
Behavioral and Psychological Symptoms in Alzheimer’s Disease

www.elsevier.com/locate/schres
Schizophrenia Researc
The effect of cognitive behavioral treatment on the positive
symptoms of schizophrenia spectrum disorders: A meta-analysis
G. Zimmermanna,c,T, J. Favrodb, V.H. Trieub, V. Pominib
aResearch Unit in Cognitive-behavioral Therapy, Institute for Psychotherapy, Department of Psychiatry, University of Lausanne, SwitzerlandbRehabilitation Unit, Department of Psychiatry, University of Lausanne, Switzerland
cDepartment of Psychology, University of Lausanne, Switzerland
Received 19 January 2005; received in revised form 24 February 2005; accepted 28 February 2005
Available online 5 April 2005
Abstract
Background: Despite the effectiveness of anti-psychotic pharmacotherapy, residual hallucinations and delusions do not
completely resolve in some medicated patients. Additional cognitive behavioral therapy (CBT) seems to improve the
management of positive symptoms. Despite promising results, the efficacy of CBT is still unclear. The present study addresses
this issue taking into account a number of newly published controlled studies.
Method: Fourteen studies including 1484 patients, published between 1990 and 2004 were identified and a meta-analysis of
their results performed.
Results: Compared to other adjunctive measures, CBT showed significant reduction in positive symptoms and there was a
higher benefit of CBT for patients suffering an acute psychotic episode versus the chronic condition (effect size of 0.57 vs.
0.27).
Discussion: CBT is a promising adjunctive treatment for positive symptoms in schizophrenia spectrum disorders. However, a
number of potentially modifying variables have not yet been examined, such as therapeutic alliance and neuropsychological
deficits.
D 2005 Elsevier B.V. All rights reserved.
Keywords: Cognitive behavioral therapy; Schizophrenia; Positive symptoms; Meta-analysis
0920-9964/$ - see front matter D 2005 Elsevier B.V. All rights reserved.
doi:10.1016/j.schres.2005.02.018
T Corresponding author. URTC - Institut Universitaire de Psy-
chotherapie, DUPA - Universite de Lausanne, Les Cedres- Site de
Cery, CH-1008 Prilly-Lausanne, Switzerland. Tel.: +41 21 643 63
15; fax: +41 21 643 65 93.
E-mail address: [email protected]
(G. Zimmermann).
1. Introduction
Despite the proven efficacy of anti-psychotic
drugs, a substantial proportion of patients (10–
60%) experience medication-resistant positive symp-
toms (Lindenmayer, 2000). Adjunctive psychological
treatments that can improve outcome are clearly
needed. Based on earlier case reports (Beck, 1952),
h 77 (2005) 1–9
G. Zimmermann et al. / Schizophrenia Research 77 (2005) 1–92
specialized cognitive behavioral approaches have
been developed to decrease patient’s distress asso-
ciated with hallucinations and delusions (Haddock et
al., 1998) and these may be useful as adjunctive
treatments.
Three recent meta-analyses have confirmed that
cognitive behavioral therapy (CBT) produces prom-
ising clinical effect on patients with schizophrenia
spectrum disorders (Gould et al., 2001; Pilling et al.,
2002; Rector and Beck, 2001). In the first empirical
review, Gould et al. (2001) indicated that the mean
effect size of CBT in reducing psychotic symptoms
was 0.65 (95% CI=0.56–0.71) across seven con-
trolled trials including 340 patients. Moreover,
follow-up analyses in four studies showed that
patients continued to improve over time (Mean
ES=0.93). However, Gould and colleagues con-
ducted statistical analysis on effect sizes without
taking sample size into account. However, effect
sizes based on large samples should play a bigger
role in any statistical analysis than those based on
smaller samples (Lipsey and Wilson, 2001; Shadish
and Haddock, 1994). In a second meta-analysis of
seven randomized clinical trials (RCTs) involving
383 subjects, group contrast analysis in six of the
seven studies demonstrated a large effect size in
favor of CBT (Mean weighted ES=0.91, SD=0.14)
(Rector and Beck, 2001). However, results of Beck’s
study rely only on six studies (including 239
patients) and among them were two with methodo-
logical limitations (absence of blind rating) that
report very large effect sizes (N0.75) in favor of
CBT (Drury et al., 1996; Pinto et al., 1999). Finally,
in a more recent meta-analysis of eight RCTs
including 393 patients, Pilling et al. (2002) con-
cluded on the basis of four suitable trials (273
patients) that CBT produce clear improvements in
mental state (Pooled fixed effect odds ratio=0.27;
95% CI=0.15–0.49) compared to all other treat-
ments. This very rigorous meta-analysis provides
promising results but unfortunately did not focus on
the improvement in positive symptoms. Furthermore,
Pilling et al. (2002) did not include three eligible
trials. The first trial was probably excluded because
of the absence of randomization (Garety et al., 1994).
Surprisingly, two other studies were not included
although continuous mental state data were available
(Pinto et al., 1999; Tarrier et al., 1993).
