The Evolution of Adult-Onset Still Disease: An Observational and Comparative Study in a Cohort of 76...
7
The Evolution of Adult-Onset Still Disease: An Observational and Comparative Study in a Cohort of 76 Italian Patients Matteo Colina, MD,* Walter Zucchini, PhD, † Giovanni Ciancio, MD,* Carlo Orzincolo, MD, ‡ Francesco Trotta, MD,* and Marcello Govoni, MD* Objectives: Adult-onset Still’s disease (AOSD) is a potentially crippling or life-threatening rare disease that may be self-limited, intermittent, and chronic. Clinical predictors of outcome are still lacking, as is information on the rate of progress of its chronic course. The main objective is to identify factors that improve our ability to predict the course of AOSD, and factors associated with the rate of progress of its chronic course. A comparison with the literature is included. Methods: A retrospective cohort observational study conducted at the tertiary-referral Rheuma- tology Unit in Ferrara, Italy. Results: Seventy-six patients (44 females and 32 males) referred to the Unit and who satisfied the criteria for AOSD were identified. Our findings on white AOSD patients are largely compatible with those previously published. Ferritin level, as well disease activity score (DAS 28 ), is associated with the rate of progression of the articular manifestations of the disease. A polyarthritis persisting over 6 months is associated with the devel- opment of a chronic articular course, irrespective of the size of the involved joints. Conclusions: Ferritin, being associated with the course of AOSD, could play a role in the diagnosis of the disease. Together with DAS 28 , it might also serve as a useful predictor for the rate of progress of the chronic course of the disease, as measured with simple erosion narrowing score. © 2011 Elsevier Inc. All rights reserved. Semin Arthritis Rheum 41:279-285 Keywords: adult-onset Still’s disease, FUO, autoinflammatory syndromes, radiologic score A dult onset Still disease (AOSD) is a rare systemic in- flammatory disorder, characterized by 4 cardinal symp- toms: quotidian or double quotidian spiking fever, ar- thritis, an evanescent salmon-pink maculopapular rash, and a white blood cell count 10,000/mm 3 , mainly neutrophilic polymorphonuclear cells ( 1-8). The incidence rate is 0.16 to 0.29 per 100,000 persons and it seems more common in the Japanese than in the French ( 1,9,10). AOSD is slightly more frequent in women than in men and affects people older than 16, de novo, or those with a history of fever of unknown origin during childhood ( 11-13). However, several cases with onset after the age of 60 have been reported ( 14,15). The etiopathogenesis is still unknown and there is evi- dence supporting both the role of genetic predisposition and the environmental factors (16). Increased levels of interleu- kin (IL)-1, IL-6, IL-18, tumor necrosis factor, and macro- phage colony-stimulating factor might play a pivotal role in its etiopathogenesis (17-22). Although traditionally consid- ered a variant of rheumatoid arthritis (RA), recent evidence suggests that AOSD could be classified in the group of poly- genic autoinflammatory syndromes (23,24). Owing to the absence of specific markers, the diagnosis of AOSD remains a clinical one and is usually made after a careful evaluation, and after exclusion of infectious, neoplastic, and other auto- immune disorders. Furthermore, the full constellation of clinical and laboratory features may not be present at the onset, so that a reliable diagnosis may be delayed for several weeks or months (13,25). *Rheumatology Section, Department of Clinical And Experimental Medicine, Uni- versity of Ferrara, Ferrara, Italy. †Institute for Statistics and Econometrics, Georg-August-Universität, Göttingen, Germany. ‡Radiology Department, Ospedale degli Infermi, Faenza, Italy. This work was supported by grants from the Fondo Regione Emilia Romagna (PG 08 23943/2008/P18). Address reprint requests to Matteo Colina, MD, Sezione di Reumatologia, Dipar- timento Medicina Clinica e Sperimentale, Università degli Studi di Ferrara, Azienda S.Anna, Corso della Giovecca, 203, 44100 Ferrara, Italy. E-mail: matteo.colina@ gmail.com. MISCELLANEOUS 279 0049-0172/11/$-see front matter © 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.semarthrit.2010.12.006
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The Evolution of Adult-Onset Still Disease: An Observational and Comparative Study in a Cohort of 76...

