The Future of Computer Applications in Biomedicine
19
24 The Future of Computer Applications in Biomedicine LAWRENCE M. F AGAN AND EDWARD H. SHORTLIFFE After reading this chapter, you should know the answers to these questions: ● What are possible future directions for biomedical informatics? ● What are the forces that are driving these changes? In this book, we have summarized the current state of biomedical informatics in a vari- ety of application areas and have reflected on the development of the field during the past 50 years. To provide a background for our discussions, we opened the book with a glimpse into the future—a vision of medical practice when individual physicians rou- tinely and conveniently use computers and electronic health records to help with infor- mation management, communication, and clinical decision making. In this chapter, we again look forward, this time concentrating on likely trends in biomedical applications of computers, on current avenues of research, and on the issues that will determine along which paths biomedical informatics will develop. 24.1 Progress in Biomedical Computing We begin by looking back at the changes in biomedical computing since the first edition of this book was published in 1990. Then we look ahead to the not-too-distant future— presenting a few scenarios that we can extrapolate from the current trends in the field. These scenarios provide perspective on the ways that computers may pervade clinical practice and the biological science laboratory. A key aspect of the clinical scenarios is the extent to which, unlike most specialized medical paraphernalia of today, medical computing applications are integrated into routine medical practice rather than used on an occasional basis. In much the same way, computers are becoming a crucial part of the analysis of data in the research laboratory, especially in the areas of genomics and proteomics, where the amount of incoming data is very large (see Chapter 22). The real- ization of a highly integrated environment depends on the solution of technological challenges, such as integrating information from multiple data sources and making the integrated information accessible to professionals when, where, and in the form that it is needed. Integration of medical and biological information also encompasses social issues, such as defining the appropriate role of computers in the workplace, resolving questions of legal liability and ethics related to biomedical computing, and assessing the effects of computer-based technology on health care costs. The chance that our 829
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of The Future of Computer Applications in Biomedicine
24The Future of Computer Applications inBiomedicine
LAWRENCE M. FAGAN AND EDWARD H. SHORTLIFFE
After reading this chapter, you should know the answers to these questions:
● What are possible future directions for biomedical informatics?● What are the forces that are driving these changes?
In this book, we have summarized the current state of biomedical informatics in a vari-ety of application areas and have reflected on the development of the field during thepast 50 years. To provide a background for our discussions, we opened the book with aglimpse into the future—a vision of medical practice when individual physicians rou-tinely and conveniently use computers and electronic health records to help with infor-mation management, communication, and clinical decision making. In this chapter, weagain look forward, this time concentrating on likely trends in biomedical applicationsof computers, on current avenues of research, and on the issues that will determinealong which paths biomedical informatics will develop.
24.1 Progress in Biomedical Computing
We begin by looking back at the changes in biomedical computing since the first editionof this book was published in 1990. Then we look ahead to the not-too-distant future—presenting a few scenarios that we can extrapolate from the current trends in the field.These scenarios provide perspective on the ways that computers may pervade clinicalpractice and the biological science laboratory. A key aspect of the clinical scenarios isthe extent to which, unlike most specialized medical paraphernalia of today, medicalcomputing applications are integrated into routine medical practice rather than used onan occasional basis. In much the same way, computers are becoming a crucial part ofthe analysis of data in the research laboratory, especially in the areas of genomics andproteomics, where the amount of incoming data is very large (see Chapter 22). The real-ization of a highly integrated environment depends on the solution of technologicalchallenges, such as integrating information from multiple data sources and making theintegrated information accessible to professionals when, where, and in the form that itis needed. Integration of medical and biological information also encompasses socialissues, such as defining the appropriate role of computers in the workplace, resolvingquestions of legal liability and ethics related to biomedical computing, and assessingthe effects of computer-based technology on health care costs. The chance that our
829

hypothetical scenarios will become reality thus depends on the resolution of a numberof technological and social issues that will be debated during the coming years.
24.1.1 Looking Back to 1990In the first edition of our book, the closing chapter included two future scenarios ofmedical care and discussed emerging topics such as the Unified Medical LanguageSystem (UMLS), integrated academic information management systems (IAIMS), andthe medical information bus (MIB). Today the UMLS is employed in informationretrieval systems as a tool for converting textual medical information into standardizedterms taken from coding schemes and terminologies such as MeSH, SNOMED, andICD and to help translate from one vocabulary to another (McCray and Miller, 1998).IAIMS sites are now scattered around the country with many different models beingimplemented. The MIB has been approved as the IEEE 1073 family of standards formedical device interconnection (Stead, 1997b) and has been incorporated into multipleinstruments at the bedside (see Chapter 17).
The scenarios we discussed in the first edition included computer-based support dur-ing both cardiac bypass surgery and long-term care of a patient with a chronic disease.Although the information-support capabilities have changed considerably in the decadesince the first version of this chapter was written, it is possible that the practice of med-icine has changed just as much. For example, less invasive alternatives to open-chestbypass surgery have become more common. Stricter criteria for admission to the hospi-tal and shorter lengths of stay once hospitalized mean that sicker patients are routinelycared for in outpatient settings. In such situations, the need for computer-based track-ing of a patient’s medical status is increased. This need has led to experiments such asthe use of wireless pen-based computers by home health care nurses for logging patientconditions and Internet-based disease management interactions between clinicians andpatients in their homes. Major attention to data protection and patient data confiden-tiality has significantly altered the technological solutions to such data management andaccess tasks (see Chapter 10).
Significant advances have been made in raw computing power (e.g., hardware andsoftware for the manipulation of three-dimensional images); interconnectivity (e.g., high-speed network backbones and wireless connections to palm-sized handheld computingdevices); the ability to store very large amounts of data (e.g., the terabyte data storagedevice shown in Figure 24.1); and the development of infrastructure—particularly in thearea of communication standards (e.g., health level 7 (HL7) and object broker architec-tures). On the other hand, the anticipated level of seamless integration between applica-tions, highly interconnected medical databases with embedded decision-support tools,and ubiquitous computing support have remained elusive but are an increasing focus ofpolicy as well as technical emphasis.
