The prevalence and clinical features of the night eating syndrome in psychiatric out-patient...
6
The prevalence and clinical features of the night eating syndrome in psychiatric out-patient population Özge Saraçlı a, ⁎ , Nuray Atasoy a , Asena Akdemir b , Olga Güriz c , Numan Konuk d , Güzin Mukaddes Sevinçer e , Handan Ankaralı f , Levent Atik a a Department of Psychiatry, Bülent Ecevit University Faculty of Medicine, Zonguldak, Turkey b Department of Psychiatry, Selçuk University Faculty of Medicine, Konya, Turkey c Department of Psychiatry, Ankara Dışkapı Yıldırım Beyazıt Education and Research Hospital, Ankara, Turkey d Department of Psychiatry, İstanbul University Cerrahpaşa Faculty of Medicine, Istanbul, Turkey e İstanbul Gelişim University, Istanbul, Turkey f Department of Biostatistics, Düzce University Faculty of Medicine, Düzce, Turkey Abstract Objective: In this study we aimed to investigate the prevalance and clinical correlations of night eating syndrome (NES) in a sample of psychiatric outpatients. Method: Four hundred thirthy three consecutive psychiatric out-patients older than 18 years were evaluated in the outpatient clinics using clinical interview according to the DSM-IV with regard to psychiatric diagnosis. Participants were also screened for presence of NES utilizing both clinical interview and self report based on Night Eating Questionnaire (NEQ) instruments. Sociodemographic and clinical features such as age, gender, education level, socioeconomic level and body mass index (BMI) were also recorded. The Body Shape Questionnaire (BSQ) and the Symptom Checklist-90 Revised (SCL-90R) were administered. Results: Based on the proposed diagnostic criteria of the NES via utilizing clinical interview method, 97 (32 male, 65 female) of the sample met diagnostic criteria for NES. The point prevalence of NES was 22.4%. No statistically significant differences were found between the two groups in terms of age, gender, marital status, education and BMI. The patients with NES had higher NEQ, BSQ and SCL-90R subscale scores than patients without NES. Prevalance of depressive disorder, impulse control disorder, and nicotine dependency was higher among patients with NES. No differences were found with regard to the medication (antipsychotics, antidepressants and mood stabilizers). Conclusion: Night eating syndrome is prevalent among psychiatric outpatients and associated with depression, impulse control disorder, and nicotine dependency. Body dissatisfaction and higher symptom severity are also other risk factors for the development of NES. © 2014 Elsevier Inc. All rights reserved. 1. Introductıon Night eating syndrome (NES) is a disorder of circadian- delayed food intake that behaviorally manifests as evening hyperphagia (EH) (the consumption of N25% of total daily food intake after the evening meal; EH) and/or nocturnal awakening and ingestion of food (NI) (N2/week; NI) with intact circadian sleep patterns [1]. The prevalence of NES has been reported to be 1–1.5% in the general population, 6–16% in patients in weight reduction programmes and 8–42% in candidates for bariatric surgery [2–4]. There are several factors related with NES such as; obesity, gender, medications, and presence of psychiatric disorders. There are few studies in the literature that have studied the presence of NES in psychiatric outpatients [5–9]. The frequencies of NES in psychiatric patients and methods of studies are shown in Table 1. Lundgren and colleagues found that 12.3% of psychiatric patients met criteria for NES Available online at www.sciencedirect.com ScienceDirect Comprehensive Psychiatry xx (2014) xxx – xxx www.elsevier.com/locate/comppsych ⁎ Corresponding author at: Bülent Ecevit Üniversitesi Psikiyatri A.D. esenköy/Kozlu/Zonguldak/Turkey. Tel.: +90 533 3450519. E-mail addresses: [email protected] (Ö. Saraçlı), [email protected] (N. Atasoy), [email protected] (A. Akdemir), [email protected] (N. Konuk), [email protected] (G.M. Sevinçer), [email protected] (H. Ankaralı), [email protected] (L. Atik). http://dx.doi.org/10.1016/j.comppsych.2014.11.007 0010-440X/© 2014 Elsevier Inc. All rights reserved.
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of The prevalence and clinical features of the night eating syndrome in psychiatric out-patient...
