
The paradox of normal neuropsychological function in schizophrenia
10
Journal of Abnormal Psychology 2000. Vol. 109, No. 4, 743-752 Copyright 2000 by the American Psychological Association, Inc. 0021-843X/00/S5.00 DOI: 10.1037//002I-843X.109.4.743 The Paradox of Normal Neuropsychological Function in Schizophrenia William S. Kremen University of California, Davis, School of Medicine and Napa State Hospital Larry J. Seidman, Stephen V. Faraone, Rosemary Toomey, and Ming T. Tsuang Massachusetts Mental Health Center, Brockton-West Roxbury Veterans Affairs Medical Center, and Harvard Institute of Psychiatric Epidemiology and Genetics Mounting evidence suggests that compromised neurocognitive function is a core feature of schizophre- nia. However, some studies have found neuropsychologically normal schizophrenia patients. To address this apparent contradiction, we blindly rated individual neuropsychological profiles of 75 schizophrenia patients and 91 control participants on the basis of methods developed by L. J. Seidman, S. V. Faraone, W. S. Kremen, J. R. Pepple, M. J. Lyons, and M. T. Tsuang (1993). Almost one-quarter of the patients were classified as neuropsychologically within normal limits (WNL). Despite significantly worse neuropsychological performance, WNL patients had higher estimated premorbid ability than did controls. Compared to a subset of controls matched on overall neuropsychological function, WNL patients had higher estimated premorbid ability and current IQs. Our results favor the view that even neuropsycho- logically normal schizophrenia patients have compromised cognitive function relative to their presumed expected or premorbid level of intellectual ability. Neuropsychological function ranging from apparently normal to widespread and dementia-like impairment is widely observed in schizophrenia (Goldstein & Shemansky, 1995: Seidman, 1990; Seidman, Cassens, Kremen, & Pepple, 1992). Multiple neuropsy- chological impairments have been observed even in the context of approximately average general intellectual functioning (Braff et al., 1991; Elliott, McKenna, Robbins, & Sahakian, 1998; Gold- William S. Kremen, Department of Psychiatry, University of California, Davis, School of Medicine and TJC Davis-Napa Psychiatric Research Center, Napa State Hospital. Larry J. Seidman, Stephen V. Faraone, Rosemary Toomey, and Ming T. Tsuang, Harvard Medical School Depart- ment of Psychiatry at Massachusetts Mental Health Center and Brockton- West Roxbury Veterans Affairs Medical Center, and Harvard Institute of Psychiatric Epidemiology and Genetics. Portions of this article were presented at the 7th biennial meeting of the International Congress on Schizophrenia Research, Santa Fe, New Mexico, April 17 to 21, 1999. Preparation of this article was supported in part by National Institute of Mental Health Grants MH43518-01 (MERIT Award) and MH46318, the Veteran's Affairs Medical Research and Health Ser- vices Research and Development Programs, and a National Alliance for Research on Schizophrenia and Depression (NARSAD) Young Investiga- tor Award. We thank Gwen Barnes, Mimi Braude, Deborha Cart, Jo-Ann Donatelli, Tova Ferro, Lisa Gabel, David Goldfinger, Robin Green, Lynda Jacobs, Denise Leville, Cathy Monaco, Anne Shore, Rob Trachtenberg, Judith Wides, John Pepple, Keith Hawkins, and Theresa Pai for their contribu- tions to the projects. We also thank Anna Mitchell, David Osser, and Larry Albert for assistance in recruiting participants at Taunton State Hospital; Sue Thiemann for statistical consultation; and Anne Hoff for helpful comments. Correspondence concerning this article should be addressed to William S. Kremen, Department of Psychiatry, University of California, Davis, School of Medicine, 4430 V Street, Sacramento, California 95817. Elec- tronic mail may be sent to [email protected]. stein, 1986; Seidman, 1983), but various proportions of schizo- phrenia patients also have been found to be neuropsychologically unimpaired (Golden et al., 1982; Palmer et al., 1997; Silverstein & Zerwic, 1985). Neuropsychologically normal schizophrenia pa- tients tend to have fewer negative symptoms, more paranoid symp- toms, and better psychosocial functioning and to receive less anticholinergic medication than their neuropsychologically im- paired counterparts (Palmer et al., 1997; Seidman et al., 1992; Silverstein & Zerwic, 1985). In apparent contradiction with the existence of neuropsychologi- cally normal schizophrenia patients is the idea thai neuropsycho- logical compromise is a core feature of schizophrenic illness. We refer to core features as dysfunctional features that reflect under- lying processes, as opposed to secondary consequences of symp- toms or treatment. Such features thus would be primary dysfunc- tions that should be present in anyone with the disorder. Evidence from several areas of research supports the notion that neuropsy- chological dysfunction is a core feature of schizophrenia. First, neuropsychological abnormalities exist prior to and at the onset of illness (Aylward, Walker, & Bettes, 1984; Hoff, Riordan, O'Donnell, Morris, & DeLisi, 1992; Jones, Rodgers, & Murray, 1994; Kremen et al., 1998). Second, compromised neuropsycho- logical function similar to deficits found in patients (although milder) is found in nonpsychotic biological relatives of schizo- phrenia patients (Cannon et al., 1994; Faraone et al., 1995; Gold- berg et al., 1993; Keefe et al., 1994; Mirsky et al., 1992). Com- promised function occurring prior to the onset of illness or in family members cannot simply reflect the effects of illness or treatment. Third, it is reasonable to postulate that a core dysfunc- tional feature would tend to be more treatment resistant than would other illness characteristics. Although neuropsychological perfor- mance may fluctuate with changes in clinical state, impairment still usually persists even when symptoms are relatively remitted 743
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of The paradox of normal neuropsychological function in schizophrenia

Journal of Abnormal Psychology2000. Vol. 109, No. 4, 743-752
Copyright 2000 by the American Psychological Association, Inc.0021-843X/00/S5.00 DOI: 10.1037//002I-843X.109.4.743
The Paradox of Normal Neuropsychological Function in Schizophrenia
William S. KremenUniversity of California, Davis, School of Medicine
and Napa State Hospital
Larry J. Seidman, Stephen V. Faraone,Rosemary Toomey, and Ming T. Tsuang
Massachusetts Mental Health Center,Brockton-West Roxbury Veterans Affairs Medical Center, and
Harvard Institute of Psychiatric Epidemiology and Genetics
Mounting evidence suggests that compromised neurocognitive function is a core feature of schizophre-
nia. However, some studies have found neuropsychologically normal schizophrenia patients. To address
this apparent contradiction, we blindly rated individual neuropsychological profiles of 75 schizophrenia
patients and 91 control participants on the basis of methods developed by L. J. Seidman, S. V. Faraone,
W. S. Kremen, J. R. Pepple, M. J. Lyons, and M. T. Tsuang (1993). Almost one-quarter of the patients
were classified as neuropsychologically within normal limits (WNL). Despite significantly worse
neuropsychological performance, WNL patients had higher estimated premorbid ability than did controls.
Compared to a subset of controls matched on overall neuropsychological function, WNL patients had
higher estimated premorbid ability and current IQs. Our results favor the view that even neuropsycho-
logically normal schizophrenia patients have compromised cognitive function relative to their presumed
expected or premorbid level of intellectual ability.
Neuropsychological function ranging from apparently normal to
widespread and dementia-like impairment is widely observed in
schizophrenia (Goldstein & Shemansky, 1995: Seidman, 1990;
Seidman, Cassens, Kremen, & Pepple, 1992). Multiple neuropsy-
chological impairments have been observed even in the context of
approximately average general intellectual functioning (Braff et
al., 1991; Elliott, McKenna, Robbins, & Sahakian, 1998; Gold-
William S. Kremen, Department of Psychiatry, University of California,
Davis, School of Medicine and TJC Davis-Napa Psychiatric Research
Center, Napa State Hospital. Larry J. Seidman, Stephen V. Faraone,
Rosemary Toomey, and Ming T. Tsuang, Harvard Medical School Depart-
ment of Psychiatry at Massachusetts Mental Health Center and Brockton-
West Roxbury Veterans Affairs Medical Center, and Harvard Institute of
Psychiatric Epidemiology and Genetics.
Portions of this article were presented at the 7th biennial meeting of the
International Congress on Schizophrenia Research, Santa Fe, New Mexico,
April 17 to 21, 1999. Preparation of this article was supported in part by
National Institute of Mental Health Grants MH43518-01 (MERIT Award)
and MH46318, the Veteran's Affairs Medical Research and Health Ser-
vices Research and Development Programs, and a National Alliance for
Research on Schizophrenia and Depression (NARSAD) Young Investiga-
tor Award.