24.1.2 Looking to the FutureDuring testimony before the U.S. House of Representatives Committee on Science in1997 concerning the future role of the Internet, one of the authors (EHS) laid out a set
830 L. M. Fagan and E. H. Shortliffe

of long-term goals for medical informatics. Like the scenarios we depicted nearly adecade ago, these goals depend on the occurrence of both technical and social changesfor their fulfillment. If the assumptions identified in Section 24.1.3 prove valid, medicalpractice in the future will incorporate aspects of the following scenarios:
● Low-cost, high-quality telemedicine: The telemedicine experiments of the mid-1990swere dependent on specialized equipment and expensive special-use communicationslines. This has evolved such that the Internet is a common vehicle for linking medicalexperts with other clinicians and patients at a distance (National Research Council,2000; Shortliffe, 2000). In the future, the Internet will be able to support clear videoimages routinely, with high-fidelity audio links to support listening to the heart and
The Future of Computer Applications in Biomedicine 831
Figure 24.1. Multi-terabyte mass storage in a tape robot facility. (Source: Reprinted by permis-sion from StorageTek, Louisville, CO. 1998.)

lungs, and common computing platforms at both ends of the links to make telemed-icine a cost-effective form of medical practice. Patients will avoid unnecessary travelfrom rural settings to major medical centers, primary care clinicians will have expertconsultation delivered to them in their offices in a highly personalized fashion, andpatients will accomplish in single office visits what now often requires multiple visitsand major inconvenience. There is reason to believe that such applications willbecome commonplace soon, with several successful demonstration projects under wayto demonstrate cost-effectiveness and a positive benefit for patients (see Chapter 14).
● Remote consultation: Quick and easy electronic access between clinical providers to dis-cuss patient cases will improve access to expert patient care and enhance patient satis-faction. For example, an attending physician, residents, and medical students in acommunity clinic who treat a patient with an unusual skin lesion will obtain immediateteleconsultation with a dermatologist at a regional medical center. The remote medicalteam will learn from the dermatologist, the expert will receive clear, diagnostic-qualityimages of the lesion, and the patient will promptly receive a specialist’s assessment. Alltoo often today, patients, when referred to major centers, experience significant delaysor fail to keep their appointments due to travel problems. Instead of sending patients tothe experts, we will improve their care by using the Internet to bring the experts tothem. Current demonstration projects in a handful of locations have shown the feasi-bility of such remote access to expertise; it remains to make the applications common-place, well integrated with routine care, and generally accepted as reimbursable clinicalactivities.
● Integrated health records: We envision the day when citizens no longer will have mul-tiple records of their health care encounters scattered throughout the offices ofnumerous physicians and the medical record rooms of multiple hospitals. Instead,their records will be linked electronically over the Internet so that each person has asingle “virtual health record”—the distributed, but unified, summary of all the healthcare they have received in their lives. Furthermore, this record will be secure, treatedwith respect and confidentiality, and released to providers only with the patient’s per-mission or during times of medical emergency according to strictly defined andenforced criteria (National Research Council, 1997). Important steps have been takenrecently to make this scenario more likely to happen. The development of a NationalHealth Information Infrastructure and adoption of nomenclature standards such asSNOMED-CT, and privacy rules such as Health Insurance Portability andAccountability Act (HIPAA) are contributing toward this goal. In 2004, PresidentBush announced a federal goal to implement ubiquitous electronic health records forall citizens within a decade. In addition, the U.S. armed services are actively pursingelectronic dog-tags that will contain abstracts of the electronic medical record of eachparticipant in the military.
● Computer-based learning: Soon, medical students on their orthopedics rotation,preparing to observe their first arthroscopic knee surgery, will be able to go theschool’s electronic learning center and use the Internet to access and manipulate athree-dimensional “virtual reality” model of the knee on a computer at the NationalInstitutes of Health. They will use new immersive technologies to “enter” the modelknee, to look from side to side to view and learn the anatomic structures and their spa-
832 L. M. Fagan and E. H. Shortliffe

tial relationships, and to manipulate the model with a simulated arthroscope, thus get-ting a surgeon’s-eye view of the procedure before experiencing the real thing. Usingthe experimental Next-Generation Internet, remote access to medical dissections isbecoming available in a limited way. In the near future, many hard-to-learn proce-dures, such as female pelvic examination, will be routinely taught to medical studentson a computer simulation/mannikin with immediate feedback rather than withpatients or living models.
● Patient and provider education: Health science schools are starting to provide distance-learning experiences via the Internet for postgraduate education, refresher courses,and home study by health science students. Eventually, clinicians will be able to pre-scribe specially selected video educational programs for patients that will be deliveredto home television sets by a direct Internet connection. Our hospitals and clinics willuse video servers over the Internet not only to deliver such materials to patients butalso to provide continuing medical and nursing education to their staffs. Providers arebeginning to make patient-oriented versions of the electronic medical records avail-able online along with relevant online information tailored to the patient’s problems(Cimino et al., 2002).
● Disease management: High-speed Internet access via Digital Subscriber Line (DSL),cable, or satellite is now being offered to most families in the United States and morethan 50 million households now have broadband connectivity. Soon, clinicians willmove beyond the simple use of telephones for managing patient problems at a dis-tance to using their visual senses as well via two-way video links. The infirm willreceive “home visits” via video links, thus avoiding unnecessary office or emergencyroom visits, and care managers will have important new tools for monitoring patientsthat emphasize prevention rather than crisis management. Early experiments showremarkable enthusiasm by patients when familiar physicians and nurses provide suchvideoconferencing interactions in the home (see Chapter 14).
