
the intention to helpseek for breast cancer symptoms
287
THE INTENTION TO HELPSEEK FOR BREAST CANCER SYMPTOMS IN AFRICAN AMERICAN WOMEN by Noreen C. Facione DISSERTATION Submitted in partial satisfaction of the requirements for the degree of DOCTOR OF PHILOSOPHY in Nursing in the GRADUATE DIVISION of the UNIVERSITY OF CALIFORNIA San Francisco Approved: Committee in Charge Deposited in the Library, University of California, San Francisco
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of the intention to helpseek for breast cancer symptoms

THE INTENTION TO HELPSEEK FOR BREAST CANCER SYMPTOMS
IN AFRICAN AMERICAN WOMEN
by
Noreen C. Facione
DISSERTATION
Submitted in partial satisfaction of the requirements for the degree of
DOCTOR OF PHILOSOPHY
in
Nursing
in the
GRADUATE DIVISION
of the
UNIVERSITY OF CALIFORNIA
San Francisco
Approved:
Committee in Charge
Deposited in the Library, University of California, San Francisco
THE INTENTION TO HELPSEEK FOR BREAST CANCER SYMPTOMS
|N AFRICAN AMERICAN WOMEN
© Copyright 1994Noreen C. Facione
All Rights Reserved

Acknowledgements
Any completed project is many people's work, and this project owes
special thanks to many people who gave support and advice. I am grateful for
the patient listening of Dr. Linda McKeever (formerly of California State U.
Fullerton) and Dr. Patricia Larson (U. California San Francisco - UCSF) who
nurtured the early framing of the research questions that were addressed in this
study. No less important were my dialogues with Drs. Gay Becker (UCSF),
Richard Snow (Stanford U.), Sarah Kagan (U. Pennsylvania), and Karen
Schumacher (UCSF) which shaped the focus of the investigation and provided
a vision of the character of the data that might be collected. Thank you, Drs.
Virginia Olesen and Afaf Meleis for providing guidance toward a feminist
perspective of women's social world at a formative stage of the project's
conceptualization. I am grateful to Dr. Jeanne McRae (Howard U.) who gave
vision to a community based study, to Dr. Heather Young (U. Washington) who
fed the vision by sharing her experience of successful community projects
guided by social behavioral theory, and to Dr. Robert Staples for providing the
opportunity to discuss race as a factor in health care access. I am indebted to
Dr. Rob Slaughter (UCSF) for his guidance in the finer points of attitudinal
measurement, and to the collaborative comments of the participating faculty of
the 1992 Oncological Nursing Research Short Course which contributed to the
strength of the study design. Thank you, Dr. Susan Gortner (UCSF), for bringing
the Philosophy of Nursing Science to life and you, Dr. Marie Cowan
iii

(U. Washington), for providing encouragement and guidance in the practical
world of research funding.
In the course of this dissertation study I was the beneficiary of guidance
from three nursing scientists whose knowledge and expertise are particularly
extraordinary: Dr. Marylin J Dodd, Dr. Afaf I Meleis, and Dr. William Holzemer.
That such a rich mentorship committee was possible is a tribute to the UCSF
School of Nursing. A delicate balance between reassurance, critique and
expectation was ever-present in their combined mentorship of my progress as
a Scientist.
Thank you, Dr. Marylin J. Dodd, for providing primary direction of this
dissertation study, and for focusing the oncological issues in the prior research
on early case-finding in breast cancer. Your unwavering engagement and belief
in the possibility of success for this ambitious endeavor sustained me when
events or demands added to the challenge of the project. Your mentoring
helped me to frame my understandings of how studies of helpseeking behavior
fit with other investigations of the breast cancer experience. I look forward to
sharing the labors of oncology nursing science with you in the future.
Thank you, Dr. William Holzemer, for always providing a much-needed
practical analysis of work accomplished, and of possible approaches to work still
needed. Your Socratic approach to conceptualization led to clear improvements
in my variable selection for this project as well as a sharpening of the variable
definitions. The initial validity and reliability evidence for measures developed
iv

as a part of this project is much indebted to your guidance. Thank you for
encouraging me to enjoy the numbers in my head.
Thank you, Dr. Afaf Meleis, for your vision of the project as necessarily
accountable to culture and gender issues. Your mentorship in this regard added
richness and increased the authenticity of the project. Our many discussions
made possible the theoretical linkage between my research objective, my
chosen methodology, and the interpretation of the data, strengthening the
potential value of the study findings. Your spirit of asking what more could be
done, trusting that practical difficulties would be worked out later, led to an
extension of the boundaries of the project. Thank you, also, for the dialogue on
the relationship between critical thinking and nursing knowledge development.
I hope its one we can continue.
A community based project is, in a very large part, the offspring of the
community. This project would not have been so successful without the efforts
of Barbara Galloway-Lee, MEd., of the San Mateo Unit of the American Cancer
Society. Thank you Barbara, for launching the focus group portion of the study
by facilitating introductions to a number of women who were community leaders
involved in health access and education projects. I thank you, along with
African American nurse researchers Dr. DeLois Weekes (UCSF), Dr. Nanny L.
Green (UCSF), Linda Woody-Wood, Dr. Gozil Shockness, and Dr. Benita Walton
Moss, for offering helpful comments on phases of the project design and the
developed survey instrument.

All of the women of the focus groups deserve special acknowledgement
for their influence on this project. They gave generously of themselves, sharing
thoughts and feelings of their own breast symptom discovery experiences as
well as narratives of their friends', relatives' and neighbors' experiences with
breast cancer. Their patient and candid efforts to analyze and critique
prospective survey items, being called upon to explain their responses to
problematic items, testifies to their commitment to the project's cultural
authenticity of measurement. I am most grateful to one of you, Ms. Mary
Flamer, who took on the job of primary research assistant and ultimately was
responsible for distributing and collecting the vast majority of the survey
questionnaires. Mary, you adopted a commitment to the project that extended
far beyond that of many project assistants, facilitating the community's
awareness of the project, and making possible the accrual of a sample that
included employed as well as unemployed women, partnered and single
women, and women who ranged across income levels. This project's service
to the community was greatly increased by your ability to offer debriefing
information and provide clarifying information when questions remained after
women completed the survey instrument. The increased community awareness
of the American Cancer Society's cancer information and patient support
services is a tribute to your efforts.
Apart from the human resources supporting the project, financial support
for the project was instrumental in supporting my full time investigative efforts as
well as providing a small remuneration to project participants, supporting the

salary of my primary research assistant, and covering the many material costs
of this survey investigation. Predoctoral fellowships from the University of
California Regents (20095-3; 34187-3) and the University of California Chancellor
(36009-3), a predoctoral scholarship in cancer nursing from the National
American Cancer Society (MPCN-24-2), a National Research Service Award
(NRSA) from the National Institute for Nursing Research, National Institutes of
Health (1 F31 NR06851-01), and a Predoctoral Fellowship in the Social
Behavioral Sciences from the California Division of the American Cancer Society
(PD-5-94). Early work also received support from a Professional Nurse
Traineeship (2A11 NU00289-16).
I would also like to acknowledge Dr. Nan Green for permitting the use of
her Perceptions of Racism scale, Dr. Kenneth Wallston and colleagues for the
use of the Chance scale from the MHLC instrument, and Dr. Krantz for the use
of the Health Opinion survey, as well as the other scientists mentioned within the
text whose work provided a base for this investigation.
Completing this project depended in no small part on the emotional
support I received from friends and colleagues at UCSF and at Santa Clara
University. Most instrumental was the support of my spouse and research
colleague Dr. Peter A. Facione. Thank you, Peter, for your tireless listening to
the day to day happenings and your willingness to provide a forum for the
continual problem solving process always necessary to a project of this size.
You provided the glue that held the work together. Thank you for believing that
this project was possible and that I was capable of leading it to completion.
vii

Since you know me best, that assessment was powerful. Just as I thank my
parents for nurturing my early intellectual development, I thank my children for
supporting my later studies. Thank you, Chris and Jerome, for always asking
how things were going, and for your patience with my stresses or my absence
from your day to day. And thank you, Carol, for sharing the growing process.
It was wonderful to know that you were always there to counsel about the
setbacks as well as the successes. Our conversations particularly helped me
to evolve a multi-disciplinary framing of the study and its findings. Thanks to all
of you for celebrating the product of all this effort.
To all of you, and there are many others who contributed whose names
I have not been able to mention individually here, I give grateful
acknowledgement. It is my hope that your contributions to this study have only
begun to bear fruit.
viii
ABSTRACT
THE INTENTION TO HELPSEEK FOR BREAST CANCER SYMPTOMS
|N|AFRICAN AMERICAN WOMEN
Noreen C. Facione
The self-discovery of a breast cancer symptom occurs within the
context of beliefs and feelings, gender roles, and social and economic
realities which may differ within culture. African American women were
chosen for study because of their later staged breast cancer at diagnosis.
The purpose of this survey research was to identify factors that influence the
timing of helpseeking for breast cancer symptoms.
Focus groups were conducted to explore possible influential factors. A
survey was then constructed from focus group data and critiqued by the
focus group women and by African American nurse researchers. The survey
was then used in a new sample (N = 352) of African American women.
Perceptions of the consequences of delaying helpseeking, health care
utilization habits, and access to services were positively and significantly
related to the intention to helpseek for a discovered breast symptom.
Religiousness, fatalistic beliefs, perceptions of social role constraints, and the
presence of a current worrisome breast symptom were significantly and
negatively related to helpseeking intention. A hierarchical multiple linear
regression model containing these variables explained 45.3% of the variance
in helpseeking intention. While younger aged, lower income, and unmarried

women were significantly less likely to intend helpseeking for a discovered
breast symptom, these demographic variables added no explained variance
to the Social behavioral model.
Variables observed to be significant to the intention to helpseek in this
sample of African American women bear striking resemblance to anecdotal
reports in the literature of the reasons women of all ethnic and racial groups
give for late helpseeking when presenting with late-staged breast cancer.
This investigation suggests the possibility of screening women for
psychosocial risk of advanced breast cancer presentation before their breast
cancer symptoms occur. Such screening could identify women who might
particularly benefit from additional guidance in monitoring their own breast
health, as well as inform providers with regard to those who might require
closer follow-up.
Mary■ in J/Dodd, KKD, RN, FAAN: Adviser
TNoreen C. Facione, MSN, RN, FNP - Candidate
TABLE OF CONTENTS
INTRODUCTION: 1
CHAPTER 1: WOMEN AT RISK FOR ADVANCED STAGE OF BREASTCANCER AT DIAGNOSIS 4
The Phenomenon of Delayed Helpseeking 5The Definition of Patient Delay 5The Prevalence of Patient Delay 7
Helpseeking's Influence on Survival 9Demographic Variables Believed Influential
to the Timing of Helpseeking 11Race and Racism - The Greater Threat
for African American Women 11
The Incidence of Breast Cancer 11
Survival of Breast Cancer 12
Socioeconomic Status - Poorer Women Againat Increased Risk 15
The Interaction Between Race and Poverty 17Older Age and Helpseeking 18Comorbidity Issues 21
CHAPTER 2: A SOCIAL BEHAVIORAL DESCRIPTION OF WOMENAT RISK FOR DELAYED HELPSEEKING 23
Cognitive and Behavioral Variables Associated with Patient Delay 23Symptom Attribution - Cues to Action 24
Presenting Symptoms of Breast Cancer 25Perceptions of the Consequences of Delayed Helpseeking 27Affective Responses to Symptom Discovery 30Perceived Behavioral Control 34
Habits of Helpseeking 36Social Normative Influences 39
Facilitating Conditions for Helpseeking 41
CHAPTER 3: THE TRIANDIS MODEL OF SOCIAL BEHAVIORAS A GUIDE TO THE STUDY OF HELPSEEKING INTENTION 44
Culturally Competent Theory 44Social Behavioral Models to Study Helpseeking Intention 45
The Triandis Model of Social Behavior 47Some Potential Limitations of the Triandis Model 53
xi

CHAPTER 4: METHODOLOGY: A THREE STEPPED PROCESS
Focus Group MethodsNew Study Variables from Focus Group SessionsPlanned Comparative Model Testing
Instrument Design Methodology - A CollaborationSurvey Methodology
Sample Inclusion and Exclusion CriteriaSurvey Sample Description
CHAPTER 5: RESULTS: FOCUS GROUP SESSIONSAND SURVEY INSTRUMENT DEVELOPMENT
Focus Group Data Phrases - Consensus and ConflictTriandis Variable Themes
Behavioral Intention
Habits of HelpseekingAffect Related to Breast Symptoms and CancerSocial Normative Influences
Perceived Consequences of Prompt VersusDelayed Helpseeking
Facilitating or Constraining InfluencesAdditional Focus Group Themes
Knowledge of Breast CancerFatalism in Relation to Breast Cancer
ReligiousnessPerceptions of Racism in the Health Care
Services Environment
Psychometric Performance of the Survey InstrumentPerformance of Developed Scales and Measures
Missing DataThe IHELP MeasureThe FEAR Measure
The CONSEQ MeasureThe HABIT MeasureThe Social Influence Measures
SOCNORMCONSTRAINT
The ACCESS MeasureThe FATE Measure
Knowledge of Symptom Presentations: TYPELimitations of the TYPE Measure
Performance of Adopted or Modified ScalesThe Religiousness Measure: RELIGThe RACISM MeasureThe AFFECT Measure
The Health Opinion Survey (HOS)The Crowne - Marlowe (CM-SD)
585862
66
6768
68
74
74
74
74
75
7677
7878
7979
8080
818282
85
8789
9090
9092
9395
96
97
98
99100101
102103
xii
CHAPTER 6: RESULTS: SURVEY OF HELPSEEKING INTENTION
Helpseeking Intention (IHELP)The Relationship of IHELP to Current SymptomatologyRelationships Between Helpseeking Intention and
Sample DemographicsAge and Helpseeking IntentionIncome and Helpseeking IntentionPartnership Status and Helpseeking IntentionResponsibility for Childcare and
Helpseeking IntentionEmployment Status and Helpseeking Intention
Social Behavioral Measures of Helpseeking IntentionKnowledge of Breast Cancer Symptom PresentationReligiousness and Helpseeking IntentionAccess to Services and Helpseeking Intention
Sub-scales of the ACCESS measure
Perceptions of Racism and Helpseeking IntentionThe Habit of Helpseeking and Helpseeking IntentionAffect and Helpseeking IntentionFear and Helpseeking IntentionFatalistic Beliefs and Helpseeking IntentionPerceptions of Consequences and
Helpseeking IntentionSocial Norms and Role Constraints on
Helpseeking IntentionModel Testing for a Combined Model of
Helpseeking IntentionVariable ModelingComparative Model TestingModel 1 - The Original Triandis Predictors
of Behavioral Intention
Model 2 - Testing the Expanded Triandis ModelModel 3 - Adding Influences Proposed
by the Focus Group WomenResidual Diagnostics for Model 3The Contribution of Demographic Variables
104104
105
107107108
108
109109
110110110111112
113114115118
119
120
121
CHAPTER 7: DISCUSSION OF RESULTS
Overview of FindingsThe Overall Intention to Helpseek
Discussion of Demographic Relationships withHelpseeking Intention
The Power of Role Related ConstraintsThe Power of BeliefsThe Power of Resources
The Power of Knowledge
126
126
127
127
129
130
132132
136136137
140143
147
150152
xiii

CHAPTER 7: DISCUSSION OF RESULTS (Continued)The Power of Affect 154
The Benefits of Triandis' Model and Philosophy of Method 155Study Limitations 158
CHAPTER 8: IMPLICATIONS FOR FUTURE RESEARCH 162
REFERENCES 167
APPENDIX A. APPENDIX TABLES 187
APPENDIX B; FOCUS GROUP MATERIALS: Consent Forms, RecruitmentMaterials, Focus Group Session Materials 193
APPENDIX C: THE SURVEY QUESTIONNAIRE 204
xiv

LIST OF TABLES: Page
Table 2 - 1: A Fear Cascade - Targets of Fear in Relation to a BreastCancer Symptom 31
Table 3 - 1: Conceptual Definitions of the Triandis' (1980) SocialBehavioral Model 49
Table 4 - 1: Scales Developed to Measure Triandis Model Variables 62
Table 4 - 2: Other Health Problems Reported by Sample Women 72
Table 5 - 1: Characteristics of Developed Scales Calculated fromSurvey Sample (N = 352) 83
Table 5 - 2: Adopted or Modified Scales Psychometric Characteristics 99
Table 6 - 1: Regression Analysis of ACCESS Sub-Scales onHelpseeking Intention 113
Table 6 - 2: Anticipated Affect in Relation to the Discovery ofa Breast Symptom 116
Table 6 - 3: Two Step Regression of Helpseeking Intention: Role StatusVariables and Perceived Role Constraints (CONSTRAINT) 124
Table 6 - 4: Study Variables Associated with the Intention toHelpseek (IHELP) 125
Table 6 - 5: Multiple Regression Analysis of Model 1 Variables 128
Table 6 - 6: Multiple Regression Analysis of Model 2 Variables 130
Table 6 - 7: Multiple Regression Analysis of Model 3 Variables 131
Table A - 1: Meta-analysis of Studies of Delayed Helpseekingfor Self-Discovered Breast Cancer Symptoms 187
Table A - 2: Demographic Descriptors of the Survey Sample (N = 352) 188
Table A - 3: The IHELP Measure-
189
Table A - 4: The IHELP Measure: Factor Analysis of Items Measuringthe Intention to Helpseek in the Event of a BreastSymptom Discovery: Oblique Rotation 190

LIST OF TABLES: Continued
PageTable A - 5: Factor Analysis of the ACCESS Scale 191
Table A - 6: Reported Behavior in Relation to a CurrentWorrisome Breast Symptom 192
LIST OF FIGURES
Figure 3 - 1:
Figure 3 - 2:
Figure 4 - 1:
Figure 6 - 1:
Figure 6 - 2:
Triandis Variables Measuring Behavioral Intention (Model 1) 53
Theoretical Expansion of Triandis Variables PredictingBehavioral Intention (Model 2) 55
Proposed Influences on Helpseeking Intention (Model 3) 65
Frequency of IHELP Scores in Symptomatic andAsymptomatic Women 106
Univariate Correlation in Best Model Explaining 45% ofVariance in Helpseeking Intention in a Sample of (n = 330)of 352 African American Women 135
INTRODUCTION
In this year of 1994, as we struggle to reform health care delivery, and
politicians seek popular issues to persuade voters, there is suddenly an
increased media focus on breast cancer. Those of us whose research
programs study breast cancer related problems hope to capitalize on this
emphasis before the spotlight moves on. There is no way to measure how
the current focus on breast cancer affected this study, perhaps by increasing
the willingness of respondents to join the focus groups or to complete the
surveys, perhaps by energizing my primary research assistant, Mary, to
recruit survey participants from the many community locations.
During the months when this study was carried out, women in the San
Francisco Bay area were generous with their ideas and feelings about a
breast cancer symptom discovery. And it was trust in God and a dedication
to helping everyone that empowered Mary, not transitory, media generated,
excitement about this important health problem for women throughout the
world. This study began as a theory-guided inquiry about health risk
behavior in a population most at risk for breast cancer death, but it became
much more. It became an inquiry molded by the community at risk, the
descriptions of the thoughts and feelings surrounding helpseeking behavior
Cast in the words of the women studied.
This study was conducted in two parts. The first was a series of four
focus group discussions with twenty-two African American women regarding
the event of a breast symptom discovery and possible breast cancer. In the

2
course of the discussions the women explored what they believed they would
think, who they would tell, how they would feel, what they would know about
the meaning of a worrisome breast symptom discovery in the context of their
lives. Lastly, they described what they thought they would do. This data was
used to construct survey items to capture a culturally relevant expression of
the factors related to helpseeking intention for a self-discovered breast
symptom. To assure that the developed survey captured the spirit and the
content of the focus groups, the developing instrument was critiqued by the
focus group women for its clarity, completeness and cultural acceptability.
Social behavioral theory, specifically the Triandis model, guided the
domain of the topics to be covered in the focus group discussion and the
scale development for the resulting questionnaire. In the second part of the
study, the newly developed survey questionnaire was used to survey a new
sample of 352 African American women. Their responses are analyzed to
explore the influences on helpseeking intention for potential breast cancer
symptoms in this at risk population.
Observed significant influences on helpseeking intention mirrored the
retrospective accounts of factors affecting the timing of helpseeking in women
with breast cancer, suggesting that women have dispositions in relation to
helpseeking that can predict their likelihood to present with advanced stage
breast cancer. Many of the variables observed to be related to low
helpseeking intention were beliefs and habits of mind, not immutable
demographics. If this array of psychological risk factors proves a stable
3
picture of the sub-group of women who seek help less promptly than others
for a potential breast cancer symptom, women might be screened to identify
those with habits of mind that put them at risk for advanced breast cancer at
diagnosis and decreased survival from the disease. Such a screening,
coupled with health care reform that makes breast symptom evaluation
possible for all women, can advance the goal of early case-finding for breast
Ca■ hCer.
CHAPTER 1
WOMEN AT RISK FOR ADVANCED STAGE OF BREAST CANCER
AT DIAGNOSIS
Untreated, a malignant breast tumor advances in stage, diminishing a
woman's chances of survival. Determining the factors which contribute to
delays in seeking help for breast cancer has been the continued focus of
cancer researchers throughout the world (Menon, Teh & Chua, 1992;
Ajekigbe, 1991; Nagadowska & Kulakowski, 1991; Neave, Mason & Kay,
1990; Rossi, et al., 1990; Machiavelli, et al., 1989; Keinan, Carmil & Rieck,
1991; Watson, et al., 1984; Mor et al., 1990). The incidence of breast cancer
continues to rise, with the United States expecting 182,000 new cases and
46,000 deaths in 1994 (ACS, 1994). England and Wales currently lead in age
adjusted death rate (28.7 per 100,000), with the United States (22.4 per
100,000) and other European countries ranking not far behind (ACS, 1994).
In light of the clearly established relationship between early case-finding and
survival, understanding the factors that determine the timing of treatment
remains of paramount importance in the effort to decrease breast cancer
mortality. Demographic and social behavioral variables associated with late
staged breast cancer at diagnosis provide the framework for investigations of
women's behavior in response to a self-discovered breast cancer symptom
and the timing of their seeking an initial provider evaluation (helpseeking).

The Phenomenon of Delayed Helpseeking
Delay in seeking a provider evaluation for self-discovered breast
cancer symptoms has been shown to significantly contribute to the stage of
breast cancer at diagnosis (Hunter, et al., 1993). This chapter is divided into
three sections: (a) the description of the phenomenon of delayed
helpseeking, its prevalence, (b) its impact on survival; and (c) demographic
variables targeting populations where delay is most observable. The
following chapter summarizes what is known about the social behavioral and
cultural variables influential to the timing of helpseeking for self-discovered
breast cancer related symptoms. Both chapters represent advances on the
research on delayed helpseeking published previously (Facione 1993a).
At least 35 research studies from 11 nations have been published in
English language journals on the topic of helpseeking or delay in helpseeking
for breast cancer symptoms since 1975. This discussion summarizes their
findings in relation to helpseeking in female cancer of the breast, no studies
having yet been reported on delayed helpseeking in the less than 1% of
breast cancer occurring in males.
The Definition of Patient Delay
In a seminal article in The American Journal of Cancer, Pack and Gallo
(1938) defined "undue patient delay" arbitrarily as "three months or more
elapsed time between discovery of symptoms and a visit to a physician."
They called for this standard measure of what they termed "patient delay" to

facilitate quantification of the phenomenon through comparison between
studies. Unfortunately, measures of diagnostic delay remain largely arbitrary
today. But there has been increasing care to separate research reports of
the phenomenon into: (a) time related to helpseeking for a self-discovered
breast symptom, and (b) time from helpseeking to diagnosis or initiation of
definitive treatment. The first time period is the domain of the patient alone.
The second is the domain of the patient, the provider, and the health care
system. Both of these time segments have important implications for a
woman's survival of breast cancer. The discussion is limited to the first, the
timing of helpseeking for self-discovered breast cancer symptoms. The
second time period, often referred to in the literature as "provider delay" is
discussed more fully elsewhere (Facione, 1993a).
Most research studies report the timing of helpseeking in terms of
categorical blocks by months, while others define a period as "patient delay"
and report the frequency of women who delay helpseeking for their breast
cancer. All studies mark the beginning of the patient delay period from the
self-discovery of symptoms. Those which mark endpoints at the first provider
consultation provide clear measures of helpseeking, while those which mark
the endpoint at biopsy, diagnosis, or first treatment unfortunately confound
the timing of helpseeking with provider and system influences.
Admittedly, the use of retrospective recall data to determine the
commencement of the patient delay period carries its own potential validity
threat. Symptomatic women might wrongly estimate or even deliberately
7
misrepresent symptom duration. Random sample selection defends against
wrong estimates or deliberate misrepresentation in quasi-experimental studies
of five year survival, theoretically distributing such individuals evenly among
sample groupings, but the potential threat to validity is greater in descriptive
behavioral studies. Many investigators, however, have observed that women
mark the timing and exact circumstances of breast symptom discovery quite
carefully (Keinan, et al., 1991; Lierman, 1988; Dodd, et al., 1992; Huguley, et
al., 1988), remembering the time and place of breast symptom discovery
quite vividly.
The Prevalence of Patient Delay
What percentage of women, diagnosed with breast cancer, delay
seeking help for their symptoms? The varying definitions of delay used by
various investigators limit the number of reported studies that can be used in
a meta-analysis of the timing of helpseeking. Thirteen breast cancer studies
published in English language journals since 1975 have examined patient
delay behavior, studied only women with confirmed breast cancer, and
reported the percentages of women who delayed for a uniform time frame of
three months or longer (Katz, et al., 1993; Menon, Teh & Chua, 1992; Rossi,
et al., 1990; Mor, et al., 1990; Freeman & Was■ ie, 1989; Samet, et al., 1988;
Vernon, et al., 1985; Huguley & Brown, 1981; MacArthur & Smith, 1981;
Nichols, et al., 1981; Adam, et al., 1980; Wilkinson et al., 1979; Dennis,
Gardner & Lim, 1975). A frequency weighted average was calculated,

equalizing the influences of differing sample sizes. This meta-analysis
estimated that 33.6% of the breast cancer women were symptomatic for three
months or more before seeking a provider evaluation. Table A-1 in Appendix
A lists the thirteen studies used for this meta-analysis comprising a total N of
9,077 breast cancer women.
There is little to suggest that delay in helpseeking is decreasing over
time. In Antonovsky & Hartman's (1974) review of patient delay behavior the
percentage of women reported to have delayed helpseeking for three months
or more ranged from 33 to 58%, but this review ranged across tumor types
and contained only three breast cancer studies. In the five most recently
published studies the reported percentage of delayed helpseeking ranged
from to 16.6% to 56%, with the frequency weighted overall percentage at
34.4% (combined n = 1,335).
The mandate for earlier case-finding in the United States can be more
concretely visualized by applying the frequency weighted percentage for the
eight USA studies (33.8%, combined n = 8,295) to the expected new breast
cancer cases for 1994. Since an estimated 60-80% of breast cancers remain
self-discovered (Katz, et al., 1993; Muskat & Huncharek, 1991; Rossi, et al.,
1990; Richardson, et al., 1992), using the 1994 estimate of 182,000 new
breast cancer cases, an estimated 109,200 to 145,600 women will newly
discover their breast cancer symptoms in 1994. Using the above meta
analysis estimate of symptom duration (33.6% for three months or more)
would predict that somewhere between 37,000 and 49,000 American women

will have their breast cancer symptoms for three months or more before
seeking an initial provider evaluation. This statistic underscores the
importance of research to identify factors influencing the timing of
helpseeking.
Helpseeking's Influence on Survival
Both patient and provider delay have direct implications for survival of
breast cancer. At least sixteen research studies published since 1975
analyzed symptom duration in relation to five and/or ten year survival, and all
concluded that delay was significantly related to decreased survival
(Richardson, et al., 1992; Nagadowska & Kulakowski, 1991; Neave, et al.,
1990; Rossi, et al., 1990; Freeman & Wasfie, 1989; Machiavelli, et al., 1989;
Huguley, et al., 1988; Charlson, 1985; Vernon, et al., 1985; Robinson, et al.,
1984; Funch, 1984; Gould-Martin, et al., 1982; Elwood & Moorehead, 1980;
Wilkinson, et al., 1979; Fisher, Redmond & Fisher, 1977; Worden & Weisman,
1975).
Although the impact of delaying helpseeking on survival is known to
differ by individual due to tumor growth rate factors, when individuals are
examined as a group, a direct and undeniable relationship is seen between
delay and survival. The consensus reported by all of the studies was that
breast tumor stage at diagnosis increased overall with delay (defined in this
case as symptom duration prior to treatment), and that increased stage of
tumor at diagnosis was associated overall with decreased survival.
10
Essentially this work provides documentation for the relationship between
delayed helpseeking and survival that was only assumed in earlier reviews of
delay behavior (Pack & Gallo, 1938; Antonovsky & Hartman, 1974; Green &
Roberts, 1974).
Fisher and colleagues (1977) observed that this relationship between
delayed helpseeking behavior and survival was not linear, suggesting that
other variables must play a part in determining survival. Biological tumor
variables such as size of tumor, steroid receptor status, histology, presence
of positive axillary nodes, and the frequency of skin and nipple involvement
have since been more fully explored in relation to symptom duration as
predictors of survival (Neave, et al., 1990; Rossi, et al., 1990; Machiavelli, et
al., 1989; Charlson, 1985; Vernon, et al., 1985).
Several studies have reported delay to be insignificant to survival once
stage of tumor at diagnosis is taken into account (Machiavelli, et al., 1989;
Charison, 1985; Vernon, et al., 1985). The ill-conceived use of statistical
methods of data analysis might be the culprit responsible for this dangerous
and illogical inference. As mentioned previously, one can expect a high
correlation between the variables "tumor stage," "tumor size/mass," and
"symptom duration" (often considered by the investigators as synonymous
with delayed helpseeking). Multiple regression data analyses which include
all of these variables, particularly hierarchical regressions where tumor stage
is introduced first as a covariate, will produce results indicating that delayed
helpseeking contributes no additional explained variance. This situation is

11
perhaps an exquisite example of when theory must guide analyses. The
fundamental concern is to reduce mortality through early case-finding and
toward that end to identify changeable variables that might be targeted for
interventions. No health care purpose is served by diminishing the
importance of the delayed helpseeking behavior variable in research reports.
Demographic Variables Believed Influential to the Timing of Helpseeking
Who are the women at risk for delayed helpseeking for breast cancer
symptoms?. Much of the research on delayed helpseeking has been focused
on the study of differences in symptom duration and stage of disease at
diagnosis between different segments of the population. Large data pools
which include demographic variables have invited this type of epidemiological
research. Observed correlations between delayed helpseeking and particular
demographic descriptors identify target groups for potential intervention
studies.
Race and Racism - The Greater Threat for African American Women
The Incidence of Breast Cancer
The number of new breast cancer cases in African American women
for 1991 was estimated at 15,000, with the number of deaths due to breast
cancer estimated as 4,850 (ACS, 1991). This represents a lower incidence
rate in African American (75.2 per 100,000) compared to Caucasian American
(88.8 per 100,000) women. The exception to this relationship is the incidence

12
of breast cancer by race in women under forty years of age. In this age
group African American women have a higher incidence rate for breast
cancer than Caucasian American women (Baquet & Rincon, 1986; Grey,
Henderson, & Pike, 1980; Krieger, 1990). It remains unclear whether this
Crossover in incidence rates which has been apparent in age-specific breast
cancer incidence data since 1969, is a result of social or biological factors.
Survival of Breast Cancer
Many investigators have reported decreased survival of breast cancer
in African American women' as compared to Caucasian American females
(Huguley & Brown, 1981; Vernon, et al., 1985; Marshall, Gregorio, & Walsh,
1986; Natarajan, et al., 1985; Dayal, Power, & Chiu, 1982). The National
Cancer Institute (NCI) data for the years 1983-1989 report that survival of
female breast cancer differs significantly by race, with Caucasian American
females having an overall five-year breast cancer survival rate of 81% and
African American women only 64% (National Cancer Institute, 1986; 1989;
Boring, Squires, & Montgomery, 1994). This gap has widened by 5% in
'Language referents to race and ethnic group change over time and
generalize without attention to diversity within populations. National Cancer
Institute statistics are currently reported in terms of the descriptors: Non
Hispanic White, Hispanic, Black, American Indian, Asian, and Other/Unknown
(Steele, et al., 1994). Self-referents for these same populations include, but
are not limited to, 'Black' and 'African American,”Latino,' etc. Ambiguities
remain as to whom is being referred to in particular contexts.
13
relation to the five-year survival rates by race reported in 1977-1979 NCI data
(Boring, et al., 1994), and the rate of 64% in African American women
represents no significant change in breast cancer five-year survival in Black
women since 1974. African American women's survival of the disease is
strikingly lower within each stage of the disease (Boring, Squires, & Tong,
1994).
Biological factors such as higher percentages of estrogen receptor
negative tumors and less well differentiated tumor histology may account for
some of this observed difference in survival by race (Valanis, Wirman, &
Hertzberg, 1987; Bain, Greenberg, & Whitaker, 1986, Natarajan, et al., 1985;
Hubay, et al., 1984; Freeman & Wasfie, 1989; Neave, et al., 1990,
Montgomery, et al., 1985; Crowe, et al., 1986; Leffall, 1981; Pegoraro, et al.,
1986). Marked differences have been seen in histologic grade of tumor in
Blacks (more undifferentiated tumors) when compared to the referent group,
Non-Hispanic Whites. There are also noted differences in tumor type. Blacks
have fewer lobular tumors, and more invasive compared to in situ ductal
tumors. However, interpretation of these differences is complicated since
increased duration of symptoms is related to both cell differentiation and
tumor invasiveness. Both of the noted differences by racial group could be a
function, in part, of symptom duration prior to diagnosis.
Nonetheless, African American women are universally reported to have
overall significantly more advanced stage of tumor at diagnosis than
American women in general (Hunter, et al., 1993; Dawson & Thompson,

14
1990; Swanson, et al., 1990; Swanson, et al., 1993; Vernon, et al., 1985;
Richardson, et al., 1992; Marshall, et al., 1982; Natarajan, et al., 1985;
Mandelblatt, et al., 1991; Saunders, 1989; Coates, et al., 1992) and
decreased overall survival of breast cancer (Farley & Flannery, 1989;
Natarajan, et al., 1985; Vernon, et al., 1985; Marshall, Gregorio, & Walsh,
1982; Dayal, Power, & Chiu, 1982; Huguley & Brown, 1981). Reports from
the NCI Surveillance, Epidemiology and End Results (SEER) Program
(Ragland, Selvin & Merrill, 1991; Bain, Greenberg & Whitaker, 1986; Boring,
Squires, & Tong, 1992), the American College of Surgeons' Commission on
Cancer (Natarajan, et al., 1985), and the Michigan Cancer Foundation
Prognostic Study (Ownby, et al., 1985) have documented larger diameter
tumors and increased numbers of positive axillary nodes in Black women in
the United States when compared to Whites.
Longer duration of symptoms prior to helpseeking is believed to
account for some of the noted difference in five year survival by race. In fact,
African American women were reported to have delayed helpseeking longer
than Caucasian American women in at least ten recently published studies
(Hunter, et al., 1993; Lauver, 1992; Coates, et al., 1992; Richardson, et al.,
1992; Mandelblatt, et al., 1991; Saunders, 1989; Ownby, et al., 1985;
Natarajan, et al., 1985; Bain, et al., 1986; Vernon, et al., 1985). In most of
these studies this group difference is simply reported, illuminating none of the
underlying reasons for the difference and thus providing no guidance for
intervention. Many of the recently reported studies analyze data from twenty

15
to forty years ago raising doubts about whether their reported results
describe the current African American population. Recently, however, Hunter
and colleagues (1993) analyzed data from the NCI's Black/White Cancer
Survival Study of women newly diagnosed in 1985-1986 (Howard, et al.,
1992). They reported that up to 50% of the excess risk for late stage at
diagnosis of breast cancer in Black women compared to White women may
be accounted for by "the intrinsic tumor biology and by the lack of current
knowledge and practices in breast cancer prevention" (1993, p. 1135).
Socioeconomic status - Poorer Women Again at Increased Risk
Fortunately, several studies have provided clues about what might be
underlie this observed difference in helpseeking between racial groups.
Poverty and diminished access to breast cancer screening and early case
finding is believed to account for much of the differences in the stage of
tumor at diagnosis by race (Dennis, et al., 1975; Ragland, et al., 1991; Dayal,
et al., 1982; Mandelblatt, et al., 1991; Richardson, et al., 1992; Freeman &
Wasfie, 1989). Others have documented that African Americans utilize health
care services proportionately less, regardless of their degree of illness
(Neighbors, 1988; Broman, 1987; Blendon, et al., 1989), attributing this to a
relative lack of monetary resources that can be spent on health care.
A study by Dayal, et al. (1982) examined factors related to survival in a
sample of 515 Caucasian American and 388 African American New York City
women treated for breast cancer between 1968 and 1977. After controlling

16
for age, stage, and socioeconomic status, racial differences in survival
became insignificant. Race and class were highly correlated in this sample,
however, and although this study is widely quoted, separation of the effects
due to race-related biological and cultural factors versus poverty per se in this
sample is not possible.
Dennis, et al., (1975) suggested that the overt racial discrimination
practices of the 1940's and 1950's, which found white doctors in some states
scheduling night office hours for Negro patients to avoid offending their White
patients (Stack, 1974), may have given way to covert racial biases in health
care environments. They reported that providers significantly delayed
treatment for the African American women compared to Caucasian American
women in their sample. Other findings suggesting prejudicial treatment by
race have been reported by other investigators. A lack of respectful
treatment was reported by 43% of the Black and Hispanic patients of a Los
Angeles medical clinic in a study reported in 1991 by Haynes. Harrell (1992)
reported Black women refusing a prenatal program to decrease low birth
weight in their infants because of disrespectful treatment by providers and
clinic staff. And as recently as February 6, 1994 an interview of African
American breast cancer survivors appeared in the Los Angeles Times
magazine telling of poor women of color receiving insensitive care from
physicians (Coleman, 1994).