We thank Gwen Barnes, Mimi Braude, Deborha Cart, Jo-Ann Donatelli,
Tova Ferro, Lisa Gabel, David Goldfinger, Robin Green, Lynda Jacobs,
Denise Leville, Cathy Monaco, Anne Shore, Rob Trachtenberg, Judith
Wides, John Pepple, Keith Hawkins, and Theresa Pai for their contribu-
tions to the projects. We also thank Anna Mitchell, David Osser, and Larry
Albert for assistance in recruiting participants at Taunton State Hospital;
Sue Thiemann for statistical consultation; and Anne Hoff for helpful
comments.
Correspondence concerning this article should be addressed to William
S. Kremen, Department of Psychiatry, University of California, Davis,
School of Medicine, 4430 V Street, Sacramento, California 95817. Elec-
tronic mail may be sent to [email protected].
stein, 1986; Seidman, 1983), but various proportions of schizo-
phrenia patients also have been found to be neuropsychologically
unimpaired (Golden et al., 1982; Palmer et al., 1997; Silverstein &
Zerwic, 1985). Neuropsychologically normal schizophrenia pa-
tients tend to have fewer negative symptoms, more paranoid symp-
toms, and better psychosocial functioning and to receive less
anticholinergic medication than their neuropsychologically im-
paired counterparts (Palmer et al., 1997; Seidman et al., 1992;
Silverstein & Zerwic, 1985).
In apparent contradiction with the existence of neuropsychologi-
cally normal schizophrenia patients is the idea thai neuropsycho-
logical compromise is a core feature of schizophrenic illness. We
refer to core features as dysfunctional features that reflect under-
lying processes, as opposed to secondary consequences of symp-
toms or treatment. Such features thus would be primary dysfunc-
tions that should be present in anyone with the disorder. Evidence
from several areas of research supports the notion that neuropsy-
chological dysfunction is a core feature of schizophrenia. First,
neuropsychological abnormalities exist prior to and at the onset of
illness (Aylward, Walker, & Bettes, 1984; Hoff, Riordan,
O'Donnell, Morris, & DeLisi, 1992; Jones, Rodgers, & Murray,
1994; Kremen et al., 1998). Second, compromised neuropsycho-
logical function similar to deficits found in patients (although
milder) is found in nonpsychotic biological relatives of schizo-
phrenia patients (Cannon et al., 1994; Faraone et al., 1995; Gold-
berg et al., 1993; Keefe et al., 1994; Mirsky et al., 1992). Com-
promised function occurring prior to the onset of illness or in
family members cannot simply reflect the effects of illness or
treatment. Third, it is reasonable to postulate that a core dysfunc-
tional feature would tend to be more treatment resistant than would
other illness characteristics. Although neuropsychological perfor-
mance may fluctuate with changes in clinical state, impairment
still usually persists even when symptoms are relatively remitted
743

744 KREMEN, SEIDMAN, FARAONE, TOOMEY, AND TSUANG
(Gold & Harvey, 1993). Taken together, this evidence is consistent
with the notion that at least some neuropsychological performance
reflects a core dysfunctional feature of schizophrenia. Despite
well-documented heterogeneity, if compromised neuropsycholog-
ical function is indeed a core feature, one must ask how it is
possible—as suggested in the aforementioned studies—to have
schizophrenia but still be neuropsychologically normal.
The clinical tradition in neuropsychology, which emphasizes the
careful description of individual cases, has advantages for discern-
ing heterogeneity but is not readily amenable to large-group data
(Marshall & Newcombe, 1984). This research-clinical distinction
is analogous to the nomothetic—idiographic distinction in person-
ality research (Allport, 1942). We have emphasized the importance
of the case study as the essence of clinical neuropsychology
(Kremen, Seidman, Pepple, Lyons, Tsuang, & Faraone, 1994;
Seidman, 1990; Seidman et al., 1993). In particular, Seidman
(1990) and Seidman et al. (1993) suggested that examination of
individual neuropsychological profiles could be a useful alterna-
tive to group analysis for making sense of heterogeneity in schizo-
phrenia. Toward the same end, Shallice, Burgess, and Frith (1991)
have characterized the individual neuropsychological profiles of a
few patients,
In this study, we used a hybrid approach involving individual
case ratings and analysis of group data derived from those ratings.
A similar approach was used in an elegant study by Palmer et al.
(1997), who identified a subgroup of schizophrenia patients as
neuropsychologically normal. We blindly rated individual neuro-
psychological profiles and compared patients rated as within nor-
mal limits (WNL) to normal control participants and to patients
rated as abnormal. Consistent with the idea of compromised neu-
rocognitive function as a core feature of the illness, we tested
whether, in comparison to controls, there would be evidence of
poorer cognitive function even in WNL schizophrenia patients.
If compromised neuropsychological function is a core feature of
schizophrenia, then those with apparently normal neuropsycholog-
ical function may have above-average levels of expected or pre-
morbid ability. The same reasoning applies to educational attain-
ment, which is likely to be attenuated by schizophrenic illness.
Indeed, we showed that chronic schizophrenia patients who were
matched one-to-one on education with controls tended to have
higher estimated premorbid ability than the controls (Kremen et
al., 1996). Therefore, we predicted that schizophrenia patients
classified as neuropsychologically WNL in this study would have
higher estimated premorbid intellectual ability in comparison to
the general intellectual ability of the controls. We also examined
the clinical and demographic correlates of neuropsychologically
normal and abnormal schizophrenia patients.
Method
Participants
All participants gave informed consent and were paid to participate.
Patients were from three Boston area public hospitals. Inclusion criteria for
patients were diagnosis of schizophrenia according to the Diagnostic and
Statistical Manual of Mental Disorders (3rd ed., rev.; DSM-IU-R; Amer-
ican Psychiatric Association, 1987), age 18 or older, English as the primary
language, and a minimum of 8 years of formal education. Exclusion criteria
were neurologic disease or damage, any insulin shock or greater than 25
lifetime electroconvuls;ve treatments, current substance abuse (within the
past 6 months), history of head injury with loss of consciousness of greater
than 5 min or with documented neurocognitive sequelae, menial retarda-
tion, and medical illnesses that may be associated with significant neuro-
cognitive impairment. Data were gathered from interviews and medical
records.
Control participants were recruited from nonprofessional hospital staff
and advertisements in the community. Except for psychopathology or
family history of psychosis, selection criteria were the same as for patients.
Controls were screened for current psychopathology with a short form of
the Minnesota Multiphasic Personality Inventory (MMPI-168; Vincent et
al., 1984) and were excluded if the score on any clinical or validity scale,
except for Masculinity-Femininity, was above 70. Further details about
ascertainment of controls are provided in previous reports (Faraone et al.,
1995; Kremen et al., 1995).
We tested 76 schizophrenia patients and 92 controls. One patient and one
control were excluded from these analyses because of incomplete neuro-
psychological profiles. Patient subgroups were as follows: 21 (28%) para-
noid, 11 (15%) disorganized, 1 (1%) catatonic, 1 (1%) residual, 41 (55%)
undifferentiated, 25 (33%) inpatients, and 50 (67%) outpatients. Demo-
graphics are shown in Table 1.
Procedures and Instruments
Assessment of psychopathology. Consensus lifetime DSM-IIl-R diag-
noses for patients were determined from interviews conducted with the
Schedule for Affective Disorders and Schizophrenia (SADS; Endicott &
Spitzer, 1978), medical record reviews, and consultation with clinicians.
As noted, in place of the interview, controls were screened for current
psychopathology with the MMPI-168.
Neuropsychological assessment. We administered a battery of neuro-
psychological tests assessing several domains of cognitive function. Be-
cause our goal was to minimize state-dependent effects and to capture
performance at its optimum level, patients were tested when they were
judged to be relatively stable clinically (i.e., at their "baseline") by the
clinical staff who were familiar with them.