The Evolution of Adult-OnsetStill Disease: An Observational and
Comparative Study in a Cohort of 76 Italian PatientsMatteo Colina, MD,* Walter Zucchini, PhD,† Giovanni Ciancio, MD,*
Carlo Orzincolo, MD,‡ Francesco Trotta, MD,* andMarcello Govoni, MD*
Objectives: Adult-onset Still’s disease (AOSD) is a potentially crippling or life-threatening raredisease that may be self-limited, intermittent, and chronic. Clinical predictors of outcome are stilllacking, as is information on the rate of progress of its chronic course. The main objective is toidentify factors that improve our ability to predict the course of AOSD, and factors associated withthe rate of progress of its chronic course. A comparison with the literature is included.Methods: A retrospective cohort observational study conducted at the tertiary-referral Rheuma-tology Unit in Ferrara, Italy.Results: Seventy-six patients (44 females and 32 males) referred to the Unit and who satisfied the criteria forAOSD were identified. Our findings on white AOSD patients are largely compatible with those previouslypublished. Ferritin level, as well disease activity score (DAS28), is associated with the rate of progression of thearticular manifestations of the disease. A polyarthritis persisting over 6 months is associated with the devel-opment of a chronic articular course, irrespective of the size of the involved joints.Conclusions: Ferritin, being associated with the course of AOSD, could play a role in the diagnosisof the disease. Together with DAS28, it might also serve as a useful predictor for the rate of progressof the chronic course of the disease, as measured with simple erosion narrowing score.© 2011 Elsevier Inc. All rights reserved. Semin Arthritis Rheum 41:279-285Keywords: adult-onset Still’s disease, FUO, autoinflammatory syndromes, radiologic score
Adult onset Still disease (AOSD) is a rare systemic in-flammatory disorder, characterized by 4 cardinal symp-toms: quotidian or double quotidian spiking fever, ar-
thritis, an evanescent salmon-pink maculopapular rash, and awhite blood cell count !10,000/mm3, mainly neutrophilicpolymorphonuclear cells (1-8). The incidence rate is 0.16 to0.29 per 100,000 persons and it seems more common in theJapanese than in the French (1,9,10). AOSD is slightly morefrequent in women than in men and affects people older than
16, de novo, or those with a history of fever of unknown originduring childhood (11-13). However, several cases with onsetafter the age of 60 have been reported (14,15).
The etiopathogenesis is still unknown and there is evi-dence supporting both the role of genetic predisposition andthe environmental factors (16). Increased levels of interleu-kin (IL)-1, IL-6, IL-18, tumor necrosis factor, and macro-phage colony-stimulating factor might play a pivotal role inits etiopathogenesis (17-22). Although traditionally consid-ered a variant of rheumatoid arthritis (RA), recent evidencesuggests that AOSD could be classified in the group of poly-genic autoinflammatory syndromes (23,24). Owing to theabsence of specific markers, the diagnosis of AOSD remainsa clinical one and is usually made after a careful evaluation,and after exclusion of infectious, neoplastic, and other auto-immune disorders. Furthermore, the full constellation ofclinical and laboratory features may not be present at theonset, so that a reliable diagnosis may be delayed for severalweeks or months (13,25).
*Rheumatology Section, Department of Clinical And Experimental Medicine, Uni-versity of Ferrara, Ferrara, Italy.†Institute for Statistics and Econometrics, Georg-August-Universität, Göttingen,Germany.‡Radiology Department, Ospedale degli Infermi, Faenza, Italy.
This work was supported by grants from the Fondo Regione Emilia Romagna (PG08 23943/2008/P18).
Address reprint requests to Matteo Colina, MD, Sezione di Reumatologia, Dipar-timento Medicina Clinica e Sperimentale, Università degli Studi di Ferrara, AziendaS.Anna, Corso della Giovecca, 203, 44100 Ferrara, Italy. E-mail: [email protected].
MISCELLANEOUS
2790049-0172/11/$-see front matter © 2011 Elsevier Inc. All rights reserved.doi:10.1016/j.semarthrit.2010.12.006

Both the clinical course and the prognosis of AOSD arehighly variable; the latter seems to be mostly influenced bythe visceral extension of the disease (4-7,26). The evolutionof the disease may be self-limited, intermittent, or chronic.Self-limited, or monocyclic disease, refers to a single episodethat subsequently fades and is followed by persistent goodhealth. The intermittent, or polycyclic, course of the diseaseis characterized by a complete remission followed by 1 ormore exacerbations. Flare-up occurrence is unpredictable.Chronic AOSD refers to a persistently active disease, usuallydue to a polyarthritic form, resembling RA (27).