17
The Interaction Between Race and Poverty
Large epidemiological studies of tumor registry data from New York,
Texas, California, Detroit, and Connecticut suggest that it is the combined
demographic descriptors of African American race and lower income that
predisposes women to late staged breast tumors at diagnosis (Richardson, et
al., 1992; Mandelblatt, et al., 1991; Farley & Flannery, 1989; Satariano, et al.,
1986; Vernon, et al., 1984). These tumor registry studies are unanimous in
reporting that the combined descriptors of African American race and lower
socioeconomic status are associated with delayed helpseeking, increased
stage of tumor at diagnosis and decreased survival. That the effects of
poverty may not be as costly for other racial groups is supported by a study
by Farley and Flannery (1989). They observed no difference in tumor stage
by socio-economic status (SES) in the Caucasian American women in their
sample but increased tumor stage in low SES African American women.
One study presents a snapshot of this key breast cancer subgroup.
Freeman & Wasfie (1989) studied a sample of 708 breast cancer patients
from a Harlem, New York, hospital center (1964-1986). All were poor, 48%
were without medical insurance, 46% were covered by Medicare or Medicaid
and the remaining 8% had private insurance, nearly all had significant co
morbid conditions (diabetes, hypertension, and ischemic heart disease) in
addition to their breast cancer. Stage Ill and stage IV tumors were seen in
43% of the study sample. Eighty-six percent presented with a self
discovered breast mass, with 12% of these also having nipple discharge,
18
pain, and breast ulceration. At least 56% of the patients delayed seeking
treatment for three months, with 29% delaying for at least six months. This
me frame for help-seeking is consistent with other reported studies of
African American women (Vernon, et al., 1985; Dennis, et al., 1975).
Freeman and Was■ ie attributed the duration of symptoms prior to helpseeking
to factors related to poverty.
Studies examining racial differences in survival in relation to
helpseeking have failed to separate the effects of environmental versus
biological influences. Clear evidence of the degree to which this difference in
survival within stage is biological (genetic predisposition, tumor histology,
hormonal response, etc.) or environmental (nutritional status, access to care,
treatment options, etc.), or both, remains to be determined.
Older Age and Helpseeking
Women who initially present with advanced breast cancer disease
(distant metastases) are more likely to be elderly according to SEER data on
the 125,000 women diagnosed between 1973 and 1984 (Yancik, et al., 1989).
This same relationship has been reported in other large scale studies (Samet,
et al., 1986; Allen, et al., 1986). Some ambiguity is introduced in this
relationship by studies reporting the percentages of women who describe
themselves as delaying the evaluation of their symptoms. In 1974
Antonovsky & Hartman reported a consensus in their reviewed studies that
older persons delayed helpseeking for cancer symptoms significantly longer

19
(all cancer sites, three of them breast studies). But contrary to the
Antonovsky & Hartman (1979) review, ten studies of breast cancer women
published since 1975 report no difference in the timing of seeking evaluation
of breast cancer symptoms by age (Menon, et al., 1992; Ajekigbe, 1991;
Rossi, et al., 1990; Adam, et al., 1980; Elwood & Moorehead, 1980; Dennis,
et.al, 1975; Huguley, et al., 1988; Worden & Weisman, 1975; Samet, et al.,
1988; Saunders, 1989). Recent studies have, however, reported that older
women are less likely to receive a breast examination from a professional
provider (PBE) than younger women (Celetano, Shapiro, & Weisman, 1982;
Senie, et al., 1981; Crawford & Cohen, 1985), and less likely to receive care
by a gynecologist rather than a general practitioner (Celetano, et al., 1982).
Two of the above studies added older age as a predictor of late staged
tumor presentation (Mandelblatt, et al., 1991; Satariano, et al., 1986). Using a
logistic model Mandelblatt and her colleagues estimated that Black, poor,
older women, receiving care in a public hospital, were 3.75 times as likely to
present with late-staged (regional and distant metastases) breast tumors than
white, younger, higher income reference group women receiving care in
private hospitals.
Only one study reported a significant association between delayed
helpseeking and older age (Nichols, et al., 1981). In their sample of British
women awaiting biopsy, age was reported to be associated with both
delayed helpseeking and eventual malignant diagnosis. That age should be
associated with malignancy is consistent with incidence curves for breast

2O
cancer, but confidence in the reported relationship between patient delay and
age in this sample is somewhat limited by the fact that only 8% of Nichols'
sample was age 65 years or older, with the "very elderly" being excluded from
sample selection.
Of particular importance is the reality of advanced tumor stage at
diagnosis in this age group. Since the treatment practices and potential for
cure of breast cancer in women of advanced age can be shown to have
improved over the years (Samet, et al., 1988; Chu, et al., 1987, Greenfield, et
al., 1987) it becomes increasingly important to understand helpseeking
behavior in this age group. That cancer of the breast remains treatable in
older women in spite of moderate delays in helpseeking is supported by a
new study from Poland. In a study of 325 Polish women over 70 years of
age, 54% of whom delayed helpseeking for more than six months,
Nagadowska and Kulakowski (1991) reported that delayed helpseeking was
associated with the number of cases that were judged to be inoperable but
not with survival overall. Delayed helpseeking was associated with increased
stage of tumor only when women had delayed for more than 24 months.
These findings are likely overstated, the sample having included only women
who were referred for surgical consideration, and excluding those believed to
have tumors too advanced for surgical treatment.

21
Comorbidity issues
Older persons have been reported to delay helpseeking because of
attributing symptoms of illness to normal aging (Samet, et al., 1988, Leventhal
& Prohaska, 1986; Frank-Stromborg, 1986). Symptoms of breast cancer are
thought to be obscured by competing health problems or more disabling
conditions (Rowe & Bradley, 1983; Crawford & Cohen, 1985; Satariano, et al.,
1989; Moritz & Satariano, 1991). In their study of Health and Functioning of
Older Women with Breast Cancer (HFW Study), Satariano and his colleagues
reported that more than 40% of the women had one or more additional,
limiting health conditions (eg. arthritis, heart disease, hypertension)
(Satariano, Ragheb, & Dupuis, 1989; Moritz & Satariano, 1991). The factors
associated with comorbidity in the breast cancer patient were advanced age,
obesity, past history of cigarette smoking, and current excessive alcohol
consumption (Satariano, 1992). These factors are easily recognizable as
among those proposed as possible risk factors for the development of breast
Ca■ hCer.
As discussed above, the Freeman & Wasfie (1989) study reported a
high incidence of comorbidity in their sample of Harlem, New York breast
cancer patients. That this apparently high rate of comorbidity is in fact a
realistic description of the comorbidity burden of older women with breast
cancer symptoms is supported by the Supplement on Aging to the United
States National Health Interview Survey (Satariano, et al., 1990, Guralnik, et
al., 1989). The survey reported that slightly more than 40% of women aged

22
55 to 84 with breast cancer had one or more additional limiting health
conditions, a similar proportion to that expected in the normal age-matched
population.
If symptoms of breast cancer are obscured by competing health
problems, it might be expected that older women with comorbid conditions
would have, on average, more advanced tumors at diagnosis. This was not
the case in the study by Moritz & Satariano (1991). In their study group of
463 older women in Detroit, the presence of comorbidity was associated with
less advanced disease. Tumor growth rates are believed to have a protective
effect against moderate helpseeking delay in this age group.
Demographic relationships can help identify groups at risk for late
staged presentation of breast cancer, but they are not adequate to guide the
interventions themselves. Even if it were the case that gender, race, age,
religious affiliation, marital status etc. were causal rather than correlated
variables for delayed helpseeking, they are not variables amenable to
change. What is needed is a better understanding of why, for instance, age
or race is correlated with delayed helpseeking in a particular study.
Researchers hopeful of increasing breast cancer survival through early case
finding must hope that the reasons why will turn out to be variables that are
amenable to change.

23
CHAPTER 2
A SOCIAL BEHAVIORAL DESCRIPTION OF WOMEN AT RISK
FOR DELAYED HELPSEEKING
Cognitive and Behavioral Variables Associated with Patient Delay
Researchers studying the personal, social and environmental variables
that influence when women seek evaluation of their discovered breast cancer
symptoms have focused on broader investigations of general illness behavior
to examine the specific experience of helpseeking for breast cancer.
Influences on the timing of helpseeking appear to be numerous and
complexly interconnected. All of the research on helpseeking for breast
cancer symptoms has been cross-sectional, it being infeasible for most
investigators to follow large numbers of symptom free women until potential
breast cancer symptoms occur and the women's helpseeking behavior can
be analyzed longitudinally. Most studies of helpseeking have relied
predominantly on chart review or tumor registry data, rather than interviewing
or surveying symptomatic or cancer-diagnosed women themselves. Few
investigators have supplied the research questions that motivated their
investigations or tested hypotheses predicting the timing of helpseeking.
That this body of literature is largely atheoretical is unfortunate in light of the
wealth of social behavioral theory available to guide such investigations.
This chapter organizes prior research on helpseeking for breast cancer
symptoms in terms of the contextual variables typically contained in social

24
behavior theories (Fishbein, 1980; Rosenstock, 1966; Triandis, 1980; Ajzen &
Madden, 1986) as an approach to structure what has been learned about
social behavioral influences on helpseeking. The current investigation
attempts to test some of these commonly observed social behavioral
influences on helpseeking in a sample drawn from a population where
prompt helpseeking is less common, African American women.
Symptom attribution - Cues to Action
Social behavioral theories of illness behavior, most notably the Health
Belief Model (Rosenstock, 1966), would suggest that a cue to action or
motivating influence will result in the increased likelihood of a behavior being
performed. In the case of helpseeking behavior, one might hypothesize that
the discovery of a breast change interpreted as a possible threat might act as
a cue to helpseeking. Therefore, interpreting a symptom as possibly breast
cancer might be hypothesized to predict more prompt helpseeking, and the
lack of this threat interpretation would predict less prompt helpseeking.
In Antonovsky and Hartman's 1974 review, high percentages of the
women in the breast cancer studies were reported as not realizing the
significance of the breast symptom that heralded the arrival of their breast
cancer. Improvement in symptom attribution is not obvious in more current
studies where wrongly attributing breast cancer symptoms to a benign
process has remained a common theme reported by investigators (Dodd, et
al., 1992; Ajekigbe, 1991; Mor, et al., 1990; Adam et al., 1980).
25
Presenting Symptoms of Breast Cancer
The most common presenting symptom of breast cancer is a lump or
mass in the breast, with or with accompanying pain. This presenting
symptom was reported to occur in from 65 to 86% of breast cancer cases in
the seven studies of helpseeking behavior which documented women's
presenting symptoms. As early as 1955, Aitken-Swann & Patterson reported
that experiencing presenting symptoms other than a lump was associated
with significantly greater patient delay. This observed relationship was
supported by seven more recent studies (Adam, et al., 1980; MacArthur &
Smith, 1981; Nichols, et al., 1981; Lierman, 1988; Gould-Martin, et al., 1982;
Richardson, et al., 1992; Feldman, et al., 1983). Two other studies observed
no difference in delay by presenting symptom (Rossi, et al., 1990; Worden &
Weisman, 1975), a difference in findings that might be somewhat attributable
to definitions of delay and small sample sizes. This common observation
suggests that women know that breast cancer commonly presents as a lump
in the breast but that they are less likely to interpret other breast cancer
symptom presentations as threatening.
The reported frequency of initial symptoms other than a lump ranged
as follows: pain (4-12%), bleeding or discharge (2-12%), dimpling or tissue
thickening (3-5%), inverted nipple (2-15%) (Rossi, et al., 1990; Adam, et al.,
1980; MacArthur & Smith, 1981; Nichols, et al., 1981; Leis, et al., 1988;
Lierman, 1988; Freeman & Wasfie, 1989; Gould-Martin, et al., 1982;
Richardson, 1992). In a study by Feldman et al. (1983), 11% (77 of 664) of

26
the women in this study reported having initial symptom presentations that
combined two or more of these symptoms, but no breast lump or mass.
Valanis, et al. (1987), in their study of the records of women who had died
from their breast cancer, observed symptom presentations other than solitary
lumps to be associated with decreased survival. They also observed that
African American women in their sample had significantly higher levels of
symptoms other than or in additional to a lump at the time of presentation of
symptoms: more skin symptoms in the form of peau d'orange (16% versus
5% in Caucasian American women), more palpable nodes (45% versus 23%),
more pain (65% versus 45%), and nipple discharge (25% versus 13%).
Conservative estimates that perhaps 15% of breast cancer cases do
not present with a breast mass would predict that 27,500 women in 1994 in
the United States will experience the onset of breast cancer with initial breast
changes other than a lump. Since these breast cancer symptoms must be
differentiated from symptoms related to normal cyclical hormonal fluctuations,
acute irritations and infections, normal maturational changes, pregnancy
changes, or fibrocystic disease, the initial misattribution of dangerous cancer
symptoms to more common, benign processes might be expected. In this
context, construing the misinterpretation of breast cancer symptoms in terms
of an easily remediated knowledge deficit would be an inadequate
representation of the problem of symptom interpretation.
This difficulty of symptom interpretation confounds the decision to
helpseek, particularly in women who have experienced prior benign breast

27
disease (Adam, et al., 1980; Gould-Martin, et al., 1982; Watson, et al., 1984;
Dodd, et al., 1992). Consideration of the difficulties of breast symptom
attribution should dictate caution regarding judging the appropriateness of
women's behavior in relation to the discovery of a breast change.
Perceptions of the Consequences of Delayed Helpseeking
Social behavioral theorists, notably Triandis (1980) and Ajzen and
Fishbein (1980), would suggest that perceiving the consequences of a given
behavior would influence one's performance of that behavior. Thus,
perceiving the consequences of delaying helpseeking for a potential breast
cancer symptom should predict more immediate helpseeking. Similarly, it
would be hypothesized that lower perceptions of consequences should result
in more delayed helpseeking. Although several investigators have found
perceptions of consequences to be influential to the performance of breast
self-examination (Nemcek, 1987; Champion, 1987), and the use of
mammography screening (Montano & Taplin, 1991), few have investigated
the consequential beliefs operative in relation to helpseeking for self
discovered breast cancer symptoms. Lauver & Chang (1991) used traditional
expectancy-value items (Fishbein, 1980) to create an expectations score,
reporting perceived consequences to be significantly associated with delayed
helpseeking. Timko (1987) reported on a significant relationship between
qualitative descriptions of lower perceived consequences and a lower
helpseeking intention.

28
Both studies utilized a design where well women were asked to
imagine a discovered breast symptom and to indicate their likelihood of
seeking immediate care. These studies are representative of those which
approach the study of helpseeking behavior through the study of the intention
to helpseek rather than helpseeking itself. Social behavioral theory (Fishbein,
1980; Triandis, 1980, Ajzen & Madden, 1986) assumes that one's stated
intention to carry out a behavior is highly predictive of one's actual
subsequent behavior, provided new influences do not occur to cause
changes in one's intention. It is desired that women have the intention to
helpseek rather than not when a breast cancer symptom is discovered, even
if this intention does not result in actual helpseeking in each and every case.
The above discussions of symptom attribution and perceptions of the
consequences of delayed helpseeking focus particular interest on a subgroup
of women who correctly attribute a symptom to breast cancer yet do not seek
an immediate provider evaluation. While a positive association between
cancer attribution and decreased patient delay is often assumed, in fact early
studies were divided on this issue. Two supported the assumption (Roberts,
1956; Harms, Plaut, & Oughterson, 1943) while one study reported an
opposite finding (Aitken-Swan & Paterson, 1955).
Current studies bearing on this question do little to illuminate the
relationship between a woman's attributing her symptom to cancer and the
timing of her helpseeking. Mor, et al. (1990) reported that breast cancer
patients attributed their symptoms to cancer more often (35.8%) than lung
29
(4.1%) or colorectal (9.1%) cancer patients, but they noted no significant
differences in the timing of helpseeking in relation to cancer attribution.
Gould-Martin (1982) and her colleagues reported that women who discovered
a breast lump while performing breast self-examination were more likely to
delay (48%) than those who discovered their lumps accidentally (38%).
Whether the self-monitoring behavior of women who practice breast self
examination might have predicted this observed difference deserves
investigation. In two studies of women's narratives of their breast cancer
symptom discovery Lierman (1988) and Dodd, et al. (1992) several women
told of attributing breast changes to cancer and yet not helpseeking. This
breast cancer population subgroup has not been the focus of any published
investigation of helpseeking behavior, so a clear description of this subgroup
has yet to be formed.
Failing to helpseek while attributing one's symptoms to cancer has not
been the focus of research. Rather anecdotal accounts hypothesize that
fatalistic beliefs and diffuse fears possibly explain this phenomenon.
Economic difficulties, lack of family support through illness, disbelief that
cancer can be cured or that one could survive a surgery, and depression also
seem plausible influences on the decision to delay seeking help for a breast
symptom, particularly if the symptom is attributed to cancer.
The concept of "denial" falls somewhere in the vicinity of discussions of
symptom attribution, although its theoretical connection remains to be
clarified. Antonovsky & Hartman (1974) proposed the possibility of a

30
continuum between denial of symptoms and hypochondriasis, suggesting
that this relationship might be captured by psychological instruments
measuring the concepts of repression and sensitization. Although denial is
commonly discussed in the coping literature, the denial of cancer symptoms
or the possibility of cancer was discussed in only two investigations of
helpseeking behavior since 1975. Denial of a symptom's relatedness to
cancer was associated with delayed helpseeking in a study by Worden &
Weisman (1975). These investigators used the criteria: "reluctance to use the
word cancer," "denial of physical incapacity," and "minimization of the
seriousness of their illness" as a measure of breast cancer denial in their
sample women. In a group of women who had delayed three months and
had palpable tumors, Wool (1986) attempted to demonstrate immature object
relation functioning, a measure of one's ability to develop strategies for reality
testing and cognitive evaluation of such things as breast cancer symptoms.
Small sample size may have limited the power to adequately test her
hypothesis.
Affective Responses to Symptom Discovery
The Green & Roberts (1974) review, which focused specifically on
breast cancer, cited a number of specific fears in relation to the discovery of
breast cancer symptoms. Table 2-1 lists these and others drawn from
anecdotal reports in the helpseeking literature. The list, although perhaps not

31
exhaustive, demonstrates numerous possible manifestations of fear in relation
to the discovery of a breast cancer symptom and the anticipated sequelae.
Table 2-1
A Fear Cascade - Targets of Fear in Relation to a Breast Cancer Symptom
Fear of doctors and hospitals Fear of abandonmentFear of ridicule Fear of loss of control
Fear of embarrassment Fear of loss of femininityFear of chemotherapy Fear of radiation therapyFear of loss of work related role Fear of being dehumanizedFear of illness Fear of losing a sexual partnerFear of the unknown of cancer Fear of painFear of the loss of a breast Fear of isolation
Fear of disfigurement Fear of surgeries/anesthesiaFear of loss of ability to mother Fear of entering a submissive roleFear of unmanageable expense Fear of cancer spreadingFear of death
Anxiety, as an affective response to the discovery of a breast cancer
symptom, has been a focus in five of the studies under review. Lauver &
Chang (1991) reported anxiety as a significant predictor of the intention to
seek care. MacFarlane & Sony (1992) assessed anxiety associated with a
breast biopsy reporting anxiety, measured by a modified version of the State
Trait Anxiety Inventory (STAI) (1970), to be significantly increased in women
who had delayed longer in contacting a physician. Three other studies
(Keinan, et al., 1991; Watson, et al., 1984; Magarey, Todd, & Blizard, 1977)
found no significant relationship between anxiety, variously measured by the
Manifest Anxiety Defensiveness Scale (Millimet, 1970) or the STAl.

32
Several possible explanations exist for the ambiguous results in these studies.
Small sample sizes, sample inclusion criteria, the study of real versus
theoretical symptoms and, particularly, the timing of data gathering limit the
confidence that can be placed in these reported findings. With what degree
of confidence can anxiety levels measured while awaiting breast biopsy
(Keinan, et al., 1991; Magarey, et al., 1977; MacFarlane & Sony, 1992) or |
during hospitalization for mastectomy (Watson, et al., 1984) be said to reflect
anxiety related to the discovery of the breast symptom itself?
Little progress has been made since Antonovsky & Hartman (1974)
broached the idea that both high and low levels of fear may be associated
with longer delays. They proposed a curvi-linear relationship between fear
and helpseeking for cancer symptoms, recognizing that the effects of fear
may differ depending on the context. Research to date has not developed a
model to predict the influence of fears and anxiety on helpseeking for breast
cancer symptoms. Knowledge of what magnitudes of fear might precipitate
or retard action, how fears might inter-relate, and which have dominant status
is also lacking.
Methodological difficulties abound in the study of affect in relation to
breast cancer symptom discovery. The investigator is likely to have access to
the symptomatic woman only after she enters the treatment environment, in
sorre cases weeks to months after her symptom discovery. It is unclear
whether generalized measures of affect are good predictors of behavior in
response to breast symptom discovery. In summary, fear and anxiety in

33
relation to helpseeking behavior would appear to more complex than
reflected in research investigations to date.
Three other affective states were suggested as possibly significant to
delayed helpseeking behavior by Antonovsky & Hartman (1974): guilt, shame,
and embarrassment. These were anecdotal responses reported as reasons
women gave for delaying professional evaluation of their symptoms.
Surprisingly, depression and anger have not been investigated as influences
on the timing of helpseeking for a discovered breast cancer symptom.
Antonovsky & Hartman (1974) viewed affective response in relation to
symptom discovery as patterned by personality trait rather than as situation
limited affective expressions. As such the individual's affective behavior
patterns were more likely to pre-date the arrival of a cancer symptom.
Personality models today continue to support this hypothesis (Costa &
McCrae, 1992; Caspi & Moffitt, 1993), suggesting that women at risk for
delayed helpseeking due to affective behavior patterns could be identified
before breast cancer symptoms occur and targeted for particular
interventions to encourage earlier helpseeking.
Of particular interest might be the relative power of affective response
to predict behavior; whether, for example, the presence of one or more of the
above affective responses will relegate all other potential influences on
helpseeking to secondary importance. Carefully crafted investigations of
wornen's affective responses to breast symptom discovery remain a focus for
future research.
34
Perceived Behavioral Control
Social behavioral theorists, most notably Ajzen and Madden (1986)
and Fishbein and Stasson (1990), have continued the debate regarding
perceptions of control or personal agency as possible influences on behavior,
achieving some consensus that perceived control is most important in the
case of predicting volitional, planned or goal-oriented behavior (Ajzen, 1985;
Ajzen & Madden, 1986; Fishbein & Stasson, 1990). Since it could be argued
that most health related behavior of concern to researchers might be
categorized as volitional, perceived control over the behavior being studied
(in this case, helpseeking) would appear to be an important focus of inquiry.
Perceptions of control over the behavior of helpseeking is a useful theoretical
umbrella under which to place studies of fatalistic beliefs and the patient
provider relationship.
Relinquishing control over one's body and life decisions have been
reported as being strong influences both on the timing of helpseeking
(Ajekigbe, 1991; Owens, Duffy, & Ashcroft, 1985) and on women's anticipated
Helpseeking for a discovered breast lump (Timko, 1987; 1984). Fears of
being forced to undergo a mutilating mastectomy was related to women's
delayed helpseeking in Ajekigbe's study of Nigerian women. Knowledge of
the breast cancer experience and its treatment demands were related to
delayed helpseeking in the women studied by Owens and colleagues (1985).
Tim Ko (1984) provided qualitative descriptions of the desire not to lose
Control of one's everyday life in women asked to imagine the discovery of a

35
breast lump and their likelihood of seeking a provider evaluation. Notably,
44.8% of the women indicated their intention to delay calling the doctor and
rather to self-monitor the symptom for a time not specified. These women
cited desires to maintain control over their day to day experiences and the
intention to retain responsibility for their own health assessment. This study
is provocative in its suggestion that asymptomatic women are not highly
inclined to intend immediate helpseeking for a breast change.
Some researchers, reporting on small sample, qualitative studies,
have reported a possible relationship between fatalistic beliefs and delayed
helpseeking for discovered breast symptoms (Dignan, et al., 1990; Perez
Stable, et al., 1992; Lierman, 1988; Goodwin, et al., 1986), some suggesting
that these beliefs may be particularly significant in the older population of
women (Lierman, 1988; Goodwin, et al., 1986). Deterministic beliefs are often
culturally bound and congruent with past life meanings. In this context, one
might trust that the events of one's life occur in relation to a force or plan
larger than and often unknown to oneself. Such beliefs are often intertwined
with religious beliefs, described in terms of "God's will," "according to nature,"
"Ptarma," "fatalismo," etc.
This metaphysical view of the world is not a minority viewpoint in many
Cultures. The effect of this influence on breast cancer survival is unknown,
but could be hypothesized to have both beneficial and non-beneficial
implications depending on the individual or the context. Some women may
be rinotivated to helpseek by trust in the certainty that they could do nothing

36
else but seek immediate evaluation for a breast cancer symptom. It just as
imaginable that other women might believe that: there is little they can do to
prevent cancer; it is their fate to develop breast cancer; or for them breast
cancer would be a death sentence. It might be hypothesized that
deterministic beliefs may interact with other beliefs about curability or the will
of God, placing some women at risk for delayed helpseeking.
Investigators in two studies examined constructs that might be
hypothesized as conceptually "close" to fatalism. Keinan, et al. (1991) used
the Beck & Weisman Hopelessness Scale (Beck, 1974) to measure
hopelessness in women undergoing biopsy for breast lumps. A small sample
size and the inclusion of women whose symptoms were physician-discovered
limit the confidence that can be placed in their report of no observable
relationship between hopelessness and delay. Worden & Weisman (1975)
reported the feeling of powerlessness as significantly influencing "lagtime" in
seeking care in their sample of 125 patients with a variety of malignant
tumors, 42 of whom were women with breast cancer.
Habits of Helpseeking
The Triandis model of social behavior stresses that habits in relation to
a behavior influence later performance of that same or other similar
behaviors. Early studies have suggested that previous general helpseeking
habits were highly influential in helpseeking for breast cancer symptoms
(King, 1951; Henderson, 1966, Hackett, Cassem, & Raker, 1973). No recent

37
studies have directly tested this hypothesis, but several have reported
relationships between breast-related diagnostic and screening behaviors and
helpseeking behavior. Having a prior history of fibrocystic (benign) breast
disease was observed to be associated with longer patient delays, although
no statistical tests of this relationship are reported (Adam, et al., 1980;
Lierman, 1988; Dodd, et al., 1992; Gould-Martin, et al., 1982).
Several researchers have reported that the practice of breast self
examination is significantly associated with prompt helpseeking for breast
cancer symptoms (Huguley & Brown, 1981; Huguley, et al., 1988; Funch,
1984) supporting the idea that breast health habits might be predictive of
helpseeking behavior in the event a breast cancer symptom is found. This
relationship is not a simple one, however, exemplified by the 20% of the
women in the study by Huguley, et al. (1988) reported as practicing breast
self-examination but delaying helpseeking for a discovered symptom for three
months or more. No investigators have yet reported relationships between
delayed helpseeking and the prior use of mammography screening or prior
experience with professional breast examination.
. Would a person with a chronic illness be more or less likely to seek
help early for a breast cancer symptom? No studies of comorbidity
influences on helpseeking are found in the literature, but theoretical
relationships between helpseeking for concurrent illness and helpseeking for
breast cancer symptoms suggest that this relationship may be more complex.
Factors like the habit of utilizing health care services, an established
38
relationship with a health care provider, and generalized trust in the health
care system would argue for early helpseeking effects. Factors like comorbid
symptoms masking symptoms of new disease, fatalism related to the illness
condition, the belief that the provider has certified one's other body systems
as healthy, reluctance to spend more financial resources on personal health
care, etc., might argue for increased patient delay. Future studies are
needed to explore these hypothetical relationships.
The habits of health care services utilization include not only
experiences with providers but also the habit of using non-traditional healing
practices. Belief in divine healing was reported to be associated with delayed
helpseeking by the Green & Roberts' 1974 review, as was a prejudice against
doctoring and the general lack of confidence in doctors. Ajekigbe (1991)
reported the use of prayer houses and spiritual healing homes (13.5%) and a
preference for herbalists (23.1%) in a study of 2,154 Nigerian women.
Traditional healers and spiritual healing is also common in African American
communities in the United States (Bailey, 1987; Thomas, 1981; Snow, 1983).
Although hypertension studies report traditional healing practices, no studies
have suggested that African American women in the United States currently
seek traditional healers for breast cancer symptoms.
Health food diets and natural cures are commonly used by persons
who experience cancer symptoms. The American Cancer Society maintains
a listing of common but scientifically unproven topical preparations and
dietary methods used by persons in the United States and Western Europe
39
(Rennecker, 1989). The proportion of women who use these cures rather
than seek immediate evaluation and treatment from a provider is not known.
Few researchers have described the self-care practices women might
try in attempting to cure their breast cancer symptoms (Lierman, 1988; Dodd,
et al., 1992). Applying antibiotic ointments to cure ulcerations on the nipple,
changing bras to correct pain under the breast, washing the nipple to clear
nipple secretions, rubbing hardened areas to soften the tissue, applying heat
to reddened, painful skin areas, removing bra padding, and pulling on the
nipple to correct nipple inversion, were all reported as self care actions
women had taken prior to helpseeking. Whether these behaviors are at all
reasonable remains to be assessed in relation to the frequency of occurrence
of benign breast symptoms in the general population.
Social Normative Influences
Contextual variables grouped under the umbrella of "social influences"
include: normative behaviors dictated by significant others (for instance,
spouses, siblings, children, providers), and perceived demands on behavior
related to social roles (Triandis, 1980, Ajzen & Fishbein, 1980). The idea that
women with breast symptoms respond to normative influences from
significant others, particularly their spouses, would predict that married or
partnered women might helpseek more promptly than non-married or non
partnered women. Two studies observed no differences in helpseeking by
marital status (Worden & Weisman, 1975; Rossi, et al., 1990). No studies

40
reported on helpseeking behavior in unmarried women with partners.
Refining the operationalization of this variable to include women in a wider
variety of partner relationships might prove more informative in future
research.
Lauver & Chang (1991) extended the definition of social normative
influence even more broadly, asking women to rate the degree to which eight
types of significant others believed they should seek immediate care for a
breast change. Social norms were not reported as significant predictors of
helpseeking n their study sample. In contrast, utilizing the Theory of
Reasoned action to predict the intention to seek care for a breast cancer
symptom, Timko (1987) reported that social normative influences were
significant predictors of the intention to helpseek.
Delaying helpseeking as a consequence of perceived social role
demands (for instance, mother, spouse, employee) has been reported in the
literature concerning women's general illness behavior (Walker & Best, 1991;
Meleis, 1991; Theorell, 1991; Facione, 1994; Bird & Fremont, 1991; Woods,
1985). Studies of helpseeking for cancer symptoms in tumor sites more
equally distributed between males and females have reported no differences
in the timing of helpseeking by gender (Zilling, Walther, & Ahren, 1990,
Mikulin & Hardcastle, 1987; Marshall, Gregorio, & Walsh, 1982; Marshall &
Funch, 1986).
But many researchers' anecdotal comments, and reports of the
reasons women give for their delayed helpseeking, suggest otherwise.

41
Devoting time and attention to the needs of someone else (Mor, et al., 1990;
Adam, et al., 1980; Dodd, et al., 1992; Worden & Weisman, 1975), taking time
to make domestic arrangements prior to the biopsy (Adam, et al., 1980),
demands associated with summer and school holidays (Adam, et al., 1980;
Lierman, 1988; Dodd, et al., 1992), work related demands (Dodd, et al.,
1992), caring for other ill family members (Adam, et al., 1980; Dodd, et al.,
1992), and the temporary presence of relatives in the home (Adam et al.,
1980) were all suggested as receiving priority over discovered breast cancer
symptoms. Significant support for the hypothesis that role responsibilities
influence helpseeking is added by Dignan, et al.'s (1990) focus group study
of helpseeking for cervical cancer symptoms. They reported women
indicating that they would seek care in relation to the need to fulfill role
responsibilities and only after child care was assured. Future investigators
should test this possible relationship between perceived and/or actual
traditional female role constraints and helpseeking for breast cancer
symptoms.
Facilitating Conditions for Helpseeking
Social behavior theory posits that one's performance of a given
behavior depends on personal and environmental factors that facilitate or
constrain the behavior. Accordingly, one could perform the behavior more
easily, more often, or more quickly and well if there were a preponderance of
factors facilitating the behavior. In contrast, even if one wishes to perform a
■ .
42
behavior, one might not be able to perform the behavior because of factors
that constrain its performance.
Few studies measured factors that might be construed as facilitating or
constraining influences on women's helpseeking behavior, and all of these
examined economic influences on helpseeking in relationship to the ability to
pay for services. A widely asserted but untested belief is that "poverty is one
of the stronger predictors of delayed helpseeking" (Bal, 1991; Freeman, 1991;
McCall, et al., 1991; Mutchler & Burr, 1991). Economic constraints were
reported as affecting women's helpseeking for breast cancer symptoms in the
above mentioned study by Ajekigbe (1991). Lauver & Chang (1991)
examined being fully covered by health insurance in relation to the intention
to helpseek for a proposed breast cancer symptom. They reported observing
no significant relationship between having insurance and helpseeking
intention. This was in contrast to a study by Gould-Martin, et al., (1982)
where lack of health insurance was associated with increased delay. One
can only speculate on the reasons for this difference in reported results.
Perhaps limiting the operational definition of resources to "full coverage
insurance" is too narrow to capture the variance in helpseeking behavior
related to economic resources.
Other studies associated delays in helpseeking with women
belonging to lower socioeconomic groups (Wilkinson, et al., 1979; Gould
Martin, et al., 1982; Farley & Flannery, 1989; Samet, et al., 1988), but none of
these interpreted this relationship in terms of the availability of health care
-
r
º
ºr
43
services. That so few studies directly addressed women's actual or perceived
access to health care services is striking, and reflects an area of major
weakness in the research to date.
The assumption that women have economic access to treatment for
breast cancer symptoms is unwarranted in many nations (Hongvivitana,
1984). This is no less true in the United States where 34.4 million Americans
are without health care coverage (Popp, 1988; Jaynes & Williams, 1988;
Lerner, 1988; Moyer, 1989), and the poor and middle class have limited
options about when and how they can obtain health care (Bal, 1991;
Freeman, 1991; Brown, 1990; 1991; Davis, 1988). The political and economic
realities of the status of women throughout the world should alert
investigators to the need to explore economic constraints to helpseeking
experienced by symptomatic women.
One can speculate that there are other constraints on helpseeking than
the ability to pay for services. Reported significant influences on health care
utilization include: geographic location of health care centers, community
transportation services, unavailability of childcare services for women
responsible for the care of children, the absence of an established health
care provider, and differences in culture, ethnic group, sexual orientation, or
gender between the women and the prospective provider (Bailey, 1987;
Stevens & Hall, 1988; Bird & Fremont, 1991; Facione, 1994 in press; Davis,
1990; Meleis, 1991). These variables have not been specifically studied in
relation to helpseeking for breast cancer symptoms.

CHAPTER 3
THE TRIANDIS MODEL OF SOCIAL BEHAVIOR
AS A GUIDE TO THE STUDY OF HELPSEEKING INTENTION
Culturally Competent Theory
The American Academy of Nursing's report entitled "Expert Panel
Report: Culturally Competent Health Care" (AAN, 1992) defined cultural
sensitivity in nursing care as an awareness of, and utilization of, knowledge
related to ethnicity, culture, gender or sexual orientation. In this context,
culturally competent nursing research in the area of health and illness
behavior might be defined as investigations that are based on knowledge and
theories that permit explanation of behavior within the context of ethnicity,
culture, gender, and sexual Orientation.
The AAN concern for cultural competency in nursing care signals the
need for research to be guided by theoretical models which clearly specify
the inter-relationships between cultural context variables and behavioral
outcomes, models that have the potential to capture the uniqueness of
diverse populations. Only then can subsequent intervention studies be
expected to respond to culturally relevant health problems and provide
effective health outcomes in today's culturally diverse society. It was within
this context of the need for cultural relevancy in research that the theoretical
model guiding this investigation was chosen.

45
Social Behavioral Models to Study Helpseeking Intention
How can we predict how a woman will respond to the discovery of a
possible breast cancer symptom? This question defies an answer when
divorced from the personal, social, environmental, and health status context
of the individual. The appreciation of the importance of all the diverse
aspects of culture as key to the development of nursing knowledge and
effective nursing care is certainly not a new perspective for either the nurse
clinician or the nurse scientist (Spector, 1991; Clinton, 1982; Lipson & Meleis,
1983; Stevens & Hall, 1988; Thompson, 1991; Funkhouser, 1990; Jemmott &
Jemmott, 1991; Meleis, Lipson, & Paul, 1992). Acknowledging the complexity
of human behavior and the range of cultural diversity within American society
today, many researchers might despair of even the possibility of a culturally
sensitive theoretical model to guide the study of health and illness behavior.
But nursing research is not for the faint at heart, and promising models which
had their beginnings in the field of social psychology continue to be
developed and tested by theorists from all disciplines including nursing
(Montano & Taplin, 1991; Lauver & Chang, 1991; Lierman, Kaspryzk, &
Benoliel, 1991; Jemmott & Jemmott, 1991).
Health behavior researchers have most frequently used Rosenstock's
Health Belief Model (HBM) (Rosenstock, 1966) to examine perceptions of the
seriousness of, susceptibility to, benefits of, and barriers to performing a
given health or illness behavior. Survey instruments based on the HBM have
typically been approached as culture-neutral rather than being developed to
:■ *

46
capture cultural variation. Not an intrinsic weakness of the HBM itself, this
communality is rather reflective of a research tradition that: tended to ignore
culture as a variable, studied predominantly Caucasian groups, designed
across-culture rather than within-culture studies, and tended to view many
aspects of diversity as deviance rather than variance. As a result, behavioral
studies utilizing the HBM frequently fail to examine powerful socio-cultural
factors such as poverty or religious beliefs that might be important to the
behavioral outcome. Most exemplary of a sustained effort to develop valid
and reliable measures is the work of Champion (1984; 1985; 1987; 1991) in
relation to breast self-examination behavior. The HBM variable that has
proven most predictive of breast self-examination is "barriers," women who
perceive barriers to performing BSE being significantly more likely not to
perform this breast cancer screening behavior. This variable consistently
predicted more variance in BSE behavior that perceived seriousness of breast
cancer, perceived susceptibility to breast cancer, or breast cancer related
health beliefs.
Two other models, the Theory of Reasoned Action and the Theory of
Planned Behavior, developed by Icek Ajzen and Martin Fishbein (Fishbein,
1980; Fishbein & Stasson, 1990, Ajzen & Madden, 1986; Ajzen & Fishbein,
1980) have also been used extensively for studies of a wide range of health
and illness behavior (Powell-Cope, et al., 1991; McCarty, 1981; Pender &
Pender, 1986; Chassin, et al., 1984; Miller, Wickoff, & Hiatt, 1992; Hendricks,
Freeman, & Sheiham, 1990; Timko, 1987, Jemmott & Jemmott, 1991). These

47
theoretical models stress consequential beliefs and social normative
influences as predictive of the intention to carry out a health-related behavior
and subsequently the performance of the behavior itself. The Theory of
Planned Behavior (Ajzen, 1987, Ajzen & Madden, 1986) adds the variable of
perceived control, one's perception of control in the situation hypothesized to
influence both one's formed intention to perform a behavior and the behavior
itself. These theories have also performed well in health behavior
investigations, commonly explaining 40-60% of the variance in the health
behavior under study (McCarty, 1981; Chassin, et al., 1981; Jemmott &
Jemmott, 1991; Timko, 1987).
The Triandis Model of Social Behavior
The Triandis model, less well known by health care researchers but
providing equally powerful results (Montano, 1986; Lauver & Chang, 1991;
Lierman, et al., 1991; Montano & Taplin, 1991), has superior promise for
culturally sensitive research (Triandis, 1977; 1980). Beginning with the
assumption that most behaviors which attract the interest of researchers are
rational, reflective behaviors (rather than reflexive, automatic behaviors), the
Triandis model builds on Kurt Lewin's Motivational Theory (1935). Arising
within the context of Triandis' research interest in cultural diversity (Triandis,
1972; 1976; Davidson, et al., 1976; Davidson & Thomson, 1976), the model
acknowledges cultural diversity as contributing to differences in behavior.

