
Examination of the substrate specificity of heparin and heparan sulfate lyases
Upload
independentCategory
view
0download
0
British lournal of HaematoIogy, 1992, 82, 391-399
The low molecular weight heparin Enoxaparin inhibits the consumption of factor VII and prothrombin activation in vivo associated with elective knee replacement surgery
FREDERICK A . O F O S U , ' . ~ JACQUES L E C L E R C , 3 FERNAND DELORME,4 SHARON c R A V E N , l S H A M I R A N S H A F A I , '
LORI FREWIN' A N D MORRIS A. B L A J C H M A N ' . ~ 'The Canadian Red Cross Society, Blood Services, Hamilton; 2Department of Pathology, McMaster University, Hamilton; 3Department of Medicine, McGill University and Montreal General Hospital, Montreal, and 4Department of Pathology, University of Montreal, Montreal
Received 23 December 1991; acceptedfor publication 19 May 1992
Summary. Patients over 40 years of age who undergo elective orthopaedic surgery have a relatively high risk for developing post-surgical deep vein thrombosis (DVT). Prophylactic use of heparin or low molecular weight hepar- ins can reduce the incidence of post-operative DVT by up to 80%. It is not known whether prophylaxis is achieved by inhibition of prothrombin activation or catalysis of thrombin inhibition in vivo. We determined the changes in concentra- tions of factor VII zymogen and thrombin-antithrombin 111 (the latter as an index of prothrombin activation) in the plasmas of 129 patients randomized to receive two daily subcutaneous injections of placebo or 30 mg of Enoxaparin after elective knee surgery. Enoxaparin reduced the fre- quency of post-surgical DVT by 70%. The concentration of
factor VII zymogen had decreased by - 50% within 24 h after the knee surgery, followed by a gradual increase to near pre- surgical values. Additionally, post-Enoxaparin plasmas had statistically significant higher concentrations of factor VII zymogen than post-placebo plasmas. Post-Enoxaparin plas- mas had significantly lower concentrations of endogenous thrombin-antithrombin I11 than comparable post-placebo plasmas. Finally, post-Enoxaparin plasmas inactivated exo- genous factor Xa and thrombin more effectively than com- parable post-placebo plasmas. As Enoxaparin moderated the generation of endogenous thrombin-antithrombin 111 after elective knee surgery, inhibition of prothrombin activation in vivo by Enoxaparin may be important for its prophylactic antithrombotic effect.
Unfractionated (UF) and low molecular weight (LMW) heparins reduce the incidence of deep venous thrombosis (DVT) associated with abdominal and orthopaedic surgery in individuals over 40 years of age (Kakkar et al, 1982; Welin- Berger et al, 1982; Leyvraz et al. 1983; Stulberg et aZ, 1984; Kakkar & Murray, 1985; Turpie et aZ, 1986: Stringer et aI, 1989; Leclerc et al, 1992). Like UF heparins from which they are derived, LMW heparins inhibit prothrombin activation in vitro by delaying the two amplification reactions usually catalysed by the initial thrombin generated endogenously (Ofosu et al, 1987, 1989; Beguin et al. 1988). On a molar basis, however, up to 20 times more LMW than UF heparins are required to delay the initiation of intrinsic prothrombin activation (Ofosu et al, 1988: Ofosu, 1990). This study is a companion study to the previously reported multicentre,
Correspondence: Dr F. A. Ofosu. Department of Pathology, McMaster University, 1200 Main Street West, Hamilton, Ontario, Canada L8N 325.
double-blind, randomized clinical trial which demonstrated that 30 mg of the LMW heparin Enoxaparin, given subcuta- neously every 12 h, reduced the incidence of DVT following elective knee surgery to less than 20% (Leclerc et al, 1992). In the previous study, 70% of patients randomized to receive placebo developed post-surgical DVT (Leclerc et al, 1992). We hypothesized that increased concentrations of tissue factor would become available following the trauma of surgery, and as a consequence, factor VII consumption and prothrombin activation would increase. Therefore, we measured the concentrations of factor VII zymogen and factor VII-related proteins (i.e. total factor VII) in the pre- and post-surgical plasmas to determine whether increased tissue factor avail- ability was associated with increased factor VII turnover, and the extent to which Enoxaparin influenced the turnover of this protein following knee surgery. The low concentration of factor VII in plasma (< 10 nM) and its short half-life favour measurement of factor VII levels as a marker of increased tissue factor availability and the associated increased coagu-
391

392
lation in vivo. We also estimated prothrombin consumption subsequent to the surgery by comparing the concentrations of endogenous thrombin-antithrombin 111 in pre-surgical with post-surgical plasmas. Our results indicate that Enoxa- parin both moderated factor VII zymogen consumption and the generation of thrombin-antithrombin 111 following elec- tive knee replacement surgery. Thus. inhibition of in viw prothrombin activation appears to be an important action for the antithrombotic effect of Enoxaparin, demonstrated by it5 ability to reduce the incidence ofD\'T associated with elective knee surgery by i O I K (Leclerc et nl. 1992 ) .
