores were statistical l y significant in
predict i ng sell F-care behaviors .
Fatients with a history of chemotherapy reported the
highest TMD at T4 (2 to 3 months after in it i at i cºn cº-f
chemotherapy) . By T5, TMI scores had decreased to a point
l ower than that at the in it i at i on cyf chemotherapy,
indicating that patients without a history of chemotherapy
had the n i gnest TNTLI scores at T 1 with TMI scores decreasing
over time. Results from this study (Dodd , 17% (3) suggest
that TML scores are different between patients who have
1 9
received prior chemotherapy and patients just beginning
chemotherapy. Based on the find ings of the study, Dodd
suggested a profile of patients and family members at risk
+ or problems cop in g : Ol der patients, patients with no
previous history of chemotherapy, and those without
recurrent disease (Dodd, 17%) .
Length of survival was linked to cop in g and mood state
in several studies ( Derogat is , Abel of f , & Mel i saratos, 1979;
Rogentine, Van Kammen, & Fox , 1977; Weisman & Worden ,
1976–77; Morris, Greer, & White, 1777; and Felton &
Revenson, 1984) . Mood state was measured by a variety of
instruments including the FON15 . Two of the studies
( Derogat is et al . , 177% , and Rogentine et al . , 1777)
reported that 1 ong-term survivors had more symptoms,
increased levels of anxiety, poorer attitudes toward
physicians, and more negative affect, but better coping
abil it y than short-term survivors. These f indings are in
contrast with other work (Weisman & Worden, 1776-77; Morris
et al . , 1977; and Felton & Revenson, 1984) that demonstrated
that short-term survivors had increased level = of anxiety
and depression ; a more negative affect ; and more trouble
cop in g than 1 ong-term survivors. The reason for the
di ++ erences between these studies may be due to trie lack of
homogeneity of research instruments measuring cop in g and
mood state .
Most of these studies have examined perf crimance status
and mood as independent constructs in cancer patients. Few
2C)
studies (Cell a , Urof i amma , & Hol l and , et al . , 1987; and
Tayl or et al . , 1985) have examined the relationship between
physical function ing and mood state in this population , and
no study has eval Liated the relationship between these two
variables over time. What is clear from the l iterature is
that mood disturbance is cºften elevated at the time of
in 1 tial diagnosis, indicating high level sof distress at
this time. Most studies f indings (Weisman & Worden ,
1776-77; Cell a , Urof lamma , & Holl and et al . , 1787; Tayl or et
al . , 1985; and Cassil eth et al., 1986) suggest that cancer
progression also causes people to experience greater mood
disturbance. What is unclear is what happens during the
course of active treatment between physical functioning and
mood state , and how do demographic variables such as age ,
gender , type of cancer , and presence of metastasis influence
physical + Lunction in g and mood state.
Chapter IV: Methods
Research Lesign
A descriptive anal ys is was performed Of C at a collected
from Oncol ogy patients in a long itudinal (four-month)
experimental study entitled "Self-Care Intervent i on to
Decrease Chemotherapy Morbidity" which tested the ability of
a specific nursing intervention to enhance self-care
practices and decrease morbidity of cancer patients
initiating chemotherapy (Dodd et al . , 1988) . The aspect of
the study reported on here focused on physical function ing
and mood state . Signed informed consent was obtained from
each participant that participated in the study as approved
by the Human Subjects Committee at the University of
Cal if ornia, San Francisco .
Sampl =
The sample consisted of 127 adult cancer patients who
were 1) 18 years of age or older ; 2) could speak and read
English ; 3) a Karnofsky performance score × 60 : 4) could
give informed consent at entry into the study : 5) had an
anticipated survival time of greater than four months
according to their primary physician ; and 6) agreed to
participate in the study. Exclusion criteria included :
receiving other cancer therapies like radiation therapy, as
well as patients with diagnoses of leukemia or AIDS.
Fatients were receiving their initial chemotherapy
treatments with at 1 east one of 5 chemotherapy agents or
their anal ogs ( i . e. , doxorub ic in , c is-platinum ,
~ *-y*-*-
cyclophosphamide, 5-fluorauracil , or methotrexate) given
al one or with other agents. Fart icipants were receiving
chemotherapy as outpatients and had no previous history of
chemotherapy treatment for their mal ignancy.
Research Setting
Fatients were referred by nurses and physicians from 18
cl in ical sites including community hospital s as well as
major medical centers from the San Francisco Bay area to Los
Angel es. Research settings included Drivate of f ices and
large out-patient c 1 in ics. The variety of settings were
sel ected to increase the external val idity of the study * =
+ i nd i ngs.
Instruments
The instruments used in this study were : the
Demographic Questionnaire, the Karnofsky Ferformance Score
(KFS) , the Fhysical Health Status Questionnaire (FHS) , and
the short form of the Fro-fi ) e Of Modd States (FDMS) .
The Demograph ic Questionnaire is a 12-item
Guest i onnaire Lised to obtain demographic informat i on about
age , gender , ethnic i ty, educational level , financial status,
mar 1 tal status, and type of cancer. (See Appendix A )
Content va idity of the quest i onnaire was established by a
panel of experts in on cology nursing .
Physical Functioning
The Karnofsky Performance Score (KFS) (See Appendix B)
measured the patient * = abil it y to accompl ish normal
activities of daily living , or their need for he ip and
nursing care (Karnofsky & Burchenal , 1947) . The KFS
consists of a series of 8 items. Farticipants were asked to
"describe your abil it i es at the present time". KFS scores
were on a 30 to 1 QQ scale collected at T 1 , T2, T3, and T4 .
A score of 1 QQ signifying adequate health status, with no
complaints and no evidence of disease and a score of 30
indicating disabil it y , with hosp it il ization needed . In
previous research studies primarily physicians, nurses , and
caregivers have completed the scale. However , for the
purpose of this study, the patients rated themselves.
Performance status was rated by two physicians and the
patients themselves (N = 100) using the KFS and Eastern
Cooperative Group (ECOG) to evaluate reliabil ity and
validity of the instruments (Con ill , Verger, & Sal amero ,
1990 ) . Correl at i on 5 were sign if i cant between the two
physicians scores (r. = .75 for KFS, .. 76 for ECOG, p < .. QQ1 )
and between physicians and patients ratings ( - 65 for KF'5,
and .5% for ECUG., p. 3. .. QQ1 ) . To test for construct validity,
the KFS has also been compared to single-item physical
qual it y of l if e scal es, such as the Katz ADL scale. The
results of this comparison found the KFS to be unbiased and
complete , with a correl at ion coefficient of .35 (Mor ,
LaLiberte, Morris, & Wiemann , 1984) . Interrater reliab 11 it y
between two physicians was . 97 in 47 interviewers. Schag,
Heinrich , & Ganz (1784) studied 273 cancer patients to test
the validity of the KFS. They reported the KFS had very
good interrater reliability among physicians (r. = .8%) .
24
The Physical Health Status Quest ionnaire (FHS) (See
Appendix C ) or "Functional Limitations Battery" was
devel oped by the Rand Corporation (Stewart, Ware , Brock , &
Davies-Avery, 1778) . Functional status is defined as both
acute and chronic functional limitations in the persuance of
normal activities of daily living .
Data was collected using the self-administered
questionnaire at T 1 , T2, T3, and T4. The FHS duestionnaire
is a 13-item scale with instructions to "circle the answer
that best describes your current abil it i es at this time".
Each question had two parts: are they able to do an
activity, and if not , how 1 ong have they been unable to do
the activity, (1) "less than one week " , (2) "one to three
weeks", or (3) "more than three weeks." The range of scores
is 13 to 27. The lower the score the more disabled the
person 1 s.
Dayton established four categories of functional
l imitations from a review of the l iterature , thereby
establish ing content val idity. The four categories are :
( 1 mobil it y , (2) physical , (3) role, and (4) self-care.
Coefficients of reproducibility were all above .90 and
internal consistency reliability was .8% ; thereby making the
rel i abil it y of the FHS scale acceptable. Test-retest
rel i abil it y was .46 or greater and gamma coefficients were
above .90 + or a l l categories. The Rand Corporation also
provided evidence of convergent and discriminant validity of
the categories of physical function ing (Stewart, Ware,
ry E.
Brook , & Davies–Avery, 1978) . In the present study,
internal consistency ranged from .83 to .85 for the four
cycles (see Table 1 ) .
The Prof ill e of Mood States (FUMS) (See Appendix II) was
devel oped by McNair, Lorr, & Dropp 1 eman ( 1971) and used
original l y with psychiatric outpatients and college
students. Administration time for the original FOMS
containing 65-items (McNair, Lorr, & Dropp 1 eman , 1771 ) , was
considered too long for ill patients ( i.e. , 15–20 minutes) .
Therefore a shorter version of the PDMS was devel oped by
Shacham ( 1983) contal ning a 37-item questionnaire with a
5-point Likert scale which halved the time to complete the
scale. The questionnaire measures six mood states
incl Lud in g : (1) tension-anxiety , (2) depression-deject iOn ,
(3) anger-hostil it y , (4) vigor-activity, (5)
fatigue-inert i a , and (6) confusion-bewilderment .
The five-point scale ranges from Q "no feel ing" to 4
"extreme feel ings". The instructions tell the patient to
"circle the number that best describes how you have been
feel ing during the past week including today." The
rational e for using a crie-week rating time was to devel OD a
range 1 ong enough to characterize the patient 's usual moods
and continuous mood responses to what is currently happen ing
in the patient ' s life, while still being short enough to
eval uate the immediate effects of treatment (McNair, Lorr, &
Droppleman, 1971) . A TML score can also be obtained by
add l ng the scores of all six factors, negatively weighing
26
vigor. The TMD score is a summary measure of distress, with
higher scores indicating more mood disturbance .
In her study of 83 cancer patients, Shacham (1783)
reported that internal consistency scores ranged from .803
to .907, and were used as standards for reducing the factors
+rom 65 to 37. The correl at i con coef f ic i ent s between the
short and long scales were all reported above .95. Internal
consistency scores, for the present study, ranged from .82
to .94 for the four cycles (see Table 1) . Little & Fenman
(178%) in their study of Veteran 's Administration (VA)
psychiatric inpatients described the short form of the FOMS
as having concurrent validity due to the instruments abil it y
to "detect diagnostic differences, clinical setting
differences , and c 1 in ical changes" (p. 46) .
Procedure
Fatients who met the criteria for the study were
approached by the Cl in ical Nurse Special ist (CNS) and
consent was obtained . At the time of consent, the patient
was randomized by the Froject Director to the experimental
or control group via a computer program. The Demographic
(Juestionnaire , the KFS , and the FOMS were administered to
the participant by the CNS or the nurse in charge in that
particular setting on entrance into the study and before the
in it i at ion of the first course of chemotherapy. The FHS
Çuest i onnaire was completed by each participant between the
first and second cycles of chemotherapy. The KFS, FHS, and
FOMS were again administered to each participant at each
subsequent cycle of chemotherapy, approximately every 3 to 4
weeks for four successive treatments. Time to complete this
information was approximately 15-20 minutes.
Data fanal ysis
Data were analyzed util izing an IBM FC and the
statistical analysis program CRUNCH. A Fearson Froduct
Moment Correl at ion was done to determine the relationship
between physical function ing and mood state at each time
point. A cone-way anal ys is of variance (ANOVA) was done to
determine differences over time for KFS, PHS, TMD scores and
+ or each D+ the 6 subscal es Of the FON15 . Fost-hoc
contrasts, using the Schef fe test were used to identify
significant differences between KFS, FHS, and FOMS subscales
scores Over time . Independent group t-tests were computed
to determine differences in physical function ing and mood
state between individual s witH breast cancer and those with
other types of cancer ; between men and women ; and between
ind i v i dual switH no evidence of metast as is and those with
evidence of metast as is .
Chapter V: Results
Sample Demograph its
Fart icipants were primarily caucasian (80%) ,
middle-aged ( mean 52 years, range 22 to 82, 5 - D - 13.3) , with
two years of college education . The majority of the
participants were female (68.5%) , married/partnered ( ò 17. ) ,
with 20% l i v i ng al One - The most common cancer diagnosis was
breast cancer (42.5%) , foll owed by lung cancer (15%) , then
ovarian (8.6%) , b 1 adder (7. Q%) , Non-Hodgk in 's lymphoma
(5.5%) , Hodgk in 's lymphoma (4.7%) , and col on cancers (3.0%) .
The number of patients with metastasis was (7%) . (See Table
2)
Study Furpose 1 : Rel at ionship Between Physical FLunction ing
and Mood State
Mean scores and standard deviations as wel 1 as the
standardized Chronbach * = Alpha for each of the scal es used
in this study are found in Table 1 .
The mean KFS scores, at each time point , were all above
80. A one-way ANOVA demonstrated that the changes in KFS
scores over time were not statistical l y sign if i cant (F (3, 51 )
= .51 p. 3. .. Q5, Figure 2) . These data indicate that patients
carried out normal act i v i ties with some effort and showed
only minor signs and symptoms of their disease .
The FHS scores ranged from 22 to 23 throughout the four
time periods. Une-way ANOVA demonstrated that the changes
in FHS scores over time were not statistical l y sign if i cant
(F (3,57) = 1.8, p. 3. .. Q5, Figure 3) . Since the highest
29
possible score on the FHS is 27, these data , along with the
KFS scores suggest that the participants exhibited a high
degree of physical function ing through four consecutive
cycles of chemotherapy.
Total Mood List Lurbance scores ranged from 18 - 2 to 14. '7.
A cone-way ANOVA, demonstrated that the changes in TMD scores
over time were not statistical l y sign if i cant (F (3,53) = .75,
p > . Q5, Figure 10) . However, TMD scores were highest at
Time 1 , suggesting that patients were the most distressed at
the in it i at ion of chemotherapy.
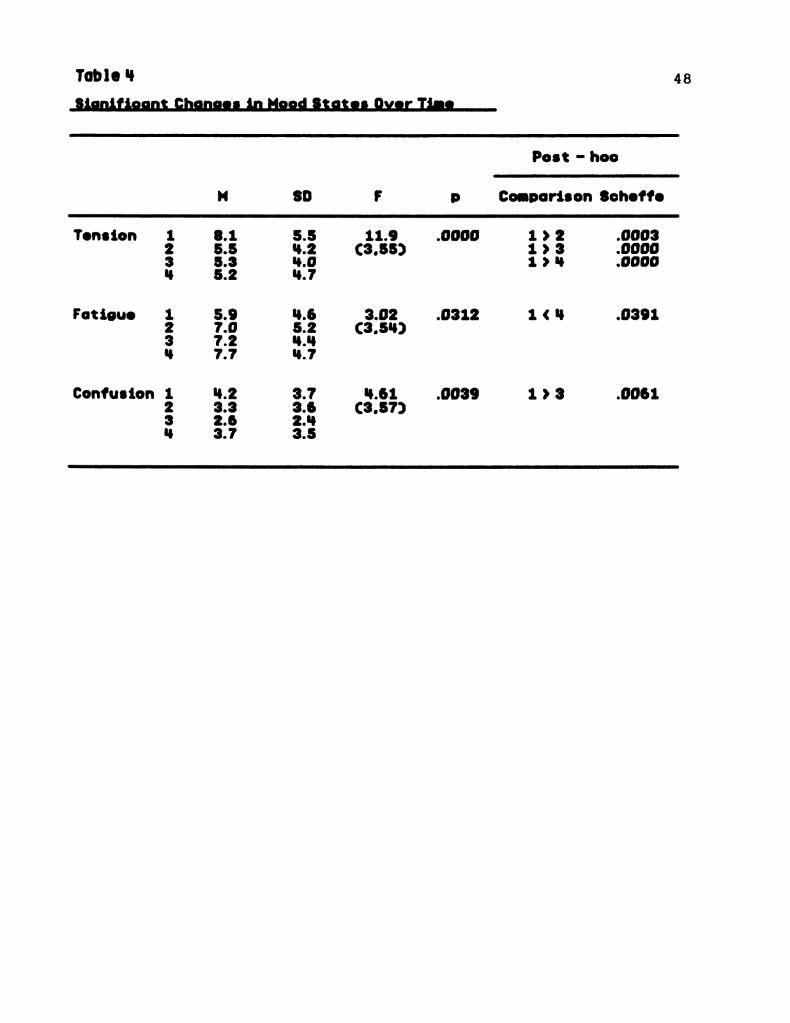
Each cº-f the subscal es Of the FOMS were eval Llated for
changes over time using a one-way ANOVA . Tension scores
decreased significantly cºver time (F (3,55) = 1 1 . 88, p.
