The limits to patient compliance with directly observed therapy for tuberculosis: a socio-medical...
13
Un i\'ersi ly of Antwerp Cahi ers Fac ul ty of Polit ical and Soc ial W I9 Editor-in-c hief: Pro f. Dr. H. Va n Pelt Thi s book is dedicaled {O RUUD PEETERS (J 95 1- 1 995 ,. A scho lar with soc iological imagi nalion . A sociomedical researc her with a grass- ro ots message. He had the rare gift of seeing th e person beh ind the di sease an d an inlimate kn owledge of sti gmalisatio n. Hennan Meulemans (Ed.) Univers/tv of Alltwerp Tuberculosis in Pakistan: The Forgotten Plague Acco Leuven I T ,e ll wipn
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of The limits to patient compliance with directly observed therapy for tuberculosis: a socio-medical...
Un iersily of Antwerp
Cahiers Fac ul ty of Polit ical and Soc ial Sc i ence~
W I9
Editor-in-chief Pro f Dr H Van Pelt
This book is dedicaled O RUUD PEETERS (J 951-1995 A scholar with soc iological imaginalion
A sociomedical researcher with a grass-roots message He had the rare gift of seeing the person behind the disease
and an inlimate knowledge of stigmalisation
Hennan Meulemans (Ed) Universtv ofAlltwerp
Tuberculosis in Pakistan The Forgotten Plague
Acco Leuven I Tell wipn
5
The limits to patient complianee with Directly Observed Therapy for tuberculosis
H Meulemal1S R Liefoog he P Mertens D Mo rteIIans S Akbar Zaidi M Farooq Soa llgi A De Muynck
51 Introduction
Persons who develop tuberculosis have to conquer not only a disease but 0 vershycome deeply entrenched prejudices Tuberculos is is a chronic infectious disease caused by the tubercJe bacillus Recently Stewart eole et al determined and anashyIysed the complete gen ome sequence of the bes t-characteri sed train of Mvcob acshyterium fubereulosis H37Rv in order to improve our understanding of the biology of this slow-growing pathogen and to help the conception of new prophylactic and therapeutic interventions (eoJe et al 1998) Tubercu losis has never been merely a biological phenomenon When the fi rst campaigns for eradicating tubercu losis were set up in the industri alised west in the 19th century TB was primarily re shygarded as a social disease (Dubos amp Dubos 1987) Whilst soci al conditions conshytributed to the contraction and spread of TB - main ly in the impoverished slums of large ei ties - cultural beliefs about the disease were cruciaJ for the social accepshytance of its sufferers In the 1940s Henry E Sigerist already summarised the esshysence of the problem There is no luberculosis without tubercle bacilli but whi le mOSl people are exposed to infec tion very few actually develop the disease A low standard of living can be as much responsible for lhe disease as the bacilli (Sigerist 1945 p 99) To this very day many policymakers and relief workers ac shyti vely involved in the control of tuberculosis have to choose between targeting the biological organism or focusing on the social aspects of the di sease
Tuberculosis is deeply rooted in the cultural system of our society The WHO Report on (he Global Tuberculosis Epidemie warned about the gravity of the epishydemie bet ween 25 and 35 milliol1 deaths each year making a total of 30 mi llion deaths during the 1990s or one quarter of all preventabie adu lt deaths (WHO 1998) However it simultaneously al erts us to the danger that stigma sends TB epidemie underground Stigmatising the sick is a complex socio-cu ltural
74 H M~LLL~I NS n
phenomenon threatening both the ue lecl ion of ncw cases and Ihe treatlllll ll or Ihe sick Ailhough curab le TB still casts an evil shadow and smially discredilS ilS vicshytim Totally elimi naling the help a patient can usually expcct to receive in norlll1 circumslances it also reduccs the patient s motivation for constant I y balt l ing agai nst the disease itse lf How cun this vilt ious circlc be broken
52 Literature
Fifty years ago Talcott Parsons approached illness in The Socia System as a form of deviant behaviour and in th at framework he elaborated the concept sick rare (Parsons 1968) Since then medical sociology has paid considerable attention to the large variability in reactions lo symptoms and illness and to the various socioshycultu ral environmental and motivational factors affecting these differences to a lesser or larger ex tern (Mechanic 1995) The study of ill ness behaviour sti ll rel ies heav ily on these early structural -functionalistic based concepts ln the 1960s Kasl and Cobb defined illness behaviour aS any activi ty undertaken by a person who feels iIJ to define the state of his health and to discover a suitable remedy (Kasl amp Cob 1966) By distinguishing betwee n the different stages of illness Suchman ilshylustrated that ill ness behaviour has a distinctly dynamic character and is a complishycated process of decision-making wi th many actors which determines the progresshysive evol ution of illness behaviour (S uchman 19651 The theoretical reference frarnework eSlablished over the course of many years on the di ffe rent stages of the iIlness and forms of care embraces many disciplines (McKinlay 1972 Conrad 1997) It has gained a distinctly eclectic nature bringing together economic demographical geographical psychological cutural and organisationa factors in causa model s to desclibe and explain the illness behaviour
A medical regimen is imposed to ensure optimum progression of illness behavshyiour ie ensure that the pat ient recovers as soon as possi ble When patients sucshyceed in conforming their illness behav iour to the medical regimen they are comshyplian t Patient eampfiollce can assu me rnany forms ra nging from demands for coshyoperation in diagnostic procedures despi te anxiety and pain through taking drugs on schedule and otherwise fo llowing a prescribed regimen to abandonment of soshycial and fami lial obligations to the needs ofthe heal th syslem (Hyde 1988) As the regimen become more complex (for exam ple more types of medical ion or higher doses have to be taken or the tleatment s duration is longer) it becomes more di fshyficult to follow the regimen strictl y and the chances of non-compliance increase
The Directly Observed Treatment Short-course (or DOTS) system impIeshyments the latest medical insights on the treatment of tuberculosis and the combat of the global epidemic (WHO 1997) 1I was developed from the collec ti ve hest pracshytices clinical trials and programm at ic operations of TB control over the past two decades The DOTS-system ac ts as the cornerstone of the Global TB Progral11l11l of the World Heal th Organisat ion and is generally considercu to be one or the 1l10s1
75rA1I HTCOl I PLlA~CE WIT H DIREC-r IY 013SERVH1T HLItAI Y
rap idly expanding and successful health interventions of the 19905 (Ravig lione et al 1997) lt seeks first and foremost 10 implemenl on the widest possible scale a standardised short-course anti-TB trcatment regi men of six to eight mont hs with direct observation of lreatment for at least the i ni tia l two months In addition to apshyplying th is medical regimen governrnent commi lment to sllstai ned TB contro sputum smear microscopy to detect in rcctio Lls cases a regular un interrupted supshypl y of quality anti-TB drugs and a monitoring and reporting system to evaluate treatment oulcomes is widely rcgarded as the fundamental basis of lhe DOTS-sysshytem (Raviglione et al 1995)
Recent literature contai ns a nu mber of synonyms for the term cOInpliance (Volmink amp Garnel 1997 p 1403) Some authors now use the term ache rence to emphasise the fac t that fo llowing a medical regimen is the independent c hoice of the patient Sometimes the term c(Jncardallee is used to stress the active exchange of information negotiation and spirit of cooperalion in the relationship bet ween illness behaviour and medical regirnen Si nce the treatment of tllberculosis does not always automaticall y imply an independent choice of the patienl and a n acti ve exchange of information between patient and carer cannot be taken for granted we prefer the term compliance in this context Moreover it conveys the fact that illshyness behaviour is essentially social behaviour As long as patients act as they should and conform to therapeutic prescriptions they can continue to fu nction soshycially without any problems However as soon as thc threshold of acceptable
norms is crossed deviant behaviour replaces legitimate illness behaviour a nd socishyet ys integrati ve capacities gradually disappear
There are many ways to deviate from the medical regimen prescribed by the DOTS-system People can ignore TB symptoms and fai l to seek treatmenl Treatshyment can be postpo ned until the disease has become very severe indeed However there are also other less radical way to be non-compliant and reduce the likelishyhood of a cure lt is qui te easy for example to forget to go to the doctor or be careshyless in keeping appointments Some people adapt rnedication to suit the msclves and simplify the treatment plan The supervision which forms all inlrinsic part of the DOTS-syslem can be changed coincidentally or iystematically etc
Accordi ng to Bayer and Wilkinson it is essentia l to take into 1ccount lhe socioshycutural context in which this dysfunctional behaviour is displ ayed (Bayer amp Wilkinson 1995) Not cveryone feels strongly about missing an appointment ad shyjust ing medication or avoiding supervision This is precisely what makes the imshyplementation of the DOTS-system so difficult and unmanageable There are plenty of reasons for discontinu ing treatment Swallowing between one and four large pills daily for six to eight months is by no rneans easy Patients rnay have to conshytend with side-effec ts such as nausea and somnolence Many fail to take their medici ne onc time because they are either homelcss or mentall y ill or due to alcoshyhol or drugs abuse
According to Weber the main reason for failing to keep up the regime n is qu ite cleal patients who commence treatment become non- infect ious and already sta rt 10 feel better after a few weeks (Weber 1996) As a result they no longel fcel the
76 11 ~U IIM - i 11 1
need to endure the discamfort s of the lreltment thereby incrcas ing the growth of multidrug-res istan t TB so that treatmcnt ncarly always I ~l ils and patients l11l0SI certuinly suffer a relapse of the di sease
Another important rea50n fo r the non-compli am behaviour of TB patien ts is re shylaled to their srigmlllisarioll Stigmatisa tion accur whcn persons arc given a negashyti ve social labe l that ident itiumles people as dev iant not because their behaviolIr vioshylaLes 11 0rl11S but because they have pers(lIla l or sac ial cha racteristics that lead IJLOshypit to exclude thern (Johnson 1995 p 2~3) Mlleh time has passed sinee Erving Goffm an plTse nted his pionccring theoretical fral1l ework for the sociologieal allalshyysis of stigm ati sat ion in 1963 (Gollrnan 19SI()) Ithough this framework initiall y resu lted in many changes in the egal area it Sllon becal11e hi ghl y relevant 10 tlll spheres of ill ness aml heal th Goffman Jistingu ished three grossly di fferent Iyres of stigma (Lemert amp Branaman 19(7) First there are abomi nations of the hody the various physical dc formitics Ncx t the re are ble mishes of individual CharaLlegraver perceived as weak wi ll domineeri ng (lr unnatuml passions treacherous anti rigid beliefs and dishonesty Fina lly there are tht lri bal stiglllas of race nation anti regraveshyligion these bei ng stigmas that can be tlan~lllitted through lineagc anel equall y contaminate allmembers of a fa l11i1 y These three types of stigma c1ea rly l11ani rest thcl11sel ves in the medical sphere
Phys ical shortcol11ings and elefolmities increase the visibility or the ill ness anel the chances of stigmatisat ion According to Stiles and Kap lan the risk for ampli fi shycnt ion of deviance i~ even disproport ionatel y greatcr on the pa rt of physicall y st igshymatised devian t actors than for those without phys ical stigmata (Stil es amp Kaplan 1996) The coughing fi t ~ sweat anacks fever phJeg lll haemoptys is the sYl11bolic symbols of ye llow sputum and blood the el11aciated skin and bone body etc which characterise a TB patient make tll berculosis very visible and threaten ing to anyone who encounters it or has impress ions of it through societys collective memory Moreover dev iations in personality structure weakness lack of wilshypower feebleness irritability anel so on contribute to stigmatisation In her essay IIIn ess as Metaphor Susan Sontag illustrated that thi s is certainly the case with TB Tuberculosis is described as the disease of bom victims of sensitive pass ive peoshyple who are not quite Iife-loving enough to surv ive (Sontag 1990 p 25) Thomas Mann s character sketch of Hans Castorp reveals that TB also affects the general daily habits and psychological structu re of the patient (Mann 1996) Finally Goffman s typology identified the tri bal stig l11as which feed on the reprehensible characteristics of an entire group The sanatori um where the group characteristi cs of TB patients are expressed par excellence veritably exude~ a permanen t threat of olltagion Grygie r describes how th is danger of contagion marked indelibly the
init iation rituals and Ii fe in the san through and through of a group of Inuit Eskishymos from the far North who were pl aced in a sanatorium more south wards in Canshyada when a TB epidemic broke out (Grygier 1994)
However although tuberculosis patien ~ are stigmati sed by their ill ness it does not mean there are no ot her apparent sources of stigmatisation The power of Lhe rHpnt = innH ( 1tfIn i middotn h hl lro n hmiddot -11 - n bull h hp r(ll rI~lt1 t n
1 II N I Cl lM ILl ANC1 Wil H DIREl- 11 Y OllSFRVED rlll RA PY 77
soei1 labeb can be ass igned to el iscredit behaviour and turn people into outcasts Ithllugh TB is undoubtedly the most important stigl11ati sing factor for the pat ient stigmatisation immediately breaks out of the medical sphere and is influenc ed by t11 anas of life from that poi nt on Research fu rthermore reveals that stigmatisashytion even continues to complicate lhe Iives of the stigmati sed even as treatmelll i mshyprovcs thei r symptoms and functioning (Link et al 1997) The stigma does not di~appea r with the disease It is perpetuated by other ~ources Si milar hypothese~ wcrc put to the test in the research carried out by Crotts et al in Australi a Al shylhough Australia has a ve ry trong framework l)f anti-discrimination legisLatioIl recent years have seen an increasing numbcr of report~ of stigmatisation af fronts 10 diglllty and discrimi nation as Cl rcsult of the hepat itis C status of indi vidual s The sligmatisat ion caused by the disease is closely related to a li festyle of inj ecting drug users the major group now at ri sk of infeclioll and the consequences genershyall y impact domestic wo rk recreational day care and Iuneral sett ings (Crofts et al 1997)
53 Methodology
531 Sampling procedure
The study is based on an oral survey carried out in onc general hospita among~ t all sputum positi ve pulmonary TB patients (n=621 ) who pre~ented themsel ves at the TB unit ie from September 1996 until October 1997 Thc patients were intershyviewed at three fixed moments at the start of the treatment af ter one month af ter two months and followed-u p till the end of the trcatment Every interview was pershyformed by a social worker belonging to a team of four Since the duration of the treatment was 8 months the last patients tiumlni shed their treatment by theend of June 1998 Duri ng lhe interviews based on questionnaires consisting predomi nantly of closed questions and a small num ber of open questions information was gat he red about the demograph ical and socio-economic protiumlle of thc patienl~ social s upport provided by diffe rent networks the patients key values their knowledge of TB and their perception of the curabil ity of the disease stigmatisation and c omplishyance
The reason for choosing the hospital ie Bethania Hospital in Sialkot (Pakistan) requi res a I itle clarificalion (see Figure I) The hospital is situated in the Punjab province at the east of the Islamabad - Lahore axis Since its foundation in 1964 as amission hospital Bcthan ia Hospital has made an enormous effort to detec t and treat tu berculosis patients from the region It is cUiTently a 215 bed front-I ine anel referral hospital providi ng medical and surgical services One hundred beds are reserveel for a specialised TB unit It has a ward for men and a ward for wamen ilS own out-patient department sputum laboratory dispensary and registration unit
11 ~ t 7lt~ I middoti rp rpt rllitprl frn01 1 (~ fr hmfnr rtrfll nf iO km around the
I1 ~ I ILicirc II 11 1
need 10 enElu re the discomforlt of the trea tment thereby increasing the grow h or multidrug-resistant TB so Iha trealmenl nea rly always fails and pat ienlS tlmos certain ly suffer a relapse of the d isca~e
Another importanI reason for Ihe non-c0mplianl behavillur of TB paticJlIs is rcshylated to their stigmatisatioll Sligmatisation occu rs whcn person are givCJl I J1cgashyti ve sociallabel that identi ri es people lt1 dev ian t nol hccallsc their behav iolIl vioshylates norms but because they have peronal or ltoc i~tI characteristics thaI 1cld jlcoshyple to exclude them (Johnson 1995 p o R3 ) Much tiJl1 ha~ passed sincc Erving GotTman presented his pionccri ng theore tical framcwork ror the suciologilal ltll1 alshyysis of stigmatisation in 1963 (Gorrlllan 1(90) Allhough Ih is fralll eworJ initia lly resulled in many changes in the lega area it soan became hi ghly relev ant to the sphcres of illness and health Goffman distinguished three gross ly di ffe rent types of stigma (Lemen amp Branaman 1997) Fi rs t there ure abominations of the body the various physical deformi lies Nex t there are blem ishes of individual charucter perceived as weak wiJ l domineeri ng or unnatural passions treacherous and rigid beliefs and dishones ty Finally there are the tri bal stigmas of race nation and reshyligion these being s ti gma~ that can be transmitted through ineage and equally conlaminate all members of a farnily These th ree types of stigma clearly mani fest themsel ves in the medieal sphere
Physical shorteom ings and dcformities increase lhe visibility of the illness and the chances of stigmatisat ion Accordi ng to Stiles and Kaplan the ri sk for amplifi shycation of devinnce is even disproportionately greater on the part of physically stigshymalised deviant ac tors than for those wi thout physical stigmata (S tiles amp Kaplan 1996) The coughing fi ts sweat attacks fe ve r phlegm haemoptysis rhe symbolic symbols of yell ow sputum and blood the emaciated skin and bone body etc which characterisc a TB patient make tu berculosis very visible and threatening to anyone who encounters it or has impressions of it through societys collective memory Moreover devi alions in persona lity structure weakness lack of will shypower feebleness irritabil ity and sa on contribute to stigmatisation In her essay IIlness (IS Metaphor Susan Sontag i lI ustrated thatthis is certainly the case with TB Tuberculosis is described as the disease of born victirn s of sensiti ve passive peoshyple who are not quile life-Iov ing enough to survive (Sontag 1990 p 25) Thomas Mann s charac ter sketch of Hans Castorp revea ls thar TB also affects the general daily habi ts and psychological structure of the patient (Mann 1996) Finally Goffman s typology idenlified the tri bal stigmas which reed on the reprehensible characteristics of an entire group The sanatorium where the group characteristics of TB patients are expressed par excellence veritably exudes a permanent threat of contagion Grygier describes how Ih is danger of contagion marked indelibly the initiation ri luals and li fe in the sun through and through of a group of Inuit Eskishymos from the far North who were placed in a sanatorium more southwards in Canshyada when a TB epidemic broke out (Grygicr 1994)
However although tuberculosis pat ients are st igmati sed by their illness it does not mean there are no other apparent sources of stigmatisation The power of the concept stigmatisation is such that it targets all social spheres where negltive
1 11I l ll) ~ II Ll Ajlc 11 H lllH ll ll (JH~~KcU I HJ KI~
soc ial labe l ~ can be assigned 10 discredit behaviour and turn people into o utcasts Although TB is undoubtedl y the most important stigmatising factor for the palien l stigmati sation immediately breab OUI of the medical sphere and is in fl ue nced by all areas of life from Ihal point on Research furthennore reveals that st igmatisashyti on even continues to complicate the lives of the sti gmati sed even as treatmenl imshyproves their sy mptoms and fu ncticlJl in g (L in k et al 1997) Thc sti gma does not disappear with the di sease It is perpetu ated by other sourees Si milar hypotheses were put to Lhe test in the research carried ()ut by Crofts et al in Austra lia AIshythough Austral ia has a very su-ong framework of anti-disc riminati on leg islation recent years have ~een an incrcasing nU lllber of reports of stigmatisation arrmnrs lo dignilY and discrimi nation as a result of the he patit i ~ C status of individll als The sligmatisation caused by Lhe disease is closely related to a lifes tyle of i njecting drug lIse rs the major group now at risk of infection and the consequences genershyaJly impact domeslic work recreational day care and funeral settings (Crofts et
al 1997)
53 Methodology
531 Sampling procedure
The sludy is based on an oral survey carried out in one genera] hospital a mongst all sputum positive pullllonary TB patients (n=621) who presented themselves at the TB unit ie from September 1996 until October J997 The patients were iOlershyviewed at three fixed moments at the start of the treatment after one month aftel two months and followed-up tiJl the end of the treatment Every inlerv iew was pershyformed by a social worker belonging to a team of four Since the duratie o of the treatment was 8 months the last patients fini shed their treatment by the end of June 1998 During lhe interviews based on questionnaires consisting predominantly 0
closed questions and a small number of open questions information was gathered about the demographical and socio-econom ic profile of the patients socia1 support provided by different networks the patients key val ues their knowledge of TB and lheir perception of the curabilily of the disease stigmatisation and compli shy
ance
The reason for choosing the hospital ie Bethania Hospital in Sialkot (Pakistan requires a little clarification (see Figure l) The hospital is situated in the Punjab province at the east of the Islamabad - LahOl-e axis Si nce its foundation in 1964 as amission hospital Bethania Hospi tal has made an enormoUS effor to detect and treat tuberculosis patients from the region It is currently a 215 bed front-li ne aod referral hospital providing medical and surgical services One hundred beds arc reserved for a speeialised TB unit It has a ward for men and a ward for wemen its own out-patienl department sputum laboratory dispcnsary and registration un it About 75 of patients are recruited from a catch ment area of 50 km around the
~ gt
Arobion Seo
u 1 1 bullbullbull 1 i 1 I I bull bull
Figurc 1 Map of PJ k i ~ lan
centre of the city of Sialkot which is described as the cul-de-sac du Pakistan et carrefour de la mondial isalion (Le Monde 24298)
Si alkot provides a unique framework for the study of TB issues in the context of a developing country (Enarson 1994) ft is a middle to large city (800000 inshyhabitants) populated by Musli ms which is gradually transforming its feu dal authoritarian relations into modern industrialised and agrarian production proshycesses and a secularised society (Za idi 1999b Zaidi 1994a) In addition to having to deal with a considerable number of public health problems it also has to conshytend wi th a serious TB epidemic resulti ng in Sisyphean tasks and feeli ngs of helpshylessness amongst all the parties concerned These ci rcumstances made the study of the tOlal cohort of TB patien ts from Bethan ia Hospital representaLive for patients from Third World countries who have been diagnosed with pulmonary tuberculoshysis (Ferraro amp Farmer 1999) The ~amrle of TB patients used in this sludy en shyabled us to a certain extent to gain a betrer underslanding of a number of elemenshytary mechanisms operating at the level of stigmati satioll compliance and TB conshytrol in an en vironment where the illness has had a devastating effect hOlh at the personal and social leve l
532 Model
The model proposed in this chapter could be desc ribed as a two-s tep modI Firsl an explanation is sought for the ways in which TB patients are stigmatisLd Many different fac tors might influence the degree of stigmalisation of a TB paticnl 111
our model (see Figu re 2) stigrnatisation is explained by fo ur variables First we hypothesise that ol der palients are more casi ly stigmatised than younger 0 nes Secshyond we tested whether or not women are stigmatised faste r than men are Th ird we included a latent construct support from fa mil y The basic hypothe sis in the model is thal an increase of support from apatients famil y will cause a decrease in stigmati sation Lastly lhe fourth model led factor that might cause stigmatisati on is a knowledge related construct It is assumed th at the less one agrees theacutelt TB i- ti
curable disease the more one wi ll be stigmatised
Figu re 2 MoJel of stigmHisalion anel compliance tor TB
llltlief3 Bltltcr2 Bdiel 1
The second step in the model is the causal explanation of compliance What are the factors that influence the illness behav iour the acceptance of the sick ro le and lhe complianee of a TB patient The model distinguishes three factors The first factor concerns compliance to therapeutic standards solely with regard to the use of medshyicine The patient has to be wi lling to be (and remain) cured and furthermore be (and remain) convinced of the usefulnes$ of the prescribed medication or the DOTS-system will not have any chances of success The two other factors are sit ushyated at a higher theoret icallevel because they refer to tbe therapeutic proces~ in general and the many profess ional requirements and obligations combi ned with feedback of repeated tes ts this complex process invol ves One factor refers to the regularity with which patients comply with their obligations in tbc succcssive stages of their treatmen t the other refers to the pOlential to persevere and complete these stages until full recovery These three factors elenrly illustrate th ree different dimensions of compliant behaviour among TB patients When implementing the DOTS-system the relevance of these factors is extremely high because the sysshytem explicitly requires the strict intake of medicine regul ar doctors visi ts and an effort sustained over many months
11 U l LLI ~J CI IL
532 1 Mal ifes lriahles
The moJel to be estimated is a non-~tandard model (Hatcher 1994 p 423) It conshysists of several mani fe t variables that account for a pan of the structural portion of the model In other word we assumc lha hese manifest variables are perfect measures for the constructs they express Before we turn our attention to the real latent constructs in lhe model we finl want 10 give an overview of its manifest variables
There Ire I lLree exoKI I ou Iwnifesl variables S~x and Ige are measured in a straighlforward way Men and women on the one hand and a patient s age exshypressed in years on the ether Occupation is measured on an ordinal seale All ocshycupat ions are placed on a soc ial stralification seale that made il possible to plaee occupations on a higher or lower sot ietal level The lower range of the scale is fo rmed by housewives unskilled and skil led labour Pakistani middle manageshyment is found in the cottage industries farmers renting their land civil servants white-coJlar workers and small business owners Finally the exeeuti ve group conshysists of land-owning farmers and large business owners
53 22 Larent COTlSrrucls
In the model we used fOlr latelll constructs Before di scussing the measurement model more deeply we concentrated on the different items for eaeh endogenous construct The family is an importan t fac tor in the social environment of the TB pashytient Therefore we tried 10 include the lt upport of lhe farnil y within the model Sinee most pat ients were married (62) we had to deal wi th both the famil y and the family-in-Iaws
Support from the family-in-Iaws was nol included extcns ively in the research We could only include a latent factor support fro m family-in-I aws based on two indicator variables We are aware th at (he lalent construct is not firml y I1Itasulnl in this way However the resullS of lhe mea ~u remen t model (see ) are acceptable (seale composite reliability P= 67) The ind icator variables from thl C0l1s1nlcl are measured on a fi ve-poi nl scale (no influence at all - strong in tluence)
The seco nd latent construct is the support a patient receives from his own 1lt1111shy
ily (seale composite reliability p= 52) This construct is based on three indicalor variables two of which ussess on a five-point seale the direc t support and inllushyence from the fam ily (strongly di scourage - strongly encourage) Besidcs l110ra l support from the family we also included financi al suppo rt Patients wen as kctl whether hey rece ived any financial support The following examples orliumlnanc ia l support were given support for transport drugs consultation fees or les l~ Thc question naire did not ask in deta il about th e ki nd of support patients received Onl y a dichotomous answer (no support anel suppo rt) was sutficiem
Stigmat isation was based on three indicator var iables (scale composilc reli abil shyity p= 64) Again the famil y plays an important role in th is construct The qllesshyti onnaire asked patients to place thell1$elves on a six-point scale (don t agrce al all
1 middot ~IIL I J I I I~ I ~ l l I I II I ~ L I~ I ~I bull bullbullbull bullbull bull bull bull
_ strongly agree) asking them to what extent they fe It that having TB is a disgrace for the fa mily Ir a person agreed strongl y with this phrase it is assumed that he feels st igmatised by his fa mil y The same goes for stigm atisation by friends Again a six point scalc was used (dont agree at all - strongly agree ) to a-sess whelher or not the patients feit stigmatised by lheir fri ends The responde nls could indi cate whether lhey agreed with the idea of very good friends leav ing lhem beshycause of their elisease The more they agreed the more stigmatised they are sup shy
posed to beo The last latent construct in the model is the patient s belief in the curabili ly of
the disease and in knowing how to handle its complexity (scale composite reliabilshyity p= 68) It is an attitudinal factor cons isting of three indicator variables in which patients were asked to gi ve their opinion on TB itself All indicators were measured on a Ii ve-point scale (strongly disagree - strongl y agree) The indicator statements dealt with the opinion on the curability of TB (TB is easy to cure) the commonness of TB (TB is a common diseasc) and wi th the difticulty of TB a~ a disease itself (TB is a difficult disease and hard to cure)
Table 3 latlnt conSlruct mcasure menl summar) (onfirmtory fac tor analy ~i s an d scalc reli shy
ability
Item t Item Description Summary Standa rdshy
ised loading
t-vulue
Support famil y-in-Iaws (p= 67)
Famlawl How much will the opi nion of y lJUr familyshy 74 102
in - Iaw~ influence yo ur dcc is ion to liumlnish or not the wholc treatment (Fi rst time)
Faml aw2 Ho much will lht Qpi nion of your fa mil yshy 69 996
in-Ia ws influ ence your decision to finish or not lhe whole tremment (Sltco nd time)
Su pport fa mily P = 52)
Fam l To what extent does your (o wnl family en shy 59 1004
cou rage or discourage you in taking daily you r medicine (Fi rl time)
Fal112 To what cX lent does yOll r (own) f~l11i1 y enshy +9 8 53
courage or discou rage yOll in taki ng daily your medi cine (Second time)
Fam3 Does you r fam ily sup port yOll liumlnancia ll y for A5 7 98
th e cost of your trealment (tran~port 1drug~ I con~u lta lion fee I tests I )
Stigmatbation (p= 64)
Stigmal It is a disgrace fOf the fumily to have a f3mshyily membcr with TB (Fi rst time)
Stigmu 2 It is a disgracegrave for the family to ha ve J fa mshyily member with TB (S econd time
Stigma ven your bes t fli cnd olllctirncs desen you when you have all infectious di seasc like TB
Belief in curabiJity of TB (p= 68)
Belief TB is easy 10 cun 80 1501 Belie fZ TB is I com mon disease 55 1099 Belief] TB is a di ffi Cll lt dicase 3nd hard to cure 57 I I 2l
Note Fit sla tist ics for mcasurelllent model of 1 1 indicators for four construCIs 2
X IK7 =14993p = 00 GFl=97 RMR = 037 CR = 96 PNFI =52 NNFI = 9J RMS I = OW
I Scale composite relinbilily p = [(I Agravef ) ~ IImiddot(eacute)][(I Agrave I ) ~ vlr( ) + I S] (lOl-o l i amp Vi 1988 p 80)
The measurement model shown in provides a reaso na bl e fit 10 the dat1 Thc ehi shysquare test of exact fit is significant where the objecti ve is to achieve a non-signifshyicant p-value However Hatcher indicates that a significant ch i-square does not ma ke the measurement mode l inadequate (Hatchcr 1994 p 289) The ehi-square ratio shows th at the ratio of the chi-square value and the degree of freedolll is lowcr than two (17) This ind icates that the chi-sguare tes t is wilhin acceptahk lilllits (Marsh et al 1988) Other favourable diagnostics incIude a goodness-or-fiumlt illdegrave X GFI) of 97 a root mean square res idual (RMR) of on a comparati vL rit illtkx CFT) of 96 a parsi mony normed fit index (PNFI) of 52 a nOn normed rit index NNFI) of 93 and a root mean square error of approxi malion (RMSEA ) of rn9
In tenns of valid ity of the constructs con vergent validity is evidcnlxd by tilegrave large and significan t loadings of the item on thei r positcd ind icators FUIhc r (v ishydence of convergent va lidity is shown in None of the correlalions betwLcll Ihl 1 shytent construClS are too high to challen ge the convergent validity oft he cons lructs
F3 F4
100
- 06 100
The discriminan t validi ly is also indicated because the conlide nce interval (plusmn two slandard errors) around the correlati on es ti mate between any two latent construclS never includes 10 (Anderson amp Gerbing 1988 p 41 6) The Varianee Extracted Test also shows the discrim inant validity of our constructs The variance extrac ted tes t compares the variance extracted from two laten t constructs with the square of the correb tion between these two constructs (FomelI amp Larcker 1981 ) Discriminant validi ty is shown when the ex plained variance is greater than the squared correlation We compared all pairs of fac tors and they all showed an iCshy
ccptable variance ex tracted
)4 Results
) 41 Description of the sample
The 62 1 pati ents were composed of 55 0( men and 45 women Seven patients out of ten were younger than 40 concuning with the global observalion that in the countries of the Eastern MeditetTanean Region around 80 of the notified smearshypositi ve TB cases in 1994 occ urred among the economically productive sector of society (15 -54 years old) (Seila 1996 p 134) Tt indicates the serious impact of tushyberculosis on the comrnun ity The skills base of the patiems was very low more than half did not receive any form of fonnal education and the problem of illi teracy aillong older female patients was particularly acute
During the fi rst 11l0nth of lreatment 80 of patien ls were hospitalised during the second month th is number dropped to onl y 48 One out of tluee regarded hospitalisation as problematic This groups di ssalisfaction was rooted both in eco~ nomic and medical causes they had to contend with financial problems absemee shyism transport costs found themseJves in dire sLrai ts doc tors were in competent the rut of he ward etc
One third of patien ls were the family breadwinner As a resuit they were very reluctant to accept the sick mIe Remarkably only one fifth of patients came from a household with more than three economically act ive persons considering lh at
roughly 70 of household eon)i steJ of si x und of ten more Illcm bers The smal nurn ber of econornicall y active person- within the ex tcnded farnilie - C311110t be atshytributed to a large nu mber of ehi ldren because rOlgh ly hal f of the pat ients had less than three children
Sixty percelt ofpalielts placed heulrh al the top oft hc standard orvuluc This is not rea ll y surprising given the fact thal the responclents were confroltcd with ~cr ishyous health prob lems which have absolu te priorit) in their dail y li ve ~ lIld prCSllll1C the recove ry of bath hea lth balallCe anu the improvement of health pOlc nlia Ic shycording to Khayat these IWO dimensions of health are tleeply motet il1 Islalnie Irashydi tion and thefiqlI of health (Khayat 1997) Tf we ZOOIll in on the largL gro llp placshying heal th at the top of the standecircll-d of valuc wc sec Ihal the followi ng vllICS arc also held in high regard falllily and marriage (thc most important aftcr hla llh ) honour and integrity religion and fait h work money (thc Icast importanI ) AIshythough female patiems and patients wilh the lowest socio-economie status atshytached most importance to health it toes not mean that t he~e groups J i-played Ihe mOSl adequate illness behav iour On the contrary the~e groups ltI nd in particlilar housewives the un skilled unernp loyed and sociall y de pri ved ofte n do Ilol J1o~ scss the most elementary knowledge abou t TB (causes sylllptoms alld eollilitlll) which is needed to pre vent infec tion or undergo routine trcatment (Grce n Il)l)) p 192-196) The concept of (external) locus of control ofte n used in rlsealh on compliant behav iour and the fa tal islic health attitude lin ked to th i alslJ applied in thi s context of TB co ntro l (Mcchanic 1983)
Throughout the analys is the operational isation ol belief in the curlli Iil Yui the disease of ten appea red as a variab Ic wi th ~e relldipit y -charactcri ~tics This vlIiahle rneasures the confi dence ~i d people have in suumll vi ng their prob lem situ alilln Trust enables Ihe complexi ry of a social system to be reduced without funher aULgt the sick can rely on thei r part ner fal11il y health worker etc to channel the ir mcdical regimen It is cJear that preci sely lhis confidence is shattered by the TB it igma thereby reducing belief in the curability orTB in genera
Correctly assessing the treatment s duration is characteri stic for patients who strongly believe in the curability of their di sease However th is element of inforshymation is certainly not common knowledge when the treatment starts_Only one in three patients is aware that the trear ment will last several months However after one mon th this number doubles and af ter two months it increases even furthcr (73 ) We established that paliems with the lowest socio-economie statu s often did not possess the Illost rudimentary objecti ve medica l knowledge_There is Iitershyally a wall between them and the cogn itive elements req ui red This wa ll cannot be tom down on y due to reasons related to soc ial strmificaLion On the other hand persons who do nol mind regular check-ups a reg imen of aw kward medication and the costs involved who (hin k it is all worthwhile and are confiden t thei r treatshyment will result in a cure are not necessarily more ski lied or have a higher professhysional rank Ir would seem that another phenomenon another mechanism is ac ti ve as far as belief in Lbe curability of TB is concerned Thinking exclusively in tems of social stratification or Iumping techniq ues of rejec tion together as ways of
bull I I I bull I ~ II ~I I ~ bull I bullbull I L bullbull I bull bull bull bull bull bull
dealing with marginal categories (Douglas 1994 p 85) does not suffice lU gain l bettel understanding of the ideal treatment condition s
Compliance has lO be viewed not only from the socio slralificatiol1 perspeclii but also from the sl ig lllarismioJl persp(crive At thc onset ofthe treatlTlent and aftel two month s treatment sevell statemenlS concern ing stigmatisation were prelgtentecl to the patients A score had to be given on a six-poi nt scale (I =dont agree at all 5=agree 6=strongly ag ree)
The two stateme nts most people i e more than 80 agreed with (score 5 or 6) both at the onset of the trearment and [WO monlhs afterwards were Jf someont has TB hejshe avoids ralking about it with ot her persons and Af ter recoverinf from TB everyone treats yO Ll the same way lS bcfore If someone contracts TB il is bes t to keep quict about it If thei r environment doesn t know anythi ng about il th~y will not treat them di fferentl y af ter they hJ ve recovered
Thc other statement many ie more than 60 agreed with both at thc begin ning of the treatment and af ter two mO IHhs was Peope who arc treated for TB should ta lk to others about it
There were three statements alrnost half of pati ent- ie more than 401r agree with both at the onset of the treatment aOl af ter two months It is a disgrace for thl famil y to have a fa mily member with TB Even your best fri ends someti me ~
desert you when you have un infectious disease li ke T B and 11 a young persol catches TB heshe will experience the consequences for the rest of hisher lirc
Thc statement only a minority ie one out of four patients agreed with both a the onset of the treatment and af ter two months was It is diffi cult to earn your Ii ing after recovering from TB The fact that only very few regarded the TB prob lem in tenns of income is re lnted to the fact that during tbis life-threatening situa ti on_ the trentment has absol ute priori ty and takes precedence over all other form of need
When the onset of the treatment is compared Nith the situation two month later there are no shifts in the statemenls ranking order This means that the firs two months of treatmen t - eg at the hospitalor contact with health carers - dOt not real ly affect their situation On the contrary the stigmatisation continues t( proliferate and feste r causi ng damage in its wake According to Goffmans termi nology it conti nues to transform TB sufferers from discreditabe tO discredilel (Goffma n 1990 p 57 ) Only two statements poi nt to a possible evolution durin~ the first two months but they do not really di sruptthe ran ki ng order in any signifi cant way Ir rerers to the statement PeopJe who are treated for TB should talk t( others about it 68 tgreed at the omet of the treatment and 78 af ter tWt months treatmenl This increase indicates that TB patients still regard opennes about their illness und breaking taboos about the subject as a norm and future ex pectati on Whilst 54 agreed at the beginning of the treatment with the state lllcn Even your best fri ends sometimes dcsert you when you have an infect ious dis ease like TB this dropped to 45 af ter lwo months treatment Ir would appea that the channels for seeking informal care do not dry up for those who respect th medical regimen
We will illustrate thatthe social Il etwork lovering the pa tien t- nlatiolls with all significant others can cithcr increasc or reduce st ig lll ati satioll iS lllilh 1 ()IJt) p 138-155) The com position of these soci al networks i- very hcterogcilcous Thcy can perhaps bes t be analy-ed by di sti nguishing the nuelear fam ily from Ihe ex shytended fa mily As far as the nuclear fam ily is cOllce rned 62 of pllicnls wcn~ married 31 were si ngle 5fr widowed anel 2 divorced For married felll aie pashytients ( 173 out of a tota l of 387 married pa tients) rclati oll) with the fa mi Iy- ill-Iaws and in particular the mother-in-Iaw were very importan t indeecl For alll10sl half of all patients (47) thc extc ll(kJ fam il y eOll1 pri -ed cighl or more perso ll- IIs li all y adu lt who all li ve under the ) (l IllC roo f In 20 of households there wen ilO ehi 1shydren (yolJnger than 12 yca r~) 327 ot households had one or two childrclI 2C1r had three or four children and 21 or had fi ve or more
542 Causal model
The proposed structural model in Figurc 2 was tested by using con veuml ntionalmaxi shymu m likel ihood est imatioll techniques Thc model~h(lwed an acecptabk fit Again the ehi -square tes t of exact fit is ~i gni tiuml ca nt but the eh i-square ratio is lower than two (07) Other favourable diagnosti c~ include a goodncss-of-tiumlt index (GFl) of 96 a rOol mean square rcs idual (R MR) of 041 a comparati ve fi l index (CF) of 97 a parsimony normed fit index iPNFI) of 72 a non normed fit index (NNFI) of 96 and a root mean squ are enOf of approximation (RMSEA) of 039 All of the path coefficients are signifi cant
Anderson and Gerbing recommend a chi-square di ffe rence tes t (CDT) in order to enhanee the confidence in the structural part of the model (Anderson amp Gerbing 1988) The CDT compares the structura l model (which is a res trictecl theoretical model MT) with an uneons trailled alternative model (Mul The relevant test statis shytics (MT has 122 df and a X2 of 17526 ML has 93 df anel a X2 of 171 89) lead to a non-significa nt CDT (X2 difference is 25 33 at 35 df) and an acceptance of M
r Thu s our restricted theoretica model (Figure 3) is preferred to the theoretica uncorrelated model
Since most of the [esH tat is ti c~ show an acceptable model we can look at the reshysu lts of the two-step model presentcd earlier Firsl we tried to model the influshyences on the degree of stigmatisation of a patient These influenees come from very different sou rces The mos important factors determi ning stigmatisation are sex and age Women are more easily stigmatised than men are This also holds for older people From the latent factors support from the family is the most im porshytant Thc more one receives SUppOrL from ones fam ily the less one is stigmalised Anothcr influence on stigmatisation comes from belief in the curability of the TB onstruct The more one believes that TB is curable the less one is stigmatised
These results sugges t that a robust position within society prevents a person from being stigmatised
We then tried to link the stigmatisation of the TB patients and the ir complianl wilh lhe directly observed therapy The restricted theoretical model reveal s that ti influence of stigmatisation on compliance only becomes clearly visible af ter intro ducing the regularity and the duration of the therapy as intervening variables closer examination compliance would appear to be a rather hybridconcept whi can take various forms and has many depths Compliance comes clearer to the [ (I when regularity and du ration are separated In the model stigmatisation with effect of -016 affects regul arity Subsequently regularity has a direct effect of on eomplianee but lhere is a stronger effect on duration and from there on comp anee The regularity and the duration of the therapy tberefore form a tandem whi ca n be brought out of balance by stigmati sation anclilo longer prov ides any gu antees for compliant behaviour
Figu re 3 Siructuralmodel of complio ncc anJ TB
SignificCllce (p-PO ll t) =0 05 =00 =000
Note Fit statistics for structural model X2n~~) =175 26 P=00 GFl =96 RMR =041 CFl =lJ
PNFl =72 NNFI =96 RMSEA =039
SS Discussion
Compliance the fin al link in the causal model is a di ffi cult concept operationalise because it refers to a complex reality The treatment of most inf uumlous diseases oceurs in a di rectly observed way (Porter amp Ogden 1997) H0 ever in practice directly observed therapies can be implemented in a variety ways For examplc DOT for sexually transmitted diseases of ten means obsef tion of a single dose of treatment whereas DOT for leprosy entails monthly ob~ valion by a health care worker of doses of ri fampicin and clofazimine Tbe 001 control strategy reeommended by the WHO for tubercul os is is based on a com nation of four types of medici ne which have to be taken together for the fi rst t
months of lrcat ment HeLlith lJre worken ensure that the I ight Ill ed icine is lak n in the right doses and fo r the cornc t length of ti me Supervis ion ean he a CLlllllshy
p ished by having the pati ent visit the cimie hosp italis ing the patient or scnuin a health care workeI to visit the pa tients home or workplace For directl y ohsnvcd therapy fe l TB it i essenti1l that superv isi on continu e~ every day for th liumlrst two months and idea lly for the entire course of the treatment The wide vltlriations in DOT-contro strategies have resulted in a situation where compliance Illci 1l111lshy
compliance have become e la~t ic eoncepls Who is campliant and who is not~ It all depends on the nature and Ihe t ve l of thc sl3ndard We cncoun tered a di vcls il y of defin itiolls with in the framew)lk or the cLJ l1lbat aga inst tube rcu l o~i-
A retrospective study (from J977) on co mpli ance of TB pat ients revealed that the default ra Ie of the out-putient population in rural Pak i~ta n amounted iO 66 Default was defined as fa ilu re to uttend the weck ly tu berc ulosis clinic fo r a period of one month (Sloan amp Sloan 1981) A fo llow-up study ( 198g-90) showed that 72 oc of the TB patients registered in Bethani a Hosp ital did not complete their 12 months trea tment coure Although the in troduction of a short-course (8 months) regimen improved the compliance default rates (56) contin ued to be high (Liefooghe et al 1995) In 1991 however 76 of TB patients reg istered in the Pakistan Institute of Chest Diseases (S indh) had kep t to the short-course reglmen for two months 2 1 had left the hospi ta l against medical advice and 3 had died (Pathan et al 1992) A study carr ied out in the lndian Wardha dislrict revealed that TB patientlt who fai]cd to take their medici ne for more than 15 days were regarded as non-comptiant because this definition is most in keeping with the adopted adshyministrative procedure (Barnhoorn amp Adriaanse 1992) In a study performed in Denver USA non-compl iance with DOT for TB was detined as foll ows (I) missing ~ 2 consecuti ve weeks of DOT (2) prolongation of treatment gt 30 days due 10 sporadic missed doses or (3 ) incarceration for presenting a th rem lO public health (Burman et al 1997) At least 18 of patients who received out-paLient DOT via the Denver Metro TubercLIl os is Clinic met at least one of these cri teria
In concusion therefore there is no golden standard for defining compliance In our study compliance the fi nal outcome which has to be explai ncd in the model is viewed from a dichotomous viewpoint On the one hand there is the category of compliant patients they com plete thei r the ra py in full and as a general rule al$o unshyderwent a sputum tes t confirming Ihem as TB negative On the other hand there is the category of non-com pliant patients they did not com plete their therapy so a sputum test was not carried out We also adopted the com pletion or fai lure to comshyplete the short -co urse direc tl y observed therapy the bas ic criterion used in the exshyam pIes given above as the key cri terion for our defi ni tion of com pliance The structural model (see Fig ure 3) demonstra tes th at it is important to systemat ically di stinguish the reguarity and the du ration of the therapy to gain a bctter undershystanding of the concept compliance Regularity is achieved when there are no or only sporadic interru ptions during the thcrapy In t hi ~ connection we refer to missed appointments or missed doses of medi cation The durarjoll of the therapy on the e ther hand refers to the treatment duration of eigh[ months which has to be
111 JIII 1 1 1III IJ IKLl 11 lH~Ult I IJ 11111lt ) ~
respected in the DOTS-regimen Two dlv iati ons are possiblc here Either Jo wn shyward the patient ends thc treatment premature1y and is regarded as d efaulter Ol upward- the period of treatment is extended because interruptions during the treatment have [0 be compenslIteti for artcrwards Both deviations from the norm indieate non-compliance Any com parison with the above referred to non-complishyance ra[es fa ils because the phenomenon is constantly regarded from di fferent anshygles Hav ing said that the folowing fac ts in our research on (non- )col11pl iancc among the 621 TB patients are worth mentioni ng
Aftel subtracti ng the nUlllbcr (l f pntients who have died (6Oc) thase who have transferred to another treaUllent centre (29r) and thc tiny group of patie nt~ where the treatmen t failed (I ) 563 pat ients remai ned According to our de liumln ition 779 of the latter group are compliant and 23 are non-compliant aresuIt which is c10sely in keepi ng with the situation at lhe lnsti tu te of Ches[ Diseases in the prov shyince of Sindh The number of in terruptions is used to indicate the regularity of the trcatment 48 of patients did not inlerrupt their treatment at all 34 in terrupted it once and 18 interrupted it various times As far as the duration of the lherapy is concerned the norm of eight months is ach ieved by 55 of patie nts [he norm i not achie ved laquo 8 months) by 33 of patients and the nonn is exceeded (gt 8 months) by 12 of patients
Broadly speaking three out of four paticnts is compliant One out of four is nOI1shycompliant interruptions during the treatmen t (because appoin tments or medicashytion is sporatlicall y missed) or failure to complete the ideal duration of treatmenl (because patients drop out too early or have to followan extended course of treatshyment) As far as establishi ng compl iance is concerned it would seem that 77 ck of patients is heading towards the WHO-target fo r global tuberculosis control namely cure 85 of the detected new smear-positive TB cases (Seita 1996 p 134)
When interpreting the results it is also important to disti nguish between ho~ p ishytalised patie nts and out-patients As we al ready stated earlier duri ng lhe rirst month of treatment 80 of patients were hospitalised Af ter the second month this number dropped to only 48 Permanent supervision at the hospital ensures that hospitalised TB patients are by definition compliant the DOTS-regime n is strictly enforced As far as non-compliance of the out-patient population is co ncerned wc noted that 17oc missed at least one appointment during the first month of treatshyment and that this number dropped 10 1I aftel thc end of the second month The first month is therefore critica especially fol patients who are not hospitalisetl Since they do not res ide at the hospi tal and only come for consultations thty enshycounter far greater difficulties internalising the norms underlying the DOTS-regishymen
The model hinges on the latent construct of stigmatisation Stigmatisation afshyfects compl iance through the Ta ndem of regu la ri ty and duration of therapy Persons who have been strongly stigmatised display more irregular illness behaviour and find it more problematic to see the ditficult and troublesome trealment through 10
[he end In th is respect il could be sa id that ending or interrup[ing the DOTS-reg imiddot
men is nol due to a Jack ol organi satioll On the contrary they are Illcchallisl llS which help to relieve thc pain of sli gmatisation ensuring that for a wh ik the TH pal ient does not have 10 he as hamed and can take a brea k when the prc-url of Ihc medical rcgimen beeomcs toa heavy (Massaro 1997) According 10 GollIllans terminology devi ali ng from the slandards of thc DOTS- rcgimen can hl rcgOl rdcJ as a technique fo r conlrolling in fo rmation The questions or whelher 10 revcal or hi de to con1iumlde in someone or keep qui et to lie or be truth ful and to who l1l hnw when and where are tricks for stoppi ng Ihe exhausting process of bleacutellllc hy socishyety They are in su mmary stra tegies to lWlwRc ( IpoiId idllltity (Schcpcr- amp Nievaard 1995 p 42-43) In Ihe mode l th rec social conditions affecl thc dcgrcc of sligmati sation of TB pat ients These co ndi lions have 10 be taken inlo account 10 reduce the lim ils to pat ienl compliancc with DOTS-strategies
The first cond it ion is rclated to the dem ()g mphico Iilloion of the pili cllt anJ comprises two variab les from the exogenous set ie gender and age FCi llalc pashytients were stigmatised more than male pat ients and older patients Wlr~ si igllwshyti sed more than young persons BOlh lin k~ are highl y significant As house wivcs or elderl y members of the ex tended fa mi Iy many have a low socio-econol11 ie Ialu For them health is above all J quest ion of physical strength (W inkvist amp Akhtar 1997) The loss of phys ical strength Ihlough tubercul osis the fact that tl1Oc who have been sl ricken wilh the diseas( can no longer perform hard labour do the housekeepmg no longer be reproducti ve etc are important contributors to stigshymat isation This is all the more so in lhe countryside where ex ternal signs of vu lshynerability often do not suffiumlce to relieve peopl e from their nonnal socill tasks in the fami ly and vill age