Frederick A . Ofosu et a1
MATE K I A LS A N D M ETH 0 D S
Materials. Asserachrom \ 'I1 : Ag kits for measuring the concentrations of factor VII-related proteins. and rabbit anti- (human factor 1'11) serum were obtained from \Vellinark Iliagnostics. Guelph. Ontario. Canada. Production of the inurine monoclonal ( 2 31-7) used as the first antibody in the enzyme linked immunosorbent assay (ELISA) for measuring the concentration of factor \ 7 I zyinogen employed pro- cedures described previously 1 Cerskus f t id. 198 5 ). Citrated platelet poor plasma from 2 5 healthy donors (ages 20-46. mean age < 3 0 ) were pooled to derive standard curves for the two factor VII ELISAs. Human placental tissue factor (Thromborel S) and Enzygnost TAT kits for measuring the concentration of thrombin-antithrombin 111 in plasma were obtained from Hoechst Canada. Montreal. Quebec. Canada. The specificity of Enzygnost TAT kits for measuring picomo- lar concentrations of thrombin-antithrornbin I11 has been established (Pelzer et d, 1988) . The monoclonal antibody coated onto microtitre plates used to quantitate factor Xa inhibition by plasma antithrombin I11 was obtained from i\merican Diagnostica. Greenwich. Conn.. L.S.A. Human 7- thrombin was generously provided by Dr J. 1V. Fenton 11. Sew York Department of Health. Albany. N.Y.. L.S.A. Kecombi- nant human factor VIIa was a gift from Janet Campbell. Novo Nordisk Canada Ltd. Toronto. Canada. Human factor 1'11 concentrate was generously provided by Dr Peter Schwartz. linmuno AG. Vienna. Austria. Dansyl-GL~-GLY-AKGCH~Cl and II-PHE-PKO-AKGCH2CI \$'ere obtained from Terachem. Toronto, Ontario. Canada. Procedures for making human factor IXa and human factor Xa have been reported pre- viously (Ofosu et ul. 19 82 ). Tween 20. p-nitrophenyl phos- phate and other reagent grade chemicals were obtained from Sigma Chemical Company. St Louis. hlo.. L.S.A. Kabbit anti- (human antithrombin 111) serum was obtained from Dako- patts, Toronto. Ontario, Canada. Goat anti-rabbit IgG to which alkaline phosphatase had been conjugated was obtained from Zymed. Toronto. Canada. CNBr-Sepharose 4 B was obtained from Pharmacia, Montreal. Quebec, Canada.
Paticvts. Patients received 3 0 rng (0.4 ml) ofEnoxaparin or 0 . 4 ml of saline every 12 h. All study medications were given by subcutaneous injection in the anterior abdominal wall. The Enoxaparin used (Laboratories Pharmuka. Filiale de Khone-Poulenc Korer, France) had a mean molecular weight of 5 . 1 h kD and an anti-factor Xa activity of 103 International [inits per mg. Injection of the study medication was generally started the morning of the first post-operative day (Day 1 ) and
was continued for up to 1 4 d. If haemostasis had not been achieved at the surgical site by the morning of Day 1 , initiation of treatment was delayed until the evening of Day 1 or the morning of Day 2 at the latest. Patients who had not achieved surgical haemostasis by the morning of Day 2 were not randomized. Adherence to the study protocol and assessment of patients' status were assessed daily by the trial nurses and investigators. The study patients did not receive any other venous thrombosis prophylaxis measures. Citrated whole blood samples were collected daily 6 h after the first injection and processed into platelet poor plasma. They were kept frozen at - 70°C until assayed.
Piitiejit strrveillance arid outcome rneasurrs. The primary outcome measure was the incidence of post-operative deep vein thrombosis. All patients underwent '151-fibrinogen leg scanning. starting on Day 1 and continued daily for 14 d or until discharge, if sooner. Patients also had repeat impedance plethysmography. starting on Day 5 and every other day until Day 14 or discharge, if sooner. Bilateral contrast venography was performed routinely at Day 1 4 or earlier if the patient was discharged, or the result of either above noninvasive test became abnormal. Patients who developed proven venous thromboembolism were treated with intra- venous heparin followed by warfarin. Patients who remained IWT-negative received no antithrombotic therapy after the study period.
ENZYME-LINKED IMMUNOSOKBENT ASSAYS
Factor \'IT zyrnogen. The murine monoclonal antibody 2 3 1-i . which reacts preferentially with factor VII zymogen (see below). was coupled to microtitre plates a t a concentra- tion of 500 ng/well in 0.1 ml of 0.1 M NaZHCOI, pH 9.6, by incubating the plates at 4°C overnight. In subsequent steps, 0 .1 ml of reagent was added to each well. Patients' plasmas (diluted 1 : 50 and 1 : 100) were added to separate wells. After incubation for 1 h at 3 7"C, the wells were washed four times with PBS/Tween 2 0 containing 1.0 mg/ml bovine serum albumin, 0.01 M Na2HPO+. 0.1 5 M NaCI, and 0.02% Tween 20. pH 7.4. [Each sample was assayed in duplicate using two different microtitre plates.] Rabbit anti-(human factor VII) serum diluted 1 in 5000 in PBS/Tween 2 0 was then added for a further 1 h incubation at 3 7°C. Following four washes with PBS/Tween 20, goat anti-rabbit IgG-alkaline phosphatase conjugate (diluted 1 : 1000) was then added. After afurther 1 h incubation at 37°C. followed by four washes with PBS/ Tween 20. p-nitrophenyl phosphate (1 mg/ml in 0 .5 M Na?CO,. 1 mM MgCI2, pH 10 .4) was added for 1 h at 37°C. The colour yield at 405 nm was then measured. The concentration of factor VII zymogen in each plasma was then determined by reference to a standard curve derived using pooled normal plasma from 2 5 healthy volunteer donors (ages 20-46) diluted 1 : 2 0 to 1 : 320.
The reactivity of factor VII (see below) and r-factor VIIa with the monoclonal antibody was also compared by ELISA. Each protein was tested at concentrations of 3 .5 and 7.0 ng/ ml in Michaelis buffer containing 1 .0 mg/ml bovine serum albumin. The two concentrations were chosen to approxi- mate that of factor VII in pooled normal plasma diluted

Moderation of in Vivo Coagulation by Enoxaparin 39 3
added to one volume of 2.0-200 n M factor Xa-antithrombin I11 in Michaelis buffer containing 1 mg/ml bovine serum albumin and 2 volumes of 2 p~ dansyl-Glu-Gly-ArgCHLC1. These samples were then diluted 1/10 or 1/20 to derive standard curves for estimating the concentration of factor Xa-antithrombin Ill generated after factor Xa had been added to each patient plasma. It was not necessary to subtract the concentrations of endogenous factor Xa-anti- thrombin 111 as none was detected in diluted patient plasmas to which no factor Xa was added.