= . QQQQ) , with the post-hoc Scheffe test indicating that the
highest tension scores were measured at T 1 (p = . QQQ3, Tab e
4, Figure 4) . Fat 1 gue scores increased sign if i cantly over
time (F (3,54) = 3.02, p = . Q312) , with the post-hoc Scheffe
test indicating that the lowest fatigue scores were reported
at T 1 (p = .03% 1 , Figure 8.) . Confusion scores decreased
over time (F (3,57) = 4.61 , p = .003%) with the post-hoc
Schef Fe test indicating that the l owest conf Lisi On scores
were reported at T3 (p = . QQ61 , Figure ?) .
In Order to determine i f there was a rel at i Cºnship
between physical function ing and mood state , Fearson 's
Froduct Moment Correl at ions were performed between KFS
scores and TML scores, and FHS scores and TML scores at each
time point . Sign if i cant negative correl at i ons were found at
each time point between KFS and TMD ( al 1 p & . Q01) and
between PHS scores and TML. scores (all p < .. QQ1 ) , indicating
that at each time period as KFS and FHS scores decreased the
TML scores increased . Thus as physical function decreased ,
the persons in this study also experienced increased mood
dist Lurbance . (See Table 3)
To determine if any of the subscal e scores on the FOMS
correl ated with either the KFS scores or the FHS scores , a
correl at i cºn matrix was done using the Fearson 's Froduct
Moment Correl at i On Coef + i C i ent . (See Table 3)
All subscale scores on the FOMS ( i . e. , tension ,
depression , anger , f at i gue, vigor, and confusion ) at T 1 and
T2 were sign if i cantly correl ated with KFS and FHS scores
(all scores p < .. Q1 ) . At T3, all subscal e scores on the
FOMS were significantly correlated with KPS scores except
for anxiety and confusion (all p < .. Q.5) . FHS scores were
only significantly correl ated with fatigue, vigor, and TMD
(all p < .. Q1 at T3) . At T4 KFS scores were significantly
correlated with all subscale scores on the FDMS ( p < .. Q.5) .
At Time 4 FHS scores were all sign if i cantly correl ated with
subscale scores on the FDM5 except + or confusion (all p &
. Q.5) . The relationship between the two measures of physical
function l ng ( i.e., KFS and FHS) were also sign if i cantly
correl ated (r. = .55 to . 6 1 , a 1 1 p < .. Q 1 ) .
Study Furpose 2 : Relationship Between flae and Physical
Funct 1 on ing and Mood State
31
To determine if anv subscale scores on the PDMS, TML.
scores, KFS scores, cr FHS scores correl ated with age , a
correl at 1 on matrix was done L1s i ng the Fears on 's Product
Moment Correl at i on Coefficient . The mood state subscal es cº-f
tension and fatigue were sign if i cantly correl ated with age
at the first two cycles of chemotherapy (T 1 and T2 ) . At T 1 ,
older participants reported less tension (r. = - . 1% , p =
. Q4) ; but at T2 more fatigue (r. =- .25 , p = . Q2) . Fhysical
function in g (FHS scores) were correlated with age at cycles
3 and 4 (T3 and T4) . Older individual = reported a decrease
in PHS scores (r. = - .22 , p = . Ç5; and r = - .24, p = . Q4) at
T3 and T4 respectively.
Study Furpose 3 : Lifference in Physical Functionina and
Mood State Between Type of Cancer . Gender ... and Metastasis.
Independent group T-tests were done to determine if
there was a difference in physical + Linction in G and mood
state between individual s with breast can cer versus
individual s with other types of cancer ; between males and
femal es; and between individual s with no evidence of
metast as is and those with evidence of metast as is .
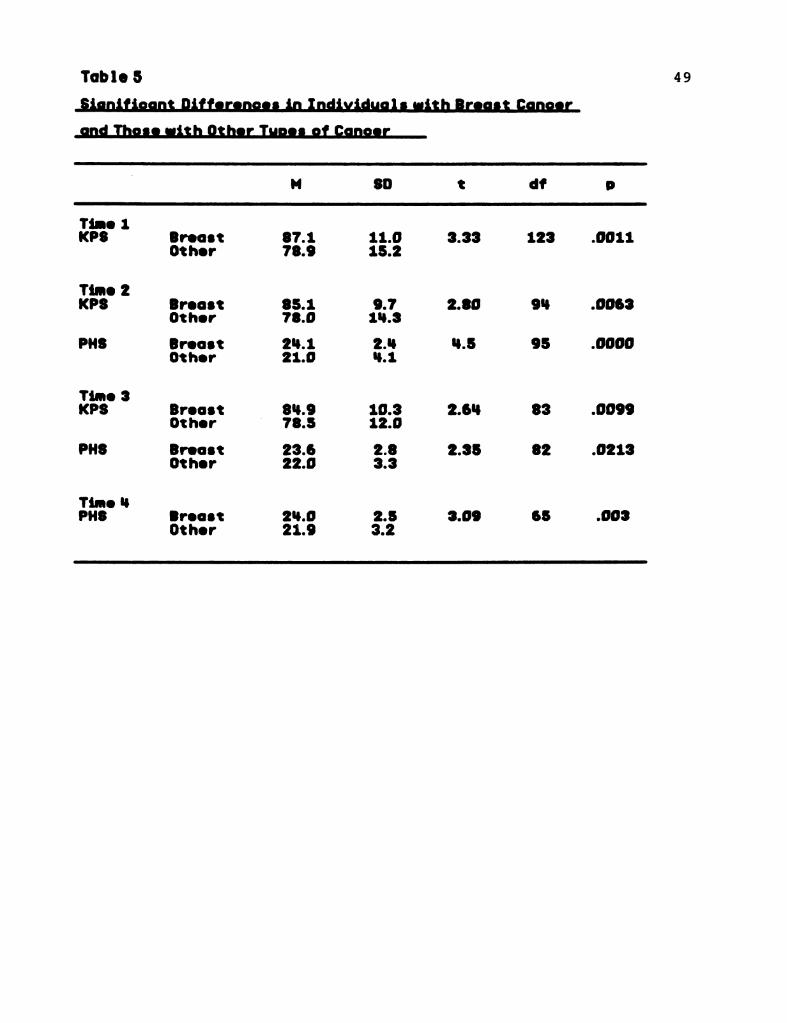
a . Results showed that individual s with breast cancer had
sign if i cantly higher K.FS and FHS scores at all four cycles
than ind 1 v i dual s with Cther types of cancer , suggest ing a
higher level of physical function i ng in breast cancer
patients. (See Tab i e 5.) There were no sign 1 + 1 cant
d if + erences in TNTLI scores between in Ci i v i Gula 1 = with breast
32
cancer and individual s with other types of cancer or in any
of the FOMS subscal e scores .
b - Women had higher KFS ( t = 3.25, p = . ØØ 16) and PHS
scores ( t = 2.1Q , p = . Q4) than men at T2, but less vigor (t.
= -2.28, p = . Q265) than men at T3, suggesting that at T2,
women had a higher level of physical function ing than men .
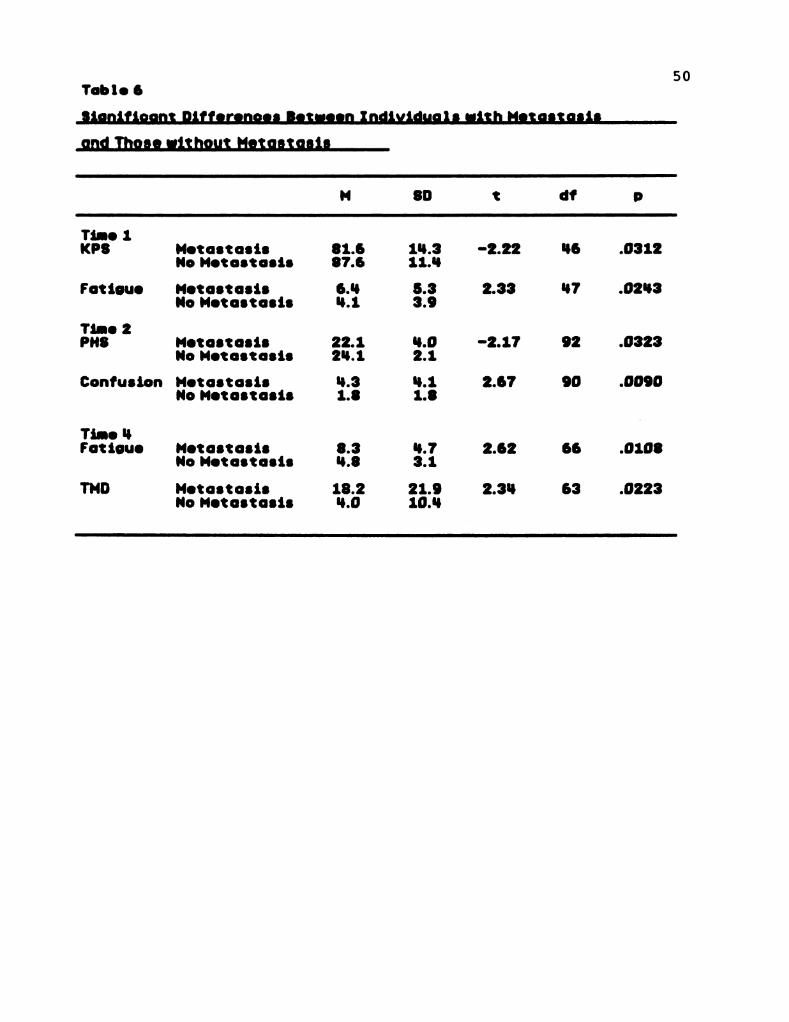
c - Sign if i cant differences in KFS and FHS scores and FDMS
scores were demonstrated in patients with evidence of
metastasis compared to individual s without evidence of
metastasis. (See Table 6) At T 1 , patients with metastasis
2 2 , p = .0312)2had significantly lower KFS scores ( t = -2.
and were more fatigued ( t = 2.33, p = . Q243) . At T2
patients with metastasis had significantly more confusion (t.
= 2.67, p = . QQ'7) and lower FHS scores ( t = -2. 17, p =
.0323) than patients without metastasis. There were no
significant differences found at T3 in any of the study
Variables. At T4, patients with metastasis had
sign if i cantly more fatigue ( t = 2.62, p = . Q1 Q8) and greater
TMD ( t = 2.34, p = .0223) than patients without metastasis.
33
Chapter VI : Discussion
Significance
The results of this study demonstrate a relationship
between decreases in physical function in g (as measured by
KFS and FHS) and increases in overal l mood disturbance (as
measured by the PDMS) during all four cycles of
chemotherapy. Fatigue, vigor , and TMD scores were highly
correl ated with KFS and PHS scores at all 4 cycles of
chemotherapy, indicating that as physical function ing
decreased , patients were more fatigued , and experienced
greater mood disturbance . The find ings of this study add to
the work of Cell a , Drofilamma, & Holl and et al . , (1987) and
Tayl or et al., (1985) in establishing a relationship between
physical function ing and mood state in patients undergoing
cancer treatment. However, the causal relationship between
def ic its in physical function ing and increases in total mood
disturbance cannot be determined from these data .
The range of mean scores of KFS (81 - 3-82 - 4) and FOMS
( 14. 7-18.2) were consistent with other study findings
that measured performance status and mood state in oncol ogy
patients (Dodd, 1788; Bukberg, Penman , & Hol 1 and , 1784:
Derogat is , Abel of f , & Mel isaratos, 1777; Cassil eth et al.,
1786 ; and McCork le & Benol iel , 1983) . While one might think
that patients undergoing chemotherapy might experience
changes in their ability to function or changes in their
mood , these data , as well as data from previous studies
(McCork 1 e & Benol i e ] , 1983; and Cassil eth et al . , 1784)
34
suggest that patients with a diagnosis of cancer or
undergoing cancer treatment continue to function wel 1 with
minimal changes in their cºveral l mood .
However, tension , depression , anger , confusion , and TMD
mean scores were highest at T 1 , suggest ing that in it i at ing
chemotherapy is a stressful event. These f indings are
similar to the findings of Musc i & Dodd (1990) and Llodd
(1790) . Ferhaps when patients recovered from their in it i al
+ ear of the unknown and over time become more knowledgeable
of the experience of receiving chemotherapy, the initial
tension and confusion dissipated .
Results of this study indicate that older individual s
reported more positive mood states, such as a lower tension
scores, at the in it i at ion of chemotherapy. However , as time
went on , older individual s reported a decrease in the level
of physical function ing. These f indings are consistent with
results from other studies that also found that increased
age was associated with better mood , but a decrease in
physical + Lunction in g (Cassil eth et al . , 1984; and Ganz ,
Schaq ... & Heinrich , 1985) . It could be that as one grows
Ol der , an individual experiences more i l l n ess and has ■ nore
contact with the health care system. Therefore, prior
experience may hel D to decrease tens 1 on level s when a new
1 | 1 ness strikes (Ganz , Schag, & Heinrich , 1785) . However,
it is well documented in the l iterature that physical
+ Lunction i ng general l y decreases as one ages , ( Mages &
Mendel sohn , 1979; and Ganz , Schag, & Heinrich , 1985) not
35
only from ill ness or treatment, but as a result of natural
aging .
Breast cancer patients reported significant i y higher
level s of physical function ing at all four time periods than
patients with other types of cancers. No studies known to
date have documented this find in g . Gender could be a
confounding variable in these f indings , although women on 1 y
had a higher level of physical function ing than men at T2 .
At Time 1 , patients with metastasis started of f with a
decrease in physical function ing (KFS) and reported
sign if i cantly more fatigue than patients without evidence of
metastasis, probably due to the metastatic disease process.
Froblems in physical function ing (FHS) persisted at T2 and a
new symptom of confusion emerged in patients with evidence
of metast as is . There were no sign if i cant differences at T3
between the two groups. Although patients with metastasis
reported significantly more mood disturbance (TML) at T4,
these scores did not change between the two groups until T4 .
Fatients with metastasis were also significantly more
fatigued at T4 than those with no evidence of metastasis.
These results support f indings from other studies (Cassil eth
et al . , 1784; Musci & Dodd, 17% and McCork le & Benol iel ,
1983) that metastatic d 1 sease produces more physical
symptoms. However , the results do not show that patients
with metast as is have greater mood dist Llrbance al drig with a
decrease in physical function in g (Tayl or , et al . , 1985; and
Cell a , Orc-fi amma, & Hol 1 and et al . , 1987) .
36
Limitat i cons
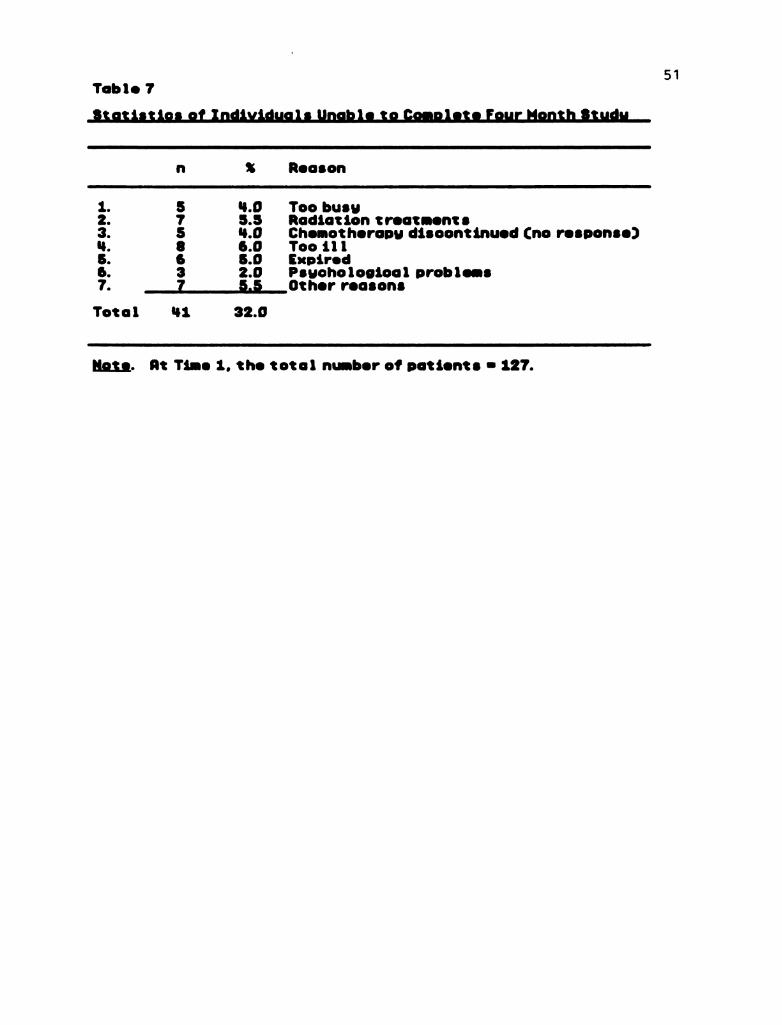
A limitation in this study and of the larger study , is
the attriticn rate of the sample over time. The sample size
at T 1 was 127 and at T4 was 7Q , which makes general ization
of these study 's findings difficult. A total of 41 patients
dropped out of the study by T4 . (See Table 7.) One could
speculate that these patients were the sick est. However , it
is important to note that the patients remain i ng in the
study at T4 (n 70) , still reported a significant amount of
+ at i gue and conf Lisi on . Another l imitat i on D+ the larger
study , which effects this study, is that the majority of
Datients were women (68%) and the most common d 1 agnosis was
breast cancer (42%) , which i imits the general ization of the
f indings to other cancer populations.