Despite these encouraging results, the issue about
CBTefficacy in the treatment of patients suffering from
psychotic disorders remains an open question (Tur-
kington et al., 2003). Furthermore, the Cochrane
library (Cormac et al., 2003) stated that CBT may
be of interest, but that other approaches, perhaps more
widely available, are just as effective. Recently,
numerous controlled trials have been completed and
thus, it is useful to further examine the effects of CBT
now that more patients have been included in trials.
The majority of the trials of CBT have been
conducted with chronic out-patients suffering from
persistent residual psychotic symptoms. However,
results of three studies have now been published in
which CBT was used with sample of in-patients
suffering from an acute psychotic episode (Drury et
al., 1996; Lewis et al., 2002; Startup et al., 2004).
Furthermore, a number of trials have included in
addition to TAU non-specific interventions as a se-
parate treatment limb to control for common effects of
psychological treatment. Thus, it would be interesting
to examine the effects of CBT related to psychotic
status of patients (chronic condition, acute episode)
and type of control conditions (treatment as usual,
non-specific intervention, waiting-list). To address
these issues, we conducted a meta-analysis to measure
the efficacy of CBT in the treatment of positive
symptoms in schizophrenia spectrum disorders.
2. Method
2.1. Literature searches
Comprehensive searches of the psychological
literature in PsycInfo, Medline, CINHAL and Francis
databases were conducted as well as studies men-
tioned in books. We obtained article abstracts by cross
referencing the following key search words: schizo-
phrenia, psychosis, cognitive behavioral therapy, CBT
and controlled trial. We examined the reference
sections of all retrieved studies, as well as in a set
of standard books on CBT.
2.2. Selection of studies
The search produced fifty-three studies. These
identified studies were included in our meta-analysis

G. Zimmermann et al. / Schizophrenia Research 77 (2005) 1–9 3
if they met the following criteria: (1) at least one CBT
group compared with a control group (waiting-list,
treatment as usual or another therapeutic treatment),
(2) studies participants meeting DSM-III R or DSM-
IV criteria for schizophrenia, schizoaffective disorder
or delusional disorder (American Psychiatric Associ-
ation, 1987, 1994), (3) at least one validated outcome
measure of positive symptoms (hallucinations and/or
delusions), (4) study results that provided sufficient
information to compute common effect size statistics
(supplemented, when necessary, by obtaining unpub-
lished information from the authors), (5) studies
completed between 1990 and 2004.
Since Marshall et al. (2000) suggested that the use
of an unpublished scale may be a source of bias in
schizophrenia trials, we only included data from
validated scales (e.g., Brief Psychiatric Rating Scale,
Comprehensive Psychopathological Rating Scale,
Maudsley Assessment of Delusions Schedule, Pos-
itive and Negative Syndrome Scale, Present State
Examination, Psychiatric Assessment Scale, Psychotic
Symptoms Rating Scales, Scale for the Assessment of
Positive Symptoms). Table 1 specifies which criteria
were used to rate positive symptoms.
2.3. Meta-analysis procedure
The key point in meta-analysis is to compute effect
size statistics capable of representing quantitative
results of a group of studies in a form that allows
comparison and synthesis (Cohen, 1988; Lipsey and
Wilson, 2001). In the current paper, the assessment of
changes in positive psychotic symptoms was the focus.
We thus calculated effect sizes (ES) on measures of
positive symptoms. Between-groups comparisons at
post-treatment, early follow-up (12 months and less)
and late follow-up (more than a year) on variables
of interest were computed using Hedge’s g (Hedges
and Ollkin, 1985). For between-subjects designs, ES
was defined as Mt�Mc /SDpooled, where SDpooled ¼ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiNt�1ð ÞSD2
t þ Nc�1ð ÞSD2c
� �= Nt�1ð Þþ Nc�1ð ÞÞð
q.Mt
is the mean of post-treatment experimental group,Mc is
the mean of post-treatment control group and SDpooled
the pooled within-group standard deviation. As it is not
unusual for studies to fail to report the means and
standard deviations needed to compute ES, a number of
different method were used to estimate ES from other
statistics that are reported (for a review, see Lipsey
and Wilson, 2001). Given that g is a slightly biased
estimate of ES particularly in small sample study
(Hedges and Ollkin, 1985), unbiased g-statistics
(unbiased g =[1� (3H (4N�9))]�g) were computed
and used in further analyses. By convention, ES were
coded such that a positive sign indicates that the CBT
group improves more than the control group. In cases
where a study used more than one validated measure
to examine positive symptoms, results of multiple
measures were standardized and averaged in order to
result in a single ES for any study. Moreover, in
studies that had more than one control condition,
comparisons of CBT and these separate conditions
were treated as individual studies.