Over these last 5 years since these goals were elucidated, we have made significantprogress toward meeting these long-term objectives for computer-assisted learning,provider and patient communication, and medical care utilizing high-speed networksand fast, commodity computers. Similar changes have been taking place in the collec-tion, interpretation, and dissemination of biological information. For example with theadvent of very fast, multiprocessor supercomputers, researchers can begin to model bio-logical processes such as the folding of a protein or the binding of a drug to a receptorsite. Some of this modeling work can be done using the high-speed Internet and distantcomputers, such as the biologically focused supercomputers in San Diego, California,and Pittsburgh, Pennsylvania. One scientist working in this area has suggested some ofthe major challenges and opportunities facing the field of computational biology:1
● A computational model of physiology: Can we create a simulation of the human bodyand estimate of the effects of medications on the diseased and nondiseased portions
The Future of Computer Applications in Biomedicine 833
1R.B. Altman in a presentation entitled “Final thoughts: Further opportunities in bioinfomatics and compu-tational biology”, presented at a conference on Bioinformatics Methods and Techniques, Stanford, CA. June23–25, 2003.
of the body with sufficient fidelity to avoid most animal and early human testing ofdrugs? Having this simulation model would bring a tremendous benefit by reducingthe number of years of testing that occurs for most drugs. However, the complexity ofthe task is daunting. Much of the pathophysiology needed to build this model isunknown, and even the parts that are known would create such a complex set of rela-tionships that the computers models may be intractable given near-term computa-tional capabilities. Furthermore, the genetic variation between individuals that isbeing studied in pharmacogenetics experiments greatly increases the complexity ofthe modeling process.
● Design of new compounds for medical and industrial use: Can we design a protein ornucleic acid to have a specified function? The determination that a particular drug canbe used to treat a medical condition has traditionally been done by testing a large col-lection of substances in the laboratory to see if any show in vitro activity. This step isthen followed by extensive animal testing. Now that we have a better understandingof protein structure, and a clearer model of how to modify the disease process, canthe drug creation process be switched to build biological custom materials to reverseor deter a pathological process?
● Engineering new biological pathways: Can we devise methods for designing and imple-menting new metabolic capabilities for treating disease? The biological metabolicpathways of various species are being mapped out quite rapidly. It is interesting toobserve the variation from species to species in pathways that perform similar meta-bolic functions for the animals. This suggests the possibility of building new meta-bolic pathways in areas such as inborn metabolic diseases. Some diseases, such assickle cell anemia, have a single flaw that must be overcome. In other genetic diseasesmultiple elements of the pathways may be missing, and there will be a need to con-struct an alternative pathway that takes into account the particular manifestations ofthe disease.
● Data mining for new knowledge: Can we ask computer programs to examine data (inthe context of our models) and create new knowledge? As we create large databasesof measurements taken during clinical care, the question arises about finding new pat-terns in those data. Exactly what effects does a drug have on various laboratory testsand measurements? If we have enough data collected across different patients but insimilar situations, will we have enough statistical power to recognize unknown rela-tionships? A large number of statistical approaches are being employed to perform astructured analysis of large data sets to learn new relationships.
These biological challenges are still likely to be unanswered as we approach the 10th edi-tion of this textbook. Because they require the development of considerable biologicalknowledge, computational techniques, and new methodologies for analysis, they likelyrepresent distant goals of biomedical computation.
24.1.3 Assumptions Underlying the ScenariosTo help you to evaluate these scenarios of the future, we must make explicit the assump-tions on which these speculations are based. In particular, we assume that health care
834 L. M. Fagan and E. H. Shortliffe
workers and life scientists will work increasingly with computers in their daily lives andthat improvements in computer technology will continue, independent of technologicaladvances in biomedical science. Furthermore, we assume that concerns about healthcare cost containment and the threat of malpractice litigation will continue to be unre-solved issues for the near term.
The technological development of medical computing depends in large part onadvances in general computing capabilities. Except in the area of medical imaging, littlecomputer technology is first developed for medical applications and then applied to therest of industry. This is especially true now that a few general-purpose microprocessorsand operating systems have become standard for all personal computers. Specializedcomputer chips will continue to be created for computationally intensive medical appli-cations, such as signal processing. In these image-processing applications, rotation, fil-tering, enhancement, and reconstruction algorithms must handle more data than can beprocessed with the standard microprocessors; thus, a market exists for specializedmachines.
It is difficult to predict whether the development of new general-purpose computerproducts will continue to follow an evolutionary trend or will undergo a paradigmshift—defined by Kuhn in his book on the nature of scientific discovery as a completechange in perspective, such as occurred with the revelation that the Earth is not flat(Kuhn, 1962). Computer processing has gone through some major shifts in directionover the last 40 years: from single-user batch processing, to timesharing on a centralresource, and then back to single-user processing, this time on local machines withaccess to specialized machines through a network. As more and more people try toaccess key Internet sites, we have moved back to a version of the timesharing model of30 years ago.
The human–machine interaction style has changed dramatically, with graphical inter-faces for novices almost completely replacing command-line interfaces. Pen, speech, andthree-dimensional interfaces have been built but have not been widely deployed, exceptin the case of pen-based datebook applications and spoken systems for very definedtasks such as airline reservations or banking. For example, Figure 24.2 shows oneapproach for using three-dimensional representations for literature retrieval. This appli-cation built at the Palo Alto Research Center (PARC) uses the three-dimensional spa-tial information to show complex trees in much greater detail than in mosttwo-dimensional layouts. There also has been a significant change from electrical tooptical methods of network transmission (fiberoptic cables) as well as a steady progres-sion from analog to digital recording of information, best illustrated by the switch fromfilm to digital images in radiology, the widespread introduction of high-speed fiber net-works, and the development of satellite communication networks. For the purposes ofthis chapter, we shall assume the continued progression of current trends rather than asignificant paradigm shift. An unanticipated discovery that is just around the cornercould, of course, quickly invalidate the assumptions.
Another subtle, but pervasive, assumption underlies this book, much of which is writ-ten by researchers in biomedical informatics. We tend to believe that more technology,thoughtfully introduced, is usually better and that computers can enhance almost anyaspect of clinical practice and biomedical research—especially information access, the
The Future of Computer Applications in Biomedicine 835

diagnostic and therapeutic components of the decision-making process, and the analy-sis of huge amounts of biological data. For example, paper documents are still themainstay of medical records in many medical settings. Still, we strive to eliminate thepaper-based components and assume that a well-designed interface (e.g., one thatallows handwritten or continuous-speech input) applied to a sufficiently fast computercan significantly improve the overall process of recording and retrieving clinical data.Although this assumption has yet to be formally verified, there is a groundswell ofdevelopment and investment activity based on successful experiments that encouragethe belief that electronic records will positively transform the way in which we providepatient care and monitor health.