Although the FHS was highly correl ated with the KFS
scores in this sample of oncol ogy patients, further studies
are needed before def in it i ve conclusions can be made on the
val idity of this instrument for Lise in an oncol ogy
popul at 1 on . One would expect that there would be a larger
degree of variabil it y in FHS scores in on cology patients,
especial l y those receiving chemotherapy due to the multiple
side effects of ten experienced . Fernaps the scoring of the
FHS should be expanded to all ow for more discrimination in
physical function ing to increase the sensitivity of the
scal e.
Cell a , Urof i amma , & Hol l and et al - , ( 1987) , Tayl or et
al . , (1985) , and Cassil eth et al . , ( 1786) have criticized
37
the PDMS as possibly missing a subset of the cancer
population due to the low level s of distress among cancer
patients in general . It would seem that persons facing a
l i fe-threatening i l l ness would demonstrate greater mood
disturbance. Cl in ical ly, the author has found that many
cancer patients do seem to take their disease and treatment
in stri de . In this study however, there was a wide
dispersion of FOMS subscale scores which provided the
opportunity for significant correl at ions to be demonstrated
even at T4, when the sample had dropped to 70. However , all
of the subscal e scores of the PDMS had large standard
deviations, suggest ing that there may be a small subset of
patients who experienced greater mood disturbance than the
group mean would suggest .
Impl ications for Fractice
Results of this study emphasize the need for health
professional s, especial l y nurses, to make ongoing
assessments of physical function ing and mood disturbance
using the patient 's self-report of the situation . Standard
self-report measurements of performance status and mood
state such as KPS, PHS, and FOMS could be implemented in the
inpatient and outpatients settings to determine changes in
Datient 's mood state and physical function ing , and to
determine changes over time . In future studies , it would be
important , even in light of the attrition at T4, to
determine how long this fatigue and confusion persisted .
The results of these measures could be eval uated by the
physician and the nurse to determine and facil it ate
intervent ions directed toward the needs of the patient .
Research studies on cancer, chemotherapy, self-care ,
survival , and coping with the side effects of chemotherapy
should continue to include measurements of physical
+ Linct i on in g and emot i cnal status to further define the
relationship between physical and emotional health .
Research is also needed to determine the best measure (s) of
physical function in g and emotional status that are
reflective of the chemotherapy patient experience.
39
References
Bukberg , J . , Penman , D . , & Holl and , J. C. ( 1784) .
Depression in hospital ized cancer patients.
Psychosomatic Medicine , 46 (3) ; 199-212.
Cassil eth , B. R. , Lusk: , E. J. , Strouse, T. B. , Mill er, D.S. ,
Brown , L.L. , Cross, F. A. , & Tenaglia, A. N. (1984) .
F’sychosocial status in chronic ill ness. New England
Journal of Medicine, 31 1, 596-511 .
Cassil eth , B. R - , LLusk , E. J. , Brown , L. L. , & Cross, F. A.
( 1786) . Fsychosocial status of cancer patients and next
of k in : Normative data from the profile of mood states.
Journal of Psychosocial Uncol pay 3 (3) × 77-195 -
Cell a , D - F - , Jacobsen, F. B. , Drav , E. J. , Holl and , J. C. ,
Silverif arb, F.M., & Rafla , S. (1987) . A brief poms
measure of distress for cancer patients. Journal of
Chronic Disease , 4Q (10) , 73%-942.
Cell a , D - F - , Orofilamma , B. , Holl and , J. C. et al . ( 1987) .
The relationship of psychol ogical distress, extents of
disease , and performance status in patients with l Lung
cancer . Cancer, 6.Q., 1661 - 1667.
Con i l l ; C . , Verger , E . , & Sal amero , M . ( 1990) .
Performance status assessment in cancer patients.
Cancer, 6.5 , 1864-1866 .
Derogat is , R. R. , Abel of f , M.D., & Mel isaratos, N. (1979) .
F’sychol og 1 cal cop in g mechanisms and survival time in
metastatic breast cancer. Journal ºf American Medical
Éassociation , 242 ( 14) , 1504-1508.
Derogat is , R. R. , Morrow, G.F., Fetting , J., Fenman, D. ,
Piasetsky, S., Schmale, A.M., Henrichs, M., & Carnicke,
C-L-. (1983) . The prevalence of psychiatric disorders
among Canter patients. Journal ci■ American Medical
fassociation , 247 (6) , 751-757.
Dodd, M. J. (1988) . Efficacy of proactive information on
self-care in chemotherapy patients. Pat lent Education
215-225º -* -and Counsel ina. , 1 1,
Dodd, M . J. ( 1788) . Fatterns of self-care in patients
with breast cancer - Western Journal of Nursing
Research , 1 Q (1) , 7-24.
Dodd, M . J . , Lovejoy, N. , Larson , F - , Stetz , K. . , Lewis, B. ,
Holz emer, B. , Hauck: , W., Paul s, S. , Lindsey, S. , &
Musc i , E. (1785) • Self-care Intervention to Decrease
Chemotherapy Morbidity. (Unpublished Manuscript) .
University of California, San Francisco.
Dodd, M - J - , Lovejoy, A., Larson, P., Musci, E., Thomas,
M - , Dibble ; S. , Hudes , M., Hauck: , W., & Kato, F.
(1970) . Coping and self-care of cancer famil ies, final
report . (Grant No. RQ1 NRQ 144) . San Francisco :
University of Cal if ornia, National Institutes
of Health .
Felton , B.J., & Revenson , T.A. (1984) . Coping with
chronic ill ness : A study of ill ness controll ability and
the influence of coping strategies on psychol ogical
adjustment - Journal of Consul ting and Clinical
F’sychol pay. , 52 (3) , 343-353.
41
Fol k man, S. , Lazarus, R. S. , Dunkel –Schetter , C. , Del Ong is ,
A . , & Gruen , R. J. (1986) - Dynamics of a stressful
encounter : Cognitive appraisal , cop in g , and encounter
outcomes. Journal of Personal it y and Scycial
Psychol cay, 50 (5) , 7%2-1003.
Frank. -Stromborg & Wright . (1984) . Ambulatory cancer
patients perception of the physical and psychosocial
changes in their lives since the diagnosis of cancer .
Cancer Nurs l ng , 117-139.
Fre idenbergs ... I . , Gordon , W . , Hibbard , M . , Levine . L. ,
Wol f , C. , & D i l l er, L. (1981-82) . Fºsychosocial aspects
of 1 i v i ng with cancer - A review of the l iterature -
International Journal of Psychiatry, 11(4) , 393-32? -
Goodman , M . ( 178%) . Managing the side effects of
Chemotherapy. Seminars in Uncol Ogy Nursing ,
5 (2) (Suppl - 1) , 27–52.
Gottschal k , L.A . (1984) . Measurement of mood and affect
in cancer patients. Cancer , 53 (Suppl - 10 ) ,
2236-2242.
Holl eb , A.I. (Ed.) (1986) - The famerican Cancer Society
Cancer Book: . New York : Doubleday and Company.
Karnofsky, [ . , 3. Burchenal , J . ( 194%) . The cl i ni cal
eval Lati on of chemotherapeutic agents in cancer . In :
C - M - Macleod (Ed : ) , Eval Liat ion of chemotherapeutic
agents. New York : Col Lumb la University Fress.
Kenneal ey, G. T. , & Mitchel 1 , M.S. (Eds.) . (1977) .
Factors that influence the therapeutic response .
Factors that influence the therapeutic response in
cancer : A comprehensive treat i se - (pp. 3–27) . New
York : Fl enum Fress.
Lazarus, R. S. , Averil 1 , J. F. , & Opton , E. M. (1974) . The
psychol ogy of coping : Issue of research and assessment .
In G.U. Coelho , D. A. , Hamberg , & J. E. Adams (Eds.) ,
Cop in a and adaptation - New York : Basic Books .
Lazarus, R. S. , & Fol k man , S. (1784) . Stress ,
appraisal , and cop ing. New York : Springer .
Little , D . , & Fenman , E. ( 178%) . Measuring sub acute mood
changes using the profile of mood states and visual
anal Ogue scales. Fºsychopathol cºsy. , 22, 42-47.
Love , R. R. , Leventhal , H . , Easter l ing , D.V., & Nerenz ,
D. R. ( 178%) . Side effects and emotional distress
during cancer chemotherapy. Cancer , 6.3, 604-6 12.
Mages , N. L. , & Mendel sohn , G. A. ( 177%) . Ef + ects D+
cancer on patients l i ves: A person ol og ical approach .
In B. C. Stone , F - Cohen , & N.E. Adler (Eds.) , Heal th
p =ychol cogy (pp. 255-284) . San Francisco :
Josey-Bass.
McCork, l e, R., & Quint-Benol iel , J . (1983) . Symptom
di stress, current concerns and mood disturbance after
diagnosis of l i fe-threaten i ng disease - Social Science
Medic ine, 17 (7) , 431-438.
A / I
43
McCorkle, R. (1786) . Evaluation of cancer management ,
final report . (Grant No. Nu■ 1 QQ1 ) . Seattle : University
of Washington , Fublic Health Services.
McNair , D . , Lorr, M . , & Dropp 1 eman, L. (1971) . EITS
Manual for the Prof i le of Mood States - San Diego -
Educational and Industrial Test ing.
Mor , V . , LaLiberte, L. , Morris, J. N. , & Wiemann , M .
(1784) . The karnofsky performance status scale.
Cancer , 53, 2002-2007.
Morris, T., Greer, H.S., & White, P. (1977) .
F’sychosocial and social adjustment to mastectomy.
Cancer, 4Q, 2381-2387.
Musc i , E. C. , & Dodd, M . J. ( 1 190 ) . Pred ict in g sel f -care
with patients and family members affective states and
family function in 9 - Oncol ogy Nursing Forum , 17 (3) ,
3%-400 .
Rogert ine, G. N. , Van Kammen, D.F., Fox , B.H., Locherty,
J. P. , Rosenblatt, J. E. , Boyd , 5 - C - , & Bunney, W. E.
( 177%) . Fsychol cog i cal factors in the progrids is of
mal ignant mel anoma : A prospective study.
F’sychosomatic Medicine , 41 (B) ; 847-655.
Schag, C. C. , Heinrich , R. L. , & Ganz , F - A - (1983) . Cancer
inventory of problem situations: An instrument for
assess in G can cer patient ‘s rehabil it at i on needs .
Journal of F =ychosºcial Uncol Gay 1(4) .
1 1-24.
44
Schag, C. C. , Heinrich , R. L. , & Ganz , F. A. ( 1 °84) .
Karnofsky performance status revisited : Reliability,
validity, and guidel ines. Journal of
Clinical Uncol ogy. , 2.(3) ; 187-173.
Shacham , 5. (1983) . A shortened version of the profile
Of mood states - Journal of Personal it y fassessment. ,
47 (3) , 305-306.
Spiegel , Li . (1986) . Fsychosocial intervent ions with
cancer Patients - Journal of Psychosocial Uncol day,
3 (4) , 83–75.
Tayl or , S.E., Lichtman , R. R. , Wood, J.V. , Bluming , A. Z. ,
Dosik , G.M., & Leibowitz, R. L. (1985) . I l l ness-related
and treatment-related factors in psychol ogical
adjustment to breast cancer. Cancer , 55, 2506-2513.
Weisman , A. L. . , & Worden , J. W. (1976–1977) . The
existential plight in cancer : Sign if i cance of the first
109 days - International Journal of Psychiatry in
Medic line , 7 (1) , 1 - 15.
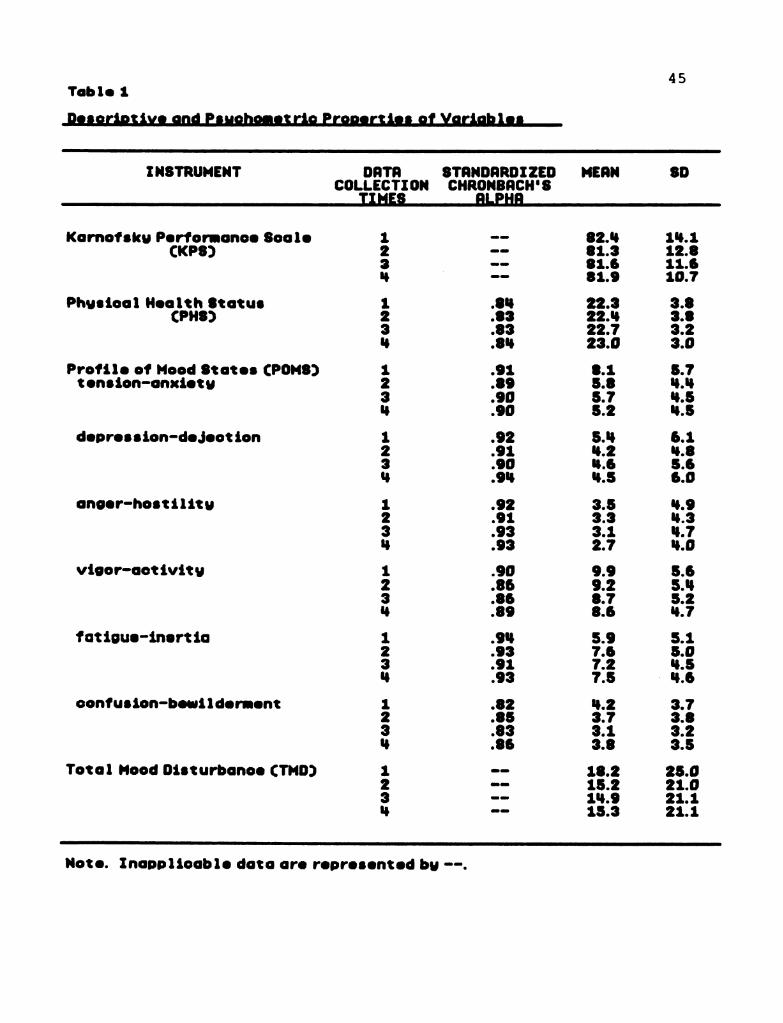
45Table 1
-Ileigriotive and Pºughomºtrio Propºrtiºn of Yariablº_
INSTRUMENT DRTR STRNDRRDIZED MERNCOLLECTION CHRONBQCH"S
IIMES Bll-PHB
Kornofsky Performance Soo leCKPSD
Physiod 1 Health StotusCPHS)
8 3 ; ;Profile of Mood States CPOM8Dtension-anxiety
depression-dejection
cºnger-hostility
vigor-dotivity
fatigue-inertio
confusion-bewilderment
9 3
Total Mood Disturbance CTMD)
9 3
- - i :
; ;
; ;Note. Inoppliocble data are represented by --.
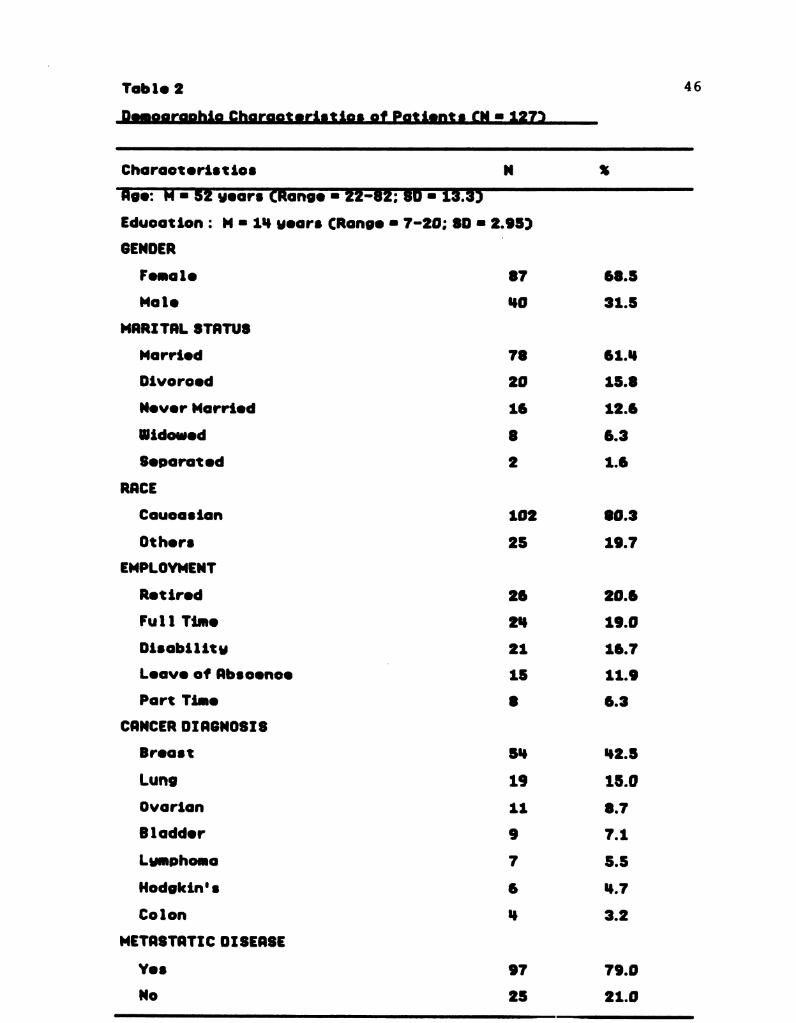
Toble 2
-Demographic charactariation of Patients (N = 1272–
Chorooteristics N %
TESTRETszycarºtkanas Ezz-82; suTI3:35Education : M = 114 years CRonge = 7-20; SD = 2.95.)