The second condition cl ose ly concerns the beiefofT8 patiel1ll in the curabifir of th eir disease We already said earlier that th is laten t construct in our research displayed features of serendi pity It is el istinct from stricl measurements ofrational med ical knowledge because it emphasises praxis ie implementing knowledge and acti ng on insights The higher the soc io-economie slatus the grealer the belief in the curabil ity of TB It is impossi ble to ignore the phenomenon of social stratifishycation when analys ing ill ness behaviollr of TB patients Patients wi th a higher proshyfessional rank have great faith in the curability of their disease The opposite also applics in equal measure unemploy ment and illileracy are cond ucive for nonshycompl iam behaviour Perhap~ the hard core of pariahs outcasts vagrants vagshyabonds tramps chronie drllnkards and drug add icts (Merton 1968 p 207) repshyresenlSthe most dangerous ri sk group for all TB control programmes When Robshyert K Merton in 1949 developcd hi s we ll-known typology of modes of adaptation by indi viduals within the cu ltu re-bearing society he discovered that these populashytion groups displ ayed retreatiII their mode of adapl3tion which implies the reshyjec tion of cul tural goals and institutional means After all why should anyone reshymain healthy And why should we lIse DOTS as Q method Does it make any difshyference) There is a negative correlat ion between belief in the curability of TB and the degree of stigmati sation Persons who are convineed they will soon be cured and capable of strictly following the medical regimen will be less stigmatised
1 ll i bull I III I 1 11 11 10-- 1 1 middot111 middotmiddot middot 1 middot _
The third condit ion is siluateel at the leve l of the social netllo rks in wh ich TB middot patients function As a general rule it can be sa id thaI persons who tcceive mor~ help from olhers are less likely 10 be stigmati sed Roughl y six out of ten pati ent~ are married and fo r married women the family-in-I aws occ upy the cen tral po- it iol in their social nelwork The model established a negati ve relationshi p betwec l support from blood re lati ve~ and support from the family-in-Iaws Solida rilYvvitl the fa mily-in-Ia ws red uces ~olidarity with biooeI relatives This app lies both il general but also in the specifi( framework of help and support in ti mes of illness The fear manied fe male TB patients have of being abancloned by their hll ~banJ and no 10nger being able to perform their domesr ic tasks should not be unMrcst i mated During a study into thc relcltion between poverty and TB in Bombay re male patients said thaI thei r husbands and mothers-in-Iaw repeated Iy sent then back to their nata l home until such lime as Ihey were cured They were often al cused of bringing the disease from their natal homes and were threatened with sep aration (Nui r et al 1997 p 8 1) The model revea led that the TB patiems who re ceived the least support from their family were stigrnatised most Th is recalls th relational natu re of all type of sti gmatisat ion People are given a negative SOCiH label or are shielded from it Your family may support you through thick and thin encourage you to do the right th ing help to fi nance treatment etc Converse l) your fam ily mayabandon you keep your situation quiet to prevent loosing fac anel keep the family reputation unb1emished
lil Pakistani society anel particularl y in l11any village and se ttl el11Cnb in th Punjab social networks and stigmati sation are inextricably li nkeel and have al enormous influence on community li fe Thc biraderi the patriarcha l nelwork 0
kinship fo rms the framework 101 social and coml11uni ty networks Special event and rites of passage such as birth the ci rcumcis ion of a son marriage allli th death of an old person si rengthen lhis solidarity within the biraderi The biradel use many other occasions to promote social and community networks and ill ne - is perhaps one of the most important When a daughter-in- Iaw becomes seriousl iJl or is hospitalised her children are either looked after by the other daughters (1
the house or are temporarily housed with other members of the birade ri If Ihe sol breadwinner of a household cannot work because he is seriously ill his nearest rel atives and olher members of his biraderi provide mora material and fi nancia l o up port These socia1 and communily links rernai n intact even after emigration Paki stanis who have emigrated to Grea t Brita in for exam ple continue to receive muc support from their biraderi (Anwar 1979) Whenever help is sought in Pakistar communities famil y and bi raderi are preferred According to a sociologic al stud carried out in Rochdale a toW D in the north of England hel p is only sOllght frOl farmer fellow viJ1 agers friend s neighbours Olher Pakistanis and the res t of 50CI ety after all possibil ities in the biraderi-network have been exhausted A TB pil tient who is admitted to hospital will initially be visited by me mbers of hi biraderi They wi llusuaJ1y be gi ven a few hundred rupees and the trad itional fru i However as news about the nature of the illness spreads within the bi rade ri cor tacts become less frequent The negative COITeiation between fa mily support an
sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more

5
The limits to patient complianee with Directly Observed Therapy for tuberculosis
H Meulemal1S R Liefoog he P Mertens D Mo rteIIans S Akbar Zaidi M Farooq Soa llgi A De Muynck
51 Introduction
Persons who develop tuberculosis have to conquer not only a disease but 0 vershycome deeply entrenched prejudices Tuberculos is is a chronic infectious disease caused by the tubercJe bacillus Recently Stewart eole et al determined and anashyIysed the complete gen ome sequence of the bes t-characteri sed train of Mvcob acshyterium fubereulosis H37Rv in order to improve our understanding of the biology of this slow-growing pathogen and to help the conception of new prophylactic and therapeutic interventions (eoJe et al 1998) Tubercu losis has never been merely a biological phenomenon When the fi rst campaigns for eradicating tubercu losis were set up in the industri alised west in the 19th century TB was primarily re shygarded as a social disease (Dubos amp Dubos 1987) Whilst soci al conditions conshytributed to the contraction and spread of TB - main ly in the impoverished slums of large ei ties - cultural beliefs about the disease were cruciaJ for the social accepshytance of its sufferers In the 1940s Henry E Sigerist already summarised the esshysence of the problem There is no luberculosis without tubercle bacilli but whi le mOSl people are exposed to infec tion very few actually develop the disease A low standard of living can be as much responsible for lhe disease as the bacilli (Sigerist 1945 p 99) To this very day many policymakers and relief workers ac shyti vely involved in the control of tuberculosis have to choose between targeting the biological organism or focusing on the social aspects of the di sease
Tuberculosis is deeply rooted in the cultural system of our society The WHO Report on (he Global Tuberculosis Epidemie warned about the gravity of the epishydemie bet ween 25 and 35 milliol1 deaths each year making a total of 30 mi llion deaths during the 1990s or one quarter of all preventabie adu lt deaths (WHO 1998) However it simultaneously al erts us to the danger that stigma sends TB epidemie underground Stigmatising the sick is a complex socio-cu ltural
74 H M~LLL~I NS n
phenomenon threatening both the ue lecl ion of ncw cases and Ihe treatlllll ll or Ihe sick Ailhough curab le TB still casts an evil shadow and smially discredilS ilS vicshytim Totally elimi naling the help a patient can usually expcct to receive in norlll1 circumslances it also reduccs the patient s motivation for constant I y balt l ing agai nst the disease itse lf How cun this vilt ious circlc be broken
52 Literature
Fifty years ago Talcott Parsons approached illness in The Socia System as a form of deviant behaviour and in th at framework he elaborated the concept sick rare (Parsons 1968) Since then medical sociology has paid considerable attention to the large variability in reactions lo symptoms and illness and to the various socioshycultu ral environmental and motivational factors affecting these differences to a lesser or larger ex tern (Mechanic 1995) The study of ill ness behaviour sti ll rel ies heav ily on these early structural -functionalistic based concepts ln the 1960s Kasl and Cobb defined illness behaviour aS any activi ty undertaken by a person who feels iIJ to define the state of his health and to discover a suitable remedy (Kasl amp Cob 1966) By distinguishing betwee n the different stages of illness Suchman ilshylustrated that ill ness behaviour has a distinctly dynamic character and is a complishycated process of decision-making wi th many actors which determines the progresshysive evol ution of illness behaviour (S uchman 19651 The theoretical reference frarnework eSlablished over the course of many years on the di ffe rent stages of the iIlness and forms of care embraces many disciplines (McKinlay 1972 Conrad 1997) It has gained a distinctly eclectic nature bringing together economic demographical geographical psychological cutural and organisationa factors in causa model s to desclibe and explain the illness behaviour
A medical regimen is imposed to ensure optimum progression of illness behavshyiour ie ensure that the pat ient recovers as soon as possi ble When patients sucshyceed in conforming their illness behav iour to the medical regimen they are comshyplian t Patient eampfiollce can assu me rnany forms ra nging from demands for coshyoperation in diagnostic procedures despi te anxiety and pain through taking drugs on schedule and otherwise fo llowing a prescribed regimen to abandonment of soshycial and fami lial obligations to the needs ofthe heal th syslem (Hyde 1988) As the regimen become more complex (for exam ple more types of medical ion or higher doses have to be taken or the tleatment s duration is longer) it becomes more di fshyficult to follow the regimen strictl y and the chances of non-compliance increase
The Directly Observed Treatment Short-course (or DOTS) system impIeshyments the latest medical insights on the treatment of tuberculosis and the combat of the global epidemic (WHO 1997) 1I was developed from the collec ti ve hest pracshytices clinical trials and programm at ic operations of TB control over the past two decades The DOTS-system ac ts as the cornerstone of the Global TB Progral11l11l of the World Heal th Organisat ion and is generally considercu to be one or the 1l10s1
75rA1I HTCOl I PLlA~CE WIT H DIREC-r IY 013SERVH1T HLItAI Y
rap idly expanding and successful health interventions of the 19905 (Ravig lione et al 1997) lt seeks first and foremost 10 implemenl on the widest possible scale a standardised short-course anti-TB trcatment regi men of six to eight mont hs with direct observation of lreatment for at least the i ni tia l two months In addition to apshyplying th is medical regimen governrnent commi lment to sllstai ned TB contro sputum smear microscopy to detect in rcctio Lls cases a regular un interrupted supshypl y of quality anti-TB drugs and a monitoring and reporting system to evaluate treatment oulcomes is widely rcgarded as the fundamental basis of lhe DOTS-sysshytem (Raviglione et al 1995)
Recent literature contai ns a nu mber of synonyms for the term cOInpliance (Volmink amp Garnel 1997 p 1403) Some authors now use the term ache rence to emphasise the fac t that fo llowing a medical regimen is the independent c hoice of the patient Sometimes the term c(Jncardallee is used to stress the active exchange of information negotiation and spirit of cooperalion in the relationship bet ween illness behaviour and medical regirnen Si nce the treatment of tllberculosis does not always automaticall y imply an independent choice of the patienl and a n acti ve exchange of information between patient and carer cannot be taken for granted we prefer the term compliance in this context Moreover it conveys the fact that illshyness behaviour is essentially social behaviour As long as patients act as they should and conform to therapeutic prescriptions they can continue to fu nction soshycially without any problems However as soon as thc threshold of acceptable
norms is crossed deviant behaviour replaces legitimate illness behaviour a nd socishyet ys integrati ve capacities gradually disappear
There are many ways to deviate from the medical regimen prescribed by the DOTS-system People can ignore TB symptoms and fai l to seek treatmenl Treatshyment can be postpo ned until the disease has become very severe indeed However there are also other less radical way to be non-compliant and reduce the likelishyhood of a cure lt is qui te easy for example to forget to go to the doctor or be careshyless in keeping appointments Some people adapt rnedication to suit the msclves and simplify the treatment plan The supervision which forms all inlrinsic part of the DOTS-syslem can be changed coincidentally or iystematically etc
Accordi ng to Bayer and Wilkinson it is essentia l to take into 1ccount lhe socioshycutural context in which this dysfunctional behaviour is displ ayed (Bayer amp Wilkinson 1995) Not cveryone feels strongly about missing an appointment ad shyjust ing medication or avoiding supervision This is precisely what makes the imshyplementation of the DOTS-system so difficult and unmanageable There are plenty of reasons for discontinu ing treatment Swallowing between one and four large pills daily for six to eight months is by no rneans easy Patients rnay have to conshytend with side-effec ts such as nausea and somnolence Many fail to take their medici ne onc time because they are either homelcss or mentall y ill or due to alcoshyhol or drugs abuse
According to Weber the main reason for failing to keep up the regime n is qu ite cleal patients who commence treatment become non- infect ious and already sta rt 10 feel better after a few weeks (Weber 1996) As a result they no longel fcel the
76 11 ~U IIM - i 11 1
need to endure the discamfort s of the lreltment thereby incrcas ing the growth of multidrug-res istan t TB so that treatmcnt ncarly always I ~l ils and patients l11l0SI certuinly suffer a relapse of the di sease
Another important rea50n fo r the non-compli am behaviour of TB patien ts is re shylaled to their srigmlllisarioll Stigmatisa tion accur whcn persons arc given a negashyti ve social labe l that ident itiumles people as dev iant not because their behaviolIr vioshylaLes 11 0rl11S but because they have pers(lIla l or sac ial cha racteristics that lead IJLOshypit to exclude thern (Johnson 1995 p 2~3) Mlleh time has passed sinee Erving Goffm an plTse nted his pionccring theoretical fral1l ework for the sociologieal allalshyysis of stigm ati sat ion in 1963 (Gollrnan 19SI()) Ithough this framework initiall y resu lted in many changes in the egal area it Sllon becal11e hi ghl y relevant 10 tlll spheres of ill ness aml heal th Goffman Jistingu ished three grossly di fferent Iyres of stigma (Lemert amp Branaman 19(7) First there are abomi nations of the hody the various physical dc formitics Ncx t the re are ble mishes of individual CharaLlegraver perceived as weak wi ll domineeri ng (lr unnatuml passions treacherous anti rigid beliefs and dishonesty Fina lly there are tht lri bal stiglllas of race nation anti regraveshyligion these bei ng stigmas that can be tlan~lllitted through lineagc anel equall y contaminate allmembers of a fa l11i1 y These three types of stigma c1ea rly l11ani rest thcl11sel ves in the medical sphere
Phys ical shortcol11ings and elefolmities increase the visibility or the ill ness anel the chances of stigmatisat ion According to Stiles and Kap lan the risk for ampli fi shycnt ion of deviance i~ even disproport ionatel y greatcr on the pa rt of physicall y st igshymatised devian t actors than for those without phys ical stigmata (Stil es amp Kaplan 1996) The coughing fi t ~ sweat anacks fever phJeg lll haemoptys is the sYl11bolic symbols of ye llow sputum and blood the el11aciated skin and bone body etc which characterise a TB patient make tll berculosis very visible and threaten ing to anyone who encounters it or has impress ions of it through societys collective memory Moreover dev iations in personality structure weakness lack of wilshypower feebleness irritability anel so on contribute to stigmatisation In her essay IIIn ess as Metaphor Susan Sontag illustrated that thi s is certainly the case with TB Tuberculosis is described as the disease of bom victims of sensitive pass ive peoshyple who are not quite Iife-loving enough to surv ive (Sontag 1990 p 25) Thomas Mann s character sketch of Hans Castorp reveals that TB also affects the general daily habits and psychological structu re of the patient (Mann 1996) Finally Goffman s typology identified the tri bal stig l11as which feed on the reprehensible characteristics of an entire group The sanatori um where the group characteristi cs of TB patients are expressed par excellence veritably exude~ a permanen t threat of olltagion Grygie r describes how th is danger of contagion marked indelibly the
init iation rituals and Ii fe in the san through and through of a group of Inuit Eskishymos from the far North who were pl aced in a sanatorium more south wards in Canshyada when a TB epidemic broke out (Grygier 1994)
However although tuberculosis patien ~ are stigmati sed by their ill ness it does not mean there are no ot her apparent sources of stigmatisation The power of Lhe rHpnt = innH ( 1tfIn i middotn h hl lro n hmiddot -11 - n bull h hp r(ll rI~lt1 t n
1 II N I Cl lM ILl ANC1 Wil H DIREl- 11 Y OllSFRVED rlll RA PY 77
soei1 labeb can be ass igned to el iscredit behaviour and turn people into outcasts Ithllugh TB is undoubtedly the most important stigl11ati sing factor for the pat ient stigmatisation immediately breaks out of the medical sphere and is influenc ed by t11 anas of life from that poi nt on Research fu rthermore reveals that stigmatisashytion even continues to complicate lhe Iives of the stigmati sed even as treatmelll i mshyprovcs thei r symptoms and functioning (Link et al 1997) The stigma does not di~appea r with the disease It is perpetuated by other ~ources Si milar hypothese~ wcrc put to the test in the research carried out by Crotts et al in Australi a Al shylhough Australia has a ve ry trong framework l)f anti-discrimination legisLatioIl recent years have seen an increasing numbcr of report~ of stigmatisation af fronts 10 diglllty and discrimi nation as Cl rcsult of the hepat itis C status of indi vidual s The sligmatisat ion caused by the disease is closely related to a li festyle of inj ecting drug users the major group now at ri sk of infeclioll and the consequences genershyall y impact domestic wo rk recreational day care and Iuneral sett ings (Crofts et al 1997)
53 Methodology
531 Sampling procedure
The study is based on an oral survey carried out in onc general hospita among~ t all sputum positi ve pulmonary TB patients (n=621 ) who pre~ented themsel ves at the TB unit ie from September 1996 until October 1997 Thc patients were intershyviewed at three fixed moments at the start of the treatment af ter one month af ter two months and followed-u p till the end of the trcatment Every interview was pershyformed by a social worker belonging to a team of four Since the duration of the treatment was 8 months the last patients tiumlni shed their treatment by theend of June 1998 Duri ng lhe interviews based on questionnaires consisting predomi nantly of closed questions and a small num ber of open questions information was gat he red about the demograph ical and socio-economic protiumlle of thc patienl~ social s upport provided by diffe rent networks the patients key values their knowledge of TB and their perception of the curabil ity of the disease stigmatisation and c omplishyance
The reason for choosing the hospital ie Bethania Hospital in Sialkot (Pakistan) requi res a I itle clarificalion (see Figure I) The hospital is situated in the Punjab province at the east of the Islamabad - Lahore axis Since its foundation in 1964 as amission hospital Bcthan ia Hospital has made an enormous effort to detec t and treat tu berculosis patients from the region It is cUiTently a 215 bed front-I ine anel referral hospital providi ng medical and surgical services One hundred beds are reserveel for a specialised TB unit It has a ward for men and a ward for wamen ilS own out-patient department sputum laboratory dispensary and registration unit
11 ~ t 7lt~ I middoti rp rpt rllitprl frn01 1 (~ fr hmfnr rtrfll nf iO km around the
I1 ~ I ILicirc II 11 1
need 10 enElu re the discomforlt of the trea tment thereby increasing the grow h or multidrug-resistant TB so Iha trealmenl nea rly always fails and pat ienlS tlmos certain ly suffer a relapse of the d isca~e
Another importanI reason for Ihe non-c0mplianl behavillur of TB paticJlIs is rcshylated to their stigmatisatioll Sligmatisation occu rs whcn person are givCJl I J1cgashyti ve sociallabel that identi ri es people lt1 dev ian t nol hccallsc their behav iolIl vioshylates norms but because they have peronal or ltoc i~tI characteristics thaI 1cld jlcoshyple to exclude them (Johnson 1995 p o R3 ) Much tiJl1 ha~ passed sincc Erving GotTman presented his pionccri ng theore tical framcwork ror the suciologilal ltll1 alshyysis of stigmatisation in 1963 (Gorrlllan 1(90) Allhough Ih is fralll eworJ initia lly resulled in many changes in the lega area it soan became hi ghly relev ant to the sphcres of illness and health Goffman distinguished three gross ly di ffe rent types of stigma (Lemen amp Branaman 1997) Fi rs t there ure abominations of the body the various physical deformi lies Nex t there are blem ishes of individual charucter perceived as weak wiJ l domineeri ng or unnatural passions treacherous and rigid beliefs and dishones ty Finally there are the tri bal stigmas of race nation and reshyligion these being s ti gma~ that can be transmitted through ineage and equally conlaminate all members of a farnily These th ree types of stigma clearly mani fest themsel ves in the medieal sphere
Physical shorteom ings and dcformities increase lhe visibility of the illness and the chances of stigmatisat ion Accordi ng to Stiles and Kaplan the ri sk for amplifi shycation of devinnce is even disproportionately greater on the part of physically stigshymalised deviant ac tors than for those wi thout physical stigmata (S tiles amp Kaplan 1996) The coughing fi ts sweat attacks fe ve r phlegm haemoptysis rhe symbolic symbols of yell ow sputum and blood the emaciated skin and bone body etc which characterisc a TB patient make tu berculosis very visible and threatening to anyone who encounters it or has impressions of it through societys collective memory Moreover devi alions in persona lity structure weakness lack of will shypower feebleness irritabil ity and sa on contribute to stigmatisation In her essay IIlness (IS Metaphor Susan Sontag i lI ustrated thatthis is certainly the case with TB Tuberculosis is described as the disease of born victirn s of sensiti ve passive peoshyple who are not quile life-Iov ing enough to survive (Sontag 1990 p 25) Thomas Mann s charac ter sketch of Hans Castorp revea ls thar TB also affects the general daily habi ts and psychological structure of the patient (Mann 1996) Finally Goffman s typology idenlified the tri bal stigmas which reed on the reprehensible characteristics of an entire group The sanatorium where the group characteristics of TB patients are expressed par excellence veritably exudes a permanent threat of contagion Grygier describes how Ih is danger of contagion marked indelibly the initiation ri luals and li fe in the sun through and through of a group of Inuit Eskishymos from the far North who were placed in a sanatorium more southwards in Canshyada when a TB epidemic broke out (Grygicr 1994)
However although tuberculosis pat ients are st igmati sed by their illness it does not mean there are no other apparent sources of stigmatisation The power of the concept stigmatisation is such that it targets all social spheres where negltive
1 11I l ll) ~ II Ll Ajlc 11 H lllH ll ll (JH~~KcU I HJ KI~
soc ial labe l ~ can be assigned 10 discredit behaviour and turn people into o utcasts Although TB is undoubtedl y the most important stigmatising factor for the palien l stigmati sation immediately breab OUI of the medical sphere and is in fl ue nced by all areas of life from Ihal point on Research furthennore reveals that st igmatisashyti on even continues to complicate the lives of the sti gmati sed even as treatmenl imshyproves their sy mptoms and fu ncticlJl in g (L in k et al 1997) Thc sti gma does not disappear with the di sease It is perpetu ated by other sourees Si milar hypotheses were put to Lhe test in the research carried ()ut by Crofts et al in Austra lia AIshythough Austral ia has a very su-ong framework of anti-disc riminati on leg islation recent years have ~een an incrcasing nU lllber of reports of stigmatisation arrmnrs lo dignilY and discrimi nation as a result of the he patit i ~ C status of individll als The sligmatisation caused by Lhe disease is closely related to a lifes tyle of i njecting drug lIse rs the major group now at risk of infection and the consequences genershyaJly impact domeslic work recreational day care and funeral settings (Crofts et
al 1997)
53 Methodology
531 Sampling procedure
The sludy is based on an oral survey carried out in one genera] hospital a mongst all sputum positive pullllonary TB patients (n=621) who presented themselves at the TB unit ie from September 1996 until October J997 The patients were iOlershyviewed at three fixed moments at the start of the treatment after one month aftel two months and followed-up tiJl the end of the treatment Every inlerv iew was pershyformed by a social worker belonging to a team of four Since the duratie o of the treatment was 8 months the last patients fini shed their treatment by the end of June 1998 During lhe interviews based on questionnaires consisting predominantly 0
closed questions and a small number of open questions information was gathered about the demographical and socio-econom ic profile of the patients socia1 support provided by different networks the patients key val ues their knowledge of TB and lheir perception of the curabilily of the disease stigmatisation and compli shy
ance
The reason for choosing the hospital ie Bethania Hospital in Sialkot (Pakistan requires a little clarification (see Figure l) The hospital is situated in the Punjab province at the east of the Islamabad - LahOl-e axis Si nce its foundation in 1964 as amission hospital Bethania Hospi tal has made an enormoUS effor to detect and treat tuberculosis patients from the region It is currently a 215 bed front-li ne aod referral hospital providing medical and surgical services One hundred beds arc reserved for a speeialised TB unit It has a ward for men and a ward for wemen its own out-patienl department sputum laboratory dispcnsary and registration un it About 75 of patients are recruited from a catch ment area of 50 km around the
~ gt
Arobion Seo
u 1 1 bullbullbull 1 i 1 I I bull bull
Figurc 1 Map of PJ k i ~ lan
centre of the city of Sialkot which is described as the cul-de-sac du Pakistan et carrefour de la mondial isalion (Le Monde 24298)
Si alkot provides a unique framework for the study of TB issues in the context of a developing country (Enarson 1994) ft is a middle to large city (800000 inshyhabitants) populated by Musli ms which is gradually transforming its feu dal authoritarian relations into modern industrialised and agrarian production proshycesses and a secularised society (Za idi 1999b Zaidi 1994a) In addition to having to deal with a considerable number of public health problems it also has to conshytend wi th a serious TB epidemic resulti ng in Sisyphean tasks and feeli ngs of helpshylessness amongst all the parties concerned These ci rcumstances made the study of the tOlal cohort of TB patien ts from Bethan ia Hospital representaLive for patients from Third World countries who have been diagnosed with pulmonary tuberculoshysis (Ferraro amp Farmer 1999) The ~amrle of TB patients used in this sludy en shyabled us to a certain extent to gain a betrer underslanding of a number of elemenshytary mechanisms operating at the level of stigmati satioll compliance and TB conshytrol in an en vironment where the illness has had a devastating effect hOlh at the personal and social leve l
532 Model
The model proposed in this chapter could be desc ribed as a two-s tep modI Firsl an explanation is sought for the ways in which TB patients are stigmatisLd Many different fac tors might influence the degree of stigmalisation of a TB paticnl 111
our model (see Figu re 2) stigrnatisation is explained by fo ur variables First we hypothesise that ol der palients are more casi ly stigmatised than younger 0 nes Secshyond we tested whether or not women are stigmatised faste r than men are Th ird we included a latent construct support from fa mil y The basic hypothe sis in the model is thal an increase of support from apatients famil y will cause a decrease in stigmati sation Lastly lhe fourth model led factor that might cause stigmatisati on is a knowledge related construct It is assumed th at the less one agrees theacutelt TB i- ti
curable disease the more one wi ll be stigmatised
Figu re 2 MoJel of stigmHisalion anel compliance tor TB
llltlief3 Bltltcr2 Bdiel 1
The second step in the model is the causal explanation of compliance What are the factors that influence the illness behav iour the acceptance of the sick ro le and lhe complianee of a TB patient The model distinguishes three factors The first factor concerns compliance to therapeutic standards solely with regard to the use of medshyicine The patient has to be wi lling to be (and remain) cured and furthermore be (and remain) convinced of the usefulnes$ of the prescribed medication or the DOTS-system will not have any chances of success The two other factors are sit ushyated at a higher theoret icallevel because they refer to tbe therapeutic proces~ in general and the many profess ional requirements and obligations combi ned with feedback of repeated tes ts this complex process invol ves One factor refers to the regularity with which patients comply with their obligations in tbc succcssive stages of their treatmen t the other refers to the pOlential to persevere and complete these stages until full recovery These three factors elenrly illustrate th ree different dimensions of compliant behaviour among TB patients When implementing the DOTS-system the relevance of these factors is extremely high because the sysshytem explicitly requires the strict intake of medicine regul ar doctors visi ts and an effort sustained over many months
11 U l LLI ~J CI IL
532 1 Mal ifes lriahles
The moJel to be estimated is a non-~tandard model (Hatcher 1994 p 423) It conshysists of several mani fe t variables that account for a pan of the structural portion of the model In other word we assumc lha hese manifest variables are perfect measures for the constructs they express Before we turn our attention to the real latent constructs in lhe model we finl want 10 give an overview of its manifest variables
There Ire I lLree exoKI I ou Iwnifesl variables S~x and Ige are measured in a straighlforward way Men and women on the one hand and a patient s age exshypressed in years on the ether Occupation is measured on an ordinal seale All ocshycupat ions are placed on a soc ial stralification seale that made il possible to plaee occupations on a higher or lower sot ietal level The lower range of the scale is fo rmed by housewives unskilled and skil led labour Pakistani middle manageshyment is found in the cottage industries farmers renting their land civil servants white-coJlar workers and small business owners Finally the exeeuti ve group conshysists of land-owning farmers and large business owners
53 22 Larent COTlSrrucls
In the model we used fOlr latelll constructs Before di scussing the measurement model more deeply we concentrated on the different items for eaeh endogenous construct The family is an importan t fac tor in the social environment of the TB pashytient Therefore we tried 10 include the lt upport of lhe farnil y within the model Sinee most pat ients were married (62) we had to deal wi th both the famil y and the family-in-Iaws
Support from the family-in-Iaws was nol included extcns ively in the research We could only include a latent factor support fro m family-in-I aws based on two indicator variables We are aware th at (he lalent construct is not firml y I1Itasulnl in this way However the resullS of lhe mea ~u remen t model (see ) are acceptable (seale composite reliability P= 67) The ind icator variables from thl C0l1s1nlcl are measured on a fi ve-poi nl scale (no influence at all - strong in tluence)
The seco nd latent construct is the support a patient receives from his own 1lt1111shy
ily (seale composite reliability p= 52) This construct is based on three indicalor variables two of which ussess on a five-point seale the direc t support and inllushyence from the fam ily (strongly di scourage - strongly encourage) Besidcs l110ra l support from the family we also included financi al suppo rt Patients wen as kctl whether hey rece ived any financial support The following examples orliumlnanc ia l support were given support for transport drugs consultation fees or les l~ Thc question naire did not ask in deta il about th e ki nd of support patients received Onl y a dichotomous answer (no support anel suppo rt) was sutficiem
Stigmat isation was based on three indicator var iables (scale composilc reli abil shyity p= 64) Again the famil y plays an important role in th is construct The qllesshyti onnaire asked patients to place thell1$elves on a six-point scale (don t agrce al all
1 middot ~IIL I J I I I~ I ~ l l I I II I ~ L I~ I ~I bull bullbullbull bullbull bull bull bull
_ strongly agree) asking them to what extent they fe It that having TB is a disgrace for the fa mily Ir a person agreed strongl y with this phrase it is assumed that he feels st igmatised by his fa mil y The same goes for stigm atisation by friends Again a six point scalc was used (dont agree at all - strongly agree ) to a-sess whelher or not the patients feit stigmatised by lheir fri ends The responde nls could indi cate whether lhey agreed with the idea of very good friends leav ing lhem beshycause of their elisease The more they agreed the more stigmatised they are sup shy
posed to beo The last latent construct in the model is the patient s belief in the curabili ly of
the disease and in knowing how to handle its complexity (scale composite reliabilshyity p= 68) It is an attitudinal factor cons isting of three indicator variables in which patients were asked to gi ve their opinion on TB itself All indicators were measured on a Ii ve-point scale (strongly disagree - strongl y agree) The indicator statements dealt with the opinion on the curability of TB (TB is easy to cure) the commonness of TB (TB is a common diseasc) and wi th the difticulty of TB a~ a disease itself (TB is a difficult disease and hard to cure)
Table 3 latlnt conSlruct mcasure menl summar) (onfirmtory fac tor analy ~i s an d scalc reli shy
ability
Item t Item Description Summary Standa rdshy
ised loading
t-vulue
Support famil y-in-Iaws (p= 67)
Famlawl How much will the opi nion of y lJUr familyshy 74 102
in - Iaw~ influence yo ur dcc is ion to liumlnish or not the wholc treatment (Fi rst time)
Faml aw2 Ho much will lht Qpi nion of your fa mil yshy 69 996
in-Ia ws influ ence your decision to finish or not lhe whole tremment (Sltco nd time)
Su pport fa mily P = 52)
Fam l To what extent does your (o wnl family en shy 59 1004
cou rage or discourage you in taking daily you r medicine (Fi rl time)
Fal112 To what cX lent does yOll r (own) f~l11i1 y enshy +9 8 53
courage or discou rage yOll in taki ng daily your medi cine (Second time)
Fam3 Does you r fam ily sup port yOll liumlnancia ll y for A5 7 98
th e cost of your trealment (tran~port 1drug~ I con~u lta lion fee I tests I )
Stigmatbation (p= 64)
Stigmal It is a disgrace fOf the fumily to have a f3mshyily membcr with TB (Fi rst time)
Stigmu 2 It is a disgracegrave for the family to ha ve J fa mshyily member with TB (S econd time
Stigma ven your bes t fli cnd olllctirncs desen you when you have all infectious di seasc like TB
Belief in curabiJity of TB (p= 68)
Belief TB is easy 10 cun 80 1501 Belie fZ TB is I com mon disease 55 1099 Belief] TB is a di ffi Cll lt dicase 3nd hard to cure 57 I I 2l
Note Fit sla tist ics for mcasurelllent model of 1 1 indicators for four construCIs 2
X IK7 =14993p = 00 GFl=97 RMR = 037 CR = 96 PNFI =52 NNFI = 9J RMS I = OW
I Scale composite relinbilily p = [(I Agravef ) ~ IImiddot(eacute)][(I Agrave I ) ~ vlr( ) + I S] (lOl-o l i amp Vi 1988 p 80)
The measurement model shown in provides a reaso na bl e fit 10 the dat1 Thc ehi shysquare test of exact fit is significant where the objecti ve is to achieve a non-signifshyicant p-value However Hatcher indicates that a significant ch i-square does not ma ke the measurement mode l inadequate (Hatchcr 1994 p 289) The ehi-square ratio shows th at the ratio of the chi-square value and the degree of freedolll is lowcr than two (17) This ind icates that the chi-sguare tes t is wilhin acceptahk lilllits (Marsh et al 1988) Other favourable diagnostics incIude a goodness-or-fiumlt illdegrave X GFI) of 97 a root mean square res idual (RMR) of on a comparati vL rit illtkx CFT) of 96 a parsi mony normed fit index (PNFI) of 52 a nOn normed rit index NNFI) of 93 and a root mean square error of approxi malion (RMSEA ) of rn9
In tenns of valid ity of the constructs con vergent validity is evidcnlxd by tilegrave large and significan t loadings of the item on thei r positcd ind icators FUIhc r (v ishydence of convergent va lidity is shown in None of the correlalions betwLcll Ihl 1 shytent construClS are too high to challen ge the convergent validity oft he cons lructs
F3 F4
100
- 06 100
The discriminan t validi ly is also indicated because the conlide nce interval (plusmn two slandard errors) around the correlati on es ti mate between any two latent construclS never includes 10 (Anderson amp Gerbing 1988 p 41 6) The Varianee Extracted Test also shows the discrim inant validity of our constructs The variance extrac ted tes t compares the variance extracted from two laten t constructs with the square of the correb tion between these two constructs (FomelI amp Larcker 1981 ) Discriminant validi ty is shown when the ex plained variance is greater than the squared correlation We compared all pairs of fac tors and they all showed an iCshy
ccptable variance ex tracted
)4 Results
) 41 Description of the sample
The 62 1 pati ents were composed of 55 0( men and 45 women Seven patients out of ten were younger than 40 concuning with the global observalion that in the countries of the Eastern MeditetTanean Region around 80 of the notified smearshypositi ve TB cases in 1994 occ urred among the economically productive sector of society (15 -54 years old) (Seila 1996 p 134) Tt indicates the serious impact of tushyberculosis on the comrnun ity The skills base of the patiems was very low more than half did not receive any form of fonnal education and the problem of illi teracy aillong older female patients was particularly acute
During the fi rst 11l0nth of lreatment 80 of patien ls were hospitalised during the second month th is number dropped to onl y 48 One out of tluee regarded hospitalisation as problematic This groups di ssalisfaction was rooted both in eco~ nomic and medical causes they had to contend with financial problems absemee shyism transport costs found themseJves in dire sLrai ts doc tors were in competent the rut of he ward etc
One third of patien ls were the family breadwinner As a resuit they were very reluctant to accept the sick mIe Remarkably only one fifth of patients came from a household with more than three economically act ive persons considering lh at
roughly 70 of household eon)i steJ of si x und of ten more Illcm bers The smal nurn ber of econornicall y active person- within the ex tcnded farnilie - C311110t be atshytributed to a large nu mber of ehi ldren because rOlgh ly hal f of the pat ients had less than three children
Sixty percelt ofpalielts placed heulrh al the top oft hc standard orvuluc This is not rea ll y surprising given the fact thal the responclents were confroltcd with ~cr ishyous health prob lems which have absolu te priorit) in their dail y li ve ~ lIld prCSllll1C the recove ry of bath hea lth balallCe anu the improvement of health pOlc nlia Ic shycording to Khayat these IWO dimensions of health are tleeply motet il1 Islalnie Irashydi tion and thefiqlI of health (Khayat 1997) Tf we ZOOIll in on the largL gro llp placshying heal th at the top of the standecircll-d of valuc wc sec Ihal the followi ng vllICS arc also held in high regard falllily and marriage (thc most important aftcr hla llh ) honour and integrity religion and fait h work money (thc Icast importanI ) AIshythough female patiems and patients wilh the lowest socio-economie status atshytached most importance to health it toes not mean that t he~e groups J i-played Ihe mOSl adequate illness behav iour On the contrary the~e groups ltI nd in particlilar housewives the un skilled unernp loyed and sociall y de pri ved ofte n do Ilol J1o~ scss the most elementary knowledge abou t TB (causes sylllptoms alld eollilitlll) which is needed to pre vent infec tion or undergo routine trcatment (Grce n Il)l)) p 192-196) The concept of (external) locus of control ofte n used in rlsealh on compliant behav iour and the fa tal islic health attitude lin ked to th i alslJ applied in thi s context of TB co ntro l (Mcchanic 1983)
Throughout the analys is the operational isation ol belief in the curlli Iil Yui the disease of ten appea red as a variab Ic wi th ~e relldipit y -charactcri ~tics This vlIiahle rneasures the confi dence ~i d people have in suumll vi ng their prob lem situ alilln Trust enables Ihe complexi ry of a social system to be reduced without funher aULgt the sick can rely on thei r part ner fal11il y health worker etc to channel the ir mcdical regimen It is cJear that preci sely lhis confidence is shattered by the TB it igma thereby reducing belief in the curability orTB in genera
Correctly assessing the treatment s duration is characteri stic for patients who strongly believe in the curability of their di sease However th is element of inforshymation is certainly not common knowledge when the treatment starts_Only one in three patients is aware that the trear ment will last several months However after one mon th this number doubles and af ter two months it increases even furthcr (73 ) We established that paliems with the lowest socio-economie statu s often did not possess the Illost rudimentary objecti ve medica l knowledge_There is Iitershyally a wall between them and the cogn itive elements req ui red This wa ll cannot be tom down on y due to reasons related to soc ial strmificaLion On the other hand persons who do nol mind regular check-ups a reg imen of aw kward medication and the costs involved who (hin k it is all worthwhile and are confiden t thei r treatshyment will result in a cure are not necessarily more ski lied or have a higher professhysional rank Ir would seem that another phenomenon another mechanism is ac ti ve as far as belief in Lbe curability of TB is concerned Thinking exclusively in tems of social stratification or Iumping techniq ues of rejec tion together as ways of
bull I I I bull I ~ II ~I I ~ bull I bullbull I L bullbull I bull bull bull bull bull bull
dealing with marginal categories (Douglas 1994 p 85) does not suffice lU gain l bettel understanding of the ideal treatment condition s
Compliance has lO be viewed not only from the socio slralificatiol1 perspeclii but also from the sl ig lllarismioJl persp(crive At thc onset ofthe treatlTlent and aftel two month s treatment sevell statemenlS concern ing stigmatisation were prelgtentecl to the patients A score had to be given on a six-poi nt scale (I =dont agree at all 5=agree 6=strongly ag ree)
The two stateme nts most people i e more than 80 agreed with (score 5 or 6) both at the onset of the trearment and [WO monlhs afterwards were Jf someont has TB hejshe avoids ralking about it with ot her persons and Af ter recoverinf from TB everyone treats yO Ll the same way lS bcfore If someone contracts TB il is bes t to keep quict about it If thei r environment doesn t know anythi ng about il th~y will not treat them di fferentl y af ter they hJ ve recovered
Thc other statement many ie more than 60 agreed with both at thc begin ning of the treatment and af ter two mO IHhs was Peope who arc treated for TB should ta lk to others about it
There were three statements alrnost half of pati ent- ie more than 401r agree with both at the onset of the treatment aOl af ter two months It is a disgrace for thl famil y to have a fa mily member with TB Even your best fri ends someti me ~
desert you when you have un infectious disease li ke T B and 11 a young persol catches TB heshe will experience the consequences for the rest of hisher lirc
Thc statement only a minority ie one out of four patients agreed with both a the onset of the treatment and af ter two months was It is diffi cult to earn your Ii ing after recovering from TB The fact that only very few regarded the TB prob lem in tenns of income is re lnted to the fact that during tbis life-threatening situa ti on_ the trentment has absol ute priori ty and takes precedence over all other form of need
When the onset of the treatment is compared Nith the situation two month later there are no shifts in the statemenls ranking order This means that the firs two months of treatmen t - eg at the hospitalor contact with health carers - dOt not real ly affect their situation On the contrary the stigmatisation continues t( proliferate and feste r causi ng damage in its wake According to Goffmans termi nology it conti nues to transform TB sufferers from discreditabe tO discredilel (Goffma n 1990 p 57 ) Only two statements poi nt to a possible evolution durin~ the first two months but they do not really di sruptthe ran ki ng order in any signifi cant way Ir rerers to the statement PeopJe who are treated for TB should talk t( others about it 68 tgreed at the omet of the treatment and 78 af ter tWt months treatmenl This increase indicates that TB patients still regard opennes about their illness und breaking taboos about the subject as a norm and future ex pectati on Whilst 54 agreed at the beginning of the treatment with the state lllcn Even your best fri ends sometimes dcsert you when you have an infect ious dis ease like TB this dropped to 45 af ter lwo months treatment Ir would appea that the channels for seeking informal care do not dry up for those who respect th medical regimen
We will illustrate thatthe social Il etwork lovering the pa tien t- nlatiolls with all significant others can cithcr increasc or reduce st ig lll ati satioll iS lllilh 1 ()IJt) p 138-155) The com position of these soci al networks i- very hcterogcilcous Thcy can perhaps bes t be analy-ed by di sti nguishing the nuelear fam ily from Ihe ex shytended fa mily As far as the nuclear fam ily is cOllce rned 62 of pllicnls wcn~ married 31 were si ngle 5fr widowed anel 2 divorced For married felll aie pashytients ( 173 out of a tota l of 387 married pa tients) rclati oll) with the fa mi Iy- ill-Iaws and in particular the mother-in-Iaw were very importan t indeecl For alll10sl half of all patients (47) thc extc ll(kJ fam il y eOll1 pri -ed cighl or more perso ll- IIs li all y adu lt who all li ve under the ) (l IllC roo f In 20 of households there wen ilO ehi 1shydren (yolJnger than 12 yca r~) 327 ot households had one or two childrclI 2C1r had three or four children and 21 or had fi ve or more
542 Causal model
The proposed structural model in Figurc 2 was tested by using con veuml ntionalmaxi shymu m likel ihood est imatioll techniques Thc model~h(lwed an acecptabk fit Again the ehi -square tes t of exact fit is ~i gni tiuml ca nt but the eh i-square ratio is lower than two (07) Other favourable diagnosti c~ include a goodncss-of-tiumlt index (GFl) of 96 a rOol mean square rcs idual (R MR) of 041 a comparati ve fi l index (CF) of 97 a parsimony normed fit index iPNFI) of 72 a non normed fit index (NNFI) of 96 and a root mean squ are enOf of approximation (RMSEA) of 039 All of the path coefficients are signifi cant
Anderson and Gerbing recommend a chi-square di ffe rence tes t (CDT) in order to enhanee the confidence in the structural part of the model (Anderson amp Gerbing 1988) The CDT compares the structura l model (which is a res trictecl theoretical model MT) with an uneons trailled alternative model (Mul The relevant test statis shytics (MT has 122 df and a X2 of 17526 ML has 93 df anel a X2 of 171 89) lead to a non-significa nt CDT (X2 difference is 25 33 at 35 df) and an acceptance of M
r Thu s our restricted theoretica model (Figure 3) is preferred to the theoretica uncorrelated model
Since most of the [esH tat is ti c~ show an acceptable model we can look at the reshysu lts of the two-step model presentcd earlier Firsl we tried to model the influshyences on the degree of stigmatisation of a patient These influenees come from very different sou rces The mos important factors determi ning stigmatisation are sex and age Women are more easily stigmatised than men are This also holds for older people From the latent factors support from the family is the most im porshytant Thc more one receives SUppOrL from ones fam ily the less one is stigmalised Anothcr influence on stigmatisation comes from belief in the curability of the TB onstruct The more one believes that TB is curable the less one is stigmatised
These results sugges t that a robust position within society prevents a person from being stigmatised
We then tried to link the stigmatisation of the TB patients and the ir complianl wilh lhe directly observed therapy The restricted theoretical model reveal s that ti influence of stigmatisation on compliance only becomes clearly visible af ter intro ducing the regularity and the duration of the therapy as intervening variables closer examination compliance would appear to be a rather hybridconcept whi can take various forms and has many depths Compliance comes clearer to the [ (I when regularity and du ration are separated In the model stigmatisation with effect of -016 affects regul arity Subsequently regularity has a direct effect of on eomplianee but lhere is a stronger effect on duration and from there on comp anee The regularity and the duration of the therapy tberefore form a tandem whi ca n be brought out of balance by stigmati sation anclilo longer prov ides any gu antees for compliant behaviour
Figu re 3 Siructuralmodel of complio ncc anJ TB
SignificCllce (p-PO ll t) =0 05 =00 =000
Note Fit statistics for structural model X2n~~) =175 26 P=00 GFl =96 RMR =041 CFl =lJ
PNFl =72 NNFI =96 RMSEA =039
SS Discussion
Compliance the fin al link in the causal model is a di ffi cult concept operationalise because it refers to a complex reality The treatment of most inf uumlous diseases oceurs in a di rectly observed way (Porter amp Ogden 1997) H0 ever in practice directly observed therapies can be implemented in a variety ways For examplc DOT for sexually transmitted diseases of ten means obsef tion of a single dose of treatment whereas DOT for leprosy entails monthly ob~ valion by a health care worker of doses of ri fampicin and clofazimine Tbe 001 control strategy reeommended by the WHO for tubercul os is is based on a com nation of four types of medici ne which have to be taken together for the fi rst t
months of lrcat ment HeLlith lJre worken ensure that the I ight Ill ed icine is lak n in the right doses and fo r the cornc t length of ti me Supervis ion ean he a CLlllllshy
p ished by having the pati ent visit the cimie hosp italis ing the patient or scnuin a health care workeI to visit the pa tients home or workplace For directl y ohsnvcd therapy fe l TB it i essenti1l that superv isi on continu e~ every day for th liumlrst two months and idea lly for the entire course of the treatment The wide vltlriations in DOT-contro strategies have resulted in a situation where compliance Illci 1l111lshy
compliance have become e la~t ic eoncepls Who is campliant and who is not~ It all depends on the nature and Ihe t ve l of thc sl3ndard We cncoun tered a di vcls il y of defin itiolls with in the framew)lk or the cLJ l1lbat aga inst tube rcu l o~i-
A retrospective study (from J977) on co mpli ance of TB pat ients revealed that the default ra Ie of the out-putient population in rural Pak i~ta n amounted iO 66 Default was defined as fa ilu re to uttend the weck ly tu berc ulosis clinic fo r a period of one month (Sloan amp Sloan 1981) A fo llow-up study ( 198g-90) showed that 72 oc of the TB patients registered in Bethani a Hosp ital did not complete their 12 months trea tment coure Although the in troduction of a short-course (8 months) regimen improved the compliance default rates (56) contin ued to be high (Liefooghe et al 1995) In 1991 however 76 of TB patients reg istered in the Pakistan Institute of Chest Diseases (S indh) had kep t to the short-course reglmen for two months 2 1 had left the hospi ta l against medical advice and 3 had died (Pathan et al 1992) A study carr ied out in the lndian Wardha dislrict revealed that TB patientlt who fai]cd to take their medici ne for more than 15 days were regarded as non-comptiant because this definition is most in keeping with the adopted adshyministrative procedure (Barnhoorn amp Adriaanse 1992) In a study performed in Denver USA non-compl iance with DOT for TB was detined as foll ows (I) missing ~ 2 consecuti ve weeks of DOT (2) prolongation of treatment gt 30 days due 10 sporadic missed doses or (3 ) incarceration for presenting a th rem lO public health (Burman et al 1997) At least 18 of patients who received out-paLient DOT via the Denver Metro TubercLIl os is Clinic met at least one of these cri teria
In concusion therefore there is no golden standard for defining compliance In our study compliance the fi nal outcome which has to be explai ncd in the model is viewed from a dichotomous viewpoint On the one hand there is the category of compliant patients they com plete thei r the ra py in full and as a general rule al$o unshyderwent a sputum tes t confirming Ihem as TB negative On the other hand there is the category of non-com pliant patients they did not com plete their therapy so a sputum test was not carried out We also adopted the com pletion or fai lure to comshyplete the short -co urse direc tl y observed therapy the bas ic criterion used in the exshyam pIes given above as the key cri terion for our defi ni tion of com pliance The structural model (see Fig ure 3) demonstra tes th at it is important to systemat ically di stinguish the reguarity and the du ration of the therapy to gain a bctter undershystanding of the concept compliance Regularity is achieved when there are no or only sporadic interru ptions during the thcrapy In t hi ~ connection we refer to missed appointments or missed doses of medi cation The durarjoll of the therapy on the e ther hand refers to the treatment duration of eigh[ months which has to be
111 JIII 1 1 1III IJ IKLl 11 lH~Ult I IJ 11111lt ) ~
respected in the DOTS-regimen Two dlv iati ons are possiblc here Either Jo wn shyward the patient ends thc treatment premature1y and is regarded as d efaulter Ol upward- the period of treatment is extended because interruptions during the treatment have [0 be compenslIteti for artcrwards Both deviations from the norm indieate non-compliance Any com parison with the above referred to non-complishyance ra[es fa ils because the phenomenon is constantly regarded from di fferent anshygles Hav ing said that the folowing fac ts in our research on (non- )col11pl iancc among the 621 TB patients are worth mentioni ng