Next, we aggregated effect sizes of the studies
following the procedures of Hedges and Ollkin (1985)
for weighting each study’s effect size by the inverse of
it’s variance, therefore giving more weight to studies
with smaller variance. To test the null hypothesis that
the population effect size was zero, 95% confidence
interval (CI) of the mean effect sizes were computed
for the population parameter. The null hypothesis was
rejected at significance level of .05 when zero was not
contained within the CI. In order to facilitate the
interpretation and to examine the practical importance
of ES, we used the widely known Binomial Effect
Size Display (BESD) developed by Rosenthal and
Rubin (1982). We used the homogeneity Q statistic to
test the assumption that all studies included in this
meta-analysis shared a common population effect size
(Hedges and Ollkin, 1985). The primary analysis used
a fixed effect model (FEM), considering that the
unique source of sampling error was the variation
resulting from the sampling of persons into studies
(Hedges, 1994; Hedges and Vevea, 1998). However,
to account for heterogeneity between treatments, a
randomized effect model (REM) was also employed
(Shadish and Haddock, 1994).
As the selective publication of positive findings
controlled trials is an important concern in meta-
analytic reviews of the literature (Lipsey and Wilson,
1993), the Fail-safe N (FSN) for the average effect
sizes was computed (Orwin, 1983). The FSN repre-
sent the number of unpublished (or unobtained)
studies with null effect sizes that would have to be
included to reduce the mean ES to a specified trivial
level.
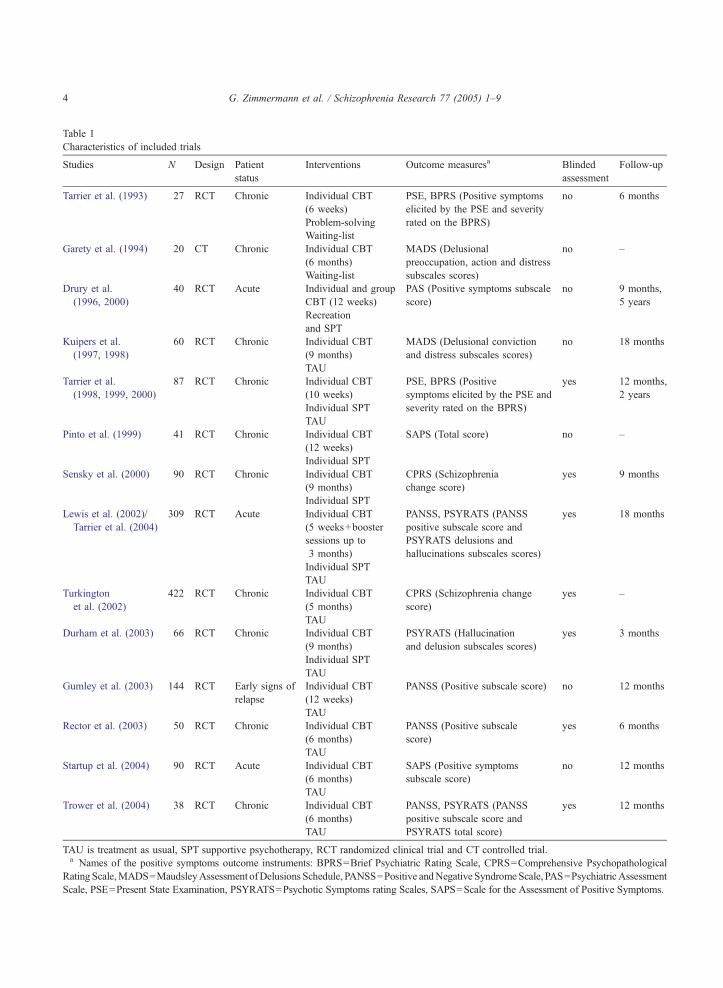
Table 1
Characteristics of included trials
Studies N Design Patient
status
Interventions Outcome measuresa Blinded
assessment
Follow-up
Tarrier et al. (1993) 27 RCT Chronic Individual CBT
(6 weeks)
PSE, BPRS (Positive symptoms
elicited by the PSE and severity
rated on the BPRS)
no 6 months
Problem-solving
Waiting-list
Garety et al. (1994) 20 CT Chronic Individual CBT
(6 months)
MADS (Delusional
preoccupation, action and distress
subscales scores)
no –
Waiting-list
Drury et al.
(1996, 2000)
40 RCT Acute Individual and group
CBT (12 weeks)
PAS (Positive symptoms subscale
score)
no 9 months,
5 years
Recreation
and SPT
Kuipers et al.
(1997, 1998)
60 RCT Chronic Individual CBT
(9 months)
MADS (Delusional conviction
and distress subscales scores)
no 18 months
TAU
Tarrier et al.