GENDER
Female 87 (58.5
Mole 10 31.5
MRRITRL STRTUS
Morried 78 61.1%
Divorced 20 15.8
Never Morried 16 12.6
Uidowed 8 6.3
Separated 2 1.6
RRCE
Coucasion 102 80.3
Others 25 19.7
EMPLOYMENT
Retired 23 20.6
Full Time 24 19.0
Discbility 21 16.7
Leave of Rbs oence-
15 11.9
Port Time 8 6.3
CRNCER DIRGNOSIS
Brecast 5\} 102.5
Lung 19 15.0
Ovorion 11 8.7
Blodder 9 7.1
Lumphomo 7 5.5
Hodgkin's 6 1.7
Colon 1, 3.2
METRSTQTIC DISEQSE
Yes 97 79.0
No 25 21.0
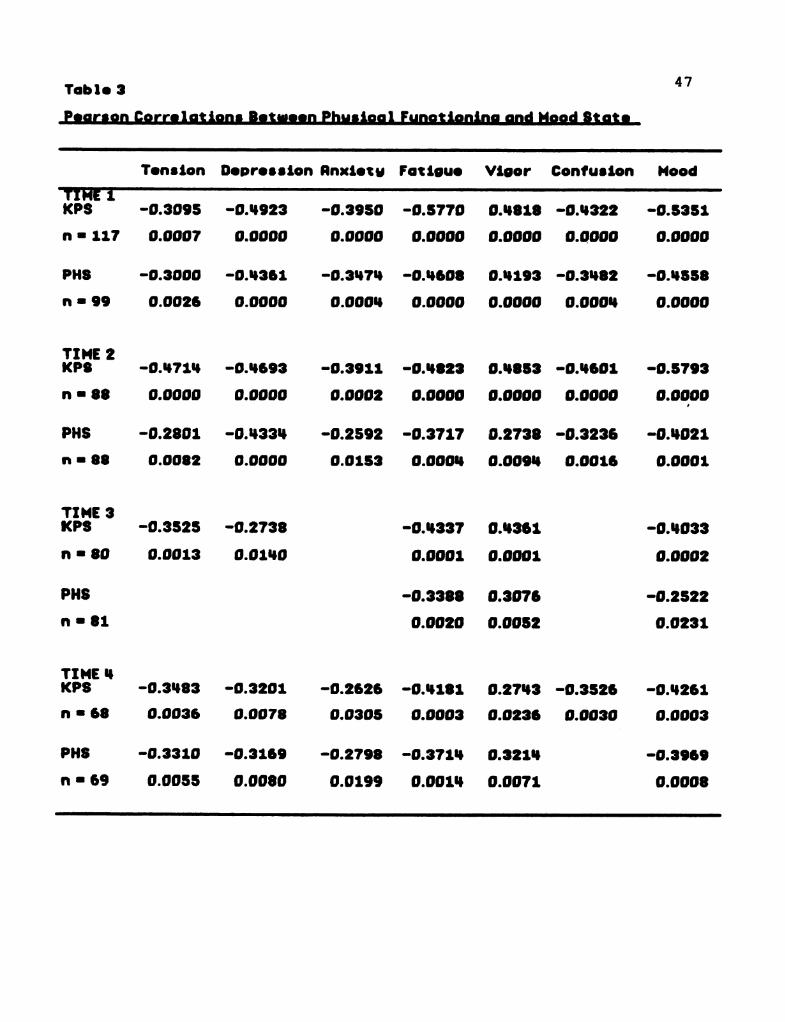
47Table 3
-Paarson Correlations. Between Philaigal fungtioning and Mood State
Tension Depression Rnxiety Fatigue Vigor Confusion Mood
TIRETIKPS -0.3095 -0.1%223 -0.3950 -0.5770 0.4818 -0.4322 -0.5351
n = 117 0.0007 0.0000 O.0000 0.0000 0.0000 0.0000 0.0000
PHS -0.3000 -0.1%361 -0.31%.71 -0.1%008 (J.M. 193 -0.3482 -0.14558
in s 99 0.0026 0.0000 0.0001} 0.0000 0.0000 0.0001} 0.0000
TIME 2KPS -0.147.10% -0.4693 -0.3911 -0.04823 (0.14853 -0.04601 -0.5793
n = 88 0.0000 0.0000 0.0002 0.0000 0.0000 0.0000 0.0000
PHS -0.2801 -0.14331, -0.2592 -0.37.17 D.2738 -0.3236 -0.1%021
in s 38 0.0082 0.0000 0.0153 0.0001} 0.009! 0.0015 0.0001
TIME 3KPS -0.3525 -0.2738 -0.4337 (0.13361 -0.1%033
n = 80 0.0013 0.01140 0.0001 0.0001 (J.0002
PHS -0.3388 (0.3076 -0.2522
in s 31 0.0020 0.0052 0.0231
TIME 14KPS -0.3483 -0.320.1 -0.2625 -0.4181 0.2743 -0.3526 -0.4261
in s 68 0.0036 0.0078 0.0305 0.0003 0.0236 (0.0030 0.0003
PHS -0.3310 -0.3169 -0.2798 -0.37.11% (J.321.1% -0.3969
in s 69 0.0055 0.0080 D.01.99 0.001" (19.0071 0.0003
Tøble tº 48
-significant Changas in Mood states over Ilma
Post - hoo
M SD F 2 Comparison Scheffe
Tension 1 8.1 5.5 11.9 .0000 1 > 2 .00032 5.5 U.2 C3,55) 1 > 3 .00003 S.3 1.0 1 > \} .00001% 5.2 14.7
Fotigue 1 5.9 13.6 3.02 .0312 1 ( 1) .03912 7.0 5.2 C3.5%)3 7.2 1.1%º 7.7 1.7
Confusion 1 1.2 3.7 lº.61 .0039 1 ) 3 .00612 3.3 3.6 C3,57)3 2.0 2.4%1% 3.7 3.5
Touble 5
-significant Diffarangas in Individuals with Bragat Cangar
—and Thoas with Qther Lupes of Canoer
M SD t dº 2
Time 1KPS Breast 87.1 11.0 3.33 123 .0011
Other 78.9 15.2
Time 2KPS Breast 85.1 9.7 2.80 91% .00053
Other 110.3
PHS Broost 214.1 2.1% 10.5 95 .0000Other 21.0 1.1
Time 3KPS Breast 80%.9 10.3 2.60% 83 .0099
Other 12.0
PHS Breast 23.6 2.8 2.35 82 .02.13Other 22.0 3.3
Time i■PHS Brecast 21.0 2.5 3.09 (35 .003
Other 21.9 3.2
50Table @
-significant Differengºs Batiusan Individuals with Hataºtaºis–
and Those without Metastasis
M SD t d'■ 2
Time 1KPS Metastosis 81.6 14.3 -2.22 136 .0312
No Met astosis 87.6 11.8%
Fatigue Metostosis 6.1% 5.3 2.33 147 .0233No Metostosis 13.1 3.9
Time 2PHS Metostasis 22.1 13.0 -2.17 92 .0323
No Metastosis 24.1 2.1
Confusion Metostosis 19.3 10.1 2.67 90 .0090No Metostosis 1.8 1.8
Time !Fotigue Metostosis 3.3 19.7 2.62 66 .01.08
No Metostosis 13.8 3.1
TMD Metostosis 18.2 21.9 2.31% 63 .0223No Metostosis 13.0 10.1%
51Table 7
-statistics of Individuals unable to complate four Month studiº
■ º % Reds on
1. 5 0.0 Too busu2. 7 S.S Rodication treatments3. 5 14.0 Chemotherapu discontinued Cno response)1%. 8 6.0 Too ill5. 6 5.0 Expired6. 3 2.0 Psychological problems7. 7 5.5 Other reosons
Total tº 1 32.0
Notº. Rt Time 1, the total number of patients - 127.
52
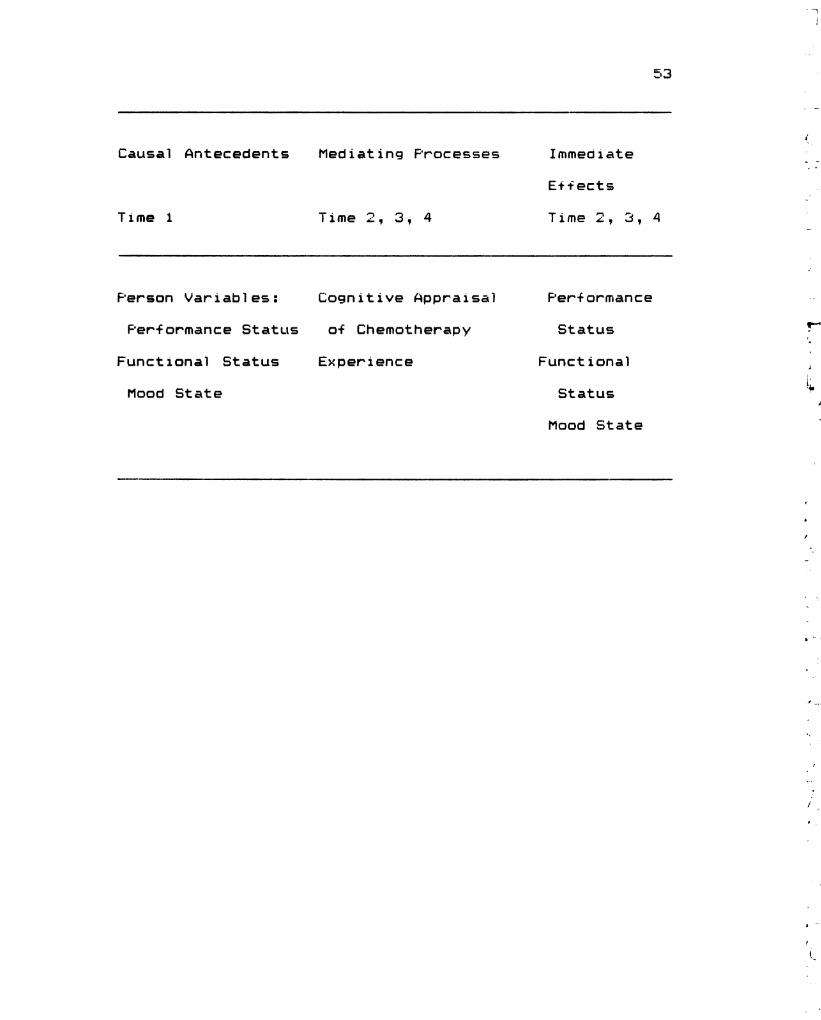
Figure 1 . Lazarus & Folk man 's Stress, Appraisal , and Cop ing
Theoretical Framework with Study Variables
Cognitive appraisal of the person toward his/her cancer
and of the chemotherapy experience can affect the
individual ‘s perception of physical function ing and mood
state at each cycle of chemotherapy.
53
Causal Antecedents
Time 1
Nied i at i ng Processes
Time 2, 3, 4
Immediate
E++ ects
Time 2, 3, 4
Ferson Variables :
Fer:f Ormance Status
Functional Status
Modd State
Cognitive Appraisal
of Chemotherapy
Experience
Perf Cºrmance
Status
Functional
Status
Mood State
–
54
Figure 2. Changes in Karnofsky Performance (KFS) Scores
Over Time
There were no sign i Fi cant changes in KFS scores over
time (F (3,61 ) = .51 1 , p = . 68.
55
Elb■ OOSEKONV/WHO-IHEdAXIS-HONHVO!
–0■ 2-0■ 7|-09-001
EHOOS
5 6
Figure 3. Changes in Fnysical Health Status (FHS) Scores
Over Time
There were no sign if i cant d 1 + + erences in FHS scores
over time (F (3,57) - 1 E 5 D. - - 1 4
57
----08ST).LVLSHLTV/EHTVOISAHc|
EHOOS
F 1 gure 4 . Changes in Tension Scores Over Time
Tension scores ( subscal e Of the FOMS) decreased
significantly over time (F (3,55) = 1 1.88, p = . Q000) , with
the post-hoc Scheffe test indicating that the highest
tension scores were measured at T 1 (p = . QQQ3) .
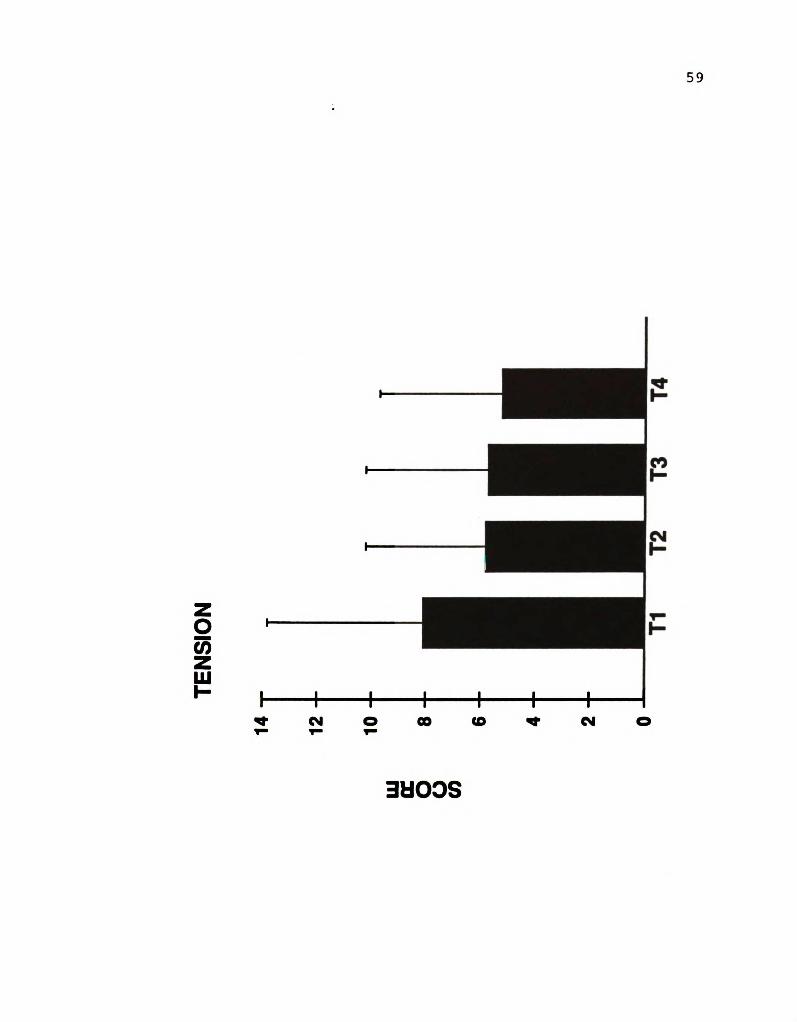
59
+0]+Z||--171
NOISNELLEHOOS
60
Figure 5. Changes in Depression Scores Over Time
There were no sign i + i cant differences in depression
scores (a subscale of the FOMS) over time (F (3,54) = .82
= . 49 ) .
D.