48
Much testing and contrasting of these various models, stressing their
relative strengths and weaknesses can be found in the research literature
(Wallston & Wallston, 1984; Godin, 1987; Liska, 1984; Miniard & Cohen,
1981; Sheppard, Hartwick, & Warshaw, 1988; Valois, Desharmais, & Godin,
1988, Warshaw & Davis, 1985; Bagozzi & Yi, 1989; Bentler & Speckart, 1979).
Variables from the models have much in common conceptually, a factor that
has encouraged researchers' eclectic creativity in their search for best models
to address particular health issues (Montano & Taplin, 1991; Lierman, et.al.,
1991). Table 3-1 lists the conceptual definitions of the variables included in
the Triandis model.
According to the model the determinants of an individual's performing
(or not performing) any given behavior (B) are: one's intention (I) to perform
(B), one's prior habit (H) of performing (B), relevant physiological arousal (P)
to perform (B), and the facilitating factors (F) in the environment that assist
(or constrain) the performance of (B). The following equation represents the
relationship between model variables as originally suggested by Triandis.
(B) = [w(■ ) + w(H)] (P) x (F)
The (w's) are weights expressing individual differences. Triandis
conceptualized (F) as being scaled between 0 and 1. When facilitating
conditions are most favorable for (B) to occur, (F) = 1. When they are most
unfavorable, (F) = 0. Similarly (P) ranges from 0 to 1. When there is no
arousal to perform (B), (P. = 0. When there is sufficient arousal to perform
(B), (P) = 1. Researchers who have tested the Triandis model to study
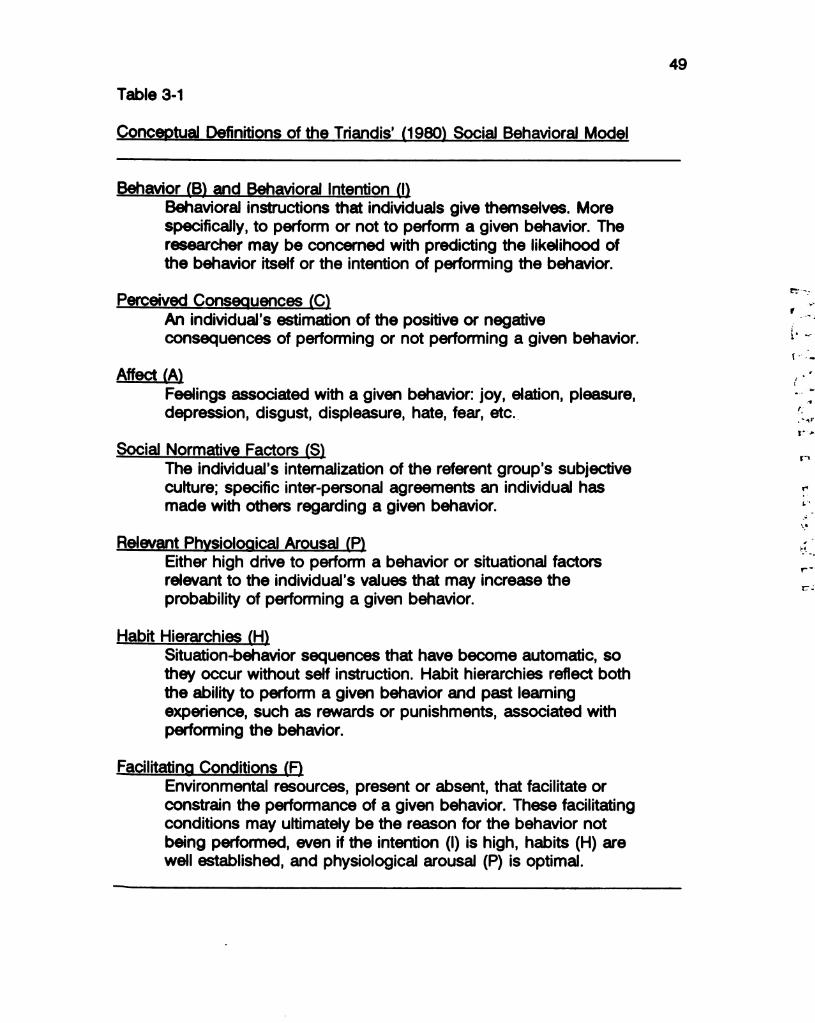
49
Table 3-1
Conceptual Definitions of the Triandis' (1980) Social Behavioral Model
Behavior (B) and Behavioral Intention (I)Behavioral instructions that individuals give themselves. Morespecifically, to perform or not to perform a given behavior. Theresearcher may be concerned with predicting the likelihood ofthe behavior itself or the intention of performing the behavior.
Perceived Consequences (C)An individual's estimation of the positive or negativeconsequences of performing or not performing a given behavior.
Affect (A)Feelings associated with a given behavior: joy, elation, pleasure,depression, disgust, displeasure, hate, fear, etc.
Social Normative Factors (S)The individual's internalization of the referent group's subjectiveculture; specific inter-personal agreements an individual hasmade with others regarding a given behavior.
Relevant Physiological Arousal (P)Either high drive to perform a behavior or situational factorsrelevant to the individual's values that may increase theprobability of performing a given behavior.
Habit Hierarchies (H)Situation-behavior sequences that have become automatic, sothey occur without self instruction. Habit hierarchies reflect boththe ability to perform a given behavior and past learningexperience, such as rewards or punishments, associated withperforming the behavior.
Facilitating Conditions (F)Environmental resources, present or absent, that facilitate orconstrain the performance of a given behavior. These facilitatingconditions may ultimately be the reason for the behavior notbeing performed, even if the intention () is high, habits (H) arewell established, and physiological arousal (P) is optimal.
prº
| -tº
º
º
tº
:

50
health and illness behaviors have chosen to express the relationship between
variables somewhat differently. Montano (1986), for instance, measured (F)
with 7-point Likert scale items measuring familiarity with immunization
procedures and access to the immunization site in his study of influenza
vaccination behavior.
Although the (P) variable seems quite central to the prediction of (B) in
Triandis' model, it has not been extensively developed, and studies testing
the model frequently omit this variable. Lauver & Chang (1991) deleted
consideration of this variable in their study of seeking care for a breast cancer
symptom, considering it to be redundant to the affect (A) variable. Montano
(1986) omitted discussion of the (P) variable, as did Valois and colleagues
(1988) in their study of exercise intention. Eliminating the (P) variable,
considering how few tests of the complete Triandis model have been
reported, would seem unwise. Within this variable would seem to lie the
motivation to perform any context relevant behavior in relation to the problem
being studied. For instance, the perception of a breast change mediated by
the interpretation of that change might be the appropriate indirect measure of
(P) for a study of helpseeking behavior.
The investigators in the studies cited above typically used multiple
regression analyses, as suggested by Triandis, to examine the predictive
power of the model. Prediction, in this discussion, refers to explanation of
shared variance in a regression analysis and as such is, strictly speaking, an

51
associational relationship rather than predictive. The equation that correctly
expresses a regression analyses of these predictor variables is:
(B) = w () + w(H) + w(F)+ w (P)
A multiple regression model is also suggested to predict the intention
(I) variable as a function of one's beliefs about the consequences (C) of
performing (or not performing) the behavior, one's affect (A) toward the
behavior, and social influences (S) one experiences in relation to the
behavior. Again the regression weights (w's) are expressions of individual
difference. This relationship is expressed in the equation:
(1) = w(C) + w(A) + w(S)
The Triandis variables typically are measured through the use of Likert
style item scales or semantic differential scales. The scales are constructed
with a balance between inclusion of all salient items and concern for
responder burden. Scale totals are used as variable values for inclusion in
the regression analysis.
Researchers are directed by Triandis to match model variable scales
with the cultural context of the intended study population. When choosing or
designing instruments to measure the model variables the researcher must
endeavor to exhaustively measure the salient, culturally relevant, aspects of
the variable that relate to whatever behavior is being studied. The
operationalization of each model variable might be expected to differ
depending on how the study population is defined in terms of gender, age,
racial/ethnic group, or class. Theoretically the amount of explained variance

52
obtainable in a given investigation is directly related to the representation of
salient aspects of each variable in the measurement tool(s). It can be seen
that this model is structured to examine health and illness behavior within
cultural groups rather than across cultural groups. The goal here is not to
measure communalities between cultural groups that account for health and
illness behavior, but rather to examine health and illness behavior in a context
that will permit unique cultural differences to be discovered and analyzed for
their power to predict the behavior under study.
That the nurse researcher may not be certain what the culturally salient
items are that should be included in the survey is a testimony to how well or
poorly we have done culturally sensitive research in the past on the particular
health or illness behavior. If salient beliefs can only be speculated upon
(such was the case with the above example), then, as was the case in this
study, preliminary qualitative key informant interview or focus group work can
be used to inform the structuring of a new instrument or the possible
modification of an existing instrument. The subsequent empirical study can
then be used to test the proposed relationships and to add support for the
generalizability of small study reports to larger, within-culture populations.
The Triandis model invites a culture specific operationalization of each
study variable. Gender issues can be explored through Triandis' (S) variable:
self-concept, social normative influences, and role constraints. The realities
of the availability and affordability of health care (Harrington & Estes, 1994;
Butler, 1988), can be modeled through measures of resource factors
**
f.tra
ra
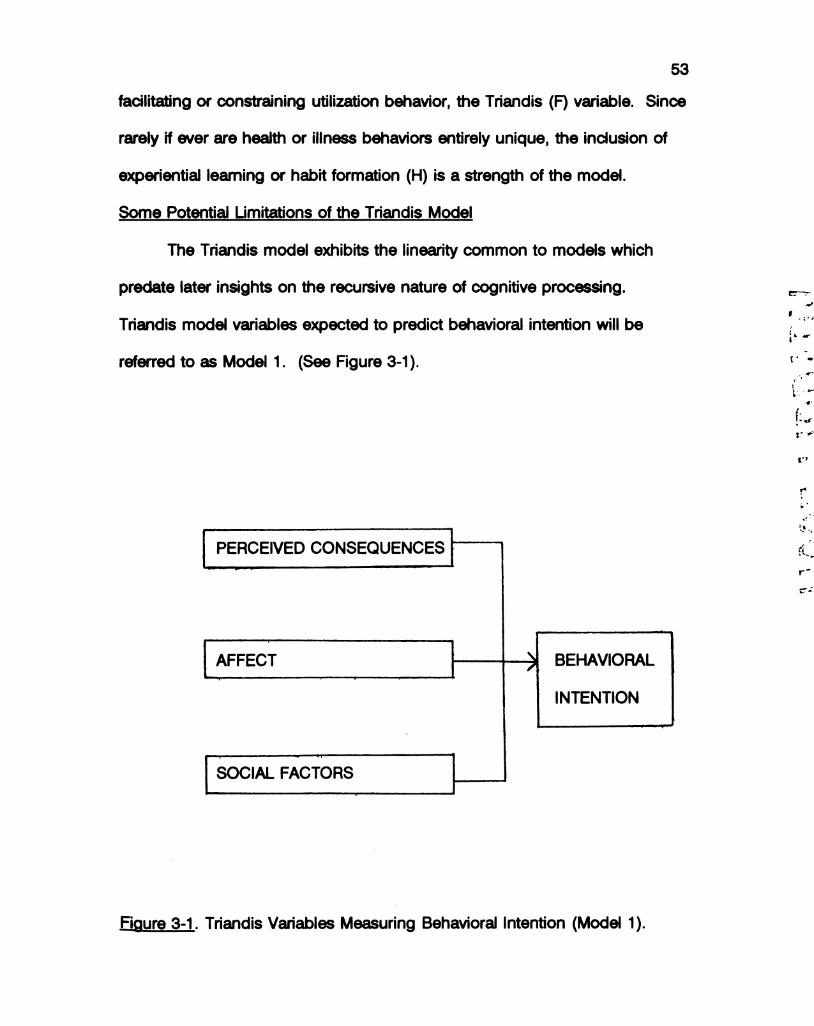
53
facilitating or constraining utilization behavior, the Triandis (F) variable. Since
rarely if ever are health or illness behaviors entirely unique, the inclusion of
experiential learning or habit formation (H) is a strength of the model.
Some Potential Limitations of the Triandis Model
The Triandis model exhibits the linearity common to models which
predate later insights on the recursive nature of cognitive processing.
Triandis model variables expected to predict behavioral intention will be
referred to as Model 1. (See Figure 3-1).
PERCEIVED CONSEQUENCES
AFFECT BEHAVIORAL
INTENTION
SOCIAL FACTORS
Figure 3-1. Triandis Variables Measuring Behavioral Intention (Model 1).

54
Critics of the model have suggested a more recursive modeling of
directional relationships between Triandis model variables (Liska, 1984;
Warshaw & Davis, 1985). Previous learning from performing the given (or a
similar) behavior might in this case be expected to influence one's
consequential beliefs about the behavior (C), one's affect toward the behavior
(A), one's perceptions of the social norm or one's role expectations in relation
to the behavior (S), the formation of the habit of performing the behavior (H),
and one's awareness of one's resources in relation to the behavior (F).
The recursivity of reflective judgment and decision-making becomes
particularly important when the concern is to predict the intention (I) to
perform a given health or illness behavior rather than the behavior (B) itself.
Rather than including only the (C), (A), and (S) variables to predict (I), the
variables (H) and (F) might also be hypothesized to explain some of the
variance in the intention to carry out the behavior (B), acknowledging one's
foreknowledge of one's available facilitating resources (F) and one's prior
behavior (H). Several groups of researchers utilizing the Triandis model to
study illness behavior have assumed a more recursive model (Godin, 1987;
Valois, et al., 1988; Montano, 1986; Lauver & Chang, 1991). Other
researchers have reported using Ajzen & Fishbein's Theory of Reasoned
Action (Ajzen & Fishbein, 1980, Fishbein, 1980) with the addition of the
Triandis model (A), (H) and/or (F) variables, effectively creating the Triandis
model (Lierman, et al., 1991; Montano & Taplin, 1991; Timko, 1987). The
theoretical expansion of the Triandis model, including all Triandis variables

55
proposed as influential to behavioral intention, will be referred to as Model 2.
(See Figure 3-2). Both Model 1 and Model 2 will be tested for their relative
contribution to the study of helpseeking intention.
PERCEIVED CONSEQUENCES
AFFECT
SOCIAL FACTORS
BEHAVIORAL
HABIT INTENTION
FACILITATING CONDITIONS
RELEVANT AROUSAL
Figure 3-2. Theoretical Expansion of Triandis Variables PredictingBehavioral Intention (Model 2).
gº
:

56
The assumption of variable independence is somewhat problematic in
the Triandis model. Miniard & Cohen (1981) point out that in models of
behavior that contain personal and social components, these components are
not independent, and therefore such models cannot be used to measure the
separate contributions of one's personal beliefs and one's social normative
beliefs on behavior. This criticism points to the likelihood of at least some
degree of collinearity between variables in the model. Multicollinearity
between model variables complicates the assessment of the explanation of
variance related to individual model variables. What is ascertainable is an
estimate of which variables contribute significantly to the explanation of the
variance in helpseeking intention and an estimate of the overall amount of
variance explained by the models tested.
One last potential limitation of Triandis' approach to culturally relevant
measurement is that measures require assessment of their validity and
reliability. Concurrent validity with other existing scales is usually
problematic, in that correlations between the developed scales and existing,
culture-neutral scales might offer little insight as to the developed scales' true
value to measure a culture-specific variable. Content validity is supported by
developing and piloting the instrument with the assistance of same-population
focus groups or key informants. Alpha coefficients of adequate magnitude,
when the instrument is subsequently used in a study sample, will add support
for the reliability of developed scales for use in other groups within the same
cultural population. Any significant change in new populations to be studied

57
theoretically requires some adaptation of the survey scales to address the
new cultural diversity.
The current study of helpseeking was conducted as described above.
A within culture design was chosen to explore helpseeking behavior in the
population most at risk for delayed helpseeking, African American women.
Focus groups were held to determine the scope and culturally relevant
concerns of African American women in relation to helpseeking for breast
cancer symptoms. The focus group data were used to develop a survey
instrument with scales corresponding to the Triandis Model variables. The
survey was then administered in a new sample of women. Scale reliabilities
were calculated and the newly developed scales were used as measures to
begin to address the question of factors influential to the timing of
helpseeking in this population. The following chapters more fully describe
this process and the results of the analyses.

58
CHAPTER 4
METHODOLOGY: A THREE STEPPED PROCESS
Chapter 3 discussed the choice of the Triandis model as superior to
guide a culture relevant study of helpseeking intention. To achieve maximal
levels of cultural relevance in measurement of the study variables a three
stepped methodology was chosen. The first step entailed focus groups to
map the cultural domain of helpseeking behavior for breast cancer
symptoms. The second step used qualitative data from these focus group
sessions to construct survey items which were then critiqued by the focus
group women. The third step used the newly developed survey questionnaire
in a new sample of women to assess helpseeking intention. This chapter
discusses the methodology of each of these steps in detail.
Focus Group Methods
This study selected as focus group participants adult, African American
women not currently being evaluated or treated for breast cancer symptoms,
and with no prior history of breast cancer. During the year prior to the start
of the project this investigator met with African American women at numerous
community settings to describe the planned investigation.
Beginning in the Fall of 1992, women who had been identified as
potentially interested in participating in the project were approached about
becoming a 'nucleus' of a focus group. A woman was chosen as the nucleus
■º
4,
:

59
of a focus group if, after being fully informed of the study, she agreed to
participate and was willing to identify four to six other women who might be
approached as possible participants in the focus group. This method of
building a focus group helped to assure that the participating women were
previously acquainted, improving the potential for frank discussion of what
were expected to be relatively intimate breast related issues. Only women
were invited to participate in the focus groups, as the presence of male
partners was believed to possibly inhibit disclosure. Participation of female
family relations were encouraged as a tactic to increase the social normative
content of the data.
After an initial telephone contact by the nucleus women or this
investigator, letters of invitation and consent forms (See Appendix B) were
mailed to each woman describing her focus group participation and providing
the time and place of the planned meeting. Focus groups and interview
sessions took place in homes, office conference rooms and a restaurant
conference room. Women participating in focus groups received a token
remuneration of $15.00 to symbolize the value of their participation and to
defray any expenses they might incur. Child care and transportation were
offered to facilitate participation, but all women chose to make their own
arrangements for these needs.
Four focus groups of three to six women were held over a six month
period. Two individual interviews were also held with women who wished to
participate but where situations precluded organization of a larger group. In
60
all, 22 African American adult women were recruited from women's
organizations, churches, or other community organizations in the Bay Area
cities of East Palo Alto, Menlo Park, Oakland, San Jose, and San Francisco.
The age of the women ranged from 20 to 76 years, distributed across the age
decades: twenties (n = 5), thirties (n = 4), forties (n = 5), fifties (n = 5), and
sixties/seventies (n = 3). Women were selected to range across family
income (under $9,999 per year to over $60,000), partnered status and
employment status in the hope that the voices of women from a wide range
of age, economic and social groups would be represented in the focus group
discussions. Acquaintance group design resulted in women of like age and
income being part of the same focus group. Half (n = 11) of the women
were currently employed outside the home. Nine were currently involved in
university courses or trade school training. Nine of the women were currently
married or partnered, four were widowed, and the remainder described
themselves as single without a current partner (n = 9).
Written invitation materials, planned questions, and planned
introductory remarks (See Appendix B) were used to standardize the
investigator effects on focus group sessions. Planned questions were guided
by the Triandis model and addressed: (a) beliefs about breast cancer in
relation to symptoms, susceptibility and treatability; (b) feelings about breast
cancer symptom discovery and the general threat of the disease; (c) social
relationships and role obligations that might influence the decision to seek
help for a discovered symptom in the breast; (d) resources available to
.
ºº
º■ . º
r

61
respond to a discovered symptom, (e) prior experiences and habits in relation
to health care system utilization both for general and breast-related visits; and
(f) family or friends' stories of breast symptom discovery or breast cancer.
The focus group discussions ran for approximately 90 to 120 minutes in
duration. Discussion in each of the focus groups was animated and moved
spontaneously from one planned topic area to another, permitting this
investigator to limit her participation to clarifying or focusing as necessary.
All focus group and interview sessions were audio-taped and
transcribed, protecting the identities of participants. Spoken phrases or
sentence groupings describing or qualifying one idea, opinion or explanation
in relation to helpseeking behavior were treated as the unit of analysis.
These will be referred to as data phrases for ease of communication in the
following text. Some data phrases were quite brief, containing only a
sentence or spoken sentence fragment. In other cases one data phrase
consisted of several sentences that the speaker used to communicate one
important idea, opinion or explanation. Data phrases were substracted from
the transcribed text and were then clustered according to their relevance to
the pre-determined categories dictated by the Triandis model. These data
phrase clusters were later used to develop scales corresponding to the study
variables, a technique described by Silverman (1993). Table 4-1 lists the
names of the developed scales corresponding to each of the Triandis Model
variables.

62
Table 4-1
Scales Developed to Measure Triandis Model Variables
Triandis Model Variable Scale Name
Behavioral Intention (I) |HELPHabit Hierarchies (H) HABITAffect (A) AFFECT, FEARSocial Normative Factors (S) SOCNORM, CONSTRAINTPerceived Consequences (C) CONSEQFacilitating Conditions (F) ACCESS
Note. Physiological Arousal (P) was measured by a dichotomous variable:Presence or absence of a current "worrisome breast symptom."
New Study Variables from Focus Group Sessions
The underlying model was not, however, treated as immutable. Rather
the investigator examined the data for other categories that might be needed
to cover the domain of helpseeking behavior in this cultural population. Data
phrases not related to the Triandis categories were analyzed for unifying
themes. The resulting groupings of data phrases lead to the addition of three
variables as possible influences on helpseeking: perceptions of racism in the
health care system (RACISM); religiousness (RELIG); and fatalistic beliefs in
relation to breast cancer (FATE). The addition of these new variables was
supported both by their spontaneous presence in all of the focus group
discussions and their anecdotal reporting by other investigators in studies of
r:*
■ - 2.º º -
■ º£rºº
f º
f
helpseeking behavior (Goodwin, et al., 1986; Lierman, 1988; Freeman &
Was■ ie, 1989, Haynes, 1991; Harrell, 1992; Richardson, et al., 1992).
Planned Comparative Model Testing
As was discussed in Chapter 3, there is some degree of behavioral
expectancy rather than intention being measured when one is asked to
estimate a behavioral intention before that intention is fully formed, (i.e. before
that behavior is likely to be performed). Recent theories of cognition would
suggest that although variables such as prior habits of helpseeking and
conditions that facilitate of constrain helpseeking might in fact play stronger
roles in the prediction of actual behavior, they nonetheless have a likely
influence on one's expectancy of performing the behavior. Knowledge of
one's prior behavioral habits and one's resources could be expected to figure
in to one's estimation of one's likely behavior. For this reason it is
hypothesized that the full list of Triandis variables (Model 2) will result in
added explained variance in helpseeking intention over the originally
hypothesized Triandis model (Model 1). Models 1 and 2 were discussed in
Chapter 3.
In this study, focus group sessions led to the addition of three
variables to the listing of potential influences on helpseeking intention:
perceptions of racism in the health care system, religiousness, and fatalistic
beliefs. A measure of knowledge of breast cancer symptoms was added in
light of the focus group women's construal of breast cancer symptoms as a
64
"lump" rather than the wider array of breast cancer presentations. This
strategy was also chosen to attempt to quantify helpseeking intention in terms
of breast cancer symptom presentation. Figure 4-1 displays all the variables
that will be explored for their influence on helpseeking intention along with
their measurement scale names. This grouping of variables will be referred to
as Model 3. It is hypothesized that the addition of these variables to the
Triandis model variables will result in additional explained variance in
helpseeking intention.
:

65
PERCEIVED CONSEQUENCES (CONSEQ)—
AFFECT (AFFECT,FEAR)—
SOCIAL FACTORS (CONSTRAINT, SOCNORM)—
HABIT (HABIT)—
RELEVANT AROUSAL (SYMPTOM)—
FACILITATING CONDITIONS (ACCESS)—
RELIGIOUSNESS (RELIG)—
FATALISTIC BELIEFS (FATE).
PERCEPTIONS OF RACISM (RACISM)—
BEHAVIORAL
INTENTION
(IHELP)
KNOWLEDGE OF SYMPTOMS (TYPE)—l
Figure 4-1. Proposed Influences on Helpseeking Intention (Model 3).
rº
º*
f
66
Instrument Design Methodology - A Collaboration
To create scales for each of the variable categories, data phrases were
reframed in the form of questions which could be answered as "true" or
"false," or as statements which could invite a four point Likert response of
"strongly agree" to "strongly disagree." Idiosyncratic jargon typical of spoken
English was avoided to maximize generalizability to the population of African
American women, a strategy suggested by survey researchers (Converse &
Presser, 1991; Spector, 1991; Henderson, et al., 1992; Triandis, 1980).
Concern for possible loss of cultural expression as a result of this strategy
was balanced by the concern of the focus groups to minimize colloquial
phrases that might be interpreted as offensive.
Focus group methodology has been suggested as one approach to
developing measurement tools with both validity and cultural sensitivity
(Ferketich, Phillips, & Verran, 1993; Triandis, 1980). Cultural sensitivity was
defined in this study in terms of three considerations: (a) validity of the
construct within the culture, (b) acceptability in terms of respect for the values
of the culture and (c) significance in terms of issues relevant to the culture
(American Academy of Nursing, 1992; Facione, 1993b). In keeping with this
philosophical approach to measurement and to validate the appropriateness
of the survey item construction, initial drafts of survey items were reviewed by
focus group women in all but the first group as a part of the group session.
The final drafts of the resulting survey were critiqued by focus group women

67
as well as a group of African American nurse researchers for
comprehensibility, cultural acceptability and scope of items.
Survey Methodology
The resulting survey questionnaire was administered by African
American research assistants to a new sample of adult African American
women (N = 352) in the southern San Francisco Bay area. African American
research assistants met with representatives of women's groups in church,
school, and community organizations. They were informed of the purpose
and methodology of the study. Entree to approach women for possible
participation was universally obtained. Women were then contacted by
posted announcements within the organizations. Research assistants also
were present within churches and organizations during meeting times to
recruit possible participants. Those women who indicated interest in the
study were given written consent forms describing their participation.
Participants were remunerated $10 for completing the survey, and all women
asked to consider participating were offered American Cancer Society
literature on breast health, cancer risk factors, breast self-examination, and
mammography. Surveys took on average 30 to 40 minutes to complete. In
some cases women took the surveys to their home for completion and
returned them at an arranged meeting time.
68
Sample Inclusion and Exclusion Criteria
Survey participants were required to be female, respond assertively to
the prompt "I would describe myself as African American or Black," be at least
eighteen years of age, reside in the San Francisco Bay Area community, be
English speaking, and be able to complete a printed survey either alone or
with assistance reading the items. Women were excluded from participating
in the survey if they were currently in treatment for breast cancer or were a
breast cancer survivor. An array of participants across income, age, social
role status, and educational levels was facilitated by targeting senior citizen
groups, business women's groups, teacher's groups, church groups, and
economic assistance programs. Some women also contacted the research
assistants after hearing of the study from others in the community, adding to
the volunteer nature of the study sample as well as to the community's sense
of ownership of the project.
Survey Sample Description
An estimated 550 women were approached as possible survey
participants. Of this number 357 surveys were administered. Of these three
were eliminated because of large amounts of incomplete data on several of
the scale measures and two were eliminated because they were received
after data analysis was complete. For the remainder of the surveys all
codable data were used in the analyses. Careful erasure, and margin

69
comments on many instruments were indications that many women had
taken considerable care in their response choices.
Some have questioned how representative the women living in
California are of women living in other part of the United States. There is an
additional question of diversity within groups, in this case the diversity of
women within the group called African American or Black. To better describe
the sample and to estimate the generalizability of reported relationships, the
women in this study were asked to report the city, state, and country where
they were born. Although 33.2% of the sample women reported being born
in the San Francisco Bay area, women reported being born in more than 148
cities in 30 states, the most common states being Texas (n = 37), Louisiana
(n = 33), Alabama (n = 11), Arkansas (n = 13), Mississippi (n = 15) and
Ohio (n = 10). Only seven of the women reported being born outside the
United States, most of these from United States protectorates. Table A - 2
(See Appendix A) lists other demographic descriptors of the sample.
Women in the sample were of a younger age overall than the
population most at risk for developing breast cancer symptoms (M = 38.65,
range 18-76 years of age, SD = 12.1, SE = 0.66). In spite of the attempts to
obtain respondents across the age categories, fewer women in the older age
groups were willing to complete the survey. In some cases where vision or
reading ability might have been a problem survey questions were read to
respondents by the research assistant or by other family members. But in
other cases the women indicated that questions about breasts were of such

70
an intimate nature that this solution was not acceptable and chose not to
participate. Because of the small representation of women in the older age
groups, reported relationships are limited in their generalizability to the older
age groupings.
On the positive side, the purpose of this study is to learn about beliefs
and values that women hold that might influence their seeking an evaluation
for a self-discovered breast change. Influencing factors that contribute to
delayed helpseeking will require social and behavioral interventions.
Knowledge about an age group young enough to permit the trial of an
intervention is preferable to knowledge about older age group women. As
these women age we will hopefully continue to know more about them as
they approach peak risk years for the development of breast cancer
symptoms.
The majority of women reported household income levels in the very
low income range, with nearly one third of the women reporting household
incomes below $10,000. This is consistent with national figures where one
third of African Americans live below the poverty level, and African American
family income is 56.1% of Caucasian American family income (Mullings,
1989).
Information on social role status was collected on three general social
role descriptions in the survey. An eight category role status variable was
constructed to model multiple role status for the three roles employee,
partnered (refers in this discussion to women with spouses and partners),

71
and child care giver. A large proportion of the sample described themselves
as currently or usually in the employee role (n = 249, 70.7%). The majority
of women described themselves as responsible for regularly providing care to
children (n = 209, 59.4%). The women in the sample were more likely to be
married or partnered (n = 200, 59.3%) than widowed or single without a
partner (n = 137, 40.7%). Most of the women held more than one social role
(n = 237, 67.3%), while less than 3% of the respondents held none of the
three social roles of employee, child care giver, or partner. Other possible
social roles associated with role burden, for instance caregiver of an elder,
were not included in the survey.• .
Incomes generally did not reflect educational level. Overall the sample
women were well educated with the mean number of reported years of
education at 13.2 in the sample (range 7-20 years of education, SD = 2.8
years, SE = .13). Only 16.76% of the women reported having less than a
high school education, with 50.85% reporting at least some college or trade
school training. Sixteen percent of the sample had graduated from college.
One hundred participants reported themselves as the only adult living
in their household. Only 29 of these women lived alone however, with 68 of
the remaining living with one to six children. The mean number of children
living in the house for the sample overall was 1.6 (range 0-12, SD = 1.6).
Although somewhat less than one third of the women were the only
adult living in their household, the others in the sample reported from one to
nine other adults living in their household. Most of these were married

72
couple households, often multi-generational family households, and in a few
cases these were women living in shelters or rehabilitation homes where
large numbers of adults live in community.
The presence of other coexisting health problems was quite common
in this study sample. Respondents were given a problem list and asked to
mark an "X" if the problem applied to them personally. Table 4-2 lists the
percentages of reported comorbid conditions.
Table 4-2
Other Health Problems Reported by Sample Women
Type of Health Problem N Percentage
High Blood Pressure 87 24.7Arthritis/Joint Problem
-
58 16.5Stomach Problem 43 12.2
Nervous Problem 39 11.1
GYN/Female Problem 32 9.1
Lung/Breathing Problem 31 8.8Bladder Problem 26 7.4
Heart Problem 25 7.1
Diabetes/Sugar Problem 22 6.3Back and Neck Problem 10. 2.8
Nineteen of the women reported being currently pregnant (5.4%).
Other serious health problems reported included thyroid problem (n = 4),
liver problems (n = 3), lupus (n = 2), sarcoidosis (n = 2), seizure disorder
(n = 1), HIV-AIDS (n = 1), multiple sclerosis (n = 1), and carotid stenosis

73
(n = 1). In all, 59.4% of the study sample (n = 209) indicated at least one
other chronic health condition, and 31.8% (n = 112) had two or more
Conditions.
Chapter 5 discusses the psychometric performance of both the newly
developed scale and the adopted scales in this survey sample. Reported
observed influences on helpseeking intention are reported in Chapter 6.
***
rº
74
CHAPTER 5
RESULTS: FOCUS GROUP SESSIONS
AND SURVEY INSTRUMENT DEVELOPMENT
Focus Group Data Phrases - Consensus and Conflict
The focus group data phrase lists, gleaned from the transcriptions of
the focus group sessions, are categorized in this chapter by study variable.
Representative themes emphasized in the development of the survey items
are Summarized.
Triandis Variable Themes
Behavioral Intention
A common assumption embedded in the focus group discussions was
that the decision to helpseek would be obvious and routine. This was true
even for women who indicated a likelihood of ignoring most other health
problems until significant discomfort or disruption of function forced them to
seek a professional examination and treatment. Typical comments about not
seeking care for symptoms were: "I usually just ignore it," and "I just hope it
will go away, even though I'm so educated and everything."
When the symptom was assumed to be specific to breast cancer, most
views could be characterized by one woman's comment "Something like a
lump is different. I go right away for something like a lump." As the
discussions progressed, women occasionally adjusted their estimates of their

75
likely helpseeking behavior. One first said she did not consider a
mastectomy a particularly traumatic surgery because "after all its not like its a
hand or something." Later the same woman said she would likely seek a
diagnosis but probably would not seek conventional treatment; "I would be
inclined to definitely want to know what's wrong...(but) I would have to think
long and hard about whether I wanted to have surgery... I would just go
ahead and try alternative... you know, look to other cultures."
The focus group women's universal expressed intention to helpseek
immediately for breast symptoms was incongruent with both their own past
helpseeking behavior and with estimates of helpseeking in the population."
Since the normative response of immediate helpseeking for cancer symptoms
is well known, concern regarding social desirability response bias led to the
decision to include a measure of social desirability in the developed survey
(Crowne & Marlowe, 1960; 1964; Reynolds, 1982).
Habits of Helpseeking
The women described using home remedies first and seeking a
professional evaluation only when their self care efforts failed. Most agreed
that most health problems could be ignored with few long term
consequences, and described ignoring symptoms that they judged not to be
"An estimated 34% of women are aware of their breast cancer symptoms
for three months or more before helpseeking, and this percentage has been
reported as high as 56% in studies with African American samples (Facione,
1993a; Freeman & Was■ ie, 1989).
76
signs of serious illness. They uniformly held that preventive care was
desirable, but defined it more as a "healthy eat, sleep and exercise regimen"
than in terms of a health screening or education visit to a provider. Doctors
were seen as "providing the answer" when the nature of the illness remained
elusive to the woman herself. Women said, "if something hangs on, then I go
see the doctor," and "If the things that I'm doing are not working, then I need
to go see if something else is wrong."
Affect Related to Breast Symptoms and Cancer
In all of the groups, women spoke of examining and monitoring
changes in their breasts and body, and of how they were often uncertain
about the meanings of some breast symptoms they experienced. Women
were divided as to whether they assumed their behavior would be calm and
deliberate or panicky and disorganized if they should discover a worrisome
change in their breast. They shared stories about helpseeking involving
themselves or their friends and family members. There were many stories of
relatives, friends and distant acquaintances who had delayed their breast
evaluation until their cancers were quite advanced. Many, but not all, of
these stories ended with the death of the woman. Often narrating these
stories of breast cancer illness or biopsy experiences led to revisiting related
expressions of emotion. Fear was the most common affective response
discussed in all of the focus groups. The women described actual or
anticipated fears related to the discovery of a breast lump, experiencing
biopsies or hearing the pathology results. Two of the 22 women told of

77
having a breast biopsy. One woman said, "The first time I felt something, I
just got a sick feeling in my stomach," and the other speculated that some
women might choose possible death over mastectomy, saying that women
might rather "live in fear of having missed a breast cancer than the fear of
going in to actually have a breast removed."
Social Normative Influences
The women envisioned that role expectations might influence some
women's helpseeking. Although some saw their partners and spouses as
involved in the self-discovery of a breast cancer symptom, saying for
example, "I would be very much influenced by my husband and what he was
thinking," others indicated that they would not involve spouses or partners in
such a discovery. An example of this position was, "I think the man I was
married to, I don't think I would have allowed him to share in my decision.
You know,...because of the breast. He would be biased a bit on the whole
thing." Sometimes conflicting normative advice regarding helpseeking was
associated with the roles of employee and mother. Employed women
generally spoke of illness as taboo in the work place. One employed women
told of her habit of talking herself into being well when she was ill. "I say to
myself, 'Now, you know you can't get sick. You are not going to get sick.' I
can do that to myself."
Role obligations of mothers were more ambiguous. Typical of views of
some of the women is the statement "If you don't take care of yourself, how
can you take care of your family!" But others' views could be characterized

78
by the comment "Being female ... society has placed that on us. We take
care of our family. You're not supposed to be taking care of yourself." There
were may testimonials of placing the health care needs of children above
personal health Care needs, both as behaviors of themselves and behavior
they'd seen in their mothers.
Perceived Consequences of Prompt Versus Delayed Helpseeking
All focus group women endorsed the belief that prompt helpseeking for
ºbreast cancer symptoms led to an improved chance of survival. One woman
summed up this knowledge in the statement "The sooner you know º
something is wrong, and the quicker you take care of it, the more likely you
are to survive." Women almost universally described themselves as likely to
be prompt helpseekers for a breast change they thought might be breast
cancer. The consequences of loss of life, work, spouse, and everyday ■
experience permeated much of the discussion.
Facilitating or Constraining Influences on Helpseeking
Economic conditions characterized the comments in this category.
"Going to the doctor, that's...for some people, they can't afford it. It's a
luxury. It's difficult to be sick and poor in America. You're in trouble." The
women were divided, however, on the issue of whether lacking the ability to
pay for a doctor's visit would affect their seeking the evaluation. "Cost
wouldn't keep me from going to the doctor. If I didn't have medical and
knew I had to get (an examination)...I'd go (to the doctor) and worry about it
later," said one woman. Other factors constraining helpseeking were spoken

79
of in these terms: "Transportation to the doctor is a big problem just in the
Black community overall," or "There are problems with the clinics... They
have lesser equipment, and you're going to take what's given."
The preceding discussion has described focus group data in relation
to Triandis model variables. The following discussion is of the focus group
data that led to the addition of several other variables to the study design.
Additional Focus Group Themes
Knowledge of Breast Cancer
Most striking was the unanimous assumption that the symptom
announcing the arrival of breast cancer would be a lump. Many comments
began with the phrase "If I were to find a lump..." This assumption colored all
focus group discussions until the investigator introduced the notion that less
often there may be other initial symptoms. There typically ensued intense
interest on the part of some of the women regarding other possible
presenting symptoms. In two of the focus groups women then offered a
narrative of a breast cancer illness experienced by someone they knew where
the presenting symptom was not a lump.
Other themes related to breast cancer knowledge were: concern for
the safety of mammography, the belief that breast cancer could be reliably
prevented by healthy lifestyle choices, and a belief that mastectomy rather
than lumpectomy would be the surgical option. One young woman (age 20)
offered her understanding that breast cancer is "usually treated by cutting it
:
º
º
80
all off" and demonstrated with a guillotine movement of her hand across her
chest. Other young aged women in the group reacted with a mixture of
disbelief and shock, necessitating information-giving by this investigator
regarding the range of treatment options in relation to stage of disease.
Fatalism in Relation to Breast Cancer
Several of the women expressed fatalistic beliefs regarding the
occurrence of or their eventual survival of breast cancer. They said, "With my
luck, it will affect me," and "If I were to find a lump, I would seriously consider
it a death sentence." Some spoke more indirectly of "people" being fatalistic,
saying, "People have that attitude that you're all going to die of something.
So they just adopt a fatalistic attitude, you know, this is going to be it."
Another said, "People think, 'I've got to die of something so if I just don't
know about it then I won't worry about it."
Religiousness
Intertwined in discussions of fate was mention of God as an active
agent in the experience of illness. One woman said that breast cancer can
come because God "sends it as a lesson." The idea that God determined
one's fate was not a negative expression of powerlessness, but rather one of
faithful trust that God would determine one's fate with compassion or in
keeping with a perhaps unknown but ultimate good. Several women also
expressed that while God's will would ultimately decide one's fate, "that didn't
mean you couldn't go to the doctor to help yourself."
-

81
Perceptions of Racism in the Health Care Services Environment
Cultural constraints on helpseeking was spoken of even more directly
in terms of the perceptions of racist treatment by some health care providers
or their staff members. "A lot of Black folks feel that things have been done
on an experimental basis. Folks have gone in (hospital) with some minor
condition and have died...And remember Tuskeegee," exemplifies the,
perhaps not inappropriate, overall distrust in the health care system that was
expressed by several of the focus group women. Although at least one
woman did not think racism was a factor in seeking help for symptoms, the
vast majority related occurrences that effectively diminished their access to
acceptable health care. "If you're Black and you go to the doctor, they think
you're on welfare," and "You don't get the kind of courtesies you deserve,"
exemplify the prejudicial treatment women described as characterizing their
past helpseeking experiences.
In conjunction with this portion of the focus group discussion,
additional comments about characteristics that increase the desirability and
comfort of a visit to a provider, women commented on the gender of the
provider being important to them in relation to discussing breast problems.
Most said that they preferred a female provider and in fact did regularly see aO
female provider.
In response to a question by this investigator regarding a preference
for seeing an African American provider, responses were more mixed. Most
women said that the race of their provider was not important. Other women

82
said that they preferred seeing an African American provider if this choice
was possible, although, they said, it typically was not possible. This lack of
choice was related to their receiving care in a clinic and having to be
attended by which ever provider was available.
Psychometric Performance of the Survey Instrument
Confidence placed on the validity of measure of a given behavioral
scale rests on its adequacy to measure the domain of the construct (content
validity), its ability to predict some external criterion (predictive validity), and
its empirical convergence with other measures of the same or related
constructs and divergence from non-related constructs (construct validity).
Reliability of the measures rests on their consistent performance across
investigations and in relation to each population studied.
Performance of Developed Scales and Measures
In the case of this investigation a number of considerations structured
the configuration of measures of the study variables. Evidence of the validity
and reliability of each of the measures varies as presented in each of the
variable discussions. Table 5-1 displays the number of items included in
each scale, mean scores, the number of usable scores in the survey sample,
an internal consistency reliability coefficient, and the item numbers
referencing each scale in the survey questionnaire for each of the developed
measures. The distribution of scores and decisions for the retention of scale

Table 5 - 1
Characteristics of Developed Scales Calculated from Survey Sample(N = 352)
Scale Name n
|HELP 347
CONSEQ 343
HABIT 348
SOCNORM 347
FATE 342
CONSTRAINT
(overall) 352
The CONSTRAINT Sub-Scales:PARTNERED 236 O6EMPLOYED 241CHILDCARE 223
ACCESS
(overall) 348
The ACCESS Sub-scales:PROV 348
COST 348
CONV 348
FEAR 336
ItemCodes”
11,3,5,7-17
P1-P20 >
H2-5,8-10 :SN1,3,4,6,7 ~
**.
FT1-3,4 * -
---
+ ºr **
SP1-5,7 --E1-4 - .FC1,2,4; ºSR1,3,4 --
* * *
B1,3,4, z---
FA1-10
FA5,6,9,10FA2,3,8;B4FA1,4,7,B1,3
A5,7,9,10,
Items Mean Range S.D. S.E. o. orin Scale
14 11.38 1-14
20 58.25 20–80
O7 18.78 7-28
O5 2.00 0-5
04 0.62 0–4
16 5.61 O-30
0.94 O-604 4.23 O-10O6 1.52 O-6
13 10.10 1-13
04 3.12 0–4
04 3.24 0-4O5 3.76 0–5
12 8.75 1-12
2.94
8.98
3.85
1.52
0.98
2.63
O.16
O.48
O.21
0.08
0.05
0.33
0.08O. 16O. 10
O.15
0.06
0.06O.O7
0.14
KR-20
.83
.79
.81
.63
.61
.76
º
.78
.7O
.61
.76
12-19
* Item Codes correspond to the item code numbers found in the rightmargin on the survey form (Appendix C).
** CONSTRAINT is a weighted composite of the three role status itemgroupings (possible sub-scales) listed below it in the table.