(1998, 1999, 2000)
87 RCT Chronic Individual CBT
(10 weeks)
PSE, BPRS (Positive
symptoms elicited by the PSE and
severity rated on the BPRS)
yes 12 months,
2 years
Individual SPT
TAU
Pinto et al. (1999) 41 RCT Chronic Individual CBT
(12 weeks)
SAPS (Total score) no –
Individual SPT
Sensky et al. (2000) 90 RCT Chronic Individual CBT
(9 months)
CPRS (Schizophrenia
change score)
yes 9 months
Individual SPT
Lewis et al. (2002)/
Tarrier et al. (2004)
309 RCT Acute Individual CBT
(5 weeks+booster
sessions up to
3 months)
PANSS, PSYRATS (PANSS
positive subscale score and
PSYRATS delusions and
hallucinations subscales scores)
yes 18 months
Individual SPT
TAU
Turkington
et al. (2002)
422 RCT Chronic Individual CBT
(5 months)
CPRS (Schizophrenia change
score)
yes –
TAU
Durham et al. (2003) 66 RCT Chronic Individual CBT
(9 months)
PSYRATS (Hallucination
and delusion subscales scores)
yes 3 months
Individual SPT
TAU
Gumley et al. (2003) 144 RCT Early signs of
relapse
Individual CBT
(12 weeks)
PANSS (Positive subscale score) no 12 months
TAU
Rector et al. (2003) 50 RCT Chronic Individual CBT
(6 months)
PANSS (Positive subscale
score)
yes 6 months
TAU
Startup et al. (2004) 90 RCT Acute Individual CBT
(6 months)
SAPS (Positive symptoms
subscale score)
no 12 months
TAU
Trower et al. (2004) 38 RCT Chronic Individual CBT
(6 months)
PANSS, PSYRATS (PANSS
positive subscale score and
PSYRATS total score)
yes 12 months
TAU
TAU is treatment as usual, SPT supportive psychotherapy, RCT randomized clinical trial and CT controlled trial.a Names of the positive symptoms outcome instruments: BPRS=Brief Psychiatric Rating Scale, CPRS=Comprehensive Psychopathological
Rating Scale,MADS=MaudsleyAssessment ofDelusions Schedule, PANSS=Positive andNegative SyndromeScale, PAS=PsychiatricAssessment
Scale, PSE=Present State Examination, PSYRATS=Psychotic Symptoms rating Scales, SAPS=Scale for the Assessment of Positive Symptoms.
G. Zimmermann et al. / Schizophrenia Research 77 (2005) 1–94

G. Zimmermann et al. / Schizophrenia Research 77 (2005) 1–9 5
3. Results
Fifteen studies involving 1504 patients (68.1% of
male, mean age of 36.02 years, SD=4.53) met the
criteria for inclusion in this analysis. Sufficient data to
compute effect size were available from twelve
published articles. For the remaining three studies
(Haddock et al., 1999; Trower et al., 2004; Turkington
et al., 2002), authors were contacted by e-mail.
Because appropriate data were not available from
the authors, one study was excluded. Table 1 provides
an overview of descriptive information about the 14
included studies involving 1484 patients.
3.1. Post-treatment
Of theses 1484 participants, a total of 1001 patients
took part in the post-treatment analyses, including 515
who received CBT and 486 a comparison treatment.
Fig. 1 plots the individual studies effect sizes that
were included in the post-treatment analysis.
Se
Turkington et a
Durham, et al. 2003 (CBT vs SPT)
Durham, et al. 2003 (CBT vs TAU)
Tarrier, et al. 1993 (CBT vs problem solving)
-0.5 0
Effect si
Fig. 1. Effect sizes for each of the studies included in the post-treatment
The fixed effect model (FEM) mean weighted ES
across all studies was 0.35 (95% CI: 0.23–0.47), the
random effect model (REM) mean weighted ES,
0.37 (95% CI: 0.23–0.52). These ES are modestly
lower than that found for the difference between
bona fide and placebo treatments (Lipsey and
Wilson, 1993) and can be classified in the small to
moderate range of effect sizes (Cohen, 1988). Over-
all, these ES imply that a typical patient in the CBT
group improved more than 64% of the control
patients and that CBT increases the success rate of
reducing positive symptoms from 41% to 59%.
Moreover, homogeneity test was not significant
(Q =21.41, p N .05) suggesting that moderating var-
iables do not play an important role in predicting the
treatment outcome. The findings can consequently be
considered as relatively robust. The FSN analysis
indicated that 14 studies with null effect sizes would
be necessary to bring the present meta-analysis
overall ES value to the 0.20 level (small effect).
Therefore, the bfile drawer problemQ is unlikely to
Garety, et al. 1994
Drury, et al. 1996
Kuipers, et al. 1997
Tarrier, et al. 1998 (CBT vs SPT)
Tarrier, et al. 1998 (CBT vs TAU)
Pinto, et al. 1999
nsky, et al. 2000
Lewis, et al. 2002 (CBT vs SPT)
Lewis, et al. 2002 (CBT vs TAU)
l. 2002
Rector, et al. 2003
Startup, et al. 2004
Trower, et al. 2004
Tarrier, et al. 1993 (CBT vs waiting list)
Combined (17)
0.5 1
ze
group contrast analysis (unblinded trials are colored in light grey).

Table 2
Post-treatment group contrast analysis details
Analysis Studies Patients Fixed effect model (FEM) Random effect model (REM) Q statistics
N N Effect sizes
(95% CI)
BESD Control vs.
CBT success rates
Effect sizes
(95% CI)
BESD Control vs.