Available online at www.sciencedirect.com
ScienceDirect
Comprehensive Psychiatry xx (2014) xxx–xxxwww.elsevier.com/locate/comppsych
The prevalence and clinical features of the night eating syndrome inpsychiatric out-patient population
Özge Saraçlıa,⁎, Nuray Atasoya, Asena Akdemirb, Olga Gürizc, Numan Konukd,Güzin Mukaddes Sevinçere, Handan Ankaralı f, Levent Atika
aDepartment of Psychiatry, Bülent Ecevit University Faculty of Medicine, Zonguldak, TurkeybDepartment of Psychiatry, Selçuk University Faculty of Medicine, Konya, Turkey
cDepartment of Psychiatry, Ankara Dışkapı Yıldırım Beyazıt Education and Research Hospital, Ankara, TurkeydDepartment of Psychiatry, İstanbul University Cerrahpaşa Faculty of Medicine, Istanbul, Turkey
eİstanbul Gelişim University, Istanbul, TurkeyfDepartment of Biostatistics, Düzce University Faculty of Medicine, Düzce, Turkey
Abstract
Objective: In this study we aimed to investigate the prevalance and clinical correlations of night eating syndrome (NES) in a sample ofpsychiatric outpatients.Method: Four hundred thirthy three consecutive psychiatric out-patients older than 18 years were evaluated in the outpatient clinics usingclinical interview according to the DSM-IV with regard to psychiatric diagnosis. Participants were also screened for presence of NES utilizingboth clinical interview and self report based on Night Eating Questionnaire (NEQ) instruments. Sociodemographic and clinical features suchas age, gender, education level, socioeconomic level and body mass index (BMI) were also recorded. The Body Shape Questionnaire (BSQ)and the Symptom Checklist-90 Revised (SCL-90R) were administered.Results: Based on the proposed diagnostic criteria of the NES via utilizing clinical interview method, 97 (32 male, 65 female) of thesample met diagnostic criteria for NES. The point prevalence of NES was 22.4%. No statistically significant differences were foundbetween the two groups in terms of age, gender, marital status, education and BMI. The patients with NES had higher NEQ, BSQ andSCL-90R subscale scores than patients without NES. Prevalance of depressive disorder, impulse control disorder, and nicotine dependencywas higher among patients with NES. No differences were found with regard to the medication (antipsychotics, antidepressants andmood stabilizers).Conclusion: Night eating syndrome is prevalent among psychiatric outpatients and associated with depression, impulse control disorder, andnicotine dependency. Body dissatisfaction and higher symptom severity are also other risk factors for the development of NES.© 2014 Elsevier Inc. All rights reserved.
1. Introductıon
Night eating syndrome (NES) is a disorder of circadian-delayed food intake that behaviorally manifests asevening hyperphagia (EH) (the consumption of N25%
⁎ Corresponding author at: Bülent Ecevit Üniversitesi Psikiyatri A.D.esenköy/Kozlu/Zonguldak/Turkey. Tel.: +90 533 3450519.
E-mail addresses: [email protected] (Ö. Saraçlı),[email protected] (N. Atasoy), [email protected] (A. Akdemir),[email protected] (N. Konuk), [email protected](G.M. Sevinçer), [email protected] (H. Ankaralı),[email protected] (L. Atik).
http://dx.doi.org/10.1016/j.comppsych.2014.11.0070010-440X/© 2014 Elsevier Inc. All rights reserved.
of total daily food intake after the evening meal; EH)and/or nocturnal awakening and ingestion of food (NI)(N2/week; NI) with intact circadian sleep patterns [1].The prevalence of NES has been reported to be 1–1.5%in the general population, 6–16% in patients in weightreduction programmes and 8–42% in candidates forbariatric surgery [2–4].
