The Inventory of Depressive Symptomatology (IDS): Clinician (IDS-C) and Self-Report (IDS-SR) ratings...
15
Introduction The Inventory of Depressive Symptomatology (IDS) was first developed as both a clinician rating (IDS-C) and a patient-completed self report (IDS-SR) in 1986 (Rush et al., 1986) in 28-item versions. Subsequently, two items were added (leaden paralysis and interperson- al rejection sensitivity) to capture all of the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) (American Psychiatric Association, 1994) atypical symptom features, which resulted in two 30- item versions (IDS-C and IDS-SR) (Rush et al., 1996). There are several reasons for developing yet anoth- er tool by which to gauge depressive symptom severity. The two major standard clinician ratings are the Hamilton Rating Scale for Depression (HRS-D) (Hamilton, 1960, 1967) and the Montgomery-Åsberg Depression Rating Scale (MADRS) (Montgomery and Åsberg, 1979). The HRS-D comes in a wide number of forms: the 6-, 17-, 21-, 24-, 28-, and 31-item versions. Psychometric reports have largely focused on the 17- item version (HRS-D 17 ) (for a review, see Yonkers and Samson, 2000). All of these different versions have several deficien- cies. Some of the items confound the types of symptoms to be rated. For example, psychic anxiety also rates irritability; pain complaints are rated with energy/fatigability. Some items are rarely encountered in depression (for example, paranoia/suspiciousness; obsessive-compulsive symptoms; derealization/ depersonalization). Other items have shown such poor performance that it has been recommended that they be deleted (for example, libido; hypochrondriasis; loss of insight; diurnal variation) (Bech et al., 1975; Rehm and O’Hara, 1985; Maier and Philipp, 1985; Nelson and Mazure, 1990). In addition, different items are given different weights. For example, sad mood is rated 0–4, but onset, middle, and late insomnia are each rated on a 0–2 scale. Several of the criterion symptoms to define DSM-IV melancholic or atypical features are also lacking (for example, distinct quality to mood, interpersonal rejection sensitivity). In addition to the above psychometric issues, no corresponding self-report is available for the HRS-D, except the Carroll Rating Scale (CRS) (Carroll et al., 1981; Feinberg and Carroll, 1985) which provides a 52-item yes/no format, but only reflects items found on the HRS-D 17 . More commonly used self-reports are the Beck Depression Inventory (BDI) (Beck et al., 1961, 1979) and the Zung Rating Scale for Depression (ZRSD) (Zung, 1965, 1985). However, the BDI has a 45 The Inventory of Depressive Symptomatology (IDS): Clinician (IDS-C) and Self-Report (IDS-SR) ratings of depressive symptoms A. JOHN RUSH, Department of Psychiatry, University of Texas Southwestern Medical Center, Dallas, USA THOMAS CARMODY, Department of Academic Computing Services, University of Texas Southwestern Medical Center, Dallas, USA PAUL-EGBERT REIMITZ, Biometrics Department, NW Organon, Oss, Netherlands ABSTRACT This paper describes the rationale and methods entailed in developing the Inventory of Depressive Symptomatology (IDS) in both clinician-rated (IDS-C) and self-reported (IDS-SR) formats. Psychometric features of the both the IDS-C and IDS-SR are presented. These scales are compared to the Hamilton Rating Scale for Depression (HRS- D) in the detection of symptom change in patients with major depressive (n = 184) or bipolar disorder (n = 141). The face validity and established psychometric features of the IDS-C and IDS-SR indicate that either may be useful in detecting symptom change, as well as in detecting residual symptoms in depressed patients. Further efforts to shorten each measure are indicated. Key words: IDS, self-report, clinician rating, depressive symptoms, major depressive disorder, bipolar disorder International Journal of Methods in Psychiatric Research, Volume 9, Number 2
Transcript of The Inventory of Depressive Symptomatology (IDS): Clinician (IDS-C) and Self-Report (IDS-SR) ratings...

IntroductionThe Inventory of Depressive Symptomatology (IDS)was first developed as both a clinician rating (IDS-C)and a patient-completed self report (IDS-SR) in 1986(Rush et al., 1986) in 28-item versions. Subsequently,two items were added (leaden paralysis and interperson-al rejection sensitivity) to capture all of the Diagnosticand Statistical Manual of Mental Disorders, Fourth Edition(DSM-IV) (American Psychiatric Association, 1994) atypical symptom features, which resulted in two 30-item versions (IDS-C and IDS-SR) (Rush et al., 1996).
There are several reasons for developing yet anoth-er tool by which to gauge depressive symptom severity.The two major standard clinician ratings are theHamilton Rating Scale for Depression (HRS-D)(Hamilton, 1960, 1967) and the Montgomery-ÅsbergDepression Rating Scale (MADRS) (Montgomery andÅsberg, 1979). The HRS-D comes in a wide number offorms: the 6-, 17-, 21-, 24-, 28-, and 31-item versions.Psychometric reports have largely focused on the 17-item version (HRS-D17) (for a review, see Yonkers andSamson, 2000).
All of these different versions have several deficien-cies. Some of the items confound the types of symptoms to be rated. For example, psychic anxiety
also rates irritability; pain complaints are rated withenergy/fatigability. Some items are rarely encounteredin depression (for example, paranoia/suspiciousness;obsessive-compulsive symptoms; derealization/ depersonalization). Other items have shown such poorperformance that it has been recommended that theybe deleted (for example, libido; hypochrondriasis; lossof insight; diurnal variation) (Bech et al., 1975; Rehmand O’Hara, 1985; Maier and Philipp, 1985; Nelsonand Mazure, 1990). In addition, different items aregiven different weights. For example, sad mood is rated0–4, but onset, middle, and late insomnia are eachrated on a 0–2 scale. Several of the criterion symptomsto define DSM-IV melancholic or atypical features arealso lacking (for example, distinct quality to mood,interpersonal rejection sensitivity).
In addition to the above psychometric issues, nocorresponding self-report is available for the HRS-D,except the Carroll Rating Scale (CRS) (Carroll et al.,1981; Feinberg and Carroll, 1985) which provides a52-item yes/no format, but only reflects items found onthe HRS-D17. More commonly used self-reports are theBeck Depression Inventory (BDI) (Beck et al., 1961,1979) and the Zung Rating Scale for Depression(ZRSD) (Zung, 1965, 1985). However, the BDI has a
45
The Inventory of Depressive Symptomatology(IDS): Clinician (IDS-C) and Self-Report(IDS-SR) ratings of depressive symptomsA. JOHN RUSH, Department of Psychiatry, University of Texas Southwestern Medical Center, Dallas, USATHOMAS CARMODY, Department of Academic Computing Services, University of Texas Southwestern
Medical Center, Dallas, USAPAUL-EGBERT REIMITZ, Biometrics Department, NW Organon, Oss, Netherlands
ABSTRACT This paper describes the rationale and methods entailed in developing the Inventory of DepressiveSymptomatology (IDS) in both clinician-rated (IDS-C) and self-reported (IDS-SR) formats. Psychometric features of theboth the IDS-C and IDS-SR are presented. These scales are compared to the Hamilton Rating Scale for Depression (HRS-D) in the detection of symptom change in patients with major depressive (n = 184) or bipolar disorder (n = 141). The facevalidity and established psychometric features of the IDS-C and IDS-SR indicate that either may be useful in detectingsymptom change, as well as in detecting residual symptoms in depressed patients. Further efforts to shorten each measureare indicated.
