
Polymorphism and Methylation of Four Genes Expressed in Salivary
This article was downloaded by: [Oklahoma State University]On: 30 November 2012, At: 10:21Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number:1072954 Registered office: Mortimer House, 37-41 Mortimer Street,London W1T 3JH, UK
Children's Health CarePublication details, including instructions forauthors and subscription information:http://www.tandfonline.com/loi/hchc20
The Influence of DepressiveSymptomatology andPediatric Chronic Illnesson the Social Responsesof Graduate Students inEducationLarry L. Mullins, John M. Chaney, Karyll L. Kiser,Britt A. Nielsen & Terry M. PaceVersion of record first published: 07 Jun 2010.
To cite this article: Larry L. Mullins, John M. Chaney, Karyll L. Kiser, Britt A.Nielsen & Terry M. Pace (1998): The Influence of Depressive Symptomatologyand Pediatric Chronic Illness on the Social Responses of Graduate Students inEducation, Children's Health Care, 27:3, 205-214
To link to this article: http://dx.doi.org/10.1207/s15326888chc2703_5
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private studypurposes. Any substantial or systematic reproduction, redistribution,reselling, loan, sub-licensing, systematic supply, or distribution in anyform to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or makeany representation that the contents will be complete or accurate orup to date. The accuracy of any instructions, formulae, and drug dosesshould be independently verified with primary sources. The publisher
shall not be liable for any loss, actions, claims, proceedings, demand, orcosts or damages whatsoever or howsoever caused arising directly orindirectly in connection with or arising out of the use of this material.
Dow
nloa
ded
by [
Okl
ahom
a St
ate
Uni
vers
ity]
at 1
0:21
30
Nov
embe
r 20
12

CHILDREN'S HEALTH CARE, 27(3), 205-214 Copyright 8 1998, Lawrence Erlbaum Associates, Inc.
The Influence of Depressive Symptomatology and Pediatric Chronic
Illness on the Social Responses of Graduate Students in Education
Larry L. Mullins and John M . Chaney Oklahoma State University
Karyll L. Kiser and Britt A. Nielsen University of Central Oklahoma
Terry M. Pace University of Oklahoma
We examined graduate education students' interpersonal responses to childhood depression in the context of pediatric chronic illness. The graduate student partici- pants, the majority (79%) of whom were actively teaching, viewed 1 of 2 films in which a child actress was portrayed as either depressed or nondepressed. Participants received either no background information or 1 of 3 descriptions of the child's illness status (i.e., having asthma, diabetes, or cancer) prior to viewing the film. Participants completed measures of personal rejection of the child and interpersonal attraction to the child based on their perceptions of the target child; participants also completed a self-report measure of depression. Results indicated that participants who viewed the depressed child perceived the child as significantly less interpersonally attractive than the nondepressed child; however, they were not more personally rejecting of her. There were no effects for illness condition. The educational and clinical implications of these findings are discussed in the context of Coyne's (1976) interpersonal model of depression.
Requests for reprints should be sent to Larry L. Mullins, Department of Psychology, 215 North Murray, Oklahoma State University, Stillwater, OK 74078. E-mail: [email protected]
Dow
nloa
ded
by [
Okl
ahom
a St
ate
Uni
vers
ity]
at 1
0:21
30
Nov
embe
r 20
12

206 MULLINS, CHANEY, KISER, NIELSEN, PACE
Early research on depression in school-age children largely focused on issues of classification, diagnosis, and treatment (e.g., Carlson & Cantwell, 1982; Kashani & Simonds, 1979; Kazdin & Petti, 1982). Later research investigated the cognitive correlates of depression, focusing on such constructs as locus of control and life stress (e.g., Lefkowitz, Tesiny, & Gordon, 1980; Mullins, Siegel, & Hodges, 1985), attributional style (e.g., Seligman et al., 1984), and control-related beliefs (e.g., Weiss et al., 1989). More recently, social, familial, and interpersonal factors in the developmental course of childhood depression have been investigated (e.g., Bell- Dolan, Reaven, & Peterson, 1993; Stark, Humphrey, Laurent, Livingston, & Christopher, 1993).