There are several factors related with NES such as;obesity, gender, medications, and presence of psychiatricdisorders. There are few studies in the literature that havestudied the presence of NES in psychiatric outpatients [5–9].The frequencies of NES in psychiatric patients and methodsof studies are shown in Table 1. Lundgren and colleaguesfound that 12.3% of psychiatric patients met criteria for NES
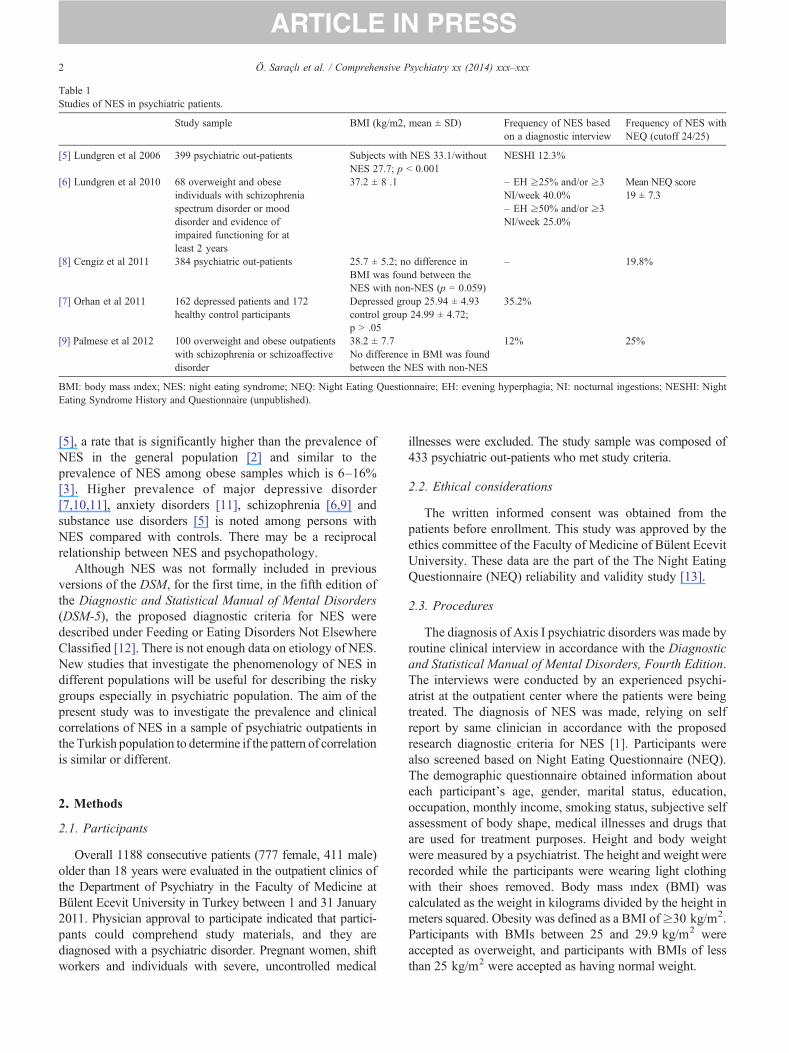
Table 1Studies of NES in psychiatric patients.
Study sample BMI (kg/m2, mean ± SD) Frequency of NES basedon a diagnostic interview
Frequency of NES withNEQ (cutoff 24/25)
[5] Lundgren et al 2006 399 psychiatric out-patients Subjects with NES 33.1/withoutNES 27.7; p b 0.001
NESHI 12.3%
[6] Lundgren et al 2010 68 overweight and obeseindividuals with schizophreniaspectrum disorder or mooddisorder and evidence ofimpaired functioning for atleast 2 years
37.2 ± 8 .1 – EH ≥25% and/or ≥3NI/week 40.0%– EH ≥50% and/or ≥3NI/week 25.0%
Mean NEQ score19 ± 7.3
[8] Cengiz et al 2011 384 psychiatric out-patients 25.7 ± 5.2; no difference inBMI was found between theNES with non-NES (p = 0.059)
– 19.8%
[7] Orhan et al 2011 162 depressed patients and 172healthy control participants
Depressed group 25.94 ± 4.93control group 24.99 ± 4.72;p N .05
35.2%
[9] Palmese et al 2012 100 overweight and obese outpatientswith schizophrenia or schizoaffectivedisorder
38.2 ± 7.7No difference in BMI was foundbetween the NES with non-NES
12% 25%
BMI: body mass ındex; NES: night eating syndrome; NEQ: Night Eating Questionnaire; EH: evening hyperphagia; NI: nocturnal ingestions; NESHI: NightEating Syndrome History and Questionnaire (unpublished).
2 Ö. Saraçlı et al. / Comprehensive Psychiatry xx (2014) xxx–xxx
[5], a rate that is significantly higher than the prevalence ofNES in the general population [2] and similar to theprevalence of NES among obese samples which is 6–16%[3]. Higher prevalence of major depressive disorder[7,10,11], anxiety disorders [11], schizophrenia [6,9] andsubstance use disorders [5] is noted among persons withNES compared with controls. There may be a reciprocalrelationship between NES and psychopathology.
Although NES was not formally included in previousversions of the DSM, for the first time, in the fifth edition ofthe Diagnostic and Statistical Manual of Mental Disorders(DSM-5), the proposed diagnostic criteria for NES weredescribed under Feeding or Eating Disorders Not ElsewhereClassified [12]. There is not enough data on etiology of NES.New studies that investigate the phenomenology of NES indifferent populations will be useful for describing the riskygroups especially in psychiatric population. The aim of thepresent study was to investigate the prevalence and clinicalcorrelations of NES in a sample of psychiatric outpatients inthe Turkish population to determine if the pattern of correlationis similar or different.