Key words: IDS, self-report, clinician rating, depressive symptoms, major depressive disorder, bipolar disorder
International Journal of Methods in Psychiatric Research, Volume 9, Number 2
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 45

Rush et al.
large number of questions that focus on cognition, andlike the ZRSD, the BDI lacks several criterion symp-toms for different subtypes.
The major clinical reason to develop these twoscales was the recognition that many depressedpatients in clinical trials and routine daily practicerespond but do not fully remit (attain an asymptomaticsymptom status) with a treatment intervention. It hasbeen our experience that patients with residual symp-toms often score between 5 and 11 on the HRS-D17.Therefore, it is our belief that the HRS-D17 is insensi-tive to lower levels of symptomatology. Yet, residualsymptoms are very important clinically. Not only arethey associated with poorer function (Miller et al.,1998) than the asymptomatic state, but they also pre-dict a worse prognosis (Faravelli et al., 1986; Thase etal., 1992; Paykel et al., 1995; Judd et al., 1998a,b).Furthermore, when these residual symptoms are suc-cessfully treated, the prognosis is improved (Fava et al.,1994, 1998a,b; Paykel et al., 1999).
Finally, from a clinical research perspective, wewished to further examine the relationship betweenself-reported and clinician-rated symptoms (see Tondoet al., 1988) in terms of the detection of treatmenteffects, and to examine factors that might result in discrepancies between these two perspectives (forexample, the presence of personality disorders). Thus,self-report and clinician ratings that examine identicalsymptoms are needed. As the IDS is available in bothformats, we also hoped to determine whether a self-report could be used by patients to detect clinically significant symptom exacerbations that might call forintervention (much as self-administered blood pressurereadings are used in the longer term management ofhypertension).
This report summarizes the available psychometricdata on both scales (Rush et al., 1996), provides newdata using the IDS in a study of bipolar disorder (n =141), in a small group of in- and outpatients withmajor depressive disorder (MDD) treated in the publicsector in Texas (n = 62), and an open 16-week trial ofnefazodone (n = 993), which was created as the run-inphase of a recently reported double-blind placebo sub-stitution discontinuation trial in outpatients withMDD (Feiger et al., 1999). Finally, we provide com-mentary of the potential for a shortened version ofeach rating scale – the Quick IDS-SR (QIDS-SR) andthe Quick IDS-C (QIDS-C). The appendix providesboth the 30-item IDS-C and the 30-item IDS-SR.They are available for use without charge by
researchers and clinicians. They have been translatedinto Dutch, French, German, Italian, Japanese,Romanian, Spanish, and most recently, Danish.
How were the IDS-C and IDS-SR developed?We set forth several specific requirements for eachitem:
• There should be equal weighting of all items (eachis scored on a 0–3 scale).
• Items should not be confounded (each item shouldmeasure only a single symptom construct). Thus,for example, there are three mood items (sad, irri-table, or anxious).
• Because we wished both IDS scales to be sensitiveto residual symptoms, a rating of ‘1’ on an item des-ignates a modest level of symptomatology.
• Items should be worded in ways that allow for selfreport with minimal inference. Thus, items anchoreach rating (0–3) to fairly concrete concepts ofseverity and duration or frequency of each symp-tom in the time period to be rated (usually the lastseven days).
• Symptom features of ‘subtypes’ (melancholic/atypical) should be included.
• Uncommon symptoms (derealization/depersonal-ization, paranoia, obsessive-compulsive symptoms,and psychotic symptoms such as hallucinations ordelusions) should not be included.
• Finally, for the time period to be rated, patientsmust decide overall whether they have had anincreased or reduced appetite, and whether theyhave had increased or decreased weight. Therefore,respondents rate only one of two items that charac-terize the direction of appetite and weight change.Scores range from 0–84 (only 28 of the 30 items arerated, with each item rated 0–3).
Following these principles, we wrote out all of theitems selected, and obtained feedback/critique frommore than a dozen, largely US, clinical researcherswho were experts in depression. The items wererevised. The resulting 28-item versions of the IDS-Cand IDS-SR were evaluated as to their psychometriccharacteristics (Rush et al., 1986, 1987; Tondo et al.,1988). Since that time, and with no change in the first28 items, we added two additional items (leaden paral-ysis; interpersonal rejection sensitivity) to create the30-item versions of both rating scales (Rush et al.,1996).
46
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 46

IDS-C and IDS-SR ratings of depressive symptoms
We subsequently developed a composite semi-structured interview that provides ratings of both theIDS-C and the HRS-D17, for use in studies that requireboth ratings, to avoid redundant questioning ofpatients (Basco and Krebaum, unpublished manu-script, 1990). Training videotapes have also beendeveloped (available upon request to the first author).
What are the psychometric features of the 30-itemIDS-C and IDS-SR?Rush et al. (1996) reported on a large psychometricstudy of the 30-item IDS-C and IDS-SR. Cronbach’salpha was 0.94 (IDS-C30) and 0.93 (IDS-SR30) for allsubjects (n = 456), which included those with MDDand normal controls, which compared with 0.89 for the HRS-D17 and 0.94 for the BDI21 in the samepopulation.
Correlation with standard scales revealed a Pearsonproduct moment correlation of 0.95 between the IDS-C30 and HRS-D17, and 0.88 between the IDS-SR30 andHRS-D17. The correlation coefficient between theIDS-C and IDS-SR was 0.91. The correlation betweenthe BDI21 and the IDS-SR30 was 0.93. The correlationbetween the IDS-SR30 and the HRS-D17 was 0.88, andthat between the BDI21 and the HRS-D17 was 0.85(Rush et al., 1996).
Factor analyses revealed a general factor, an anxietyfactor, and an atypical symptom feature factor for theIDS-C; and a general factor, an anxious/atypical factor,and a sleep factor for the IDS-SR. In subsequent largefactor analyses (Gullion and Rush, 1998) using allitems from the BDI21, HRS-D17, IDS-C30, and IDS-SR30,10 discrete factors were obtained that largely reflectedthe DSM-IV criterion symptoms for a major depressiveepisode. Interestingly, the IDS-SR30 and IDS-C30 itemsprovided a broader ‘coverage’ of these factors than dideither the BDI21 or the HRS-D17.