61
NOISSEE|d|E|C.EHO3)S
Figure & . Changes in Anger Scores Over T 1 me
There were no sign if i cant d if + erences in anger scores
(a sub scal e Df the FOMS) Over time (F (3,54) .3% , p = . 76 ) .
wº
/(r-, -
s
63
HEISONV/-01
EHOOS
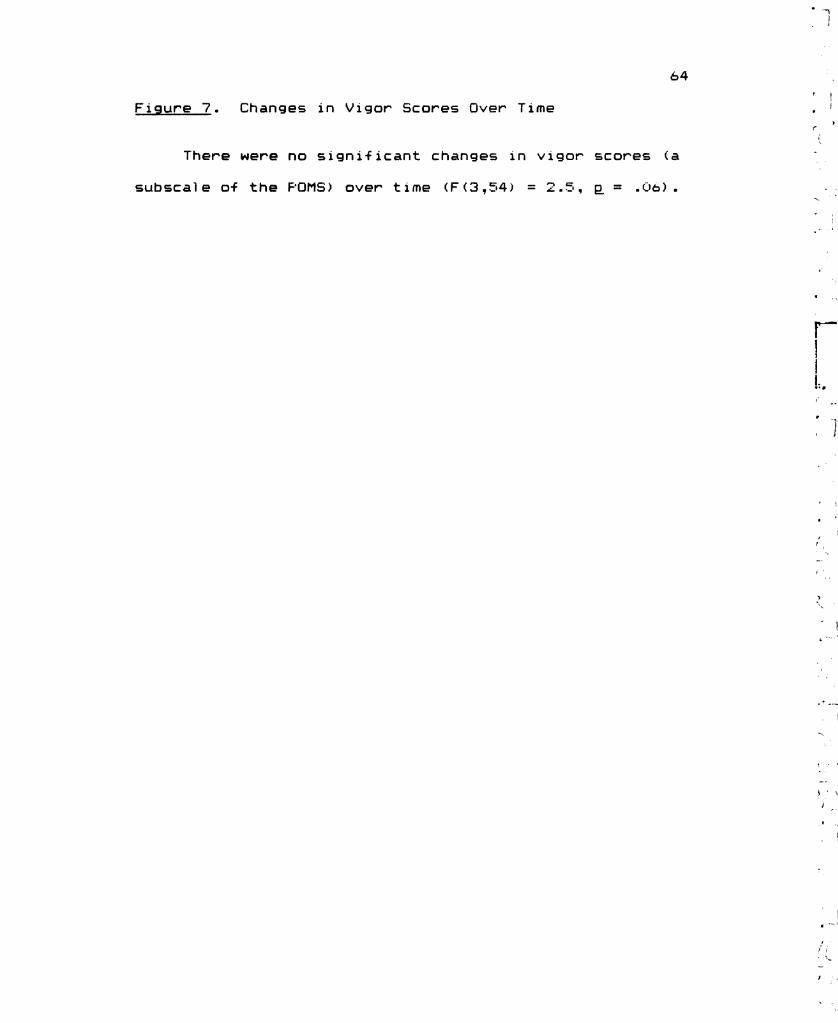
64r
Figure 7 . Changes in Vigor Scores Over Time
There were no sign if i cant changes in v i g or scores ( a-
subscale of the FDMS) over time (F (3,54) = 2.5 , p = . Q6) .
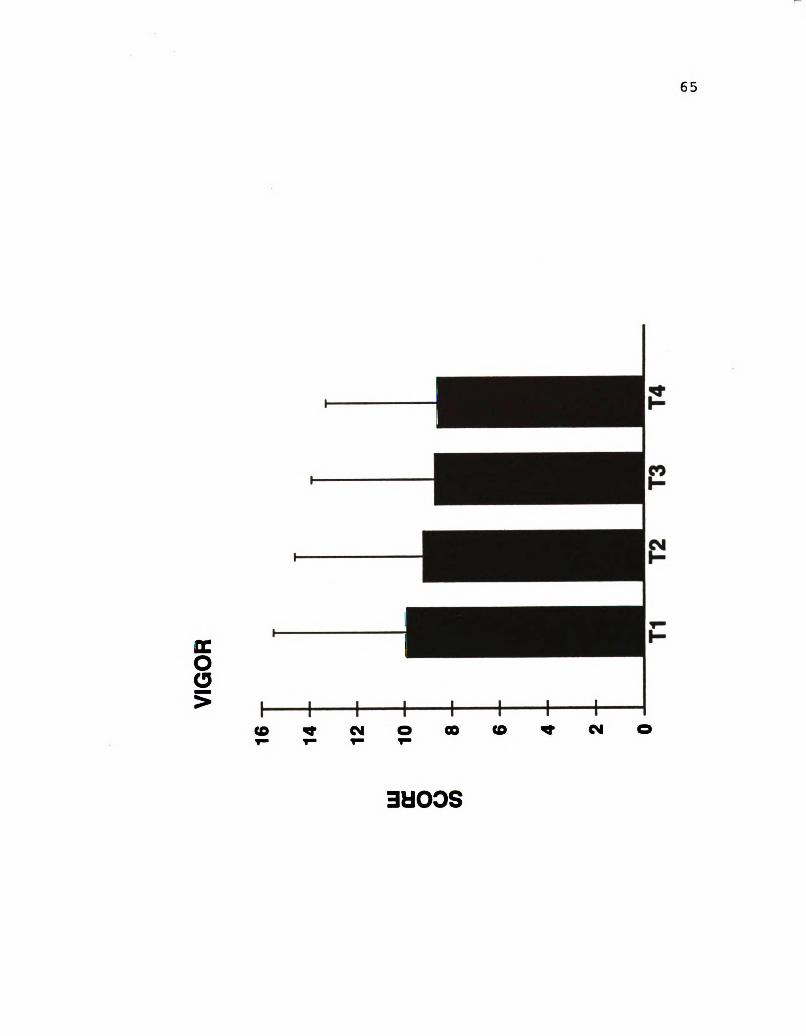
65
EHOOS
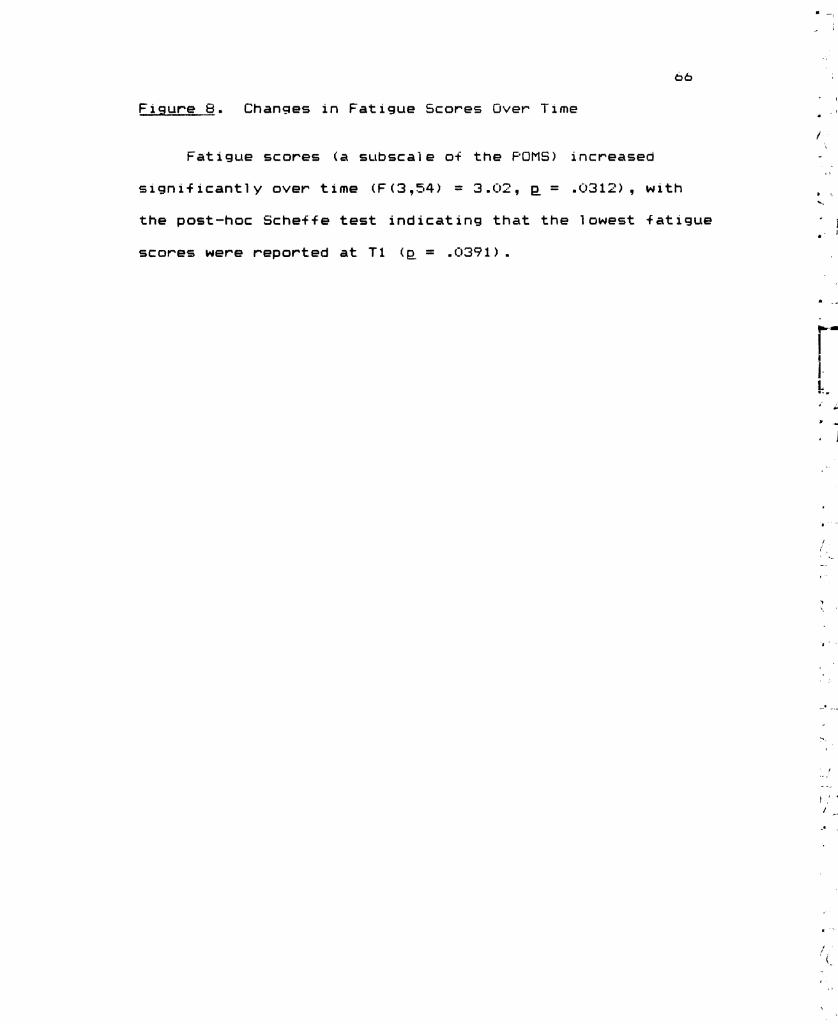
66
Figure 8 - Changes in F at i gue Scores Over Time
Fat i gue scores ( a sub scal e c-f the FOMS) increased
significantly over time (F (3,54) = 3. Q2, p = . Q312) , with
the post-hoc Sche+fe test indicating that the lowest fatigue
scores were reported at T 1 (p = .03% 1 ) .
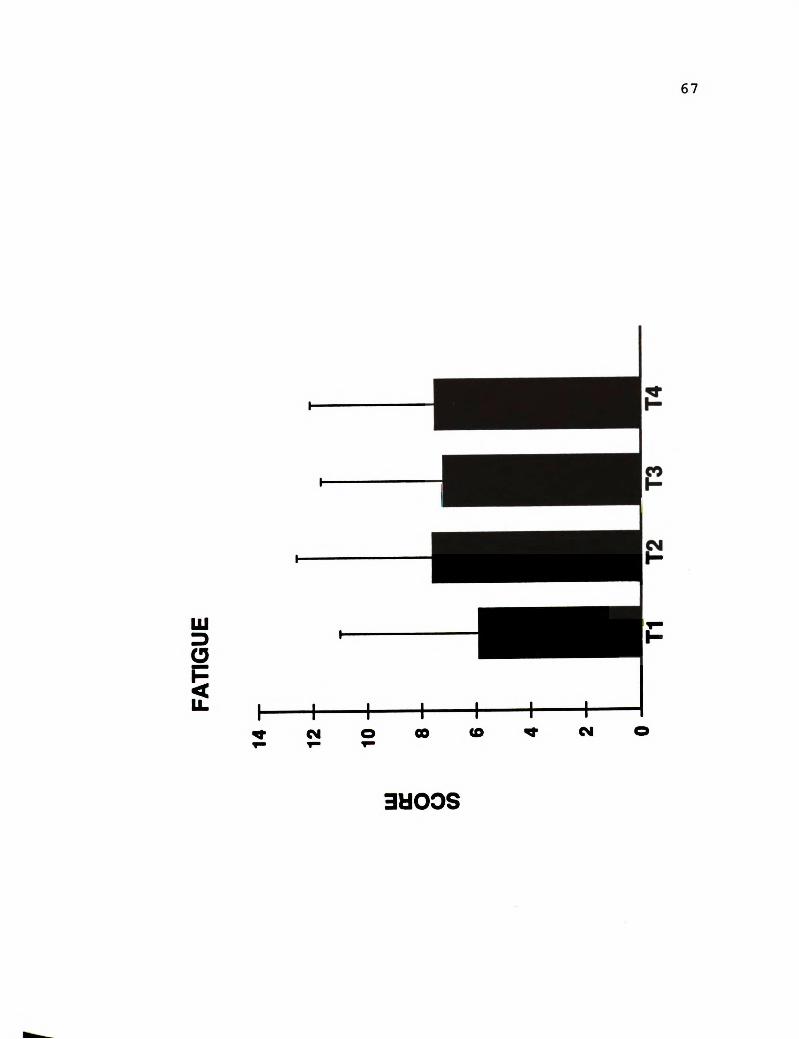
67
ETSOLLVE
EEOC)S
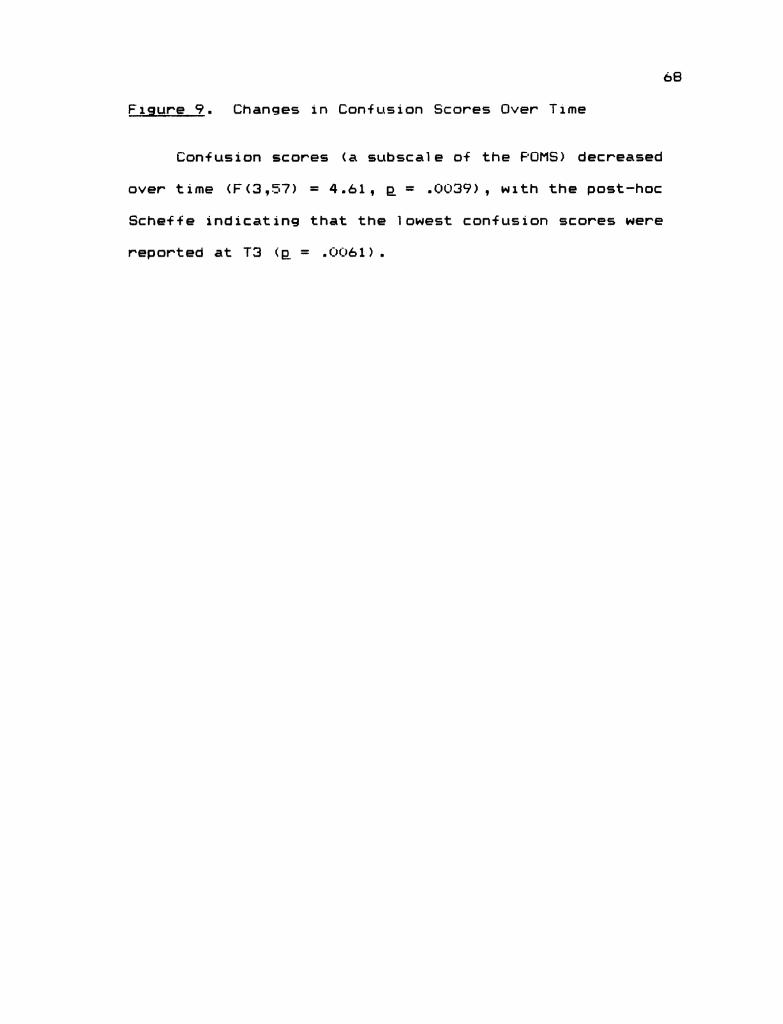
68
Figure 2. Changes in Confusion Scores Over Time
Conf Lisi On scores (a sub scal e dif the FOMS) decreased
over time (F (3,57) = 4.61 , p = . QQ3%) , with the post-hoc
Schef + e indicating that the l owest confusion scores were
reported at T3 (p = . QQ61 ) .
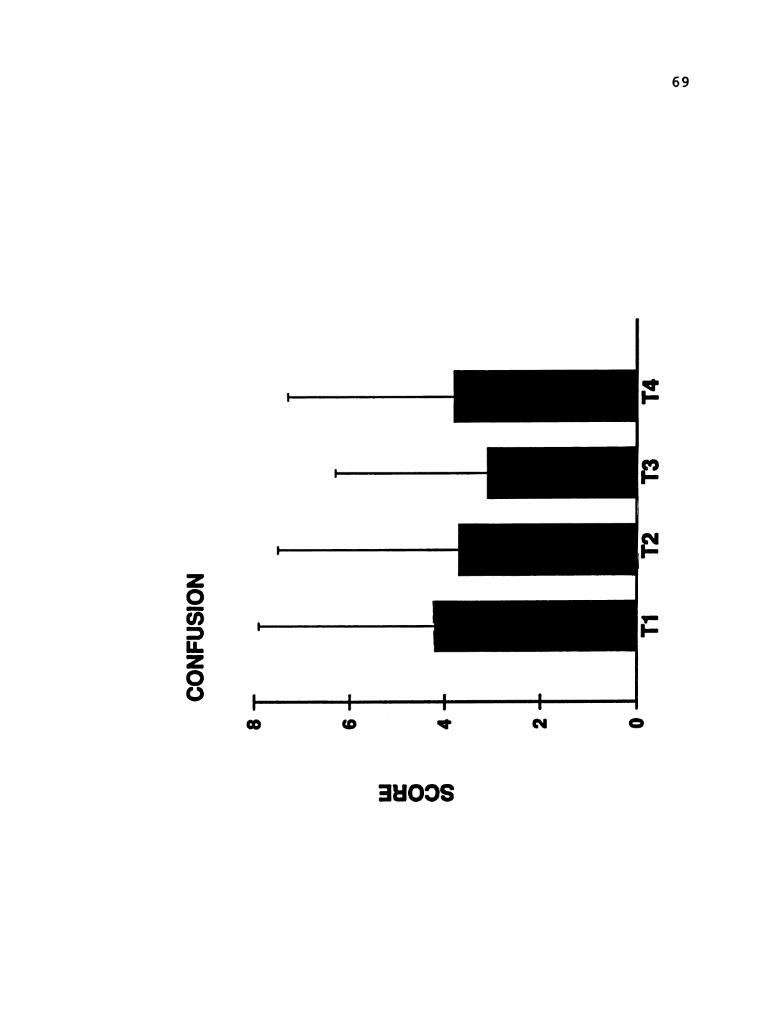
69
NOISTEINOSOEHOOS
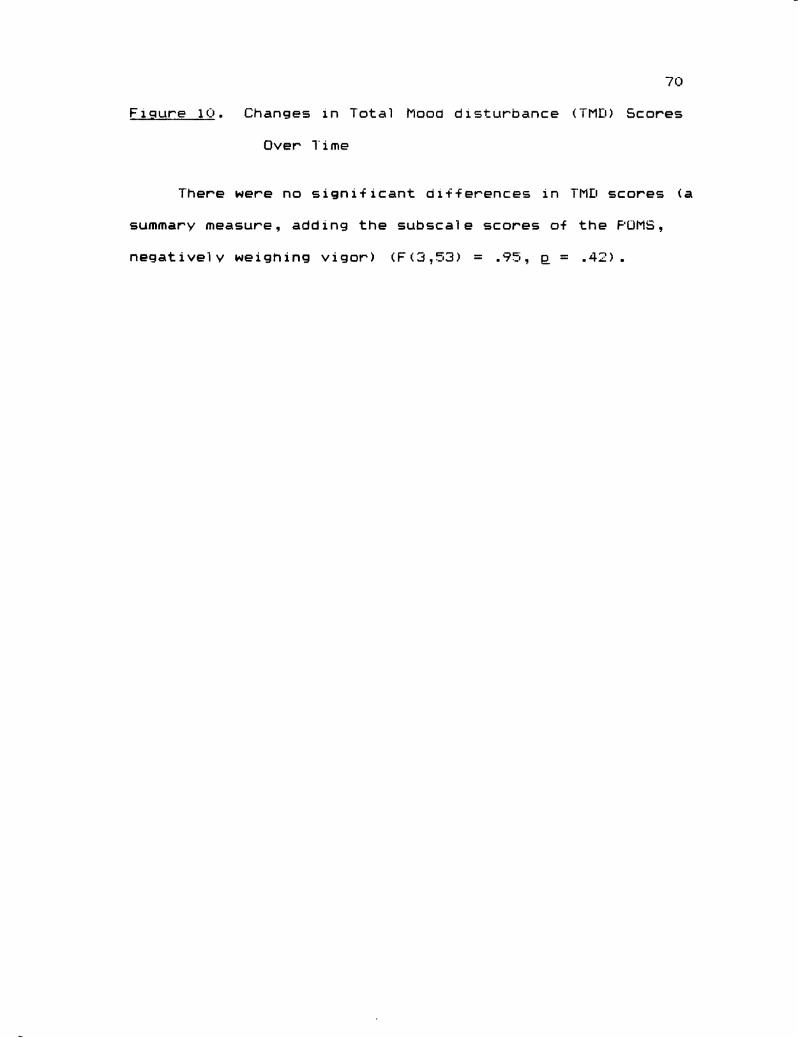
70
F i gure 1 Q - Changes in Total Plood dist Lurbance (TMI) Scores
Over Time
There were no sign if i cant ci i f + erences in TML scores (a
summary measure , adding the sub scale scores of the FUP15,
negatively weigning vigor ) (F (3,53) = .75 , p = .42) .