Reactivity of factor V l l zymogen. and proteolysed factor Vl l with the monoclonal antibody 231-7 and rabbit anti-human factor VII. The monoclonal antibody (300 mg) was coupled to 30 g of CNBr-Sepharose 4B and packed into a 2.5 x 100 cm column. The column was equilibrated with 0.05 M Tris-HCI. 0.145 M NaCI, pH 7.4 and 5000 units of reconstituted human factor VII concentrate filtered through the affinity column. The column was developed with the equilibrating buffer until the OD at 280 nm was <0.01. The column was next developed with 30 ml of 0.05 M Tris-HCI containing 2 M
NaCI, pH 7.4. Factor VII still bound to the column was eluted with 30 ml of 0.1 M sodium citrate, pH 3.5 in 5 ml fractions into test tubes containing 1 ml of 2 M Tris. The eluate was immediately dialysed against 20 mM Tris-HCI. pH 7.4, applied on a Pharmacia MonoQ FPLC column, and eluted with a NaCl gradient made in the same buffer. Factor VII eluted at 0.22 M NaCl concentration. Factor VII (final concentration 200 nM) was incubated with 20 nM human factor IXa or 20 nM human factor Xa, crude human placental tissue factor (Thromborel S) diluted 1 : 10 in Michaelis buffer, and 5 mM CaCI2 at 3 7°C. After incubation times varying from 30 s to 1 h, proteolysis of factor VII was halted by adding EDTA and dansyl-Glu-Gly-ArgCH2Cl to final concentra- tions of 5 mM and 1 PM, respectively. Factor VII (1 00 nM) was also digested with a-chymotrypsin (1 : 100 enzyme to sub- strate ratio) for incubations varying from 30 s to 1 h and the reaction was stopped with 5 mM phenylmethyl sulphonyl fluoride. The products obtained (300 ng/channel) were assessed after 0.1% SDS-polyacrylamide gel electrophoresis and Western blotting. Two antibodies (each at a final concentration of 1 pg/ml) were used to identify the proteoly- tic products of factor VII obtained: the monoclonal antibody 23 1- 7; and the IgG fraction from rabbit polyclonal antibodies to factor VII affinity purified on factor VII-Sepharose 4B.
Statistical analysis. The Wilcoxon Rank Sum Test was used to determine whether differences between sets of assay values were statistically significant. The only information available when the plasmas were assayed were names of the patients and the dates the blood samples were collected and processed. The randomization code, and information on the DVT status of patients, became available after all assays had been completed.
1 : 100 and 1 : 5 0 respectively. The colour yield obtained with both concentrations of factor VII was at least twice that of r- factor VIIa. suggesting that factor VIIa reacted less effectively with the monoclonal antibody than factor VII.
Factor Vll-related antigen and endogenous thrombin-antith- rombin I l l . Asserachrom VII: Ag kits were used to determine the concentrations of factor VII-related antigens in patient plasmas diluted 1 : 50 and 1 : 100. The pooled plasma used to estimate the concentrations of factor VII zymogen was also used to derive the standard curves for this assay, and identical dilutions as those used for the factor VII zymogen assays were also employed. The concentration of endogenous TAT in patient plasmas was determined using Enzygnost TAT kits. The manufacturer's instructions were rigorously followed for each ELISA.
Inhibition of exogenous thrombin and exogenousfactor Xa. We determined how the surgery, and surgery plus Enoxaparin. altered the inactivation of exogenous factor Xa or thrombin in each patient plasma. This was accomplished by comparing the capacity of the plasma to inactivate the two enzymes before and after surgery. To determine the concentration of added thrombin inactivated by each plasma, it was necessary to first determine the concentration of endogenous throm- bin-antithrombin I11 in that plasma using the Enzygnost TAT kits as above. Alpha-thrombin (2 nM) in Michaelis buffer, containing 1 mg/ml fatty acid-free bovine serum albumin, was then added to an equal volume of the plasma under study. Michaelis buffer consisted of 36 mM sodium acetate, 36 mM sodium barbital, 145 mM sodium chloride, at pH 7.4. The thrombin and plasma had separately been pre-incubated to 37°C. After a 30 s incubation at 37°C D-Phe-Pro- ArgCH2CI was added to a final concentration of 1 PM to inactivate residual thrombin. After a further incubation at 3 7°C for 10 min, the concentration of thrombin-antithrom- bin Ill in each plasma was then determined using the Enzygnost TAT kit. The concentation of endogenous throm- bin-antithrombin I11 in each plasma was subtracted from the value obtained after thrombin had been added to that plasma, i.e. exogenous thrombin-antithrombin 111. The resulting figure was the concentration of added thrombin inactivated by antithrombin II in that plasma.