People frequently criticize medical professionals for being technocrats—for encour-aging an increase in mechanization and electronic gadgetry that tends to alienate bothworkers and patients. Such increases fuel the concern that modern medicine is becom-ing increasingly impersonal and sterile. How do we meld the automated environmentsproposed in this chapter’s introductory scenarios with our wistful memories of kindlyfamily doctors making house calls and attending their patients’ weddings, christenings,bar mitzvahs, and the like? The reality, of course, is that the trend away from such tra-ditional images predated the introduction of computers in medicine and has resultedmore from modern pressures on health care financing and the need for subspecializa-
836 L. M. Fagan and E. H. Shortliffe
Figure 24.2. Three-dimensional representation of the MeSH tree using the InformationVisualizer Toolkit created at Xerox PARC. A portion of a citation about breast cancer is shownin the foreground. (Source: Reprinted from Hearst/Karadi, SIGIR’97, courtesy of ACM.)
tion to deal with an increasingly complex subject area. The role for computers and otherinformation technologies results as much from these pressures as it does from a blindfaith that all technology is good, useful, and worth the associated costs. Many argue, infact, that the prudent use of computing technology will introduce the kinds of efficien-cies needed if clinicians are to return to an era in which more relaxed time spent withpatients is feasible.
Once medical computing applications have been shown to be effective, the technolo-gies will need to be evaluated carefully and consistently before their routine adoption.We need to know that the benefits exceed the costs, both financial and sociological. Thedebate about where and how computers should be used is even more complex in devel-oping countries, where advanced technology might partially compensate for shortagesin medical expertise but where scarce health care resources might be more effectivelyemployed to provide sanitation, antibiotics, and basic medical supplies. Nonetheless, thescenarios above were painted with the assumptions that there will be an increased appli-cation of computers in all aspects of medicine and that the key difference between thefuture and today will be that computers will become ubiquitous and that they will havea high degree of interconnection and an increased ability to interoperate.
24.2 Integration of Computer-Based Technologies
Most of the individual capabilities described in the preceding scenarios exist today in pro-totype form. What does not exist is an environment that brings together a large variety ofcomputer-based support tools. The removal of barriers to integration requires both tech-nological advances, such as the development of standards for data sharing and commu-nication (see Chapter 7), and a better understanding of sociological issues, such as whencomputer use may be inappropriate or how the need for coordinated planning can over-come logistical barriers to connecting heterogeneous resources in a seamless fashion.
We can begin to assess the degree of connectivity in a medical center by asking sim-ple questions. Can the laboratory computer communicate results to the computer thatprovides decision support, without a person having to reenter the data? Do the pro-grams that provide decision support use the same terms to describe symptoms as dothose that professionals use to perform electronic searches of citation databases? Dophysicians and other health personnel use computers to get information without think-ing about the fact that they are using a computer system, just as they pick up a medicalchart and use it without first thinking about the format of the paper documents?
Computer systems must be integrated into the medical setting in three ways. First,applications must fit the existing information flow in the settings where they are to beused. If the machine sits in a corner of the clinic, out of the normal traffic flow, and ifthere is another way to accomplish the specific task, then the computer system is likelyto be ignored. Likewise, programs that arbitrarily constrain physicians to unnaturalprocedures for entering and accessing information are less likely to be used. User inter-faces should be flexible and intuitive; just as the fields of a paper medical form can becompleted in an arbitrary order, data-entry programs should allow users to enter infor-mation in any order.
The Future of Computer Applications in Biomedicine 837

Surgeons attempting so-called telepresence surgery over the Internet, bringing special-ized expertise to an operating room possibly hundreds of miles away, will be unable to assistin the procedure if the movements they make with hand devices at one end are not instantlyreflected in what they see happening with the actual instruments at the other end of thelink. How do we ensure interoperability across the many networks that now span our coun-try (National Research Council, 2000)? Can we guarantee adequate response time for thetelesurgery application not only on the major backbone networks but also on the last seg-ments of wire, cable, or wireless network that come into offices and other remote settings?
Second, computer systems should provide common access to all computer-basedresources, so a user cannot tell where one program ends and another starts. In thisbook, we have described such diverse applications as computed tomographic scanningand bibliographic searching. Many of these systems have been developed independ-ently, and most are completely incompatible. In the future, the radiologists’ picturearchiving and communications system (PACS) workstation (see Chapter 18) shoulddeliver more than just images—for example, a radiologist may wish also to search eas-ily for references on unusual presentations of a specific disease process and to includethese references in a paper being composed with a text editor. Ideally, users should nothave to switch between computers, to stop one program and to start another, or evento use different sets of commands to obtain all the information they need. That thedesired information resources may exist on multiple machines in different parts of themedical center or the country should be invisible to the user.
Third, the user interface must be both consistent across applications and easy touse, which may require multiple interface modalities, such as pointing, flexible spokennatural-language interfaces, and text input. Both at the user interface and internally,programs should use a common terminology to refer to frequently used concepts,such as a diagnosis, a symptom, or a laboratory test value.