The management of AOSD is primarily directed at theacute phase, while in the chronic forms RA-like arthritisrepresents the major problem (28,29). Thus the availabil-ity of reliable predictors for a chronic course might enablethe identification of patients with a poorer prognosis andhence warrant an early aggressive therapy.
In this study, the clinical features of a cohort of Italianpatients were followed up in a single tertiary referral centerand investigated, with special emphasis on patterns of diseasecourse and potential clinical predictors for the outcomes.The rate of progression of articular disease was also assessed.We compare our findings with those in the literature.
METHODS
Patient SelectionThe present study initially used a retrospective cohort design.All the patients diagnosed as having AOSD by physicians of theSection of Rheumatology, Department of Clinical and Experi-
mental Medicine, University of Ferrara, since 1985, were in-cluded. All the patients satisfied the 1992 Yamaguchi classifica-tion criteria (30). Since 1990, outcome data have beenprospectively recorded with regard to the clinical course, bloodtests results, and therapeutic regimens. Nineteen patients weretested for mediteranean fever mutations and all resulted nega-tive. Articular imaging (by conventional radiograms and/ormagnetic resonancewithgadolinium)wasperformedaccordingto clinical indication. Between May and June 2009 we con-ducted the last follow-up evaluations. For the study we haveconsidered only those patients whose diagnosis was still con-firmed in this period (31).
To identify the 5 articles that provided the data inFigures 1 to 3, a computerized literature search was con-ducted using Medline, PubMed, EMBase and CochraneCentral Register of Controlled Trials (CENTRAL) forarticles published in English (up to October 2010) apply-ing the MeSH terms and keywords “adult-onset Still dis-ease,” “fever of unknown origin,” and “autoinflammatorydiseases.” Boolean operators (NOT; AND; OR) wereused in succession to narrow and widen the search.
Only studies that published the raw data (or percent-ages, from which the counts could be computed) wereincluded. Of these, the 5 studies with the largest samplesizes were selected.
Determination of Disease ActivitySystemic and articular disease activity were determinedusing clinical, laboratory, and, in selected cases, radio-
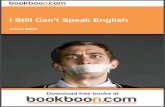
Figure 1 Incidence (number of cases and sample size), percentages, and 95% confidence intervals of clinical characteristics forour sample and those of the 5 largest previously published studies. Caption: 1: Masson and coworkers (4); 2: Ohta and coworkers(3); 3: Pouchot and coworkers (5); 4: Fautrel and coworkers (39); 5: Zeng and coworkers (8); 6: Colina and coworkers.
280 Evolution of adult-onset Still disease

graphic criteria. Active systemic disease required 2 ormore of the following: temperature higher than 39°C;typical rash; serositis; leukocytosis !10,000/mm3 (withneutrophilia !90%); reticuloendothelial involvement; orelevation of erythrosedimentation rate (ESR; normalvalue: "20 mm/h). Active articular disease, instead, re-quired 2 or more of the following: morning stiffness !30minutes, polyarthralgias, or synovial effusion. Duringeach visit the Health Assessment Questionnaire (HAQ)was administrated to patients who presented articular in-volvement and disease activity score (DAS28) was calcu-lated.
Classification of Patients by Disease PatternPatients were classified according to the types of articularor systemic pattern they presented at the onset of thedisease and during the follow-up. Classification was basedon review of case history by the authors (MC, GC). Indi-viduals with systemic disease were also subdivided inmonocyclic and polycyclic patterns. In the latter case, asymptom-free period of at least 2 months between 2 re-lapses had to be present. Chronic articular course has beencharacterized by the persistence of joint symptoms. Inpatients with articular disease we performed radiographsof affected joints every year to determine the evolutionof the disease. The Simple Erosions Narrowing Score(SENS) was used to score the radiographs (32,33). Radio-logic pictures were read with the assistance of an expertskeletal radiologist (CO).