*

items is discussed below for each scale. Scales were studied
psychometrically using interactive statistical software (Crunch4, 1991) with the
capability of performing distributional analyses, factor analytic analyses and
internal consistency estimation.
Missing Data
Three cases were omitted from analysis due to large amounts of
missing data. Two of these also contained scales where all answers were
marked "TRUE/YES" or all "False/No." The third had only one response
marked per page. These surveys were judged to have no possible usable
data. Thirteen other surveys had large amounts of missing data, that is they
were missing entire scales as though the respondent had missed the page.
These surveys were coded as possible and no coding was done for missing
scales. In a limited number of other surveys, an occasional scale (RACISM
and FEAR) was responded to as all "True/Strongly Agree." These surveys
were coded as marked. The rationale for this decision stems from the fact
that items on these scale are framed roughly equally from the positive and
negative perspective. Scores from scales marked in this way were typically in
the mid range of the scale distribution and not particularly influential in data
analyses. This investigator also wished to retain these scales out of respect
for the respondent in the, albeit unlikely, event that these were her actual
responses.
Other missing data were relatively rare in this survey study. Missing
data occurred in the form of a skipped response on any particular scale. If

ae*■
*

85
the scale was coded on a four point Likert "Strongly Agree...."Strongly
Disagree" continuum, missing data was coded 2.4 so as not to influence the
overall agreement or disagreement in relation to the concept being
measured. If the items were dichotomous items scored directionally in
relation to helpseeking intention, then the mean response score per item for
the remaining items was calculated and used to estimate the missing item
score. These estimates were retained as missing data when frequencies of ºresponse for individual items are reported in text and appendices tables. ~.
gº-sº
The IHELP Measure ~The dependent variable, the intention to helpseek for breast cancer :
**
related symptoms (IHELP), was measured by 14 items (See Appendix A,
Table A - 3). Because of the dichotomous scoring of the items, the Kuder- 2.
Richardson (KR-20) coefficient was used to estimate the internal consistency º
of the measure (KR-20 = .83). The items appeared intermittently in the -
survey, beginning in the second half. They were interrupted by the AFFECT
and CONSEQ scales and items assessing breast cancer symptom knowledge
and the existence of comorbid conditions. In the complete survey (See
Appendix C), items 1-5 are followed a page later by items 6-13 (no new
instructions), and item 14 appears as one of the last of the 215 items in the
Survey.
Converse and Presser have described how respondents "bring their
answers to an item into line with what they have said to another item (1986,
p.40). The IHELP items were interspersed throughout the survey to

86
theoretically increase the number of times the respondent would need to
think again about her likely behavior in relation to a breast symptom
discovery.
Responses were coded "True" = 0, "False" = 1, except in the case of
items 2, 6, 9, and 11 which were reverse coded ("False" = 0, "True" = 1). For
item 14, "not sure" = 0. This item was presented in a slightly different format
in the questionnaire and, for the sake of scale symmetry, might better have :
been presented in the format "All things considered I am not sure that I would :have a discovered breast change checked immediately by a doctor" r(True = 0, False = 1). Future investigations might test this adapted form of :
º
the item.
The items measuring IHELP were studied using an interactive internal - -
.*
consistency statistical package (Crunch4, 1991) to assess the scale -dimensions and internal consistency. Two items were eliminated early in the º
analysis because of negative factor loadings and negative effects on the
Kuder-Richardson - 20 reliability coefficient, suggesting that these items may
be inviting ambiguous interpretation. The possibility of shortening the IHELP
measure to ten items was evidenced by several possible groupings of ten
|HELP items achieving KR-20 coefficients of .80 or higher and having factor
loadings above .300. Ultimately, however, it was determined to retain all
fourteen items in the measure of IHELP in this study. All of the fourteen
retained items have high face validity. Elimination of any of these items
would have been relatively arbitrary, and there was no advantage to

*-

87
shortening the IHELP measure when nothing was to be gained in internal
consistency and data collection was already complete.
The KR-20 for the resulting fourteen item IHELP scale was .83 and the
mean homogeneity ratio was .261. Item-Total correlations ranged from .366 -
.589. Table A - 4 (See Appendix A) displays the factor analysis of the
responses to the 14 IHELP items based on 347 non-missing cases. An
oblique rotation was determined as most theoretically appropriate since the º
dimensions of IHELP were not expected to be entirely discrete factors. :An examination of the three retained factors strongly suggests that the ..
items cluster in relation to coping style. Factor 1 items can be seen to have 2.
the Common theme of immediate or aggressive action, action in response to
the appraised threat of the breast symptom discovery. Factor 2 items º
Commonly describe detachment or disassociation, a disengagement from the r
symptom discovery situation. Lastly, Factor 3 items all describe an avowed gº
inaction, the intent to do nothing in response to the symptom discovery,
perhaps a denial of the need to helpseek. Items in each of these clusters
were examined for estimations of their internal consistency as possible future
sub-scales with resulting KR-20 internal consistencies of .78 (Factor 1), .68
(Factor 2), and .67 (Factor 3).
The FEAR Measure
As discussed above, affective influences on helpseeking have proven
particularly enigmatic in prior research. Although women describe fears and
anxiety, as well as an assortment of other emotions as integral to the

ae”■
**
º
s
~~~~

88
experience of discovering a breast cancer symptom, prior studies have failed
to describe individual differences in helpseeking in terms of these emotional
responses. In an attempt to connect fear to various aspects of the symptom
discovery and helpseeking experience, a second measure of affect was
constructed.* The number of data phrases describing emotion in the focus
group facilitated construction of this second measure.”
One item (A11, Appendix C) was judged as too complexly worded and
open to ambiguity of response and dropped from the scale. The resulting
twelve items were dichotomously scored items exploring the objective targets
of the fear response in relation to symptom discovery (eg. surgery, death,
loss of function, worse disease, etc.). The summed score of these twelve
items was used as an indicator of the magnitude of fear (FEAR). A second
measure of affect which spans an array of emotional responses to the self
discovery of a breast symptom was constructed from a modification of an
analog scale by Timko (1984; 1987).
* The second of the affect variable measures (AFFECT) is discussed
below in the section on adopted and modified scale measures.
* Focus group affect data phrases were often strikingly similar to the
qualitative data phrases reported by Timko (1987) and Lauver & Angerame
(1993), supporting their likely generalizability across populations of women.
My framing of additional items was doubtless influenced by knowledge of the
relevant prior work of these researchers.

89
The CONSEQ Measure
Twenty items were used to measure perceptions of consequences
related to the timing of helpseeking [P1-P20, Appendix C]. Respondents
were asked to imagine for a moment that they had just discovered a problem
in their breast. After each CONSEQ item respondents were asked to check
one of four boxes ranging from "Definitely Yes" to "Definitely No" to describe
what they thought would happen if they "waited a while before having the
change in (your) breast examined by a doctor." The score for perceived
consequences (CONSEQ) was derived by summing the scores for all twenty
items. The possible scores for CONSEQ ranged from 20 to 80 and the
median possible score was 50.
All but four of the CONSEQ items were drawn from focus group data
phrases. The remaining four were adopted from Timko's (1984) behavioral
beliefs measure [P1;10-11;17]. These items seemed to capture the spirit of
the focus group and were more succinct at describing these four aspects of
potential consequences than the focus group data phrases. The score for
CONSEQ is the sum of the 20 item responses and was considered to be a
measure of the magnitude of the possible consequences that might arise as
a result of "waiting awhile."
Notable was the degree to which many of the focus group data
phrases echoed those reported by Timko (1987) in her study of the intention
to helpseek for a presumed breast lump, and those in the qualitative study of
helpseeking intention by Lauver & Angerame's (1993). This suggests that the

----***
90
domain of consequential beliefs relative to helpseeking for breast cancer has
been well enumerated in the literature.
The HABIT Measure
Respondents were given 4-point Likert style items with choices ranging
from "Strongly Agree" to "Strongly Disagree." Scores for HABIT were derived
by summing the seven items, with possible scores for HABIT ranging from 7
to 28. Twelve items to measure the habit of helpseeking for health related
problems were deved rom focus group data phrases. Seven of these items
were determined to be the most internally consistent measure of HABIT [H2
5,8–10]. There are four positive frames describing regular, routine
helpseeking, and three negative frames ("only when it's serious," "I really have
to be hurting," and "I usually ignore my sickness..."). Responses are on a
four point Likert with anchors from "Strongly Agree" to "Strongly Disagree."
The Social Influence Measures
SOCNORM. The Triandis variable of Social Factors was divided into
two conceptual parts for measurement. The first was social normative
influences (SOCNORM) on helpseeking intention. Although some ambiguity
existed and was described by focus group women regarding whether its wise
to place trust in a health care provider, the normative belief is that a women
who believes she may have a breast cancer symptom should best have it
evaluated immediately by a provider. But the idea that the social normative
response will influence the performance of a behavior includes the
consideration of how public versus private the performance of the behavior

···:

91
might be. The discovery of a breast symptom is a private rather than public
event. Social norms may be less influential in the case of helpseeking for
discovery of a breast symptom than, for instance, helpseeking for engine
trouble in the fast lane of the freeway.
The items constructed for the SOCNORM Scale differ from the classic
expectancy-value format where one is asked what normative behavior one
expected each of one's key social contacts to avow, and second be asked
how likely one would be to value this directive. The scale then resembles a
check list of persons' expected normative directives and one's valuing of the
directives. Scoring is done by multiplying expectancies and values and
summing the items. Problems arise when expected norms are either not
known or not valued. In the case of this investigation, problems arose more
fundamentally in that the focus group women found prototypes of this
measure displeasingly repetitive, frustrating to complete, and/or construed the
question framing as insulting to their intellect. For these reasons, it was
decided to abandon the classical expectancy-value construction and to again
use the method of constructing items from focus group data phrases,
emphasizing the social versus private nature of behavioral responses in
relation to the symptom discovery.
Seven items were initially included in the survey. Two were eliminated
to improve internal consistency of the measure. The remaining five items
were retained as a measure of social factors influencing helpseeking
[SN1,3,4,6,7, Appendix C] preceded by the instructions: "How would the
º
:
ºr.

º

92
people in your life be important if you thought you might have a problem in
one of your breasts?" Each item was dichotomously scored, asking the
respondent to circle "True" or "False." The five items were summed to derive
a possible SOCNORM score of 0 to 5, with 0 corresponding to lower social
normative influence and 5 corresponding to higher social normative influence.
CONSTRAINT. Another theoretical dimension of social factors in the
Triandis Model is one's role expectations in relation to the behavior. In the
context of female roles it was decided to explore this variable in terms of the
frequently held roles of: spouse or partner, employee, or one responsible for
taking care of children living in the home. The descriptor "mother" was not
the operational definition used as it was too narrow to include grandmothers,
sisters, aunts and other women who were assuming the role of caring for
children in the home.
Items were constructed to address possible perceived constraints on
helpseeking associated with each of these roles. Separate items ascertained
the women's status regarding which roles they held. Only those currently
holding roles were asked to complete items about role related constraint on
helpseeking. Six of the eight items developed for the childcare section were
retained as the measure of CHILDCARE, six of the seven spouse or partner
items retained to measure PARTNERED, and all four of the items constructed
to measure EMPLOYED.
To create an overall role related constraint on helpseeking score
(CONSTRAINT), first the four EMPLOYED items (E1-E4, Appendix C] were

——————
•,■
~~~~.

93
dichotomized to reduce them to the same level of measurement as the items
measuring CHILDCARE [FC1,FC2,FC4; SR1,SR3,SR4] and PARTNERED
[SP1-SP5,SP7]. The three scores were then standardized so each
contributed equal amounts to the CONSTRAINT measure. CONSTRAINT was
calculated by adding together the standardized scores for each of the roles
the women held. Scores of "0" were given to women for each role she did
not hold, assuming she would not experience any role related constraint on
helpseeking associated with that role. The following formula was used to
allow a possible 12 point contribution from each of the three components of
CONSTRAINT:
CONSTRAINT = (PARTNERED “2) + (CHILDCARE * 2) + (EMPLOYED “ 3)
The resulting measure of perceived role related constraint on
helpseeking intention was skewed to the right with most women reporting low
levels of constraints on helpseeking related to the roles held. The estimate of
internal consistency coefficient of .76 (KR-20) was computed by analyzing the
responses for all 16 CONSTRAINT items. For this analyses, only the
responses of women who held all three roles were available for analysis (n =
123) as only they had responded to all 16 of the CONSTRAINT items.
The ACCESS Measure
The items measuring access to health care services combined four
items suggested by Berkanovic et al., (1982) with ten additional items
developed from focus group data phrases. The decision to combine these
item groupings was empirically supported by significant correlation (r. = .52,

º

94
p <.01) between the Berkanovic items and the focus group items, and by an
overall KR-20 internal consistency coefficient of .76 for the 14 items.
Access to health care services (ACCESS) was measured with these 14
dichotomously scored items, with item responses associated with lack of
access scored "0" and those indicating access to services scored "1." The
possible range of scores on the scale was therefore 0 through 14, with a-----
score of "0" theoretically reporting lowest access to services and a score of º
"14" reporting highest access. £º-
A factor analysis of these items provided an added insight to the …components of access being addressed by the scale. The analysis resulted :-in retention of three factors, grouping the items into three categories that ******
corresponded to theoretical aspects of access: Factor 1 contained items *::::referring to the strength of the patient provider relationship (PROV), Factor 2 ‘.…
-
grouped items related to the cost of services (COST), and Factor 3 to the -->º
convenience of services (CONV). One item, B2, (See Appendix C) was
eliminated because it did not load as expected primarily on the CONV sub- º
scale. Eliminating this item also raised the KR-20 for the overall ACCESS
measure to .78. Table A - 4 (See Appendix A) displays the factor analysis
results for the overall measure of ACCESS as well as the KR-20 internal
reliability coefficients for the sub-scale measures of COST, PROV, and CONV.
Kuder-Richardson reliability coefficients are high for the sub-scales,
particularly in consideration of their short length and dichotomous scoring.
The shortness of the sub-scales will prove an advantage for minimizing


95
responder burden should the validity and reliability of these sub-scales hold
up under replication.
The FATE Measure
Since no measure of fatalistic beliefs was identified from the literature,
it was decided to explore using the Chance scale (Form B) of the Wallston,
Wallston, & DeVellis (1978) Multidimensional Health Locus of Control Scales
(MHLC). The MHLC scales were developed for use in studies of expected
behavior and as such offered promise in a study of intended helpseeking
behavior. Since the Chance scale is not a measure of fatalism, but rather a
measure of external chance, several items developed from the focus group
data phrases to measure fatalism in relation to breast cancer were also
included in the survey.
Analysis of the data for this group of items did not, however, strongly
support an advantage of combining focus group fatalism items with the
Chance MHLC items. The focus group fatalism items correlated well with the
Chance MHLC items (r = .39, p <.01), offering support for the convergent
validity of these two close constructs. Factor analysis suggests that the four
focus group items are a separate dimension from the MHLC Chance items.
Also the a reliability of the Chance scale alone in this sample was .58, (lower
than the internal consistency of .67-77 reported by Wallston, et al.), while
the focus group fatalism items achieved an a of .61. Combining the MHLC
Chance items and the focus group items achieves only an a coefficient of
.68, not a remarkable improvement.

*-
*
r
* *
-
w
----■ ~~~~■ ~~~~~~…•
•··
96
In light of these analyses it was determined to retain only the four
focus group generated items as the measure of FATE particularly as this
achieved a measure specific to breast cancer. These four items are coded
FT1 - FT4 in the survey (Appendix C). The FATE score was computed by
summing the four items, and the scores ranged from 0 (less fatalistic) through
4 (more fatalistic).
Knowledge of Symptom Presentations: (TYPE)
One influence on the intention to helpseek might be the interpretation
of the breast change itself, as requiring or not requiring a provider evaluation.
This aspect of helpseeking behavior is often approached in terms of
'knowledge measures' (EVAXX, 1980; Champion, 1991), and in this study was
approached in terms of knowledge of the possible presenting symptoms of
breast cancer. The literature has reported that women evaluate breast lumps
as needing provider examination more quickly than other breast cancer
related symptoms. In order to explore potential differences in helpseeking
intention by symptom type, the women in this sample were provided with a
list of breast symptoms all of which can be symptoms of breast cancer (See
Appendix C, Items Y1 - Y14). The women were asked to respond "Yes" or
"No" to the following: "Here is a list of possible changes you might notice in
your breast. Which of the changes would make you decide to get your
breast checked right away by a doctor or nurse?" "Yes" responses were
scores as '1' and "No" responses '0'. Frequencies of "Yes" and "No"
responses were tabulated.

97
Potential measurement problems were observed to occur in relation to
this method of measuring symptom knowledge. Clarification questions asked
of the research assistants indicated that at least some of the women thought
the listing was a symptom checklist asking about symptoms they might be
currently experiencing. Although the instructions to this portion of the survey
appear to be clear and concise, many of the women (n = 51, 14.5%)
responded "No" to every symptom presentation, a response that is
inconsistent with the overall high intention to helpseek in the sample. The
reason why respondents may have misinterpreted the instructions was not
readily apparent. If this were the case, however, then the percentage
estimates of helpseeking for each symptom might be underestimates of
actual symptom specific helpseeking intention.
On the other hand, 36.6% (n = 101) of the women responded
affirmatively to all of the symptom descriptions. This response may reflect
actual helpseeking intention, but there is a concern that listing the symptom
presentations may have resulted in an inflated estimate of women's overall
knowledge of breast cancer symptoms. A measure of helpseeking intention
in relation to the array of possible breast cancer symptoms, one that does not
cue the respondent yet extracts a full description of the respondents'
knowledge, remains for future investigations.
Limitations of the TYPE Measure. This scale development portion of
the study was necessary to begin the process of achieving culturally reliable
and valid measures of the variables studied. The completion of this sizable
***
*...*****, sew"*******
a. **** * * * *
*_***
* *-* **** * * *
****

*-

98
survey questionnaire with minimal missing data was also of key importance to
provide adequate power for psychometric evaluation of the scales. That this
was achievable suggests that the responder burden was not excessive for the
entire survey instrument. The evidence for the content validity of these
measures rests at this time on the strength of the collaborative focus group
process and on support from qualitative investigations in the literature. All
developed scales attained reliability coefficients of adequate magnitude for
placing initial confidence in them as consistent measures. Further evidence
for the validity and reliability of all the newly developed measures must await
repeated investigations.
The remainder of the analyses in this investigation will use the newly
developed independent variable measures to study differences in helpseeking
intention as measured by the newly developed IHELP scale. These findings
will await replication in an independent and randomly selected sample of
African American women, building on these first efforts at culturally relevant
measurement scales to advance the strength of each.
Performance of Adopted or Modified Scales
Several scales developed by other investigators were used as
independent measures or as measures to assess the validity of developed
scales. The distributions of scores on these measures in the survey sample
are displayed in Table 5-2.
****
*...***- *
º*... -º
rºsa-- *

----
re
º
-
-

99
Table 5-2
Adopted or Modified Scales Psychometric Characteristics
Author Scale Name n Items Mean Range SD SE a■ kR-20
Strayhorn, RELIG 352 12 42.16 13-6O 9.70 0.52 .90
Weideman & Larson (1990)
Green, RACISM 351 12 29.68 13-48 5.55 0.30 .82 * *
(1991) º
Timko AFFECT 314 14 60.37 O-112 22.91 1.29 .87 º:(1984- Modified from affective adjective list) º
Crowne & CM-SD 349 13 8.1 1 1-13 2.82 0.15 .68 ..Marlowe (1960) º
Krantz, HOS 347 9 5.95 0-9 2.21 O. 12 .69
Baum & Wideman, 1980) *
Wallston, CHLC 350 6 2.44 0–6 1.61 0.09 .58 …”Wallston & Devellis (1978)
The Religiousness Measure: RELIG
A revision of Kauffman's (1979) Religiousness scale (Strayhorn, et al.,
1990) was adopted without revision to measure religiousness in this study
sample. The measure contains twelve items, each scored as a possible 5
points. The range of scores is from 12 which represents choices
corresponding to "less religious" on each of the twelve items, to 60 which
represents choices corresponding to "more religious." The median possible
score on the instrument is 36.
*
**

1OO
The reliability coefficient of .90 observed in this study sample was
somewhat higher than the .88 reported by Strayhorn and colleagues. Their
description of a two factor scale containing intrinsic and extrinsic descriptors
of religiousness was also observed in this sample, with the exception that
three of the items loaded on the opposite factor from that reported by
Strayhorn and colleagues.****
The RACISM Measure •. --*~~~
Perceptions of racism were measured with Green's (1991) "Perceptions º: --->* - -
Related to Racism and Health and/or Health Care" sub-scale. Green's scale …-* * *
items were constructed from statements reported in qualitative studies of ----.
African American women's pregnancy and health care experiences. Green'se
scale was minimally modified for this study by removing references to ---.* ~ *
pregnancy. The addition of two additional focus group items to the scale ---increased the Chronbach's a reliability coefficient from .80 to .82. These ~~
additional items were added more to assure that all important content from
the focus group data phrases were included in the survey. Ultimately it was
decided to retain the entire twelve items as the measure of RACISM, although
this combined scale can be reduced to eight items and still achieve a
Chronbach's a reliability of .80. Such a reduction might be advisable for
future study to reduce responder burden.
-
Response choices ranged from "Strongly Agree" to "Strongly Disagree"
in a 4-point Likert format. The lowest possible score on the scale was 12

~_^

101
signifying lowest perceptions of racism, and the highest score a 48 signifying
the highest perception of racism.
The AFFECT Measure
Achieving a better understanding of affective response to discovery of
a breast symptom was an important focus of this study since other
investigations have failed to explain how affect and helpseeking interact.
Measures of affective response to the discovery of a breast change were
limited to Timko's measure which coupled affective terms (eg. pessimistic and
hopeless, fearful and apprehensive, surprised and curious, etc.) and asked
respondents to mark whether they might feel the emotion on a seven point
continuum from "Extremely" to "Not at all." It was decided to include a
measure of affect similar to Timko's as a way of assessing total affective state
and as a way to explore differences between differing affective descriptors."
Because coupled prompts are to be avoided if possible since
respondents might relate differently to each of the two components (Converse
& Presser, 1986), fourteen of the affective terms included in the Timko scale
were separated into single affect items and converted to analog scales
anchored with "Extremely" and "Not at all."
Women were asked: Imagine for a moment that you are bathing and
you notice that there is a definite change in one of your breasts. "Discovering
“Although this measure is not, strictly speaking, an adopted measure, it is
discussed here because of its strong influence on the measure constructed
for this study.

--
aea
…--

102
the change in my breast would make me feel:" The word "change" was used
rather than "lump" or "problem" or "trouble" to minimally prejudice the
interpretation of the breast symptom to which this scenario was alluding.
These instructions were followed by the analog measures of the fourteen
affective terms. The analog scales were scored along an 8.00 centimeter
continuum [Items T1-T14, Appendix C]. A total level of affect score (AFFECT)
was calculated by summing the values on the 14 items. The possible range
of the score for AFFECT was 0 to 112, the mid-point on this scale being 56.
The distribution of this scale measure was normal (SW test of Normality
= .96, p <.01) in the survey sample. Cronbach's a was quite high (.87) for a
scale which is clearly measuring a multi-dimensional construct.
The Health Opinion Survey (HOS)
Since the Behavioral Involvement Scale of Krantz's Health Opinion
Survey (HOS-H) has been described as being predictive of "being a clinic
user" (Krantz, et al., 1980; Dinning & Crampton, 1989), it was decided to
include this measure in the survey as a test of the convergent validity of the
developed HABIT scale. Focus group women found the items
comprehensible and culturally acceptable. Scores on the HOS-H scale were
significantly correlated with those on the HABIT scale (r = .25, p <.03) as
hypothesized, offering concurrent validity support for the newly developed
HABIT Scale.
****
...**********
r. --"

e-+==
~|~~~
■

103
The Crowne-Marlowe Measure (CM-SD)
The Reynolds (1982) short form of the Crowne-Marlowe Social
Desirability Scale (1960) was judged acceptable for inclusion in the survey by
the focus group participants. This was of particular importance to this
investigator because the possibility of alienating the survey women by the
inclusion of items that could be perceived as reflecting negatively on oneself.
Concern that these items might appear to survey participants as disjointed
from the health related focus of the remainder of the survey were also not
realized. This scale performed moderately well in the study sample,
achieving a Chronbach's a reliability of .68. The mean score of 8.11 was
notably higher than that reported for Reynolds' undergraduate students
(M = 5.67, SD = 3.20). This difference in means may be attributable to
cultural differences in the samples or actual differences in social desirability
response bias between groups.


104
CHAPTER 6
RESULTS: SURVEY OF HELPSEEKING INTENTION
Helpseeking Intention (IHELP)
Overall the women in the sample had the expectancy of immediate
helpseeking for a self-discovered breast cancer symptom. The possible
range of scores for the IHELP measure was 0 to 14 with 0 representing
choices intending against helpseeking on all 14 items and 14 representing
choices intending toward helpseeking on all 14 items. Scores for IHELP in
the survey sample ranged from 1 to 14, (M = 11.38, SD = 2.94, SE = 0.16).
Since the majority of women with breast cancer have been reported to
seek immediate provider evaluation for their self-discovered breast cancer
symptoms, usually within a month (Richardson, et al. 1992; Samet, et.al,
1988), a skewed distribution in the direction of higher intention to helpseek
was anticipated for the IHELP measure. In fact, a highly skewed distribution
for IHELP was observed in the survey sample. Less than 8% of the women in
the sample were generally disposed against helpseeking for a self-discovered
breast symptom, (that is, responded against helpseeking on at least half of
the IHELP items).
The overall correlation between the Crowne-Marlowe CM-SD measure
and the measure of IHELP was r = 0.18, p <.01, suggesting that social
desirability response bias may have accounted for as little as 3.4% of the
variance in the IHELP measure. That a significant correlation was observed

i

105
between IHELP scores and scores on the social desirability measure is not
surprising given that immediate helpseeking for a suspected cancer symptom
is the normative response and one might expect a self report measure to be
somewhat biased in the direction of the normative behavior.
The Relationship of IHELP to Current Symptomatology
The performance of the IHELP measure was further explored in relation****
women's descriptions of their current symptomatology. More than one third º
of the sample (n = 122, 34.7%) responded positively to the item "I have a r:change in my breast right now that sometimes worries me." As the º:proportion of women currently monitoring a possible breast symptom has not --.been reported in the literature, the large size of this sub-group was not *****
anticipated. For the purposes of these analyses, these women will be º-:referred to as "symptomatic," and compared with those who indicated no ºcurrent awareness of changes in their breast, "asymptomatic." The term Tº
"symptomatic" applies only to the self-report of a breast change in that no
assessment of women's symptoms was carried out in this survey study. This
context was judged to be the most authentic for a study of helpseeking
intention, given that self-description of "having a change in the breast that
worries me" is the context in which the decision to helpseek must be made.
Symptomatic women had lower scores on the IHELP measure
(M = 10.03, SD = 3.27, SE = 0.30, n = 122) as compared to asymptomatic
women (M = 12.17, SD = 2.39, SE = 0.16, n = 221). This difference in
scores was significant by t-test, t|(193) = - 6.35, p < .01. Figure 6-1 provides

106
a visual display of the differences in the distribution of IHELP in these two
groups. Social desirability response bias was observed to differ significantly
in relation to IHELP scores. The IHELP scores of symptomatic women were
independent of the CM-SD scores (r. = 0.06, p <.49) although IHELP was
minimally correlated with the CM-SD in the asymptomatic group (r. = 0.26,
p <.01) explaining potentially 6.7% of the variance in this group's IHELP
SCOre.
1OO------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
1 2 3 4 5 6 7 8 9 10 1 1 12 13 14
Symptomatic . . . . . |HELP ScoreAsymptomatic .
Figure 6-1Frequencies of IHELP Scores in Symptomatic and Asymptomatic Women
107
Women who indicated that they were currently monitoring a breast
change that worried them were asked additional exploratory questions about
their behavior in relation to that breast change. The frequencies of these
responses are recorded in Table A - 6 (See Appendix A).
Descriptions of the symptom as something other than a lump in the
majority of these women (59.8%) could be interpreted as signifying that the
breast changes concerning the women were relatively benign or even normal
fluctuations in breast tissue. Breast symptoms, however, were of relatively
frequent concern to the women in the sample. Slightly more than half
(50.8%) were concerned enough about their breast changes to consult a
provider, and a third (33.9%) of these breast changes were biopsied.
In spite of the fact that breast changes are most often benign, there
was a strong concern in the symptomatic women that the breast change they
were experiencing might be cancer. Of the 62 women who had had their
breast changes evaluated by a doctor or a nurse provider, 21 women (33.9%)
were still concerned that the change might be breast cancer. In fact nine
(42.9%) of the 21 women who had had a biopsy for the breast change were
still concerned that the change might be cancer.
Relationships between Helpseeking Intention and Sample Demographics
Age and Helpseeking Intention
Age was significantly related to the intention to helpseek measure with
younger women indicating lower helpseeking intention than older women (r. =

108
0.26, p <.01). Because women over age 60 were under-represented in this
sample, an extrapolated relationship of higher helpseeking intention cannot
be generalized to this group of women as a curvilinear effect for age has not
been tested with this sample selection.
Income and Helpseeking Intention
There was a direct and positive correlation between the IHELP score
and reported family income. An analysis of variance by family income
showed significantly lower IHELP scores in women with reported family
incomes at or below $9,999 when compared to women reporting family
income at $40,000 or higher, F(6,314) = 8.17, p <.01.
Partnership Status and Helpseeking Intention
An analysis of variance showed significant differences in the IHELP
measure by partnered status, F(3,331) = 6.70, p <.01. By Scheffé post hoc
analyses, there was no significant difference in IHELP score between
currently married women (M = 12.19) and women who were widowed
(M = 12.86). Both of these groups were significantly higher in helpseeking
intention than single women whether partnered (M = 10.84, p <.01) or
unpartnered (M = 10.93, p<.01). This finding echoes other studies reporting
women with spouses less likely to delay helpseeking (Lierman, 1988; Dodd,
et al., 1992).
In order to attempt to separate age and partnership role effects, an
analysis of the variance in age among partnership groups were examined. It
was observed that married or widowed women were significantly older overall

109
(M = 43.3 years of age, SD = 11.8) than the single women (M = 35.5 years
of age, SD = 11.3) (t = 5.99, p <.01). However, single women with partners
were not significantly different in age from married women. These
observations suggest that it is partnership status rather than age that is
related to the lower helpseeking intention in single women with partners.
Responsibility for Childcare and Helpseeking Intention
Being responsible for childcare was dichotomously modeled
(YESCHILD = "1") for the following analyses. Women who reported
themselves as responsible for childcare scored significantly lower on the
|HELP measure (t = 12.92, p <.01) than those with no childcare
responsibilities. There were no age related effects in the significantly lower
helpseeking intention observed in women with childcare responsibilities
(t = - 1.97, p <.01). The number of children living in the household was not
significantly related to helpseeking intention (r. = - 0.11, p <.08), nor was
there an observed relationship between the number of adults living in the
household and helpseeking intention (r. = - 0.10, p <.17).
Employment Status and Helpseeking Intention
Nearly half (48.58%) of the sample women were currently employed
outside the home, and more than two thirds (71.02%) reported that they
customarily worked outside the home. An analysis of variance in helpseeking
intention by employment status showed that the sample women currently
working outside the home scored significantly higher in helpseeking intention
than women who reported themselves as usually not working outside the

110
home, F(2,330) = 7.320, Scheffé p <.01. An examination of age in relation to
employment groups showed that there was no significance in age between
the employment groups, (F(3,322) = 2.176, p <.115), thus there are no
confounding age effects in this observed relationship between holding the
role of employee and higher helpseeking intention.
Social Behavioral Measures of Helpseeking Intention
Knowledge of Breast Cancer Symptom Presentation
Overall, sample women indicated moderate helpseeking intention for
the majority of listed breast symptoms [See Items Y1-Y14, Appendix C]. The
symptoms most frequently indicated as cues to helpseeking were: "a new
lump I never had before" (n = 238, 67.6%), "a lump I knew I had in my breast
getting bigger" (n = 243, 69.0%), "a little blood coming from my nipple" (n =
236, 67.0%), and "constant pain in my breast" (n = 238, 67.6%). "Persistent
itching in my breast" (n=165, 46.9%), "clear drainage from my nipple" (n =
197, 56.0%), "a dimpling in the skin of one of my breasts" (n = 197, 56.0%),
and "one of my nipples beginning to sink inward" (n = 205, 58.2%) were least
selected as likely to motivate helpseeking.
Religiousness and Helpseeking Intention
The women in the survey sample described themselves as religious
overall, scoring from 13 to 60 (M = 42.16, SD = 9.70) on the religiousness
measure. This observation supports the accepted belief of the prevalence of
religiousness in the African American community (Chatters, Levin, & Taylor,
1992; Gallop, 1984). Religiousness and age were correlated in the sample

111
(r. = 0.36, p <.01) with older women describing themselves as more religious.
Religiousness and helpseeking were also observed to be minimally related
overall (r. = 0.22, p <.01), explaining potentially 4.9% of the variance in the
|HELP measure.
Access to Services and Helpseeking Intention
It was expected that women would describe lack of access to health
care services in general as a result of the documented lack of access in lower
income and particularly in African American populations (Blendon, et al.,
1989; Merrill, 1991; Steiner, 1991; McCoy, et al., 1991), and in light of the
general consensus of the focus group women that access to services is a
pervasive problem in the African American community.
Scores on the ACCESS scale were somewhat of a surprise as a result
of this expectation (range = 1 to 13, M = 10.10, SD = 2.78). This negative
skewing of the ACCESS measure (skewness = - 0.95) might be indicative of
the fact that lack of access has been overstated in other investigations, but
other explanations might be more likely. Possibly it is the case that this
sample, being recruited in community organizations, has an over
representation of women who are able to access all types of services
including health care services. Similarly, the geographic location of the
sample in a metropolitan area should increase relative access to services in
comparison to women residing in more remote geographic areas. If this is
the case then the measure of ACCESS in this study sample may be over
estimate of ACCESS in the larger population of African American women.

112
In this study ACCESS was the variable chosen to operationalize the
Triandis model variable Facilitating Conditions. In accordance with the
Triandis model, those persons with lack of access to health care services
should be observed to helpseek less often. If intention formation is indeed a
non-linear process and knowledge of lack of access enters into one's
intention formation, then lack of access might also be expected to influence
one's helpseeking intention. In the current study, helpseeking intention as
measured by IHELP was significantly and strongly related to the overall
ACCESS measure (r = 0.46, p <.01). This supports the hypothesis that
reported perceptions of access to services influences helpseeking intention.
This observed relationship is reported in terms of perceptions of access
because the sample women's actual access to services was not directly
assessed. This indirect measure of access is more appropriate in examining
decision-making in relation to helpseeking, however, because it is one's
perceptions and beliefs of the situational context that influence one's
decisions, not the external, objective reality of the context.
Sub-scales of the ACCESS measure. As described in Chapter 5, the
factor analysis of the overall ACCESS scale (Table A - 5) provided three sub
scales corresponding to aspects of access that have been hypothesized to
influence the utilization of health care services (Hongvivitana, 1984). These
three sub-scales were: the patient provider relationship (PROV), concern with
the cost of care (COST), and the convenience of utilizing the services
(CONV). All three of the sub-scale measures were significantly correlated
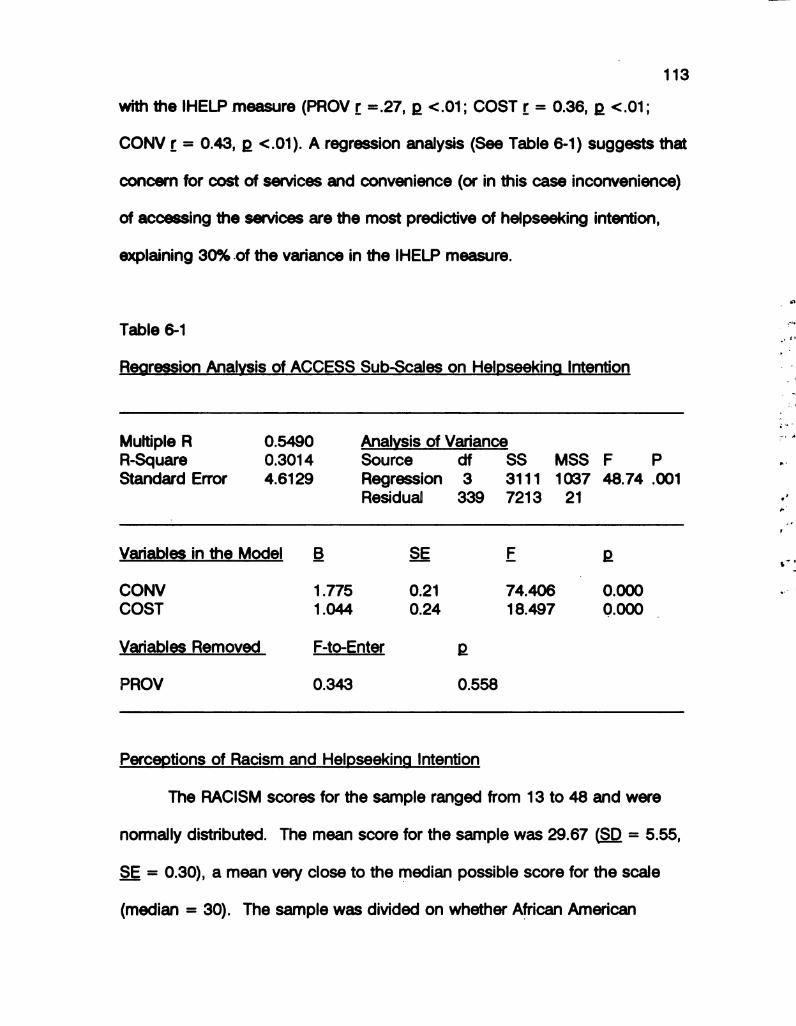
113
with the IHELP measure (PROV r =.27, p <.01; COST r = 0.36, p <.01;
CONV r = 0.43, p <.01). A regression analysis (See Table 6-1) suggests that
concern for cost of services and convenience (or in this case inconvenience)
of accessing the services are the most predictive of helpseeking intention,
explaining 30% of the variance in the IHELP measure.
Table 6-1 :Regression Analysis of ACCESS Sub-Scales on Helpseeking Intention !-
iMultiple R 0.5490 Analysis of Variance ºf a
R-Square O.3014 Source Clf SS MSS F P sº
Standard Error 4.6129 Regression 3 311 1 1 037 48.74 .001
Residual 339 7213 21 !.,”
Variables in the Model B SE E p ***
CONV 1.775 0.21 74.406 O.OOO r
COST 1.044 0.24 18,497 0.000
Variables Removed F-to-Enter p
PROV 0.343 O.558
Perceptions of Racism and Helpseeking Intention
The RACISM scores for the sample ranged from 13 to 48 and were
normally distributed. The mean score for the sample was 29.67 (SD = 5.55,
SE = 0.30), a mean very close to the median possible score for the scale
(median = 30). The sample was divided on whether African American
114
women experienced racist treatment in the health care system. The Green
(1991) scale is not a personal report scale. Women respond regarding what
they think "Black women experience" rather than regarding what they
themselves experience, or how they have perceived their own previous health
care encounters. As such it is a somewhat more indirect measure of
personal perceptions than other variable measures in the study.
In the focus group discussions the hypothesis was raised that lower
income women experience more racism in the health care system than higher
income women. This hypothesis was tested in the survey sample but no
significant difference in RACISM scores by family income was observed,
F(6,318) = 0.94, p <.46). The median of score on RACISM and the normal
distribution of these scores indicate that half of the sample women perceived
at least some degree of racism in the health care system. There was no
significant relationship observed between perceptions of racism in the health
care system and helpseeking intention (r. = -0.07, p <.18).
The Habit of Helpseeking and Helpseeking Intention
The HABIT measure was normally distributed with a range of 7 to 28
and a mean score of 18.78 (SW Test of Normally - 0.97, p <.01). Higher
HABIT scores were significantly related to higher helpseeking intention in the
survey sample (r = 0.39, p <.01), supporting the hypothesis that having the
habit of helpseeking for more general illness problems would influence one's
intention to helpseek for the specific problem of a breast symptom.
****

115
Women in the focus group discussions proposed a relationship
between perceptions of racism in the health care system and general
helpseeking habits. It was hypothesized that higher perceptions of racism
would result in more reluctance to utilize health care services and therefore a
lower score on the HABIT scale. This hypothesis was not supported in the
study sample; RACISM scores were not related to HABIT scores at or beyond
the .05 level of probability (r = - 0.10, p <.13).
Affect and Helpseeking Intention
Table 6-2 displays the means and distributions for each of the affective
terms and for the total level of affect (AFFECT) anticipated in relation to a
breast symptom discovery. Each of the individual affective terms showed a
non-normal distribution, that is, women tended to mark their responses near
one or the other of the anchors "Extremely" or "Not at all." The scores
spanned the range of possible scores (0.0 to 8.0) for each of the items.
Mean scores above 4.0 indicated that the women on average expected that
they would experience the particular affective response in the event of
discovering a change in their breast, and those below 4.0 indicating that they
would not likely experience the emotion.