Aftel subtracti ng the nUlllbcr (l f pntients who have died (6Oc) thase who have transferred to another treaUllent centre (29r) and thc tiny group of patie nt~ where the treatmen t failed (I ) 563 pat ients remai ned According to our de liumln ition 779 of the latter group are compliant and 23 are non-compliant aresuIt which is c10sely in keepi ng with the situation at lhe lnsti tu te of Ches[ Diseases in the prov shyince of Sindh The number of in terruptions is used to indicate the regularity of the trcatment 48 of patients did not inlerrupt their treatment at all 34 in terrupted it once and 18 interrupted it various times As far as the duration of the lherapy is concerned the norm of eight months is ach ieved by 55 of patie nts [he norm i not achie ved laquo 8 months) by 33 of patients and the nonn is exceeded (gt 8 months) by 12 of patients
Broadly speaking three out of four paticnts is compliant One out of four is nOI1shycompliant interruptions during the treatmen t (because appoin tments or medicashytion is sporatlicall y missed) or failure to complete the ideal duration of treatmenl (because patients drop out too early or have to followan extended course of treatshyment) As far as establishi ng compl iance is concerned it would seem that 77 ck of patients is heading towards the WHO-target fo r global tuberculosis control namely cure 85 of the detected new smear-positive TB cases (Seita 1996 p 134)
When interpreting the results it is also important to disti nguish between ho~ p ishytalised patie nts and out-patients As we al ready stated earlier duri ng lhe rirst month of treatment 80 of patients were hospitalised Af ter the second month this number dropped to only 48 Permanent supervision at the hospital ensures that hospitalised TB patients are by definition compliant the DOTS-regime n is strictly enforced As far as non-compliance of the out-patient population is co ncerned wc noted that 17oc missed at least one appointment during the first month of treatshyment and that this number dropped 10 1I aftel thc end of the second month The first month is therefore critica especially fol patients who are not hospitalisetl Since they do not res ide at the hospi tal and only come for consultations thty enshycounter far greater difficulties internalising the norms underlying the DOTS-regishymen
The model hinges on the latent construct of stigmatisation Stigmatisation afshyfects compl iance through the Ta ndem of regu la ri ty and duration of therapy Persons who have been strongly stigmatised display more irregular illness behaviour and find it more problematic to see the ditficult and troublesome trealment through 10
[he end In th is respect il could be sa id that ending or interrup[ing the DOTS-reg imiddot
men is nol due to a Jack ol organi satioll On the contrary they are Illcchallisl llS which help to relieve thc pain of sli gmatisation ensuring that for a wh ik the TH pal ient does not have 10 he as hamed and can take a brea k when the prc-url of Ihc medical rcgimen beeomcs toa heavy (Massaro 1997) According 10 GollIllans terminology devi ali ng from the slandards of thc DOTS- rcgimen can hl rcgOl rdcJ as a technique fo r conlrolling in fo rmation The questions or whelher 10 revcal or hi de to con1iumlde in someone or keep qui et to lie or be truth ful and to who l1l hnw when and where are tricks for stoppi ng Ihe exhausting process of bleacutellllc hy socishyety They are in su mmary stra tegies to lWlwRc ( IpoiId idllltity (Schcpcr- amp Nievaard 1995 p 42-43) In Ihe mode l th rec social conditions affecl thc dcgrcc of sligmati sation of TB pat ients These co ndi lions have 10 be taken inlo account 10 reduce the lim ils to pat ienl compliancc with DOTS-strategies
The first cond it ion is rclated to the dem ()g mphico Iilloion of the pili cllt anJ comprises two variab les from the exogenous set ie gender and age FCi llalc pashytients were stigmatised more than male pat ients and older patients Wlr~ si igllwshyti sed more than young persons BOlh lin k~ are highl y significant As house wivcs or elderl y members of the ex tended fa mi Iy many have a low socio-econol11 ie Ialu For them health is above all J quest ion of physical strength (W inkvist amp Akhtar 1997) The loss of phys ical strength Ihlough tubercul osis the fact that tl1Oc who have been sl ricken wilh the diseas( can no longer perform hard labour do the housekeepmg no longer be reproducti ve etc are important contributors to stigshymat isation This is all the more so in lhe countryside where ex ternal signs of vu lshynerability often do not suffiumlce to relieve peopl e from their nonnal socill tasks in the fami ly and vill age
The second condition cl ose ly concerns the beiefofT8 patiel1ll in the curabifir of th eir disease We already said earlier that th is laten t construct in our research displayed features of serendi pity It is el istinct from stricl measurements ofrational med ical knowledge because it emphasises praxis ie implementing knowledge and acti ng on insights The higher the soc io-economie slatus the grealer the belief in the curabil ity of TB It is impossi ble to ignore the phenomenon of social stratifishycation when analys ing ill ness behaviollr of TB patients Patients wi th a higher proshyfessional rank have great faith in the curability of their disease The opposite also applics in equal measure unemploy ment and illileracy are cond ucive for nonshycompl iam behaviour Perhap~ the hard core of pariahs outcasts vagrants vagshyabonds tramps chronie drllnkards and drug add icts (Merton 1968 p 207) repshyresenlSthe most dangerous ri sk group for all TB control programmes When Robshyert K Merton in 1949 developcd hi s we ll-known typology of modes of adaptation by indi viduals within the cu ltu re-bearing society he discovered that these populashytion groups displ ayed retreatiII their mode of adapl3tion which implies the reshyjec tion of cul tural goals and institutional means After all why should anyone reshymain healthy And why should we lIse DOTS as Q method Does it make any difshyference) There is a negative correlat ion between belief in the curability of TB and the degree of stigmati sation Persons who are convineed they will soon be cured and capable of strictly following the medical regimen will be less stigmatised
1 ll i bull I III I 1 11 11 10-- 1 1 middot111 middotmiddot middot 1 middot _
The third condit ion is siluateel at the leve l of the social netllo rks in wh ich TB middot patients function As a general rule it can be sa id thaI persons who tcceive mor~ help from olhers are less likely 10 be stigmati sed Roughl y six out of ten pati ent~ are married and fo r married women the family-in-I aws occ upy the cen tral po- it iol in their social nelwork The model established a negati ve relationshi p betwec l support from blood re lati ve~ and support from the family-in-Iaws Solida rilYvvitl the fa mily-in-Ia ws red uces ~olidarity with biooeI relatives This app lies both il general but also in the specifi( framework of help and support in ti mes of illness The fear manied fe male TB patients have of being abancloned by their hll ~banJ and no 10nger being able to perform their domesr ic tasks should not be unMrcst i mated During a study into thc relcltion between poverty and TB in Bombay re male patients said thaI thei r husbands and mothers-in-Iaw repeated Iy sent then back to their nata l home until such lime as Ihey were cured They were often al cused of bringing the disease from their natal homes and were threatened with sep aration (Nui r et al 1997 p 8 1) The model revea led that the TB patiems who re ceived the least support from their family were stigrnatised most Th is recalls th relational natu re of all type of sti gmatisat ion People are given a negative SOCiH label or are shielded from it Your family may support you through thick and thin encourage you to do the right th ing help to fi nance treatment etc Converse l) your fam ily mayabandon you keep your situation quiet to prevent loosing fac anel keep the family reputation unb1emished
lil Pakistani society anel particularl y in l11any village and se ttl el11Cnb in th Punjab social networks and stigmati sation are inextricably li nkeel and have al enormous influence on community li fe Thc biraderi the patriarcha l nelwork 0
kinship fo rms the framework 101 social and coml11uni ty networks Special event and rites of passage such as birth the ci rcumcis ion of a son marriage allli th death of an old person si rengthen lhis solidarity within the biraderi The biradel use many other occasions to promote social and community networks and ill ne - is perhaps one of the most important When a daughter-in- Iaw becomes seriousl iJl or is hospitalised her children are either looked after by the other daughters (1
the house or are temporarily housed with other members of the birade ri If Ihe sol breadwinner of a household cannot work because he is seriously ill his nearest rel atives and olher members of his biraderi provide mora material and fi nancia l o up port These socia1 and communily links rernai n intact even after emigration Paki stanis who have emigrated to Grea t Brita in for exam ple continue to receive muc support from their biraderi (Anwar 1979) Whenever help is sought in Pakistar communities famil y and bi raderi are preferred According to a sociologic al stud carried out in Rochdale a toW D in the north of England hel p is only sOllght frOl farmer fellow viJ1 agers friend s neighbours Olher Pakistanis and the res t of 50CI ety after all possibil ities in the biraderi-network have been exhausted A TB pil tient who is admitted to hospital will initially be visited by me mbers of hi biraderi They wi llusuaJ1y be gi ven a few hundred rupees and the trad itional fru i However as news about the nature of the illness spreads within the bi rade ri cor tacts become less frequent The negative COITeiation between fa mily support an
sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more
74 H M~LLL~I NS n
phenomenon threatening both the ue lecl ion of ncw cases and Ihe treatlllll ll or Ihe sick Ailhough curab le TB still casts an evil shadow and smially discredilS ilS vicshytim Totally elimi naling the help a patient can usually expcct to receive in norlll1 circumslances it also reduccs the patient s motivation for constant I y balt l ing agai nst the disease itse lf How cun this vilt ious circlc be broken
52 Literature
Fifty years ago Talcott Parsons approached illness in The Socia System as a form of deviant behaviour and in th at framework he elaborated the concept sick rare (Parsons 1968) Since then medical sociology has paid considerable attention to the large variability in reactions lo symptoms and illness and to the various socioshycultu ral environmental and motivational factors affecting these differences to a lesser or larger ex tern (Mechanic 1995) The study of ill ness behaviour sti ll rel ies heav ily on these early structural -functionalistic based concepts ln the 1960s Kasl and Cobb defined illness behaviour aS any activi ty undertaken by a person who feels iIJ to define the state of his health and to discover a suitable remedy (Kasl amp Cob 1966) By distinguishing betwee n the different stages of illness Suchman ilshylustrated that ill ness behaviour has a distinctly dynamic character and is a complishycated process of decision-making wi th many actors which determines the progresshysive evol ution of illness behaviour (S uchman 19651 The theoretical reference frarnework eSlablished over the course of many years on the di ffe rent stages of the iIlness and forms of care embraces many disciplines (McKinlay 1972 Conrad 1997) It has gained a distinctly eclectic nature bringing together economic demographical geographical psychological cutural and organisationa factors in causa model s to desclibe and explain the illness behaviour
A medical regimen is imposed to ensure optimum progression of illness behavshyiour ie ensure that the pat ient recovers as soon as possi ble When patients sucshyceed in conforming their illness behav iour to the medical regimen they are comshyplian t Patient eampfiollce can assu me rnany forms ra nging from demands for coshyoperation in diagnostic procedures despi te anxiety and pain through taking drugs on schedule and otherwise fo llowing a prescribed regimen to abandonment of soshycial and fami lial obligations to the needs ofthe heal th syslem (Hyde 1988) As the regimen become more complex (for exam ple more types of medical ion or higher doses have to be taken or the tleatment s duration is longer) it becomes more di fshyficult to follow the regimen strictl y and the chances of non-compliance increase
The Directly Observed Treatment Short-course (or DOTS) system impIeshyments the latest medical insights on the treatment of tuberculosis and the combat of the global epidemic (WHO 1997) 1I was developed from the collec ti ve hest pracshytices clinical trials and programm at ic operations of TB control over the past two decades The DOTS-system ac ts as the cornerstone of the Global TB Progral11l11l of the World Heal th Organisat ion and is generally considercu to be one or the 1l10s1
75rA1I HTCOl I PLlA~CE WIT H DIREC-r IY 013SERVH1T HLItAI Y
rap idly expanding and successful health interventions of the 19905 (Ravig lione et al 1997) lt seeks first and foremost 10 implemenl on the widest possible scale a standardised short-course anti-TB trcatment regi men of six to eight mont hs with direct observation of lreatment for at least the i ni tia l two months In addition to apshyplying th is medical regimen governrnent commi lment to sllstai ned TB contro sputum smear microscopy to detect in rcctio Lls cases a regular un interrupted supshypl y of quality anti-TB drugs and a monitoring and reporting system to evaluate treatment oulcomes is widely rcgarded as the fundamental basis of lhe DOTS-sysshytem (Raviglione et al 1995)
Recent literature contai ns a nu mber of synonyms for the term cOInpliance (Volmink amp Garnel 1997 p 1403) Some authors now use the term ache rence to emphasise the fac t that fo llowing a medical regimen is the independent c hoice of the patient Sometimes the term c(Jncardallee is used to stress the active exchange of information negotiation and spirit of cooperalion in the relationship bet ween illness behaviour and medical regirnen Si nce the treatment of tllberculosis does not always automaticall y imply an independent choice of the patienl and a n acti ve exchange of information between patient and carer cannot be taken for granted we prefer the term compliance in this context Moreover it conveys the fact that illshyness behaviour is essentially social behaviour As long as patients act as they should and conform to therapeutic prescriptions they can continue to fu nction soshycially without any problems However as soon as thc threshold of acceptable
norms is crossed deviant behaviour replaces legitimate illness behaviour a nd socishyet ys integrati ve capacities gradually disappear
There are many ways to deviate from the medical regimen prescribed by the DOTS-system People can ignore TB symptoms and fai l to seek treatmenl Treatshyment can be postpo ned until the disease has become very severe indeed However there are also other less radical way to be non-compliant and reduce the likelishyhood of a cure lt is qui te easy for example to forget to go to the doctor or be careshyless in keeping appointments Some people adapt rnedication to suit the msclves and simplify the treatment plan The supervision which forms all inlrinsic part of the DOTS-syslem can be changed coincidentally or iystematically etc
Accordi ng to Bayer and Wilkinson it is essentia l to take into 1ccount lhe socioshycutural context in which this dysfunctional behaviour is displ ayed (Bayer amp Wilkinson 1995) Not cveryone feels strongly about missing an appointment ad shyjust ing medication or avoiding supervision This is precisely what makes the imshyplementation of the DOTS-system so difficult and unmanageable There are plenty of reasons for discontinu ing treatment Swallowing between one and four large pills daily for six to eight months is by no rneans easy Patients rnay have to conshytend with side-effec ts such as nausea and somnolence Many fail to take their medici ne onc time because they are either homelcss or mentall y ill or due to alcoshyhol or drugs abuse
According to Weber the main reason for failing to keep up the regime n is qu ite cleal patients who commence treatment become non- infect ious and already sta rt 10 feel better after a few weeks (Weber 1996) As a result they no longel fcel the
76 11 ~U IIM - i 11 1
need to endure the discamfort s of the lreltment thereby incrcas ing the growth of multidrug-res istan t TB so that treatmcnt ncarly always I ~l ils and patients l11l0SI certuinly suffer a relapse of the di sease
Another important rea50n fo r the non-compli am behaviour of TB patien ts is re shylaled to their srigmlllisarioll Stigmatisa tion accur whcn persons arc given a negashyti ve social labe l that ident itiumles people as dev iant not because their behaviolIr vioshylaLes 11 0rl11S but because they have pers(lIla l or sac ial cha racteristics that lead IJLOshypit to exclude thern (Johnson 1995 p 2~3) Mlleh time has passed sinee Erving Goffm an plTse nted his pionccring theoretical fral1l ework for the sociologieal allalshyysis of stigm ati sat ion in 1963 (Gollrnan 19SI()) Ithough this framework initiall y resu lted in many changes in the egal area it Sllon becal11e hi ghl y relevant 10 tlll spheres of ill ness aml heal th Goffman Jistingu ished three grossly di fferent Iyres of stigma (Lemert amp Branaman 19(7) First there are abomi nations of the hody the various physical dc formitics Ncx t the re are ble mishes of individual CharaLlegraver perceived as weak wi ll domineeri ng (lr unnatuml passions treacherous anti rigid beliefs and dishonesty Fina lly there are tht lri bal stiglllas of race nation anti regraveshyligion these bei ng stigmas that can be tlan~lllitted through lineagc anel equall y contaminate allmembers of a fa l11i1 y These three types of stigma c1ea rly l11ani rest thcl11sel ves in the medical sphere
Phys ical shortcol11ings and elefolmities increase the visibility or the ill ness anel the chances of stigmatisat ion According to Stiles and Kap lan the risk for ampli fi shycnt ion of deviance i~ even disproport ionatel y greatcr on the pa rt of physicall y st igshymatised devian t actors than for those without phys ical stigmata (Stil es amp Kaplan 1996) The coughing fi t ~ sweat anacks fever phJeg lll haemoptys is the sYl11bolic symbols of ye llow sputum and blood the el11aciated skin and bone body etc which characterise a TB patient make tll berculosis very visible and threaten ing to anyone who encounters it or has impress ions of it through societys collective memory Moreover dev iations in personality structure weakness lack of wilshypower feebleness irritability anel so on contribute to stigmatisation In her essay IIIn ess as Metaphor Susan Sontag illustrated that thi s is certainly the case with TB Tuberculosis is described as the disease of bom victims of sensitive pass ive peoshyple who are not quite Iife-loving enough to surv ive (Sontag 1990 p 25) Thomas Mann s character sketch of Hans Castorp reveals that TB also affects the general daily habits and psychological structu re of the patient (Mann 1996) Finally Goffman s typology identified the tri bal stig l11as which feed on the reprehensible characteristics of an entire group The sanatori um where the group characteristi cs of TB patients are expressed par excellence veritably exude~ a permanen t threat of olltagion Grygie r describes how th is danger of contagion marked indelibly the
init iation rituals and Ii fe in the san through and through of a group of Inuit Eskishymos from the far North who were pl aced in a sanatorium more south wards in Canshyada when a TB epidemic broke out (Grygier 1994)
However although tuberculosis patien ~ are stigmati sed by their ill ness it does not mean there are no ot her apparent sources of stigmatisation The power of Lhe rHpnt = innH ( 1tfIn i middotn h hl lro n hmiddot -11 - n bull h hp r(ll rI~lt1 t n
1 II N I Cl lM ILl ANC1 Wil H DIREl- 11 Y OllSFRVED rlll RA PY 77
soei1 labeb can be ass igned to el iscredit behaviour and turn people into outcasts Ithllugh TB is undoubtedly the most important stigl11ati sing factor for the pat ient stigmatisation immediately breaks out of the medical sphere and is influenc ed by t11 anas of life from that poi nt on Research fu rthermore reveals that stigmatisashytion even continues to complicate lhe Iives of the stigmati sed even as treatmelll i mshyprovcs thei r symptoms and functioning (Link et al 1997) The stigma does not di~appea r with the disease It is perpetuated by other ~ources Si milar hypothese~ wcrc put to the test in the research carried out by Crotts et al in Australi a Al shylhough Australia has a ve ry trong framework l)f anti-discrimination legisLatioIl recent years have seen an increasing numbcr of report~ of stigmatisation af fronts 10 diglllty and discrimi nation as Cl rcsult of the hepat itis C status of indi vidual s The sligmatisat ion caused by the disease is closely related to a li festyle of inj ecting drug users the major group now at ri sk of infeclioll and the consequences genershyall y impact domestic wo rk recreational day care and Iuneral sett ings (Crofts et al 1997)
53 Methodology
531 Sampling procedure
The study is based on an oral survey carried out in onc general hospita among~ t all sputum positi ve pulmonary TB patients (n=621 ) who pre~ented themsel ves at the TB unit ie from September 1996 until October 1997 Thc patients were intershyviewed at three fixed moments at the start of the treatment af ter one month af ter two months and followed-u p till the end of the trcatment Every interview was pershyformed by a social worker belonging to a team of four Since the duration of the treatment was 8 months the last patients tiumlni shed their treatment by theend of June 1998 Duri ng lhe interviews based on questionnaires consisting predomi nantly of closed questions and a small num ber of open questions information was gat he red about the demograph ical and socio-economic protiumlle of thc patienl~ social s upport provided by diffe rent networks the patients key values their knowledge of TB and their perception of the curabil ity of the disease stigmatisation and c omplishyance
The reason for choosing the hospital ie Bethania Hospital in Sialkot (Pakistan) requi res a I itle clarificalion (see Figure I) The hospital is situated in the Punjab province at the east of the Islamabad - Lahore axis Since its foundation in 1964 as amission hospital Bcthan ia Hospital has made an enormous effort to detec t and treat tu berculosis patients from the region It is cUiTently a 215 bed front-I ine anel referral hospital providi ng medical and surgical services One hundred beds are reserveel for a specialised TB unit It has a ward for men and a ward for wamen ilS own out-patient department sputum laboratory dispensary and registration unit
11 ~ t 7lt~ I middoti rp rpt rllitprl frn01 1 (~ fr hmfnr rtrfll nf iO km around the
I1 ~ I ILicirc II 11 1
need 10 enElu re the discomforlt of the trea tment thereby increasing the grow h or multidrug-resistant TB so Iha trealmenl nea rly always fails and pat ienlS tlmos certain ly suffer a relapse of the d isca~e
Another importanI reason for Ihe non-c0mplianl behavillur of TB paticJlIs is rcshylated to their stigmatisatioll Sligmatisation occu rs whcn person are givCJl I J1cgashyti ve sociallabel that identi ri es people lt1 dev ian t nol hccallsc their behav iolIl vioshylates norms but because they have peronal or ltoc i~tI characteristics thaI 1cld jlcoshyple to exclude them (Johnson 1995 p o R3 ) Much tiJl1 ha~ passed sincc Erving GotTman presented his pionccri ng theore tical framcwork ror the suciologilal ltll1 alshyysis of stigmatisation in 1963 (Gorrlllan 1(90) Allhough Ih is fralll eworJ initia lly resulled in many changes in the lega area it soan became hi ghly relev ant to the sphcres of illness and health Goffman distinguished three gross ly di ffe rent types of stigma (Lemen amp Branaman 1997) Fi rs t there ure abominations of the body the various physical deformi lies Nex t there are blem ishes of individual charucter perceived as weak wiJ l domineeri ng or unnatural passions treacherous and rigid beliefs and dishones ty Finally there are the tri bal stigmas of race nation and reshyligion these being s ti gma~ that can be transmitted through ineage and equally conlaminate all members of a farnily These th ree types of stigma clearly mani fest themsel ves in the medieal sphere
Physical shorteom ings and dcformities increase lhe visibility of the illness and the chances of stigmatisat ion Accordi ng to Stiles and Kaplan the ri sk for amplifi shycation of devinnce is even disproportionately greater on the part of physically stigshymalised deviant ac tors than for those wi thout physical stigmata (S tiles amp Kaplan 1996) The coughing fi ts sweat attacks fe ve r phlegm haemoptysis rhe symbolic symbols of yell ow sputum and blood the emaciated skin and bone body etc which characterisc a TB patient make tu berculosis very visible and threatening to anyone who encounters it or has impressions of it through societys collective memory Moreover devi alions in persona lity structure weakness lack of will shypower feebleness irritabil ity and sa on contribute to stigmatisation In her essay IIlness (IS Metaphor Susan Sontag i lI ustrated thatthis is certainly the case with TB Tuberculosis is described as the disease of born victirn s of sensiti ve passive peoshyple who are not quile life-Iov ing enough to survive (Sontag 1990 p 25) Thomas Mann s charac ter sketch of Hans Castorp revea ls thar TB also affects the general daily habi ts and psychological structure of the patient (Mann 1996) Finally Goffman s typology idenlified the tri bal stigmas which reed on the reprehensible characteristics of an entire group The sanatorium where the group characteristics of TB patients are expressed par excellence veritably exudes a permanent threat of contagion Grygier describes how Ih is danger of contagion marked indelibly the initiation ri luals and li fe in the sun through and through of a group of Inuit Eskishymos from the far North who were placed in a sanatorium more southwards in Canshyada when a TB epidemic broke out (Grygicr 1994)
However although tuberculosis pat ients are st igmati sed by their illness it does not mean there are no other apparent sources of stigmatisation The power of the concept stigmatisation is such that it targets all social spheres where negltive
1 11I l ll) ~ II Ll Ajlc 11 H lllH ll ll (JH~~KcU I HJ KI~
soc ial labe l ~ can be assigned 10 discredit behaviour and turn people into o utcasts Although TB is undoubtedl y the most important stigmatising factor for the palien l stigmati sation immediately breab OUI of the medical sphere and is in fl ue nced by all areas of life from Ihal point on Research furthennore reveals that st igmatisashyti on even continues to complicate the lives of the sti gmati sed even as treatmenl imshyproves their sy mptoms and fu ncticlJl in g (L in k et al 1997) Thc sti gma does not disappear with the di sease It is perpetu ated by other sourees Si milar hypotheses were put to Lhe test in the research carried ()ut by Crofts et al in Austra lia AIshythough Austral ia has a very su-ong framework of anti-disc riminati on leg islation recent years have ~een an incrcasing nU lllber of reports of stigmatisation arrmnrs lo dignilY and discrimi nation as a result of the he patit i ~ C status of individll als The sligmatisation caused by Lhe disease is closely related to a lifes tyle of i njecting drug lIse rs the major group now at risk of infection and the consequences genershyaJly impact domeslic work recreational day care and funeral settings (Crofts et
al 1997)
53 Methodology
531 Sampling procedure
The sludy is based on an oral survey carried out in one genera] hospital a mongst all sputum positive pullllonary TB patients (n=621) who presented themselves at the TB unit ie from September 1996 until October J997 The patients were iOlershyviewed at three fixed moments at the start of the treatment after one month aftel two months and followed-up tiJl the end of the treatment Every inlerv iew was pershyformed by a social worker belonging to a team of four Since the duratie o of the treatment was 8 months the last patients fini shed their treatment by the end of June 1998 During lhe interviews based on questionnaires consisting predominantly 0
closed questions and a small number of open questions information was gathered about the demographical and socio-econom ic profile of the patients socia1 support provided by different networks the patients key val ues their knowledge of TB and lheir perception of the curabilily of the disease stigmatisation and compli shy
ance
The reason for choosing the hospital ie Bethania Hospital in Sialkot (Pakistan requires a little clarification (see Figure l) The hospital is situated in the Punjab province at the east of the Islamabad - LahOl-e axis Si nce its foundation in 1964 as amission hospital Bethania Hospi tal has made an enormoUS effor to detect and treat tuberculosis patients from the region It is currently a 215 bed front-li ne aod referral hospital providing medical and surgical services One hundred beds arc reserved for a speeialised TB unit It has a ward for men and a ward for wemen its own out-patienl department sputum laboratory dispcnsary and registration un it About 75 of patients are recruited from a catch ment area of 50 km around the
~ gt
Arobion Seo
u 1 1 bullbullbull 1 i 1 I I bull bull
Figurc 1 Map of PJ k i ~ lan
centre of the city of Sialkot which is described as the cul-de-sac du Pakistan et carrefour de la mondial isalion (Le Monde 24298)
Si alkot provides a unique framework for the study of TB issues in the context of a developing country (Enarson 1994) ft is a middle to large city (800000 inshyhabitants) populated by Musli ms which is gradually transforming its feu dal authoritarian relations into modern industrialised and agrarian production proshycesses and a secularised society (Za idi 1999b Zaidi 1994a) In addition to having to deal with a considerable number of public health problems it also has to conshytend wi th a serious TB epidemic resulti ng in Sisyphean tasks and feeli ngs of helpshylessness amongst all the parties concerned These ci rcumstances made the study of the tOlal cohort of TB patien ts from Bethan ia Hospital representaLive for patients from Third World countries who have been diagnosed with pulmonary tuberculoshysis (Ferraro amp Farmer 1999) The ~amrle of TB patients used in this sludy en shyabled us to a certain extent to gain a betrer underslanding of a number of elemenshytary mechanisms operating at the level of stigmati satioll compliance and TB conshytrol in an en vironment where the illness has had a devastating effect hOlh at the personal and social leve l
532 Model
The model proposed in this chapter could be desc ribed as a two-s tep modI Firsl an explanation is sought for the ways in which TB patients are stigmatisLd Many different fac tors might influence the degree of stigmalisation of a TB paticnl 111
our model (see Figu re 2) stigrnatisation is explained by fo ur variables First we hypothesise that ol der palients are more casi ly stigmatised than younger 0 nes Secshyond we tested whether or not women are stigmatised faste r than men are Th ird we included a latent construct support from fa mil y The basic hypothe sis in the model is thal an increase of support from apatients famil y will cause a decrease in stigmati sation Lastly lhe fourth model led factor that might cause stigmatisati on is a knowledge related construct It is assumed th at the less one agrees theacutelt TB i- ti
curable disease the more one wi ll be stigmatised
Figu re 2 MoJel of stigmHisalion anel compliance tor TB
llltlief3 Bltltcr2 Bdiel 1
The second step in the model is the causal explanation of compliance What are the factors that influence the illness behav iour the acceptance of the sick ro le and lhe complianee of a TB patient The model distinguishes three factors The first factor concerns compliance to therapeutic standards solely with regard to the use of medshyicine The patient has to be wi lling to be (and remain) cured and furthermore be (and remain) convinced of the usefulnes$ of the prescribed medication or the DOTS-system will not have any chances of success The two other factors are sit ushyated at a higher theoret icallevel because they refer to tbe therapeutic proces~ in general and the many profess ional requirements and obligations combi ned with feedback of repeated tes ts this complex process invol ves One factor refers to the regularity with which patients comply with their obligations in tbc succcssive stages of their treatmen t the other refers to the pOlential to persevere and complete these stages until full recovery These three factors elenrly illustrate th ree different dimensions of compliant behaviour among TB patients When implementing the DOTS-system the relevance of these factors is extremely high because the sysshytem explicitly requires the strict intake of medicine regul ar doctors visi ts and an effort sustained over many months
11 U l LLI ~J CI IL
532 1 Mal ifes lriahles
The moJel to be estimated is a non-~tandard model (Hatcher 1994 p 423) It conshysists of several mani fe t variables that account for a pan of the structural portion of the model In other word we assumc lha hese manifest variables are perfect measures for the constructs they express Before we turn our attention to the real latent constructs in lhe model we finl want 10 give an overview of its manifest variables
There Ire I lLree exoKI I ou Iwnifesl variables S~x and Ige are measured in a straighlforward way Men and women on the one hand and a patient s age exshypressed in years on the ether Occupation is measured on an ordinal seale All ocshycupat ions are placed on a soc ial stralification seale that made il possible to plaee occupations on a higher or lower sot ietal level The lower range of the scale is fo rmed by housewives unskilled and skil led labour Pakistani middle manageshyment is found in the cottage industries farmers renting their land civil servants white-coJlar workers and small business owners Finally the exeeuti ve group conshysists of land-owning farmers and large business owners
53 22 Larent COTlSrrucls
In the model we used fOlr latelll constructs Before di scussing the measurement model more deeply we concentrated on the different items for eaeh endogenous construct The family is an importan t fac tor in the social environment of the TB pashytient Therefore we tried 10 include the lt upport of lhe farnil y within the model Sinee most pat ients were married (62) we had to deal wi th both the famil y and the family-in-Iaws
Support from the family-in-Iaws was nol included extcns ively in the research We could only include a latent factor support fro m family-in-I aws based on two indicator variables We are aware th at (he lalent construct is not firml y I1Itasulnl in this way However the resullS of lhe mea ~u remen t model (see ) are acceptable (seale composite reliability P= 67) The ind icator variables from thl C0l1s1nlcl are measured on a fi ve-poi nl scale (no influence at all - strong in tluence)
The seco nd latent construct is the support a patient receives from his own 1lt1111shy
ily (seale composite reliability p= 52) This construct is based on three indicalor variables two of which ussess on a five-point seale the direc t support and inllushyence from the fam ily (strongly di scourage - strongly encourage) Besidcs l110ra l support from the family we also included financi al suppo rt Patients wen as kctl whether hey rece ived any financial support The following examples orliumlnanc ia l support were given support for transport drugs consultation fees or les l~ Thc question naire did not ask in deta il about th e ki nd of support patients received Onl y a dichotomous answer (no support anel suppo rt) was sutficiem
Stigmat isation was based on three indicator var iables (scale composilc reli abil shyity p= 64) Again the famil y plays an important role in th is construct The qllesshyti onnaire asked patients to place thell1$elves on a six-point scale (don t agrce al all
1 middot ~IIL I J I I I~ I ~ l l I I II I ~ L I~ I ~I bull bullbullbull bullbull bull bull bull
_ strongly agree) asking them to what extent they fe It that having TB is a disgrace for the fa mily Ir a person agreed strongl y with this phrase it is assumed that he feels st igmatised by his fa mil y The same goes for stigm atisation by friends Again a six point scalc was used (dont agree at all - strongly agree ) to a-sess whelher or not the patients feit stigmatised by lheir fri ends The responde nls could indi cate whether lhey agreed with the idea of very good friends leav ing lhem beshycause of their elisease The more they agreed the more stigmatised they are sup shy
posed to beo The last latent construct in the model is the patient s belief in the curabili ly of
the disease and in knowing how to handle its complexity (scale composite reliabilshyity p= 68) It is an attitudinal factor cons isting of three indicator variables in which patients were asked to gi ve their opinion on TB itself All indicators were measured on a Ii ve-point scale (strongly disagree - strongl y agree) The indicator statements dealt with the opinion on the curability of TB (TB is easy to cure) the commonness of TB (TB is a common diseasc) and wi th the difticulty of TB a~ a disease itself (TB is a difficult disease and hard to cure)
Table 3 latlnt conSlruct mcasure menl summar) (onfirmtory fac tor analy ~i s an d scalc reli shy
ability
Item t Item Description Summary Standa rdshy
ised loading
t-vulue
Support famil y-in-Iaws (p= 67)
Famlawl How much will the opi nion of y lJUr familyshy 74 102
in - Iaw~ influence yo ur dcc is ion to liumlnish or not the wholc treatment (Fi rst time)
Faml aw2 Ho much will lht Qpi nion of your fa mil yshy 69 996
in-Ia ws influ ence your decision to finish or not lhe whole tremment (Sltco nd time)
Su pport fa mily P = 52)
Fam l To what extent does your (o wnl family en shy 59 1004
cou rage or discourage you in taking daily you r medicine (Fi rl time)
Fal112 To what cX lent does yOll r (own) f~l11i1 y enshy +9 8 53
courage or discou rage yOll in taki ng daily your medi cine (Second time)
Fam3 Does you r fam ily sup port yOll liumlnancia ll y for A5 7 98
th e cost of your trealment (tran~port 1drug~ I con~u lta lion fee I tests I )
Stigmatbation (p= 64)
Stigmal It is a disgrace fOf the fumily to have a f3mshyily membcr with TB (Fi rst time)
Stigmu 2 It is a disgracegrave for the family to ha ve J fa mshyily member with TB (S econd time
Stigma ven your bes t fli cnd olllctirncs desen you when you have all infectious di seasc like TB
Belief in curabiJity of TB (p= 68)
Belief TB is easy 10 cun 80 1501 Belie fZ TB is I com mon disease 55 1099 Belief] TB is a di ffi Cll lt dicase 3nd hard to cure 57 I I 2l
Note Fit sla tist ics for mcasurelllent model of 1 1 indicators for four construCIs 2
X IK7 =14993p = 00 GFl=97 RMR = 037 CR = 96 PNFI =52 NNFI = 9J RMS I = OW
I Scale composite relinbilily p = [(I Agravef ) ~ IImiddot(eacute)][(I Agrave I ) ~ vlr( ) + I S] (lOl-o l i amp Vi 1988 p 80)
The measurement model shown in provides a reaso na bl e fit 10 the dat1 Thc ehi shysquare test of exact fit is significant where the objecti ve is to achieve a non-signifshyicant p-value However Hatcher indicates that a significant ch i-square does not ma ke the measurement mode l inadequate (Hatchcr 1994 p 289) The ehi-square ratio shows th at the ratio of the chi-square value and the degree of freedolll is lowcr than two (17) This ind icates that the chi-sguare tes t is wilhin acceptahk lilllits (Marsh et al 1988) Other favourable diagnostics incIude a goodness-or-fiumlt illdegrave X GFI) of 97 a root mean square res idual (RMR) of on a comparati vL rit illtkx CFT) of 96 a parsi mony normed fit index (PNFI) of 52 a nOn normed rit index NNFI) of 93 and a root mean square error of approxi malion (RMSEA ) of rn9
In tenns of valid ity of the constructs con vergent validity is evidcnlxd by tilegrave large and significan t loadings of the item on thei r positcd ind icators FUIhc r (v ishydence of convergent va lidity is shown in None of the correlalions betwLcll Ihl 1 shytent construClS are too high to challen ge the convergent validity oft he cons lructs
F3 F4
100
- 06 100
The discriminan t validi ly is also indicated because the conlide nce interval (plusmn two slandard errors) around the correlati on es ti mate between any two latent construclS never includes 10 (Anderson amp Gerbing 1988 p 41 6) The Varianee Extracted Test also shows the discrim inant validity of our constructs The variance extrac ted tes t compares the variance extracted from two laten t constructs with the square of the correb tion between these two constructs (FomelI amp Larcker 1981 ) Discriminant validi ty is shown when the ex plained variance is greater than the squared correlation We compared all pairs of fac tors and they all showed an iCshy
ccptable variance ex tracted
)4 Results
) 41 Description of the sample
The 62 1 pati ents were composed of 55 0( men and 45 women Seven patients out of ten were younger than 40 concuning with the global observalion that in the countries of the Eastern MeditetTanean Region around 80 of the notified smearshypositi ve TB cases in 1994 occ urred among the economically productive sector of society (15 -54 years old) (Seila 1996 p 134) Tt indicates the serious impact of tushyberculosis on the comrnun ity The skills base of the patiems was very low more than half did not receive any form of fonnal education and the problem of illi teracy aillong older female patients was particularly acute
During the fi rst 11l0nth of lreatment 80 of patien ls were hospitalised during the second month th is number dropped to onl y 48 One out of tluee regarded hospitalisation as problematic This groups di ssalisfaction was rooted both in eco~ nomic and medical causes they had to contend with financial problems absemee shyism transport costs found themseJves in dire sLrai ts doc tors were in competent the rut of he ward etc
One third of patien ls were the family breadwinner As a resuit they were very reluctant to accept the sick mIe Remarkably only one fifth of patients came from a household with more than three economically act ive persons considering lh at
roughly 70 of household eon)i steJ of si x und of ten more Illcm bers The smal nurn ber of econornicall y active person- within the ex tcnded farnilie - C311110t be atshytributed to a large nu mber of ehi ldren because rOlgh ly hal f of the pat ients had less than three children
Sixty percelt ofpalielts placed heulrh al the top oft hc standard orvuluc This is not rea ll y surprising given the fact thal the responclents were confroltcd with ~cr ishyous health prob lems which have absolu te priorit) in their dail y li ve ~ lIld prCSllll1C the recove ry of bath hea lth balallCe anu the improvement of health pOlc nlia Ic shycording to Khayat these IWO dimensions of health are tleeply motet il1 Islalnie Irashydi tion and thefiqlI of health (Khayat 1997) Tf we ZOOIll in on the largL gro llp placshying heal th at the top of the standecircll-d of valuc wc sec Ihal the followi ng vllICS arc also held in high regard falllily and marriage (thc most important aftcr hla llh ) honour and integrity religion and fait h work money (thc Icast importanI ) AIshythough female patiems and patients wilh the lowest socio-economie status atshytached most importance to health it toes not mean that t he~e groups J i-played Ihe mOSl adequate illness behav iour On the contrary the~e groups ltI nd in particlilar housewives the un skilled unernp loyed and sociall y de pri ved ofte n do Ilol J1o~ scss the most elementary knowledge abou t TB (causes sylllptoms alld eollilitlll) which is needed to pre vent infec tion or undergo routine trcatment (Grce n Il)l)) p 192-196) The concept of (external) locus of control ofte n used in rlsealh on compliant behav iour and the fa tal islic health attitude lin ked to th i alslJ applied in thi s context of TB co ntro l (Mcchanic 1983)
Throughout the analys is the operational isation ol belief in the curlli Iil Yui the disease of ten appea red as a variab Ic wi th ~e relldipit y -charactcri ~tics This vlIiahle rneasures the confi dence ~i d people have in suumll vi ng their prob lem situ alilln Trust enables Ihe complexi ry of a social system to be reduced without funher aULgt the sick can rely on thei r part ner fal11il y health worker etc to channel the ir mcdical regimen It is cJear that preci sely lhis confidence is shattered by the TB it igma thereby reducing belief in the curability orTB in genera
Correctly assessing the treatment s duration is characteri stic for patients who strongly believe in the curability of their di sease However th is element of inforshymation is certainly not common knowledge when the treatment starts_Only one in three patients is aware that the trear ment will last several months However after one mon th this number doubles and af ter two months it increases even furthcr (73 ) We established that paliems with the lowest socio-economie statu s often did not possess the Illost rudimentary objecti ve medica l knowledge_There is Iitershyally a wall between them and the cogn itive elements req ui red This wa ll cannot be tom down on y due to reasons related to soc ial strmificaLion On the other hand persons who do nol mind regular check-ups a reg imen of aw kward medication and the costs involved who (hin k it is all worthwhile and are confiden t thei r treatshyment will result in a cure are not necessarily more ski lied or have a higher professhysional rank Ir would seem that another phenomenon another mechanism is ac ti ve as far as belief in Lbe curability of TB is concerned Thinking exclusively in tems of social stratification or Iumping techniq ues of rejec tion together as ways of
bull I I I bull I ~ II ~I I ~ bull I bullbull I L bullbull I bull bull bull bull bull bull
dealing with marginal categories (Douglas 1994 p 85) does not suffice lU gain l bettel understanding of the ideal treatment condition s
Compliance has lO be viewed not only from the socio slralificatiol1 perspeclii but also from the sl ig lllarismioJl persp(crive At thc onset ofthe treatlTlent and aftel two month s treatment sevell statemenlS concern ing stigmatisation were prelgtentecl to the patients A score had to be given on a six-poi nt scale (I =dont agree at all 5=agree 6=strongly ag ree)
The two stateme nts most people i e more than 80 agreed with (score 5 or 6) both at the onset of the trearment and [WO monlhs afterwards were Jf someont has TB hejshe avoids ralking about it with ot her persons and Af ter recoverinf from TB everyone treats yO Ll the same way lS bcfore If someone contracts TB il is bes t to keep quict about it If thei r environment doesn t know anythi ng about il th~y will not treat them di fferentl y af ter they hJ ve recovered
Thc other statement many ie more than 60 agreed with both at thc begin ning of the treatment and af ter two mO IHhs was Peope who arc treated for TB should ta lk to others about it
There were three statements alrnost half of pati ent- ie more than 401r agree with both at the onset of the treatment aOl af ter two months It is a disgrace for thl famil y to have a fa mily member with TB Even your best fri ends someti me ~
desert you when you have un infectious disease li ke T B and 11 a young persol catches TB heshe will experience the consequences for the rest of hisher lirc
Thc statement only a minority ie one out of four patients agreed with both a the onset of the treatment and af ter two months was It is diffi cult to earn your Ii ing after recovering from TB The fact that only very few regarded the TB prob lem in tenns of income is re lnted to the fact that during tbis life-threatening situa ti on_ the trentment has absol ute priori ty and takes precedence over all other form of need
When the onset of the treatment is compared Nith the situation two month later there are no shifts in the statemenls ranking order This means that the firs two months of treatmen t - eg at the hospitalor contact with health carers - dOt not real ly affect their situation On the contrary the stigmatisation continues t( proliferate and feste r causi ng damage in its wake According to Goffmans termi nology it conti nues to transform TB sufferers from discreditabe tO discredilel (Goffma n 1990 p 57 ) Only two statements poi nt to a possible evolution durin~ the first two months but they do not really di sruptthe ran ki ng order in any signifi cant way Ir rerers to the statement PeopJe who are treated for TB should talk t( others about it 68 tgreed at the omet of the treatment and 78 af ter tWt months treatmenl This increase indicates that TB patients still regard opennes about their illness und breaking taboos about the subject as a norm and future ex pectati on Whilst 54 agreed at the beginning of the treatment with the state lllcn Even your best fri ends sometimes dcsert you when you have an infect ious dis ease like TB this dropped to 45 af ter lwo months treatment Ir would appea that the channels for seeking informal care do not dry up for those who respect th medical regimen
We will illustrate thatthe social Il etwork lovering the pa tien t- nlatiolls with all significant others can cithcr increasc or reduce st ig lll ati satioll iS lllilh 1 ()IJt) p 138-155) The com position of these soci al networks i- very hcterogcilcous Thcy can perhaps bes t be analy-ed by di sti nguishing the nuelear fam ily from Ihe ex shytended fa mily As far as the nuclear fam ily is cOllce rned 62 of pllicnls wcn~ married 31 were si ngle 5fr widowed anel 2 divorced For married felll aie pashytients ( 173 out of a tota l of 387 married pa tients) rclati oll) with the fa mi Iy- ill-Iaws and in particular the mother-in-Iaw were very importan t indeecl For alll10sl half of all patients (47) thc extc ll(kJ fam il y eOll1 pri -ed cighl or more perso ll- IIs li all y adu lt who all li ve under the ) (l IllC roo f In 20 of households there wen ilO ehi 1shydren (yolJnger than 12 yca r~) 327 ot households had one or two childrclI 2C1r had three or four children and 21 or had fi ve or more
542 Causal model
The proposed structural model in Figurc 2 was tested by using con veuml ntionalmaxi shymu m likel ihood est imatioll techniques Thc model~h(lwed an acecptabk fit Again the ehi -square tes t of exact fit is ~i gni tiuml ca nt but the eh i-square ratio is lower than two (07) Other favourable diagnosti c~ include a goodncss-of-tiumlt index (GFl) of 96 a rOol mean square rcs idual (R MR) of 041 a comparati ve fi l index (CF) of 97 a parsimony normed fit index iPNFI) of 72 a non normed fit index (NNFI) of 96 and a root mean squ are enOf of approximation (RMSEA) of 039 All of the path coefficients are signifi cant
Anderson and Gerbing recommend a chi-square di ffe rence tes t (CDT) in order to enhanee the confidence in the structural part of the model (Anderson amp Gerbing 1988) The CDT compares the structura l model (which is a res trictecl theoretical model MT) with an uneons trailled alternative model (Mul The relevant test statis shytics (MT has 122 df and a X2 of 17526 ML has 93 df anel a X2 of 171 89) lead to a non-significa nt CDT (X2 difference is 25 33 at 35 df) and an acceptance of M
r Thu s our restricted theoretica model (Figure 3) is preferred to the theoretica uncorrelated model
Since most of the [esH tat is ti c~ show an acceptable model we can look at the reshysu lts of the two-step model presentcd earlier Firsl we tried to model the influshyences on the degree of stigmatisation of a patient These influenees come from very different sou rces The mos important factors determi ning stigmatisation are sex and age Women are more easily stigmatised than men are This also holds for older people From the latent factors support from the family is the most im porshytant Thc more one receives SUppOrL from ones fam ily the less one is stigmalised Anothcr influence on stigmatisation comes from belief in the curability of the TB onstruct The more one believes that TB is curable the less one is stigmatised
These results sugges t that a robust position within society prevents a person from being stigmatised
We then tried to link the stigmatisation of the TB patients and the ir complianl wilh lhe directly observed therapy The restricted theoretical model reveal s that ti influence of stigmatisation on compliance only becomes clearly visible af ter intro ducing the regularity and the duration of the therapy as intervening variables closer examination compliance would appear to be a rather hybridconcept whi can take various forms and has many depths Compliance comes clearer to the [ (I when regularity and du ration are separated In the model stigmatisation with effect of -016 affects regul arity Subsequently regularity has a direct effect of on eomplianee but lhere is a stronger effect on duration and from there on comp anee The regularity and the duration of the therapy tberefore form a tandem whi ca n be brought out of balance by stigmati sation anclilo longer prov ides any gu antees for compliant behaviour
Figu re 3 Siructuralmodel of complio ncc anJ TB
SignificCllce (p-PO ll t) =0 05 =00 =000
Note Fit statistics for structural model X2n~~) =175 26 P=00 GFl =96 RMR =041 CFl =lJ
PNFl =72 NNFI =96 RMSEA =039
SS Discussion
Compliance the fin al link in the causal model is a di ffi cult concept operationalise because it refers to a complex reality The treatment of most inf uumlous diseases oceurs in a di rectly observed way (Porter amp Ogden 1997) H0 ever in practice directly observed therapies can be implemented in a variety ways For examplc DOT for sexually transmitted diseases of ten means obsef tion of a single dose of treatment whereas DOT for leprosy entails monthly ob~ valion by a health care worker of doses of ri fampicin and clofazimine Tbe 001 control strategy reeommended by the WHO for tubercul os is is based on a com nation of four types of medici ne which have to be taken together for the fi rst t
months of lrcat ment HeLlith lJre worken ensure that the I ight Ill ed icine is lak n in the right doses and fo r the cornc t length of ti me Supervis ion ean he a CLlllllshy
p ished by having the pati ent visit the cimie hosp italis ing the patient or scnuin a health care workeI to visit the pa tients home or workplace For directl y ohsnvcd therapy fe l TB it i essenti1l that superv isi on continu e~ every day for th liumlrst two months and idea lly for the entire course of the treatment The wide vltlriations in DOT-contro strategies have resulted in a situation where compliance Illci 1l111lshy
compliance have become e la~t ic eoncepls Who is campliant and who is not~ It all depends on the nature and Ihe t ve l of thc sl3ndard We cncoun tered a di vcls il y of defin itiolls with in the framew)lk or the cLJ l1lbat aga inst tube rcu l o~i-
A retrospective study (from J977) on co mpli ance of TB pat ients revealed that the default ra Ie of the out-putient population in rural Pak i~ta n amounted iO 66 Default was defined as fa ilu re to uttend the weck ly tu berc ulosis clinic fo r a period of one month (Sloan amp Sloan 1981) A fo llow-up study ( 198g-90) showed that 72 oc of the TB patients registered in Bethani a Hosp ital did not complete their 12 months trea tment coure Although the in troduction of a short-course (8 months) regimen improved the compliance default rates (56) contin ued to be high (Liefooghe et al 1995) In 1991 however 76 of TB patients reg istered in the Pakistan Institute of Chest Diseases (S indh) had kep t to the short-course reglmen for two months 2 1 had left the hospi ta l against medical advice and 3 had died (Pathan et al 1992) A study carr ied out in the lndian Wardha dislrict revealed that TB patientlt who fai]cd to take their medici ne for more than 15 days were regarded as non-comptiant because this definition is most in keeping with the adopted adshyministrative procedure (Barnhoorn amp Adriaanse 1992) In a study performed in Denver USA non-compl iance with DOT for TB was detined as foll ows (I) missing ~ 2 consecuti ve weeks of DOT (2) prolongation of treatment gt 30 days due 10 sporadic missed doses or (3 ) incarceration for presenting a th rem lO public health (Burman et al 1997) At least 18 of patients who received out-paLient DOT via the Denver Metro TubercLIl os is Clinic met at least one of these cri teria