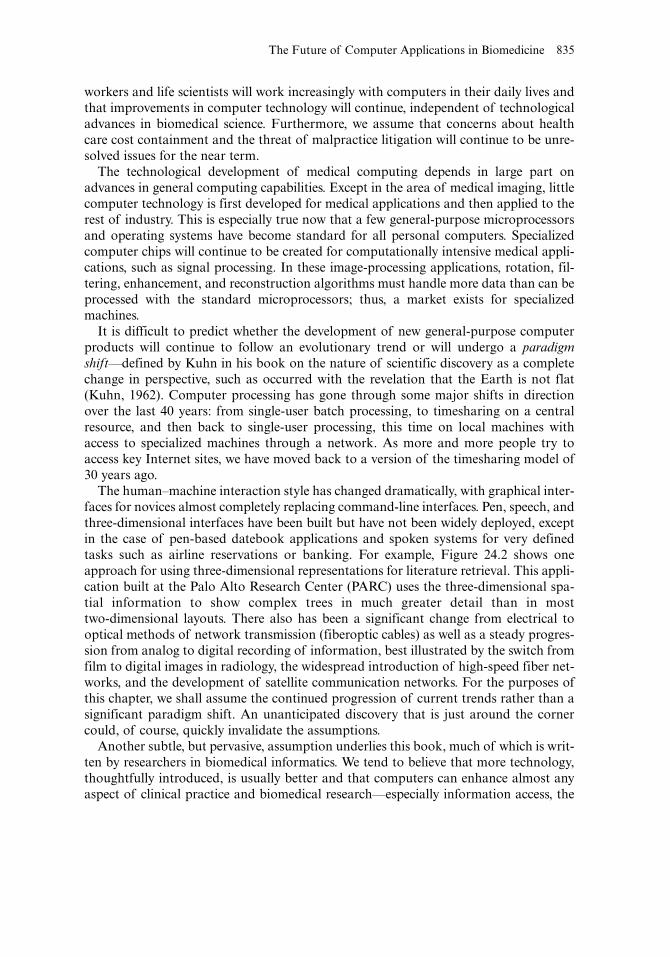
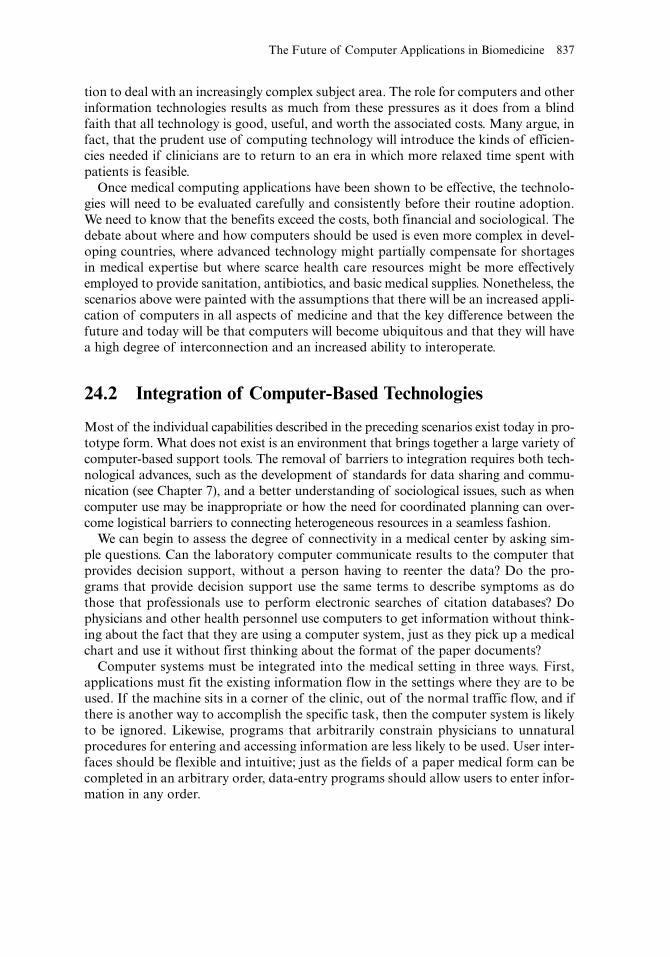
We are seeing increasing amounts of medical information packed into smaller, morepowerful computers, such as hand-sized personal digital assistants (PDAs). The config-uration of computers is starting to change. Figure 24.3 shows a computer system that isworn attached to the body. Using spoken input or a keypad mounted on the arm alongwith a heads-up display, the computer is inherently as mobile as the person using thesystem. Although this device may seem far in the future for medical care, a less sophis-ticated version of this equipment is used everyday in the rental car business to check-inreturning cars and print receipts. Although the rental car business is far more structuredthan medical practice, the example shows that this type of technological change can besuccessfully integrated into the workplace.
Figure 24.4 is a fanciful figure from Wired Magazine that hints at the future effects ofnanotechnology. Technology is not quite at the Fantastic Voyage level where miniaturerobots flow through the body repairing problems, but the field of microelectromechan-ical systems (MEMS) has created methods to build very small sensors and miniaturemechanical devices. In the figure, the illustrator imagines miniature devices being usedas an intervention to remove “smart dust” household sensors that might have been acci-dentally inhaled. Certainly, the ability to build sensors and treatment devices at such asmall scale will influence future medical care, especially in the management of chronicdiseases such as diabetes.
838 L. M. Fagan and E. H. Shortliffe
24.3 Future Role of Computers in Health Care andBiomedicine
As we discussed in the previous section, fulfillment of the opening scenarios in thischapter will require significant technological changes. Equally important are the orga-nizational and attitudinal changes that will be necessary to implement the new tech-nologies as they emerge. Health professionals, health institutions, medical systemdevelopers, and society as a whole must carefully consider the appropriate role of com-puters in medicine and assess the potential benefits of computers in terms of improvedaccess to information, enhanced communication, increased efficiency of health caredelivery, and higher quality of medical care.
Although the potential benefits of using computers are many, there are also potentialcosts, only some of which are monetary. For example, computer-based medical recordsystems will never exactly replicate the flexibility of current paper-based systems. Thisflexibility includes the ability to create progress notes about patients, using any words inany order and in any format, with or without diagrams, to record the information.
The Future of Computer Applications in Biomedicine 839
Figure 24.3. A wearable computer, including monacle display, voice input, belt-mounted centralprocessing unit, and hand-mounted keypad. (Source: Photograph by Lawrence M. Fagan.Xybernaut, Mobile Assistant, and MA IV are registered trademarks of Xybernaut Corporation.)