2. Methods
2.1. Participants
Overall 1188 consecutive patients (777 female, 411 male)older than 18 years were evaluated in the outpatient clinics ofthe Department of Psychiatry in the Faculty of Medicine atBülent Ecevit University in Turkey between 1 and 31 January2011. Physician approval to participate indicated that partici-pants could comprehend study materials, and they arediagnosed with a psychiatric disorder. Pregnant women, shiftworkers and individuals with severe, uncontrolled medical
illnesses were excluded. The study sample was composed of433 psychiatric out-patients who met study criteria.
2.2. Ethical considerations
The written informed consent was obtained from thepatients before enrollment. This study was approved by theethics committee of the Faculty of Medicine of Bülent EcevitUniversity. These data are the part of the The Night EatingQuestionnaire (NEQ) reliability and validity study [13].
2.3. Procedures
The diagnosis of Axis I psychiatric disorders was made byroutine clinical interview in accordance with the Diagnosticand Statistical Manual of Mental Disorders, Fourth Edition.The interviews were conducted by an experienced psychi-atrist at the outpatient center where the patients were beingtreated. The diagnosis of NES was made, relying on selfreport by same clinician in accordance with the proposedresearch diagnostic criteria for NES [1]. Participants werealso screened based on Night Eating Questionnaire (NEQ).The demographic questionnaire obtained information abouteach participant's age, gender, marital status, education,occupation, monthly income, smoking status, subjective selfassessment of body shape, medical illnesses and drugs thatare used for treatment purposes. Height and body weightwere measured by a psychiatrist. The height and weight wererecorded while the participants were wearing light clothingwith their shoes removed. Body mass ındex (BMI) wascalculated as the weight in kilograms divided by the height inmeters squared. Obesity was defined as a BMI of≥30 kg/m2.Participants with BMIs between 25 and 29.9 kg/m2 wereaccepted as overweight, and participants with BMIs of lessthan 25 kg/m2 were accepted as having normal weight.

3Ö. Saraçlı et al. / Comprehensive Psychiatry xx (2014) xxx–xxx
2.4. Measures
2.4.1. The Night Eating Questionnaire (NEQ)Developed byAllison and colleagues [14], the Night Eating
Questionnaire is designed as a Likert scale self-report measureto assess the presence and frequency of night eating behaviors.The primary behaviors evaluated by the NEQ are: eveninghyperphagia, nocturnal awakenings with ingestion of food,morning anoreksia, initial insomnia, and mood disturbances.The Turkish version ofNEQhas been demonstrated to be validand reliable in the Turkish psychiatric population with aCronbach's α = 0.69 [13].
2.4.2. The Body Shape Questionnaire (BSQ)The BSQ is a 34-item self-report questionnaire that
assesses body image and concerns about body shape. Theparticipants have to respond to items regarding how theyhave felt about their body shape in the last few weeks,choosing among 6 degrees of severity. Higher scores reflectgreater body dissatisfaction. The reliability and validity ofBSQ for Turkish population were shown by Akdemir et al. asit is in its original version [15,16].
2.4.3. The Symptom Checklist-90 Revised (SCL-90R)The SCL-90R is a well-established, self-report, clinical
rating scale that assesses outpatient symptomatic psycholog-ical disturbance [17,18]. It comprises the following 9 primarysymptom scales and one additional item: somatization,obsession–compulsion, interpersonal sensitivity, depression,anxiety, hostility, phobic anxiety, paranoid ideation, psychoti-cism, and the additional item of eating and sleep disorder scale.
2.5. Statistical and data analyses
For the comparison of continuous variables, Student's t-testwas used. The values were presented as the mean ± thestandard deviation (SD) and percentages. For comparisonbetween the groups, the chi-square test and Fisher's exact testwere used. The Pearson correlation was used to determine thesignificance of correlations between NEQ, BSQ, BMI, andSCL-90R scores. The odds ratios and the 95% confidenceintervals (CIs) were calculated, and a p value of b0.05 wasconsidered as statistically significant. Data were computerizedwith the use of the Statistical Packages for the Social Sciencessoftware (SPSS v.15.0; SPSS Inc., Chicago, IL, USA).
3. Results
Enrolled participants are on average 37.75 ± 12.02 yearsold, 70.7% of them (n = 306) are female; and 65.8% of them(n = 285) are married. Participants' BMI's ranged from 16.6to 48.0 kg/m2 (mean = 27.4 ± 5.4). The mean BMI for thesample was 27.4 ± 5.4. The demographic characteristics ofthe patients are presented in Table 2.