116
Table 6-2
Anticipated Affect in Relation to the Discovery of a Breast Symptom
Affect item Mean Median SD SE
Angry 2.91 1.55 2.96 .16Surprised 5.47 6.93 2.37 .13Annoyed 3.52 3.35 3.12 .17Embarrassed 1.64 O.55 2.37 .13
Ashamed 1.61 O.60 2.36 .13
Panicky 4.77 5.79 3.04 .16Afraid 5.46 6.89 2.76 .15Shocked 4.81 5.93 2.99 .16
Anxious 4.67 5.95 3.11 .17Worried 5.87 7.20 2.53 . 13
Hopeless 1.90 O.7O 2.49 .13Sad 3.90 3.90 3.10 .17
Concerned 6.43 7.40 2.27 . 12
Depressed 3.84 3.90 3.01 .16Total Affect 56.82 60.51 24.99 135
Note: n = 344, Missing cases = 8
The affective term most often selected as likely to be experienced was
"Concern." The median response of 7.40 is an indication of how many of the
sample believed that they would experience extreme or near extreme
concern, and how few of the women anticipated being "Not at all concerned."
Other terms describing expected high levels of affect were "Surprise," "Fear,"
and "Worry," while "Panicky," "Anxious," and "Shocked" were nearly as often
identified.
117
Women were least likely to expect affect described as "Embarrassed,"
"Ashamed," or "Hopeless." Median scores on all three of these affective
responses were below 1.0, indicating that half of the respondents marked the
analog scale near the anchor reading "Not at all" for these affective
descriptors.
Overall affect (AFFECT), calculated by summing the analog scale
scores, was not related to the IHELP measure in the survey sample sº
(r. = -0.02, p <.79). Other investigators have hypothesized that an equivocal **
relationship between affect and actual helpseeking might indicate that strong
affect is as likely to motivate women to helpseek for a discovered symptom
as it is to paralyze their active response to the threat of a discovered
symptom. The scatterplot of the IHELP and AFFECT measures was *
examined for evidence of the curvilinear relationship proposed by Antonovsky
and Hartman (1974) to exist between these two variables, but no such-
curvilinear relationship was observed.
Examination of each varied affective response in relation to IHELP
resulted in weak correlations between high anticipation of two of the emotions
and the IHELP measure. Women who reported they would be angry
(r = - 0.12, p <.03) or feel ashamed (r = - 0.10, p <.06) scored lower on the
|HELP measure. Reports of likely lack of concern was also correlated with
low helpseeking scores (r. = 0.16, p <.01).
Other support for this significant relationship between the emotions
anger and shame and decreased helpseeking intention was seen in the

118
scoring of several additional items measuring the expectation of these two
emotional responses (See items A1, A2 in Appendix C, Survey
Questionnaire). In order to explore affect as fully as possible in relation to
helpseeking, additional affect items derived from focus group data phrases
addressing anger, embarrassment, shame, depression, and fear were
included in the survey questionnaire. As single item measures they have
limited reliability and can be regarded only as exploratory, but they are
presented here because of their congruence with the above analog scale
findings, adding support for the observation that certain emotions may have
more influence on the timing of helpseeking than others.
The item measuring anger asked women to indicate how they thought
they would feel if they discovered a problem in one of their breasts ("True" or
"False"): "I would feel mostly angry that this had happened to me." Women
who responded "True" scored significantly lower on the IHELP scale
(t = -3.59, p <.01). Similarly women who responded "True" to the statement:
"I would feel ashamed that I did something to make the breast problem
happen" scored significantly lower on the IHELP measure (t = - 6.52, p<.01).
Fear and Helpseeking Intention-
The FEAR scale used 12 Likert-style items to examine fear in relation to
different aspects of the symptom discovery, diagnosis and treatment
experience. There was no observed relationship between the overall FEAR
score (range = 1 to 12, M = 8.75, SD = 2.63) and the IHELP measure
(r = 0.09, p <.12). This result is similar to the non-significant or somewhat
se
twº-"
*** *
.*
* * * *
****
- *gas-- *
-----
!---
****

119
ambiguous findings of other investigators who have tried to study the
relationship between fear and helpseeking behavior (Antonovsky & Hartman,
1974; Magarey, et al., 1977, Mor, et al., 1990).
In an attempt to further illuminate the theoretical relationship between
fear and the timing of helpseeking, an examination of individual items relating
to fear was carried out. One high fear item (A15, See Appendix C] was
associated with significantly lower helpseeking intention scores: "I would
mostly be afraid of the pain I might experience" (t = - 3.35, p <.01). Two
high fear items [La3, A14] were associated with significantly higher
helpseeking scores: "I would be afraid I might lose my breast" (t = 2.26,
p <.03), and " would be afraid if I didn't go immediately it would get worse"
(t = 3.01, p. <.01). Three low fear items [A6; A11; LA4] were associated with
significantly lower helpseeking scores: "I would never panic" (t = 2.64,
p <.01); "I would rather live in fear of having missed a breast cancer than
facing the fear of having a breast removed" (t = 4.62, p <.01); and "I don't
think I would be afraid if I discovered a breast problem" (t = 3.58, p <.01).
These items are included here to advance investigators' potential
understanding of affect in relation to helpseeking for future investigations.
Fatalistic Beliefs and Helpseeking Intention
The respondents scores were not evenly distributed on the FATE
measure (range = 1 to 4, M = 0.62, SD = .98), with many fewer women
responding in the direction of high fatalism. Women scoring high in fatalism
were significantly less likely to intend helpseeking in relation to a breast

120
symptom discovery as measured by the IHELP measure (r = - 0.47, p <.01).
This correlation suggests that as much as 22.1% of the variance in the IHELP
measure could be explained by the FATE score. The items measuring
fatalism in this study were specific to beliefs of powerlessness in relation to
developing breast cancer and perhaps dying from the disease. To the extent
that this measure of fatalism proves to be a valid measure in relation to breast
cancer, fatalism may have a negative influence on a woman's intention to
helpseek for breast cancer symptoms and correspondingly to her survival of
the disease.
Perceptions of Consequences and Helpseeking Intention
The distribution of CONSEQ was normally distributed in the survey
sample, with the mean of 58.25 substantially above the median score for the
scale (median = 50). Women in the sample generally perceived negative
consequences to be associated with delayed helpseeking. Scores on the
CONSEQ scale were significantly and positively related to the IHELP measure
in the survey sample (r = 0.49, p <.01), potentially explaining as much as
23% of the variance in helpseeking intention.
All CONSEQ items were largely endorsed in the direction of negative
consequences as an expected result of delayed helpseeking. Most women
reported that they would worry if they put off a breast evaluation (83.8%).
Most realized that delaying helpseeking would not prevent an undesirable
diagnosis (77.1%). And most indicated that waiting would not permit them to

121
avoid surgery (73.3%). Most agreed with the statement that the breast
problem was not likely to go away if untreated (86.7%).
Fewer women agreed that "the chance of losing (my) breast" would
increase (59.0%), that they would be "more likely to need major surgery"
(55.0%), or that "their condition would become more serious or get worse"
(66.3%). More than a third of the sample (n = 126, 37.8%) responded
negatively to the consequence of "possible death."
Social Norms and Role Constraints on Helpseeking Intention
Social norm scores (SOCNORM) for the sample ranged from 0 to 5,
but were not normally distributed, with more women indicating lower social
influence in relation to a breast problem (M = 2.0, SD = 1.52). SOCNORM
was significantly and negatively related to the IHELP measure
(r. = - 0.30, p <.01).
The second measure of social influences on helpseeking intention
(CONSTRAINT) examined social role related constraint on helpseeking
behavior in relation to three common social roles (sub-scales): being
employed (EMPLOYED); being married or partnered (PARTNERED); and
being responsible for child care (CHILDCARE). Since age effects confounded
some of these observed relationships, differences in the amount of role
related constraints were examined in relation to helpseeking intention within
each role grouping. For each of the CONSTRAINT sub-scales, high scores
indicated high perception of role-related constraints on helpseeking.

122
Overall, women who were responsible for childcare generally perceived
little constraint on their helpseeking. The CHILDCARE mean was 1.52 (range
0 to 6, SD = 1.44). Higher CHILDCARE scores, however, were significantly
associated with lower scores on the IHELP measure (r. = - 0.49, p <.01),
suggesting that those women who did perceive childcare related constraints
on helpseeking were less likely to intend helpseeking for breast cancer
*symptoms. ***
* º
A similar relationship was observed in regard to perceptions of partner *---***
or spouse related constraints on helpseeking (PARTNERED). Although most º
women perceived little partner-related constraint on their helpseeking --.
(M = 0.94, range 0 to 6, SD = 1.27), those women who did report higher
perceptions of partner or spouse related constraint scored significantly lower zº
in helpseeking intention (r. = - 0.49, p <.01). ~~
Employed women had significantly higher IHELP scores than -->
unemployed women (t = 7.32, p <.01), and sample women overall reported
low levels of employment related constraints (EMPLOYED) on helpseeking
(M = 4.23, range 0-10, SD = 2.51). However, in those women who reported
higher perceptions of employee-related constraints on helpseeking, these
perceptions were significantly and inversely related to helpseeking intention
(r. = - 0.44, p <.01).
The construction of the overall perceived role-related constraints
measure (CONSTRAINT) was discussed previously in Chapter 5. Scores on
CONSTRAINT ranged from 0 to 30, where 0 represented the lowest reported

123
perceived constraint on helpseeking and 30 the highest. Scores were not
normally distributed, with the majority of women reporting an overall low
perceived constraint on helpseeking (M = 5.66, SD = 6.13, SE = 0.33).
Respondents' scores on the CONSTRAINT measure were significantly
and negatively related to their IHELP scores (r = - 0.45, p < .01). This
degree of association suggests that CONSTRAINT scores could explain as
much as 20.4% of the variance in helpseeking intention as measured by the º:
|HELP measure. This observed finding is compatible with the reported º***
influence on helpseeking behavior itself in studies in the literature (Adam, et --al., 1980; Lierman, 1988; Dodd, et al., 1992). --.
To explore the relative influence of role status and role related
constraints on the intention to helpseek, the IHELP measure was regressed -:- º º
on the three dichotomously scored role status variables: having childcare --responsibilities (YES-CHILD), being a spouse or partner (YES-PARTNER), and - *
being customarily employed outside the home (YES-EMPLOY) in a standard
multiple linear regression analysis. The three role status variables were
entered together in the first step of the model. The coefficient of
determination (R*) for these variables was 0.089 indicating that together they
explained 8.9% of the variance in IHELP. In the second step the
CONSTRAINT variable was entered into the model. The addition of
CONSTRAINT at Step 2 resulted in 23.1% (or an additional 14.2%) explained
variance. The regression demonstrates that although role status is a
significant predictor of helpseeking intention, it is not as strong a predictor as

124
perceived role related constraints. All of the variance explained in the IHELP
measure related to being responsible for childcare (YES-CHILD) was shared
with CONSTRAINT, but additional variance in IHELP was explained by the
variables measuring role status for spouse or partner (YES-PARTNER) and
being employed (YES-EMPLOY). Table 6-3 displays this regression analysis.
Table 6–3
Two Step Regression of Helpseeking Intention: Role Status Variables andPerceived Role Constraints (CONSTRAINT)
Variables Beta E p Unique Variance Bº
YES-CHILD -0.13 5.50 0.02 0.022YES-PARTNER 0.20 13.96 O.O1 O.051YES-EMPLOY O. 14 6.22 0.01 0.034
(Step 1) .089
CONSTRAINT -0.421 59.66 0.000 0.189
(Step 2) .231
Overall F = 24.22 Significance of F: p <.01
Table 6–4 lists all of the study variables observed to be related to
helpseeking intention as measured by the IHELP measure and the possible
explained variance in IHELP associated with each. These variables are not
independent of each other and as a result several variables may be
accounting for the same measured variance (collinearity between variables).
Each of these variables is important, however, as each represents a possible

125
approach for an intervention designed to increase African American women's
helpseeking intention in response to the discovery of a potential breast
cancer symptom.
Table 6–4
Study Variables Associated with the Intention to Helpseek (IHELP)
Social Behavioral Variables: --
Study Variable Statistic p R*/Eta” º
ACCESS r = 0.46 <.O1 .21 IHABIT r = 0.39 <.O1 .15 --.CONSTRAINT r = - 0.43 <.O1 .19 ---SOCNORM r = - 0.30 <.01 .09
CONSEQ r = 0.49 . <.O1 .24 º
FATE r = - 0.47 <.01 .22 :RELIG r = 0.23 <.O1 .05 * g
Demographic Variables: zº,Study Variable Statistic p R*/Eta”
AGE r = 0.26 <.01 .O7EDUC r = 0.19 <.O1 .04
SYMPTOM t = - 6.35 <.01 .11HOUSEHOLD INCOME F = 8.17 <.01 .14
RELATIONSHIPS* E = 7.44 <.01 .07
* This refers to the categorical demographic measure: Married, Widowed,Single with Partner, Single Without Partner.

126
Model Testing for a Combined Model of Helpseeking Intention
A comparative analysis was carried out of the three proposed models
for predicting helpseeking intention discussed in Chapter 3. Model 1
contains the variables proposed to predict helpseeking intention in the
original Triandis model: perceived consequences of delaying helpseeking
(CONSEQ), two measures of affect (AFFECT; FEAR), and two measures of
social normative influences (SOCNORM; CONSTRAINT). Model 2 is a º
theoretically driven expansion of Model 1, adding the variables habit of ºhelpseeking (HABIT), physiological arousal to helpseek (SYMPTOM), and --
facilitating or constraining conditions in relation to helpseeking (ACCESS). :-Model 3 comprises all of the Model 2 variables, as well as additional variables ***-
derived from the focus group portion of this study: religiousness (RELIG), z:perceptions of racism in the health care system (RACISM), fatalistic beliefs in …relation to breast cancer (FATE), and knowledge of breast cancer symptoms I.
(TYPE).
Variable Modeling
Scatter plots of the dependent variable and each of the independent
variables were examined to check linearity assumptions of regression
analyses. The demographic variables age (AGE) and educational level
(EDUC) were maintained as continuous variables. INCOME was modeled by
the dummy variables LOWINC (reported family income of $9,999 or lower)
and MIDINC (reported family income of $10,000 to $39,999), using women
with reported family incomes above $40,000 as the reference group.
127
Dichotomous variables were coded 'O' to indicate absence of the
characteristic and '1' for presence of the characteristic. These were: being
symptomatic, that is, reporting current self-monitoring of a symptom
(SYMPTOM), having a partner or spouse (YES-PARTNER), currently or usually
employed (YES-EMPLOY), and having the responsibility for childcare
(YES-CHILD).
Comparative Model Testing :
All three models were built using the same approach. First a full * * *
* * *
regression model was built for each of the models to ascertain the maximum
explained variance from the model variables. Forward, backward and --.
stepwise methods were used to study possible shared variance effects *-*-
among the model variables. Interaction terms were explored for model main -:~ *
effects. The same correlation matrix, including all of the main effects ºvariables to be tested in the respective models, was used to formulate all I
three of the regression models.
To ascertain the influence on social desirability effects in the
measurement of the dependent variable, IHELP, all three of the models were
rerun with the inclusion of the Crowne Marlowe social desirability (CM-SD)
scale scores as an additional independent variable. In no case did the CM-SD
score variable attain a significant F statistic to remain in the model.
Model 1 - The Original Triandis Predictors of Behavioral Intention
According to the Triandis model (MODEL 1), the intention to perform a
behavior, i.e. helpseek for a self-discovered breast symptom, will be

128
influenced by perceptions of the consequences (CONSEQ), affective
responses (FEAR, AFFECT), and social normative factors (SOCNORM;
CONSTRAINT). Model 1 was tested by regressing the intention to helpseek
(IHELP) on the five independent variable measures. The simultaneous
multiple regression analysis accounted for 31.48% of the variance in IHELP.
Exploration of interactions between the models main effects did not result in
an improved formulation of the model. The E tests for CONSEQ and ºº *
CONSTRAINT were significant at the p3.01 level, with these two variables * -
**
accounting for 31.7% of the variance in IHELP. Table 6-5 displays this --
analysis. --.
Table 6-5 -:~ *
Multiple Regression Analysis of Model 1 Variables ºI
Multiple R O.56 Overall Equation F = 61.33R-Square O.31 Significance of F p <.01
Variable Beta E p
CONSEQ O.37 27.01 .01CONSTRAINT -0.30 30.92 .01
Constant O 23.92 .01

129
Model 2 - Testing the Expanded Triandis Model
Model 2 added the variables HABIT, SYMPTOM, and ACCESS (Step 2
of the regression analysis), with a resulting 10.7% increase in the explanation
of variance in IHELP over Model 1. The F tests for the variables from Model 1
remained significant, with the addition of three model variables, HABIT,
ACCESS, and the interaction between being symptomatic and perceiving role
related constraints on helpseeking (SYMP"CONSTR). These five variables
explained 42.2% of the variance in IHELP. The inclusion of the interaction
between SYMPTOM and CONSTRAINT (SYMP"CONSTR) in the model
suggests that perceived constraints on helpseeking related to role
expectations were more influential on helpseeking intention in Women who
were currently symptomatic. The additional explained variance in Model 2
supports the theoretical expansion of the Triandis variables to model a less
linear decision-making process in the formation of intention for helpseeking
behavior. Table 6-6 displays this analysis.
º º
ºº
--
::º

130
Table 6-6
Multiple Regression Analysis of Model 2 Variables
Multiple R 0.650 Overall Equation F = 44.97R-Square 0.422 Significance of F p <.01
Variable Beta E p R*.
CONSEQ 0.19 14.54 .01 2.CONSTRAINT -0.232 20.14 .01 * *
(Step 1) .315 - * *
**
HABIT O.179 . 14.13 .01 .."ACCESS 0.229 20.25 .01 . .SYMP*CONSTR -0.138 7.64 .O1 ---Constant O 12.19 .01 * *-
-
(Step 2) .422
* º
* * *
* º
One additional variable passed the tolerance test to enter the model, ºthe interaction between HABIT and ACCESS. The inclusion of this interaction ~~
variable, however, introduced serious structural multicollinearity into the
model evidenced by a beta coefficient of opposite sign than the known
relationship with the dependent variable. Since both of these variables were
represented in the model as main effects, no further attempts at model fitting
in this regard were carried out.
Model 3 - Adding Influences Proposed by the Focus Group Women
The Triandis model, as previously reported in the literature, appears to
explain significant amounts of variance in the helpseeking measure. Model 3
was examined for the additional contribution of variables derived from the

131
focus group data phrases by adding the variables RACISM, RELIG, and FATE
at Step 3 of the regression analysis. The F test for one additional main
effects variable was significant at the p <.01 level, FATE, as was the
interaction between FATE and RELIG (FATE"RELIG). The model including
the interaction variable best described the data, improving the R* explained
variance for the IHELP measure to 45.26%. Table 6-7 displays this analysis.
Table 6-7
Multiple Regression Analysis of Model 3 Variables
Multiple R 0.673 Overall Equation F = 42.160R-Square 0.4526 Significance of F p <.01
Variable Beta E p R*
CONSEQ O.17 12.62 .01CONSTRAINT –0.17 10.20 .O1
(Step 1) .315
HABIT 0.19. 16.73 .01ACCESS 0.20 15.64 .01
SYMP*CONSTR -0.11 4.82 .03
(Step 2) 42.2
FATE*RELIG -0.20 15.58 .01
Constant O 13.16 .01
(Step 3) 45.3

132
Residual Diagnostics for Model 3
Studentized residuals were plotted against hat-values to visually
identify observations with possibly extreme influence. Cook's Distance
statistics for these potentially influential observations were then examined as
well as covariance ratios to ascertain whether any observations had undue
influence on the beta coefficients of the regression equation. Three
observations with high Studentized residuals, hat-values or Cook's Distance
statistics were identified as influential to the regression coefficients (Fox,
1991; Achen, 1982). The data were checked for these observations and
found to be correctly coded. These three individuals were all found to have
helpseeking scores more than two standard deviations below the mean.
Since these women could be described as displaying a more intense level of
the disposition being measured, it was determined that these observations
should not be deleted from the data. Rather they were judged to provide
important input to the calculation of the beta coefficients because they were
scores of women who were highly indisposed toward helpseeking.
Scatterplots were also examined of all independent variable values
against the raw residuals as a final check of the assumption of linearity. All
plots were found to be consistent with this assumption.
The Contribution of Demographic Variables
Lastly the demographic variables AGE, EDUC, INCOME, YES-CHILD,
YES-PARTNER, and YES-EMPLOY were entered into the regression analysis

133
at Step 4 to ascertain whether any additional variance could be explained by
these variables. socia behavioral theorists (Triandis, 1980, Ajzen & Fishbein,
1980) posit that all demographic individual differences will be expressed in
terms of the measures of belief and attitude in the model, thus no additional
explained variance is expected if the belief and attitudinal variables are
inclusive enough to cover the domain. In this investigation, no additionalº
variance in IHELP was explained by the addition of the demographic 2.
variables. This observation supports the claims of the social behavioral :
theorists and adds evidence for the goodness of fit of this social behavioral -
model of helpseeking intention. -:Separation of the effects of poverty and cultural beliefs has rarely been * * *
possible in prior investigations of health behavior. In order to attempt to -:explore the relative influences of poverty and social behavioral beliefs, one ºlast regression maneuver was carried out. The household income variables I.
(LOWINC, MIDINC) were forced to enter Model 3. Next variables were
removed from the model to discover which shared explained variance with
the income measure. Each of three model variables, ACCESS, CONSEQ,
and FATE"RELIG, shared large amounts of variance with the dummy variable
LOWINC, rendering LOWINC insignificant when either of the three remained
in the model. The variables HABIT, CONSTRAINT and SYMP*CONSTR
shared less variance with the income variables. A model containing these
three and the income variables explained 33.7% of the variance in IHELP,

134
whereas the model containing the income variables alone explained only
10.5%.
Figure 6 - 2 on the following page displays the relationships between
the significant model variables and the IHELP measure (Model 3), the 'best'
model of the data in this investigation. This model's structure draws strong
support from the Triandis model of social behavior but adds two new focus
group variables.

135
* Perceptions of Consequencesof Delaying Helpseeking
* Access to Services
* Habit of Helpseeking
* Role Related Constraints
on Helpseeking
* Currently Symptomatic
HelpseekingIntentionR* = .453
+ Fatalistic Beliefs
[3 = O.17
■ 3 = 0.20
■ 3 = 0.19
■ 3 = –0.17
■ 3 = –0.11
B = -0.20
about Breast Cancery
+ Religiousness
Figure 6-2: Univariate Correlation in Best ModelExplaining 45% of Variance in Helpseeking Intentionin a Sample (n = 330) of 352 African American Women.
* Variables from Original or Theoretically Expanded Triandis Model+ Variables from Focus Group Data
136
CHAPTER 7
DISCUSSION OF RESULTs
Overview of Findings
The self-discovery of a breast cancer symptom occurs within the
context of beliefs and feelings, gender roles, and social and economic
realities which may differ within culture. African American women were
chosen for this study population because of their later staged breast cancer
at diagnosis. The purpose of this survey research was to identify factors that
influence the timing of their helpseeking for breast cancer symptoms.
Focus groups were conducted to explore possible influential factors. A
survey was then constructed from focus group data critiqued by the focus
group women and African American nurse researchers. The survey was then
used in a new sample of African American women (N = 352).
Perceptions of the consequences of delaying helpseeking, health care
utilization habits, and access to services were positively and significantly
related to the intention to helpseek for a discovered breast symptom.
Fatalistic beliefs in relation to breast cancer, religiousness, perceptions of
social role constraints on helpseeking, and a current worrisome breast
symptom were significantly and negatively related to helpseeking intention. A
hierarchical multiple linear regression model containing these variables
explained 45.3% of the variance in helpseeking intention. While younger
aged, lower income, and unmarried women were significantly less likely to
º

137
intend helpseeking for a discovered breast symptom, adding these
demographic variables to the social behavioral model contributed no increase
in explained variance.
This study has been a productive initial investigation of factors
influencing African American women's helpseeking intention for self
discovered breast cancer symptoms. Although the observed relationships atº
times have particular salience to African American women, more often they 2appear to apply more broadly to gender related behavior. To the extent that -
women share gender role responsibilities, relative poverty, and perceptions º
about the threat of breast cancer, the African American women in this sample -:***-
have provided a picture of helpseeking behavior that begins to characterize
the phenomenon of helpseeking in their sisters of other American cultural º:- '
*-*.}
groups. **---,
*
The Overall Intention to Helpseek
Overall, women in the sample were inclined to helpseek immediately
for a breast change they judged to be worrisome, but a minority of the
women indicated significantly lower intention to helpseek. Assuming that all
the women in the sample understood breast cancer to be a threat to life, it
might have been anticipated that when asked whether they were likely to
seek a provider evaluation of a breast symptom, all of the women in the
sample would have responded affirmatively. The fact many women
138
responded negatively to multiple helpseeking items and that 8% responded
negatively to at least half of the helpseeking items is of great interest.
The analysis of the IHELP scale suggested that perhaps more was
being measured than simply an overall likelihood of helpseeking. The factor
analysis of the IHELP measure led to three item clusters strongly suggestive
of coping strategies in relation to the stressful experience of breast symptom
discovery. They were termed in this investigation: immediate action,
detachment or disassociation, and avowed inaction. These three
conceptualizations bring to mind three of the coping style categories of the
Folkman & Lazarus model (1984), Confrontative Coping, Distancing, and
Escape/Avoidance, respectively. Should this prove to be the case with further
investigation of this measure, the tool might provide not only an overall
estimate of helpseeking intention but some clues to how women might be
likely to cope with a discovered breast symptom.
Warshaw & Davis (1985) described the distinction between "formed
intention" and "expectancy" in relation to measures of planned behavior,
raising the issue of whether it is intention or expectancy that is being targeted
by the IHELP measure. More exploration of the tool will be needed to
determine the response to this query. Perhaps women who are currently
monitoring a worrisome change in their breast have a more fully formed
intention in relation to helpseeking, whereas, in women without breast
symptoms, expectancy of behavior is more often being measured. A better
139
term for the phenomenon being explored may be "the likelihood of
helpseeking." To date there are no prior investigations in the literature where
differences in helpseeking intention between these two groups of women has
been described or measured.
Women in this sample who described themselves as currently
monitoring a change in their breast reported less likelihood of helpseeking
than asymptomatic women. In this sample, women monitoring a breast
change comprised one third of the survey sample. Since this percentage has
not been reported elsewhere in the literature, and in light of the non-random
nature of the sample selection, the validity of this estimate should be an
important focus of future investigations.
Significant differences in helpseeking intention were observed between
women without breast symptoms and women who were currently monitoring
a breast change, with symptomatic women indicating lower helpseeking
intention. This observed difference suggests that women with asymptomatic
breasts might tend to misjudge the complexity of the decision to seek a
provider evaluation and over estimate the promptness and appropriateness of
their helpseeking for potential breast cancer symptoms. More important for
symptomatic women, educational campaigns targeting women who are
currently monitoring a change in their breast might possibly decrease the
time to initial provider evaluation for these women.
It would appear that both the influence of social desirability response
bias and the tendency to overstate the intention to helpseek in the absence of

140
proximity to experiencing actual symptoms make measurement of the
intention to helpseek especially difficult and certainly more complex than
described by other investigators of helpseeking. Nonetheless, the observed
differences described above suggest that the IHELP tool is measuring
important aspects of helpseeking intention, adding support for its validity.
Discussion of Demographic Relationships with Helpseeking Intention .An analysis of demographic data on the survey sample indicates that
lower income women in the sample were more likely to indicate lower ..
intention of helpseeking for a breast cancer symptom. This observation is ..consistent with other investigator's reports of lower income women presenting e-º-
with later staged breast cancer symptoms (Richardson, et al., 1992; º4.
Mandelblatt, et al., 1991; Farley & Flannery, 1989). Of significance here is *that the women in the sample were already displaying the potential effect of º
their poverty on their potential survival from breast cancer by expressing an
overall lower intention to helpseek for a discovered breast symptom in the
form of a lower IHELP score. Certainly this lower IHELP score is
understandable in the context of a family income below $9,999 per year and
the relatively high cost of living in the San Francisco Bay area. To intend to
spend resources for the evaluation of a breast symptom that may prove to be
benign would require prioritizing this potential need above the needs of
Others and above One's own needs that were not breast health related.

141
Younger women in the sample were less likely to intend to helpseek.
Since the age range of the women did not include large numbers of women
above the age of 55, this observed relationship exists within the spectrum of
women in the pre and peri-menopausal years and can not be generalized to
older aged women. Helpseeking intention might well be curvi-linear in
distribution with both younger and older aged women less likely to intend
helpseeking, but not enough data points in the older aged group were .available to examine this possibility.
The absence in the literature of a longitudinal study of helpseeking º
intention by age, for any specific health problem, precludes a clear * *
understanding of the implications of the observed difference in helpseeking
intention by age in the current investigation. It is not known whether persons
modify their attitudes about seeking evaluation for symptoms as they age and
gain health and illness related knowledge and experience; or whether the .
shared health and illness wisdom of each age cohort remains relatively stable
as the cohort ages; or whether individual differences between persons'
helpseeking behavior remains relatively stable throughout life. If the first
situation is true, a person's helpseeking intention could be expected to
developmentally increase without intervention. If the second is true, an
intervention to improve helpseeking intention could target a particular age
cohort with measures designed to modify the collective wisdom about the
value of helpseeking. If the third situation is true, then target groups must be
screened for individuals at risk for delayed helpseeking for symptoms

142
suggestive of breast cancer. Since most biopsychosocial models of behavior
would suggest that several of these situations might exert influence, planned
interventions would require multiple foci. Some interventions might target age
cohorts for educational intervention to modify belief and behavioral influences
on helpseeking. Others might emphasize individual screening of biologically
high risk women to identify those at risk of delayed helpseeking. The
observed relationships in the present study suggest screening might focus on
perceived constraints on helpseeking related to social roles, fatalistic beliefs
about breast cancer, and underestimates of the consequences of delayed
helpseeking.
Lastly, perceptions of racism in the health care environment was not
observed to significantly influence helpseeking intention in the sample
women. This finding is encouraging, as the need to interact with individuals
and institutions that potentially or actually exhibit racism is an ever-present
context for African American women in the United States. Scholar Derek Bell,
in his work Faces at the Bottom of the Well, characterizes racism as an
"integral, permanent and indestructible component" of American society
(1992, p. ix). Although some might hope he is mistaken, perceptions of
racism in the health care environment reported by this study's sample women
support his contention.
Few studies have explored the degree to which a woman might decide
not to have a health screening visit in order to avoid a potentially unpleasant
racist encounter. In the current study, however, concern that she might

143
experience a racist encounter is apparently of little consequence when
deciding whether or not to seek help for a breast symptom.
The Power of Role-Related Constraints
A higher helpseeking intention was observed in women who were
currently or usually employed. A complete interpretation of this observed
relationship will require further study. It may be that employed women and .
those usually employed have increased access to health care insurance,
making the cost factors related to helpseeking less prohibitive. But so many
low income jobs fail to provide health care benefits that this seems a doubtful ºexplanation. Perhaps a relationship could be charted in relation to the *-
likelihood of private or Medicaid health insurance benefits for those employed :or recently employed when compared to those who have been more :disenfranchised from the work/benefits environment. I
Another offered explanation of similar findings is that women who do
not often leave their homes are over-represented in the unemployed group,
but this objection is mitigated somewhat by the sample selection method that
recruited women from other organization settings outside the home. Further
study of the relationship between employee role and helpseeking intention
will be needed to confirm and clarify this observed relationship.
Reported social normative influences on more immediate helpseeking
were observed to be significantly if weakly related to lower helpseeking
intention in the study sample. One explanation of this unexpected

144
observation is that the measure of SOCNORM was actually indicative of
something other than normative influences on helpseeking. As described in
Chapter 5, the SOCNORM measure was altered from the classical
expectancy-value format because of an apparent cultural unacceptability of
what were described by focus group women as tedious, repetitive and
condescending questions. Indeed, this reaction to the expectancy-value
measurement format is probably not unique to African American women, and
more study populations might in fact reject it if given the opportunity to :
critique measures in advance.
The sample women's responses to the SOCNORM items could be * -
interpreted to be expressing autonomy, a message that was present in the
focus groups as well. For instance, several items judged by focus group :4.
women as offensive and deleted from the final survey questionnaire were
criticized because they seemed to infer that a woman could not make her …
own decision about helpseeking and would have to be told what to do by
others. Perhaps this cultural interpretation remained in spite of item
deletions. It seemed important to focus group women that it be understood
that African American women make their own decisions. This importance o:
this message is conveyed vividly in the words of the African American poet
Audre Lorde in her collection of essays about her liver cancer experience,
A Burst of Light: "...I have a right to decide what happens to my own body,
not because I know more than anybody else, but because it is my body. And

145
I have a right to acquire the information that can help me make those crucial
decisions" (Lorde, 1990, p.35).
Women's concern that investigators as well as providers adequately
acknowledge their autonomy of decision emerges as particularly important in
discussions of illness behavior, and perhaps was not dealt with directly
enough in the current investigation. Similarly, a valid and acceptable
measure of social normative influences on the decision to helpseek in Africanº
American respondents requires further development.
Holding particular social roles were observed to influence helpseekingº
intention in the sample women in this study. Having a spouse or being a .widow was associated with increased helpseeking intention compared to
* *
being single with or without a partner. Having the responsibility for providing º
care for children was associated with an overall decreased helpseeking ºintention. And being employed was associated with an overall increased
helpseeking intention. But in terms of all three of these roles, the attitude that
holding the social role constrained helpseeking was universally associated
with lower helpseeking intention. The perception of role constraints on
helpseeking was observed to be a stronger influence on helpseeking
intention than simply holding the gender role, suggesting that such
perceptions of gender role related constraints on health and illness behavior
might put some women at particular risk for delayed helpseeking for breast
CanCer.

146
Had only the holding of gender roles been examined in this study, the
observed relationships between role status and helpseeking intention would
have simply served as indications of groups to be targeted wn behavioral
interventions to improve helpseeking intention. Since the study also
measured attitudes toward helpseeking in relation to each of the roles,
guidance as to the nature of the intervention is also forthcoming. The
relationships observed between perceived role constraints and helpseeking, º
while explicated by the African American women in the sample have clear -
implications for women of other population groups. Gender behavior theory º
can be used to guide interventions to modify attitudes about the value of .helpseeking in the context of social role demands.
Focus group women suggested married women might project differing ºrole expectations in relation to immediate helpseeking for a breast symptom ºthan single women. This relationship was, in fact, observed in the survey
sample. The hypotheses focus group women offered were that unmarried
women were more uncertain of their intimacy relationships, would feel more
threat in relation to a potential illness that might disfigure them, would worry
about the loss of a sexual relationship, and/or would be more concerned
about stigmatization because of a breast symptom evaluation. Since these
issues were beyond the scope of the current investigation, these hypotheses
must await further research.

147
The Power of Beliefs
Perceptions of consequences for delaying helpseeking for breast
cancer symptoms were generally but universally acknowledged by the
women in the study sample. Although not helpseeking was associated with
"worry" about the symptom in more than 80% of the women, only one half to
two thirds of the women endorsed the consequence of the likelihood of more
serious disease or extensive breast surgery as a result of delayed t
helpseeking. Approximately 25% suggested that they might avoid a cancer
diagnosis if they delayed. And more than a third disavowed the
consequence of death as an increased possibility of delay. .It is possible that this disavowal of death as a consequence of delay is **.
a reflection of women's knowledge that most breast symptoms are benign. º*
But although one is not likely to die from a discovered breast symptom, º"possible death" is clearly within the range of logical outcomes if the symptom 3.
is cancer-related, particularly if treatment is delayed. Studies observing that
the exacerbation of a previously discovered symptom was what eventually
motivated helpseeking in women who initially delayed (Lierman, 1988; Dodd,
et al., 1992) raise concern about consequential beliefs that deny a potential
threat to life in relation to delaying evaluation of breast symptoms. Why a
minority of women might not anticipate the likely advance of their breast
disease with delayed helpseeking is beyond the scope of the current
investigation.

148
The majority of the women's responses in relation to the seriousness of
the imagined breast symptoms, the likelihood that they would indeed signal
the arrival of breast cancer, are strangely consistent with a resignation to the
relentlessness of breast cancer being portrayed in recent breast cancer
'survivor' stories in the media. Yet, for many, this assessment of
consequences stopped short of endorsing an advancing disease likely to
threaten life. This view of the breast cancer threat seems congruent with the
popular knowledge about breast cancer presented in the media, and with the
reported increased belief on the part of African Americans compared to
Caucasian Americans that cancer is not preventable (Jepson, et al., 1991).
Overall fatalism in relation to breast cancer was not observed in this
study sample. Rather, the minority of women with higher fatalism scores
were significantly less likely to intend helpseeking. This study finding is
supported by anecdotal reports of fatalistic beliefs in women who present
with late staged breast cancer.
In September of 1992 the National Cancer Institute (NCI) projected a
one in eight lifetime probability of American women developing breast cancer.
Although this estimate was extrapolated based on a life expectancy of 95+
years without death from some other cause, many women immediately
contacted the cancer society for information on breast cancer risk interpreting
the statistic to mean that one in eight women would develop breast cancer in
their immediate future. The statistic "one in eight" when applied in one time
frame across any homogenous group would signal a 12.5% incidence level.