A high correspondence between the IDS-C and IDS-SR was reflected in the item-by-item comparison (Tondoet al., 1988). Only four items (irritability, negative viewof self, and psychomotor agitation/retardation) werescored slightly higher with the IDS-SR28 than with theIDS-C28. The overall relationship between the IDS-C28
and IDS-SR28 total score was found to beIDS-C28 = 4.9 + 0.7 (IDS-SR28). In general, theIDS-SR30 scores are about one to two points higher thantotal scores on the IDS-C30 (Rush et al., 1996).
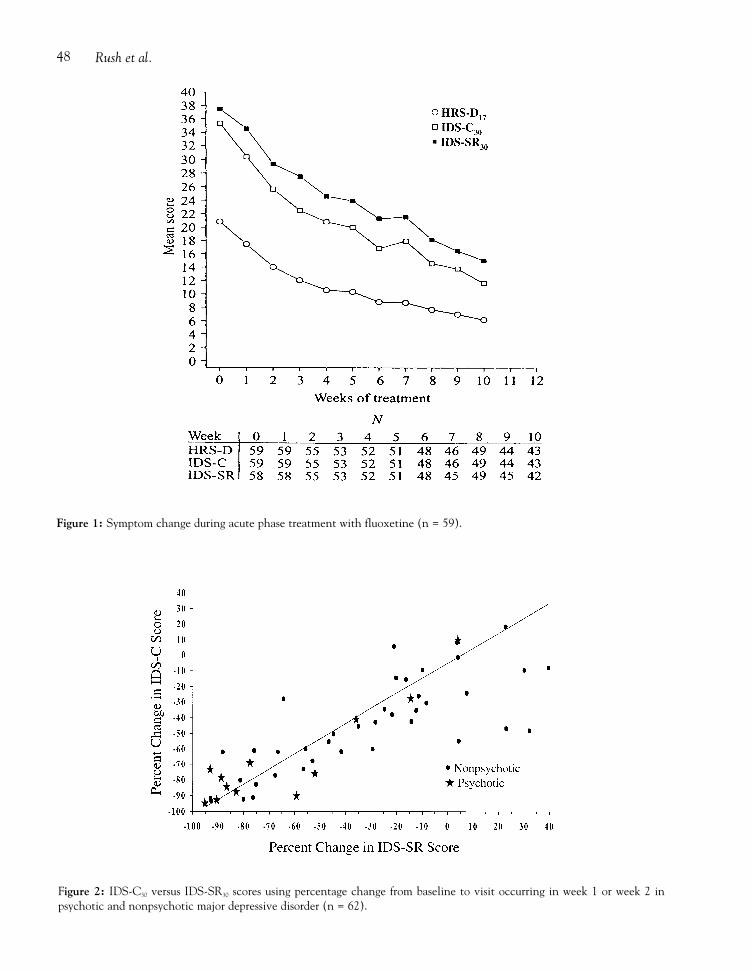
Are the IDS-C and IDS-SR sensitive to change?Rush et al. (1996) (Figure 1) found an equivalent
degree of sensitivity to change in a 10-week acutephase treatment trial of fluoxetine (n = 59). The slopesof both the IDS-C and IDS-SR were visually steeperthan that for the HRS-D17 obtained at the same time,suggesting at least an equivalent, if not greater, sensi-tivity to change than with the HRS-D17. We developedthresholds for both scales (depressed: IDS-C30 = ≥13 orIDS-SR30 ≥18; non-depressed = IDS-C30 <13 or IDS-SR30 <18).
Figure 2 shows the results from baseline to secondvisit in a small group (n = 62) of inpatients and outpa-tients with MDD seen and treated in the public sectorin Texas (Biggs et al., in press). This finding suggeststhat the IDS-SR30 might substitute for the IDS-C30 as achange measure. Figure 3 also reveals near-equivalentsensitivity to detecting change in patients (n = 141)with bipolar disorder (Rush, Hatef, Nolen, Suppes,McElroy, Altshuler, Denicoff, Keck, Post, unpublisheddata, 2000). Table 1 shows that both the IDS-C andIDS-SR differentiate depressed, manic, mixed andminimally-symptomatic (euthymic) states encoun-tered in patients with bipolar disorder (Rush et al.,unpublished data, 2000).
To further compare the HRS-D24 with the IDS-SR30,we took advantage of a published dataset in which out-patients with non-psychotic MDD were treated withnefazodone (up to 600 mg/day) (Feiger et al., 1999). Inthis open treatment trial, both IDS-SR30 and HRS-D24
were collected on each occasion (see Table 2). As canbe seen, the ratio of the IDS-SR30 total score to theHRS-D24 total score was nearly constant at 1.47 (range1.44–1.50) across all measurement occasions, whichindicates that the two scales are equivalently sensitivein detecting symptom reduction in this outpatientsample.
We then compared the status of patients at exit usingthe HRS-D24 and the IDS-C30. As can be seen in Table3, the IDS-C found that while 22.5% of the sample weredeclared responders by the HRS-D24 (≥50% reductionfrom baseline), the IDS-C30 found them to not have a≥50% decrease in IDS-C30 total scores. This finding isconsistent with the notion that the HRS-D is not assensitive to residual symptoms as is the IDS-C30.
Can the IDS be shortened?At the suggestion of Dr Per Bech, we tried to mirrorthe six-item Hamilton Rating Scale (Bech et al., 1975,1981; O’Sullivan et al., 1997) by selecting items fromthe IDS-C and IDS-SR that measured identical symp-toms: sad mood (item 5); concentration (item 15);
47
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 47
Rush et al.48
Figure 1: Symptom change during acute phase treatment with fluoxetine (n = 59).
Figure 2: IDS-C30 versus IDS-SR30 scores using percentage change from baseline to visit occurring in week 1 or week 2 in psychotic and nonpsychotic major depressive disorder (n = 62).
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 48

IDS-C and IDS-SR ratings of depressive symptoms 49
Figure 3: Change in IDS-C30 and IDS-SR30 total scores in bipolar disorder (n = 141).