Over the course of the study, some changes were made in the test
battery. Tests included in the present analyses are those given to most of
the participants. For general verbal ability, we used the Wechsler Adult
Intelligence Scale—Revised (WAIS-R; Wechsler, 1981) Vocabulary
subtest and the Wide-Range Achievement Test—Revised (WRAT-R; Jas-
tak & Wilkinson, 1984) Reading and Spelling subtests. For general visual-
spatial ability, we used the WAIS-R Block Design subtest, the Hooper
Visual Organization Test (Hooper, 1983), and Judgment of Line Orienta-
tion (Benton, Hamsher, Vamey, & Spreen, 1983). For verbal declarative
memory, we used the Wechsler Memory Scale (WMS; Wechsler, 1945) or
the Wechsler Memory Scale—Revised (WMS-R; Wechsler, 1987) Logical
Memories subtest. The WMS-R was published after the study began, and
the decision was made to switch from the WMS to the WMS-R. Conse-
quently, not all participants were administered the same version. We
calculated each participant's score as a percentage of the maximum pos-
sible score because the stories composing the Logical Memories subtest
differ slightly on the two test versions. These scores were calculated for
immediate recall, delayed recall, and the percentage retained from imme-
diate to delayed recall. For abstraction-executive function, we used the
number of perseveration and categories on the Wisconsin Card Sorting
Test (Heaton, 1981) and the number of total misses on the Visual-Verbal
Test (Feldman & Drasgow, 1981). For executive-motor function, we used
the total score and number of perseverations on Graphic Sequencing and
the Manual Position Sequencing total score. For perceptual—motor speed,
we used the WAIS-R Digit Symbol subtest and the time on Parts A and B
of the Trail Making Test (War Department, 1944). For mental control-
encoding, we used the WAIS-R Digit Span subtest and the WRAT-R
Arithmetic subtest. For sustained attention-vigilance, we used die number
of digits detected (regardless of ear of report accuracy) and number of
digits correct (based on ear of report) on the Dichotic Listening Test
NEUROPSYCHOLOGICAL FUNCTION IN SCHIZOPHRENIA 745
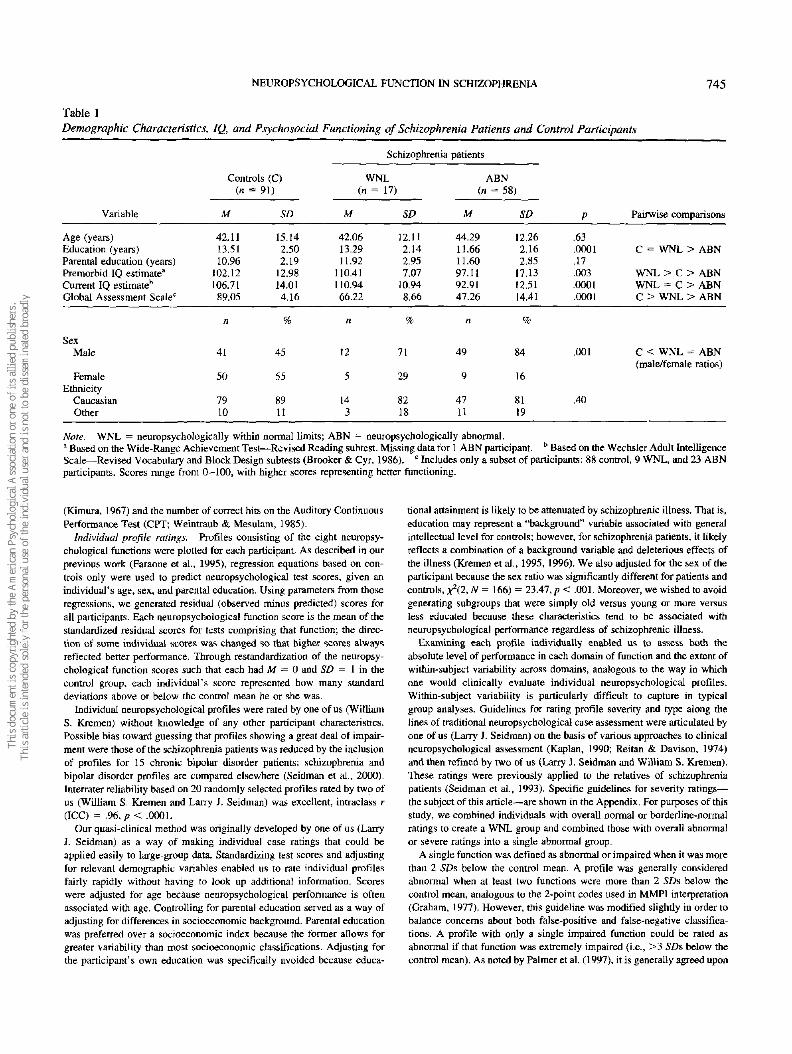
Table 1
Demographic Characteristics, 1Q, and Psychosocial Functioning of Schizophrenia Patients and Control Participants
Schizophrenia patients
Controls (C)
Variable
Age (years)Education (years)
Parental education (years)Premorbid IQ estimate3
Current IQ estimate11
Global Assessment Scalec
SexMale
FemaleEthnicity
Caucasian
Other
(n =
M
42.1113.51
10.96102.12
106.7189.05
n
41
50
79
10
91)
SD
15.14
2.502.19
12.9814.014.16
%
45
55
8911
WNL
(« =
M
42.0613.2911.92
110.411 10.9466.22
n
12
5
14
3
17)
SD
12.112.142.957.07
10.94
8.66
%
71
29
8218
ABN
(n =
M
44.29
11.6611.6097.1192.91
47.26
n
49
9
47
11
'58)
SD
12.262.162.85
17.1312.5114.41
%
84
16
8119
P
.63
.0001
.17
.003
.0001
.0001
.001
.40
Pairwise comparisons
C = WNL > ABN
WNL > C> ABN
WNL = C> ABNC > WNL > ABN
C < WNL = ABN(male/female ratios)
Note. WNL = neuropsychologically within normal limits; ABN = neuropsychologically abnormal.a Based on the Wide-Range Achievement Test—Revised Reading subtest. Missing data for 1 ABN participant. b Based on the Wechsler Adult IntelligenceScale—Revised Vocabulary and Block Design subtests (Brooker & Cyr, 1986). c Includes only a subset of participants: 88 control, 9 WNL, and 23 ABN .participants. Scores range from 0-100, with higher scores representing better functioning.
(Kimura, 1967) and the number of correct hits on the Auditory Continuous
Performance Test (CRT; Weintraub & Mesulam, 1985).
Individual profile ratings. Profiles consisting of the eight neuropsy-
chological functions were plotted for each participant. As described in our
previous work (Faraone et al, 1995), regression equations based on con-
trols only were used to predict neuropsychological test scores, given an
individual's age, sex, and parental education. Using parameters from those
regressions, we generated residual (observed minus predicted) scores for
all participants. Each neuropsychological function score is the mean of the
standardized residual scores for tests comprising that function; the direc-
tion of some individual scores was changed so that higher scores always
reflected better performance. Through restandardizatioii of the neuropsy-
chological function scores such that each had M = 0 and SD = I in die
control group, each individual's score represented how many standard
deviations above or below the control mean he or she was.
Individual neuropsychological profiles were rated by one of us (William
S. Kremen) without knowledge of any other participant characteristics.
Possible bias toward guessing that profiles showing a great deal of impair-
ment were those of the schizophrenia patients was reduced by the inclusion
of profiles for 15 chronic bipolar disorder patients; schizophrenia and
bipolar disorder profiles are compared elsewhere (Seidman et al., 2000).
Interrater reliability based on 20 randomly selected profiles rated by two of
us (William S, Kremen and Larry J. Seidman) was excellent, intraclass r
(ICC) = .96, p< .0001.
Our quasi-clinical method was originally developed by one of us (Larry
J. Seidman) as a way of making individual case ratings that could be
applied easily to large-group data. Standardizing test scores and adjusting
for relevant demographic variables enabled us to rate individual profiles
fairly rapidly without having to look up additional information. Scores
were adjusted for age because neuropsychological performance is often
associated with age. Controlling for parental education served as a way of
adjusting for differences in socioeconomic background. Parental education
was preferred over a socioeconomic index because the former allows for
greater variability than most socioeconomic classifications. Adjusting for
the participant's own education was specifically avoided because educa-
tional attainment is likely to be attenuated by schizophrenic illness. That is,
education may represent a "background" variable associated with general
intellectual level for controls; however, for schizophrenia patients, it likely
reflects a combination of a background variable and deleterious effects of
the illness (Kremen et al., 1995, 1996). We also adjusted for the sex of the
participant because the sex ratio was significantly different for patients and
controls, ^(2, N= 166) = 23.47, p < .001. Moreover, we wished to avoid
generating subgroups that were simply old versus young or more versus
less educated because these characteristics tend to be associated with
neuropsychological performance regardless of schizophrenic illness.
Examining each profile individually enabled us to assess both the
absolute level of performance in each domain of function and the extent of
within-subject variability across domains, analogous to the way in which
one would clinically evaluate individual neuropsychological profiles.
Within-subject variability is particularly difficult to capture in typical
group analyses. Guidelines for rating profile severity and type along the
lines of traditional neuropsychological case assessment were articulated by
one of us (Larry J. Seidman) on the basis of various approaches to clinical
neuropsychological assessment (Kaplan, 1990; Reitan & Davison, 1974)
and then refined by two of us (Larry J. Seidman and William S. Kremen).
These ratings were previously applied to the relatives of schizophrenia
patients (Seidman et al., 1993). Specific guidelines for severity ratings—
the subject of this article—are shown in the Appendix, For purposes of this
study, we combined individuals with overall normal or borderline-normal
ratings to create a WNL group and combined those with overall abnormal
or severe ratings into a single abnormal group.