CBT success rates
Chronic condition 10 798 0.27 (0.11–0.42) .433–.567 0.27 (0.11–0.42) .433–.567 8.72, p N .05
Acute episode 3 203 0.57 (0.31–0.83) .363–.637 0.57 (0.31–0.83) .363–.637 1.50, p N .05
Q is a homogeneity statistic ( p N .05 indicates homogeneity).
G. Zimmermann et al. / Schizophrenia Research 77 (2005) 1–96
influence the overall result, even though only
published studies were used.
As methodological heterogeneity between studies
may result in different conclusions about treatment
efficacy (Kazdin, 1994), we compared studies with
and without blind outcome assessment (see Fig. 1).
Results indicated that the FEM and REM mean
weighted ES were 0.54 (95% CI: 0.29–0.79) across
studies without blind assessment and 0.29 (95% CI:
0.15–0.43) across studies with blind assessment.
However, an independent sample t-test revealed that
the difference between unbiased ES from blinded and
unblinded trials is non-significant (t(15)=�0.91,
p N .05).
Table 2 lists the FEM and REM mean weighted
ES for studies conducted with stabilized patients
suffering from chronic positive psychotic symptoms
and patients in acute psychotic episodes, as well as
the number of studies contributing to the ES, its 95%
CI, the BSED and the Q homogeneity statistic. Table
3 makes a distinction between comparison treatments
Table 3
Post-treatment group contrast analysis details according to different types
Analysis Studies Patients Fixed effect model (FEM)
N N Effect sizes
(95% CI)
BESD Co
CBT succ
CBT vs. non-specific treatment
Chronic condition 5 246 0.32 (0.06–0.57) .421–.579
Acute episode 2 104 0.69 (0.30–1.09) .337–.663
All conditions 7 350 0.42 (0.21–0.64) .397–.603
CBT vs. treatment as usual
Chronic condition 6 569 0.26 (0.09–0.43) .436–.565
Acute episode 2 133 0.48 (0.13–0.82) .383–.617
All conditions 8 702 0.30 (0.15–0.46) .423–.577
CBT vs. waiting-list
Chronic condition 2 47 0.55 (0.04–1.14) .367–.633
Q is a homogeneity statistic ( p N .05 indicates homogeneity).
categorized as non-specific treatment, treatment as
usual and waiting-list and provides identical statistics
than Table 2. As can be seen in Table 2, mean
weight ES were larger for patients in the acute phase
than for patients in the chronic phase of the disorder.
In the acute state, these ES were in the moderate to
large range of effects sizes, whereas for patients in
the chronic state they were in the small to moderate
range. Moreover, results reported in Table 3 indi-
cated that mean weight ES in favor of CBT were in
the moderate range when compared to waiting-list
and in the small to moderate range when compared
to non-specific treatment and treatment as usual.
However, two-way ANOVA using unbiased ES as
the dependent variable and patient status (chronic vs.
acute) and control treatment format (non-specific,
treatment as usual, waiting-list) as independent
variables, did not show any significant group effects
(patient status: F(1, 16)=1.08, p N .05; control treat-
ment format: F(2, 15)= .30, p N .05) and interaction
effects (F(2, 15)= .76, p N .05).
of control condition
Random effect model (REM) Q statistics
ntrol vs.
ess rates
Effect sizes
(95% CI)
BESD Control vs.
CBT success rates
0.31 (0.02–0.61) .423–.577 5.99, p N .05
0.69 (0.30–1.09) .337–.663 0.85, p N .05
0.43 (0.18–0.68) .395–.605 9.32, p N .05
0.30 (0.07–0.53) .426–.574 9.52, p N .05
0.48 (0.13–0.82) .383–.617 0.01, p N .05
0.32 (0.15–0.50) .421–.579 10.75, p N .05
0.55 (0.04–1.14) .367–.633 0.64, p N .05

G. Zimmermann et al. / Schizophrenia Research 77 (2005) 1–9 7
3.2. Follow-up
Of the 14 studies included, 11 studies reported
follow-up data. A total 540 patients took part in the
early follow-up analyses (256 with CBT and 284 with
comparison treatment), and a total 353 patients took
part in the late follow-up analyses (127 with CBT and
226 with comparison treatment).
At early follow-up (3–12 months), the FEM and
REM mean weight ES were 0.40 (95% CI: 0.24–
0.57), indicating that the CBT efficacy was even
slightly better compared with immediately post-treat-
ment data. The homogeneity test was not statistically
significant (Q =12.80, p N .05). Furthermore, results at
late follow-up (N12 months) suggested that this gain
was essentially maintained over an extended period
(N12 months) after the end of treatment (ES=0.33,
95% CI: 0.14–0.51 / Q =2.77, p N .05).
4. Discussion
This review provides effect size analyses for
controlled studies of cognitive behavioral treatments
of positive symptoms in schizophrenia spectrum
disorders published during the last 15 years. This
meta-analysis using a sample of 14 outcome published
studies supports the general conclusion that CBT is a
promising approach for adjunctive treatment of
positive symptoms in patients with schizophrenia.