Statistical AnalysisFor comparing our findings with those in the literature,we computed 95% confidence intervals for binomial pro-portions using the Agresti-Coull method (34) imple-mented in the library “binom” of the package R (35). Twomethods were applied in the follow-up analysis: Fisher’sexact test and the nonparametric “bootstrap Kolmogorov-Smirnov test” to test for equality of the distributions ofthe serum ferritin, as well as those of ESR and C-reactiveprotein. The test, which does not assume that the data arenormally distributed, is described in (36) and was imple-mented using function “ks.boot” of the R library “Match-ing.” A logistic regression, implemented using the R func-tion “glm,” was applied to assess whether the ferritinserum level is significantly associated with the progressionof the disease. A generalized linear model was used toidentify the predictors for the rate of progress of the artic-ular disease. This was used instead of a normal regressionmodel because the observations that we are analyzing arecounts (nonnegative integers), namely, the annual in-crease in the number of erosions, joint space narrowings(JSNs), and SENS. We used a negative binomial responseinstead of the usual Poisson because the counts are over-dispersed. The R library “gamlss” (37) was used for thecomputations. The model was initially fitted using thepredictors: serum ferritin level, HAQ, and DAS28 (all ob-tained at the time of diagnosis), number of years followingdiagnosis, and gender. In a second phase the model wasrefitted using only that subset of predictors that were
Figure 2 Incidence (number of cases and sample size), percentages, and 95% confidence intervals of laboratory characteristicsfor our sample and those of the 5 largest previously published studies. Caption: 1: Masson and coworkers (4); 2: Ohta andcoworkers (3); 3: Pouchot and coworkers (5); 4: Fautrel and coworkers (39); 5: Zeng and coworkers (8); 6: Colina and coworkers.
M. Colina et al. 281

clearly associated with the rate of progress. QQ plots ofthe quantile residuals (37) were used to check the fit of themodels.
RESULTS
Seventy-six European patients (44 females and 32 males)with a follow-up of at least 2 years who satisfied the crite-ria for AOSD were identified. Five patients had been ex-cluded from the study because they did not meet theserequirements. Five patients presented an episode of feverof unknown origin during childhood. In those cases fe-ver of unknown origin was considered to be the firstsymptom of the disease. The range of age at onset was 11to 70 years; the mean and standard deviation were 36 and14 years, respectively. The age distribution has a peak inthe interval of 20 to 30 years and then diminishes gradu-ally. The mean diagnostic delay was 21 months (SD 25);the large SD is explained by long delays, which reached upto 10 years, reflecting the possible diagnostic difficulties.Onset manifestations were as follows: fever in all the cases,articular symptoms in 55 patients (72%), rash in 44(58%), sore throat in 28 (37%), myalgias in 8 (13%), andhemophagocytic syndrome in 2 patients (3%). Typicalcutaneous manifestations were present in most cases, butwe observed some exceptions: fixed plaques (2 cases), ec-zematous lesions (2 cases), acneic lesions at trunk and rootof arms. Cutaneous dermographism was observed duringfollow-up in 19 patients (31%). Figures 1 to 3 display thefindings (cases and sample size) and 95% confidence in-tervals for the proportions of clinical and laboratory char-
acteristics for our sample as well as for the samples in the5 largest previously published studies. All the reportedclinical and laboratory characteristics were presentthroughout the course of the disease. The clinical coursesin AOSD patients were the following: monocyclic sys-temic pattern in 20 cases (26%), polycyclic systemic pat-tern in 23 cases (30%), and chronic articular pattern inthe remaining 33 (44%).
Symptoms, physical examination, and laboratory find-ings at the time of diagnosis and 6 months later for the 23patients with chronic systemic course and for the 33 pa-tients with chronic articular course are summarized inTable 1. There are no statistical differences between the 2groups, not even in the ferritin level, at the time of diag-nosis. Very clear are the differences between the distribu-tions of symptoms at the time of diagnosis and those after6 months; for example, the percentage of patients withrash decreased from 100% to 0%, etc. However, thisenormous reduction, which is attributable to therapy, isnot surprising.