In the adult depression literature, aspects of interpersonal and social functioning have become increasingly acknowledged as salient factors in the genesis and maintenance of affective disorders. Much of this research originates from the interpersonal theory of depression described by Coyne (1976). Coyne and others (e.g., Hammen & Peters, 1977, 1978) postulated that depressive symptoms are, in part, maintained by the social responses of others. The primary premise of the model is that the depressed individual interacts with other people in ways that elicit subtle criticism and rejection, which are then observed by the depressed individual, thereby contributing further to and confirming feelings of worthlessness. Much support for Coyne's model has been garnered from a number of studies involving adults (e.g., Gotlib & Beatty, 1985; Hokanson, Rubert, Welker, Hollander, & Hedeen, 1989).
Extending this model to child populations, Mullins and colleagues (Mullins, Peterson, Wonderlich, & Reaven, 1986) found evidence that similar interpersonal processes may also occur with depressed children. After viewing a film of a depressed child model, college students clearly perceived the child in strikingly negative terms across anumber of interpersonal dimensions. Using a similar analog design, such findings have been replicated with child peers (Peterson, Mullins, & Johnson, 1985), grade school teachers (Peterson, Wonderlich, Reaven, & Mullins, 1987), and medical students (Youll, Mullins, Calkins, & Johnson, 1991) serving as observers of the child. Research conducted in naturalistic settings has also indicated that negative social responding of this type also takes place with depressed adolescents (Connolly, Geller, Marton, & Kutcher, 1992; Sacco & MacLeod, 1990). Furthermore, recent data suggested that grade school teachers evidence negative social responses to students manifesting depressive symptomatology (Mullins et al., 1995; Pace, Mullins, & Beesley, 1994). Both of these studies found that teacher ratings of personal rejection and interpersonal attractiveness were significantly associated with higher levels of children's self-reported depressive symptomatology. Collectively, the aforementioned results warrant concern. Teach- ers who inadvertently reinforce and thereby maintain or exacerbate depressive symptoms may place children who exhibit even subtle depressive-type behaviors at risk.
Dow
nloa
ded
by [
Okl
ahom
a St
ate
Uni
vers
ity]
at 1
0:21
30
Nov
embe
r 20
12
SOCIAL RESPONSES TO DEPRESSION AND ILLNESS 207
If indeed teachers respond negatively to children with depressive symptoms, what responses may be elicited toward those children who evidence medical problems or a disabling condition? In many classroom settings, chronically ill children and handicapped children increasingly make up a portion of the student population. Indeed, inclusion rules and least-restrictive environment legislation have heightened the likelihood that chronically ill children will be a part of the regular classroom setting. Given these circumstances, the child with a chronic illness provides a target stimulus in the classroom ecosystem for social responding. However, little direct data exist to support the argument that teachers would be either more or less rejecting of the chronically ill child. Most interesting, in our previous analog studies, interaction effects were found for external life stress conditions. In essence, participants watching the child in high-depression-high- stress conditions were rated more positively than high depression alone conditions. Thus, it may be that presence of external stress in a child's life results in a different attribution for the child's depression, thereby lessening the negative effect of the depressive stimulus target. To the extent that the chronically ill child is by definition in a stressful situation, negative perceptions may be similarly attenuated.
In this study, the variable of chronic illness was introduced. In addition, a new target sample of participants was utilized, that of graduate students in education, the majority of whom were teaching full time. It was hypothesized that chronic illness would potentially serve as an "explanation7' for child depression, altering attributions made by participants, and thereby attenuate negative social responding.