In concusion therefore there is no golden standard for defining compliance In our study compliance the fi nal outcome which has to be explai ncd in the model is viewed from a dichotomous viewpoint On the one hand there is the category of compliant patients they com plete thei r the ra py in full and as a general rule al$o unshyderwent a sputum tes t confirming Ihem as TB negative On the other hand there is the category of non-com pliant patients they did not com plete their therapy so a sputum test was not carried out We also adopted the com pletion or fai lure to comshyplete the short -co urse direc tl y observed therapy the bas ic criterion used in the exshyam pIes given above as the key cri terion for our defi ni tion of com pliance The structural model (see Fig ure 3) demonstra tes th at it is important to systemat ically di stinguish the reguarity and the du ration of the therapy to gain a bctter undershystanding of the concept compliance Regularity is achieved when there are no or only sporadic interru ptions during the thcrapy In t hi ~ connection we refer to missed appointments or missed doses of medi cation The durarjoll of the therapy on the e ther hand refers to the treatment duration of eigh[ months which has to be
111 JIII 1 1 1III IJ IKLl 11 lH~Ult I IJ 11111lt ) ~
respected in the DOTS-regimen Two dlv iati ons are possiblc here Either Jo wn shyward the patient ends thc treatment premature1y and is regarded as d efaulter Ol upward- the period of treatment is extended because interruptions during the treatment have [0 be compenslIteti for artcrwards Both deviations from the norm indieate non-compliance Any com parison with the above referred to non-complishyance ra[es fa ils because the phenomenon is constantly regarded from di fferent anshygles Hav ing said that the folowing fac ts in our research on (non- )col11pl iancc among the 621 TB patients are worth mentioni ng
Aftel subtracti ng the nUlllbcr (l f pntients who have died (6Oc) thase who have transferred to another treaUllent centre (29r) and thc tiny group of patie nt~ where the treatmen t failed (I ) 563 pat ients remai ned According to our de liumln ition 779 of the latter group are compliant and 23 are non-compliant aresuIt which is c10sely in keepi ng with the situation at lhe lnsti tu te of Ches[ Diseases in the prov shyince of Sindh The number of in terruptions is used to indicate the regularity of the trcatment 48 of patients did not inlerrupt their treatment at all 34 in terrupted it once and 18 interrupted it various times As far as the duration of the lherapy is concerned the norm of eight months is ach ieved by 55 of patie nts [he norm i not achie ved laquo 8 months) by 33 of patients and the nonn is exceeded (gt 8 months) by 12 of patients
Broadly speaking three out of four paticnts is compliant One out of four is nOI1shycompliant interruptions during the treatmen t (because appoin tments or medicashytion is sporatlicall y missed) or failure to complete the ideal duration of treatmenl (because patients drop out too early or have to followan extended course of treatshyment) As far as establishi ng compl iance is concerned it would seem that 77 ck of patients is heading towards the WHO-target fo r global tuberculosis control namely cure 85 of the detected new smear-positive TB cases (Seita 1996 p 134)
When interpreting the results it is also important to disti nguish between ho~ p ishytalised patie nts and out-patients As we al ready stated earlier duri ng lhe rirst month of treatment 80 of patients were hospitalised Af ter the second month this number dropped to only 48 Permanent supervision at the hospital ensures that hospitalised TB patients are by definition compliant the DOTS-regime n is strictly enforced As far as non-compliance of the out-patient population is co ncerned wc noted that 17oc missed at least one appointment during the first month of treatshyment and that this number dropped 10 1I aftel thc end of the second month The first month is therefore critica especially fol patients who are not hospitalisetl Since they do not res ide at the hospi tal and only come for consultations thty enshycounter far greater difficulties internalising the norms underlying the DOTS-regishymen
The model hinges on the latent construct of stigmatisation Stigmatisation afshyfects compl iance through the Ta ndem of regu la ri ty and duration of therapy Persons who have been strongly stigmatised display more irregular illness behaviour and find it more problematic to see the ditficult and troublesome trealment through 10
[he end In th is respect il could be sa id that ending or interrup[ing the DOTS-reg imiddot
men is nol due to a Jack ol organi satioll On the contrary they are Illcchallisl llS which help to relieve thc pain of sli gmatisation ensuring that for a wh ik the TH pal ient does not have 10 he as hamed and can take a brea k when the prc-url of Ihc medical rcgimen beeomcs toa heavy (Massaro 1997) According 10 GollIllans terminology devi ali ng from the slandards of thc DOTS- rcgimen can hl rcgOl rdcJ as a technique fo r conlrolling in fo rmation The questions or whelher 10 revcal or hi de to con1iumlde in someone or keep qui et to lie or be truth ful and to who l1l hnw when and where are tricks for stoppi ng Ihe exhausting process of bleacutellllc hy socishyety They are in su mmary stra tegies to lWlwRc ( IpoiId idllltity (Schcpcr- amp Nievaard 1995 p 42-43) In Ihe mode l th rec social conditions affecl thc dcgrcc of sligmati sation of TB pat ients These co ndi lions have 10 be taken inlo account 10 reduce the lim ils to pat ienl compliancc with DOTS-strategies
The first cond it ion is rclated to the dem ()g mphico Iilloion of the pili cllt anJ comprises two variab les from the exogenous set ie gender and age FCi llalc pashytients were stigmatised more than male pat ients and older patients Wlr~ si igllwshyti sed more than young persons BOlh lin k~ are highl y significant As house wivcs or elderl y members of the ex tended fa mi Iy many have a low socio-econol11 ie Ialu For them health is above all J quest ion of physical strength (W inkvist amp Akhtar 1997) The loss of phys ical strength Ihlough tubercul osis the fact that tl1Oc who have been sl ricken wilh the diseas( can no longer perform hard labour do the housekeepmg no longer be reproducti ve etc are important contributors to stigshymat isation This is all the more so in lhe countryside where ex ternal signs of vu lshynerability often do not suffiumlce to relieve peopl e from their nonnal socill tasks in the fami ly and vill age
The second condition cl ose ly concerns the beiefofT8 patiel1ll in the curabifir of th eir disease We already said earlier that th is laten t construct in our research displayed features of serendi pity It is el istinct from stricl measurements ofrational med ical knowledge because it emphasises praxis ie implementing knowledge and acti ng on insights The higher the soc io-economie slatus the grealer the belief in the curabil ity of TB It is impossi ble to ignore the phenomenon of social stratifishycation when analys ing ill ness behaviollr of TB patients Patients wi th a higher proshyfessional rank have great faith in the curability of their disease The opposite also applics in equal measure unemploy ment and illileracy are cond ucive for nonshycompl iam behaviour Perhap~ the hard core of pariahs outcasts vagrants vagshyabonds tramps chronie drllnkards and drug add icts (Merton 1968 p 207) repshyresenlSthe most dangerous ri sk group for all TB control programmes When Robshyert K Merton in 1949 developcd hi s we ll-known typology of modes of adaptation by indi viduals within the cu ltu re-bearing society he discovered that these populashytion groups displ ayed retreatiII their mode of adapl3tion which implies the reshyjec tion of cul tural goals and institutional means After all why should anyone reshymain healthy And why should we lIse DOTS as Q method Does it make any difshyference) There is a negative correlat ion between belief in the curability of TB and the degree of stigmati sation Persons who are convineed they will soon be cured and capable of strictly following the medical regimen will be less stigmatised
1 ll i bull I III I 1 11 11 10-- 1 1 middot111 middotmiddot middot 1 middot _
The third condit ion is siluateel at the leve l of the social netllo rks in wh ich TB middot patients function As a general rule it can be sa id thaI persons who tcceive mor~ help from olhers are less likely 10 be stigmati sed Roughl y six out of ten pati ent~ are married and fo r married women the family-in-I aws occ upy the cen tral po- it iol in their social nelwork The model established a negati ve relationshi p betwec l support from blood re lati ve~ and support from the family-in-Iaws Solida rilYvvitl the fa mily-in-Ia ws red uces ~olidarity with biooeI relatives This app lies both il general but also in the specifi( framework of help and support in ti mes of illness The fear manied fe male TB patients have of being abancloned by their hll ~banJ and no 10nger being able to perform their domesr ic tasks should not be unMrcst i mated During a study into thc relcltion between poverty and TB in Bombay re male patients said thaI thei r husbands and mothers-in-Iaw repeated Iy sent then back to their nata l home until such lime as Ihey were cured They were often al cused of bringing the disease from their natal homes and were threatened with sep aration (Nui r et al 1997 p 8 1) The model revea led that the TB patiems who re ceived the least support from their family were stigrnatised most Th is recalls th relational natu re of all type of sti gmatisat ion People are given a negative SOCiH label or are shielded from it Your family may support you through thick and thin encourage you to do the right th ing help to fi nance treatment etc Converse l) your fam ily mayabandon you keep your situation quiet to prevent loosing fac anel keep the family reputation unb1emished
lil Pakistani society anel particularl y in l11any village and se ttl el11Cnb in th Punjab social networks and stigmati sation are inextricably li nkeel and have al enormous influence on community li fe Thc biraderi the patriarcha l nelwork 0
kinship fo rms the framework 101 social and coml11uni ty networks Special event and rites of passage such as birth the ci rcumcis ion of a son marriage allli th death of an old person si rengthen lhis solidarity within the biraderi The biradel use many other occasions to promote social and community networks and ill ne - is perhaps one of the most important When a daughter-in- Iaw becomes seriousl iJl or is hospitalised her children are either looked after by the other daughters (1
the house or are temporarily housed with other members of the birade ri If Ihe sol breadwinner of a household cannot work because he is seriously ill his nearest rel atives and olher members of his biraderi provide mora material and fi nancia l o up port These socia1 and communily links rernai n intact even after emigration Paki stanis who have emigrated to Grea t Brita in for exam ple continue to receive muc support from their biraderi (Anwar 1979) Whenever help is sought in Pakistar communities famil y and bi raderi are preferred According to a sociologic al stud carried out in Rochdale a toW D in the north of England hel p is only sOllght frOl farmer fellow viJ1 agers friend s neighbours Olher Pakistanis and the res t of 50CI ety after all possibil ities in the biraderi-network have been exhausted A TB pil tient who is admitted to hospital will initially be visited by me mbers of hi biraderi They wi llusuaJ1y be gi ven a few hundred rupees and the trad itional fru i However as news about the nature of the illness spreads within the bi rade ri cor tacts become less frequent The negative COITeiation between fa mily support an
sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more
76 11 ~U IIM - i 11 1
need to endure the discamfort s of the lreltment thereby incrcas ing the growth of multidrug-res istan t TB so that treatmcnt ncarly always I ~l ils and patients l11l0SI certuinly suffer a relapse of the di sease
Another important rea50n fo r the non-compli am behaviour of TB patien ts is re shylaled to their srigmlllisarioll Stigmatisa tion accur whcn persons arc given a negashyti ve social labe l that ident itiumles people as dev iant not because their behaviolIr vioshylaLes 11 0rl11S but because they have pers(lIla l or sac ial cha racteristics that lead IJLOshypit to exclude thern (Johnson 1995 p 2~3) Mlleh time has passed sinee Erving Goffm an plTse nted his pionccring theoretical fral1l ework for the sociologieal allalshyysis of stigm ati sat ion in 1963 (Gollrnan 19SI()) Ithough this framework initiall y resu lted in many changes in the egal area it Sllon becal11e hi ghl y relevant 10 tlll spheres of ill ness aml heal th Goffman Jistingu ished three grossly di fferent Iyres of stigma (Lemert amp Branaman 19(7) First there are abomi nations of the hody the various physical dc formitics Ncx t the re are ble mishes of individual CharaLlegraver perceived as weak wi ll domineeri ng (lr unnatuml passions treacherous anti rigid beliefs and dishonesty Fina lly there are tht lri bal stiglllas of race nation anti regraveshyligion these bei ng stigmas that can be tlan~lllitted through lineagc anel equall y contaminate allmembers of a fa l11i1 y These three types of stigma c1ea rly l11ani rest thcl11sel ves in the medical sphere
Phys ical shortcol11ings and elefolmities increase the visibility or the ill ness anel the chances of stigmatisat ion According to Stiles and Kap lan the risk for ampli fi shycnt ion of deviance i~ even disproport ionatel y greatcr on the pa rt of physicall y st igshymatised devian t actors than for those without phys ical stigmata (Stil es amp Kaplan 1996) The coughing fi t ~ sweat anacks fever phJeg lll haemoptys is the sYl11bolic symbols of ye llow sputum and blood the el11aciated skin and bone body etc which characterise a TB patient make tll berculosis very visible and threaten ing to anyone who encounters it or has impress ions of it through societys collective memory Moreover dev iations in personality structure weakness lack of wilshypower feebleness irritability anel so on contribute to stigmatisation In her essay IIIn ess as Metaphor Susan Sontag illustrated that thi s is certainly the case with TB Tuberculosis is described as the disease of bom victims of sensitive pass ive peoshyple who are not quite Iife-loving enough to surv ive (Sontag 1990 p 25) Thomas Mann s character sketch of Hans Castorp reveals that TB also affects the general daily habits and psychological structu re of the patient (Mann 1996) Finally Goffman s typology identified the tri bal stig l11as which feed on the reprehensible characteristics of an entire group The sanatori um where the group characteristi cs of TB patients are expressed par excellence veritably exude~ a permanen t threat of olltagion Grygie r describes how th is danger of contagion marked indelibly the
init iation rituals and Ii fe in the san through and through of a group of Inuit Eskishymos from the far North who were pl aced in a sanatorium more south wards in Canshyada when a TB epidemic broke out (Grygier 1994)
However although tuberculosis patien ~ are stigmati sed by their ill ness it does not mean there are no ot her apparent sources of stigmatisation The power of Lhe rHpnt = innH ( 1tfIn i middotn h hl lro n hmiddot -11 - n bull h hp r(ll rI~lt1 t n
1 II N I Cl lM ILl ANC1 Wil H DIREl- 11 Y OllSFRVED rlll RA PY 77
soei1 labeb can be ass igned to el iscredit behaviour and turn people into outcasts Ithllugh TB is undoubtedly the most important stigl11ati sing factor for the pat ient stigmatisation immediately breaks out of the medical sphere and is influenc ed by t11 anas of life from that poi nt on Research fu rthermore reveals that stigmatisashytion even continues to complicate lhe Iives of the stigmati sed even as treatmelll i mshyprovcs thei r symptoms and functioning (Link et al 1997) The stigma does not di~appea r with the disease It is perpetuated by other ~ources Si milar hypothese~ wcrc put to the test in the research carried out by Crotts et al in Australi a Al shylhough Australia has a ve ry trong framework l)f anti-discrimination legisLatioIl recent years have seen an increasing numbcr of report~ of stigmatisation af fronts 10 diglllty and discrimi nation as Cl rcsult of the hepat itis C status of indi vidual s The sligmatisat ion caused by the disease is closely related to a li festyle of inj ecting drug users the major group now at ri sk of infeclioll and the consequences genershyall y impact domestic wo rk recreational day care and Iuneral sett ings (Crofts et al 1997)
53 Methodology
531 Sampling procedure
The study is based on an oral survey carried out in onc general hospita among~ t all sputum positi ve pulmonary TB patients (n=621 ) who pre~ented themsel ves at the TB unit ie from September 1996 until October 1997 Thc patients were intershyviewed at three fixed moments at the start of the treatment af ter one month af ter two months and followed-u p till the end of the trcatment Every interview was pershyformed by a social worker belonging to a team of four Since the duration of the treatment was 8 months the last patients tiumlni shed their treatment by theend of June 1998 Duri ng lhe interviews based on questionnaires consisting predomi nantly of closed questions and a small num ber of open questions information was gat he red about the demograph ical and socio-economic protiumlle of thc patienl~ social s upport provided by diffe rent networks the patients key values their knowledge of TB and their perception of the curabil ity of the disease stigmatisation and c omplishyance
The reason for choosing the hospital ie Bethania Hospital in Sialkot (Pakistan) requi res a I itle clarificalion (see Figure I) The hospital is situated in the Punjab province at the east of the Islamabad - Lahore axis Since its foundation in 1964 as amission hospital Bcthan ia Hospital has made an enormous effort to detec t and treat tu berculosis patients from the region It is cUiTently a 215 bed front-I ine anel referral hospital providi ng medical and surgical services One hundred beds are reserveel for a specialised TB unit It has a ward for men and a ward for wamen ilS own out-patient department sputum laboratory dispensary and registration unit
11 ~ t 7lt~ I middoti rp rpt rllitprl frn01 1 (~ fr hmfnr rtrfll nf iO km around the
I1 ~ I ILicirc II 11 1
need 10 enElu re the discomforlt of the trea tment thereby increasing the grow h or multidrug-resistant TB so Iha trealmenl nea rly always fails and pat ienlS tlmos certain ly suffer a relapse of the d isca~e
Another importanI reason for Ihe non-c0mplianl behavillur of TB paticJlIs is rcshylated to their stigmatisatioll Sligmatisation occu rs whcn person are givCJl I J1cgashyti ve sociallabel that identi ri es people lt1 dev ian t nol hccallsc their behav iolIl vioshylates norms but because they have peronal or ltoc i~tI characteristics thaI 1cld jlcoshyple to exclude them (Johnson 1995 p o R3 ) Much tiJl1 ha~ passed sincc Erving GotTman presented his pionccri ng theore tical framcwork ror the suciologilal ltll1 alshyysis of stigmatisation in 1963 (Gorrlllan 1(90) Allhough Ih is fralll eworJ initia lly resulled in many changes in the lega area it soan became hi ghly relev ant to the sphcres of illness and health Goffman distinguished three gross ly di ffe rent types of stigma (Lemen amp Branaman 1997) Fi rs t there ure abominations of the body the various physical deformi lies Nex t there are blem ishes of individual charucter perceived as weak wiJ l domineeri ng or unnatural passions treacherous and rigid beliefs and dishones ty Finally there are the tri bal stigmas of race nation and reshyligion these being s ti gma~ that can be transmitted through ineage and equally conlaminate all members of a farnily These th ree types of stigma clearly mani fest themsel ves in the medieal sphere
Physical shorteom ings and dcformities increase lhe visibility of the illness and the chances of stigmatisat ion Accordi ng to Stiles and Kaplan the ri sk for amplifi shycation of devinnce is even disproportionately greater on the part of physically stigshymalised deviant ac tors than for those wi thout physical stigmata (S tiles amp Kaplan 1996) The coughing fi ts sweat attacks fe ve r phlegm haemoptysis rhe symbolic symbols of yell ow sputum and blood the emaciated skin and bone body etc which characterisc a TB patient make tu berculosis very visible and threatening to anyone who encounters it or has impressions of it through societys collective memory Moreover devi alions in persona lity structure weakness lack of will shypower feebleness irritabil ity and sa on contribute to stigmatisation In her essay IIlness (IS Metaphor Susan Sontag i lI ustrated thatthis is certainly the case with TB Tuberculosis is described as the disease of born victirn s of sensiti ve passive peoshyple who are not quile life-Iov ing enough to survive (Sontag 1990 p 25) Thomas Mann s charac ter sketch of Hans Castorp revea ls thar TB also affects the general daily habi ts and psychological structure of the patient (Mann 1996) Finally Goffman s typology idenlified the tri bal stigmas which reed on the reprehensible characteristics of an entire group The sanatorium where the group characteristics of TB patients are expressed par excellence veritably exudes a permanent threat of contagion Grygier describes how Ih is danger of contagion marked indelibly the initiation ri luals and li fe in the sun through and through of a group of Inuit Eskishymos from the far North who were placed in a sanatorium more southwards in Canshyada when a TB epidemic broke out (Grygicr 1994)
However although tuberculosis pat ients are st igmati sed by their illness it does not mean there are no other apparent sources of stigmatisation The power of the concept stigmatisation is such that it targets all social spheres where negltive
1 11I l ll) ~ II Ll Ajlc 11 H lllH ll ll (JH~~KcU I HJ KI~
soc ial labe l ~ can be assigned 10 discredit behaviour and turn people into o utcasts Although TB is undoubtedl y the most important stigmatising factor for the palien l stigmati sation immediately breab OUI of the medical sphere and is in fl ue nced by all areas of life from Ihal point on Research furthennore reveals that st igmatisashyti on even continues to complicate the lives of the sti gmati sed even as treatmenl imshyproves their sy mptoms and fu ncticlJl in g (L in k et al 1997) Thc sti gma does not disappear with the di sease It is perpetu ated by other sourees Si milar hypotheses were put to Lhe test in the research carried ()ut by Crofts et al in Austra lia AIshythough Austral ia has a very su-ong framework of anti-disc riminati on leg islation recent years have ~een an incrcasing nU lllber of reports of stigmatisation arrmnrs lo dignilY and discrimi nation as a result of the he patit i ~ C status of individll als The sligmatisation caused by Lhe disease is closely related to a lifes tyle of i njecting drug lIse rs the major group now at risk of infection and the consequences genershyaJly impact domeslic work recreational day care and funeral settings (Crofts et
al 1997)
53 Methodology
531 Sampling procedure
The sludy is based on an oral survey carried out in one genera] hospital a mongst all sputum positive pullllonary TB patients (n=621) who presented themselves at the TB unit ie from September 1996 until October J997 The patients were iOlershyviewed at three fixed moments at the start of the treatment after one month aftel two months and followed-up tiJl the end of the treatment Every inlerv iew was pershyformed by a social worker belonging to a team of four Since the duratie o of the treatment was 8 months the last patients fini shed their treatment by the end of June 1998 During lhe interviews based on questionnaires consisting predominantly 0
closed questions and a small number of open questions information was gathered about the demographical and socio-econom ic profile of the patients socia1 support provided by different networks the patients key val ues their knowledge of TB and lheir perception of the curabilily of the disease stigmatisation and compli shy
ance
The reason for choosing the hospital ie Bethania Hospital in Sialkot (Pakistan requires a little clarification (see Figure l) The hospital is situated in the Punjab province at the east of the Islamabad - LahOl-e axis Si nce its foundation in 1964 as amission hospital Bethania Hospi tal has made an enormoUS effor to detect and treat tuberculosis patients from the region It is currently a 215 bed front-li ne aod referral hospital providing medical and surgical services One hundred beds arc reserved for a speeialised TB unit It has a ward for men and a ward for wemen its own out-patienl department sputum laboratory dispcnsary and registration un it About 75 of patients are recruited from a catch ment area of 50 km around the
~ gt
Arobion Seo
u 1 1 bullbullbull 1 i 1 I I bull bull
Figurc 1 Map of PJ k i ~ lan
centre of the city of Sialkot which is described as the cul-de-sac du Pakistan et carrefour de la mondial isalion (Le Monde 24298)
Si alkot provides a unique framework for the study of TB issues in the context of a developing country (Enarson 1994) ft is a middle to large city (800000 inshyhabitants) populated by Musli ms which is gradually transforming its feu dal authoritarian relations into modern industrialised and agrarian production proshycesses and a secularised society (Za idi 1999b Zaidi 1994a) In addition to having to deal with a considerable number of public health problems it also has to conshytend wi th a serious TB epidemic resulti ng in Sisyphean tasks and feeli ngs of helpshylessness amongst all the parties concerned These ci rcumstances made the study of the tOlal cohort of TB patien ts from Bethan ia Hospital representaLive for patients from Third World countries who have been diagnosed with pulmonary tuberculoshysis (Ferraro amp Farmer 1999) The ~amrle of TB patients used in this sludy en shyabled us to a certain extent to gain a betrer underslanding of a number of elemenshytary mechanisms operating at the level of stigmati satioll compliance and TB conshytrol in an en vironment where the illness has had a devastating effect hOlh at the personal and social leve l
532 Model
The model proposed in this chapter could be desc ribed as a two-s tep modI Firsl an explanation is sought for the ways in which TB patients are stigmatisLd Many different fac tors might influence the degree of stigmalisation of a TB paticnl 111
our model (see Figu re 2) stigrnatisation is explained by fo ur variables First we hypothesise that ol der palients are more casi ly stigmatised than younger 0 nes Secshyond we tested whether or not women are stigmatised faste r than men are Th ird we included a latent construct support from fa mil y The basic hypothe sis in the model is thal an increase of support from apatients famil y will cause a decrease in stigmati sation Lastly lhe fourth model led factor that might cause stigmatisati on is a knowledge related construct It is assumed th at the less one agrees theacutelt TB i- ti
curable disease the more one wi ll be stigmatised
Figu re 2 MoJel of stigmHisalion anel compliance tor TB
llltlief3 Bltltcr2 Bdiel 1
The second step in the model is the causal explanation of compliance What are the factors that influence the illness behav iour the acceptance of the sick ro le and lhe complianee of a TB patient The model distinguishes three factors The first factor concerns compliance to therapeutic standards solely with regard to the use of medshyicine The patient has to be wi lling to be (and remain) cured and furthermore be (and remain) convinced of the usefulnes$ of the prescribed medication or the DOTS-system will not have any chances of success The two other factors are sit ushyated at a higher theoret icallevel because they refer to tbe therapeutic proces~ in general and the many profess ional requirements and obligations combi ned with feedback of repeated tes ts this complex process invol ves One factor refers to the regularity with which patients comply with their obligations in tbc succcssive stages of their treatmen t the other refers to the pOlential to persevere and complete these stages until full recovery These three factors elenrly illustrate th ree different dimensions of compliant behaviour among TB patients When implementing the DOTS-system the relevance of these factors is extremely high because the sysshytem explicitly requires the strict intake of medicine regul ar doctors visi ts and an effort sustained over many months
11 U l LLI ~J CI IL
532 1 Mal ifes lriahles
The moJel to be estimated is a non-~tandard model (Hatcher 1994 p 423) It conshysists of several mani fe t variables that account for a pan of the structural portion of the model In other word we assumc lha hese manifest variables are perfect measures for the constructs they express Before we turn our attention to the real latent constructs in lhe model we finl want 10 give an overview of its manifest variables
There Ire I lLree exoKI I ou Iwnifesl variables S~x and Ige are measured in a straighlforward way Men and women on the one hand and a patient s age exshypressed in years on the ether Occupation is measured on an ordinal seale All ocshycupat ions are placed on a soc ial stralification seale that made il possible to plaee occupations on a higher or lower sot ietal level The lower range of the scale is fo rmed by housewives unskilled and skil led labour Pakistani middle manageshyment is found in the cottage industries farmers renting their land civil servants white-coJlar workers and small business owners Finally the exeeuti ve group conshysists of land-owning farmers and large business owners
53 22 Larent COTlSrrucls
In the model we used fOlr latelll constructs Before di scussing the measurement model more deeply we concentrated on the different items for eaeh endogenous construct The family is an importan t fac tor in the social environment of the TB pashytient Therefore we tried 10 include the lt upport of lhe farnil y within the model Sinee most pat ients were married (62) we had to deal wi th both the famil y and the family-in-Iaws
Support from the family-in-Iaws was nol included extcns ively in the research We could only include a latent factor support fro m family-in-I aws based on two indicator variables We are aware th at (he lalent construct is not firml y I1Itasulnl in this way However the resullS of lhe mea ~u remen t model (see ) are acceptable (seale composite reliability P= 67) The ind icator variables from thl C0l1s1nlcl are measured on a fi ve-poi nl scale (no influence at all - strong in tluence)
The seco nd latent construct is the support a patient receives from his own 1lt1111shy
ily (seale composite reliability p= 52) This construct is based on three indicalor variables two of which ussess on a five-point seale the direc t support and inllushyence from the fam ily (strongly di scourage - strongly encourage) Besidcs l110ra l support from the family we also included financi al suppo rt Patients wen as kctl whether hey rece ived any financial support The following examples orliumlnanc ia l support were given support for transport drugs consultation fees or les l~ Thc question naire did not ask in deta il about th e ki nd of support patients received Onl y a dichotomous answer (no support anel suppo rt) was sutficiem
Stigmat isation was based on three indicator var iables (scale composilc reli abil shyity p= 64) Again the famil y plays an important role in th is construct The qllesshyti onnaire asked patients to place thell1$elves on a six-point scale (don t agrce al all
1 middot ~IIL I J I I I~ I ~ l l I I II I ~ L I~ I ~I bull bullbullbull bullbull bull bull bull
_ strongly agree) asking them to what extent they fe It that having TB is a disgrace for the fa mily Ir a person agreed strongl y with this phrase it is assumed that he feels st igmatised by his fa mil y The same goes for stigm atisation by friends Again a six point scalc was used (dont agree at all - strongly agree ) to a-sess whelher or not the patients feit stigmatised by lheir fri ends The responde nls could indi cate whether lhey agreed with the idea of very good friends leav ing lhem beshycause of their elisease The more they agreed the more stigmatised they are sup shy
posed to beo The last latent construct in the model is the patient s belief in the curabili ly of
the disease and in knowing how to handle its complexity (scale composite reliabilshyity p= 68) It is an attitudinal factor cons isting of three indicator variables in which patients were asked to gi ve their opinion on TB itself All indicators were measured on a Ii ve-point scale (strongly disagree - strongl y agree) The indicator statements dealt with the opinion on the curability of TB (TB is easy to cure) the commonness of TB (TB is a common diseasc) and wi th the difticulty of TB a~ a disease itself (TB is a difficult disease and hard to cure)
Table 3 latlnt conSlruct mcasure menl summar) (onfirmtory fac tor analy ~i s an d scalc reli shy
ability
Item t Item Description Summary Standa rdshy
ised loading
t-vulue
Support famil y-in-Iaws (p= 67)
Famlawl How much will the opi nion of y lJUr familyshy 74 102
in - Iaw~ influence yo ur dcc is ion to liumlnish or not the wholc treatment (Fi rst time)
Faml aw2 Ho much will lht Qpi nion of your fa mil yshy 69 996
in-Ia ws influ ence your decision to finish or not lhe whole tremment (Sltco nd time)
Su pport fa mily P = 52)
Fam l To what extent does your (o wnl family en shy 59 1004
cou rage or discourage you in taking daily you r medicine (Fi rl time)
Fal112 To what cX lent does yOll r (own) f~l11i1 y enshy +9 8 53
courage or discou rage yOll in taki ng daily your medi cine (Second time)
Fam3 Does you r fam ily sup port yOll liumlnancia ll y for A5 7 98
th e cost of your trealment (tran~port 1drug~ I con~u lta lion fee I tests I )
Stigmatbation (p= 64)
Stigmal It is a disgrace fOf the fumily to have a f3mshyily membcr with TB (Fi rst time)
Stigmu 2 It is a disgracegrave for the family to ha ve J fa mshyily member with TB (S econd time
Stigma ven your bes t fli cnd olllctirncs desen you when you have all infectious di seasc like TB
Belief in curabiJity of TB (p= 68)
Belief TB is easy 10 cun 80 1501 Belie fZ TB is I com mon disease 55 1099 Belief] TB is a di ffi Cll lt dicase 3nd hard to cure 57 I I 2l
Note Fit sla tist ics for mcasurelllent model of 1 1 indicators for four construCIs 2
X IK7 =14993p = 00 GFl=97 RMR = 037 CR = 96 PNFI =52 NNFI = 9J RMS I = OW
I Scale composite relinbilily p = [(I Agravef ) ~ IImiddot(eacute)][(I Agrave I ) ~ vlr( ) + I S] (lOl-o l i amp Vi 1988 p 80)
The measurement model shown in provides a reaso na bl e fit 10 the dat1 Thc ehi shysquare test of exact fit is significant where the objecti ve is to achieve a non-signifshyicant p-value However Hatcher indicates that a significant ch i-square does not ma ke the measurement mode l inadequate (Hatchcr 1994 p 289) The ehi-square ratio shows th at the ratio of the chi-square value and the degree of freedolll is lowcr than two (17) This ind icates that the chi-sguare tes t is wilhin acceptahk lilllits (Marsh et al 1988) Other favourable diagnostics incIude a goodness-or-fiumlt illdegrave X GFI) of 97 a root mean square res idual (RMR) of on a comparati vL rit illtkx CFT) of 96 a parsi mony normed fit index (PNFI) of 52 a nOn normed rit index NNFI) of 93 and a root mean square error of approxi malion (RMSEA ) of rn9
In tenns of valid ity of the constructs con vergent validity is evidcnlxd by tilegrave large and significan t loadings of the item on thei r positcd ind icators FUIhc r (v ishydence of convergent va lidity is shown in None of the correlalions betwLcll Ihl 1 shytent construClS are too high to challen ge the convergent validity oft he cons lructs
F3 F4
100
- 06 100
The discriminan t validi ly is also indicated because the conlide nce interval (plusmn two slandard errors) around the correlati on es ti mate between any two latent construclS never includes 10 (Anderson amp Gerbing 1988 p 41 6) The Varianee Extracted Test also shows the discrim inant validity of our constructs The variance extrac ted tes t compares the variance extracted from two laten t constructs with the square of the correb tion between these two constructs (FomelI amp Larcker 1981 ) Discriminant validi ty is shown when the ex plained variance is greater than the squared correlation We compared all pairs of fac tors and they all showed an iCshy
ccptable variance ex tracted
)4 Results
) 41 Description of the sample
The 62 1 pati ents were composed of 55 0( men and 45 women Seven patients out of ten were younger than 40 concuning with the global observalion that in the countries of the Eastern MeditetTanean Region around 80 of the notified smearshypositi ve TB cases in 1994 occ urred among the economically productive sector of society (15 -54 years old) (Seila 1996 p 134) Tt indicates the serious impact of tushyberculosis on the comrnun ity The skills base of the patiems was very low more than half did not receive any form of fonnal education and the problem of illi teracy aillong older female patients was particularly acute
During the fi rst 11l0nth of lreatment 80 of patien ls were hospitalised during the second month th is number dropped to onl y 48 One out of tluee regarded hospitalisation as problematic This groups di ssalisfaction was rooted both in eco~ nomic and medical causes they had to contend with financial problems absemee shyism transport costs found themseJves in dire sLrai ts doc tors were in competent the rut of he ward etc
One third of patien ls were the family breadwinner As a resuit they were very reluctant to accept the sick mIe Remarkably only one fifth of patients came from a household with more than three economically act ive persons considering lh at
roughly 70 of household eon)i steJ of si x und of ten more Illcm bers The smal nurn ber of econornicall y active person- within the ex tcnded farnilie - C311110t be atshytributed to a large nu mber of ehi ldren because rOlgh ly hal f of the pat ients had less than three children
Sixty percelt ofpalielts placed heulrh al the top oft hc standard orvuluc This is not rea ll y surprising given the fact thal the responclents were confroltcd with ~cr ishyous health prob lems which have absolu te priorit) in their dail y li ve ~ lIld prCSllll1C the recove ry of bath hea lth balallCe anu the improvement of health pOlc nlia Ic shycording to Khayat these IWO dimensions of health are tleeply motet il1 Islalnie Irashydi tion and thefiqlI of health (Khayat 1997) Tf we ZOOIll in on the largL gro llp placshying heal th at the top of the standecircll-d of valuc wc sec Ihal the followi ng vllICS arc also held in high regard falllily and marriage (thc most important aftcr hla llh ) honour and integrity religion and fait h work money (thc Icast importanI ) AIshythough female patiems and patients wilh the lowest socio-economie status atshytached most importance to health it toes not mean that t he~e groups J i-played Ihe mOSl adequate illness behav iour On the contrary the~e groups ltI nd in particlilar housewives the un skilled unernp loyed and sociall y de pri ved ofte n do Ilol J1o~ scss the most elementary knowledge abou t TB (causes sylllptoms alld eollilitlll) which is needed to pre vent infec tion or undergo routine trcatment (Grce n Il)l)) p 192-196) The concept of (external) locus of control ofte n used in rlsealh on compliant behav iour and the fa tal islic health attitude lin ked to th i alslJ applied in thi s context of TB co ntro l (Mcchanic 1983)
Throughout the analys is the operational isation ol belief in the curlli Iil Yui the disease of ten appea red as a variab Ic wi th ~e relldipit y -charactcri ~tics This vlIiahle rneasures the confi dence ~i d people have in suumll vi ng their prob lem situ alilln Trust enables Ihe complexi ry of a social system to be reduced without funher aULgt the sick can rely on thei r part ner fal11il y health worker etc to channel the ir mcdical regimen It is cJear that preci sely lhis confidence is shattered by the TB it igma thereby reducing belief in the curability orTB in genera
Correctly assessing the treatment s duration is characteri stic for patients who strongly believe in the curability of their di sease However th is element of inforshymation is certainly not common knowledge when the treatment starts_Only one in three patients is aware that the trear ment will last several months However after one mon th this number doubles and af ter two months it increases even furthcr (73 ) We established that paliems with the lowest socio-economie statu s often did not possess the Illost rudimentary objecti ve medica l knowledge_There is Iitershyally a wall between them and the cogn itive elements req ui red This wa ll cannot be tom down on y due to reasons related to soc ial strmificaLion On the other hand persons who do nol mind regular check-ups a reg imen of aw kward medication and the costs involved who (hin k it is all worthwhile and are confiden t thei r treatshyment will result in a cure are not necessarily more ski lied or have a higher professhysional rank Ir would seem that another phenomenon another mechanism is ac ti ve as far as belief in Lbe curability of TB is concerned Thinking exclusively in tems of social stratification or Iumping techniq ues of rejec tion together as ways of
bull I I I bull I ~ II ~I I ~ bull I bullbull I L bullbull I bull bull bull bull bull bull
dealing with marginal categories (Douglas 1994 p 85) does not suffice lU gain l bettel understanding of the ideal treatment condition s
Compliance has lO be viewed not only from the socio slralificatiol1 perspeclii but also from the sl ig lllarismioJl persp(crive At thc onset ofthe treatlTlent and aftel two month s treatment sevell statemenlS concern ing stigmatisation were prelgtentecl to the patients A score had to be given on a six-poi nt scale (I =dont agree at all 5=agree 6=strongly ag ree)
The two stateme nts most people i e more than 80 agreed with (score 5 or 6) both at the onset of the trearment and [WO monlhs afterwards were Jf someont has TB hejshe avoids ralking about it with ot her persons and Af ter recoverinf from TB everyone treats yO Ll the same way lS bcfore If someone contracts TB il is bes t to keep quict about it If thei r environment doesn t know anythi ng about il th~y will not treat them di fferentl y af ter they hJ ve recovered
Thc other statement many ie more than 60 agreed with both at thc begin ning of the treatment and af ter two mO IHhs was Peope who arc treated for TB should ta lk to others about it
There were three statements alrnost half of pati ent- ie more than 401r agree with both at the onset of the treatment aOl af ter two months It is a disgrace for thl famil y to have a fa mily member with TB Even your best fri ends someti me ~
desert you when you have un infectious disease li ke T B and 11 a young persol catches TB heshe will experience the consequences for the rest of hisher lirc
Thc statement only a minority ie one out of four patients agreed with both a the onset of the treatment and af ter two months was It is diffi cult to earn your Ii ing after recovering from TB The fact that only very few regarded the TB prob lem in tenns of income is re lnted to the fact that during tbis life-threatening situa ti on_ the trentment has absol ute priori ty and takes precedence over all other form of need
When the onset of the treatment is compared Nith the situation two month later there are no shifts in the statemenls ranking order This means that the firs two months of treatmen t - eg at the hospitalor contact with health carers - dOt not real ly affect their situation On the contrary the stigmatisation continues t( proliferate and feste r causi ng damage in its wake According to Goffmans termi nology it conti nues to transform TB sufferers from discreditabe tO discredilel (Goffma n 1990 p 57 ) Only two statements poi nt to a possible evolution durin~ the first two months but they do not really di sruptthe ran ki ng order in any signifi cant way Ir rerers to the statement PeopJe who are treated for TB should talk t( others about it 68 tgreed at the omet of the treatment and 78 af ter tWt months treatmenl This increase indicates that TB patients still regard opennes about their illness und breaking taboos about the subject as a norm and future ex pectati on Whilst 54 agreed at the beginning of the treatment with the state lllcn Even your best fri ends sometimes dcsert you when you have an infect ious dis ease like TB this dropped to 45 af ter lwo months treatment Ir would appea that the channels for seeking informal care do not dry up for those who respect th medical regimen
We will illustrate thatthe social Il etwork lovering the pa tien t- nlatiolls with all significant others can cithcr increasc or reduce st ig lll ati satioll iS lllilh 1 ()IJt) p 138-155) The com position of these soci al networks i- very hcterogcilcous Thcy can perhaps bes t be analy-ed by di sti nguishing the nuelear fam ily from Ihe ex shytended fa mily As far as the nuclear fam ily is cOllce rned 62 of pllicnls wcn~ married 31 were si ngle 5fr widowed anel 2 divorced For married felll aie pashytients ( 173 out of a tota l of 387 married pa tients) rclati oll) with the fa mi Iy- ill-Iaws and in particular the mother-in-Iaw were very importan t indeecl For alll10sl half of all patients (47) thc extc ll(kJ fam il y eOll1 pri -ed cighl or more perso ll- IIs li all y adu lt who all li ve under the ) (l IllC roo f In 20 of households there wen ilO ehi 1shydren (yolJnger than 12 yca r~) 327 ot households had one or two childrclI 2C1r had three or four children and 21 or had fi ve or more
542 Causal model
The proposed structural model in Figurc 2 was tested by using con veuml ntionalmaxi shymu m likel ihood est imatioll techniques Thc model~h(lwed an acecptabk fit Again the ehi -square tes t of exact fit is ~i gni tiuml ca nt but the eh i-square ratio is lower than two (07) Other favourable diagnosti c~ include a goodncss-of-tiumlt index (GFl) of 96 a rOol mean square rcs idual (R MR) of 041 a comparati ve fi l index (CF) of 97 a parsimony normed fit index iPNFI) of 72 a non normed fit index (NNFI) of 96 and a root mean squ are enOf of approximation (RMSEA) of 039 All of the path coefficients are signifi cant
Anderson and Gerbing recommend a chi-square di ffe rence tes t (CDT) in order to enhanee the confidence in the structural part of the model (Anderson amp Gerbing 1988) The CDT compares the structura l model (which is a res trictecl theoretical model MT) with an uneons trailled alternative model (Mul The relevant test statis shytics (MT has 122 df and a X2 of 17526 ML has 93 df anel a X2 of 171 89) lead to a non-significa nt CDT (X2 difference is 25 33 at 35 df) and an acceptance of M
r Thu s our restricted theoretica model (Figure 3) is preferred to the theoretica uncorrelated model
Since most of the [esH tat is ti c~ show an acceptable model we can look at the reshysu lts of the two-step model presentcd earlier Firsl we tried to model the influshyences on the degree of stigmatisation of a patient These influenees come from very different sou rces The mos important factors determi ning stigmatisation are sex and age Women are more easily stigmatised than men are This also holds for older people From the latent factors support from the family is the most im porshytant Thc more one receives SUppOrL from ones fam ily the less one is stigmalised Anothcr influence on stigmatisation comes from belief in the curability of the TB onstruct The more one believes that TB is curable the less one is stigmatised
These results sugges t that a robust position within society prevents a person from being stigmatised
We then tried to link the stigmatisation of the TB patients and the ir complianl wilh lhe directly observed therapy The restricted theoretical model reveal s that ti influence of stigmatisation on compliance only becomes clearly visible af ter intro ducing the regularity and the duration of the therapy as intervening variables closer examination compliance would appear to be a rather hybridconcept whi can take various forms and has many depths Compliance comes clearer to the [ (I when regularity and du ration are separated In the model stigmatisation with effect of -016 affects regul arity Subsequently regularity has a direct effect of on eomplianee but lhere is a stronger effect on duration and from there on comp anee The regularity and the duration of the therapy tberefore form a tandem whi ca n be brought out of balance by stigmati sation anclilo longer prov ides any gu antees for compliant behaviour
Figu re 3 Siructuralmodel of complio ncc anJ TB
SignificCllce (p-PO ll t) =0 05 =00 =000
Note Fit statistics for structural model X2n~~) =175 26 P=00 GFl =96 RMR =041 CFl =lJ
PNFl =72 NNFI =96 RMSEA =039
SS Discussion
Compliance the fin al link in the causal model is a di ffi cult concept operationalise because it refers to a complex reality The treatment of most inf uumlous diseases oceurs in a di rectly observed way (Porter amp Ogden 1997) H0 ever in practice directly observed therapies can be implemented in a variety ways For examplc DOT for sexually transmitted diseases of ten means obsef tion of a single dose of treatment whereas DOT for leprosy entails monthly ob~ valion by a health care worker of doses of ri fampicin and clofazimine Tbe 001 control strategy reeommended by the WHO for tubercul os is is based on a com nation of four types of medici ne which have to be taken together for the fi rst t
months of lrcat ment HeLlith lJre worken ensure that the I ight Ill ed icine is lak n in the right doses and fo r the cornc t length of ti me Supervis ion ean he a CLlllllshy
p ished by having the pati ent visit the cimie hosp italis ing the patient or scnuin a health care workeI to visit the pa tients home or workplace For directl y ohsnvcd therapy fe l TB it i essenti1l that superv isi on continu e~ every day for th liumlrst two months and idea lly for the entire course of the treatment The wide vltlriations in DOT-contro strategies have resulted in a situation where compliance Illci 1l111lshy
compliance have become e la~t ic eoncepls Who is campliant and who is not~ It all depends on the nature and Ihe t ve l of thc sl3ndard We cncoun tered a di vcls il y of defin itiolls with in the framew)lk or the cLJ l1lbat aga inst tube rcu l o~i-
A retrospective study (from J977) on co mpli ance of TB pat ients revealed that the default ra Ie of the out-putient population in rural Pak i~ta n amounted iO 66 Default was defined as fa ilu re to uttend the weck ly tu berc ulosis clinic fo r a period of one month (Sloan amp Sloan 1981) A fo llow-up study ( 198g-90) showed that 72 oc of the TB patients registered in Bethani a Hosp ital did not complete their 12 months trea tment coure Although the in troduction of a short-course (8 months) regimen improved the compliance default rates (56) contin ued to be high (Liefooghe et al 1995) In 1991 however 76 of TB patients reg istered in the Pakistan Institute of Chest Diseases (S indh) had kep t to the short-course reglmen for two months 2 1 had left the hospi ta l against medical advice and 3 had died (Pathan et al 1992) A study carr ied out in the lndian Wardha dislrict revealed that TB patientlt who fai]cd to take their medici ne for more than 15 days were regarded as non-comptiant because this definition is most in keeping with the adopted adshyministrative procedure (Barnhoorn amp Adriaanse 1992) In a study performed in Denver USA non-compl iance with DOT for TB was detined as foll ows (I) missing ~ 2 consecuti ve weeks of DOT (2) prolongation of treatment gt 30 days due 10 sporadic missed doses or (3 ) incarceration for presenting a th rem lO public health (Burman et al 1997) At least 18 of patients who received out-paLient DOT via the Denver Metro TubercLIl os is Clinic met at least one of these cri teria
In concusion therefore there is no golden standard for defining compliance In our study compliance the fi nal outcome which has to be explai ncd in the model is viewed from a dichotomous viewpoint On the one hand there is the category of compliant patients they com plete thei r the ra py in full and as a general rule al$o unshyderwent a sputum tes t confirming Ihem as TB negative On the other hand there is the category of non-com pliant patients they did not com plete their therapy so a sputum test was not carried out We also adopted the com pletion or fai lure to comshyplete the short -co urse direc tl y observed therapy the bas ic criterion used in the exshyam pIes given above as the key cri terion for our defi ni tion of com pliance The structural model (see Fig ure 3) demonstra tes th at it is important to systemat ically di stinguish the reguarity and the du ration of the therapy to gain a bctter undershystanding of the concept compliance Regularity is achieved when there are no or only sporadic interru ptions during the thcrapy In t hi ~ connection we refer to missed appointments or missed doses of medi cation The durarjoll of the therapy on the e ther hand refers to the treatment duration of eigh[ months which has to be
111 JIII 1 1 1III IJ IKLl 11 lH~Ult I IJ 11111lt ) ~
respected in the DOTS-regimen Two dlv iati ons are possiblc here Either Jo wn shyward the patient ends thc treatment premature1y and is regarded as d efaulter Ol upward- the period of treatment is extended because interruptions during the treatment have [0 be compenslIteti for artcrwards Both deviations from the norm indieate non-compliance Any com parison with the above referred to non-complishyance ra[es fa ils because the phenomenon is constantly regarded from di fferent anshygles Hav ing said that the folowing fac ts in our research on (non- )col11pl iancc among the 621 TB patients are worth mentioni ng
Aftel subtracti ng the nUlllbcr (l f pntients who have died (6Oc) thase who have transferred to another treaUllent centre (29r) and thc tiny group of patie nt~ where the treatmen t failed (I ) 563 pat ients remai ned According to our de liumln ition 779 of the latter group are compliant and 23 are non-compliant aresuIt which is c10sely in keepi ng with the situation at lhe lnsti tu te of Ches[ Diseases in the prov shyince of Sindh The number of in terruptions is used to indicate the regularity of the trcatment 48 of patients did not inlerrupt their treatment at all 34 in terrupted it once and 18 interrupted it various times As far as the duration of the lherapy is concerned the norm of eight months is ach ieved by 55 of patie nts [he norm i not achie ved laquo 8 months) by 33 of patients and the nonn is exceeded (gt 8 months) by 12 of patients
Broadly speaking three out of four paticnts is compliant One out of four is nOI1shycompliant interruptions during the treatmen t (because appoin tments or medicashytion is sporatlicall y missed) or failure to complete the ideal duration of treatmenl (because patients drop out too early or have to followan extended course of treatshyment) As far as establishi ng compl iance is concerned it would seem that 77 ck of patients is heading towards the WHO-target fo r global tuberculosis control namely cure 85 of the detected new smear-positive TB cases (Seita 1996 p 134)
When interpreting the results it is also important to disti nguish between ho~ p ishytalised patie nts and out-patients As we al ready stated earlier duri ng lhe rirst month of treatment 80 of patients were hospitalised Af ter the second month this number dropped to only 48 Permanent supervision at the hospital ensures that hospitalised TB patients are by definition compliant the DOTS-regime n is strictly enforced As far as non-compliance of the out-patient population is co ncerned wc noted that 17oc missed at least one appointment during the first month of treatshyment and that this number dropped 10 1I aftel thc end of the second month The first month is therefore critica especially fol patients who are not hospitalisetl Since they do not res ide at the hospi tal and only come for consultations thty enshycounter far greater difficulties internalising the norms underlying the DOTS-regishymen
The model hinges on the latent construct of stigmatisation Stigmatisation afshyfects compl iance through the Ta ndem of regu la ri ty and duration of therapy Persons who have been strongly stigmatised display more irregular illness behaviour and find it more problematic to see the ditficult and troublesome trealment through 10
[he end In th is respect il could be sa id that ending or interrup[ing the DOTS-reg imiddot