149
In actuality, a cancer free, 60 year old, African American woman's risk of
developing breast cancer sometime during the remainder of her life is 2%
(NCI, 1992).
A misunderstanding of relative risk for breast cancer, coupled with any
disposition toward fatalism regarding one's inability to survive the disease
once it is diagnosed, would predict a powerful potential effect on a woman's
behavior in the event of a breast symptom discovery. The measure of
fatalism (FATE) used in this study targeted specific attitudes about breast
cancer framed in terms of denial of personal control, indicated by its
correlation with the Chance MHLC scale. While being religious in itself did
not predict lower levels of helpseeking intention, the interaction of high
fatalism and high religiousness was strongly associated with lower levels of
helpseeking intention.
Interventions to improve helpseeking intention in relation to possible
strongly seated beliefs about one's susceptibility and perhaps one's destiny
regarding breast cancer are in the realm of experimental interventions. Such
beliefs are only one part of an individual's epistemological framework which
guides overall life experience. The epistemological framework may be
proving highly beneficial overall to the individual's health concerns as well as
more general life issues. The challenge of an intervention would be to
integrate new ideas into the existing framework to make appropriate
helpseeking for breast symptoms more possible for individuals where
helpseeking intention is least. Current intervention projects like "En Acción
2.

150
Contra el Cancer" directed at countering fatalism in relation to cancer illness
in Latinos may offer insight into the likelihood of the success of such
interventions (Perez-Stable, et al., 1992).
The Power of Resources
The overall description of high access to health care services is
somewhat puzzling. The literature is uniformly descriptive of a relative lack of
access to services in the African American population, and reports of general
lack of access to services was anticipated in this sample which included large
numbers of low income women. One explanation is that the group of women
surveyed were women who were, in fact, more able to access services than
other women in the community. This is possible given the volunteer nature of
the sample selection which would have under represented women who have
difficulty accessing community services in general. Another possibility is that
the women's assessment of their access to services were within the Context
of their individual socio-cultural experience, and were thus rated adequate. If
the conditions of their access to services were evaluated by women from
other socio-cultural environments, perhaps the ratings of access adequacy
might have been different.
The current study did not include an objective evaluation of women's
assess to services, but it would appear that women's perceptions of their
access is a potential influential to their decision to seek an evaluation for a
breast symptom. The examination of the particular components of the
151
access scale showed concern for the cost of the services and practical
problems with actually using the health care agency were more likely to be
associated with decreased helpseeking intention than the woman's
relationship with the provider.
Women's self-report of lack of access to services and lower habits of
health care services utilization may indicate a real unavailability of diagnostic
and treatment services. But it may also indicate a relative lack of experience
in the strategies needed to attain health care for potentially serious illness. If
early case-finding for breast cancer is the desired outcome, all women will
need to know how to achieve an evaluation o a discovered breast symptom
without fearing the risk of devastating financial repercussions.
The habit of health care utilization is theoretically one of several
influences on helpseeking behavior for breast cancer symptoms, but if one
considers for a moment what types of factors might go into the formation of a
habit in relation to a given behavior, it is possible to see that a measure of
health care utilization habits may potentially be an indirect and composite
measure of several influences, among them one's past health problems or
one's prior access to services. To habitually engage in a behavior one must
have the economic resources to do it, the practical capacity to do it, have
time to do it in the context of one's other role responsibilities, tolerate or
perhaps even enjoy doing it. One might argue that to do it reliably and often
one must see some very particular benefit from doing it. Since those who do
not have the habit of generally helpseeking for illness problems might have
152
any number of reasons why this is the case, a clear interpretation of the .
observed relationship between habit and helpseeking intention is problematic.
To the extent that habits of utilization are predictive of helpseeking,
women who do not frequently utilize the health care system will be at
increased risk for delayed helpseeking for a breast cancer symptom.
The observed shared variance between household income, access to
services, misperceptions of the consequences of delayed helpseeking, and
high religiousness coupled with fatalistic beliefs about breast cancer gives
insight into which of the variables here observed to influence helpseeking
intention might be embedded in poverty. These are in contrast to other
effects observed as significant which span the income range, namely
perceptions of constraints related to social roles, the current monitoring of a ºf
breast change, and habits of health care utilization. yº*
The Power of Knowledge
Women in this sample indicated only a moderate level of helpseeking
intention by breast cancer symptom presentation. Several breast cancer
symptom presentations were apparently unrecognized by slightly over 40% of
the sample women. Because of the possibility that a misinterpretation of
directions for completing this scale may have occurred at least in some of the
women, this estimate may be higher than the actual proportion.
Earlier studies have suggested that African Americans may be less
knowledgeable about cancer symptoms than Caucasian Americans (EVAXX,

153
1980), and that African American's general knowledge about cancer risk and
the need for prompt treatment is es than that of Caucasian Americans
(Jepson, et al., 1991; Denniston, 1981). This investigation studied only
African Americans so no comparative evaluation can be suggested.
However, this study sample's knowledge of potential breast cancer symptoms
generally mirrored reports of symptom knowledge in studies of other
population groups, namely knowledge of the most common presentation of a
breast mass and less awareness of other symptom presentations.
Sample women were more likely to intend helpseeking in relation to a
mass or 'lump' presentation, supporting the findings of other researchers
(MacArthur & Smith, 1981; Nichols, et al., 1981; Lierman, 1988; Feldman, et
al., 1983; Richardson, et al., 1992; Gould-Martin, et al., 1982), and suggesting º
that African American women are more similar to than different from other ;populations of women that have been studied in regard to their knowledge of }
breast symptom presentation. Since there are no reported surveys of
Caucasian women's intention to helpseek for the array of breast cancer
symptom presentations, it can not be determined whether the percentage of
the sample indicating that they were not likely to seek an evaluation for a
dimpling in the skin of their breast (44%) or for a developing nipple retraction
(41.8%) was more or less than it might be in other populations of women.
154
The POWer of Affect
An examination of a scatterplot of the raw residuals of the model and
the values for AFFECT and FEAR revealed no suggestion of a curvilinear
relationship to support Antonovsky & Hartman's proposal that affect is higher
at both extremes of the time frame for helpseeking (1974). There were no
significant relationships observed between affect and helpseeking intention.
Only two of the affect analog measures were significantly related to
helpseeking intention. Both high expectations of anger and high expectations
of shame were associated with lower helpseeking intention. This represents
the first empirical measure of anticipated affect in relation to helpseeking
intention, although shame was anecdotally reported as related to delayed
helpseeking by Antonovsky & Hartman (1974). Anger in relation to discovery
of a breast symptom has not been addressed in studies of the timing of
helpseeking. An exploration of fear in relation to events surrounding
symptom discovery did not provide new insight into how this affective
response might influence helpseeking. Methodological considerations related
to imagined breast symptom discovery versus actual breast cancer
experience may have limited the ability to access potential influences related
to fear as well as other affective responses.
One on-going dialogue among social behavioral theorists is the
discussion of whether affective influences are subsumed by the measures of
perceived consequences and social normative influences (Ajzen & Fishbein,
1980) or whether affect needs to be included in the model individually. The
-

155
affect variables in this model failed to enter the model, adding empirical
support for Ajzen and Fishbein position. But this lack of observed systematic
relationship between emotion and helpseeking intention remains
unsatisfactory in relation to experiential knowledge that one's affective state
can indeed influence one's behavior, and the shared hypothesis on the part
of women and researchers alike that affect has some, albeit complex,
relationship to helpseeking intention.
Perhaps affect becomes an active influence only in symptomatic
conditions. Were this the case, measurement of affect, at the time it is
exerting an influence on helpseeking presents formidable measurement
problems. Although further exploration of the possible effects of affect on
helpseeking remains important, the potential to translate such an
understanding to a designed intervention remains challenging.
The Benefits of Triandis' Model and Philosophy of Method
The Triandis model purporting to predict behavioral intentions in terms
of only three variables, perceived consequences, affect and social factors.
Other variables such as habits, facilitating environmental conditions and
physiological arousal are only deemed influentia after a formed intention is
reached, mediating the ability to carry out the intended behavior. In this
study it was hypothesized that, in fact, intention formation or at least
behavioral expectancy is not so linear a process. All of the Triandis model
variables were rather believed to be potentially significant to the intention to
t *
y

156
helpseek. Model testing supported the belief that, at least in the case of
helpseeking intention, the larger variable list provides a better model of the
data than the original Triandis model.
Following Triandis' philosophy of methodology to cany Out a Culture
specific investigation of behavior, or in this case helpseeking behavioral
intention, offered additional value. In the course of preliminary work to create
culturally relevant measures of the study variables, additional variables
emerged as potentially significant and worthy of exploration. Two of these
additional variables proved to add to the explanation of variance in
helpseeking intention and were retained in the construction of the best model
of helpseeking intention.
Guided by both the original model put forth by Triandis and his º
philosophy of within-culture measurement, this investigation resulted in a ;}model with the potential to offer significant explanation of helpseeking in
African American women. The combination of variable measures attained in
this investigation, taken together, could account for as much as 46% of the
variance in African American women's helpseeking intention for self
discovered breast Cancer symptoms. Additional explanation of variance is
potentially possible if measurement problems can be solved for several other
variables still suspected as potentially influential to helpseeking intention.
The model of helpseeking intention has particular power when
compared with the anecdotal reports in the literature of women who present
with late staged breast cancer. The reported observation that poorer women
*

157
have more advanced staged breast cancer is common in the literature
(Mandelblatt, et al., 1991; Richardson, et al., 1992; Freeman & Was■ ie, 1989).
The implications are more chilling when even in advance of symptoms poor
women envision themselves as less likely (less able?) to helpseek in the
event that they discover a worrisome change in their breast.
At least one study of the timing of helpseeking for breast cancer
symptoms suggested that women's descriptions of social role constraints as
reasons why they delayed helpseeking were simply rationalizations for
inappropriate behavior and denial of obvious illness (Adam, et al., 1980). The
women in this study described their social role obligations as constraining onl
their helpseeking even in the absence of symptoms, although this effect was
even more powerful in women who were currently monitoring a worrisome
change in their breast. Rather than creating a post hoc rationalization of
;irrational behavior, the current study suggests that women are more likely at
risk for late staged tumor presentation as a result of pre-existing role
perceptions that dictate their health behavior.
These and other similarities between the modeling of helpseeking
intention in these well women and the descriptions of women who present
with later staged tumors suggest that women at risk for delayed helpseeking
can be identified prior to developing breast cancer symptoms, and
interventions can be directed at encouraging a reformulation of that intention
to improve the timing of helpseeking.

158
Study Limitations
Because African Americans comprise only 10% of the population of the
United States, locating a randomly selected sample of African Americans for
survey research can prove quite difficult and expensive (Smith, 1993). Even if
the researcher concentrates the search for participants in areas where large
numbers of African American families live, the number of households
contacted must exceed the needed number of participants by several fold.
These practical considerations guided the sample selection for this
investigation which relied on community group contacts and snowball
techniques. As a result, the volunteer nature of this sample may have had an
effect on the estimates or the effect sizes of observed relationships, and
perhaps possibly on the significance of the relationships themselves. Future
studies replicating aspects of this investigation in randomly selected samples
:will be needed to add support for the observations reported here.
Methodological problems and practical considerations emerge in the
selection of samples to represent all parts of the population being studied.
These deserve consideration. Populations seen to be at potential risk for
higher incidence of breast cancer or delayed helpseeking are traditionally
least represented in study samples: the elderly, the poor, and women of
color. Community based research improves sample representation of these
groups somewhat, but those who are housebound or homeless, without
transportation, and too engaged in procuring essential needs to participate in
research studies remain relatively voiceless in the study results. Offering

159
some reimbursement for time spent participating in research and bringing the
study to the neighborhood were part of this study's design to include a full
range of voices. Even with these considerations, older women found
participation too problematic.
It is not clear whether the women in the sample were voicing their own
beliefs about the influences on helpseeking intention or the popularly held
beliefs of the larger cultural group of which they are members. Although
each of the survey items were framed in terms of a personal response, when
a personal response was not forthcoming women may have voiced the
collective wisdom instead This response bias is related but different than the
classic social desirability response bias assessed by the CM-SD scale in this
study. The collective wisdom, as expressed by the focus group women, was
the expectancy of helpseeking as soon as possible for all threatening
symptoms, regardless of other responsibilies to family or employer, in spite
of fear, without regard to economic realities, even if access to services is
problematic. Responses that verbalize the collective wisdom would
universally underestimate the potential ‘true score' of an individual women in
relation to all these variables. This would suggest that all reported
relationships in this study may be under estimated in the woman who is
actually engaged in a helpseeking decision. That this is true is supported by
the lower scores for helpseeking in symptomatic women in the survey
sample.

160
Survey design, while advantageous for broad explorations of many
potential inter-related variables, limits the depth of understanding possible in
relation to any one relationship. Although social behavioral theory offers
hypothetical explanations of the relationships, further investigations, narrower
in scope and richer in qualitative data, will be needed to enrich the
understanding of the relationships here suggested as possibly significant to
helpseeking behavior. These future investigations should focus on evaluating
the findings of the current study as well as searching for theoretically sound
ways to translate them in to behavioral interventions to influence helpseeking
intention. Although the intention-behavior relationship is supported by
numerous investigations of other health related behaviors, longitudinal
investigations are needed to understand whether and how helpseeking
intention changes over time and how well it predicts helpseeking behavior for
breast cancer symptoms.
The observed difference in helpseeking intention in relation to age
raises some concern, and a complete interpretation of this relationship is
beyond the scope of the current study. Since longitudinal studies of
helpseeking intention have yet to be carried out, this relationship remains
unexplained. There were relatively few women over age 60 in this sample
limiting the generalizability of findings. Future studies of older age group
women should explore study variables as they apply to this population,
expanding role related constraints to include roles held by the older aged
group. Studies with samples than span across the age range should explore

161
the possibility of a curvilinear relationship between age and helpseeking
intention. Hypothetically both younger and older aged women might have
lower helpseeking intention for diverse reasons.
The necessary omission, due to measurement problems, of a measure
of knowledge of symptom presentations limited the ability to test this
expected influence in the present investigation. Since such a measure must
fully assess knowledge of symptom presentation without providing cues to
respondents of possible breast cancer symptoms, such a measure is
particularly problematic for survey research methodology.

162
CHAPTER 8
IMPLICATIONS FOR FUTURE RESEARCH
Breast cancer remains primarily a cancer of women. The study of
behavior in relation to breast cancer should be mindful of gender
considerations. In past investigations, information regarding role obligations
and gender specific meanings associated with breast cancer and breast
symptoms appear more to have been thrust upon the investigators than
actively sought as part of the planned research. Future investigations should
centralize gender issues as part of the environment to be studied in relation
to breast symptom discovery. Similarly, providers should explore potential
health risks associated with perceived role-related constraints on health
behavior.
The African American women in this sample have provided a picture of
the contextual variables potentially influencing helpseeking intention in their
lives. These variables are doubtless expressed in unique ways within the
African American community, some of them proving potentially less or more
influential than they might be in other ethnic or racial groups. But the
influences suggested as potentially influential to the timing of helpseeking
resonate with the common experience of the wider population of women as
wives, mothers, grandmothers, aunts, lovers, employees, and selves. In this
respect, the picture drawn by the sample women points to a more general
understanding of the problem of women's behavioral dilemma in response to

163
a discovered breast symptom. Whereas interventions to assist women to
deal with the problem would best be expressed within the cultural experience
in which they live, the theoretical model to guide such interventions can be
envisioned to transcend the dimensions of particular population groups.
The differences in helpseeking intention in relation to current
symptomatology suggests that asymptomatic women may underestimate the
complexity of their helpseeking response. These women may hear education
messages about the need to seek a prompt evaluation and assume a
behavioral response that is less likely once the symptom actually appears.
Additional investigations targeting symptomatic women may help
investigators to learn more about this change in helpseeking intention.
Future studies might particularly target women who describe themselves as
having symptoms as best informants of the intention to helpseek for breast
cancer symptoms, selecting them at random in the community at large and
not just within the health care system.
It has been suggested previously that investigators should focus their
inquiry on helpseeking singularly on the group of women who indicate the
intention to delay helpseeking, since it may be here that the strongest factors
influencing delay are concentrated (Facione 1993a). Since it is difficult to
locate large numbers of these women, perhaps a more practical population
for study would be those women currently monitoring a breast change. In
the current study the percentage of women currently monitoring a breast
symptom was approximately 34%. In a randomly selected sample, this

164
percentage might be considerably less, but these women are likely to be
more in touch with the factors influencing their decision to helpseek than
women who are less immersed in the experience. Separating the
observations these two groups of women in future studies should provide
clarifying insights on the phenomenon of helpseeking.
The issues of access to evaluation and treatment for a discovered
breast symptom cannot be overlooked. Ideally an objective measure of
access to care should be incorporated into future study designs to permit
control of this variable in behavioral studies of helpseeking behavior. No
further studies are necessary to point out the fact that later staged breast
cancer is seen in poorer women. Rather, studies which quantify the relative
influence of perceived or actual access on actual or intended helpseeking
behavior would provide support for those who would argue for changes in
the health care delivery system to equalize access for all persons.
A realistic look at the possibility of racial or cultural bias influencing
helpseeking is warranted in every health care setting where gatekeeper
groups might limit access to health care. Further investigations will be
needed to explore what additions or modifications of the picture will be
needed to best understand the particular cultural experience of Latinas,
Native Americans, Asian Americans, European Americans, and women of
Other cºura groups.
Antonovsky & Hartman (1974) viewed behavioral response in relation
to symptom discovery as patterned by personality trait. Personality models
165
today continue to support this hypothesis (Costa & McCrae, 1992; Caspi &
Moffitt, 1993), suggesting that personality measures might identify women at
risk for delayed helpseeking before breast cancer symptoms occur.
Helpseeking intention might also be examined in relation to the full range of
coping strategies likely to be employed in response to the discovery of a
breast cancer symptom, perhaps guided by a coping model such as that of
Folkman & Lazarus (1988). Personal differences in coping strategies might
be expected to be associated with differences in helpseeking intention.
Further development of the IHELP scale to encompass other possible coping
strategies might improve the variance, validity and reliability of the measure.
A future longitudinal study to trace the continuity between helpseeking
intention and actual helpseeking behavior would add support to this observed
relationship but seems unlikely considering the likely cost of following a large
enough cohort of women until breast symptoms developed in a sufficient
number to examine this relationship. But if the strength of the intention
behavior relationship holds in the case of helpseeking behavior to the degree
that it has been shown in studies of mammography screening and other
health behavior, demonstrating a pre-set psychosocial condition for late
helpseeking and delayed diagnosis could have powerful implications for
screening programs and individual provider visits. The ability to screen all
women for psychologically related risk of delayed helpseeking would be a
particularly important addition to cancer screening. Given the cost of treating
advanced staged breast cancer, such screening would be likely to be cost
166
effective, particularly for women at higher biological risk for the development
of breast cancer.
The development of a valid and reliable tool to identify women least
likely to helpseek immediately for a discovered breast symptom could assist
providers to identify women who might particularly benefit from more frequent
screening or more guidance in relation to helpseeking behavior, breast
cancer symptom presentation, counseling for role related stress, and
information about new treatment options.

167
REFERENCES
Achen, C. H. (1982). Interpreting and Using Regression. Newbury Park, CA:Sage.
Adam, S.A., Horner, J. K., & Vessey, M. P. (1980). Delay in treatment forbreast cancer. Community Medicine, 2, 195 - 201.
Aitken-Swan, J. & Paterson, R. (1955). The cancer patient: Delay in seekingadvice. British Medical Journal, 1, 623 - 627.
Ajekigbe, A. T. (1991). Fear of mastectomy: The most common factorresponsible for late presentation of carcinoma of the breast in Nigeria.
Clinical Oncology, 3, 78 - 80.
Ajzen, l. (1985). From intentions to actions: A theory of planned behavior. InJ. Kuhl & J. Beckman (Eds.), Action Control (pp. 11 - 39). Berlain:Springer-Verlag.
Ajzen, l. (1987) Attitudes, traits, and actions: Dispositional prediction ofbehavior in personality and social psychology. Advances inExperimental Social Psychology, 20, 1 - 63.
Ajzen, I. & Fishbein, M. (1980). Understanding Attitudes and PredictingSocial Behavior (pp. 1 - 279). Englewood Cliffs, NJ: Prentice Hall.
Ajzen, I. & Madden, T. J. (1986). Prediction of goal-directed behavior:Attitudes, intentions, and perceived behavioral control. Journal ofExperimental Psychology, 22, 453 - 474.
Allan, C., Cox, E. B., Manton, K. G., & Cohen, H. J. (1986). Breast cancer inthe elderly: Current patterns of care. Journal of the American GeriatricSociety, 31, 637 - 642.
-
American Academy of Nursing. (1992). AAN Expert panel report: CulturallyCompetent Health Care. Nursing Outlook, 40, 277 - 283.
American Cancer Society. (1991). Cancer Facts and Figures for MinorityAmericans 1991 (pp. 1 - 15). Atlanta, GA: American Cancer Society.
American Cancer Society. (1994). Cancer Facts & Figures (pp. 1 - 28).Atlanta, GA: American Cancer Society.

168
American Cancer Society. (1994). California 1993 Cancer Facts and Figures(pp.1 - 30). Atlanta, GA: American Cancer Society.
American Joint Committee on Cancer. (1988). Manual for Staging of Cancer(pp. 145 - 148). Third edition.
Antonovsky, A. & Hartman, H. (1974). Delay in the detection of cancer: Areview of the literature. Health Education Monographs, 2, 98 - 128.
Bagozzi, R. P. & Yi, Y. (1989). The degree of intention formation as amoderator to the attitude-behavior relationship. Social PsychologyQuarterly, 52(4), 266 - 279.
Bailey, E. J. (1987). Sociocultural factors and health care-seeking behavioramong black Americans. Journal of the National Medical Association,79(4), 389 - 392.
Bain, R. P., Greenberg, R. S., & Whitaker, J. P. (1986). Racial differences insurvival of women with breast cancer. Journal of Chronic Disease,39(8), 631 - 642.
Bal, D. G. (1991). Prevention and changing demographics: The underservedand cancer. Cancer, 67, 1814 - 1816.
Baquet, C. R. & Ringen, K. (1986). Cancer Among Blacks (pp. 42).Washington, DC: National Cancer Institute.
Beck, A. T. & Weisman, A. (1974). The measurement of pessimism: Thehopelessness scale. Journal of Consulting and Clinical Psychology, 42,861 - 869.
Bell, D. (1992). Faces at the Bottom of the Well. New York: Basic Books.
Bentler, P.M. & Speckart, G. (1979). Models of attitude-behavior relations.Psychology Review, 86(5), 452 - 464.
Berkanovic, E., Telesky, C., & Reeder, S. (1981). Structural and socialpsychological factors in the decision to seek medical care forsymptoms. Medical Care, 19(7), 693 - 709.
Bird, C. E. & Fremont, A. M. (1991). Gender, time use and health. Journal ofHealth and Social Behavior, 32, 114 - 129.

169
Blendon, R. J., Aiken, L. H., Freeman, H. E., & Corey, C. R. (1989). Access tomedical care for black and white Americans: A matter of continuingconcern. Journal of the American Medical Association, 261(2),278 - 281.
Bloom, J. R., Hates, W. A., Saunders, F., & Flatt, S. (1987). Cancerawareness and secondary prevention in black Americans: Implicationsfor intervention. Family Community Health, 10(3), 19 - 30.
Boring, C. C., Squires, T. S., & Heath, C. W. (1992). Cancer statistics forAfrican Americans. Cancer, 42(1), 7 - 17.
Boring, C. C., Squires, T. S., & Montgomery, (1994). Cancer Statistics 1994.Ca - A Cancer Journal for Clinicians, 44(1), 7 - 26.
Boring, C. C., Squires, T. S., & Tong, T. (1993). Cancer Statistics, 1993.CA - A Cancer Journal for Clinicians, 43(1), 7 - 26.
Broman, C. L. (1987). Race differences in professional helpseeking. AmericanJournal of Community Psychology, 15(4), 473 - 489.
Brown, E. R. (1990). Health access issues. In L. E. Irwin, J. Stern, J. Steinfeld,L. Breslow, H. Crothers, & D. Fink (Eds.), Cancer and the Underserved:An Agenda for Changes in the 1990's (pp.93 - 104). Proceedings ofthe Conference November 3–4, 1989. Oakland, CA: American CancerSociety.
Brown, L. D. (1991). The medically uninsured: Problems, policies, andpolitics. In L. D. Brown (Ed.), Health Policy and the Disadvantaged(pp. 169 - 183). Durham: Duke University Press.
Butler, P. A. (1988). Too Poor to be Sick: Access to Medical Care for theUninsured. American Public Health Association.
Caspi, A. & Moffitt, T. E. (1993). When do individual differences matter?A paradoxical theory of personality coherence. Psychological Inquiry,4(4), 247 - 271.
Celetano, D. D., Shapiro, S., & Weisman, C. (1982). Cancer preventivescreening behavior among elderly women. Preventive Medicine, 11,454 - 463.
Champion, V. L. (1984). Instrument development for health belief modelConstructs. Advances in Nursing Science, 6(3), 73 - 85.

170
Champion, V. L. (1985). Use of the Health Belief Model in determiningfrequency of breast self-examination. Research in Nursing and Health,8(4), 373 - 379.
Champion, V. L. (1987). The relationship of breast self-examination to healthbelief model variables. Research in Nursing and Health, 10(6),375 - 382.
Champion, V. (1991). The relationship of selected variables to breast cancerdetection behaviors in women 35 and older. Oncology Nursing Forum,18(4), 733 - 739.
Charison, M. E. (1985). Delay in the treatment of carcinoma of the breast.Surgery, Gynecology & Obstetrics, 160, 393 - 399.
Chassin, L., Presson, C. C., Sherman, S.J., Cirty, E., & Olshavsky, R. W.(1984). Journal of Applied Social Psychology, 14(3), 224 - 243.
Chatters, L. M., Levin, J. S., & Taylor, R. J. (1992). Antecedents anddimensions of religious involvement among older Black adults. Journalof Gerontology, 47(6), S269 - S278.
Chu, J., Diehr, P. & Feigl, P., Glae■ ke, G., Begg, C., Glickman, A., & Ford, L.(1987). The effect of age on the care of women with breast cancer incommunity hospitals. Journal of Gerontology, 42, 185 - 190.
Clinton, J. H. (1982). Ethnicity: The development of an empirical construct forCross Cultural research. Western Journal of Nursing Research, 4,281 - 300.
Coates, R. J., Bransfield, D. D., Wesley, M., Hankey, B., Eley, W., Greenberg,R. S., Flanders, D., Hunter, C. P., Edwards, B. K., Forman, M., Chen, V.W., Reynolds, P., Boyd, P., Austin, D., Muss, H., Blacklow, R. S.(1992). Differences between Black and White women with breastcancer in time from symptom recognition to medical consultation.Journal of the National Cancer Institute, 84(12), 938 - 950.
Coleman, W. (1994). Sisters in arms. Los Angeles Times News Magazine,(pp. 4 - 5) February 6, 1994.
Converse, J. M. & Presser, S. (1986). Survey Questions, (pp. 9 - 79).Newbury Park: Sage Publications.
Costa, P. T., & McCrae, R. R. (1992). The Revised NEO Personality InventoryManual. Odessa, FL: Psychological Assessment Resources.

171
Crawford, J. & Cohen, H. J. (1985). Aging and neoplasia. Annual Review ofGerontology and Geriatrics, 4, 3 - 32.
Crowne, D. P. & Marlowe, D. (1960). A new scale of social desirabilityindependent of psychopathology. Journal of Consulting Psychology,24(4), 349 - 354.
Crowne, D. P. & Marlowe, D. (1964). The Approval Motive. New York, NY:John Wiley.
Crunch Software (1991). CrunchA. Oakland, CA: New England Software.
Davidson, A. R., Jaccard, J. J., Triandis, H. C., Morales, M. L., Dias-Guerrero,R. (1976). Cross-cultural model testing: Toward a solution of the eticemic dilemma. International Journal of Psychology, 11(1), 1 - 13.
Davidson A. R. & Thomson E. (1980). Cross-cultural studies of attitudes andbeliefs. In H. Triandis & R. W. Brislin (Eds.), Handbook of CrossCultural Psychology: Vol. 5: Boston: Allyn & Bacon.
Davis, A. (1990). Sick and tired of being sick and tired: The politics of blackwomen's health. In E. C. White (Ed.), Black Women's Health Book,
(pp. 18 - 26). Seattle: Seal Press.
Davis, J. E. (1988). National initiatives for care of the medically needy.Journal of the American Medical Association, 259(21), 3171 - 3173.
Dawson, D. A. & Thompson, G. B. (1990). Breast Cancer Risk Factors andScreening: United States, 1987. DHHS Publication Number PHS90-1500. Washington, DC: U.S. Government Printing Office.
Dayal, H. H., Power, R. N., & Chiu, C. (1982). Race and socio-economicstatus in survival from breast cancer. Journal of Chronic Disease, 35,675 - 683.
Dean, K. J., Holst, E., & Wagner, M. G. (1983). Self-care for common illnessesin Denmark. Medical Care, 21(10), 1012 - 1032.
Dennis, C. R., Gardner, B., & Lim. (1975). Analysis of survival and recurrencevs. patient and doctor delay in treatment of breast cancer. Cancer, 35,714 - 72O.
Denniston, R. W. (1981). Cancer knowledge, attitudes, and practices amongBlack Americans. Cancer Among Black Populations, (pp. 225-235).New York, NY: Alan B. Liss, Inc.
º
*
172
Dignan, M., Michielutte, R., Sharp, P., Bahnson, J., Young, L., & Beal, P.(1990). The role of focus groups in health education for cervical canceramong minority women. Journal of Community Health, 15(6),369 - 375.
Dinning, W. D. & Crampton, J. (1989). The Krantz Health Opinion Survey:Correlation with preventive health behaviors and intentions.Psychological Reports, 64, 59 - 64.
Dodd, M. J., Lovejoy, N., Stetz, K., Larsen, P. Linsey, A. M., Musci, E., Lewis,B., Hauck, W., Paul, S., & Holzemer, W. (1988-1992). Self-careinterventions to decrease chemotherapy morbidity. Funded NationalInstitute of Health, National Cancer Institute RO1 CA 48312.
Elwood, J. M. & Moorehead, W. P. (1980). Delay in diagnosis and longtermsurvival in breast cancer. British Medical Journal, 280, 1291 - 1294.
EVAXX, Inc. (1980). Black American's attitudes toward cancer and cancertests. Cancer, 31(4), 212 - 218.
Facione, N. C. (1994). An exploration of role overload and health: Themarried mother in the waged labor force. Health Care for WomenInternational, 15(2), 157 - 167.
Facione, N. C. (1993a). Delay versus helpseeking for breast cancersymptoms: A critical review of the literature on patient and providerdelay. Social Science & Medicine, 36(12), 1521 - 1534.
Facione, N. C. (1993b). The Triandis model for the study of health and illnessbehavior: A social behavior theory with sensitivity to diversity.Advances in Nursing Science, 15(3), 49 - 58.
Farley, T. A. & Flannery, J. T. (1987) Late stage diagnosis of breast cancer inwomen of lower socioeconomic status: Public health implications.American Journal of Public Health, 79, 1508 - 1512.
Feldman, J. G., Saunders, M., et al. (1983). The effects of patient delay andsymptoms to treatment failure in patients with breast cancer. Cancer,51, 1226 - 1229.
Ferketich, S., Phillips, L., & Verran, J. (1993). Development and administrationof a survey instrument for cross cultural research. Research in Nursing& Health, 16, 227 - 230.

173
Fishbein, M. H. (1980). A Theory of Reasoned Action: Some applications andimplications. In H. E. Howe (Ed.), Beliefs, Attitudes, and Values:Nebraska Symposium on Motivation 1979 (pp. 65 - 116). Lincoln, NB:University of Nebraska Press.
Fishbein, M. & Stasson, M. (1990). The role of desires, self-predictions, andperceived control in the prediction of training session attendance.Journal of Applied Psychology, 2003), 173 - 198.
Fisher, E. R., Redmond, C., & Fisher, B. (1977). A perspective concerning therelation of duration of symptoms to treatment failure in patients withbreast cancer. Cancer, 40, 3160 - 3167.
Folkman, S. & Lazarus, R. S. (1988). The relationship between coping andemotion: Implications for theory and research. Social Science &Medicine, 26(3), 309 - 317.
Fox, S. A. & Stein, J. A. (1991) The effect of physician-patient communicationon mammography utilization by different ethnic groups. Medical Care,29(11), 1065 - 1082.
Frank-Stromborg, M. (1986). The role of the nurse in early detection ofcancer. Population sixty-six years of age and older. Oncology NursingForum, 13(3), 66 - 74.
Freeman, H. (1991). Race, poverty and cancer. Journal of the NationalCancer Institute, 83(8), 526 - 527.
Freeman, H. P. & Was■ ie, T. J. (1989). Cancer of the breast in poor blackwomen. Cancer, 63(12), 2562 - 2569.
Funch, D. P. (1984). The role of patient delay in the evaluation of breastself-examination. Journal of Psychosocial Oncology, 2, 31 - 39.
Funkhouser, S. W. & Moser, D. K. (1990). Is health care racist? Advances inNursing Science, 12(2), 47-55.
Gallup, G. (1984). Religion in America, Princeton, NJ: Princeton ReligionResearch Center.
-
Godin, G. (1987). Importance of the emotional aspect of attitude to predictintention. Psychology Reports, 61, 719 - 723.
174
Goodwin, J. S., Samet, J. M., Key, C. R., Humble, C., Kutvirt, D., & Hunt, C.(1986). Stage at diagnosis of cancer varies with the age of the patient.
Journal of the American Geriatric Society, 34, 20 - 26.
Gould-Martin, K. Paganini-Hill, A., Mack, T., & Ross, R. K. (1982). Behavioraland biological determinants of surgical stage of breast cancer.Preventive Medicine, 11, 429 - 440.
Green, L. W. & Roberts, B. J. (1974). The research literature on why womendelay in seeking medical care for breast symptoms. Health EducationMonographs, 2, 129 - 177.
Green, N (1991). Stress, Self-Esteem and Racism as Factors Associated withLow Birth Weight and Pre-term Delivery in African American Women.(Unpublished Doctoral Dissertation. University of California, SanFrancisco.
Greenfield, S., Blanco, D. M., Elashoff, R. M. & Ganz, P. A. (1987). Patterns ofCare related to age of breast cancer patients. Journal of the AmericanMedical Association, 20, 2766 - 2770.
Grey, G. E., Henderson, B. E., & Pike, M. C. (1980). Changing ratio of breastcancer incidence rates with age of black females compared with whitefemales in the United States. Journal of the National Cancer Institute,64, 461 - 463.
Guralnik, J. M. LaCroix, A. Z., Everett, D. F., & Kovar, M. G. (1989). Aging inthe Eighties. The Prevalence of Comorbidity and its Association withDisability. Hyattsville, MD; National Center for Health Statistics,Advance Data from vital and health statistics: No. 170.
Hackett, T. P. Cassem, N. H., & Raker, J. W. Patient delay in cancer. (1973).New England Journal of Medicine, 289, 14 - 20.
Harms, C. R., Plaut, J. A., & Oughterson, A. W. (1943). Delay in the treatmentof Cancer. Journal of the American Medical Association, 121, 335 - 338.
Harrell, S. B. (1992). The meaning of prenatal care to African Americanwomen. Paper presented at the Sixth Annual Black NursesSymposium. University of California, San Francisco, February, 1992.
Harrington, C. & Estes, C. L. (1994). Health Policy and Nursing, (pp. 349 -383). Boston: Jones & Bartlett.
175
Haynes, M. A. (1991). Making cancer prevention effective for African -Americans. Statistical Bulletin, 72(2), 18 - 22.
Henderson, J. G. (1966). Denial and repression as factors in the delay ofpatients with cancer presenting themselves to a physician. Annals ofthe New York Academy of Science, 125, 856 - 864.
Henderson, D. J., Sampselle, C., Mayes, F., & Oakley, D. (1992), TowardCulturally sensitive research in a multicultural society. Health Care forWomen International, 13, 339 - 350.
Hendricks, S.J., Freeman, R., & Sheiham, A. (1989). Why inner city motherstake their children for routine medical and dental examinations.
Community Dental Health, 7, 33 - 41.
Hongvivitana, T. (1984). Data analysis: Social science perspective. EvaluatingPreventive Health Care in South-East Asia (pp. 139-150). South-eastAsia Regional Office Technical Publication No. 4. New Delhi: WorldHealth Organization.
Hubay, C. A., Arafah, B., Gordon, N. H., Guyton, S. P., & Crowe, J. P. (1984).Hormone receptors: An update and application. Surgical Clinics ofNorth America, 64, 1155 - 1172.
Huguley, C. M. & Brown, R. L. (1981). The value of breast self examination.Cancer, 47, 989 - 995.
Huguley, C. M., Brown, R. L., Greenberg, R. S., & Clark, W. S. (1988). Breastself-examination and survival from breast cancer. Cancer, 62, 1389 -1396.
Hunter, C. P., Redmond, C. K., Chen, V. W., Austin, D. F., Greenberg, R. S.Correa, P., Muss, H. B., Forman, M. R., Wesley, M. N., Blacklow, R. S.,Kurman, R. J., Dignam, J. J., Edwards, B. K., Shapiro, S. (1993).Breast cancer: Factors associated with stage at diagnosis in Black andWhite women. Journal of the National Cancer Institute, 85(14), 1129 -1137.
Jaynes, G. D. & Williams, R. M. (1988). A Common Destiny: Blacks andAmerican Society, (p.394). Report from the Committee on the Statusof Black Americans. Washington, DC: National Academy of Sciences.
Jemmott, L. S. & Jemmott, J. B. (1991). Applying the Theory of ReasonedAction to Aids Risk Behavior: Condom use among black women.Nursing Research, 40(4), 228 - 234.

176
Jepson, C., Kessler, L. G., Portnoy, B., & Gibbs, T. (1991). Black and Whitedifferences in cancer presentation, knowledge and behavior. AmericanJournal of Public Health, 81(4), 501 - 504.
Katz, S.J., Hislip, G., Thomas, D. B., & Larson, E. B. (1993). Delay fromsymptom to diagnosis and treatment of breast cancer in WashingtonState and British Columbia. Medical Care, 31(3), 264 - 268.
Kauffman, J. H. (1979). Social correlates of spiritual maturity among NorthAmerican Mennonites. In D. O.Mobe (Ed.), Spiritual Well-being:Sociological Perspectives (pp. 237 - 254). Washington, DC: UniversityPress of America.
Keinan, G., Carmil, D., & Rieck, M. (1991). Predicting women's delay inseeking medical care after discovery of a lump in the breast: The roleof personality and behavior patterns. Behavioral Medicine, 17(4),177 - 183.
King, R. A. & Leach, J. E. (1951). Habits of medical care. Cancer, 4,221 - 225.
Krantz, D. S., Baum, A., & Wideman, M. (1980). Assessment of processes forself treatment and information in health care. Journal of Personalityand Social Psychology, 39(15), 977 - 990.
Krieger, N. (1990). Social class and the black/white crossover in theage-specific incidence of breast cancer. A study linking census-deriveddata to population-based registry records. American Journal ofEpidemiology, 131(5), 804 - 814.
Lauver, D. (1992). Psychosocial variables, race, and intention to seek care forbreast cancer symptoms. Nursing Research, 41(4), 236 - 241.
Lauver, D. & Angerame, M. (1993). Women's expectations about seeking carefor breast cancer symptoms. Oncology Nursing Forum, 2003),519 - 525.
Lauver, D. & Chang, A. (1991). Testing theoretical explanations of intentionsto seek care for a breast cancer symptom. J of Applied SocialPsychology, 21(17), 1440 - 1458.
Leffall, L. D. (1981). Breast cancer in black women. CA, 31, 208 - 211.