The concentration of factor Xa-antithrombin Ill generated after factor Xa was added to each plasma was determined as follows. To 50 pl of plasma was added 50 pl of 100 nM factor Xa in Michaelis buffer containing 1 mg/ml bovine serum albumin. The enzyme and plasma had been separately pre- incubated to 3 7°C. After a 60 s incubation at 3 7"C, 100 pl of 2 PM dansyl-Glu-Gly-ArgCH2CI was added to inactivate the free factor Xa then present in the reaction mixture. The reaction mixture was diluted 1 in 10 and 1 in 20, and the concentration of factor Xa-antithrombin Ill generated was then determined by the ELISA for factor Xa-antithrombin I11 described previously (Ofosu et al, 1990). Each sample was assayed in duplicate using two different plates. Note, how- ever. that the monoclonal antibody to factor Xa/factor X was used to coat the microtitre plates in this study. The previous method employed the IgG fraction from sheep anti-(human factor X) serum affinity purified on factor X-Sepharose 4B (Ofosu et al, 1990). One volume of pooled normal plasma was
RESULTS
Reactivity of factor VII, factor Vlla and chymotrypsin digested factor V l l with anti-factor V l l antibodies The polyclonal anti-factor VII antibodies reacted with factor
394 Frederick A . Ofosu et a1
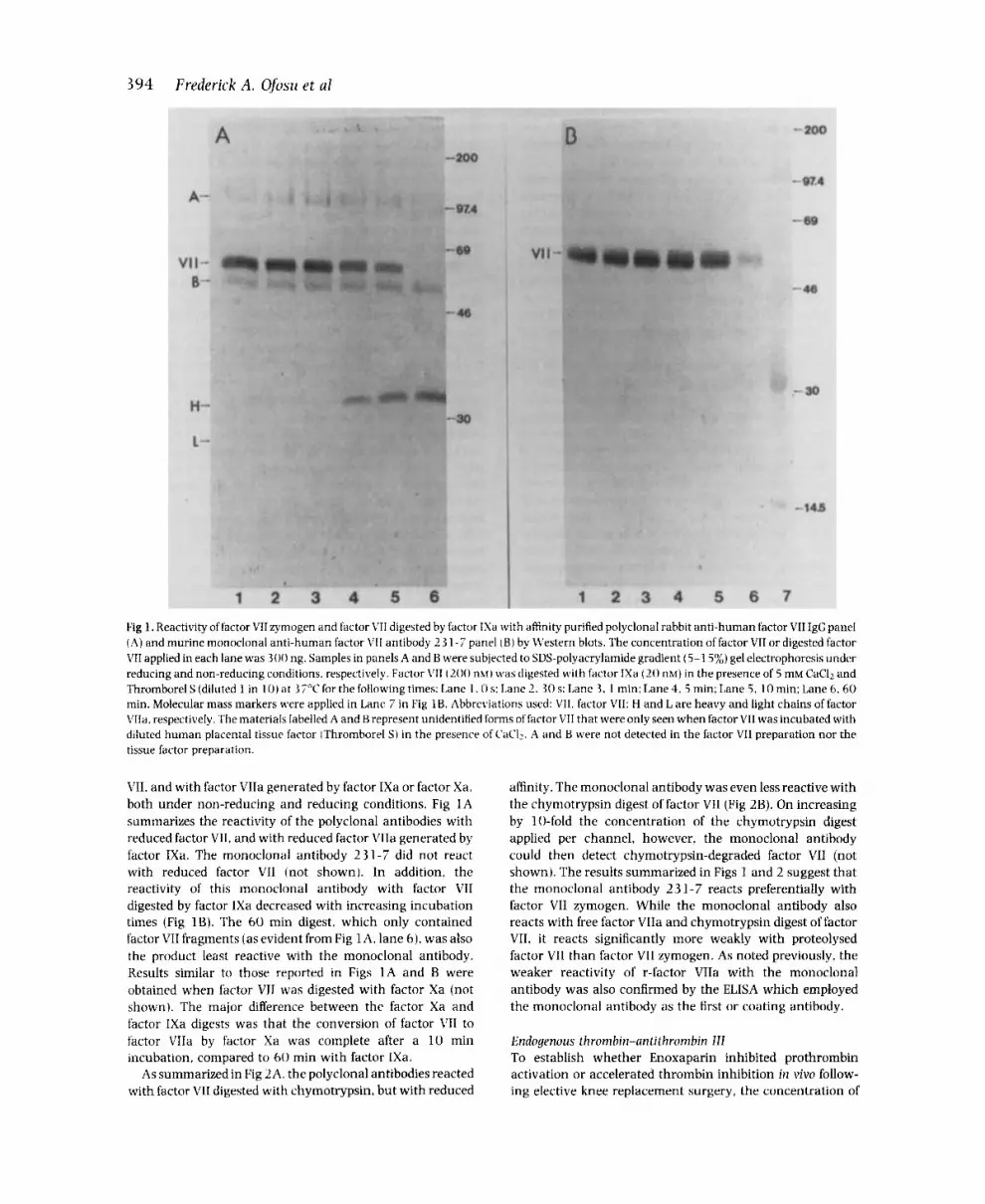
Fig 1. Reactivity of factor VIIzymogen and factor VII digested by factor INa with affinity purified polyclonal rabbit anti-human factor VII IgC panel (A) and murine monoclonal anti-human factor V I I antibody 2 3 1 - i panel ( B ) by U’estern blots. The concentration of factor VII or digested factor VII applied in each lane was 300 ng. Samples in panels A and B were subjected to SDS-polyacrylamide gradient (5-1 5%) gel electrophoresis under reducing and non-reducing conditions. respectively. Factor \’I1 ( 2 0 0 mi) was digested with factor IXa (20 nM) in the presence of 5 mM CaCll and Thromborel S (diluted 1 in 1 0 ) at 37°C for the following times: Lane 1,O s : Lane 2 , 3 0 s: Lane 3. 1 min: Lane 4, 5 min; Lane 5 , 10 min; Lane 6. 60 min. Molecular mass markers were applied in Lane 7 in Fig 1B. Abbreviations used: VII. factor VII: H and L are heavy and light chains of factor LTa. respectively. The materials labelled A and B represent unidentified forms of factor VII that were only seen when factor VII was incubated with diluted human placental tissur factor (Thromborel S) in the presence of CaCI:. A and B were not detected in the factor V11 preparation nor the tissue factor preparation.
VII, and with factor VIIa generated by factor IXa or factor Xa, both under non-reducing and reducing conditions. Fig 1A summariaes the reactivity of the polyclonal antibodies with reduced factor VII. and with reduced factor VIIa generated by factor IXa. The monoclonal antibody 231-7 did not react with reduced factor VII (not shown). In addition, the reactivity of this monoclonal antibody with factor VII digested by factor IXa decreased with increasing incubation times (Fig IB). The 60 min digest. which only contained factor VII fragments (as evident from Fig 1A. lane 6). was also the product least reactive with the monoclonal antibody. Kesults similar to those reported in Figs 1A and B were obtained when factor VII was digested with factor Xa (not shown). The major difference between the factor Xa and factor IXa digests was that the conversion of factor L’II to factor VIIa by factor Xa was complete after a 10 min incubation. compared to 60 min with factor IXa.