Moreover, the therapeutic effects are preserved at
follow-up, suggesting that the CBT has long-term
effects (Garety et al., 2000).
The global mean weighted effect size of 0.37 is
considered as modest, which is not surprising,
according to Tarrier and Wykes (2004), given the
severity of the disorder. This effect size dropped
even to 0.29 when we considered only blinded trials,
indicating that methodological flaws could make it
premature to identify psychological treatment as
efficacious. The effect size in the current study is
two and half times lower than the mean weighted
between-group effect size reported in the study of
Rector and Beck (2001). However, results of Beck’s
study rely only on six studies (including 239
patients) among which two report very large effect
sizes (N0.75) in favor of CBT (Drury et al., 1996;
Pinto et al., 1999). Furthermore, our results show
that CBT has a better effect on patients in an acute
psychotic episode (mean weighed ES=0.57) than on
stabilized chronic patients suffering from persistent
psychotic symptoms (mean weighted ES=0.27).
However, this difference was not statistically sig-
nificant, and the inclusion of the Drury et al. (1996)
study presenting some methodological limitations
might have conducted to an overestimation of effect
size in acutely ill patients. Moreover, a replication of
Drury’s study with a greater methodological rigor
failed to show the superiority of CBT over suppor-
tive counseling on acutely psychotic in-patients
(Haddock et al., 1999).
The comparison group designed to control non-
specific effects of therapy exposure differ greatly
between studies, ranging from waiting-list (Tarrier et
al., 1993; Garety et al., 1994) to manual-based and
supervised supportive counseling (Tarrier et al., 1998;
Lewis et al., 2002). Further effect sizes analyses
indicate, as expected, that CBT is more superior to
waiting-list than to non-specific intervention (mostly
defined as supportive therapy) and treatment as usual.
Interestingly, effects of CBT are slightly less pro-
nounced when it is compared with treatment as usual
rather than with non-specific treatment, such as
supportive counseling. However, differences between
comparison groups were non-significant.
Several limitations of this study are acknowledged.
First, a number of studies have included non-specific
treatment in addition to standard psychiatric care.
While other treatments could be considered as placebo
treatment, these non-specific interventions are also
heterogeneous between studies (supportive counsel-
ing, befriending, problem solving). Secondly, we did
not completely investigate the methodological quality
of each trial, and methodological differences have
been shown to interfere with the detection of a true
treatment effect (Kazdin, 1994; Kazdin and Bass,
1989). In this study, unblinded trials were associated
with an increased estimate of 86% of effect size.
Consequently, stringent controlled blind trials are
recommended for future randomized clinical trials
evaluating CBT. Finally, a relatively small number of
studies available for the meta-analysis made exami-
nation of many variables of interest statistically
underpowered.
Despite the importance of research in psychother-
apy indicating that the quality of the therapeutic

G. Zimmermann et al. / Schizophrenia Research 77 (2005) 1–98
relationship is one of the strongest predictor of a
successful outcome, there is growing bias in psycho-
therapy towards bempirically supported treatmentsQdependent on the medical model. Further research is
needed to address some unexamined potentially
important variables (for example alliance, competence
of therapist, treatment dosage). Finally, recent studies
suggest that schizophrenic patients present with a
deficit in source monitoring (Keefe et al., 2002) and
that memory distortions are associated with psychotic
symptoms (Clancy et al., 2002). Thus, combining
CBT with training for specific neuropsychological
deficits associated with auditory hallucinations or
delusions may also be important for future research
trials.
Acknowledgements
We thank Kerry Ross and Douglas Turkington for
providing data.
References
American Psychiatric Association, 1987. Diagnostic and Statistical
Manual of Mental Disorders: DSM-III-R, 3rd revised ed.
American Psychiatric Association, Washington, DC.
American Psychiatric Association, 1994. Diagnostic and Statistical
Manual of Mental Disorders: DSM-IV, 4th ed. American
Psychiatric Association, Washington, DC.
Beck, A.T., 1952. Successful outpatient psychotheraphy of a
chronic schizophrenic with a delusion based on borrowed guilt.
Psychiatry 15, 305–312.
Clancy, S.A., McNally, R.J., Schacter, D.L., Lenzenweger,
M.F., Pitman, R.K., 2002. Memory distortion in people re-
porting abduction by aliens. J. Abnorm. Psychology 111 (3),
455–461.
Cohen, J., 1988. Statistical Power Analysis for the Behavioral
Sciences, 2nd ed. Academic Press, New York.
Cormac, I., Campbell, C., Silveira Da Mota Neto, J., 2003.
Cognitive behaviour therapy for schizophrenia. Cochrane Data-
base Syst. Rev. 3, 14.
Drury, V., Birchwood, M., Cochrane, R., MacMillan, F., 1996.
Cognitive therapy and recovery from acute psychosis: a
controlled trial. I. Impact on psychotic symptoms. Br. J.
Psychiatry 169, 593–601.
Drury, V., Birchwood, M., Cochrane, R., 2000. Cognitive therapy
and recovery from acute psychosis: a controlled trial. 3. Five-
year follow-up. Br. J. Psychiatry 177, 8–14.