177
Leis, H. P., Greene, F. L., Cammarata, A., & Hilfer, S. E. (1988). Nippledischarge: Surgical significance. Southern Medical Journal, 81(1),20 - 26.
Lerner, M. (1988). Access to the American health care system: Consequencesfor cancer control. CA, 39, 289 - 295.
Leventhal, E. A. & Prohaska, T. (1986). Age, symptom interpretation, andhealth behavior. Journal of the American Geriatric Society, 34, 185-191.
Lewin, K. (1935). A Dynamic Theory of Personality: Selected Papers.Translated by D. K. Adams & K. E. Zener. New York: McGraw Hill.
Lewis, O. (1966). The culture of poverty. Scientific American, 215(4), 19 - 25.
Lierman, L. M. (1988). Discovery of breast changes. Cancer Nursing, 11(6),352 - 361.
Lierman, L. M., Kaspryzk, D., & Benoliel, J. Q. (1991). Understandingadherence to breast self-examination in older women. Western Journal
of Nursing Research, 13(1), 46 - 66.
Lipson, J. G. & Meleis, A. l. (1983). Issues in health care of Middle Easternpatients. Western Journal of Medicine, 139(6), 854 - 861.
Liska, A. E. (1984). A critical examination of the causal structure of theFishbein/Ajzen attitude-behavior model. Social Science Quarterly,47(1), 61 - 74.
Lorde, A. (1990). Living with cancer. In, E. C. White, (Ed.). The BlackWomen's Health Book, (pp. 27- 37). Seattle, WA: Seal Press.
MacArthur, C. & Smith, A. (1981). Delay in breast cancer and the nature ofpresenting symptoms. The Lancet, I(8220), 601 - 603.
MacFarlane, E. M. & Sony, S. D. (1992). Women, breast lump discovery, andassociated stress. Health Care for Women International, 13, 23 - 32.
Machiavelli, M., Leone, B., Romero, A., Perez, J., Vallejo, C., Bianco, A.,Rodriguez, R., Estevez, R., Chacon, R., Dansky, C., Alvarez, L., Xynos,F., & Rabinovich, M. (1989). Relation between delay and survival in 596patients with breast cancer. Oncology, 46(2), 78 - 82.

178
Magarey, C. J., Todd, P. B., & Blizard, P. J. (1977). Psycho-social factorsinfluencing delay and breast self-examination in women with symptomsof breast cancer. Social Science and Medicine, 11, 229 - 232.
Mandelblatt, J., Andrews, H., Kerner, J., Zauber, A., & Burnett, W. (1991).Determinants of late stage diagnosis of breast and cervical cancer: Theimpact of age, race, Social class, and hospital type. American Journalof Public Health, 81(5), 646 – 649.
Marshall, J. R., Gregorio, D. I., & Walsh, D. (1982). Sex differences in illnessbehavior. Care seeking among cancer patients. Journal of Health andSocial Behavior, 23, 197 - 204.
Marshall, J. R. & Funch, D. P. (1986). Gender and illness behavior amongcolorectal cancer patients. Women and Health, 11, 67 - 82.
McCall, N., Rice, T., Boismier, J., & West, R. (1991). Private health insuranceand medical care utilization: Evidence from the Medicare population.Inquiry, 28(3), 276-287.
McCarty, D. (1981). Changing contraceptive usage intentions: A test of theFishbein Model of Intention. Journal of Applied Psychology, 11(3),192 - 211.
McCoy, C. B., Nielson, B. B., Chitwood, D. D., Zavertnik, J. J., & Khoury, E. L.(1991). Increasing the cancer screening of the medically underservedin South Florida. Cancer, 67, 1808 - 1813.
Meleis, A. l. (1991). Between two cultures: Identity, roles, and health. HealthCare of Women International, 12, 365 - 377.
Meleis, A.I., Lipson, J.G., & Paul, S.M.(1992). Ethnicity and health among fiveMiddle Eastern immigrant groups. Nursing Research, 41(2), 98 - 103.
Menon, M., Teh, C. H., & Chua, C. L. (1992). Clinical and Social problems inyoung women with breast carcinoma. Australian and New ZealandJournal of Surgery, 62, 364 - 367.
Merrill, J. M. (1991). Access to high-tech health care. Cancer, 67, 1750 -1752.
Mikulin, T. & Hardcastle, J. D. (1987). Gastric cancer - Delay in diagnosis andits causes. European Journal of Cancer and Clinical Oncology, 23(11),1683 - 1690.
179
Miller, P., Wikoff, R., & Hiatt, A. (1992). Fishbein’s Model of Reasoned Actionand compliance behavior of hypertensive patients. Nursing Research,41(2), 104 - 109.
Millimet, C. R. (1970). Manifest anxiety-defensiveness scale: First factor of theMMP revisited. Psychology Report, 27, 603 - 609.
Miniard, P. W. & Cohen, J. B. (1981). An examination of the Fishbein-Ajzenbehavioral-intentions model's concepts and measures. Journal ofExperimental Social Psychology, 17, 309 - 339.
Montano, D. E. (1986). Predicting and understanding influenza vaccinationbehavior. Medical Care, 24(5), 438 - 453.
Montano, D. E. & Taplin, S. H. (1991). A test of an expanded theory ofreasoned action to predict mammography participation. Social Scienceand Medicine, 32(6), 733 - 741.
Montgomery, A. C. V., McClelland, R. A., Skilton, R. A., & Easton, D. (1985).Risk factors and clinical data related to oestrogen receptor status inwomen presenting with breast cancer. British Journal of Surgery, 72,626 - 628.
Mor, V., Masterson-Allen, S., Goldberg, R., Guadagnoli, E., & Wool, M. S.(1990). Prediagnostic symptom recognition and help-seeking amongcancer patients. Journal of Community Health, 15(4), 253 - 266.
Moritz, D. & Satariano, W. A. (1991). Factors associated with stage of breastcancer at diagnosis in women ages 55-84. Presented at the AnnualMeetings of the Society for Epidemiologic Research. Buffalo, NY.
Moyer, M. E. (1989). Data watch: A revised look at the number of uninsuredAmericans. Health Affaires, 8, 102 - 110.
Mullings, L. (1989). Inequality and African-American health status: Policiesand prospects. In W. van Horne (Ed.), Race: Twentieth CenturyDilemmas - Twenty-first Century Prognoses (pp. 154 - 182). Madison:University of Wisconsin Institute on Race and Ethnicity.
Muscat, J. E. & Huncharek, M. S. (1991). Breast self-examination and extentof disease: A population-based study. Cancer Detection andPrevention, 15(2), 155 - 159.

18O
Mutchler, J. E. & Burr, J. A. (1991). Racial differences in health and healthCare service utilization in later life: The effect of socioeconomic status.
Journal of Health and Social Behavior, 32, 342 - 356.
Nagadowska, M. & Kulakowski, A. (1991). Breast cancer in elderly women:Characteristics of the disease. European Journal of Surgical Oncology,17, 609 - 614.
Natarajan, N., Nemoto, T., Mettlin, C., & Murphy, G. P. (1985). Race-relateddifferences in breast cancer patients. Cancer, 56, 1704 - 1709.
National Cancer Institute. (1986). Cancer Among Blacks and other Minorities:Statistical Profiles. DHHS Pub. No. (NCI) 86-2785. Washington, DC:U. S. Government Printing Office.
National Cancer Institute. (1989). 1987 Annual Cancer Statistics Review1973-1986. NIH Publication no. 89-2789. Bethesda: National CancerInstitute.
National Cancer Institute. (1992). Lifetime probability of breast cancer inAmerican women. Bethesda, MD: Statement from the Office of CancerCommunications. September 25, 1992.
Neave, L. M., Mason, B. H., & Kay, R. G. (1990). Does delay in diagnosis ofbreast cancer affect survival? Breast Cancer Research and Treatment,15(2), 103 - 108.
Neighbors, H. V. (1988). The helpseeking behavior of Black Americans.Journal of the National Medical Association, 80(9), 1009 - 1012.
Nemcek, M. A. (1990). Health beliefs and breast self-examination amongBlack women. Health Values, 14(5), 41 - 52.
Nichols, S., Waters, W. E., Fraser, J. D., Wheeler, M. J., & Ingham, S. K.(1981). Delay in presentation of breast symptoms for consultantinvestigation. Community Medicine, 3, 217 - 225.
Owens, R. G., Duffy, J. E., & Ashcroft, J. J. (1985). Women's responses todetection of breast lumps: A British study. Health Education Journal,44(2), 69-70.
Ownby, H. E., et al. (1985). Racial differences in breast cancer patients.Journal of the National Cancer Institute, 75, 55 - 59.
**
181
Pack, G. T. & Gallo, J. S. (1938). Culpability for delay in treatment of cancer.American Journal of Cancer, 33, 443 - 462.
Pegoraro, R. J., Nirmul, D., Reinach, S. G., Jordaan, J. P., & Joubert, S. M.(1986). Breast cancer prognosis in three different racial groups inrelation to steroid hormone receptor status. Breast Cancer Researchand Treatment, 7, 111 - 118.
Pender, N. J. & Pender, A. R. (1986). Attitudes, subjective norms, andintentions to engage in health behaviors. Nursing Research, 35(1),15 - 18.
Perez-Stable, E. J., Sabogal, F., Otero-Sabogal, R., Hiatt, R. A. & McPhee, S.J. (1992). Misconceptions about cancer among Latinos and Anglos.Journal of the American Medical Association, 268(22), 3219 - 3223.
Popp, S. R. (1988). Health care for the poor. Where has all the money gone?Journal of Nursing Administration, 18, 8 - 11.
Powell-Cope, G. M., Lierman, L. M., Kasprzyk, D., Young, H. M., & Benoliel, J.Q. (1991). The Theory of Reasoned Action in prediction of breast selfexamination: A comparison of two studies. Health Care for WomenInternational, 12, 51 - 61.
Ragland, K. E., Selvin, S., & Merrill, D. W. (1991). Black-white differences instage-specific cancer survival: Analysis of seven selected sites.American Journal Of Epidemiology, 133(7), 672 - 682.
Ray, J. J. (1984). The reliability of short social desirability scales. The Journalof Social Psychology, 123, 133 - 134.
Renneker, M. (1989). Understanding Cancer. Palo Alto, CA: Bull Publishing.
Reynolds, W. M. (1982). Development of reliable and valid short forms of theMarlowe-Crowne Social Desirability Scale. Journal of ClinicalPsychology, 38(1), 119 - 124.
Rice, D. P. (1990). Poverty. In L. E. Irwin, J. Stern, J. Steinfeld, L. Breslow, H.Crothers, & D. Fink (Eds.). Cancer and the Underserved: An Agendafor Change in the 1990's (pp. 63 - 78). Proceedings of the ConferenceNovember 3–4, 1989. Oakland, CA: American Cancer Society.

182
Richardson, J. L., Langholz, B., Bernstein, L., Burciaga, C., Danley, K, &Ross, R. K. (1992). Stage and delay in breast cancer diagnosis byrace, Socioeconomic status, age and year. British Journal of Cancer,65, 922 - 926.
Roberts, B. J. (1956). A study of selected factors and their association withaction for medical care. (Unpublished doctoral dissertation). HarvardUniversity. Cambridge.
Robinson, E., Mohilever, J., Zidan, J., & Sapir, D. (1984). Delay in diagnosisof cancer. Cancer, 54, 1454-1460.
Rosenstock, I. M. (1966). Why people use health services. Milbank MemorialFund Quarterly, 44(Suppl.), 94 - 123.
Rossi, S., Cinini, C., Di Pietro, C., Lombardi, C., Crucitti, A., Bellatone, R., &Crucitti, F. (1990). Diagnostic delay in breast cancer: Correlation withdisease state and prognosis. Tumori, 76, 559-562.
Rowe, J. W. & Bradley, E. C. (1983). The elderly cancer patient:Pathophysiological considerations. In R. Yancik et al. (Eds.),Perspectives on Prevention and Treatment of Cancer in the Elderly.New York: Raven Press.
Samet, J. M., Hunt, W. C., Lerchen, M. L., & Goodwin, J. S. (1988). Delay inseeking care for cancer symptoms: A population-based study of elderlyNew Mexicans. Journal of the National Cancer Institute, 80, 432 - 438.
Samet, J. S., Samet, J. M., Key, C. R., Humble, C., Kutvirt, D., & Hunt, C.(1986). Stage at diagnosis of cancer varies with the age of the patient.Journal of the American Geriatric Society, 34, 20 - 24.
Satariano, W. A. (1992). Comorbidity and functional status in older womenwith breast cancer: Implications for screening, treatment, andprognosis. Journal of Gerontology, 47, Spec. No.: 24 - 31.
Satariano, W. A., Belle, S. H. & Swanson, G. M. (1986). The severity of breastcancer at diagnosis: A comparison of age and extent of disease inBlack and White women. American Journal of Public Health, 76(7),779 - 782.
Satariano, W. A., Ragheb, N. E., Branch, L. G., & Swanson, G. M. (1990).Difficulties in physical functioning reported by middle aged and elderlywomen with breast cancer. A case comparison. Journal ofGerontology, 45(1), M3 - M11.

183
Satariano, W. A., Ragheb, N. E., & Dupuis, M. (1989). Comorbidity in olderwomen with breast cancer: An epidemiologic approach. In R. Yancik &J. Yates (Eds.), Cancer in the Elderly: Approaches to Early Detectionand Treatment (pp. 71 - 101). New York: Springer.
Saunders, L. D. (1989). Differences in the timeliness of diagnosis, breast andCervical cancer, San Francisco 1974-85. American Journal of PublicHealth, 79(1), 69 - 73.
Senie, R. T., Rosen, P. P., Lesser, M. L., & Kinne, D. W. (1981). Breastself-examination and medical examination related to breast cancer
stage. American Journal of Public Health, 71, 583 - 590.
Sheppard, B. H., Hartwick, J., & Warshaw, P.R. (1988). The Theory ofReasoned Action: A meta-analysis of past research withrecommendations for modifications and future research. Journal of
Consumer Research, 15, 325 - 343.
Silverman, D. (1993). Interpreting Qualitative Data, (pp. 115 - 143). London:Sage.
Smith, A. W. (1993). Survey research on African Americans: Methodologicalinnovations. In, J. H. Stanfield & R. M. Dennis (Eds.), Race andEthnicity in Research Methods, (pp. 217 - 229). Newbury Park, CA:Sage.
Snow, L. F. (1983). Traditional health beliefs and practices among lower classBlack Americans. Western Journal of Medicine, 139, 820 - 828.
Spector, R. E. (1991). Cultural Diversity in Health and Illness. 3rd ed. Norwalk,CN: Appleton & Lange.
Stack, C. B. (1974). All Our Kin: Strategies for Survival in a Black Community,New York: Harper & Row.
Steele, G. D., Osteem, R. T., Winchester, D. P., Murphey, G. P., & Menck, H.R. (1994). Clinical highlights from the National Cancer Data Base,1994. Ca - A Cancer Journal for Clinicians, 44(2), 71 - 95.
Steiner, C. B. (1991). Access to cancer prevention, detection, and treatment.Cancer, 67, 1736 - 1740.
Stevens, P. E. & Hall, J. M. (1988). Stigma, health beliefs and experienceswith health Care in lesbian women. Image: Journal of Nursing
Scholarship, 2002), 69 - 73.

184
Strayhorn, J. M., Weideman, C. S. & Larson, D. (1990). A measure ofreligiousness and its relation to parent and child mental healthvariables. Journal of Community Psychology, 18, 34 - 43.
Swanson, G. M., Ragheb, N. E., Lin, C., Hankey, B. F., Miller, B., Horn-Ross,P., White, E., Liff, J. M., Harlan, L. C., McWhorter, W. P., Mullan, P. B.,Key, C. R. (1993). Breast cancer among Black and White women in the1980's. Cancer, 72, 788 - 798.
Swanson, G. M., Satariano, E. R., Satariano, W. A., & Treatt, B. A. (1990).Racial differences in the early detection of breast cancer inmetropolitan Detroit, 1978 - 1987. Cancer, 66, 1297 - 1301.
Theorell, T. (1991). Psychosocial cardiovascular risks--On the double loads inwomen. Psychotherapy and Psychosomatics, 55, 81 - 89.
Thomas, D. N. (1981). Black American patient care. In G. Henderson & M.Primeaux (Eds.), Transcultural Health Care (pp. 209 - 223). Menlo Park,CA: Addison Wesley.
Thompson JL. (1991). Exploring gender and culture with Khmer refugeewomen: Reflections on participatory feminist research. Advances inNursing Science, 13(3), 30 - 48.
Timko, C. (1984). Seeking medical care for breast cancer symptoms:Predicting intentions to engage in prompt or delay behavior.(Unpublished doctoral dissertation, University of Massachusetts,Amherst.
Timko, C. (1987). Seeking medical care for a breast cancer symptom:Determinants of intentions to engage in prompt or delay behavior.Health Psychology, 6(4), 305 - 328.
Triandis, H. C. (1977). Interpersonal Behavior (pp. 1 - 37, 64 - 93, 194 - 234,277 - 311). Monterey, CA: Brooks/Cole Publishing.
Triandis, H. C. (1980). Values, attitudes, and interpersonal behavior. In H. E.Howe (Ed.), Beliefs, Attitudes, and Values: Nebraska Symposium onMotivation, 1979, (pp. 195 - 259). Lincoln, Nebraska: University ofNebraska Press.
Triandis HC. (1972). The Analysis of Subjective Culture. New York, NY: Wiley.
Triandis HC. (1976). Variations in Black and White Perceptions of the SocialEnvironment. Champaign, IL: University of Illinois.
185
Valanis, B., Wirman, J, & Hertzberg, V. S. (1987). Social and biological factorsin relation to survival among black vs. white women with breast cancer.Breast Cancer Research and Treatment, 9, 135 - 144.
Valois P, Desharnais R, Godin G. (1988). A comparison of the Fishbein andAjzen and the Triandis attitudinal models for the prediction of exerciseintention and behavior. Journal of Behavioral Medicine, 11(5),459 - 472.
Vernon, S. W., Tilley, B. C., Neale, A. V., & Steinfeldt, L. (1985). Ethnicity,survival, and delay in seeking treatment for symptoms of breastcancer. Cancer, 55, 1563 - 1571.
Walker, L. O. & Best, M. A. (1991). Well being of mothers with infant children:A preliminary comparison of employed women and homemakers.Women and Health, 17(1), 71 - 89.
Wallston, B. S. & Wallston, K. A. (1984). Social psychological models ofhealth behavior: An examination and integration. In A. Baum, S. E.Taylor, & J. E. Singer (Eds.), Handbook of Psychology and Health:Vol.4. Hillsdale, NJ: Lawrence Erlbaum.
-
Wallston, K.A., Wallston, B. S., & DeVellis, R. (1978). Development of themultidimensional Health Locus of Control (MHLC) scales. HealthEducation Monographs, 6, 161 - 170.
Warshaw, P. R. & Davis, F. D. (1985). Disentangling behavioral intention andbehavioral expectation. Journal of Experimental Social Psychology, 21,213 - 228.
Watson, M., Greer, S., Blake, S., & Shrapnell, K. (1984). Reaction to adiagnosis of breast cancer: Relationship between denial, delay andrates of psychological morbidity. Cancer, 53, 2008 - 2012.
Wilkinson, G. S., Edgerton, F., Wallace, H. J., Reese, P., Patterson, J., &Priori, R. (1979). Delay, stage of disease and survival from breastcancer. Journal of Chronic Disease, 32, 365 - 373.
Wool, M. (1986). Extreme denial in breast cancer patients and capacity forobject relations. Psychotherapy and Psychosomatics, 46, 196 - 204.
Woods, N. F. (1985). Employment, family roles and mental ill health in youngmarried women. Nursing Research, 34, 4 - 10.

186
Worden, J. W. & Weisman, A. D. (1975). Psychosocial components of lagtimein Cancer diagnosis. Journal of Psychosomatic Research, 19, 69 - 79.
Yancik, R., Ries, L. G., & Yates, J. W. (1989). Breast cancer in aging women.A population-based study of contrasts in stage, surgery, and survival.Cancer, 63(5), 976 - 981.
Zilling, T. L., Walther, B. S., & Ahren. B. (1990). Delay in diagnosing of gastriccancer. A prospective study evaluating doctors' and patients' delayand its influence on five year survival. Anticancer Research, 10(2A),411 - 416.

187
Appendix A:
Table A - 1
Meta-Analysis of Studies of Delayed Helpseeking for Self-Discovered BreastCancer Symptoms
Author & Year Sample % of Women Delaying ºReference Published (N) 3 Months or More (N)
Dennis, Gardner, 1975 237 48.0 (114)& Lim
(USA)Wilkinson, et.al. 1979 1784 31.9 (569)
(USA)Adam, et.al. 1980 162 9.9 (16)
(Great Britain)-
Nichols, et.al. 1981 72 40.0 (29)(Great Britain)
- -
MacArthur 1981 145 31.0 (45)& Smith
(Great Britain)Huguley & Brown 1981 2092 20.5 (429)
º
(USA) -Vernon, et:al. 1985 3061 44.0 (1347)
º
(USA)Samet, et.al. 1988 189 , 24.6 (46)
(USA)Freeman 1989 193 56.0 (108)
-
& Wasfie y
(USA)Mor, et.al. 1990 298 32.0 (95)
(USA)-
Rossi, et.al. 1990 189 35.5 (67)(ITALY)
Menon, Teh, & 1992 359 39.0 (140)Chua (Singapore)
Katz, et. al. 1993 296 16.6 (49)(USA)Total Sample N = 9077 Total Delaying 3 Months = 3054
Note. Overall Relative Frequency of 3 Months Delay = 33.6%

Table A - 2
Demographic Descriptors of the Survey Sample (N=352)
Age in Years18–2526-30
31-3536-4041–45
46–50
51-5556–60
61-6565+
Missing
■ l48
42
64
54
35
29
2223134
18
Employment Status nNow EmployedUsually but not
now employedUsually NOT
employedMissing
171
79
8418
Household income n$9,999 or below10,000 to 19,99920,000 to 29,99930,000 to 39,99940,000 to 49,99950,000 or aboveMissing
Cumulative Freq.4890
154
208243272
294318
330
334
352
7%13.6411.93
18.1815.34
9.94
8.24
6.256.53
3.69
1.15
5.11
Cumulative Frequency171
250
334352
Cumulative Frequency
%48.58
22.44
23.865.12
%31.8214.49
13.35
9.665.68
15.91
9.09
Partnered Status
MarriedWidowed
Not partneredSingle/partneredMissing
11251
47
34
2O
56
32
■ l121
17
12079
15
112163
210
244
26432O
352
Cumulative Frequency121
138258337
352
%34.38
4.8234.0922.45
4.26
Cumulative 9%13.6425.57
43.7559.0969.0377.27
83.5290.3493.75
94.89
100.00
Cumulative 9%48.58
71.02
94.89
100.00
Cumulative 9%31.8246.31
59.66
69.3275.OO
90.91
100.00
Cumulative 9%34.38
39.2073.3095.74
100.00

189
Table A-3
|HELP Measure: (Kuder Richardson - 20 = 83)
Instructions: Here is a list of some of the things that a woman might do if shefound a problem in her breast: Circle YES or No to show what you might do:
% True 9%. False Missing1. 34.7 62.5 2.8 Try not to think about it.2. 86.7 10.8 2.5 Get the breast checked immediately by a
doctor.”
3. 9.1 88.4 2.5 Just ignore it.4. 24.7 71.9 3.4 Wait and pray about it.5. 19.3 76.4 4.3 Wait to see if the problem got worse,
then get it checked.6. 86.4 11.6 2.0 If I found a breast lump I think I would
go right in to the doctor.”7. 10.5 86.6 2.8 I'd probably do nothing about a breast
change because you have to die ofsomething.
8. 20.2 76.4 3.4 If I could avoid it, I would not go to thedoctor.
9. 82.1 15.1 2.8 I would be on the phone to the doctor rightaway.”
10. 8.2 88.9 2.8 If I had a problem with my breast I wouldjust refuse to deal with it.
11. 75.0 22.4 2.6 I cannot imagine myself doing anything butcalling the doctor immediately.”
12. 25.6 71.9 2.5 would just hope the breast problem wouldgo away.
13. 18.2 81.5 0.3 If I had a change in my breast, I wouldprobably wait to see if things got worsebefore I had my breast examined by adoctor.
14. All things considered, when I think about whether I would have my breastchange checked by a doctor.17.1% I am not sure that I would have it checked immediately.”78.4% I am very sure that I would have my breast checked
immediately.4.5% (Missing data)
Note: * Indicates reverse coding.
S.
-
º
o

190
Table A - 4
|HELP Measure: Factor Analysis of Items Measuring the Intention to Helpseekin the Event of a Breast Symptom Discovery: Oblique Rotation
EigenValue Percent Cumulative Percent of Variance
Factors: 4.482 32.0 32.01.730 12.4 44.4
1.096 7.8 52.2
Item Number. Factor 1 Factor 2 Factor 3
17 O.791 O.OO4 -0. 10614 O.761 O.088 -0.25516 O.721 -0.063 O.194
10 O.661 -0.054 O. 196
5 O.509 0.359 O.OO71 0.404 0.139 0.234
3 -O.O7O O.745 –0.089
9 0.243 0.669 –0.024
8 -0.012 0.629 0.034
7 0.084 O,535 O. 122
15 -0. 102 0.496 0.35813 –0.073 0.102 O.788
11 –0.028 O.O67 O.776
12 0.319 –0.040 0.610

191
Table A - 5
Factor Analysis of the ACCESS Scale
Factors:
Eigenvalue Percentage Cumulative Percent of Variance
Varimax rotated factor loadings
Items:
FA5FA10FAQFA6FA2FA3FA8B4FA1B3FA7B1
FA4
3.722 28.6 28.61.384 10.6 39.3
1.230 9.5 48.7
Factor 1 Factor 2 Factor 3 Sub-Scale KR-20
O.804 O. 113 0.001
O.739 0.081 -0.026 PROV .65
0.576 O. 156 O.251 (Factor 1)O.477 O.199 O.212
O. 121 O.776 O. 122 COST .70
–0.076 O.737 0.244 (Factor 2)O.219 O.655 O.348
O. 187 0.605 -O.O95 CONV .61
O. 138 -0.004 O.725 (Factor 3)–0.076 O. 115 O.645O.265 O. 193 O.634
O.264 0.239 O.546
O.291 0.010 O.287

Table A - 6
Reported Behavior in Relation to a Current Worrisome Breast Symptom.
Behavior True
n(%)
The change is a lump: 34 (27.9)Have had prior breast changes: 31 (25.4)Has been examined by a Dr/Ns: 62 (50.8)Had had a biopsy: 21 (17.2)Concerned it might be cancer: 33 (27.0)Discussed breast change
with a friend or relative: 31 (25.4)
False
n(%)
73 (59.8)77 (63.1)50 (41.0)82 (67.2)75 (61.5)
72 (59.0)
Missingn(%)
15 (12.3)14 (11.5)10 (8.2)19 (15.6)14 (11.5)
19 (15.6)
s

193
Appendix B - 1:
Letter of Invitation to Participate in Focus Group Session
Date:
Ms.
| and my colleague, Professor Marylin Dodd, PhD, are nurse researchers atthe University of California, San Francisco. The American Cancer Society andthe National Institute of Health have both provided funding to help support astudy we are beginning. The study will increase understanding of howwomen decide to have breast examinations and what they think about breastcancer. Our study is dedicated especially to African American womenbecause of the need for today's health care research to clearly and correctlypresent the perspectives of both women and persons of color. The womenwho will be asked to participate in this particular study will be communitywomen like yourself, not breast cancer patients.
Barbara Galloway-Lee,MSW, a friend and colleague from the San Mateo Unitof the American Cancer Society, suggested that we contact you as a womanwho might be interested in participating in one of several discussion groupswe will be holding as a first phase of the study. Each discussion groupwould be small, only three or four women and a discussion leader. Themeeting would be arranged near your home at a convenient time. Yourparticipation would be strictly voluntary, and carries no obligation forcontinued involvement in the study.
Because this research is about humans, women humans in particular, aconsent form explaining your participation is also included to inform youcompletely and help you decide if you would like to participate in this firstphase of the study. I would welcome hearing from you at (415) 697-0144,and we will set up a convenient time for a group meeting.
Most sincerely,
Noreen FacionePhD Candidate
Department of Physiological NursingUniversity of California, San Francisco
º

194
Appendix B - 2: Focus Group Narrative Introduction
I'd like to introduce myself to all of you. My name is Noreen Facione,and I am a nurse researcher from the University of California, San Francisco.As I hope you all know from the copy of the consent form I mailed with yourinvitation letter, this focus group meeting is part of the first phase of aresearch project about how women decide to go to have a breastexamination. And the women who will participate in the second phase of thestudy will all be African American women. I'm sure you know that breastcancer is becoming more common in all groups of women. Because of thisincreasing threat we have chosen to study this very critical problem inwomen's health. I guess I could have chosen to work on a common malehealth problem, but ... this is another example of the year of the woman.
You may be wondering why a white woman would be involved in astudy about black women, so let me explain my interest. Black women haveless chance of getting breast cancer than white women, but when they getbreast cancer, they have a lower chance of survival than any other racialgroup. That is the reason why this study begins by focusing on AfricanAmericans. Future studies will take what we learn from this study and extendit to other groups of women.
I have a second reason for being particularly interested in the health ofAfrican Americans. My family has four African American members. I havebeen concerned for a long time that fewer research dollars have been spenton African Americans. So I'm especially glad to be involved in this study.
Our purpose tonight is to make sure that when the second phase ofthe study gets done, it asks all the right questions so that the women in thestudy get to tell their real story. The study will be a questionnaire. Throughour discussion tonight I hope to learn what questions need to be in thatquestionnaire.
We are going to be on a first name basis. I've made name cards forthose of us who are meeting for the first time. I will be tape recording ourdiscussion. This is necessary because I want to be sure to benefit fromeverything all of you have to say. After the session all names will be removedfrom the tape to be sure to protect your privacy. I will also be taking somenotes because I can't rely on the tape alone, in case it malfunctions. Butplease try not to speak at the same time as someone else because the tapewill not be able to record your comments, and we don't want to lose any ofyour valuable ideas.
Are there any questions? This is strictly voluntary, so if there are noquestions and everyone wishes to continue please sign a copy of the consentform. If you would like to know more about how the study progresses, leaveme a note on this short survey I am giving to each of you to fill out. Therestrooms are around to the left. If you have to leave for some reason, justgo ahead and leave quietly, so there is no interruption in the discussion. Letme say thanks in advance for participating.

195
Appendix B - 3:
Questions Guiding Focus Group Sessions(Ask questions in whatever order seems best for flow of discussion)
-
1. I'd like us to start this discussion by taking a moment for eachof us to remember back to some time in our adult lives when
we've been sick. Using that memory, I'd like us to talk a littleabout what it is like to deal with being sick. What kind of thingsdo we do? How do we decide whether we need to see a doctoror nurse?
2. Now another little exercise. I'd like to have you imagine for amoment that you have just discovered a change in your breastthat worries you. To make this more real, maybe we could allmentally put ourselves in the place where we sometimes checkour breasts. What I'd like us to talk about now are the feelingsthat we would have all around that kind of a discovery? Ifyou've had a real experience with a breast change in the pastyou can use that experience to get in touch with what your realfeelings were, but there's no reason you have to share any pastexperiences.
3. We've talked about the feelings we'd have about finding abreast change. Now let's talk about what we think we might do
-
if we discovered such a change.
4. Take time out to discuss breast changes, if this issue arises.
5. What kinds of reasons might a woman have for waiting awhilebefore having the breast checked by a nurse or doctor?
6. What kinds of reasons might a woman have for having thebreast checked by a nurse or doctor right away?
7. How would the opinions of others affect your decision on what*
to do if you discovered a change in your breast that worried-
you?
8. ls there anything (else) about being a wife or a mother or alover, for instance, that would influence your decision aboutwhether to get the breast change checked?
9. Would the cost be a factor in your decision about whether tohave your breast checked?

196
Appendix B - 4: CHR Approved Consent Form for Focus Group Participation
SEEKING EXAMINATIONS FOR BREAST SYMPTOMSUNIVERSITY OF CALIFORNIA, SAN FRANCISCO
CONSENT TO BE A RESEARCH PARTICIPANTIN A FOCUS GROUP SESSION
Purpose of the Study: Marylin Dodd, RN, PhD and Noreen Facione, RN,MSN at the University of California, San Francisco School of Nursing havedeveloped this study to learn about how women decide when to get a breastexamination and what difficulties they might have obtaining that examination.They want to use this information to write a survey questionnaire of women'sthoughts, opinions, and feelings about getting breast examinations and aboutbreast CanCer.
Procedures: If I agree to participate in this study, the following will happen:I will participate in a discussion with three to four other women. In thediscussion I and the other women will discuss our thoughts, opinions andfeelings about health care check-ups, breast examinations, the difficultiesassociated with getting health care examinations, our feelings about breastcancer, and any other related issues that women in the group think should beincluded in the discussion. Participation in the first discussion meeting willtake about two hours. A discussion leader will guide the discussion byasking general questions, so I will not have to do any work to lead thediscussion. I understand that I don't have to talk at all if I decide I don't want
to. I will not be required to respond to any particular question, and if I wishto stop participating in the discussion I can leave at any time.
After the discussion ideas are used to write the questionnaire I will be askedwhat I think about the questionnaire, whether its easy to understand, andwhether it includes all the ideas that were talked about in the discussion
group. I can give my opinions in a second meeting of my discussion groupor I can give them to Ms. Noreen Facione in a telephone conversation. Mycomments will help make sure the questionnaire really asks the questions ourgroup of women thought were important.
Risks: Although none of the discussion questions are intended to make meuncomfortable or embarrassed, since the discussion will be about breastexaminations, it is possible that I might be uncomfortable with some part ofthe discussion.
Benefits: The discussion leader is knowledgeable about breast examinationsand mammography examinations. If I wish, she will provide me withinformation about how to examine my own breasts, guidelines for when
º*


197
should obtain a professional breast examination and information about lowcost mammography examinations, but only if I want her to provide thisinformation.
Alternatives: If I choose not to participate in this study, I can still receiveinformation about breast self examination, guidelines for when I should obtaina professional breast examination and information about where to obtain lowcost mammogram, but only if I desire this information. I would not need toparticipate in any discussion groups.
Costs: I will not be charged anything for any part of the discussion meeting.Coffee, tea or refreshments during the discussion group will be paid for bythe nurse researcher. The information or teaching about breast examinationsis free of charge and so are any information booklets I might want.
Reimbursement: There will be a reimbursement of $15.00 for each womanparticipating in this study.
Questions: This study has been explained to me by Ms. Noreen Facione orand my questions have been answered. If I have
other questions about the study, I may call Ms. Noreen Facione at (415) 697O144, or Dr. Marylin Dodd at (415) 476-4320, Monday through Friday, 9:00a.m. to 5:00 p.m. or at
. If for some reason I do not want to call Ms.
Facione or Dr. Dodd, I may contact the Committee on Human Research,which is concerned with the protection of human volunteers in researchprojects. I may reach the committee office between 8:00 a.m. and 5:00 p.m.by calling (415) 476-1814 or by writing the Committee on Human Research,P. O. Box 0616, University of California, San Francisco, CA, 94143.
Consent: I have been given copies of this consent form and the ExperimentalSubjects' Bill of Rights to keep.PARTICIPATION IN RESEARCH IS VOLUNTARY. I have the right to refuse toparticipate in this study or to stop participating in the at any time without anynegative consequences.
If I wish to participate I should sign below:
Date Participant's-
Signature
Participant's Telephone Person Obtaining Consent3-31-93


198
Appendix B - 5: CHR Approved Consent Form for Survey Participation
PARTICIPANT'S CONSENT FORM
§ § §The African American Women's
Breast Health Survey-
§ $ §
The questions in this survey were developed by Marylin Dodd, RN,PhD and Noreen Facione, RN, MSN at the University of California, SanFrancisco School of Nursing with the help and guidance of women in the SanFrancisco Bay Area Black community. The survey asks questions about: 1)how women see themselves in terms of their family roles, religious, beliefsand, health needs, 2) how women decide whether to go to the doctor forgeneral health problems and breast examinations, 3) difficulties women mighthave about going to the doctor, and 4) thoughts and feelings women haveabout breast cancer.
If you decide to participate in this survey, the following will happen:You will be asked to read and answer the questions in the survey
questionnaire. If, for some reason you choose not to answer a particularquestion, you may leave it blank. It will take about 45 minutes to completethe survey questionnaire. Although none of the survey questions areintended to make you uncomfortable or embarrassed, since the survey isabout breast examinations, it is possible that you might be uncomfortablewith some of the questions. After you complete the survey you willimmediately be given $10.00 cash for your time and effort contributed tocomplete the questionnaire. If you wish, you can receive printed informationabout how to examine your own breasts, guidelines for when you shouldobtain a professional breast examination and information about low costmammograms. You will be able to receive this information whether youagreed to participate in this survey or not. There is no cost to you forparticipating in the study or for information about breast health examinations.
You have the right to refuse to participate in this study or to stopparticipating in the at any time without any negative consequences. Toprotect your privacy, this consent form it will be kept in a locked file andnever connected with the answers you write on the survey questionnaire.Your answers will be counted with the answers of the other women who
participate in the survey, and this information will be used to help designbreast health projects that meet the needs of African American women.Please ask any questions you might still have to help you decide whether youwould like to participate by completing the survey questionnaire.

199
Appendix B - 5 (Continued):
You have been given a copy of this consent form and the ExperimentalSubjects' Bill of Rights to keep. If you would like to participate in thisstudy by completing the survey questionnaire please show your consentby signing here:
Date Participant's Signature
Participant's Telephone Person Obtaining Consent8-1-93

2OO
Appendix B - 5 (Continued):
UNIVERSITY OF CALIFORNIA, SAN FRANCISCO
EXPERIMENTAL SUBJECT’S
BILL OF RIGHTS
The rights below are the rights of every person who is asked to be in aresearch study. As an experimental subject I have the following rights:
1) To be told what the study is trying to find out,2) To be told what will happen to me and whether any of the
procedures, drugs, or devices is different from what would beused in standard practice,
3) To be told about the frequent and/or important risks, side effects, ordiscomforts of the things that will happen to me for researchpurposes,
4) To be told if I can expect any benefit from participating, and, if so,what the benefit might be,
5) To be told of the other choices I have and how they may be betteror worse than being in the study,
6) To be allowed to ask any questions concerning the study bothbefore agreeing to be involved and during the course of thestudy,
7) To be told what sort of medical treatment is available if anycomplications arise,
8) To refuse to participate at all, or to change my mind aboutparticipation after the study is started. This decision will notaffect my right to receive the care I would receive if I were not inthe study,
9) To receive a copy of the signed and dated consent form,10) To be free of pressure when considering whether I wish to agree to
be in the study.
If I have other questions: I may call Ms. Noreen Facione at (415) 697-0144,or Dr. Marylin Dodd at (415) 476-4320, Monday through Friday, 9:00 a.m. to5:00 p.m. or at
-
I may also contact the Committee on Human Research, which is concernedwith the protection of human volunteers in research projects. I may reach thecommittee office between 8:00 a.m. and 5:00 p.m. by calling (415) 476-1814or by writing: Committee on Human Research, P. O. Box 0962
University of California, San FranciscoSan Francisco, CA, 94143.
■

201
Appendix B - 6:
Script for Research Assistants to Introduce Survey Study to Leaders ofCommunity Organizations
Ms./Dr./Mr.
I and my colleagues, Noreen Facione, RN, MS, Professor Marylin Dodd, PhD,are researchers at the University of California, San Francisco. The AmericanCancer Society and the National Institute of Health have both providedfunding to help support a study to increase understanding of how womendecide to have breast examinations and what they think about breast cancer.I would like to tell you all about this study and ask you whether we mightinvite women members of your church (or women's group, school, worksetting) to participate in the study. Please feel free to interrupt me to ask anyquestions you wish. Our study is dedicated especially to African Americanwomen. This is because African American women are diagnosed at a laterstage of breast cancer and their survival of breast cancer is poorer than othergroups of women. We have undertaken this study because of the need forthis breast cancer study to clearly and correctly represent the perspectives ofAfrican American women themselves.
In the first part of the study which is already complete, African Americanwomen from the Bay area community collaborated with us to design a surveyquestionnaire. (Show the questionnaire for review). This is the questionnairethat we will use for the second part of the study. We would like to ask thewomen in your church (or women's group, school, work setting) if they wouldlike to participate in the second phase of this study by completing thequestionnaire. First they will receive a consent form (show consent form andexperimental subjects Bill of Rights), and questions they have about the studywill be answered by myself or one of the other members of the study team. Ifa woman chooses to participate she will complete the questionnaire and begiven an immediate $10.00 cash reimbursement for her participation. Womenmay refuse to participate or change their mind at any time. All the women wecontact will be offered printed materials from the American Cancer society,but may refuse those as well. The women we contact will be treated with theutmost courtesy at all times by our study group. If any type of problem arisesor if you would like to withdraw your permission to contact women throughthis organization you may contact Noreen Facione from 9 am to 5 pm at(415) 697-0144 or Marylin Dodd at (415) 476-4320. Or if you wish you maycontact the Committee on Human Research at UCSF (415) 476-1814. (Showwhere these numbers appear on the consent for and provide copy to beretained at the setting).