Thus, one of three different types of chronic illness conditions or a condition with no chronic illness was introduced to graduate students in education before their viewing one of two videotapes, that of a depressed or nondepressed child actress. The three disease conditions included asthma, diabetes, and cancer. It was hypothesized that the depressed target child would be more rejected than the nondepressed child, replicating the results of our previous research. It was further hypothesized that the depressed actress identified as having a chronic illness would be less rejected than the depressed actress identified as having no chronic illness. No hypotheses were made concerning the effects of type of illness on social responding.
METHOD
Participants
Participants were obtained from a university in a large metropolitan area in central Oklahoma. A total of 138 graduate students enrolled in educational courses consented to participate. Consent from all participants was obtained in accordance with the policies of the university institutional review board, and the participants
Dow
nloa
ded
by [
Okl
ahom
a St
ate
Uni
vers
ity]
at 1
0:21
30
Nov
embe
r 20
12

were treated in compliance with American Psychological Association ethical standards. Approximately 96% of the participants were White; the remaining participants were African American (2%), Native American (I%), and Asian American (1%). There were 105 women and 30 men (with 3 individuals not responding) who participated in this study. The average age of the participants was 35 years (SD = 8.66). Eighty-six (62%) participants were married; 34 (25%) were single; 16 (12%) were divorced; 1 (0.7%) was separated; and 1 (0.7%) was widowed. The mean number of children in the home was 1.1 (SD = 1.15), and 58 (42%) of the participants had no children in the home. Twenty-four (18%) partici- pants reported a family income of $20,000 or below, and 104 (73%) participants reported a family income of more than $20,000.
The educational specializations of the participants were as follows: elementary education, 55 (40%); secondary education, 28 (20%); special education, 10 (7%); and other, 42 (32%). One individual did not respond to this item. Five participants had master's degrees; the remaining 133 participants had bachelor's degrees. Thirty-five (25%) participants reported that at least one family member had a chronic illness, and 56 (41%) participants reported at least one family member had apsychiatric disorder. A total of 108 (79%) participants were teaching school, and the mean number of years of involvement as a teacher was 5.5 years (SD = 5.69) for all participants. Thus, the majority of graduate student participants in this study were actively teaching and had done so for a relatively lengthy period of time. The participants with teaching experience reported an average of 3.9 (SD = 8.65) students with a chronic illness in their classrooms during their teaching careers.
Measures
Teacher ratings of personal rejection and interpersonal attraction. Ten items on 7-point Likert-type scales (1 = very much so to 7 = not at all) were used to assess the degree to which participants personally rejected a child (e.g., "Indicate your willingness to supervise her in an hour-long daily structured activity for a year."). Personal rejection items were developed from those of Hammen and Peters (1978); higher scores reflected greater rejection. Educator perceptions of the physical-interpersonal attractiveness of a child were measured using 20 items on 7-point Likert-style scales. These scales are anchored with adjectives that represent extremes of physical or interpersonal characteristics (e.g., cute to plain); higher scores indicate lower interpersonal attraction. Personal rejection and interpersonal attraction measures have been utilized in previous research (Mullins et a]., 1986; Pace et a]., 1994; Peterson et a]., 1987). Both scales have been found to have acceptable reliability (coefficient a = .93-.98).
Dow
nloa
ded
by [
Okl
ahom
a St
ate
Uni
vers
ity]
at 1
0:21
30
Nov
embe
r 20
12

SOCIAL RESPONSES TO DEPRESSION AND ILLNESS 209
Beck Depression Inventory. Given that depression has been found to influ- ence perceptions of child pathology, the Beck Depression Inventory (BDI; Beck & Steer, 1987) was used to assess level of depressive symptomatology in the partici- pants. The BDI is a self-report measure of depression used to evaluate current level of depressive symptomatology. The inventory consists of 21 items, with responses scored from 0 to 3 based on the intensity of depressive symptoms experienced during the previous week. High reliability has been found for both measures internal consistency and stability, and comparisons of BDI scores to clinical diagnoses yield a high degree of validity for adults. In this study, the participants' scores on the BDI ranged from 0 to 24 with a mean score of 5.4 (SD = 4.33). Thus, the sample could be best typified as nondepressed.