Based on the proposed diagnostic criteria of the NES viautilizing clinical interview method, 97 (32 male, 65 female)of the sample met full diagnostic criteria for NES. The point
prevalence ofNES, based on the total group of 433 participants,was 22.4%. In comparison, using data obtained from the self-report measure the NEQ, 40% of the patients scored 18 andabove; 19.4% scored 25 and above and 9.0% scored 30 andabove. The average Night Eating Questionnaire (NEQ) scorefor the sample was 18.00 ± 7.7 points (out of 52 points).
When the patients with NES (n = 97) were compared withthose without NES (n = 336) with regard to age, gender, maritalstatus, education, height, weight, and BMI; no statisticallysignificant differences were found between the two groups(Table 2). The rate of patients with NESwas not different on thebasis of BMI classification (Table 2, p = 0.106).
When the subjective self-perception of the patient'scategory of BMI was analyzed, 48% of the participantsperceived their weight accurately, 40.4% of them under-estimated, and 11.5% of them overestimated their categoryof BMI. BSQ mean score was significantly higher inoverestimating group than accurate and underestimatinggroups (respectively p b 0.001 and p b 0.001). NEQ meanscore was significantly higher in overestimating group thanaccurate (p = 0.028). Also NES diagnosis was more frequentin overestimating group than accurate and underestimatinggroup (36.0, 19.7, and 21.7% respectively; p = 0.044).
The patients with NES had higher NEQ, BSQ, andSCL-90R subscales scores than patients without NES(Table 2). The difference was statistically significant(p b 0.001). There was a positive correlation between NEQand BSQ total score (r = 0.367, p b 0.001) when controllingfor BMI; between BMI and BSQ total score (r = 0.302p b 0.001); and between SCL-90 R general severity indexscore and BSQ (r = 0.428 p b 0.001) and NEQ total scores(r = 0.549 p b 0.001).
Table 3 presents the rate of psychiatric diagnosis betweengroups (with NES vs. without NES). Intermittent explosivedisorder (six patients), pathological gambling (five patients),and trichotillomania (three patients) were classified asimpulse control disorder. Prevalence of depressive disorderand impulse control disorder were higher among patientswith NES (p b 0.001). Prevalence of nicotine dependencywas higher in those with NES as well (p = 0.004). Anxietydisorder was reported at higher rates among patients withoutNES (p b 0.001). No differences were found with regard tothe medication used as antipsychotics, antidepressants andmood stabilizers (p N 0.05).
4. Dıscussıon
The present study investigated the prevalance and clinicalcorrelations of NES in a sample of psychiatric outpatients.Within this population, based on a diagnostic interview,22.4% met the criteria for NES. When we analyzed thefrequencies of NES in psychiatric patients and methods ofstudies as shown in Table 1, compatible with the literature,the frequencies of NES with self-report of NEQ waereshigher than clinical diagnosis [9]. The difference between the

Table 2Demographic and clinical characteristics in participants with and without NES.
NES-positive individuals (n = 97) NES-negative individuals (n = 336) p
Age (year) (mean ± SD) 37.34 ± 11.2 37.87 ± 12.3 0.702⁎
Gender n (%) Male 32 (33%) 95 (28.3%) 0.373⁎⁎
Female 65 (67%) 241 (71.7%)Education (year) (mean ± SD) 7.88 ± 3.3 8.21 ± 3.7 0.420⁎
Income (monthly) (mean ± SD) 1164 ± 757 1339 ± 939 0.146⁎
Marital status n (%) Single 25 (25.8%) 91 (27.1%) 0.054⁎⁎
Married 59 (60.8%) 226 (67.3%)Divorced–widowed 13 (13.4%) 19 (5.7%)
Height (mean ± SD) 1.65 ± 0.09 1.64 ± 0.08 0.317⁎
Weight (mean ± SD) 76.53 ± 15.8 73.97 ± 16.1 0.168⁎
BMI (mean ± SD) 28.1 ± 5.9 27.3 ± 5.3 0.216⁎
Normal (BMI b 25) n (%) 33 (34.4%) 108 (32.2%) 0.106⁎⁎
Overweight (25–29.9) n (%) 26 (27.1%) 130 (38.8%)Obese (BMI N 30) n (%) 37 (38.5%) 97 (29.0%)
Waist circumference (mean ± SD) 92.0 ± 13.5 91.4 ± 15.1 0.734⁎
Hip circumference (mean ± SD) 107.65 ± 11.9 105.91 ± 11.1 0.186⁎
NEQ (mean ± SD) 27.4 ± 7.0 15.2 ± 5.4 b0.001⁎
BSQ (mean ± SD) 94.4 ± 43.5 66.0 ± 32.2 b0.001⁎
SCL-90R General Severity Index (mean ± SD) 1.8 ± 0.7 1.1 ± 0.7 b0.001⁎
Somatization 2.1 ± 1.0 1.4 ± 0.9 b0.001⁎
Obsession–compulsion 1.9 ± 0.7 1.3 ± 0.8 b0.001⁎
Interpersonal sensitivity 2.0 ± 0.9 1.2 ± 0.8 b0.001⁎
Depression 1.9 ± 0.8 1.3 ± 0.8 b0.001⁎
Anxiety 1.8 ± 0.9 1.2 ± 0.8 b0.001⁎
Hostility 1.7 ± 1.0 1.1 ± 0.9 b0.001⁎
Phobic anxiety 1.4 ± 0.9 0.8 ± 0.7 b0.001⁎
Paranoid ideation 1.8 ± 1.0 1.1 ± 0.8 b0.001⁎
Psychoticism 1.4 ± 0.9 0.8 ± 0.7 b0.001⁎
Eating and sleep disorder 1.8 ± 0.8 1.1 ± 0.7 b0.001⁎
⁎ Student's t-test.⁎⁎ The chi-square test.