Table 1: The IDS in bipolar disorder (n = 141)
Euthymic Depressed Manic Mixed(n = 30) (n = 61) (n = 14) (n = 36)
IDS-C30 9.7 ± 6.1 29.5 ± 12.3 11.4 ± 7.6 29.7 ± 15.0
IDS-SR30 10.2 ± 7.9 31.4 ± 12.2 13.2 ± 8.9 30.1 ± 14.1
Table 2: Total IDS-SR30 and HRS-D24 scores by visit (acute phase trial of nefazodone in MDD)
Week (n) IDS-SR30 HRS-D24 I/H Ratio
0 (646) 39.5 ± 8.7 26.9 ± 5.0 1.471 (594) 35.5 ± 9.7 24.0 ± 6.2 1.482 (595) 32.9 ± 10.2 22.2 ± 6.6 1.483 (582) 30.1 ± 11.3 20.7 ± 7.7 1.454 (575) 28.5 ± 11.6 19.8 ± 7.9 1.446 (554) 26.0 ± 12.3 17.5 ± 8.3 1.488 (517) 23.6 ± 12.6 15.8 ± 8.5 1.4910 (502) 21.4 ± 12.5 14.5 ± 8.7 1.4712 (506) 19.1 ± 13.0 12.9 ± 9.0 1.47Last visit (637) 21.1 ± 13.9 14.1 ± 9.7 1.50
IDS-SR ÷ HRS-D24 = 1.475 (average) (range: 1.44 to 1.50)
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 49

Rush et al.
guilt/self-criticism (item 16); suicidal ideation (item18); interest (item 19); and energy (item 20); plus thehighest score on any one sleep item (early, middle, lateinsomnia or hypersomnia) (items 1–4); the maximumscore on any one of the appetite/weight changes (items11–14); and the highest score on either of the psy-chomotor (agitation/retardation) items (23 and 24).We called the items so selected Quick IDS (or QIDS)(total score range = 0–27).
We used an existing dataset that included 122 out-patients treated with either fluoxetine or nefazodoneand calculated correlations at exit between the QIDSand the HRS-D17 (Rush et al., 1998). The correlationbetween the QIDS-C and the IDS-C30 was 0.93. The
QIDS-SR correlated 0.94 with the IDS-SR30, suggest-ing the likely possibility that shortened versions ofboth the IDS-C and IDS-SR may be feasible. In fact,the QIDS-C correlated 0.88 with the HRS-D17 in thissample, and the QIDS-SR correlated 0.72 with theHRS-D17. Figure 4 shows the percentage improvementin the QIDS-C corresponding highly to the percentageimprovement (baseline to exit) with the HRS-D17 inthis sample (n = 122).
ConclusionsTo date, the IDS-C30 and the IDS-SR30 have substantialface validity. Concurrent and discriminative validityhave been demonstrated in patients with major depres-sive and bipolar disorders. In both measures, factors aresimilar (but not identical) and include an anxiety anda general factor. Interestingly, the IDS-SR30 seems to beas sensitive to change as both the IDS-C30 and theHRS-D. To date, the IDS-C30 and IDS-SR30 bothappear to detect residual symptoms that may be lesswell detected by the HRS-D, although more work isneeded in this area. The possibility of using the IDS-SR30 as a substitute for a clinician rating is raised byseveral post hoc analyses that have been conducted.Moreover, it may be feasible to develop a QIDS-C anda QIDS-SR, which, in turn, could facilitate the mea-surement of symptoms in the daily care of patients withmood disorders.
50
Table 3: Is the IDS-C30 more sensitive than the HRS-D17
(12-week open trial of nefazodone; n = 993)
Exit HRS-D17 Exit IDS-C30
Response* Response 41.9%Response Non-response 22.5%Non-response Response 4.3%Non-response Non-response 31.3%
*Response defined as ≥50% reduction from baseline inHRS-D17 or IDS-C30, respectively.
Figure 4: HRS-D17 versus QIDS-C using percent improvement from baseline to exit (n = 122).
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 50

IDS-C and IDS-SR ratings of depressive symptoms
Appendix
INVENTORY OF DEPRESSIVE SYMPTOMATOLOGY(CLINICIAN-RATED) (IDS-C)
Name:Todays date:
Please circle one response to each item that best describesthe patient for the last seven days.
1. Sleep Onset Insomnia:
0 Never takes longer than 30 minutes to fall alseep.1 Takes at least 30 minutes to fall asleep, less than half the
time.2 Takes at least 30 minutes to fall aseep, more than half the
time.3 Takes more than 60 minutes to fall asleep, more than
half the time.
2. Mid-Nocturnal Insomnia:
0 Does not wake up at night.1 Restless, light sleep with few awakenings.2 Wakes up at least once a night, but goes back to sleep
easily.3 Awakens more than once a night and stays
awake for 20 minutes or more, more than half the time.
3. Early Morning Insomnia:
0 Less than half the time, awakens no more than 30 minutes before necessary.
1 More than half the time, awakens more than 30 minutes before need be.
2 Awakens at least one hour before need be, more thanhalf the time.
3 Awakens at least two hours before need be, more thanhalf the time.
4. Hypersomnia:
0 Sleeps no longer than 7-8 hours/night, without naps.1 Sleeps no longer than 10 hours in a 24 hour period
(include naps).
2 Sleeps no longer than 12 hours in a 24 hour period(include naps).
3 Sleeps longer than 12 hours in a 24 hour period(include naps).
5. Mood (Sad):
0 Does not feel sad.1 Feels sad less than half the time.2 Feels sad more than half the time.3 Feels intensely sad virtually all of the time.
6. Mood (Irritable):
0 Does not feel irritable.1 Feels irritable less than half the time.2 Feels irritable more than half the time.3 Feels extremely irritable virtually all of the time.
7. Mood (Anxious):
0 Does not feel anxious or tense.1 Feels anxious/tense less than half the time.2 Feels anxious/tense more than half the time.3 Feels extremely anxious/tense virtually all of the time.
8. Reactivity of Mood:
0 Mood brightens to normal level and lasts several hourswhen good events occur.
1 Mood brightens but does not feel like normal self whengood events occur.
2 Mood brightens only somewhat with few selected,extremely desired events.
3 Mood does not brighten at all, even when very good ordesired events occur.
9. Mood Variation:
0 Notes no regular relationship between mood and timeof day.
1 Mood often relates to time of day due toenvironmental circumstances.
2 For most of week, mood appears more related to time ofday than to events.
3 Mood is clearly, predictably, better or worse at a fixedtime each day.
51
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 51

Rush et al.
9a.Is mood typically worse in morning, afternoon, or night(circle one).
9b. Is mood variation attributed to environment by thepatient? (yes or no) (circle one).
10. Quality of Mood:
0 Mood is virtually identical to feelings associated withbereavement or is undisturbed.
1 Mood is largely like sadness in bereavement, although itmay lack explanation, be associated with more anxiety,or be much more intense.