As summarized in Fig 2A. the polyclonal antibodies reacted with factor VII digested with chymotrypsin, but with reduced
affinity. The monoclonal antibody was even less reactive with the chymotrypsin digest of factor VII (Fig 2B). On increasing by 10-fold the concentration of the chymotrypsin digest applied per channel, however, the monoclonal antibody could then detect chymotrypsin-degraded factor VII (not shown). The results summarized in Figs 1 and 2 suggest that the monoclonal antibody 2 3 1-7 reacts preferentially with factor VII zymogen. While the monoclonal antibody also reacts with free factor VIIa and chymotrypsin digest of factor VII. it reacts significantly more weakly with proteolysed factor VII than factor VII zymogen. As noted previously, the weaker reactivity of r-factor VIIa with the monoclonal antibody was also confirmed by the ELISA which employed the monoclonal antibody as the first or coating antibody.
Endogenous thrombin-antithrombin 111 To establish whether Enoxaparin inhibited prothrombin activation or accelerated thrombin inhibition in vivo follow- ing elective knee replacement surgery, the concentration of

Moderation of in Vivo Coagulation by Enoxaparin 3 9 5
Fig 2. Reactivity of factor VII and factor VII digested with chymotrypsin with polyclonal rabbit anti-human factor VII IgG (panel A) and the monoclonal anti-factor VII antibody 231-7 (panel B) assessed by Western blots. The substrate to enzyme ratio (weight: weight) was 100: 1 . The samples were not reduced before electrophoresis. The concentration of factor VII or its digestion products was applied in each lane was 300 ng. Lane 1, factor VII; Lanes 2-6 were factor VII digests obtained after 0. 1 , 10. 30 and 60 min incubations, respectively. Molecular mass markers were applied in Lane 7. Abbreviations: VII, factor VII; p. proteolysed factor VII (likely representing factor VII with the gla-domain cleaved).
endogenous thrombin-antithrombin I11 was determined in each pre- and post-surgical plasma and the results summar- ized in Fig 3 . As shown in Fig 3A, the concentration of endogenous thrombin-antithrombin I11 (mean f SEM) in pre-surgical plasma samples of patients on Enoxaparin and placebo were less than SO PM. Following surgery, the concentrations of endogenous thrombin-antithrombin I11 had increased in each post-surgical plasma, and significantly more was generated in plasmas of patients who received the placebo than in plasmas of patients who received Enoxaparin (with P values <O.O5 for the difference between plasmas of patients on Enoxaparin versus placebo for all post-surgical days except day 1).
The concentrations (mean f SEM) of endogenous throm- bin-antithrombin I11 in the pre- and post-surgical plasma samples of patients who remained DVT free on Enoxaparin or placebo, and patients on placebo who developed post- operative DVT are summarized in Fig 3B. For each post- surgical day, the concentrations of endogenous thrombin- antithrombin 111 in the plasmas of patients receiving Enoxa- parin who remained DVT-negative were lower than those of patients who received placebo injections. In none of the three
groups had the mean concentration of the endogenous thrombin-antithrombin I11 level returned to the pre-surgical value by the seventh post-operative day. The concentrations of endogenous thrombin-antithrombin I11 in the plasma of DVT-positive Enoxaparin patients are not presented in Fig 3B for the following reasons. Ofthe 11 patients in this group, pre- and post-surgical plasma samples were available from three to eight of the patients. When a diagnosis of DVT was confirmed, the patients then received therapeutic doses of heparin and subsequent warfarin. Therefore, blood from these patients was then no longer available for this study after they developed DVT.
Factor Vll consumption in vivo Table I summarizes the concentrations of factor VII in the pre- operative plasmas of patients randomized to receive placebo or Enoxaparin. Whether patients who developed post-opera- tive DVT received Enoxaparin or placebo, the differences between the pre-operative total factor VII (factor VII-related antigen) and factor VII zymogen averaged 20 .2 unit/ml (P<O.OS) for the DVT positive group. In contrast, the difference between these two measures of plasma factor VII

396 Frederick A . Ofosu et al A 2 5 0
200
r F
4 u) 1 5 0 3
w 100 0 0 0 z w 50
0 P R E l 2 3 4 5 6 7
DAY
250/
P R E l 2 3 4 5 6 7 DAY
Fig 3 . ( A ) Changes in the concentration of endogenous thrombin- antithrombin 111 ITAT) in plasmas of patients randomized to receive Enoxaparin (broken lines) or placebo (solid lines). The mean i SEhI are reported. The number of samples analysed at each time point varied between 37 and 60 . IB) Changes in the concentration (mean +SEMI of endogenous thrombin-antithrombin Ill ITAT) in plasmas of DVT negative Enoxaparin patients (broken lines. r I = 31- 18): DVT negative placebo patients (solid lines. r i = 19-17): and DYT positive placebo patients (dotted lines, n= 2 1-3 3 ) patients.
concentration was < 0. I unitlml for patients who remained DVT-negative (P>O.O5).
Fig 3A summarizes the changes in factor VII zymogen concentration (mean & SEM) associated with elective knee surgery. The surgery led to massive consumption of factor VII zymogen. and the lowest concentration was noted in plasmas obtained after the first post-operative injection of Enoxaparin or placebo. In addition, higher factor VII zymogen concentra- tions were observed in all post-Enoxaparin plasmas than in the post-placebo plasmas ( P < 0 . 0 5 for the differences between Enoxaparin versus placebo plasmas on days 1, 2 , 5. 6 and 7 ) . These results suggest that Enoxaparin moderates the consumption of factor VII zymogen in vivo following knee surgery. The changes in the concentration of total factor VII- related proteins in the two plasma groups were also deter- mined and the results summarized in Fig 4B. With one exception, the mean concentration of factor VII-related proteins in the plasma samples of patients who received
A 1 . 5 0
-1 E
'E 1 . 0 . s L
3
N - - - > a f 0 . 5 0
0
0 1 . 5 0
-1 E
= 1 . 0 \ v) L
a - c - - > a
0 . 5 0
0
P R E l 2 3 4 5 6 7 DAY
P R E l 2 3 4 5 6 7 DAY
Fig 4. Changes in the concentration (meanfSEM) of factor VII zymogen ( A ) and total factor VII-related proteins (B) in plasmas of patients randomized to receive either Enoxaparin (broken lines) or placebo (solid lines) after knee replacement surgery. The total number of samples assayed at each point in time varied from 37 to 59.
placebo were lower than those patients on Enoxaparin. However. the differences between the concentrations of factor VII-related proteins in the plasmas of patients on Enoxaparin and placebo were not statistically significant.