4 Ö. Saraçlı et al. / Comprehensive Psychiatry xx (2014) xxx–xxx
studies may be related to the employment of differentdiagnostic criteria and methods. Palmese et al. speculate thatmajor discrepancy between the interview and NEQ may berelated to poor understanding and/or misinterpretation ofsome questions by some patients with schizophrenia [9].
Remarkably, the frequency of NES based on NEQ cutoff25 and above found in this sample (19.4%) was identical tothose previously recorded in a sample of psychiatric patients
Table 3The psychiatric diagnoses among patients with or without NES.
NES-positive individuals(n = 97) n (%)
Anxiety disorders⁎ 29 (29.9)Major depression⁎ 32 (33.0%)Bipolar disorder 14 (14.4)Psychotic disorder 7 (7.2)Somatoform disorder 1 (1.0)Impulse control disorder⁎ 7 (7.2)Adjustment disorder 4 (4.1)Alcohol dependence 3 (3.1)Nicotine dependence⁎⁎ 46 (47.4%)
The chi-square test and Fisher's exact t est.⁎ p b 0.001.⁎⁎ p = 0.004.
by Cengiz et al. (19.8%) in Turkey [8]. But, our figure ishigher than that of Lundgreen et al, who reported theprevalence as 12.3% among general psychiatric samples [5].Another study of Ludgren et al. reported a NES rate of 40%when diagnosis was based on the proposed diagnosticcriteria in patients with serious mental illnesses [6]. Thisdifference may be due to the cultural factors or severity ofpsychiatric illness severity in the study sample. In our
NES-negative individuals(n = 336) n (%)
Total(N = 433)n (%)
157 (46.7) 186 (43.0)62 (18.5%) 94 (21.7%)43 (12.8) 57 (13.2)40 (11.9) 47 (10.9)16 (4.8) 17 (3.9)7 (2.1) 14 (3.2)7 (2.1) 11 (2.5)4 (1.2) 7 (1.6)
105 (31.3%) 151 (34.9%)

5Ö. Saraçlı et al. / Comprehensive Psychiatry xx (2014) xxx–xxx
sample, we did not assess severe psychiatric patients; but wefound out that general severity index and also subscalesscores were higher in NES positive patients.
It is important to describe other risk factors that mayaffect the development of NES. Data regarding therelationship between gender and NES are limited. Someauthors found NES prevalence to be comparable betweengenders [3,4,19]. On the other hand, three studies havereported male sex as a risk factor for NES [7,20,21]. Wedid not find any relationship between gender and NES inour study.
The degree of BMI was also reported as a risk factor forNES in the literature. However, BMI was not differentbetween the groups of our study sample. In the literature, it isfrequently noted that obesity or higher BMI commonlycorrelates with NES in general population [2,3,19]. In thestudies that have compared NES with non-NES inpsychiatric participants, BMI was greater in the NES groupin only one study [6]. Lundgren and colleagues reported that,although their sample was, on average, overweight (meanBMI = 29.1 kg/m2), obese psychiatric patients (i.e. thosewith a BMI of ≥30 kg/m2) were five times more likely tomeet the criteria for NES compared to non-obese (i.e. thosewith a BMI of 18.5–25.9 kg/m2) psychiatric patients [6].BMI was not found to be significantly different betweenpsychiatric participants with-NES and without-NES in theprevious studies [6–8]. This result may be explained with thehigher prevalance of BMI in psychiatric outpatientscompared to the community sample. Future studies areneeded to examine the prospective changes in weight amongpsychiatric outpatients with NES of all weight ranges.