The persistence of active articular manifestations after6 months was found to be strongly associated with achronic course (P value "0.001); in particular, it is worthobserving that, after 6 months, a polyarthritis was associ-ated with chronic articular course in all the cases. Thegender of patients was nearly significant at the 5% levelwith an indication that males are more likely to experiencea chronic course. The other variables that were consid-ered, but that were not significant, were as follows: defer-vescence "3 days, articular manifestations at onset, rash,
Figure 3 Incidence (number of cases and sample size), percentages, and 95% confidence intervals of our sample and those ofthe 2 previous studies. Captions: 1: Masson and coworkers (4); 2: Pouchot and coworkers (5); 3: Colina and coworkers.
282 Evolution of adult-onset Still disease

lymphoadenomegalies !3, ESR, C-reactive protein.Only ferritin was significant (P " 0.002); higher levels offerritin are associated with the chronic course. To exam-ine the relationship in the reverse order, we also applied alogistic regression with the course of the disease as depen-dent variable and ferritin level as an independent variable.The hypothesis that there is no relationship was rejected(P " 0.01); the probability of a chronic course increaseswith increasing levels of ferritin.
To identify the factors associated with the rate of prog-ress of the articular disease, observations were made oneach patient annually following diagnosis. We recordedthe number of erosions, the number of JSNs, and theSENS, the latter being the sum of the first 2. The annual
increase in each of the above counts was analyzed. Thepredictors considered were ferritin level, HAQ, andDAS28 (all measured at the time of diagnosis), gender, andthe duration of the disease.
The mean annual increase in SENS is associated withferritin level (P value "0.001) and DAS28 (P value "0.001); SENS increases faster for higher levels of these 2predictors. The same applies separately to erosions (P val-ues "0.001 and 0.08, respectively) and JSN (P valuesboth "0.001). The mean annual increase slows downwith time (measured here by the number of years follow-ing diagnosis) for JSN (P value " 0.001) and SENS (Pvalue # 0.002). Figure 4 displays how the mean annualincrease in the number of erosions, in JSN and in SENS,
Table 1 Clinical and Laboratory Characteristics at the Time of Diagnosis and 6 months Later for Chronic Systemic andChronic Articular Course
Symptoms and LabFindings
Policyclic (23 Patients) Chronic Articular (33 Patients)
At Time ofDiagnosis
After 6Months
At Time ofDiagnosis
After 6Months
Articular manifestationArthralgie 26% 57% 21% 33%Mono-oligo arthritis 48% 43% 30% 67%Poliarthritis 26% 0% 49% 0%
Defervescenzae "3 daysYes 43% NA 30% NA
RashYes 100% 0% 88% 9%
Lymphoadenomegalies !3Yes 57% 13% 64% 15
ESRMean (SD) 84 (25) 28 (24) 81 (27) 31 (21)
CRPMean (SD) 7.8 (4.8) 3.1 (2.5) 7.4 (5.0) 6.4 (6.6)
FerritinMean (SD) 3645 (6204) 229 (97) 7242 (9806) 1593 (3643)
Figure 4 The dependence of the mean annual increase in the number of erosions, JSN, and SENS on DAS28, ferritin, and yearpost diagnosis. Caption: Left panel: annual increase as a function of DAS, for ferritin level # 4000 ng/mL, and 5 years postdiagnosis; middle panel: annual increase as a function of ferritin, for DAS28 # 4 and 5 years post diagnosis; right panel: annualincrease as a function of year post diagnosis, for ferritin level # 4000 ng/mL and DAS28 # 4.
M. Colina et al. 283

depends on each of the 3 predictors, in each case forselected constant levels of the remaining 2 predictors. So,for example, the left panel in Figure 4 shows how themean annual increase of erosions of JSN and of SENSdepend on DAS in the fifth year after diagnosis and for aferritin level of 4000 ng/mL. The curve changes if a dif-ferent year, or a different ferritin level, is selected, al-though its general shape remains the same.
DISCUSSION
AOSD represents a potentially crippling or life-threaten-ing disease in young adults. Although rare, it has beenidentified with increasing frequency worldwide since itsfirst extensive description in 1971 (38).
There are currently several classification criteria forAOSD, but those of Yamaguchi are the most used. How-ever, it is worth recalling that the latter are not specified indetail. In particular, the exclusion criteria provide onlygeneral recommendations and there is no precise list ofdiagnoses or set of laboratory tests to be performed. Thesecond important limitation is that serum ferritin and itsglycosylated component are not included as is in Fautrel’sproposed criteria (39).