men is nol due to a Jack ol organi satioll On the contrary they are Illcchallisl llS which help to relieve thc pain of sli gmatisation ensuring that for a wh ik the TH pal ient does not have 10 he as hamed and can take a brea k when the prc-url of Ihc medical rcgimen beeomcs toa heavy (Massaro 1997) According 10 GollIllans terminology devi ali ng from the slandards of thc DOTS- rcgimen can hl rcgOl rdcJ as a technique fo r conlrolling in fo rmation The questions or whelher 10 revcal or hi de to con1iumlde in someone or keep qui et to lie or be truth ful and to who l1l hnw when and where are tricks for stoppi ng Ihe exhausting process of bleacutellllc hy socishyety They are in su mmary stra tegies to lWlwRc ( IpoiId idllltity (Schcpcr- amp Nievaard 1995 p 42-43) In Ihe mode l th rec social conditions affecl thc dcgrcc of sligmati sation of TB pat ients These co ndi lions have 10 be taken inlo account 10 reduce the lim ils to pat ienl compliancc with DOTS-strategies
The first cond it ion is rclated to the dem ()g mphico Iilloion of the pili cllt anJ comprises two variab les from the exogenous set ie gender and age FCi llalc pashytients were stigmatised more than male pat ients and older patients Wlr~ si igllwshyti sed more than young persons BOlh lin k~ are highl y significant As house wivcs or elderl y members of the ex tended fa mi Iy many have a low socio-econol11 ie Ialu For them health is above all J quest ion of physical strength (W inkvist amp Akhtar 1997) The loss of phys ical strength Ihlough tubercul osis the fact that tl1Oc who have been sl ricken wilh the diseas( can no longer perform hard labour do the housekeepmg no longer be reproducti ve etc are important contributors to stigshymat isation This is all the more so in lhe countryside where ex ternal signs of vu lshynerability often do not suffiumlce to relieve peopl e from their nonnal socill tasks in the fami ly and vill age
The second condition cl ose ly concerns the beiefofT8 patiel1ll in the curabifir of th eir disease We already said earlier that th is laten t construct in our research displayed features of serendi pity It is el istinct from stricl measurements ofrational med ical knowledge because it emphasises praxis ie implementing knowledge and acti ng on insights The higher the soc io-economie slatus the grealer the belief in the curabil ity of TB It is impossi ble to ignore the phenomenon of social stratifishycation when analys ing ill ness behaviollr of TB patients Patients wi th a higher proshyfessional rank have great faith in the curability of their disease The opposite also applics in equal measure unemploy ment and illileracy are cond ucive for nonshycompl iam behaviour Perhap~ the hard core of pariahs outcasts vagrants vagshyabonds tramps chronie drllnkards and drug add icts (Merton 1968 p 207) repshyresenlSthe most dangerous ri sk group for all TB control programmes When Robshyert K Merton in 1949 developcd hi s we ll-known typology of modes of adaptation by indi viduals within the cu ltu re-bearing society he discovered that these populashytion groups displ ayed retreatiII their mode of adapl3tion which implies the reshyjec tion of cul tural goals and institutional means After all why should anyone reshymain healthy And why should we lIse DOTS as Q method Does it make any difshyference) There is a negative correlat ion between belief in the curability of TB and the degree of stigmati sation Persons who are convineed they will soon be cured and capable of strictly following the medical regimen will be less stigmatised
1 ll i bull I III I 1 11 11 10-- 1 1 middot111 middotmiddot middot 1 middot _
The third condit ion is siluateel at the leve l of the social netllo rks in wh ich TB middot patients function As a general rule it can be sa id thaI persons who tcceive mor~ help from olhers are less likely 10 be stigmati sed Roughl y six out of ten pati ent~ are married and fo r married women the family-in-I aws occ upy the cen tral po- it iol in their social nelwork The model established a negati ve relationshi p betwec l support from blood re lati ve~ and support from the family-in-Iaws Solida rilYvvitl the fa mily-in-Ia ws red uces ~olidarity with biooeI relatives This app lies both il general but also in the specifi( framework of help and support in ti mes of illness The fear manied fe male TB patients have of being abancloned by their hll ~banJ and no 10nger being able to perform their domesr ic tasks should not be unMrcst i mated During a study into thc relcltion between poverty and TB in Bombay re male patients said thaI thei r husbands and mothers-in-Iaw repeated Iy sent then back to their nata l home until such lime as Ihey were cured They were often al cused of bringing the disease from their natal homes and were threatened with sep aration (Nui r et al 1997 p 8 1) The model revea led that the TB patiems who re ceived the least support from their family were stigrnatised most Th is recalls th relational natu re of all type of sti gmatisat ion People are given a negative SOCiH label or are shielded from it Your family may support you through thick and thin encourage you to do the right th ing help to fi nance treatment etc Converse l) your fam ily mayabandon you keep your situation quiet to prevent loosing fac anel keep the family reputation unb1emished
lil Pakistani society anel particularl y in l11any village and se ttl el11Cnb in th Punjab social networks and stigmati sation are inextricably li nkeel and have al enormous influence on community li fe Thc biraderi the patriarcha l nelwork 0
kinship fo rms the framework 101 social and coml11uni ty networks Special event and rites of passage such as birth the ci rcumcis ion of a son marriage allli th death of an old person si rengthen lhis solidarity within the biraderi The biradel use many other occasions to promote social and community networks and ill ne - is perhaps one of the most important When a daughter-in- Iaw becomes seriousl iJl or is hospitalised her children are either looked after by the other daughters (1
the house or are temporarily housed with other members of the birade ri If Ihe sol breadwinner of a household cannot work because he is seriously ill his nearest rel atives and olher members of his biraderi provide mora material and fi nancia l o up port These socia1 and communily links rernai n intact even after emigration Paki stanis who have emigrated to Grea t Brita in for exam ple continue to receive muc support from their biraderi (Anwar 1979) Whenever help is sought in Pakistar communities famil y and bi raderi are preferred According to a sociologic al stud carried out in Rochdale a toW D in the north of England hel p is only sOllght frOl farmer fellow viJ1 agers friend s neighbours Olher Pakistanis and the res t of 50CI ety after all possibil ities in the biraderi-network have been exhausted A TB pil tient who is admitted to hospital will initially be visited by me mbers of hi biraderi They wi llusuaJ1y be gi ven a few hundred rupees and the trad itional fru i However as news about the nature of the illness spreads within the bi rade ri cor tacts become less frequent The negative COITeiation between fa mily support an
sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more

I1 ~ I ILicirc II 11 1
need 10 enElu re the discomforlt of the trea tment thereby increasing the grow h or multidrug-resistant TB so Iha trealmenl nea rly always fails and pat ienlS tlmos certain ly suffer a relapse of the d isca~e
Another importanI reason for Ihe non-c0mplianl behavillur of TB paticJlIs is rcshylated to their stigmatisatioll Sligmatisation occu rs whcn person are givCJl I J1cgashyti ve sociallabel that identi ri es people lt1 dev ian t nol hccallsc their behav iolIl vioshylates norms but because they have peronal or ltoc i~tI characteristics thaI 1cld jlcoshyple to exclude them (Johnson 1995 p o R3 ) Much tiJl1 ha~ passed sincc Erving GotTman presented his pionccri ng theore tical framcwork ror the suciologilal ltll1 alshyysis of stigmatisation in 1963 (Gorrlllan 1(90) Allhough Ih is fralll eworJ initia lly resulled in many changes in the lega area it soan became hi ghly relev ant to the sphcres of illness and health Goffman distinguished three gross ly di ffe rent types of stigma (Lemen amp Branaman 1997) Fi rs t there ure abominations of the body the various physical deformi lies Nex t there are blem ishes of individual charucter perceived as weak wiJ l domineeri ng or unnatural passions treacherous and rigid beliefs and dishones ty Finally there are the tri bal stigmas of race nation and reshyligion these being s ti gma~ that can be transmitted through ineage and equally conlaminate all members of a farnily These th ree types of stigma clearly mani fest themsel ves in the medieal sphere
Physical shorteom ings and dcformities increase lhe visibility of the illness and the chances of stigmatisat ion Accordi ng to Stiles and Kaplan the ri sk for amplifi shycation of devinnce is even disproportionately greater on the part of physically stigshymalised deviant ac tors than for those wi thout physical stigmata (S tiles amp Kaplan 1996) The coughing fi ts sweat attacks fe ve r phlegm haemoptysis rhe symbolic symbols of yell ow sputum and blood the emaciated skin and bone body etc which characterisc a TB patient make tu berculosis very visible and threatening to anyone who encounters it or has impressions of it through societys collective memory Moreover devi alions in persona lity structure weakness lack of will shypower feebleness irritabil ity and sa on contribute to stigmatisation In her essay IIlness (IS Metaphor Susan Sontag i lI ustrated thatthis is certainly the case with TB Tuberculosis is described as the disease of born victirn s of sensiti ve passive peoshyple who are not quile life-Iov ing enough to survive (Sontag 1990 p 25) Thomas Mann s charac ter sketch of Hans Castorp revea ls thar TB also affects the general daily habi ts and psychological structure of the patient (Mann 1996) Finally Goffman s typology idenlified the tri bal stigmas which reed on the reprehensible characteristics of an entire group The sanatorium where the group characteristics of TB patients are expressed par excellence veritably exudes a permanent threat of contagion Grygier describes how Ih is danger of contagion marked indelibly the initiation ri luals and li fe in the sun through and through of a group of Inuit Eskishymos from the far North who were placed in a sanatorium more southwards in Canshyada when a TB epidemic broke out (Grygicr 1994)
However although tuberculosis pat ients are st igmati sed by their illness it does not mean there are no other apparent sources of stigmatisation The power of the concept stigmatisation is such that it targets all social spheres where negltive
1 11I l ll) ~ II Ll Ajlc 11 H lllH ll ll (JH~~KcU I HJ KI~
soc ial labe l ~ can be assigned 10 discredit behaviour and turn people into o utcasts Although TB is undoubtedl y the most important stigmatising factor for the palien l stigmati sation immediately breab OUI of the medical sphere and is in fl ue nced by all areas of life from Ihal point on Research furthennore reveals that st igmatisashyti on even continues to complicate the lives of the sti gmati sed even as treatmenl imshyproves their sy mptoms and fu ncticlJl in g (L in k et al 1997) Thc sti gma does not disappear with the di sease It is perpetu ated by other sourees Si milar hypotheses were put to Lhe test in the research carried ()ut by Crofts et al in Austra lia AIshythough Austral ia has a very su-ong framework of anti-disc riminati on leg islation recent years have ~een an incrcasing nU lllber of reports of stigmatisation arrmnrs lo dignilY and discrimi nation as a result of the he patit i ~ C status of individll als The sligmatisation caused by Lhe disease is closely related to a lifes tyle of i njecting drug lIse rs the major group now at risk of infection and the consequences genershyaJly impact domeslic work recreational day care and funeral settings (Crofts et
al 1997)
53 Methodology
531 Sampling procedure
The sludy is based on an oral survey carried out in one genera] hospital a mongst all sputum positive pullllonary TB patients (n=621) who presented themselves at the TB unit ie from September 1996 until October J997 The patients were iOlershyviewed at three fixed moments at the start of the treatment after one month aftel two months and followed-up tiJl the end of the treatment Every inlerv iew was pershyformed by a social worker belonging to a team of four Since the duratie o of the treatment was 8 months the last patients fini shed their treatment by the end of June 1998 During lhe interviews based on questionnaires consisting predominantly 0
closed questions and a small number of open questions information was gathered about the demographical and socio-econom ic profile of the patients socia1 support provided by different networks the patients key val ues their knowledge of TB and lheir perception of the curabilily of the disease stigmatisation and compli shy
ance
The reason for choosing the hospital ie Bethania Hospital in Sialkot (Pakistan requires a little clarification (see Figure l) The hospital is situated in the Punjab province at the east of the Islamabad - LahOl-e axis Si nce its foundation in 1964 as amission hospital Bethania Hospi tal has made an enormoUS effor to detect and treat tuberculosis patients from the region It is currently a 215 bed front-li ne aod referral hospital providing medical and surgical services One hundred beds arc reserved for a speeialised TB unit It has a ward for men and a ward for wemen its own out-patienl department sputum laboratory dispcnsary and registration un it About 75 of patients are recruited from a catch ment area of 50 km around the
~ gt
Arobion Seo
u 1 1 bullbullbull 1 i 1 I I bull bull
Figurc 1 Map of PJ k i ~ lan
centre of the city of Sialkot which is described as the cul-de-sac du Pakistan et carrefour de la mondial isalion (Le Monde 24298)
Si alkot provides a unique framework for the study of TB issues in the context of a developing country (Enarson 1994) ft is a middle to large city (800000 inshyhabitants) populated by Musli ms which is gradually transforming its feu dal authoritarian relations into modern industrialised and agrarian production proshycesses and a secularised society (Za idi 1999b Zaidi 1994a) In addition to having to deal with a considerable number of public health problems it also has to conshytend wi th a serious TB epidemic resulti ng in Sisyphean tasks and feeli ngs of helpshylessness amongst all the parties concerned These ci rcumstances made the study of the tOlal cohort of TB patien ts from Bethan ia Hospital representaLive for patients from Third World countries who have been diagnosed with pulmonary tuberculoshysis (Ferraro amp Farmer 1999) The ~amrle of TB patients used in this sludy en shyabled us to a certain extent to gain a betrer underslanding of a number of elemenshytary mechanisms operating at the level of stigmati satioll compliance and TB conshytrol in an en vironment where the illness has had a devastating effect hOlh at the personal and social leve l
532 Model
The model proposed in this chapter could be desc ribed as a two-s tep modI Firsl an explanation is sought for the ways in which TB patients are stigmatisLd Many different fac tors might influence the degree of stigmalisation of a TB paticnl 111
our model (see Figu re 2) stigrnatisation is explained by fo ur variables First we hypothesise that ol der palients are more casi ly stigmatised than younger 0 nes Secshyond we tested whether or not women are stigmatised faste r than men are Th ird we included a latent construct support from fa mil y The basic hypothe sis in the model is thal an increase of support from apatients famil y will cause a decrease in stigmati sation Lastly lhe fourth model led factor that might cause stigmatisati on is a knowledge related construct It is assumed th at the less one agrees theacutelt TB i- ti
curable disease the more one wi ll be stigmatised
Figu re 2 MoJel of stigmHisalion anel compliance tor TB
llltlief3 Bltltcr2 Bdiel 1
The second step in the model is the causal explanation of compliance What are the factors that influence the illness behav iour the acceptance of the sick ro le and lhe complianee of a TB patient The model distinguishes three factors The first factor concerns compliance to therapeutic standards solely with regard to the use of medshyicine The patient has to be wi lling to be (and remain) cured and furthermore be (and remain) convinced of the usefulnes$ of the prescribed medication or the DOTS-system will not have any chances of success The two other factors are sit ushyated at a higher theoret icallevel because they refer to tbe therapeutic proces~ in general and the many profess ional requirements and obligations combi ned with feedback of repeated tes ts this complex process invol ves One factor refers to the regularity with which patients comply with their obligations in tbc succcssive stages of their treatmen t the other refers to the pOlential to persevere and complete these stages until full recovery These three factors elenrly illustrate th ree different dimensions of compliant behaviour among TB patients When implementing the DOTS-system the relevance of these factors is extremely high because the sysshytem explicitly requires the strict intake of medicine regul ar doctors visi ts and an effort sustained over many months
11 U l LLI ~J CI IL
532 1 Mal ifes lriahles
The moJel to be estimated is a non-~tandard model (Hatcher 1994 p 423) It conshysists of several mani fe t variables that account for a pan of the structural portion of the model In other word we assumc lha hese manifest variables are perfect measures for the constructs they express Before we turn our attention to the real latent constructs in lhe model we finl want 10 give an overview of its manifest variables
There Ire I lLree exoKI I ou Iwnifesl variables S~x and Ige are measured in a straighlforward way Men and women on the one hand and a patient s age exshypressed in years on the ether Occupation is measured on an ordinal seale All ocshycupat ions are placed on a soc ial stralification seale that made il possible to plaee occupations on a higher or lower sot ietal level The lower range of the scale is fo rmed by housewives unskilled and skil led labour Pakistani middle manageshyment is found in the cottage industries farmers renting their land civil servants white-coJlar workers and small business owners Finally the exeeuti ve group conshysists of land-owning farmers and large business owners
53 22 Larent COTlSrrucls
In the model we used fOlr latelll constructs Before di scussing the measurement model more deeply we concentrated on the different items for eaeh endogenous construct The family is an importan t fac tor in the social environment of the TB pashytient Therefore we tried 10 include the lt upport of lhe farnil y within the model Sinee most pat ients were married (62) we had to deal wi th both the famil y and the family-in-Iaws
Support from the family-in-Iaws was nol included extcns ively in the research We could only include a latent factor support fro m family-in-I aws based on two indicator variables We are aware th at (he lalent construct is not firml y I1Itasulnl in this way However the resullS of lhe mea ~u remen t model (see ) are acceptable (seale composite reliability P= 67) The ind icator variables from thl C0l1s1nlcl are measured on a fi ve-poi nl scale (no influence at all - strong in tluence)
The seco nd latent construct is the support a patient receives from his own 1lt1111shy
ily (seale composite reliability p= 52) This construct is based on three indicalor variables two of which ussess on a five-point seale the direc t support and inllushyence from the fam ily (strongly di scourage - strongly encourage) Besidcs l110ra l support from the family we also included financi al suppo rt Patients wen as kctl whether hey rece ived any financial support The following examples orliumlnanc ia l support were given support for transport drugs consultation fees or les l~ Thc question naire did not ask in deta il about th e ki nd of support patients received Onl y a dichotomous answer (no support anel suppo rt) was sutficiem
Stigmat isation was based on three indicator var iables (scale composilc reli abil shyity p= 64) Again the famil y plays an important role in th is construct The qllesshyti onnaire asked patients to place thell1$elves on a six-point scale (don t agrce al all
1 middot ~IIL I J I I I~ I ~ l l I I II I ~ L I~ I ~I bull bullbullbull bullbull bull bull bull
_ strongly agree) asking them to what extent they fe It that having TB is a disgrace for the fa mily Ir a person agreed strongl y with this phrase it is assumed that he feels st igmatised by his fa mil y The same goes for stigm atisation by friends Again a six point scalc was used (dont agree at all - strongly agree ) to a-sess whelher or not the patients feit stigmatised by lheir fri ends The responde nls could indi cate whether lhey agreed with the idea of very good friends leav ing lhem beshycause of their elisease The more they agreed the more stigmatised they are sup shy
posed to beo The last latent construct in the model is the patient s belief in the curabili ly of
the disease and in knowing how to handle its complexity (scale composite reliabilshyity p= 68) It is an attitudinal factor cons isting of three indicator variables in which patients were asked to gi ve their opinion on TB itself All indicators were measured on a Ii ve-point scale (strongly disagree - strongl y agree) The indicator statements dealt with the opinion on the curability of TB (TB is easy to cure) the commonness of TB (TB is a common diseasc) and wi th the difticulty of TB a~ a disease itself (TB is a difficult disease and hard to cure)
Table 3 latlnt conSlruct mcasure menl summar) (onfirmtory fac tor analy ~i s an d scalc reli shy
ability
Item t Item Description Summary Standa rdshy
ised loading
t-vulue
Support famil y-in-Iaws (p= 67)
Famlawl How much will the opi nion of y lJUr familyshy 74 102
in - Iaw~ influence yo ur dcc is ion to liumlnish or not the wholc treatment (Fi rst time)
Faml aw2 Ho much will lht Qpi nion of your fa mil yshy 69 996
in-Ia ws influ ence your decision to finish or not lhe whole tremment (Sltco nd time)
Su pport fa mily P = 52)
Fam l To what extent does your (o wnl family en shy 59 1004
cou rage or discourage you in taking daily you r medicine (Fi rl time)
Fal112 To what cX lent does yOll r (own) f~l11i1 y enshy +9 8 53
courage or discou rage yOll in taki ng daily your medi cine (Second time)
Fam3 Does you r fam ily sup port yOll liumlnancia ll y for A5 7 98
th e cost of your trealment (tran~port 1drug~ I con~u lta lion fee I tests I )
Stigmatbation (p= 64)
Stigmal It is a disgrace fOf the fumily to have a f3mshyily membcr with TB (Fi rst time)
Stigmu 2 It is a disgracegrave for the family to ha ve J fa mshyily member with TB (S econd time
Stigma ven your bes t fli cnd olllctirncs desen you when you have all infectious di seasc like TB
Belief in curabiJity of TB (p= 68)
Belief TB is easy 10 cun 80 1501 Belie fZ TB is I com mon disease 55 1099 Belief] TB is a di ffi Cll lt dicase 3nd hard to cure 57 I I 2l
Note Fit sla tist ics for mcasurelllent model of 1 1 indicators for four construCIs 2
X IK7 =14993p = 00 GFl=97 RMR = 037 CR = 96 PNFI =52 NNFI = 9J RMS I = OW
I Scale composite relinbilily p = [(I Agravef ) ~ IImiddot(eacute)][(I Agrave I ) ~ vlr( ) + I S] (lOl-o l i amp Vi 1988 p 80)
The measurement model shown in provides a reaso na bl e fit 10 the dat1 Thc ehi shysquare test of exact fit is significant where the objecti ve is to achieve a non-signifshyicant p-value However Hatcher indicates that a significant ch i-square does not ma ke the measurement mode l inadequate (Hatchcr 1994 p 289) The ehi-square ratio shows th at the ratio of the chi-square value and the degree of freedolll is lowcr than two (17) This ind icates that the chi-sguare tes t is wilhin acceptahk lilllits (Marsh et al 1988) Other favourable diagnostics incIude a goodness-or-fiumlt illdegrave X GFI) of 97 a root mean square res idual (RMR) of on a comparati vL rit illtkx CFT) of 96 a parsi mony normed fit index (PNFI) of 52 a nOn normed rit index NNFI) of 93 and a root mean square error of approxi malion (RMSEA ) of rn9
In tenns of valid ity of the constructs con vergent validity is evidcnlxd by tilegrave large and significan t loadings of the item on thei r positcd ind icators FUIhc r (v ishydence of convergent va lidity is shown in None of the correlalions betwLcll Ihl 1 shytent construClS are too high to challen ge the convergent validity oft he cons lructs
F3 F4
100
- 06 100
The discriminan t validi ly is also indicated because the conlide nce interval (plusmn two slandard errors) around the correlati on es ti mate between any two latent construclS never includes 10 (Anderson amp Gerbing 1988 p 41 6) The Varianee Extracted Test also shows the discrim inant validity of our constructs The variance extrac ted tes t compares the variance extracted from two laten t constructs with the square of the correb tion between these two constructs (FomelI amp Larcker 1981 ) Discriminant validi ty is shown when the ex plained variance is greater than the squared correlation We compared all pairs of fac tors and they all showed an iCshy
ccptable variance ex tracted
)4 Results
) 41 Description of the sample
The 62 1 pati ents were composed of 55 0( men and 45 women Seven patients out of ten were younger than 40 concuning with the global observalion that in the countries of the Eastern MeditetTanean Region around 80 of the notified smearshypositi ve TB cases in 1994 occ urred among the economically productive sector of society (15 -54 years old) (Seila 1996 p 134) Tt indicates the serious impact of tushyberculosis on the comrnun ity The skills base of the patiems was very low more than half did not receive any form of fonnal education and the problem of illi teracy aillong older female patients was particularly acute
During the fi rst 11l0nth of lreatment 80 of patien ls were hospitalised during the second month th is number dropped to onl y 48 One out of tluee regarded hospitalisation as problematic This groups di ssalisfaction was rooted both in eco~ nomic and medical causes they had to contend with financial problems absemee shyism transport costs found themseJves in dire sLrai ts doc tors were in competent the rut of he ward etc
One third of patien ls were the family breadwinner As a resuit they were very reluctant to accept the sick mIe Remarkably only one fifth of patients came from a household with more than three economically act ive persons considering lh at
roughly 70 of household eon)i steJ of si x und of ten more Illcm bers The smal nurn ber of econornicall y active person- within the ex tcnded farnilie - C311110t be atshytributed to a large nu mber of ehi ldren because rOlgh ly hal f of the pat ients had less than three children
Sixty percelt ofpalielts placed heulrh al the top oft hc standard orvuluc This is not rea ll y surprising given the fact thal the responclents were confroltcd with ~cr ishyous health prob lems which have absolu te priorit) in their dail y li ve ~ lIld prCSllll1C the recove ry of bath hea lth balallCe anu the improvement of health pOlc nlia Ic shycording to Khayat these IWO dimensions of health are tleeply motet il1 Islalnie Irashydi tion and thefiqlI of health (Khayat 1997) Tf we ZOOIll in on the largL gro llp placshying heal th at the top of the standecircll-d of valuc wc sec Ihal the followi ng vllICS arc also held in high regard falllily and marriage (thc most important aftcr hla llh ) honour and integrity religion and fait h work money (thc Icast importanI ) AIshythough female patiems and patients wilh the lowest socio-economie status atshytached most importance to health it toes not mean that t he~e groups J i-played Ihe mOSl adequate illness behav iour On the contrary the~e groups ltI nd in particlilar housewives the un skilled unernp loyed and sociall y de pri ved ofte n do Ilol J1o~ scss the most elementary knowledge abou t TB (causes sylllptoms alld eollilitlll) which is needed to pre vent infec tion or undergo routine trcatment (Grce n Il)l)) p 192-196) The concept of (external) locus of control ofte n used in rlsealh on compliant behav iour and the fa tal islic health attitude lin ked to th i alslJ applied in thi s context of TB co ntro l (Mcchanic 1983)
Throughout the analys is the operational isation ol belief in the curlli Iil Yui the disease of ten appea red as a variab Ic wi th ~e relldipit y -charactcri ~tics This vlIiahle rneasures the confi dence ~i d people have in suumll vi ng their prob lem situ alilln Trust enables Ihe complexi ry of a social system to be reduced without funher aULgt the sick can rely on thei r part ner fal11il y health worker etc to channel the ir mcdical regimen It is cJear that preci sely lhis confidence is shattered by the TB it igma thereby reducing belief in the curability orTB in genera
Correctly assessing the treatment s duration is characteri stic for patients who strongly believe in the curability of their di sease However th is element of inforshymation is certainly not common knowledge when the treatment starts_Only one in three patients is aware that the trear ment will last several months However after one mon th this number doubles and af ter two months it increases even furthcr (73 ) We established that paliems with the lowest socio-economie statu s often did not possess the Illost rudimentary objecti ve medica l knowledge_There is Iitershyally a wall between them and the cogn itive elements req ui red This wa ll cannot be tom down on y due to reasons related to soc ial strmificaLion On the other hand persons who do nol mind regular check-ups a reg imen of aw kward medication and the costs involved who (hin k it is all worthwhile and are confiden t thei r treatshyment will result in a cure are not necessarily more ski lied or have a higher professhysional rank Ir would seem that another phenomenon another mechanism is ac ti ve as far as belief in Lbe curability of TB is concerned Thinking exclusively in tems of social stratification or Iumping techniq ues of rejec tion together as ways of
bull I I I bull I ~ II ~I I ~ bull I bullbull I L bullbull I bull bull bull bull bull bull
dealing with marginal categories (Douglas 1994 p 85) does not suffice lU gain l bettel understanding of the ideal treatment condition s
Compliance has lO be viewed not only from the socio slralificatiol1 perspeclii but also from the sl ig lllarismioJl persp(crive At thc onset ofthe treatlTlent and aftel two month s treatment sevell statemenlS concern ing stigmatisation were prelgtentecl to the patients A score had to be given on a six-poi nt scale (I =dont agree at all 5=agree 6=strongly ag ree)
The two stateme nts most people i e more than 80 agreed with (score 5 or 6) both at the onset of the trearment and [WO monlhs afterwards were Jf someont has TB hejshe avoids ralking about it with ot her persons and Af ter recoverinf from TB everyone treats yO Ll the same way lS bcfore If someone contracts TB il is bes t to keep quict about it If thei r environment doesn t know anythi ng about il th~y will not treat them di fferentl y af ter they hJ ve recovered
Thc other statement many ie more than 60 agreed with both at thc begin ning of the treatment and af ter two mO IHhs was Peope who arc treated for TB should ta lk to others about it
There were three statements alrnost half of pati ent- ie more than 401r agree with both at the onset of the treatment aOl af ter two months It is a disgrace for thl famil y to have a fa mily member with TB Even your best fri ends someti me ~
desert you when you have un infectious disease li ke T B and 11 a young persol catches TB heshe will experience the consequences for the rest of hisher lirc
Thc statement only a minority ie one out of four patients agreed with both a the onset of the treatment and af ter two months was It is diffi cult to earn your Ii ing after recovering from TB The fact that only very few regarded the TB prob lem in tenns of income is re lnted to the fact that during tbis life-threatening situa ti on_ the trentment has absol ute priori ty and takes precedence over all other form of need
When the onset of the treatment is compared Nith the situation two month later there are no shifts in the statemenls ranking order This means that the firs two months of treatmen t - eg at the hospitalor contact with health carers - dOt not real ly affect their situation On the contrary the stigmatisation continues t( proliferate and feste r causi ng damage in its wake According to Goffmans termi nology it conti nues to transform TB sufferers from discreditabe tO discredilel (Goffma n 1990 p 57 ) Only two statements poi nt to a possible evolution durin~ the first two months but they do not really di sruptthe ran ki ng order in any signifi cant way Ir rerers to the statement PeopJe who are treated for TB should talk t( others about it 68 tgreed at the omet of the treatment and 78 af ter tWt months treatmenl This increase indicates that TB patients still regard opennes about their illness und breaking taboos about the subject as a norm and future ex pectati on Whilst 54 agreed at the beginning of the treatment with the state lllcn Even your best fri ends sometimes dcsert you when you have an infect ious dis ease like TB this dropped to 45 af ter lwo months treatment Ir would appea that the channels for seeking informal care do not dry up for those who respect th medical regimen
We will illustrate thatthe social Il etwork lovering the pa tien t- nlatiolls with all significant others can cithcr increasc or reduce st ig lll ati satioll iS lllilh 1 ()IJt) p 138-155) The com position of these soci al networks i- very hcterogcilcous Thcy can perhaps bes t be analy-ed by di sti nguishing the nuelear fam ily from Ihe ex shytended fa mily As far as the nuclear fam ily is cOllce rned 62 of pllicnls wcn~ married 31 were si ngle 5fr widowed anel 2 divorced For married felll aie pashytients ( 173 out of a tota l of 387 married pa tients) rclati oll) with the fa mi Iy- ill-Iaws and in particular the mother-in-Iaw were very importan t indeecl For alll10sl half of all patients (47) thc extc ll(kJ fam il y eOll1 pri -ed cighl or more perso ll- IIs li all y adu lt who all li ve under the ) (l IllC roo f In 20 of households there wen ilO ehi 1shydren (yolJnger than 12 yca r~) 327 ot households had one or two childrclI 2C1r had three or four children and 21 or had fi ve or more
542 Causal model
The proposed structural model in Figurc 2 was tested by using con veuml ntionalmaxi shymu m likel ihood est imatioll techniques Thc model~h(lwed an acecptabk fit Again the ehi -square tes t of exact fit is ~i gni tiuml ca nt but the eh i-square ratio is lower than two (07) Other favourable diagnosti c~ include a goodncss-of-tiumlt index (GFl) of 96 a rOol mean square rcs idual (R MR) of 041 a comparati ve fi l index (CF) of 97 a parsimony normed fit index iPNFI) of 72 a non normed fit index (NNFI) of 96 and a root mean squ are enOf of approximation (RMSEA) of 039 All of the path coefficients are signifi cant
Anderson and Gerbing recommend a chi-square di ffe rence tes t (CDT) in order to enhanee the confidence in the structural part of the model (Anderson amp Gerbing 1988) The CDT compares the structura l model (which is a res trictecl theoretical model MT) with an uneons trailled alternative model (Mul The relevant test statis shytics (MT has 122 df and a X2 of 17526 ML has 93 df anel a X2 of 171 89) lead to a non-significa nt CDT (X2 difference is 25 33 at 35 df) and an acceptance of M
r Thu s our restricted theoretica model (Figure 3) is preferred to the theoretica uncorrelated model
Since most of the [esH tat is ti c~ show an acceptable model we can look at the reshysu lts of the two-step model presentcd earlier Firsl we tried to model the influshyences on the degree of stigmatisation of a patient These influenees come from very different sou rces The mos important factors determi ning stigmatisation are sex and age Women are more easily stigmatised than men are This also holds for older people From the latent factors support from the family is the most im porshytant Thc more one receives SUppOrL from ones fam ily the less one is stigmalised Anothcr influence on stigmatisation comes from belief in the curability of the TB onstruct The more one believes that TB is curable the less one is stigmatised
These results sugges t that a robust position within society prevents a person from being stigmatised
We then tried to link the stigmatisation of the TB patients and the ir complianl wilh lhe directly observed therapy The restricted theoretical model reveal s that ti influence of stigmatisation on compliance only becomes clearly visible af ter intro ducing the regularity and the duration of the therapy as intervening variables closer examination compliance would appear to be a rather hybridconcept whi can take various forms and has many depths Compliance comes clearer to the [ (I when regularity and du ration are separated In the model stigmatisation with effect of -016 affects regul arity Subsequently regularity has a direct effect of on eomplianee but lhere is a stronger effect on duration and from there on comp anee The regularity and the duration of the therapy tberefore form a tandem whi ca n be brought out of balance by stigmati sation anclilo longer prov ides any gu antees for compliant behaviour
Figu re 3 Siructuralmodel of complio ncc anJ TB
SignificCllce (p-PO ll t) =0 05 =00 =000
Note Fit statistics for structural model X2n~~) =175 26 P=00 GFl =96 RMR =041 CFl =lJ
PNFl =72 NNFI =96 RMSEA =039
SS Discussion
Compliance the fin al link in the causal model is a di ffi cult concept operationalise because it refers to a complex reality The treatment of most inf uumlous diseases oceurs in a di rectly observed way (Porter amp Ogden 1997) H0 ever in practice directly observed therapies can be implemented in a variety ways For examplc DOT for sexually transmitted diseases of ten means obsef tion of a single dose of treatment whereas DOT for leprosy entails monthly ob~ valion by a health care worker of doses of ri fampicin and clofazimine Tbe 001 control strategy reeommended by the WHO for tubercul os is is based on a com nation of four types of medici ne which have to be taken together for the fi rst t
months of lrcat ment HeLlith lJre worken ensure that the I ight Ill ed icine is lak n in the right doses and fo r the cornc t length of ti me Supervis ion ean he a CLlllllshy
p ished by having the pati ent visit the cimie hosp italis ing the patient or scnuin a health care workeI to visit the pa tients home or workplace For directl y ohsnvcd therapy fe l TB it i essenti1l that superv isi on continu e~ every day for th liumlrst two months and idea lly for the entire course of the treatment The wide vltlriations in DOT-contro strategies have resulted in a situation where compliance Illci 1l111lshy
compliance have become e la~t ic eoncepls Who is campliant and who is not~ It all depends on the nature and Ihe t ve l of thc sl3ndard We cncoun tered a di vcls il y of defin itiolls with in the framew)lk or the cLJ l1lbat aga inst tube rcu l o~i-
A retrospective study (from J977) on co mpli ance of TB pat ients revealed that the default ra Ie of the out-putient population in rural Pak i~ta n amounted iO 66 Default was defined as fa ilu re to uttend the weck ly tu berc ulosis clinic fo r a period of one month (Sloan amp Sloan 1981) A fo llow-up study ( 198g-90) showed that 72 oc of the TB patients registered in Bethani a Hosp ital did not complete their 12 months trea tment coure Although the in troduction of a short-course (8 months) regimen improved the compliance default rates (56) contin ued to be high (Liefooghe et al 1995) In 1991 however 76 of TB patients reg istered in the Pakistan Institute of Chest Diseases (S indh) had kep t to the short-course reglmen for two months 2 1 had left the hospi ta l against medical advice and 3 had died (Pathan et al 1992) A study carr ied out in the lndian Wardha dislrict revealed that TB patientlt who fai]cd to take their medici ne for more than 15 days were regarded as non-comptiant because this definition is most in keeping with the adopted adshyministrative procedure (Barnhoorn amp Adriaanse 1992) In a study performed in Denver USA non-compl iance with DOT for TB was detined as foll ows (I) missing ~ 2 consecuti ve weeks of DOT (2) prolongation of treatment gt 30 days due 10 sporadic missed doses or (3 ) incarceration for presenting a th rem lO public health (Burman et al 1997) At least 18 of patients who received out-paLient DOT via the Denver Metro TubercLIl os is Clinic met at least one of these cri teria
In concusion therefore there is no golden standard for defining compliance In our study compliance the fi nal outcome which has to be explai ncd in the model is viewed from a dichotomous viewpoint On the one hand there is the category of compliant patients they com plete thei r the ra py in full and as a general rule al$o unshyderwent a sputum tes t confirming Ihem as TB negative On the other hand there is the category of non-com pliant patients they did not com plete their therapy so a sputum test was not carried out We also adopted the com pletion or fai lure to comshyplete the short -co urse direc tl y observed therapy the bas ic criterion used in the exshyam pIes given above as the key cri terion for our defi ni tion of com pliance The structural model (see Fig ure 3) demonstra tes th at it is important to systemat ically di stinguish the reguarity and the du ration of the therapy to gain a bctter undershystanding of the concept compliance Regularity is achieved when there are no or only sporadic interru ptions during the thcrapy In t hi ~ connection we refer to missed appointments or missed doses of medi cation The durarjoll of the therapy on the e ther hand refers to the treatment duration of eigh[ months which has to be
111 JIII 1 1 1III IJ IKLl 11 lH~Ult I IJ 11111lt ) ~
respected in the DOTS-regimen Two dlv iati ons are possiblc here Either Jo wn shyward the patient ends thc treatment premature1y and is regarded as d efaulter Ol upward- the period of treatment is extended because interruptions during the treatment have [0 be compenslIteti for artcrwards Both deviations from the norm indieate non-compliance Any com parison with the above referred to non-complishyance ra[es fa ils because the phenomenon is constantly regarded from di fferent anshygles Hav ing said that the folowing fac ts in our research on (non- )col11pl iancc among the 621 TB patients are worth mentioni ng
Aftel subtracti ng the nUlllbcr (l f pntients who have died (6Oc) thase who have transferred to another treaUllent centre (29r) and thc tiny group of patie nt~ where the treatmen t failed (I ) 563 pat ients remai ned According to our de liumln ition 779 of the latter group are compliant and 23 are non-compliant aresuIt which is c10sely in keepi ng with the situation at lhe lnsti tu te of Ches[ Diseases in the prov shyince of Sindh The number of in terruptions is used to indicate the regularity of the trcatment 48 of patients did not inlerrupt their treatment at all 34 in terrupted it once and 18 interrupted it various times As far as the duration of the lherapy is concerned the norm of eight months is ach ieved by 55 of patie nts [he norm i not achie ved laquo 8 months) by 33 of patients and the nonn is exceeded (gt 8 months) by 12 of patients
Broadly speaking three out of four paticnts is compliant One out of four is nOI1shycompliant interruptions during the treatmen t (because appoin tments or medicashytion is sporatlicall y missed) or failure to complete the ideal duration of treatmenl (because patients drop out too early or have to followan extended course of treatshyment) As far as establishi ng compl iance is concerned it would seem that 77 ck of patients is heading towards the WHO-target fo r global tuberculosis control namely cure 85 of the detected new smear-positive TB cases (Seita 1996 p 134)
When interpreting the results it is also important to disti nguish between ho~ p ishytalised patie nts and out-patients As we al ready stated earlier duri ng lhe rirst month of treatment 80 of patients were hospitalised Af ter the second month this number dropped to only 48 Permanent supervision at the hospital ensures that hospitalised TB patients are by definition compliant the DOTS-regime n is strictly enforced As far as non-compliance of the out-patient population is co ncerned wc noted that 17oc missed at least one appointment during the first month of treatshyment and that this number dropped 10 1I aftel thc end of the second month The first month is therefore critica especially fol patients who are not hospitalisetl Since they do not res ide at the hospi tal and only come for consultations thty enshycounter far greater difficulties internalising the norms underlying the DOTS-regishymen
The model hinges on the latent construct of stigmatisation Stigmatisation afshyfects compl iance through the Ta ndem of regu la ri ty and duration of therapy Persons who have been strongly stigmatised display more irregular illness behaviour and find it more problematic to see the ditficult and troublesome trealment through 10
[he end In th is respect il could be sa id that ending or interrup[ing the DOTS-reg imiddot
men is nol due to a Jack ol organi satioll On the contrary they are Illcchallisl llS which help to relieve thc pain of sli gmatisation ensuring that for a wh ik the TH pal ient does not have 10 he as hamed and can take a brea k when the prc-url of Ihc medical rcgimen beeomcs toa heavy (Massaro 1997) According 10 GollIllans terminology devi ali ng from the slandards of thc DOTS- rcgimen can hl rcgOl rdcJ as a technique fo r conlrolling in fo rmation The questions or whelher 10 revcal or hi de to con1iumlde in someone or keep qui et to lie or be truth ful and to who l1l hnw when and where are tricks for stoppi ng Ihe exhausting process of bleacutellllc hy socishyety They are in su mmary stra tegies to lWlwRc ( IpoiId idllltity (Schcpcr- amp Nievaard 1995 p 42-43) In Ihe mode l th rec social conditions affecl thc dcgrcc of sligmati sation of TB pat ients These co ndi lions have 10 be taken inlo account 10 reduce the lim ils to pat ienl compliancc with DOTS-strategies
The first cond it ion is rclated to the dem ()g mphico Iilloion of the pili cllt anJ comprises two variab les from the exogenous set ie gender and age FCi llalc pashytients were stigmatised more than male pat ients and older patients Wlr~ si igllwshyti sed more than young persons BOlh lin k~ are highl y significant As house wivcs or elderl y members of the ex tended fa mi Iy many have a low socio-econol11 ie Ialu For them health is above all J quest ion of physical strength (W inkvist amp Akhtar 1997) The loss of phys ical strength Ihlough tubercul osis the fact that tl1Oc who have been sl ricken wilh the diseas( can no longer perform hard labour do the housekeepmg no longer be reproducti ve etc are important contributors to stigshymat isation This is all the more so in lhe countryside where ex ternal signs of vu lshynerability often do not suffiumlce to relieve peopl e from their nonnal socill tasks in the fami ly and vill age
The second condition cl ose ly concerns the beiefofT8 patiel1ll in the curabifir of th eir disease We already said earlier that th is laten t construct in our research displayed features of serendi pity It is el istinct from stricl measurements ofrational med ical knowledge because it emphasises praxis ie implementing knowledge and acti ng on insights The higher the soc io-economie slatus the grealer the belief in the curabil ity of TB It is impossi ble to ignore the phenomenon of social stratifishycation when analys ing ill ness behaviollr of TB patients Patients wi th a higher proshyfessional rank have great faith in the curability of their disease The opposite also applics in equal measure unemploy ment and illileracy are cond ucive for nonshycompl iam behaviour Perhap~ the hard core of pariahs outcasts vagrants vagshyabonds tramps chronie drllnkards and drug add icts (Merton 1968 p 207) repshyresenlSthe most dangerous ri sk group for all TB control programmes When Robshyert K Merton in 1949 developcd hi s we ll-known typology of modes of adaptation by indi viduals within the cu ltu re-bearing society he discovered that these populashytion groups displ ayed retreatiII their mode of adapl3tion which implies the reshyjec tion of cul tural goals and institutional means After all why should anyone reshymain healthy And why should we lIse DOTS as Q method Does it make any difshyference) There is a negative correlat ion between belief in the curability of TB and the degree of stigmati sation Persons who are convineed they will soon be cured and capable of strictly following the medical regimen will be less stigmatised
1 ll i bull I III I 1 11 11 10-- 1 1 middot111 middotmiddot middot 1 middot _
The third condit ion is siluateel at the leve l of the social netllo rks in wh ich TB middot patients function As a general rule it can be sa id thaI persons who tcceive mor~ help from olhers are less likely 10 be stigmati sed Roughl y six out of ten pati ent~ are married and fo r married women the family-in-I aws occ upy the cen tral po- it iol in their social nelwork The model established a negati ve relationshi p betwec l support from blood re lati ve~ and support from the family-in-Iaws Solida rilYvvitl the fa mily-in-Ia ws red uces ~olidarity with biooeI relatives This app lies both il general but also in the specifi( framework of help and support in ti mes of illness The fear manied fe male TB patients have of being abancloned by their hll ~banJ and no 10nger being able to perform their domesr ic tasks should not be unMrcst i mated During a study into thc relcltion between poverty and TB in Bombay re male patients said thaI thei r husbands and mothers-in-Iaw repeated Iy sent then back to their nata l home until such lime as Ihey were cured They were often al cused of bringing the disease from their natal homes and were threatened with sep aration (Nui r et al 1997 p 8 1) The model revea led that the TB patiems who re ceived the least support from their family were stigrnatised most Th is recalls th relational natu re of all type of sti gmatisat ion People are given a negative SOCiH label or are shielded from it Your family may support you through thick and thin encourage you to do the right th ing help to fi nance treatment etc Converse l) your fam ily mayabandon you keep your situation quiet to prevent loosing fac anel keep the family reputation unb1emished
lil Pakistani society anel particularl y in l11any village and se ttl el11Cnb in th Punjab social networks and stigmati sation are inextricably li nkeel and have al enormous influence on community li fe Thc biraderi the patriarcha l nelwork 0
kinship fo rms the framework 101 social and coml11uni ty networks Special event and rites of passage such as birth the ci rcumcis ion of a son marriage allli th death of an old person si rengthen lhis solidarity within the biraderi The biradel use many other occasions to promote social and community networks and ill ne - is perhaps one of the most important When a daughter-in- Iaw becomes seriousl iJl or is hospitalised her children are either looked after by the other daughters (1
the house or are temporarily housed with other members of the birade ri If Ihe sol breadwinner of a household cannot work because he is seriously ill his nearest rel atives and olher members of his biraderi provide mora material and fi nancia l o up port These socia1 and communily links rernai n intact even after emigration Paki stanis who have emigrated to Grea t Brita in for exam ple continue to receive muc support from their biraderi (Anwar 1979) Whenever help is sought in Pakistar communities famil y and bi raderi are preferred According to a sociologic al stud carried out in Rochdale a toW D in the north of England hel p is only sOllght frOl farmer fellow viJ1 agers friend s neighbours Olher Pakistanis and the res t of 50CI ety after all possibil ities in the biraderi-network have been exhausted A TB pil tient who is admitted to hospital will initially be visited by me mbers of hi biraderi They wi llusuaJ1y be gi ven a few hundred rupees and the trad itional fru i However as news about the nature of the illness spreads within the bi rade ri cor tacts become less frequent The negative COITeiation between fa mily support an
sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more
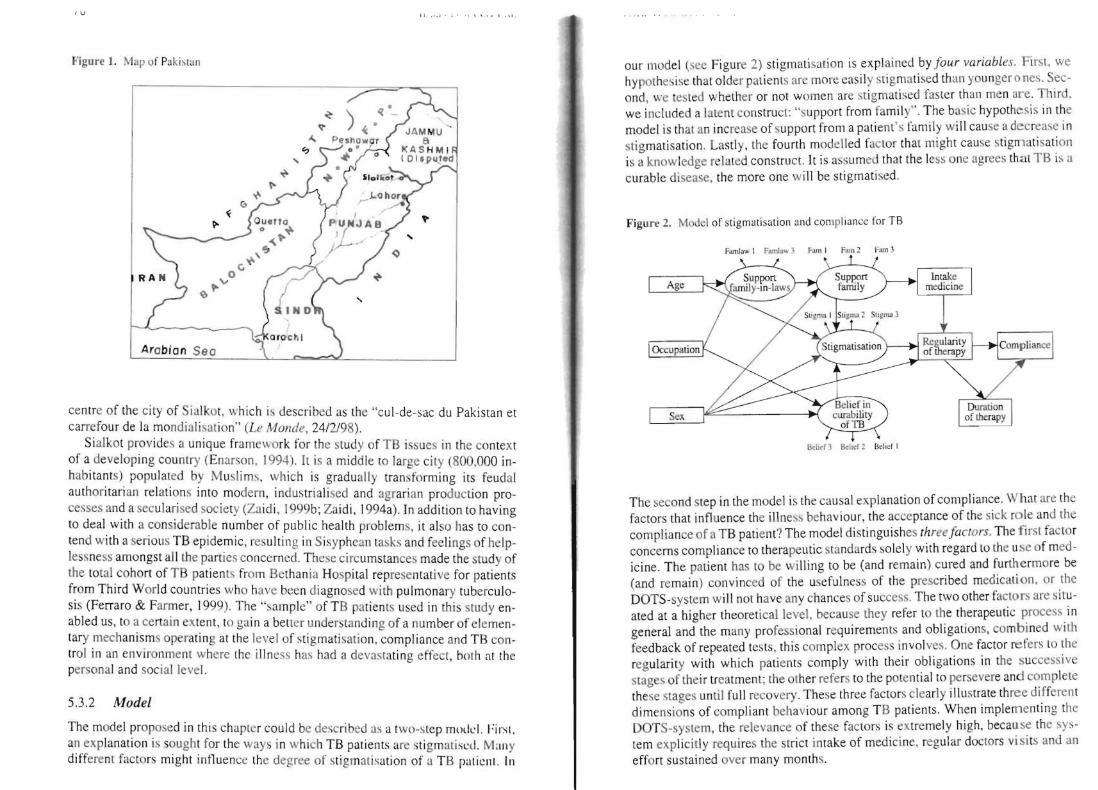
~ gt
Arobion Seo
u 1 1 bullbullbull 1 i 1 I I bull bull
Figurc 1 Map of PJ k i ~ lan
centre of the city of Sialkot which is described as the cul-de-sac du Pakistan et carrefour de la mondial isalion (Le Monde 24298)
Si alkot provides a unique framework for the study of TB issues in the context of a developing country (Enarson 1994) ft is a middle to large city (800000 inshyhabitants) populated by Musli ms which is gradually transforming its feu dal authoritarian relations into modern industrialised and agrarian production proshycesses and a secularised society (Za idi 1999b Zaidi 1994a) In addition to having to deal with a considerable number of public health problems it also has to conshytend wi th a serious TB epidemic resulti ng in Sisyphean tasks and feeli ngs of helpshylessness amongst all the parties concerned These ci rcumstances made the study of the tOlal cohort of TB patien ts from Bethan ia Hospital representaLive for patients from Third World countries who have been diagnosed with pulmonary tuberculoshysis (Ferraro amp Farmer 1999) The ~amrle of TB patients used in this sludy en shyabled us to a certain extent to gain a betrer underslanding of a number of elemenshytary mechanisms operating at the level of stigmati satioll compliance and TB conshytrol in an en vironment where the illness has had a devastating effect hOlh at the personal and social leve l
532 Model
The model proposed in this chapter could be desc ribed as a two-s tep modI Firsl an explanation is sought for the ways in which TB patients are stigmatisLd Many different fac tors might influence the degree of stigmalisation of a TB paticnl 111
our model (see Figu re 2) stigrnatisation is explained by fo ur variables First we hypothesise that ol der palients are more casi ly stigmatised than younger 0 nes Secshyond we tested whether or not women are stigmatised faste r than men are Th ird we included a latent construct support from fa mil y The basic hypothe sis in the model is thal an increase of support from apatients famil y will cause a decrease in stigmati sation Lastly lhe fourth model led factor that might cause stigmatisati on is a knowledge related construct It is assumed th at the less one agrees theacutelt TB i- ti
curable disease the more one wi ll be stigmatised
Figu re 2 MoJel of stigmHisalion anel compliance tor TB
llltlief3 Bltltcr2 Bdiel 1
The second step in the model is the causal explanation of compliance What are the factors that influence the illness behav iour the acceptance of the sick ro le and lhe complianee of a TB patient The model distinguishes three factors The first factor concerns compliance to therapeutic standards solely with regard to the use of medshyicine The patient has to be wi lling to be (and remain) cured and furthermore be (and remain) convinced of the usefulnes$ of the prescribed medication or the DOTS-system will not have any chances of success The two other factors are sit ushyated at a higher theoret icallevel because they refer to tbe therapeutic proces~ in general and the many profess ional requirements and obligations combi ned with feedback of repeated tes ts this complex process invol ves One factor refers to the regularity with which patients comply with their obligations in tbc succcssive stages of their treatmen t the other refers to the pOlential to persevere and complete these stages until full recovery These three factors elenrly illustrate th ree different dimensions of compliant behaviour among TB patients When implementing the DOTS-system the relevance of these factors is extremely high because the sysshytem explicitly requires the strict intake of medicine regul ar doctors visi ts and an effort sustained over many months
11 U l LLI ~J CI IL
532 1 Mal ifes lriahles
The moJel to be estimated is a non-~tandard model (Hatcher 1994 p 423) It conshysists of several mani fe t variables that account for a pan of the structural portion of the model In other word we assumc lha hese manifest variables are perfect measures for the constructs they express Before we turn our attention to the real latent constructs in lhe model we finl want 10 give an overview of its manifest variables