For each post-surgical day. the concentrations of total factor VII-related proteins exceeded those of factor VII zymogen. The differences between the concentrations of total factor VII-related antigen and factor VII zymogen in the post- operative plasmas of patients on placebo were significantly different (E' varying from 0.0007 to 0.03). In contrast, there were no statistically significant differences between the concentrations of total factor VII-related antigen and factor VII zymogen in comparable plasmas of patients on Enoxa- parin. Since proteolysed factor VII was less reactive with the monoclonal than polyclonal antibodies by Western blotting and ELISA. these results suggest a greater in vivo factor VTT zymogen turnover (consumption) in patients on placebo than patients on Enoxaparin. While the forms of proteolysed factor VII in post-surgical plasmas were unidentified, the proteo- lysed factor VII moieties generated in vivo in the plasmas of patients on placebo also appeared to be less reactive with the monoclonal than the polyclonal antibodies.

Moderation of in Vivo Coagulation by Enoxaparin 397
500
I, 400
300 r u) 2
4 200 ; 8 w 100
0
Table I. Summary of the concentrations (in units/ml of plasma) of total factor VII (FVIIT) and factor VII zymogen (FVIIz) in the pre-operative plasmas of patients randomized to receive placebo or Enoxaparin after elective knee surgery.
Patients [FVIIT]* [FVIIz] * P
All patients 1 .27 f0 .05 (75) 1 .14 f0 .07 (75) 0.028 All DVT positive 1.25f0.06 (26) 1.04f0.06 (26) 0.042 DVT positive placebo 1 .32 f0 .08 (20) 1.12f0.06 (20) 0.088 DVT positive Enoxaparin 1 .05 f0 .12 (6) 0 .78f0.13 (6) 0.262 All DVT negative 1.27f0.07 (49) 1 .19f0.06 (49) 0.266 DVT negative placebo 1.2410.08 (19) 1.16f0.11 (19) 0.509 DVT negative Enoxaparin 1.2910.09 (30) 1.2210.08 (30) 0.312
* The values reported are the mean f SEM. The numbers in parentheses are the numbers of pre-operative samples that were assayed.
P R E l 2 3 4 5 6 7 DAY
Fig 5. The capacity of antithrombin I11 in pre- and post-surgical plasma samples to inactivate added thrombin (reported as exogenous thrombin-antithrombin 111 DVT). Symbols: broken line, plasmas of patients receiving Enoxaparin (n = 3 3-60); and solid lines, plasmas of patients receiving placebo ( n = 39-61). The values reported are mean f SEM.
lnhibition of exogenous a-thrombin and exogenous factor Xa The capacity of each post-surgical plasma to inactivate exogenous a-thrombin was compared with that of the pre- surgical plasma, and the results obtained are summarized in Fig 5. Before surgery, the plasmas of each of the two groups of patients inactivated a third of the added thrombin. Based on the inhibition of exogenous thrombin by the post-placebo plasma, the knee surgery did not alter the capacity of the patients’ plasma to inactivate exogenous thrombin. Post- Enoxaparin plasmas of DVT-negative patients inactivated 30-400/, more a-thrombin than the pre-surgical plasmas and post-placebo plasmas (P<O.O5). Thus, subcutaneous injec- tion of Enoxaparin increased the intrinsic capacity of plasmas to inactivate thrombin ex vivo.
The capacity of the pre-surgical and post-surgical plasma samples to inactivate exogenous factor Xa were determined and the results summarized in Fig 6. The pre-operative plasmas of the two groups of patients inactivated exogenous factor Xa to the same extent. The post-placebo plasmas inactivated exogenous factor Xa to the same extent as the pre-operative plasmas. Subcutaneous injections of Enoxa-
20
F 5
4 ; s 5
15 - X
u) 10 3
w
0
I
I I
P R E l 2 3 4 5 6 7 DAY
Fig 6. The capacity of antithrombin 111 in pre- and post-surgical plasma samples of patients randomized to receive either Enoxaparin (broken lines, n=28-47) or placebo (solid lines, n=31-54) to inactivate exogenous factor Xa. The values reported are mean+ SEM.
parin increased by three- to four-fold the intrinsic capacity of the patients’ plasmas to inactivate exogenous factor Xa. The anti-factor Xa activity resulting from the injection of Enoxa- parin averaged 0.22 + 0.01 International units (Leclerc et al, 1992).
DISCUSSION
This study determined how elective knee surgery influences the turnover of factor VII and prothrombin in patients randomized to receive placebo or prophylactically effective dose of Enoxaparin. The surgery markedly increased the turnover of factor VII zymogen and the generation of endogenous thrombin-antithrombin 111, a marker we used to assess prothrombin turnover. Neither the concentration of factor VII zymogen (Fig 4A) nor that of endogenous throm- bin-antithrombin I11 (Fig 3 ) had returned to the pre- operative value by the seventh post-operative day. These results imply that there is sustained rather than periodic increase in in vivo coagulation following knee surgery.

398 Frederick A. Ofosu et a1
Nonetheless, the intensity of post-operative in vivo coagula- tion decreased with time in the two groups of patients. When compared to patients injected with placebo, the twice daily injections of Enoxaparin moderated the turnover of factor VII zymogen and decreased the production of endogenous thrombin-antithrombin 111 in vivo.