In the present study, we found that body dissatisfactionand night eating problems were higher in over-estimatinggroup than others. In agreement with our findings, Lundgrenet al. found that night eaters had higher concerns aboutdietary restraint, weight, body shape, and eating [22].
In contrast with the aforementioned studies, it was alsoreported that NES does not involve the same degree of over-concern with body weight or shape as BED [10]. There is aneed for further studies on this issue.
We found that there was a positive correlation betweenNEQ and BSQ total score (r = 0.367, p b 0.001) aftercontrolling for BMI. In addition, there was a positivecorrelation between BMI and BSQ total score (r = 0.302p b 0.001). This correlation shows that body dissatisfactionis an important feature of NES. We think that bodydissatisfaction may affect eating behaviors in some waysbut it is important to distinguish the origin of the higher BSQscore, which can stem from changing the eating pattern ofthe higher BMI or NEQ as mentioned in literature [23].
Another finding of our study that needed to be explainedwas the presence of comorbid psychiatric disorders withinNES groups. We have found that depressive disorder (33 and18.5%, p b 0.001) and impulse control disorders (7.2 and2.1%, p b 0.001) were higher in patients with NES thanwithout NES. Consistent with our study, depression rates in
NES patients were higher and the symptoms and diagnosis ofdepression were generally more frequent among individualswith NES in the previous studies [10,19]. In a descriptivestudy of NES, de Zwaan and colleagues found that 56% ofpatients had a lifetime history of a major depressive disorder,which was higher than the rate seen among the healthycontrol group [11]. Orhan et al. found that the rates of NES indepression outpatients (35.2%) were higher when comparedto the healthy control (19.2%) participants [7]. In anotherstudy from Turkey, in contrast to our study, Cengiz et al.found that there was no relationship between psychiatricdisorders and NES. However, their study was undertaken ingeneral psychiatric population [8].
Turkish culture leads to low rates of alcohol dependence,but high rates of nicotine dependence. We think that thiscultural feature may have led fewer people to be diagnosedwith alcohol use disorders in our study (n = 3, 4 respective-ly). However nicotine dependence was more frequent in theNES group (p = 0.004). On the contrary, Lundgren et al.found out that 30.6% of the patients with NES met criteriafor a lifetime substance use disorder, compared with 8.3% ofnon-night eaters [5]. Considering the high percentage ofimpulse control disorder, and nicotine use in NES group, wethink that these findings may indicate that presence ofanother risky behavior in addition to bad eating behaviormay contribute to the development of NES. We could notfind any literature that supports our finding.
The prevalence of NES is high among those withpsychiatric disorders [5,6], particularly in those with bulimianervosa [24], sleep disorders [22] and schizophrenia [9]. Wefound no relationship between these psychiatric diagnosisand NES in our psychiatric outpatient sample. It is importantto investigate the effects of medicines on NES. It wasreported that patients with NES were more likely to beprescribed more than one atypical antipsychotic than patientswithout NES (38.8 vs. 30.8%, respectively) [5]. In oursample we found no relationship between the use ofmedicines (antipsychotics, antidepressants, mood stabilizers)and the presence of NES. We suggest that new studies thatinvestigate especially the effect of atypical antipsychoticsamong NES groups are needed, and these studies should takethe relation between these medications and higher body massindex into consideration.
There are various limitations in our study. Absence ofnormal controls is an important limitation. Several otherfactors may explain the high prevalence of NES in thissample, including life stress, sleep disturbance, culturalissues. Pychiatric patients face daily life stressors includingpoor health, limited financial resources, and stigma whichcould increase the likelihood of nocturnal ingestions of food.We did not analyze these issues. The high prevalence,however, could also be due to the sample size. Future studiesare needed to corroborate these findings in a largerpopulation, to understand why this population is under anincreased risk for NES, and to determine the effects of NESon health outcomes among psychiatric patients.

6 Ö. Saraçlı et al. / Comprehensive Psychiatry xx (2014) xxx–xxx
References
[1] Allison KC, Lundgren JD, O'Reardon JP, Geliebter A, Gluck ME,Vinai P, et al. Proposed diagnostic criteria for night eating syndrome.Int J Eat Disord 2010;43:241-7.
[2] Rand CSW, Macgregor MD, Stunkard AJ. The night eating syndromein the general population and among post-operative obesity surgerypatients. Int J Eat Disord 1997;22:65-9.
[3] Cerú-Björk C, Andersson I, Rössner S. Night eating and nocturnaleating-two different or similar syndromes among obese patients? Int JObes Relat Metab Disord 2001;25:365-72.