As far our study is concerned, the findings summarizedin Figures 1 to 3 exhibit some inconsistencies with previ-ous studies. Possible explanations include a selection biasdue to diverse sensitivity in collecting anamnestic data bydifferent clinicians, and also different genetic back-grounds. Since we regard AOSD as being principally afebrile disease, it is of some concern that in 2 studies theproportion of patients with spiking fever was estimated asbeing clearly below 1 (Fig. 1). For example, Fautrel andcoworkers reported fever in only 85% of subjects. Thisdifference might be due to referral bias, considering thenonrheumatologic selection of the patients in that work.We also conjecture that lower proportions that we ob-served for arthritic involvement of knees, ankles, elbows,and shoulders (Fig. 3) might be explained by the fact thatwe prescribed imaging of these joints only when clinicallyindicated. Again, different genetic backgrounds mightalso play a role.
The long-term natural history of AOSD is not yet fullyknown, principally due to paucity of evidence.
Of the 3 courses of AOSD, chronic articular disease hasthe worst prognosis quoad valetudinem because of theerosivity of articular involvement. In contrast to RA, ero-sions are not an early event, which is not surprising con-sidering that in AOSD the 2 major prognostic factors forearly erosive poliarthritis, namely rheumatoid factor andanticyclic citrullinated peptides antibodies, are absent.
Our study has demonstrated that serum ferritin isstrongly associated with a poorer prognosis. Ferritin is anacute phase reactant, produced by the hystiocytes-macro-phage system under stimulation of IL-1", IL-18, tumornecrosis factor-#, and IL-6, and is also released by dam-aged hepatocytes (40). The usefulness of elevated serum
ferritin concentrations as a diagnostic tool is limited by itsoccurrence at very high levels in other diseases, therebyreducing its specificity for AOSD. The comparison offerritin levels between those patients with chronic sys-temic and chronic articular course also weakens the casefor regarding ferritin as a prognostic marker, but does notcontradict the fact that ferritin levels differed significantlywhen all 3 courses were considered. Thus our data suggestthat ferritin might yet be a useful prognostic factor (41-43), perhaps in combination with others.
In conclusion, our findings on white AOSD patientsare largely compatible with those previously published. Anotable difference is the association of ferritin level,DAS28, and years from diagnosis with the rate of progres-sion of the articular manifestations of the disease. Weobserved that an active polyarthritis persisting over 6months from the onset, irrespective of the size of theinvolved joints, is associated with the development of achronic articular course. This could be considered tauto-logic, but it is worth considering that, as for early RA, thepersistence of joint symptoms over time is the most reli-able chronicity index. It is also very interesting to noticethat a mono-oligoarthritis may also actively persist andrequire aggressive treatments. In our opinion patientswith a systemic form of the disease should be closely mon-itored because this subset exhibits the worst prognosisquod vitam (44-46).
This study is not valid for epidemiologic purposes be-cause of a large proportion of patients came from otherdistricts. Furthermore, this is an observational study inwhich there was no control over the selection of patients.It is also worth observing that there were large overlaps inthe distributions of ferritin for the different courses,which thus reduce its effectiveness as a predictor. Ofcourse, prospective studies, involving a larger number ofAOSD patients, are needed to confirm our findings re-garding prognostic factors. As the disease is rare, definitiveresults might require a multicenter study.
REFERENCES
1. Esdaile JM. Adult Still’s disease. In: Hochberg MC, Silman AJ,Smolen JS, Weinblatt ME, Weisman MH, editors. Rheumatol-ogy, 4th ed. London: Mosby; 2008. p. 785-92.
2. Efthimiou P, Paik PK, Bielory L. Diagnosis and management ofadult onset Still’s disease. Ann Rheum Dis 2006;65:564-72.
3. Ohta A, Yamaguchi M, Tsunematsu T, Kasukawa R, MizushimaH, Kashiwagi H, et al. Adult Still’s disease: a multicenter survey ofJapanese patients. J Rheumatol 1990;17:1058-63.
4. Masson C, Le Loët X, Lioté F, Renou P, Dubost JJ, Boissier MC,et al. Adult Still’s disease: Part I. Manifestations and complica-tions in sixty-five cases in France. Rev Rhum Engl Ed 1995;62:748-57.