There Ire I lLree exoKI I ou Iwnifesl variables S~x and Ige are measured in a straighlforward way Men and women on the one hand and a patient s age exshypressed in years on the ether Occupation is measured on an ordinal seale All ocshycupat ions are placed on a soc ial stralification seale that made il possible to plaee occupations on a higher or lower sot ietal level The lower range of the scale is fo rmed by housewives unskilled and skil led labour Pakistani middle manageshyment is found in the cottage industries farmers renting their land civil servants white-coJlar workers and small business owners Finally the exeeuti ve group conshysists of land-owning farmers and large business owners
53 22 Larent COTlSrrucls
In the model we used fOlr latelll constructs Before di scussing the measurement model more deeply we concentrated on the different items for eaeh endogenous construct The family is an importan t fac tor in the social environment of the TB pashytient Therefore we tried 10 include the lt upport of lhe farnil y within the model Sinee most pat ients were married (62) we had to deal wi th both the famil y and the family-in-Iaws
Support from the family-in-Iaws was nol included extcns ively in the research We could only include a latent factor support fro m family-in-I aws based on two indicator variables We are aware th at (he lalent construct is not firml y I1Itasulnl in this way However the resullS of lhe mea ~u remen t model (see ) are acceptable (seale composite reliability P= 67) The ind icator variables from thl C0l1s1nlcl are measured on a fi ve-poi nl scale (no influence at all - strong in tluence)
The seco nd latent construct is the support a patient receives from his own 1lt1111shy
ily (seale composite reliability p= 52) This construct is based on three indicalor variables two of which ussess on a five-point seale the direc t support and inllushyence from the fam ily (strongly di scourage - strongly encourage) Besidcs l110ra l support from the family we also included financi al suppo rt Patients wen as kctl whether hey rece ived any financial support The following examples orliumlnanc ia l support were given support for transport drugs consultation fees or les l~ Thc question naire did not ask in deta il about th e ki nd of support patients received Onl y a dichotomous answer (no support anel suppo rt) was sutficiem
Stigmat isation was based on three indicator var iables (scale composilc reli abil shyity p= 64) Again the famil y plays an important role in th is construct The qllesshyti onnaire asked patients to place thell1$elves on a six-point scale (don t agrce al all
1 middot ~IIL I J I I I~ I ~ l l I I II I ~ L I~ I ~I bull bullbullbull bullbull bull bull bull
_ strongly agree) asking them to what extent they fe It that having TB is a disgrace for the fa mily Ir a person agreed strongl y with this phrase it is assumed that he feels st igmatised by his fa mil y The same goes for stigm atisation by friends Again a six point scalc was used (dont agree at all - strongly agree ) to a-sess whelher or not the patients feit stigmatised by lheir fri ends The responde nls could indi cate whether lhey agreed with the idea of very good friends leav ing lhem beshycause of their elisease The more they agreed the more stigmatised they are sup shy
posed to beo The last latent construct in the model is the patient s belief in the curabili ly of
the disease and in knowing how to handle its complexity (scale composite reliabilshyity p= 68) It is an attitudinal factor cons isting of three indicator variables in which patients were asked to gi ve their opinion on TB itself All indicators were measured on a Ii ve-point scale (strongly disagree - strongl y agree) The indicator statements dealt with the opinion on the curability of TB (TB is easy to cure) the commonness of TB (TB is a common diseasc) and wi th the difticulty of TB a~ a disease itself (TB is a difficult disease and hard to cure)
Table 3 latlnt conSlruct mcasure menl summar) (onfirmtory fac tor analy ~i s an d scalc reli shy
ability
Item t Item Description Summary Standa rdshy
ised loading
t-vulue
Support famil y-in-Iaws (p= 67)
Famlawl How much will the opi nion of y lJUr familyshy 74 102
in - Iaw~ influence yo ur dcc is ion to liumlnish or not the wholc treatment (Fi rst time)
Faml aw2 Ho much will lht Qpi nion of your fa mil yshy 69 996
in-Ia ws influ ence your decision to finish or not lhe whole tremment (Sltco nd time)
Su pport fa mily P = 52)
Fam l To what extent does your (o wnl family en shy 59 1004
cou rage or discourage you in taking daily you r medicine (Fi rl time)
Fal112 To what cX lent does yOll r (own) f~l11i1 y enshy +9 8 53
courage or discou rage yOll in taki ng daily your medi cine (Second time)
Fam3 Does you r fam ily sup port yOll liumlnancia ll y for A5 7 98
th e cost of your trealment (tran~port 1drug~ I con~u lta lion fee I tests I )
Stigmatbation (p= 64)
Stigmal It is a disgrace fOf the fumily to have a f3mshyily membcr with TB (Fi rst time)
Stigmu 2 It is a disgracegrave for the family to ha ve J fa mshyily member with TB (S econd time
Stigma ven your bes t fli cnd olllctirncs desen you when you have all infectious di seasc like TB
Belief in curabiJity of TB (p= 68)
Belief TB is easy 10 cun 80 1501 Belie fZ TB is I com mon disease 55 1099 Belief] TB is a di ffi Cll lt dicase 3nd hard to cure 57 I I 2l
Note Fit sla tist ics for mcasurelllent model of 1 1 indicators for four construCIs 2
X IK7 =14993p = 00 GFl=97 RMR = 037 CR = 96 PNFI =52 NNFI = 9J RMS I = OW
I Scale composite relinbilily p = [(I Agravef ) ~ IImiddot(eacute)][(I Agrave I ) ~ vlr( ) + I S] (lOl-o l i amp Vi 1988 p 80)
The measurement model shown in provides a reaso na bl e fit 10 the dat1 Thc ehi shysquare test of exact fit is significant where the objecti ve is to achieve a non-signifshyicant p-value However Hatcher indicates that a significant ch i-square does not ma ke the measurement mode l inadequate (Hatchcr 1994 p 289) The ehi-square ratio shows th at the ratio of the chi-square value and the degree of freedolll is lowcr than two (17) This ind icates that the chi-sguare tes t is wilhin acceptahk lilllits (Marsh et al 1988) Other favourable diagnostics incIude a goodness-or-fiumlt illdegrave X GFI) of 97 a root mean square res idual (RMR) of on a comparati vL rit illtkx CFT) of 96 a parsi mony normed fit index (PNFI) of 52 a nOn normed rit index NNFI) of 93 and a root mean square error of approxi malion (RMSEA ) of rn9
In tenns of valid ity of the constructs con vergent validity is evidcnlxd by tilegrave large and significan t loadings of the item on thei r positcd ind icators FUIhc r (v ishydence of convergent va lidity is shown in None of the correlalions betwLcll Ihl 1 shytent construClS are too high to challen ge the convergent validity oft he cons lructs
F3 F4
100
- 06 100
The discriminan t validi ly is also indicated because the conlide nce interval (plusmn two slandard errors) around the correlati on es ti mate between any two latent construclS never includes 10 (Anderson amp Gerbing 1988 p 41 6) The Varianee Extracted Test also shows the discrim inant validity of our constructs The variance extrac ted tes t compares the variance extracted from two laten t constructs with the square of the correb tion between these two constructs (FomelI amp Larcker 1981 ) Discriminant validi ty is shown when the ex plained variance is greater than the squared correlation We compared all pairs of fac tors and they all showed an iCshy
ccptable variance ex tracted
)4 Results
) 41 Description of the sample
The 62 1 pati ents were composed of 55 0( men and 45 women Seven patients out of ten were younger than 40 concuning with the global observalion that in the countries of the Eastern MeditetTanean Region around 80 of the notified smearshypositi ve TB cases in 1994 occ urred among the economically productive sector of society (15 -54 years old) (Seila 1996 p 134) Tt indicates the serious impact of tushyberculosis on the comrnun ity The skills base of the patiems was very low more than half did not receive any form of fonnal education and the problem of illi teracy aillong older female patients was particularly acute
During the fi rst 11l0nth of lreatment 80 of patien ls were hospitalised during the second month th is number dropped to onl y 48 One out of tluee regarded hospitalisation as problematic This groups di ssalisfaction was rooted both in eco~ nomic and medical causes they had to contend with financial problems absemee shyism transport costs found themseJves in dire sLrai ts doc tors were in competent the rut of he ward etc
One third of patien ls were the family breadwinner As a resuit they were very reluctant to accept the sick mIe Remarkably only one fifth of patients came from a household with more than three economically act ive persons considering lh at
roughly 70 of household eon)i steJ of si x und of ten more Illcm bers The smal nurn ber of econornicall y active person- within the ex tcnded farnilie - C311110t be atshytributed to a large nu mber of ehi ldren because rOlgh ly hal f of the pat ients had less than three children
Sixty percelt ofpalielts placed heulrh al the top oft hc standard orvuluc This is not rea ll y surprising given the fact thal the responclents were confroltcd with ~cr ishyous health prob lems which have absolu te priorit) in their dail y li ve ~ lIld prCSllll1C the recove ry of bath hea lth balallCe anu the improvement of health pOlc nlia Ic shycording to Khayat these IWO dimensions of health are tleeply motet il1 Islalnie Irashydi tion and thefiqlI of health (Khayat 1997) Tf we ZOOIll in on the largL gro llp placshying heal th at the top of the standecircll-d of valuc wc sec Ihal the followi ng vllICS arc also held in high regard falllily and marriage (thc most important aftcr hla llh ) honour and integrity religion and fait h work money (thc Icast importanI ) AIshythough female patiems and patients wilh the lowest socio-economie status atshytached most importance to health it toes not mean that t he~e groups J i-played Ihe mOSl adequate illness behav iour On the contrary the~e groups ltI nd in particlilar housewives the un skilled unernp loyed and sociall y de pri ved ofte n do Ilol J1o~ scss the most elementary knowledge abou t TB (causes sylllptoms alld eollilitlll) which is needed to pre vent infec tion or undergo routine trcatment (Grce n Il)l)) p 192-196) The concept of (external) locus of control ofte n used in rlsealh on compliant behav iour and the fa tal islic health attitude lin ked to th i alslJ applied in thi s context of TB co ntro l (Mcchanic 1983)
Throughout the analys is the operational isation ol belief in the curlli Iil Yui the disease of ten appea red as a variab Ic wi th ~e relldipit y -charactcri ~tics This vlIiahle rneasures the confi dence ~i d people have in suumll vi ng their prob lem situ alilln Trust enables Ihe complexi ry of a social system to be reduced without funher aULgt the sick can rely on thei r part ner fal11il y health worker etc to channel the ir mcdical regimen It is cJear that preci sely lhis confidence is shattered by the TB it igma thereby reducing belief in the curability orTB in genera
Correctly assessing the treatment s duration is characteri stic for patients who strongly believe in the curability of their di sease However th is element of inforshymation is certainly not common knowledge when the treatment starts_Only one in three patients is aware that the trear ment will last several months However after one mon th this number doubles and af ter two months it increases even furthcr (73 ) We established that paliems with the lowest socio-economie statu s often did not possess the Illost rudimentary objecti ve medica l knowledge_There is Iitershyally a wall between them and the cogn itive elements req ui red This wa ll cannot be tom down on y due to reasons related to soc ial strmificaLion On the other hand persons who do nol mind regular check-ups a reg imen of aw kward medication and the costs involved who (hin k it is all worthwhile and are confiden t thei r treatshyment will result in a cure are not necessarily more ski lied or have a higher professhysional rank Ir would seem that another phenomenon another mechanism is ac ti ve as far as belief in Lbe curability of TB is concerned Thinking exclusively in tems of social stratification or Iumping techniq ues of rejec tion together as ways of
bull I I I bull I ~ II ~I I ~ bull I bullbull I L bullbull I bull bull bull bull bull bull
dealing with marginal categories (Douglas 1994 p 85) does not suffice lU gain l bettel understanding of the ideal treatment condition s
Compliance has lO be viewed not only from the socio slralificatiol1 perspeclii but also from the sl ig lllarismioJl persp(crive At thc onset ofthe treatlTlent and aftel two month s treatment sevell statemenlS concern ing stigmatisation were prelgtentecl to the patients A score had to be given on a six-poi nt scale (I =dont agree at all 5=agree 6=strongly ag ree)
The two stateme nts most people i e more than 80 agreed with (score 5 or 6) both at the onset of the trearment and [WO monlhs afterwards were Jf someont has TB hejshe avoids ralking about it with ot her persons and Af ter recoverinf from TB everyone treats yO Ll the same way lS bcfore If someone contracts TB il is bes t to keep quict about it If thei r environment doesn t know anythi ng about il th~y will not treat them di fferentl y af ter they hJ ve recovered
Thc other statement many ie more than 60 agreed with both at thc begin ning of the treatment and af ter two mO IHhs was Peope who arc treated for TB should ta lk to others about it
There were three statements alrnost half of pati ent- ie more than 401r agree with both at the onset of the treatment aOl af ter two months It is a disgrace for thl famil y to have a fa mily member with TB Even your best fri ends someti me ~
desert you when you have un infectious disease li ke T B and 11 a young persol catches TB heshe will experience the consequences for the rest of hisher lirc
Thc statement only a minority ie one out of four patients agreed with both a the onset of the treatment and af ter two months was It is diffi cult to earn your Ii ing after recovering from TB The fact that only very few regarded the TB prob lem in tenns of income is re lnted to the fact that during tbis life-threatening situa ti on_ the trentment has absol ute priori ty and takes precedence over all other form of need
When the onset of the treatment is compared Nith the situation two month later there are no shifts in the statemenls ranking order This means that the firs two months of treatmen t - eg at the hospitalor contact with health carers - dOt not real ly affect their situation On the contrary the stigmatisation continues t( proliferate and feste r causi ng damage in its wake According to Goffmans termi nology it conti nues to transform TB sufferers from discreditabe tO discredilel (Goffma n 1990 p 57 ) Only two statements poi nt to a possible evolution durin~ the first two months but they do not really di sruptthe ran ki ng order in any signifi cant way Ir rerers to the statement PeopJe who are treated for TB should talk t( others about it 68 tgreed at the omet of the treatment and 78 af ter tWt months treatmenl This increase indicates that TB patients still regard opennes about their illness und breaking taboos about the subject as a norm and future ex pectati on Whilst 54 agreed at the beginning of the treatment with the state lllcn Even your best fri ends sometimes dcsert you when you have an infect ious dis ease like TB this dropped to 45 af ter lwo months treatment Ir would appea that the channels for seeking informal care do not dry up for those who respect th medical regimen
We will illustrate thatthe social Il etwork lovering the pa tien t- nlatiolls with all significant others can cithcr increasc or reduce st ig lll ati satioll iS lllilh 1 ()IJt) p 138-155) The com position of these soci al networks i- very hcterogcilcous Thcy can perhaps bes t be analy-ed by di sti nguishing the nuelear fam ily from Ihe ex shytended fa mily As far as the nuclear fam ily is cOllce rned 62 of pllicnls wcn~ married 31 were si ngle 5fr widowed anel 2 divorced For married felll aie pashytients ( 173 out of a tota l of 387 married pa tients) rclati oll) with the fa mi Iy- ill-Iaws and in particular the mother-in-Iaw were very importan t indeecl For alll10sl half of all patients (47) thc extc ll(kJ fam il y eOll1 pri -ed cighl or more perso ll- IIs li all y adu lt who all li ve under the ) (l IllC roo f In 20 of households there wen ilO ehi 1shydren (yolJnger than 12 yca r~) 327 ot households had one or two childrclI 2C1r had three or four children and 21 or had fi ve or more
542 Causal model
The proposed structural model in Figurc 2 was tested by using con veuml ntionalmaxi shymu m likel ihood est imatioll techniques Thc model~h(lwed an acecptabk fit Again the ehi -square tes t of exact fit is ~i gni tiuml ca nt but the eh i-square ratio is lower than two (07) Other favourable diagnosti c~ include a goodncss-of-tiumlt index (GFl) of 96 a rOol mean square rcs idual (R MR) of 041 a comparati ve fi l index (CF) of 97 a parsimony normed fit index iPNFI) of 72 a non normed fit index (NNFI) of 96 and a root mean squ are enOf of approximation (RMSEA) of 039 All of the path coefficients are signifi cant
Anderson and Gerbing recommend a chi-square di ffe rence tes t (CDT) in order to enhanee the confidence in the structural part of the model (Anderson amp Gerbing 1988) The CDT compares the structura l model (which is a res trictecl theoretical model MT) with an uneons trailled alternative model (Mul The relevant test statis shytics (MT has 122 df and a X2 of 17526 ML has 93 df anel a X2 of 171 89) lead to a non-significa nt CDT (X2 difference is 25 33 at 35 df) and an acceptance of M
r Thu s our restricted theoretica model (Figure 3) is preferred to the theoretica uncorrelated model
Since most of the [esH tat is ti c~ show an acceptable model we can look at the reshysu lts of the two-step model presentcd earlier Firsl we tried to model the influshyences on the degree of stigmatisation of a patient These influenees come from very different sou rces The mos important factors determi ning stigmatisation are sex and age Women are more easily stigmatised than men are This also holds for older people From the latent factors support from the family is the most im porshytant Thc more one receives SUppOrL from ones fam ily the less one is stigmalised Anothcr influence on stigmatisation comes from belief in the curability of the TB onstruct The more one believes that TB is curable the less one is stigmatised
These results sugges t that a robust position within society prevents a person from being stigmatised
We then tried to link the stigmatisation of the TB patients and the ir complianl wilh lhe directly observed therapy The restricted theoretical model reveal s that ti influence of stigmatisation on compliance only becomes clearly visible af ter intro ducing the regularity and the duration of the therapy as intervening variables closer examination compliance would appear to be a rather hybridconcept whi can take various forms and has many depths Compliance comes clearer to the [ (I when regularity and du ration are separated In the model stigmatisation with effect of -016 affects regul arity Subsequently regularity has a direct effect of on eomplianee but lhere is a stronger effect on duration and from there on comp anee The regularity and the duration of the therapy tberefore form a tandem whi ca n be brought out of balance by stigmati sation anclilo longer prov ides any gu antees for compliant behaviour
Figu re 3 Siructuralmodel of complio ncc anJ TB
SignificCllce (p-PO ll t) =0 05 =00 =000
Note Fit statistics for structural model X2n~~) =175 26 P=00 GFl =96 RMR =041 CFl =lJ
PNFl =72 NNFI =96 RMSEA =039
SS Discussion
Compliance the fin al link in the causal model is a di ffi cult concept operationalise because it refers to a complex reality The treatment of most inf uumlous diseases oceurs in a di rectly observed way (Porter amp Ogden 1997) H0 ever in practice directly observed therapies can be implemented in a variety ways For examplc DOT for sexually transmitted diseases of ten means obsef tion of a single dose of treatment whereas DOT for leprosy entails monthly ob~ valion by a health care worker of doses of ri fampicin and clofazimine Tbe 001 control strategy reeommended by the WHO for tubercul os is is based on a com nation of four types of medici ne which have to be taken together for the fi rst t
months of lrcat ment HeLlith lJre worken ensure that the I ight Ill ed icine is lak n in the right doses and fo r the cornc t length of ti me Supervis ion ean he a CLlllllshy
p ished by having the pati ent visit the cimie hosp italis ing the patient or scnuin a health care workeI to visit the pa tients home or workplace For directl y ohsnvcd therapy fe l TB it i essenti1l that superv isi on continu e~ every day for th liumlrst two months and idea lly for the entire course of the treatment The wide vltlriations in DOT-contro strategies have resulted in a situation where compliance Illci 1l111lshy
compliance have become e la~t ic eoncepls Who is campliant and who is not~ It all depends on the nature and Ihe t ve l of thc sl3ndard We cncoun tered a di vcls il y of defin itiolls with in the framew)lk or the cLJ l1lbat aga inst tube rcu l o~i-
A retrospective study (from J977) on co mpli ance of TB pat ients revealed that the default ra Ie of the out-putient population in rural Pak i~ta n amounted iO 66 Default was defined as fa ilu re to uttend the weck ly tu berc ulosis clinic fo r a period of one month (Sloan amp Sloan 1981) A fo llow-up study ( 198g-90) showed that 72 oc of the TB patients registered in Bethani a Hosp ital did not complete their 12 months trea tment coure Although the in troduction of a short-course (8 months) regimen improved the compliance default rates (56) contin ued to be high (Liefooghe et al 1995) In 1991 however 76 of TB patients reg istered in the Pakistan Institute of Chest Diseases (S indh) had kep t to the short-course reglmen for two months 2 1 had left the hospi ta l against medical advice and 3 had died (Pathan et al 1992) A study carr ied out in the lndian Wardha dislrict revealed that TB patientlt who fai]cd to take their medici ne for more than 15 days were regarded as non-comptiant because this definition is most in keeping with the adopted adshyministrative procedure (Barnhoorn amp Adriaanse 1992) In a study performed in Denver USA non-compl iance with DOT for TB was detined as foll ows (I) missing ~ 2 consecuti ve weeks of DOT (2) prolongation of treatment gt 30 days due 10 sporadic missed doses or (3 ) incarceration for presenting a th rem lO public health (Burman et al 1997) At least 18 of patients who received out-paLient DOT via the Denver Metro TubercLIl os is Clinic met at least one of these cri teria
In concusion therefore there is no golden standard for defining compliance In our study compliance the fi nal outcome which has to be explai ncd in the model is viewed from a dichotomous viewpoint On the one hand there is the category of compliant patients they com plete thei r the ra py in full and as a general rule al$o unshyderwent a sputum tes t confirming Ihem as TB negative On the other hand there is the category of non-com pliant patients they did not com plete their therapy so a sputum test was not carried out We also adopted the com pletion or fai lure to comshyplete the short -co urse direc tl y observed therapy the bas ic criterion used in the exshyam pIes given above as the key cri terion for our defi ni tion of com pliance The structural model (see Fig ure 3) demonstra tes th at it is important to systemat ically di stinguish the reguarity and the du ration of the therapy to gain a bctter undershystanding of the concept compliance Regularity is achieved when there are no or only sporadic interru ptions during the thcrapy In t hi ~ connection we refer to missed appointments or missed doses of medi cation The durarjoll of the therapy on the e ther hand refers to the treatment duration of eigh[ months which has to be
111 JIII 1 1 1III IJ IKLl 11 lH~Ult I IJ 11111lt ) ~
respected in the DOTS-regimen Two dlv iati ons are possiblc here Either Jo wn shyward the patient ends thc treatment premature1y and is regarded as d efaulter Ol upward- the period of treatment is extended because interruptions during the treatment have [0 be compenslIteti for artcrwards Both deviations from the norm indieate non-compliance Any com parison with the above referred to non-complishyance ra[es fa ils because the phenomenon is constantly regarded from di fferent anshygles Hav ing said that the folowing fac ts in our research on (non- )col11pl iancc among the 621 TB patients are worth mentioni ng
Aftel subtracti ng the nUlllbcr (l f pntients who have died (6Oc) thase who have transferred to another treaUllent centre (29r) and thc tiny group of patie nt~ where the treatmen t failed (I ) 563 pat ients remai ned According to our de liumln ition 779 of the latter group are compliant and 23 are non-compliant aresuIt which is c10sely in keepi ng with the situation at lhe lnsti tu te of Ches[ Diseases in the prov shyince of Sindh The number of in terruptions is used to indicate the regularity of the trcatment 48 of patients did not inlerrupt their treatment at all 34 in terrupted it once and 18 interrupted it various times As far as the duration of the lherapy is concerned the norm of eight months is ach ieved by 55 of patie nts [he norm i not achie ved laquo 8 months) by 33 of patients and the nonn is exceeded (gt 8 months) by 12 of patients
Broadly speaking three out of four paticnts is compliant One out of four is nOI1shycompliant interruptions during the treatmen t (because appoin tments or medicashytion is sporatlicall y missed) or failure to complete the ideal duration of treatmenl (because patients drop out too early or have to followan extended course of treatshyment) As far as establishi ng compl iance is concerned it would seem that 77 ck of patients is heading towards the WHO-target fo r global tuberculosis control namely cure 85 of the detected new smear-positive TB cases (Seita 1996 p 134)
When interpreting the results it is also important to disti nguish between ho~ p ishytalised patie nts and out-patients As we al ready stated earlier duri ng lhe rirst month of treatment 80 of patients were hospitalised Af ter the second month this number dropped to only 48 Permanent supervision at the hospital ensures that hospitalised TB patients are by definition compliant the DOTS-regime n is strictly enforced As far as non-compliance of the out-patient population is co ncerned wc noted that 17oc missed at least one appointment during the first month of treatshyment and that this number dropped 10 1I aftel thc end of the second month The first month is therefore critica especially fol patients who are not hospitalisetl Since they do not res ide at the hospi tal and only come for consultations thty enshycounter far greater difficulties internalising the norms underlying the DOTS-regishymen
The model hinges on the latent construct of stigmatisation Stigmatisation afshyfects compl iance through the Ta ndem of regu la ri ty and duration of therapy Persons who have been strongly stigmatised display more irregular illness behaviour and find it more problematic to see the ditficult and troublesome trealment through 10
[he end In th is respect il could be sa id that ending or interrup[ing the DOTS-reg imiddot
men is nol due to a Jack ol organi satioll On the contrary they are Illcchallisl llS which help to relieve thc pain of sli gmatisation ensuring that for a wh ik the TH pal ient does not have 10 he as hamed and can take a brea k when the prc-url of Ihc medical rcgimen beeomcs toa heavy (Massaro 1997) According 10 GollIllans terminology devi ali ng from the slandards of thc DOTS- rcgimen can hl rcgOl rdcJ as a technique fo r conlrolling in fo rmation The questions or whelher 10 revcal or hi de to con1iumlde in someone or keep qui et to lie or be truth ful and to who l1l hnw when and where are tricks for stoppi ng Ihe exhausting process of bleacutellllc hy socishyety They are in su mmary stra tegies to lWlwRc ( IpoiId idllltity (Schcpcr- amp Nievaard 1995 p 42-43) In Ihe mode l th rec social conditions affecl thc dcgrcc of sligmati sation of TB pat ients These co ndi lions have 10 be taken inlo account 10 reduce the lim ils to pat ienl compliancc with DOTS-strategies
The first cond it ion is rclated to the dem ()g mphico Iilloion of the pili cllt anJ comprises two variab les from the exogenous set ie gender and age FCi llalc pashytients were stigmatised more than male pat ients and older patients Wlr~ si igllwshyti sed more than young persons BOlh lin k~ are highl y significant As house wivcs or elderl y members of the ex tended fa mi Iy many have a low socio-econol11 ie Ialu For them health is above all J quest ion of physical strength (W inkvist amp Akhtar 1997) The loss of phys ical strength Ihlough tubercul osis the fact that tl1Oc who have been sl ricken wilh the diseas( can no longer perform hard labour do the housekeepmg no longer be reproducti ve etc are important contributors to stigshymat isation This is all the more so in lhe countryside where ex ternal signs of vu lshynerability often do not suffiumlce to relieve peopl e from their nonnal socill tasks in the fami ly and vill age
The second condition cl ose ly concerns the beiefofT8 patiel1ll in the curabifir of th eir disease We already said earlier that th is laten t construct in our research displayed features of serendi pity It is el istinct from stricl measurements ofrational med ical knowledge because it emphasises praxis ie implementing knowledge and acti ng on insights The higher the soc io-economie slatus the grealer the belief in the curabil ity of TB It is impossi ble to ignore the phenomenon of social stratifishycation when analys ing ill ness behaviollr of TB patients Patients wi th a higher proshyfessional rank have great faith in the curability of their disease The opposite also applics in equal measure unemploy ment and illileracy are cond ucive for nonshycompl iam behaviour Perhap~ the hard core of pariahs outcasts vagrants vagshyabonds tramps chronie drllnkards and drug add icts (Merton 1968 p 207) repshyresenlSthe most dangerous ri sk group for all TB control programmes When Robshyert K Merton in 1949 developcd hi s we ll-known typology of modes of adaptation by indi viduals within the cu ltu re-bearing society he discovered that these populashytion groups displ ayed retreatiII their mode of adapl3tion which implies the reshyjec tion of cul tural goals and institutional means After all why should anyone reshymain healthy And why should we lIse DOTS as Q method Does it make any difshyference) There is a negative correlat ion between belief in the curability of TB and the degree of stigmati sation Persons who are convineed they will soon be cured and capable of strictly following the medical regimen will be less stigmatised
1 ll i bull I III I 1 11 11 10-- 1 1 middot111 middotmiddot middot 1 middot _
The third condit ion is siluateel at the leve l of the social netllo rks in wh ich TB middot patients function As a general rule it can be sa id thaI persons who tcceive mor~ help from olhers are less likely 10 be stigmati sed Roughl y six out of ten pati ent~ are married and fo r married women the family-in-I aws occ upy the cen tral po- it iol in their social nelwork The model established a negati ve relationshi p betwec l support from blood re lati ve~ and support from the family-in-Iaws Solida rilYvvitl the fa mily-in-Ia ws red uces ~olidarity with biooeI relatives This app lies both il general but also in the specifi( framework of help and support in ti mes of illness The fear manied fe male TB patients have of being abancloned by their hll ~banJ and no 10nger being able to perform their domesr ic tasks should not be unMrcst i mated During a study into thc relcltion between poverty and TB in Bombay re male patients said thaI thei r husbands and mothers-in-Iaw repeated Iy sent then back to their nata l home until such lime as Ihey were cured They were often al cused of bringing the disease from their natal homes and were threatened with sep aration (Nui r et al 1997 p 8 1) The model revea led that the TB patiems who re ceived the least support from their family were stigrnatised most Th is recalls th relational natu re of all type of sti gmatisat ion People are given a negative SOCiH label or are shielded from it Your family may support you through thick and thin encourage you to do the right th ing help to fi nance treatment etc Converse l) your fam ily mayabandon you keep your situation quiet to prevent loosing fac anel keep the family reputation unb1emished
lil Pakistani society anel particularl y in l11any village and se ttl el11Cnb in th Punjab social networks and stigmati sation are inextricably li nkeel and have al enormous influence on community li fe Thc biraderi the patriarcha l nelwork 0
kinship fo rms the framework 101 social and coml11uni ty networks Special event and rites of passage such as birth the ci rcumcis ion of a son marriage allli th death of an old person si rengthen lhis solidarity within the biraderi The biradel use many other occasions to promote social and community networks and ill ne - is perhaps one of the most important When a daughter-in- Iaw becomes seriousl iJl or is hospitalised her children are either looked after by the other daughters (1
the house or are temporarily housed with other members of the birade ri If Ihe sol breadwinner of a household cannot work because he is seriously ill his nearest rel atives and olher members of his biraderi provide mora material and fi nancia l o up port These socia1 and communily links rernai n intact even after emigration Paki stanis who have emigrated to Grea t Brita in for exam ple continue to receive muc support from their biraderi (Anwar 1979) Whenever help is sought in Pakistar communities famil y and bi raderi are preferred According to a sociologic al stud carried out in Rochdale a toW D in the north of England hel p is only sOllght frOl farmer fellow viJ1 agers friend s neighbours Olher Pakistanis and the res t of 50CI ety after all possibil ities in the biraderi-network have been exhausted A TB pil tient who is admitted to hospital will initially be visited by me mbers of hi biraderi They wi llusuaJ1y be gi ven a few hundred rupees and the trad itional fru i However as news about the nature of the illness spreads within the bi rade ri cor tacts become less frequent The negative COITeiation between fa mily support an
sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more
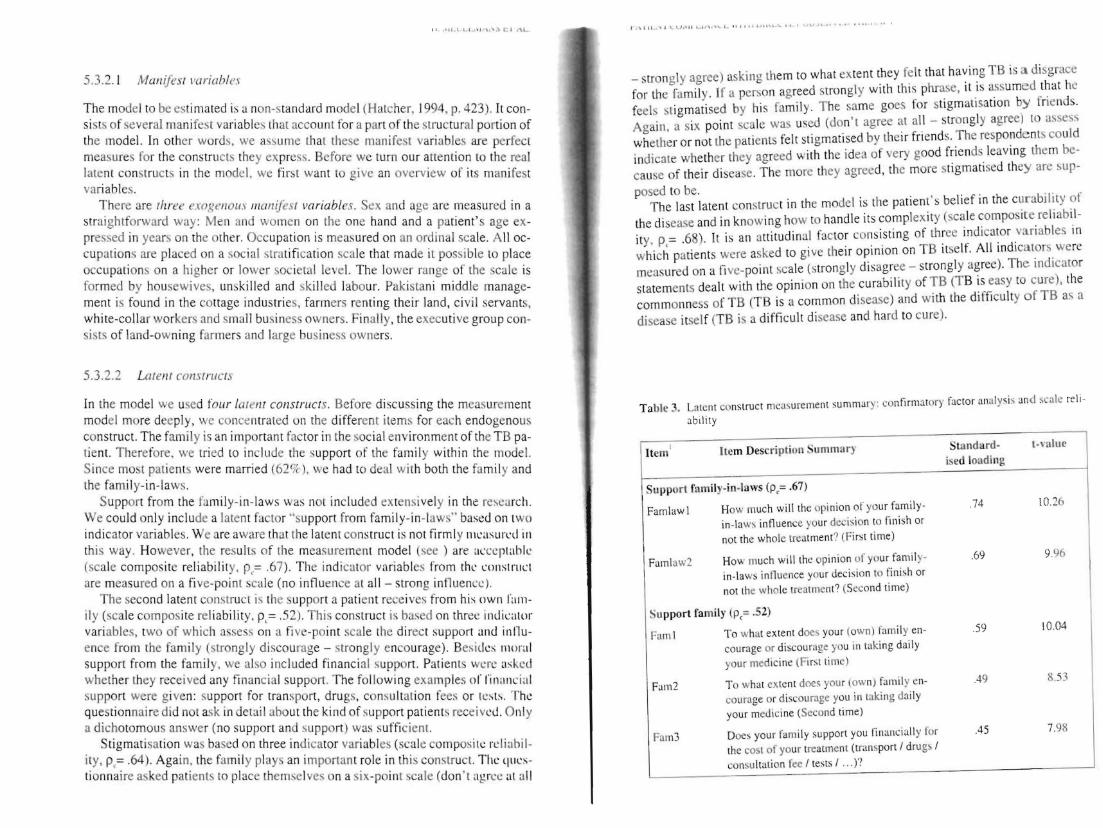
11 U l LLI ~J CI IL
532 1 Mal ifes lriahles
The moJel to be estimated is a non-~tandard model (Hatcher 1994 p 423) It conshysists of several mani fe t variables that account for a pan of the structural portion of the model In other word we assumc lha hese manifest variables are perfect measures for the constructs they express Before we turn our attention to the real latent constructs in lhe model we finl want 10 give an overview of its manifest variables
There Ire I lLree exoKI I ou Iwnifesl variables S~x and Ige are measured in a straighlforward way Men and women on the one hand and a patient s age exshypressed in years on the ether Occupation is measured on an ordinal seale All ocshycupat ions are placed on a soc ial stralification seale that made il possible to plaee occupations on a higher or lower sot ietal level The lower range of the scale is fo rmed by housewives unskilled and skil led labour Pakistani middle manageshyment is found in the cottage industries farmers renting their land civil servants white-coJlar workers and small business owners Finally the exeeuti ve group conshysists of land-owning farmers and large business owners
53 22 Larent COTlSrrucls
In the model we used fOlr latelll constructs Before di scussing the measurement model more deeply we concentrated on the different items for eaeh endogenous construct The family is an importan t fac tor in the social environment of the TB pashytient Therefore we tried 10 include the lt upport of lhe farnil y within the model Sinee most pat ients were married (62) we had to deal wi th both the famil y and the family-in-Iaws
Support from the family-in-Iaws was nol included extcns ively in the research We could only include a latent factor support fro m family-in-I aws based on two indicator variables We are aware th at (he lalent construct is not firml y I1Itasulnl in this way However the resullS of lhe mea ~u remen t model (see ) are acceptable (seale composite reliability P= 67) The ind icator variables from thl C0l1s1nlcl are measured on a fi ve-poi nl scale (no influence at all - strong in tluence)
The seco nd latent construct is the support a patient receives from his own 1lt1111shy
ily (seale composite reliability p= 52) This construct is based on three indicalor variables two of which ussess on a five-point seale the direc t support and inllushyence from the fam ily (strongly di scourage - strongly encourage) Besidcs l110ra l support from the family we also included financi al suppo rt Patients wen as kctl whether hey rece ived any financial support The following examples orliumlnanc ia l support were given support for transport drugs consultation fees or les l~ Thc question naire did not ask in deta il about th e ki nd of support patients received Onl y a dichotomous answer (no support anel suppo rt) was sutficiem
Stigmat isation was based on three indicator var iables (scale composilc reli abil shyity p= 64) Again the famil y plays an important role in th is construct The qllesshyti onnaire asked patients to place thell1$elves on a six-point scale (don t agrce al all
1 middot ~IIL I J I I I~ I ~ l l I I II I ~ L I~ I ~I bull bullbullbull bullbull bull bull bull
_ strongly agree) asking them to what extent they fe It that having TB is a disgrace for the fa mily Ir a person agreed strongl y with this phrase it is assumed that he feels st igmatised by his fa mil y The same goes for stigm atisation by friends Again a six point scalc was used (dont agree at all - strongly agree ) to a-sess whelher or not the patients feit stigmatised by lheir fri ends The responde nls could indi cate whether lhey agreed with the idea of very good friends leav ing lhem beshycause of their elisease The more they agreed the more stigmatised they are sup shy
posed to beo The last latent construct in the model is the patient s belief in the curabili ly of
the disease and in knowing how to handle its complexity (scale composite reliabilshyity p= 68) It is an attitudinal factor cons isting of three indicator variables in which patients were asked to gi ve their opinion on TB itself All indicators were measured on a Ii ve-point scale (strongly disagree - strongl y agree) The indicator statements dealt with the opinion on the curability of TB (TB is easy to cure) the commonness of TB (TB is a common diseasc) and wi th the difticulty of TB a~ a disease itself (TB is a difficult disease and hard to cure)
Table 3 latlnt conSlruct mcasure menl summar) (onfirmtory fac tor analy ~i s an d scalc reli shy
ability
Item t Item Description Summary Standa rdshy
ised loading
t-vulue
Support famil y-in-Iaws (p= 67)
Famlawl How much will the opi nion of y lJUr familyshy 74 102
in - Iaw~ influence yo ur dcc is ion to liumlnish or not the wholc treatment (Fi rst time)
Faml aw2 Ho much will lht Qpi nion of your fa mil yshy 69 996
in-Ia ws influ ence your decision to finish or not lhe whole tremment (Sltco nd time)
Su pport fa mily P = 52)
Fam l To what extent does your (o wnl family en shy 59 1004
cou rage or discourage you in taking daily you r medicine (Fi rl time)
Fal112 To what cX lent does yOll r (own) f~l11i1 y enshy +9 8 53
courage or discou rage yOll in taki ng daily your medi cine (Second time)
Fam3 Does you r fam ily sup port yOll liumlnancia ll y for A5 7 98
th e cost of your trealment (tran~port 1drug~ I con~u lta lion fee I tests I )
Stigmatbation (p= 64)
Stigmal It is a disgrace fOf the fumily to have a f3mshyily membcr with TB (Fi rst time)
Stigmu 2 It is a disgracegrave for the family to ha ve J fa mshyily member with TB (S econd time
Stigma ven your bes t fli cnd olllctirncs desen you when you have all infectious di seasc like TB
Belief in curabiJity of TB (p= 68)
Belief TB is easy 10 cun 80 1501 Belie fZ TB is I com mon disease 55 1099 Belief] TB is a di ffi Cll lt dicase 3nd hard to cure 57 I I 2l
Note Fit sla tist ics for mcasurelllent model of 1 1 indicators for four construCIs 2
X IK7 =14993p = 00 GFl=97 RMR = 037 CR = 96 PNFI =52 NNFI = 9J RMS I = OW
I Scale composite relinbilily p = [(I Agravef ) ~ IImiddot(eacute)][(I Agrave I ) ~ vlr( ) + I S] (lOl-o l i amp Vi 1988 p 80)
The measurement model shown in provides a reaso na bl e fit 10 the dat1 Thc ehi shysquare test of exact fit is significant where the objecti ve is to achieve a non-signifshyicant p-value However Hatcher indicates that a significant ch i-square does not ma ke the measurement mode l inadequate (Hatchcr 1994 p 289) The ehi-square ratio shows th at the ratio of the chi-square value and the degree of freedolll is lowcr than two (17) This ind icates that the chi-sguare tes t is wilhin acceptahk lilllits (Marsh et al 1988) Other favourable diagnostics incIude a goodness-or-fiumlt illdegrave X GFI) of 97 a root mean square res idual (RMR) of on a comparati vL rit illtkx CFT) of 96 a parsi mony normed fit index (PNFI) of 52 a nOn normed rit index NNFI) of 93 and a root mean square error of approxi malion (RMSEA ) of rn9
In tenns of valid ity of the constructs con vergent validity is evidcnlxd by tilegrave large and significan t loadings of the item on thei r positcd ind icators FUIhc r (v ishydence of convergent va lidity is shown in None of the correlalions betwLcll Ihl 1 shytent construClS are too high to challen ge the convergent validity oft he cons lructs
F3 F4
100
- 06 100
The discriminan t validi ly is also indicated because the conlide nce interval (plusmn two slandard errors) around the correlati on es ti mate between any two latent construclS never includes 10 (Anderson amp Gerbing 1988 p 41 6) The Varianee Extracted Test also shows the discrim inant validity of our constructs The variance extrac ted tes t compares the variance extracted from two laten t constructs with the square of the correb tion between these two constructs (FomelI amp Larcker 1981 ) Discriminant validi ty is shown when the ex plained variance is greater than the squared correlation We compared all pairs of fac tors and they all showed an iCshy
ccptable variance ex tracted
)4 Results
) 41 Description of the sample
The 62 1 pati ents were composed of 55 0( men and 45 women Seven patients out of ten were younger than 40 concuning with the global observalion that in the countries of the Eastern MeditetTanean Region around 80 of the notified smearshypositi ve TB cases in 1994 occ urred among the economically productive sector of society (15 -54 years old) (Seila 1996 p 134) Tt indicates the serious impact of tushyberculosis on the comrnun ity The skills base of the patiems was very low more than half did not receive any form of fonnal education and the problem of illi teracy aillong older female patients was particularly acute
During the fi rst 11l0nth of lreatment 80 of patien ls were hospitalised during the second month th is number dropped to onl y 48 One out of tluee regarded hospitalisation as problematic This groups di ssalisfaction was rooted both in eco~ nomic and medical causes they had to contend with financial problems absemee shyism transport costs found themseJves in dire sLrai ts doc tors were in competent the rut of he ward etc
One third of patien ls were the family breadwinner As a resuit they were very reluctant to accept the sick mIe Remarkably only one fifth of patients came from a household with more than three economically act ive persons considering lh at
roughly 70 of household eon)i steJ of si x und of ten more Illcm bers The smal nurn ber of econornicall y active person- within the ex tcnded farnilie - C311110t be atshytributed to a large nu mber of ehi ldren because rOlgh ly hal f of the pat ients had less than three children
Sixty percelt ofpalielts placed heulrh al the top oft hc standard orvuluc This is not rea ll y surprising given the fact thal the responclents were confroltcd with ~cr ishyous health prob lems which have absolu te priorit) in their dail y li ve ~ lIld prCSllll1C the recove ry of bath hea lth balallCe anu the improvement of health pOlc nlia Ic shycording to Khayat these IWO dimensions of health are tleeply motet il1 Islalnie Irashydi tion and thefiqlI of health (Khayat 1997) Tf we ZOOIll in on the largL gro llp placshying heal th at the top of the standecircll-d of valuc wc sec Ihal the followi ng vllICS arc also held in high regard falllily and marriage (thc most important aftcr hla llh ) honour and integrity religion and fait h work money (thc Icast importanI ) AIshythough female patiems and patients wilh the lowest socio-economie status atshytached most importance to health it toes not mean that t he~e groups J i-played Ihe mOSl adequate illness behav iour On the contrary the~e groups ltI nd in particlilar housewives the un skilled unernp loyed and sociall y de pri ved ofte n do Ilol J1o~ scss the most elementary knowledge abou t TB (causes sylllptoms alld eollilitlll) which is needed to pre vent infec tion or undergo routine trcatment (Grce n Il)l)) p 192-196) The concept of (external) locus of control ofte n used in rlsealh on compliant behav iour and the fa tal islic health attitude lin ked to th i alslJ applied in thi s context of TB co ntro l (Mcchanic 1983)
Throughout the analys is the operational isation ol belief in the curlli Iil Yui the disease of ten appea red as a variab Ic wi th ~e relldipit y -charactcri ~tics This vlIiahle rneasures the confi dence ~i d people have in suumll vi ng their prob lem situ alilln Trust enables Ihe complexi ry of a social system to be reduced without funher aULgt the sick can rely on thei r part ner fal11il y health worker etc to channel the ir mcdical regimen It is cJear that preci sely lhis confidence is shattered by the TB it igma thereby reducing belief in the curability orTB in genera
Correctly assessing the treatment s duration is characteri stic for patients who strongly believe in the curability of their di sease However th is element of inforshymation is certainly not common knowledge when the treatment starts_Only one in three patients is aware that the trear ment will last several months However after one mon th this number doubles and af ter two months it increases even furthcr (73 ) We established that paliems with the lowest socio-economie statu s often did not possess the Illost rudimentary objecti ve medica l knowledge_There is Iitershyally a wall between them and the cogn itive elements req ui red This wa ll cannot be tom down on y due to reasons related to soc ial strmificaLion On the other hand persons who do nol mind regular check-ups a reg imen of aw kward medication and the costs involved who (hin k it is all worthwhile and are confiden t thei r treatshyment will result in a cure are not necessarily more ski lied or have a higher professhysional rank Ir would seem that another phenomenon another mechanism is ac ti ve as far as belief in Lbe curability of TB is concerned Thinking exclusively in tems of social stratification or Iumping techniq ues of rejec tion together as ways of
bull I I I bull I ~ II ~I I ~ bull I bullbull I L bullbull I bull bull bull bull bull bull
dealing with marginal categories (Douglas 1994 p 85) does not suffice lU gain l bettel understanding of the ideal treatment condition s
Compliance has lO be viewed not only from the socio slralificatiol1 perspeclii but also from the sl ig lllarismioJl persp(crive At thc onset ofthe treatlTlent and aftel two month s treatment sevell statemenlS concern ing stigmatisation were prelgtentecl to the patients A score had to be given on a six-poi nt scale (I =dont agree at all 5=agree 6=strongly ag ree)
The two stateme nts most people i e more than 80 agreed with (score 5 or 6) both at the onset of the trearment and [WO monlhs afterwards were Jf someont has TB hejshe avoids ralking about it with ot her persons and Af ter recoverinf from TB everyone treats yO Ll the same way lS bcfore If someone contracts TB il is bes t to keep quict about it If thei r environment doesn t know anythi ng about il th~y will not treat them di fferentl y af ter they hJ ve recovered
Thc other statement many ie more than 60 agreed with both at thc begin ning of the treatment and af ter two mO IHhs was Peope who arc treated for TB should ta lk to others about it
There were three statements alrnost half of pati ent- ie more than 401r agree with both at the onset of the treatment aOl af ter two months It is a disgrace for thl famil y to have a fa mily member with TB Even your best fri ends someti me ~
desert you when you have un infectious disease li ke T B and 11 a young persol catches TB heshe will experience the consequences for the rest of hisher lirc
Thc statement only a minority ie one out of four patients agreed with both a the onset of the treatment and af ter two months was It is diffi cult to earn your Ii ing after recovering from TB The fact that only very few regarded the TB prob lem in tenns of income is re lnted to the fact that during tbis life-threatening situa ti on_ the trentment has absol ute priori ty and takes precedence over all other form of need
When the onset of the treatment is compared Nith the situation two month later there are no shifts in the statemenls ranking order This means that the firs two months of treatmen t - eg at the hospitalor contact with health carers - dOt not real ly affect their situation On the contrary the stigmatisation continues t( proliferate and feste r causi ng damage in its wake According to Goffmans termi nology it conti nues to transform TB sufferers from discreditabe tO discredilel (Goffma n 1990 p 57 ) Only two statements poi nt to a possible evolution durin~ the first two months but they do not really di sruptthe ran ki ng order in any signifi cant way Ir rerers to the statement PeopJe who are treated for TB should talk t( others about it 68 tgreed at the omet of the treatment and 78 af ter tWt months treatmenl This increase indicates that TB patients still regard opennes about their illness und breaking taboos about the subject as a norm and future ex pectati on Whilst 54 agreed at the beginning of the treatment with the state lllcn Even your best fri ends sometimes dcsert you when you have an infect ious dis ease like TB this dropped to 45 af ter lwo months treatment Ir would appea that the channels for seeking informal care do not dry up for those who respect th medical regimen
We will illustrate thatthe social Il etwork lovering the pa tien t- nlatiolls with all significant others can cithcr increasc or reduce st ig lll ati satioll iS lllilh 1 ()IJt) p 138-155) The com position of these soci al networks i- very hcterogcilcous Thcy can perhaps bes t be analy-ed by di sti nguishing the nuelear fam ily from Ihe ex shytended fa mily As far as the nuclear fam ily is cOllce rned 62 of pllicnls wcn~ married 31 were si ngle 5fr widowed anel 2 divorced For married felll aie pashytients ( 173 out of a tota l of 387 married pa tients) rclati oll) with the fa mi Iy- ill-Iaws and in particular the mother-in-Iaw were very importan t indeecl For alll10sl half of all patients (47) thc extc ll(kJ fam il y eOll1 pri -ed cighl or more perso ll- IIs li all y adu lt who all li ve under the ) (l IllC roo f In 20 of households there wen ilO ehi 1shydren (yolJnger than 12 yca r~) 327 ot households had one or two childrclI 2C1r had three or four children and 21 or had fi ve or more
542 Causal model
The proposed structural model in Figurc 2 was tested by using con veuml ntionalmaxi shymu m likel ihood est imatioll techniques Thc model~h(lwed an acecptabk fit Again the ehi -square tes t of exact fit is ~i gni tiuml ca nt but the eh i-square ratio is lower than two (07) Other favourable diagnosti c~ include a goodncss-of-tiumlt index (GFl) of 96 a rOol mean square rcs idual (R MR) of 041 a comparati ve fi l index (CF) of 97 a parsimony normed fit index iPNFI) of 72 a non normed fit index (NNFI) of 96 and a root mean squ are enOf of approximation (RMSEA) of 039 All of the path coefficients are signifi cant
Anderson and Gerbing recommend a chi-square di ffe rence tes t (CDT) in order to enhanee the confidence in the structural part of the model (Anderson amp Gerbing 1988) The CDT compares the structura l model (which is a res trictecl theoretical model MT) with an uneons trailled alternative model (Mul The relevant test statis shytics (MT has 122 df and a X2 of 17526 ML has 93 df anel a X2 of 171 89) lead to a non-significa nt CDT (X2 difference is 25 33 at 35 df) and an acceptance of M
r Thu s our restricted theoretica model (Figure 3) is preferred to the theoretica uncorrelated model
Since most of the [esH tat is ti c~ show an acceptable model we can look at the reshysu lts of the two-step model presentcd earlier Firsl we tried to model the influshyences on the degree of stigmatisation of a patient These influenees come from very different sou rces The mos important factors determi ning stigmatisation are sex and age Women are more easily stigmatised than men are This also holds for older people From the latent factors support from the family is the most im porshytant Thc more one receives SUppOrL from ones fam ily the less one is stigmalised Anothcr influence on stigmatisation comes from belief in the curability of the TB onstruct The more one believes that TB is curable the less one is stigmatised
These results sugges t that a robust position within society prevents a person from being stigmatised
We then tried to link the stigmatisation of the TB patients and the ir complianl wilh lhe directly observed therapy The restricted theoretical model reveal s that ti influence of stigmatisation on compliance only becomes clearly visible af ter intro ducing the regularity and the duration of the therapy as intervening variables closer examination compliance would appear to be a rather hybridconcept whi can take various forms and has many depths Compliance comes clearer to the [ (I when regularity and du ration are separated In the model stigmatisation with effect of -016 affects regul arity Subsequently regularity has a direct effect of on eomplianee but lhere is a stronger effect on duration and from there on comp anee The regularity and the duration of the therapy tberefore form a tandem whi ca n be brought out of balance by stigmati sation anclilo longer prov ides any gu antees for compliant behaviour
Figu re 3 Siructuralmodel of complio ncc anJ TB
SignificCllce (p-PO ll t) =0 05 =00 =000
Note Fit statistics for structural model X2n~~) =175 26 P=00 GFl =96 RMR =041 CFl =lJ
PNFl =72 NNFI =96 RMSEA =039
SS Discussion
Compliance the fin al link in the causal model is a di ffi cult concept operationalise because it refers to a complex reality The treatment of most inf uumlous diseases oceurs in a di rectly observed way (Porter amp Ogden 1997) H0 ever in practice directly observed therapies can be implemented in a variety ways For examplc DOT for sexually transmitted diseases of ten means obsef tion of a single dose of treatment whereas DOT for leprosy entails monthly ob~ valion by a health care worker of doses of ri fampicin and clofazimine Tbe 001 control strategy reeommended by the WHO for tubercul os is is based on a com nation of four types of medici ne which have to be taken together for the fi rst t
months of lrcat ment HeLlith lJre worken ensure that the I ight Ill ed icine is lak n in the right doses and fo r the cornc t length of ti me Supervis ion ean he a CLlllllshy
p ished by having the pati ent visit the cimie hosp italis ing the patient or scnuin a health care workeI to visit the pa tients home or workplace For directl y ohsnvcd therapy fe l TB it i essenti1l that superv isi on continu e~ every day for th liumlrst two months and idea lly for the entire course of the treatment The wide vltlriations in DOT-contro strategies have resulted in a situation where compliance Illci 1l111lshy
compliance have become e la~t ic eoncepls Who is campliant and who is not~ It all depends on the nature and Ihe t ve l of thc sl3ndard We cncoun tered a di vcls il y of defin itiolls with in the framew)lk or the cLJ l1lbat aga inst tube rcu l o~i-