2O2
Appendix B - 6 Continued:
ls there a possibility that the women in your organization might like to hearabout this study and decide whether they might like to participate?
2.
(if No: Thank the contact person, leave a card with contact information in the-
event there is reconsideration or the need for further information about the-
study.)
(If Yes.) Ask the following questions as appropriate:ls there someone else that organizes meetings of the women in your
church (or women's group, school, work setting) who we should work with tocontact women about the study?
ls there a planned meeting where we could tell women about thestudy?
ls there a newsletter (newsletter ads will appear as the flyer contentbelow)?
May we post information flyers in a location you feel appropriate?
Would you like to be the person who women contact if they want to hearmore about the study, or should it be a member of this study team? (Flyer.attached).
(Record in writing for other team members the exact method of contactauthorized by the organization member.)
Contacts will begin.....(clarify approximate or actual date of planned contactto potential participants). Thank you for facilitating our contacting womenwho might potentially like to participate in this study. Would you like a
º
summary of the study results? (Record Yes or No and name of person to f
whom the summary should be directed.)

…--

203
Appendix B - 7:
Posted Flyer to Advertise the Study
§ UCSF #
African American Women's
Breast Health Survey
A study planned especially to hear the opinions ofAfrican American women regarding their health care andtheir approach to breast health is recruiting adult, AfricanAmerican women participants now! The results of thestudy will be used to design a breast cancer educationand screening program with particular attention to theneeds of African American women. We would like you tobe one of the women who contributes to this study.
The questionnaire for this study was developed withthe help of African American women in your community.If you decide to participate in the study, you will be paidan immediate $10.00 cash for the 30 - 45 minutes it willtake you to fill out the questionnaire. There are no otherobligations.
If you would like to hear more about this study:Contact Noreen Facione at (415) 697-0144. Participationis totally voluntary, and you can change your mind at anytime.
This project is funded in part by the American Cancer Societyand by the National Center for Nursing Research.

204
Appendix C. Survey Questionnaire
$ $ §
The African American Women’s
Breast Health Survey
§ $ $
Begin Here:
If you describe yourself as Black or AfricanAmerican, are a woman who is at least eighteenyears of age, and have read and signed aconsent form to be a participant in this study,please read each of the following questionscarefully, and answer what is most true for youpersonally. There are no right or wronganswers. What's important is how youpersonally think or feel about each question.
Please Continue


205
THERE IS NO NEED TO WRITE YOUR NAME ANYWHERE ON THIS SURVEY.
The following information will help us to understand something about the group ofwomen who took part in this research. Please ignore these small coding numbers. ,
1. I would describe myself as a Black (or an African American) woman.(Circle ONE) TRUE FALSE (D1)
2. My age is years. [D2,
3. I was born in (City), (State, [D34)
(Country). (DS)
4. Circle the highest grade in school completed:Grade School High School College Grad School
1 2 3 4 5 6 7 8 9 10 1 1 12 1 2 3 4 1 2 3 4 [D6,
5. I am currently: (Mark an X)MarriedWidowed
Single, without a partnerSingle, with a partner [Dr.
6 . I am: (Mark an X)Currently employed outside the home.Usually employed outside the home, but not currently.Usually not employed outside the home. (D8,
7. How many adults (including yourself) currently live in your household?
8. How many children currently live in your household? [D10
9. Our household income is: (Mark an X)Less than $9,999 a year.$10,000 to $19,999 a year.$20,000 to $29,999 a year.$30,000 to $39,999 a year.$40,000 to $49,999 a year.$50,000 to $59,999 a year.More than $60,000 a year. (D11)
=10. People in my family ask me for advice about their health.(Circle ONE) TRUE FALSE [D12]
* Please go on to the next page $

2O6
HEALTH OPINIONS: Circle AGREE or DISAGREE to show your opinion. Even ifyou don't completely agree or disagree with a statement, choose the one answer thatComes the closest to what you believe.
~….CircleYour Response.…
Except for serious illness, it's generally better AGREE DISAGREEto take care of your own health than to seek ■ ki,
professional help.
It is better to rely on the judgements of doctors AGREE DISAGREE(who are experts) than to rely on "common sense" ■ k2.
in taking care of your own body.
Clinics and hospitals are good places to go for AGREE DISAGREEhelp since it's best for medical experts to take ■ cº
responsibility for health Care.
Learning how to cure some of your illness without AGREE DISAGREEcontacting a physician is a good idea. (K4]
It's almost always better to seek professional AGREE DISAGREEhelp than to try to treat yourself. ■ º
Learning how to cure some of your illness AGREE DISAGREEwithout contacting a physician may create (K6)
more harm than good.
Recovery is usually quicker under the care AGREE DISAGREEof a doctor or nurse than when patients ■ ky;
take care of themselves.
If it costs the same, I'd rather have a AGREE DISAGREEdoctor or nurse give me treatment than [ke]
to do the same treatment myself.
It is better to rely less on physicians AGREE DISAGREEand more on your own common sense when ■ kg)
it comes to caring for your body.
* Please go on to the next page &

-■ -■ -■ -**·
*■|×·
*
*■ ae■■
·-----**…----…-■■ *■■
■● *-----·*aeºº,i!
2O7
RELIGIOUS PRACTICES: Mark an "X" on the line beside the answer that is mostCorrect for you personally. (Choose One)
How religious would you say you are? not at allnot very much
_ somewhat_ pretty much
very much (R1)
To what extent are you conscious of not at allto a small extent
to a moderate extent
to a large extent
some religious goal or purpose in lifewhich serves to give direction to your life?
to a very large extent [R2)
How often do you study the Bible, or other ■ leVer
religious literature privately? seldomoccasionallyabout once a week
daily [R3]
Other than at mealtime, how often several times per daydo you pray to God privately? daily
occasionallySeldom
neVer [R]
How often do you experience or feel God's neVer
approval for some good act you seldomhave done? occasionally
often
very often ■ R5,
How often do you experience God's ■ leVer
disapproval for some undesirable act you seldomhave done? occasionally
often
very often [R&
* Please go on to the next page &


208
RELIGIOUS PRACTICES (Continued): (Choose One)
On the average, how often have you neVer sattended religious worship services a few times a yearSunday morning and/or other days) Once or twice a month 1.
during the last year? weekly, or almost weekly*
more than Once a week [Rn
s
How large a part of your income do none
you donate per year to a church or areligious organization?
a very small part of my incomea small part of my incomea medium part of my incomea large part of my income [Rel s
... ."
How often do you serve a church or neVe■
other religious organization in Sunday a few times a yearschool teaching, church project Once Or twice a monthleadership, or other responsibilities? weekly or almost weekly
more than once a week tRol
How would you describe the nature no relationshipof your relationship to God? distant relationship
between distant and close º
relationship s
close relationship-
very close relationship [Rio,
When you are tempted to do very oftensomething wrong, how often do you oftenask God for strength to do it right? sometimes º
Seldom
neVer [R11)
When you have decisions to make, in very oftenyour everyday life, how often do you often *
ask yourself what God would want sometimesyou to do, or ask God for help seldomin making the decision? neVer ■ R12)
* Please go on to the next page $

l
l

209
Listed below are a number of statements concerning PERSONAL ATTITUDES. Readeach item, and decide whether the statement is true or false for you personally.(Circle One)
True False It is sometimes hard for me to go on with my workif I am not encouraged. [M1)
True False | sometimes feel resentful when I don't get my way. (M2)
True False On a few occasions, I have given up on doing somethingbecause I thought too little of my ability. (M3)
True False There have been times when I felt like rebelling againstpeople in authority even though I knew they were right. [M4]
True False No matter who I'm talking to, I'm always a good listener.
True False There have been occasions when I took advantage ofSOmeOne. [M6,
True False I am always willing to admit it when I make a mistake.
True False | sometimes try to get even, rather than forgive and forget.
Tru False I am always courteous, even to people who are disagreeable.
True False I have never been annoyed when people expressed ideas verydifferent from my own. [M10
True False There have been times when I was quite jealous of thegood fortune of another. IM11)
True False I am sometimes irritated by people who ask favors of me.
True False I have never deliberately said something that hurt someone'sfeelings. [M13)
* Please go on to the next page &
i


210
These items are statements about your PERSONAL BELIEFS, so there are no rightOr wrong answers. Circle AGREE or DISAGREE to show which answer comes theclosest to what you believe. Please try to answer even if you do not completelyagree or disagree. (Circle One)
Often I feel that no matter what I do, if AGREE DISAGREE [.I'm going to get sick, I will get sick. [c1) -
It seems that my health is greatly influenced AGREE DISAGREE ºby accidental happenings. ■ cal
When I am sick, I just have to let nature AGREE DISAGREErun its course. (C3) -
******------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------ .
If its meant to be, I will stay healthy. AGREE DISAGREE
When I stay healthy, I am just plain lucky. AGREE DISAGREE
Even when I take care of my self, its easy AGREE DISAGREEto get sick. (C6,
{T§ Complete the next 4 questions only if you are currently employed outside the ºhome. If you are not currently employed outside the home, you may go on to the º
next page. (CHECK ONE)-
1. Finding time to go to the doctor would depend on whether I could get off work.
Strongly Agree Agree Disagree Strongly Disagree *
2. When I get sick I always say, "I can't afford to be home sick, so I'm not sick!" *
Strongly Agree Agree Disagree Strongly Disagree-
3. My work would not interfere with a doctor's appointment.
Strongly Agree Agree Disagree Strongly Disagree *
4. I probably wouldn't take time off from work just to get my breasts checked.
Strongly Agree Agree Disagree Strongly Disagree (E4)
$ Please go on to the next page &

211
GETTING TO THE DOCTOR. Draw a circle around TRUE or FALSE to Show which ismost correct for you. (Circle One)
Transportation to the doctor is a TRUE FALSE
big problem for me. IFA1)
I have health insurance or MediCal TRUE FALSEto help pay for my doctor visits. (FA2)
Its often difficult to see a doctor TRUE FALSEwhen I'm able to go. (B1)
| usually don't have to make any special TRUE FALSEarrangements in order to go to the doctor. (B2)
The doctors I need to see are located in TRUE FALSEinconvenient places. (B3)
I don't worry much about the cost when TRUE FALSEI think about going to the doctor. (B4)
I don't go to the doctor because I don't TRUE FALSEhave health insurance. IfA9,
The place where I go to see the doctor is TRUE FALSEalways crowded. (FAA)
| have a doctor | feel comfortable with. TRUE FALSE
| get my health care in a well-equiped facility. TRUE FALSE
The emergency room is the only place I can find TRUE FALSEa doctor when I need One. (FAn
I don't go to the doctor because I don't have TRUE FALSEthe money. (FAB)
I don't receive much personal attention when TRUE FALSE
I go to see the doctor. ".
I know I can do a lot to keep myself TRUE FALSEfrom getting sick. !crl
If it's meant to be, I will stay healthy. TRUE FALSE ICS)
* Please go on to the next page &

212
PERCEPTIONS: Mark an "X" in the space following the word that best tells how youfeel about each of the following statements.
Black women have fewer options for health care than white women.
Strongly Agree Agree Disagree Strongly Disagree [Rn)
I haven't always gotten the kind of courtesies I should have in a white doctor's office.
Strongly Agree Agree Disagree Strongly Disagree (R21
Black women experience negative attitudes when they go to white doctor's offices.
Strongly Agree Agree Disagree_ Strongly Disagree toil
Doctors treat black women and white women the same.
Strongly Agree Agree Disagree_ Strongly Disagree (G2)
Racism is a problem in my life.
Strongly Agree Agree Disagree Strongly Disagree (G3)
Sometimes, in a white doctor's office, if you are black its as if you don't belong there.
Strongly Agree Agree Disagree Strongly Disagree (G4)
Racial discrimination in a doctor's office is common.
Strongly Agree Agree Disagree Strongly Disagree IG5)
In most hospitals, black women and white women get the same kind of care.
Strongly Agree Agree Disagree Strongly Disagree (G6)
Doctors and nurses act the same way to white women and black women.
Strongly Agree Agree Disagree Strongly Disagree IG7,
If a black woman comes to a doctor's office its assumed that she's on welfare.
Strongly Agree Agree Disagree Strongly Disagree (G6
I am not affected by racial discrimination.
Strongly Agree Agree Disagree Strongly Disagree [Go]
Black women can receive the care they want equally as white women.
Strongly Agree Agree Disagree Strongly Disagree (G10)
* Please go on to the next page $

: *-
º
* *- -
a
--- -"
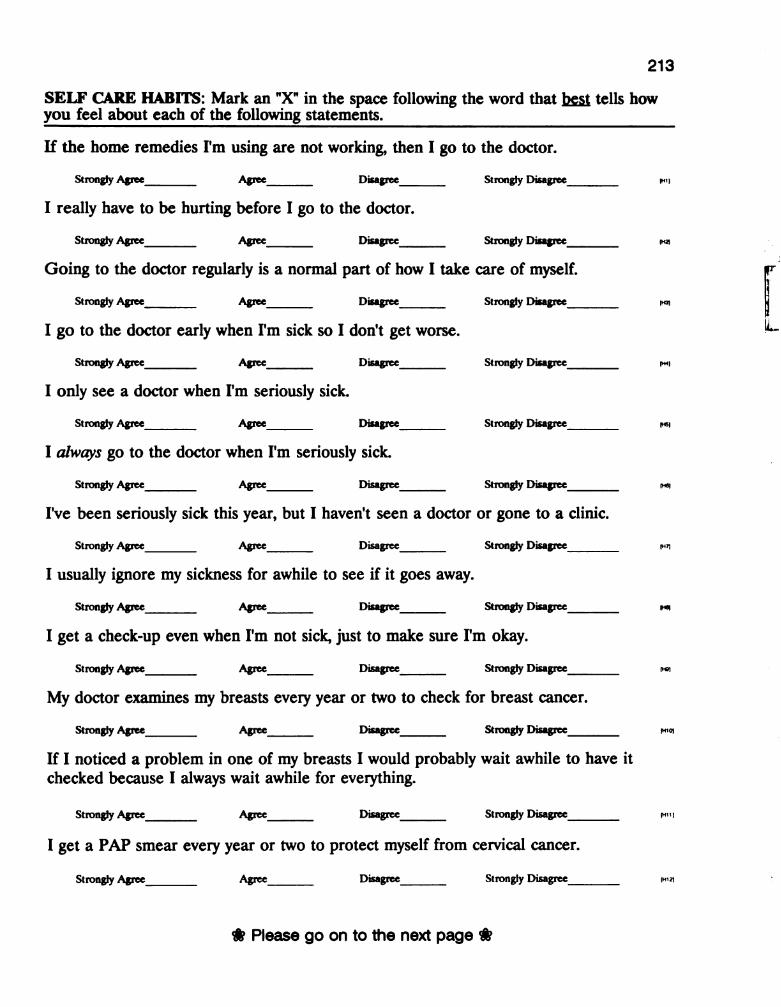
213
SELF CARE HABITS: Mark an "X" in the space following the word that best tells howyou feel about each of the following statements.
If the home remedies I'm using are not working, then I go to the doctor.
Strongly Agree Agree Disagree Strongly Disagree [H1]
I really have to be hurting before I go to the doctor.
Strongly Agree Agree Disagree Strongly Disagree [H2]
Going to the doctor regularly is a normal part of how I take care of myself.
Strongly Agree Agree Disagree Strongly Disagree IH3)
I go to the doctor early when I'm sick so I don't get worse.
Strongly Agree Agree Disagree Strongly Disagree [H4)
I only see a doctor when I'm seriously sick.
Strongly Agree Agree Disagree Strongly Disagree [H5)
I always go to the doctor when I'm seriously sick.
Strongly Agree Agree Disagree Strongly Disagree (H6)
I've been seriously sick this year, but I haven't seen a doctor or gone to a clinic.
Strongly Agree Agree Disagree Strongly Disagree (Hn
I usually ignore my sickness for awhile to see if it goes away.
Strongly Agree Agree Disagree Strongly Disagree [H6)
I get a check-up even when I'm not sick, just to make sure I'm okay.
Strongly Agree Agree Disagree Strongly Disagree ■ ºo)
My doctor examines my breasts every year or two to check for breast cancer.
Strongly Agree Agree Disagree Strongly Disagree [H10)
If I noticed a problem in one of my breasts I would probably wait awhile to have itchecked because I always wait awhile for everything.
Strongly Agree Agree Disagree Strongly Disagree [H11)
I get a PAP smear every year or two to protect myself from cervical cancer.
Strongly Agree Agree Disagree Strongly Disagree [H12]
* Please go on to the next page $
:

--
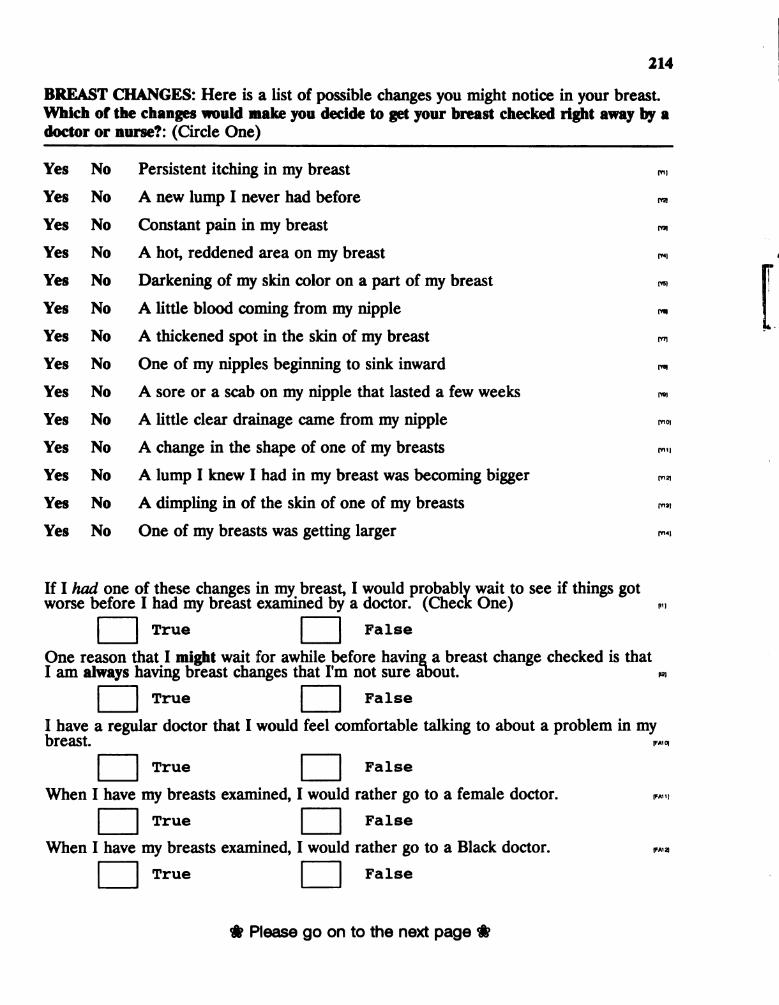
214
BREAST CHANGES: Here is a list of possible changes you might notice in your breast.Which of the changes would make you decide to get your breast checked right away by adoctor or nurse?: (Circle One)
Yes No Persistent itching in my breast tril
Yes No A new lump I never had before trz.
Yes No Constant pain in my breast [Yo!
Yes No A hot, reddened area on my breast [Y4]
Yes No Darkening of my skin color on a part of my breast ■ ys)
Yes No A little blood coming from my nipple [we]
Yes No A thickened spot in the skin of my breast [Yn
Yes No One of my nipples beginning to sink inward Tre
Yes No A sore or a scab on my nipple that lasted a few weeks [Yo!
Yes No A little clear drainage came from my nipple Trio)
Yes No A change in the shape of one of my breasts [Y11,
Yes No A lump I knew I had in my breast was becoming bigger [Y12,
Yes No A dimpling in of the skin of one of my breasts [Y13]
Yes No One of my breasts was getting larger Triº,
If I had one of these changes in my breast, I would Pº wait to see if things gotworse before I had my breast examined by a doctor. (Check One) [1]
True False
One reason that I might wait for awhile before having a breast change checked is thatI am always having breast changes that I'm not sure about. [12]
True False
; have a regular doctor that I would feel comfortable talking to about a problem in myreaSt. [FAtol
True False
When I have my breasts examined, I would rather go to a female doctor. IFA11]
True False
When I have my breasts examined, I would rather go to a Black doctor. FA12,
True False
* Please go on to the next page &
--
ss
*.

215
Imagine for a moment that you have just noticed a problem in one of your breasts.Consider each of the statements below carefully. Mark an "X" to show what you thinkwould happen if you waited awhile rather than have the change in your breast examinedby a doctor.
Definitely : Probably Probably DefinitelyYes i Yes i No i No
I would avoid unpleasant medical procedures.-
(P11
I would be more likely to need major surgery.- [P21
I would avoid undesirable interactions with a physician.- - -
IP3)
The breast problem would go away. [P4)
I would avoid an undesirable diagnosis.- -
(P5)
I would minimize the need for more involved treatment | | | | Pe.
There would be an increased chance of losing my breast.- -
(Pn
I would avoid a major disruption to my life in general.- - -
r
The problem would have time to grow or spread.- - -
; "
I would avoid upsetting my family. : Piq
I would save money.
I might avoid having a surgery.
I would avoid looking like a hypochondriac.---------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------
I would convince myself that it was nothing serious.
Nothing would happen.
* Please go on to the next page $


216
This part of the questionnaire asks you to describe your FEELINGS. Imagine for a momentthat you have just discovered a problem in your breast. Beside each "feeling word" thereis a line between "extremely" and "not at all." Extremely means that you would feel thefeeling very, very strongly. Not at all means that you would not have the feeling at all.
Imagine for a moment that you are bathing and you notice that there is a definite changein one of your breasts. Discovering the change in my breast would make me feel:
(Mark an "X" somewhere on the line to show how you think you would feel.)
Angry: Extremely Not at all [T11
Surprised: Extremely Not at all [72]
Annoyed: Extremely Not at all Ital
Embarrassed: Extremely Not at all IT4)
Ashamed: Extremely Not at all (T5)
Panicky: Extremely Not at all [T6]
Afraid: Extremely Not at all [T]
Shocked: Extremely Not at all [TS
Anxious: Extremely Not at all ITQ)
Worried: Extremely Not at all [T10]
Hopeless: Extremely Not at all ■ till
Sad: Extremely Not at all IT12]
Concerned: Extremely Not at all ■ tial
Depressed: Extremely Not at all [Ti4]
* Please go on to the next page $

------
■

217
How do you think you would FEEL if you discovered a problem in one of your breasts:(Circle One)
TRUE FALSE I would feel mostly angry that this had happened to me. *
I would feel ashamed that I did something to make theTRUE FALSE breast problem happen. ...
TRUE FALSE I would be embarrassed to get the breast problem checked. *
TRUE FALSE I would be so depressed, I would probably do nothing about it. ...
TRUE FALSE I would be more afraid if I didn't go to the doctor. *.
Thinking about any kind of serious illness, especially one like cancer,TRUE FALSE always makes me feel afraid. . . .
TRUE FALSE I would never panic. *
TRUE FALSE I would feel anxious until I found out if it was serious. wn.
I would be happier if I didn't know whether the change in my breastTRUE FALSE was breast cancer. (A8)
TRUE FALSE I'd be afraid because this might mean I have breast cancer. [A2]
TRUE FALSE I'd be afraid because I might need surgery on my breast. [A10.
I would rather live in fear of having missed a breast cancer ratherTRUE FALSE than facing the fear of having a breast removed. (A11)
TRUE FALSE I'd be afraid that this breast problem might threaten my life. A12,
TRUE FALSE I would not be afraid of diagnostic tests or medical treatments. ...
I'd be afraid that I would not be able to take care of all myTRUE FALSE responsibilities if I get ill myself. (A13)
I would be afraid if I didn't go to the doctor immediately it wouldTRUE FALSE get worse. -"
TRUE FALSE I would be afraid I might lose my breast. *
TRUE FALSE I would mostly be afraid of the pain I might experience. --
TRUE FALSE I don't think I would be afraid if I discovered a breast problem. ...
* Please go on to the next page &


218
Do you have any of the health problems listed below?(Mark an X on the line to show that the problem applies to you personally.)
A Blood Pressure Problem Arthritis (Crnº-2,
A Nervous Condition A Diabetes/Sugar Problem (Crnº-4)
A Stomach Problem A Heart Problem ICmé-6,
A GYN/Female Problem A Cancer Problem (Crny-8)
A Lung/Breathing Problem A Bladder Problem ■ cro-tol
Are you pregnant at this time? Yes No (Cm11)
If you are troubled by some other health problem not mentioned and would like to name
it, what is it? (Cºn12.
§ Complete the next group of questions ONLY IF YOU ARE RESPONSIBLE FORTAKING CARE OF CHILDREN CURRENTLY LIVING INSIDE YOUR HOME. If you are notcurrently responsible for children living in your home, you may go on to the next page.
Which is most correct for you personally?(Circle One)
TRUE FALSE
TRUE FALSE
TRUE FALSE
TRUE FALSE
TRUE FALSE
TRUE FALSE
TRUE FALSE
| usually have to take the children with me when I go to the doctor.(FC1)
| usually take the children to the doctor right away when they'resick, but for myself, I usually wait. (Srij
I don't go to the doctor because there is no one to watch thechildren. [Fe2,
The children are not a problem when I have to go to the doctor. ra.
I am usually too busy with my children to go to the doctor or theclinic when I'm sick. [Fowl
Even though I have lots of people to take care of, I would not delayhaving my own breasts checked. [sº]
I would probably wait a while before having my breast examinedbecause I would need to make sure that the people who depend onme were taken care of first. [80]
* Please go on to the next page $


219
Here is a list of some of the things that a woman might do if she found a problem in her
YES
YES
YES
YES
YES
YES
YES
NO Try not to think about it. ■ º
NO Check it periodically myself to make sure it didn't change. ■ º
NO Get the breast checked immediately by a doctor. [6]
NO Try taking medication for it. ■ el
NO Just ignore it. [In
NO Wait and pray about it. [16]
NO Wait to see if the problem got worse, then get it checked. ■ ol
$ if you do not have a spouse or partner at the moment, you can go on to the nextpage. If you do currently have a spouse or partner. (Circle One)
TRUE
TRUE
TRUE
TRUE
TRUE
TRUE
TRUE
FALSE
FALSE
FALSE
FALSE
FALSE
FALSE
FALSE
If I discovered a change in my breast that worried me, myspouse/partner would want me to have my breast checkedimmediately. [Sp1)
My spouse/partner probably wouldn't want me to have my breastchecked. (Spal
I would not share my worry about my breast with myspouse/partner. (spal
I would probably have to put off having my breast checked becauseof my spouse/partner. [Sp4)
What my spouse/partner wanted would not affect what I decided todo about getting my breast checked. [Spé,
I would probably have my breasts examined sooner because of myspouse/partner. [Spé,
I would be afraid of losing my spouse/partner if I had a problem inmy breast. [Spy]
* Please go on to the next page &


220
How would THE PEOPLE IN YOUR LIFE be important if you thought you might have
TRUE
TRUE
TRUE
TRUE
TRUE
TRUE
TRUE
TRUE
TRUE
TRUE
TRUE
TRUE
TRUE
TRUE
TRUE
FALSE
FALSE
FALSE
FALSE
FALSE
FALSE
FALSE
FALSE
FALSE
FALSE
FALSE
FALSE
FALSE
FALSE
FALSE
I would probably talk about the breast change with someone closeto me before I decided whether to have it examined by a doctor.
If I mentioned a problem with my breast to the person closest to me,this person would probably say "Don't hesitate, go have it checked."
I would talk with my girl friends about my breast problem and theywould help me decide what to do.
| listen to the advise of others about whether I need to go to thedoctor.
I would keep the discovery of a breast change to myself untildecided what to do about it.
I have a friend or relative who is a nurse that I would ask about
the breast change to help me decide what to do.
Being female, you take care of your family, you take care of yourspouse or partner, but you're not supposed to worry about takingcare of yourself.
| always tell my mother or sister about changes in my body, and shetells me when I need to see the doctor.
If I found a breast lump I think I would go right in to the doctor.
I'd probably do nothing about a breast change because you haveto die of something.
If I could avoid it, I would not go to the doctor.[12]
I would be on the phone to the doctor right away. (113)
If I had a problem with my breast I would just refuse to deal with it.tº 4,
| cannot imagine myself doing anything but calling the doctorimmediately. [15]
I would just hope the breast problem would go away. ■ ite,
$ Please go on to the next page $
221
What you think is most correct for you? (Circle One)
TRUE
TRUE
TRUE
FALSE
FALSE
FALSE
If anyone is going to get breast cancerit will probably be me. ■ ful
If I had a lump in my breast I'd think"Well, I have to die of something." Fiz.
If I did get breast cancer, there wouldn'tbe much l could do about it. [Fal
Sometimes I think I'm destined to get
* The first person I would tell about a problem in my breast would be:(Check Only One) Husband/Partner
GirlfriendDoctor/NurseSister/MotherOther (What relation is this person
to you?)No One. (G1)
$ All things considered, when I think about whether I would have my breast changechecked by a doctor: (Choose Only One)
I am not sure that I would have it checked immediately.I am very sure that I would have my breast checked immediately.
■ in
$ I have a change in my breast right now that sometimes worries me.
YES NO
(G21
If you answered "YES" to this last question about having a change in your breast right nowthat sometimes worries you, which is most correct for you? (Circle One)
YESYESYESYESYESYES
YES
YES
NO I am worried that this change might be breast cancer. (G3)
NO A doctor or nurse has checked the change in my breast. [Gº]
NO I don't think I'm very likely to get breast cancer. [Gº]
NO The change in my breast is a lump. (G6)
NO I have had a biopsy or a surgery for this breast change. (Gin
NO I have asked a friend or family member what I should do about thechange in my breast. IG-6,
NO I get so many changes in my breasts, this one doesn't worry memuch. [Gº]
NO I can't financially afford to deal with my breast problem now. [Gºto|
* Please go on to the last page &
222
$ if there is something else you would like to say about breast problemsthat we forgot to ask please write us some comments So we caninclude your ideas:
§ $ $
THANK YOU VERY MUCH FOR YOURPARTICIPATION IN THIS PROJECT.
§ $ $
INFORMATION ABOUT BREAST EXAMINATIONSAND MAMMOGRAPHY ARE AVAILABLE WHEN
YOU RETURN THIS SURVEY

-- º--- is - ■
- - - - Cº, ºv. M G in * - \ ... I
º ".- - - - º -- ----- º
- - º - * -- - - º, -- - --
º –– “ - / is ºr 1/2 º' Cº- -"C/º ºv : J ‘. . -- - C. *** * º + - - -
ºvº --, -º-, - -
tº Raº--
º■ º º in . . .-º º/º sº. `
- -
sº tº lº■■ *\º C- -, -, - ■ º ‘. . . . . .
- * ,- - - º º, L | D R A R Y - L º -- sº ---
-
-º, yº
- --> º, * * --- ". In º * M: vº * I - _*-
-º, - - ~~ ■ º º L | º -, 1. "... º
-º - º A
l ---- -- * . -- -> º -- --------- º *** - - *. - --- --■ -
- ºvº º 1, º, º - 2 - tº ■ º. -\ -- ",
º º A Nºv º - W. ºld ** *.-
º - º – 1/ º -- - -- ~ ■ º - ), ■ º ■ º tº -- -- º !- º --- -
- I C º º ºº/ º \- sº ºf ~ º-
* º – - –º - - - - -
* ... º ■ º tº a Lº - - -- ~ ºnfººd º º, Yººn * - ■ º | Q: v \, gº º, ... " " -
-k Of ony - - - -
ºf Y -- - irculotion des * > . . `-- * vºn -- * -- RETURNIo the º lifornio Library & º \- -- * . . . University of Co ---
| l - - - - n or to the º 1. Yº--- -
■ º s - N REGIONAL LIBRARY FACILITY º t º -º - - - -
RTHER-
ion -- - º
- º º/º º - * *º 400, Richmond Field Stotio --- º º A--- - - - - - - - - -"C. -- iversity of Colifornio -* , , , * :
-º, | {} º * R º -- -
| University CA 94804–4698 (10 . º º-
º º, L. º -- Richmond, S *. --
- - -
- - - -AY
-UQ * -
- - -- * DAFTER7 DAY º/1 - .
-a º L - * º ALL BOOKS MAYBE ºd by colling 7.1/101. -ºn
º- • 2-month loons moy be sº- º sº - ...'
- - - º - -
--- - ■ º º º -\. º -- (510) 642 6753 chorged by bringing-
º - º -ºf º sº º - • 1-yed loons moy be re L– * -- -* º - * 12 ºn
-~
Y; ) º --- º L tº R_* books to NRLF smoy be mode 4 - - º/ -- tº- -
-
d rechorge- º
* * - - - * * * Cls on-
** *-*. -- - - -• Renew fe .* -\ * - - --- sº
-
-,- -
doys prior to due dote. --- ~"U/º > | - º - - --- -| ºv : * * - BELOW * Lºº
º ºn tº DUE AS STAMPED º, ---, - .
* cº■ º. \º
- - *~ - * -- ~--- -- -
º-
~ ; - º º IT - -". 'le _MAR 2 9 2001 v \■
- -º, t º ■
---- º º *L `… --- w * - \ -> -
º - ~ *- -- - -
- º T s A tº Ni / sº L:- , , º º ~ -
t (0. º, ºr dººr.- -
-- *
- - - • * - - , T:
º º ■-
º º -
-- A. R_Y º * , -- -- ----- º --º
º tº - |- * , -- -tº-º- – -
--- - - º -- : ºn| º - - -
C º, - -º ~ º-> l■
-º, * . - ºº, ..º -y --- -- -- -ºncº º tº
~~ *—''''“ -º--
º
... * *- º r-/
r - -- Lºs - J.- º, º
- - ---■ t ºncºco º-
º º - - - --
vº■ J 17 º, * *- ºn * ,■ º, º 'º, sº º ** 12,000 (11/95) ---
'''' { º y º º -- - - º |-
º |- --- -- ■ -- .* º . C & ºr -
º | º º º, Li C. ■ ' ■ - ** --- º, ■ º º As ºf vº Q || ||- º - - º
-* – s T * - º – 2 ” * - º, - ... as \- º- * º -- - --- - - - * ---------, > - " - º |- º (0. º º l"º ■ º \º º º
ºvº º * * \ º ~ *- *- --
Lº Rººº º, ºn º * \, , , ■ º º- º * , p º º
-tº
-º º ºil, ■ º 'y. º Cº. *- º º r a - ! -- - ■ - o |* > - - - - º
- - -> ) wº- - - º ---, --
.." º Oil º- * * º º - º a º, º º * º
-º, L^ - *
- - - -- - º -
| * , - sº º-
º º - -, º -( º º º º i■ ■ º -- ■ º- sº ºvºi () * : * * ºn tº > *
-- - -º -> Dº ºs º * * * * * --º, sº ."º *\º º º'c - -* - --- - -- - - - *- º - - - - -() º º º, - -- *
-

º - - - : ; * - *** - - ... I - - * > *
-> 1 ºf v . . . . " . . . .-- , -- . . . ... t -- º * * * * ~ * * * * * * –– º - , , y
• * . . . . tgº ■ º * -º , ºr * . . ." .***
º* - - - - - - - - , , * -
-\ * , … 7–* º ". . . /* Not to be taken * . , ■ º f/ ... ',º º * , , from the room. º
- *-
* , * -- |-- ºr sº tº . ~ *, *, C & ". . . .* f = -
-
■ "-- .* *
I■ º © ■ º lºGºl - * ! t -
* . – ' -- * - -- tº* - - -4
º º: * º! > * | | º R * º | *
--* ... -- ; f - -- * 1 º -*-
- -* ºn . . . . . . ; * * * * * , a zº º -- - º * . -- * - - * * * * * * . - r 1 * : * * * * . . ; * *
º .."- • * , º - * s º 63294O … • * - . :- - - - º
º \ - º
-> -º, 7 | |||| - *.* * * º
* → - * - ; : )• º * / , a º * , --> * , * -- - -
- sJ º - º * * º | | º t º **** -- :
* * ---- * . - * --- ... • ** -- - *...* º . .- -- * -- • *. -. . . . . . . . . , 3 1378 00832 9406 – sº
** * . . º º - - --- -- ‘.* . , -
º *- * - sº * * * * * * * * * * * 'º - º - - * , º .* * * * * * * * **\, , , , , , , , * . . ºº: ■ , , , * -- * . . . .” --- ~ º-■ ,* . ■ * * * * * . . . -- *. - --- º * . *- * . . * , ; ; ; ; , t º … - - -
*- : º *.* º, ;-) -- -J.' * l
º, ■ º; : * * * * * - - .. l, ar *** *** - - |
1. | * -º * * : " ": -" |-
|-º, * * ~~ º r—--- * . | | in tº a * - ? º L
*| º * * * ~~- J - -
, - -- - -
| * - * - * - * f ; ºº º * : * >
... ºn º º .* --
y - - - - - - - -, ** * s - * * * * *
\ -- ºr, • * / º'
º * [ ] s*. ‘. . . . . . * - -- ** * ** *. ---, - . “ ~ : ... " º - * *---
• * * * . . . . ] -- // * > tº vºn IT & ---* * . - * *- - * - , -º -
- * * * * -- - * º . . , ºr -º,
- - • * * * * * * * * --
* . *º '', -* A . º
o * .* y º , , … wº (".." ... ', i■ º º --º º * - / . • * * * º ~ *... .Y. is Cº. //* --- J -ºº º
ºf , *
* * * ~~*
- º º --" * * - - * - º, L ■ º s –" ºw º
* ----- **| —l -
■-*--->
º ■- - * *- ! > - *-* - - * * - ----- *
* * * - * \! \, li º ! º, * sº .*. º' ºf ■ |! -- - -
* * * º º *. º *...* ■ lº (. º*
-
º º A■* * * * º ** -* .*
- –
-.* -** * : * ** Y º
º --> ■ º -*º t * / --> º rº----- - * º ... / ~"
------ * . -** - sº !---
-- * --
----. , , , !, | … " * * * * * - - s ‘. . | |* , , – 1 . . . . . . . . . . . . . .
- - **
* * * . . .-
"… . .V.
- *º * , , , -- * * s cº, º i■ /", º ..". " ---> º
~” a º f * *** * - f --- .*-º * * *~~ * - º * . . . . . . . . . . º º,
º*-
- , , ,º • *
* | *.--
* *
! -- e
º- - * * * * • *-- -A. º. Y. M. . . . –-
** º- ". . . . . . . . . . . " ! sº{` i■ ... "... * -
e - - º ~ *.*,--- .*- - - -* * * * -
* , . . "t * ---
- * * * * * * * *- º !, º º * º
-
- -
* * - - * * * * * > . * * º* - - - - - - - - - - -
- * * * - * . . . . . . yº • , , * . . . . . . . ~ * ºº- --- * * - . *- -- -- *
** - - º -
{f
* * * * * * * * * *-- * * * * * ~ *-* :
*





