[infractionated heparin and L,MW heparins reduce the frequency of DVT associated with orthopaedic surgery by 50% or more. Recent reports demonstrate that the concen- trations of endogenous thrombin-antithrombin 111 in patient plasmas increase markedly after surgery (Bogaty-Yver & Samama. 1989: Buller & ten Cate, 1989: Hoeck et al. 1989) . The precise mechanism(s) by which UF and LMW heparins prevent DVT after orthopaedic surgery are not known. Results of studies on the mechanisms for the in vitro anticoagulant actions of IJF and LMW heparins identify some potential ways by which UF and LMW heparins could prevent DVT in man. UF and LMW heparins simultaneously delay the onset of factor X, factor V and prothrombin activation irz vitro primarily by catalysing the inhibition of endogenous throm- bin (Ofosu ef a]. 1987. 1988: Beguin et al , 1988) . When prothrombin and factor X activation begin in heparinized plasma. UF and LMW heparins catalyse the inhibition of the two enzymes (Beguin et RI. 1988: Ofosu et nl. 1988. 1989. 1990). UF and LMW heparins. which catalyse the inhibition of both thrombin and factor Xa. suppress prothrombin activation in vitro more effectively than dermatan sulphate. which only catalyses thrombin inhibition. or the pentasac- charide with high affinity to antithrombin 111. which only catalysesfactor Xa inhibition (Ofosu et r r l , 19x8. 1990: Ofosu. 1990).
This present study investigated whether the net effect of subcutaneous injections of Enoxaparin on in vivo coagulation was to inhibit prothrombin activation or to catalyse the inhibition of thrombin by antithrombin 111. The degree to which Enoxaparin influences prothrombin activation can be best assessed by measuring the endogenous concentrations of both prothrombin fragment 1 + 2 and thrombin-antithrom- bin 111. The first parameter estimates the concentration of prothrombin converted to prothrombin fragment 1 + 2 and thrombin in vivo. The second parameter estimates how efficiently the thrombin generated in vivo is neutralized by antithrombin 11. We did not measure the concentrations of prothrombin fragment 1 + 2 as the commercial kits for measuring this parameter were not available at the time this study was conducted.
Post-Enoxaparin plasma samples inactivated exogenous thrombin more effectively than post-placebo samples (Fig 5 ). Based on this observation, higher concentrations of throm- bin-antithrombin 111 would be found in post-Enoxaparin than in post-placebo plasmas if the same concentrations of prothrombin were converted to thrombin in the two groups of patients. The lower concentration of thrombin-antithrom- bin 111 present in post-Enoxaparin versus post-placebo plas- mas (Fig 3 ) implies that the net action of Enoxaparin on in vivo coagulation is to inhibit prothrombin activation. We must point out that if Enoxaparin also accelerates the clearance of thrombin-antithrombin 111 in v i m this could account for the lower levels of endogenous thrombin-
antithrombin III found in the plasmas of patients who received Enoxaparin instead of placebo. However, we are unaware of studies demonstrating that LMW heparins accelerate the clearance of thrombin-antithrombin 111. Con- sistent with the possibility that less thrombin was generated in vivo after Enoxaparin. the LMW heparin also appeared to moderate factor VII zymogen consumption in vivo. In this context. it is noteworthy that the mean difference between total factor VII-related antigen and factor VII zymogen in the pre-operative plasmas of patients who developed post-opera- tive DVT was 2 0 . 2 units/ml, compared to 10.1 unit/ml for patients who remained DVT-negative. While the reasons for the apparent greater factor VII proteolysis in pre-operative plasmas of patients who developed DVT are unknown, this degree of factor VII proteolysis in vivo may be a risk factor for post-operative DVT.
Whether Enoxaparin also moderated factor V, factor VIII. factor IX. and factor X activation following orthopaedic surgery was not determined in this study. Therefore, the precise mechanisms by which Enoxaparin moderates pro- thrombin activation and moderates the proteolysis of factor VII zymogen cannot be stated. Plasmas of patients receiving Enoxaparin inactivated both exogenous thrombin and factor Xa more effectively than plasmas of patients on placebo. The increased capacity of plasma of the former patients to inactivate exogenous factor Xa is consistent with the results of previous studies (Planes et al, 1986; Samama et al, 1988; Leclerc et al, 1992) . We could clearly demonstrate increased thrombin inhibition by all post-surgical plasmas in this study only when the enzyme was added to an equal volume of undiluted patient plasma. As reported previously, higher dilutions of plasma markedly decrease the catalytic efficiency of UF and LMW heparins, and dermatan sulphate on thrombin inhibition (Fernandez et al, 1987).
The results of this study can be summarized as follows. (1) Elective knee surgery increases in vivo coagulation. a conse- quence demonstrated by increased factor VII consumption and increased concentrations of endogenous thrombin- antithrombin 111. ( 2 ) Compared to the effects of placebo, Enoxaparin appears to moderate in vivo prothrombin con- sumption following knee surgery. ( 3 ) Subcutaneous injec- tions of this LMW heparin enhance the intrinsic capacity of the patients' plasmas to inactivate both exogenous a- thrombin and factor Xa. We conclude that inhibition of in vivo prothrombin activation appears to be a n important action for the antithrombotic effect ofthis LMW heparin after knee surgery.
ACKNOWLEDGMENTS
This work was supported in part by Canadian Red Cross Society, Blood Services Grant HA-03-89. and a grant from Rhdne-Poulenc. Montreal, Canada. The generous donation of the Enzygnost TAT kits by Dr H. Pelzer. Behringwerke AG, Marburg, Germany. to measure exogenous thrombin inhibi- tion is gratefully acknowledged. The technical contributions of Helen B. Ofosu, Teresa Kelly and Azra Ali in assaying patient samples are also gratefully acknowledged.

Moderation of in Vivo Coagulation by Enoxaparin 399 REFERENCES
Beguin. S.. Lindhout, T. & Hemker, H.C. (1988) The mode of action of heparin in plasma. Thrombosis and Huemostusis, 60, 457-462.
Rogaty-Yver U. & Samama, M. (1989) Thrombin antithrombin I11 complexes for the detection of post-operative hypercoagulable state in surgical patients receiving heparin prophylaxis. Thrombo- sis and Haemostasis. 61, 538.
Buller, H.R & ten Cate, J.W. (1989) Acquired antithrombin 111 deficiency. Laboratory diagnosis, incidence, clinical implications and treatment with antithrombin I11 concentrate. American Journal of Medicine. 87, (Suppl 3B), 445-485.