A single function was defined as abnormal or impaired when it was more
than 2 SDs below the control mean. A profile was generally considered
abnormal when at least two functions were more than 2 SDs below the
control mean, analogous to the 2-point codes used in MMPI interpretation
(Graham, 1977). However, this guideline was modified slightly in order to
balance concerns about both false-positive and false-negative classifica-
tions. A profile with only a single impaired function could be rated as
abnormal if that function was extremely impaired (i.e., >3 SDs below the
control mean). As noted by Palmer et al. (1997), it is generally agreed upon

746 KREMEN, SEIDMAN, FARAONE, TOOMEY, AND TSUANG
that there are likely to be too many false positives if overall cognitive
abnormality is based on only a single impaired function (American Acad-
emy of Neurology, 1991; American Psychiatric Association, 1987; Heaton,
Grant, & Matthews, 1991; McKhann et al.. 1984), On the other hand, we
believed that 3 or more SDs below the control mean reflected impairment
that was extreme enough to warrant classification as abnormal. We also
considered sizable discrepancies between domains of function to indicate
compromised neuropsychological function, even if neither function was
more than 2 SDs below the control mean. Such discrepancies also had to
be considered neuropsychologically meaningful. For example, verbal
memory function that was only slightly below the control mean but that
was 2 or more SDs below a person's general verbal ability would be
considered to reflect compromised verbal memory function. By these
definitions, performance may be compromised without being technically
abnormal or impaired.
Estimating change from expected or premorbid level of function. In
accord with our definition of terms, the performance of patients with no
functions greater than 2 SDs. below the control mean might still be judged
to reflect decline or compromised functioning relative to their expected or
premorbid level of ability. It should also be noted that premorbid ability
was not used in making profile severity ratings. On the basis of previous
work by our group and others, we used WRAT-R Reading scores as an
estimate of premorbid intellectual ability (Dalby & Williams, 1986; Kre-
men et al., 1995, 1996). The discrepancies between standardized scores on
the WRAT-R Reading and current IQ based on age-scaled Vocabulary and
Block Design subtests (Brooker & Cyr, 1986) served as one index of
decline from premorbid level of function. Because educational attainment
is likely to be attenuated by schizophrenic illness, we also examined
discrepancies between standardized scores on WRAT-R Reading and
education.
Tf schizophrenia is conceptualized as a neurodevelopmental disorder
(Feinberg, 1982; Seidman, 1990; Weinberger, 1987), then premorbid may
not be an entirely appropriate construct. We use the term to refer to the
period prior to the onset of florid psychotic symptoms. Premorbid ability
thus refers to the putative expected level of ability had the individual not
had schizophrenia or genes predisposing him or her to schizophrenia (for
a more detailed discussion, see Kremen et al., 1995, 1996).
Substance use ratings. We rated substance use on a 0-4 scale derived
from relevant sections of the SADS, with questions modified for rating
both lifetime (prior to the past 6 months) and current (past 6 months) use.
Individuals with current alcohol ratings of 3 (abuse, with duration of 6
months to 5 years) or higher or current drug ratings of 2 (regular use) or
higher were excluded, fnterrater reliability based on 20 cases was excellent,
ICCs ̂ .95, ps < .0001. There was too little variability in current drug use
to compute a meaningful ICC; ratings were 0 in all cases, except for one
participant, who received ratings of 0 and 1. See Faraone et al. (1995) for
additional details about these ratings.
Symptom ratings. Symptoms were assessed with the Scale for the
Assessment of Negative Symptoms (SANS; Andreasen, 1983) and the
Scale for the Assessment of Positive Symptoms (SAPS; Andreasen, 1984).
We examined Negative, Reality Distortion (Delusions and Hallucinations),
and Disorganization (Positive Formal Thought Disorder and Bizarre Be-
havior) dimensions from global SANS and SAPS scores (Arndt, Alliger, &
Andreasen, 1991; Liddle, 1987; Toomey et al., 1997). The Inattention
subscale was omitted because of its redundancy with cognitive function.
Psychosocial functioning. The Global Assessment Scale (GAS; Endi-
cott, Spitzer, Fleiss, & Cohen, 1976) was used as a general index of
psychosocial functioning.
Data Analysis
Controls and patient subgroups were compared by means of univariate
analyses of variance (ANOVAs). Significant ANOVAs were followed by
r tests for pairwise comparisons. For demographic and clinical character-
istics that were categorical variables, chi-square tests were used. Neuro-
psychological functions were also analyzed with Kruskal-Wallis tests
followed by Wilcoxon rank sum tests for pairwise comparisons. All sig-
nificant differences remained significant with these nonparametric tests
(results available on request), thus eliminating any concerns about distri-
butional properties of the measures or unbalanced designs in which group
sizes differ substantially. Given the consistency of results, we report only
the results of the parametric tests. All tests were two-tailed.
Results
Neuropsychological Profiles
Seventeen (23%) of the schizophrenia patients and 84 (92%) of
the controls were classified as having neuropsychological profiles
that were WNL, )f(\, N = 166) - 83.70, p < .001. Note that the
analyses reported here are based on the entire control group,
including the seven controls (8%) who were classified as neuro-
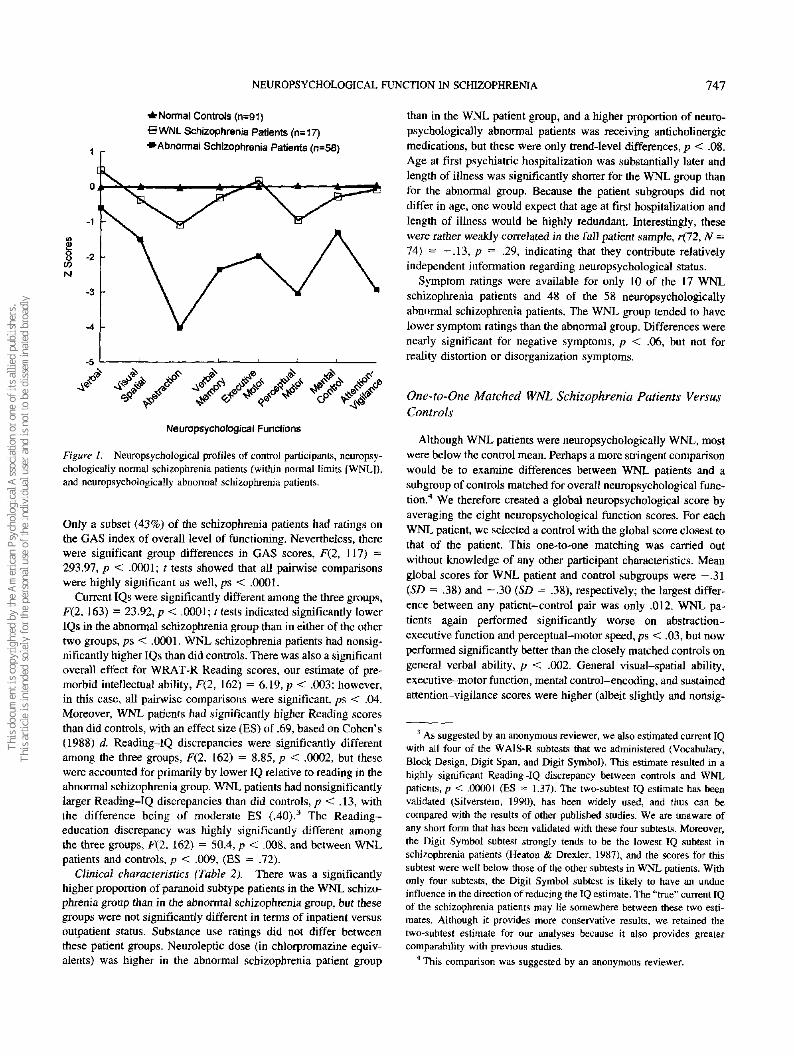
psychologically abnormal. Figure 1 depicts the mean neuropsy-
chological profiles for controls, WNL schizophrenia patients, and
neuropsychologically abnormal schizophrenia patients (n — 58;
77%). Differences in each of the eight neuropsychological func-
tions, as determined by univariate ANOVAs, were significant at or
beyond the .0001 level.1 These differences (and those for the
nonparametric results) would remain significant even with a con-
servative Bonferroni correction.