Computer-based systems limit flexibility in return for increased legibility and access tothe information and for the ability to use the information for other purposes, such asclinical research studies that use multiple patient databases. We see the same pattern inthe use of automated bank-teller machines. There are only a few ways to complete acash withdrawal transaction through a sequence of button pushes, but there are a largenumber of ways in which we can make this request of a human teller. Automated tellersare available at 3:00 A.M. in the morning, however; human tellers are not.
The idea that computer approaches would require the additional structuring ofmedical records was perceived by Lawrence Weed more than 30 years ago (Weed,1969). Weed noted that, for medical records to be useful, they had to be indexedsuch that important information could be extracted. In particular, he proposed thatthe medical record be organized according to the patient’s current problems—theproblem-oriented medical record (POMR). Variations of the POMR have become astandard feature of medical record keeping, regardless of whether computers areused. In the problem-oriented medical information system (PROMIS), a computer-based implementation of the POMR, such rigid and time-consuming indexing of
840 L. M. Fagan and E. H. Shortliffe
Figure 24.4. Amusing illustration of miniature robotic devices used as a treatment of accidentalinhalation of “smart dust” robotic sensors. (Source: Illustration by Chuck Henderson. Reprintedby permission from Wired Magazine. This illustration appeared in the April, 2004 issue.)

patient problems was required that clinicians ultimately proved reluctant to use thesystem. Standardization provides benefits but exacts costs in terms of decreasedflexibility; it makes information more accessible but restricts freedom to pursuealternate means to accomplish the same result. It is unlikely that new computerinnovations will ever eliminate this trade-off.
Similarly, the use of computers requires trade-offs with respect to confidentiality ofmedical information. Legitimate users can more conveniently access computer-basedrecords in well-designed systems. Without sufficient security and policy measures, how-ever, unauthorized users may threaten the confidentiality and integrity of databases.Fortunately, with adequate attention to security issues, modern methods backed by effec-tive security policies can ensure that patient data are kept with greater confidentiality incomputer systems than they are in the paper charts of hospital wards. The growing vol-ume of clinical data stored electronically, widespread remote access capabilities, and thetrend toward secondary and tertiary uses of clinical information result in the need forongoing attention to concerns of security and confidentiality (see Chapter 10).
Earlier fears that computers could replace physicians have not been borne out, andcomputers are likely to remain decision-support tools rather than substitute decisionmakers (Shortliffe, 1989). It is more likely that computers will be used increasingly tomonitor the quality of health care delivered and to help evaluate physician performance.Greater automation will therefore change the nature of medical practice in nontrivialways. The challenge for system developers and users will be to identify the solution thatprovides the optimal balance between flexibility and standardization.
Computers in the future are likely to have even a greater influence on the practice ofbiology in the research laboratory. Exponential increases in the availability of experi-mental data necessitate computational support. Examples include cross-species investi-gation of DNA sequences, analysis of microarray data, and simulation of cellularfunction. Just as clinicians need to adjust their practice to accommodate computationalsupport, biologists need to provide a computational infrastructure for the collection,analysis, and dissemination of laboratory data. An exceptional illustration of the powerof computers is in the field of pharmacogenetics, where clinical and biological data arecombined to determine individual responses to drug therapy. This requires the develop-ment of terminologies to support these disparate data sources, a complex databaseschema to store the information, and intelligent searching function to highlight the keyrelationships. It is likely that these types of biological and clinical applications will be afocus of research and development in the coming decades.
24.4 Forces Affecting the Future of Medical Computing
In this book, we have identified several important factors that affect the current and futurerole of computers in medicine. These factors include advances in biotechnology and com-puter hardware and software, changes in the background of health professionals, changesin the medicolegal climate, and changing strategies for health care reimbursement. The rel-ative strengths of these forces will determine how likely it is that the scenarios we proposedwill take place and how quickly we can expect such changes to occur.
The Future of Computer Applications in Biomedicine 841

24.4.1 Changes in Computers and Biomedical TechnologyModern computers are smaller, less expensive, and more powerful than were their pred-ecessors. Although microchip designers are approaching the physical limits on howclose together electronic elements can be placed, these trends will continue. By the timea new microprocessor chip or memory chip is adapted for use in new computer systems,manufacturers are creating samples of the next generation of chips. The most importantramification of current trends in microcomputer technology is that it is now possible toinclude a microprocessor and memory in most pieces of medical equipment.
The ability to connect multiple devices over high-speed networks has enabled a dra-matic change in the way medical computer systems are designed. It is now practical todevelop systems in which multiple data storage devices are accessed by complex comput-ers that sort and abstract the numerous patient data that are generated. This design con-trasts with the traditional approach in which health professionals would need to gatherinformation from many different devices or locations in the medical center to obtain acomplete picture of a patient’s status. Relatively low-cost computer workstations or net-work-based terminals now allow information to be manipulated at each patient’s bedside,as well as at other work areas in medical centers and ambulatory clinics.
High-speed networks and private intranets allow physicians in private offices to con-nect to computers in the hospitals where they admit patients or to repositories of datafrom multiple care settings and systems.
We have much more data to transmit over the network, such as those from digitizedradiology images, online reports, and computer-based charting of the patient’s condition.In the future, even faster networks and larger storage devices will be necessary to managethe overwhelming volume of data that will be created by all-digital clinical data systems.
24.4.2 Changes in the Background of Health Professionalsand BiologistsComputers will continue to be made faster and less expensive and will have more fea-tures; however, sufficient computing power now exists for most applications. Thus, thelimitations on the pervasiveness of computers in medicine do not hinge as crucially onthe development of new hardware as they did in the past. The availability of relativelyinexpensive and powerful computers is changing health care workers’ familiarity withmachines by exposing these people to computers in all aspects of their daily lives. Thisincreased familiarity in turn increases acceptance of computers in the workplace,another crucial determinant of how computers will fare in the next 15 years.