Ceskus. A.L.. Birchall. K.J.. Clarke, B.J.. Ofosu, F A . , Modi, G.J. & Blajchman. M.A. (1985) Immunodepletion of plasma factor VII using a monoclonal antibody. British Journal of Haematology, 61,
Fernandez, F.A., Buchanan. M.R.. Hirsh, J. , Fenton. J.W. I1 & Ofosu. F.A. (1 987) Catalysis of thrombin inhibition provides an index for estimating the antithrombotic potential of glycosaminoglycans in rabbits. Thrombosis and Haemostasis, 57, 286-293.
Hoeck, J.A., Normohamed. M.T.. ten Cate, J.W., Buller, H.R., Knipscheer. H.C., Hamelynck. K.J., Marti. R.I. & Sturk. A. (1989) Thrombin-antithrombin 111 complexes in the prediction of deep vein thrombosis following total hip replacement. Thrombosis and Huemostasis, 62, 10 50- 1 0 5 2.
Kakkar. V.V.. Djazaeri, B.. Fok. J.. Fletcher, J., Scully, M.F. & Westick, J. (1982) Low molecular weight heparin and prevention of post- operative deep vein thrombosis. British Medical Journal, 284, 375- 379.
Kakkar. V.V. & Murray, M.J.G. (1985) Efficacy and safety of low molecular weight heparin (CY2 1 6) in preventing post-operative venous thrornboembolism: a cooperative study. British Journal of Surgery, 72, 786-791.
Leclerc, J.R.. Geerts, W.. Desjardins, L.. Jobin, F., Laroche, F., Delmore. F.. Haviernick, S., Atkinson, S. & Bourgouin, J. (1992) Prevention of venous thromboembolism after major knee surgery using a low molecular weight heparin fragment (Enoxaparin). Thrombosis and Haemostasis. In press.
Leyvraz, R.. Richard, 7.. Bachman. F.. van Melle, C., Treyvand, J.M., Livio, J.J. & Candardjis, G. (1983) Adjusted versus fixed-dose subcutaneous heparin in the prevention of deep vein thrombosis after total hip replacement. New England lournal of Medicine, 309, 9 54-9 58.
Ofosu. F A . (1990) In vitro and ex vivo activities of CY216: comparison with other low molecular weight heparins. Haemostu- sis. 20, 180-1 92.
Ofosu, FA.. Choay, J., Anvari, N., Smith, L.M. & Blajchman, M.A. ( 1 990) Inhibition of factor X and factor V activation by dermatan sulfate and the pentasaccharide with high affinity to antithrombin 111. European Journal of Biochemistry, 193, 485-493.
467-47 5.
Ofosu, F.A., Hirsh, J., Esmon, C.T.. Fenton, J.W.. I1 & Blajchman. M A . (1 989) Unfractionated heparin inhibits thrombin-catalyzed ampli- fication reactions more efficiently than those catalyzed by factor Xa. Biochemical Journal. 257, 143-150.
Ofosu. F A , Modi, G.. Cerskus. A.L., Hirsh. J. & Blajchman, M.A. (1982) Heparin with low affinity to antithrombin 111 inhibits the activation of prothrombin in plasma. Thrombosis Research. 28, 487-497.
Ofosu, F A . , Sie, P., Modi. G.J., Fernandez, F.. Buchanan, M.R.. Blajchman. M A . , Boneu, B. & Hirsch. J. (1987) The inhibition of thrombin-dependent feedback reactions is critical to the expression of the anticoagulant effects of heparin. Biochemical Journal. 243.
Ofosu. F.A.. Smith, L.M., Anvari, N. & Blajchman. M.A. (1988) An approach to assigning in vitro potency to unfractionated and low molecular weight heparins based on the inhibition of prothrombin activation and catalysis of thrombin inhibition. Thrombosis and Haemostasis, 60, 193-198.
Pelzer, H., Schwarz, A. & Heimburger, N. ( 1 988) Determination of thrombin-antithrombin I11 complex in plasma with an enzyme- linked immunosorbent assay. Thrombosis and Huemostusis. 59, 101-1 06.
Planes, A,, Vochelle, N., Ferru. J., Przyrawski, D., Clerc, J.. Fagola. M. &Planes, M. (1986) Enoxaparin low molecular weight heparin: Its use in the prevention of deep venous thrombosis following total hip replacement. Huemostasis, 16, 152-1 58.
Samama, M., Bernard, P., Bonnardot, J.P.. Combe-Tamzali. S., Lansom. Y. & Tissot. E. (1988) Low molecular weight heparin compared with unfractionated heparin thrice daily in prevention of post-operative thrombosis. A randomized, multicentre trial. British Journal of Surgery, 75, 128-131.
Stringer, M.D., Steadman. C.A.. Hedges, A.R., Thomas, E.M., Morley, T.R. & Kakkar, V.V. (1989) Deep vein thrombosis after elective knee surgery. An incidence study in 31 2 patients. Journal of Bone and Joint Surgery. 71-B, 492-497.
Stulberg, B.N.. Insall, J.N.. Williams, G.W. & Ghelman, B. (1984) Deep vein thrombosis following total knee replacement. Journal of Bone and Joint Surgery, 66A. 194-201.
Turpie. A.G.G., Levine, M., Hirsh, J., Carter, C., Jay, R.M.. Powers, P.J.. Andrew, M.. Gull, R. & Gent, M. (1986) A randomized controlled trial of a low molecular weight heparin (Enoxaparin) to prevent deep-vein thrombosis in patients undergoing elective hip surgery. New England Journal of Medicine, 31 5, 925-929.
Welin-Berger. T.. Bygdeman, S. & Mebius. C. (1982) Deep vein thrombosis following hip surgery: relationship to activated factor X activity: effect of heparin and dextran. Acta Orthopaedica Scandinavica. 53, 93 7-947.
579-588.
Copyright © 2022 FDOKUMEN




