2 Less than half the time, mood is qualitatively distinctfrom grief and therefore difficult to explain to others.
3 Mood is qualitatively distinct from grief nearly all of thetime. Complete either 11 or 12 (not both)
11. Appetite (Decreased):
0 No change from usual appetite.1 Eats somewhat less often and/or lesser amounts than
usual.2 Eats much less than usual and only with personal effort.3 Eats rarely within a 24-hour period, and only with
extreme personal effort or with persuasion by others.
12. Appetite (increased):
0 No change from usual appetite.1 More frequently feels a need to eat than usual.2 Regularly eats more often and/or greater amounts than
usual.3 Feels driven to overeat at and between meals.
Complete either 13 or 14 (not both)
13. Weight (Decrease) Within The Last Two Weeks:
0 Has experienced no weight change.1 Feels as if some slight weight loss occurred.2 Has lost 2 pounds or more.3 Has lost 5 pounds or more.
14. Weight (increase) Within the Last Two Weeks:
0 Has experienced no weight change.1 Feels as if some slight weight gain has occurred.2 Has gained 2 pounds or more.3 Has gained 5 pounds or more.
15. Concentration/Decision Making:
0 No change in usual capacity to concentrate and decide.1 Occasionally feels indecisive or notes that
attention often wanders.2 Most of the time struggles to focus attention or
make decisions.3 Cannot concentrate well enough to read or
cannot make even minor decisions.
16. Outlook (Self):
0 Sees self as equally worthwhile and deserving as others.1 Is more self-blaming than usual.2 Largely believes that he/she causes problems for others.3 Ruminates over major and minor defects in self.
17. Outlook (Future):
0 Views future with usual optimism.1 Occasionally has pessimistic outlook that can be
dispelled by others or events.2 Largely pessimistic for the near future.3 Sees no hope for self/situation anytime in the future.
18. Suicidal Ideation:
0 Does not think of suicide or death.1 Feels life is empty or is not worth living.2 Thinks of suicide/death several times a week for several
minutes.3 Thinks of suicide/death several times a day in depth, or
has made specific plans, or attempted suicide.
19. Involvement:
0 No change from usual level of interest in other peopleand activities.
1 Notices a reduction in former interests/activities.2 Finds only one or two former interests remain.3 Has virtually no interest in formerly pursued activities.
20. Energy/Fatiguability:
0 No change in usual level of energy.1 Tires more easily than usual. 2 Makes significant personal effort to initiate or maintain
usual daily activities.
52
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 52

IDS-C and IDS-SR ratings of depressive symptoms
3 Unable to carry out most of usual daily activities due tolack of energy.
21. Pleasure/Enjoyment (exclude sexual activities):
0 Participates in and derives usual sense of enjoymentfrom pleasurable activities.
1 Does not feel usual enjoyment from pleasurable activities.2 Rarely derives pleasure from any activities.3 Is unable to register any sense of pleasure/enjoyment
from anything.
22. Sexual Interest: Has usual interest in or derives usualpleasure from sex.
1 Has near usual interest in or derives some pleasure fromsex.
2 Has little desire for or rarely derives pleasure from sex.3 Has absolutely no interest in or derives no pleasure from
sex.
23. Psychomotor Slowing:
0 Normal speed of thinking, gesturing, and speaking.1 Patient notes slowed thinking, and voice modulation is
reduced.2 Takes several seconds to respond to most questions;
reports slowed thinking.3 Is largely unresponsive to most questions without strong
encouragement.
24. Psychomotor Agitation:
0 No increased speed or disorganization in thinking or gesturing.
1 Fidgets, wrings hands and shifts positions often.2 Describes impulse to move about and displays motor
restlessness.3 Unable to stay seated. Paces about with or without
permission.
25. Somatic Complaints:
0 States there is no feeling of limb heaviness or pains.1 Complains of headaches, abdominal, back or joint pains
that are intermittent and not disabling.2 Complains that the above pains are present most of the
time.
3 Functional impairment results from the above pains.
26. Sympathetic Arousal:
0 Reports no palpitations, tremors, blurred vision, tinnitusor increased sweating, dyspnea, hot and cold flashes,chest pain.
1 The above are mild and only intermittently present.2 The above are moderate and present more than half the
time.3 The above result in functional impairment.
27. Panic/Phobic Symptoms:
0 Has neither panic episodes nor phobic symptoms.1 Has mild panic episodes or phobias that do not usually
alter behavior or incapacitate.2 Has significant panic episodes or phobias that modify
behavior but do not incapacitate.3 Has incapacitating panic episodes at least once a week
or severe phobias that lead to complete and regularavoidance behavior.
28. Gastrointestinal:
0 Has no change in usual bowel habits.1 Has intermittent constipation and/or diarrhea that is
mild.2 Has diarrhea and/or constipation most of the time that
does not impair functioning.3 Has intermittent presence of constipation and/or
diarrhea that requires treatment or causes functionalimpairment.
29. Interpersonal Sensitivity:
0 Has not felt easily rejected, slighted, criticized or hurtby others at all.
1 Occasionally feels rejected, slighted, criticized or hurtby others.
2 Often feels rejected, slighted, criticized or hurt by others, but with only slight effects on social/occupational functioning.
3 Often feels rejected, slighted, criticized or hurt by others that results in impaired social/occupational functioning.
53
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 53

Rush et al.
30. Leaden Paralysis/Physical Energy:
0 Does not experience the physical sensation of feelingweighted down and without physical energy.
1 Occasionally experiences periods of feeling physicallyweighted down and without physical energy, but without a negative effect on work, school, or activitylevel.
2 Feels physically weighted down (without physicalenergy) more than half the time.
3 Feels physically weighted down (without physicalenergy) most of the time, several hours per day, severaldays per week.
Range 0–84 score.© Copyright retained by A. John Rush MD. This scale may be used for research or clinical purposes withpermission from Dr Rush.
INVENTORY OF DEPRESSIVE SYMPTOMATOLOGY (SELF-REPORT) (IDS-SR)
NAME:
TODAY'S DATE
Please circle the one response to each item that bestdescribes you for the past seven days.
1 . Falling Asleep:
0 I never take longer than 30 minutes to fall asleep.1 I take at least 30 minutes to fall asleep, less than half
the time.2 I take at least 30 minutes to fall asleep, more than half
the time.3 I take more than 60 minutes to fall asleep, more than
half the time.
2. Sleep During the Night:
0 I do not wake up at night.1 I have a restless, light sleep with a few brief awakenings
each night.2 I wake up at least once a night, but I go back to sleep
easily.3 I awaken more than once a night and stay awake for 20
minutes or more, more than half the time.