Since the early 1970s, people have increasingly interacted with computers in theirdaily lives to perform financial transactions, to make travel arrangements, and even topurchase groceries. In many situations, people do not use the computer themselves butrather talk to an intermediary, such as an airline reservation agent or bank clerk. Largecomputer systems are so deeply integrated into many business practices that it is notuncommon to hear, “I can’t help you—the computer is down.” This switch to computer-based record keeping for most financial transactions is so pervasive that you would besurprised and concerned if you were to receive a monthly bank statement that was writ-
842 L. M. Fagan and E. H. Shortliffe

ten out in longhand. Within the last 10 years, many mediated computer-based transac-tions have been replaced by direct contact between a consumer and a computer system.We can withdraw cash from automated bank tellers, request a trip routing from a com-puter at the rental car stand, or obtain an account balance by a touch-tone telephone.As described in almost every chapter in this book, the acceptance of the Internet modelof interaction is cutting out intermediary steps and allowing users to access large onlinedatabases directly from home or work.
Young health care workers today have been exposed to computers throughout their edu-cation. Many college courses assign projects that must be carried out using the computer.It is difficult to determine how the current hodgepodge of computers in the medical settingwill bias these users. It may be that, when the integrated system becomes available, healthcare professionals will not use the system fully because of previous negative experiences inless sophisticated environments. On the other hand, familiarity with computers and withtheir operation may prepare users to accept well-designed, easy-to-use systems.
24.4.3 Legal ConsiderationsThe number of malpractice lawsuits and the sizes of the settlements have increased inrecent years. Today, the specter of potential legal action hangs over every medical inter-action. Computers can either exacerbate or alleviate this situation. The computer-baseddiagnostic system may provide a reminder of a rare but life-threatening disease thatmight have been overlooked in the differential diagnosis. On the other hand, decision-support systems might generate warnings that, if ignored by health care workers, couldbe used as evidence against those workers in a court action (see Chapter 10).
During the last few years, there has been a national-level focus on the cause of med-ical errors during the diagnostic and treatment process. The Institute of Medicine(IOM) has performed several key studies in this area (Kohn, 1999; Committee onQuality of Health Care in America, 2001; Aspden, 2003). These studies showed aseries of issues with the medical process that can lead to medical errors. One of theresults of these studies has been new requirements to track errors and near misses.The second IOM report suggested that the number of errors would be reduced by thewidespread introduction of information technology. The 2003 IOM report laid outpossible data standards that would help to increase patient safety. In 2004, the gov-ernment increased its efforts to promote a National Health InformationInfrastructure that will provide mechanisms to interlink medical records at diverseinstitutions, and thus decrease the possibilities of errors or repeated tests because ofincreased access to clinical information.
24.4.4 Health Care FinancingSome people assume that the continuing evolution of computer hardware and softwareis the most important force influencing the development of medical computing. Socialissues such as health care financing and the legal aspects of medicine, however, proba-bly outweigh the technological factors. Perhaps the strongest force at work today is the pressure to control health care costs. Health care financing influences all choices
The Future of Computer Applications in Biomedicine 843

regarding the acquisition and maintenance of high-technology equipment and information systems.
Current schemes for health care financing have been designed to slow the rate ofgrowth of health care costs. These policies translate into pressure to reduce costs inevery aspect of medical diagnosis and treatment, such as to substitute ambulatory carefor hospitalizations, to shorten hospital stays, to select less expensive surgical proce-dures, and to order fewer laboratory tests. As incentives for making optimal decisionsin these areas increase, there is a greater need for computers that can collect, store,interpret, and present data during the decision-making process.
Order-entry systems routinely screen test orders against criteria for test ordering andquestion or cancel tests that do not meet the criteria. A more sophisticated clinicaldecision-support system might serve as an adjunct to an order management system,assessing which tests are most appropriate to order for specific patients who requireexpensive workups (e.g., custom-tailored evaluation of thyroid function). Such a sys-tem might also evaluate drug orders and suggest less expensive substitutes that areequally effective while checking for drug–drug interactions, and so on.
It is now common that computers are used by health plans to enforce a particularstyle of care through concurrent or post hoc review of the medical decision-makingprocess, including decisions about length of stay and tests performed. Thus, one forcepromoting the use of computers by clinicians is the knowledge that computers are oftenused by insurers to review these clinicians’ decisions after the fact. The clinicians mayprefer to know what the computer system will advise beforehand so that they can be pre-pared to justify intentional deviations from the norm. Increasingly, health care admin-istrators and medical practice directors are requiring use of clinical systems by cliniciansto understand and manage clinical interventions and outcomes in response to decreas-ing reimbursement for services and managed care contracting arrangements.
In the United States, an entire new and thriving industry has evolved in response toefforts to manage health care costs more effectively: pharmacy benefits managers(PBMs). Highly dependent on computer technology to manage their business functions,the PBMs manage the prescription benefits for insured individuals, working with retailpharmacies but also providing mail-order options and encouraging appropriate conver-sion to generic equivalents that can greatly reduce the cost of care for insurers (and forthe employers who are the PBM’s clients). Note that the PBMs, like managed careorganizations, must distinguish between their customers (generally employers) and theirmembers (employees and their families who receive their medical insurance through theemployee’s work). PBMs are only one example of new industries that have evolved inpart because of the unusual nature of health care financing in the United States whencompared with other parts of the world (see Chapter 23).
Although the use of computer technology can help health professionals to cope withthe growing complexity of medical practice, it also contributes to the increasing cost ofhealth care. Studies are beginning to show the benefits of outpatient computerizedpatient order entry (Johnston, 2003). Some computers are so embedded in the clinicalenvironment, especially in complex environments such as operating rooms or intensivecare units, that it is hard to show a decrease in patient morbidity or mortality due to thecomputers alone. Large numbers of devices are already being used in these settings, and
844 L. M. Fagan and E. H. Shortliffe

patients are often treated for multiple concurrent problems. Even if patient-monitoringequipment could help health care workers to recognize potentially dangerous situationsearlier than they otherwise would, showing that the computer system affected the out-come would be difficult. At the other extreme are devices that can be shown to make adifference, but whose cost is very high, such as computed tomography and magnetic res-onance imaging systems. Because they replace invasive techniques (which have a signif-icant potential for causing harm) or provide information that is available from no othersource, there has been little debate about the utility of these new modalities. Instead, thehigh cost of this equipment has focused attention on how best to distribute these newresources. Demonstrating the return on investment in computer technology is a majorchallenge to widespread implementation of health care computer systems in light oftheir often staggering capital cost and the expense of staff resources required to supportthe many clinical users and to implement, integrate, manage, and maintain increasinglycomplex distributed systems and networks. No matter how computer systems are usedin the future, we will need to evaluate the influence of the computer application onhealth care financing and to assess the new technology in light of alternative uses ofresources.