Pairwise comparisons showed that neuropsychologically abnor-
mal schizophrenia patients were substantially impaired on all
neuropsychological functions compared with controls or WNL
patients, all ps < .004. Comparisons of controls and WNL patients
revealed highly significant differences in abstraction-executive
function, 1(106) = 4.19, p < .0001, and perceptual-motor speed,
((106) - 3.71, p < .0003. General verbal ability was nearly
significantly different, r(l06) = -1.97, p < .052, but in the
opposite direction; that is, WNL patients scored somewhat higher
than controls.2
Correlates of Neuropsychological Performance
Demographics, IQ, and psychosocial functioning (control and
patient subgroups) (Table I). In considering these comparisons,
it should be recalled that neuropsychological test scores were
adjusted for age, sex, and parental education. There were no
differences in age, F(2, 163) = 0.47,^ = .63, parental education,
F(2, 163) = 1.77, p = .17, or ethnicity, j^(2, N = 164) = 1.82,
p — .40. As indicated in the Method section, there was a signifi-
cantly higher proportion of men in the patient groups than in the
control group, but the sex ratio was not significantly different
between the patient groups. There were highly significant differ-
ences in participants' own education. F(2, 163) = 11.33, p <
.0001. Educational attainment was lower in the abnormal schizo-
phrenia group than in either of the other two groups, /?s < .02, but
it did not differ between controls and WNL schizophrenia patients.
1 Raw scores for individual tests composing each function are available
on request.2 Controls and WNL patients did not differ in declarative memory, p =
.26. As suggested by an anonymous reviewer, inclusion of the percent
retained score could have obscured group differences, but the results were
essentially unchanged for immediate recall alone, p = .21.
NEUROPSYCHOLOGICAL FUNCTION IN SCHIZOPHRENIA 747
^Normal Controls (n=91)
eWNL Schizophrenia Patients (n=17)
1 •Abnormal Schizophrenia Patients (n=58)
Neuropsychological Functions
Figure I. Neuropsychological profiles of control participants, neuropsy-
chologically normal schizophrenia patients (within normal limits [WNL]},and neuropsychologically abnormal schizophrenia patients.
Only a subset (43%) of the schizophrenia patients had ratings on
the GAS index of overall level of functioning. Nevertheless, there
were significant group differences in GAS scores, F(2, 117) =
293.97, p < .0001; t tests showed that all pairwise comparisons
were highly significant as well, ps < .0001.
Current IQs were significantly different among the three groups,
F(2, 163) = 23.92, p < .0001; t tests indicated significantly lower
IQs in the abnormal schizophrenia group than in either of the other
two groups, ps < .0001. WNL schizophrenia patients had nonsig-
nificantly higher IQs than did controls. There was also a significant
overall effect for WRAT-R Reading scores, our estimate of pre-
morbid intellectual ability, F(2, 162) = 6.19, p < .003; however,
in this case, all pairwise comparisons were significant, ps < .04.
Moreover, WNL patients had significantly higher Reading scores
than did controls, with an effect size (ES) of .69, based on Cohen's
(1988) d. Reading-IQ discrepancies were significantly different
among the three groups, F(2, 162) = 8.85, p < .0002, but these
were accounted for primarily by lower IQ relative to reading in the
abnormal schizophrenia group. WNL patients had nonsignificantly
larger Reading-TQ discrepancies than did controls, p < .13, with
the difference being of moderate ES (.40).3 The Reading-
education discrepancy was highly significantly different among
the three groups, F(2. 162) = 50.4, p < .008, and between WNL
patients and controls, p < .009, (ES = .72).
Clinical characteristics (Table 2). There was a significantly
higher proportion of paranoid subtype patients in the WNL schizo-
phrenia group than in the abnormal schizophrenia group, but these
groups were not significantly different in terms of inpatient versus
outpatient status. Substance use ratings did not differ between
these patient groups. Neuroleptic dose (in chlorpromazine equiv-
alents) was higher in the abnormal schizophrenia patient group
than in the WNL patient group, and a higher proportion of neuro-
psychologically abnormal patients was receiving anticholinergic
medications, but these were only trend-level differences, p < .08.
Age at first psychiatric hospitalization was substantially later and
length of illness was significantly shorter for the WNL group than
for the abnormal group. Because the patient subgroups did not
differ in age, one would expect that age at first hospitalization and
length of illness would be highly redundant. Interestingly, these
were rather weakly correlated in the full patient sample, r(72, N =
74) = — .13, p = .29, indicating that they contribute relatively
independent information regarding neuropsychological status.
Symptom ratings were available for only 10 of the 17 WNL
schizophrenia patients and 48 of the 58 neuropsychologically
abnormal schizophrenia patients. The WNL group tended to have
lower symptom ratings than the abnormal group. Differences were
nearly significant for negative symptoms, p < .06, but not for
reality distortion or disorganization symptoms.
One-to-One Matched WNL Schizophrenia Patients Versus
Controls
Although WNL patients were neuropsychologically WNL, most
were below the control mean. Perhaps a more stringent comparison
would be to examine differences between WNL patients and a
subgroup of controls matched for overall neuropsychological func-
tion.4 We therefore created a global neuropsychological score by
averaging the eight neuropsychological function scores. For each
WNL patient, we selected a control with the global score closest to
that of the patient. This one-to-one matching was carried out
without knowledge of any other participant characteristics. Mean
global scores for WNL patient and control subgroups were —.31
(SD = .38) and -.30 (SD = .38), respectively; the largest differ-
ence between any patient-control pair was only .012. WNL pa-
tients again performed significantly worse on abstraction-
executive function and perceptual-motor speed, ps < .03, but now
performed significantly better than the closely matched controls on
general verbal ability, p < .002. General visual-spatial ability,
executive-motor function, mental control—encoding, and sustained
attention-vigilance scores were higher (albeit slightly and nonsig-
3 As suggested by an anonymous reviewer, we also estimated current IQwith all four of the WAIS-R subtests that we administered (Vocabulary,
Block Design, Digit Span, and Digit Symbol). This estimate resulted in ahighly significant Reading-IQ discrepancy between controls and WNLpatients, p < .00001 (ES = 1.37). The two-subtest IQ estimate has beenvalidated (Silverstein, 1990), has been widely used, and thus can be
compared with the results of other published studies. We are unaware ofany short form that has been validated with these four subtests. Moreover,the Digit Symbol subtest strongly tends to be the lowest IQ subtest in
schizophrenia patients (Heaton & Drexler, 1987), and the scores for thissubtest were well below those of the other subtests in WNL patients. Withonly four subtests, the Digit Symbol subtest is likely to have an undueinfluence in the direction of reducing the IQ estimate. The "true" current IQof the schizophrenia patients may lie somewhere between these two esti-mates. Although it provides more conservative results, we retained thetwo-subtest estimate for our analyses because it also provides greatercomparability with previous studies.
4 This comparison was suggested by an anonymous reviewer.

748 KREMEN, SEIDMAN, FARAONE, TOOMEY, AND TSUANG
Table 2
Clinical Characteristics of Neuropsychologically Normal and
Impaired Schizophrenia Patients
Schizophrenia patients
WNL(n = 17)
ABN
(n = 58)
Variable M SD M SD
Substance use history*Alcohol 1.59 1.54 1.93 1.35 .22Drug 0.53 1.01 2.18 1.31 .18
Age at first psychiatrichospitalization (years)6 29.18 8.04 22.58 5.28 .005
Length of illness (years)1" 14.11 11.94 22.21 10.50 .009Symptom ratings6
Negative 1.07 1.30 1.80 1.05 .06Reality Distortion 1.90 1.45 2.18 1.51 .60Disorganization 0.90 0.88 1.44 1.05 .14
Neuroleptic dosed 378.13 269.25 659.65 600.84 .08
Paranoid subtypeOutpatientsReceiving anticholinergicse
n
9
144
%
538224
n
12
3627
%
21
6248
.009
.12
.08
Note. WNL — neuropsychologically within normal limits; ABN = neu-ropsychologically abnormal.a Substance use ratings were from 0 (never or occasional) to 4 (heavyor sustained abuse). h Missing data for 1 ABN participant. c Basedon the Scale tor the Assessment of Negative Symptoms (SANS) and theScale for the Assessment of Positive Symptoms (SAPS) and includingonly a subset of participants: 10 WNL and 48 ABN participants.Negative - mean of SANS subscales except Inattention; Reality Dis-tortion = mean of SAPS Delusions and Hallucinations subscales;Disorganization — mean of SAPS Bizarre Behavior and Positive FormalThought Disorder subscales. d Measured in milligrams of chlorprom-azine equivalents. Missing data for 1 WNL participant and 1 ABNparticipant. Results are based on the Kruskal-Wallis chi-square test; theI test was significant at the .01 level, but the distribution of dosagevalues deviated substantially from normality. c Missing data for 2ABN participants.
nificantly) in WNL patients than in controls.5 Educational attain-
ment was slightly higher in WNL patients, p = .10, and both
current IQs (110.9 vs. 98.6), p < .004, and WRAT-R Reading
scores (110.4 vs. 95.8), p < .002, were significantly higher in
WNL patients than in controls. GAS scores were substantially
lower in WNL patients than in the matched controls, p < .0001.