3. Waking Up Too Early:
0 Most of the time, I awaken no more than 30 minutesbefore I need to get up.
1 More than half the time, I awaken more than 30 minutes before I need to get up.
2 I almost always awaken at least one hour or so before Ineed to, but I go back to sleep eventually.
3 I awaken at least one hour before I need to, and can'tgo back to sleep.
4. Sleeping Too Much:
0 I sleep no longer than 7-8 hours/night, withoutnapping during the day.
1 I sleep no longer than 10 hours in a 24-hour periodincluding naps.
2 I sleep no longer than 12 hours in a 24-hour periodincluding naps.
3 I sleep longer than 12 hours in a 24-hour periodincluding naps.
5. Feeling Sad:
0 I do not feel sad1 I feel sad less than half the time.2 I feel sad more than half the time.3 I feel sad nearly all of the time.
6. Feeling Irritable:
0 I do not feel irritable.1 I feel irritable less than half the time.2 I feel irritable more than half the time.3 I feel extremely irritable nearly all of the time.
7. Feeling Anxious or Tense:
0 I do not feel anxious or tense.1 I feel anxious (tense) less than half the time.2 I feel anxious (tense) more than half the time.3 I feel extremely anxious (tense) nearly all of the
time.8. Response of Your Mood to Good or Desired Events:
0 My mood brightens to a normal level which lasts forseveral hours when good events occur.
1 My mood brightens but I do not feel like my normal selfwhen good events occur.
54
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 54

IDS-C and IDS-SR ratings of depressive symptoms
2 My mood brightens only somewhat to a rather limitedrange of desired events.
3 My mood does not brighten at all, even when very goodor desired events occur in my life.
9. Mood in Relation to the Time of Day:
0 There is no regular relationship between my mood andthe time of day.
1 My mood often relates to the time of day because ofenvironmental events (e.g., being alone, working).
2 In general, my mood is more related to the time of daythan to environmental events.
3 My mood is clearly and predictably better or worse at aparticular time each day.
9a. Is your mood typically worse in the morning, afternoonor night? (circle one)
9a. Is your mood variation attributed to the environment?(yes or no) (circle one)
10. The Quality of Your Mood:
0 The mood (internal feelings) that I experience is verymuch a normal mood.
1 My mood is sad, but this sadness is pretty much like thesad mood I would feel if someone close to me died orleft.
2 My mood is sad, but this sadness has a rather differentquality to it than the sadness I would feel if someoneclose to me died or left.
3 My mood is sad, but this sadness is different from thetype of sadness associated with grief or loss.
Please complete either 11 or 12 (not both)
11. Decreased Appetite:
0 There is no change in my usual appetite.1 I eat somewhat less often or lesser amounts of food than
usual.2 I eat much less than usual and only with personal effort.3 I rarely eat within a 24-hour period, and only with
extreme personal effort or when others persuade me toeat.
12. Increased Appetite:
0 There is no change from my usual appetite.
1 I feel a need to eat more frequently than usual.2 I regularly eat more often and/or greater amounts of
food than usual.3 I feel driven to overeat both at mealtime and
between meals.
Please complete either 13 or 14 (not both)
13. Within the Last Two Weeks:
0 I have not had a change in my weight.1 I feel as if I've had a slight weight loss.2 I have lost 2 pounds or more.3 I have lost 5 pounds or more.
14. Within the Last Two Weeks:
0 I have not had a change in my weight.1 I feel as if I've had a slight weight gain.2 I have gained 2 pounds or more.3 I have gained 5 pounds or more.
15. Concentration/Decision Making:
0 There is no change in my usual capacity to concentrateor make decisions.
1 I occasionally feel indecisive or find that my attentionwanders.
2 Most of the time, I struggle to focus my attention or tomake decisions.
3 I cannot concentrate well enough to read or cannotmake even minor decisions.
16. View of Myself:
0 I see myself as equally worthwhile and deserving asother people.
1 I am more self-blaming than usual.2 I largely believe that I cause problems for others.3 I think almost constantly about major and minor
defects in myself.
17. View of My Future:
0 I have an optimistic view of my future.1 I am occasionally pessimistic about my future, but for
the most part I believe things will get better.2 I'm pretty certain that my immediate future
(1–2 months) does not hold much promise of goodthings for me.
55
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 55
Rush et al.
3 I see no hope of anything good happening to me anytime in the future.
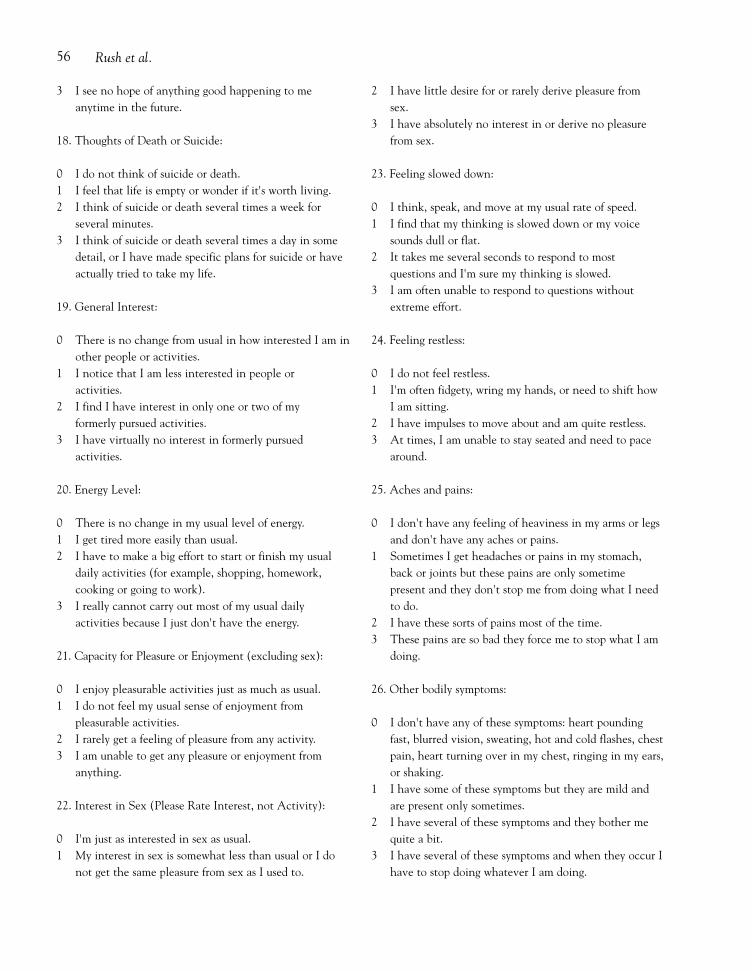
18. Thoughts of Death or Suicide:
0 I do not think of suicide or death.1 I feel that life is empty or wonder if it's worth living.2 I think of suicide or death several times a week for
several minutes.3 I think of suicide or death several times a day in some
detail, or I have made specific plans for suicide or haveactually tried to take my life.