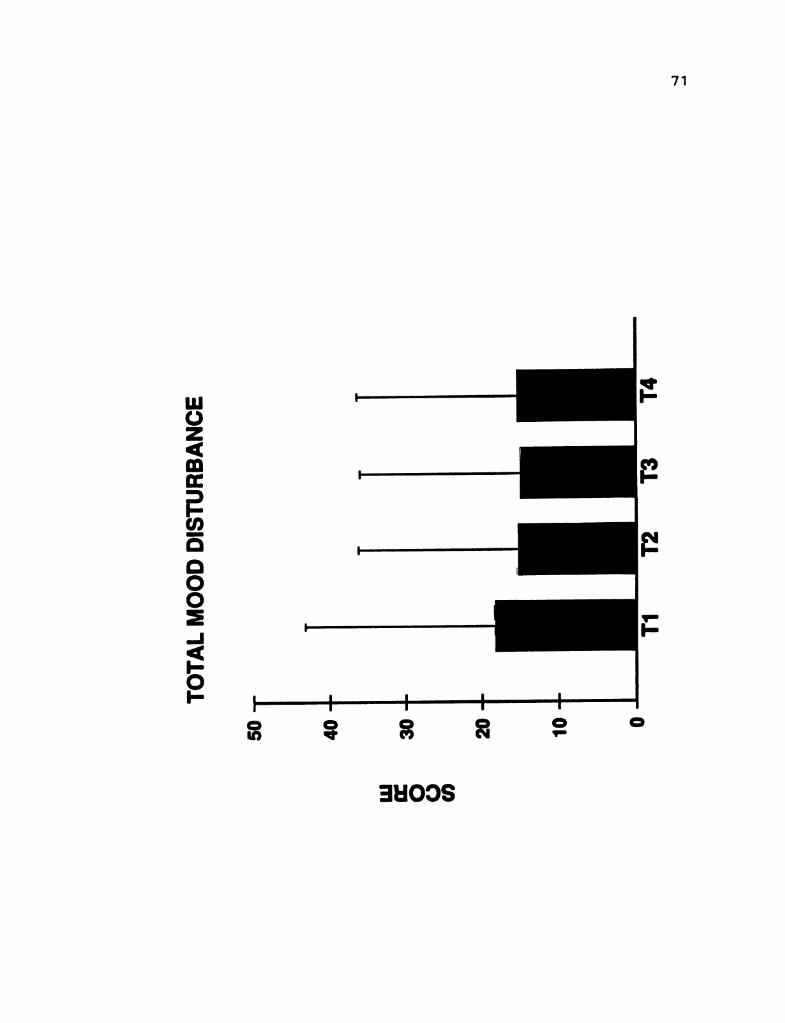
71
--09
EKONVERHTISICICIOOWTVILO1
EHOOS
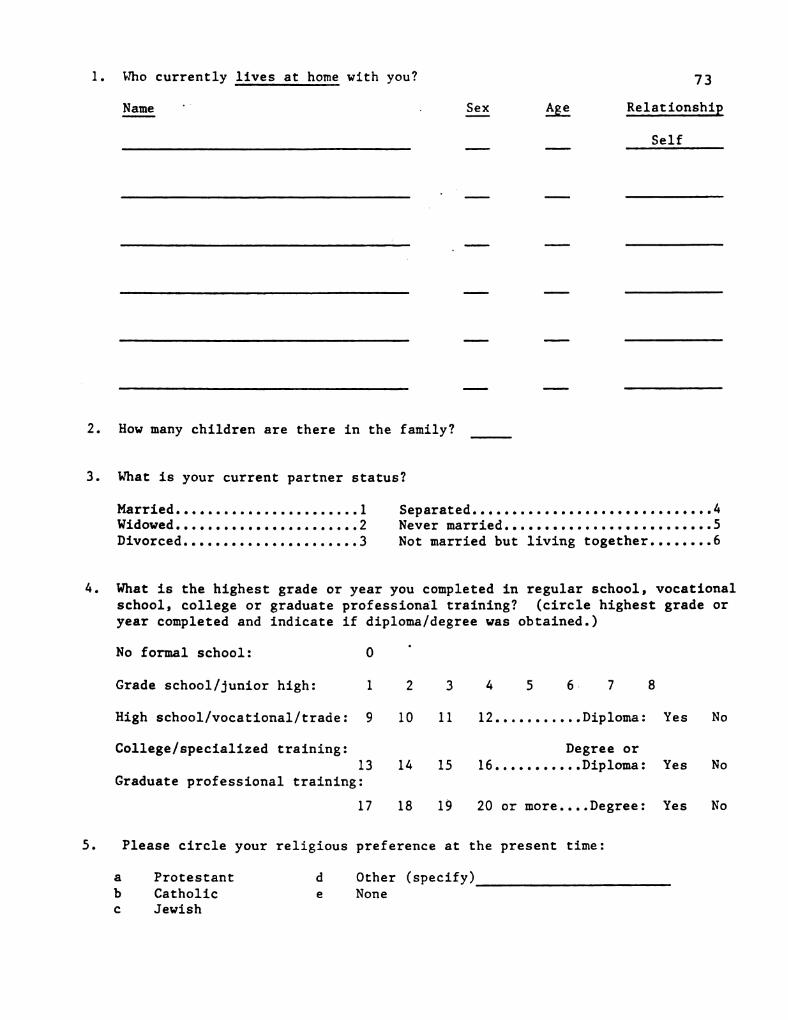
1.
2.
3.
5.
Who currently lives at home with you? 73
Name- - -
Sex Age Relationship
Self
How many children are there in the family?
What is your current partner status?
Married. . . . . . . . . . . . . . . . . . . . . . . 1 Separated. . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4Widowed. . . . . . . . . . . . . . . . . . . . . . .2 Never married. . . . . . . . . . . . . . . . . . . . . . . . . .5Divorced. . . . . . . . . . . . . . . . . . . . . .3 Not married but living together. . . . . . . .6
What is the highest grade or year you completed in regular school, vocationalschool, college or graduate professional training? (circle highest grade oryear completed and indicate if diploma/degree was obtained.)
No formal school: O
Grade school/junior high: l 2 3 4 5 6 7 8
High school/vocational/trade: 9 10 1 1 12. . . . . . . . . . . Diploma: Yes No
College/specialized training: Degree or13 14 15 16. . . . . . . . . . . Diploma: Yes No
Graduate professional training:
17 18 19 20 or more.... Degree: Yes No
Please circle your religious preference at the present time:
a Protestant d Other (specify)b Catholic e NoneC Jewish
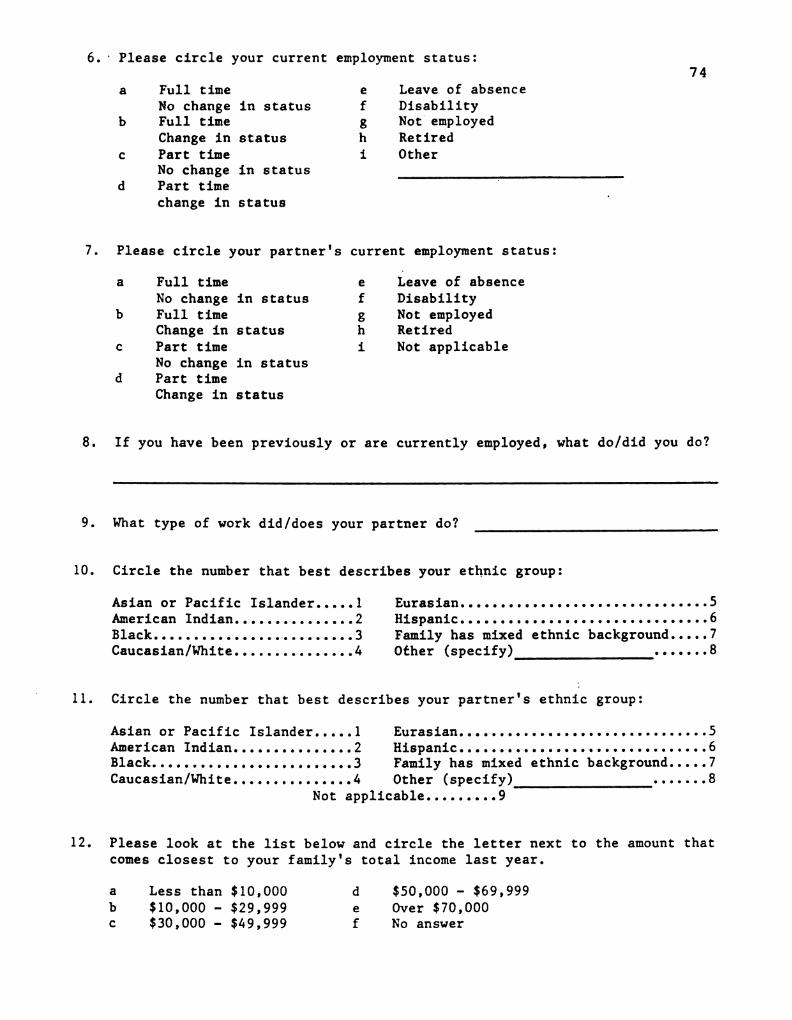
74
10.
11.
12.
Full timeNo changeFull time
Change inPart time
No changePart time
change in
in status
Statu S
in status
Statu S
iPlease circle your current employment status:
Leave of absence
DisabilityNot employedRetiredOther
Please circle your partner's current employment status:
a
b
Full timeNo changeFull timeChange inPart time
No changePart time
Change in
in status
Statu S
in status
Status
iLeave of absenceDisabilityNot employedRetired
Not applicable
If you have been previously or are currently employed, what do/did you do?
What type of work did/does your partner do?
Circle the number that best describes your ethnic group:
Asian or Pacific Islander..... 1American Indian. . . . . . . . . . . . . . .2Black. . . . . . . . . . . . . . . . . . . . . . . . .3Caucasian/White. . . . . . . . . . . . . . .4
Eurasian. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Hispanic. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6Family has mixed ethnic background. . . . . 7Other (specify) 8
Circle the number that best describes your partner's ethnic group:
Asian or Pacific Islander. . . . .American Indian. . . . . . . . . . . . . . .Black. .
l23
Caucasian/White. . . . . . . . . . . . . . .4
Eurasian. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Hispanic. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .6Family has mixed ethnic background. . . . . 7
8Other (specify)Not applicable . . . . . . . . .9
Please look at the list below and circle the letter next to the amount thatcomes closest to your family's total income last year.
a
bC
Less than$10,000 –$30,000 –
$10,000$29,999$49,999
de
f
$50,000 – $69,999Over $70,000No answer
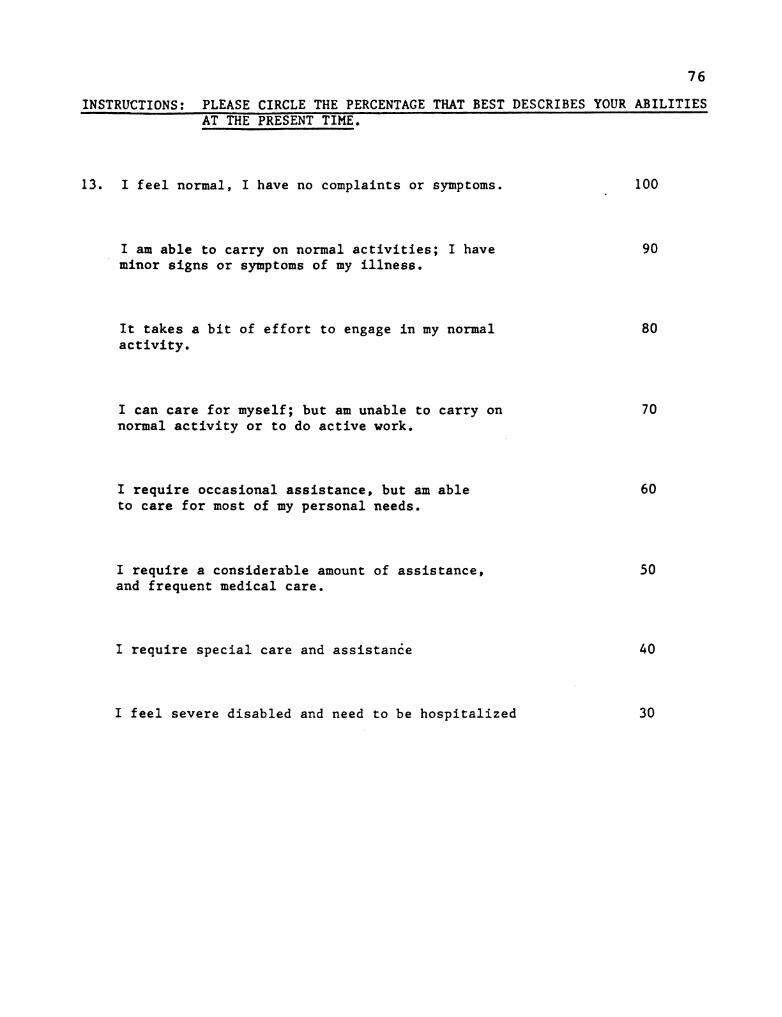
76
INSTRUCTIONS: PLEASE CIRCLE THE PERCENTAGE THAT BEST DESCRIBES YOUR ABILITIESAT THE PRESENT TIME.
13. I feel normal, I have no complaints or symptoms.-
100
I am able to carry on normal activities; I have 90minor signs or symptoms of my illness.
It takes a bit of effort to engage in my normal 80activity.
I can care for myself; but am unable to carry on 70normal activity or to do active work.
I require occasional assistance, but am able 60to care for most of my personal needs.
I require a considerable amount of assistance, 50and frequent medical care.