Design and Procedure
Adult participants from graduate education courses were randomly assigned to view one of two films in which a child actress was portrayed as either depressed or nondepressed. These films have been used in previous research (e.g., Mullins et al., 1986) and have been judged by expert raters to accurately depict the desired role condition, that is, depressed versus nondepressed. Prior to viewing the film, participants received, through random assignment, either no background informa- tion or one of three descriptions of the child's illness status (i.e., having asthma, diabetes, or cancer). After viewing the film, participants then completed measures of personal rejection and interpersonal attraction based on their perceptions about the child actress. In addition, the participants completed the BDI.
RESULTS
Prior to analysis, the variables were examined for accuracy of dataentry and missing values. Two cases were omitted from the analysis due to missing data for the dependent measures, leaving 136 participants. Also, demographic factors were examined for group differences. Analyses of demographic data indicated that participants in each condition did not differ significantly in terms of age, F(7, 128) = .99, p = .44; sex, x2(7, n = 133) = 4.50, p = .72; or marital status, X2(28, n = 136) = 30.96, p = .32. Scores on interpersonal attraction and personal rejection did not significantly correlate with any of the demographic data (e.g., age, sex, years of education, years of teaching) with all ps greater than .05. Additionally, no signifi- cant effects were found for specialized training, that is, special education teachers versus general education, F(2,133) = 1 . 5 8 , ~ = 21 ; or for prior teaching experience, F(1, 133) = .91, p = .40, on the two dependent variables.
Dow
nloa
ded
by [
Okl
ahom
a St
ate
Uni
vers
ity]
at 1
0:21
30
Nov
embe
r 20
12
21 0 MULLINS, CHANEY, KISER, NIELSEN, PACE
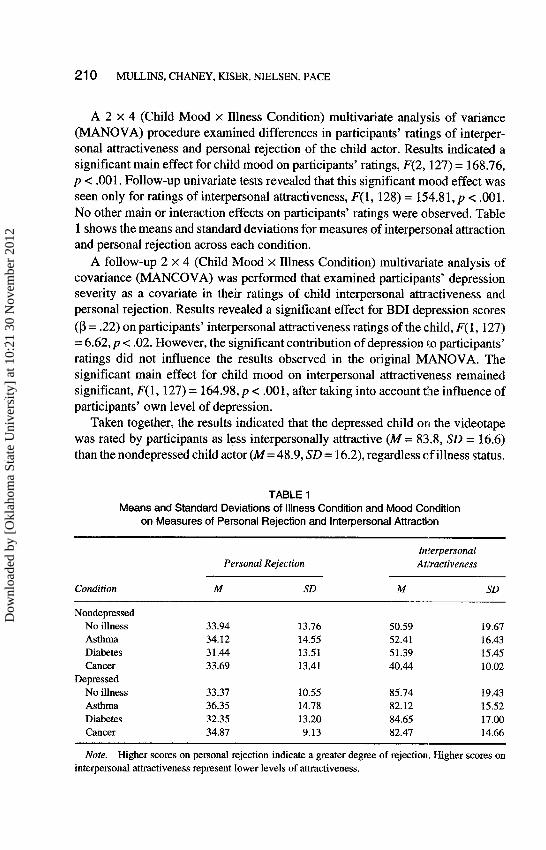
A 2 x 4 (Child Mood x Illness Condition) multivariate analysis of variance (MANOVA) procedure examined differences in participants' ratings of interper- sonal attractiveness and personal rejection of the child actor. Results indicated a significant main effect for child mood on participants' ratings, F(2, 127) = 168.76, p < .001. Follow-up univariate tests revealed that this significant mood effect was seen only for ratings of interpersonal attractiveness, F(1, 128) = 154.8 1, p c .001. No other main or interaction effects on participants' ratings were observed. Table 1 shows the means and standard deviations for measures of interpersonal attraction and personal rejection across each condition.