19. General Interest:
0 There is no change from usual in how interested I am inother people or activities.
1 I notice that I am less interested in people or activities.
2 I find I have interest in only one or two of myformerly pursued activities.
3 I have virtually no interest in formerly pursuedactivities.
20. Energy Level:
0 There is no change in my usual level of energy.1 I get tired more easily than usual.2 I have to make a big effort to start or finish my usual
daily activities (for example, shopping, homework, cooking or going to work).
3 I really cannot carry out most of my usual dailyactivities because I just don't have the energy.
21. Capacity for Pleasure or Enjoyment (excluding sex):
0 I enjoy pleasurable activities just as much as usual.1 I do not feel my usual sense of enjoyment from
pleasurable activities.2 I rarely get a feeling of pleasure from any activity.3 I am unable to get any pleasure or enjoyment from
anything.
22. Interest in Sex (Please Rate Interest, not Activity):
0 I'm just as interested in sex as usual.1 My interest in sex is somewhat less than usual or I do
not get the same pleasure from sex as I used to.
2 I have little desire for or rarely derive pleasure from sex.
3 I have absolutely no interest in or derive no pleasurefrom sex.
23. Feeling slowed down:
0 I think, speak, and move at my usual rate of speed.1 I find that my thinking is slowed down or my voice
sounds dull or flat.2 It takes me several seconds to respond to most
questions and I'm sure my thinking is slowed.3 I am often unable to respond to questions without
extreme effort.
24. Feeling restless:
0 I do not feel restless.1 I'm often fidgety, wring my hands, or need to shift how
I am sitting.2 I have impulses to move about and am quite restless.3 At times, I am unable to stay seated and need to pace
around.
25. Aches and pains:
0 I don't have any feeling of heaviness in my arms or legsand don't have any aches or pains.
1 Sometimes I get headaches or pains in my stomach,back or joints but these pains are only sometime present and they don't stop me from doing what I needto do.
2 I have these sorts of pains most of the time.3 These pains are so bad they force me to stop what I am
doing.
26. Other bodily symptoms:
0 I don't have any of these symptoms: heart poundingfast, blurred vision, sweating, hot and cold flashes, chestpain, heart turning over in my chest, ringing in my ears,or shaking.
1 I have some of these symptoms but they are mild andare present only sometimes.
2 I have several of these symptoms and they bother mequite a bit.
3 I have several of these symptoms and when they occur Ihave to stop doing whatever I am doing.
56
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 56

IDS-C and IDS-SR ratings of depressive symptoms
27. Panic/Phobic symptoms:
0 I have no spells of panic or specific fears (phobia) (suchas animals or heights).
1 I have mild panic episodes or fears that do not usuallychange my behavior or stop me from functioning.
2 I have significant panic episodes or fears that force meto change my behavior but do not stop me from func-tioning.
3 I have panic episodes at least once a week or severefears that stop me from carrying on my daily activities.
28. Constipation/diarrhea:
0 There is no change in my usual bowel habits.1 I have intermittent constipation or diarrhea which is
mild.2 I have diarrhea or constipation most of the time but it
does not interfere with my day-to-day functioning.3 I have constipation or diarrhea for which I take medi-
cine or which interferes with my day-to-day activities.
29. Interpersonal Sensitivity:
0 I have not felt easily rejected, slighted, criticized or hurtby others at all.
1 I have occasionally felt rejected, slighted, criticized orhurt by others.
2 I have often felt rejected, slighted, criticized or hurt byothers, but these feelings have had only slight effects onmy relationships or work.
3 I have often felt rejected, slighted, criticized or hurt byothers and these feelings have impaired my relation-ships and work.
30. Leaden Paralysis/Physical Energy:
0 I have not experienced the physical sensation of feelingweighted down and without physical energy.
1 I have occasionally experienced periods of feeling physi-cally weighted down and without physical energy, but
without a negative effect on work, school, or activitylevel.
2 I feel physically weighted down (without physical ener-gy) more than half the time. I feel physically weighteddown (without physical energy) most of the time, sever-al hours per day, several days per week.
Thank you
Range 0–84 Score:
© Copyright retained by A. John Rush MD. This scale may be used for research or clinical purposes with permission from Dr Rush.
AcknowledgementsThe work reported herein was supported in part by agrant from the National Institute of Mental Health(MH-53799), by Mental Health Connections, a part-nership between Dallas County Mental Health andMental Retardation (MHRM) and the Department ofPsychiatry of the University of Texas SouthwesternMedical Center, which receives funding from theTexas State Legislature and the Dallas CountyHospital District, and by the Sara M. and Charles E.Seay Center for Basic and Applied Research inPsychiatry. We gratefully acknowledge the secretarialsupport of David Savage and Fast Word, Inc., Dallas,Texas and the administrative support of Kenneth Z.Altshuler, MD, Stanton Sharp Distinguished Chair,Professor and Chairman, Department of Psychiatry,University of Texas Southwestern Medical Center,Dallas, TX.
Presented in part at the ECST Strasbourg ForumVIII, Issues of Concern in the Standardisation andHarmonization of Psychotropic Drug Trials in Europe,Strasbourg, France, 9–10 June 1999.
57
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 57

Rush et al.
ReferencesAmerican Psychiatric Association. Diagnostic and Statistical
Manual of Mental Disorders, Fourth Edition.Washington, DC: American Psychiatric Association,1994.
Bech P, Gram LF, Dein E, Jacobsen O, Vitger J, Bolwig TG.Quantitative rating of depressive states – correlationsbetween clinical assessment, Beck’s self-rating scale andHamilton’s objective rating scale. Acta Psychiatr Scand1975; 51: 161–70.
Bech P, Allerup P, Gram LF, Reisby N, Rosenberg R,Jacobsen O, Nagy A. The Hamilton Depression Scale.Evaluation of objectivity using logistic models. ActaPsychiatr Scand 1981; 63: 290–9.
Beck AT, Ward CH, Mendelson M, Mock JE, Erbaugh JK.An inventory for measuring depression. Arch GenPsychiatry 1961; 4: 561–71.
Beck AT, Rush AJ, Shaw BF, Emery G. Cognitive Therapy ofDepression. New York: Guilford Press, 1979.
Biggs MM, Shores-Wilson K, Rush AJ, Carmody TJ, TrivediMH, Crismon ML, Toprac MG, Mason M. A comparisonof alternative assessments of depressive symptom severity:a pilot study. Psychiatry Res, in press.
Carroll BJ, Feinberg M, Smouse PE, Rawson SG, Greden JF.The Carroll Rating Scale for Depression. I. Development,reliability and validation. Br J Psychiatry 1981; 138:194–200.