A retrospective study (from J977) on co mpli ance of TB pat ients revealed that the default ra Ie of the out-putient population in rural Pak i~ta n amounted iO 66 Default was defined as fa ilu re to uttend the weck ly tu berc ulosis clinic fo r a period of one month (Sloan amp Sloan 1981) A fo llow-up study ( 198g-90) showed that 72 oc of the TB patients registered in Bethani a Hosp ital did not complete their 12 months trea tment coure Although the in troduction of a short-course (8 months) regimen improved the compliance default rates (56) contin ued to be high (Liefooghe et al 1995) In 1991 however 76 of TB patients reg istered in the Pakistan Institute of Chest Diseases (S indh) had kep t to the short-course reglmen for two months 2 1 had left the hospi ta l against medical advice and 3 had died (Pathan et al 1992) A study carr ied out in the lndian Wardha dislrict revealed that TB patientlt who fai]cd to take their medici ne for more than 15 days were regarded as non-comptiant because this definition is most in keeping with the adopted adshyministrative procedure (Barnhoorn amp Adriaanse 1992) In a study performed in Denver USA non-compl iance with DOT for TB was detined as foll ows (I) missing ~ 2 consecuti ve weeks of DOT (2) prolongation of treatment gt 30 days due 10 sporadic missed doses or (3 ) incarceration for presenting a th rem lO public health (Burman et al 1997) At least 18 of patients who received out-paLient DOT via the Denver Metro TubercLIl os is Clinic met at least one of these cri teria
In concusion therefore there is no golden standard for defining compliance In our study compliance the fi nal outcome which has to be explai ncd in the model is viewed from a dichotomous viewpoint On the one hand there is the category of compliant patients they com plete thei r the ra py in full and as a general rule al$o unshyderwent a sputum tes t confirming Ihem as TB negative On the other hand there is the category of non-com pliant patients they did not com plete their therapy so a sputum test was not carried out We also adopted the com pletion or fai lure to comshyplete the short -co urse direc tl y observed therapy the bas ic criterion used in the exshyam pIes given above as the key cri terion for our defi ni tion of com pliance The structural model (see Fig ure 3) demonstra tes th at it is important to systemat ically di stinguish the reguarity and the du ration of the therapy to gain a bctter undershystanding of the concept compliance Regularity is achieved when there are no or only sporadic interru ptions during the thcrapy In t hi ~ connection we refer to missed appointments or missed doses of medi cation The durarjoll of the therapy on the e ther hand refers to the treatment duration of eigh[ months which has to be
111 JIII 1 1 1III IJ IKLl 11 lH~Ult I IJ 11111lt ) ~
respected in the DOTS-regimen Two dlv iati ons are possiblc here Either Jo wn shyward the patient ends thc treatment premature1y and is regarded as d efaulter Ol upward- the period of treatment is extended because interruptions during the treatment have [0 be compenslIteti for artcrwards Both deviations from the norm indieate non-compliance Any com parison with the above referred to non-complishyance ra[es fa ils because the phenomenon is constantly regarded from di fferent anshygles Hav ing said that the folowing fac ts in our research on (non- )col11pl iancc among the 621 TB patients are worth mentioni ng
Aftel subtracti ng the nUlllbcr (l f pntients who have died (6Oc) thase who have transferred to another treaUllent centre (29r) and thc tiny group of patie nt~ where the treatmen t failed (I ) 563 pat ients remai ned According to our de liumln ition 779 of the latter group are compliant and 23 are non-compliant aresuIt which is c10sely in keepi ng with the situation at lhe lnsti tu te of Ches[ Diseases in the prov shyince of Sindh The number of in terruptions is used to indicate the regularity of the trcatment 48 of patients did not inlerrupt their treatment at all 34 in terrupted it once and 18 interrupted it various times As far as the duration of the lherapy is concerned the norm of eight months is ach ieved by 55 of patie nts [he norm i not achie ved laquo 8 months) by 33 of patients and the nonn is exceeded (gt 8 months) by 12 of patients
Broadly speaking three out of four paticnts is compliant One out of four is nOI1shycompliant interruptions during the treatmen t (because appoin tments or medicashytion is sporatlicall y missed) or failure to complete the ideal duration of treatmenl (because patients drop out too early or have to followan extended course of treatshyment) As far as establishi ng compl iance is concerned it would seem that 77 ck of patients is heading towards the WHO-target fo r global tuberculosis control namely cure 85 of the detected new smear-positive TB cases (Seita 1996 p 134)
When interpreting the results it is also important to disti nguish between ho~ p ishytalised patie nts and out-patients As we al ready stated earlier duri ng lhe rirst month of treatment 80 of patients were hospitalised Af ter the second month this number dropped to only 48 Permanent supervision at the hospital ensures that hospitalised TB patients are by definition compliant the DOTS-regime n is strictly enforced As far as non-compliance of the out-patient population is co ncerned wc noted that 17oc missed at least one appointment during the first month of treatshyment and that this number dropped 10 1I aftel thc end of the second month The first month is therefore critica especially fol patients who are not hospitalisetl Since they do not res ide at the hospi tal and only come for consultations thty enshycounter far greater difficulties internalising the norms underlying the DOTS-regishymen
The model hinges on the latent construct of stigmatisation Stigmatisation afshyfects compl iance through the Ta ndem of regu la ri ty and duration of therapy Persons who have been strongly stigmatised display more irregular illness behaviour and find it more problematic to see the ditficult and troublesome trealment through 10
[he end In th is respect il could be sa id that ending or interrup[ing the DOTS-reg imiddot
men is nol due to a Jack ol organi satioll On the contrary they are Illcchallisl llS which help to relieve thc pain of sli gmatisation ensuring that for a wh ik the TH pal ient does not have 10 he as hamed and can take a brea k when the prc-url of Ihc medical rcgimen beeomcs toa heavy (Massaro 1997) According 10 GollIllans terminology devi ali ng from the slandards of thc DOTS- rcgimen can hl rcgOl rdcJ as a technique fo r conlrolling in fo rmation The questions or whelher 10 revcal or hi de to con1iumlde in someone or keep qui et to lie or be truth ful and to who l1l hnw when and where are tricks for stoppi ng Ihe exhausting process of bleacutellllc hy socishyety They are in su mmary stra tegies to lWlwRc ( IpoiId idllltity (Schcpcr- amp Nievaard 1995 p 42-43) In Ihe mode l th rec social conditions affecl thc dcgrcc of sligmati sation of TB pat ients These co ndi lions have 10 be taken inlo account 10 reduce the lim ils to pat ienl compliancc with DOTS-strategies
The first cond it ion is rclated to the dem ()g mphico Iilloion of the pili cllt anJ comprises two variab les from the exogenous set ie gender and age FCi llalc pashytients were stigmatised more than male pat ients and older patients Wlr~ si igllwshyti sed more than young persons BOlh lin k~ are highl y significant As house wivcs or elderl y members of the ex tended fa mi Iy many have a low socio-econol11 ie Ialu For them health is above all J quest ion of physical strength (W inkvist amp Akhtar 1997) The loss of phys ical strength Ihlough tubercul osis the fact that tl1Oc who have been sl ricken wilh the diseas( can no longer perform hard labour do the housekeepmg no longer be reproducti ve etc are important contributors to stigshymat isation This is all the more so in lhe countryside where ex ternal signs of vu lshynerability often do not suffiumlce to relieve peopl e from their nonnal socill tasks in the fami ly and vill age
The second condition cl ose ly concerns the beiefofT8 patiel1ll in the curabifir of th eir disease We already said earlier that th is laten t construct in our research displayed features of serendi pity It is el istinct from stricl measurements ofrational med ical knowledge because it emphasises praxis ie implementing knowledge and acti ng on insights The higher the soc io-economie slatus the grealer the belief in the curabil ity of TB It is impossi ble to ignore the phenomenon of social stratifishycation when analys ing ill ness behaviollr of TB patients Patients wi th a higher proshyfessional rank have great faith in the curability of their disease The opposite also applics in equal measure unemploy ment and illileracy are cond ucive for nonshycompl iam behaviour Perhap~ the hard core of pariahs outcasts vagrants vagshyabonds tramps chronie drllnkards and drug add icts (Merton 1968 p 207) repshyresenlSthe most dangerous ri sk group for all TB control programmes When Robshyert K Merton in 1949 developcd hi s we ll-known typology of modes of adaptation by indi viduals within the cu ltu re-bearing society he discovered that these populashytion groups displ ayed retreatiII their mode of adapl3tion which implies the reshyjec tion of cul tural goals and institutional means After all why should anyone reshymain healthy And why should we lIse DOTS as Q method Does it make any difshyference) There is a negative correlat ion between belief in the curability of TB and the degree of stigmati sation Persons who are convineed they will soon be cured and capable of strictly following the medical regimen will be less stigmatised
1 ll i bull I III I 1 11 11 10-- 1 1 middot111 middotmiddot middot 1 middot _
The third condit ion is siluateel at the leve l of the social netllo rks in wh ich TB middot patients function As a general rule it can be sa id thaI persons who tcceive mor~ help from olhers are less likely 10 be stigmati sed Roughl y six out of ten pati ent~ are married and fo r married women the family-in-I aws occ upy the cen tral po- it iol in their social nelwork The model established a negati ve relationshi p betwec l support from blood re lati ve~ and support from the family-in-Iaws Solida rilYvvitl the fa mily-in-Ia ws red uces ~olidarity with biooeI relatives This app lies both il general but also in the specifi( framework of help and support in ti mes of illness The fear manied fe male TB patients have of being abancloned by their hll ~banJ and no 10nger being able to perform their domesr ic tasks should not be unMrcst i mated During a study into thc relcltion between poverty and TB in Bombay re male patients said thaI thei r husbands and mothers-in-Iaw repeated Iy sent then back to their nata l home until such lime as Ihey were cured They were often al cused of bringing the disease from their natal homes and were threatened with sep aration (Nui r et al 1997 p 8 1) The model revea led that the TB patiems who re ceived the least support from their family were stigrnatised most Th is recalls th relational natu re of all type of sti gmatisat ion People are given a negative SOCiH label or are shielded from it Your family may support you through thick and thin encourage you to do the right th ing help to fi nance treatment etc Converse l) your fam ily mayabandon you keep your situation quiet to prevent loosing fac anel keep the family reputation unb1emished
lil Pakistani society anel particularl y in l11any village and se ttl el11Cnb in th Punjab social networks and stigmati sation are inextricably li nkeel and have al enormous influence on community li fe Thc biraderi the patriarcha l nelwork 0
kinship fo rms the framework 101 social and coml11uni ty networks Special event and rites of passage such as birth the ci rcumcis ion of a son marriage allli th death of an old person si rengthen lhis solidarity within the biraderi The biradel use many other occasions to promote social and community networks and ill ne - is perhaps one of the most important When a daughter-in- Iaw becomes seriousl iJl or is hospitalised her children are either looked after by the other daughters (1
the house or are temporarily housed with other members of the birade ri If Ihe sol breadwinner of a household cannot work because he is seriously ill his nearest rel atives and olher members of his biraderi provide mora material and fi nancia l o up port These socia1 and communily links rernai n intact even after emigration Paki stanis who have emigrated to Grea t Brita in for exam ple continue to receive muc support from their biraderi (Anwar 1979) Whenever help is sought in Pakistar communities famil y and bi raderi are preferred According to a sociologic al stud carried out in Rochdale a toW D in the north of England hel p is only sOllght frOl farmer fellow viJ1 agers friend s neighbours Olher Pakistanis and the res t of 50CI ety after all possibil ities in the biraderi-network have been exhausted A TB pil tient who is admitted to hospital will initially be visited by me mbers of hi biraderi They wi llusuaJ1y be gi ven a few hundred rupees and the trad itional fru i However as news about the nature of the illness spreads within the bi rade ri cor tacts become less frequent The negative COITeiation between fa mily support an
sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more
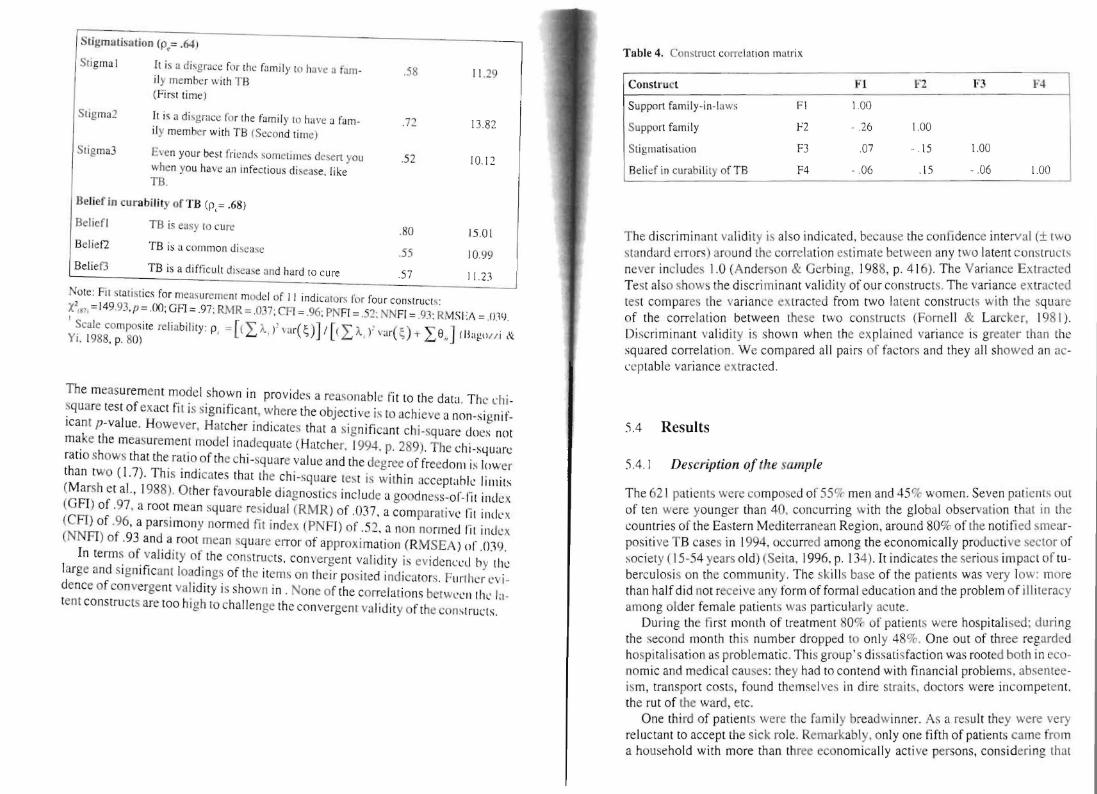
Stigmatbation (p= 64)
Stigmal It is a disgrace fOf the fumily to have a f3mshyily membcr with TB (Fi rst time)
Stigmu 2 It is a disgracegrave for the family to ha ve J fa mshyily member with TB (S econd time
Stigma ven your bes t fli cnd olllctirncs desen you when you have all infectious di seasc like TB
Belief in curabiJity of TB (p= 68)
Belief TB is easy 10 cun 80 1501 Belie fZ TB is I com mon disease 55 1099 Belief] TB is a di ffi Cll lt dicase 3nd hard to cure 57 I I 2l
Note Fit sla tist ics for mcasurelllent model of 1 1 indicators for four construCIs 2
X IK7 =14993p = 00 GFl=97 RMR = 037 CR = 96 PNFI =52 NNFI = 9J RMS I = OW
I Scale composite relinbilily p = [(I Agravef ) ~ IImiddot(eacute)][(I Agrave I ) ~ vlr( ) + I S] (lOl-o l i amp Vi 1988 p 80)
The measurement model shown in provides a reaso na bl e fit 10 the dat1 Thc ehi shysquare test of exact fit is significant where the objecti ve is to achieve a non-signifshyicant p-value However Hatcher indicates that a significant ch i-square does not ma ke the measurement mode l inadequate (Hatchcr 1994 p 289) The ehi-square ratio shows th at the ratio of the chi-square value and the degree of freedolll is lowcr than two (17) This ind icates that the chi-sguare tes t is wilhin acceptahk lilllits (Marsh et al 1988) Other favourable diagnostics incIude a goodness-or-fiumlt illdegrave X GFI) of 97 a root mean square res idual (RMR) of on a comparati vL rit illtkx CFT) of 96 a parsi mony normed fit index (PNFI) of 52 a nOn normed rit index NNFI) of 93 and a root mean square error of approxi malion (RMSEA ) of rn9
In tenns of valid ity of the constructs con vergent validity is evidcnlxd by tilegrave large and significan t loadings of the item on thei r positcd ind icators FUIhc r (v ishydence of convergent va lidity is shown in None of the correlalions betwLcll Ihl 1 shytent construClS are too high to challen ge the convergent validity oft he cons lructs
F3 F4
100
- 06 100
The discriminan t validi ly is also indicated because the conlide nce interval (plusmn two slandard errors) around the correlati on es ti mate between any two latent construclS never includes 10 (Anderson amp Gerbing 1988 p 41 6) The Varianee Extracted Test also shows the discrim inant validity of our constructs The variance extrac ted tes t compares the variance extracted from two laten t constructs with the square of the correb tion between these two constructs (FomelI amp Larcker 1981 ) Discriminant validi ty is shown when the ex plained variance is greater than the squared correlation We compared all pairs of fac tors and they all showed an iCshy
ccptable variance ex tracted
)4 Results
) 41 Description of the sample
The 62 1 pati ents were composed of 55 0( men and 45 women Seven patients out of ten were younger than 40 concuning with the global observalion that in the countries of the Eastern MeditetTanean Region around 80 of the notified smearshypositi ve TB cases in 1994 occ urred among the economically productive sector of society (15 -54 years old) (Seila 1996 p 134) Tt indicates the serious impact of tushyberculosis on the comrnun ity The skills base of the patiems was very low more than half did not receive any form of fonnal education and the problem of illi teracy aillong older female patients was particularly acute
During the fi rst 11l0nth of lreatment 80 of patien ls were hospitalised during the second month th is number dropped to onl y 48 One out of tluee regarded hospitalisation as problematic This groups di ssalisfaction was rooted both in eco~ nomic and medical causes they had to contend with financial problems absemee shyism transport costs found themseJves in dire sLrai ts doc tors were in competent the rut of he ward etc
One third of patien ls were the family breadwinner As a resuit they were very reluctant to accept the sick mIe Remarkably only one fifth of patients came from a household with more than three economically act ive persons considering lh at
roughly 70 of household eon)i steJ of si x und of ten more Illcm bers The smal nurn ber of econornicall y active person- within the ex tcnded farnilie - C311110t be atshytributed to a large nu mber of ehi ldren because rOlgh ly hal f of the pat ients had less than three children
Sixty percelt ofpalielts placed heulrh al the top oft hc standard orvuluc This is not rea ll y surprising given the fact thal the responclents were confroltcd with ~cr ishyous health prob lems which have absolu te priorit) in their dail y li ve ~ lIld prCSllll1C the recove ry of bath hea lth balallCe anu the improvement of health pOlc nlia Ic shycording to Khayat these IWO dimensions of health are tleeply motet il1 Islalnie Irashydi tion and thefiqlI of health (Khayat 1997) Tf we ZOOIll in on the largL gro llp placshying heal th at the top of the standecircll-d of valuc wc sec Ihal the followi ng vllICS arc also held in high regard falllily and marriage (thc most important aftcr hla llh ) honour and integrity religion and fait h work money (thc Icast importanI ) AIshythough female patiems and patients wilh the lowest socio-economie status atshytached most importance to health it toes not mean that t he~e groups J i-played Ihe mOSl adequate illness behav iour On the contrary the~e groups ltI nd in particlilar housewives the un skilled unernp loyed and sociall y de pri ved ofte n do Ilol J1o~ scss the most elementary knowledge abou t TB (causes sylllptoms alld eollilitlll) which is needed to pre vent infec tion or undergo routine trcatment (Grce n Il)l)) p 192-196) The concept of (external) locus of control ofte n used in rlsealh on compliant behav iour and the fa tal islic health attitude lin ked to th i alslJ applied in thi s context of TB co ntro l (Mcchanic 1983)
Throughout the analys is the operational isation ol belief in the curlli Iil Yui the disease of ten appea red as a variab Ic wi th ~e relldipit y -charactcri ~tics This vlIiahle rneasures the confi dence ~i d people have in suumll vi ng their prob lem situ alilln Trust enables Ihe complexi ry of a social system to be reduced without funher aULgt the sick can rely on thei r part ner fal11il y health worker etc to channel the ir mcdical regimen It is cJear that preci sely lhis confidence is shattered by the TB it igma thereby reducing belief in the curability orTB in genera
Correctly assessing the treatment s duration is characteri stic for patients who strongly believe in the curability of their di sease However th is element of inforshymation is certainly not common knowledge when the treatment starts_Only one in three patients is aware that the trear ment will last several months However after one mon th this number doubles and af ter two months it increases even furthcr (73 ) We established that paliems with the lowest socio-economie statu s often did not possess the Illost rudimentary objecti ve medica l knowledge_There is Iitershyally a wall between them and the cogn itive elements req ui red This wa ll cannot be tom down on y due to reasons related to soc ial strmificaLion On the other hand persons who do nol mind regular check-ups a reg imen of aw kward medication and the costs involved who (hin k it is all worthwhile and are confiden t thei r treatshyment will result in a cure are not necessarily more ski lied or have a higher professhysional rank Ir would seem that another phenomenon another mechanism is ac ti ve as far as belief in Lbe curability of TB is concerned Thinking exclusively in tems of social stratification or Iumping techniq ues of rejec tion together as ways of
bull I I I bull I ~ II ~I I ~ bull I bullbull I L bullbull I bull bull bull bull bull bull
dealing with marginal categories (Douglas 1994 p 85) does not suffice lU gain l bettel understanding of the ideal treatment condition s
Compliance has lO be viewed not only from the socio slralificatiol1 perspeclii but also from the sl ig lllarismioJl persp(crive At thc onset ofthe treatlTlent and aftel two month s treatment sevell statemenlS concern ing stigmatisation were prelgtentecl to the patients A score had to be given on a six-poi nt scale (I =dont agree at all 5=agree 6=strongly ag ree)
The two stateme nts most people i e more than 80 agreed with (score 5 or 6) both at the onset of the trearment and [WO monlhs afterwards were Jf someont has TB hejshe avoids ralking about it with ot her persons and Af ter recoverinf from TB everyone treats yO Ll the same way lS bcfore If someone contracts TB il is bes t to keep quict about it If thei r environment doesn t know anythi ng about il th~y will not treat them di fferentl y af ter they hJ ve recovered
Thc other statement many ie more than 60 agreed with both at thc begin ning of the treatment and af ter two mO IHhs was Peope who arc treated for TB should ta lk to others about it
There were three statements alrnost half of pati ent- ie more than 401r agree with both at the onset of the treatment aOl af ter two months It is a disgrace for thl famil y to have a fa mily member with TB Even your best fri ends someti me ~
desert you when you have un infectious disease li ke T B and 11 a young persol catches TB heshe will experience the consequences for the rest of hisher lirc
Thc statement only a minority ie one out of four patients agreed with both a the onset of the treatment and af ter two months was It is diffi cult to earn your Ii ing after recovering from TB The fact that only very few regarded the TB prob lem in tenns of income is re lnted to the fact that during tbis life-threatening situa ti on_ the trentment has absol ute priori ty and takes precedence over all other form of need
When the onset of the treatment is compared Nith the situation two month later there are no shifts in the statemenls ranking order This means that the firs two months of treatmen t - eg at the hospitalor contact with health carers - dOt not real ly affect their situation On the contrary the stigmatisation continues t( proliferate and feste r causi ng damage in its wake According to Goffmans termi nology it conti nues to transform TB sufferers from discreditabe tO discredilel (Goffma n 1990 p 57 ) Only two statements poi nt to a possible evolution durin~ the first two months but they do not really di sruptthe ran ki ng order in any signifi cant way Ir rerers to the statement PeopJe who are treated for TB should talk t( others about it 68 tgreed at the omet of the treatment and 78 af ter tWt months treatmenl This increase indicates that TB patients still regard opennes about their illness und breaking taboos about the subject as a norm and future ex pectati on Whilst 54 agreed at the beginning of the treatment with the state lllcn Even your best fri ends sometimes dcsert you when you have an infect ious dis ease like TB this dropped to 45 af ter lwo months treatment Ir would appea that the channels for seeking informal care do not dry up for those who respect th medical regimen
We will illustrate thatthe social Il etwork lovering the pa tien t- nlatiolls with all significant others can cithcr increasc or reduce st ig lll ati satioll iS lllilh 1 ()IJt) p 138-155) The com position of these soci al networks i- very hcterogcilcous Thcy can perhaps bes t be analy-ed by di sti nguishing the nuelear fam ily from Ihe ex shytended fa mily As far as the nuclear fam ily is cOllce rned 62 of pllicnls wcn~ married 31 were si ngle 5fr widowed anel 2 divorced For married felll aie pashytients ( 173 out of a tota l of 387 married pa tients) rclati oll) with the fa mi Iy- ill-Iaws and in particular the mother-in-Iaw were very importan t indeecl For alll10sl half of all patients (47) thc extc ll(kJ fam il y eOll1 pri -ed cighl or more perso ll- IIs li all y adu lt who all li ve under the ) (l IllC roo f In 20 of households there wen ilO ehi 1shydren (yolJnger than 12 yca r~) 327 ot households had one or two childrclI 2C1r had three or four children and 21 or had fi ve or more
542 Causal model
The proposed structural model in Figurc 2 was tested by using con veuml ntionalmaxi shymu m likel ihood est imatioll techniques Thc model~h(lwed an acecptabk fit Again the ehi -square tes t of exact fit is ~i gni tiuml ca nt but the eh i-square ratio is lower than two (07) Other favourable diagnosti c~ include a goodncss-of-tiumlt index (GFl) of 96 a rOol mean square rcs idual (R MR) of 041 a comparati ve fi l index (CF) of 97 a parsimony normed fit index iPNFI) of 72 a non normed fit index (NNFI) of 96 and a root mean squ are enOf of approximation (RMSEA) of 039 All of the path coefficients are signifi cant
Anderson and Gerbing recommend a chi-square di ffe rence tes t (CDT) in order to enhanee the confidence in the structural part of the model (Anderson amp Gerbing 1988) The CDT compares the structura l model (which is a res trictecl theoretical model MT) with an uneons trailled alternative model (Mul The relevant test statis shytics (MT has 122 df and a X2 of 17526 ML has 93 df anel a X2 of 171 89) lead to a non-significa nt CDT (X2 difference is 25 33 at 35 df) and an acceptance of M
r Thu s our restricted theoretica model (Figure 3) is preferred to the theoretica uncorrelated model
Since most of the [esH tat is ti c~ show an acceptable model we can look at the reshysu lts of the two-step model presentcd earlier Firsl we tried to model the influshyences on the degree of stigmatisation of a patient These influenees come from very different sou rces The mos important factors determi ning stigmatisation are sex and age Women are more easily stigmatised than men are This also holds for older people From the latent factors support from the family is the most im porshytant Thc more one receives SUppOrL from ones fam ily the less one is stigmalised Anothcr influence on stigmatisation comes from belief in the curability of the TB onstruct The more one believes that TB is curable the less one is stigmatised
These results sugges t that a robust position within society prevents a person from being stigmatised
We then tried to link the stigmatisation of the TB patients and the ir complianl wilh lhe directly observed therapy The restricted theoretical model reveal s that ti influence of stigmatisation on compliance only becomes clearly visible af ter intro ducing the regularity and the duration of the therapy as intervening variables closer examination compliance would appear to be a rather hybridconcept whi can take various forms and has many depths Compliance comes clearer to the [ (I when regularity and du ration are separated In the model stigmatisation with effect of -016 affects regul arity Subsequently regularity has a direct effect of on eomplianee but lhere is a stronger effect on duration and from there on comp anee The regularity and the duration of the therapy tberefore form a tandem whi ca n be brought out of balance by stigmati sation anclilo longer prov ides any gu antees for compliant behaviour
Figu re 3 Siructuralmodel of complio ncc anJ TB
SignificCllce (p-PO ll t) =0 05 =00 =000
Note Fit statistics for structural model X2n~~) =175 26 P=00 GFl =96 RMR =041 CFl =lJ
PNFl =72 NNFI =96 RMSEA =039
SS Discussion
Compliance the fin al link in the causal model is a di ffi cult concept operationalise because it refers to a complex reality The treatment of most inf uumlous diseases oceurs in a di rectly observed way (Porter amp Ogden 1997) H0 ever in practice directly observed therapies can be implemented in a variety ways For examplc DOT for sexually transmitted diseases of ten means obsef tion of a single dose of treatment whereas DOT for leprosy entails monthly ob~ valion by a health care worker of doses of ri fampicin and clofazimine Tbe 001 control strategy reeommended by the WHO for tubercul os is is based on a com nation of four types of medici ne which have to be taken together for the fi rst t
months of lrcat ment HeLlith lJre worken ensure that the I ight Ill ed icine is lak n in the right doses and fo r the cornc t length of ti me Supervis ion ean he a CLlllllshy
p ished by having the pati ent visit the cimie hosp italis ing the patient or scnuin a health care workeI to visit the pa tients home or workplace For directl y ohsnvcd therapy fe l TB it i essenti1l that superv isi on continu e~ every day for th liumlrst two months and idea lly for the entire course of the treatment The wide vltlriations in DOT-contro strategies have resulted in a situation where compliance Illci 1l111lshy
compliance have become e la~t ic eoncepls Who is campliant and who is not~ It all depends on the nature and Ihe t ve l of thc sl3ndard We cncoun tered a di vcls il y of defin itiolls with in the framew)lk or the cLJ l1lbat aga inst tube rcu l o~i-
A retrospective study (from J977) on co mpli ance of TB pat ients revealed that the default ra Ie of the out-putient population in rural Pak i~ta n amounted iO 66 Default was defined as fa ilu re to uttend the weck ly tu berc ulosis clinic fo r a period of one month (Sloan amp Sloan 1981) A fo llow-up study ( 198g-90) showed that 72 oc of the TB patients registered in Bethani a Hosp ital did not complete their 12 months trea tment coure Although the in troduction of a short-course (8 months) regimen improved the compliance default rates (56) contin ued to be high (Liefooghe et al 1995) In 1991 however 76 of TB patients reg istered in the Pakistan Institute of Chest Diseases (S indh) had kep t to the short-course reglmen for two months 2 1 had left the hospi ta l against medical advice and 3 had died (Pathan et al 1992) A study carr ied out in the lndian Wardha dislrict revealed that TB patientlt who fai]cd to take their medici ne for more than 15 days were regarded as non-comptiant because this definition is most in keeping with the adopted adshyministrative procedure (Barnhoorn amp Adriaanse 1992) In a study performed in Denver USA non-compl iance with DOT for TB was detined as foll ows (I) missing ~ 2 consecuti ve weeks of DOT (2) prolongation of treatment gt 30 days due 10 sporadic missed doses or (3 ) incarceration for presenting a th rem lO public health (Burman et al 1997) At least 18 of patients who received out-paLient DOT via the Denver Metro TubercLIl os is Clinic met at least one of these cri teria
In concusion therefore there is no golden standard for defining compliance In our study compliance the fi nal outcome which has to be explai ncd in the model is viewed from a dichotomous viewpoint On the one hand there is the category of compliant patients they com plete thei r the ra py in full and as a general rule al$o unshyderwent a sputum tes t confirming Ihem as TB negative On the other hand there is the category of non-com pliant patients they did not com plete their therapy so a sputum test was not carried out We also adopted the com pletion or fai lure to comshyplete the short -co urse direc tl y observed therapy the bas ic criterion used in the exshyam pIes given above as the key cri terion for our defi ni tion of com pliance The structural model (see Fig ure 3) demonstra tes th at it is important to systemat ically di stinguish the reguarity and the du ration of the therapy to gain a bctter undershystanding of the concept compliance Regularity is achieved when there are no or only sporadic interru ptions during the thcrapy In t hi ~ connection we refer to missed appointments or missed doses of medi cation The durarjoll of the therapy on the e ther hand refers to the treatment duration of eigh[ months which has to be
111 JIII 1 1 1III IJ IKLl 11 lH~Ult I IJ 11111lt ) ~
respected in the DOTS-regimen Two dlv iati ons are possiblc here Either Jo wn shyward the patient ends thc treatment premature1y and is regarded as d efaulter Ol upward- the period of treatment is extended because interruptions during the treatment have [0 be compenslIteti for artcrwards Both deviations from the norm indieate non-compliance Any com parison with the above referred to non-complishyance ra[es fa ils because the phenomenon is constantly regarded from di fferent anshygles Hav ing said that the folowing fac ts in our research on (non- )col11pl iancc among the 621 TB patients are worth mentioni ng
Aftel subtracti ng the nUlllbcr (l f pntients who have died (6Oc) thase who have transferred to another treaUllent centre (29r) and thc tiny group of patie nt~ where the treatmen t failed (I ) 563 pat ients remai ned According to our de liumln ition 779 of the latter group are compliant and 23 are non-compliant aresuIt which is c10sely in keepi ng with the situation at lhe lnsti tu te of Ches[ Diseases in the prov shyince of Sindh The number of in terruptions is used to indicate the regularity of the trcatment 48 of patients did not inlerrupt their treatment at all 34 in terrupted it once and 18 interrupted it various times As far as the duration of the lherapy is concerned the norm of eight months is ach ieved by 55 of patie nts [he norm i not achie ved laquo 8 months) by 33 of patients and the nonn is exceeded (gt 8 months) by 12 of patients
Broadly speaking three out of four paticnts is compliant One out of four is nOI1shycompliant interruptions during the treatmen t (because appoin tments or medicashytion is sporatlicall y missed) or failure to complete the ideal duration of treatmenl (because patients drop out too early or have to followan extended course of treatshyment) As far as establishi ng compl iance is concerned it would seem that 77 ck of patients is heading towards the WHO-target fo r global tuberculosis control namely cure 85 of the detected new smear-positive TB cases (Seita 1996 p 134)
When interpreting the results it is also important to disti nguish between ho~ p ishytalised patie nts and out-patients As we al ready stated earlier duri ng lhe rirst month of treatment 80 of patients were hospitalised Af ter the second month this number dropped to only 48 Permanent supervision at the hospital ensures that hospitalised TB patients are by definition compliant the DOTS-regime n is strictly enforced As far as non-compliance of the out-patient population is co ncerned wc noted that 17oc missed at least one appointment during the first month of treatshyment and that this number dropped 10 1I aftel thc end of the second month The first month is therefore critica especially fol patients who are not hospitalisetl Since they do not res ide at the hospi tal and only come for consultations thty enshycounter far greater difficulties internalising the norms underlying the DOTS-regishymen
The model hinges on the latent construct of stigmatisation Stigmatisation afshyfects compl iance through the Ta ndem of regu la ri ty and duration of therapy Persons who have been strongly stigmatised display more irregular illness behaviour and find it more problematic to see the ditficult and troublesome trealment through 10
[he end In th is respect il could be sa id that ending or interrup[ing the DOTS-reg imiddot
men is nol due to a Jack ol organi satioll On the contrary they are Illcchallisl llS which help to relieve thc pain of sli gmatisation ensuring that for a wh ik the TH pal ient does not have 10 he as hamed and can take a brea k when the prc-url of Ihc medical rcgimen beeomcs toa heavy (Massaro 1997) According 10 GollIllans terminology devi ali ng from the slandards of thc DOTS- rcgimen can hl rcgOl rdcJ as a technique fo r conlrolling in fo rmation The questions or whelher 10 revcal or hi de to con1iumlde in someone or keep qui et to lie or be truth ful and to who l1l hnw when and where are tricks for stoppi ng Ihe exhausting process of bleacutellllc hy socishyety They are in su mmary stra tegies to lWlwRc ( IpoiId idllltity (Schcpcr- amp Nievaard 1995 p 42-43) In Ihe mode l th rec social conditions affecl thc dcgrcc of sligmati sation of TB pat ients These co ndi lions have 10 be taken inlo account 10 reduce the lim ils to pat ienl compliancc with DOTS-strategies
The first cond it ion is rclated to the dem ()g mphico Iilloion of the pili cllt anJ comprises two variab les from the exogenous set ie gender and age FCi llalc pashytients were stigmatised more than male pat ients and older patients Wlr~ si igllwshyti sed more than young persons BOlh lin k~ are highl y significant As house wivcs or elderl y members of the ex tended fa mi Iy many have a low socio-econol11 ie Ialu For them health is above all J quest ion of physical strength (W inkvist amp Akhtar 1997) The loss of phys ical strength Ihlough tubercul osis the fact that tl1Oc who have been sl ricken wilh the diseas( can no longer perform hard labour do the housekeepmg no longer be reproducti ve etc are important contributors to stigshymat isation This is all the more so in lhe countryside where ex ternal signs of vu lshynerability often do not suffiumlce to relieve peopl e from their nonnal socill tasks in the fami ly and vill age
The second condition cl ose ly concerns the beiefofT8 patiel1ll in the curabifir of th eir disease We already said earlier that th is laten t construct in our research displayed features of serendi pity It is el istinct from stricl measurements ofrational med ical knowledge because it emphasises praxis ie implementing knowledge and acti ng on insights The higher the soc io-economie slatus the grealer the belief in the curabil ity of TB It is impossi ble to ignore the phenomenon of social stratifishycation when analys ing ill ness behaviollr of TB patients Patients wi th a higher proshyfessional rank have great faith in the curability of their disease The opposite also applics in equal measure unemploy ment and illileracy are cond ucive for nonshycompl iam behaviour Perhap~ the hard core of pariahs outcasts vagrants vagshyabonds tramps chronie drllnkards and drug add icts (Merton 1968 p 207) repshyresenlSthe most dangerous ri sk group for all TB control programmes When Robshyert K Merton in 1949 developcd hi s we ll-known typology of modes of adaptation by indi viduals within the cu ltu re-bearing society he discovered that these populashytion groups displ ayed retreatiII their mode of adapl3tion which implies the reshyjec tion of cul tural goals and institutional means After all why should anyone reshymain healthy And why should we lIse DOTS as Q method Does it make any difshyference) There is a negative correlat ion between belief in the curability of TB and the degree of stigmati sation Persons who are convineed they will soon be cured and capable of strictly following the medical regimen will be less stigmatised
1 ll i bull I III I 1 11 11 10-- 1 1 middot111 middotmiddot middot 1 middot _
The third condit ion is siluateel at the leve l of the social netllo rks in wh ich TB middot patients function As a general rule it can be sa id thaI persons who tcceive mor~ help from olhers are less likely 10 be stigmati sed Roughl y six out of ten pati ent~ are married and fo r married women the family-in-I aws occ upy the cen tral po- it iol in their social nelwork The model established a negati ve relationshi p betwec l support from blood re lati ve~ and support from the family-in-Iaws Solida rilYvvitl the fa mily-in-Ia ws red uces ~olidarity with biooeI relatives This app lies both il general but also in the specifi( framework of help and support in ti mes of illness The fear manied fe male TB patients have of being abancloned by their hll ~banJ and no 10nger being able to perform their domesr ic tasks should not be unMrcst i mated During a study into thc relcltion between poverty and TB in Bombay re male patients said thaI thei r husbands and mothers-in-Iaw repeated Iy sent then back to their nata l home until such lime as Ihey were cured They were often al cused of bringing the disease from their natal homes and were threatened with sep aration (Nui r et al 1997 p 8 1) The model revea led that the TB patiems who re ceived the least support from their family were stigrnatised most Th is recalls th relational natu re of all type of sti gmatisat ion People are given a negative SOCiH label or are shielded from it Your family may support you through thick and thin encourage you to do the right th ing help to fi nance treatment etc Converse l) your fam ily mayabandon you keep your situation quiet to prevent loosing fac anel keep the family reputation unb1emished
lil Pakistani society anel particularl y in l11any village and se ttl el11Cnb in th Punjab social networks and stigmati sation are inextricably li nkeel and have al enormous influence on community li fe Thc biraderi the patriarcha l nelwork 0
kinship fo rms the framework 101 social and coml11uni ty networks Special event and rites of passage such as birth the ci rcumcis ion of a son marriage allli th death of an old person si rengthen lhis solidarity within the biraderi The biradel use many other occasions to promote social and community networks and ill ne - is perhaps one of the most important When a daughter-in- Iaw becomes seriousl iJl or is hospitalised her children are either looked after by the other daughters (1
the house or are temporarily housed with other members of the birade ri If Ihe sol breadwinner of a household cannot work because he is seriously ill his nearest rel atives and olher members of his biraderi provide mora material and fi nancia l o up port These socia1 and communily links rernai n intact even after emigration Paki stanis who have emigrated to Grea t Brita in for exam ple continue to receive muc support from their biraderi (Anwar 1979) Whenever help is sought in Pakistar communities famil y and bi raderi are preferred According to a sociologic al stud carried out in Rochdale a toW D in the north of England hel p is only sOllght frOl farmer fellow viJ1 agers friend s neighbours Olher Pakistanis and the res t of 50CI ety after all possibil ities in the biraderi-network have been exhausted A TB pil tient who is admitted to hospital will initially be visited by me mbers of hi biraderi They wi llusuaJ1y be gi ven a few hundred rupees and the trad itional fru i However as news about the nature of the illness spreads within the bi rade ri cor tacts become less frequent The negative COITeiation between fa mily support an
sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more
roughly 70 of household eon)i steJ of si x und of ten more Illcm bers The smal nurn ber of econornicall y active person- within the ex tcnded farnilie - C311110t be atshytributed to a large nu mber of ehi ldren because rOlgh ly hal f of the pat ients had less than three children
Sixty percelt ofpalielts placed heulrh al the top oft hc standard orvuluc This is not rea ll y surprising given the fact thal the responclents were confroltcd with ~cr ishyous health prob lems which have absolu te priorit) in their dail y li ve ~ lIld prCSllll1C the recove ry of bath hea lth balallCe anu the improvement of health pOlc nlia Ic shycording to Khayat these IWO dimensions of health are tleeply motet il1 Islalnie Irashydi tion and thefiqlI of health (Khayat 1997) Tf we ZOOIll in on the largL gro llp placshying heal th at the top of the standecircll-d of valuc wc sec Ihal the followi ng vllICS arc also held in high regard falllily and marriage (thc most important aftcr hla llh ) honour and integrity religion and fait h work money (thc Icast importanI ) AIshythough female patiems and patients wilh the lowest socio-economie status atshytached most importance to health it toes not mean that t he~e groups J i-played Ihe mOSl adequate illness behav iour On the contrary the~e groups ltI nd in particlilar housewives the un skilled unernp loyed and sociall y de pri ved ofte n do Ilol J1o~ scss the most elementary knowledge abou t TB (causes sylllptoms alld eollilitlll) which is needed to pre vent infec tion or undergo routine trcatment (Grce n Il)l)) p 192-196) The concept of (external) locus of control ofte n used in rlsealh on compliant behav iour and the fa tal islic health attitude lin ked to th i alslJ applied in thi s context of TB co ntro l (Mcchanic 1983)
Throughout the analys is the operational isation ol belief in the curlli Iil Yui the disease of ten appea red as a variab Ic wi th ~e relldipit y -charactcri ~tics This vlIiahle rneasures the confi dence ~i d people have in suumll vi ng their prob lem situ alilln Trust enables Ihe complexi ry of a social system to be reduced without funher aULgt the sick can rely on thei r part ner fal11il y health worker etc to channel the ir mcdical regimen It is cJear that preci sely lhis confidence is shattered by the TB it igma thereby reducing belief in the curability orTB in genera
Correctly assessing the treatment s duration is characteri stic for patients who strongly believe in the curability of their di sease However th is element of inforshymation is certainly not common knowledge when the treatment starts_Only one in three patients is aware that the trear ment will last several months However after one mon th this number doubles and af ter two months it increases even furthcr (73 ) We established that paliems with the lowest socio-economie statu s often did not possess the Illost rudimentary objecti ve medica l knowledge_There is Iitershyally a wall between them and the cogn itive elements req ui red This wa ll cannot be tom down on y due to reasons related to soc ial strmificaLion On the other hand persons who do nol mind regular check-ups a reg imen of aw kward medication and the costs involved who (hin k it is all worthwhile and are confiden t thei r treatshyment will result in a cure are not necessarily more ski lied or have a higher professhysional rank Ir would seem that another phenomenon another mechanism is ac ti ve as far as belief in Lbe curability of TB is concerned Thinking exclusively in tems of social stratification or Iumping techniq ues of rejec tion together as ways of
bull I I I bull I ~ II ~I I ~ bull I bullbull I L bullbull I bull bull bull bull bull bull
dealing with marginal categories (Douglas 1994 p 85) does not suffice lU gain l bettel understanding of the ideal treatment condition s
Compliance has lO be viewed not only from the socio slralificatiol1 perspeclii but also from the sl ig lllarismioJl persp(crive At thc onset ofthe treatlTlent and aftel two month s treatment sevell statemenlS concern ing stigmatisation were prelgtentecl to the patients A score had to be given on a six-poi nt scale (I =dont agree at all 5=agree 6=strongly ag ree)
The two stateme nts most people i e more than 80 agreed with (score 5 or 6) both at the onset of the trearment and [WO monlhs afterwards were Jf someont has TB hejshe avoids ralking about it with ot her persons and Af ter recoverinf from TB everyone treats yO Ll the same way lS bcfore If someone contracts TB il is bes t to keep quict about it If thei r environment doesn t know anythi ng about il th~y will not treat them di fferentl y af ter they hJ ve recovered
Thc other statement many ie more than 60 agreed with both at thc begin ning of the treatment and af ter two mO IHhs was Peope who arc treated for TB should ta lk to others about it
There were three statements alrnost half of pati ent- ie more than 401r agree with both at the onset of the treatment aOl af ter two months It is a disgrace for thl famil y to have a fa mily member with TB Even your best fri ends someti me ~
desert you when you have un infectious disease li ke T B and 11 a young persol catches TB heshe will experience the consequences for the rest of hisher lirc
Thc statement only a minority ie one out of four patients agreed with both a the onset of the treatment and af ter two months was It is diffi cult to earn your Ii ing after recovering from TB The fact that only very few regarded the TB prob lem in tenns of income is re lnted to the fact that during tbis life-threatening situa ti on_ the trentment has absol ute priori ty and takes precedence over all other form of need
When the onset of the treatment is compared Nith the situation two month later there are no shifts in the statemenls ranking order This means that the firs two months of treatmen t - eg at the hospitalor contact with health carers - dOt not real ly affect their situation On the contrary the stigmatisation continues t( proliferate and feste r causi ng damage in its wake According to Goffmans termi nology it conti nues to transform TB sufferers from discreditabe tO discredilel (Goffma n 1990 p 57 ) Only two statements poi nt to a possible evolution durin~ the first two months but they do not really di sruptthe ran ki ng order in any signifi cant way Ir rerers to the statement PeopJe who are treated for TB should talk t( others about it 68 tgreed at the omet of the treatment and 78 af ter tWt months treatmenl This increase indicates that TB patients still regard opennes about their illness und breaking taboos about the subject as a norm and future ex pectati on Whilst 54 agreed at the beginning of the treatment with the state lllcn Even your best fri ends sometimes dcsert you when you have an infect ious dis ease like TB this dropped to 45 af ter lwo months treatment Ir would appea that the channels for seeking informal care do not dry up for those who respect th medical regimen
We will illustrate thatthe social Il etwork lovering the pa tien t- nlatiolls with all significant others can cithcr increasc or reduce st ig lll ati satioll iS lllilh 1 ()IJt) p 138-155) The com position of these soci al networks i- very hcterogcilcous Thcy can perhaps bes t be analy-ed by di sti nguishing the nuelear fam ily from Ihe ex shytended fa mily As far as the nuclear fam ily is cOllce rned 62 of pllicnls wcn~ married 31 were si ngle 5fr widowed anel 2 divorced For married felll aie pashytients ( 173 out of a tota l of 387 married pa tients) rclati oll) with the fa mi Iy- ill-Iaws and in particular the mother-in-Iaw were very importan t indeecl For alll10sl half of all patients (47) thc extc ll(kJ fam il y eOll1 pri -ed cighl or more perso ll- IIs li all y adu lt who all li ve under the ) (l IllC roo f In 20 of households there wen ilO ehi 1shydren (yolJnger than 12 yca r~) 327 ot households had one or two childrclI 2C1r had three or four children and 21 or had fi ve or more
542 Causal model
The proposed structural model in Figurc 2 was tested by using con veuml ntionalmaxi shymu m likel ihood est imatioll techniques Thc model~h(lwed an acecptabk fit Again the ehi -square tes t of exact fit is ~i gni tiuml ca nt but the eh i-square ratio is lower than two (07) Other favourable diagnosti c~ include a goodncss-of-tiumlt index (GFl) of 96 a rOol mean square rcs idual (R MR) of 041 a comparati ve fi l index (CF) of 97 a parsimony normed fit index iPNFI) of 72 a non normed fit index (NNFI) of 96 and a root mean squ are enOf of approximation (RMSEA) of 039 All of the path coefficients are signifi cant
Anderson and Gerbing recommend a chi-square di ffe rence tes t (CDT) in order to enhanee the confidence in the structural part of the model (Anderson amp Gerbing 1988) The CDT compares the structura l model (which is a res trictecl theoretical model MT) with an uneons trailled alternative model (Mul The relevant test statis shytics (MT has 122 df and a X2 of 17526 ML has 93 df anel a X2 of 171 89) lead to a non-significa nt CDT (X2 difference is 25 33 at 35 df) and an acceptance of M
r Thu s our restricted theoretica model (Figure 3) is preferred to the theoretica uncorrelated model
Since most of the [esH tat is ti c~ show an acceptable model we can look at the reshysu lts of the two-step model presentcd earlier Firsl we tried to model the influshyences on the degree of stigmatisation of a patient These influenees come from very different sou rces The mos important factors determi ning stigmatisation are sex and age Women are more easily stigmatised than men are This also holds for older people From the latent factors support from the family is the most im porshytant Thc more one receives SUppOrL from ones fam ily the less one is stigmalised Anothcr influence on stigmatisation comes from belief in the curability of the TB onstruct The more one believes that TB is curable the less one is stigmatised
These results sugges t that a robust position within society prevents a person from being stigmatised
We then tried to link the stigmatisation of the TB patients and the ir complianl wilh lhe directly observed therapy The restricted theoretical model reveal s that ti influence of stigmatisation on compliance only becomes clearly visible af ter intro ducing the regularity and the duration of the therapy as intervening variables closer examination compliance would appear to be a rather hybridconcept whi can take various forms and has many depths Compliance comes clearer to the [ (I when regularity and du ration are separated In the model stigmatisation with effect of -016 affects regul arity Subsequently regularity has a direct effect of on eomplianee but lhere is a stronger effect on duration and from there on comp anee The regularity and the duration of the therapy tberefore form a tandem whi ca n be brought out of balance by stigmati sation anclilo longer prov ides any gu antees for compliant behaviour
Figu re 3 Siructuralmodel of complio ncc anJ TB
SignificCllce (p-PO ll t) =0 05 =00 =000
Note Fit statistics for structural model X2n~~) =175 26 P=00 GFl =96 RMR =041 CFl =lJ
PNFl =72 NNFI =96 RMSEA =039
SS Discussion
Compliance the fin al link in the causal model is a di ffi cult concept operationalise because it refers to a complex reality The treatment of most inf uumlous diseases oceurs in a di rectly observed way (Porter amp Ogden 1997) H0 ever in practice directly observed therapies can be implemented in a variety ways For examplc DOT for sexually transmitted diseases of ten means obsef tion of a single dose of treatment whereas DOT for leprosy entails monthly ob~ valion by a health care worker of doses of ri fampicin and clofazimine Tbe 001 control strategy reeommended by the WHO for tubercul os is is based on a com nation of four types of medici ne which have to be taken together for the fi rst t
months of lrcat ment HeLlith lJre worken ensure that the I ight Ill ed icine is lak n in the right doses and fo r the cornc t length of ti me Supervis ion ean he a CLlllllshy
p ished by having the pati ent visit the cimie hosp italis ing the patient or scnuin a health care workeI to visit the pa tients home or workplace For directl y ohsnvcd therapy fe l TB it i essenti1l that superv isi on continu e~ every day for th liumlrst two months and idea lly for the entire course of the treatment The wide vltlriations in DOT-contro strategies have resulted in a situation where compliance Illci 1l111lshy
compliance have become e la~t ic eoncepls Who is campliant and who is not~ It all depends on the nature and Ihe t ve l of thc sl3ndard We cncoun tered a di vcls il y of defin itiolls with in the framew)lk or the cLJ l1lbat aga inst tube rcu l o~i-