Discussion
Neuropsychologically Normal Status Does Not Preclude
Compromised Neurocognitive Function
Despite being classified as neuropsychologically WNL, the
WNL patients still manifested poorer overall neuropsychological
performance than did controls, with deficits accounted for primar-
ily by abstract!on-executive function and perceptual-motor speed.
In contrast to the neuropsychological differences, both groups had
similar levels of educational attainment, and WNL patients had
significantly higher estimated premorbid intellectual ability than
did controls. Compared with a subgroup of controls who were
matched one-to-one on global neuropsychological function, WNL
patients had both significantly higher estimated premorbid intel-
lectual ability and current IQ but still had significantly poorer
abstraction-executive function and perceptual-motor speed.
Suggestive of a decline from premorbid level of function,
schizophrenia patients in a previous study by our group (which
included a subset of participants in this study) had significantly
larger Reading-IQ discrepancies than did controls (Kremen et al.,
1996).6 These discrepancies were nonsignificantly larger in WNL
patients than in controls, although there was a moderate ES of .40.
Consistent with our argument that educational attainment is atten-
uated by schizophrenic illness (Kremen et al., 1996), WNL pa-
tients had higher Reading scores than did the control group as a
whole, relative to their level of education (ES = .72). When WNL
patients were compared with a subset of matched controls, there
were even greater differences in educational attainment, [Q, and
WRAT-R Reading scores; all of these were higher in WNL pa-
tients, despite the persistence of the abstraction-executive and
perceptual-motor speed deficits. Differences in discrepancy scores
for these matched groups were reduced for Reading-IQ (ES = .24)
but not for Reading-education (ES = .70). Thus, WNL patients
may have relatively little decline in general intellectual function,
but they still appear to have attenuated educational attainment and
compromised neuropsychological function relative to expected or
premorbid ability.
On the basis of studies of both schizophrenia patients and their
biological relatives, we have argued that even prodromal symp-
toms are likely to result in reduced educational attainment or
neuropsychological deficits or both (Faraone et al., 1995; Kremen
et al., 1995, 1996). In contrast, Palmer et al. (1997) reasoned that
onset of illness after the completion of typical formal education
meant that the illness was unlikely to have interfered with educa-
tional attainment. However, even with age of onset that was much
later than that in the neuropsychologically abnormal patients, our
data strongly suggest that WNL patients still had reduced educa-
tional attainment.
Elliott et al. (1998) also found significantly impaired perfor-
mance on a variety of neuropsychological tests in schizophrenia
patients of similar age and with similar current and estimated
premorbid IQs as our WNL patients. Even genetically at-risk
individuals (including discordant monozygotic twins) manifest
neuropsychological deficits relative to controls or to estimates of
expected intellectual ability based on WRAT-R Reading scores
(e.g., Faraone et al., 1995; Goldberg et al., 1990; Kremen et al.,
1995). Thus, schizophrenia without at least some degree of com-
promised neurocognitive function relative to expected or premor-
bid ability seems unlikely.
5 Simple CPTs are prone to ceiling effects in controls, but it was the
more difficult Dichotic Listening Test that accounted for most of the
variance in the attention-vigilance function.6 There were 44 schizophrenia patients and 44 controls in the previous
study of Kremen et al. (1996), and these individuals are also included in
this study. However, neuropsychological function was not examined in the
earlier article.

NEUROPSYCHOLOGICAL FUNCTION IN SCHIZOPHRENIA 749
Other Clinical and Demographic Correlates of
Neuropsychological Performance
Essentially, the pattern of clinical and demographic correlates is
consistent with WNL patients having a milder illness than neuro-
psychologically abnormal patients. Consistent with this view, the
WNL patients had much later age of onset and shorter duration of
illness than did the abnormal patients. Sex differences might
impact the age-of-onset findings (cf. Goldstein, 1995), but this
notion is difficult to gauge because a majority of the patients were
men and the scores were adjusted for sex.
The difference in the proportions of paranoid subtype patients in
our neuropsychologically abnormal and WNL schizophrenia
groups is consistent with several (e.g., Kremen, Seidman, Gold-
stein, Faraone, & Tsuang, 1994; Seidman et al., 1992; Silverstein
& Zerwic, 1985), but not all (Palmer et al., 1997), studies suggest-
ing better functioning in paranoid patients. Symptom differences
between WNL and abnormal patients were relatively weak, but
GAS ratings were quite different. This finding is consistent with
other data showing that cognitive function tends to be a better
predictor of psychosocial functioning than does symptomatology
(Green, 1996).
Limitations
Because data for symptom and GAS ratings were available for
only a subset of participants, conclusions regarding these variables
must be considered more tentative than conclusions about other
variables. We could not include visual-spatial declarative memory
because during the study we began using an updated version of the
test that was not comparable to the older version. Although we
cannot be certain, on the basis of previous findings (Saykin et al.,
1991; Seidman et al., 1992), it seems unlikely that this addition
would have greatly altered the neuropsychological results.
A generalized deficit in the schizophrenia patients could lead to
misinterpretation of our results (Chapman & Chapman, 1978).
Relatively poorer performance on particular neuropsychological
functions compared with that of others might, for example, be a
reflection of differences in task difficulty rather than specific
abilities. We believe that several factors argue against this expla-
nation in this study. First, attention-vigilance was worse than
mental control-encoding in the neuropsychologically abnormal
patients but was slightly better than mental control-encoding in
the WNL patients. This pattern suggests a double dissociation of
function. Second, (he WNL group cannot be said to have a gen-
eralized deficit because they performed nonsignificantly better
than the controls on two functions (verbal ability and executive-
motor function). Compared with controls matched on global neu-
ropsychological performance, WNL patients had significantly bet-
ter verbal ability and nonsignificantly better performance on four
other neuropsychological functions. If differences are attributable
to task difficulty or other psychometric properties, the results
should be in the same direction in each group. Finally, in contrast
to our results, schizophrenia patients studied by Saykin et al.
(1991, 1994) showed their most prominent deficits in declarative
memory. Because we used very similar tests, we also should have
observed the most prominent relative deficiencies in memory if
that pattern were primarily a function of task difficulty or some
other psychometric property.
It should be noted that with a cross-sectional design, we can
only infer decline from expected or premorbid ability levels based
on the observed discrepancies. Although we cannot know when
declines may have occurred or whether score discrepancies have
always been present and do not reflect change over time, inferring
decline seems the most parsimonious explanation. Moreover, lon-
gitudinal studies in which premorbid cognitive data were available
have indicated declines after the onset of psychosis (Goldman et
al., 1999; Schwartzman & Douglas, 1962).
Although relatively stable, our patient sample was a very
chronic one. It is possible that some patients early in the course of
illness do not experience any neuropsychological decline from
premorbid levels. Goldman et al. (1999) recently studied first-
episode patients who had improved neuropsychological function
after 3 years of illness. Current functioning was average (.2 SD
below the control mean), but their grade school achievement test
scores averaged 2 grades above grade level. These longitudinal
results for young, nonchronic patients strongly suggest decline
from superior to approximately average levels of function. Thus,
results from both chronic and first-episode patients support our
contention that compromised neuropsychological function is in-
deed a core feature of schizophrenia. Moreover, most studies have
not found evidence of progressive neuropsychological deteriora-
tion (Hoff et al., 1999: Hyde et al., 1994; Rund, 1998), at least not
before age 50 (Fucetola et al., 2000).
Summary
Although we classified almost one-quarter of a group of chronic
schizophrenia patients as being neuropsychologically WNL, our
findings were consistent with the notion that even these apparently
unimpaired patifents had compromised neuropsychological func-
tion relative to their expected or premorbid level of intellectual
ability. These findings support the hypothesis that compromised
neuropsychological function is a core feature of illness that is
present in virtually all individuals with schizophrenia. Further
understanding of the neural underpinnings of compromised neu-
ropsychological function in schizophrenia will be necessary to
understand whether or not the same sort of neuropsychological
compromise underlies all cases of schizophrenia and the extent to
which neural substrates for neuropsychological dysfunction and
traditional signs and symptoms may overlap. Finally, longitudinal
studies will be necessary to fully understand if and how neuropsy-
chological function changes over the course of illness, how it may
influence psychosocial functioning, and how neuropsychological
change is affected by level of premorbid intellectual ability.
References
Allport, G. \V. (1942). The use of personal documents in psychological
science. New York: Social Science Research Council.
American Academy of Neurology. (1991). Nomenclature and research case
definitions for neurologic manifestations of human immunodeficiency
virus-type ] (HIV-1) infection: Report of a working group of the
American Academy of Neurology AIDS Task Force. Neurology, 41.
778-785.