24.5 Looking Back: What Have We Learned?
An introductory book can only scratch the surface of a field as varied and complex asbiomedical informatics. In each chapter, we have examined technical questions abouthow a system works (or ought to work); we must also view each area in light of thehealth care trends and the social and fiscal issues that shape the ways in which clinicalcare is delivered now and in the future. In this chapter, we have emphasized the richsocial and technological context in which biomedical informatics moves ahead both asa scientific discipline and as a set of methodologies, devices, and complex systems thatserve health care workers and, through them, their patients. One of the most importantchanges is the increase in the use of computers to help with the analysis of biologicaldata. As more clinically important genetic data come online, new application areas suchas pharmacogenetics are influencing clinical care. This type of new application that spansclinical and biological data is clearly the start of a new trend in informatics. Glimpses ofthe future can be at once both exciting and frightening—exciting when we see how emerg-ing technologies can address the frequently cited problems that confound current healthcare practices but frightening when we realize that methodologies must be applied wiselyand with sensitivity if patients are to receive the humane and cost-sensitive health carethat they have every right to expect. The question is not whether computer technologieswill play a pervasive role in the health care environment of the future, but how we canensure that future systems are designed and implemented effectively to optimize tech-nology’s role as a stimulus and support for the health care system and for individualpractitioners. The outcomes of the process will depend as much on health care planners,practitioners, and policymakers as they will on the efforts of system developers and bio-medical informatics professionals. It is to all such individuals that this book has beendedicated.
The Future of Computer Applications in Biomedicine 845

Suggested Readings
Altman R.B. (2001). Challenges for intelligent systems in biology. IEEE Intelligent Systems, 16(2):2001, 14–18.
In this summary article, R.B. Altman lays out some major future challenges for biocomputation.
http: //www.citl.org/research/ ACPOE_Executive_Preview.pdf (Web site accessed July 9, 2004).This Web site provides an executive summary of the cost/ benefits of Ambulatory ComputerizedProvider Order Entry. See Johnston (2003) for the full report.
Committee on Quality of Health Care in America, Institute of Medicine, Crossing the QualityChasm: A New Health System for the 21st Century. Washington, D.C.: National AcademiesPress.
This report discussed structural changes to the practice of medicine to address some of the issuesdiscussed in the IOM report, To Err is Human.
Stead W.W., et al. (Eds.) (1998). Focus on an agenda for biomedical informatics. Journal of theAmerican Medical Informatics Association, 5(5):395–420. Special Issue.
The 1998 Scientific Symposium of the American College of Medical Informatics (ACMI) wasdevoted to developing visions for the future of health care and biomedicine and a strategic agendafor health and biomedical informatics in support of those visions. The first five articles containedin this special issue illustrate these findings and continue to be timely.
Questions for Discussion
1. Select an area of biomedicine with which you are familiar. Based on what you havelearned in this book, propose a scenario for that area that takes place 20 years in thefuture. Be sure to think about how issues of system integration, networking, andchanges in workflow will affect the evolution of computers in the setting you describe.
2. Imagine that you are a patient visiting a health care facility at which the physicianshave made a major commitment to computer-based tools. How would you react tothe following situations?a. Before you are ushered into the examining room, the nurse takes your blood pres-
sure and pulse in a work area and then enters the information into a computer ter-minal located in the nursing station adjacent to the waiting room.
b. While the physician interviews you, he or she occasionally types information intoa computer workstation that is facing the physician; you cannot see the screen.
c. While the physician interviews you, he or she occasionally uses a mouse-pointingdevice to enter information into a computer workstation located such that, whenfacing the physician, you cannot see the screen.
d. While the physician interviews you, he or she occasionally uses a mouse-pointingdevice to enter information into a computer workstation that you both can see.While doing so, the physician explains the data being reviewed and entered.
e. While the physician interviews you, he or she enters information into a clipboard-sized computer terminal that responds to finger touch and requires no keyboardtyping.
846 L. M. Fagan and E. H. Shortliffe

f. While the physician interviews you, he or she occasionally stops to dictate aphrase. A speech-understanding interface processes what is being said and storesthe infor mation in a medical record system.
g. There is no computer in the examining room, but you notice that between visits,the physician uses a workstation in the office to review and enter patient data.
Now imagine that you are the physician in each situation. How would you reactin each case? What do your answers to these questions tell you about the potentialeffect of computers on patient–physician rapport? What insight have you gainedregarding how interactive technologies could affect the patient–physicianencounter? Did you have different reactions to scenarios c and d? Do you believethat most people would respond to these two situations as you did?
3. You are the medical director of a 30-physician multispecialty group practice. Thepractice is physician-owned and managed and maintains a tight affiliation with anearby academic medical center. You are considering implementing an ambulatorymedical record system to support your practice operations. Discuss at least eight sig-nificant challenges you will face, considering technology, user, legal, and financial fac-tors. How will you address each issue?
4. Defend or refute the following proposition: “Knowledge-based clinical systems willbe widely used and generally accepted by clinician users within the next 5 years.”
5. You are asked to design a pharmacogenetic system that can help to understand whichpatients will respond to particular medicines. You need to design a database of studiesthat relate descriptions of the medical conditions, medications, and genetic sequences.Which terminologies would you choose for each of these data types? What are some keyelements that would need to be included in the database schemas? What problems doyou anticipate having in the design of the data structures for this task?
The Future of Computer Applications in Biomedicine 847