Feinberg M, Carroll BJ. The Carroll Rating Scale forDepression. In N Sartorius and TA Ban (eds) Assessmentof Depression. New York: Springer-Verlag, pp. 188–200,1985.
Faravelli C, Ambonetti A, Pallanti S, Pazzagli A. Depressiverelapses and incomplete recovery from index episode. AmJ Psychiatry 1986; 143: 888–91.
Fava GA, Grandi S, Zielezny M, Canestrari R, Morphy MA.Cognitive behavioral treatment of residual symptoms inprimary major depressive disorder. Am J Psychiatry 1994;151: 1295–9.
Fava GA, Rafanelli C, Grandi S, Conti S, Belluardo P.Prevention of recurrent depression with cognitive behav-ioral therapy: preliminary findings. Arch Gen Psychiatry1998a; 55: 816–20.
Fava GA, Rafanelli C, Grandi S, Canestrari R, Morphy M.A. Six-year outcome for cognitive behavioral treatmentof residual symptoms in major depression. Am JPsychiatry 1998b; 155: 1443–5.
Feiger AD, Bielski RJ, Bremner J, Heiser JF, Trivedi M,Wilcox CS, Roberts DL, Kensler TT, McQuade RD,Kaplita SB, Archibald DG. Double-blind, placebo-substi-tution study of nefazodone in the prevention of relapseduring continuation treatment of outpatients with majordepression. Int Clin Psychopharmacol 1999; 14: 19–28.
Gullion CM, Rush AJ. Toward a generalizable model ofsymptoms in major depressive disorder. Biol Psychiatry1998; 44: 959–72.
Hamilton M. A rating scale for depression. J NeurolNeurosurg Psychiatry 1960; 12: 56–62.
Hamilton M. Development of a rating scale for primarydepressive illness. Br J Soc Clin Psychol 1967; 6: 278–96.
Judd LL, Akiskal HS, Maser JD, Zeller PJ, Endicott J, CoryellW, Paulus MP, Kunovac JL, Leon AC, Mueller TI, RiceJA, Keller MB. A prospective 12-year study of subsyndro-mal and syndromal depressive symptoms in unipolarmajor depressive disorders. Arch Gen Psychiatry 1998a;55: 694–700.
Judd LL, Akiskal HS, Maser JD, Zeller PJ, Endicott J, CoryellW, Paulus MP, Kunovac JL, Leon AC, Mueller TI, RiceJA, Keller MB. Major depressive disorder: a prospectivestudy of residual subthreshold depressive symptoms as pre-dictor of rapid relapse. J Affect Disord 1998b; 50: 97–108
Maier W, Philipp M. Comparative analysis of observerdepression scales. Acta Psychiatr Scand 1985; 72: 239–45.
Miller IW, Keitner GI, Schatzberg AF, Klein DN, Thase ME,Rush AJ, Markowitz J, Schlager DS, Kornstein SG, DavisSM, Harrison WM, Keller MB. The treatment of chronicdepression, part 3: psychosocial functioning before andafter treatment with sertraline or imipramine. J ClinPsychiatry 1998; 59: 608–19.
Montgomery SA, Åsberg M. A new depression scaledesigned to be sensitive to change. Br J Psychiatry 1979;134: 382–9.
Nelson JC, Mazure CM. A scale for rating tricyclic responsein major depression: the TRIM. J Clin Psychopharmacol1990; 10: 252–60.
O’Sullivan RL, Fava M, Agustin CM, Baer L, Rosenbaum JF.Sensitivity of the six-item Hamilton Depression RatingScale. Acta Psychiatr Scand 1997; 95: 379–84.
Paykel ES, Ramana R, Cooper Z, Hayhurst H, Kerr J,Barocka A. Residual symptoms after partial remission: animportant outcome in depression. Psychol Med 1995; 25:1171–80.
Paykel ES, Scott J, Teasdale JD, Johnson AL, Garland A,Moore R, Jenaway A, Cornwall PL, Hayhurst H, AbbottR, Pope M. Prevention of relapse in residual depression bycognitive therapy. a controlled trial. Arch Gen Psychiatry1999; 56: 829–35.
Rehm LP, O’Hara MW. Item characteristics of the HamiltonRating Scale for Depression. J Psychiatr Res 1985; 19:31–41.
Rush AJ, Armitage R, Gillin JC, Yonkers KA, Winokur A,Moldofsky H, Vogel GW, Kaplita SB, Fleming JB,Montplaisir J, Erman MK, Albala BJ, McQuade RD.Comparative effects of nefazodone and fluoxetine onsleep in outpatients with major depressive disorder. BiolPsychiatry 1998; 44: 3–14.
Rush AJ, Giles DE, Schlesser MA, Fulton CL, WeissenburgerJE, Burns CT. The Inventory for DepressiveSymptomatology (IDS): preliminary findings. PsychiatryRes 1986; 18: 65–87.
58
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 58

IDS-C and IDS-SR ratings of depressive symptoms
Rush AJ, Gullion CM, Basco MR, Jarrett RB, Trivedi MH.The Inventory of Depressive Symptomatology (IDS): psy-chometric properties. Psychol Med 1996; 26: 477–86.
Rush AJ, Hiser W, Giles DE. A comparison of self-reportedversus clinician-rated symptoms in depression. J ClinPsychiatry 1987; 48: 246–248.
Thase ME, Simons AD, McGeary J, Cahalane JF, Hughes C,Harden T, Friedman E. Relapse after cognitive behaviortherapy of depression: potential implications for longercourses of treatment. Am J Psychiatry 1992; 149:1046–52.
Tondo L, Burrai C, Scamonatti L, Weissenburger JE, RushAJ. Comparison between clinician-rated and self-report-ed depressive symptoms in Italian psychiatric patients.Neuropsychobiology 1988; 19, 1–5.
Yonkers K, Samson J. Mood disorders. In AmericanPsychiatric Association ed. Handbook of PsychiatricMeasures. Washington, DC: American PsychiatricAssociation, 2000
Zung WWK. A self-rating depression scale. Arch GenPsychiatry 1965; 12: 63–70.
Zung WWK. Zung self-rating depression scale and depressionstatus inventory. In N Sartorius, TA Ban (eds).Assessment of Depression. New York: Springer-Verlag,pp. 2217–31, 1985.
Correspondence to A. John Rush, Department ofPsychiatry, University of Texas Southwestern MedicalCenter, 5323 Harry Hines Blvd., Dallas, TX 75390-9086, USA. Telephone (+1) 214-648-4600. Fax (+1)214-648-4612. Email [email protected].
59
IJMPR 9(2) 3rd mb 3/8/97 12:15 pm Page 59