I require special care and assistance 40
I feel severe disabled and need to be hospitalized 30
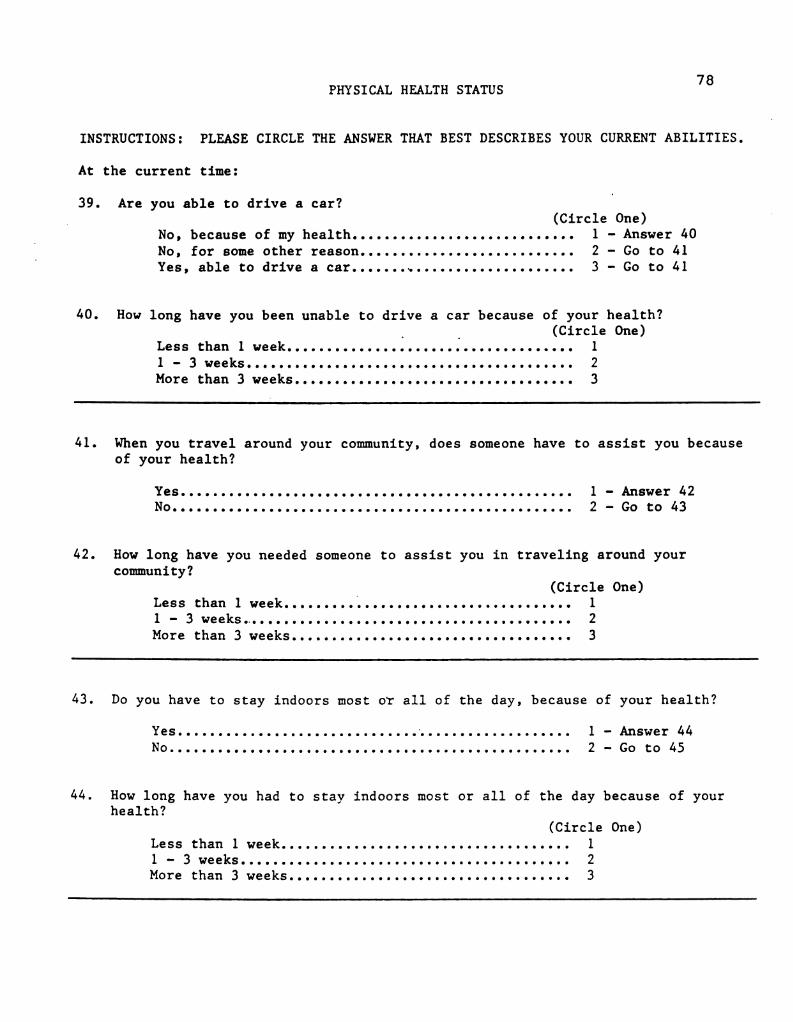
PHYSICAL HEALTH STATUS 78
INSTRUCTIONS: PLEASE CIRCLE THE ANSWER THAT BEST DESCRIBES YOUR CURRENT ABILITIES.
At the current time:
39. Are you able to drive a car?(Circle One)
No, because of my health. . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 - Answer 40No, for some other reason. . . . . . . . . . . . . . . . . . . . . . . . . . . 2 - Go to 41Yes, able to drive a car. . . . . . . . . . . . . . . . . . . . . . . . . . . . 3 - Go to 41
40. How long have you been unable to drive a car because of your health?-
(Circle One)Less than 1 week. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1l
-3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
More than 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
41. When you travel around your community, does someone have to assist you becauseof your health?
Yes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . l - Answer 42No. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
-Go to 43
42. How long have you needed someone to assist you in traveling around yourcommunity?
(Circle One)Less than 1 week. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
-3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
More than 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
43. Do you have to stay indoors most or all of the day, because of your health?
Yes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 - Answer 44No. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 - Go to 45
44. How long have you had to stay indoors most or all of the day because of yourhealth?
(Circle One)Less than 1 week. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 - 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2More than 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
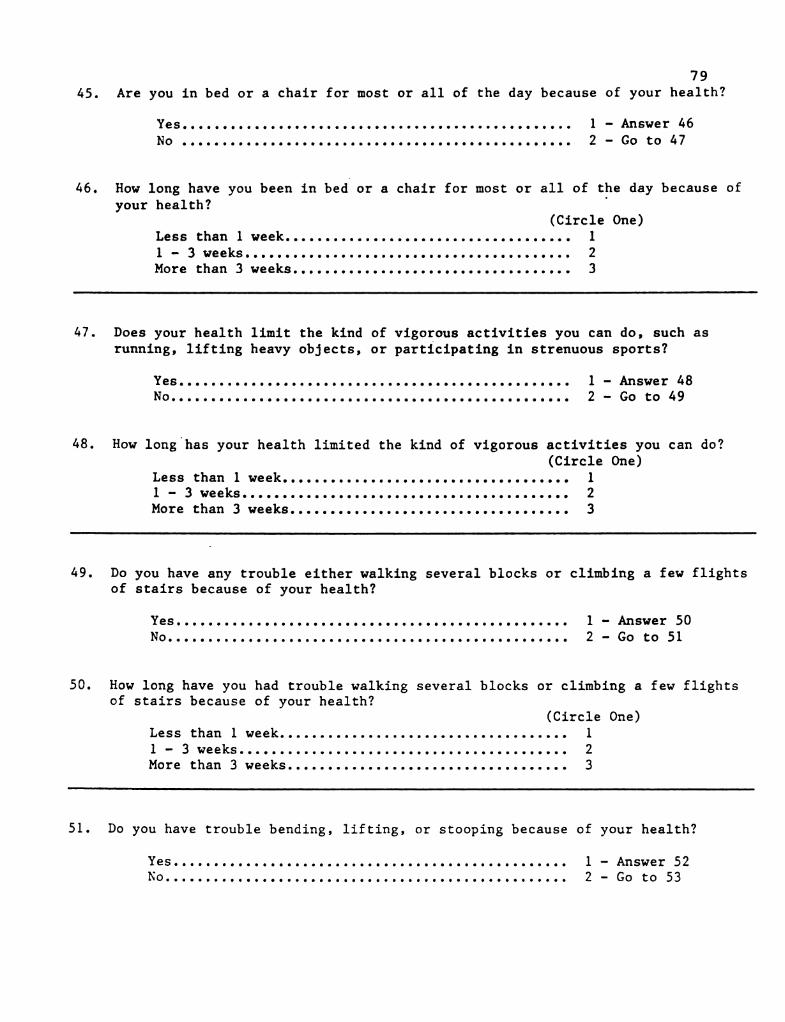
79Are you in bed or a chair for most or all of the day because of your health?45.
Yes. . . . . . . . . . . . . . . . . - - - - - - - - - - - e e e e e º e e - e. e. • e º e º 'º - - - - 1 - Answer 46No e e - e. e. e. e. e. e. e. e e - e. e. e. e. e. e. e. e. e. e. e. e. e. • e º e - e. e. e º 'º - e - - - - - - e - - - - 2 - Go to 47
46. How long have you been in bed or a chair for most or all of the day because ofyour health?
(Circle One)Less than 1 week. . . . . . . . . . . . . . . e - e. e. e. e. e. e e s - e. e. e. e. e. e. e. e. ... 11 - 3 weeks. . . . . . . . . . . . . . . . - - - - - - - - - - - - - - - - - - - - - - - - - 2More than 3 weeks. . . . . . . . . . . . . . . . . . . - - - - - - - - . . . . . . . . 3
47. Does your health limit the kind of vigorous activities you can do, such asrunning, lifting heavy objects, or participating in strenuous sports?
Yes. . . . . . . . . . . . . . . . . . . . - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 1 - Answer 48No - - - - - - - - - - - • e º 'o - e º 'o e º e - e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. - - - - - - - 2 - Go to 49
48. How long has your health limited the kind of vigorous activities you can do?(Circle One)
Less than 1 week. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . l1 - 3 weeks. . . . - - - - - e e º e e - e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. 2More than 3 weeks. . . . . . . . e - e. e. e. e. e. e. e. e. e. e. e. e. e. . . . . . . . . . . . . 3
49. Do you have any trouble either walking several blocks or climbing a few flightsof stairs because of your health?
Yes. . . . . . . . . . . . . . . . . . . . . . e e o e e - e. e. e. e. e. e. e. e. e. e. e. e. e. . . . . . . . . 1 - Answer 50No. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . e e e º e º e e s e ... 2 - Go to 51
50. How long have you had trouble walking several blocks or climbing a few flightsof stairs because of your health?
(Circle One)Less than 1 week. . . . . . . . - - - - - - - - - - - - - - - - - - - - - - - - - - - ... 11 - 3 weeks. . . . . . . . . . . . . . . . . . . . . . . e e º e º 'º e s e e º 'º e e . . . . 2More than 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
51. Do you have trouble bending, lifting, or stooping because of your health?
1 - Answer 52No. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2 – Go to 53
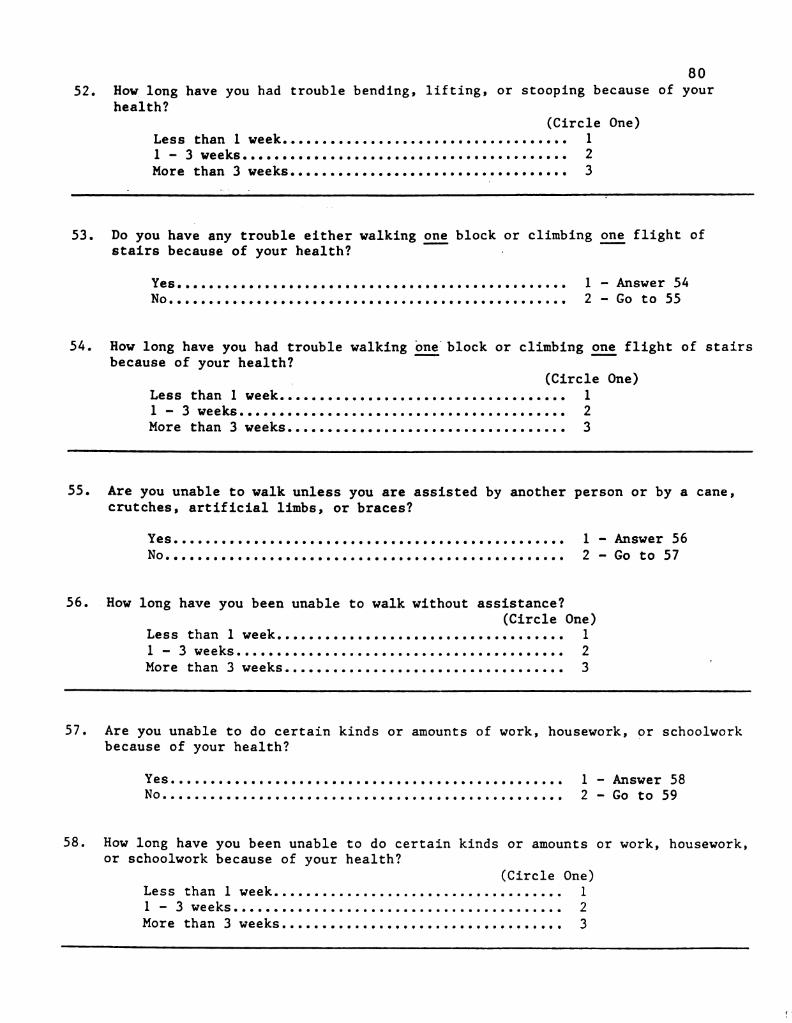
80How long have you had trouble bending, lifting, or stooping because of your52.health?
(Circle One)Less than 1 week. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 - 3 weeks. . . . . . . . . . - - - - - - - - - - e e s e º e º e o 'º e º e º 'º - e. e. e. e. e. 2More than 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
53. Do you have any trouble either walking one block or climbing one flight ofstairs because of your health?
-
Yes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1 – Answer 54No. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
-Go to 55
54. How long have you had trouble walking one block or climbing one flight of stairsbecause of your health?
(Circle One)Less than 1 week. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1l
-3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
More than 3 weeks. . . . . . . . . e c e e s - e. e. e. e. . . . . . . . . . . . . . . . . 3
55. Are you unable to walk unless you are assisted by another person or by a cane,crutches, artificial limbs, or braces?
Yes. . . . . . . . . . . . . . . . . . . . - - - - - - e e - e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. 1 - Answer 56No. . . . . . . . . . . . . . . . . . . . - - - - - - - e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. 2 - Go to 57
56. How long have you been unable to walk without assistance?(Circle One)
Less than 1 week. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . l1 - 3 weeks. . . . . . e e - e. e. e. e. e. e. e. e. e. e. e - e. e. e. e. e. e. e. e. e. e. e. e. e. e. e º 'o - e. e. 2More than 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
57. Are you unable to do certain kinds or amounts of work, housework, or schoolworkbecause of your health?
Yes. . . . . . . . . . . . . . . . . . . . . . . . . . . . e - e. e. e. e. e. e. e. e. e. e. e. e. . . . . . . . 1 - Answer 58No. . . . . . . . . . . . . . . . . . . . . . . . . . - - - - - - - - - - - - - - - - - - - - - - . . 2 – Go to 59
58. How long have you been unable to do certain kinds or amounts or work, housework,or schoolwork because of your health?
(Circle One)Less than 1 week. . . . . . . . . . . . . . . . . . . - - - - - - - - - - - - - - - - - l1 - 3 weeks. . . . . . . . • * * * * * * * * * * ~ * - e. e. e. e. e s - e. e. e. e. e. e. e. e. e. e. e. e. 2More than 3 weeks. . . . . . . . . . . • e º e º e - e. e. e. e. e. e. e. e. e. e. e. e. e. e. e. ... 3
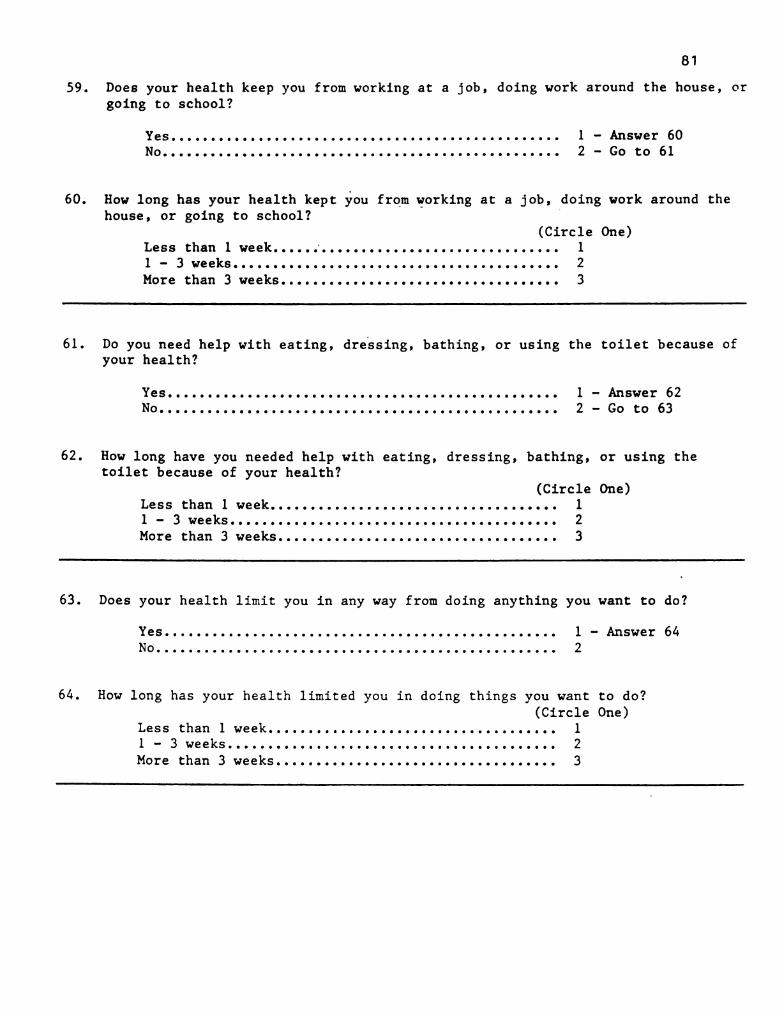
81
59.
60.
Does your health keep you from working at a job, doing work around the house, orgoing to school?
1 - Answer 602 – Go to 61
Yes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .No. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
How long has your health kept you from working at a job, doing work around thehouse, or going to school?
(Circle One)Less than 1 week. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 - 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2More than 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
61.
62.
Do you need help with eating, dressing, bathing, or using the toilet because ofyour health?
1 – Answer 622 – Go to 63
Yes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .No. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
How long have you needed help with eating, dressing, bathing, or using thetoilet because of your health?
(Circle One)Less than 1 week. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 - 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2More than 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
63.
64.
Does your health limit you in any way from doing anything you want to do?