Durham, R.C., Guthrie, M., Morton, R.V., Reid, D.A., Treliving,
L.R., Fowler, D., Macdonald, R.R., 2003. Tayside–Fife clinical
trial of cognitive-behavioural therapy for medication-resistant
psychotic symptoms. Results to 3-month follow-up. Br. J.
Psychiatry 182, 303–311.
Garety, P.A., Kuipers, L., Fowler, D., Chamberlain, F., Dunn, G.,
1994. Cognitive behavioural therapy for drug-resistant psycho-
sis. Br. J. Med. Psychol. 67, 259–271.
Garety, P.A., Fowler, D., Kuipers, E., 2000. Cognitive-behavioral
therapy for medication-resistant symptoms. Schizophr. Bull. 26
(1), 73–86.
Gould, R.A., Mueser, K.T., Bolton, E., Mays, V., Goff, D., 2001.
Cognitive therapy for psychosis in schizophrenia: an effect size
analysis. Schizophr. Res. 48 (2-3), 335–342.
Gumley, A., O’Grady, M., McNay, L., Reilly, J., Power, K., Norrie,
J., 2003. Early intervention for relapse in schizophrenia: results
of a 12-month randomized controlled trial of cognitive
behavioural therapy. Psychol. Med. 33 (3), 419–431.
Haddock, G., Tarrier, N., Spaulding, W., Yusupoff, L., Kinney, C.,
McCarthy, E., 1998. Individual cognitive-behavior therapy in
the treatment of hallucinations and delusions: a review. Clin.
Psychol. Rev. 18 (7), 821–838.
Haddock, G., Tarrier, N., Morrisson, A.P., Hopkins, R., Drake,
R., Lewis, S., 1999. A pilot study evaluating the effective-
ness of individual inpatient cognitive-behavioural therapy in
early psychosis. Soc. Psychiatry Psychiatr. Epidemiol. 34,
254–258.
Hedges, L.V., 1994. Statistical considerations. In: Cooper, H.,
Hedges, L.V. (Eds.), The Handbook of Research Synthesis.
Russel Sage Foundation, New York, pp. 29–38.
Hedges, L.V., Ollkin, I., 1985. Statistical Methods for Meta-
analysis. Academic Press, New York.
Hedges, L.V., Vevea, J.L., 1998. Fixed- and random effects models
in meta-analysis. Psychol. Methods 3, 486–504.
Kazdin, A.E., 1994. Methodology, design and evaluation in
psychotherapy research. In: Bergin, A.E., Garfield, S.L.
(Eds.), Handbook of Psychotherapy and Behavior Change, 4th
ed. John Wiley & Sons, New York, pp. 19–71.
Kazdin, A.E., Bass, D., 1989. Power to detect differences between
alternative treatments in comparative psychotherapy outcome
research. J. Consult. Clin. Psychol. 51 (1), 138–147.
Keefe, R.S.E., Arnold, M.C., Bayen, U.J., McEvoy, J.P., Wilson,
W.H., 2002. Source-monitoring deficits for self-generated
stimuli ion schizophrenia: multinomial modeling of data from
three sources. Schizophr. Res. 57, 51–67.
Kuipers, E., Garety, P., Fowler, D., Dunn, G., Bebbington, P.,
Freeman, D., Hadley, C., 1997. London–East Anglia rando-
mised controlled trial of cognitive-behavioural therapy for
psychosis: I. Effects of the treatment phase. Br. J. Psychiatry
171, 319–327.
Kuipers, E., Fowler, D., Garety, P., Chisholm, D., Freeman, D.,
Dunn, G., Bebbington, P., Hadley, C., 1998. London–East
Anglia randomised controlled trial of cognitive-behavioural
therapy for psychosis: III. Follow-up and economic evaluation
at 18 months. Br. J. Psychiatry 173, 61–68.
Lewis, S., Tarrier, N., Haddock, G., Bentall, R., Kinderman, P.,
Kingdon, D., Siddle, R., Drake, R., Everitt, J., Leadley, K.,
Benn, A., Grazebrook, K., Haley, C., Akhtar, S., Davies, L.,
Palmer, S., Faragher, B., Dunn, G., 2002. Randomised
G. Zimmermann et al. / Schizophrenia Research 77 (2005) 1–9 9
controlled trial of cognitive-behavioural therapy in early
schizophrenia: acute-phase outcomes. Br. J. Psychiatry 43
(Supplementum 43), s91–s97.
Lindenmayer, J.-P., 2000. Treatment refractory schizophrenia.
Psychiatr. Q. 71 (4), 373–384.
Lipsey, M.W., Wilson, D.B., 1993. The efficacy of psychological,
educational, and behavioral treatment. Confirmation from meta-
analysis. Am. Psychol. 48 (12), 1181–1209.
Lipsey, M.W., Wilson, D.B., 2001. Practical Meta-analysis. Sage,
Thousand Oaks, CA.