American Psychiatric Association. (19S7). Diagnostic and statistical man-
ual of mental disorders (3rd ed., rev.). Washington, DC: American
Psychiatric Press.

750 KREMEN, SEIDMAN, FARAONE, TOOMEY, AND TSUANG
Andreasen, N. C. (1983). Scale for the Assessment of Negative Symptoms
(SANS). Iowa City: University of Iowa.
Andreasen, N. C, (1984). Scale for the Assessment of Positive Symptoms
(SAPS). Iowa City: University of Iowa.
Arndt, S., Alliger, R. J., & Andreasen, N. C, (1991), The distinction of
positive and negative symptoms: The failure of a two-dimensional
model. British Journal of Psychiatry, 158, 317-322.
Aylward, E., Walker, E., & Bettes, B. (1984). Intelligence in schizophre-
nia: Meta-analysis of the research. Schizophrenia Bulletin, W, 430-459.
Benton, A. L, Hamsher. K,, Varney, N. R., & Spreen, O. (1983). Contri-
butions to neuropsychological assessment. New York: Oxford Univer-
sity Press.
Braff, D. L., Heaton, R., Kuck, J., Cullum, M., MoranviHe, J., Grant, L, &
Zisook, S. (1991). The generalized pattern of neuropsychological defi-
cits in outpatients with chronic schizophrenia with heterogeneous Wis-
consin Card Sorting Test results. Archives of General Psychiatry, 48,
891-898.
Brooker, B. H., & Cyr, J. J. (1986). Tables for clinicians to use to convert
WAIS-R short forms. Journal of Clinical Psychology, 42, 982-986.
Cannon, T, D., Zorrilla, L. E., Shtasel, D., Gur, R. E., Gur, R. C., Marco,
E. J., Moberg, P., & Price, A. (1994). Neuropsychological functioning in
siblings discordant for schizophrenia and healthy volunteers. Archives of
General Psychiatry, 51. 651-661.
Chapman, L. 1, & Chapman, J. P. (1978). The measurement of differential
deficit. Journal of Psychiatric Research, 14, 303-311.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences.
Hillsdale, NJ: Erlbaum.
Dalby, J. T., & Williams, R. (1986). Preserved reading and spelling ability
in psychotic disorders. Psychological Medicine, 16, 171-175.
Elliott, R,, McKenna, P. J., Robbins, T. W., & Sahakian, B. I. (1998).
Specific neuropsychological deficits in schizophrenic patients with pre-
served intellectual function. Cognitive Neuropsychiatry, 3, 45-70.
Endicott, S., & Spitzer, R. L. (1978). A diagnostic interview: The Schedule
for Affective Disorders and Schizophrenia. Archives of General Psychi-
atry, 35, 837-844.
Endicott, J., Spitzer, R. L., Fleiss, J. L., & Cohen, J. (1976). The Global
Assessment Scale: A procedure for measuring overall severity of a
psychiatric disturbance. Archives of General Psychiatry, 33, 766-771.
Faraone, S. V., Seidman, L, J,, Kremen, W. S., Pepple, 3. R., Lyons, M. J.,
& Tsuang, M. T. (1995). Neuropsychological functioning among the
nonpsychotic relatives of schizophrenic patients: A diagnostic efficiency
analysis. Journal of Abnormal Psychology, 104, 286-304.
Feinberg, I. (1982). Schizophrenia: Caused by a fault in programmed
synaptic elimination during adolescence? Journal of Psychiatric Re-
search, 4, 319-334.
Feldman, M. J., & Drasgow, J. (1981). The Visual-Verbal Test. Los
Angeles: Western Psychological Services. (Original work published
1959)
Fucetola, R., Seidman, L. J., Kremen, W. S., Faraone, S. V., Goldstein,
J. M., & Tsuang, M. T. (2000). Age and neuropsychological function in
schizophrenia: A decline in executive abilities beyond that observed in
normal volunteers. Biological Psychiatry, 48, 137-146.
Gold, J. M., & Harvey, P. D. (1993). Cognitive deficits in schizophrenia.
Psychiatric Clinics of North America, 16, 295-312.
Goldberg, T. E., Ragland, D., Torrey, E. F., Gold, J. M., Bigelow, L. B., &
Weinberger, D. R. (1990). Neuropsychological assessment of monozy-
gotic twins discordant for schizophrenia. Archives of General Psychia-
try, 47, 1066-1072.
Goldberg, T. E., Torrey, E. F., Gold, J. M., Ragland, J. D.. Bigelow, L. B.,
& Weinberger, D. R. (1993). Learning and memory in monozygotic
twins discordant for schizophrenia. Psychological Medicine, 23,11-85.
Golden, C., Maclnnes, W., Ariel, R., Ruedrich, S., Chu, C.-C., Coffman, J.?
Graber, B., & Bloch, S. (1982). Cross-validation of the ability of the
Luria-Nebraska neuropsychological battery to differentiate chronic
schizophrenics with and without ventricular enlargement. Journal of
Consulting and Clinical Psychology, 50, 87-95.
Goldman, R. S., Bates, J., Bilder, R. M., Conley, J., Reiter, G., Pappadopu-
los, E., Robinson, D., Alvir, J. M. A., Lieberman, J., & Schooler, N.
(1999). Reverse cohort analysis of preserved neurocognitive function in
first-episode schizophrenia (.Abstract]. Schizophrenia Research, 36, 131.
Goldstein, G. (1986). The neuropsychology of schizophrenia. In 1. Grant &
K. M. Adams (Eds.), Neuropsychological assessment of neuropsychiat-
ric disorders (pp. 147-171). New York: Oxford University Press.
Goldstein. J. M. (1995). The impact of gender on understanding the
epidemiology of schizophrenia. In M. Seeman (Ed.), Gender and psy-
chopathology (pp. 159-199). Washington, DC: American Psychiatric
Press.
Goldstein, G., & Shemansky, W. J. (1995). Influences on cognitive heter-
ogeneity in schizophrenia. Schizophrenia Research, 18, 59-69.
Graham, J. R. (1977). The. MMPl: A practical guide. New York: Oxford
University Press.
Green, M. F. (1996). What are the functional consequences of neurocog-
nitive deficits in schizophrenia? American Journal of Psychiatry, 153,
321-330.
Heaton, R. K. (1981). Wisconsin Card Sorting Test manual. Odessa, FL:
Psychological Assessment Resources.
Heaton, R. K., & Drexler, M. (1987). Clinical neuropsychological findings
in schizophrenia and aging. In N. E. Miller & G. D. Cohen (Eds.),
Schizophrenia and aging: Schizophrenia, paranoia, and schizophreni-
form disorders in later life (pp. 145-161). New York: Guilford Press.
Heaton, R. K., Grant, I., & Matthews, C. G. (1991), Comprehensive norms
for an expanded Halstead-Reitan Battery: Demographic corrections,
research findings, and clinical applications. Odessa, FL: Psychological
Assessment Resources.
Hoff, A. L., Riordan, H., O'Donnell, D. W., Moms, L., & DeLisi, L. E.
(1992). Neuropsychological functioning of first-episode schizophreni-
form patients. American Journal of Psychiatry, 149, 898-903.
Hoff, A. L., Sakuma, M., Wieneke, M., Horon, R., Kushner, M., & DeLisi,
I.. E. (1999). A longitudinal neuropsychological follow-up study of
patients with first episode schizophrenia. American Journal of Psychi-
atry, {56, 1336-1341.
Hooper, H. E. (1983). Hooper Visual Organization Test (VOT) manual.
Los Angeles: Western Psychological Services.
Hyde, T., Nawroz, S., Goldberg, T., Bigelow, L., Strong, D., Ostrem, J.,
Weinberger, D., & Kleinman, J. (1994). Is there cognitive decline in
schizophrenia? A cross-sectional study. British Journal of Psychiatry,
J64, 494-500.
Jastak, S., & Wilkinson, G. (1984). The Wide Range Achievement Test-
revised. Wilmington, DE: Jastak Associates.
Jones, P., Rodgers, B., & Murray, R. M. (1994). Child developmental risk
factors for adult schizophrenia in the British 1946 birth cohort. Lancet,
344, 1398-1402.
Kaplan, E. F. (1990). The process approach to neuropsychological assess-
ment of psychiatric patients. Journal of Neuropsychiatry and Clinical
Neurosciences, 2, 72—87,
Keefe, R. S., Silverman, J. M., Lees Roitman, S. E., Harvey, P. D., Duncan,
M. A., Alroy, D., Siever, L. J., Davis, K. L., & Mohs, R. C. (1994).
Performance of nonpsychotic relatives of schizophrenic patients on
cognitive tests. Psychiatry Research, 53, 1-12.
Kimura, D. (1967). Functional asymmetry of the brain in dichotic listening.
Cortex, 3, 163-178.