1 - Answer 642
Yes. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .No. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
How long has your health limited you in doing things you want to do?(Circle One)
Less than 1 week. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11 - 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2More than 3 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3
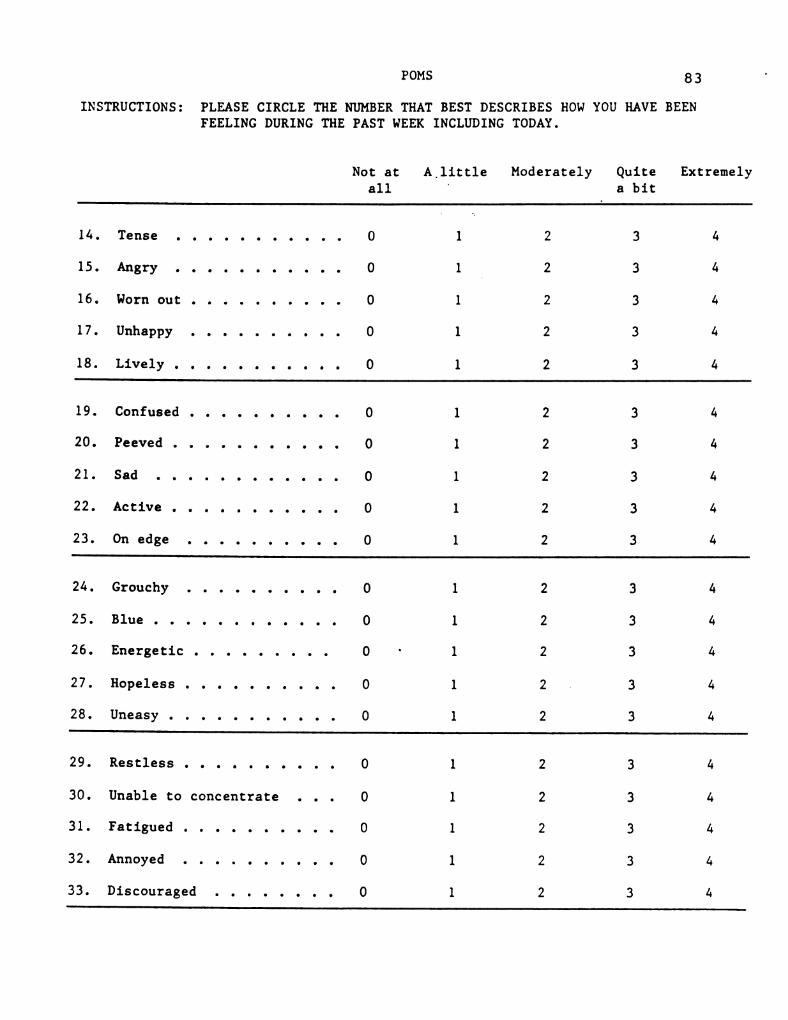
POMS 83
INSTRUCTIONS: PLEASE CIRCLE THE NUMBER THAT BEST DESCRIBES HOW YOU HAVE BEENFEELING DURING THE PAST WEEK INCLUDING TODAY.
Not at A. little Moderately Quite Extremelyall
-a bit
14. Tense . . . . . . . . . . . 0 1 2 3 4
15. Angry - - e - e. e. e. e. 0 1 2 3 4
16. Worn out . . . . . . . . . . 0 l 2 3 4
17. Unhappy . . . . . . . . . . O l 2 3 4
18. Lively . . . . . . . . . . . 0 l 2 3 4
19. Confused . . . . . . . . . . O l 2 3 4
20. Peeved . . . . . . . . . . . O l 2 3 4
21. Sad . . . . . . . . . . . . O l 2 3 4
22. Active . . . . . . . . . . . 0 l 2 3 4
23. On edge . . . . . . . . . . 0 l 2 3 4
24. Grouchy . . . . . . . . . . 0 1 2 3 4
25. Blue . . . . . . . . . . . . 0 l 2 3 4
26. Energetic . . . . . . . . . 0- l 2 3 4
27. Hopeless . . . . . . . . . . O l 2 . 3 4
28. Uneasy . . . . . . . . . . . 0 l 2 3 4
29. Restless . . . . . . . . . . O l 2 3 4
30. Unable to concentrate . . . O l 2 3 4
31. Fatigued . . . . . . . . . . O l 2 3 4
32. Annoyed . . . . . . . . . . O l 2 3 4
33. Discouraged . . . . . . . . 0 l 2 3 4
84(Continued)
Not at A little Moderately Quite Extremelyall a bit
34. Resentful . . . . O l 2 3 4
35. Nervous . . . . . 0 1 2 3 4
36. Miserable . . . . . O l 2 3 4
37. Cheerful . . . . . O l 2 3 4
38. Bitter . . . . . . . . 0 l 2 3 4
39. Exhausted . . . . . . O l 2 3 4
40. Anxious . . . 0 l 2 3 4
41. Helpless . . . . . . 0 l 2 3 4
42. Weary . . . . . . . 0 l 2 3 4
43. Bewildered . . . . . O l 2 3 4
44. Furious . . . . . . . O l 2 3 4
45. Full of pep . . . 0 1 2 3 4
46. Worthless . . . . . 0 l 2 3 4
47. Forgetful . . . . . . 0 l 2 3 4
48. Vigorous . . . 0 l 2 3 4
49. Uncertain about things . 0 l 2 3 4
50. Bushed . . . 0 l 2 3 4
* → - ? ~.cº L_ `. —r- & |-- C. * > ( ). --- º
-
--- <!-- -
s sºon” L. Jºs *T/C * Dºlls ºvºgº º -- ~/C & Csº º ºº ~~ º, sº 1.
-
z - -*//*@ ºf ºne cº■ º º Sºnºcºlº■ /º. Q sº tº C).7g/■ . !/?ºld S->
Y ºl. º/ºutcº .- º* º
*~ 1. -> -
º -S º ar O)) cº º ~ ** - ( ) .* *.. - & º * –
%, O) le s T- °, L. B RARY Sº [-r] *, * // A-2 s T- º } L. B RARY S. º
º [T] & – 4, ---, -º |- l º, […] & --- o, -r- sº L(* ~ -f | | | ~ * º * - - - Sº
- - -*/ ~ _
% -- sº ºvº. 9 in ºr TúC º º vº gº º is ºº >, >( ) *- 2
**, Sº- ~, º, ºf ! . . . ~, '4 sº ~y12. Sº * ~ 2 N ºf S nº.71/11////? 2 *
... -- *.S. 0.05/01/11/ / ////(J 2- S. - - - - - - - !. () }} } }//?". // 'Q-- ~ y, 7/7, fly
■ º sº, "Sº a cºncº sº. , 9 sº º, cºy 7& º º º °o sº º, .* ‘’’.
* I jº Ole ºn tº ■ º. Ole sº tº& (). > - *— %) -r- C a sº
- -Q - -
~ C | ~ f º-
C, | | ~ * ºº - /C % y – – S. ºvº 3 IT * -- sº C t /(
7. º - - º A-Tºvº 3 in * -º ~ S- * 1. º. *** -
º 42. Nº º 1. S’ ~) - º, -º * * , , , , , (TN º, ,º -1.- Cº.) 1/11/ º 2. * * * * * * * * * * 0.757-21/?" / / ///? (J
-º Fine ºld S &-
.Nº *4. º 7 1//■ º º º,-
\*~ - -~ º, A- &- º * * * A- -º- -
- -.** º C i Y _º - ? } Sº- -
º, L | B RA R_Y sº L. J º, ..) le_sº […] º, y L ■ B RA R_Y Sº ºr- º, 4- / le º T
y - - –– - y ~ L l --2 > ‘o ~ o C. &o, | || sº cº- ^c, […] sº LN, ■ º L. sº cº-, , , , º […] * -->º, NS (/C º-' sºvº gº º s' T.C 2 *----' sº ºv-S e- *º º, ~ * ...sº º ~ º, sº º, s
-42, -º º 2. º. * / / / > 2 - * º jº
º º 2 < C■■ ,- -
*S dºl■ !-
!/?" --
*Y.1//, //, //C/º () *- -º-, 4-4 tº -'y º º/7 incº gº, sº º, º/rºncº º º-
1. * *- -
J. -S- 1. º %5 *-oº, O - º - - º * *sº ■ º. L. BRARY is ■ ºlº, O/) sº [-º, L1 BRARY is fir- “… . /
C –––L.
------- -
L.- * ~&*
- »
s -°o | || 3. Q- > °C, --r- ** ºs ºvºgº º-' º■ C * I s ATuvº■ ºf T * –– * - C º■
*-
º, º º, Sº* 4, Nº. ºf 77/71 f ■ , 12, Sº
ºº,Sºft,nº gº tº º/?tº C■ . º/■ ºn CA■ J 2.
- * : * ~ **... sºut■ º 2.S *
-4- sº º º A- * sº
-
-
2 º º º- * * c º
-º, O/ º %, L. B. RARY sº —r- º O/) s […] º,º, L■ B RA R_Y sº L-
| • * | |- - -~
---c o &
- * -
". º vo ■ º r- o” º, […] sº -*º, L. sº >T * Wºwºg in º. L. sº . ■ /C 2 *-*-' sº ºv’■ gº º Sº -2 º' q.” -
( ) & - - ry ~ 2 * ! --* . . Sº 'a sº º, sº º, 3 -y
**S ºut■ º º C■ .tº ■ º, º º■ *@ ºf .
º Sº 4-
sº % & /…/■ c■ , ■ o Nº ºt A-2 sº º “CisSº 'º. -> 9. * º * t- º
c º º, * x * ºº ‘’’.
tº sº fºr lº O/] sº […]” LIBRARY is ºr ■ º, O) ºn tº~ L– O. […] sº –– •o - r & L. º sº –– 'o
--
~ * (* º r * º º-
+.- C - ºvugin º -- * I■ o ■ º ls A-Tºvº 9 17 * -º
º, sº gº º/ºr ” sº º, º nºt ■ º C. *.cºncº lsº -- ~~~~ Sº º, C).7///7.1/10/■ o sº -- *- º _º-
* 'º º *A sº º * cy ->
”, L. BRARY sº----
º, O) le s T- º, L1 BRARY sº L º, O) le sº ■L.º -
\
º
o, -r- > (* […] sº---
o, —r- S- y º, T º| | -- c- * - * L-
| ~ * * . º ~~! -
1-1 %, º U■ C º'-'º ºvº gº º º i■ ( º sº ºf~
2. - -& ) ~ *
- !, -> **, Sº ~, 72 -** ~y *1. Sºº, Nº º, Sº º * 12 -º
º ºf S yº y ºrºf 2 <! --~~~~ 1. Jºy' 21/?". / º 2. * Y, Z/7, fºr ºff ºf C■ º *. ºº sº cºnciº º 4. 0.05'101/11/ *S. Sº, ºr º /.../■ ciº■ o 2
wsº -º- º º º º … º. º
*, * , <- º, p .* * > * a tº &- º,-■ º tºº tº º, . /le s ■ º tºº sº,
sº º —r- ~ º sº - - - 'o • r- ~ - *2-º ~s v. N. º L. º c-, 1/7 º, ■ º- º~ A R v \{ { º º' c-7 , /* º ■
-
S AR v × 9 T º, sº (10 º-
j v \{ {} IT º, º L'C º,º . Sº º
º - ºr a-
~, f4. - Sº 7- - º ºº/º º º - *** - - - ** Jºy'■ J1/11////(J 2.s. C■ . **, *7-zº-■ ºº. **º A- .Nº º C 7//7”//c■ . To & Cº. º º º, º/7 ºf Clººd sº
O)) º º &A R_Y "… O/2 ºrºº Li B R A R Y sº
- º, ~ * .** f ~ -- -- -
“, t A * lº ■ º º, L! ■ º ■ A. R_ Sº - r = %, t .* º B ~ R_Y _º-> -- - º - -
| – º-
wº* }
(). ■ º º L. | > Q- - &- (? r- -
C. - f - (* & * - ~ *
º' ºvº gº º º■ C º' -- ºvug in º. -- –- * t
sº
º-º, s !/. ->º: , ºr º, NT º, sº º, º f ; ; ; º º º, NT -º º■ ºvº º º■ º Tº dº */ºf Q J 2. * * * * * *- -,
- -
S sº cºncº º-
Yº sº, º ■ º*-
- *- * º -S- º-
n *- - º y- -*.* 2. º -.* * *º
-
..))) 2 º r — ”, 1_ | ■ º RA R_Y º ■ ' rºl º t)/2 . º F----, ”,
-L ■ º ■ º A■e
º
º■9
~S’ H *, -- Lº ºvºv ºvº º ”, tº ' -7 sº 4, - - - - º
º º, tºsº - + *O º O- º | •o —r- º |-- º
-r ~ […] * º * -7 º* º ~ -*-
Aºvº. 9 in º, - * I■ o – Sº AR5 vº; 9 T º sº < (■ ( º,--
*
º, sº tº sº * > 1, N
nº.71/ º/ºr S ºs-
º cºn■ º- 2.s C■ .
-----, -- * -JJ) 77.1/11/////Sº sº Sº lºcºco is ºw
-
Q º º/7 ºncºco sº.st- -> º ~sº- - - º º º
O) sº tº º BRARY_sº | | |º O) is º, Librass sº L.* -sº-~ S- ‘…. º o -- ->
º […] º A-Tº: vº 9 IT º L. sº - /C º º º A ºf vº G 7 º,-> sº - /Cº-y º - -
º s w º º º º sº* Sº ojº■ (, *2 S
-º, Sº º/wº º C■ . A.
CO º dº º sº Sw ºil/7C■ , ■ º - 2 º º S & 1//, //, //- N + º 4. - --> -º-
- 4 *~-º- º, ~ º, o º
º- º *- - -
s º2- O/7 sº º, L ■ B RA R_Y º | º, O) º,!- L ■ ■ º RA |-
L. O) | –– ()-
J
c - -- º, º --- *o --
º■ c º […] sº A Rivº G 17 º L J's º/C * I ºvº gº º, L.ººp, sº º ºn tº º, sºº º s
- 1- ºr º, Nº - -
- º }}}.}//?" / / ///?” (J 2.s - -> * UW'■ 21/?? / / //?” (J ºSºnº ■ º. " º/?2Sº & 4, cº º, º º■ /º ºf* Q t- º º,
- • */ A- -º
LIBRARY--> *1. sº 4
L. º Ole sº-", Leº jº Ole sºº º, º […] *. RA s ■ º º, - tºcº - -
*- ºO•o> ze > z- sº ---
º, L. sº ~/C * I ºvºgri º L. sº - C º, ■ ºlº sº.º ~ () º
-*1 = %, sº 12, Sº ºcºncº º, cºlºn*/º 3. C■ .º I//■ º■ co sº cºlº /-
-z/. S
tº tºº tº O) sº tºº Lºlº .)))~. r- c º S -> r- - -
ºvº, a tº º L– s ~/C º, ■ is sººn".-- º ~/C º, Iº * QJ. ~ º ( )º O 7,2 *- -
72 -N * sº 71. º -*/º 42.sº C■ . - - - - *** cºlº. º 2.9-
sº º, º/rºncº sº º- - *- sº */
12. ~~
1.
-* >C■ .&■ ºfººd -S º9. ~ º() º
O) le º tº LIBRARY sº O) le sº […] ”, Li BRARY ~ L.& •o 2 C
->
~->
º- -- > C- […] o O -- ººº ºvugin * -- sº - C * - sº ºvug in º. |- s º/C
º * -y sº º,
12 Sº º/” º -N ~y -º sº }}}} y º/” º º -yo º on■ oºn. º sº cºncisco º, cºlºr. º Sº, º& Tº º
*º 1. 1.-º- ^1. N º- º O 2 º º, C ** O 2 ~
s L. º, º / → º, L■ B RARY s L. º, -- / * sº ■ º- ”, L. B. RA- - - º --- -
ºº
sº -
Or ~ *o - ~[…] º º, ----o -** r º
-(* º **T/C *. [] . ■ ºvº gº º, -- - C - ºgº º L–*/
- -s ºº 7. º- º º
-y -sº on º/”
f º, sº-
4 º' º/ºr 5 *.s.ºncºco sº, cºpiº A/º/, Q º, cºncº is a Q is *.4- ºº~ º &- º º 4- sº ºtº tº Ole tº tº 22- --
* , -- sº Q. […] cº -- > O- c-
f º C. ~ + º º º* * º *.-
* * –– -… […] s º/C *-- ºvºgº º L. Jºs ~/C º 'º ºvº> dº y "…
º, sº º 2 º s* - 42 sº '4, sº-
*/2 - -
º 2 - º--------- S 00001/11//
Sº tº º ºr ■ co Ø dºwn. º sº, c)º ■ ººncºco º 4. º –*- sº- ººº º 9.
sº ■ º Libºº s L. º, O■ ) sº T- * LeRºy t * . )))º º O c•o sº - - -
º *.ºvºi g : T º, L. J S. c- FOR REFERENCE º | | | sº * I■ º º ■ ºsº
º, sº |º ºº/º- º C■ .
º º
O) le s º LIB Not To Be TAKEN FROM THE ROOM [- º, Lib RARY sº --º, º º | º car. --- - - - º: –– o, -r- º L–º, ■ º sºon º
-
ºvºº gº º |- s º/C
J.
º
Odº fºunci■ co*–
-ºr "--- - - -- -
º, Sº Yºlº / / // C 2 º'--
*S ºutº■ º- 2 * .S.
-º, º dº */º º, cºncisco º, * 'S' ºl, c\,://ºnsº º, ->
-º s º, *~
1.
* … O/) , º, . " sº, º 0/1. º. º. iiºnS --> º- * * º r—— º, LI ■ º R A R Y _º ----, "º. * * - * –– º, L ! º R A.