Marshall, M., Lockwood, A., Bradley, C., Adams, C., Joy, C.,
Fenton, M., 2000. Unpublished rating scales: a major source of
bias in randomised controlled trials of treatments for schizo-
phrenia. Br. J. Psychiatry 176, 249–252.
Orwin, R.G., 1983. A fail-safe N for effect size in meta-analysis.
J. Educ. Stat. 8, 157–159.
Pilling, S., Bebbington, P., Kuipers, E., Garety, P., Geddes, J.,
Orbach, G., Morgan, C., 2002. Psychological treatments in
schizophrenia: I. Meta-analysis of family intervention and
cognitive behaviour therapy. Psychol. Med. 32 (5), 763–782.
Pinto, A., Pia, S.L., Mennella, R., Giorgio, D., DeSimone, L., 1999.
Cognitive-behavioral therapy and clozapine for clients with
treatment-refractory schizophrenia. Psychiatr. Serv. 50 (7),
901–904.
Rector, N.A., Beck, A.T., 2001. Cognitive behavioral therapy for
schizophrenia: an empirical review. J. Nerv. Ment. Dis. 189 (5),
278–287.
Rector, N.A., Seeman, M.V., Segal, Z.V., 2003. Cognitive therapy
for schizophrenia: a preliminary randomized controlled trial.
Schizophr. Res. 63 (1-2), 1–11.
Rosenthal, R., Rubin, D.B., 1982. A simple, general purpose
display of magnitude of experimental effect. J. Educ. Psychol.
74 (2), 166–169.
Sensky, T., Turkington, D., Kingdon, D., Scott, J.L., Scott, J.,
Siddle, R., O’Carroll, M., Barnes, T.R., 2000. A randomized
controlled trial of cognitive-behavioral therapy for persistent
symptoms in schizophrenia resistant to medication. Arch. Gen.
Psychiatry 57 (2), 165–172.
Shadish, W.R., Haddock, C.K., 1994. Combining estimates of
effect size. In: Cooper, H., Hedges, L.V. (Eds.), The Handbook
of Research Synthesis. Russel Sage Foundation, New York,
pp. 261–281.
Startup, M., Jackson, M.C., Bendix, S., 2004. North Wales
randomized controlled trial of cognitive behaviour therapy for
acute schizophrenia spectrum disorders: outcomes at 6 and 12
months. Psychol. Med. 34, 413–422.
Tarrier, N., Wykes, T., 2004. Is there evidence that cognitive
behaviour therapy is an effective treatment for schizophre-
nia? A cautious or cautionary tale? Behav. Res. Ther. 42,
1377–1401.
Tarrier, N., Beckett, R., Harwood, S., Baker, A., et al., 1993. A trial
of two cognitive-behavioural methods of treating drug-resistant
residual psychotic symptoms in schizophrenic patients: I.
Outcome. Br. J. Psychiatry 162, 524–532.
Tarrier, N., Yusupoff, L., Kinney, C., McCarthy, E., Gledhill, A.,
Haddock, G., Morris, J., 1998. Randomised controlled trial of
intensive cognitive behaviour therapy for patients with chronic
schizophrenia. Br. Med. J. 317, 303–307.
Tarrier, N., Wittkowski, A., Kinney, C., McCarthy, E., Morris, J.,
Humphreys, L., 1999. Durability of the effects of cognitive-
behavioural therapy in the treatment of chronic schizophrenia:
12 month follow-up. Br. J. Psychiatry 174, 500–504.
Tarrier, N., Kinney, C., McCarthy, E., Humphreys, L., Wittkowski,
A., Morris, J., 2000. Two-year follow-up of cognitive-behav-
ioral therapy and supportive counseling in the treatment of
persistent symptoms in chronic schizophrenia. J. Consult. Clin.
Psychol. 68 (5), 917–922.
Tarrier, N., Lewis, S., Haddock, G., Bental, R., Drake, R.,
Kinderman, P., Kingdon, D., Siddle, R., Everitt, B., Leadley,
K., Benn, A., Grazebrook, K., Haley, C., Akhtar, S., Davies, L.,
Palmer, S., Dunn, G., 2004. Cognitive-behavioural therapy in
first episode and early schizophrenia. 18-month follow-up of a
randomised controlled trial. Br. J. Psychiatry 184, 231–239.
Trower, P., Birchwood, M., Meaden, A., Byrne, S., Nelson, A.,
Ross, K., 2004. Cognitive therapy for command hallucinations:
randomised controlled trial. Br. J. Psychiatry 184, 312–320.
Turkington, D., Kingdon, D., Turner, T., 2002. Effectiveness of a
brief cognitive-behavioural therapy intervention in the treatment
of schizophrenia. Br. J. Psychiatry 180, 523–527.
Turkington, D., McKenna, P.J., Cannon, M., McKenzie, K., Sims,
A., 2003. Is cognitive-behavioural therapy a worthwhile treat-
ment for psychosis? Br. J. Psychiatry 182, 477–479.
Copyright © 2022 FDOKUMEN



