Kremen, W. S., Buka, S. L., Seidman, L. J., Goldstein, J. M., Koren, D., &
Tsuang, M. T. (1998). IQ decline during childhood and adult psychotic
symptoms in a community sample: A 19-year longitudinal study. Amer-
ican Journal of Psychiatry, 155, 672-679.
Kremen, W. S., Seidman, L. J., Faraone, S. V., Pepple, J. R., Lyons, M. J.,
& Tsuang, M. T. (1995). The '3 Rs' and neuropsychological function in
NEUROPSYCHOLOGICAL FUNCTION IN SCHIZOPHRENIA 751
schizophrenia: A test of the matching fallacy in biological relatives.
Psychiatry Research, 56, 135-143.
Kremen, W. S., Seidman, L. J., Faraone, S. V., Pepple, J. R., Lyons, M. J.,
& Tsuang, M. T. (1996). The "3 Rs" and neuropsychological function in
schizophrenia: An empirical test of the matching fallacy. Neuropsychol-
ogy, JO, 22-31.
Kremen, W. S., Seidman, L. J., Goldstein, J. M., Faraone, S. V., & Tsuang,
M. T, (1994). Systematized delusions and neuropsychological function
in paranoid and nonparanoid schizophrenia. Schizophrenia Research,
12, 223-236.
Kremen, W. S., Seidman, L. J,, Pepple, J. R., Lyons, M. J., Tsuang. M. T.,
& Faraone, S. V. (1994). Neuropsychological risk indicators for schizo-
phrenia: A review of family studies. Schizophrenia Bulletin, 20, 103-
119.
Liddle, P. F. (1987). The symptoms of chronic schizophrenia. A re-
examination of the positive-negative dichotomy. British Journal of
Psychiatry, 151, 145-151.
Marshall, J. C., & Newcombe, F. (1984). Putative problems and pure
progress in neuropsychological single-case studies. Journal of Clinical
Neuropsychology, 6, 65-70.
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., &
Stadlan, E. M. (1984). Clinical diagnosis of Alzheimer's disease: Report
of the NINCSD-ADRDA work group under the auspices of Department
of Health and Human Services Task Force on Alzheimer's Disease.
Neurology, 34, 939-944.
Mirsky, A. F., Locnhead, S. J.t Jones, B. P., Kugelmass, S., Walsh, D., &
Kendler, K. S. (1992). On familial factors in the attentional deficit in
schizophrenia: A review and report of two new subject samples. Journal
of Psychiatric Research, 26, 383-403.
Palmer, B. W., Heaton, R. K., Paulsen, J. S., Kuck, J., Braff, D., Harris,
M. J., Zisook, S., & Jeste, D. V. (1997). Is it possible to be schizophrenic
yet neuropsychologically normal? Neuropsychology, 11, 437-446.
Reitan, R. M., & Davison, L, A. (1974). Clinical neuropsychology: Cur-
rent status and applications. New York: Wiley,
Rund, B. R. (1998). A review of longitudinal studies of cognitive functions
in schizophrenia patients. Schizophrenia Bulletin, 24, 425-435.
Saykin, A. J., Gur, R. C., Gur, R. E., Mozley, P. D., Mozley, L. H.,
Resnick, S. M., Kester, B., & Stafiniak, P. (1991). Neuropsychological
function in schizophrenia: Selective impairment in memory and learn-
ing. Archives of General Psychiatry, 48, 618-624.
Saykin, A. J., Shtasel, D. L., Gur, R. E., Kester, D. B., Mozley, L. H.,
Stafiniak, P., & Gur, R. C. (1994), Neuropsychological deficits in
neuroleptic naive patients with first-episode schizophrenia. Archives of
General Psychiatry, 51, 124-131.
Schwartzman, A. E., & Douglas, V. I. (1962). Intellectual loss in schizo-
phrenia: Part I. Canadian Journal of Psychology, 16, 1-10.
Seidman, L- J. (1983). Schizophrenia and brain dysfunction: An integration
of recent neurodiagnostic findings. Psychological Bulletin, 94, 195-238.
Seidman, L. J. (1990). The neuropsychology of schizophrenia: A neuro-
developmental and case study approach. Journal of Neuropsychiatry and
Clinical Neurosciences, 2, 301-312.
Seidman, L. J., Cassens, G., Kremen, W. S., & Pepple, J. R. (1992). The
neuropsychology of schizophrenia. In R. F. White (Ed.), Clinical syn-
dromes in adult neuropsychology: The practitioner's handbook (pp.
381-449). Amsterdam: Elsevier.
Seidman, L. J., Faraone, S. V., Kremen, W. S., Pepple, J. R., Lyons, M. J.,
& Tsuang, M. T. (1993). Neuropsychological dysfunctions in the non-
psychotic first-degree relatives of schizophrenic patients. Poster session
presented at the 8th annual meeting of the Society for Research and
Psychopathology, Chicago.
Seidman, L. J., Kremen, W. S., Koren, D., Faraone, S. V., Toomey, R., &
Tsuang, M. T. (2000). A comparative profile analysis of neuropsycho-
logical function in schizophrenia and bipolar psychoses. Manuscript
submitted for publication.
Shallice, T., Burgess, P. W., & Frith, C. D. (1991). Can the neuropsycho-
logical case-study approach be applied to schizophrenia? Psychological
Medicine, 21, 661-673.
Silverstein, A. B. (1990). Short forms of individual intelligence tests.
Journal of Consulting ana" Clinical Psychology, 2, 3-11.
Silverstein, M. L., & Zerwic, M. J. (1985). Clinical psychopathologic
symptoms in neuropsychologically impaired and intact schizophrenics.
Journal of Counseling and Clinical Psychology, 53, 267-268.
Toomey, R., Kremen, W. S., Simpson, J, C., Samson, J. A., Seidman, L. J.,
Lyons, M. J., Faraone, S. V., & Tsuang, M. T. (1997). Revisiting the
factor structure for positive and negative symptoms: Evidence from a
large heterogeneous group of psychiatric patients. American Journal of
Psychiatry, 154, 371-377.
Vincent, K. R., Castillo, I. M., Hauser, R. L, Zapata, J. A., Stuart, H. J.,
Cohn, C. K., & O'Shanick, G. J. (1984). MMP1-168 codebook. Nor-
wood, NJ: Ablex.
War Department. (1944). Army Individual Test Battery. Manual of direc-
tions and scoring. Washington, DC: Adjutant General's Office.
Wechsler, D. (1945). A standardized memory scale for clinical use. Jour-
nal of Psychology, 19, 87-95.
Wechsler, D. (1981). Manual for the Wechsler Adult Intelligence Scale-
revised. San Antonio, TX: Psychological Corporation.
Wechsler, D. (1987). Manual for the Wechsler Memory Scale—revised.
San Antonio, TX: Psychological Corporation.
Weinberger, D. R. (1987). Implications of normal brain development for
the pathogenesis of schizophrenia. Archives of General Psychiatry, 44,
660-669.
Weintraub, S., & Mesulam, M.-M. (1985). Mental state assessment of
young and elderly adults in behavioral neurology. In M.-M. Mesulam
(Ed.), Principles of behavioral neurology (pp. 71-124). Philadelphia,
PA: F. A. Davis.
(Appendix follows}

752 KREMEN, SEIDMAN, FARAONE, TOOMEY, AND TSUANG
Appendix
Guidelines for Rating Severity of Individual Neuropsychologicai Profiles (Based on Eight Functions)
This information is based on that given by Seidman et al. (1993).
NormalExpect within-subject variability of up to 1 to 2 SDs across functionsExpect function scores that are down to 1 SD below the control meanA single function may be close to or equal to 2 SDs below the control mean
Borderline NormalA single function that is ^2 and ^3 SDs below the control meanTwo functions that are ^1.5 and ^2 SDs below the control meanA single function that is ^1.5 SDs and s2 SDs below the control mean but also well below all other functions (difference of ^2 SDs,)
Examples: Verbal score = I and verbal memory = -1.5; one function is 2.5 SDs below another, but the more impaired function is only 1.5 SDsbelow the control mean (suggests selective impairment in the context of a mild severity level)
AbnormalA single function that is >3 SDs below the control meanTwo or three functions that are >2 SDs below the control meanTwo or more functions that are >1 SD and ^2 SDs below the control mean, with at least 4 SDs between the highest and lowest functions
Examples: Both visual memory and visual-spatial functions are >2 SDs below the control means, but the rest of the profile is relatively flat andwell within the average range; abstraction = -1.5, attention-vigilance - -1.8, and verbal = 2.2, making a 4-5D difference between thehighest and lowest scores
SevereFour or more functions that are >2 SDs below the control mean
Received May 17, 1999
Revision received March 1, 2000
Accepted June 8, 2000 •




