[4] Allison KC, Wadden TA, Sarwer DB, Fabricatore AN, Crerand C,Gibbons L, et al. Night eating syndrome and binge eating disorderamong persons seeking bariatric surgery: prevalence and relatedfeatures. Obesity 2006;14:77-82.
[5] Lundgren JD, Allison KC, Crow S, O'Reardon JP, Berg KC, Galbraith J,et al. Prevalence of the night eating syndrome in a psychiatric population.Am J Psychiatry 2006;163:156-8.
[6] Lundgren JD, Rempfer MV, Brown CE, Goetz J, Hamera E. Theprevalence of night eating syndrome and binge eating disorder amongoverweight and obese individuals with serious mental illness.Psychiatry Res 2010;175:233-6.
[7] Orhan FÖ, Özer UG, Özer A, Altunören Ö, Çelik M, Karaaslan MF.Night eating syndrome among patients with depression. Isr JPsychiatry Relat Sci 2011;48:212-7.
[8] Cengiz Y, Toker SG, Karamustafalıoğlu KO, Bakım B, Özçelik B.Prevalence of night eating syndrome and comorbidity with otherpsychiatric disorders in psychiatric outpatient population. YeniSymposium, 49; 2011. p. 83-8.
[9] Palmese LB, Ratliff JC, Reutenauer EL, Tonizzo KM, Grilo CM,Tek C. Prevalence of night eating in obese individuals withschizophrenia and schizoaffective disorder. Compr Psychiatry2013;54:276-81.
[10] Allison KC, Grilo CM, Masheb RM, Stunkard AJ. Binge eatingdisorder and night eating syndrome: a comparative study of disorderedeating. J Consult Clin Psychol 2005;73:1107-15.
[11] De Zwaan M, Roerig D, Crosby R, Karaz S, Mitchell J. Nighttimeeating: a descriptive study. Int J Eat Disord 2006;39:224-32.
[12] DSM-5 development [webpage on the Internet]. Arlington, VA:American Psychiatric Association; 2012 [Available from:, http://www.dsm5.org/ProposedRevision/Pages/proposedrevision.aspx?rid=26.Accessed February 7, 2013].
[13] AtasoyN, SaraçlıÖ,KonukN,AnkaralıH,Güriz SO,AkdemirA, et al. Thereliability and validity of Turkish version of The Night EatingQuestionnairein psychiatric outpatient population. Anatol J Psychiatry 2014;15:238-47.
[14] Allison KC, Lundgren JD, O'Reardon JP, Martino NS, Sarwer DB,Wadden TA, et al. The Night Eating Questionnaire (NEQ):psychometric properties of a measure of severity of the night eatingsyndrome. Eat Behav 2008;9:62-72.
[15] Akdemir A, Inandi T, Akbas D, Karaoglan Kahilogullari A, Eren M,Canpolat BI. Validity and reliability of a Turkish version of the bodyshape questionnaire among female high school students: preliminaryexamination. Eur Eat Disord Rev 2012;20:114-5.
[16] Cooper PJ, Taylor MJ, Cooper Z, Fairburn CG. Development andvalidation of the body shape questionnaire. Int J Eat Disord 1987;6:485-94.
[17] Derogatis LR. SCL-90: Administration, scoring and proceduremanual-1 for the revised version. Baltimore, MD: John HopkinsUniv., School of Medicine, Clinical Psychometrics Unit; 1977.
[18] Dağ I. Belirti Tarama Listesi (SCL-90R)’nin üniversite öğrencileri içingüvenirliği ve geçerliği. Turk Psikiyatri Derg 1991;2:5-12.
[19] Gluck ME, Geliebter A, Satov T. Night eating syndrome is associatedwith depression, low self-esteem, reduced daytime hunger, and lessweight loss in obese outpatients. Obes Res 2001;9:264-7.
[20] Grilo CM, Masheb RM. Night-time eating in men and women withbinge eating disorder. Behav Res Ther 2004;42:397-407.
[21] Aronoff NJ, Geliebter A, Zammit G. Gender and body mass index asrelated to the night-eating syndrome in obese outpatients. J Am DietAssoc 2001;101:102-4.
[22] Lundgren JD, Allison KC, O’Reardon JP, Stunkard AJ. A descriptivestudy of non-obese persons with night eating syndrome and a weight-matched comparison group. Eat Behav 2008;9:343-51.
[23] Johnson F, Cooke L, Croker H, Wardle J. Changing perceptions ofweight in Great Britain: comparison of two population surveys. BMJ2008;337:a494 [10].
[24] Lundgren JD, Shapiro JR, Bulik CM. Night eating patterns of patients withbulimia nervosa: a preliminary report. Eat Weight Disord 2008;13:171-5.