A follow-up 2 x 4 (Child Mood x Illness Condition) multivariate analysis of covariance (MANCOVA) was performed that examined participants' depression severity as a covariate in their ratings of child interpersonal attractiveness and personal rejection. Results revealed a significant effect for BDI depression scores (p = .22) on participants' interpersonal attractiveness ratings of the child, F(1, 127) = 6.62, p < .02. However, the significant contribution of depression to participants' ratings did not influence the results observed in the original MANOVA. The significant main effect for child mood on interpersonal attractiveness remained significant, F(l, 127) = 164.98, p < ,001, after taking into account the influence of participants' own level of depression.
Taken together, the results indicated that the depressed child on the videotape was rated by participants as less interpersonally attractive (M = 83.8, SD = 16.6) than the nondepressed child actor (M = 48.9, SD = 16.2), regardless of illness status.
TABLE 1 Means and Standard Deviations of Illness Condition and Mood Condition
on Measures of Personal Rejection and Interpersonal Attraction
Condition
Interpersonal Personal Rejection Attractiveness
M SD M SD
Nondepressed No illness 33.94 13.76 50.59 19.67 Asthma 34.12 14.55 52.41 16.43 Diabetes 31.44 13.51 51.39 15.45 Cancer 33.69 13.41 40.44 10.02
Depressed No illness 33.37 10.55 85.74 19.43 Asthma 36.35 14.78 82.12 15.52 Diabetes 32.35 13.20 84.65 17.00 Cancer 34.87 9.13 82.47 14.66
Note. Higher scores on personal rejection indicate a greater degree of rejection. Higher scores on interpersonal attractiveness represent lower levels of attractiveness.
Dow
nloa
ded
by [
Okl
ahom
a St
ate
Uni
vers
ity]
at 1
0:21
30
Nov
embe
r 20
12
SOCIAL RESPONSES TO DEPRESSION AND ILLNESS 21 1
Also, despite the significant influence of participants' depression on their percep- tions of the child actor, child depressed mood continued to have a robust effect on participants' ratings of child interpersonal attractiveness. Thus, participants' de- pression and child mood on the videotape had significant, independent effects on participants' ratings of child interpersonal attractiveness. No relation was found between the child's illness status and ratings of personal rejection or interpersonal attractiveness.
DISCUSSION
This study examined the influence of depressive symptomatology and chronic illness in children on the social responses of graduate students in education courses. The results indicate that depressive symptomatology in children was found to be associated with only one type of negative social responding on the part of the graduate students in education, specifically, on the interpersonal attraction measure. Thus, participants who watched the depressed child actress perceived her to be less interpersonally and physically attractive than the child in the nondepressed condi- tion. Contrary to previous findings (e.g., Mullins et al., 1986; Peterson et al., 1987), the graduate student participants did not personally reject the child in the depressed condition. This pattern of results suggests that although the graduate student participants perceived the child to be less interpersonally attractive, they would not engage in rejecting behavior toward her. Thus, the results of this study only partially support Coyne's (1976) interpersonal model of depression, which posits that significant others respond to the depressed individual with a variety of negative social responses.
No support was found for the second hypothesis of this study. Although we found an effect for mood and the interpersonal attraction measure, there was no effect for the chronic illness condition. Thus, knowledge of the child having a chronic illness did not influence their perception of the child actress; more specifi- cally, knowledge that she had a chronic illness did not attenuate the negative ratings of interpersonal attraction.
There are a number of possible explanations for these results. First, the infor- mation about the child's chronic illness may not have been made salient for participants in the context of the brief written scenario. Thus, it may be necessary to introduce the chronic illness information in the video itself, with discussion of the impact of that illneks on the child's life. Further, it may well be that because none of the chronic illnesses noted have any obvious physical stigmata, participants may not have perceived the child as any different. Inclusion of a child with a visible handicapping condition might have helped clarify this issue.