A retrospective study (from J977) on co mpli ance of TB pat ients revealed that the default ra Ie of the out-putient population in rural Pak i~ta n amounted iO 66 Default was defined as fa ilu re to uttend the weck ly tu berc ulosis clinic fo r a period of one month (Sloan amp Sloan 1981) A fo llow-up study ( 198g-90) showed that 72 oc of the TB patients registered in Bethani a Hosp ital did not complete their 12 months trea tment coure Although the in troduction of a short-course (8 months) regimen improved the compliance default rates (56) contin ued to be high (Liefooghe et al 1995) In 1991 however 76 of TB patients reg istered in the Pakistan Institute of Chest Diseases (S indh) had kep t to the short-course reglmen for two months 2 1 had left the hospi ta l against medical advice and 3 had died (Pathan et al 1992) A study carr ied out in the lndian Wardha dislrict revealed that TB patientlt who fai]cd to take their medici ne for more than 15 days were regarded as non-comptiant because this definition is most in keeping with the adopted adshyministrative procedure (Barnhoorn amp Adriaanse 1992) In a study performed in Denver USA non-compl iance with DOT for TB was detined as foll ows (I) missing ~ 2 consecuti ve weeks of DOT (2) prolongation of treatment gt 30 days due 10 sporadic missed doses or (3 ) incarceration for presenting a th rem lO public health (Burman et al 1997) At least 18 of patients who received out-paLient DOT via the Denver Metro TubercLIl os is Clinic met at least one of these cri teria
In concusion therefore there is no golden standard for defining compliance In our study compliance the fi nal outcome which has to be explai ncd in the model is viewed from a dichotomous viewpoint On the one hand there is the category of compliant patients they com plete thei r the ra py in full and as a general rule al$o unshyderwent a sputum tes t confirming Ihem as TB negative On the other hand there is the category of non-com pliant patients they did not com plete their therapy so a sputum test was not carried out We also adopted the com pletion or fai lure to comshyplete the short -co urse direc tl y observed therapy the bas ic criterion used in the exshyam pIes given above as the key cri terion for our defi ni tion of com pliance The structural model (see Fig ure 3) demonstra tes th at it is important to systemat ically di stinguish the reguarity and the du ration of the therapy to gain a bctter undershystanding of the concept compliance Regularity is achieved when there are no or only sporadic interru ptions during the thcrapy In t hi ~ connection we refer to missed appointments or missed doses of medi cation The durarjoll of the therapy on the e ther hand refers to the treatment duration of eigh[ months which has to be
111 JIII 1 1 1III IJ IKLl 11 lH~Ult I IJ 11111lt ) ~
respected in the DOTS-regimen Two dlv iati ons are possiblc here Either Jo wn shyward the patient ends thc treatment premature1y and is regarded as d efaulter Ol upward- the period of treatment is extended because interruptions during the treatment have [0 be compenslIteti for artcrwards Both deviations from the norm indieate non-compliance Any com parison with the above referred to non-complishyance ra[es fa ils because the phenomenon is constantly regarded from di fferent anshygles Hav ing said that the folowing fac ts in our research on (non- )col11pl iancc among the 621 TB patients are worth mentioni ng
Aftel subtracti ng the nUlllbcr (l f pntients who have died (6Oc) thase who have transferred to another treaUllent centre (29r) and thc tiny group of patie nt~ where the treatmen t failed (I ) 563 pat ients remai ned According to our de liumln ition 779 of the latter group are compliant and 23 are non-compliant aresuIt which is c10sely in keepi ng with the situation at lhe lnsti tu te of Ches[ Diseases in the prov shyince of Sindh The number of in terruptions is used to indicate the regularity of the trcatment 48 of patients did not inlerrupt their treatment at all 34 in terrupted it once and 18 interrupted it various times As far as the duration of the lherapy is concerned the norm of eight months is ach ieved by 55 of patie nts [he norm i not achie ved laquo 8 months) by 33 of patients and the nonn is exceeded (gt 8 months) by 12 of patients
Broadly speaking three out of four paticnts is compliant One out of four is nOI1shycompliant interruptions during the treatmen t (because appoin tments or medicashytion is sporatlicall y missed) or failure to complete the ideal duration of treatmenl (because patients drop out too early or have to followan extended course of treatshyment) As far as establishi ng compl iance is concerned it would seem that 77 ck of patients is heading towards the WHO-target fo r global tuberculosis control namely cure 85 of the detected new smear-positive TB cases (Seita 1996 p 134)
When interpreting the results it is also important to disti nguish between ho~ p ishytalised patie nts and out-patients As we al ready stated earlier duri ng lhe rirst month of treatment 80 of patients were hospitalised Af ter the second month this number dropped to only 48 Permanent supervision at the hospital ensures that hospitalised TB patients are by definition compliant the DOTS-regime n is strictly enforced As far as non-compliance of the out-patient population is co ncerned wc noted that 17oc missed at least one appointment during the first month of treatshyment and that this number dropped 10 1I aftel thc end of the second month The first month is therefore critica especially fol patients who are not hospitalisetl Since they do not res ide at the hospi tal and only come for consultations thty enshycounter far greater difficulties internalising the norms underlying the DOTS-regishymen
The model hinges on the latent construct of stigmatisation Stigmatisation afshyfects compl iance through the Ta ndem of regu la ri ty and duration of therapy Persons who have been strongly stigmatised display more irregular illness behaviour and find it more problematic to see the ditficult and troublesome trealment through 10
[he end In th is respect il could be sa id that ending or interrup[ing the DOTS-reg imiddot
men is nol due to a Jack ol organi satioll On the contrary they are Illcchallisl llS which help to relieve thc pain of sli gmatisation ensuring that for a wh ik the TH pal ient does not have 10 he as hamed and can take a brea k when the prc-url of Ihc medical rcgimen beeomcs toa heavy (Massaro 1997) According 10 GollIllans terminology devi ali ng from the slandards of thc DOTS- rcgimen can hl rcgOl rdcJ as a technique fo r conlrolling in fo rmation The questions or whelher 10 revcal or hi de to con1iumlde in someone or keep qui et to lie or be truth ful and to who l1l hnw when and where are tricks for stoppi ng Ihe exhausting process of bleacutellllc hy socishyety They are in su mmary stra tegies to lWlwRc ( IpoiId idllltity (Schcpcr- amp Nievaard 1995 p 42-43) In Ihe mode l th rec social conditions affecl thc dcgrcc of sligmati sation of TB pat ients These co ndi lions have 10 be taken inlo account 10 reduce the lim ils to pat ienl compliancc with DOTS-strategies
The first cond it ion is rclated to the dem ()g mphico Iilloion of the pili cllt anJ comprises two variab les from the exogenous set ie gender and age FCi llalc pashytients were stigmatised more than male pat ients and older patients Wlr~ si igllwshyti sed more than young persons BOlh lin k~ are highl y significant As house wivcs or elderl y members of the ex tended fa mi Iy many have a low socio-econol11 ie Ialu For them health is above all J quest ion of physical strength (W inkvist amp Akhtar 1997) The loss of phys ical strength Ihlough tubercul osis the fact that tl1Oc who have been sl ricken wilh the diseas( can no longer perform hard labour do the housekeepmg no longer be reproducti ve etc are important contributors to stigshymat isation This is all the more so in lhe countryside where ex ternal signs of vu lshynerability often do not suffiumlce to relieve peopl e from their nonnal socill tasks in the fami ly and vill age
The second condition cl ose ly concerns the beiefofT8 patiel1ll in the curabifir of th eir disease We already said earlier that th is laten t construct in our research displayed features of serendi pity It is el istinct from stricl measurements ofrational med ical knowledge because it emphasises praxis ie implementing knowledge and acti ng on insights The higher the soc io-economie slatus the grealer the belief in the curabil ity of TB It is impossi ble to ignore the phenomenon of social stratifishycation when analys ing ill ness behaviollr of TB patients Patients wi th a higher proshyfessional rank have great faith in the curability of their disease The opposite also applics in equal measure unemploy ment and illileracy are cond ucive for nonshycompl iam behaviour Perhap~ the hard core of pariahs outcasts vagrants vagshyabonds tramps chronie drllnkards and drug add icts (Merton 1968 p 207) repshyresenlSthe most dangerous ri sk group for all TB control programmes When Robshyert K Merton in 1949 developcd hi s we ll-known typology of modes of adaptation by indi viduals within the cu ltu re-bearing society he discovered that these populashytion groups displ ayed retreatiII their mode of adapl3tion which implies the reshyjec tion of cul tural goals and institutional means After all why should anyone reshymain healthy And why should we lIse DOTS as Q method Does it make any difshyference) There is a negative correlat ion between belief in the curability of TB and the degree of stigmati sation Persons who are convineed they will soon be cured and capable of strictly following the medical regimen will be less stigmatised
1 ll i bull I III I 1 11 11 10-- 1 1 middot111 middotmiddot middot 1 middot _
The third condit ion is siluateel at the leve l of the social netllo rks in wh ich TB middot patients function As a general rule it can be sa id thaI persons who tcceive mor~ help from olhers are less likely 10 be stigmati sed Roughl y six out of ten pati ent~ are married and fo r married women the family-in-I aws occ upy the cen tral po- it iol in their social nelwork The model established a negati ve relationshi p betwec l support from blood re lati ve~ and support from the family-in-Iaws Solida rilYvvitl the fa mily-in-Ia ws red uces ~olidarity with biooeI relatives This app lies both il general but also in the specifi( framework of help and support in ti mes of illness The fear manied fe male TB patients have of being abancloned by their hll ~banJ and no 10nger being able to perform their domesr ic tasks should not be unMrcst i mated During a study into thc relcltion between poverty and TB in Bombay re male patients said thaI thei r husbands and mothers-in-Iaw repeated Iy sent then back to their nata l home until such lime as Ihey were cured They were often al cused of bringing the disease from their natal homes and were threatened with sep aration (Nui r et al 1997 p 8 1) The model revea led that the TB patiems who re ceived the least support from their family were stigrnatised most Th is recalls th relational natu re of all type of sti gmatisat ion People are given a negative SOCiH label or are shielded from it Your family may support you through thick and thin encourage you to do the right th ing help to fi nance treatment etc Converse l) your fam ily mayabandon you keep your situation quiet to prevent loosing fac anel keep the family reputation unb1emished
lil Pakistani society anel particularl y in l11any village and se ttl el11Cnb in th Punjab social networks and stigmati sation are inextricably li nkeel and have al enormous influence on community li fe Thc biraderi the patriarcha l nelwork 0
kinship fo rms the framework 101 social and coml11uni ty networks Special event and rites of passage such as birth the ci rcumcis ion of a son marriage allli th death of an old person si rengthen lhis solidarity within the biraderi The biradel use many other occasions to promote social and community networks and ill ne - is perhaps one of the most important When a daughter-in- Iaw becomes seriousl iJl or is hospitalised her children are either looked after by the other daughters (1
the house or are temporarily housed with other members of the birade ri If Ihe sol breadwinner of a household cannot work because he is seriously ill his nearest rel atives and olher members of his biraderi provide mora material and fi nancia l o up port These socia1 and communily links rernai n intact even after emigration Paki stanis who have emigrated to Grea t Brita in for exam ple continue to receive muc support from their biraderi (Anwar 1979) Whenever help is sought in Pakistar communities famil y and bi raderi are preferred According to a sociologic al stud carried out in Rochdale a toW D in the north of England hel p is only sOllght frOl farmer fellow viJ1 agers friend s neighbours Olher Pakistanis and the res t of 50CI ety after all possibil ities in the biraderi-network have been exhausted A TB pil tient who is admitted to hospital will initially be visited by me mbers of hi biraderi They wi llusuaJ1y be gi ven a few hundred rupees and the trad itional fru i However as news about the nature of the illness spreads within the bi rade ri cor tacts become less frequent The negative COITeiation between fa mily support an
sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more
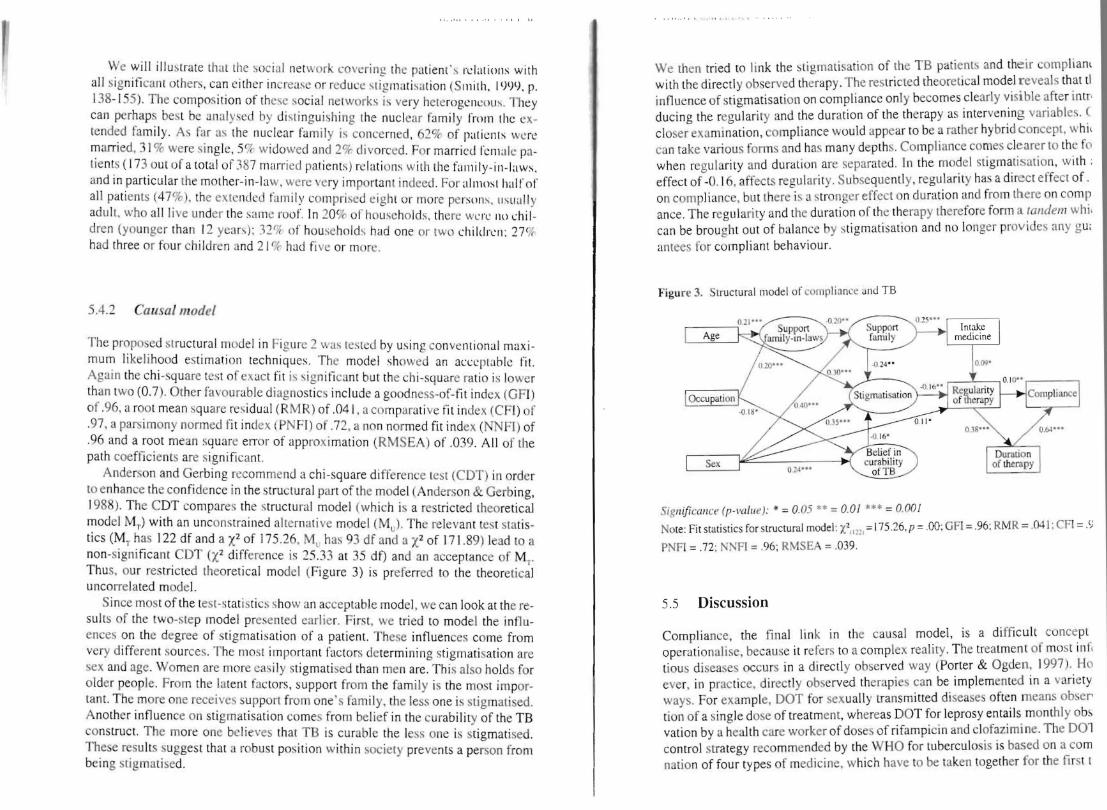
We will illustrate thatthe social Il etwork lovering the pa tien t- nlatiolls with all significant others can cithcr increasc or reduce st ig lll ati satioll iS lllilh 1 ()IJt) p 138-155) The com position of these soci al networks i- very hcterogcilcous Thcy can perhaps bes t be analy-ed by di sti nguishing the nuelear fam ily from Ihe ex shytended fa mily As far as the nuclear fam ily is cOllce rned 62 of pllicnls wcn~ married 31 were si ngle 5fr widowed anel 2 divorced For married felll aie pashytients ( 173 out of a tota l of 387 married pa tients) rclati oll) with the fa mi Iy- ill-Iaws and in particular the mother-in-Iaw were very importan t indeecl For alll10sl half of all patients (47) thc extc ll(kJ fam il y eOll1 pri -ed cighl or more perso ll- IIs li all y adu lt who all li ve under the ) (l IllC roo f In 20 of households there wen ilO ehi 1shydren (yolJnger than 12 yca r~) 327 ot households had one or two childrclI 2C1r had three or four children and 21 or had fi ve or more
542 Causal model
The proposed structural model in Figurc 2 was tested by using con veuml ntionalmaxi shymu m likel ihood est imatioll techniques Thc model~h(lwed an acecptabk fit Again the ehi -square tes t of exact fit is ~i gni tiuml ca nt but the eh i-square ratio is lower than two (07) Other favourable diagnosti c~ include a goodncss-of-tiumlt index (GFl) of 96 a rOol mean square rcs idual (R MR) of 041 a comparati ve fi l index (CF) of 97 a parsimony normed fit index iPNFI) of 72 a non normed fit index (NNFI) of 96 and a root mean squ are enOf of approximation (RMSEA) of 039 All of the path coefficients are signifi cant
Anderson and Gerbing recommend a chi-square di ffe rence tes t (CDT) in order to enhanee the confidence in the structural part of the model (Anderson amp Gerbing 1988) The CDT compares the structura l model (which is a res trictecl theoretical model MT) with an uneons trailled alternative model (Mul The relevant test statis shytics (MT has 122 df and a X2 of 17526 ML has 93 df anel a X2 of 171 89) lead to a non-significa nt CDT (X2 difference is 25 33 at 35 df) and an acceptance of M
r Thu s our restricted theoretica model (Figure 3) is preferred to the theoretica uncorrelated model
Since most of the [esH tat is ti c~ show an acceptable model we can look at the reshysu lts of the two-step model presentcd earlier Firsl we tried to model the influshyences on the degree of stigmatisation of a patient These influenees come from very different sou rces The mos important factors determi ning stigmatisation are sex and age Women are more easily stigmatised than men are This also holds for older people From the latent factors support from the family is the most im porshytant Thc more one receives SUppOrL from ones fam ily the less one is stigmalised Anothcr influence on stigmatisation comes from belief in the curability of the TB onstruct The more one believes that TB is curable the less one is stigmatised
These results sugges t that a robust position within society prevents a person from being stigmatised
We then tried to link the stigmatisation of the TB patients and the ir complianl wilh lhe directly observed therapy The restricted theoretical model reveal s that ti influence of stigmatisation on compliance only becomes clearly visible af ter intro ducing the regularity and the duration of the therapy as intervening variables closer examination compliance would appear to be a rather hybridconcept whi can take various forms and has many depths Compliance comes clearer to the [ (I when regularity and du ration are separated In the model stigmatisation with effect of -016 affects regul arity Subsequently regularity has a direct effect of on eomplianee but lhere is a stronger effect on duration and from there on comp anee The regularity and the duration of the therapy tberefore form a tandem whi ca n be brought out of balance by stigmati sation anclilo longer prov ides any gu antees for compliant behaviour
Figu re 3 Siructuralmodel of complio ncc anJ TB
SignificCllce (p-PO ll t) =0 05 =00 =000
Note Fit statistics for structural model X2n~~) =175 26 P=00 GFl =96 RMR =041 CFl =lJ
PNFl =72 NNFI =96 RMSEA =039
SS Discussion
Compliance the fin al link in the causal model is a di ffi cult concept operationalise because it refers to a complex reality The treatment of most inf uumlous diseases oceurs in a di rectly observed way (Porter amp Ogden 1997) H0 ever in practice directly observed therapies can be implemented in a variety ways For examplc DOT for sexually transmitted diseases of ten means obsef tion of a single dose of treatment whereas DOT for leprosy entails monthly ob~ valion by a health care worker of doses of ri fampicin and clofazimine Tbe 001 control strategy reeommended by the WHO for tubercul os is is based on a com nation of four types of medici ne which have to be taken together for the fi rst t
months of lrcat ment HeLlith lJre worken ensure that the I ight Ill ed icine is lak n in the right doses and fo r the cornc t length of ti me Supervis ion ean he a CLlllllshy
p ished by having the pati ent visit the cimie hosp italis ing the patient or scnuin a health care workeI to visit the pa tients home or workplace For directl y ohsnvcd therapy fe l TB it i essenti1l that superv isi on continu e~ every day for th liumlrst two months and idea lly for the entire course of the treatment The wide vltlriations in DOT-contro strategies have resulted in a situation where compliance Illci 1l111lshy
compliance have become e la~t ic eoncepls Who is campliant and who is not~ It all depends on the nature and Ihe t ve l of thc sl3ndard We cncoun tered a di vcls il y of defin itiolls with in the framew)lk or the cLJ l1lbat aga inst tube rcu l o~i-
A retrospective study (from J977) on co mpli ance of TB pat ients revealed that the default ra Ie of the out-putient population in rural Pak i~ta n amounted iO 66 Default was defined as fa ilu re to uttend the weck ly tu berc ulosis clinic fo r a period of one month (Sloan amp Sloan 1981) A fo llow-up study ( 198g-90) showed that 72 oc of the TB patients registered in Bethani a Hosp ital did not complete their 12 months trea tment coure Although the in troduction of a short-course (8 months) regimen improved the compliance default rates (56) contin ued to be high (Liefooghe et al 1995) In 1991 however 76 of TB patients reg istered in the Pakistan Institute of Chest Diseases (S indh) had kep t to the short-course reglmen for two months 2 1 had left the hospi ta l against medical advice and 3 had died (Pathan et al 1992) A study carr ied out in the lndian Wardha dislrict revealed that TB patientlt who fai]cd to take their medici ne for more than 15 days were regarded as non-comptiant because this definition is most in keeping with the adopted adshyministrative procedure (Barnhoorn amp Adriaanse 1992) In a study performed in Denver USA non-compl iance with DOT for TB was detined as foll ows (I) missing ~ 2 consecuti ve weeks of DOT (2) prolongation of treatment gt 30 days due 10 sporadic missed doses or (3 ) incarceration for presenting a th rem lO public health (Burman et al 1997) At least 18 of patients who received out-paLient DOT via the Denver Metro TubercLIl os is Clinic met at least one of these cri teria
In concusion therefore there is no golden standard for defining compliance In our study compliance the fi nal outcome which has to be explai ncd in the model is viewed from a dichotomous viewpoint On the one hand there is the category of compliant patients they com plete thei r the ra py in full and as a general rule al$o unshyderwent a sputum tes t confirming Ihem as TB negative On the other hand there is the category of non-com pliant patients they did not com plete their therapy so a sputum test was not carried out We also adopted the com pletion or fai lure to comshyplete the short -co urse direc tl y observed therapy the bas ic criterion used in the exshyam pIes given above as the key cri terion for our defi ni tion of com pliance The structural model (see Fig ure 3) demonstra tes th at it is important to systemat ically di stinguish the reguarity and the du ration of the therapy to gain a bctter undershystanding of the concept compliance Regularity is achieved when there are no or only sporadic interru ptions during the thcrapy In t hi ~ connection we refer to missed appointments or missed doses of medi cation The durarjoll of the therapy on the e ther hand refers to the treatment duration of eigh[ months which has to be
111 JIII 1 1 1III IJ IKLl 11 lH~Ult I IJ 11111lt ) ~
respected in the DOTS-regimen Two dlv iati ons are possiblc here Either Jo wn shyward the patient ends thc treatment premature1y and is regarded as d efaulter Ol upward- the period of treatment is extended because interruptions during the treatment have [0 be compenslIteti for artcrwards Both deviations from the norm indieate non-compliance Any com parison with the above referred to non-complishyance ra[es fa ils because the phenomenon is constantly regarded from di fferent anshygles Hav ing said that the folowing fac ts in our research on (non- )col11pl iancc among the 621 TB patients are worth mentioni ng
Aftel subtracti ng the nUlllbcr (l f pntients who have died (6Oc) thase who have transferred to another treaUllent centre (29r) and thc tiny group of patie nt~ where the treatmen t failed (I ) 563 pat ients remai ned According to our de liumln ition 779 of the latter group are compliant and 23 are non-compliant aresuIt which is c10sely in keepi ng with the situation at lhe lnsti tu te of Ches[ Diseases in the prov shyince of Sindh The number of in terruptions is used to indicate the regularity of the trcatment 48 of patients did not inlerrupt their treatment at all 34 in terrupted it once and 18 interrupted it various times As far as the duration of the lherapy is concerned the norm of eight months is ach ieved by 55 of patie nts [he norm i not achie ved laquo 8 months) by 33 of patients and the nonn is exceeded (gt 8 months) by 12 of patients
Broadly speaking three out of four paticnts is compliant One out of four is nOI1shycompliant interruptions during the treatmen t (because appoin tments or medicashytion is sporatlicall y missed) or failure to complete the ideal duration of treatmenl (because patients drop out too early or have to followan extended course of treatshyment) As far as establishi ng compl iance is concerned it would seem that 77 ck of patients is heading towards the WHO-target fo r global tuberculosis control namely cure 85 of the detected new smear-positive TB cases (Seita 1996 p 134)
When interpreting the results it is also important to disti nguish between ho~ p ishytalised patie nts and out-patients As we al ready stated earlier duri ng lhe rirst month of treatment 80 of patients were hospitalised Af ter the second month this number dropped to only 48 Permanent supervision at the hospital ensures that hospitalised TB patients are by definition compliant the DOTS-regime n is strictly enforced As far as non-compliance of the out-patient population is co ncerned wc noted that 17oc missed at least one appointment during the first month of treatshyment and that this number dropped 10 1I aftel thc end of the second month The first month is therefore critica especially fol patients who are not hospitalisetl Since they do not res ide at the hospi tal and only come for consultations thty enshycounter far greater difficulties internalising the norms underlying the DOTS-regishymen
The model hinges on the latent construct of stigmatisation Stigmatisation afshyfects compl iance through the Ta ndem of regu la ri ty and duration of therapy Persons who have been strongly stigmatised display more irregular illness behaviour and find it more problematic to see the ditficult and troublesome trealment through 10
[he end In th is respect il could be sa id that ending or interrup[ing the DOTS-reg imiddot
men is nol due to a Jack ol organi satioll On the contrary they are Illcchallisl llS which help to relieve thc pain of sli gmatisation ensuring that for a wh ik the TH pal ient does not have 10 he as hamed and can take a brea k when the prc-url of Ihc medical rcgimen beeomcs toa heavy (Massaro 1997) According 10 GollIllans terminology devi ali ng from the slandards of thc DOTS- rcgimen can hl rcgOl rdcJ as a technique fo r conlrolling in fo rmation The questions or whelher 10 revcal or hi de to con1iumlde in someone or keep qui et to lie or be truth ful and to who l1l hnw when and where are tricks for stoppi ng Ihe exhausting process of bleacutellllc hy socishyety They are in su mmary stra tegies to lWlwRc ( IpoiId idllltity (Schcpcr- amp Nievaard 1995 p 42-43) In Ihe mode l th rec social conditions affecl thc dcgrcc of sligmati sation of TB pat ients These co ndi lions have 10 be taken inlo account 10 reduce the lim ils to pat ienl compliancc with DOTS-strategies
The first cond it ion is rclated to the dem ()g mphico Iilloion of the pili cllt anJ comprises two variab les from the exogenous set ie gender and age FCi llalc pashytients were stigmatised more than male pat ients and older patients Wlr~ si igllwshyti sed more than young persons BOlh lin k~ are highl y significant As house wivcs or elderl y members of the ex tended fa mi Iy many have a low socio-econol11 ie Ialu For them health is above all J quest ion of physical strength (W inkvist amp Akhtar 1997) The loss of phys ical strength Ihlough tubercul osis the fact that tl1Oc who have been sl ricken wilh the diseas( can no longer perform hard labour do the housekeepmg no longer be reproducti ve etc are important contributors to stigshymat isation This is all the more so in lhe countryside where ex ternal signs of vu lshynerability often do not suffiumlce to relieve peopl e from their nonnal socill tasks in the fami ly and vill age
The second condition cl ose ly concerns the beiefofT8 patiel1ll in the curabifir of th eir disease We already said earlier that th is laten t construct in our research displayed features of serendi pity It is el istinct from stricl measurements ofrational med ical knowledge because it emphasises praxis ie implementing knowledge and acti ng on insights The higher the soc io-economie slatus the grealer the belief in the curabil ity of TB It is impossi ble to ignore the phenomenon of social stratifishycation when analys ing ill ness behaviollr of TB patients Patients wi th a higher proshyfessional rank have great faith in the curability of their disease The opposite also applics in equal measure unemploy ment and illileracy are cond ucive for nonshycompl iam behaviour Perhap~ the hard core of pariahs outcasts vagrants vagshyabonds tramps chronie drllnkards and drug add icts (Merton 1968 p 207) repshyresenlSthe most dangerous ri sk group for all TB control programmes When Robshyert K Merton in 1949 developcd hi s we ll-known typology of modes of adaptation by indi viduals within the cu ltu re-bearing society he discovered that these populashytion groups displ ayed retreatiII their mode of adapl3tion which implies the reshyjec tion of cul tural goals and institutional means After all why should anyone reshymain healthy And why should we lIse DOTS as Q method Does it make any difshyference) There is a negative correlat ion between belief in the curability of TB and the degree of stigmati sation Persons who are convineed they will soon be cured and capable of strictly following the medical regimen will be less stigmatised
1 ll i bull I III I 1 11 11 10-- 1 1 middot111 middotmiddot middot 1 middot _
The third condit ion is siluateel at the leve l of the social netllo rks in wh ich TB middot patients function As a general rule it can be sa id thaI persons who tcceive mor~ help from olhers are less likely 10 be stigmati sed Roughl y six out of ten pati ent~ are married and fo r married women the family-in-I aws occ upy the cen tral po- it iol in their social nelwork The model established a negati ve relationshi p betwec l support from blood re lati ve~ and support from the family-in-Iaws Solida rilYvvitl the fa mily-in-Ia ws red uces ~olidarity with biooeI relatives This app lies both il general but also in the specifi( framework of help and support in ti mes of illness The fear manied fe male TB patients have of being abancloned by their hll ~banJ and no 10nger being able to perform their domesr ic tasks should not be unMrcst i mated During a study into thc relcltion between poverty and TB in Bombay re male patients said thaI thei r husbands and mothers-in-Iaw repeated Iy sent then back to their nata l home until such lime as Ihey were cured They were often al cused of bringing the disease from their natal homes and were threatened with sep aration (Nui r et al 1997 p 8 1) The model revea led that the TB patiems who re ceived the least support from their family were stigrnatised most Th is recalls th relational natu re of all type of sti gmatisat ion People are given a negative SOCiH label or are shielded from it Your family may support you through thick and thin encourage you to do the right th ing help to fi nance treatment etc Converse l) your fam ily mayabandon you keep your situation quiet to prevent loosing fac anel keep the family reputation unb1emished
lil Pakistani society anel particularl y in l11any village and se ttl el11Cnb in th Punjab social networks and stigmati sation are inextricably li nkeel and have al enormous influence on community li fe Thc biraderi the patriarcha l nelwork 0
kinship fo rms the framework 101 social and coml11uni ty networks Special event and rites of passage such as birth the ci rcumcis ion of a son marriage allli th death of an old person si rengthen lhis solidarity within the biraderi The biradel use many other occasions to promote social and community networks and ill ne - is perhaps one of the most important When a daughter-in- Iaw becomes seriousl iJl or is hospitalised her children are either looked after by the other daughters (1
the house or are temporarily housed with other members of the birade ri If Ihe sol breadwinner of a household cannot work because he is seriously ill his nearest rel atives and olher members of his biraderi provide mora material and fi nancia l o up port These socia1 and communily links rernai n intact even after emigration Paki stanis who have emigrated to Grea t Brita in for exam ple continue to receive muc support from their biraderi (Anwar 1979) Whenever help is sought in Pakistar communities famil y and bi raderi are preferred According to a sociologic al stud carried out in Rochdale a toW D in the north of England hel p is only sOllght frOl farmer fellow viJ1 agers friend s neighbours Olher Pakistanis and the res t of 50CI ety after all possibil ities in the biraderi-network have been exhausted A TB pil tient who is admitted to hospital will initially be visited by me mbers of hi biraderi They wi llusuaJ1y be gi ven a few hundred rupees and the trad itional fru i However as news about the nature of the illness spreads within the bi rade ri cor tacts become less frequent The negative COITeiation between fa mily support an
sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more
months of lrcat ment HeLlith lJre worken ensure that the I ight Ill ed icine is lak n in the right doses and fo r the cornc t length of ti me Supervis ion ean he a CLlllllshy
p ished by having the pati ent visit the cimie hosp italis ing the patient or scnuin a health care workeI to visit the pa tients home or workplace For directl y ohsnvcd therapy fe l TB it i essenti1l that superv isi on continu e~ every day for th liumlrst two months and idea lly for the entire course of the treatment The wide vltlriations in DOT-contro strategies have resulted in a situation where compliance Illci 1l111lshy
compliance have become e la~t ic eoncepls Who is campliant and who is not~ It all depends on the nature and Ihe t ve l of thc sl3ndard We cncoun tered a di vcls il y of defin itiolls with in the framew)lk or the cLJ l1lbat aga inst tube rcu l o~i-
A retrospective study (from J977) on co mpli ance of TB pat ients revealed that the default ra Ie of the out-putient population in rural Pak i~ta n amounted iO 66 Default was defined as fa ilu re to uttend the weck ly tu berc ulosis clinic fo r a period of one month (Sloan amp Sloan 1981) A fo llow-up study ( 198g-90) showed that 72 oc of the TB patients registered in Bethani a Hosp ital did not complete their 12 months trea tment coure Although the in troduction of a short-course (8 months) regimen improved the compliance default rates (56) contin ued to be high (Liefooghe et al 1995) In 1991 however 76 of TB patients reg istered in the Pakistan Institute of Chest Diseases (S indh) had kep t to the short-course reglmen for two months 2 1 had left the hospi ta l against medical advice and 3 had died (Pathan et al 1992) A study carr ied out in the lndian Wardha dislrict revealed that TB patientlt who fai]cd to take their medici ne for more than 15 days were regarded as non-comptiant because this definition is most in keeping with the adopted adshyministrative procedure (Barnhoorn amp Adriaanse 1992) In a study performed in Denver USA non-compl iance with DOT for TB was detined as foll ows (I) missing ~ 2 consecuti ve weeks of DOT (2) prolongation of treatment gt 30 days due 10 sporadic missed doses or (3 ) incarceration for presenting a th rem lO public health (Burman et al 1997) At least 18 of patients who received out-paLient DOT via the Denver Metro TubercLIl os is Clinic met at least one of these cri teria
In concusion therefore there is no golden standard for defining compliance In our study compliance the fi nal outcome which has to be explai ncd in the model is viewed from a dichotomous viewpoint On the one hand there is the category of compliant patients they com plete thei r the ra py in full and as a general rule al$o unshyderwent a sputum tes t confirming Ihem as TB negative On the other hand there is the category of non-com pliant patients they did not com plete their therapy so a sputum test was not carried out We also adopted the com pletion or fai lure to comshyplete the short -co urse direc tl y observed therapy the bas ic criterion used in the exshyam pIes given above as the key cri terion for our defi ni tion of com pliance The structural model (see Fig ure 3) demonstra tes th at it is important to systemat ically di stinguish the reguarity and the du ration of the therapy to gain a bctter undershystanding of the concept compliance Regularity is achieved when there are no or only sporadic interru ptions during the thcrapy In t hi ~ connection we refer to missed appointments or missed doses of medi cation The durarjoll of the therapy on the e ther hand refers to the treatment duration of eigh[ months which has to be
111 JIII 1 1 1III IJ IKLl 11 lH~Ult I IJ 11111lt ) ~
respected in the DOTS-regimen Two dlv iati ons are possiblc here Either Jo wn shyward the patient ends thc treatment premature1y and is regarded as d efaulter Ol upward- the period of treatment is extended because interruptions during the treatment have [0 be compenslIteti for artcrwards Both deviations from the norm indieate non-compliance Any com parison with the above referred to non-complishyance ra[es fa ils because the phenomenon is constantly regarded from di fferent anshygles Hav ing said that the folowing fac ts in our research on (non- )col11pl iancc among the 621 TB patients are worth mentioni ng
Aftel subtracti ng the nUlllbcr (l f pntients who have died (6Oc) thase who have transferred to another treaUllent centre (29r) and thc tiny group of patie nt~ where the treatmen t failed (I ) 563 pat ients remai ned According to our de liumln ition 779 of the latter group are compliant and 23 are non-compliant aresuIt which is c10sely in keepi ng with the situation at lhe lnsti tu te of Ches[ Diseases in the prov shyince of Sindh The number of in terruptions is used to indicate the regularity of the trcatment 48 of patients did not inlerrupt their treatment at all 34 in terrupted it once and 18 interrupted it various times As far as the duration of the lherapy is concerned the norm of eight months is ach ieved by 55 of patie nts [he norm i not achie ved laquo 8 months) by 33 of patients and the nonn is exceeded (gt 8 months) by 12 of patients
Broadly speaking three out of four paticnts is compliant One out of four is nOI1shycompliant interruptions during the treatmen t (because appoin tments or medicashytion is sporatlicall y missed) or failure to complete the ideal duration of treatmenl (because patients drop out too early or have to followan extended course of treatshyment) As far as establishi ng compl iance is concerned it would seem that 77 ck of patients is heading towards the WHO-target fo r global tuberculosis control namely cure 85 of the detected new smear-positive TB cases (Seita 1996 p 134)
When interpreting the results it is also important to disti nguish between ho~ p ishytalised patie nts and out-patients As we al ready stated earlier duri ng lhe rirst month of treatment 80 of patients were hospitalised Af ter the second month this number dropped to only 48 Permanent supervision at the hospital ensures that hospitalised TB patients are by definition compliant the DOTS-regime n is strictly enforced As far as non-compliance of the out-patient population is co ncerned wc noted that 17oc missed at least one appointment during the first month of treatshyment and that this number dropped 10 1I aftel thc end of the second month The first month is therefore critica especially fol patients who are not hospitalisetl Since they do not res ide at the hospi tal and only come for consultations thty enshycounter far greater difficulties internalising the norms underlying the DOTS-regishymen
The model hinges on the latent construct of stigmatisation Stigmatisation afshyfects compl iance through the Ta ndem of regu la ri ty and duration of therapy Persons who have been strongly stigmatised display more irregular illness behaviour and find it more problematic to see the ditficult and troublesome trealment through 10
[he end In th is respect il could be sa id that ending or interrup[ing the DOTS-reg imiddot
men is nol due to a Jack ol organi satioll On the contrary they are Illcchallisl llS which help to relieve thc pain of sli gmatisation ensuring that for a wh ik the TH pal ient does not have 10 he as hamed and can take a brea k when the prc-url of Ihc medical rcgimen beeomcs toa heavy (Massaro 1997) According 10 GollIllans terminology devi ali ng from the slandards of thc DOTS- rcgimen can hl rcgOl rdcJ as a technique fo r conlrolling in fo rmation The questions or whelher 10 revcal or hi de to con1iumlde in someone or keep qui et to lie or be truth ful and to who l1l hnw when and where are tricks for stoppi ng Ihe exhausting process of bleacutellllc hy socishyety They are in su mmary stra tegies to lWlwRc ( IpoiId idllltity (Schcpcr- amp Nievaard 1995 p 42-43) In Ihe mode l th rec social conditions affecl thc dcgrcc of sligmati sation of TB pat ients These co ndi lions have 10 be taken inlo account 10 reduce the lim ils to pat ienl compliancc with DOTS-strategies
The first cond it ion is rclated to the dem ()g mphico Iilloion of the pili cllt anJ comprises two variab les from the exogenous set ie gender and age FCi llalc pashytients were stigmatised more than male pat ients and older patients Wlr~ si igllwshyti sed more than young persons BOlh lin k~ are highl y significant As house wivcs or elderl y members of the ex tended fa mi Iy many have a low socio-econol11 ie Ialu For them health is above all J quest ion of physical strength (W inkvist amp Akhtar 1997) The loss of phys ical strength Ihlough tubercul osis the fact that tl1Oc who have been sl ricken wilh the diseas( can no longer perform hard labour do the housekeepmg no longer be reproducti ve etc are important contributors to stigshymat isation This is all the more so in lhe countryside where ex ternal signs of vu lshynerability often do not suffiumlce to relieve peopl e from their nonnal socill tasks in the fami ly and vill age
The second condition cl ose ly concerns the beiefofT8 patiel1ll in the curabifir of th eir disease We already said earlier that th is laten t construct in our research displayed features of serendi pity It is el istinct from stricl measurements ofrational med ical knowledge because it emphasises praxis ie implementing knowledge and acti ng on insights The higher the soc io-economie slatus the grealer the belief in the curabil ity of TB It is impossi ble to ignore the phenomenon of social stratifishycation when analys ing ill ness behaviollr of TB patients Patients wi th a higher proshyfessional rank have great faith in the curability of their disease The opposite also applics in equal measure unemploy ment and illileracy are cond ucive for nonshycompl iam behaviour Perhap~ the hard core of pariahs outcasts vagrants vagshyabonds tramps chronie drllnkards and drug add icts (Merton 1968 p 207) repshyresenlSthe most dangerous ri sk group for all TB control programmes When Robshyert K Merton in 1949 developcd hi s we ll-known typology of modes of adaptation by indi viduals within the cu ltu re-bearing society he discovered that these populashytion groups displ ayed retreatiII their mode of adapl3tion which implies the reshyjec tion of cul tural goals and institutional means After all why should anyone reshymain healthy And why should we lIse DOTS as Q method Does it make any difshyference) There is a negative correlat ion between belief in the curability of TB and the degree of stigmati sation Persons who are convineed they will soon be cured and capable of strictly following the medical regimen will be less stigmatised
1 ll i bull I III I 1 11 11 10-- 1 1 middot111 middotmiddot middot 1 middot _
The third condit ion is siluateel at the leve l of the social netllo rks in wh ich TB middot patients function As a general rule it can be sa id thaI persons who tcceive mor~ help from olhers are less likely 10 be stigmati sed Roughl y six out of ten pati ent~ are married and fo r married women the family-in-I aws occ upy the cen tral po- it iol in their social nelwork The model established a negati ve relationshi p betwec l support from blood re lati ve~ and support from the family-in-Iaws Solida rilYvvitl the fa mily-in-Ia ws red uces ~olidarity with biooeI relatives This app lies both il general but also in the specifi( framework of help and support in ti mes of illness The fear manied fe male TB patients have of being abancloned by their hll ~banJ and no 10nger being able to perform their domesr ic tasks should not be unMrcst i mated During a study into thc relcltion between poverty and TB in Bombay re male patients said thaI thei r husbands and mothers-in-Iaw repeated Iy sent then back to their nata l home until such lime as Ihey were cured They were often al cused of bringing the disease from their natal homes and were threatened with sep aration (Nui r et al 1997 p 8 1) The model revea led that the TB patiems who re ceived the least support from their family were stigrnatised most Th is recalls th relational natu re of all type of sti gmatisat ion People are given a negative SOCiH label or are shielded from it Your family may support you through thick and thin encourage you to do the right th ing help to fi nance treatment etc Converse l) your fam ily mayabandon you keep your situation quiet to prevent loosing fac anel keep the family reputation unb1emished
lil Pakistani society anel particularl y in l11any village and se ttl el11Cnb in th Punjab social networks and stigmati sation are inextricably li nkeel and have al enormous influence on community li fe Thc biraderi the patriarcha l nelwork 0
kinship fo rms the framework 101 social and coml11uni ty networks Special event and rites of passage such as birth the ci rcumcis ion of a son marriage allli th death of an old person si rengthen lhis solidarity within the biraderi The biradel use many other occasions to promote social and community networks and ill ne - is perhaps one of the most important When a daughter-in- Iaw becomes seriousl iJl or is hospitalised her children are either looked after by the other daughters (1
the house or are temporarily housed with other members of the birade ri If Ihe sol breadwinner of a household cannot work because he is seriously ill his nearest rel atives and olher members of his biraderi provide mora material and fi nancia l o up port These socia1 and communily links rernai n intact even after emigration Paki stanis who have emigrated to Grea t Brita in for exam ple continue to receive muc support from their biraderi (Anwar 1979) Whenever help is sought in Pakistar communities famil y and bi raderi are preferred According to a sociologic al stud carried out in Rochdale a toW D in the north of England hel p is only sOllght frOl farmer fellow viJ1 agers friend s neighbours Olher Pakistanis and the res t of 50CI ety after all possibil ities in the biraderi-network have been exhausted A TB pil tient who is admitted to hospital will initially be visited by me mbers of hi biraderi They wi llusuaJ1y be gi ven a few hundred rupees and the trad itional fru i However as news about the nature of the illness spreads within the bi rade ri cor tacts become less frequent The negative COITeiation between fa mily support an
sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more
men is nol due to a Jack ol organi satioll On the contrary they are Illcchallisl llS which help to relieve thc pain of sli gmatisation ensuring that for a wh ik the TH pal ient does not have 10 he as hamed and can take a brea k when the prc-url of Ihc medical rcgimen beeomcs toa heavy (Massaro 1997) According 10 GollIllans terminology devi ali ng from the slandards of thc DOTS- rcgimen can hl rcgOl rdcJ as a technique fo r conlrolling in fo rmation The questions or whelher 10 revcal or hi de to con1iumlde in someone or keep qui et to lie or be truth ful and to who l1l hnw when and where are tricks for stoppi ng Ihe exhausting process of bleacutellllc hy socishyety They are in su mmary stra tegies to lWlwRc ( IpoiId idllltity (Schcpcr- amp Nievaard 1995 p 42-43) In Ihe mode l th rec social conditions affecl thc dcgrcc of sligmati sation of TB pat ients These co ndi lions have 10 be taken inlo account 10 reduce the lim ils to pat ienl compliancc with DOTS-strategies
The first cond it ion is rclated to the dem ()g mphico Iilloion of the pili cllt anJ comprises two variab les from the exogenous set ie gender and age FCi llalc pashytients were stigmatised more than male pat ients and older patients Wlr~ si igllwshyti sed more than young persons BOlh lin k~ are highl y significant As house wivcs or elderl y members of the ex tended fa mi Iy many have a low socio-econol11 ie Ialu For them health is above all J quest ion of physical strength (W inkvist amp Akhtar 1997) The loss of phys ical strength Ihlough tubercul osis the fact that tl1Oc who have been sl ricken wilh the diseas( can no longer perform hard labour do the housekeepmg no longer be reproducti ve etc are important contributors to stigshymat isation This is all the more so in lhe countryside where ex ternal signs of vu lshynerability often do not suffiumlce to relieve peopl e from their nonnal socill tasks in the fami ly and vill age
The second condition cl ose ly concerns the beiefofT8 patiel1ll in the curabifir of th eir disease We already said earlier that th is laten t construct in our research displayed features of serendi pity It is el istinct from stricl measurements ofrational med ical knowledge because it emphasises praxis ie implementing knowledge and acti ng on insights The higher the soc io-economie slatus the grealer the belief in the curabil ity of TB It is impossi ble to ignore the phenomenon of social stratifishycation when analys ing ill ness behaviollr of TB patients Patients wi th a higher proshyfessional rank have great faith in the curability of their disease The opposite also applics in equal measure unemploy ment and illileracy are cond ucive for nonshycompl iam behaviour Perhap~ the hard core of pariahs outcasts vagrants vagshyabonds tramps chronie drllnkards and drug add icts (Merton 1968 p 207) repshyresenlSthe most dangerous ri sk group for all TB control programmes When Robshyert K Merton in 1949 developcd hi s we ll-known typology of modes of adaptation by indi viduals within the cu ltu re-bearing society he discovered that these populashytion groups displ ayed retreatiII their mode of adapl3tion which implies the reshyjec tion of cul tural goals and institutional means After all why should anyone reshymain healthy And why should we lIse DOTS as Q method Does it make any difshyference) There is a negative correlat ion between belief in the curability of TB and the degree of stigmati sation Persons who are convineed they will soon be cured and capable of strictly following the medical regimen will be less stigmatised
1 ll i bull I III I 1 11 11 10-- 1 1 middot111 middotmiddot middot 1 middot _
The third condit ion is siluateel at the leve l of the social netllo rks in wh ich TB middot patients function As a general rule it can be sa id thaI persons who tcceive mor~ help from olhers are less likely 10 be stigmati sed Roughl y six out of ten pati ent~ are married and fo r married women the family-in-I aws occ upy the cen tral po- it iol in their social nelwork The model established a negati ve relationshi p betwec l support from blood re lati ve~ and support from the family-in-Iaws Solida rilYvvitl the fa mily-in-Ia ws red uces ~olidarity with biooeI relatives This app lies both il general but also in the specifi( framework of help and support in ti mes of illness The fear manied fe male TB patients have of being abancloned by their hll ~banJ and no 10nger being able to perform their domesr ic tasks should not be unMrcst i mated During a study into thc relcltion between poverty and TB in Bombay re male patients said thaI thei r husbands and mothers-in-Iaw repeated Iy sent then back to their nata l home until such lime as Ihey were cured They were often al cused of bringing the disease from their natal homes and were threatened with sep aration (Nui r et al 1997 p 8 1) The model revea led that the TB patiems who re ceived the least support from their family were stigrnatised most Th is recalls th relational natu re of all type of sti gmatisat ion People are given a negative SOCiH label or are shielded from it Your family may support you through thick and thin encourage you to do the right th ing help to fi nance treatment etc Converse l) your fam ily mayabandon you keep your situation quiet to prevent loosing fac anel keep the family reputation unb1emished
lil Pakistani society anel particularl y in l11any village and se ttl el11Cnb in th Punjab social networks and stigmati sation are inextricably li nkeel and have al enormous influence on community li fe Thc biraderi the patriarcha l nelwork 0
kinship fo rms the framework 101 social and coml11uni ty networks Special event and rites of passage such as birth the ci rcumcis ion of a son marriage allli th death of an old person si rengthen lhis solidarity within the biraderi The biradel use many other occasions to promote social and community networks and ill ne - is perhaps one of the most important When a daughter-in- Iaw becomes seriousl iJl or is hospitalised her children are either looked after by the other daughters (1
the house or are temporarily housed with other members of the birade ri If Ihe sol breadwinner of a household cannot work because he is seriously ill his nearest rel atives and olher members of his biraderi provide mora material and fi nancia l o up port These socia1 and communily links rernai n intact even after emigration Paki stanis who have emigrated to Grea t Brita in for exam ple continue to receive muc support from their biraderi (Anwar 1979) Whenever help is sought in Pakistar communities famil y and bi raderi are preferred According to a sociologic al stud carried out in Rochdale a toW D in the north of England hel p is only sOllght frOl farmer fellow viJ1 agers friend s neighbours Olher Pakistanis and the res t of 50CI ety after all possibil ities in the biraderi-network have been exhausted A TB pil tient who is admitted to hospital will initially be visited by me mbers of hi biraderi They wi llusuaJ1y be gi ven a few hundred rupees and the trad itional fru i However as news about the nature of the illness spreads within the bi rade ri cor tacts become less frequent The negative COITeiation between fa mily support an
sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more

sligmati sation in case of TB i Jeep ly I)l)led in Pakistani soc iety Stiglllalis~lli(l1l erodes solidarity within soeial nClworb and serious ly ill1pair~ lhe ei vil slalu of TB patients The soc iologie1 model of the trealment of infeetious disc~l scs (Douglas 1994 p 85) whieh is required to mke the DOTS- medical rcg illlcn ltlCshycepted a~ a standard of care ror all TB ptients can only be devel opcd iI wc rCL lgshynise these subtIe socia mec hanisms
56 Conclusion
Pat ient corn pliance wilh the DOTS- Ill etl i c~d regimcn is an absolute condilion IOf
combati ng the tu berculos i ~ -c piJemic bll th in count ri es with high and low kwis of welfare For TB pat ients eO lllpliance means regu larl y taki ng different medicines for a long period of ti me under medical su perv ision Mony methods are used to make ill ness behaviour a compliant a~ poss ibl e Illass media campaigns hea lth educarion and counsel ing mobil is~1ti o n of fa mi Iy members local liaison persons vol unIeers or fi eld workers as supervisors ma lJed or telephone reminders of apshypointments and fo llow-up to missed appointments selec tion of CLles (meals other da il y rhythms ) to program menla ll y the intake of medic i nes serving-up medishycines in well-organised containers financial incenti ves etc
In our research we establ ished that compiance is thwarted by many conditions Economic demographical geograp hical psyc hological and socio-cultural factors have an impact on ill ness beha viour [I is hardly possible to identify which of these factors is decisive Moreover these factors differ according to lhe con text or TB Our empirical materia ill ustraled that the study of compJiance is impossible withshyout (he sociol srratiflc(Iioll-persfJ ecri e Someone who is economically vulnerashybie unskill ed and unemployed poor and socially lhreatened will also be the first to abandon the DOTS -regimen A low soci o-economie status is an important predicshyto r of non-compliance and is therefore aften used as a criterion for the selective app lication of the DOTS-strategy
Furthermore nol only the social stratifical ion-perspec ti ve bUL also the srigmatishysation perspecrive increases insigh t into the rnechanisms of rejee tiol1 of nonns and non- complianee of TB patients T B patients are stigmatised because lheir ilness disrupts their Jives and causes insecurities It threatens thei r social relations and 50shy
cia l structure beeause their illness bears the hallmark of a sub-culture of poverty weakness and lack of hygiene TB graduall y and surreplitiously erodes the support affo rded by social networks The socia l network canrlot hold out against so much socia l censure Furtherrnore fri encls fail to musIer support and are afraid of beshyeoming ostracised too Complete ly distraughl patients who are already in a preshycarious situation from the vcry beginn ing are stigmat ised even further
The only way to break thi s vicious circ le is to develop lhe DOTS-strategy u the standard of care and a service to all TB patients ra ther than being seen as a proceshydure of last resorts fo r non-compliant patients (Fujiwara et al 1997 Nolan 1997)
Thc ud vanlage~ of uni versaly appying the DOTS-strategy wil undoubtedly inshyIre a~e even fun her when lhe sli gmali~ alion perspecti ve is in volved in lhe analysis of non-cornpl iance of TB patients There is a real dange r that the patients reached by sdecti ve DOTS-prograrnrnouml will be sl igrn atiscd even more