5. Pouchot J, Sampalis JS, Beaudet F, Carette S, Décary F, Salusin-sky-Sternbach M, et al. Adult Still’s disease: manifestations, dis-ease course, and outcome in 62 patients. Medicine 1991;70:118-36.
6. Wouters JM, van de Putte LB. Adult-onset Still’s disease: clinicaland laboratory features, treatment and progress in 45 cases. QJ Med 1986;61:1055-65.
284 Evolution of adult-onset Still disease

7. Reginato AJ, Schumacher HR Jr, Baker DG, O’Connor CR, Fer-reiros J. Adult onset Still’s disease: experience in 23 patients andliterature review with emphasis on organ failure. Semin ArthritisRheum 1987;17:39-57.
8. Zeng T, Zou YQ, Wu MF, Yang CD. Clinical features and prog-nosis of adult-onset Still’s disease: 61 cases from China. J Rheu-matol 2009;36:1026-31.
9. Magadur-Joly G, Billaud E, Barrier JH, Pennec YL, Masson C,Renou P, et al. Epidemiology of adult Still’s disease: estimate ofthe incidence by a retrospective study in west France. Ann RheumDis 1995;54:587-90.
10. Wakai K, Ohta A, Tamakoshi A, Ohno Y, Kawamura T, Aoki R,et al. Estimated prevalence and incidence of adult Still’s disease:findings by a nationwide epidemiological survey in Japan. J Epi-demiol 1997;7:221-5.
11. Ohta A, Yamaguchi M, Kaneoka H, Nagayoshi T, Hiida M.Adult Still’s disease: review of 228 cases from the literature.J Rheumatol 1987;14:1139-46.
12. Kahn MF. Adult Still’s disease. Still many issues unresolved.J Rheumatol 1996;23:2015-6.
13. Fautrel B. Adult-onset Still disease. Best Pract Res Clin Rheuma-tol 2008;22:773-92.
14. Wouters JM, van Rijswijk MH, van de Putte LB. Adult onsetStill’s disease in the elderly: a report of two cases. J Rheumatol1985;12:791-3.
15. Uson J, Pena JM, del Arco A, Barbado FJ, Vazquez JJ. Still’sdisease in a 72-year old man. J Rheumatol 1993;20:1608.
16. Arlet JB, Le Thi Huong DB, Pochot J, Piette JC. Physiopatholo-gie de la maladie de Still de l’adulte. Rev Med Interne 2005;26:549-56.
17. Efthimiou P, Kontzias A, Ward CM, Ogden NS. Adult-onsetStill’s disease: can recent advances in our understanding of itspathogenesis lead to targeted therapy? Nat Clin Pract Rheumatol2007;3:328-35.
18. Hoshino T, Ohta A, Yang D, Kawamoto M, Kikuchi M, Inoue Y,et al. Elevated serum interleukin 6, interferon-gamma, and tumornecrosis factor-alpha levels in patients with Still’s disease. J Rheu-matol 1998;25:396-8.
19. Dinarello CA. IL-18: a TH1-inducing, proinflammatory cyto-kine and new member of the IL-1 family. J Allergy Clin Immunol1999;103:11-24.
20. Kawashima M, Yamamura M, Taniai M, Yamauchi H, TanimotoT, Kurimoto M, et al. Levels of interleukin-18 and its bindinginhibitors in the blood circulation of patients with adult-onsetStill’s disease. Arthritis Rheum 2001;44:550-60.
21. Kawaguchi Y, Terajima H, Harigai M, Hara M, Kamatani N.Interleukin-18 as a novel diagnostic marker and indicator of dis-ease severity in adult-onset Still’s disease. Arthritis Rheum 2001;44:1716-7.
22. Choi JH, Such CH, Lee YM, et al. Serum cytokine profiles inpatients with adult onset Still’s disease. J Rheumatol 2003;30:2422-7.
23. Chen DY, Lan JL, Lin FJ, Hsieh TY. Proinflammatory cytokineprofiles in sera and pathological tissues of patients with activeuntreated adult onset Still’s disease. J Rheumatol 2005;53:320-7.
24. Masters SL, Simon A, Aksentijevic I, Kastner DL. Horror auto-inflammaticus: the molecular pathophisiology of autoinflamma-tory disease. Annu Rev Immunol 2009;27:621-8.