What other factors might explain the findings? Perhaps the use of graduate students in education, the majority of whom were experienced teachers and all pursuing master's degrees, introduced a unique sample. Thus, it is possible that the
Dow
nloa
ded
by [
Okl
ahom
a St
ate
Uni
vers
ity]
at 1
0:21
30
Nov
embe
r 20
12

2 12 MULLINS, CHANEY, KISER, NIELSEN, PACE
participants represented a more ''cu1tura11y sensitive" group, one less prone to developing differential attitudes based on personal attributes. In addition, this sample of students may have been quite sensitive to issues of inclusion. The fact that the participants did not personally reject the depressed child partially supports this notion. Our past research (e.g., Mullins et al., 1995; Pace et al., 1994; Peterson et al., 1987) has consistently revealed a relation between depression in children and rejection by teachers in laboratory settings and in the actual classroom context. This contrasting finding in the current research strongly supports the need to further investigate whether advanced education mitigates negative social responding.
Certainly, this study is limited by its analog nature and inclusion of only female targets in the video. Future research is needed that focuses on teacher responses to children with chronic illness and handicapping conditions in naturalistic settings, that is, actual classroom settings. Although teachers may endorse a positive social response toward depressed children in the laboratory setting or paper-and-pencil tasks, their behavior in the classroom may be more negative. In this manner, we can further assess the means by which negative social responding can be potentially attenuated, particularly for at-risk children.
IMPLICATIONS FOR PRACTICE
Our past research strongly suggests that influential agents in a child's life-adults, peers, and teachers-potentially harbor negative perceptions of children evidencing depressive symptomatology. To the extent these perceptions are communicated via direct behavior, at-risk children may become further depressed. The results, al- though partially inconsistent with our previous work, suggest a number of inter- vention strategies. First, teachers should be educated about the social respond- ing-depression link, thus heightening their own awareness about this issue. Teachers may then be better able to monitor their own responses to a given child and hopefully inhibit behaviors that communicate criticism or dislike. Clinicians who provide therapeutic intervention for depressed children also need to consider intervention in a wider variety of social contexts, including the classroom. This may require behavioral observations in the classroom and direct consultation with teachers. Finally, parents need education about the influence of negative social responding. The parent who communicates to his or her unhappy-and possibly depressed--child that "your teachers really do care about you" may be invalidating the child's veridical perception that they are not wholly liked an~d accepted by significant others in their social environment.
ACKNOWLEDGMENTS
We appreciate Judith Lepuschitz, John Westerman, and Odus Rice for their help in securing participants for the study.
Dow
nloa
ded
by [
Okl
ahom
a St
ate
Uni
vers
ity]
at 1
0:21
30
Nov
embe
r 20
12

SOCIAL RESPONSES TO DEPRESSION AND ILLNESS 21 3
REFERENCES
Beck, A. T., &Steer, R. A. (1987). BeckDepression Inventory manual. San Antonio, TX: Psychological Corporation.
Bell-Dolan, D., Reaven, N., & Peterson, L. (1993). Depression and social functioning: A multidimen- sional study of the linkages. Journal of Clinical Child Psychology, 22, 306-315.
Carlson, G. A., & Cantwell, D. P. (1982). A survey of depressive symptoms, syndrome and disorder in a child psychiatric population. Journal of Child Psychology and Psychiatry, 21, 19-25.
Connolly, J., Geller, S., Marton, M., & Kutcher, S. (1992). Peer responses to social interaction with depressed adolescents. Journal of Clinical Child Psychology, 21, 365-370.
Coyne, J. C. (1976). Depression and the response of others. Journal of Abnormal Psychology, 85, 186193.
Gotlib, I. H., & Beatty, M. E. (1985). Negative responses to depression: The role of attributional style. Cognitive Therapy and Research, 9, 91-103.
Hammen, C. L., & Peters, S. D. (1977). Differential responses to male and female depressive reactions. Journal of Consulting and Clinical Psychology, 45, 994-1001.
Hammen, C. L., & Peters, S. D. (1978). Interpersonal consequences of depression: Responses to men and women enacting a depressed role. Journal of Abnormal Psychology, 87,322-332.
Hokanson, J. E., Rubert, M. P., Welker, R. A., Hollander, G. R., & Hedeen, C. (1989). Interpersonal concomitants and antecedents of depression among college students. Journal of Abnormal Psychol- ogy, 98,209-217.
Kashani, J., & Simonds, J. F. (1979). The incidence of depression in children. American Journal of Psychiatry, 136, 1203-1205.
Kazdin, A. E., & Petti, T. A. (1982). Self-report and interview measures of childhood and adolescent depression. Journal of Child Psychology and Psychiatry, 23, 437-457.
Lefkowitz, M. M., Tesiny, E. P., &Gordon, N. H. (1980). Childhood depression, family income, and locus of control. Journal of Nervous and Mental Disease, 168,732-735.
Mullins, L. L., Chard, S., Hartman, V. L., Bowlby, D., Rich, L., &Burke, C. (1995). The relationship between depressive symptomatology in school children and the social responses of teachers. Jouml of Clinical Child Psychology, 24, 474-482.
Mullins, L. L., Peterson, L., Wonderlich, S. A., & Reaven, N. M. (1986). The influence of depressive symptomatology in children on the social responses and perceptions of adults. Journal of Clinical Child Psychology, 15,233-240.
Mullins, L. L., Siege], L. J., & Hodges, K. (1985). Cognitive problem solving and life event correlates of depressive symptoms in children. Journal of Abnormal Child Psychology, 13, 305-314.
Pace, T. M., Mullins, L. L., & Beesley, D. (1994, August). Teachers' social responding to depressive symptomatology in children-A test of the interpersonal theory of depression. Paper presented at the meeting of the American Psychological Association, Los Angeles.
Peterson, L., Mullins, L. L., & Ridley-Johnson, R. (1985). Childhood depression: Peer reactions to depression and life stress. Journal of Abnormal Child Psychology, 13, 597409.
Peterson, L., Wonderlich, S. A,, Reaven, N. M., & Mullins, L. L. (1987). Adult educators' response to depression and stress in children. J o u m l of Social and Clinical Psychology, 5, 51-58.
Sacco, W. P., & MacLeod, V. A. (1990). Interpersonal responses of primary caregivers to pregnant adolescents differing on depression level. Journal of Clinical Child Psychology, 19, 265-270.
Seligman, M. E. P., Peterson, C., Kaslow, N. J., Tannenbaum, R. L., Allay, L. B., & Abramson, L. Y. (1984). Attributional style and depressive symptoms among children. Journal ofAbnorma1 Psychol- ogy, 93,235-238.
Stark, K. D., Humphrey, L. L., Laurent, J., Livingston, R., & Christopher, J. (1993). Cognitive, behavioral, and family fbctors in the differentiation of depression and anxiety disorders during childhood. Journal of Consulting and Clinical Psychology, 61, 878-886.
Dow
nloa
ded
by [
Okl
ahom
a St
ate
Uni
vers
ity]
at 1
0:21
30
Nov
embe
r 20
12
21 4 MULLINS, CHANEY, KISER, NIELSEN, PACE
Weiss, J. R., Stevens, J. S., Curry, J. F., Cohen, K., Craighead, W. E., Burlingame, W. V., Smith, A., Weiss, B., & Parmelee, D. X. (1989). Control-related cognitions and depression among inpatient children and adolescents. Journal of the American Academy of Child and Adolescent Psychiatry, 28, 358-363.
Youll, L. K., Mullins, L. L., Calkins, D., & Johnson, J. (1991, August). Medical students' social responding to children. Paper presented at the meeting of the American Psychological Association, San Francisco.
Dow
nloa
ded
by [
Okl
ahom
a St
ate
Uni
vers
ity]
at 1
0:21
30
Nov
embe
r 20
12
Copyright © 2022 FDOKUMEN




