25. Wung PK, Pipeling MR, Wigley FM. “Still” ill? Am J Med 2008;121:491-3.
26. Masson C, Le Loët X, Lioté F, Renou P, Dubost JJ, Boissier MC,et al. Adult Still’s disease: part II. Management, outcome andprognostic factors. Rev Rhum Engl Ed 1995;62:758-65.
27. Cush JJ, Medgser TA Jr, Christy WC, et al. Adult-onset Still’sdisease: clinical course and outcome. Arthritis Rheum 1987;30:186-94.
28. Bagnari V, Colina M, Ciancio G, Govoni M, Trotta F. Adult-onset Still’s disease: a review. Rheumatol Int 2010;30:855-62.
29. Efthimiou P, Georgy S. Pathogenesis and management of adult-onset Still’s disease. Semin Arthritis Rheum 2006;36:144-52.
30. Yamaguchi M, Ohta A, Tsunematsu T, Kasukawa R, MizushimaY, Kashiwagi H, et al. Preliminary criteria for classification ofadult Still’s disease. J Rheumatol 1992;19:424-30.
31. Trotta F, Dovigo L, Scapoli G, Cavazzini L, Castoldi G. Immu-noblastic malignant lymphoma in adult onset Still’s disease.J Rheumatol 1993;20:1788-92.
32. van der Heijde D, Dankert T, Nieman F, Rau R, Boers M. Reli-ability and sensitivity to change of a simplification of the Sharp/van der Heijde radiological assessment in rheumatoid arthritis.Rheumatology 1999;38:941-7.
33. Dias EM, Lukas C, Landewé R, Fatenejad S, van der Heijde D.Reliability and sensitivity to change of the Simple Erosion Nar-rowing Score compared with the Sharp-van der Heijde methodfor scoring radiographs in rheumatoid arthritis. Ann Rheum Dis2008;67:375-9.
34. Agresti A, Coull BA. Approximate is better than “exact” for inter-val estimation of binomial proportions. Am Stat 1998;52:119-26.
35. Ihaka R, Gentleman R. R: a language for data analysis and graph-ics. J Comput Graph Stat 1996;5:299-314.
36. Abadie A. Bootstrap tests for distributional treatment effects ininstrumental variable models. JASA 2002;97:284-92.
37. Rigby RA, Stasinopoulos DM. Generalized additive models forlocation, scale and shape (with discussion). J Roy Stat Soc C App2005;54:507-54.
38. Bywaters EG. Still’s disease in the adult. Ann Rheum Dis 1971;30:121-33.
39. Fautrel B, Zing E, Golmard JL, Le Moël G, Bissery A, Rioux C, etal. Proposal for a new set of classification criteria for adult-onsetStill disease. Medicine 2002;81:194-200.
40. Zandman-Goddard G, Shoenfeld Y. Ferritin in autoimmune dis-eases. Autoimmun Rev 2007;6:457-63.
41. Fautrel B, Le Moël G, Saint-Marcoux B, Taupin P, Vignes S,Rozenberg S, et al. Diagnostic value of ferritin and glycosylatedferritin in adult onset Still’s disease. J Rheumatol 2001;28:322-9.
42. Lee MH, Means RT Jr. Extremely elevated serum ferritin levels ina university hospital: associated diseases and clinical significance.Am J Med 1995;98:566-71.
43. Lee SW, Park YB, Song JS, Lee SK. The mid-range of the adjustedlevel of ferritin can predict the chronic course in patients withadult onset Still’s disease. J Rheumatol 2009;36:156-62.
44. Colina M, Govoni M, Trotta F. Fatal myocarditis in adult-onsetStill disease with diffuse intravascular coagulation. Rheumatol Int2009;29:1355-7.
45. Dhote R, Simon J, Papo T, Detournay B, Sailler L, Andre MH, etal. Reactive hemophagocytic syndrome in adult systemic disease:report of twenty-six cases and literature review. Arthritis Rheum2003;15:633-9.
46. Arlet JB, Le Thi Huong D, Marinho A, Amoura Z, Wechsler B,Papo T, et al. Reactive haemophagocytic syndrome in adult-onsetStill’s disease: a report of six patients and a review of the literature.Ann Rheum Dis 2006;65:1596-601.
M. Colina et al. 285